User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Mycoplasma pneumoniae
Mycoplasma pneumoniae is a cell wall–deficient pleomorphic bacterium and well-reported cause of respiratory tract infection in the school-aged child. Symptoms are variable, and clinical presentations run the gamut from upper respiratory (usually self-limited) and lower respiratory tract involvement (pneumonia) to unusual manifestations including nervous system disease (encephalitis, cerebellar ataxia, transverse myelitis), hemolytic anemia, Stevens-Johnson syndrome, and myocarditis/pericarditis.
Pneumonia occurs in 10% of infected school-aged children, and cough can persist for 3-4 weeks; some children wheeze in the setting of Mycoplasma infection. Radiographic patterns of disease are variable; patchy alveolar infiltrates with small pleural effusions are often described. Consolidated pneumonia, large effusions, and hilar adenopathy are uncommonly reported, and severe disease has been described in certain patient populations, including those with sickle cell disease, children with Down syndrome, and those with immunodeficiencies. The acute chest presentation has been associated with M. pneumoniae in children with sickle cell anemia and prolonged hospitalizations (mean, 10 days), and the need for transfusion and mechanical ventilation was noted in 82% and 6%, respectively, in one study (Pediatrics 2003;112(1 Pt 1):87-95). Community clusters of pneumonia are reported in school-aged children, and in Rhode Island, an outbreak was reported in children from four schools; 76 had pneumonia and 3 had encephalitis (J. Infect. Dis. 2008;198:1365-74).

Considering this is a common pathogen, there are a number of questions regarding the scope of disease and impact of treatment that are incompletely answered. The first problem is that it is hard to confirm diagnostically. Culture is technically difficult, the organism takes up to 3 weeks to grow, and the diagnostic test is offered in very few labs. The old-fashioned cold agglutinin test has a low sensitivity and specificity; an increase in titers can be seen during a variety of viral infections. Polymerase chain reaction (PCR) on respiratory secretions is increasingly available; sensitivity and specificity are said to be 80% and 100%, respectively. The organism can persist in the respiratory tract for several weeks though, even after treatment, so PCR can remain positive for 2-3 weeks. This makes it hard to use PCR to confirm M. pneumoniae as the etiologic agent, especially in the setting of unusual clinical presentations. Serologic testing is often ordered and hard to interpret. False positive IgM antibody tests are not uncommon, and IgM antibody can persist for months. Outside of PCR and culture, acute and convalescent specimens can be used diagnostically, and a fourfold IgG antibody rise is consistent with acute infection.
Macrolides are regarded as the preferred treatment for M. pneumoniae pneumonia, but several studies question whether treatment impacts the clinical course. This may be due to the inherent difficulty of confirming M. pneumoniae as the etiologic agent, as most studies used serology to confirm the diagnosis. In countries outside the United States, macrolide resistance is well reported, and this may be underappreciated in the United States. We recently cared for a teenager with Down syndrome with pneumonia caused by M. pneumoniae who had a protracted clinical course. Fever and hypoxemia were persistent over a several-week period despite two courses of azithromycin and exclusion of virus, bacteria, and fungal pathogens. Bronchoalveolar lavage was performed, M. pneumoniae was detected by PCR, and macrolide resistance was confirmed. Levofloxacin was given, and she recovered over the next week.
Macrolide resistance is commonly reported outside the United States; rates in China are reported to be greater than 90%, in Japan 80%, and in Europe, between 15% and 25%. A recent study from Greg Storch and his colleagues (Pediatr. Infect. Dis. J. 2012;31:409-10) documented macrolide resistance in 8% of respiratory samples collected between 2007 and 2010 (49 patients; mean age, 10 years), noting the resistance rate was 3% in 2007-2008 and 15% in 2009-2010. A recently published study of data from Canada reported that 12.1% of M. pneumoniae–positive specimens collected between 2010 and January 2012 carried nucleotide mutations associated with macrolide resistance in the 23S rRNA gene (Emerg. Infect. Dis. 2013 September [doi: 10.3201/eid1909.121466]). Anecdotal studies suggest that patients with macrolide-resistant M. pneumoniae infection clinically improve when given doxycycline (or minocycline) or levofloxacin.
A number of clinical questions regarding M. pneumoniae may be answered more definitively in the future, but we need more easily available diagnostics (PCR is a good start), routinely accessible susceptibility data, and a good randomized controlled study to investigate the question of whether treatment shortens the course of disease.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri-Kansas City. She said she has no conflicts of interest to disclose. E-mail her at pdnews@frontlinemedcom.com.
Mycoplasma pneumoniae is a cell wall–deficient pleomorphic bacterium and well-reported cause of respiratory tract infection in the school-aged child. Symptoms are variable, and clinical presentations run the gamut from upper respiratory (usually self-limited) and lower respiratory tract involvement (pneumonia) to unusual manifestations including nervous system disease (encephalitis, cerebellar ataxia, transverse myelitis), hemolytic anemia, Stevens-Johnson syndrome, and myocarditis/pericarditis.
Pneumonia occurs in 10% of infected school-aged children, and cough can persist for 3-4 weeks; some children wheeze in the setting of Mycoplasma infection. Radiographic patterns of disease are variable; patchy alveolar infiltrates with small pleural effusions are often described. Consolidated pneumonia, large effusions, and hilar adenopathy are uncommonly reported, and severe disease has been described in certain patient populations, including those with sickle cell disease, children with Down syndrome, and those with immunodeficiencies. The acute chest presentation has been associated with M. pneumoniae in children with sickle cell anemia and prolonged hospitalizations (mean, 10 days), and the need for transfusion and mechanical ventilation was noted in 82% and 6%, respectively, in one study (Pediatrics 2003;112(1 Pt 1):87-95). Community clusters of pneumonia are reported in school-aged children, and in Rhode Island, an outbreak was reported in children from four schools; 76 had pneumonia and 3 had encephalitis (J. Infect. Dis. 2008;198:1365-74).
Considering this is a common pathogen, there are a number of questions regarding the scope of disease and impact of treatment that are incompletely answered. The first problem is that it is hard to confirm diagnostically. Culture is technically difficult, the organism takes up to 3 weeks to grow, and the diagnostic test is offered in very few labs. The old-fashioned cold agglutinin test has a low sensitivity and specificity; an increase in titers can be seen during a variety of viral infections. Polymerase chain reaction (PCR) on respiratory secretions is increasingly available; sensitivity and specificity are said to be 80% and 100%, respectively. The organism can persist in the respiratory tract for several weeks though, even after treatment, so PCR can remain positive for 2-3 weeks. This makes it hard to use PCR to confirm M. pneumoniae as the etiologic agent, especially in the setting of unusual clinical presentations. Serologic testing is often ordered and hard to interpret. False positive IgM antibody tests are not uncommon, and IgM antibody can persist for months. Outside of PCR and culture, acute and convalescent specimens can be used diagnostically, and a fourfold IgG antibody rise is consistent with acute infection.
Macrolides are regarded as the preferred treatment for M. pneumoniae pneumonia, but several studies question whether treatment impacts the clinical course. This may be due to the inherent difficulty of confirming M. pneumoniae as the etiologic agent, as most studies used serology to confirm the diagnosis. In countries outside the United States, macrolide resistance is well reported, and this may be underappreciated in the United States. We recently cared for a teenager with Down syndrome with pneumonia caused by M. pneumoniae who had a protracted clinical course. Fever and hypoxemia were persistent over a several-week period despite two courses of azithromycin and exclusion of virus, bacteria, and fungal pathogens. Bronchoalveolar lavage was performed, M. pneumoniae was detected by PCR, and macrolide resistance was confirmed. Levofloxacin was given, and she recovered over the next week.
Macrolide resistance is commonly reported outside the United States; rates in China are reported to be greater than 90%, in Japan 80%, and in Europe, between 15% and 25%. A recent study from Greg Storch and his colleagues (Pediatr. Infect. Dis. J. 2012;31:409-10) documented macrolide resistance in 8% of respiratory samples collected between 2007 and 2010 (49 patients; mean age, 10 years), noting the resistance rate was 3% in 2007-2008 and 15% in 2009-2010. A recently published study of data from Canada reported that 12.1% of M. pneumoniae–positive specimens collected between 2010 and January 2012 carried nucleotide mutations associated with macrolide resistance in the 23S rRNA gene (Emerg. Infect. Dis. 2013 September [doi: 10.3201/eid1909.121466]). Anecdotal studies suggest that patients with macrolide-resistant M. pneumoniae infection clinically improve when given doxycycline (or minocycline) or levofloxacin.
A number of clinical questions regarding M. pneumoniae may be answered more definitively in the future, but we need more easily available diagnostics (PCR is a good start), routinely accessible susceptibility data, and a good randomized controlled study to investigate the question of whether treatment shortens the course of disease.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri-Kansas City. She said she has no conflicts of interest to disclose. E-mail her at pdnews@frontlinemedcom.com.
Mycoplasma pneumoniae is a cell wall–deficient pleomorphic bacterium and well-reported cause of respiratory tract infection in the school-aged child. Symptoms are variable, and clinical presentations run the gamut from upper respiratory (usually self-limited) and lower respiratory tract involvement (pneumonia) to unusual manifestations including nervous system disease (encephalitis, cerebellar ataxia, transverse myelitis), hemolytic anemia, Stevens-Johnson syndrome, and myocarditis/pericarditis.
Pneumonia occurs in 10% of infected school-aged children, and cough can persist for 3-4 weeks; some children wheeze in the setting of Mycoplasma infection. Radiographic patterns of disease are variable; patchy alveolar infiltrates with small pleural effusions are often described. Consolidated pneumonia, large effusions, and hilar adenopathy are uncommonly reported, and severe disease has been described in certain patient populations, including those with sickle cell disease, children with Down syndrome, and those with immunodeficiencies. The acute chest presentation has been associated with M. pneumoniae in children with sickle cell anemia and prolonged hospitalizations (mean, 10 days), and the need for transfusion and mechanical ventilation was noted in 82% and 6%, respectively, in one study (Pediatrics 2003;112(1 Pt 1):87-95). Community clusters of pneumonia are reported in school-aged children, and in Rhode Island, an outbreak was reported in children from four schools; 76 had pneumonia and 3 had encephalitis (J. Infect. Dis. 2008;198:1365-74).
Considering this is a common pathogen, there are a number of questions regarding the scope of disease and impact of treatment that are incompletely answered. The first problem is that it is hard to confirm diagnostically. Culture is technically difficult, the organism takes up to 3 weeks to grow, and the diagnostic test is offered in very few labs. The old-fashioned cold agglutinin test has a low sensitivity and specificity; an increase in titers can be seen during a variety of viral infections. Polymerase chain reaction (PCR) on respiratory secretions is increasingly available; sensitivity and specificity are said to be 80% and 100%, respectively. The organism can persist in the respiratory tract for several weeks though, even after treatment, so PCR can remain positive for 2-3 weeks. This makes it hard to use PCR to confirm M. pneumoniae as the etiologic agent, especially in the setting of unusual clinical presentations. Serologic testing is often ordered and hard to interpret. False positive IgM antibody tests are not uncommon, and IgM antibody can persist for months. Outside of PCR and culture, acute and convalescent specimens can be used diagnostically, and a fourfold IgG antibody rise is consistent with acute infection.
Macrolides are regarded as the preferred treatment for M. pneumoniae pneumonia, but several studies question whether treatment impacts the clinical course. This may be due to the inherent difficulty of confirming M. pneumoniae as the etiologic agent, as most studies used serology to confirm the diagnosis. In countries outside the United States, macrolide resistance is well reported, and this may be underappreciated in the United States. We recently cared for a teenager with Down syndrome with pneumonia caused by M. pneumoniae who had a protracted clinical course. Fever and hypoxemia were persistent over a several-week period despite two courses of azithromycin and exclusion of virus, bacteria, and fungal pathogens. Bronchoalveolar lavage was performed, M. pneumoniae was detected by PCR, and macrolide resistance was confirmed. Levofloxacin was given, and she recovered over the next week.
Macrolide resistance is commonly reported outside the United States; rates in China are reported to be greater than 90%, in Japan 80%, and in Europe, between 15% and 25%. A recent study from Greg Storch and his colleagues (Pediatr. Infect. Dis. J. 2012;31:409-10) documented macrolide resistance in 8% of respiratory samples collected between 2007 and 2010 (49 patients; mean age, 10 years), noting the resistance rate was 3% in 2007-2008 and 15% in 2009-2010. A recently published study of data from Canada reported that 12.1% of M. pneumoniae–positive specimens collected between 2010 and January 2012 carried nucleotide mutations associated with macrolide resistance in the 23S rRNA gene (Emerg. Infect. Dis. 2013 September [doi: 10.3201/eid1909.121466]). Anecdotal studies suggest that patients with macrolide-resistant M. pneumoniae infection clinically improve when given doxycycline (or minocycline) or levofloxacin.
A number of clinical questions regarding M. pneumoniae may be answered more definitively in the future, but we need more easily available diagnostics (PCR is a good start), routinely accessible susceptibility data, and a good randomized controlled study to investigate the question of whether treatment shortens the course of disease.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri-Kansas City. She said she has no conflicts of interest to disclose. E-mail her at pdnews@frontlinemedcom.com.

Nonmedical exemption population clusters factor into 2010 California pertussis outbreak
California communities with higher numbers of nonmedically exempt school children experienced higher rates of pertussis cases in 2010.
Between 2000 and 2010, California nonmedical exemption rates went from less than 1.0% to 2.33%, with some schools reporting unvaccinated populations of 84% in 2010, according to the Centers for Disease Control and Prevention. At 9,120 cases of pertussis and 10 subsequent deaths in 2010, California recorded more statewide incidences of the disease since 1947, just after the pertussis-containing vaccines were introduced in the United States.
Investigators led by Jessica E. Atwell, M.P.H., of the Johns Hopkins Bloomberg School of Public Health, Baltimore, recently reported data linking the two phenomena. "Our findings suggest that communities with large numbers of intentionally unvaccinated or undervaccinated persons can lead to pertussis outbreaks," Ms. Atwell and her colleagues wrote (Pediatrics 2013;132:624-30).
The 2010 outbreak previously has been attributed to waning immunity, susceptibility in the infant population, better detection rates, and adaptation by the circulating strains, yet the role of the choice to forego immunization had not previously been investigated, according to the study authors. To determine the relationship, Ms. Atwell and her team evaluated the spatial clustering of nonmedical exemptions for kindergartners in the state between the 2005-2006 and 2009-2010 school years and compared it with the space-time clustering of pertussis cases reported in the state in 2010.
Pertussis outbreak data from the California Department of Public Health were "geocoded" and aggregated, as were the school’s exact locations, to protect patient privacy. Data for the number of kindergartners enrolled in the state, and the number of kindergartners with nonmedical exemptions also were tabulated. School enrollment and the number of nonmedical exemptions also were aggregated to the census tract level.
The investigators calculated nonmedical exemption rates by dividing the nonmedically exempted children by the total number of kindergartners enrolled in each census tract. They used spatial scan statistics to identify clusters of monthly pertussis cases, and multivariate logistic regression to determine the odds ratios (OR) for pertussis cases within or out of nonmedical exemption clusters, and to compare various demographic characteristics of each tract.
The data indicated that census tracts within a cluster of nonmedical exemptions were more likely to also be within locations with pertussis case clusters (OR, 2.47). This was true even after researchers adjusted for covariates such as race, population density, average family size, education, and income (OR, 1.73). Ms. Atwell and her team also found that the pertussis incidence rate ratio (IRR) was higher within nonmedical exemption clusters than it was outside of them (IRR, 1.20) and that the associated risk remained after adjusting for covariates (IRR, 1.12).
Two statistically significant clusters of pertussis cases, spanning from May 2010 to October 2010, and from July 2010 to November 2010, existed in central California with 3,783 observed cases out of an expected level of 1,835 (relative risk, 2.91), and in San Diego County with 980 vs. an expected level of 391 (RR, 2.71). Reported pertussis rates statewide in 2010 varied monthly from less than 100 in January to more than 1,000 in August. Nonmedical exemptions and clusters of pertussis cases, according to the authors, were associated with high socioeconomic status, lower average family size, higher education levels, lower percentages of racial or ethnic minorities, and higher income levels statewide.
Nonmedical exemption data in California does not include specifics as to which vaccines were or were not given, or any dosages; therefore, the authors wrote "it is possible that some children with a nonmedical exemption were completely vaccinated against pertussis." They suggested that "future studies should attempt to analyze varying rates of vaccine avoidance for specific antigens to determine the magnitude of impact within populations with high nonmedical exemptions."
Because their study did not include homeschooled children, the authors concluded that additional analysis should be explored. They also cited the need for future studies to include data on subgroups of the various case definitions which, in California, includes acute cough illness of any duration with polymerase chain reaction detection of Bordetella pertussis–specific nucleic acid, or one or more typical pertussis symptoms that can be epidemiologically linked to a confirmed case.
The authors did not report any relevant disclosures. The CDC funded the collection of vaccine-preventable disease and immunization data at the California Department of Public Health.
California communities with higher numbers of nonmedically exempt school children experienced higher rates of pertussis cases in 2010.
Between 2000 and 2010, California nonmedical exemption rates went from less than 1.0% to 2.33%, with some schools reporting unvaccinated populations of 84% in 2010, according to the Centers for Disease Control and Prevention. At 9,120 cases of pertussis and 10 subsequent deaths in 2010, California recorded more statewide incidences of the disease since 1947, just after the pertussis-containing vaccines were introduced in the United States.
Investigators led by Jessica E. Atwell, M.P.H., of the Johns Hopkins Bloomberg School of Public Health, Baltimore, recently reported data linking the two phenomena. "Our findings suggest that communities with large numbers of intentionally unvaccinated or undervaccinated persons can lead to pertussis outbreaks," Ms. Atwell and her colleagues wrote (Pediatrics 2013;132:624-30).
The 2010 outbreak previously has been attributed to waning immunity, susceptibility in the infant population, better detection rates, and adaptation by the circulating strains, yet the role of the choice to forego immunization had not previously been investigated, according to the study authors. To determine the relationship, Ms. Atwell and her team evaluated the spatial clustering of nonmedical exemptions for kindergartners in the state between the 2005-2006 and 2009-2010 school years and compared it with the space-time clustering of pertussis cases reported in the state in 2010.
Pertussis outbreak data from the California Department of Public Health were "geocoded" and aggregated, as were the school’s exact locations, to protect patient privacy. Data for the number of kindergartners enrolled in the state, and the number of kindergartners with nonmedical exemptions also were tabulated. School enrollment and the number of nonmedical exemptions also were aggregated to the census tract level.
The investigators calculated nonmedical exemption rates by dividing the nonmedically exempted children by the total number of kindergartners enrolled in each census tract. They used spatial scan statistics to identify clusters of monthly pertussis cases, and multivariate logistic regression to determine the odds ratios (OR) for pertussis cases within or out of nonmedical exemption clusters, and to compare various demographic characteristics of each tract.
The data indicated that census tracts within a cluster of nonmedical exemptions were more likely to also be within locations with pertussis case clusters (OR, 2.47). This was true even after researchers adjusted for covariates such as race, population density, average family size, education, and income (OR, 1.73). Ms. Atwell and her team also found that the pertussis incidence rate ratio (IRR) was higher within nonmedical exemption clusters than it was outside of them (IRR, 1.20) and that the associated risk remained after adjusting for covariates (IRR, 1.12).
Two statistically significant clusters of pertussis cases, spanning from May 2010 to October 2010, and from July 2010 to November 2010, existed in central California with 3,783 observed cases out of an expected level of 1,835 (relative risk, 2.91), and in San Diego County with 980 vs. an expected level of 391 (RR, 2.71). Reported pertussis rates statewide in 2010 varied monthly from less than 100 in January to more than 1,000 in August. Nonmedical exemptions and clusters of pertussis cases, according to the authors, were associated with high socioeconomic status, lower average family size, higher education levels, lower percentages of racial or ethnic minorities, and higher income levels statewide.
Nonmedical exemption data in California does not include specifics as to which vaccines were or were not given, or any dosages; therefore, the authors wrote "it is possible that some children with a nonmedical exemption were completely vaccinated against pertussis." They suggested that "future studies should attempt to analyze varying rates of vaccine avoidance for specific antigens to determine the magnitude of impact within populations with high nonmedical exemptions."
Because their study did not include homeschooled children, the authors concluded that additional analysis should be explored. They also cited the need for future studies to include data on subgroups of the various case definitions which, in California, includes acute cough illness of any duration with polymerase chain reaction detection of Bordetella pertussis–specific nucleic acid, or one or more typical pertussis symptoms that can be epidemiologically linked to a confirmed case.
The authors did not report any relevant disclosures. The CDC funded the collection of vaccine-preventable disease and immunization data at the California Department of Public Health.
California communities with higher numbers of nonmedically exempt school children experienced higher rates of pertussis cases in 2010.
Between 2000 and 2010, California nonmedical exemption rates went from less than 1.0% to 2.33%, with some schools reporting unvaccinated populations of 84% in 2010, according to the Centers for Disease Control and Prevention. At 9,120 cases of pertussis and 10 subsequent deaths in 2010, California recorded more statewide incidences of the disease since 1947, just after the pertussis-containing vaccines were introduced in the United States.
Investigators led by Jessica E. Atwell, M.P.H., of the Johns Hopkins Bloomberg School of Public Health, Baltimore, recently reported data linking the two phenomena. "Our findings suggest that communities with large numbers of intentionally unvaccinated or undervaccinated persons can lead to pertussis outbreaks," Ms. Atwell and her colleagues wrote (Pediatrics 2013;132:624-30).
The 2010 outbreak previously has been attributed to waning immunity, susceptibility in the infant population, better detection rates, and adaptation by the circulating strains, yet the role of the choice to forego immunization had not previously been investigated, according to the study authors. To determine the relationship, Ms. Atwell and her team evaluated the spatial clustering of nonmedical exemptions for kindergartners in the state between the 2005-2006 and 2009-2010 school years and compared it with the space-time clustering of pertussis cases reported in the state in 2010.
Pertussis outbreak data from the California Department of Public Health were "geocoded" and aggregated, as were the school’s exact locations, to protect patient privacy. Data for the number of kindergartners enrolled in the state, and the number of kindergartners with nonmedical exemptions also were tabulated. School enrollment and the number of nonmedical exemptions also were aggregated to the census tract level.
The investigators calculated nonmedical exemption rates by dividing the nonmedically exempted children by the total number of kindergartners enrolled in each census tract. They used spatial scan statistics to identify clusters of monthly pertussis cases, and multivariate logistic regression to determine the odds ratios (OR) for pertussis cases within or out of nonmedical exemption clusters, and to compare various demographic characteristics of each tract.
The data indicated that census tracts within a cluster of nonmedical exemptions were more likely to also be within locations with pertussis case clusters (OR, 2.47). This was true even after researchers adjusted for covariates such as race, population density, average family size, education, and income (OR, 1.73). Ms. Atwell and her team also found that the pertussis incidence rate ratio (IRR) was higher within nonmedical exemption clusters than it was outside of them (IRR, 1.20) and that the associated risk remained after adjusting for covariates (IRR, 1.12).
Two statistically significant clusters of pertussis cases, spanning from May 2010 to October 2010, and from July 2010 to November 2010, existed in central California with 3,783 observed cases out of an expected level of 1,835 (relative risk, 2.91), and in San Diego County with 980 vs. an expected level of 391 (RR, 2.71). Reported pertussis rates statewide in 2010 varied monthly from less than 100 in January to more than 1,000 in August. Nonmedical exemptions and clusters of pertussis cases, according to the authors, were associated with high socioeconomic status, lower average family size, higher education levels, lower percentages of racial or ethnic minorities, and higher income levels statewide.
Nonmedical exemption data in California does not include specifics as to which vaccines were or were not given, or any dosages; therefore, the authors wrote "it is possible that some children with a nonmedical exemption were completely vaccinated against pertussis." They suggested that "future studies should attempt to analyze varying rates of vaccine avoidance for specific antigens to determine the magnitude of impact within populations with high nonmedical exemptions."
Because their study did not include homeschooled children, the authors concluded that additional analysis should be explored. They also cited the need for future studies to include data on subgroups of the various case definitions which, in California, includes acute cough illness of any duration with polymerase chain reaction detection of Bordetella pertussis–specific nucleic acid, or one or more typical pertussis symptoms that can be epidemiologically linked to a confirmed case.
The authors did not report any relevant disclosures. The CDC funded the collection of vaccine-preventable disease and immunization data at the California Department of Public Health.
FROM PEDIATRICS
Major finding: Nonmedical exemption population clusters were 2.5 times more likely to overlap with regional pertussis case clusters in California.
Data source: Multivariate logistic regression analyses of nonmedical exemptions for California kindergartners during 2005-2010, compared with the state’s pertussis case clusters.
Disclosures: The authors did not report any relevant disclosures. The CDC funded the collection of vaccine-preventable disease and immunization data at the Calif. Dept. of Public Health.

Autoantibodies play role in myositis classification, treatment
LAS VEGAS – Autoantibodies and autoantibody subsets can be particularly helpful for classifying and treating patients with myositis, including those with myositis-associated interstitial lung disease, according to Dr. Chester V. Oddis.
Many autoantibody subsets are phenotypically and clinically well defined, and have clinical relevance, said Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh.
Serological classification isn’t always accurate or routinely available for all clinicians, but this may change in the near future as improved techniques for autoantibody detection become available, he said at Perspectives in Rheumatic Diseases 2013.
Anti-MDA-5 and interstitial lung disease
One autoantibody that has gained attention in recent years is anti-MDA-5, also known as anti-CADM-140, which is often seen in patients with amyopathic dermatomyositis (ADM).
Patients with ADM represent a subset of dermatomyositis patients who have cutaneous manifestations of dermatomyositis for 6 months or longer and have no clinical evidence of proximal muscle weakness but may have mild serum muscle enzyme abnormalities. More extensive muscle testing in these patients generally demonstrates no or minimal abnormalities. However, these patients should not be considered to have simply a benign cutaneous form of disease; in fact, they have a frequency of malignancy similar to that of patients with classic dermatomyositis (14% in one series of nearly 300 patients, compared with 15% in classic dermatomyositis).
In addition, ADM patients also have a relatively high frequency of lung disease, Dr. Oddis said. In a published review of the literature of nearly 200 patients with ADM, 10% had interstitial lung disease (ILD) – an important point given that the rash of dermatomyositis may be subtle and missed, he noted.
The Asian population seems to be particularly at risk for this complication. Two studies in recent years have demonstrated that Japanese ADM patients with anti-MDA-5 present with rapidly progressive ILD. A 2011 study showed an increased incidence of acute or subacute interstitial pneumonitis in Chinese patients. Other studies have shown similar findings in Korean and other Asian populations, Dr. Oddis noted.
The presence of anti-MDA-5 represents a novel cutaneous phenotype involving palmar papules and cutaneous ulcerations, severe vasculopathy, and rapidly progressive ILD. The target autoantigen in these cases is MDA-5, which is involved in innate immune defense against viruses, he explained, noting that this supports the possibility that a viral trigger plays a role in the disease.
"I think this complication is filtering into the U.S. population, as we have seen it in our myositis cohort," Dr. Oddis said of the anti-MDA-5 association with ADM and severe ILD. He noted that he recently cared for a 70-year-old white male with "double pneumonia" (a finding that "should always raise suspicion of autoimmune ILD") in June of 2012, a rash of dermatomyositis in September of 2012, and vasculitic skin changes in January of 2013. He presented without muscle weakness.
Anti-synthetase syndrome and ILD
Another autoantibody myositis subset involves the anti-synthetases, including PL-7, PL-12, EJ, and Jo-1.
Patients with anti-synthetase syndrome are generally a clinically homogeneous patient population characterized by fever, myositis, arthritis, Raynaud’s phenomenon, mechanic’s hands, and ILD. About 30%-40% of myositis patients have ILD, which is a significant contributor to morbidity and mortality.
Anti-Jo-1 is found in 50%-75% of these patients, and the coexistence of Ro52 may portend worse prognosis, Dr. Oddis said.
There are certain clinical features of ILD in polymyositis and dermatomyositis, including progressive dyspnea with or without nonproductive cough, lack of digital clubbing (unlike in idiopathic pulmonary fibrosis), and lack of pleuritis and pleural effusion in most cases (unlike in systemic lupus erythematosus). However, presentation can be variable, with about one-third of patients developing ILD before muscle or skin manifestations are apparent. Some patients present with acute disease (acute respiratory distress syndrome), and others present with subacute disease that is chronic and slowly progressing or asymptomatic.
It is important to understand when making a diagnosis of autoimmune ILD that not all patients will present with the classic anti-synthetase syndrome, Dr. Oddis said.
In some cases, patients will have an "incomplete" clinical syndrome with ILD alone or ILD with only subtle connective tissue disease findings, myositis-specific autoantibodies in the absence of myositis, and/or a negative antinuclear antibody (ANA) test, he explained.
The initial symptoms in patients may vary depending on the anti-synthetase autoantibody that is present. In a University of Pittsburgh study, for example, Jo-1 was found in 60% of cases; non-Jo-1 synthetase positive cases more often experienced Raynaud’s as their initial symptom, less often experienced muscle and joint problems as their initial symptom, and had a longer delay in diagnosis, compared with Jo-1 patients. Survival was also decreased, compared with Jo-1 patients.
As for ANA, about half of patients tested positive, whereas 72% demonstrated positive anti-cytoplasmic staining on indirect immunofluorescence.
The diagnosis of autoimmune ILD can be missed when there is a failure to recognize "incomplete" clinical syndromes, when there is a failure to order or detect myositis-specific autoantibodies – even in patients without myositis – and when a negative ANA is considered to be reassuring, Dr. Oddis said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – Autoantibodies and autoantibody subsets can be particularly helpful for classifying and treating patients with myositis, including those with myositis-associated interstitial lung disease, according to Dr. Chester V. Oddis.
Many autoantibody subsets are phenotypically and clinically well defined, and have clinical relevance, said Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh.
Serological classification isn’t always accurate or routinely available for all clinicians, but this may change in the near future as improved techniques for autoantibody detection become available, he said at Perspectives in Rheumatic Diseases 2013.
Anti-MDA-5 and interstitial lung disease
One autoantibody that has gained attention in recent years is anti-MDA-5, also known as anti-CADM-140, which is often seen in patients with amyopathic dermatomyositis (ADM).
Patients with ADM represent a subset of dermatomyositis patients who have cutaneous manifestations of dermatomyositis for 6 months or longer and have no clinical evidence of proximal muscle weakness but may have mild serum muscle enzyme abnormalities. More extensive muscle testing in these patients generally demonstrates no or minimal abnormalities. However, these patients should not be considered to have simply a benign cutaneous form of disease; in fact, they have a frequency of malignancy similar to that of patients with classic dermatomyositis (14% in one series of nearly 300 patients, compared with 15% in classic dermatomyositis).
In addition, ADM patients also have a relatively high frequency of lung disease, Dr. Oddis said. In a published review of the literature of nearly 200 patients with ADM, 10% had interstitial lung disease (ILD) – an important point given that the rash of dermatomyositis may be subtle and missed, he noted.
The Asian population seems to be particularly at risk for this complication. Two studies in recent years have demonstrated that Japanese ADM patients with anti-MDA-5 present with rapidly progressive ILD. A 2011 study showed an increased incidence of acute or subacute interstitial pneumonitis in Chinese patients. Other studies have shown similar findings in Korean and other Asian populations, Dr. Oddis noted.
The presence of anti-MDA-5 represents a novel cutaneous phenotype involving palmar papules and cutaneous ulcerations, severe vasculopathy, and rapidly progressive ILD. The target autoantigen in these cases is MDA-5, which is involved in innate immune defense against viruses, he explained, noting that this supports the possibility that a viral trigger plays a role in the disease.
"I think this complication is filtering into the U.S. population, as we have seen it in our myositis cohort," Dr. Oddis said of the anti-MDA-5 association with ADM and severe ILD. He noted that he recently cared for a 70-year-old white male with "double pneumonia" (a finding that "should always raise suspicion of autoimmune ILD") in June of 2012, a rash of dermatomyositis in September of 2012, and vasculitic skin changes in January of 2013. He presented without muscle weakness.
Anti-synthetase syndrome and ILD
Another autoantibody myositis subset involves the anti-synthetases, including PL-7, PL-12, EJ, and Jo-1.
Patients with anti-synthetase syndrome are generally a clinically homogeneous patient population characterized by fever, myositis, arthritis, Raynaud’s phenomenon, mechanic’s hands, and ILD. About 30%-40% of myositis patients have ILD, which is a significant contributor to morbidity and mortality.
Anti-Jo-1 is found in 50%-75% of these patients, and the coexistence of Ro52 may portend worse prognosis, Dr. Oddis said.
There are certain clinical features of ILD in polymyositis and dermatomyositis, including progressive dyspnea with or without nonproductive cough, lack of digital clubbing (unlike in idiopathic pulmonary fibrosis), and lack of pleuritis and pleural effusion in most cases (unlike in systemic lupus erythematosus). However, presentation can be variable, with about one-third of patients developing ILD before muscle or skin manifestations are apparent. Some patients present with acute disease (acute respiratory distress syndrome), and others present with subacute disease that is chronic and slowly progressing or asymptomatic.
It is important to understand when making a diagnosis of autoimmune ILD that not all patients will present with the classic anti-synthetase syndrome, Dr. Oddis said.
In some cases, patients will have an "incomplete" clinical syndrome with ILD alone or ILD with only subtle connective tissue disease findings, myositis-specific autoantibodies in the absence of myositis, and/or a negative antinuclear antibody (ANA) test, he explained.
The initial symptoms in patients may vary depending on the anti-synthetase autoantibody that is present. In a University of Pittsburgh study, for example, Jo-1 was found in 60% of cases; non-Jo-1 synthetase positive cases more often experienced Raynaud’s as their initial symptom, less often experienced muscle and joint problems as their initial symptom, and had a longer delay in diagnosis, compared with Jo-1 patients. Survival was also decreased, compared with Jo-1 patients.
As for ANA, about half of patients tested positive, whereas 72% demonstrated positive anti-cytoplasmic staining on indirect immunofluorescence.
The diagnosis of autoimmune ILD can be missed when there is a failure to recognize "incomplete" clinical syndromes, when there is a failure to order or detect myositis-specific autoantibodies – even in patients without myositis – and when a negative ANA is considered to be reassuring, Dr. Oddis said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – Autoantibodies and autoantibody subsets can be particularly helpful for classifying and treating patients with myositis, including those with myositis-associated interstitial lung disease, according to Dr. Chester V. Oddis.
Many autoantibody subsets are phenotypically and clinically well defined, and have clinical relevance, said Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh.
Serological classification isn’t always accurate or routinely available for all clinicians, but this may change in the near future as improved techniques for autoantibody detection become available, he said at Perspectives in Rheumatic Diseases 2013.
Anti-MDA-5 and interstitial lung disease
One autoantibody that has gained attention in recent years is anti-MDA-5, also known as anti-CADM-140, which is often seen in patients with amyopathic dermatomyositis (ADM).
Patients with ADM represent a subset of dermatomyositis patients who have cutaneous manifestations of dermatomyositis for 6 months or longer and have no clinical evidence of proximal muscle weakness but may have mild serum muscle enzyme abnormalities. More extensive muscle testing in these patients generally demonstrates no or minimal abnormalities. However, these patients should not be considered to have simply a benign cutaneous form of disease; in fact, they have a frequency of malignancy similar to that of patients with classic dermatomyositis (14% in one series of nearly 300 patients, compared with 15% in classic dermatomyositis).
In addition, ADM patients also have a relatively high frequency of lung disease, Dr. Oddis said. In a published review of the literature of nearly 200 patients with ADM, 10% had interstitial lung disease (ILD) – an important point given that the rash of dermatomyositis may be subtle and missed, he noted.
The Asian population seems to be particularly at risk for this complication. Two studies in recent years have demonstrated that Japanese ADM patients with anti-MDA-5 present with rapidly progressive ILD. A 2011 study showed an increased incidence of acute or subacute interstitial pneumonitis in Chinese patients. Other studies have shown similar findings in Korean and other Asian populations, Dr. Oddis noted.
The presence of anti-MDA-5 represents a novel cutaneous phenotype involving palmar papules and cutaneous ulcerations, severe vasculopathy, and rapidly progressive ILD. The target autoantigen in these cases is MDA-5, which is involved in innate immune defense against viruses, he explained, noting that this supports the possibility that a viral trigger plays a role in the disease.
"I think this complication is filtering into the U.S. population, as we have seen it in our myositis cohort," Dr. Oddis said of the anti-MDA-5 association with ADM and severe ILD. He noted that he recently cared for a 70-year-old white male with "double pneumonia" (a finding that "should always raise suspicion of autoimmune ILD") in June of 2012, a rash of dermatomyositis in September of 2012, and vasculitic skin changes in January of 2013. He presented without muscle weakness.
Anti-synthetase syndrome and ILD
Another autoantibody myositis subset involves the anti-synthetases, including PL-7, PL-12, EJ, and Jo-1.
Patients with anti-synthetase syndrome are generally a clinically homogeneous patient population characterized by fever, myositis, arthritis, Raynaud’s phenomenon, mechanic’s hands, and ILD. About 30%-40% of myositis patients have ILD, which is a significant contributor to morbidity and mortality.
Anti-Jo-1 is found in 50%-75% of these patients, and the coexistence of Ro52 may portend worse prognosis, Dr. Oddis said.
There are certain clinical features of ILD in polymyositis and dermatomyositis, including progressive dyspnea with or without nonproductive cough, lack of digital clubbing (unlike in idiopathic pulmonary fibrosis), and lack of pleuritis and pleural effusion in most cases (unlike in systemic lupus erythematosus). However, presentation can be variable, with about one-third of patients developing ILD before muscle or skin manifestations are apparent. Some patients present with acute disease (acute respiratory distress syndrome), and others present with subacute disease that is chronic and slowly progressing or asymptomatic.
It is important to understand when making a diagnosis of autoimmune ILD that not all patients will present with the classic anti-synthetase syndrome, Dr. Oddis said.
In some cases, patients will have an "incomplete" clinical syndrome with ILD alone or ILD with only subtle connective tissue disease findings, myositis-specific autoantibodies in the absence of myositis, and/or a negative antinuclear antibody (ANA) test, he explained.
The initial symptoms in patients may vary depending on the anti-synthetase autoantibody that is present. In a University of Pittsburgh study, for example, Jo-1 was found in 60% of cases; non-Jo-1 synthetase positive cases more often experienced Raynaud’s as their initial symptom, less often experienced muscle and joint problems as their initial symptom, and had a longer delay in diagnosis, compared with Jo-1 patients. Survival was also decreased, compared with Jo-1 patients.
As for ANA, about half of patients tested positive, whereas 72% demonstrated positive anti-cytoplasmic staining on indirect immunofluorescence.
The diagnosis of autoimmune ILD can be missed when there is a failure to recognize "incomplete" clinical syndromes, when there is a failure to order or detect myositis-specific autoantibodies – even in patients without myositis – and when a negative ANA is considered to be reassuring, Dr. Oddis said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
AT PERSPECTIVES IN RHEUMATIC DISEASES 2013
Flu outlook 2013-2014: Don’t hesitate. Vaccinate!
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).

This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).
This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).
This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
AT THE NFID ANNUAL INFLUENZA PRESS CONFERENCE

Limited data support multiple myositis treatment options
LAS VEGAS – Corticosteroids remain the initial treatment of choice for myositis and myositis-associated interstitial lung disease, but immunosuppressive agents, intravenous immunoglobulin, and biologics can also play a role in the treatment of one or both of these conditions, according to Dr. Chester V. Oddis.
For myositis in general, Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh, recommends an initial divided dose of 30 mg of prednisone twice daily, continued until serum creatine kinase (CK) levels fall to normal. At that time, the total daily prednisone dose can be consolidated into a single morning dose, he said at Perspectives in Rheumatic Diseases 2013.

The prednisone can then be tapered by 25% every 3-4 weeks down to a 5- to 10-mg daily maintenance dose that is continued until active disease is suppressed for 12 months. This is a general guideline that helps prevent disease flares, he noted.
Keep in mind that improvement in strength generally lags behind improvement in CK levels, he added.
Nonsteroidal immunosuppressives
Not all patients will need an additional immunosuppressive agent, but for those who do, methotrexate is a good option, Dr. Oddis said, noting that methotrexate is the drug he is most comfortable using in those cases.
The literature also supports the combined use of methotrexate and azathioprine, which when given together have been shown to be effective in treatment-resistant myositis and in those who failed either of the drugs alone.
"So that’s a regimen you might want to think about," he said.
Another immunosuppressive option is mycophenolate mofetil (MMF), which has been shown in several small studies and case series to be of benefit. In one study, 6 of 10 patients with dermatomyositis successfully tapered corticosteroids with MMF, and 10 of 12 in another study experienced improvement in cutaneous features of the disease.
The use of intravenous immunoglobulin (IVIg) as add-on therapy with MMF was effective in severe refractory patients, including four with polymyositis and three with dermatomyositis. In a retrospective review of 50 patients with juvenile dermatomyositis, MMF for 12 months was well tolerated, improved skin and muscle, and proved to be steroid-sparing, Dr. Oddis said.
Cyclosporine, tacrolimus, and cyclophosphamide are other immunosuppressive options.
While cyclophosphamide is more often used for myositis-associated interstitial lung disease (ILD), it can be of benefit for refractory skin disease, and can be useful in non-ILD myositis cases that involve severe skin disease.
The only available controlled data for IVIg alone are from a study published more than 20 years ago, but that randomized, double-blind, placebo-controlled study showed that treatment was safe, effective, and steroid sparing in 15 patients with dermatomyositis, he said.
Biologics
As for biologics, anti–tumor necrosis factor–alpha (anti-TNF-alpha) therapy and B-cell therapy have both been considered. Anti-TNF-alpha therapy makes sense because TNF-alpha and other proinflammatory cytokines are increased in muscle tissue of myositis patients; TNF-alpha is toxic to myofibers and prevents their regeneration; and TNF-alpha enhances other inflammatory cytokines in both dermatomyositis and polymyositis, but data are lacking on whether targeting TNF-alpha is worthwhile.
B cell therapy, on the other hand, is showing promise. In one open-label pilot study, rituximab was effective in seven patients with refractory dermatomyositis, and in others it was effective in anti-synthetase syndrome. Rituximab also was effective in two studies for refractory myositis and dermatomyositis rash, and it induced longstanding remission in some of the patients. In another study, however, rituximab was not effective for dermatomyositis rash.
The multicenter Rituximab in Myositis (RIM) study, the largest ever done in myositis, evaluated rituximab for the treatment of refractory adult and juvenile dermatomyositis and adult polymyositis patients.
Although the primary and secondary endpoints of the RIM study were not achieved, 83% of refractory adult and juvenile myositis patients met the definition of improvement, there was a significant corticosteroid sparing effect between the baseline dose and the dose at study conclusion, and treatment was generally well tolerated, he said.
Other targets that are being explored include interleukin-6 and type 1 IFN genes. Findings suggest that coordinated dysregulation of type 1 IFN signaling and IL-6 production are contributors to dermatomyositis pathogenesis, he explained.
Treating myositis patients with ILD
The treatment approach to these patients is somewhat similar to those without ILD, with corticosteroids as initial treatment, Dr. Oddis said.
Cyclophosphamide and azathioprine have been used early on, and also in corticosteroid resistant cases, but with variable results. Cyclophosphamide can be given orally or by IV for 3-6 months.
MMF has been used with success in connective tissue disease–associated ILD, and based on small studies it appears to be effective in myositis-associated ILD as well.
Cyclosporine and tacrolimus have been used in both adult and pediatric patients with promising, steroid-sparing results, he said, noting that the use of anti-T-cell therapy in myositis-associated ILD makes sense, because findings from multiple studies have implicated activated CD8-positive T-cells in myositis-associated ILD.
"It’s an exciting time for therapeutic interventions in myositis, but even though we have all these therapeutic options, we have to temper our enthusiasm with what they do long term," he said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – Corticosteroids remain the initial treatment of choice for myositis and myositis-associated interstitial lung disease, but immunosuppressive agents, intravenous immunoglobulin, and biologics can also play a role in the treatment of one or both of these conditions, according to Dr. Chester V. Oddis.
For myositis in general, Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh, recommends an initial divided dose of 30 mg of prednisone twice daily, continued until serum creatine kinase (CK) levels fall to normal. At that time, the total daily prednisone dose can be consolidated into a single morning dose, he said at Perspectives in Rheumatic Diseases 2013.
The prednisone can then be tapered by 25% every 3-4 weeks down to a 5- to 10-mg daily maintenance dose that is continued until active disease is suppressed for 12 months. This is a general guideline that helps prevent disease flares, he noted.
Keep in mind that improvement in strength generally lags behind improvement in CK levels, he added.
Nonsteroidal immunosuppressives
Not all patients will need an additional immunosuppressive agent, but for those who do, methotrexate is a good option, Dr. Oddis said, noting that methotrexate is the drug he is most comfortable using in those cases.
The literature also supports the combined use of methotrexate and azathioprine, which when given together have been shown to be effective in treatment-resistant myositis and in those who failed either of the drugs alone.
"So that’s a regimen you might want to think about," he said.
Another immunosuppressive option is mycophenolate mofetil (MMF), which has been shown in several small studies and case series to be of benefit. In one study, 6 of 10 patients with dermatomyositis successfully tapered corticosteroids with MMF, and 10 of 12 in another study experienced improvement in cutaneous features of the disease.
The use of intravenous immunoglobulin (IVIg) as add-on therapy with MMF was effective in severe refractory patients, including four with polymyositis and three with dermatomyositis. In a retrospective review of 50 patients with juvenile dermatomyositis, MMF for 12 months was well tolerated, improved skin and muscle, and proved to be steroid-sparing, Dr. Oddis said.
Cyclosporine, tacrolimus, and cyclophosphamide are other immunosuppressive options.
While cyclophosphamide is more often used for myositis-associated interstitial lung disease (ILD), it can be of benefit for refractory skin disease, and can be useful in non-ILD myositis cases that involve severe skin disease.
The only available controlled data for IVIg alone are from a study published more than 20 years ago, but that randomized, double-blind, placebo-controlled study showed that treatment was safe, effective, and steroid sparing in 15 patients with dermatomyositis, he said.
Biologics
As for biologics, anti–tumor necrosis factor–alpha (anti-TNF-alpha) therapy and B-cell therapy have both been considered. Anti-TNF-alpha therapy makes sense because TNF-alpha and other proinflammatory cytokines are increased in muscle tissue of myositis patients; TNF-alpha is toxic to myofibers and prevents their regeneration; and TNF-alpha enhances other inflammatory cytokines in both dermatomyositis and polymyositis, but data are lacking on whether targeting TNF-alpha is worthwhile.
B cell therapy, on the other hand, is showing promise. In one open-label pilot study, rituximab was effective in seven patients with refractory dermatomyositis, and in others it was effective in anti-synthetase syndrome. Rituximab also was effective in two studies for refractory myositis and dermatomyositis rash, and it induced longstanding remission in some of the patients. In another study, however, rituximab was not effective for dermatomyositis rash.
The multicenter Rituximab in Myositis (RIM) study, the largest ever done in myositis, evaluated rituximab for the treatment of refractory adult and juvenile dermatomyositis and adult polymyositis patients.
Although the primary and secondary endpoints of the RIM study were not achieved, 83% of refractory adult and juvenile myositis patients met the definition of improvement, there was a significant corticosteroid sparing effect between the baseline dose and the dose at study conclusion, and treatment was generally well tolerated, he said.
Other targets that are being explored include interleukin-6 and type 1 IFN genes. Findings suggest that coordinated dysregulation of type 1 IFN signaling and IL-6 production are contributors to dermatomyositis pathogenesis, he explained.
Treating myositis patients with ILD
The treatment approach to these patients is somewhat similar to those without ILD, with corticosteroids as initial treatment, Dr. Oddis said.
Cyclophosphamide and azathioprine have been used early on, and also in corticosteroid resistant cases, but with variable results. Cyclophosphamide can be given orally or by IV for 3-6 months.
MMF has been used with success in connective tissue disease–associated ILD, and based on small studies it appears to be effective in myositis-associated ILD as well.
Cyclosporine and tacrolimus have been used in both adult and pediatric patients with promising, steroid-sparing results, he said, noting that the use of anti-T-cell therapy in myositis-associated ILD makes sense, because findings from multiple studies have implicated activated CD8-positive T-cells in myositis-associated ILD.
"It’s an exciting time for therapeutic interventions in myositis, but even though we have all these therapeutic options, we have to temper our enthusiasm with what they do long term," he said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – Corticosteroids remain the initial treatment of choice for myositis and myositis-associated interstitial lung disease, but immunosuppressive agents, intravenous immunoglobulin, and biologics can also play a role in the treatment of one or both of these conditions, according to Dr. Chester V. Oddis.
For myositis in general, Dr. Oddis, professor of medicine and associate director of the rheumatology fellowship training program at the University of Pittsburgh, recommends an initial divided dose of 30 mg of prednisone twice daily, continued until serum creatine kinase (CK) levels fall to normal. At that time, the total daily prednisone dose can be consolidated into a single morning dose, he said at Perspectives in Rheumatic Diseases 2013.
The prednisone can then be tapered by 25% every 3-4 weeks down to a 5- to 10-mg daily maintenance dose that is continued until active disease is suppressed for 12 months. This is a general guideline that helps prevent disease flares, he noted.
Keep in mind that improvement in strength generally lags behind improvement in CK levels, he added.
Nonsteroidal immunosuppressives
Not all patients will need an additional immunosuppressive agent, but for those who do, methotrexate is a good option, Dr. Oddis said, noting that methotrexate is the drug he is most comfortable using in those cases.
The literature also supports the combined use of methotrexate and azathioprine, which when given together have been shown to be effective in treatment-resistant myositis and in those who failed either of the drugs alone.
"So that’s a regimen you might want to think about," he said.
Another immunosuppressive option is mycophenolate mofetil (MMF), which has been shown in several small studies and case series to be of benefit. In one study, 6 of 10 patients with dermatomyositis successfully tapered corticosteroids with MMF, and 10 of 12 in another study experienced improvement in cutaneous features of the disease.
The use of intravenous immunoglobulin (IVIg) as add-on therapy with MMF was effective in severe refractory patients, including four with polymyositis and three with dermatomyositis. In a retrospective review of 50 patients with juvenile dermatomyositis, MMF for 12 months was well tolerated, improved skin and muscle, and proved to be steroid-sparing, Dr. Oddis said.
Cyclosporine, tacrolimus, and cyclophosphamide are other immunosuppressive options.
While cyclophosphamide is more often used for myositis-associated interstitial lung disease (ILD), it can be of benefit for refractory skin disease, and can be useful in non-ILD myositis cases that involve severe skin disease.
The only available controlled data for IVIg alone are from a study published more than 20 years ago, but that randomized, double-blind, placebo-controlled study showed that treatment was safe, effective, and steroid sparing in 15 patients with dermatomyositis, he said.
Biologics
As for biologics, anti–tumor necrosis factor–alpha (anti-TNF-alpha) therapy and B-cell therapy have both been considered. Anti-TNF-alpha therapy makes sense because TNF-alpha and other proinflammatory cytokines are increased in muscle tissue of myositis patients; TNF-alpha is toxic to myofibers and prevents their regeneration; and TNF-alpha enhances other inflammatory cytokines in both dermatomyositis and polymyositis, but data are lacking on whether targeting TNF-alpha is worthwhile.
B cell therapy, on the other hand, is showing promise. In one open-label pilot study, rituximab was effective in seven patients with refractory dermatomyositis, and in others it was effective in anti-synthetase syndrome. Rituximab also was effective in two studies for refractory myositis and dermatomyositis rash, and it induced longstanding remission in some of the patients. In another study, however, rituximab was not effective for dermatomyositis rash.
The multicenter Rituximab in Myositis (RIM) study, the largest ever done in myositis, evaluated rituximab for the treatment of refractory adult and juvenile dermatomyositis and adult polymyositis patients.
Although the primary and secondary endpoints of the RIM study were not achieved, 83% of refractory adult and juvenile myositis patients met the definition of improvement, there was a significant corticosteroid sparing effect between the baseline dose and the dose at study conclusion, and treatment was generally well tolerated, he said.
Other targets that are being explored include interleukin-6 and type 1 IFN genes. Findings suggest that coordinated dysregulation of type 1 IFN signaling and IL-6 production are contributors to dermatomyositis pathogenesis, he explained.
Treating myositis patients with ILD
The treatment approach to these patients is somewhat similar to those without ILD, with corticosteroids as initial treatment, Dr. Oddis said.
Cyclophosphamide and azathioprine have been used early on, and also in corticosteroid resistant cases, but with variable results. Cyclophosphamide can be given orally or by IV for 3-6 months.
MMF has been used with success in connective tissue disease–associated ILD, and based on small studies it appears to be effective in myositis-associated ILD as well.
Cyclosporine and tacrolimus have been used in both adult and pediatric patients with promising, steroid-sparing results, he said, noting that the use of anti-T-cell therapy in myositis-associated ILD makes sense, because findings from multiple studies have implicated activated CD8-positive T-cells in myositis-associated ILD.
"It’s an exciting time for therapeutic interventions in myositis, but even though we have all these therapeutic options, we have to temper our enthusiasm with what they do long term," he said.
Dr. Oddis has served on an advisory board for Questcor.
The meeting was held by Global Academy for Medical Education. GAME and this news organization are owned by Frontline Medical Communications.
AT PERSPECTIVES IN RHEUMATIC DISEASES 2013

Obstructive sleep apnea: A diagnostic and treatment guide
CASE 1 Mr. M, age 59, has diabetes, hypertension, hyperlipidemia, and obesity, with a body mass index (BMI) of 37 kg/m2. His hyperlipidemia is well controlled with atorvastatin. He also takes hydrochlorothiazide, lisinopril, metformin, and glyburide, but neither his hypertension nor his glucose levels are well controlled. Mr. M does not exercise, and acknowledges eating a high-calorie diet.
Mr. M reports that his wife has begun complaining about his loud snoring, and that he’s been falling asleep at work. He says he has 2 to 3 alcoholic drinks per week, and doesn’t smoke or take any other drugs.
CASE 2 Ms. C, age 35, is seeking treatment for early morning headaches that began several months ago. She describes a constant dull pain over the frontal area that occurs almost every day and typically resolves in 2 to 3 hours. The pain is not affected by postural changes, she says.
She also reports fatigue, daytime sleepiness, and anxiety. Ms. C has a normal BMI (24 kg/m2), takes no medication, and has no prior history of migraine or tension headaches. She denies any alcohol or recreational drug use.
If Mr. M and Ms. C were your patients, what would your next step be?
Obstructive sleep apnea (OSA) is characterized by repeated cycles of partial airway obstruction, hypoxemia, sympathetic discharge, and arousal to restore ventilation. In addition to fragmented sleep and daytime sleepiness, this common sleep disorder is associated with a decreased functional capacity1-3 and an increased risk for accidents, arrhythmias, myocardial infarction (MI), stroke, and death.4-6 In the Wisconsin Sleep Cohort, an 18-year follow-up study, the estimated hazard ratio for patients with severe OSA was 3.0 for all-cause mortality (95% CI; P-trend <.008) and 5.2 for cardiovascular death (95% CI; P=.003).7
The prevalence of OSA in the United States is 3% to 7% for males and 2% to 5% for females, with higher rates among those older than 65 years. But these figures apply only to those with an OSA diagnosis. An additional 5% of the general population is believed to have undiagnosed OSA.4,8
Arriving at an OSA diagnosis may not be difficult with a patient like Mr. M, who is obese and has classic symptoms. But it is important to consider OSA in patients who, like Ms. C, are not overweight and whose chief complaint appears to be unrelated to sleep.
This review—of risk factors, common (and uncommon) symptoms, diagnostic criteria, and treatment for OSA—highlights key indicators and optimal therapies.
The OSA profile: Risk factors and presenting symptoms
Obesity is perhaps the best-known risk factor for OSA: About 70% of patients with OSA are obese, and 40% of obese individuals have OSA. Approximately 60% of those with OSA have metabolic syndrome.9-12 But it is important to remember that individuals with normal or even low BMI may develop OSA, as well.
Other possible contributing factors include alcohol use, smoking, nasal congestion, menopause, polycystic ovary disease, and a genetic predisposition. And OSA may cause or worsen a wide range of conditions, including hypertension, congestive heart failure, atrial fibrillation, stroke, and nocturnal arrhythmias.8,13
Symptoms may be classic—or not
A bed partner’s complaint about a patient’s snoring, typically followed by arousal and gasping for air, is often the first indication of OSA. Loud snoring and daytime sleepiness are the most common symptoms. But not all patients present with these classic symptoms. Some may complain of irritability, difficulty concentrating, daily headaches, and nocturia.
Because the symptoms of OSA are not highly specific, a wide differential diagnosis must be considered, including numerous causes of excessive daytime sleepiness and conditions, such as panic attacks, pulmonary disease, and gastroesophageal reflux disease, which can interfere with sleep (TABLE 1).8,13
What to include in the medical history and work-up
When you suspect OSA or another sleep disorder, the medical history should include a complete review of systems. The social history needs to include information regarding alcohol intake, use of sedatives, and recreational drugs. If possible, interview the patient’s bed partner, as well.
Examine upper airway anatomy. In performing a physical exam, pay special attention to blood pressure, BMI, and upper airway anatomy. Assess for conditions that can cause obstruction, such as nasal congestion, septal deviation, retrognathia (malocclusion of the mouth due to an abnormal posterior position of the maxilla or mandible), macroglossia (an unusually large tongue), dental malocclusion, enlarged lymphoid tissue and tonsils, large uvula, low hanging soft palate, and a large neck circumference (>40 cm for females and >43 cm for males).13
Order blood tests. Routine blood tests do not support an OSA diagnosis, but they help rule out or identify other conditions associated or mimicking OSA, such as anemia, hypothyroidism, diabetes, liver disease, and kidney disease. Suggested labs include a comprehensive metabolic profile, complete blood count, and thyroid-stimulating hormone test.
Sleep studies are needed for a definitive diagnosis
Conducted overnight in a sleep lab, polysomnography (PSG) uses respiratory effort, respiratory air flow, and peripheral oximetry to identify and quantify episodes of apnea and hypopnea (reported as the apnea-hypopnea index, or AHI). PSG also records brain electrical activity (electroencephalogram), heart rhythm (electrocardiogram), eye movement (electro-oculogram), and muscle activation (electromyogram)—studies used to identify other sleep disorders, such as restless leg syndrome, narcolepsy, parasomnias, and disturbances in rapid-eye movement
(REM) sleep.
Home monitoring. For patients who are unable or unwilling to undergo an overnight sleep study, home portable monitoring is a less expensive alternative. The monitor—a small wireless device—provides data for calculating the AHI and the presence and degree of oxygen desaturation.14 Unlike PSG, which can identify the amount of pressure needed for continuous positive airway pressure (CPAP) therapy, findings from a portable monitor are not sufficient to rule out other sleep disorders to determine whether CPAP is required.15
Evaluating daytime sleepiness. Several tools have been used to evaluate daytime sleepiness. The Epworth Sleepiness Scale (ESS), a quick 8-item screening questionnaire, determines the average person’s level of sleepiness during the day. It ranges from 0 to 24 points, with 10 being normal. Although the ESS has been used extensively in OSA research, recent studies found that it has a low sensitivity (54%) and specificity (57%) for scores >10 and does not correlate well with hypopnea and apnea measurements.16,17

Two additional tools, the Berlin and STOP questionnaires, can also be used to screen for OSA. Both questionnaires have about a 50% positive predictive value and a 70% negative predictive value.18,19
Diagnosing and classifying OSA
Diagnostic criteria developed by the American Academy of Sleep Medicine (AASM) are based on reported and observed symptoms and PSG recordings of hypopnea and apneic episodes. Of the 4 criteria (A through D), patients must meet either A, B, and D or C and D (TABLE 2).15
The AASM further classifies OSA as mild, moderate, or severe (TABLE 3)15 based on the AHI as well as on clinical findings, including oxygen desaturation and arrhythmias. Patients with severe OSA have excessive daytime sleepiness (EDS) that interferes with their normal activities, 15 as well as severe oxygen desaturation, moderate to severe cardiac arrhythmias, and significant risk for hypertension, MI, stroke, and cor pulmonale.
CASE 1 An examination of Mr. M’s upper airway anatomy reveals a neck circumference of 44 cm and normal oropharynx. The results of his lab tests were only significant for elevated blood sugar (234 mg/dL) and glycosylated hemoglobin (9.2%). Because he presents with classic symptoms of OSA, he receives a referral for PSG. He is found to have an AHI of 49, consistent with severe sleep apnea.
CASE 2 A system review of Ms. C finds no fever, nausea, vomiting, weakness, vision changes, or neurological symptoms. A Patient Health Questionnaire-9 (depression screen) is normal, as are her lab tests and a brain MRI with and without contrast. After an extensive work-up for headaches finds nothing, OSA is considered, in light of her daytime sleepiness—and she, too, is referred for PSG. This patient has moderate OSA, with an AHI of 27.
Initiating treatment: What’s best?
Ideally, treatment of OSA would reverse EDS and fatigue, restore full cognitive function, reduce the risk of accidents associated with OSA, and minimize its harmful cardiovascular and pulmonary effects. In fact, while OSA can be managed and its effects ameliorated, all available treatments have limitations and a cure remains elusive.
Let patients know that our understanding of OSA is limited, that treatment may not reverse or eliminate all the risks associated with this condition, and that compliance can be challenging. You can also tell them that, while more and better studies are needed, several modalities have been found to successfully treat OSA.
What to expect from lifestyle modification
Recommend lifestyle changes, such as weight loss, regular exercise early in the day, greater emphasis on sleep hygiene (eg, using the bed only for sleeping and sexual activity), and avoidance of sedating drugs and alcohol for patients with OSA.20,21
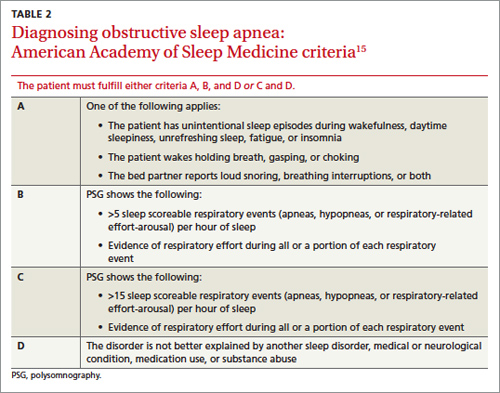
The beneficial effect of weight loss on OSA has been demonstrated in studies of both bariatric surgery and conventional weight loss therapies.21-23 While early studies of bariatric surgery were often limited by small size, ambiguous classification of OSA, and selection and follow-up biases, more recent trials show that while OSA symptoms frequently improve postoperatively, the disorder typically persists despite significant reductions in both BMI and AHI.24 Weight reduction should be strongly encouraged for obese patients, however, not only to improve OSA symptoms, but also to reduce the risk for other diseases.
Avoidance of alcohol. Alcohol has adverse effects on sleep: It shortens sleep latency, increases slow-wave sleep, suppresses REM and parasympathetic nerve activity,25 and can exacerbate OSA. Driving simulation studies have found that, compared with healthy individuals, those with untreated OSA are more susceptible to the effects of alcohol and at higher risk for accidents after just one drink.26
CPAP improves sleep, but some problems persist
CPAP supplies a flow of positive air pressure, adjusted to the level needed to keep the airway open, delivered through a facial device best suited to the patient’s anatomy, physiology, and comfort.
Multiple studies have demonstrated the effectiveness of CPAP in reducing symptoms of moderate to severe OSA, compared with placebo and other treatment modalities such as oral devices, surgical procedures, and medications. CPAP reduces AHI, blood pressure, and cardiac arrhythmias. It improves sleep efficiency, oxygen saturation, and self-reported sleep and well-being.27-30 While it ameliorates many of the harmful effects of OSA, it does not improve or reverse all of them. (See “Peripheral neuropathy linked to obstructive sleep apnea?”)
A Cochrane review of 36 randomized controlled trials with a combined total of more than 1700 patients demonstrated the superiority of CPAP vs control in several measures, such as subjective daytime sleepiness, quality of life, cognitive function, and blood pressure.28 On specific parameters of OSA, such as snoring and EDS, studies yielded mixed results.
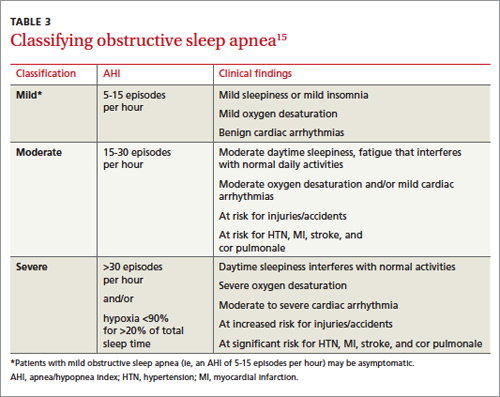
CPAP has been found to decrease work-related injuries and morbidity and mortality associated with motor vehicle accidents linked to EDS.30-32 However, no study of CPAP has demonstrated a long-term reduction in morbidity and mortality. And no standards define the minimum number of sleep hours and/or frequency of CPAP use that is required to obtain specific benefits.
Patient compliance is poor. Part of the problem is that CPAP is difficult to use, which affects compliance. Poor patient compliance is a major barrier to evaluating its long-term benefits. (The video below, "CPAP Patients Tips from the FDA", can help ensure that patients use CPAP safely and effectively.) Studies estimate that 65% to 89% of patients with CPAP devices use them for at least 4 hours a night for 70% of nights, but that about half of those for whom CPAP is prescribed stop using it after 2 to 3 years.33-36 Several risk factors and comorbid conditions, including advanced age, diabetes, obesity, smoking, and especially, depression, are associated with decreased compliance.13
Improving CPAP compliance continues to be a challenge, highlighting the importance of treating not only OSA but all comorbidities, particularly depression. Short-term studies have found behavioral modification to be a promising means of improving CPAP compliance.33-36
Although not a first-line therapy, bilevel positive airway pressure (BiPAP), which delivers both inspiratory and expiratory pressure via a face device, can be tried in patients unable to tolerate CPAP.37 Studies are limited and it has been used in patients with complex OSA.
Oral appliances are a CPAP alternative
Mandibular repositioning devices (MRDs) and tongue-retaining devices are alternatives to CPAP.38 Although both types of oral appliance are beneficial, they are less effective than CPAP.28
MRDs, which are more commonly used than tongue-retaining devices, are available in several models. An MRD can be custom-made to hold the lower jaw in a forward position during sleep, enlarge the space behind the tongue, and put tension on the walls of the pharynx and the palate to reduce collapse.38
Tongue-retaining devices—splints that hold the tongue in place to keep the airway open—can be used for mild to moderate OSA, and for patients unable to tolerate CPAP.38,39
Studies comparing MRDs and tongue-retaining devices found no statistically significant difference in their ability to reduce AHI, but patients tolerated MRDs better.38,39 Nonetheless, both devices can cause dental discomfort, temporomandibular joint pain, dry mouth or excessive salivation, gum irritation, bruxism, and long-term occlusal changes.38
Is surgery an option?
Numerous surgical techniques are available for treating OSA, all aimed at relieving the obstruction by removing or bypassing it or increasing airway size. These include uvulopalatopharyngoplasty, which resects the uvula, retrolingual, and palatine tonsillar tissue; septoplasty; rhinoplasty; nasal turbinate reduction; nasal polypectomy palatal advancement pharyngoplasty; tonsillectomy; adenoidectomy; palatal implants; tongue reduction; genioglossus advancement; and maxillomandibular advancement.
The choice of modality depends on the patient’s anatomy and physiology, and is selected only after a full evaluation by a head and neck surgeon who specializes in surgical treatment of OSA.40,41 There is a paucity of reliable studies on the results of such procedures, but a Cochrane review of the existing literature concluded that surgery is only indicated for severe cases of sleep apnea in patients who have an anatomic obstruction.40
Too little evidence of medications’ efficacy
Numerous drugs have been tested for the treatment of OSA. Two Cochrane reviews looked at multiple trials of more than 20 drugs, in meta-analyses encompassing more than 500 patients.42,43 Ten drugs—eszopiclone, paroxetine, acetazolamide, ondansetron-fluoxetine combination, naltrexone, and fluticasone nasal spray among them—showed a statistically significant reduction in AHI, and a few showed a subjective benefit in daytime sleepiness. However, the studies were very small and of short duration and the reviewers concluded that evidence is insufficient to recommend drug therapy for OSA.
CASE 1 CPAP was prescribed for Mr. M. He tolerated it well and after 2 weeks, he reported feeling refreshed upon awakening, having less daytime somnolence and being better able to concentrate at work. His hypertension and glucose control improved, but he continues to struggle with his weight.
CASE 2 Ms. C started CPAP and within a week, her morning headaches and irritability resolved.
CORRESPONDENCE
Cecilia Gutierrez, MD, 200 West Arbor Drive, Mail Code 8809, San Diego, CA 92103; cagutierrez@ucsd.edu
1. Dempsey JA, Veasey SC, Morgan BJ, et al. Pathophysiology of sleep apnea. Physiol Rev. 2010;90:47-112.
2. Jenkinson C, Stradling J, Petersen S. Comparison of three measures of quality of life outcome in the evaluation of continuous positive airways pressure therapy for sleep apnoea. J Sleep Res. 1997;6:199-204.
3. Satela MJ. Neuropsychological impairment and quality of life in obstructive sleep apnea. Clin Chest Med. 2003;24:249-259.
4. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217-1239.
5. Yaggi HK, Concato J, Kernan W, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034-2041.
6. Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046-1053.
7. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;3:1071-1078.
8. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:136-143.
9. Coughlin SR, Mawdsley L, Mugarza JA, et al. Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Eur Heart J. 2004;25:735-741.
10. Basta M, Vgontzas AN. Metabolic abnormalities in obesity and sleep apnea are in a continuum. Sleep Med. 2007;8:5-7.
11. Peppard PE, Young T, Palta M, et al. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284:3015-3021.
12. Parish JM, Adam T, Facchiano L. Relationship of metabolic syndrome and obstructive sleep apnea. J Clin Sleep Med. 2007;3:467-472.
13. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013-2016.
14. Skomro RP, Gjevre J, Reid J, et al. Outcomes of home-base diagnosis and treatment of obstructive sleep apnea. Chest. 2010;138:257-263.
15. Iber C, Ancoli-Israel S, Chesson AL Jr, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Westchester, IL: American Academy of Sleep Medicine; 2007.
16. Johns MW. Sensitivity and specificity of the multiple sleep maintenance tests, the maintenance of wakefulness tests and the Epworth sleepiness scale: failure of the MSLT as a gold standard. J Sleep Res. 2000;9:5-11.
17. Hesselbacher S, Subramanian S, Allen J, et al. Body mass index, gender, and ethnic variations alter the clinical implication of the Epworth sleepiness scale in patients with suspected of obstructive sleep apnea. Open Respir Med J. 2012;6:2020-2027.
18. Ahmadi N, Chung S, Gibbs A, et al. The Berlin questionnaire for sleep apnea in a sleep clinic population: relationship to polysomnographic measurement of respiratory disturbance. Sleep Breath. 2008;12:38-45.
19. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108:812-821.
20. Shneerson J, Wright J. Lifestyle modification for obstructive sleep apnoea. Cochrane Database Syst Rev. 2001;(1):CD002875.
21. Barvaux VA, Aubert G, Rodenstein DO. Weight loss as treatment for obstructive sleep apnea. Sleep Med Rev. 2000;4:435-452.
22. Buchwald H, Avidor H, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
23. Dixon JB, Schachter LM, O’Brien PE, et al. Surgical vs. conventional therapy for weight loss treatment of obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;308:1142-1149.
24. Greenburg A, Lettieri C, Arn E. Effects of surgical weight loss on measures of obstructive sleep apnea: a meta-analysis. Am J Med. 2009;122:535-542.
25. Sagawa Y, Kondo H, Matsubuchi N. Alcohol has a dose-related effect on parasympathetic nerve activity during sleep. Alcohol Clin Exp Res. 2011;35:2093-2100.
26. Vakulin A, Baulk SD, Catcheside PG, et al. Effects of alcohol and sleep restriction on simulated driving performance in untreated patients with obstructive sleep apnea. Ann Intern Med. 2009;151:447-455.
27. Patel SR, White DP, Malhotra A, et al. Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: results of a meta-analysis. Arch Intern Med. 2003;163:565-571.
28. Giles TL, Lasserson TJ, Smith BH, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;(3):CD001106.
29. Simantirakis EN, Schiza SI, Marketou ME, et al. Severe bradyarrhythmias in patients with sleep apnoea: the effect of continuous positive airway pressure treatment: a long-term evaluation using an insertable loop recorder. Eur Heart J. 2004;25:1070-1076.
30. Marshall NS, Barnes M, Travier N, et al. Continuous positive airway pressure reduces daytime sleepiness in mild to moderate obstructive sleep apnoea: a meta-analysis. Thorax. 2006;61:430-434.
31. Findley L, Smith C, Hooper J, et al. Treatment with nasal CPAP decreases automobile accidents in patient with sleep apnea. Am J Respir Crit Care Med. 2000;161:857-859.
32. Barbe F, Sunyer J, de la Pena A, et al. Effects of continuous positive airway pressure on the risk of road accidents in sleep apnea patients. Respiration. 2007;74:44-49.
33. Sin DD, Mayers I, Man GC, et al. Long Term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population based study. Chest. 2002;121:430-435.
34. Cormican LJ, Williams A. Sleep disordered breathing and its treatment in congestive heart failure. Heart. 2005;91:1265-1270.
35. Lindberg E, Berne C, Elmasry A, et al. CPAP treatment of a population-based sample—what are the benefits and the treatment compliance? Sleep Med. 2006;7:553-560.
36. Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnea-hypopnea syndrome (SAHS). Sleep Med. 2003;7:81-99.
37. Blau A, Minx M, Peter JG, et al. Auto bi-level pressure relief-PAP is as effective as CPAP in OSA patients—a pilot study. Sleep Breath. 2012;16:773-739.
38. Chan AS, Lee RW, Cistulli PA. Dental appliance treatment for obstructive sleep apnea. Chest. 2007;132:693-699.
39. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29:240-243.
40. Sundaram S, Bridgman SA, Lim J, et al. Surgery for obstructive sleep apnoea. Cochrane Database Syst Rev. 2005;(4):CD001004.
41. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33:1396-1407.
42. Smith I, Lasserson TJ, Wright JJ. Drug therapy for obstructive sleep apnea in adults. Cochrane Database Syst Rev. 2006;():CD003002. Review.
43. Mason M, Welsh EJ, Smith I. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2013;(5): CD003002.
CASE 1 Mr. M, age 59, has diabetes, hypertension, hyperlipidemia, and obesity, with a body mass index (BMI) of 37 kg/m2. His hyperlipidemia is well controlled with atorvastatin. He also takes hydrochlorothiazide, lisinopril, metformin, and glyburide, but neither his hypertension nor his glucose levels are well controlled. Mr. M does not exercise, and acknowledges eating a high-calorie diet.
Mr. M reports that his wife has begun complaining about his loud snoring, and that he’s been falling asleep at work. He says he has 2 to 3 alcoholic drinks per week, and doesn’t smoke or take any other drugs.
CASE 2 Ms. C, age 35, is seeking treatment for early morning headaches that began several months ago. She describes a constant dull pain over the frontal area that occurs almost every day and typically resolves in 2 to 3 hours. The pain is not affected by postural changes, she says.
She also reports fatigue, daytime sleepiness, and anxiety. Ms. C has a normal BMI (24 kg/m2), takes no medication, and has no prior history of migraine or tension headaches. She denies any alcohol or recreational drug use.
If Mr. M and Ms. C were your patients, what would your next step be?
Obstructive sleep apnea (OSA) is characterized by repeated cycles of partial airway obstruction, hypoxemia, sympathetic discharge, and arousal to restore ventilation. In addition to fragmented sleep and daytime sleepiness, this common sleep disorder is associated with a decreased functional capacity1-3 and an increased risk for accidents, arrhythmias, myocardial infarction (MI), stroke, and death.4-6 In the Wisconsin Sleep Cohort, an 18-year follow-up study, the estimated hazard ratio for patients with severe OSA was 3.0 for all-cause mortality (95% CI; P-trend <.008) and 5.2 for cardiovascular death (95% CI; P=.003).7
The prevalence of OSA in the United States is 3% to 7% for males and 2% to 5% for females, with higher rates among those older than 65 years. But these figures apply only to those with an OSA diagnosis. An additional 5% of the general population is believed to have undiagnosed OSA.4,8
Arriving at an OSA diagnosis may not be difficult with a patient like Mr. M, who is obese and has classic symptoms. But it is important to consider OSA in patients who, like Ms. C, are not overweight and whose chief complaint appears to be unrelated to sleep.
This review—of risk factors, common (and uncommon) symptoms, diagnostic criteria, and treatment for OSA—highlights key indicators and optimal therapies.
The OSA profile: Risk factors and presenting symptoms
Obesity is perhaps the best-known risk factor for OSA: About 70% of patients with OSA are obese, and 40% of obese individuals have OSA. Approximately 60% of those with OSA have metabolic syndrome.9-12 But it is important to remember that individuals with normal or even low BMI may develop OSA, as well.
Other possible contributing factors include alcohol use, smoking, nasal congestion, menopause, polycystic ovary disease, and a genetic predisposition. And OSA may cause or worsen a wide range of conditions, including hypertension, congestive heart failure, atrial fibrillation, stroke, and nocturnal arrhythmias.8,13
Symptoms may be classic—or not
A bed partner’s complaint about a patient’s snoring, typically followed by arousal and gasping for air, is often the first indication of OSA. Loud snoring and daytime sleepiness are the most common symptoms. But not all patients present with these classic symptoms. Some may complain of irritability, difficulty concentrating, daily headaches, and nocturia.
Because the symptoms of OSA are not highly specific, a wide differential diagnosis must be considered, including numerous causes of excessive daytime sleepiness and conditions, such as panic attacks, pulmonary disease, and gastroesophageal reflux disease, which can interfere with sleep (TABLE 1).8,13
What to include in the medical history and work-up
When you suspect OSA or another sleep disorder, the medical history should include a complete review of systems. The social history needs to include information regarding alcohol intake, use of sedatives, and recreational drugs. If possible, interview the patient’s bed partner, as well.
Examine upper airway anatomy. In performing a physical exam, pay special attention to blood pressure, BMI, and upper airway anatomy. Assess for conditions that can cause obstruction, such as nasal congestion, septal deviation, retrognathia (malocclusion of the mouth due to an abnormal posterior position of the maxilla or mandible), macroglossia (an unusually large tongue), dental malocclusion, enlarged lymphoid tissue and tonsils, large uvula, low hanging soft palate, and a large neck circumference (>40 cm for females and >43 cm for males).13
Order blood tests. Routine blood tests do not support an OSA diagnosis, but they help rule out or identify other conditions associated or mimicking OSA, such as anemia, hypothyroidism, diabetes, liver disease, and kidney disease. Suggested labs include a comprehensive metabolic profile, complete blood count, and thyroid-stimulating hormone test.
Sleep studies are needed for a definitive diagnosis
Conducted overnight in a sleep lab, polysomnography (PSG) uses respiratory effort, respiratory air flow, and peripheral oximetry to identify and quantify episodes of apnea and hypopnea (reported as the apnea-hypopnea index, or AHI). PSG also records brain electrical activity (electroencephalogram), heart rhythm (electrocardiogram), eye movement (electro-oculogram), and muscle activation (electromyogram)—studies used to identify other sleep disorders, such as restless leg syndrome, narcolepsy, parasomnias, and disturbances in rapid-eye movement
(REM) sleep.
Home monitoring. For patients who are unable or unwilling to undergo an overnight sleep study, home portable monitoring is a less expensive alternative. The monitor—a small wireless device—provides data for calculating the AHI and the presence and degree of oxygen desaturation.14 Unlike PSG, which can identify the amount of pressure needed for continuous positive airway pressure (CPAP) therapy, findings from a portable monitor are not sufficient to rule out other sleep disorders to determine whether CPAP is required.15
Evaluating daytime sleepiness. Several tools have been used to evaluate daytime sleepiness. The Epworth Sleepiness Scale (ESS), a quick 8-item screening questionnaire, determines the average person’s level of sleepiness during the day. It ranges from 0 to 24 points, with 10 being normal. Although the ESS has been used extensively in OSA research, recent studies found that it has a low sensitivity (54%) and specificity (57%) for scores >10 and does not correlate well with hypopnea and apnea measurements.16,17
Two additional tools, the Berlin and STOP questionnaires, can also be used to screen for OSA. Both questionnaires have about a 50% positive predictive value and a 70% negative predictive value.18,19
Diagnosing and classifying OSA
Diagnostic criteria developed by the American Academy of Sleep Medicine (AASM) are based on reported and observed symptoms and PSG recordings of hypopnea and apneic episodes. Of the 4 criteria (A through D), patients must meet either A, B, and D or C and D (TABLE 2).15
The AASM further classifies OSA as mild, moderate, or severe (TABLE 3)15 based on the AHI as well as on clinical findings, including oxygen desaturation and arrhythmias. Patients with severe OSA have excessive daytime sleepiness (EDS) that interferes with their normal activities, 15 as well as severe oxygen desaturation, moderate to severe cardiac arrhythmias, and significant risk for hypertension, MI, stroke, and cor pulmonale.
CASE 1 An examination of Mr. M’s upper airway anatomy reveals a neck circumference of 44 cm and normal oropharynx. The results of his lab tests were only significant for elevated blood sugar (234 mg/dL) and glycosylated hemoglobin (9.2%). Because he presents with classic symptoms of OSA, he receives a referral for PSG. He is found to have an AHI of 49, consistent with severe sleep apnea.
CASE 2 A system review of Ms. C finds no fever, nausea, vomiting, weakness, vision changes, or neurological symptoms. A Patient Health Questionnaire-9 (depression screen) is normal, as are her lab tests and a brain MRI with and without contrast. After an extensive work-up for headaches finds nothing, OSA is considered, in light of her daytime sleepiness—and she, too, is referred for PSG. This patient has moderate OSA, with an AHI of 27.
Initiating treatment: What’s best?
Ideally, treatment of OSA would reverse EDS and fatigue, restore full cognitive function, reduce the risk of accidents associated with OSA, and minimize its harmful cardiovascular and pulmonary effects. In fact, while OSA can be managed and its effects ameliorated, all available treatments have limitations and a cure remains elusive.
Let patients know that our understanding of OSA is limited, that treatment may not reverse or eliminate all the risks associated with this condition, and that compliance can be challenging. You can also tell them that, while more and better studies are needed, several modalities have been found to successfully treat OSA.
What to expect from lifestyle modification
Recommend lifestyle changes, such as weight loss, regular exercise early in the day, greater emphasis on sleep hygiene (eg, using the bed only for sleeping and sexual activity), and avoidance of sedating drugs and alcohol for patients with OSA.20,21
The beneficial effect of weight loss on OSA has been demonstrated in studies of both bariatric surgery and conventional weight loss therapies.21-23 While early studies of bariatric surgery were often limited by small size, ambiguous classification of OSA, and selection and follow-up biases, more recent trials show that while OSA symptoms frequently improve postoperatively, the disorder typically persists despite significant reductions in both BMI and AHI.24 Weight reduction should be strongly encouraged for obese patients, however, not only to improve OSA symptoms, but also to reduce the risk for other diseases.
Avoidance of alcohol. Alcohol has adverse effects on sleep: It shortens sleep latency, increases slow-wave sleep, suppresses REM and parasympathetic nerve activity,25 and can exacerbate OSA. Driving simulation studies have found that, compared with healthy individuals, those with untreated OSA are more susceptible to the effects of alcohol and at higher risk for accidents after just one drink.26
CPAP improves sleep, but some problems persist
CPAP supplies a flow of positive air pressure, adjusted to the level needed to keep the airway open, delivered through a facial device best suited to the patient’s anatomy, physiology, and comfort.
Multiple studies have demonstrated the effectiveness of CPAP in reducing symptoms of moderate to severe OSA, compared with placebo and other treatment modalities such as oral devices, surgical procedures, and medications. CPAP reduces AHI, blood pressure, and cardiac arrhythmias. It improves sleep efficiency, oxygen saturation, and self-reported sleep and well-being.27-30 While it ameliorates many of the harmful effects of OSA, it does not improve or reverse all of them. (See “Peripheral neuropathy linked to obstructive sleep apnea?”)
A Cochrane review of 36 randomized controlled trials with a combined total of more than 1700 patients demonstrated the superiority of CPAP vs control in several measures, such as subjective daytime sleepiness, quality of life, cognitive function, and blood pressure.28 On specific parameters of OSA, such as snoring and EDS, studies yielded mixed results.
CPAP has been found to decrease work-related injuries and morbidity and mortality associated with motor vehicle accidents linked to EDS.30-32 However, no study of CPAP has demonstrated a long-term reduction in morbidity and mortality. And no standards define the minimum number of sleep hours and/or frequency of CPAP use that is required to obtain specific benefits.
Patient compliance is poor. Part of the problem is that CPAP is difficult to use, which affects compliance. Poor patient compliance is a major barrier to evaluating its long-term benefits. (The video below, "CPAP Patients Tips from the FDA", can help ensure that patients use CPAP safely and effectively.) Studies estimate that 65% to 89% of patients with CPAP devices use them for at least 4 hours a night for 70% of nights, but that about half of those for whom CPAP is prescribed stop using it after 2 to 3 years.33-36 Several risk factors and comorbid conditions, including advanced age, diabetes, obesity, smoking, and especially, depression, are associated with decreased compliance.13
Improving CPAP compliance continues to be a challenge, highlighting the importance of treating not only OSA but all comorbidities, particularly depression. Short-term studies have found behavioral modification to be a promising means of improving CPAP compliance.33-36
Although not a first-line therapy, bilevel positive airway pressure (BiPAP), which delivers both inspiratory and expiratory pressure via a face device, can be tried in patients unable to tolerate CPAP.37 Studies are limited and it has been used in patients with complex OSA.
Oral appliances are a CPAP alternative
Mandibular repositioning devices (MRDs) and tongue-retaining devices are alternatives to CPAP.38 Although both types of oral appliance are beneficial, they are less effective than CPAP.28
MRDs, which are more commonly used than tongue-retaining devices, are available in several models. An MRD can be custom-made to hold the lower jaw in a forward position during sleep, enlarge the space behind the tongue, and put tension on the walls of the pharynx and the palate to reduce collapse.38
Tongue-retaining devices—splints that hold the tongue in place to keep the airway open—can be used for mild to moderate OSA, and for patients unable to tolerate CPAP.38,39
Studies comparing MRDs and tongue-retaining devices found no statistically significant difference in their ability to reduce AHI, but patients tolerated MRDs better.38,39 Nonetheless, both devices can cause dental discomfort, temporomandibular joint pain, dry mouth or excessive salivation, gum irritation, bruxism, and long-term occlusal changes.38
Is surgery an option?
Numerous surgical techniques are available for treating OSA, all aimed at relieving the obstruction by removing or bypassing it or increasing airway size. These include uvulopalatopharyngoplasty, which resects the uvula, retrolingual, and palatine tonsillar tissue; septoplasty; rhinoplasty; nasal turbinate reduction; nasal polypectomy palatal advancement pharyngoplasty; tonsillectomy; adenoidectomy; palatal implants; tongue reduction; genioglossus advancement; and maxillomandibular advancement.
The choice of modality depends on the patient’s anatomy and physiology, and is selected only after a full evaluation by a head and neck surgeon who specializes in surgical treatment of OSA.40,41 There is a paucity of reliable studies on the results of such procedures, but a Cochrane review of the existing literature concluded that surgery is only indicated for severe cases of sleep apnea in patients who have an anatomic obstruction.40
Too little evidence of medications’ efficacy
Numerous drugs have been tested for the treatment of OSA. Two Cochrane reviews looked at multiple trials of more than 20 drugs, in meta-analyses encompassing more than 500 patients.42,43 Ten drugs—eszopiclone, paroxetine, acetazolamide, ondansetron-fluoxetine combination, naltrexone, and fluticasone nasal spray among them—showed a statistically significant reduction in AHI, and a few showed a subjective benefit in daytime sleepiness. However, the studies were very small and of short duration and the reviewers concluded that evidence is insufficient to recommend drug therapy for OSA.
CASE 1 CPAP was prescribed for Mr. M. He tolerated it well and after 2 weeks, he reported feeling refreshed upon awakening, having less daytime somnolence and being better able to concentrate at work. His hypertension and glucose control improved, but he continues to struggle with his weight.
CASE 2 Ms. C started CPAP and within a week, her morning headaches and irritability resolved.
CORRESPONDENCE
Cecilia Gutierrez, MD, 200 West Arbor Drive, Mail Code 8809, San Diego, CA 92103; cagutierrez@ucsd.edu
CASE 1 Mr. M, age 59, has diabetes, hypertension, hyperlipidemia, and obesity, with a body mass index (BMI) of 37 kg/m2. His hyperlipidemia is well controlled with atorvastatin. He also takes hydrochlorothiazide, lisinopril, metformin, and glyburide, but neither his hypertension nor his glucose levels are well controlled. Mr. M does not exercise, and acknowledges eating a high-calorie diet.
Mr. M reports that his wife has begun complaining about his loud snoring, and that he’s been falling asleep at work. He says he has 2 to 3 alcoholic drinks per week, and doesn’t smoke or take any other drugs.
CASE 2 Ms. C, age 35, is seeking treatment for early morning headaches that began several months ago. She describes a constant dull pain over the frontal area that occurs almost every day and typically resolves in 2 to 3 hours. The pain is not affected by postural changes, she says.
She also reports fatigue, daytime sleepiness, and anxiety. Ms. C has a normal BMI (24 kg/m2), takes no medication, and has no prior history of migraine or tension headaches. She denies any alcohol or recreational drug use.
If Mr. M and Ms. C were your patients, what would your next step be?
Obstructive sleep apnea (OSA) is characterized by repeated cycles of partial airway obstruction, hypoxemia, sympathetic discharge, and arousal to restore ventilation. In addition to fragmented sleep and daytime sleepiness, this common sleep disorder is associated with a decreased functional capacity1-3 and an increased risk for accidents, arrhythmias, myocardial infarction (MI), stroke, and death.4-6 In the Wisconsin Sleep Cohort, an 18-year follow-up study, the estimated hazard ratio for patients with severe OSA was 3.0 for all-cause mortality (95% CI; P-trend <.008) and 5.2 for cardiovascular death (95% CI; P=.003).7
The prevalence of OSA in the United States is 3% to 7% for males and 2% to 5% for females, with higher rates among those older than 65 years. But these figures apply only to those with an OSA diagnosis. An additional 5% of the general population is believed to have undiagnosed OSA.4,8
Arriving at an OSA diagnosis may not be difficult with a patient like Mr. M, who is obese and has classic symptoms. But it is important to consider OSA in patients who, like Ms. C, are not overweight and whose chief complaint appears to be unrelated to sleep.
This review—of risk factors, common (and uncommon) symptoms, diagnostic criteria, and treatment for OSA—highlights key indicators and optimal therapies.
The OSA profile: Risk factors and presenting symptoms
Obesity is perhaps the best-known risk factor for OSA: About 70% of patients with OSA are obese, and 40% of obese individuals have OSA. Approximately 60% of those with OSA have metabolic syndrome.9-12 But it is important to remember that individuals with normal or even low BMI may develop OSA, as well.
Other possible contributing factors include alcohol use, smoking, nasal congestion, menopause, polycystic ovary disease, and a genetic predisposition. And OSA may cause or worsen a wide range of conditions, including hypertension, congestive heart failure, atrial fibrillation, stroke, and nocturnal arrhythmias.8,13
Symptoms may be classic—or not
A bed partner’s complaint about a patient’s snoring, typically followed by arousal and gasping for air, is often the first indication of OSA. Loud snoring and daytime sleepiness are the most common symptoms. But not all patients present with these classic symptoms. Some may complain of irritability, difficulty concentrating, daily headaches, and nocturia.
Because the symptoms of OSA are not highly specific, a wide differential diagnosis must be considered, including numerous causes of excessive daytime sleepiness and conditions, such as panic attacks, pulmonary disease, and gastroesophageal reflux disease, which can interfere with sleep (TABLE 1).8,13
What to include in the medical history and work-up
When you suspect OSA or another sleep disorder, the medical history should include a complete review of systems. The social history needs to include information regarding alcohol intake, use of sedatives, and recreational drugs. If possible, interview the patient’s bed partner, as well.
Examine upper airway anatomy. In performing a physical exam, pay special attention to blood pressure, BMI, and upper airway anatomy. Assess for conditions that can cause obstruction, such as nasal congestion, septal deviation, retrognathia (malocclusion of the mouth due to an abnormal posterior position of the maxilla or mandible), macroglossia (an unusually large tongue), dental malocclusion, enlarged lymphoid tissue and tonsils, large uvula, low hanging soft palate, and a large neck circumference (>40 cm for females and >43 cm for males).13
Order blood tests. Routine blood tests do not support an OSA diagnosis, but they help rule out or identify other conditions associated or mimicking OSA, such as anemia, hypothyroidism, diabetes, liver disease, and kidney disease. Suggested labs include a comprehensive metabolic profile, complete blood count, and thyroid-stimulating hormone test.
Sleep studies are needed for a definitive diagnosis
Conducted overnight in a sleep lab, polysomnography (PSG) uses respiratory effort, respiratory air flow, and peripheral oximetry to identify and quantify episodes of apnea and hypopnea (reported as the apnea-hypopnea index, or AHI). PSG also records brain electrical activity (electroencephalogram), heart rhythm (electrocardiogram), eye movement (electro-oculogram), and muscle activation (electromyogram)—studies used to identify other sleep disorders, such as restless leg syndrome, narcolepsy, parasomnias, and disturbances in rapid-eye movement
(REM) sleep.
Home monitoring. For patients who are unable or unwilling to undergo an overnight sleep study, home portable monitoring is a less expensive alternative. The monitor—a small wireless device—provides data for calculating the AHI and the presence and degree of oxygen desaturation.14 Unlike PSG, which can identify the amount of pressure needed for continuous positive airway pressure (CPAP) therapy, findings from a portable monitor are not sufficient to rule out other sleep disorders to determine whether CPAP is required.15
Evaluating daytime sleepiness. Several tools have been used to evaluate daytime sleepiness. The Epworth Sleepiness Scale (ESS), a quick 8-item screening questionnaire, determines the average person’s level of sleepiness during the day. It ranges from 0 to 24 points, with 10 being normal. Although the ESS has been used extensively in OSA research, recent studies found that it has a low sensitivity (54%) and specificity (57%) for scores >10 and does not correlate well with hypopnea and apnea measurements.16,17
Two additional tools, the Berlin and STOP questionnaires, can also be used to screen for OSA. Both questionnaires have about a 50% positive predictive value and a 70% negative predictive value.18,19
Diagnosing and classifying OSA
Diagnostic criteria developed by the American Academy of Sleep Medicine (AASM) are based on reported and observed symptoms and PSG recordings of hypopnea and apneic episodes. Of the 4 criteria (A through D), patients must meet either A, B, and D or C and D (TABLE 2).15
The AASM further classifies OSA as mild, moderate, or severe (TABLE 3)15 based on the AHI as well as on clinical findings, including oxygen desaturation and arrhythmias. Patients with severe OSA have excessive daytime sleepiness (EDS) that interferes with their normal activities, 15 as well as severe oxygen desaturation, moderate to severe cardiac arrhythmias, and significant risk for hypertension, MI, stroke, and cor pulmonale.
CASE 1 An examination of Mr. M’s upper airway anatomy reveals a neck circumference of 44 cm and normal oropharynx. The results of his lab tests were only significant for elevated blood sugar (234 mg/dL) and glycosylated hemoglobin (9.2%). Because he presents with classic symptoms of OSA, he receives a referral for PSG. He is found to have an AHI of 49, consistent with severe sleep apnea.
CASE 2 A system review of Ms. C finds no fever, nausea, vomiting, weakness, vision changes, or neurological symptoms. A Patient Health Questionnaire-9 (depression screen) is normal, as are her lab tests and a brain MRI with and without contrast. After an extensive work-up for headaches finds nothing, OSA is considered, in light of her daytime sleepiness—and she, too, is referred for PSG. This patient has moderate OSA, with an AHI of 27.
Initiating treatment: What’s best?
Ideally, treatment of OSA would reverse EDS and fatigue, restore full cognitive function, reduce the risk of accidents associated with OSA, and minimize its harmful cardiovascular and pulmonary effects. In fact, while OSA can be managed and its effects ameliorated, all available treatments have limitations and a cure remains elusive.
Let patients know that our understanding of OSA is limited, that treatment may not reverse or eliminate all the risks associated with this condition, and that compliance can be challenging. You can also tell them that, while more and better studies are needed, several modalities have been found to successfully treat OSA.
What to expect from lifestyle modification
Recommend lifestyle changes, such as weight loss, regular exercise early in the day, greater emphasis on sleep hygiene (eg, using the bed only for sleeping and sexual activity), and avoidance of sedating drugs and alcohol for patients with OSA.20,21
The beneficial effect of weight loss on OSA has been demonstrated in studies of both bariatric surgery and conventional weight loss therapies.21-23 While early studies of bariatric surgery were often limited by small size, ambiguous classification of OSA, and selection and follow-up biases, more recent trials show that while OSA symptoms frequently improve postoperatively, the disorder typically persists despite significant reductions in both BMI and AHI.24 Weight reduction should be strongly encouraged for obese patients, however, not only to improve OSA symptoms, but also to reduce the risk for other diseases.
Avoidance of alcohol. Alcohol has adverse effects on sleep: It shortens sleep latency, increases slow-wave sleep, suppresses REM and parasympathetic nerve activity,25 and can exacerbate OSA. Driving simulation studies have found that, compared with healthy individuals, those with untreated OSA are more susceptible to the effects of alcohol and at higher risk for accidents after just one drink.26
CPAP improves sleep, but some problems persist
CPAP supplies a flow of positive air pressure, adjusted to the level needed to keep the airway open, delivered through a facial device best suited to the patient’s anatomy, physiology, and comfort.
Multiple studies have demonstrated the effectiveness of CPAP in reducing symptoms of moderate to severe OSA, compared with placebo and other treatment modalities such as oral devices, surgical procedures, and medications. CPAP reduces AHI, blood pressure, and cardiac arrhythmias. It improves sleep efficiency, oxygen saturation, and self-reported sleep and well-being.27-30 While it ameliorates many of the harmful effects of OSA, it does not improve or reverse all of them. (See “Peripheral neuropathy linked to obstructive sleep apnea?”)
A Cochrane review of 36 randomized controlled trials with a combined total of more than 1700 patients demonstrated the superiority of CPAP vs control in several measures, such as subjective daytime sleepiness, quality of life, cognitive function, and blood pressure.28 On specific parameters of OSA, such as snoring and EDS, studies yielded mixed results.
CPAP has been found to decrease work-related injuries and morbidity and mortality associated with motor vehicle accidents linked to EDS.30-32 However, no study of CPAP has demonstrated a long-term reduction in morbidity and mortality. And no standards define the minimum number of sleep hours and/or frequency of CPAP use that is required to obtain specific benefits.
Patient compliance is poor. Part of the problem is that CPAP is difficult to use, which affects compliance. Poor patient compliance is a major barrier to evaluating its long-term benefits. (The video below, "CPAP Patients Tips from the FDA", can help ensure that patients use CPAP safely and effectively.) Studies estimate that 65% to 89% of patients with CPAP devices use them for at least 4 hours a night for 70% of nights, but that about half of those for whom CPAP is prescribed stop using it after 2 to 3 years.33-36 Several risk factors and comorbid conditions, including advanced age, diabetes, obesity, smoking, and especially, depression, are associated with decreased compliance.13
Improving CPAP compliance continues to be a challenge, highlighting the importance of treating not only OSA but all comorbidities, particularly depression. Short-term studies have found behavioral modification to be a promising means of improving CPAP compliance.33-36
Although not a first-line therapy, bilevel positive airway pressure (BiPAP), which delivers both inspiratory and expiratory pressure via a face device, can be tried in patients unable to tolerate CPAP.37 Studies are limited and it has been used in patients with complex OSA.
Oral appliances are a CPAP alternative
Mandibular repositioning devices (MRDs) and tongue-retaining devices are alternatives to CPAP.38 Although both types of oral appliance are beneficial, they are less effective than CPAP.28
MRDs, which are more commonly used than tongue-retaining devices, are available in several models. An MRD can be custom-made to hold the lower jaw in a forward position during sleep, enlarge the space behind the tongue, and put tension on the walls of the pharynx and the palate to reduce collapse.38
Tongue-retaining devices—splints that hold the tongue in place to keep the airway open—can be used for mild to moderate OSA, and for patients unable to tolerate CPAP.38,39
Studies comparing MRDs and tongue-retaining devices found no statistically significant difference in their ability to reduce AHI, but patients tolerated MRDs better.38,39 Nonetheless, both devices can cause dental discomfort, temporomandibular joint pain, dry mouth or excessive salivation, gum irritation, bruxism, and long-term occlusal changes.38
Is surgery an option?
Numerous surgical techniques are available for treating OSA, all aimed at relieving the obstruction by removing or bypassing it or increasing airway size. These include uvulopalatopharyngoplasty, which resects the uvula, retrolingual, and palatine tonsillar tissue; septoplasty; rhinoplasty; nasal turbinate reduction; nasal polypectomy palatal advancement pharyngoplasty; tonsillectomy; adenoidectomy; palatal implants; tongue reduction; genioglossus advancement; and maxillomandibular advancement.
The choice of modality depends on the patient’s anatomy and physiology, and is selected only after a full evaluation by a head and neck surgeon who specializes in surgical treatment of OSA.40,41 There is a paucity of reliable studies on the results of such procedures, but a Cochrane review of the existing literature concluded that surgery is only indicated for severe cases of sleep apnea in patients who have an anatomic obstruction.40
Too little evidence of medications’ efficacy
Numerous drugs have been tested for the treatment of OSA. Two Cochrane reviews looked at multiple trials of more than 20 drugs, in meta-analyses encompassing more than 500 patients.42,43 Ten drugs—eszopiclone, paroxetine, acetazolamide, ondansetron-fluoxetine combination, naltrexone, and fluticasone nasal spray among them—showed a statistically significant reduction in AHI, and a few showed a subjective benefit in daytime sleepiness. However, the studies were very small and of short duration and the reviewers concluded that evidence is insufficient to recommend drug therapy for OSA.
CASE 1 CPAP was prescribed for Mr. M. He tolerated it well and after 2 weeks, he reported feeling refreshed upon awakening, having less daytime somnolence and being better able to concentrate at work. His hypertension and glucose control improved, but he continues to struggle with his weight.
CASE 2 Ms. C started CPAP and within a week, her morning headaches and irritability resolved.
CORRESPONDENCE
Cecilia Gutierrez, MD, 200 West Arbor Drive, Mail Code 8809, San Diego, CA 92103; cagutierrez@ucsd.edu
1. Dempsey JA, Veasey SC, Morgan BJ, et al. Pathophysiology of sleep apnea. Physiol Rev. 2010;90:47-112.
2. Jenkinson C, Stradling J, Petersen S. Comparison of three measures of quality of life outcome in the evaluation of continuous positive airways pressure therapy for sleep apnoea. J Sleep Res. 1997;6:199-204.
3. Satela MJ. Neuropsychological impairment and quality of life in obstructive sleep apnea. Clin Chest Med. 2003;24:249-259.
4. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217-1239.
5. Yaggi HK, Concato J, Kernan W, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034-2041.
6. Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046-1053.
7. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;3:1071-1078.
8. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:136-143.
9. Coughlin SR, Mawdsley L, Mugarza JA, et al. Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Eur Heart J. 2004;25:735-741.
10. Basta M, Vgontzas AN. Metabolic abnormalities in obesity and sleep apnea are in a continuum. Sleep Med. 2007;8:5-7.
11. Peppard PE, Young T, Palta M, et al. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284:3015-3021.
12. Parish JM, Adam T, Facchiano L. Relationship of metabolic syndrome and obstructive sleep apnea. J Clin Sleep Med. 2007;3:467-472.
13. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013-2016.
14. Skomro RP, Gjevre J, Reid J, et al. Outcomes of home-base diagnosis and treatment of obstructive sleep apnea. Chest. 2010;138:257-263.
15. Iber C, Ancoli-Israel S, Chesson AL Jr, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Westchester, IL: American Academy of Sleep Medicine; 2007.
16. Johns MW. Sensitivity and specificity of the multiple sleep maintenance tests, the maintenance of wakefulness tests and the Epworth sleepiness scale: failure of the MSLT as a gold standard. J Sleep Res. 2000;9:5-11.
17. Hesselbacher S, Subramanian S, Allen J, et al. Body mass index, gender, and ethnic variations alter the clinical implication of the Epworth sleepiness scale in patients with suspected of obstructive sleep apnea. Open Respir Med J. 2012;6:2020-2027.
18. Ahmadi N, Chung S, Gibbs A, et al. The Berlin questionnaire for sleep apnea in a sleep clinic population: relationship to polysomnographic measurement of respiratory disturbance. Sleep Breath. 2008;12:38-45.
19. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108:812-821.
20. Shneerson J, Wright J. Lifestyle modification for obstructive sleep apnoea. Cochrane Database Syst Rev. 2001;(1):CD002875.
21. Barvaux VA, Aubert G, Rodenstein DO. Weight loss as treatment for obstructive sleep apnea. Sleep Med Rev. 2000;4:435-452.
22. Buchwald H, Avidor H, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
23. Dixon JB, Schachter LM, O’Brien PE, et al. Surgical vs. conventional therapy for weight loss treatment of obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;308:1142-1149.
24. Greenburg A, Lettieri C, Arn E. Effects of surgical weight loss on measures of obstructive sleep apnea: a meta-analysis. Am J Med. 2009;122:535-542.
25. Sagawa Y, Kondo H, Matsubuchi N. Alcohol has a dose-related effect on parasympathetic nerve activity during sleep. Alcohol Clin Exp Res. 2011;35:2093-2100.
26. Vakulin A, Baulk SD, Catcheside PG, et al. Effects of alcohol and sleep restriction on simulated driving performance in untreated patients with obstructive sleep apnea. Ann Intern Med. 2009;151:447-455.
27. Patel SR, White DP, Malhotra A, et al. Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: results of a meta-analysis. Arch Intern Med. 2003;163:565-571.
28. Giles TL, Lasserson TJ, Smith BH, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;(3):CD001106.
29. Simantirakis EN, Schiza SI, Marketou ME, et al. Severe bradyarrhythmias in patients with sleep apnoea: the effect of continuous positive airway pressure treatment: a long-term evaluation using an insertable loop recorder. Eur Heart J. 2004;25:1070-1076.
30. Marshall NS, Barnes M, Travier N, et al. Continuous positive airway pressure reduces daytime sleepiness in mild to moderate obstructive sleep apnoea: a meta-analysis. Thorax. 2006;61:430-434.
31. Findley L, Smith C, Hooper J, et al. Treatment with nasal CPAP decreases automobile accidents in patient with sleep apnea. Am J Respir Crit Care Med. 2000;161:857-859.
32. Barbe F, Sunyer J, de la Pena A, et al. Effects of continuous positive airway pressure on the risk of road accidents in sleep apnea patients. Respiration. 2007;74:44-49.
33. Sin DD, Mayers I, Man GC, et al. Long Term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population based study. Chest. 2002;121:430-435.
34. Cormican LJ, Williams A. Sleep disordered breathing and its treatment in congestive heart failure. Heart. 2005;91:1265-1270.
35. Lindberg E, Berne C, Elmasry A, et al. CPAP treatment of a population-based sample—what are the benefits and the treatment compliance? Sleep Med. 2006;7:553-560.
36. Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnea-hypopnea syndrome (SAHS). Sleep Med. 2003;7:81-99.
37. Blau A, Minx M, Peter JG, et al. Auto bi-level pressure relief-PAP is as effective as CPAP in OSA patients—a pilot study. Sleep Breath. 2012;16:773-739.
38. Chan AS, Lee RW, Cistulli PA. Dental appliance treatment for obstructive sleep apnea. Chest. 2007;132:693-699.
39. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29:240-243.
40. Sundaram S, Bridgman SA, Lim J, et al. Surgery for obstructive sleep apnoea. Cochrane Database Syst Rev. 2005;(4):CD001004.
41. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33:1396-1407.
42. Smith I, Lasserson TJ, Wright JJ. Drug therapy for obstructive sleep apnea in adults. Cochrane Database Syst Rev. 2006;():CD003002. Review.
43. Mason M, Welsh EJ, Smith I. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2013;(5): CD003002.
1. Dempsey JA, Veasey SC, Morgan BJ, et al. Pathophysiology of sleep apnea. Physiol Rev. 2010;90:47-112.
2. Jenkinson C, Stradling J, Petersen S. Comparison of three measures of quality of life outcome in the evaluation of continuous positive airways pressure therapy for sleep apnoea. J Sleep Res. 1997;6:199-204.
3. Satela MJ. Neuropsychological impairment and quality of life in obstructive sleep apnea. Clin Chest Med. 2003;24:249-259.
4. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217-1239.
5. Yaggi HK, Concato J, Kernan W, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034-2041.
6. Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046-1053.
7. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;3:1071-1078.
8. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:136-143.
9. Coughlin SR, Mawdsley L, Mugarza JA, et al. Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Eur Heart J. 2004;25:735-741.
10. Basta M, Vgontzas AN. Metabolic abnormalities in obesity and sleep apnea are in a continuum. Sleep Med. 2007;8:5-7.
11. Peppard PE, Young T, Palta M, et al. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284:3015-3021.
12. Parish JM, Adam T, Facchiano L. Relationship of metabolic syndrome and obstructive sleep apnea. J Clin Sleep Med. 2007;3:467-472.
13. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013-2016.
14. Skomro RP, Gjevre J, Reid J, et al. Outcomes of home-base diagnosis and treatment of obstructive sleep apnea. Chest. 2010;138:257-263.
15. Iber C, Ancoli-Israel S, Chesson AL Jr, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Westchester, IL: American Academy of Sleep Medicine; 2007.
16. Johns MW. Sensitivity and specificity of the multiple sleep maintenance tests, the maintenance of wakefulness tests and the Epworth sleepiness scale: failure of the MSLT as a gold standard. J Sleep Res. 2000;9:5-11.
17. Hesselbacher S, Subramanian S, Allen J, et al. Body mass index, gender, and ethnic variations alter the clinical implication of the Epworth sleepiness scale in patients with suspected of obstructive sleep apnea. Open Respir Med J. 2012;6:2020-2027.
18. Ahmadi N, Chung S, Gibbs A, et al. The Berlin questionnaire for sleep apnea in a sleep clinic population: relationship to polysomnographic measurement of respiratory disturbance. Sleep Breath. 2008;12:38-45.
19. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108:812-821.
20. Shneerson J, Wright J. Lifestyle modification for obstructive sleep apnoea. Cochrane Database Syst Rev. 2001;(1):CD002875.
21. Barvaux VA, Aubert G, Rodenstein DO. Weight loss as treatment for obstructive sleep apnea. Sleep Med Rev. 2000;4:435-452.
22. Buchwald H, Avidor H, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
23. Dixon JB, Schachter LM, O’Brien PE, et al. Surgical vs. conventional therapy for weight loss treatment of obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;308:1142-1149.
24. Greenburg A, Lettieri C, Arn E. Effects of surgical weight loss on measures of obstructive sleep apnea: a meta-analysis. Am J Med. 2009;122:535-542.
25. Sagawa Y, Kondo H, Matsubuchi N. Alcohol has a dose-related effect on parasympathetic nerve activity during sleep. Alcohol Clin Exp Res. 2011;35:2093-2100.
26. Vakulin A, Baulk SD, Catcheside PG, et al. Effects of alcohol and sleep restriction on simulated driving performance in untreated patients with obstructive sleep apnea. Ann Intern Med. 2009;151:447-455.
27. Patel SR, White DP, Malhotra A, et al. Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: results of a meta-analysis. Arch Intern Med. 2003;163:565-571.
28. Giles TL, Lasserson TJ, Smith BH, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;(3):CD001106.
29. Simantirakis EN, Schiza SI, Marketou ME, et al. Severe bradyarrhythmias in patients with sleep apnoea: the effect of continuous positive airway pressure treatment: a long-term evaluation using an insertable loop recorder. Eur Heart J. 2004;25:1070-1076.
30. Marshall NS, Barnes M, Travier N, et al. Continuous positive airway pressure reduces daytime sleepiness in mild to moderate obstructive sleep apnoea: a meta-analysis. Thorax. 2006;61:430-434.
31. Findley L, Smith C, Hooper J, et al. Treatment with nasal CPAP decreases automobile accidents in patient with sleep apnea. Am J Respir Crit Care Med. 2000;161:857-859.
32. Barbe F, Sunyer J, de la Pena A, et al. Effects of continuous positive airway pressure on the risk of road accidents in sleep apnea patients. Respiration. 2007;74:44-49.
33. Sin DD, Mayers I, Man GC, et al. Long Term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population based study. Chest. 2002;121:430-435.
34. Cormican LJ, Williams A. Sleep disordered breathing and its treatment in congestive heart failure. Heart. 2005;91:1265-1270.
35. Lindberg E, Berne C, Elmasry A, et al. CPAP treatment of a population-based sample—what are the benefits and the treatment compliance? Sleep Med. 2006;7:553-560.
36. Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnea-hypopnea syndrome (SAHS). Sleep Med. 2003;7:81-99.
37. Blau A, Minx M, Peter JG, et al. Auto bi-level pressure relief-PAP is as effective as CPAP in OSA patients—a pilot study. Sleep Breath. 2012;16:773-739.
38. Chan AS, Lee RW, Cistulli PA. Dental appliance treatment for obstructive sleep apnea. Chest. 2007;132:693-699.
39. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29:240-243.
40. Sundaram S, Bridgman SA, Lim J, et al. Surgery for obstructive sleep apnoea. Cochrane Database Syst Rev. 2005;(4):CD001004.
41. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33:1396-1407.
42. Smith I, Lasserson TJ, Wright JJ. Drug therapy for obstructive sleep apnea in adults. Cochrane Database Syst Rev. 2006;():CD003002. Review.
43. Mason M, Welsh EJ, Smith I. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2013;(5): CD003002.

Don't mind the noise-- they're just trying to sleep
Two years ago, a house guest apologized to my wife and me as he prepared to turn in for the evening. He was sorry to subject us to his noisy CPAP machine, he said. Last year at a family reunion, my sleepy brother-in-law blamed his lethargy on sleep apnea, and another in-law chimed in to say that CPAP worked great for her.
If my family and friends are any indication, we seem to be surrounded by people with obstructive sleep apnea (OSA), due almost entirely to the steep rise in obesity over the past 30 years.
It is alarming to know that OSA is associated with traffic accidents, worsening of diabetes and hypertension, atrial fibrillation, and a higher risk of death. What we don’t yet know is whether these major health problems are caused by sleep apnea or whether they’re fellow travelers. (In “Obstructive sleep apnea: A diagnostic and treatment guide” on page 565, Gutierrez and Brady present an evidence-based summary of symptoms, diagnostic criteria, and treatment modalities. And in “Peripheral neuropathy linked to obstructive sleep apnea?” on page 577, Schmidt et al highlight a lesser known association with OSA.)
There is excellent evidence that CPAP and, in some cases, dental devices, can alleviate daytime sleepiness in patients with OSA. But more randomized trials are needed to determine whether treatment of OSA can improve hypertension, diabetes control, and atrial fibrillation, as well as prevent excess mortality.
Recent trials offer a glimmer of hope. One found that CPAP therapy led to small but significant blood pressure reductions in patients with treatment-resistant hypertension.1 Another demonstrated that CPAP led to improvement in lipid profiles and hemoglobin A1c in obese patients with diabetes.2 But many more studies are needed to know how effective sleep apnea treatments are in reducing the significant morbidity and mortality associated with OSA.
Sleep medicine is a young specialty, so it is not surprising that high-quality randomized trials of sleep apnea are in their infancy. (The American Academy of Sleep Medicine was founded in 1975 and the American Board of Sleep Medicine was established in 1991.) Because the science is evolving, I encourage you to stay abreast of new developments in the field. In the meantime, nothing works better for improving sleep apnea, hypertension, and diabetes than good old-fashioned weight loss!
1. Lozano L, Tovar JL, Sampo G, et al. Continuous positive airway pressure treatment in sleep apnea patients with resistant hypertension: a randomized, controlled trial. J Hypertens. 2010;28:2161-2168.
2. Weinstock TG, Wang X, Rueschman M, et al. A controlled trial of CPAP therapy on metabolic control in individuals with impaired glucose tolerance and sleep apnea. Sleep. 2012;35:617B-625B.
Two years ago, a house guest apologized to my wife and me as he prepared to turn in for the evening. He was sorry to subject us to his noisy CPAP machine, he said. Last year at a family reunion, my sleepy brother-in-law blamed his lethargy on sleep apnea, and another in-law chimed in to say that CPAP worked great for her.
If my family and friends are any indication, we seem to be surrounded by people with obstructive sleep apnea (OSA), due almost entirely to the steep rise in obesity over the past 30 years.
It is alarming to know that OSA is associated with traffic accidents, worsening of diabetes and hypertension, atrial fibrillation, and a higher risk of death. What we don’t yet know is whether these major health problems are caused by sleep apnea or whether they’re fellow travelers. (In “Obstructive sleep apnea: A diagnostic and treatment guide” on page 565, Gutierrez and Brady present an evidence-based summary of symptoms, diagnostic criteria, and treatment modalities. And in “Peripheral neuropathy linked to obstructive sleep apnea?” on page 577, Schmidt et al highlight a lesser known association with OSA.)
There is excellent evidence that CPAP and, in some cases, dental devices, can alleviate daytime sleepiness in patients with OSA. But more randomized trials are needed to determine whether treatment of OSA can improve hypertension, diabetes control, and atrial fibrillation, as well as prevent excess mortality.
Recent trials offer a glimmer of hope. One found that CPAP therapy led to small but significant blood pressure reductions in patients with treatment-resistant hypertension.1 Another demonstrated that CPAP led to improvement in lipid profiles and hemoglobin A1c in obese patients with diabetes.2 But many more studies are needed to know how effective sleep apnea treatments are in reducing the significant morbidity and mortality associated with OSA.
Sleep medicine is a young specialty, so it is not surprising that high-quality randomized trials of sleep apnea are in their infancy. (The American Academy of Sleep Medicine was founded in 1975 and the American Board of Sleep Medicine was established in 1991.) Because the science is evolving, I encourage you to stay abreast of new developments in the field. In the meantime, nothing works better for improving sleep apnea, hypertension, and diabetes than good old-fashioned weight loss!
Two years ago, a house guest apologized to my wife and me as he prepared to turn in for the evening. He was sorry to subject us to his noisy CPAP machine, he said. Last year at a family reunion, my sleepy brother-in-law blamed his lethargy on sleep apnea, and another in-law chimed in to say that CPAP worked great for her.
If my family and friends are any indication, we seem to be surrounded by people with obstructive sleep apnea (OSA), due almost entirely to the steep rise in obesity over the past 30 years.
It is alarming to know that OSA is associated with traffic accidents, worsening of diabetes and hypertension, atrial fibrillation, and a higher risk of death. What we don’t yet know is whether these major health problems are caused by sleep apnea or whether they’re fellow travelers. (In “Obstructive sleep apnea: A diagnostic and treatment guide” on page 565, Gutierrez and Brady present an evidence-based summary of symptoms, diagnostic criteria, and treatment modalities. And in “Peripheral neuropathy linked to obstructive sleep apnea?” on page 577, Schmidt et al highlight a lesser known association with OSA.)
There is excellent evidence that CPAP and, in some cases, dental devices, can alleviate daytime sleepiness in patients with OSA. But more randomized trials are needed to determine whether treatment of OSA can improve hypertension, diabetes control, and atrial fibrillation, as well as prevent excess mortality.
Recent trials offer a glimmer of hope. One found that CPAP therapy led to small but significant blood pressure reductions in patients with treatment-resistant hypertension.1 Another demonstrated that CPAP led to improvement in lipid profiles and hemoglobin A1c in obese patients with diabetes.2 But many more studies are needed to know how effective sleep apnea treatments are in reducing the significant morbidity and mortality associated with OSA.
Sleep medicine is a young specialty, so it is not surprising that high-quality randomized trials of sleep apnea are in their infancy. (The American Academy of Sleep Medicine was founded in 1975 and the American Board of Sleep Medicine was established in 1991.) Because the science is evolving, I encourage you to stay abreast of new developments in the field. In the meantime, nothing works better for improving sleep apnea, hypertension, and diabetes than good old-fashioned weight loss!
1. Lozano L, Tovar JL, Sampo G, et al. Continuous positive airway pressure treatment in sleep apnea patients with resistant hypertension: a randomized, controlled trial. J Hypertens. 2010;28:2161-2168.
2. Weinstock TG, Wang X, Rueschman M, et al. A controlled trial of CPAP therapy on metabolic control in individuals with impaired glucose tolerance and sleep apnea. Sleep. 2012;35:617B-625B.
1. Lozano L, Tovar JL, Sampo G, et al. Continuous positive airway pressure treatment in sleep apnea patients with resistant hypertension: a randomized, controlled trial. J Hypertens. 2010;28:2161-2168.
2. Weinstock TG, Wang X, Rueschman M, et al. A controlled trial of CPAP therapy on metabolic control in individuals with impaired glucose tolerance and sleep apnea. Sleep. 2012;35:617B-625B.
Obstructive sleep apnea is a risk factor for Barrett’s esophagus
Obstructive sleep apnea is a risk factor for Barrett’s esophagus, according to findings published online September 11 in Clinical Gastroenterology and Hepatology.
Researchers from the Mayo Clinic in Rochester, Minn., studied 7,482 patients who had undergone both a diagnostic polysomnogram and esophagogastroduodenoscopy from January 2000 to November 2011.
"In this subset of patients, the presence of OSA [obstructive sleep apnea] was associated with an 80% increased risk of [Barrett’s esophagus], compared to subjects without OSA and [Barrett’s esophagus]," wrote study author Dr. Prasad G. Iyer and his colleagues (Clin. Gastroenterol. Hepatol. 2013 September;11:1108-14.e5).

Several overlapping risk factors exist for obstructive sleep apnea and Barrett’s esophagus (BE), including obesity, gastroesophageal reflux disease (GERD), male gender, and older age. This study was designed to explore whether there is a relationship between obstructive sleep apnea and Barrett’s esophagus independent of these factors.
Subjects were categorized into four groups: diagnosis of BE but not OSA; OSA but not BE; both; or neither. Of the 7,482 patients, 2,480 did not have a diagnosis of OSA or BE; 83 had BE but not OSA; 4,641 had OSA but not BE; and 278 had a diagnosis of both.
The study authors used univariable models assessing age, sex, body mass index, GERD, and smoking history to determine the association between OSA and BE. GERD and OSA were associated with Barrett’s esophagus. A multiple-variable analysis was performed to observe the association of OSA with BE, adjusting for other factors. Patients with OSA were about 80% more at risk for having Barrett’s esophagus than were subjects without OSA or Barrett’s esophagus.
"This association was dose dependent, with an increase in severity of OSA being associated with an increased risk of Barrett’s esophagus," wrote the authors.
Additionally, since "the association of [Barrett’s esophagus] and OSA could be confounded by gastroesophageal reflux," the researchers also performed analyses to determine whether this relationship was independent of a GERD diagnosis. In a univariate analysis, both OSA and GERD were associated with BE, and in a multiple-variable analysis demonstrated that "both OSA and GERD were "independently associated with an increased risk of Barrett’s esophagus."
Dr. Iyer and his colleagues cited a few limitations to this study. First, the study’s design did not allow for exploration of a specific mechanism for how OSA predisposes individuals to Barrett’s esophagus. Second, the ability to accurately assess the association of OSA with GERD was limited by a lack of an established clinical definition of GERD. Finally, the use of ICD-9 codes to diagnose conditions may have resulted in overestimates in the sample.
The authors concluded that further research is needed to confirm that these findings can be applied to the general population and to explore whether treatment for OSA may help reverse this risk.
They also added that given the "asymptomatic nature" of Barrett’s esophagus and the higher risk of esophageal adenocarcinoma, patients with OSA may benefit from BE screening.
Dr. Iyer and his colleagues disclosed that this study was supported in part by the American College of Gastroenterology, the National Institute of Diabetes, Digestive and Kidney Disease; and the Edward C. Rosenow Endowed Professorship Internal Medicine Residency Award at the Mayo Clinic.
Obstructive sleep apnea is a risk factor for Barrett’s esophagus, according to findings published online September 11 in Clinical Gastroenterology and Hepatology.
Researchers from the Mayo Clinic in Rochester, Minn., studied 7,482 patients who had undergone both a diagnostic polysomnogram and esophagogastroduodenoscopy from January 2000 to November 2011.
"In this subset of patients, the presence of OSA [obstructive sleep apnea] was associated with an 80% increased risk of [Barrett’s esophagus], compared to subjects without OSA and [Barrett’s esophagus]," wrote study author Dr. Prasad G. Iyer and his colleagues (Clin. Gastroenterol. Hepatol. 2013 September;11:1108-14.e5).
Several overlapping risk factors exist for obstructive sleep apnea and Barrett’s esophagus (BE), including obesity, gastroesophageal reflux disease (GERD), male gender, and older age. This study was designed to explore whether there is a relationship between obstructive sleep apnea and Barrett’s esophagus independent of these factors.
Subjects were categorized into four groups: diagnosis of BE but not OSA; OSA but not BE; both; or neither. Of the 7,482 patients, 2,480 did not have a diagnosis of OSA or BE; 83 had BE but not OSA; 4,641 had OSA but not BE; and 278 had a diagnosis of both.
The study authors used univariable models assessing age, sex, body mass index, GERD, and smoking history to determine the association between OSA and BE. GERD and OSA were associated with Barrett’s esophagus. A multiple-variable analysis was performed to observe the association of OSA with BE, adjusting for other factors. Patients with OSA were about 80% more at risk for having Barrett’s esophagus than were subjects without OSA or Barrett’s esophagus.
"This association was dose dependent, with an increase in severity of OSA being associated with an increased risk of Barrett’s esophagus," wrote the authors.
Additionally, since "the association of [Barrett’s esophagus] and OSA could be confounded by gastroesophageal reflux," the researchers also performed analyses to determine whether this relationship was independent of a GERD diagnosis. In a univariate analysis, both OSA and GERD were associated with BE, and in a multiple-variable analysis demonstrated that "both OSA and GERD were "independently associated with an increased risk of Barrett’s esophagus."
Dr. Iyer and his colleagues cited a few limitations to this study. First, the study’s design did not allow for exploration of a specific mechanism for how OSA predisposes individuals to Barrett’s esophagus. Second, the ability to accurately assess the association of OSA with GERD was limited by a lack of an established clinical definition of GERD. Finally, the use of ICD-9 codes to diagnose conditions may have resulted in overestimates in the sample.
The authors concluded that further research is needed to confirm that these findings can be applied to the general population and to explore whether treatment for OSA may help reverse this risk.
They also added that given the "asymptomatic nature" of Barrett’s esophagus and the higher risk of esophageal adenocarcinoma, patients with OSA may benefit from BE screening.
Dr. Iyer and his colleagues disclosed that this study was supported in part by the American College of Gastroenterology, the National Institute of Diabetes, Digestive and Kidney Disease; and the Edward C. Rosenow Endowed Professorship Internal Medicine Residency Award at the Mayo Clinic.
Obstructive sleep apnea is a risk factor for Barrett’s esophagus, according to findings published online September 11 in Clinical Gastroenterology and Hepatology.
Researchers from the Mayo Clinic in Rochester, Minn., studied 7,482 patients who had undergone both a diagnostic polysomnogram and esophagogastroduodenoscopy from January 2000 to November 2011.
"In this subset of patients, the presence of OSA [obstructive sleep apnea] was associated with an 80% increased risk of [Barrett’s esophagus], compared to subjects without OSA and [Barrett’s esophagus]," wrote study author Dr. Prasad G. Iyer and his colleagues (Clin. Gastroenterol. Hepatol. 2013 September;11:1108-14.e5).
Several overlapping risk factors exist for obstructive sleep apnea and Barrett’s esophagus (BE), including obesity, gastroesophageal reflux disease (GERD), male gender, and older age. This study was designed to explore whether there is a relationship between obstructive sleep apnea and Barrett’s esophagus independent of these factors.
Subjects were categorized into four groups: diagnosis of BE but not OSA; OSA but not BE; both; or neither. Of the 7,482 patients, 2,480 did not have a diagnosis of OSA or BE; 83 had BE but not OSA; 4,641 had OSA but not BE; and 278 had a diagnosis of both.
The study authors used univariable models assessing age, sex, body mass index, GERD, and smoking history to determine the association between OSA and BE. GERD and OSA were associated with Barrett’s esophagus. A multiple-variable analysis was performed to observe the association of OSA with BE, adjusting for other factors. Patients with OSA were about 80% more at risk for having Barrett’s esophagus than were subjects without OSA or Barrett’s esophagus.
"This association was dose dependent, with an increase in severity of OSA being associated with an increased risk of Barrett’s esophagus," wrote the authors.
Additionally, since "the association of [Barrett’s esophagus] and OSA could be confounded by gastroesophageal reflux," the researchers also performed analyses to determine whether this relationship was independent of a GERD diagnosis. In a univariate analysis, both OSA and GERD were associated with BE, and in a multiple-variable analysis demonstrated that "both OSA and GERD were "independently associated with an increased risk of Barrett’s esophagus."
Dr. Iyer and his colleagues cited a few limitations to this study. First, the study’s design did not allow for exploration of a specific mechanism for how OSA predisposes individuals to Barrett’s esophagus. Second, the ability to accurately assess the association of OSA with GERD was limited by a lack of an established clinical definition of GERD. Finally, the use of ICD-9 codes to diagnose conditions may have resulted in overestimates in the sample.
The authors concluded that further research is needed to confirm that these findings can be applied to the general population and to explore whether treatment for OSA may help reverse this risk.
They also added that given the "asymptomatic nature" of Barrett’s esophagus and the higher risk of esophageal adenocarcinoma, patients with OSA may benefit from BE screening.
Dr. Iyer and his colleagues disclosed that this study was supported in part by the American College of Gastroenterology, the National Institute of Diabetes, Digestive and Kidney Disease; and the Edward C. Rosenow Endowed Professorship Internal Medicine Residency Award at the Mayo Clinic.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Major finding: The presence of OSA was associated with an 80% increased risk of Barrett’s esophagus, compared with subjects without OSA.
Data source: A case-control study of 7,482 patients who underwent both a polysomnogram and esophagogastroduodenoscopy and were screened for OSA and BE using ICD-9 codes.
Disclosures: The study was supported in part by the American College of Gastroenterology, the National Institute of Diabetes, Digestive and Kidney Disease; and the Edward C. Rosenow Endowed Professorship Internal Medicine Residency Award at the Mayo Clinic.

Start sleep apnea therapy with CPAP, not surgery
First-line treatment for adults with obstructive sleep apnea should be continuous positive airway pressure therapy or a mandibular advancement device, according to the American College of Physicians’ clinical practice guideline published online Sept. 24 in Annals of Internal Medicine.
In contrast, no surgical procedures or pharmacologic agents should be considered as first-line treatment, because there is insufficient evidence supporting those approaches, said Dr. Amir Qaseem, director of clinical policy at the ACP, Philadelphia, and his associates on the clinical guidelines committee.

Overweight and obese patients with obstructive sleep apnea (OSA) should be encouraged to lose weight, because that has been shown to improve symptoms and reduce scores on the Apnea-Hypopnea Index. Weight loss also confers many other health benefits, they added, while carrying minimal risk of adverse effects.
Those are the chief recommendations of the clinical practice guideline, which was compiled "to present information on both the benefits and harms of interventions" to all clinicians who treat adults with OSA. The guideline is based on a rigorous review of the evidence regarding OSA published in the literature from 1966 through 2012.
Overall, the evidence concerning hard clinical outcomes for any intervention for OSA was extremely limited.
Continuous positive airway pressure (CPAP) was the most extensively studied intervention for OSA, but the evidence from most studies was considered to be only of moderate quality. Studies assessed only the treatment’s effect on immediate outcomes and did not evaluate longer term outcomes such as cardiovascular illness or mortality. In addition, studies that examined CPAP’s effect on quality of life "were inconsistent and therefore inconclusive."
Nevertheless, the balance of evidence does show that CPAP is more effective than are control conditions or sham CPAP at improving scores on the apnea-hypopnea index, which measures the number of apneic and hypopneic episodes per hour of monitored sleep. CPAP also improved scores on the Epworth Sleepiness Scale, a self-administered questionnaire in which patients rate their likelihood of dozing off during various situations.
CPAP also is effective at improving oxygen saturation and reducing scores on the arousal index, which measures the frequency of arousals per hour of sleep using electroencephalography. However, there were insufficient data to compare the different types of CPAP, such as fixed CPAP, auto-CPAP, flexible bilevel CPAP, or CPAP with humidification.
There also was insufficient evidence to directly compare CPAP against other interventions, Dr. Qaseem and his colleagues said (Ann. Intern. Med. 2013;159:471-83).
The guideline recommends that mandibular or dental advancement devices to position the patient’s jaw while sleeping are a useful alternative for those who prefer this intervention to CPAP or for those who cannot tolerate or adhere to CPAP. Moderate-quality evidence showed that mandibular advancement devices improve scores on the apnea-hypopnea index and the arousal index.
However, that recommendation is considered "weak," because the overall data supporting the use of mandibular advancement devices are of low quality.
The data also were insufficient to recommend the use of any pharmacologic agents as a first-line therapy for OSA, or indeed as any therapy for the condition. Those include mirtazapine, xylometazoline, fluticasone, paroxetine, pantoprazole, steroids, acetazolamide, and protriptyline.
Only seven studies assessed surgical interventions for OSA. They were of varied quality, and their outcomes were inconsistent, so, the evidence is insufficient to support any surgery as first-line treatment. The procedures assessed in the studies included uvulopalatopharyngoplasty (UPPP); laser-assisted uvulopalatoplasty; radiofrequency ablation; and various combinations of pharyngoplasty, tonsillectomy, adenoidectomy, genioglossal advancement septoplasty, ablation of the nasal turbinates, and other nasal surgeries.
However, there was some evidence to suggest that UPPP and tracheostomy reduced mortality in patients with OSA.
The guideline strongly recommends that all OSA patients who are overweight or obese should be encouraged to lose weight. The evidence, albeit of low quality, shows that any intensive weight-loss intervention helps improve OSA symptoms and scores on the apnea-hypopnea index.
Finally, the evidence was insufficient to assess the potential benefits of positional therapy, oropharyngeal exercise, palatal implants, or atrial overdrive pacing for patients who already have dual-chamber pacemakers, Dr. Qaseem and his associates said.
The guideline was supported entirely by the American College of Physicians. The investigators had no relevant conflicts of interest.
Obesity is
epidemic in the United States
and “recommending to patients that they lose weight” is not a particularly
effective intervention. The real take-home message from this study is that
there is poor evidence for all treatments, but that the only studies showing a decreased
mortality were those involving surgery. Noninvasive remedies should generally
be preferred when deemed effective. Many patients find CPAP and oral appliances
uncomfortable and compliance rates with these treatments are poor. Obstructive
sleep apnea presents with a wide spectrum of symptoms, and occasionally, an
emergency tracheotomy may be lifesaving for a moribund patient. Patients with
severe OSA have a three- to sixfold increase in all-cause mortality. Motor
vehicle accidents are a major cause of death in patients with severe OSA. It
should also be emphasized that patients with OSA are best evaluated with a formal
sleep study to quantitate the degree of sleep apnea. OSA is a serious health
problem for which a variety of treatments are available. Although surgery is
rarely the first-line therapy, it plays an important role for patients with
particularly severe OSA, some of whom will require a tracheotomy, and in patients
for whom medical therapy is intolerable, not complied with, or ineffective.
Dr. Mark
Weissler is the J.P. Riddle Distinguished Professor of Otolaryngology – head
and neck surgery, University of North Carolina,
Chapel Hill.
Obesity is
epidemic in the United States
and “recommending to patients that they lose weight” is not a particularly
effective intervention. The real take-home message from this study is that
there is poor evidence for all treatments, but that the only studies showing a decreased
mortality were those involving surgery. Noninvasive remedies should generally
be preferred when deemed effective. Many patients find CPAP and oral appliances
uncomfortable and compliance rates with these treatments are poor. Obstructive
sleep apnea presents with a wide spectrum of symptoms, and occasionally, an
emergency tracheotomy may be lifesaving for a moribund patient. Patients with
severe OSA have a three- to sixfold increase in all-cause mortality. Motor
vehicle accidents are a major cause of death in patients with severe OSA. It
should also be emphasized that patients with OSA are best evaluated with a formal
sleep study to quantitate the degree of sleep apnea. OSA is a serious health
problem for which a variety of treatments are available. Although surgery is
rarely the first-line therapy, it plays an important role for patients with
particularly severe OSA, some of whom will require a tracheotomy, and in patients
for whom medical therapy is intolerable, not complied with, or ineffective.
Dr. Mark
Weissler is the J.P. Riddle Distinguished Professor of Otolaryngology – head
and neck surgery, University of North Carolina,
Chapel Hill.
Obesity is
epidemic in the United States
and “recommending to patients that they lose weight” is not a particularly
effective intervention. The real take-home message from this study is that
there is poor evidence for all treatments, but that the only studies showing a decreased
mortality were those involving surgery. Noninvasive remedies should generally
be preferred when deemed effective. Many patients find CPAP and oral appliances
uncomfortable and compliance rates with these treatments are poor. Obstructive
sleep apnea presents with a wide spectrum of symptoms, and occasionally, an
emergency tracheotomy may be lifesaving for a moribund patient. Patients with
severe OSA have a three- to sixfold increase in all-cause mortality. Motor
vehicle accidents are a major cause of death in patients with severe OSA. It
should also be emphasized that patients with OSA are best evaluated with a formal
sleep study to quantitate the degree of sleep apnea. OSA is a serious health
problem for which a variety of treatments are available. Although surgery is
rarely the first-line therapy, it plays an important role for patients with
particularly severe OSA, some of whom will require a tracheotomy, and in patients
for whom medical therapy is intolerable, not complied with, or ineffective.
Dr. Mark
Weissler is the J.P. Riddle Distinguished Professor of Otolaryngology – head
and neck surgery, University of North Carolina,
Chapel Hill.
First-line treatment for adults with obstructive sleep apnea should be continuous positive airway pressure therapy or a mandibular advancement device, according to the American College of Physicians’ clinical practice guideline published online Sept. 24 in Annals of Internal Medicine.
In contrast, no surgical procedures or pharmacologic agents should be considered as first-line treatment, because there is insufficient evidence supporting those approaches, said Dr. Amir Qaseem, director of clinical policy at the ACP, Philadelphia, and his associates on the clinical guidelines committee.
Overweight and obese patients with obstructive sleep apnea (OSA) should be encouraged to lose weight, because that has been shown to improve symptoms and reduce scores on the Apnea-Hypopnea Index. Weight loss also confers many other health benefits, they added, while carrying minimal risk of adverse effects.
Those are the chief recommendations of the clinical practice guideline, which was compiled "to present information on both the benefits and harms of interventions" to all clinicians who treat adults with OSA. The guideline is based on a rigorous review of the evidence regarding OSA published in the literature from 1966 through 2012.
Overall, the evidence concerning hard clinical outcomes for any intervention for OSA was extremely limited.
Continuous positive airway pressure (CPAP) was the most extensively studied intervention for OSA, but the evidence from most studies was considered to be only of moderate quality. Studies assessed only the treatment’s effect on immediate outcomes and did not evaluate longer term outcomes such as cardiovascular illness or mortality. In addition, studies that examined CPAP’s effect on quality of life "were inconsistent and therefore inconclusive."
Nevertheless, the balance of evidence does show that CPAP is more effective than are control conditions or sham CPAP at improving scores on the apnea-hypopnea index, which measures the number of apneic and hypopneic episodes per hour of monitored sleep. CPAP also improved scores on the Epworth Sleepiness Scale, a self-administered questionnaire in which patients rate their likelihood of dozing off during various situations.
CPAP also is effective at improving oxygen saturation and reducing scores on the arousal index, which measures the frequency of arousals per hour of sleep using electroencephalography. However, there were insufficient data to compare the different types of CPAP, such as fixed CPAP, auto-CPAP, flexible bilevel CPAP, or CPAP with humidification.
There also was insufficient evidence to directly compare CPAP against other interventions, Dr. Qaseem and his colleagues said (Ann. Intern. Med. 2013;159:471-83).
The guideline recommends that mandibular or dental advancement devices to position the patient’s jaw while sleeping are a useful alternative for those who prefer this intervention to CPAP or for those who cannot tolerate or adhere to CPAP. Moderate-quality evidence showed that mandibular advancement devices improve scores on the apnea-hypopnea index and the arousal index.
However, that recommendation is considered "weak," because the overall data supporting the use of mandibular advancement devices are of low quality.
The data also were insufficient to recommend the use of any pharmacologic agents as a first-line therapy for OSA, or indeed as any therapy for the condition. Those include mirtazapine, xylometazoline, fluticasone, paroxetine, pantoprazole, steroids, acetazolamide, and protriptyline.
Only seven studies assessed surgical interventions for OSA. They were of varied quality, and their outcomes were inconsistent, so, the evidence is insufficient to support any surgery as first-line treatment. The procedures assessed in the studies included uvulopalatopharyngoplasty (UPPP); laser-assisted uvulopalatoplasty; radiofrequency ablation; and various combinations of pharyngoplasty, tonsillectomy, adenoidectomy, genioglossal advancement septoplasty, ablation of the nasal turbinates, and other nasal surgeries.
However, there was some evidence to suggest that UPPP and tracheostomy reduced mortality in patients with OSA.
The guideline strongly recommends that all OSA patients who are overweight or obese should be encouraged to lose weight. The evidence, albeit of low quality, shows that any intensive weight-loss intervention helps improve OSA symptoms and scores on the apnea-hypopnea index.
Finally, the evidence was insufficient to assess the potential benefits of positional therapy, oropharyngeal exercise, palatal implants, or atrial overdrive pacing for patients who already have dual-chamber pacemakers, Dr. Qaseem and his associates said.
The guideline was supported entirely by the American College of Physicians. The investigators had no relevant conflicts of interest.
First-line treatment for adults with obstructive sleep apnea should be continuous positive airway pressure therapy or a mandibular advancement device, according to the American College of Physicians’ clinical practice guideline published online Sept. 24 in Annals of Internal Medicine.
In contrast, no surgical procedures or pharmacologic agents should be considered as first-line treatment, because there is insufficient evidence supporting those approaches, said Dr. Amir Qaseem, director of clinical policy at the ACP, Philadelphia, and his associates on the clinical guidelines committee.
Overweight and obese patients with obstructive sleep apnea (OSA) should be encouraged to lose weight, because that has been shown to improve symptoms and reduce scores on the Apnea-Hypopnea Index. Weight loss also confers many other health benefits, they added, while carrying minimal risk of adverse effects.
Those are the chief recommendations of the clinical practice guideline, which was compiled "to present information on both the benefits and harms of interventions" to all clinicians who treat adults with OSA. The guideline is based on a rigorous review of the evidence regarding OSA published in the literature from 1966 through 2012.
Overall, the evidence concerning hard clinical outcomes for any intervention for OSA was extremely limited.
Continuous positive airway pressure (CPAP) was the most extensively studied intervention for OSA, but the evidence from most studies was considered to be only of moderate quality. Studies assessed only the treatment’s effect on immediate outcomes and did not evaluate longer term outcomes such as cardiovascular illness or mortality. In addition, studies that examined CPAP’s effect on quality of life "were inconsistent and therefore inconclusive."
Nevertheless, the balance of evidence does show that CPAP is more effective than are control conditions or sham CPAP at improving scores on the apnea-hypopnea index, which measures the number of apneic and hypopneic episodes per hour of monitored sleep. CPAP also improved scores on the Epworth Sleepiness Scale, a self-administered questionnaire in which patients rate their likelihood of dozing off during various situations.
CPAP also is effective at improving oxygen saturation and reducing scores on the arousal index, which measures the frequency of arousals per hour of sleep using electroencephalography. However, there were insufficient data to compare the different types of CPAP, such as fixed CPAP, auto-CPAP, flexible bilevel CPAP, or CPAP with humidification.
There also was insufficient evidence to directly compare CPAP against other interventions, Dr. Qaseem and his colleagues said (Ann. Intern. Med. 2013;159:471-83).
The guideline recommends that mandibular or dental advancement devices to position the patient’s jaw while sleeping are a useful alternative for those who prefer this intervention to CPAP or for those who cannot tolerate or adhere to CPAP. Moderate-quality evidence showed that mandibular advancement devices improve scores on the apnea-hypopnea index and the arousal index.
However, that recommendation is considered "weak," because the overall data supporting the use of mandibular advancement devices are of low quality.
The data also were insufficient to recommend the use of any pharmacologic agents as a first-line therapy for OSA, or indeed as any therapy for the condition. Those include mirtazapine, xylometazoline, fluticasone, paroxetine, pantoprazole, steroids, acetazolamide, and protriptyline.
Only seven studies assessed surgical interventions for OSA. They were of varied quality, and their outcomes were inconsistent, so, the evidence is insufficient to support any surgery as first-line treatment. The procedures assessed in the studies included uvulopalatopharyngoplasty (UPPP); laser-assisted uvulopalatoplasty; radiofrequency ablation; and various combinations of pharyngoplasty, tonsillectomy, adenoidectomy, genioglossal advancement septoplasty, ablation of the nasal turbinates, and other nasal surgeries.
However, there was some evidence to suggest that UPPP and tracheostomy reduced mortality in patients with OSA.
The guideline strongly recommends that all OSA patients who are overweight or obese should be encouraged to lose weight. The evidence, albeit of low quality, shows that any intensive weight-loss intervention helps improve OSA symptoms and scores on the apnea-hypopnea index.
Finally, the evidence was insufficient to assess the potential benefits of positional therapy, oropharyngeal exercise, palatal implants, or atrial overdrive pacing for patients who already have dual-chamber pacemakers, Dr. Qaseem and his associates said.
The guideline was supported entirely by the American College of Physicians. The investigators had no relevant conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Major finding: First-line therapy for adults with obstructive sleep apnea should be CPAP or a mandibular advancement device; surgery and pharmacotherapy do not appear to be effective, and weight loss is strongly recommended for patients who are overweight or obese.
Data source: The guideline was based on a systematic review of the literature regarding obstructive sleep apnea from 1966 through 2010.
Disclosures: The guideline was supported entirely by the American College of Physicians. The investigators had no relevant conflicts of interest.

Study sheds light on exacerbation risks with RA lung disease
An older age at the time of diagnosis and treatment with methotrexate were significantly associated with an increased risk of developing "acute exacerbation" of rheumatoid arthritis–associated interstitial lung disease in a retrospective cohort study of 51 patients.
The other risk factor associated with the development of acute exacerbation (AE) was a specific pattern on high-resolution CT scan, which was also associated with poorer survival, reported Dr. Hironao Hozumi, of Hamamatsu (Japan) University, and associates.
Overall, survival was also significantly lower among those who developed AE, according to the study. As far as the authors know, this is the first study to investigate the risk factors and prognosis associated with AE in patients who have been diagnosed with rheumatoid arthritis–associated interstitial lung disease (RA-ILD). Until this study, risk factors and prognosis for AEs in patients with RA-ILD have been unclear, they said.
AE is "a recently established and an increasingly recognized occurrence" in people with idiopathic pulmonary fibrosis, and it also affects people with other types of interstitial lung diseases, including those associated with collagen vascular disease, the authors noted. It was defined in the study as "acute deterioration in respiratory status, with newly developed bilateral ground-glass opacities and/or consolidations" visible on chest x-ray or CT scans.
The retrospective case-control study evaluated medical records and images of 51 patients consecutively diagnosed with RA-ILD at Hamamatsu University Hospital between 1995 and 2012. The median ages at the time of the RA and ILD diagnoses were 61 and 62 years, respectively. A majority (57%) of the patients were men. The patients had been followed for a median of 8.5 years (range, 1-17 years) before being diagnosed with AE (BMJ Open 2013;3:e003132).
During the observation period of 1-11 years, 11 of the 51 patients (22%) developed AE at a median age of 72 years (range, 60-86 years). In a univariate Cox hazard analysis, an older age at ILD diagnosis was associated with an 11% increased risk for AE occurrence.
Of the 11 patients who developed AE, 7 (64%) died of respiratory failure during the initial episode of AE, compared with 2 (5%) of the 40 patients who did not develop AE.
There was a usual interstitial pneumonia (UIP) pattern on high-resolution CT in 14 (27%) of the 51 patients. This pattern was found in 6 (55%) of the patients who had AE, compared with 8 (20%) of the 40 patients with no AE, a significant difference. This comparison gave a hazard ratio of 1.95 in a univariate Cox hazard analysis. For AE occurrence, a UIP pattern on high-resolution CT had a positive predictive value of 43% and a negative predictive value of 87%. The 1-year incidence of AE was 6.5% among those with a UIP pattern on high-resolution CT, compared with an overall rate of 2.8% in the study.
The overall 5-year survival was 90% for all the patients, but there was a significant difference among those with or without the UIP pattern (70% vs. 97%). Patients’ risk of death more than doubled with an AE occurrence (hazard ratio, 2.47).
The use of methotrexate was associated with a threefold increased risk of developing AE (HR, 3.04) in a univariate Cox hazard analysis. Of 10 patients treated with methotrexate, 6 (55%) in the AE group used the drug (including 5 who had been treated for at least 3 years and 1 treated for 1 year), compared with 4 (10%) in the non-AE group, a significant difference. Although methotrexate was discontinued, the respiratory condition of all six patients in the AE group continued to deteriorate and they had poor responses to corticosteroid therapy.
The authors found no associations with disease activity and the development of AE, so RA activity may not be related to the development of AE, the authors wrote. However, they noted that methotrexate "possibly accelerates the fibroproliferative process of RA-ILD."
There also were no significant differences in factors that included sex, age at the time of diagnosis of RA or RA-ILD, smoking habits, and other factors between those who did and did not develop an AE.
The investigators said that the limitations of the study included the retrospective design and the small sample size, and that "larger prospective studies investigating AEs in RA-ILD are indicated."
The authors had no disclosures to report. The study was partly funded by a grant from Japan’s Ministry of Health, Labor, and Welfare to the Diffuse Lung Diseases Research Group.
An older age at the time of diagnosis and treatment with methotrexate were significantly associated with an increased risk of developing "acute exacerbation" of rheumatoid arthritis–associated interstitial lung disease in a retrospective cohort study of 51 patients.
The other risk factor associated with the development of acute exacerbation (AE) was a specific pattern on high-resolution CT scan, which was also associated with poorer survival, reported Dr. Hironao Hozumi, of Hamamatsu (Japan) University, and associates.
Overall, survival was also significantly lower among those who developed AE, according to the study. As far as the authors know, this is the first study to investigate the risk factors and prognosis associated with AE in patients who have been diagnosed with rheumatoid arthritis–associated interstitial lung disease (RA-ILD). Until this study, risk factors and prognosis for AEs in patients with RA-ILD have been unclear, they said.
AE is "a recently established and an increasingly recognized occurrence" in people with idiopathic pulmonary fibrosis, and it also affects people with other types of interstitial lung diseases, including those associated with collagen vascular disease, the authors noted. It was defined in the study as "acute deterioration in respiratory status, with newly developed bilateral ground-glass opacities and/or consolidations" visible on chest x-ray or CT scans.
The retrospective case-control study evaluated medical records and images of 51 patients consecutively diagnosed with RA-ILD at Hamamatsu University Hospital between 1995 and 2012. The median ages at the time of the RA and ILD diagnoses were 61 and 62 years, respectively. A majority (57%) of the patients were men. The patients had been followed for a median of 8.5 years (range, 1-17 years) before being diagnosed with AE (BMJ Open 2013;3:e003132).
During the observation period of 1-11 years, 11 of the 51 patients (22%) developed AE at a median age of 72 years (range, 60-86 years). In a univariate Cox hazard analysis, an older age at ILD diagnosis was associated with an 11% increased risk for AE occurrence.
Of the 11 patients who developed AE, 7 (64%) died of respiratory failure during the initial episode of AE, compared with 2 (5%) of the 40 patients who did not develop AE.
There was a usual interstitial pneumonia (UIP) pattern on high-resolution CT in 14 (27%) of the 51 patients. This pattern was found in 6 (55%) of the patients who had AE, compared with 8 (20%) of the 40 patients with no AE, a significant difference. This comparison gave a hazard ratio of 1.95 in a univariate Cox hazard analysis. For AE occurrence, a UIP pattern on high-resolution CT had a positive predictive value of 43% and a negative predictive value of 87%. The 1-year incidence of AE was 6.5% among those with a UIP pattern on high-resolution CT, compared with an overall rate of 2.8% in the study.
The overall 5-year survival was 90% for all the patients, but there was a significant difference among those with or without the UIP pattern (70% vs. 97%). Patients’ risk of death more than doubled with an AE occurrence (hazard ratio, 2.47).
The use of methotrexate was associated with a threefold increased risk of developing AE (HR, 3.04) in a univariate Cox hazard analysis. Of 10 patients treated with methotrexate, 6 (55%) in the AE group used the drug (including 5 who had been treated for at least 3 years and 1 treated for 1 year), compared with 4 (10%) in the non-AE group, a significant difference. Although methotrexate was discontinued, the respiratory condition of all six patients in the AE group continued to deteriorate and they had poor responses to corticosteroid therapy.
The authors found no associations with disease activity and the development of AE, so RA activity may not be related to the development of AE, the authors wrote. However, they noted that methotrexate "possibly accelerates the fibroproliferative process of RA-ILD."
There also were no significant differences in factors that included sex, age at the time of diagnosis of RA or RA-ILD, smoking habits, and other factors between those who did and did not develop an AE.
The investigators said that the limitations of the study included the retrospective design and the small sample size, and that "larger prospective studies investigating AEs in RA-ILD are indicated."
The authors had no disclosures to report. The study was partly funded by a grant from Japan’s Ministry of Health, Labor, and Welfare to the Diffuse Lung Diseases Research Group.
An older age at the time of diagnosis and treatment with methotrexate were significantly associated with an increased risk of developing "acute exacerbation" of rheumatoid arthritis–associated interstitial lung disease in a retrospective cohort study of 51 patients.
The other risk factor associated with the development of acute exacerbation (AE) was a specific pattern on high-resolution CT scan, which was also associated with poorer survival, reported Dr. Hironao Hozumi, of Hamamatsu (Japan) University, and associates.
Overall, survival was also significantly lower among those who developed AE, according to the study. As far as the authors know, this is the first study to investigate the risk factors and prognosis associated with AE in patients who have been diagnosed with rheumatoid arthritis–associated interstitial lung disease (RA-ILD). Until this study, risk factors and prognosis for AEs in patients with RA-ILD have been unclear, they said.
AE is "a recently established and an increasingly recognized occurrence" in people with idiopathic pulmonary fibrosis, and it also affects people with other types of interstitial lung diseases, including those associated with collagen vascular disease, the authors noted. It was defined in the study as "acute deterioration in respiratory status, with newly developed bilateral ground-glass opacities and/or consolidations" visible on chest x-ray or CT scans.
The retrospective case-control study evaluated medical records and images of 51 patients consecutively diagnosed with RA-ILD at Hamamatsu University Hospital between 1995 and 2012. The median ages at the time of the RA and ILD diagnoses were 61 and 62 years, respectively. A majority (57%) of the patients were men. The patients had been followed for a median of 8.5 years (range, 1-17 years) before being diagnosed with AE (BMJ Open 2013;3:e003132).
During the observation period of 1-11 years, 11 of the 51 patients (22%) developed AE at a median age of 72 years (range, 60-86 years). In a univariate Cox hazard analysis, an older age at ILD diagnosis was associated with an 11% increased risk for AE occurrence.
Of the 11 patients who developed AE, 7 (64%) died of respiratory failure during the initial episode of AE, compared with 2 (5%) of the 40 patients who did not develop AE.
There was a usual interstitial pneumonia (UIP) pattern on high-resolution CT in 14 (27%) of the 51 patients. This pattern was found in 6 (55%) of the patients who had AE, compared with 8 (20%) of the 40 patients with no AE, a significant difference. This comparison gave a hazard ratio of 1.95 in a univariate Cox hazard analysis. For AE occurrence, a UIP pattern on high-resolution CT had a positive predictive value of 43% and a negative predictive value of 87%. The 1-year incidence of AE was 6.5% among those with a UIP pattern on high-resolution CT, compared with an overall rate of 2.8% in the study.
The overall 5-year survival was 90% for all the patients, but there was a significant difference among those with or without the UIP pattern (70% vs. 97%). Patients’ risk of death more than doubled with an AE occurrence (hazard ratio, 2.47).
The use of methotrexate was associated with a threefold increased risk of developing AE (HR, 3.04) in a univariate Cox hazard analysis. Of 10 patients treated with methotrexate, 6 (55%) in the AE group used the drug (including 5 who had been treated for at least 3 years and 1 treated for 1 year), compared with 4 (10%) in the non-AE group, a significant difference. Although methotrexate was discontinued, the respiratory condition of all six patients in the AE group continued to deteriorate and they had poor responses to corticosteroid therapy.
The authors found no associations with disease activity and the development of AE, so RA activity may not be related to the development of AE, the authors wrote. However, they noted that methotrexate "possibly accelerates the fibroproliferative process of RA-ILD."
There also were no significant differences in factors that included sex, age at the time of diagnosis of RA or RA-ILD, smoking habits, and other factors between those who did and did not develop an AE.
The investigators said that the limitations of the study included the retrospective design and the small sample size, and that "larger prospective studies investigating AEs in RA-ILD are indicated."
The authors had no disclosures to report. The study was partly funded by a grant from Japan’s Ministry of Health, Labor, and Welfare to the Diffuse Lung Diseases Research Group.
FROM BMJ OPEN
Major finding: The use of methotrexate was associated with a threefold increased risk of developing acute exacerbation of RA-ILD (HR, 3.04) in a univariate Cox hazard analysis.
Data source: A retrospective case-control study that looked at the medical records and images of 51 patients diagnosed with RA-ILD at an academic hospital in Japan between 1995 and 2012.
Disclosures: The authors had no disclosures to report. The study was partly funded by a grant from Japan’s Ministry of Health, Labor, and Welfare to the Diffuse Lung Diseases Research Group.