User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Youths turning to e-cigarettes over traditional smokes
Students in grades 6-12 who have never smoked traditional cigarettes are trying e-cigarettes in greater numbers, potentially justifying the Food and Drug Administration’s proposal to broaden its tobacco oversight to include e-cigarettes.
The number of middle- to high-school-aged children who have never smoked but have used e-cigarettes increased threefold between 2011 and 2013 from 79,000 to 263,000, based on an analysis of the Centers for Disease Control and Prevention’s (CDC’s) National Youth Tobacco Survey from 2011, 2012, and 2013. In addition, among those who have tried e-cigarettes, 43.9% said they intended to smoke conventional cigarettes, according to a report published online Aug. 20 in Nicotine & Tobacco Research.

"The increasing number of young people who use e-cigarettes should be a concern for parents and the public health community, especially since youth e-cigarette users were nearly twice as likely to have intentions to smoke conventional cigarettes, compared with youth who never tried e-cigarettes," Rebecca Bunnell, Sc.D., associate director of the CDC’s Office on Smoking and Health, and her colleagues reported (Nicotine Tob. Res. 2014 Aug. 20 [doi: 10.1093/ntr/ntu166]).
Research also found connections between the number of tobacco ads to which youths were exposed and the likelihood of intention to smoke cigarettes. Of students who said they had no exposure to such advertising, 13% reported that they intended to smoke, compared with 20.4% of those who reported exposure to one or two ads and 25.6% among those reporting exposure to three or four ads.
The Food and Drug Administration currently is reviewing comments on a proposed rule that would broaden its regulatory authority over tobacco products to include e-cigarettes. Various medical societies have called for that regulation to cover advertising of e-cigarettes as well as other related products, such as refill containers.
The authors reported no conflicts of interest.
Students in grades 6-12 who have never smoked traditional cigarettes are trying e-cigarettes in greater numbers, potentially justifying the Food and Drug Administration’s proposal to broaden its tobacco oversight to include e-cigarettes.
The number of middle- to high-school-aged children who have never smoked but have used e-cigarettes increased threefold between 2011 and 2013 from 79,000 to 263,000, based on an analysis of the Centers for Disease Control and Prevention’s (CDC’s) National Youth Tobacco Survey from 2011, 2012, and 2013. In addition, among those who have tried e-cigarettes, 43.9% said they intended to smoke conventional cigarettes, according to a report published online Aug. 20 in Nicotine & Tobacco Research.
"The increasing number of young people who use e-cigarettes should be a concern for parents and the public health community, especially since youth e-cigarette users were nearly twice as likely to have intentions to smoke conventional cigarettes, compared with youth who never tried e-cigarettes," Rebecca Bunnell, Sc.D., associate director of the CDC’s Office on Smoking and Health, and her colleagues reported (Nicotine Tob. Res. 2014 Aug. 20 [doi: 10.1093/ntr/ntu166]).
Research also found connections between the number of tobacco ads to which youths were exposed and the likelihood of intention to smoke cigarettes. Of students who said they had no exposure to such advertising, 13% reported that they intended to smoke, compared with 20.4% of those who reported exposure to one or two ads and 25.6% among those reporting exposure to three or four ads.
The Food and Drug Administration currently is reviewing comments on a proposed rule that would broaden its regulatory authority over tobacco products to include e-cigarettes. Various medical societies have called for that regulation to cover advertising of e-cigarettes as well as other related products, such as refill containers.
The authors reported no conflicts of interest.
Students in grades 6-12 who have never smoked traditional cigarettes are trying e-cigarettes in greater numbers, potentially justifying the Food and Drug Administration’s proposal to broaden its tobacco oversight to include e-cigarettes.
The number of middle- to high-school-aged children who have never smoked but have used e-cigarettes increased threefold between 2011 and 2013 from 79,000 to 263,000, based on an analysis of the Centers for Disease Control and Prevention’s (CDC’s) National Youth Tobacco Survey from 2011, 2012, and 2013. In addition, among those who have tried e-cigarettes, 43.9% said they intended to smoke conventional cigarettes, according to a report published online Aug. 20 in Nicotine & Tobacco Research.
"The increasing number of young people who use e-cigarettes should be a concern for parents and the public health community, especially since youth e-cigarette users were nearly twice as likely to have intentions to smoke conventional cigarettes, compared with youth who never tried e-cigarettes," Rebecca Bunnell, Sc.D., associate director of the CDC’s Office on Smoking and Health, and her colleagues reported (Nicotine Tob. Res. 2014 Aug. 20 [doi: 10.1093/ntr/ntu166]).
Research also found connections between the number of tobacco ads to which youths were exposed and the likelihood of intention to smoke cigarettes. Of students who said they had no exposure to such advertising, 13% reported that they intended to smoke, compared with 20.4% of those who reported exposure to one or two ads and 25.6% among those reporting exposure to three or four ads.
The Food and Drug Administration currently is reviewing comments on a proposed rule that would broaden its regulatory authority over tobacco products to include e-cigarettes. Various medical societies have called for that regulation to cover advertising of e-cigarettes as well as other related products, such as refill containers.
The authors reported no conflicts of interest.
FROM NICOTINE & TOBACCO RESEARCH

Smokers not so welcome in the house anymore
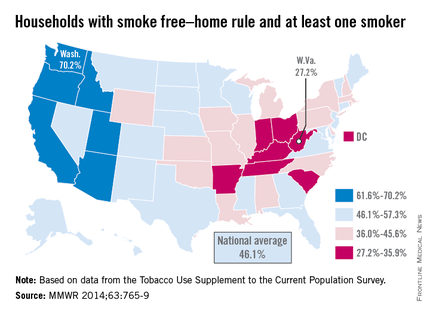
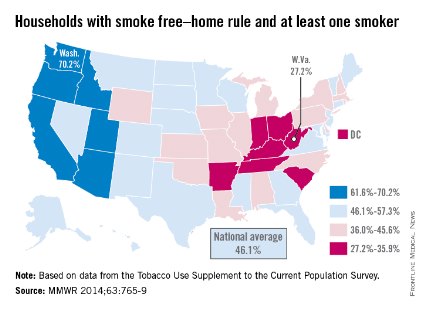
The national prevalence of households with a rule against smoking indoors and at least one adult smoker increased nearly fivefold from 1992 to 2011, the Centers for Disease Control and Prevention reported Sept. 4.
Washington had the highest rate of smokers forced to go outside in 2010-2011, with 70.2% of households with at least one adult smoker staying smoke free. Utah was second at 68.4%, and California was third at 67.9%. West Virginia reported the lowest rate of smoke-free households that had at least one adult smoker, with only 27.2% staying smoke free in 2010-2011. Kentucky was next with a reported rate of 29.3%, and Indiana was next with 31.4% (MMWR 2014;63:765-9).
The national rate of smoke-free households with at least one adult smoker was 46.1% in 2010-2011, compared with 9.6% in 1992-1993. For all households, 83% were smoke free in 2010-2011, compared with 43% in 1992-1993. The smoke-free home rate for households without an adult smoker was 91.4% in 2010-2011, up from 56.7% in 1992-1993, according to the CDC.
Although progress has been made on keeping homes smoke free, approximately 88 million U.S. residents 3 years or older were exposed to secondhand smoke during 2007-2008, the CDC investigators said.
The analysis was based on data from the Tobacco Use Supplement to the Current Population Survey.
The national prevalence of households with a rule against smoking indoors and at least one adult smoker increased nearly fivefold from 1992 to 2011, the Centers for Disease Control and Prevention reported Sept. 4.
Washington had the highest rate of smokers forced to go outside in 2010-2011, with 70.2% of households with at least one adult smoker staying smoke free. Utah was second at 68.4%, and California was third at 67.9%. West Virginia reported the lowest rate of smoke-free households that had at least one adult smoker, with only 27.2% staying smoke free in 2010-2011. Kentucky was next with a reported rate of 29.3%, and Indiana was next with 31.4% (MMWR 2014;63:765-9).
The national rate of smoke-free households with at least one adult smoker was 46.1% in 2010-2011, compared with 9.6% in 1992-1993. For all households, 83% were smoke free in 2010-2011, compared with 43% in 1992-1993. The smoke-free home rate for households without an adult smoker was 91.4% in 2010-2011, up from 56.7% in 1992-1993, according to the CDC.
Although progress has been made on keeping homes smoke free, approximately 88 million U.S. residents 3 years or older were exposed to secondhand smoke during 2007-2008, the CDC investigators said.
The analysis was based on data from the Tobacco Use Supplement to the Current Population Survey.
The national prevalence of households with a rule against smoking indoors and at least one adult smoker increased nearly fivefold from 1992 to 2011, the Centers for Disease Control and Prevention reported Sept. 4.
Washington had the highest rate of smokers forced to go outside in 2010-2011, with 70.2% of households with at least one adult smoker staying smoke free. Utah was second at 68.4%, and California was third at 67.9%. West Virginia reported the lowest rate of smoke-free households that had at least one adult smoker, with only 27.2% staying smoke free in 2010-2011. Kentucky was next with a reported rate of 29.3%, and Indiana was next with 31.4% (MMWR 2014;63:765-9).
The national rate of smoke-free households with at least one adult smoker was 46.1% in 2010-2011, compared with 9.6% in 1992-1993. For all households, 83% were smoke free in 2010-2011, compared with 43% in 1992-1993. The smoke-free home rate for households without an adult smoker was 91.4% in 2010-2011, up from 56.7% in 1992-1993, according to the CDC.
Although progress has been made on keeping homes smoke free, approximately 88 million U.S. residents 3 years or older were exposed to secondhand smoke during 2007-2008, the CDC investigators said.
The analysis was based on data from the Tobacco Use Supplement to the Current Population Survey.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
CDC: Time is running out to contain Ebola virus
Despite some signs of hope, the "window of opportunity" to contain and end the current Ebola virus outbreak in West Africa is shutting, causing the situation to worsen "significantly," according to officials at the Centers for Disease Control and Prevention.
"This is really the first epidemic of Ebola the world has ever known," Dr. Thomas Frieden, CDC director, said during a media briefing.

The prevailing belief, according to Dr. Frieden, is that the virus’s rapid spread is not due to mutation but instead to cultural and logistical obstacles.
"It’s not spreading in new ways, according to everything that we know," Dr. Frieden said. "It’s spreading through just two routes: people caring for other people ... and unsafe burial practices. ... That is really the Achilles’ heel. We know how it spreads; we know how to stop it. The challenge is to do that everywhere it is needed."
The Ebola virus is transmitted primarily through body fluids, but it also can be spread through contact with contaminated objects such as needles. Ebola is not spread through the air or by water.
Noting that rapid response is essential, and that data are lacking as to the actual numbers of those infected with the virus, Dr. Frieden outlined three key things that are needed to stem the epidemic: more resources; technical expertise in both health care management and logistics; and a coordinated global approach to ending the outbreak.
Dr. Frieden said it was a paradox that "the more the world isolates these countries, the harder it will be for them to control these outbreaks, the more cases there will be, and the less safe other countries will be. Like it or not, we’re connected."
The area currently experiencing outbreaks includes the countries of Guinea, Liberia, Sierra Leone, and Nigeria, with what Dr. Frieden said is a "dense, forested region that is the epicenter" located where the borders of all but Nigeria meet. The remote area is not serviced by radio or television and is rife with what Dr. Frieden called "misconceptions" about how the disease is transmitted.
"We can turn this around. Sometimes the problem can seem so large, it’s hard to get started, but we can chip away at the challenges, one by one," he said, inviting anyone with experience working in austere conditions, either as a health care provider or manager of an under-resourced facility, to consider volunteering his or her services, noting that the longer the crisis continues, the less stable the local communities will be.

In addition to nearly $20 million in aid from the U.S. Agency for International Development, for goods ranging from personal protection gear to resources for safer burials, the CDC will continue to support efforts by the World Health Organization (WHO) to contain the epidemic within the year, by deploying top CDC epidemic intelligence teams to help with tracking, treatment, and screening, he said.
The need for global coordination is not due to a lack of willingness from local officials and personnel to respond, according to Dr. Frieden.
"The countries are willing. In an Ebola treatment unit run by Doctors Without Borders, more than 90% of the staff are locals," Dr. Frieden said of one of the stops on his tour of West Africa. "Each of the presidents [of the affected countries] said the same thing to me: ‘Tell us what to do and we will do it. If we can’t do it, help us to do it. Teach us to care for Ebola patients and to manage the system more effectively.’ They need the world to work with them."
According to WHO, more than 1,400 patients have died of Ebola virus infection to date in this outbreak, making this the largest Ebola outbreak ever recorded. There are still "significant gaps in reporting in some intense transmission areas," and that the number of cases ultimately may top 20,000, according to WHO, which noted this outbreak has featured the infection and deaths of "an unprecedented number of health care workers."
There are no vaccines for Ebola approved by the Food and Drug Administration, although the National Institute of Allergy and Infectious Diseases currently is attempting to develop one.
As to treatments, ZMapp, a trio of monoclonal antibodies that was successfully used to treat two American health workers who were infected with Ebola, also has shown promise in a controlled trial with primates. According to ZMapp’s manufacturer, Mapp Biopharmaceuticals, the supply of the drug is currently exhausted and there is as yet no date for when more will be available.
On Twitter @whitneymcknight
Despite some signs of hope, the "window of opportunity" to contain and end the current Ebola virus outbreak in West Africa is shutting, causing the situation to worsen "significantly," according to officials at the Centers for Disease Control and Prevention.
"This is really the first epidemic of Ebola the world has ever known," Dr. Thomas Frieden, CDC director, said during a media briefing.
The prevailing belief, according to Dr. Frieden, is that the virus’s rapid spread is not due to mutation but instead to cultural and logistical obstacles.
"It’s not spreading in new ways, according to everything that we know," Dr. Frieden said. "It’s spreading through just two routes: people caring for other people ... and unsafe burial practices. ... That is really the Achilles’ heel. We know how it spreads; we know how to stop it. The challenge is to do that everywhere it is needed."
The Ebola virus is transmitted primarily through body fluids, but it also can be spread through contact with contaminated objects such as needles. Ebola is not spread through the air or by water.
Noting that rapid response is essential, and that data are lacking as to the actual numbers of those infected with the virus, Dr. Frieden outlined three key things that are needed to stem the epidemic: more resources; technical expertise in both health care management and logistics; and a coordinated global approach to ending the outbreak.
Dr. Frieden said it was a paradox that "the more the world isolates these countries, the harder it will be for them to control these outbreaks, the more cases there will be, and the less safe other countries will be. Like it or not, we’re connected."
The area currently experiencing outbreaks includes the countries of Guinea, Liberia, Sierra Leone, and Nigeria, with what Dr. Frieden said is a "dense, forested region that is the epicenter" located where the borders of all but Nigeria meet. The remote area is not serviced by radio or television and is rife with what Dr. Frieden called "misconceptions" about how the disease is transmitted.
"We can turn this around. Sometimes the problem can seem so large, it’s hard to get started, but we can chip away at the challenges, one by one," he said, inviting anyone with experience working in austere conditions, either as a health care provider or manager of an under-resourced facility, to consider volunteering his or her services, noting that the longer the crisis continues, the less stable the local communities will be.
In addition to nearly $20 million in aid from the U.S. Agency for International Development, for goods ranging from personal protection gear to resources for safer burials, the CDC will continue to support efforts by the World Health Organization (WHO) to contain the epidemic within the year, by deploying top CDC epidemic intelligence teams to help with tracking, treatment, and screening, he said.
The need for global coordination is not due to a lack of willingness from local officials and personnel to respond, according to Dr. Frieden.
"The countries are willing. In an Ebola treatment unit run by Doctors Without Borders, more than 90% of the staff are locals," Dr. Frieden said of one of the stops on his tour of West Africa. "Each of the presidents [of the affected countries] said the same thing to me: ‘Tell us what to do and we will do it. If we can’t do it, help us to do it. Teach us to care for Ebola patients and to manage the system more effectively.’ They need the world to work with them."
According to WHO, more than 1,400 patients have died of Ebola virus infection to date in this outbreak, making this the largest Ebola outbreak ever recorded. There are still "significant gaps in reporting in some intense transmission areas," and that the number of cases ultimately may top 20,000, according to WHO, which noted this outbreak has featured the infection and deaths of "an unprecedented number of health care workers."
There are no vaccines for Ebola approved by the Food and Drug Administration, although the National Institute of Allergy and Infectious Diseases currently is attempting to develop one.
As to treatments, ZMapp, a trio of monoclonal antibodies that was successfully used to treat two American health workers who were infected with Ebola, also has shown promise in a controlled trial with primates. According to ZMapp’s manufacturer, Mapp Biopharmaceuticals, the supply of the drug is currently exhausted and there is as yet no date for when more will be available.
On Twitter @whitneymcknight
Despite some signs of hope, the "window of opportunity" to contain and end the current Ebola virus outbreak in West Africa is shutting, causing the situation to worsen "significantly," according to officials at the Centers for Disease Control and Prevention.
"This is really the first epidemic of Ebola the world has ever known," Dr. Thomas Frieden, CDC director, said during a media briefing.
The prevailing belief, according to Dr. Frieden, is that the virus’s rapid spread is not due to mutation but instead to cultural and logistical obstacles.
"It’s not spreading in new ways, according to everything that we know," Dr. Frieden said. "It’s spreading through just two routes: people caring for other people ... and unsafe burial practices. ... That is really the Achilles’ heel. We know how it spreads; we know how to stop it. The challenge is to do that everywhere it is needed."
The Ebola virus is transmitted primarily through body fluids, but it also can be spread through contact with contaminated objects such as needles. Ebola is not spread through the air or by water.
Noting that rapid response is essential, and that data are lacking as to the actual numbers of those infected with the virus, Dr. Frieden outlined three key things that are needed to stem the epidemic: more resources; technical expertise in both health care management and logistics; and a coordinated global approach to ending the outbreak.
Dr. Frieden said it was a paradox that "the more the world isolates these countries, the harder it will be for them to control these outbreaks, the more cases there will be, and the less safe other countries will be. Like it or not, we’re connected."
The area currently experiencing outbreaks includes the countries of Guinea, Liberia, Sierra Leone, and Nigeria, with what Dr. Frieden said is a "dense, forested region that is the epicenter" located where the borders of all but Nigeria meet. The remote area is not serviced by radio or television and is rife with what Dr. Frieden called "misconceptions" about how the disease is transmitted.
"We can turn this around. Sometimes the problem can seem so large, it’s hard to get started, but we can chip away at the challenges, one by one," he said, inviting anyone with experience working in austere conditions, either as a health care provider or manager of an under-resourced facility, to consider volunteering his or her services, noting that the longer the crisis continues, the less stable the local communities will be.
In addition to nearly $20 million in aid from the U.S. Agency for International Development, for goods ranging from personal protection gear to resources for safer burials, the CDC will continue to support efforts by the World Health Organization (WHO) to contain the epidemic within the year, by deploying top CDC epidemic intelligence teams to help with tracking, treatment, and screening, he said.
The need for global coordination is not due to a lack of willingness from local officials and personnel to respond, according to Dr. Frieden.
"The countries are willing. In an Ebola treatment unit run by Doctors Without Borders, more than 90% of the staff are locals," Dr. Frieden said of one of the stops on his tour of West Africa. "Each of the presidents [of the affected countries] said the same thing to me: ‘Tell us what to do and we will do it. If we can’t do it, help us to do it. Teach us to care for Ebola patients and to manage the system more effectively.’ They need the world to work with them."
According to WHO, more than 1,400 patients have died of Ebola virus infection to date in this outbreak, making this the largest Ebola outbreak ever recorded. There are still "significant gaps in reporting in some intense transmission areas," and that the number of cases ultimately may top 20,000, according to WHO, which noted this outbreak has featured the infection and deaths of "an unprecedented number of health care workers."
There are no vaccines for Ebola approved by the Food and Drug Administration, although the National Institute of Allergy and Infectious Diseases currently is attempting to develop one.
As to treatments, ZMapp, a trio of monoclonal antibodies that was successfully used to treat two American health workers who were infected with Ebola, also has shown promise in a controlled trial with primates. According to ZMapp’s manufacturer, Mapp Biopharmaceuticals, the supply of the drug is currently exhausted and there is as yet no date for when more will be available.
On Twitter @whitneymcknight
FROM A CDC TELECONFERENCE

COPPS-2 curtails colchicine enthusiasm in cardiac surgery
Patients undergoing cardiac surgery who took colchicine had significantly less postpericardiotomy syndrome than did those on placebo, but this protective effect did not extend to postoperative atrial fibrillation and pericardial or pleural effusions in the double-blind COPPS-2 trial.
The failure of colchicine to prevent postoperative atrial fibrillation (AF) was probably due to more frequent adverse events (36 vs. 21 with placebo), especially gastrointestinal intolerance (26 vs. 12), and drug discontinuation (39 vs. 32), since a prespecified on-treatment analysis showed a significant reduction in AF in patients tolerating the drug, Dr. Massimo Imazio reported at the annual congress of the European Society of Cardiology.

"The high rate of adverse effects is a reason for concern and suggests that colchicine should be considered only in well-selected patients," Dr. Imazio and his associates wrote in an article on COPPS-2 simultaneously published online (JAMA 2014 [doi:10.1001/jama.2014.11026]).
Colchicine has been a promising strategy for postpericardiotomy syndrome prevention, besting methylprednisolone and aspirin in a large meta-analysis (Am. J. Cardiol. 2011;108:575-9).
In the largest trial, COPPS (Colchicine for the Prevention of the Postpericardiotomy Syndrome), Dr. Imazio reported that colchicine significantly reduced the incidence of postpericardiotomy syndrome (8.9% vs. 21.1%), postoperative pericardial effusions (relative risk reduction, 43.9%), and pleural effusions (RRR, 52.3%) at 12 months, compared with placebo (Am. Heart J. 2011;162:527-32 and Eur. Heart J. 2010;31:2749-54). Colchicine was given for 1 month, beginning on the third postoperative day with a 1-mg twice-daily loading dose.
In COPPS-2, the 360 consecutive candidates for cardiac surgery also were given colchicine or placebo for 1 month, but treatment was started 48-72 hours before surgery to pretreat patients and improve colchicine’s ability to prevent postoperative systemic inflammation and its complications.
Colchicine also was administered using weight-based dosing (0.5 mg twice daily in patients weighing at least 70 kg or 0.5 mg once daily in those under 70 kg), and they avoided the loading dose in an effort to improve adherence.
"However, we observed a 2-fold increase of adverse effects and study drug discontinuations compared with those reported in the COPPS trial, likely due to significant vulnerability of patients in the perioperative phase, when the use of antibiotics and proton pump inhibitors is common and also increases the risk of gastrointestinal effects (e.g., diarrhea)," explained Dr. Imazio of Maria Vittoria Hospital and the University of Torino (Italy).
Still, colchicine provided significant protection in the COPPS-2 primary outcome of postpericardiotomy syndrome, compared with placebo (19.4% vs. 29.4%; 95% confidence interval, 1.1%-18.7%). The number needed to treat was 10.
The outcome did not differ significantly among predetermined subgroups based on age, sex, and presence or absence of pericardial effusion, although colchicine was especially efficacious in the setting of systemic inflammation with elevated C-reactive protein, the authors noted.
The intention-to-treat analysis revealed no significant differences between the colchicine and placebo groups for postoperative AF (33.9% vs. 41.7%; 95% CI, –2.2%-17.6%) or postoperative pericardial/pleural effusion (57.2% vs. 58.9%; 95% CI, –8.5%-11.7%).
The prespecified on-treatment analysis, however, showed a 14.2% absolute difference in postoperative AF, favoring colchicine over placebo (27% vs. 41.2%; 95% CI, 3.3%-24.7%).
"While the efficacy of colchicine for postpericardiotomy syndrome prevention is confirmed, the extent of efficacy for postoperative AF needs to be further investigated in future trials," Dr. Imazio stated.
Ongoing studies also will better clarify the potential of colchicine using lower doses that may be better tolerated.
The 360 patients were evenly randomized from 11 centers in Italy between March 2012 and March 2014. Their mean age was 67.5 years, 69% were men, and 36% had planned valvular surgery. Key exclusion criteria were absence of sinus rhythm at enrollment, urgent cardiac surgery, cardiac transplantation, and contraindications to colchicine.
COPPS-2 was supported by the Italian National Health Service and FARGIM. Acarpia provided the study drug. Dr. Imazio reported no conflicts of interest. A coauthor reported consultancy for Servier, serving on an advisory board for Boehringer Ingelheim, and lecturer fees from Abbott, AstraZeneca, Merck, Serono, Richter Gedeon, and Teva.
Patients undergoing cardiac surgery who took colchicine had significantly less postpericardiotomy syndrome than did those on placebo, but this protective effect did not extend to postoperative atrial fibrillation and pericardial or pleural effusions in the double-blind COPPS-2 trial.
The failure of colchicine to prevent postoperative atrial fibrillation (AF) was probably due to more frequent adverse events (36 vs. 21 with placebo), especially gastrointestinal intolerance (26 vs. 12), and drug discontinuation (39 vs. 32), since a prespecified on-treatment analysis showed a significant reduction in AF in patients tolerating the drug, Dr. Massimo Imazio reported at the annual congress of the European Society of Cardiology.
"The high rate of adverse effects is a reason for concern and suggests that colchicine should be considered only in well-selected patients," Dr. Imazio and his associates wrote in an article on COPPS-2 simultaneously published online (JAMA 2014 [doi:10.1001/jama.2014.11026]).
Colchicine has been a promising strategy for postpericardiotomy syndrome prevention, besting methylprednisolone and aspirin in a large meta-analysis (Am. J. Cardiol. 2011;108:575-9).
In the largest trial, COPPS (Colchicine for the Prevention of the Postpericardiotomy Syndrome), Dr. Imazio reported that colchicine significantly reduced the incidence of postpericardiotomy syndrome (8.9% vs. 21.1%), postoperative pericardial effusions (relative risk reduction, 43.9%), and pleural effusions (RRR, 52.3%) at 12 months, compared with placebo (Am. Heart J. 2011;162:527-32 and Eur. Heart J. 2010;31:2749-54). Colchicine was given for 1 month, beginning on the third postoperative day with a 1-mg twice-daily loading dose.
In COPPS-2, the 360 consecutive candidates for cardiac surgery also were given colchicine or placebo for 1 month, but treatment was started 48-72 hours before surgery to pretreat patients and improve colchicine’s ability to prevent postoperative systemic inflammation and its complications.
Colchicine also was administered using weight-based dosing (0.5 mg twice daily in patients weighing at least 70 kg or 0.5 mg once daily in those under 70 kg), and they avoided the loading dose in an effort to improve adherence.
"However, we observed a 2-fold increase of adverse effects and study drug discontinuations compared with those reported in the COPPS trial, likely due to significant vulnerability of patients in the perioperative phase, when the use of antibiotics and proton pump inhibitors is common and also increases the risk of gastrointestinal effects (e.g., diarrhea)," explained Dr. Imazio of Maria Vittoria Hospital and the University of Torino (Italy).
Still, colchicine provided significant protection in the COPPS-2 primary outcome of postpericardiotomy syndrome, compared with placebo (19.4% vs. 29.4%; 95% confidence interval, 1.1%-18.7%). The number needed to treat was 10.
The outcome did not differ significantly among predetermined subgroups based on age, sex, and presence or absence of pericardial effusion, although colchicine was especially efficacious in the setting of systemic inflammation with elevated C-reactive protein, the authors noted.
The intention-to-treat analysis revealed no significant differences between the colchicine and placebo groups for postoperative AF (33.9% vs. 41.7%; 95% CI, –2.2%-17.6%) or postoperative pericardial/pleural effusion (57.2% vs. 58.9%; 95% CI, –8.5%-11.7%).
The prespecified on-treatment analysis, however, showed a 14.2% absolute difference in postoperative AF, favoring colchicine over placebo (27% vs. 41.2%; 95% CI, 3.3%-24.7%).
"While the efficacy of colchicine for postpericardiotomy syndrome prevention is confirmed, the extent of efficacy for postoperative AF needs to be further investigated in future trials," Dr. Imazio stated.
Ongoing studies also will better clarify the potential of colchicine using lower doses that may be better tolerated.
The 360 patients were evenly randomized from 11 centers in Italy between March 2012 and March 2014. Their mean age was 67.5 years, 69% were men, and 36% had planned valvular surgery. Key exclusion criteria were absence of sinus rhythm at enrollment, urgent cardiac surgery, cardiac transplantation, and contraindications to colchicine.
COPPS-2 was supported by the Italian National Health Service and FARGIM. Acarpia provided the study drug. Dr. Imazio reported no conflicts of interest. A coauthor reported consultancy for Servier, serving on an advisory board for Boehringer Ingelheim, and lecturer fees from Abbott, AstraZeneca, Merck, Serono, Richter Gedeon, and Teva.
Patients undergoing cardiac surgery who took colchicine had significantly less postpericardiotomy syndrome than did those on placebo, but this protective effect did not extend to postoperative atrial fibrillation and pericardial or pleural effusions in the double-blind COPPS-2 trial.
The failure of colchicine to prevent postoperative atrial fibrillation (AF) was probably due to more frequent adverse events (36 vs. 21 with placebo), especially gastrointestinal intolerance (26 vs. 12), and drug discontinuation (39 vs. 32), since a prespecified on-treatment analysis showed a significant reduction in AF in patients tolerating the drug, Dr. Massimo Imazio reported at the annual congress of the European Society of Cardiology.
"The high rate of adverse effects is a reason for concern and suggests that colchicine should be considered only in well-selected patients," Dr. Imazio and his associates wrote in an article on COPPS-2 simultaneously published online (JAMA 2014 [doi:10.1001/jama.2014.11026]).
Colchicine has been a promising strategy for postpericardiotomy syndrome prevention, besting methylprednisolone and aspirin in a large meta-analysis (Am. J. Cardiol. 2011;108:575-9).
In the largest trial, COPPS (Colchicine for the Prevention of the Postpericardiotomy Syndrome), Dr. Imazio reported that colchicine significantly reduced the incidence of postpericardiotomy syndrome (8.9% vs. 21.1%), postoperative pericardial effusions (relative risk reduction, 43.9%), and pleural effusions (RRR, 52.3%) at 12 months, compared with placebo (Am. Heart J. 2011;162:527-32 and Eur. Heart J. 2010;31:2749-54). Colchicine was given for 1 month, beginning on the third postoperative day with a 1-mg twice-daily loading dose.
In COPPS-2, the 360 consecutive candidates for cardiac surgery also were given colchicine or placebo for 1 month, but treatment was started 48-72 hours before surgery to pretreat patients and improve colchicine’s ability to prevent postoperative systemic inflammation and its complications.
Colchicine also was administered using weight-based dosing (0.5 mg twice daily in patients weighing at least 70 kg or 0.5 mg once daily in those under 70 kg), and they avoided the loading dose in an effort to improve adherence.
"However, we observed a 2-fold increase of adverse effects and study drug discontinuations compared with those reported in the COPPS trial, likely due to significant vulnerability of patients in the perioperative phase, when the use of antibiotics and proton pump inhibitors is common and also increases the risk of gastrointestinal effects (e.g., diarrhea)," explained Dr. Imazio of Maria Vittoria Hospital and the University of Torino (Italy).
Still, colchicine provided significant protection in the COPPS-2 primary outcome of postpericardiotomy syndrome, compared with placebo (19.4% vs. 29.4%; 95% confidence interval, 1.1%-18.7%). The number needed to treat was 10.
The outcome did not differ significantly among predetermined subgroups based on age, sex, and presence or absence of pericardial effusion, although colchicine was especially efficacious in the setting of systemic inflammation with elevated C-reactive protein, the authors noted.
The intention-to-treat analysis revealed no significant differences between the colchicine and placebo groups for postoperative AF (33.9% vs. 41.7%; 95% CI, –2.2%-17.6%) or postoperative pericardial/pleural effusion (57.2% vs. 58.9%; 95% CI, –8.5%-11.7%).
The prespecified on-treatment analysis, however, showed a 14.2% absolute difference in postoperative AF, favoring colchicine over placebo (27% vs. 41.2%; 95% CI, 3.3%-24.7%).
"While the efficacy of colchicine for postpericardiotomy syndrome prevention is confirmed, the extent of efficacy for postoperative AF needs to be further investigated in future trials," Dr. Imazio stated.
Ongoing studies also will better clarify the potential of colchicine using lower doses that may be better tolerated.
The 360 patients were evenly randomized from 11 centers in Italy between March 2012 and March 2014. Their mean age was 67.5 years, 69% were men, and 36% had planned valvular surgery. Key exclusion criteria were absence of sinus rhythm at enrollment, urgent cardiac surgery, cardiac transplantation, and contraindications to colchicine.
COPPS-2 was supported by the Italian National Health Service and FARGIM. Acarpia provided the study drug. Dr. Imazio reported no conflicts of interest. A coauthor reported consultancy for Servier, serving on an advisory board for Boehringer Ingelheim, and lecturer fees from Abbott, AstraZeneca, Merck, Serono, Richter Gedeon, and Teva.
FROM THE ESC CONGRESS 2014
Key clinical point: Perioperative use of colchicine should be considered only in well-selected patients.
Major finding: Perioperative colchicine use cut the incidence of postpericardiotomy syndrome, but not postoperative atrial fibrillation or pericardial/pleural effusion.
Data source: Double-blind, randomized clinical trial in 360 consecutive candidates for heart surgery.
Disclosures: COPPS-2 was supported by the Italian National Health Service and FARGIM. Acarpia provided the study drug. Dr. Imazio reported no conflicts of interest. A coauthor reported consultancy for Servier, serving on an advisory board for Boehringer Ingelheim, and lecturer fees from Abbott, AstraZeneca, Merck, Serono, Richter Gedeon, and Teva.

Aortic dissection associated with obstructive sleep apnea syndrome
Aortic dissection is significantly associated with obstructive sleep apnea, according to a Chinese study that found 81.7% of patients with Stanford’s type B aortic dissection have obstructive sleep apnea, compared with 67.2% of controls with suspected sleep apnea but no aortic disease.
A cross-sectional study in 82 patients with aortic dissection (AD), compared with 116 controls, showed individuals with aortic dissection had a higher apnea-hypopnea index, higher Berlin scores (75.6% vs. 54.3% high risk), a higher mean 4% oxygen desaturation index (16 vs. 7 events/hour), and a lower oxygen saturation during sleep (average, 87% vs. 93%). All findings were statistically significant.
"Recently, Saruhara et al. showed that patients with aortic diseases frequently suffered from moderate to severe OSAS [obstructive sleep apnea syndrome] and recommended that screening for OSAS may be helpful for early detection of patients with aortic disease," wrote Dr. Xuemin Zhang of the Peking University People’s Hospital and colleagues, in the 7 Aug. online edition of the Annals of Vascular Surgery [doi:10.1016/j.avsg.2014.07.014].
"Our results suggest that there is a strong association between OSAS and AD, supporting OSAS as an independent risk factor for type B AD."
The study was supported by a grant from the Foundation of Peking University People’s Hospital for Clinical Trial. There were no conflicts of interest declared.
Aortic dissection is significantly associated with obstructive sleep apnea, according to a Chinese study that found 81.7% of patients with Stanford’s type B aortic dissection have obstructive sleep apnea, compared with 67.2% of controls with suspected sleep apnea but no aortic disease.
A cross-sectional study in 82 patients with aortic dissection (AD), compared with 116 controls, showed individuals with aortic dissection had a higher apnea-hypopnea index, higher Berlin scores (75.6% vs. 54.3% high risk), a higher mean 4% oxygen desaturation index (16 vs. 7 events/hour), and a lower oxygen saturation during sleep (average, 87% vs. 93%). All findings were statistically significant.
"Recently, Saruhara et al. showed that patients with aortic diseases frequently suffered from moderate to severe OSAS [obstructive sleep apnea syndrome] and recommended that screening for OSAS may be helpful for early detection of patients with aortic disease," wrote Dr. Xuemin Zhang of the Peking University People’s Hospital and colleagues, in the 7 Aug. online edition of the Annals of Vascular Surgery [doi:10.1016/j.avsg.2014.07.014].
"Our results suggest that there is a strong association between OSAS and AD, supporting OSAS as an independent risk factor for type B AD."
The study was supported by a grant from the Foundation of Peking University People’s Hospital for Clinical Trial. There were no conflicts of interest declared.
Aortic dissection is significantly associated with obstructive sleep apnea, according to a Chinese study that found 81.7% of patients with Stanford’s type B aortic dissection have obstructive sleep apnea, compared with 67.2% of controls with suspected sleep apnea but no aortic disease.
A cross-sectional study in 82 patients with aortic dissection (AD), compared with 116 controls, showed individuals with aortic dissection had a higher apnea-hypopnea index, higher Berlin scores (75.6% vs. 54.3% high risk), a higher mean 4% oxygen desaturation index (16 vs. 7 events/hour), and a lower oxygen saturation during sleep (average, 87% vs. 93%). All findings were statistically significant.
"Recently, Saruhara et al. showed that patients with aortic diseases frequently suffered from moderate to severe OSAS [obstructive sleep apnea syndrome] and recommended that screening for OSAS may be helpful for early detection of patients with aortic disease," wrote Dr. Xuemin Zhang of the Peking University People’s Hospital and colleagues, in the 7 Aug. online edition of the Annals of Vascular Surgery [doi:10.1016/j.avsg.2014.07.014].
"Our results suggest that there is a strong association between OSAS and AD, supporting OSAS as an independent risk factor for type B AD."
The study was supported by a grant from the Foundation of Peking University People’s Hospital for Clinical Trial. There were no conflicts of interest declared.
FROM ANNALS OF VASCULAR SURGERY
Major finding: Aortic dissection is significantly associated with obstructive sleep apnea, with 81.7% of patients with Stanford’s type B aortic dissection having obstructive sleep apnea, compared with 67.2% of controls with suspected sleep apnea but no aortic disease.
Data source: A cross-sectional study in 82 patients with aortic dissection and 116 controls.
Disclosures: The study was supported by a grant from the Foundation of Peking University People’s Hospital for Clinical Trial. There were no conflicts of interest declared.
NIH set to begin human testing on experimental Ebola vaccine
The National Institute of Allergy and Infectious Diseases will begin human testing of a new vaccine developed to prevent contracting the deadly Ebola virus.
The vaccine is the first of several phase I treatments to go into clinical trials on humans. The hope is that the vaccine ultimately will be used to stem the tide of Ebola infections in western Africa, where the virus already has claimed more than 1,400 lives since the outbreak began in March.
"There is an urgent need for a protective Ebola vaccine, and it is important to establish that a vaccine is safe and spurs the immune system to react in a way necessary to protect against infection," Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said in a statement. "The [National Institutes of Health] is playing a key role in accelerating the development and testing of investigational Ebola vaccines."
The testing will take place at the National Institutes of Health Clinical Center in Maryland, where the vaccine – developed jointly by the NIAID and GlaxoSmithKline – will be administered to 20 healthy adults who have not contracted the Ebola virus. Ten adults will receive an intramuscular injection, while the other ten will receive the same injection in a higher dosage. All participants in the trial, which has been dubbed VRC 207, are between the ages of 18 and 50.
Once phase I trials are complete, the next step will be to test the vaccine on a larger number of people in phase II studies. Phase III trials would determine whether the vaccine is effective. The VRC 207 trial is expected to begin in October.
"Today we know the best way to prevent the spread of Ebola infection is through public health measures, including good infection control practices, isolation, contact tracing, quarantine, and provision of personal protective equipment," Dr. Fauci said in the statement. "However, a vaccine will ultimately be an important tool in the prevention effort. The launch of phase I Ebola vaccine studies is the first step in a long process."
Additionally, the NIH has partnered with a British consortium to test the NIAID/GSK vaccine on healthy adults in the United Kingdom. Permission to test the vaccine in the western African nations of Gambia and Mali is still pending approval from authorities in those countries. The U.K. trial is scheduled to begin in September.
The NIAID anticipates that initial safety and immunogenicity data from the phase I trials should be available by late 2014.
The National Institute of Allergy and Infectious Diseases will begin human testing of a new vaccine developed to prevent contracting the deadly Ebola virus.
The vaccine is the first of several phase I treatments to go into clinical trials on humans. The hope is that the vaccine ultimately will be used to stem the tide of Ebola infections in western Africa, where the virus already has claimed more than 1,400 lives since the outbreak began in March.
"There is an urgent need for a protective Ebola vaccine, and it is important to establish that a vaccine is safe and spurs the immune system to react in a way necessary to protect against infection," Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said in a statement. "The [National Institutes of Health] is playing a key role in accelerating the development and testing of investigational Ebola vaccines."
The testing will take place at the National Institutes of Health Clinical Center in Maryland, where the vaccine – developed jointly by the NIAID and GlaxoSmithKline – will be administered to 20 healthy adults who have not contracted the Ebola virus. Ten adults will receive an intramuscular injection, while the other ten will receive the same injection in a higher dosage. All participants in the trial, which has been dubbed VRC 207, are between the ages of 18 and 50.
Once phase I trials are complete, the next step will be to test the vaccine on a larger number of people in phase II studies. Phase III trials would determine whether the vaccine is effective. The VRC 207 trial is expected to begin in October.
"Today we know the best way to prevent the spread of Ebola infection is through public health measures, including good infection control practices, isolation, contact tracing, quarantine, and provision of personal protective equipment," Dr. Fauci said in the statement. "However, a vaccine will ultimately be an important tool in the prevention effort. The launch of phase I Ebola vaccine studies is the first step in a long process."
Additionally, the NIH has partnered with a British consortium to test the NIAID/GSK vaccine on healthy adults in the United Kingdom. Permission to test the vaccine in the western African nations of Gambia and Mali is still pending approval from authorities in those countries. The U.K. trial is scheduled to begin in September.
The NIAID anticipates that initial safety and immunogenicity data from the phase I trials should be available by late 2014.
The National Institute of Allergy and Infectious Diseases will begin human testing of a new vaccine developed to prevent contracting the deadly Ebola virus.
The vaccine is the first of several phase I treatments to go into clinical trials on humans. The hope is that the vaccine ultimately will be used to stem the tide of Ebola infections in western Africa, where the virus already has claimed more than 1,400 lives since the outbreak began in March.
"There is an urgent need for a protective Ebola vaccine, and it is important to establish that a vaccine is safe and spurs the immune system to react in a way necessary to protect against infection," Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said in a statement. "The [National Institutes of Health] is playing a key role in accelerating the development and testing of investigational Ebola vaccines."
The testing will take place at the National Institutes of Health Clinical Center in Maryland, where the vaccine – developed jointly by the NIAID and GlaxoSmithKline – will be administered to 20 healthy adults who have not contracted the Ebola virus. Ten adults will receive an intramuscular injection, while the other ten will receive the same injection in a higher dosage. All participants in the trial, which has been dubbed VRC 207, are between the ages of 18 and 50.
Once phase I trials are complete, the next step will be to test the vaccine on a larger number of people in phase II studies. Phase III trials would determine whether the vaccine is effective. The VRC 207 trial is expected to begin in October.
"Today we know the best way to prevent the spread of Ebola infection is through public health measures, including good infection control practices, isolation, contact tracing, quarantine, and provision of personal protective equipment," Dr. Fauci said in the statement. "However, a vaccine will ultimately be an important tool in the prevention effort. The launch of phase I Ebola vaccine studies is the first step in a long process."
Additionally, the NIH has partnered with a British consortium to test the NIAID/GSK vaccine on healthy adults in the United Kingdom. Permission to test the vaccine in the western African nations of Gambia and Mali is still pending approval from authorities in those countries. The U.K. trial is scheduled to begin in September.
The NIAID anticipates that initial safety and immunogenicity data from the phase I trials should be available by late 2014.
A sustained postdischarge smoking cessation intervention ups likelihood of quitting
A sustained postdischarge smoking cessation intervention was more effective than standard recommendations regarding smoking cessation for hospitalized adults with a desire to quit smoking in the randomized, controlled Hospital-Initiated Assistance for Nicotine Dependence (Helping HAND) trial.
The 198 patients who were assigned to receive sustained care were more likely than the 199 who received standard care to use counseling (37% vs. 23%; relative risk, 1.63) and pharmacotherapy (79% vs. 59%; RR, 1.34) after discharge.

Those who received sustained care also were more likely to have biochemically validated, 7-day tobacco abstinence at 6 months (26% vs. 15%; RR, 1.71; number needed to treat, 9.4), Dr. Nancy A. Rigotti, who is director of the Tobacco Research and Treatment Center at Massachusetts General Hospital, Boston, and her colleagues reported online Aug. 20 in JAMA.
Patients in the study had a mean age of 53 years. Those assigned to the sustained-care group had an initial inpatient visit and received five supportive, automated, interactive phone calls and their choice of any approved smoking cessation medication or combination of medications for up to 90 days after discharge. The control group received recommendations for postdischarge pharmacotherapy and smoking cessation counseling, the investigators said (JAMA 2014;312:719-28).
"These findings, if replicated, suggest a translatable, low-cost approach to achieving sustained smoking cessation after a hospital stay," they concluded.
This study was supported by the National Heart, Lung, and Blood Institute and the Department of Veterans Affairs, and is part of the Consortium of Hospitals Advancing Research on Tobacco initiative, which is jointly sponsored by the National Cancer Institute, the NHLBI, and other federal agencies. Dr. Rigotti was an unpaid consultant for Pfizer and Alere Wellbeing regarding smoking cessation, received royalties from UpToDate for reviews on smoking cessation, and received travel reimbursement from Pfizer. Several coauthors were paid consultants for or received grants from Pfizer, and one coauthor was a paid consultant on tobacco policy for CVS.
A sustained postdischarge smoking cessation intervention was more effective than standard recommendations regarding smoking cessation for hospitalized adults with a desire to quit smoking in the randomized, controlled Hospital-Initiated Assistance for Nicotine Dependence (Helping HAND) trial.
The 198 patients who were assigned to receive sustained care were more likely than the 199 who received standard care to use counseling (37% vs. 23%; relative risk, 1.63) and pharmacotherapy (79% vs. 59%; RR, 1.34) after discharge.
Those who received sustained care also were more likely to have biochemically validated, 7-day tobacco abstinence at 6 months (26% vs. 15%; RR, 1.71; number needed to treat, 9.4), Dr. Nancy A. Rigotti, who is director of the Tobacco Research and Treatment Center at Massachusetts General Hospital, Boston, and her colleagues reported online Aug. 20 in JAMA.
Patients in the study had a mean age of 53 years. Those assigned to the sustained-care group had an initial inpatient visit and received five supportive, automated, interactive phone calls and their choice of any approved smoking cessation medication or combination of medications for up to 90 days after discharge. The control group received recommendations for postdischarge pharmacotherapy and smoking cessation counseling, the investigators said (JAMA 2014;312:719-28).
"These findings, if replicated, suggest a translatable, low-cost approach to achieving sustained smoking cessation after a hospital stay," they concluded.
This study was supported by the National Heart, Lung, and Blood Institute and the Department of Veterans Affairs, and is part of the Consortium of Hospitals Advancing Research on Tobacco initiative, which is jointly sponsored by the National Cancer Institute, the NHLBI, and other federal agencies. Dr. Rigotti was an unpaid consultant for Pfizer and Alere Wellbeing regarding smoking cessation, received royalties from UpToDate for reviews on smoking cessation, and received travel reimbursement from Pfizer. Several coauthors were paid consultants for or received grants from Pfizer, and one coauthor was a paid consultant on tobacco policy for CVS.
A sustained postdischarge smoking cessation intervention was more effective than standard recommendations regarding smoking cessation for hospitalized adults with a desire to quit smoking in the randomized, controlled Hospital-Initiated Assistance for Nicotine Dependence (Helping HAND) trial.
The 198 patients who were assigned to receive sustained care were more likely than the 199 who received standard care to use counseling (37% vs. 23%; relative risk, 1.63) and pharmacotherapy (79% vs. 59%; RR, 1.34) after discharge.
Those who received sustained care also were more likely to have biochemically validated, 7-day tobacco abstinence at 6 months (26% vs. 15%; RR, 1.71; number needed to treat, 9.4), Dr. Nancy A. Rigotti, who is director of the Tobacco Research and Treatment Center at Massachusetts General Hospital, Boston, and her colleagues reported online Aug. 20 in JAMA.
Patients in the study had a mean age of 53 years. Those assigned to the sustained-care group had an initial inpatient visit and received five supportive, automated, interactive phone calls and their choice of any approved smoking cessation medication or combination of medications for up to 90 days after discharge. The control group received recommendations for postdischarge pharmacotherapy and smoking cessation counseling, the investigators said (JAMA 2014;312:719-28).
"These findings, if replicated, suggest a translatable, low-cost approach to achieving sustained smoking cessation after a hospital stay," they concluded.
This study was supported by the National Heart, Lung, and Blood Institute and the Department of Veterans Affairs, and is part of the Consortium of Hospitals Advancing Research on Tobacco initiative, which is jointly sponsored by the National Cancer Institute, the NHLBI, and other federal agencies. Dr. Rigotti was an unpaid consultant for Pfizer and Alere Wellbeing regarding smoking cessation, received royalties from UpToDate for reviews on smoking cessation, and received travel reimbursement from Pfizer. Several coauthors were paid consultants for or received grants from Pfizer, and one coauthor was a paid consultant on tobacco policy for CVS.
FROM JAMA
Key clinical point: Sustained support upon hospital discharge helps people quit smoking.
Major finding: More patients in the intervention group had biochemically validated 7-day tobacco abstinence at 6 months (26% vs. 15%, relative risk, 1.71, number needed to treat, 9.4).
Data source: The randomized, controlled Helping HAND trial involving 397 patients.
Disclosures: This study was supported by the National Heart, Lung, and Blood Institute and the Department of Veterans Affairs. Dr. Rigotti was an unpaid consultant for Pfizer and Alere Wellbeing regarding smoking cessation, received royalties from UpToDate for reviews on smoking cessation, and received travel reimbursement from Pfizer. Several coauthors were paid consultants for or received grants from Pfizer, and one coauthor was a paid consultant on tobacco policy for CVS.

Testosterone replacement enhances aerobic capacity in mobility-limited men
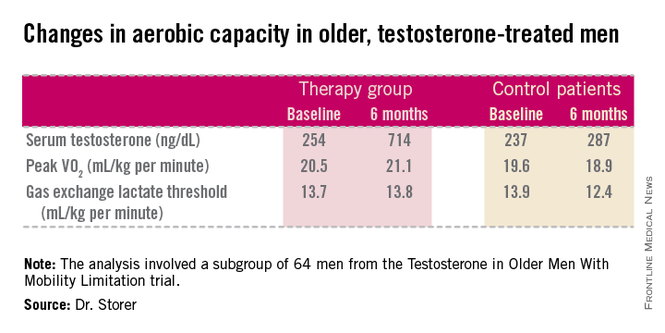
CHICAGO – Testosterone replacement therapy in mobility-impaired, sedentary older men with low testosterone levels improved two different measures of aerobic capacity in a placebo-controlled, randomized 6-month clinical trial.
The age-related decline in peak oxygen uptake during exercise, or peak VO2, was 3.4-fold less in the testosterone-treated men than would be expected based on published population norms. Moreover, the rate of decline in peak VO2 in placebo-treated controls was nearly twice the expected rate for the age-matched general population; this accelerated decline was probably due to their limited mobility and low testosterone levels, Thomas W. Storer, Ph.D., said at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
"This study is the first to show enhanced endurance performance as a result of testosterone therapy in men who have difficulty performing some physical tasks but are otherwise healthy. This is something we think is going to be clinically meaningful," said Dr. Storer, director of the exercise physiology and physical performance laboratory at Brigham and Women’s Hospital, Boston.
He presented an analysis of a subset of participants in the prospective, randomized Testosterone in Older Men With Mobility Limitation (TOM) trial, in which subjects with low total or free testosterone levels were placed on 10 mg/day of testosterone gel or placebo gel for 6 months. The subgroup consisted of 64 men, mean age 73, who underwent formal testing of aerobic capacity via measurement of changes over time in peak VO2 and gas exchange lactate threshold during symptom-limited exercise cycling.
The gas exchange lactate threshold is a good functional measure of the ability to do work over a prolonged period. The rate remained steady during the 6-month study in the testosterone-treated men but declined significantly – and to a greater-than-expected extent based on normative values – in the placebo-treated controls (see chart).

"We think the mechanisms involved in this benefit are many," Dr. Storer said in an interview. Among them are testosterone’s demonstrated ability to increase muscle mass and thereby generate more force during exercise; increased RBC formation; stimulation of tissue capillarity in order to allow more blood flow to the exercising muscle; and stimulation of mitochondrial biogenesis, which increases oxygen uptake by muscle tissue.
However, he added that although these results are quite promising, he doesn’t think this work is ready for prime time application in daily clinical practice. He plans to further evaluate the safety of this treatment and the durability of the effects in a study with larger patient numbers and longer treatment.
The study was funded by the National Institute on Aging, the Claude D. Pepper Older Americans Independence Center, and Boston University. Dr. Storer reported having no relevant financial conflicts.
CHICAGO – Testosterone replacement therapy in mobility-impaired, sedentary older men with low testosterone levels improved two different measures of aerobic capacity in a placebo-controlled, randomized 6-month clinical trial.
The age-related decline in peak oxygen uptake during exercise, or peak VO2, was 3.4-fold less in the testosterone-treated men than would be expected based on published population norms. Moreover, the rate of decline in peak VO2 in placebo-treated controls was nearly twice the expected rate for the age-matched general population; this accelerated decline was probably due to their limited mobility and low testosterone levels, Thomas W. Storer, Ph.D., said at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
"This study is the first to show enhanced endurance performance as a result of testosterone therapy in men who have difficulty performing some physical tasks but are otherwise healthy. This is something we think is going to be clinically meaningful," said Dr. Storer, director of the exercise physiology and physical performance laboratory at Brigham and Women’s Hospital, Boston.
He presented an analysis of a subset of participants in the prospective, randomized Testosterone in Older Men With Mobility Limitation (TOM) trial, in which subjects with low total or free testosterone levels were placed on 10 mg/day of testosterone gel or placebo gel for 6 months. The subgroup consisted of 64 men, mean age 73, who underwent formal testing of aerobic capacity via measurement of changes over time in peak VO2 and gas exchange lactate threshold during symptom-limited exercise cycling.
The gas exchange lactate threshold is a good functional measure of the ability to do work over a prolonged period. The rate remained steady during the 6-month study in the testosterone-treated men but declined significantly – and to a greater-than-expected extent based on normative values – in the placebo-treated controls (see chart).
"We think the mechanisms involved in this benefit are many," Dr. Storer said in an interview. Among them are testosterone’s demonstrated ability to increase muscle mass and thereby generate more force during exercise; increased RBC formation; stimulation of tissue capillarity in order to allow more blood flow to the exercising muscle; and stimulation of mitochondrial biogenesis, which increases oxygen uptake by muscle tissue.
However, he added that although these results are quite promising, he doesn’t think this work is ready for prime time application in daily clinical practice. He plans to further evaluate the safety of this treatment and the durability of the effects in a study with larger patient numbers and longer treatment.
The study was funded by the National Institute on Aging, the Claude D. Pepper Older Americans Independence Center, and Boston University. Dr. Storer reported having no relevant financial conflicts.
CHICAGO – Testosterone replacement therapy in mobility-impaired, sedentary older men with low testosterone levels improved two different measures of aerobic capacity in a placebo-controlled, randomized 6-month clinical trial.
The age-related decline in peak oxygen uptake during exercise, or peak VO2, was 3.4-fold less in the testosterone-treated men than would be expected based on published population norms. Moreover, the rate of decline in peak VO2 in placebo-treated controls was nearly twice the expected rate for the age-matched general population; this accelerated decline was probably due to their limited mobility and low testosterone levels, Thomas W. Storer, Ph.D., said at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
"This study is the first to show enhanced endurance performance as a result of testosterone therapy in men who have difficulty performing some physical tasks but are otherwise healthy. This is something we think is going to be clinically meaningful," said Dr. Storer, director of the exercise physiology and physical performance laboratory at Brigham and Women’s Hospital, Boston.
He presented an analysis of a subset of participants in the prospective, randomized Testosterone in Older Men With Mobility Limitation (TOM) trial, in which subjects with low total or free testosterone levels were placed on 10 mg/day of testosterone gel or placebo gel for 6 months. The subgroup consisted of 64 men, mean age 73, who underwent formal testing of aerobic capacity via measurement of changes over time in peak VO2 and gas exchange lactate threshold during symptom-limited exercise cycling.
The gas exchange lactate threshold is a good functional measure of the ability to do work over a prolonged period. The rate remained steady during the 6-month study in the testosterone-treated men but declined significantly – and to a greater-than-expected extent based on normative values – in the placebo-treated controls (see chart).
"We think the mechanisms involved in this benefit are many," Dr. Storer said in an interview. Among them are testosterone’s demonstrated ability to increase muscle mass and thereby generate more force during exercise; increased RBC formation; stimulation of tissue capillarity in order to allow more blood flow to the exercising muscle; and stimulation of mitochondrial biogenesis, which increases oxygen uptake by muscle tissue.
However, he added that although these results are quite promising, he doesn’t think this work is ready for prime time application in daily clinical practice. He plans to further evaluate the safety of this treatment and the durability of the effects in a study with larger patient numbers and longer treatment.
The study was funded by the National Institute on Aging, the Claude D. Pepper Older Americans Independence Center, and Boston University. Dr. Storer reported having no relevant financial conflicts.
AT ICE/ENDO 2014
Key clinical point: Testosterone replacement therapy neutralizes the age-related decline in aerobic capacity in older men with low testosterone and mobility limitation.
Major finding: The age-related decline in peak VO2 in testosterone takers was 3.4-fold less than expected based on age-related norms.
Data source: A subanalysis of data from the randomized, prospective TOM trial, in which participants with low testosterone were randomized to 10 mg/day of testosterone gel or placebo for 6 months.
Disclosures: TOM was funded by the National Institute on Aging, the Claude D. Pepper Older Americans Independence Center, and Boston University.
WHO to push for public ban of e-cigarettes
The use of electronic cigarettes, like that of their tobacco-containing cousins, should be banned in public indoor spaces, the World Health Organization recommends.
Users of electronic nicotine delivery systems devices (ENDS), such as e-cigarettes, should "be legally requested not to use ENDS indoors, especially where smoking is banned, until exhaled vapor is proved to be not harmful to bystanders and reasonable evidence exists that smoke-free policy enforcement is not undermined," according to a WHO report published Aug. 26.

The report is intended to provide a framework for governments to follow when developing regulations around e-cigarettes. It is on the agenda for the upcoming 6th Conference of the Parties to the WHO Framework Convention on Tobacco Control in Moscow Oct. 13-18.
The report recommends that manufacturers be prohibited from making any health claims related to ENDS, specifically identifying claims that e-cigarettes are smoking cessation products. The report notes that there is anecdotal evidence to suggest e-cigarettes have been effective in helping people quit smoking but "their efficacy has not been systematically evaluated yet." WHO recommends that approved and proven cessation products should be tried first, with e-cigarettes being a last resort. Recent guidelines from the American Heart Association echoed that sentiment.
The WHO guidance is in line with recent recommendations made to the Food and Drug Administration from various medical societies in advocating for strict oversight in marketing to ensure that children are not targeted. The FDA is considering broadening its tobacco oversight to include e-cigarettes.
The use of electronic cigarettes, like that of their tobacco-containing cousins, should be banned in public indoor spaces, the World Health Organization recommends.
Users of electronic nicotine delivery systems devices (ENDS), such as e-cigarettes, should "be legally requested not to use ENDS indoors, especially where smoking is banned, until exhaled vapor is proved to be not harmful to bystanders and reasonable evidence exists that smoke-free policy enforcement is not undermined," according to a WHO report published Aug. 26.
The report is intended to provide a framework for governments to follow when developing regulations around e-cigarettes. It is on the agenda for the upcoming 6th Conference of the Parties to the WHO Framework Convention on Tobacco Control in Moscow Oct. 13-18.
The report recommends that manufacturers be prohibited from making any health claims related to ENDS, specifically identifying claims that e-cigarettes are smoking cessation products. The report notes that there is anecdotal evidence to suggest e-cigarettes have been effective in helping people quit smoking but "their efficacy has not been systematically evaluated yet." WHO recommends that approved and proven cessation products should be tried first, with e-cigarettes being a last resort. Recent guidelines from the American Heart Association echoed that sentiment.
The WHO guidance is in line with recent recommendations made to the Food and Drug Administration from various medical societies in advocating for strict oversight in marketing to ensure that children are not targeted. The FDA is considering broadening its tobacco oversight to include e-cigarettes.
The use of electronic cigarettes, like that of their tobacco-containing cousins, should be banned in public indoor spaces, the World Health Organization recommends.
Users of electronic nicotine delivery systems devices (ENDS), such as e-cigarettes, should "be legally requested not to use ENDS indoors, especially where smoking is banned, until exhaled vapor is proved to be not harmful to bystanders and reasonable evidence exists that smoke-free policy enforcement is not undermined," according to a WHO report published Aug. 26.
The report is intended to provide a framework for governments to follow when developing regulations around e-cigarettes. It is on the agenda for the upcoming 6th Conference of the Parties to the WHO Framework Convention on Tobacco Control in Moscow Oct. 13-18.
The report recommends that manufacturers be prohibited from making any health claims related to ENDS, specifically identifying claims that e-cigarettes are smoking cessation products. The report notes that there is anecdotal evidence to suggest e-cigarettes have been effective in helping people quit smoking but "their efficacy has not been systematically evaluated yet." WHO recommends that approved and proven cessation products should be tried first, with e-cigarettes being a last resort. Recent guidelines from the American Heart Association echoed that sentiment.
The WHO guidance is in line with recent recommendations made to the Food and Drug Administration from various medical societies in advocating for strict oversight in marketing to ensure that children are not targeted. The FDA is considering broadening its tobacco oversight to include e-cigarettes.

When Patients Ask for Antibiotics, Arm Them With Handouts
Drug store and supermarket shelves display aisle after aisle of OTC medications that alleviate the common symptoms of upper respiratory infections. Despite the easy availability of symptom relief, a significant number of people consult clinicians in primary care offices, emergency departments (EDs), and walk-in or convenient care clinics for help when they feel that they’re “coming down with something.” During these visits, many of these patients expect, and sometimes demand, antibiotics.
Antibiotics may be viewed by the patient as a quick fix, with the demand undoubtedly fueled by busy lifestyles, long work hours, and little time for patients to stay home while ill. Patients so inclined may “doctor shop” if their demands are not met; clinicians know better but may feel pressure to “satisfy the customer” and may rationalize that an antibiotic might prove helpful in a particular case.
Lee et al studied outpatient antibiotic prescribing in the United States for acute respiratory tract infections (ARTI), including acute nasopharyngitis, upper respiratory tract infection, bronchitis, influenza, pharyngitis, and sinusitis. In 2000, antibiotics were prescribed during outpatient visits for ARTI to 64% of patients; by 2010, that percentage had increased to 73%.1 Although antibiotics are neither effective nor appropriate for the treatment of ARTI, most of which are viral infections, they are commonly prescribed. Further, while 17% of ARTI prescriptions in 2000 were for broad-spectrum antibiotics, that percentage jumped to 46% in 2010.1,2
Patient insistence on antibiotics may stem either from little knowledge of or little regard for the health problems caused by unnecessary antibiotic use. For example, one study found that 19.3% of drug-related ED visits were related to systemic antibiotics; nearly 80% of those were for allergic reactions.3,4 With an estimated 50% of antibiotic prescriptions considered inappropriate, the overuse of antibiotics creates unnecessary personal health risks and health care expenditures. Further, a more serious consequence of this overuse is the growing public health problem of antibiotic resistance (see Figure 1).1,2

Clinicians are ideally positioned to address these issues by incorporating effective, proactive strategies into selected patient encounters to specifically explain appropriate versus inappropriate antibiotic use.
Continue for patient handouts >>
One approach is to merge accurate, powerful messages about antibiotics with helpful information about effective OTC products to both enlighten patients and offer them the symptomatic relief they seek. The CDC has taken the lead in this area with its “Get Smart: Know When Antibiotics Work” initiative, which includes a variety of materials for both health care providers and patients.5
Inspired by the unmet need for written communications that explain viral and bacterial illnesses in simple terms and the reasons why taking antibiotics for the former is a bad idea, we developed two handouts for adult patients who present to the clinician’s office with viral respiratory illnesses.
The first is entitled “Prescription for Recovery From Your Viral Respiratory Illness” [download PDF]. Intended to be duplicated and designed with primary care use in mind, it can be customized for specialty use as well.
This “prescription” handout addresses common complaints of fever, pain (eg, sore throat, body aches, headache), cough, congestion (chest, nose, sinuses), and sneezing/runny nose. Clinicians can check off the appropriate treatments for an individual patient, who can use it as a handy reference to purchase the recommended OTC products and/or for selecting products or preparing helpful remedies at home. Blank lines at the bottom provide space for you to write in your OTC preferences and allow you to customize patient instructions.
The second patient handout is entitled “Antibiotics: When You Need Them, When You Don’t, and What to Take When You Don’t” [download PDF]. This focused patient teaching tool offers an overview of
• Viral and bacterial respiratory illnesses and what the patient should do if he or she has one or the other (including when to see a clinician)
• Some helpful OTC and home treatments for symptoms of viral respiratory illnesses
• When antibiotics are indicated and when they’re not—and why
• The serious problems caused by unnecessary use of antibiotics.
This brief guide can be used as a general informational handout that can, for example, be given, mailed, or e-mailed to all adult patients at the start of cold and flu season and retained by them for reference. It can also be provided along with the “prescription” handout to patients with ARTIs who visit your office. In the latter situation, the patient leaves your office with concrete information and guidance for appropriate care of his or her viral respiratory illness—but without a prescription for antibiotics. As with the “prescription” handout, this brief guide may be duplicated or customized as needed.
To download the handouts: Click here.
REFERENCES
1. Lee GC, Reveles KR, Attridge RT, et al. Outpatient antibiotic prescribing in the United States: 2000-2010. BMC Med. 2014;12:96.
2. CDC. Antibiotics: will they work when you really need them? www.cdc.gov/getsmart/healthcare/factsheets/antibiotics.html#MustAct. Accessed August 14, 2014.
3. Shehab N, Patel P, Srinivasan A, Budnitz D. Emergency department visits for antibiotic associated adverse events. Clin Infect Dis. 2008;47:735-743.
4. CDC. Adverse drug events from select medication classes. www.cdc.gov/MedicationSafety/program_focus_activities.html. Accessed August 4, 2014.
5. CDC. Get smart: know when antibiotics work. www.cdc.gov/getsmart/. Accessed August 14, 2014.
Drug store and supermarket shelves display aisle after aisle of OTC medications that alleviate the common symptoms of upper respiratory infections. Despite the easy availability of symptom relief, a significant number of people consult clinicians in primary care offices, emergency departments (EDs), and walk-in or convenient care clinics for help when they feel that they’re “coming down with something.” During these visits, many of these patients expect, and sometimes demand, antibiotics.
Antibiotics may be viewed by the patient as a quick fix, with the demand undoubtedly fueled by busy lifestyles, long work hours, and little time for patients to stay home while ill. Patients so inclined may “doctor shop” if their demands are not met; clinicians know better but may feel pressure to “satisfy the customer” and may rationalize that an antibiotic might prove helpful in a particular case.
Lee et al studied outpatient antibiotic prescribing in the United States for acute respiratory tract infections (ARTI), including acute nasopharyngitis, upper respiratory tract infection, bronchitis, influenza, pharyngitis, and sinusitis. In 2000, antibiotics were prescribed during outpatient visits for ARTI to 64% of patients; by 2010, that percentage had increased to 73%.1 Although antibiotics are neither effective nor appropriate for the treatment of ARTI, most of which are viral infections, they are commonly prescribed. Further, while 17% of ARTI prescriptions in 2000 were for broad-spectrum antibiotics, that percentage jumped to 46% in 2010.1,2
Patient insistence on antibiotics may stem either from little knowledge of or little regard for the health problems caused by unnecessary antibiotic use. For example, one study found that 19.3% of drug-related ED visits were related to systemic antibiotics; nearly 80% of those were for allergic reactions.3,4 With an estimated 50% of antibiotic prescriptions considered inappropriate, the overuse of antibiotics creates unnecessary personal health risks and health care expenditures. Further, a more serious consequence of this overuse is the growing public health problem of antibiotic resistance (see Figure 1).1,2
Clinicians are ideally positioned to address these issues by incorporating effective, proactive strategies into selected patient encounters to specifically explain appropriate versus inappropriate antibiotic use.
Continue for patient handouts >>
One approach is to merge accurate, powerful messages about antibiotics with helpful information about effective OTC products to both enlighten patients and offer them the symptomatic relief they seek. The CDC has taken the lead in this area with its “Get Smart: Know When Antibiotics Work” initiative, which includes a variety of materials for both health care providers and patients.5
Inspired by the unmet need for written communications that explain viral and bacterial illnesses in simple terms and the reasons why taking antibiotics for the former is a bad idea, we developed two handouts for adult patients who present to the clinician’s office with viral respiratory illnesses.
The first is entitled “Prescription for Recovery From Your Viral Respiratory Illness” [download PDF]. Intended to be duplicated and designed with primary care use in mind, it can be customized for specialty use as well.
This “prescription” handout addresses common complaints of fever, pain (eg, sore throat, body aches, headache), cough, congestion (chest, nose, sinuses), and sneezing/runny nose. Clinicians can check off the appropriate treatments for an individual patient, who can use it as a handy reference to purchase the recommended OTC products and/or for selecting products or preparing helpful remedies at home. Blank lines at the bottom provide space for you to write in your OTC preferences and allow you to customize patient instructions.
The second patient handout is entitled “Antibiotics: When You Need Them, When You Don’t, and What to Take When You Don’t” [download PDF]. This focused patient teaching tool offers an overview of
• Viral and bacterial respiratory illnesses and what the patient should do if he or she has one or the other (including when to see a clinician)
• Some helpful OTC and home treatments for symptoms of viral respiratory illnesses
• When antibiotics are indicated and when they’re not—and why
• The serious problems caused by unnecessary use of antibiotics.
This brief guide can be used as a general informational handout that can, for example, be given, mailed, or e-mailed to all adult patients at the start of cold and flu season and retained by them for reference. It can also be provided along with the “prescription” handout to patients with ARTIs who visit your office. In the latter situation, the patient leaves your office with concrete information and guidance for appropriate care of his or her viral respiratory illness—but without a prescription for antibiotics. As with the “prescription” handout, this brief guide may be duplicated or customized as needed.
To download the handouts: Click here.
REFERENCES
1. Lee GC, Reveles KR, Attridge RT, et al. Outpatient antibiotic prescribing in the United States: 2000-2010. BMC Med. 2014;12:96.
2. CDC. Antibiotics: will they work when you really need them? www.cdc.gov/getsmart/healthcare/factsheets/antibiotics.html#MustAct. Accessed August 14, 2014.
3. Shehab N, Patel P, Srinivasan A, Budnitz D. Emergency department visits for antibiotic associated adverse events. Clin Infect Dis. 2008;47:735-743.
4. CDC. Adverse drug events from select medication classes. www.cdc.gov/MedicationSafety/program_focus_activities.html. Accessed August 4, 2014.
5. CDC. Get smart: know when antibiotics work. www.cdc.gov/getsmart/. Accessed August 14, 2014.
Drug store and supermarket shelves display aisle after aisle of OTC medications that alleviate the common symptoms of upper respiratory infections. Despite the easy availability of symptom relief, a significant number of people consult clinicians in primary care offices, emergency departments (EDs), and walk-in or convenient care clinics for help when they feel that they’re “coming down with something.” During these visits, many of these patients expect, and sometimes demand, antibiotics.
Antibiotics may be viewed by the patient as a quick fix, with the demand undoubtedly fueled by busy lifestyles, long work hours, and little time for patients to stay home while ill. Patients so inclined may “doctor shop” if their demands are not met; clinicians know better but may feel pressure to “satisfy the customer” and may rationalize that an antibiotic might prove helpful in a particular case.
Lee et al studied outpatient antibiotic prescribing in the United States for acute respiratory tract infections (ARTI), including acute nasopharyngitis, upper respiratory tract infection, bronchitis, influenza, pharyngitis, and sinusitis. In 2000, antibiotics were prescribed during outpatient visits for ARTI to 64% of patients; by 2010, that percentage had increased to 73%.1 Although antibiotics are neither effective nor appropriate for the treatment of ARTI, most of which are viral infections, they are commonly prescribed. Further, while 17% of ARTI prescriptions in 2000 were for broad-spectrum antibiotics, that percentage jumped to 46% in 2010.1,2
Patient insistence on antibiotics may stem either from little knowledge of or little regard for the health problems caused by unnecessary antibiotic use. For example, one study found that 19.3% of drug-related ED visits were related to systemic antibiotics; nearly 80% of those were for allergic reactions.3,4 With an estimated 50% of antibiotic prescriptions considered inappropriate, the overuse of antibiotics creates unnecessary personal health risks and health care expenditures. Further, a more serious consequence of this overuse is the growing public health problem of antibiotic resistance (see Figure 1).1,2
Clinicians are ideally positioned to address these issues by incorporating effective, proactive strategies into selected patient encounters to specifically explain appropriate versus inappropriate antibiotic use.
Continue for patient handouts >>
One approach is to merge accurate, powerful messages about antibiotics with helpful information about effective OTC products to both enlighten patients and offer them the symptomatic relief they seek. The CDC has taken the lead in this area with its “Get Smart: Know When Antibiotics Work” initiative, which includes a variety of materials for both health care providers and patients.5
Inspired by the unmet need for written communications that explain viral and bacterial illnesses in simple terms and the reasons why taking antibiotics for the former is a bad idea, we developed two handouts for adult patients who present to the clinician’s office with viral respiratory illnesses.
The first is entitled “Prescription for Recovery From Your Viral Respiratory Illness” [download PDF]. Intended to be duplicated and designed with primary care use in mind, it can be customized for specialty use as well.
This “prescription” handout addresses common complaints of fever, pain (eg, sore throat, body aches, headache), cough, congestion (chest, nose, sinuses), and sneezing/runny nose. Clinicians can check off the appropriate treatments for an individual patient, who can use it as a handy reference to purchase the recommended OTC products and/or for selecting products or preparing helpful remedies at home. Blank lines at the bottom provide space for you to write in your OTC preferences and allow you to customize patient instructions.
The second patient handout is entitled “Antibiotics: When You Need Them, When You Don’t, and What to Take When You Don’t” [download PDF]. This focused patient teaching tool offers an overview of
• Viral and bacterial respiratory illnesses and what the patient should do if he or she has one or the other (including when to see a clinician)
• Some helpful OTC and home treatments for symptoms of viral respiratory illnesses
• When antibiotics are indicated and when they’re not—and why
• The serious problems caused by unnecessary use of antibiotics.
This brief guide can be used as a general informational handout that can, for example, be given, mailed, or e-mailed to all adult patients at the start of cold and flu season and retained by them for reference. It can also be provided along with the “prescription” handout to patients with ARTIs who visit your office. In the latter situation, the patient leaves your office with concrete information and guidance for appropriate care of his or her viral respiratory illness—but without a prescription for antibiotics. As with the “prescription” handout, this brief guide may be duplicated or customized as needed.
To download the handouts: Click here.
REFERENCES
1. Lee GC, Reveles KR, Attridge RT, et al. Outpatient antibiotic prescribing in the United States: 2000-2010. BMC Med. 2014;12:96.
2. CDC. Antibiotics: will they work when you really need them? www.cdc.gov/getsmart/healthcare/factsheets/antibiotics.html#MustAct. Accessed August 14, 2014.
3. Shehab N, Patel P, Srinivasan A, Budnitz D. Emergency department visits for antibiotic associated adverse events. Clin Infect Dis. 2008;47:735-743.
4. CDC. Adverse drug events from select medication classes. www.cdc.gov/MedicationSafety/program_focus_activities.html. Accessed August 4, 2014.
5. CDC. Get smart: know when antibiotics work. www.cdc.gov/getsmart/. Accessed August 14, 2014.