User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Preventive treatment delays first seizure onset in tuberous sclerosis complex
according to research presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. This treatment strategy reduces the risk and severity of epilepsy, said the investigators.
As much as 90% of patients with TSC have epilepsy. Seizures generally start during infancy and are often resistant to medication. Clinicians are increasingly able to diagnose TSC prenatally, thus creating an opportunity for pursuing preventive strategies.
In the multicenter EPISTOP trial, Katarzyna Kotulska, MD, head of neurology and epileptology at Children’s Memorial Health Institute in Warsaw, and colleagues compared the efficacy and safety of preventive vigabatrin treatment with those of conventional vigabatrin treatment in infants with TSC. The researchers followed 94 infants with TSC and without a history of seizures with monthly video EEG. Conventional treatment was initiated after the first electrographic or clinical seizure, and preventive treatment was administered when epileptiform discharges were visible on EEG but before the first seizure.
Six sites randomly assigned patients to treatment in a equal groups in a randomized, controlled trial. At four other sites, treatment allocation was fixed in an open-label trial. All patients were followed until age 2 years. The study’s primary endpoint was the time to first clinical seizure.
A total of 53 patients participated in the randomized, controlled trial, and 41 participated in the open-label study; 79 patients completed the study. Of this group, 25 received preventive treatment, 25 received conventional treatment, and 22 patients had seizures before epileptiform activity was detected on EEG. Seven patients had neither seizures nor abnormal EEG.
The time to first clinical seizure was significantly longer in patients who received preventive treatment, compared with those who received conventional treatment. In the randomized, controlled trial, time to first seizure was 364 days in the preventive treatment group and 124 days in the conventional treatment group. In the open-label trial, time to first seizure was 426 days in the preventive treatment group and 106 days in the conventional treatment group.
A pooled analysis indicated that, at 24 months, preventive treatment significantly reduced the risk of clinical seizures (odds ratio, 0.21), drug-resistant epilepsy (OR, 0.23), and infantile spasms (OR, 0). The investigators did not record any adverse events related to preventive treatment.
The study was funded by the 7th Framework Program of the European Union. Dr. Kotulska did not report any disclosures.
SOURCE: Kotulska K et al. CNS-ICNA 2020, Abstract PL13.
according to research presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. This treatment strategy reduces the risk and severity of epilepsy, said the investigators.
As much as 90% of patients with TSC have epilepsy. Seizures generally start during infancy and are often resistant to medication. Clinicians are increasingly able to diagnose TSC prenatally, thus creating an opportunity for pursuing preventive strategies.
In the multicenter EPISTOP trial, Katarzyna Kotulska, MD, head of neurology and epileptology at Children’s Memorial Health Institute in Warsaw, and colleagues compared the efficacy and safety of preventive vigabatrin treatment with those of conventional vigabatrin treatment in infants with TSC. The researchers followed 94 infants with TSC and without a history of seizures with monthly video EEG. Conventional treatment was initiated after the first electrographic or clinical seizure, and preventive treatment was administered when epileptiform discharges were visible on EEG but before the first seizure.
Six sites randomly assigned patients to treatment in a equal groups in a randomized, controlled trial. At four other sites, treatment allocation was fixed in an open-label trial. All patients were followed until age 2 years. The study’s primary endpoint was the time to first clinical seizure.
A total of 53 patients participated in the randomized, controlled trial, and 41 participated in the open-label study; 79 patients completed the study. Of this group, 25 received preventive treatment, 25 received conventional treatment, and 22 patients had seizures before epileptiform activity was detected on EEG. Seven patients had neither seizures nor abnormal EEG.
The time to first clinical seizure was significantly longer in patients who received preventive treatment, compared with those who received conventional treatment. In the randomized, controlled trial, time to first seizure was 364 days in the preventive treatment group and 124 days in the conventional treatment group. In the open-label trial, time to first seizure was 426 days in the preventive treatment group and 106 days in the conventional treatment group.
A pooled analysis indicated that, at 24 months, preventive treatment significantly reduced the risk of clinical seizures (odds ratio, 0.21), drug-resistant epilepsy (OR, 0.23), and infantile spasms (OR, 0). The investigators did not record any adverse events related to preventive treatment.
The study was funded by the 7th Framework Program of the European Union. Dr. Kotulska did not report any disclosures.
SOURCE: Kotulska K et al. CNS-ICNA 2020, Abstract PL13.
according to research presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. This treatment strategy reduces the risk and severity of epilepsy, said the investigators.
As much as 90% of patients with TSC have epilepsy. Seizures generally start during infancy and are often resistant to medication. Clinicians are increasingly able to diagnose TSC prenatally, thus creating an opportunity for pursuing preventive strategies.
In the multicenter EPISTOP trial, Katarzyna Kotulska, MD, head of neurology and epileptology at Children’s Memorial Health Institute in Warsaw, and colleagues compared the efficacy and safety of preventive vigabatrin treatment with those of conventional vigabatrin treatment in infants with TSC. The researchers followed 94 infants with TSC and without a history of seizures with monthly video EEG. Conventional treatment was initiated after the first electrographic or clinical seizure, and preventive treatment was administered when epileptiform discharges were visible on EEG but before the first seizure.
Six sites randomly assigned patients to treatment in a equal groups in a randomized, controlled trial. At four other sites, treatment allocation was fixed in an open-label trial. All patients were followed until age 2 years. The study’s primary endpoint was the time to first clinical seizure.
A total of 53 patients participated in the randomized, controlled trial, and 41 participated in the open-label study; 79 patients completed the study. Of this group, 25 received preventive treatment, 25 received conventional treatment, and 22 patients had seizures before epileptiform activity was detected on EEG. Seven patients had neither seizures nor abnormal EEG.
The time to first clinical seizure was significantly longer in patients who received preventive treatment, compared with those who received conventional treatment. In the randomized, controlled trial, time to first seizure was 364 days in the preventive treatment group and 124 days in the conventional treatment group. In the open-label trial, time to first seizure was 426 days in the preventive treatment group and 106 days in the conventional treatment group.
A pooled analysis indicated that, at 24 months, preventive treatment significantly reduced the risk of clinical seizures (odds ratio, 0.21), drug-resistant epilepsy (OR, 0.23), and infantile spasms (OR, 0). The investigators did not record any adverse events related to preventive treatment.
The study was funded by the 7th Framework Program of the European Union. Dr. Kotulska did not report any disclosures.
SOURCE: Kotulska K et al. CNS-ICNA 2020, Abstract PL13.
FROM CNS-ICNA 2020
Comorbidity burden is greater among children with tics than children with stereotypies
, according to an analysis presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. The former also are younger at their first visit than are the latter. Compared with children with tics, children with stereotypies also have fewer comorbidities and receive fewer recommendations for interventions. This difference between groups may not merely reflect the younger age at presentation of children with stereotypies (e.g., at an age before a comorbidity is manifest). “At least in our population, it does seem to reflect an overall lower burden of comorbidities,” said Shannon Dean, MD, PhD, assistant professor of neurology at the Kennedy Krieger Institute of Johns Hopkins University in Baltimore.

Common pediatric movement disorders
Tics (i.e., short-lasting, sudden, repetitive movements) and stereotypies (i.e., rhythmic, fixed, deliberate, but purposeless movements) are common pediatric movement disorders with favorable prognoses. The disorders share several comorbidities, the most common of which are ADHD, anxiety, and obsessive-compulsive disorder (OCD). Dr. Dean and colleagues examined differences in comorbidity burden, resource use, and need for intervention between children with tics and those with stereotypies.
The investigators performed a retrospective chart review and identified 63 children diagnosed with stereotypies. They matched each of these children, by age when possible, with a child first diagnosed with a chronic or provisional tic disorder during the same year. All patients presented to the University of Rochester (N.Y.) Child Neurology Clinic between 2003 and 2016. Dr. Dean and colleagues excluded children with diagnoses for which stereotypies are considered a secondary feature (e.g., autism, intellectual disability, and blindness). They also excluded children who had tics and stereotypies.
The researchers examined the groups’ total number of visits, comorbidities, and recommended interventions. They also analyzed data from a follow-up survey that were available for 20 of the 63 patients with stereotypies. They tested continuous or discrete variables for normal distribution and used T tests or Mann–Whitney U as appropriate. To analyze categorical data, they used chi squared or Fisher’s exact test for groups smaller than five.
Differing rates of intervention
Children with stereotypies were younger at first visit (mean age, 5.6 years vs. 7.1 years) and at last visit (mean age, 6.5 years vs. 9.8 years) and had fewer total visits (1.8 vs. 4.5), compared with children with tics.
The three most common comorbidities in the population were more prevalent among patients with tics than among patients with stereotypies. The prevalence of ADHD was 27% among patients with stereotypies and 48% among patients with tics. The prevalence of OCD was 8% among children with stereotypies and 41% among children with tics. The prevalence of anxiety was 21% among children with stereotypies and 63% among children with tics. Children with stereotypies also had fewer neuropsychiatric comorbidities overall than did children with tics (0.7 per patient versus 1.9 per patient).
The clinicians had recommended at least one medication for tics in 22% of the children with tics. No medication is available for children with stereotypies. The clinicians recommended behavioral therapy for 13% of the children with tics, but for none of the children with stereotypies, “because none of them had functional impairment that would warrant intervention,” said Dr. Dean. The clinicians also made more recommendations for pharmaceutical and behavioral treatments for comorbidities in patients with tics than in patients with stereotypies.
When the investigators examined the follow-up survey data, they found that patients with stereotypies were older at last contact than patients with tics. Last contact was defined as the time of the survey for patients with stereotypies and the time of the last clinic visit for patients with tics. When Dr. Dean and colleagues examined the three most common comorbidities, however, they again found that the burden was greater among patients with tics (1.5 per patient) than among patients with stereotypies (0.8 per patient).
The study was funded by the T32 Experimental Therapeutics Training Grant from the University of Rochester, N.Y. Dr. Dean did not report any disclosures.
SOURCE: Dean S et al. CNS-ICNA 2020. Abstract PL52.
, according to an analysis presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. The former also are younger at their first visit than are the latter. Compared with children with tics, children with stereotypies also have fewer comorbidities and receive fewer recommendations for interventions. This difference between groups may not merely reflect the younger age at presentation of children with stereotypies (e.g., at an age before a comorbidity is manifest). “At least in our population, it does seem to reflect an overall lower burden of comorbidities,” said Shannon Dean, MD, PhD, assistant professor of neurology at the Kennedy Krieger Institute of Johns Hopkins University in Baltimore.
Common pediatric movement disorders
Tics (i.e., short-lasting, sudden, repetitive movements) and stereotypies (i.e., rhythmic, fixed, deliberate, but purposeless movements) are common pediatric movement disorders with favorable prognoses. The disorders share several comorbidities, the most common of which are ADHD, anxiety, and obsessive-compulsive disorder (OCD). Dr. Dean and colleagues examined differences in comorbidity burden, resource use, and need for intervention between children with tics and those with stereotypies.
The investigators performed a retrospective chart review and identified 63 children diagnosed with stereotypies. They matched each of these children, by age when possible, with a child first diagnosed with a chronic or provisional tic disorder during the same year. All patients presented to the University of Rochester (N.Y.) Child Neurology Clinic between 2003 and 2016. Dr. Dean and colleagues excluded children with diagnoses for which stereotypies are considered a secondary feature (e.g., autism, intellectual disability, and blindness). They also excluded children who had tics and stereotypies.
The researchers examined the groups’ total number of visits, comorbidities, and recommended interventions. They also analyzed data from a follow-up survey that were available for 20 of the 63 patients with stereotypies. They tested continuous or discrete variables for normal distribution and used T tests or Mann–Whitney U as appropriate. To analyze categorical data, they used chi squared or Fisher’s exact test for groups smaller than five.
Differing rates of intervention
Children with stereotypies were younger at first visit (mean age, 5.6 years vs. 7.1 years) and at last visit (mean age, 6.5 years vs. 9.8 years) and had fewer total visits (1.8 vs. 4.5), compared with children with tics.
The three most common comorbidities in the population were more prevalent among patients with tics than among patients with stereotypies. The prevalence of ADHD was 27% among patients with stereotypies and 48% among patients with tics. The prevalence of OCD was 8% among children with stereotypies and 41% among children with tics. The prevalence of anxiety was 21% among children with stereotypies and 63% among children with tics. Children with stereotypies also had fewer neuropsychiatric comorbidities overall than did children with tics (0.7 per patient versus 1.9 per patient).
The clinicians had recommended at least one medication for tics in 22% of the children with tics. No medication is available for children with stereotypies. The clinicians recommended behavioral therapy for 13% of the children with tics, but for none of the children with stereotypies, “because none of them had functional impairment that would warrant intervention,” said Dr. Dean. The clinicians also made more recommendations for pharmaceutical and behavioral treatments for comorbidities in patients with tics than in patients with stereotypies.
When the investigators examined the follow-up survey data, they found that patients with stereotypies were older at last contact than patients with tics. Last contact was defined as the time of the survey for patients with stereotypies and the time of the last clinic visit for patients with tics. When Dr. Dean and colleagues examined the three most common comorbidities, however, they again found that the burden was greater among patients with tics (1.5 per patient) than among patients with stereotypies (0.8 per patient).
The study was funded by the T32 Experimental Therapeutics Training Grant from the University of Rochester, N.Y. Dr. Dean did not report any disclosures.
SOURCE: Dean S et al. CNS-ICNA 2020. Abstract PL52.
, according to an analysis presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. The former also are younger at their first visit than are the latter. Compared with children with tics, children with stereotypies also have fewer comorbidities and receive fewer recommendations for interventions. This difference between groups may not merely reflect the younger age at presentation of children with stereotypies (e.g., at an age before a comorbidity is manifest). “At least in our population, it does seem to reflect an overall lower burden of comorbidities,” said Shannon Dean, MD, PhD, assistant professor of neurology at the Kennedy Krieger Institute of Johns Hopkins University in Baltimore.
Common pediatric movement disorders
Tics (i.e., short-lasting, sudden, repetitive movements) and stereotypies (i.e., rhythmic, fixed, deliberate, but purposeless movements) are common pediatric movement disorders with favorable prognoses. The disorders share several comorbidities, the most common of which are ADHD, anxiety, and obsessive-compulsive disorder (OCD). Dr. Dean and colleagues examined differences in comorbidity burden, resource use, and need for intervention between children with tics and those with stereotypies.
The investigators performed a retrospective chart review and identified 63 children diagnosed with stereotypies. They matched each of these children, by age when possible, with a child first diagnosed with a chronic or provisional tic disorder during the same year. All patients presented to the University of Rochester (N.Y.) Child Neurology Clinic between 2003 and 2016. Dr. Dean and colleagues excluded children with diagnoses for which stereotypies are considered a secondary feature (e.g., autism, intellectual disability, and blindness). They also excluded children who had tics and stereotypies.
The researchers examined the groups’ total number of visits, comorbidities, and recommended interventions. They also analyzed data from a follow-up survey that were available for 20 of the 63 patients with stereotypies. They tested continuous or discrete variables for normal distribution and used T tests or Mann–Whitney U as appropriate. To analyze categorical data, they used chi squared or Fisher’s exact test for groups smaller than five.
Differing rates of intervention
Children with stereotypies were younger at first visit (mean age, 5.6 years vs. 7.1 years) and at last visit (mean age, 6.5 years vs. 9.8 years) and had fewer total visits (1.8 vs. 4.5), compared with children with tics.
The three most common comorbidities in the population were more prevalent among patients with tics than among patients with stereotypies. The prevalence of ADHD was 27% among patients with stereotypies and 48% among patients with tics. The prevalence of OCD was 8% among children with stereotypies and 41% among children with tics. The prevalence of anxiety was 21% among children with stereotypies and 63% among children with tics. Children with stereotypies also had fewer neuropsychiatric comorbidities overall than did children with tics (0.7 per patient versus 1.9 per patient).
The clinicians had recommended at least one medication for tics in 22% of the children with tics. No medication is available for children with stereotypies. The clinicians recommended behavioral therapy for 13% of the children with tics, but for none of the children with stereotypies, “because none of them had functional impairment that would warrant intervention,” said Dr. Dean. The clinicians also made more recommendations for pharmaceutical and behavioral treatments for comorbidities in patients with tics than in patients with stereotypies.
When the investigators examined the follow-up survey data, they found that patients with stereotypies were older at last contact than patients with tics. Last contact was defined as the time of the survey for patients with stereotypies and the time of the last clinic visit for patients with tics. When Dr. Dean and colleagues examined the three most common comorbidities, however, they again found that the burden was greater among patients with tics (1.5 per patient) than among patients with stereotypies (0.8 per patient).
The study was funded by the T32 Experimental Therapeutics Training Grant from the University of Rochester, N.Y. Dr. Dean did not report any disclosures.
SOURCE: Dean S et al. CNS-ICNA 2020. Abstract PL52.
FROM CNS-ICNA 2020
Outpatient visits rebound for most specialties to pre-COVID-19 levels
, according to new data.
Overall visits plunged by almost 60% at the low point in late March and did not start recovering until late June, when visits were still off by 10%. Visits began to rise again – by 2% over the March 1 baseline – around Labor Day.
As of Oct. 4, visits had returned to that March 1 baseline, which was slightly higher than in late February, according to data analyzed by Harvard University, the Commonwealth Fund, and the healthcare technology company Phreesia, which helps medical practices with patient registration, insurance verification, and payments, and has data on 50,000 providers in all 50 states.
The study was published online by the Commonwealth Fund.
In-person visits are still down 6% from the March 1 baseline. Telemedicine visits – which surged in mid-April to account for some 13%-14% of visits – have subsided to 6% of visits.
Many states reopened businesses and lifted travel restrictions in early September, benefiting medical practices in some areas. But clinicians in some regions are still facing rising COVID-19 cases, as well as “the challenges of keeping patients and clinicians safe while also maintaining revenue,” wrote the report authors.
Some specialties are still hard hit. For the week starting Oct. 4, visits to pulmonologists were off 20% from March 1. Otolaryngology visits were down 17%, and behavioral health visits were down 14%. Cardiology, allergy/immunology, neurology, gastroenterology, and endocrinology also saw drops of 5%-10% from March.
Patients were flocking to dermatologists, however. Visits were up 17% over baseline. Primary care also was popular, with a 13% increase over March 1.
At the height of the pandemic shutdown in late March, Medicare beneficiaries stayed away from doctors the most. Visits dipped 63%, compared with 56% for the commercially insured, and 52% for those on Medicaid. Now, Medicare visits are up 3% over baseline, while Medicaid visits are down 1% and commercially insured visits have risen 1% from March.
The over-65 age group did not have the steepest drop in visits when analyzed by age. Children aged 3-17 years saw the biggest decline at the height of the shutdown. Infants to 5-year-olds have still not returned to prepandemic visit levels. Those visits are off by 10%-18%. The 65-and-older group is up 4% from March.
Larger practices – with more than six clinicians – have seen the biggest rebound, after having had the largest dip in visits, from a decline of 53% in late March to a 14% rise over that baseline. Practices with fewer than five clinicians are still 6% down from the March baseline.
Wide variation in telemedicine use
The researchers reported a massive gap in the percentage of various specialties that are using telemedicine. At the top end are behavioral health specialists, where 41% of visits are by telemedicine.
The next-closest specialty is endocrinology, which has 14% of visits via telemedicine, on par with rheumatology, neurology, and gastroenterology. At the low end: ophthalmology, with zero virtual visits; otolaryngology (1%), orthopedics (1%), surgery (2%), and dermatology and ob.gyn., both at 3%.
Smaller practices – with fewer than five clinicians – never adopted telemedicine at the rate of the larger practices. During the mid-April peak, about 10% of the smaller practices were using telemedicine in adult primary care practices, compared with 19% of those primary care practices with more than six clinicians.
The gap persists. Currently, 9% of the larger practices are using telemedicine, compared with 4% of small practices.
One-third of all provider organizations analyzed never-adopted telemedicine. And while use continues, it is now mostly minimal. At the April peak, 35% of the practices with telemedicine reported heavy use – that is, in more than 20% of visits. In September, 9% said they had such heavy use.
A version of this article originally appeared on Medscape.com.
, according to new data.
Overall visits plunged by almost 60% at the low point in late March and did not start recovering until late June, when visits were still off by 10%. Visits began to rise again – by 2% over the March 1 baseline – around Labor Day.
As of Oct. 4, visits had returned to that March 1 baseline, which was slightly higher than in late February, according to data analyzed by Harvard University, the Commonwealth Fund, and the healthcare technology company Phreesia, which helps medical practices with patient registration, insurance verification, and payments, and has data on 50,000 providers in all 50 states.
The study was published online by the Commonwealth Fund.
In-person visits are still down 6% from the March 1 baseline. Telemedicine visits – which surged in mid-April to account for some 13%-14% of visits – have subsided to 6% of visits.
Many states reopened businesses and lifted travel restrictions in early September, benefiting medical practices in some areas. But clinicians in some regions are still facing rising COVID-19 cases, as well as “the challenges of keeping patients and clinicians safe while also maintaining revenue,” wrote the report authors.
Some specialties are still hard hit. For the week starting Oct. 4, visits to pulmonologists were off 20% from March 1. Otolaryngology visits were down 17%, and behavioral health visits were down 14%. Cardiology, allergy/immunology, neurology, gastroenterology, and endocrinology also saw drops of 5%-10% from March.
Patients were flocking to dermatologists, however. Visits were up 17% over baseline. Primary care also was popular, with a 13% increase over March 1.
At the height of the pandemic shutdown in late March, Medicare beneficiaries stayed away from doctors the most. Visits dipped 63%, compared with 56% for the commercially insured, and 52% for those on Medicaid. Now, Medicare visits are up 3% over baseline, while Medicaid visits are down 1% and commercially insured visits have risen 1% from March.
The over-65 age group did not have the steepest drop in visits when analyzed by age. Children aged 3-17 years saw the biggest decline at the height of the shutdown. Infants to 5-year-olds have still not returned to prepandemic visit levels. Those visits are off by 10%-18%. The 65-and-older group is up 4% from March.
Larger practices – with more than six clinicians – have seen the biggest rebound, after having had the largest dip in visits, from a decline of 53% in late March to a 14% rise over that baseline. Practices with fewer than five clinicians are still 6% down from the March baseline.
Wide variation in telemedicine use
The researchers reported a massive gap in the percentage of various specialties that are using telemedicine. At the top end are behavioral health specialists, where 41% of visits are by telemedicine.
The next-closest specialty is endocrinology, which has 14% of visits via telemedicine, on par with rheumatology, neurology, and gastroenterology. At the low end: ophthalmology, with zero virtual visits; otolaryngology (1%), orthopedics (1%), surgery (2%), and dermatology and ob.gyn., both at 3%.
Smaller practices – with fewer than five clinicians – never adopted telemedicine at the rate of the larger practices. During the mid-April peak, about 10% of the smaller practices were using telemedicine in adult primary care practices, compared with 19% of those primary care practices with more than six clinicians.
The gap persists. Currently, 9% of the larger practices are using telemedicine, compared with 4% of small practices.
One-third of all provider organizations analyzed never-adopted telemedicine. And while use continues, it is now mostly minimal. At the April peak, 35% of the practices with telemedicine reported heavy use – that is, in more than 20% of visits. In September, 9% said they had such heavy use.
A version of this article originally appeared on Medscape.com.
, according to new data.
Overall visits plunged by almost 60% at the low point in late March and did not start recovering until late June, when visits were still off by 10%. Visits began to rise again – by 2% over the March 1 baseline – around Labor Day.
As of Oct. 4, visits had returned to that March 1 baseline, which was slightly higher than in late February, according to data analyzed by Harvard University, the Commonwealth Fund, and the healthcare technology company Phreesia, which helps medical practices with patient registration, insurance verification, and payments, and has data on 50,000 providers in all 50 states.
The study was published online by the Commonwealth Fund.
In-person visits are still down 6% from the March 1 baseline. Telemedicine visits – which surged in mid-April to account for some 13%-14% of visits – have subsided to 6% of visits.
Many states reopened businesses and lifted travel restrictions in early September, benefiting medical practices in some areas. But clinicians in some regions are still facing rising COVID-19 cases, as well as “the challenges of keeping patients and clinicians safe while also maintaining revenue,” wrote the report authors.
Some specialties are still hard hit. For the week starting Oct. 4, visits to pulmonologists were off 20% from March 1. Otolaryngology visits were down 17%, and behavioral health visits were down 14%. Cardiology, allergy/immunology, neurology, gastroenterology, and endocrinology also saw drops of 5%-10% from March.
Patients were flocking to dermatologists, however. Visits were up 17% over baseline. Primary care also was popular, with a 13% increase over March 1.
At the height of the pandemic shutdown in late March, Medicare beneficiaries stayed away from doctors the most. Visits dipped 63%, compared with 56% for the commercially insured, and 52% for those on Medicaid. Now, Medicare visits are up 3% over baseline, while Medicaid visits are down 1% and commercially insured visits have risen 1% from March.
The over-65 age group did not have the steepest drop in visits when analyzed by age. Children aged 3-17 years saw the biggest decline at the height of the shutdown. Infants to 5-year-olds have still not returned to prepandemic visit levels. Those visits are off by 10%-18%. The 65-and-older group is up 4% from March.
Larger practices – with more than six clinicians – have seen the biggest rebound, after having had the largest dip in visits, from a decline of 53% in late March to a 14% rise over that baseline. Practices with fewer than five clinicians are still 6% down from the March baseline.
Wide variation in telemedicine use
The researchers reported a massive gap in the percentage of various specialties that are using telemedicine. At the top end are behavioral health specialists, where 41% of visits are by telemedicine.
The next-closest specialty is endocrinology, which has 14% of visits via telemedicine, on par with rheumatology, neurology, and gastroenterology. At the low end: ophthalmology, with zero virtual visits; otolaryngology (1%), orthopedics (1%), surgery (2%), and dermatology and ob.gyn., both at 3%.
Smaller practices – with fewer than five clinicians – never adopted telemedicine at the rate of the larger practices. During the mid-April peak, about 10% of the smaller practices were using telemedicine in adult primary care practices, compared with 19% of those primary care practices with more than six clinicians.
The gap persists. Currently, 9% of the larger practices are using telemedicine, compared with 4% of small practices.
One-third of all provider organizations analyzed never-adopted telemedicine. And while use continues, it is now mostly minimal. At the April peak, 35% of the practices with telemedicine reported heavy use – that is, in more than 20% of visits. In September, 9% said they had such heavy use.
A version of this article originally appeared on Medscape.com.
Teen vaping in the time of COVID-19
It’s an electronic cigarette maker’s dream, but a public health nightmare: The confluence of social isolation and anxiety resulting from the COVID-19 pandemic has the potential to make recent progress against e-cigarette use among teens go up in smoke.

“Stress and worsening mental health issues are well-known predisposing factors for smoking, both in quantity and frequency and in relapse,” said Mary Cataletto, MD, FCCP, clinical professor of pediatrics at New York University Winthrop Hospital, Mineola, during a webinar on e-cigarettes and vaping with asthma in the time of COVID-19, hosted by the Allergy & Asthma Network.
Prior to the pandemic, public health experts appeared to be making inroads into curbing e-cigarette use, according to results of the 2020 National Youth Tobacco Survey, a cross-sectional school-based survey of students from grades 6 to 12.
“In 2020, approximately 1 in 5 high school students and 1 in 20 middle school students currently used e-cigarettes. By comparison, in 2019, 27.5% of high school students (4.11 million) and 10.5% of middle school students (1.24 million) reported current e-cigarette use,” wrote Brian A. King, PhD, MPH, and colleagues, in an article reporting those results.
“We definitely believe that there was a real decline that occurred up until March. Those data from the National Youth Tobacco Survey were collected prior to youth leaving school settings and prior to the implementation of social distancing and other measures,” said Dr. King, deputy director for research translation in the Office on Smoking and Health within the National Center for Chronic Disease Prevention and Health Promotion at the Centers for Disease Control and Prevention.
“That said, the jury’s still out on what’s going to happen with youth use during the coming year, particularly during the COVID-19 pandemic” he said in an interview.
Flavor of the moment
Even though the data through March 2020 showed a distinct decline in e-cigarette use, Dr. King and colleagues found that 3.6 million U.S. adolescents still currently used e-cigarettes in 2020; among current users, more than 80% reported using flavored e-cigarettes.
Dr. Cataletto said in an interview that the 2020 National Youth Tobacco Survey continues to report widespread use of flavored e-cigarettes among young smokers despite Food and Drug Administration admonitions to manufacturers and retailers to remove unauthorized e-cigarettes from the market.
On Jan. 2, 2020, the FDA reported a finalized enforcement policy directed against “unauthorized flavored cartridge-based e-cigarettes that appeal to children, including fruit and mint.”
But as Dr. King and other investigators also mentioned in a separate analysis of e-cigarette unit sales, that enforcement policy applies only to prefilled cartridge e-cigarette products, such as those made by JUUL, and that while sales of mint- or fruit-flavored products of this type declined from September 2014 to May 2020, there was an increase in the sale of disposable e-cigarettes with flavors other than menthol or tobacco.
Dr. Cataletto pointed out that this vaping trend has coincided with the COVID-19 pandemic, noting that, on March 13, 2020, just 2 days after the World Health Organization declared that spread of COVID-19 was officially a pandemic, 16 states closed schools, leaving millions of middle school– and high school–age children at loose ends. She said: “This raised a number of concerns. Would students who used e-cigarettes be at increased risk of COVID-19? Would e-cigarette use increase again due to the social isolation and anxiety as predicted for tobacco smokers? How would access and availability impact e-cigarette use?
“It’s possible that use may go down, because youth may have less access to their typical social sources or other manners in which they obtain the product.” Dr. King said. “Alternatively, youth may have more disposable time on their hands and may be open to other sources of access to these products, and so use could increase.”
There is evidence to suggest that the latter scenario may be true, according to investigators who surveyed more than 1,000 Canadian adolescents about alcohol use, binge drinking, cannabis use, and vaping in the 3 weeks directly before and after social distancing measures took effect.
The investigators found that the frequency of both alcohol and cannabis use increased during social isolation, and that, although about half of respondents reported solitary substance use, 32% reported using substances with peers via technology, and 24% reported using substances face to face, despite social distancing mandates, reported Tara M. Dumas, PhD, from Huron University College, London, Ont.
“These authors suggest that teens who feared loss of friendships during quarantine might be more willing to engage in risky behaviors such as face to face substance use to maintain social status, while solitary substance use was related to both COVID19 fears and depressive symptomatology,” Dr. Cataletto said.
E-cigarettes and COVID-19
A recent survey of 4,351 adolescents and young adults in the United States showed that a COVID-19 diagnosis was five times more likely among those who had ever used e-cigarettes, seven times more likely among conventional cigarette and e-cigarette uses, and nearly seven times more likely among those who had used both within the past 30 days .
Perhaps not surprisingly, adolescents and young adults with asthma who also vape may be at especially high risk for COVID-19, but the exact effect may be hard to pin down with current levels of evidence.
“Prior to the pandemic we did see both new-onset asthma and asthma exacerbations in teens who reported either vaping or dual use with tobacco products,” Dr. Cataletto said. “However, numbers were small, were confounded by the bias of subspecialty practice, and the onset of the pandemic, which affected not only face-to-face visits but the opportunity to perform pulmonary function testing for a number of months.”
Dr. King noted: “There is an emerging body of science that does indicate that there could be some respiratory risks related to e-cigarette use, particularly among certain populations. ... That said, there’s no conclusive link between e-cigarette use and specific disease outcomes, which typically requires a robust body of different science conducted in multiple settings.”
He said that e-cigarette vapors contain ultrafine particles and heavy metals that can be inhaled deeply into the lungs, both of which have previously been associated with respiratory risk, including complications from asthma.
An ounce of prevention
“When it comes to cessation, we do know that about 50% of youth who are using tobacco products including e-cigarettes, want to quit, and about the same proportion make an effort to quit, so there’s certainly a will there, but we don’t clearly have an evidence-based way,” Dr. King said.
Combinations of behavioral interventions including face-to-face consultations and digital or telephone support can be helpful, Dr. Cataletto said, but both she and Dr. King agree that prevention is the most effective method of reducing e-cigarette use among teens and young adults, including peer support and education efforts.
Asked how she gets her patients to report honestly about their habits, Dr. Cataletto acknowledged that “this is a challenge for many kids. Some are unaware that many of the commercially available e-cigarette products contain nicotine and they are not ‘just vaping flavoring.’ Ongoing education is important, and it is happening in schools, in pediatrician’s offices, at home and in the community.”
Dr. Cataletto and Dr. King reported no relevant conflicts of interest. Dr. Cataletto serves on the editorial advisory board for Chest Physician.
It’s an electronic cigarette maker’s dream, but a public health nightmare: The confluence of social isolation and anxiety resulting from the COVID-19 pandemic has the potential to make recent progress against e-cigarette use among teens go up in smoke.
“Stress and worsening mental health issues are well-known predisposing factors for smoking, both in quantity and frequency and in relapse,” said Mary Cataletto, MD, FCCP, clinical professor of pediatrics at New York University Winthrop Hospital, Mineola, during a webinar on e-cigarettes and vaping with asthma in the time of COVID-19, hosted by the Allergy & Asthma Network.
Prior to the pandemic, public health experts appeared to be making inroads into curbing e-cigarette use, according to results of the 2020 National Youth Tobacco Survey, a cross-sectional school-based survey of students from grades 6 to 12.
“In 2020, approximately 1 in 5 high school students and 1 in 20 middle school students currently used e-cigarettes. By comparison, in 2019, 27.5% of high school students (4.11 million) and 10.5% of middle school students (1.24 million) reported current e-cigarette use,” wrote Brian A. King, PhD, MPH, and colleagues, in an article reporting those results.
“We definitely believe that there was a real decline that occurred up until March. Those data from the National Youth Tobacco Survey were collected prior to youth leaving school settings and prior to the implementation of social distancing and other measures,” said Dr. King, deputy director for research translation in the Office on Smoking and Health within the National Center for Chronic Disease Prevention and Health Promotion at the Centers for Disease Control and Prevention.
“That said, the jury’s still out on what’s going to happen with youth use during the coming year, particularly during the COVID-19 pandemic” he said in an interview.
Flavor of the moment
Even though the data through March 2020 showed a distinct decline in e-cigarette use, Dr. King and colleagues found that 3.6 million U.S. adolescents still currently used e-cigarettes in 2020; among current users, more than 80% reported using flavored e-cigarettes.
Dr. Cataletto said in an interview that the 2020 National Youth Tobacco Survey continues to report widespread use of flavored e-cigarettes among young smokers despite Food and Drug Administration admonitions to manufacturers and retailers to remove unauthorized e-cigarettes from the market.
On Jan. 2, 2020, the FDA reported a finalized enforcement policy directed against “unauthorized flavored cartridge-based e-cigarettes that appeal to children, including fruit and mint.”
But as Dr. King and other investigators also mentioned in a separate analysis of e-cigarette unit sales, that enforcement policy applies only to prefilled cartridge e-cigarette products, such as those made by JUUL, and that while sales of mint- or fruit-flavored products of this type declined from September 2014 to May 2020, there was an increase in the sale of disposable e-cigarettes with flavors other than menthol or tobacco.
Dr. Cataletto pointed out that this vaping trend has coincided with the COVID-19 pandemic, noting that, on March 13, 2020, just 2 days after the World Health Organization declared that spread of COVID-19 was officially a pandemic, 16 states closed schools, leaving millions of middle school– and high school–age children at loose ends. She said: “This raised a number of concerns. Would students who used e-cigarettes be at increased risk of COVID-19? Would e-cigarette use increase again due to the social isolation and anxiety as predicted for tobacco smokers? How would access and availability impact e-cigarette use?
“It’s possible that use may go down, because youth may have less access to their typical social sources or other manners in which they obtain the product.” Dr. King said. “Alternatively, youth may have more disposable time on their hands and may be open to other sources of access to these products, and so use could increase.”
There is evidence to suggest that the latter scenario may be true, according to investigators who surveyed more than 1,000 Canadian adolescents about alcohol use, binge drinking, cannabis use, and vaping in the 3 weeks directly before and after social distancing measures took effect.
The investigators found that the frequency of both alcohol and cannabis use increased during social isolation, and that, although about half of respondents reported solitary substance use, 32% reported using substances with peers via technology, and 24% reported using substances face to face, despite social distancing mandates, reported Tara M. Dumas, PhD, from Huron University College, London, Ont.
“These authors suggest that teens who feared loss of friendships during quarantine might be more willing to engage in risky behaviors such as face to face substance use to maintain social status, while solitary substance use was related to both COVID19 fears and depressive symptomatology,” Dr. Cataletto said.
E-cigarettes and COVID-19
A recent survey of 4,351 adolescents and young adults in the United States showed that a COVID-19 diagnosis was five times more likely among those who had ever used e-cigarettes, seven times more likely among conventional cigarette and e-cigarette uses, and nearly seven times more likely among those who had used both within the past 30 days .
Perhaps not surprisingly, adolescents and young adults with asthma who also vape may be at especially high risk for COVID-19, but the exact effect may be hard to pin down with current levels of evidence.
“Prior to the pandemic we did see both new-onset asthma and asthma exacerbations in teens who reported either vaping or dual use with tobacco products,” Dr. Cataletto said. “However, numbers were small, were confounded by the bias of subspecialty practice, and the onset of the pandemic, which affected not only face-to-face visits but the opportunity to perform pulmonary function testing for a number of months.”
Dr. King noted: “There is an emerging body of science that does indicate that there could be some respiratory risks related to e-cigarette use, particularly among certain populations. ... That said, there’s no conclusive link between e-cigarette use and specific disease outcomes, which typically requires a robust body of different science conducted in multiple settings.”
He said that e-cigarette vapors contain ultrafine particles and heavy metals that can be inhaled deeply into the lungs, both of which have previously been associated with respiratory risk, including complications from asthma.
An ounce of prevention
“When it comes to cessation, we do know that about 50% of youth who are using tobacco products including e-cigarettes, want to quit, and about the same proportion make an effort to quit, so there’s certainly a will there, but we don’t clearly have an evidence-based way,” Dr. King said.
Combinations of behavioral interventions including face-to-face consultations and digital or telephone support can be helpful, Dr. Cataletto said, but both she and Dr. King agree that prevention is the most effective method of reducing e-cigarette use among teens and young adults, including peer support and education efforts.
Asked how she gets her patients to report honestly about their habits, Dr. Cataletto acknowledged that “this is a challenge for many kids. Some are unaware that many of the commercially available e-cigarette products contain nicotine and they are not ‘just vaping flavoring.’ Ongoing education is important, and it is happening in schools, in pediatrician’s offices, at home and in the community.”
Dr. Cataletto and Dr. King reported no relevant conflicts of interest. Dr. Cataletto serves on the editorial advisory board for Chest Physician.
It’s an electronic cigarette maker’s dream, but a public health nightmare: The confluence of social isolation and anxiety resulting from the COVID-19 pandemic has the potential to make recent progress against e-cigarette use among teens go up in smoke.
“Stress and worsening mental health issues are well-known predisposing factors for smoking, both in quantity and frequency and in relapse,” said Mary Cataletto, MD, FCCP, clinical professor of pediatrics at New York University Winthrop Hospital, Mineola, during a webinar on e-cigarettes and vaping with asthma in the time of COVID-19, hosted by the Allergy & Asthma Network.
Prior to the pandemic, public health experts appeared to be making inroads into curbing e-cigarette use, according to results of the 2020 National Youth Tobacco Survey, a cross-sectional school-based survey of students from grades 6 to 12.
“In 2020, approximately 1 in 5 high school students and 1 in 20 middle school students currently used e-cigarettes. By comparison, in 2019, 27.5% of high school students (4.11 million) and 10.5% of middle school students (1.24 million) reported current e-cigarette use,” wrote Brian A. King, PhD, MPH, and colleagues, in an article reporting those results.
“We definitely believe that there was a real decline that occurred up until March. Those data from the National Youth Tobacco Survey were collected prior to youth leaving school settings and prior to the implementation of social distancing and other measures,” said Dr. King, deputy director for research translation in the Office on Smoking and Health within the National Center for Chronic Disease Prevention and Health Promotion at the Centers for Disease Control and Prevention.
“That said, the jury’s still out on what’s going to happen with youth use during the coming year, particularly during the COVID-19 pandemic” he said in an interview.
Flavor of the moment
Even though the data through March 2020 showed a distinct decline in e-cigarette use, Dr. King and colleagues found that 3.6 million U.S. adolescents still currently used e-cigarettes in 2020; among current users, more than 80% reported using flavored e-cigarettes.
Dr. Cataletto said in an interview that the 2020 National Youth Tobacco Survey continues to report widespread use of flavored e-cigarettes among young smokers despite Food and Drug Administration admonitions to manufacturers and retailers to remove unauthorized e-cigarettes from the market.
On Jan. 2, 2020, the FDA reported a finalized enforcement policy directed against “unauthorized flavored cartridge-based e-cigarettes that appeal to children, including fruit and mint.”
But as Dr. King and other investigators also mentioned in a separate analysis of e-cigarette unit sales, that enforcement policy applies only to prefilled cartridge e-cigarette products, such as those made by JUUL, and that while sales of mint- or fruit-flavored products of this type declined from September 2014 to May 2020, there was an increase in the sale of disposable e-cigarettes with flavors other than menthol or tobacco.
Dr. Cataletto pointed out that this vaping trend has coincided with the COVID-19 pandemic, noting that, on March 13, 2020, just 2 days after the World Health Organization declared that spread of COVID-19 was officially a pandemic, 16 states closed schools, leaving millions of middle school– and high school–age children at loose ends. She said: “This raised a number of concerns. Would students who used e-cigarettes be at increased risk of COVID-19? Would e-cigarette use increase again due to the social isolation and anxiety as predicted for tobacco smokers? How would access and availability impact e-cigarette use?
“It’s possible that use may go down, because youth may have less access to their typical social sources or other manners in which they obtain the product.” Dr. King said. “Alternatively, youth may have more disposable time on their hands and may be open to other sources of access to these products, and so use could increase.”
There is evidence to suggest that the latter scenario may be true, according to investigators who surveyed more than 1,000 Canadian adolescents about alcohol use, binge drinking, cannabis use, and vaping in the 3 weeks directly before and after social distancing measures took effect.
The investigators found that the frequency of both alcohol and cannabis use increased during social isolation, and that, although about half of respondents reported solitary substance use, 32% reported using substances with peers via technology, and 24% reported using substances face to face, despite social distancing mandates, reported Tara M. Dumas, PhD, from Huron University College, London, Ont.
“These authors suggest that teens who feared loss of friendships during quarantine might be more willing to engage in risky behaviors such as face to face substance use to maintain social status, while solitary substance use was related to both COVID19 fears and depressive symptomatology,” Dr. Cataletto said.
E-cigarettes and COVID-19
A recent survey of 4,351 adolescents and young adults in the United States showed that a COVID-19 diagnosis was five times more likely among those who had ever used e-cigarettes, seven times more likely among conventional cigarette and e-cigarette uses, and nearly seven times more likely among those who had used both within the past 30 days .
Perhaps not surprisingly, adolescents and young adults with asthma who also vape may be at especially high risk for COVID-19, but the exact effect may be hard to pin down with current levels of evidence.
“Prior to the pandemic we did see both new-onset asthma and asthma exacerbations in teens who reported either vaping or dual use with tobacco products,” Dr. Cataletto said. “However, numbers were small, were confounded by the bias of subspecialty practice, and the onset of the pandemic, which affected not only face-to-face visits but the opportunity to perform pulmonary function testing for a number of months.”
Dr. King noted: “There is an emerging body of science that does indicate that there could be some respiratory risks related to e-cigarette use, particularly among certain populations. ... That said, there’s no conclusive link between e-cigarette use and specific disease outcomes, which typically requires a robust body of different science conducted in multiple settings.”
He said that e-cigarette vapors contain ultrafine particles and heavy metals that can be inhaled deeply into the lungs, both of which have previously been associated with respiratory risk, including complications from asthma.
An ounce of prevention
“When it comes to cessation, we do know that about 50% of youth who are using tobacco products including e-cigarettes, want to quit, and about the same proportion make an effort to quit, so there’s certainly a will there, but we don’t clearly have an evidence-based way,” Dr. King said.
Combinations of behavioral interventions including face-to-face consultations and digital or telephone support can be helpful, Dr. Cataletto said, but both she and Dr. King agree that prevention is the most effective method of reducing e-cigarette use among teens and young adults, including peer support and education efforts.
Asked how she gets her patients to report honestly about their habits, Dr. Cataletto acknowledged that “this is a challenge for many kids. Some are unaware that many of the commercially available e-cigarette products contain nicotine and they are not ‘just vaping flavoring.’ Ongoing education is important, and it is happening in schools, in pediatrician’s offices, at home and in the community.”
Dr. Cataletto and Dr. King reported no relevant conflicts of interest. Dr. Cataletto serves on the editorial advisory board for Chest Physician.
EMA panel backs peanut allergy desensitizing powder Palforzia
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
When the only clinical choices are ‘lose-lose’
Among the many tolls inflicted on health care workers by COVID-19 is one that is not as easily measured as rates of death or disease, but is no less tangible: moral injury. This is the term by which we describe the psychological, social, and spiritual impact of high-stakes situations that lead to the betrayal or transgression of our own deeply held moral beliefs and values.

The current pandemic has provided innumerable such situations that can increase the risk for moral injury, whether we deal directly with patients infected by the coronavirus or not. Telling family members they cannot visit critically ill loved ones. Delaying code activities, even momentarily, to get fully protected with personal protective equipment. Seeing patients who have delayed their necessary or preventive care. Using video rather than touch to reassure people.
Knowing that we are following guidelines from the Centers for Disease Control and Prevention does not stop our feelings of guilt. The longer this pandemic goes on, the more likely it is that these situations will begin to take a toll on us.
For most of us, being exposed to moral injuries is new; they have historically been most associated with severe traumatic wartime experiences. Soldiers, philosophers, and writers have described the ethical dilemmas inherent in war for as long as recorded history. But the use of this term is a more recent development, which the Moral Injury Project at Syracuse (N.Y.) University describes as probably originating in the Vietnam War–era writings of veteran and peace activist Camillo “Mac” Bica and psychiatrist Jonathan Shay. Examples of wartime events that have been thought to lead to moral injury include: causing the harm or death of civilians, knowingly but without alternatives, or accidentally; failing to provide medical aid to an injured civilian or service member; and following orders that were illegal, immoral, and/or against the rules of engagement or the Geneva Conventions.
However, the occurrence of moral injuries in modern health care is increasingly being reported, primarily as an adverse effect of health care inefficiencies that can contribute to burnout. COVID-19 has now provided an array of additional stressors that can cause moral injuries among health care workers. A recent guidance document on moral injury published by the American Psychiatric Association noted that, in the context of a public health disaster, such as COVID-19, it is sometimes necessary to transition from ordinary standards of care to those more appropriate in a crisis, as in wartime. This forces us all to confront challenging questions for which there may be no clear answers, and to make “lose-lose” choices in which no one involved – patients, family, or clinicians – ends up feeling satisfied or even comfortable.
Our lives have been altered significantly, and for many, completely turned upside down by enormous sacrifices and tragic losses. Globally, physicians account for over half of healthcare worker deaths. In the United States alone, over 900 health care workers have died of COVID-19.
Most of us have felt the symptoms of moral injury: frustration, anger, disgust, guilt. A recent report describes three levels of stressors in health care occurring during the pandemic, which are not dissimilar to those wartime events described previously.
- Severe moral stressors, such as the denial of treatment to a COVID-19 patient owing to lack of resources, the inability to provide optimal care to non–COVID-19 patients for many reasons, and concern about passing COVID to loved ones.
- Moderate moral stressors, such as preventing visitors, especially to dying patients, triaging patients for healthcare services with inadequate information, and trying to solve the tension between the need for self-preservation and the need to treat.
- Lower-level but common moral challenges, especially in the community – for example, seeing others not protecting the community by hoarding food, gathering for large parties, and not social distancing or wearing masks. Such stressors lead to frustration and contempt, especially from healthcare workers making personal sacrifices and who may be at risk for infection caused by these behaviors.
Every one of us is affected by these stressors. I certainly am.
What are the outcomes? We know that moral injuries are a risk factor for the development of mental health problems and burnout, and not surprisingly we are seeing that mental health problems, suicidality, and substance use disorders have increased markedly during COVID-19, as recently detailed by the CDC.

Common emotions that occur in response to moral injuries are: feelings of guilt, shame, anger, sadness, anxiety, and disgust; intrapersonal outcomes, including lowered self-esteem, high self-criticism, and beliefs about being bad, damaged, unworthy, failing, or weak; interpersonal outcomes, including loss of faith in people, avoidance of intimacy, and lack of trust in authority figures; and existential and spiritual outcomes, including loss of faith in previous religious beliefs and no longer believing in a just world.
Moral injuries tend to originate primarily from systems-based problems, as we have seen with the lack of concerted national approaches to the pandemic. On the positive side, solutions typically also involve systems-based changes, which in this case may mean changes in leadership styles nationally and locally, as well as changes in the culture of medicine and the way healthcare is practiced and managed in the modern era. We are starting to see some of those changes with the increased use of telemedicine and health technologies, as well as more of a focus on the well-being of health care workers, now deemed “essential.”
As individuals, we are not helpless. There are things we can do in our workplaces to create change. I suggest:
- Acknowledge that you, like me, are affected by these stressors. This is not a secret, and you should not be ashamed of your feelings.
- Talk with your colleagues, loved ones, and friends about how you and they are affected. You are not alone. Encourage others to share their thoughts, stories, and feelings.
- Put this topic on your meeting and departmental agendas and discuss these moral issues openly with your colleagues. Allow sufficient time to engage in open dialogue.
- Work out ways of assisting those who are in high-risk situations, especially for moderate to severe injuries. Be supportive toward those affected.
- Modify policies and change rosters and rotate staff between high- and low-stress roles. Protect and support at-risk colleagues.
- Think about difficult ethical decisions in advance so they can be made by groups, not individuals, and certainly not “on the fly.”
- Keep everyone in your workplace constantly informed, especially of impending staff or equipment shortages.
- Maintain your inherent self-care and resilience with rest, good nutrition, sleep, exercise, love, caring, socialization, and work-life balance.
- Be prepared to access the many professional support services available in our community if you are intensely distressed or if the above suggestions are not enough.
Remember, we are in this together and will find strength in each other. This too will pass.
This article first appeared on Medscape.com.
Among the many tolls inflicted on health care workers by COVID-19 is one that is not as easily measured as rates of death or disease, but is no less tangible: moral injury. This is the term by which we describe the psychological, social, and spiritual impact of high-stakes situations that lead to the betrayal or transgression of our own deeply held moral beliefs and values.
The current pandemic has provided innumerable such situations that can increase the risk for moral injury, whether we deal directly with patients infected by the coronavirus or not. Telling family members they cannot visit critically ill loved ones. Delaying code activities, even momentarily, to get fully protected with personal protective equipment. Seeing patients who have delayed their necessary or preventive care. Using video rather than touch to reassure people.
Knowing that we are following guidelines from the Centers for Disease Control and Prevention does not stop our feelings of guilt. The longer this pandemic goes on, the more likely it is that these situations will begin to take a toll on us.
For most of us, being exposed to moral injuries is new; they have historically been most associated with severe traumatic wartime experiences. Soldiers, philosophers, and writers have described the ethical dilemmas inherent in war for as long as recorded history. But the use of this term is a more recent development, which the Moral Injury Project at Syracuse (N.Y.) University describes as probably originating in the Vietnam War–era writings of veteran and peace activist Camillo “Mac” Bica and psychiatrist Jonathan Shay. Examples of wartime events that have been thought to lead to moral injury include: causing the harm or death of civilians, knowingly but without alternatives, or accidentally; failing to provide medical aid to an injured civilian or service member; and following orders that were illegal, immoral, and/or against the rules of engagement or the Geneva Conventions.
However, the occurrence of moral injuries in modern health care is increasingly being reported, primarily as an adverse effect of health care inefficiencies that can contribute to burnout. COVID-19 has now provided an array of additional stressors that can cause moral injuries among health care workers. A recent guidance document on moral injury published by the American Psychiatric Association noted that, in the context of a public health disaster, such as COVID-19, it is sometimes necessary to transition from ordinary standards of care to those more appropriate in a crisis, as in wartime. This forces us all to confront challenging questions for which there may be no clear answers, and to make “lose-lose” choices in which no one involved – patients, family, or clinicians – ends up feeling satisfied or even comfortable.
Our lives have been altered significantly, and for many, completely turned upside down by enormous sacrifices and tragic losses. Globally, physicians account for over half of healthcare worker deaths. In the United States alone, over 900 health care workers have died of COVID-19.
Most of us have felt the symptoms of moral injury: frustration, anger, disgust, guilt. A recent report describes three levels of stressors in health care occurring during the pandemic, which are not dissimilar to those wartime events described previously.
- Severe moral stressors, such as the denial of treatment to a COVID-19 patient owing to lack of resources, the inability to provide optimal care to non–COVID-19 patients for many reasons, and concern about passing COVID to loved ones.
- Moderate moral stressors, such as preventing visitors, especially to dying patients, triaging patients for healthcare services with inadequate information, and trying to solve the tension between the need for self-preservation and the need to treat.
- Lower-level but common moral challenges, especially in the community – for example, seeing others not protecting the community by hoarding food, gathering for large parties, and not social distancing or wearing masks. Such stressors lead to frustration and contempt, especially from healthcare workers making personal sacrifices and who may be at risk for infection caused by these behaviors.
Every one of us is affected by these stressors. I certainly am.
What are the outcomes? We know that moral injuries are a risk factor for the development of mental health problems and burnout, and not surprisingly we are seeing that mental health problems, suicidality, and substance use disorders have increased markedly during COVID-19, as recently detailed by the CDC.
Common emotions that occur in response to moral injuries are: feelings of guilt, shame, anger, sadness, anxiety, and disgust; intrapersonal outcomes, including lowered self-esteem, high self-criticism, and beliefs about being bad, damaged, unworthy, failing, or weak; interpersonal outcomes, including loss of faith in people, avoidance of intimacy, and lack of trust in authority figures; and existential and spiritual outcomes, including loss of faith in previous religious beliefs and no longer believing in a just world.
Moral injuries tend to originate primarily from systems-based problems, as we have seen with the lack of concerted national approaches to the pandemic. On the positive side, solutions typically also involve systems-based changes, which in this case may mean changes in leadership styles nationally and locally, as well as changes in the culture of medicine and the way healthcare is practiced and managed in the modern era. We are starting to see some of those changes with the increased use of telemedicine and health technologies, as well as more of a focus on the well-being of health care workers, now deemed “essential.”
As individuals, we are not helpless. There are things we can do in our workplaces to create change. I suggest:
- Acknowledge that you, like me, are affected by these stressors. This is not a secret, and you should not be ashamed of your feelings.
- Talk with your colleagues, loved ones, and friends about how you and they are affected. You are not alone. Encourage others to share their thoughts, stories, and feelings.
- Put this topic on your meeting and departmental agendas and discuss these moral issues openly with your colleagues. Allow sufficient time to engage in open dialogue.
- Work out ways of assisting those who are in high-risk situations, especially for moderate to severe injuries. Be supportive toward those affected.
- Modify policies and change rosters and rotate staff between high- and low-stress roles. Protect and support at-risk colleagues.
- Think about difficult ethical decisions in advance so they can be made by groups, not individuals, and certainly not “on the fly.”
- Keep everyone in your workplace constantly informed, especially of impending staff or equipment shortages.
- Maintain your inherent self-care and resilience with rest, good nutrition, sleep, exercise, love, caring, socialization, and work-life balance.
- Be prepared to access the many professional support services available in our community if you are intensely distressed or if the above suggestions are not enough.
Remember, we are in this together and will find strength in each other. This too will pass.
This article first appeared on Medscape.com.
Among the many tolls inflicted on health care workers by COVID-19 is one that is not as easily measured as rates of death or disease, but is no less tangible: moral injury. This is the term by which we describe the psychological, social, and spiritual impact of high-stakes situations that lead to the betrayal or transgression of our own deeply held moral beliefs and values.
The current pandemic has provided innumerable such situations that can increase the risk for moral injury, whether we deal directly with patients infected by the coronavirus or not. Telling family members they cannot visit critically ill loved ones. Delaying code activities, even momentarily, to get fully protected with personal protective equipment. Seeing patients who have delayed their necessary or preventive care. Using video rather than touch to reassure people.
Knowing that we are following guidelines from the Centers for Disease Control and Prevention does not stop our feelings of guilt. The longer this pandemic goes on, the more likely it is that these situations will begin to take a toll on us.
For most of us, being exposed to moral injuries is new; they have historically been most associated with severe traumatic wartime experiences. Soldiers, philosophers, and writers have described the ethical dilemmas inherent in war for as long as recorded history. But the use of this term is a more recent development, which the Moral Injury Project at Syracuse (N.Y.) University describes as probably originating in the Vietnam War–era writings of veteran and peace activist Camillo “Mac” Bica and psychiatrist Jonathan Shay. Examples of wartime events that have been thought to lead to moral injury include: causing the harm or death of civilians, knowingly but without alternatives, or accidentally; failing to provide medical aid to an injured civilian or service member; and following orders that were illegal, immoral, and/or against the rules of engagement or the Geneva Conventions.
However, the occurrence of moral injuries in modern health care is increasingly being reported, primarily as an adverse effect of health care inefficiencies that can contribute to burnout. COVID-19 has now provided an array of additional stressors that can cause moral injuries among health care workers. A recent guidance document on moral injury published by the American Psychiatric Association noted that, in the context of a public health disaster, such as COVID-19, it is sometimes necessary to transition from ordinary standards of care to those more appropriate in a crisis, as in wartime. This forces us all to confront challenging questions for which there may be no clear answers, and to make “lose-lose” choices in which no one involved – patients, family, or clinicians – ends up feeling satisfied or even comfortable.
Our lives have been altered significantly, and for many, completely turned upside down by enormous sacrifices and tragic losses. Globally, physicians account for over half of healthcare worker deaths. In the United States alone, over 900 health care workers have died of COVID-19.
Most of us have felt the symptoms of moral injury: frustration, anger, disgust, guilt. A recent report describes three levels of stressors in health care occurring during the pandemic, which are not dissimilar to those wartime events described previously.
- Severe moral stressors, such as the denial of treatment to a COVID-19 patient owing to lack of resources, the inability to provide optimal care to non–COVID-19 patients for many reasons, and concern about passing COVID to loved ones.
- Moderate moral stressors, such as preventing visitors, especially to dying patients, triaging patients for healthcare services with inadequate information, and trying to solve the tension between the need for self-preservation and the need to treat.
- Lower-level but common moral challenges, especially in the community – for example, seeing others not protecting the community by hoarding food, gathering for large parties, and not social distancing or wearing masks. Such stressors lead to frustration and contempt, especially from healthcare workers making personal sacrifices and who may be at risk for infection caused by these behaviors.
Every one of us is affected by these stressors. I certainly am.
What are the outcomes? We know that moral injuries are a risk factor for the development of mental health problems and burnout, and not surprisingly we are seeing that mental health problems, suicidality, and substance use disorders have increased markedly during COVID-19, as recently detailed by the CDC.
Common emotions that occur in response to moral injuries are: feelings of guilt, shame, anger, sadness, anxiety, and disgust; intrapersonal outcomes, including lowered self-esteem, high self-criticism, and beliefs about being bad, damaged, unworthy, failing, or weak; interpersonal outcomes, including loss of faith in people, avoidance of intimacy, and lack of trust in authority figures; and existential and spiritual outcomes, including loss of faith in previous religious beliefs and no longer believing in a just world.
Moral injuries tend to originate primarily from systems-based problems, as we have seen with the lack of concerted national approaches to the pandemic. On the positive side, solutions typically also involve systems-based changes, which in this case may mean changes in leadership styles nationally and locally, as well as changes in the culture of medicine and the way healthcare is practiced and managed in the modern era. We are starting to see some of those changes with the increased use of telemedicine and health technologies, as well as more of a focus on the well-being of health care workers, now deemed “essential.”
As individuals, we are not helpless. There are things we can do in our workplaces to create change. I suggest:
- Acknowledge that you, like me, are affected by these stressors. This is not a secret, and you should not be ashamed of your feelings.
- Talk with your colleagues, loved ones, and friends about how you and they are affected. You are not alone. Encourage others to share their thoughts, stories, and feelings.
- Put this topic on your meeting and departmental agendas and discuss these moral issues openly with your colleagues. Allow sufficient time to engage in open dialogue.
- Work out ways of assisting those who are in high-risk situations, especially for moderate to severe injuries. Be supportive toward those affected.
- Modify policies and change rosters and rotate staff between high- and low-stress roles. Protect and support at-risk colleagues.
- Think about difficult ethical decisions in advance so they can be made by groups, not individuals, and certainly not “on the fly.”
- Keep everyone in your workplace constantly informed, especially of impending staff or equipment shortages.
- Maintain your inherent self-care and resilience with rest, good nutrition, sleep, exercise, love, caring, socialization, and work-life balance.
- Be prepared to access the many professional support services available in our community if you are intensely distressed or if the above suggestions are not enough.
Remember, we are in this together and will find strength in each other. This too will pass.
This article first appeared on Medscape.com.
Scrubs ad that insulted women and DOs pulled after outcry
A video that advertised scrubs but denigrated women and DOs has been removed from the company’s website after fierce backlash.
On Tuesday Kevin Klauer, DO, EJD, directed this tweet to the medical uniform company Figs: “@wearfigs REMOVE YOUR DO offensive web ad immediately or the @AOAforDOs will proceed promptly with a defamation lawsuit on behalf of our members and profession.”
Also on Tuesday, the American Association of Colleges of Osteopathic Medicine demanded a public apology.
The video ad featured a woman carrying a “Medical Terminology for Dummies” book upside down while modeling the pink scrubs from all angles and dancing. At one point in the ad, the camera zooms in on the badge clipped to her waistband that read “DO.”
Agnieszka Solberg, MD, a vascular and interventional radiologist and assistant clinical professor at the University of North Dakota in Grand Forks, was among those voicing pointed criticism on social media.
“This was another hit for our DO colleagues,” she said in an interview, emphasizing that MDs and DOs provide the same level of care.
AACOM tweeted: “We are outraged women physicians & doctors of osteopathic medicine are still attacked in ignorant marketing campaigns. A company like @wearfigs should be ashamed for promoting these stereotypes. We demand the respect we’ve earned AND a public apology.”
Dr. Solberg says this is not the first offense by the company. She said she had stopped buying the company’s scrubs a year ago because the ads “have been portraying female providers as dumb and silly. This was the final straw.”
She said the timing of the ad is suspect as DOs had been swept into a storm of negativity earlier this month, as Medscape Medical News reported, when some questioned the qualifications of President Donald Trump’s physician, Sean Conley, who is a DO.
The scrubs ad ignited criticism across specialties, provider levels, and genders.
Jessica K. Willett, MD, tweeted: “As women physicians in 2020, we still struggle to be taken seriously compared to our male counterparts, as we battle stereotypes like THIS EXACT ONE. We expect the brands we support to reflect the badasses we are.”
The company responded to her tweet: “Thank you so much for the feedback! Totally not our intent – we’re taking down both the men’s and women’s versions of this ASAP! I really appreciate you taking the time to share this.”
The company did not respond to a request for comment but issued an apology on social media: “A lot of you guys have pointed out an insensitive video we had on our site – we are incredibly sorry for any hurt this has caused you, especially our female DOs (who are amazing!) FIGS is a female founded company whose only mission is to make you guys feel awesome.”
The Los Angeles–based company, which Forbes estimated will make $250 million in sales this year, was founded by co-CEOs Heather Hasson and Trina Spear.
A med student wrote on Twitter: “As a female and a DO student, how would I ever “feel awesome” about myself knowing that this is how you view me??? And how you want others to view me??? Women and DO’s have fought stereotypes way too long for you to go ahead and put this out there. Do better.”
Even the company’s apology was tinged with disrespect, some noted, with the use of “you guys” and for what it didn’t include.
As Liesl Young, MD, tweeted: “We are not “guys”, we are women. MD = DO. We stand together.”
Dr. Solberg said the apology came across as an apology that feelings were hurt. It should have detailed the changes the company would make to prevent another incident and address the processes that led to the video.
Dr. Solberg said she is seeing something positive come from the whole incident in that, “women are taking up the torch of feminism in such a volatile and divisive time.”
Dr. Solberg reported no relevant financial relationships.
This article first appeared on Medscape.com.
A video that advertised scrubs but denigrated women and DOs has been removed from the company’s website after fierce backlash.
On Tuesday Kevin Klauer, DO, EJD, directed this tweet to the medical uniform company Figs: “@wearfigs REMOVE YOUR DO offensive web ad immediately or the @AOAforDOs will proceed promptly with a defamation lawsuit on behalf of our members and profession.”
Also on Tuesday, the American Association of Colleges of Osteopathic Medicine demanded a public apology.
The video ad featured a woman carrying a “Medical Terminology for Dummies” book upside down while modeling the pink scrubs from all angles and dancing. At one point in the ad, the camera zooms in on the badge clipped to her waistband that read “DO.”
Agnieszka Solberg, MD, a vascular and interventional radiologist and assistant clinical professor at the University of North Dakota in Grand Forks, was among those voicing pointed criticism on social media.
“This was another hit for our DO colleagues,” she said in an interview, emphasizing that MDs and DOs provide the same level of care.
AACOM tweeted: “We are outraged women physicians & doctors of osteopathic medicine are still attacked in ignorant marketing campaigns. A company like @wearfigs should be ashamed for promoting these stereotypes. We demand the respect we’ve earned AND a public apology.”
Dr. Solberg says this is not the first offense by the company. She said she had stopped buying the company’s scrubs a year ago because the ads “have been portraying female providers as dumb and silly. This was the final straw.”
She said the timing of the ad is suspect as DOs had been swept into a storm of negativity earlier this month, as Medscape Medical News reported, when some questioned the qualifications of President Donald Trump’s physician, Sean Conley, who is a DO.
The scrubs ad ignited criticism across specialties, provider levels, and genders.
Jessica K. Willett, MD, tweeted: “As women physicians in 2020, we still struggle to be taken seriously compared to our male counterparts, as we battle stereotypes like THIS EXACT ONE. We expect the brands we support to reflect the badasses we are.”
The company responded to her tweet: “Thank you so much for the feedback! Totally not our intent – we’re taking down both the men’s and women’s versions of this ASAP! I really appreciate you taking the time to share this.”
The company did not respond to a request for comment but issued an apology on social media: “A lot of you guys have pointed out an insensitive video we had on our site – we are incredibly sorry for any hurt this has caused you, especially our female DOs (who are amazing!) FIGS is a female founded company whose only mission is to make you guys feel awesome.”
The Los Angeles–based company, which Forbes estimated will make $250 million in sales this year, was founded by co-CEOs Heather Hasson and Trina Spear.
A med student wrote on Twitter: “As a female and a DO student, how would I ever “feel awesome” about myself knowing that this is how you view me??? And how you want others to view me??? Women and DO’s have fought stereotypes way too long for you to go ahead and put this out there. Do better.”
Even the company’s apology was tinged with disrespect, some noted, with the use of “you guys” and for what it didn’t include.
As Liesl Young, MD, tweeted: “We are not “guys”, we are women. MD = DO. We stand together.”
Dr. Solberg said the apology came across as an apology that feelings were hurt. It should have detailed the changes the company would make to prevent another incident and address the processes that led to the video.
Dr. Solberg said she is seeing something positive come from the whole incident in that, “women are taking up the torch of feminism in such a volatile and divisive time.”
Dr. Solberg reported no relevant financial relationships.
This article first appeared on Medscape.com.
A video that advertised scrubs but denigrated women and DOs has been removed from the company’s website after fierce backlash.
On Tuesday Kevin Klauer, DO, EJD, directed this tweet to the medical uniform company Figs: “@wearfigs REMOVE YOUR DO offensive web ad immediately or the @AOAforDOs will proceed promptly with a defamation lawsuit on behalf of our members and profession.”
Also on Tuesday, the American Association of Colleges of Osteopathic Medicine demanded a public apology.
The video ad featured a woman carrying a “Medical Terminology for Dummies” book upside down while modeling the pink scrubs from all angles and dancing. At one point in the ad, the camera zooms in on the badge clipped to her waistband that read “DO.”
Agnieszka Solberg, MD, a vascular and interventional radiologist and assistant clinical professor at the University of North Dakota in Grand Forks, was among those voicing pointed criticism on social media.
“This was another hit for our DO colleagues,” she said in an interview, emphasizing that MDs and DOs provide the same level of care.
AACOM tweeted: “We are outraged women physicians & doctors of osteopathic medicine are still attacked in ignorant marketing campaigns. A company like @wearfigs should be ashamed for promoting these stereotypes. We demand the respect we’ve earned AND a public apology.”
Dr. Solberg says this is not the first offense by the company. She said she had stopped buying the company’s scrubs a year ago because the ads “have been portraying female providers as dumb and silly. This was the final straw.”
She said the timing of the ad is suspect as DOs had been swept into a storm of negativity earlier this month, as Medscape Medical News reported, when some questioned the qualifications of President Donald Trump’s physician, Sean Conley, who is a DO.
The scrubs ad ignited criticism across specialties, provider levels, and genders.
Jessica K. Willett, MD, tweeted: “As women physicians in 2020, we still struggle to be taken seriously compared to our male counterparts, as we battle stereotypes like THIS EXACT ONE. We expect the brands we support to reflect the badasses we are.”
The company responded to her tweet: “Thank you so much for the feedback! Totally not our intent – we’re taking down both the men’s and women’s versions of this ASAP! I really appreciate you taking the time to share this.”
The company did not respond to a request for comment but issued an apology on social media: “A lot of you guys have pointed out an insensitive video we had on our site – we are incredibly sorry for any hurt this has caused you, especially our female DOs (who are amazing!) FIGS is a female founded company whose only mission is to make you guys feel awesome.”
The Los Angeles–based company, which Forbes estimated will make $250 million in sales this year, was founded by co-CEOs Heather Hasson and Trina Spear.
A med student wrote on Twitter: “As a female and a DO student, how would I ever “feel awesome” about myself knowing that this is how you view me??? And how you want others to view me??? Women and DO’s have fought stereotypes way too long for you to go ahead and put this out there. Do better.”
Even the company’s apology was tinged with disrespect, some noted, with the use of “you guys” and for what it didn’t include.
As Liesl Young, MD, tweeted: “We are not “guys”, we are women. MD = DO. We stand together.”
Dr. Solberg said the apology came across as an apology that feelings were hurt. It should have detailed the changes the company would make to prevent another incident and address the processes that led to the video.
Dr. Solberg said she is seeing something positive come from the whole incident in that, “women are taking up the torch of feminism in such a volatile and divisive time.”
Dr. Solberg reported no relevant financial relationships.
This article first appeared on Medscape.com.
NMOSD challenges in children
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
FROM CNS-ICNA 2020
Worldwide measles vaccination is flagging
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
FROM CNS-ICNA 2020
Latest week brings 44,000 more children with COVID-19
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
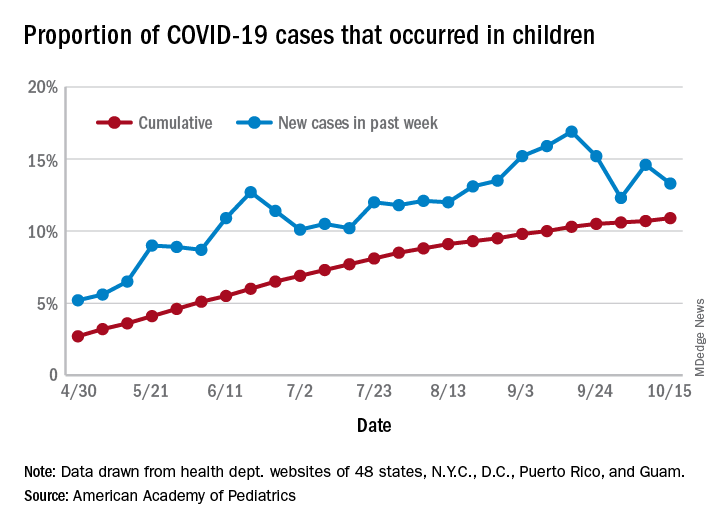
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.