User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Demand for COVID vaccines expected to get heated – and fast
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Rap music mention of mental health topics more than doubles

Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
FROM JAMA PEDIATRICS
New child COVID-19 cases down in last weekly count
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association. 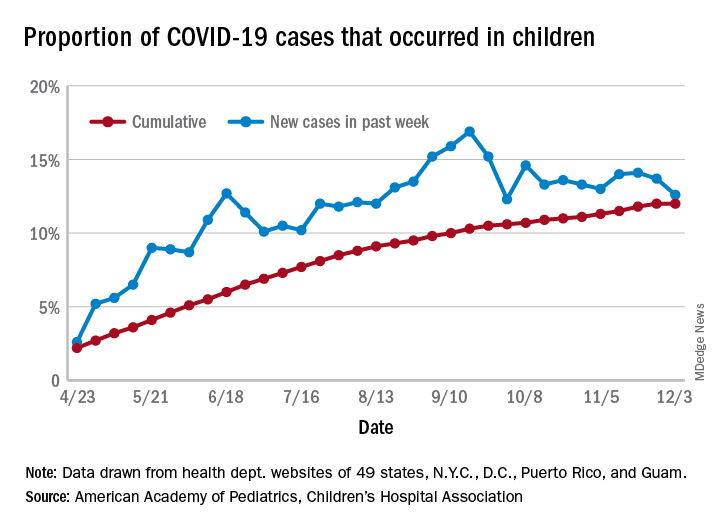
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
New residency matching sets record, says NRMP
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
Biden chooses California Attorney General Xavier Becerra to head HHS

If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
COVID-19: Hand sanitizer poisonings soar, psych patients at high risk
Cases of poisoning – intentional and unintentional – from ingestion of alcohol-based hand sanitizer have soared during the COVID-19 pandemic.
In the United Kingdom alone, alcohol-based hand sanitizer poisonings reported to the National Poisons Information Service jumped 157% – from 155 between January 1 and September 16, 2019, to 398 between Jan. 1 and Sept. 14, 2020, new research shows.
More needs to be done to protect those at risk of unintentional and intentional swallowing of alcohol-based hand sanitizer, including children, people with dementia/confusion, and those with mental health issues, according to Georgia Richards, DPhil student, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
“If providers are supplying alcohol-based hand sanitizers in the community to reduce the spread of SARS-CoV-2, Ms. Richards said in an interview.
The study was published online Dec. 1 in BMJ Evidence-Based Medicine.
European, U.S. poisoning rates soar
In the paper Ms. Richards described two deaths that occurred in hospitals in England.
In one case, a 30-year-old woman, detained in a psychiatric unit who received the antidepressant venlafaxine was found dead in her hospital bed with a container of hand-sanitizing gel beside her.
“The gel was readily accessible to patients on the ward from a communal dispenser, and patients were allowed to fill cups or other containers with it to keep in their rooms,” Ms. Richards reported.
A postmortem analysis found a high level of alcohol in her blood (214 mg of alcohol in 100 mL of blood). The medical cause of death was listed as “ingestion of alcohol and venlafaxine.” The coroner concluded that the combination of these substances suppressed the patient’s breathing, leading to her death.
The other case involved a 76-year-old man who unintentionally swallowed an unknown quantity of alcohol-based hand-sanitizing foam attached to the foot of his hospital bed.
The patient had a history of agitation and depression and was treated with antidepressants. He had become increasingly confused over the preceding 9 months, possibly because of vascular dementia.
His blood ethanol concentration was 463 mg/dL (100 mmol/L) initially and 354 mg/dL (77mmol/L) 10 hours later. He was admitted to the ICU, where he received lorazepam and haloperidol and treated with ventilation, with a plan to allow the alcohol to be naturally metabolized.
The patient developed complications and died 6 days later. The primary causes of death were bronchopneumonia and acute alcohol toxicity, secondary to acute delirium and coronary artery disease.
Since COVID-19 started, alcohol-based hand sanitizers are among the most sought-after commodities around the world. The volume of these products – now found in homes, hospitals, schools, workplaces, and elsewhere – “may be a cause for concern,” Ms. Richards wrote.
Yet, warnings about the toxicity and lethality of intentional or unintentional ingestion of these products have not been widely disseminated, she noted.
To reduce the risk of harm, Ms. Richards suggested educating the public and health care professionals, improving warning labels on products, and increasing the awareness and reporting of such exposures to public health authorities.
“While governments and public health authorities have successfully heightened our awareness of, and need for, better hand hygiene during the COVID-19 outbreak, they must also make the public aware of the potential harms and encourage the reporting of such harms to poisons information centers,” she noted.
Increases in alcohol-based hand sanitizer poisoning during the pandemic have also been reported in the United States.
The American Association of Poison Control Centers reports that data from the National Poison Data System show 32,892 hand sanitizer exposure cases reported to the 55 U.S. poison control centers from Jan. 1 to Nov. 15, 2020 – an increase of 73%, compared with the same time period during the previous year.
An increase in self-harm
Weighing in on this issue, Robert Bassett, DO, associate medical director of the Poison Control Center at Children’s Hospital of Philadelphia, said in an interview that “cleaning agents and disinfectants have been around for eons and their potential for toxicity hasn’t changed.
“Now with COVID, and this hypervigilance when it comes to cleanliness, there is increased access and the exposure risk has gone up,” he said.
“One of the sad casualties of an overstressed health care system and a globally depressed environment is worsening behavioral health emergencies and, as part of that, the risk of self-harm goes up,” Dr. Bassett added.
“The consensus is that there has been an exacerbation of behavioral health emergencies and behavioral health needs since COVID started and hand sanitizers are readily accessible to someone who may be looking to self-harm,” he said.
This research had no specific funding. Ms. Richards is the editorial registrar of BMJ Evidence Based Medicine and is developing a website to track preventable deaths. Dr. Bassett disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Cases of poisoning – intentional and unintentional – from ingestion of alcohol-based hand sanitizer have soared during the COVID-19 pandemic.
In the United Kingdom alone, alcohol-based hand sanitizer poisonings reported to the National Poisons Information Service jumped 157% – from 155 between January 1 and September 16, 2019, to 398 between Jan. 1 and Sept. 14, 2020, new research shows.
More needs to be done to protect those at risk of unintentional and intentional swallowing of alcohol-based hand sanitizer, including children, people with dementia/confusion, and those with mental health issues, according to Georgia Richards, DPhil student, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
“If providers are supplying alcohol-based hand sanitizers in the community to reduce the spread of SARS-CoV-2, Ms. Richards said in an interview.
The study was published online Dec. 1 in BMJ Evidence-Based Medicine.
European, U.S. poisoning rates soar
In the paper Ms. Richards described two deaths that occurred in hospitals in England.
In one case, a 30-year-old woman, detained in a psychiatric unit who received the antidepressant venlafaxine was found dead in her hospital bed with a container of hand-sanitizing gel beside her.
“The gel was readily accessible to patients on the ward from a communal dispenser, and patients were allowed to fill cups or other containers with it to keep in their rooms,” Ms. Richards reported.
A postmortem analysis found a high level of alcohol in her blood (214 mg of alcohol in 100 mL of blood). The medical cause of death was listed as “ingestion of alcohol and venlafaxine.” The coroner concluded that the combination of these substances suppressed the patient’s breathing, leading to her death.
The other case involved a 76-year-old man who unintentionally swallowed an unknown quantity of alcohol-based hand-sanitizing foam attached to the foot of his hospital bed.
The patient had a history of agitation and depression and was treated with antidepressants. He had become increasingly confused over the preceding 9 months, possibly because of vascular dementia.
His blood ethanol concentration was 463 mg/dL (100 mmol/L) initially and 354 mg/dL (77mmol/L) 10 hours later. He was admitted to the ICU, where he received lorazepam and haloperidol and treated with ventilation, with a plan to allow the alcohol to be naturally metabolized.
The patient developed complications and died 6 days later. The primary causes of death were bronchopneumonia and acute alcohol toxicity, secondary to acute delirium and coronary artery disease.
Since COVID-19 started, alcohol-based hand sanitizers are among the most sought-after commodities around the world. The volume of these products – now found in homes, hospitals, schools, workplaces, and elsewhere – “may be a cause for concern,” Ms. Richards wrote.
Yet, warnings about the toxicity and lethality of intentional or unintentional ingestion of these products have not been widely disseminated, she noted.
To reduce the risk of harm, Ms. Richards suggested educating the public and health care professionals, improving warning labels on products, and increasing the awareness and reporting of such exposures to public health authorities.
“While governments and public health authorities have successfully heightened our awareness of, and need for, better hand hygiene during the COVID-19 outbreak, they must also make the public aware of the potential harms and encourage the reporting of such harms to poisons information centers,” she noted.
Increases in alcohol-based hand sanitizer poisoning during the pandemic have also been reported in the United States.
The American Association of Poison Control Centers reports that data from the National Poison Data System show 32,892 hand sanitizer exposure cases reported to the 55 U.S. poison control centers from Jan. 1 to Nov. 15, 2020 – an increase of 73%, compared with the same time period during the previous year.
An increase in self-harm
Weighing in on this issue, Robert Bassett, DO, associate medical director of the Poison Control Center at Children’s Hospital of Philadelphia, said in an interview that “cleaning agents and disinfectants have been around for eons and their potential for toxicity hasn’t changed.
“Now with COVID, and this hypervigilance when it comes to cleanliness, there is increased access and the exposure risk has gone up,” he said.
“One of the sad casualties of an overstressed health care system and a globally depressed environment is worsening behavioral health emergencies and, as part of that, the risk of self-harm goes up,” Dr. Bassett added.
“The consensus is that there has been an exacerbation of behavioral health emergencies and behavioral health needs since COVID started and hand sanitizers are readily accessible to someone who may be looking to self-harm,” he said.
This research had no specific funding. Ms. Richards is the editorial registrar of BMJ Evidence Based Medicine and is developing a website to track preventable deaths. Dr. Bassett disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Cases of poisoning – intentional and unintentional – from ingestion of alcohol-based hand sanitizer have soared during the COVID-19 pandemic.
In the United Kingdom alone, alcohol-based hand sanitizer poisonings reported to the National Poisons Information Service jumped 157% – from 155 between January 1 and September 16, 2019, to 398 between Jan. 1 and Sept. 14, 2020, new research shows.
More needs to be done to protect those at risk of unintentional and intentional swallowing of alcohol-based hand sanitizer, including children, people with dementia/confusion, and those with mental health issues, according to Georgia Richards, DPhil student, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
“If providers are supplying alcohol-based hand sanitizers in the community to reduce the spread of SARS-CoV-2, Ms. Richards said in an interview.
The study was published online Dec. 1 in BMJ Evidence-Based Medicine.
European, U.S. poisoning rates soar
In the paper Ms. Richards described two deaths that occurred in hospitals in England.
In one case, a 30-year-old woman, detained in a psychiatric unit who received the antidepressant venlafaxine was found dead in her hospital bed with a container of hand-sanitizing gel beside her.
“The gel was readily accessible to patients on the ward from a communal dispenser, and patients were allowed to fill cups or other containers with it to keep in their rooms,” Ms. Richards reported.
A postmortem analysis found a high level of alcohol in her blood (214 mg of alcohol in 100 mL of blood). The medical cause of death was listed as “ingestion of alcohol and venlafaxine.” The coroner concluded that the combination of these substances suppressed the patient’s breathing, leading to her death.
The other case involved a 76-year-old man who unintentionally swallowed an unknown quantity of alcohol-based hand-sanitizing foam attached to the foot of his hospital bed.
The patient had a history of agitation and depression and was treated with antidepressants. He had become increasingly confused over the preceding 9 months, possibly because of vascular dementia.
His blood ethanol concentration was 463 mg/dL (100 mmol/L) initially and 354 mg/dL (77mmol/L) 10 hours later. He was admitted to the ICU, where he received lorazepam and haloperidol and treated with ventilation, with a plan to allow the alcohol to be naturally metabolized.
The patient developed complications and died 6 days later. The primary causes of death were bronchopneumonia and acute alcohol toxicity, secondary to acute delirium and coronary artery disease.
Since COVID-19 started, alcohol-based hand sanitizers are among the most sought-after commodities around the world. The volume of these products – now found in homes, hospitals, schools, workplaces, and elsewhere – “may be a cause for concern,” Ms. Richards wrote.
Yet, warnings about the toxicity and lethality of intentional or unintentional ingestion of these products have not been widely disseminated, she noted.
To reduce the risk of harm, Ms. Richards suggested educating the public and health care professionals, improving warning labels on products, and increasing the awareness and reporting of such exposures to public health authorities.
“While governments and public health authorities have successfully heightened our awareness of, and need for, better hand hygiene during the COVID-19 outbreak, they must also make the public aware of the potential harms and encourage the reporting of such harms to poisons information centers,” she noted.
Increases in alcohol-based hand sanitizer poisoning during the pandemic have also been reported in the United States.
The American Association of Poison Control Centers reports that data from the National Poison Data System show 32,892 hand sanitizer exposure cases reported to the 55 U.S. poison control centers from Jan. 1 to Nov. 15, 2020 – an increase of 73%, compared with the same time period during the previous year.
An increase in self-harm
Weighing in on this issue, Robert Bassett, DO, associate medical director of the Poison Control Center at Children’s Hospital of Philadelphia, said in an interview that “cleaning agents and disinfectants have been around for eons and their potential for toxicity hasn’t changed.
“Now with COVID, and this hypervigilance when it comes to cleanliness, there is increased access and the exposure risk has gone up,” he said.
“One of the sad casualties of an overstressed health care system and a globally depressed environment is worsening behavioral health emergencies and, as part of that, the risk of self-harm goes up,” Dr. Bassett added.
“The consensus is that there has been an exacerbation of behavioral health emergencies and behavioral health needs since COVID started and hand sanitizers are readily accessible to someone who may be looking to self-harm,” he said.
This research had no specific funding. Ms. Richards is the editorial registrar of BMJ Evidence Based Medicine and is developing a website to track preventable deaths. Dr. Bassett disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Infant’s COVID-19–related myocardial injury reversed
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.

and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
FROM JACC CASE REPORTS
Key clinical point: Children presenting with COVID-19 should be tested for heart failure.
Major finding: A 2-month-old infant with COVID-19 had acute but reversible myocardial injury.
Study details: Single case report.
Disclosures: Dr. Sharma, MD, has no relevant financial relationships to disclose.
Source: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
FDA clears first drug for rare genetic causes of severe obesity
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
Understanding and addressing suicide risk in LGBTQ+ youth
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
FROM AAP 2020
Watch for cognitive traps that lead diagnostics astray
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and

“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.

Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and
“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.
Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and
“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.
Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
FROM AAP 2020
