User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Updated recommendations released on COVID-19 and pediatric ALL
The main threat to the vast majority of children with acute lymphoblastic leukemia still remains the ALL itself, according to updated recommendations released by the Leukemia Committee of the French Society for the Fight Against Cancers and Leukemias in Children and Adolescents (SFCE).

“The situation of the current COVID-19 pandemic is continuously evolving. We thus have taken the more recent knowledge into account to update the previous recommendations from the Leukemia Committee,” Jérémie Rouger-Gaudichon, MD, of Pediatric Hemato-Immuno-Oncology Unit, Centre Hospitalier Universitaire, Caen (France), and colleagues wrote on behalf of the SFCE.
The updated recommendations are based on data collected in a real-time prospective survey among the 30 SFCE centers since April 2020. As of December 2020, 127 cases of COVID-19 were reported, most of them being enrolled in the PEDONCOVID study (NCT04433871) according to the report. Of these, eight patients required hospitalization in intensive care unit and one patient with relapsed acute lymphoblastic leukemia (ALL) died from ARDS with multiorgan failure. This confirms earlier reports that SARS-CoV-2 infection can be severe in some children with cancer and/or having hematopoietic stem cell transplant (HSCT), according to the report, which was published online in Bulletin du Cancer.
Recommendations
General recommendations were provided in the report, including the following:
- Test for SARS-CoV-2 (preferably by PCR or at least by immunological tests, on nasopharyngeal swab) before starting intensive induction chemotherapy or other intensive phase of treatment, for ALL patients, with or without symptoms.
- Delay systemic treatment if possible (e.g., absence of major hyperleukocytosis) in positive patients. During later phases, if patients test positive, tests should be repeated over time until negativity, especially before the beginning of an intensive course.
- Isolate any COVID-19–negative child or adolescent to allow treatment to continue (facial mask, social distancing, barrier measures, no contact with individuals suspected of COVID-19 or COVID-19–positive), in particular for patients to be allografted.
- Limit visitation to parents and potentially siblings in patients slated for HSCT and follow all necessary sanitary procedures for those visits.
The report provides a lengthy discussion of more detailed recommendations, including the following for first-line treatment of ALL:
- For patients with high-risk ALL, an individualized decision regarding transplantation and its timing should weigh the risks of transplantation in an epidemic context of COVID-19 against the risk linked to ALL.
- Minimizing hospital visits by the use of home blood tests and partial use of telemedicine may be considered.
- A physical examination should be performed regularly to avoid any delay in the diagnosis of treatment complications or relapse and preventative measures for SARS-CoV-2 should be applied in the home.
Patients with relapsed ALL may be at more risk from the effects of COVID-19 disease, according to the others, so for ALL patients receiving second-line or more treatment the recommendations include the following:
- Testing must be performed before starting a chemotherapy block, and postponing chemotherapy in case of positive test should be discussed in accordance with each specific situation and benefits/risks ratio regarding the leukemia.
- First-relapse patients should follow the INTREALL treatment protocol as much as possible and those who reach appropriate complete remission should be considered promptly for allogeneic transplantation, despite the pandemic.
- Second relapse and refractory relapses require testing and negative results for inclusion in phase I-II trials being conducted by most if not all academic or industrial promoters.
- The indication for treatment with CAR-T cells must be weighed with the center that would perform the procedure to determine the feasibility of performing all necessary procedures including apheresis and manufacturing.
In the case of a SARS-CoV-2 infection diagnosis during the treatment of ALL, discussions should occur with regard to stopping and/or postponing all chemotherapies, according to the severity of the ALL, the stage of treatment and the severity of clinical and/or radiological signs. In addition, any specific anti-COVID-19 treatment must be discussed with the infectious diseases team, according to the report.
“Fortunately, SARS-CoV-2 infection appears nevertheless to be mild in most children with cancer/ALL. Thus, the main threat to the vast majority of children with ALL still remains the ALL itself. Long-term data including well-matched case-control studies will tell if treatment delays/modifications due to COVID-19 have impacted the outcome if children with ALL,” the authors stated. However, “despite extremely rapid advances obtained in less than one year, our knowledge of SARS-CoV-2 and its complications is still incomplete,” they concluded, adding that the recommendations will likely need to be updated within another few months.
The authors reported that they had no conflicts of interest.
The main threat to the vast majority of children with acute lymphoblastic leukemia still remains the ALL itself, according to updated recommendations released by the Leukemia Committee of the French Society for the Fight Against Cancers and Leukemias in Children and Adolescents (SFCE).
“The situation of the current COVID-19 pandemic is continuously evolving. We thus have taken the more recent knowledge into account to update the previous recommendations from the Leukemia Committee,” Jérémie Rouger-Gaudichon, MD, of Pediatric Hemato-Immuno-Oncology Unit, Centre Hospitalier Universitaire, Caen (France), and colleagues wrote on behalf of the SFCE.
The updated recommendations are based on data collected in a real-time prospective survey among the 30 SFCE centers since April 2020. As of December 2020, 127 cases of COVID-19 were reported, most of them being enrolled in the PEDONCOVID study (NCT04433871) according to the report. Of these, eight patients required hospitalization in intensive care unit and one patient with relapsed acute lymphoblastic leukemia (ALL) died from ARDS with multiorgan failure. This confirms earlier reports that SARS-CoV-2 infection can be severe in some children with cancer and/or having hematopoietic stem cell transplant (HSCT), according to the report, which was published online in Bulletin du Cancer.
Recommendations
General recommendations were provided in the report, including the following:
- Test for SARS-CoV-2 (preferably by PCR or at least by immunological tests, on nasopharyngeal swab) before starting intensive induction chemotherapy or other intensive phase of treatment, for ALL patients, with or without symptoms.
- Delay systemic treatment if possible (e.g., absence of major hyperleukocytosis) in positive patients. During later phases, if patients test positive, tests should be repeated over time until negativity, especially before the beginning of an intensive course.
- Isolate any COVID-19–negative child or adolescent to allow treatment to continue (facial mask, social distancing, barrier measures, no contact with individuals suspected of COVID-19 or COVID-19–positive), in particular for patients to be allografted.
- Limit visitation to parents and potentially siblings in patients slated for HSCT and follow all necessary sanitary procedures for those visits.
The report provides a lengthy discussion of more detailed recommendations, including the following for first-line treatment of ALL:
- For patients with high-risk ALL, an individualized decision regarding transplantation and its timing should weigh the risks of transplantation in an epidemic context of COVID-19 against the risk linked to ALL.
- Minimizing hospital visits by the use of home blood tests and partial use of telemedicine may be considered.
- A physical examination should be performed regularly to avoid any delay in the diagnosis of treatment complications or relapse and preventative measures for SARS-CoV-2 should be applied in the home.
Patients with relapsed ALL may be at more risk from the effects of COVID-19 disease, according to the others, so for ALL patients receiving second-line or more treatment the recommendations include the following:
- Testing must be performed before starting a chemotherapy block, and postponing chemotherapy in case of positive test should be discussed in accordance with each specific situation and benefits/risks ratio regarding the leukemia.
- First-relapse patients should follow the INTREALL treatment protocol as much as possible and those who reach appropriate complete remission should be considered promptly for allogeneic transplantation, despite the pandemic.
- Second relapse and refractory relapses require testing and negative results for inclusion in phase I-II trials being conducted by most if not all academic or industrial promoters.
- The indication for treatment with CAR-T cells must be weighed with the center that would perform the procedure to determine the feasibility of performing all necessary procedures including apheresis and manufacturing.
In the case of a SARS-CoV-2 infection diagnosis during the treatment of ALL, discussions should occur with regard to stopping and/or postponing all chemotherapies, according to the severity of the ALL, the stage of treatment and the severity of clinical and/or radiological signs. In addition, any specific anti-COVID-19 treatment must be discussed with the infectious diseases team, according to the report.
“Fortunately, SARS-CoV-2 infection appears nevertheless to be mild in most children with cancer/ALL. Thus, the main threat to the vast majority of children with ALL still remains the ALL itself. Long-term data including well-matched case-control studies will tell if treatment delays/modifications due to COVID-19 have impacted the outcome if children with ALL,” the authors stated. However, “despite extremely rapid advances obtained in less than one year, our knowledge of SARS-CoV-2 and its complications is still incomplete,” they concluded, adding that the recommendations will likely need to be updated within another few months.
The authors reported that they had no conflicts of interest.
The main threat to the vast majority of children with acute lymphoblastic leukemia still remains the ALL itself, according to updated recommendations released by the Leukemia Committee of the French Society for the Fight Against Cancers and Leukemias in Children and Adolescents (SFCE).
“The situation of the current COVID-19 pandemic is continuously evolving. We thus have taken the more recent knowledge into account to update the previous recommendations from the Leukemia Committee,” Jérémie Rouger-Gaudichon, MD, of Pediatric Hemato-Immuno-Oncology Unit, Centre Hospitalier Universitaire, Caen (France), and colleagues wrote on behalf of the SFCE.
The updated recommendations are based on data collected in a real-time prospective survey among the 30 SFCE centers since April 2020. As of December 2020, 127 cases of COVID-19 were reported, most of them being enrolled in the PEDONCOVID study (NCT04433871) according to the report. Of these, eight patients required hospitalization in intensive care unit and one patient with relapsed acute lymphoblastic leukemia (ALL) died from ARDS with multiorgan failure. This confirms earlier reports that SARS-CoV-2 infection can be severe in some children with cancer and/or having hematopoietic stem cell transplant (HSCT), according to the report, which was published online in Bulletin du Cancer.
Recommendations
General recommendations were provided in the report, including the following:
- Test for SARS-CoV-2 (preferably by PCR or at least by immunological tests, on nasopharyngeal swab) before starting intensive induction chemotherapy or other intensive phase of treatment, for ALL patients, with or without symptoms.
- Delay systemic treatment if possible (e.g., absence of major hyperleukocytosis) in positive patients. During later phases, if patients test positive, tests should be repeated over time until negativity, especially before the beginning of an intensive course.
- Isolate any COVID-19–negative child or adolescent to allow treatment to continue (facial mask, social distancing, barrier measures, no contact with individuals suspected of COVID-19 or COVID-19–positive), in particular for patients to be allografted.
- Limit visitation to parents and potentially siblings in patients slated for HSCT and follow all necessary sanitary procedures for those visits.
The report provides a lengthy discussion of more detailed recommendations, including the following for first-line treatment of ALL:
- For patients with high-risk ALL, an individualized decision regarding transplantation and its timing should weigh the risks of transplantation in an epidemic context of COVID-19 against the risk linked to ALL.
- Minimizing hospital visits by the use of home blood tests and partial use of telemedicine may be considered.
- A physical examination should be performed regularly to avoid any delay in the diagnosis of treatment complications or relapse and preventative measures for SARS-CoV-2 should be applied in the home.
Patients with relapsed ALL may be at more risk from the effects of COVID-19 disease, according to the others, so for ALL patients receiving second-line or more treatment the recommendations include the following:
- Testing must be performed before starting a chemotherapy block, and postponing chemotherapy in case of positive test should be discussed in accordance with each specific situation and benefits/risks ratio regarding the leukemia.
- First-relapse patients should follow the INTREALL treatment protocol as much as possible and those who reach appropriate complete remission should be considered promptly for allogeneic transplantation, despite the pandemic.
- Second relapse and refractory relapses require testing and negative results for inclusion in phase I-II trials being conducted by most if not all academic or industrial promoters.
- The indication for treatment with CAR-T cells must be weighed with the center that would perform the procedure to determine the feasibility of performing all necessary procedures including apheresis and manufacturing.
In the case of a SARS-CoV-2 infection diagnosis during the treatment of ALL, discussions should occur with regard to stopping and/or postponing all chemotherapies, according to the severity of the ALL, the stage of treatment and the severity of clinical and/or radiological signs. In addition, any specific anti-COVID-19 treatment must be discussed with the infectious diseases team, according to the report.
“Fortunately, SARS-CoV-2 infection appears nevertheless to be mild in most children with cancer/ALL. Thus, the main threat to the vast majority of children with ALL still remains the ALL itself. Long-term data including well-matched case-control studies will tell if treatment delays/modifications due to COVID-19 have impacted the outcome if children with ALL,” the authors stated. However, “despite extremely rapid advances obtained in less than one year, our knowledge of SARS-CoV-2 and its complications is still incomplete,” they concluded, adding that the recommendations will likely need to be updated within another few months.
The authors reported that they had no conflicts of interest.
FROM BULLETIN DU CANCER
School refusal and COVID-19: The pediatrician's role
Hooray for back to school! But not for everyone. ... what to do with those who have trouble transitioning back?

As we have now passed a year since COVID-19–related shutdowns were implemented throughout the United States; and with returns to in-person schooling continuing to vary based on location, many of us either in our personal lives, or through conversations with patients and families, are experiencing a yearning for the “good old days” of fully in-person schooling. As the place where children and adolescents spend a good portion of their waking hours, school is integral to not just children’s academic development, but to emotional and social development as well. One interesting phenomenon I’ve seen working with many children and families is that the strong desire to go back to school is not universal. Some of my patients are perfectly happy to be doing “remote schooling”, as it reduces the stress that they were experiencing in this setting before the pandemic.1 These families find themselves wondering – how will I get my child to return to school? As we (hopefully) turn the corner toward a return to normalcy, I believe many of us may find ourselves counseling families on whether a return to in-person schooling is in their child’s best interest. Even when a family decides it is best for their child to return, we might encounter scenarios in which children and adolescents outright refuse to go to school, or engage in avoidant behavior, which is broadly known as “school refusal.” Discussion of a treatment approach to this often challenging clinical scenario is warranted.
The first step in addressing the issue is defining it. School refusal is not a “diagnosis” in psychiatric lexicon, rather it describes a behavior which may be a symptom or manifestation of any number of underlying factors. One helpful definition proposed is (a) missing 25% of total school time for at least 2 weeks or (b) experiencing difficulty attending school such that there is significant interference in the child’s or family’s daily routine for at least 2 weeks, or (c) missing at least 10 days of school over a period of 15 weeks.2 The common thread of this, and any other definition, is sustained absenteeism or avoidance with significant impact to education, family life, or both. It is estimated that the prevalence of this phenomenon is between 1% and 2% of school-aged children.
Next to consider is what might be prompting or underlying the behavior. A comprehensive evaluation approach should include consideration of environmental factors such as bullying and learning difficulties, as well as presence of an anxiety or depressive disorder. Awareness of whether the child/adolescent has a 504 plan or individualized education program (IEP) is vital, as these can be marshaled for additional support. Family factors, including parental illness (medical and/or psychiatric), should also be considered. As school avoidance behaviors often include somatic symptoms of anxiety such as palpitations, shortness of breath, and abdominal pain; a rule out of medical etiology is recommended, as well as a caution to consider both medical and behavioral factors simultaneously, as focus on either separately can lead to missing the other.
Separation anxiety and social anxiety disorders are two specific conditions that may manifest in school refusal and should be evaluated for specifically. Separation anxiety is characterized by developmentally inappropriate, excessive worry or distress associated with separation from a primary caregiver or major attachment figure. Social anxiety is characterized by excessive fear or worry about being negatively evaluated by others in social situations.3 One publicly available tool that can be helpful for screening for a variety of anxiety disorders in children and adolescents is the SCARED.4 The PHQ-9 Adolescent5 is one such screening instrument for depression, which can be a driving factor or co-occur in children with school refusal.
When it comes to treatment, the best evidence out there is for a cognitive-behavioral therapy (CBT)–based approach motivated toward a return to the school setting as soon as possible.6,7 This will involve looking at how thoughts, behaviors, and feelings are interacting with each other in the clinical scenario and how these might be challenged or changed in a positive manner. Coping and problem-solving skills are often incorporated. This approach may also involve gradual exposure to the anxiety-producing situation in a hierarchical fashion starting with less anxiety-provoking scenarios and moving toward increasingly challenging ones. CBT for school refusal is likely most effective when including both school and family involvement to ensure consistency across settings. Making sure that there are not inadvertent reinforcing factors motivating staying home (for instance unrestricted access to electronic devices) is an important step to consider. If anxiety or depression is moderately to severely impairing – which is frequently the case when school refusal comes to clinical attention, consider use of medication as part of the treatment strategy. Selective serotonin reuptake inhibitors as a class are the most commonly used medications and deserve strong consideration.
To summarize, school refusal can occur for a variety of reasons. Early identification and comprehensive treatment taking into account child and family preference and using a multimodal approach to encourage and support a quick return to the school environment is considered best practice.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. See, for example: www.npr.org/2021/03/08/971457441/as-many-parents-fret-over-remote-learning-some-find-their-kids-are-thriving.
2. Kearney CA. Educ Psychol Rev. 2008;20:257-82.
3. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, Va.: American Psychiatric Association, 2013.
4. Available at: www.pediatricbipolar.pitt.edu/resources/instruments.
5. Available at: www.aacap.org/App_Themes/AACAP/docs/member_resources/toolbox_for_clinical_practice_and_outcomes/symptoms/GLAD-PC_PHQ-9.pdf.
6. Elliott JG and Place M. J Child Psychol Psychiatry. 2019;60(1):4-15.
7. Prabhuswamy M. J Paed Child Health. 2018;54(10):1117-20.
Hooray for back to school! But not for everyone. ... what to do with those who have trouble transitioning back?
As we have now passed a year since COVID-19–related shutdowns were implemented throughout the United States; and with returns to in-person schooling continuing to vary based on location, many of us either in our personal lives, or through conversations with patients and families, are experiencing a yearning for the “good old days” of fully in-person schooling. As the place where children and adolescents spend a good portion of their waking hours, school is integral to not just children’s academic development, but to emotional and social development as well. One interesting phenomenon I’ve seen working with many children and families is that the strong desire to go back to school is not universal. Some of my patients are perfectly happy to be doing “remote schooling”, as it reduces the stress that they were experiencing in this setting before the pandemic.1 These families find themselves wondering – how will I get my child to return to school? As we (hopefully) turn the corner toward a return to normalcy, I believe many of us may find ourselves counseling families on whether a return to in-person schooling is in their child’s best interest. Even when a family decides it is best for their child to return, we might encounter scenarios in which children and adolescents outright refuse to go to school, or engage in avoidant behavior, which is broadly known as “school refusal.” Discussion of a treatment approach to this often challenging clinical scenario is warranted.
The first step in addressing the issue is defining it. School refusal is not a “diagnosis” in psychiatric lexicon, rather it describes a behavior which may be a symptom or manifestation of any number of underlying factors. One helpful definition proposed is (a) missing 25% of total school time for at least 2 weeks or (b) experiencing difficulty attending school such that there is significant interference in the child’s or family’s daily routine for at least 2 weeks, or (c) missing at least 10 days of school over a period of 15 weeks.2 The common thread of this, and any other definition, is sustained absenteeism or avoidance with significant impact to education, family life, or both. It is estimated that the prevalence of this phenomenon is between 1% and 2% of school-aged children.
Next to consider is what might be prompting or underlying the behavior. A comprehensive evaluation approach should include consideration of environmental factors such as bullying and learning difficulties, as well as presence of an anxiety or depressive disorder. Awareness of whether the child/adolescent has a 504 plan or individualized education program (IEP) is vital, as these can be marshaled for additional support. Family factors, including parental illness (medical and/or psychiatric), should also be considered. As school avoidance behaviors often include somatic symptoms of anxiety such as palpitations, shortness of breath, and abdominal pain; a rule out of medical etiology is recommended, as well as a caution to consider both medical and behavioral factors simultaneously, as focus on either separately can lead to missing the other.
Separation anxiety and social anxiety disorders are two specific conditions that may manifest in school refusal and should be evaluated for specifically. Separation anxiety is characterized by developmentally inappropriate, excessive worry or distress associated with separation from a primary caregiver or major attachment figure. Social anxiety is characterized by excessive fear or worry about being negatively evaluated by others in social situations.3 One publicly available tool that can be helpful for screening for a variety of anxiety disorders in children and adolescents is the SCARED.4 The PHQ-9 Adolescent5 is one such screening instrument for depression, which can be a driving factor or co-occur in children with school refusal.
When it comes to treatment, the best evidence out there is for a cognitive-behavioral therapy (CBT)–based approach motivated toward a return to the school setting as soon as possible.6,7 This will involve looking at how thoughts, behaviors, and feelings are interacting with each other in the clinical scenario and how these might be challenged or changed in a positive manner. Coping and problem-solving skills are often incorporated. This approach may also involve gradual exposure to the anxiety-producing situation in a hierarchical fashion starting with less anxiety-provoking scenarios and moving toward increasingly challenging ones. CBT for school refusal is likely most effective when including both school and family involvement to ensure consistency across settings. Making sure that there are not inadvertent reinforcing factors motivating staying home (for instance unrestricted access to electronic devices) is an important step to consider. If anxiety or depression is moderately to severely impairing – which is frequently the case when school refusal comes to clinical attention, consider use of medication as part of the treatment strategy. Selective serotonin reuptake inhibitors as a class are the most commonly used medications and deserve strong consideration.
To summarize, school refusal can occur for a variety of reasons. Early identification and comprehensive treatment taking into account child and family preference and using a multimodal approach to encourage and support a quick return to the school environment is considered best practice.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. See, for example: www.npr.org/2021/03/08/971457441/as-many-parents-fret-over-remote-learning-some-find-their-kids-are-thriving.
2. Kearney CA. Educ Psychol Rev. 2008;20:257-82.
3. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, Va.: American Psychiatric Association, 2013.
4. Available at: www.pediatricbipolar.pitt.edu/resources/instruments.
5. Available at: www.aacap.org/App_Themes/AACAP/docs/member_resources/toolbox_for_clinical_practice_and_outcomes/symptoms/GLAD-PC_PHQ-9.pdf.
6. Elliott JG and Place M. J Child Psychol Psychiatry. 2019;60(1):4-15.
7. Prabhuswamy M. J Paed Child Health. 2018;54(10):1117-20.
Hooray for back to school! But not for everyone. ... what to do with those who have trouble transitioning back?
As we have now passed a year since COVID-19–related shutdowns were implemented throughout the United States; and with returns to in-person schooling continuing to vary based on location, many of us either in our personal lives, or through conversations with patients and families, are experiencing a yearning for the “good old days” of fully in-person schooling. As the place where children and adolescents spend a good portion of their waking hours, school is integral to not just children’s academic development, but to emotional and social development as well. One interesting phenomenon I’ve seen working with many children and families is that the strong desire to go back to school is not universal. Some of my patients are perfectly happy to be doing “remote schooling”, as it reduces the stress that they were experiencing in this setting before the pandemic.1 These families find themselves wondering – how will I get my child to return to school? As we (hopefully) turn the corner toward a return to normalcy, I believe many of us may find ourselves counseling families on whether a return to in-person schooling is in their child’s best interest. Even when a family decides it is best for their child to return, we might encounter scenarios in which children and adolescents outright refuse to go to school, or engage in avoidant behavior, which is broadly known as “school refusal.” Discussion of a treatment approach to this often challenging clinical scenario is warranted.
The first step in addressing the issue is defining it. School refusal is not a “diagnosis” in psychiatric lexicon, rather it describes a behavior which may be a symptom or manifestation of any number of underlying factors. One helpful definition proposed is (a) missing 25% of total school time for at least 2 weeks or (b) experiencing difficulty attending school such that there is significant interference in the child’s or family’s daily routine for at least 2 weeks, or (c) missing at least 10 days of school over a period of 15 weeks.2 The common thread of this, and any other definition, is sustained absenteeism or avoidance with significant impact to education, family life, or both. It is estimated that the prevalence of this phenomenon is between 1% and 2% of school-aged children.
Next to consider is what might be prompting or underlying the behavior. A comprehensive evaluation approach should include consideration of environmental factors such as bullying and learning difficulties, as well as presence of an anxiety or depressive disorder. Awareness of whether the child/adolescent has a 504 plan or individualized education program (IEP) is vital, as these can be marshaled for additional support. Family factors, including parental illness (medical and/or psychiatric), should also be considered. As school avoidance behaviors often include somatic symptoms of anxiety such as palpitations, shortness of breath, and abdominal pain; a rule out of medical etiology is recommended, as well as a caution to consider both medical and behavioral factors simultaneously, as focus on either separately can lead to missing the other.
Separation anxiety and social anxiety disorders are two specific conditions that may manifest in school refusal and should be evaluated for specifically. Separation anxiety is characterized by developmentally inappropriate, excessive worry or distress associated with separation from a primary caregiver or major attachment figure. Social anxiety is characterized by excessive fear or worry about being negatively evaluated by others in social situations.3 One publicly available tool that can be helpful for screening for a variety of anxiety disorders in children and adolescents is the SCARED.4 The PHQ-9 Adolescent5 is one such screening instrument for depression, which can be a driving factor or co-occur in children with school refusal.
When it comes to treatment, the best evidence out there is for a cognitive-behavioral therapy (CBT)–based approach motivated toward a return to the school setting as soon as possible.6,7 This will involve looking at how thoughts, behaviors, and feelings are interacting with each other in the clinical scenario and how these might be challenged or changed in a positive manner. Coping and problem-solving skills are often incorporated. This approach may also involve gradual exposure to the anxiety-producing situation in a hierarchical fashion starting with less anxiety-provoking scenarios and moving toward increasingly challenging ones. CBT for school refusal is likely most effective when including both school and family involvement to ensure consistency across settings. Making sure that there are not inadvertent reinforcing factors motivating staying home (for instance unrestricted access to electronic devices) is an important step to consider. If anxiety or depression is moderately to severely impairing – which is frequently the case when school refusal comes to clinical attention, consider use of medication as part of the treatment strategy. Selective serotonin reuptake inhibitors as a class are the most commonly used medications and deserve strong consideration.
To summarize, school refusal can occur for a variety of reasons. Early identification and comprehensive treatment taking into account child and family preference and using a multimodal approach to encourage and support a quick return to the school environment is considered best practice.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. See, for example: www.npr.org/2021/03/08/971457441/as-many-parents-fret-over-remote-learning-some-find-their-kids-are-thriving.
2. Kearney CA. Educ Psychol Rev. 2008;20:257-82.
3. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, Va.: American Psychiatric Association, 2013.
4. Available at: www.pediatricbipolar.pitt.edu/resources/instruments.
5. Available at: www.aacap.org/App_Themes/AACAP/docs/member_resources/toolbox_for_clinical_practice_and_outcomes/symptoms/GLAD-PC_PHQ-9.pdf.
6. Elliott JG and Place M. J Child Psychol Psychiatry. 2019;60(1):4-15.
7. Prabhuswamy M. J Paed Child Health. 2018;54(10):1117-20.
AAP issues five recommendations for common dermatologic problems
The American Academy of Pediatrics recently issued five recommendations for the most common dermatologic problems in primary care pediatrics.
Topics include diagnostic and management strategies for a variety of conditions, including atopic dermatitis, fungal infections, and autoimmune conditions.
The AAP Section on Dermatology created the recommendations, which were then reviewed and approved by “more than a dozen relevant AAP committees, councils, and sections,” before final approval by the AAP executive committee and board of directors.
The final list represents a collaborative effort with the Choosing Wisely initiative of the American Board of Internal Medicine Foundation, which aims “to promote conversations between clinicians and patients by helping patients choose care that is supported by evidence, not duplicative of other tests or procedures already received, free from harm, [and] truly necessary.”
Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego, said that the recommendations are “a fine set of suggestions to help health care providers with some of their pediatric dermatology issues.”
• To begin, the AAP recommended against use of combination topical steroid antifungals for candida skin infections, diaper dermatitis, and tinea corporis, despite approvals for these indications.
“Many providers are unaware that the combination products contain a relatively high-potency topical steroid,” the AAP wrote, noting that “combination products are also often expensive and not covered by pharmacy plans.”
Diaper dermatitis responds best to barrier creams and ointments alone, according to the AAP. If needed, a topical, low-potency steroid may be used no more than twice a day, and tapered with improvement. Similarly, the AAP recommended a separate, low-potency steroid for tinea corporis if pruritus is severe.
• In contrast with this call for minimal treatment intensity, the AAP recommended a more intensive approach to tinea capitis, advising against topical medications alone.
“Topical treatments cannot penetrate the hair shaft itself, which is where the infection lies; thus, monotherapy with topical medications is insufficient to effectively treat the infection,” the AAP wrote. “This insufficient treatment can lead to increased health care costs resulting from multiple visits and the prescribing of ineffective medications.”
While medicated shampoos may still be used as adjunctive treatments for tinea capitis, the AAP recommended primary therapy with either griseofulvin or terbinafine, slightly favoring terbinafine because of adequate efficacy, lesser expense, and shorter regimen.
According to Dr. Eichenfield, a more thorough workup should also be considered.
“Consider culturing possible tinea capitis, so that oral antifungals can be used judiciously and not used for other scaling scalp diagnoses,” he said.
• For most cases of atopic dermatitis, the AAP advised against oral or injected corticosteroids, despite rapid efficacy, because of potential for adverse events, such as adrenal suppression, growth retardation, and disease worsening upon discontinuation. Instead, they recommended topical therapies, “good skin care practices,” and if necessary, “phototherapy and/or steroid-sparing systemic agents.”
“Systemic corticosteroids should only be prescribed for severe flares once all other treatment options have been exhausted and should be limited to a short course for the purpose of bridging to a steroid-sparing agent,” the AAP wrote.
Dr. Eichenfield emphasized this point, noting that new therapies have expanded treatment options.
“Be aware of the advances in atopic dermatitis,” he said, “with newer topical medications and with a new systemic biologic agent approved for moderate to severe refractory atopic dermatitis for ages 6 and older.”
• Turning to diagnostic strategies, the AAP recommended against routine laboratory testing for associated autoimmune diseases among patients with vitiligo, unless clinical signs and/or symptoms of such diseases are present.
“There is no convincing evidence that extensive workups in the absence of specific clinical suspicion improves outcomes for patients and may in fact beget additional costs and harms,” the AAP wrote. “Although many studies suggest ordering these tests, it is based largely on the increased cosegregation of vitiligo and thyroid disease and not on improved outcomes from having identified an abnormal laboratory test result.”
• Similarly, the AAP advised practitioners to avoid routinely testing patients with alopecia areata for other diseases if relevant symptoms and signs aren’t present.
“As in the case of vitiligo, it is more common to find thyroid autoantibodies or subclinical hypothyroidism than overt thyroid disease, unless there are clinically suspicious findings,” the AAP wrote. “Patients identified as having subclinical hypothyroidism are not currently treated and may even have resolution of the abnormal TSH.”
Before drawing blood, Dr. Eichenfield suggested that clinicians first ask the right questions.
“Be comfortable with screening questions about growth, weight, or activity changes to assist with decisions for thyroid screening in a patient with vitiligo or alopecia areata,” he said.
Choosing Wisely is an initiative of the American Board of Internal Medicine. The AAP and Dr. Eichenfield reported no conflicts of interest.
The American Academy of Pediatrics recently issued five recommendations for the most common dermatologic problems in primary care pediatrics.
Topics include diagnostic and management strategies for a variety of conditions, including atopic dermatitis, fungal infections, and autoimmune conditions.
The AAP Section on Dermatology created the recommendations, which were then reviewed and approved by “more than a dozen relevant AAP committees, councils, and sections,” before final approval by the AAP executive committee and board of directors.
The final list represents a collaborative effort with the Choosing Wisely initiative of the American Board of Internal Medicine Foundation, which aims “to promote conversations between clinicians and patients by helping patients choose care that is supported by evidence, not duplicative of other tests or procedures already received, free from harm, [and] truly necessary.”
Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego, said that the recommendations are “a fine set of suggestions to help health care providers with some of their pediatric dermatology issues.”
• To begin, the AAP recommended against use of combination topical steroid antifungals for candida skin infections, diaper dermatitis, and tinea corporis, despite approvals for these indications.
“Many providers are unaware that the combination products contain a relatively high-potency topical steroid,” the AAP wrote, noting that “combination products are also often expensive and not covered by pharmacy plans.”
Diaper dermatitis responds best to barrier creams and ointments alone, according to the AAP. If needed, a topical, low-potency steroid may be used no more than twice a day, and tapered with improvement. Similarly, the AAP recommended a separate, low-potency steroid for tinea corporis if pruritus is severe.
• In contrast with this call for minimal treatment intensity, the AAP recommended a more intensive approach to tinea capitis, advising against topical medications alone.
“Topical treatments cannot penetrate the hair shaft itself, which is where the infection lies; thus, monotherapy with topical medications is insufficient to effectively treat the infection,” the AAP wrote. “This insufficient treatment can lead to increased health care costs resulting from multiple visits and the prescribing of ineffective medications.”
While medicated shampoos may still be used as adjunctive treatments for tinea capitis, the AAP recommended primary therapy with either griseofulvin or terbinafine, slightly favoring terbinafine because of adequate efficacy, lesser expense, and shorter regimen.
According to Dr. Eichenfield, a more thorough workup should also be considered.
“Consider culturing possible tinea capitis, so that oral antifungals can be used judiciously and not used for other scaling scalp diagnoses,” he said.
• For most cases of atopic dermatitis, the AAP advised against oral or injected corticosteroids, despite rapid efficacy, because of potential for adverse events, such as adrenal suppression, growth retardation, and disease worsening upon discontinuation. Instead, they recommended topical therapies, “good skin care practices,” and if necessary, “phototherapy and/or steroid-sparing systemic agents.”
“Systemic corticosteroids should only be prescribed for severe flares once all other treatment options have been exhausted and should be limited to a short course for the purpose of bridging to a steroid-sparing agent,” the AAP wrote.
Dr. Eichenfield emphasized this point, noting that new therapies have expanded treatment options.
“Be aware of the advances in atopic dermatitis,” he said, “with newer topical medications and with a new systemic biologic agent approved for moderate to severe refractory atopic dermatitis for ages 6 and older.”
• Turning to diagnostic strategies, the AAP recommended against routine laboratory testing for associated autoimmune diseases among patients with vitiligo, unless clinical signs and/or symptoms of such diseases are present.
“There is no convincing evidence that extensive workups in the absence of specific clinical suspicion improves outcomes for patients and may in fact beget additional costs and harms,” the AAP wrote. “Although many studies suggest ordering these tests, it is based largely on the increased cosegregation of vitiligo and thyroid disease and not on improved outcomes from having identified an abnormal laboratory test result.”
• Similarly, the AAP advised practitioners to avoid routinely testing patients with alopecia areata for other diseases if relevant symptoms and signs aren’t present.
“As in the case of vitiligo, it is more common to find thyroid autoantibodies or subclinical hypothyroidism than overt thyroid disease, unless there are clinically suspicious findings,” the AAP wrote. “Patients identified as having subclinical hypothyroidism are not currently treated and may even have resolution of the abnormal TSH.”
Before drawing blood, Dr. Eichenfield suggested that clinicians first ask the right questions.
“Be comfortable with screening questions about growth, weight, or activity changes to assist with decisions for thyroid screening in a patient with vitiligo or alopecia areata,” he said.
Choosing Wisely is an initiative of the American Board of Internal Medicine. The AAP and Dr. Eichenfield reported no conflicts of interest.
The American Academy of Pediatrics recently issued five recommendations for the most common dermatologic problems in primary care pediatrics.
Topics include diagnostic and management strategies for a variety of conditions, including atopic dermatitis, fungal infections, and autoimmune conditions.
The AAP Section on Dermatology created the recommendations, which were then reviewed and approved by “more than a dozen relevant AAP committees, councils, and sections,” before final approval by the AAP executive committee and board of directors.
The final list represents a collaborative effort with the Choosing Wisely initiative of the American Board of Internal Medicine Foundation, which aims “to promote conversations between clinicians and patients by helping patients choose care that is supported by evidence, not duplicative of other tests or procedures already received, free from harm, [and] truly necessary.”
Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego, said that the recommendations are “a fine set of suggestions to help health care providers with some of their pediatric dermatology issues.”
• To begin, the AAP recommended against use of combination topical steroid antifungals for candida skin infections, diaper dermatitis, and tinea corporis, despite approvals for these indications.
“Many providers are unaware that the combination products contain a relatively high-potency topical steroid,” the AAP wrote, noting that “combination products are also often expensive and not covered by pharmacy plans.”
Diaper dermatitis responds best to barrier creams and ointments alone, according to the AAP. If needed, a topical, low-potency steroid may be used no more than twice a day, and tapered with improvement. Similarly, the AAP recommended a separate, low-potency steroid for tinea corporis if pruritus is severe.
• In contrast with this call for minimal treatment intensity, the AAP recommended a more intensive approach to tinea capitis, advising against topical medications alone.
“Topical treatments cannot penetrate the hair shaft itself, which is where the infection lies; thus, monotherapy with topical medications is insufficient to effectively treat the infection,” the AAP wrote. “This insufficient treatment can lead to increased health care costs resulting from multiple visits and the prescribing of ineffective medications.”
While medicated shampoos may still be used as adjunctive treatments for tinea capitis, the AAP recommended primary therapy with either griseofulvin or terbinafine, slightly favoring terbinafine because of adequate efficacy, lesser expense, and shorter regimen.
According to Dr. Eichenfield, a more thorough workup should also be considered.
“Consider culturing possible tinea capitis, so that oral antifungals can be used judiciously and not used for other scaling scalp diagnoses,” he said.
• For most cases of atopic dermatitis, the AAP advised against oral or injected corticosteroids, despite rapid efficacy, because of potential for adverse events, such as adrenal suppression, growth retardation, and disease worsening upon discontinuation. Instead, they recommended topical therapies, “good skin care practices,” and if necessary, “phototherapy and/or steroid-sparing systemic agents.”
“Systemic corticosteroids should only be prescribed for severe flares once all other treatment options have been exhausted and should be limited to a short course for the purpose of bridging to a steroid-sparing agent,” the AAP wrote.
Dr. Eichenfield emphasized this point, noting that new therapies have expanded treatment options.
“Be aware of the advances in atopic dermatitis,” he said, “with newer topical medications and with a new systemic biologic agent approved for moderate to severe refractory atopic dermatitis for ages 6 and older.”
• Turning to diagnostic strategies, the AAP recommended against routine laboratory testing for associated autoimmune diseases among patients with vitiligo, unless clinical signs and/or symptoms of such diseases are present.
“There is no convincing evidence that extensive workups in the absence of specific clinical suspicion improves outcomes for patients and may in fact beget additional costs and harms,” the AAP wrote. “Although many studies suggest ordering these tests, it is based largely on the increased cosegregation of vitiligo and thyroid disease and not on improved outcomes from having identified an abnormal laboratory test result.”
• Similarly, the AAP advised practitioners to avoid routinely testing patients with alopecia areata for other diseases if relevant symptoms and signs aren’t present.
“As in the case of vitiligo, it is more common to find thyroid autoantibodies or subclinical hypothyroidism than overt thyroid disease, unless there are clinically suspicious findings,” the AAP wrote. “Patients identified as having subclinical hypothyroidism are not currently treated and may even have resolution of the abnormal TSH.”
Before drawing blood, Dr. Eichenfield suggested that clinicians first ask the right questions.
“Be comfortable with screening questions about growth, weight, or activity changes to assist with decisions for thyroid screening in a patient with vitiligo or alopecia areata,” he said.
Choosing Wisely is an initiative of the American Board of Internal Medicine. The AAP and Dr. Eichenfield reported no conflicts of interest.
FROM CHOOSING WISELY AND THE AAP
Fauci worries about possible post–COVID-19 ‘mental health pandemic’
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.

Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.
Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.
Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
The siesta solution
Are you a napper? Unless you’re retired that may sound like a ridiculous question. When could you possibly fit in the time to doze off for even 20 minutes? I suspect there may be one or two of you who, although you are still working, have found a way to schedule a nap into your schedules. The rest of us must wait until we no longer have clinical responsibilities.

In my experience, you regular nappers seem to be the lucky few who have discovered the art of nodding off after lunch and waking up refreshed and ready to take on a full afternoon of patients. We in the unlucky majority may have tried taking a nap but run the risk of its flowing into a deep slumber the length of which we can’t control. Or, more likely, we find that we wake feeling groggy and disoriented and, even worse, the daytime nod off has messed up our nighttime schedule.
Well, it turns out the ability to take daytime naps and reap their cardiometabolic benefits is not just luck but has a significant genetic component. Investigators at Massachusetts General Hospital in Boston have recently published a study in which they report finding more than a score of gene regions that determine a person’s propensity to take daytime naps.. The researchers have also unearthed preliminary evidence supporting a link between daytime napping and cardiometabolic health. My mother began napping when my sister and I were infants and never gave it up. Unfortunately, I seem to have ended up on the wrong side of the genomic shuffle.
Although this new research is interesting, I don’t think the investigators have enough information to answer one of the questions that every pediatrician fields multiple times each week. “When should my toddler grow out of his afternoon nap?” Although it looks like we may be getting closer to a gene-based answer, I have always couched my reply in terms of behavior modification and the fostering of habit-forming associations.
As a child begins to transition from multiple short naps interspersed with feedings to a pattern of two distinct naps, I suggest to parents that they begin to think of the afternoon nap as a siesta. In other words, the nap is something that always comes immediately after lunch with no intervening shenanigans. No playtime, no Teletubbies videos, no quick trips to the grocery store, nothing, nada, zip.
At least for me, lunch has always been soporific. And I suspect we will learn eventually that association cuts across the entire genetic landscape to one degree or another. It makes sense to take advantage of that association and remove all other distractions. For some parents, that means creating the illusion that they too are taking a siesta: No TV, no phone calls. Imagine that the whole household has suddenly moved to Spain for the next hour or two. If you’ve ever been a tourist in rural Spain and tried to do anything, buy anything, or visit a museum between 2 and 4 p.m. you’ve got the idea.
When the child is young he or she will probably fall asleep as long as his parents have been reasonably successful at maintaining sleep hygiene practices. As the child is gaining more stamina and gives up the morning nap, the siesta will remain as a quiet time because that’s the way it’s always been in the household. The child may sleep or play quietly, or be read a sleep-inducing story because no other options will be available until some predetermined time. An hour is usually reasonable. If sleep hasn’t overtaken them, an earlier bedtime will probably be in order. The child will outgrow the napping part of the siesta when his or her sleep need is gone. But, the siesta/quiet time can remain as an option until all-day school intervenes. This scheme works if you can get parents to appropriately prioritize their child’s sleep needs. That’s not always an easy sell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Are you a napper? Unless you’re retired that may sound like a ridiculous question. When could you possibly fit in the time to doze off for even 20 minutes? I suspect there may be one or two of you who, although you are still working, have found a way to schedule a nap into your schedules. The rest of us must wait until we no longer have clinical responsibilities.
In my experience, you regular nappers seem to be the lucky few who have discovered the art of nodding off after lunch and waking up refreshed and ready to take on a full afternoon of patients. We in the unlucky majority may have tried taking a nap but run the risk of its flowing into a deep slumber the length of which we can’t control. Or, more likely, we find that we wake feeling groggy and disoriented and, even worse, the daytime nod off has messed up our nighttime schedule.
Well, it turns out the ability to take daytime naps and reap their cardiometabolic benefits is not just luck but has a significant genetic component. Investigators at Massachusetts General Hospital in Boston have recently published a study in which they report finding more than a score of gene regions that determine a person’s propensity to take daytime naps.. The researchers have also unearthed preliminary evidence supporting a link between daytime napping and cardiometabolic health. My mother began napping when my sister and I were infants and never gave it up. Unfortunately, I seem to have ended up on the wrong side of the genomic shuffle.
Although this new research is interesting, I don’t think the investigators have enough information to answer one of the questions that every pediatrician fields multiple times each week. “When should my toddler grow out of his afternoon nap?” Although it looks like we may be getting closer to a gene-based answer, I have always couched my reply in terms of behavior modification and the fostering of habit-forming associations.
As a child begins to transition from multiple short naps interspersed with feedings to a pattern of two distinct naps, I suggest to parents that they begin to think of the afternoon nap as a siesta. In other words, the nap is something that always comes immediately after lunch with no intervening shenanigans. No playtime, no Teletubbies videos, no quick trips to the grocery store, nothing, nada, zip.
At least for me, lunch has always been soporific. And I suspect we will learn eventually that association cuts across the entire genetic landscape to one degree or another. It makes sense to take advantage of that association and remove all other distractions. For some parents, that means creating the illusion that they too are taking a siesta: No TV, no phone calls. Imagine that the whole household has suddenly moved to Spain for the next hour or two. If you’ve ever been a tourist in rural Spain and tried to do anything, buy anything, or visit a museum between 2 and 4 p.m. you’ve got the idea.
When the child is young he or she will probably fall asleep as long as his parents have been reasonably successful at maintaining sleep hygiene practices. As the child is gaining more stamina and gives up the morning nap, the siesta will remain as a quiet time because that’s the way it’s always been in the household. The child may sleep or play quietly, or be read a sleep-inducing story because no other options will be available until some predetermined time. An hour is usually reasonable. If sleep hasn’t overtaken them, an earlier bedtime will probably be in order. The child will outgrow the napping part of the siesta when his or her sleep need is gone. But, the siesta/quiet time can remain as an option until all-day school intervenes. This scheme works if you can get parents to appropriately prioritize their child’s sleep needs. That’s not always an easy sell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Are you a napper? Unless you’re retired that may sound like a ridiculous question. When could you possibly fit in the time to doze off for even 20 minutes? I suspect there may be one or two of you who, although you are still working, have found a way to schedule a nap into your schedules. The rest of us must wait until we no longer have clinical responsibilities.
In my experience, you regular nappers seem to be the lucky few who have discovered the art of nodding off after lunch and waking up refreshed and ready to take on a full afternoon of patients. We in the unlucky majority may have tried taking a nap but run the risk of its flowing into a deep slumber the length of which we can’t control. Or, more likely, we find that we wake feeling groggy and disoriented and, even worse, the daytime nod off has messed up our nighttime schedule.
Well, it turns out the ability to take daytime naps and reap their cardiometabolic benefits is not just luck but has a significant genetic component. Investigators at Massachusetts General Hospital in Boston have recently published a study in which they report finding more than a score of gene regions that determine a person’s propensity to take daytime naps.. The researchers have also unearthed preliminary evidence supporting a link between daytime napping and cardiometabolic health. My mother began napping when my sister and I were infants and never gave it up. Unfortunately, I seem to have ended up on the wrong side of the genomic shuffle.
Although this new research is interesting, I don’t think the investigators have enough information to answer one of the questions that every pediatrician fields multiple times each week. “When should my toddler grow out of his afternoon nap?” Although it looks like we may be getting closer to a gene-based answer, I have always couched my reply in terms of behavior modification and the fostering of habit-forming associations.
As a child begins to transition from multiple short naps interspersed with feedings to a pattern of two distinct naps, I suggest to parents that they begin to think of the afternoon nap as a siesta. In other words, the nap is something that always comes immediately after lunch with no intervening shenanigans. No playtime, no Teletubbies videos, no quick trips to the grocery store, nothing, nada, zip.
At least for me, lunch has always been soporific. And I suspect we will learn eventually that association cuts across the entire genetic landscape to one degree or another. It makes sense to take advantage of that association and remove all other distractions. For some parents, that means creating the illusion that they too are taking a siesta: No TV, no phone calls. Imagine that the whole household has suddenly moved to Spain for the next hour or two. If you’ve ever been a tourist in rural Spain and tried to do anything, buy anything, or visit a museum between 2 and 4 p.m. you’ve got the idea.
When the child is young he or she will probably fall asleep as long as his parents have been reasonably successful at maintaining sleep hygiene practices. As the child is gaining more stamina and gives up the morning nap, the siesta will remain as a quiet time because that’s the way it’s always been in the household. The child may sleep or play quietly, or be read a sleep-inducing story because no other options will be available until some predetermined time. An hour is usually reasonable. If sleep hasn’t overtaken them, an earlier bedtime will probably be in order. The child will outgrow the napping part of the siesta when his or her sleep need is gone. But, the siesta/quiet time can remain as an option until all-day school intervenes. This scheme works if you can get parents to appropriately prioritize their child’s sleep needs. That’s not always an easy sell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Decline in child COVID-19 cases picks up after 2-week slowdown
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.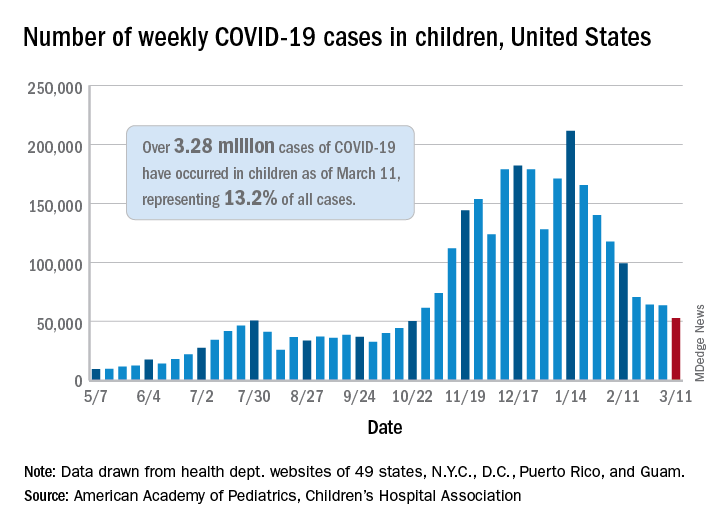
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
First pill for COVID-19 could be ready by year’s end
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.

Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
Is pediatric subspecialty training financially worth it?
Pursuing fellowship training is often financially costly in terms of lifetime earnings, compared with starting a career as a general pediatrician immediately after residency, a report suggests.
Researchers found that most pediatric subspecialists – including those practicing neurology, pulmonology, and adolescent medicine – do not see a financial return from additional training because of the delays in receiving increased compensation and the repayment of educational debt.
“Most pediatric subspecialists don’t experience a relative increase in compensation after training compared to a general pediatrician, so there isn’t a financial benefit to additional training,” lead author Eva Catenaccio, MD, from the division of pediatric neurology, department of neurology, Johns Hopkins University, Baltimore, told this news organization.
The findings, published online March 8 in Pediatrics, contribute to the ongoing debate about the length of pediatric fellowship training programs. The data also provide evidence for the potential effect of a pediatric subspecialty loan repayment program.
Pediatric subspecialty training rarely pays off
However, not all practitioners in pediatric subspecialties would find themselves in the red relative to their generalist peers. Three subspecialties had a positive financial return: cardiology, critical care, and neonatology. Dr. Catenaccio explained that this may be because these subspecialties tend to be “inpatient procedure oriented, which are often more [lucrative] than outpatient cognitive–oriented subspecialties, such as pediatric infectious diseases, endocrinology, or adolescent medicine.”
Enrolling in a pediatric fellowship program resulted in lifetime financial returns that ranged from an increase of $852,129 for cardiology, relative to general pediatrics, to a loss of $1,594,366 for adolescent medicine, researchers found.
For the study, researchers calculated the financial returns of 15 pediatric subspecialties – emergency medicine, neurology, cardiology, critical care, neonatology, hematology and oncology, pulmonology, hospitalist medicine, allergy and immunology, gastroenterology, rheumatology, nephrology, adolescent medicine, infectious diseases, and endocrinology – in comparison with returns of private practice general pediatrics on the basis of 2018-2019 data on fellowship stipends, compensation, and educational debt.
They obtained most of the data from the Association of American Medical Colleges Survey of Resident/Fellow Stipends and Benefits, AAMC’s annual Medical School Faculty Salary Report, and the AAMC Medical School Graduation Questionnaire.
Richard Mink, MD, department of pediatrics, Harbor-UCLA Medical Center, Torrance, Calif., noted that it would have been helpful to have also compared the lifetime earnings of practitioners in pediatric subspecialties to academic general pediatricians and not just those in private practice.
The financial gap has worsened
To better understand which aspects of fellowship training have the greatest effect on lifetime compensation, Dr. Catenaccio and colleagues evaluated the potential effects of shortening fellowship length, eliminating school debt, and implementing a federal loan repayment plan. These changes enhanced the returns of cardiology, critical care, and neonatology – subspecialties that had already seen financial returns before these changes – and resulted in a positive financial return for emergency medicine.
The changes also narrowed the financial gap between subspecialties and general pediatrics. However, the remaining subspecialties still earned less than private practice pediatrics.
The new study is an update to a 2011 report, which reflected 2007-2008 data for 11 subspecialties. This time around, the researchers included the subspecialty of hospitalist medicine, which was approved as a board-certified subspecialty by the American Board of Pediatrics in 2014, as well as neurology, allergy and immunology, and adolescent medicine.
“I was most surprised that the additional pediatric subspecialties we included since the 2011 report followed the same general trend, with pediatric subspecialty training having a lower lifetime earning potential than general pediatrics,” Dr. Catenaccio said.
Comparing results from the two study periods showed that the financial gap between general pediatrics and subspecialty pediatrics worsened over time. For example, the financial return for pediatric endocrinology decreased an additional $500,000 between 2007 and 2018.
The researchers believe a combination of increased educational debt burden, slow growth in compensation, and changing interest rates over time have caused the financial differences between general pediatrics and subspecialty pediatrics to become more pronounced.
‘Pediatric subspecialty training is worth it!’
Despite the financial gaps, Dr. Catenaccio and colleagues say pediatric subspecialty training is still worthwhile but that policymakers should address these financial differences to help guide workforce distribution in a way that meets the needs of patients.
“I think pediatric subspecialty training is worth it,” said Dr. Catenaccio, who’s pursuing pediatric subspecialty training. “There are so many factors that go into choosing a specialty or subspecialty in medicine, including the desire to care for a particular patient population, interest in certain diseases or organ systems, lifestyle considerations, and research opportunities.”
But it’s also important for trainees to be aware of economic considerations in their decision-making.
Dr. Mink, who wrote an accompanying commentary, agrees that young clinicians should not make career decisions on the basis of metrics such as lifetime earning measures.
“I think people who go into pediatrics have decided that money is not the driving force,” said Dr. Mink. He noted that pediatricians are usually not paid well, compared with other specialists. “To me the important thing is you have to like what you’re doing.”
A 2020 study found that trainees who chose a career in pediatric pulmonology, a subspecialty, said that financial considerations were not the driving factor in their decision-making. Nevertheless, Dr. Mink also believes young clinicians should take into account their educational debt.
The further widening of the financial gap between general pediatrics and pediatric subspecialties could lead to shortages in the pediatric subspecialty workforce.
The authors and Dr. Mink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pursuing fellowship training is often financially costly in terms of lifetime earnings, compared with starting a career as a general pediatrician immediately after residency, a report suggests.
Researchers found that most pediatric subspecialists – including those practicing neurology, pulmonology, and adolescent medicine – do not see a financial return from additional training because of the delays in receiving increased compensation and the repayment of educational debt.
“Most pediatric subspecialists don’t experience a relative increase in compensation after training compared to a general pediatrician, so there isn’t a financial benefit to additional training,” lead author Eva Catenaccio, MD, from the division of pediatric neurology, department of neurology, Johns Hopkins University, Baltimore, told this news organization.
The findings, published online March 8 in Pediatrics, contribute to the ongoing debate about the length of pediatric fellowship training programs. The data also provide evidence for the potential effect of a pediatric subspecialty loan repayment program.
Pediatric subspecialty training rarely pays off
However, not all practitioners in pediatric subspecialties would find themselves in the red relative to their generalist peers. Three subspecialties had a positive financial return: cardiology, critical care, and neonatology. Dr. Catenaccio explained that this may be because these subspecialties tend to be “inpatient procedure oriented, which are often more [lucrative] than outpatient cognitive–oriented subspecialties, such as pediatric infectious diseases, endocrinology, or adolescent medicine.”
Enrolling in a pediatric fellowship program resulted in lifetime financial returns that ranged from an increase of $852,129 for cardiology, relative to general pediatrics, to a loss of $1,594,366 for adolescent medicine, researchers found.
For the study, researchers calculated the financial returns of 15 pediatric subspecialties – emergency medicine, neurology, cardiology, critical care, neonatology, hematology and oncology, pulmonology, hospitalist medicine, allergy and immunology, gastroenterology, rheumatology, nephrology, adolescent medicine, infectious diseases, and endocrinology – in comparison with returns of private practice general pediatrics on the basis of 2018-2019 data on fellowship stipends, compensation, and educational debt.
They obtained most of the data from the Association of American Medical Colleges Survey of Resident/Fellow Stipends and Benefits, AAMC’s annual Medical School Faculty Salary Report, and the AAMC Medical School Graduation Questionnaire.
Richard Mink, MD, department of pediatrics, Harbor-UCLA Medical Center, Torrance, Calif., noted that it would have been helpful to have also compared the lifetime earnings of practitioners in pediatric subspecialties to academic general pediatricians and not just those in private practice.
The financial gap has worsened
To better understand which aspects of fellowship training have the greatest effect on lifetime compensation, Dr. Catenaccio and colleagues evaluated the potential effects of shortening fellowship length, eliminating school debt, and implementing a federal loan repayment plan. These changes enhanced the returns of cardiology, critical care, and neonatology – subspecialties that had already seen financial returns before these changes – and resulted in a positive financial return for emergency medicine.
The changes also narrowed the financial gap between subspecialties and general pediatrics. However, the remaining subspecialties still earned less than private practice pediatrics.
The new study is an update to a 2011 report, which reflected 2007-2008 data for 11 subspecialties. This time around, the researchers included the subspecialty of hospitalist medicine, which was approved as a board-certified subspecialty by the American Board of Pediatrics in 2014, as well as neurology, allergy and immunology, and adolescent medicine.
“I was most surprised that the additional pediatric subspecialties we included since the 2011 report followed the same general trend, with pediatric subspecialty training having a lower lifetime earning potential than general pediatrics,” Dr. Catenaccio said.
Comparing results from the two study periods showed that the financial gap between general pediatrics and subspecialty pediatrics worsened over time. For example, the financial return for pediatric endocrinology decreased an additional $500,000 between 2007 and 2018.
The researchers believe a combination of increased educational debt burden, slow growth in compensation, and changing interest rates over time have caused the financial differences between general pediatrics and subspecialty pediatrics to become more pronounced.
‘Pediatric subspecialty training is worth it!’
Despite the financial gaps, Dr. Catenaccio and colleagues say pediatric subspecialty training is still worthwhile but that policymakers should address these financial differences to help guide workforce distribution in a way that meets the needs of patients.
“I think pediatric subspecialty training is worth it,” said Dr. Catenaccio, who’s pursuing pediatric subspecialty training. “There are so many factors that go into choosing a specialty or subspecialty in medicine, including the desire to care for a particular patient population, interest in certain diseases or organ systems, lifestyle considerations, and research opportunities.”
But it’s also important for trainees to be aware of economic considerations in their decision-making.
Dr. Mink, who wrote an accompanying commentary, agrees that young clinicians should not make career decisions on the basis of metrics such as lifetime earning measures.
“I think people who go into pediatrics have decided that money is not the driving force,” said Dr. Mink. He noted that pediatricians are usually not paid well, compared with other specialists. “To me the important thing is you have to like what you’re doing.”
A 2020 study found that trainees who chose a career in pediatric pulmonology, a subspecialty, said that financial considerations were not the driving factor in their decision-making. Nevertheless, Dr. Mink also believes young clinicians should take into account their educational debt.
The further widening of the financial gap between general pediatrics and pediatric subspecialties could lead to shortages in the pediatric subspecialty workforce.
The authors and Dr. Mink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pursuing fellowship training is often financially costly in terms of lifetime earnings, compared with starting a career as a general pediatrician immediately after residency, a report suggests.
Researchers found that most pediatric subspecialists – including those practicing neurology, pulmonology, and adolescent medicine – do not see a financial return from additional training because of the delays in receiving increased compensation and the repayment of educational debt.
“Most pediatric subspecialists don’t experience a relative increase in compensation after training compared to a general pediatrician, so there isn’t a financial benefit to additional training,” lead author Eva Catenaccio, MD, from the division of pediatric neurology, department of neurology, Johns Hopkins University, Baltimore, told this news organization.
The findings, published online March 8 in Pediatrics, contribute to the ongoing debate about the length of pediatric fellowship training programs. The data also provide evidence for the potential effect of a pediatric subspecialty loan repayment program.
Pediatric subspecialty training rarely pays off
However, not all practitioners in pediatric subspecialties would find themselves in the red relative to their generalist peers. Three subspecialties had a positive financial return: cardiology, critical care, and neonatology. Dr. Catenaccio explained that this may be because these subspecialties tend to be “inpatient procedure oriented, which are often more [lucrative] than outpatient cognitive–oriented subspecialties, such as pediatric infectious diseases, endocrinology, or adolescent medicine.”
Enrolling in a pediatric fellowship program resulted in lifetime financial returns that ranged from an increase of $852,129 for cardiology, relative to general pediatrics, to a loss of $1,594,366 for adolescent medicine, researchers found.
For the study, researchers calculated the financial returns of 15 pediatric subspecialties – emergency medicine, neurology, cardiology, critical care, neonatology, hematology and oncology, pulmonology, hospitalist medicine, allergy and immunology, gastroenterology, rheumatology, nephrology, adolescent medicine, infectious diseases, and endocrinology – in comparison with returns of private practice general pediatrics on the basis of 2018-2019 data on fellowship stipends, compensation, and educational debt.
They obtained most of the data from the Association of American Medical Colleges Survey of Resident/Fellow Stipends and Benefits, AAMC’s annual Medical School Faculty Salary Report, and the AAMC Medical School Graduation Questionnaire.
Richard Mink, MD, department of pediatrics, Harbor-UCLA Medical Center, Torrance, Calif., noted that it would have been helpful to have also compared the lifetime earnings of practitioners in pediatric subspecialties to academic general pediatricians and not just those in private practice.
The financial gap has worsened
To better understand which aspects of fellowship training have the greatest effect on lifetime compensation, Dr. Catenaccio and colleagues evaluated the potential effects of shortening fellowship length, eliminating school debt, and implementing a federal loan repayment plan. These changes enhanced the returns of cardiology, critical care, and neonatology – subspecialties that had already seen financial returns before these changes – and resulted in a positive financial return for emergency medicine.
The changes also narrowed the financial gap between subspecialties and general pediatrics. However, the remaining subspecialties still earned less than private practice pediatrics.
The new study is an update to a 2011 report, which reflected 2007-2008 data for 11 subspecialties. This time around, the researchers included the subspecialty of hospitalist medicine, which was approved as a board-certified subspecialty by the American Board of Pediatrics in 2014, as well as neurology, allergy and immunology, and adolescent medicine.
“I was most surprised that the additional pediatric subspecialties we included since the 2011 report followed the same general trend, with pediatric subspecialty training having a lower lifetime earning potential than general pediatrics,” Dr. Catenaccio said.
Comparing results from the two study periods showed that the financial gap between general pediatrics and subspecialty pediatrics worsened over time. For example, the financial return for pediatric endocrinology decreased an additional $500,000 between 2007 and 2018.
The researchers believe a combination of increased educational debt burden, slow growth in compensation, and changing interest rates over time have caused the financial differences between general pediatrics and subspecialty pediatrics to become more pronounced.
‘Pediatric subspecialty training is worth it!’
Despite the financial gaps, Dr. Catenaccio and colleagues say pediatric subspecialty training is still worthwhile but that policymakers should address these financial differences to help guide workforce distribution in a way that meets the needs of patients.
“I think pediatric subspecialty training is worth it,” said Dr. Catenaccio, who’s pursuing pediatric subspecialty training. “There are so many factors that go into choosing a specialty or subspecialty in medicine, including the desire to care for a particular patient population, interest in certain diseases or organ systems, lifestyle considerations, and research opportunities.”
But it’s also important for trainees to be aware of economic considerations in their decision-making.
Dr. Mink, who wrote an accompanying commentary, agrees that young clinicians should not make career decisions on the basis of metrics such as lifetime earning measures.
“I think people who go into pediatrics have decided that money is not the driving force,” said Dr. Mink. He noted that pediatricians are usually not paid well, compared with other specialists. “To me the important thing is you have to like what you’re doing.”
A 2020 study found that trainees who chose a career in pediatric pulmonology, a subspecialty, said that financial considerations were not the driving factor in their decision-making. Nevertheless, Dr. Mink also believes young clinicians should take into account their educational debt.
The further widening of the financial gap between general pediatrics and pediatric subspecialties could lead to shortages in the pediatric subspecialty workforce.
The authors and Dr. Mink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Infantile hemangiomas: Accurate diagnosis is crucial
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Helping parents deal with children’s transition to in-person school
This spring may bring an unusual transition for families: a return to in-person school after nearly a year in a virtual classroom. This will undoubtedly come as a welcome relief to many parents worried about their children’s education and development and struggling with running school from home. But it is important for parents to remember that transitions, even happy ones, are difficult. You can help parents to anticipate what may be challenging about this transition for their children so that they are all prepared and can diminish struggles and support their children’s mastery.
Be curious about their children’s thoughts and feelings

Parents should adopt a truly curious and open-minded approach with their children. Remind parents that, while they are experts on their own children, they should not assume they know what their children are thinking or feeling about the return to school. Some children, especially ones struggling with learning problems or difficulty with peers, will have grown very comfortable being at home with parents or siblings. Some children, especially pre- and early teens, may have changed substantially in the year and might feel uncertain about returning to a prior team or group of friends. Some children may feel concerned about leaving a pet at home alone. Some children may be going to a new school and be anxious about facing such a big transition without the usual planning and supports. Those on a college track may be worried they are “behind” academically or in college preparation.
Parents can show up when and where their children are most likely to talk, perhaps bath time or bedtime for younger children or in the car together with their adolescents. They can ask: “Have you been thinking about what it might be like to go back to school? Have your friends been chatting about it?” They might be curious together about what might have changed in a year. What might be really great about being back in a classroom? What might they miss about home school? And what might be new? Are you worried about the work, any of your friends, or not being home? If children can begin to anticipate both the good and the difficult, they will be better equipped to face and manage the challenges and appreciate the delights.
Children in elementary school are built to master new situations but are also prone to anxiety about new expectations and demands. Parents can be calmly curious about what their thoughts, feelings, and questions are and look for answers together. Often all they need is to see parents being calm in the face of uncertainty, bearing the strong feelings that may come, and preserving curiosity and compassion. Adolescents may be grieving the things they have missed, or they may have concerns about relationships and practical matters such as the implications for applying to college. Parents can offer compassion and validation and help them to devise their own strategies to face the practical challenges they are concerned about.
Be mindful of their children’s vulnerabilities
While most children will find the transition back to school easier than they may anticipate, there will be some for whom the transition will be very challenging. Children who have been bullied at school may have found themselves able to concentrate and learn free of the fear and stress of a classmate’s taunts or stares. Children with learning disabilities or ADHD have probably struggled with online school, but they have also likely established strategies and supports during the year that have enabled them to get enough individualized help to get their work done. These children are vulnerable to falling behind and getting discouraged when these supports are lost, and possibly not replaced with new ones in the chaos of transition. Parents should reassure their children that they will work with the school to make sure that they can succeed in the classroom as they did at home.

Children with an inhibited or shy temperament might have found that it was easier to focus and listen in the comfortable setting of home than in a busy, stimulating classroom. Children who suffer from anxiety disorders that may make separating from parents or managing the performance and social demands of school extra difficult will find the return to school especially challenging. Some younger children may have experienced the emergence of an anxiety disorder during the past year, and the return to school may mark the challenge that brings heretofore quiet symptoms into full relief.
These children have all enjoyed being able to avoid the discomfort of certain anxiety-provoking situations, and they may be particularly stressed by anticipating a return to school. Younger children may begin to have stomach aches and other physical complaints as the return to school gets close, older children may seem more withdrawn or irritable or begin discussing ways to continue school from home. Parents should help their children try to identify and describe their worries. For anxious children, having a chance to practice may be very helpful. Visiting their school, especially if it is a new school, or having a planned hangout with a friend (with appropriate precautions) is the kind of exposure that can lessen anticipatory anxiety. If this is not enough, parents should not hesitate to bring in other caring, supportive adults, such as school counselors or therapists that may be essential to helping their children face and manage what may be intense anxiety.
Consider routines to support their transition
Just as parents begin to return their children to an earlier bedtime toward the end of summer, it will be helpful to consider how changing certain routines will support their children now. If children will need to get up earlier to be ready for a bus or a team practice, they should start moving bedtime and wake-up time earlier gradually. Uniforms or backpacks that have not been seen for a year should be dug out. Children who are planning a return to a sport may benefit from gradually increasing their exercise or starting training now. This will have the added benefit of improving sleep and energy and fortifying children for the challenges of change. Parents might consider reaching out to other parents in the same class as their children and having a virtual conversation to share their thoughts.
If their family has developed some new “COVID routines” that they have come to enjoy, they should find a way to preserve them. Perhaps they are having dinner together more often or have established a family game night or Netflix night. Help parents consider how to avoid falling back into overscheduling their children and themselves. If they created a time to Zoom with distant or vulnerable loved ones, they might decide to continue this. School may determine some of their routines, but they should also prioritize their family connections and well-being in deciding how to schedule their days.
Find opportunity for mastery and meaning
As parents are listening, validating, and planning with their children, they might use this time to reflect on valuable lessons. They might point out the value of patience: Adjusting to change takes time and happens in fits and starts. It has been 12 months since many of the pandemic changes started and it will take more than a few days to adjust as schools reopen. They might point out how proud they are of what their children have been able to learn, build, or do during this year, what they admire about them. It may be a time to consider what their family may have lost and gained during the past year, what they are eager to leave behind, and what they might like to keep. And it is also a chance for parents to observe that change is an inevitable part of life (especially when growing up). It is always challenging, and often brings loss and sadness. But if we pay attention, there are also the green shoots of what is new and possible.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
This spring may bring an unusual transition for families: a return to in-person school after nearly a year in a virtual classroom. This will undoubtedly come as a welcome relief to many parents worried about their children’s education and development and struggling with running school from home. But it is important for parents to remember that transitions, even happy ones, are difficult. You can help parents to anticipate what may be challenging about this transition for their children so that they are all prepared and can diminish struggles and support their children’s mastery.
Be curious about their children’s thoughts and feelings
Parents should adopt a truly curious and open-minded approach with their children. Remind parents that, while they are experts on their own children, they should not assume they know what their children are thinking or feeling about the return to school. Some children, especially ones struggling with learning problems or difficulty with peers, will have grown very comfortable being at home with parents or siblings. Some children, especially pre- and early teens, may have changed substantially in the year and might feel uncertain about returning to a prior team or group of friends. Some children may feel concerned about leaving a pet at home alone. Some children may be going to a new school and be anxious about facing such a big transition without the usual planning and supports. Those on a college track may be worried they are “behind” academically or in college preparation.
Parents can show up when and where their children are most likely to talk, perhaps bath time or bedtime for younger children or in the car together with their adolescents. They can ask: “Have you been thinking about what it might be like to go back to school? Have your friends been chatting about it?” They might be curious together about what might have changed in a year. What might be really great about being back in a classroom? What might they miss about home school? And what might be new? Are you worried about the work, any of your friends, or not being home? If children can begin to anticipate both the good and the difficult, they will be better equipped to face and manage the challenges and appreciate the delights.
Children in elementary school are built to master new situations but are also prone to anxiety about new expectations and demands. Parents can be calmly curious about what their thoughts, feelings, and questions are and look for answers together. Often all they need is to see parents being calm in the face of uncertainty, bearing the strong feelings that may come, and preserving curiosity and compassion. Adolescents may be grieving the things they have missed, or they may have concerns about relationships and practical matters such as the implications for applying to college. Parents can offer compassion and validation and help them to devise their own strategies to face the practical challenges they are concerned about.
Be mindful of their children’s vulnerabilities
While most children will find the transition back to school easier than they may anticipate, there will be some for whom the transition will be very challenging. Children who have been bullied at school may have found themselves able to concentrate and learn free of the fear and stress of a classmate’s taunts or stares. Children with learning disabilities or ADHD have probably struggled with online school, but they have also likely established strategies and supports during the year that have enabled them to get enough individualized help to get their work done. These children are vulnerable to falling behind and getting discouraged when these supports are lost, and possibly not replaced with new ones in the chaos of transition. Parents should reassure their children that they will work with the school to make sure that they can succeed in the classroom as they did at home.
Children with an inhibited or shy temperament might have found that it was easier to focus and listen in the comfortable setting of home than in a busy, stimulating classroom. Children who suffer from anxiety disorders that may make separating from parents or managing the performance and social demands of school extra difficult will find the return to school especially challenging. Some younger children may have experienced the emergence of an anxiety disorder during the past year, and the return to school may mark the challenge that brings heretofore quiet symptoms into full relief.
These children have all enjoyed being able to avoid the discomfort of certain anxiety-provoking situations, and they may be particularly stressed by anticipating a return to school. Younger children may begin to have stomach aches and other physical complaints as the return to school gets close, older children may seem more withdrawn or irritable or begin discussing ways to continue school from home. Parents should help their children try to identify and describe their worries. For anxious children, having a chance to practice may be very helpful. Visiting their school, especially if it is a new school, or having a planned hangout with a friend (with appropriate precautions) is the kind of exposure that can lessen anticipatory anxiety. If this is not enough, parents should not hesitate to bring in other caring, supportive adults, such as school counselors or therapists that may be essential to helping their children face and manage what may be intense anxiety.
Consider routines to support their transition
Just as parents begin to return their children to an earlier bedtime toward the end of summer, it will be helpful to consider how changing certain routines will support their children now. If children will need to get up earlier to be ready for a bus or a team practice, they should start moving bedtime and wake-up time earlier gradually. Uniforms or backpacks that have not been seen for a year should be dug out. Children who are planning a return to a sport may benefit from gradually increasing their exercise or starting training now. This will have the added benefit of improving sleep and energy and fortifying children for the challenges of change. Parents might consider reaching out to other parents in the same class as their children and having a virtual conversation to share their thoughts.
If their family has developed some new “COVID routines” that they have come to enjoy, they should find a way to preserve them. Perhaps they are having dinner together more often or have established a family game night or Netflix night. Help parents consider how to avoid falling back into overscheduling their children and themselves. If they created a time to Zoom with distant or vulnerable loved ones, they might decide to continue this. School may determine some of their routines, but they should also prioritize their family connections and well-being in deciding how to schedule their days.
Find opportunity for mastery and meaning
As parents are listening, validating, and planning with their children, they might use this time to reflect on valuable lessons. They might point out the value of patience: Adjusting to change takes time and happens in fits and starts. It has been 12 months since many of the pandemic changes started and it will take more than a few days to adjust as schools reopen. They might point out how proud they are of what their children have been able to learn, build, or do during this year, what they admire about them. It may be a time to consider what their family may have lost and gained during the past year, what they are eager to leave behind, and what they might like to keep. And it is also a chance for parents to observe that change is an inevitable part of life (especially when growing up). It is always challenging, and often brings loss and sadness. But if we pay attention, there are also the green shoots of what is new and possible.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
This spring may bring an unusual transition for families: a return to in-person school after nearly a year in a virtual classroom. This will undoubtedly come as a welcome relief to many parents worried about their children’s education and development and struggling with running school from home. But it is important for parents to remember that transitions, even happy ones, are difficult. You can help parents to anticipate what may be challenging about this transition for their children so that they are all prepared and can diminish struggles and support their children’s mastery.
Be curious about their children’s thoughts and feelings
Parents should adopt a truly curious and open-minded approach with their children. Remind parents that, while they are experts on their own children, they should not assume they know what their children are thinking or feeling about the return to school. Some children, especially ones struggling with learning problems or difficulty with peers, will have grown very comfortable being at home with parents or siblings. Some children, especially pre- and early teens, may have changed substantially in the year and might feel uncertain about returning to a prior team or group of friends. Some children may feel concerned about leaving a pet at home alone. Some children may be going to a new school and be anxious about facing such a big transition without the usual planning and supports. Those on a college track may be worried they are “behind” academically or in college preparation.
Parents can show up when and where their children are most likely to talk, perhaps bath time or bedtime for younger children or in the car together with their adolescents. They can ask: “Have you been thinking about what it might be like to go back to school? Have your friends been chatting about it?” They might be curious together about what might have changed in a year. What might be really great about being back in a classroom? What might they miss about home school? And what might be new? Are you worried about the work, any of your friends, or not being home? If children can begin to anticipate both the good and the difficult, they will be better equipped to face and manage the challenges and appreciate the delights.
Children in elementary school are built to master new situations but are also prone to anxiety about new expectations and demands. Parents can be calmly curious about what their thoughts, feelings, and questions are and look for answers together. Often all they need is to see parents being calm in the face of uncertainty, bearing the strong feelings that may come, and preserving curiosity and compassion. Adolescents may be grieving the things they have missed, or they may have concerns about relationships and practical matters such as the implications for applying to college. Parents can offer compassion and validation and help them to devise their own strategies to face the practical challenges they are concerned about.
Be mindful of their children’s vulnerabilities
While most children will find the transition back to school easier than they may anticipate, there will be some for whom the transition will be very challenging. Children who have been bullied at school may have found themselves able to concentrate and learn free of the fear and stress of a classmate’s taunts or stares. Children with learning disabilities or ADHD have probably struggled with online school, but they have also likely established strategies and supports during the year that have enabled them to get enough individualized help to get their work done. These children are vulnerable to falling behind and getting discouraged when these supports are lost, and possibly not replaced with new ones in the chaos of transition. Parents should reassure their children that they will work with the school to make sure that they can succeed in the classroom as they did at home.
Children with an inhibited or shy temperament might have found that it was easier to focus and listen in the comfortable setting of home than in a busy, stimulating classroom. Children who suffer from anxiety disorders that may make separating from parents or managing the performance and social demands of school extra difficult will find the return to school especially challenging. Some younger children may have experienced the emergence of an anxiety disorder during the past year, and the return to school may mark the challenge that brings heretofore quiet symptoms into full relief.
These children have all enjoyed being able to avoid the discomfort of certain anxiety-provoking situations, and they may be particularly stressed by anticipating a return to school. Younger children may begin to have stomach aches and other physical complaints as the return to school gets close, older children may seem more withdrawn or irritable or begin discussing ways to continue school from home. Parents should help their children try to identify and describe their worries. For anxious children, having a chance to practice may be very helpful. Visiting their school, especially if it is a new school, or having a planned hangout with a friend (with appropriate precautions) is the kind of exposure that can lessen anticipatory anxiety. If this is not enough, parents should not hesitate to bring in other caring, supportive adults, such as school counselors or therapists that may be essential to helping their children face and manage what may be intense anxiety.
Consider routines to support their transition
Just as parents begin to return their children to an earlier bedtime toward the end of summer, it will be helpful to consider how changing certain routines will support their children now. If children will need to get up earlier to be ready for a bus or a team practice, they should start moving bedtime and wake-up time earlier gradually. Uniforms or backpacks that have not been seen for a year should be dug out. Children who are planning a return to a sport may benefit from gradually increasing their exercise or starting training now. This will have the added benefit of improving sleep and energy and fortifying children for the challenges of change. Parents might consider reaching out to other parents in the same class as their children and having a virtual conversation to share their thoughts.
If their family has developed some new “COVID routines” that they have come to enjoy, they should find a way to preserve them. Perhaps they are having dinner together more often or have established a family game night or Netflix night. Help parents consider how to avoid falling back into overscheduling their children and themselves. If they created a time to Zoom with distant or vulnerable loved ones, they might decide to continue this. School may determine some of their routines, but they should also prioritize their family connections and well-being in deciding how to schedule their days.
Find opportunity for mastery and meaning
As parents are listening, validating, and planning with their children, they might use this time to reflect on valuable lessons. They might point out the value of patience: Adjusting to change takes time and happens in fits and starts. It has been 12 months since many of the pandemic changes started and it will take more than a few days to adjust as schools reopen. They might point out how proud they are of what their children have been able to learn, build, or do during this year, what they admire about them. It may be a time to consider what their family may have lost and gained during the past year, what they are eager to leave behind, and what they might like to keep. And it is also a chance for parents to observe that change is an inevitable part of life (especially when growing up). It is always challenging, and often brings loss and sadness. But if we pay attention, there are also the green shoots of what is new and possible.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.