User login
Virus Alerts
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
The Reality of Today

SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
Tough Negotiations Avert B.C. Hospitalist Walkout
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
The Coming Windfall
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
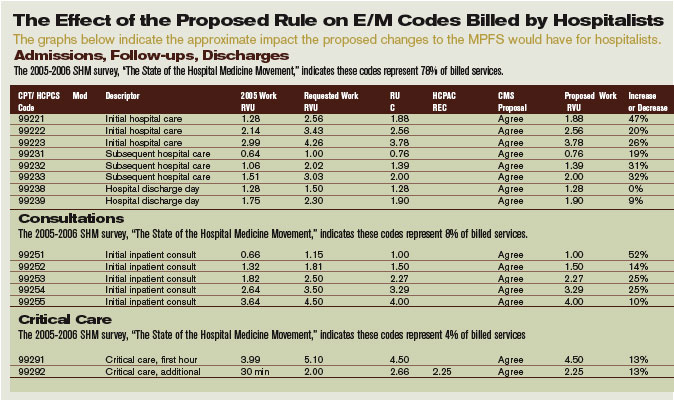
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
Clinical approach to patients with neuropathic pain
Lung Cancer Gender Gap
Aquatic Antagonists: Stingray Injury
ECT wipes out 30 years of memories
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.
Locum Terrans

Dr. Mann looked out the reinforced window at the acutely curving horizon. He saw a vista of lifeless craters under a harsh gray sky. Robotic equipment excavated along the sides of the craters for rare minerals. For about the thousandth time he asked himself what he was doing on this god-forsaken asteroid. He looked down at his scheduling terminal. Three patients were listed on his roster for the day: two burns and a fracture. They were all basic humanoids—what a bore.
When Hugh Mann was hired as a locum, he was excited. He had trained in humanoid medicine as well as xeno-geno-biology. He was in the top half of his class at the University of Ganymede—no easy accomplishment in a galaxy of overachieving life forms. His minority status as a native Terran had helped him get into school, but his sheer determination and long hours had made him successful.
He had served during the Great Rigellian War, followed by 10 solar standard years of private practice on Ios-3. Now he was getting fed up with the assortment of life forms he was treating. Dealing with the usual high platinum levels, impacted crillobars, and tentacular torsion had grown old. Even the few human patients who were grateful for a physician of their own species wasn’t enough to keep him satisfied.
When the invitation to work for Pro Lo—interstellar Locums—arrived on his screen, he was ready for adventure. An asteroid mine in the outer ring of Nebulon sounded exotic. He knew the choice locations went to those doctors who had worked with the company for years, but it was worth the risk. Or so he had thought. The mine colony was dull. There was no nightlife, not even any vaguely humanoid females for recreation. Two more weeks and his three-month tour of duty would be over. It had been at best unexciting, but he had made some serious dinars. Maybe the next assignment would be more interesting.
His self-pity was interrupted by his greatest source of annoyance. It was the pathetic excuse for a robot assistant with which he had been saddled. Some perverse designer had come up with the Old Chap 7. Perhaps the basic model had been a fairly functional assistant—175 years ago. This one had been modified to resemble an old Earth-style English butler, down to the bowler, umbrella (like it ever rained on this rock) and “Cheerio!” vernacular. He shook his head in dismay. The robot looked at him and printed out “Stiff upper lip old bean.” Dr. Mann just groaned. Worse than its pseudo-British façade, the robotic unit was severely out of date. The data banks were loaded with the Annals of Interstellar Medicine for the past 500 years, but nothing for the past three decades. That might be interesting for an archivist, but he had never seen any value in studying history. He’d taken to calling the robot Jeeves.
Dr. Mann looked out the window again at the star-filled sky. Suddenly there was a great flash of light at the horizon line. Alarms started to blare. A message came across the screen. A small asteroid had hit an Imperial transport vehicle. An emergency docking at mine base Nebulon was requested.
The mine’s director, an obstreperous Vegan named Weezul, barged into Dr. Mann’s clinic space, nervously rubbing his furry tentacles.
“Get ready for action,” he bellowed. “We have a VILF coming.”
A very important life form? This was what Dr. Mann had been waiting for. Then the bad news: The vessel had been transporting the Rigellian ambassador. This was bad news on multiple fronts. Dr. Mann had never treated a Rigellian, though he’d seen a lot of them incinerated during the war. They were allies—at least for now.
Dr. Mann called Jeeves over, and they reviewed what information there was about these enormous creatures. The Rigellian races evolved in a low gravity environment and were huge—often 24 meters or longer. They were aquatic and had two lower limbs and four upper. They had a circulatory system with a carbon monoxide-based metabolism and some strange religious beliefs about modern medicine.
The damaged ship’s lifeboat landed with two passengers—the captain and the Rigellian ambassador himself—as well as an entourage of support, translator, and protocol robots. Talk about extreme VILFs!
The captain’s injury seemed minor. An Iogan, his thick outer cortex had been lacerated. Iogans tend to have an unpleasant personality, and the captain was no exception. His rigid mouth worked to form Lingua words Dr. Mann could understand: “Don’t worry about me you fool, see to the ambassador.” Good advice, coming from a creature that looked like a giant lima bean.
The ambassador lay floating in a large, rapidly improvised tub of clear oil, supporting its large body in the higher artificial gravity of the asteroid. It would take hours to decrease the radial spin of the mine to diminish the gravitational pull to more tolerable levels. The left lower appendage was out of alignment. Donning a somewhat snug space suit, Dr. Mann climbed into the tub. With great difficulty he manipulated the injured limb. To his credit, the ambassador never winced. Dr. Mann had no way to image the limb with its tough cartilage. It would not fit into the mine’s limited scanner facility, and the portable unit would not function in liquid. Using an elastic waterproof wrap he managed to put the limb back into alignment. He hoped it would be sufficient.
Dr. Mann wanted to give the ambassador something for pain. The protocol robot came forward. “Rigellians will accept no medicine that is not derived from their home world.” Dr. Mann never liked to have a patient of any life form in pain, but if the ambassador could stand it, so could he.
Dr. Mann climbed out of the tank and checked on the captain. Jeeves had finished the dressing and had administered Iogian pain medication from stock. “I hope you are not allergic,” Dr. Mann quipped to the captain, who glared in response.
It looked like the emergency was over. Dr. Mann was pleased with himself.
Suddenly, though, things got ugly. It started with the captain. His normally green skin became spotted with blue wheals. It looked like an allergic reaction to the pain medication. Dr. Mann had Jeeves administer Moruvian pineal extract. It usually did the trick on these sentient legumes.
Dr. Mann thought he’d better check the ambassador. When he walked over to the tank something seemed wrong. The injured limb had grown to twice its normal size, and the ambassador seemed to be struggling to respire. A grim realization hit Dr. Mann: A clot had formed in the limb and embolized to the ambassador’s breathing apparatus.
Dr. Mann ran to Jeeves and accessed the medical data banks. There was nothing about the Rigellian coagulation cascade. Jeeves’ bank had only a few vague references to Rigellian physiology. The species refusal to use medication only made things worse. If he did not act quickly his patient might die. And Dr. Mann did not want to be responsible for a resumption of interstellar conflict.
He stared at Jeeves. He had never seen a robot look nervous before, but the Old Chap 7 was showing some odd behavior, taking off his hat and spinning his umbrella. Dr. Mann tried to concentrate. He had Jeeves pull up everything he had on the treatment of embolism. The modern treatment was to inject clot-eating bacteria, modified to the specie. This was out of the question; the nearest xeno-genome lab was two days from the asteroid.
He looked further back in the medical journals. Before bacteria lysis it was Q-beam radiation, and before that mini-robots with lasers. He had no Q-beam facility and rigging up mini-robots with lasers would take at least two days.
Jeeves poked him with his umbrella. What was wrong with the crazy robot? Dr. Mann had gone all the way back to the 20th century looking for an option. Then it hit him. He had read about something called an IVC filter. Perhaps he could fashion something to block the ambassador’s oversize vessel—but what? Jeeves poked him again.
Dr. Mann grabbed the umbrella from the robot and was about to snap it in two when an idea hit him. He pulled the fabric from the metal skeleton, ran to the radiation sterilizer, and sanitized the remains of the umbrella. One hour later it was inserted in the ambassador’s main vessel, ready to catch any further errant clot. Hopefully he’d live until a cruiser with a well-stocked sickbay arrived
Dr. Mann stared at Jeeves. Perhaps he had been wrong about his robot assistant. It had helped save the ambassador. Then Dr. Mann checked the captain, noticing for the first time how ancient the being looked. The captain had worsened acutely, its breathing labored, a sick wheezing sound coming past the rigid fiber that made up the upper part of its mouth.
Dr. Mann grabbed an intubation tube. The captain needed to be on a ventilator. Luckily Dr. Mann had had experience with this type of geriatric vegetable-like creature. He tried three times unsuccessfully, but managed on the fourth to slide the tube pass the rigid maxilla.
Dr. Mann sat on the floor. He was exhausted by the efforts of the day, especially the stressful intubation. Jeeves rolled over to him, and placed his bowler on Dr. Mann’s head. With a sly robotic wink his print out read, “Stiff upper lip, old bean” TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
Dr. Mann looked out the reinforced window at the acutely curving horizon. He saw a vista of lifeless craters under a harsh gray sky. Robotic equipment excavated along the sides of the craters for rare minerals. For about the thousandth time he asked himself what he was doing on this god-forsaken asteroid. He looked down at his scheduling terminal. Three patients were listed on his roster for the day: two burns and a fracture. They were all basic humanoids—what a bore.
When Hugh Mann was hired as a locum, he was excited. He had trained in humanoid medicine as well as xeno-geno-biology. He was in the top half of his class at the University of Ganymede—no easy accomplishment in a galaxy of overachieving life forms. His minority status as a native Terran had helped him get into school, but his sheer determination and long hours had made him successful.
He had served during the Great Rigellian War, followed by 10 solar standard years of private practice on Ios-3. Now he was getting fed up with the assortment of life forms he was treating. Dealing with the usual high platinum levels, impacted crillobars, and tentacular torsion had grown old. Even the few human patients who were grateful for a physician of their own species wasn’t enough to keep him satisfied.
When the invitation to work for Pro Lo—interstellar Locums—arrived on his screen, he was ready for adventure. An asteroid mine in the outer ring of Nebulon sounded exotic. He knew the choice locations went to those doctors who had worked with the company for years, but it was worth the risk. Or so he had thought. The mine colony was dull. There was no nightlife, not even any vaguely humanoid females for recreation. Two more weeks and his three-month tour of duty would be over. It had been at best unexciting, but he had made some serious dinars. Maybe the next assignment would be more interesting.
His self-pity was interrupted by his greatest source of annoyance. It was the pathetic excuse for a robot assistant with which he had been saddled. Some perverse designer had come up with the Old Chap 7. Perhaps the basic model had been a fairly functional assistant—175 years ago. This one had been modified to resemble an old Earth-style English butler, down to the bowler, umbrella (like it ever rained on this rock) and “Cheerio!” vernacular. He shook his head in dismay. The robot looked at him and printed out “Stiff upper lip old bean.” Dr. Mann just groaned. Worse than its pseudo-British façade, the robotic unit was severely out of date. The data banks were loaded with the Annals of Interstellar Medicine for the past 500 years, but nothing for the past three decades. That might be interesting for an archivist, but he had never seen any value in studying history. He’d taken to calling the robot Jeeves.
Dr. Mann looked out the window again at the star-filled sky. Suddenly there was a great flash of light at the horizon line. Alarms started to blare. A message came across the screen. A small asteroid had hit an Imperial transport vehicle. An emergency docking at mine base Nebulon was requested.
The mine’s director, an obstreperous Vegan named Weezul, barged into Dr. Mann’s clinic space, nervously rubbing his furry tentacles.
“Get ready for action,” he bellowed. “We have a VILF coming.”
A very important life form? This was what Dr. Mann had been waiting for. Then the bad news: The vessel had been transporting the Rigellian ambassador. This was bad news on multiple fronts. Dr. Mann had never treated a Rigellian, though he’d seen a lot of them incinerated during the war. They were allies—at least for now.
Dr. Mann called Jeeves over, and they reviewed what information there was about these enormous creatures. The Rigellian races evolved in a low gravity environment and were huge—often 24 meters or longer. They were aquatic and had two lower limbs and four upper. They had a circulatory system with a carbon monoxide-based metabolism and some strange religious beliefs about modern medicine.
The damaged ship’s lifeboat landed with two passengers—the captain and the Rigellian ambassador himself—as well as an entourage of support, translator, and protocol robots. Talk about extreme VILFs!
The captain’s injury seemed minor. An Iogan, his thick outer cortex had been lacerated. Iogans tend to have an unpleasant personality, and the captain was no exception. His rigid mouth worked to form Lingua words Dr. Mann could understand: “Don’t worry about me you fool, see to the ambassador.” Good advice, coming from a creature that looked like a giant lima bean.
The ambassador lay floating in a large, rapidly improvised tub of clear oil, supporting its large body in the higher artificial gravity of the asteroid. It would take hours to decrease the radial spin of the mine to diminish the gravitational pull to more tolerable levels. The left lower appendage was out of alignment. Donning a somewhat snug space suit, Dr. Mann climbed into the tub. With great difficulty he manipulated the injured limb. To his credit, the ambassador never winced. Dr. Mann had no way to image the limb with its tough cartilage. It would not fit into the mine’s limited scanner facility, and the portable unit would not function in liquid. Using an elastic waterproof wrap he managed to put the limb back into alignment. He hoped it would be sufficient.
Dr. Mann wanted to give the ambassador something for pain. The protocol robot came forward. “Rigellians will accept no medicine that is not derived from their home world.” Dr. Mann never liked to have a patient of any life form in pain, but if the ambassador could stand it, so could he.
Dr. Mann climbed out of the tank and checked on the captain. Jeeves had finished the dressing and had administered Iogian pain medication from stock. “I hope you are not allergic,” Dr. Mann quipped to the captain, who glared in response.
It looked like the emergency was over. Dr. Mann was pleased with himself.
Suddenly, though, things got ugly. It started with the captain. His normally green skin became spotted with blue wheals. It looked like an allergic reaction to the pain medication. Dr. Mann had Jeeves administer Moruvian pineal extract. It usually did the trick on these sentient legumes.
Dr. Mann thought he’d better check the ambassador. When he walked over to the tank something seemed wrong. The injured limb had grown to twice its normal size, and the ambassador seemed to be struggling to respire. A grim realization hit Dr. Mann: A clot had formed in the limb and embolized to the ambassador’s breathing apparatus.
Dr. Mann ran to Jeeves and accessed the medical data banks. There was nothing about the Rigellian coagulation cascade. Jeeves’ bank had only a few vague references to Rigellian physiology. The species refusal to use medication only made things worse. If he did not act quickly his patient might die. And Dr. Mann did not want to be responsible for a resumption of interstellar conflict.
He stared at Jeeves. He had never seen a robot look nervous before, but the Old Chap 7 was showing some odd behavior, taking off his hat and spinning his umbrella. Dr. Mann tried to concentrate. He had Jeeves pull up everything he had on the treatment of embolism. The modern treatment was to inject clot-eating bacteria, modified to the specie. This was out of the question; the nearest xeno-genome lab was two days from the asteroid.
He looked further back in the medical journals. Before bacteria lysis it was Q-beam radiation, and before that mini-robots with lasers. He had no Q-beam facility and rigging up mini-robots with lasers would take at least two days.
Jeeves poked him with his umbrella. What was wrong with the crazy robot? Dr. Mann had gone all the way back to the 20th century looking for an option. Then it hit him. He had read about something called an IVC filter. Perhaps he could fashion something to block the ambassador’s oversize vessel—but what? Jeeves poked him again.
Dr. Mann grabbed the umbrella from the robot and was about to snap it in two when an idea hit him. He pulled the fabric from the metal skeleton, ran to the radiation sterilizer, and sanitized the remains of the umbrella. One hour later it was inserted in the ambassador’s main vessel, ready to catch any further errant clot. Hopefully he’d live until a cruiser with a well-stocked sickbay arrived
Dr. Mann stared at Jeeves. Perhaps he had been wrong about his robot assistant. It had helped save the ambassador. Then Dr. Mann checked the captain, noticing for the first time how ancient the being looked. The captain had worsened acutely, its breathing labored, a sick wheezing sound coming past the rigid fiber that made up the upper part of its mouth.
Dr. Mann grabbed an intubation tube. The captain needed to be on a ventilator. Luckily Dr. Mann had had experience with this type of geriatric vegetable-like creature. He tried three times unsuccessfully, but managed on the fourth to slide the tube pass the rigid maxilla.
Dr. Mann sat on the floor. He was exhausted by the efforts of the day, especially the stressful intubation. Jeeves rolled over to him, and placed his bowler on Dr. Mann’s head. With a sly robotic wink his print out read, “Stiff upper lip, old bean” TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
Dr. Mann looked out the reinforced window at the acutely curving horizon. He saw a vista of lifeless craters under a harsh gray sky. Robotic equipment excavated along the sides of the craters for rare minerals. For about the thousandth time he asked himself what he was doing on this god-forsaken asteroid. He looked down at his scheduling terminal. Three patients were listed on his roster for the day: two burns and a fracture. They were all basic humanoids—what a bore.
When Hugh Mann was hired as a locum, he was excited. He had trained in humanoid medicine as well as xeno-geno-biology. He was in the top half of his class at the University of Ganymede—no easy accomplishment in a galaxy of overachieving life forms. His minority status as a native Terran had helped him get into school, but his sheer determination and long hours had made him successful.
He had served during the Great Rigellian War, followed by 10 solar standard years of private practice on Ios-3. Now he was getting fed up with the assortment of life forms he was treating. Dealing with the usual high platinum levels, impacted crillobars, and tentacular torsion had grown old. Even the few human patients who were grateful for a physician of their own species wasn’t enough to keep him satisfied.
When the invitation to work for Pro Lo—interstellar Locums—arrived on his screen, he was ready for adventure. An asteroid mine in the outer ring of Nebulon sounded exotic. He knew the choice locations went to those doctors who had worked with the company for years, but it was worth the risk. Or so he had thought. The mine colony was dull. There was no nightlife, not even any vaguely humanoid females for recreation. Two more weeks and his three-month tour of duty would be over. It had been at best unexciting, but he had made some serious dinars. Maybe the next assignment would be more interesting.
His self-pity was interrupted by his greatest source of annoyance. It was the pathetic excuse for a robot assistant with which he had been saddled. Some perverse designer had come up with the Old Chap 7. Perhaps the basic model had been a fairly functional assistant—175 years ago. This one had been modified to resemble an old Earth-style English butler, down to the bowler, umbrella (like it ever rained on this rock) and “Cheerio!” vernacular. He shook his head in dismay. The robot looked at him and printed out “Stiff upper lip old bean.” Dr. Mann just groaned. Worse than its pseudo-British façade, the robotic unit was severely out of date. The data banks were loaded with the Annals of Interstellar Medicine for the past 500 years, but nothing for the past three decades. That might be interesting for an archivist, but he had never seen any value in studying history. He’d taken to calling the robot Jeeves.
Dr. Mann looked out the window again at the star-filled sky. Suddenly there was a great flash of light at the horizon line. Alarms started to blare. A message came across the screen. A small asteroid had hit an Imperial transport vehicle. An emergency docking at mine base Nebulon was requested.
The mine’s director, an obstreperous Vegan named Weezul, barged into Dr. Mann’s clinic space, nervously rubbing his furry tentacles.
“Get ready for action,” he bellowed. “We have a VILF coming.”
A very important life form? This was what Dr. Mann had been waiting for. Then the bad news: The vessel had been transporting the Rigellian ambassador. This was bad news on multiple fronts. Dr. Mann had never treated a Rigellian, though he’d seen a lot of them incinerated during the war. They were allies—at least for now.
Dr. Mann called Jeeves over, and they reviewed what information there was about these enormous creatures. The Rigellian races evolved in a low gravity environment and were huge—often 24 meters or longer. They were aquatic and had two lower limbs and four upper. They had a circulatory system with a carbon monoxide-based metabolism and some strange religious beliefs about modern medicine.
The damaged ship’s lifeboat landed with two passengers—the captain and the Rigellian ambassador himself—as well as an entourage of support, translator, and protocol robots. Talk about extreme VILFs!
The captain’s injury seemed minor. An Iogan, his thick outer cortex had been lacerated. Iogans tend to have an unpleasant personality, and the captain was no exception. His rigid mouth worked to form Lingua words Dr. Mann could understand: “Don’t worry about me you fool, see to the ambassador.” Good advice, coming from a creature that looked like a giant lima bean.
The ambassador lay floating in a large, rapidly improvised tub of clear oil, supporting its large body in the higher artificial gravity of the asteroid. It would take hours to decrease the radial spin of the mine to diminish the gravitational pull to more tolerable levels. The left lower appendage was out of alignment. Donning a somewhat snug space suit, Dr. Mann climbed into the tub. With great difficulty he manipulated the injured limb. To his credit, the ambassador never winced. Dr. Mann had no way to image the limb with its tough cartilage. It would not fit into the mine’s limited scanner facility, and the portable unit would not function in liquid. Using an elastic waterproof wrap he managed to put the limb back into alignment. He hoped it would be sufficient.
Dr. Mann wanted to give the ambassador something for pain. The protocol robot came forward. “Rigellians will accept no medicine that is not derived from their home world.” Dr. Mann never liked to have a patient of any life form in pain, but if the ambassador could stand it, so could he.
Dr. Mann climbed out of the tank and checked on the captain. Jeeves had finished the dressing and had administered Iogian pain medication from stock. “I hope you are not allergic,” Dr. Mann quipped to the captain, who glared in response.
It looked like the emergency was over. Dr. Mann was pleased with himself.
Suddenly, though, things got ugly. It started with the captain. His normally green skin became spotted with blue wheals. It looked like an allergic reaction to the pain medication. Dr. Mann had Jeeves administer Moruvian pineal extract. It usually did the trick on these sentient legumes.
Dr. Mann thought he’d better check the ambassador. When he walked over to the tank something seemed wrong. The injured limb had grown to twice its normal size, and the ambassador seemed to be struggling to respire. A grim realization hit Dr. Mann: A clot had formed in the limb and embolized to the ambassador’s breathing apparatus.
Dr. Mann ran to Jeeves and accessed the medical data banks. There was nothing about the Rigellian coagulation cascade. Jeeves’ bank had only a few vague references to Rigellian physiology. The species refusal to use medication only made things worse. If he did not act quickly his patient might die. And Dr. Mann did not want to be responsible for a resumption of interstellar conflict.
He stared at Jeeves. He had never seen a robot look nervous before, but the Old Chap 7 was showing some odd behavior, taking off his hat and spinning his umbrella. Dr. Mann tried to concentrate. He had Jeeves pull up everything he had on the treatment of embolism. The modern treatment was to inject clot-eating bacteria, modified to the specie. This was out of the question; the nearest xeno-genome lab was two days from the asteroid.
He looked further back in the medical journals. Before bacteria lysis it was Q-beam radiation, and before that mini-robots with lasers. He had no Q-beam facility and rigging up mini-robots with lasers would take at least two days.
Jeeves poked him with his umbrella. What was wrong with the crazy robot? Dr. Mann had gone all the way back to the 20th century looking for an option. Then it hit him. He had read about something called an IVC filter. Perhaps he could fashion something to block the ambassador’s oversize vessel—but what? Jeeves poked him again.
Dr. Mann grabbed the umbrella from the robot and was about to snap it in two when an idea hit him. He pulled the fabric from the metal skeleton, ran to the radiation sterilizer, and sanitized the remains of the umbrella. One hour later it was inserted in the ambassador’s main vessel, ready to catch any further errant clot. Hopefully he’d live until a cruiser with a well-stocked sickbay arrived
Dr. Mann stared at Jeeves. Perhaps he had been wrong about his robot assistant. It had helped save the ambassador. Then Dr. Mann checked the captain, noticing for the first time how ancient the being looked. The captain had worsened acutely, its breathing labored, a sick wheezing sound coming past the rigid fiber that made up the upper part of its mouth.
Dr. Mann grabbed an intubation tube. The captain needed to be on a ventilator. Luckily Dr. Mann had had experience with this type of geriatric vegetable-like creature. He tried three times unsuccessfully, but managed on the fourth to slide the tube pass the rigid maxilla.
Dr. Mann sat on the floor. He was exhausted by the efforts of the day, especially the stressful intubation. Jeeves rolled over to him, and placed his bowler on Dr. Mann’s head. With a sly robotic wink his print out read, “Stiff upper lip, old bean” TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
Production-Based Compensation for Hospitalists Overlooked Too Often?

Should hospitalists, or doctors in general, be compensated based on their production? This question has received increased attention in the last few years. A major criticism of production-based compensation is that it is essentially a system that pays doctors for doing more, not for doing better. There is a growing interest in shifting at least some of physician (and hospital) compensation to a system based on the quality of care delivered.
At this point it isn’t entirely clear how all of this will play out in the coming years. What is clear is that for the time being the financial health of our practices is very dependent on our production (as well as other factors such as financial support from a hospital). So until Medicare and other payers change their system of physician reimbursement, I think it can be a good idea in many practices for at least some of a hospitalist’s income to be based on production because that helps connect him/her to the economic health of the practice.
In my May 2006 column (p. 50) I suggested that you consider production-based compensation because it can allow you and your partners to take more control of decisions about how hard you want to work and when you want to add additional doctors to your group. Most production-based compensation formulas allow doctors in the same group to work different amounts, such as working a different number of days on the schedule, and carrying different patient loads. In contrast, groups in which the hospitalists have a fixed salary (or one with a very small production-based component) usually require the doctors to work the same number of days on the schedule, and try to ensure all doctors have similar daily patient load.
When I discuss this idea with hospitalists around the country they often express concern that it would be too risky to go on a production-based salary system. They say things like, “I can’t go on production because I can’t control how many patients are referred to our practice.”
While it’s true that we have little control over patient volume from one day to the next, we have significant control over volume for any lengthy interval such as a year. If you provide good service to referring doctors and usually accept referrals graciously you will have a much higher volume than if you regularly resist referrals.
And I’ll bet that the majority of the other doctors at your hospital can’t precisely control their patient volume, but their compensation is based entirely on individual production. This is true of many emergency department and radiology practices, and some medical subspecialty groups. Why should hospitalist practice be different?
Another misconception about production-based compensation is that it is synonymous with foregoing any financial support from your hospital or other sponsoring institution. It isn’t. You can still pay individual doctors on productivity and include financial support from the hospital. For example, if the doctors are paid $55 for every wRVU generated, then $40 of that might come from professional fee collections, and $15 from the hospital (employer).
Others fear that a salary based on production will cause doctors to work at unreasonably high workloads, leading to poor patient care or patient satisfaction, or less efficient use of hospital resources (e.g., keep patients in the hospital longer). This is a potential risk, but not a common problem in my experience. There can also be concern that compensation based on productivity will cause the doctors within a group to compete with one another for patients (and income), leading to stress within the group. This is an uncommon problem, and—if it occurs within your group—it probably means that there are too many doctors in your practice (or that you should market the practice to attract more patients) rather than proving that productivity-based compensation is a bad idea.
But an explanation that clarifies objections to productivity-based compensation certainly isn’t enough of a reason to support it. You need to be convinced of some of its benefits. Hospitalists who aren’t used to being paid based in part or in whole on production tend to see it as a very stressful—or even oppressive—way to be paid. But I hope to convince you it is actually liberating.
In the absence of a production component, many groups try hard to ensure that every doctor works the same amount. For example, a group that pays a fixed annual salary to all doctors typically encourages or insists that each doctor must work almost the same amount. But when paid on production, each doctor in the group can, within reasonable boundaries, decide how much he or she wants to work. Of course all of the group’s work must be taken care of, but in nearly every group some doctors are probably willing to work a little more and others a little less than the average workload for the group.
Nearly 15 years ago, before I married and had children, I got hooked on the idea of learning to fly airplanes. Wow, did I enjoy it. But it is pretty time consuming to get a pilot’s license, to say nothing of the expense. There were a number of days that I was to be the admitting doctor for our practice, but great weather and an available plane and instructor would lure me away. On a number of occasions at 4 or 5 p.m. I called my partner who had gone home for the day and said, “Chuck, would you be willing to cover admissions so I can go flying?” He usually said “sure,” at which point I’d tell him that there were already two patients waiting in the ED.
This system made both of us happy. After nine months I was a licensed pilot and for that year my partner had a much higher income than I did. We both got what we wanted, and paying ourselves on production is what made this possible. If we were in a group with a fixed salary I can’t imagine he would have been willing to help me out so often (if ever), and I would have been limited to taking flying lessons only on my days off. Or I would have needed to pay my partner back by making up the evenings he covered for me.
My point in telling this story is that so many people think of paying hospitalists based entirely, or in part, on production is just a way to get them to maintain unreasonably high work loads. But I think it simply liberates the doctor to decide for himself what the right workload is, while owning the economic consequences of that choice. It allowed me the opportunity to work less.
A few hospitalists paid on production might choose badly and choose to work at an unreasonable (or unsafe) pace, but nearly all will make reasonable decisions. And members of a group can periodically adjust their workload up or down according to their need at the time; there is no requirement to work at the same load year after year. In fact, my partners and I in Florida didn’t even keep track of precisely how often each of us was on call over the year because there wasn’t any reason it needed to be the same for each person. (We did make some effort to distribute call evenly, but didn’t worry when it never worked out just right because each doctor could take more or less call and see a corresponding change in income).
I realize that there is no perfect compensation system, and one based on production can have shortcomings. But I think too many hospitalists assume the only reasonable system is one such as a fixed annual salary, or an hourly rate, or some method that intentionally avoids paying for productivity. You should think about how liberating productivity compensation can be. Basing a significant portion (say 40% or more—or even 100%) on productivity might be a good idea for you.
And there is nothing about productivity-based compensation that interferes with also providing financial reward for good quality of care. I’m a fan of both. If payers increasingly use quality of care as the basis for physician reimbursement in the future, individual physician compensation formulas should be based more on quality than production. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Should hospitalists, or doctors in general, be compensated based on their production? This question has received increased attention in the last few years. A major criticism of production-based compensation is that it is essentially a system that pays doctors for doing more, not for doing better. There is a growing interest in shifting at least some of physician (and hospital) compensation to a system based on the quality of care delivered.
At this point it isn’t entirely clear how all of this will play out in the coming years. What is clear is that for the time being the financial health of our practices is very dependent on our production (as well as other factors such as financial support from a hospital). So until Medicare and other payers change their system of physician reimbursement, I think it can be a good idea in many practices for at least some of a hospitalist’s income to be based on production because that helps connect him/her to the economic health of the practice.
In my May 2006 column (p. 50) I suggested that you consider production-based compensation because it can allow you and your partners to take more control of decisions about how hard you want to work and when you want to add additional doctors to your group. Most production-based compensation formulas allow doctors in the same group to work different amounts, such as working a different number of days on the schedule, and carrying different patient loads. In contrast, groups in which the hospitalists have a fixed salary (or one with a very small production-based component) usually require the doctors to work the same number of days on the schedule, and try to ensure all doctors have similar daily patient load.
When I discuss this idea with hospitalists around the country they often express concern that it would be too risky to go on a production-based salary system. They say things like, “I can’t go on production because I can’t control how many patients are referred to our practice.”
While it’s true that we have little control over patient volume from one day to the next, we have significant control over volume for any lengthy interval such as a year. If you provide good service to referring doctors and usually accept referrals graciously you will have a much higher volume than if you regularly resist referrals.
And I’ll bet that the majority of the other doctors at your hospital can’t precisely control their patient volume, but their compensation is based entirely on individual production. This is true of many emergency department and radiology practices, and some medical subspecialty groups. Why should hospitalist practice be different?
Another misconception about production-based compensation is that it is synonymous with foregoing any financial support from your hospital or other sponsoring institution. It isn’t. You can still pay individual doctors on productivity and include financial support from the hospital. For example, if the doctors are paid $55 for every wRVU generated, then $40 of that might come from professional fee collections, and $15 from the hospital (employer).
Others fear that a salary based on production will cause doctors to work at unreasonably high workloads, leading to poor patient care or patient satisfaction, or less efficient use of hospital resources (e.g., keep patients in the hospital longer). This is a potential risk, but not a common problem in my experience. There can also be concern that compensation based on productivity will cause the doctors within a group to compete with one another for patients (and income), leading to stress within the group. This is an uncommon problem, and—if it occurs within your group—it probably means that there are too many doctors in your practice (or that you should market the practice to attract more patients) rather than proving that productivity-based compensation is a bad idea.
But an explanation that clarifies objections to productivity-based compensation certainly isn’t enough of a reason to support it. You need to be convinced of some of its benefits. Hospitalists who aren’t used to being paid based in part or in whole on production tend to see it as a very stressful—or even oppressive—way to be paid. But I hope to convince you it is actually liberating.
In the absence of a production component, many groups try hard to ensure that every doctor works the same amount. For example, a group that pays a fixed annual salary to all doctors typically encourages or insists that each doctor must work almost the same amount. But when paid on production, each doctor in the group can, within reasonable boundaries, decide how much he or she wants to work. Of course all of the group’s work must be taken care of, but in nearly every group some doctors are probably willing to work a little more and others a little less than the average workload for the group.
Nearly 15 years ago, before I married and had children, I got hooked on the idea of learning to fly airplanes. Wow, did I enjoy it. But it is pretty time consuming to get a pilot’s license, to say nothing of the expense. There were a number of days that I was to be the admitting doctor for our practice, but great weather and an available plane and instructor would lure me away. On a number of occasions at 4 or 5 p.m. I called my partner who had gone home for the day and said, “Chuck, would you be willing to cover admissions so I can go flying?” He usually said “sure,” at which point I’d tell him that there were already two patients waiting in the ED.
This system made both of us happy. After nine months I was a licensed pilot and for that year my partner had a much higher income than I did. We both got what we wanted, and paying ourselves on production is what made this possible. If we were in a group with a fixed salary I can’t imagine he would have been willing to help me out so often (if ever), and I would have been limited to taking flying lessons only on my days off. Or I would have needed to pay my partner back by making up the evenings he covered for me.
My point in telling this story is that so many people think of paying hospitalists based entirely, or in part, on production is just a way to get them to maintain unreasonably high work loads. But I think it simply liberates the doctor to decide for himself what the right workload is, while owning the economic consequences of that choice. It allowed me the opportunity to work less.
A few hospitalists paid on production might choose badly and choose to work at an unreasonable (or unsafe) pace, but nearly all will make reasonable decisions. And members of a group can periodically adjust their workload up or down according to their need at the time; there is no requirement to work at the same load year after year. In fact, my partners and I in Florida didn’t even keep track of precisely how often each of us was on call over the year because there wasn’t any reason it needed to be the same for each person. (We did make some effort to distribute call evenly, but didn’t worry when it never worked out just right because each doctor could take more or less call and see a corresponding change in income).
I realize that there is no perfect compensation system, and one based on production can have shortcomings. But I think too many hospitalists assume the only reasonable system is one such as a fixed annual salary, or an hourly rate, or some method that intentionally avoids paying for productivity. You should think about how liberating productivity compensation can be. Basing a significant portion (say 40% or more—or even 100%) on productivity might be a good idea for you.
And there is nothing about productivity-based compensation that interferes with also providing financial reward for good quality of care. I’m a fan of both. If payers increasingly use quality of care as the basis for physician reimbursement in the future, individual physician compensation formulas should be based more on quality than production. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Should hospitalists, or doctors in general, be compensated based on their production? This question has received increased attention in the last few years. A major criticism of production-based compensation is that it is essentially a system that pays doctors for doing more, not for doing better. There is a growing interest in shifting at least some of physician (and hospital) compensation to a system based on the quality of care delivered.
At this point it isn’t entirely clear how all of this will play out in the coming years. What is clear is that for the time being the financial health of our practices is very dependent on our production (as well as other factors such as financial support from a hospital). So until Medicare and other payers change their system of physician reimbursement, I think it can be a good idea in many practices for at least some of a hospitalist’s income to be based on production because that helps connect him/her to the economic health of the practice.
In my May 2006 column (p. 50) I suggested that you consider production-based compensation because it can allow you and your partners to take more control of decisions about how hard you want to work and when you want to add additional doctors to your group. Most production-based compensation formulas allow doctors in the same group to work different amounts, such as working a different number of days on the schedule, and carrying different patient loads. In contrast, groups in which the hospitalists have a fixed salary (or one with a very small production-based component) usually require the doctors to work the same number of days on the schedule, and try to ensure all doctors have similar daily patient load.
When I discuss this idea with hospitalists around the country they often express concern that it would be too risky to go on a production-based salary system. They say things like, “I can’t go on production because I can’t control how many patients are referred to our practice.”
While it’s true that we have little control over patient volume from one day to the next, we have significant control over volume for any lengthy interval such as a year. If you provide good service to referring doctors and usually accept referrals graciously you will have a much higher volume than if you regularly resist referrals.
And I’ll bet that the majority of the other doctors at your hospital can’t precisely control their patient volume, but their compensation is based entirely on individual production. This is true of many emergency department and radiology practices, and some medical subspecialty groups. Why should hospitalist practice be different?
Another misconception about production-based compensation is that it is synonymous with foregoing any financial support from your hospital or other sponsoring institution. It isn’t. You can still pay individual doctors on productivity and include financial support from the hospital. For example, if the doctors are paid $55 for every wRVU generated, then $40 of that might come from professional fee collections, and $15 from the hospital (employer).
Others fear that a salary based on production will cause doctors to work at unreasonably high workloads, leading to poor patient care or patient satisfaction, or less efficient use of hospital resources (e.g., keep patients in the hospital longer). This is a potential risk, but not a common problem in my experience. There can also be concern that compensation based on productivity will cause the doctors within a group to compete with one another for patients (and income), leading to stress within the group. This is an uncommon problem, and—if it occurs within your group—it probably means that there are too many doctors in your practice (or that you should market the practice to attract more patients) rather than proving that productivity-based compensation is a bad idea.
But an explanation that clarifies objections to productivity-based compensation certainly isn’t enough of a reason to support it. You need to be convinced of some of its benefits. Hospitalists who aren’t used to being paid based in part or in whole on production tend to see it as a very stressful—or even oppressive—way to be paid. But I hope to convince you it is actually liberating.
In the absence of a production component, many groups try hard to ensure that every doctor works the same amount. For example, a group that pays a fixed annual salary to all doctors typically encourages or insists that each doctor must work almost the same amount. But when paid on production, each doctor in the group can, within reasonable boundaries, decide how much he or she wants to work. Of course all of the group’s work must be taken care of, but in nearly every group some doctors are probably willing to work a little more and others a little less than the average workload for the group.
Nearly 15 years ago, before I married and had children, I got hooked on the idea of learning to fly airplanes. Wow, did I enjoy it. But it is pretty time consuming to get a pilot’s license, to say nothing of the expense. There were a number of days that I was to be the admitting doctor for our practice, but great weather and an available plane and instructor would lure me away. On a number of occasions at 4 or 5 p.m. I called my partner who had gone home for the day and said, “Chuck, would you be willing to cover admissions so I can go flying?” He usually said “sure,” at which point I’d tell him that there were already two patients waiting in the ED.
This system made both of us happy. After nine months I was a licensed pilot and for that year my partner had a much higher income than I did. We both got what we wanted, and paying ourselves on production is what made this possible. If we were in a group with a fixed salary I can’t imagine he would have been willing to help me out so often (if ever), and I would have been limited to taking flying lessons only on my days off. Or I would have needed to pay my partner back by making up the evenings he covered for me.
My point in telling this story is that so many people think of paying hospitalists based entirely, or in part, on production is just a way to get them to maintain unreasonably high work loads. But I think it simply liberates the doctor to decide for himself what the right workload is, while owning the economic consequences of that choice. It allowed me the opportunity to work less.
A few hospitalists paid on production might choose badly and choose to work at an unreasonable (or unsafe) pace, but nearly all will make reasonable decisions. And members of a group can periodically adjust their workload up or down according to their need at the time; there is no requirement to work at the same load year after year. In fact, my partners and I in Florida didn’t even keep track of precisely how often each of us was on call over the year because there wasn’t any reason it needed to be the same for each person. (We did make some effort to distribute call evenly, but didn’t worry when it never worked out just right because each doctor could take more or less call and see a corresponding change in income).
I realize that there is no perfect compensation system, and one based on production can have shortcomings. But I think too many hospitalists assume the only reasonable system is one such as a fixed annual salary, or an hourly rate, or some method that intentionally avoids paying for productivity. You should think about how liberating productivity compensation can be. Basing a significant portion (say 40% or more—or even 100%) on productivity might be a good idea for you.
And there is nothing about productivity-based compensation that interferes with also providing financial reward for good quality of care. I’m a fan of both. If payers increasingly use quality of care as the basis for physician reimbursement in the future, individual physician compensation formulas should be based more on quality than production. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.