User login
Driving with dementia: How to assess safety behind the wheel
Mr. D, age 75, presents to your office with a 5-year history of gradually declining memory. His wife reports he is having difficulty with word finding, managing his finances, and shopping, and he needs supervision when using the stove. Nonetheless, he enjoys playing golf and drives himself to the golf course 3 times a week. He is compliant with his chronic medical therapy for hypertension, hypercholesterolemia, and asthma.
Patients with dementia who continue to drive pose a potential danger on the road, worry their families, and present challenges to clinicians. Most people would agree that patients with moderate or severe dementia should not drive, but a careful evaluation is required to assess whether a patient such as Mr. D with mild dementia remains fit to drive.
This article explores how dementia exacerbates age-related changes in driving ability and discusses how to assess driving in patients with dementia. Our goal is to help clinicians sort through data from in-office physical and cognitive assessments, family caregivers/informants’ reports, and (when available) on-road testing. We also discuss:
- guidelines for assessing older drivers that can help balance patients’ need for autonomy with public safety
- strategies for discussing driving cessation with patients and their families.
Driving: A privilege, not a right
Driving is central to older adults’ autonomy, and >75% of persons age ≥75 rely on driving as their primary mode of transportation.1 Driving cessation in this population has been associated with a 3-fold decrease in out-of-home activity2 and a 2.5-fold increase in depressive symptoms.3 Nonetheless, some 4.5 million Americans have Alzheimer’s disease (AD),4 and dementia poses a substantial risk to safe driving.
Although driving must be sacrificed when personal and public safety is at risk, most physicians perceive an uncomfortable conflict of interest between patient confidentiality and public safety.5 Assessing driving safety of patients with dementia can undermine the doctor-patient relationship and pose hardships for patients.
Mr. D has a 5-year history of memory problems that affect his daily functioning, yet he continues to drive. A longitudinal study of persons with dementia found that among the 29% who were driving at baseline, more than one-half were still behind the wheel 2 years later.6
Age and driving safety. Even in the absence of dementia, driving ability declines with aging (Tables 1 and 2).7,8 Older persons may self-regulate and restrict their driving to shorter distances, with fewer trips at night, on high-speed roads, or in unfamiliar situations. Their driving is rarely aggressive and they are unlikely to speed, but they may drive more slowly than other traffic.7,8 Although the overall rate of motor vehicle collisions declines with age:
- the rate of collisions per mile driven increases after age 659
- drivers age >65 have the highest fatality rate per mile driven among adults age ≥25.10
A dementia diagnosis is not sufficient to withdraw driving privileges, according to American Medical Association (AMA)/National Highway Traffic Safety Administration (NHTSA) guidelines. These recommend that you base decisions on the individual’s driving ability, and—when you have concerns—factor in a focused medical assessment and formal assessment of driving skills.10
Table 1
Age-related changes that may affect driving fitness
| Decreased physical capabilities, including declining muscle tone, flexibility, and reaction time |
| Decreased hearing and visual acuity |
| Increased fragility, resulting in longer time to heal should injuries occur |
| Increased medication use with possible side effect of drowsiness |
| Source: References 7,8 |
Table 2
Older drivers’ common traffic violations leading to crashes*
| Failure to obey traffic signals, including stop signs and red lights |
| Unsafe left turns (driver may inaccurately judge speed of oncoming vehicle) |
| Inappropriate turns (such as difficulty judging distance from oncoming cars, wide or narrow turns, or not timing the turn correctly with traffic lights) |
| Unsafe passing |
| Failure to yield |
| * These errors often lead to multivehicle accidents Source: References 7,8 |
CASE CONTINUED: Cognitive deficits quantified
You perform a Mini-Mental State Examination (MMSE). Mr. D scores 24/30, losing 1 point for orientation, 2 points for attention, 2 points for recall, and 1 point for copying. This score, along with his history, indicates mild dementia, although he claims he is a safe driver. On further cognitive testing, Mr. D completes the Trails A test in 90 seconds and Trails B test in 250 seconds (well below 1.5 standard deviations of the norm for his age and education).11 On the clock-drawing task, he drew a poorly organized clock, with unequal spaces between numbers and hands pointing to “10” and “11” instead of properly indicating “10 after 11.”
Mr. D and his wife live in a rural area, 5 miles from the nearest grocery store. His wife never drove, and she relies on him for weekly shopping trips and to drive her to her bridge club. She denies any problems with his driving but states, “Other drivers have become so aggressive; they’re always honking at him.” Their daughter denies that Mr. D has driving problems but admits that for the last 2 years she has refused to allow her child to ride in his car.
Focused in-office assessment
Information to assess driving ability can come from the patient, family caregiver/informant, and clinical judgment. Patients with dementia are notoriously inaccurate in self-reported driving ability, either for lack of insight or as a testament to the importance of driving to their autonomy. Caregivers often are more accurate in describing a patient’s driving, but other agendas may color their responses.
In a study of patients with very mild or mild AD, 94% reported themselves as safe drivers, whereas on-road driving instructors rated <50% of drivers in these groups as safe. Caregivers were better able to classify driving performance, but 36% of their ratings were incorrect.12
Cognitive assessment. To assess older drivers’ cognition, AMA/NHTSA’s Guide to Assessing and Counseling Older Drivers recommends the Trail-Making Test, Part B and the clock-drawing test.10 The Canadian Medical Association suggests the MMSE.13 Both guides say that abnormalities in these tests indicate a need for more detailed testing, including referral to specialized driving assessment and retesting at regular intervals (Algorithm). Retest patients with mild dementia at least every 6 months or sooner when dementia severity increases noticeably14 (Box 1).6,15
The MMSE is widely used to screen for cognitive impairment and identify dementia or delirium, but it is not a diagnostic tool or proxy driving test. A patient with dementia may produce a high MMSE score and yet be an unsafe driver. For example, well-educated patients or those with vascular or frontotemporal dementia may retain cognitive abilities as measured by the MMSE until later in the disease.
Considerable effort has been put into developing tools to help clinicians quickly and accurately differentiate safe from unsafe drivers by assessing cognition. Unfortunately, no consistent link has been found between cognitive test results and driving outcome measures. A systematic review of office-based predictors of fitness to drive in dementia found 5 studies showing an association between MMSE scores and driving and 5 studies showing no such association.16 Thus, although the AMA/NHTSA guide recommends the MMSE, Trails B, and clock-drawing tests, cognitive tests—including these—are not sufficient to assess driving ability.
Severity of dementia. International consensus groups have attempted to create guidelines for patients with dementia who drive. American, Canadian, and Australian groups suggest that a diagnosis of moderate to severe dementia precludes driving, and the driver’s licenses of persons with these conditions should be revoked.17
In general, AD is considered severe when the MMSE score is <10 or the patient becomes dependent on a caregiver for survival.18 AD of moderate severity is more difficult to define, but a Canadian consensus conference suggested a practical approach: Patients with AD would be considered to have moderate to severe dementia and should not drive when they cannot independently perform multiple instrumental activities of daily living or any of the basic activities of daily living.19
Some dementias may impair driving more quickly than AD does. For example, hallucinations may occur early in Lewy body dementia, as may impulsivity in frontotemporal dementia and motor impairment in vascular dementia.
Mrs. Y visits your office for a follow-up regarding mild Alzheimer’s disease (AD), which was diagnosed 2 years ago. She passed an on-road test 3 months ago and has an Mini-Mental State Examination score of 24/30. Over the last month she has become depressed, with insomnia and mild psychomotor retardation. She occasionally has hallucinations.
Behavioral and psychological symptoms such as agitation, aggression, hallucinations, apathy, depression, and anxiety are common neuropsychiatric sequelae of AD. Little is known about the risks these symptoms pose to road safety, but we recommend that clinicians strongly consider the potential for impaired driving.
In a longitudinal study, cognitive impairment and behavioral disturbances—especially agitation, apathy, and hallucinations—were strong predictors of driving cessation among patients with dementia.6 Furthermore, a case crossover study of patients with dementia found a 54% increase in risk of motor vehicle collisions associated with the use of psychotropic medications.15
Consider all aspects of the patient’s clinical status, including neuropsychiatric symptoms, psychotropic medications, comorbid medical conditions (including hearing and vision impairment), and concomitant therapy for medical conditions. Any could change a safe driver with mild dementia into an unsafe driver.
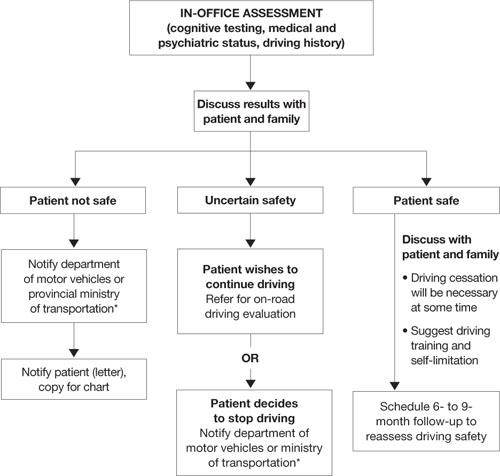
Algorithm: 3 options for drivers with dementia, based on in-office assessment
* Observe legislation or statutes that address reporting unsafe drivers to the department of motor vehicles or ministry of transportation
On-road driving tests
Because some individuals with mild dementia can drive safely for extended periods, international recommendations for assessing the driver with dementia emphasize on-road driving tests.10,13,20–22 American10 and Canadian guidelines13 suggest that a dementia diagnosis is not sufficient to withdraw licensure.
A formal driving assessment is necessary to establish road safety for patients with mild dementia except when the need for license withdrawal is evident, such as when the patient has:
- a history of major driving problems (such as crashes or driving the wrong way on a highway)
- significant contraindications to driving on the history or physical examination (such as severe inattention or psychosis).
Challenges of on-road testing. On-road tests may be the gold standard, but they are not without clinical problems.
Need to retest. Because almost all dementias are progressive and driving skills deteriorate over time, most guidelines recommend periodic retesting. For patients with dementia who pass on-road evaluations, limited evidence supports retesting every 6 months.14 Take an individual approach, however, because of the various rates at which the dementias progress.
Testing vs real world conditions. Structured on-road testing is not equivalent to unstructured real-world driving, in which the patient often must navigate without instruction or assistance.
Rural vs urban driving. Road tests conducted in urban areas assess skills associated with complex conditions and the need to respond quickly to crises. They might not assess as well rural driving, which requires sustained attention on monotonous roads.
Inaccessibility. Cost and lack of availability of on-road tests, particularly in rural areas, limit the number of patients whose performance can be evaluated.
CASE CONTINUED: Distressing results
Mr. D has a history of decline in cognition and function, objective cognitive difficulties, and a subtle history of driving problems. You refer him for a specialized on-road test, and the report indicates that he failed. Errors included wide turns, driving too slowly, getting caught in an intersection twice during red lights while attempting to turn left, driving on the shoulder, and failing to signal lane changes. You review the results with Mr. D and his wife and recommend that he cease driving immediately.
Mr. D is furious, and his wife is dismayed. He demands to know how he can continue to play golf, which is his only form of exercise and recreation. Will she have to give up her bridge club? How will they shop for food? They request permission to at least to drive to the grocery store during the daytime.
You explain that no system allows individuals to drive only at certain times, and for the sake of safety you cannot grant them special permission. You discuss alternatives, such as asking their daughter for assistance with grocery shopping and taking taxis or ride-sharing with friends who play golf and bridge.
Remain firm, but ease the blow
Driving cessation orders distress patients, families, and clinicians. A failed road test clearly indicates unsafe driving, and driving cessation is critical to public safety.
A review by Man-Son-Hing et al23 found that drivers with dementia performed worse than nondemented controls in all studies that examined driving performance (on-road, simulator, or caregiver report). Simulators showed problems such as off-road driving, deviation from posted speed, and more time to negotiate left turns.24
By comparison, only 1 of 3 studies using state crash records showed an increased risk of collisions in persons with dementia compared with controls.23 From a research perspective, however, studies that use state-reported collisions to assess driving risk are confounded by driving restrictions on persons with dementia.
Mr. D wants to continue driving with restrictions. No studies have shown reduced crash rates when drivers with dementia used compensatory strategies such as restrictions, retraining/education, having a passenger “co-pilot,” on-board navigation, or cognitive enhancers.23
If Mr. D had passed the road test, the situation would have been more ambiguous. Two studies have examined on-road driving performance over time in patients with early-stage dementia.25,26 Both studies followed drivers prospectively for 2 years, and those with mild dementia (vs very mild or no dementia) were most likely to show a decline in driving skills:
- All participants with mild dementia were rated as “not safe” by the end of 2 years by Duchek et al.25
- Median time to “failure” (or a rating of unsafe) was 324 days for drivers with mild dementia vs 605 days for those with very mild dementia, as reported by Ott et al.26
Mr. D’s passionate plea for reconsideration highlights the need for communities to develop alternate transportation for seniors whose driving becomes unsafe (Box 2).
Legal liability? Physicians often are concerned about legal responsibilities and risks involved in reporting unsafe drivers. Be aware of local statutes or legislations regarding mandatory reporting of patients you deem unsafe to drive.17 These laws usually protect physicians from lawsuits related to violating patient confidentiality. Civil lawsuits remain possible, however, if clinicians fail to report an unsafe driver who subsequently is involved in a motor vehicle collision.27
1. Meet with family first. Help them assume a positive and supportive role. Explain concretely and empathically your concern for the safety of the patient and others. Clearly outline your findings that the patient is not fit to drive, and explain that the law requires you to report the patient to the authorities.
Remind family members that the goal of driving assessment is to prevent a collision, and they carry some responsibility because they are aware of the potential risk of letting their family member continue to drive. If necessary, have family members witness a repeat performance by the patient on the most revealing test. Discuss the importance of finding alternate transportation to reduce the risk of isolation and depression that can follow driving cessation.
2. Meet with patient. Having the family present can be helpful, but ask them to assume a supportive role. Give the patient a positive role by recognizing that he or she has been a responsible driver, and part of this responsibility is to stop driving before an accident occurs. Acknowledge that it is normal to be unhappy upon learning that one’s driving privileges are being revoked.
Sometimes it helps to give the patient a prescription in their name that says, “Do not drive.” Families who receive a copy may find this very helpful, too, for reminding the patient later about what you said.
If your patient argues with your position, remain firm and do not argue. Indicate that you have made notes on the meeting and are notifying the authorities about the patient’s unsafe driving. You can add that your chart could be subpoenaed and the patient may be legally liable and financially responsible should he or she continue to drive and have a collision.
3. Talk about transportation options. Family members could share driving responsibilities. Taxi rides can cost less than maintaining a car if the patient drives <4,000 km (2,500 miles) per year. Suggest that patients or families find volunteer drivers or contact helpful taxi drivers a day before an outing is planned.
4. If patient refuses to comply, meet with the family again and encourage them to remove the patient’s opportunity to drive (confiscate the keys, disable the car, or remove the car altogether).
Provide a written statement to the patient and family outlining why the patient can no longer drive. Indicate that it is your legal responsibility to report unsafe drivers, and you intend to notify the authorities regarding the patient’s driving status. If the patient remains noncompliant, continue to encourage family to remove the opportunity to drive.
Related resources
- Physician’s guide to assessing and counseling older drivers. American Medical Association and the National Highway Traffic Safety Administration, 2003. www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook.
- Determining medical fitness to operate motor vehicles. Canadian Medical Association. 2006. www.cma.ca/index.cfm/ci_id/18223/la_id/1.htm.
- Canadian Driving Research Initiative for Vehicular Safety in the Elderly (CanDRIVE). www.candrive.ca.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rapoport receives grant/research support from the Canadian Institute of Health Research and the Ontario Neurotrauma Foundation.
1. Stowell-Ritter A, Straight A, Evans EL. Understanding senior transportation: report and analysis of a survey of consumers age 50+. Washington, DC: American Association of Retired Persons; 2002.
2. Marottoli RA, de Leon CFM, Glass TA, et al. Consequences of driving cessation: decreased out-of-home activity levels. J Gerontol B Psychol Sci Soc Sci 2000;55(6):S334-40.
3. Marottoli RA, Mendes de Leon CF, Glass TA, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven EPESE. Established Populations for Epidemiologic Studies of the Elderly. J Am Geriatr Soc 1997;45(2):202-6.
4. Hebert LE, Scherr PA, Bienias JL, et al. Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol 2003;60(8):1119-22.
5. Jang RW, Man-Son-Hing M, Molnar FJ, et al. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J Gen Intern Med 2007;22(4):531-43.
6. Herrmann N, Rapoport MJ, Sambrook R, et al. Predictors of driving cessation in mild-to-moderate dementia. CMAJ 2006;175(6):591-5.
7. Hedlund J. Countermeasures that work: a highway safety countermeasure guide for state highway safety offices. Washington, DC: National Highway Traffic Safety Administration; 2006.
8. Dobbs B. Medical conditions and driving: a review of the literature (1960-2000). Washington, DC: National Highway Traffic Safety Administration; 2005. Available at: http://www.nhtsa.dot.gov/people/injury/research/Medical_Condition_Driving/pages/TRD.html. Accessed September 29, 2008.
9. Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev 2003;35(2):227-35.
10. Physician’s guide to assessing and counseling older drivers. Washington, DC: National Highway Traffic Safety Administration; 2003. Available at: http://www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook. Accessed September 29, 2008.
11. Yeudall LT, Reddon JR, Gill DM, et al. Normative data for the Halstead-Reitan neuropsychological tests stratified by age and sex. J Clin Psychol 1987;43(3):346-67.
12. Brown LB, Ott BR, Papandonatos GD, et al. Prediction of on-road driving performance in patients with early Alzheimer’s disease. J Am Geriatr Soc 2005;53(1):94-8.
13. Determining medical fitness to operate motor vehicles. CMA driver’s guide. 7th ed. Ottawa, Ontario, Canada: Canadian Medical Association; 2006.
14. Molnar FJ, Patel A, Marshall SC, et al. Systematic review of the optimal frequency of follow-up in persons with mild dementia who continue to drive. Alzheimer Dis Assoc Disord 2006;20(4):295-7.
15. Rapoport MJ, Herrmann N, Molnar FJ, et al. Psychotropic medications and motor vehicle collisions in patients with dementia (letter). J Am Geriatr Soc 2008;56(10):1968-70.
16. Molnar FJ, Patel A, Marshall SC, et al. Clinical utility of office-based cognitive predictors of fitness to drive in persons with dementia: a systematic review. J Am Geriatr Soc 2006;54(12):1809-24.
17. Rapoport MJ, Herrmann N, Molnar FJ, et al. Sharing the responsibility for assessing the risk of the driver with dementia. CMAJ. 2007;177(6):599-601.
18. Herrmann N, Gauthier S, Lysy PG. Clinical practice guidelines for severe Alzheimer’s disease. Alzheimers Dement 2007;3(4):385-97.
19. Hogan DB, Bailey P, Carswell A, et al. Management of mild to moderate Alzheimer’s disease and dementia. Alzheimers Dement 2007;3(4):355-84.
19. Assessing fitness to drive for commercial and private vehicle drivers. Sydney, Australia: National Library of Australia; 2006. Available at: http://www.austroads.com.au/aftd/index.html. Accessed November 4, 2008.
21. Medical aspects of fitness to drive. A guide for medical practitioners. Wellington, New Zealand: Land Transport Safety Authority; 2002. Available at: http://www.transfund.govt.nz/licensing/docs/ltsa-medical-aspects.pdf. Accessed September 29, 2008.
22. At a glance guide to the current medical standards of fitness to drive. Swansea, UK: Drivers Medical Group, Driver and Vehicle Licensing Agency; 2008. Available at: http://www.dvla.gov.uk/medical/ataglance.aspx. Accessed September 29, 2008.
23. Man-Son-Hing M, Marshall SC, Molnar FJ, Wilson KG. Systematic review of driving risk and the efficacy of compensatory strategies in persons with dementia. J Am Geriatr Soc 2007;55(6):878-84.
24. Cox DJ, Quillian WC, Thorndike FP, et al. Evaluating driving performance of outpatients with Alzheimer disease. J Am Board Fam Pract 1998;11(4):264-71.
25. Duchek JM, Carr DB, Hunt L, et al. Longitudinal driving performance in early-stage dementia of the Alzheimer type. J Am Geriatr Soc 2003;51(10):1342-7.
26. Ott BR, Heindel WC, Papandonatos GD, et al. A longitudinal study of drivers with Alzheimer disease. Neurology 2008;70(14):1171-8.
27. Molnar FJ, Byszewski AM, Marshall SC, Man-Son-Hing M. In-office evaluation of medical fitness to drive: practical approaches for assessing older people. Can Fam Physician 2005;51:372-9.
Mr. D, age 75, presents to your office with a 5-year history of gradually declining memory. His wife reports he is having difficulty with word finding, managing his finances, and shopping, and he needs supervision when using the stove. Nonetheless, he enjoys playing golf and drives himself to the golf course 3 times a week. He is compliant with his chronic medical therapy for hypertension, hypercholesterolemia, and asthma.
Patients with dementia who continue to drive pose a potential danger on the road, worry their families, and present challenges to clinicians. Most people would agree that patients with moderate or severe dementia should not drive, but a careful evaluation is required to assess whether a patient such as Mr. D with mild dementia remains fit to drive.
This article explores how dementia exacerbates age-related changes in driving ability and discusses how to assess driving in patients with dementia. Our goal is to help clinicians sort through data from in-office physical and cognitive assessments, family caregivers/informants’ reports, and (when available) on-road testing. We also discuss:
- guidelines for assessing older drivers that can help balance patients’ need for autonomy with public safety
- strategies for discussing driving cessation with patients and their families.
Driving: A privilege, not a right
Driving is central to older adults’ autonomy, and >75% of persons age ≥75 rely on driving as their primary mode of transportation.1 Driving cessation in this population has been associated with a 3-fold decrease in out-of-home activity2 and a 2.5-fold increase in depressive symptoms.3 Nonetheless, some 4.5 million Americans have Alzheimer’s disease (AD),4 and dementia poses a substantial risk to safe driving.
Although driving must be sacrificed when personal and public safety is at risk, most physicians perceive an uncomfortable conflict of interest between patient confidentiality and public safety.5 Assessing driving safety of patients with dementia can undermine the doctor-patient relationship and pose hardships for patients.
Mr. D has a 5-year history of memory problems that affect his daily functioning, yet he continues to drive. A longitudinal study of persons with dementia found that among the 29% who were driving at baseline, more than one-half were still behind the wheel 2 years later.6
Age and driving safety. Even in the absence of dementia, driving ability declines with aging (Tables 1 and 2).7,8 Older persons may self-regulate and restrict their driving to shorter distances, with fewer trips at night, on high-speed roads, or in unfamiliar situations. Their driving is rarely aggressive and they are unlikely to speed, but they may drive more slowly than other traffic.7,8 Although the overall rate of motor vehicle collisions declines with age:
- the rate of collisions per mile driven increases after age 659
- drivers age >65 have the highest fatality rate per mile driven among adults age ≥25.10
A dementia diagnosis is not sufficient to withdraw driving privileges, according to American Medical Association (AMA)/National Highway Traffic Safety Administration (NHTSA) guidelines. These recommend that you base decisions on the individual’s driving ability, and—when you have concerns—factor in a focused medical assessment and formal assessment of driving skills.10
Table 1
Age-related changes that may affect driving fitness
| Decreased physical capabilities, including declining muscle tone, flexibility, and reaction time |
| Decreased hearing and visual acuity |
| Increased fragility, resulting in longer time to heal should injuries occur |
| Increased medication use with possible side effect of drowsiness |
| Source: References 7,8 |
Table 2
Older drivers’ common traffic violations leading to crashes*
| Failure to obey traffic signals, including stop signs and red lights |
| Unsafe left turns (driver may inaccurately judge speed of oncoming vehicle) |
| Inappropriate turns (such as difficulty judging distance from oncoming cars, wide or narrow turns, or not timing the turn correctly with traffic lights) |
| Unsafe passing |
| Failure to yield |
| * These errors often lead to multivehicle accidents Source: References 7,8 |
CASE CONTINUED: Cognitive deficits quantified
You perform a Mini-Mental State Examination (MMSE). Mr. D scores 24/30, losing 1 point for orientation, 2 points for attention, 2 points for recall, and 1 point for copying. This score, along with his history, indicates mild dementia, although he claims he is a safe driver. On further cognitive testing, Mr. D completes the Trails A test in 90 seconds and Trails B test in 250 seconds (well below 1.5 standard deviations of the norm for his age and education).11 On the clock-drawing task, he drew a poorly organized clock, with unequal spaces between numbers and hands pointing to “10” and “11” instead of properly indicating “10 after 11.”
Mr. D and his wife live in a rural area, 5 miles from the nearest grocery store. His wife never drove, and she relies on him for weekly shopping trips and to drive her to her bridge club. She denies any problems with his driving but states, “Other drivers have become so aggressive; they’re always honking at him.” Their daughter denies that Mr. D has driving problems but admits that for the last 2 years she has refused to allow her child to ride in his car.
Focused in-office assessment
Information to assess driving ability can come from the patient, family caregiver/informant, and clinical judgment. Patients with dementia are notoriously inaccurate in self-reported driving ability, either for lack of insight or as a testament to the importance of driving to their autonomy. Caregivers often are more accurate in describing a patient’s driving, but other agendas may color their responses.
In a study of patients with very mild or mild AD, 94% reported themselves as safe drivers, whereas on-road driving instructors rated <50% of drivers in these groups as safe. Caregivers were better able to classify driving performance, but 36% of their ratings were incorrect.12
Cognitive assessment. To assess older drivers’ cognition, AMA/NHTSA’s Guide to Assessing and Counseling Older Drivers recommends the Trail-Making Test, Part B and the clock-drawing test.10 The Canadian Medical Association suggests the MMSE.13 Both guides say that abnormalities in these tests indicate a need for more detailed testing, including referral to specialized driving assessment and retesting at regular intervals (Algorithm). Retest patients with mild dementia at least every 6 months or sooner when dementia severity increases noticeably14 (Box 1).6,15
The MMSE is widely used to screen for cognitive impairment and identify dementia or delirium, but it is not a diagnostic tool or proxy driving test. A patient with dementia may produce a high MMSE score and yet be an unsafe driver. For example, well-educated patients or those with vascular or frontotemporal dementia may retain cognitive abilities as measured by the MMSE until later in the disease.
Considerable effort has been put into developing tools to help clinicians quickly and accurately differentiate safe from unsafe drivers by assessing cognition. Unfortunately, no consistent link has been found between cognitive test results and driving outcome measures. A systematic review of office-based predictors of fitness to drive in dementia found 5 studies showing an association between MMSE scores and driving and 5 studies showing no such association.16 Thus, although the AMA/NHTSA guide recommends the MMSE, Trails B, and clock-drawing tests, cognitive tests—including these—are not sufficient to assess driving ability.
Severity of dementia. International consensus groups have attempted to create guidelines for patients with dementia who drive. American, Canadian, and Australian groups suggest that a diagnosis of moderate to severe dementia precludes driving, and the driver’s licenses of persons with these conditions should be revoked.17
In general, AD is considered severe when the MMSE score is <10 or the patient becomes dependent on a caregiver for survival.18 AD of moderate severity is more difficult to define, but a Canadian consensus conference suggested a practical approach: Patients with AD would be considered to have moderate to severe dementia and should not drive when they cannot independently perform multiple instrumental activities of daily living or any of the basic activities of daily living.19
Some dementias may impair driving more quickly than AD does. For example, hallucinations may occur early in Lewy body dementia, as may impulsivity in frontotemporal dementia and motor impairment in vascular dementia.
Mrs. Y visits your office for a follow-up regarding mild Alzheimer’s disease (AD), which was diagnosed 2 years ago. She passed an on-road test 3 months ago and has an Mini-Mental State Examination score of 24/30. Over the last month she has become depressed, with insomnia and mild psychomotor retardation. She occasionally has hallucinations.
Behavioral and psychological symptoms such as agitation, aggression, hallucinations, apathy, depression, and anxiety are common neuropsychiatric sequelae of AD. Little is known about the risks these symptoms pose to road safety, but we recommend that clinicians strongly consider the potential for impaired driving.
In a longitudinal study, cognitive impairment and behavioral disturbances—especially agitation, apathy, and hallucinations—were strong predictors of driving cessation among patients with dementia.6 Furthermore, a case crossover study of patients with dementia found a 54% increase in risk of motor vehicle collisions associated with the use of psychotropic medications.15
Consider all aspects of the patient’s clinical status, including neuropsychiatric symptoms, psychotropic medications, comorbid medical conditions (including hearing and vision impairment), and concomitant therapy for medical conditions. Any could change a safe driver with mild dementia into an unsafe driver.
Algorithm: 3 options for drivers with dementia, based on in-office assessment
* Observe legislation or statutes that address reporting unsafe drivers to the department of motor vehicles or ministry of transportation
On-road driving tests
Because some individuals with mild dementia can drive safely for extended periods, international recommendations for assessing the driver with dementia emphasize on-road driving tests.10,13,20–22 American10 and Canadian guidelines13 suggest that a dementia diagnosis is not sufficient to withdraw licensure.
A formal driving assessment is necessary to establish road safety for patients with mild dementia except when the need for license withdrawal is evident, such as when the patient has:
- a history of major driving problems (such as crashes or driving the wrong way on a highway)
- significant contraindications to driving on the history or physical examination (such as severe inattention or psychosis).
Challenges of on-road testing. On-road tests may be the gold standard, but they are not without clinical problems.
Need to retest. Because almost all dementias are progressive and driving skills deteriorate over time, most guidelines recommend periodic retesting. For patients with dementia who pass on-road evaluations, limited evidence supports retesting every 6 months.14 Take an individual approach, however, because of the various rates at which the dementias progress.
Testing vs real world conditions. Structured on-road testing is not equivalent to unstructured real-world driving, in which the patient often must navigate without instruction or assistance.
Rural vs urban driving. Road tests conducted in urban areas assess skills associated with complex conditions and the need to respond quickly to crises. They might not assess as well rural driving, which requires sustained attention on monotonous roads.
Inaccessibility. Cost and lack of availability of on-road tests, particularly in rural areas, limit the number of patients whose performance can be evaluated.
CASE CONTINUED: Distressing results
Mr. D has a history of decline in cognition and function, objective cognitive difficulties, and a subtle history of driving problems. You refer him for a specialized on-road test, and the report indicates that he failed. Errors included wide turns, driving too slowly, getting caught in an intersection twice during red lights while attempting to turn left, driving on the shoulder, and failing to signal lane changes. You review the results with Mr. D and his wife and recommend that he cease driving immediately.
Mr. D is furious, and his wife is dismayed. He demands to know how he can continue to play golf, which is his only form of exercise and recreation. Will she have to give up her bridge club? How will they shop for food? They request permission to at least to drive to the grocery store during the daytime.
You explain that no system allows individuals to drive only at certain times, and for the sake of safety you cannot grant them special permission. You discuss alternatives, such as asking their daughter for assistance with grocery shopping and taking taxis or ride-sharing with friends who play golf and bridge.
Remain firm, but ease the blow
Driving cessation orders distress patients, families, and clinicians. A failed road test clearly indicates unsafe driving, and driving cessation is critical to public safety.
A review by Man-Son-Hing et al23 found that drivers with dementia performed worse than nondemented controls in all studies that examined driving performance (on-road, simulator, or caregiver report). Simulators showed problems such as off-road driving, deviation from posted speed, and more time to negotiate left turns.24
By comparison, only 1 of 3 studies using state crash records showed an increased risk of collisions in persons with dementia compared with controls.23 From a research perspective, however, studies that use state-reported collisions to assess driving risk are confounded by driving restrictions on persons with dementia.
Mr. D wants to continue driving with restrictions. No studies have shown reduced crash rates when drivers with dementia used compensatory strategies such as restrictions, retraining/education, having a passenger “co-pilot,” on-board navigation, or cognitive enhancers.23
If Mr. D had passed the road test, the situation would have been more ambiguous. Two studies have examined on-road driving performance over time in patients with early-stage dementia.25,26 Both studies followed drivers prospectively for 2 years, and those with mild dementia (vs very mild or no dementia) were most likely to show a decline in driving skills:
- All participants with mild dementia were rated as “not safe” by the end of 2 years by Duchek et al.25
- Median time to “failure” (or a rating of unsafe) was 324 days for drivers with mild dementia vs 605 days for those with very mild dementia, as reported by Ott et al.26
Mr. D’s passionate plea for reconsideration highlights the need for communities to develop alternate transportation for seniors whose driving becomes unsafe (Box 2).
Legal liability? Physicians often are concerned about legal responsibilities and risks involved in reporting unsafe drivers. Be aware of local statutes or legislations regarding mandatory reporting of patients you deem unsafe to drive.17 These laws usually protect physicians from lawsuits related to violating patient confidentiality. Civil lawsuits remain possible, however, if clinicians fail to report an unsafe driver who subsequently is involved in a motor vehicle collision.27
1. Meet with family first. Help them assume a positive and supportive role. Explain concretely and empathically your concern for the safety of the patient and others. Clearly outline your findings that the patient is not fit to drive, and explain that the law requires you to report the patient to the authorities.
Remind family members that the goal of driving assessment is to prevent a collision, and they carry some responsibility because they are aware of the potential risk of letting their family member continue to drive. If necessary, have family members witness a repeat performance by the patient on the most revealing test. Discuss the importance of finding alternate transportation to reduce the risk of isolation and depression that can follow driving cessation.
2. Meet with patient. Having the family present can be helpful, but ask them to assume a supportive role. Give the patient a positive role by recognizing that he or she has been a responsible driver, and part of this responsibility is to stop driving before an accident occurs. Acknowledge that it is normal to be unhappy upon learning that one’s driving privileges are being revoked.
Sometimes it helps to give the patient a prescription in their name that says, “Do not drive.” Families who receive a copy may find this very helpful, too, for reminding the patient later about what you said.
If your patient argues with your position, remain firm and do not argue. Indicate that you have made notes on the meeting and are notifying the authorities about the patient’s unsafe driving. You can add that your chart could be subpoenaed and the patient may be legally liable and financially responsible should he or she continue to drive and have a collision.
3. Talk about transportation options. Family members could share driving responsibilities. Taxi rides can cost less than maintaining a car if the patient drives <4,000 km (2,500 miles) per year. Suggest that patients or families find volunteer drivers or contact helpful taxi drivers a day before an outing is planned.
4. If patient refuses to comply, meet with the family again and encourage them to remove the patient’s opportunity to drive (confiscate the keys, disable the car, or remove the car altogether).
Provide a written statement to the patient and family outlining why the patient can no longer drive. Indicate that it is your legal responsibility to report unsafe drivers, and you intend to notify the authorities regarding the patient’s driving status. If the patient remains noncompliant, continue to encourage family to remove the opportunity to drive.
Related resources
- Physician’s guide to assessing and counseling older drivers. American Medical Association and the National Highway Traffic Safety Administration, 2003. www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook.
- Determining medical fitness to operate motor vehicles. Canadian Medical Association. 2006. www.cma.ca/index.cfm/ci_id/18223/la_id/1.htm.
- Canadian Driving Research Initiative for Vehicular Safety in the Elderly (CanDRIVE). www.candrive.ca.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rapoport receives grant/research support from the Canadian Institute of Health Research and the Ontario Neurotrauma Foundation.
Mr. D, age 75, presents to your office with a 5-year history of gradually declining memory. His wife reports he is having difficulty with word finding, managing his finances, and shopping, and he needs supervision when using the stove. Nonetheless, he enjoys playing golf and drives himself to the golf course 3 times a week. He is compliant with his chronic medical therapy for hypertension, hypercholesterolemia, and asthma.
Patients with dementia who continue to drive pose a potential danger on the road, worry their families, and present challenges to clinicians. Most people would agree that patients with moderate or severe dementia should not drive, but a careful evaluation is required to assess whether a patient such as Mr. D with mild dementia remains fit to drive.
This article explores how dementia exacerbates age-related changes in driving ability and discusses how to assess driving in patients with dementia. Our goal is to help clinicians sort through data from in-office physical and cognitive assessments, family caregivers/informants’ reports, and (when available) on-road testing. We also discuss:
- guidelines for assessing older drivers that can help balance patients’ need for autonomy with public safety
- strategies for discussing driving cessation with patients and their families.
Driving: A privilege, not a right
Driving is central to older adults’ autonomy, and >75% of persons age ≥75 rely on driving as their primary mode of transportation.1 Driving cessation in this population has been associated with a 3-fold decrease in out-of-home activity2 and a 2.5-fold increase in depressive symptoms.3 Nonetheless, some 4.5 million Americans have Alzheimer’s disease (AD),4 and dementia poses a substantial risk to safe driving.
Although driving must be sacrificed when personal and public safety is at risk, most physicians perceive an uncomfortable conflict of interest between patient confidentiality and public safety.5 Assessing driving safety of patients with dementia can undermine the doctor-patient relationship and pose hardships for patients.
Mr. D has a 5-year history of memory problems that affect his daily functioning, yet he continues to drive. A longitudinal study of persons with dementia found that among the 29% who were driving at baseline, more than one-half were still behind the wheel 2 years later.6
Age and driving safety. Even in the absence of dementia, driving ability declines with aging (Tables 1 and 2).7,8 Older persons may self-regulate and restrict their driving to shorter distances, with fewer trips at night, on high-speed roads, or in unfamiliar situations. Their driving is rarely aggressive and they are unlikely to speed, but they may drive more slowly than other traffic.7,8 Although the overall rate of motor vehicle collisions declines with age:
- the rate of collisions per mile driven increases after age 659
- drivers age >65 have the highest fatality rate per mile driven among adults age ≥25.10
A dementia diagnosis is not sufficient to withdraw driving privileges, according to American Medical Association (AMA)/National Highway Traffic Safety Administration (NHTSA) guidelines. These recommend that you base decisions on the individual’s driving ability, and—when you have concerns—factor in a focused medical assessment and formal assessment of driving skills.10
Table 1
Age-related changes that may affect driving fitness
| Decreased physical capabilities, including declining muscle tone, flexibility, and reaction time |
| Decreased hearing and visual acuity |
| Increased fragility, resulting in longer time to heal should injuries occur |
| Increased medication use with possible side effect of drowsiness |
| Source: References 7,8 |
Table 2
Older drivers’ common traffic violations leading to crashes*
| Failure to obey traffic signals, including stop signs and red lights |
| Unsafe left turns (driver may inaccurately judge speed of oncoming vehicle) |
| Inappropriate turns (such as difficulty judging distance from oncoming cars, wide or narrow turns, or not timing the turn correctly with traffic lights) |
| Unsafe passing |
| Failure to yield |
| * These errors often lead to multivehicle accidents Source: References 7,8 |
CASE CONTINUED: Cognitive deficits quantified
You perform a Mini-Mental State Examination (MMSE). Mr. D scores 24/30, losing 1 point for orientation, 2 points for attention, 2 points for recall, and 1 point for copying. This score, along with his history, indicates mild dementia, although he claims he is a safe driver. On further cognitive testing, Mr. D completes the Trails A test in 90 seconds and Trails B test in 250 seconds (well below 1.5 standard deviations of the norm for his age and education).11 On the clock-drawing task, he drew a poorly organized clock, with unequal spaces between numbers and hands pointing to “10” and “11” instead of properly indicating “10 after 11.”
Mr. D and his wife live in a rural area, 5 miles from the nearest grocery store. His wife never drove, and she relies on him for weekly shopping trips and to drive her to her bridge club. She denies any problems with his driving but states, “Other drivers have become so aggressive; they’re always honking at him.” Their daughter denies that Mr. D has driving problems but admits that for the last 2 years she has refused to allow her child to ride in his car.
Focused in-office assessment
Information to assess driving ability can come from the patient, family caregiver/informant, and clinical judgment. Patients with dementia are notoriously inaccurate in self-reported driving ability, either for lack of insight or as a testament to the importance of driving to their autonomy. Caregivers often are more accurate in describing a patient’s driving, but other agendas may color their responses.
In a study of patients with very mild or mild AD, 94% reported themselves as safe drivers, whereas on-road driving instructors rated <50% of drivers in these groups as safe. Caregivers were better able to classify driving performance, but 36% of their ratings were incorrect.12
Cognitive assessment. To assess older drivers’ cognition, AMA/NHTSA’s Guide to Assessing and Counseling Older Drivers recommends the Trail-Making Test, Part B and the clock-drawing test.10 The Canadian Medical Association suggests the MMSE.13 Both guides say that abnormalities in these tests indicate a need for more detailed testing, including referral to specialized driving assessment and retesting at regular intervals (Algorithm). Retest patients with mild dementia at least every 6 months or sooner when dementia severity increases noticeably14 (Box 1).6,15
The MMSE is widely used to screen for cognitive impairment and identify dementia or delirium, but it is not a diagnostic tool or proxy driving test. A patient with dementia may produce a high MMSE score and yet be an unsafe driver. For example, well-educated patients or those with vascular or frontotemporal dementia may retain cognitive abilities as measured by the MMSE until later in the disease.
Considerable effort has been put into developing tools to help clinicians quickly and accurately differentiate safe from unsafe drivers by assessing cognition. Unfortunately, no consistent link has been found between cognitive test results and driving outcome measures. A systematic review of office-based predictors of fitness to drive in dementia found 5 studies showing an association between MMSE scores and driving and 5 studies showing no such association.16 Thus, although the AMA/NHTSA guide recommends the MMSE, Trails B, and clock-drawing tests, cognitive tests—including these—are not sufficient to assess driving ability.
Severity of dementia. International consensus groups have attempted to create guidelines for patients with dementia who drive. American, Canadian, and Australian groups suggest that a diagnosis of moderate to severe dementia precludes driving, and the driver’s licenses of persons with these conditions should be revoked.17
In general, AD is considered severe when the MMSE score is <10 or the patient becomes dependent on a caregiver for survival.18 AD of moderate severity is more difficult to define, but a Canadian consensus conference suggested a practical approach: Patients with AD would be considered to have moderate to severe dementia and should not drive when they cannot independently perform multiple instrumental activities of daily living or any of the basic activities of daily living.19
Some dementias may impair driving more quickly than AD does. For example, hallucinations may occur early in Lewy body dementia, as may impulsivity in frontotemporal dementia and motor impairment in vascular dementia.
Mrs. Y visits your office for a follow-up regarding mild Alzheimer’s disease (AD), which was diagnosed 2 years ago. She passed an on-road test 3 months ago and has an Mini-Mental State Examination score of 24/30. Over the last month she has become depressed, with insomnia and mild psychomotor retardation. She occasionally has hallucinations.
Behavioral and psychological symptoms such as agitation, aggression, hallucinations, apathy, depression, and anxiety are common neuropsychiatric sequelae of AD. Little is known about the risks these symptoms pose to road safety, but we recommend that clinicians strongly consider the potential for impaired driving.
In a longitudinal study, cognitive impairment and behavioral disturbances—especially agitation, apathy, and hallucinations—were strong predictors of driving cessation among patients with dementia.6 Furthermore, a case crossover study of patients with dementia found a 54% increase in risk of motor vehicle collisions associated with the use of psychotropic medications.15
Consider all aspects of the patient’s clinical status, including neuropsychiatric symptoms, psychotropic medications, comorbid medical conditions (including hearing and vision impairment), and concomitant therapy for medical conditions. Any could change a safe driver with mild dementia into an unsafe driver.
Algorithm: 3 options for drivers with dementia, based on in-office assessment
* Observe legislation or statutes that address reporting unsafe drivers to the department of motor vehicles or ministry of transportation
On-road driving tests
Because some individuals with mild dementia can drive safely for extended periods, international recommendations for assessing the driver with dementia emphasize on-road driving tests.10,13,20–22 American10 and Canadian guidelines13 suggest that a dementia diagnosis is not sufficient to withdraw licensure.
A formal driving assessment is necessary to establish road safety for patients with mild dementia except when the need for license withdrawal is evident, such as when the patient has:
- a history of major driving problems (such as crashes or driving the wrong way on a highway)
- significant contraindications to driving on the history or physical examination (such as severe inattention or psychosis).
Challenges of on-road testing. On-road tests may be the gold standard, but they are not without clinical problems.
Need to retest. Because almost all dementias are progressive and driving skills deteriorate over time, most guidelines recommend periodic retesting. For patients with dementia who pass on-road evaluations, limited evidence supports retesting every 6 months.14 Take an individual approach, however, because of the various rates at which the dementias progress.
Testing vs real world conditions. Structured on-road testing is not equivalent to unstructured real-world driving, in which the patient often must navigate without instruction or assistance.
Rural vs urban driving. Road tests conducted in urban areas assess skills associated with complex conditions and the need to respond quickly to crises. They might not assess as well rural driving, which requires sustained attention on monotonous roads.
Inaccessibility. Cost and lack of availability of on-road tests, particularly in rural areas, limit the number of patients whose performance can be evaluated.
CASE CONTINUED: Distressing results
Mr. D has a history of decline in cognition and function, objective cognitive difficulties, and a subtle history of driving problems. You refer him for a specialized on-road test, and the report indicates that he failed. Errors included wide turns, driving too slowly, getting caught in an intersection twice during red lights while attempting to turn left, driving on the shoulder, and failing to signal lane changes. You review the results with Mr. D and his wife and recommend that he cease driving immediately.
Mr. D is furious, and his wife is dismayed. He demands to know how he can continue to play golf, which is his only form of exercise and recreation. Will she have to give up her bridge club? How will they shop for food? They request permission to at least to drive to the grocery store during the daytime.
You explain that no system allows individuals to drive only at certain times, and for the sake of safety you cannot grant them special permission. You discuss alternatives, such as asking their daughter for assistance with grocery shopping and taking taxis or ride-sharing with friends who play golf and bridge.
Remain firm, but ease the blow
Driving cessation orders distress patients, families, and clinicians. A failed road test clearly indicates unsafe driving, and driving cessation is critical to public safety.
A review by Man-Son-Hing et al23 found that drivers with dementia performed worse than nondemented controls in all studies that examined driving performance (on-road, simulator, or caregiver report). Simulators showed problems such as off-road driving, deviation from posted speed, and more time to negotiate left turns.24
By comparison, only 1 of 3 studies using state crash records showed an increased risk of collisions in persons with dementia compared with controls.23 From a research perspective, however, studies that use state-reported collisions to assess driving risk are confounded by driving restrictions on persons with dementia.
Mr. D wants to continue driving with restrictions. No studies have shown reduced crash rates when drivers with dementia used compensatory strategies such as restrictions, retraining/education, having a passenger “co-pilot,” on-board navigation, or cognitive enhancers.23
If Mr. D had passed the road test, the situation would have been more ambiguous. Two studies have examined on-road driving performance over time in patients with early-stage dementia.25,26 Both studies followed drivers prospectively for 2 years, and those with mild dementia (vs very mild or no dementia) were most likely to show a decline in driving skills:
- All participants with mild dementia were rated as “not safe” by the end of 2 years by Duchek et al.25
- Median time to “failure” (or a rating of unsafe) was 324 days for drivers with mild dementia vs 605 days for those with very mild dementia, as reported by Ott et al.26
Mr. D’s passionate plea for reconsideration highlights the need for communities to develop alternate transportation for seniors whose driving becomes unsafe (Box 2).
Legal liability? Physicians often are concerned about legal responsibilities and risks involved in reporting unsafe drivers. Be aware of local statutes or legislations regarding mandatory reporting of patients you deem unsafe to drive.17 These laws usually protect physicians from lawsuits related to violating patient confidentiality. Civil lawsuits remain possible, however, if clinicians fail to report an unsafe driver who subsequently is involved in a motor vehicle collision.27
1. Meet with family first. Help them assume a positive and supportive role. Explain concretely and empathically your concern for the safety of the patient and others. Clearly outline your findings that the patient is not fit to drive, and explain that the law requires you to report the patient to the authorities.
Remind family members that the goal of driving assessment is to prevent a collision, and they carry some responsibility because they are aware of the potential risk of letting their family member continue to drive. If necessary, have family members witness a repeat performance by the patient on the most revealing test. Discuss the importance of finding alternate transportation to reduce the risk of isolation and depression that can follow driving cessation.
2. Meet with patient. Having the family present can be helpful, but ask them to assume a supportive role. Give the patient a positive role by recognizing that he or she has been a responsible driver, and part of this responsibility is to stop driving before an accident occurs. Acknowledge that it is normal to be unhappy upon learning that one’s driving privileges are being revoked.
Sometimes it helps to give the patient a prescription in their name that says, “Do not drive.” Families who receive a copy may find this very helpful, too, for reminding the patient later about what you said.
If your patient argues with your position, remain firm and do not argue. Indicate that you have made notes on the meeting and are notifying the authorities about the patient’s unsafe driving. You can add that your chart could be subpoenaed and the patient may be legally liable and financially responsible should he or she continue to drive and have a collision.
3. Talk about transportation options. Family members could share driving responsibilities. Taxi rides can cost less than maintaining a car if the patient drives <4,000 km (2,500 miles) per year. Suggest that patients or families find volunteer drivers or contact helpful taxi drivers a day before an outing is planned.
4. If patient refuses to comply, meet with the family again and encourage them to remove the patient’s opportunity to drive (confiscate the keys, disable the car, or remove the car altogether).
Provide a written statement to the patient and family outlining why the patient can no longer drive. Indicate that it is your legal responsibility to report unsafe drivers, and you intend to notify the authorities regarding the patient’s driving status. If the patient remains noncompliant, continue to encourage family to remove the opportunity to drive.
Related resources
- Physician’s guide to assessing and counseling older drivers. American Medical Association and the National Highway Traffic Safety Administration, 2003. www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook.
- Determining medical fitness to operate motor vehicles. Canadian Medical Association. 2006. www.cma.ca/index.cfm/ci_id/18223/la_id/1.htm.
- Canadian Driving Research Initiative for Vehicular Safety in the Elderly (CanDRIVE). www.candrive.ca.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rapoport receives grant/research support from the Canadian Institute of Health Research and the Ontario Neurotrauma Foundation.
1. Stowell-Ritter A, Straight A, Evans EL. Understanding senior transportation: report and analysis of a survey of consumers age 50+. Washington, DC: American Association of Retired Persons; 2002.
2. Marottoli RA, de Leon CFM, Glass TA, et al. Consequences of driving cessation: decreased out-of-home activity levels. J Gerontol B Psychol Sci Soc Sci 2000;55(6):S334-40.
3. Marottoli RA, Mendes de Leon CF, Glass TA, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven EPESE. Established Populations for Epidemiologic Studies of the Elderly. J Am Geriatr Soc 1997;45(2):202-6.
4. Hebert LE, Scherr PA, Bienias JL, et al. Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol 2003;60(8):1119-22.
5. Jang RW, Man-Son-Hing M, Molnar FJ, et al. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J Gen Intern Med 2007;22(4):531-43.
6. Herrmann N, Rapoport MJ, Sambrook R, et al. Predictors of driving cessation in mild-to-moderate dementia. CMAJ 2006;175(6):591-5.
7. Hedlund J. Countermeasures that work: a highway safety countermeasure guide for state highway safety offices. Washington, DC: National Highway Traffic Safety Administration; 2006.
8. Dobbs B. Medical conditions and driving: a review of the literature (1960-2000). Washington, DC: National Highway Traffic Safety Administration; 2005. Available at: http://www.nhtsa.dot.gov/people/injury/research/Medical_Condition_Driving/pages/TRD.html. Accessed September 29, 2008.
9. Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev 2003;35(2):227-35.
10. Physician’s guide to assessing and counseling older drivers. Washington, DC: National Highway Traffic Safety Administration; 2003. Available at: http://www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook. Accessed September 29, 2008.
11. Yeudall LT, Reddon JR, Gill DM, et al. Normative data for the Halstead-Reitan neuropsychological tests stratified by age and sex. J Clin Psychol 1987;43(3):346-67.
12. Brown LB, Ott BR, Papandonatos GD, et al. Prediction of on-road driving performance in patients with early Alzheimer’s disease. J Am Geriatr Soc 2005;53(1):94-8.
13. Determining medical fitness to operate motor vehicles. CMA driver’s guide. 7th ed. Ottawa, Ontario, Canada: Canadian Medical Association; 2006.
14. Molnar FJ, Patel A, Marshall SC, et al. Systematic review of the optimal frequency of follow-up in persons with mild dementia who continue to drive. Alzheimer Dis Assoc Disord 2006;20(4):295-7.
15. Rapoport MJ, Herrmann N, Molnar FJ, et al. Psychotropic medications and motor vehicle collisions in patients with dementia (letter). J Am Geriatr Soc 2008;56(10):1968-70.
16. Molnar FJ, Patel A, Marshall SC, et al. Clinical utility of office-based cognitive predictors of fitness to drive in persons with dementia: a systematic review. J Am Geriatr Soc 2006;54(12):1809-24.
17. Rapoport MJ, Herrmann N, Molnar FJ, et al. Sharing the responsibility for assessing the risk of the driver with dementia. CMAJ. 2007;177(6):599-601.
18. Herrmann N, Gauthier S, Lysy PG. Clinical practice guidelines for severe Alzheimer’s disease. Alzheimers Dement 2007;3(4):385-97.
19. Hogan DB, Bailey P, Carswell A, et al. Management of mild to moderate Alzheimer’s disease and dementia. Alzheimers Dement 2007;3(4):355-84.
19. Assessing fitness to drive for commercial and private vehicle drivers. Sydney, Australia: National Library of Australia; 2006. Available at: http://www.austroads.com.au/aftd/index.html. Accessed November 4, 2008.
21. Medical aspects of fitness to drive. A guide for medical practitioners. Wellington, New Zealand: Land Transport Safety Authority; 2002. Available at: http://www.transfund.govt.nz/licensing/docs/ltsa-medical-aspects.pdf. Accessed September 29, 2008.
22. At a glance guide to the current medical standards of fitness to drive. Swansea, UK: Drivers Medical Group, Driver and Vehicle Licensing Agency; 2008. Available at: http://www.dvla.gov.uk/medical/ataglance.aspx. Accessed September 29, 2008.
23. Man-Son-Hing M, Marshall SC, Molnar FJ, Wilson KG. Systematic review of driving risk and the efficacy of compensatory strategies in persons with dementia. J Am Geriatr Soc 2007;55(6):878-84.
24. Cox DJ, Quillian WC, Thorndike FP, et al. Evaluating driving performance of outpatients with Alzheimer disease. J Am Board Fam Pract 1998;11(4):264-71.
25. Duchek JM, Carr DB, Hunt L, et al. Longitudinal driving performance in early-stage dementia of the Alzheimer type. J Am Geriatr Soc 2003;51(10):1342-7.
26. Ott BR, Heindel WC, Papandonatos GD, et al. A longitudinal study of drivers with Alzheimer disease. Neurology 2008;70(14):1171-8.
27. Molnar FJ, Byszewski AM, Marshall SC, Man-Son-Hing M. In-office evaluation of medical fitness to drive: practical approaches for assessing older people. Can Fam Physician 2005;51:372-9.
1. Stowell-Ritter A, Straight A, Evans EL. Understanding senior transportation: report and analysis of a survey of consumers age 50+. Washington, DC: American Association of Retired Persons; 2002.
2. Marottoli RA, de Leon CFM, Glass TA, et al. Consequences of driving cessation: decreased out-of-home activity levels. J Gerontol B Psychol Sci Soc Sci 2000;55(6):S334-40.
3. Marottoli RA, Mendes de Leon CF, Glass TA, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven EPESE. Established Populations for Epidemiologic Studies of the Elderly. J Am Geriatr Soc 1997;45(2):202-6.
4. Hebert LE, Scherr PA, Bienias JL, et al. Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol 2003;60(8):1119-22.
5. Jang RW, Man-Son-Hing M, Molnar FJ, et al. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J Gen Intern Med 2007;22(4):531-43.
6. Herrmann N, Rapoport MJ, Sambrook R, et al. Predictors of driving cessation in mild-to-moderate dementia. CMAJ 2006;175(6):591-5.
7. Hedlund J. Countermeasures that work: a highway safety countermeasure guide for state highway safety offices. Washington, DC: National Highway Traffic Safety Administration; 2006.
8. Dobbs B. Medical conditions and driving: a review of the literature (1960-2000). Washington, DC: National Highway Traffic Safety Administration; 2005. Available at: http://www.nhtsa.dot.gov/people/injury/research/Medical_Condition_Driving/pages/TRD.html. Accessed September 29, 2008.
9. Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev 2003;35(2):227-35.
10. Physician’s guide to assessing and counseling older drivers. Washington, DC: National Highway Traffic Safety Administration; 2003. Available at: http://www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook. Accessed September 29, 2008.
11. Yeudall LT, Reddon JR, Gill DM, et al. Normative data for the Halstead-Reitan neuropsychological tests stratified by age and sex. J Clin Psychol 1987;43(3):346-67.
12. Brown LB, Ott BR, Papandonatos GD, et al. Prediction of on-road driving performance in patients with early Alzheimer’s disease. J Am Geriatr Soc 2005;53(1):94-8.
13. Determining medical fitness to operate motor vehicles. CMA driver’s guide. 7th ed. Ottawa, Ontario, Canada: Canadian Medical Association; 2006.
14. Molnar FJ, Patel A, Marshall SC, et al. Systematic review of the optimal frequency of follow-up in persons with mild dementia who continue to drive. Alzheimer Dis Assoc Disord 2006;20(4):295-7.
15. Rapoport MJ, Herrmann N, Molnar FJ, et al. Psychotropic medications and motor vehicle collisions in patients with dementia (letter). J Am Geriatr Soc 2008;56(10):1968-70.
16. Molnar FJ, Patel A, Marshall SC, et al. Clinical utility of office-based cognitive predictors of fitness to drive in persons with dementia: a systematic review. J Am Geriatr Soc 2006;54(12):1809-24.
17. Rapoport MJ, Herrmann N, Molnar FJ, et al. Sharing the responsibility for assessing the risk of the driver with dementia. CMAJ. 2007;177(6):599-601.
18. Herrmann N, Gauthier S, Lysy PG. Clinical practice guidelines for severe Alzheimer’s disease. Alzheimers Dement 2007;3(4):385-97.
19. Hogan DB, Bailey P, Carswell A, et al. Management of mild to moderate Alzheimer’s disease and dementia. Alzheimers Dement 2007;3(4):355-84.
19. Assessing fitness to drive for commercial and private vehicle drivers. Sydney, Australia: National Library of Australia; 2006. Available at: http://www.austroads.com.au/aftd/index.html. Accessed November 4, 2008.
21. Medical aspects of fitness to drive. A guide for medical practitioners. Wellington, New Zealand: Land Transport Safety Authority; 2002. Available at: http://www.transfund.govt.nz/licensing/docs/ltsa-medical-aspects.pdf. Accessed September 29, 2008.
22. At a glance guide to the current medical standards of fitness to drive. Swansea, UK: Drivers Medical Group, Driver and Vehicle Licensing Agency; 2008. Available at: http://www.dvla.gov.uk/medical/ataglance.aspx. Accessed September 29, 2008.
23. Man-Son-Hing M, Marshall SC, Molnar FJ, Wilson KG. Systematic review of driving risk and the efficacy of compensatory strategies in persons with dementia. J Am Geriatr Soc 2007;55(6):878-84.
24. Cox DJ, Quillian WC, Thorndike FP, et al. Evaluating driving performance of outpatients with Alzheimer disease. J Am Board Fam Pract 1998;11(4):264-71.
25. Duchek JM, Carr DB, Hunt L, et al. Longitudinal driving performance in early-stage dementia of the Alzheimer type. J Am Geriatr Soc 2003;51(10):1342-7.
26. Ott BR, Heindel WC, Papandonatos GD, et al. A longitudinal study of drivers with Alzheimer disease. Neurology 2008;70(14):1171-8.
27. Molnar FJ, Byszewski AM, Marshall SC, Man-Son-Hing M. In-office evaluation of medical fitness to drive: practical approaches for assessing older people. Can Fam Physician 2005;51:372-9.
Novel agent more effective than standard therapy in NHL
Preliminary results of a phase 3 study indicate that pixantrone is more effective than standard chemotherapy in patients with advanced, relapsed, aggressive non-Hodgkin lymphoma (NHL).
The phase 3 EXTEND PIX301 trial enrolled 140 NHL patients from 130 sites in 17 countries. Patients had received 2 or more prior therapies and were sensitive to anthracycline treatment.
They were randomized to receive either pixantrone or another single-agent drug currently used in this patient population and selected by a physician. The trial assessed patients’ complete remission or unconfirmed complete remission rate, overall survival, and progression-free survival.
Twenty percent of patients who received pixantrone achieved either a confirmed or unconfirmed complete remission, compared to 5.7% of patients on standard chemotherapy. Eleven percent of pixantrone patients’ remissions were confirmed, whereas none of the standard chemotherapy remissions were.
The overall response rate was 37.1% with pixantrone and 14.3% for patients on standard chemotherapy. Response rates were determined by an independent assessment panel that was blinded to treatment assignments.
Complete safety information for this study is not yet available. However, the study was monitored on an ongoing basis by an independent Data Safety Monitoring Committee, and no serious concerns were raised. The most common serious toxicities (> 5%) observed in previous trials of pixantrone include grade 3 and 4 neutropenia and febrile neutropenia.
Seventy-four percent of patients enrolled in this study discontinued therapy due to disease progression or death, the majority of which were in the standard chemotherapy control arm.
This study was funded by Cell Therapeutics, Inc., the company developing pixantrone.
Cell Therapeutics says it plans to submit complete study data for presentation at a major scientific conference. The organization also plans to request a pre-New Drug Application meeting with the FDA and expects to begin submission of a rolling New Drug Application to the FDA in early 2009.
Pixantrone is an antitumor agent that contains an aza-anthracenedione molecular structure, which differentiates it from anthracycline chemotherapy agents. ![]()
Preliminary results of a phase 3 study indicate that pixantrone is more effective than standard chemotherapy in patients with advanced, relapsed, aggressive non-Hodgkin lymphoma (NHL).
The phase 3 EXTEND PIX301 trial enrolled 140 NHL patients from 130 sites in 17 countries. Patients had received 2 or more prior therapies and were sensitive to anthracycline treatment.
They were randomized to receive either pixantrone or another single-agent drug currently used in this patient population and selected by a physician. The trial assessed patients’ complete remission or unconfirmed complete remission rate, overall survival, and progression-free survival.
Twenty percent of patients who received pixantrone achieved either a confirmed or unconfirmed complete remission, compared to 5.7% of patients on standard chemotherapy. Eleven percent of pixantrone patients’ remissions were confirmed, whereas none of the standard chemotherapy remissions were.
The overall response rate was 37.1% with pixantrone and 14.3% for patients on standard chemotherapy. Response rates were determined by an independent assessment panel that was blinded to treatment assignments.
Complete safety information for this study is not yet available. However, the study was monitored on an ongoing basis by an independent Data Safety Monitoring Committee, and no serious concerns were raised. The most common serious toxicities (> 5%) observed in previous trials of pixantrone include grade 3 and 4 neutropenia and febrile neutropenia.
Seventy-four percent of patients enrolled in this study discontinued therapy due to disease progression or death, the majority of which were in the standard chemotherapy control arm.
This study was funded by Cell Therapeutics, Inc., the company developing pixantrone.
Cell Therapeutics says it plans to submit complete study data for presentation at a major scientific conference. The organization also plans to request a pre-New Drug Application meeting with the FDA and expects to begin submission of a rolling New Drug Application to the FDA in early 2009.
Pixantrone is an antitumor agent that contains an aza-anthracenedione molecular structure, which differentiates it from anthracycline chemotherapy agents. ![]()
Preliminary results of a phase 3 study indicate that pixantrone is more effective than standard chemotherapy in patients with advanced, relapsed, aggressive non-Hodgkin lymphoma (NHL).
The phase 3 EXTEND PIX301 trial enrolled 140 NHL patients from 130 sites in 17 countries. Patients had received 2 or more prior therapies and were sensitive to anthracycline treatment.
They were randomized to receive either pixantrone or another single-agent drug currently used in this patient population and selected by a physician. The trial assessed patients’ complete remission or unconfirmed complete remission rate, overall survival, and progression-free survival.
Twenty percent of patients who received pixantrone achieved either a confirmed or unconfirmed complete remission, compared to 5.7% of patients on standard chemotherapy. Eleven percent of pixantrone patients’ remissions were confirmed, whereas none of the standard chemotherapy remissions were.
The overall response rate was 37.1% with pixantrone and 14.3% for patients on standard chemotherapy. Response rates were determined by an independent assessment panel that was blinded to treatment assignments.
Complete safety information for this study is not yet available. However, the study was monitored on an ongoing basis by an independent Data Safety Monitoring Committee, and no serious concerns were raised. The most common serious toxicities (> 5%) observed in previous trials of pixantrone include grade 3 and 4 neutropenia and febrile neutropenia.
Seventy-four percent of patients enrolled in this study discontinued therapy due to disease progression or death, the majority of which were in the standard chemotherapy control arm.
This study was funded by Cell Therapeutics, Inc., the company developing pixantrone.
Cell Therapeutics says it plans to submit complete study data for presentation at a major scientific conference. The organization also plans to request a pre-New Drug Application meeting with the FDA and expects to begin submission of a rolling New Drug Application to the FDA in early 2009.
Pixantrone is an antitumor agent that contains an aza-anthracenedione molecular structure, which differentiates it from anthracycline chemotherapy agents. ![]()
Proceedings of the Ethical Challenges in Surgical Innovation Summit
Supplement Editors:
Allen Bashour, MD, and Eric Kodish, MD
Contents
Most of the articles in this supplement were developed from audio transcripts of the summit’s presentations and panel discussions. The transcripts were edited by the Cleveland Clinic Journal of Medicine staff for clarity and conciseness, and were then review and revised/approved by the respective speaker or panelists. Exceptions are the articles followed by an asterisk (*) below, which were submitted as manuscripts by their authors.
From the summit directors*
Eric Kodish, MD, and Allen Bashour, MD
Editors and contributors
Welcome—Ethics in surgical innovation: Vigorous discussion will foster future progress
Delos M. Cosgrove, MD
Panel 1: Surgical Innovation and Ethical Dilemmas
Surgical innovation and ethical dilemmas: Precautions and proximity*
Joseph J. Fins, MD
Surgical innovation and ethical dilemmas: A panel discussion
Isador Lieberman, MD; James Herndon, MD; Joseph Hahn, MD; Joseph J. Fins, MD; and Ali Rezai, MD
Panel 2: Transplant Innovation and Ethical Challenges
Pushing the envelope in transplantation: Three lives at stake*
Pauline W. Chen, MD
Transplant innovation and ethical challenges: What have we learned? A collection of perspectives and panel discussion
Denton A. Cooley, MD; John J. Fung, MD, PhD; James B. Young, MD; Thomas E. Starzl, MD, PhD; Mark Siegler, MD; and Pauline W. Chen, MD
We have come far, but selecting organ recipients remains an ethical minefield—Denton A. Cooley, MD
Despite the odds, the transplant field has progressed rapidly—John J. Fung, MD, PhD
A continued need for evidence-based guidance—James B. Young, MD
What does—and does not—spur innovation?—Thomas E. Starzl, MD, PhD
Panel discussion—Moderated by Mark Siegler, MD
Keynote Address
Medical professionalism in a commercialized health care market*
Arnold S. Relman, MD
Panel 3: Inside the Operating Room
Inside the operating room—balancing the risks and benefi ts of new surgical procedures: A collection of perspectives and panel discussion
Joel D. Cooper, MD; Ralph V. Clayman, MD; Thomas M. Krummel, MD; Philip R. Schauer, MD; Christopher Thompson, MD, MHES; and Jonathan D. Moreno, PhD
How should we introduce and evaluate new procedures?—Joel D. Cooper, MD
Idea to implementation: A personal perspective on the development of laparoscopic nephrectomy—Ralph V. Clayman, MD
Special perspectives in infants and children—Thomas M. Krummel, MD
Bariatric surgery: What role for ethics as established procedures approach new frontiers?—Philip R. Schauer, MD
Natural orifice transluminal endoscopic surgery: Too much too soon?—Christopher Thompson, MD, MHES
Panel discussion—Moderated by Jonathan D. Moreno, PhD
Keynote Address
Will the United States maintain its position as a world leader in medical technology?
Thomas J. Fogarty, MD
Panel 4: Outside the Operating Room
Outside the operating room—economic, regulatory, and legal challenges: A collection of perspectives and panel discussion
Lawrence K. Altman, MD; Michael A. Mussallem; Rebecca Dresser, JD; Paul A. Lombardo, PhD, JD; Peter A. Ubel, MD; and Christopher L. White, Esq
Preface—Lawrence K. Altman, MD (Moderator)
A device company perspective: Serving patients is the key to sustainable success—Michael A. Mussallem
A regulatory and legal perspective: Issues in off-label device use—Rebecca Dresser, JD
A historical perspective: The more things change, the more they remain the same—Paul A. Lombardo, PhD, JD
An economic value perspective: Setting limits on health care can be ethical—Peter A. Ubel, MD
An industry perspective: Proactive self-regulation through an industry code of ethics—Christopher L. White, Esq
Panel discussion—Moderated by Lawrence K. Altman, MD
Panel 5: New Surgical Devices and Ethical Challenges
New surgical devices and ethical challenges: A collection of perspectives and panel discussion
Daniel Schultz, MD; Mary H. McGrath, MD, MPH; Thomas H. Murray, PhD; Roy K. Greenberg, MD; and Thomas J. Fogarty, MD
An FDA perspective on device regulation—Daniel Schultz, MD
Responsibilities of the media, FDA, and professional societies—Mary H. McGrath, MD, MPH
Promoting swift, safe, and smart innovation—Thomas H. Murray, PhD
Panel discussion—Moderated by Roy K. Greenberg, MD
Supplement Editors:
Allen Bashour, MD, and Eric Kodish, MD
Contents
Most of the articles in this supplement were developed from audio transcripts of the summit’s presentations and panel discussions. The transcripts were edited by the Cleveland Clinic Journal of Medicine staff for clarity and conciseness, and were then review and revised/approved by the respective speaker or panelists. Exceptions are the articles followed by an asterisk (*) below, which were submitted as manuscripts by their authors.
From the summit directors*
Eric Kodish, MD, and Allen Bashour, MD
Editors and contributors
Welcome—Ethics in surgical innovation: Vigorous discussion will foster future progress
Delos M. Cosgrove, MD
Panel 1: Surgical Innovation and Ethical Dilemmas
Surgical innovation and ethical dilemmas: Precautions and proximity*
Joseph J. Fins, MD
Surgical innovation and ethical dilemmas: A panel discussion
Isador Lieberman, MD; James Herndon, MD; Joseph Hahn, MD; Joseph J. Fins, MD; and Ali Rezai, MD
Panel 2: Transplant Innovation and Ethical Challenges
Pushing the envelope in transplantation: Three lives at stake*
Pauline W. Chen, MD
Transplant innovation and ethical challenges: What have we learned? A collection of perspectives and panel discussion
Denton A. Cooley, MD; John J. Fung, MD, PhD; James B. Young, MD; Thomas E. Starzl, MD, PhD; Mark Siegler, MD; and Pauline W. Chen, MD
We have come far, but selecting organ recipients remains an ethical minefield—Denton A. Cooley, MD
Despite the odds, the transplant field has progressed rapidly—John J. Fung, MD, PhD
A continued need for evidence-based guidance—James B. Young, MD
What does—and does not—spur innovation?—Thomas E. Starzl, MD, PhD
Panel discussion—Moderated by Mark Siegler, MD
Keynote Address
Medical professionalism in a commercialized health care market*
Arnold S. Relman, MD
Panel 3: Inside the Operating Room
Inside the operating room—balancing the risks and benefi ts of new surgical procedures: A collection of perspectives and panel discussion
Joel D. Cooper, MD; Ralph V. Clayman, MD; Thomas M. Krummel, MD; Philip R. Schauer, MD; Christopher Thompson, MD, MHES; and Jonathan D. Moreno, PhD
How should we introduce and evaluate new procedures?—Joel D. Cooper, MD
Idea to implementation: A personal perspective on the development of laparoscopic nephrectomy—Ralph V. Clayman, MD
Special perspectives in infants and children—Thomas M. Krummel, MD
Bariatric surgery: What role for ethics as established procedures approach new frontiers?—Philip R. Schauer, MD
Natural orifice transluminal endoscopic surgery: Too much too soon?—Christopher Thompson, MD, MHES
Panel discussion—Moderated by Jonathan D. Moreno, PhD
Keynote Address
Will the United States maintain its position as a world leader in medical technology?
Thomas J. Fogarty, MD
Panel 4: Outside the Operating Room
Outside the operating room—economic, regulatory, and legal challenges: A collection of perspectives and panel discussion
Lawrence K. Altman, MD; Michael A. Mussallem; Rebecca Dresser, JD; Paul A. Lombardo, PhD, JD; Peter A. Ubel, MD; and Christopher L. White, Esq
Preface—Lawrence K. Altman, MD (Moderator)
A device company perspective: Serving patients is the key to sustainable success—Michael A. Mussallem
A regulatory and legal perspective: Issues in off-label device use—Rebecca Dresser, JD
A historical perspective: The more things change, the more they remain the same—Paul A. Lombardo, PhD, JD
An economic value perspective: Setting limits on health care can be ethical—Peter A. Ubel, MD
An industry perspective: Proactive self-regulation through an industry code of ethics—Christopher L. White, Esq
Panel discussion—Moderated by Lawrence K. Altman, MD
Panel 5: New Surgical Devices and Ethical Challenges
New surgical devices and ethical challenges: A collection of perspectives and panel discussion
Daniel Schultz, MD; Mary H. McGrath, MD, MPH; Thomas H. Murray, PhD; Roy K. Greenberg, MD; and Thomas J. Fogarty, MD
An FDA perspective on device regulation—Daniel Schultz, MD
Responsibilities of the media, FDA, and professional societies—Mary H. McGrath, MD, MPH
Promoting swift, safe, and smart innovation—Thomas H. Murray, PhD
Panel discussion—Moderated by Roy K. Greenberg, MD
Supplement Editors:
Allen Bashour, MD, and Eric Kodish, MD
Contents
Most of the articles in this supplement were developed from audio transcripts of the summit’s presentations and panel discussions. The transcripts were edited by the Cleveland Clinic Journal of Medicine staff for clarity and conciseness, and were then review and revised/approved by the respective speaker or panelists. Exceptions are the articles followed by an asterisk (*) below, which were submitted as manuscripts by their authors.
From the summit directors*
Eric Kodish, MD, and Allen Bashour, MD
Editors and contributors
Welcome—Ethics in surgical innovation: Vigorous discussion will foster future progress
Delos M. Cosgrove, MD
Panel 1: Surgical Innovation and Ethical Dilemmas
Surgical innovation and ethical dilemmas: Precautions and proximity*
Joseph J. Fins, MD
Surgical innovation and ethical dilemmas: A panel discussion
Isador Lieberman, MD; James Herndon, MD; Joseph Hahn, MD; Joseph J. Fins, MD; and Ali Rezai, MD
Panel 2: Transplant Innovation and Ethical Challenges
Pushing the envelope in transplantation: Three lives at stake*
Pauline W. Chen, MD
Transplant innovation and ethical challenges: What have we learned? A collection of perspectives and panel discussion
Denton A. Cooley, MD; John J. Fung, MD, PhD; James B. Young, MD; Thomas E. Starzl, MD, PhD; Mark Siegler, MD; and Pauline W. Chen, MD
We have come far, but selecting organ recipients remains an ethical minefield—Denton A. Cooley, MD
Despite the odds, the transplant field has progressed rapidly—John J. Fung, MD, PhD
A continued need for evidence-based guidance—James B. Young, MD
What does—and does not—spur innovation?—Thomas E. Starzl, MD, PhD
Panel discussion—Moderated by Mark Siegler, MD
Keynote Address
Medical professionalism in a commercialized health care market*
Arnold S. Relman, MD
Panel 3: Inside the Operating Room
Inside the operating room—balancing the risks and benefi ts of new surgical procedures: A collection of perspectives and panel discussion
Joel D. Cooper, MD; Ralph V. Clayman, MD; Thomas M. Krummel, MD; Philip R. Schauer, MD; Christopher Thompson, MD, MHES; and Jonathan D. Moreno, PhD
How should we introduce and evaluate new procedures?—Joel D. Cooper, MD
Idea to implementation: A personal perspective on the development of laparoscopic nephrectomy—Ralph V. Clayman, MD
Special perspectives in infants and children—Thomas M. Krummel, MD
Bariatric surgery: What role for ethics as established procedures approach new frontiers?—Philip R. Schauer, MD
Natural orifice transluminal endoscopic surgery: Too much too soon?—Christopher Thompson, MD, MHES
Panel discussion—Moderated by Jonathan D. Moreno, PhD
Keynote Address
Will the United States maintain its position as a world leader in medical technology?
Thomas J. Fogarty, MD
Panel 4: Outside the Operating Room
Outside the operating room—economic, regulatory, and legal challenges: A collection of perspectives and panel discussion
Lawrence K. Altman, MD; Michael A. Mussallem; Rebecca Dresser, JD; Paul A. Lombardo, PhD, JD; Peter A. Ubel, MD; and Christopher L. White, Esq
Preface—Lawrence K. Altman, MD (Moderator)
A device company perspective: Serving patients is the key to sustainable success—Michael A. Mussallem
A regulatory and legal perspective: Issues in off-label device use—Rebecca Dresser, JD
A historical perspective: The more things change, the more they remain the same—Paul A. Lombardo, PhD, JD
An economic value perspective: Setting limits on health care can be ethical—Peter A. Ubel, MD
An industry perspective: Proactive self-regulation through an industry code of ethics—Christopher L. White, Esq
Panel discussion—Moderated by Lawrence K. Altman, MD
Panel 5: New Surgical Devices and Ethical Challenges
New surgical devices and ethical challenges: A collection of perspectives and panel discussion
Daniel Schultz, MD; Mary H. McGrath, MD, MPH; Thomas H. Murray, PhD; Roy K. Greenberg, MD; and Thomas J. Fogarty, MD
An FDA perspective on device regulation—Daniel Schultz, MD
Responsibilities of the media, FDA, and professional societies—Mary H. McGrath, MD, MPH
Promoting swift, safe, and smart innovation—Thomas H. Murray, PhD
Panel discussion—Moderated by Roy K. Greenberg, MD
From the summit directors
Surgical innovation lives on the border between tradition and regulation in a vaguely defined frontier. Over the course of many centuries, a framework for clinical medical ethics has developed with broad consensus regarding fiduciary obligations between patient and doctor, the principles of beneficence and nonmaleficence, and, more recently, respect for persons and autonomy. During the past century, a parallel set of ethical and regulatory norms has developed surrounding the ethics of research involving human subjects. While both sets of frameworks—those governing clinical ethics and those governing research ethics—contribute to understanding the ethical challenges that arise in the course of surgical innovation, neither is alone sufficient to provide clear guidance.
We decided that further discourse would help resolve some of the ambiguity that exists between the frameworks of clinical ethics and research ethics, and we set out to convene a summit meeting to provide a forum for this discourse. It was our hope that bringing together some of the nation’s foremost surgical innovators with leading bioethicists would catalyze a series of presentations and discussions to create a meaningful ethical framework for thinking about surgical innovation. The summit took place May 8–9, 2008, at Cleveland Clinic, and we were not disappointed. We now have the pleasure of presenting the proceedings in text form.
The summit’s five panel presentations and discussions and two keynote addresses shared the objective of educating participants about moral dilemmas that often arise in the conduct of device development and other innovations in surgery. Panelists suggested potential solutions to the challenges of protecting patients from risk without hindering creativity and progress.
The ethical challenges faced by surgical innovators will not go away. As we develop and refine technology, including new devices, procedures, and transplants, new problems will arise. Two examples of complicated issues on the horizon are robotic surgery and natural orifice transluminal endoscopic surgery (NOTES). While the specific developments will change, the ethical basis of our actions should remain constant. We need to always ask the same questions:
- Is this in the best interests of the patient?
- Have we been thoughtful and effective in the process of informed consent?
- Will our actions be consistent with our own professional integrity?
Our hope is that these proceedings will prompt the necessary next steps: further development of these ideas, writing of papers and convening of more meetings, and, most importantly, further innovation to continue helping patients.
Surgical innovation lives on the border between tradition and regulation in a vaguely defined frontier. Over the course of many centuries, a framework for clinical medical ethics has developed with broad consensus regarding fiduciary obligations between patient and doctor, the principles of beneficence and nonmaleficence, and, more recently, respect for persons and autonomy. During the past century, a parallel set of ethical and regulatory norms has developed surrounding the ethics of research involving human subjects. While both sets of frameworks—those governing clinical ethics and those governing research ethics—contribute to understanding the ethical challenges that arise in the course of surgical innovation, neither is alone sufficient to provide clear guidance.
We decided that further discourse would help resolve some of the ambiguity that exists between the frameworks of clinical ethics and research ethics, and we set out to convene a summit meeting to provide a forum for this discourse. It was our hope that bringing together some of the nation’s foremost surgical innovators with leading bioethicists would catalyze a series of presentations and discussions to create a meaningful ethical framework for thinking about surgical innovation. The summit took place May 8–9, 2008, at Cleveland Clinic, and we were not disappointed. We now have the pleasure of presenting the proceedings in text form.
The summit’s five panel presentations and discussions and two keynote addresses shared the objective of educating participants about moral dilemmas that often arise in the conduct of device development and other innovations in surgery. Panelists suggested potential solutions to the challenges of protecting patients from risk without hindering creativity and progress.
The ethical challenges faced by surgical innovators will not go away. As we develop and refine technology, including new devices, procedures, and transplants, new problems will arise. Two examples of complicated issues on the horizon are robotic surgery and natural orifice transluminal endoscopic surgery (NOTES). While the specific developments will change, the ethical basis of our actions should remain constant. We need to always ask the same questions:
- Is this in the best interests of the patient?
- Have we been thoughtful and effective in the process of informed consent?
- Will our actions be consistent with our own professional integrity?
Our hope is that these proceedings will prompt the necessary next steps: further development of these ideas, writing of papers and convening of more meetings, and, most importantly, further innovation to continue helping patients.
Surgical innovation lives on the border between tradition and regulation in a vaguely defined frontier. Over the course of many centuries, a framework for clinical medical ethics has developed with broad consensus regarding fiduciary obligations between patient and doctor, the principles of beneficence and nonmaleficence, and, more recently, respect for persons and autonomy. During the past century, a parallel set of ethical and regulatory norms has developed surrounding the ethics of research involving human subjects. While both sets of frameworks—those governing clinical ethics and those governing research ethics—contribute to understanding the ethical challenges that arise in the course of surgical innovation, neither is alone sufficient to provide clear guidance.
We decided that further discourse would help resolve some of the ambiguity that exists between the frameworks of clinical ethics and research ethics, and we set out to convene a summit meeting to provide a forum for this discourse. It was our hope that bringing together some of the nation’s foremost surgical innovators with leading bioethicists would catalyze a series of presentations and discussions to create a meaningful ethical framework for thinking about surgical innovation. The summit took place May 8–9, 2008, at Cleveland Clinic, and we were not disappointed. We now have the pleasure of presenting the proceedings in text form.
The summit’s five panel presentations and discussions and two keynote addresses shared the objective of educating participants about moral dilemmas that often arise in the conduct of device development and other innovations in surgery. Panelists suggested potential solutions to the challenges of protecting patients from risk without hindering creativity and progress.
The ethical challenges faced by surgical innovators will not go away. As we develop and refine technology, including new devices, procedures, and transplants, new problems will arise. Two examples of complicated issues on the horizon are robotic surgery and natural orifice transluminal endoscopic surgery (NOTES). While the specific developments will change, the ethical basis of our actions should remain constant. We need to always ask the same questions:
- Is this in the best interests of the patient?
- Have we been thoughtful and effective in the process of informed consent?
- Will our actions be consistent with our own professional integrity?
Our hope is that these proceedings will prompt the necessary next steps: further development of these ideas, writing of papers and convening of more meetings, and, most importantly, further innovation to continue helping patients.
Ethics in surgical innovation: Vigorous discussion will foster future progress
Welcome to Cleveland Clinic. We are delighted to have you here, and I am sure this is going to be a very interesting and provocative meeting.
In 1873 Sir John Eric Erichsen, surgeon to Queen Victoria, wrote that “although methods of practice may be modified and varied, and even improved to some extent,” “the knife cannot always have fresh fields for conquest.” How wrong he was.
Surgical innovation has continued without a break from Erichsen’s day to ours. In 1873 only 2.5% of the population survived to age 65. Over the past 100 years, surgical innovation has helped to extend the average life expectancy to 76 years.
AN UNRULY TRADITION
Surgical innovation has happened largely without rules and by its own unruly tradition. In some ways, it is the last frontier in medicine. Today surgical innovation is arguably defined and barely regulated. Technical variation is the norm, and every patient is different. The boundary between taking an alternative approach and embarking on a novel human experimentation may be finely shaded. No surgical equivalent to the Food and Drug Administration monitors the operating room. Professional ethics and common sense guide routine intraoperative intervention.
Formal research projects are carried out in compliance with the institutional review board (IRB) and the usual ethical and regulatory standards for human subjects research. Between these two posts lies a large, vaguely defined field. That is where this symposium will be spending the majority of its time.
Surgical progress is problem-driven and rarely planned. It has often taken place under stress or in response to contingent need or opportunity.
In our own lifetimes we have seen the development of cardiac surgery in a virtually rule-free environment. Surgery for coronary artery disease did not develop out of a surgical protocol but arose out of new knowledge of the disease mechanism and improvements in imaging, anesthesia, extracorporeal oxygenation, and a combination of gifted surgeons and experienced surgical teams. It was immediately accepted as therapy. There are similar examples in every surgical field.
Over the past 40 years only 10% to 20% of surgical techniques have undergone clinical trials. Transplant is a classic example. Cardiac transplant moved forward without clinical trials, and it is unlikely that clinical trials will ever be done. The laparoscopic revolution came about in the same way.
A REGULATORY BALANCING ACT
Regulation is necessary, but where and how much? In a recent speech here at Cleveland Clinic, Anne Mulcahy, chief executive officer of Xerox, said, “Most great things happen by accident and experimentation. The moment you try to streamline and keep everything captive to very focused and disciplined outcomes, you lose your ability to really invent.”
On the other hand, we cannot let surgery devolve into what a past president of the Canadian Medical Association called “a chaos of techniques devoid of moral purpose.”
Finding the right balance will be difficult. All of this makes this symposium on ethics in surgical innovation relevant, necessary, and likely to be of interest well beyond these rooms. The profession of surgery has everything to gain from a frank discussion of the issues surrounding innovation. A solid grasp of ethics will improve our practice, protect our patients, and foster progress and innovation as we go forward.
You have a wonderful opportunity to discuss with some of the finest innovators in surgery—who are here in this room—the ethical and moral dilemmas of innovation. We cannot, on the one hand, proceed completely without plan; on the other hand, we cannot regulate innovation out of existence. In the end, it is about our patients, and their interest has to be placed first.
Thank you for joining us. I am sure you are going to have an excellent symposium.
Welcome to Cleveland Clinic. We are delighted to have you here, and I am sure this is going to be a very interesting and provocative meeting.
In 1873 Sir John Eric Erichsen, surgeon to Queen Victoria, wrote that “although methods of practice may be modified and varied, and even improved to some extent,” “the knife cannot always have fresh fields for conquest.” How wrong he was.
Surgical innovation has continued without a break from Erichsen’s day to ours. In 1873 only 2.5% of the population survived to age 65. Over the past 100 years, surgical innovation has helped to extend the average life expectancy to 76 years.
AN UNRULY TRADITION
Surgical innovation has happened largely without rules and by its own unruly tradition. In some ways, it is the last frontier in medicine. Today surgical innovation is arguably defined and barely regulated. Technical variation is the norm, and every patient is different. The boundary between taking an alternative approach and embarking on a novel human experimentation may be finely shaded. No surgical equivalent to the Food and Drug Administration monitors the operating room. Professional ethics and common sense guide routine intraoperative intervention.
Formal research projects are carried out in compliance with the institutional review board (IRB) and the usual ethical and regulatory standards for human subjects research. Between these two posts lies a large, vaguely defined field. That is where this symposium will be spending the majority of its time.
Surgical progress is problem-driven and rarely planned. It has often taken place under stress or in response to contingent need or opportunity.
In our own lifetimes we have seen the development of cardiac surgery in a virtually rule-free environment. Surgery for coronary artery disease did not develop out of a surgical protocol but arose out of new knowledge of the disease mechanism and improvements in imaging, anesthesia, extracorporeal oxygenation, and a combination of gifted surgeons and experienced surgical teams. It was immediately accepted as therapy. There are similar examples in every surgical field.
Over the past 40 years only 10% to 20% of surgical techniques have undergone clinical trials. Transplant is a classic example. Cardiac transplant moved forward without clinical trials, and it is unlikely that clinical trials will ever be done. The laparoscopic revolution came about in the same way.
A REGULATORY BALANCING ACT
Regulation is necessary, but where and how much? In a recent speech here at Cleveland Clinic, Anne Mulcahy, chief executive officer of Xerox, said, “Most great things happen by accident and experimentation. The moment you try to streamline and keep everything captive to very focused and disciplined outcomes, you lose your ability to really invent.”
On the other hand, we cannot let surgery devolve into what a past president of the Canadian Medical Association called “a chaos of techniques devoid of moral purpose.”
Finding the right balance will be difficult. All of this makes this symposium on ethics in surgical innovation relevant, necessary, and likely to be of interest well beyond these rooms. The profession of surgery has everything to gain from a frank discussion of the issues surrounding innovation. A solid grasp of ethics will improve our practice, protect our patients, and foster progress and innovation as we go forward.
You have a wonderful opportunity to discuss with some of the finest innovators in surgery—who are here in this room—the ethical and moral dilemmas of innovation. We cannot, on the one hand, proceed completely without plan; on the other hand, we cannot regulate innovation out of existence. In the end, it is about our patients, and their interest has to be placed first.
Thank you for joining us. I am sure you are going to have an excellent symposium.
Welcome to Cleveland Clinic. We are delighted to have you here, and I am sure this is going to be a very interesting and provocative meeting.
In 1873 Sir John Eric Erichsen, surgeon to Queen Victoria, wrote that “although methods of practice may be modified and varied, and even improved to some extent,” “the knife cannot always have fresh fields for conquest.” How wrong he was.
Surgical innovation has continued without a break from Erichsen’s day to ours. In 1873 only 2.5% of the population survived to age 65. Over the past 100 years, surgical innovation has helped to extend the average life expectancy to 76 years.
AN UNRULY TRADITION
Surgical innovation has happened largely without rules and by its own unruly tradition. In some ways, it is the last frontier in medicine. Today surgical innovation is arguably defined and barely regulated. Technical variation is the norm, and every patient is different. The boundary between taking an alternative approach and embarking on a novel human experimentation may be finely shaded. No surgical equivalent to the Food and Drug Administration monitors the operating room. Professional ethics and common sense guide routine intraoperative intervention.
Formal research projects are carried out in compliance with the institutional review board (IRB) and the usual ethical and regulatory standards for human subjects research. Between these two posts lies a large, vaguely defined field. That is where this symposium will be spending the majority of its time.
Surgical progress is problem-driven and rarely planned. It has often taken place under stress or in response to contingent need or opportunity.
In our own lifetimes we have seen the development of cardiac surgery in a virtually rule-free environment. Surgery for coronary artery disease did not develop out of a surgical protocol but arose out of new knowledge of the disease mechanism and improvements in imaging, anesthesia, extracorporeal oxygenation, and a combination of gifted surgeons and experienced surgical teams. It was immediately accepted as therapy. There are similar examples in every surgical field.
Over the past 40 years only 10% to 20% of surgical techniques have undergone clinical trials. Transplant is a classic example. Cardiac transplant moved forward without clinical trials, and it is unlikely that clinical trials will ever be done. The laparoscopic revolution came about in the same way.
A REGULATORY BALANCING ACT
Regulation is necessary, but where and how much? In a recent speech here at Cleveland Clinic, Anne Mulcahy, chief executive officer of Xerox, said, “Most great things happen by accident and experimentation. The moment you try to streamline and keep everything captive to very focused and disciplined outcomes, you lose your ability to really invent.”
On the other hand, we cannot let surgery devolve into what a past president of the Canadian Medical Association called “a chaos of techniques devoid of moral purpose.”
Finding the right balance will be difficult. All of this makes this symposium on ethics in surgical innovation relevant, necessary, and likely to be of interest well beyond these rooms. The profession of surgery has everything to gain from a frank discussion of the issues surrounding innovation. A solid grasp of ethics will improve our practice, protect our patients, and foster progress and innovation as we go forward.
You have a wonderful opportunity to discuss with some of the finest innovators in surgery—who are here in this room—the ethical and moral dilemmas of innovation. We cannot, on the one hand, proceed completely without plan; on the other hand, we cannot regulate innovation out of existence. In the end, it is about our patients, and their interest has to be placed first.
Thank you for joining us. I am sure you are going to have an excellent symposium.
Surgical innovation and ethical dilemmas: Precautions and proximity
No! I am not Prince Hamlet, nor was meant to be;
Am an attendant lord, one that will do
To swell a progress, start a scene or two…
—T.S. Eliot, The Love Song of J. Alfred Prufrock
Let me start by thanking the organizers for their invitation to be here and to start this off. I am not sure if that invitation was an act of kindness or of throwing a fellow bioethicist to the lions, as we will be addressing a complicated set of issues upon which well-intentioned folks disagree and sometimes disagree with a passion.
What I would like to do is to lay out some of the inherent ethical problems related to surgical innovation. I will argue that some of these problems are unique to surgery and that others relate to how we have chosen to define categories like research and practice. Other problems involve how we view the proportionality of risks and benefits in surgical research. I will argue that we have falsely analogized surgical progress to progress made in other areas of biomedical research and misunderstood the highly personal, or proximate, nature of surgical inquiry. Without appreciating the import of what I will call “surgical proximity,” we will be unable to adequately address ethical issues in surgical innovation.
PROBLEMS OR DILEMMAS?
So let me begin with the title of our session, “Surgical Innovation and Ethical Dilemmas,” and why this juxta position is counterproductive. A colleague long ago taught me to distinguish problems from dilemmas—the former being resolvable, the latter intractable, often involving a choice between two equally unfavorable choices.
Although I may be making too much of the semantics, I do think the title betrays a presumption that surgical innovation invariably forces adversarial choices. It tends to dichotomize ethical reflection, pitting those who favor prudence against those who endorse progress, or it creates too stark a difference between ethical issues in surgical practice and those encountered in the conduct of surgical research.
Even therapeutic, validated surgery in many ways has the potential to become innovative, if not outright experimental. Patients may have anatomical differences that require surgical improvisation, or complications may arise during “routine” surgery, creating the need for an imaginative response.1 At what point do these departures from expected care become novel interventions, innovative or even experimental? A routine case with an unexpected turn can even become a case report opening up a new field of endeavor.
For instance, the field of stereotactic functional neurosurgery was born out of a “routine” case of ablative surgery for Parkinson’s disease in the 1980s, when the French neurosurgeon Alim Benabid was using electrodes to determine which areas of the brain should be destroyed. As he was mapping the thalamus, he noted that the tremor of his patient abated. This led him to wonder if one could treat drug-resistant Parkinson’s with electrical stimulation instead of destructive lesioning.2 Benabid’s translational insight during an ordinary case led to the development of the rather extraordinary field of stereotactic functional neurosurgery and neuromodulation.3,4
Another example from an earlier era comes from the life work of neurosurgeon Wilder Penfield, who did pioneering work in the surgical treatment of epilepsy. Here, the accumulation of experience from “routine care” led to generalizable knowledge, much like hypotheses are validated in experimental work. In Penfield’s case, his clinical use of electrical stimulation to plan resections of scar tissue causing epilepsy led him to map the human homunculus, a magnificent achievement of profound importance.5,6
So let us avoid simplistic and confounding demarcations. Instead of dichotomizing innovation and prudence—or surgical research and surgical practice—let us try to start our deliberations with an eye toward a more synthetic approach. Like most things in nature and in biology, ethics too is on a continuum with gradations that can fit into an Aristotelian taxonomy. Let us emulate what Aristotle called phronesis, or practical wisdom, these next 2 days so that we achieve constructive outcomes, or what the pragmatists would call instrumental goods.7
If we are successful in laying out the ethical issues in this clinically pragmatic fashion, we can turn intractable “dilemmas” into problems amenable to resolution through the particularistic invocation of ethical principles as they relate to the surgical context.8 If we follow this inductive method of moral problem solving, we will avoid sweeping ethical generalizations, or categoricals, that can misrepresent the complexity of innovative research and deprive society of its benefits.9
INNOVATION VS PRUDENCE: A FALSE DICHOTOMY
So let us start by understanding the presuppositions that led to the expectation that dilemmas will descend upon those who engage in surgical innovation. In my view, this expectation begins with what is called the precautionary principle, a concept with some currency in the realm of environmental ethics.10
The precautionary principle urges caution and prudence when facing unknowns and is an antecedent sort of utilitarianism. One makes judgments about the advisability of actions based on a prior assessment of foreseeable risks and benefits. If the risks are excessive or exceed benefits, the precautionary principle urges care, caution, and even avoidance of a given course of action.
When the precautionary principle is implicitly invoked in making judgments about research, the objective is to pursue a degree of safety that is comparable to that of established therapy. But interventions that have progressed to being deemed “therapeutic” have of course achieved a requisite degree of both safety and efficacy—that is what makes them therapeutic, as opposed to investigational, interventions. One cannot know before one has conducted a clinical trial, and completed statistical analysis, whether a new surgical advance or device meets these expectations. Because of this lack of knowledge, there is an inherent degree of risk in any novel intervention.
The challenge posed by innovation or novelty creates the possibility of untoward events. It leads to invocation of the precautionary principle, which, echoing the admonitions of the philosopher Hans Jonas, urges us to “give greater weight to the prognosis of doom than to that of bliss.”11,12
This is not a bad way to go through life, assuming one wants to emulate T.S. Eliot’s J. Alfred Prufrock, who lamentably “measured out my life with coffee spoons.”13 Unlike the surgeon, who must make decisions in real time, Eliot’s protagonist could not move forward. Despite his desire to avoid the indecision of Prince Hamlet, alluded to in this paper’s epigraph, Prufrock was paralyzed by doubts and fears, with “time yet for a hundred indecisions, and for a hundred visions and revisions.”13
Despite Eliot’s invocation of “a patient etherised upon a table,”13 the poem shares little with the surgical life. It has much more in common with the precautionary principle. Like Prufrock, the precautionary principle favors what is known— the status quo—as what is unknown is invariably more risky than the familiar. Needless to say, this is antithetical to innovation because discovery invariably requires scenarios that involve novelty and unknown risks. When faced with the certain security of stasis or the potential dangers of innovation, the precautionary principle will invariably choose stasis, leading us, as the legal scholar Cass Sunstein notes, “in no direction at all.”14
Seen through the prism of the precautionary principle, then, surgical innovation invariably presents a dilemma. Discovery and innovation are fundamentally at odds with the precautionary principle, because of their potential for risk.15
The challenge posed by the precautionary principle—which, to be fair, is seen in all areas of clinical research—becomes even more pronounced in surgical research because of the size and scope of clinical trials. As is well appreciated here, compared with drug trials, surgical trials are small. Sometimes they can involve a single subject, whereas drug trials may include thousands of participants. Because of drug trials’ large volume of subjects, therapeutic effects can be small to justify ongoing research. In a surgical trial or a device trial, the number of subjects is smaller, so the therapeutic impact has to be larger to warrant further development and ongoing study. This burden of scale increases the probability of reciprocally large adverse effects. This potential for disaster magnifies the impact of the precautionary principle and may lead to a distortion in ethical judgment along the lines of Hans Jonas’ admonition.12
By all of this I am not suggesting that we abandon precautions and prudence. Instead, my point is to explicate the additional challenges faced by surgical research and the sway of the precautionary principle over this area of inquiry and innovation. By being explicit about the impact of this principle, we can be cognizant of its potential to distort judgments about risks and benefits. Only then can we hope to balance the pursuit of progress with that of safety.
SURGICAL RESPONSIBILITY
These distortions also need to be recognized, and made explicit, because surgical research, more so than pharmacologic research, is much more personal and intimate. This point becomes clear if we consider a surgical trial that does not succeed.
In the surgical arena, such failures are taken to heart and personalized. Unlike trials that involve drugs, surgical research is more proximate. It is not just the failure of a drug or of pharmacology; it is also possibly the failure of the operator, the surgeon who did not achieve the desired goal because of poor execution of surgical technique.
This crucial difference in medical versus surgical cultures is captured by Charles Bosk in his magisterial sociological study of surgery, Forgive and Remember: Managing Medical Failure. In a discussion of morbidity and mortality rounds, Bosk writes:
The specific nature of surgical treatment links the action of the physician and the response of the patient more intimately than in other areas of medicine....When the patient of an internist dies, the natural question his colleagues ask is, “What happened?” When the patient of a surgeon dies, his colleagues ask, “What did you do?”16
As in clinical surgical practice, in surgical research, it is the personal and individualized mediation of the surgeon that is central to the intervention. Here the intermediary is neither a drug nor its bioavailability; rather, it is the operator’s technique plus or minus the operative design and the reliability of an instrument or a device. In either case, the contribution is more proximate and personal, stemming from the actions of individual surgeons and the work of their hands.
History is instructive on this theme of surgical causality and personal culpability if we consider the life of Harvey Cushing, a Cleveland native whose ashes are buried nearby in Lake View Cemetery.17 Cushing was a gifted and innovative surgeon whose technique handling tissues changed how the brain was approached operatively. He is acknowledged as the father of neurosurgery, having created a professional nexus to institutionalize and carry on his innovative work.18
Cushing’s greatest innovation was probably in his individual efforts as a working surgeon. Over the course of his lifetime, he made the resection of brain tumors a safe and sometimes effective treatment for an otherwise dread disease. Michael Bliss, Cushing’s most recent biographer, reports mortality data from more than 2,400 surgeries done by Cushing during his operative lifetime.17 Early in his career (from 1896 to 1911), while he was at Johns Hopkins, Cushing’s case mortality rate was 24.7%. During his later years at the Brigham Hospital, it was 16.2%. By 1930–1931 it was down to 8.8%.
These were extraordinary statistics: no one matched Cushing’s numbers, or his ability to do what he did. Bliss cites mortality data from his surgical contemporaries in the late 1920s as ranging from approximately 35% to 45%. By the numbers Bliss compares Cushing’s talent—his truly brilliant outlier performance—to that of his Jazz Age contemporary, Babe Ruth, who also had outsized talent compared with his peers.17
Cushing himself, a collegiate second baseman at Yale, linked sport and statistics in a most telling way. Documenting his ongoing surgical progress was a hedge against failure and lightened the emotional burdens of the surgical suite. Cushing observed: “A neurosurgeon’s responsibilities would be insufferable if he did not feel that his knowledge of an intricate subject was constantly growing—that his game was improving.”17
This quote and Cushing’s operative statistics point to his nascent effort to engage in evidence-based research and speaks to the spectacular difference that a surgical innovator can make. The extraordinary results achieved by Cushing in his day also suggest that surgeons are not fungible at the vanguard of discovery. History tells us, as contemporary assessments of current research cannot, that only Harvey Cushing could achieve Cushingoid results.
A second point that stems from Cushing’s comment about the burdens of operative work and surgical research is how personally taxing that responsibility can be. Without making progress, he said, the “responsibilities would be insufferable”17 (my italics).
Even the great Harvey Cushing perceived the weight of these burdens, suggesting that any effort to depersonalize the ethics of surgical innovation would be naïve. The singularity of Cushing’s surgical accomplishments (his operative excellence as compared with his peer group) and the felt weight of these achievements suggest that surgical innovation is highly personal and proximate to the surgical researcher in a way that is distinct for surgical innovation. This relationship of operative causality and personal culpability can be subsumed under what I will call surgical proximity.
SURGICAL PROXIMITY
Surgical proximity has several implications for the conduct of research. In this section I will address two issues: conflicts of interest and clinical equipoise.
Surgical proximity and conflicts of interest
As the Cushing example illustrates, at least at the outset of a clinical trial the surgeon himself is part of the actual design of the trial. The same surgical method in the hands of one of his contemporaries would have led to a dramatically different result. The surgeon who is at the forefront of innovation becomes an experimental variable until the methods can be generalized.
The importance of the operator as an essential ingredient in early surgical research points to a key difference with pharmaceutical trials, where the purity of the drug-based intervention can be maintained. This difference has implications for the “rebuttable presumption” stance promulgated by the Association of American Medical Colleges (AAMC), which looks askance at innovators conducting clinical trials if they have a conflict of interest, such as intellectual property rights for their discoveries.19,20
In many cases, the work that surgical innovators do, as in the case of device development, could not be done without collaborations with industry. Taking the surgical talent of the potentially conflicted—but highly talented—innovator out of the equation may be counterproductive.
Time does not allow me to fully address the conflict-of-interest issue in this forum; suffice it to say that the differential knowledge, skill, and talent of early surgical innovators may be the difference between a trial’s early success or failure. The role of such innovators should neither be truncated or precluded nor be viewed a priori in a prejudicial fashion. Instead, their talents and vision should be welcomed as instrumental to the potential success of the work, managed of course with the proper degree of transparency and disclosure.
As I have noted previously,4,21 if the rationale for a conflict of interest is to allow laudable work to continue that otherwise could not occur without the personal intervention, and talents, of a surgical innovator, it seems prejudicial to view the conflict of interest as disqualifying until proven otherwise. This view is consistent with the legal framework of the US Constitution, which explicitly authorizes Congress “to promote the Progress of Science and the useful Arts, by securing for limited Times to Authors and Inventors the exclusive Right to their respective Writings and Discoveries.”22 It is also embedded in the Patent Act of 1790,23 which balances the patent’s period of exclusivity against the inventor’s obligation to share and disseminate expertise. This role for the innovator is also consistent with the intent and incentives within the framework of the Bayh-Dole Act of 1980,24 which was passed with the expectation that industrial partnerships would move ideas from the bench to the bedside.
I hope that others at this conference will be able to return to the issue of conflicts of interest and how the question of surgical proximity may, or may not, alter our ethical judgments about the surgeon’s role in research where there may be a conflict of interest.
Surgical proximity and equipoise
Surgical proximity also has an impact on clinical equipoise, the ethical neutrality about outcomes felt necessary for the conduct of clinical trials.25 The surgeon’s sense of causality and proximity to the operative act makes surgical research different because the equipoise, which exists objectively about the research questions at hand, may not exist in the mind of the surgical researcher. Let me explain.
Taking a patient to surgery is highly consequential. As we have seen from Bosk’s work,16 surgeons feel a sense of responsibility for their operative acts and surgical work. This felt responsibility, inculcated in surgical training and surgical culture, obligates the surgeon to make a proportionality judgment about bringing a patient to the operating room, be it for research or for clinical practice. In this way, surgical investigators have determined, at least in their own minds, that net benefits outweigh net risks, thus breaching clinical equipoise.
It is hard for a surgeon to commit to an operative procedure—be it for clinical care or for research— with all its attendant risks if he or she does not believe that the intervention is safe and effective. We can appreciate the importance of the surgeon’s perspective on the utility of any proposed operation if we consider the opposing question of futility in clinical practice.26 Whereas internists or intensivists might be compelled by families to continue aggressive intensive care, surgeons cannot be compelled to take a patient to the operating room when they deem that the risks outweigh the benefits. Because the surgeon is such a proximate moral agent, he or she will be held culpable for the actions that occur in theater. This degree of responsibility is accompanied by a retained degree of discretion—an almost old-world paternalistic discretion27—to counter the demands for disproportionate care.
This same sense of culpability and responsibility informs the surgeon’s willingness to take any patient to the operating room. In the case of research, this willingness becomes an issue of concern because it means that in the surgeon’s mind, favorable operative proportionality has been achieved.
This process of self-regulation28 can have implications for the informed-consent process because surgeons believe in their work and can exert a strong dynamic transference on subjects who may be desperate for cure.29 Because of this potential bias, surgical research may become especially prone to a therapeutic misconception. That is, if the surgeon is willing to take the risks of doing an innovative procedure in the operating room, then it has crossed some sort of internal threshold of proportionality in which the risks, whatever they are, have become acceptable given the putative benefits. Given what Bosk has written about surgical failure,16 a high bar is crossed when a surgeon takes a patient to the operating room for a novel procedure, even though motivations at that bar may occasionally be mixed.* (*Lest I be misconstrued as too idealistic, this burdens-vs-benefits equation may be fueled by a complex mosaic of motivations and may not always be informed fully by patient-centered benefits. If the surgeon is the innovator and the inventor, these benefits may be for the pursuit of a hypothesis and associated with potential fame or fortune. But even in these cases, judgments about proportionality are informed by surgical proximity. [For more on the ethics of conflicts of interest, see references 4 and 21.])
FROM SURGICAL RESEARCH TO EDUCATION
This leads to my closing observations about transitions in surgical research, when the work of the pioneering surgeon is bequeathed to the broader surgical community to pick up the torch—or scalpel—and expand the work.
This takes me away from research and, fittingly here at a medical school dedicated to research training, brings me to medical education. To transcend the personal dimensions of surgical innovation—and the courage and vision of the founders—and sustain it more broadly, innovators also have to become educators of future surgeons, organizers of talent, and moral exemplars for the next generation. They have to appreciate that the work that they started, if it is important, will not be completed during their tenure but that future generations will carry it forward and expand upon it. They also have to prepare the next generation with the tools and orientation to appreciate their vision and to embrace what Thomas Kuhn might call new scientific paradigms.30
On several occasions Wilder Penfield, who founded the Montreal Neurological Institute, wrote with regret about Victor Horsley, the neurosurgeon at Queens Square in London. Penfield viewed Horsley as the founder of his field, but Horsley left no disciples. In his autobiography, fittingly entitled No Man Alone, Penfield noted that Horsley, “the most distinguished pioneer neurosurgeon, had died in 1916 without having established a school of neurosurgery.”5 This is in contrast to the discipline-building work of Cushing.
It is not an accident that Dr. Cushing founded a field full of trainees and protégés, of which my co-panelists are descendants. It was intentional and part of his ethos of being truly innovative. And it is not an accident that the distinguished surgical innovators at this symposium have also created institutional structures to continue their work for decades to come. Their achievements have transcended the individual innovator and have become systematic. It is said that Dr. Thomas Starzl launched a field.31 Dr. Denton Cooley founded the Texas Heart Institute.32 Dr. Thomas Fogarty started the Fogarty Institute for Innovation, whose mission statement explicitly notes that it is “an educational non-profit that mentors, trains and inspires the next generation of medical innovators.”33 Each of these pioneers, I believe, appreciates the need for continuity and dissemination.
But even here there is something that we nonsurgeons need to understand: although the work transcends the individual surgeon, the ties remain personal and linked to the impact and legacy of founders. Take, for example, highly prized membership in the Denton A. Cooley Cardiovascular Surgical Society.34 This too is about the importance of individuals and surgical proximity, but here it is transgenerational.
CONCLUSION
If we truly want to continue the dialogue begun here today, we need to understand these social and professional networks and the importance of surgical proximity in transmitting both methods and values. The proximate nature of surgical research—and the causality and responsibility that accrues to the surgeon—makes surgical research different than other areas of biomedical inquiry. This difference has implications for risk-benefit analysis, conflicts of interest, and clinical equipoise. I hope that my colleagues return to these themes in the coming days so that the regulation of this important area of research can be informed by a deeper understanding of the ethics of surgical discovery and innovation.35
Acknowledgments
Dr. Fins gratefully acknowledges the invitation to participate in this symposium, the helpful suggestions of Dr. Eric Kodish, and partial grant support of the Weill Cornell Medical College Research Ethics Core, NIH Clinical & Translational Science Center UL1-RR024966.
- Frader JE, Caniano DA. Research and innovation in surgery. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:216–241.
- Speelman JD, Bosch DA. Resurgence of functional neurosurgery for Parkinson’s disease: a historical perspective. Mov Disord 1998; 13:582–588.
- Holstein WJ. Rewiring the brain: how a bright idea became an innovative medical device. US News & World Report. March 1, 1999:52–53.
- Fins JJ, Schachter M. Investigators, industry, and the heuristic device: ethics, patent law, and clinical innovation. Account Res 2001; 8:219–233.
- Penfield W. No Man Alone: A Neurosurgeon’s Life. Boston, MA: Little Brown; 1977.
- Feindel W. The contributions of Wilder Penfield to the functional anatomy of the human brain. Hum Neurobiol 1982; 1:231–234.
- Aristotle. The Nicomachean Ethics. Weldon JEC, trans. Amherst, NY: Prometheus Books; 1987.
- Fins JJ, Bacchetta MD, Miller FG. Clinical pragmatism: a method of moral problem solving. Kennedy Inst Ethics J 1997; 7:129–145.
- Miller FG, Fins JJ. Protecting human subjects in brain research: a pragmatic perspective. In: Illes J, ed. Neuroethics: Defining the Issues in Theory, Practice and Policy. New York, NY: Oxford University Press; 2005.
- Pollan M. The year in ideas: A to Z.; precautionary principle. New York Times. December 9, 2001.
- van den Belt H. Debating the precautionary principle: “guilty until proven innocent” or “innocent until proven guilty”? Plant Physiol 2003; 132:1122–1126.
- Jonas H. The Imperative of Responsibility: In Search of an Ethics for the Technological Age. Chicago, IL: University of Chicago Press; 1985:34.
- Eliot TS. The Love Song of J. Alfred Prufrock. In: Abrams MH, ed. The Norton Anthology of English Literature. Vol 2. 4th ed. New York, NY: W.W. Norton & Co; 1979:2259–2264.
- Sunstein CR. The paralyzing principle. Regulation. Winter 2002– 2003; 25(4):32–37.
- Holm S, Harris J. Precautionary principle stifles discovery. Nature 1999; 400:398.
- Bosk C. Forgive and Remember: Managing Medical Failure. Chicago, IL: University of Chicago Press; 1979:29–30.
- Bliss M. Harvey Cushing: A Life in Surgery. Oxford, UK: Oxford University Press; 2005.
- Pinkus RL. Mistakes as a social construct: an historical approach. Kennedy Inst Ethics J 2001; 11:117–133.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress I: policy and guidelines for the oversight of individual financial interests in human subjects research. Acad Med 2003; 78:225–236.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress II: principles and recommendations for oversight of an institution’s financial interests in human subjects research. Acad Med 2003; 78:237– 245.
- Fins JJ. Disclose and justify: intellectual property, conflicts of interest, and neurosurgery. Congress Quarterly (Official Newsmagazine of the Congress of Neurological Surgeons) 2007; 8(3):34–36.
- U.S. Constitution, art. I, §8, cl. 8; see also id. at art. I, §8, cl. 18.
- Patent Act of 1790, ch. 7, 1 Stat. 109–111 (1790).
- Patent and Trademark Act Amendments of 1980 (Bayh-Dole Act); Pub L No. 96-517. Codified as 35 USC §§200–212 (1994).
- Freedman B. Equipoise and the ethics of clinical research. N Engl J Med 1987; 317:141–145.
- Callahan D. Necessity, futility, and the good society. J Am Geriatr Soc 1994; 42:866–867.
- Katz J. The Silent World of Doctor and Patient. New York, NY: Free Press; 1984.
- Jones RS, Fletcher JC. Self-regulation of surgical practice and research. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:255–279.
- Kim SY. Assessing and communicating the risks and benefits of gene transfer clinical trials. Curr Opin Mol Ther 2006; 8:384– 389.
- Kuhn TS. The Structure of Scientific Revolutions. 2nd ed. Chicago, IL: University of Chicago Press; 1970.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon. Pittsburgh, PA: University of Pittsburgh Press; 2003.
- Twenty Five Years of Excellence: A History of the Texas Heart Institute. Houston, TX: Texas Heart Institute Foundation; 1989.
- Fogarty Institute for Innovation Web site. Available at: http://01659a8. netsolhost.com/aboutus.html. Accessed June 6, 2008.
- Denton A. Cooley Cardiovascular Surgical Society Web site. Available at: http://www.cooleysociety.com/about.html. Accessed June 6, 2008.
- de Melo-Martín I, Palmer LI, Fins JJ. Viewpoint: developing a research ethics consultation service to foster responsive and responsible clinical research. Acad Med 2007; 82:900–904.
No! I am not Prince Hamlet, nor was meant to be;
Am an attendant lord, one that will do
To swell a progress, start a scene or two…
—T.S. Eliot, The Love Song of J. Alfred Prufrock
Let me start by thanking the organizers for their invitation to be here and to start this off. I am not sure if that invitation was an act of kindness or of throwing a fellow bioethicist to the lions, as we will be addressing a complicated set of issues upon which well-intentioned folks disagree and sometimes disagree with a passion.
What I would like to do is to lay out some of the inherent ethical problems related to surgical innovation. I will argue that some of these problems are unique to surgery and that others relate to how we have chosen to define categories like research and practice. Other problems involve how we view the proportionality of risks and benefits in surgical research. I will argue that we have falsely analogized surgical progress to progress made in other areas of biomedical research and misunderstood the highly personal, or proximate, nature of surgical inquiry. Without appreciating the import of what I will call “surgical proximity,” we will be unable to adequately address ethical issues in surgical innovation.
PROBLEMS OR DILEMMAS?
So let me begin with the title of our session, “Surgical Innovation and Ethical Dilemmas,” and why this juxta position is counterproductive. A colleague long ago taught me to distinguish problems from dilemmas—the former being resolvable, the latter intractable, often involving a choice between two equally unfavorable choices.
Although I may be making too much of the semantics, I do think the title betrays a presumption that surgical innovation invariably forces adversarial choices. It tends to dichotomize ethical reflection, pitting those who favor prudence against those who endorse progress, or it creates too stark a difference between ethical issues in surgical practice and those encountered in the conduct of surgical research.
Even therapeutic, validated surgery in many ways has the potential to become innovative, if not outright experimental. Patients may have anatomical differences that require surgical improvisation, or complications may arise during “routine” surgery, creating the need for an imaginative response.1 At what point do these departures from expected care become novel interventions, innovative or even experimental? A routine case with an unexpected turn can even become a case report opening up a new field of endeavor.
For instance, the field of stereotactic functional neurosurgery was born out of a “routine” case of ablative surgery for Parkinson’s disease in the 1980s, when the French neurosurgeon Alim Benabid was using electrodes to determine which areas of the brain should be destroyed. As he was mapping the thalamus, he noted that the tremor of his patient abated. This led him to wonder if one could treat drug-resistant Parkinson’s with electrical stimulation instead of destructive lesioning.2 Benabid’s translational insight during an ordinary case led to the development of the rather extraordinary field of stereotactic functional neurosurgery and neuromodulation.3,4
Another example from an earlier era comes from the life work of neurosurgeon Wilder Penfield, who did pioneering work in the surgical treatment of epilepsy. Here, the accumulation of experience from “routine care” led to generalizable knowledge, much like hypotheses are validated in experimental work. In Penfield’s case, his clinical use of electrical stimulation to plan resections of scar tissue causing epilepsy led him to map the human homunculus, a magnificent achievement of profound importance.5,6
So let us avoid simplistic and confounding demarcations. Instead of dichotomizing innovation and prudence—or surgical research and surgical practice—let us try to start our deliberations with an eye toward a more synthetic approach. Like most things in nature and in biology, ethics too is on a continuum with gradations that can fit into an Aristotelian taxonomy. Let us emulate what Aristotle called phronesis, or practical wisdom, these next 2 days so that we achieve constructive outcomes, or what the pragmatists would call instrumental goods.7
If we are successful in laying out the ethical issues in this clinically pragmatic fashion, we can turn intractable “dilemmas” into problems amenable to resolution through the particularistic invocation of ethical principles as they relate to the surgical context.8 If we follow this inductive method of moral problem solving, we will avoid sweeping ethical generalizations, or categoricals, that can misrepresent the complexity of innovative research and deprive society of its benefits.9
INNOVATION VS PRUDENCE: A FALSE DICHOTOMY
So let us start by understanding the presuppositions that led to the expectation that dilemmas will descend upon those who engage in surgical innovation. In my view, this expectation begins with what is called the precautionary principle, a concept with some currency in the realm of environmental ethics.10
The precautionary principle urges caution and prudence when facing unknowns and is an antecedent sort of utilitarianism. One makes judgments about the advisability of actions based on a prior assessment of foreseeable risks and benefits. If the risks are excessive or exceed benefits, the precautionary principle urges care, caution, and even avoidance of a given course of action.
When the precautionary principle is implicitly invoked in making judgments about research, the objective is to pursue a degree of safety that is comparable to that of established therapy. But interventions that have progressed to being deemed “therapeutic” have of course achieved a requisite degree of both safety and efficacy—that is what makes them therapeutic, as opposed to investigational, interventions. One cannot know before one has conducted a clinical trial, and completed statistical analysis, whether a new surgical advance or device meets these expectations. Because of this lack of knowledge, there is an inherent degree of risk in any novel intervention.
The challenge posed by innovation or novelty creates the possibility of untoward events. It leads to invocation of the precautionary principle, which, echoing the admonitions of the philosopher Hans Jonas, urges us to “give greater weight to the prognosis of doom than to that of bliss.”11,12
This is not a bad way to go through life, assuming one wants to emulate T.S. Eliot’s J. Alfred Prufrock, who lamentably “measured out my life with coffee spoons.”13 Unlike the surgeon, who must make decisions in real time, Eliot’s protagonist could not move forward. Despite his desire to avoid the indecision of Prince Hamlet, alluded to in this paper’s epigraph, Prufrock was paralyzed by doubts and fears, with “time yet for a hundred indecisions, and for a hundred visions and revisions.”13
Despite Eliot’s invocation of “a patient etherised upon a table,”13 the poem shares little with the surgical life. It has much more in common with the precautionary principle. Like Prufrock, the precautionary principle favors what is known— the status quo—as what is unknown is invariably more risky than the familiar. Needless to say, this is antithetical to innovation because discovery invariably requires scenarios that involve novelty and unknown risks. When faced with the certain security of stasis or the potential dangers of innovation, the precautionary principle will invariably choose stasis, leading us, as the legal scholar Cass Sunstein notes, “in no direction at all.”14
Seen through the prism of the precautionary principle, then, surgical innovation invariably presents a dilemma. Discovery and innovation are fundamentally at odds with the precautionary principle, because of their potential for risk.15
The challenge posed by the precautionary principle—which, to be fair, is seen in all areas of clinical research—becomes even more pronounced in surgical research because of the size and scope of clinical trials. As is well appreciated here, compared with drug trials, surgical trials are small. Sometimes they can involve a single subject, whereas drug trials may include thousands of participants. Because of drug trials’ large volume of subjects, therapeutic effects can be small to justify ongoing research. In a surgical trial or a device trial, the number of subjects is smaller, so the therapeutic impact has to be larger to warrant further development and ongoing study. This burden of scale increases the probability of reciprocally large adverse effects. This potential for disaster magnifies the impact of the precautionary principle and may lead to a distortion in ethical judgment along the lines of Hans Jonas’ admonition.12
By all of this I am not suggesting that we abandon precautions and prudence. Instead, my point is to explicate the additional challenges faced by surgical research and the sway of the precautionary principle over this area of inquiry and innovation. By being explicit about the impact of this principle, we can be cognizant of its potential to distort judgments about risks and benefits. Only then can we hope to balance the pursuit of progress with that of safety.
SURGICAL RESPONSIBILITY
These distortions also need to be recognized, and made explicit, because surgical research, more so than pharmacologic research, is much more personal and intimate. This point becomes clear if we consider a surgical trial that does not succeed.
In the surgical arena, such failures are taken to heart and personalized. Unlike trials that involve drugs, surgical research is more proximate. It is not just the failure of a drug or of pharmacology; it is also possibly the failure of the operator, the surgeon who did not achieve the desired goal because of poor execution of surgical technique.
This crucial difference in medical versus surgical cultures is captured by Charles Bosk in his magisterial sociological study of surgery, Forgive and Remember: Managing Medical Failure. In a discussion of morbidity and mortality rounds, Bosk writes:
The specific nature of surgical treatment links the action of the physician and the response of the patient more intimately than in other areas of medicine....When the patient of an internist dies, the natural question his colleagues ask is, “What happened?” When the patient of a surgeon dies, his colleagues ask, “What did you do?”16
As in clinical surgical practice, in surgical research, it is the personal and individualized mediation of the surgeon that is central to the intervention. Here the intermediary is neither a drug nor its bioavailability; rather, it is the operator’s technique plus or minus the operative design and the reliability of an instrument or a device. In either case, the contribution is more proximate and personal, stemming from the actions of individual surgeons and the work of their hands.
History is instructive on this theme of surgical causality and personal culpability if we consider the life of Harvey Cushing, a Cleveland native whose ashes are buried nearby in Lake View Cemetery.17 Cushing was a gifted and innovative surgeon whose technique handling tissues changed how the brain was approached operatively. He is acknowledged as the father of neurosurgery, having created a professional nexus to institutionalize and carry on his innovative work.18
Cushing’s greatest innovation was probably in his individual efforts as a working surgeon. Over the course of his lifetime, he made the resection of brain tumors a safe and sometimes effective treatment for an otherwise dread disease. Michael Bliss, Cushing’s most recent biographer, reports mortality data from more than 2,400 surgeries done by Cushing during his operative lifetime.17 Early in his career (from 1896 to 1911), while he was at Johns Hopkins, Cushing’s case mortality rate was 24.7%. During his later years at the Brigham Hospital, it was 16.2%. By 1930–1931 it was down to 8.8%.
These were extraordinary statistics: no one matched Cushing’s numbers, or his ability to do what he did. Bliss cites mortality data from his surgical contemporaries in the late 1920s as ranging from approximately 35% to 45%. By the numbers Bliss compares Cushing’s talent—his truly brilliant outlier performance—to that of his Jazz Age contemporary, Babe Ruth, who also had outsized talent compared with his peers.17
Cushing himself, a collegiate second baseman at Yale, linked sport and statistics in a most telling way. Documenting his ongoing surgical progress was a hedge against failure and lightened the emotional burdens of the surgical suite. Cushing observed: “A neurosurgeon’s responsibilities would be insufferable if he did not feel that his knowledge of an intricate subject was constantly growing—that his game was improving.”17
This quote and Cushing’s operative statistics point to his nascent effort to engage in evidence-based research and speaks to the spectacular difference that a surgical innovator can make. The extraordinary results achieved by Cushing in his day also suggest that surgeons are not fungible at the vanguard of discovery. History tells us, as contemporary assessments of current research cannot, that only Harvey Cushing could achieve Cushingoid results.
A second point that stems from Cushing’s comment about the burdens of operative work and surgical research is how personally taxing that responsibility can be. Without making progress, he said, the “responsibilities would be insufferable”17 (my italics).
Even the great Harvey Cushing perceived the weight of these burdens, suggesting that any effort to depersonalize the ethics of surgical innovation would be naïve. The singularity of Cushing’s surgical accomplishments (his operative excellence as compared with his peer group) and the felt weight of these achievements suggest that surgical innovation is highly personal and proximate to the surgical researcher in a way that is distinct for surgical innovation. This relationship of operative causality and personal culpability can be subsumed under what I will call surgical proximity.
SURGICAL PROXIMITY
Surgical proximity has several implications for the conduct of research. In this section I will address two issues: conflicts of interest and clinical equipoise.
Surgical proximity and conflicts of interest
As the Cushing example illustrates, at least at the outset of a clinical trial the surgeon himself is part of the actual design of the trial. The same surgical method in the hands of one of his contemporaries would have led to a dramatically different result. The surgeon who is at the forefront of innovation becomes an experimental variable until the methods can be generalized.
The importance of the operator as an essential ingredient in early surgical research points to a key difference with pharmaceutical trials, where the purity of the drug-based intervention can be maintained. This difference has implications for the “rebuttable presumption” stance promulgated by the Association of American Medical Colleges (AAMC), which looks askance at innovators conducting clinical trials if they have a conflict of interest, such as intellectual property rights for their discoveries.19,20
In many cases, the work that surgical innovators do, as in the case of device development, could not be done without collaborations with industry. Taking the surgical talent of the potentially conflicted—but highly talented—innovator out of the equation may be counterproductive.
Time does not allow me to fully address the conflict-of-interest issue in this forum; suffice it to say that the differential knowledge, skill, and talent of early surgical innovators may be the difference between a trial’s early success or failure. The role of such innovators should neither be truncated or precluded nor be viewed a priori in a prejudicial fashion. Instead, their talents and vision should be welcomed as instrumental to the potential success of the work, managed of course with the proper degree of transparency and disclosure.
As I have noted previously,4,21 if the rationale for a conflict of interest is to allow laudable work to continue that otherwise could not occur without the personal intervention, and talents, of a surgical innovator, it seems prejudicial to view the conflict of interest as disqualifying until proven otherwise. This view is consistent with the legal framework of the US Constitution, which explicitly authorizes Congress “to promote the Progress of Science and the useful Arts, by securing for limited Times to Authors and Inventors the exclusive Right to their respective Writings and Discoveries.”22 It is also embedded in the Patent Act of 1790,23 which balances the patent’s period of exclusivity against the inventor’s obligation to share and disseminate expertise. This role for the innovator is also consistent with the intent and incentives within the framework of the Bayh-Dole Act of 1980,24 which was passed with the expectation that industrial partnerships would move ideas from the bench to the bedside.
I hope that others at this conference will be able to return to the issue of conflicts of interest and how the question of surgical proximity may, or may not, alter our ethical judgments about the surgeon’s role in research where there may be a conflict of interest.
Surgical proximity and equipoise
Surgical proximity also has an impact on clinical equipoise, the ethical neutrality about outcomes felt necessary for the conduct of clinical trials.25 The surgeon’s sense of causality and proximity to the operative act makes surgical research different because the equipoise, which exists objectively about the research questions at hand, may not exist in the mind of the surgical researcher. Let me explain.
Taking a patient to surgery is highly consequential. As we have seen from Bosk’s work,16 surgeons feel a sense of responsibility for their operative acts and surgical work. This felt responsibility, inculcated in surgical training and surgical culture, obligates the surgeon to make a proportionality judgment about bringing a patient to the operating room, be it for research or for clinical practice. In this way, surgical investigators have determined, at least in their own minds, that net benefits outweigh net risks, thus breaching clinical equipoise.
It is hard for a surgeon to commit to an operative procedure—be it for clinical care or for research— with all its attendant risks if he or she does not believe that the intervention is safe and effective. We can appreciate the importance of the surgeon’s perspective on the utility of any proposed operation if we consider the opposing question of futility in clinical practice.26 Whereas internists or intensivists might be compelled by families to continue aggressive intensive care, surgeons cannot be compelled to take a patient to the operating room when they deem that the risks outweigh the benefits. Because the surgeon is such a proximate moral agent, he or she will be held culpable for the actions that occur in theater. This degree of responsibility is accompanied by a retained degree of discretion—an almost old-world paternalistic discretion27—to counter the demands for disproportionate care.
This same sense of culpability and responsibility informs the surgeon’s willingness to take any patient to the operating room. In the case of research, this willingness becomes an issue of concern because it means that in the surgeon’s mind, favorable operative proportionality has been achieved.
This process of self-regulation28 can have implications for the informed-consent process because surgeons believe in their work and can exert a strong dynamic transference on subjects who may be desperate for cure.29 Because of this potential bias, surgical research may become especially prone to a therapeutic misconception. That is, if the surgeon is willing to take the risks of doing an innovative procedure in the operating room, then it has crossed some sort of internal threshold of proportionality in which the risks, whatever they are, have become acceptable given the putative benefits. Given what Bosk has written about surgical failure,16 a high bar is crossed when a surgeon takes a patient to the operating room for a novel procedure, even though motivations at that bar may occasionally be mixed.* (*Lest I be misconstrued as too idealistic, this burdens-vs-benefits equation may be fueled by a complex mosaic of motivations and may not always be informed fully by patient-centered benefits. If the surgeon is the innovator and the inventor, these benefits may be for the pursuit of a hypothesis and associated with potential fame or fortune. But even in these cases, judgments about proportionality are informed by surgical proximity. [For more on the ethics of conflicts of interest, see references 4 and 21.])
FROM SURGICAL RESEARCH TO EDUCATION
This leads to my closing observations about transitions in surgical research, when the work of the pioneering surgeon is bequeathed to the broader surgical community to pick up the torch—or scalpel—and expand the work.
This takes me away from research and, fittingly here at a medical school dedicated to research training, brings me to medical education. To transcend the personal dimensions of surgical innovation—and the courage and vision of the founders—and sustain it more broadly, innovators also have to become educators of future surgeons, organizers of talent, and moral exemplars for the next generation. They have to appreciate that the work that they started, if it is important, will not be completed during their tenure but that future generations will carry it forward and expand upon it. They also have to prepare the next generation with the tools and orientation to appreciate their vision and to embrace what Thomas Kuhn might call new scientific paradigms.30
On several occasions Wilder Penfield, who founded the Montreal Neurological Institute, wrote with regret about Victor Horsley, the neurosurgeon at Queens Square in London. Penfield viewed Horsley as the founder of his field, but Horsley left no disciples. In his autobiography, fittingly entitled No Man Alone, Penfield noted that Horsley, “the most distinguished pioneer neurosurgeon, had died in 1916 without having established a school of neurosurgery.”5 This is in contrast to the discipline-building work of Cushing.
It is not an accident that Dr. Cushing founded a field full of trainees and protégés, of which my co-panelists are descendants. It was intentional and part of his ethos of being truly innovative. And it is not an accident that the distinguished surgical innovators at this symposium have also created institutional structures to continue their work for decades to come. Their achievements have transcended the individual innovator and have become systematic. It is said that Dr. Thomas Starzl launched a field.31 Dr. Denton Cooley founded the Texas Heart Institute.32 Dr. Thomas Fogarty started the Fogarty Institute for Innovation, whose mission statement explicitly notes that it is “an educational non-profit that mentors, trains and inspires the next generation of medical innovators.”33 Each of these pioneers, I believe, appreciates the need for continuity and dissemination.
But even here there is something that we nonsurgeons need to understand: although the work transcends the individual surgeon, the ties remain personal and linked to the impact and legacy of founders. Take, for example, highly prized membership in the Denton A. Cooley Cardiovascular Surgical Society.34 This too is about the importance of individuals and surgical proximity, but here it is transgenerational.
CONCLUSION
If we truly want to continue the dialogue begun here today, we need to understand these social and professional networks and the importance of surgical proximity in transmitting both methods and values. The proximate nature of surgical research—and the causality and responsibility that accrues to the surgeon—makes surgical research different than other areas of biomedical inquiry. This difference has implications for risk-benefit analysis, conflicts of interest, and clinical equipoise. I hope that my colleagues return to these themes in the coming days so that the regulation of this important area of research can be informed by a deeper understanding of the ethics of surgical discovery and innovation.35
Acknowledgments
Dr. Fins gratefully acknowledges the invitation to participate in this symposium, the helpful suggestions of Dr. Eric Kodish, and partial grant support of the Weill Cornell Medical College Research Ethics Core, NIH Clinical & Translational Science Center UL1-RR024966.
No! I am not Prince Hamlet, nor was meant to be;
Am an attendant lord, one that will do
To swell a progress, start a scene or two…
—T.S. Eliot, The Love Song of J. Alfred Prufrock
Let me start by thanking the organizers for their invitation to be here and to start this off. I am not sure if that invitation was an act of kindness or of throwing a fellow bioethicist to the lions, as we will be addressing a complicated set of issues upon which well-intentioned folks disagree and sometimes disagree with a passion.
What I would like to do is to lay out some of the inherent ethical problems related to surgical innovation. I will argue that some of these problems are unique to surgery and that others relate to how we have chosen to define categories like research and practice. Other problems involve how we view the proportionality of risks and benefits in surgical research. I will argue that we have falsely analogized surgical progress to progress made in other areas of biomedical research and misunderstood the highly personal, or proximate, nature of surgical inquiry. Without appreciating the import of what I will call “surgical proximity,” we will be unable to adequately address ethical issues in surgical innovation.
PROBLEMS OR DILEMMAS?
So let me begin with the title of our session, “Surgical Innovation and Ethical Dilemmas,” and why this juxta position is counterproductive. A colleague long ago taught me to distinguish problems from dilemmas—the former being resolvable, the latter intractable, often involving a choice between two equally unfavorable choices.
Although I may be making too much of the semantics, I do think the title betrays a presumption that surgical innovation invariably forces adversarial choices. It tends to dichotomize ethical reflection, pitting those who favor prudence against those who endorse progress, or it creates too stark a difference between ethical issues in surgical practice and those encountered in the conduct of surgical research.
Even therapeutic, validated surgery in many ways has the potential to become innovative, if not outright experimental. Patients may have anatomical differences that require surgical improvisation, or complications may arise during “routine” surgery, creating the need for an imaginative response.1 At what point do these departures from expected care become novel interventions, innovative or even experimental? A routine case with an unexpected turn can even become a case report opening up a new field of endeavor.
For instance, the field of stereotactic functional neurosurgery was born out of a “routine” case of ablative surgery for Parkinson’s disease in the 1980s, when the French neurosurgeon Alim Benabid was using electrodes to determine which areas of the brain should be destroyed. As he was mapping the thalamus, he noted that the tremor of his patient abated. This led him to wonder if one could treat drug-resistant Parkinson’s with electrical stimulation instead of destructive lesioning.2 Benabid’s translational insight during an ordinary case led to the development of the rather extraordinary field of stereotactic functional neurosurgery and neuromodulation.3,4
Another example from an earlier era comes from the life work of neurosurgeon Wilder Penfield, who did pioneering work in the surgical treatment of epilepsy. Here, the accumulation of experience from “routine care” led to generalizable knowledge, much like hypotheses are validated in experimental work. In Penfield’s case, his clinical use of electrical stimulation to plan resections of scar tissue causing epilepsy led him to map the human homunculus, a magnificent achievement of profound importance.5,6
So let us avoid simplistic and confounding demarcations. Instead of dichotomizing innovation and prudence—or surgical research and surgical practice—let us try to start our deliberations with an eye toward a more synthetic approach. Like most things in nature and in biology, ethics too is on a continuum with gradations that can fit into an Aristotelian taxonomy. Let us emulate what Aristotle called phronesis, or practical wisdom, these next 2 days so that we achieve constructive outcomes, or what the pragmatists would call instrumental goods.7
If we are successful in laying out the ethical issues in this clinically pragmatic fashion, we can turn intractable “dilemmas” into problems amenable to resolution through the particularistic invocation of ethical principles as they relate to the surgical context.8 If we follow this inductive method of moral problem solving, we will avoid sweeping ethical generalizations, or categoricals, that can misrepresent the complexity of innovative research and deprive society of its benefits.9
INNOVATION VS PRUDENCE: A FALSE DICHOTOMY
So let us start by understanding the presuppositions that led to the expectation that dilemmas will descend upon those who engage in surgical innovation. In my view, this expectation begins with what is called the precautionary principle, a concept with some currency in the realm of environmental ethics.10
The precautionary principle urges caution and prudence when facing unknowns and is an antecedent sort of utilitarianism. One makes judgments about the advisability of actions based on a prior assessment of foreseeable risks and benefits. If the risks are excessive or exceed benefits, the precautionary principle urges care, caution, and even avoidance of a given course of action.
When the precautionary principle is implicitly invoked in making judgments about research, the objective is to pursue a degree of safety that is comparable to that of established therapy. But interventions that have progressed to being deemed “therapeutic” have of course achieved a requisite degree of both safety and efficacy—that is what makes them therapeutic, as opposed to investigational, interventions. One cannot know before one has conducted a clinical trial, and completed statistical analysis, whether a new surgical advance or device meets these expectations. Because of this lack of knowledge, there is an inherent degree of risk in any novel intervention.
The challenge posed by innovation or novelty creates the possibility of untoward events. It leads to invocation of the precautionary principle, which, echoing the admonitions of the philosopher Hans Jonas, urges us to “give greater weight to the prognosis of doom than to that of bliss.”11,12
This is not a bad way to go through life, assuming one wants to emulate T.S. Eliot’s J. Alfred Prufrock, who lamentably “measured out my life with coffee spoons.”13 Unlike the surgeon, who must make decisions in real time, Eliot’s protagonist could not move forward. Despite his desire to avoid the indecision of Prince Hamlet, alluded to in this paper’s epigraph, Prufrock was paralyzed by doubts and fears, with “time yet for a hundred indecisions, and for a hundred visions and revisions.”13
Despite Eliot’s invocation of “a patient etherised upon a table,”13 the poem shares little with the surgical life. It has much more in common with the precautionary principle. Like Prufrock, the precautionary principle favors what is known— the status quo—as what is unknown is invariably more risky than the familiar. Needless to say, this is antithetical to innovation because discovery invariably requires scenarios that involve novelty and unknown risks. When faced with the certain security of stasis or the potential dangers of innovation, the precautionary principle will invariably choose stasis, leading us, as the legal scholar Cass Sunstein notes, “in no direction at all.”14
Seen through the prism of the precautionary principle, then, surgical innovation invariably presents a dilemma. Discovery and innovation are fundamentally at odds with the precautionary principle, because of their potential for risk.15
The challenge posed by the precautionary principle—which, to be fair, is seen in all areas of clinical research—becomes even more pronounced in surgical research because of the size and scope of clinical trials. As is well appreciated here, compared with drug trials, surgical trials are small. Sometimes they can involve a single subject, whereas drug trials may include thousands of participants. Because of drug trials’ large volume of subjects, therapeutic effects can be small to justify ongoing research. In a surgical trial or a device trial, the number of subjects is smaller, so the therapeutic impact has to be larger to warrant further development and ongoing study. This burden of scale increases the probability of reciprocally large adverse effects. This potential for disaster magnifies the impact of the precautionary principle and may lead to a distortion in ethical judgment along the lines of Hans Jonas’ admonition.12
By all of this I am not suggesting that we abandon precautions and prudence. Instead, my point is to explicate the additional challenges faced by surgical research and the sway of the precautionary principle over this area of inquiry and innovation. By being explicit about the impact of this principle, we can be cognizant of its potential to distort judgments about risks and benefits. Only then can we hope to balance the pursuit of progress with that of safety.
SURGICAL RESPONSIBILITY
These distortions also need to be recognized, and made explicit, because surgical research, more so than pharmacologic research, is much more personal and intimate. This point becomes clear if we consider a surgical trial that does not succeed.
In the surgical arena, such failures are taken to heart and personalized. Unlike trials that involve drugs, surgical research is more proximate. It is not just the failure of a drug or of pharmacology; it is also possibly the failure of the operator, the surgeon who did not achieve the desired goal because of poor execution of surgical technique.
This crucial difference in medical versus surgical cultures is captured by Charles Bosk in his magisterial sociological study of surgery, Forgive and Remember: Managing Medical Failure. In a discussion of morbidity and mortality rounds, Bosk writes:
The specific nature of surgical treatment links the action of the physician and the response of the patient more intimately than in other areas of medicine....When the patient of an internist dies, the natural question his colleagues ask is, “What happened?” When the patient of a surgeon dies, his colleagues ask, “What did you do?”16
As in clinical surgical practice, in surgical research, it is the personal and individualized mediation of the surgeon that is central to the intervention. Here the intermediary is neither a drug nor its bioavailability; rather, it is the operator’s technique plus or minus the operative design and the reliability of an instrument or a device. In either case, the contribution is more proximate and personal, stemming from the actions of individual surgeons and the work of their hands.
History is instructive on this theme of surgical causality and personal culpability if we consider the life of Harvey Cushing, a Cleveland native whose ashes are buried nearby in Lake View Cemetery.17 Cushing was a gifted and innovative surgeon whose technique handling tissues changed how the brain was approached operatively. He is acknowledged as the father of neurosurgery, having created a professional nexus to institutionalize and carry on his innovative work.18
Cushing’s greatest innovation was probably in his individual efforts as a working surgeon. Over the course of his lifetime, he made the resection of brain tumors a safe and sometimes effective treatment for an otherwise dread disease. Michael Bliss, Cushing’s most recent biographer, reports mortality data from more than 2,400 surgeries done by Cushing during his operative lifetime.17 Early in his career (from 1896 to 1911), while he was at Johns Hopkins, Cushing’s case mortality rate was 24.7%. During his later years at the Brigham Hospital, it was 16.2%. By 1930–1931 it was down to 8.8%.
These were extraordinary statistics: no one matched Cushing’s numbers, or his ability to do what he did. Bliss cites mortality data from his surgical contemporaries in the late 1920s as ranging from approximately 35% to 45%. By the numbers Bliss compares Cushing’s talent—his truly brilliant outlier performance—to that of his Jazz Age contemporary, Babe Ruth, who also had outsized talent compared with his peers.17
Cushing himself, a collegiate second baseman at Yale, linked sport and statistics in a most telling way. Documenting his ongoing surgical progress was a hedge against failure and lightened the emotional burdens of the surgical suite. Cushing observed: “A neurosurgeon’s responsibilities would be insufferable if he did not feel that his knowledge of an intricate subject was constantly growing—that his game was improving.”17
This quote and Cushing’s operative statistics point to his nascent effort to engage in evidence-based research and speaks to the spectacular difference that a surgical innovator can make. The extraordinary results achieved by Cushing in his day also suggest that surgeons are not fungible at the vanguard of discovery. History tells us, as contemporary assessments of current research cannot, that only Harvey Cushing could achieve Cushingoid results.
A second point that stems from Cushing’s comment about the burdens of operative work and surgical research is how personally taxing that responsibility can be. Without making progress, he said, the “responsibilities would be insufferable”17 (my italics).
Even the great Harvey Cushing perceived the weight of these burdens, suggesting that any effort to depersonalize the ethics of surgical innovation would be naïve. The singularity of Cushing’s surgical accomplishments (his operative excellence as compared with his peer group) and the felt weight of these achievements suggest that surgical innovation is highly personal and proximate to the surgical researcher in a way that is distinct for surgical innovation. This relationship of operative causality and personal culpability can be subsumed under what I will call surgical proximity.
SURGICAL PROXIMITY
Surgical proximity has several implications for the conduct of research. In this section I will address two issues: conflicts of interest and clinical equipoise.
Surgical proximity and conflicts of interest
As the Cushing example illustrates, at least at the outset of a clinical trial the surgeon himself is part of the actual design of the trial. The same surgical method in the hands of one of his contemporaries would have led to a dramatically different result. The surgeon who is at the forefront of innovation becomes an experimental variable until the methods can be generalized.
The importance of the operator as an essential ingredient in early surgical research points to a key difference with pharmaceutical trials, where the purity of the drug-based intervention can be maintained. This difference has implications for the “rebuttable presumption” stance promulgated by the Association of American Medical Colleges (AAMC), which looks askance at innovators conducting clinical trials if they have a conflict of interest, such as intellectual property rights for their discoveries.19,20
In many cases, the work that surgical innovators do, as in the case of device development, could not be done without collaborations with industry. Taking the surgical talent of the potentially conflicted—but highly talented—innovator out of the equation may be counterproductive.
Time does not allow me to fully address the conflict-of-interest issue in this forum; suffice it to say that the differential knowledge, skill, and talent of early surgical innovators may be the difference between a trial’s early success or failure. The role of such innovators should neither be truncated or precluded nor be viewed a priori in a prejudicial fashion. Instead, their talents and vision should be welcomed as instrumental to the potential success of the work, managed of course with the proper degree of transparency and disclosure.
As I have noted previously,4,21 if the rationale for a conflict of interest is to allow laudable work to continue that otherwise could not occur without the personal intervention, and talents, of a surgical innovator, it seems prejudicial to view the conflict of interest as disqualifying until proven otherwise. This view is consistent with the legal framework of the US Constitution, which explicitly authorizes Congress “to promote the Progress of Science and the useful Arts, by securing for limited Times to Authors and Inventors the exclusive Right to their respective Writings and Discoveries.”22 It is also embedded in the Patent Act of 1790,23 which balances the patent’s period of exclusivity against the inventor’s obligation to share and disseminate expertise. This role for the innovator is also consistent with the intent and incentives within the framework of the Bayh-Dole Act of 1980,24 which was passed with the expectation that industrial partnerships would move ideas from the bench to the bedside.
I hope that others at this conference will be able to return to the issue of conflicts of interest and how the question of surgical proximity may, or may not, alter our ethical judgments about the surgeon’s role in research where there may be a conflict of interest.
Surgical proximity and equipoise
Surgical proximity also has an impact on clinical equipoise, the ethical neutrality about outcomes felt necessary for the conduct of clinical trials.25 The surgeon’s sense of causality and proximity to the operative act makes surgical research different because the equipoise, which exists objectively about the research questions at hand, may not exist in the mind of the surgical researcher. Let me explain.
Taking a patient to surgery is highly consequential. As we have seen from Bosk’s work,16 surgeons feel a sense of responsibility for their operative acts and surgical work. This felt responsibility, inculcated in surgical training and surgical culture, obligates the surgeon to make a proportionality judgment about bringing a patient to the operating room, be it for research or for clinical practice. In this way, surgical investigators have determined, at least in their own minds, that net benefits outweigh net risks, thus breaching clinical equipoise.
It is hard for a surgeon to commit to an operative procedure—be it for clinical care or for research— with all its attendant risks if he or she does not believe that the intervention is safe and effective. We can appreciate the importance of the surgeon’s perspective on the utility of any proposed operation if we consider the opposing question of futility in clinical practice.26 Whereas internists or intensivists might be compelled by families to continue aggressive intensive care, surgeons cannot be compelled to take a patient to the operating room when they deem that the risks outweigh the benefits. Because the surgeon is such a proximate moral agent, he or she will be held culpable for the actions that occur in theater. This degree of responsibility is accompanied by a retained degree of discretion—an almost old-world paternalistic discretion27—to counter the demands for disproportionate care.
This same sense of culpability and responsibility informs the surgeon’s willingness to take any patient to the operating room. In the case of research, this willingness becomes an issue of concern because it means that in the surgeon’s mind, favorable operative proportionality has been achieved.
This process of self-regulation28 can have implications for the informed-consent process because surgeons believe in their work and can exert a strong dynamic transference on subjects who may be desperate for cure.29 Because of this potential bias, surgical research may become especially prone to a therapeutic misconception. That is, if the surgeon is willing to take the risks of doing an innovative procedure in the operating room, then it has crossed some sort of internal threshold of proportionality in which the risks, whatever they are, have become acceptable given the putative benefits. Given what Bosk has written about surgical failure,16 a high bar is crossed when a surgeon takes a patient to the operating room for a novel procedure, even though motivations at that bar may occasionally be mixed.* (*Lest I be misconstrued as too idealistic, this burdens-vs-benefits equation may be fueled by a complex mosaic of motivations and may not always be informed fully by patient-centered benefits. If the surgeon is the innovator and the inventor, these benefits may be for the pursuit of a hypothesis and associated with potential fame or fortune. But even in these cases, judgments about proportionality are informed by surgical proximity. [For more on the ethics of conflicts of interest, see references 4 and 21.])
FROM SURGICAL RESEARCH TO EDUCATION
This leads to my closing observations about transitions in surgical research, when the work of the pioneering surgeon is bequeathed to the broader surgical community to pick up the torch—or scalpel—and expand the work.
This takes me away from research and, fittingly here at a medical school dedicated to research training, brings me to medical education. To transcend the personal dimensions of surgical innovation—and the courage and vision of the founders—and sustain it more broadly, innovators also have to become educators of future surgeons, organizers of talent, and moral exemplars for the next generation. They have to appreciate that the work that they started, if it is important, will not be completed during their tenure but that future generations will carry it forward and expand upon it. They also have to prepare the next generation with the tools and orientation to appreciate their vision and to embrace what Thomas Kuhn might call new scientific paradigms.30
On several occasions Wilder Penfield, who founded the Montreal Neurological Institute, wrote with regret about Victor Horsley, the neurosurgeon at Queens Square in London. Penfield viewed Horsley as the founder of his field, but Horsley left no disciples. In his autobiography, fittingly entitled No Man Alone, Penfield noted that Horsley, “the most distinguished pioneer neurosurgeon, had died in 1916 without having established a school of neurosurgery.”5 This is in contrast to the discipline-building work of Cushing.
It is not an accident that Dr. Cushing founded a field full of trainees and protégés, of which my co-panelists are descendants. It was intentional and part of his ethos of being truly innovative. And it is not an accident that the distinguished surgical innovators at this symposium have also created institutional structures to continue their work for decades to come. Their achievements have transcended the individual innovator and have become systematic. It is said that Dr. Thomas Starzl launched a field.31 Dr. Denton Cooley founded the Texas Heart Institute.32 Dr. Thomas Fogarty started the Fogarty Institute for Innovation, whose mission statement explicitly notes that it is “an educational non-profit that mentors, trains and inspires the next generation of medical innovators.”33 Each of these pioneers, I believe, appreciates the need for continuity and dissemination.
But even here there is something that we nonsurgeons need to understand: although the work transcends the individual surgeon, the ties remain personal and linked to the impact and legacy of founders. Take, for example, highly prized membership in the Denton A. Cooley Cardiovascular Surgical Society.34 This too is about the importance of individuals and surgical proximity, but here it is transgenerational.
CONCLUSION
If we truly want to continue the dialogue begun here today, we need to understand these social and professional networks and the importance of surgical proximity in transmitting both methods and values. The proximate nature of surgical research—and the causality and responsibility that accrues to the surgeon—makes surgical research different than other areas of biomedical inquiry. This difference has implications for risk-benefit analysis, conflicts of interest, and clinical equipoise. I hope that my colleagues return to these themes in the coming days so that the regulation of this important area of research can be informed by a deeper understanding of the ethics of surgical discovery and innovation.35
Acknowledgments
Dr. Fins gratefully acknowledges the invitation to participate in this symposium, the helpful suggestions of Dr. Eric Kodish, and partial grant support of the Weill Cornell Medical College Research Ethics Core, NIH Clinical & Translational Science Center UL1-RR024966.
- Frader JE, Caniano DA. Research and innovation in surgery. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:216–241.
- Speelman JD, Bosch DA. Resurgence of functional neurosurgery for Parkinson’s disease: a historical perspective. Mov Disord 1998; 13:582–588.
- Holstein WJ. Rewiring the brain: how a bright idea became an innovative medical device. US News & World Report. March 1, 1999:52–53.
- Fins JJ, Schachter M. Investigators, industry, and the heuristic device: ethics, patent law, and clinical innovation. Account Res 2001; 8:219–233.
- Penfield W. No Man Alone: A Neurosurgeon’s Life. Boston, MA: Little Brown; 1977.
- Feindel W. The contributions of Wilder Penfield to the functional anatomy of the human brain. Hum Neurobiol 1982; 1:231–234.
- Aristotle. The Nicomachean Ethics. Weldon JEC, trans. Amherst, NY: Prometheus Books; 1987.
- Fins JJ, Bacchetta MD, Miller FG. Clinical pragmatism: a method of moral problem solving. Kennedy Inst Ethics J 1997; 7:129–145.
- Miller FG, Fins JJ. Protecting human subjects in brain research: a pragmatic perspective. In: Illes J, ed. Neuroethics: Defining the Issues in Theory, Practice and Policy. New York, NY: Oxford University Press; 2005.
- Pollan M. The year in ideas: A to Z.; precautionary principle. New York Times. December 9, 2001.
- van den Belt H. Debating the precautionary principle: “guilty until proven innocent” or “innocent until proven guilty”? Plant Physiol 2003; 132:1122–1126.
- Jonas H. The Imperative of Responsibility: In Search of an Ethics for the Technological Age. Chicago, IL: University of Chicago Press; 1985:34.
- Eliot TS. The Love Song of J. Alfred Prufrock. In: Abrams MH, ed. The Norton Anthology of English Literature. Vol 2. 4th ed. New York, NY: W.W. Norton & Co; 1979:2259–2264.
- Sunstein CR. The paralyzing principle. Regulation. Winter 2002– 2003; 25(4):32–37.
- Holm S, Harris J. Precautionary principle stifles discovery. Nature 1999; 400:398.
- Bosk C. Forgive and Remember: Managing Medical Failure. Chicago, IL: University of Chicago Press; 1979:29–30.
- Bliss M. Harvey Cushing: A Life in Surgery. Oxford, UK: Oxford University Press; 2005.
- Pinkus RL. Mistakes as a social construct: an historical approach. Kennedy Inst Ethics J 2001; 11:117–133.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress I: policy and guidelines for the oversight of individual financial interests in human subjects research. Acad Med 2003; 78:225–236.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress II: principles and recommendations for oversight of an institution’s financial interests in human subjects research. Acad Med 2003; 78:237– 245.
- Fins JJ. Disclose and justify: intellectual property, conflicts of interest, and neurosurgery. Congress Quarterly (Official Newsmagazine of the Congress of Neurological Surgeons) 2007; 8(3):34–36.
- U.S. Constitution, art. I, §8, cl. 8; see also id. at art. I, §8, cl. 18.
- Patent Act of 1790, ch. 7, 1 Stat. 109–111 (1790).
- Patent and Trademark Act Amendments of 1980 (Bayh-Dole Act); Pub L No. 96-517. Codified as 35 USC §§200–212 (1994).
- Freedman B. Equipoise and the ethics of clinical research. N Engl J Med 1987; 317:141–145.
- Callahan D. Necessity, futility, and the good society. J Am Geriatr Soc 1994; 42:866–867.
- Katz J. The Silent World of Doctor and Patient. New York, NY: Free Press; 1984.
- Jones RS, Fletcher JC. Self-regulation of surgical practice and research. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:255–279.
- Kim SY. Assessing and communicating the risks and benefits of gene transfer clinical trials. Curr Opin Mol Ther 2006; 8:384– 389.
- Kuhn TS. The Structure of Scientific Revolutions. 2nd ed. Chicago, IL: University of Chicago Press; 1970.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon. Pittsburgh, PA: University of Pittsburgh Press; 2003.
- Twenty Five Years of Excellence: A History of the Texas Heart Institute. Houston, TX: Texas Heart Institute Foundation; 1989.
- Fogarty Institute for Innovation Web site. Available at: http://01659a8. netsolhost.com/aboutus.html. Accessed June 6, 2008.
- Denton A. Cooley Cardiovascular Surgical Society Web site. Available at: http://www.cooleysociety.com/about.html. Accessed June 6, 2008.
- de Melo-Martín I, Palmer LI, Fins JJ. Viewpoint: developing a research ethics consultation service to foster responsive and responsible clinical research. Acad Med 2007; 82:900–904.
- Frader JE, Caniano DA. Research and innovation in surgery. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:216–241.
- Speelman JD, Bosch DA. Resurgence of functional neurosurgery for Parkinson’s disease: a historical perspective. Mov Disord 1998; 13:582–588.
- Holstein WJ. Rewiring the brain: how a bright idea became an innovative medical device. US News & World Report. March 1, 1999:52–53.
- Fins JJ, Schachter M. Investigators, industry, and the heuristic device: ethics, patent law, and clinical innovation. Account Res 2001; 8:219–233.
- Penfield W. No Man Alone: A Neurosurgeon’s Life. Boston, MA: Little Brown; 1977.
- Feindel W. The contributions of Wilder Penfield to the functional anatomy of the human brain. Hum Neurobiol 1982; 1:231–234.
- Aristotle. The Nicomachean Ethics. Weldon JEC, trans. Amherst, NY: Prometheus Books; 1987.
- Fins JJ, Bacchetta MD, Miller FG. Clinical pragmatism: a method of moral problem solving. Kennedy Inst Ethics J 1997; 7:129–145.
- Miller FG, Fins JJ. Protecting human subjects in brain research: a pragmatic perspective. In: Illes J, ed. Neuroethics: Defining the Issues in Theory, Practice and Policy. New York, NY: Oxford University Press; 2005.
- Pollan M. The year in ideas: A to Z.; precautionary principle. New York Times. December 9, 2001.
- van den Belt H. Debating the precautionary principle: “guilty until proven innocent” or “innocent until proven guilty”? Plant Physiol 2003; 132:1122–1126.
- Jonas H. The Imperative of Responsibility: In Search of an Ethics for the Technological Age. Chicago, IL: University of Chicago Press; 1985:34.
- Eliot TS. The Love Song of J. Alfred Prufrock. In: Abrams MH, ed. The Norton Anthology of English Literature. Vol 2. 4th ed. New York, NY: W.W. Norton & Co; 1979:2259–2264.
- Sunstein CR. The paralyzing principle. Regulation. Winter 2002– 2003; 25(4):32–37.
- Holm S, Harris J. Precautionary principle stifles discovery. Nature 1999; 400:398.
- Bosk C. Forgive and Remember: Managing Medical Failure. Chicago, IL: University of Chicago Press; 1979:29–30.
- Bliss M. Harvey Cushing: A Life in Surgery. Oxford, UK: Oxford University Press; 2005.
- Pinkus RL. Mistakes as a social construct: an historical approach. Kennedy Inst Ethics J 2001; 11:117–133.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress I: policy and guidelines for the oversight of individual financial interests in human subjects research. Acad Med 2003; 78:225–236.
- AAMC Task Force on Financial Conflicts of Interest in Clinical Research. Protecting subjects, preserving trust, promoting progress II: principles and recommendations for oversight of an institution’s financial interests in human subjects research. Acad Med 2003; 78:237– 245.
- Fins JJ. Disclose and justify: intellectual property, conflicts of interest, and neurosurgery. Congress Quarterly (Official Newsmagazine of the Congress of Neurological Surgeons) 2007; 8(3):34–36.
- U.S. Constitution, art. I, §8, cl. 8; see also id. at art. I, §8, cl. 18.
- Patent Act of 1790, ch. 7, 1 Stat. 109–111 (1790).
- Patent and Trademark Act Amendments of 1980 (Bayh-Dole Act); Pub L No. 96-517. Codified as 35 USC §§200–212 (1994).
- Freedman B. Equipoise and the ethics of clinical research. N Engl J Med 1987; 317:141–145.
- Callahan D. Necessity, futility, and the good society. J Am Geriatr Soc 1994; 42:866–867.
- Katz J. The Silent World of Doctor and Patient. New York, NY: Free Press; 1984.
- Jones RS, Fletcher JC. Self-regulation of surgical practice and research. In: McCullough LB, Jones JW, Brody BA, eds. Surgical Ethics. New York, NY: Oxford University Press; 1998:255–279.
- Kim SY. Assessing and communicating the risks and benefits of gene transfer clinical trials. Curr Opin Mol Ther 2006; 8:384– 389.
- Kuhn TS. The Structure of Scientific Revolutions. 2nd ed. Chicago, IL: University of Chicago Press; 1970.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon. Pittsburgh, PA: University of Pittsburgh Press; 2003.
- Twenty Five Years of Excellence: A History of the Texas Heart Institute. Houston, TX: Texas Heart Institute Foundation; 1989.
- Fogarty Institute for Innovation Web site. Available at: http://01659a8. netsolhost.com/aboutus.html. Accessed June 6, 2008.
- Denton A. Cooley Cardiovascular Surgical Society Web site. Available at: http://www.cooleysociety.com/about.html. Accessed June 6, 2008.
- de Melo-Martín I, Palmer LI, Fins JJ. Viewpoint: developing a research ethics consultation service to foster responsive and responsible clinical research. Acad Med 2007; 82:900–904.
Surgical innovation and ethical dilemmas: A panel discussion
END RESULTS: WHY SO ELUSIVE STILL?
Dr. Isador Lieberman, Moderator: Let me begin this discussion with a 1910 quote from Ernest Codman, a general surgeon at Massachusetts General Hospital, who stated:
In 1900 I became interested in what I called the “end result” idea, which was merely the commonsense notion that every hospital should follow every patient it treats long enough to determine whether or not the treatment has been successful, and then should inquire, “If not, why not?” with a view to preventing similar failure in the future.
My questions to the panel are: What has changed in the last 100 years? Are we documenting our end results? Have we gone wrong and, if so, where have we gone wrong?
Dr. James Herndon: Although Codman’s ideas in this area were not well received at the time, today we do have some “end result” ideas. We have outcomes data, but I would argue that they are far too limited and not to the level required in the 21st century. I have asked myself many times why the surgical profession has not focused on this issue more than it has. I agree with Dr. [Joseph] Fins’ comments in his presentation [see previous article in this supplement] that it would be nice to have a bottom-up approach rather than a top-down approach, but I do not see a change until we as physicians step up to the plate and make a change.
Why haven’t we? There are a number of reasons. The malpractice climate in the United States has been one major factor. Surgeons fear disclosure. The relationship between a surgeon and the patient is professional and private, and physicians do not want transparency—they do not want their patient or anyone to know that an adverse event or bad outcome has occurred.
Also, doctors, especially surgeons, are reluctant to use guidelines or follow protocols. I participated a number of years ago in an American Academy of Orthopaedic Surgeons project called MODEMS; it was an attempt to set up guidelines for orthopedic surgeons to manage back pain, shoulder pain, and other orthopedic conditions. By the time we finished we had accomplished nothing, because the protocols and guidelines were so extensive that almost any type of management for any patient would be compliant.
Additionally, hospitals in the United States have become more like for-profit businesses, with a focus on short-term profits and with short tenures for their chief executive officers (CEOs)—4 or 5 years, on average. With nearly 50% of US hospitals bordering on bankruptcy, they are not able or willing to invest in major patient safety protocols and guidelines because the CEOs do not see a short-term benefit to them. Witness the fact that only 15% of US hospitals have computerized physician order entry systems and electronic medical records. From what I have read, it takes about 5 years before a hospital recoups such investments from the resulting safety improvements and efficiencies.
These are some, but by no means all, of the reasons we do not have appropriate outcomes in all specialty fields. My plea is that physicians lead the effort to measure and report outcomes down the road.
Dr. Lieberman: Dr. Hahn, why do you think we have not kept up with Dr. Codman’s premise from 100 years ago?
Dr. Joseph Hahn: We hold a yearly Medical Innovation Summit at the Cleveland Clinic, and what has emerged from many of those meetings is a lack of interest in paying for outcomes analyses. The providers, the government, and industry all say that they do not have the money for these analyses. So the first reason that Codman’s premise has not been lived up to is that the source of funding remains undetermined. Second, most surgical innovations have been geared toward inventing devices to overcome very specific problems that arise during or following surgery rather than toward substantiating the worth of a procedure through collection of evidence. A third reason involves the pressure that investors place on industry to make money, which tends to lead to investments in getting products to market rather than outcomes research. With all of these factors and the pressures from so many directions, the surgical profession hasn’t stepped back to thoroughly consider what we are doing to our patients and just how worthwhile it is.
Dr. Lieberman: Who do you think should be paying for outcomes analyses?
Dr. Hahn: I think the government should. The role of government is to take care of its citizens. The Centers for Medicare and Medicaid Services (CMS) does its best with the information it has, but it admits that it pays for some procedures without knowing whether or not they are truly worthwhile. An example is the use of artificial discs in the cervical spine. I am sure that the artificial disc manufacturers made a case for their product to CMS by claiming it was associated with less pain and resulted in a superior outcome compared to fusion using bone from the hip, regardless of whether they had the scientific evidence to prove it.
Dr. Lieberman: Dr. Fins, would you like to weigh in on Codman’s “end result” premise?
Dr. Joseph Fins: I would just point out that the history is not homogeneous. I have been involved in deep brain stimulation work, and the legacy of psychosurgery has been an egregious lack of outcomes studies, but now we do have outcomes studies and scales. For example, there is now the Yale-Brown Obsessive Compulsive Scale to rate the severity of symptoms in obsessive-compulsive disorder. In our deep brain stimulation study,1 we are using a coma recovery scale, and the Food and Drug Administration’s (FDA’s) investigational device exemption (IDE) process requires us to produce outcomes data to protect potential subjects. It may be an example of neuropsychiatric exceptionalism that neurology and psychiatry are areas of increased focus while somatic therapies are somehow presumed to be okay.
Dr. Hahn: FDA may be requiring the outcomes data, but I have not heard that they are willing to pay for it.
Dr. Fins: You are correct.
Dr. Ali Rezai: Part of the problem is the translation of rapid scientific discoveries and technological advances into the field, and education has a role here. Surgeons’ reluctance to integrate guidelines and outcomes measures into practice must be addressed very early in their training—in medical school—and then continued throughout residency and fellowship programs. The same early and continuing approach should be taken with respect to how to conduct and properly interpret a clinical trial.
Dr. Herndon: That is a good point. Surgical education programs have slipped a bit in the past 5 to 10 years, at least in orthopedics. With the reductions in residents’ work hours and the fast pace of residency programs, our residents spend most of their time in the operating room, struggling to master the multitude of procedures in orthopedics. As a result, they are not discussing outcomes or adequately following patients long-term after surgery. I have a hard time getting our faculty to bring residents into their offices so that the residents can examine patients and see why they are operating on certain kinds of patients, as well as the types of follow-up information that can and should be obtained from patients. Training today is so oriented to operative techniques that residencies have difficulty dealing with these other important issues.
WHO DEFINES THE INDICATIONS?
Dr. Lieberman: As new devices and new techniques emerge, who defines their indications? The inventor of the device, a government authority that may or may not have the medical background, patient advocacy groups, or the device manufacturer? And how should we regulate those indications?
Dr. Fins: I would echo Dr. Wilder Penfield’s words, “No man alone.” The orthopedic surgeon or neurosurgeon does not have to do this alone; it is really about teams. And those teams can and should include biostatisticians, recognizing that the biostatistician needs to fully understand what the surgeon is doing. There also has to be attention given to patients’ individualistic outcomes. I recently met with some FDA staff and learned that the FDA is very interested in novel methodologies to better understand what counts as an outcome for individual patients. So I think indications should be guided by individualistic outcomes coupled with the surgical possibilities and with the rigorous biostatistical methods that are now evolving. A conference like this represents an opportunity to generalize the conversation and support more collaboration on indications going forward.
Dr. Rezai: Indications should be defined using a team-oriented approach. Part of the problem of psychosurgery in the past was that the surgeon was defining indications without collaborating with the psychiatrist. In my field of deep brain stimulation and brain pacemakers, everything we have done for the past 20 years—surgery for Parkinson’s disease, depression, obsessive-compulsive disorder, traumatic brain injury, epilepsy—has involved working closely with neurologists, epileptologists, brain injury specialists, psychiatrists, and psychologists to agree on indications. These teams also need to have close partnerships with ethicists. Teamwork is a vital aspect of proper development of an indication.
Dr. Hahn: It has to be the clinicians who set forth the indications. Of course, that may be done by a team of clinicians, but as a surgeon I certainly do not want the manufacturers of an artificial disc telling me what they think the indications for an artificial disc are.
As for the role of patients, some of them are very well informed about their problem. I cannot tell you how many have shown up in my office with reprints of articles I have written. This is a trend that has really mushroomed over the past 10 years. But even though patients are catching up, they are still at a disadvantage. Patients are going to have a say, but it is still the clinicians whose role is to decide the indications and then provide patients with a risk-benefit analysis.
Dr. Herndon: I agree. Although patients are becoming more involved in the process, real shared decision-making has not yet happened in my field.
More broadly, I feel that our professional organizations have to become more actively involved in the process of defining indications. Otherwise, after the innovators develop a device or procedure that will significantly change the approach to a particular problem, it will enter the market at large without any critical assessment of the technology involved and without accounting for the learning curve for each individual surgeon.
Take the example of minimally invasive total hip replacement, which involves a 1-inch incision in the front of the hip and a 1-inch incision in the back of the hip. The learning curve for this procedure appears to be about 40 cases, based on the opinion of experts around the country. Yet when this minimally invasive approach emerged, every surgeon who had been performing total hip replacements wanted this new operation at his or her fingertips because patients were demanding it. Some surgeons adopted it too quickly, without adequate training. I know one distraught surgeon who abandoned the procedure because of numerous failures during his first 100 cases. He returned to the standard hip replacement approach.
Our profession cannot let this experience continue or proliferate. Yet the professional organizations in orthopedics have walked away from technology assessment because industry does not want it; technology assessment is not in industry’s best interest. We have had a number of conflicts in our professional organizations when attempting to move technology assessment forward. It is also very expensive to do.
Finally, indications can sometimes be governed more by economics than by science. I was asked to write a letter to the editor about two technologies for managing intertrochanteric fractures of the hip that were recently featured in the Journal of Bone and Joint Surgery.2,3 One technology involves a compression screw that has been shown to be effective in outcomes studies. The other is an intramedullary nail that has not been well studied and has no proven benefit over the compression screw. In doing research for my letter,4 I found that Medicare assigns more relative value units (RVUs) for the intramedullary nail than for the compression screw. In Boston, the total dollar difference in RVUs between the two is $300: the surgeon makes $1,500 for the procedure that involves the intramedullary nail versus $1,200 for using the compression screw. Not surprisingly, use of the intramedullary nail has been climbing rapidly in the United States without any evidence to justify its use over the other, less expensive technique.
CREDENTIALING: CAN IT KEEP PACE WITH INNOVATION?
Dr. Fins: I agree that surgical competence and regulation—self-regulation or professional regulation—are big issues. One of my greatest fears is that surgeons will do procedures they are not trained to do, and cause great harm as a result. We are hearing about this now with the resurgence of psychosurgery in China.
It strikes me as interesting that the field of neurosurgery is as yet undifferentiated and that there is no subspecialty certification in stereotactic neurosurgery. This is in contrast to invasive cardiology on the medical side, where physicians who do catheterizations and electrophysiologic studies have special additional training.
As innovations develop, we have to track qualifications and credentialing along the way. There should be provisions to grandfather surgeons in if they are in a post-training point in their career, but we have to ensure that the new technology is matched by the operator’s skill. This is particularly pertinent in light of the concept of “surgical proximity”5 and the importance of the individual operator; this is not comparable to just disseminating a new drug.
Dr. Lieberman: Who should do the credentialing? Should it be the government or our profession?
Dr. Fins: Recertification or credentialing should be by peers—the American College of Surgeons and the surgical boards. Of course, funders or payors may request an additional level of certification to do certain procedures, which I would endorse as a safety measure and to help ensure a minimal standard of care for innovative interventions.
Dr. Hahn: But it is not so simple. There is a blurring of surgical expertise once surgeons complete their training. Spine surgery used to be done by either neurosurgeons or orthopedic surgeons; now we have spine surgeons. What we neurosurgeons started to see with that change was that our neurosurgery trainees were being told they could not get on hospital staffs because they did not have credentials in spine surgery or, to take another example, in pediatric surgery. Well, the neurosurgery board made a conscious decision to not offer certificates of added qualification (CAQs). We challenged the hospitals in court and won. But the overriding message is that it is all about economics.
Dr. Herndon: In orthopedics we now have two CAQs—one in hand surgery and one (starting in 2009) in sports medicine. The hand surgeons have not noticed any adverse effect because they do not generate as much revenue as the spine surgeons do. Most orthopedic surgeons start as general orthopedists and then change their practice characteristics as their practices mature. Over time they may focus on one particular area, such as arthroscopic knee surgery or total hip or knee replacement, which makes it difficult for them to pass a general orthopedic examination. Our board recognized this trend and developed oral and written board exams with case reviews concentrating on the surgeon’s self-chosen specialty. We do not need the CAQs because they have been misused, and we as a profession have been letting others misuse them. Again, I think we need to get back to controlling the process ourselves.
Dr. Hahn: What do you do when a surgeon has finished training and then becomes interested in performing a new procedure developed since the time of his or her training? This can really be a challenge when the surgeon hears of a new procedure, goes and takes a 3-day training seminar on it, and comes back believing that he or she is ready to perform the procedure. I have had creative surgeons on staff who want to try a new procedure but have never done any cases, believing that the new technology alone will suffice. What we finally decided to do in these instances was to put in place other staff to proctor these cases to ensure that no harm was coming to patients.
Dr. Herndon: I admire that approach, because we as a profession have to educate our colleagues about whatever new procedures they are about to use in their practice. There is a learning curve for every operation, and learning on one’s own, at the expense of patients, is not appropriate. Should we have experienced colleagues work with surgeons on new procedures until they have performed the 40 or so cases necessary to be proficient? Should we send surgeons to other institutions to do their 40 cases under experienced supervision? I am not sure what the best approach is, but this is a question that a forum like this should begin to address.
HOW MUCH RISK IS ACCEPTABLE?
Dr. Lieberman: Let’s build on this issue of credentialing by turning to the concept of risk. What is an acceptable level of risk with a new device? Is a 50% risk of an adverse outcome appropriate? What about 10%? And who determines the acceptable risk? The profession? The regulatory bodies? Patients?
Dr. Fins: Our expectation about risks in clinical practice should evolve from what was anticipated and actually observed in the clinical trial of an intervention. Adverse events should be envisioned prospectively in the design of a trial, with the magnitude of risks delineated in the protocol. Any unexpected risks that occur, even if small, could be a major reporting issue. Beyond that, it is difficult to say what an acceptable level of risk is without a particularistic clinical trial. Whatever the risk of an intervention, the assessment of the risk must account for regional variation, variation among surgeons, and also systems issues.
The Institute of Medicine report, To Err is Human, attributed medical errors to faulty systems, processes, and conditions. So when we think about errors and risk, we have to consider more than just the individual operator. Just as To Err is Human analogized medical errors to airplane crashes, we might think of surgical retraining in the context of how pilots get retrained using flight simulators. If pilots have not flown a particular aircraft in a long time, they lose their flight certification for that type of craft and then must be retrained to operate it.
As surgical technology gets more advanced, specific, and nuanced, the discordance between one’s training and the potential things one can do becomes greater. Paradoxically, innovation can at least potentially make situations more dangerous in that the operator may not be able to perform the task with the improved technology. For example, pilots who know how to fly a Cessna can fly another simply constructed plane, but if they attempt to fly a higher-technology aircraft, like an F-16, they have a greater risk of having a catastrophic event even though the F-16 flies better, faster, and higher.
Dr. Lieberman: But are you willing to identify a level of acceptable risk?
Dr. Fins: It is based on the patient’s preference, after informed consent. An acceptable level of risk is the level that people are willing to accept. What I am concerned about is the variance around a known risk, whatever it may be, that is attributable to human errors that may be preventable through training or by solving systems problems.
Dr. Lieberman: Dr. Rezai, you place needles into the brain. Who should decide the risk of that action? You? The patient? And what do you feel is an acceptable risk level?
Dr. Rezai: It is a complex question, of course, and a number of variables come into play. Whether or not the patient’s condition is life-threatening or disabling is a very important factor in the risk-benefit ratio. Regulatory guidance from the FDA is strong with respect to defining device-related adverse effects as serious or nonserious, and our peers, both surgeons and nonsurgeons, help to further dictate the risk and tolerability of a procedure and its alternatives. For example, in considering a surgical procedure, one must weigh its risk against the risks of medications to treat the disorder, such as side effects, the ease of medication adherence, and the number of emergency room visits that may result from adverse effects of the medications.
Determining acceptable risk rests fundamentally and first with the patient and then with the surgeon and his or her peers (surgeons and nonsurgeons) in conjunction with regulatory components and oversight. All of these factors contribute.
In my field of deep brain stimulation, the threshold for acceptable risk can be high since we see patients with chronic conditions in whom all previous medication attempts have failed, many of whom are disabled, intractable to current therapies, and with a significant compromise of quality of life. Examples include wheelchair-dependent patients with severe Parkinson’s disease, severely depressed patients who will not leave the house and have attempted suicide, and obsessive-compulsive disorder patients who need 10 hours just to take a shower. This type of intractability to current therapies and the suffering of patients and families with limited options and little hope infl uence assessments of procedural risk.
Dr. Hahn: Performing a controlled clinical trial of a surgical procedure is difficult at best. I recall a clinical trial in which patients with parkinsonism were to be randomized either to have stem cells implanted in their brain or to undergo a sham operation with no stem cells. Well, very few patients signed up for the trial because everyone wanted the stem cells. So, obtaining a large enough denominator to define the risk of, for example, hemorrhage from sticking a needle into a vessel is almost impossible.
Dr. Herndon: Except when there are risks of serious life-threatening events, I believe the patient is the one who makes the decision after having the risks fully explained to him or her. Surgeons are educated in a system in which we learn to accept complications. It is the risk of doing business. We have not learned very well how to differentiate a complication from an adverse event or an error. We must learn to do that. We live with complications every day. Those complications must be conveyed to patients so that they understand what they are about to undergo, what can happen, and what cannot happen. The patient is the ultimate decider, in my opinion.
Dr. Lieberman: That reminds me of something one of my mentors often said: “If you are going to run with the big dogs, expect to get bitten in the butt once in a while.”
ETHICAL DILEMMAS ARISING FROM NEW OPTIONS
Question from audience: In my specialty, we have a non-life-threatening condition with a well-established 25% recurrence rate after traditional surgery with sutures, and a 25% rate of reoperation. A device comes along and it improves the outcomes so that the recurrence rate declines to 10%, but along with the extra costs of doing the procedure with the device, there is also a complication rate of about 10% that requires reoperation with the device, and a few of those patients actually end up worse. Ethically, how should the clinician proceed in this situation? The old way, or the new way that improves outcomes but at a higher cost and risk?
Dr. Fins: Based on the size of the populations, is the difference in the combined rates of recurrence and complications between the traditional and new methods (25% vs 20%) statistically significant?
Response from questioner: The difference is probably not statistically significant.
Dr. Fins: Okay, so you are saying that the numbers are basically equal. That is the first consideration, but there is a nuance to one of the variables, and that is an improvement in quality of life with one of the treatments. Measuring its significance is subjective. A patient may place greater emphasis on quality of life than would somebody who is not a beneficiary of the operation. That is why I said before that biostatistical input that goes beyond crude measures of mortality or reoperation rates can be very helpful. The risk of reoperation may be one that the patient is willing to take for a chance at an improvement in quality of life.
There is a wonderful book by Howard Brody called The Healer’s Power6 in which he writes about the physician’s power to frame a question so as to engineer outcomes. While that is not something that Brody endorses, he does endorse the use of the physician’s power to guide patients using good informed consent, providing direction without being so determinative that patients feel compelled to choose the physician’s recommendation. Patients should be able to decline your recommendation while still having the benefit of your counsel. And in a case like this, your counsel should include variables that may seem “softer” or more difficult to quantify than crude measures such as mortality or reoperation rates.
Dr. Rezai: You have to compare multiple outcomes between the two approaches—surgical time, recovery time, patient quality of life (as assessed by scales), family quality of life, time to return to work, etc. I think it is important to try new technologies because the failure rate or the complication rate may be reduced over time, but only if you evaluate the failures and then restrategize. Only in doing so can you reduce risk, and if the benefit profile and the risk profile prove to be good, then the new technology should be pushed forward.
Dr. Herndon: If the volume of procedures performed by the surgeon is important with respect to outcomes with either one of these two procedures, that should be taken into account. Also, if a new procedure carries a higher complication rate than the traditional procedure, I think that more cohort studies from large centers are needed to gauge the true complication rate before the new technology enters the general market. Continued surveillance, such as with a postmarket registry of outcomes with these procedures, would also be helpful to make adjustments in the future if necessary.
Dr. Hahn: If you looked at the early experience of Med tronic with pacers, you would be amazed at the number of deaths and complications that occurred during the first 3 years. But we do not even think about that now.
CAN INNOVATION HAPPEN WITHOUT INCENTIVES?
Question from audience: Dr. Hahn alluded earlier to the infl uence of money. All of you on the panel are institutionally based, and you are used to practicing with colleagues. I would suggest that surgery today is really not an individual sport, but that is the way it is practiced in much of the nation. Would we be better off if we developed a system that removed us from direct financial influence? Can we get the money out of the equation so that people have motives other than direct personal gain?
Dr. Hahn: I went to an institutional review board (IRB) retreat that included, of course, some IRB members who were not clinicians. They asked the same question that you just did: Why would you even expect to get anything for what you invent? I think that is naïve. People who work hard and invent things deserve to reap a reward. The challenge lies in working with industry, which may try to convince us to use its innovations without our input, as opposed to working with us to identify a clinical problem and trying to solve it together. In that way, the end product and the logic behind its use will be better.
I will give you an example from when I was head of surgery here. A company made a voice-activated table that would obey the surgeon’s commands, such as “left,” “right,” “up,” or “down.” I asked the representative why such a product was needed, and he responded that the surgeon wants to be in total control of the operating room. I told him we do not change the position of the table very often. After a 2-week trial, the table was a dud. He fired the entire group that was working on the project. It was a case of a company simply trying to come up with a product it could sell.
The opposite scenario is if I invent the latest and greatest stent for the carotids and I want to use it. The question becomes how to strike a balance: how to protect the patients while at the same time rewarding the inventor. Another challenge is that device companies want you to stay on their scientific advisory board and they will pay you for it.
These questions are a big concern, and we have spent a lot of time on these issues at Cleveland Clinic. In fact, we held our own conference on biomedical confl icts of interest in September 2006 with attendees from around the country to discuss the necessary firewalls for ensuring that data are not contaminated, that the surgeon-inventor does not fudge data so that his innovation will make it to the marketplace, etc. At that conference, a number of people spoke about Vioxx. I am a surgeon, and my take on the COX-2 inhibitors is that a lot of my patients take these drugs and think they are wonderful, but there are some problems and risks. What is wrong with explaining to patients the risks and complications of these drugs, making your own recommendation about their use (unless you are receiving money from their manufacturers, which you would need to disclose to patients), and then letting patients make their own informed decisions? Personally, I was on Bextra for 3 years and was furious when it was pulled from the market because nobody gave me a choice whether or not to continue using it.
Dr. Lieberman: Let’s explore this concept a little deeper. We know that innovation is so important, but how do we encourage clinicians to innovate in this environment? Dr. Hahn, you served as chairman of CC Innovations, which is Cleveland Clinic’s technology commercialization arm. What were some of the strategies you came across in that role?
Dr. Hahn: We look for creative staff. We tell them up front that we want them to come to Cleveland Clinic and invent things. Our mission is literally to work on problems and take solutions to our patients. The culture here is meant to be creative. As a part of that culture, we welcome working with industry, as opposed to industry thrusting its innovations on us.
We are averaging more than 200 invention disclosures per year. More than 500 of our staff are involved with various industrial partners, and we are not going to hide that. In fact, we are going to make it public. The thought is that we owe it to our patients to work on their problems. At the same time, we owe it to our patients to say when we are working with industry on a particular product and explain to them why we think it would work in their case, if we think it would. While doing so, we need to make it clear that we will be happy to refer them for a second opinion if they would like. If I have a patient who wants a second opinion, I will offer to make the phone call for them and get them in. I think that is an advantage of the model we have here.
The reality is that there are some procedures that can only be done by one surgeon here, a surgeon who may have helped develop the procedure or some technology involved in it. Are we going to tell that surgeon that he or she cannot perform the procedure on anyone? That does not make sense. So you need to have a management plan that puts in place firewalls to protect the data on that procedure from any possible contamination.
So yes, we do reward staff who are doing innovation, and we do work with industry, and we do tell our patients we are doing it, and we do build firewalls to protect the data.
Dr. Lieberman: How about the rest of the panel? What are your thoughts on providing incentives for innovation?
Dr. Fins: Money is a key issue. The way the landscape is now structured, collaborations with industry are part of the mix. Under the Bayh-Dole Act of 1980, institutions are granted intellectual property rights to ideas or inventions developed by their researchers, and then the institutions can enter into contracts with industry to move the innovations forward. If industry support of research were removed, we would have to double the budget of the National Institutes of Health to compensate.
On the other hand, industry support can sometimes prove to be a disincentive to innovation in that it may engineer certain kinds of research or deprive investigators of tools they may need to do more basic science types of research. It is an academic freedom issue. At a translational level, industry may be helpful and catalytic. But sometimes it pushes an investigator to work for a short-term innovative application at the expense of a more speculative, riskier innovation.
We need to acknowledge that industry collaborations are part and parcel of the universe and focus on working with industry to moderate its influences. At the same time, we must use our leverage on the investigative side of the equation to pursue academic freedom and to leverage industry resources to perhaps pay for some of the care that innovative devices make possible. For example, contracting agreements could be drawn up so that money came back to the populations that participated in a clinical trial, or to a community that otherwise may need the device but cannot afford it. I think we have to create some type of charitable impulse to moderate the excesses of the profits and use them for the common good.
Dr. Herndon: I would like to touch on disclosure. The orthopedic implant industry has been required by law to disclose its relationships with orthopedic surgeons, including the amount of money that surgeons may be getting from industry. This requirement has had unintended consequences that underscore the importance of disclosure. First, some of the monetary awards, whether market-driven or not, are quite excessive. Second, reviewing the contracts for royalties has led to the discovery that many are not supported by patents or intellectual property rights. Third, these disclosures have revealed that certain surgeons who work at major US institutions, and who thus have an obligation to pay the institution some of the monies from their research, have not disclosed their relationships for years and have kept those monies solely for themselves. So this disclosure requirement has brought many things to light.
Dr. Rezai: As long as there is human disease and suffering, innovation will continue. It has in the past and it will in the future. Most innovators have it in their genes and in their blood. They can be taught to innovate, but they have to have the intrinsic curiosity and the creative mind to be an innovator. Institutional support of innovation is important, as is respect for the process that must be followed, including transparency and disclosure. If you put all these together, then innovation can be facilitated.
IF TESTING MOVES OFFSHORE, CAN ETHICS FOLLOW?
Dr. Lieberman: I am going to paint a scenario on which I would like each panelist to briefly comment. New Device X is backed by a big vendor. It is a great device, but because of all the regulatory issues in the United States, it is taken to China or South America and is being implanted there, where the regulatory environment is much more lenient. Can we rationalize this practice? How is it possibly ethical?
Dr. Fins: I can answer in 5 seconds: we shouldn’t do it.
Dr. Rezai: This is a reality we are facing with increasing rules and regulations in the United States. You have to engage the process, and it takes time. If you have colleagues who can follow clinical trials outside the United States, you can have the device tested outside and then bring it back to the United States. Unfortunately, the reality is that the regulatory process can be slow, so more testing will be done abroad, in my opinion.
Dr. Hahn: I disagree with Dr. Fins. This may be the only way to get the trials started, and we then are able to use some of the offshore data to approach the FDA for approval. I do not think that it is taking advantage of anybody; it is a way of getting things through the system.
Dr. Herndon: The door has been opened, and it is only going to increase. My only request would be that the investigators who do this function as they would here in the United States, under IRB controls and the other kinds of oversight that they would expect and demand of themselves in their own institutions.
- Schiff ND, Giacino JT, Kalmar K, et al. Behavioral improvements with thalamic stimulation after severe traumatic brain injury. Nature 2007; 448:600–603.
- Forte ML, Virnig BA, Kane RL, et al. Geographic variation in device use for intertrochanteric hip fractures. J Bone Joint Surg Am 2008; 90:691–699.
- Anglen JO, Weinstein JN. Nail or plate fixation of intertrochanteric hip fractures: changing pattern of practice. A review of the American Board of Orthopaedic Surgery database. J Bone Joint Surg Am 2008; 90:700–707.
- Herndon JH. Technology assessment and adoption in orthopaedics [letter]. J Bone Joint Surg Am 2008; 90e. http://www.ejbjs.org/cgi/eletters/90/4/689. Published April 1, 2008. Accessed August 25, 2008.
- Fins JJ. Surgical innovation and ethical dilemmas: precautions and proximity. Cleve Clin J Med 2008; 75(suppl 6):S7–S12.
- Brody H. The Healer’s Power. New Haven, CT: Yale University Press; 1992.
END RESULTS: WHY SO ELUSIVE STILL?
Dr. Isador Lieberman, Moderator: Let me begin this discussion with a 1910 quote from Ernest Codman, a general surgeon at Massachusetts General Hospital, who stated:
In 1900 I became interested in what I called the “end result” idea, which was merely the commonsense notion that every hospital should follow every patient it treats long enough to determine whether or not the treatment has been successful, and then should inquire, “If not, why not?” with a view to preventing similar failure in the future.
My questions to the panel are: What has changed in the last 100 years? Are we documenting our end results? Have we gone wrong and, if so, where have we gone wrong?
Dr. James Herndon: Although Codman’s ideas in this area were not well received at the time, today we do have some “end result” ideas. We have outcomes data, but I would argue that they are far too limited and not to the level required in the 21st century. I have asked myself many times why the surgical profession has not focused on this issue more than it has. I agree with Dr. [Joseph] Fins’ comments in his presentation [see previous article in this supplement] that it would be nice to have a bottom-up approach rather than a top-down approach, but I do not see a change until we as physicians step up to the plate and make a change.
Why haven’t we? There are a number of reasons. The malpractice climate in the United States has been one major factor. Surgeons fear disclosure. The relationship between a surgeon and the patient is professional and private, and physicians do not want transparency—they do not want their patient or anyone to know that an adverse event or bad outcome has occurred.
Also, doctors, especially surgeons, are reluctant to use guidelines or follow protocols. I participated a number of years ago in an American Academy of Orthopaedic Surgeons project called MODEMS; it was an attempt to set up guidelines for orthopedic surgeons to manage back pain, shoulder pain, and other orthopedic conditions. By the time we finished we had accomplished nothing, because the protocols and guidelines were so extensive that almost any type of management for any patient would be compliant.
Additionally, hospitals in the United States have become more like for-profit businesses, with a focus on short-term profits and with short tenures for their chief executive officers (CEOs)—4 or 5 years, on average. With nearly 50% of US hospitals bordering on bankruptcy, they are not able or willing to invest in major patient safety protocols and guidelines because the CEOs do not see a short-term benefit to them. Witness the fact that only 15% of US hospitals have computerized physician order entry systems and electronic medical records. From what I have read, it takes about 5 years before a hospital recoups such investments from the resulting safety improvements and efficiencies.
These are some, but by no means all, of the reasons we do not have appropriate outcomes in all specialty fields. My plea is that physicians lead the effort to measure and report outcomes down the road.
Dr. Lieberman: Dr. Hahn, why do you think we have not kept up with Dr. Codman’s premise from 100 years ago?
Dr. Joseph Hahn: We hold a yearly Medical Innovation Summit at the Cleveland Clinic, and what has emerged from many of those meetings is a lack of interest in paying for outcomes analyses. The providers, the government, and industry all say that they do not have the money for these analyses. So the first reason that Codman’s premise has not been lived up to is that the source of funding remains undetermined. Second, most surgical innovations have been geared toward inventing devices to overcome very specific problems that arise during or following surgery rather than toward substantiating the worth of a procedure through collection of evidence. A third reason involves the pressure that investors place on industry to make money, which tends to lead to investments in getting products to market rather than outcomes research. With all of these factors and the pressures from so many directions, the surgical profession hasn’t stepped back to thoroughly consider what we are doing to our patients and just how worthwhile it is.
Dr. Lieberman: Who do you think should be paying for outcomes analyses?
Dr. Hahn: I think the government should. The role of government is to take care of its citizens. The Centers for Medicare and Medicaid Services (CMS) does its best with the information it has, but it admits that it pays for some procedures without knowing whether or not they are truly worthwhile. An example is the use of artificial discs in the cervical spine. I am sure that the artificial disc manufacturers made a case for their product to CMS by claiming it was associated with less pain and resulted in a superior outcome compared to fusion using bone from the hip, regardless of whether they had the scientific evidence to prove it.
Dr. Lieberman: Dr. Fins, would you like to weigh in on Codman’s “end result” premise?
Dr. Joseph Fins: I would just point out that the history is not homogeneous. I have been involved in deep brain stimulation work, and the legacy of psychosurgery has been an egregious lack of outcomes studies, but now we do have outcomes studies and scales. For example, there is now the Yale-Brown Obsessive Compulsive Scale to rate the severity of symptoms in obsessive-compulsive disorder. In our deep brain stimulation study,1 we are using a coma recovery scale, and the Food and Drug Administration’s (FDA’s) investigational device exemption (IDE) process requires us to produce outcomes data to protect potential subjects. It may be an example of neuropsychiatric exceptionalism that neurology and psychiatry are areas of increased focus while somatic therapies are somehow presumed to be okay.
Dr. Hahn: FDA may be requiring the outcomes data, but I have not heard that they are willing to pay for it.
Dr. Fins: You are correct.
Dr. Ali Rezai: Part of the problem is the translation of rapid scientific discoveries and technological advances into the field, and education has a role here. Surgeons’ reluctance to integrate guidelines and outcomes measures into practice must be addressed very early in their training—in medical school—and then continued throughout residency and fellowship programs. The same early and continuing approach should be taken with respect to how to conduct and properly interpret a clinical trial.
Dr. Herndon: That is a good point. Surgical education programs have slipped a bit in the past 5 to 10 years, at least in orthopedics. With the reductions in residents’ work hours and the fast pace of residency programs, our residents spend most of their time in the operating room, struggling to master the multitude of procedures in orthopedics. As a result, they are not discussing outcomes or adequately following patients long-term after surgery. I have a hard time getting our faculty to bring residents into their offices so that the residents can examine patients and see why they are operating on certain kinds of patients, as well as the types of follow-up information that can and should be obtained from patients. Training today is so oriented to operative techniques that residencies have difficulty dealing with these other important issues.
WHO DEFINES THE INDICATIONS?
Dr. Lieberman: As new devices and new techniques emerge, who defines their indications? The inventor of the device, a government authority that may or may not have the medical background, patient advocacy groups, or the device manufacturer? And how should we regulate those indications?
Dr. Fins: I would echo Dr. Wilder Penfield’s words, “No man alone.” The orthopedic surgeon or neurosurgeon does not have to do this alone; it is really about teams. And those teams can and should include biostatisticians, recognizing that the biostatistician needs to fully understand what the surgeon is doing. There also has to be attention given to patients’ individualistic outcomes. I recently met with some FDA staff and learned that the FDA is very interested in novel methodologies to better understand what counts as an outcome for individual patients. So I think indications should be guided by individualistic outcomes coupled with the surgical possibilities and with the rigorous biostatistical methods that are now evolving. A conference like this represents an opportunity to generalize the conversation and support more collaboration on indications going forward.
Dr. Rezai: Indications should be defined using a team-oriented approach. Part of the problem of psychosurgery in the past was that the surgeon was defining indications without collaborating with the psychiatrist. In my field of deep brain stimulation and brain pacemakers, everything we have done for the past 20 years—surgery for Parkinson’s disease, depression, obsessive-compulsive disorder, traumatic brain injury, epilepsy—has involved working closely with neurologists, epileptologists, brain injury specialists, psychiatrists, and psychologists to agree on indications. These teams also need to have close partnerships with ethicists. Teamwork is a vital aspect of proper development of an indication.
Dr. Hahn: It has to be the clinicians who set forth the indications. Of course, that may be done by a team of clinicians, but as a surgeon I certainly do not want the manufacturers of an artificial disc telling me what they think the indications for an artificial disc are.
As for the role of patients, some of them are very well informed about their problem. I cannot tell you how many have shown up in my office with reprints of articles I have written. This is a trend that has really mushroomed over the past 10 years. But even though patients are catching up, they are still at a disadvantage. Patients are going to have a say, but it is still the clinicians whose role is to decide the indications and then provide patients with a risk-benefit analysis.
Dr. Herndon: I agree. Although patients are becoming more involved in the process, real shared decision-making has not yet happened in my field.
More broadly, I feel that our professional organizations have to become more actively involved in the process of defining indications. Otherwise, after the innovators develop a device or procedure that will significantly change the approach to a particular problem, it will enter the market at large without any critical assessment of the technology involved and without accounting for the learning curve for each individual surgeon.
Take the example of minimally invasive total hip replacement, which involves a 1-inch incision in the front of the hip and a 1-inch incision in the back of the hip. The learning curve for this procedure appears to be about 40 cases, based on the opinion of experts around the country. Yet when this minimally invasive approach emerged, every surgeon who had been performing total hip replacements wanted this new operation at his or her fingertips because patients were demanding it. Some surgeons adopted it too quickly, without adequate training. I know one distraught surgeon who abandoned the procedure because of numerous failures during his first 100 cases. He returned to the standard hip replacement approach.
Our profession cannot let this experience continue or proliferate. Yet the professional organizations in orthopedics have walked away from technology assessment because industry does not want it; technology assessment is not in industry’s best interest. We have had a number of conflicts in our professional organizations when attempting to move technology assessment forward. It is also very expensive to do.
Finally, indications can sometimes be governed more by economics than by science. I was asked to write a letter to the editor about two technologies for managing intertrochanteric fractures of the hip that were recently featured in the Journal of Bone and Joint Surgery.2,3 One technology involves a compression screw that has been shown to be effective in outcomes studies. The other is an intramedullary nail that has not been well studied and has no proven benefit over the compression screw. In doing research for my letter,4 I found that Medicare assigns more relative value units (RVUs) for the intramedullary nail than for the compression screw. In Boston, the total dollar difference in RVUs between the two is $300: the surgeon makes $1,500 for the procedure that involves the intramedullary nail versus $1,200 for using the compression screw. Not surprisingly, use of the intramedullary nail has been climbing rapidly in the United States without any evidence to justify its use over the other, less expensive technique.
CREDENTIALING: CAN IT KEEP PACE WITH INNOVATION?
Dr. Fins: I agree that surgical competence and regulation—self-regulation or professional regulation—are big issues. One of my greatest fears is that surgeons will do procedures they are not trained to do, and cause great harm as a result. We are hearing about this now with the resurgence of psychosurgery in China.
It strikes me as interesting that the field of neurosurgery is as yet undifferentiated and that there is no subspecialty certification in stereotactic neurosurgery. This is in contrast to invasive cardiology on the medical side, where physicians who do catheterizations and electrophysiologic studies have special additional training.
As innovations develop, we have to track qualifications and credentialing along the way. There should be provisions to grandfather surgeons in if they are in a post-training point in their career, but we have to ensure that the new technology is matched by the operator’s skill. This is particularly pertinent in light of the concept of “surgical proximity”5 and the importance of the individual operator; this is not comparable to just disseminating a new drug.
Dr. Lieberman: Who should do the credentialing? Should it be the government or our profession?
Dr. Fins: Recertification or credentialing should be by peers—the American College of Surgeons and the surgical boards. Of course, funders or payors may request an additional level of certification to do certain procedures, which I would endorse as a safety measure and to help ensure a minimal standard of care for innovative interventions.
Dr. Hahn: But it is not so simple. There is a blurring of surgical expertise once surgeons complete their training. Spine surgery used to be done by either neurosurgeons or orthopedic surgeons; now we have spine surgeons. What we neurosurgeons started to see with that change was that our neurosurgery trainees were being told they could not get on hospital staffs because they did not have credentials in spine surgery or, to take another example, in pediatric surgery. Well, the neurosurgery board made a conscious decision to not offer certificates of added qualification (CAQs). We challenged the hospitals in court and won. But the overriding message is that it is all about economics.
Dr. Herndon: In orthopedics we now have two CAQs—one in hand surgery and one (starting in 2009) in sports medicine. The hand surgeons have not noticed any adverse effect because they do not generate as much revenue as the spine surgeons do. Most orthopedic surgeons start as general orthopedists and then change their practice characteristics as their practices mature. Over time they may focus on one particular area, such as arthroscopic knee surgery or total hip or knee replacement, which makes it difficult for them to pass a general orthopedic examination. Our board recognized this trend and developed oral and written board exams with case reviews concentrating on the surgeon’s self-chosen specialty. We do not need the CAQs because they have been misused, and we as a profession have been letting others misuse them. Again, I think we need to get back to controlling the process ourselves.
Dr. Hahn: What do you do when a surgeon has finished training and then becomes interested in performing a new procedure developed since the time of his or her training? This can really be a challenge when the surgeon hears of a new procedure, goes and takes a 3-day training seminar on it, and comes back believing that he or she is ready to perform the procedure. I have had creative surgeons on staff who want to try a new procedure but have never done any cases, believing that the new technology alone will suffice. What we finally decided to do in these instances was to put in place other staff to proctor these cases to ensure that no harm was coming to patients.
Dr. Herndon: I admire that approach, because we as a profession have to educate our colleagues about whatever new procedures they are about to use in their practice. There is a learning curve for every operation, and learning on one’s own, at the expense of patients, is not appropriate. Should we have experienced colleagues work with surgeons on new procedures until they have performed the 40 or so cases necessary to be proficient? Should we send surgeons to other institutions to do their 40 cases under experienced supervision? I am not sure what the best approach is, but this is a question that a forum like this should begin to address.
HOW MUCH RISK IS ACCEPTABLE?
Dr. Lieberman: Let’s build on this issue of credentialing by turning to the concept of risk. What is an acceptable level of risk with a new device? Is a 50% risk of an adverse outcome appropriate? What about 10%? And who determines the acceptable risk? The profession? The regulatory bodies? Patients?
Dr. Fins: Our expectation about risks in clinical practice should evolve from what was anticipated and actually observed in the clinical trial of an intervention. Adverse events should be envisioned prospectively in the design of a trial, with the magnitude of risks delineated in the protocol. Any unexpected risks that occur, even if small, could be a major reporting issue. Beyond that, it is difficult to say what an acceptable level of risk is without a particularistic clinical trial. Whatever the risk of an intervention, the assessment of the risk must account for regional variation, variation among surgeons, and also systems issues.
The Institute of Medicine report, To Err is Human, attributed medical errors to faulty systems, processes, and conditions. So when we think about errors and risk, we have to consider more than just the individual operator. Just as To Err is Human analogized medical errors to airplane crashes, we might think of surgical retraining in the context of how pilots get retrained using flight simulators. If pilots have not flown a particular aircraft in a long time, they lose their flight certification for that type of craft and then must be retrained to operate it.
As surgical technology gets more advanced, specific, and nuanced, the discordance between one’s training and the potential things one can do becomes greater. Paradoxically, innovation can at least potentially make situations more dangerous in that the operator may not be able to perform the task with the improved technology. For example, pilots who know how to fly a Cessna can fly another simply constructed plane, but if they attempt to fly a higher-technology aircraft, like an F-16, they have a greater risk of having a catastrophic event even though the F-16 flies better, faster, and higher.
Dr. Lieberman: But are you willing to identify a level of acceptable risk?
Dr. Fins: It is based on the patient’s preference, after informed consent. An acceptable level of risk is the level that people are willing to accept. What I am concerned about is the variance around a known risk, whatever it may be, that is attributable to human errors that may be preventable through training or by solving systems problems.
Dr. Lieberman: Dr. Rezai, you place needles into the brain. Who should decide the risk of that action? You? The patient? And what do you feel is an acceptable risk level?
Dr. Rezai: It is a complex question, of course, and a number of variables come into play. Whether or not the patient’s condition is life-threatening or disabling is a very important factor in the risk-benefit ratio. Regulatory guidance from the FDA is strong with respect to defining device-related adverse effects as serious or nonserious, and our peers, both surgeons and nonsurgeons, help to further dictate the risk and tolerability of a procedure and its alternatives. For example, in considering a surgical procedure, one must weigh its risk against the risks of medications to treat the disorder, such as side effects, the ease of medication adherence, and the number of emergency room visits that may result from adverse effects of the medications.
Determining acceptable risk rests fundamentally and first with the patient and then with the surgeon and his or her peers (surgeons and nonsurgeons) in conjunction with regulatory components and oversight. All of these factors contribute.
In my field of deep brain stimulation, the threshold for acceptable risk can be high since we see patients with chronic conditions in whom all previous medication attempts have failed, many of whom are disabled, intractable to current therapies, and with a significant compromise of quality of life. Examples include wheelchair-dependent patients with severe Parkinson’s disease, severely depressed patients who will not leave the house and have attempted suicide, and obsessive-compulsive disorder patients who need 10 hours just to take a shower. This type of intractability to current therapies and the suffering of patients and families with limited options and little hope infl uence assessments of procedural risk.
Dr. Hahn: Performing a controlled clinical trial of a surgical procedure is difficult at best. I recall a clinical trial in which patients with parkinsonism were to be randomized either to have stem cells implanted in their brain or to undergo a sham operation with no stem cells. Well, very few patients signed up for the trial because everyone wanted the stem cells. So, obtaining a large enough denominator to define the risk of, for example, hemorrhage from sticking a needle into a vessel is almost impossible.
Dr. Herndon: Except when there are risks of serious life-threatening events, I believe the patient is the one who makes the decision after having the risks fully explained to him or her. Surgeons are educated in a system in which we learn to accept complications. It is the risk of doing business. We have not learned very well how to differentiate a complication from an adverse event or an error. We must learn to do that. We live with complications every day. Those complications must be conveyed to patients so that they understand what they are about to undergo, what can happen, and what cannot happen. The patient is the ultimate decider, in my opinion.
Dr. Lieberman: That reminds me of something one of my mentors often said: “If you are going to run with the big dogs, expect to get bitten in the butt once in a while.”
ETHICAL DILEMMAS ARISING FROM NEW OPTIONS
Question from audience: In my specialty, we have a non-life-threatening condition with a well-established 25% recurrence rate after traditional surgery with sutures, and a 25% rate of reoperation. A device comes along and it improves the outcomes so that the recurrence rate declines to 10%, but along with the extra costs of doing the procedure with the device, there is also a complication rate of about 10% that requires reoperation with the device, and a few of those patients actually end up worse. Ethically, how should the clinician proceed in this situation? The old way, or the new way that improves outcomes but at a higher cost and risk?
Dr. Fins: Based on the size of the populations, is the difference in the combined rates of recurrence and complications between the traditional and new methods (25% vs 20%) statistically significant?
Response from questioner: The difference is probably not statistically significant.
Dr. Fins: Okay, so you are saying that the numbers are basically equal. That is the first consideration, but there is a nuance to one of the variables, and that is an improvement in quality of life with one of the treatments. Measuring its significance is subjective. A patient may place greater emphasis on quality of life than would somebody who is not a beneficiary of the operation. That is why I said before that biostatistical input that goes beyond crude measures of mortality or reoperation rates can be very helpful. The risk of reoperation may be one that the patient is willing to take for a chance at an improvement in quality of life.
There is a wonderful book by Howard Brody called The Healer’s Power6 in which he writes about the physician’s power to frame a question so as to engineer outcomes. While that is not something that Brody endorses, he does endorse the use of the physician’s power to guide patients using good informed consent, providing direction without being so determinative that patients feel compelled to choose the physician’s recommendation. Patients should be able to decline your recommendation while still having the benefit of your counsel. And in a case like this, your counsel should include variables that may seem “softer” or more difficult to quantify than crude measures such as mortality or reoperation rates.
Dr. Rezai: You have to compare multiple outcomes between the two approaches—surgical time, recovery time, patient quality of life (as assessed by scales), family quality of life, time to return to work, etc. I think it is important to try new technologies because the failure rate or the complication rate may be reduced over time, but only if you evaluate the failures and then restrategize. Only in doing so can you reduce risk, and if the benefit profile and the risk profile prove to be good, then the new technology should be pushed forward.
Dr. Herndon: If the volume of procedures performed by the surgeon is important with respect to outcomes with either one of these two procedures, that should be taken into account. Also, if a new procedure carries a higher complication rate than the traditional procedure, I think that more cohort studies from large centers are needed to gauge the true complication rate before the new technology enters the general market. Continued surveillance, such as with a postmarket registry of outcomes with these procedures, would also be helpful to make adjustments in the future if necessary.
Dr. Hahn: If you looked at the early experience of Med tronic with pacers, you would be amazed at the number of deaths and complications that occurred during the first 3 years. But we do not even think about that now.
CAN INNOVATION HAPPEN WITHOUT INCENTIVES?
Question from audience: Dr. Hahn alluded earlier to the infl uence of money. All of you on the panel are institutionally based, and you are used to practicing with colleagues. I would suggest that surgery today is really not an individual sport, but that is the way it is practiced in much of the nation. Would we be better off if we developed a system that removed us from direct financial influence? Can we get the money out of the equation so that people have motives other than direct personal gain?
Dr. Hahn: I went to an institutional review board (IRB) retreat that included, of course, some IRB members who were not clinicians. They asked the same question that you just did: Why would you even expect to get anything for what you invent? I think that is naïve. People who work hard and invent things deserve to reap a reward. The challenge lies in working with industry, which may try to convince us to use its innovations without our input, as opposed to working with us to identify a clinical problem and trying to solve it together. In that way, the end product and the logic behind its use will be better.
I will give you an example from when I was head of surgery here. A company made a voice-activated table that would obey the surgeon’s commands, such as “left,” “right,” “up,” or “down.” I asked the representative why such a product was needed, and he responded that the surgeon wants to be in total control of the operating room. I told him we do not change the position of the table very often. After a 2-week trial, the table was a dud. He fired the entire group that was working on the project. It was a case of a company simply trying to come up with a product it could sell.
The opposite scenario is if I invent the latest and greatest stent for the carotids and I want to use it. The question becomes how to strike a balance: how to protect the patients while at the same time rewarding the inventor. Another challenge is that device companies want you to stay on their scientific advisory board and they will pay you for it.
These questions are a big concern, and we have spent a lot of time on these issues at Cleveland Clinic. In fact, we held our own conference on biomedical confl icts of interest in September 2006 with attendees from around the country to discuss the necessary firewalls for ensuring that data are not contaminated, that the surgeon-inventor does not fudge data so that his innovation will make it to the marketplace, etc. At that conference, a number of people spoke about Vioxx. I am a surgeon, and my take on the COX-2 inhibitors is that a lot of my patients take these drugs and think they are wonderful, but there are some problems and risks. What is wrong with explaining to patients the risks and complications of these drugs, making your own recommendation about their use (unless you are receiving money from their manufacturers, which you would need to disclose to patients), and then letting patients make their own informed decisions? Personally, I was on Bextra for 3 years and was furious when it was pulled from the market because nobody gave me a choice whether or not to continue using it.
Dr. Lieberman: Let’s explore this concept a little deeper. We know that innovation is so important, but how do we encourage clinicians to innovate in this environment? Dr. Hahn, you served as chairman of CC Innovations, which is Cleveland Clinic’s technology commercialization arm. What were some of the strategies you came across in that role?
Dr. Hahn: We look for creative staff. We tell them up front that we want them to come to Cleveland Clinic and invent things. Our mission is literally to work on problems and take solutions to our patients. The culture here is meant to be creative. As a part of that culture, we welcome working with industry, as opposed to industry thrusting its innovations on us.
We are averaging more than 200 invention disclosures per year. More than 500 of our staff are involved with various industrial partners, and we are not going to hide that. In fact, we are going to make it public. The thought is that we owe it to our patients to work on their problems. At the same time, we owe it to our patients to say when we are working with industry on a particular product and explain to them why we think it would work in their case, if we think it would. While doing so, we need to make it clear that we will be happy to refer them for a second opinion if they would like. If I have a patient who wants a second opinion, I will offer to make the phone call for them and get them in. I think that is an advantage of the model we have here.
The reality is that there are some procedures that can only be done by one surgeon here, a surgeon who may have helped develop the procedure or some technology involved in it. Are we going to tell that surgeon that he or she cannot perform the procedure on anyone? That does not make sense. So you need to have a management plan that puts in place firewalls to protect the data on that procedure from any possible contamination.
So yes, we do reward staff who are doing innovation, and we do work with industry, and we do tell our patients we are doing it, and we do build firewalls to protect the data.
Dr. Lieberman: How about the rest of the panel? What are your thoughts on providing incentives for innovation?
Dr. Fins: Money is a key issue. The way the landscape is now structured, collaborations with industry are part of the mix. Under the Bayh-Dole Act of 1980, institutions are granted intellectual property rights to ideas or inventions developed by their researchers, and then the institutions can enter into contracts with industry to move the innovations forward. If industry support of research were removed, we would have to double the budget of the National Institutes of Health to compensate.
On the other hand, industry support can sometimes prove to be a disincentive to innovation in that it may engineer certain kinds of research or deprive investigators of tools they may need to do more basic science types of research. It is an academic freedom issue. At a translational level, industry may be helpful and catalytic. But sometimes it pushes an investigator to work for a short-term innovative application at the expense of a more speculative, riskier innovation.
We need to acknowledge that industry collaborations are part and parcel of the universe and focus on working with industry to moderate its influences. At the same time, we must use our leverage on the investigative side of the equation to pursue academic freedom and to leverage industry resources to perhaps pay for some of the care that innovative devices make possible. For example, contracting agreements could be drawn up so that money came back to the populations that participated in a clinical trial, or to a community that otherwise may need the device but cannot afford it. I think we have to create some type of charitable impulse to moderate the excesses of the profits and use them for the common good.
Dr. Herndon: I would like to touch on disclosure. The orthopedic implant industry has been required by law to disclose its relationships with orthopedic surgeons, including the amount of money that surgeons may be getting from industry. This requirement has had unintended consequences that underscore the importance of disclosure. First, some of the monetary awards, whether market-driven or not, are quite excessive. Second, reviewing the contracts for royalties has led to the discovery that many are not supported by patents or intellectual property rights. Third, these disclosures have revealed that certain surgeons who work at major US institutions, and who thus have an obligation to pay the institution some of the monies from their research, have not disclosed their relationships for years and have kept those monies solely for themselves. So this disclosure requirement has brought many things to light.
Dr. Rezai: As long as there is human disease and suffering, innovation will continue. It has in the past and it will in the future. Most innovators have it in their genes and in their blood. They can be taught to innovate, but they have to have the intrinsic curiosity and the creative mind to be an innovator. Institutional support of innovation is important, as is respect for the process that must be followed, including transparency and disclosure. If you put all these together, then innovation can be facilitated.
IF TESTING MOVES OFFSHORE, CAN ETHICS FOLLOW?
Dr. Lieberman: I am going to paint a scenario on which I would like each panelist to briefly comment. New Device X is backed by a big vendor. It is a great device, but because of all the regulatory issues in the United States, it is taken to China or South America and is being implanted there, where the regulatory environment is much more lenient. Can we rationalize this practice? How is it possibly ethical?
Dr. Fins: I can answer in 5 seconds: we shouldn’t do it.
Dr. Rezai: This is a reality we are facing with increasing rules and regulations in the United States. You have to engage the process, and it takes time. If you have colleagues who can follow clinical trials outside the United States, you can have the device tested outside and then bring it back to the United States. Unfortunately, the reality is that the regulatory process can be slow, so more testing will be done abroad, in my opinion.
Dr. Hahn: I disagree with Dr. Fins. This may be the only way to get the trials started, and we then are able to use some of the offshore data to approach the FDA for approval. I do not think that it is taking advantage of anybody; it is a way of getting things through the system.
Dr. Herndon: The door has been opened, and it is only going to increase. My only request would be that the investigators who do this function as they would here in the United States, under IRB controls and the other kinds of oversight that they would expect and demand of themselves in their own institutions.
END RESULTS: WHY SO ELUSIVE STILL?
Dr. Isador Lieberman, Moderator: Let me begin this discussion with a 1910 quote from Ernest Codman, a general surgeon at Massachusetts General Hospital, who stated:
In 1900 I became interested in what I called the “end result” idea, which was merely the commonsense notion that every hospital should follow every patient it treats long enough to determine whether or not the treatment has been successful, and then should inquire, “If not, why not?” with a view to preventing similar failure in the future.
My questions to the panel are: What has changed in the last 100 years? Are we documenting our end results? Have we gone wrong and, if so, where have we gone wrong?
Dr. James Herndon: Although Codman’s ideas in this area were not well received at the time, today we do have some “end result” ideas. We have outcomes data, but I would argue that they are far too limited and not to the level required in the 21st century. I have asked myself many times why the surgical profession has not focused on this issue more than it has. I agree with Dr. [Joseph] Fins’ comments in his presentation [see previous article in this supplement] that it would be nice to have a bottom-up approach rather than a top-down approach, but I do not see a change until we as physicians step up to the plate and make a change.
Why haven’t we? There are a number of reasons. The malpractice climate in the United States has been one major factor. Surgeons fear disclosure. The relationship between a surgeon and the patient is professional and private, and physicians do not want transparency—they do not want their patient or anyone to know that an adverse event or bad outcome has occurred.
Also, doctors, especially surgeons, are reluctant to use guidelines or follow protocols. I participated a number of years ago in an American Academy of Orthopaedic Surgeons project called MODEMS; it was an attempt to set up guidelines for orthopedic surgeons to manage back pain, shoulder pain, and other orthopedic conditions. By the time we finished we had accomplished nothing, because the protocols and guidelines were so extensive that almost any type of management for any patient would be compliant.
Additionally, hospitals in the United States have become more like for-profit businesses, with a focus on short-term profits and with short tenures for their chief executive officers (CEOs)—4 or 5 years, on average. With nearly 50% of US hospitals bordering on bankruptcy, they are not able or willing to invest in major patient safety protocols and guidelines because the CEOs do not see a short-term benefit to them. Witness the fact that only 15% of US hospitals have computerized physician order entry systems and electronic medical records. From what I have read, it takes about 5 years before a hospital recoups such investments from the resulting safety improvements and efficiencies.
These are some, but by no means all, of the reasons we do not have appropriate outcomes in all specialty fields. My plea is that physicians lead the effort to measure and report outcomes down the road.
Dr. Lieberman: Dr. Hahn, why do you think we have not kept up with Dr. Codman’s premise from 100 years ago?
Dr. Joseph Hahn: We hold a yearly Medical Innovation Summit at the Cleveland Clinic, and what has emerged from many of those meetings is a lack of interest in paying for outcomes analyses. The providers, the government, and industry all say that they do not have the money for these analyses. So the first reason that Codman’s premise has not been lived up to is that the source of funding remains undetermined. Second, most surgical innovations have been geared toward inventing devices to overcome very specific problems that arise during or following surgery rather than toward substantiating the worth of a procedure through collection of evidence. A third reason involves the pressure that investors place on industry to make money, which tends to lead to investments in getting products to market rather than outcomes research. With all of these factors and the pressures from so many directions, the surgical profession hasn’t stepped back to thoroughly consider what we are doing to our patients and just how worthwhile it is.
Dr. Lieberman: Who do you think should be paying for outcomes analyses?
Dr. Hahn: I think the government should. The role of government is to take care of its citizens. The Centers for Medicare and Medicaid Services (CMS) does its best with the information it has, but it admits that it pays for some procedures without knowing whether or not they are truly worthwhile. An example is the use of artificial discs in the cervical spine. I am sure that the artificial disc manufacturers made a case for their product to CMS by claiming it was associated with less pain and resulted in a superior outcome compared to fusion using bone from the hip, regardless of whether they had the scientific evidence to prove it.
Dr. Lieberman: Dr. Fins, would you like to weigh in on Codman’s “end result” premise?
Dr. Joseph Fins: I would just point out that the history is not homogeneous. I have been involved in deep brain stimulation work, and the legacy of psychosurgery has been an egregious lack of outcomes studies, but now we do have outcomes studies and scales. For example, there is now the Yale-Brown Obsessive Compulsive Scale to rate the severity of symptoms in obsessive-compulsive disorder. In our deep brain stimulation study,1 we are using a coma recovery scale, and the Food and Drug Administration’s (FDA’s) investigational device exemption (IDE) process requires us to produce outcomes data to protect potential subjects. It may be an example of neuropsychiatric exceptionalism that neurology and psychiatry are areas of increased focus while somatic therapies are somehow presumed to be okay.
Dr. Hahn: FDA may be requiring the outcomes data, but I have not heard that they are willing to pay for it.
Dr. Fins: You are correct.
Dr. Ali Rezai: Part of the problem is the translation of rapid scientific discoveries and technological advances into the field, and education has a role here. Surgeons’ reluctance to integrate guidelines and outcomes measures into practice must be addressed very early in their training—in medical school—and then continued throughout residency and fellowship programs. The same early and continuing approach should be taken with respect to how to conduct and properly interpret a clinical trial.
Dr. Herndon: That is a good point. Surgical education programs have slipped a bit in the past 5 to 10 years, at least in orthopedics. With the reductions in residents’ work hours and the fast pace of residency programs, our residents spend most of their time in the operating room, struggling to master the multitude of procedures in orthopedics. As a result, they are not discussing outcomes or adequately following patients long-term after surgery. I have a hard time getting our faculty to bring residents into their offices so that the residents can examine patients and see why they are operating on certain kinds of patients, as well as the types of follow-up information that can and should be obtained from patients. Training today is so oriented to operative techniques that residencies have difficulty dealing with these other important issues.
WHO DEFINES THE INDICATIONS?
Dr. Lieberman: As new devices and new techniques emerge, who defines their indications? The inventor of the device, a government authority that may or may not have the medical background, patient advocacy groups, or the device manufacturer? And how should we regulate those indications?
Dr. Fins: I would echo Dr. Wilder Penfield’s words, “No man alone.” The orthopedic surgeon or neurosurgeon does not have to do this alone; it is really about teams. And those teams can and should include biostatisticians, recognizing that the biostatistician needs to fully understand what the surgeon is doing. There also has to be attention given to patients’ individualistic outcomes. I recently met with some FDA staff and learned that the FDA is very interested in novel methodologies to better understand what counts as an outcome for individual patients. So I think indications should be guided by individualistic outcomes coupled with the surgical possibilities and with the rigorous biostatistical methods that are now evolving. A conference like this represents an opportunity to generalize the conversation and support more collaboration on indications going forward.
Dr. Rezai: Indications should be defined using a team-oriented approach. Part of the problem of psychosurgery in the past was that the surgeon was defining indications without collaborating with the psychiatrist. In my field of deep brain stimulation and brain pacemakers, everything we have done for the past 20 years—surgery for Parkinson’s disease, depression, obsessive-compulsive disorder, traumatic brain injury, epilepsy—has involved working closely with neurologists, epileptologists, brain injury specialists, psychiatrists, and psychologists to agree on indications. These teams also need to have close partnerships with ethicists. Teamwork is a vital aspect of proper development of an indication.
Dr. Hahn: It has to be the clinicians who set forth the indications. Of course, that may be done by a team of clinicians, but as a surgeon I certainly do not want the manufacturers of an artificial disc telling me what they think the indications for an artificial disc are.
As for the role of patients, some of them are very well informed about their problem. I cannot tell you how many have shown up in my office with reprints of articles I have written. This is a trend that has really mushroomed over the past 10 years. But even though patients are catching up, they are still at a disadvantage. Patients are going to have a say, but it is still the clinicians whose role is to decide the indications and then provide patients with a risk-benefit analysis.
Dr. Herndon: I agree. Although patients are becoming more involved in the process, real shared decision-making has not yet happened in my field.
More broadly, I feel that our professional organizations have to become more actively involved in the process of defining indications. Otherwise, after the innovators develop a device or procedure that will significantly change the approach to a particular problem, it will enter the market at large without any critical assessment of the technology involved and without accounting for the learning curve for each individual surgeon.
Take the example of minimally invasive total hip replacement, which involves a 1-inch incision in the front of the hip and a 1-inch incision in the back of the hip. The learning curve for this procedure appears to be about 40 cases, based on the opinion of experts around the country. Yet when this minimally invasive approach emerged, every surgeon who had been performing total hip replacements wanted this new operation at his or her fingertips because patients were demanding it. Some surgeons adopted it too quickly, without adequate training. I know one distraught surgeon who abandoned the procedure because of numerous failures during his first 100 cases. He returned to the standard hip replacement approach.
Our profession cannot let this experience continue or proliferate. Yet the professional organizations in orthopedics have walked away from technology assessment because industry does not want it; technology assessment is not in industry’s best interest. We have had a number of conflicts in our professional organizations when attempting to move technology assessment forward. It is also very expensive to do.
Finally, indications can sometimes be governed more by economics than by science. I was asked to write a letter to the editor about two technologies for managing intertrochanteric fractures of the hip that were recently featured in the Journal of Bone and Joint Surgery.2,3 One technology involves a compression screw that has been shown to be effective in outcomes studies. The other is an intramedullary nail that has not been well studied and has no proven benefit over the compression screw. In doing research for my letter,4 I found that Medicare assigns more relative value units (RVUs) for the intramedullary nail than for the compression screw. In Boston, the total dollar difference in RVUs between the two is $300: the surgeon makes $1,500 for the procedure that involves the intramedullary nail versus $1,200 for using the compression screw. Not surprisingly, use of the intramedullary nail has been climbing rapidly in the United States without any evidence to justify its use over the other, less expensive technique.
CREDENTIALING: CAN IT KEEP PACE WITH INNOVATION?
Dr. Fins: I agree that surgical competence and regulation—self-regulation or professional regulation—are big issues. One of my greatest fears is that surgeons will do procedures they are not trained to do, and cause great harm as a result. We are hearing about this now with the resurgence of psychosurgery in China.
It strikes me as interesting that the field of neurosurgery is as yet undifferentiated and that there is no subspecialty certification in stereotactic neurosurgery. This is in contrast to invasive cardiology on the medical side, where physicians who do catheterizations and electrophysiologic studies have special additional training.
As innovations develop, we have to track qualifications and credentialing along the way. There should be provisions to grandfather surgeons in if they are in a post-training point in their career, but we have to ensure that the new technology is matched by the operator’s skill. This is particularly pertinent in light of the concept of “surgical proximity”5 and the importance of the individual operator; this is not comparable to just disseminating a new drug.
Dr. Lieberman: Who should do the credentialing? Should it be the government or our profession?
Dr. Fins: Recertification or credentialing should be by peers—the American College of Surgeons and the surgical boards. Of course, funders or payors may request an additional level of certification to do certain procedures, which I would endorse as a safety measure and to help ensure a minimal standard of care for innovative interventions.
Dr. Hahn: But it is not so simple. There is a blurring of surgical expertise once surgeons complete their training. Spine surgery used to be done by either neurosurgeons or orthopedic surgeons; now we have spine surgeons. What we neurosurgeons started to see with that change was that our neurosurgery trainees were being told they could not get on hospital staffs because they did not have credentials in spine surgery or, to take another example, in pediatric surgery. Well, the neurosurgery board made a conscious decision to not offer certificates of added qualification (CAQs). We challenged the hospitals in court and won. But the overriding message is that it is all about economics.
Dr. Herndon: In orthopedics we now have two CAQs—one in hand surgery and one (starting in 2009) in sports medicine. The hand surgeons have not noticed any adverse effect because they do not generate as much revenue as the spine surgeons do. Most orthopedic surgeons start as general orthopedists and then change their practice characteristics as their practices mature. Over time they may focus on one particular area, such as arthroscopic knee surgery or total hip or knee replacement, which makes it difficult for them to pass a general orthopedic examination. Our board recognized this trend and developed oral and written board exams with case reviews concentrating on the surgeon’s self-chosen specialty. We do not need the CAQs because they have been misused, and we as a profession have been letting others misuse them. Again, I think we need to get back to controlling the process ourselves.
Dr. Hahn: What do you do when a surgeon has finished training and then becomes interested in performing a new procedure developed since the time of his or her training? This can really be a challenge when the surgeon hears of a new procedure, goes and takes a 3-day training seminar on it, and comes back believing that he or she is ready to perform the procedure. I have had creative surgeons on staff who want to try a new procedure but have never done any cases, believing that the new technology alone will suffice. What we finally decided to do in these instances was to put in place other staff to proctor these cases to ensure that no harm was coming to patients.
Dr. Herndon: I admire that approach, because we as a profession have to educate our colleagues about whatever new procedures they are about to use in their practice. There is a learning curve for every operation, and learning on one’s own, at the expense of patients, is not appropriate. Should we have experienced colleagues work with surgeons on new procedures until they have performed the 40 or so cases necessary to be proficient? Should we send surgeons to other institutions to do their 40 cases under experienced supervision? I am not sure what the best approach is, but this is a question that a forum like this should begin to address.
HOW MUCH RISK IS ACCEPTABLE?
Dr. Lieberman: Let’s build on this issue of credentialing by turning to the concept of risk. What is an acceptable level of risk with a new device? Is a 50% risk of an adverse outcome appropriate? What about 10%? And who determines the acceptable risk? The profession? The regulatory bodies? Patients?
Dr. Fins: Our expectation about risks in clinical practice should evolve from what was anticipated and actually observed in the clinical trial of an intervention. Adverse events should be envisioned prospectively in the design of a trial, with the magnitude of risks delineated in the protocol. Any unexpected risks that occur, even if small, could be a major reporting issue. Beyond that, it is difficult to say what an acceptable level of risk is without a particularistic clinical trial. Whatever the risk of an intervention, the assessment of the risk must account for regional variation, variation among surgeons, and also systems issues.
The Institute of Medicine report, To Err is Human, attributed medical errors to faulty systems, processes, and conditions. So when we think about errors and risk, we have to consider more than just the individual operator. Just as To Err is Human analogized medical errors to airplane crashes, we might think of surgical retraining in the context of how pilots get retrained using flight simulators. If pilots have not flown a particular aircraft in a long time, they lose their flight certification for that type of craft and then must be retrained to operate it.
As surgical technology gets more advanced, specific, and nuanced, the discordance between one’s training and the potential things one can do becomes greater. Paradoxically, innovation can at least potentially make situations more dangerous in that the operator may not be able to perform the task with the improved technology. For example, pilots who know how to fly a Cessna can fly another simply constructed plane, but if they attempt to fly a higher-technology aircraft, like an F-16, they have a greater risk of having a catastrophic event even though the F-16 flies better, faster, and higher.
Dr. Lieberman: But are you willing to identify a level of acceptable risk?
Dr. Fins: It is based on the patient’s preference, after informed consent. An acceptable level of risk is the level that people are willing to accept. What I am concerned about is the variance around a known risk, whatever it may be, that is attributable to human errors that may be preventable through training or by solving systems problems.
Dr. Lieberman: Dr. Rezai, you place needles into the brain. Who should decide the risk of that action? You? The patient? And what do you feel is an acceptable risk level?
Dr. Rezai: It is a complex question, of course, and a number of variables come into play. Whether or not the patient’s condition is life-threatening or disabling is a very important factor in the risk-benefit ratio. Regulatory guidance from the FDA is strong with respect to defining device-related adverse effects as serious or nonserious, and our peers, both surgeons and nonsurgeons, help to further dictate the risk and tolerability of a procedure and its alternatives. For example, in considering a surgical procedure, one must weigh its risk against the risks of medications to treat the disorder, such as side effects, the ease of medication adherence, and the number of emergency room visits that may result from adverse effects of the medications.
Determining acceptable risk rests fundamentally and first with the patient and then with the surgeon and his or her peers (surgeons and nonsurgeons) in conjunction with regulatory components and oversight. All of these factors contribute.
In my field of deep brain stimulation, the threshold for acceptable risk can be high since we see patients with chronic conditions in whom all previous medication attempts have failed, many of whom are disabled, intractable to current therapies, and with a significant compromise of quality of life. Examples include wheelchair-dependent patients with severe Parkinson’s disease, severely depressed patients who will not leave the house and have attempted suicide, and obsessive-compulsive disorder patients who need 10 hours just to take a shower. This type of intractability to current therapies and the suffering of patients and families with limited options and little hope infl uence assessments of procedural risk.
Dr. Hahn: Performing a controlled clinical trial of a surgical procedure is difficult at best. I recall a clinical trial in which patients with parkinsonism were to be randomized either to have stem cells implanted in their brain or to undergo a sham operation with no stem cells. Well, very few patients signed up for the trial because everyone wanted the stem cells. So, obtaining a large enough denominator to define the risk of, for example, hemorrhage from sticking a needle into a vessel is almost impossible.
Dr. Herndon: Except when there are risks of serious life-threatening events, I believe the patient is the one who makes the decision after having the risks fully explained to him or her. Surgeons are educated in a system in which we learn to accept complications. It is the risk of doing business. We have not learned very well how to differentiate a complication from an adverse event or an error. We must learn to do that. We live with complications every day. Those complications must be conveyed to patients so that they understand what they are about to undergo, what can happen, and what cannot happen. The patient is the ultimate decider, in my opinion.
Dr. Lieberman: That reminds me of something one of my mentors often said: “If you are going to run with the big dogs, expect to get bitten in the butt once in a while.”
ETHICAL DILEMMAS ARISING FROM NEW OPTIONS
Question from audience: In my specialty, we have a non-life-threatening condition with a well-established 25% recurrence rate after traditional surgery with sutures, and a 25% rate of reoperation. A device comes along and it improves the outcomes so that the recurrence rate declines to 10%, but along with the extra costs of doing the procedure with the device, there is also a complication rate of about 10% that requires reoperation with the device, and a few of those patients actually end up worse. Ethically, how should the clinician proceed in this situation? The old way, or the new way that improves outcomes but at a higher cost and risk?
Dr. Fins: Based on the size of the populations, is the difference in the combined rates of recurrence and complications between the traditional and new methods (25% vs 20%) statistically significant?
Response from questioner: The difference is probably not statistically significant.
Dr. Fins: Okay, so you are saying that the numbers are basically equal. That is the first consideration, but there is a nuance to one of the variables, and that is an improvement in quality of life with one of the treatments. Measuring its significance is subjective. A patient may place greater emphasis on quality of life than would somebody who is not a beneficiary of the operation. That is why I said before that biostatistical input that goes beyond crude measures of mortality or reoperation rates can be very helpful. The risk of reoperation may be one that the patient is willing to take for a chance at an improvement in quality of life.
There is a wonderful book by Howard Brody called The Healer’s Power6 in which he writes about the physician’s power to frame a question so as to engineer outcomes. While that is not something that Brody endorses, he does endorse the use of the physician’s power to guide patients using good informed consent, providing direction without being so determinative that patients feel compelled to choose the physician’s recommendation. Patients should be able to decline your recommendation while still having the benefit of your counsel. And in a case like this, your counsel should include variables that may seem “softer” or more difficult to quantify than crude measures such as mortality or reoperation rates.
Dr. Rezai: You have to compare multiple outcomes between the two approaches—surgical time, recovery time, patient quality of life (as assessed by scales), family quality of life, time to return to work, etc. I think it is important to try new technologies because the failure rate or the complication rate may be reduced over time, but only if you evaluate the failures and then restrategize. Only in doing so can you reduce risk, and if the benefit profile and the risk profile prove to be good, then the new technology should be pushed forward.
Dr. Herndon: If the volume of procedures performed by the surgeon is important with respect to outcomes with either one of these two procedures, that should be taken into account. Also, if a new procedure carries a higher complication rate than the traditional procedure, I think that more cohort studies from large centers are needed to gauge the true complication rate before the new technology enters the general market. Continued surveillance, such as with a postmarket registry of outcomes with these procedures, would also be helpful to make adjustments in the future if necessary.
Dr. Hahn: If you looked at the early experience of Med tronic with pacers, you would be amazed at the number of deaths and complications that occurred during the first 3 years. But we do not even think about that now.
CAN INNOVATION HAPPEN WITHOUT INCENTIVES?
Question from audience: Dr. Hahn alluded earlier to the infl uence of money. All of you on the panel are institutionally based, and you are used to practicing with colleagues. I would suggest that surgery today is really not an individual sport, but that is the way it is practiced in much of the nation. Would we be better off if we developed a system that removed us from direct financial influence? Can we get the money out of the equation so that people have motives other than direct personal gain?
Dr. Hahn: I went to an institutional review board (IRB) retreat that included, of course, some IRB members who were not clinicians. They asked the same question that you just did: Why would you even expect to get anything for what you invent? I think that is naïve. People who work hard and invent things deserve to reap a reward. The challenge lies in working with industry, which may try to convince us to use its innovations without our input, as opposed to working with us to identify a clinical problem and trying to solve it together. In that way, the end product and the logic behind its use will be better.
I will give you an example from when I was head of surgery here. A company made a voice-activated table that would obey the surgeon’s commands, such as “left,” “right,” “up,” or “down.” I asked the representative why such a product was needed, and he responded that the surgeon wants to be in total control of the operating room. I told him we do not change the position of the table very often. After a 2-week trial, the table was a dud. He fired the entire group that was working on the project. It was a case of a company simply trying to come up with a product it could sell.
The opposite scenario is if I invent the latest and greatest stent for the carotids and I want to use it. The question becomes how to strike a balance: how to protect the patients while at the same time rewarding the inventor. Another challenge is that device companies want you to stay on their scientific advisory board and they will pay you for it.
These questions are a big concern, and we have spent a lot of time on these issues at Cleveland Clinic. In fact, we held our own conference on biomedical confl icts of interest in September 2006 with attendees from around the country to discuss the necessary firewalls for ensuring that data are not contaminated, that the surgeon-inventor does not fudge data so that his innovation will make it to the marketplace, etc. At that conference, a number of people spoke about Vioxx. I am a surgeon, and my take on the COX-2 inhibitors is that a lot of my patients take these drugs and think they are wonderful, but there are some problems and risks. What is wrong with explaining to patients the risks and complications of these drugs, making your own recommendation about their use (unless you are receiving money from their manufacturers, which you would need to disclose to patients), and then letting patients make their own informed decisions? Personally, I was on Bextra for 3 years and was furious when it was pulled from the market because nobody gave me a choice whether or not to continue using it.
Dr. Lieberman: Let’s explore this concept a little deeper. We know that innovation is so important, but how do we encourage clinicians to innovate in this environment? Dr. Hahn, you served as chairman of CC Innovations, which is Cleveland Clinic’s technology commercialization arm. What were some of the strategies you came across in that role?
Dr. Hahn: We look for creative staff. We tell them up front that we want them to come to Cleveland Clinic and invent things. Our mission is literally to work on problems and take solutions to our patients. The culture here is meant to be creative. As a part of that culture, we welcome working with industry, as opposed to industry thrusting its innovations on us.
We are averaging more than 200 invention disclosures per year. More than 500 of our staff are involved with various industrial partners, and we are not going to hide that. In fact, we are going to make it public. The thought is that we owe it to our patients to work on their problems. At the same time, we owe it to our patients to say when we are working with industry on a particular product and explain to them why we think it would work in their case, if we think it would. While doing so, we need to make it clear that we will be happy to refer them for a second opinion if they would like. If I have a patient who wants a second opinion, I will offer to make the phone call for them and get them in. I think that is an advantage of the model we have here.
The reality is that there are some procedures that can only be done by one surgeon here, a surgeon who may have helped develop the procedure or some technology involved in it. Are we going to tell that surgeon that he or she cannot perform the procedure on anyone? That does not make sense. So you need to have a management plan that puts in place firewalls to protect the data on that procedure from any possible contamination.
So yes, we do reward staff who are doing innovation, and we do work with industry, and we do tell our patients we are doing it, and we do build firewalls to protect the data.
Dr. Lieberman: How about the rest of the panel? What are your thoughts on providing incentives for innovation?
Dr. Fins: Money is a key issue. The way the landscape is now structured, collaborations with industry are part of the mix. Under the Bayh-Dole Act of 1980, institutions are granted intellectual property rights to ideas or inventions developed by their researchers, and then the institutions can enter into contracts with industry to move the innovations forward. If industry support of research were removed, we would have to double the budget of the National Institutes of Health to compensate.
On the other hand, industry support can sometimes prove to be a disincentive to innovation in that it may engineer certain kinds of research or deprive investigators of tools they may need to do more basic science types of research. It is an academic freedom issue. At a translational level, industry may be helpful and catalytic. But sometimes it pushes an investigator to work for a short-term innovative application at the expense of a more speculative, riskier innovation.
We need to acknowledge that industry collaborations are part and parcel of the universe and focus on working with industry to moderate its influences. At the same time, we must use our leverage on the investigative side of the equation to pursue academic freedom and to leverage industry resources to perhaps pay for some of the care that innovative devices make possible. For example, contracting agreements could be drawn up so that money came back to the populations that participated in a clinical trial, or to a community that otherwise may need the device but cannot afford it. I think we have to create some type of charitable impulse to moderate the excesses of the profits and use them for the common good.
Dr. Herndon: I would like to touch on disclosure. The orthopedic implant industry has been required by law to disclose its relationships with orthopedic surgeons, including the amount of money that surgeons may be getting from industry. This requirement has had unintended consequences that underscore the importance of disclosure. First, some of the monetary awards, whether market-driven or not, are quite excessive. Second, reviewing the contracts for royalties has led to the discovery that many are not supported by patents or intellectual property rights. Third, these disclosures have revealed that certain surgeons who work at major US institutions, and who thus have an obligation to pay the institution some of the monies from their research, have not disclosed their relationships for years and have kept those monies solely for themselves. So this disclosure requirement has brought many things to light.
Dr. Rezai: As long as there is human disease and suffering, innovation will continue. It has in the past and it will in the future. Most innovators have it in their genes and in their blood. They can be taught to innovate, but they have to have the intrinsic curiosity and the creative mind to be an innovator. Institutional support of innovation is important, as is respect for the process that must be followed, including transparency and disclosure. If you put all these together, then innovation can be facilitated.
IF TESTING MOVES OFFSHORE, CAN ETHICS FOLLOW?
Dr. Lieberman: I am going to paint a scenario on which I would like each panelist to briefly comment. New Device X is backed by a big vendor. It is a great device, but because of all the regulatory issues in the United States, it is taken to China or South America and is being implanted there, where the regulatory environment is much more lenient. Can we rationalize this practice? How is it possibly ethical?
Dr. Fins: I can answer in 5 seconds: we shouldn’t do it.
Dr. Rezai: This is a reality we are facing with increasing rules and regulations in the United States. You have to engage the process, and it takes time. If you have colleagues who can follow clinical trials outside the United States, you can have the device tested outside and then bring it back to the United States. Unfortunately, the reality is that the regulatory process can be slow, so more testing will be done abroad, in my opinion.
Dr. Hahn: I disagree with Dr. Fins. This may be the only way to get the trials started, and we then are able to use some of the offshore data to approach the FDA for approval. I do not think that it is taking advantage of anybody; it is a way of getting things through the system.
Dr. Herndon: The door has been opened, and it is only going to increase. My only request would be that the investigators who do this function as they would here in the United States, under IRB controls and the other kinds of oversight that they would expect and demand of themselves in their own institutions.
- Schiff ND, Giacino JT, Kalmar K, et al. Behavioral improvements with thalamic stimulation after severe traumatic brain injury. Nature 2007; 448:600–603.
- Forte ML, Virnig BA, Kane RL, et al. Geographic variation in device use for intertrochanteric hip fractures. J Bone Joint Surg Am 2008; 90:691–699.
- Anglen JO, Weinstein JN. Nail or plate fixation of intertrochanteric hip fractures: changing pattern of practice. A review of the American Board of Orthopaedic Surgery database. J Bone Joint Surg Am 2008; 90:700–707.
- Herndon JH. Technology assessment and adoption in orthopaedics [letter]. J Bone Joint Surg Am 2008; 90e. http://www.ejbjs.org/cgi/eletters/90/4/689. Published April 1, 2008. Accessed August 25, 2008.
- Fins JJ. Surgical innovation and ethical dilemmas: precautions and proximity. Cleve Clin J Med 2008; 75(suppl 6):S7–S12.
- Brody H. The Healer’s Power. New Haven, CT: Yale University Press; 1992.
- Schiff ND, Giacino JT, Kalmar K, et al. Behavioral improvements with thalamic stimulation after severe traumatic brain injury. Nature 2007; 448:600–603.
- Forte ML, Virnig BA, Kane RL, et al. Geographic variation in device use for intertrochanteric hip fractures. J Bone Joint Surg Am 2008; 90:691–699.
- Anglen JO, Weinstein JN. Nail or plate fixation of intertrochanteric hip fractures: changing pattern of practice. A review of the American Board of Orthopaedic Surgery database. J Bone Joint Surg Am 2008; 90:700–707.
- Herndon JH. Technology assessment and adoption in orthopaedics [letter]. J Bone Joint Surg Am 2008; 90e. http://www.ejbjs.org/cgi/eletters/90/4/689. Published April 1, 2008. Accessed August 25, 2008.
- Fins JJ. Surgical innovation and ethical dilemmas: precautions and proximity. Cleve Clin J Med 2008; 75(suppl 6):S7–S12.
- Brody H. The Healer’s Power. New Haven, CT: Yale University Press; 1992.
Pushing the envelope in transplantation: Three lives at stake
Anyone involved in transplantation has witnessed the Lazarean awakening of many of our patients. On the verge of dying, these patients receive a transplant then go home to their loved ones, to their communities, and to the rest of their life.
Transplantation has always straddled the border between life and death; it has always pushed the biological envelope.
But it has also always pushed the ethical envelope.
How? In forcing all of us, not just transplant surgeons, to reconsider some of our most fundamental ethical dilemmas:
- What is death?
- Can we extend life?
- Whose life do we extend?
- At what price the extension of life?
- Just because we can extend life, should we?
And every one of these dilemmas is further complicated by another issue unique to transplantation. At stake in every transplant is not just the patient’s life, but three lives—the patient, the donor, and the person on the waiting list who likely died because the organ went to your patient, not her or him.
While we are not focusing today on organ donation or allocation, let us not forget that transplantation is unique in this regard. There are always three patients to consider.
What we will focus on today are transplant and post-transplant innovations. To help introduce the discussion, I would like to share a narrative that I believe illuminates ethical dilemmas that go hand-in-hand with transplantation’s innovations.
THE STORY OF MAX
Max was the tiny embodiment of a biological keystone cop. In utero he had developed a gaping defect of his abdominal wall. His intestines twisted around themselves, and the obstetricians had to deliver Max emergently. The pediatric surgeons immediately removed the gangrenous remnants of nearly his entire bowel.
At 10 months, Max received a liver and small bowel transplant. The transplanted organs worked initially; with a small feeding tube inserted directly into his gut, Max digested for the first time in his life tablespoons of food, albeit a chalky liquid supplement.
But Max, within 2 months of his transplant, had again become a permanent resident in the pediatric intensive care unit. Achieving the right balance of immunosuppression so Max could keep the transplanted organs and yet maintain sufficient immunity to fight off infection had become an impossible task.
I was in my fellowship at the time of Max’s transplant; and Eric, an attending surgeon with a square jaw and dark Dick Tracy looks, led the surgical team’s management of Max’s case.
As Max became sicker, Eric spent more hours with his tiny patient. I found him by Max’s bedside at 3:00 in the morning and then at 7:00 the next night, his hair, clothes, and personal aura in a state that reflected obliviousness to his own care. Just by being with Max so much, Eric knew all the particularities of that baby, all his idiosyncratic reactions, every significant lab result of Max’s entire life.
At first I found Eric’s dedication inspiring, almost thrilling in a martyred saint kind of way. And Max seemed to call out to any of us who hoped to be divinely touched. During rounds, Max giggled at me, as if he understood that playing with him was infinitely more interesting than arguing over doses of medication with other doctors. Spurred on by Max’s cause, I raced to uncover test results before Eric, as if my quicker response would translate into an equal or greater enthusiasm for Max’s plight. I nagged the radiology technicians to give me Max’s x-rays hot off the presses. I set the alarms on my beeper to see Max in the middle of the night and on mornings long before any member of the surgical team, particularly Eric, arrived.
Despite my enthusiastic attentions, Max became sicker. We gave Max higher doses of steroids, and his big, shiny black eyes turned into a pair of hyphens on the rolling swells of his face. His tiny body became engorged with fluid from repeated infections, and Max’s once buttery skin slowly became the ridiculously inadequate biological grounding for monitors and catheters. The nurses took to using the bed around him to clip wires and anchor dressings, and they hung mechanized pumps on tall IV poles which stood like skeletal beasts of burden crowded around Max’s bed.
Through all of Max’s crises, Eric never let up. But Max was going to die soon if we could not find the source of his infections. Eric finally decided to take Max to the operating room, worried about a hidden infection around his transplanted intestines. “We’ve got to take him back to the OR,” he said to us. Eric looked at us then asked rhetorically, “I mean, is there any other option?” We all understood what Eric was really asking. Were we doing enough? Was it our fault?
That trip to the OR would be the first of almost a dozen. Under searing heat lamps we snipped the sutures that held a plastic abdominal patch in place and uncovered the small cavity filled with congealed organs. We picked away at the block-like mass, terrified of inadvertently cutting a hole in his transplanted intestine and creating another source of infection. Then, finding nothing and too scared to cause any more damage, we whipstitched a piece of plastic back to the edge of Max’s abdominal wall. Over time, it became harder and harder to find untouched flesh where we could place a new stitch.
Over a month later Max died of a massive fungal infection. I mentioned his death to Jaimie, a pragmatic and brilliant head nurse who possessed more insight into our patients and hospital politics than most of the physicians.
“Maybe it was a good thing, huh?” Jaimie responded flatly. She walked out of the room and I could hear her asking aloud, “I mean, how much can you do to a person?”
THE EARLY TRANSPLANT ERA, DESPITE BLEAKER OUTCOMES, HAS LESSONS TO TEACH
I grew up, surgically speaking, at a time when transplant science fiction had become standard of care, when patients transplanted a decade or more earlier would routinely drop by clinic to say hello, and when patients on the brink of death could expect a full recovery.
But it was not always this way. And it took courageous individuals navigating the difficult relationship between innovation and ethics to get us here.
What is extraordinary about this panel is that these surgeons not only were at the forefront of transplantation’s history but also remain deeply involved in its future. Over the next hour roughly, they will give us an extraordinary look into the intersection of innovation and ethics in the past, present, and future of transplant surgery.
I hope you are eager as I am to hear what they have to share with us.
Anyone involved in transplantation has witnessed the Lazarean awakening of many of our patients. On the verge of dying, these patients receive a transplant then go home to their loved ones, to their communities, and to the rest of their life.
Transplantation has always straddled the border between life and death; it has always pushed the biological envelope.
But it has also always pushed the ethical envelope.
How? In forcing all of us, not just transplant surgeons, to reconsider some of our most fundamental ethical dilemmas:
- What is death?
- Can we extend life?
- Whose life do we extend?
- At what price the extension of life?
- Just because we can extend life, should we?
And every one of these dilemmas is further complicated by another issue unique to transplantation. At stake in every transplant is not just the patient’s life, but three lives—the patient, the donor, and the person on the waiting list who likely died because the organ went to your patient, not her or him.
While we are not focusing today on organ donation or allocation, let us not forget that transplantation is unique in this regard. There are always three patients to consider.
What we will focus on today are transplant and post-transplant innovations. To help introduce the discussion, I would like to share a narrative that I believe illuminates ethical dilemmas that go hand-in-hand with transplantation’s innovations.
THE STORY OF MAX
Max was the tiny embodiment of a biological keystone cop. In utero he had developed a gaping defect of his abdominal wall. His intestines twisted around themselves, and the obstetricians had to deliver Max emergently. The pediatric surgeons immediately removed the gangrenous remnants of nearly his entire bowel.
At 10 months, Max received a liver and small bowel transplant. The transplanted organs worked initially; with a small feeding tube inserted directly into his gut, Max digested for the first time in his life tablespoons of food, albeit a chalky liquid supplement.
But Max, within 2 months of his transplant, had again become a permanent resident in the pediatric intensive care unit. Achieving the right balance of immunosuppression so Max could keep the transplanted organs and yet maintain sufficient immunity to fight off infection had become an impossible task.
I was in my fellowship at the time of Max’s transplant; and Eric, an attending surgeon with a square jaw and dark Dick Tracy looks, led the surgical team’s management of Max’s case.
As Max became sicker, Eric spent more hours with his tiny patient. I found him by Max’s bedside at 3:00 in the morning and then at 7:00 the next night, his hair, clothes, and personal aura in a state that reflected obliviousness to his own care. Just by being with Max so much, Eric knew all the particularities of that baby, all his idiosyncratic reactions, every significant lab result of Max’s entire life.
At first I found Eric’s dedication inspiring, almost thrilling in a martyred saint kind of way. And Max seemed to call out to any of us who hoped to be divinely touched. During rounds, Max giggled at me, as if he understood that playing with him was infinitely more interesting than arguing over doses of medication with other doctors. Spurred on by Max’s cause, I raced to uncover test results before Eric, as if my quicker response would translate into an equal or greater enthusiasm for Max’s plight. I nagged the radiology technicians to give me Max’s x-rays hot off the presses. I set the alarms on my beeper to see Max in the middle of the night and on mornings long before any member of the surgical team, particularly Eric, arrived.
Despite my enthusiastic attentions, Max became sicker. We gave Max higher doses of steroids, and his big, shiny black eyes turned into a pair of hyphens on the rolling swells of his face. His tiny body became engorged with fluid from repeated infections, and Max’s once buttery skin slowly became the ridiculously inadequate biological grounding for monitors and catheters. The nurses took to using the bed around him to clip wires and anchor dressings, and they hung mechanized pumps on tall IV poles which stood like skeletal beasts of burden crowded around Max’s bed.
Through all of Max’s crises, Eric never let up. But Max was going to die soon if we could not find the source of his infections. Eric finally decided to take Max to the operating room, worried about a hidden infection around his transplanted intestines. “We’ve got to take him back to the OR,” he said to us. Eric looked at us then asked rhetorically, “I mean, is there any other option?” We all understood what Eric was really asking. Were we doing enough? Was it our fault?
That trip to the OR would be the first of almost a dozen. Under searing heat lamps we snipped the sutures that held a plastic abdominal patch in place and uncovered the small cavity filled with congealed organs. We picked away at the block-like mass, terrified of inadvertently cutting a hole in his transplanted intestine and creating another source of infection. Then, finding nothing and too scared to cause any more damage, we whipstitched a piece of plastic back to the edge of Max’s abdominal wall. Over time, it became harder and harder to find untouched flesh where we could place a new stitch.
Over a month later Max died of a massive fungal infection. I mentioned his death to Jaimie, a pragmatic and brilliant head nurse who possessed more insight into our patients and hospital politics than most of the physicians.
“Maybe it was a good thing, huh?” Jaimie responded flatly. She walked out of the room and I could hear her asking aloud, “I mean, how much can you do to a person?”
THE EARLY TRANSPLANT ERA, DESPITE BLEAKER OUTCOMES, HAS LESSONS TO TEACH
I grew up, surgically speaking, at a time when transplant science fiction had become standard of care, when patients transplanted a decade or more earlier would routinely drop by clinic to say hello, and when patients on the brink of death could expect a full recovery.
But it was not always this way. And it took courageous individuals navigating the difficult relationship between innovation and ethics to get us here.
What is extraordinary about this panel is that these surgeons not only were at the forefront of transplantation’s history but also remain deeply involved in its future. Over the next hour roughly, they will give us an extraordinary look into the intersection of innovation and ethics in the past, present, and future of transplant surgery.
I hope you are eager as I am to hear what they have to share with us.
Anyone involved in transplantation has witnessed the Lazarean awakening of many of our patients. On the verge of dying, these patients receive a transplant then go home to their loved ones, to their communities, and to the rest of their life.
Transplantation has always straddled the border between life and death; it has always pushed the biological envelope.
But it has also always pushed the ethical envelope.
How? In forcing all of us, not just transplant surgeons, to reconsider some of our most fundamental ethical dilemmas:
- What is death?
- Can we extend life?
- Whose life do we extend?
- At what price the extension of life?
- Just because we can extend life, should we?
And every one of these dilemmas is further complicated by another issue unique to transplantation. At stake in every transplant is not just the patient’s life, but three lives—the patient, the donor, and the person on the waiting list who likely died because the organ went to your patient, not her or him.
While we are not focusing today on organ donation or allocation, let us not forget that transplantation is unique in this regard. There are always three patients to consider.
What we will focus on today are transplant and post-transplant innovations. To help introduce the discussion, I would like to share a narrative that I believe illuminates ethical dilemmas that go hand-in-hand with transplantation’s innovations.
THE STORY OF MAX
Max was the tiny embodiment of a biological keystone cop. In utero he had developed a gaping defect of his abdominal wall. His intestines twisted around themselves, and the obstetricians had to deliver Max emergently. The pediatric surgeons immediately removed the gangrenous remnants of nearly his entire bowel.
At 10 months, Max received a liver and small bowel transplant. The transplanted organs worked initially; with a small feeding tube inserted directly into his gut, Max digested for the first time in his life tablespoons of food, albeit a chalky liquid supplement.
But Max, within 2 months of his transplant, had again become a permanent resident in the pediatric intensive care unit. Achieving the right balance of immunosuppression so Max could keep the transplanted organs and yet maintain sufficient immunity to fight off infection had become an impossible task.
I was in my fellowship at the time of Max’s transplant; and Eric, an attending surgeon with a square jaw and dark Dick Tracy looks, led the surgical team’s management of Max’s case.
As Max became sicker, Eric spent more hours with his tiny patient. I found him by Max’s bedside at 3:00 in the morning and then at 7:00 the next night, his hair, clothes, and personal aura in a state that reflected obliviousness to his own care. Just by being with Max so much, Eric knew all the particularities of that baby, all his idiosyncratic reactions, every significant lab result of Max’s entire life.
At first I found Eric’s dedication inspiring, almost thrilling in a martyred saint kind of way. And Max seemed to call out to any of us who hoped to be divinely touched. During rounds, Max giggled at me, as if he understood that playing with him was infinitely more interesting than arguing over doses of medication with other doctors. Spurred on by Max’s cause, I raced to uncover test results before Eric, as if my quicker response would translate into an equal or greater enthusiasm for Max’s plight. I nagged the radiology technicians to give me Max’s x-rays hot off the presses. I set the alarms on my beeper to see Max in the middle of the night and on mornings long before any member of the surgical team, particularly Eric, arrived.
Despite my enthusiastic attentions, Max became sicker. We gave Max higher doses of steroids, and his big, shiny black eyes turned into a pair of hyphens on the rolling swells of his face. His tiny body became engorged with fluid from repeated infections, and Max’s once buttery skin slowly became the ridiculously inadequate biological grounding for monitors and catheters. The nurses took to using the bed around him to clip wires and anchor dressings, and they hung mechanized pumps on tall IV poles which stood like skeletal beasts of burden crowded around Max’s bed.
Through all of Max’s crises, Eric never let up. But Max was going to die soon if we could not find the source of his infections. Eric finally decided to take Max to the operating room, worried about a hidden infection around his transplanted intestines. “We’ve got to take him back to the OR,” he said to us. Eric looked at us then asked rhetorically, “I mean, is there any other option?” We all understood what Eric was really asking. Were we doing enough? Was it our fault?
That trip to the OR would be the first of almost a dozen. Under searing heat lamps we snipped the sutures that held a plastic abdominal patch in place and uncovered the small cavity filled with congealed organs. We picked away at the block-like mass, terrified of inadvertently cutting a hole in his transplanted intestine and creating another source of infection. Then, finding nothing and too scared to cause any more damage, we whipstitched a piece of plastic back to the edge of Max’s abdominal wall. Over time, it became harder and harder to find untouched flesh where we could place a new stitch.
Over a month later Max died of a massive fungal infection. I mentioned his death to Jaimie, a pragmatic and brilliant head nurse who possessed more insight into our patients and hospital politics than most of the physicians.
“Maybe it was a good thing, huh?” Jaimie responded flatly. She walked out of the room and I could hear her asking aloud, “I mean, how much can you do to a person?”
THE EARLY TRANSPLANT ERA, DESPITE BLEAKER OUTCOMES, HAS LESSONS TO TEACH
I grew up, surgically speaking, at a time when transplant science fiction had become standard of care, when patients transplanted a decade or more earlier would routinely drop by clinic to say hello, and when patients on the brink of death could expect a full recovery.
But it was not always this way. And it took courageous individuals navigating the difficult relationship between innovation and ethics to get us here.
What is extraordinary about this panel is that these surgeons not only were at the forefront of transplantation’s history but also remain deeply involved in its future. Over the next hour roughly, they will give us an extraordinary look into the intersection of innovation and ethics in the past, present, and future of transplant surgery.
I hope you are eager as I am to hear what they have to share with us.
Transplant innovation and ethical challenges: What have we learned?
We have come far, but selecting organ recipients remains an ethical minefield
By Denton A. Cooley, MD
Only 40 years ago, on December 3, 1967, the world was electrified by news of the first cardiac transplantation, performed in Cape Town, South Africa, by the renowned Dr. Christiaan Barnard.
We have progressed considerably since that time, but not all issues have been settled. After several attempts by Dr. Norman Shumway and by Dr. Adrian Kantrowitz in this country, we in Houston performed the first successful cardiac transplantation in the United States in April 1968. Initially we were impressed with the results, and we embarked upon a very active cardiac transplant program, performing as many as had been done in total around the world. But after we had done some 15 or 20 cardiac transplants, the discouraging news began to emerge that the patients were not surviving long: our longest survived for only 2 years.
As a result, our group in Houston, like others, declared a moratorium on cardiac transplantation. The only group that continued throughout this era was at Stanford University under Shumway, who had some success with immunosuppressive drugs. In the early 1980s, a new immunosuppressant, cyclosporine, appeared that was used for kidney transplantation, which reinvigorated us and others to use this drug for cardiac transplantation. Since then, under the direction of my colleague, Dr. Bud Frazier, we have performed more than 1,000 cardiac transplantations at the Texas Heart Institute.
From the beginning, we were called upon to identify appropriate donors and suitable recipients. Although we rely on certain objective factors, such as age, weight, body size, gender, and blood type, many other issues must also be considered. Fortunately, the modern concept of brain death has now been accepted not only by the public and ethicists, but also by the legal community; in contrast, at one time it was considered homicidal to remove a beating heart. I credit Christiaan Barnard with having the courage to remove a beating heart from a 26-year-old donor who had suffered irreversible brain damage. Many of us had wanted to get into the transplant program but we could not identify a donor.
The following case illustrates some of the other ethical complexities that we continue to struggle with today.
CASE STUDY: A 17-YEAR-OLD WITH HEART FAILURE AND A DESTRUCTIVE LIFESTYLE
Several years ago, a 17-year-old Latin American boy came to our clinic in heart failure. He was very disarming, but when we looked into his background we found that he had dropped out of high school after 1 year and was living with a girlfriend who was 2 months pregnant by him and already had a 2-year-old child. The patient’s cardiomyopathy was related to cocaine and alcohol abuse. Nevertheless, his stepfather was eligible for Texas Medicaid, and he was accepted for cardiac transplantation.
After the transplantation, he abided by the immunosuppressive drug regimen while he was under our care. Then he moved to Fort Wayne, Indiana, where Indiana Medicaid would not honor his Texas Medicaid coverage. So our hospital had to send him his immunosuppressive drugs, which he used rather sporadically.
While in Indiana, he was incarcerated for assault and battery on his girlfriend. He began to have heart failure but did not qualify to have the biopsies required for proper study of rejection of his heart. He returned to our clinic and was scheduled for catheterization the next day when he went into acute cardiac failure. He had emergency late-night implantation of a percutaneous ventricular assist device, which required catheterizing the left atrium by perforating the interatrial septum, taking the oxygenated blood out of the left atrium, and pumping it back into the aorta with a centrifugal pump. His heart began to recover, and the device was removed after 72 hours.
At this point he needed another transplantation. Our medical review board considered his eligibility and turned him down, citing that others on our waiting list were more deserving of a transplant and that retransplantation has a poorer success rate than initial transplantation.
EACH CASE POSES PROBLEMS, BUT A RECORD OF SUCCESS EMERGES
Although this patient could be viewed as a sort of sociopath, he nevertheless is a young man who is incapacitated and in need of heroic measures. His case illustrates the kind of nonmedical problems that face those of us who are actively involved in cardiac transplantation. It can be very difficult to find solutions to the myriad social, economic, legal, and ethical issues.
We perform about 50 transplants a year in our institution, and every one of them has some issue. Nevertheless, we just honored 25 patients who have survived more than 20 years with cardiac transplantation.
Despite the odds, the transplant field has progressed rapidly
By John J. Fung, MD, PhD
Dr. Pauline Chen’s clinical vignette [see previous article in this supplement] unfortunately still typifies small bowel transplantation. One would not expect to hear that kind of story today for a kidney or liver transplant, but in the early 1970s it was typical.
‘WHY WOULD ANY YOUNG PHYSICIAN WANT TO GET INVOLVED IN THIS?’
Dr. Cooley’s comments about the moratorium on cardiac transplantation brought back memories for me, particularly from when I was studying liver transplantation in the 1970s. There was almost uniform mortality in transplants performed in the late 1960s and early ’70s. One wonders why any young physician would have wanted to get involved in transplantation at that time. I was a fellow training with Dr. Thomas Starzl at the University of Pittsburgh and remember him saying, “Just make it work, then let everybody else figure out why.” I think that typifies the surgical mentality.
We perform transplantations because we know that the alternative is prolonged morbidity and death. Knowing that we can provide a touch of hope is why we move forward in this field.
The technology of transplantation has developed through aggressive scientific developments in the laboratory. It is fascinating that all this has developed in only 50 years. If we had proceeded in a very stepwise manner, we probably would not be even a tenth as far along in the field as we are now.
Heart, lung, liver, and kidney transplantation are now all pretty routine. Intestinal transplantation is in the developing phase. The Cleveland Clinic is currently involved in facial transplantation, which has some different ethical issues related to identity.
Everything in transplantation relates to ethics, from issues about using marginal donor grafts or using beating-heart donors when someone has not been declared brain dead, to issues in patient selection, which often depends on social, economic (ie, insurance coverage), and psychosocial factors such as substance abuse and nonadherence issues.
ETHICAL INSIGHTS FROM TRANSPLANTS IN HIV-POSITIVE PATIENTS
An ethical area of particular interest to me that the Cleveland Clinic has also been involved with is transplanting patients who are HIV-positive. This has always been an enigma: why would we want to transplant an HIV-positive patient? Before the advent of antiviral therapies for HIV in the mid-1990s, mortality rates were very high, with patients suffering miserable deaths from Kaposi sarcoma, the JC virus leukoencephalopathies, and other debilitating opportunistic infections.
When I first arrived at the University of Pittsburgh as a fellow, Dr. Starzl was telling us about this mystery virus disease; when they retrospectively analyzed specimens from organ recipients and donors, they realized that HIV was being transmitted to patients from donors as well as from blood transfusions. The exposure to health care providers was also substantial: an average of 20 to 30 units of blood was used for a liver transplant.
Patients who were HIV-positive were excluded from transplants even through the mid-1990s. I remember evaluating standard listing criteria for transplant recipients at a conference and hearing transplant surgeons say that HIV is an absolute contraindication to transplant. I said, “Wait a minute, this is 1997; you cannot say that. Given that attitude, patients with HIV will never be transplanted.” The New England Journal of Medicine had just published a major paper about the extent of survival in patients being treated with highly active antiretroviral therapy.
So we then started a prospective study of transplantation in HIV-positive patients, and long-term follow-up has shown that these patients can do very well. Interestingly, transplantation offers a new approach to treating HIV-positive patients, in terms of immune reconstitution and the ability of immunosuppressive agents to restore immune competency by preventing the T-cell apoptosis initiated by HIV infection.
A continued need for evidence-based guidance
By James B. Young, MD
Speaking as the lone internist on this panel, and also as a clinical trialist and evidence-based clinical practitioner, the greatest ethical challenge I see for transplantation is how to move the field forward in terms of garnering evidence that can help us treat patients and keep them alive. Nobody will deny that heart transplantation is life-saving therapy: my patients with end-stage ischemic cardiomyopathy can be dramatically transformed by a heart transplant after being near death. The questions now are how best to gain the data to guide the next round of innovations in transplant medicine and how to know when the time is right to attempt those innovations.
A HISTORICAL GLANCE AT HEART TRANSPLANTATION
Dr. Sharon Hunt, who was one of the first heart transplant cardiologists and worked with Dr. Norman Shumway, almost singlehandedly moved the field of cardiac transplantation forward. She recently chronicled its history,1 and this sort of historical review yields a couple of insights. First, fewer heart transplants are being done in the United States in this decade than in the 1990s,2 in large part because other effective interventions for heart failure have been developed. However, the number of heart transplants is in fact on the rise again.2 Second, survival rates in heart transplant have improved substantially in recent years compared with earlier eras, as documented by registry data from the International Society for Heart and Lung Transplantation.3
Among other things, we have learned how to improve the operation, better choose and preserve hearts, and better match hearts to recipients. We now can use hearts from older donors and allow older patients to undergo transplantation. One of the keys to the better survival rates is a dramatic change in the use of medications. Cyclosporine allowed for successful heart transplantation in the 1980s, and we have since seen the advent of agents such as tacrolimus, rapamycin, and mycophenolate mofetil. We rely less on the early immunosuppressants, such as prednisone and azathioprine.
Despite these successes from a survival standpoint, problems still need to be addressed. For instance, at 5 years, virtually every patient following a heart transplant develops hypertension and dyslipidemia, 1 in 3 has renal dysfunction (some requiring dialysis or transplant), 1 in 3 has diabetes, and some develop a strange allograft arteriopathy.3
THE CHALLENGE OF EVALUATING A BOUTIQUE SCIENCE
Heart transplantation is a bit of a boutique science. Although relatively few heart transplants are performed compared with liver or kidney transplants, heart transplantation is a dramatic operation limited by many ethical challenges surrounding organ donor supply and utilization.
As for any boutique science, questions arise about how to evaluate it with the rigor of regulatory authority—from both the Food and Drug Administration (FDA) perspective and the institutional review board (IRB) perspective—without large clinical trials. Suppose that Dr. Cooley wants to make a minor modification in his immunosuppressive protocol because of an observation of a high incidence of renal failure at the 5-year point; does that ethically demand a large randomized clinical trial?
How can we design clinical trials to help determine which direction to take in immunosuppression intensification or utilization protocols? Other challenges include evaluating outcomes (such as coronary artery vasculopathy) from databases, and then figuring out good and bad practices. For example, databases show us that a donor history of diabetes increases the recipient’s long-term risk of developing coronary artery vasculopathy.3 Receiving a heart from a male donor also increases risk.3 Better understanding the panoply of adverse events and what leads to better outcomes will give us a sense of how to proceed and can drive the design of clinical trials.
OTHER ETHICAL CHALLENGES
From an ethical standpoint, how do we change practice? We have data on outcomes at 5, 10, and even 20 years. The half-life of a heart transplanted today is 12.5 years, whereas it used to be about 7 years.3 Although it is clear that we have made progress, it is a challenge to determine exactly how to make subtle changes in practice, such as addressing polypharmacy post-transplant.
Developing schemes that enable major innovation, particularly through coordination among medical and surgical teams, is another challenge. For example, we are working with preservation techniques that use a beating heart for transplantation. From solid evidence based on animal models, we believe this preparation can allow preservation of a heart for up to 12 hours. To some, that may beg a number of questions: Why do we need to do a clinical trial in humans? Why does the FDA need to regulate us? Why do we even need to answer to an IRB? Why not just make the change to alleviate the problem of donor organ supply?
What does—and does not—spur innovation?
By Thomas E. Starzl, MD, PhD
LESSONS FROM THE CODMAN ANALYSIS OF FAILURES
Dr. Ernest Codman was a Harvard Medical School professor in the early 20th century who tried to introduce a system of analyzing failures at Massachusetts General Hospital and other Harvard-affiliated hospitals. As a result, he was metaphorically ridden out of town on a rail.
Codman recommended that complications and failures be classified as one of the following:
- An error in diagnosis
- An error in judgment
- An error in technique (if a surgical or a medicalproblem)
- An error in management.
Only one escape hatch existed that did not indictthe surgical or medical team as culpable: the disease. At the time, nothing could be done for many diseases, including cancer, heart disease, renal failure, and bowel insufficiency.
This is a type of analysis that can be brought to a mortality and morbidity conference and will not accept a lot of alibis; it forces the group to always look at what could have been done to prevent a complication or death. Some practitioners always want to blame some factor other than themselves: sometimes the patient, by being deemed noncompliant, is even held responsible for his or her own complication or death.
I think the Codman analysis of failures is a good starting point for discussing innovations, especially since true breakthroughs come in those cases where the failure falls into the category of being caused by the disease itself, not by a medical or surgical error. And that is surely where transplantation falls.
PROGRESS DOES NOT ALWAYS REQUIRE FULL UNDERSTANDING
Transplantation was first successfully performed in the context of breaking through the donor-recipient genetic barrier on January 6, 1959, when Joseph Murray and his team at the the Brigham Hospital performed a kidney transplant using the patient’s fraternal twin as a donor. This event was reproduced in Paris by Jean Hamburger and his team on June 14, 1959, and then on three or four other occasions in the next several years in patients who received sublethal total body irradiation. This was at a time when no pharmacological immunosuppression was available, so no follow-up treatment was offered.
Astoundingly, the first case—the fraternal twin— lived for more than 20 years, and the French case for 25 years, without ever being treated with immunosuppression. They were inexplicably tolerant. When immunosuppressive drugs were developed and survival rates improved, the questions around these early cases were never answered: Why did those transplantations work? What were the mechanisms of engraftment? What was the relationship of engraftment to tolerance? Without answering those questions, there was no way to make other big leaps in improvement of what was already proved in principle—that is, the feasibility of actually doing this kind of treatment. Improvements in patient and graft survival were dependent almost entirely on better drugs.
RANDOMIZED TRIALS HAVE A DUBIOUS RECORD IN TRANSPLANTATION
I know this will offend just about everyone here, but I have no confidence in evidence-based therapy if we are talking about randomized trials. None of the great advances in transplantation has had anything to do with randomized trials. In my opinion, randomized trials in transplantation have done nothing but confuse the issue and have very nearly made it impossible for the better immunosuppressants to be brought on board. Cyclosporine offered a tremendous step forward, but the randomized trials, carried out mostly in Europe, did not reveal much difference in outcome from treatment with azathioprine, at least as assessed by patient and graft survival. The same thing occurred when tacrolimus emerged; randomized multicenter trials actually delayed the widespread use of this superior drug for at least half a dozen years.
IN THE BIG PICTURE, MONEY IS HOBBLING INNOVATION
Earlier it was debated whether money drives everything. I do not believe that money drives everything in medicine in Europe, and it certainly has little to do with driving improvements in Asia. But money does drive everything in the United States, although the real question is whether it has to be that way.
I believe that innovation is somehow built within our genome. Many of the great advances in transplantation, the elucidation of principles, and the relatively recent discovery of the mechanisms of alloengraftment were achieved without grant support. The researchers involved could not have asked for National Institutes of Health funding because their ideas were so far out of the box that they probably would have been rejected or stolen.
I wonder to what extent the vast amount of money available for research is actually a disincentive for genuine advancements. Part of the problem is that the power of allocation is put in the hands of anonymous peer-review committees. That system generates droves of people to pursue money allocated to a certain area to learn more and more about less and less, in the vague hope that acquiring enough details will result in a realistic concept. Sometimes the picture simply becomes more confused.
Another problem is that we have produced far more scientists than jobs, so that funding becomes the first priority because it is the only means of employment. In earlier days, what drove people more often was that they were confronted with a child who was dying and the central questions was, “How can I treat this patient?” They did laboratory research on their own to produce evidence that a new innovative idea could work. I believe that if you have experiments that show that you can keep a heart beating on a preservation device for 12 hours, and you can put it in a dog and it works well, that is the evidence you need to proceed. How are you going to do a randomized trial—hang on to an organ and let it beat for 12 hours just so it conforms with some protocol? That is nonsense.
There was a period when clinical journals—Surgery of Gynecology and Obstetrics, Annals of Surgery, Annals of Internal Medicine, New England Journal of Medicine, and others—published front-running discoveries. That ended about 25 years ago when it became more important to learn about details. The journals then became superfluous, and for another reason as well: money drove the wheel more and more. Hospital and program administrators expected the publications to be advertisements, and the minute that articles started promoting something rather than reporting facts, they lost value. Today the impact factors of the surgical journals are at about 2 or 3, meaning that their articles are cited infrequently and have little real influence on the practice of medicine.
How did we reach this point where money drives everything? I think the page was turned in the very early 1990s, and it had to do with how medical practice is governed, especially in academic hospitals. Half of the health care in this country is now provided by hospitals that are associated with medical schools. Those hospitals and basic research laboratories are where our young people will assimilate their ideals. If that climate is not right, then we are raising the wrong kind of doctors.
Earlier researchers looked at a problem and thought, “Here’s a question that has to do with this patient before my eyes, and I must find some way to solve it. Let’s go to the laboratory.” Today there is a real danger that they are thinking, “I need to advance my career, so let’s see how I can get some money. A little research will be a stepping stone to my professional development.” Our discussion of medical and surgical ethics today should take place within this framework.
Panel discussion
Moderated by Mark Siegler, MD
WERE FINANCES A DRIVER OF EARLY TRANSPLANT INNOVATION?
Dr. Mark Siegler: It is clear that there are more ethical and less ethical ways to introduce innovations. I am reminded of an article in JAMA by Francis Moore in the late 1980s in which he warned that one of the things to look at for any new innovation was the ethical climate of the institution.4 He cautioned us to be very aware of the driving force behind an innovation. Is it to improve patient care? To save lives that otherwise would be lost? Or is it primarily for the self-aggrandizement of an investigator or the financial goals of an institution?
I also remember the chapter in Dr. Starzl’s book The Puzzle People5 about the anguish involved in introducing liver transplantation. It seems that financial considerations were not the driver of major steps forward in introducing liver transplantation, in Dr. Starzl’s case, or heart transplantation, in Dr. Cooley’s case. Would you comment?
Dr. Thomas Starzl: Actually, not only were we not driven by economic gain, we expected fi nancial penalty for focusing on transplantation. If ever there was a field that developed against the grain, that was costly to people who worked in it, whose engagement meant that for most of their career they would work for substandard income compared with their peers—even those peers in academic medicine, let alone those in private practice—it would be transplantation.
It was not until 1973, when the end-stage renal disease (ESRD) program began under Medicare, that cash for transplantation started to become available. The real cash streams did not start until the middle to late 1980s when nonrenal organs became the cash cows. To be fair, no new technology can be assimilated into the health care system unless it at least pays for itself. But you can go beyond that and create baronial kingdoms, and I think that is where you can go wrong.
Dr. Denton Cooley: I would add that those of us privileged to spend our entire career in academic settings have an opportunity that others may not have. A lot of brilliant people in private practice are capable of doing many things but do not have an institution to represent and protect them. I have also always felt that those of us in these positions have an obligation to become innovators. Surgeons who merely see how many appendectomies or cholecystectomies they can perform are being very derelict of their responsibility to the institution.
MEASURING SUCCESS IN HEART TRANSPLANTATION
Dr. Siegler: Dr. Cooley, what is the current success rate for heart transplants?
Dr. Cooley: Nationwide, around 90% of recipients survive 12 months. Of those, maybe half are still alive 5 years later. Of course, we do not know what the future will hold. It is interesting that the fi rst sign of rejection seems to be coronary occlusive disease. It is a different type of coronary occlusive disease than is seen in atherosclerosis: it is diffuse, involving the entire extent of the coronary circulation, and is not really amenable to coronary bypass or other interventional procedures.
Dr. Siegler: We are now at about the 40th anniversary of the first human heart transplants, an extraordinary and historic innovation. Dr. Cooley, do you think the timing was right in 1968 when you did the fi rst heart transplant in the United States? In retrospect, would you have done the first transplant sooner or maybe even a couple of years later?
Dr. Cooley: You can argue it both ways. Should we have waited for further developments? At the time, heart transplantation seemed to work fairly well in animals, but we never really know until it reaches the clinical level. It was probably as opportune a time as any. We knew something about organ rejection at the time, and we had immunosuppressive drugs, although they were not as effective as they are today. The news electrified the world. I think we were pretty well prepared for this spectacular event.
Dr. Siegler: When would have been the optimal time to do a clinical trial in order to achieve evidence-based medicine in heart transplantation? Would it have been during the big breakthroughs of Shumway, Barnard, and Cooley, or now, when we have the general strategy and can find out how we can do better?
Dr. James Young: I would not have done a randomized trial at that time. The patients who were getting transplanted then were nearly dead; all other management was futile. In 1970, Life magazine listed the 102 heart transplants that had been done around the world up to that point, and maybe only 2 or 3 of the patients were still alive. That prompted the moratorium that Dr. Cooley referred to.
As ethical clinicians, we are supposed to do our best to make our patients feel better and make them live longer. Sometimes you have to do something radical. On that basis, one can argue that we should not transplant “the walking wounded,” that instead we should save organs for patients who are truly terminal without some sort of ventricular replacement therapy. But today we are getting away from transplanting only dying patients, so we need randomized trials to find out how we are doing in transplanting outpatients. That is the setting in which trials are now needed.
THE ETHICS OF ‘LETTING GO’
Question from audience: Dr. Chen’s story [see previous article] raised the issue of the ethics of “letting go” of one’s patient. I wonder if in transplantation, especially when innovative procedures are involved, a commitment to the procedure itself might sometimes conflict with the need to let go of the patient.
Dr. John Fung: In the United States, we measure efficacy and benefits in different ways than people do in other parts of the world. Here, for a child with a biliary atresia—the most common reason for liver transplantation—we expend hundreds of thousands of dollars for a liver transplant, which is usually able to save the child’s life. But in China, a severely ill child is viewed as a medical and economic liability and will be allowed to die so the family can have another child.
It is also not only the ethics of letting go. We all deal with letting go, not just in transplant medicine. It is also the ethics of actually getting a patient into the system. In the case of transplanting a newborn, as in Dr. Chen’s narrative, should they even have embarked on that?
Dr. Pauline Chen: For me, the story illustrates the remarkable connection and profound attachment between a surgeon and his or her patient. The fact that three patients are really involved in transplantation—the donor, the recipient, and the patient still on the waiting list because the organ went to the recipient instead—also motivates the team with a sense of obligation to the two unseen patients.
If there is a lesson about the ethics of letting go, I think it is that we often fail to talk about these issues among ourselves. Perhaps if we had discussed end-of-life care or palliative care in Max’s case, we might have had more insight into the pressures we felt in considering the lives of three separate people. And those discussions might have—or might not have— changed the situation.
Dr. Starzl: I agree completely with the preceding comments. All kinds of motivations might cause a surgeon to cling too long—the ones that were mentioned as well as some ignoble ones, such as vanity, in terms of looking at one’s survival numbers.
I would also like to take a much larger view. Some years ago in Colorado, the governor at the time, Richard Lamm, thought that intensive care units (ICUs) were harmful—that they were economically draining, did not serve society, and prolonged suffering. My position, which was really the opposite, was that maybe he was right in his philosophy but transplantation had, in a sense, changed all that. Transplantation took desperate people who were in the ICU, with no chance of coming out, and dramatically returned them to wonderful health.
As procedures get better, this scenario happens more and more often. I agree that there is a time when you realize that no intervention will work and you should stop treatment. That is a bitter pill. But it is very hard to define when that moment occurs.
Dr. Chen: There also may be somewhat of a generational difference in approach.
Most surgeons will fully acknowledge that they stand on the shoulders of giants, and that holds particularly true in a field like transplantation. When I was training in liver transplantation, for example, 80% to 90% of the patients could fully expect to survive 5 years. For my vintage of surgeons, then, death and failure were rarities and they were truly a sort of enemy, whereas surgeons like Dr. Starzl and Dr. Cooley have seen so much more and are far more used to all the variations of outcomes. Because of that breadth of experience that you have, I think you are wiser than my generation of surgeons, for whom death often has to be ablated at all costs. I think it follows, then, that you would also have a better sense of when to stop.
Dr. Starzl: There is a generational change—there is no doubt about it.
IS TRANSPLANT ETHICAL WHEN A LIFE IS NOT AT STAKE?
Question from audience: What are the ethical implications of non-lifesaving transplants, specifically of the hand and face?
Dr. Young: I have been on many peer-review committees charged with looking at this issue. Although the ethics can be very troubling, I have resolved important questions in my mind by examining them through the context of human suffering. Our mission as physicians and caregivers is to relieve suffering, which can take the form of pain, a shortened lifespan, or even a debilitating disfigurement of the face or a severe limitation, such as after traumatic amputation. Looking at the issue this way, I am less troubled than I was initially, when I viewed these kinds of transplantations as simply altering physical appearance or extending ability.
Dr. Starzl: The next big movement in transplantation is going to be in composite tissue allotransplantation—that is, transplantation of the face, limbs, etc. Mechanisms of alloengraftment have recently been uncovered such that it is now possible to formulate protocols that use either very light immunosuppression (avoiding the 20% or 25% rate of renal failure at 5 years that we heard about from Dr. Young) or no immunosuppression at all.6 Without the heavy burden of immunosuppression, this type of transplantation can become worthwhile. Putting a new hand or face on someone is astounding: it changes the morphology of the brain, which can be observed with functional magnetic resonance imaging. It changes the soul, if that is what you want to think of when talking about the brain. I think it will be very important.
Dr. Siegler: This extraordinary panel has not only discussed events from 50 years ago; each of the panelists spoke of a future that is rich in promise and innovation—and in ethical issues. It reminds me of a remarkable letter written in 1794 by Thomas Jefferson to John Adams, which says, “We should never return to earlier times when all scientific progress was proscribed as innovation.” More than 200 years later, Jefferson’s insight remains modern and relevant.
- Hunt SA. Taking heart—cardiac transplantation past, present, and future. N Engl J Med 2006; 355:231–235.
- Heart and Lung Transplantation in the United States, 1997-2006(Chapter VI). In: 2007 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Data 1997-2006. Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Rockville, MD. Available at: http://www.ustransplant.org/annual_reports/current. Accessed July 22, 2008.
- Taylor DO, Edwards LB, Boucek MM, et al. Registry of the International Society for Heart and Lung Transplantation: twenty-second official adult heart transplant report—2005. J Heart Lung Transplant 2005; 24:945–955.
- Moore FD. The desperate case: CARE (costs, applicability, research, ethics). JAMA 1989; 261:1483–1484.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon.Pittsburgh, PA: University of Pittsburgh Press; 1992.
- Starzl TE. Immunosuppressive therapy and tolerance of organ allografts. N Engl J Med 2008; 358:407–411.
We have come far, but selecting organ recipients remains an ethical minefield
By Denton A. Cooley, MD
Only 40 years ago, on December 3, 1967, the world was electrified by news of the first cardiac transplantation, performed in Cape Town, South Africa, by the renowned Dr. Christiaan Barnard.
We have progressed considerably since that time, but not all issues have been settled. After several attempts by Dr. Norman Shumway and by Dr. Adrian Kantrowitz in this country, we in Houston performed the first successful cardiac transplantation in the United States in April 1968. Initially we were impressed with the results, and we embarked upon a very active cardiac transplant program, performing as many as had been done in total around the world. But after we had done some 15 or 20 cardiac transplants, the discouraging news began to emerge that the patients were not surviving long: our longest survived for only 2 years.
As a result, our group in Houston, like others, declared a moratorium on cardiac transplantation. The only group that continued throughout this era was at Stanford University under Shumway, who had some success with immunosuppressive drugs. In the early 1980s, a new immunosuppressant, cyclosporine, appeared that was used for kidney transplantation, which reinvigorated us and others to use this drug for cardiac transplantation. Since then, under the direction of my colleague, Dr. Bud Frazier, we have performed more than 1,000 cardiac transplantations at the Texas Heart Institute.
From the beginning, we were called upon to identify appropriate donors and suitable recipients. Although we rely on certain objective factors, such as age, weight, body size, gender, and blood type, many other issues must also be considered. Fortunately, the modern concept of brain death has now been accepted not only by the public and ethicists, but also by the legal community; in contrast, at one time it was considered homicidal to remove a beating heart. I credit Christiaan Barnard with having the courage to remove a beating heart from a 26-year-old donor who had suffered irreversible brain damage. Many of us had wanted to get into the transplant program but we could not identify a donor.
The following case illustrates some of the other ethical complexities that we continue to struggle with today.
CASE STUDY: A 17-YEAR-OLD WITH HEART FAILURE AND A DESTRUCTIVE LIFESTYLE
Several years ago, a 17-year-old Latin American boy came to our clinic in heart failure. He was very disarming, but when we looked into his background we found that he had dropped out of high school after 1 year and was living with a girlfriend who was 2 months pregnant by him and already had a 2-year-old child. The patient’s cardiomyopathy was related to cocaine and alcohol abuse. Nevertheless, his stepfather was eligible for Texas Medicaid, and he was accepted for cardiac transplantation.
After the transplantation, he abided by the immunosuppressive drug regimen while he was under our care. Then he moved to Fort Wayne, Indiana, where Indiana Medicaid would not honor his Texas Medicaid coverage. So our hospital had to send him his immunosuppressive drugs, which he used rather sporadically.
While in Indiana, he was incarcerated for assault and battery on his girlfriend. He began to have heart failure but did not qualify to have the biopsies required for proper study of rejection of his heart. He returned to our clinic and was scheduled for catheterization the next day when he went into acute cardiac failure. He had emergency late-night implantation of a percutaneous ventricular assist device, which required catheterizing the left atrium by perforating the interatrial septum, taking the oxygenated blood out of the left atrium, and pumping it back into the aorta with a centrifugal pump. His heart began to recover, and the device was removed after 72 hours.
At this point he needed another transplantation. Our medical review board considered his eligibility and turned him down, citing that others on our waiting list were more deserving of a transplant and that retransplantation has a poorer success rate than initial transplantation.
EACH CASE POSES PROBLEMS, BUT A RECORD OF SUCCESS EMERGES
Although this patient could be viewed as a sort of sociopath, he nevertheless is a young man who is incapacitated and in need of heroic measures. His case illustrates the kind of nonmedical problems that face those of us who are actively involved in cardiac transplantation. It can be very difficult to find solutions to the myriad social, economic, legal, and ethical issues.
We perform about 50 transplants a year in our institution, and every one of them has some issue. Nevertheless, we just honored 25 patients who have survived more than 20 years with cardiac transplantation.
Despite the odds, the transplant field has progressed rapidly
By John J. Fung, MD, PhD
Dr. Pauline Chen’s clinical vignette [see previous article in this supplement] unfortunately still typifies small bowel transplantation. One would not expect to hear that kind of story today for a kidney or liver transplant, but in the early 1970s it was typical.
‘WHY WOULD ANY YOUNG PHYSICIAN WANT TO GET INVOLVED IN THIS?’
Dr. Cooley’s comments about the moratorium on cardiac transplantation brought back memories for me, particularly from when I was studying liver transplantation in the 1970s. There was almost uniform mortality in transplants performed in the late 1960s and early ’70s. One wonders why any young physician would have wanted to get involved in transplantation at that time. I was a fellow training with Dr. Thomas Starzl at the University of Pittsburgh and remember him saying, “Just make it work, then let everybody else figure out why.” I think that typifies the surgical mentality.
We perform transplantations because we know that the alternative is prolonged morbidity and death. Knowing that we can provide a touch of hope is why we move forward in this field.
The technology of transplantation has developed through aggressive scientific developments in the laboratory. It is fascinating that all this has developed in only 50 years. If we had proceeded in a very stepwise manner, we probably would not be even a tenth as far along in the field as we are now.
Heart, lung, liver, and kidney transplantation are now all pretty routine. Intestinal transplantation is in the developing phase. The Cleveland Clinic is currently involved in facial transplantation, which has some different ethical issues related to identity.
Everything in transplantation relates to ethics, from issues about using marginal donor grafts or using beating-heart donors when someone has not been declared brain dead, to issues in patient selection, which often depends on social, economic (ie, insurance coverage), and psychosocial factors such as substance abuse and nonadherence issues.
ETHICAL INSIGHTS FROM TRANSPLANTS IN HIV-POSITIVE PATIENTS
An ethical area of particular interest to me that the Cleveland Clinic has also been involved with is transplanting patients who are HIV-positive. This has always been an enigma: why would we want to transplant an HIV-positive patient? Before the advent of antiviral therapies for HIV in the mid-1990s, mortality rates were very high, with patients suffering miserable deaths from Kaposi sarcoma, the JC virus leukoencephalopathies, and other debilitating opportunistic infections.
When I first arrived at the University of Pittsburgh as a fellow, Dr. Starzl was telling us about this mystery virus disease; when they retrospectively analyzed specimens from organ recipients and donors, they realized that HIV was being transmitted to patients from donors as well as from blood transfusions. The exposure to health care providers was also substantial: an average of 20 to 30 units of blood was used for a liver transplant.
Patients who were HIV-positive were excluded from transplants even through the mid-1990s. I remember evaluating standard listing criteria for transplant recipients at a conference and hearing transplant surgeons say that HIV is an absolute contraindication to transplant. I said, “Wait a minute, this is 1997; you cannot say that. Given that attitude, patients with HIV will never be transplanted.” The New England Journal of Medicine had just published a major paper about the extent of survival in patients being treated with highly active antiretroviral therapy.
So we then started a prospective study of transplantation in HIV-positive patients, and long-term follow-up has shown that these patients can do very well. Interestingly, transplantation offers a new approach to treating HIV-positive patients, in terms of immune reconstitution and the ability of immunosuppressive agents to restore immune competency by preventing the T-cell apoptosis initiated by HIV infection.
A continued need for evidence-based guidance
By James B. Young, MD
Speaking as the lone internist on this panel, and also as a clinical trialist and evidence-based clinical practitioner, the greatest ethical challenge I see for transplantation is how to move the field forward in terms of garnering evidence that can help us treat patients and keep them alive. Nobody will deny that heart transplantation is life-saving therapy: my patients with end-stage ischemic cardiomyopathy can be dramatically transformed by a heart transplant after being near death. The questions now are how best to gain the data to guide the next round of innovations in transplant medicine and how to know when the time is right to attempt those innovations.
A HISTORICAL GLANCE AT HEART TRANSPLANTATION
Dr. Sharon Hunt, who was one of the first heart transplant cardiologists and worked with Dr. Norman Shumway, almost singlehandedly moved the field of cardiac transplantation forward. She recently chronicled its history,1 and this sort of historical review yields a couple of insights. First, fewer heart transplants are being done in the United States in this decade than in the 1990s,2 in large part because other effective interventions for heart failure have been developed. However, the number of heart transplants is in fact on the rise again.2 Second, survival rates in heart transplant have improved substantially in recent years compared with earlier eras, as documented by registry data from the International Society for Heart and Lung Transplantation.3
Among other things, we have learned how to improve the operation, better choose and preserve hearts, and better match hearts to recipients. We now can use hearts from older donors and allow older patients to undergo transplantation. One of the keys to the better survival rates is a dramatic change in the use of medications. Cyclosporine allowed for successful heart transplantation in the 1980s, and we have since seen the advent of agents such as tacrolimus, rapamycin, and mycophenolate mofetil. We rely less on the early immunosuppressants, such as prednisone and azathioprine.
Despite these successes from a survival standpoint, problems still need to be addressed. For instance, at 5 years, virtually every patient following a heart transplant develops hypertension and dyslipidemia, 1 in 3 has renal dysfunction (some requiring dialysis or transplant), 1 in 3 has diabetes, and some develop a strange allograft arteriopathy.3
THE CHALLENGE OF EVALUATING A BOUTIQUE SCIENCE
Heart transplantation is a bit of a boutique science. Although relatively few heart transplants are performed compared with liver or kidney transplants, heart transplantation is a dramatic operation limited by many ethical challenges surrounding organ donor supply and utilization.
As for any boutique science, questions arise about how to evaluate it with the rigor of regulatory authority—from both the Food and Drug Administration (FDA) perspective and the institutional review board (IRB) perspective—without large clinical trials. Suppose that Dr. Cooley wants to make a minor modification in his immunosuppressive protocol because of an observation of a high incidence of renal failure at the 5-year point; does that ethically demand a large randomized clinical trial?
How can we design clinical trials to help determine which direction to take in immunosuppression intensification or utilization protocols? Other challenges include evaluating outcomes (such as coronary artery vasculopathy) from databases, and then figuring out good and bad practices. For example, databases show us that a donor history of diabetes increases the recipient’s long-term risk of developing coronary artery vasculopathy.3 Receiving a heart from a male donor also increases risk.3 Better understanding the panoply of adverse events and what leads to better outcomes will give us a sense of how to proceed and can drive the design of clinical trials.
OTHER ETHICAL CHALLENGES
From an ethical standpoint, how do we change practice? We have data on outcomes at 5, 10, and even 20 years. The half-life of a heart transplanted today is 12.5 years, whereas it used to be about 7 years.3 Although it is clear that we have made progress, it is a challenge to determine exactly how to make subtle changes in practice, such as addressing polypharmacy post-transplant.
Developing schemes that enable major innovation, particularly through coordination among medical and surgical teams, is another challenge. For example, we are working with preservation techniques that use a beating heart for transplantation. From solid evidence based on animal models, we believe this preparation can allow preservation of a heart for up to 12 hours. To some, that may beg a number of questions: Why do we need to do a clinical trial in humans? Why does the FDA need to regulate us? Why do we even need to answer to an IRB? Why not just make the change to alleviate the problem of donor organ supply?
What does—and does not—spur innovation?
By Thomas E. Starzl, MD, PhD
LESSONS FROM THE CODMAN ANALYSIS OF FAILURES
Dr. Ernest Codman was a Harvard Medical School professor in the early 20th century who tried to introduce a system of analyzing failures at Massachusetts General Hospital and other Harvard-affiliated hospitals. As a result, he was metaphorically ridden out of town on a rail.
Codman recommended that complications and failures be classified as one of the following:
- An error in diagnosis
- An error in judgment
- An error in technique (if a surgical or a medicalproblem)
- An error in management.
Only one escape hatch existed that did not indictthe surgical or medical team as culpable: the disease. At the time, nothing could be done for many diseases, including cancer, heart disease, renal failure, and bowel insufficiency.
This is a type of analysis that can be brought to a mortality and morbidity conference and will not accept a lot of alibis; it forces the group to always look at what could have been done to prevent a complication or death. Some practitioners always want to blame some factor other than themselves: sometimes the patient, by being deemed noncompliant, is even held responsible for his or her own complication or death.
I think the Codman analysis of failures is a good starting point for discussing innovations, especially since true breakthroughs come in those cases where the failure falls into the category of being caused by the disease itself, not by a medical or surgical error. And that is surely where transplantation falls.
PROGRESS DOES NOT ALWAYS REQUIRE FULL UNDERSTANDING
Transplantation was first successfully performed in the context of breaking through the donor-recipient genetic barrier on January 6, 1959, when Joseph Murray and his team at the the Brigham Hospital performed a kidney transplant using the patient’s fraternal twin as a donor. This event was reproduced in Paris by Jean Hamburger and his team on June 14, 1959, and then on three or four other occasions in the next several years in patients who received sublethal total body irradiation. This was at a time when no pharmacological immunosuppression was available, so no follow-up treatment was offered.
Astoundingly, the first case—the fraternal twin— lived for more than 20 years, and the French case for 25 years, without ever being treated with immunosuppression. They were inexplicably tolerant. When immunosuppressive drugs were developed and survival rates improved, the questions around these early cases were never answered: Why did those transplantations work? What were the mechanisms of engraftment? What was the relationship of engraftment to tolerance? Without answering those questions, there was no way to make other big leaps in improvement of what was already proved in principle—that is, the feasibility of actually doing this kind of treatment. Improvements in patient and graft survival were dependent almost entirely on better drugs.
RANDOMIZED TRIALS HAVE A DUBIOUS RECORD IN TRANSPLANTATION
I know this will offend just about everyone here, but I have no confidence in evidence-based therapy if we are talking about randomized trials. None of the great advances in transplantation has had anything to do with randomized trials. In my opinion, randomized trials in transplantation have done nothing but confuse the issue and have very nearly made it impossible for the better immunosuppressants to be brought on board. Cyclosporine offered a tremendous step forward, but the randomized trials, carried out mostly in Europe, did not reveal much difference in outcome from treatment with azathioprine, at least as assessed by patient and graft survival. The same thing occurred when tacrolimus emerged; randomized multicenter trials actually delayed the widespread use of this superior drug for at least half a dozen years.
IN THE BIG PICTURE, MONEY IS HOBBLING INNOVATION
Earlier it was debated whether money drives everything. I do not believe that money drives everything in medicine in Europe, and it certainly has little to do with driving improvements in Asia. But money does drive everything in the United States, although the real question is whether it has to be that way.
I believe that innovation is somehow built within our genome. Many of the great advances in transplantation, the elucidation of principles, and the relatively recent discovery of the mechanisms of alloengraftment were achieved without grant support. The researchers involved could not have asked for National Institutes of Health funding because their ideas were so far out of the box that they probably would have been rejected or stolen.
I wonder to what extent the vast amount of money available for research is actually a disincentive for genuine advancements. Part of the problem is that the power of allocation is put in the hands of anonymous peer-review committees. That system generates droves of people to pursue money allocated to a certain area to learn more and more about less and less, in the vague hope that acquiring enough details will result in a realistic concept. Sometimes the picture simply becomes more confused.
Another problem is that we have produced far more scientists than jobs, so that funding becomes the first priority because it is the only means of employment. In earlier days, what drove people more often was that they were confronted with a child who was dying and the central questions was, “How can I treat this patient?” They did laboratory research on their own to produce evidence that a new innovative idea could work. I believe that if you have experiments that show that you can keep a heart beating on a preservation device for 12 hours, and you can put it in a dog and it works well, that is the evidence you need to proceed. How are you going to do a randomized trial—hang on to an organ and let it beat for 12 hours just so it conforms with some protocol? That is nonsense.
There was a period when clinical journals—Surgery of Gynecology and Obstetrics, Annals of Surgery, Annals of Internal Medicine, New England Journal of Medicine, and others—published front-running discoveries. That ended about 25 years ago when it became more important to learn about details. The journals then became superfluous, and for another reason as well: money drove the wheel more and more. Hospital and program administrators expected the publications to be advertisements, and the minute that articles started promoting something rather than reporting facts, they lost value. Today the impact factors of the surgical journals are at about 2 or 3, meaning that their articles are cited infrequently and have little real influence on the practice of medicine.
How did we reach this point where money drives everything? I think the page was turned in the very early 1990s, and it had to do with how medical practice is governed, especially in academic hospitals. Half of the health care in this country is now provided by hospitals that are associated with medical schools. Those hospitals and basic research laboratories are where our young people will assimilate their ideals. If that climate is not right, then we are raising the wrong kind of doctors.
Earlier researchers looked at a problem and thought, “Here’s a question that has to do with this patient before my eyes, and I must find some way to solve it. Let’s go to the laboratory.” Today there is a real danger that they are thinking, “I need to advance my career, so let’s see how I can get some money. A little research will be a stepping stone to my professional development.” Our discussion of medical and surgical ethics today should take place within this framework.
Panel discussion
Moderated by Mark Siegler, MD
WERE FINANCES A DRIVER OF EARLY TRANSPLANT INNOVATION?
Dr. Mark Siegler: It is clear that there are more ethical and less ethical ways to introduce innovations. I am reminded of an article in JAMA by Francis Moore in the late 1980s in which he warned that one of the things to look at for any new innovation was the ethical climate of the institution.4 He cautioned us to be very aware of the driving force behind an innovation. Is it to improve patient care? To save lives that otherwise would be lost? Or is it primarily for the self-aggrandizement of an investigator or the financial goals of an institution?
I also remember the chapter in Dr. Starzl’s book The Puzzle People5 about the anguish involved in introducing liver transplantation. It seems that financial considerations were not the driver of major steps forward in introducing liver transplantation, in Dr. Starzl’s case, or heart transplantation, in Dr. Cooley’s case. Would you comment?
Dr. Thomas Starzl: Actually, not only were we not driven by economic gain, we expected fi nancial penalty for focusing on transplantation. If ever there was a field that developed against the grain, that was costly to people who worked in it, whose engagement meant that for most of their career they would work for substandard income compared with their peers—even those peers in academic medicine, let alone those in private practice—it would be transplantation.
It was not until 1973, when the end-stage renal disease (ESRD) program began under Medicare, that cash for transplantation started to become available. The real cash streams did not start until the middle to late 1980s when nonrenal organs became the cash cows. To be fair, no new technology can be assimilated into the health care system unless it at least pays for itself. But you can go beyond that and create baronial kingdoms, and I think that is where you can go wrong.
Dr. Denton Cooley: I would add that those of us privileged to spend our entire career in academic settings have an opportunity that others may not have. A lot of brilliant people in private practice are capable of doing many things but do not have an institution to represent and protect them. I have also always felt that those of us in these positions have an obligation to become innovators. Surgeons who merely see how many appendectomies or cholecystectomies they can perform are being very derelict of their responsibility to the institution.
MEASURING SUCCESS IN HEART TRANSPLANTATION
Dr. Siegler: Dr. Cooley, what is the current success rate for heart transplants?
Dr. Cooley: Nationwide, around 90% of recipients survive 12 months. Of those, maybe half are still alive 5 years later. Of course, we do not know what the future will hold. It is interesting that the fi rst sign of rejection seems to be coronary occlusive disease. It is a different type of coronary occlusive disease than is seen in atherosclerosis: it is diffuse, involving the entire extent of the coronary circulation, and is not really amenable to coronary bypass or other interventional procedures.
Dr. Siegler: We are now at about the 40th anniversary of the first human heart transplants, an extraordinary and historic innovation. Dr. Cooley, do you think the timing was right in 1968 when you did the fi rst heart transplant in the United States? In retrospect, would you have done the first transplant sooner or maybe even a couple of years later?
Dr. Cooley: You can argue it both ways. Should we have waited for further developments? At the time, heart transplantation seemed to work fairly well in animals, but we never really know until it reaches the clinical level. It was probably as opportune a time as any. We knew something about organ rejection at the time, and we had immunosuppressive drugs, although they were not as effective as they are today. The news electrified the world. I think we were pretty well prepared for this spectacular event.
Dr. Siegler: When would have been the optimal time to do a clinical trial in order to achieve evidence-based medicine in heart transplantation? Would it have been during the big breakthroughs of Shumway, Barnard, and Cooley, or now, when we have the general strategy and can find out how we can do better?
Dr. James Young: I would not have done a randomized trial at that time. The patients who were getting transplanted then were nearly dead; all other management was futile. In 1970, Life magazine listed the 102 heart transplants that had been done around the world up to that point, and maybe only 2 or 3 of the patients were still alive. That prompted the moratorium that Dr. Cooley referred to.
As ethical clinicians, we are supposed to do our best to make our patients feel better and make them live longer. Sometimes you have to do something radical. On that basis, one can argue that we should not transplant “the walking wounded,” that instead we should save organs for patients who are truly terminal without some sort of ventricular replacement therapy. But today we are getting away from transplanting only dying patients, so we need randomized trials to find out how we are doing in transplanting outpatients. That is the setting in which trials are now needed.
THE ETHICS OF ‘LETTING GO’
Question from audience: Dr. Chen’s story [see previous article] raised the issue of the ethics of “letting go” of one’s patient. I wonder if in transplantation, especially when innovative procedures are involved, a commitment to the procedure itself might sometimes conflict with the need to let go of the patient.
Dr. John Fung: In the United States, we measure efficacy and benefits in different ways than people do in other parts of the world. Here, for a child with a biliary atresia—the most common reason for liver transplantation—we expend hundreds of thousands of dollars for a liver transplant, which is usually able to save the child’s life. But in China, a severely ill child is viewed as a medical and economic liability and will be allowed to die so the family can have another child.
It is also not only the ethics of letting go. We all deal with letting go, not just in transplant medicine. It is also the ethics of actually getting a patient into the system. In the case of transplanting a newborn, as in Dr. Chen’s narrative, should they even have embarked on that?
Dr. Pauline Chen: For me, the story illustrates the remarkable connection and profound attachment between a surgeon and his or her patient. The fact that three patients are really involved in transplantation—the donor, the recipient, and the patient still on the waiting list because the organ went to the recipient instead—also motivates the team with a sense of obligation to the two unseen patients.
If there is a lesson about the ethics of letting go, I think it is that we often fail to talk about these issues among ourselves. Perhaps if we had discussed end-of-life care or palliative care in Max’s case, we might have had more insight into the pressures we felt in considering the lives of three separate people. And those discussions might have—or might not have— changed the situation.
Dr. Starzl: I agree completely with the preceding comments. All kinds of motivations might cause a surgeon to cling too long—the ones that were mentioned as well as some ignoble ones, such as vanity, in terms of looking at one’s survival numbers.
I would also like to take a much larger view. Some years ago in Colorado, the governor at the time, Richard Lamm, thought that intensive care units (ICUs) were harmful—that they were economically draining, did not serve society, and prolonged suffering. My position, which was really the opposite, was that maybe he was right in his philosophy but transplantation had, in a sense, changed all that. Transplantation took desperate people who were in the ICU, with no chance of coming out, and dramatically returned them to wonderful health.
As procedures get better, this scenario happens more and more often. I agree that there is a time when you realize that no intervention will work and you should stop treatment. That is a bitter pill. But it is very hard to define when that moment occurs.
Dr. Chen: There also may be somewhat of a generational difference in approach.
Most surgeons will fully acknowledge that they stand on the shoulders of giants, and that holds particularly true in a field like transplantation. When I was training in liver transplantation, for example, 80% to 90% of the patients could fully expect to survive 5 years. For my vintage of surgeons, then, death and failure were rarities and they were truly a sort of enemy, whereas surgeons like Dr. Starzl and Dr. Cooley have seen so much more and are far more used to all the variations of outcomes. Because of that breadth of experience that you have, I think you are wiser than my generation of surgeons, for whom death often has to be ablated at all costs. I think it follows, then, that you would also have a better sense of when to stop.
Dr. Starzl: There is a generational change—there is no doubt about it.
IS TRANSPLANT ETHICAL WHEN A LIFE IS NOT AT STAKE?
Question from audience: What are the ethical implications of non-lifesaving transplants, specifically of the hand and face?
Dr. Young: I have been on many peer-review committees charged with looking at this issue. Although the ethics can be very troubling, I have resolved important questions in my mind by examining them through the context of human suffering. Our mission as physicians and caregivers is to relieve suffering, which can take the form of pain, a shortened lifespan, or even a debilitating disfigurement of the face or a severe limitation, such as after traumatic amputation. Looking at the issue this way, I am less troubled than I was initially, when I viewed these kinds of transplantations as simply altering physical appearance or extending ability.
Dr. Starzl: The next big movement in transplantation is going to be in composite tissue allotransplantation—that is, transplantation of the face, limbs, etc. Mechanisms of alloengraftment have recently been uncovered such that it is now possible to formulate protocols that use either very light immunosuppression (avoiding the 20% or 25% rate of renal failure at 5 years that we heard about from Dr. Young) or no immunosuppression at all.6 Without the heavy burden of immunosuppression, this type of transplantation can become worthwhile. Putting a new hand or face on someone is astounding: it changes the morphology of the brain, which can be observed with functional magnetic resonance imaging. It changes the soul, if that is what you want to think of when talking about the brain. I think it will be very important.
Dr. Siegler: This extraordinary panel has not only discussed events from 50 years ago; each of the panelists spoke of a future that is rich in promise and innovation—and in ethical issues. It reminds me of a remarkable letter written in 1794 by Thomas Jefferson to John Adams, which says, “We should never return to earlier times when all scientific progress was proscribed as innovation.” More than 200 years later, Jefferson’s insight remains modern and relevant.
We have come far, but selecting organ recipients remains an ethical minefield
By Denton A. Cooley, MD
Only 40 years ago, on December 3, 1967, the world was electrified by news of the first cardiac transplantation, performed in Cape Town, South Africa, by the renowned Dr. Christiaan Barnard.
We have progressed considerably since that time, but not all issues have been settled. After several attempts by Dr. Norman Shumway and by Dr. Adrian Kantrowitz in this country, we in Houston performed the first successful cardiac transplantation in the United States in April 1968. Initially we were impressed with the results, and we embarked upon a very active cardiac transplant program, performing as many as had been done in total around the world. But after we had done some 15 or 20 cardiac transplants, the discouraging news began to emerge that the patients were not surviving long: our longest survived for only 2 years.
As a result, our group in Houston, like others, declared a moratorium on cardiac transplantation. The only group that continued throughout this era was at Stanford University under Shumway, who had some success with immunosuppressive drugs. In the early 1980s, a new immunosuppressant, cyclosporine, appeared that was used for kidney transplantation, which reinvigorated us and others to use this drug for cardiac transplantation. Since then, under the direction of my colleague, Dr. Bud Frazier, we have performed more than 1,000 cardiac transplantations at the Texas Heart Institute.
From the beginning, we were called upon to identify appropriate donors and suitable recipients. Although we rely on certain objective factors, such as age, weight, body size, gender, and blood type, many other issues must also be considered. Fortunately, the modern concept of brain death has now been accepted not only by the public and ethicists, but also by the legal community; in contrast, at one time it was considered homicidal to remove a beating heart. I credit Christiaan Barnard with having the courage to remove a beating heart from a 26-year-old donor who had suffered irreversible brain damage. Many of us had wanted to get into the transplant program but we could not identify a donor.
The following case illustrates some of the other ethical complexities that we continue to struggle with today.
CASE STUDY: A 17-YEAR-OLD WITH HEART FAILURE AND A DESTRUCTIVE LIFESTYLE
Several years ago, a 17-year-old Latin American boy came to our clinic in heart failure. He was very disarming, but when we looked into his background we found that he had dropped out of high school after 1 year and was living with a girlfriend who was 2 months pregnant by him and already had a 2-year-old child. The patient’s cardiomyopathy was related to cocaine and alcohol abuse. Nevertheless, his stepfather was eligible for Texas Medicaid, and he was accepted for cardiac transplantation.
After the transplantation, he abided by the immunosuppressive drug regimen while he was under our care. Then he moved to Fort Wayne, Indiana, where Indiana Medicaid would not honor his Texas Medicaid coverage. So our hospital had to send him his immunosuppressive drugs, which he used rather sporadically.
While in Indiana, he was incarcerated for assault and battery on his girlfriend. He began to have heart failure but did not qualify to have the biopsies required for proper study of rejection of his heart. He returned to our clinic and was scheduled for catheterization the next day when he went into acute cardiac failure. He had emergency late-night implantation of a percutaneous ventricular assist device, which required catheterizing the left atrium by perforating the interatrial septum, taking the oxygenated blood out of the left atrium, and pumping it back into the aorta with a centrifugal pump. His heart began to recover, and the device was removed after 72 hours.
At this point he needed another transplantation. Our medical review board considered his eligibility and turned him down, citing that others on our waiting list were more deserving of a transplant and that retransplantation has a poorer success rate than initial transplantation.
EACH CASE POSES PROBLEMS, BUT A RECORD OF SUCCESS EMERGES
Although this patient could be viewed as a sort of sociopath, he nevertheless is a young man who is incapacitated and in need of heroic measures. His case illustrates the kind of nonmedical problems that face those of us who are actively involved in cardiac transplantation. It can be very difficult to find solutions to the myriad social, economic, legal, and ethical issues.
We perform about 50 transplants a year in our institution, and every one of them has some issue. Nevertheless, we just honored 25 patients who have survived more than 20 years with cardiac transplantation.
Despite the odds, the transplant field has progressed rapidly
By John J. Fung, MD, PhD
Dr. Pauline Chen’s clinical vignette [see previous article in this supplement] unfortunately still typifies small bowel transplantation. One would not expect to hear that kind of story today for a kidney or liver transplant, but in the early 1970s it was typical.
‘WHY WOULD ANY YOUNG PHYSICIAN WANT TO GET INVOLVED IN THIS?’
Dr. Cooley’s comments about the moratorium on cardiac transplantation brought back memories for me, particularly from when I was studying liver transplantation in the 1970s. There was almost uniform mortality in transplants performed in the late 1960s and early ’70s. One wonders why any young physician would have wanted to get involved in transplantation at that time. I was a fellow training with Dr. Thomas Starzl at the University of Pittsburgh and remember him saying, “Just make it work, then let everybody else figure out why.” I think that typifies the surgical mentality.
We perform transplantations because we know that the alternative is prolonged morbidity and death. Knowing that we can provide a touch of hope is why we move forward in this field.
The technology of transplantation has developed through aggressive scientific developments in the laboratory. It is fascinating that all this has developed in only 50 years. If we had proceeded in a very stepwise manner, we probably would not be even a tenth as far along in the field as we are now.
Heart, lung, liver, and kidney transplantation are now all pretty routine. Intestinal transplantation is in the developing phase. The Cleveland Clinic is currently involved in facial transplantation, which has some different ethical issues related to identity.
Everything in transplantation relates to ethics, from issues about using marginal donor grafts or using beating-heart donors when someone has not been declared brain dead, to issues in patient selection, which often depends on social, economic (ie, insurance coverage), and psychosocial factors such as substance abuse and nonadherence issues.
ETHICAL INSIGHTS FROM TRANSPLANTS IN HIV-POSITIVE PATIENTS
An ethical area of particular interest to me that the Cleveland Clinic has also been involved with is transplanting patients who are HIV-positive. This has always been an enigma: why would we want to transplant an HIV-positive patient? Before the advent of antiviral therapies for HIV in the mid-1990s, mortality rates were very high, with patients suffering miserable deaths from Kaposi sarcoma, the JC virus leukoencephalopathies, and other debilitating opportunistic infections.
When I first arrived at the University of Pittsburgh as a fellow, Dr. Starzl was telling us about this mystery virus disease; when they retrospectively analyzed specimens from organ recipients and donors, they realized that HIV was being transmitted to patients from donors as well as from blood transfusions. The exposure to health care providers was also substantial: an average of 20 to 30 units of blood was used for a liver transplant.
Patients who were HIV-positive were excluded from transplants even through the mid-1990s. I remember evaluating standard listing criteria for transplant recipients at a conference and hearing transplant surgeons say that HIV is an absolute contraindication to transplant. I said, “Wait a minute, this is 1997; you cannot say that. Given that attitude, patients with HIV will never be transplanted.” The New England Journal of Medicine had just published a major paper about the extent of survival in patients being treated with highly active antiretroviral therapy.
So we then started a prospective study of transplantation in HIV-positive patients, and long-term follow-up has shown that these patients can do very well. Interestingly, transplantation offers a new approach to treating HIV-positive patients, in terms of immune reconstitution and the ability of immunosuppressive agents to restore immune competency by preventing the T-cell apoptosis initiated by HIV infection.
A continued need for evidence-based guidance
By James B. Young, MD
Speaking as the lone internist on this panel, and also as a clinical trialist and evidence-based clinical practitioner, the greatest ethical challenge I see for transplantation is how to move the field forward in terms of garnering evidence that can help us treat patients and keep them alive. Nobody will deny that heart transplantation is life-saving therapy: my patients with end-stage ischemic cardiomyopathy can be dramatically transformed by a heart transplant after being near death. The questions now are how best to gain the data to guide the next round of innovations in transplant medicine and how to know when the time is right to attempt those innovations.
A HISTORICAL GLANCE AT HEART TRANSPLANTATION
Dr. Sharon Hunt, who was one of the first heart transplant cardiologists and worked with Dr. Norman Shumway, almost singlehandedly moved the field of cardiac transplantation forward. She recently chronicled its history,1 and this sort of historical review yields a couple of insights. First, fewer heart transplants are being done in the United States in this decade than in the 1990s,2 in large part because other effective interventions for heart failure have been developed. However, the number of heart transplants is in fact on the rise again.2 Second, survival rates in heart transplant have improved substantially in recent years compared with earlier eras, as documented by registry data from the International Society for Heart and Lung Transplantation.3
Among other things, we have learned how to improve the operation, better choose and preserve hearts, and better match hearts to recipients. We now can use hearts from older donors and allow older patients to undergo transplantation. One of the keys to the better survival rates is a dramatic change in the use of medications. Cyclosporine allowed for successful heart transplantation in the 1980s, and we have since seen the advent of agents such as tacrolimus, rapamycin, and mycophenolate mofetil. We rely less on the early immunosuppressants, such as prednisone and azathioprine.
Despite these successes from a survival standpoint, problems still need to be addressed. For instance, at 5 years, virtually every patient following a heart transplant develops hypertension and dyslipidemia, 1 in 3 has renal dysfunction (some requiring dialysis or transplant), 1 in 3 has diabetes, and some develop a strange allograft arteriopathy.3
THE CHALLENGE OF EVALUATING A BOUTIQUE SCIENCE
Heart transplantation is a bit of a boutique science. Although relatively few heart transplants are performed compared with liver or kidney transplants, heart transplantation is a dramatic operation limited by many ethical challenges surrounding organ donor supply and utilization.
As for any boutique science, questions arise about how to evaluate it with the rigor of regulatory authority—from both the Food and Drug Administration (FDA) perspective and the institutional review board (IRB) perspective—without large clinical trials. Suppose that Dr. Cooley wants to make a minor modification in his immunosuppressive protocol because of an observation of a high incidence of renal failure at the 5-year point; does that ethically demand a large randomized clinical trial?
How can we design clinical trials to help determine which direction to take in immunosuppression intensification or utilization protocols? Other challenges include evaluating outcomes (such as coronary artery vasculopathy) from databases, and then figuring out good and bad practices. For example, databases show us that a donor history of diabetes increases the recipient’s long-term risk of developing coronary artery vasculopathy.3 Receiving a heart from a male donor also increases risk.3 Better understanding the panoply of adverse events and what leads to better outcomes will give us a sense of how to proceed and can drive the design of clinical trials.
OTHER ETHICAL CHALLENGES
From an ethical standpoint, how do we change practice? We have data on outcomes at 5, 10, and even 20 years. The half-life of a heart transplanted today is 12.5 years, whereas it used to be about 7 years.3 Although it is clear that we have made progress, it is a challenge to determine exactly how to make subtle changes in practice, such as addressing polypharmacy post-transplant.
Developing schemes that enable major innovation, particularly through coordination among medical and surgical teams, is another challenge. For example, we are working with preservation techniques that use a beating heart for transplantation. From solid evidence based on animal models, we believe this preparation can allow preservation of a heart for up to 12 hours. To some, that may beg a number of questions: Why do we need to do a clinical trial in humans? Why does the FDA need to regulate us? Why do we even need to answer to an IRB? Why not just make the change to alleviate the problem of donor organ supply?
What does—and does not—spur innovation?
By Thomas E. Starzl, MD, PhD
LESSONS FROM THE CODMAN ANALYSIS OF FAILURES
Dr. Ernest Codman was a Harvard Medical School professor in the early 20th century who tried to introduce a system of analyzing failures at Massachusetts General Hospital and other Harvard-affiliated hospitals. As a result, he was metaphorically ridden out of town on a rail.
Codman recommended that complications and failures be classified as one of the following:
- An error in diagnosis
- An error in judgment
- An error in technique (if a surgical or a medicalproblem)
- An error in management.
Only one escape hatch existed that did not indictthe surgical or medical team as culpable: the disease. At the time, nothing could be done for many diseases, including cancer, heart disease, renal failure, and bowel insufficiency.
This is a type of analysis that can be brought to a mortality and morbidity conference and will not accept a lot of alibis; it forces the group to always look at what could have been done to prevent a complication or death. Some practitioners always want to blame some factor other than themselves: sometimes the patient, by being deemed noncompliant, is even held responsible for his or her own complication or death.
I think the Codman analysis of failures is a good starting point for discussing innovations, especially since true breakthroughs come in those cases where the failure falls into the category of being caused by the disease itself, not by a medical or surgical error. And that is surely where transplantation falls.
PROGRESS DOES NOT ALWAYS REQUIRE FULL UNDERSTANDING
Transplantation was first successfully performed in the context of breaking through the donor-recipient genetic barrier on January 6, 1959, when Joseph Murray and his team at the the Brigham Hospital performed a kidney transplant using the patient’s fraternal twin as a donor. This event was reproduced in Paris by Jean Hamburger and his team on June 14, 1959, and then on three or four other occasions in the next several years in patients who received sublethal total body irradiation. This was at a time when no pharmacological immunosuppression was available, so no follow-up treatment was offered.
Astoundingly, the first case—the fraternal twin— lived for more than 20 years, and the French case for 25 years, without ever being treated with immunosuppression. They were inexplicably tolerant. When immunosuppressive drugs were developed and survival rates improved, the questions around these early cases were never answered: Why did those transplantations work? What were the mechanisms of engraftment? What was the relationship of engraftment to tolerance? Without answering those questions, there was no way to make other big leaps in improvement of what was already proved in principle—that is, the feasibility of actually doing this kind of treatment. Improvements in patient and graft survival were dependent almost entirely on better drugs.
RANDOMIZED TRIALS HAVE A DUBIOUS RECORD IN TRANSPLANTATION
I know this will offend just about everyone here, but I have no confidence in evidence-based therapy if we are talking about randomized trials. None of the great advances in transplantation has had anything to do with randomized trials. In my opinion, randomized trials in transplantation have done nothing but confuse the issue and have very nearly made it impossible for the better immunosuppressants to be brought on board. Cyclosporine offered a tremendous step forward, but the randomized trials, carried out mostly in Europe, did not reveal much difference in outcome from treatment with azathioprine, at least as assessed by patient and graft survival. The same thing occurred when tacrolimus emerged; randomized multicenter trials actually delayed the widespread use of this superior drug for at least half a dozen years.
IN THE BIG PICTURE, MONEY IS HOBBLING INNOVATION
Earlier it was debated whether money drives everything. I do not believe that money drives everything in medicine in Europe, and it certainly has little to do with driving improvements in Asia. But money does drive everything in the United States, although the real question is whether it has to be that way.
I believe that innovation is somehow built within our genome. Many of the great advances in transplantation, the elucidation of principles, and the relatively recent discovery of the mechanisms of alloengraftment were achieved without grant support. The researchers involved could not have asked for National Institutes of Health funding because their ideas were so far out of the box that they probably would have been rejected or stolen.
I wonder to what extent the vast amount of money available for research is actually a disincentive for genuine advancements. Part of the problem is that the power of allocation is put in the hands of anonymous peer-review committees. That system generates droves of people to pursue money allocated to a certain area to learn more and more about less and less, in the vague hope that acquiring enough details will result in a realistic concept. Sometimes the picture simply becomes more confused.
Another problem is that we have produced far more scientists than jobs, so that funding becomes the first priority because it is the only means of employment. In earlier days, what drove people more often was that they were confronted with a child who was dying and the central questions was, “How can I treat this patient?” They did laboratory research on their own to produce evidence that a new innovative idea could work. I believe that if you have experiments that show that you can keep a heart beating on a preservation device for 12 hours, and you can put it in a dog and it works well, that is the evidence you need to proceed. How are you going to do a randomized trial—hang on to an organ and let it beat for 12 hours just so it conforms with some protocol? That is nonsense.
There was a period when clinical journals—Surgery of Gynecology and Obstetrics, Annals of Surgery, Annals of Internal Medicine, New England Journal of Medicine, and others—published front-running discoveries. That ended about 25 years ago when it became more important to learn about details. The journals then became superfluous, and for another reason as well: money drove the wheel more and more. Hospital and program administrators expected the publications to be advertisements, and the minute that articles started promoting something rather than reporting facts, they lost value. Today the impact factors of the surgical journals are at about 2 or 3, meaning that their articles are cited infrequently and have little real influence on the practice of medicine.
How did we reach this point where money drives everything? I think the page was turned in the very early 1990s, and it had to do with how medical practice is governed, especially in academic hospitals. Half of the health care in this country is now provided by hospitals that are associated with medical schools. Those hospitals and basic research laboratories are where our young people will assimilate their ideals. If that climate is not right, then we are raising the wrong kind of doctors.
Earlier researchers looked at a problem and thought, “Here’s a question that has to do with this patient before my eyes, and I must find some way to solve it. Let’s go to the laboratory.” Today there is a real danger that they are thinking, “I need to advance my career, so let’s see how I can get some money. A little research will be a stepping stone to my professional development.” Our discussion of medical and surgical ethics today should take place within this framework.
Panel discussion
Moderated by Mark Siegler, MD
WERE FINANCES A DRIVER OF EARLY TRANSPLANT INNOVATION?
Dr. Mark Siegler: It is clear that there are more ethical and less ethical ways to introduce innovations. I am reminded of an article in JAMA by Francis Moore in the late 1980s in which he warned that one of the things to look at for any new innovation was the ethical climate of the institution.4 He cautioned us to be very aware of the driving force behind an innovation. Is it to improve patient care? To save lives that otherwise would be lost? Or is it primarily for the self-aggrandizement of an investigator or the financial goals of an institution?
I also remember the chapter in Dr. Starzl’s book The Puzzle People5 about the anguish involved in introducing liver transplantation. It seems that financial considerations were not the driver of major steps forward in introducing liver transplantation, in Dr. Starzl’s case, or heart transplantation, in Dr. Cooley’s case. Would you comment?
Dr. Thomas Starzl: Actually, not only were we not driven by economic gain, we expected fi nancial penalty for focusing on transplantation. If ever there was a field that developed against the grain, that was costly to people who worked in it, whose engagement meant that for most of their career they would work for substandard income compared with their peers—even those peers in academic medicine, let alone those in private practice—it would be transplantation.
It was not until 1973, when the end-stage renal disease (ESRD) program began under Medicare, that cash for transplantation started to become available. The real cash streams did not start until the middle to late 1980s when nonrenal organs became the cash cows. To be fair, no new technology can be assimilated into the health care system unless it at least pays for itself. But you can go beyond that and create baronial kingdoms, and I think that is where you can go wrong.
Dr. Denton Cooley: I would add that those of us privileged to spend our entire career in academic settings have an opportunity that others may not have. A lot of brilliant people in private practice are capable of doing many things but do not have an institution to represent and protect them. I have also always felt that those of us in these positions have an obligation to become innovators. Surgeons who merely see how many appendectomies or cholecystectomies they can perform are being very derelict of their responsibility to the institution.
MEASURING SUCCESS IN HEART TRANSPLANTATION
Dr. Siegler: Dr. Cooley, what is the current success rate for heart transplants?
Dr. Cooley: Nationwide, around 90% of recipients survive 12 months. Of those, maybe half are still alive 5 years later. Of course, we do not know what the future will hold. It is interesting that the fi rst sign of rejection seems to be coronary occlusive disease. It is a different type of coronary occlusive disease than is seen in atherosclerosis: it is diffuse, involving the entire extent of the coronary circulation, and is not really amenable to coronary bypass or other interventional procedures.
Dr. Siegler: We are now at about the 40th anniversary of the first human heart transplants, an extraordinary and historic innovation. Dr. Cooley, do you think the timing was right in 1968 when you did the fi rst heart transplant in the United States? In retrospect, would you have done the first transplant sooner or maybe even a couple of years later?
Dr. Cooley: You can argue it both ways. Should we have waited for further developments? At the time, heart transplantation seemed to work fairly well in animals, but we never really know until it reaches the clinical level. It was probably as opportune a time as any. We knew something about organ rejection at the time, and we had immunosuppressive drugs, although they were not as effective as they are today. The news electrified the world. I think we were pretty well prepared for this spectacular event.
Dr. Siegler: When would have been the optimal time to do a clinical trial in order to achieve evidence-based medicine in heart transplantation? Would it have been during the big breakthroughs of Shumway, Barnard, and Cooley, or now, when we have the general strategy and can find out how we can do better?
Dr. James Young: I would not have done a randomized trial at that time. The patients who were getting transplanted then were nearly dead; all other management was futile. In 1970, Life magazine listed the 102 heart transplants that had been done around the world up to that point, and maybe only 2 or 3 of the patients were still alive. That prompted the moratorium that Dr. Cooley referred to.
As ethical clinicians, we are supposed to do our best to make our patients feel better and make them live longer. Sometimes you have to do something radical. On that basis, one can argue that we should not transplant “the walking wounded,” that instead we should save organs for patients who are truly terminal without some sort of ventricular replacement therapy. But today we are getting away from transplanting only dying patients, so we need randomized trials to find out how we are doing in transplanting outpatients. That is the setting in which trials are now needed.
THE ETHICS OF ‘LETTING GO’
Question from audience: Dr. Chen’s story [see previous article] raised the issue of the ethics of “letting go” of one’s patient. I wonder if in transplantation, especially when innovative procedures are involved, a commitment to the procedure itself might sometimes conflict with the need to let go of the patient.
Dr. John Fung: In the United States, we measure efficacy and benefits in different ways than people do in other parts of the world. Here, for a child with a biliary atresia—the most common reason for liver transplantation—we expend hundreds of thousands of dollars for a liver transplant, which is usually able to save the child’s life. But in China, a severely ill child is viewed as a medical and economic liability and will be allowed to die so the family can have another child.
It is also not only the ethics of letting go. We all deal with letting go, not just in transplant medicine. It is also the ethics of actually getting a patient into the system. In the case of transplanting a newborn, as in Dr. Chen’s narrative, should they even have embarked on that?
Dr. Pauline Chen: For me, the story illustrates the remarkable connection and profound attachment between a surgeon and his or her patient. The fact that three patients are really involved in transplantation—the donor, the recipient, and the patient still on the waiting list because the organ went to the recipient instead—also motivates the team with a sense of obligation to the two unseen patients.
If there is a lesson about the ethics of letting go, I think it is that we often fail to talk about these issues among ourselves. Perhaps if we had discussed end-of-life care or palliative care in Max’s case, we might have had more insight into the pressures we felt in considering the lives of three separate people. And those discussions might have—or might not have— changed the situation.
Dr. Starzl: I agree completely with the preceding comments. All kinds of motivations might cause a surgeon to cling too long—the ones that were mentioned as well as some ignoble ones, such as vanity, in terms of looking at one’s survival numbers.
I would also like to take a much larger view. Some years ago in Colorado, the governor at the time, Richard Lamm, thought that intensive care units (ICUs) were harmful—that they were economically draining, did not serve society, and prolonged suffering. My position, which was really the opposite, was that maybe he was right in his philosophy but transplantation had, in a sense, changed all that. Transplantation took desperate people who were in the ICU, with no chance of coming out, and dramatically returned them to wonderful health.
As procedures get better, this scenario happens more and more often. I agree that there is a time when you realize that no intervention will work and you should stop treatment. That is a bitter pill. But it is very hard to define when that moment occurs.
Dr. Chen: There also may be somewhat of a generational difference in approach.
Most surgeons will fully acknowledge that they stand on the shoulders of giants, and that holds particularly true in a field like transplantation. When I was training in liver transplantation, for example, 80% to 90% of the patients could fully expect to survive 5 years. For my vintage of surgeons, then, death and failure were rarities and they were truly a sort of enemy, whereas surgeons like Dr. Starzl and Dr. Cooley have seen so much more and are far more used to all the variations of outcomes. Because of that breadth of experience that you have, I think you are wiser than my generation of surgeons, for whom death often has to be ablated at all costs. I think it follows, then, that you would also have a better sense of when to stop.
Dr. Starzl: There is a generational change—there is no doubt about it.
IS TRANSPLANT ETHICAL WHEN A LIFE IS NOT AT STAKE?
Question from audience: What are the ethical implications of non-lifesaving transplants, specifically of the hand and face?
Dr. Young: I have been on many peer-review committees charged with looking at this issue. Although the ethics can be very troubling, I have resolved important questions in my mind by examining them through the context of human suffering. Our mission as physicians and caregivers is to relieve suffering, which can take the form of pain, a shortened lifespan, or even a debilitating disfigurement of the face or a severe limitation, such as after traumatic amputation. Looking at the issue this way, I am less troubled than I was initially, when I viewed these kinds of transplantations as simply altering physical appearance or extending ability.
Dr. Starzl: The next big movement in transplantation is going to be in composite tissue allotransplantation—that is, transplantation of the face, limbs, etc. Mechanisms of alloengraftment have recently been uncovered such that it is now possible to formulate protocols that use either very light immunosuppression (avoiding the 20% or 25% rate of renal failure at 5 years that we heard about from Dr. Young) or no immunosuppression at all.6 Without the heavy burden of immunosuppression, this type of transplantation can become worthwhile. Putting a new hand or face on someone is astounding: it changes the morphology of the brain, which can be observed with functional magnetic resonance imaging. It changes the soul, if that is what you want to think of when talking about the brain. I think it will be very important.
Dr. Siegler: This extraordinary panel has not only discussed events from 50 years ago; each of the panelists spoke of a future that is rich in promise and innovation—and in ethical issues. It reminds me of a remarkable letter written in 1794 by Thomas Jefferson to John Adams, which says, “We should never return to earlier times when all scientific progress was proscribed as innovation.” More than 200 years later, Jefferson’s insight remains modern and relevant.
- Hunt SA. Taking heart—cardiac transplantation past, present, and future. N Engl J Med 2006; 355:231–235.
- Heart and Lung Transplantation in the United States, 1997-2006(Chapter VI). In: 2007 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Data 1997-2006. Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Rockville, MD. Available at: http://www.ustransplant.org/annual_reports/current. Accessed July 22, 2008.
- Taylor DO, Edwards LB, Boucek MM, et al. Registry of the International Society for Heart and Lung Transplantation: twenty-second official adult heart transplant report—2005. J Heart Lung Transplant 2005; 24:945–955.
- Moore FD. The desperate case: CARE (costs, applicability, research, ethics). JAMA 1989; 261:1483–1484.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon.Pittsburgh, PA: University of Pittsburgh Press; 1992.
- Starzl TE. Immunosuppressive therapy and tolerance of organ allografts. N Engl J Med 2008; 358:407–411.
- Hunt SA. Taking heart—cardiac transplantation past, present, and future. N Engl J Med 2006; 355:231–235.
- Heart and Lung Transplantation in the United States, 1997-2006(Chapter VI). In: 2007 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Data 1997-2006. Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Rockville, MD. Available at: http://www.ustransplant.org/annual_reports/current. Accessed July 22, 2008.
- Taylor DO, Edwards LB, Boucek MM, et al. Registry of the International Society for Heart and Lung Transplantation: twenty-second official adult heart transplant report—2005. J Heart Lung Transplant 2005; 24:945–955.
- Moore FD. The desperate case: CARE (costs, applicability, research, ethics). JAMA 1989; 261:1483–1484.
- Starzl TE. The Puzzle People: Memoirs of a Transplant Surgeon.Pittsburgh, PA: University of Pittsburgh Press; 1992.
- Starzl TE. Immunosuppressive therapy and tolerance of organ allografts. N Engl J Med 2008; 358:407–411.
Medical professionalism in a commercialized health care market*
Medical professionalism in the United States is facing a crisis, just as serious as the crisis facing the health care system, and the two crises are interrelated.
To understand today’s crisis in medical professionalism requires knowing what a profession is and what role it plays in modern society. Freidson1 considered a profession to be one of three options modern society has for controlling and organizing work. The other two options are the free market and management by organizations such as government or private businesses. Freidson suggested that medical work was totally unsuited for control by the market or by government or business and, therefore, the practice of medicine could only be conducted properly as a profession.
According to Freidson,1 a profession is highly specialized and grounded in a body of knowledge and skills that is given special status in the labor force, its members are certified through a formal educational program controlled by the profession, and qualified members are granted exclusive jurisdiction and a sheltered position in the labor market. Perhaps most important, professionals have an ideology that assigns a higher priority to doing useful and needed work than to economic rewards, an ideology that focuses more on the quality and social benefits of work than its profitability.
Although this ideology is the most important part of medical professionalism, it is what is now most at risk. The science and technology of medicine and the special place that medical practice holds in the labor market are not presently threatened. The expanding professional health care responsibilities of nurses and the increase in other health workers such as physician assistants and technicians are changing the mix of the health care workforce, but the central role of the physician as the manager and provider of medical services is not likely to be challenged.
Endangered are the ethical foundations of medicine, including the commitment of physicians to put the needs of patients ahead of personal gain, to deal with patients honestly, competently, and compassionately, and to avoid conflicts of interest that could undermine public trust in the altruism of medicine. It is this commitment, what Freidson called the “soul” of the profession,1 that is eroding, even while its scientific and technical authority grows stronger. Ironically, medical science and technology are flourishing, even as the moral foundations of the medical profession lose their influence on the behavior of physicians.
This undermining of professional values was an inevitable result of the change in the scientific, economic, legal, and social environment in which medicine is now being practiced. A major reason for the decline of medical professional values is the growing commercialization of the US health care system.2 Health care has become a $2 trillion industry,2 largely shaped by the entry and growth of innumerable private investor-owned businesses that sell health insurance and deliver medical care with a primary concern for the maximization of their income. To survive in this new medical market, most nonprofit medical institutions act like their for-profit competitors, and the behavior of nonprofits and for-profits has become less and less distinguishable. In no other health care system in the world do investors and business considerations play such an important role. In no other country are the organizations that provide medical care so driven by income and profit-generating considerations. This uniquely US development is an important cause of the health cost crisis that is destabilizing the entire economy, and it has played a major part in eroding the ethical commitments of physicians.
Many physicians have contributed to this transformation by accepting the view that medical practice is also in essence a business. Medical practice is now widely viewed as a demanding and technical business that requires extensive, credentialed education and great personal responsibilities—but a business nevertheless. This change in attitude has important consequences. In business, increasing shareholder value through increased revenue and increased profit is the primary goal. However, medical professionalism requires that physicians give even greater primacy to the medical needs of patients and to the public health of the society in which their patients live. When physicians think of themselves as being primarily in business, professional values recede and the practice of medicine changes.
Physicians have always been concerned with earning a comfortable living, and there have always been some who were driven by greed, but the current focus on moneymaking and the seductions of financial rewards have changed the climate of US medical practice at the expense of professional altruism and the moral commitment to patients.3 The vast amount of money in the US medical care system and the manifold opportunities for physicians to earn high incomes have made it almost impossible for many to function as true fiduciaries for patients.
The essence of medicine is so different from that of ordinary business that they are inherently at odds. Business concepts of good management may be useful in medical practice, but only to a degree. The fundamental ethos of medical practice contrasts sharply with that of ordinary commerce, and market principles do not apply to the relationship between physician and patient.4 Such insights have not stopped the advance of the “medical-industrial complex,”5 or prevented the growing domination of market ideology over medical professionalism.
Other forces in the new environment have also been eroding medical professionalism. The growth of technology and specialization is attracting more physicians into specialties and away from primary care.6 The greater economic rewards of procedural specialties are particularly appealing to new graduates who enter practice burdened with large educational debts. Specialization is not necessarily incompatible with ethical professional practice, but it often reduces the opportunities for personal interactions between physicians and patients and thus weakens the bond between physicians and patients. It is too easy for even the best specialists to behave simply as skilled technicians, focused exclusively on their patients’ narrow medical problems and unmindful of their professional obligations to the whole person they are serving.
The law also has played a major role in the decline of medical professionalism. The 1975 Supreme Court ruling that the professions were not protected from antitrust law7 undermined the traditional restraint that medical professional societies had always placed on the commercial behavior of physicians, such as advertising and investing in the products they prescribe or facilities they recommend. Having lost some initial legal battles and fearing the financial costs of losing more, organized medicine now hesitates to require physicians to behave differently from business people. It asks only that physicians’ business activities should be legal, disclosed to patients, and not inconsistent with patients’ interests. Until forced by antitrust concerns to change its ethical code in 1980, the American Medical Association had held that “in the practice of medicine a physician should limit the source of his professional income to medical services actually rendered by him, or under his supervision, to his patients” and that “the practice of medicine should not be commercialized, nor treated as a commodity in trade.”8 These sentiments reflecting the spirit of professionalism are now gone.
Professionalism is also compromised by the failure of physicians to exercise self-regulation that would be supported by law. Many physicians are reluctant to identify incompetent or unethical colleagues. Such behavior also undermines the public’s trust in the profession.
Yet another deprofessionalizing force has been the growing influence of the pharmaceutical industry on the practice of medicine. This industry now uses its enormous financial resources to help shape the postgraduate and continuing medical education of physicians in ways that serve its marketing purposes.9 Physicians and medical educational institutions aid and abet this influence by accepting, sometimes even soliciting, financial help and other favors from the industry, thus relinquishing what should be their professional responsibility for self-education. A medical profession that is being educated by an industry that sells the drugs physicians prescribe and other tools physicians use is abdicating its ethical commitment to serve as the independent fiduciary for its patients.10
The preservation of independent professionalism and its ethical commitment to patients still are very important because physicians are at the center of the health care system and the public must be able to depend on and trust physicians. There is currently much concern about the paternalism and elitism of medicine, and this concern is often used to justify policies seeking to establish so-called consumer-directed health care.11 Although there undoubtedly is a need for patients to have more information and responsibility for their health care choices, without trustworthy and accountable professional guidance from physicians, the health care system could not function. In the absence of physicians’ commitment to professional values, health care becomes just another industry that may, by continuing along its present course, be heading toward bankruptcy.
Physicians should not accept the industrialization of medical care, but should work instead toward major reforms that will restore the health care system to its proper role as a social service that society provides to all. Virtually every other advanced nation has achieved that goal. An essential part of the needed reforms is a rededication of physicians to the ethical professional principles on which the practice of medicine should rest. Such reforms will require public and political initiatives12 and the active participation of the medical profession.
Medical professionalism cannot survive in the current commercialized health care market. The continued privatization of health care and the continued prevalence and intrusion of market forces in the practice of medicine will not only bankrupt the health care system, but also will inevitably undermine the ethical foundations of medical practice and dissolve the moral precepts that have historically defined the medical profession. Physicians who care about these values must support major reform of both the insurance and the delivery sides of the health care system.2 It is the one policy option most likely to preserve the integrity and values of the medical profession.
ADDENDUM
The foregoing commentary, published last year in JAMA, explains why I am concerned about the “ethical challenges in surgical innovation,” the subject of this conference. Although the legal status of patent applications for surgical methods (“process patents”) has not yet been fully defined,13 such applications fortunately are relatively rare. The great majority of surgical techniques are not patented and are freely available to surgeons—as they should be. However, the devices, equipment, and implants that may be an essential part of new surgical techniques can be and are patented, and may therefore be profitable. If these patented items are developed by a staff physician or are the product of collaboration between such a physician and a company, should financial benefits accrue to the physician involved? Some say yes. They seem convinced that without some sort of financial incentive—royalties, direct payments from the manufacturer, or equity interest in the manufacturer—physicians would simply not be motivated to do innovative work, and the “translational” research essential for medical progress would languish.
I strongly disagree with this view, but unfortunately it has gained considerable influence in academic medicine in recent years, despite the fact that it conflicts with medical professional ethics. Court interpretation of antitrust law in 19757 forced the American Medical Association to abandon its long-standing ethical injunction against practicing physicians earning income from financial interests in the medical products they use or prescribe. However, antitrust legislation is not relevant here, and no legal restraints prevent medical schools, teaching hospitals, and similar medical institutions from regulating or even prohibiting such outside earnings by their full-time salaried staff. These earnings constitute a clear conflict of interest, and there is a growing national consensus that such conflicts not only should be publicly disclosed but should be regulated by the institutions employing the physicians. If the institutions do not do this job, many now believe the government should.
What is the evidence that personal financial rewards are necessary incentives for physicians to work on “translational” research? I submit that there is little or none—only an assumption. But the fact is that even before commercialization began to transform health care 3 or 4 decades ago, and even before salaried academic physicians began to earn substantial outside income from their financial ties to device and drug manufacturers, “translational” research was thriving. In the 2 or 3 decades after World War II, salaried academic physicians conducted applied medical and surgical research, often in cooperation with industry but usually without any personal gain. It is true that today there is much more “translational” research going on, but that is probably explained by the greater number of researchers working now and the much greater public and private investment in research. It does not follow that the recent growth in applied biomedical investigation would not have occurred without personal financial incentives to academic physicians and surgeons. Such an assumption not only ignores medical history but demeans the professional values that we physicians swear to live by.
If we continue to encourage, or even allow, practicing physicians and surgeons to be entrepreneurs and have financial interests in the products they use and prescribe, we will surely undermine the ethical traditions of our profession, as I have argued in the above JAMA commentary. But beyond this ethical catastrophe, such policy would surely destroy the credibility and integrity of the whole US medical research enterprise, with dire consequences for society. I believe it is time for our best clinical research institutions to insist that research cooperation with industry be conducted in a much more professional and controlled manner. Academic-industrial cooperation can often facilitate advances in research, but any financial gains for the academic side should flow to institutions, not individuals, and should be strictly regulated by law to ensure that the public interest is protected and the integrity of the medical profession preserved.
I refuse to believe that academic physicians will stop their search for innovative devices and methods for treating their patients if they are not given extra financial rewards beyond their salaries. Of course, they need to be paid well and they need the time and resources required for their research, but that should be the responsibility of their institutions, not of industry. The present shortage of time and resources for research in not-for-profit medical institutions must be addressed, but turning the responsibility over to the free market of medical entrepreneurialism is not the answer. It will lead only to a dead end for our profession and for the public stake in medical research. This is a challenge that the best and strongest US medical institutions must face up to, but government will also need to help. Our country depends on a vibrant but socially responsible and trustworthy medical research sector. That is an objective that unregulated commercial markets and private interests cannot achieve. We need academic institutions, supported by public policies, to lead the way.
- Freidson E. Professionalism: The Third Logic. Chicago, IL: University of Chicago Press; 2001.
- Relman AS. A Second Opinion: Rescuing America’s Health Care. New York, NY: Public Affairs; 2007.
- Special section: commercialism in medicine. Camb Q Healthc Ethics 2007; 16:368–445.
- Arrow KJ. Uncertainty and the welfare economics of medical care. Am Econ Rev 1963; 53:941–973.
- Relman AS. The new medical-industrial complex. N Engl J Med 1980; 303:963–997.
- Bodenheimer T. Primary care: will it survive? N Engl J Med 2006; 355:861–863.
- Goldfarb v Virginia State Bar, 421 US 773 (1975).
- American Medical Association. Opinions and Reports of the Judicial Council. Chicago, IL: American Medical Association; 1966.
- DeAngelis CD. Rainbow to dark clouds. JAMA 2005; 294:1107.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA 2001; 285:2009–2012.
- Herzlinger RE, ed. Consumer-Driven Health Care: Implications for Providers, Payers and Policy-Makers. San Francisco, CA: Jossey-Bass; 2004.
- Cohen JJ, Cruess S, Davidson C. Alliance between society and medicine: the public’s stake in medical professionalism. JAMA 2007; 298:670–673.
- Kesselheim AS, Mello MM. Medical-process patents—monopolizing the delivery of health care. N Engl J Med 2006; 355:2036– 2041.
Medical professionalism in the United States is facing a crisis, just as serious as the crisis facing the health care system, and the two crises are interrelated.
To understand today’s crisis in medical professionalism requires knowing what a profession is and what role it plays in modern society. Freidson1 considered a profession to be one of three options modern society has for controlling and organizing work. The other two options are the free market and management by organizations such as government or private businesses. Freidson suggested that medical work was totally unsuited for control by the market or by government or business and, therefore, the practice of medicine could only be conducted properly as a profession.
According to Freidson,1 a profession is highly specialized and grounded in a body of knowledge and skills that is given special status in the labor force, its members are certified through a formal educational program controlled by the profession, and qualified members are granted exclusive jurisdiction and a sheltered position in the labor market. Perhaps most important, professionals have an ideology that assigns a higher priority to doing useful and needed work than to economic rewards, an ideology that focuses more on the quality and social benefits of work than its profitability.
Although this ideology is the most important part of medical professionalism, it is what is now most at risk. The science and technology of medicine and the special place that medical practice holds in the labor market are not presently threatened. The expanding professional health care responsibilities of nurses and the increase in other health workers such as physician assistants and technicians are changing the mix of the health care workforce, but the central role of the physician as the manager and provider of medical services is not likely to be challenged.
Endangered are the ethical foundations of medicine, including the commitment of physicians to put the needs of patients ahead of personal gain, to deal with patients honestly, competently, and compassionately, and to avoid conflicts of interest that could undermine public trust in the altruism of medicine. It is this commitment, what Freidson called the “soul” of the profession,1 that is eroding, even while its scientific and technical authority grows stronger. Ironically, medical science and technology are flourishing, even as the moral foundations of the medical profession lose their influence on the behavior of physicians.
This undermining of professional values was an inevitable result of the change in the scientific, economic, legal, and social environment in which medicine is now being practiced. A major reason for the decline of medical professional values is the growing commercialization of the US health care system.2 Health care has become a $2 trillion industry,2 largely shaped by the entry and growth of innumerable private investor-owned businesses that sell health insurance and deliver medical care with a primary concern for the maximization of their income. To survive in this new medical market, most nonprofit medical institutions act like their for-profit competitors, and the behavior of nonprofits and for-profits has become less and less distinguishable. In no other health care system in the world do investors and business considerations play such an important role. In no other country are the organizations that provide medical care so driven by income and profit-generating considerations. This uniquely US development is an important cause of the health cost crisis that is destabilizing the entire economy, and it has played a major part in eroding the ethical commitments of physicians.
Many physicians have contributed to this transformation by accepting the view that medical practice is also in essence a business. Medical practice is now widely viewed as a demanding and technical business that requires extensive, credentialed education and great personal responsibilities—but a business nevertheless. This change in attitude has important consequences. In business, increasing shareholder value through increased revenue and increased profit is the primary goal. However, medical professionalism requires that physicians give even greater primacy to the medical needs of patients and to the public health of the society in which their patients live. When physicians think of themselves as being primarily in business, professional values recede and the practice of medicine changes.
Physicians have always been concerned with earning a comfortable living, and there have always been some who were driven by greed, but the current focus on moneymaking and the seductions of financial rewards have changed the climate of US medical practice at the expense of professional altruism and the moral commitment to patients.3 The vast amount of money in the US medical care system and the manifold opportunities for physicians to earn high incomes have made it almost impossible for many to function as true fiduciaries for patients.
The essence of medicine is so different from that of ordinary business that they are inherently at odds. Business concepts of good management may be useful in medical practice, but only to a degree. The fundamental ethos of medical practice contrasts sharply with that of ordinary commerce, and market principles do not apply to the relationship between physician and patient.4 Such insights have not stopped the advance of the “medical-industrial complex,”5 or prevented the growing domination of market ideology over medical professionalism.
Other forces in the new environment have also been eroding medical professionalism. The growth of technology and specialization is attracting more physicians into specialties and away from primary care.6 The greater economic rewards of procedural specialties are particularly appealing to new graduates who enter practice burdened with large educational debts. Specialization is not necessarily incompatible with ethical professional practice, but it often reduces the opportunities for personal interactions between physicians and patients and thus weakens the bond between physicians and patients. It is too easy for even the best specialists to behave simply as skilled technicians, focused exclusively on their patients’ narrow medical problems and unmindful of their professional obligations to the whole person they are serving.
The law also has played a major role in the decline of medical professionalism. The 1975 Supreme Court ruling that the professions were not protected from antitrust law7 undermined the traditional restraint that medical professional societies had always placed on the commercial behavior of physicians, such as advertising and investing in the products they prescribe or facilities they recommend. Having lost some initial legal battles and fearing the financial costs of losing more, organized medicine now hesitates to require physicians to behave differently from business people. It asks only that physicians’ business activities should be legal, disclosed to patients, and not inconsistent with patients’ interests. Until forced by antitrust concerns to change its ethical code in 1980, the American Medical Association had held that “in the practice of medicine a physician should limit the source of his professional income to medical services actually rendered by him, or under his supervision, to his patients” and that “the practice of medicine should not be commercialized, nor treated as a commodity in trade.”8 These sentiments reflecting the spirit of professionalism are now gone.
Professionalism is also compromised by the failure of physicians to exercise self-regulation that would be supported by law. Many physicians are reluctant to identify incompetent or unethical colleagues. Such behavior also undermines the public’s trust in the profession.
Yet another deprofessionalizing force has been the growing influence of the pharmaceutical industry on the practice of medicine. This industry now uses its enormous financial resources to help shape the postgraduate and continuing medical education of physicians in ways that serve its marketing purposes.9 Physicians and medical educational institutions aid and abet this influence by accepting, sometimes even soliciting, financial help and other favors from the industry, thus relinquishing what should be their professional responsibility for self-education. A medical profession that is being educated by an industry that sells the drugs physicians prescribe and other tools physicians use is abdicating its ethical commitment to serve as the independent fiduciary for its patients.10
The preservation of independent professionalism and its ethical commitment to patients still are very important because physicians are at the center of the health care system and the public must be able to depend on and trust physicians. There is currently much concern about the paternalism and elitism of medicine, and this concern is often used to justify policies seeking to establish so-called consumer-directed health care.11 Although there undoubtedly is a need for patients to have more information and responsibility for their health care choices, without trustworthy and accountable professional guidance from physicians, the health care system could not function. In the absence of physicians’ commitment to professional values, health care becomes just another industry that may, by continuing along its present course, be heading toward bankruptcy.
Physicians should not accept the industrialization of medical care, but should work instead toward major reforms that will restore the health care system to its proper role as a social service that society provides to all. Virtually every other advanced nation has achieved that goal. An essential part of the needed reforms is a rededication of physicians to the ethical professional principles on which the practice of medicine should rest. Such reforms will require public and political initiatives12 and the active participation of the medical profession.
Medical professionalism cannot survive in the current commercialized health care market. The continued privatization of health care and the continued prevalence and intrusion of market forces in the practice of medicine will not only bankrupt the health care system, but also will inevitably undermine the ethical foundations of medical practice and dissolve the moral precepts that have historically defined the medical profession. Physicians who care about these values must support major reform of both the insurance and the delivery sides of the health care system.2 It is the one policy option most likely to preserve the integrity and values of the medical profession.
ADDENDUM
The foregoing commentary, published last year in JAMA, explains why I am concerned about the “ethical challenges in surgical innovation,” the subject of this conference. Although the legal status of patent applications for surgical methods (“process patents”) has not yet been fully defined,13 such applications fortunately are relatively rare. The great majority of surgical techniques are not patented and are freely available to surgeons—as they should be. However, the devices, equipment, and implants that may be an essential part of new surgical techniques can be and are patented, and may therefore be profitable. If these patented items are developed by a staff physician or are the product of collaboration between such a physician and a company, should financial benefits accrue to the physician involved? Some say yes. They seem convinced that without some sort of financial incentive—royalties, direct payments from the manufacturer, or equity interest in the manufacturer—physicians would simply not be motivated to do innovative work, and the “translational” research essential for medical progress would languish.
I strongly disagree with this view, but unfortunately it has gained considerable influence in academic medicine in recent years, despite the fact that it conflicts with medical professional ethics. Court interpretation of antitrust law in 19757 forced the American Medical Association to abandon its long-standing ethical injunction against practicing physicians earning income from financial interests in the medical products they use or prescribe. However, antitrust legislation is not relevant here, and no legal restraints prevent medical schools, teaching hospitals, and similar medical institutions from regulating or even prohibiting such outside earnings by their full-time salaried staff. These earnings constitute a clear conflict of interest, and there is a growing national consensus that such conflicts not only should be publicly disclosed but should be regulated by the institutions employing the physicians. If the institutions do not do this job, many now believe the government should.
What is the evidence that personal financial rewards are necessary incentives for physicians to work on “translational” research? I submit that there is little or none—only an assumption. But the fact is that even before commercialization began to transform health care 3 or 4 decades ago, and even before salaried academic physicians began to earn substantial outside income from their financial ties to device and drug manufacturers, “translational” research was thriving. In the 2 or 3 decades after World War II, salaried academic physicians conducted applied medical and surgical research, often in cooperation with industry but usually without any personal gain. It is true that today there is much more “translational” research going on, but that is probably explained by the greater number of researchers working now and the much greater public and private investment in research. It does not follow that the recent growth in applied biomedical investigation would not have occurred without personal financial incentives to academic physicians and surgeons. Such an assumption not only ignores medical history but demeans the professional values that we physicians swear to live by.
If we continue to encourage, or even allow, practicing physicians and surgeons to be entrepreneurs and have financial interests in the products they use and prescribe, we will surely undermine the ethical traditions of our profession, as I have argued in the above JAMA commentary. But beyond this ethical catastrophe, such policy would surely destroy the credibility and integrity of the whole US medical research enterprise, with dire consequences for society. I believe it is time for our best clinical research institutions to insist that research cooperation with industry be conducted in a much more professional and controlled manner. Academic-industrial cooperation can often facilitate advances in research, but any financial gains for the academic side should flow to institutions, not individuals, and should be strictly regulated by law to ensure that the public interest is protected and the integrity of the medical profession preserved.
I refuse to believe that academic physicians will stop their search for innovative devices and methods for treating their patients if they are not given extra financial rewards beyond their salaries. Of course, they need to be paid well and they need the time and resources required for their research, but that should be the responsibility of their institutions, not of industry. The present shortage of time and resources for research in not-for-profit medical institutions must be addressed, but turning the responsibility over to the free market of medical entrepreneurialism is not the answer. It will lead only to a dead end for our profession and for the public stake in medical research. This is a challenge that the best and strongest US medical institutions must face up to, but government will also need to help. Our country depends on a vibrant but socially responsible and trustworthy medical research sector. That is an objective that unregulated commercial markets and private interests cannot achieve. We need academic institutions, supported by public policies, to lead the way.
Medical professionalism in the United States is facing a crisis, just as serious as the crisis facing the health care system, and the two crises are interrelated.
To understand today’s crisis in medical professionalism requires knowing what a profession is and what role it plays in modern society. Freidson1 considered a profession to be one of three options modern society has for controlling and organizing work. The other two options are the free market and management by organizations such as government or private businesses. Freidson suggested that medical work was totally unsuited for control by the market or by government or business and, therefore, the practice of medicine could only be conducted properly as a profession.
According to Freidson,1 a profession is highly specialized and grounded in a body of knowledge and skills that is given special status in the labor force, its members are certified through a formal educational program controlled by the profession, and qualified members are granted exclusive jurisdiction and a sheltered position in the labor market. Perhaps most important, professionals have an ideology that assigns a higher priority to doing useful and needed work than to economic rewards, an ideology that focuses more on the quality and social benefits of work than its profitability.
Although this ideology is the most important part of medical professionalism, it is what is now most at risk. The science and technology of medicine and the special place that medical practice holds in the labor market are not presently threatened. The expanding professional health care responsibilities of nurses and the increase in other health workers such as physician assistants and technicians are changing the mix of the health care workforce, but the central role of the physician as the manager and provider of medical services is not likely to be challenged.
Endangered are the ethical foundations of medicine, including the commitment of physicians to put the needs of patients ahead of personal gain, to deal with patients honestly, competently, and compassionately, and to avoid conflicts of interest that could undermine public trust in the altruism of medicine. It is this commitment, what Freidson called the “soul” of the profession,1 that is eroding, even while its scientific and technical authority grows stronger. Ironically, medical science and technology are flourishing, even as the moral foundations of the medical profession lose their influence on the behavior of physicians.
This undermining of professional values was an inevitable result of the change in the scientific, economic, legal, and social environment in which medicine is now being practiced. A major reason for the decline of medical professional values is the growing commercialization of the US health care system.2 Health care has become a $2 trillion industry,2 largely shaped by the entry and growth of innumerable private investor-owned businesses that sell health insurance and deliver medical care with a primary concern for the maximization of their income. To survive in this new medical market, most nonprofit medical institutions act like their for-profit competitors, and the behavior of nonprofits and for-profits has become less and less distinguishable. In no other health care system in the world do investors and business considerations play such an important role. In no other country are the organizations that provide medical care so driven by income and profit-generating considerations. This uniquely US development is an important cause of the health cost crisis that is destabilizing the entire economy, and it has played a major part in eroding the ethical commitments of physicians.
Many physicians have contributed to this transformation by accepting the view that medical practice is also in essence a business. Medical practice is now widely viewed as a demanding and technical business that requires extensive, credentialed education and great personal responsibilities—but a business nevertheless. This change in attitude has important consequences. In business, increasing shareholder value through increased revenue and increased profit is the primary goal. However, medical professionalism requires that physicians give even greater primacy to the medical needs of patients and to the public health of the society in which their patients live. When physicians think of themselves as being primarily in business, professional values recede and the practice of medicine changes.
Physicians have always been concerned with earning a comfortable living, and there have always been some who were driven by greed, but the current focus on moneymaking and the seductions of financial rewards have changed the climate of US medical practice at the expense of professional altruism and the moral commitment to patients.3 The vast amount of money in the US medical care system and the manifold opportunities for physicians to earn high incomes have made it almost impossible for many to function as true fiduciaries for patients.
The essence of medicine is so different from that of ordinary business that they are inherently at odds. Business concepts of good management may be useful in medical practice, but only to a degree. The fundamental ethos of medical practice contrasts sharply with that of ordinary commerce, and market principles do not apply to the relationship between physician and patient.4 Such insights have not stopped the advance of the “medical-industrial complex,”5 or prevented the growing domination of market ideology over medical professionalism.
Other forces in the new environment have also been eroding medical professionalism. The growth of technology and specialization is attracting more physicians into specialties and away from primary care.6 The greater economic rewards of procedural specialties are particularly appealing to new graduates who enter practice burdened with large educational debts. Specialization is not necessarily incompatible with ethical professional practice, but it often reduces the opportunities for personal interactions between physicians and patients and thus weakens the bond between physicians and patients. It is too easy for even the best specialists to behave simply as skilled technicians, focused exclusively on their patients’ narrow medical problems and unmindful of their professional obligations to the whole person they are serving.
The law also has played a major role in the decline of medical professionalism. The 1975 Supreme Court ruling that the professions were not protected from antitrust law7 undermined the traditional restraint that medical professional societies had always placed on the commercial behavior of physicians, such as advertising and investing in the products they prescribe or facilities they recommend. Having lost some initial legal battles and fearing the financial costs of losing more, organized medicine now hesitates to require physicians to behave differently from business people. It asks only that physicians’ business activities should be legal, disclosed to patients, and not inconsistent with patients’ interests. Until forced by antitrust concerns to change its ethical code in 1980, the American Medical Association had held that “in the practice of medicine a physician should limit the source of his professional income to medical services actually rendered by him, or under his supervision, to his patients” and that “the practice of medicine should not be commercialized, nor treated as a commodity in trade.”8 These sentiments reflecting the spirit of professionalism are now gone.
Professionalism is also compromised by the failure of physicians to exercise self-regulation that would be supported by law. Many physicians are reluctant to identify incompetent or unethical colleagues. Such behavior also undermines the public’s trust in the profession.
Yet another deprofessionalizing force has been the growing influence of the pharmaceutical industry on the practice of medicine. This industry now uses its enormous financial resources to help shape the postgraduate and continuing medical education of physicians in ways that serve its marketing purposes.9 Physicians and medical educational institutions aid and abet this influence by accepting, sometimes even soliciting, financial help and other favors from the industry, thus relinquishing what should be their professional responsibility for self-education. A medical profession that is being educated by an industry that sells the drugs physicians prescribe and other tools physicians use is abdicating its ethical commitment to serve as the independent fiduciary for its patients.10
The preservation of independent professionalism and its ethical commitment to patients still are very important because physicians are at the center of the health care system and the public must be able to depend on and trust physicians. There is currently much concern about the paternalism and elitism of medicine, and this concern is often used to justify policies seeking to establish so-called consumer-directed health care.11 Although there undoubtedly is a need for patients to have more information and responsibility for their health care choices, without trustworthy and accountable professional guidance from physicians, the health care system could not function. In the absence of physicians’ commitment to professional values, health care becomes just another industry that may, by continuing along its present course, be heading toward bankruptcy.
Physicians should not accept the industrialization of medical care, but should work instead toward major reforms that will restore the health care system to its proper role as a social service that society provides to all. Virtually every other advanced nation has achieved that goal. An essential part of the needed reforms is a rededication of physicians to the ethical professional principles on which the practice of medicine should rest. Such reforms will require public and political initiatives12 and the active participation of the medical profession.
Medical professionalism cannot survive in the current commercialized health care market. The continued privatization of health care and the continued prevalence and intrusion of market forces in the practice of medicine will not only bankrupt the health care system, but also will inevitably undermine the ethical foundations of medical practice and dissolve the moral precepts that have historically defined the medical profession. Physicians who care about these values must support major reform of both the insurance and the delivery sides of the health care system.2 It is the one policy option most likely to preserve the integrity and values of the medical profession.
ADDENDUM
The foregoing commentary, published last year in JAMA, explains why I am concerned about the “ethical challenges in surgical innovation,” the subject of this conference. Although the legal status of patent applications for surgical methods (“process patents”) has not yet been fully defined,13 such applications fortunately are relatively rare. The great majority of surgical techniques are not patented and are freely available to surgeons—as they should be. However, the devices, equipment, and implants that may be an essential part of new surgical techniques can be and are patented, and may therefore be profitable. If these patented items are developed by a staff physician or are the product of collaboration between such a physician and a company, should financial benefits accrue to the physician involved? Some say yes. They seem convinced that without some sort of financial incentive—royalties, direct payments from the manufacturer, or equity interest in the manufacturer—physicians would simply not be motivated to do innovative work, and the “translational” research essential for medical progress would languish.
I strongly disagree with this view, but unfortunately it has gained considerable influence in academic medicine in recent years, despite the fact that it conflicts with medical professional ethics. Court interpretation of antitrust law in 19757 forced the American Medical Association to abandon its long-standing ethical injunction against practicing physicians earning income from financial interests in the medical products they use or prescribe. However, antitrust legislation is not relevant here, and no legal restraints prevent medical schools, teaching hospitals, and similar medical institutions from regulating or even prohibiting such outside earnings by their full-time salaried staff. These earnings constitute a clear conflict of interest, and there is a growing national consensus that such conflicts not only should be publicly disclosed but should be regulated by the institutions employing the physicians. If the institutions do not do this job, many now believe the government should.
What is the evidence that personal financial rewards are necessary incentives for physicians to work on “translational” research? I submit that there is little or none—only an assumption. But the fact is that even before commercialization began to transform health care 3 or 4 decades ago, and even before salaried academic physicians began to earn substantial outside income from their financial ties to device and drug manufacturers, “translational” research was thriving. In the 2 or 3 decades after World War II, salaried academic physicians conducted applied medical and surgical research, often in cooperation with industry but usually without any personal gain. It is true that today there is much more “translational” research going on, but that is probably explained by the greater number of researchers working now and the much greater public and private investment in research. It does not follow that the recent growth in applied biomedical investigation would not have occurred without personal financial incentives to academic physicians and surgeons. Such an assumption not only ignores medical history but demeans the professional values that we physicians swear to live by.
If we continue to encourage, or even allow, practicing physicians and surgeons to be entrepreneurs and have financial interests in the products they use and prescribe, we will surely undermine the ethical traditions of our profession, as I have argued in the above JAMA commentary. But beyond this ethical catastrophe, such policy would surely destroy the credibility and integrity of the whole US medical research enterprise, with dire consequences for society. I believe it is time for our best clinical research institutions to insist that research cooperation with industry be conducted in a much more professional and controlled manner. Academic-industrial cooperation can often facilitate advances in research, but any financial gains for the academic side should flow to institutions, not individuals, and should be strictly regulated by law to ensure that the public interest is protected and the integrity of the medical profession preserved.
I refuse to believe that academic physicians will stop their search for innovative devices and methods for treating their patients if they are not given extra financial rewards beyond their salaries. Of course, they need to be paid well and they need the time and resources required for their research, but that should be the responsibility of their institutions, not of industry. The present shortage of time and resources for research in not-for-profit medical institutions must be addressed, but turning the responsibility over to the free market of medical entrepreneurialism is not the answer. It will lead only to a dead end for our profession and for the public stake in medical research. This is a challenge that the best and strongest US medical institutions must face up to, but government will also need to help. Our country depends on a vibrant but socially responsible and trustworthy medical research sector. That is an objective that unregulated commercial markets and private interests cannot achieve. We need academic institutions, supported by public policies, to lead the way.
- Freidson E. Professionalism: The Third Logic. Chicago, IL: University of Chicago Press; 2001.
- Relman AS. A Second Opinion: Rescuing America’s Health Care. New York, NY: Public Affairs; 2007.
- Special section: commercialism in medicine. Camb Q Healthc Ethics 2007; 16:368–445.
- Arrow KJ. Uncertainty and the welfare economics of medical care. Am Econ Rev 1963; 53:941–973.
- Relman AS. The new medical-industrial complex. N Engl J Med 1980; 303:963–997.
- Bodenheimer T. Primary care: will it survive? N Engl J Med 2006; 355:861–863.
- Goldfarb v Virginia State Bar, 421 US 773 (1975).
- American Medical Association. Opinions and Reports of the Judicial Council. Chicago, IL: American Medical Association; 1966.
- DeAngelis CD. Rainbow to dark clouds. JAMA 2005; 294:1107.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA 2001; 285:2009–2012.
- Herzlinger RE, ed. Consumer-Driven Health Care: Implications for Providers, Payers and Policy-Makers. San Francisco, CA: Jossey-Bass; 2004.
- Cohen JJ, Cruess S, Davidson C. Alliance between society and medicine: the public’s stake in medical professionalism. JAMA 2007; 298:670–673.
- Kesselheim AS, Mello MM. Medical-process patents—monopolizing the delivery of health care. N Engl J Med 2006; 355:2036– 2041.
- Freidson E. Professionalism: The Third Logic. Chicago, IL: University of Chicago Press; 2001.
- Relman AS. A Second Opinion: Rescuing America’s Health Care. New York, NY: Public Affairs; 2007.
- Special section: commercialism in medicine. Camb Q Healthc Ethics 2007; 16:368–445.
- Arrow KJ. Uncertainty and the welfare economics of medical care. Am Econ Rev 1963; 53:941–973.
- Relman AS. The new medical-industrial complex. N Engl J Med 1980; 303:963–997.
- Bodenheimer T. Primary care: will it survive? N Engl J Med 2006; 355:861–863.
- Goldfarb v Virginia State Bar, 421 US 773 (1975).
- American Medical Association. Opinions and Reports of the Judicial Council. Chicago, IL: American Medical Association; 1966.
- DeAngelis CD. Rainbow to dark clouds. JAMA 2005; 294:1107.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA 2001; 285:2009–2012.
- Herzlinger RE, ed. Consumer-Driven Health Care: Implications for Providers, Payers and Policy-Makers. San Francisco, CA: Jossey-Bass; 2004.
- Cohen JJ, Cruess S, Davidson C. Alliance between society and medicine: the public’s stake in medical professionalism. JAMA 2007; 298:670–673.
- Kesselheim AS, Mello MM. Medical-process patents—monopolizing the delivery of health care. N Engl J Med 2006; 355:2036– 2041.