User login
Helping patients cope with traumatic loss
When tragedies like the Aurora, Colo., and Newtown, Conn., shootings occur, we wonder whether people can ever overcome their grief and find a way to move on with their lives. Froma Walsh, Ph.D., a leading authority on family resilience, has developed an approach that can be used to strengthen families and communities that have suffered such tragedies.
Dr. Walsh is the codirector and cofounder of the Chicago Center for Family Health, and the Mose and Sylvia Firestone Professor Emerita in the school of social service administration and department of psychiatry at the University of Chicago.

Resilience originally was described as individual resilience. Dr. Walsh, who has broadened that concept, provides us with important steps to understand how to help heal families and communities that suffer from unimaginable trauma and loss.
Individual resilience
Beginning in the 1960s, British psychiatrist Sir Michael Rutter studied youth from inner-city London and on the Isle of Wight. Even though they experienced many risk factors, 25% of the children had a good outcome. The children who showed individual resilience had the following characteristics: an easy temperament; female; a positive school climate; self-mastery; self-efficacy; planning skills; and a warm, close, personal relationship with an adult.
From 1955 to 1985, American researchers Emmy E. Werner, Ph.D., and Ruth S. Smith, Ph.D., studied a high-risk population of children in Hawaii and found that 36% showed individual resilience, despite their risk factors. Resilient personal characteristics found in this study were similar: being female, socially responsible, adaptable, tolerant, achievement oriented, a good communicator, and having good self-esteem as well as a caring environment inside and outside the family.
Acquiring resilient qualities
After traumatic events happen, how do people cope? How does the coping process result in growth? We are all familiar with the saying: "What doesn’t break you makes you stronger." This is resilience. How can we help families and communities become stronger?
Family resilience
Dr. Walsh developed the concept of family resilience and a practice framework, identifying key family processes that clinicians can target to strengthen family resilience. She is quick to point out that resilience does not lie in specific characteristics, but rather in family processes that promote resilience. These family processes include a family belief system that pulls family members together and forward, the ability to have hope, a spiritual or value orientation to draw meaning and new purpose out of a tragedy, being able to organize family life to meet challenges, reaching out to extended kin and community networks, collaborative problem solving, and clear communication between members.
Her article, "Traumatic loss and major disasters: strengthening family and community resilience," identifies ways that professionals can help families cope with traumatic loss (Fam. Process 2007;46:207-27). She identifies nine aspects of family life as being key factors in families being able to cope well with traumatic loss:.
• Making meaning of traumatic loss experience. Families ask "Why us?" Families need to make sense of their experiences in a way that allows them to live on. "New meaning" highlights the strengths of the survivors and shows a "new way" of relating to the world and to others. As psychiatrists, we can support the family in finding their own meaning, by helping them examine their beliefs about blame, responsibility, or negligence; and helping them come to terms with accountability and limits of control in the situation.
• Hope. Families need to regain hope in their future possibilities. How does this family want to continue and what does this family want to become? Although they cannot change what has happened, we can support their efforts to "master the possible" by promoting active agency in doing all they can as they move forward.
• Transcendence and spirituality. Families can use their personal values and faith communities for support and to help with forgiveness. Honoring those who died with memorials, anniversary remembrances, and celebrations of milestones in recovery will facilitate healing and growth. These rituals help affirm social values of goodness and compassion. "Recovery is a journey of the heart and spirit, bringing survivors back to the fullness of life," Dr. Walsh wrote in her article.
• Flexibility and stability. Flexibility allows adaptation in the family and allows it to stabilize. Families need to buffer the upheaval and restore security, reliability, and continuity in daily routines. They might need to construct a "new normal" in their lives.
• Connectedness. Each family member has her own adaptation to loss, but family members need to remain mutually supportive. If relationships have prior unresolved conflicts, distress can be worse. Family therapy can prove helpful.
• Extended kin and social resources. Reach out to friends, neighbors, health care providers, clergy and congregational support, school teachers and counselors, employers and coworkers, and neighborhood or community organizations. Multifamily community support groups can help families exchange information, share painful memories and feelings, provide mutual support, and encourage hope and efforts for recovery.
• Clear, consistent information. Families often need help to clarify facts and circumstances of traumatic events and to help their children understand, as age appropriate.
• Emotional sharing and support. Families and the community will experience a wide range of feelings. It is important to allow painful or unacceptable feelings to be expressed and supported, even when differences are viewed as threatening, to avoid the risk of future somatic and emotional disturbance, destructive behavior, or substance abuse. Journals and artwork are helpful, especially with children.
• Collaborative problem solving. Family and communities can coordinate collaborative efforts to promote recovery and resilience. Learning from their experience, they can take steps proactively to prevent future tragedies. One mother who lost a child in the Newtown massacre said she wanted her family and her community to be defined not by their tragedy and suffering, but by the way they are responding, by galvanizing action to stop gun violence.
Community resilience
Community resilience is promoted by Dr. Judith Landau and Jack Saul, Ph.D. in a book edited by Dr. Walsh and Monica McGoldrick, Ph.D., called "Living Beyond Loss: Death in the Family" (see list of further reading below). Community members can create a support system that connects individuals and families. Community support provides a highly connected and reality based understanding. Ongoing support groups can respond accurately to the community needs. Perhaps the community might create a neighborhood resource center or a public space to gather, a witness project, or a community website. Such interventions can have a long-lasting positive impact on the community and the families.
Professional resilience
Compassion fatigue can occur when witnessing trauma and in experiencing ongoing distress. Mental health professionals cannot heal all wounds, but we can create a safe haven for family and community members to share pain and their seeking a new path.
Kaethe Weingarten, Ph.D., has developed a compassionate witnessing project aimed at helping professionals understand the importance of "witnessing" suffering and struggle. She encourages professionals to become aware of their own responses to witnessing trauma and to develop tools to cope with the effects of witnessing trauma.
A family resilience approach is a very positive and constructive way that we can use to teach families how to make sense of what has happened and how to move forward, as difficult as that may currently seem to be.
Further reading:
Here is a list of additional reading you can do to help patients who are facing unimaginable loss:
• "Common Shock: Witnessing Violence Every Day," (New York: Dutton, 2003)
• "Family Resilience: A Framework for Clinical Practice," (Family Process 2003;42:1-18)
• "Living Beyond Loss: Death in the Family," (New York: Norton, 2004, 2nd ed.).
• "Resilience Concepts and Findings: Implications for Family Therapy," (J. Family Therapy 1999;21:119-44).
• "Strengthening Family Resilience," (New York: Guilford Press, 2006)
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. E-mail Dr. Heru at cpnews@elsevier.com.
When tragedies like the Aurora, Colo., and Newtown, Conn., shootings occur, we wonder whether people can ever overcome their grief and find a way to move on with their lives. Froma Walsh, Ph.D., a leading authority on family resilience, has developed an approach that can be used to strengthen families and communities that have suffered such tragedies.
Dr. Walsh is the codirector and cofounder of the Chicago Center for Family Health, and the Mose and Sylvia Firestone Professor Emerita in the school of social service administration and department of psychiatry at the University of Chicago.
Resilience originally was described as individual resilience. Dr. Walsh, who has broadened that concept, provides us with important steps to understand how to help heal families and communities that suffer from unimaginable trauma and loss.
Individual resilience
Beginning in the 1960s, British psychiatrist Sir Michael Rutter studied youth from inner-city London and on the Isle of Wight. Even though they experienced many risk factors, 25% of the children had a good outcome. The children who showed individual resilience had the following characteristics: an easy temperament; female; a positive school climate; self-mastery; self-efficacy; planning skills; and a warm, close, personal relationship with an adult.
From 1955 to 1985, American researchers Emmy E. Werner, Ph.D., and Ruth S. Smith, Ph.D., studied a high-risk population of children in Hawaii and found that 36% showed individual resilience, despite their risk factors. Resilient personal characteristics found in this study were similar: being female, socially responsible, adaptable, tolerant, achievement oriented, a good communicator, and having good self-esteem as well as a caring environment inside and outside the family.
Acquiring resilient qualities
After traumatic events happen, how do people cope? How does the coping process result in growth? We are all familiar with the saying: "What doesn’t break you makes you stronger." This is resilience. How can we help families and communities become stronger?
Family resilience
Dr. Walsh developed the concept of family resilience and a practice framework, identifying key family processes that clinicians can target to strengthen family resilience. She is quick to point out that resilience does not lie in specific characteristics, but rather in family processes that promote resilience. These family processes include a family belief system that pulls family members together and forward, the ability to have hope, a spiritual or value orientation to draw meaning and new purpose out of a tragedy, being able to organize family life to meet challenges, reaching out to extended kin and community networks, collaborative problem solving, and clear communication between members.
Her article, "Traumatic loss and major disasters: strengthening family and community resilience," identifies ways that professionals can help families cope with traumatic loss (Fam. Process 2007;46:207-27). She identifies nine aspects of family life as being key factors in families being able to cope well with traumatic loss:.
• Making meaning of traumatic loss experience. Families ask "Why us?" Families need to make sense of their experiences in a way that allows them to live on. "New meaning" highlights the strengths of the survivors and shows a "new way" of relating to the world and to others. As psychiatrists, we can support the family in finding their own meaning, by helping them examine their beliefs about blame, responsibility, or negligence; and helping them come to terms with accountability and limits of control in the situation.
• Hope. Families need to regain hope in their future possibilities. How does this family want to continue and what does this family want to become? Although they cannot change what has happened, we can support their efforts to "master the possible" by promoting active agency in doing all they can as they move forward.
• Transcendence and spirituality. Families can use their personal values and faith communities for support and to help with forgiveness. Honoring those who died with memorials, anniversary remembrances, and celebrations of milestones in recovery will facilitate healing and growth. These rituals help affirm social values of goodness and compassion. "Recovery is a journey of the heart and spirit, bringing survivors back to the fullness of life," Dr. Walsh wrote in her article.
• Flexibility and stability. Flexibility allows adaptation in the family and allows it to stabilize. Families need to buffer the upheaval and restore security, reliability, and continuity in daily routines. They might need to construct a "new normal" in their lives.
• Connectedness. Each family member has her own adaptation to loss, but family members need to remain mutually supportive. If relationships have prior unresolved conflicts, distress can be worse. Family therapy can prove helpful.
• Extended kin and social resources. Reach out to friends, neighbors, health care providers, clergy and congregational support, school teachers and counselors, employers and coworkers, and neighborhood or community organizations. Multifamily community support groups can help families exchange information, share painful memories and feelings, provide mutual support, and encourage hope and efforts for recovery.
• Clear, consistent information. Families often need help to clarify facts and circumstances of traumatic events and to help their children understand, as age appropriate.
• Emotional sharing and support. Families and the community will experience a wide range of feelings. It is important to allow painful or unacceptable feelings to be expressed and supported, even when differences are viewed as threatening, to avoid the risk of future somatic and emotional disturbance, destructive behavior, or substance abuse. Journals and artwork are helpful, especially with children.
• Collaborative problem solving. Family and communities can coordinate collaborative efforts to promote recovery and resilience. Learning from their experience, they can take steps proactively to prevent future tragedies. One mother who lost a child in the Newtown massacre said she wanted her family and her community to be defined not by their tragedy and suffering, but by the way they are responding, by galvanizing action to stop gun violence.
Community resilience
Community resilience is promoted by Dr. Judith Landau and Jack Saul, Ph.D. in a book edited by Dr. Walsh and Monica McGoldrick, Ph.D., called "Living Beyond Loss: Death in the Family" (see list of further reading below). Community members can create a support system that connects individuals and families. Community support provides a highly connected and reality based understanding. Ongoing support groups can respond accurately to the community needs. Perhaps the community might create a neighborhood resource center or a public space to gather, a witness project, or a community website. Such interventions can have a long-lasting positive impact on the community and the families.
Professional resilience
Compassion fatigue can occur when witnessing trauma and in experiencing ongoing distress. Mental health professionals cannot heal all wounds, but we can create a safe haven for family and community members to share pain and their seeking a new path.
Kaethe Weingarten, Ph.D., has developed a compassionate witnessing project aimed at helping professionals understand the importance of "witnessing" suffering and struggle. She encourages professionals to become aware of their own responses to witnessing trauma and to develop tools to cope with the effects of witnessing trauma.
A family resilience approach is a very positive and constructive way that we can use to teach families how to make sense of what has happened and how to move forward, as difficult as that may currently seem to be.
Further reading:
Here is a list of additional reading you can do to help patients who are facing unimaginable loss:
• "Common Shock: Witnessing Violence Every Day," (New York: Dutton, 2003)
• "Family Resilience: A Framework for Clinical Practice," (Family Process 2003;42:1-18)
• "Living Beyond Loss: Death in the Family," (New York: Norton, 2004, 2nd ed.).
• "Resilience Concepts and Findings: Implications for Family Therapy," (J. Family Therapy 1999;21:119-44).
• "Strengthening Family Resilience," (New York: Guilford Press, 2006)
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. E-mail Dr. Heru at cpnews@elsevier.com.
When tragedies like the Aurora, Colo., and Newtown, Conn., shootings occur, we wonder whether people can ever overcome their grief and find a way to move on with their lives. Froma Walsh, Ph.D., a leading authority on family resilience, has developed an approach that can be used to strengthen families and communities that have suffered such tragedies.
Dr. Walsh is the codirector and cofounder of the Chicago Center for Family Health, and the Mose and Sylvia Firestone Professor Emerita in the school of social service administration and department of psychiatry at the University of Chicago.
Resilience originally was described as individual resilience. Dr. Walsh, who has broadened that concept, provides us with important steps to understand how to help heal families and communities that suffer from unimaginable trauma and loss.
Individual resilience
Beginning in the 1960s, British psychiatrist Sir Michael Rutter studied youth from inner-city London and on the Isle of Wight. Even though they experienced many risk factors, 25% of the children had a good outcome. The children who showed individual resilience had the following characteristics: an easy temperament; female; a positive school climate; self-mastery; self-efficacy; planning skills; and a warm, close, personal relationship with an adult.
From 1955 to 1985, American researchers Emmy E. Werner, Ph.D., and Ruth S. Smith, Ph.D., studied a high-risk population of children in Hawaii and found that 36% showed individual resilience, despite their risk factors. Resilient personal characteristics found in this study were similar: being female, socially responsible, adaptable, tolerant, achievement oriented, a good communicator, and having good self-esteem as well as a caring environment inside and outside the family.
Acquiring resilient qualities
After traumatic events happen, how do people cope? How does the coping process result in growth? We are all familiar with the saying: "What doesn’t break you makes you stronger." This is resilience. How can we help families and communities become stronger?
Family resilience
Dr. Walsh developed the concept of family resilience and a practice framework, identifying key family processes that clinicians can target to strengthen family resilience. She is quick to point out that resilience does not lie in specific characteristics, but rather in family processes that promote resilience. These family processes include a family belief system that pulls family members together and forward, the ability to have hope, a spiritual or value orientation to draw meaning and new purpose out of a tragedy, being able to organize family life to meet challenges, reaching out to extended kin and community networks, collaborative problem solving, and clear communication between members.
Her article, "Traumatic loss and major disasters: strengthening family and community resilience," identifies ways that professionals can help families cope with traumatic loss (Fam. Process 2007;46:207-27). She identifies nine aspects of family life as being key factors in families being able to cope well with traumatic loss:.
• Making meaning of traumatic loss experience. Families ask "Why us?" Families need to make sense of their experiences in a way that allows them to live on. "New meaning" highlights the strengths of the survivors and shows a "new way" of relating to the world and to others. As psychiatrists, we can support the family in finding their own meaning, by helping them examine their beliefs about blame, responsibility, or negligence; and helping them come to terms with accountability and limits of control in the situation.
• Hope. Families need to regain hope in their future possibilities. How does this family want to continue and what does this family want to become? Although they cannot change what has happened, we can support their efforts to "master the possible" by promoting active agency in doing all they can as they move forward.
• Transcendence and spirituality. Families can use their personal values and faith communities for support and to help with forgiveness. Honoring those who died with memorials, anniversary remembrances, and celebrations of milestones in recovery will facilitate healing and growth. These rituals help affirm social values of goodness and compassion. "Recovery is a journey of the heart and spirit, bringing survivors back to the fullness of life," Dr. Walsh wrote in her article.
• Flexibility and stability. Flexibility allows adaptation in the family and allows it to stabilize. Families need to buffer the upheaval and restore security, reliability, and continuity in daily routines. They might need to construct a "new normal" in their lives.
• Connectedness. Each family member has her own adaptation to loss, but family members need to remain mutually supportive. If relationships have prior unresolved conflicts, distress can be worse. Family therapy can prove helpful.
• Extended kin and social resources. Reach out to friends, neighbors, health care providers, clergy and congregational support, school teachers and counselors, employers and coworkers, and neighborhood or community organizations. Multifamily community support groups can help families exchange information, share painful memories and feelings, provide mutual support, and encourage hope and efforts for recovery.
• Clear, consistent information. Families often need help to clarify facts and circumstances of traumatic events and to help their children understand, as age appropriate.
• Emotional sharing and support. Families and the community will experience a wide range of feelings. It is important to allow painful or unacceptable feelings to be expressed and supported, even when differences are viewed as threatening, to avoid the risk of future somatic and emotional disturbance, destructive behavior, or substance abuse. Journals and artwork are helpful, especially with children.
• Collaborative problem solving. Family and communities can coordinate collaborative efforts to promote recovery and resilience. Learning from their experience, they can take steps proactively to prevent future tragedies. One mother who lost a child in the Newtown massacre said she wanted her family and her community to be defined not by their tragedy and suffering, but by the way they are responding, by galvanizing action to stop gun violence.
Community resilience
Community resilience is promoted by Dr. Judith Landau and Jack Saul, Ph.D. in a book edited by Dr. Walsh and Monica McGoldrick, Ph.D., called "Living Beyond Loss: Death in the Family" (see list of further reading below). Community members can create a support system that connects individuals and families. Community support provides a highly connected and reality based understanding. Ongoing support groups can respond accurately to the community needs. Perhaps the community might create a neighborhood resource center or a public space to gather, a witness project, or a community website. Such interventions can have a long-lasting positive impact on the community and the families.
Professional resilience
Compassion fatigue can occur when witnessing trauma and in experiencing ongoing distress. Mental health professionals cannot heal all wounds, but we can create a safe haven for family and community members to share pain and their seeking a new path.
Kaethe Weingarten, Ph.D., has developed a compassionate witnessing project aimed at helping professionals understand the importance of "witnessing" suffering and struggle. She encourages professionals to become aware of their own responses to witnessing trauma and to develop tools to cope with the effects of witnessing trauma.
A family resilience approach is a very positive and constructive way that we can use to teach families how to make sense of what has happened and how to move forward, as difficult as that may currently seem to be.
Further reading:
Here is a list of additional reading you can do to help patients who are facing unimaginable loss:
• "Common Shock: Witnessing Violence Every Day," (New York: Dutton, 2003)
• "Family Resilience: A Framework for Clinical Practice," (Family Process 2003;42:1-18)
• "Living Beyond Loss: Death in the Family," (New York: Norton, 2004, 2nd ed.).
• "Resilience Concepts and Findings: Implications for Family Therapy," (J. Family Therapy 1999;21:119-44).
• "Strengthening Family Resilience," (New York: Guilford Press, 2006)
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. E-mail Dr. Heru at cpnews@elsevier.com.
Paclitaxel-eluting stent approved for PAD
The Food and Drug Administration has approved a new paclitaxel-eluting stent indciated for the treatment of peripheral artery disease.
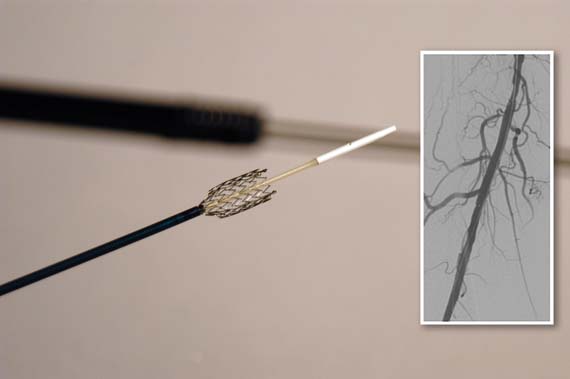
The Zilver PTX Drug-Eluting Peripheral Stent, which is manufactured by Cook Medical of Bloomington, Ind., is the first drug-eluting stent to win approval for this indication.
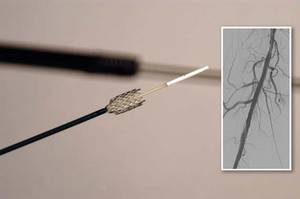
The approval was based on findings from both a randomized controlled trial and on a registry study, which together comprised more than 1,200 patients.
According to an FDA press statement, the studies indicate that treatment with the stent "is at least as safe as treatment with percutaneous transluminal angioplasty (PTA) and significantly more effective."
The randomized trial included a total of 479 patients who had a single stenotic lesion less than 140 mm in one or both of the femoropopliteal arteries.
The patients were randomized to the paclitaxel-eluting stent or to PTA. If the transluminal procedure failed, then the patients received either the paclitaxel-eluting stent or a bare-metal stent.
After 12 months, 83% of the arteries treated with the drug-eluting stent were still open, compared with 33% of those in the PTA group.
In those patients who had the stent placed after a failed PTA, 90% of arteries were open, compared with 73% in those who got the bare-metal stent.
In October 2011, the FDA's Circulatory System Devices Panel voted 11 to 0 that the benefits of the Zilver PTX stent outweighed its risks as a treatment for patients with symptomatic atherosclerotic stenosis of the femoropopliteal arteries on the basis of that trial.
This past October, the 3-year results of the study were presented at the Vascular Interventional Advances 2012 meeting in Las Vegas. The results showed that there was a 70.7% primary patency seen for the paclitaxel-eluting stent, compared with 49.1% for PTA and bare-metal stents.
The registry study followed 767 patients for 24 months. These patients had a maximum of four stents placed; the stents could be utilized to treat a single lesion or to treat multiple lesions.
At 12 months, the fracture rate was 1.5%; fractures were not associated with any clinical problems. The rate of stent thrombosis was 2.8% at 12 months and 3.5% at 24 months.
"The clinical study demonstrated that the [the paclitaxel-eluting stent] is more effective than the use of balloon angioplasty for the treatment of symptomatic peripheral artery disease in above-the-knee femoropopliteal artery," Christy Foreman, director of the Office of Device Evaluation at the FDA's Center for Devices and Radiological Health, said in the statement.
"This approval expands the treatment options for patients suffering from symptomatic peripheral artery disease," she added.
In both studies, the most common major adverse event was restenosis requiring additional treatment to reestablish adequate flow in the artery.
The device is contraindicated in patients with stenoses that cannot be dilated to permit passage of the catheter or proper placement of the stent.
It is also contraindicated in patients who cannot receive recommended drug therapy due to bleeding disorders, or women who are pregnant, breastfeeding, or planning to become pregnant in the next 5 years.
The FDA will now require the manufacturer to conduct a 5-year postapproval study of 900 patients to further evaluate the stent's safety and efficacy.
The banging noise you hear emanating from your radiologic imaging area is not the MRI machine, but nails being pounded into the coffin of the fem-pop bypass graft operation. Incremental but significant progress has been made in treating SFA occlusive disease over the last decade from POBA to tools that facilitate crossing/reentry of CTOs to bare-metal/covered stenting to DES. The Zilver PTX trial and registry have resulted in commercial approval of a long enough, large enough self-expanding stent to be useful in peripheral interventions.
| Dr. Brian Rubin |
Treated lesions included ISRs as well as primary atherosclerotic lesions, and data from both trials showed near-identical 12 and 24 month results, with Zilver PTX resulting in primary patency rates 15-20% higher than results with bare-metal stenting alone. As of mid-November 2012, the complete FDA 57-page PDF of both studies is available online and should be required reading While most surgeons would claim their 12 month fem-AK pop bypass patency to be better than the 83% primary patency reported for Zilver PTX, multiple recent published reports suggest otherwise.
A number of important issues remain unresolved including: 1. how much will each stent cost? (the grapevine has it that the pricing will be surprisingly low) 2. am I really limited to a maximum of 14 cm treated length per leg? (probably not since paclitaxel levels peaked at less than 30 minutes, were gone within a few hours and were very low anyway 3. what antiplatelet therapy is required? (still to be determined- ASA alone is probably adequate) and 4. how do I treat smaller diameter vessels? (Zilver PTX is only approved in 6-8 mm diameters). Although 3-year data have recently been reported, the long-term outcomes after DES remain unknown at this time.
While fem-pop bypass may still find limited utility and needs to remain in the surgical armamentarium, the commercial approval of Zilver PTX stents has nibbled away again at the difference in outcomes between endovascular and open surgical therapy for SFA occlusive disease.
If other studies including long-term outcome reports confirm these initial salutary results, the fem-pop graft will soon follow the utilization curve of open aortic surgery and become an endangered operation.
Dr. Brian Rubin is a professor of the department of surgery at the Washington University School of Medicine, St. Louis.
The banging noise you hear emanating from your radiologic imaging area is not the MRI machine, but nails being pounded into the coffin of the fem-pop bypass graft operation. Incremental but significant progress has been made in treating SFA occlusive disease over the last decade from POBA to tools that facilitate crossing/reentry of CTOs to bare-metal/covered stenting to DES. The Zilver PTX trial and registry have resulted in commercial approval of a long enough, large enough self-expanding stent to be useful in peripheral interventions.
| Dr. Brian Rubin |
Treated lesions included ISRs as well as primary atherosclerotic lesions, and data from both trials showed near-identical 12 and 24 month results, with Zilver PTX resulting in primary patency rates 15-20% higher than results with bare-metal stenting alone. As of mid-November 2012, the complete FDA 57-page PDF of both studies is available online and should be required reading While most surgeons would claim their 12 month fem-AK pop bypass patency to be better than the 83% primary patency reported for Zilver PTX, multiple recent published reports suggest otherwise.
A number of important issues remain unresolved including: 1. how much will each stent cost? (the grapevine has it that the pricing will be surprisingly low) 2. am I really limited to a maximum of 14 cm treated length per leg? (probably not since paclitaxel levels peaked at less than 30 minutes, were gone within a few hours and were very low anyway 3. what antiplatelet therapy is required? (still to be determined- ASA alone is probably adequate) and 4. how do I treat smaller diameter vessels? (Zilver PTX is only approved in 6-8 mm diameters). Although 3-year data have recently been reported, the long-term outcomes after DES remain unknown at this time.
While fem-pop bypass may still find limited utility and needs to remain in the surgical armamentarium, the commercial approval of Zilver PTX stents has nibbled away again at the difference in outcomes between endovascular and open surgical therapy for SFA occlusive disease.
If other studies including long-term outcome reports confirm these initial salutary results, the fem-pop graft will soon follow the utilization curve of open aortic surgery and become an endangered operation.
Dr. Brian Rubin is a professor of the department of surgery at the Washington University School of Medicine, St. Louis.
The banging noise you hear emanating from your radiologic imaging area is not the MRI machine, but nails being pounded into the coffin of the fem-pop bypass graft operation. Incremental but significant progress has been made in treating SFA occlusive disease over the last decade from POBA to tools that facilitate crossing/reentry of CTOs to bare-metal/covered stenting to DES. The Zilver PTX trial and registry have resulted in commercial approval of a long enough, large enough self-expanding stent to be useful in peripheral interventions.
| Dr. Brian Rubin |
Treated lesions included ISRs as well as primary atherosclerotic lesions, and data from both trials showed near-identical 12 and 24 month results, with Zilver PTX resulting in primary patency rates 15-20% higher than results with bare-metal stenting alone. As of mid-November 2012, the complete FDA 57-page PDF of both studies is available online and should be required reading While most surgeons would claim their 12 month fem-AK pop bypass patency to be better than the 83% primary patency reported for Zilver PTX, multiple recent published reports suggest otherwise.
A number of important issues remain unresolved including: 1. how much will each stent cost? (the grapevine has it that the pricing will be surprisingly low) 2. am I really limited to a maximum of 14 cm treated length per leg? (probably not since paclitaxel levels peaked at less than 30 minutes, were gone within a few hours and were very low anyway 3. what antiplatelet therapy is required? (still to be determined- ASA alone is probably adequate) and 4. how do I treat smaller diameter vessels? (Zilver PTX is only approved in 6-8 mm diameters). Although 3-year data have recently been reported, the long-term outcomes after DES remain unknown at this time.
While fem-pop bypass may still find limited utility and needs to remain in the surgical armamentarium, the commercial approval of Zilver PTX stents has nibbled away again at the difference in outcomes between endovascular and open surgical therapy for SFA occlusive disease.
If other studies including long-term outcome reports confirm these initial salutary results, the fem-pop graft will soon follow the utilization curve of open aortic surgery and become an endangered operation.
Dr. Brian Rubin is a professor of the department of surgery at the Washington University School of Medicine, St. Louis.
The Food and Drug Administration has approved a new paclitaxel-eluting stent indciated for the treatment of peripheral artery disease.
The Zilver PTX Drug-Eluting Peripheral Stent, which is manufactured by Cook Medical of Bloomington, Ind., is the first drug-eluting stent to win approval for this indication.
The approval was based on findings from both a randomized controlled trial and on a registry study, which together comprised more than 1,200 patients.
According to an FDA press statement, the studies indicate that treatment with the stent "is at least as safe as treatment with percutaneous transluminal angioplasty (PTA) and significantly more effective."
The randomized trial included a total of 479 patients who had a single stenotic lesion less than 140 mm in one or both of the femoropopliteal arteries.
The patients were randomized to the paclitaxel-eluting stent or to PTA. If the transluminal procedure failed, then the patients received either the paclitaxel-eluting stent or a bare-metal stent.
After 12 months, 83% of the arteries treated with the drug-eluting stent were still open, compared with 33% of those in the PTA group.
In those patients who had the stent placed after a failed PTA, 90% of arteries were open, compared with 73% in those who got the bare-metal stent.
In October 2011, the FDA's Circulatory System Devices Panel voted 11 to 0 that the benefits of the Zilver PTX stent outweighed its risks as a treatment for patients with symptomatic atherosclerotic stenosis of the femoropopliteal arteries on the basis of that trial.
This past October, the 3-year results of the study were presented at the Vascular Interventional Advances 2012 meeting in Las Vegas. The results showed that there was a 70.7% primary patency seen for the paclitaxel-eluting stent, compared with 49.1% for PTA and bare-metal stents.
The registry study followed 767 patients for 24 months. These patients had a maximum of four stents placed; the stents could be utilized to treat a single lesion or to treat multiple lesions.
At 12 months, the fracture rate was 1.5%; fractures were not associated with any clinical problems. The rate of stent thrombosis was 2.8% at 12 months and 3.5% at 24 months.
"The clinical study demonstrated that the [the paclitaxel-eluting stent] is more effective than the use of balloon angioplasty for the treatment of symptomatic peripheral artery disease in above-the-knee femoropopliteal artery," Christy Foreman, director of the Office of Device Evaluation at the FDA's Center for Devices and Radiological Health, said in the statement.
"This approval expands the treatment options for patients suffering from symptomatic peripheral artery disease," she added.
In both studies, the most common major adverse event was restenosis requiring additional treatment to reestablish adequate flow in the artery.
The device is contraindicated in patients with stenoses that cannot be dilated to permit passage of the catheter or proper placement of the stent.
It is also contraindicated in patients who cannot receive recommended drug therapy due to bleeding disorders, or women who are pregnant, breastfeeding, or planning to become pregnant in the next 5 years.
The FDA will now require the manufacturer to conduct a 5-year postapproval study of 900 patients to further evaluate the stent's safety and efficacy.
The Food and Drug Administration has approved a new paclitaxel-eluting stent indciated for the treatment of peripheral artery disease.
The Zilver PTX Drug-Eluting Peripheral Stent, which is manufactured by Cook Medical of Bloomington, Ind., is the first drug-eluting stent to win approval for this indication.
The approval was based on findings from both a randomized controlled trial and on a registry study, which together comprised more than 1,200 patients.
According to an FDA press statement, the studies indicate that treatment with the stent "is at least as safe as treatment with percutaneous transluminal angioplasty (PTA) and significantly more effective."
The randomized trial included a total of 479 patients who had a single stenotic lesion less than 140 mm in one or both of the femoropopliteal arteries.
The patients were randomized to the paclitaxel-eluting stent or to PTA. If the transluminal procedure failed, then the patients received either the paclitaxel-eluting stent or a bare-metal stent.
After 12 months, 83% of the arteries treated with the drug-eluting stent were still open, compared with 33% of those in the PTA group.
In those patients who had the stent placed after a failed PTA, 90% of arteries were open, compared with 73% in those who got the bare-metal stent.
In October 2011, the FDA's Circulatory System Devices Panel voted 11 to 0 that the benefits of the Zilver PTX stent outweighed its risks as a treatment for patients with symptomatic atherosclerotic stenosis of the femoropopliteal arteries on the basis of that trial.
This past October, the 3-year results of the study were presented at the Vascular Interventional Advances 2012 meeting in Las Vegas. The results showed that there was a 70.7% primary patency seen for the paclitaxel-eluting stent, compared with 49.1% for PTA and bare-metal stents.
The registry study followed 767 patients for 24 months. These patients had a maximum of four stents placed; the stents could be utilized to treat a single lesion or to treat multiple lesions.
At 12 months, the fracture rate was 1.5%; fractures were not associated with any clinical problems. The rate of stent thrombosis was 2.8% at 12 months and 3.5% at 24 months.
"The clinical study demonstrated that the [the paclitaxel-eluting stent] is more effective than the use of balloon angioplasty for the treatment of symptomatic peripheral artery disease in above-the-knee femoropopliteal artery," Christy Foreman, director of the Office of Device Evaluation at the FDA's Center for Devices and Radiological Health, said in the statement.
"This approval expands the treatment options for patients suffering from symptomatic peripheral artery disease," she added.
In both studies, the most common major adverse event was restenosis requiring additional treatment to reestablish adequate flow in the artery.
The device is contraindicated in patients with stenoses that cannot be dilated to permit passage of the catheter or proper placement of the stent.
It is also contraindicated in patients who cannot receive recommended drug therapy due to bleeding disorders, or women who are pregnant, breastfeeding, or planning to become pregnant in the next 5 years.
The FDA will now require the manufacturer to conduct a 5-year postapproval study of 900 patients to further evaluate the stent's safety and efficacy.
Thirty-day readmissions and the posthospital syndrome
Most of us struggle to be proficient in that fine art of balancing high-quality, cost-effective medical care, patient and family satisfaction, and length of stay. One, or even two, of these without the other, just won’t cut muster these days, and with the CMS Hospital Readmissions Reduction Program, the pressure is on to cut readmissions within 30 days of discharge, or else! (Section 3025 of the Affordable Care Act requires the CMS to reduce payments to acute care hospitals with excessive readmission rates as of Oct. 1, 2012.)
Realistically, we all know that even if we provide the best medical care possible, there will always be patients with chronic, end-stage disease whom we will never "fix." The best we can do is optimize the quality of their lives until they die or are readmitted and the cycle begins again. But there may be much more we as hospitalists can do to optimize the overall care of our patients to improve their outcomes, and save our hospitals a great deal of money at the same time.
"Post-Hospital Syndrome – An Acquired, Transient Condition of Generalized Risk" an article published Jan. 10 in the New England Journal of Medicine, gives excellent insight into underappreciated factors that result in readmission to the hospital (N. Engl. J. Med. 2013;368:100-2). Approximately one-fifth of Medicare patients admitted to a hospital require readmission within 30 days, surprisingly often for conditions completely unrelated to the original reason for admission. For instance, among patients initially admitted for heart failure, only 37% of readmissions within 30 days were for worsening heart failure. Likewise, after a hospitalization for a COPD exacerbation, only 36% of readmissions within 30 days were for another exacerbation.
Regardless of the original reason for admission, common causes of readmission include infection, gastrointestinal conditions, metabolic derangements, mental illness, trauma, heart failure, COPD, and pneumonia. And, despite what would seem intuitive, the severity of the initial illness did not help predict which patients would require readmission.
Sleep deprivation is a major contributor to postdischarge morbidity. Polysomnographic studies have demonstrated a reduction in REM sleep and an increase in non-REM sleep in hospitalized patients. Sleep deprivation is known to adversely impact immune function, cardiac risk, and even the coagulation cascade, in addition to the more obvious things such as mental function, ability to ambulate safely, and emotional well-being.
Inadequate nutrition is another culprit. Between being NPO for procedures, which are commonly rescheduled, feeling too sick (or too groggy) to eat, and the increased catabolic demands of many acute illnesses, the pendulum often swings far away from a homeostasis into a potentially dangerous zone, despite how the patient may look at first glance. Some potential consequences of poor nutrition include impaired wound healing, increased infection risk, and decreased cardiac and respiratory function.
Other factors, such as uncontrolled pain, a host of new medications – with myriad side effects – and deconditioning from lying in bed for prolonged periods also play key roles in setting patients up for a potentially debilitating vulnerability that often results in yet another acute illness requiring hospitalization not long after their initial discharge.
We ought to start thinking about discharge planning when we first admit patients. Based on this article, we need to include innovative ways to decrease the posthospital syndrome. There are some simple things we can do: Optimize pain control, get them out of bed as soon as possible, and create an environment to facilitate peaceful sleep. For example, we can easily minimize interruptions during early morning hours for vital sign checks and blood draws in stable patients. (Do we really need routine follow-up lab to be drawn at 6 a.m. in every patient?)
We should all think about our workflow and what we can do differently to minimize the physiologic vulnerability of our patients at discharge so they can be safely discharged (and stay discharged).
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care.
Most of us struggle to be proficient in that fine art of balancing high-quality, cost-effective medical care, patient and family satisfaction, and length of stay. One, or even two, of these without the other, just won’t cut muster these days, and with the CMS Hospital Readmissions Reduction Program, the pressure is on to cut readmissions within 30 days of discharge, or else! (Section 3025 of the Affordable Care Act requires the CMS to reduce payments to acute care hospitals with excessive readmission rates as of Oct. 1, 2012.)
Realistically, we all know that even if we provide the best medical care possible, there will always be patients with chronic, end-stage disease whom we will never "fix." The best we can do is optimize the quality of their lives until they die or are readmitted and the cycle begins again. But there may be much more we as hospitalists can do to optimize the overall care of our patients to improve their outcomes, and save our hospitals a great deal of money at the same time.
"Post-Hospital Syndrome – An Acquired, Transient Condition of Generalized Risk" an article published Jan. 10 in the New England Journal of Medicine, gives excellent insight into underappreciated factors that result in readmission to the hospital (N. Engl. J. Med. 2013;368:100-2). Approximately one-fifth of Medicare patients admitted to a hospital require readmission within 30 days, surprisingly often for conditions completely unrelated to the original reason for admission. For instance, among patients initially admitted for heart failure, only 37% of readmissions within 30 days were for worsening heart failure. Likewise, after a hospitalization for a COPD exacerbation, only 36% of readmissions within 30 days were for another exacerbation.
Regardless of the original reason for admission, common causes of readmission include infection, gastrointestinal conditions, metabolic derangements, mental illness, trauma, heart failure, COPD, and pneumonia. And, despite what would seem intuitive, the severity of the initial illness did not help predict which patients would require readmission.
Sleep deprivation is a major contributor to postdischarge morbidity. Polysomnographic studies have demonstrated a reduction in REM sleep and an increase in non-REM sleep in hospitalized patients. Sleep deprivation is known to adversely impact immune function, cardiac risk, and even the coagulation cascade, in addition to the more obvious things such as mental function, ability to ambulate safely, and emotional well-being.
Inadequate nutrition is another culprit. Between being NPO for procedures, which are commonly rescheduled, feeling too sick (or too groggy) to eat, and the increased catabolic demands of many acute illnesses, the pendulum often swings far away from a homeostasis into a potentially dangerous zone, despite how the patient may look at first glance. Some potential consequences of poor nutrition include impaired wound healing, increased infection risk, and decreased cardiac and respiratory function.
Other factors, such as uncontrolled pain, a host of new medications – with myriad side effects – and deconditioning from lying in bed for prolonged periods also play key roles in setting patients up for a potentially debilitating vulnerability that often results in yet another acute illness requiring hospitalization not long after their initial discharge.
We ought to start thinking about discharge planning when we first admit patients. Based on this article, we need to include innovative ways to decrease the posthospital syndrome. There are some simple things we can do: Optimize pain control, get them out of bed as soon as possible, and create an environment to facilitate peaceful sleep. For example, we can easily minimize interruptions during early morning hours for vital sign checks and blood draws in stable patients. (Do we really need routine follow-up lab to be drawn at 6 a.m. in every patient?)
We should all think about our workflow and what we can do differently to minimize the physiologic vulnerability of our patients at discharge so they can be safely discharged (and stay discharged).
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care.
Most of us struggle to be proficient in that fine art of balancing high-quality, cost-effective medical care, patient and family satisfaction, and length of stay. One, or even two, of these without the other, just won’t cut muster these days, and with the CMS Hospital Readmissions Reduction Program, the pressure is on to cut readmissions within 30 days of discharge, or else! (Section 3025 of the Affordable Care Act requires the CMS to reduce payments to acute care hospitals with excessive readmission rates as of Oct. 1, 2012.)
Realistically, we all know that even if we provide the best medical care possible, there will always be patients with chronic, end-stage disease whom we will never "fix." The best we can do is optimize the quality of their lives until they die or are readmitted and the cycle begins again. But there may be much more we as hospitalists can do to optimize the overall care of our patients to improve their outcomes, and save our hospitals a great deal of money at the same time.
"Post-Hospital Syndrome – An Acquired, Transient Condition of Generalized Risk" an article published Jan. 10 in the New England Journal of Medicine, gives excellent insight into underappreciated factors that result in readmission to the hospital (N. Engl. J. Med. 2013;368:100-2). Approximately one-fifth of Medicare patients admitted to a hospital require readmission within 30 days, surprisingly often for conditions completely unrelated to the original reason for admission. For instance, among patients initially admitted for heart failure, only 37% of readmissions within 30 days were for worsening heart failure. Likewise, after a hospitalization for a COPD exacerbation, only 36% of readmissions within 30 days were for another exacerbation.
Regardless of the original reason for admission, common causes of readmission include infection, gastrointestinal conditions, metabolic derangements, mental illness, trauma, heart failure, COPD, and pneumonia. And, despite what would seem intuitive, the severity of the initial illness did not help predict which patients would require readmission.
Sleep deprivation is a major contributor to postdischarge morbidity. Polysomnographic studies have demonstrated a reduction in REM sleep and an increase in non-REM sleep in hospitalized patients. Sleep deprivation is known to adversely impact immune function, cardiac risk, and even the coagulation cascade, in addition to the more obvious things such as mental function, ability to ambulate safely, and emotional well-being.
Inadequate nutrition is another culprit. Between being NPO for procedures, which are commonly rescheduled, feeling too sick (or too groggy) to eat, and the increased catabolic demands of many acute illnesses, the pendulum often swings far away from a homeostasis into a potentially dangerous zone, despite how the patient may look at first glance. Some potential consequences of poor nutrition include impaired wound healing, increased infection risk, and decreased cardiac and respiratory function.
Other factors, such as uncontrolled pain, a host of new medications – with myriad side effects – and deconditioning from lying in bed for prolonged periods also play key roles in setting patients up for a potentially debilitating vulnerability that often results in yet another acute illness requiring hospitalization not long after their initial discharge.
We ought to start thinking about discharge planning when we first admit patients. Based on this article, we need to include innovative ways to decrease the posthospital syndrome. There are some simple things we can do: Optimize pain control, get them out of bed as soon as possible, and create an environment to facilitate peaceful sleep. For example, we can easily minimize interruptions during early morning hours for vital sign checks and blood draws in stable patients. (Do we really need routine follow-up lab to be drawn at 6 a.m. in every patient?)
We should all think about our workflow and what we can do differently to minimize the physiologic vulnerability of our patients at discharge so they can be safely discharged (and stay discharged).
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care.

The power of culture
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.

Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.
Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.
Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.

Lab test for multiple gastroenteritis pathogens cleared for use
A test that can detect multiple causes of infectious gastroenteritis in one stool sample has been cleared for marketing by the Food and Drug Administration.
The xTAG Gastrointestinal Pathogen Panel (GPP), a multiplexed nucleic acid test, is the "first test that can simultaneously detect 11 common viral, bacterial, and parasitic causes of infectious gastroenteritis from a single patient sample," the agency said in a Jan. 14 statement announcing the approval.

The xTAG GPP tests for the bacteria Campylobacter, Clostridium difficile toxin A/B, Escherichia coli O157, enterotoxigenic E. coli (ETEC) LT/ST, Salmonella, Shigella, and Shiga-like toxin-producing E. coli (STEC) stx1/stx2; the viruses norovirus and rotavirus A; and the parasites Cryptosporidium and Giardia lamblia.
This test can help clinicians identify and treat the cause of gastroenteritis in patients more quickly, and "could also allow clinicians and public health professionals to more quickly identify and investigate the source of potential gastroenteritis outbreaks," Alberto Gutierrez, Ph.D., director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health, said in the statement.
In studies conducted by the manufacturer, Luminex, results of the xTAG GPP were "comparable" with the results of individual tests for the 11 pathogens in stool samples from 1,407 patients with suspected infectious gastroenteritis, 313 samples from pediatric patients with suspected infectious gastroenteritis, and 203 samples from patients with confirmed cases of infectious gastroenteritis, according to the FDA. Because of the risk of false positives, "all positive results from the xTAG GPP need to be confirmed by additional testing," the agency’s announcement said.
The test, which is now available in the United States, can provide multiple results within 5 hours. It is the first and most comprehensive multiplexed product of its kind in the United States, according to a statement from Luminex.
The FDA cites data from the Centers for Disease Control and Prevention reporting that the number of deaths associated with gastroenteritis increased from nearly 7,000 to more than 17,000 per year between 1999 and 2007 in the United States. Two-thirds of the deaths were attributed to norovirus and C. difficile.
A test that can detect multiple causes of infectious gastroenteritis in one stool sample has been cleared for marketing by the Food and Drug Administration.
The xTAG Gastrointestinal Pathogen Panel (GPP), a multiplexed nucleic acid test, is the "first test that can simultaneously detect 11 common viral, bacterial, and parasitic causes of infectious gastroenteritis from a single patient sample," the agency said in a Jan. 14 statement announcing the approval.
The xTAG GPP tests for the bacteria Campylobacter, Clostridium difficile toxin A/B, Escherichia coli O157, enterotoxigenic E. coli (ETEC) LT/ST, Salmonella, Shigella, and Shiga-like toxin-producing E. coli (STEC) stx1/stx2; the viruses norovirus and rotavirus A; and the parasites Cryptosporidium and Giardia lamblia.
This test can help clinicians identify and treat the cause of gastroenteritis in patients more quickly, and "could also allow clinicians and public health professionals to more quickly identify and investigate the source of potential gastroenteritis outbreaks," Alberto Gutierrez, Ph.D., director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health, said in the statement.
In studies conducted by the manufacturer, Luminex, results of the xTAG GPP were "comparable" with the results of individual tests for the 11 pathogens in stool samples from 1,407 patients with suspected infectious gastroenteritis, 313 samples from pediatric patients with suspected infectious gastroenteritis, and 203 samples from patients with confirmed cases of infectious gastroenteritis, according to the FDA. Because of the risk of false positives, "all positive results from the xTAG GPP need to be confirmed by additional testing," the agency’s announcement said.
The test, which is now available in the United States, can provide multiple results within 5 hours. It is the first and most comprehensive multiplexed product of its kind in the United States, according to a statement from Luminex.
The FDA cites data from the Centers for Disease Control and Prevention reporting that the number of deaths associated with gastroenteritis increased from nearly 7,000 to more than 17,000 per year between 1999 and 2007 in the United States. Two-thirds of the deaths were attributed to norovirus and C. difficile.
A test that can detect multiple causes of infectious gastroenteritis in one stool sample has been cleared for marketing by the Food and Drug Administration.
The xTAG Gastrointestinal Pathogen Panel (GPP), a multiplexed nucleic acid test, is the "first test that can simultaneously detect 11 common viral, bacterial, and parasitic causes of infectious gastroenteritis from a single patient sample," the agency said in a Jan. 14 statement announcing the approval.
The xTAG GPP tests for the bacteria Campylobacter, Clostridium difficile toxin A/B, Escherichia coli O157, enterotoxigenic E. coli (ETEC) LT/ST, Salmonella, Shigella, and Shiga-like toxin-producing E. coli (STEC) stx1/stx2; the viruses norovirus and rotavirus A; and the parasites Cryptosporidium and Giardia lamblia.
This test can help clinicians identify and treat the cause of gastroenteritis in patients more quickly, and "could also allow clinicians and public health professionals to more quickly identify and investigate the source of potential gastroenteritis outbreaks," Alberto Gutierrez, Ph.D., director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health, said in the statement.
In studies conducted by the manufacturer, Luminex, results of the xTAG GPP were "comparable" with the results of individual tests for the 11 pathogens in stool samples from 1,407 patients with suspected infectious gastroenteritis, 313 samples from pediatric patients with suspected infectious gastroenteritis, and 203 samples from patients with confirmed cases of infectious gastroenteritis, according to the FDA. Because of the risk of false positives, "all positive results from the xTAG GPP need to be confirmed by additional testing," the agency’s announcement said.
The test, which is now available in the United States, can provide multiple results within 5 hours. It is the first and most comprehensive multiplexed product of its kind in the United States, according to a statement from Luminex.
The FDA cites data from the Centers for Disease Control and Prevention reporting that the number of deaths associated with gastroenteritis increased from nearly 7,000 to more than 17,000 per year between 1999 and 2007 in the United States. Two-thirds of the deaths were attributed to norovirus and C. difficile.
TORS: Postop bleeding risk rises with antithrombotic use
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY; HEAD AND NECK SURGERY FOUNDATION
Major Finding: Approximately three-quarters of patients (8 of 11) who underwent TORS and experienced some postop bleeding were on an antithrombotic medication.
Data Source: A review of 147 consecutive patients at a single surgery center.
Disclosures: Dr. Asher said he had no relevant financial conflicts.
Statins cut risk of hepatocellular carcinoma
Statin therapy taken to prevent cardiovascular events also appears to protect against hepatocellular carcinoma, reducing the overall risk for the cancer by 37%, according to the results of a systematic review and meta-analysis.
In a meta-analysis of all the studies in the literature that have examined statins’ effect on HCC risk, use of the drugs was associated with a pronounced and consistent risk reduction (48%) in Asian populations, as well as a still-significant reduction (33%) in Western populations, reported Dr. Siddharth Singh and his associates at the Mayo Clinic, Rochester, Minn.
Video source: American Gastroenterological Association's YouTube page
At present, "it does not seem prudent to prescribe statins for chemoprevention" of HCC in the general population, mainly because of the high number of people who would need to be treated to prevent a single case of HCC. "However, in patients with multiple risk factors, such as East Asian men who have chronic HBV [hepatitis B virus] infection, statins may have a clinically relevant chemoprotective effect against HCC, the investigators said (Gastroenterology 2012 Oct. 15 [doi: 10.1053/j.gastro.2012.10.005]).
Prospective cohort studies or randomized clinical trials of the issue are warranted in populations at high risk for HCC, they noted.
The results of preclinical studies have suggested that statins may decrease the risk of cancers, perhaps because their antiproliferative, proapoptotic, antiangiogenic, immunomodulatory, and anti-infective effects may prevent cancer growth. But clinical studies have produced conflicting results.
Dr. Singh and his colleagues performed a systematic review of the literature for studies that clearly defined statin exposure, reported HCC risk, and either reported relative risks or odds ratios for the development of HCC or provided the data so those risks could be calculated. They then performed a meta-analysis of 10 studies: 7 observational studies and 3 that reported pooled data from 26 randomized clinical trials.
Most of the studies were considered to be of high quality. Most of them accounted for various potential confounders such as patient age; sex; medication use; and the presence of viral hepatitis, cirrhosis, diabetes, or alcoholic liver disease. The likelihood of selection bias and of publication bias in the included studies was judged to be very low.
Altogether the 10 studies included 1,459,417 subjects and 4,298 cases of HCC.
In an initial analysis of the data, the use of statins was associated with a significant 41% reduction in the rate of HCC. After the data were adjusted to account for several potential confounders, the risk reduction was altered slightly, but a robust 37% reduction in HCC rate remained.
The investigators also performed an analysis of the data based on the location of the studies, because the epidemiology of HCC is so different between Western and Asian populations. They found that statin use correlated with a 48% reduction in the rate of HCC in Asian populations, where viral hepatitis is the primary risk factor for the disease, and a 33% reduction in the rate of HCC in Western populations, where the metabolic syndrome, nonalcoholic fatty liver disease, and alcohol-related cirrhosis are the primary risk factors.
The researchers also performed sensitivity analyses according to the studies’ design (cohort vs. case control) and quality (high vs. low). Both cohort and case-control studies confirmed a protective effect of statins against the development of HCC, as did both high-quality and low-quality studies.
In a final sensitivity analysis, each study was serially excluded from the meta-analysis to determine whether any one study was having a dominant effect on the odds ratios. None of the studies was found to markedly affect the outcomes of the analyses.
The study design didn’t permit separate analyses of the protective effects of statins by drug type or by dose or duration of therapy.
The studies included in this meta-analysis were too heterogeneous to allow the investigators to calculate an overall number needed to treat. But the studies restricted to Asian patients were homogeneous and did allow this calculation for men of Asian ethnicity.
Dr. Singh and his associates determined that 5,209 East Asian men would need to be treated with statins to prevent 1 case of HCC per year. For very-high-risk Asian men with chronic HBV-associated cirrhosis, the number needed to treat with statins to prevent 1 case of HCC per year would be 57.
No financial conflicts of interest were reported.
Statin therapy taken to prevent cardiovascular events also appears to protect against hepatocellular carcinoma, reducing the overall risk for the cancer by 37%, according to the results of a systematic review and meta-analysis.
In a meta-analysis of all the studies in the literature that have examined statins’ effect on HCC risk, use of the drugs was associated with a pronounced and consistent risk reduction (48%) in Asian populations, as well as a still-significant reduction (33%) in Western populations, reported Dr. Siddharth Singh and his associates at the Mayo Clinic, Rochester, Minn.
Video source: American Gastroenterological Association's YouTube page
At present, "it does not seem prudent to prescribe statins for chemoprevention" of HCC in the general population, mainly because of the high number of people who would need to be treated to prevent a single case of HCC. "However, in patients with multiple risk factors, such as East Asian men who have chronic HBV [hepatitis B virus] infection, statins may have a clinically relevant chemoprotective effect against HCC, the investigators said (Gastroenterology 2012 Oct. 15 [doi: 10.1053/j.gastro.2012.10.005]).
Prospective cohort studies or randomized clinical trials of the issue are warranted in populations at high risk for HCC, they noted.
The results of preclinical studies have suggested that statins may decrease the risk of cancers, perhaps because their antiproliferative, proapoptotic, antiangiogenic, immunomodulatory, and anti-infective effects may prevent cancer growth. But clinical studies have produced conflicting results.
Dr. Singh and his colleagues performed a systematic review of the literature for studies that clearly defined statin exposure, reported HCC risk, and either reported relative risks or odds ratios for the development of HCC or provided the data so those risks could be calculated. They then performed a meta-analysis of 10 studies: 7 observational studies and 3 that reported pooled data from 26 randomized clinical trials.
Most of the studies were considered to be of high quality. Most of them accounted for various potential confounders such as patient age; sex; medication use; and the presence of viral hepatitis, cirrhosis, diabetes, or alcoholic liver disease. The likelihood of selection bias and of publication bias in the included studies was judged to be very low.
Altogether the 10 studies included 1,459,417 subjects and 4,298 cases of HCC.
In an initial analysis of the data, the use of statins was associated with a significant 41% reduction in the rate of HCC. After the data were adjusted to account for several potential confounders, the risk reduction was altered slightly, but a robust 37% reduction in HCC rate remained.
The investigators also performed an analysis of the data based on the location of the studies, because the epidemiology of HCC is so different between Western and Asian populations. They found that statin use correlated with a 48% reduction in the rate of HCC in Asian populations, where viral hepatitis is the primary risk factor for the disease, and a 33% reduction in the rate of HCC in Western populations, where the metabolic syndrome, nonalcoholic fatty liver disease, and alcohol-related cirrhosis are the primary risk factors.
The researchers also performed sensitivity analyses according to the studies’ design (cohort vs. case control) and quality (high vs. low). Both cohort and case-control studies confirmed a protective effect of statins against the development of HCC, as did both high-quality and low-quality studies.
In a final sensitivity analysis, each study was serially excluded from the meta-analysis to determine whether any one study was having a dominant effect on the odds ratios. None of the studies was found to markedly affect the outcomes of the analyses.
The study design didn’t permit separate analyses of the protective effects of statins by drug type or by dose or duration of therapy.
The studies included in this meta-analysis were too heterogeneous to allow the investigators to calculate an overall number needed to treat. But the studies restricted to Asian patients were homogeneous and did allow this calculation for men of Asian ethnicity.
Dr. Singh and his associates determined that 5,209 East Asian men would need to be treated with statins to prevent 1 case of HCC per year. For very-high-risk Asian men with chronic HBV-associated cirrhosis, the number needed to treat with statins to prevent 1 case of HCC per year would be 57.
No financial conflicts of interest were reported.
Statin therapy taken to prevent cardiovascular events also appears to protect against hepatocellular carcinoma, reducing the overall risk for the cancer by 37%, according to the results of a systematic review and meta-analysis.
In a meta-analysis of all the studies in the literature that have examined statins’ effect on HCC risk, use of the drugs was associated with a pronounced and consistent risk reduction (48%) in Asian populations, as well as a still-significant reduction (33%) in Western populations, reported Dr. Siddharth Singh and his associates at the Mayo Clinic, Rochester, Minn.
Video source: American Gastroenterological Association's YouTube page
At present, "it does not seem prudent to prescribe statins for chemoprevention" of HCC in the general population, mainly because of the high number of people who would need to be treated to prevent a single case of HCC. "However, in patients with multiple risk factors, such as East Asian men who have chronic HBV [hepatitis B virus] infection, statins may have a clinically relevant chemoprotective effect against HCC, the investigators said (Gastroenterology 2012 Oct. 15 [doi: 10.1053/j.gastro.2012.10.005]).
Prospective cohort studies or randomized clinical trials of the issue are warranted in populations at high risk for HCC, they noted.
The results of preclinical studies have suggested that statins may decrease the risk of cancers, perhaps because their antiproliferative, proapoptotic, antiangiogenic, immunomodulatory, and anti-infective effects may prevent cancer growth. But clinical studies have produced conflicting results.
Dr. Singh and his colleagues performed a systematic review of the literature for studies that clearly defined statin exposure, reported HCC risk, and either reported relative risks or odds ratios for the development of HCC or provided the data so those risks could be calculated. They then performed a meta-analysis of 10 studies: 7 observational studies and 3 that reported pooled data from 26 randomized clinical trials.
Most of the studies were considered to be of high quality. Most of them accounted for various potential confounders such as patient age; sex; medication use; and the presence of viral hepatitis, cirrhosis, diabetes, or alcoholic liver disease. The likelihood of selection bias and of publication bias in the included studies was judged to be very low.
Altogether the 10 studies included 1,459,417 subjects and 4,298 cases of HCC.
In an initial analysis of the data, the use of statins was associated with a significant 41% reduction in the rate of HCC. After the data were adjusted to account for several potential confounders, the risk reduction was altered slightly, but a robust 37% reduction in HCC rate remained.
The investigators also performed an analysis of the data based on the location of the studies, because the epidemiology of HCC is so different between Western and Asian populations. They found that statin use correlated with a 48% reduction in the rate of HCC in Asian populations, where viral hepatitis is the primary risk factor for the disease, and a 33% reduction in the rate of HCC in Western populations, where the metabolic syndrome, nonalcoholic fatty liver disease, and alcohol-related cirrhosis are the primary risk factors.
The researchers also performed sensitivity analyses according to the studies’ design (cohort vs. case control) and quality (high vs. low). Both cohort and case-control studies confirmed a protective effect of statins against the development of HCC, as did both high-quality and low-quality studies.
In a final sensitivity analysis, each study was serially excluded from the meta-analysis to determine whether any one study was having a dominant effect on the odds ratios. None of the studies was found to markedly affect the outcomes of the analyses.
The study design didn’t permit separate analyses of the protective effects of statins by drug type or by dose or duration of therapy.
The studies included in this meta-analysis were too heterogeneous to allow the investigators to calculate an overall number needed to treat. But the studies restricted to Asian patients were homogeneous and did allow this calculation for men of Asian ethnicity.
Dr. Singh and his associates determined that 5,209 East Asian men would need to be treated with statins to prevent 1 case of HCC per year. For very-high-risk Asian men with chronic HBV-associated cirrhosis, the number needed to treat with statins to prevent 1 case of HCC per year would be 57.
No financial conflicts of interest were reported.
FROM GASTROENTEROLOGY
Major Finding: Statin therapy reduced the risk of developing hepatocellular carcinoma by 37% overall; the risk reduction was stronger (48%) in Asian populations but still significant (33%) in Western populations.
Data Source: A systematic review and meta-analysis of 10 observational studies or randomized clinical trials involving 1,459,417 subjects, of whom 4,298 developed HCC during follow-up.
Disclosures: No financial conflicts of interest were reported.
Case of the Month
A 56-year-old Hispanic female with a past medical history significant for basal cell carcinoma presented with a history of itchy, erythematous papules on her right cheek. Four days prior, she presented for suture removal after reconstruction with an island pedicle flap following Mohs micrographic surgery. She experienced a similar rash on her forearm following another surgery in the past.
a) Cellulitis
b) Contact dermatitis
c) Herpes simplex virus
Diagnosis: Contact dermatitis secondary to Mastisol and Steri-Strips

Contact dermatitis is a localized, pruritic, erythematous rash that occurs after contact with a certain allergen or irritant. The disorder is typically classified as either allergic contact dermatitis or irritant contact dermatitis.
Allergic contact dermatitis is a T cell–mediated, type-IV, delayed-type hypersensitivity reaction that requires prior sensitization with the causative agent before the patient becomes allergic to it. The typical rash of pruritus, erythema, edema, and vesicle formation occurs with further exposures.
The mechanism of immune response to a particular allergen requires that the antigen be of low molecular weight (less than 500 d) in order to penetrate the stratum corneum and gain access to the immunologic system. CD4, CD8, T regulatory cells, and natural killer T cells have all been implicated.
The process is composed of an afferent (sensitization) phase and an efferent (elicitation) phase.
Common haptens or immunogenic agents include nickel, urushiol from poison ivy resin, ultraviolet light, dyes, and fragrances.
This patient revealed a history of a similar reaction to the one presented in this case following wound dressing on her forearm with two products: Steri-Strips and Mastisol liquid adhesive. Unfortunately, she did not reveal this history until she had experienced the reaction a second time. The patient was instructed to apply hydrocortisone 1% cream twice daily to the red areas only and to follow up with a clinic visit in 4-5 days. Documentation of her allergy was included in her medical record.
This case was submitted by Dr. Keyvan Nouri; Dr. Katlein Franca; Jennifer Ledon; and Jessica Savas of the University of Miami.
–Donna Bilu Martin, M.D.
A 56-year-old Hispanic female with a past medical history significant for basal cell carcinoma presented with a history of itchy, erythematous papules on her right cheek. Four days prior, she presented for suture removal after reconstruction with an island pedicle flap following Mohs micrographic surgery. She experienced a similar rash on her forearm following another surgery in the past.
a) Cellulitis
b) Contact dermatitis
c) Herpes simplex virus
Diagnosis: Contact dermatitis secondary to Mastisol and Steri-Strips
Contact dermatitis is a localized, pruritic, erythematous rash that occurs after contact with a certain allergen or irritant. The disorder is typically classified as either allergic contact dermatitis or irritant contact dermatitis.
Allergic contact dermatitis is a T cell–mediated, type-IV, delayed-type hypersensitivity reaction that requires prior sensitization with the causative agent before the patient becomes allergic to it. The typical rash of pruritus, erythema, edema, and vesicle formation occurs with further exposures.
The mechanism of immune response to a particular allergen requires that the antigen be of low molecular weight (less than 500 d) in order to penetrate the stratum corneum and gain access to the immunologic system. CD4, CD8, T regulatory cells, and natural killer T cells have all been implicated.
The process is composed of an afferent (sensitization) phase and an efferent (elicitation) phase.
Common haptens or immunogenic agents include nickel, urushiol from poison ivy resin, ultraviolet light, dyes, and fragrances.
This patient revealed a history of a similar reaction to the one presented in this case following wound dressing on her forearm with two products: Steri-Strips and Mastisol liquid adhesive. Unfortunately, she did not reveal this history until she had experienced the reaction a second time. The patient was instructed to apply hydrocortisone 1% cream twice daily to the red areas only and to follow up with a clinic visit in 4-5 days. Documentation of her allergy was included in her medical record.
This case was submitted by Dr. Keyvan Nouri; Dr. Katlein Franca; Jennifer Ledon; and Jessica Savas of the University of Miami.
–Donna Bilu Martin, M.D.
A 56-year-old Hispanic female with a past medical history significant for basal cell carcinoma presented with a history of itchy, erythematous papules on her right cheek. Four days prior, she presented for suture removal after reconstruction with an island pedicle flap following Mohs micrographic surgery. She experienced a similar rash on her forearm following another surgery in the past.
a) Cellulitis
b) Contact dermatitis
c) Herpes simplex virus
Diagnosis: Contact dermatitis secondary to Mastisol and Steri-Strips
Contact dermatitis is a localized, pruritic, erythematous rash that occurs after contact with a certain allergen or irritant. The disorder is typically classified as either allergic contact dermatitis or irritant contact dermatitis.
Allergic contact dermatitis is a T cell–mediated, type-IV, delayed-type hypersensitivity reaction that requires prior sensitization with the causative agent before the patient becomes allergic to it. The typical rash of pruritus, erythema, edema, and vesicle formation occurs with further exposures.
The mechanism of immune response to a particular allergen requires that the antigen be of low molecular weight (less than 500 d) in order to penetrate the stratum corneum and gain access to the immunologic system. CD4, CD8, T regulatory cells, and natural killer T cells have all been implicated.
The process is composed of an afferent (sensitization) phase and an efferent (elicitation) phase.
Common haptens or immunogenic agents include nickel, urushiol from poison ivy resin, ultraviolet light, dyes, and fragrances.
This patient revealed a history of a similar reaction to the one presented in this case following wound dressing on her forearm with two products: Steri-Strips and Mastisol liquid adhesive. Unfortunately, she did not reveal this history until she had experienced the reaction a second time. The patient was instructed to apply hydrocortisone 1% cream twice daily to the red areas only and to follow up with a clinic visit in 4-5 days. Documentation of her allergy was included in her medical record.
This case was submitted by Dr. Keyvan Nouri; Dr. Katlein Franca; Jennifer Ledon; and Jessica Savas of the University of Miami.
–Donna Bilu Martin, M.D.

FDA approves plasma product

The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
Academic Hospitalist Balanced Scorecard
The field of hospital medicine, now the fastest growing specialty in medical history,[1] was born out of pressure to improve the efficiency and quality of clinical care in US hospitals.[2] Delivering safe and high‐value clinical care is a central goal of the field and has been an essential component of its growth and success.
The clinical demands on academic hospitalists have grown recently, fueled by the need to staff services previously covered by housestaff, whose hours are now restricted. Despite these new demands, expectations have grown in other arenas as well. Academic hospitalist groups (AHGs) are often expected to make significant contributions in quality improvement, patient safety, education, research, and administration. With broad expectations beyond clinical care, AHGs face unique challenges. Groups that focus mainly on providing coverage and improving clinical performance may find that they are unable to fully contribute in these other domains. To be successful, AHGs must develop strategies that balance their energies, resources, and performance.
The balanced scorecard (BSC) was introduced by Kaplan and Norton in 1992 to allow corporations to view their performance broadly, rather than narrowly focusing on financial measures. The BSC requires organizations to develop a balanced portfolio of performance metrics across 4 key perspectives: financial, customers, internal processes, and learning and growth. Metrics within these perspectives should help answer fundamental questions about the organization (Table 1).[3] Over time, the BSC evolved from a performance measurement tool to a strategic management system.[4] Successful organizations translate their mission and vision to specific strategic objectives in each of the 4 perspectives, delineate how these objectives will help the organization reach its vision with a strategy map,[5] and then utilize the BSC to track and monitor performance to ensure that the vision is achieved.[6]
| BSC Perspective | Traditional Questions[3] | Questions Revised for AHCs |
|---|---|---|
| ||
| Financial | How do we look to our shareholders? | What financial condition must we be in to allow us to accomplish our mission? |
| Customers | How do customers see us? | How do we ensure that our services and products add the level of value desired by our stakeholders? |
| Internal processes | What must we excel at? | How do we produce our products and services to add maximum value for our customers and stakeholders? |
| Learning and growth | How can we continue to improve and create value? | How do we ensure that we change and improve in order to achieve our vision? |
Although originally conceived for businesses, the BSC has found its way into the healthcare industry, with reports of successful implementation in organizations ranging from individual departments to research collaboratives[7] to national healthcare systems.[8] However, there are few reports of BSC implementation in academic health centers.[9, 10] Because most academic centers are not‐for‐profit, Zelman suggests that the 4 BSC perspectives be modified to better fit their unique characteristics (Table 1).[11] To the best of our knowledge, there is no literature describing the development of a BSC in an academic hospitalist group. In this article, we describe the development of, and early experiences with, an academic hospital medicine BSC developed as part of a strategic planning initiative.
METHODS
The University of California, San Francisco (UCSF) Division of Hospital Medicine (DHM) was established in 2005. Currently, there are more than 50 faculty members, having doubled in the last 4 years. In addition to staffing several housestaff and nonhousestaff clinical services, faculty are involved in a wide variety of nonclinical endeavors at local and national levels. They participate and lead initiatives in education, faculty development, patient safety, care efficiency, quality improvement, information technology, and global health. There is an active research enterprise that generates nearly $5 million in grant funding annually.
Needs Assessment
During a division retreat in 2009, faculty identified several areas in need of improvement, including: clinical care processes, educational promotion, faculty development, and work‐life balance. Based on these needs, divisional mission and vision statements were created (Table 2).
|
| Our mission: to provide the highest quality clinical care, education, research, and innovation in academic hospital medicine. |
| Our vision: to be the best division of hospital medicine by promoting excellence, integrity, innovation, and professional satisfaction among our faculty, trainees, and staff. |
Division leadership made it a priority to create a strategic plan to address these wide‐ranging issues. To accomplish this, we recognized the need to develop a formal way of translating our vision into specific and measurable objectives, establish systems of performance measurement, improve accountability, and effectively communicate these strategic goals to the group. Based on these needs, we set out to develop a divisional BSC.
Development
At the time of BSC development, the DHM was organized into 4 functional areas: quality and safety, education, faculty development, and academics and research. A task force was formed, comprised of 8 senior faculty representing these key areas. The mission and vision statements were used as the foundation for the development of division goals and objectives. The group was careful to choose objectives within each of the 4 BSC perspectives for academic centers, as defined by Zelman (Table 1). The taskforce then brainstormed specific metrics that would track performance within the 4 functional areas. The only stipulation during this process was that the metrics had to meet the following criteria:
- Important to the division and to the individual faculty members
- Measurable through either current or developed processes
- Data are valid and their validity trusted by the faculty members
- Amenable to improvement by faculty (ie, through their individual action they could impact the metric)
From the subsequent list of metrics, we used a modified Delphi method to rank‐order them by importance to arrive at our final set of metrics. Kaplan and Norton noted that focusing on a manageable number of metrics (ie, a handful in each BSC perspective) is important for an achievable strategic vision.[6] With the metrics chosen, we identified data sources or developed new systems to collect data for which there was no current source. We assigned individuals responsible for collecting and analyzing the data, identified local or national benchmarks, if available, and established performance targets for the coming year, when possible.
The BSC is updated quarterly, and results are presented to the division during a noon meeting and posted on the division website. Metrics are re‐evaluated on a yearly basis. They are continued, modified, or discarded depending on performance and/or changes in strategic priorities.
The initial BSC focused on division‐wide metrics and performance. Early efforts to develop the scorecard were framed as experimental, with no clear decision taken regarding how metrics might ultimately be used to improve performance (ie, how public to make both individual and group results, whether to tie bonus payments to performance).
RESULTS
There were 41 initial metrics considered by the division BSC task force (Table 3). Of these, 16 were chosen for the initial BSC through the modified Delphi method. Over the past 2 years, these initial metrics have been modified to reflect current strategic goals and objectives. Figure 1 illustrates the BSC for fiscal year (FY) 2012. An online version of this, complete with graphical representations of the data and metric definitions, can be found at
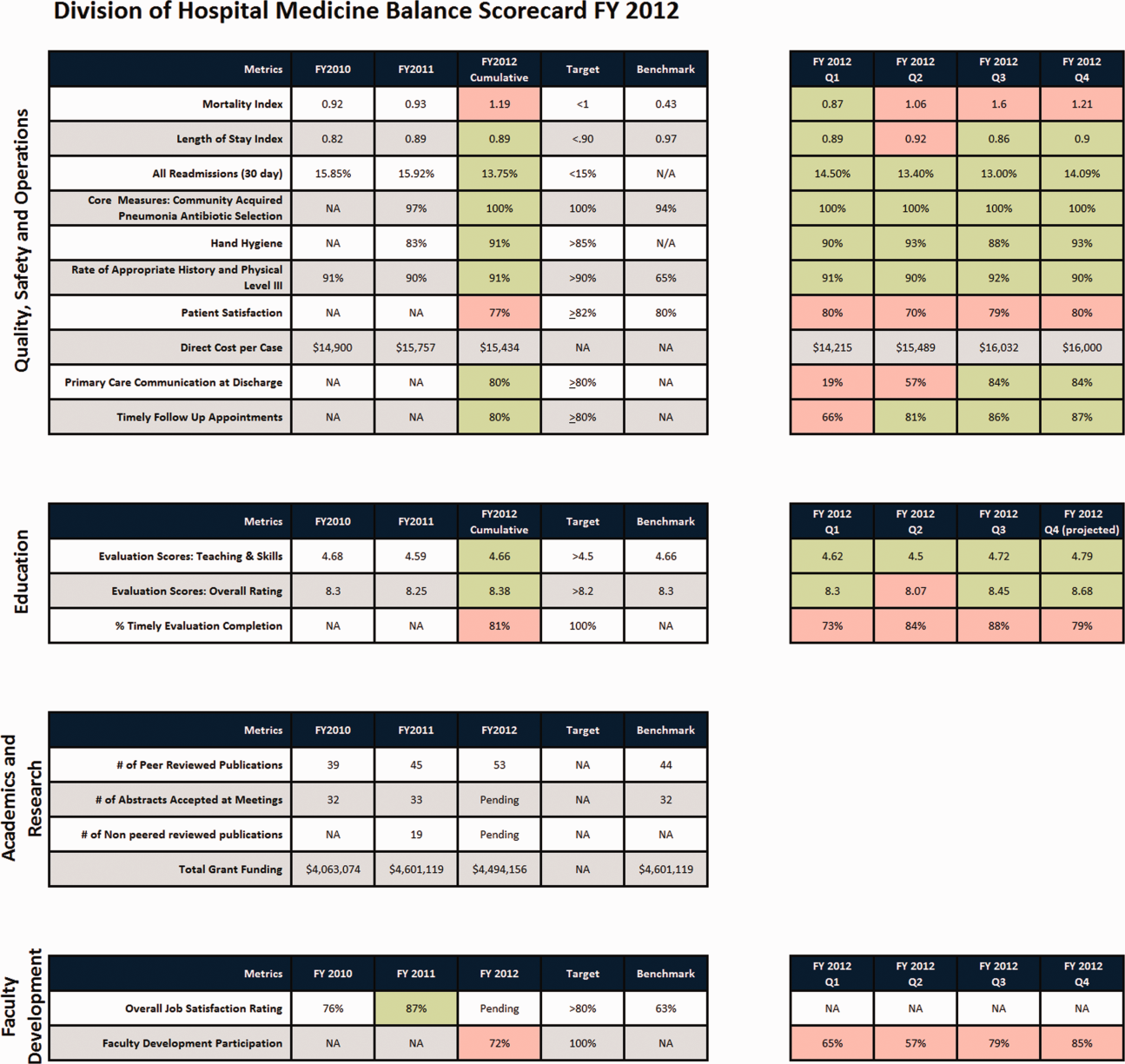
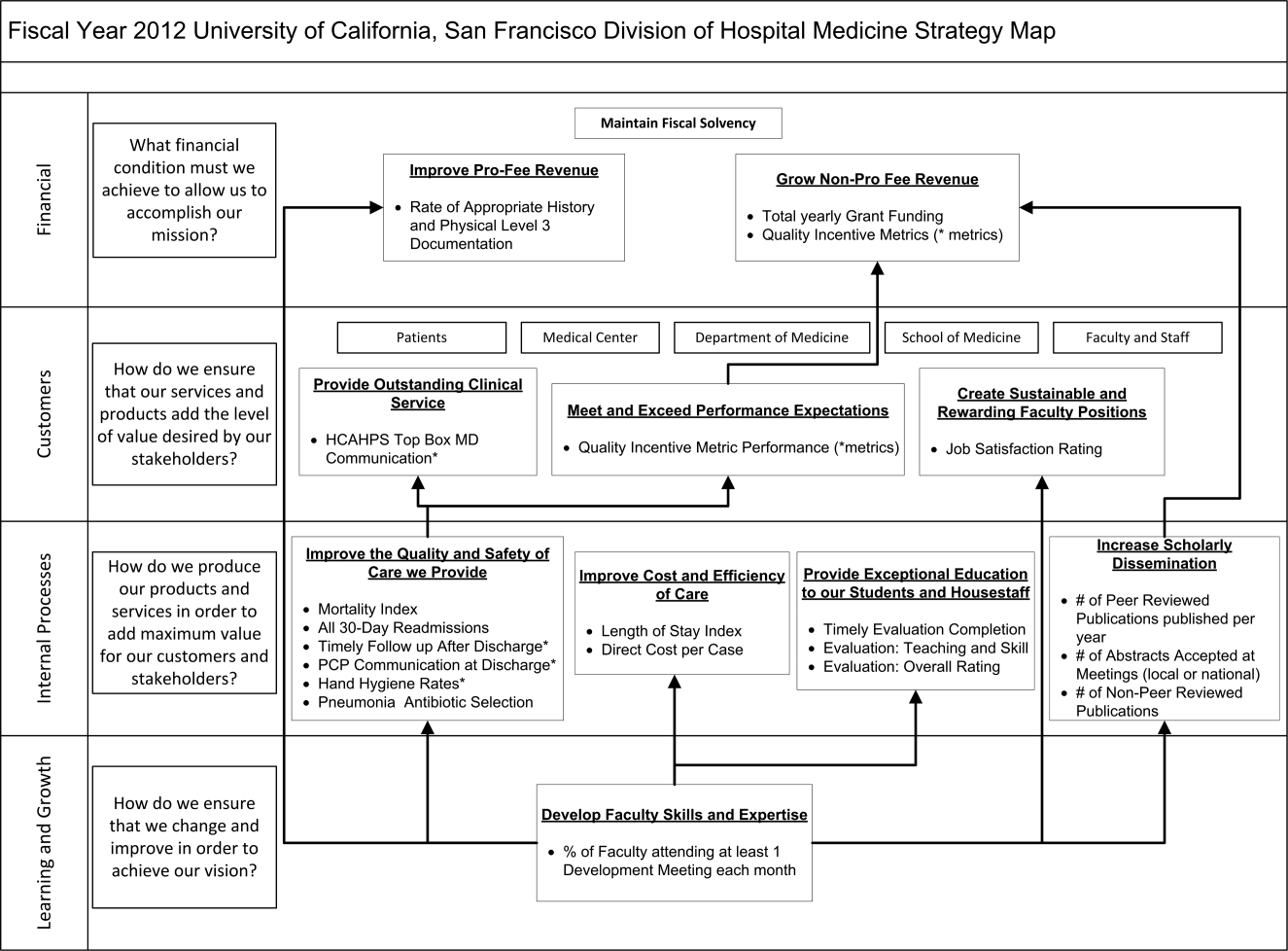
| Quality, Safety, and Operations | Education | Academics and Research | Faculty Development |
|---|---|---|---|
| |||
| Appropriate level of care | CME courses taught | Abstracts accepted | Attendance and participation |
| Billing and documentation | Curriculum development | Academic reputation | Being an agent of change |
| Clinical efficiency | Student/housestaff feedback | Grant funding | Division citizenship |
| Clinical professionalism | Mentoring | Mentorship | Job satisfaction |
| Communication | Quality of teaching rounds | Papers published | Mentorship |
| Core measures performance | Participation in national organizations | Committees and task forces | |
| Practice evidence‐based medicine | |||
| Fund of knowledge | |||
| Guideline adherence | |||
| Unplanned transfers to ICU | |||
| Implementation and initiation of projects | |||
| Length of stay | |||
| Medical errors | |||
| Mortality | |||
| Multidisciplinary approach to patient care | |||
| Multisource feedback evaluations | |||
| Never events | |||
| Patient‐centered care | |||
| Patient satisfaction | |||
| Practice‐based learning | |||
| Procedures | |||
| Readmissions | |||
| Reputation and expertise | |||
| Seeing patient on the day of admission | |||
| Quality of transfers of care | |||
DISCUSSION
Like many hospitalist groups, our division has experienced tremendous growth, both in our numbers and the breadth of roles that we fill. With this growth has come increasing expectations in multiple domains, competing priorities, and limited resources. We successfully developed a BSC as a tool to help our division reach its vision: balancing high quality clinical care, education, academics, and faculty development while maintaining a strong sense of community. We have found that the BSC has helped us meet several key goals.
The first goal was to allow for a broad view of our performance. This is the BSC's most basic function, and we saw immediate and tangible benefits. The scorecard provided a broad snapshot of our performance in a single place. For example, in the clinical domain, we saw that our direct cost per case was increasing despite our adjusted average length of stay remaining stable from FY2010‐FY2011. In academics and research, we saw that the number of abstracts accepted at national meetings increased by almost 30% in FY2011 (Figure 1).
The second goal was to create transparency and accountability. By measuring performance and displaying it on the division Web site, the BSC has promoted transparency. If performance does not meet our targets, the division as a whole becomes accountable. Leadership must understand why performance fell short and initiate changes to improve it. For instance, the rising direct cost per case has spurred the development of a high‐value care committee tasked with finding ways of reducing cost while providing high‐quality care.[12]
The third goal was to communicate goals and engage our faculty. As our division has grown, ensuring a shared vision among our entire faculty became an increasing challenge. The BSC functions as a communication platform between leadership and faculty, and yielded multiple benefits. As the metrics were born out of our mission and vision, the BSC has become a tangible representation of our core values. Moreover, individual faculty can see that they are part of a greater, high‐performing organization and realize they can impact the group's performance through their individual effort. For example, this has helped promote receptivity to carefully disseminated individual performance measures for billing and documentation, and patient satisfaction, in conjunction with faculty development in these areas.
The fourth goal was to ensure that we use data to guide strategic decisions. We felt that strategic decisions needed to be based on objective, rather than perceived or anecdotal, information. This meant translating our vision into measurable objectives that would drive performance improvement. For example, before the BSC, we were committed to the dissemination of our research and innovations. Yet, we quickly realized that we did not have a system to collect even basic data on academic performancea deficit we filled by leveraging information gathered from online databases and faculty curricula vitae. These data allowed us, for the first time, to objectively reflect on this as a strategic goal and to have an ongoing mechanism to monitor academic productivity.
Lessons Learned/Keys to Success
With our initial experience, we have gained insight that may be helpful to other AHGs considering implementing a BSC. First, and most importantly, AHGs should take the necessary time to build consensus and buy‐in. Particularly in areas where data are analyzed for the first time, faculty are often wary about the validity of the data or the purpose and utility of performance measurement. Faculty may be concerned about how collection of performance data could affect promotion or create a hostile and competitive work environment.
This concern grows when one moves from division‐wide to individual data. It is inevitable that the collection and dissemination of performance data will create some level of discomfort among faculty members, which can be a force for improvement or for angst. These issues should be anticipated, discussed, and actively managed. It is critical to be transparent with how data will be used. We have made clear that the transition from group to individual performance data, and from simple transparency to incentives, will be done thoughtfully and with tremendous input from our faculty. This tension can also be mitigated by choosing metrics that are internally driven, rather than determined by external groups (ie, following the principle that the measures should be important to the division and individual faculty members).
Next, the process of developing a mature BSC takes time. Much of our first year was spent developing systems for measurement, collecting data, and determining appropriate comparators and targets. The data in the first BSC functioned mainly as a baseline marker of performance. Some metrics, particularly in education and academics, had no national or local benchmarks. In these cases we identified comparable groups (such as other medical teaching services or other well‐established AHGs) or merely used our prior year's performance as a benchmark. Also, some of our metrics did not initially have performance targets. In most instances, this was because this was the first time that we looked at these data, and it was unclear what an appropriate target would be until more data became available.
Moving into our third year, we are seeing a natural evolution in the BSC's use. Some metrics that were initially chosen have been replaced or modified to reflect changing goals and priorities. Functional directors participate in choosing and developing performance metrics in their area. Previously, there was no formal structure for these groups to develop and measure strategic objectives and be accountable for performance improvement. They are now expected to define goals with measurable outcomes, to report progress to division leadership, and to develop their own scorecard to track performance. Each group chooses 2 to 4 metrics within their domain that are the most important for the division to improve on, which are then included in the division BSC.
We have also made efforts to build synergy between our BSC and performance goals set by external groups. Although continuing to favor metrics that are internally driven and meaningful to our faculty, we recognize that our goals must also reflect the needs and interests of broader stakeholders. For example, hand hygiene rates and patient satisfaction scores are UCSF medical center and divisional priorities (the former includes them in a financial incentive system for managers, staff, and many physicians) and are incorporated into the BSC as division‐wide incentive metrics.
Limitations
Our project has several limitations. It was conducted at a single institution, and our metrics may not be generalizable to other groups. However, the main goal of this article was not to focus on specific metrics but the process that we undertook to choose and develop them. Other institutions will likely identify different metrics based on their specific strategic objectives. We are also early in our experience with the BSC, and it is still not clear what effect it will have on the desired outcomes for our objectives. However, Henriksen recently reported that implementing a BSC at a large academic health center, in parallel with other performance improvement initiatives, resulted in substantial improvement in their chosen performance metrics.[13]
Despite the several years of development, we still view this as an early version of a BSC. To fully realize its benefits, an organization must choose metrics that will not simply measure performance but drive it. Our current BSC relies primarily on lagging measures, which show what our performance has been, and includes few leading metrics, which can predict trends in performance. As explained by Kaplan and Norton, this type of BSC risks skewing toward controlling rather than driving performance.[14] A mature BSC will include a mix of leading and lagging indicators, the combination illustrating a logical progression from measurement to performance. For instance, we measure total grant funding per year, which is a lagging indicator. However, to be most effective we could measure the percent of faculty who have attended grant‐writing workshops, the number of new grant sources identified, or the number of grant proposals submitted each quarter. These leading indicators would allow us to see performance trends that could be improved before the final outcome, total grant funding, is realized.
Finally, the issues surrounding the acceptability of this overall strategy will likely hinge on how we implement the more complex steps that relate to transparency, individual attribution, and perhaps ultimately incentives. Success in this area depends as much on culture as on strategy.
Next Steps
The next major step in the evolution of the BSC, and part of a broader faculty development program, will be the development of individual BSCs. They will be created using a similar methodology and allow faculty to reflect on their performance compared to peers and recognized benchmarks. Ideally, this will allow hospitalists in our group to establish personal strategic plans and monitor their performance over time. Individualizing these BSCs will be critical; although a research‐oriented faculty member might be striving for more than 5 publications and a large grant in a year, a clinician‐educator may seek outstanding teaching reviews and completion of a key quality improvement project. Both efforts need to be highly valued, and the divisional BSC should roll up these varied individual goals into a balanced whole.
In conclusion, we successfully developed and implemented a BSC to aid in strategic planning. The BSC ensures that we make strategic decisions using data, identify internally driven objectives, develop systems of performance measurement, and increase transparency and accountability. Our hope is that this description of the development of our BSC will be useful to other groups considering a similar endeavor.
Acknowledgments
The authors thank Noori Dhillon, Sadaf Akbaryar, Katie Quinn, Gerri Berg, and Maria Novelero for data collection and analysis. The authors also thank the faculty and staff who participated in the development process of the BSC.
Disclosure
Nothing to report.
- . The hospitalist field turns 15: new opportunities and challenges. J Hosp Med. 2011;6(4):E1–E4.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , . The balanced scorecard—measures that drive performance. Harv Bus Rev. 1992;70(1):71–79.
- , . Using the balanced scorecard as a strategic management system. Harv Bus Rev. 1996;74(1):75–85.
- , . Having trouble with your strategy? Then map it. Harv Bus Rev. 2000;78:167–176, 202.
- , . Putting the balanced scorecard to work. Harv Bus Rev. 1993;71:134–147.
- , , , et al. Development and implementation of a performance measure tool in an academic pediatric research network. Contemp Clin Trials. 2010;31(5):429–437.
- , . Lives in the balance: an analysis of the balanced scorecard (BSC) in healthcare organizations. Int J Prod Perform Manag. 2007;57(1):6–21.
- , . The “Balanced Scorecard”: development and implementation in an academic clinical department. Acad Med. 1999;74(2):114–122.
- . Introducing a balanced scorecard management system in a university anesthesiology department. Anesth Analg. 2002;95(6):1731–1738, table of contents.
- , , , , . Issues for academic health centers to consider before implementing a balanced‐scorecard effort. Acad Med. 1999;74(12):1269–1277.
- , . Cents and sensitivity—teaching physicians to think about costs. N Engl J Med. 2012;367(2):99–101.
- , , , et al. 10‐year experience integrating strategic performance improvement initiatives: can the balanced scorecard, Six Sigma, and team training all thrive in a single hospital? In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3. Performance and Tools. Rockville, MD: Agency for Healthcare Research and Quality; 2008. Available at: http://www.ncbi.nlm.nih.gov/books/NBK43660. Accessed 15 June 2011.
- , . Linking the balanced scorecard to strategy. Calif Manage Rev. 1996;39(1):53–79.
The field of hospital medicine, now the fastest growing specialty in medical history,[1] was born out of pressure to improve the efficiency and quality of clinical care in US hospitals.[2] Delivering safe and high‐value clinical care is a central goal of the field and has been an essential component of its growth and success.
The clinical demands on academic hospitalists have grown recently, fueled by the need to staff services previously covered by housestaff, whose hours are now restricted. Despite these new demands, expectations have grown in other arenas as well. Academic hospitalist groups (AHGs) are often expected to make significant contributions in quality improvement, patient safety, education, research, and administration. With broad expectations beyond clinical care, AHGs face unique challenges. Groups that focus mainly on providing coverage and improving clinical performance may find that they are unable to fully contribute in these other domains. To be successful, AHGs must develop strategies that balance their energies, resources, and performance.
The balanced scorecard (BSC) was introduced by Kaplan and Norton in 1992 to allow corporations to view their performance broadly, rather than narrowly focusing on financial measures. The BSC requires organizations to develop a balanced portfolio of performance metrics across 4 key perspectives: financial, customers, internal processes, and learning and growth. Metrics within these perspectives should help answer fundamental questions about the organization (Table 1).[3] Over time, the BSC evolved from a performance measurement tool to a strategic management system.[4] Successful organizations translate their mission and vision to specific strategic objectives in each of the 4 perspectives, delineate how these objectives will help the organization reach its vision with a strategy map,[5] and then utilize the BSC to track and monitor performance to ensure that the vision is achieved.[6]
| BSC Perspective | Traditional Questions[3] | Questions Revised for AHCs |
|---|---|---|
| ||
| Financial | How do we look to our shareholders? | What financial condition must we be in to allow us to accomplish our mission? |
| Customers | How do customers see us? | How do we ensure that our services and products add the level of value desired by our stakeholders? |
| Internal processes | What must we excel at? | How do we produce our products and services to add maximum value for our customers and stakeholders? |
| Learning and growth | How can we continue to improve and create value? | How do we ensure that we change and improve in order to achieve our vision? |
Although originally conceived for businesses, the BSC has found its way into the healthcare industry, with reports of successful implementation in organizations ranging from individual departments to research collaboratives[7] to national healthcare systems.[8] However, there are few reports of BSC implementation in academic health centers.[9, 10] Because most academic centers are not‐for‐profit, Zelman suggests that the 4 BSC perspectives be modified to better fit their unique characteristics (Table 1).[11] To the best of our knowledge, there is no literature describing the development of a BSC in an academic hospitalist group. In this article, we describe the development of, and early experiences with, an academic hospital medicine BSC developed as part of a strategic planning initiative.
METHODS
The University of California, San Francisco (UCSF) Division of Hospital Medicine (DHM) was established in 2005. Currently, there are more than 50 faculty members, having doubled in the last 4 years. In addition to staffing several housestaff and nonhousestaff clinical services, faculty are involved in a wide variety of nonclinical endeavors at local and national levels. They participate and lead initiatives in education, faculty development, patient safety, care efficiency, quality improvement, information technology, and global health. There is an active research enterprise that generates nearly $5 million in grant funding annually.
Needs Assessment
During a division retreat in 2009, faculty identified several areas in need of improvement, including: clinical care processes, educational promotion, faculty development, and work‐life balance. Based on these needs, divisional mission and vision statements were created (Table 2).
|
| Our mission: to provide the highest quality clinical care, education, research, and innovation in academic hospital medicine. |
| Our vision: to be the best division of hospital medicine by promoting excellence, integrity, innovation, and professional satisfaction among our faculty, trainees, and staff. |
Division leadership made it a priority to create a strategic plan to address these wide‐ranging issues. To accomplish this, we recognized the need to develop a formal way of translating our vision into specific and measurable objectives, establish systems of performance measurement, improve accountability, and effectively communicate these strategic goals to the group. Based on these needs, we set out to develop a divisional BSC.
Development
At the time of BSC development, the DHM was organized into 4 functional areas: quality and safety, education, faculty development, and academics and research. A task force was formed, comprised of 8 senior faculty representing these key areas. The mission and vision statements were used as the foundation for the development of division goals and objectives. The group was careful to choose objectives within each of the 4 BSC perspectives for academic centers, as defined by Zelman (Table 1). The taskforce then brainstormed specific metrics that would track performance within the 4 functional areas. The only stipulation during this process was that the metrics had to meet the following criteria:
- Important to the division and to the individual faculty members
- Measurable through either current or developed processes
- Data are valid and their validity trusted by the faculty members
- Amenable to improvement by faculty (ie, through their individual action they could impact the metric)
From the subsequent list of metrics, we used a modified Delphi method to rank‐order them by importance to arrive at our final set of metrics. Kaplan and Norton noted that focusing on a manageable number of metrics (ie, a handful in each BSC perspective) is important for an achievable strategic vision.[6] With the metrics chosen, we identified data sources or developed new systems to collect data for which there was no current source. We assigned individuals responsible for collecting and analyzing the data, identified local or national benchmarks, if available, and established performance targets for the coming year, when possible.
The BSC is updated quarterly, and results are presented to the division during a noon meeting and posted on the division website. Metrics are re‐evaluated on a yearly basis. They are continued, modified, or discarded depending on performance and/or changes in strategic priorities.
The initial BSC focused on division‐wide metrics and performance. Early efforts to develop the scorecard were framed as experimental, with no clear decision taken regarding how metrics might ultimately be used to improve performance (ie, how public to make both individual and group results, whether to tie bonus payments to performance).
RESULTS
There were 41 initial metrics considered by the division BSC task force (Table 3). Of these, 16 were chosen for the initial BSC through the modified Delphi method. Over the past 2 years, these initial metrics have been modified to reflect current strategic goals and objectives. Figure 1 illustrates the BSC for fiscal year (FY) 2012. An online version of this, complete with graphical representations of the data and metric definitions, can be found at
| Quality, Safety, and Operations | Education | Academics and Research | Faculty Development |
|---|---|---|---|
| |||
| Appropriate level of care | CME courses taught | Abstracts accepted | Attendance and participation |
| Billing and documentation | Curriculum development | Academic reputation | Being an agent of change |
| Clinical efficiency | Student/housestaff feedback | Grant funding | Division citizenship |
| Clinical professionalism | Mentoring | Mentorship | Job satisfaction |
| Communication | Quality of teaching rounds | Papers published | Mentorship |
| Core measures performance | Participation in national organizations | Committees and task forces | |
| Practice evidence‐based medicine | |||
| Fund of knowledge | |||
| Guideline adherence | |||
| Unplanned transfers to ICU | |||
| Implementation and initiation of projects | |||
| Length of stay | |||
| Medical errors | |||
| Mortality | |||
| Multidisciplinary approach to patient care | |||
| Multisource feedback evaluations | |||
| Never events | |||
| Patient‐centered care | |||
| Patient satisfaction | |||
| Practice‐based learning | |||
| Procedures | |||
| Readmissions | |||
| Reputation and expertise | |||
| Seeing patient on the day of admission | |||
| Quality of transfers of care | |||
DISCUSSION
Like many hospitalist groups, our division has experienced tremendous growth, both in our numbers and the breadth of roles that we fill. With this growth has come increasing expectations in multiple domains, competing priorities, and limited resources. We successfully developed a BSC as a tool to help our division reach its vision: balancing high quality clinical care, education, academics, and faculty development while maintaining a strong sense of community. We have found that the BSC has helped us meet several key goals.
The first goal was to allow for a broad view of our performance. This is the BSC's most basic function, and we saw immediate and tangible benefits. The scorecard provided a broad snapshot of our performance in a single place. For example, in the clinical domain, we saw that our direct cost per case was increasing despite our adjusted average length of stay remaining stable from FY2010‐FY2011. In academics and research, we saw that the number of abstracts accepted at national meetings increased by almost 30% in FY2011 (Figure 1).
The second goal was to create transparency and accountability. By measuring performance and displaying it on the division Web site, the BSC has promoted transparency. If performance does not meet our targets, the division as a whole becomes accountable. Leadership must understand why performance fell short and initiate changes to improve it. For instance, the rising direct cost per case has spurred the development of a high‐value care committee tasked with finding ways of reducing cost while providing high‐quality care.[12]
The third goal was to communicate goals and engage our faculty. As our division has grown, ensuring a shared vision among our entire faculty became an increasing challenge. The BSC functions as a communication platform between leadership and faculty, and yielded multiple benefits. As the metrics were born out of our mission and vision, the BSC has become a tangible representation of our core values. Moreover, individual faculty can see that they are part of a greater, high‐performing organization and realize they can impact the group's performance through their individual effort. For example, this has helped promote receptivity to carefully disseminated individual performance measures for billing and documentation, and patient satisfaction, in conjunction with faculty development in these areas.
The fourth goal was to ensure that we use data to guide strategic decisions. We felt that strategic decisions needed to be based on objective, rather than perceived or anecdotal, information. This meant translating our vision into measurable objectives that would drive performance improvement. For example, before the BSC, we were committed to the dissemination of our research and innovations. Yet, we quickly realized that we did not have a system to collect even basic data on academic performancea deficit we filled by leveraging information gathered from online databases and faculty curricula vitae. These data allowed us, for the first time, to objectively reflect on this as a strategic goal and to have an ongoing mechanism to monitor academic productivity.
Lessons Learned/Keys to Success
With our initial experience, we have gained insight that may be helpful to other AHGs considering implementing a BSC. First, and most importantly, AHGs should take the necessary time to build consensus and buy‐in. Particularly in areas where data are analyzed for the first time, faculty are often wary about the validity of the data or the purpose and utility of performance measurement. Faculty may be concerned about how collection of performance data could affect promotion or create a hostile and competitive work environment.
This concern grows when one moves from division‐wide to individual data. It is inevitable that the collection and dissemination of performance data will create some level of discomfort among faculty members, which can be a force for improvement or for angst. These issues should be anticipated, discussed, and actively managed. It is critical to be transparent with how data will be used. We have made clear that the transition from group to individual performance data, and from simple transparency to incentives, will be done thoughtfully and with tremendous input from our faculty. This tension can also be mitigated by choosing metrics that are internally driven, rather than determined by external groups (ie, following the principle that the measures should be important to the division and individual faculty members).
Next, the process of developing a mature BSC takes time. Much of our first year was spent developing systems for measurement, collecting data, and determining appropriate comparators and targets. The data in the first BSC functioned mainly as a baseline marker of performance. Some metrics, particularly in education and academics, had no national or local benchmarks. In these cases we identified comparable groups (such as other medical teaching services or other well‐established AHGs) or merely used our prior year's performance as a benchmark. Also, some of our metrics did not initially have performance targets. In most instances, this was because this was the first time that we looked at these data, and it was unclear what an appropriate target would be until more data became available.
Moving into our third year, we are seeing a natural evolution in the BSC's use. Some metrics that were initially chosen have been replaced or modified to reflect changing goals and priorities. Functional directors participate in choosing and developing performance metrics in their area. Previously, there was no formal structure for these groups to develop and measure strategic objectives and be accountable for performance improvement. They are now expected to define goals with measurable outcomes, to report progress to division leadership, and to develop their own scorecard to track performance. Each group chooses 2 to 4 metrics within their domain that are the most important for the division to improve on, which are then included in the division BSC.
We have also made efforts to build synergy between our BSC and performance goals set by external groups. Although continuing to favor metrics that are internally driven and meaningful to our faculty, we recognize that our goals must also reflect the needs and interests of broader stakeholders. For example, hand hygiene rates and patient satisfaction scores are UCSF medical center and divisional priorities (the former includes them in a financial incentive system for managers, staff, and many physicians) and are incorporated into the BSC as division‐wide incentive metrics.
Limitations
Our project has several limitations. It was conducted at a single institution, and our metrics may not be generalizable to other groups. However, the main goal of this article was not to focus on specific metrics but the process that we undertook to choose and develop them. Other institutions will likely identify different metrics based on their specific strategic objectives. We are also early in our experience with the BSC, and it is still not clear what effect it will have on the desired outcomes for our objectives. However, Henriksen recently reported that implementing a BSC at a large academic health center, in parallel with other performance improvement initiatives, resulted in substantial improvement in their chosen performance metrics.[13]
Despite the several years of development, we still view this as an early version of a BSC. To fully realize its benefits, an organization must choose metrics that will not simply measure performance but drive it. Our current BSC relies primarily on lagging measures, which show what our performance has been, and includes few leading metrics, which can predict trends in performance. As explained by Kaplan and Norton, this type of BSC risks skewing toward controlling rather than driving performance.[14] A mature BSC will include a mix of leading and lagging indicators, the combination illustrating a logical progression from measurement to performance. For instance, we measure total grant funding per year, which is a lagging indicator. However, to be most effective we could measure the percent of faculty who have attended grant‐writing workshops, the number of new grant sources identified, or the number of grant proposals submitted each quarter. These leading indicators would allow us to see performance trends that could be improved before the final outcome, total grant funding, is realized.
Finally, the issues surrounding the acceptability of this overall strategy will likely hinge on how we implement the more complex steps that relate to transparency, individual attribution, and perhaps ultimately incentives. Success in this area depends as much on culture as on strategy.
Next Steps
The next major step in the evolution of the BSC, and part of a broader faculty development program, will be the development of individual BSCs. They will be created using a similar methodology and allow faculty to reflect on their performance compared to peers and recognized benchmarks. Ideally, this will allow hospitalists in our group to establish personal strategic plans and monitor their performance over time. Individualizing these BSCs will be critical; although a research‐oriented faculty member might be striving for more than 5 publications and a large grant in a year, a clinician‐educator may seek outstanding teaching reviews and completion of a key quality improvement project. Both efforts need to be highly valued, and the divisional BSC should roll up these varied individual goals into a balanced whole.
In conclusion, we successfully developed and implemented a BSC to aid in strategic planning. The BSC ensures that we make strategic decisions using data, identify internally driven objectives, develop systems of performance measurement, and increase transparency and accountability. Our hope is that this description of the development of our BSC will be useful to other groups considering a similar endeavor.
Acknowledgments
The authors thank Noori Dhillon, Sadaf Akbaryar, Katie Quinn, Gerri Berg, and Maria Novelero for data collection and analysis. The authors also thank the faculty and staff who participated in the development process of the BSC.
Disclosure
Nothing to report.
The field of hospital medicine, now the fastest growing specialty in medical history,[1] was born out of pressure to improve the efficiency and quality of clinical care in US hospitals.[2] Delivering safe and high‐value clinical care is a central goal of the field and has been an essential component of its growth and success.
The clinical demands on academic hospitalists have grown recently, fueled by the need to staff services previously covered by housestaff, whose hours are now restricted. Despite these new demands, expectations have grown in other arenas as well. Academic hospitalist groups (AHGs) are often expected to make significant contributions in quality improvement, patient safety, education, research, and administration. With broad expectations beyond clinical care, AHGs face unique challenges. Groups that focus mainly on providing coverage and improving clinical performance may find that they are unable to fully contribute in these other domains. To be successful, AHGs must develop strategies that balance their energies, resources, and performance.
The balanced scorecard (BSC) was introduced by Kaplan and Norton in 1992 to allow corporations to view their performance broadly, rather than narrowly focusing on financial measures. The BSC requires organizations to develop a balanced portfolio of performance metrics across 4 key perspectives: financial, customers, internal processes, and learning and growth. Metrics within these perspectives should help answer fundamental questions about the organization (Table 1).[3] Over time, the BSC evolved from a performance measurement tool to a strategic management system.[4] Successful organizations translate their mission and vision to specific strategic objectives in each of the 4 perspectives, delineate how these objectives will help the organization reach its vision with a strategy map,[5] and then utilize the BSC to track and monitor performance to ensure that the vision is achieved.[6]
| BSC Perspective | Traditional Questions[3] | Questions Revised for AHCs |
|---|---|---|
| ||
| Financial | How do we look to our shareholders? | What financial condition must we be in to allow us to accomplish our mission? |
| Customers | How do customers see us? | How do we ensure that our services and products add the level of value desired by our stakeholders? |
| Internal processes | What must we excel at? | How do we produce our products and services to add maximum value for our customers and stakeholders? |
| Learning and growth | How can we continue to improve and create value? | How do we ensure that we change and improve in order to achieve our vision? |
Although originally conceived for businesses, the BSC has found its way into the healthcare industry, with reports of successful implementation in organizations ranging from individual departments to research collaboratives[7] to national healthcare systems.[8] However, there are few reports of BSC implementation in academic health centers.[9, 10] Because most academic centers are not‐for‐profit, Zelman suggests that the 4 BSC perspectives be modified to better fit their unique characteristics (Table 1).[11] To the best of our knowledge, there is no literature describing the development of a BSC in an academic hospitalist group. In this article, we describe the development of, and early experiences with, an academic hospital medicine BSC developed as part of a strategic planning initiative.
METHODS
The University of California, San Francisco (UCSF) Division of Hospital Medicine (DHM) was established in 2005. Currently, there are more than 50 faculty members, having doubled in the last 4 years. In addition to staffing several housestaff and nonhousestaff clinical services, faculty are involved in a wide variety of nonclinical endeavors at local and national levels. They participate and lead initiatives in education, faculty development, patient safety, care efficiency, quality improvement, information technology, and global health. There is an active research enterprise that generates nearly $5 million in grant funding annually.
Needs Assessment
During a division retreat in 2009, faculty identified several areas in need of improvement, including: clinical care processes, educational promotion, faculty development, and work‐life balance. Based on these needs, divisional mission and vision statements were created (Table 2).
|
| Our mission: to provide the highest quality clinical care, education, research, and innovation in academic hospital medicine. |
| Our vision: to be the best division of hospital medicine by promoting excellence, integrity, innovation, and professional satisfaction among our faculty, trainees, and staff. |
Division leadership made it a priority to create a strategic plan to address these wide‐ranging issues. To accomplish this, we recognized the need to develop a formal way of translating our vision into specific and measurable objectives, establish systems of performance measurement, improve accountability, and effectively communicate these strategic goals to the group. Based on these needs, we set out to develop a divisional BSC.
Development
At the time of BSC development, the DHM was organized into 4 functional areas: quality and safety, education, faculty development, and academics and research. A task force was formed, comprised of 8 senior faculty representing these key areas. The mission and vision statements were used as the foundation for the development of division goals and objectives. The group was careful to choose objectives within each of the 4 BSC perspectives for academic centers, as defined by Zelman (Table 1). The taskforce then brainstormed specific metrics that would track performance within the 4 functional areas. The only stipulation during this process was that the metrics had to meet the following criteria:
- Important to the division and to the individual faculty members
- Measurable through either current or developed processes
- Data are valid and their validity trusted by the faculty members
- Amenable to improvement by faculty (ie, through their individual action they could impact the metric)
From the subsequent list of metrics, we used a modified Delphi method to rank‐order them by importance to arrive at our final set of metrics. Kaplan and Norton noted that focusing on a manageable number of metrics (ie, a handful in each BSC perspective) is important for an achievable strategic vision.[6] With the metrics chosen, we identified data sources or developed new systems to collect data for which there was no current source. We assigned individuals responsible for collecting and analyzing the data, identified local or national benchmarks, if available, and established performance targets for the coming year, when possible.
The BSC is updated quarterly, and results are presented to the division during a noon meeting and posted on the division website. Metrics are re‐evaluated on a yearly basis. They are continued, modified, or discarded depending on performance and/or changes in strategic priorities.
The initial BSC focused on division‐wide metrics and performance. Early efforts to develop the scorecard were framed as experimental, with no clear decision taken regarding how metrics might ultimately be used to improve performance (ie, how public to make both individual and group results, whether to tie bonus payments to performance).
RESULTS
There were 41 initial metrics considered by the division BSC task force (Table 3). Of these, 16 were chosen for the initial BSC through the modified Delphi method. Over the past 2 years, these initial metrics have been modified to reflect current strategic goals and objectives. Figure 1 illustrates the BSC for fiscal year (FY) 2012. An online version of this, complete with graphical representations of the data and metric definitions, can be found at
| Quality, Safety, and Operations | Education | Academics and Research | Faculty Development |
|---|---|---|---|
| |||
| Appropriate level of care | CME courses taught | Abstracts accepted | Attendance and participation |
| Billing and documentation | Curriculum development | Academic reputation | Being an agent of change |
| Clinical efficiency | Student/housestaff feedback | Grant funding | Division citizenship |
| Clinical professionalism | Mentoring | Mentorship | Job satisfaction |
| Communication | Quality of teaching rounds | Papers published | Mentorship |
| Core measures performance | Participation in national organizations | Committees and task forces | |
| Practice evidence‐based medicine | |||
| Fund of knowledge | |||
| Guideline adherence | |||
| Unplanned transfers to ICU | |||
| Implementation and initiation of projects | |||
| Length of stay | |||
| Medical errors | |||
| Mortality | |||
| Multidisciplinary approach to patient care | |||
| Multisource feedback evaluations | |||
| Never events | |||
| Patient‐centered care | |||
| Patient satisfaction | |||
| Practice‐based learning | |||
| Procedures | |||
| Readmissions | |||
| Reputation and expertise | |||
| Seeing patient on the day of admission | |||
| Quality of transfers of care | |||
DISCUSSION
Like many hospitalist groups, our division has experienced tremendous growth, both in our numbers and the breadth of roles that we fill. With this growth has come increasing expectations in multiple domains, competing priorities, and limited resources. We successfully developed a BSC as a tool to help our division reach its vision: balancing high quality clinical care, education, academics, and faculty development while maintaining a strong sense of community. We have found that the BSC has helped us meet several key goals.
The first goal was to allow for a broad view of our performance. This is the BSC's most basic function, and we saw immediate and tangible benefits. The scorecard provided a broad snapshot of our performance in a single place. For example, in the clinical domain, we saw that our direct cost per case was increasing despite our adjusted average length of stay remaining stable from FY2010‐FY2011. In academics and research, we saw that the number of abstracts accepted at national meetings increased by almost 30% in FY2011 (Figure 1).
The second goal was to create transparency and accountability. By measuring performance and displaying it on the division Web site, the BSC has promoted transparency. If performance does not meet our targets, the division as a whole becomes accountable. Leadership must understand why performance fell short and initiate changes to improve it. For instance, the rising direct cost per case has spurred the development of a high‐value care committee tasked with finding ways of reducing cost while providing high‐quality care.[12]
The third goal was to communicate goals and engage our faculty. As our division has grown, ensuring a shared vision among our entire faculty became an increasing challenge. The BSC functions as a communication platform between leadership and faculty, and yielded multiple benefits. As the metrics were born out of our mission and vision, the BSC has become a tangible representation of our core values. Moreover, individual faculty can see that they are part of a greater, high‐performing organization and realize they can impact the group's performance through their individual effort. For example, this has helped promote receptivity to carefully disseminated individual performance measures for billing and documentation, and patient satisfaction, in conjunction with faculty development in these areas.
The fourth goal was to ensure that we use data to guide strategic decisions. We felt that strategic decisions needed to be based on objective, rather than perceived or anecdotal, information. This meant translating our vision into measurable objectives that would drive performance improvement. For example, before the BSC, we were committed to the dissemination of our research and innovations. Yet, we quickly realized that we did not have a system to collect even basic data on academic performancea deficit we filled by leveraging information gathered from online databases and faculty curricula vitae. These data allowed us, for the first time, to objectively reflect on this as a strategic goal and to have an ongoing mechanism to monitor academic productivity.
Lessons Learned/Keys to Success
With our initial experience, we have gained insight that may be helpful to other AHGs considering implementing a BSC. First, and most importantly, AHGs should take the necessary time to build consensus and buy‐in. Particularly in areas where data are analyzed for the first time, faculty are often wary about the validity of the data or the purpose and utility of performance measurement. Faculty may be concerned about how collection of performance data could affect promotion or create a hostile and competitive work environment.
This concern grows when one moves from division‐wide to individual data. It is inevitable that the collection and dissemination of performance data will create some level of discomfort among faculty members, which can be a force for improvement or for angst. These issues should be anticipated, discussed, and actively managed. It is critical to be transparent with how data will be used. We have made clear that the transition from group to individual performance data, and from simple transparency to incentives, will be done thoughtfully and with tremendous input from our faculty. This tension can also be mitigated by choosing metrics that are internally driven, rather than determined by external groups (ie, following the principle that the measures should be important to the division and individual faculty members).
Next, the process of developing a mature BSC takes time. Much of our first year was spent developing systems for measurement, collecting data, and determining appropriate comparators and targets. The data in the first BSC functioned mainly as a baseline marker of performance. Some metrics, particularly in education and academics, had no national or local benchmarks. In these cases we identified comparable groups (such as other medical teaching services or other well‐established AHGs) or merely used our prior year's performance as a benchmark. Also, some of our metrics did not initially have performance targets. In most instances, this was because this was the first time that we looked at these data, and it was unclear what an appropriate target would be until more data became available.
Moving into our third year, we are seeing a natural evolution in the BSC's use. Some metrics that were initially chosen have been replaced or modified to reflect changing goals and priorities. Functional directors participate in choosing and developing performance metrics in their area. Previously, there was no formal structure for these groups to develop and measure strategic objectives and be accountable for performance improvement. They are now expected to define goals with measurable outcomes, to report progress to division leadership, and to develop their own scorecard to track performance. Each group chooses 2 to 4 metrics within their domain that are the most important for the division to improve on, which are then included in the division BSC.
We have also made efforts to build synergy between our BSC and performance goals set by external groups. Although continuing to favor metrics that are internally driven and meaningful to our faculty, we recognize that our goals must also reflect the needs and interests of broader stakeholders. For example, hand hygiene rates and patient satisfaction scores are UCSF medical center and divisional priorities (the former includes them in a financial incentive system for managers, staff, and many physicians) and are incorporated into the BSC as division‐wide incentive metrics.
Limitations
Our project has several limitations. It was conducted at a single institution, and our metrics may not be generalizable to other groups. However, the main goal of this article was not to focus on specific metrics but the process that we undertook to choose and develop them. Other institutions will likely identify different metrics based on their specific strategic objectives. We are also early in our experience with the BSC, and it is still not clear what effect it will have on the desired outcomes for our objectives. However, Henriksen recently reported that implementing a BSC at a large academic health center, in parallel with other performance improvement initiatives, resulted in substantial improvement in their chosen performance metrics.[13]
Despite the several years of development, we still view this as an early version of a BSC. To fully realize its benefits, an organization must choose metrics that will not simply measure performance but drive it. Our current BSC relies primarily on lagging measures, which show what our performance has been, and includes few leading metrics, which can predict trends in performance. As explained by Kaplan and Norton, this type of BSC risks skewing toward controlling rather than driving performance.[14] A mature BSC will include a mix of leading and lagging indicators, the combination illustrating a logical progression from measurement to performance. For instance, we measure total grant funding per year, which is a lagging indicator. However, to be most effective we could measure the percent of faculty who have attended grant‐writing workshops, the number of new grant sources identified, or the number of grant proposals submitted each quarter. These leading indicators would allow us to see performance trends that could be improved before the final outcome, total grant funding, is realized.
Finally, the issues surrounding the acceptability of this overall strategy will likely hinge on how we implement the more complex steps that relate to transparency, individual attribution, and perhaps ultimately incentives. Success in this area depends as much on culture as on strategy.
Next Steps
The next major step in the evolution of the BSC, and part of a broader faculty development program, will be the development of individual BSCs. They will be created using a similar methodology and allow faculty to reflect on their performance compared to peers and recognized benchmarks. Ideally, this will allow hospitalists in our group to establish personal strategic plans and monitor their performance over time. Individualizing these BSCs will be critical; although a research‐oriented faculty member might be striving for more than 5 publications and a large grant in a year, a clinician‐educator may seek outstanding teaching reviews and completion of a key quality improvement project. Both efforts need to be highly valued, and the divisional BSC should roll up these varied individual goals into a balanced whole.
In conclusion, we successfully developed and implemented a BSC to aid in strategic planning. The BSC ensures that we make strategic decisions using data, identify internally driven objectives, develop systems of performance measurement, and increase transparency and accountability. Our hope is that this description of the development of our BSC will be useful to other groups considering a similar endeavor.
Acknowledgments
The authors thank Noori Dhillon, Sadaf Akbaryar, Katie Quinn, Gerri Berg, and Maria Novelero for data collection and analysis. The authors also thank the faculty and staff who participated in the development process of the BSC.
Disclosure
Nothing to report.
- . The hospitalist field turns 15: new opportunities and challenges. J Hosp Med. 2011;6(4):E1–E4.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , . The balanced scorecard—measures that drive performance. Harv Bus Rev. 1992;70(1):71–79.
- , . Using the balanced scorecard as a strategic management system. Harv Bus Rev. 1996;74(1):75–85.
- , . Having trouble with your strategy? Then map it. Harv Bus Rev. 2000;78:167–176, 202.
- , . Putting the balanced scorecard to work. Harv Bus Rev. 1993;71:134–147.
- , , , et al. Development and implementation of a performance measure tool in an academic pediatric research network. Contemp Clin Trials. 2010;31(5):429–437.
- , . Lives in the balance: an analysis of the balanced scorecard (BSC) in healthcare organizations. Int J Prod Perform Manag. 2007;57(1):6–21.
- , . The “Balanced Scorecard”: development and implementation in an academic clinical department. Acad Med. 1999;74(2):114–122.
- . Introducing a balanced scorecard management system in a university anesthesiology department. Anesth Analg. 2002;95(6):1731–1738, table of contents.
- , , , , . Issues for academic health centers to consider before implementing a balanced‐scorecard effort. Acad Med. 1999;74(12):1269–1277.
- , . Cents and sensitivity—teaching physicians to think about costs. N Engl J Med. 2012;367(2):99–101.
- , , , et al. 10‐year experience integrating strategic performance improvement initiatives: can the balanced scorecard, Six Sigma, and team training all thrive in a single hospital? In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3. Performance and Tools. Rockville, MD: Agency for Healthcare Research and Quality; 2008. Available at: http://www.ncbi.nlm.nih.gov/books/NBK43660. Accessed 15 June 2011.
- , . Linking the balanced scorecard to strategy. Calif Manage Rev. 1996;39(1):53–79.
- . The hospitalist field turns 15: new opportunities and challenges. J Hosp Med. 2011;6(4):E1–E4.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , . The balanced scorecard—measures that drive performance. Harv Bus Rev. 1992;70(1):71–79.
- , . Using the balanced scorecard as a strategic management system. Harv Bus Rev. 1996;74(1):75–85.
- , . Having trouble with your strategy? Then map it. Harv Bus Rev. 2000;78:167–176, 202.
- , . Putting the balanced scorecard to work. Harv Bus Rev. 1993;71:134–147.
- , , , et al. Development and implementation of a performance measure tool in an academic pediatric research network. Contemp Clin Trials. 2010;31(5):429–437.
- , . Lives in the balance: an analysis of the balanced scorecard (BSC) in healthcare organizations. Int J Prod Perform Manag. 2007;57(1):6–21.
- , . The “Balanced Scorecard”: development and implementation in an academic clinical department. Acad Med. 1999;74(2):114–122.
- . Introducing a balanced scorecard management system in a university anesthesiology department. Anesth Analg. 2002;95(6):1731–1738, table of contents.
- , , , , . Issues for academic health centers to consider before implementing a balanced‐scorecard effort. Acad Med. 1999;74(12):1269–1277.
- , . Cents and sensitivity—teaching physicians to think about costs. N Engl J Med. 2012;367(2):99–101.
- , , , et al. 10‐year experience integrating strategic performance improvement initiatives: can the balanced scorecard, Six Sigma, and team training all thrive in a single hospital? In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3. Performance and Tools. Rockville, MD: Agency for Healthcare Research and Quality; 2008. Available at: http://www.ncbi.nlm.nih.gov/books/NBK43660. Accessed 15 June 2011.
- , . Linking the balanced scorecard to strategy. Calif Manage Rev. 1996;39(1):53–79.