User login
Product News: 09 2014
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at cutis@frontlinemedcom.com.
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at cutis@frontlinemedcom.com.
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at cutis@frontlinemedcom.com.

Subcutaneous Panniculitislike T-Cell Lymphoma
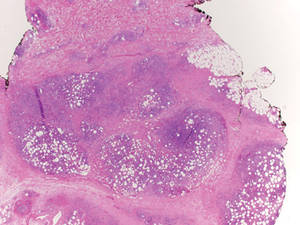
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
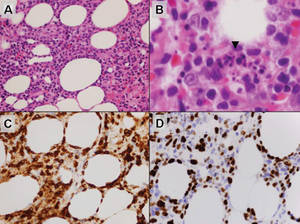
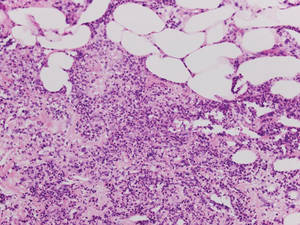
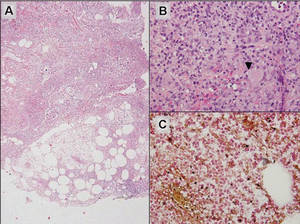
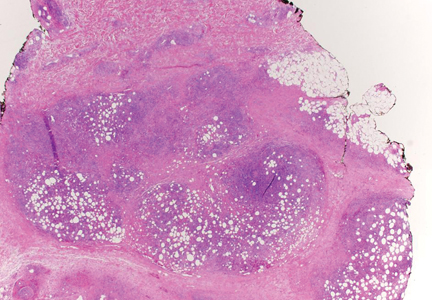
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
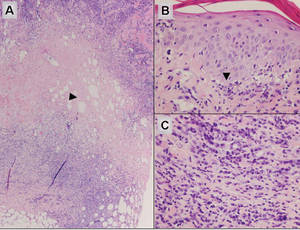
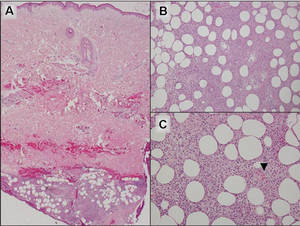
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
|
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
|
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
Five reasons physicians will use mobile health for patient care
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.

But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.
But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.
But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.

Calcipotriene–Betamethasone Dipropionate Topical Suspension in the Management of Psoriasis: A Status Report on Available Data With an Overview of Practical Clinical Application
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
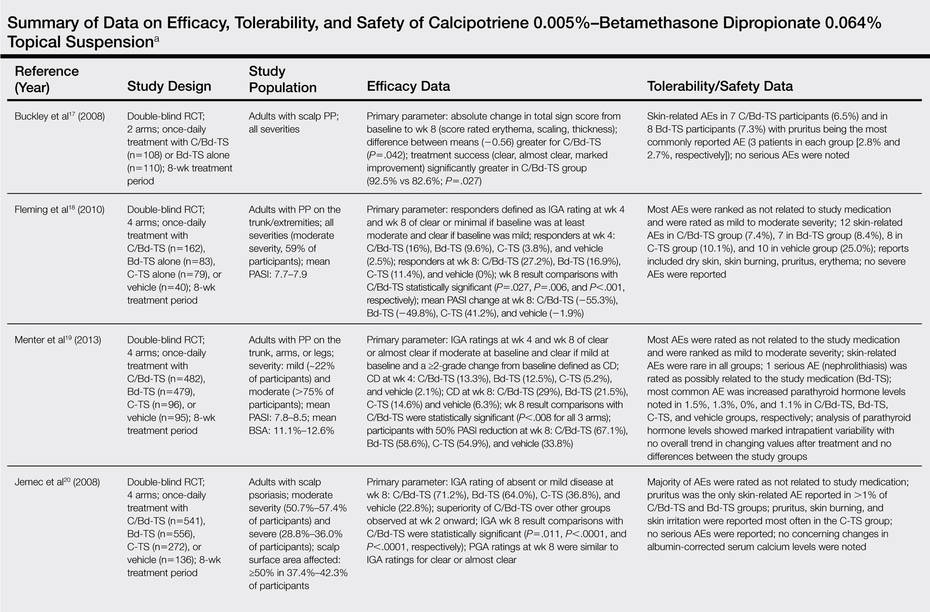
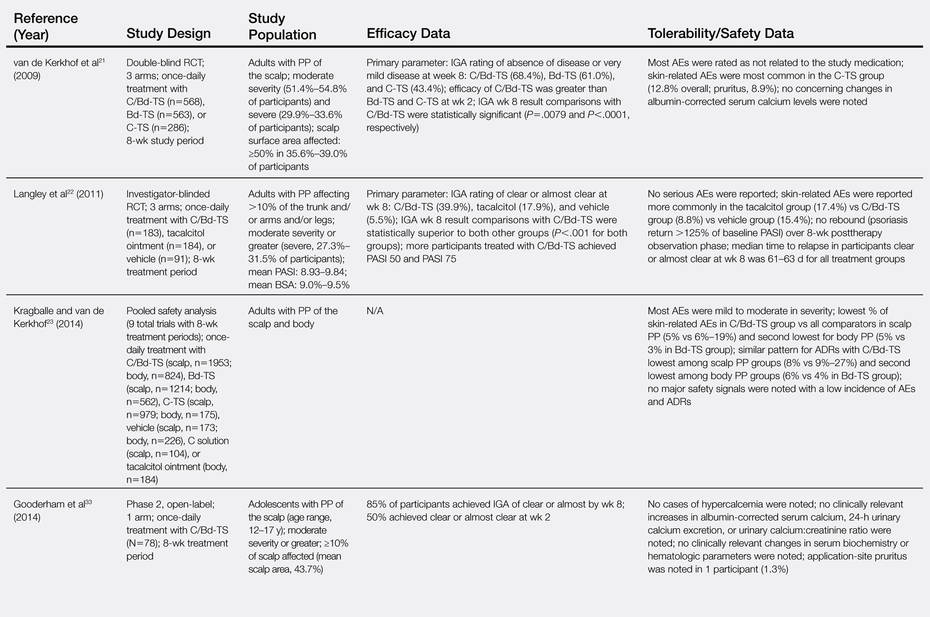
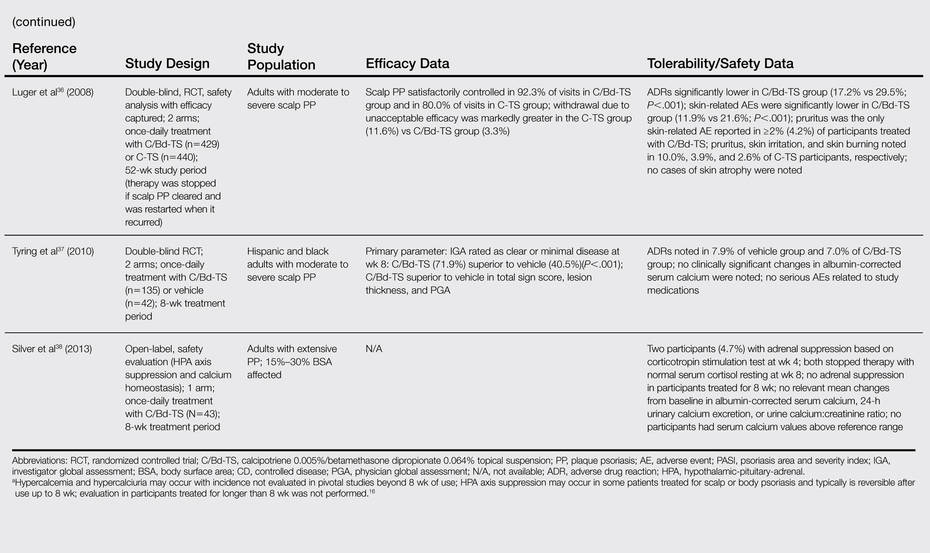
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
Practice Points
- Calcipotriene 0.005%–betamethasone dipropionate 0.064% topical suspension (C/Bd-TS) applied once daily has been shown in multiple studies to be effective, well tolerated, and safe for the treatment of plaque psoriasis (PP) involving the scalp and/or other body sites such as the trunk and extremities. Studies have included all severities of PP, with both investigator and subject assessments shown to be favorable overall.
- Most studies were completed in adults over a duration of 8 weeks; however, clinical trials also have been performed with C/Bd-TS in adults treated for up to 52 weeks for scalp psoriasis, in a subgroup of Hispanic/Latino and black/African American adult patients with scalp psoriasis, and in adolescents with scalp psoriasis.
- Studies evaluating application of C/Bd-TS once daily for PP affecting nonscalp sites have primarily involved use on the trunk and extremities.
- The adaptability for scalp and body application allows for use in many cases of a single topical product without needing to prescribe a second leave-on medication specifically for use on the scalp.
Fats may hold key to new malaria treatment
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.” ![]()
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.” ![]()
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.” ![]()
Re-analyses of RCTs may reveal different conclusions

Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials. ![]()
Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials. ![]()
Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials. ![]()
NICE recommends eculizumab for aHUS despite cost

Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Recommendations for managing SCD lack supporting evidence

Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance. ![]()
Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance. ![]()
Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance. ![]()
Statins do not worsen diabetes microvascular complications, may be protective
Contrary to expectations, statin use before the development of type II diabetes did not worsen microvascular complications such as retinopathy, neuropathy, and gangrene of the foot.
In fact, despite concerns that statins have been seen to increase glucose levels and the risk of diabetes development, they may provide a protective effect from these conditions in newly developed diabetic patients, according to an analysis of data from more than 60,000 individuals in the Danish Patient Registry.

"The cumulative incidences of diabetic retinopathy, diabetic neuropathy, and gangrene were reduced in statin users compared with non–statin users, but [the] risk of diabetic nephropathy was similar for all patients with diabetes," stated Dr. Sune F. Nielsen, Ph.D., and Dr. Børge G. Nordestgaard of the Herlev Hospital, Copenhagen University Hospital. However, they did find that statin use, as previously seen, did significantly increase the risk of developing diabetes in the first place. Their study was published online Sept. 10 in the Lancet Diabetes & Endocrinology (2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
The researchers performed a nested matched study of all men and women living in Denmark who were diagnosed with incident diabetes during 1996-2009 at age 40 years or older, and assessed their outcomes through use of the Danish Civil Registration System, the Danish Patient Registry, and the Danish Registry of Medicinal Product Statistics. After exclusions, 62,716 patients with diabetes were randomly selected for the study: 15,679 statin users and 47,037 non–statin users. The primary outcome was the incidence of diabetic retinopathy, diabetic neuropathy, diabetic nephropathy, and gangrene of the foot. The design "captured 100% of individuals in Denmark who had ever used a statin within the time frame of the study."
Follow-up was censored at date of death for 9,560 individuals. During 215,725 person-years of follow-up, diabetic retinopathy was recorded in 2,866 patients, diabetic neuropathy in 1,406, diabetic nephropathy in 1,248, and gangrene of the foot in 2,392.
Over a median follow-up of 2.7 years, statin users were significantly less likely to be diagnosed with diabetic neuropathy (hazard ratio, 0.66; 95% confidence interval, 0.57-0.75: P less than .0001) and diabetic retinopathy (HR, 0.60; 95% CI 0.54-0.66: P less than .0001) than were those who had not received statins. However, no difference was noted in the incidence of diabetic nephropathy (HR, 0.97; 95% CI, 0.85-1.10; P = .62).
In contrast, the researchers found that statin use significantly increased the risk of developing diabetes in people who did not have the disease when the study began. When they compared a random selection of 272,994 non–statin users with 90,998 statin users, the multivariable adjusted hazard ratio for the risk of developing diabetes was 1.17 (95% CI, 1.14-1.21). These results are similar to those seen in previous randomized studies of statin use.
"In conclusion, we found no evidence that statin use is associated with an increased risk of microvascular disease; this result is important and clinically reassuring on its own. Whether or not statins are protective against some forms of microvascular disease, a possibility raised by these data, and by which mechanism, will need to be addressed in studies similar to ours, or in Mendelian randomization studies," said Dr. Nielsen and Dr. Nordestgaard. "Ideally, however, this question should be addressed in the setting of a randomized controlled trial," they added.
Dr. Nordestgaard has received consultancy fees or lecture honoraria from AstraZeneca, Pfizer, and Merck, and Dr. Nielsen declared no competing interests. The work was supported by Herlev Hospital, Copenhagen University Hospital.
Pharmacoepidemiological studies need cautious interpretation and can be regarded only as hypothesis generating; Dr. Nielsen and Dr. Nordestgaard are appropriately circumspect.
The study has many strengths, such as its size, the quality and coverage of the national registry, and external validity – i.e., statin use was associated with an increased risk of diabetes, an effect size similar to that reported in randomized trials of statins. However, important weaknesses of the study include the absence of data on important predictors of microvascular disease – e.g., hemoglobin A1c, urine albumin, and blood pressure. For now, any benefit of statins on microvascular complications remains unproven.
Dr. David Preiss, of the University of Glasgow (Scotland), is cochair of the Scottish Lipid Forum, whose annual meeting is supported by grants from pharmaceutical companies including MSD, AstraZeneca, and Sanofi. The remarks are taken from his accompanying commentary (Lancet Diabetes Endocrinol. 2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
Pharmacoepidemiological studies need cautious interpretation and can be regarded only as hypothesis generating; Dr. Nielsen and Dr. Nordestgaard are appropriately circumspect.
The study has many strengths, such as its size, the quality and coverage of the national registry, and external validity – i.e., statin use was associated with an increased risk of diabetes, an effect size similar to that reported in randomized trials of statins. However, important weaknesses of the study include the absence of data on important predictors of microvascular disease – e.g., hemoglobin A1c, urine albumin, and blood pressure. For now, any benefit of statins on microvascular complications remains unproven.
Dr. David Preiss, of the University of Glasgow (Scotland), is cochair of the Scottish Lipid Forum, whose annual meeting is supported by grants from pharmaceutical companies including MSD, AstraZeneca, and Sanofi. The remarks are taken from his accompanying commentary (Lancet Diabetes Endocrinol. 2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
Pharmacoepidemiological studies need cautious interpretation and can be regarded only as hypothesis generating; Dr. Nielsen and Dr. Nordestgaard are appropriately circumspect.
The study has many strengths, such as its size, the quality and coverage of the national registry, and external validity – i.e., statin use was associated with an increased risk of diabetes, an effect size similar to that reported in randomized trials of statins. However, important weaknesses of the study include the absence of data on important predictors of microvascular disease – e.g., hemoglobin A1c, urine albumin, and blood pressure. For now, any benefit of statins on microvascular complications remains unproven.
Dr. David Preiss, of the University of Glasgow (Scotland), is cochair of the Scottish Lipid Forum, whose annual meeting is supported by grants from pharmaceutical companies including MSD, AstraZeneca, and Sanofi. The remarks are taken from his accompanying commentary (Lancet Diabetes Endocrinol. 2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
Contrary to expectations, statin use before the development of type II diabetes did not worsen microvascular complications such as retinopathy, neuropathy, and gangrene of the foot.
In fact, despite concerns that statins have been seen to increase glucose levels and the risk of diabetes development, they may provide a protective effect from these conditions in newly developed diabetic patients, according to an analysis of data from more than 60,000 individuals in the Danish Patient Registry.
"The cumulative incidences of diabetic retinopathy, diabetic neuropathy, and gangrene were reduced in statin users compared with non–statin users, but [the] risk of diabetic nephropathy was similar for all patients with diabetes," stated Dr. Sune F. Nielsen, Ph.D., and Dr. Børge G. Nordestgaard of the Herlev Hospital, Copenhagen University Hospital. However, they did find that statin use, as previously seen, did significantly increase the risk of developing diabetes in the first place. Their study was published online Sept. 10 in the Lancet Diabetes & Endocrinology (2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
The researchers performed a nested matched study of all men and women living in Denmark who were diagnosed with incident diabetes during 1996-2009 at age 40 years or older, and assessed their outcomes through use of the Danish Civil Registration System, the Danish Patient Registry, and the Danish Registry of Medicinal Product Statistics. After exclusions, 62,716 patients with diabetes were randomly selected for the study: 15,679 statin users and 47,037 non–statin users. The primary outcome was the incidence of diabetic retinopathy, diabetic neuropathy, diabetic nephropathy, and gangrene of the foot. The design "captured 100% of individuals in Denmark who had ever used a statin within the time frame of the study."
Follow-up was censored at date of death for 9,560 individuals. During 215,725 person-years of follow-up, diabetic retinopathy was recorded in 2,866 patients, diabetic neuropathy in 1,406, diabetic nephropathy in 1,248, and gangrene of the foot in 2,392.
Over a median follow-up of 2.7 years, statin users were significantly less likely to be diagnosed with diabetic neuropathy (hazard ratio, 0.66; 95% confidence interval, 0.57-0.75: P less than .0001) and diabetic retinopathy (HR, 0.60; 95% CI 0.54-0.66: P less than .0001) than were those who had not received statins. However, no difference was noted in the incidence of diabetic nephropathy (HR, 0.97; 95% CI, 0.85-1.10; P = .62).
In contrast, the researchers found that statin use significantly increased the risk of developing diabetes in people who did not have the disease when the study began. When they compared a random selection of 272,994 non–statin users with 90,998 statin users, the multivariable adjusted hazard ratio for the risk of developing diabetes was 1.17 (95% CI, 1.14-1.21). These results are similar to those seen in previous randomized studies of statin use.
"In conclusion, we found no evidence that statin use is associated with an increased risk of microvascular disease; this result is important and clinically reassuring on its own. Whether or not statins are protective against some forms of microvascular disease, a possibility raised by these data, and by which mechanism, will need to be addressed in studies similar to ours, or in Mendelian randomization studies," said Dr. Nielsen and Dr. Nordestgaard. "Ideally, however, this question should be addressed in the setting of a randomized controlled trial," they added.
Dr. Nordestgaard has received consultancy fees or lecture honoraria from AstraZeneca, Pfizer, and Merck, and Dr. Nielsen declared no competing interests. The work was supported by Herlev Hospital, Copenhagen University Hospital.
Contrary to expectations, statin use before the development of type II diabetes did not worsen microvascular complications such as retinopathy, neuropathy, and gangrene of the foot.
In fact, despite concerns that statins have been seen to increase glucose levels and the risk of diabetes development, they may provide a protective effect from these conditions in newly developed diabetic patients, according to an analysis of data from more than 60,000 individuals in the Danish Patient Registry.
"The cumulative incidences of diabetic retinopathy, diabetic neuropathy, and gangrene were reduced in statin users compared with non–statin users, but [the] risk of diabetic nephropathy was similar for all patients with diabetes," stated Dr. Sune F. Nielsen, Ph.D., and Dr. Børge G. Nordestgaard of the Herlev Hospital, Copenhagen University Hospital. However, they did find that statin use, as previously seen, did significantly increase the risk of developing diabetes in the first place. Their study was published online Sept. 10 in the Lancet Diabetes & Endocrinology (2014 Sept. 10 [doi: 10.1016/S2213-8587(14)70173-1]).
The researchers performed a nested matched study of all men and women living in Denmark who were diagnosed with incident diabetes during 1996-2009 at age 40 years or older, and assessed their outcomes through use of the Danish Civil Registration System, the Danish Patient Registry, and the Danish Registry of Medicinal Product Statistics. After exclusions, 62,716 patients with diabetes were randomly selected for the study: 15,679 statin users and 47,037 non–statin users. The primary outcome was the incidence of diabetic retinopathy, diabetic neuropathy, diabetic nephropathy, and gangrene of the foot. The design "captured 100% of individuals in Denmark who had ever used a statin within the time frame of the study."
Follow-up was censored at date of death for 9,560 individuals. During 215,725 person-years of follow-up, diabetic retinopathy was recorded in 2,866 patients, diabetic neuropathy in 1,406, diabetic nephropathy in 1,248, and gangrene of the foot in 2,392.
Over a median follow-up of 2.7 years, statin users were significantly less likely to be diagnosed with diabetic neuropathy (hazard ratio, 0.66; 95% confidence interval, 0.57-0.75: P less than .0001) and diabetic retinopathy (HR, 0.60; 95% CI 0.54-0.66: P less than .0001) than were those who had not received statins. However, no difference was noted in the incidence of diabetic nephropathy (HR, 0.97; 95% CI, 0.85-1.10; P = .62).
In contrast, the researchers found that statin use significantly increased the risk of developing diabetes in people who did not have the disease when the study began. When they compared a random selection of 272,994 non–statin users with 90,998 statin users, the multivariable adjusted hazard ratio for the risk of developing diabetes was 1.17 (95% CI, 1.14-1.21). These results are similar to those seen in previous randomized studies of statin use.
"In conclusion, we found no evidence that statin use is associated with an increased risk of microvascular disease; this result is important and clinically reassuring on its own. Whether or not statins are protective against some forms of microvascular disease, a possibility raised by these data, and by which mechanism, will need to be addressed in studies similar to ours, or in Mendelian randomization studies," said Dr. Nielsen and Dr. Nordestgaard. "Ideally, however, this question should be addressed in the setting of a randomized controlled trial," they added.
Dr. Nordestgaard has received consultancy fees or lecture honoraria from AstraZeneca, Pfizer, and Merck, and Dr. Nielsen declared no competing interests. The work was supported by Herlev Hospital, Copenhagen University Hospital.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Key clinical point: Statins may protect against microvascular complications in diabetes patients.
Major finding: Statin users were significantly less likely to be diagnosed with diabetic neuropathy (HR, 0.66) and diabetic retinopathy (HR, 0.60) than non–statin users.
Data source: A registry study compared 62,716 patients with diabetes: 15,679 statin users and 47,037 non–statin users.
Disclosures: Dr. Nordestgaard has received consultancy fees or lecture honoraria from AstraZeneca, Pfizer, and Merck, and Dr. Nielsen declared no competing interests. The work was supported by Herlev Hospital, Copenhagen University Hospital.
NHLBI expert panel issues guideline on sickle cell disease
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.

Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.
Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.
Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
FROM JAMA
Major finding: The two most widely available disease-modifying therapies for SCD, hydroxyurea and long-term transfusions, are underused, in large part because no evidence-based treatment protocols have been devised until now.
Data source: A review of the literature and compilation of management guidelines "to assist health care professionals in the management of common issues of sickle cell disease."
Disclosures: The National Heart, Lung, and Blood Institute sponsored the development of this guideline. All expert panel members served voluntarily. Many reported numerous ties to industry sources.
