User login
From the Washington Office: Who we are and what we do
Senior staff of the Division of Advocacy and Health Policy was recently approached and asked to consider contributing a monthly column for ACS Surgery News. Unanimously, we agreed that it was imperative to do so and with this inaugural column, we embark on such an endeavor.
As many Fellows may be unfamiliar with the College’s Washington, DC, office and the Division of Advocacy and Health Policy, we thought it might be instructive with our first contribution to provide an overview of the office. However, being mindful of the proximity to the November elections, I will also refer Fellows to Election 2014: Issue-based considerations from a surgeon’s perspective in the Sept. 30th edition of the ACS Advocate for a quick refresher on some of the cogent issues expected to impact surgeons and their patients in the 114th Congress.
The ACS offices in Washington, DC, are located at 20 F St., NW, on the “Senate side” of Capitol Hill. The Division of Advocacy and Health Policy consists of 20 staff members working in the following areas: Legislative and Political Affairs, Quality Affairs, and Regulatory Affairs and State Affairs.
The Legislative and Political Affairs section currently consists of a Deputy Director, John Hedstrom, JD; as well as Manager of Political Affairs, Sara Morse; and lobbyists Matt Coffron and Heather Smith. Obviously, their focus is upon working toward the passage of legislation that furthers the College’s objectives of assuring access to quality surgical care. In the course of doing so, ACS staff routinely interface and work with not only individual members of Congress but also with congressional staff representing those individual members as well as the committee staff of the major committees of jurisdiction for our issues: 1) House Committee on Energy and Commerce; 2) House Ways and Means Committee; and 3) Senate Finance Committee. This section supports the College’s Legislative Committee.
ACSPA-SurgeonsPAC and the ACSPA-SurgeonsVoice platform of the Health Policy Advisory Council are managed by this section as well. The access to legislators facilitated by SurgeonsPAC enables us to have an opportunity to frame the argument on the issues affecting surgical patients and the practice of surgery. SurgeonsVoice provides resources for Fellows to develop relationships with their individual senators and representatives such that they too can actively participate in advocacy both at home via in-district meetings and here on Capitol Hill.
Though legislation and its attendant politics frequently garner more attention, it is the sections of Quality Affairs and Regulatory Affairs that concentrate on the effects of that successful legislation that becomes law and thus impacts surgeons and their patients. Staffing these sections are Manager of Regulatory Affairs, Vinita Ollapaly, JD; Manager of Quality Affairs, Jill Sage, MPH; as well as Sana Gokak, MPH; Neha Agrawal and Sarah Kurusz. Specific activities of this section include support of the General Surgery Coding and Reimbursement Committee and the annual ACS response to the Medicare Physician Fee Schedule proposed rule. This year that rule included proposals to eliminate 10- and 90-day global codes and to eliminate an exemption in the Open Payments (“Sunshine Act”) for physicians who serve as speakers at accredited CME programs. These areas of the ACS also assist Fellows in understanding and maintaining compliance with the Physician Quality Reporting System (PQRS). An excellent example of their work product can be found in the September issue of the ACS Bulletin entitled, “The benefits of PQRS participation and what the College is doing on your behalf (p. 28).
The State Affairs section moved to the Washington, DC, office from Chicago just over a year ago. Jon Sutton, who has been with ACS for 16 years, heads up this section and is assisted by Justin Rosen and Tara Leystra, MPH. Current active projects on which Jon and his team are engaged include obtaining coverage for bariatric surgery in the essential benefit packages of the various state exchanges, passage of the Uniform Emergency Volunteer Health Practitioners Act, as well as supporting the legislative and regulatory advocacy efforts of state chapters. The State Affairs section also supports the ACS delegation to the AMA House of Delegates and administers the State Lobby Day grant program.
The Director of the Division of Advocacy and Health Policy is Christian Shalgian, who has been with ACS for more than 16 years. Frank Opelka, MD, FACS (Medical Director for Quality and Health Policy) and I (Medical Director for Advocacy) are extremely pleased to have joined him this past June and look forward to assisting our Fellows and the College with challenges facing healthcare in the near and long-term future. We also look forward to contributing to ACS Surgery News as a means by which to communicate with you about our efforts relative to same.
Until next month …..
Dr. Bailey is a Pediatric Surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Senior staff of the Division of Advocacy and Health Policy was recently approached and asked to consider contributing a monthly column for ACS Surgery News. Unanimously, we agreed that it was imperative to do so and with this inaugural column, we embark on such an endeavor.
As many Fellows may be unfamiliar with the College’s Washington, DC, office and the Division of Advocacy and Health Policy, we thought it might be instructive with our first contribution to provide an overview of the office. However, being mindful of the proximity to the November elections, I will also refer Fellows to Election 2014: Issue-based considerations from a surgeon’s perspective in the Sept. 30th edition of the ACS Advocate for a quick refresher on some of the cogent issues expected to impact surgeons and their patients in the 114th Congress.
The ACS offices in Washington, DC, are located at 20 F St., NW, on the “Senate side” of Capitol Hill. The Division of Advocacy and Health Policy consists of 20 staff members working in the following areas: Legislative and Political Affairs, Quality Affairs, and Regulatory Affairs and State Affairs.
The Legislative and Political Affairs section currently consists of a Deputy Director, John Hedstrom, JD; as well as Manager of Political Affairs, Sara Morse; and lobbyists Matt Coffron and Heather Smith. Obviously, their focus is upon working toward the passage of legislation that furthers the College’s objectives of assuring access to quality surgical care. In the course of doing so, ACS staff routinely interface and work with not only individual members of Congress but also with congressional staff representing those individual members as well as the committee staff of the major committees of jurisdiction for our issues: 1) House Committee on Energy and Commerce; 2) House Ways and Means Committee; and 3) Senate Finance Committee. This section supports the College’s Legislative Committee.
ACSPA-SurgeonsPAC and the ACSPA-SurgeonsVoice platform of the Health Policy Advisory Council are managed by this section as well. The access to legislators facilitated by SurgeonsPAC enables us to have an opportunity to frame the argument on the issues affecting surgical patients and the practice of surgery. SurgeonsVoice provides resources for Fellows to develop relationships with their individual senators and representatives such that they too can actively participate in advocacy both at home via in-district meetings and here on Capitol Hill.
Though legislation and its attendant politics frequently garner more attention, it is the sections of Quality Affairs and Regulatory Affairs that concentrate on the effects of that successful legislation that becomes law and thus impacts surgeons and their patients. Staffing these sections are Manager of Regulatory Affairs, Vinita Ollapaly, JD; Manager of Quality Affairs, Jill Sage, MPH; as well as Sana Gokak, MPH; Neha Agrawal and Sarah Kurusz. Specific activities of this section include support of the General Surgery Coding and Reimbursement Committee and the annual ACS response to the Medicare Physician Fee Schedule proposed rule. This year that rule included proposals to eliminate 10- and 90-day global codes and to eliminate an exemption in the Open Payments (“Sunshine Act”) for physicians who serve as speakers at accredited CME programs. These areas of the ACS also assist Fellows in understanding and maintaining compliance with the Physician Quality Reporting System (PQRS). An excellent example of their work product can be found in the September issue of the ACS Bulletin entitled, “The benefits of PQRS participation and what the College is doing on your behalf (p. 28).
The State Affairs section moved to the Washington, DC, office from Chicago just over a year ago. Jon Sutton, who has been with ACS for 16 years, heads up this section and is assisted by Justin Rosen and Tara Leystra, MPH. Current active projects on which Jon and his team are engaged include obtaining coverage for bariatric surgery in the essential benefit packages of the various state exchanges, passage of the Uniform Emergency Volunteer Health Practitioners Act, as well as supporting the legislative and regulatory advocacy efforts of state chapters. The State Affairs section also supports the ACS delegation to the AMA House of Delegates and administers the State Lobby Day grant program.
The Director of the Division of Advocacy and Health Policy is Christian Shalgian, who has been with ACS for more than 16 years. Frank Opelka, MD, FACS (Medical Director for Quality and Health Policy) and I (Medical Director for Advocacy) are extremely pleased to have joined him this past June and look forward to assisting our Fellows and the College with challenges facing healthcare in the near and long-term future. We also look forward to contributing to ACS Surgery News as a means by which to communicate with you about our efforts relative to same.
Until next month …..
Dr. Bailey is a Pediatric Surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Senior staff of the Division of Advocacy and Health Policy was recently approached and asked to consider contributing a monthly column for ACS Surgery News. Unanimously, we agreed that it was imperative to do so and with this inaugural column, we embark on such an endeavor.
As many Fellows may be unfamiliar with the College’s Washington, DC, office and the Division of Advocacy and Health Policy, we thought it might be instructive with our first contribution to provide an overview of the office. However, being mindful of the proximity to the November elections, I will also refer Fellows to Election 2014: Issue-based considerations from a surgeon’s perspective in the Sept. 30th edition of the ACS Advocate for a quick refresher on some of the cogent issues expected to impact surgeons and their patients in the 114th Congress.
The ACS offices in Washington, DC, are located at 20 F St., NW, on the “Senate side” of Capitol Hill. The Division of Advocacy and Health Policy consists of 20 staff members working in the following areas: Legislative and Political Affairs, Quality Affairs, and Regulatory Affairs and State Affairs.
The Legislative and Political Affairs section currently consists of a Deputy Director, John Hedstrom, JD; as well as Manager of Political Affairs, Sara Morse; and lobbyists Matt Coffron and Heather Smith. Obviously, their focus is upon working toward the passage of legislation that furthers the College’s objectives of assuring access to quality surgical care. In the course of doing so, ACS staff routinely interface and work with not only individual members of Congress but also with congressional staff representing those individual members as well as the committee staff of the major committees of jurisdiction for our issues: 1) House Committee on Energy and Commerce; 2) House Ways and Means Committee; and 3) Senate Finance Committee. This section supports the College’s Legislative Committee.
ACSPA-SurgeonsPAC and the ACSPA-SurgeonsVoice platform of the Health Policy Advisory Council are managed by this section as well. The access to legislators facilitated by SurgeonsPAC enables us to have an opportunity to frame the argument on the issues affecting surgical patients and the practice of surgery. SurgeonsVoice provides resources for Fellows to develop relationships with their individual senators and representatives such that they too can actively participate in advocacy both at home via in-district meetings and here on Capitol Hill.
Though legislation and its attendant politics frequently garner more attention, it is the sections of Quality Affairs and Regulatory Affairs that concentrate on the effects of that successful legislation that becomes law and thus impacts surgeons and their patients. Staffing these sections are Manager of Regulatory Affairs, Vinita Ollapaly, JD; Manager of Quality Affairs, Jill Sage, MPH; as well as Sana Gokak, MPH; Neha Agrawal and Sarah Kurusz. Specific activities of this section include support of the General Surgery Coding and Reimbursement Committee and the annual ACS response to the Medicare Physician Fee Schedule proposed rule. This year that rule included proposals to eliminate 10- and 90-day global codes and to eliminate an exemption in the Open Payments (“Sunshine Act”) for physicians who serve as speakers at accredited CME programs. These areas of the ACS also assist Fellows in understanding and maintaining compliance with the Physician Quality Reporting System (PQRS). An excellent example of their work product can be found in the September issue of the ACS Bulletin entitled, “The benefits of PQRS participation and what the College is doing on your behalf (p. 28).
The State Affairs section moved to the Washington, DC, office from Chicago just over a year ago. Jon Sutton, who has been with ACS for 16 years, heads up this section and is assisted by Justin Rosen and Tara Leystra, MPH. Current active projects on which Jon and his team are engaged include obtaining coverage for bariatric surgery in the essential benefit packages of the various state exchanges, passage of the Uniform Emergency Volunteer Health Practitioners Act, as well as supporting the legislative and regulatory advocacy efforts of state chapters. The State Affairs section also supports the ACS delegation to the AMA House of Delegates and administers the State Lobby Day grant program.
The Director of the Division of Advocacy and Health Policy is Christian Shalgian, who has been with ACS for more than 16 years. Frank Opelka, MD, FACS (Medical Director for Quality and Health Policy) and I (Medical Director for Advocacy) are extremely pleased to have joined him this past June and look forward to assisting our Fellows and the College with challenges facing healthcare in the near and long-term future. We also look forward to contributing to ACS Surgery News as a means by which to communicate with you about our efforts relative to same.
Until next month …..
Dr. Bailey is a Pediatric Surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.

The Rural Surgeon: Critical staff ‘wearing many hats’
In my recent travels to ACS state chapter gatherings and in my meeting with rural surgeons in a variety of settings, I have heard on many occasions a particular theme of concern: the lack of resources, in particular, personnel resources available in rural hospitals. A shortage of nurses, assistants, and support staff of all kinds has emerged as a serious, continuing challenge for surgeons who work in small communities.
Rural surgery still “gets it done” in spite of resource challenges. Actually, rural surgeons perform more procedures per year with more variety in procedure types than did their urban peers, in spite of limited resources (J. Am. Coll. Surg. 2005;201:732-6).

Resource shortage for rural practices is a common subject on the rural surgery Listserv. Rural surgeons might exclaim, “We have done so much with so little for so long that we are now expected to do everything with nothing forever!” Nursing and support personnel are key resources that can be in short supply.
The rural surgery Listserv has hosted a contest inviting rural surgeons to complete the following statement: “You know you are a rural surgeon if … (YKYAARSI).” At a recent rural surgery dinner at a scientific meeting, we had a little fun amidst all of the serious topics. The winner surgeon read his winning entry: “You know you are a rural surgeon if your first OR assistant is also the OR director, the director of nursing, the DRG coordinator, the director of QA for the ER, the coordinator of emergency preparedness, the committee coordinator for the annual hospital Christmas party, the chairwoman of the committee for quality measures, the best enema nurse, and the best interpreter of the local jargon, such as ‘casophagus’ (esophagus), ‘whistle’ (penis), ‘physic’ (enema), ‘hepmotoma’ (hematoma ), and ‘toodinitis’ (vaginal infection).” Laughter and cheers followed.
Is this hyperbole? The winning YKYAARSI entry is likely closer to reality for many rural surgeons than might be supposed by those who practice in institutions with abundant personnel resources. In small community hospitals, one dedicated staff nurse can have many roles and many jobs.
Early in my career, I practiced with a true team. Individuals had specific roles. My physician assistants assisted me during operations and on rounds. The OR head nurse “ran the board.” The director of surgical services coordinated all functions of the OR from an office. The emergency room was under the management of a veteran emergency nurse. Patients received outstanding bedside nursing care on the surgical floors and in the ICU. IV teams developed and provided valuable services. Skilled lab techs drew blood. An administrative assistant coordinated social events and fund raising. Clearly, trained individuals focused on their areas of expertise.
Gradually, this structure changed. Individuals had to assume many different roles and fill positions that were otherwise unfamiliar to them. The nursing and support personnel resources available for surgery started to diminish significantly.
Today, the concept of team is reduced to single individuals “wearing many hats.” They have all accepted the additional roles to support their hospitals and then made sincere efforts to perform well. The added responsibilities have stressed these well-intentioned nurses, technicians, and assistants both physically and emotionally. Frequently circumstances prevented them from being resources for surgery, straining surgical performance and patient care. I have experienced such situations firsthand, and I have no doubt many readers have as well.
The YKYAARSI winning entry came to life at my critical access hospital. The OR charge nurse became the director for surgical services, ob.gyn., and the emergency department. Previously, this capable nurse would either circulate my cases or be the first assistant. She also took call. She had the greatest skill starting IVs. With the additional duties outside of the OR, this “resource” nearly disappeared, depriving the practice of her abilities and experience. Providing overall quality care became even more challenging. The new “director of almost everything” also led efforts to raise funds for the hospital building campaign. In addition, she developed and coordinated a half-marathon to lift spirits and get pledges for the hospital. In spite of being encouraged to the contrary by hospital administration, even this smart, determined nurse fell behind, and was no longer a resource for surgery.
Like other rural surgeons in similar circumstances, I persisted and adapted to working with less, but I recognize that this situation is not ideal, and perhaps in the long run, not sustainable.
The root of the problem of limited personnel resources for rural surgery is multifactorial and the topic for another column. If you have experienced a personnel shortage or a situation of critical staff “wearing many hats” and would like to contribute to this discussion, please feel free to e-mail me.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.
In my recent travels to ACS state chapter gatherings and in my meeting with rural surgeons in a variety of settings, I have heard on many occasions a particular theme of concern: the lack of resources, in particular, personnel resources available in rural hospitals. A shortage of nurses, assistants, and support staff of all kinds has emerged as a serious, continuing challenge for surgeons who work in small communities.
Rural surgery still “gets it done” in spite of resource challenges. Actually, rural surgeons perform more procedures per year with more variety in procedure types than did their urban peers, in spite of limited resources (J. Am. Coll. Surg. 2005;201:732-6).
Resource shortage for rural practices is a common subject on the rural surgery Listserv. Rural surgeons might exclaim, “We have done so much with so little for so long that we are now expected to do everything with nothing forever!” Nursing and support personnel are key resources that can be in short supply.
The rural surgery Listserv has hosted a contest inviting rural surgeons to complete the following statement: “You know you are a rural surgeon if … (YKYAARSI).” At a recent rural surgery dinner at a scientific meeting, we had a little fun amidst all of the serious topics. The winner surgeon read his winning entry: “You know you are a rural surgeon if your first OR assistant is also the OR director, the director of nursing, the DRG coordinator, the director of QA for the ER, the coordinator of emergency preparedness, the committee coordinator for the annual hospital Christmas party, the chairwoman of the committee for quality measures, the best enema nurse, and the best interpreter of the local jargon, such as ‘casophagus’ (esophagus), ‘whistle’ (penis), ‘physic’ (enema), ‘hepmotoma’ (hematoma ), and ‘toodinitis’ (vaginal infection).” Laughter and cheers followed.
Is this hyperbole? The winning YKYAARSI entry is likely closer to reality for many rural surgeons than might be supposed by those who practice in institutions with abundant personnel resources. In small community hospitals, one dedicated staff nurse can have many roles and many jobs.
Early in my career, I practiced with a true team. Individuals had specific roles. My physician assistants assisted me during operations and on rounds. The OR head nurse “ran the board.” The director of surgical services coordinated all functions of the OR from an office. The emergency room was under the management of a veteran emergency nurse. Patients received outstanding bedside nursing care on the surgical floors and in the ICU. IV teams developed and provided valuable services. Skilled lab techs drew blood. An administrative assistant coordinated social events and fund raising. Clearly, trained individuals focused on their areas of expertise.
Gradually, this structure changed. Individuals had to assume many different roles and fill positions that were otherwise unfamiliar to them. The nursing and support personnel resources available for surgery started to diminish significantly.
Today, the concept of team is reduced to single individuals “wearing many hats.” They have all accepted the additional roles to support their hospitals and then made sincere efforts to perform well. The added responsibilities have stressed these well-intentioned nurses, technicians, and assistants both physically and emotionally. Frequently circumstances prevented them from being resources for surgery, straining surgical performance and patient care. I have experienced such situations firsthand, and I have no doubt many readers have as well.
The YKYAARSI winning entry came to life at my critical access hospital. The OR charge nurse became the director for surgical services, ob.gyn., and the emergency department. Previously, this capable nurse would either circulate my cases or be the first assistant. She also took call. She had the greatest skill starting IVs. With the additional duties outside of the OR, this “resource” nearly disappeared, depriving the practice of her abilities and experience. Providing overall quality care became even more challenging. The new “director of almost everything” also led efforts to raise funds for the hospital building campaign. In addition, she developed and coordinated a half-marathon to lift spirits and get pledges for the hospital. In spite of being encouraged to the contrary by hospital administration, even this smart, determined nurse fell behind, and was no longer a resource for surgery.
Like other rural surgeons in similar circumstances, I persisted and adapted to working with less, but I recognize that this situation is not ideal, and perhaps in the long run, not sustainable.
The root of the problem of limited personnel resources for rural surgery is multifactorial and the topic for another column. If you have experienced a personnel shortage or a situation of critical staff “wearing many hats” and would like to contribute to this discussion, please feel free to e-mail me.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.
In my recent travels to ACS state chapter gatherings and in my meeting with rural surgeons in a variety of settings, I have heard on many occasions a particular theme of concern: the lack of resources, in particular, personnel resources available in rural hospitals. A shortage of nurses, assistants, and support staff of all kinds has emerged as a serious, continuing challenge for surgeons who work in small communities.
Rural surgery still “gets it done” in spite of resource challenges. Actually, rural surgeons perform more procedures per year with more variety in procedure types than did their urban peers, in spite of limited resources (J. Am. Coll. Surg. 2005;201:732-6).
Resource shortage for rural practices is a common subject on the rural surgery Listserv. Rural surgeons might exclaim, “We have done so much with so little for so long that we are now expected to do everything with nothing forever!” Nursing and support personnel are key resources that can be in short supply.
The rural surgery Listserv has hosted a contest inviting rural surgeons to complete the following statement: “You know you are a rural surgeon if … (YKYAARSI).” At a recent rural surgery dinner at a scientific meeting, we had a little fun amidst all of the serious topics. The winner surgeon read his winning entry: “You know you are a rural surgeon if your first OR assistant is also the OR director, the director of nursing, the DRG coordinator, the director of QA for the ER, the coordinator of emergency preparedness, the committee coordinator for the annual hospital Christmas party, the chairwoman of the committee for quality measures, the best enema nurse, and the best interpreter of the local jargon, such as ‘casophagus’ (esophagus), ‘whistle’ (penis), ‘physic’ (enema), ‘hepmotoma’ (hematoma ), and ‘toodinitis’ (vaginal infection).” Laughter and cheers followed.
Is this hyperbole? The winning YKYAARSI entry is likely closer to reality for many rural surgeons than might be supposed by those who practice in institutions with abundant personnel resources. In small community hospitals, one dedicated staff nurse can have many roles and many jobs.
Early in my career, I practiced with a true team. Individuals had specific roles. My physician assistants assisted me during operations and on rounds. The OR head nurse “ran the board.” The director of surgical services coordinated all functions of the OR from an office. The emergency room was under the management of a veteran emergency nurse. Patients received outstanding bedside nursing care on the surgical floors and in the ICU. IV teams developed and provided valuable services. Skilled lab techs drew blood. An administrative assistant coordinated social events and fund raising. Clearly, trained individuals focused on their areas of expertise.
Gradually, this structure changed. Individuals had to assume many different roles and fill positions that were otherwise unfamiliar to them. The nursing and support personnel resources available for surgery started to diminish significantly.
Today, the concept of team is reduced to single individuals “wearing many hats.” They have all accepted the additional roles to support their hospitals and then made sincere efforts to perform well. The added responsibilities have stressed these well-intentioned nurses, technicians, and assistants both physically and emotionally. Frequently circumstances prevented them from being resources for surgery, straining surgical performance and patient care. I have experienced such situations firsthand, and I have no doubt many readers have as well.
The YKYAARSI winning entry came to life at my critical access hospital. The OR charge nurse became the director for surgical services, ob.gyn., and the emergency department. Previously, this capable nurse would either circulate my cases or be the first assistant. She also took call. She had the greatest skill starting IVs. With the additional duties outside of the OR, this “resource” nearly disappeared, depriving the practice of her abilities and experience. Providing overall quality care became even more challenging. The new “director of almost everything” also led efforts to raise funds for the hospital building campaign. In addition, she developed and coordinated a half-marathon to lift spirits and get pledges for the hospital. In spite of being encouraged to the contrary by hospital administration, even this smart, determined nurse fell behind, and was no longer a resource for surgery.
Like other rural surgeons in similar circumstances, I persisted and adapted to working with less, but I recognize that this situation is not ideal, and perhaps in the long run, not sustainable.
The root of the problem of limited personnel resources for rural surgery is multifactorial and the topic for another column. If you have experienced a personnel shortage or a situation of critical staff “wearing many hats” and would like to contribute to this discussion, please feel free to e-mail me.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.

The Rural Surgeon: Thanksgiving
Thanksgiving will soon be here and celebrated joyfully with food, friends, and family in many homes around the country. Football, as well, has become a big part of this tradition on the fourth Thursday of November, an official holiday proclaimed by Abraham Lincoln in 1863. The first Thanksgiving was at Plymouth Plantation in 1621. It is unknown if any rural surgeons were present then. During this holiday, many rural surgeons will be giving thanks for more than food, friends, family, and football.
Twenty-five percent of the population is rural and fewer than 10% of surgeons practice in rural locations. This fact is complicated by the advanced age of the surgeons (~55 y/o) with more than 60% of them planning to retire in less than 10 years. The changes to all aspects of health care today, such as the Affordable Care Act, ACOs, and EMRs, affect the rural health care environment more profoundly and actually promote the deterioration of rural surgical practices. In recent years, rural surgeons have had few reasons to give thanks for the trajectory of their professional situation and fewer yet for the degree of acknowledgment of their challenges by the profession as a whole.

In the past 2 years, thanks to the tireless efforts of a few activists and enlightened leadership in the College, the ACS is now reaching out to rural surgeons, to recognize and to represent them. An important first step was the establishment of the Advisory Council on Rural Surgery, with its pillars for member services, education, quality, advocacy, as well as communication. The Council is chaired by Dr. Tyler Hughes.
Some critics might conclude that this council is just another group of surgeons more concerned about appearances and prominent positions than making an impact on the professional lives of rural surgeons. But such a conclusion would be wrong. Since its inception, the ACRS has worked relentlessly to identify and address the needs of rural surgeons. Efforts of all the pillars have involved education, along with local and national engagement of rural surgeons with emphasis on training, recruitment, and retention. The ACRS has stressed and promoted the value and quality found in rural surgical practices. Members of the Council have generously given their time and enthusiasm to advance these goals.
One of the major roles played by ACRS members has been contributing articles on the realities of a rural practice for the ACS Bulletin’s regular column, “Dispatches from rural surgeons.” Member services chair Dr. Mike Sarap wrote the initial article “The value of chapter membership: The rural surgeon’s perspective,” detailing chapter membership benefits. It concluded that patient care would benefit from a united, networked surgical community. Local ACS chapters can be a foundation of community and professional support among rural surgeons.
Dr. Mark Savarise, advocacy chair, wrote the feature article, “CPT 2012 brings with it new codes and code changes,” that provided invaluable information to rural surgeons, who otherwise would have struggled to secure it. Recently, Dr. Savarise wrote “ACS intervenes to resolve questions about the 96-hour rule” on an issue of great concern to rural surgeons. These efforts to raise awareness, articulate concerns, advocate for change, and inform members about issues are among the most important tasks of the ACRS.
The ACRS also emphasizes continuing education for rural surgeons. Rural surgery symposiums and skills courses over the years attest to that fact and acknowledge the ACRS connection with the Mithoefer Center, Cooperstown, NY, and the Nora Institute in Chicago, IL. ACRS council member, Dr. David Borgstrom, “Rural surgical practice requires a new training model, offers great opportunities” in another Bulletin rural surgery dispatch. The article describes the existing and emerging training programs, ranging from rural surgery rotations and dedicated rural surgery tracks to immersion and fellowship opportunities. The ACS has hosted a series of regional meetings such as the ACS Surgical Healthcare Quality Forum Iowa in June 2014 to engage the surgical community to share ideas on training and workforce needs, maintenance of quality care, and staff retention. In addition, ACS has introduced the Transition to Practice Program in General Surgery, which has been established in several institutions to help residents move into rural surgical practice. This program offers clinical training but also practice management training tailored to rural surgery.
ACRS quality chair, Dr. Don Nakayama, professor and chair at West Virginia University, Morgantown, has collected standards criteria for rural surgery centers of excellence and is composing a verification document for rural surgical practices. This document will assist rural surgeons and be instrumental in maintaining resources and quality in their practices. Once implemented by the ACS, the verification process for rural surgery, like the well-established program for trauma, will enable the highest standards required for the inspiring quality and for better outcomes. This new verification process and its standards give the rural surgeon a basis for the best practice.
The College has stepped up its advocacy efforts to have an impact on policy and legislation to support all surgeons. The ACS Washington office is vital and Dr. Pat Bailey, ACS medical director of advocacy, has worked with the ACRS to make sure the concerns of rural surgeons are incorporated into the advocacy strategy.
One of the four pillars of the ACRS is communication. The rural surgeons listserv was developed in by the ACRS in 2012 and has been a great success. With more than 1,000 members, and several million emails exchanged, the listserv has become meeting place for the community of rural surgeons. During the numerous rural listserv discussions and threads, many of the emails expressed thanks and appreciation. One rural surgeon volunteered, “This is the most tangible, personally applicable arm of the College I have been exposed to in nearly 40 years as a Fellow.” The conversation continued with this sentiment, “I am terrifically gratified to find that the guilt I have suffered all these years (30+) is misplaced.” As the thread continued, the word thanks appeared multiple times. The communication mission of the ACRS will continue with the development of the ACS Communities platform.
The ACS support for rural surgeons came at an ideal time. And for many in the community, this support is a cause for thankfulness.
In participating in the listserv, rural surgeons identified many topics of interest and some actual concerns to them. Call and locum tenens coverage were the most prominent potential issues. The ACS leadership is aware of both subjects and is currently investigating each one. These matters are vital to rural surgeons, and this publication, ACS Surgery News, invites rural surgeons (or any reader) to respond with any additional information. A productive dialogue could follow and be useful to the ACS. Regardless, the ACS will continue without interruption the process of support rural surgeons.
By its actions, the ACS gives living proof to its motto – “inspiring quality, highest standards, better outcomes” – which now have improved chances for surgeons to continue their work in rural communities. Rural surgeons have experienced the true meaning of ACS Fellowship. Indeed, during this Thanksgiving, rural surgeons will be giving thanks for food, friends, family, and the calling to the surgical profession. Rural surgeons will also be grateful for their College and its personal support of their profession and their practices. Thank you and Happy Thanksgiving to everyone.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.
Thanksgiving will soon be here and celebrated joyfully with food, friends, and family in many homes around the country. Football, as well, has become a big part of this tradition on the fourth Thursday of November, an official holiday proclaimed by Abraham Lincoln in 1863. The first Thanksgiving was at Plymouth Plantation in 1621. It is unknown if any rural surgeons were present then. During this holiday, many rural surgeons will be giving thanks for more than food, friends, family, and football.
Twenty-five percent of the population is rural and fewer than 10% of surgeons practice in rural locations. This fact is complicated by the advanced age of the surgeons (~55 y/o) with more than 60% of them planning to retire in less than 10 years. The changes to all aspects of health care today, such as the Affordable Care Act, ACOs, and EMRs, affect the rural health care environment more profoundly and actually promote the deterioration of rural surgical practices. In recent years, rural surgeons have had few reasons to give thanks for the trajectory of their professional situation and fewer yet for the degree of acknowledgment of their challenges by the profession as a whole.
In the past 2 years, thanks to the tireless efforts of a few activists and enlightened leadership in the College, the ACS is now reaching out to rural surgeons, to recognize and to represent them. An important first step was the establishment of the Advisory Council on Rural Surgery, with its pillars for member services, education, quality, advocacy, as well as communication. The Council is chaired by Dr. Tyler Hughes.
Some critics might conclude that this council is just another group of surgeons more concerned about appearances and prominent positions than making an impact on the professional lives of rural surgeons. But such a conclusion would be wrong. Since its inception, the ACRS has worked relentlessly to identify and address the needs of rural surgeons. Efforts of all the pillars have involved education, along with local and national engagement of rural surgeons with emphasis on training, recruitment, and retention. The ACRS has stressed and promoted the value and quality found in rural surgical practices. Members of the Council have generously given their time and enthusiasm to advance these goals.
One of the major roles played by ACRS members has been contributing articles on the realities of a rural practice for the ACS Bulletin’s regular column, “Dispatches from rural surgeons.” Member services chair Dr. Mike Sarap wrote the initial article “The value of chapter membership: The rural surgeon’s perspective,” detailing chapter membership benefits. It concluded that patient care would benefit from a united, networked surgical community. Local ACS chapters can be a foundation of community and professional support among rural surgeons.
Dr. Mark Savarise, advocacy chair, wrote the feature article, “CPT 2012 brings with it new codes and code changes,” that provided invaluable information to rural surgeons, who otherwise would have struggled to secure it. Recently, Dr. Savarise wrote “ACS intervenes to resolve questions about the 96-hour rule” on an issue of great concern to rural surgeons. These efforts to raise awareness, articulate concerns, advocate for change, and inform members about issues are among the most important tasks of the ACRS.
The ACRS also emphasizes continuing education for rural surgeons. Rural surgery symposiums and skills courses over the years attest to that fact and acknowledge the ACRS connection with the Mithoefer Center, Cooperstown, NY, and the Nora Institute in Chicago, IL. ACRS council member, Dr. David Borgstrom, “Rural surgical practice requires a new training model, offers great opportunities” in another Bulletin rural surgery dispatch. The article describes the existing and emerging training programs, ranging from rural surgery rotations and dedicated rural surgery tracks to immersion and fellowship opportunities. The ACS has hosted a series of regional meetings such as the ACS Surgical Healthcare Quality Forum Iowa in June 2014 to engage the surgical community to share ideas on training and workforce needs, maintenance of quality care, and staff retention. In addition, ACS has introduced the Transition to Practice Program in General Surgery, which has been established in several institutions to help residents move into rural surgical practice. This program offers clinical training but also practice management training tailored to rural surgery.
ACRS quality chair, Dr. Don Nakayama, professor and chair at West Virginia University, Morgantown, has collected standards criteria for rural surgery centers of excellence and is composing a verification document for rural surgical practices. This document will assist rural surgeons and be instrumental in maintaining resources and quality in their practices. Once implemented by the ACS, the verification process for rural surgery, like the well-established program for trauma, will enable the highest standards required for the inspiring quality and for better outcomes. This new verification process and its standards give the rural surgeon a basis for the best practice.
The College has stepped up its advocacy efforts to have an impact on policy and legislation to support all surgeons. The ACS Washington office is vital and Dr. Pat Bailey, ACS medical director of advocacy, has worked with the ACRS to make sure the concerns of rural surgeons are incorporated into the advocacy strategy.
One of the four pillars of the ACRS is communication. The rural surgeons listserv was developed in by the ACRS in 2012 and has been a great success. With more than 1,000 members, and several million emails exchanged, the listserv has become meeting place for the community of rural surgeons. During the numerous rural listserv discussions and threads, many of the emails expressed thanks and appreciation. One rural surgeon volunteered, “This is the most tangible, personally applicable arm of the College I have been exposed to in nearly 40 years as a Fellow.” The conversation continued with this sentiment, “I am terrifically gratified to find that the guilt I have suffered all these years (30+) is misplaced.” As the thread continued, the word thanks appeared multiple times. The communication mission of the ACRS will continue with the development of the ACS Communities platform.
The ACS support for rural surgeons came at an ideal time. And for many in the community, this support is a cause for thankfulness.
In participating in the listserv, rural surgeons identified many topics of interest and some actual concerns to them. Call and locum tenens coverage were the most prominent potential issues. The ACS leadership is aware of both subjects and is currently investigating each one. These matters are vital to rural surgeons, and this publication, ACS Surgery News, invites rural surgeons (or any reader) to respond with any additional information. A productive dialogue could follow and be useful to the ACS. Regardless, the ACS will continue without interruption the process of support rural surgeons.
By its actions, the ACS gives living proof to its motto – “inspiring quality, highest standards, better outcomes” – which now have improved chances for surgeons to continue their work in rural communities. Rural surgeons have experienced the true meaning of ACS Fellowship. Indeed, during this Thanksgiving, rural surgeons will be giving thanks for food, friends, family, and the calling to the surgical profession. Rural surgeons will also be grateful for their College and its personal support of their profession and their practices. Thank you and Happy Thanksgiving to everyone.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.
Thanksgiving will soon be here and celebrated joyfully with food, friends, and family in many homes around the country. Football, as well, has become a big part of this tradition on the fourth Thursday of November, an official holiday proclaimed by Abraham Lincoln in 1863. The first Thanksgiving was at Plymouth Plantation in 1621. It is unknown if any rural surgeons were present then. During this holiday, many rural surgeons will be giving thanks for more than food, friends, family, and football.
Twenty-five percent of the population is rural and fewer than 10% of surgeons practice in rural locations. This fact is complicated by the advanced age of the surgeons (~55 y/o) with more than 60% of them planning to retire in less than 10 years. The changes to all aspects of health care today, such as the Affordable Care Act, ACOs, and EMRs, affect the rural health care environment more profoundly and actually promote the deterioration of rural surgical practices. In recent years, rural surgeons have had few reasons to give thanks for the trajectory of their professional situation and fewer yet for the degree of acknowledgment of their challenges by the profession as a whole.
In the past 2 years, thanks to the tireless efforts of a few activists and enlightened leadership in the College, the ACS is now reaching out to rural surgeons, to recognize and to represent them. An important first step was the establishment of the Advisory Council on Rural Surgery, with its pillars for member services, education, quality, advocacy, as well as communication. The Council is chaired by Dr. Tyler Hughes.
Some critics might conclude that this council is just another group of surgeons more concerned about appearances and prominent positions than making an impact on the professional lives of rural surgeons. But such a conclusion would be wrong. Since its inception, the ACRS has worked relentlessly to identify and address the needs of rural surgeons. Efforts of all the pillars have involved education, along with local and national engagement of rural surgeons with emphasis on training, recruitment, and retention. The ACRS has stressed and promoted the value and quality found in rural surgical practices. Members of the Council have generously given their time and enthusiasm to advance these goals.
One of the major roles played by ACRS members has been contributing articles on the realities of a rural practice for the ACS Bulletin’s regular column, “Dispatches from rural surgeons.” Member services chair Dr. Mike Sarap wrote the initial article “The value of chapter membership: The rural surgeon’s perspective,” detailing chapter membership benefits. It concluded that patient care would benefit from a united, networked surgical community. Local ACS chapters can be a foundation of community and professional support among rural surgeons.
Dr. Mark Savarise, advocacy chair, wrote the feature article, “CPT 2012 brings with it new codes and code changes,” that provided invaluable information to rural surgeons, who otherwise would have struggled to secure it. Recently, Dr. Savarise wrote “ACS intervenes to resolve questions about the 96-hour rule” on an issue of great concern to rural surgeons. These efforts to raise awareness, articulate concerns, advocate for change, and inform members about issues are among the most important tasks of the ACRS.
The ACRS also emphasizes continuing education for rural surgeons. Rural surgery symposiums and skills courses over the years attest to that fact and acknowledge the ACRS connection with the Mithoefer Center, Cooperstown, NY, and the Nora Institute in Chicago, IL. ACRS council member, Dr. David Borgstrom, “Rural surgical practice requires a new training model, offers great opportunities” in another Bulletin rural surgery dispatch. The article describes the existing and emerging training programs, ranging from rural surgery rotations and dedicated rural surgery tracks to immersion and fellowship opportunities. The ACS has hosted a series of regional meetings such as the ACS Surgical Healthcare Quality Forum Iowa in June 2014 to engage the surgical community to share ideas on training and workforce needs, maintenance of quality care, and staff retention. In addition, ACS has introduced the Transition to Practice Program in General Surgery, which has been established in several institutions to help residents move into rural surgical practice. This program offers clinical training but also practice management training tailored to rural surgery.
ACRS quality chair, Dr. Don Nakayama, professor and chair at West Virginia University, Morgantown, has collected standards criteria for rural surgery centers of excellence and is composing a verification document for rural surgical practices. This document will assist rural surgeons and be instrumental in maintaining resources and quality in their practices. Once implemented by the ACS, the verification process for rural surgery, like the well-established program for trauma, will enable the highest standards required for the inspiring quality and for better outcomes. This new verification process and its standards give the rural surgeon a basis for the best practice.
The College has stepped up its advocacy efforts to have an impact on policy and legislation to support all surgeons. The ACS Washington office is vital and Dr. Pat Bailey, ACS medical director of advocacy, has worked with the ACRS to make sure the concerns of rural surgeons are incorporated into the advocacy strategy.
One of the four pillars of the ACRS is communication. The rural surgeons listserv was developed in by the ACRS in 2012 and has been a great success. With more than 1,000 members, and several million emails exchanged, the listserv has become meeting place for the community of rural surgeons. During the numerous rural listserv discussions and threads, many of the emails expressed thanks and appreciation. One rural surgeon volunteered, “This is the most tangible, personally applicable arm of the College I have been exposed to in nearly 40 years as a Fellow.” The conversation continued with this sentiment, “I am terrifically gratified to find that the guilt I have suffered all these years (30+) is misplaced.” As the thread continued, the word thanks appeared multiple times. The communication mission of the ACRS will continue with the development of the ACS Communities platform.
The ACS support for rural surgeons came at an ideal time. And for many in the community, this support is a cause for thankfulness.
In participating in the listserv, rural surgeons identified many topics of interest and some actual concerns to them. Call and locum tenens coverage were the most prominent potential issues. The ACS leadership is aware of both subjects and is currently investigating each one. These matters are vital to rural surgeons, and this publication, ACS Surgery News, invites rural surgeons (or any reader) to respond with any additional information. A productive dialogue could follow and be useful to the ACS. Regardless, the ACS will continue without interruption the process of support rural surgeons.
By its actions, the ACS gives living proof to its motto – “inspiring quality, highest standards, better outcomes” – which now have improved chances for surgeons to continue their work in rural communities. Rural surgeons have experienced the true meaning of ACS Fellowship. Indeed, during this Thanksgiving, rural surgeons will be giving thanks for food, friends, family, and the calling to the surgical profession. Rural surgeons will also be grateful for their College and its personal support of their profession and their practices. Thank you and Happy Thanksgiving to everyone.
Dr. Caropreso is a general surgeon at Keokuk (Iowa) Area Hospital and Clinical Professor of Surgery at the University of Iowa Carver College of Medicine. He has practiced surgery in the rural communities of Mason City, Iowa; Keokuk, Iowa; and Carthage, Ill., for 37 years.

A post-Thanksgiving post
In the wake of the grand jury’s decision not to indict Officer Darren Wilson for the death of Michael Brown in Ferguson, Mo., an artist/comedian named Joe Veix made a brilliant fake mock-up of what the New York Times’ banner page would look like the following day. The fake headline says, “Everything’s ... Awful,” (expletive deleted) and it calls out the endlessly scatological nature of the opinion pages. It captured the bleakness of the moment. The world-on-fire sentiment is one that I often feel, particularly when calamities, man-made or otherwise, strike.
So the Thanksgiving holiday was a welcome break from the world. It was a time to retreat from the world.
Starting with the peaceful drive from Providence, R.I., to New York, we insulated ourselves briefly from the 24-hour news cycle, the bad news, the critics and thought pieces, and the criticisms of the thought pieces. We managed to tune out our phones, those instruments of endless mind-numbing connectivity, and enjoy each other’s company. We listened to music, told stories, spent time together in the kitchen making old family favorites. We talked about our anxieties and aspirations. We shared stories of our childhood and sibling rivalry, and the curious relationship of parents and children. We had dinner with friends of a friend, strangers who welcomed us into their home. We made new friends, got well fed, and drank plenty of hot apple cider and whiskey. We basked in love and affection, and went to bed that night content as pigs in a very warm blanket.
The holiday was enough, for the briefest of moments, to be at peace with the mess of the human condition.
This left me thinking of the ultimate big-level picture of the condition we are in. In 1990, the spacecraft Voyager 1 left our atmosphere, and when it was about 4 billion miles away, it took a snapshot of Earth, seen here.
It is this image that inspired Carl Sagan to write the following passage. Every reading of it leaves me with different measures but always the same combination of conflicting emotions: of sadness, and insignificance, of awe, and gratitude, and hope.
“From this distant vantage point, the Earth might not seem of any particular interest. But for us, it’s different. Consider again that dot. That’s here, that’s home, that’s us. On it everyone you love, everyone you know, everyone you ever heard of, every human being who ever was, lived out their lives. The aggregate of our joy and suffering, thousands of confident religions, ideologies, and economic doctrines, every hunter and forager, every hero and coward, every creator and destroyer of civilization, every king and peasant, every young couple in love, every mother and father, hopeful child, inventor and explorer, every teacher of morals, every corrupt politician, every “superstar,” every “supreme leader,” every saint and sinner in the history of our species lived there – on the mote of dust suspended in a sunbeam.”
Dr. Chan practices rheumatology in Pawtucket, R.I.
In the wake of the grand jury’s decision not to indict Officer Darren Wilson for the death of Michael Brown in Ferguson, Mo., an artist/comedian named Joe Veix made a brilliant fake mock-up of what the New York Times’ banner page would look like the following day. The fake headline says, “Everything’s ... Awful,” (expletive deleted) and it calls out the endlessly scatological nature of the opinion pages. It captured the bleakness of the moment. The world-on-fire sentiment is one that I often feel, particularly when calamities, man-made or otherwise, strike.
So the Thanksgiving holiday was a welcome break from the world. It was a time to retreat from the world.
Starting with the peaceful drive from Providence, R.I., to New York, we insulated ourselves briefly from the 24-hour news cycle, the bad news, the critics and thought pieces, and the criticisms of the thought pieces. We managed to tune out our phones, those instruments of endless mind-numbing connectivity, and enjoy each other’s company. We listened to music, told stories, spent time together in the kitchen making old family favorites. We talked about our anxieties and aspirations. We shared stories of our childhood and sibling rivalry, and the curious relationship of parents and children. We had dinner with friends of a friend, strangers who welcomed us into their home. We made new friends, got well fed, and drank plenty of hot apple cider and whiskey. We basked in love and affection, and went to bed that night content as pigs in a very warm blanket.
The holiday was enough, for the briefest of moments, to be at peace with the mess of the human condition.
This left me thinking of the ultimate big-level picture of the condition we are in. In 1990, the spacecraft Voyager 1 left our atmosphere, and when it was about 4 billion miles away, it took a snapshot of Earth, seen here.
It is this image that inspired Carl Sagan to write the following passage. Every reading of it leaves me with different measures but always the same combination of conflicting emotions: of sadness, and insignificance, of awe, and gratitude, and hope.
“From this distant vantage point, the Earth might not seem of any particular interest. But for us, it’s different. Consider again that dot. That’s here, that’s home, that’s us. On it everyone you love, everyone you know, everyone you ever heard of, every human being who ever was, lived out their lives. The aggregate of our joy and suffering, thousands of confident religions, ideologies, and economic doctrines, every hunter and forager, every hero and coward, every creator and destroyer of civilization, every king and peasant, every young couple in love, every mother and father, hopeful child, inventor and explorer, every teacher of morals, every corrupt politician, every “superstar,” every “supreme leader,” every saint and sinner in the history of our species lived there – on the mote of dust suspended in a sunbeam.”
Dr. Chan practices rheumatology in Pawtucket, R.I.
In the wake of the grand jury’s decision not to indict Officer Darren Wilson for the death of Michael Brown in Ferguson, Mo., an artist/comedian named Joe Veix made a brilliant fake mock-up of what the New York Times’ banner page would look like the following day. The fake headline says, “Everything’s ... Awful,” (expletive deleted) and it calls out the endlessly scatological nature of the opinion pages. It captured the bleakness of the moment. The world-on-fire sentiment is one that I often feel, particularly when calamities, man-made or otherwise, strike.
So the Thanksgiving holiday was a welcome break from the world. It was a time to retreat from the world.
Starting with the peaceful drive from Providence, R.I., to New York, we insulated ourselves briefly from the 24-hour news cycle, the bad news, the critics and thought pieces, and the criticisms of the thought pieces. We managed to tune out our phones, those instruments of endless mind-numbing connectivity, and enjoy each other’s company. We listened to music, told stories, spent time together in the kitchen making old family favorites. We talked about our anxieties and aspirations. We shared stories of our childhood and sibling rivalry, and the curious relationship of parents and children. We had dinner with friends of a friend, strangers who welcomed us into their home. We made new friends, got well fed, and drank plenty of hot apple cider and whiskey. We basked in love and affection, and went to bed that night content as pigs in a very warm blanket.
The holiday was enough, for the briefest of moments, to be at peace with the mess of the human condition.
This left me thinking of the ultimate big-level picture of the condition we are in. In 1990, the spacecraft Voyager 1 left our atmosphere, and when it was about 4 billion miles away, it took a snapshot of Earth, seen here.
It is this image that inspired Carl Sagan to write the following passage. Every reading of it leaves me with different measures but always the same combination of conflicting emotions: of sadness, and insignificance, of awe, and gratitude, and hope.
“From this distant vantage point, the Earth might not seem of any particular interest. But for us, it’s different. Consider again that dot. That’s here, that’s home, that’s us. On it everyone you love, everyone you know, everyone you ever heard of, every human being who ever was, lived out their lives. The aggregate of our joy and suffering, thousands of confident religions, ideologies, and economic doctrines, every hunter and forager, every hero and coward, every creator and destroyer of civilization, every king and peasant, every young couple in love, every mother and father, hopeful child, inventor and explorer, every teacher of morals, every corrupt politician, every “superstar,” every “supreme leader,” every saint and sinner in the history of our species lived there – on the mote of dust suspended in a sunbeam.”
Dr. Chan practices rheumatology in Pawtucket, R.I.

First randomized evidence for kinase inhibitor use in AML

Photo courtesy of ASH
SAN FRANCISCO—Researchers have presented the first randomized evidence that kinase inhibitors are effective in the treatment of acute myeloid leukemia
(AML).
The multikinase inhibitor sorafenib improved event-free and relapse-free survival in younger patients.
“Interestingly, at this point in time, we can see no clear overall survival benefit for patients treated in the sorafenib arm,” said trial investigator Christoph Röllig, MD, of the Universitätsklinikum Dresden in Germany.
Dr Röllig, representing the Study Alliance Leukemia, presented data on sorafenib from the SORAML trial during the plenary session of the 2014 ASH Annual Meeting (abstract 6). Some funding for this trial was provided by Bayer Healthcare, the company developing sorafenib.
Dr Röllig explained that support for sorafenib’s clinical efficacy in AML was based primarily on case series and a few early phase clinical and nonrandomized
trials.
An earlier randomized study with sorafenib in older AML patients showed no beneficial antileukemic effect with the addition of the agent, and the treatment was associated with significant morbidity.
However, because the biology of AML and drug tolerance are different in younger people, the Study Alliance Leukemia decided to test the drug in a younger
patient population.
They randomized 276 newly diagnosed AML patients aged 60 years or younger to receive 2 cycles of induction chemotherapy with an anthracycline and cytarabine plus either sorafenib or placebo.
The sorafenib dose was 800 mg per day orally. All patients received at least one dose of study medication, forming the statistical analysis set.
Once in complete remission, intermediate-risk patients with a family donor and high-risk patients with a matched donor went on to stem cell transplant.
All other patients proceeded to high-dose cytarabine-based consolidation treatment plus sorafenib or placebo followed by 1 year of maintenance treatment with sorafenib or placebo.
The primary endpoint was event-free survival (EFS). An event was defined as primary treatment failure, relapse, or death.
Patients in each arm were a median age of 50 years, 17% were FLT3-ITD positive, and 33% were NPM1 mutated.
The complete response (CR) rate was 60% in the sorafenib arm and 59% in the placebo arm. Patients with FLT3-ITD mutation achieved a 57% CR rate with sorafenib and a 52% CR rate with placebo.
After a median follow-up of 3 years, investigators observed “significant prolongation of event-free survival in the sorafenib arm,” Dr Röllig said.
Patients on the sorafenib arm had a median EFS of 40% compared with 22% on the placebo arm, or 21 months compared with 9 months (P=0.013).
Patients were censored at the time of transplant. However, uncensored results were very similar, Dr Röllig noted, “with an even greater advantage for sorafenib.”
Fifty-six percent of sorafenib-treated patients were relapse-free and alive after 3 years, compared with 38% of patients on placebo (P=0.017).
The 3-year overall survival was 63% in the sorafenib arm and 56% in the placebo arm (P=0.382).
An exploratory analysis of FLT3-ITD patients revealed that 1-year EFS for sorafenib-treated patients was 54%, and, for placebo-treated patients, it was 50%.
“The reasons for potential efficacy of sorafenib in this mainly FLT3-ITD-negative population must remain speculative,” Dr Röllig said. “We can speculate that the inhibition of other kinases apart from FLT3 might be responsible for the efficacy of this drug in this patient population.”
Sorafenib significantly increased the risk of grade 3 or greater hand-foot syndrome (P<0.001), diarrhea (P=0.001), bleeding (P=0.016), rash (P=0.045), liver toxicity (P=0.048), and fever (P=0.035).
Dr Röllig indicated a confirmatory trial would be desirable in order to establish sorafenib in the AML treatment armamentarium. ![]()
Photo courtesy of ASH
SAN FRANCISCO—Researchers have presented the first randomized evidence that kinase inhibitors are effective in the treatment of acute myeloid leukemia
(AML).
The multikinase inhibitor sorafenib improved event-free and relapse-free survival in younger patients.
“Interestingly, at this point in time, we can see no clear overall survival benefit for patients treated in the sorafenib arm,” said trial investigator Christoph Röllig, MD, of the Universitätsklinikum Dresden in Germany.
Dr Röllig, representing the Study Alliance Leukemia, presented data on sorafenib from the SORAML trial during the plenary session of the 2014 ASH Annual Meeting (abstract 6). Some funding for this trial was provided by Bayer Healthcare, the company developing sorafenib.
Dr Röllig explained that support for sorafenib’s clinical efficacy in AML was based primarily on case series and a few early phase clinical and nonrandomized
trials.
An earlier randomized study with sorafenib in older AML patients showed no beneficial antileukemic effect with the addition of the agent, and the treatment was associated with significant morbidity.
However, because the biology of AML and drug tolerance are different in younger people, the Study Alliance Leukemia decided to test the drug in a younger
patient population.
They randomized 276 newly diagnosed AML patients aged 60 years or younger to receive 2 cycles of induction chemotherapy with an anthracycline and cytarabine plus either sorafenib or placebo.
The sorafenib dose was 800 mg per day orally. All patients received at least one dose of study medication, forming the statistical analysis set.
Once in complete remission, intermediate-risk patients with a family donor and high-risk patients with a matched donor went on to stem cell transplant.
All other patients proceeded to high-dose cytarabine-based consolidation treatment plus sorafenib or placebo followed by 1 year of maintenance treatment with sorafenib or placebo.
The primary endpoint was event-free survival (EFS). An event was defined as primary treatment failure, relapse, or death.
Patients in each arm were a median age of 50 years, 17% were FLT3-ITD positive, and 33% were NPM1 mutated.
The complete response (CR) rate was 60% in the sorafenib arm and 59% in the placebo arm. Patients with FLT3-ITD mutation achieved a 57% CR rate with sorafenib and a 52% CR rate with placebo.
After a median follow-up of 3 years, investigators observed “significant prolongation of event-free survival in the sorafenib arm,” Dr Röllig said.
Patients on the sorafenib arm had a median EFS of 40% compared with 22% on the placebo arm, or 21 months compared with 9 months (P=0.013).
Patients were censored at the time of transplant. However, uncensored results were very similar, Dr Röllig noted, “with an even greater advantage for sorafenib.”
Fifty-six percent of sorafenib-treated patients were relapse-free and alive after 3 years, compared with 38% of patients on placebo (P=0.017).
The 3-year overall survival was 63% in the sorafenib arm and 56% in the placebo arm (P=0.382).
An exploratory analysis of FLT3-ITD patients revealed that 1-year EFS for sorafenib-treated patients was 54%, and, for placebo-treated patients, it was 50%.
“The reasons for potential efficacy of sorafenib in this mainly FLT3-ITD-negative population must remain speculative,” Dr Röllig said. “We can speculate that the inhibition of other kinases apart from FLT3 might be responsible for the efficacy of this drug in this patient population.”
Sorafenib significantly increased the risk of grade 3 or greater hand-foot syndrome (P<0.001), diarrhea (P=0.001), bleeding (P=0.016), rash (P=0.045), liver toxicity (P=0.048), and fever (P=0.035).
Dr Röllig indicated a confirmatory trial would be desirable in order to establish sorafenib in the AML treatment armamentarium. ![]()
Photo courtesy of ASH
SAN FRANCISCO—Researchers have presented the first randomized evidence that kinase inhibitors are effective in the treatment of acute myeloid leukemia
(AML).
The multikinase inhibitor sorafenib improved event-free and relapse-free survival in younger patients.
“Interestingly, at this point in time, we can see no clear overall survival benefit for patients treated in the sorafenib arm,” said trial investigator Christoph Röllig, MD, of the Universitätsklinikum Dresden in Germany.
Dr Röllig, representing the Study Alliance Leukemia, presented data on sorafenib from the SORAML trial during the plenary session of the 2014 ASH Annual Meeting (abstract 6). Some funding for this trial was provided by Bayer Healthcare, the company developing sorafenib.
Dr Röllig explained that support for sorafenib’s clinical efficacy in AML was based primarily on case series and a few early phase clinical and nonrandomized
trials.
An earlier randomized study with sorafenib in older AML patients showed no beneficial antileukemic effect with the addition of the agent, and the treatment was associated with significant morbidity.
However, because the biology of AML and drug tolerance are different in younger people, the Study Alliance Leukemia decided to test the drug in a younger
patient population.
They randomized 276 newly diagnosed AML patients aged 60 years or younger to receive 2 cycles of induction chemotherapy with an anthracycline and cytarabine plus either sorafenib or placebo.
The sorafenib dose was 800 mg per day orally. All patients received at least one dose of study medication, forming the statistical analysis set.
Once in complete remission, intermediate-risk patients with a family donor and high-risk patients with a matched donor went on to stem cell transplant.
All other patients proceeded to high-dose cytarabine-based consolidation treatment plus sorafenib or placebo followed by 1 year of maintenance treatment with sorafenib or placebo.
The primary endpoint was event-free survival (EFS). An event was defined as primary treatment failure, relapse, or death.
Patients in each arm were a median age of 50 years, 17% were FLT3-ITD positive, and 33% were NPM1 mutated.
The complete response (CR) rate was 60% in the sorafenib arm and 59% in the placebo arm. Patients with FLT3-ITD mutation achieved a 57% CR rate with sorafenib and a 52% CR rate with placebo.
After a median follow-up of 3 years, investigators observed “significant prolongation of event-free survival in the sorafenib arm,” Dr Röllig said.
Patients on the sorafenib arm had a median EFS of 40% compared with 22% on the placebo arm, or 21 months compared with 9 months (P=0.013).
Patients were censored at the time of transplant. However, uncensored results were very similar, Dr Röllig noted, “with an even greater advantage for sorafenib.”
Fifty-six percent of sorafenib-treated patients were relapse-free and alive after 3 years, compared with 38% of patients on placebo (P=0.017).
The 3-year overall survival was 63% in the sorafenib arm and 56% in the placebo arm (P=0.382).
An exploratory analysis of FLT3-ITD patients revealed that 1-year EFS for sorafenib-treated patients was 54%, and, for placebo-treated patients, it was 50%.
“The reasons for potential efficacy of sorafenib in this mainly FLT3-ITD-negative population must remain speculative,” Dr Röllig said. “We can speculate that the inhibition of other kinases apart from FLT3 might be responsible for the efficacy of this drug in this patient population.”
Sorafenib significantly increased the risk of grade 3 or greater hand-foot syndrome (P<0.001), diarrhea (P=0.001), bleeding (P=0.016), rash (P=0.045), liver toxicity (P=0.048), and fever (P=0.035).
Dr Röllig indicated a confirmatory trial would be desirable in order to establish sorafenib in the AML treatment armamentarium. ![]()
Antibody shows activity in relapsed/refractory NHL
SAN FRANCISCO—The anti-CD19 antibody M0R208 has demonstrated encouraging single-agent activity in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to a presenter at the 2014 ASH Annual Meeting.
“It is encouraging to see results in an NHL study that selects a different target than CD20,” said Kristie Blum, MD, of The Ohio State University in Columbus.
“In particular, it is good to see activity in elderly large-cell lymphoma patients.”
MOR208 is an Fc-engineered humanized monoclonal antibody that targets the CD19 antigen.
“It possesses significantly enhanced antibody-dependent cell-mediated cytotoxicity, a key mechanism for tumor cell killing,” Dr Blum explained. “We have seen previous responses in diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL).”
In fact, MOR208 recently received fast-track designation from the US Food and Drug Administration to treat DLBCL.
At ASH, Dr Blum reported on a non-randomized, phase 2a study designed to assess the efficacy and safety of single-agent MOR208 in adults with relapsed or refractory NHL (abstract 3089). The trial was sponsored by MorphoSys AG, the company developing MOR208.
The study included 89 patients—35 with DLBCL, 31 with FL, 12 with mantle cell lymphoma (MCL), and 11 with other indolent NHLs (iNHLs). The patients had a median age of 67 years, were previously treated with rituximab, and were not candidates for high-dose therapy with stem cell support.
The patients were treated over 56 days. MOR208 was given intravenously at 12 mg/kg as 8 weekly doses on days 1, 8, 15, and 22 of each cycle. Patients with at least stable disease continued treatment for another cycle.
After completing 12 weekly doses of treatment, responding patients received maintenance MOR208 every 2 or 4 weeks, depending on the investigator’s decision, until progression.
The results showed overall response rates of 26% for DLBCL patients, 23% for FL patients, and 36% in iNHL patients. No MCL patients responded.
There were 2 complete responses in the DLBCL cohort and 1 complete response each in the FL and iNHL cohorts. Response duration reached 13.8 months.
The drug was well-tolerated with an acceptable toxicity profile, Dr Blum said. The most frequently reported treatment-emergent adverse events of any grade were thrombocytopenia, anemia, and neutropenia, all at 9%.
Infusion-related reactions were reported in 9% of patients and were typically grade 1 or 2. There have been no treatment-related deaths.
Protocols are being developed for trials that combine MOR208 with other anti-lymphoma therapies, with plans to open phase 1/2 trials by mid-2015.
“We plan to take the drug forward in combination with bendamustine or lenalidomide plus rituximab,” Dr Blum said. “By adding the drug into a bendamustine-rituximab combination, we will hit 2 different targets and may see synergistic cell killing.” ![]()
SAN FRANCISCO—The anti-CD19 antibody M0R208 has demonstrated encouraging single-agent activity in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to a presenter at the 2014 ASH Annual Meeting.
“It is encouraging to see results in an NHL study that selects a different target than CD20,” said Kristie Blum, MD, of The Ohio State University in Columbus.
“In particular, it is good to see activity in elderly large-cell lymphoma patients.”
MOR208 is an Fc-engineered humanized monoclonal antibody that targets the CD19 antigen.
“It possesses significantly enhanced antibody-dependent cell-mediated cytotoxicity, a key mechanism for tumor cell killing,” Dr Blum explained. “We have seen previous responses in diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL).”
In fact, MOR208 recently received fast-track designation from the US Food and Drug Administration to treat DLBCL.
At ASH, Dr Blum reported on a non-randomized, phase 2a study designed to assess the efficacy and safety of single-agent MOR208 in adults with relapsed or refractory NHL (abstract 3089). The trial was sponsored by MorphoSys AG, the company developing MOR208.
The study included 89 patients—35 with DLBCL, 31 with FL, 12 with mantle cell lymphoma (MCL), and 11 with other indolent NHLs (iNHLs). The patients had a median age of 67 years, were previously treated with rituximab, and were not candidates for high-dose therapy with stem cell support.
The patients were treated over 56 days. MOR208 was given intravenously at 12 mg/kg as 8 weekly doses on days 1, 8, 15, and 22 of each cycle. Patients with at least stable disease continued treatment for another cycle.
After completing 12 weekly doses of treatment, responding patients received maintenance MOR208 every 2 or 4 weeks, depending on the investigator’s decision, until progression.
The results showed overall response rates of 26% for DLBCL patients, 23% for FL patients, and 36% in iNHL patients. No MCL patients responded.
There were 2 complete responses in the DLBCL cohort and 1 complete response each in the FL and iNHL cohorts. Response duration reached 13.8 months.
The drug was well-tolerated with an acceptable toxicity profile, Dr Blum said. The most frequently reported treatment-emergent adverse events of any grade were thrombocytopenia, anemia, and neutropenia, all at 9%.
Infusion-related reactions were reported in 9% of patients and were typically grade 1 or 2. There have been no treatment-related deaths.
Protocols are being developed for trials that combine MOR208 with other anti-lymphoma therapies, with plans to open phase 1/2 trials by mid-2015.
“We plan to take the drug forward in combination with bendamustine or lenalidomide plus rituximab,” Dr Blum said. “By adding the drug into a bendamustine-rituximab combination, we will hit 2 different targets and may see synergistic cell killing.” ![]()
SAN FRANCISCO—The anti-CD19 antibody M0R208 has demonstrated encouraging single-agent activity in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to a presenter at the 2014 ASH Annual Meeting.
“It is encouraging to see results in an NHL study that selects a different target than CD20,” said Kristie Blum, MD, of The Ohio State University in Columbus.
“In particular, it is good to see activity in elderly large-cell lymphoma patients.”
MOR208 is an Fc-engineered humanized monoclonal antibody that targets the CD19 antigen.
“It possesses significantly enhanced antibody-dependent cell-mediated cytotoxicity, a key mechanism for tumor cell killing,” Dr Blum explained. “We have seen previous responses in diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL).”
In fact, MOR208 recently received fast-track designation from the US Food and Drug Administration to treat DLBCL.
At ASH, Dr Blum reported on a non-randomized, phase 2a study designed to assess the efficacy and safety of single-agent MOR208 in adults with relapsed or refractory NHL (abstract 3089). The trial was sponsored by MorphoSys AG, the company developing MOR208.
The study included 89 patients—35 with DLBCL, 31 with FL, 12 with mantle cell lymphoma (MCL), and 11 with other indolent NHLs (iNHLs). The patients had a median age of 67 years, were previously treated with rituximab, and were not candidates for high-dose therapy with stem cell support.
The patients were treated over 56 days. MOR208 was given intravenously at 12 mg/kg as 8 weekly doses on days 1, 8, 15, and 22 of each cycle. Patients with at least stable disease continued treatment for another cycle.
After completing 12 weekly doses of treatment, responding patients received maintenance MOR208 every 2 or 4 weeks, depending on the investigator’s decision, until progression.
The results showed overall response rates of 26% for DLBCL patients, 23% for FL patients, and 36% in iNHL patients. No MCL patients responded.
There were 2 complete responses in the DLBCL cohort and 1 complete response each in the FL and iNHL cohorts. Response duration reached 13.8 months.
The drug was well-tolerated with an acceptable toxicity profile, Dr Blum said. The most frequently reported treatment-emergent adverse events of any grade were thrombocytopenia, anemia, and neutropenia, all at 9%.
Infusion-related reactions were reported in 9% of patients and were typically grade 1 or 2. There have been no treatment-related deaths.
Protocols are being developed for trials that combine MOR208 with other anti-lymphoma therapies, with plans to open phase 1/2 trials by mid-2015.
“We plan to take the drug forward in combination with bendamustine or lenalidomide plus rituximab,” Dr Blum said. “By adding the drug into a bendamustine-rituximab combination, we will hit 2 different targets and may see synergistic cell killing.” ![]()
FDA approves drug for HCM
The US Food and Drug Administration (FDA) has approved denosumab (XGEVA) to treat hypercalcemia of malignancy (HCM) that is refractory to bisphosphonate therapy.
HCM results from cancer-driven increases in bone resorption. If left untreated, the condition can lead to renal failure, progressive mental impairment, coma, and death.
Denosumab works by binding to RANK ligand, a protein essential for the formation, function, and survival of osteoclasts.
The drug prevents RANK ligand from activating its receptor, RANK, on the surface of osteoclasts, thereby decreasing bone destruction and calcium release.
Denosumab previously received FDA approval to treat giant cell tumor of the bone and for the prevention of skeletal-related events in patients with bone metastases from solid tumors.
The FDA’s approval of denosumab for HCM is based on positive results from an open-label, single-arm study, which enrolled 33 patients with advanced cancer and persistent hypercalcemia after recent bisphosphonate treatment.
The primary endpoint was the proportion of patients with a response, defined as albumin-corrected serum calcium (CSC) < 11.5 mg/dL (2.9 mmol/L; adverse events grade < 1) within 10 days of the first dose of denosumab.
Secondary endpoints included the proportion of patients who experienced a complete response (defined as CSC < 10.8 mg/dL [2.7 mmol/L]) by day 10, time to response, and response duration (defined as the number of days from the first occurrence of CSC < 11.5 mg/dL).
The primary endpoint was met. At day 10, the response rate was 63.6%. Likewise, the overall complete response rate was 63.6%. The estimated median time to response was 9 days, and the median duration of response was 104 days.
The most common adverse events were nausea, dyspnea, decreased appetite, headache, peripheral edema, vomiting, anemia, constipation, and diarrhea.
Potential safety risks
Patients with HCM should receive 120 mg of denosumab as a subcutaneous injection every 4 weeks with additional doses of 120 mg on days 8 and 15 of the first month of therapy.
Pre-existing hypocalcemia must be corrected prior to initiating denosumab therapy. The drug can cause severe, symptomatic hypocalcemia, and fatal cases have been reported.
Physicians should monitor patients’ calcium levels and administer calcium, magnesium, and vitamin D as necessary. Levels should be monitored more frequently when denosumab is given with other drugs that can lower calcium levels. Patients should be advised to contact a healthcare professional if they experience symptoms of hypocalcemia.
Osteonecrosis of the jaw can occur in patients receiving denosumab. Patients who are suspected of having or who develop osteonecrosis of the jaw while on treatment should receive care by a dentist or an oral surgeon.
Atypical femoral fracture has been reported with denosumab, so patients should be advised to report new or unusual thigh, hip, or groin pain. Patients presenting with an atypical femur fracture should be assessed for signs of fracture in the contralateral limb. Physicians should consider interrupting denosumab pending a risk/benefit assessment.
Denosumab can cause fetal harm when administered to a pregnant woman. Physicians should advise females of reproductive potential to use highly effective contraception during therapy and for at least 5 months after the last dose of denosumab.
Amgen, the company developing denosumab, markets the drug as both XGEVA and Prolia (for different indications). Patients receiving XGEVA should not take Prolia.
For more information on denosumab (XGEVA), visit www.xgeva.com. ![]()
The US Food and Drug Administration (FDA) has approved denosumab (XGEVA) to treat hypercalcemia of malignancy (HCM) that is refractory to bisphosphonate therapy.
HCM results from cancer-driven increases in bone resorption. If left untreated, the condition can lead to renal failure, progressive mental impairment, coma, and death.
Denosumab works by binding to RANK ligand, a protein essential for the formation, function, and survival of osteoclasts.
The drug prevents RANK ligand from activating its receptor, RANK, on the surface of osteoclasts, thereby decreasing bone destruction and calcium release.
Denosumab previously received FDA approval to treat giant cell tumor of the bone and for the prevention of skeletal-related events in patients with bone metastases from solid tumors.
The FDA’s approval of denosumab for HCM is based on positive results from an open-label, single-arm study, which enrolled 33 patients with advanced cancer and persistent hypercalcemia after recent bisphosphonate treatment.
The primary endpoint was the proportion of patients with a response, defined as albumin-corrected serum calcium (CSC) < 11.5 mg/dL (2.9 mmol/L; adverse events grade < 1) within 10 days of the first dose of denosumab.
Secondary endpoints included the proportion of patients who experienced a complete response (defined as CSC < 10.8 mg/dL [2.7 mmol/L]) by day 10, time to response, and response duration (defined as the number of days from the first occurrence of CSC < 11.5 mg/dL).
The primary endpoint was met. At day 10, the response rate was 63.6%. Likewise, the overall complete response rate was 63.6%. The estimated median time to response was 9 days, and the median duration of response was 104 days.
The most common adverse events were nausea, dyspnea, decreased appetite, headache, peripheral edema, vomiting, anemia, constipation, and diarrhea.
Potential safety risks
Patients with HCM should receive 120 mg of denosumab as a subcutaneous injection every 4 weeks with additional doses of 120 mg on days 8 and 15 of the first month of therapy.
Pre-existing hypocalcemia must be corrected prior to initiating denosumab therapy. The drug can cause severe, symptomatic hypocalcemia, and fatal cases have been reported.
Physicians should monitor patients’ calcium levels and administer calcium, magnesium, and vitamin D as necessary. Levels should be monitored more frequently when denosumab is given with other drugs that can lower calcium levels. Patients should be advised to contact a healthcare professional if they experience symptoms of hypocalcemia.
Osteonecrosis of the jaw can occur in patients receiving denosumab. Patients who are suspected of having or who develop osteonecrosis of the jaw while on treatment should receive care by a dentist or an oral surgeon.
Atypical femoral fracture has been reported with denosumab, so patients should be advised to report new or unusual thigh, hip, or groin pain. Patients presenting with an atypical femur fracture should be assessed for signs of fracture in the contralateral limb. Physicians should consider interrupting denosumab pending a risk/benefit assessment.
Denosumab can cause fetal harm when administered to a pregnant woman. Physicians should advise females of reproductive potential to use highly effective contraception during therapy and for at least 5 months after the last dose of denosumab.
Amgen, the company developing denosumab, markets the drug as both XGEVA and Prolia (for different indications). Patients receiving XGEVA should not take Prolia.
For more information on denosumab (XGEVA), visit www.xgeva.com. ![]()
The US Food and Drug Administration (FDA) has approved denosumab (XGEVA) to treat hypercalcemia of malignancy (HCM) that is refractory to bisphosphonate therapy.
HCM results from cancer-driven increases in bone resorption. If left untreated, the condition can lead to renal failure, progressive mental impairment, coma, and death.
Denosumab works by binding to RANK ligand, a protein essential for the formation, function, and survival of osteoclasts.
The drug prevents RANK ligand from activating its receptor, RANK, on the surface of osteoclasts, thereby decreasing bone destruction and calcium release.
Denosumab previously received FDA approval to treat giant cell tumor of the bone and for the prevention of skeletal-related events in patients with bone metastases from solid tumors.
The FDA’s approval of denosumab for HCM is based on positive results from an open-label, single-arm study, which enrolled 33 patients with advanced cancer and persistent hypercalcemia after recent bisphosphonate treatment.
The primary endpoint was the proportion of patients with a response, defined as albumin-corrected serum calcium (CSC) < 11.5 mg/dL (2.9 mmol/L; adverse events grade < 1) within 10 days of the first dose of denosumab.
Secondary endpoints included the proportion of patients who experienced a complete response (defined as CSC < 10.8 mg/dL [2.7 mmol/L]) by day 10, time to response, and response duration (defined as the number of days from the first occurrence of CSC < 11.5 mg/dL).
The primary endpoint was met. At day 10, the response rate was 63.6%. Likewise, the overall complete response rate was 63.6%. The estimated median time to response was 9 days, and the median duration of response was 104 days.
The most common adverse events were nausea, dyspnea, decreased appetite, headache, peripheral edema, vomiting, anemia, constipation, and diarrhea.
Potential safety risks
Patients with HCM should receive 120 mg of denosumab as a subcutaneous injection every 4 weeks with additional doses of 120 mg on days 8 and 15 of the first month of therapy.
Pre-existing hypocalcemia must be corrected prior to initiating denosumab therapy. The drug can cause severe, symptomatic hypocalcemia, and fatal cases have been reported.
Physicians should monitor patients’ calcium levels and administer calcium, magnesium, and vitamin D as necessary. Levels should be monitored more frequently when denosumab is given with other drugs that can lower calcium levels. Patients should be advised to contact a healthcare professional if they experience symptoms of hypocalcemia.
Osteonecrosis of the jaw can occur in patients receiving denosumab. Patients who are suspected of having or who develop osteonecrosis of the jaw while on treatment should receive care by a dentist or an oral surgeon.
Atypical femoral fracture has been reported with denosumab, so patients should be advised to report new or unusual thigh, hip, or groin pain. Patients presenting with an atypical femur fracture should be assessed for signs of fracture in the contralateral limb. Physicians should consider interrupting denosumab pending a risk/benefit assessment.
Denosumab can cause fetal harm when administered to a pregnant woman. Physicians should advise females of reproductive potential to use highly effective contraception during therapy and for at least 5 months after the last dose of denosumab.
Amgen, the company developing denosumab, markets the drug as both XGEVA and Prolia (for different indications). Patients receiving XGEVA should not take Prolia.
For more information on denosumab (XGEVA), visit www.xgeva.com. ![]()
Combo may enhance spleen reductions in MF

the 2014 ASH Annual Meeting
SAN FRANCISCO—Combination therapy with ruxolitinib and panobinostat shows signs of efficacy in myelofibrosis (MF), according to research
presented at the 2014 ASH Annual Meeting.
“Targeting multiple components of the JAK/STAT pathway, as well as parallel signaling pathways that may also be involved in the pathogenesis of myelofibrosis, has the potential to have a synergistic therapeutic effect on the underlying disease,” said Jean-Jacques Kiladjian MD, PhD, of the Hôpital Saint-Louis and Université Paris Diderot in Paris, France.
Ruxolitinib, a potent JAK1/JAK2 inhibitor, demonstrated rapid and durable reductions in splenomegaly and MF-related symptoms, improved quality of life, and provided a survival advantage in the phase 3 COMFORT studies.
Panobinostat, a potent oral pan-deacetylase inhibitor, reduced spleen size, symptoms, and JAK2V617F allele burden in patients with MF in phase 1 and phase 2 studies.
The combination of ruxolitinib and panobinostat demonstrated synergistic anti-MF activity in a phase 1b study.
At ASH, Dr Kiladjian presented updated results from the expansion phase of this trial (abstract 711). This study was sponsored by Novartis, the company developing ruxolitinib.
The treatment schedule was ruxolitinib at 5 mg to 15 mg twice daily and panobinostat at 10 mg to 25 mg once daily 3 times per week on days 2, 4, and 6 every other week in a 28-day cycle.
A dose-escalation phase included 38 patients with a median age of 63 years, and an expansion phase included 23 patients with a median age of 67 years.
The recommended phase 2 dose was 15 mg of ruxolitinib twice daily and 25 mg of panobinostat twice weekly, every other week.
“Changes in spleen size were seen in the escalation phase, even at low doses,” Dr Kiladjian said. “Some patients completely eliminated splenomegaly.”
The expansion phase showed similar results. At 24 weeks, more than 85% of patients had a 50% or greater reduction in splenomegaly. Some 59% of patients achieved a 50% or greater reduction in palpable spleen length.
“We saw some JAK2 inhibition and reduction in bone marrow fibrosis, as well as significant reduction in several cytokines related to inflammation,” Dr Kiladjian said.
The most common hematologic adverse events were anemia and thrombocytopenia. There were few neutropenias.
“We saw quite remarkably stable levels of hemoglobin and platelets,” Dr Kiladjian said.
Non-hematologic adverse events were primarily gastrointestinal toxicity associated with panobinostat, including grade 3 or 4 diarrhea and asthenia.
“The rates of adverse events observed in this trial are in line with the expected and known adverse events of these 2 agents when used as monotherapies,” Dr Kiladjian said.
“The combination of ruxolitinib and panobinostat was well-tolerated and resulted in substantial reductions in splenomegaly. Most patients treated at the [recommended phase 2 dose] of combination therapy achieved a spleen response.”
Dr Kiladjian therefore encouraged further exploration of this “favorable” combination. ![]()
the 2014 ASH Annual Meeting
SAN FRANCISCO—Combination therapy with ruxolitinib and panobinostat shows signs of efficacy in myelofibrosis (MF), according to research
presented at the 2014 ASH Annual Meeting.
“Targeting multiple components of the JAK/STAT pathway, as well as parallel signaling pathways that may also be involved in the pathogenesis of myelofibrosis, has the potential to have a synergistic therapeutic effect on the underlying disease,” said Jean-Jacques Kiladjian MD, PhD, of the Hôpital Saint-Louis and Université Paris Diderot in Paris, France.
Ruxolitinib, a potent JAK1/JAK2 inhibitor, demonstrated rapid and durable reductions in splenomegaly and MF-related symptoms, improved quality of life, and provided a survival advantage in the phase 3 COMFORT studies.
Panobinostat, a potent oral pan-deacetylase inhibitor, reduced spleen size, symptoms, and JAK2V617F allele burden in patients with MF in phase 1 and phase 2 studies.
The combination of ruxolitinib and panobinostat demonstrated synergistic anti-MF activity in a phase 1b study.
At ASH, Dr Kiladjian presented updated results from the expansion phase of this trial (abstract 711). This study was sponsored by Novartis, the company developing ruxolitinib.
The treatment schedule was ruxolitinib at 5 mg to 15 mg twice daily and panobinostat at 10 mg to 25 mg once daily 3 times per week on days 2, 4, and 6 every other week in a 28-day cycle.
A dose-escalation phase included 38 patients with a median age of 63 years, and an expansion phase included 23 patients with a median age of 67 years.
The recommended phase 2 dose was 15 mg of ruxolitinib twice daily and 25 mg of panobinostat twice weekly, every other week.
“Changes in spleen size were seen in the escalation phase, even at low doses,” Dr Kiladjian said. “Some patients completely eliminated splenomegaly.”
The expansion phase showed similar results. At 24 weeks, more than 85% of patients had a 50% or greater reduction in splenomegaly. Some 59% of patients achieved a 50% or greater reduction in palpable spleen length.
“We saw some JAK2 inhibition and reduction in bone marrow fibrosis, as well as significant reduction in several cytokines related to inflammation,” Dr Kiladjian said.
The most common hematologic adverse events were anemia and thrombocytopenia. There were few neutropenias.
“We saw quite remarkably stable levels of hemoglobin and platelets,” Dr Kiladjian said.
Non-hematologic adverse events were primarily gastrointestinal toxicity associated with panobinostat, including grade 3 or 4 diarrhea and asthenia.
“The rates of adverse events observed in this trial are in line with the expected and known adverse events of these 2 agents when used as monotherapies,” Dr Kiladjian said.
“The combination of ruxolitinib and panobinostat was well-tolerated and resulted in substantial reductions in splenomegaly. Most patients treated at the [recommended phase 2 dose] of combination therapy achieved a spleen response.”
Dr Kiladjian therefore encouraged further exploration of this “favorable” combination. ![]()
the 2014 ASH Annual Meeting
SAN FRANCISCO—Combination therapy with ruxolitinib and panobinostat shows signs of efficacy in myelofibrosis (MF), according to research
presented at the 2014 ASH Annual Meeting.
“Targeting multiple components of the JAK/STAT pathway, as well as parallel signaling pathways that may also be involved in the pathogenesis of myelofibrosis, has the potential to have a synergistic therapeutic effect on the underlying disease,” said Jean-Jacques Kiladjian MD, PhD, of the Hôpital Saint-Louis and Université Paris Diderot in Paris, France.
Ruxolitinib, a potent JAK1/JAK2 inhibitor, demonstrated rapid and durable reductions in splenomegaly and MF-related symptoms, improved quality of life, and provided a survival advantage in the phase 3 COMFORT studies.
Panobinostat, a potent oral pan-deacetylase inhibitor, reduced spleen size, symptoms, and JAK2V617F allele burden in patients with MF in phase 1 and phase 2 studies.
The combination of ruxolitinib and panobinostat demonstrated synergistic anti-MF activity in a phase 1b study.
At ASH, Dr Kiladjian presented updated results from the expansion phase of this trial (abstract 711). This study was sponsored by Novartis, the company developing ruxolitinib.
The treatment schedule was ruxolitinib at 5 mg to 15 mg twice daily and panobinostat at 10 mg to 25 mg once daily 3 times per week on days 2, 4, and 6 every other week in a 28-day cycle.
A dose-escalation phase included 38 patients with a median age of 63 years, and an expansion phase included 23 patients with a median age of 67 years.
The recommended phase 2 dose was 15 mg of ruxolitinib twice daily and 25 mg of panobinostat twice weekly, every other week.
“Changes in spleen size were seen in the escalation phase, even at low doses,” Dr Kiladjian said. “Some patients completely eliminated splenomegaly.”
The expansion phase showed similar results. At 24 weeks, more than 85% of patients had a 50% or greater reduction in splenomegaly. Some 59% of patients achieved a 50% or greater reduction in palpable spleen length.
“We saw some JAK2 inhibition and reduction in bone marrow fibrosis, as well as significant reduction in several cytokines related to inflammation,” Dr Kiladjian said.
The most common hematologic adverse events were anemia and thrombocytopenia. There were few neutropenias.
“We saw quite remarkably stable levels of hemoglobin and platelets,” Dr Kiladjian said.
Non-hematologic adverse events were primarily gastrointestinal toxicity associated with panobinostat, including grade 3 or 4 diarrhea and asthenia.
“The rates of adverse events observed in this trial are in line with the expected and known adverse events of these 2 agents when used as monotherapies,” Dr Kiladjian said.
“The combination of ruxolitinib and panobinostat was well-tolerated and resulted in substantial reductions in splenomegaly. Most patients treated at the [recommended phase 2 dose] of combination therapy achieved a spleen response.”
Dr Kiladjian therefore encouraged further exploration of this “favorable” combination. ![]()
Osteoporosis medication use down in older women
Even as the number of women aged 50 years and older continues to rise, the percentage who are taking osteoporosis medications has fallen by one-third since 2004-2005, the Agency for Healthcare Research and Quality reported.
In 2004-2005, 15% of all women aged 50 years and over were using some form of prescribed osteoporosis drug, but that number had dropped to 10% by 2010-2011, according to data from the Medical Expenditure Panel Survey. The total number of women aged 50 and older increased from 47.8 million to 55.2 million over that same time period.

In 2010-2011, 8.3% of all women aged at least 50 years were using bisphosphonates, down from a high of 12.3% in 2006-2007 but up from 5.6% in 2000-2001. Use of the next most popular form of osteoporosis medication, the selective estrogen receptor modulators (SERMS), declined from 4.2% of all older women in 2002-2003 to 1.6% in 2010-2011, the AHRQ said.
Data for denosumab (Prolia), a fully human monoclonal antibody drug approved for the treatment of osteoporosis, were not available in the MEPS during the analysis period.
Even as the number of women aged 50 years and older continues to rise, the percentage who are taking osteoporosis medications has fallen by one-third since 2004-2005, the Agency for Healthcare Research and Quality reported.
In 2004-2005, 15% of all women aged 50 years and over were using some form of prescribed osteoporosis drug, but that number had dropped to 10% by 2010-2011, according to data from the Medical Expenditure Panel Survey. The total number of women aged 50 and older increased from 47.8 million to 55.2 million over that same time period.
In 2010-2011, 8.3% of all women aged at least 50 years were using bisphosphonates, down from a high of 12.3% in 2006-2007 but up from 5.6% in 2000-2001. Use of the next most popular form of osteoporosis medication, the selective estrogen receptor modulators (SERMS), declined from 4.2% of all older women in 2002-2003 to 1.6% in 2010-2011, the AHRQ said.
Data for denosumab (Prolia), a fully human monoclonal antibody drug approved for the treatment of osteoporosis, were not available in the MEPS during the analysis period.
Even as the number of women aged 50 years and older continues to rise, the percentage who are taking osteoporosis medications has fallen by one-third since 2004-2005, the Agency for Healthcare Research and Quality reported.
In 2004-2005, 15% of all women aged 50 years and over were using some form of prescribed osteoporosis drug, but that number had dropped to 10% by 2010-2011, according to data from the Medical Expenditure Panel Survey. The total number of women aged 50 and older increased from 47.8 million to 55.2 million over that same time period.
In 2010-2011, 8.3% of all women aged at least 50 years were using bisphosphonates, down from a high of 12.3% in 2006-2007 but up from 5.6% in 2000-2001. Use of the next most popular form of osteoporosis medication, the selective estrogen receptor modulators (SERMS), declined from 4.2% of all older women in 2002-2003 to 1.6% in 2010-2011, the AHRQ said.
Data for denosumab (Prolia), a fully human monoclonal antibody drug approved for the treatment of osteoporosis, were not available in the MEPS during the analysis period.
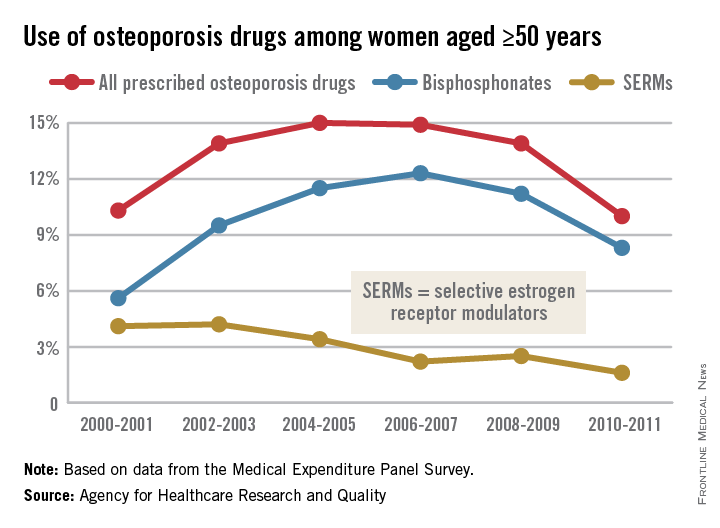
The Spectrum of Pigmented Purpuric Dermatosis and Mycosis Fungoides: Atypical T-Cell Dyscrasia
Case Report
A healthy 17-year-old adolescent boy with an unremarkable medical history presented with an asymptomatic fixed rash on the abdomen, buttocks, and legs. The rash initially developed in a small area on the right leg 2 years prior and had slowly progressed. He was not currently taking any medications and did not participate in intense physical activity. Multiple biopsies had previously been performed by an outside physician, the most recent one demonstrating an interface and superficial perivascular lymphocytic infiltrate with extravasated red blood cells consistent with pigmented purpura. He did not respond to treatment with intralesional corticosteroids, high-potency topical steroids, or high-dose oral prednisone.
Clinical examination revealed multiple annular purpuric patches on the abdomen, buttocks, and legs that covered approximately 20% of the body surface area (Figure 1). Over several follow-up visits, a few of the lesions evolved from patches to thin plaques. There was no adenopathy or hepatosplenomegaly. Three additional biopsies taken over the next 4 months demonstrated a mixture of small mature lymphocytes with some atypical lymphocytes in the dermis and epidermis exhibiting diminished CD7 staining and lymphocytes lining up at the dermoepidermal junction. T-cell receptor g gene rearrangements demonstrated the same clonal population in all 3 specimens. The patient was diagnosed with stage IB mycosis fungoides (MF) of the pigmented purpura–like variant. Marked improvement of the lesions was noted after 6 weeks of psoralen plus UVA therapy 3 times weekly (Figure 2). Treatment was continued for 6 months but was discontinued due to the international shortage of methoxsalen. Two months after discontinuation, most of the lesions had completely resolved (Figure 3).
|


Comment
Mycoses fungoides is a rare cutaneous lymphoma that affects approximately 2000 patients in the United States.1 Only 5% of all cases are known to occur in the first 2 decades of life,2 and even fewer cases pre-sent with pigmented purpura, usually of the lichenoid variant.3 Although the patches and plaques of MF can masquerade as many other dermatoses (eg, dermatophytosis, psoriasis, dermatitis), there have been few reports of patients presenting with lesions with the clinical appearance of pigmented purpuric dermatosis (PPD).4 As with the many cases of early MF, which are histologically indistinguishable from dermatitis, the pigmented purpura–like variant of MF initially may have the histologic appearance of pigmented purpura and generally evolves to the histologic appearance of MF over time.
Similar to our case, there have been reports of clinical and histologic diagnosis of PPD preceding the histologic diagnosis of MF. In a small cohort study of 3 young men, Barnhill and Braverman5 first demonstrated the progression of PPD to MF over a 12-year period. The age of onset ranged from 14 to 30 years, with a mean age of 24.3 years. Biopsies in all 3 patients were consistent with PPD for many years prior to the diagnosis of MF, with an average length of time to diagnosis of 8.4 years. Atypical from most cases of PPD, the patients in this study demonstrated extensive involvement of the trunk, arms, and legs.5 It has been suggested that atypical PPD is a variant of PPD that evolves into MF over many years; however, we believe that PPD is a variant of MF, similar to the way an indolent dermatitis may evolve to classical MF over time. If characterized by a T-cell clone, this period preceding the diagnosis of cutaneous T-cell lymphoma could be characterized as a cutaneous T-cell lymphoid dyscrasia.
Guitart and Magro6 noted multiple chronic conditions that are associated with T-cell clones, including PPD. These conditions occurred without a known trigger, were unresponsive to topical therapies, and often did not meet diagnostic criteria for MF. The investigators felt the criteria that may indicate a cutaneous T-cell lymphoid dyscrasia include widespread distribution, lymphocytic infiltrate, diminished CD7 and CD62L expression, and clonality. Lymphocytes may be small without notable atypia.6
In a study of 43 patients with PPD, Magro et al3 found monoclonality and diminished CD7 expression in 18 participants, correlating with large surface area involvement. Approximately 40% of patients had histologic findings consistent with MF, suggesting that T-cell gene rearrangement studies should be obtained for prognostic evaluation in patients with widespread disease.3

| 
|
To facilitate proper patient care, histopathology and molecular markers should be evaluated in conjunction with the clinical picture. A considerable increase in the size of the body surface area affected by purpuric patches combined with the presence of poikilodermatous changes and pruritus as well as disease lasting longer than 1 year should prompt an increased clinical suspicion of MF in patients with PPD.4,5 Histologically, the presence of Pautrier microabscesses, large cerebriform lymphocytes, and intraepidermal lymphocytic atypia extending beyond the dermis also would support a diagnosis of MF.3 Given the morphologic appearance and distribution of the lesions in our patient combined with epidermotropism, diminished CD7 expression, and monoclonality seen on pathology, we favored a diagnosis of MF. It would not be unreasonable to call this clonal variant of PPD a T-cell lymphoid dyscrasia. We appreciate that both PPD and MF will respond to phototherapy.7
Conclusion
We propose that there is a spectrum of disease presenting as PPD or MF sitting at either end of that spectrum and an intermediate stage, where not all criteria for cutaneous lymphoma are met, characterized as cutaneous T-cell lymphoid dyscrasia. Until the potential for evolution of PPD to malignant disease is better understood, patients with unusual presentations of pigmented purpura should be further evaluated for MF.
1. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol. 2007;143:854-859.
2. Koch SE, Zackheim HS, Williams ML, et al. Mycosis fungoides beginning in childhood and adolescence. J Am Acad Dermatol. 1987;17:563-570.
3. Magro CM, Schaefer JT, Crowson AN, et al. Pigmented purpuric dermatosis: classification by phenotypic and molecular profiles. Am J Clin Pathol. 2007;128:218-229.
4. Hanna S, Walsh N, D’Intino Y, et al. Mycosis fungoides presenting as pigmented purpuric dermatitis. Pediatr Dermatol. 2006;23:350-354.
5. Barnhill RL, Braverman IM. Progression of pigmented purpura-like eruptions to mycosis fungoides: report of three cases. J Am Acad Dermatol. 1988;19(1, pt 1):25-31.
6. Guitart J, Magro C. Cutaneous T-cell lymphoid dyscrasia: a unifying term for idiopathic chronic dermatoses with persistent T-cell clones. Arch Dermatol. 2007;143:921-932.
7. Seckin D, Yazici Z, Senol A, et al. A case of Schamberg’s disease responding dramatically to PUVA treatment. Photodermatol Photoimmunol Photomed. 2008;24:95-96.
Case Report
A healthy 17-year-old adolescent boy with an unremarkable medical history presented with an asymptomatic fixed rash on the abdomen, buttocks, and legs. The rash initially developed in a small area on the right leg 2 years prior and had slowly progressed. He was not currently taking any medications and did not participate in intense physical activity. Multiple biopsies had previously been performed by an outside physician, the most recent one demonstrating an interface and superficial perivascular lymphocytic infiltrate with extravasated red blood cells consistent with pigmented purpura. He did not respond to treatment with intralesional corticosteroids, high-potency topical steroids, or high-dose oral prednisone.
Clinical examination revealed multiple annular purpuric patches on the abdomen, buttocks, and legs that covered approximately 20% of the body surface area (Figure 1). Over several follow-up visits, a few of the lesions evolved from patches to thin plaques. There was no adenopathy or hepatosplenomegaly. Three additional biopsies taken over the next 4 months demonstrated a mixture of small mature lymphocytes with some atypical lymphocytes in the dermis and epidermis exhibiting diminished CD7 staining and lymphocytes lining up at the dermoepidermal junction. T-cell receptor g gene rearrangements demonstrated the same clonal population in all 3 specimens. The patient was diagnosed with stage IB mycosis fungoides (MF) of the pigmented purpura–like variant. Marked improvement of the lesions was noted after 6 weeks of psoralen plus UVA therapy 3 times weekly (Figure 2). Treatment was continued for 6 months but was discontinued due to the international shortage of methoxsalen. Two months after discontinuation, most of the lesions had completely resolved (Figure 3).
|
Comment
Mycoses fungoides is a rare cutaneous lymphoma that affects approximately 2000 patients in the United States.1 Only 5% of all cases are known to occur in the first 2 decades of life,2 and even fewer cases pre-sent with pigmented purpura, usually of the lichenoid variant.3 Although the patches and plaques of MF can masquerade as many other dermatoses (eg, dermatophytosis, psoriasis, dermatitis), there have been few reports of patients presenting with lesions with the clinical appearance of pigmented purpuric dermatosis (PPD).4 As with the many cases of early MF, which are histologically indistinguishable from dermatitis, the pigmented purpura–like variant of MF initially may have the histologic appearance of pigmented purpura and generally evolves to the histologic appearance of MF over time.
Similar to our case, there have been reports of clinical and histologic diagnosis of PPD preceding the histologic diagnosis of MF. In a small cohort study of 3 young men, Barnhill and Braverman5 first demonstrated the progression of PPD to MF over a 12-year period. The age of onset ranged from 14 to 30 years, with a mean age of 24.3 years. Biopsies in all 3 patients were consistent with PPD for many years prior to the diagnosis of MF, with an average length of time to diagnosis of 8.4 years. Atypical from most cases of PPD, the patients in this study demonstrated extensive involvement of the trunk, arms, and legs.5 It has been suggested that atypical PPD is a variant of PPD that evolves into MF over many years; however, we believe that PPD is a variant of MF, similar to the way an indolent dermatitis may evolve to classical MF over time. If characterized by a T-cell clone, this period preceding the diagnosis of cutaneous T-cell lymphoma could be characterized as a cutaneous T-cell lymphoid dyscrasia.
Guitart and Magro6 noted multiple chronic conditions that are associated with T-cell clones, including PPD. These conditions occurred without a known trigger, were unresponsive to topical therapies, and often did not meet diagnostic criteria for MF. The investigators felt the criteria that may indicate a cutaneous T-cell lymphoid dyscrasia include widespread distribution, lymphocytic infiltrate, diminished CD7 and CD62L expression, and clonality. Lymphocytes may be small without notable atypia.6
In a study of 43 patients with PPD, Magro et al3 found monoclonality and diminished CD7 expression in 18 participants, correlating with large surface area involvement. Approximately 40% of patients had histologic findings consistent with MF, suggesting that T-cell gene rearrangement studies should be obtained for prognostic evaluation in patients with widespread disease.3
|
|
|
To facilitate proper patient care, histopathology and molecular markers should be evaluated in conjunction with the clinical picture. A considerable increase in the size of the body surface area affected by purpuric patches combined with the presence of poikilodermatous changes and pruritus as well as disease lasting longer than 1 year should prompt an increased clinical suspicion of MF in patients with PPD.4,5 Histologically, the presence of Pautrier microabscesses, large cerebriform lymphocytes, and intraepidermal lymphocytic atypia extending beyond the dermis also would support a diagnosis of MF.3 Given the morphologic appearance and distribution of the lesions in our patient combined with epidermotropism, diminished CD7 expression, and monoclonality seen on pathology, we favored a diagnosis of MF. It would not be unreasonable to call this clonal variant of PPD a T-cell lymphoid dyscrasia. We appreciate that both PPD and MF will respond to phototherapy.7
Conclusion
We propose that there is a spectrum of disease presenting as PPD or MF sitting at either end of that spectrum and an intermediate stage, where not all criteria for cutaneous lymphoma are met, characterized as cutaneous T-cell lymphoid dyscrasia. Until the potential for evolution of PPD to malignant disease is better understood, patients with unusual presentations of pigmented purpura should be further evaluated for MF.
Case Report
A healthy 17-year-old adolescent boy with an unremarkable medical history presented with an asymptomatic fixed rash on the abdomen, buttocks, and legs. The rash initially developed in a small area on the right leg 2 years prior and had slowly progressed. He was not currently taking any medications and did not participate in intense physical activity. Multiple biopsies had previously been performed by an outside physician, the most recent one demonstrating an interface and superficial perivascular lymphocytic infiltrate with extravasated red blood cells consistent with pigmented purpura. He did not respond to treatment with intralesional corticosteroids, high-potency topical steroids, or high-dose oral prednisone.
Clinical examination revealed multiple annular purpuric patches on the abdomen, buttocks, and legs that covered approximately 20% of the body surface area (Figure 1). Over several follow-up visits, a few of the lesions evolved from patches to thin plaques. There was no adenopathy or hepatosplenomegaly. Three additional biopsies taken over the next 4 months demonstrated a mixture of small mature lymphocytes with some atypical lymphocytes in the dermis and epidermis exhibiting diminished CD7 staining and lymphocytes lining up at the dermoepidermal junction. T-cell receptor g gene rearrangements demonstrated the same clonal population in all 3 specimens. The patient was diagnosed with stage IB mycosis fungoides (MF) of the pigmented purpura–like variant. Marked improvement of the lesions was noted after 6 weeks of psoralen plus UVA therapy 3 times weekly (Figure 2). Treatment was continued for 6 months but was discontinued due to the international shortage of methoxsalen. Two months after discontinuation, most of the lesions had completely resolved (Figure 3).
|
Comment
Mycoses fungoides is a rare cutaneous lymphoma that affects approximately 2000 patients in the United States.1 Only 5% of all cases are known to occur in the first 2 decades of life,2 and even fewer cases pre-sent with pigmented purpura, usually of the lichenoid variant.3 Although the patches and plaques of MF can masquerade as many other dermatoses (eg, dermatophytosis, psoriasis, dermatitis), there have been few reports of patients presenting with lesions with the clinical appearance of pigmented purpuric dermatosis (PPD).4 As with the many cases of early MF, which are histologically indistinguishable from dermatitis, the pigmented purpura–like variant of MF initially may have the histologic appearance of pigmented purpura and generally evolves to the histologic appearance of MF over time.
Similar to our case, there have been reports of clinical and histologic diagnosis of PPD preceding the histologic diagnosis of MF. In a small cohort study of 3 young men, Barnhill and Braverman5 first demonstrated the progression of PPD to MF over a 12-year period. The age of onset ranged from 14 to 30 years, with a mean age of 24.3 years. Biopsies in all 3 patients were consistent with PPD for many years prior to the diagnosis of MF, with an average length of time to diagnosis of 8.4 years. Atypical from most cases of PPD, the patients in this study demonstrated extensive involvement of the trunk, arms, and legs.5 It has been suggested that atypical PPD is a variant of PPD that evolves into MF over many years; however, we believe that PPD is a variant of MF, similar to the way an indolent dermatitis may evolve to classical MF over time. If characterized by a T-cell clone, this period preceding the diagnosis of cutaneous T-cell lymphoma could be characterized as a cutaneous T-cell lymphoid dyscrasia.
Guitart and Magro6 noted multiple chronic conditions that are associated with T-cell clones, including PPD. These conditions occurred without a known trigger, were unresponsive to topical therapies, and often did not meet diagnostic criteria for MF. The investigators felt the criteria that may indicate a cutaneous T-cell lymphoid dyscrasia include widespread distribution, lymphocytic infiltrate, diminished CD7 and CD62L expression, and clonality. Lymphocytes may be small without notable atypia.6
In a study of 43 patients with PPD, Magro et al3 found monoclonality and diminished CD7 expression in 18 participants, correlating with large surface area involvement. Approximately 40% of patients had histologic findings consistent with MF, suggesting that T-cell gene rearrangement studies should be obtained for prognostic evaluation in patients with widespread disease.3
|
|
|
To facilitate proper patient care, histopathology and molecular markers should be evaluated in conjunction with the clinical picture. A considerable increase in the size of the body surface area affected by purpuric patches combined with the presence of poikilodermatous changes and pruritus as well as disease lasting longer than 1 year should prompt an increased clinical suspicion of MF in patients with PPD.4,5 Histologically, the presence of Pautrier microabscesses, large cerebriform lymphocytes, and intraepidermal lymphocytic atypia extending beyond the dermis also would support a diagnosis of MF.3 Given the morphologic appearance and distribution of the lesions in our patient combined with epidermotropism, diminished CD7 expression, and monoclonality seen on pathology, we favored a diagnosis of MF. It would not be unreasonable to call this clonal variant of PPD a T-cell lymphoid dyscrasia. We appreciate that both PPD and MF will respond to phototherapy.7
Conclusion
We propose that there is a spectrum of disease presenting as PPD or MF sitting at either end of that spectrum and an intermediate stage, where not all criteria for cutaneous lymphoma are met, characterized as cutaneous T-cell lymphoid dyscrasia. Until the potential for evolution of PPD to malignant disease is better understood, patients with unusual presentations of pigmented purpura should be further evaluated for MF.
1. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol. 2007;143:854-859.
2. Koch SE, Zackheim HS, Williams ML, et al. Mycosis fungoides beginning in childhood and adolescence. J Am Acad Dermatol. 1987;17:563-570.
3. Magro CM, Schaefer JT, Crowson AN, et al. Pigmented purpuric dermatosis: classification by phenotypic and molecular profiles. Am J Clin Pathol. 2007;128:218-229.
4. Hanna S, Walsh N, D’Intino Y, et al. Mycosis fungoides presenting as pigmented purpuric dermatitis. Pediatr Dermatol. 2006;23:350-354.
5. Barnhill RL, Braverman IM. Progression of pigmented purpura-like eruptions to mycosis fungoides: report of three cases. J Am Acad Dermatol. 1988;19(1, pt 1):25-31.
6. Guitart J, Magro C. Cutaneous T-cell lymphoid dyscrasia: a unifying term for idiopathic chronic dermatoses with persistent T-cell clones. Arch Dermatol. 2007;143:921-932.
7. Seckin D, Yazici Z, Senol A, et al. A case of Schamberg’s disease responding dramatically to PUVA treatment. Photodermatol Photoimmunol Photomed. 2008;24:95-96.
1. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol. 2007;143:854-859.
2. Koch SE, Zackheim HS, Williams ML, et al. Mycosis fungoides beginning in childhood and adolescence. J Am Acad Dermatol. 1987;17:563-570.
3. Magro CM, Schaefer JT, Crowson AN, et al. Pigmented purpuric dermatosis: classification by phenotypic and molecular profiles. Am J Clin Pathol. 2007;128:218-229.
4. Hanna S, Walsh N, D’Intino Y, et al. Mycosis fungoides presenting as pigmented purpuric dermatitis. Pediatr Dermatol. 2006;23:350-354.
5. Barnhill RL, Braverman IM. Progression of pigmented purpura-like eruptions to mycosis fungoides: report of three cases. J Am Acad Dermatol. 1988;19(1, pt 1):25-31.
6. Guitart J, Magro C. Cutaneous T-cell lymphoid dyscrasia: a unifying term for idiopathic chronic dermatoses with persistent T-cell clones. Arch Dermatol. 2007;143:921-932.
7. Seckin D, Yazici Z, Senol A, et al. A case of Schamberg’s disease responding dramatically to PUVA treatment. Photodermatol Photoimmunol Photomed. 2008;24:95-96.
Practice Points
- Pigmented purpuric dermatosis may lie on a spectrum with mycosis fungoides (MF).
- Pigmented purpuric dermatosis of MF should be closely followed and likely treated as MF.
- Pigmented purpuric dermatosis may have T-cell gene rearrangements that may or may not be associated with MF.
