User login
Oral cancer survival lower with positive margins, public insurance
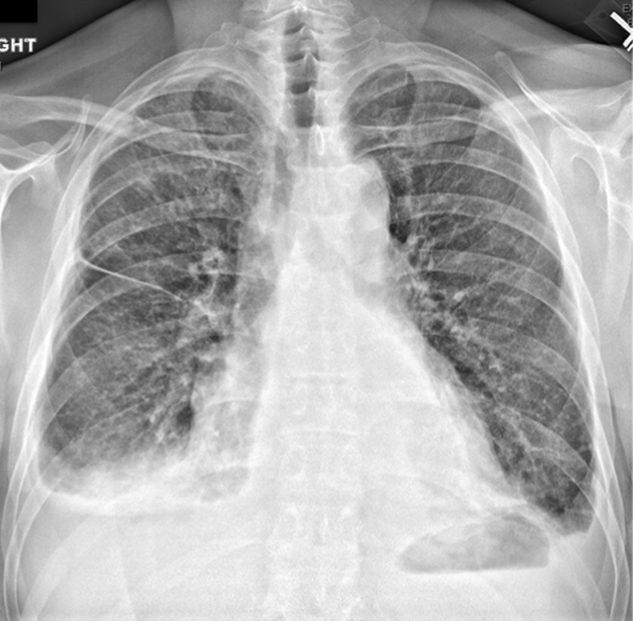
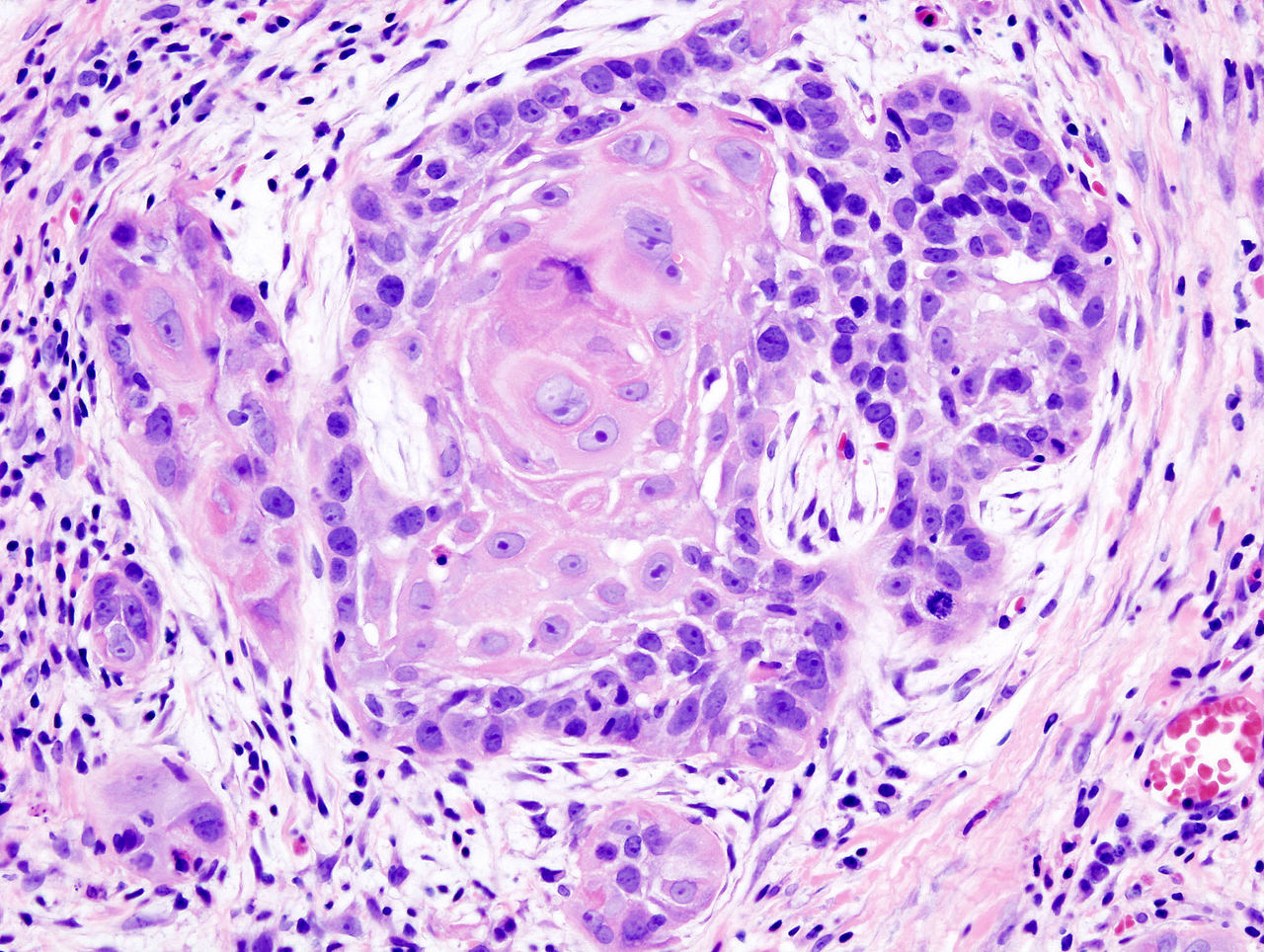
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
Key clinical point: Treatment factors such as neck dissection, tumor margins, type of insurance, and health care facility impact 5-year survival after surgery for early stage oral cavity cancer.
Major finding: Radiation, chemotherapy, positive tumor margin, nonacademic facility, and nonprivate insurance were significantly associated with lower 5-year survival.
Data source: Retrospective study of 6,830 patients in National Cancer Data Base who underwent surgery to treat stage I or II oral cavity squamous cell cancer.
Disclosures: The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
Focus on Seizures
Seizure Safety Tips
Nicotinamide cuts rate of nonmelanoma skin cancer in those at high risk
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
FROM THE ASCO 2015 PRESSCAST
Key clinical point: Nicotinamide, an inexpensive oral vitamin, protects against nonmelanoma skin cancer in patients at high risk.
Major finding: Patients taking nicotinamide had a 23% lower rate of new basal cell and squamous cell carcinomas.
Data source: A randomized, placebo-controlled phase III trial among 386 patients with past nonmelanoma skin cancers.
Disclosures: Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Managing open wounds in ob.gyn.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.

An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.

Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.
An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.
Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.
An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.
Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.

Adding mAb to treatment extends PFS in MM

Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Modified T cells may treat GVHD
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Company stops phase 3 PTCL trial

for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()
for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()
for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()
Equation provides new insight into blood flow

Engineers have devised an equation that yields simple predictions as to how quickly blood cells will migrate away from blood-vessel walls, how they will behave when they collide with each other, and how they will segregate during flow.
In the long run, these insights could help practitioners manipulate the mechanics of blood to design better blood transfusions, new techniques for drug delivery, and new processes for isolating blood-borne tumor cells.
Mike Graham, PhD, of the University of Wisconsin-Madison, and his colleagues described this work in Physical Review Letters.
“I’m really excited about this paper because it’s the first analytical theory for this phenomenon,” Dr Graham said. “It’s not very common that theory is ahead of experiments, but we’re in that position now.”
Dr Graham and his colleagues created complex computer simulations that showed how relatively stiff white blood cells and platelets interact with more flexible red blood cells.
As the different cells collide during blood flow, white cells tend to be pushed toward the walls of a blood vessel. This segregation process, called margination, creates some advantages; for example, letting white blood cells quickly exit the blood vessel to head to the site of an injury or infection.
However, the mechanical details of blood could spell both good news and bad in areas ranging from drug delivery to blood disorders to the spread of disease.
“I view my role as providing a fundamental basis of understanding for practitioners and for other engineers who are more directly connected with applications,” Dr Graham said.
Now, he is aiming to draw a firmer connection between mechanical insights and the biological functions they might impact. His group is working to refine the new equation to suit more complex flow situations and pursuing an experimental collaboration with Wilbur Lam, MD, PhD, a hematologist at Georgia Tech and Emory University in Atlanta.
Building on Dr Graham’s theoretical and simulation work, Dr Lam’s research group is creating microfluidic devices to study the behavior of blood cells. Dr Lam has developed a way to grow endothelial cells inside the artificial channels of the microfluidic devices.
“I think, together, our labs have really stumbled on how fluid mechanics may be able to explain a lot of the biological phenomena we see in blood,” Dr Lam said. “This can be related to a new way of understanding inflammation, infections, even transfusion medicine. It really pervades many different problems we see in hematology.”
Dr Graham said that capturing the physical nuances of blood vessels’ shape, size, and relative stiffness has tremendous value, even given the myriad other forces at work in the human body.
“We’d like to be able to convince practitioners that you don’t have to worry about all the details to capture the fundamental understanding of what’s going on,” Dr Graham said. “It’s extremely challenging to incorporate all the phenomena that might be important into a simulation. You have to make your case convincingly—if you want somebody to apply this research—that you’ve kept the important parts.”
Both researchers pointed out that sickle cell anemia has long been understood as both a mechanical and a biological problem. The defective red blood cells the disease causes are not only misshapen, but also stiffer than healthy red blood cells, meaning they block blood flow.
Yet, on a more detailed mechanical level, Drs Graham and Lam believe that sickle cells may literally poke and irritate the inner walls of blood vessels. If so, that would make sickle cell anemia not just a blood disorder but a disorder of the entire circulatory system. Their combined research strengths now create an opportunity to test that hypothesis.
“Biologists and hematologists have known for decades that these cells can get stuck, but what is less understood is that the blood vessel walls in the entire patient are really inflamed, and we don’t really know why,” Dr Lam said.
The researchers noted that a better understanding of blood-flow mechanics could help to make blood transfusions safer as well. Transfusions can sometimes set off heart attacks or lung damage, and the medical community isn’t entirely sure why. Dr Lam wants to find out if certain cells in stored, donated blood have mechanical properties that put patients at greater risk.
Though the collaboration between Drs Graham and Lam is still in an early stage, both researchers see the possibility of opening a new frontier in blood research.
“This would be a whole new category of things we could be looking at, and that’s why it’s so exciting,” Dr Lam said. “Suddenly, we have applications where the mechanics can be just as important.” ![]()
Engineers have devised an equation that yields simple predictions as to how quickly blood cells will migrate away from blood-vessel walls, how they will behave when they collide with each other, and how they will segregate during flow.
In the long run, these insights could help practitioners manipulate the mechanics of blood to design better blood transfusions, new techniques for drug delivery, and new processes for isolating blood-borne tumor cells.
Mike Graham, PhD, of the University of Wisconsin-Madison, and his colleagues described this work in Physical Review Letters.
“I’m really excited about this paper because it’s the first analytical theory for this phenomenon,” Dr Graham said. “It’s not very common that theory is ahead of experiments, but we’re in that position now.”
Dr Graham and his colleagues created complex computer simulations that showed how relatively stiff white blood cells and platelets interact with more flexible red blood cells.
As the different cells collide during blood flow, white cells tend to be pushed toward the walls of a blood vessel. This segregation process, called margination, creates some advantages; for example, letting white blood cells quickly exit the blood vessel to head to the site of an injury or infection.
However, the mechanical details of blood could spell both good news and bad in areas ranging from drug delivery to blood disorders to the spread of disease.
“I view my role as providing a fundamental basis of understanding for practitioners and for other engineers who are more directly connected with applications,” Dr Graham said.
Now, he is aiming to draw a firmer connection between mechanical insights and the biological functions they might impact. His group is working to refine the new equation to suit more complex flow situations and pursuing an experimental collaboration with Wilbur Lam, MD, PhD, a hematologist at Georgia Tech and Emory University in Atlanta.
Building on Dr Graham’s theoretical and simulation work, Dr Lam’s research group is creating microfluidic devices to study the behavior of blood cells. Dr Lam has developed a way to grow endothelial cells inside the artificial channels of the microfluidic devices.
“I think, together, our labs have really stumbled on how fluid mechanics may be able to explain a lot of the biological phenomena we see in blood,” Dr Lam said. “This can be related to a new way of understanding inflammation, infections, even transfusion medicine. It really pervades many different problems we see in hematology.”
Dr Graham said that capturing the physical nuances of blood vessels’ shape, size, and relative stiffness has tremendous value, even given the myriad other forces at work in the human body.
“We’d like to be able to convince practitioners that you don’t have to worry about all the details to capture the fundamental understanding of what’s going on,” Dr Graham said. “It’s extremely challenging to incorporate all the phenomena that might be important into a simulation. You have to make your case convincingly—if you want somebody to apply this research—that you’ve kept the important parts.”
Both researchers pointed out that sickle cell anemia has long been understood as both a mechanical and a biological problem. The defective red blood cells the disease causes are not only misshapen, but also stiffer than healthy red blood cells, meaning they block blood flow.
Yet, on a more detailed mechanical level, Drs Graham and Lam believe that sickle cells may literally poke and irritate the inner walls of blood vessels. If so, that would make sickle cell anemia not just a blood disorder but a disorder of the entire circulatory system. Their combined research strengths now create an opportunity to test that hypothesis.
“Biologists and hematologists have known for decades that these cells can get stuck, but what is less understood is that the blood vessel walls in the entire patient are really inflamed, and we don’t really know why,” Dr Lam said.
The researchers noted that a better understanding of blood-flow mechanics could help to make blood transfusions safer as well. Transfusions can sometimes set off heart attacks or lung damage, and the medical community isn’t entirely sure why. Dr Lam wants to find out if certain cells in stored, donated blood have mechanical properties that put patients at greater risk.
Though the collaboration between Drs Graham and Lam is still in an early stage, both researchers see the possibility of opening a new frontier in blood research.
“This would be a whole new category of things we could be looking at, and that’s why it’s so exciting,” Dr Lam said. “Suddenly, we have applications where the mechanics can be just as important.” ![]()
Engineers have devised an equation that yields simple predictions as to how quickly blood cells will migrate away from blood-vessel walls, how they will behave when they collide with each other, and how they will segregate during flow.
In the long run, these insights could help practitioners manipulate the mechanics of blood to design better blood transfusions, new techniques for drug delivery, and new processes for isolating blood-borne tumor cells.
Mike Graham, PhD, of the University of Wisconsin-Madison, and his colleagues described this work in Physical Review Letters.
“I’m really excited about this paper because it’s the first analytical theory for this phenomenon,” Dr Graham said. “It’s not very common that theory is ahead of experiments, but we’re in that position now.”
Dr Graham and his colleagues created complex computer simulations that showed how relatively stiff white blood cells and platelets interact with more flexible red blood cells.
As the different cells collide during blood flow, white cells tend to be pushed toward the walls of a blood vessel. This segregation process, called margination, creates some advantages; for example, letting white blood cells quickly exit the blood vessel to head to the site of an injury or infection.
However, the mechanical details of blood could spell both good news and bad in areas ranging from drug delivery to blood disorders to the spread of disease.
“I view my role as providing a fundamental basis of understanding for practitioners and for other engineers who are more directly connected with applications,” Dr Graham said.
Now, he is aiming to draw a firmer connection between mechanical insights and the biological functions they might impact. His group is working to refine the new equation to suit more complex flow situations and pursuing an experimental collaboration with Wilbur Lam, MD, PhD, a hematologist at Georgia Tech and Emory University in Atlanta.
Building on Dr Graham’s theoretical and simulation work, Dr Lam’s research group is creating microfluidic devices to study the behavior of blood cells. Dr Lam has developed a way to grow endothelial cells inside the artificial channels of the microfluidic devices.
“I think, together, our labs have really stumbled on how fluid mechanics may be able to explain a lot of the biological phenomena we see in blood,” Dr Lam said. “This can be related to a new way of understanding inflammation, infections, even transfusion medicine. It really pervades many different problems we see in hematology.”
Dr Graham said that capturing the physical nuances of blood vessels’ shape, size, and relative stiffness has tremendous value, even given the myriad other forces at work in the human body.
“We’d like to be able to convince practitioners that you don’t have to worry about all the details to capture the fundamental understanding of what’s going on,” Dr Graham said. “It’s extremely challenging to incorporate all the phenomena that might be important into a simulation. You have to make your case convincingly—if you want somebody to apply this research—that you’ve kept the important parts.”
Both researchers pointed out that sickle cell anemia has long been understood as both a mechanical and a biological problem. The defective red blood cells the disease causes are not only misshapen, but also stiffer than healthy red blood cells, meaning they block blood flow.
Yet, on a more detailed mechanical level, Drs Graham and Lam believe that sickle cells may literally poke and irritate the inner walls of blood vessels. If so, that would make sickle cell anemia not just a blood disorder but a disorder of the entire circulatory system. Their combined research strengths now create an opportunity to test that hypothesis.
“Biologists and hematologists have known for decades that these cells can get stuck, but what is less understood is that the blood vessel walls in the entire patient are really inflamed, and we don’t really know why,” Dr Lam said.
The researchers noted that a better understanding of blood-flow mechanics could help to make blood transfusions safer as well. Transfusions can sometimes set off heart attacks or lung damage, and the medical community isn’t entirely sure why. Dr Lam wants to find out if certain cells in stored, donated blood have mechanical properties that put patients at greater risk.
Though the collaboration between Drs Graham and Lam is still in an early stage, both researchers see the possibility of opening a new frontier in blood research.
“This would be a whole new category of things we could be looking at, and that’s why it’s so exciting,” Dr Lam said. “Suddenly, we have applications where the mechanics can be just as important.” ![]()
A coat with a clue
A 59‐year‐old man with a history of hypertension was admitted with 6 months of shortness of breath, night sweats, and debilitating fatigue. His symptoms were initially mild and would persist for weeks at a time, after which he would feel better for several days. Over the 2 weeks prior to admission his symptoms had progressed, and he had become dyspneic with minimal exertion.
Progressive dyspnea has a broad differential that includes diseases of the heart (eg, congestive heart failure, aortic stenosis, constrictive pericarditis), lung (eg, chronic obstructive pulmonary disease, interstitial lung disease, pulmonary hypertension, pleural effusion), and blood (eg, anemia).
Night sweats suggest an inflammatory condition, but do not help prioritize infection, malignancy, or autoimmunity. Any of those conditions can be relapsing and remitting, at least in their early phases, but the return to normalcy raises the possibility of hypersensitivity pneumonitis from a periodic exposure.
The 6‐month duration makes typical bacterial and viral infections less likely and suggests indolent infections such as mycobacteria, fungi, or human immunodeficiency virus. Lymphoma or chronic leukemia could cause dyspnea through pleural or pulmonary involvement or from anemia. Autoimmune conditions such as systemic lupus erythematosus or adult Still's disease could also present with this course.
On admission, he described progressive orthopnea, lower extremity edema, and a 15‐lb weight gain. He denied chest pain or palpitations. His symptoms did not correlate with environmental or occupational exposures. He had been diagnosed with essential hypertension a few years earlier but was not taking any medications. He worked as an editor for a newspaper and had traveled throughout California. He never used tobacco and drank alcohol in moderation. He previously smoked marijuana. His father died of Alzheimer's disease, and his mother and 2 siblings were healthy.
Orthopnea, lower extremity edema, and weight gain suggest volume overload, which can result from heart failure, cirrhosis, renal failure, or nephrotic syndrome. The untreated hypertension is a principal risk factor for heart failure. Subacute bacterial endocarditis is an important consideration in a patient with suspected heart failure and night sweats. Travel through the central valley of California may have exposed him to coccidiodomycosis, which can cause chronic pulmonary and extrapulmonary infection.
Physical examination revealed a chronically ill‐appearing man in mild respiratory distress. His temperature was 37.2C, heart rate was 83 bpm, and blood pressure was 168/81 mm Hg. His oxygen saturation was 97% with a respiratory rate of 17 while breathing ambient air. Bilateral chemosis was present. He had crackles at the lung bases. There was a 2/6 systolic murmur loudest at the left lower sternal border with apical radiation. His jugular venous pressure was 2 cm above the sternal angle at 45. He had mild pitting edema of both lower extremities. His abdomen was soft and nondistended. He demonstrated full range of motion of all extremities and had no rashes. He was alert and oriented to person, place, and time. There were no cranial nerve deficits. His strength, sensation and coordination were intact, and he had a normal gait.
Chemosis (conjunctival edema) usually represents conjunctival irritation from an allergic, infectious, or toxic process. It can also be seen in cases of increased ophthalmic venous pressure such as hyperthyroid ophthalmopathy, superior vena cava syndrome, or carotid‐cavernous sinus fistula. The crackles, weight gain, borderline jugular venous distention, and edema suggest some systemic volume overload, but not enough to produce chemosis.
The location and timing of the murmur suggests regurgitation through the mitral or tricuspid valve, a ventricular septal defect, or hypertrophic cardiomyopathy. Tricuspid regurgitation may indicate pulmonary hypertension with right ventricular failure. Despite the absence of fever, subacute bacterial endocarditis remains a concern.
Laboratory evaluation revealed a white blood cell count of 9600/L, hemoglobin of 8.7 g/dL, and platelet count of 522,000/L. Mean corpuscular volume was 88 fL. Serum chemistries were normal; serum creatinine was 1.2 mg/dL. Serum albumin was 2.6 g/dL. A urinalysis was normal. An electrocardiogram demonstrated normal sinus rhythm and left ventricular hypertrophy (LVH). A chest x‐ray revealed interstitial edema and small bilateral pleural effusions. A transthoracic echocardiogram demonstrated normal left ventricular systolic function, an ejection fraction of 65%, mild LVH, and mild diastolic dysfunction. Mild mitral regurgitation, a mildly dilated left atrium, and a minimal pericardial effusion were also noted. A renal ultrasound revealed an atrophic left kidney without arterial flow. He was treated with diuretics for presumed heart failure related to diastolic dysfunction. His dyspnea partially improved, and he was discharged.
Heart failure with preserved ejection fraction may be contributing to his dyspnea but is unlikely to be entirely explanatory given the laboratory abnormalities. The absence of valvular vegetations on transthoracic echocardiogram lowers the probability of bacterial endocarditis. The interstitial pulmonary markings may represent pulmonary edema but alternatively could reflect interstitial lung disease, lymphangitic spread of cancer, infection (eg, Pneumocystis jiroveci), or diffuse alveolar hemorrhage.
Anemia may also be contributing to his dyspnea. There is no evidence of bleeding on history, examination, or imaging. Hemolysis is unlikely given the absence of jaundice, splenomegaly, or a known predisposing condition. The normocytic anemia may also arise from chronic inflammation. Severe anemia can cause high output heart failure, but usually the hemoglobin level is much lower and the echocardiogram would have suggestive findings. Thrombocytosis suggests inflammation, a primary myeloproliferative disorder, or severe iron deficiency (not suspected here). His hypoalbuminemia is further evidence of chronic inflammation especially in the absence of nephropathy, hepatopathy, or a protein‐losing enteropathy.
An atrophic kidney may be congenital or result from long‐standing unilateral renal ischemia, infection, or obstruction. Diminished arterial flow in a middle‐aged man with hypertension may simply reflect atherosclerotic renal artery stenosis, but mass effect within the left renal artery from thrombus, infection, or cancer cannot be ruled out.
Four weeks later he was readmitted for progressive dyspnea and persistent night sweats. He was afebrile, fatigued, and in marked respiratory distress. The remainder of his physical examination was unchanged. Laboratory evaluation revealed a white blood cell count of 20,000/L with neutrophilic predominance, hemoglobin of 11 g/dL, and platelet count of 614,000/L. Creatinine was 1.4 mg/dL. Erythrocyte sedimentation rate (ESR) was greater than 100 mm/h, and C‐reactive protein (CRP) was 44 mg/L. Blood cultures were negative. Chest x‐ray (Figure 1) revealed persistent interstitial edema and increased bilateral pleural effusions.
Although clinical and radiologic features continue to suggest heart failure, the marked respiratory distress and persistent chest x‐ray abnormalities imply that a superimposed process is affecting the lungs. The night sweats, neutrophilia, and elevated ESR and CRP strongly suggest an inflammatory state from infection, malignancy, or autoimmunity.
A computed tomography (CT) scan of the lungs would help assess for interstitial lung disease, lymphangitic carcinomatosis and septic emboli. Blood cultures should be repeated to definitively exclude subacute endocarditis. A peripheral blood smear is needed to evaluate for hematologic malignancy. Finally, human immunodeficiency virus antibody testing is indicated.
CT of the abdomen and pelvis demonstrated left renal artery stenosis, an atrophic left kidney, right kidney edema with mild perinephric stranding, and mild‐to‐moderate right hydroureter without an obstructing mass or calculus. There was mild splenomegaly and mesenteric lymphadenopathy up to 3 cm in diameter. The distal thoracic and suprarenal abdominal aorta had crescentic high‐density wall thickening. There were small sclerotic densities of the proximal femora, pelvic girdle, and thoracolumbar spine (Figure 2). Contrast chest CT demonstrated severe wall thickening of his entire thoracic aorta. There was also cardiomegaly, mild interlobular septal thickening, small bilateral pleural effusions, a 3.2‐cm right upper lobe paratracheal lymph node, and nodular pleural thickening (Figure 3).

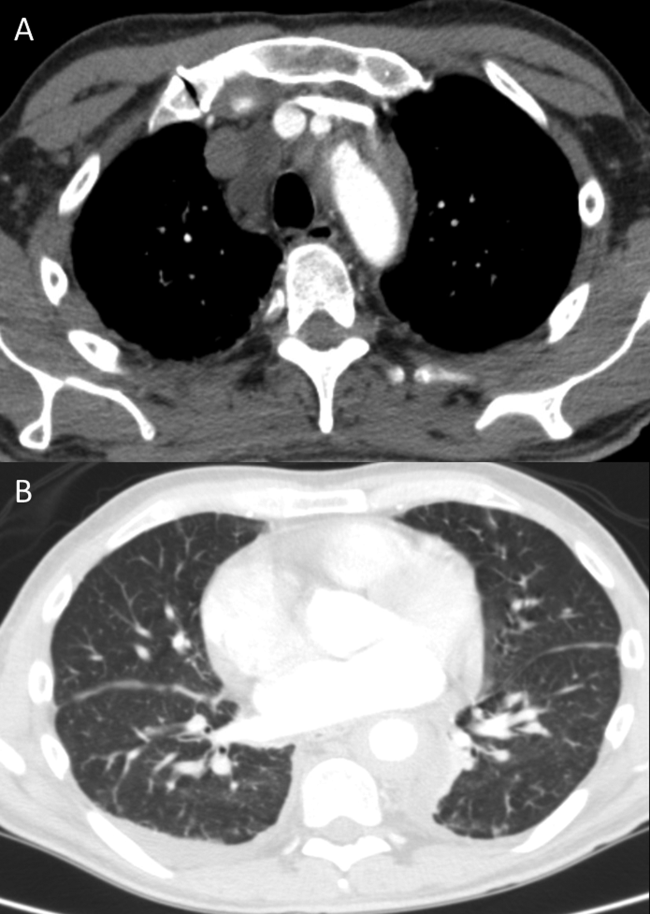
Diffuse aortopathy is caused by inflammatory, infectious, or infiltrative processes. Large vessel vasculitides such as Behet's disease, giant cell arteritis, and Takayasu's arteritis are unlikely, as the patient lacks the associated clinical findings or epidemiology. Imaging does not reveal preexisting aortic pathology, such as an aneurysm or atherosclerotic plaque, which could predispose him to bacterial endovascular infection.
Urinary system dilation without an obvious obstruction could be explained by retroperitoneal fibrosis. Generalized lymphadenopathy, (suspected) retroperitoneal fibrosis, sclerotic bone lesions, and cardiopulmonary disease collectively suggest a widespread infiltrative process. Lymphoma may lead to lymphadenopathy and bone lesions but would not explain the aortopathy. He lacks risk factors for infections like tuberculosis or tertiary syphilis, a well‐known cause of aortopathy in the past.
Widespread multisystem involvement invites consideration of nonmalignant, noninfectious infiltrative disorders such as immunoglobulin G4‐related disease (IgG4‐RD), histiocytoses such as Erdheim‐Chester disease (ECD), systemic mastocytosis (SM), and sarcoidosis. ECD is a disorder of non‐Langerhans histiocytes that infiltrate the aorta, bones, retroperitoneum, lungs, myocardium, and periorbital structures. Perinephric stranding is sometimes seen in this condition. The lymphoplasmacytes in IgG4‐RD and noncaseating granulomas of sarcoidosis infiltrate many of the same organs. Common sites infiltrated by mast cells in SM include the bone and lymph nodes. Among these diseases, ECD and IgG4‐RD more commonly manifest with aortic and retroperitoneal infiltration and thus are prioritized on this differential diagnosis.
A positron emission tomography (PET) scan revealed abnormal fluordeoxyglucose uptake involving the thoracic aorta, right apical pleural surface, perinephric soft tissue, and various marrow spaces. Core needle biopsy of a sclerotic lesion in the right ischium demonstrated focal marrow replacement by a fibrohistiocytic process. No malignant cells or pathogenic organisms were identified. Biopsy of the right kidney revealed chronic interstitial nephritis with features of megalocytic interstitial nephritis (histiocytic inflammation) and arteriolar nephrosclerosis. A transbronchial biopsy demonstrated alveolar tissue with focal intra‐alveolar hemorrhage and organization, but no malignancy, atypia, or pathogenic organisms.
The biopsy results do not support infection, lymphoma, or carcinoma. The absence of noncaseating granulomas and mastocytes on multiple biopsies essentially rules out sarcoidosis and SM, respectively. None of the characteristic pathologic features of IgG4‐RDlymphoplasmacytic infiltrate, obliterative phlebitis, and fibrosiswere observed. The pulmonary pathology points to injury, but not the underlying cause. The bone and kidney tissue samples reveal histiocytic infiltration.
The abnormalities of the aorta, bone, lung, kidney, and retroperitoneum can be explained by the diffuse histiocytic involvement seen in ECD. The perinephric stranding detected on CT and perinephric inflammation on the PET scan may reflect the hairy kidney of ECD, which is a result of histiocytic infiltration. It is possible that the chemosis relates to exophthalmos from histiocytic orbital infiltrates. Sensitivity for detecting orbital pathology on a PET scan is limited because of the high signal from the adjacent brain.
ECD should be distinguished from Langerhans cell histiocytosis (LCH) by immunohistologic staining and microscopic characteristics of the histiocytes. LCH usually does not involve the aorta, and it more commonly involves the skin.
Serum IgG4 was within normal limits, and immunohistochemical staining of pathology specimens for IgG4 was negative. The BRAF V600E mutation, which is present in the majority of patients with ECD, was detected in a subsequent right perinephric biopsy specimen. The patient was diagnosed with ECD.
Prednisone and pegylated interferon‐ led to a rapid improvement in his symptoms. As the prednisone was tapered, he developed bilateral periorbital swelling. Magnetic resonance imaging (MRI) revealed well‐circumscribed, intraorbital soft tissue masses with partial encasement of his optic nerves and superior ophthalmic veins, as well as infiltration of his transverse sinuses, consistent with intracranial manifestations of ECD. There was no evidence of pituitary, hypothalamic, or other brain parenchymal infiltration. His dyspnea, night sweats, and hypertension improved; however, 3 months into therapy he developed an extensive rash. Interferon was discontinued. Vemurafinib, a serine kinase inhibitor that targets the BRAF mutation, was prescribed with subsequent resolution of the rash.
COMMENTARY
This patient suffered from a chronic, progressive, inflammatory illness. Although the disease initially appeared to be confined to the heart and lungs, laboratory testing signaled a more systemic condition, and subsequent imaging demonstrated involvement of a disparate group of organs. Subacute disease processes with elevated markers of inflammation and diffuse organ involvement often fall into 1 of 3 categories: infectious, autoimmune, or neoplastic. The histiocytoses inhabit a fourth and easily overlooked category that can be described as infiltrative. Infiltrative diseases are a heterogeneous group of conditions that cause illness when cells or substances not normally found in tissues lead to organ dysfunction.
Although traditional teaching has focused on sarcoidosis, amyloidosis, and hemochromatosis as the primary representatives of this category, the medical literature describes a number of other infiltrative disease processes. IgG4‐RD is a fibroinflammatory disorder characterized by space‐occupying lesions, a lymphoplasmacytic infiltrate of IgG4‐positive plasma cells, and storiform (matted and irregularly whorled microscopic pattern) fibrosis.[1] IgG4‐RD, like sarcoidosis, blurs the categorical line between infiltrative and autoimmune diseases. Other infiltrative cellular disorders, such as histiocytosis and mastocytosis, exist on a spectrum between monoclonal proliferation and neoplastic invasion.
The histiocytoses represent a diverse group of disorders with an evolving nomenclature, characterized by localized or diffuse infiltration of macrophages, monocytes, and dendritic cells (Table 1). ECD is a rare, non‐Langerhans histiocytosis characterized by excessive recruitment and activation of histiocytes through kinase signaling pathways.[2, 3] Immunohistochemical staining for CD68, CD163, and Factor XIIIa, with lack of staining for CD1a, S100, and CD207, supports the diagnosis.[3] Mutations in the BRAF V600E gene (a protein kinase involved in cell proliferation) represent the most likely etiology of this overactivation. An estimated 38% to 100% of patients with ECD harbor this mutation, with detection rates influenced by the sensitivity of testing techniques.[3] The serine kinase inhibitor vemurafinib targets this mutation, and early experience with this agent in ECD demonstrates encouraging results.[4]
| Dendritic cell disorders |
| Langerhans cell histiocytosis |
| Secondary dendritic cell processes |
| Juvenile xanthogranuloma and related disorders (including Erdheim‐Chester disease) |
| Solitary histiocytomas with a dendritic phenotype |
| Macrophage‐related disorders |
| Primary hemophagocytic lymphohistiocytosis (familial and sporadic) |
| Secondary hemophagocytic syndromes |
| Sinus histiocytosis with massive lymphadenopathy (Rosai‐Dorfman disease) |
| Solitary histiocytoma with a macrophage phenotype |
| Malignant histiocytic disorders |
| Monocyte‐related leukemias |
| Extramedullary monocytic tumor or sarcoma |
| Dendritic cell‐related histiocytic sarcoma |
| Macrophage‐related histiocytic sarcoma |
ECD presents heterogeneously, occurring most commonly between the ages of 40 and 70 years. Nonspecific symptoms include weakness, fatigue, fever, chills, weight loss, and night sweats. Typical sites of involvement include the bone, central nervous system, cardiovascular system, lungs, and retroperitoneum. Bone involvement is nearly universal, and bone pain is the most common presenting symptom. Symmetric diaphyseal and metaphyseal osteosclerotic lesions may be seen on x‐rays, bone scan, PET, CT, and MRI.[3] Approximately 50% of patients have extraskeletal involvement at diagnosis.[5] Neurologic manifestations may result from invasion of histiocytes into the facial bones, orbits, meninges, and intracranial vessels, as eventually developed in this patient. Diabetes insipidus is the most common neurologic manifestation of ECD, followed by exophthalmos, cerebellar ataxia, panhypopituitarism, and papilledema.[6, 7] Approximately 75% of patients eventually suffer from cardiovascular disease, including hypertension, congestive heart failure, acute myocardial infarction, valvular dysfunction, pericardial infiltration, and cardiac tamponade.[8] Vascular involvement includes perivascular infiltration and periaortic fibrosis, resulting in the coated aorta seen in 20% of patients with ECD.[3] Pulmonary manifestations of ECD include interstitial, pleural, and consolidative lung disease. A review of high‐resolution chest CTs of patients with ECD demonstrated that greater than half had evidence of parenchymal lung disease, with interlobular septal thickening being the most common finding.[9] Infiltration and fibrosis of retroperitoneal structures is common. Infiltration of perinephric fat creates irregular renal borders, appearing radiographically as hairy kidneys.
Arriving at the diagnosis in this case proved to be challenging because the early presentation was consistent with congestive heart failure. As the patient's conditioned deteriorated, imaging suggested multisystem involvement. It was the extensive aortopathy in particularnot the less specific bone, kidney, lymph node, or pulmonary findingsthat allowed the clinicians to hone the extensive differential diagnosis. The coated aorta is a finding that has been strongly associated with ECD; few other conditions coat the aorta in a similar fashion.[10] In most mysteries, the perpetrator's coat conceals his identity; however, in this story the coat gave it away.
KEY LEARNING POINTS
- Subacute, inflammatory, multiorgan disease is usually explained by 3 categoriesinfection, autoimmunity, and neoplasiabut a fourth category, infiltrative disorders, sometimes warrants consideration.
- ECD presents heterogeneously, ranging from localized disease to widespread organ infiltration. The classic presentation includes bone pain, diabetes insipidus, and exophthalmos.
- Characteristic radiological findings that suggest ECD include long bone osteosclerosis, a coated aorta from periaortic infiltration, and hairy kidneys from perinephric infiltration.
Disclosure
Nothing to report
- , , IgG4‐related disease. N Engl J Med. 2012;366(6):539–551.
- , , , Diagnosing Erdheim‐Chester disease. Ann Rheum Dis. 2013;72(7):e19.
- , , , et al. Consensus guidelines for the diagnosis and clinical management of Erdheim‐Chester disease. Blood. 2014;124(4):483–492.
- , , , et al. The efficacy of vemurafenib in Erdheim‐Chester Disease and Langerhans Cell Histiocytosis: preliminary results from VE‐Basket Study. Blood. 2014;124(21):635.
- , , , et al. Erdheim‐Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996;75(3):157–169.
- , , , et al. Neurological manifestations and neuroradiological presentation of Erdheim‐Chester disease: report of 6 cases and systematic review of the literature. J Neurol. 2006;253(10):1267–1277.
- , , , et al. Cerebral, facial, and orbital involvement in Erdheim‐Chester disease: CT and MR imaging findings. Radiology. 2010;255(2):586–594.
- , , , et al. Images in cardiovascular medicine. Cardiac involvement in Erdheim‐Chester disease: magnetic resonance and computed tomographic scan imaging in a monocentric series of 37 patients. Circulation. 2009;119(25):e597–e598.
- , , , et al. Pulmonary involvement in Erdheim‐Chester disease: a single‐center study of thirty‐four patients and a review of the literature. Arthritis Rheum. 2010;62(11):3504–3512.
- , , , et al. “Coated aorta”: a new sign of Erdheim‐Chester disease. J Rheumatol. 2000;27(6):1550–1553.
A 59‐year‐old man with a history of hypertension was admitted with 6 months of shortness of breath, night sweats, and debilitating fatigue. His symptoms were initially mild and would persist for weeks at a time, after which he would feel better for several days. Over the 2 weeks prior to admission his symptoms had progressed, and he had become dyspneic with minimal exertion.
Progressive dyspnea has a broad differential that includes diseases of the heart (eg, congestive heart failure, aortic stenosis, constrictive pericarditis), lung (eg, chronic obstructive pulmonary disease, interstitial lung disease, pulmonary hypertension, pleural effusion), and blood (eg, anemia).
Night sweats suggest an inflammatory condition, but do not help prioritize infection, malignancy, or autoimmunity. Any of those conditions can be relapsing and remitting, at least in their early phases, but the return to normalcy raises the possibility of hypersensitivity pneumonitis from a periodic exposure.
The 6‐month duration makes typical bacterial and viral infections less likely and suggests indolent infections such as mycobacteria, fungi, or human immunodeficiency virus. Lymphoma or chronic leukemia could cause dyspnea through pleural or pulmonary involvement or from anemia. Autoimmune conditions such as systemic lupus erythematosus or adult Still's disease could also present with this course.
On admission, he described progressive orthopnea, lower extremity edema, and a 15‐lb weight gain. He denied chest pain or palpitations. His symptoms did not correlate with environmental or occupational exposures. He had been diagnosed with essential hypertension a few years earlier but was not taking any medications. He worked as an editor for a newspaper and had traveled throughout California. He never used tobacco and drank alcohol in moderation. He previously smoked marijuana. His father died of Alzheimer's disease, and his mother and 2 siblings were healthy.
Orthopnea, lower extremity edema, and weight gain suggest volume overload, which can result from heart failure, cirrhosis, renal failure, or nephrotic syndrome. The untreated hypertension is a principal risk factor for heart failure. Subacute bacterial endocarditis is an important consideration in a patient with suspected heart failure and night sweats. Travel through the central valley of California may have exposed him to coccidiodomycosis, which can cause chronic pulmonary and extrapulmonary infection.
Physical examination revealed a chronically ill‐appearing man in mild respiratory distress. His temperature was 37.2C, heart rate was 83 bpm, and blood pressure was 168/81 mm Hg. His oxygen saturation was 97% with a respiratory rate of 17 while breathing ambient air. Bilateral chemosis was present. He had crackles at the lung bases. There was a 2/6 systolic murmur loudest at the left lower sternal border with apical radiation. His jugular venous pressure was 2 cm above the sternal angle at 45. He had mild pitting edema of both lower extremities. His abdomen was soft and nondistended. He demonstrated full range of motion of all extremities and had no rashes. He was alert and oriented to person, place, and time. There were no cranial nerve deficits. His strength, sensation and coordination were intact, and he had a normal gait.
Chemosis (conjunctival edema) usually represents conjunctival irritation from an allergic, infectious, or toxic process. It can also be seen in cases of increased ophthalmic venous pressure such as hyperthyroid ophthalmopathy, superior vena cava syndrome, or carotid‐cavernous sinus fistula. The crackles, weight gain, borderline jugular venous distention, and edema suggest some systemic volume overload, but not enough to produce chemosis.
The location and timing of the murmur suggests regurgitation through the mitral or tricuspid valve, a ventricular septal defect, or hypertrophic cardiomyopathy. Tricuspid regurgitation may indicate pulmonary hypertension with right ventricular failure. Despite the absence of fever, subacute bacterial endocarditis remains a concern.
Laboratory evaluation revealed a white blood cell count of 9600/L, hemoglobin of 8.7 g/dL, and platelet count of 522,000/L. Mean corpuscular volume was 88 fL. Serum chemistries were normal; serum creatinine was 1.2 mg/dL. Serum albumin was 2.6 g/dL. A urinalysis was normal. An electrocardiogram demonstrated normal sinus rhythm and left ventricular hypertrophy (LVH). A chest x‐ray revealed interstitial edema and small bilateral pleural effusions. A transthoracic echocardiogram demonstrated normal left ventricular systolic function, an ejection fraction of 65%, mild LVH, and mild diastolic dysfunction. Mild mitral regurgitation, a mildly dilated left atrium, and a minimal pericardial effusion were also noted. A renal ultrasound revealed an atrophic left kidney without arterial flow. He was treated with diuretics for presumed heart failure related to diastolic dysfunction. His dyspnea partially improved, and he was discharged.
Heart failure with preserved ejection fraction may be contributing to his dyspnea but is unlikely to be entirely explanatory given the laboratory abnormalities. The absence of valvular vegetations on transthoracic echocardiogram lowers the probability of bacterial endocarditis. The interstitial pulmonary markings may represent pulmonary edema but alternatively could reflect interstitial lung disease, lymphangitic spread of cancer, infection (eg, Pneumocystis jiroveci), or diffuse alveolar hemorrhage.
Anemia may also be contributing to his dyspnea. There is no evidence of bleeding on history, examination, or imaging. Hemolysis is unlikely given the absence of jaundice, splenomegaly, or a known predisposing condition. The normocytic anemia may also arise from chronic inflammation. Severe anemia can cause high output heart failure, but usually the hemoglobin level is much lower and the echocardiogram would have suggestive findings. Thrombocytosis suggests inflammation, a primary myeloproliferative disorder, or severe iron deficiency (not suspected here). His hypoalbuminemia is further evidence of chronic inflammation especially in the absence of nephropathy, hepatopathy, or a protein‐losing enteropathy.
An atrophic kidney may be congenital or result from long‐standing unilateral renal ischemia, infection, or obstruction. Diminished arterial flow in a middle‐aged man with hypertension may simply reflect atherosclerotic renal artery stenosis, but mass effect within the left renal artery from thrombus, infection, or cancer cannot be ruled out.
Four weeks later he was readmitted for progressive dyspnea and persistent night sweats. He was afebrile, fatigued, and in marked respiratory distress. The remainder of his physical examination was unchanged. Laboratory evaluation revealed a white blood cell count of 20,000/L with neutrophilic predominance, hemoglobin of 11 g/dL, and platelet count of 614,000/L. Creatinine was 1.4 mg/dL. Erythrocyte sedimentation rate (ESR) was greater than 100 mm/h, and C‐reactive protein (CRP) was 44 mg/L. Blood cultures were negative. Chest x‐ray (Figure 1) revealed persistent interstitial edema and increased bilateral pleural effusions.
Although clinical and radiologic features continue to suggest heart failure, the marked respiratory distress and persistent chest x‐ray abnormalities imply that a superimposed process is affecting the lungs. The night sweats, neutrophilia, and elevated ESR and CRP strongly suggest an inflammatory state from infection, malignancy, or autoimmunity.
A computed tomography (CT) scan of the lungs would help assess for interstitial lung disease, lymphangitic carcinomatosis and septic emboli. Blood cultures should be repeated to definitively exclude subacute endocarditis. A peripheral blood smear is needed to evaluate for hematologic malignancy. Finally, human immunodeficiency virus antibody testing is indicated.
CT of the abdomen and pelvis demonstrated left renal artery stenosis, an atrophic left kidney, right kidney edema with mild perinephric stranding, and mild‐to‐moderate right hydroureter without an obstructing mass or calculus. There was mild splenomegaly and mesenteric lymphadenopathy up to 3 cm in diameter. The distal thoracic and suprarenal abdominal aorta had crescentic high‐density wall thickening. There were small sclerotic densities of the proximal femora, pelvic girdle, and thoracolumbar spine (Figure 2). Contrast chest CT demonstrated severe wall thickening of his entire thoracic aorta. There was also cardiomegaly, mild interlobular septal thickening, small bilateral pleural effusions, a 3.2‐cm right upper lobe paratracheal lymph node, and nodular pleural thickening (Figure 3).
Diffuse aortopathy is caused by inflammatory, infectious, or infiltrative processes. Large vessel vasculitides such as Behet's disease, giant cell arteritis, and Takayasu's arteritis are unlikely, as the patient lacks the associated clinical findings or epidemiology. Imaging does not reveal preexisting aortic pathology, such as an aneurysm or atherosclerotic plaque, which could predispose him to bacterial endovascular infection.
Urinary system dilation without an obvious obstruction could be explained by retroperitoneal fibrosis. Generalized lymphadenopathy, (suspected) retroperitoneal fibrosis, sclerotic bone lesions, and cardiopulmonary disease collectively suggest a widespread infiltrative process. Lymphoma may lead to lymphadenopathy and bone lesions but would not explain the aortopathy. He lacks risk factors for infections like tuberculosis or tertiary syphilis, a well‐known cause of aortopathy in the past.
Widespread multisystem involvement invites consideration of nonmalignant, noninfectious infiltrative disorders such as immunoglobulin G4‐related disease (IgG4‐RD), histiocytoses such as Erdheim‐Chester disease (ECD), systemic mastocytosis (SM), and sarcoidosis. ECD is a disorder of non‐Langerhans histiocytes that infiltrate the aorta, bones, retroperitoneum, lungs, myocardium, and periorbital structures. Perinephric stranding is sometimes seen in this condition. The lymphoplasmacytes in IgG4‐RD and noncaseating granulomas of sarcoidosis infiltrate many of the same organs. Common sites infiltrated by mast cells in SM include the bone and lymph nodes. Among these diseases, ECD and IgG4‐RD more commonly manifest with aortic and retroperitoneal infiltration and thus are prioritized on this differential diagnosis.
A positron emission tomography (PET) scan revealed abnormal fluordeoxyglucose uptake involving the thoracic aorta, right apical pleural surface, perinephric soft tissue, and various marrow spaces. Core needle biopsy of a sclerotic lesion in the right ischium demonstrated focal marrow replacement by a fibrohistiocytic process. No malignant cells or pathogenic organisms were identified. Biopsy of the right kidney revealed chronic interstitial nephritis with features of megalocytic interstitial nephritis (histiocytic inflammation) and arteriolar nephrosclerosis. A transbronchial biopsy demonstrated alveolar tissue with focal intra‐alveolar hemorrhage and organization, but no malignancy, atypia, or pathogenic organisms.
The biopsy results do not support infection, lymphoma, or carcinoma. The absence of noncaseating granulomas and mastocytes on multiple biopsies essentially rules out sarcoidosis and SM, respectively. None of the characteristic pathologic features of IgG4‐RDlymphoplasmacytic infiltrate, obliterative phlebitis, and fibrosiswere observed. The pulmonary pathology points to injury, but not the underlying cause. The bone and kidney tissue samples reveal histiocytic infiltration.
The abnormalities of the aorta, bone, lung, kidney, and retroperitoneum can be explained by the diffuse histiocytic involvement seen in ECD. The perinephric stranding detected on CT and perinephric inflammation on the PET scan may reflect the hairy kidney of ECD, which is a result of histiocytic infiltration. It is possible that the chemosis relates to exophthalmos from histiocytic orbital infiltrates. Sensitivity for detecting orbital pathology on a PET scan is limited because of the high signal from the adjacent brain.
ECD should be distinguished from Langerhans cell histiocytosis (LCH) by immunohistologic staining and microscopic characteristics of the histiocytes. LCH usually does not involve the aorta, and it more commonly involves the skin.
Serum IgG4 was within normal limits, and immunohistochemical staining of pathology specimens for IgG4 was negative. The BRAF V600E mutation, which is present in the majority of patients with ECD, was detected in a subsequent right perinephric biopsy specimen. The patient was diagnosed with ECD.
Prednisone and pegylated interferon‐ led to a rapid improvement in his symptoms. As the prednisone was tapered, he developed bilateral periorbital swelling. Magnetic resonance imaging (MRI) revealed well‐circumscribed, intraorbital soft tissue masses with partial encasement of his optic nerves and superior ophthalmic veins, as well as infiltration of his transverse sinuses, consistent with intracranial manifestations of ECD. There was no evidence of pituitary, hypothalamic, or other brain parenchymal infiltration. His dyspnea, night sweats, and hypertension improved; however, 3 months into therapy he developed an extensive rash. Interferon was discontinued. Vemurafinib, a serine kinase inhibitor that targets the BRAF mutation, was prescribed with subsequent resolution of the rash.
COMMENTARY
This patient suffered from a chronic, progressive, inflammatory illness. Although the disease initially appeared to be confined to the heart and lungs, laboratory testing signaled a more systemic condition, and subsequent imaging demonstrated involvement of a disparate group of organs. Subacute disease processes with elevated markers of inflammation and diffuse organ involvement often fall into 1 of 3 categories: infectious, autoimmune, or neoplastic. The histiocytoses inhabit a fourth and easily overlooked category that can be described as infiltrative. Infiltrative diseases are a heterogeneous group of conditions that cause illness when cells or substances not normally found in tissues lead to organ dysfunction.
Although traditional teaching has focused on sarcoidosis, amyloidosis, and hemochromatosis as the primary representatives of this category, the medical literature describes a number of other infiltrative disease processes. IgG4‐RD is a fibroinflammatory disorder characterized by space‐occupying lesions, a lymphoplasmacytic infiltrate of IgG4‐positive plasma cells, and storiform (matted and irregularly whorled microscopic pattern) fibrosis.[1] IgG4‐RD, like sarcoidosis, blurs the categorical line between infiltrative and autoimmune diseases. Other infiltrative cellular disorders, such as histiocytosis and mastocytosis, exist on a spectrum between monoclonal proliferation and neoplastic invasion.
The histiocytoses represent a diverse group of disorders with an evolving nomenclature, characterized by localized or diffuse infiltration of macrophages, monocytes, and dendritic cells (Table 1). ECD is a rare, non‐Langerhans histiocytosis characterized by excessive recruitment and activation of histiocytes through kinase signaling pathways.[2, 3] Immunohistochemical staining for CD68, CD163, and Factor XIIIa, with lack of staining for CD1a, S100, and CD207, supports the diagnosis.[3] Mutations in the BRAF V600E gene (a protein kinase involved in cell proliferation) represent the most likely etiology of this overactivation. An estimated 38% to 100% of patients with ECD harbor this mutation, with detection rates influenced by the sensitivity of testing techniques.[3] The serine kinase inhibitor vemurafinib targets this mutation, and early experience with this agent in ECD demonstrates encouraging results.[4]
| Dendritic cell disorders |
| Langerhans cell histiocytosis |
| Secondary dendritic cell processes |
| Juvenile xanthogranuloma and related disorders (including Erdheim‐Chester disease) |
| Solitary histiocytomas with a dendritic phenotype |
| Macrophage‐related disorders |
| Primary hemophagocytic lymphohistiocytosis (familial and sporadic) |
| Secondary hemophagocytic syndromes |
| Sinus histiocytosis with massive lymphadenopathy (Rosai‐Dorfman disease) |
| Solitary histiocytoma with a macrophage phenotype |
| Malignant histiocytic disorders |
| Monocyte‐related leukemias |
| Extramedullary monocytic tumor or sarcoma |
| Dendritic cell‐related histiocytic sarcoma |
| Macrophage‐related histiocytic sarcoma |
ECD presents heterogeneously, occurring most commonly between the ages of 40 and 70 years. Nonspecific symptoms include weakness, fatigue, fever, chills, weight loss, and night sweats. Typical sites of involvement include the bone, central nervous system, cardiovascular system, lungs, and retroperitoneum. Bone involvement is nearly universal, and bone pain is the most common presenting symptom. Symmetric diaphyseal and metaphyseal osteosclerotic lesions may be seen on x‐rays, bone scan, PET, CT, and MRI.[3] Approximately 50% of patients have extraskeletal involvement at diagnosis.[5] Neurologic manifestations may result from invasion of histiocytes into the facial bones, orbits, meninges, and intracranial vessels, as eventually developed in this patient. Diabetes insipidus is the most common neurologic manifestation of ECD, followed by exophthalmos, cerebellar ataxia, panhypopituitarism, and papilledema.[6, 7] Approximately 75% of patients eventually suffer from cardiovascular disease, including hypertension, congestive heart failure, acute myocardial infarction, valvular dysfunction, pericardial infiltration, and cardiac tamponade.[8] Vascular involvement includes perivascular infiltration and periaortic fibrosis, resulting in the coated aorta seen in 20% of patients with ECD.[3] Pulmonary manifestations of ECD include interstitial, pleural, and consolidative lung disease. A review of high‐resolution chest CTs of patients with ECD demonstrated that greater than half had evidence of parenchymal lung disease, with interlobular septal thickening being the most common finding.[9] Infiltration and fibrosis of retroperitoneal structures is common. Infiltration of perinephric fat creates irregular renal borders, appearing radiographically as hairy kidneys.
Arriving at the diagnosis in this case proved to be challenging because the early presentation was consistent with congestive heart failure. As the patient's conditioned deteriorated, imaging suggested multisystem involvement. It was the extensive aortopathy in particularnot the less specific bone, kidney, lymph node, or pulmonary findingsthat allowed the clinicians to hone the extensive differential diagnosis. The coated aorta is a finding that has been strongly associated with ECD; few other conditions coat the aorta in a similar fashion.[10] In most mysteries, the perpetrator's coat conceals his identity; however, in this story the coat gave it away.
KEY LEARNING POINTS
- Subacute, inflammatory, multiorgan disease is usually explained by 3 categoriesinfection, autoimmunity, and neoplasiabut a fourth category, infiltrative disorders, sometimes warrants consideration.
- ECD presents heterogeneously, ranging from localized disease to widespread organ infiltration. The classic presentation includes bone pain, diabetes insipidus, and exophthalmos.
- Characteristic radiological findings that suggest ECD include long bone osteosclerosis, a coated aorta from periaortic infiltration, and hairy kidneys from perinephric infiltration.
Disclosure
Nothing to report
A 59‐year‐old man with a history of hypertension was admitted with 6 months of shortness of breath, night sweats, and debilitating fatigue. His symptoms were initially mild and would persist for weeks at a time, after which he would feel better for several days. Over the 2 weeks prior to admission his symptoms had progressed, and he had become dyspneic with minimal exertion.
Progressive dyspnea has a broad differential that includes diseases of the heart (eg, congestive heart failure, aortic stenosis, constrictive pericarditis), lung (eg, chronic obstructive pulmonary disease, interstitial lung disease, pulmonary hypertension, pleural effusion), and blood (eg, anemia).
Night sweats suggest an inflammatory condition, but do not help prioritize infection, malignancy, or autoimmunity. Any of those conditions can be relapsing and remitting, at least in their early phases, but the return to normalcy raises the possibility of hypersensitivity pneumonitis from a periodic exposure.
The 6‐month duration makes typical bacterial and viral infections less likely and suggests indolent infections such as mycobacteria, fungi, or human immunodeficiency virus. Lymphoma or chronic leukemia could cause dyspnea through pleural or pulmonary involvement or from anemia. Autoimmune conditions such as systemic lupus erythematosus or adult Still's disease could also present with this course.
On admission, he described progressive orthopnea, lower extremity edema, and a 15‐lb weight gain. He denied chest pain or palpitations. His symptoms did not correlate with environmental or occupational exposures. He had been diagnosed with essential hypertension a few years earlier but was not taking any medications. He worked as an editor for a newspaper and had traveled throughout California. He never used tobacco and drank alcohol in moderation. He previously smoked marijuana. His father died of Alzheimer's disease, and his mother and 2 siblings were healthy.
Orthopnea, lower extremity edema, and weight gain suggest volume overload, which can result from heart failure, cirrhosis, renal failure, or nephrotic syndrome. The untreated hypertension is a principal risk factor for heart failure. Subacute bacterial endocarditis is an important consideration in a patient with suspected heart failure and night sweats. Travel through the central valley of California may have exposed him to coccidiodomycosis, which can cause chronic pulmonary and extrapulmonary infection.
Physical examination revealed a chronically ill‐appearing man in mild respiratory distress. His temperature was 37.2C, heart rate was 83 bpm, and blood pressure was 168/81 mm Hg. His oxygen saturation was 97% with a respiratory rate of 17 while breathing ambient air. Bilateral chemosis was present. He had crackles at the lung bases. There was a 2/6 systolic murmur loudest at the left lower sternal border with apical radiation. His jugular venous pressure was 2 cm above the sternal angle at 45. He had mild pitting edema of both lower extremities. His abdomen was soft and nondistended. He demonstrated full range of motion of all extremities and had no rashes. He was alert and oriented to person, place, and time. There were no cranial nerve deficits. His strength, sensation and coordination were intact, and he had a normal gait.
Chemosis (conjunctival edema) usually represents conjunctival irritation from an allergic, infectious, or toxic process. It can also be seen in cases of increased ophthalmic venous pressure such as hyperthyroid ophthalmopathy, superior vena cava syndrome, or carotid‐cavernous sinus fistula. The crackles, weight gain, borderline jugular venous distention, and edema suggest some systemic volume overload, but not enough to produce chemosis.
The location and timing of the murmur suggests regurgitation through the mitral or tricuspid valve, a ventricular septal defect, or hypertrophic cardiomyopathy. Tricuspid regurgitation may indicate pulmonary hypertension with right ventricular failure. Despite the absence of fever, subacute bacterial endocarditis remains a concern.
Laboratory evaluation revealed a white blood cell count of 9600/L, hemoglobin of 8.7 g/dL, and platelet count of 522,000/L. Mean corpuscular volume was 88 fL. Serum chemistries were normal; serum creatinine was 1.2 mg/dL. Serum albumin was 2.6 g/dL. A urinalysis was normal. An electrocardiogram demonstrated normal sinus rhythm and left ventricular hypertrophy (LVH). A chest x‐ray revealed interstitial edema and small bilateral pleural effusions. A transthoracic echocardiogram demonstrated normal left ventricular systolic function, an ejection fraction of 65%, mild LVH, and mild diastolic dysfunction. Mild mitral regurgitation, a mildly dilated left atrium, and a minimal pericardial effusion were also noted. A renal ultrasound revealed an atrophic left kidney without arterial flow. He was treated with diuretics for presumed heart failure related to diastolic dysfunction. His dyspnea partially improved, and he was discharged.
Heart failure with preserved ejection fraction may be contributing to his dyspnea but is unlikely to be entirely explanatory given the laboratory abnormalities. The absence of valvular vegetations on transthoracic echocardiogram lowers the probability of bacterial endocarditis. The interstitial pulmonary markings may represent pulmonary edema but alternatively could reflect interstitial lung disease, lymphangitic spread of cancer, infection (eg, Pneumocystis jiroveci), or diffuse alveolar hemorrhage.
Anemia may also be contributing to his dyspnea. There is no evidence of bleeding on history, examination, or imaging. Hemolysis is unlikely given the absence of jaundice, splenomegaly, or a known predisposing condition. The normocytic anemia may also arise from chronic inflammation. Severe anemia can cause high output heart failure, but usually the hemoglobin level is much lower and the echocardiogram would have suggestive findings. Thrombocytosis suggests inflammation, a primary myeloproliferative disorder, or severe iron deficiency (not suspected here). His hypoalbuminemia is further evidence of chronic inflammation especially in the absence of nephropathy, hepatopathy, or a protein‐losing enteropathy.
An atrophic kidney may be congenital or result from long‐standing unilateral renal ischemia, infection, or obstruction. Diminished arterial flow in a middle‐aged man with hypertension may simply reflect atherosclerotic renal artery stenosis, but mass effect within the left renal artery from thrombus, infection, or cancer cannot be ruled out.
Four weeks later he was readmitted for progressive dyspnea and persistent night sweats. He was afebrile, fatigued, and in marked respiratory distress. The remainder of his physical examination was unchanged. Laboratory evaluation revealed a white blood cell count of 20,000/L with neutrophilic predominance, hemoglobin of 11 g/dL, and platelet count of 614,000/L. Creatinine was 1.4 mg/dL. Erythrocyte sedimentation rate (ESR) was greater than 100 mm/h, and C‐reactive protein (CRP) was 44 mg/L. Blood cultures were negative. Chest x‐ray (Figure 1) revealed persistent interstitial edema and increased bilateral pleural effusions.
Although clinical and radiologic features continue to suggest heart failure, the marked respiratory distress and persistent chest x‐ray abnormalities imply that a superimposed process is affecting the lungs. The night sweats, neutrophilia, and elevated ESR and CRP strongly suggest an inflammatory state from infection, malignancy, or autoimmunity.
A computed tomography (CT) scan of the lungs would help assess for interstitial lung disease, lymphangitic carcinomatosis and septic emboli. Blood cultures should be repeated to definitively exclude subacute endocarditis. A peripheral blood smear is needed to evaluate for hematologic malignancy. Finally, human immunodeficiency virus antibody testing is indicated.
CT of the abdomen and pelvis demonstrated left renal artery stenosis, an atrophic left kidney, right kidney edema with mild perinephric stranding, and mild‐to‐moderate right hydroureter without an obstructing mass or calculus. There was mild splenomegaly and mesenteric lymphadenopathy up to 3 cm in diameter. The distal thoracic and suprarenal abdominal aorta had crescentic high‐density wall thickening. There were small sclerotic densities of the proximal femora, pelvic girdle, and thoracolumbar spine (Figure 2). Contrast chest CT demonstrated severe wall thickening of his entire thoracic aorta. There was also cardiomegaly, mild interlobular septal thickening, small bilateral pleural effusions, a 3.2‐cm right upper lobe paratracheal lymph node, and nodular pleural thickening (Figure 3).
Diffuse aortopathy is caused by inflammatory, infectious, or infiltrative processes. Large vessel vasculitides such as Behet's disease, giant cell arteritis, and Takayasu's arteritis are unlikely, as the patient lacks the associated clinical findings or epidemiology. Imaging does not reveal preexisting aortic pathology, such as an aneurysm or atherosclerotic plaque, which could predispose him to bacterial endovascular infection.
Urinary system dilation without an obvious obstruction could be explained by retroperitoneal fibrosis. Generalized lymphadenopathy, (suspected) retroperitoneal fibrosis, sclerotic bone lesions, and cardiopulmonary disease collectively suggest a widespread infiltrative process. Lymphoma may lead to lymphadenopathy and bone lesions but would not explain the aortopathy. He lacks risk factors for infections like tuberculosis or tertiary syphilis, a well‐known cause of aortopathy in the past.
Widespread multisystem involvement invites consideration of nonmalignant, noninfectious infiltrative disorders such as immunoglobulin G4‐related disease (IgG4‐RD), histiocytoses such as Erdheim‐Chester disease (ECD), systemic mastocytosis (SM), and sarcoidosis. ECD is a disorder of non‐Langerhans histiocytes that infiltrate the aorta, bones, retroperitoneum, lungs, myocardium, and periorbital structures. Perinephric stranding is sometimes seen in this condition. The lymphoplasmacytes in IgG4‐RD and noncaseating granulomas of sarcoidosis infiltrate many of the same organs. Common sites infiltrated by mast cells in SM include the bone and lymph nodes. Among these diseases, ECD and IgG4‐RD more commonly manifest with aortic and retroperitoneal infiltration and thus are prioritized on this differential diagnosis.
A positron emission tomography (PET) scan revealed abnormal fluordeoxyglucose uptake involving the thoracic aorta, right apical pleural surface, perinephric soft tissue, and various marrow spaces. Core needle biopsy of a sclerotic lesion in the right ischium demonstrated focal marrow replacement by a fibrohistiocytic process. No malignant cells or pathogenic organisms were identified. Biopsy of the right kidney revealed chronic interstitial nephritis with features of megalocytic interstitial nephritis (histiocytic inflammation) and arteriolar nephrosclerosis. A transbronchial biopsy demonstrated alveolar tissue with focal intra‐alveolar hemorrhage and organization, but no malignancy, atypia, or pathogenic organisms.
The biopsy results do not support infection, lymphoma, or carcinoma. The absence of noncaseating granulomas and mastocytes on multiple biopsies essentially rules out sarcoidosis and SM, respectively. None of the characteristic pathologic features of IgG4‐RDlymphoplasmacytic infiltrate, obliterative phlebitis, and fibrosiswere observed. The pulmonary pathology points to injury, but not the underlying cause. The bone and kidney tissue samples reveal histiocytic infiltration.
The abnormalities of the aorta, bone, lung, kidney, and retroperitoneum can be explained by the diffuse histiocytic involvement seen in ECD. The perinephric stranding detected on CT and perinephric inflammation on the PET scan may reflect the hairy kidney of ECD, which is a result of histiocytic infiltration. It is possible that the chemosis relates to exophthalmos from histiocytic orbital infiltrates. Sensitivity for detecting orbital pathology on a PET scan is limited because of the high signal from the adjacent brain.
ECD should be distinguished from Langerhans cell histiocytosis (LCH) by immunohistologic staining and microscopic characteristics of the histiocytes. LCH usually does not involve the aorta, and it more commonly involves the skin.
Serum IgG4 was within normal limits, and immunohistochemical staining of pathology specimens for IgG4 was negative. The BRAF V600E mutation, which is present in the majority of patients with ECD, was detected in a subsequent right perinephric biopsy specimen. The patient was diagnosed with ECD.
Prednisone and pegylated interferon‐ led to a rapid improvement in his symptoms. As the prednisone was tapered, he developed bilateral periorbital swelling. Magnetic resonance imaging (MRI) revealed well‐circumscribed, intraorbital soft tissue masses with partial encasement of his optic nerves and superior ophthalmic veins, as well as infiltration of his transverse sinuses, consistent with intracranial manifestations of ECD. There was no evidence of pituitary, hypothalamic, or other brain parenchymal infiltration. His dyspnea, night sweats, and hypertension improved; however, 3 months into therapy he developed an extensive rash. Interferon was discontinued. Vemurafinib, a serine kinase inhibitor that targets the BRAF mutation, was prescribed with subsequent resolution of the rash.
COMMENTARY
This patient suffered from a chronic, progressive, inflammatory illness. Although the disease initially appeared to be confined to the heart and lungs, laboratory testing signaled a more systemic condition, and subsequent imaging demonstrated involvement of a disparate group of organs. Subacute disease processes with elevated markers of inflammation and diffuse organ involvement often fall into 1 of 3 categories: infectious, autoimmune, or neoplastic. The histiocytoses inhabit a fourth and easily overlooked category that can be described as infiltrative. Infiltrative diseases are a heterogeneous group of conditions that cause illness when cells or substances not normally found in tissues lead to organ dysfunction.
Although traditional teaching has focused on sarcoidosis, amyloidosis, and hemochromatosis as the primary representatives of this category, the medical literature describes a number of other infiltrative disease processes. IgG4‐RD is a fibroinflammatory disorder characterized by space‐occupying lesions, a lymphoplasmacytic infiltrate of IgG4‐positive plasma cells, and storiform (matted and irregularly whorled microscopic pattern) fibrosis.[1] IgG4‐RD, like sarcoidosis, blurs the categorical line between infiltrative and autoimmune diseases. Other infiltrative cellular disorders, such as histiocytosis and mastocytosis, exist on a spectrum between monoclonal proliferation and neoplastic invasion.
The histiocytoses represent a diverse group of disorders with an evolving nomenclature, characterized by localized or diffuse infiltration of macrophages, monocytes, and dendritic cells (Table 1). ECD is a rare, non‐Langerhans histiocytosis characterized by excessive recruitment and activation of histiocytes through kinase signaling pathways.[2, 3] Immunohistochemical staining for CD68, CD163, and Factor XIIIa, with lack of staining for CD1a, S100, and CD207, supports the diagnosis.[3] Mutations in the BRAF V600E gene (a protein kinase involved in cell proliferation) represent the most likely etiology of this overactivation. An estimated 38% to 100% of patients with ECD harbor this mutation, with detection rates influenced by the sensitivity of testing techniques.[3] The serine kinase inhibitor vemurafinib targets this mutation, and early experience with this agent in ECD demonstrates encouraging results.[4]
| Dendritic cell disorders |
| Langerhans cell histiocytosis |
| Secondary dendritic cell processes |
| Juvenile xanthogranuloma and related disorders (including Erdheim‐Chester disease) |
| Solitary histiocytomas with a dendritic phenotype |
| Macrophage‐related disorders |
| Primary hemophagocytic lymphohistiocytosis (familial and sporadic) |
| Secondary hemophagocytic syndromes |
| Sinus histiocytosis with massive lymphadenopathy (Rosai‐Dorfman disease) |
| Solitary histiocytoma with a macrophage phenotype |
| Malignant histiocytic disorders |
| Monocyte‐related leukemias |
| Extramedullary monocytic tumor or sarcoma |
| Dendritic cell‐related histiocytic sarcoma |
| Macrophage‐related histiocytic sarcoma |
ECD presents heterogeneously, occurring most commonly between the ages of 40 and 70 years. Nonspecific symptoms include weakness, fatigue, fever, chills, weight loss, and night sweats. Typical sites of involvement include the bone, central nervous system, cardiovascular system, lungs, and retroperitoneum. Bone involvement is nearly universal, and bone pain is the most common presenting symptom. Symmetric diaphyseal and metaphyseal osteosclerotic lesions may be seen on x‐rays, bone scan, PET, CT, and MRI.[3] Approximately 50% of patients have extraskeletal involvement at diagnosis.[5] Neurologic manifestations may result from invasion of histiocytes into the facial bones, orbits, meninges, and intracranial vessels, as eventually developed in this patient. Diabetes insipidus is the most common neurologic manifestation of ECD, followed by exophthalmos, cerebellar ataxia, panhypopituitarism, and papilledema.[6, 7] Approximately 75% of patients eventually suffer from cardiovascular disease, including hypertension, congestive heart failure, acute myocardial infarction, valvular dysfunction, pericardial infiltration, and cardiac tamponade.[8] Vascular involvement includes perivascular infiltration and periaortic fibrosis, resulting in the coated aorta seen in 20% of patients with ECD.[3] Pulmonary manifestations of ECD include interstitial, pleural, and consolidative lung disease. A review of high‐resolution chest CTs of patients with ECD demonstrated that greater than half had evidence of parenchymal lung disease, with interlobular septal thickening being the most common finding.[9] Infiltration and fibrosis of retroperitoneal structures is common. Infiltration of perinephric fat creates irregular renal borders, appearing radiographically as hairy kidneys.
Arriving at the diagnosis in this case proved to be challenging because the early presentation was consistent with congestive heart failure. As the patient's conditioned deteriorated, imaging suggested multisystem involvement. It was the extensive aortopathy in particularnot the less specific bone, kidney, lymph node, or pulmonary findingsthat allowed the clinicians to hone the extensive differential diagnosis. The coated aorta is a finding that has been strongly associated with ECD; few other conditions coat the aorta in a similar fashion.[10] In most mysteries, the perpetrator's coat conceals his identity; however, in this story the coat gave it away.
KEY LEARNING POINTS
- Subacute, inflammatory, multiorgan disease is usually explained by 3 categoriesinfection, autoimmunity, and neoplasiabut a fourth category, infiltrative disorders, sometimes warrants consideration.
- ECD presents heterogeneously, ranging from localized disease to widespread organ infiltration. The classic presentation includes bone pain, diabetes insipidus, and exophthalmos.
- Characteristic radiological findings that suggest ECD include long bone osteosclerosis, a coated aorta from periaortic infiltration, and hairy kidneys from perinephric infiltration.
Disclosure
Nothing to report
- , , IgG4‐related disease. N Engl J Med. 2012;366(6):539–551.
- , , , Diagnosing Erdheim‐Chester disease. Ann Rheum Dis. 2013;72(7):e19.
- , , , et al. Consensus guidelines for the diagnosis and clinical management of Erdheim‐Chester disease. Blood. 2014;124(4):483–492.
- , , , et al. The efficacy of vemurafenib in Erdheim‐Chester Disease and Langerhans Cell Histiocytosis: preliminary results from VE‐Basket Study. Blood. 2014;124(21):635.
- , , , et al. Erdheim‐Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996;75(3):157–169.
- , , , et al. Neurological manifestations and neuroradiological presentation of Erdheim‐Chester disease: report of 6 cases and systematic review of the literature. J Neurol. 2006;253(10):1267–1277.
- , , , et al. Cerebral, facial, and orbital involvement in Erdheim‐Chester disease: CT and MR imaging findings. Radiology. 2010;255(2):586–594.
- , , , et al. Images in cardiovascular medicine. Cardiac involvement in Erdheim‐Chester disease: magnetic resonance and computed tomographic scan imaging in a monocentric series of 37 patients. Circulation. 2009;119(25):e597–e598.
- , , , et al. Pulmonary involvement in Erdheim‐Chester disease: a single‐center study of thirty‐four patients and a review of the literature. Arthritis Rheum. 2010;62(11):3504–3512.
- , , , et al. “Coated aorta”: a new sign of Erdheim‐Chester disease. J Rheumatol. 2000;27(6):1550–1553.
- , , IgG4‐related disease. N Engl J Med. 2012;366(6):539–551.
- , , , Diagnosing Erdheim‐Chester disease. Ann Rheum Dis. 2013;72(7):e19.
- , , , et al. Consensus guidelines for the diagnosis and clinical management of Erdheim‐Chester disease. Blood. 2014;124(4):483–492.
- , , , et al. The efficacy of vemurafenib in Erdheim‐Chester Disease and Langerhans Cell Histiocytosis: preliminary results from VE‐Basket Study. Blood. 2014;124(21):635.
- , , , et al. Erdheim‐Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996;75(3):157–169.
- , , , et al. Neurological manifestations and neuroradiological presentation of Erdheim‐Chester disease: report of 6 cases and systematic review of the literature. J Neurol. 2006;253(10):1267–1277.
- , , , et al. Cerebral, facial, and orbital involvement in Erdheim‐Chester disease: CT and MR imaging findings. Radiology. 2010;255(2):586–594.
- , , , et al. Images in cardiovascular medicine. Cardiac involvement in Erdheim‐Chester disease: magnetic resonance and computed tomographic scan imaging in a monocentric series of 37 patients. Circulation. 2009;119(25):e597–e598.
- , , , et al. Pulmonary involvement in Erdheim‐Chester disease: a single‐center study of thirty‐four patients and a review of the literature. Arthritis Rheum. 2010;62(11):3504–3512.
- , , , et al. “Coated aorta”: a new sign of Erdheim‐Chester disease. J Rheumatol. 2000;27(6):1550–1553.