User login
Nursing Home Residents Likely to Suffer Fractures
NEW YORK - Older adults living in long-term care are more than twice as likely as their peers living at home to suffer a fracture, and a new guideline endorsed by the Scientific Advisory Council of Osteoporosis Canada explains how to reduce their risk.
Residents of long-term care tend to be frailer and have more health problems than similar people who live on their own, which explains the higher risk of fractures in long-term care facilities, said lead author Dr. Alexandra Papaioannou of McMaster University and Hamilton Health Sciences in Hamilton, Ontario.
"Up to a third of seniors in long-term care suffer a fracture," often of the hip or spine, she said. For these residents, "long-term care is their home, the nurses know them, and acute care can be a frightening traumatic experience for residents."
The authors developed the new guideline based on input from older people and their families, who most wanted to avoid pain, loss of activity, and hospitalization, Papaioannou said. They also studied published literature on the risks and benefits of strategies to prevent fracture.
The guideline strongly recommends calcium supplementation of 1200 mg or three servings of dairy daily for people older than 70. These calcium levels reduce hip fracture risk and slightly reduce the risk of other fractures, but they may also cause gastrointestinal side effects. For residents who want to avoid these, supplementation may not be a good option, the authors write.
Residents at high risk of fracture, i.e., those with prior fracture of the hip or spine, more than one prior fracture, or one prior fracture and recent use of glucocorticoids, should also take daily vitamin D3 supplements, which are more affordable than vitamin D2, the authors wrote online September 14 in CMAJ.
They also recommend that high-risk residents take alendronate weekly, or risedronate weekly or monthly, as first-line therapy to prevent fractures, as long as they do not have difficulty swallowing and can remain upright for 30 minutes after administration, and they do not have severe renal insufficiency.
For residents who are at high risk of fractures and who have difficulty taking oral medications, they recommend zoledronic acid or denosumab as first-line therapy.
High-risk residents who are mobile should wear hip-protectors, which can protect against fracture in the event of a fall. Low-risk residents who are mobile may wear the devices, depending on their values and preferences.
Balance, strength, and functional exercise can help prevent falls for low-risk residents, and may be useful for high-risk residents, but the exercise itself increases the risk of fall slightly.
Lastly, the authors recommend that all residents have "multifactorial interventions" that are tailored to each individual and include medication reviews, environmental hazard assessment, assistive device use, exercise, and educational interventions for staff.
"Many residents have multiple medical conditions and we need to make sure that they include their lifespan and goals of care in the assessment," Papaioannou said. "The goals of those with short lifespans may be very different from those with longer lifespans."
These recommendations are similar to those for residential care facilities in Australia and the ones made by the Society for Post-Acute and Long-Term Care Medicine in the U.S., the authors point out.
"The document is an excellent guide on how to identify patients at risk, who should be treated and how," said Dr. Gustavo Duque, director of the Musculoskeletal Ageing Research Program at the University of Sydney in Australia.
Doctors often reduce medications for residents who are admitted to nursing homes without realizing that those with osteoporosis or previous fractures are more likely to suffer a fracture at their new residence than in the community, Duque, who was not involved in writing the new guideline, said by email.
"Ceasing osteoporosis treatment has demonstrated to increase the risk of fractures," Duque said. "Unfortunately we see that situation every day."
NEW YORK - Older adults living in long-term care are more than twice as likely as their peers living at home to suffer a fracture, and a new guideline endorsed by the Scientific Advisory Council of Osteoporosis Canada explains how to reduce their risk.
Residents of long-term care tend to be frailer and have more health problems than similar people who live on their own, which explains the higher risk of fractures in long-term care facilities, said lead author Dr. Alexandra Papaioannou of McMaster University and Hamilton Health Sciences in Hamilton, Ontario.
"Up to a third of seniors in long-term care suffer a fracture," often of the hip or spine, she said. For these residents, "long-term care is their home, the nurses know them, and acute care can be a frightening traumatic experience for residents."
The authors developed the new guideline based on input from older people and their families, who most wanted to avoid pain, loss of activity, and hospitalization, Papaioannou said. They also studied published literature on the risks and benefits of strategies to prevent fracture.
The guideline strongly recommends calcium supplementation of 1200 mg or three servings of dairy daily for people older than 70. These calcium levels reduce hip fracture risk and slightly reduce the risk of other fractures, but they may also cause gastrointestinal side effects. For residents who want to avoid these, supplementation may not be a good option, the authors write.
Residents at high risk of fracture, i.e., those with prior fracture of the hip or spine, more than one prior fracture, or one prior fracture and recent use of glucocorticoids, should also take daily vitamin D3 supplements, which are more affordable than vitamin D2, the authors wrote online September 14 in CMAJ.
They also recommend that high-risk residents take alendronate weekly, or risedronate weekly or monthly, as first-line therapy to prevent fractures, as long as they do not have difficulty swallowing and can remain upright for 30 minutes after administration, and they do not have severe renal insufficiency.
For residents who are at high risk of fractures and who have difficulty taking oral medications, they recommend zoledronic acid or denosumab as first-line therapy.
High-risk residents who are mobile should wear hip-protectors, which can protect against fracture in the event of a fall. Low-risk residents who are mobile may wear the devices, depending on their values and preferences.
Balance, strength, and functional exercise can help prevent falls for low-risk residents, and may be useful for high-risk residents, but the exercise itself increases the risk of fall slightly.
Lastly, the authors recommend that all residents have "multifactorial interventions" that are tailored to each individual and include medication reviews, environmental hazard assessment, assistive device use, exercise, and educational interventions for staff.
"Many residents have multiple medical conditions and we need to make sure that they include their lifespan and goals of care in the assessment," Papaioannou said. "The goals of those with short lifespans may be very different from those with longer lifespans."
These recommendations are similar to those for residential care facilities in Australia and the ones made by the Society for Post-Acute and Long-Term Care Medicine in the U.S., the authors point out.
"The document is an excellent guide on how to identify patients at risk, who should be treated and how," said Dr. Gustavo Duque, director of the Musculoskeletal Ageing Research Program at the University of Sydney in Australia.
Doctors often reduce medications for residents who are admitted to nursing homes without realizing that those with osteoporosis or previous fractures are more likely to suffer a fracture at their new residence than in the community, Duque, who was not involved in writing the new guideline, said by email.
"Ceasing osteoporosis treatment has demonstrated to increase the risk of fractures," Duque said. "Unfortunately we see that situation every day."
NEW YORK - Older adults living in long-term care are more than twice as likely as their peers living at home to suffer a fracture, and a new guideline endorsed by the Scientific Advisory Council of Osteoporosis Canada explains how to reduce their risk.
Residents of long-term care tend to be frailer and have more health problems than similar people who live on their own, which explains the higher risk of fractures in long-term care facilities, said lead author Dr. Alexandra Papaioannou of McMaster University and Hamilton Health Sciences in Hamilton, Ontario.
"Up to a third of seniors in long-term care suffer a fracture," often of the hip or spine, she said. For these residents, "long-term care is their home, the nurses know them, and acute care can be a frightening traumatic experience for residents."
The authors developed the new guideline based on input from older people and their families, who most wanted to avoid pain, loss of activity, and hospitalization, Papaioannou said. They also studied published literature on the risks and benefits of strategies to prevent fracture.
The guideline strongly recommends calcium supplementation of 1200 mg or three servings of dairy daily for people older than 70. These calcium levels reduce hip fracture risk and slightly reduce the risk of other fractures, but they may also cause gastrointestinal side effects. For residents who want to avoid these, supplementation may not be a good option, the authors write.
Residents at high risk of fracture, i.e., those with prior fracture of the hip or spine, more than one prior fracture, or one prior fracture and recent use of glucocorticoids, should also take daily vitamin D3 supplements, which are more affordable than vitamin D2, the authors wrote online September 14 in CMAJ.
They also recommend that high-risk residents take alendronate weekly, or risedronate weekly or monthly, as first-line therapy to prevent fractures, as long as they do not have difficulty swallowing and can remain upright for 30 minutes after administration, and they do not have severe renal insufficiency.
For residents who are at high risk of fractures and who have difficulty taking oral medications, they recommend zoledronic acid or denosumab as first-line therapy.
High-risk residents who are mobile should wear hip-protectors, which can protect against fracture in the event of a fall. Low-risk residents who are mobile may wear the devices, depending on their values and preferences.
Balance, strength, and functional exercise can help prevent falls for low-risk residents, and may be useful for high-risk residents, but the exercise itself increases the risk of fall slightly.
Lastly, the authors recommend that all residents have "multifactorial interventions" that are tailored to each individual and include medication reviews, environmental hazard assessment, assistive device use, exercise, and educational interventions for staff.
"Many residents have multiple medical conditions and we need to make sure that they include their lifespan and goals of care in the assessment," Papaioannou said. "The goals of those with short lifespans may be very different from those with longer lifespans."
These recommendations are similar to those for residential care facilities in Australia and the ones made by the Society for Post-Acute and Long-Term Care Medicine in the U.S., the authors point out.
"The document is an excellent guide on how to identify patients at risk, who should be treated and how," said Dr. Gustavo Duque, director of the Musculoskeletal Ageing Research Program at the University of Sydney in Australia.
Doctors often reduce medications for residents who are admitted to nursing homes without realizing that those with osteoporosis or previous fractures are more likely to suffer a fracture at their new residence than in the community, Duque, who was not involved in writing the new guideline, said by email.
"Ceasing osteoporosis treatment has demonstrated to increase the risk of fractures," Duque said. "Unfortunately we see that situation every day."
ACP guidelines aim to improve PE diagnosis

Photo by Angela Mary Butler
Clinicians should stratify patients with suspected acute pulmonary embolism (PE) to ensure use of the appropriate diagnostic strategy, according to guidelines from the American College of Physicians (ACP).
The ACP’s guidelines, published in Annals of Internal Medicine, are designed to help clinicians identify patients who should undergo diagnostic testing for PE—D-dimer and imaging—and those who should not.
“The use of computed tomography (CT) for the evaluation of patients with suspected pulmonary embolism is increasing, despite no evidence that this increased use has led to improved patient outcomes, while exposing patients to unnecessary risks and expense,” said ACP President Wayne J. Riley, MD.
“ACP’s advice is designed to help physicians identify patients for whom a PE is so unlikely that they need no further testing, for whom plasma D-dimer testing can provide additional risk stratification, and for whom imaging is indicated because of their high risk and clinical presentation.”
The guidelines say the first step for clinicians evaluating patients with suspected acute PE is to use a validated clinical prediction rule to estimate the patients’ pre-test probability of PE. The Wells and Geneva rules have been validated and are considered equally accurate in predicting the probability of PE.
In patients who have a low pre-test probability of PE, clinicians should apply the Pulmonary Embolism Rule-Out Criteria (PERC) rule. Clinicians should not obtain D-dimer tests or imaging studies in patients with a low pre-test probability of PE and who meet all 8 PERC.
Patients who have an intermediate pre-test probability of PE or patients with low pre-test probability of PE who do not meet all PERC should have a high sensitivity D-dimer test as the initial step in diagnosis.
Clinicians should not use imaging as the initial test in patients who have a low or intermediate pre-test probability of PE.
Since normal D-dimer levels increase with age, clinicians should use age-adjusted D-dimer thresholds (age times 10 ng/mL rather than a generic 500 ng/mL) in patients older than 50 years to determine whether imaging is warranted.
Clinicians should not use imaging in low- or intermediate-risk patients with a D-dimer below the age-adjusted cutoff.
“While highly sensitive, plasma D-dimer testing is nonspecific, and false-positives can lead to unnecessary imaging,” said guideline author Ali S. Raja, MD, of Massachusetts General Hospital in Boston.
“The use of an age-adjusted threshold resulted in maintenance of sensitivities with improved specificities in all age groups.”
Patients with high pre-test probability of PE should undergo imaging with CT pulmonary angiography. Clinicians should reserve V/Q scans for patients who have a contraindication for CT pulmonary angiography or if CT pulmonary angiography is not available.
Clinicians should avoid obtaining a D-dimer measurement in patients with a high pre-test probability of PE. ![]()
Photo by Angela Mary Butler
Clinicians should stratify patients with suspected acute pulmonary embolism (PE) to ensure use of the appropriate diagnostic strategy, according to guidelines from the American College of Physicians (ACP).
The ACP’s guidelines, published in Annals of Internal Medicine, are designed to help clinicians identify patients who should undergo diagnostic testing for PE—D-dimer and imaging—and those who should not.
“The use of computed tomography (CT) for the evaluation of patients with suspected pulmonary embolism is increasing, despite no evidence that this increased use has led to improved patient outcomes, while exposing patients to unnecessary risks and expense,” said ACP President Wayne J. Riley, MD.
“ACP’s advice is designed to help physicians identify patients for whom a PE is so unlikely that they need no further testing, for whom plasma D-dimer testing can provide additional risk stratification, and for whom imaging is indicated because of their high risk and clinical presentation.”
The guidelines say the first step for clinicians evaluating patients with suspected acute PE is to use a validated clinical prediction rule to estimate the patients’ pre-test probability of PE. The Wells and Geneva rules have been validated and are considered equally accurate in predicting the probability of PE.
In patients who have a low pre-test probability of PE, clinicians should apply the Pulmonary Embolism Rule-Out Criteria (PERC) rule. Clinicians should not obtain D-dimer tests or imaging studies in patients with a low pre-test probability of PE and who meet all 8 PERC.
Patients who have an intermediate pre-test probability of PE or patients with low pre-test probability of PE who do not meet all PERC should have a high sensitivity D-dimer test as the initial step in diagnosis.
Clinicians should not use imaging as the initial test in patients who have a low or intermediate pre-test probability of PE.
Since normal D-dimer levels increase with age, clinicians should use age-adjusted D-dimer thresholds (age times 10 ng/mL rather than a generic 500 ng/mL) in patients older than 50 years to determine whether imaging is warranted.
Clinicians should not use imaging in low- or intermediate-risk patients with a D-dimer below the age-adjusted cutoff.
“While highly sensitive, plasma D-dimer testing is nonspecific, and false-positives can lead to unnecessary imaging,” said guideline author Ali S. Raja, MD, of Massachusetts General Hospital in Boston.
“The use of an age-adjusted threshold resulted in maintenance of sensitivities with improved specificities in all age groups.”
Patients with high pre-test probability of PE should undergo imaging with CT pulmonary angiography. Clinicians should reserve V/Q scans for patients who have a contraindication for CT pulmonary angiography or if CT pulmonary angiography is not available.
Clinicians should avoid obtaining a D-dimer measurement in patients with a high pre-test probability of PE. ![]()
Photo by Angela Mary Butler
Clinicians should stratify patients with suspected acute pulmonary embolism (PE) to ensure use of the appropriate diagnostic strategy, according to guidelines from the American College of Physicians (ACP).
The ACP’s guidelines, published in Annals of Internal Medicine, are designed to help clinicians identify patients who should undergo diagnostic testing for PE—D-dimer and imaging—and those who should not.
“The use of computed tomography (CT) for the evaluation of patients with suspected pulmonary embolism is increasing, despite no evidence that this increased use has led to improved patient outcomes, while exposing patients to unnecessary risks and expense,” said ACP President Wayne J. Riley, MD.
“ACP’s advice is designed to help physicians identify patients for whom a PE is so unlikely that they need no further testing, for whom plasma D-dimer testing can provide additional risk stratification, and for whom imaging is indicated because of their high risk and clinical presentation.”
The guidelines say the first step for clinicians evaluating patients with suspected acute PE is to use a validated clinical prediction rule to estimate the patients’ pre-test probability of PE. The Wells and Geneva rules have been validated and are considered equally accurate in predicting the probability of PE.
In patients who have a low pre-test probability of PE, clinicians should apply the Pulmonary Embolism Rule-Out Criteria (PERC) rule. Clinicians should not obtain D-dimer tests or imaging studies in patients with a low pre-test probability of PE and who meet all 8 PERC.
Patients who have an intermediate pre-test probability of PE or patients with low pre-test probability of PE who do not meet all PERC should have a high sensitivity D-dimer test as the initial step in diagnosis.
Clinicians should not use imaging as the initial test in patients who have a low or intermediate pre-test probability of PE.
Since normal D-dimer levels increase with age, clinicians should use age-adjusted D-dimer thresholds (age times 10 ng/mL rather than a generic 500 ng/mL) in patients older than 50 years to determine whether imaging is warranted.
Clinicians should not use imaging in low- or intermediate-risk patients with a D-dimer below the age-adjusted cutoff.
“While highly sensitive, plasma D-dimer testing is nonspecific, and false-positives can lead to unnecessary imaging,” said guideline author Ali S. Raja, MD, of Massachusetts General Hospital in Boston.
“The use of an age-adjusted threshold resulted in maintenance of sensitivities with improved specificities in all age groups.”
Patients with high pre-test probability of PE should undergo imaging with CT pulmonary angiography. Clinicians should reserve V/Q scans for patients who have a contraindication for CT pulmonary angiography or if CT pulmonary angiography is not available.
Clinicians should avoid obtaining a D-dimer measurement in patients with a high pre-test probability of PE. ![]()
Nonviral gene transfer of CARs tested in humans
Photo courtesy of MDACC
NEW YORK—Researchers have used a nonviral approach to create chimeric antigen receptor (CAR) T cells and tested these cells in safety trials.
Patients with advanced lymphoma or leukemia were infused with the nonvirally modified CD19-directed CAR T cells after autologous or allogeneic hematopoietic stem cell transplant (HSCT).
Eighty-six percent of autologous HSCT recipients were alive 24 months after infusion, and 53% of allogeneic HSCT recipients were alive with a median follow-up of 6.5 months.
“Gratifyingly, the patients have not demonstrated any acute or late toxicity to these CAR T-cell infusions,” said Laurence Cooper, MD, PhD, formerly of MD Anderson Cancer Center (MDACC) in Houston, Texas, and now with Ziopharm Oncology.
Dr Cooper presented these results at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Some of the technology he described was conducted at MDACC. Dr Cooper is currently a visiting scientist there and will continue to supervise the development of this technology.
Dr Cooper said the appeal of this nonviral approach, which is a modified Sleeping Beauty approach, “is it essentially avoids the complexity of making a virus, a lentivirus or a retrovirus, it can be done at quite low cost, and really allows for a nimbleness to this system.”
Using a simple blood draw of 200 cc of peripheral blood—the process does not require apheresis—the T cells can be expanded on a feeder cell layer and genetically reprogrammed.
Sleeping Beauty system
The researchers reprogrammed the T cells using a 2-plasmid Sleeping Beauty system, which is a transposon/transposase system.
The transposon DNA plasmid codes for the cargo load, which, in this case, is the CAR. At the same time, the transposase DNA plasmid is electroporated, “which is really the secret sauce of the transposition event,” Dr Cooper explained.
After electroporation, the transposon/transposase are co-cultured with K562-derived artificial antigen-presenting cells (aAPC) and expanded with the integrated transposon of K562-aAPC. In this case, CD19 is on the aAPC.
CD19 is co-expressed with other co-stimulatory molecules, CD86 and 4-1BB ligand.
In addition, the researchers added a molecule of interleukin 15 that’s sewn in frame to the Fc region of an immunoglobulin that then activates the T cell in the context of these co-stimulatory molecules.
The T cells that have stable integrants of the CAR grow out over time. And those that have transient expression of the CAR die by neglect.
“By day 14, most of the T cells have the CAR sewn into the genome and are stably expressed,” Dr Cooper said.
The CAR used for these safety trials at MDACC targets CD19 and uses mouse scFv held in frame with an immunoglobulin 4 Fc (IgG4Fc) stalk.
It’s tunneled through the T-cell membrane and has 2 costimulatory molecules, signal 1 delivered by phosphorylation of the immunoreceptor tyrosine-based activation motif in CD3ζ and signal 2 by the costimulatory domain CD28.
The researchers tested the CD19 CARs in 2 clinical settings—one with T cells that were patient-derived and infused after autologous HSCT, and the second with T cells that were derived from a third party and infused after allogeneic HSCT.
Infusion after autologous HSCT
The researchers first tried the CARs in 7 non-Hodgkin lymphoma patients who had an autologous HSCT. Their median age was 52 (range, 36-61).
Five patients received a starting CAR T-cell dose of 5x108 cells/m2, and 2 received 5x109 cells/m2.
Six patients (86%) remain alive and are in complete remission (CR) at a median follow-up of 24 months.
Infusion after allogeneic HSCT
The researchers expanded the investigation to a wider cohort of 19 patients who had undergone allogeneic HSCT.
Seventeen patients had advanced CD19-positive acute lymphoblastic leukemia, and 2 had non-Hodgkin lymphoma. Their median age was 35 (range, 21-56).
All patients were on graft-versus-host disease (GVHD) prophylaxis with tacrolimus at the time of CAR infusion. A subset of these allogeneic transplant patients had haploidentical donors rather than matched sibling donors.
Five patients received a CAR T-cell dose of 106, 6 patients received 107, 5 received 5x107, and 3 received 5x108 cells/m2 based on recipient body surface area.
Fifty-eight percent of patients (11/19) achieved a CR, and 10 remain alive a median of 6.5 months after CAR T-cell infusion.
Three patients developed GVHD, 1 with steroid-refractory acute liver disease, 1 with grade 2 acute skin disease, and 1 with chronic limited skin disease. The incidence of GVHD was lower than historical controls at MDACC, Dr Cooper said.
“[G]ratifyingly, in this clinical setting of minimal disease, patients did not have any acute or late toxicity from these infusions,” he added.
And the rate of cytomegalovirus reactivation after CAR T-cell infusion was 24%, compared with 41% for patients after transplant at MDACC without CAR T-cell infusion.
Eight patients received haploidentical HSCT followed by CAR T-cell infusion, and 75% (6/8) remain in CR.
Persistence of infused T cells
The researchers used 2 forms of PCR—qPCR and droplet PCR—to map the fate of the CARs.
“Roughly speaking, for these patients, and this is in line with the literature, in terms of those T cells that are activated through CD28 in contrast to 4-1BB, these T cells are, on average, living about 28 or so days post-infusion,” Dr Cooper noted.
He said this is similar to results observed with CARs being tested at the National Cancer Institute and Memorial Sloan-Kettering Cancer Center. ![]()
Photo courtesy of MDACC
NEW YORK—Researchers have used a nonviral approach to create chimeric antigen receptor (CAR) T cells and tested these cells in safety trials.
Patients with advanced lymphoma or leukemia were infused with the nonvirally modified CD19-directed CAR T cells after autologous or allogeneic hematopoietic stem cell transplant (HSCT).
Eighty-six percent of autologous HSCT recipients were alive 24 months after infusion, and 53% of allogeneic HSCT recipients were alive with a median follow-up of 6.5 months.
“Gratifyingly, the patients have not demonstrated any acute or late toxicity to these CAR T-cell infusions,” said Laurence Cooper, MD, PhD, formerly of MD Anderson Cancer Center (MDACC) in Houston, Texas, and now with Ziopharm Oncology.
Dr Cooper presented these results at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Some of the technology he described was conducted at MDACC. Dr Cooper is currently a visiting scientist there and will continue to supervise the development of this technology.
Dr Cooper said the appeal of this nonviral approach, which is a modified Sleeping Beauty approach, “is it essentially avoids the complexity of making a virus, a lentivirus or a retrovirus, it can be done at quite low cost, and really allows for a nimbleness to this system.”
Using a simple blood draw of 200 cc of peripheral blood—the process does not require apheresis—the T cells can be expanded on a feeder cell layer and genetically reprogrammed.
Sleeping Beauty system
The researchers reprogrammed the T cells using a 2-plasmid Sleeping Beauty system, which is a transposon/transposase system.
The transposon DNA plasmid codes for the cargo load, which, in this case, is the CAR. At the same time, the transposase DNA plasmid is electroporated, “which is really the secret sauce of the transposition event,” Dr Cooper explained.
After electroporation, the transposon/transposase are co-cultured with K562-derived artificial antigen-presenting cells (aAPC) and expanded with the integrated transposon of K562-aAPC. In this case, CD19 is on the aAPC.
CD19 is co-expressed with other co-stimulatory molecules, CD86 and 4-1BB ligand.
In addition, the researchers added a molecule of interleukin 15 that’s sewn in frame to the Fc region of an immunoglobulin that then activates the T cell in the context of these co-stimulatory molecules.
The T cells that have stable integrants of the CAR grow out over time. And those that have transient expression of the CAR die by neglect.
“By day 14, most of the T cells have the CAR sewn into the genome and are stably expressed,” Dr Cooper said.
The CAR used for these safety trials at MDACC targets CD19 and uses mouse scFv held in frame with an immunoglobulin 4 Fc (IgG4Fc) stalk.
It’s tunneled through the T-cell membrane and has 2 costimulatory molecules, signal 1 delivered by phosphorylation of the immunoreceptor tyrosine-based activation motif in CD3ζ and signal 2 by the costimulatory domain CD28.
The researchers tested the CD19 CARs in 2 clinical settings—one with T cells that were patient-derived and infused after autologous HSCT, and the second with T cells that were derived from a third party and infused after allogeneic HSCT.
Infusion after autologous HSCT
The researchers first tried the CARs in 7 non-Hodgkin lymphoma patients who had an autologous HSCT. Their median age was 52 (range, 36-61).
Five patients received a starting CAR T-cell dose of 5x108 cells/m2, and 2 received 5x109 cells/m2.
Six patients (86%) remain alive and are in complete remission (CR) at a median follow-up of 24 months.
Infusion after allogeneic HSCT
The researchers expanded the investigation to a wider cohort of 19 patients who had undergone allogeneic HSCT.
Seventeen patients had advanced CD19-positive acute lymphoblastic leukemia, and 2 had non-Hodgkin lymphoma. Their median age was 35 (range, 21-56).
All patients were on graft-versus-host disease (GVHD) prophylaxis with tacrolimus at the time of CAR infusion. A subset of these allogeneic transplant patients had haploidentical donors rather than matched sibling donors.
Five patients received a CAR T-cell dose of 106, 6 patients received 107, 5 received 5x107, and 3 received 5x108 cells/m2 based on recipient body surface area.
Fifty-eight percent of patients (11/19) achieved a CR, and 10 remain alive a median of 6.5 months after CAR T-cell infusion.
Three patients developed GVHD, 1 with steroid-refractory acute liver disease, 1 with grade 2 acute skin disease, and 1 with chronic limited skin disease. The incidence of GVHD was lower than historical controls at MDACC, Dr Cooper said.
“[G]ratifyingly, in this clinical setting of minimal disease, patients did not have any acute or late toxicity from these infusions,” he added.
And the rate of cytomegalovirus reactivation after CAR T-cell infusion was 24%, compared with 41% for patients after transplant at MDACC without CAR T-cell infusion.
Eight patients received haploidentical HSCT followed by CAR T-cell infusion, and 75% (6/8) remain in CR.
Persistence of infused T cells
The researchers used 2 forms of PCR—qPCR and droplet PCR—to map the fate of the CARs.
“Roughly speaking, for these patients, and this is in line with the literature, in terms of those T cells that are activated through CD28 in contrast to 4-1BB, these T cells are, on average, living about 28 or so days post-infusion,” Dr Cooper noted.
He said this is similar to results observed with CARs being tested at the National Cancer Institute and Memorial Sloan-Kettering Cancer Center. ![]()
Photo courtesy of MDACC
NEW YORK—Researchers have used a nonviral approach to create chimeric antigen receptor (CAR) T cells and tested these cells in safety trials.
Patients with advanced lymphoma or leukemia were infused with the nonvirally modified CD19-directed CAR T cells after autologous or allogeneic hematopoietic stem cell transplant (HSCT).
Eighty-six percent of autologous HSCT recipients were alive 24 months after infusion, and 53% of allogeneic HSCT recipients were alive with a median follow-up of 6.5 months.
“Gratifyingly, the patients have not demonstrated any acute or late toxicity to these CAR T-cell infusions,” said Laurence Cooper, MD, PhD, formerly of MD Anderson Cancer Center (MDACC) in Houston, Texas, and now with Ziopharm Oncology.
Dr Cooper presented these results at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Some of the technology he described was conducted at MDACC. Dr Cooper is currently a visiting scientist there and will continue to supervise the development of this technology.
Dr Cooper said the appeal of this nonviral approach, which is a modified Sleeping Beauty approach, “is it essentially avoids the complexity of making a virus, a lentivirus or a retrovirus, it can be done at quite low cost, and really allows for a nimbleness to this system.”
Using a simple blood draw of 200 cc of peripheral blood—the process does not require apheresis—the T cells can be expanded on a feeder cell layer and genetically reprogrammed.
Sleeping Beauty system
The researchers reprogrammed the T cells using a 2-plasmid Sleeping Beauty system, which is a transposon/transposase system.
The transposon DNA plasmid codes for the cargo load, which, in this case, is the CAR. At the same time, the transposase DNA plasmid is electroporated, “which is really the secret sauce of the transposition event,” Dr Cooper explained.
After electroporation, the transposon/transposase are co-cultured with K562-derived artificial antigen-presenting cells (aAPC) and expanded with the integrated transposon of K562-aAPC. In this case, CD19 is on the aAPC.
CD19 is co-expressed with other co-stimulatory molecules, CD86 and 4-1BB ligand.
In addition, the researchers added a molecule of interleukin 15 that’s sewn in frame to the Fc region of an immunoglobulin that then activates the T cell in the context of these co-stimulatory molecules.
The T cells that have stable integrants of the CAR grow out over time. And those that have transient expression of the CAR die by neglect.
“By day 14, most of the T cells have the CAR sewn into the genome and are stably expressed,” Dr Cooper said.
The CAR used for these safety trials at MDACC targets CD19 and uses mouse scFv held in frame with an immunoglobulin 4 Fc (IgG4Fc) stalk.
It’s tunneled through the T-cell membrane and has 2 costimulatory molecules, signal 1 delivered by phosphorylation of the immunoreceptor tyrosine-based activation motif in CD3ζ and signal 2 by the costimulatory domain CD28.
The researchers tested the CD19 CARs in 2 clinical settings—one with T cells that were patient-derived and infused after autologous HSCT, and the second with T cells that were derived from a third party and infused after allogeneic HSCT.
Infusion after autologous HSCT
The researchers first tried the CARs in 7 non-Hodgkin lymphoma patients who had an autologous HSCT. Their median age was 52 (range, 36-61).
Five patients received a starting CAR T-cell dose of 5x108 cells/m2, and 2 received 5x109 cells/m2.
Six patients (86%) remain alive and are in complete remission (CR) at a median follow-up of 24 months.
Infusion after allogeneic HSCT
The researchers expanded the investigation to a wider cohort of 19 patients who had undergone allogeneic HSCT.
Seventeen patients had advanced CD19-positive acute lymphoblastic leukemia, and 2 had non-Hodgkin lymphoma. Their median age was 35 (range, 21-56).
All patients were on graft-versus-host disease (GVHD) prophylaxis with tacrolimus at the time of CAR infusion. A subset of these allogeneic transplant patients had haploidentical donors rather than matched sibling donors.
Five patients received a CAR T-cell dose of 106, 6 patients received 107, 5 received 5x107, and 3 received 5x108 cells/m2 based on recipient body surface area.
Fifty-eight percent of patients (11/19) achieved a CR, and 10 remain alive a median of 6.5 months after CAR T-cell infusion.
Three patients developed GVHD, 1 with steroid-refractory acute liver disease, 1 with grade 2 acute skin disease, and 1 with chronic limited skin disease. The incidence of GVHD was lower than historical controls at MDACC, Dr Cooper said.
“[G]ratifyingly, in this clinical setting of minimal disease, patients did not have any acute or late toxicity from these infusions,” he added.
And the rate of cytomegalovirus reactivation after CAR T-cell infusion was 24%, compared with 41% for patients after transplant at MDACC without CAR T-cell infusion.
Eight patients received haploidentical HSCT followed by CAR T-cell infusion, and 75% (6/8) remain in CR.
Persistence of infused T cells
The researchers used 2 forms of PCR—qPCR and droplet PCR—to map the fate of the CARs.
“Roughly speaking, for these patients, and this is in line with the literature, in terms of those T cells that are activated through CD28 in contrast to 4-1BB, these T cells are, on average, living about 28 or so days post-infusion,” Dr Cooper noted.
He said this is similar to results observed with CARs being tested at the National Cancer Institute and Memorial Sloan-Kettering Cancer Center. ![]()
Problems in pediatric cancer care in Europe

Photo by Logan Tuttle
VIENNA—Despite progress made in recent years, there are “major problems” in pediatric oncology care in Europe, according to a report from the European Society for Paediatric Oncology (SIOPE).
Cancer is still the first cause of death by disease in children age 1 and older in Europe, and more than 300,000 European citizens are pediatric cancer survivors.
These individuals have a higher risk of death at 5 years after diagnosis than that of the general population.
“This is a serious problem for patients, their families, and for health services, with major inequalities existing across Europe,” said SIOPE President Gilles Vassal, MD, PhD, of the Institut Gustave Roussy in Villejuif, France.
“Add to this the fact that 35% of such cancers normally occur before the child is 5 years old and that many pediatric cancers are difficult to treat, and you will understand why we thought it essential to try to tackle this problem in a practical way.”
The resulting report, “The SIOPE Strategic Plan: A European Cancer Plan for Children and Adolescents,” was recently presented at the 2015 European Cancer Congress.
Problem-solving
The report was drawn up after widespread consultation, including discussions with parents, patients, and survivors. It sets out existing problems and proposes solutions to tackle them.
Among these problems are poor access to new drugs for pediatric patients; lack of funding; disparities across Europe in access to treatment and, hence, survival; and the fact that pediatric oncology has been relatively isolated from the adult oncology community.
With the goal of fixing these problems, the report sets out a number of goals and lists the key factors that will be necessary in order to achieve them.
These include a commitment of all funding bodies to finance projects and structures of relevance to pediatric oncology; a strong partnership with patients, parents, and survivors, including better communication and dissemination of information; better collaboration with adult oncology; and transparent partnerships with industry.
Understanding biology
“One of the most important objectives focuses on increasing our knowledge of the biology of pediatric tumors,” said SIOPE President-Elect Martin Schrappe, MD, of the University of Kiel, Germany.
“Cancers in adults result from a multistep process, usually after exposure to external carcinogens such as tobacco, alcohol, and diet, and often progress over many years. Pediatric malignancies develop early in life and over a much shorter time period. This suggests that fewer and stronger events are required for them to progress. Compared with adult cancers, most of them show fewer genetic defects and have a lower genetic complexity.”
“Major progress has been made in understanding pediatric tumor biology, and this has led to the discovery of some unique cancer hallmarks. Now, we need to use modern, innovative technologies to further decipher the mechanisms of pediatric tumor development, progression, and relapse, and speed up its translation to the clinic.”
To do this effectively and fairly, according to the report, interactions need to be strengthened at several levels—between networks of basic research teams, between basic scientists and clinical researchers, and by increasing the involvement of patients and parents in the search for personalized treatments. SIOPE plans to monitor progress through research into outcomes.
Improving quality of life
Another important issue for SIOPE is improving the quality of life for survivors.
“We believe that, in 2020, there will be nearly half a million European pediatric cancer survivors, and many of them will have side effects that are severe enough to affect their daily lives,” Dr Schrappe said. “While the fact that so many survive is a cause for rejoicing, we have a duty to provide them with optimal long-term care so that the rest of their lives may be as normal as possible.”
“One way of doing this would be the creation of a ‘survivorship passport’ for each child and adolescent cured of a cancer. This would contain a history of their disease and treatment, together with relevant follow-up measures aimed at improving their quality of life and a database for storing the clinical data [that would] facilitate monitoring and research.” ![]()
Photo by Logan Tuttle
VIENNA—Despite progress made in recent years, there are “major problems” in pediatric oncology care in Europe, according to a report from the European Society for Paediatric Oncology (SIOPE).
Cancer is still the first cause of death by disease in children age 1 and older in Europe, and more than 300,000 European citizens are pediatric cancer survivors.
These individuals have a higher risk of death at 5 years after diagnosis than that of the general population.
“This is a serious problem for patients, their families, and for health services, with major inequalities existing across Europe,” said SIOPE President Gilles Vassal, MD, PhD, of the Institut Gustave Roussy in Villejuif, France.
“Add to this the fact that 35% of such cancers normally occur before the child is 5 years old and that many pediatric cancers are difficult to treat, and you will understand why we thought it essential to try to tackle this problem in a practical way.”
The resulting report, “The SIOPE Strategic Plan: A European Cancer Plan for Children and Adolescents,” was recently presented at the 2015 European Cancer Congress.
Problem-solving
The report was drawn up after widespread consultation, including discussions with parents, patients, and survivors. It sets out existing problems and proposes solutions to tackle them.
Among these problems are poor access to new drugs for pediatric patients; lack of funding; disparities across Europe in access to treatment and, hence, survival; and the fact that pediatric oncology has been relatively isolated from the adult oncology community.
With the goal of fixing these problems, the report sets out a number of goals and lists the key factors that will be necessary in order to achieve them.
These include a commitment of all funding bodies to finance projects and structures of relevance to pediatric oncology; a strong partnership with patients, parents, and survivors, including better communication and dissemination of information; better collaboration with adult oncology; and transparent partnerships with industry.
Understanding biology
“One of the most important objectives focuses on increasing our knowledge of the biology of pediatric tumors,” said SIOPE President-Elect Martin Schrappe, MD, of the University of Kiel, Germany.
“Cancers in adults result from a multistep process, usually after exposure to external carcinogens such as tobacco, alcohol, and diet, and often progress over many years. Pediatric malignancies develop early in life and over a much shorter time period. This suggests that fewer and stronger events are required for them to progress. Compared with adult cancers, most of them show fewer genetic defects and have a lower genetic complexity.”
“Major progress has been made in understanding pediatric tumor biology, and this has led to the discovery of some unique cancer hallmarks. Now, we need to use modern, innovative technologies to further decipher the mechanisms of pediatric tumor development, progression, and relapse, and speed up its translation to the clinic.”
To do this effectively and fairly, according to the report, interactions need to be strengthened at several levels—between networks of basic research teams, between basic scientists and clinical researchers, and by increasing the involvement of patients and parents in the search for personalized treatments. SIOPE plans to monitor progress through research into outcomes.
Improving quality of life
Another important issue for SIOPE is improving the quality of life for survivors.
“We believe that, in 2020, there will be nearly half a million European pediatric cancer survivors, and many of them will have side effects that are severe enough to affect their daily lives,” Dr Schrappe said. “While the fact that so many survive is a cause for rejoicing, we have a duty to provide them with optimal long-term care so that the rest of their lives may be as normal as possible.”
“One way of doing this would be the creation of a ‘survivorship passport’ for each child and adolescent cured of a cancer. This would contain a history of their disease and treatment, together with relevant follow-up measures aimed at improving their quality of life and a database for storing the clinical data [that would] facilitate monitoring and research.” ![]()
Photo by Logan Tuttle
VIENNA—Despite progress made in recent years, there are “major problems” in pediatric oncology care in Europe, according to a report from the European Society for Paediatric Oncology (SIOPE).
Cancer is still the first cause of death by disease in children age 1 and older in Europe, and more than 300,000 European citizens are pediatric cancer survivors.
These individuals have a higher risk of death at 5 years after diagnosis than that of the general population.
“This is a serious problem for patients, their families, and for health services, with major inequalities existing across Europe,” said SIOPE President Gilles Vassal, MD, PhD, of the Institut Gustave Roussy in Villejuif, France.
“Add to this the fact that 35% of such cancers normally occur before the child is 5 years old and that many pediatric cancers are difficult to treat, and you will understand why we thought it essential to try to tackle this problem in a practical way.”
The resulting report, “The SIOPE Strategic Plan: A European Cancer Plan for Children and Adolescents,” was recently presented at the 2015 European Cancer Congress.
Problem-solving
The report was drawn up after widespread consultation, including discussions with parents, patients, and survivors. It sets out existing problems and proposes solutions to tackle them.
Among these problems are poor access to new drugs for pediatric patients; lack of funding; disparities across Europe in access to treatment and, hence, survival; and the fact that pediatric oncology has been relatively isolated from the adult oncology community.
With the goal of fixing these problems, the report sets out a number of goals and lists the key factors that will be necessary in order to achieve them.
These include a commitment of all funding bodies to finance projects and structures of relevance to pediatric oncology; a strong partnership with patients, parents, and survivors, including better communication and dissemination of information; better collaboration with adult oncology; and transparent partnerships with industry.
Understanding biology
“One of the most important objectives focuses on increasing our knowledge of the biology of pediatric tumors,” said SIOPE President-Elect Martin Schrappe, MD, of the University of Kiel, Germany.
“Cancers in adults result from a multistep process, usually after exposure to external carcinogens such as tobacco, alcohol, and diet, and often progress over many years. Pediatric malignancies develop early in life and over a much shorter time period. This suggests that fewer and stronger events are required for them to progress. Compared with adult cancers, most of them show fewer genetic defects and have a lower genetic complexity.”
“Major progress has been made in understanding pediatric tumor biology, and this has led to the discovery of some unique cancer hallmarks. Now, we need to use modern, innovative technologies to further decipher the mechanisms of pediatric tumor development, progression, and relapse, and speed up its translation to the clinic.”
To do this effectively and fairly, according to the report, interactions need to be strengthened at several levels—between networks of basic research teams, between basic scientists and clinical researchers, and by increasing the involvement of patients and parents in the search for personalized treatments. SIOPE plans to monitor progress through research into outcomes.
Improving quality of life
Another important issue for SIOPE is improving the quality of life for survivors.
“We believe that, in 2020, there will be nearly half a million European pediatric cancer survivors, and many of them will have side effects that are severe enough to affect their daily lives,” Dr Schrappe said. “While the fact that so many survive is a cause for rejoicing, we have a duty to provide them with optimal long-term care so that the rest of their lives may be as normal as possible.”
“One way of doing this would be the creation of a ‘survivorship passport’ for each child and adolescent cured of a cancer. This would contain a history of their disease and treatment, together with relevant follow-up measures aimed at improving their quality of life and a database for storing the clinical data [that would] facilitate monitoring and research.” ![]()
CHMP endorses expanded indication for azacitidine

Image by Lance Liotta
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for azacitidine for injection (Vidaza).
The CHMP is recommending that azacitidine be approved to treat adults age 65 and older with acute myeloid leukemia (AML) who are not eligible for hematopoietic stem cell transplant (HSCT) and have more than 30% blasts according to the WHO classification.
The CHMP’s recommendation will be reviewed by the European Commission (EC). The EC usually follows the CHMP’s recommendations and is expected to deliver its final decision in 2 months.
The CHMP said this new indication for azacitidine would bring significant clinical benefit in comparison with existing therapies. If the EC follows the CHMP’s recommendation, azacitidine will receive extended market protection in all its indications for an additional year throughout the European Economic Area.
Azacitidine is already approved in the European Economic Area for the treatment of HSCT-ineligible adults diagnosed with intermediate-2- and high-risk myelodysplastic syndromes; chronic myelomonocytic leukemia with 10%-29% marrow blasts without myeloproliferative disorder; or AML with 20%-30% blasts and multi-lineage dysplasia.
AML-001 trial
The CHMP’s recommendation to expand the indication of azacitidine in AML was based on data from the AML-001 trial. This randomized study included patients age 65 and older with newly diagnosed or secondary AML with greater than 30% blasts.
Patients were pre-selected to receive 1 of 3 regimens per investigator’s choice. This included intensive chemotherapy (standard 7+3 regimen), low-dose cytarabine (20 mg subcutaneously twice a day for 10 days of each 28-day cycle) or best supportive care only.
Patients were then randomized to receive either azacitidine (75 mg/m2/day subcutaneously for 7 days of each 28-day cycle, n=241) or their predetermined conventional care regimen (CCR, n=247).
Median overall survival, the study’s primary endpoint, was 10.4 months for patients receiving azacitidine and 6.5 months for patients receiving CCR (hazard ratio=0.85, P=0.1009).
One-year survival rates with azacitidine and CCR were 46.5% and 34.2%, respectively.
Grade 3/4 anemia occurred in 16% of patients who received azacitidine, 5% who received best supportive care, 23% who received low-dose cytarabine, and 14% who received intensive chemotherapy.
Grade 3/4 neutropenia occurred in 26%, 5%, 25%, and 33%, respectively. Grade 3/4 febrile neutropenia occurred in 28%, 28%, 30%, and 31%, respectively. And grade 3/4 thrombocytopenia occurred in 24%, 5%, 28%, and 21%, respectively. ![]()
Image by Lance Liotta
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for azacitidine for injection (Vidaza).
The CHMP is recommending that azacitidine be approved to treat adults age 65 and older with acute myeloid leukemia (AML) who are not eligible for hematopoietic stem cell transplant (HSCT) and have more than 30% blasts according to the WHO classification.
The CHMP’s recommendation will be reviewed by the European Commission (EC). The EC usually follows the CHMP’s recommendations and is expected to deliver its final decision in 2 months.
The CHMP said this new indication for azacitidine would bring significant clinical benefit in comparison with existing therapies. If the EC follows the CHMP’s recommendation, azacitidine will receive extended market protection in all its indications for an additional year throughout the European Economic Area.
Azacitidine is already approved in the European Economic Area for the treatment of HSCT-ineligible adults diagnosed with intermediate-2- and high-risk myelodysplastic syndromes; chronic myelomonocytic leukemia with 10%-29% marrow blasts without myeloproliferative disorder; or AML with 20%-30% blasts and multi-lineage dysplasia.
AML-001 trial
The CHMP’s recommendation to expand the indication of azacitidine in AML was based on data from the AML-001 trial. This randomized study included patients age 65 and older with newly diagnosed or secondary AML with greater than 30% blasts.
Patients were pre-selected to receive 1 of 3 regimens per investigator’s choice. This included intensive chemotherapy (standard 7+3 regimen), low-dose cytarabine (20 mg subcutaneously twice a day for 10 days of each 28-day cycle) or best supportive care only.
Patients were then randomized to receive either azacitidine (75 mg/m2/day subcutaneously for 7 days of each 28-day cycle, n=241) or their predetermined conventional care regimen (CCR, n=247).
Median overall survival, the study’s primary endpoint, was 10.4 months for patients receiving azacitidine and 6.5 months for patients receiving CCR (hazard ratio=0.85, P=0.1009).
One-year survival rates with azacitidine and CCR were 46.5% and 34.2%, respectively.
Grade 3/4 anemia occurred in 16% of patients who received azacitidine, 5% who received best supportive care, 23% who received low-dose cytarabine, and 14% who received intensive chemotherapy.
Grade 3/4 neutropenia occurred in 26%, 5%, 25%, and 33%, respectively. Grade 3/4 febrile neutropenia occurred in 28%, 28%, 30%, and 31%, respectively. And grade 3/4 thrombocytopenia occurred in 24%, 5%, 28%, and 21%, respectively. ![]()
Image by Lance Liotta
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for azacitidine for injection (Vidaza).
The CHMP is recommending that azacitidine be approved to treat adults age 65 and older with acute myeloid leukemia (AML) who are not eligible for hematopoietic stem cell transplant (HSCT) and have more than 30% blasts according to the WHO classification.
The CHMP’s recommendation will be reviewed by the European Commission (EC). The EC usually follows the CHMP’s recommendations and is expected to deliver its final decision in 2 months.
The CHMP said this new indication for azacitidine would bring significant clinical benefit in comparison with existing therapies. If the EC follows the CHMP’s recommendation, azacitidine will receive extended market protection in all its indications for an additional year throughout the European Economic Area.
Azacitidine is already approved in the European Economic Area for the treatment of HSCT-ineligible adults diagnosed with intermediate-2- and high-risk myelodysplastic syndromes; chronic myelomonocytic leukemia with 10%-29% marrow blasts without myeloproliferative disorder; or AML with 20%-30% blasts and multi-lineage dysplasia.
AML-001 trial
The CHMP’s recommendation to expand the indication of azacitidine in AML was based on data from the AML-001 trial. This randomized study included patients age 65 and older with newly diagnosed or secondary AML with greater than 30% blasts.
Patients were pre-selected to receive 1 of 3 regimens per investigator’s choice. This included intensive chemotherapy (standard 7+3 regimen), low-dose cytarabine (20 mg subcutaneously twice a day for 10 days of each 28-day cycle) or best supportive care only.
Patients were then randomized to receive either azacitidine (75 mg/m2/day subcutaneously for 7 days of each 28-day cycle, n=241) or their predetermined conventional care regimen (CCR, n=247).
Median overall survival, the study’s primary endpoint, was 10.4 months for patients receiving azacitidine and 6.5 months for patients receiving CCR (hazard ratio=0.85, P=0.1009).
One-year survival rates with azacitidine and CCR were 46.5% and 34.2%, respectively.
Grade 3/4 anemia occurred in 16% of patients who received azacitidine, 5% who received best supportive care, 23% who received low-dose cytarabine, and 14% who received intensive chemotherapy.
Grade 3/4 neutropenia occurred in 26%, 5%, 25%, and 33%, respectively. Grade 3/4 febrile neutropenia occurred in 28%, 28%, 30%, and 31%, respectively. And grade 3/4 thrombocytopenia occurred in 24%, 5%, 28%, and 21%, respectively. ![]()
My go-to Web resources for quick ICD-10 coding questions
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
New composite measure improves warfarin anticoagulation monitoring
A new composite measure that incorporates both time in therapeutic range and international normalized ratio variability appears to be more accurate than either of these tests alone at monitoring warfarin anticoagulation, according to a report published online Sept. 29 in Circulation: Cardiovascular Quality and Outcomes.
Time in therapeutic range (TTR) and international normalized ratio (INR) variability track two different aspects of anticoagulation control. TTR measures the percentage of time that patients spend within the therapeutic range while taking warfarin, which reflects the amount of time that treatment intensity was appropriate. INR variability measures variations in the stability of warfarin’s anticoagulation effects over time. Most clinicians monitor their patients using one or the other of these measures, usually TTR. A composite measure that combines the two “would encourage providers to focus on all components of anticoagulation control, not just those measured by the current standard of care, TTR,” said Dr. Zayd Razouki of the Center for Health Services Research in Primary Care, Durham (N.C.) Veterans Affairs Medical Center, and his associates.

It is important to note that a substantial number of patients taking warfarin could be classified as having poor control of anticoagulation by one of these measures, but good control by the other. Combining TTR with INR variability would ensure that both appropriate intensity and appropriate stability of warfarin therapy were being used to judge each patient’s anticoagulation control, they noted.
The investigators devised such a measure, a summary score they called WCM (warfarin composite measure). They then compared the performance of all three measures at predicting major warfarin-related complications, using as a sample population 40,404 participants in the Veterans Affairs Study to Improve Anticoagulation (VARIA). These study subjects were aged 65 years or older (mean age 76), had been taking warfarin for at least 6 months to treat atrial fibrillation, and were followed for an average of 14 months for the development of ischemic stroke, major bleeding, and fatal bleeding.
A total of 3.1% of these patients developed ischemic stroke, 6.4% developed major bleeding, and 0.9% developed fatal bleeding while taking warfarin. After the data were adjusted to account for numerous potential confounding factors, WCM correlated most closely with risk for adverse warfarin-related clinical events, Dr. Razouki and his associates wrote (Circ Cardiovasc Qual Outcomes. 2015 Sep 29. doi:10.1161/circoutcomes.115.001789).
Their findings also indicate that WCM may be a more accurate measure of a clinic’s or a medical system’s performance at monitoring anticoagulation than either their average TTR or INR variability alone.
The study results may not be generalizable to all populations, because this VA sample was overwhelmingly male (98%), the investigators added.
A new composite measure that incorporates both time in therapeutic range and international normalized ratio variability appears to be more accurate than either of these tests alone at monitoring warfarin anticoagulation, according to a report published online Sept. 29 in Circulation: Cardiovascular Quality and Outcomes.
Time in therapeutic range (TTR) and international normalized ratio (INR) variability track two different aspects of anticoagulation control. TTR measures the percentage of time that patients spend within the therapeutic range while taking warfarin, which reflects the amount of time that treatment intensity was appropriate. INR variability measures variations in the stability of warfarin’s anticoagulation effects over time. Most clinicians monitor their patients using one or the other of these measures, usually TTR. A composite measure that combines the two “would encourage providers to focus on all components of anticoagulation control, not just those measured by the current standard of care, TTR,” said Dr. Zayd Razouki of the Center for Health Services Research in Primary Care, Durham (N.C.) Veterans Affairs Medical Center, and his associates.
It is important to note that a substantial number of patients taking warfarin could be classified as having poor control of anticoagulation by one of these measures, but good control by the other. Combining TTR with INR variability would ensure that both appropriate intensity and appropriate stability of warfarin therapy were being used to judge each patient’s anticoagulation control, they noted.
The investigators devised such a measure, a summary score they called WCM (warfarin composite measure). They then compared the performance of all three measures at predicting major warfarin-related complications, using as a sample population 40,404 participants in the Veterans Affairs Study to Improve Anticoagulation (VARIA). These study subjects were aged 65 years or older (mean age 76), had been taking warfarin for at least 6 months to treat atrial fibrillation, and were followed for an average of 14 months for the development of ischemic stroke, major bleeding, and fatal bleeding.
A total of 3.1% of these patients developed ischemic stroke, 6.4% developed major bleeding, and 0.9% developed fatal bleeding while taking warfarin. After the data were adjusted to account for numerous potential confounding factors, WCM correlated most closely with risk for adverse warfarin-related clinical events, Dr. Razouki and his associates wrote (Circ Cardiovasc Qual Outcomes. 2015 Sep 29. doi:10.1161/circoutcomes.115.001789).
Their findings also indicate that WCM may be a more accurate measure of a clinic’s or a medical system’s performance at monitoring anticoagulation than either their average TTR or INR variability alone.
The study results may not be generalizable to all populations, because this VA sample was overwhelmingly male (98%), the investigators added.
A new composite measure that incorporates both time in therapeutic range and international normalized ratio variability appears to be more accurate than either of these tests alone at monitoring warfarin anticoagulation, according to a report published online Sept. 29 in Circulation: Cardiovascular Quality and Outcomes.
Time in therapeutic range (TTR) and international normalized ratio (INR) variability track two different aspects of anticoagulation control. TTR measures the percentage of time that patients spend within the therapeutic range while taking warfarin, which reflects the amount of time that treatment intensity was appropriate. INR variability measures variations in the stability of warfarin’s anticoagulation effects over time. Most clinicians monitor their patients using one or the other of these measures, usually TTR. A composite measure that combines the two “would encourage providers to focus on all components of anticoagulation control, not just those measured by the current standard of care, TTR,” said Dr. Zayd Razouki of the Center for Health Services Research in Primary Care, Durham (N.C.) Veterans Affairs Medical Center, and his associates.
It is important to note that a substantial number of patients taking warfarin could be classified as having poor control of anticoagulation by one of these measures, but good control by the other. Combining TTR with INR variability would ensure that both appropriate intensity and appropriate stability of warfarin therapy were being used to judge each patient’s anticoagulation control, they noted.
The investigators devised such a measure, a summary score they called WCM (warfarin composite measure). They then compared the performance of all three measures at predicting major warfarin-related complications, using as a sample population 40,404 participants in the Veterans Affairs Study to Improve Anticoagulation (VARIA). These study subjects were aged 65 years or older (mean age 76), had been taking warfarin for at least 6 months to treat atrial fibrillation, and were followed for an average of 14 months for the development of ischemic stroke, major bleeding, and fatal bleeding.
A total of 3.1% of these patients developed ischemic stroke, 6.4% developed major bleeding, and 0.9% developed fatal bleeding while taking warfarin. After the data were adjusted to account for numerous potential confounding factors, WCM correlated most closely with risk for adverse warfarin-related clinical events, Dr. Razouki and his associates wrote (Circ Cardiovasc Qual Outcomes. 2015 Sep 29. doi:10.1161/circoutcomes.115.001789).
Their findings also indicate that WCM may be a more accurate measure of a clinic’s or a medical system’s performance at monitoring anticoagulation than either their average TTR or INR variability alone.
The study results may not be generalizable to all populations, because this VA sample was overwhelmingly male (98%), the investigators added.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
Key clinical point: A composite measure that combines TTR with INR variability appears more accurate than either of these individual tests at monitoring warfarin anticoagulation.
Major finding: Of the participants, 3.1% developed ischemic stroke, 6.4% developed major bleeding, and 0.9% developed fatal bleeding while taking warfarin.
Data source: A secondary analysis of data from the Veterans Affairs Study to Improve Anticoagulation, involving 40,404 VA patients taking warfarin for AF during a 2-year period.
Disclosures: This study was supported by the Durham VA Medical Center and VA Health Service Research and Development. Dr. Razouki and his associates reported having no relevant financial disclosures.
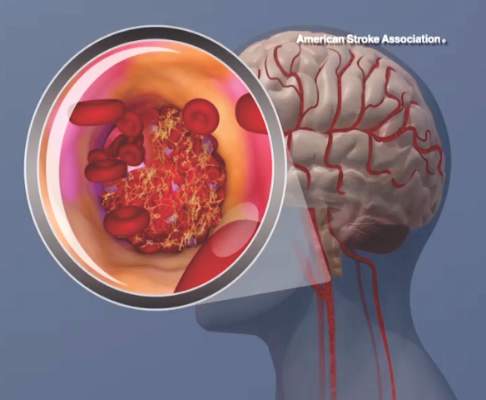
Mind your ABCDs, and your Es, when caring for a ‘difficult patient’
Much has been written about “the difficult patient” in the medical literature.1,2 Also labeled as a “heartsink patient,” “hateful patient,” and “black hole,” they possess characteristics that evoke powerful, often negative, emotional responses in providers that can be counter-therapeutic. “The difficult provider” also is thought to contribute to the failure of the patient encounter,3 and providers may have limited awareness of these patient–provider characteristics that can lead to such interactions. Early identification of these characteristics is essential to implementing effective interventions for the care of a difficult patient.
The mnemonic ABCD highlights patient characteristics that suggest you are dealing with a difficult patient (Table).
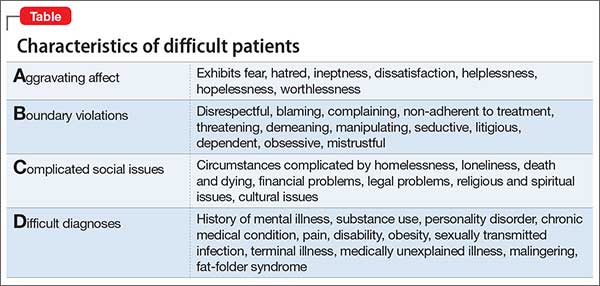
7 Negatives that affect the provider–patient relationship
The 7 Es highlight negative provider-related variables that contribute to perceived and actual difficulty providing care. As a psychiatrist doing consultation-liaison work, this memory device also can be a tool to educate physician–colleagues, nursing staff, and other members of the treatment team.
Expertise. Lack of basic knowledge or experience with your patient’s condition and circumstances, or not being familiar with available resources, could limit your confidence, be counter-productive, and lead to inappropriate care.
Experiences. Current and past life experiences could negatively color a provider’s feelings, thoughts, and interactions with the patient. Negative interpersonal experiences could manifest as countertransference.
Empathy. The inability to empathize makes it difficult to understand the patient, creating distance between you and the patient.
Engagement level. A lack of rapport and ineffective communication leads to a patient feeling misunderstood and unsatisfied with the clinical interaction.
Emotions. Feeling tired, angry, or resentful harms the provider–patient interaction.
Environment. A stressful, loud, pressured environment filled with distractions can undermine the provider–patient relationship.
Extra help. Limited access to, and the unavailability of, social services, housing, and similar resources could make an already difficult situation seem impossible to solve. Working without such help can lead to feelings of helplessness and hopelessness for you and your patient.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this publication/presentation are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
1. Strous RD, Ulman A, Kotler M. The hateful patient revisited: relevance for 21st century medicine. Eur J Intern Med. 2006;17(6):387-393.
2. Smith S. Dealing with the difficult patient. Postgrad Med J. 1995;71(841):653-657.
3. Hawken SJ. Strategies for dealing with the challenging patient. N Z Fam Physician. 2005;32(4):266-269.
Much has been written about “the difficult patient” in the medical literature.1,2 Also labeled as a “heartsink patient,” “hateful patient,” and “black hole,” they possess characteristics that evoke powerful, often negative, emotional responses in providers that can be counter-therapeutic. “The difficult provider” also is thought to contribute to the failure of the patient encounter,3 and providers may have limited awareness of these patient–provider characteristics that can lead to such interactions. Early identification of these characteristics is essential to implementing effective interventions for the care of a difficult patient.
The mnemonic ABCD highlights patient characteristics that suggest you are dealing with a difficult patient (Table).
7 Negatives that affect the provider–patient relationship
The 7 Es highlight negative provider-related variables that contribute to perceived and actual difficulty providing care. As a psychiatrist doing consultation-liaison work, this memory device also can be a tool to educate physician–colleagues, nursing staff, and other members of the treatment team.
Expertise. Lack of basic knowledge or experience with your patient’s condition and circumstances, or not being familiar with available resources, could limit your confidence, be counter-productive, and lead to inappropriate care.
Experiences. Current and past life experiences could negatively color a provider’s feelings, thoughts, and interactions with the patient. Negative interpersonal experiences could manifest as countertransference.
Empathy. The inability to empathize makes it difficult to understand the patient, creating distance between you and the patient.
Engagement level. A lack of rapport and ineffective communication leads to a patient feeling misunderstood and unsatisfied with the clinical interaction.
Emotions. Feeling tired, angry, or resentful harms the provider–patient interaction.
Environment. A stressful, loud, pressured environment filled with distractions can undermine the provider–patient relationship.
Extra help. Limited access to, and the unavailability of, social services, housing, and similar resources could make an already difficult situation seem impossible to solve. Working without such help can lead to feelings of helplessness and hopelessness for you and your patient.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this publication/presentation are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
Much has been written about “the difficult patient” in the medical literature.1,2 Also labeled as a “heartsink patient,” “hateful patient,” and “black hole,” they possess characteristics that evoke powerful, often negative, emotional responses in providers that can be counter-therapeutic. “The difficult provider” also is thought to contribute to the failure of the patient encounter,3 and providers may have limited awareness of these patient–provider characteristics that can lead to such interactions. Early identification of these characteristics is essential to implementing effective interventions for the care of a difficult patient.
The mnemonic ABCD highlights patient characteristics that suggest you are dealing with a difficult patient (Table).
7 Negatives that affect the provider–patient relationship
The 7 Es highlight negative provider-related variables that contribute to perceived and actual difficulty providing care. As a psychiatrist doing consultation-liaison work, this memory device also can be a tool to educate physician–colleagues, nursing staff, and other members of the treatment team.
Expertise. Lack of basic knowledge or experience with your patient’s condition and circumstances, or not being familiar with available resources, could limit your confidence, be counter-productive, and lead to inappropriate care.
Experiences. Current and past life experiences could negatively color a provider’s feelings, thoughts, and interactions with the patient. Negative interpersonal experiences could manifest as countertransference.
Empathy. The inability to empathize makes it difficult to understand the patient, creating distance between you and the patient.
Engagement level. A lack of rapport and ineffective communication leads to a patient feeling misunderstood and unsatisfied with the clinical interaction.
Emotions. Feeling tired, angry, or resentful harms the provider–patient interaction.
Environment. A stressful, loud, pressured environment filled with distractions can undermine the provider–patient relationship.
Extra help. Limited access to, and the unavailability of, social services, housing, and similar resources could make an already difficult situation seem impossible to solve. Working without such help can lead to feelings of helplessness and hopelessness for you and your patient.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this publication/presentation are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
1. Strous RD, Ulman A, Kotler M. The hateful patient revisited: relevance for 21st century medicine. Eur J Intern Med. 2006;17(6):387-393.
2. Smith S. Dealing with the difficult patient. Postgrad Med J. 1995;71(841):653-657.
3. Hawken SJ. Strategies for dealing with the challenging patient. N Z Fam Physician. 2005;32(4):266-269.
1. Strous RD, Ulman A, Kotler M. The hateful patient revisited: relevance for 21st century medicine. Eur J Intern Med. 2006;17(6):387-393.
2. Smith S. Dealing with the difficult patient. Postgrad Med J. 1995;71(841):653-657.
3. Hawken SJ. Strategies for dealing with the challenging patient. N Z Fam Physician. 2005;32(4):266-269.
Postpartum preeclampsia, mother dies: $6.9M settlement

Postpartum preeclampsia, mother dies: $6.9M settlement
Four days after delivery of a healthy child, a 31-year-old mother went to the emergency department (ED) reporting tightness in her chest, difficulty breathing, and swelling in her lower extremities. Pulmonary embolism was ruled out and she was discharged. When she returned 3 days later, her legs were more swollen than before and her systolic blood pressure was 160 mm Hg. She was sent home again. Four days later, she suffered a seizure at home, in the ambulance during transport, and at the hospital. She was transferred to another facility a few days later where she died a week after transfer.
Estate’s Claim The ED physicians and hospital staff were negligent in not diagnosing and treating postpartum preeclampsia. This led to seizures, brain damage, and death. Antihypertensive and antiseizure medications would have prevented her death.
Defendant’s defense The actions taken were reasonable because she had no symptoms of preeclampsia during pregnancy or delivery.
Verdict A $6.9 million Illinois settlement was reached.
Ovary not removed; cyst develops
A 38-year-old woman underwent what was planned as total hysterectomy with bilateral salpingo-oophorectomy. The procedure was prophylactic: she had been treated for stage 3 breast cancer and her family history put her at high risk for developing ovarian cancer. Two days after surgery, the pathology report noted only 1 ovary.
Two months later, the patient went to the ED with right lower quadrant pain. It was determined that she had an ovarian cyst. She underwent additional surgery to remove the right ovary.
Patient’s claim The gynecologist was negligent in failing to remove the patient’s right ovary.
Physician’s defense Failure to remove the ovary was due to the patient’s abnormal anatomy.
Verdict A $250,000 Missouri verdict was returned.
Microcephaly not detected before birth
At 19 weeks’ gestation, an ultrasonographic anatomy scan showed that both hands of the fetus were clenched tightly. Amniocentesis results were reported as normal. No further fetal testing was ordered.
At birth, the baby was found to have Dandy Walker Variant, a severe brain malformation. The child has difficulty moving, is cognitively impaired, and requires a feeding tube and 24-hour care.
Parents’ claim Seen on ultrasonography, the fetus’ clenched fists were a sign of possible fetal abnormality. The maternal-fetal medicine (MFM) specialist who evaluated the ultrasound and amniocentesis and the ObGyn should have recommended fetal magnetic resonance imaging, which would have shown the microcephaly. If the parents had known of the abnormality, they would have terminated the pregnancy.
Defendant’s defense The case was settled during trial.
Verdict A $6 million New Jersey settlement was reached, including $5 million from the MFM and $1 million from the ObGyn.
Injury during hydrothermal ablation
When a 41-year-old woman underwent hydrothermal ablation to treat menorrhagia, her uterus was perforated and hot saline solution injured her intestines. During repair surgery, 21 inches of bowel were resected and a colostomy was created, which was reversed 8 months later.
Patient’s claim The gynecologist was negligent in performing the ablation. The manufacturer produced a poorly designed device.
Defendant’s defense The rupture was spontaneous. The procedure was properly performed. The device is safe.
Verdict A $2 million Kansas verdict was returned. The gynecologist was found 60% at fault and the manufacturer was 40% at fault. The patient’s net recovery was $322,300 due to the state cap.
Postpartum preeclampsia, mother dies: $6.9M settlement
Four days after delivery of a healthy child, a 31-year-old mother went to the emergency department (ED) reporting tightness in her chest, difficulty breathing, and swelling in her lower extremities. Pulmonary embolism was ruled out and she was discharged. When she returned 3 days later, her legs were more swollen than before and her systolic blood pressure was 160 mm Hg. She was sent home again. Four days later, she suffered a seizure at home, in the ambulance during transport, and at the hospital. She was transferred to another facility a few days later where she died a week after transfer.
Estate’s Claim The ED physicians and hospital staff were negligent in not diagnosing and treating postpartum preeclampsia. This led to seizures, brain damage, and death. Antihypertensive and antiseizure medications would have prevented her death.
Defendant’s defense The actions taken were reasonable because she had no symptoms of preeclampsia during pregnancy or delivery.
Verdict A $6.9 million Illinois settlement was reached.
Ovary not removed; cyst develops
A 38-year-old woman underwent what was planned as total hysterectomy with bilateral salpingo-oophorectomy. The procedure was prophylactic: she had been treated for stage 3 breast cancer and her family history put her at high risk for developing ovarian cancer. Two days after surgery, the pathology report noted only 1 ovary.
Two months later, the patient went to the ED with right lower quadrant pain. It was determined that she had an ovarian cyst. She underwent additional surgery to remove the right ovary.
Patient’s claim The gynecologist was negligent in failing to remove the patient’s right ovary.
Physician’s defense Failure to remove the ovary was due to the patient’s abnormal anatomy.
Verdict A $250,000 Missouri verdict was returned.
Microcephaly not detected before birth
At 19 weeks’ gestation, an ultrasonographic anatomy scan showed that both hands of the fetus were clenched tightly. Amniocentesis results were reported as normal. No further fetal testing was ordered.
At birth, the baby was found to have Dandy Walker Variant, a severe brain malformation. The child has difficulty moving, is cognitively impaired, and requires a feeding tube and 24-hour care.
Parents’ claim Seen on ultrasonography, the fetus’ clenched fists were a sign of possible fetal abnormality. The maternal-fetal medicine (MFM) specialist who evaluated the ultrasound and amniocentesis and the ObGyn should have recommended fetal magnetic resonance imaging, which would have shown the microcephaly. If the parents had known of the abnormality, they would have terminated the pregnancy.
Defendant’s defense The case was settled during trial.
Verdict A $6 million New Jersey settlement was reached, including $5 million from the MFM and $1 million from the ObGyn.
Injury during hydrothermal ablation
When a 41-year-old woman underwent hydrothermal ablation to treat menorrhagia, her uterus was perforated and hot saline solution injured her intestines. During repair surgery, 21 inches of bowel were resected and a colostomy was created, which was reversed 8 months later.
Patient’s claim The gynecologist was negligent in performing the ablation. The manufacturer produced a poorly designed device.
Defendant’s defense The rupture was spontaneous. The procedure was properly performed. The device is safe.
Verdict A $2 million Kansas verdict was returned. The gynecologist was found 60% at fault and the manufacturer was 40% at fault. The patient’s net recovery was $322,300 due to the state cap.
Postpartum preeclampsia, mother dies: $6.9M settlement
Four days after delivery of a healthy child, a 31-year-old mother went to the emergency department (ED) reporting tightness in her chest, difficulty breathing, and swelling in her lower extremities. Pulmonary embolism was ruled out and she was discharged. When she returned 3 days later, her legs were more swollen than before and her systolic blood pressure was 160 mm Hg. She was sent home again. Four days later, she suffered a seizure at home, in the ambulance during transport, and at the hospital. She was transferred to another facility a few days later where she died a week after transfer.
Estate’s Claim The ED physicians and hospital staff were negligent in not diagnosing and treating postpartum preeclampsia. This led to seizures, brain damage, and death. Antihypertensive and antiseizure medications would have prevented her death.
Defendant’s defense The actions taken were reasonable because she had no symptoms of preeclampsia during pregnancy or delivery.
Verdict A $6.9 million Illinois settlement was reached.
Ovary not removed; cyst develops
A 38-year-old woman underwent what was planned as total hysterectomy with bilateral salpingo-oophorectomy. The procedure was prophylactic: she had been treated for stage 3 breast cancer and her family history put her at high risk for developing ovarian cancer. Two days after surgery, the pathology report noted only 1 ovary.
Two months later, the patient went to the ED with right lower quadrant pain. It was determined that she had an ovarian cyst. She underwent additional surgery to remove the right ovary.
Patient’s claim The gynecologist was negligent in failing to remove the patient’s right ovary.
Physician’s defense Failure to remove the ovary was due to the patient’s abnormal anatomy.
Verdict A $250,000 Missouri verdict was returned.
Microcephaly not detected before birth
At 19 weeks’ gestation, an ultrasonographic anatomy scan showed that both hands of the fetus were clenched tightly. Amniocentesis results were reported as normal. No further fetal testing was ordered.
At birth, the baby was found to have Dandy Walker Variant, a severe brain malformation. The child has difficulty moving, is cognitively impaired, and requires a feeding tube and 24-hour care.
Parents’ claim Seen on ultrasonography, the fetus’ clenched fists were a sign of possible fetal abnormality. The maternal-fetal medicine (MFM) specialist who evaluated the ultrasound and amniocentesis and the ObGyn should have recommended fetal magnetic resonance imaging, which would have shown the microcephaly. If the parents had known of the abnormality, they would have terminated the pregnancy.
Defendant’s defense The case was settled during trial.
Verdict A $6 million New Jersey settlement was reached, including $5 million from the MFM and $1 million from the ObGyn.
Injury during hydrothermal ablation
When a 41-year-old woman underwent hydrothermal ablation to treat menorrhagia, her uterus was perforated and hot saline solution injured her intestines. During repair surgery, 21 inches of bowel were resected and a colostomy was created, which was reversed 8 months later.
Patient’s claim The gynecologist was negligent in performing the ablation. The manufacturer produced a poorly designed device.
Defendant’s defense The rupture was spontaneous. The procedure was properly performed. The device is safe.
Verdict A $2 million Kansas verdict was returned. The gynecologist was found 60% at fault and the manufacturer was 40% at fault. The patient’s net recovery was $322,300 due to the state cap.
In This Article
- Ovary not removed; cyst develops
- Microcephaly not detected before birth
- Injury during hydrothermal ablation

Mastering finance for your practice—without an MBA
Being a caring, knowledgeable clinician is vital for patient care, but having such skill does not necessarily mean that running a medical practice comes easy— especially if you do not have a basic background in business. Financial fundamentals are rarely taught in residency and, with administrative burdens increasingly placed on physicians in solo and small practices, it isn’t surprising that many practitioners feel underprepared.
Fortunately, it doesn’t take a master’s degree in business administration to conquer these challenges. You just need some understanding of key operating principles.
Accounting basics
It isn’t personal; it’s only business. Delineate the point at which personal finances stop and business finances begin. Make sure that you have a business checking account and credit card, and run all your business expenses through those accounts—never through your personal accounts. That policy will save you time if your practice is audited and, more important, will help you be efficient by guiding your focus to the right set of numbers by which to manage the practice.
Set up a system to track transactions. Many businesses use the accounting software QuickBooks; the program can generate sophisticated reports, and many banks can export data to it automatically. But QuickBooks might be more complicated than what you need to get started; a simple spreadsheet program, such as Excel, might suffice. By working through the numbers yourself, you gain a more intimate knowledge of the state of your finances.
Assemble a team of experts to assist you, at least in the beginning, with building a core knowledge base and good habits. Don’t think that this absolves you of responsibility, however: Ultimately, you sign off on what your advisors recommend. For example, an accountant can prepare your tax return, but you review and approve it, and a financial advisor might recommend certain investments, but only you can authorize them. You might work with a banker for a business loan or a bookkeeper to help you with your day-to-day record-keeping, but no one can give you the critical thinking you need to maximize your financial success.
The devil is in those details
Delve into your practice’s profit/loss statement, or create one if it doesn’t exist. Understanding these data is critical for maintaining financial health. Without knowing how much money you are taking in and where it is going, you cannot be confident that your business model is viable.
Revenue is easier to digest because it typically derives from only a few sources: professional fees and interest and, perhaps, speaking engagements, consultation to trainees, teaching, and rental income.
Expenses. Getting a grasp of where the money goes is more challenging. Common examples of costs of running a practice include, but aren’t limited to, the list in the Table.
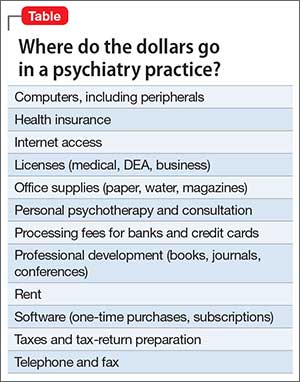
By doing this basic profit/loss math, you will see how much money should be left over (profit) at the end of the month. To confirm, reconcile your numbers with your monthly business checking account statement; QuickBooks does this semi-automatically, or you can do it by hand. Reconciliation might feel uncomfortable if you are a novice to accounting, but spending a few moments to catch an error now is far less onerous than remedying what began as a small mistake and compounded to a big one over the years.
Other financial reports, such as a balance sheet and a statement of cash flow, are useful for giving you a sense of your practice’s long-term financial health. Typically, however, they are unnecessary during early stages of establishing a practice—and the work they require can be overwhelming.
After you’re done with the math
Based on your financial analysis of the practice, you will be able to pay yourself a salary based on the profit (that is, revenue minus expenses). Before you take your salary, however:
• Consider keeping enough in your business checking account to pay next month’s bills.
• Remember to adjust your monthly compensation downward by 20% to 50% to withhold for payroll and estimated federal and state taxes.
• Look into tax-advantaged business benefit plans. A retirement account, certain savings plans (eg, flexible spending accounts for dependent care or health care), a commuter plan, and life insurance paid for by the business can make your income go further. Some of these benefits are available only to employees of corporations; crunch the numbers, however, and discuss with your accountant whether the cost of incorporating is worthwhile.
• Determine whether hiring an assistant, or adding an additional one, will increase your bottom line. You incur significant expenses by hiring an employee—salary, payroll taxes, and time spent training, to name a few—but doing so might be worth it if the time that he (she) saves you opens up billable hours for seeing patients.
Good care requires a solid foundation
Caring for people who are suffering, while being financially successful, are not contradictory goals. Although you deal with a person’s private, intense feelings when you provide care, you also have an obligation to ensure the financial health of your practice.
Disclosure
Dr. Braslow is the founder of Luminello.com.
Being a caring, knowledgeable clinician is vital for patient care, but having such skill does not necessarily mean that running a medical practice comes easy— especially if you do not have a basic background in business. Financial fundamentals are rarely taught in residency and, with administrative burdens increasingly placed on physicians in solo and small practices, it isn’t surprising that many practitioners feel underprepared.
Fortunately, it doesn’t take a master’s degree in business administration to conquer these challenges. You just need some understanding of key operating principles.
Accounting basics
It isn’t personal; it’s only business. Delineate the point at which personal finances stop and business finances begin. Make sure that you have a business checking account and credit card, and run all your business expenses through those accounts—never through your personal accounts. That policy will save you time if your practice is audited and, more important, will help you be efficient by guiding your focus to the right set of numbers by which to manage the practice.
Set up a system to track transactions. Many businesses use the accounting software QuickBooks; the program can generate sophisticated reports, and many banks can export data to it automatically. But QuickBooks might be more complicated than what you need to get started; a simple spreadsheet program, such as Excel, might suffice. By working through the numbers yourself, you gain a more intimate knowledge of the state of your finances.
Assemble a team of experts to assist you, at least in the beginning, with building a core knowledge base and good habits. Don’t think that this absolves you of responsibility, however: Ultimately, you sign off on what your advisors recommend. For example, an accountant can prepare your tax return, but you review and approve it, and a financial advisor might recommend certain investments, but only you can authorize them. You might work with a banker for a business loan or a bookkeeper to help you with your day-to-day record-keeping, but no one can give you the critical thinking you need to maximize your financial success.
The devil is in those details
Delve into your practice’s profit/loss statement, or create one if it doesn’t exist. Understanding these data is critical for maintaining financial health. Without knowing how much money you are taking in and where it is going, you cannot be confident that your business model is viable.
Revenue is easier to digest because it typically derives from only a few sources: professional fees and interest and, perhaps, speaking engagements, consultation to trainees, teaching, and rental income.
Expenses. Getting a grasp of where the money goes is more challenging. Common examples of costs of running a practice include, but aren’t limited to, the list in the Table.
By doing this basic profit/loss math, you will see how much money should be left over (profit) at the end of the month. To confirm, reconcile your numbers with your monthly business checking account statement; QuickBooks does this semi-automatically, or you can do it by hand. Reconciliation might feel uncomfortable if you are a novice to accounting, but spending a few moments to catch an error now is far less onerous than remedying what began as a small mistake and compounded to a big one over the years.
Other financial reports, such as a balance sheet and a statement of cash flow, are useful for giving you a sense of your practice’s long-term financial health. Typically, however, they are unnecessary during early stages of establishing a practice—and the work they require can be overwhelming.
After you’re done with the math
Based on your financial analysis of the practice, you will be able to pay yourself a salary based on the profit (that is, revenue minus expenses). Before you take your salary, however:
• Consider keeping enough in your business checking account to pay next month’s bills.
• Remember to adjust your monthly compensation downward by 20% to 50% to withhold for payroll and estimated federal and state taxes.
• Look into tax-advantaged business benefit plans. A retirement account, certain savings plans (eg, flexible spending accounts for dependent care or health care), a commuter plan, and life insurance paid for by the business can make your income go further. Some of these benefits are available only to employees of corporations; crunch the numbers, however, and discuss with your accountant whether the cost of incorporating is worthwhile.
• Determine whether hiring an assistant, or adding an additional one, will increase your bottom line. You incur significant expenses by hiring an employee—salary, payroll taxes, and time spent training, to name a few—but doing so might be worth it if the time that he (she) saves you opens up billable hours for seeing patients.
Good care requires a solid foundation
Caring for people who are suffering, while being financially successful, are not contradictory goals. Although you deal with a person’s private, intense feelings when you provide care, you also have an obligation to ensure the financial health of your practice.
Disclosure
Dr. Braslow is the founder of Luminello.com.
Being a caring, knowledgeable clinician is vital for patient care, but having such skill does not necessarily mean that running a medical practice comes easy— especially if you do not have a basic background in business. Financial fundamentals are rarely taught in residency and, with administrative burdens increasingly placed on physicians in solo and small practices, it isn’t surprising that many practitioners feel underprepared.
Fortunately, it doesn’t take a master’s degree in business administration to conquer these challenges. You just need some understanding of key operating principles.
Accounting basics
It isn’t personal; it’s only business. Delineate the point at which personal finances stop and business finances begin. Make sure that you have a business checking account and credit card, and run all your business expenses through those accounts—never through your personal accounts. That policy will save you time if your practice is audited and, more important, will help you be efficient by guiding your focus to the right set of numbers by which to manage the practice.
Set up a system to track transactions. Many businesses use the accounting software QuickBooks; the program can generate sophisticated reports, and many banks can export data to it automatically. But QuickBooks might be more complicated than what you need to get started; a simple spreadsheet program, such as Excel, might suffice. By working through the numbers yourself, you gain a more intimate knowledge of the state of your finances.
Assemble a team of experts to assist you, at least in the beginning, with building a core knowledge base and good habits. Don’t think that this absolves you of responsibility, however: Ultimately, you sign off on what your advisors recommend. For example, an accountant can prepare your tax return, but you review and approve it, and a financial advisor might recommend certain investments, but only you can authorize them. You might work with a banker for a business loan or a bookkeeper to help you with your day-to-day record-keeping, but no one can give you the critical thinking you need to maximize your financial success.
The devil is in those details
Delve into your practice’s profit/loss statement, or create one if it doesn’t exist. Understanding these data is critical for maintaining financial health. Without knowing how much money you are taking in and where it is going, you cannot be confident that your business model is viable.
Revenue is easier to digest because it typically derives from only a few sources: professional fees and interest and, perhaps, speaking engagements, consultation to trainees, teaching, and rental income.
Expenses. Getting a grasp of where the money goes is more challenging. Common examples of costs of running a practice include, but aren’t limited to, the list in the Table.
By doing this basic profit/loss math, you will see how much money should be left over (profit) at the end of the month. To confirm, reconcile your numbers with your monthly business checking account statement; QuickBooks does this semi-automatically, or you can do it by hand. Reconciliation might feel uncomfortable if you are a novice to accounting, but spending a few moments to catch an error now is far less onerous than remedying what began as a small mistake and compounded to a big one over the years.
Other financial reports, such as a balance sheet and a statement of cash flow, are useful for giving you a sense of your practice’s long-term financial health. Typically, however, they are unnecessary during early stages of establishing a practice—and the work they require can be overwhelming.
After you’re done with the math
Based on your financial analysis of the practice, you will be able to pay yourself a salary based on the profit (that is, revenue minus expenses). Before you take your salary, however:
• Consider keeping enough in your business checking account to pay next month’s bills.
• Remember to adjust your monthly compensation downward by 20% to 50% to withhold for payroll and estimated federal and state taxes.
• Look into tax-advantaged business benefit plans. A retirement account, certain savings plans (eg, flexible spending accounts for dependent care or health care), a commuter plan, and life insurance paid for by the business can make your income go further. Some of these benefits are available only to employees of corporations; crunch the numbers, however, and discuss with your accountant whether the cost of incorporating is worthwhile.
• Determine whether hiring an assistant, or adding an additional one, will increase your bottom line. You incur significant expenses by hiring an employee—salary, payroll taxes, and time spent training, to name a few—but doing so might be worth it if the time that he (she) saves you opens up billable hours for seeing patients.
Good care requires a solid foundation
Caring for people who are suffering, while being financially successful, are not contradictory goals. Although you deal with a person’s private, intense feelings when you provide care, you also have an obligation to ensure the financial health of your practice.
Disclosure
Dr. Braslow is the founder of Luminello.com.