User login
Differences in Care, Outcomes for In-Hospital Versus Community-Onset Stroke
Clinical question: Are there any differences in care and outcomes for in-hospital versus community-onset stroke?
Background: In-hospital stroke accounts for 4%-17% of all strokes. Hospitalists and other non-neurological services have to identify and treat subsequent stroke in their patients. There is not much literature detailing the differences between hospitalized stroke patients and those admitted for stroke.
Study design: Prospective cohort study.
Setting: All regional stroke centers in Ontario, Canada.
Synopsis: During a period of nine years, 973 in-hospital and 28,837 community-acquired stroke patients were followed. Compared to community-acquired stroke patients, in-hospital stroke patients had longer time to confirmatory neuroimaging, lower use of thrombolysis, lower use of investigational tests, and longer length of stay, and they were more likely to be disabled or dead at discharge. The two cohorts had similar mortality outcomes after discharge at 30 days and one year, after adjusting for multiple factors. Interestingly, in-hospital stroke patients were more likely to be given the proper medications for secondary prevention at discharge.
The study was limited in that the authors were unable to research why in-hospital patients did not get timely diagnosis and comparable treatment. The admission diagnoses were not enough for the authors to determine if that condition mattered in care. Secondary analysis found that in-hospital stroke patients were older and had more comorbidities (i.e., diabetes, hypertension, hyperlipidemia, and atrial fibrillation). The primary reason in-hospital stroke patients did not get thrombolysis was because of a contraindication.
Bottom line: In-hospital stroke patients have increased lengths of stay and more disability compared to community-onset stroke patients.
Citation: Saltman AP, Silver FL, Fang J, Stamplecoski M, Kapral MK. Care and outcomes of patients with in-hospital stroke. JAMA Neurol. 2015;72(7):749-755.
Clinical question: Are there any differences in care and outcomes for in-hospital versus community-onset stroke?
Background: In-hospital stroke accounts for 4%-17% of all strokes. Hospitalists and other non-neurological services have to identify and treat subsequent stroke in their patients. There is not much literature detailing the differences between hospitalized stroke patients and those admitted for stroke.
Study design: Prospective cohort study.
Setting: All regional stroke centers in Ontario, Canada.
Synopsis: During a period of nine years, 973 in-hospital and 28,837 community-acquired stroke patients were followed. Compared to community-acquired stroke patients, in-hospital stroke patients had longer time to confirmatory neuroimaging, lower use of thrombolysis, lower use of investigational tests, and longer length of stay, and they were more likely to be disabled or dead at discharge. The two cohorts had similar mortality outcomes after discharge at 30 days and one year, after adjusting for multiple factors. Interestingly, in-hospital stroke patients were more likely to be given the proper medications for secondary prevention at discharge.
The study was limited in that the authors were unable to research why in-hospital patients did not get timely diagnosis and comparable treatment. The admission diagnoses were not enough for the authors to determine if that condition mattered in care. Secondary analysis found that in-hospital stroke patients were older and had more comorbidities (i.e., diabetes, hypertension, hyperlipidemia, and atrial fibrillation). The primary reason in-hospital stroke patients did not get thrombolysis was because of a contraindication.
Bottom line: In-hospital stroke patients have increased lengths of stay and more disability compared to community-onset stroke patients.
Citation: Saltman AP, Silver FL, Fang J, Stamplecoski M, Kapral MK. Care and outcomes of patients with in-hospital stroke. JAMA Neurol. 2015;72(7):749-755.
Clinical question: Are there any differences in care and outcomes for in-hospital versus community-onset stroke?
Background: In-hospital stroke accounts for 4%-17% of all strokes. Hospitalists and other non-neurological services have to identify and treat subsequent stroke in their patients. There is not much literature detailing the differences between hospitalized stroke patients and those admitted for stroke.
Study design: Prospective cohort study.
Setting: All regional stroke centers in Ontario, Canada.
Synopsis: During a period of nine years, 973 in-hospital and 28,837 community-acquired stroke patients were followed. Compared to community-acquired stroke patients, in-hospital stroke patients had longer time to confirmatory neuroimaging, lower use of thrombolysis, lower use of investigational tests, and longer length of stay, and they were more likely to be disabled or dead at discharge. The two cohorts had similar mortality outcomes after discharge at 30 days and one year, after adjusting for multiple factors. Interestingly, in-hospital stroke patients were more likely to be given the proper medications for secondary prevention at discharge.
The study was limited in that the authors were unable to research why in-hospital patients did not get timely diagnosis and comparable treatment. The admission diagnoses were not enough for the authors to determine if that condition mattered in care. Secondary analysis found that in-hospital stroke patients were older and had more comorbidities (i.e., diabetes, hypertension, hyperlipidemia, and atrial fibrillation). The primary reason in-hospital stroke patients did not get thrombolysis was because of a contraindication.
Bottom line: In-hospital stroke patients have increased lengths of stay and more disability compared to community-onset stroke patients.
Citation: Saltman AP, Silver FL, Fang J, Stamplecoski M, Kapral MK. Care and outcomes of patients with in-hospital stroke. JAMA Neurol. 2015;72(7):749-755.
Tips for Hospitalists on Improving Diagnostic Skills
Case
A 67-year-old man presents to the hospital with persistent, subjective fevers and malaise for one month, subacute onset of dyspnea, and nonproductive cough for the preceding six days. The patient is a nonsmoker, denies sick contacts, and has had no foreign travel. What would be the best approach to making the diagnosis while working to enhance diagnostic skills?
Diagnostic Reasoning
With clinical experience, making a diagnosis can become so routine that physicians might not contemplate their problem-solving strategies. Diagnostic reasoning is the process of thinking about a clinical problem to form a diagnosis. Experienced clinicians typically rely upon nonanalytic reasoning (i.e., pattern recognition) for straightforward problems, reverting to analytic reasoning if a pattern is not recognized.
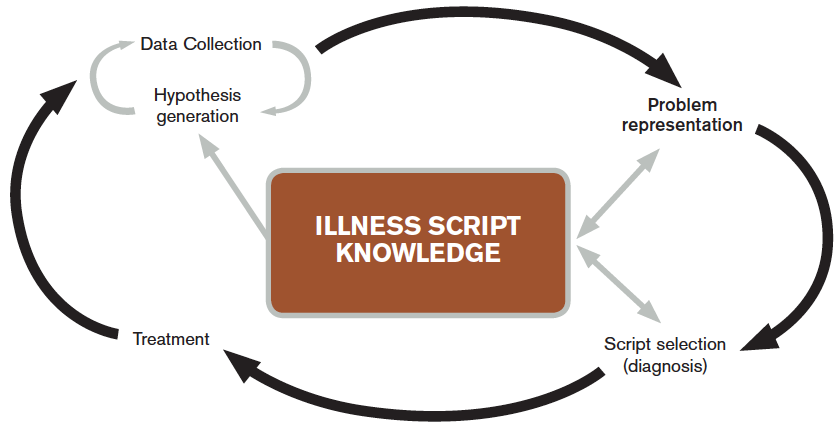
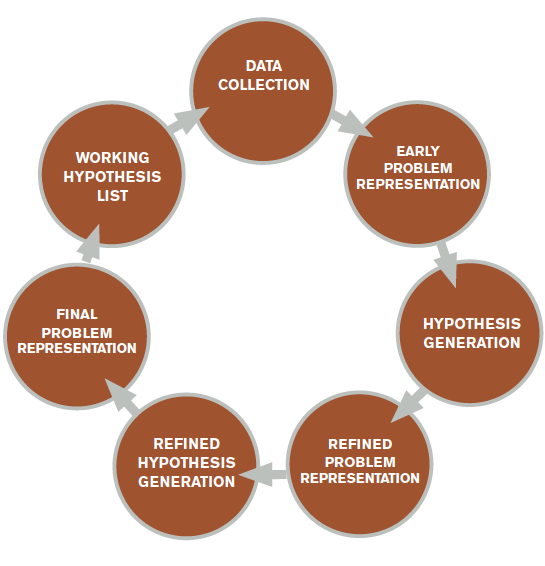
The literature describes five steps in the reasoning process (see Figure 1). In the early stages of data collection, hypotheses emerge that feed back into data collection behaviors as the clinician seeks confirmatory evidence. This complex interplay between data collection and hypothesis generation/elimination leads to a more clearly defined understanding of the patient’s presentation. The synthesis of the patient’s presentation, including epidemiologic risk factors, symptoms, signs, and laboratory and radiologic studies, is called the “problem representation.” After a clinician conceives the problem representation, he or she reviews the mental representations of diseases (i.e., illness scripts) to determine hypotheses by finding disease presentations that best match the formulated problem representation (see Figure 2).
Analytic and nonanalytic reasoning. In what is known as the dual process theory, diagnostic reasoning is believed to occur both analytically and nonanalytically.1 Nonanalytic reasoning is often exemplified by rapid, subconscious “pattern recognition” and is developed through clinical experience and other nonclinical learning experiences (e.g. reading).
Conversely, analytic reasoning, the “slow,” conscious, cognitive processing, is typically utilized when a patient presentation is complicated or does not fit a known disease pattern. Clinicians apply both strategies to make diagnoses in evaluating complex cases.
In the outlined case, while the symptoms of fever and cough might lead to the diagnosis of community-acquired pneumonia (CAP), the time course seems unusually long. This atypical pattern for CAP could trigger analytic reasoning, leading to new considerations such as tuberculosis (TB).
Case Continued
On examination, the patient has severe rigors and diaphoresis, as well as a fever of 39.4°C and a heart rate of 102 bpm. Full examination discloses mild end-expiratory wheezes and bronchial breath sounds in the right lower lobe. The remainder of his examination is normal. Labs reveal WBC 8.5x103, hemoglobin 11g/dL, MCV of 92 fL, and platelet count 22,000 mm3. Blood cultures, sputum cultures, and respiratory virus microarray are normal. The chest X-ray (CXR) is unremarkable.
Further history reveals that the patient is a sheepherder living in a primitive earthen structure in the rural mountains of western New Mexico.
Problem representation revisited. With additional historical, laboratory, and radiological data collected, further interpretation and synthesis occur. Salient elements are highlighted and prioritized, irrelevant details are discarded, and data of uncertain relevance are reevaluated as additional data are gathered. The problem representation—an interpreted, subjective mental model of a patient’s clinical presentation—is updated and reformulated. The verbal expression of the problem representation is variously called the assessment, summary statement, or “one-liner.” Within this summary statement, and fundamental to the creation of a strong problem representation, is the incorporation of “semantic qualifiers.”
“Semantic qualifiers” (e.g. acute vs. chronic or unremitting vs. relapsing) are paired, opposing descriptive adjectives that can be used to compare and contrast diagnostic considerations.² Clinicians distinguish between diseases using key signs and symptoms and use these descriptors to assist with this discrimination in hypothesis generation. An example for this patient would be: A 67-year-old sheepherder living in rural New Mexico presents with persistent fevers and malaise for one month, along with subacute development of nonproductive cough and dyspnea, sepsis, anemia, and thrombocytopenia.
Note how the incorporation of epidemiologic information (sheepherder living in an earthen structure in rural New Mexico) creates a context in which the additional problems can be framed (persistent malaise, subacute cough). In this case, the persistent fevers help the clinician to narrow possibilities in the differential diagnosis and create focused hypotheses.
Although the benefit of teaching accurate and thorough problem representation seems self-evident, studies have not demonstrated that improved problem representation enhances diagnostic accuracy; however, we believe that there is still value in adapting and teaching this skill.3
Hypothesis refinement and the differential diagnosis. Initial hypotheses occur early in data collection, as the patient’s history and physical examination findings trigger connections to clinicians’ bank of known diseases (e.g. orthopnea triggers congestive heart failure). As the clinician collects additional data, he or she refines these hypotheses, changing the likelihood based on “fit” of the problem representation with known diseases or illness scripts.
When employing analytic reasoning processes, clinicians may benefit from using organizational frameworks to assist with hypothesis generation (see Table 1). For this patient, possible hypotheses could include CAP, TB, lymphoma, lung neoplasm, or other indolent pulmonary infection.

Illness scripts. Once discrete hypotheses (e.g. CAP, pulmonary embolism) have been generated, clinicians need a method to accurately compare disease processes. This can be done through the use of an illness script. Illness scripts are mental representations of diseases and are likely to include epidemiology, typical and atypical patterns of presentation, and distinguishing features.
For example, a clinician’s illness script for a typical presentation of bacterial CAP likely includes fever, productive cough, pleuritic chest discomfort, and infiltrate on CXR. Clinician educators who teach illness scripts should ensure that students understand that diseases have atypical presentations, even though they may only teach them the prototypical one. Conceptualizing diseases in this fashion allows clinicians to seek the disease with the “script” that best matches the patient’s story (i.e., clinical presentation).
In this case, the clinician is now thinking of causes of persistent fever + nonproductive cough + dyspnea + anemia + thrombocytopenia; possibilities include lymphoma or unusual infection (e.g. tick-borne relapsing fever, or TBRF).
Case Resolution and Script Selection
As the clinician processes the case, a known illness script of TBRF matches the patient’s clinical presentation, and a peripheral smear is ordered. The smear reveals presence of spirochetal organisms, later confirmed by PCR to be Borrelia hermsii, confirming the diagnosis of TBRF.
Errors in Clinical Reasoning
Although most clinicians are quite accurate in typical presentations of common diseases, they are more likely to commit diagnostic errors when faced with uncommon diseases, atypical presentations, and/or challenging contexts. The following sections categorize a selection of some common errors and offer some expert opinion from the literature on avoiding them.
Common diagnostic errors. Clinicians use heuristics, or mental shortcuts, which can occasionally induce diagnostic errors. By definition, the fundamental problem in all diagnostic error is premature closure, or acceptance of a diagnosis before it is fully verified. In the case presented, the clinician may have accepted the diagnosis of CAP without recognizing other possible diagnoses.
Two common heuristics/biases that can sometimes lead to premature closure are the availability and anchoring biases. Availability bias means that the diagnoses easily thought of—and often most recent in the memory—are more likely to be assigned to a patient problem. The diagnosis of pulmonary embolism would be more “available” in a patient with fever, dyspnea, and normal CXR, especially if the clinician recently had seen a patient with PE. Anchoring bias occurs when early information is relied upon to make clinical judgments and the clinician fixates on a diagnosis despite acquiring additional or contrary information. For example, a clinician may rely upon a diagnosis of CAP based on the sign-out from a colleague, despite the one-month history of symptoms, rather than broadening the differential.
Clinician-focused methods to reduce diagnostic errors. Multiple methods exist that may mitigate diagnostic errors, although definitive proof of their value is still lacking, owing to the difficulty involved in studying such errors due to the multitude of causes.4 In our opinion, building a mental database of illness scripts by reading and seeing patients, as well as being metacognitive, are the best methods for individual clinicians to use to reduce their errors (see “deliberate practice” below).
Metacognition, or thinking about one’s thinking, is another method of reducing errors and can be characterized by “reflection in action” (reflection in real time) and “reflection on action” (reflection after an event).5 For example, taking a few moments at the end of a week on clinical service to reflect on the hospital course and diagnostic paths of the most complex patient presentations (reflection on action) is an exercise used to reduce errors.
For reflection in action, a clinician may pause when confronted with paradoxical findings for a current patient’s presentation (e.g. elevated jugular veinous pressure and crackles on exam but normal b-type natriuretic peptide), and “think aloud” (see below) to ensure he or she is processing all of the appropriate elements of the case.5
In the case presented above, the time course might have initiated reflection into erroneous decision-making at the moment the clinician thought that CAP was a possibility (reflection in action). Although direct evidence is inconclusive as to whether these techniques improve diagnostic accuracy, engaging in metacognitive exercises remains a cornerstone of seasoned clinical reasoning experts.6
Teaching and Learning Principles
Making a commitment. During a patient presentation, it is often helpful to ask a learner to develop a two- to four-item prioritized differential diagnosis list based on likelihood and/or lethality. Have the learner describe which diagnosis is most likely (i.e., the working diagnosis), in addition to the reasons “for” or “against” certain hypotheses. Once the diagnosis has been determined, combine commitment with an exercise in metacognition by asking the learner, “Why do you think that your initial diagnosis of Q-fever was incorrect?” Clinical educators may then follow up with teaching pearls and their approach to this type of case (see Table 1).
Think aloud: In this method, an instructor expresses his or her thoughts aloud in real time.7 By modeling this technique, attending physicians allow learners to observe the process of developing a differential diagnosis and plan. For example, during the admission process, instructors could verbalize their approach to fever in a systematic fashion (see Table 1) after the trainee has completed the presentation: “At this point I am considering an infectious cause such as pneumonia, given the respiratory symptoms, although the one-month history of fever and malaise makes me think that I should keep neoplasm and an unusual infection on my list of possibilities.”
Conversely, instructors can ask trainees to voice their thoughts aloud to better understand their reasoning processes. By using this method, instructors can also support, correct, or reinforce the trainees’ appropriate use of knowledge in the clinical reasoning process.
Deliberate practice. To improve diagnostic skills, trainees must engage in deliberate practice, defined as intentional, repetitious practice aimed at improving performance.8 To facilitate this, a trainee should evaluate as many patients as possible and present to an experienced clinician with subsequent feedback. Trainees are likely to miss subtle historical or examination points (e.g. the history of sheepherding) because their illness scripts are limited or incompletely developed. Teachers should emphasize the importance of developing broad and deep illness scripts, so learners will, hopefully, become more aware of their limitations and recognize what they do not know.
Key Takeaways
Clinicians solve diagnostic problems using both nonanalytic and analytic reasoning processes. Although evidence is inconclusive, some clinical reasoning experts suggest the use of reflective strategies to enhance diagnostic accuracy, especially in complicated cases.9 To prevent premature closure, we encourage hospitalists to perform an analytic “double-check” before determining their final diagnosis.
Furthermore, the clinical reasoning literature suggests that knowledge and its organization are key to expert performance.10 In diagnostic reasoning, this key knowledge has been termed “illness scripts.” Thus, the task of the aspiring expert diagnostician is to learn the key features of diseases and focus on discriminating features, starting with typical presentations of common diseases and working up to atypical presentations of uncommon diseases.
Engaging in deliberate practice, seeking feedback on diagnostic accuracy, and reflecting upon your own reasoning process can provide valuable information for improving future diagnostic reasoning. The ultimate goal of these practices is to enhance diagnostic skills in order to avoid errors and improve patient care.
Bottom Line
Diagnosis is a challenging task. Diagnostic accuracy may be enhanced by expanding the learner’s knowledge of illness scripts and using an analytic double-check to confirm initial diagnoses determined by nonanalytic reasoning.
Drs. Rendon, Roesch, and Rao are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Rencic is a hospitalist in the department of internal medicine at Tufts University School of Medicine in Boston.
References
- Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. 2005;39(1):98-106.
- Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217-2225.
- Nendaz MR, Bordage G. Promoting diagnostic problem representation. Med Educ. 2002;36(8):760-766.
- Norman GR, Eva KW. Diagnostic error and clinical reasoning. Med Educ. 2010;44(1):94-100.
- Schön DA. The Reflective Practitioner: How Professionals Think in Action. London: Temple Smith; 1983.
- Croskerry P. Achieving quality in clinical decision making: cognitive strategies and detection of bias. Acad Emerg Med. 2002;9(11):1184-1204.
- Van Someren MW, Burnard YF, Sandberg JAC. The Think Aloud Method: A Practical Guide to Modelling Cognitive Processes. London: Academic Press; 1994.
- Ericsson KA, Krampe RT, Tesch-Romer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363-406.
- Mamede S, Schmidt HG, Penaforte JC. Effects of reflective practice on the accuracy of medical diagnoses. Med Educ. 2008;42(5):468-475.
- Elstein, AS, Shulman LS, Sprafka SA. Medical Problem Solving: An Analysis of Clinical Reasoning. Cambridge, Mass.: Harvard University Press; 1978.
- Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med. 2010;85(7):1118-1124.
- Rencic J. Twelve tips for teaching expertise in clinical reasoning. Med Teach. 2011;33(11):887-892.
Case
A 67-year-old man presents to the hospital with persistent, subjective fevers and malaise for one month, subacute onset of dyspnea, and nonproductive cough for the preceding six days. The patient is a nonsmoker, denies sick contacts, and has had no foreign travel. What would be the best approach to making the diagnosis while working to enhance diagnostic skills?
Diagnostic Reasoning
With clinical experience, making a diagnosis can become so routine that physicians might not contemplate their problem-solving strategies. Diagnostic reasoning is the process of thinking about a clinical problem to form a diagnosis. Experienced clinicians typically rely upon nonanalytic reasoning (i.e., pattern recognition) for straightforward problems, reverting to analytic reasoning if a pattern is not recognized.
The literature describes five steps in the reasoning process (see Figure 1). In the early stages of data collection, hypotheses emerge that feed back into data collection behaviors as the clinician seeks confirmatory evidence. This complex interplay between data collection and hypothesis generation/elimination leads to a more clearly defined understanding of the patient’s presentation. The synthesis of the patient’s presentation, including epidemiologic risk factors, symptoms, signs, and laboratory and radiologic studies, is called the “problem representation.” After a clinician conceives the problem representation, he or she reviews the mental representations of diseases (i.e., illness scripts) to determine hypotheses by finding disease presentations that best match the formulated problem representation (see Figure 2).
Analytic and nonanalytic reasoning. In what is known as the dual process theory, diagnostic reasoning is believed to occur both analytically and nonanalytically.1 Nonanalytic reasoning is often exemplified by rapid, subconscious “pattern recognition” and is developed through clinical experience and other nonclinical learning experiences (e.g. reading).
Conversely, analytic reasoning, the “slow,” conscious, cognitive processing, is typically utilized when a patient presentation is complicated or does not fit a known disease pattern. Clinicians apply both strategies to make diagnoses in evaluating complex cases.
In the outlined case, while the symptoms of fever and cough might lead to the diagnosis of community-acquired pneumonia (CAP), the time course seems unusually long. This atypical pattern for CAP could trigger analytic reasoning, leading to new considerations such as tuberculosis (TB).
Case Continued
On examination, the patient has severe rigors and diaphoresis, as well as a fever of 39.4°C and a heart rate of 102 bpm. Full examination discloses mild end-expiratory wheezes and bronchial breath sounds in the right lower lobe. The remainder of his examination is normal. Labs reveal WBC 8.5x103, hemoglobin 11g/dL, MCV of 92 fL, and platelet count 22,000 mm3. Blood cultures, sputum cultures, and respiratory virus microarray are normal. The chest X-ray (CXR) is unremarkable.
Further history reveals that the patient is a sheepherder living in a primitive earthen structure in the rural mountains of western New Mexico.
Problem representation revisited. With additional historical, laboratory, and radiological data collected, further interpretation and synthesis occur. Salient elements are highlighted and prioritized, irrelevant details are discarded, and data of uncertain relevance are reevaluated as additional data are gathered. The problem representation—an interpreted, subjective mental model of a patient’s clinical presentation—is updated and reformulated. The verbal expression of the problem representation is variously called the assessment, summary statement, or “one-liner.” Within this summary statement, and fundamental to the creation of a strong problem representation, is the incorporation of “semantic qualifiers.”
“Semantic qualifiers” (e.g. acute vs. chronic or unremitting vs. relapsing) are paired, opposing descriptive adjectives that can be used to compare and contrast diagnostic considerations.² Clinicians distinguish between diseases using key signs and symptoms and use these descriptors to assist with this discrimination in hypothesis generation. An example for this patient would be: A 67-year-old sheepherder living in rural New Mexico presents with persistent fevers and malaise for one month, along with subacute development of nonproductive cough and dyspnea, sepsis, anemia, and thrombocytopenia.
Note how the incorporation of epidemiologic information (sheepherder living in an earthen structure in rural New Mexico) creates a context in which the additional problems can be framed (persistent malaise, subacute cough). In this case, the persistent fevers help the clinician to narrow possibilities in the differential diagnosis and create focused hypotheses.
Although the benefit of teaching accurate and thorough problem representation seems self-evident, studies have not demonstrated that improved problem representation enhances diagnostic accuracy; however, we believe that there is still value in adapting and teaching this skill.3
Hypothesis refinement and the differential diagnosis. Initial hypotheses occur early in data collection, as the patient’s history and physical examination findings trigger connections to clinicians’ bank of known diseases (e.g. orthopnea triggers congestive heart failure). As the clinician collects additional data, he or she refines these hypotheses, changing the likelihood based on “fit” of the problem representation with known diseases or illness scripts.
When employing analytic reasoning processes, clinicians may benefit from using organizational frameworks to assist with hypothesis generation (see Table 1). For this patient, possible hypotheses could include CAP, TB, lymphoma, lung neoplasm, or other indolent pulmonary infection.
Illness scripts. Once discrete hypotheses (e.g. CAP, pulmonary embolism) have been generated, clinicians need a method to accurately compare disease processes. This can be done through the use of an illness script. Illness scripts are mental representations of diseases and are likely to include epidemiology, typical and atypical patterns of presentation, and distinguishing features.
For example, a clinician’s illness script for a typical presentation of bacterial CAP likely includes fever, productive cough, pleuritic chest discomfort, and infiltrate on CXR. Clinician educators who teach illness scripts should ensure that students understand that diseases have atypical presentations, even though they may only teach them the prototypical one. Conceptualizing diseases in this fashion allows clinicians to seek the disease with the “script” that best matches the patient’s story (i.e., clinical presentation).
In this case, the clinician is now thinking of causes of persistent fever + nonproductive cough + dyspnea + anemia + thrombocytopenia; possibilities include lymphoma or unusual infection (e.g. tick-borne relapsing fever, or TBRF).
Case Resolution and Script Selection
As the clinician processes the case, a known illness script of TBRF matches the patient’s clinical presentation, and a peripheral smear is ordered. The smear reveals presence of spirochetal organisms, later confirmed by PCR to be Borrelia hermsii, confirming the diagnosis of TBRF.
Errors in Clinical Reasoning
Although most clinicians are quite accurate in typical presentations of common diseases, they are more likely to commit diagnostic errors when faced with uncommon diseases, atypical presentations, and/or challenging contexts. The following sections categorize a selection of some common errors and offer some expert opinion from the literature on avoiding them.
Common diagnostic errors. Clinicians use heuristics, or mental shortcuts, which can occasionally induce diagnostic errors. By definition, the fundamental problem in all diagnostic error is premature closure, or acceptance of a diagnosis before it is fully verified. In the case presented, the clinician may have accepted the diagnosis of CAP without recognizing other possible diagnoses.
Two common heuristics/biases that can sometimes lead to premature closure are the availability and anchoring biases. Availability bias means that the diagnoses easily thought of—and often most recent in the memory—are more likely to be assigned to a patient problem. The diagnosis of pulmonary embolism would be more “available” in a patient with fever, dyspnea, and normal CXR, especially if the clinician recently had seen a patient with PE. Anchoring bias occurs when early information is relied upon to make clinical judgments and the clinician fixates on a diagnosis despite acquiring additional or contrary information. For example, a clinician may rely upon a diagnosis of CAP based on the sign-out from a colleague, despite the one-month history of symptoms, rather than broadening the differential.
Clinician-focused methods to reduce diagnostic errors. Multiple methods exist that may mitigate diagnostic errors, although definitive proof of their value is still lacking, owing to the difficulty involved in studying such errors due to the multitude of causes.4 In our opinion, building a mental database of illness scripts by reading and seeing patients, as well as being metacognitive, are the best methods for individual clinicians to use to reduce their errors (see “deliberate practice” below).
Metacognition, or thinking about one’s thinking, is another method of reducing errors and can be characterized by “reflection in action” (reflection in real time) and “reflection on action” (reflection after an event).5 For example, taking a few moments at the end of a week on clinical service to reflect on the hospital course and diagnostic paths of the most complex patient presentations (reflection on action) is an exercise used to reduce errors.
For reflection in action, a clinician may pause when confronted with paradoxical findings for a current patient’s presentation (e.g. elevated jugular veinous pressure and crackles on exam but normal b-type natriuretic peptide), and “think aloud” (see below) to ensure he or she is processing all of the appropriate elements of the case.5
In the case presented above, the time course might have initiated reflection into erroneous decision-making at the moment the clinician thought that CAP was a possibility (reflection in action). Although direct evidence is inconclusive as to whether these techniques improve diagnostic accuracy, engaging in metacognitive exercises remains a cornerstone of seasoned clinical reasoning experts.6
Teaching and Learning Principles
Making a commitment. During a patient presentation, it is often helpful to ask a learner to develop a two- to four-item prioritized differential diagnosis list based on likelihood and/or lethality. Have the learner describe which diagnosis is most likely (i.e., the working diagnosis), in addition to the reasons “for” or “against” certain hypotheses. Once the diagnosis has been determined, combine commitment with an exercise in metacognition by asking the learner, “Why do you think that your initial diagnosis of Q-fever was incorrect?” Clinical educators may then follow up with teaching pearls and their approach to this type of case (see Table 1).
Think aloud: In this method, an instructor expresses his or her thoughts aloud in real time.7 By modeling this technique, attending physicians allow learners to observe the process of developing a differential diagnosis and plan. For example, during the admission process, instructors could verbalize their approach to fever in a systematic fashion (see Table 1) after the trainee has completed the presentation: “At this point I am considering an infectious cause such as pneumonia, given the respiratory symptoms, although the one-month history of fever and malaise makes me think that I should keep neoplasm and an unusual infection on my list of possibilities.”
Conversely, instructors can ask trainees to voice their thoughts aloud to better understand their reasoning processes. By using this method, instructors can also support, correct, or reinforce the trainees’ appropriate use of knowledge in the clinical reasoning process.
Deliberate practice. To improve diagnostic skills, trainees must engage in deliberate practice, defined as intentional, repetitious practice aimed at improving performance.8 To facilitate this, a trainee should evaluate as many patients as possible and present to an experienced clinician with subsequent feedback. Trainees are likely to miss subtle historical or examination points (e.g. the history of sheepherding) because their illness scripts are limited or incompletely developed. Teachers should emphasize the importance of developing broad and deep illness scripts, so learners will, hopefully, become more aware of their limitations and recognize what they do not know.
Key Takeaways
Clinicians solve diagnostic problems using both nonanalytic and analytic reasoning processes. Although evidence is inconclusive, some clinical reasoning experts suggest the use of reflective strategies to enhance diagnostic accuracy, especially in complicated cases.9 To prevent premature closure, we encourage hospitalists to perform an analytic “double-check” before determining their final diagnosis.
Furthermore, the clinical reasoning literature suggests that knowledge and its organization are key to expert performance.10 In diagnostic reasoning, this key knowledge has been termed “illness scripts.” Thus, the task of the aspiring expert diagnostician is to learn the key features of diseases and focus on discriminating features, starting with typical presentations of common diseases and working up to atypical presentations of uncommon diseases.
Engaging in deliberate practice, seeking feedback on diagnostic accuracy, and reflecting upon your own reasoning process can provide valuable information for improving future diagnostic reasoning. The ultimate goal of these practices is to enhance diagnostic skills in order to avoid errors and improve patient care.
Bottom Line
Diagnosis is a challenging task. Diagnostic accuracy may be enhanced by expanding the learner’s knowledge of illness scripts and using an analytic double-check to confirm initial diagnoses determined by nonanalytic reasoning.
Drs. Rendon, Roesch, and Rao are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Rencic is a hospitalist in the department of internal medicine at Tufts University School of Medicine in Boston.
References
- Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. 2005;39(1):98-106.
- Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217-2225.
- Nendaz MR, Bordage G. Promoting diagnostic problem representation. Med Educ. 2002;36(8):760-766.
- Norman GR, Eva KW. Diagnostic error and clinical reasoning. Med Educ. 2010;44(1):94-100.
- Schön DA. The Reflective Practitioner: How Professionals Think in Action. London: Temple Smith; 1983.
- Croskerry P. Achieving quality in clinical decision making: cognitive strategies and detection of bias. Acad Emerg Med. 2002;9(11):1184-1204.
- Van Someren MW, Burnard YF, Sandberg JAC. The Think Aloud Method: A Practical Guide to Modelling Cognitive Processes. London: Academic Press; 1994.
- Ericsson KA, Krampe RT, Tesch-Romer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363-406.
- Mamede S, Schmidt HG, Penaforte JC. Effects of reflective practice on the accuracy of medical diagnoses. Med Educ. 2008;42(5):468-475.
- Elstein, AS, Shulman LS, Sprafka SA. Medical Problem Solving: An Analysis of Clinical Reasoning. Cambridge, Mass.: Harvard University Press; 1978.
- Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med. 2010;85(7):1118-1124.
- Rencic J. Twelve tips for teaching expertise in clinical reasoning. Med Teach. 2011;33(11):887-892.
Case
A 67-year-old man presents to the hospital with persistent, subjective fevers and malaise for one month, subacute onset of dyspnea, and nonproductive cough for the preceding six days. The patient is a nonsmoker, denies sick contacts, and has had no foreign travel. What would be the best approach to making the diagnosis while working to enhance diagnostic skills?
Diagnostic Reasoning
With clinical experience, making a diagnosis can become so routine that physicians might not contemplate their problem-solving strategies. Diagnostic reasoning is the process of thinking about a clinical problem to form a diagnosis. Experienced clinicians typically rely upon nonanalytic reasoning (i.e., pattern recognition) for straightforward problems, reverting to analytic reasoning if a pattern is not recognized.
The literature describes five steps in the reasoning process (see Figure 1). In the early stages of data collection, hypotheses emerge that feed back into data collection behaviors as the clinician seeks confirmatory evidence. This complex interplay between data collection and hypothesis generation/elimination leads to a more clearly defined understanding of the patient’s presentation. The synthesis of the patient’s presentation, including epidemiologic risk factors, symptoms, signs, and laboratory and radiologic studies, is called the “problem representation.” After a clinician conceives the problem representation, he or she reviews the mental representations of diseases (i.e., illness scripts) to determine hypotheses by finding disease presentations that best match the formulated problem representation (see Figure 2).
Analytic and nonanalytic reasoning. In what is known as the dual process theory, diagnostic reasoning is believed to occur both analytically and nonanalytically.1 Nonanalytic reasoning is often exemplified by rapid, subconscious “pattern recognition” and is developed through clinical experience and other nonclinical learning experiences (e.g. reading).
Conversely, analytic reasoning, the “slow,” conscious, cognitive processing, is typically utilized when a patient presentation is complicated or does not fit a known disease pattern. Clinicians apply both strategies to make diagnoses in evaluating complex cases.
In the outlined case, while the symptoms of fever and cough might lead to the diagnosis of community-acquired pneumonia (CAP), the time course seems unusually long. This atypical pattern for CAP could trigger analytic reasoning, leading to new considerations such as tuberculosis (TB).
Case Continued
On examination, the patient has severe rigors and diaphoresis, as well as a fever of 39.4°C and a heart rate of 102 bpm. Full examination discloses mild end-expiratory wheezes and bronchial breath sounds in the right lower lobe. The remainder of his examination is normal. Labs reveal WBC 8.5x103, hemoglobin 11g/dL, MCV of 92 fL, and platelet count 22,000 mm3. Blood cultures, sputum cultures, and respiratory virus microarray are normal. The chest X-ray (CXR) is unremarkable.
Further history reveals that the patient is a sheepherder living in a primitive earthen structure in the rural mountains of western New Mexico.
Problem representation revisited. With additional historical, laboratory, and radiological data collected, further interpretation and synthesis occur. Salient elements are highlighted and prioritized, irrelevant details are discarded, and data of uncertain relevance are reevaluated as additional data are gathered. The problem representation—an interpreted, subjective mental model of a patient’s clinical presentation—is updated and reformulated. The verbal expression of the problem representation is variously called the assessment, summary statement, or “one-liner.” Within this summary statement, and fundamental to the creation of a strong problem representation, is the incorporation of “semantic qualifiers.”
“Semantic qualifiers” (e.g. acute vs. chronic or unremitting vs. relapsing) are paired, opposing descriptive adjectives that can be used to compare and contrast diagnostic considerations.² Clinicians distinguish between diseases using key signs and symptoms and use these descriptors to assist with this discrimination in hypothesis generation. An example for this patient would be: A 67-year-old sheepherder living in rural New Mexico presents with persistent fevers and malaise for one month, along with subacute development of nonproductive cough and dyspnea, sepsis, anemia, and thrombocytopenia.
Note how the incorporation of epidemiologic information (sheepherder living in an earthen structure in rural New Mexico) creates a context in which the additional problems can be framed (persistent malaise, subacute cough). In this case, the persistent fevers help the clinician to narrow possibilities in the differential diagnosis and create focused hypotheses.
Although the benefit of teaching accurate and thorough problem representation seems self-evident, studies have not demonstrated that improved problem representation enhances diagnostic accuracy; however, we believe that there is still value in adapting and teaching this skill.3
Hypothesis refinement and the differential diagnosis. Initial hypotheses occur early in data collection, as the patient’s history and physical examination findings trigger connections to clinicians’ bank of known diseases (e.g. orthopnea triggers congestive heart failure). As the clinician collects additional data, he or she refines these hypotheses, changing the likelihood based on “fit” of the problem representation with known diseases or illness scripts.
When employing analytic reasoning processes, clinicians may benefit from using organizational frameworks to assist with hypothesis generation (see Table 1). For this patient, possible hypotheses could include CAP, TB, lymphoma, lung neoplasm, or other indolent pulmonary infection.
Illness scripts. Once discrete hypotheses (e.g. CAP, pulmonary embolism) have been generated, clinicians need a method to accurately compare disease processes. This can be done through the use of an illness script. Illness scripts are mental representations of diseases and are likely to include epidemiology, typical and atypical patterns of presentation, and distinguishing features.
For example, a clinician’s illness script for a typical presentation of bacterial CAP likely includes fever, productive cough, pleuritic chest discomfort, and infiltrate on CXR. Clinician educators who teach illness scripts should ensure that students understand that diseases have atypical presentations, even though they may only teach them the prototypical one. Conceptualizing diseases in this fashion allows clinicians to seek the disease with the “script” that best matches the patient’s story (i.e., clinical presentation).
In this case, the clinician is now thinking of causes of persistent fever + nonproductive cough + dyspnea + anemia + thrombocytopenia; possibilities include lymphoma or unusual infection (e.g. tick-borne relapsing fever, or TBRF).
Case Resolution and Script Selection
As the clinician processes the case, a known illness script of TBRF matches the patient’s clinical presentation, and a peripheral smear is ordered. The smear reveals presence of spirochetal organisms, later confirmed by PCR to be Borrelia hermsii, confirming the diagnosis of TBRF.
Errors in Clinical Reasoning
Although most clinicians are quite accurate in typical presentations of common diseases, they are more likely to commit diagnostic errors when faced with uncommon diseases, atypical presentations, and/or challenging contexts. The following sections categorize a selection of some common errors and offer some expert opinion from the literature on avoiding them.
Common diagnostic errors. Clinicians use heuristics, or mental shortcuts, which can occasionally induce diagnostic errors. By definition, the fundamental problem in all diagnostic error is premature closure, or acceptance of a diagnosis before it is fully verified. In the case presented, the clinician may have accepted the diagnosis of CAP without recognizing other possible diagnoses.
Two common heuristics/biases that can sometimes lead to premature closure are the availability and anchoring biases. Availability bias means that the diagnoses easily thought of—and often most recent in the memory—are more likely to be assigned to a patient problem. The diagnosis of pulmonary embolism would be more “available” in a patient with fever, dyspnea, and normal CXR, especially if the clinician recently had seen a patient with PE. Anchoring bias occurs when early information is relied upon to make clinical judgments and the clinician fixates on a diagnosis despite acquiring additional or contrary information. For example, a clinician may rely upon a diagnosis of CAP based on the sign-out from a colleague, despite the one-month history of symptoms, rather than broadening the differential.
Clinician-focused methods to reduce diagnostic errors. Multiple methods exist that may mitigate diagnostic errors, although definitive proof of their value is still lacking, owing to the difficulty involved in studying such errors due to the multitude of causes.4 In our opinion, building a mental database of illness scripts by reading and seeing patients, as well as being metacognitive, are the best methods for individual clinicians to use to reduce their errors (see “deliberate practice” below).
Metacognition, or thinking about one’s thinking, is another method of reducing errors and can be characterized by “reflection in action” (reflection in real time) and “reflection on action” (reflection after an event).5 For example, taking a few moments at the end of a week on clinical service to reflect on the hospital course and diagnostic paths of the most complex patient presentations (reflection on action) is an exercise used to reduce errors.
For reflection in action, a clinician may pause when confronted with paradoxical findings for a current patient’s presentation (e.g. elevated jugular veinous pressure and crackles on exam but normal b-type natriuretic peptide), and “think aloud” (see below) to ensure he or she is processing all of the appropriate elements of the case.5
In the case presented above, the time course might have initiated reflection into erroneous decision-making at the moment the clinician thought that CAP was a possibility (reflection in action). Although direct evidence is inconclusive as to whether these techniques improve diagnostic accuracy, engaging in metacognitive exercises remains a cornerstone of seasoned clinical reasoning experts.6
Teaching and Learning Principles
Making a commitment. During a patient presentation, it is often helpful to ask a learner to develop a two- to four-item prioritized differential diagnosis list based on likelihood and/or lethality. Have the learner describe which diagnosis is most likely (i.e., the working diagnosis), in addition to the reasons “for” or “against” certain hypotheses. Once the diagnosis has been determined, combine commitment with an exercise in metacognition by asking the learner, “Why do you think that your initial diagnosis of Q-fever was incorrect?” Clinical educators may then follow up with teaching pearls and their approach to this type of case (see Table 1).
Think aloud: In this method, an instructor expresses his or her thoughts aloud in real time.7 By modeling this technique, attending physicians allow learners to observe the process of developing a differential diagnosis and plan. For example, during the admission process, instructors could verbalize their approach to fever in a systematic fashion (see Table 1) after the trainee has completed the presentation: “At this point I am considering an infectious cause such as pneumonia, given the respiratory symptoms, although the one-month history of fever and malaise makes me think that I should keep neoplasm and an unusual infection on my list of possibilities.”
Conversely, instructors can ask trainees to voice their thoughts aloud to better understand their reasoning processes. By using this method, instructors can also support, correct, or reinforce the trainees’ appropriate use of knowledge in the clinical reasoning process.
Deliberate practice. To improve diagnostic skills, trainees must engage in deliberate practice, defined as intentional, repetitious practice aimed at improving performance.8 To facilitate this, a trainee should evaluate as many patients as possible and present to an experienced clinician with subsequent feedback. Trainees are likely to miss subtle historical or examination points (e.g. the history of sheepherding) because their illness scripts are limited or incompletely developed. Teachers should emphasize the importance of developing broad and deep illness scripts, so learners will, hopefully, become more aware of their limitations and recognize what they do not know.
Key Takeaways
Clinicians solve diagnostic problems using both nonanalytic and analytic reasoning processes. Although evidence is inconclusive, some clinical reasoning experts suggest the use of reflective strategies to enhance diagnostic accuracy, especially in complicated cases.9 To prevent premature closure, we encourage hospitalists to perform an analytic “double-check” before determining their final diagnosis.
Furthermore, the clinical reasoning literature suggests that knowledge and its organization are key to expert performance.10 In diagnostic reasoning, this key knowledge has been termed “illness scripts.” Thus, the task of the aspiring expert diagnostician is to learn the key features of diseases and focus on discriminating features, starting with typical presentations of common diseases and working up to atypical presentations of uncommon diseases.
Engaging in deliberate practice, seeking feedback on diagnostic accuracy, and reflecting upon your own reasoning process can provide valuable information for improving future diagnostic reasoning. The ultimate goal of these practices is to enhance diagnostic skills in order to avoid errors and improve patient care.
Bottom Line
Diagnosis is a challenging task. Diagnostic accuracy may be enhanced by expanding the learner’s knowledge of illness scripts and using an analytic double-check to confirm initial diagnoses determined by nonanalytic reasoning.
Drs. Rendon, Roesch, and Rao are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Rencic is a hospitalist in the department of internal medicine at Tufts University School of Medicine in Boston.
References
- Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. 2005;39(1):98-106.
- Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217-2225.
- Nendaz MR, Bordage G. Promoting diagnostic problem representation. Med Educ. 2002;36(8):760-766.
- Norman GR, Eva KW. Diagnostic error and clinical reasoning. Med Educ. 2010;44(1):94-100.
- Schön DA. The Reflective Practitioner: How Professionals Think in Action. London: Temple Smith; 1983.
- Croskerry P. Achieving quality in clinical decision making: cognitive strategies and detection of bias. Acad Emerg Med. 2002;9(11):1184-1204.
- Van Someren MW, Burnard YF, Sandberg JAC. The Think Aloud Method: A Practical Guide to Modelling Cognitive Processes. London: Academic Press; 1994.
- Ericsson KA, Krampe RT, Tesch-Romer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363-406.
- Mamede S, Schmidt HG, Penaforte JC. Effects of reflective practice on the accuracy of medical diagnoses. Med Educ. 2008;42(5):468-475.
- Elstein, AS, Shulman LS, Sprafka SA. Medical Problem Solving: An Analysis of Clinical Reasoning. Cambridge, Mass.: Harvard University Press; 1978.
- Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med. 2010;85(7):1118-1124.
- Rencic J. Twelve tips for teaching expertise in clinical reasoning. Med Teach. 2011;33(11):887-892.
Hospitalists Can Join SHM's New 'Fight the Resistance' Campaign
In June, Eric Howell, MD, SFHM, SHM’s senior physician advisor, attended a White House forum on antibiotic resistance. That day, SHM committed to empowering hospitalists to fight antibiotic resistance through better prescribing behaviors.
In a blog post on The Hospital Leader, Dr. Howell wrote, “This isn’t limited to a single hospital. There are now more than 44,000 hospitalists nationwide and every one of us plays an important role in antibiotic stewardship. The bedside is the front line of this fight against antibiotic resistance.”
Now, hospitalists everywhere can join Dr. Howell at the front line of protecting patients from the many harms of overprescribing antibiotics, with SHM’s new
“Fight the Resistance” campaign.
At the heart of the campaign are three posters intended to remind all hospital-based staff about the need for antibiotic stewardship. The posters are available for download now, and a large-format version of one of the posters is included in the November issue of The Hospitalist.
SHM encourages hospitalists to post these posters in their hospitals as a reminder to use antibiotics only when necessary—and for only as long as necessary.
SHM will be hosting a social media-driven contest encouraging hospitalists to share pictures of the posters on the wall in their hospital, using the #FightTheResistance hashtag.
For more information, visit www.fighttheresistance.org.
In June, Eric Howell, MD, SFHM, SHM’s senior physician advisor, attended a White House forum on antibiotic resistance. That day, SHM committed to empowering hospitalists to fight antibiotic resistance through better prescribing behaviors.
In a blog post on The Hospital Leader, Dr. Howell wrote, “This isn’t limited to a single hospital. There are now more than 44,000 hospitalists nationwide and every one of us plays an important role in antibiotic stewardship. The bedside is the front line of this fight against antibiotic resistance.”
Now, hospitalists everywhere can join Dr. Howell at the front line of protecting patients from the many harms of overprescribing antibiotics, with SHM’s new
“Fight the Resistance” campaign.
At the heart of the campaign are three posters intended to remind all hospital-based staff about the need for antibiotic stewardship. The posters are available for download now, and a large-format version of one of the posters is included in the November issue of The Hospitalist.
SHM encourages hospitalists to post these posters in their hospitals as a reminder to use antibiotics only when necessary—and for only as long as necessary.
SHM will be hosting a social media-driven contest encouraging hospitalists to share pictures of the posters on the wall in their hospital, using the #FightTheResistance hashtag.
For more information, visit www.fighttheresistance.org.
In June, Eric Howell, MD, SFHM, SHM’s senior physician advisor, attended a White House forum on antibiotic resistance. That day, SHM committed to empowering hospitalists to fight antibiotic resistance through better prescribing behaviors.
In a blog post on The Hospital Leader, Dr. Howell wrote, “This isn’t limited to a single hospital. There are now more than 44,000 hospitalists nationwide and every one of us plays an important role in antibiotic stewardship. The bedside is the front line of this fight against antibiotic resistance.”
Now, hospitalists everywhere can join Dr. Howell at the front line of protecting patients from the many harms of overprescribing antibiotics, with SHM’s new
“Fight the Resistance” campaign.
At the heart of the campaign are three posters intended to remind all hospital-based staff about the need for antibiotic stewardship. The posters are available for download now, and a large-format version of one of the posters is included in the November issue of The Hospitalist.
SHM encourages hospitalists to post these posters in their hospitals as a reminder to use antibiotics only when necessary—and for only as long as necessary.
SHM will be hosting a social media-driven contest encouraging hospitalists to share pictures of the posters on the wall in their hospital, using the #FightTheResistance hashtag.
For more information, visit www.fighttheresistance.org.
Society of Hospital Medicine Resources Provide Quality Improvement Tips
Whether you’ve been tasked with leading a major quality improvement program or simply want to make a few things better for your patients, SHM has resources for every scale of quality improvement initiative, all created by national experts in their fields.
1. Attend an SHM Quality Improvement Webinar
The last of SHM’s live quality improvement webinars, “Elevating Provider Experience to Improve Patient Experience,” will be presented at 2 p.m. EST on Nov. 11, by Mark Rudolph, MD, SFHM. You can visit the archives of our other quality improvement webinars on topics like improving patient discharge, managing diabetes in the hospital, and general principles of quality improvement.
2. Tune in to RADEO: SHM’s New Opioid Stewardship Mentored Implementation Program
SHM has introduced RADEO: Reducing Adverse Drug Events related to Opioids, a new implementation guide and mentored implementation program designed to empower hospitalists to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression, and death.
SHM is recruiting now for participants in the mentored implementation program, and the guide is available online.
3. Download a New QI Resource
When you download a quality improvement toolkit or resource from SHM, you can be confident you are getting the best guidance from the national authorities on improving care for hospitalized patients.
SHM provides materials on the most pressing issues in hospital medicine, including:
- End-of-life care;
- Opioid monitoring;
- Antibiotic stewardship;
- Post-acute care;
- Veinous thromboembolism (VTE);
- Pain management; and
- Congestive heart failure (CHF).
To download, visit www.hospitalmedicine.org/qi.
Whether you’ve been tasked with leading a major quality improvement program or simply want to make a few things better for your patients, SHM has resources for every scale of quality improvement initiative, all created by national experts in their fields.
1. Attend an SHM Quality Improvement Webinar
The last of SHM’s live quality improvement webinars, “Elevating Provider Experience to Improve Patient Experience,” will be presented at 2 p.m. EST on Nov. 11, by Mark Rudolph, MD, SFHM. You can visit the archives of our other quality improvement webinars on topics like improving patient discharge, managing diabetes in the hospital, and general principles of quality improvement.
2. Tune in to RADEO: SHM’s New Opioid Stewardship Mentored Implementation Program
SHM has introduced RADEO: Reducing Adverse Drug Events related to Opioids, a new implementation guide and mentored implementation program designed to empower hospitalists to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression, and death.
SHM is recruiting now for participants in the mentored implementation program, and the guide is available online.
3. Download a New QI Resource
When you download a quality improvement toolkit or resource from SHM, you can be confident you are getting the best guidance from the national authorities on improving care for hospitalized patients.
SHM provides materials on the most pressing issues in hospital medicine, including:
- End-of-life care;
- Opioid monitoring;
- Antibiotic stewardship;
- Post-acute care;
- Veinous thromboembolism (VTE);
- Pain management; and
- Congestive heart failure (CHF).
To download, visit www.hospitalmedicine.org/qi.
Whether you’ve been tasked with leading a major quality improvement program or simply want to make a few things better for your patients, SHM has resources for every scale of quality improvement initiative, all created by national experts in their fields.
1. Attend an SHM Quality Improvement Webinar
The last of SHM’s live quality improvement webinars, “Elevating Provider Experience to Improve Patient Experience,” will be presented at 2 p.m. EST on Nov. 11, by Mark Rudolph, MD, SFHM. You can visit the archives of our other quality improvement webinars on topics like improving patient discharge, managing diabetes in the hospital, and general principles of quality improvement.
2. Tune in to RADEO: SHM’s New Opioid Stewardship Mentored Implementation Program
SHM has introduced RADEO: Reducing Adverse Drug Events related to Opioids, a new implementation guide and mentored implementation program designed to empower hospitalists to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression, and death.
SHM is recruiting now for participants in the mentored implementation program, and the guide is available online.
3. Download a New QI Resource
When you download a quality improvement toolkit or resource from SHM, you can be confident you are getting the best guidance from the national authorities on improving care for hospitalized patients.
SHM provides materials on the most pressing issues in hospital medicine, including:
- End-of-life care;
- Opioid monitoring;
- Antibiotic stewardship;
- Post-acute care;
- Veinous thromboembolism (VTE);
- Pain management; and
- Congestive heart failure (CHF).
To download, visit www.hospitalmedicine.org/qi.
Start Planning for Hospital Medicine 2016
At the end of the year, many hospitalists still have funds left in their CME stipends. Now is the time to plan for 2016.
SHM’s annual meeting, Hospital Medicine 2016 (HM16), is the premier destination for hospitalists looking to brush up on skills, learn the latest clinical and management concepts, and grow their network in a growing field. Last year, more than one in 10 meeting attendees said they would recommend SHM’s annual meeting to a colleague.
The meeting is divided into two sections: a day of in-depth pre-courses and the official program. This year’s pre-courses include:
- ABIM Maintenance of Certification and board preparation;
- Bedside procedures;
- Point-of-care ultrasound for the hospitalist;
- Perioperative Medicine: Spy into the world of perioperative medicine;
- The Highly Effective Hospital Medicine Group: Using SHM’s key characteristics to drive performance; and
- Advanced interactive critical care.
The official meeting’s content is broken up into separate tracks, making it easier for hospitalists to schedule their sessions based on their roles and interests in the hospital medicine movement. HM16 tracks feature many favorites, with updated content and three entirely new tracks.
- Academic/Research: This combined track is for hospitalists who practice in academic medical centers, as well as for those in any setting who are interested in research.
- Clinical: The clinical track focuses on essential topics in adult clinical medicine, emphasizing recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery.
- NEW! Co-Management/Perioperative Medicine: This hospitalist core competency increases in complexity, yet many physicians were not even taught the basics in residency. This new track explores the perioperative and consultative medicine questions that challenge hospitalists on a daily basis.
- Doctor-Patient Relationship: As service is a quality outcome, this track is dedicated to giving frontline hospitalists practical skills for success in enhancing the doctor-patient relationship and information on what to do when the therapeutic relationship fails.
- NEW! Health IT for Hospitalists: Health information technology has changed the practice of medicine. While the potential is great, the result is often inefficiency and frustration, coupled with a lack of improvement in quality and safety. All hospitalists need to properly utilize the available technology and engage in improving these systems.
- Pediatric: The 2016 pediatric track focuses on “The Edges of the Practice” and will highlight hot topics and issues for pediatric hospitalists who take care of newborns and/or adolescents.
- NEW! Post-Acute Care: The post-acute care track targets two audiences. The first—mainstream hospitalists—are increasingly being asked to assume responsibility for the full episode of care, including the post-acute care services after discharge.
- Potpourri: The potpourri track offers presentations on a variety of nonclinical topics of interest to the practicing hospitalist. Topics include medical-legal aspects of hospital medicine, best practices and strategies to improve sleep in the hospital, and personal professional optimization.
- Practice Management: The importance of organizational infrastructure related to the practice of hospital medicine is well recognized, and information in this area continues to accumulate.
- Quality: Given the importance of quality and patient safety in the delivery of healthcare, the quality track is offered to address the imperatives around development and implementation of improvement efforts in the hospital.
- Rapid Fire: The rapid fire track is designed to provide participants with “rapid bursts” of content and to address specific questions framed by the Annual Meeting Committee.
- Workshops: Workshop track topics were submitted by SHM members, peer reviewed, and selected based on their relevancy to hospitalists, designed engagement and interaction with participants, presenter experience, and clarity of submission.
- Young Hospitalists: Inspired by SHM Past President Eric Howell’s vision to increase the hospital medicine “pipeline,” this track is dedicated to new hospitalists, residents, and medical students—the future of SHM.
For details, visit www.hospitalmedicine2016.org.
Call for HM16 RIV Abstracts
Seize the opportunity to present your research, innovative ideas, and clinical stories to a national audience at HM16.
Visit the submission site for full details. To ensure success, SHM strongly recommends that you complete your submission well ahead of the deadline of Wednesday, Dec. 1, 2015, at 11:30 p.m. EST.
For details, visit www.hospitalmedicine2016.org.
At the end of the year, many hospitalists still have funds left in their CME stipends. Now is the time to plan for 2016.
SHM’s annual meeting, Hospital Medicine 2016 (HM16), is the premier destination for hospitalists looking to brush up on skills, learn the latest clinical and management concepts, and grow their network in a growing field. Last year, more than one in 10 meeting attendees said they would recommend SHM’s annual meeting to a colleague.
The meeting is divided into two sections: a day of in-depth pre-courses and the official program. This year’s pre-courses include:
- ABIM Maintenance of Certification and board preparation;
- Bedside procedures;
- Point-of-care ultrasound for the hospitalist;
- Perioperative Medicine: Spy into the world of perioperative medicine;
- The Highly Effective Hospital Medicine Group: Using SHM’s key characteristics to drive performance; and
- Advanced interactive critical care.
The official meeting’s content is broken up into separate tracks, making it easier for hospitalists to schedule their sessions based on their roles and interests in the hospital medicine movement. HM16 tracks feature many favorites, with updated content and three entirely new tracks.
- Academic/Research: This combined track is for hospitalists who practice in academic medical centers, as well as for those in any setting who are interested in research.
- Clinical: The clinical track focuses on essential topics in adult clinical medicine, emphasizing recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery.
- NEW! Co-Management/Perioperative Medicine: This hospitalist core competency increases in complexity, yet many physicians were not even taught the basics in residency. This new track explores the perioperative and consultative medicine questions that challenge hospitalists on a daily basis.
- Doctor-Patient Relationship: As service is a quality outcome, this track is dedicated to giving frontline hospitalists practical skills for success in enhancing the doctor-patient relationship and information on what to do when the therapeutic relationship fails.
- NEW! Health IT for Hospitalists: Health information technology has changed the practice of medicine. While the potential is great, the result is often inefficiency and frustration, coupled with a lack of improvement in quality and safety. All hospitalists need to properly utilize the available technology and engage in improving these systems.
- Pediatric: The 2016 pediatric track focuses on “The Edges of the Practice” and will highlight hot topics and issues for pediatric hospitalists who take care of newborns and/or adolescents.
- NEW! Post-Acute Care: The post-acute care track targets two audiences. The first—mainstream hospitalists—are increasingly being asked to assume responsibility for the full episode of care, including the post-acute care services after discharge.
- Potpourri: The potpourri track offers presentations on a variety of nonclinical topics of interest to the practicing hospitalist. Topics include medical-legal aspects of hospital medicine, best practices and strategies to improve sleep in the hospital, and personal professional optimization.
- Practice Management: The importance of organizational infrastructure related to the practice of hospital medicine is well recognized, and information in this area continues to accumulate.
- Quality: Given the importance of quality and patient safety in the delivery of healthcare, the quality track is offered to address the imperatives around development and implementation of improvement efforts in the hospital.
- Rapid Fire: The rapid fire track is designed to provide participants with “rapid bursts” of content and to address specific questions framed by the Annual Meeting Committee.
- Workshops: Workshop track topics were submitted by SHM members, peer reviewed, and selected based on their relevancy to hospitalists, designed engagement and interaction with participants, presenter experience, and clarity of submission.
- Young Hospitalists: Inspired by SHM Past President Eric Howell’s vision to increase the hospital medicine “pipeline,” this track is dedicated to new hospitalists, residents, and medical students—the future of SHM.
For details, visit www.hospitalmedicine2016.org.
Call for HM16 RIV Abstracts
Seize the opportunity to present your research, innovative ideas, and clinical stories to a national audience at HM16.
Visit the submission site for full details. To ensure success, SHM strongly recommends that you complete your submission well ahead of the deadline of Wednesday, Dec. 1, 2015, at 11:30 p.m. EST.
For details, visit www.hospitalmedicine2016.org.
At the end of the year, many hospitalists still have funds left in their CME stipends. Now is the time to plan for 2016.
SHM’s annual meeting, Hospital Medicine 2016 (HM16), is the premier destination for hospitalists looking to brush up on skills, learn the latest clinical and management concepts, and grow their network in a growing field. Last year, more than one in 10 meeting attendees said they would recommend SHM’s annual meeting to a colleague.
The meeting is divided into two sections: a day of in-depth pre-courses and the official program. This year’s pre-courses include:
- ABIM Maintenance of Certification and board preparation;
- Bedside procedures;
- Point-of-care ultrasound for the hospitalist;
- Perioperative Medicine: Spy into the world of perioperative medicine;
- The Highly Effective Hospital Medicine Group: Using SHM’s key characteristics to drive performance; and
- Advanced interactive critical care.
The official meeting’s content is broken up into separate tracks, making it easier for hospitalists to schedule their sessions based on their roles and interests in the hospital medicine movement. HM16 tracks feature many favorites, with updated content and three entirely new tracks.
- Academic/Research: This combined track is for hospitalists who practice in academic medical centers, as well as for those in any setting who are interested in research.
- Clinical: The clinical track focuses on essential topics in adult clinical medicine, emphasizing recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery.
- NEW! Co-Management/Perioperative Medicine: This hospitalist core competency increases in complexity, yet many physicians were not even taught the basics in residency. This new track explores the perioperative and consultative medicine questions that challenge hospitalists on a daily basis.
- Doctor-Patient Relationship: As service is a quality outcome, this track is dedicated to giving frontline hospitalists practical skills for success in enhancing the doctor-patient relationship and information on what to do when the therapeutic relationship fails.
- NEW! Health IT for Hospitalists: Health information technology has changed the practice of medicine. While the potential is great, the result is often inefficiency and frustration, coupled with a lack of improvement in quality and safety. All hospitalists need to properly utilize the available technology and engage in improving these systems.
- Pediatric: The 2016 pediatric track focuses on “The Edges of the Practice” and will highlight hot topics and issues for pediatric hospitalists who take care of newborns and/or adolescents.
- NEW! Post-Acute Care: The post-acute care track targets two audiences. The first—mainstream hospitalists—are increasingly being asked to assume responsibility for the full episode of care, including the post-acute care services after discharge.
- Potpourri: The potpourri track offers presentations on a variety of nonclinical topics of interest to the practicing hospitalist. Topics include medical-legal aspects of hospital medicine, best practices and strategies to improve sleep in the hospital, and personal professional optimization.
- Practice Management: The importance of organizational infrastructure related to the practice of hospital medicine is well recognized, and information in this area continues to accumulate.
- Quality: Given the importance of quality and patient safety in the delivery of healthcare, the quality track is offered to address the imperatives around development and implementation of improvement efforts in the hospital.
- Rapid Fire: The rapid fire track is designed to provide participants with “rapid bursts” of content and to address specific questions framed by the Annual Meeting Committee.
- Workshops: Workshop track topics were submitted by SHM members, peer reviewed, and selected based on their relevancy to hospitalists, designed engagement and interaction with participants, presenter experience, and clarity of submission.
- Young Hospitalists: Inspired by SHM Past President Eric Howell’s vision to increase the hospital medicine “pipeline,” this track is dedicated to new hospitalists, residents, and medical students—the future of SHM.
For details, visit www.hospitalmedicine2016.org.
Call for HM16 RIV Abstracts
Seize the opportunity to present your research, innovative ideas, and clinical stories to a national audience at HM16.
Visit the submission site for full details. To ensure success, SHM strongly recommends that you complete your submission well ahead of the deadline of Wednesday, Dec. 1, 2015, at 11:30 p.m. EST.
For details, visit www.hospitalmedicine2016.org.
Mark Your Calendar: Dates for Hospitalists
There are always ways to get more involved in the hospital medicine movement, and deadlines for some of them are approaching:
- November 22 – Fellows and Senior Fellows Applications: Interested in earning the only designations specifically for hospitalists? Start your application today; it can take some time to assemble and submit.
- December 31 – Membership Ambassadors: Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
- February 15, 2016 – Student Hospitalist Scholarship: Are you an aspiring medical student who’s joined the hospitalist movement? Apply for the Student Hospitalist Scholarship and receive a stipend to support your research over the summer of 2016.
There are always ways to get more involved in the hospital medicine movement, and deadlines for some of them are approaching:
- November 22 – Fellows and Senior Fellows Applications: Interested in earning the only designations specifically for hospitalists? Start your application today; it can take some time to assemble and submit.
- December 31 – Membership Ambassadors: Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
- February 15, 2016 – Student Hospitalist Scholarship: Are you an aspiring medical student who’s joined the hospitalist movement? Apply for the Student Hospitalist Scholarship and receive a stipend to support your research over the summer of 2016.
There are always ways to get more involved in the hospital medicine movement, and deadlines for some of them are approaching:
- November 22 – Fellows and Senior Fellows Applications: Interested in earning the only designations specifically for hospitalists? Start your application today; it can take some time to assemble and submit.
- December 31 – Membership Ambassadors: Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
- February 15, 2016 – Student Hospitalist Scholarship: Are you an aspiring medical student who’s joined the hospitalist movement? Apply for the Student Hospitalist Scholarship and receive a stipend to support your research over the summer of 2016.
Society of Hospital Medicine Nearing 15,000 Members
More than 14,000 hospitalists are now members of SHM, and we expect to welcome the 15,000th member early in 2016. SHM will celebrate this milestone for the hospital medicine movement at Hospital Medicine 2016, so stay tuned to learn the identity of the 15,000th member!
More than 14,000 hospitalists are now members of SHM, and we expect to welcome the 15,000th member early in 2016. SHM will celebrate this milestone for the hospital medicine movement at Hospital Medicine 2016, so stay tuned to learn the identity of the 15,000th member!
More than 14,000 hospitalists are now members of SHM, and we expect to welcome the 15,000th member early in 2016. SHM will celebrate this milestone for the hospital medicine movement at Hospital Medicine 2016, so stay tuned to learn the identity of the 15,000th member!
Holiday Discounts for SHM Merchandise
Looking for the perfect holiday gift for a hospitalist friend or colleague? Think about a stainless steel SHM coffee tumbler or a cozy SHM hoodie. All SHM merchandise is currently 10% off. To start your SHM shopping, click “eStore”.
Looking for the perfect holiday gift for a hospitalist friend or colleague? Think about a stainless steel SHM coffee tumbler or a cozy SHM hoodie. All SHM merchandise is currently 10% off. To start your SHM shopping, click “eStore”.
Looking for the perfect holiday gift for a hospitalist friend or colleague? Think about a stainless steel SHM coffee tumbler or a cozy SHM hoodie. All SHM merchandise is currently 10% off. To start your SHM shopping, click “eStore”.
Maintenance of Certification Process Should Ensure Physicians Deliver Quality Care

When the American Board of Internal Medicine (ABIM) announced changes to its Maintenance of Certification (MOC) process in early 2014, the response was overwhelmingly negative. Individual physicians and medical societies criticized ABIM for adding significant time and expense to MOC, and loudly challenged the program’s effectiveness, relevance, and value.
After months of backlash, ABIM issued an apology in February and rolled back or delayed some of the MOC changes. In a letter to diplomates, ABIM President and Chief Executive Officer Richard J. Baron, MD, acknowledged that some of the criticism of ABIM was legitimate and that “some believe ABIM has turned a deaf ear to practicing physicians.” He said, “We got it wrong and sincerely apologize. We are sorry.”
Despite ABIM’s apology, the conversation about MOC continues to rage—and for good reason.
Though the medical community needs a formal process like MOC to ensure that physicians at all stages of their careers are knowledgeable, qualified, and capable of handling their patients’ care, it’s not clear that the current MOC process delivers those outcomes. I’m certain there are individuals who, over the course of seven or 10 years, complete their training modules, pass an exam, and still do not practice according to the most current, evidence-based guidelines. Just because we know the information needed to pass an exam doesn’t mean we actively use that knowledge to deliver quality care to patients.
To bridge this gap, certifying organizations like ABIM and the American Board of Family Medicine (ABFM) should consider how to better integrate the MOC process into physicians’ daily practice of medicine, so that actual patient care and outcomes are used to determine whether or not an individual is recertified.
Done well, this integration would solve multiple problems.
New Approach Required
Instead of measuring our test-taking ability, it would tie certification directly to how we care for patients: weighing whether or not we use current, evidence-based practices to achieve optimal outcomes. It also would address the problem of testing physicians’ knowledge on topics that fall outside their normal scope of practice. For example, as I have focused my career in hospital medicine, I no longer practice in pediatrics or OB/GYN, but those topics are still included in my family medicine board examination. When I was recertified in 2013, I spent a lot more time preparing for that section of the exam than for the areas in which I practice daily.
In fact, a better-integrated MOC process could help reduce the significant investment of time and money associated with recertification. Not only do most physicians need to take time off from practicing to prepare for the exam, but we also must bear the direct costs of the test itself, along with the necessary test preparation materials.
According to a study released in July by the University of California at San Francisco and Stanford University, ABIM’s latest MOC requirements will cost individual physicians more than $23,600 over 10 years, with the costs in some subspecialties exceeding $40,000. Of those costs, $9 out of every $10 is associated with the demand the process makes on a physician’s time. In announcing the study, the lead author said, “We estimate that ABIM MOC will cost 33.7 million physician-hours over 10 years. Efforts to reform MOC and lower its costs should focus on making the most efficient use of physician time.”
A Simple SPARK
Until MOC is reformed, physicians seeking recertification have no option but to continue under the current process. To help members with test preparation, SHM has launched SPARK, an online tool to prepare physicians for the ABIM/ABFM Focused Practice in Hospital Medicine (FPHM) exam. It is available to SHM members at a significant discount. SPARK features 175 vignette-style, single best answer, multiple-choice questions, complete with answers, cohort comparison, discussion, references, and quizzing capabilities. This first edition targets gaps in other available tools like palliative care, ethics and decision-making, patient safety, peri-operative care, consultative co-management, quality, cost, and clinical reasoning.
The first iteration of SPARK has launched. From here, we will expand SPARK to include preparation materials for the remainder of the family medicine/internal medicine sections of the MOC exam. As the only FPHM MOC preparation tool created by hospitalists for hospitalists, we believe SPARK provides an effective and more affordable alternative to the test preparation tools offered directly through ABIM and ABFM.
Although the concept of MOC is a valid one, the process should be improved to ensure that physicians maintain the knowledge necessary to deliver high quality care. As we work toward further reforms, we hope SPARK will ease the preparation process for our members.

When the American Board of Internal Medicine (ABIM) announced changes to its Maintenance of Certification (MOC) process in early 2014, the response was overwhelmingly negative. Individual physicians and medical societies criticized ABIM for adding significant time and expense to MOC, and loudly challenged the program’s effectiveness, relevance, and value.
After months of backlash, ABIM issued an apology in February and rolled back or delayed some of the MOC changes. In a letter to diplomates, ABIM President and Chief Executive Officer Richard J. Baron, MD, acknowledged that some of the criticism of ABIM was legitimate and that “some believe ABIM has turned a deaf ear to practicing physicians.” He said, “We got it wrong and sincerely apologize. We are sorry.”
Despite ABIM’s apology, the conversation about MOC continues to rage—and for good reason.
Though the medical community needs a formal process like MOC to ensure that physicians at all stages of their careers are knowledgeable, qualified, and capable of handling their patients’ care, it’s not clear that the current MOC process delivers those outcomes. I’m certain there are individuals who, over the course of seven or 10 years, complete their training modules, pass an exam, and still do not practice according to the most current, evidence-based guidelines. Just because we know the information needed to pass an exam doesn’t mean we actively use that knowledge to deliver quality care to patients.
To bridge this gap, certifying organizations like ABIM and the American Board of Family Medicine (ABFM) should consider how to better integrate the MOC process into physicians’ daily practice of medicine, so that actual patient care and outcomes are used to determine whether or not an individual is recertified.
Done well, this integration would solve multiple problems.
New Approach Required
Instead of measuring our test-taking ability, it would tie certification directly to how we care for patients: weighing whether or not we use current, evidence-based practices to achieve optimal outcomes. It also would address the problem of testing physicians’ knowledge on topics that fall outside their normal scope of practice. For example, as I have focused my career in hospital medicine, I no longer practice in pediatrics or OB/GYN, but those topics are still included in my family medicine board examination. When I was recertified in 2013, I spent a lot more time preparing for that section of the exam than for the areas in which I practice daily.
In fact, a better-integrated MOC process could help reduce the significant investment of time and money associated with recertification. Not only do most physicians need to take time off from practicing to prepare for the exam, but we also must bear the direct costs of the test itself, along with the necessary test preparation materials.
According to a study released in July by the University of California at San Francisco and Stanford University, ABIM’s latest MOC requirements will cost individual physicians more than $23,600 over 10 years, with the costs in some subspecialties exceeding $40,000. Of those costs, $9 out of every $10 is associated with the demand the process makes on a physician’s time. In announcing the study, the lead author said, “We estimate that ABIM MOC will cost 33.7 million physician-hours over 10 years. Efforts to reform MOC and lower its costs should focus on making the most efficient use of physician time.”
A Simple SPARK
Until MOC is reformed, physicians seeking recertification have no option but to continue under the current process. To help members with test preparation, SHM has launched SPARK, an online tool to prepare physicians for the ABIM/ABFM Focused Practice in Hospital Medicine (FPHM) exam. It is available to SHM members at a significant discount. SPARK features 175 vignette-style, single best answer, multiple-choice questions, complete with answers, cohort comparison, discussion, references, and quizzing capabilities. This first edition targets gaps in other available tools like palliative care, ethics and decision-making, patient safety, peri-operative care, consultative co-management, quality, cost, and clinical reasoning.
The first iteration of SPARK has launched. From here, we will expand SPARK to include preparation materials for the remainder of the family medicine/internal medicine sections of the MOC exam. As the only FPHM MOC preparation tool created by hospitalists for hospitalists, we believe SPARK provides an effective and more affordable alternative to the test preparation tools offered directly through ABIM and ABFM.
Although the concept of MOC is a valid one, the process should be improved to ensure that physicians maintain the knowledge necessary to deliver high quality care. As we work toward further reforms, we hope SPARK will ease the preparation process for our members.
When the American Board of Internal Medicine (ABIM) announced changes to its Maintenance of Certification (MOC) process in early 2014, the response was overwhelmingly negative. Individual physicians and medical societies criticized ABIM for adding significant time and expense to MOC, and loudly challenged the program’s effectiveness, relevance, and value.
After months of backlash, ABIM issued an apology in February and rolled back or delayed some of the MOC changes. In a letter to diplomates, ABIM President and Chief Executive Officer Richard J. Baron, MD, acknowledged that some of the criticism of ABIM was legitimate and that “some believe ABIM has turned a deaf ear to practicing physicians.” He said, “We got it wrong and sincerely apologize. We are sorry.”
Despite ABIM’s apology, the conversation about MOC continues to rage—and for good reason.
Though the medical community needs a formal process like MOC to ensure that physicians at all stages of their careers are knowledgeable, qualified, and capable of handling their patients’ care, it’s not clear that the current MOC process delivers those outcomes. I’m certain there are individuals who, over the course of seven or 10 years, complete their training modules, pass an exam, and still do not practice according to the most current, evidence-based guidelines. Just because we know the information needed to pass an exam doesn’t mean we actively use that knowledge to deliver quality care to patients.
To bridge this gap, certifying organizations like ABIM and the American Board of Family Medicine (ABFM) should consider how to better integrate the MOC process into physicians’ daily practice of medicine, so that actual patient care and outcomes are used to determine whether or not an individual is recertified.
Done well, this integration would solve multiple problems.
New Approach Required
Instead of measuring our test-taking ability, it would tie certification directly to how we care for patients: weighing whether or not we use current, evidence-based practices to achieve optimal outcomes. It also would address the problem of testing physicians’ knowledge on topics that fall outside their normal scope of practice. For example, as I have focused my career in hospital medicine, I no longer practice in pediatrics or OB/GYN, but those topics are still included in my family medicine board examination. When I was recertified in 2013, I spent a lot more time preparing for that section of the exam than for the areas in which I practice daily.
In fact, a better-integrated MOC process could help reduce the significant investment of time and money associated with recertification. Not only do most physicians need to take time off from practicing to prepare for the exam, but we also must bear the direct costs of the test itself, along with the necessary test preparation materials.
According to a study released in July by the University of California at San Francisco and Stanford University, ABIM’s latest MOC requirements will cost individual physicians more than $23,600 over 10 years, with the costs in some subspecialties exceeding $40,000. Of those costs, $9 out of every $10 is associated with the demand the process makes on a physician’s time. In announcing the study, the lead author said, “We estimate that ABIM MOC will cost 33.7 million physician-hours over 10 years. Efforts to reform MOC and lower its costs should focus on making the most efficient use of physician time.”
A Simple SPARK
Until MOC is reformed, physicians seeking recertification have no option but to continue under the current process. To help members with test preparation, SHM has launched SPARK, an online tool to prepare physicians for the ABIM/ABFM Focused Practice in Hospital Medicine (FPHM) exam. It is available to SHM members at a significant discount. SPARK features 175 vignette-style, single best answer, multiple-choice questions, complete with answers, cohort comparison, discussion, references, and quizzing capabilities. This first edition targets gaps in other available tools like palliative care, ethics and decision-making, patient safety, peri-operative care, consultative co-management, quality, cost, and clinical reasoning.
The first iteration of SPARK has launched. From here, we will expand SPARK to include preparation materials for the remainder of the family medicine/internal medicine sections of the MOC exam. As the only FPHM MOC preparation tool created by hospitalists for hospitalists, we believe SPARK provides an effective and more affordable alternative to the test preparation tools offered directly through ABIM and ABFM.
Although the concept of MOC is a valid one, the process should be improved to ensure that physicians maintain the knowledge necessary to deliver high quality care. As we work toward further reforms, we hope SPARK will ease the preparation process for our members.
When Should Hospitalists Order Continuous Cardiac Monitoring?
Case
Two patients on continuous cardiac monitoring (CCM) are admitted to the hospital. One is a 56-year-old man with hemodynamically stable sepsis secondary to pneumonia. There is no sign of arrhythmia on initial evaluation. The second patient is a 67-year-old man with a history of coronary artery disease (CAD) admitted with chest pain. Should these patients be admitted with CCM?
Overview
CCM was first introduced in hospitals in the early 1960s for heart rate and rhythm monitoring in coronary ICUs. Since that time, CCM has been widely used in the hospital setting among critically and noncritically ill patients. Some hospitals have a limited capacity for monitoring, which is dictated by bed or technology availability. Other hospitals have the ability to monitor any patient.
Guidelines from the American College of Cardiology (ACC) in 1991 and the American Heart Association (AHA) in 2004 guide inpatient use of CCM. These guidelines make recommendations based on the likelihood of patient benefit—will likely benefit, may benefit, unlikely to benefit—and are primarily based on expert opinion; rigorous clinical trial data is not available.1,2 Based on these guidelines, patients with primary cardiac diagnoses, including acute coronary syndrome (ACS), post-cardiac surgery, and arrhythmia, are the most likely to benefit from monitoring.2,3
In practical use, many hospitalists use CCM to detect signs of hemodynamic instability.3 Currently there is no data to support the idea that CCM is a safe or equivalent method of detecting hemodynamic instability compared to close clinical evaluation and frequent vital sign measurement. In fact, physicians overestimate the utility of CCM in guiding management decisions, and witnessed clinical deterioration is a more frequent factor in the decision to escalate the level of care of a patient.3,4
Guideline Recommendations
CCM is intended to identify life-threatening arrhythmias, ischemia, and QT prolongation (see Figure 1). The AHA guidelines address which patients will benefit from CCM; the main indications include an acute cardiac diagnosis or critical illness.1
In addition, the AHA guidelines provide recommendations for the duration of monitoring. These recommendations vary from time-limited monitoring (e.g. unexplained syncope) to a therapeutic-based recommendation (e.g. high-grade atrioventricular block requiring pacemaker placement).
The guidelines also identify a subset of patients who are unlikely to benefit from monitoring (Class III), including low-risk post-operative patients, patients with rate-controlled atrial fibrillation, and patients undergoing hemodialysis without other indications for monitoring.
Several studies have examined the frequency of CCM use. In one study of 236 admissions to a community hospital general ward population, approximately 50% of the 745 monitoring days were not indicated by ACC/AHA guidelines.5 In this study, only 5% of telemetry events occurred in patients without indications, and none of these events required any specific therapy.5 Thus, improved adherence to the ACC/AHA guidelines can decrease CCM use in patients who are unlikely to benefit.
Life-threatening arrhythmia detection. Cleverley and colleagues reported that patients who suffered a cardiac arrest on noncritical care units had a higher survival to hospital discharge if they were on CCM during the event.6 However, a similar study recently showed no benefit to cardiac monitoring for in-hospital arrest if patients were monitored remotely.7 Patients who experience a cardiac arrest in a noncritical care area may benefit from direct cardiac monitoring, though larger studies are needed to assess all potential confounding effects, including nurse-to-patient ratios, location of monitoring (remote or unit-based), advanced cardiac life support response times, and whether the event was witnessed.
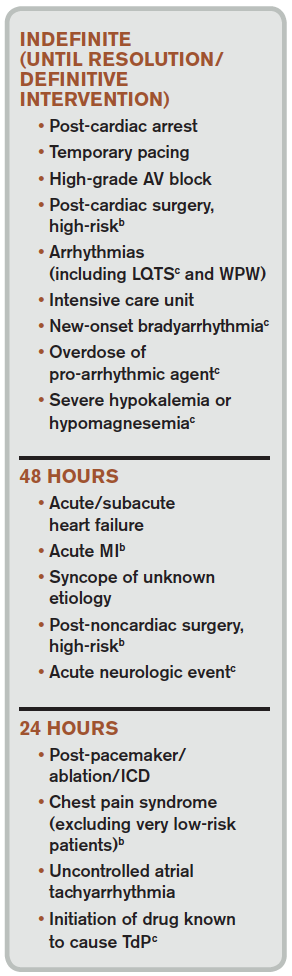
Bottom line: AHA guidelines recommend use of CCM in patients with a higher likelihood of developing a life-threatening arrhythmia, including those with an ACS, those experiencing post-cardiac arrest, or those who are critically ill. Medical ward patients who should be monitored include those with acute or subacute congestive heart failure, syncope of unknown etiology, and uncontrolled atrial fibrillation.1
Ischemia surveillance. Computerized ST-segment monitoring has been available for high-risk post-operative patients and those with acute cardiac events since the mid-1980s. When properly used, it offers the ability to detect “silent” ischemia, which is associated with increased in-hospital complications and worse patient outcomes.
Computerized ST-segment monitoring is often associated with a high rate of false positive alarms, however, and has not been universally adopted. Recommendations for its use are based on expert opinion, because no randomized trial has shown that increasing the sensitivity of ischemia detection improves patient outcomes.
Bottom line: AHA guidelines recommend ST-segment monitoring in patients with early ACS and post-acute MI as well as in patients at high risk for silent ischemia, including high-risk post-operative patients.1
QT-interval monitoring. A corrected QT-interval (QTc) greater than 0.50 milliseconds correlates with a higher risk for torsades de pointes and is associated with higher mortality. In critically ill patients in a large academic medical center, guideline-based QT-interval monitoring showed poor specificity for predicting the development of QTc prolongation; however, the risk of QTc prolongation increased with the presence of multiple risk factors.8
Bottom line: AHA guidelines recommend QT-interval monitoring in patients with risk factors for QTc-prolongation, including those starting QTc-prolonging drugs, those with overdose of pro-arrhythmic drugs, those with new-onset bradyarrhythmias, those with severe hypokalemia or hypomagnesemia, and those who have experienced acute neurologic events.1
Recommendations Outside of Guidelines
Patients admitted to medical services for noncardiac diagnoses have a high rate of telemetry use and a perceived benefit associated with cardiac monitoring.3 Although guidelines for noncardiac patients to direct hospitalists on when to use this technology are lacking, there may be some utility in monitoring certain subsets of inpatients.
Sepsis. Patients with hemodynamically stable sepsis develop atrial fibrillation at a higher rate than patients without sepsis and have higher in-hospital mortality. Patients at highest risk are those who are elderly or have severe sepsis.7 CCM can identify atrial fibrillation in real time, which may allow for earlier intervention; however, it is important to consider that other modalities, such as patient symptoms, physical exam, and standard EKG, are potentially as effective at detecting atrial fibrillation as CCM.
Bottom line: Our recommendation is to use CCM in patients who are at higher risk, including elderly patients and those with severe sepsis, until sepsis has resolved and/or the patient is hemodynamically stable for 24 hours.
Alcohol withdrawal. Patients with severe alcohol withdrawal have an increased incidence of arrhythmia and ischemia during the detoxification process. Specifically, patients with delirium tremens and seizures are at higher risk for significant QTc prolongation and tachyarrhythmias.9
Bottom line: Our recommendation is to use CCM in patients with severe alcohol withdrawal and to discontinue monitoring once withdrawal has resolved.
COPD. Patients with COPD exacerbations have a high risk of in-hospital and long-term mortality. The highest risk for mortality appears to be in patients presenting with atrial or ventricular arrhythmias and those over 65 years old.10 There is no clear evidence that beta-agonist use in COPD exacerbations increases arrhythmias other than sinus tachycardia or is associated with worse outcomes.11
Bottom line: Our recommendation is to use CCM only in patients with COPD exacerbation who have other indications as described in the AHA guidelines.
CCM Disadvantages
Alarm fatigue. Alarm fatigue is defined as the desensitization of a clinician to an alarm stimulus, resulting from sensory overload and causing the response of an alarm to be delayed or dismissed.12 In 2014, the Emergency Care Research Institute named alarm hazards as the number one health technology hazard, noting that numerous alarms on a daily basis can lead to desensitization and “alarm fatigue.”
CCM, and the overuse of CCM in particular, contribute to alarm fatigue, which can lead to patient safety issues, including delays in treatment, medication errors, and potentially death.
Increased cost. Because telemetry requires specialized equipment and trained monitoring staff, cost can be significant. In addition to equipment, cost includes time spent by providers, nurses, and technicians interpreting the images and discussing findings with consultants, as well as the additional studies obtained as a result of identified arrhythmias.
Studies on CCM cost vary widely, with conservative estimates of approximately $53 to as much as $1,400 per patient per day in some hospitals.13
Lack of specificity. Because of the high sensitivity and low specificity of CCM, use of CCM in low-risk patients without indications increases the risk of misinterpreting false-positive findings as clinically significant. This can lead to errors in management, including overtesting, unnecessary consultation with subspecialists, and the potential for inappropriate invasive procedures.1
High-Value CCM Use
Because of the low value associated with cardiac monitoring in many patients and the high sensitivity of the guidelines to capture patients at high risk for cardiac events, many hospitals have sought to limit the overuse of this technology. The most successful interventions have targeted the electronic ordering system by requiring an indication and hardwiring an order duration based on guideline recommendations. In a recent study, this intervention led to a 70% decrease in usage and reported $4.8 million cost savings without increasing the rate of in-hospital rapid response or cardiac arrest.14
Systems-level interventions to decrease inappropriate initiation and facilitate discontinuation of cardiac monitoring are a proven way to increase compliance with guidelines and decrease the overuse of CCM.
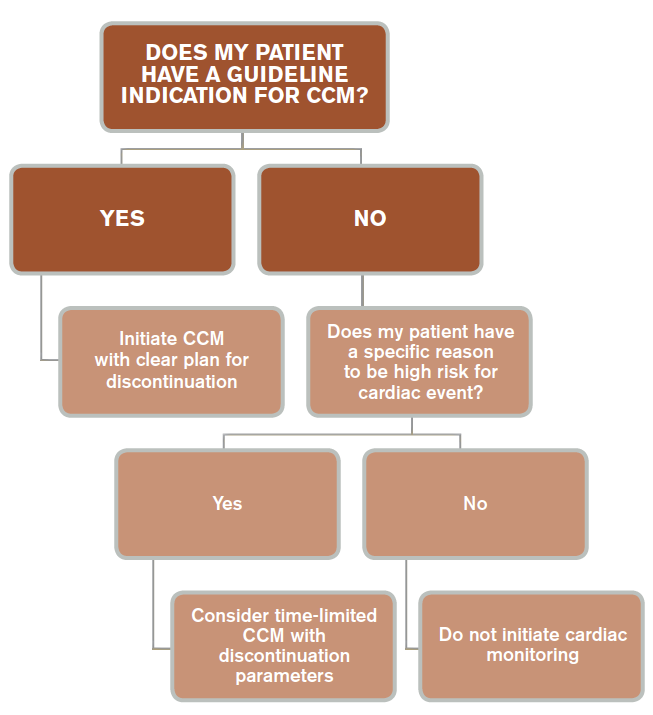
Back to the Case
According to AHA guidelines, the only patient who has an indication for CCM is the 67-year-old man with known CAD and chest pain, and, accordingly, the patient was placed on CCM. The patient underwent evaluation for ACS, and monitoring was discontinued after 24 hours when ACS was ruled out. The 56-year-old man with sepsis responded to treatment of pneumonia and was not placed on CCM.
In general, patients admitted with acute cardiac-related diseases should be placed on CCM. Guidelines are lacking with respect to many noncardiac diseases, and we recommend a time-limited duration (typically 24 hours) if CCM is ordered for a patient with a special circumstance outside of guidelines (see Figure 3).
Key Takeaway
Hospitalists should use continuous cardiac monitoring for specific indications and not routinely for all patients.
Drs. Lacy and Rendon are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Davis is a resident in internal medicine at UNM, and Dr. Tolstrup is a cardiologist at UNM.
References
- Drew BJ, Califf RM, Funk M, et al. Practice standards for electrocardiographic monitoring in hospital settings: an American Heart Association scientific statement from the Councils on Cardiovascular Nursing, Clinical Cardiology, and Cardiovascular Disease in the Young: endorsed by the International Society of Computerized Electrocardiology and the American Association of Critical-Care Nurses. Circulation. 2004;110(17):2721-2746. doi:10.1161/01.CIR.0000145144.56673.59.
- Recommended guidelines for in-hospital cardiac monitoring of adults for detection of arrhythmia. Emergency Cardiac Care Committee members. J Am Coll Cardiol. 1991;18(6):1431-1433.
- Najafi N, Auerbach A. Use and outcomes of telemetry monitoring on a medicine service. Arch Intern Med. 2012;172(17):1349-1350. doi:10.1001/archinternmed.2012.3163.
- Estrada CA, Rosman HS, Prasad NK, et al. Role of telemetry monitoring in the non-intensive care unit. Am J Cardiol. 1995;76(12):960-965.
- Curry JP, Hanson CW III, Russell MW, Hanna C, Devine G, Ochroch EA. The use and effectiveness of electrocardiographic telemetry monitoring in a community hospital general care setting. Anesth Analg. 2003;97(5):1483-1487.
- Cleverley K, Mousavi N, Stronger L, et al. The impact of telemetry on survival of in-hospital cardiac arrests in non-critical care patients. Resuscitation. 2013;84(7):878-882. doi:10.1016/j.resuscitation.2013.01.038.
- Walkey AJ, Greiner MA, Heckbert SR, et al. Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors. Am Heart J. 2013;165(6):949-955.e3. doi:10.1016/j.ahj.2013.03.020.
- Pickham D, Helfenbein E, Shinn JA, Chan G, Funk M, Drew BJ. How many patients need QT interval monitoring in critical care units? Preliminary report of the QT in Practice study. J Electrocardiol. 2010;43(6):572-576. doi:10.1016/j.jelectrocard.2010.05.016.
- Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227. doi:2006/13/smw-11319.
- Fuso L, Incalzi RA, Pistelli R, et al. Predicting mortality of patients hospitalized for acutely exacerbated chronic obstructive pulmonary disease. Am J Med. 1995;98(3):272-277.
- Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004;125(6):2309-2321.
- McCartney PR. Clinical alarm management. MCN Am J Matern Child Nurs. 2012;37(3):202. doi:10.1097/NMC.0b013e31824c5b4a.
- Benjamin EM, Klugman RA, Luckmann R, Fairchild DG, Abookire SA. Impact of cardiac telemetry on patient safety and cost. Am J Manag Care. 2013;19(6):e225-e232.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854. doi:10.1001/jamainternmed.2014.4491.
Case
Two patients on continuous cardiac monitoring (CCM) are admitted to the hospital. One is a 56-year-old man with hemodynamically stable sepsis secondary to pneumonia. There is no sign of arrhythmia on initial evaluation. The second patient is a 67-year-old man with a history of coronary artery disease (CAD) admitted with chest pain. Should these patients be admitted with CCM?
Overview
CCM was first introduced in hospitals in the early 1960s for heart rate and rhythm monitoring in coronary ICUs. Since that time, CCM has been widely used in the hospital setting among critically and noncritically ill patients. Some hospitals have a limited capacity for monitoring, which is dictated by bed or technology availability. Other hospitals have the ability to monitor any patient.
Guidelines from the American College of Cardiology (ACC) in 1991 and the American Heart Association (AHA) in 2004 guide inpatient use of CCM. These guidelines make recommendations based on the likelihood of patient benefit—will likely benefit, may benefit, unlikely to benefit—and are primarily based on expert opinion; rigorous clinical trial data is not available.1,2 Based on these guidelines, patients with primary cardiac diagnoses, including acute coronary syndrome (ACS), post-cardiac surgery, and arrhythmia, are the most likely to benefit from monitoring.2,3
In practical use, many hospitalists use CCM to detect signs of hemodynamic instability.3 Currently there is no data to support the idea that CCM is a safe or equivalent method of detecting hemodynamic instability compared to close clinical evaluation and frequent vital sign measurement. In fact, physicians overestimate the utility of CCM in guiding management decisions, and witnessed clinical deterioration is a more frequent factor in the decision to escalate the level of care of a patient.3,4
Guideline Recommendations
CCM is intended to identify life-threatening arrhythmias, ischemia, and QT prolongation (see Figure 1). The AHA guidelines address which patients will benefit from CCM; the main indications include an acute cardiac diagnosis or critical illness.1
In addition, the AHA guidelines provide recommendations for the duration of monitoring. These recommendations vary from time-limited monitoring (e.g. unexplained syncope) to a therapeutic-based recommendation (e.g. high-grade atrioventricular block requiring pacemaker placement).
The guidelines also identify a subset of patients who are unlikely to benefit from monitoring (Class III), including low-risk post-operative patients, patients with rate-controlled atrial fibrillation, and patients undergoing hemodialysis without other indications for monitoring.
Several studies have examined the frequency of CCM use. In one study of 236 admissions to a community hospital general ward population, approximately 50% of the 745 monitoring days were not indicated by ACC/AHA guidelines.5 In this study, only 5% of telemetry events occurred in patients without indications, and none of these events required any specific therapy.5 Thus, improved adherence to the ACC/AHA guidelines can decrease CCM use in patients who are unlikely to benefit.
Life-threatening arrhythmia detection. Cleverley and colleagues reported that patients who suffered a cardiac arrest on noncritical care units had a higher survival to hospital discharge if they were on CCM during the event.6 However, a similar study recently showed no benefit to cardiac monitoring for in-hospital arrest if patients were monitored remotely.7 Patients who experience a cardiac arrest in a noncritical care area may benefit from direct cardiac monitoring, though larger studies are needed to assess all potential confounding effects, including nurse-to-patient ratios, location of monitoring (remote or unit-based), advanced cardiac life support response times, and whether the event was witnessed.
Bottom line: AHA guidelines recommend use of CCM in patients with a higher likelihood of developing a life-threatening arrhythmia, including those with an ACS, those experiencing post-cardiac arrest, or those who are critically ill. Medical ward patients who should be monitored include those with acute or subacute congestive heart failure, syncope of unknown etiology, and uncontrolled atrial fibrillation.1
Ischemia surveillance. Computerized ST-segment monitoring has been available for high-risk post-operative patients and those with acute cardiac events since the mid-1980s. When properly used, it offers the ability to detect “silent” ischemia, which is associated with increased in-hospital complications and worse patient outcomes.
Computerized ST-segment monitoring is often associated with a high rate of false positive alarms, however, and has not been universally adopted. Recommendations for its use are based on expert opinion, because no randomized trial has shown that increasing the sensitivity of ischemia detection improves patient outcomes.
Bottom line: AHA guidelines recommend ST-segment monitoring in patients with early ACS and post-acute MI as well as in patients at high risk for silent ischemia, including high-risk post-operative patients.1
QT-interval monitoring. A corrected QT-interval (QTc) greater than 0.50 milliseconds correlates with a higher risk for torsades de pointes and is associated with higher mortality. In critically ill patients in a large academic medical center, guideline-based QT-interval monitoring showed poor specificity for predicting the development of QTc prolongation; however, the risk of QTc prolongation increased with the presence of multiple risk factors.8
Bottom line: AHA guidelines recommend QT-interval monitoring in patients with risk factors for QTc-prolongation, including those starting QTc-prolonging drugs, those with overdose of pro-arrhythmic drugs, those with new-onset bradyarrhythmias, those with severe hypokalemia or hypomagnesemia, and those who have experienced acute neurologic events.1
Recommendations Outside of Guidelines
Patients admitted to medical services for noncardiac diagnoses have a high rate of telemetry use and a perceived benefit associated with cardiac monitoring.3 Although guidelines for noncardiac patients to direct hospitalists on when to use this technology are lacking, there may be some utility in monitoring certain subsets of inpatients.
Sepsis. Patients with hemodynamically stable sepsis develop atrial fibrillation at a higher rate than patients without sepsis and have higher in-hospital mortality. Patients at highest risk are those who are elderly or have severe sepsis.7 CCM can identify atrial fibrillation in real time, which may allow for earlier intervention; however, it is important to consider that other modalities, such as patient symptoms, physical exam, and standard EKG, are potentially as effective at detecting atrial fibrillation as CCM.
Bottom line: Our recommendation is to use CCM in patients who are at higher risk, including elderly patients and those with severe sepsis, until sepsis has resolved and/or the patient is hemodynamically stable for 24 hours.
Alcohol withdrawal. Patients with severe alcohol withdrawal have an increased incidence of arrhythmia and ischemia during the detoxification process. Specifically, patients with delirium tremens and seizures are at higher risk for significant QTc prolongation and tachyarrhythmias.9
Bottom line: Our recommendation is to use CCM in patients with severe alcohol withdrawal and to discontinue monitoring once withdrawal has resolved.
COPD. Patients with COPD exacerbations have a high risk of in-hospital and long-term mortality. The highest risk for mortality appears to be in patients presenting with atrial or ventricular arrhythmias and those over 65 years old.10 There is no clear evidence that beta-agonist use in COPD exacerbations increases arrhythmias other than sinus tachycardia or is associated with worse outcomes.11
Bottom line: Our recommendation is to use CCM only in patients with COPD exacerbation who have other indications as described in the AHA guidelines.
CCM Disadvantages
Alarm fatigue. Alarm fatigue is defined as the desensitization of a clinician to an alarm stimulus, resulting from sensory overload and causing the response of an alarm to be delayed or dismissed.12 In 2014, the Emergency Care Research Institute named alarm hazards as the number one health technology hazard, noting that numerous alarms on a daily basis can lead to desensitization and “alarm fatigue.”
CCM, and the overuse of CCM in particular, contribute to alarm fatigue, which can lead to patient safety issues, including delays in treatment, medication errors, and potentially death.
Increased cost. Because telemetry requires specialized equipment and trained monitoring staff, cost can be significant. In addition to equipment, cost includes time spent by providers, nurses, and technicians interpreting the images and discussing findings with consultants, as well as the additional studies obtained as a result of identified arrhythmias.
Studies on CCM cost vary widely, with conservative estimates of approximately $53 to as much as $1,400 per patient per day in some hospitals.13
Lack of specificity. Because of the high sensitivity and low specificity of CCM, use of CCM in low-risk patients without indications increases the risk of misinterpreting false-positive findings as clinically significant. This can lead to errors in management, including overtesting, unnecessary consultation with subspecialists, and the potential for inappropriate invasive procedures.1
High-Value CCM Use
Because of the low value associated with cardiac monitoring in many patients and the high sensitivity of the guidelines to capture patients at high risk for cardiac events, many hospitals have sought to limit the overuse of this technology. The most successful interventions have targeted the electronic ordering system by requiring an indication and hardwiring an order duration based on guideline recommendations. In a recent study, this intervention led to a 70% decrease in usage and reported $4.8 million cost savings without increasing the rate of in-hospital rapid response or cardiac arrest.14
Systems-level interventions to decrease inappropriate initiation and facilitate discontinuation of cardiac monitoring are a proven way to increase compliance with guidelines and decrease the overuse of CCM.
Back to the Case
According to AHA guidelines, the only patient who has an indication for CCM is the 67-year-old man with known CAD and chest pain, and, accordingly, the patient was placed on CCM. The patient underwent evaluation for ACS, and monitoring was discontinued after 24 hours when ACS was ruled out. The 56-year-old man with sepsis responded to treatment of pneumonia and was not placed on CCM.
In general, patients admitted with acute cardiac-related diseases should be placed on CCM. Guidelines are lacking with respect to many noncardiac diseases, and we recommend a time-limited duration (typically 24 hours) if CCM is ordered for a patient with a special circumstance outside of guidelines (see Figure 3).
Key Takeaway
Hospitalists should use continuous cardiac monitoring for specific indications and not routinely for all patients.
Drs. Lacy and Rendon are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Davis is a resident in internal medicine at UNM, and Dr. Tolstrup is a cardiologist at UNM.
References
- Drew BJ, Califf RM, Funk M, et al. Practice standards for electrocardiographic monitoring in hospital settings: an American Heart Association scientific statement from the Councils on Cardiovascular Nursing, Clinical Cardiology, and Cardiovascular Disease in the Young: endorsed by the International Society of Computerized Electrocardiology and the American Association of Critical-Care Nurses. Circulation. 2004;110(17):2721-2746. doi:10.1161/01.CIR.0000145144.56673.59.
- Recommended guidelines for in-hospital cardiac monitoring of adults for detection of arrhythmia. Emergency Cardiac Care Committee members. J Am Coll Cardiol. 1991;18(6):1431-1433.
- Najafi N, Auerbach A. Use and outcomes of telemetry monitoring on a medicine service. Arch Intern Med. 2012;172(17):1349-1350. doi:10.1001/archinternmed.2012.3163.
- Estrada CA, Rosman HS, Prasad NK, et al. Role of telemetry monitoring in the non-intensive care unit. Am J Cardiol. 1995;76(12):960-965.
- Curry JP, Hanson CW III, Russell MW, Hanna C, Devine G, Ochroch EA. The use and effectiveness of electrocardiographic telemetry monitoring in a community hospital general care setting. Anesth Analg. 2003;97(5):1483-1487.
- Cleverley K, Mousavi N, Stronger L, et al. The impact of telemetry on survival of in-hospital cardiac arrests in non-critical care patients. Resuscitation. 2013;84(7):878-882. doi:10.1016/j.resuscitation.2013.01.038.
- Walkey AJ, Greiner MA, Heckbert SR, et al. Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors. Am Heart J. 2013;165(6):949-955.e3. doi:10.1016/j.ahj.2013.03.020.
- Pickham D, Helfenbein E, Shinn JA, Chan G, Funk M, Drew BJ. How many patients need QT interval monitoring in critical care units? Preliminary report of the QT in Practice study. J Electrocardiol. 2010;43(6):572-576. doi:10.1016/j.jelectrocard.2010.05.016.
- Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227. doi:2006/13/smw-11319.
- Fuso L, Incalzi RA, Pistelli R, et al. Predicting mortality of patients hospitalized for acutely exacerbated chronic obstructive pulmonary disease. Am J Med. 1995;98(3):272-277.
- Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004;125(6):2309-2321.
- McCartney PR. Clinical alarm management. MCN Am J Matern Child Nurs. 2012;37(3):202. doi:10.1097/NMC.0b013e31824c5b4a.
- Benjamin EM, Klugman RA, Luckmann R, Fairchild DG, Abookire SA. Impact of cardiac telemetry on patient safety and cost. Am J Manag Care. 2013;19(6):e225-e232.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854. doi:10.1001/jamainternmed.2014.4491.
Case
Two patients on continuous cardiac monitoring (CCM) are admitted to the hospital. One is a 56-year-old man with hemodynamically stable sepsis secondary to pneumonia. There is no sign of arrhythmia on initial evaluation. The second patient is a 67-year-old man with a history of coronary artery disease (CAD) admitted with chest pain. Should these patients be admitted with CCM?
Overview
CCM was first introduced in hospitals in the early 1960s for heart rate and rhythm monitoring in coronary ICUs. Since that time, CCM has been widely used in the hospital setting among critically and noncritically ill patients. Some hospitals have a limited capacity for monitoring, which is dictated by bed or technology availability. Other hospitals have the ability to monitor any patient.
Guidelines from the American College of Cardiology (ACC) in 1991 and the American Heart Association (AHA) in 2004 guide inpatient use of CCM. These guidelines make recommendations based on the likelihood of patient benefit—will likely benefit, may benefit, unlikely to benefit—and are primarily based on expert opinion; rigorous clinical trial data is not available.1,2 Based on these guidelines, patients with primary cardiac diagnoses, including acute coronary syndrome (ACS), post-cardiac surgery, and arrhythmia, are the most likely to benefit from monitoring.2,3
In practical use, many hospitalists use CCM to detect signs of hemodynamic instability.3 Currently there is no data to support the idea that CCM is a safe or equivalent method of detecting hemodynamic instability compared to close clinical evaluation and frequent vital sign measurement. In fact, physicians overestimate the utility of CCM in guiding management decisions, and witnessed clinical deterioration is a more frequent factor in the decision to escalate the level of care of a patient.3,4
Guideline Recommendations
CCM is intended to identify life-threatening arrhythmias, ischemia, and QT prolongation (see Figure 1). The AHA guidelines address which patients will benefit from CCM; the main indications include an acute cardiac diagnosis or critical illness.1
In addition, the AHA guidelines provide recommendations for the duration of monitoring. These recommendations vary from time-limited monitoring (e.g. unexplained syncope) to a therapeutic-based recommendation (e.g. high-grade atrioventricular block requiring pacemaker placement).
The guidelines also identify a subset of patients who are unlikely to benefit from monitoring (Class III), including low-risk post-operative patients, patients with rate-controlled atrial fibrillation, and patients undergoing hemodialysis without other indications for monitoring.
Several studies have examined the frequency of CCM use. In one study of 236 admissions to a community hospital general ward population, approximately 50% of the 745 monitoring days were not indicated by ACC/AHA guidelines.5 In this study, only 5% of telemetry events occurred in patients without indications, and none of these events required any specific therapy.5 Thus, improved adherence to the ACC/AHA guidelines can decrease CCM use in patients who are unlikely to benefit.
Life-threatening arrhythmia detection. Cleverley and colleagues reported that patients who suffered a cardiac arrest on noncritical care units had a higher survival to hospital discharge if they were on CCM during the event.6 However, a similar study recently showed no benefit to cardiac monitoring for in-hospital arrest if patients were monitored remotely.7 Patients who experience a cardiac arrest in a noncritical care area may benefit from direct cardiac monitoring, though larger studies are needed to assess all potential confounding effects, including nurse-to-patient ratios, location of monitoring (remote or unit-based), advanced cardiac life support response times, and whether the event was witnessed.
Bottom line: AHA guidelines recommend use of CCM in patients with a higher likelihood of developing a life-threatening arrhythmia, including those with an ACS, those experiencing post-cardiac arrest, or those who are critically ill. Medical ward patients who should be monitored include those with acute or subacute congestive heart failure, syncope of unknown etiology, and uncontrolled atrial fibrillation.1
Ischemia surveillance. Computerized ST-segment monitoring has been available for high-risk post-operative patients and those with acute cardiac events since the mid-1980s. When properly used, it offers the ability to detect “silent” ischemia, which is associated with increased in-hospital complications and worse patient outcomes.
Computerized ST-segment monitoring is often associated with a high rate of false positive alarms, however, and has not been universally adopted. Recommendations for its use are based on expert opinion, because no randomized trial has shown that increasing the sensitivity of ischemia detection improves patient outcomes.
Bottom line: AHA guidelines recommend ST-segment monitoring in patients with early ACS and post-acute MI as well as in patients at high risk for silent ischemia, including high-risk post-operative patients.1
QT-interval monitoring. A corrected QT-interval (QTc) greater than 0.50 milliseconds correlates with a higher risk for torsades de pointes and is associated with higher mortality. In critically ill patients in a large academic medical center, guideline-based QT-interval monitoring showed poor specificity for predicting the development of QTc prolongation; however, the risk of QTc prolongation increased with the presence of multiple risk factors.8
Bottom line: AHA guidelines recommend QT-interval monitoring in patients with risk factors for QTc-prolongation, including those starting QTc-prolonging drugs, those with overdose of pro-arrhythmic drugs, those with new-onset bradyarrhythmias, those with severe hypokalemia or hypomagnesemia, and those who have experienced acute neurologic events.1
Recommendations Outside of Guidelines
Patients admitted to medical services for noncardiac diagnoses have a high rate of telemetry use and a perceived benefit associated with cardiac monitoring.3 Although guidelines for noncardiac patients to direct hospitalists on when to use this technology are lacking, there may be some utility in monitoring certain subsets of inpatients.
Sepsis. Patients with hemodynamically stable sepsis develop atrial fibrillation at a higher rate than patients without sepsis and have higher in-hospital mortality. Patients at highest risk are those who are elderly or have severe sepsis.7 CCM can identify atrial fibrillation in real time, which may allow for earlier intervention; however, it is important to consider that other modalities, such as patient symptoms, physical exam, and standard EKG, are potentially as effective at detecting atrial fibrillation as CCM.
Bottom line: Our recommendation is to use CCM in patients who are at higher risk, including elderly patients and those with severe sepsis, until sepsis has resolved and/or the patient is hemodynamically stable for 24 hours.
Alcohol withdrawal. Patients with severe alcohol withdrawal have an increased incidence of arrhythmia and ischemia during the detoxification process. Specifically, patients with delirium tremens and seizures are at higher risk for significant QTc prolongation and tachyarrhythmias.9
Bottom line: Our recommendation is to use CCM in patients with severe alcohol withdrawal and to discontinue monitoring once withdrawal has resolved.
COPD. Patients with COPD exacerbations have a high risk of in-hospital and long-term mortality. The highest risk for mortality appears to be in patients presenting with atrial or ventricular arrhythmias and those over 65 years old.10 There is no clear evidence that beta-agonist use in COPD exacerbations increases arrhythmias other than sinus tachycardia or is associated with worse outcomes.11
Bottom line: Our recommendation is to use CCM only in patients with COPD exacerbation who have other indications as described in the AHA guidelines.
CCM Disadvantages
Alarm fatigue. Alarm fatigue is defined as the desensitization of a clinician to an alarm stimulus, resulting from sensory overload and causing the response of an alarm to be delayed or dismissed.12 In 2014, the Emergency Care Research Institute named alarm hazards as the number one health technology hazard, noting that numerous alarms on a daily basis can lead to desensitization and “alarm fatigue.”
CCM, and the overuse of CCM in particular, contribute to alarm fatigue, which can lead to patient safety issues, including delays in treatment, medication errors, and potentially death.
Increased cost. Because telemetry requires specialized equipment and trained monitoring staff, cost can be significant. In addition to equipment, cost includes time spent by providers, nurses, and technicians interpreting the images and discussing findings with consultants, as well as the additional studies obtained as a result of identified arrhythmias.
Studies on CCM cost vary widely, with conservative estimates of approximately $53 to as much as $1,400 per patient per day in some hospitals.13
Lack of specificity. Because of the high sensitivity and low specificity of CCM, use of CCM in low-risk patients without indications increases the risk of misinterpreting false-positive findings as clinically significant. This can lead to errors in management, including overtesting, unnecessary consultation with subspecialists, and the potential for inappropriate invasive procedures.1
High-Value CCM Use
Because of the low value associated with cardiac monitoring in many patients and the high sensitivity of the guidelines to capture patients at high risk for cardiac events, many hospitals have sought to limit the overuse of this technology. The most successful interventions have targeted the electronic ordering system by requiring an indication and hardwiring an order duration based on guideline recommendations. In a recent study, this intervention led to a 70% decrease in usage and reported $4.8 million cost savings without increasing the rate of in-hospital rapid response or cardiac arrest.14
Systems-level interventions to decrease inappropriate initiation and facilitate discontinuation of cardiac monitoring are a proven way to increase compliance with guidelines and decrease the overuse of CCM.
Back to the Case
According to AHA guidelines, the only patient who has an indication for CCM is the 67-year-old man with known CAD and chest pain, and, accordingly, the patient was placed on CCM. The patient underwent evaluation for ACS, and monitoring was discontinued after 24 hours when ACS was ruled out. The 56-year-old man with sepsis responded to treatment of pneumonia and was not placed on CCM.
In general, patients admitted with acute cardiac-related diseases should be placed on CCM. Guidelines are lacking with respect to many noncardiac diseases, and we recommend a time-limited duration (typically 24 hours) if CCM is ordered for a patient with a special circumstance outside of guidelines (see Figure 3).
Key Takeaway
Hospitalists should use continuous cardiac monitoring for specific indications and not routinely for all patients.
Drs. Lacy and Rendon are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque. Dr. Davis is a resident in internal medicine at UNM, and Dr. Tolstrup is a cardiologist at UNM.
References
- Drew BJ, Califf RM, Funk M, et al. Practice standards for electrocardiographic monitoring in hospital settings: an American Heart Association scientific statement from the Councils on Cardiovascular Nursing, Clinical Cardiology, and Cardiovascular Disease in the Young: endorsed by the International Society of Computerized Electrocardiology and the American Association of Critical-Care Nurses. Circulation. 2004;110(17):2721-2746. doi:10.1161/01.CIR.0000145144.56673.59.
- Recommended guidelines for in-hospital cardiac monitoring of adults for detection of arrhythmia. Emergency Cardiac Care Committee members. J Am Coll Cardiol. 1991;18(6):1431-1433.
- Najafi N, Auerbach A. Use and outcomes of telemetry monitoring on a medicine service. Arch Intern Med. 2012;172(17):1349-1350. doi:10.1001/archinternmed.2012.3163.
- Estrada CA, Rosman HS, Prasad NK, et al. Role of telemetry monitoring in the non-intensive care unit. Am J Cardiol. 1995;76(12):960-965.
- Curry JP, Hanson CW III, Russell MW, Hanna C, Devine G, Ochroch EA. The use and effectiveness of electrocardiographic telemetry monitoring in a community hospital general care setting. Anesth Analg. 2003;97(5):1483-1487.
- Cleverley K, Mousavi N, Stronger L, et al. The impact of telemetry on survival of in-hospital cardiac arrests in non-critical care patients. Resuscitation. 2013;84(7):878-882. doi:10.1016/j.resuscitation.2013.01.038.
- Walkey AJ, Greiner MA, Heckbert SR, et al. Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors. Am Heart J. 2013;165(6):949-955.e3. doi:10.1016/j.ahj.2013.03.020.
- Pickham D, Helfenbein E, Shinn JA, Chan G, Funk M, Drew BJ. How many patients need QT interval monitoring in critical care units? Preliminary report of the QT in Practice study. J Electrocardiol. 2010;43(6):572-576. doi:10.1016/j.jelectrocard.2010.05.016.
- Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227. doi:2006/13/smw-11319.
- Fuso L, Incalzi RA, Pistelli R, et al. Predicting mortality of patients hospitalized for acutely exacerbated chronic obstructive pulmonary disease. Am J Med. 1995;98(3):272-277.
- Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004;125(6):2309-2321.
- McCartney PR. Clinical alarm management. MCN Am J Matern Child Nurs. 2012;37(3):202. doi:10.1097/NMC.0b013e31824c5b4a.
- Benjamin EM, Klugman RA, Luckmann R, Fairchild DG, Abookire SA. Impact of cardiac telemetry on patient safety and cost. Am J Manag Care. 2013;19(6):e225-e232.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854. doi:10.1001/jamainternmed.2014.4491.