User login
What psychiatrists must know to make the mandated transition to ICD-10
Just as psychiatrists are adapting to DSM-5, they have to cope with implementation of the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). This challenge raises questions: What is the importance of understanding ICD-10? How will it affect the practice of psychiatry?
Furthermore, how does ICD-10 relate to DSM-5 and Current Procedural Terminology (CPT)? How does it differ from ICD-9? What are the ICD-10-Clinical Modification (CM) and ICD-10-Procedures (PCS)?Learning the essence of the changes, and understanding what impact they have on your clinical work, are necessary to ensure that your practice keeps pace with professional and legal standards of care. The effort involved is not onerous, however, and can improve the quality and efficiency of your care and how you document it.
In this article, we provide you with an overview of ICD-10; highlight major changes of the new classification; explain its relevance to clinical practice; and offer guidelines for implementing it effectively. We also emphasize that a good understanding of DSM-5 facilitates appreciation of ICD-10 and makes its implementation fairly easy and straightforward.
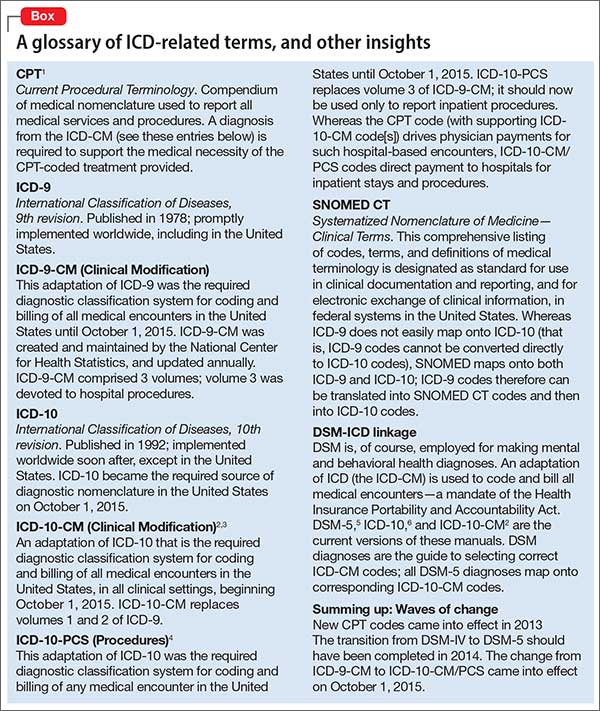
To begin, we provide a glossary of ICD-related terms and a review of additional definitions, distinctions, and dates (Box).1-6
Major changes from ICD-9
No question: ICD-10 is going to significantly influence your practice and your reimbursement. Furthermore, a number of revisions in ICD-10 have the potential to meaningfully improve clinical documentation and communication and to enhance your ability to precisely describe the complexity of your patients—with implications for billing.
ICD-10 differs from ICD-9 in organization, structure, code composition, and level of detail. In addition, ICD-10 makes some changes in terminology and definitions, with the goal of improving precision.
ICD-10 also is much larger than ICD-9.The total number of medical diagnostic codes has increased more than 5-fold—from approximately 13,000 to 69,000. This expansion allows for greater specificity in diagnosis and enables differentiation of an initial clinical encounter from a subsequent encounter.
To accommodate the expansion in the number of codes, the 5-digit numeric codes used in ICD-9 have been replaced in ICD-10 by 7-digit alphanumeric codes:
- the first digit always is a letter
- the second and third digits are numbers followed by a decimal point
- the fourth though seventh digits can be letters or numbers
- the first 3 digits denote the diagnostic category
- the fourth through sixth digits provide diagnostic detail
- the seventh digit provides information about the nature of the encounter (eg, initial, subsequent, or sequel, denoted respectively by “A,” “D,” and “S” in the seventh digit).
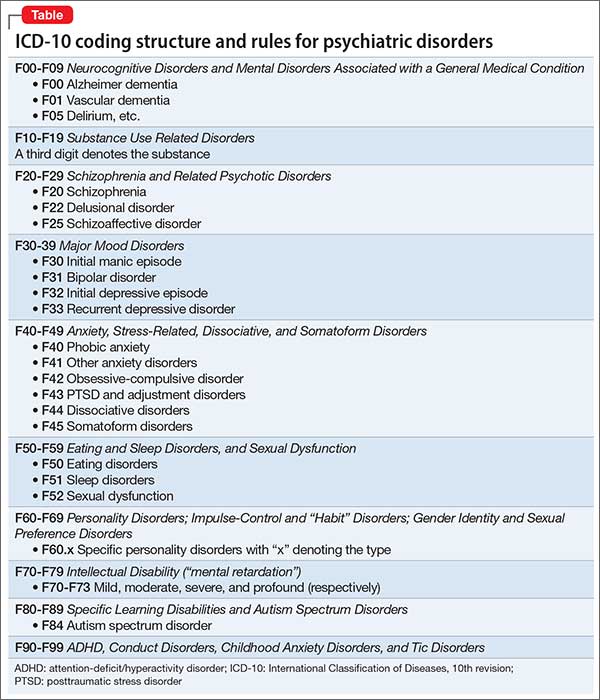
The number of 3-digit categories for psychiatric disorders has increased from 30 in ICD-9 (290-319) to 100 in ICD-10 (F00-F99). Only the first 5 digits are used for the section on mental disorders in ICD-10, with the first digit always “F” and the second digit a number denoting the broad type of disorders. The second and third digits in conjunction define the major category of the disorder; the fourth and fifth digits provide additional descriptive detail about the disorder (Table).
ICD-9 ‘V’ codes are out
What were called “V” codes in ICD-9—factors that influence health status and contact with health services—have been replaced by “Z” codes in ICD-10. These “Z” codes provide greater detail and precision than “V” codes provided.
Examples of “Z” codes relevant to psychiatry are:
Z00 General psychiatric examination (eg, of a person who does not have a complaint or diagnosis)
Z03 Examination for suspected mental and behavioral disorder
Z04 Examination for medicolegal or other purposes; Z04.8 is relevant laboratory testing, such as drug testing of urine or blood
Z50 Care involving rehabilitation (substance use disorder, etc.)
Z60 Problem related to social environment
Z61 Problem related to negative life events in childhood
Z63 Problem related to primary support group, including family circumstances
Z64-Z65 Problem related to other psychosocial circumstances
Z70-Z71 Condition requiring counseling, not elsewhere classified
Z73 Problem related to difficulty with life management (burnout, stress, role conflict, etc.)
Z75 Problem related to medical facilities and other aspects of health care (eg, awaiting admission)
Z81 Family history of mental or behavioral disorders
Z85-Z91 Personal history of various disorders (must be absent or in full remission at the moment); Z86.51, for example, refers to a history of combat and operational stress reaction.
Greater precision is now possible when coding for treatment-related adverse effects. A particular adverse effect now is coded under the relevant system, along with its attribution to the specific substance. Obesity attributable to antipsychotic treatment,7,8 for example, is coded as E66.1.
Integrating DSM-5 and ICD-10
Because DSM-5 lists corresponding ICD-10-CM codes for all disorders, you will find it much easier than other physicians to implement ICD-10. DSM-5 includes ICD-9-CM and ICD-10-CM codes for each DSM-5 disorder (for example, the ICD-9-CM code for schizophrenia is 295.x; the ICD-10-CM code is F20.9).9
Furthermore, a number of changes from ICD-9-CM to ICD-10-CM enable documentation of greater diagnostic specificity; for example, DSM-5 schizoaffective disorder, bipolar type, and schizoaffective disorder, depressive type, are distinctly coded as F25.0 and F25.1, respectively, in ICD-10-CM, whereas both were coded as 295.7 in ICD-9-CM.10
You will continue to use DSM-5 criteria to guide your diagnostic process, translating the DSM-5 diagnosis (diagnoses) into corresponding ICD-10-CM codes. Experience with DSM-5 substantially simplifies the transition to ICD-10.
Key differences between DSM-5 and ICD-10
There are notable differences in organization and content between DSM-5 and ICD-10.
The 20 chapters in DSM-5 begin with neurodevelopmental disorders; neurocognitive disorders are toward the end (ie, childhood to late life). In contrast, neurocognitive disorders (ie, “dementia”) appear at the beginning of ICD-10; neurodevelopmental disorders are at the end.
Elimination of schizophrenia subtypes in DSM-5 necessitates coding of all schizophrenia as F20.9 in ICD-10-CM because F20.0-F20.8 are specific subtypes. DSM-5 schizophreniform disorder is coded F20.81.
Substance abuse and substance dependence continue to be separate in ICD-10-CM, but they are combined in a single category of substance use disorders in DSM-5. The correct ICD-10-CM code (ie, abuse vs dependence) is determined by the severity of the substance use disorder: “Mild” coding as abuse (F1x.1) and “moderate” and “severe” coding as dependence (F2x.2), with x denoting the substance abused.
There can be multiple applicable diagnoses associated with a clinical encounter, as there was with ICD-9-CM. Give precedence to the diagnosis that best represents the nature of the presenting problem; list other diagnoses in the order of their relevance. DSM-5 and ICD-10-CM are similar in this regard.
ICD-10-CM uses only subtypes, in contrast to the use of subtypes and specifiers in DSM-5 to describe variability in disorders across patients. It is possible, however, to code certain DSM-5 specifiers in ICD-10-CM. (This is discussed in the “Recording Procedures” section of the DSM-5 text and summarized at the beginning of the manual, and appears in the “Appendix.”) To code the catatonia specifier in the context of schizoaffective disorder, depressive type, for example, use ICD-10-CM code F25.1 for the disorder and add code F06.1 for the catatonia specifier.11
How will ICD-10 affect your practice?
As of October 1, 2015, all health care facilities were to have become ICD-10 compliant. Furthermore, any Health Insurance Portability and Accountability Act-covered entity must use ICD-10-CM codes if it expects to be reimbursed for health care services.
Mental health practitioners might think that the transition from ICD-9-CM to ICD-10-CM involves only billers and coders, not them. They are wrong. All clinicians are responsible for documenting their diagnostic and treatment services properly. Medical records must contain adequate information to support any diagnostic (ICD-10-CM) and treatment (CPT) codes that are applied to a given clinical encounter.
The greater detail and specificity that are provided by ICD-10-CM allow more accurate recording of clinical complexity, which, in turn, influences reimbursement. However, good documentation is necessary for proper coding. Because clinicians are ultimately responsible for proper diagnostic coding, good understanding of ICD-10-CM is essential to be able to code properly.
Similar to the expansion of ICD-10-CM (from volumes 1 and 2 of ICD-9-CM), ICD-10-PCS has undergone similar expansion (from volume 3 of ICD-9-CM), with a corresponding increase in specificity. For example, there are now 5 distinct codes for electroconvulsive therapy (GZB0ZZZ-GZB4ZZZ) that distinguish unilateral from bilateral electrode placement and single from multiple stimulations.
DSM-5 will continue to be the frameworkfor psychiatric assessment and diagnosis. ICD-10-CM will be the coding system to accurately denote DSM-5 diagnoses. The Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics recognize DSM-5 as the means to identify proper ICD-10-CM codes for mental disorders. CMS also has announced that, although ICD-10-CM codes are necessary for reimbursement, use of an incorrect code will not be the basis for denying a Medicare claim for 1 year.
Making ICD-10 part of practice
Here are several keys to implementing ICD-10 with minimum pain and maximum benefit.
Multiple diagnosis codes should be listed in the order of their relevance to the clinical encounter.
Visit type. The seventh character of the ICD-10-CM code denotes the type of visit (initial, subsequent, or sequela) and must be provided:
- An initial encounter is one in which the patient first receives active treatment.
- A subsequent encounter refers to a follow-up visit in which the patient receives routine care during the healing or recovery phase.
- A sequel encounter is one in which a patient receives treatment for complications or conditions that arise as a direct result of the initial condition.
The transition to ICD-10 should be facilitated by adoption of DSM-5. Continue using DSM-5 to determine the correct diagnosis or diagnoses of the mental disorder, then apply the corresponding ICD-10-CM code(s). The better you understand and apply DSM-5, the more precise you can be in utilizing the greater specificity and accuracy afforded by ICD-10-CM coding.
Document well. Good understanding of the structure and organization of ICD-10-CM facilitates efficient, comprehensive documentation. This, in turn, will foster better clinical communication and appropriate reimbursement.
Know your payers—in particular, their policies regarding differential reimbursement for clinical complexity (based on ICD-10-CM/PCS). Medical practices that are part of an accountable care organization, and those that have risk-adjusted contracts must pay special attention to documenting clinical complexity when coding.
Know your electronic health care record, understand what tools it offers to efficiently translate DSM-5 diagnoses into appropriate ICD-10-CM codes, and use those tools efficiently.
Review your medical record documentation for the top 20 conditions in your practice, in the context of their definition in ICD-10-CM.
If you have coders who do ICD-10-CM coding for you, review a few patient charts with them to compare your sense of the patient’s clinical complexity and their coding based on your documentation.
Changes in DSM-5 have encouraged clinicians to improve their assessment of patients and provide measurement-based care. The significant changes in ICD-10-CM should provide the impetus for you to hone your ability to provide documentation. Sufficient flexibility exists within guidelines to permit individualization of the style of documentation.
Because all DSM-5 diagnoses map to appropriate ICD-10-CM codes, effective use of DSM-5 should make the transition to ICD-10 easy.
Bottom Line
Compared with ICD-9, definitions of mental health diagnoses have been improved in ICD-10, and more elaborate code descriptions in ICD-10-CM provide for greater precision when you report a diagnosis. The result? More accurate and efficient documentation of the care you provide and better reimbursement. Understanding what impact the changes in ICD-10 will have on your clinical work will ensure that your practice keeps pace with professional and legal standards of care.
Related Resources
• Blue Cross Blue Shield of Michigan ICD-10 update: mental and behavioral health ICD-10-CM codes. http://www.bcbsm.com/content/dam/public/Providers/Documents/help/faqs/icd10-update-mentalhealth.pdf.
• American Psychiatric Association ICD-10 tutorial. http://www.psychiatry.org/psychiatrists/practice/dsm/icd-10.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 5th edition. Washington DC: American Psychiatric Association; 2013.
2. World Health Organization. The ICD-10 classification of mental and behavioral disorders: clinical descriptions and diagnostic guidelines. Geneva, Switzerland: World Health Organization; 1992.
3. American Medical Association. ICD-10-CM 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
4. American Medical Association. CPT-2016, professional edition. Chicago, IL: American Medical Association; 2015.
5. American Medical Association. ICD-10-CM expert for physicians 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
6. American Medical Association. ICD-10-PCS mapping to ICD-9-CM volume 3. Chicago, IL: American Medical Association; 2015.
7. Tandon R, Halbreich U. The second-generation ‘atypical’ antipsychotics: similar efficacy but different neuroendocrine side-effects. Psychoneuroendocrinology. 2003;28(suppl 1):1-7.
8. Tandon R. Antipsychotics in the treatment of schizophrenia: an overview. J Clin Psychiatry. 2011;72(suppl 1):4-8.
9. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3-10.
10. Malaspina D, Owens MJ, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150(1):21-25.
11. Tandon R, Heckers S, Bustillo J, et al. Catatonia in DSM-5. Schizophr Res. 2013;150(1):26-30.
Just as psychiatrists are adapting to DSM-5, they have to cope with implementation of the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). This challenge raises questions: What is the importance of understanding ICD-10? How will it affect the practice of psychiatry?
Furthermore, how does ICD-10 relate to DSM-5 and Current Procedural Terminology (CPT)? How does it differ from ICD-9? What are the ICD-10-Clinical Modification (CM) and ICD-10-Procedures (PCS)?Learning the essence of the changes, and understanding what impact they have on your clinical work, are necessary to ensure that your practice keeps pace with professional and legal standards of care. The effort involved is not onerous, however, and can improve the quality and efficiency of your care and how you document it.
In this article, we provide you with an overview of ICD-10; highlight major changes of the new classification; explain its relevance to clinical practice; and offer guidelines for implementing it effectively. We also emphasize that a good understanding of DSM-5 facilitates appreciation of ICD-10 and makes its implementation fairly easy and straightforward.
To begin, we provide a glossary of ICD-related terms and a review of additional definitions, distinctions, and dates (Box).1-6
Major changes from ICD-9
No question: ICD-10 is going to significantly influence your practice and your reimbursement. Furthermore, a number of revisions in ICD-10 have the potential to meaningfully improve clinical documentation and communication and to enhance your ability to precisely describe the complexity of your patients—with implications for billing.
ICD-10 differs from ICD-9 in organization, structure, code composition, and level of detail. In addition, ICD-10 makes some changes in terminology and definitions, with the goal of improving precision.
ICD-10 also is much larger than ICD-9.The total number of medical diagnostic codes has increased more than 5-fold—from approximately 13,000 to 69,000. This expansion allows for greater specificity in diagnosis and enables differentiation of an initial clinical encounter from a subsequent encounter.
To accommodate the expansion in the number of codes, the 5-digit numeric codes used in ICD-9 have been replaced in ICD-10 by 7-digit alphanumeric codes:
- the first digit always is a letter
- the second and third digits are numbers followed by a decimal point
- the fourth though seventh digits can be letters or numbers
- the first 3 digits denote the diagnostic category
- the fourth through sixth digits provide diagnostic detail
- the seventh digit provides information about the nature of the encounter (eg, initial, subsequent, or sequel, denoted respectively by “A,” “D,” and “S” in the seventh digit).
The number of 3-digit categories for psychiatric disorders has increased from 30 in ICD-9 (290-319) to 100 in ICD-10 (F00-F99). Only the first 5 digits are used for the section on mental disorders in ICD-10, with the first digit always “F” and the second digit a number denoting the broad type of disorders. The second and third digits in conjunction define the major category of the disorder; the fourth and fifth digits provide additional descriptive detail about the disorder (Table).
ICD-9 ‘V’ codes are out
What were called “V” codes in ICD-9—factors that influence health status and contact with health services—have been replaced by “Z” codes in ICD-10. These “Z” codes provide greater detail and precision than “V” codes provided.
Examples of “Z” codes relevant to psychiatry are:
Z00 General psychiatric examination (eg, of a person who does not have a complaint or diagnosis)
Z03 Examination for suspected mental and behavioral disorder
Z04 Examination for medicolegal or other purposes; Z04.8 is relevant laboratory testing, such as drug testing of urine or blood
Z50 Care involving rehabilitation (substance use disorder, etc.)
Z60 Problem related to social environment
Z61 Problem related to negative life events in childhood
Z63 Problem related to primary support group, including family circumstances
Z64-Z65 Problem related to other psychosocial circumstances
Z70-Z71 Condition requiring counseling, not elsewhere classified
Z73 Problem related to difficulty with life management (burnout, stress, role conflict, etc.)
Z75 Problem related to medical facilities and other aspects of health care (eg, awaiting admission)
Z81 Family history of mental or behavioral disorders
Z85-Z91 Personal history of various disorders (must be absent or in full remission at the moment); Z86.51, for example, refers to a history of combat and operational stress reaction.
Greater precision is now possible when coding for treatment-related adverse effects. A particular adverse effect now is coded under the relevant system, along with its attribution to the specific substance. Obesity attributable to antipsychotic treatment,7,8 for example, is coded as E66.1.
Integrating DSM-5 and ICD-10
Because DSM-5 lists corresponding ICD-10-CM codes for all disorders, you will find it much easier than other physicians to implement ICD-10. DSM-5 includes ICD-9-CM and ICD-10-CM codes for each DSM-5 disorder (for example, the ICD-9-CM code for schizophrenia is 295.x; the ICD-10-CM code is F20.9).9
Furthermore, a number of changes from ICD-9-CM to ICD-10-CM enable documentation of greater diagnostic specificity; for example, DSM-5 schizoaffective disorder, bipolar type, and schizoaffective disorder, depressive type, are distinctly coded as F25.0 and F25.1, respectively, in ICD-10-CM, whereas both were coded as 295.7 in ICD-9-CM.10
You will continue to use DSM-5 criteria to guide your diagnostic process, translating the DSM-5 diagnosis (diagnoses) into corresponding ICD-10-CM codes. Experience with DSM-5 substantially simplifies the transition to ICD-10.
Key differences between DSM-5 and ICD-10
There are notable differences in organization and content between DSM-5 and ICD-10.
The 20 chapters in DSM-5 begin with neurodevelopmental disorders; neurocognitive disorders are toward the end (ie, childhood to late life). In contrast, neurocognitive disorders (ie, “dementia”) appear at the beginning of ICD-10; neurodevelopmental disorders are at the end.
Elimination of schizophrenia subtypes in DSM-5 necessitates coding of all schizophrenia as F20.9 in ICD-10-CM because F20.0-F20.8 are specific subtypes. DSM-5 schizophreniform disorder is coded F20.81.
Substance abuse and substance dependence continue to be separate in ICD-10-CM, but they are combined in a single category of substance use disorders in DSM-5. The correct ICD-10-CM code (ie, abuse vs dependence) is determined by the severity of the substance use disorder: “Mild” coding as abuse (F1x.1) and “moderate” and “severe” coding as dependence (F2x.2), with x denoting the substance abused.
There can be multiple applicable diagnoses associated with a clinical encounter, as there was with ICD-9-CM. Give precedence to the diagnosis that best represents the nature of the presenting problem; list other diagnoses in the order of their relevance. DSM-5 and ICD-10-CM are similar in this regard.
ICD-10-CM uses only subtypes, in contrast to the use of subtypes and specifiers in DSM-5 to describe variability in disorders across patients. It is possible, however, to code certain DSM-5 specifiers in ICD-10-CM. (This is discussed in the “Recording Procedures” section of the DSM-5 text and summarized at the beginning of the manual, and appears in the “Appendix.”) To code the catatonia specifier in the context of schizoaffective disorder, depressive type, for example, use ICD-10-CM code F25.1 for the disorder and add code F06.1 for the catatonia specifier.11
How will ICD-10 affect your practice?
As of October 1, 2015, all health care facilities were to have become ICD-10 compliant. Furthermore, any Health Insurance Portability and Accountability Act-covered entity must use ICD-10-CM codes if it expects to be reimbursed for health care services.
Mental health practitioners might think that the transition from ICD-9-CM to ICD-10-CM involves only billers and coders, not them. They are wrong. All clinicians are responsible for documenting their diagnostic and treatment services properly. Medical records must contain adequate information to support any diagnostic (ICD-10-CM) and treatment (CPT) codes that are applied to a given clinical encounter.
The greater detail and specificity that are provided by ICD-10-CM allow more accurate recording of clinical complexity, which, in turn, influences reimbursement. However, good documentation is necessary for proper coding. Because clinicians are ultimately responsible for proper diagnostic coding, good understanding of ICD-10-CM is essential to be able to code properly.
Similar to the expansion of ICD-10-CM (from volumes 1 and 2 of ICD-9-CM), ICD-10-PCS has undergone similar expansion (from volume 3 of ICD-9-CM), with a corresponding increase in specificity. For example, there are now 5 distinct codes for electroconvulsive therapy (GZB0ZZZ-GZB4ZZZ) that distinguish unilateral from bilateral electrode placement and single from multiple stimulations.
DSM-5 will continue to be the frameworkfor psychiatric assessment and diagnosis. ICD-10-CM will be the coding system to accurately denote DSM-5 diagnoses. The Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics recognize DSM-5 as the means to identify proper ICD-10-CM codes for mental disorders. CMS also has announced that, although ICD-10-CM codes are necessary for reimbursement, use of an incorrect code will not be the basis for denying a Medicare claim for 1 year.
Making ICD-10 part of practice
Here are several keys to implementing ICD-10 with minimum pain and maximum benefit.
Multiple diagnosis codes should be listed in the order of their relevance to the clinical encounter.
Visit type. The seventh character of the ICD-10-CM code denotes the type of visit (initial, subsequent, or sequela) and must be provided:
- An initial encounter is one in which the patient first receives active treatment.
- A subsequent encounter refers to a follow-up visit in which the patient receives routine care during the healing or recovery phase.
- A sequel encounter is one in which a patient receives treatment for complications or conditions that arise as a direct result of the initial condition.
The transition to ICD-10 should be facilitated by adoption of DSM-5. Continue using DSM-5 to determine the correct diagnosis or diagnoses of the mental disorder, then apply the corresponding ICD-10-CM code(s). The better you understand and apply DSM-5, the more precise you can be in utilizing the greater specificity and accuracy afforded by ICD-10-CM coding.
Document well. Good understanding of the structure and organization of ICD-10-CM facilitates efficient, comprehensive documentation. This, in turn, will foster better clinical communication and appropriate reimbursement.
Know your payers—in particular, their policies regarding differential reimbursement for clinical complexity (based on ICD-10-CM/PCS). Medical practices that are part of an accountable care organization, and those that have risk-adjusted contracts must pay special attention to documenting clinical complexity when coding.
Know your electronic health care record, understand what tools it offers to efficiently translate DSM-5 diagnoses into appropriate ICD-10-CM codes, and use those tools efficiently.
Review your medical record documentation for the top 20 conditions in your practice, in the context of their definition in ICD-10-CM.
If you have coders who do ICD-10-CM coding for you, review a few patient charts with them to compare your sense of the patient’s clinical complexity and their coding based on your documentation.
Changes in DSM-5 have encouraged clinicians to improve their assessment of patients and provide measurement-based care. The significant changes in ICD-10-CM should provide the impetus for you to hone your ability to provide documentation. Sufficient flexibility exists within guidelines to permit individualization of the style of documentation.
Because all DSM-5 diagnoses map to appropriate ICD-10-CM codes, effective use of DSM-5 should make the transition to ICD-10 easy.
Bottom Line
Compared with ICD-9, definitions of mental health diagnoses have been improved in ICD-10, and more elaborate code descriptions in ICD-10-CM provide for greater precision when you report a diagnosis. The result? More accurate and efficient documentation of the care you provide and better reimbursement. Understanding what impact the changes in ICD-10 will have on your clinical work will ensure that your practice keeps pace with professional and legal standards of care.
Related Resources
• Blue Cross Blue Shield of Michigan ICD-10 update: mental and behavioral health ICD-10-CM codes. http://www.bcbsm.com/content/dam/public/Providers/Documents/help/faqs/icd10-update-mentalhealth.pdf.
• American Psychiatric Association ICD-10 tutorial. http://www.psychiatry.org/psychiatrists/practice/dsm/icd-10.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Just as psychiatrists are adapting to DSM-5, they have to cope with implementation of the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). This challenge raises questions: What is the importance of understanding ICD-10? How will it affect the practice of psychiatry?
Furthermore, how does ICD-10 relate to DSM-5 and Current Procedural Terminology (CPT)? How does it differ from ICD-9? What are the ICD-10-Clinical Modification (CM) and ICD-10-Procedures (PCS)?Learning the essence of the changes, and understanding what impact they have on your clinical work, are necessary to ensure that your practice keeps pace with professional and legal standards of care. The effort involved is not onerous, however, and can improve the quality and efficiency of your care and how you document it.
In this article, we provide you with an overview of ICD-10; highlight major changes of the new classification; explain its relevance to clinical practice; and offer guidelines for implementing it effectively. We also emphasize that a good understanding of DSM-5 facilitates appreciation of ICD-10 and makes its implementation fairly easy and straightforward.
To begin, we provide a glossary of ICD-related terms and a review of additional definitions, distinctions, and dates (Box).1-6
Major changes from ICD-9
No question: ICD-10 is going to significantly influence your practice and your reimbursement. Furthermore, a number of revisions in ICD-10 have the potential to meaningfully improve clinical documentation and communication and to enhance your ability to precisely describe the complexity of your patients—with implications for billing.
ICD-10 differs from ICD-9 in organization, structure, code composition, and level of detail. In addition, ICD-10 makes some changes in terminology and definitions, with the goal of improving precision.
ICD-10 also is much larger than ICD-9.The total number of medical diagnostic codes has increased more than 5-fold—from approximately 13,000 to 69,000. This expansion allows for greater specificity in diagnosis and enables differentiation of an initial clinical encounter from a subsequent encounter.
To accommodate the expansion in the number of codes, the 5-digit numeric codes used in ICD-9 have been replaced in ICD-10 by 7-digit alphanumeric codes:
- the first digit always is a letter
- the second and third digits are numbers followed by a decimal point
- the fourth though seventh digits can be letters or numbers
- the first 3 digits denote the diagnostic category
- the fourth through sixth digits provide diagnostic detail
- the seventh digit provides information about the nature of the encounter (eg, initial, subsequent, or sequel, denoted respectively by “A,” “D,” and “S” in the seventh digit).
The number of 3-digit categories for psychiatric disorders has increased from 30 in ICD-9 (290-319) to 100 in ICD-10 (F00-F99). Only the first 5 digits are used for the section on mental disorders in ICD-10, with the first digit always “F” and the second digit a number denoting the broad type of disorders. The second and third digits in conjunction define the major category of the disorder; the fourth and fifth digits provide additional descriptive detail about the disorder (Table).
ICD-9 ‘V’ codes are out
What were called “V” codes in ICD-9—factors that influence health status and contact with health services—have been replaced by “Z” codes in ICD-10. These “Z” codes provide greater detail and precision than “V” codes provided.
Examples of “Z” codes relevant to psychiatry are:
Z00 General psychiatric examination (eg, of a person who does not have a complaint or diagnosis)
Z03 Examination for suspected mental and behavioral disorder
Z04 Examination for medicolegal or other purposes; Z04.8 is relevant laboratory testing, such as drug testing of urine or blood
Z50 Care involving rehabilitation (substance use disorder, etc.)
Z60 Problem related to social environment
Z61 Problem related to negative life events in childhood
Z63 Problem related to primary support group, including family circumstances
Z64-Z65 Problem related to other psychosocial circumstances
Z70-Z71 Condition requiring counseling, not elsewhere classified
Z73 Problem related to difficulty with life management (burnout, stress, role conflict, etc.)
Z75 Problem related to medical facilities and other aspects of health care (eg, awaiting admission)
Z81 Family history of mental or behavioral disorders
Z85-Z91 Personal history of various disorders (must be absent or in full remission at the moment); Z86.51, for example, refers to a history of combat and operational stress reaction.
Greater precision is now possible when coding for treatment-related adverse effects. A particular adverse effect now is coded under the relevant system, along with its attribution to the specific substance. Obesity attributable to antipsychotic treatment,7,8 for example, is coded as E66.1.
Integrating DSM-5 and ICD-10
Because DSM-5 lists corresponding ICD-10-CM codes for all disorders, you will find it much easier than other physicians to implement ICD-10. DSM-5 includes ICD-9-CM and ICD-10-CM codes for each DSM-5 disorder (for example, the ICD-9-CM code for schizophrenia is 295.x; the ICD-10-CM code is F20.9).9
Furthermore, a number of changes from ICD-9-CM to ICD-10-CM enable documentation of greater diagnostic specificity; for example, DSM-5 schizoaffective disorder, bipolar type, and schizoaffective disorder, depressive type, are distinctly coded as F25.0 and F25.1, respectively, in ICD-10-CM, whereas both were coded as 295.7 in ICD-9-CM.10
You will continue to use DSM-5 criteria to guide your diagnostic process, translating the DSM-5 diagnosis (diagnoses) into corresponding ICD-10-CM codes. Experience with DSM-5 substantially simplifies the transition to ICD-10.
Key differences between DSM-5 and ICD-10
There are notable differences in organization and content between DSM-5 and ICD-10.
The 20 chapters in DSM-5 begin with neurodevelopmental disorders; neurocognitive disorders are toward the end (ie, childhood to late life). In contrast, neurocognitive disorders (ie, “dementia”) appear at the beginning of ICD-10; neurodevelopmental disorders are at the end.
Elimination of schizophrenia subtypes in DSM-5 necessitates coding of all schizophrenia as F20.9 in ICD-10-CM because F20.0-F20.8 are specific subtypes. DSM-5 schizophreniform disorder is coded F20.81.
Substance abuse and substance dependence continue to be separate in ICD-10-CM, but they are combined in a single category of substance use disorders in DSM-5. The correct ICD-10-CM code (ie, abuse vs dependence) is determined by the severity of the substance use disorder: “Mild” coding as abuse (F1x.1) and “moderate” and “severe” coding as dependence (F2x.2), with x denoting the substance abused.
There can be multiple applicable diagnoses associated with a clinical encounter, as there was with ICD-9-CM. Give precedence to the diagnosis that best represents the nature of the presenting problem; list other diagnoses in the order of their relevance. DSM-5 and ICD-10-CM are similar in this regard.
ICD-10-CM uses only subtypes, in contrast to the use of subtypes and specifiers in DSM-5 to describe variability in disorders across patients. It is possible, however, to code certain DSM-5 specifiers in ICD-10-CM. (This is discussed in the “Recording Procedures” section of the DSM-5 text and summarized at the beginning of the manual, and appears in the “Appendix.”) To code the catatonia specifier in the context of schizoaffective disorder, depressive type, for example, use ICD-10-CM code F25.1 for the disorder and add code F06.1 for the catatonia specifier.11
How will ICD-10 affect your practice?
As of October 1, 2015, all health care facilities were to have become ICD-10 compliant. Furthermore, any Health Insurance Portability and Accountability Act-covered entity must use ICD-10-CM codes if it expects to be reimbursed for health care services.
Mental health practitioners might think that the transition from ICD-9-CM to ICD-10-CM involves only billers and coders, not them. They are wrong. All clinicians are responsible for documenting their diagnostic and treatment services properly. Medical records must contain adequate information to support any diagnostic (ICD-10-CM) and treatment (CPT) codes that are applied to a given clinical encounter.
The greater detail and specificity that are provided by ICD-10-CM allow more accurate recording of clinical complexity, which, in turn, influences reimbursement. However, good documentation is necessary for proper coding. Because clinicians are ultimately responsible for proper diagnostic coding, good understanding of ICD-10-CM is essential to be able to code properly.
Similar to the expansion of ICD-10-CM (from volumes 1 and 2 of ICD-9-CM), ICD-10-PCS has undergone similar expansion (from volume 3 of ICD-9-CM), with a corresponding increase in specificity. For example, there are now 5 distinct codes for electroconvulsive therapy (GZB0ZZZ-GZB4ZZZ) that distinguish unilateral from bilateral electrode placement and single from multiple stimulations.
DSM-5 will continue to be the frameworkfor psychiatric assessment and diagnosis. ICD-10-CM will be the coding system to accurately denote DSM-5 diagnoses. The Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics recognize DSM-5 as the means to identify proper ICD-10-CM codes for mental disorders. CMS also has announced that, although ICD-10-CM codes are necessary for reimbursement, use of an incorrect code will not be the basis for denying a Medicare claim for 1 year.
Making ICD-10 part of practice
Here are several keys to implementing ICD-10 with minimum pain and maximum benefit.
Multiple diagnosis codes should be listed in the order of their relevance to the clinical encounter.
Visit type. The seventh character of the ICD-10-CM code denotes the type of visit (initial, subsequent, or sequela) and must be provided:
- An initial encounter is one in which the patient first receives active treatment.
- A subsequent encounter refers to a follow-up visit in which the patient receives routine care during the healing or recovery phase.
- A sequel encounter is one in which a patient receives treatment for complications or conditions that arise as a direct result of the initial condition.
The transition to ICD-10 should be facilitated by adoption of DSM-5. Continue using DSM-5 to determine the correct diagnosis or diagnoses of the mental disorder, then apply the corresponding ICD-10-CM code(s). The better you understand and apply DSM-5, the more precise you can be in utilizing the greater specificity and accuracy afforded by ICD-10-CM coding.
Document well. Good understanding of the structure and organization of ICD-10-CM facilitates efficient, comprehensive documentation. This, in turn, will foster better clinical communication and appropriate reimbursement.
Know your payers—in particular, their policies regarding differential reimbursement for clinical complexity (based on ICD-10-CM/PCS). Medical practices that are part of an accountable care organization, and those that have risk-adjusted contracts must pay special attention to documenting clinical complexity when coding.
Know your electronic health care record, understand what tools it offers to efficiently translate DSM-5 diagnoses into appropriate ICD-10-CM codes, and use those tools efficiently.
Review your medical record documentation for the top 20 conditions in your practice, in the context of their definition in ICD-10-CM.
If you have coders who do ICD-10-CM coding for you, review a few patient charts with them to compare your sense of the patient’s clinical complexity and their coding based on your documentation.
Changes in DSM-5 have encouraged clinicians to improve their assessment of patients and provide measurement-based care. The significant changes in ICD-10-CM should provide the impetus for you to hone your ability to provide documentation. Sufficient flexibility exists within guidelines to permit individualization of the style of documentation.
Because all DSM-5 diagnoses map to appropriate ICD-10-CM codes, effective use of DSM-5 should make the transition to ICD-10 easy.
Bottom Line
Compared with ICD-9, definitions of mental health diagnoses have been improved in ICD-10, and more elaborate code descriptions in ICD-10-CM provide for greater precision when you report a diagnosis. The result? More accurate and efficient documentation of the care you provide and better reimbursement. Understanding what impact the changes in ICD-10 will have on your clinical work will ensure that your practice keeps pace with professional and legal standards of care.
Related Resources
• Blue Cross Blue Shield of Michigan ICD-10 update: mental and behavioral health ICD-10-CM codes. http://www.bcbsm.com/content/dam/public/Providers/Documents/help/faqs/icd10-update-mentalhealth.pdf.
• American Psychiatric Association ICD-10 tutorial. http://www.psychiatry.org/psychiatrists/practice/dsm/icd-10.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 5th edition. Washington DC: American Psychiatric Association; 2013.
2. World Health Organization. The ICD-10 classification of mental and behavioral disorders: clinical descriptions and diagnostic guidelines. Geneva, Switzerland: World Health Organization; 1992.
3. American Medical Association. ICD-10-CM 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
4. American Medical Association. CPT-2016, professional edition. Chicago, IL: American Medical Association; 2015.
5. American Medical Association. ICD-10-CM expert for physicians 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
6. American Medical Association. ICD-10-PCS mapping to ICD-9-CM volume 3. Chicago, IL: American Medical Association; 2015.
7. Tandon R, Halbreich U. The second-generation ‘atypical’ antipsychotics: similar efficacy but different neuroendocrine side-effects. Psychoneuroendocrinology. 2003;28(suppl 1):1-7.
8. Tandon R. Antipsychotics in the treatment of schizophrenia: an overview. J Clin Psychiatry. 2011;72(suppl 1):4-8.
9. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3-10.
10. Malaspina D, Owens MJ, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150(1):21-25.
11. Tandon R, Heckers S, Bustillo J, et al. Catatonia in DSM-5. Schizophr Res. 2013;150(1):26-30.
1. Diagnostic and statistical manual of mental disorders, 5th edition. Washington DC: American Psychiatric Association; 2013.
2. World Health Organization. The ICD-10 classification of mental and behavioral disorders: clinical descriptions and diagnostic guidelines. Geneva, Switzerland: World Health Organization; 1992.
3. American Medical Association. ICD-10-CM 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
4. American Medical Association. CPT-2016, professional edition. Chicago, IL: American Medical Association; 2015.
5. American Medical Association. ICD-10-CM expert for physicians 2016: the complete official code set. Chicago, IL: American Medical Association; 2015.
6. American Medical Association. ICD-10-PCS mapping to ICD-9-CM volume 3. Chicago, IL: American Medical Association; 2015.
7. Tandon R, Halbreich U. The second-generation ‘atypical’ antipsychotics: similar efficacy but different neuroendocrine side-effects. Psychoneuroendocrinology. 2003;28(suppl 1):1-7.
8. Tandon R. Antipsychotics in the treatment of schizophrenia: an overview. J Clin Psychiatry. 2011;72(suppl 1):4-8.
9. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3-10.
10. Malaspina D, Owens MJ, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150(1):21-25.
11. Tandon R, Heckers S, Bustillo J, et al. Catatonia in DSM-5. Schizophr Res. 2013;150(1):26-30.

Isolated Brachialis Muscle Atrophy
Isolated brachialis muscle atrophy has been rarely reported. Among the few cases in the literature, 1 was attributed to a presumed compartment syndrome,1 1 to a displaced clavicle fracture,2 and 3 to neuralgic amyotrophy.3,4 We present a case of isolated brachialis muscle atrophy of unknown etiology, the presentation of which is consistent with neuralgic amyotrophy, also known as Parsonage-Turner syndrome or brachial plexitis. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old right-handed highway worker presented for evaluation of right-arm muscle atrophy. One year earlier, while lifting heavy bags at work, he felt a painful strain in his right arm, although there was no bruising or swelling. Approximately 4 weeks after this incident, he developed right shoulder pain and began to notice a slight decrease in the muscle mass of his right anterior arm. On evaluation at an outside facility, the physician noted some brachialis muscle atrophy. His shoulder pain was attributed to acromioclavicular joint problems. After an initial trial of physical therapy that did not alleviate this joint pain, an acromioclavicular joint resection was performed, and his pain improved. The brachialis muscle atrophy continued to progress, however. Over the course of the next 6 months, the patient noticed a continually decreasing muscle mass in his right arm, as well as arm fatigue with routine recreational activities. On follow-up, again at an outside institution, the treating physicians noted continued atrophy of the distal arm corresponding to the region of the brachialis musculature. Magnetic resonance imaging showed continuity of the brachialis muscle and tendon, with muscle atrophy. The patient was able to return to work, although with a subjective decrease in right elbow flexion strength.
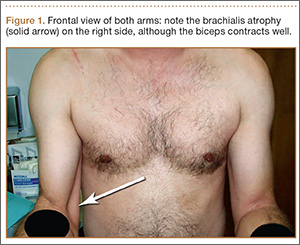
On presentation at our institution, the patient complained of right arm weakness with heavy use but did not have pain or sensory complaints. His medical history was otherwise unremarkable. Physical examination revealed obvious wasting of the right brachialis muscle, most notable on the lateral aspect of the distal arm (Figures 1, 2A, 2B). His biceps muscle was functioning with full strength and had a normal bulk. He had a normal range of active and passive motion, including full extension and flexion of both elbows, as well as complete pronosupination of the forearms. There was no focal tenderness. Manual muscle testing of both upper extremities was completely normal except for 4/5 flexion strength of the right elbow. Neurovascular examination also revealed normal findings, including intact sensation over the radiolateral forearm. A second magnetic resonance image showed that the brachialis muscle had completely atrophied. Because the clinical examination and imaging studies both indicated isolated brachialis atrophy without deficit elsewhere along the musculocutaneous nerve, electromyography was not performed. The patient was fully functional and working at his usual occupation, and no further intervention was recommended.

Discussion
Isolated wasting of the brachialis muscle is extremely rare with few reports in the literature. Farmer and colleagues1 reported a case of brachialis atrophy that was presumed to have resulted from exercise-induced chronic compartment syndrome. In that case, the patient developed a prodrome of arm pain followed by brachialis muscle atrophy. This patient was treated with oral anti-inflammatory agents with improvement in pain but without recovery of the brachialis muscle. While this case was attributed to compartment syndrome, it is likely that it represented neuralgic amyotrophy because there was no evidence of elbow flexion contracture, which would have accompanied true necrosis of the brachialis muscle as seen in compartment syndrome. However, acute compartment syndrome of the brachialis muscle after minor trauma has been reported.5 In that case, full-scale compartment syndrome was treated with rapid fasciotomy, with complete recovery of the brachialis.
Isolated brachialis atrophy has also been described in the setting of a displaced midshaft clavicle fracture in an elite athlete.2 Two fracture fragments were thought to have injured the brachial plexus, separately causing brachialis atrophy and altered sensation over the clavicular head of the deltoid muscle. Atrophy remained 1 year after injury.
Although it had been occasionally reported, the first large series of patients with sporadic neuralgic amyotrophy in the upper extremity was reported by Parsonage and Turner6 in 1948. They described 136 patients who developed flaccid paralysis and atrophy of various muscles of the shoulder girdle and/or upper extremity. This was generally preceded by acute pain in the shoulder girdle, often associated with antecedent viral infection, stress, illness, or other precipitating factors.
To our knowledge, there have been 3 other reported cases of neuralgic amyotrophy of the brachialis muscle. Watson and colleagues3 presented 2 patients with nonspecific, neurogenic shoulder pain after which an indolent, progressive atrophy of the brachialis muscle ensued.3 Van Tongel and colleagues4 described a more traditional case of Parsonage-Turner syndrome, with bilateral wasting of the shoulder girdle that also exhibited unilateral brachialis atrophy without affecting other muscles in the arm.4 Our case, with shoulder pain followed by muscle atrophy, fits the pattern of neuralgic amyotrophy.
Others have similarly described isolated wasting of 1 muscle with the sparing of other muscles with a common innervation. Isolated atrophy of the extensor or flexor pollicis longus has been reported as variants of either posterior or anterior interosseous neuropathy, respectively.7,8 Nerve fibers in the brachial plexus destined to innervate muscles supplied by the anterior interosseous nerve may be the cause of the motor deficit in cases of anterior interosseous nerve palsy, which seem to be associated with brachial plexitis.9
We present a case of isolated brachialis muscle atrophy after a minor trauma that may have resulted from Parsonage-Turner syndrome or a variant of brachial plexitis. The constellation of shoulder and arm pain, with subsequent muscle atrophy, makes this diagnosis likely.
1. Farmer KW, McFarland EG, Sonin A, Cosgarea AJ, Roehrig GJ. Isolated necrosis of the brachialis muscle due to exercise. Orthopedics. 2002;25(6):682-684.
2. Rüst CA, Knechtle B, Knechtle P, Rosemann T. Atrophy of the brachialis muscle after a displaced clavicle fracture in an Ironman triathlete: case report. J Brachial Plex Periph Nerve Inj. 2011;6(1):e44-e47.
3. Watson BV, Rose-Innes A, Engstrom JW, Brown JD. Isolated brachialis wasting: an unusual presentation of neuralgic amyotrophy. Muscle Nerve. 2001;24(12):1699-1702.
4. Van Tongel A, Schreurs M, Bruyninckx F, Debeer P. Bilateral Parsonage-Turner syndrome with unilateral brachialis muscle wasting: a case report. J Shoulder Elbow Surg. 2010;19(8):e14-e16.
5. Jenkins NH, Mintowt-Czyz WJ. Compression of the biceps-brachialis compartment after trivial trauma. J Bone Joint Surg Br. 1986;68(3):374.
6. Parsonage MJ, Turner JW. Neuralgic amyotrophy; the shoulder-girdle syndrome. Lancet. 1948;1(6513):973-978.
7. Horton TC. Isolated paralysis of the extensor pollicis longus muscle: a further variation of posterior interosseous nerve palsy. J Hand Surg Br. 2000;25(2):225-226.
8. Hill NA, Howard FM, Huffer BR. The incomplete anterior interosseous nerve syndrome. J Hand Surg Am. 1985;10(1):4-16.
9. Rennels GD, Ochoa J. Neuralgic amyotrophy manifesting as anterior interosseous nerve palsy. Muscle Nerve. 1980;3(2):160-164.
Isolated brachialis muscle atrophy has been rarely reported. Among the few cases in the literature, 1 was attributed to a presumed compartment syndrome,1 1 to a displaced clavicle fracture,2 and 3 to neuralgic amyotrophy.3,4 We present a case of isolated brachialis muscle atrophy of unknown etiology, the presentation of which is consistent with neuralgic amyotrophy, also known as Parsonage-Turner syndrome or brachial plexitis. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old right-handed highway worker presented for evaluation of right-arm muscle atrophy. One year earlier, while lifting heavy bags at work, he felt a painful strain in his right arm, although there was no bruising or swelling. Approximately 4 weeks after this incident, he developed right shoulder pain and began to notice a slight decrease in the muscle mass of his right anterior arm. On evaluation at an outside facility, the physician noted some brachialis muscle atrophy. His shoulder pain was attributed to acromioclavicular joint problems. After an initial trial of physical therapy that did not alleviate this joint pain, an acromioclavicular joint resection was performed, and his pain improved. The brachialis muscle atrophy continued to progress, however. Over the course of the next 6 months, the patient noticed a continually decreasing muscle mass in his right arm, as well as arm fatigue with routine recreational activities. On follow-up, again at an outside institution, the treating physicians noted continued atrophy of the distal arm corresponding to the region of the brachialis musculature. Magnetic resonance imaging showed continuity of the brachialis muscle and tendon, with muscle atrophy. The patient was able to return to work, although with a subjective decrease in right elbow flexion strength.
On presentation at our institution, the patient complained of right arm weakness with heavy use but did not have pain or sensory complaints. His medical history was otherwise unremarkable. Physical examination revealed obvious wasting of the right brachialis muscle, most notable on the lateral aspect of the distal arm (Figures 1, 2A, 2B). His biceps muscle was functioning with full strength and had a normal bulk. He had a normal range of active and passive motion, including full extension and flexion of both elbows, as well as complete pronosupination of the forearms. There was no focal tenderness. Manual muscle testing of both upper extremities was completely normal except for 4/5 flexion strength of the right elbow. Neurovascular examination also revealed normal findings, including intact sensation over the radiolateral forearm. A second magnetic resonance image showed that the brachialis muscle had completely atrophied. Because the clinical examination and imaging studies both indicated isolated brachialis atrophy without deficit elsewhere along the musculocutaneous nerve, electromyography was not performed. The patient was fully functional and working at his usual occupation, and no further intervention was recommended.
Discussion
Isolated wasting of the brachialis muscle is extremely rare with few reports in the literature. Farmer and colleagues1 reported a case of brachialis atrophy that was presumed to have resulted from exercise-induced chronic compartment syndrome. In that case, the patient developed a prodrome of arm pain followed by brachialis muscle atrophy. This patient was treated with oral anti-inflammatory agents with improvement in pain but without recovery of the brachialis muscle. While this case was attributed to compartment syndrome, it is likely that it represented neuralgic amyotrophy because there was no evidence of elbow flexion contracture, which would have accompanied true necrosis of the brachialis muscle as seen in compartment syndrome. However, acute compartment syndrome of the brachialis muscle after minor trauma has been reported.5 In that case, full-scale compartment syndrome was treated with rapid fasciotomy, with complete recovery of the brachialis.
Isolated brachialis atrophy has also been described in the setting of a displaced midshaft clavicle fracture in an elite athlete.2 Two fracture fragments were thought to have injured the brachial plexus, separately causing brachialis atrophy and altered sensation over the clavicular head of the deltoid muscle. Atrophy remained 1 year after injury.
Although it had been occasionally reported, the first large series of patients with sporadic neuralgic amyotrophy in the upper extremity was reported by Parsonage and Turner6 in 1948. They described 136 patients who developed flaccid paralysis and atrophy of various muscles of the shoulder girdle and/or upper extremity. This was generally preceded by acute pain in the shoulder girdle, often associated with antecedent viral infection, stress, illness, or other precipitating factors.
To our knowledge, there have been 3 other reported cases of neuralgic amyotrophy of the brachialis muscle. Watson and colleagues3 presented 2 patients with nonspecific, neurogenic shoulder pain after which an indolent, progressive atrophy of the brachialis muscle ensued.3 Van Tongel and colleagues4 described a more traditional case of Parsonage-Turner syndrome, with bilateral wasting of the shoulder girdle that also exhibited unilateral brachialis atrophy without affecting other muscles in the arm.4 Our case, with shoulder pain followed by muscle atrophy, fits the pattern of neuralgic amyotrophy.
Others have similarly described isolated wasting of 1 muscle with the sparing of other muscles with a common innervation. Isolated atrophy of the extensor or flexor pollicis longus has been reported as variants of either posterior or anterior interosseous neuropathy, respectively.7,8 Nerve fibers in the brachial plexus destined to innervate muscles supplied by the anterior interosseous nerve may be the cause of the motor deficit in cases of anterior interosseous nerve palsy, which seem to be associated with brachial plexitis.9
We present a case of isolated brachialis muscle atrophy after a minor trauma that may have resulted from Parsonage-Turner syndrome or a variant of brachial plexitis. The constellation of shoulder and arm pain, with subsequent muscle atrophy, makes this diagnosis likely.
Isolated brachialis muscle atrophy has been rarely reported. Among the few cases in the literature, 1 was attributed to a presumed compartment syndrome,1 1 to a displaced clavicle fracture,2 and 3 to neuralgic amyotrophy.3,4 We present a case of isolated brachialis muscle atrophy of unknown etiology, the presentation of which is consistent with neuralgic amyotrophy, also known as Parsonage-Turner syndrome or brachial plexitis. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old right-handed highway worker presented for evaluation of right-arm muscle atrophy. One year earlier, while lifting heavy bags at work, he felt a painful strain in his right arm, although there was no bruising or swelling. Approximately 4 weeks after this incident, he developed right shoulder pain and began to notice a slight decrease in the muscle mass of his right anterior arm. On evaluation at an outside facility, the physician noted some brachialis muscle atrophy. His shoulder pain was attributed to acromioclavicular joint problems. After an initial trial of physical therapy that did not alleviate this joint pain, an acromioclavicular joint resection was performed, and his pain improved. The brachialis muscle atrophy continued to progress, however. Over the course of the next 6 months, the patient noticed a continually decreasing muscle mass in his right arm, as well as arm fatigue with routine recreational activities. On follow-up, again at an outside institution, the treating physicians noted continued atrophy of the distal arm corresponding to the region of the brachialis musculature. Magnetic resonance imaging showed continuity of the brachialis muscle and tendon, with muscle atrophy. The patient was able to return to work, although with a subjective decrease in right elbow flexion strength.
On presentation at our institution, the patient complained of right arm weakness with heavy use but did not have pain or sensory complaints. His medical history was otherwise unremarkable. Physical examination revealed obvious wasting of the right brachialis muscle, most notable on the lateral aspect of the distal arm (Figures 1, 2A, 2B). His biceps muscle was functioning with full strength and had a normal bulk. He had a normal range of active and passive motion, including full extension and flexion of both elbows, as well as complete pronosupination of the forearms. There was no focal tenderness. Manual muscle testing of both upper extremities was completely normal except for 4/5 flexion strength of the right elbow. Neurovascular examination also revealed normal findings, including intact sensation over the radiolateral forearm. A second magnetic resonance image showed that the brachialis muscle had completely atrophied. Because the clinical examination and imaging studies both indicated isolated brachialis atrophy without deficit elsewhere along the musculocutaneous nerve, electromyography was not performed. The patient was fully functional and working at his usual occupation, and no further intervention was recommended.
Discussion
Isolated wasting of the brachialis muscle is extremely rare with few reports in the literature. Farmer and colleagues1 reported a case of brachialis atrophy that was presumed to have resulted from exercise-induced chronic compartment syndrome. In that case, the patient developed a prodrome of arm pain followed by brachialis muscle atrophy. This patient was treated with oral anti-inflammatory agents with improvement in pain but without recovery of the brachialis muscle. While this case was attributed to compartment syndrome, it is likely that it represented neuralgic amyotrophy because there was no evidence of elbow flexion contracture, which would have accompanied true necrosis of the brachialis muscle as seen in compartment syndrome. However, acute compartment syndrome of the brachialis muscle after minor trauma has been reported.5 In that case, full-scale compartment syndrome was treated with rapid fasciotomy, with complete recovery of the brachialis.
Isolated brachialis atrophy has also been described in the setting of a displaced midshaft clavicle fracture in an elite athlete.2 Two fracture fragments were thought to have injured the brachial plexus, separately causing brachialis atrophy and altered sensation over the clavicular head of the deltoid muscle. Atrophy remained 1 year after injury.
Although it had been occasionally reported, the first large series of patients with sporadic neuralgic amyotrophy in the upper extremity was reported by Parsonage and Turner6 in 1948. They described 136 patients who developed flaccid paralysis and atrophy of various muscles of the shoulder girdle and/or upper extremity. This was generally preceded by acute pain in the shoulder girdle, often associated with antecedent viral infection, stress, illness, or other precipitating factors.
To our knowledge, there have been 3 other reported cases of neuralgic amyotrophy of the brachialis muscle. Watson and colleagues3 presented 2 patients with nonspecific, neurogenic shoulder pain after which an indolent, progressive atrophy of the brachialis muscle ensued.3 Van Tongel and colleagues4 described a more traditional case of Parsonage-Turner syndrome, with bilateral wasting of the shoulder girdle that also exhibited unilateral brachialis atrophy without affecting other muscles in the arm.4 Our case, with shoulder pain followed by muscle atrophy, fits the pattern of neuralgic amyotrophy.
Others have similarly described isolated wasting of 1 muscle with the sparing of other muscles with a common innervation. Isolated atrophy of the extensor or flexor pollicis longus has been reported as variants of either posterior or anterior interosseous neuropathy, respectively.7,8 Nerve fibers in the brachial plexus destined to innervate muscles supplied by the anterior interosseous nerve may be the cause of the motor deficit in cases of anterior interosseous nerve palsy, which seem to be associated with brachial plexitis.9
We present a case of isolated brachialis muscle atrophy after a minor trauma that may have resulted from Parsonage-Turner syndrome or a variant of brachial plexitis. The constellation of shoulder and arm pain, with subsequent muscle atrophy, makes this diagnosis likely.
1. Farmer KW, McFarland EG, Sonin A, Cosgarea AJ, Roehrig GJ. Isolated necrosis of the brachialis muscle due to exercise. Orthopedics. 2002;25(6):682-684.
2. Rüst CA, Knechtle B, Knechtle P, Rosemann T. Atrophy of the brachialis muscle after a displaced clavicle fracture in an Ironman triathlete: case report. J Brachial Plex Periph Nerve Inj. 2011;6(1):e44-e47.
3. Watson BV, Rose-Innes A, Engstrom JW, Brown JD. Isolated brachialis wasting: an unusual presentation of neuralgic amyotrophy. Muscle Nerve. 2001;24(12):1699-1702.
4. Van Tongel A, Schreurs M, Bruyninckx F, Debeer P. Bilateral Parsonage-Turner syndrome with unilateral brachialis muscle wasting: a case report. J Shoulder Elbow Surg. 2010;19(8):e14-e16.
5. Jenkins NH, Mintowt-Czyz WJ. Compression of the biceps-brachialis compartment after trivial trauma. J Bone Joint Surg Br. 1986;68(3):374.
6. Parsonage MJ, Turner JW. Neuralgic amyotrophy; the shoulder-girdle syndrome. Lancet. 1948;1(6513):973-978.
7. Horton TC. Isolated paralysis of the extensor pollicis longus muscle: a further variation of posterior interosseous nerve palsy. J Hand Surg Br. 2000;25(2):225-226.
8. Hill NA, Howard FM, Huffer BR. The incomplete anterior interosseous nerve syndrome. J Hand Surg Am. 1985;10(1):4-16.
9. Rennels GD, Ochoa J. Neuralgic amyotrophy manifesting as anterior interosseous nerve palsy. Muscle Nerve. 1980;3(2):160-164.
1. Farmer KW, McFarland EG, Sonin A, Cosgarea AJ, Roehrig GJ. Isolated necrosis of the brachialis muscle due to exercise. Orthopedics. 2002;25(6):682-684.
2. Rüst CA, Knechtle B, Knechtle P, Rosemann T. Atrophy of the brachialis muscle after a displaced clavicle fracture in an Ironman triathlete: case report. J Brachial Plex Periph Nerve Inj. 2011;6(1):e44-e47.
3. Watson BV, Rose-Innes A, Engstrom JW, Brown JD. Isolated brachialis wasting: an unusual presentation of neuralgic amyotrophy. Muscle Nerve. 2001;24(12):1699-1702.
4. Van Tongel A, Schreurs M, Bruyninckx F, Debeer P. Bilateral Parsonage-Turner syndrome with unilateral brachialis muscle wasting: a case report. J Shoulder Elbow Surg. 2010;19(8):e14-e16.
5. Jenkins NH, Mintowt-Czyz WJ. Compression of the biceps-brachialis compartment after trivial trauma. J Bone Joint Surg Br. 1986;68(3):374.
6. Parsonage MJ, Turner JW. Neuralgic amyotrophy; the shoulder-girdle syndrome. Lancet. 1948;1(6513):973-978.
7. Horton TC. Isolated paralysis of the extensor pollicis longus muscle: a further variation of posterior interosseous nerve palsy. J Hand Surg Br. 2000;25(2):225-226.
8. Hill NA, Howard FM, Huffer BR. The incomplete anterior interosseous nerve syndrome. J Hand Surg Am. 1985;10(1):4-16.
9. Rennels GD, Ochoa J. Neuralgic amyotrophy manifesting as anterior interosseous nerve palsy. Muscle Nerve. 1980;3(2):160-164.

FDA approves lesinurad for uric acid lowering in gout
Lesinurad (Zurampic) has been approved to treat hyperuricemia associated with gout, when used in combination with a xanthine oxidase inhibitor, the Food and Drug Administration announced on Dec. 22.
Lesinurad promotes uric acid excretion by inhibiting the function of transporter proteins involved in uric acid reabsorption in the kidney.
“Zurampic provides a new treatment option for the millions of people who may develop gout over their lifetimes,” said Dr. Badrul Chowdhury, director of the Division of Pulmonary, Allergy, and Rheumatology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s safety and efficacy were evaluated in 1,537 participants in three randomized, placebo-controlled studies of its use in combination with a xanthine oxidase inhibitor. Participants treated for up to 12 months with lesinurad experienced reduced serum uric acid levels, compared with participants given placebo.
The most common adverse reactions in the clinical trials were headache, influenza, increased blood creatinine, and gastroesophageal reflux disease. Lesinurad has a boxed warning that provides important safety information, including the risk for acute renal failure, which is more common when lesinurad is used without a xanthine oxidase inhibitor and with higher-than-approved doses.
The FDA also said in its statement that the agency is requiring a postmarketing study to further evaluate the renal and cardiovascular safety of lesinurad.
Zurampic is manufactured by AstraZeneca Pharmaceuticals.
On Twitter @maryjodales
Lesinurad (Zurampic) has been approved to treat hyperuricemia associated with gout, when used in combination with a xanthine oxidase inhibitor, the Food and Drug Administration announced on Dec. 22.
Lesinurad promotes uric acid excretion by inhibiting the function of transporter proteins involved in uric acid reabsorption in the kidney.
“Zurampic provides a new treatment option for the millions of people who may develop gout over their lifetimes,” said Dr. Badrul Chowdhury, director of the Division of Pulmonary, Allergy, and Rheumatology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s safety and efficacy were evaluated in 1,537 participants in three randomized, placebo-controlled studies of its use in combination with a xanthine oxidase inhibitor. Participants treated for up to 12 months with lesinurad experienced reduced serum uric acid levels, compared with participants given placebo.
The most common adverse reactions in the clinical trials were headache, influenza, increased blood creatinine, and gastroesophageal reflux disease. Lesinurad has a boxed warning that provides important safety information, including the risk for acute renal failure, which is more common when lesinurad is used without a xanthine oxidase inhibitor and with higher-than-approved doses.
The FDA also said in its statement that the agency is requiring a postmarketing study to further evaluate the renal and cardiovascular safety of lesinurad.
Zurampic is manufactured by AstraZeneca Pharmaceuticals.
On Twitter @maryjodales
Lesinurad (Zurampic) has been approved to treat hyperuricemia associated with gout, when used in combination with a xanthine oxidase inhibitor, the Food and Drug Administration announced on Dec. 22.
Lesinurad promotes uric acid excretion by inhibiting the function of transporter proteins involved in uric acid reabsorption in the kidney.
“Zurampic provides a new treatment option for the millions of people who may develop gout over their lifetimes,” said Dr. Badrul Chowdhury, director of the Division of Pulmonary, Allergy, and Rheumatology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s safety and efficacy were evaluated in 1,537 participants in three randomized, placebo-controlled studies of its use in combination with a xanthine oxidase inhibitor. Participants treated for up to 12 months with lesinurad experienced reduced serum uric acid levels, compared with participants given placebo.
The most common adverse reactions in the clinical trials were headache, influenza, increased blood creatinine, and gastroesophageal reflux disease. Lesinurad has a boxed warning that provides important safety information, including the risk for acute renal failure, which is more common when lesinurad is used without a xanthine oxidase inhibitor and with higher-than-approved doses.
The FDA also said in its statement that the agency is requiring a postmarketing study to further evaluate the renal and cardiovascular safety of lesinurad.
Zurampic is manufactured by AstraZeneca Pharmaceuticals.
On Twitter @maryjodales
16 New Year’s resolutions for psychiatrists in 2016
Such decisions can be made at any time, but the dawn of a year is a powerful signal of a new beginning—another lease on life, a potential turning point. Imbedded in those resolutions is a subliminal sense of urgency to correct one’s long-neglected shortcomings as the calendar ruthlessly points to inevitable aging and the relentless march of time.
A psychiatric perspective
For psychiatrists, New Year’s resolutions transcend the (often ephemeral) impulse to go on a diet or buy a membership at the local gym. We have a unique perspective on the challenges that our patients face every day as they cope with the complex demands of life despite their anxiety, depression, or psychosis.
We are aware of the many unmet needs in managing complex neuropsychiatric brain disorders and the major challenges of erasing the burdensome stigma that engulfs our patients and the practice of psychiatry itself—despite its noble mission of repairing fractured brains, mending tortured souls, and restoring peace of mind and wellness. We are proud of our clinical and scientific accomplishments but are painfully cognizant of our limitations and the huge chasm between what we know and what we will eventually know once the brain reveals its glorious mysteries through neuroscientific research.
What can you resolve?
Here is my proposed list of pragmatic resolutions that most psychiatrists would regard as part of a perpetual to-do list—a must-do bucket of cherished goals and brave new horizons to bring complete mental health for our patients and immeasurable gratification for us, who dream of cures for brain disorders that trigger various ailments of the mind.
- Practice like a physician to emphasize the medical foundation of psychiatry: Always check on a patient’s physical health, and monitor his (her) cardiometabolic status. Wear the symbolic white coat that often enhances the physician−patient relationship.
- Dedicate a significant percentage of your practice to the sickest patients. There are enough non-physician mental health professionals to handle the walking wounded and worried well.
- Advocate relentlessly throughout your sphere of influence, and publicly, for true parity between psychiatric and non-mental medical disorders—not only for insurance coverage but for overall societal acceptance and compassion as well.
- Lobby vigorously for hospitalization instead of imprisonment of the seriously mentally ill because psychosis is a brain disease, not a criminal offense.
- Adopt evidence-based psychiatric practice whenever possible to achieve the best outcomes. Judiciously implement off-label practices, however, if no evidence-based treatments exist for a suffering patient.
- Avoid senseless and irrational polypharmacy but do not hesitate to use rational, beneficial combination therapy.
- Provide 1 hour a week of pro bono psychiatric work for the indigent and underserved. The rewards of giving what amounts to 1 week a year are immeasurably more gratifying than a few more dollars in your bank account.
- Resist calling an ill person a ‘client’ or ‘consumer’—at least until oncologists and cardiologists start doing so. Refuse to give up your medical identify in the many de-medicalized mental health clinics.
- Never let a patient leave your office without some psychotherapy, even as part of a 15-minute med-check.
- Stay current and on the cutting edge of evolving psychiatric practice by logging into PubMed every day (even briefly) to read a few abstracts of the latest studies related to patients you saw that day.
- Think like a neurologist by identifying the neural circuits of psychiatric symptoms. Act like a cardiologist by doing everything medically possible to prevent recurrence of psychotic, manic, or depressive episodes because they damage brain tissue just as a myocardial infarction damages the heart.
- Support research with words, money, and passion. Psychiatric neuroscientific breakthroughs generate superior treatments, erase stigma, and advance the quality of life for patients. Donate annually to the researchers of your choice, at the medical school where you were trained, or at a nonprofit research institute.
- Make time to write for publication, annually, at least 1 case report or a letter to the editor about observations from your practice. You can contribute immensely to the discovery process by sharing novel clinical insights.
- Never give up on any patient or set expectations too low, regardless of the diagnosis or severity of illness. Giving up destroys hope and ushers in despondency. Get a second opinion if you run out of options for a patient.
- Always set remission followed by recovery as the therapeutic goal for every patient. Let the patient know this and ask him (her) commit to that goal with you.
- Be genuinely proud to be a psychiatrist. You assess and rectify disorders of the mind, the most complex and magical product of the human brain that determines who we are and how we think, emote, communicate, verbalize, empathize, love, hate, remember, plan, problem-solve, and, of course, make resolutions.
Back to diet and exercise—for our patients and for us!
It’s OK to include, among your New Year’s resolutions, a pledge to strongly encourage patients to diet and exercise. Given the tendency of many of them to gain weight and die prematurely as a consequence of obesity-related cardiometabolic risk factors, you should urge them to eat healthy and exercise every time you see them, not only on New Year’s Day.
Such decisions can be made at any time, but the dawn of a year is a powerful signal of a new beginning—another lease on life, a potential turning point. Imbedded in those resolutions is a subliminal sense of urgency to correct one’s long-neglected shortcomings as the calendar ruthlessly points to inevitable aging and the relentless march of time.
A psychiatric perspective
For psychiatrists, New Year’s resolutions transcend the (often ephemeral) impulse to go on a diet or buy a membership at the local gym. We have a unique perspective on the challenges that our patients face every day as they cope with the complex demands of life despite their anxiety, depression, or psychosis.
We are aware of the many unmet needs in managing complex neuropsychiatric brain disorders and the major challenges of erasing the burdensome stigma that engulfs our patients and the practice of psychiatry itself—despite its noble mission of repairing fractured brains, mending tortured souls, and restoring peace of mind and wellness. We are proud of our clinical and scientific accomplishments but are painfully cognizant of our limitations and the huge chasm between what we know and what we will eventually know once the brain reveals its glorious mysteries through neuroscientific research.
What can you resolve?
Here is my proposed list of pragmatic resolutions that most psychiatrists would regard as part of a perpetual to-do list—a must-do bucket of cherished goals and brave new horizons to bring complete mental health for our patients and immeasurable gratification for us, who dream of cures for brain disorders that trigger various ailments of the mind.
- Practice like a physician to emphasize the medical foundation of psychiatry: Always check on a patient’s physical health, and monitor his (her) cardiometabolic status. Wear the symbolic white coat that often enhances the physician−patient relationship.
- Dedicate a significant percentage of your practice to the sickest patients. There are enough non-physician mental health professionals to handle the walking wounded and worried well.
- Advocate relentlessly throughout your sphere of influence, and publicly, for true parity between psychiatric and non-mental medical disorders—not only for insurance coverage but for overall societal acceptance and compassion as well.
- Lobby vigorously for hospitalization instead of imprisonment of the seriously mentally ill because psychosis is a brain disease, not a criminal offense.
- Adopt evidence-based psychiatric practice whenever possible to achieve the best outcomes. Judiciously implement off-label practices, however, if no evidence-based treatments exist for a suffering patient.
- Avoid senseless and irrational polypharmacy but do not hesitate to use rational, beneficial combination therapy.
- Provide 1 hour a week of pro bono psychiatric work for the indigent and underserved. The rewards of giving what amounts to 1 week a year are immeasurably more gratifying than a few more dollars in your bank account.
- Resist calling an ill person a ‘client’ or ‘consumer’—at least until oncologists and cardiologists start doing so. Refuse to give up your medical identify in the many de-medicalized mental health clinics.
- Never let a patient leave your office without some psychotherapy, even as part of a 15-minute med-check.
- Stay current and on the cutting edge of evolving psychiatric practice by logging into PubMed every day (even briefly) to read a few abstracts of the latest studies related to patients you saw that day.
- Think like a neurologist by identifying the neural circuits of psychiatric symptoms. Act like a cardiologist by doing everything medically possible to prevent recurrence of psychotic, manic, or depressive episodes because they damage brain tissue just as a myocardial infarction damages the heart.
- Support research with words, money, and passion. Psychiatric neuroscientific breakthroughs generate superior treatments, erase stigma, and advance the quality of life for patients. Donate annually to the researchers of your choice, at the medical school where you were trained, or at a nonprofit research institute.
- Make time to write for publication, annually, at least 1 case report or a letter to the editor about observations from your practice. You can contribute immensely to the discovery process by sharing novel clinical insights.
- Never give up on any patient or set expectations too low, regardless of the diagnosis or severity of illness. Giving up destroys hope and ushers in despondency. Get a second opinion if you run out of options for a patient.
- Always set remission followed by recovery as the therapeutic goal for every patient. Let the patient know this and ask him (her) commit to that goal with you.
- Be genuinely proud to be a psychiatrist. You assess and rectify disorders of the mind, the most complex and magical product of the human brain that determines who we are and how we think, emote, communicate, verbalize, empathize, love, hate, remember, plan, problem-solve, and, of course, make resolutions.
Back to diet and exercise—for our patients and for us!
It’s OK to include, among your New Year’s resolutions, a pledge to strongly encourage patients to diet and exercise. Given the tendency of many of them to gain weight and die prematurely as a consequence of obesity-related cardiometabolic risk factors, you should urge them to eat healthy and exercise every time you see them, not only on New Year’s Day.
Such decisions can be made at any time, but the dawn of a year is a powerful signal of a new beginning—another lease on life, a potential turning point. Imbedded in those resolutions is a subliminal sense of urgency to correct one’s long-neglected shortcomings as the calendar ruthlessly points to inevitable aging and the relentless march of time.
A psychiatric perspective
For psychiatrists, New Year’s resolutions transcend the (often ephemeral) impulse to go on a diet or buy a membership at the local gym. We have a unique perspective on the challenges that our patients face every day as they cope with the complex demands of life despite their anxiety, depression, or psychosis.
We are aware of the many unmet needs in managing complex neuropsychiatric brain disorders and the major challenges of erasing the burdensome stigma that engulfs our patients and the practice of psychiatry itself—despite its noble mission of repairing fractured brains, mending tortured souls, and restoring peace of mind and wellness. We are proud of our clinical and scientific accomplishments but are painfully cognizant of our limitations and the huge chasm between what we know and what we will eventually know once the brain reveals its glorious mysteries through neuroscientific research.
What can you resolve?
Here is my proposed list of pragmatic resolutions that most psychiatrists would regard as part of a perpetual to-do list—a must-do bucket of cherished goals and brave new horizons to bring complete mental health for our patients and immeasurable gratification for us, who dream of cures for brain disorders that trigger various ailments of the mind.
- Practice like a physician to emphasize the medical foundation of psychiatry: Always check on a patient’s physical health, and monitor his (her) cardiometabolic status. Wear the symbolic white coat that often enhances the physician−patient relationship.
- Dedicate a significant percentage of your practice to the sickest patients. There are enough non-physician mental health professionals to handle the walking wounded and worried well.
- Advocate relentlessly throughout your sphere of influence, and publicly, for true parity between psychiatric and non-mental medical disorders—not only for insurance coverage but for overall societal acceptance and compassion as well.
- Lobby vigorously for hospitalization instead of imprisonment of the seriously mentally ill because psychosis is a brain disease, not a criminal offense.
- Adopt evidence-based psychiatric practice whenever possible to achieve the best outcomes. Judiciously implement off-label practices, however, if no evidence-based treatments exist for a suffering patient.
- Avoid senseless and irrational polypharmacy but do not hesitate to use rational, beneficial combination therapy.
- Provide 1 hour a week of pro bono psychiatric work for the indigent and underserved. The rewards of giving what amounts to 1 week a year are immeasurably more gratifying than a few more dollars in your bank account.
- Resist calling an ill person a ‘client’ or ‘consumer’—at least until oncologists and cardiologists start doing so. Refuse to give up your medical identify in the many de-medicalized mental health clinics.
- Never let a patient leave your office without some psychotherapy, even as part of a 15-minute med-check.
- Stay current and on the cutting edge of evolving psychiatric practice by logging into PubMed every day (even briefly) to read a few abstracts of the latest studies related to patients you saw that day.
- Think like a neurologist by identifying the neural circuits of psychiatric symptoms. Act like a cardiologist by doing everything medically possible to prevent recurrence of psychotic, manic, or depressive episodes because they damage brain tissue just as a myocardial infarction damages the heart.
- Support research with words, money, and passion. Psychiatric neuroscientific breakthroughs generate superior treatments, erase stigma, and advance the quality of life for patients. Donate annually to the researchers of your choice, at the medical school where you were trained, or at a nonprofit research institute.
- Make time to write for publication, annually, at least 1 case report or a letter to the editor about observations from your practice. You can contribute immensely to the discovery process by sharing novel clinical insights.
- Never give up on any patient or set expectations too low, regardless of the diagnosis or severity of illness. Giving up destroys hope and ushers in despondency. Get a second opinion if you run out of options for a patient.
- Always set remission followed by recovery as the therapeutic goal for every patient. Let the patient know this and ask him (her) commit to that goal with you.
- Be genuinely proud to be a psychiatrist. You assess and rectify disorders of the mind, the most complex and magical product of the human brain that determines who we are and how we think, emote, communicate, verbalize, empathize, love, hate, remember, plan, problem-solve, and, of course, make resolutions.
Back to diet and exercise—for our patients and for us!
It’s OK to include, among your New Year’s resolutions, a pledge to strongly encourage patients to diet and exercise. Given the tendency of many of them to gain weight and die prematurely as a consequence of obesity-related cardiometabolic risk factors, you should urge them to eat healthy and exercise every time you see them, not only on New Year’s Day.
A checklist of approaches for alleviating behavioral problems in dementia
Dementia—“major neurocognitive disorder” in DSM-5—manifests as progressive decline in cognitive function.In tandem with that decline, approximately 80% of nursing home patients with dementia exhibit behavioral disturbances,1 including irritability, insomnia, wandering, and repetitive questioning.1,2 These disturbances can erode their quality of life and can frustrate caregivers and providers.3
Causative pathology
Before designing a therapeutic intervention for cognitively impaired people with behavioral disturbances, a precise diagnosis of the causative pathology must be determined. This affords therapies that specifically address the patient’s problems. Other related and unrelated somatic or mental health concerns should be identified to specify the optimal approach.
Patients in whom dementia is suspected require that a thorough medical, psychiatric, substance use, and family history be taken to identify predisposing factors for their illness2; exhaustive review of the history might reveal drug interactions or polypharmacy that can cause or exacerbate symptoms, including behavioral manifestations. Physical examination, cognitive function testing, laboratory tests, and neuroimaging also help reveal the etiologic diagnosis of the dementia.1,3
Identifying the diagnosis directs the treatment; for example, a behaviorally discontrolled person with a cognitive, stroke-induced encephalopathy requires an entirely different regimen than a comparatively compromised individual with Alzheimer’s disease or frontotemporal dementia. Early detection of dementia also is helpful for managing its cognitive and behavioral problems more effectively.1Once a diagnosis of dementia is established, it might be behavioral symptoms and poor insight that become more worrisome to the patient’s caregivers and providers than cognitive deficits. Your task is then to apply behavioral approaches to management, with consistency, to maximize, at all times, the patient’s safety and comfort.4
How you approach behavioral management is important
Consider these interventions:
- Ensure that you appropriately treat associated depression, pain, and somatic illness—whether related or unrelated to dementia.
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
- Provide family and caregivers with disease education, social support, and management tips1,2; be respectful to family members in all interactions.3
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
Minimize psychosocial and environmental stressors
- Avoid unnecessary environmental changes, such as rearranging or refurbishing the patient’s living space.1
- As noted, ensure that the patient is comfortable and safe in his (her) surroundings, such as providing wall-mounted handrails and other aids for ambulation.
- Provide access to television, proper lighting, and other indicated life-enhancing devices.1,2
- Consider a pet for the patient; pets can be an important adjunct in providing comfort.
- Provide music to reduce agitation and anxiety.4
- Appeal to institutional administration to provide a higher staff−patient ratio for comfort and security.2,5
- Because social contact is helpful to build a pleasant environment, preserve opportunities for the patient to communicate with others, and facilitate socialization by encouraging friendly interactions.1
- Provide stimulation and diversion with social activities, support programs, and physical exercise—sources of interaction that can promote health and improve sleep.
- Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.2,5
- Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.1
- Provide access to television, proper lighting, and other indicated life-enhancing devices.Provide music to reduce agitation and anxiety.Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.
Other considerations
- Identify and treat primary and secondary causes of the underlying major neurocognitive disorder.
- Use an integrative, multidisciplinary approach to manage behavioral problems in dementia.
- Utilize a social worker’s expertise to faciliate family, financial, or related social issues and better cooperation. This promotes comfort for patients, families, and staff.
- Physical therapy aids in maintaining physical function, especially preservation of gait, balance, and range of motion. Thus, with greater stability avoiding a fall can be a life-saving event.
- Socialization, mental outlook, and emotional health are improved by occupational therapist interventions.
- Individual psychotherapy helps to improve self-esteem and personal adjustment. Group activities reinforces interpersonal connections.
- Refer the family and caregivers for supportive therapy and education on dementia; such resources help minimize deleterious effects of the patient’s behavioral problems on those key people.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tampi RR, Williamson D, Muralee S, et al. Behavioral and psychological symptoms of dementia: part I—epidemiology, neurobiology, heritability, and evaluation. Clinical Geriatrics. 2011;19:41-46.
2. Hulme C, Wright J, Crocker T, et al. Non-pharmacological approaches for dementia that informal carers might try or access: a systematic review. Int J Geriatr Psychiatry. 2010;25(7):756-763.
3. Perkins R. Evidence-based practice interventions for managing behavioral and psychological symptoms of dementia in nursing home residents. Ann Longterm Care. 2012;20(12):24.
4. Desai AK, Grossberg GT. Recognition and management of behavioral disturbances in dementia. Prim Care Companion J Clin Psychiatry. 2001;3(3):93-109.
5. Douglas S, James I, Ballard C. Non-pharmacological interventions in dementia. Advances in Psychiatric Treatment. 2004;10(3):171-177.
Dementia—“major neurocognitive disorder” in DSM-5—manifests as progressive decline in cognitive function.In tandem with that decline, approximately 80% of nursing home patients with dementia exhibit behavioral disturbances,1 including irritability, insomnia, wandering, and repetitive questioning.1,2 These disturbances can erode their quality of life and can frustrate caregivers and providers.3
Causative pathology
Before designing a therapeutic intervention for cognitively impaired people with behavioral disturbances, a precise diagnosis of the causative pathology must be determined. This affords therapies that specifically address the patient’s problems. Other related and unrelated somatic or mental health concerns should be identified to specify the optimal approach.
Patients in whom dementia is suspected require that a thorough medical, psychiatric, substance use, and family history be taken to identify predisposing factors for their illness2; exhaustive review of the history might reveal drug interactions or polypharmacy that can cause or exacerbate symptoms, including behavioral manifestations. Physical examination, cognitive function testing, laboratory tests, and neuroimaging also help reveal the etiologic diagnosis of the dementia.1,3
Identifying the diagnosis directs the treatment; for example, a behaviorally discontrolled person with a cognitive, stroke-induced encephalopathy requires an entirely different regimen than a comparatively compromised individual with Alzheimer’s disease or frontotemporal dementia. Early detection of dementia also is helpful for managing its cognitive and behavioral problems more effectively.1Once a diagnosis of dementia is established, it might be behavioral symptoms and poor insight that become more worrisome to the patient’s caregivers and providers than cognitive deficits. Your task is then to apply behavioral approaches to management, with consistency, to maximize, at all times, the patient’s safety and comfort.4
How you approach behavioral management is important
Consider these interventions:
- Ensure that you appropriately treat associated depression, pain, and somatic illness—whether related or unrelated to dementia.
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
- Provide family and caregivers with disease education, social support, and management tips1,2; be respectful to family members in all interactions.3
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
Minimize psychosocial and environmental stressors
- Avoid unnecessary environmental changes, such as rearranging or refurbishing the patient’s living space.1
- As noted, ensure that the patient is comfortable and safe in his (her) surroundings, such as providing wall-mounted handrails and other aids for ambulation.
- Provide access to television, proper lighting, and other indicated life-enhancing devices.1,2
- Consider a pet for the patient; pets can be an important adjunct in providing comfort.
- Provide music to reduce agitation and anxiety.4
- Appeal to institutional administration to provide a higher staff−patient ratio for comfort and security.2,5
- Because social contact is helpful to build a pleasant environment, preserve opportunities for the patient to communicate with others, and facilitate socialization by encouraging friendly interactions.1
- Provide stimulation and diversion with social activities, support programs, and physical exercise—sources of interaction that can promote health and improve sleep.
- Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.2,5
- Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.1
- Provide access to television, proper lighting, and other indicated life-enhancing devices.Provide music to reduce agitation and anxiety.Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.
Other considerations
- Identify and treat primary and secondary causes of the underlying major neurocognitive disorder.
- Use an integrative, multidisciplinary approach to manage behavioral problems in dementia.
- Utilize a social worker’s expertise to faciliate family, financial, or related social issues and better cooperation. This promotes comfort for patients, families, and staff.
- Physical therapy aids in maintaining physical function, especially preservation of gait, balance, and range of motion. Thus, with greater stability avoiding a fall can be a life-saving event.
- Socialization, mental outlook, and emotional health are improved by occupational therapist interventions.
- Individual psychotherapy helps to improve self-esteem and personal adjustment. Group activities reinforces interpersonal connections.
- Refer the family and caregivers for supportive therapy and education on dementia; such resources help minimize deleterious effects of the patient’s behavioral problems on those key people.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dementia—“major neurocognitive disorder” in DSM-5—manifests as progressive decline in cognitive function.In tandem with that decline, approximately 80% of nursing home patients with dementia exhibit behavioral disturbances,1 including irritability, insomnia, wandering, and repetitive questioning.1,2 These disturbances can erode their quality of life and can frustrate caregivers and providers.3
Causative pathology
Before designing a therapeutic intervention for cognitively impaired people with behavioral disturbances, a precise diagnosis of the causative pathology must be determined. This affords therapies that specifically address the patient’s problems. Other related and unrelated somatic or mental health concerns should be identified to specify the optimal approach.
Patients in whom dementia is suspected require that a thorough medical, psychiatric, substance use, and family history be taken to identify predisposing factors for their illness2; exhaustive review of the history might reveal drug interactions or polypharmacy that can cause or exacerbate symptoms, including behavioral manifestations. Physical examination, cognitive function testing, laboratory tests, and neuroimaging also help reveal the etiologic diagnosis of the dementia.1,3
Identifying the diagnosis directs the treatment; for example, a behaviorally discontrolled person with a cognitive, stroke-induced encephalopathy requires an entirely different regimen than a comparatively compromised individual with Alzheimer’s disease or frontotemporal dementia. Early detection of dementia also is helpful for managing its cognitive and behavioral problems more effectively.1Once a diagnosis of dementia is established, it might be behavioral symptoms and poor insight that become more worrisome to the patient’s caregivers and providers than cognitive deficits. Your task is then to apply behavioral approaches to management, with consistency, to maximize, at all times, the patient’s safety and comfort.4
How you approach behavioral management is important
Consider these interventions:
- Ensure that you appropriately treat associated depression, pain, and somatic illness—whether related or unrelated to dementia.
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
- Provide family and caregivers with disease education, social support, and management tips1,2; be respectful to family members in all interactions.3
- Offer caregivers and staff a plan for attending to supportive measures, including nutrition, hydration, and socialization.
Minimize psychosocial and environmental stressors
- Avoid unnecessary environmental changes, such as rearranging or refurbishing the patient’s living space.1
- As noted, ensure that the patient is comfortable and safe in his (her) surroundings, such as providing wall-mounted handrails and other aids for ambulation.
- Provide access to television, proper lighting, and other indicated life-enhancing devices.1,2
- Consider a pet for the patient; pets can be an important adjunct in providing comfort.
- Provide music to reduce agitation and anxiety.4
- Appeal to institutional administration to provide a higher staff−patient ratio for comfort and security.2,5
- Because social contact is helpful to build a pleasant environment, preserve opportunities for the patient to communicate with others, and facilitate socialization by encouraging friendly interactions.1
- Provide stimulation and diversion with social activities, support programs, and physical exercise—sources of interaction that can promote health and improve sleep.
- Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.2,5
- Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.1
- Provide access to television, proper lighting, and other indicated life-enhancing devices.Provide music to reduce agitation and anxiety.Redirection and validation are helpful to divert a patient’s attention from stressful situations and keep him (her) calm.Pharmacotherapy should be implemented if psychosocial methods of behavioral management fail or the patient’s behavior becomes threatening.
Other considerations
- Identify and treat primary and secondary causes of the underlying major neurocognitive disorder.
- Use an integrative, multidisciplinary approach to manage behavioral problems in dementia.
- Utilize a social worker’s expertise to faciliate family, financial, or related social issues and better cooperation. This promotes comfort for patients, families, and staff.
- Physical therapy aids in maintaining physical function, especially preservation of gait, balance, and range of motion. Thus, with greater stability avoiding a fall can be a life-saving event.
- Socialization, mental outlook, and emotional health are improved by occupational therapist interventions.
- Individual psychotherapy helps to improve self-esteem and personal adjustment. Group activities reinforces interpersonal connections.
- Refer the family and caregivers for supportive therapy and education on dementia; such resources help minimize deleterious effects of the patient’s behavioral problems on those key people.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tampi RR, Williamson D, Muralee S, et al. Behavioral and psychological symptoms of dementia: part I—epidemiology, neurobiology, heritability, and evaluation. Clinical Geriatrics. 2011;19:41-46.
2. Hulme C, Wright J, Crocker T, et al. Non-pharmacological approaches for dementia that informal carers might try or access: a systematic review. Int J Geriatr Psychiatry. 2010;25(7):756-763.
3. Perkins R. Evidence-based practice interventions for managing behavioral and psychological symptoms of dementia in nursing home residents. Ann Longterm Care. 2012;20(12):24.
4. Desai AK, Grossberg GT. Recognition and management of behavioral disturbances in dementia. Prim Care Companion J Clin Psychiatry. 2001;3(3):93-109.
5. Douglas S, James I, Ballard C. Non-pharmacological interventions in dementia. Advances in Psychiatric Treatment. 2004;10(3):171-177.
1. Tampi RR, Williamson D, Muralee S, et al. Behavioral and psychological symptoms of dementia: part I—epidemiology, neurobiology, heritability, and evaluation. Clinical Geriatrics. 2011;19:41-46.
2. Hulme C, Wright J, Crocker T, et al. Non-pharmacological approaches for dementia that informal carers might try or access: a systematic review. Int J Geriatr Psychiatry. 2010;25(7):756-763.
3. Perkins R. Evidence-based practice interventions for managing behavioral and psychological symptoms of dementia in nursing home residents. Ann Longterm Care. 2012;20(12):24.
4. Desai AK, Grossberg GT. Recognition and management of behavioral disturbances in dementia. Prim Care Companion J Clin Psychiatry. 2001;3(3):93-109.
5. Douglas S, James I, Ballard C. Non-pharmacological interventions in dementia. Advances in Psychiatric Treatment. 2004;10(3):171-177.
Self-directed learning
Never before in history has medicine progressed as quickly as it does today. The half-life of knowledge and practices is shortening, and the ocean of literature continues to amass every day. In this context, it is simply not possible for training programs to teach in didactics everything residents must know to become competent, much less excellent, doctors. Self-directed learning has become a critical part of residents’ education.
How can we make self-directed learning a more successful process? Attending physicians are likely to answer with the old saying, ‘You can lead a horse to water, but you can’t make it drink!’ While this saying points to the fact that self-directed learning requires a thirsty horse, it takes for granted the role of the guide in showing where water is plentiful. We argue that residents’ self-directed learning can be made more successful by recognizing the role of attendings in this process.

In an era of infinite resources, the limiting factor to learning has become time. The more we learn, the more humbled we are by the vastness of what we don’t know. Self-directed learners must be smart in deciding what should be learned. Herein lies the value of attendings, who, whether we are aware or not, shape our learning simply by virtue of their example. We would do well to pay closer attention to them. No textbook can replace their vast experience, which allows them to hone in on relevant details, to quickly develop comprehensive differentials, or revise plans.
But this learning cannot be based on simply observing and blindly emulating our teachers. We refer to Dr. Bloom’s taxonomy for levels of cognitive learning, in saying that these steps will only get us to the most basic levels of learning, which is “knowing” a disease to the extent that we can apply that knowledge in patient care. These can be acquired without significant mental effort; just by listening to morning reports, reading quick tidbits in between taking care of patients, etc. The goal, however, should be utilizing this basic knowledge as a foundation to develop higher levels of learning, namely Analysis, Synthesis, and Evaluation.
An example for analysis would be quickly going over each of the differentials in a disease and learning what distinguishes them. Synthesis is integrating different ideas and creating a customized plan for the particular patient that is found in no book. Lastly, evaluation is the level of cognition needed to be able to appraise and critique the large volume of opinion that we come across, establish our own opinion, and be able to defend it.
Here again our attendings are valuable resources who can guide us in reaching each of these levels. We must be willing to challenge ourselves by challenging our attendings when things do not make sense. It means always questioning why your attending physician made one medical decision versus another. It means also to challenge what we think we know, in order to discover what we don’t know. … Returning to the old adage, perhaps the key to self-directed learning is for the horse to learn his masters’ ways to the well, so he may adapt to an ever-changing environment.
Dr. Hung and Dr. Ramakrishna are pediatric residents at the Metrohealth Medical Center in Cleveland, Ohio. Email them at pdnews@frontlinemedcom.com.
Never before in history has medicine progressed as quickly as it does today. The half-life of knowledge and practices is shortening, and the ocean of literature continues to amass every day. In this context, it is simply not possible for training programs to teach in didactics everything residents must know to become competent, much less excellent, doctors. Self-directed learning has become a critical part of residents’ education.
How can we make self-directed learning a more successful process? Attending physicians are likely to answer with the old saying, ‘You can lead a horse to water, but you can’t make it drink!’ While this saying points to the fact that self-directed learning requires a thirsty horse, it takes for granted the role of the guide in showing where water is plentiful. We argue that residents’ self-directed learning can be made more successful by recognizing the role of attendings in this process.
In an era of infinite resources, the limiting factor to learning has become time. The more we learn, the more humbled we are by the vastness of what we don’t know. Self-directed learners must be smart in deciding what should be learned. Herein lies the value of attendings, who, whether we are aware or not, shape our learning simply by virtue of their example. We would do well to pay closer attention to them. No textbook can replace their vast experience, which allows them to hone in on relevant details, to quickly develop comprehensive differentials, or revise plans.
But this learning cannot be based on simply observing and blindly emulating our teachers. We refer to Dr. Bloom’s taxonomy for levels of cognitive learning, in saying that these steps will only get us to the most basic levels of learning, which is “knowing” a disease to the extent that we can apply that knowledge in patient care. These can be acquired without significant mental effort; just by listening to morning reports, reading quick tidbits in between taking care of patients, etc. The goal, however, should be utilizing this basic knowledge as a foundation to develop higher levels of learning, namely Analysis, Synthesis, and Evaluation.
An example for analysis would be quickly going over each of the differentials in a disease and learning what distinguishes them. Synthesis is integrating different ideas and creating a customized plan for the particular patient that is found in no book. Lastly, evaluation is the level of cognition needed to be able to appraise and critique the large volume of opinion that we come across, establish our own opinion, and be able to defend it.
Here again our attendings are valuable resources who can guide us in reaching each of these levels. We must be willing to challenge ourselves by challenging our attendings when things do not make sense. It means always questioning why your attending physician made one medical decision versus another. It means also to challenge what we think we know, in order to discover what we don’t know. … Returning to the old adage, perhaps the key to self-directed learning is for the horse to learn his masters’ ways to the well, so he may adapt to an ever-changing environment.
Dr. Hung and Dr. Ramakrishna are pediatric residents at the Metrohealth Medical Center in Cleveland, Ohio. Email them at pdnews@frontlinemedcom.com.
Never before in history has medicine progressed as quickly as it does today. The half-life of knowledge and practices is shortening, and the ocean of literature continues to amass every day. In this context, it is simply not possible for training programs to teach in didactics everything residents must know to become competent, much less excellent, doctors. Self-directed learning has become a critical part of residents’ education.
How can we make self-directed learning a more successful process? Attending physicians are likely to answer with the old saying, ‘You can lead a horse to water, but you can’t make it drink!’ While this saying points to the fact that self-directed learning requires a thirsty horse, it takes for granted the role of the guide in showing where water is plentiful. We argue that residents’ self-directed learning can be made more successful by recognizing the role of attendings in this process.
In an era of infinite resources, the limiting factor to learning has become time. The more we learn, the more humbled we are by the vastness of what we don’t know. Self-directed learners must be smart in deciding what should be learned. Herein lies the value of attendings, who, whether we are aware or not, shape our learning simply by virtue of their example. We would do well to pay closer attention to them. No textbook can replace their vast experience, which allows them to hone in on relevant details, to quickly develop comprehensive differentials, or revise plans.
But this learning cannot be based on simply observing and blindly emulating our teachers. We refer to Dr. Bloom’s taxonomy for levels of cognitive learning, in saying that these steps will only get us to the most basic levels of learning, which is “knowing” a disease to the extent that we can apply that knowledge in patient care. These can be acquired without significant mental effort; just by listening to morning reports, reading quick tidbits in between taking care of patients, etc. The goal, however, should be utilizing this basic knowledge as a foundation to develop higher levels of learning, namely Analysis, Synthesis, and Evaluation.
An example for analysis would be quickly going over each of the differentials in a disease and learning what distinguishes them. Synthesis is integrating different ideas and creating a customized plan for the particular patient that is found in no book. Lastly, evaluation is the level of cognition needed to be able to appraise and critique the large volume of opinion that we come across, establish our own opinion, and be able to defend it.
Here again our attendings are valuable resources who can guide us in reaching each of these levels. We must be willing to challenge ourselves by challenging our attendings when things do not make sense. It means always questioning why your attending physician made one medical decision versus another. It means also to challenge what we think we know, in order to discover what we don’t know. … Returning to the old adage, perhaps the key to self-directed learning is for the horse to learn his masters’ ways to the well, so he may adapt to an ever-changing environment.
Dr. Hung and Dr. Ramakrishna are pediatric residents at the Metrohealth Medical Center in Cleveland, Ohio. Email them at pdnews@frontlinemedcom.com.

A PEARL of wisdom about writing ‘Pearls’
Since 2005, I’ve had the opportunity to review “Pearls” articles submitted for publication in Current Psychiatry. In that time, I have read many worthwhile papers written by authors who may not be entirely clear about what constitutes a “Pearl." The mnemonic PEARL could help authors:
- decide if their article or idea is appropriate for “Pearls”
- construct the article to conform to the “Pearls” format.
Easy to remember. Lengthy, highly detailed articles may be helpful and informative but are not consistent with the purpose of “Pearls.
Alert. A “Pearl” should alert a physician to identify a problem, diagnosis, or adverse effect that they might otherwise miss or take unnecessary time to identify. Classic examples are the “handshake diagnosis” of hyperthyroidism,1 or the “3 little words that can diagnose mild cognitive impairment.”2
References. A professional article of any length should include references. References add immediate credibility to the information presented. For a “Pearl,” even 1 reference is acceptable. A writer can easily search PubMed and the Internet to find references to confirm or support their ideas.
Less is more. Architect Mies van der Rohe’s minimalist concept applies to “Pearls.” A “Pearl”—like its namesake—is small, polished, and valuable. Simplicity is its essence.
I hope this mnemonic is useful for clinicians interested in sharing their ideas or experiences to help others in the field. I look forward to reviewing many more “Pearls.”
1. Bedell SE, Graboys TB. Hand to hand. J Gen Intern Med. 2002;17(8):653-656.
2. Steenland NK, Auman CM, Patel PM, et al. Development of a rapid screening instrument for mild cognitive impairment and undiagnosed dementia. J Alzheimers Dis. 2008;15(3):419-427.
Since 2005, I’ve had the opportunity to review “Pearls” articles submitted for publication in Current Psychiatry. In that time, I have read many worthwhile papers written by authors who may not be entirely clear about what constitutes a “Pearl." The mnemonic PEARL could help authors:
- decide if their article or idea is appropriate for “Pearls”
- construct the article to conform to the “Pearls” format.
Easy to remember. Lengthy, highly detailed articles may be helpful and informative but are not consistent with the purpose of “Pearls.
Alert. A “Pearl” should alert a physician to identify a problem, diagnosis, or adverse effect that they might otherwise miss or take unnecessary time to identify. Classic examples are the “handshake diagnosis” of hyperthyroidism,1 or the “3 little words that can diagnose mild cognitive impairment.”2
References. A professional article of any length should include references. References add immediate credibility to the information presented. For a “Pearl,” even 1 reference is acceptable. A writer can easily search PubMed and the Internet to find references to confirm or support their ideas.
Less is more. Architect Mies van der Rohe’s minimalist concept applies to “Pearls.” A “Pearl”—like its namesake—is small, polished, and valuable. Simplicity is its essence.
I hope this mnemonic is useful for clinicians interested in sharing their ideas or experiences to help others in the field. I look forward to reviewing many more “Pearls.”
Since 2005, I’ve had the opportunity to review “Pearls” articles submitted for publication in Current Psychiatry. In that time, I have read many worthwhile papers written by authors who may not be entirely clear about what constitutes a “Pearl." The mnemonic PEARL could help authors:
- decide if their article or idea is appropriate for “Pearls”
- construct the article to conform to the “Pearls” format.
Easy to remember. Lengthy, highly detailed articles may be helpful and informative but are not consistent with the purpose of “Pearls.
Alert. A “Pearl” should alert a physician to identify a problem, diagnosis, or adverse effect that they might otherwise miss or take unnecessary time to identify. Classic examples are the “handshake diagnosis” of hyperthyroidism,1 or the “3 little words that can diagnose mild cognitive impairment.”2
References. A professional article of any length should include references. References add immediate credibility to the information presented. For a “Pearl,” even 1 reference is acceptable. A writer can easily search PubMed and the Internet to find references to confirm or support their ideas.
Less is more. Architect Mies van der Rohe’s minimalist concept applies to “Pearls.” A “Pearl”—like its namesake—is small, polished, and valuable. Simplicity is its essence.
I hope this mnemonic is useful for clinicians interested in sharing their ideas or experiences to help others in the field. I look forward to reviewing many more “Pearls.”
1. Bedell SE, Graboys TB. Hand to hand. J Gen Intern Med. 2002;17(8):653-656.
2. Steenland NK, Auman CM, Patel PM, et al. Development of a rapid screening instrument for mild cognitive impairment and undiagnosed dementia. J Alzheimers Dis. 2008;15(3):419-427.
1. Bedell SE, Graboys TB. Hand to hand. J Gen Intern Med. 2002;17(8):653-656.
2. Steenland NK, Auman CM, Patel PM, et al. Development of a rapid screening instrument for mild cognitive impairment and undiagnosed dementia. J Alzheimers Dis. 2008;15(3):419-427.
Guidance for parents of LGBT youth
Two years ago, a mother of one of my patients asked me for advice. She knew that her daughter identified as lesbian, and she was fully supportive. One day, her daughter wanted to go to a sleepover at a female friend’s house. Her first reaction was to say yes, but then she had second thoughts: If her daughter were straight, and this friend were male, she would not allow her to go because of the potential for sexual activity. When she told her daughter she could not attend the sleepover, her daughter accused her of not letting her go because of her sexual orientation. And now, the dilemma: In her effort to be fair and consistent with her values, the mother is being accused of discrimination. What should she do?
Parents play an irreplaceable role in the life of any teen, especially in the lives of teens that identify as lesbian, gay, bisexual, or transgender (LGBT). But many LGBT youth face serious challenges with their parents. They face the potential of parental rejection of their sexual or gender identity. At the very worst, teens may face homelessness if they come out to homophobic parents.1 Youth whose parents are accepting, nevertheless, are less likely to have mental health problems or engage in substance use.2

As a clinical provider for children and adolescents, caregivers will ask you for advice on how to address parenting challenges. Because LGBT youth are at risk for many adverse health outcomes, and parental support is paramount in preventing them, this is an opportunity for you to help this vulnerable population.
If parents ask you how to be supportive of their LGBT children, here are some recommendations, which are based on an intervention by colleagues at the University of Utah:3
1. Let their affection show. Receiving news that a child is LGBT can be emotionally intense for parents.4 Because of this emotional intensity, parents may react negatively and neglect to show their love for their child, which is what the child is seeking. Parents showing affection is the first step in supporting their LGBT child. Remind parents to tell their child that they love them no matter what.
2. Avoid rejecting behaviors. This is sometimes hard, because some forms of rejection can be quite subtle. Avoid saying anything that may indicate a negative view of LGBT people, even if it is not intended. For example, saying that something is “gay” may seem innocent enough, but it sends the message that being gay is something to be ashamed of.
3. Express their pain away from their child. Evidence shows that minimizing a child’s exposure to parental conflict and stress is associated with better coping with these devastating events.5 Parents should avoid telling their children that news of their sexual orientation or gender identity upsets them, as this is another form of rejecting behavior.
4. Do good before they feel good. Previous studies suggest that changes in behavior can occur even though a person may feel otherwise.6 Negative feelings about a child’s sexual orientation or gender identity can last months or years.7 It’s okay to have these feelings, but showing support such as telling their child how they still love them can ultimately lead to acceptance.
Although it is important for parents to accept their child, it is only half the battle. If you remember Baumrind’s theory on parenting, there are two sides of parenting. The first side involves parents showing their affection, love, and support for their children, which I described earlier. The other side involves managing a child’s behaviors, whether parents create an environment that makes it difficult to engage in behaviors they disapprove of or teach their children how to make the right decision.8 Many LGBT youth engage in risky behaviors because it’s a way of coping in a homophobic environment. The parents’ job is to teach their children healthier coping strategies.
Research on this aspect of parenting in LGBT youth is still at its infancy, and some of it is not reassuring. One important behavior, parental monitoring, which is “a set of correlated parenting behaviors involving attention to and tracking of the child’s whereabouts, activities, and adaptations,”9 can prevent conduct disorders, substance use, and mental health problems in the typical teenager.10 Unfortunately, we don’t find the same results for sexual minorities. One study suggests that parental monitoring may not prevent high-risk sexual behavior for young gay males, even if the parent is aware of the young man’s sexual orientation.11
This doesn’t mean that parental monitoring isn’t helpful. This just means that parenting LGBT youth is different than parenting heterosexual youth. It’s not enough for parents to just accept their child’s sexual orientation. They also must help them make the right decisions taking into consideration the effect of stigma and discrimination on sexual minorities. There are a couple of things you can suggest to your parents to help them raise their LGBT children:
1. Be proactive. Join organizations that support parents of LGBT youth such as Parents, Families, and Friends of Lesbians and Gays (PFLAG). Also, parents must be aware of their children’s behavior. If they are acting depressed, seek help. Having depression or anxiety increases the chances of engaging in risky behaviors, so the earlier parents address this, the better.
2. Make their child know what their views are on high risk-behaviors, such as substance use or having unprotected sex. They need to communicate their expectations clearly. If parents believe that drinking alcohol before the legal age is wrong, they should clearly let their children know that.
3. Make it easier for their child to tell parents what’s going on in their lives. Parents have to gain their children’s trust, be accessible (don’t answer texts while talking to them!), and be an active listener. LGBT youth may not ask parents for advice because they feel that because their parents are straight or cisgender, their life experiences do not apply. Being a member of an organization like PLFAG can be helpful, because parents can ask other parents who have experience raising LGBT youth for advice that works.
4. If parents’ children do something wrong, they should talk to them about how their actions were risky. Children will listen to parents if they view their parenting as legitimate and fair, which can only happen if there is a strong parent-child relationship. Being supportive of a child’s sexual orientation or gender identity is key here. And for the next time, it’s always good to role-play a scenario (for example, what to do if someone tries to make them drink at a party).
Parents of LGBT youth face many challenges. You can help these parents by encouraging them to accept and support their child’s sexual orientation or gender identity and provide parenting strategies relevant for LGBT youth. Most important of all, encourage them to seek support through organizations like PFLAG. With this support, parents can encourage healthy development in LGBT youth.
Resources for parents of LGBT youth
• The Centers for Disease Control and Prevention (CDC) has information on the health of LGBT Youth and advice on parental monitoring in general.
• The Family Acceptance Project is a project researching ways to improve parent-child relationships in LGBT Youth.
• PFLAG is an organization that provides support for families of LGBT youth.
• Lead with Love is a film about how various types of families react to their children coming out to them.
References
1. J Sex Res. 2004 Nov;41(4):329-42.
2. Aust N Z J Psychiatry. 2010 Sep;44(9):774-83.
3. Huebner D. “Leading with Love: Interventions to Support Families of Lesbian, Gay, and Bisexual Adolescents,” The Register Report, Vol. 39. National Register of Health Service Psychologists, Spring 2013.
4. J GLBT Fam Stud. 2014 Jan;10(1-2):36-57.
5. Prof Psychol Res Pr. 2008 Apr;39(2):113-21.
6. “Behaviorism: Classic Studies” (Casper, Wyo: Endeavor Books/Mountain States Litho, 2009).
7. Journal of LGBT Issues in Counseling. 2008;2(2):126-58.
8. Genet Psychol Monogr. 1967;75(1):43-88.
9. Clin Child Fam Psychol Rev. 1998 Mar;1(1):61-75.
10. “Parental Monitoring of Adolescents: Current Perspectives for Researchers and Practitioners” (New York: Columbia University Press, 2010).
11. AIDS Behav. 2014 Aug;18(8):1604-14.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of UPMC and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at pdnews@frontlinemedcom.com.
Two years ago, a mother of one of my patients asked me for advice. She knew that her daughter identified as lesbian, and she was fully supportive. One day, her daughter wanted to go to a sleepover at a female friend’s house. Her first reaction was to say yes, but then she had second thoughts: If her daughter were straight, and this friend were male, she would not allow her to go because of the potential for sexual activity. When she told her daughter she could not attend the sleepover, her daughter accused her of not letting her go because of her sexual orientation. And now, the dilemma: In her effort to be fair and consistent with her values, the mother is being accused of discrimination. What should she do?
Parents play an irreplaceable role in the life of any teen, especially in the lives of teens that identify as lesbian, gay, bisexual, or transgender (LGBT). But many LGBT youth face serious challenges with their parents. They face the potential of parental rejection of their sexual or gender identity. At the very worst, teens may face homelessness if they come out to homophobic parents.1 Youth whose parents are accepting, nevertheless, are less likely to have mental health problems or engage in substance use.2
As a clinical provider for children and adolescents, caregivers will ask you for advice on how to address parenting challenges. Because LGBT youth are at risk for many adverse health outcomes, and parental support is paramount in preventing them, this is an opportunity for you to help this vulnerable population.
If parents ask you how to be supportive of their LGBT children, here are some recommendations, which are based on an intervention by colleagues at the University of Utah:3
1. Let their affection show. Receiving news that a child is LGBT can be emotionally intense for parents.4 Because of this emotional intensity, parents may react negatively and neglect to show their love for their child, which is what the child is seeking. Parents showing affection is the first step in supporting their LGBT child. Remind parents to tell their child that they love them no matter what.
2. Avoid rejecting behaviors. This is sometimes hard, because some forms of rejection can be quite subtle. Avoid saying anything that may indicate a negative view of LGBT people, even if it is not intended. For example, saying that something is “gay” may seem innocent enough, but it sends the message that being gay is something to be ashamed of.
3. Express their pain away from their child. Evidence shows that minimizing a child’s exposure to parental conflict and stress is associated with better coping with these devastating events.5 Parents should avoid telling their children that news of their sexual orientation or gender identity upsets them, as this is another form of rejecting behavior.
4. Do good before they feel good. Previous studies suggest that changes in behavior can occur even though a person may feel otherwise.6 Negative feelings about a child’s sexual orientation or gender identity can last months or years.7 It’s okay to have these feelings, but showing support such as telling their child how they still love them can ultimately lead to acceptance.
Although it is important for parents to accept their child, it is only half the battle. If you remember Baumrind’s theory on parenting, there are two sides of parenting. The first side involves parents showing their affection, love, and support for their children, which I described earlier. The other side involves managing a child’s behaviors, whether parents create an environment that makes it difficult to engage in behaviors they disapprove of or teach their children how to make the right decision.8 Many LGBT youth engage in risky behaviors because it’s a way of coping in a homophobic environment. The parents’ job is to teach their children healthier coping strategies.
Research on this aspect of parenting in LGBT youth is still at its infancy, and some of it is not reassuring. One important behavior, parental monitoring, which is “a set of correlated parenting behaviors involving attention to and tracking of the child’s whereabouts, activities, and adaptations,”9 can prevent conduct disorders, substance use, and mental health problems in the typical teenager.10 Unfortunately, we don’t find the same results for sexual minorities. One study suggests that parental monitoring may not prevent high-risk sexual behavior for young gay males, even if the parent is aware of the young man’s sexual orientation.11
This doesn’t mean that parental monitoring isn’t helpful. This just means that parenting LGBT youth is different than parenting heterosexual youth. It’s not enough for parents to just accept their child’s sexual orientation. They also must help them make the right decisions taking into consideration the effect of stigma and discrimination on sexual minorities. There are a couple of things you can suggest to your parents to help them raise their LGBT children:
1. Be proactive. Join organizations that support parents of LGBT youth such as Parents, Families, and Friends of Lesbians and Gays (PFLAG). Also, parents must be aware of their children’s behavior. If they are acting depressed, seek help. Having depression or anxiety increases the chances of engaging in risky behaviors, so the earlier parents address this, the better.
2. Make their child know what their views are on high risk-behaviors, such as substance use or having unprotected sex. They need to communicate their expectations clearly. If parents believe that drinking alcohol before the legal age is wrong, they should clearly let their children know that.
3. Make it easier for their child to tell parents what’s going on in their lives. Parents have to gain their children’s trust, be accessible (don’t answer texts while talking to them!), and be an active listener. LGBT youth may not ask parents for advice because they feel that because their parents are straight or cisgender, their life experiences do not apply. Being a member of an organization like PLFAG can be helpful, because parents can ask other parents who have experience raising LGBT youth for advice that works.
4. If parents’ children do something wrong, they should talk to them about how their actions were risky. Children will listen to parents if they view their parenting as legitimate and fair, which can only happen if there is a strong parent-child relationship. Being supportive of a child’s sexual orientation or gender identity is key here. And for the next time, it’s always good to role-play a scenario (for example, what to do if someone tries to make them drink at a party).
Parents of LGBT youth face many challenges. You can help these parents by encouraging them to accept and support their child’s sexual orientation or gender identity and provide parenting strategies relevant for LGBT youth. Most important of all, encourage them to seek support through organizations like PFLAG. With this support, parents can encourage healthy development in LGBT youth.
Resources for parents of LGBT youth
• The Centers for Disease Control and Prevention (CDC) has information on the health of LGBT Youth and advice on parental monitoring in general.
• The Family Acceptance Project is a project researching ways to improve parent-child relationships in LGBT Youth.
• PFLAG is an organization that provides support for families of LGBT youth.
• Lead with Love is a film about how various types of families react to their children coming out to them.
References
1. J Sex Res. 2004 Nov;41(4):329-42.
2. Aust N Z J Psychiatry. 2010 Sep;44(9):774-83.
3. Huebner D. “Leading with Love: Interventions to Support Families of Lesbian, Gay, and Bisexual Adolescents,” The Register Report, Vol. 39. National Register of Health Service Psychologists, Spring 2013.
4. J GLBT Fam Stud. 2014 Jan;10(1-2):36-57.
5. Prof Psychol Res Pr. 2008 Apr;39(2):113-21.
6. “Behaviorism: Classic Studies” (Casper, Wyo: Endeavor Books/Mountain States Litho, 2009).
7. Journal of LGBT Issues in Counseling. 2008;2(2):126-58.
8. Genet Psychol Monogr. 1967;75(1):43-88.
9. Clin Child Fam Psychol Rev. 1998 Mar;1(1):61-75.
10. “Parental Monitoring of Adolescents: Current Perspectives for Researchers and Practitioners” (New York: Columbia University Press, 2010).
11. AIDS Behav. 2014 Aug;18(8):1604-14.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of UPMC and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at pdnews@frontlinemedcom.com.
Two years ago, a mother of one of my patients asked me for advice. She knew that her daughter identified as lesbian, and she was fully supportive. One day, her daughter wanted to go to a sleepover at a female friend’s house. Her first reaction was to say yes, but then she had second thoughts: If her daughter were straight, and this friend were male, she would not allow her to go because of the potential for sexual activity. When she told her daughter she could not attend the sleepover, her daughter accused her of not letting her go because of her sexual orientation. And now, the dilemma: In her effort to be fair and consistent with her values, the mother is being accused of discrimination. What should she do?
Parents play an irreplaceable role in the life of any teen, especially in the lives of teens that identify as lesbian, gay, bisexual, or transgender (LGBT). But many LGBT youth face serious challenges with their parents. They face the potential of parental rejection of their sexual or gender identity. At the very worst, teens may face homelessness if they come out to homophobic parents.1 Youth whose parents are accepting, nevertheless, are less likely to have mental health problems or engage in substance use.2
As a clinical provider for children and adolescents, caregivers will ask you for advice on how to address parenting challenges. Because LGBT youth are at risk for many adverse health outcomes, and parental support is paramount in preventing them, this is an opportunity for you to help this vulnerable population.
If parents ask you how to be supportive of their LGBT children, here are some recommendations, which are based on an intervention by colleagues at the University of Utah:3
1. Let their affection show. Receiving news that a child is LGBT can be emotionally intense for parents.4 Because of this emotional intensity, parents may react negatively and neglect to show their love for their child, which is what the child is seeking. Parents showing affection is the first step in supporting their LGBT child. Remind parents to tell their child that they love them no matter what.
2. Avoid rejecting behaviors. This is sometimes hard, because some forms of rejection can be quite subtle. Avoid saying anything that may indicate a negative view of LGBT people, even if it is not intended. For example, saying that something is “gay” may seem innocent enough, but it sends the message that being gay is something to be ashamed of.
3. Express their pain away from their child. Evidence shows that minimizing a child’s exposure to parental conflict and stress is associated with better coping with these devastating events.5 Parents should avoid telling their children that news of their sexual orientation or gender identity upsets them, as this is another form of rejecting behavior.
4. Do good before they feel good. Previous studies suggest that changes in behavior can occur even though a person may feel otherwise.6 Negative feelings about a child’s sexual orientation or gender identity can last months or years.7 It’s okay to have these feelings, but showing support such as telling their child how they still love them can ultimately lead to acceptance.
Although it is important for parents to accept their child, it is only half the battle. If you remember Baumrind’s theory on parenting, there are two sides of parenting. The first side involves parents showing their affection, love, and support for their children, which I described earlier. The other side involves managing a child’s behaviors, whether parents create an environment that makes it difficult to engage in behaviors they disapprove of or teach their children how to make the right decision.8 Many LGBT youth engage in risky behaviors because it’s a way of coping in a homophobic environment. The parents’ job is to teach their children healthier coping strategies.
Research on this aspect of parenting in LGBT youth is still at its infancy, and some of it is not reassuring. One important behavior, parental monitoring, which is “a set of correlated parenting behaviors involving attention to and tracking of the child’s whereabouts, activities, and adaptations,”9 can prevent conduct disorders, substance use, and mental health problems in the typical teenager.10 Unfortunately, we don’t find the same results for sexual minorities. One study suggests that parental monitoring may not prevent high-risk sexual behavior for young gay males, even if the parent is aware of the young man’s sexual orientation.11
This doesn’t mean that parental monitoring isn’t helpful. This just means that parenting LGBT youth is different than parenting heterosexual youth. It’s not enough for parents to just accept their child’s sexual orientation. They also must help them make the right decisions taking into consideration the effect of stigma and discrimination on sexual minorities. There are a couple of things you can suggest to your parents to help them raise their LGBT children:
1. Be proactive. Join organizations that support parents of LGBT youth such as Parents, Families, and Friends of Lesbians and Gays (PFLAG). Also, parents must be aware of their children’s behavior. If they are acting depressed, seek help. Having depression or anxiety increases the chances of engaging in risky behaviors, so the earlier parents address this, the better.
2. Make their child know what their views are on high risk-behaviors, such as substance use or having unprotected sex. They need to communicate their expectations clearly. If parents believe that drinking alcohol before the legal age is wrong, they should clearly let their children know that.
3. Make it easier for their child to tell parents what’s going on in their lives. Parents have to gain their children’s trust, be accessible (don’t answer texts while talking to them!), and be an active listener. LGBT youth may not ask parents for advice because they feel that because their parents are straight or cisgender, their life experiences do not apply. Being a member of an organization like PLFAG can be helpful, because parents can ask other parents who have experience raising LGBT youth for advice that works.
4. If parents’ children do something wrong, they should talk to them about how their actions were risky. Children will listen to parents if they view their parenting as legitimate and fair, which can only happen if there is a strong parent-child relationship. Being supportive of a child’s sexual orientation or gender identity is key here. And for the next time, it’s always good to role-play a scenario (for example, what to do if someone tries to make them drink at a party).
Parents of LGBT youth face many challenges. You can help these parents by encouraging them to accept and support their child’s sexual orientation or gender identity and provide parenting strategies relevant for LGBT youth. Most important of all, encourage them to seek support through organizations like PFLAG. With this support, parents can encourage healthy development in LGBT youth.
Resources for parents of LGBT youth
• The Centers for Disease Control and Prevention (CDC) has information on the health of LGBT Youth and advice on parental monitoring in general.
• The Family Acceptance Project is a project researching ways to improve parent-child relationships in LGBT Youth.
• PFLAG is an organization that provides support for families of LGBT youth.
• Lead with Love is a film about how various types of families react to their children coming out to them.
References
1. J Sex Res. 2004 Nov;41(4):329-42.
2. Aust N Z J Psychiatry. 2010 Sep;44(9):774-83.
3. Huebner D. “Leading with Love: Interventions to Support Families of Lesbian, Gay, and Bisexual Adolescents,” The Register Report, Vol. 39. National Register of Health Service Psychologists, Spring 2013.
4. J GLBT Fam Stud. 2014 Jan;10(1-2):36-57.
5. Prof Psychol Res Pr. 2008 Apr;39(2):113-21.
6. “Behaviorism: Classic Studies” (Casper, Wyo: Endeavor Books/Mountain States Litho, 2009).
7. Journal of LGBT Issues in Counseling. 2008;2(2):126-58.
8. Genet Psychol Monogr. 1967;75(1):43-88.
9. Clin Child Fam Psychol Rev. 1998 Mar;1(1):61-75.
10. “Parental Monitoring of Adolescents: Current Perspectives for Researchers and Practitioners” (New York: Columbia University Press, 2010).
11. AIDS Behav. 2014 Aug;18(8):1604-14.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of UPMC and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at pdnews@frontlinemedcom.com.

Parental Perceptions of Nighttime Communication Are Strong Predictors of Patient Experience
Clinical question: How does parental perception of overnight pediatric inpatient care affect the overall patient experience?
Background: Restrictions on resident duty hours have become progressively more stringent as attention to the effects of resident fatigue on patient safety has increased. In 2011, the Accreditation Council for Graduate Medical Education (ACGME) limited total weekly duty hours to 80 and reduced shifts for junior trainees to a maximum of 16 hours. As a result, a majority of teaching hospitals have instituted “night float,” or night team models, for overnight coverage of pediatric inpatients. The rapid adoption of night float inpatient coverage models has raised concerns about training residents in a structure that may not foster patient ownership and may promote shift worker mentality. Although communication between healthcare providers and patients/caregivers is known to be a key driver of patient satisfaction, little is known about the quality of communication overnight in the era of night float teams.
Study design: Prospective cohort study utilizing survey methodology.
Setting: Two general pediatric units at a 395-bed, urban, freestanding children’s teaching hospital.
Synopsis: A randomly selected subset of children (0-17 years) with English-speaking parents/caregivers admitted to two general pediatric units was studied over an 18-month period. Both general pediatric and subspecialty service patients, including adolescent, immunology, hematology, and rheumatology, were included. Researchers administered written surveys on weekday (Monday-Thursday) evenings prior to discharge, and surveys were collected either later that evening or in the morning. The surveys included 29 questions that used a five-point Likert scale to assess communication and experience.
These questions covered the following constructs:
- Parent understanding of the medical plan;
- Parent communication and experience with nighttime doctors;
- Parent communication and experience with nighttime nurses;
- Parent perceptions of nighttime interactions between doctors and nurses; and
- Parent overall experience of care during hospitalization.
An open question addressing whether parents had anything else to share about communication during the hospitalization was included. The primary outcome measure was the so-called “top-box” rating of overall experience of care during the hospitalization (from construct five). This outcome was dichotomous based on whether the parent had given the highest rating or not for all five questions in that construct (either “excellent” or “strongly agree”).
A top-box rating of overall experience of care was found to be associated with high mean construct scores regarding communication and experience with doctors (4.85) and nurses (4.87). Top-box overall experience ratings were also associated with top ratings for coordination between daytime and nighttime nurses and for teamwork between nighttime doctors and nurses. Multivariable analysis showed that parents’ rating of direct communications with doctors and nurses and perceived teamwork and communication between doctors and nurses were significant predictors of top-box overall experience.
Bottom line: Parents’ perceptions of direct communications with nighttime doctors and nurses and their perceived teamwork and communication were strong predictors of overall experience of care during pediatric hospitalization.
Citation: Khan A, Rogers JE, Melvin P, et al. Physician and nurse nighttime communication and parents’ hospital experience. Pediatrics. 2015;136(5):e1249-1258.

Clinical question: How does parental perception of overnight pediatric inpatient care affect the overall patient experience?
Background: Restrictions on resident duty hours have become progressively more stringent as attention to the effects of resident fatigue on patient safety has increased. In 2011, the Accreditation Council for Graduate Medical Education (ACGME) limited total weekly duty hours to 80 and reduced shifts for junior trainees to a maximum of 16 hours. As a result, a majority of teaching hospitals have instituted “night float,” or night team models, for overnight coverage of pediatric inpatients. The rapid adoption of night float inpatient coverage models has raised concerns about training residents in a structure that may not foster patient ownership and may promote shift worker mentality. Although communication between healthcare providers and patients/caregivers is known to be a key driver of patient satisfaction, little is known about the quality of communication overnight in the era of night float teams.
Study design: Prospective cohort study utilizing survey methodology.
Setting: Two general pediatric units at a 395-bed, urban, freestanding children’s teaching hospital.
Synopsis: A randomly selected subset of children (0-17 years) with English-speaking parents/caregivers admitted to two general pediatric units was studied over an 18-month period. Both general pediatric and subspecialty service patients, including adolescent, immunology, hematology, and rheumatology, were included. Researchers administered written surveys on weekday (Monday-Thursday) evenings prior to discharge, and surveys were collected either later that evening or in the morning. The surveys included 29 questions that used a five-point Likert scale to assess communication and experience.
These questions covered the following constructs:
- Parent understanding of the medical plan;
- Parent communication and experience with nighttime doctors;
- Parent communication and experience with nighttime nurses;
- Parent perceptions of nighttime interactions between doctors and nurses; and
- Parent overall experience of care during hospitalization.
An open question addressing whether parents had anything else to share about communication during the hospitalization was included. The primary outcome measure was the so-called “top-box” rating of overall experience of care during the hospitalization (from construct five). This outcome was dichotomous based on whether the parent had given the highest rating or not for all five questions in that construct (either “excellent” or “strongly agree”).
A top-box rating of overall experience of care was found to be associated with high mean construct scores regarding communication and experience with doctors (4.85) and nurses (4.87). Top-box overall experience ratings were also associated with top ratings for coordination between daytime and nighttime nurses and for teamwork between nighttime doctors and nurses. Multivariable analysis showed that parents’ rating of direct communications with doctors and nurses and perceived teamwork and communication between doctors and nurses were significant predictors of top-box overall experience.
Bottom line: Parents’ perceptions of direct communications with nighttime doctors and nurses and their perceived teamwork and communication were strong predictors of overall experience of care during pediatric hospitalization.
Citation: Khan A, Rogers JE, Melvin P, et al. Physician and nurse nighttime communication and parents’ hospital experience. Pediatrics. 2015;136(5):e1249-1258.
Clinical question: How does parental perception of overnight pediatric inpatient care affect the overall patient experience?
Background: Restrictions on resident duty hours have become progressively more stringent as attention to the effects of resident fatigue on patient safety has increased. In 2011, the Accreditation Council for Graduate Medical Education (ACGME) limited total weekly duty hours to 80 and reduced shifts for junior trainees to a maximum of 16 hours. As a result, a majority of teaching hospitals have instituted “night float,” or night team models, for overnight coverage of pediatric inpatients. The rapid adoption of night float inpatient coverage models has raised concerns about training residents in a structure that may not foster patient ownership and may promote shift worker mentality. Although communication between healthcare providers and patients/caregivers is known to be a key driver of patient satisfaction, little is known about the quality of communication overnight in the era of night float teams.
Study design: Prospective cohort study utilizing survey methodology.
Setting: Two general pediatric units at a 395-bed, urban, freestanding children’s teaching hospital.
Synopsis: A randomly selected subset of children (0-17 years) with English-speaking parents/caregivers admitted to two general pediatric units was studied over an 18-month period. Both general pediatric and subspecialty service patients, including adolescent, immunology, hematology, and rheumatology, were included. Researchers administered written surveys on weekday (Monday-Thursday) evenings prior to discharge, and surveys were collected either later that evening or in the morning. The surveys included 29 questions that used a five-point Likert scale to assess communication and experience.
These questions covered the following constructs:
- Parent understanding of the medical plan;
- Parent communication and experience with nighttime doctors;
- Parent communication and experience with nighttime nurses;
- Parent perceptions of nighttime interactions between doctors and nurses; and
- Parent overall experience of care during hospitalization.
An open question addressing whether parents had anything else to share about communication during the hospitalization was included. The primary outcome measure was the so-called “top-box” rating of overall experience of care during the hospitalization (from construct five). This outcome was dichotomous based on whether the parent had given the highest rating or not for all five questions in that construct (either “excellent” or “strongly agree”).
A top-box rating of overall experience of care was found to be associated with high mean construct scores regarding communication and experience with doctors (4.85) and nurses (4.87). Top-box overall experience ratings were also associated with top ratings for coordination between daytime and nighttime nurses and for teamwork between nighttime doctors and nurses. Multivariable analysis showed that parents’ rating of direct communications with doctors and nurses and perceived teamwork and communication between doctors and nurses were significant predictors of top-box overall experience.
Bottom line: Parents’ perceptions of direct communications with nighttime doctors and nurses and their perceived teamwork and communication were strong predictors of overall experience of care during pediatric hospitalization.
Citation: Khan A, Rogers JE, Melvin P, et al. Physician and nurse nighttime communication and parents’ hospital experience. Pediatrics. 2015;136(5):e1249-1258.
Statin may reduce vaso-occlusive pain in SCD

Photo courtesy of the CDC
ORLANDO, FL—In a small study, the cholesterol-lowering medication simvastatin reduced the frequency of vaso-occlusive pain in adults and children with sickle cell disease (SCD).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain after 3 months of treatment with simvastatin.
There was a slight overall decrease in the intensity of pain as well, but this was not statistically significant.
Still, investigators observed a decrease in biomarkers of inflammation and said the drug appeared to be safe for this patient population.
The team believes these preliminary data suggest the need to conduct a larger, randomized trial of simvastatin in SCD.
Carolyn C. Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California, presented the data at the 2015 ASH Annual Meeting (abstract 545).*
“Vaso-occlusive pain is a clinical hallmark and major cause of morbidity in sickle cell disease,” Dr Hoppe said. “Triggered by polymerization and hemolysis, vaso-occlusion involves multiple pathways.”
Similarly, although statins are best known for their cholesterol-inhibiting ability, they also inhibit oxidative stress and inflammation.
With this in mind, Dr Hoppe and her colleagues previously tested simvastatin in a phase 1 study of SCD patients who were 13 years of age or older.
The investigators found the safety profile to be acceptable, and they observed an improvement in biomarkers of inflammation. So they decided to carry out the current study.
This was a single-center, uncontrolled trial that enrolled SCD patients ages 10 and older. They received once-daily oral simvastatin (40 mg) for 3 months.
The primary outcome measure was the frequency and intensity of vaso-occlusive pain, as recorded by daily electronic pain diaries, before and after simvastatin treatment.
Clinical laboratory studies and plasma biomarkers were evaluated at baseline, at 0.5, 1, 2, and 3 months during treatment, as well as 1 month after the discontinuation of simvastatin.
Results
Nineteen patients completed the study. They had a mean age of 19 (range, 10-34), and 13 were female. Seventeen had HbSS genotype, and 2 had S/β0 thalassemia. Ten patients were receiving hydroxyurea.
The simvastatin adherence rate was 85%, and the adherence to using the daily pain diary was 73%.
Dr Hoppe said there were no new safety issues or drug-related adverse events in this trial. There was no myalgia or myopathy. One subject did experience transient facial swelling that may have been drug-related.
The patients’ total cholesterol decreased by 20% from baseline. There was a significant decrease in both LDL and HDL cholesterol (P<0.001 for both).
Creatinine kinase remained stable during treatment, as did hemoglobin levels.
Dr Hoppe noted that the study was not designed to include an assessment of fetal hemoglobin, so she and her colleagues did not have data on that measure for all the patients, but the team did observe an increase in fetal hemoglobin levels from baseline among the patients who were receiving hydroxyurea.
The investigators observed a decrease from baseline in markers of hemolysis—absolute reticulocyte count (P=0.006) and total bilirubin (P=0.02).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain from baseline (P=0.005) and a 10% decrease in the intensity of pain (which was not significant).
There was a 59% decrease in hsCRP (P=0.003), an 18% decrease in sE-selectin (P=0.01), a 5% decrease in sICAM (P=0.03), and a 17% decrease in VEGF (P=0.05). There was no significant effect on plasma nitric oxide metabolites, sVCAM1, or P-selectin levels.
“These results are basically preliminary data to give clinical support for a larger, randomized trial of simvastatin to assess its clinical efficacy in SCD,” Dr Hoppe concluded.
She reported receiving research funding and consultancy payments from Eli Lilly and Company, and another investigator involved in this study is an employee of Pharmacyclics LLC. ![]()
*Data in the abstract differ from the data presented.
Photo courtesy of the CDC
ORLANDO, FL—In a small study, the cholesterol-lowering medication simvastatin reduced the frequency of vaso-occlusive pain in adults and children with sickle cell disease (SCD).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain after 3 months of treatment with simvastatin.
There was a slight overall decrease in the intensity of pain as well, but this was not statistically significant.
Still, investigators observed a decrease in biomarkers of inflammation and said the drug appeared to be safe for this patient population.
The team believes these preliminary data suggest the need to conduct a larger, randomized trial of simvastatin in SCD.
Carolyn C. Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California, presented the data at the 2015 ASH Annual Meeting (abstract 545).*
“Vaso-occlusive pain is a clinical hallmark and major cause of morbidity in sickle cell disease,” Dr Hoppe said. “Triggered by polymerization and hemolysis, vaso-occlusion involves multiple pathways.”
Similarly, although statins are best known for their cholesterol-inhibiting ability, they also inhibit oxidative stress and inflammation.
With this in mind, Dr Hoppe and her colleagues previously tested simvastatin in a phase 1 study of SCD patients who were 13 years of age or older.
The investigators found the safety profile to be acceptable, and they observed an improvement in biomarkers of inflammation. So they decided to carry out the current study.
This was a single-center, uncontrolled trial that enrolled SCD patients ages 10 and older. They received once-daily oral simvastatin (40 mg) for 3 months.
The primary outcome measure was the frequency and intensity of vaso-occlusive pain, as recorded by daily electronic pain diaries, before and after simvastatin treatment.
Clinical laboratory studies and plasma biomarkers were evaluated at baseline, at 0.5, 1, 2, and 3 months during treatment, as well as 1 month after the discontinuation of simvastatin.
Results
Nineteen patients completed the study. They had a mean age of 19 (range, 10-34), and 13 were female. Seventeen had HbSS genotype, and 2 had S/β0 thalassemia. Ten patients were receiving hydroxyurea.
The simvastatin adherence rate was 85%, and the adherence to using the daily pain diary was 73%.
Dr Hoppe said there were no new safety issues or drug-related adverse events in this trial. There was no myalgia or myopathy. One subject did experience transient facial swelling that may have been drug-related.
The patients’ total cholesterol decreased by 20% from baseline. There was a significant decrease in both LDL and HDL cholesterol (P<0.001 for both).
Creatinine kinase remained stable during treatment, as did hemoglobin levels.
Dr Hoppe noted that the study was not designed to include an assessment of fetal hemoglobin, so she and her colleagues did not have data on that measure for all the patients, but the team did observe an increase in fetal hemoglobin levels from baseline among the patients who were receiving hydroxyurea.
The investigators observed a decrease from baseline in markers of hemolysis—absolute reticulocyte count (P=0.006) and total bilirubin (P=0.02).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain from baseline (P=0.005) and a 10% decrease in the intensity of pain (which was not significant).
There was a 59% decrease in hsCRP (P=0.003), an 18% decrease in sE-selectin (P=0.01), a 5% decrease in sICAM (P=0.03), and a 17% decrease in VEGF (P=0.05). There was no significant effect on plasma nitric oxide metabolites, sVCAM1, or P-selectin levels.
“These results are basically preliminary data to give clinical support for a larger, randomized trial of simvastatin to assess its clinical efficacy in SCD,” Dr Hoppe concluded.
She reported receiving research funding and consultancy payments from Eli Lilly and Company, and another investigator involved in this study is an employee of Pharmacyclics LLC. ![]()
*Data in the abstract differ from the data presented.
Photo courtesy of the CDC
ORLANDO, FL—In a small study, the cholesterol-lowering medication simvastatin reduced the frequency of vaso-occlusive pain in adults and children with sickle cell disease (SCD).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain after 3 months of treatment with simvastatin.
There was a slight overall decrease in the intensity of pain as well, but this was not statistically significant.
Still, investigators observed a decrease in biomarkers of inflammation and said the drug appeared to be safe for this patient population.
The team believes these preliminary data suggest the need to conduct a larger, randomized trial of simvastatin in SCD.
Carolyn C. Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California, presented the data at the 2015 ASH Annual Meeting (abstract 545).*
“Vaso-occlusive pain is a clinical hallmark and major cause of morbidity in sickle cell disease,” Dr Hoppe said. “Triggered by polymerization and hemolysis, vaso-occlusion involves multiple pathways.”
Similarly, although statins are best known for their cholesterol-inhibiting ability, they also inhibit oxidative stress and inflammation.
With this in mind, Dr Hoppe and her colleagues previously tested simvastatin in a phase 1 study of SCD patients who were 13 years of age or older.
The investigators found the safety profile to be acceptable, and they observed an improvement in biomarkers of inflammation. So they decided to carry out the current study.
This was a single-center, uncontrolled trial that enrolled SCD patients ages 10 and older. They received once-daily oral simvastatin (40 mg) for 3 months.
The primary outcome measure was the frequency and intensity of vaso-occlusive pain, as recorded by daily electronic pain diaries, before and after simvastatin treatment.
Clinical laboratory studies and plasma biomarkers were evaluated at baseline, at 0.5, 1, 2, and 3 months during treatment, as well as 1 month after the discontinuation of simvastatin.
Results
Nineteen patients completed the study. They had a mean age of 19 (range, 10-34), and 13 were female. Seventeen had HbSS genotype, and 2 had S/β0 thalassemia. Ten patients were receiving hydroxyurea.
The simvastatin adherence rate was 85%, and the adherence to using the daily pain diary was 73%.
Dr Hoppe said there were no new safety issues or drug-related adverse events in this trial. There was no myalgia or myopathy. One subject did experience transient facial swelling that may have been drug-related.
The patients’ total cholesterol decreased by 20% from baseline. There was a significant decrease in both LDL and HDL cholesterol (P<0.001 for both).
Creatinine kinase remained stable during treatment, as did hemoglobin levels.
Dr Hoppe noted that the study was not designed to include an assessment of fetal hemoglobin, so she and her colleagues did not have data on that measure for all the patients, but the team did observe an increase in fetal hemoglobin levels from baseline among the patients who were receiving hydroxyurea.
The investigators observed a decrease from baseline in markers of hemolysis—absolute reticulocyte count (P=0.006) and total bilirubin (P=0.02).
Overall, there was a 46% decrease in the frequency of vaso-occlusive pain from baseline (P=0.005) and a 10% decrease in the intensity of pain (which was not significant).
There was a 59% decrease in hsCRP (P=0.003), an 18% decrease in sE-selectin (P=0.01), a 5% decrease in sICAM (P=0.03), and a 17% decrease in VEGF (P=0.05). There was no significant effect on plasma nitric oxide metabolites, sVCAM1, or P-selectin levels.
“These results are basically preliminary data to give clinical support for a larger, randomized trial of simvastatin to assess its clinical efficacy in SCD,” Dr Hoppe concluded.
She reported receiving research funding and consultancy payments from Eli Lilly and Company, and another investigator involved in this study is an employee of Pharmacyclics LLC. ![]()
*Data in the abstract differ from the data presented.