User login
How malaria fools the immune system

infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have reconstructed how malaria parasite proteins bind to the antibodies that act as the first line of defense against the parasite.
The team described the binding of immunoglobulin M (IgM) to Plasmodium falciparum erythrocyte membrane protein-1 (PfEMP1).
They said their findings, published in Cell Reports, may provide valuable knowledge for the design of antimalarial drugs.
One strategy the malaria parasite Plasmodium falciparum uses to amplify its probability of spreading is the formation of rosette-shaped clusters of uninfected red blood cells (RBCs) surrounding a malaria-infected RBC.
Since the parasite in the central cell of the rosette can easily infect the surrounding cells, the rosette enhances the infection. Rosetting is associated with severe malaria and high fever.
One of the key players in the formation of the rosette is PfEMP1. PfEMP1 sticks out of the infected RBC and deceives one of the first defenses against malaria—IgM antibodies.
IgMs bind to the parasite or parasite-infected cells and call other immune molecules, like the complement system, for backup.
With the current study, researchers have shown that IgMs bind 1 or 2 PfEMP1 proteins, forming a bouquet-type shape on the surface of the infected cells.
Plasmodium falciparum exploits these IgMs to its own advantage because the bouquet attracts more RBCs, facilitating the formation of rosettes. Moreover, the IgMs in the bouquet are not able to bind the complement system and destroy the infected cell.
“The bond between PfEMP1s and IgMs is like the perfect Velcro—not too loose, not too strong,” said Ulf Skoglund, PhD, of Okinawa Institute for Science and Technology Graduate University in Japan.
“It is devilishly engineered to fool our immune system.”
The technique Dr Skoglund and his colleagues used to assess this bond allowed them to have a unique view of the proteins’ conformation.
“We have seen that PfEMP1 is a stiff, C-shaped protein,” he said. “Being stiff is an advantage. If it was floppy, it would not work so well. IgM, instead, assume 3 conformations: extended, bell, and turtle shape.”
Dr Skoglund and his colleagues believe that having this 3D structural model of the PfEMP1 and IgM complex can help scientists design antimalarial treatments that can break down or wash out malaria rosettes without hurting the patient. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have reconstructed how malaria parasite proteins bind to the antibodies that act as the first line of defense against the parasite.
The team described the binding of immunoglobulin M (IgM) to Plasmodium falciparum erythrocyte membrane protein-1 (PfEMP1).
They said their findings, published in Cell Reports, may provide valuable knowledge for the design of antimalarial drugs.
One strategy the malaria parasite Plasmodium falciparum uses to amplify its probability of spreading is the formation of rosette-shaped clusters of uninfected red blood cells (RBCs) surrounding a malaria-infected RBC.
Since the parasite in the central cell of the rosette can easily infect the surrounding cells, the rosette enhances the infection. Rosetting is associated with severe malaria and high fever.
One of the key players in the formation of the rosette is PfEMP1. PfEMP1 sticks out of the infected RBC and deceives one of the first defenses against malaria—IgM antibodies.
IgMs bind to the parasite or parasite-infected cells and call other immune molecules, like the complement system, for backup.
With the current study, researchers have shown that IgMs bind 1 or 2 PfEMP1 proteins, forming a bouquet-type shape on the surface of the infected cells.
Plasmodium falciparum exploits these IgMs to its own advantage because the bouquet attracts more RBCs, facilitating the formation of rosettes. Moreover, the IgMs in the bouquet are not able to bind the complement system and destroy the infected cell.
“The bond between PfEMP1s and IgMs is like the perfect Velcro—not too loose, not too strong,” said Ulf Skoglund, PhD, of Okinawa Institute for Science and Technology Graduate University in Japan.
“It is devilishly engineered to fool our immune system.”
The technique Dr Skoglund and his colleagues used to assess this bond allowed them to have a unique view of the proteins’ conformation.
“We have seen that PfEMP1 is a stiff, C-shaped protein,” he said. “Being stiff is an advantage. If it was floppy, it would not work so well. IgM, instead, assume 3 conformations: extended, bell, and turtle shape.”
Dr Skoglund and his colleagues believe that having this 3D structural model of the PfEMP1 and IgM complex can help scientists design antimalarial treatments that can break down or wash out malaria rosettes without hurting the patient. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have reconstructed how malaria parasite proteins bind to the antibodies that act as the first line of defense against the parasite.
The team described the binding of immunoglobulin M (IgM) to Plasmodium falciparum erythrocyte membrane protein-1 (PfEMP1).
They said their findings, published in Cell Reports, may provide valuable knowledge for the design of antimalarial drugs.
One strategy the malaria parasite Plasmodium falciparum uses to amplify its probability of spreading is the formation of rosette-shaped clusters of uninfected red blood cells (RBCs) surrounding a malaria-infected RBC.
Since the parasite in the central cell of the rosette can easily infect the surrounding cells, the rosette enhances the infection. Rosetting is associated with severe malaria and high fever.
One of the key players in the formation of the rosette is PfEMP1. PfEMP1 sticks out of the infected RBC and deceives one of the first defenses against malaria—IgM antibodies.
IgMs bind to the parasite or parasite-infected cells and call other immune molecules, like the complement system, for backup.
With the current study, researchers have shown that IgMs bind 1 or 2 PfEMP1 proteins, forming a bouquet-type shape on the surface of the infected cells.
Plasmodium falciparum exploits these IgMs to its own advantage because the bouquet attracts more RBCs, facilitating the formation of rosettes. Moreover, the IgMs in the bouquet are not able to bind the complement system and destroy the infected cell.
“The bond between PfEMP1s and IgMs is like the perfect Velcro—not too loose, not too strong,” said Ulf Skoglund, PhD, of Okinawa Institute for Science and Technology Graduate University in Japan.
“It is devilishly engineered to fool our immune system.”
The technique Dr Skoglund and his colleagues used to assess this bond allowed them to have a unique view of the proteins’ conformation.
“We have seen that PfEMP1 is a stiff, C-shaped protein,” he said. “Being stiff is an advantage. If it was floppy, it would not work so well. IgM, instead, assume 3 conformations: extended, bell, and turtle shape.”
Dr Skoglund and his colleagues believe that having this 3D structural model of the PfEMP1 and IgM complex can help scientists design antimalarial treatments that can break down or wash out malaria rosettes without hurting the patient. ![]()
Endocrine Society issues first-ever guidelines for primary adrenal insufficiency
New guidelines on the diagnosis and management of primary adrenal insufficiency stress the importance of early recognition and the need to prevent life-threatening adrenal crises in these patients.
These are the first clinical practice guidelines on primary adrenal insufficiency (PAI), also known as Addison’s disease, issued by Endocrine Society (J Clin Endocrinol Metab. 2016 Jan 13:jc20151710 [Epub ahead of print]).
“Because it’s a rare disease and symptoms can mimic common conditions, adrenal insufficiency is often, at least initially, overlooked,” guideline co-author Dr. Deborah Merke, a senior investigator with the National Institutes of Health Clinical Center in Bethesda, Md., said. “So the main goal of these clinical practice guidelines is to improve patient care.”
The guidelines suggest clinicians should have a low diagnostic threshold in acutely ill patients with unexplained symptoms or signs suggestive of PAI such as volume depletion, hypotension, hyponatremia, hyperkalemia, fever, abdominal pain, hyperpigmentation, or, especially in children, hypoglycemia.
This low diagnostic threshold for PAI should also be extended to pregnant women with unexplained persistent nausea, fatigue, and hypotension.
For adult patients with a suspected adrenal crisis, an immediate parenteral injection of hydrocortisone 100 mg should be given, followed by appropriate fluid resuscitation and 200 mg of hydrocortisone for 24 hours, according to the guidelines, which were co-sponsored by the European Society of Endocrinology and American Association for Clinical Chemistry.
Despite a known association between adrenal crisis and mortality, there is a knowledge gap regarding how to prevent, recognize, and reduce the risk of these life-threatening events, Dr. Merke said.
To that end, the task force has taken a page from the diabetes community in recommending all PAI patients carry steroid emergency identification cards and be equipped with a glucocorticoid injection kit for emergency use and be educated on how to use it.
The guidelines also advocate education about stress dosing to counter the increased demand for corticosteroids during periods of stress, which can encompass something as common as the flu.
“Just like diabetics carry around emergency medicines, it’s important for patients with adrenal insufficiency to carry around an emergency kit and to realize that should they start to get sick, they need to increase their doses,” she said. “There often seems to be a lack of awareness among physicians as well that these patients have a potentially life-threatening condition, should they get a common illness.”
One of the key unanswered clinical questions the task force sought to address was whether the widely used high-dose (250 mcg) corticotropin stimulation test, also known as the adrenocorticotropin (ACTH) or short Synacthen test, should be replaced by the low-dose test (1 mcg) to diagnosis PAI.
Despite a review of published data and a systematic review commissioned by the task force, “We didn’t come up with much scientific evidence to say we should be changing the historic standard,” Dr. Merke said.
The systematic review identified only five studies of high-dose corticotropin testing specifically in PAI and none of low-dose testing. The low-dose test has shown higher sensitivity in the detection of adrenal insufficiency in critically ill patients and secondary adrenal insufficiency, but the limited available data suggest it does not provide better diagnostic accuracy for PAI than the high-dose test.
As a result, the guidelines recommend the standard, short corticotropin test (250 mcg for adults and children aged at least 2 years) as the “gold standard” diagnostic test to establish a PAI diagnosis.
The low-dose (1 mcg) test is recommended only when corticotropin is in short supply, which is not typically a problem in the United States, she said.
If corticotropin testing isn’t feasible, a combination of a morning plasma ACTH and cortisol levels (less than 5 mcg/dL) can be used as an initial screening, though confirmatory testing with corticotropin stimulation is strongly recommended.
Glucocorticoid therapy is recommended in all patients with confirmed PAI based on the highest quality of evidence, with a clear preference given for the short-acting steroids, Dr. Merke observed.
Hydrocortisone 15 mg-25 mg or cortisone acetate 20 mg-35 mg given in two to three divided doses per day is suggested for adults, with the highest dose to be given in the morning. Once- or twice-daily prednisolone 3 mg-5 mg is suggested as an alternative.
Hydrocortisone is also suggested over cortisone acetate, prednisolone, or prednisone for pregnant women and recommended for children (about 8 mg/m2 per day), but the evidence supporting these items was of low quality.
The guidelines suggest against using dexamethasone, the longest-acting glucocorticoid, because of the potential long-term side effects of overt-treatment and the frequent appearance of cushingoid side effects. They also recommend against dexamethasone in pregnant women because it is not inactivated in the placenta.
The guidelines are also quite clear in their suggestion against hormonal monitoring of glucocorticoid replacement and instead favor adjusting treatment based only on clinical response.
“This is a very important suggestion that we made because often clinicians use ACTH to adjust doses and this commonly results in overreplacement and there are side effects to overreplacement,” including weight gain, insomnia, and peripheral edema, Dr. Merke said.
A second systematic review commissioned by the task force involving 15 observational studies of glucocorticoid replacement regimens uncovered very sparse data on mortality, bone density, and incidence of adrenal crisis.
It has been suggested that newer extended-release and dual-release glucocorticoid formulations may result in higher health-reality quality of life than once-, twice-, or thrice-daily regimens, but once again, the evidence was insufficient to support a specific recommendation.
Dr. Merke acknowledged that many of the guidelines recommendations were ungraded or best practices, reflecting the lack of randomized clinical trials in PAI.
“I think that’s why it was so important for us to do this,” she said. “We had a group of experts that were very familiar with this disease providing guidance, but I think it’s also one reason why physicians out there in practice get confused about exactly what to do because of the lack of hard evidence. ... It does certainly cry for the need for more studies in these rare diseases.”
The guidelines were funded by the Endocrine Society, and the authors reported receiving no external funding or remuneration.
New guidelines on the diagnosis and management of primary adrenal insufficiency stress the importance of early recognition and the need to prevent life-threatening adrenal crises in these patients.
These are the first clinical practice guidelines on primary adrenal insufficiency (PAI), also known as Addison’s disease, issued by Endocrine Society (J Clin Endocrinol Metab. 2016 Jan 13:jc20151710 [Epub ahead of print]).
“Because it’s a rare disease and symptoms can mimic common conditions, adrenal insufficiency is often, at least initially, overlooked,” guideline co-author Dr. Deborah Merke, a senior investigator with the National Institutes of Health Clinical Center in Bethesda, Md., said. “So the main goal of these clinical practice guidelines is to improve patient care.”
The guidelines suggest clinicians should have a low diagnostic threshold in acutely ill patients with unexplained symptoms or signs suggestive of PAI such as volume depletion, hypotension, hyponatremia, hyperkalemia, fever, abdominal pain, hyperpigmentation, or, especially in children, hypoglycemia.
This low diagnostic threshold for PAI should also be extended to pregnant women with unexplained persistent nausea, fatigue, and hypotension.
For adult patients with a suspected adrenal crisis, an immediate parenteral injection of hydrocortisone 100 mg should be given, followed by appropriate fluid resuscitation and 200 mg of hydrocortisone for 24 hours, according to the guidelines, which were co-sponsored by the European Society of Endocrinology and American Association for Clinical Chemistry.
Despite a known association between adrenal crisis and mortality, there is a knowledge gap regarding how to prevent, recognize, and reduce the risk of these life-threatening events, Dr. Merke said.
To that end, the task force has taken a page from the diabetes community in recommending all PAI patients carry steroid emergency identification cards and be equipped with a glucocorticoid injection kit for emergency use and be educated on how to use it.
The guidelines also advocate education about stress dosing to counter the increased demand for corticosteroids during periods of stress, which can encompass something as common as the flu.
“Just like diabetics carry around emergency medicines, it’s important for patients with adrenal insufficiency to carry around an emergency kit and to realize that should they start to get sick, they need to increase their doses,” she said. “There often seems to be a lack of awareness among physicians as well that these patients have a potentially life-threatening condition, should they get a common illness.”
One of the key unanswered clinical questions the task force sought to address was whether the widely used high-dose (250 mcg) corticotropin stimulation test, also known as the adrenocorticotropin (ACTH) or short Synacthen test, should be replaced by the low-dose test (1 mcg) to diagnosis PAI.
Despite a review of published data and a systematic review commissioned by the task force, “We didn’t come up with much scientific evidence to say we should be changing the historic standard,” Dr. Merke said.
The systematic review identified only five studies of high-dose corticotropin testing specifically in PAI and none of low-dose testing. The low-dose test has shown higher sensitivity in the detection of adrenal insufficiency in critically ill patients and secondary adrenal insufficiency, but the limited available data suggest it does not provide better diagnostic accuracy for PAI than the high-dose test.
As a result, the guidelines recommend the standard, short corticotropin test (250 mcg for adults and children aged at least 2 years) as the “gold standard” diagnostic test to establish a PAI diagnosis.
The low-dose (1 mcg) test is recommended only when corticotropin is in short supply, which is not typically a problem in the United States, she said.
If corticotropin testing isn’t feasible, a combination of a morning plasma ACTH and cortisol levels (less than 5 mcg/dL) can be used as an initial screening, though confirmatory testing with corticotropin stimulation is strongly recommended.
Glucocorticoid therapy is recommended in all patients with confirmed PAI based on the highest quality of evidence, with a clear preference given for the short-acting steroids, Dr. Merke observed.
Hydrocortisone 15 mg-25 mg or cortisone acetate 20 mg-35 mg given in two to three divided doses per day is suggested for adults, with the highest dose to be given in the morning. Once- or twice-daily prednisolone 3 mg-5 mg is suggested as an alternative.
Hydrocortisone is also suggested over cortisone acetate, prednisolone, or prednisone for pregnant women and recommended for children (about 8 mg/m2 per day), but the evidence supporting these items was of low quality.
The guidelines suggest against using dexamethasone, the longest-acting glucocorticoid, because of the potential long-term side effects of overt-treatment and the frequent appearance of cushingoid side effects. They also recommend against dexamethasone in pregnant women because it is not inactivated in the placenta.
The guidelines are also quite clear in their suggestion against hormonal monitoring of glucocorticoid replacement and instead favor adjusting treatment based only on clinical response.
“This is a very important suggestion that we made because often clinicians use ACTH to adjust doses and this commonly results in overreplacement and there are side effects to overreplacement,” including weight gain, insomnia, and peripheral edema, Dr. Merke said.
A second systematic review commissioned by the task force involving 15 observational studies of glucocorticoid replacement regimens uncovered very sparse data on mortality, bone density, and incidence of adrenal crisis.
It has been suggested that newer extended-release and dual-release glucocorticoid formulations may result in higher health-reality quality of life than once-, twice-, or thrice-daily regimens, but once again, the evidence was insufficient to support a specific recommendation.
Dr. Merke acknowledged that many of the guidelines recommendations were ungraded or best practices, reflecting the lack of randomized clinical trials in PAI.
“I think that’s why it was so important for us to do this,” she said. “We had a group of experts that were very familiar with this disease providing guidance, but I think it’s also one reason why physicians out there in practice get confused about exactly what to do because of the lack of hard evidence. ... It does certainly cry for the need for more studies in these rare diseases.”
The guidelines were funded by the Endocrine Society, and the authors reported receiving no external funding or remuneration.
New guidelines on the diagnosis and management of primary adrenal insufficiency stress the importance of early recognition and the need to prevent life-threatening adrenal crises in these patients.
These are the first clinical practice guidelines on primary adrenal insufficiency (PAI), also known as Addison’s disease, issued by Endocrine Society (J Clin Endocrinol Metab. 2016 Jan 13:jc20151710 [Epub ahead of print]).
“Because it’s a rare disease and symptoms can mimic common conditions, adrenal insufficiency is often, at least initially, overlooked,” guideline co-author Dr. Deborah Merke, a senior investigator with the National Institutes of Health Clinical Center in Bethesda, Md., said. “So the main goal of these clinical practice guidelines is to improve patient care.”
The guidelines suggest clinicians should have a low diagnostic threshold in acutely ill patients with unexplained symptoms or signs suggestive of PAI such as volume depletion, hypotension, hyponatremia, hyperkalemia, fever, abdominal pain, hyperpigmentation, or, especially in children, hypoglycemia.
This low diagnostic threshold for PAI should also be extended to pregnant women with unexplained persistent nausea, fatigue, and hypotension.
For adult patients with a suspected adrenal crisis, an immediate parenteral injection of hydrocortisone 100 mg should be given, followed by appropriate fluid resuscitation and 200 mg of hydrocortisone for 24 hours, according to the guidelines, which were co-sponsored by the European Society of Endocrinology and American Association for Clinical Chemistry.
Despite a known association between adrenal crisis and mortality, there is a knowledge gap regarding how to prevent, recognize, and reduce the risk of these life-threatening events, Dr. Merke said.
To that end, the task force has taken a page from the diabetes community in recommending all PAI patients carry steroid emergency identification cards and be equipped with a glucocorticoid injection kit for emergency use and be educated on how to use it.
The guidelines also advocate education about stress dosing to counter the increased demand for corticosteroids during periods of stress, which can encompass something as common as the flu.
“Just like diabetics carry around emergency medicines, it’s important for patients with adrenal insufficiency to carry around an emergency kit and to realize that should they start to get sick, they need to increase their doses,” she said. “There often seems to be a lack of awareness among physicians as well that these patients have a potentially life-threatening condition, should they get a common illness.”
One of the key unanswered clinical questions the task force sought to address was whether the widely used high-dose (250 mcg) corticotropin stimulation test, also known as the adrenocorticotropin (ACTH) or short Synacthen test, should be replaced by the low-dose test (1 mcg) to diagnosis PAI.
Despite a review of published data and a systematic review commissioned by the task force, “We didn’t come up with much scientific evidence to say we should be changing the historic standard,” Dr. Merke said.
The systematic review identified only five studies of high-dose corticotropin testing specifically in PAI and none of low-dose testing. The low-dose test has shown higher sensitivity in the detection of adrenal insufficiency in critically ill patients and secondary adrenal insufficiency, but the limited available data suggest it does not provide better diagnostic accuracy for PAI than the high-dose test.
As a result, the guidelines recommend the standard, short corticotropin test (250 mcg for adults and children aged at least 2 years) as the “gold standard” diagnostic test to establish a PAI diagnosis.
The low-dose (1 mcg) test is recommended only when corticotropin is in short supply, which is not typically a problem in the United States, she said.
If corticotropin testing isn’t feasible, a combination of a morning plasma ACTH and cortisol levels (less than 5 mcg/dL) can be used as an initial screening, though confirmatory testing with corticotropin stimulation is strongly recommended.
Glucocorticoid therapy is recommended in all patients with confirmed PAI based on the highest quality of evidence, with a clear preference given for the short-acting steroids, Dr. Merke observed.
Hydrocortisone 15 mg-25 mg or cortisone acetate 20 mg-35 mg given in two to three divided doses per day is suggested for adults, with the highest dose to be given in the morning. Once- or twice-daily prednisolone 3 mg-5 mg is suggested as an alternative.
Hydrocortisone is also suggested over cortisone acetate, prednisolone, or prednisone for pregnant women and recommended for children (about 8 mg/m2 per day), but the evidence supporting these items was of low quality.
The guidelines suggest against using dexamethasone, the longest-acting glucocorticoid, because of the potential long-term side effects of overt-treatment and the frequent appearance of cushingoid side effects. They also recommend against dexamethasone in pregnant women because it is not inactivated in the placenta.
The guidelines are also quite clear in their suggestion against hormonal monitoring of glucocorticoid replacement and instead favor adjusting treatment based only on clinical response.
“This is a very important suggestion that we made because often clinicians use ACTH to adjust doses and this commonly results in overreplacement and there are side effects to overreplacement,” including weight gain, insomnia, and peripheral edema, Dr. Merke said.
A second systematic review commissioned by the task force involving 15 observational studies of glucocorticoid replacement regimens uncovered very sparse data on mortality, bone density, and incidence of adrenal crisis.
It has been suggested that newer extended-release and dual-release glucocorticoid formulations may result in higher health-reality quality of life than once-, twice-, or thrice-daily regimens, but once again, the evidence was insufficient to support a specific recommendation.
Dr. Merke acknowledged that many of the guidelines recommendations were ungraded or best practices, reflecting the lack of randomized clinical trials in PAI.
“I think that’s why it was so important for us to do this,” she said. “We had a group of experts that were very familiar with this disease providing guidance, but I think it’s also one reason why physicians out there in practice get confused about exactly what to do because of the lack of hard evidence. ... It does certainly cry for the need for more studies in these rare diseases.”
The guidelines were funded by the Endocrine Society, and the authors reported receiving no external funding or remuneration.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM

AHA: Bariatric surgery slashes heart failure exacerbations
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Bariatric surgery in obese patients with heart failure results in a dramatic reduction in ED visits and hospital admission for heart failure.
Major finding: The combined rate of ED visits and hospital admissions for heart failure dropped by 44% during the 2 years after a large group of patients with heart failure underwent bariatric surgery for obesity.
Data source: This case-control study compared the rates of ED visits and hospital admissions for worsening heart failure in 1,664 patients with heart failure during the 2 years before and 2 years after they underwent bariatric surgery for obesity.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study, which utilized publicly available patient data.
San Diego Hospitalist Weijen Chang, MD, SFHM, Offers Suggestions on Things to Do at HM16
Weijen Chang, MD, SFHM, associate clinical professor at the University of California at San Diego, has a concern: If people attending HM16 don’t get out and about, he worries, they might leave with the impression that his town is sort of, well, normal.
“San Diego is a very laid-back place in general,” says Dr. Chang, director of the hospitalist service in the La Jolla location of the UCSD Health System and longtime pediatrics editor for The Hospitalist. “I think tourists end up being in very touristy areas and don’t generally get a sense of that.”
Read more about the new tracks, speakers at HM16.
Like a good doctor, he’s here to offer a cure. Here are Dr. Chang’s tips for seeing the city. Some are fairly standard and, yes, even a little touristy. But some do give you a taste of that true San Diego vibe, if you’re up for it. He hopes you are.
Mission Beach, Pacific Beach
“Mission Beach is kind of funky,” Dr. Chang says. “Pacific Beach is a little less funky, but it kind of gives you that sort of funky San Diego feeling that a lot of people don’t get when they’re in touristy areas.”
If you make it to Pacific Beach, he says, keep an eye out for “Slomo,” the nickname of a neurologist-turned-Rollerblader who constantly skates up and down the promenade and is nationally known.
“He’s kind of like a fixture,” Dr. Chang says. “Literally, he’s there every single day.”
Harbor Cruise
“If you don’t have access to a car, a really fun and easy thing is a harbor cruise,” Dr. Chang says. “It takes you around all the different ships in the harbor.”
The cruise also goes to Coronado, an island just across the San Diego Bay from downtown.
Lunch at Hotel del Coronado
For those willing to hitch a ride via Uber, Lyft, or a regular taxi—you don’t really need a car to see quite a bit in San Diego—this is a good option. “It’s not super-expensive, and you could see the hotel and walk around the beach there,” Dr. Chang says.
Torrey Pines State Natural Reserve, La Jolla Cove
Torrey Pines is north of downtown and is a good choice for a family outing, Dr. Chang suggests.
“It’s a beautiful hike. They have cliffs in that area. It’s a good family thing to do because the whole family can hike along,” he says. “They have a museum there.”
And beautiful Torrey pine trees are unique to that area.
Also, La Jolla Cove is an option. It’s a touristy spot but a “really pretty” one, Dr. Chang adds.
Balboa Park, Gaslamp Quarter, Little Italy
Dr. Chang suggests Panama 66, a restaurant in Balboa Park.
“It’s in a sculpture garden, and there’s usually a live band playing,” he says. “You can buy a beer or glass of wine and have dinner, too. Or you can just get a couple snacks and hang out and listen to music. That’s sort of my speed when it comes to nightlife. And I imagine for most doctors, it’s sort of their speed.”
There’s also the Old Globe theater in the park. Attendees might want to catch a show. “Just walking around Balboa Park at night is kind of fun,” he says.
Hitting the Gaslamp Quarter, a trendy restaurant and shop area near the convention center, is a nice, “easy thing to do,” he says. One spot there worth checking out is a new speakeasy-style place called Prohibition.
“It’s quieter; it’s got nice jazz and is a little more laid-back than perhaps a big loud, bustling bar would be,” he notes.
Little Italy, a long walk or a taxi ride from the conference, is an area “that some people overlook that has a lot of nice restaurants and bars. And it’s a little more laid-back than the Gaslamp,” Dr. Chang says. “The Gaslamp can sometimes be a little bit overwhelming.”
Coronado, Mission Beach
If you want suggestions for seeing a great sunset, he says, Coronado and Mission Beach would be worthwhile, but “anywhere along the westward-facing beach is pretty spectacular.”

Thomas R. Collins is a freelance writer in South Florida.
Weijen Chang, MD, SFHM, associate clinical professor at the University of California at San Diego, has a concern: If people attending HM16 don’t get out and about, he worries, they might leave with the impression that his town is sort of, well, normal.
“San Diego is a very laid-back place in general,” says Dr. Chang, director of the hospitalist service in the La Jolla location of the UCSD Health System and longtime pediatrics editor for The Hospitalist. “I think tourists end up being in very touristy areas and don’t generally get a sense of that.”
Read more about the new tracks, speakers at HM16.
Like a good doctor, he’s here to offer a cure. Here are Dr. Chang’s tips for seeing the city. Some are fairly standard and, yes, even a little touristy. But some do give you a taste of that true San Diego vibe, if you’re up for it. He hopes you are.
Mission Beach, Pacific Beach
“Mission Beach is kind of funky,” Dr. Chang says. “Pacific Beach is a little less funky, but it kind of gives you that sort of funky San Diego feeling that a lot of people don’t get when they’re in touristy areas.”
If you make it to Pacific Beach, he says, keep an eye out for “Slomo,” the nickname of a neurologist-turned-Rollerblader who constantly skates up and down the promenade and is nationally known.
“He’s kind of like a fixture,” Dr. Chang says. “Literally, he’s there every single day.”
Harbor Cruise
“If you don’t have access to a car, a really fun and easy thing is a harbor cruise,” Dr. Chang says. “It takes you around all the different ships in the harbor.”
The cruise also goes to Coronado, an island just across the San Diego Bay from downtown.
Lunch at Hotel del Coronado
For those willing to hitch a ride via Uber, Lyft, or a regular taxi—you don’t really need a car to see quite a bit in San Diego—this is a good option. “It’s not super-expensive, and you could see the hotel and walk around the beach there,” Dr. Chang says.
Torrey Pines State Natural Reserve, La Jolla Cove
Torrey Pines is north of downtown and is a good choice for a family outing, Dr. Chang suggests.
“It’s a beautiful hike. They have cliffs in that area. It’s a good family thing to do because the whole family can hike along,” he says. “They have a museum there.”
And beautiful Torrey pine trees are unique to that area.
Also, La Jolla Cove is an option. It’s a touristy spot but a “really pretty” one, Dr. Chang adds.
Balboa Park, Gaslamp Quarter, Little Italy
Dr. Chang suggests Panama 66, a restaurant in Balboa Park.
“It’s in a sculpture garden, and there’s usually a live band playing,” he says. “You can buy a beer or glass of wine and have dinner, too. Or you can just get a couple snacks and hang out and listen to music. That’s sort of my speed when it comes to nightlife. And I imagine for most doctors, it’s sort of their speed.”
There’s also the Old Globe theater in the park. Attendees might want to catch a show. “Just walking around Balboa Park at night is kind of fun,” he says.
Hitting the Gaslamp Quarter, a trendy restaurant and shop area near the convention center, is a nice, “easy thing to do,” he says. One spot there worth checking out is a new speakeasy-style place called Prohibition.
“It’s quieter; it’s got nice jazz and is a little more laid-back than perhaps a big loud, bustling bar would be,” he notes.
Little Italy, a long walk or a taxi ride from the conference, is an area “that some people overlook that has a lot of nice restaurants and bars. And it’s a little more laid-back than the Gaslamp,” Dr. Chang says. “The Gaslamp can sometimes be a little bit overwhelming.”
Coronado, Mission Beach
If you want suggestions for seeing a great sunset, he says, Coronado and Mission Beach would be worthwhile, but “anywhere along the westward-facing beach is pretty spectacular.”
Thomas R. Collins is a freelance writer in South Florida.
Weijen Chang, MD, SFHM, associate clinical professor at the University of California at San Diego, has a concern: If people attending HM16 don’t get out and about, he worries, they might leave with the impression that his town is sort of, well, normal.
“San Diego is a very laid-back place in general,” says Dr. Chang, director of the hospitalist service in the La Jolla location of the UCSD Health System and longtime pediatrics editor for The Hospitalist. “I think tourists end up being in very touristy areas and don’t generally get a sense of that.”
Read more about the new tracks, speakers at HM16.
Like a good doctor, he’s here to offer a cure. Here are Dr. Chang’s tips for seeing the city. Some are fairly standard and, yes, even a little touristy. But some do give you a taste of that true San Diego vibe, if you’re up for it. He hopes you are.
Mission Beach, Pacific Beach
“Mission Beach is kind of funky,” Dr. Chang says. “Pacific Beach is a little less funky, but it kind of gives you that sort of funky San Diego feeling that a lot of people don’t get when they’re in touristy areas.”
If you make it to Pacific Beach, he says, keep an eye out for “Slomo,” the nickname of a neurologist-turned-Rollerblader who constantly skates up and down the promenade and is nationally known.
“He’s kind of like a fixture,” Dr. Chang says. “Literally, he’s there every single day.”
Harbor Cruise
“If you don’t have access to a car, a really fun and easy thing is a harbor cruise,” Dr. Chang says. “It takes you around all the different ships in the harbor.”
The cruise also goes to Coronado, an island just across the San Diego Bay from downtown.
Lunch at Hotel del Coronado
For those willing to hitch a ride via Uber, Lyft, or a regular taxi—you don’t really need a car to see quite a bit in San Diego—this is a good option. “It’s not super-expensive, and you could see the hotel and walk around the beach there,” Dr. Chang says.
Torrey Pines State Natural Reserve, La Jolla Cove
Torrey Pines is north of downtown and is a good choice for a family outing, Dr. Chang suggests.
“It’s a beautiful hike. They have cliffs in that area. It’s a good family thing to do because the whole family can hike along,” he says. “They have a museum there.”
And beautiful Torrey pine trees are unique to that area.
Also, La Jolla Cove is an option. It’s a touristy spot but a “really pretty” one, Dr. Chang adds.
Balboa Park, Gaslamp Quarter, Little Italy
Dr. Chang suggests Panama 66, a restaurant in Balboa Park.
“It’s in a sculpture garden, and there’s usually a live band playing,” he says. “You can buy a beer or glass of wine and have dinner, too. Or you can just get a couple snacks and hang out and listen to music. That’s sort of my speed when it comes to nightlife. And I imagine for most doctors, it’s sort of their speed.”
There’s also the Old Globe theater in the park. Attendees might want to catch a show. “Just walking around Balboa Park at night is kind of fun,” he says.
Hitting the Gaslamp Quarter, a trendy restaurant and shop area near the convention center, is a nice, “easy thing to do,” he says. One spot there worth checking out is a new speakeasy-style place called Prohibition.
“It’s quieter; it’s got nice jazz and is a little more laid-back than perhaps a big loud, bustling bar would be,” he notes.
Little Italy, a long walk or a taxi ride from the conference, is an area “that some people overlook that has a lot of nice restaurants and bars. And it’s a little more laid-back than the Gaslamp,” Dr. Chang says. “The Gaslamp can sometimes be a little bit overwhelming.”
Coronado, Mission Beach
If you want suggestions for seeing a great sunset, he says, Coronado and Mission Beach would be worthwhile, but “anywhere along the westward-facing beach is pretty spectacular.”
Thomas R. Collins is a freelance writer in South Florida.

Monitoring drug release with nanoparticles

Image courtesy of PNAS
Researchers say they have devised a system that allows for real-time monitoring of drug release.
The team created a luminescent nanoparticle and attached it to the anticancer drug doxorubicin, which allowed them to visualize the drug’s arrival in cancer cells.
Thus far, the team has only tested this system in vitro, but animal studies are currently underway.
“We really want to see what’s going on when we give chemo drugs, and this work paves the way for the exciting endeavor,” said Mingjun Zhang, PhD, of The Ohio State University in Columbus.
He and his colleagues described their work in Nature Nanotechnology.
The researchers noted that peptide nanoparticles with fluorescence properties are highly sought after because they are biodegradable and considered safe. However, peptides have limited intrinsic optical properties and therefore don’t make effective imaging probes.
In an attempt to overcome the imaging problem without compromising safety, the researchers created tryptophan–phenylalanine dipeptide nanoparticles (DNPs).
“Composed of natural amino acids, the nanoparticle is inherently biocompatible,” Dr Zhang said. “Our biological machines can easily take care of it.”
In addition, the DNPs proved photostable and could maintain their luminescence for extended periods of time.
To test the imaging capabilities of the DNPs, the researchers modified the nanoparticles with MUC1 aptamers so they would recognize the overexpressed MUC1 proteins on A549 human carcinoma epithelial cells.
Experiments showed these DNP/aptamer conjugates could effectively target and light up the cancer cells.
The researchers then tested the DNPs’ ability to monitor drug release by hitching the nanoparticles to doxorubicin. In experiments with A549 cells, the team was able to visualize the doxorubicin inside the cells.
Dr Zhang and his colleagues said the DNPs could be effective with other drugs as well. In fact, the team hopes this method might one day provide patients and their doctors with information on how well and how quickly a medication is working. ![]()
Image courtesy of PNAS
Researchers say they have devised a system that allows for real-time monitoring of drug release.
The team created a luminescent nanoparticle and attached it to the anticancer drug doxorubicin, which allowed them to visualize the drug’s arrival in cancer cells.
Thus far, the team has only tested this system in vitro, but animal studies are currently underway.
“We really want to see what’s going on when we give chemo drugs, and this work paves the way for the exciting endeavor,” said Mingjun Zhang, PhD, of The Ohio State University in Columbus.
He and his colleagues described their work in Nature Nanotechnology.
The researchers noted that peptide nanoparticles with fluorescence properties are highly sought after because they are biodegradable and considered safe. However, peptides have limited intrinsic optical properties and therefore don’t make effective imaging probes.
In an attempt to overcome the imaging problem without compromising safety, the researchers created tryptophan–phenylalanine dipeptide nanoparticles (DNPs).
“Composed of natural amino acids, the nanoparticle is inherently biocompatible,” Dr Zhang said. “Our biological machines can easily take care of it.”
In addition, the DNPs proved photostable and could maintain their luminescence for extended periods of time.
To test the imaging capabilities of the DNPs, the researchers modified the nanoparticles with MUC1 aptamers so they would recognize the overexpressed MUC1 proteins on A549 human carcinoma epithelial cells.
Experiments showed these DNP/aptamer conjugates could effectively target and light up the cancer cells.
The researchers then tested the DNPs’ ability to monitor drug release by hitching the nanoparticles to doxorubicin. In experiments with A549 cells, the team was able to visualize the doxorubicin inside the cells.
Dr Zhang and his colleagues said the DNPs could be effective with other drugs as well. In fact, the team hopes this method might one day provide patients and their doctors with information on how well and how quickly a medication is working. ![]()
Image courtesy of PNAS
Researchers say they have devised a system that allows for real-time monitoring of drug release.
The team created a luminescent nanoparticle and attached it to the anticancer drug doxorubicin, which allowed them to visualize the drug’s arrival in cancer cells.
Thus far, the team has only tested this system in vitro, but animal studies are currently underway.
“We really want to see what’s going on when we give chemo drugs, and this work paves the way for the exciting endeavor,” said Mingjun Zhang, PhD, of The Ohio State University in Columbus.
He and his colleagues described their work in Nature Nanotechnology.
The researchers noted that peptide nanoparticles with fluorescence properties are highly sought after because they are biodegradable and considered safe. However, peptides have limited intrinsic optical properties and therefore don’t make effective imaging probes.
In an attempt to overcome the imaging problem without compromising safety, the researchers created tryptophan–phenylalanine dipeptide nanoparticles (DNPs).
“Composed of natural amino acids, the nanoparticle is inherently biocompatible,” Dr Zhang said. “Our biological machines can easily take care of it.”
In addition, the DNPs proved photostable and could maintain their luminescence for extended periods of time.
To test the imaging capabilities of the DNPs, the researchers modified the nanoparticles with MUC1 aptamers so they would recognize the overexpressed MUC1 proteins on A549 human carcinoma epithelial cells.
Experiments showed these DNP/aptamer conjugates could effectively target and light up the cancer cells.
The researchers then tested the DNPs’ ability to monitor drug release by hitching the nanoparticles to doxorubicin. In experiments with A549 cells, the team was able to visualize the doxorubicin inside the cells.
Dr Zhang and his colleagues said the DNPs could be effective with other drugs as well. In fact, the team hopes this method might one day provide patients and their doctors with information on how well and how quickly a medication is working. ![]()
Oral Leukoedema with Mucosal Desquamation Caused by Toothpaste Containing Sodium Lauryl Sulfate
To the Editor:
A 34-year-old woman presented for evaluation of dry mouth and painless peeling of the oral mucosa of 2 months’ duration. She denied any other skin eruptions, dry eyes, vulvar or vaginal pain, or recent hair loss. A recent antinuclear antibodies test was negative. The patient’s medical history was otherwise unremarkable and her current medications included multivitamins only.
Oral examination revealed peeling gray-white tissue on the buccal mucosa and mouth floor (Figure 1). After the tissue was manually removed with a tongue blade, the mucosal base was normal in color and texture. The patient denied bruxism, biting of the mucosa or other oral trauma, or use of tobacco or nonsteroidal anti-inflammatory drugs.

Biopsies from the buccal mucosa were performed to rule out erosive lichen planus and autoimmune blistering disorders. Microscopy revealed parakeratosis and intracellular edema of the mucosa. An intraepithelial cleft at the parakeratotic surface also was present (Figure 2). Minimal inflammation was noted. Fungal staining and direct immunofluorescence were negative.
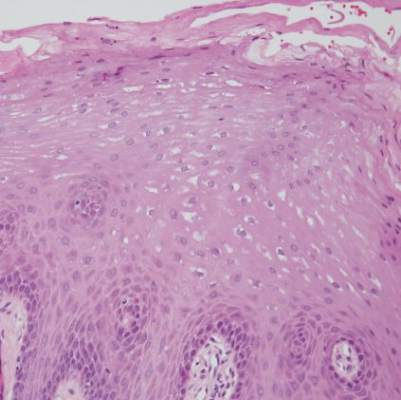
The gray-white clinical appearance of the oral mucosa resembled leukoedema, but the peeling phenomenon was uncharacteristic. Histologically, leukoedema typically has a parakeratotic and acanthotic epithelium with marked intracellular edema of the spinous layer.1,2 Our patient demonstrated intracellular edema with the additional finding of a superficial intraepithelial cleft. These features were consistent with the observed mucosal sloughing and normal tissue base and led to our diagnosis of leukoedema with mucosal desquamation. This clinical and histologic picture was previously described in another report, but a causative agent could not be identified.2
Because leukoedema can be secondary to chemical or mechanical trauma,3 we hypothesized that the patient’s toothpaste may be the causative agent. After discontinuing use of her regular toothpaste and keeping the rest of her oral hygiene routine unchanged, the patient’s condition resolved within 2 days. The patient could not identify how long she had been using the toothpaste before symptoms began.
Our case as well as a report in the literature suggest that leukoedema with mucosal desquamation may be the result of contact mucositis to dental hygiene products.3 Reports in the dental literature suggest that a possible cause for oral mucosal desquamation is sensitivity to sodium lauryl sulfate (SLS),1,4 an ingredient used in some toothpastes, including the one used by our patient. The patient has since switched to a non–SLS-containing toothpaste and has remained asymptomatic. She was unwilling to reintroduce an SLS-containing product for further evaluation.
Sodium lauryl sulfate is a strong anionic detergent that is commonly used as a foaming agent in dentifrices.4 In products with higher concentrations of SLS, the incidence of oral epithelial desquamation increases. Triclosan has been shown to protect against this irritant phenomenon.5 Interestingly, the SLS-containing toothpaste used by our patient did not contain triclosan.
Although leukoedema and mucosal desquamation induced by oral care products are well-described in the dental literature, it is important for dermatologists to be aware of this phenomenon, as the differential diagnosis includes autoimmune blistering disorders and erosive lichen planus, for which dermatology referral may be requested. Further studies of SLS and other toothpaste ingredients are needed to establish if sloughing of the oral mucosa is primarily caused by SLS or another ingredient.
- Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. Philadelphia, PA: WB Saunders; 1983.
- Zegarelli DJ, Silvers DN. Shedding oral mucosa. Cutis. 1994;54:323-326.
- Archard HO, Carlson KP, Stanley HR. Leukoedema of the human oral mucosa. Oral Surg Oral Med Oral Pathol. 1971;25:717-728.
- Herlofson BB, Barkvoll P. Desquamative effect of sodium lauryl sulfate on oral mucosa. a preliminary study. Acta Odontol Scand. 1993;51:39-43.
- Skaare A, Eide G, Herlofson B, et al. The effect of toothpaste containing triclosan on oral mucosal desquamation. a model study. J Clin Periodontology. 1996;23:1100-1103.
To the Editor:
A 34-year-old woman presented for evaluation of dry mouth and painless peeling of the oral mucosa of 2 months’ duration. She denied any other skin eruptions, dry eyes, vulvar or vaginal pain, or recent hair loss. A recent antinuclear antibodies test was negative. The patient’s medical history was otherwise unremarkable and her current medications included multivitamins only.
Oral examination revealed peeling gray-white tissue on the buccal mucosa and mouth floor (Figure 1). After the tissue was manually removed with a tongue blade, the mucosal base was normal in color and texture. The patient denied bruxism, biting of the mucosa or other oral trauma, or use of tobacco or nonsteroidal anti-inflammatory drugs.
Biopsies from the buccal mucosa were performed to rule out erosive lichen planus and autoimmune blistering disorders. Microscopy revealed parakeratosis and intracellular edema of the mucosa. An intraepithelial cleft at the parakeratotic surface also was present (Figure 2). Minimal inflammation was noted. Fungal staining and direct immunofluorescence were negative.
The gray-white clinical appearance of the oral mucosa resembled leukoedema, but the peeling phenomenon was uncharacteristic. Histologically, leukoedema typically has a parakeratotic and acanthotic epithelium with marked intracellular edema of the spinous layer.1,2 Our patient demonstrated intracellular edema with the additional finding of a superficial intraepithelial cleft. These features were consistent with the observed mucosal sloughing and normal tissue base and led to our diagnosis of leukoedema with mucosal desquamation. This clinical and histologic picture was previously described in another report, but a causative agent could not be identified.2
Because leukoedema can be secondary to chemical or mechanical trauma,3 we hypothesized that the patient’s toothpaste may be the causative agent. After discontinuing use of her regular toothpaste and keeping the rest of her oral hygiene routine unchanged, the patient’s condition resolved within 2 days. The patient could not identify how long she had been using the toothpaste before symptoms began.
Our case as well as a report in the literature suggest that leukoedema with mucosal desquamation may be the result of contact mucositis to dental hygiene products.3 Reports in the dental literature suggest that a possible cause for oral mucosal desquamation is sensitivity to sodium lauryl sulfate (SLS),1,4 an ingredient used in some toothpastes, including the one used by our patient. The patient has since switched to a non–SLS-containing toothpaste and has remained asymptomatic. She was unwilling to reintroduce an SLS-containing product for further evaluation.
Sodium lauryl sulfate is a strong anionic detergent that is commonly used as a foaming agent in dentifrices.4 In products with higher concentrations of SLS, the incidence of oral epithelial desquamation increases. Triclosan has been shown to protect against this irritant phenomenon.5 Interestingly, the SLS-containing toothpaste used by our patient did not contain triclosan.
Although leukoedema and mucosal desquamation induced by oral care products are well-described in the dental literature, it is important for dermatologists to be aware of this phenomenon, as the differential diagnosis includes autoimmune blistering disorders and erosive lichen planus, for which dermatology referral may be requested. Further studies of SLS and other toothpaste ingredients are needed to establish if sloughing of the oral mucosa is primarily caused by SLS or another ingredient.
To the Editor:
A 34-year-old woman presented for evaluation of dry mouth and painless peeling of the oral mucosa of 2 months’ duration. She denied any other skin eruptions, dry eyes, vulvar or vaginal pain, or recent hair loss. A recent antinuclear antibodies test was negative. The patient’s medical history was otherwise unremarkable and her current medications included multivitamins only.
Oral examination revealed peeling gray-white tissue on the buccal mucosa and mouth floor (Figure 1). After the tissue was manually removed with a tongue blade, the mucosal base was normal in color and texture. The patient denied bruxism, biting of the mucosa or other oral trauma, or use of tobacco or nonsteroidal anti-inflammatory drugs.
Biopsies from the buccal mucosa were performed to rule out erosive lichen planus and autoimmune blistering disorders. Microscopy revealed parakeratosis and intracellular edema of the mucosa. An intraepithelial cleft at the parakeratotic surface also was present (Figure 2). Minimal inflammation was noted. Fungal staining and direct immunofluorescence were negative.
The gray-white clinical appearance of the oral mucosa resembled leukoedema, but the peeling phenomenon was uncharacteristic. Histologically, leukoedema typically has a parakeratotic and acanthotic epithelium with marked intracellular edema of the spinous layer.1,2 Our patient demonstrated intracellular edema with the additional finding of a superficial intraepithelial cleft. These features were consistent with the observed mucosal sloughing and normal tissue base and led to our diagnosis of leukoedema with mucosal desquamation. This clinical and histologic picture was previously described in another report, but a causative agent could not be identified.2
Because leukoedema can be secondary to chemical or mechanical trauma,3 we hypothesized that the patient’s toothpaste may be the causative agent. After discontinuing use of her regular toothpaste and keeping the rest of her oral hygiene routine unchanged, the patient’s condition resolved within 2 days. The patient could not identify how long she had been using the toothpaste before symptoms began.
Our case as well as a report in the literature suggest that leukoedema with mucosal desquamation may be the result of contact mucositis to dental hygiene products.3 Reports in the dental literature suggest that a possible cause for oral mucosal desquamation is sensitivity to sodium lauryl sulfate (SLS),1,4 an ingredient used in some toothpastes, including the one used by our patient. The patient has since switched to a non–SLS-containing toothpaste and has remained asymptomatic. She was unwilling to reintroduce an SLS-containing product for further evaluation.
Sodium lauryl sulfate is a strong anionic detergent that is commonly used as a foaming agent in dentifrices.4 In products with higher concentrations of SLS, the incidence of oral epithelial desquamation increases. Triclosan has been shown to protect against this irritant phenomenon.5 Interestingly, the SLS-containing toothpaste used by our patient did not contain triclosan.
Although leukoedema and mucosal desquamation induced by oral care products are well-described in the dental literature, it is important for dermatologists to be aware of this phenomenon, as the differential diagnosis includes autoimmune blistering disorders and erosive lichen planus, for which dermatology referral may be requested. Further studies of SLS and other toothpaste ingredients are needed to establish if sloughing of the oral mucosa is primarily caused by SLS or another ingredient.
- Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. Philadelphia, PA: WB Saunders; 1983.
- Zegarelli DJ, Silvers DN. Shedding oral mucosa. Cutis. 1994;54:323-326.
- Archard HO, Carlson KP, Stanley HR. Leukoedema of the human oral mucosa. Oral Surg Oral Med Oral Pathol. 1971;25:717-728.
- Herlofson BB, Barkvoll P. Desquamative effect of sodium lauryl sulfate on oral mucosa. a preliminary study. Acta Odontol Scand. 1993;51:39-43.
- Skaare A, Eide G, Herlofson B, et al. The effect of toothpaste containing triclosan on oral mucosal desquamation. a model study. J Clin Periodontology. 1996;23:1100-1103.
- Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. Philadelphia, PA: WB Saunders; 1983.
- Zegarelli DJ, Silvers DN. Shedding oral mucosa. Cutis. 1994;54:323-326.
- Archard HO, Carlson KP, Stanley HR. Leukoedema of the human oral mucosa. Oral Surg Oral Med Oral Pathol. 1971;25:717-728.
- Herlofson BB, Barkvoll P. Desquamative effect of sodium lauryl sulfate on oral mucosa. a preliminary study. Acta Odontol Scand. 1993;51:39-43.
- Skaare A, Eide G, Herlofson B, et al. The effect of toothpaste containing triclosan on oral mucosal desquamation. a model study. J Clin Periodontology. 1996;23:1100-1103.

ADHD, Part 2: How important is a teacher’s assessment?
Dr. David Pickar and Dr. Lillian M. Beard address the importance of flagging ADHD in the classroom, addressing family resistance to treatment, and situations that might call for the involvement of other mental health colleagues.
“I find a lot of resistance [to the ADHD diagnosis], particularly among African American families,” says Dr. Beard, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
“An untreated ADHD kid is difficult for the teacher, but it is toughest on the kid,” says Dr. Pickar, adjunct professor of psychiatry at Johns Hopkins University, Baltimore. “Families may not hear it all, but a doctor pays a lot of attention to what the teacher is saying about that child in the classroom.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. David Pickar and Dr. Lillian M. Beard address the importance of flagging ADHD in the classroom, addressing family resistance to treatment, and situations that might call for the involvement of other mental health colleagues.
“I find a lot of resistance [to the ADHD diagnosis], particularly among African American families,” says Dr. Beard, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
“An untreated ADHD kid is difficult for the teacher, but it is toughest on the kid,” says Dr. Pickar, adjunct professor of psychiatry at Johns Hopkins University, Baltimore. “Families may not hear it all, but a doctor pays a lot of attention to what the teacher is saying about that child in the classroom.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. David Pickar and Dr. Lillian M. Beard address the importance of flagging ADHD in the classroom, addressing family resistance to treatment, and situations that might call for the involvement of other mental health colleagues.
“I find a lot of resistance [to the ADHD diagnosis], particularly among African American families,” says Dr. Beard, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
“An untreated ADHD kid is difficult for the teacher, but it is toughest on the kid,” says Dr. Pickar, adjunct professor of psychiatry at Johns Hopkins University, Baltimore. “Families may not hear it all, but a doctor pays a lot of attention to what the teacher is saying about that child in the classroom.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

ADHD, Part 1: Is prevalence overstated in children?
Primary care physicians are on the front lines for diagnosing and prescribing to treat attention-deficit/hyperactivity disorder in children. In this video, Dr. David Pickar and Dr. Lillian M. Beard discuss what primary care physicians should know to feel confident when diagnosing and treating ADHD.
“[The first time] you see a patient with ADHD respond to stimulants, you see it is lifesaving … [the result] takes your breath away,” Dr. Pickar says.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Primary care physicians are on the front lines for diagnosing and prescribing to treat attention-deficit/hyperactivity disorder in children. In this video, Dr. David Pickar and Dr. Lillian M. Beard discuss what primary care physicians should know to feel confident when diagnosing and treating ADHD.
“[The first time] you see a patient with ADHD respond to stimulants, you see it is lifesaving … [the result] takes your breath away,” Dr. Pickar says.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Primary care physicians are on the front lines for diagnosing and prescribing to treat attention-deficit/hyperactivity disorder in children. In this video, Dr. David Pickar and Dr. Lillian M. Beard discuss what primary care physicians should know to feel confident when diagnosing and treating ADHD.
“[The first time] you see a patient with ADHD respond to stimulants, you see it is lifesaving … [the result] takes your breath away,” Dr. Pickar says.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Collaborative Care, Part 2: What is 'enough' team care training?
Medical students are better prepared for practice when they learn to integrate mental health and team-based care in the academic setting.
“All schools of health professions’ education are moving in that direction,” says Dr. Lawrence “Bopper” Deyton, senior associate dean for public health at George Washington University, Washington. “Nobody has it perfect yet, but I think we’re seeing changes in that direction.”
In this installment of Mental Health Consult, Dr. Deyton and Dr. April Barbour, director of general internal medicine and the primary care residency program at George Washington University, Washington, discuss approaches to teaching integrated mental health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Medical students are better prepared for practice when they learn to integrate mental health and team-based care in the academic setting.
“All schools of health professions’ education are moving in that direction,” says Dr. Lawrence “Bopper” Deyton, senior associate dean for public health at George Washington University, Washington. “Nobody has it perfect yet, but I think we’re seeing changes in that direction.”
In this installment of Mental Health Consult, Dr. Deyton and Dr. April Barbour, director of general internal medicine and the primary care residency program at George Washington University, Washington, discuss approaches to teaching integrated mental health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Medical students are better prepared for practice when they learn to integrate mental health and team-based care in the academic setting.
“All schools of health professions’ education are moving in that direction,” says Dr. Lawrence “Bopper” Deyton, senior associate dean for public health at George Washington University, Washington. “Nobody has it perfect yet, but I think we’re seeing changes in that direction.”
In this installment of Mental Health Consult, Dr. Deyton and Dr. April Barbour, director of general internal medicine and the primary care residency program at George Washington University, Washington, discuss approaches to teaching integrated mental health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Understanding the Deeds’ family tragedy
Last week, the Washington Post reported that Virginia state Sen. Creigh Deeds has filed a $6 million wrongful death lawsuit against the state of Virginia and the mental health agency that employed an evaluator who saw his son during a psychiatric crisis. In November 2013, Sen. Deeds’ son, Gus, had been brought to an emergency department for evaluation. He was judged to be both psychotic and dangerous, but a bed could not be located for him within the state-mandated 6-hour time frame, and Gus Deeds was released. Soon after, he repeatedly stabbed his father, then took his own life with a firearm.
My knowledge of the case is limited to what has been reported in the media, but as a psychiatrist practicing in Maryland where there are no time limits on locating beds, the story is unthinkable. Why would a very ill and very violent – and perhaps very treatable – young man be released from an emergency department because the gong went off in someone’s ill-conceived game of human “beat the clock?” While I have no inside knowledge of the Deeds’ family tragedy, I do want to talk about the Virginia laws that may have enabled a predictable calamity.

Most psychiatrists are familiar with the practice of psychiatric boarding, or holding a patient in the emergency department for a prolonged period of time because a bed cannot be located on a psychiatry inpatient unit. It’s not unusual for EDs to take many hours, or even several days, to transfer psychiatry patients to treatment units. In some places, it can take even longer. In Vermont, where the state hospital was demolished by a tropical storm, there were instances when patients remained in the ED for up to 6 weeks. On Native American reservations without hospital facilities, very ill psychiatric patients may be housed in jails, again for weeks, while an appropriate hospital bed is located off the reservation. Boarding is, by any measure, inhumane, and in 2014, the Washington state Supreme Court ruled it unlawful, though it did not say exactly where the patients were to be held pending bed availability.
With the civil rights of patients in mind, there is something to be said for mandating that beds be located for patients in a timely manner, and for the patient who is distressed, 6 hours may seem to be quite a long enough time. A drop-dead time, however, leaves no room for unforeseen issues, or even for the possibility that medication could be administered in the ED that might avert the need for an involuntary admission. A time limit of this type forces an immediate decision before a thoughtful assessment can be done and other interventions can be explored. In 2014, as one response to the Deeds’ family tragedy, the law was changed to lengthen the period to 8 hours.
In Virginia, the logistics of admitting a patient are more complex than in most states. Any citizen who is concerned about another person’s mental state and safety can apply to a magistrate for an emergency custody order. The patient is then transported by the sheriff, and the clock starts ticking on the 8-hour time frame. In the ED, the patient is seen by the emergency physician, but regardless of how obviously ill and dangerous the patient is, the physician has no authority to involuntarily admit a psychiatric patient. An outside agency – a local community service board (CSB) – is contacted, and an emergency services staff person is summoned to evaluate the patient, perform preadmission screening, and locate a bed.
Virginia is divided into 41 catchment areas, each served by a community service board. Each CSB is required to have crisis staff who assess patients for civil commitment. Virginia is a state with both urban and rural areas consisting of nearly 43,000 square miles. While the CSB prescreener drives in, performs the evaluation, and searches for an available bed, the clock continues to tick.
The qualifications to be a screener are not precise. The website in the county where Gus Deeds lived advertises: “QUALIFICATIONS: Master’s Degree in human services related field, mental health and/or substance abuse experience; or equivalent combination of education and experience including BSN RN’s with Psychiatric Nursing experience in outpatient or inpatient settings. Extensive knowledge of the DSM, mental health and substance abuse assessments, treatment, crisis assessment and intervention strategies for clients of all ages; must be certified or eligible to be certified as a prescreener by the CSB and Virginia DBHDS” (Department of Behavioral Health & Developmental Services). The prescreener has the authority to override the ED physician and release a patient the physician believes should be admitted.
It’s not uncommon to hear people compare the treatment of an acute myocardial infarction to the treatment of an agitated psychosis, especially when the topic of parity is raised. Could one imagine a scenario where an ED physician could not admit a patient with chest pain without first waiting hours for an outside consultant to come – a consultant who was not even a physician? Presumably, this is not an issue meant to defy parity but to prevent financial conflicts of interest in situations where patient civil rights are a sensitive concern.
Given all the obstacles, what’s surprising is that the vast majority of the time, if it’s determined that a patient needs involuntary admission, a temporary detention order (TDO) is issued and a bed is located. A study done in 2013 looked at the outcome of TDOs issued in a 3-month period. Of an estimated 5,000 TDOs, beds were located for 98.5% of the patients. Still, 72 patients who had been found to be in need of admission were released because beds could not be found before the emergency custody order expired. The practice of releasing patients in crisis has been assigned its own jargon: “streeting.” It’s not quite that simple, however: Not everyone was released as the gong struck. In 273 instances, patients were admitted after the TDO expired, with an average time to admission of just over 16 hours.
A major issue is that Virginia, like nearly all states, has a shortage of psychiatric beds. In Virginia, the problems may be unnecessarily complex with the added requirement to pull in an outside agency and not leave admission decisions to ED clinicians, coupled with a short time limit for transport, treatment, and admission of a complex, sometimes dangerous patient population. According to the Post article, the Deeds suit is particularly troublesome, because beds were available: The CSB prescreener did not call every available hospital, and he attempted to contact one nearby hospital by fax. The fax number he had was wrong, so the request for the bed was never received by the facility. But the facility did, in fact, have a bed. What hasn’t been legislated is how fast a screener needs to drive to the hospital, or how fast he or she is expected to dial for beds, or what happens if he gets a flat tire or if the responses don’t come fast enough.
Tragedy often leads to change, and laws in Virginia changed after the Virginia Tech shootings, and again after the Deeds’ family tragedy. Legislative gaps remain, however, and bed shortages, time limits, and the requirement for an outside agency assessment continue to leave room for the possibility of more tragedy. Clearly, there is more to be done.
With thanks to Dr. Anita Everett for her consultation.
Dr. Miller is coauthor of the forthcoming book, “Committed: The Battle Over Involuntary Psychiatric Care.”
Last week, the Washington Post reported that Virginia state Sen. Creigh Deeds has filed a $6 million wrongful death lawsuit against the state of Virginia and the mental health agency that employed an evaluator who saw his son during a psychiatric crisis. In November 2013, Sen. Deeds’ son, Gus, had been brought to an emergency department for evaluation. He was judged to be both psychotic and dangerous, but a bed could not be located for him within the state-mandated 6-hour time frame, and Gus Deeds was released. Soon after, he repeatedly stabbed his father, then took his own life with a firearm.
My knowledge of the case is limited to what has been reported in the media, but as a psychiatrist practicing in Maryland where there are no time limits on locating beds, the story is unthinkable. Why would a very ill and very violent – and perhaps very treatable – young man be released from an emergency department because the gong went off in someone’s ill-conceived game of human “beat the clock?” While I have no inside knowledge of the Deeds’ family tragedy, I do want to talk about the Virginia laws that may have enabled a predictable calamity.
Most psychiatrists are familiar with the practice of psychiatric boarding, or holding a patient in the emergency department for a prolonged period of time because a bed cannot be located on a psychiatry inpatient unit. It’s not unusual for EDs to take many hours, or even several days, to transfer psychiatry patients to treatment units. In some places, it can take even longer. In Vermont, where the state hospital was demolished by a tropical storm, there were instances when patients remained in the ED for up to 6 weeks. On Native American reservations without hospital facilities, very ill psychiatric patients may be housed in jails, again for weeks, while an appropriate hospital bed is located off the reservation. Boarding is, by any measure, inhumane, and in 2014, the Washington state Supreme Court ruled it unlawful, though it did not say exactly where the patients were to be held pending bed availability.
With the civil rights of patients in mind, there is something to be said for mandating that beds be located for patients in a timely manner, and for the patient who is distressed, 6 hours may seem to be quite a long enough time. A drop-dead time, however, leaves no room for unforeseen issues, or even for the possibility that medication could be administered in the ED that might avert the need for an involuntary admission. A time limit of this type forces an immediate decision before a thoughtful assessment can be done and other interventions can be explored. In 2014, as one response to the Deeds’ family tragedy, the law was changed to lengthen the period to 8 hours.
In Virginia, the logistics of admitting a patient are more complex than in most states. Any citizen who is concerned about another person’s mental state and safety can apply to a magistrate for an emergency custody order. The patient is then transported by the sheriff, and the clock starts ticking on the 8-hour time frame. In the ED, the patient is seen by the emergency physician, but regardless of how obviously ill and dangerous the patient is, the physician has no authority to involuntarily admit a psychiatric patient. An outside agency – a local community service board (CSB) – is contacted, and an emergency services staff person is summoned to evaluate the patient, perform preadmission screening, and locate a bed.
Virginia is divided into 41 catchment areas, each served by a community service board. Each CSB is required to have crisis staff who assess patients for civil commitment. Virginia is a state with both urban and rural areas consisting of nearly 43,000 square miles. While the CSB prescreener drives in, performs the evaluation, and searches for an available bed, the clock continues to tick.
The qualifications to be a screener are not precise. The website in the county where Gus Deeds lived advertises: “QUALIFICATIONS: Master’s Degree in human services related field, mental health and/or substance abuse experience; or equivalent combination of education and experience including BSN RN’s with Psychiatric Nursing experience in outpatient or inpatient settings. Extensive knowledge of the DSM, mental health and substance abuse assessments, treatment, crisis assessment and intervention strategies for clients of all ages; must be certified or eligible to be certified as a prescreener by the CSB and Virginia DBHDS” (Department of Behavioral Health & Developmental Services). The prescreener has the authority to override the ED physician and release a patient the physician believes should be admitted.
It’s not uncommon to hear people compare the treatment of an acute myocardial infarction to the treatment of an agitated psychosis, especially when the topic of parity is raised. Could one imagine a scenario where an ED physician could not admit a patient with chest pain without first waiting hours for an outside consultant to come – a consultant who was not even a physician? Presumably, this is not an issue meant to defy parity but to prevent financial conflicts of interest in situations where patient civil rights are a sensitive concern.
Given all the obstacles, what’s surprising is that the vast majority of the time, if it’s determined that a patient needs involuntary admission, a temporary detention order (TDO) is issued and a bed is located. A study done in 2013 looked at the outcome of TDOs issued in a 3-month period. Of an estimated 5,000 TDOs, beds were located for 98.5% of the patients. Still, 72 patients who had been found to be in need of admission were released because beds could not be found before the emergency custody order expired. The practice of releasing patients in crisis has been assigned its own jargon: “streeting.” It’s not quite that simple, however: Not everyone was released as the gong struck. In 273 instances, patients were admitted after the TDO expired, with an average time to admission of just over 16 hours.
A major issue is that Virginia, like nearly all states, has a shortage of psychiatric beds. In Virginia, the problems may be unnecessarily complex with the added requirement to pull in an outside agency and not leave admission decisions to ED clinicians, coupled with a short time limit for transport, treatment, and admission of a complex, sometimes dangerous patient population. According to the Post article, the Deeds suit is particularly troublesome, because beds were available: The CSB prescreener did not call every available hospital, and he attempted to contact one nearby hospital by fax. The fax number he had was wrong, so the request for the bed was never received by the facility. But the facility did, in fact, have a bed. What hasn’t been legislated is how fast a screener needs to drive to the hospital, or how fast he or she is expected to dial for beds, or what happens if he gets a flat tire or if the responses don’t come fast enough.
Tragedy often leads to change, and laws in Virginia changed after the Virginia Tech shootings, and again after the Deeds’ family tragedy. Legislative gaps remain, however, and bed shortages, time limits, and the requirement for an outside agency assessment continue to leave room for the possibility of more tragedy. Clearly, there is more to be done.
With thanks to Dr. Anita Everett for her consultation.
Dr. Miller is coauthor of the forthcoming book, “Committed: The Battle Over Involuntary Psychiatric Care.”
Last week, the Washington Post reported that Virginia state Sen. Creigh Deeds has filed a $6 million wrongful death lawsuit against the state of Virginia and the mental health agency that employed an evaluator who saw his son during a psychiatric crisis. In November 2013, Sen. Deeds’ son, Gus, had been brought to an emergency department for evaluation. He was judged to be both psychotic and dangerous, but a bed could not be located for him within the state-mandated 6-hour time frame, and Gus Deeds was released. Soon after, he repeatedly stabbed his father, then took his own life with a firearm.
My knowledge of the case is limited to what has been reported in the media, but as a psychiatrist practicing in Maryland where there are no time limits on locating beds, the story is unthinkable. Why would a very ill and very violent – and perhaps very treatable – young man be released from an emergency department because the gong went off in someone’s ill-conceived game of human “beat the clock?” While I have no inside knowledge of the Deeds’ family tragedy, I do want to talk about the Virginia laws that may have enabled a predictable calamity.
Most psychiatrists are familiar with the practice of psychiatric boarding, or holding a patient in the emergency department for a prolonged period of time because a bed cannot be located on a psychiatry inpatient unit. It’s not unusual for EDs to take many hours, or even several days, to transfer psychiatry patients to treatment units. In some places, it can take even longer. In Vermont, where the state hospital was demolished by a tropical storm, there were instances when patients remained in the ED for up to 6 weeks. On Native American reservations without hospital facilities, very ill psychiatric patients may be housed in jails, again for weeks, while an appropriate hospital bed is located off the reservation. Boarding is, by any measure, inhumane, and in 2014, the Washington state Supreme Court ruled it unlawful, though it did not say exactly where the patients were to be held pending bed availability.
With the civil rights of patients in mind, there is something to be said for mandating that beds be located for patients in a timely manner, and for the patient who is distressed, 6 hours may seem to be quite a long enough time. A drop-dead time, however, leaves no room for unforeseen issues, or even for the possibility that medication could be administered in the ED that might avert the need for an involuntary admission. A time limit of this type forces an immediate decision before a thoughtful assessment can be done and other interventions can be explored. In 2014, as one response to the Deeds’ family tragedy, the law was changed to lengthen the period to 8 hours.
In Virginia, the logistics of admitting a patient are more complex than in most states. Any citizen who is concerned about another person’s mental state and safety can apply to a magistrate for an emergency custody order. The patient is then transported by the sheriff, and the clock starts ticking on the 8-hour time frame. In the ED, the patient is seen by the emergency physician, but regardless of how obviously ill and dangerous the patient is, the physician has no authority to involuntarily admit a psychiatric patient. An outside agency – a local community service board (CSB) – is contacted, and an emergency services staff person is summoned to evaluate the patient, perform preadmission screening, and locate a bed.
Virginia is divided into 41 catchment areas, each served by a community service board. Each CSB is required to have crisis staff who assess patients for civil commitment. Virginia is a state with both urban and rural areas consisting of nearly 43,000 square miles. While the CSB prescreener drives in, performs the evaluation, and searches for an available bed, the clock continues to tick.
The qualifications to be a screener are not precise. The website in the county where Gus Deeds lived advertises: “QUALIFICATIONS: Master’s Degree in human services related field, mental health and/or substance abuse experience; or equivalent combination of education and experience including BSN RN’s with Psychiatric Nursing experience in outpatient or inpatient settings. Extensive knowledge of the DSM, mental health and substance abuse assessments, treatment, crisis assessment and intervention strategies for clients of all ages; must be certified or eligible to be certified as a prescreener by the CSB and Virginia DBHDS” (Department of Behavioral Health & Developmental Services). The prescreener has the authority to override the ED physician and release a patient the physician believes should be admitted.
It’s not uncommon to hear people compare the treatment of an acute myocardial infarction to the treatment of an agitated psychosis, especially when the topic of parity is raised. Could one imagine a scenario where an ED physician could not admit a patient with chest pain without first waiting hours for an outside consultant to come – a consultant who was not even a physician? Presumably, this is not an issue meant to defy parity but to prevent financial conflicts of interest in situations where patient civil rights are a sensitive concern.
Given all the obstacles, what’s surprising is that the vast majority of the time, if it’s determined that a patient needs involuntary admission, a temporary detention order (TDO) is issued and a bed is located. A study done in 2013 looked at the outcome of TDOs issued in a 3-month period. Of an estimated 5,000 TDOs, beds were located for 98.5% of the patients. Still, 72 patients who had been found to be in need of admission were released because beds could not be found before the emergency custody order expired. The practice of releasing patients in crisis has been assigned its own jargon: “streeting.” It’s not quite that simple, however: Not everyone was released as the gong struck. In 273 instances, patients were admitted after the TDO expired, with an average time to admission of just over 16 hours.
A major issue is that Virginia, like nearly all states, has a shortage of psychiatric beds. In Virginia, the problems may be unnecessarily complex with the added requirement to pull in an outside agency and not leave admission decisions to ED clinicians, coupled with a short time limit for transport, treatment, and admission of a complex, sometimes dangerous patient population. According to the Post article, the Deeds suit is particularly troublesome, because beds were available: The CSB prescreener did not call every available hospital, and he attempted to contact one nearby hospital by fax. The fax number he had was wrong, so the request for the bed was never received by the facility. But the facility did, in fact, have a bed. What hasn’t been legislated is how fast a screener needs to drive to the hospital, or how fast he or she is expected to dial for beds, or what happens if he gets a flat tire or if the responses don’t come fast enough.
Tragedy often leads to change, and laws in Virginia changed after the Virginia Tech shootings, and again after the Deeds’ family tragedy. Legislative gaps remain, however, and bed shortages, time limits, and the requirement for an outside agency assessment continue to leave room for the possibility of more tragedy. Clearly, there is more to be done.
With thanks to Dr. Anita Everett for her consultation.
Dr. Miller is coauthor of the forthcoming book, “Committed: The Battle Over Involuntary Psychiatric Care.”
