User login
A 60-year-old man with forehead swelling
A 60-year-old man presented to our emergency department with a 4-day history of frontal headaches he described as “stinging.” He had also had a large swollen area on his forehead for the past 8 weeks.
He denied fevers, chills, nausea, vomiting, blurry vision, tinnitus, and neck pain, as well as any recent sinus infection, intransanal cocaine use, rhinorrhea, or head trauma. A month ago, he had presented to our emergency department with forehead swelling but no headaches. At that time, the swelling was thought to be an allergic reaction to lisinopril or metformin, medications he takes for hypertension and type 2 diabetes. He had been discharged home with a prescription for a course of prednisone in tapering doses, but that had failed to resolve the swelling.
Physical examination revealed a well-circumscribed area of swelling, 3 by 4 cm, in the central forehead (Figure 1). The area was warm, erythematous, fluctuant, and tender to palpation. The nasal septum was intact and the nasal mucosa appeared pink and healthy. The remainder of the examination was unremarkable.
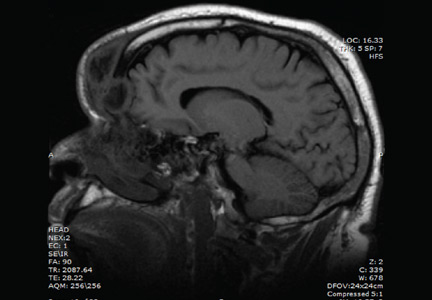
He was afebrile and hemodynamically stable. His peripheral white blood cell count was mildly elevated at 11.1 × 109. Computed tomography of the brain and sinuses revealed a fluid collection in the frontal scalp associated with erosion of the anterior frontal sinus with posterior extension and enhancement of the adjacent meninges. Magnetic resonance imaging (Figure 2) revealed similar findings. A diagnosis of Pott puffy tumor was made based on the imaging findings.
The name of this condition is misleading, as it is not a neoplasm but an infection. It requires urgent antibiotic therapy and surgical management because of the high risk of the infection spreading to the brain. Our patient was started on a broad-spectrum antibiotic regimen of intravenous vancomycin, ceftriaxone, and metronidazole pending tissue culture to identify the causative organism.
POTT PUFFY TUMOR: A BRIEF OVERVIEW
First described in 1760 by Sir Percivall Pott,1 the same English surgeon who first described tuberculosis of the spine, Pott puffy tumor is a well-demarcated area of swelling that occurs when a frontal sinus infection breaks through the anterior portion of the frontal sinus and forms an abscess between the frontal bone and periosteum with associated osteomyelitis.2 Though rare in adults (it is more common in children and adolescents),3 Pott puffy tumor is caused by conditions often encountered in internal medicine practice, such as bacterial sinusitis, head trauma, and intranasal cocaine use.
The infection can spread to the brain either directly by destruction of the posterior frontal sinus (as in our patient) or by way of the veins that drain the frontal sinus. Meningitis, epidural empyema, frontal lobe abscess, and cavernous sinus thrombosis2 have all been described. Intracranial complications are seen in nearly 100% of children and adolescents with Pott puffy tumor. The rate in adults is 30%,4,5 which is much lower but is nevertheless worrisome because patients can be initially misdiagnosed with scalp abscess,3 cellulitis, or epidermoid cyst,4 and then sent home from the emergency department or physician’s office. In a case series of 32 adult patients with Pott puffy tumor, nearly 45% were initially misdiagnosed, most often by an internist, dermatologist, ophthalmologist, or emergency room physician.4
The most common infective organisms are streptococci, staphylococci, and anaerobes,4 but Haemophilus, Aspergillus species, and invasive mucormycosis have also been described.
MANAGEMENT OPTIONS
Because of the risk of spread of the infection to the brain, rapid initiation of a broad-spectrum antibiotic is warranted in all patients with Pott puffy tumor pending results of tissue culture. Antibiotics may be necessary for at least 4 to 6 weeks to resolve osteomyelitis of the frontal bone and to decrease inflammation before surgery.6
Endoscopic sinus surgery is routinely done to drain the infected sinus and to remove or debride infected bone. Patients with intracranial extension of infection may require a combined endoscopic and neurosurgical approach.
OUTCOME
Our patient’s puffy tumor spontaneously ruptured externally on hospital day 3, and the purulent fluid was sent for culture that grew Streptococcus anginosus. His headaches improved almost immediately after this occurred. The antibiotic regimen was narrowed to ceftriaxone and metronidazole, and 1 week later he was discharged home with instructions to complete a 6-week course of antibiotics. Three weeks after he was discharged, he returned for outpatient endoscopic sinus surgery. At a follow-up visit 2 weeks after surgery, the forehead swelling had resolved, and he was well.
- Tattersall R, Tattersall R. Pott’s puffy tumor. Lancet 2002; 359:1060–1063.
- Forgie SE, Marrie TJ. Pott’s puffy tumor. Am J Med 2008; 121:1041–1042.
- Grewal HS, Dangaych NS, Esposito A. A tumor that is not a tumor but it sure can kill! Am J Case Rep 2012; 13:133–136.
- Akiyama K, Karaki M, Mori N. Evaluation of adult Pott’s puffy tumor: our five cases and 27 literature cases. Laryngoscope 2012; 122:2382–2388.
- Suwan PT, Mogal S, Chaudhary S. Pott’s puffy tumor: an uncommon clinical entity. Case Rep Pediatr 2012; 2012:386104.
- Lauria RA, Laffitte Fernandes F, Brito TP, Pereira PS, Chone CT. Extensive frontoparietal abscess: complication of frontal sinusitis (Pott’s puffy tumor). Case Rep Otolaryngol 2014; 2014:632464.
A 60-year-old man presented to our emergency department with a 4-day history of frontal headaches he described as “stinging.” He had also had a large swollen area on his forehead for the past 8 weeks.
He denied fevers, chills, nausea, vomiting, blurry vision, tinnitus, and neck pain, as well as any recent sinus infection, intransanal cocaine use, rhinorrhea, or head trauma. A month ago, he had presented to our emergency department with forehead swelling but no headaches. At that time, the swelling was thought to be an allergic reaction to lisinopril or metformin, medications he takes for hypertension and type 2 diabetes. He had been discharged home with a prescription for a course of prednisone in tapering doses, but that had failed to resolve the swelling.
Physical examination revealed a well-circumscribed area of swelling, 3 by 4 cm, in the central forehead (Figure 1). The area was warm, erythematous, fluctuant, and tender to palpation. The nasal septum was intact and the nasal mucosa appeared pink and healthy. The remainder of the examination was unremarkable.
He was afebrile and hemodynamically stable. His peripheral white blood cell count was mildly elevated at 11.1 × 109. Computed tomography of the brain and sinuses revealed a fluid collection in the frontal scalp associated with erosion of the anterior frontal sinus with posterior extension and enhancement of the adjacent meninges. Magnetic resonance imaging (Figure 2) revealed similar findings. A diagnosis of Pott puffy tumor was made based on the imaging findings.
The name of this condition is misleading, as it is not a neoplasm but an infection. It requires urgent antibiotic therapy and surgical management because of the high risk of the infection spreading to the brain. Our patient was started on a broad-spectrum antibiotic regimen of intravenous vancomycin, ceftriaxone, and metronidazole pending tissue culture to identify the causative organism.
POTT PUFFY TUMOR: A BRIEF OVERVIEW
First described in 1760 by Sir Percivall Pott,1 the same English surgeon who first described tuberculosis of the spine, Pott puffy tumor is a well-demarcated area of swelling that occurs when a frontal sinus infection breaks through the anterior portion of the frontal sinus and forms an abscess between the frontal bone and periosteum with associated osteomyelitis.2 Though rare in adults (it is more common in children and adolescents),3 Pott puffy tumor is caused by conditions often encountered in internal medicine practice, such as bacterial sinusitis, head trauma, and intranasal cocaine use.
The infection can spread to the brain either directly by destruction of the posterior frontal sinus (as in our patient) or by way of the veins that drain the frontal sinus. Meningitis, epidural empyema, frontal lobe abscess, and cavernous sinus thrombosis2 have all been described. Intracranial complications are seen in nearly 100% of children and adolescents with Pott puffy tumor. The rate in adults is 30%,4,5 which is much lower but is nevertheless worrisome because patients can be initially misdiagnosed with scalp abscess,3 cellulitis, or epidermoid cyst,4 and then sent home from the emergency department or physician’s office. In a case series of 32 adult patients with Pott puffy tumor, nearly 45% were initially misdiagnosed, most often by an internist, dermatologist, ophthalmologist, or emergency room physician.4
The most common infective organisms are streptococci, staphylococci, and anaerobes,4 but Haemophilus, Aspergillus species, and invasive mucormycosis have also been described.
MANAGEMENT OPTIONS
Because of the risk of spread of the infection to the brain, rapid initiation of a broad-spectrum antibiotic is warranted in all patients with Pott puffy tumor pending results of tissue culture. Antibiotics may be necessary for at least 4 to 6 weeks to resolve osteomyelitis of the frontal bone and to decrease inflammation before surgery.6
Endoscopic sinus surgery is routinely done to drain the infected sinus and to remove or debride infected bone. Patients with intracranial extension of infection may require a combined endoscopic and neurosurgical approach.
OUTCOME
Our patient’s puffy tumor spontaneously ruptured externally on hospital day 3, and the purulent fluid was sent for culture that grew Streptococcus anginosus. His headaches improved almost immediately after this occurred. The antibiotic regimen was narrowed to ceftriaxone and metronidazole, and 1 week later he was discharged home with instructions to complete a 6-week course of antibiotics. Three weeks after he was discharged, he returned for outpatient endoscopic sinus surgery. At a follow-up visit 2 weeks after surgery, the forehead swelling had resolved, and he was well.
A 60-year-old man presented to our emergency department with a 4-day history of frontal headaches he described as “stinging.” He had also had a large swollen area on his forehead for the past 8 weeks.
He denied fevers, chills, nausea, vomiting, blurry vision, tinnitus, and neck pain, as well as any recent sinus infection, intransanal cocaine use, rhinorrhea, or head trauma. A month ago, he had presented to our emergency department with forehead swelling but no headaches. At that time, the swelling was thought to be an allergic reaction to lisinopril or metformin, medications he takes for hypertension and type 2 diabetes. He had been discharged home with a prescription for a course of prednisone in tapering doses, but that had failed to resolve the swelling.
Physical examination revealed a well-circumscribed area of swelling, 3 by 4 cm, in the central forehead (Figure 1). The area was warm, erythematous, fluctuant, and tender to palpation. The nasal septum was intact and the nasal mucosa appeared pink and healthy. The remainder of the examination was unremarkable.
He was afebrile and hemodynamically stable. His peripheral white blood cell count was mildly elevated at 11.1 × 109. Computed tomography of the brain and sinuses revealed a fluid collection in the frontal scalp associated with erosion of the anterior frontal sinus with posterior extension and enhancement of the adjacent meninges. Magnetic resonance imaging (Figure 2) revealed similar findings. A diagnosis of Pott puffy tumor was made based on the imaging findings.
The name of this condition is misleading, as it is not a neoplasm but an infection. It requires urgent antibiotic therapy and surgical management because of the high risk of the infection spreading to the brain. Our patient was started on a broad-spectrum antibiotic regimen of intravenous vancomycin, ceftriaxone, and metronidazole pending tissue culture to identify the causative organism.
POTT PUFFY TUMOR: A BRIEF OVERVIEW
First described in 1760 by Sir Percivall Pott,1 the same English surgeon who first described tuberculosis of the spine, Pott puffy tumor is a well-demarcated area of swelling that occurs when a frontal sinus infection breaks through the anterior portion of the frontal sinus and forms an abscess between the frontal bone and periosteum with associated osteomyelitis.2 Though rare in adults (it is more common in children and adolescents),3 Pott puffy tumor is caused by conditions often encountered in internal medicine practice, such as bacterial sinusitis, head trauma, and intranasal cocaine use.
The infection can spread to the brain either directly by destruction of the posterior frontal sinus (as in our patient) or by way of the veins that drain the frontal sinus. Meningitis, epidural empyema, frontal lobe abscess, and cavernous sinus thrombosis2 have all been described. Intracranial complications are seen in nearly 100% of children and adolescents with Pott puffy tumor. The rate in adults is 30%,4,5 which is much lower but is nevertheless worrisome because patients can be initially misdiagnosed with scalp abscess,3 cellulitis, or epidermoid cyst,4 and then sent home from the emergency department or physician’s office. In a case series of 32 adult patients with Pott puffy tumor, nearly 45% were initially misdiagnosed, most often by an internist, dermatologist, ophthalmologist, or emergency room physician.4
The most common infective organisms are streptococci, staphylococci, and anaerobes,4 but Haemophilus, Aspergillus species, and invasive mucormycosis have also been described.
MANAGEMENT OPTIONS
Because of the risk of spread of the infection to the brain, rapid initiation of a broad-spectrum antibiotic is warranted in all patients with Pott puffy tumor pending results of tissue culture. Antibiotics may be necessary for at least 4 to 6 weeks to resolve osteomyelitis of the frontal bone and to decrease inflammation before surgery.6
Endoscopic sinus surgery is routinely done to drain the infected sinus and to remove or debride infected bone. Patients with intracranial extension of infection may require a combined endoscopic and neurosurgical approach.
OUTCOME
Our patient’s puffy tumor spontaneously ruptured externally on hospital day 3, and the purulent fluid was sent for culture that grew Streptococcus anginosus. His headaches improved almost immediately after this occurred. The antibiotic regimen was narrowed to ceftriaxone and metronidazole, and 1 week later he was discharged home with instructions to complete a 6-week course of antibiotics. Three weeks after he was discharged, he returned for outpatient endoscopic sinus surgery. At a follow-up visit 2 weeks after surgery, the forehead swelling had resolved, and he was well.
- Tattersall R, Tattersall R. Pott’s puffy tumor. Lancet 2002; 359:1060–1063.
- Forgie SE, Marrie TJ. Pott’s puffy tumor. Am J Med 2008; 121:1041–1042.
- Grewal HS, Dangaych NS, Esposito A. A tumor that is not a tumor but it sure can kill! Am J Case Rep 2012; 13:133–136.
- Akiyama K, Karaki M, Mori N. Evaluation of adult Pott’s puffy tumor: our five cases and 27 literature cases. Laryngoscope 2012; 122:2382–2388.
- Suwan PT, Mogal S, Chaudhary S. Pott’s puffy tumor: an uncommon clinical entity. Case Rep Pediatr 2012; 2012:386104.
- Lauria RA, Laffitte Fernandes F, Brito TP, Pereira PS, Chone CT. Extensive frontoparietal abscess: complication of frontal sinusitis (Pott’s puffy tumor). Case Rep Otolaryngol 2014; 2014:632464.
- Tattersall R, Tattersall R. Pott’s puffy tumor. Lancet 2002; 359:1060–1063.
- Forgie SE, Marrie TJ. Pott’s puffy tumor. Am J Med 2008; 121:1041–1042.
- Grewal HS, Dangaych NS, Esposito A. A tumor that is not a tumor but it sure can kill! Am J Case Rep 2012; 13:133–136.
- Akiyama K, Karaki M, Mori N. Evaluation of adult Pott’s puffy tumor: our five cases and 27 literature cases. Laryngoscope 2012; 122:2382–2388.
- Suwan PT, Mogal S, Chaudhary S. Pott’s puffy tumor: an uncommon clinical entity. Case Rep Pediatr 2012; 2012:386104.
- Lauria RA, Laffitte Fernandes F, Brito TP, Pereira PS, Chone CT. Extensive frontoparietal abscess: complication of frontal sinusitis (Pott’s puffy tumor). Case Rep Otolaryngol 2014; 2014:632464.
Obesity and exercise
Obesity means having a body mass index (BMI) of 30 or higher. Being obese increases your risk of health problems including high blood pressure, diabetes, cholesterol, arthritis, cancer, and cardiovascular diseases such as stroke and heart attack. You can reduce these risks by losing weight.
The healthy way to lose weight is to eat fewer calories, eat less processed food and more whole foods, and exercise regularly. A dietitian can help you create a flexible and balanced eating plan to help you meet your goals.
When beginning an exercise plan, start slowly with a combination of aerobic, resistance, flexibility, and balance exercises. A combined aerobic and resistance exercise program will likely result in more weight loss than either alone.

Aerobic exercises should be the foundation of your program. Choose exercises that involve large muscle groups, such as walking. Walking is the easiest way for most people to start exercising, but you can also consider other exercises such as stationary bicycling, slow jogging, and water aerobics.
Resistance training involves lifting weights using either weight machines or free weights (dumbbells).
Flexibility exercises are a type of stretching that improves the movements of your muscles, joints, and ligaments.
Balance exercises improve your stability and reduce the chance of falling or other injuries. These exercises can be done without any equipment. For example, with single-leg balance, you balance on one foot for 15 seconds. A stand-sit involves standing up and sitting down without using your hands.
Your provider will design an exercise program for you that includes the frequency, intensity, time, and types of exercise. Typically, you’ll want to lose about 10% of your weight over a 6-month period. Be sure to set SMART goals (Specific, Measurable, Attainable, Realistic, Timely) to sustain the self-discipline required for long-term success. Also consider tracking your physical activity using a wearable device (eg, Fitbit) or a smartphone app. It lets you see your progress over time, helps you set new goals, and helps keep you motivated.
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints available by calling 216-444-2661.
For patient information on hundreds of health topics, visit the Center for Consumer Health Information website, www.clevelandclinic.org/health.
Obesity means having a body mass index (BMI) of 30 or higher. Being obese increases your risk of health problems including high blood pressure, diabetes, cholesterol, arthritis, cancer, and cardiovascular diseases such as stroke and heart attack. You can reduce these risks by losing weight.
The healthy way to lose weight is to eat fewer calories, eat less processed food and more whole foods, and exercise regularly. A dietitian can help you create a flexible and balanced eating plan to help you meet your goals.
When beginning an exercise plan, start slowly with a combination of aerobic, resistance, flexibility, and balance exercises. A combined aerobic and resistance exercise program will likely result in more weight loss than either alone.
Aerobic exercises should be the foundation of your program. Choose exercises that involve large muscle groups, such as walking. Walking is the easiest way for most people to start exercising, but you can also consider other exercises such as stationary bicycling, slow jogging, and water aerobics.
Resistance training involves lifting weights using either weight machines or free weights (dumbbells).
Flexibility exercises are a type of stretching that improves the movements of your muscles, joints, and ligaments.
Balance exercises improve your stability and reduce the chance of falling or other injuries. These exercises can be done without any equipment. For example, with single-leg balance, you balance on one foot for 15 seconds. A stand-sit involves standing up and sitting down without using your hands.
Your provider will design an exercise program for you that includes the frequency, intensity, time, and types of exercise. Typically, you’ll want to lose about 10% of your weight over a 6-month period. Be sure to set SMART goals (Specific, Measurable, Attainable, Realistic, Timely) to sustain the self-discipline required for long-term success. Also consider tracking your physical activity using a wearable device (eg, Fitbit) or a smartphone app. It lets you see your progress over time, helps you set new goals, and helps keep you motivated.
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints available by calling 216-444-2661.
For patient information on hundreds of health topics, visit the Center for Consumer Health Information website, www.clevelandclinic.org/health.
Obesity means having a body mass index (BMI) of 30 or higher. Being obese increases your risk of health problems including high blood pressure, diabetes, cholesterol, arthritis, cancer, and cardiovascular diseases such as stroke and heart attack. You can reduce these risks by losing weight.
The healthy way to lose weight is to eat fewer calories, eat less processed food and more whole foods, and exercise regularly. A dietitian can help you create a flexible and balanced eating plan to help you meet your goals.
When beginning an exercise plan, start slowly with a combination of aerobic, resistance, flexibility, and balance exercises. A combined aerobic and resistance exercise program will likely result in more weight loss than either alone.
Aerobic exercises should be the foundation of your program. Choose exercises that involve large muscle groups, such as walking. Walking is the easiest way for most people to start exercising, but you can also consider other exercises such as stationary bicycling, slow jogging, and water aerobics.
Resistance training involves lifting weights using either weight machines or free weights (dumbbells).
Flexibility exercises are a type of stretching that improves the movements of your muscles, joints, and ligaments.
Balance exercises improve your stability and reduce the chance of falling or other injuries. These exercises can be done without any equipment. For example, with single-leg balance, you balance on one foot for 15 seconds. A stand-sit involves standing up and sitting down without using your hands.
Your provider will design an exercise program for you that includes the frequency, intensity, time, and types of exercise. Typically, you’ll want to lose about 10% of your weight over a 6-month period. Be sure to set SMART goals (Specific, Measurable, Attainable, Realistic, Timely) to sustain the self-discipline required for long-term success. Also consider tracking your physical activity using a wearable device (eg, Fitbit) or a smartphone app. It lets you see your progress over time, helps you set new goals, and helps keep you motivated.
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints available by calling 216-444-2661.
For patient information on hundreds of health topics, visit the Center for Consumer Health Information website, www.clevelandclinic.org/health.

Tailor chronic pain interventions to the patient’s clinical profile

February 2016 Digital Edition
Table of Contents
- A Prescription for Music Lessons
- A New View for the VA
- Management of Diabetic Foot Ulcers: A Review
- Monitoring Heat Injuries in a Hazmat Environment
- Hyponatremia Secondary to Lisinopril in a Veteran Patient
- Clinical Video Telehealth for Gait and Balance
- Asymptomatic but Time for a Hip Revision
- Impact of Interprofessional Care Teams on Metabolic Parameters in Patients

Table of Contents
- A Prescription for Music Lessons
- A New View for the VA
- Management of Diabetic Foot Ulcers: A Review
- Monitoring Heat Injuries in a Hazmat Environment
- Hyponatremia Secondary to Lisinopril in a Veteran Patient
- Clinical Video Telehealth for Gait and Balance
- Asymptomatic but Time for a Hip Revision
- Impact of Interprofessional Care Teams on Metabolic Parameters in Patients
Table of Contents
- A Prescription for Music Lessons
- A New View for the VA
- Management of Diabetic Foot Ulcers: A Review
- Monitoring Heat Injuries in a Hazmat Environment
- Hyponatremia Secondary to Lisinopril in a Veteran Patient
- Clinical Video Telehealth for Gait and Balance
- Asymptomatic but Time for a Hip Revision
- Impact of Interprofessional Care Teams on Metabolic Parameters in Patients

Adoption of Choosing Wisely Recommendations Slow to Catch On
Clinical question: Have the Choosing Wisely campaign recommendations led to changes in practice?

Background: The Choosing Wisely campaign aims to reduce the incidence of low-value care by providing evidence-based recommendations for common clinical situations. The rate of adoption of these recommendations is unknown.
Study design: Retrospective review.
Setting: Anthem insurance members.
Synopsis: The study examined the claims data from 25 million Anthem insurance members to compare the rate of services that were targeted by seven Choosing Wisely campaign recommendations before and after the recommendations were published in 2012.
Investigators found the incidence of two of the services declined after the Choosing Wisely recommendations were published; the other five services remained stable or increased slightly. Furthermore, the declines were statistically significant but not a marked absolute difference, with the incidence of head imaging in patients with uncomplicated headaches going down to 13.4% from 14.9% and the use of cardiac imaging in the absence of cardiac disease declining to 9.7% from 10.8%.
The main limitations are the narrow population of Anthem insurance members and the lack of specific data that could help answer why clinical practice has not changed, but that could be the aim of future studies.
Bottom line: Choosing Wisely recommendations have not been adopted on a population level; widespread implementation likely will require financial incentives, provider-level data feedback, and systems interventions.
Citation: Rosenberg A, Agiro A, Gottlieb M, et al. Early trends among seven recommendations from the Choosing Wisely campaign. JAMA Intern Med. 2015;175(12):1913-1920. doi:10.1001/jamainternmed.2015.5441.
Clinical question: Have the Choosing Wisely campaign recommendations led to changes in practice?
Background: The Choosing Wisely campaign aims to reduce the incidence of low-value care by providing evidence-based recommendations for common clinical situations. The rate of adoption of these recommendations is unknown.
Study design: Retrospective review.
Setting: Anthem insurance members.
Synopsis: The study examined the claims data from 25 million Anthem insurance members to compare the rate of services that were targeted by seven Choosing Wisely campaign recommendations before and after the recommendations were published in 2012.
Investigators found the incidence of two of the services declined after the Choosing Wisely recommendations were published; the other five services remained stable or increased slightly. Furthermore, the declines were statistically significant but not a marked absolute difference, with the incidence of head imaging in patients with uncomplicated headaches going down to 13.4% from 14.9% and the use of cardiac imaging in the absence of cardiac disease declining to 9.7% from 10.8%.
The main limitations are the narrow population of Anthem insurance members and the lack of specific data that could help answer why clinical practice has not changed, but that could be the aim of future studies.
Bottom line: Choosing Wisely recommendations have not been adopted on a population level; widespread implementation likely will require financial incentives, provider-level data feedback, and systems interventions.
Citation: Rosenberg A, Agiro A, Gottlieb M, et al. Early trends among seven recommendations from the Choosing Wisely campaign. JAMA Intern Med. 2015;175(12):1913-1920. doi:10.1001/jamainternmed.2015.5441.
Clinical question: Have the Choosing Wisely campaign recommendations led to changes in practice?
Background: The Choosing Wisely campaign aims to reduce the incidence of low-value care by providing evidence-based recommendations for common clinical situations. The rate of adoption of these recommendations is unknown.
Study design: Retrospective review.
Setting: Anthem insurance members.
Synopsis: The study examined the claims data from 25 million Anthem insurance members to compare the rate of services that were targeted by seven Choosing Wisely campaign recommendations before and after the recommendations were published in 2012.
Investigators found the incidence of two of the services declined after the Choosing Wisely recommendations were published; the other five services remained stable or increased slightly. Furthermore, the declines were statistically significant but not a marked absolute difference, with the incidence of head imaging in patients with uncomplicated headaches going down to 13.4% from 14.9% and the use of cardiac imaging in the absence of cardiac disease declining to 9.7% from 10.8%.
The main limitations are the narrow population of Anthem insurance members and the lack of specific data that could help answer why clinical practice has not changed, but that could be the aim of future studies.
Bottom line: Choosing Wisely recommendations have not been adopted on a population level; widespread implementation likely will require financial incentives, provider-level data feedback, and systems interventions.
Citation: Rosenberg A, Agiro A, Gottlieb M, et al. Early trends among seven recommendations from the Choosing Wisely campaign. JAMA Intern Med. 2015;175(12):1913-1920. doi:10.1001/jamainternmed.2015.5441.

Standard BMI inadequate for ALL patients

Photo by Bill Branson
New research suggests that body mass index (BMI) is an inadequate method for estimating changes in body fat and obesity in children with acute lymphoblastic leukemia (ALL).
Investigators found a discrepancy between BMI and body composition in this population, and the cause of this appeared to be increases in body fat with simultaneous loss of lean muscle mass during treatment.
The team reported these findings in Leukemia & Lymphoma.
With previous work, the investigators found that obese children diagnosed with high-risk ALL had a 50% greater risk of their disease recurring compared with children who were not obese.
“In my lab, we’ve seen a direct interaction between fat cells and leukemia cells that may help explain this increased risk of disease relapse,” said study author Steven Mittelman, MD, PhD, of Children’s Hospital Los Angeles in California.
“It appears that the fat cells ‘protect’ leukemia cells, making them less susceptible to chemotherapy and making an accurate measure of body fat essential.”
To determine if BMI accurately reflects body fat in ALL, the investigators analyzed 50 patients. They were predominantly Hispanic, between the ages of 10 to 21, and had newly diagnosed high-risk B-precursor ALL or T-cell ALL.
The team measured the percentage of total body fat and lean muscle mass at the time of diagnosis, at the end of induction, and at the end of delayed intensification. They also calculated BMI Z-score—a measure of how a given child’s BMI deviates from a population of children of the same age and sex—at these time points.
The investigators said sarcopenic obesity—gain in body fat percentage with loss of lean muscle mass—was “surprisingly common” during ALL treatment.
And sarcopenic obesity resulted in poor correlation between changes in BMI Z-score and body fat percentage overall (r=-0.05), within the time points (r=0.02), and within patients (r=-0.09, all not significant). BMI Z-score and body fat percentage changed in opposite directions in more than 50% of interval assessments.
“We found that change in BMI did not reflect changes in body fat or obesity,” said Etan Orgel, MD, of Children’s Hospital Los Angeles.
“In some patients, reaching a ‘healthy’ BMI was due solely to loss of muscle even while body fat continued to rise. Based on these results, we believe that evaluation of obesity in patients with leukemia should include direct measures of body composition.” ![]()
Photo by Bill Branson
New research suggests that body mass index (BMI) is an inadequate method for estimating changes in body fat and obesity in children with acute lymphoblastic leukemia (ALL).
Investigators found a discrepancy between BMI and body composition in this population, and the cause of this appeared to be increases in body fat with simultaneous loss of lean muscle mass during treatment.
The team reported these findings in Leukemia & Lymphoma.
With previous work, the investigators found that obese children diagnosed with high-risk ALL had a 50% greater risk of their disease recurring compared with children who were not obese.
“In my lab, we’ve seen a direct interaction between fat cells and leukemia cells that may help explain this increased risk of disease relapse,” said study author Steven Mittelman, MD, PhD, of Children’s Hospital Los Angeles in California.
“It appears that the fat cells ‘protect’ leukemia cells, making them less susceptible to chemotherapy and making an accurate measure of body fat essential.”
To determine if BMI accurately reflects body fat in ALL, the investigators analyzed 50 patients. They were predominantly Hispanic, between the ages of 10 to 21, and had newly diagnosed high-risk B-precursor ALL or T-cell ALL.
The team measured the percentage of total body fat and lean muscle mass at the time of diagnosis, at the end of induction, and at the end of delayed intensification. They also calculated BMI Z-score—a measure of how a given child’s BMI deviates from a population of children of the same age and sex—at these time points.
The investigators said sarcopenic obesity—gain in body fat percentage with loss of lean muscle mass—was “surprisingly common” during ALL treatment.
And sarcopenic obesity resulted in poor correlation between changes in BMI Z-score and body fat percentage overall (r=-0.05), within the time points (r=0.02), and within patients (r=-0.09, all not significant). BMI Z-score and body fat percentage changed in opposite directions in more than 50% of interval assessments.
“We found that change in BMI did not reflect changes in body fat or obesity,” said Etan Orgel, MD, of Children’s Hospital Los Angeles.
“In some patients, reaching a ‘healthy’ BMI was due solely to loss of muscle even while body fat continued to rise. Based on these results, we believe that evaluation of obesity in patients with leukemia should include direct measures of body composition.” ![]()
Photo by Bill Branson
New research suggests that body mass index (BMI) is an inadequate method for estimating changes in body fat and obesity in children with acute lymphoblastic leukemia (ALL).
Investigators found a discrepancy between BMI and body composition in this population, and the cause of this appeared to be increases in body fat with simultaneous loss of lean muscle mass during treatment.
The team reported these findings in Leukemia & Lymphoma.
With previous work, the investigators found that obese children diagnosed with high-risk ALL had a 50% greater risk of their disease recurring compared with children who were not obese.
“In my lab, we’ve seen a direct interaction between fat cells and leukemia cells that may help explain this increased risk of disease relapse,” said study author Steven Mittelman, MD, PhD, of Children’s Hospital Los Angeles in California.
“It appears that the fat cells ‘protect’ leukemia cells, making them less susceptible to chemotherapy and making an accurate measure of body fat essential.”
To determine if BMI accurately reflects body fat in ALL, the investigators analyzed 50 patients. They were predominantly Hispanic, between the ages of 10 to 21, and had newly diagnosed high-risk B-precursor ALL or T-cell ALL.
The team measured the percentage of total body fat and lean muscle mass at the time of diagnosis, at the end of induction, and at the end of delayed intensification. They also calculated BMI Z-score—a measure of how a given child’s BMI deviates from a population of children of the same age and sex—at these time points.
The investigators said sarcopenic obesity—gain in body fat percentage with loss of lean muscle mass—was “surprisingly common” during ALL treatment.
And sarcopenic obesity resulted in poor correlation between changes in BMI Z-score and body fat percentage overall (r=-0.05), within the time points (r=0.02), and within patients (r=-0.09, all not significant). BMI Z-score and body fat percentage changed in opposite directions in more than 50% of interval assessments.
“We found that change in BMI did not reflect changes in body fat or obesity,” said Etan Orgel, MD, of Children’s Hospital Los Angeles.
“In some patients, reaching a ‘healthy’ BMI was due solely to loss of muscle even while body fat continued to rise. Based on these results, we believe that evaluation of obesity in patients with leukemia should include direct measures of body composition.” ![]()
NICE issues draft guideline for NHL

a cancer patient
Photo courtesy of NCI/
Mathews Media Group
The National Institute for Health and Care Excellence (NICE) has issued a draft guideline for the diagnosis and management of non-Hodgkin lymphoma (NHL).
The guideline, which is open for consultation, covers adults and young people who are referred to secondary care with suspected NHL or who have newly diagnosed or relapsed NHL.
It contains recommendations for the management of 6 different NHL subtypes—diffuse large B-cell lymphoma, mantle cell lymphoma, follicular lymphoma, MALT lymphoma, Burkitt lymphoma, and peripheral T-cell lymphoma.
The guideline considers which method of biopsy is most appropriate, which diagnostic test most suitable, how the stage of disease is best assessed, and what treatment is likely to be most effective.
It also proposes recommendations for how best to support patients who complete their treatment. These include the provision of end-of-treatment summaries to be discussed with the patient and an increase in education on the possible relapse/late side-effects of their treatment.
“This draft guideline is now open for consultation,” said Mark Baker, director of the Centre of Clinical Practice at NICE.
“We want to hear from patients and all those who provide care for people with non-Hodgkin’s lymphoma in the NHS [National Health Service] so that we can produce a guideline which will support everyone who diagnoses, treats, and has to live with this disease.”
The consultation closes on March 11, 2016, with the final guideline expected in the summer. ![]()
a cancer patient
Photo courtesy of NCI/
Mathews Media Group
The National Institute for Health and Care Excellence (NICE) has issued a draft guideline for the diagnosis and management of non-Hodgkin lymphoma (NHL).
The guideline, which is open for consultation, covers adults and young people who are referred to secondary care with suspected NHL or who have newly diagnosed or relapsed NHL.
It contains recommendations for the management of 6 different NHL subtypes—diffuse large B-cell lymphoma, mantle cell lymphoma, follicular lymphoma, MALT lymphoma, Burkitt lymphoma, and peripheral T-cell lymphoma.
The guideline considers which method of biopsy is most appropriate, which diagnostic test most suitable, how the stage of disease is best assessed, and what treatment is likely to be most effective.
It also proposes recommendations for how best to support patients who complete their treatment. These include the provision of end-of-treatment summaries to be discussed with the patient and an increase in education on the possible relapse/late side-effects of their treatment.
“This draft guideline is now open for consultation,” said Mark Baker, director of the Centre of Clinical Practice at NICE.
“We want to hear from patients and all those who provide care for people with non-Hodgkin’s lymphoma in the NHS [National Health Service] so that we can produce a guideline which will support everyone who diagnoses, treats, and has to live with this disease.”
The consultation closes on March 11, 2016, with the final guideline expected in the summer. ![]()
a cancer patient
Photo courtesy of NCI/
Mathews Media Group
The National Institute for Health and Care Excellence (NICE) has issued a draft guideline for the diagnosis and management of non-Hodgkin lymphoma (NHL).
The guideline, which is open for consultation, covers adults and young people who are referred to secondary care with suspected NHL or who have newly diagnosed or relapsed NHL.
It contains recommendations for the management of 6 different NHL subtypes—diffuse large B-cell lymphoma, mantle cell lymphoma, follicular lymphoma, MALT lymphoma, Burkitt lymphoma, and peripheral T-cell lymphoma.
The guideline considers which method of biopsy is most appropriate, which diagnostic test most suitable, how the stage of disease is best assessed, and what treatment is likely to be most effective.
It also proposes recommendations for how best to support patients who complete their treatment. These include the provision of end-of-treatment summaries to be discussed with the patient and an increase in education on the possible relapse/late side-effects of their treatment.
“This draft guideline is now open for consultation,” said Mark Baker, director of the Centre of Clinical Practice at NICE.
“We want to hear from patients and all those who provide care for people with non-Hodgkin’s lymphoma in the NHS [National Health Service] so that we can produce a guideline which will support everyone who diagnoses, treats, and has to live with this disease.”
The consultation closes on March 11, 2016, with the final guideline expected in the summer. ![]()
Minor residual staining found adequate for colonoscopy
A Boston Bowel Preparation Scale (BBPS) score of 2 – indicating mild residual staining and small stool fragments – was as good as the optimal preparation score of 3 for visualizing polyps and adenomas larger than 5 mm and advanced adenomas during colonoscopy, researchers said.
A score of 2 might increase the chances of missing smaller polyps, but is adequate for detecting clinically significant masses, Dr. Brian Clark of Yale University, New Haven, Conn., and his associates reported in the February issue of Gastroenterology. But a score of 1 – meaning that there is enough staining or stool to obscure the mucosa – significantly increased the chances of missing adenomas larger than 5 mm, they said. Patients should undergo early repeat colonoscopy if their BBPS score is 1 or 0 in any colon segment, they emphasized.
Source: American Gastroenterological Association
Bowel preparation for colonoscopy is considered adequate if endoscopists can detect polyps larger than 5 mm, but no prior study had quantified the amount of preparation needed. This prospective observational study assessed adequate preparation in terms of the BBPS, which scores each of three colon segments on a scale of 0 (solid stool covering the mucosa) to 3 points (entire mucosa seen well, with no residual staining). Study participants included 438 men aged 50-75 years who underwent screening or surveillance colonoscopy at a single Veterans Affairs center, followed by repeat colonoscopies within 60 days performed by different blinded endoscopists. The investigators excluded patients who scored 0 in all colon segments or had familial polyposis syndrome, inflammatory bowel disease, polyps so large that they could not be completely removed, or a history of colonic or rectal resection. In all, they analyzed 1,161 colon segments (Gastroenterology. 2015 Dec 7. doi: 10.1053/j.gastro.2015.09.041).
Endoscopists missed about 5% of adenomas greater than 5 mm, regardless of whether BBPS scores were 2 or 3 in a model that accounted for age, reason for colonoscopy, colon segment, number of polyps removed in the first examination, and endoscopist performing the procedure, the researchers said. But when BBPS scores were 1, endoscopists missed 16% of adenomas larger than 5 mm, a difference of about 10%. Furthermore, 43% of screening and surveillance intervals would have been incorrect had they been based solely on an initial examination for which scores were 1 in at least one segment. In contrast, only about 15% of intervals would have been incorrect for patients who scored 2 or 3 in all segments.
In all, 80% of patients were sufficiently prepared, having scored at least 2 in all segments on the first examination. “Determining whether a patient’s preparation quality is adequate is one of the most common and important decisions made by gastroenterologists each day,” the researchers said. Between 25% and 30% of screening and surveillance colonoscopies occur at “inappropriately shortened intervals,” often because of uncertainty about what constitutes adequate visualization, they added. Defining adequate visualization based on bowel preparation could save billions of dollars in health care costs every year, minimize complications from unnecessary procedures, and pinpoint those patients who truly need an early repeat colonoscopy to help prevent interval colorectal cancer, they emphasized.
The National Institutes of Health funded the study. The investigators had no disclosures.
We have seen a dramatic increase in attention to improving the adenoma detection rate (ADR) during colonoscopy because patients of endoscopists with a higher ADR have a lower risk of colorectal cancer after colonoscopy. One major contributor to missed adenomas is inadequate bowel preparation, though little was known about how best to define adequacy.

|
| Dr. Jason Domonitz |
Clark and colleagues’ elegant tandem colonoscopy study helps address this knowledge gap using the Boston Bowel Preparation Scale (BBPS), a validated instrument that is easy to implement. They hypothesized that a BBPS colon-segment score of 2 was noninferior to a score of 3 for identifying adenomas greater than 5 mm, but that a BBPS colon-segment score of 1 would be inferior to scores of 2 or 3. Their findings support this hypothesis and give us long overdue data that we can now use to define an adequate bowel preparation. Given that the adenoma miss rate was 16% when the segment score was 1, but only about 5% with higher scores, it is reasonable to recommend repeat colonoscopy within 12 months if any segment score is less than 2. Otherwise, standard surveillance intervals should be recommended. Finally, unless and until other scoring systems are similarly validated, these findings should encourage the widespread adoption of the BBPS.
Dr. Jason A. Dominitz, AGAF, is the national program director for gastroenterology for the Veterans Health Administration and is professor of medicine in the division of gastroenterology at the University of Washington, Seattle. He has no conflicts of interest.
We have seen a dramatic increase in attention to improving the adenoma detection rate (ADR) during colonoscopy because patients of endoscopists with a higher ADR have a lower risk of colorectal cancer after colonoscopy. One major contributor to missed adenomas is inadequate bowel preparation, though little was known about how best to define adequacy.
|
|
| Dr. Jason Domonitz |
Clark and colleagues’ elegant tandem colonoscopy study helps address this knowledge gap using the Boston Bowel Preparation Scale (BBPS), a validated instrument that is easy to implement. They hypothesized that a BBPS colon-segment score of 2 was noninferior to a score of 3 for identifying adenomas greater than 5 mm, but that a BBPS colon-segment score of 1 would be inferior to scores of 2 or 3. Their findings support this hypothesis and give us long overdue data that we can now use to define an adequate bowel preparation. Given that the adenoma miss rate was 16% when the segment score was 1, but only about 5% with higher scores, it is reasonable to recommend repeat colonoscopy within 12 months if any segment score is less than 2. Otherwise, standard surveillance intervals should be recommended. Finally, unless and until other scoring systems are similarly validated, these findings should encourage the widespread adoption of the BBPS.
Dr. Jason A. Dominitz, AGAF, is the national program director for gastroenterology for the Veterans Health Administration and is professor of medicine in the division of gastroenterology at the University of Washington, Seattle. He has no conflicts of interest.
We have seen a dramatic increase in attention to improving the adenoma detection rate (ADR) during colonoscopy because patients of endoscopists with a higher ADR have a lower risk of colorectal cancer after colonoscopy. One major contributor to missed adenomas is inadequate bowel preparation, though little was known about how best to define adequacy.
|
|
| Dr. Jason Domonitz |
Clark and colleagues’ elegant tandem colonoscopy study helps address this knowledge gap using the Boston Bowel Preparation Scale (BBPS), a validated instrument that is easy to implement. They hypothesized that a BBPS colon-segment score of 2 was noninferior to a score of 3 for identifying adenomas greater than 5 mm, but that a BBPS colon-segment score of 1 would be inferior to scores of 2 or 3. Their findings support this hypothesis and give us long overdue data that we can now use to define an adequate bowel preparation. Given that the adenoma miss rate was 16% when the segment score was 1, but only about 5% with higher scores, it is reasonable to recommend repeat colonoscopy within 12 months if any segment score is less than 2. Otherwise, standard surveillance intervals should be recommended. Finally, unless and until other scoring systems are similarly validated, these findings should encourage the widespread adoption of the BBPS.
Dr. Jason A. Dominitz, AGAF, is the national program director for gastroenterology for the Veterans Health Administration and is professor of medicine in the division of gastroenterology at the University of Washington, Seattle. He has no conflicts of interest.
A Boston Bowel Preparation Scale (BBPS) score of 2 – indicating mild residual staining and small stool fragments – was as good as the optimal preparation score of 3 for visualizing polyps and adenomas larger than 5 mm and advanced adenomas during colonoscopy, researchers said.
A score of 2 might increase the chances of missing smaller polyps, but is adequate for detecting clinically significant masses, Dr. Brian Clark of Yale University, New Haven, Conn., and his associates reported in the February issue of Gastroenterology. But a score of 1 – meaning that there is enough staining or stool to obscure the mucosa – significantly increased the chances of missing adenomas larger than 5 mm, they said. Patients should undergo early repeat colonoscopy if their BBPS score is 1 or 0 in any colon segment, they emphasized.
Source: American Gastroenterological Association
Bowel preparation for colonoscopy is considered adequate if endoscopists can detect polyps larger than 5 mm, but no prior study had quantified the amount of preparation needed. This prospective observational study assessed adequate preparation in terms of the BBPS, which scores each of three colon segments on a scale of 0 (solid stool covering the mucosa) to 3 points (entire mucosa seen well, with no residual staining). Study participants included 438 men aged 50-75 years who underwent screening or surveillance colonoscopy at a single Veterans Affairs center, followed by repeat colonoscopies within 60 days performed by different blinded endoscopists. The investigators excluded patients who scored 0 in all colon segments or had familial polyposis syndrome, inflammatory bowel disease, polyps so large that they could not be completely removed, or a history of colonic or rectal resection. In all, they analyzed 1,161 colon segments (Gastroenterology. 2015 Dec 7. doi: 10.1053/j.gastro.2015.09.041).
Endoscopists missed about 5% of adenomas greater than 5 mm, regardless of whether BBPS scores were 2 or 3 in a model that accounted for age, reason for colonoscopy, colon segment, number of polyps removed in the first examination, and endoscopist performing the procedure, the researchers said. But when BBPS scores were 1, endoscopists missed 16% of adenomas larger than 5 mm, a difference of about 10%. Furthermore, 43% of screening and surveillance intervals would have been incorrect had they been based solely on an initial examination for which scores were 1 in at least one segment. In contrast, only about 15% of intervals would have been incorrect for patients who scored 2 or 3 in all segments.
In all, 80% of patients were sufficiently prepared, having scored at least 2 in all segments on the first examination. “Determining whether a patient’s preparation quality is adequate is one of the most common and important decisions made by gastroenterologists each day,” the researchers said. Between 25% and 30% of screening and surveillance colonoscopies occur at “inappropriately shortened intervals,” often because of uncertainty about what constitutes adequate visualization, they added. Defining adequate visualization based on bowel preparation could save billions of dollars in health care costs every year, minimize complications from unnecessary procedures, and pinpoint those patients who truly need an early repeat colonoscopy to help prevent interval colorectal cancer, they emphasized.
The National Institutes of Health funded the study. The investigators had no disclosures.
A Boston Bowel Preparation Scale (BBPS) score of 2 – indicating mild residual staining and small stool fragments – was as good as the optimal preparation score of 3 for visualizing polyps and adenomas larger than 5 mm and advanced adenomas during colonoscopy, researchers said.
A score of 2 might increase the chances of missing smaller polyps, but is adequate for detecting clinically significant masses, Dr. Brian Clark of Yale University, New Haven, Conn., and his associates reported in the February issue of Gastroenterology. But a score of 1 – meaning that there is enough staining or stool to obscure the mucosa – significantly increased the chances of missing adenomas larger than 5 mm, they said. Patients should undergo early repeat colonoscopy if their BBPS score is 1 or 0 in any colon segment, they emphasized.
Source: American Gastroenterological Association
Bowel preparation for colonoscopy is considered adequate if endoscopists can detect polyps larger than 5 mm, but no prior study had quantified the amount of preparation needed. This prospective observational study assessed adequate preparation in terms of the BBPS, which scores each of three colon segments on a scale of 0 (solid stool covering the mucosa) to 3 points (entire mucosa seen well, with no residual staining). Study participants included 438 men aged 50-75 years who underwent screening or surveillance colonoscopy at a single Veterans Affairs center, followed by repeat colonoscopies within 60 days performed by different blinded endoscopists. The investigators excluded patients who scored 0 in all colon segments or had familial polyposis syndrome, inflammatory bowel disease, polyps so large that they could not be completely removed, or a history of colonic or rectal resection. In all, they analyzed 1,161 colon segments (Gastroenterology. 2015 Dec 7. doi: 10.1053/j.gastro.2015.09.041).
Endoscopists missed about 5% of adenomas greater than 5 mm, regardless of whether BBPS scores were 2 or 3 in a model that accounted for age, reason for colonoscopy, colon segment, number of polyps removed in the first examination, and endoscopist performing the procedure, the researchers said. But when BBPS scores were 1, endoscopists missed 16% of adenomas larger than 5 mm, a difference of about 10%. Furthermore, 43% of screening and surveillance intervals would have been incorrect had they been based solely on an initial examination for which scores were 1 in at least one segment. In contrast, only about 15% of intervals would have been incorrect for patients who scored 2 or 3 in all segments.
In all, 80% of patients were sufficiently prepared, having scored at least 2 in all segments on the first examination. “Determining whether a patient’s preparation quality is adequate is one of the most common and important decisions made by gastroenterologists each day,” the researchers said. Between 25% and 30% of screening and surveillance colonoscopies occur at “inappropriately shortened intervals,” often because of uncertainty about what constitutes adequate visualization, they added. Defining adequate visualization based on bowel preparation could save billions of dollars in health care costs every year, minimize complications from unnecessary procedures, and pinpoint those patients who truly need an early repeat colonoscopy to help prevent interval colorectal cancer, they emphasized.
The National Institutes of Health funded the study. The investigators had no disclosures.
FROM GASTROENTEROLOGY
Key clinical point: Minor residual staining that does not obscure the bowel mucosa is adequate for detection of adenomas greater than 5 mm during surveillance or screening colonoscopy.
Major finding: Endoscopists missed about 5% of clinically significant adenomas, regardless of whether the Boston Bowel Preparation Score was 2 (minor residual staining) or 3 (entire mucosa seen well).
Data source: A blinded prospective observational study of 438 men at a single Veterans Affairs center.
Disclosures: The National Institutes of Health funded the study. The investigators had no disclosures.

Drug combo held up in real-world HCV study
A 12-week, ribavirin-free regimen achieved sustained virologic response for 85% of patients with genotype 1 hepatitis C virus (HCV) infection, researchers reported in the February issue of Gastroenterology.
“This represents one of the first applications of a highly effective HCV regimen outside clinical trials,” said Dr. Mark S. Sulkowski of John Hopkins University in Baltimore and his associates. Adding ribavirin to the simeprevir and sofosbuvir combination regimen did not improve sustained virologic response (SVR), but patients were less likely to achieve it if they had cirrhosis, current or prior hepatic decompensation, or a history of failing other protease inhibitors, the investigators said.

Novel hepatitis C therapies have yielded “substantially lower” rates of SVR and more side effects in everyday practice than in clinical trials, the investigators noted. To better understand how some of newest HCV drugs perform in the real world, they conducted an observational cohort study of the safety, tolerability, and efficacy of simeprevir plus sofosbuvir for treating genotype 1 HCV infections in academic and nonacademic settings (HCV-TARGET) (Gastroenterology 2015 doi: 10.1053/j.gastro.2015.10.013).
A total of 836 patients received once-daily simeprevir (150 mg) and sofosbuvir (400 mg), and 169 of them also received ribavirin. Most (61%) patients had genotype 1a infection and were white (76%), male (61%), and cirrhotic (59%); 13% were black. Patients usually were treatment experienced, having failed peginterferon and ribavirin either with (12%) or without (46%) telaprevir or boceprevir, the researchers said.
In all, 675 (84%) patients achieved SVR after 12 weeks of treatment (SVR12; 95% confidence interval, 81%-87%). Adding ribavirin to the combination PI regimen did not improve SVR, regardless of cirrhosis status, genetic subtype, or treatment history. However, crude SVR12 rates were only 75% for patients with hepatic decompensation and 81% for those with cirrhosis, and these patients had significantly lower adjusted odds of achieving SVR, compared with other patients. In hindsight, decompensated and cirrhotic patients might have needed 24 weeks of treatment, as the Food and Drug Administration now recommends based on the COSMOS trial results (Lancet. 2014;384[9956]:1756-65), the investigators said.
The adjusted model did not uncover a link between genotype 1 subtype and SVR, but only about 10% of patients were tested for the Q80K polymorphism, which is more common in genotype 1a infections and is associated with treatment resistance, the investigators noted. Crude SVR12 rates were 92% for patients with genotype 1b infection and 86% for those with 1a infection, they said.
Only 3% of patients stopped treatment; 2% did so because of side effects, and ribavirin did not significantly affect rates of treatment discontinuation, said the investigators. The most common side effects were fatigue, headache, nausea, rash, and insomnia. Serious adverse events affected 5% of patients and included gastrointestinal bleeding (0.5%), hepatic failure or encephalopathy (1.2%), and infections (1.1%).
Taken together, these results show that simeprevir and sofosbuvir effectively translate from the clinical trial setting into clinical practice, said the researchers. “Additional research is needed to understand which patients may benefit from different treatment regimens or longer treatment durations,” they emphasized.
The study was supported by the University of Florida at Gainesville, the University of North Carolina at Chapel Hill, AbbVie, Bristol-Myers Squibb, Gilead, Janssen, Kadmon, Merck, Vertex, and the National Institutes of Health. Dr. Sulkowski reported grants and personal fees from Gilead, Janssen, Achillion, Abbvie, Merck, and Bristol-Myers Squibb. Of 14 coinvestigators, 13 reported financial relationships with a number of pharmaceutical companies.
A 12-week, ribavirin-free regimen achieved sustained virologic response for 85% of patients with genotype 1 hepatitis C virus (HCV) infection, researchers reported in the February issue of Gastroenterology.
“This represents one of the first applications of a highly effective HCV regimen outside clinical trials,” said Dr. Mark S. Sulkowski of John Hopkins University in Baltimore and his associates. Adding ribavirin to the simeprevir and sofosbuvir combination regimen did not improve sustained virologic response (SVR), but patients were less likely to achieve it if they had cirrhosis, current or prior hepatic decompensation, or a history of failing other protease inhibitors, the investigators said.
Novel hepatitis C therapies have yielded “substantially lower” rates of SVR and more side effects in everyday practice than in clinical trials, the investigators noted. To better understand how some of newest HCV drugs perform in the real world, they conducted an observational cohort study of the safety, tolerability, and efficacy of simeprevir plus sofosbuvir for treating genotype 1 HCV infections in academic and nonacademic settings (HCV-TARGET) (Gastroenterology 2015 doi: 10.1053/j.gastro.2015.10.013).
A total of 836 patients received once-daily simeprevir (150 mg) and sofosbuvir (400 mg), and 169 of them also received ribavirin. Most (61%) patients had genotype 1a infection and were white (76%), male (61%), and cirrhotic (59%); 13% were black. Patients usually were treatment experienced, having failed peginterferon and ribavirin either with (12%) or without (46%) telaprevir or boceprevir, the researchers said.
In all, 675 (84%) patients achieved SVR after 12 weeks of treatment (SVR12; 95% confidence interval, 81%-87%). Adding ribavirin to the combination PI regimen did not improve SVR, regardless of cirrhosis status, genetic subtype, or treatment history. However, crude SVR12 rates were only 75% for patients with hepatic decompensation and 81% for those with cirrhosis, and these patients had significantly lower adjusted odds of achieving SVR, compared with other patients. In hindsight, decompensated and cirrhotic patients might have needed 24 weeks of treatment, as the Food and Drug Administration now recommends based on the COSMOS trial results (Lancet. 2014;384[9956]:1756-65), the investigators said.
The adjusted model did not uncover a link between genotype 1 subtype and SVR, but only about 10% of patients were tested for the Q80K polymorphism, which is more common in genotype 1a infections and is associated with treatment resistance, the investigators noted. Crude SVR12 rates were 92% for patients with genotype 1b infection and 86% for those with 1a infection, they said.
Only 3% of patients stopped treatment; 2% did so because of side effects, and ribavirin did not significantly affect rates of treatment discontinuation, said the investigators. The most common side effects were fatigue, headache, nausea, rash, and insomnia. Serious adverse events affected 5% of patients and included gastrointestinal bleeding (0.5%), hepatic failure or encephalopathy (1.2%), and infections (1.1%).
Taken together, these results show that simeprevir and sofosbuvir effectively translate from the clinical trial setting into clinical practice, said the researchers. “Additional research is needed to understand which patients may benefit from different treatment regimens or longer treatment durations,” they emphasized.
The study was supported by the University of Florida at Gainesville, the University of North Carolina at Chapel Hill, AbbVie, Bristol-Myers Squibb, Gilead, Janssen, Kadmon, Merck, Vertex, and the National Institutes of Health. Dr. Sulkowski reported grants and personal fees from Gilead, Janssen, Achillion, Abbvie, Merck, and Bristol-Myers Squibb. Of 14 coinvestigators, 13 reported financial relationships with a number of pharmaceutical companies.
A 12-week, ribavirin-free regimen achieved sustained virologic response for 85% of patients with genotype 1 hepatitis C virus (HCV) infection, researchers reported in the February issue of Gastroenterology.
“This represents one of the first applications of a highly effective HCV regimen outside clinical trials,” said Dr. Mark S. Sulkowski of John Hopkins University in Baltimore and his associates. Adding ribavirin to the simeprevir and sofosbuvir combination regimen did not improve sustained virologic response (SVR), but patients were less likely to achieve it if they had cirrhosis, current or prior hepatic decompensation, or a history of failing other protease inhibitors, the investigators said.
Novel hepatitis C therapies have yielded “substantially lower” rates of SVR and more side effects in everyday practice than in clinical trials, the investigators noted. To better understand how some of newest HCV drugs perform in the real world, they conducted an observational cohort study of the safety, tolerability, and efficacy of simeprevir plus sofosbuvir for treating genotype 1 HCV infections in academic and nonacademic settings (HCV-TARGET) (Gastroenterology 2015 doi: 10.1053/j.gastro.2015.10.013).
A total of 836 patients received once-daily simeprevir (150 mg) and sofosbuvir (400 mg), and 169 of them also received ribavirin. Most (61%) patients had genotype 1a infection and were white (76%), male (61%), and cirrhotic (59%); 13% were black. Patients usually were treatment experienced, having failed peginterferon and ribavirin either with (12%) or without (46%) telaprevir or boceprevir, the researchers said.
In all, 675 (84%) patients achieved SVR after 12 weeks of treatment (SVR12; 95% confidence interval, 81%-87%). Adding ribavirin to the combination PI regimen did not improve SVR, regardless of cirrhosis status, genetic subtype, or treatment history. However, crude SVR12 rates were only 75% for patients with hepatic decompensation and 81% for those with cirrhosis, and these patients had significantly lower adjusted odds of achieving SVR, compared with other patients. In hindsight, decompensated and cirrhotic patients might have needed 24 weeks of treatment, as the Food and Drug Administration now recommends based on the COSMOS trial results (Lancet. 2014;384[9956]:1756-65), the investigators said.
The adjusted model did not uncover a link between genotype 1 subtype and SVR, but only about 10% of patients were tested for the Q80K polymorphism, which is more common in genotype 1a infections and is associated with treatment resistance, the investigators noted. Crude SVR12 rates were 92% for patients with genotype 1b infection and 86% for those with 1a infection, they said.
Only 3% of patients stopped treatment; 2% did so because of side effects, and ribavirin did not significantly affect rates of treatment discontinuation, said the investigators. The most common side effects were fatigue, headache, nausea, rash, and insomnia. Serious adverse events affected 5% of patients and included gastrointestinal bleeding (0.5%), hepatic failure or encephalopathy (1.2%), and infections (1.1%).
Taken together, these results show that simeprevir and sofosbuvir effectively translate from the clinical trial setting into clinical practice, said the researchers. “Additional research is needed to understand which patients may benefit from different treatment regimens or longer treatment durations,” they emphasized.
The study was supported by the University of Florida at Gainesville, the University of North Carolina at Chapel Hill, AbbVie, Bristol-Myers Squibb, Gilead, Janssen, Kadmon, Merck, Vertex, and the National Institutes of Health. Dr. Sulkowski reported grants and personal fees from Gilead, Janssen, Achillion, Abbvie, Merck, and Bristol-Myers Squibb. Of 14 coinvestigators, 13 reported financial relationships with a number of pharmaceutical companies.
FROM GASTROENTEROLOGY
Key clinical point: Twelve weeks of simeprevir and sofosbuvir cured about 85% of real-world patients with genotype 1 hepatitis C virus infection.
Major finding: The unadjusted rate of SVR12 was 85% (95% CI, 82%-88%).
Data source: An analysis of an observational cohort study of protease inhibitor combination regimen with or without ribavirin for 836 patients (HCV-TARGET).
Disclosures: The study was supported by the University of Florida at Gainesville, the University of North Carolina at Chapel Hill, AbbVie, Bristol-Myers Squibb, Gilead, Janssen, Kadmon, Merck, Vertex, and the National Institutes of Health. Dr. Sulkowski reported grants and personal fees from Gilead, Janssen, Achillion, Abbvie, Merck, and Bristol-Myers Squibb. Of 14 coinvestigators, 13 reported financial relationships with a number of pharmaceutical companies.
