User login
Study Shows an Increase in Older Americans that Take at Least Five Medications
(Reuters Health) - The proportion of older Americans taking at least five medications or supplements went up in a recent study.
The increase in people using multiple medications - known as polypharmacy - paralleled an increase in the number of older Americans at risk for major drug interactions, researchers found.
"That's a concern from a public health standpoint, because it's getting worse," said Dima Qato, the study's lead author from the University of Illinois at Chicago.
Qato and her colleagues previously reported that polypharmacy is common among older Americans. More than half were taking prescription and nonprescription medications between 2005 and 2006.
There have been a lot of changes in U.S. regulations and the pharmacy market since that time, however. Some of those changes include new and less expensive generic drugs and the implementation of Medicare Part D, which is the prescription component of the government-run health insurance program for the elderly or disabled.
To evaluate the change in polypharmacy over time, the researchers compared the 2005-2006 results to data collected from 2010-2011.
Participants in the study were between the ages of 62 and 85 and were living at home. The researchers interviewed 2,351 people in 2005-2006 and 2,206 in 2010-2011.
Overall, about 67 percent were taking five or more medications or supplements in 2010-2011, up from about 53 percent in 2005-2006.
Use of cholesterol-lowering statins rose from about 34 percent to about 46 percent, the researchers reported in JAMA Internal Medicine. The proportion of people taking blood-thinning medications also increased, from about 33 percent to 43 percent, and use of omega-3 fish oil pills rose from about 5 percent to about 19 percent.
Along with the increase in polypharmacy, the researchers found the risk of major drug interactions nearly doubled, going from about 8 percent to about 15 percent.
"I think we have to keep in mind that while it's important to improve access to medications, we need to make sure they're used safely," said Qato.
On one hand, the new results can be seen as positive, said Dr. Michael Steinman, a gerontologist at the University of California, San Francisco.
We're treating more people with medications that could potentially help them," he said. "But when people have four or five chronic conditions, medications quickly balloon to a large number."
It's important to ensure clear communication between everyone involved in a patient's care, including the patient, said Steinman, who wrote an editorial accompanying the new study.
"You can get rid of problems and excess medications by talking with your doctors," he said.
A separate study reported in the same issue of the journal found that nearly 42 percent of adults did not tell their doctors about the use of complementary or alternative medicine, which includes - among other things - supplements, herbs, homeopathy, special diets and acupuncture.
Many patients said they didn't tell their doctors about these alternative medicines because they weren't asked or because their doctors didn't need to know that information, write Judy Juo and Pamela Jo Johnson, of the University of Minnesota in Minneapolis.
"If a person is talking with their doctor about the medications they're using, they should be talking about all the medications they're using," said Steinman.
(Reuters Health) - The proportion of older Americans taking at least five medications or supplements went up in a recent study.
The increase in people using multiple medications - known as polypharmacy - paralleled an increase in the number of older Americans at risk for major drug interactions, researchers found.
"That's a concern from a public health standpoint, because it's getting worse," said Dima Qato, the study's lead author from the University of Illinois at Chicago.
Qato and her colleagues previously reported that polypharmacy is common among older Americans. More than half were taking prescription and nonprescription medications between 2005 and 2006.
There have been a lot of changes in U.S. regulations and the pharmacy market since that time, however. Some of those changes include new and less expensive generic drugs and the implementation of Medicare Part D, which is the prescription component of the government-run health insurance program for the elderly or disabled.
To evaluate the change in polypharmacy over time, the researchers compared the 2005-2006 results to data collected from 2010-2011.
Participants in the study were between the ages of 62 and 85 and were living at home. The researchers interviewed 2,351 people in 2005-2006 and 2,206 in 2010-2011.
Overall, about 67 percent were taking five or more medications or supplements in 2010-2011, up from about 53 percent in 2005-2006.
Use of cholesterol-lowering statins rose from about 34 percent to about 46 percent, the researchers reported in JAMA Internal Medicine. The proportion of people taking blood-thinning medications also increased, from about 33 percent to 43 percent, and use of omega-3 fish oil pills rose from about 5 percent to about 19 percent.
Along with the increase in polypharmacy, the researchers found the risk of major drug interactions nearly doubled, going from about 8 percent to about 15 percent.
"I think we have to keep in mind that while it's important to improve access to medications, we need to make sure they're used safely," said Qato.
On one hand, the new results can be seen as positive, said Dr. Michael Steinman, a gerontologist at the University of California, San Francisco.
We're treating more people with medications that could potentially help them," he said. "But when people have four or five chronic conditions, medications quickly balloon to a large number."
It's important to ensure clear communication between everyone involved in a patient's care, including the patient, said Steinman, who wrote an editorial accompanying the new study.
"You can get rid of problems and excess medications by talking with your doctors," he said.
A separate study reported in the same issue of the journal found that nearly 42 percent of adults did not tell their doctors about the use of complementary or alternative medicine, which includes - among other things - supplements, herbs, homeopathy, special diets and acupuncture.
Many patients said they didn't tell their doctors about these alternative medicines because they weren't asked or because their doctors didn't need to know that information, write Judy Juo and Pamela Jo Johnson, of the University of Minnesota in Minneapolis.
"If a person is talking with their doctor about the medications they're using, they should be talking about all the medications they're using," said Steinman.
(Reuters Health) - The proportion of older Americans taking at least five medications or supplements went up in a recent study.
The increase in people using multiple medications - known as polypharmacy - paralleled an increase in the number of older Americans at risk for major drug interactions, researchers found.
"That's a concern from a public health standpoint, because it's getting worse," said Dima Qato, the study's lead author from the University of Illinois at Chicago.
Qato and her colleagues previously reported that polypharmacy is common among older Americans. More than half were taking prescription and nonprescription medications between 2005 and 2006.
There have been a lot of changes in U.S. regulations and the pharmacy market since that time, however. Some of those changes include new and less expensive generic drugs and the implementation of Medicare Part D, which is the prescription component of the government-run health insurance program for the elderly or disabled.
To evaluate the change in polypharmacy over time, the researchers compared the 2005-2006 results to data collected from 2010-2011.
Participants in the study were between the ages of 62 and 85 and were living at home. The researchers interviewed 2,351 people in 2005-2006 and 2,206 in 2010-2011.
Overall, about 67 percent were taking five or more medications or supplements in 2010-2011, up from about 53 percent in 2005-2006.
Use of cholesterol-lowering statins rose from about 34 percent to about 46 percent, the researchers reported in JAMA Internal Medicine. The proportion of people taking blood-thinning medications also increased, from about 33 percent to 43 percent, and use of omega-3 fish oil pills rose from about 5 percent to about 19 percent.
Along with the increase in polypharmacy, the researchers found the risk of major drug interactions nearly doubled, going from about 8 percent to about 15 percent.
"I think we have to keep in mind that while it's important to improve access to medications, we need to make sure they're used safely," said Qato.
On one hand, the new results can be seen as positive, said Dr. Michael Steinman, a gerontologist at the University of California, San Francisco.
We're treating more people with medications that could potentially help them," he said. "But when people have four or five chronic conditions, medications quickly balloon to a large number."
It's important to ensure clear communication between everyone involved in a patient's care, including the patient, said Steinman, who wrote an editorial accompanying the new study.
"You can get rid of problems and excess medications by talking with your doctors," he said.
A separate study reported in the same issue of the journal found that nearly 42 percent of adults did not tell their doctors about the use of complementary or alternative medicine, which includes - among other things - supplements, herbs, homeopathy, special diets and acupuncture.
Many patients said they didn't tell their doctors about these alternative medicines because they weren't asked or because their doctors didn't need to know that information, write Judy Juo and Pamela Jo Johnson, of the University of Minnesota in Minneapolis.
"If a person is talking with their doctor about the medications they're using, they should be talking about all the medications they're using," said Steinman.
Tool predicts risks of DAPT with ‘modest accuracy’

Researchers believe a new tool could help physicians predict the risks and benefits of extended dual antiplatelet therapy (DAPT) in patients who have undergone percutaneous coronary intervention (PCI).
The team said the tool, known as the DAPT Score, exhibited “modest accuracy” for determining which patients were at high risk for late ischemic events and would therefore benefit most from longer-term DAPT therapy.
The DAPT Score also proved somewhat accurate for identifying patients who were at high risk of late bleeding events and might be harmed by continuing DAPT for more than a year after PCI.
Still, the researchers said the scoring system requires further validation and prospective evaluation to assess its potential effects on patient care.
Robert W. Yeh, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts, and his colleagues reported these results in JAMA.
“Dual antiplatelet therapy is standard for patients following coronary stent procedures, but we haven’t had good tools to help us determine how long we should be treating individual patients,” Dr Yeh said.
So he and his colleagues set out to identify factors that would predict whether the expected benefit of reduced ischemia would outweigh the expected increase in bleeding associated with continuing DAPT for more than a year after PCI.
The team used 11,648 patients treated on the DAPT study to create the DAPT Score. Patients in this trial had a drug-eluting stent placed, then received 12 months of open-label thienopyridine plus aspirin. After that, they were randomized to 18 months of continued thienopyridine plus aspirin or placebo plus aspirin.
The DAPT Score was designed to distinguish ischemic and bleeding risk 12 to 30 months after PCI. Patients are given a numerical score (-2 to 10) based on certain risk factors. They receive:
- 1 point each for myocardial infarction at presentation, prior myocardial infarction or PCI, diabetes, stent diameter less than 3 mm, smoking, and paclitaxel-eluting stent
- 2 points each for history of congestive heart failure/low ejection fraction and vein graft intervention
- −1 point for age 65 to younger than 75
- −2 points for age 75 or older.
The researchers validated the DAPT Score in 8136 patients from the PROTECT trial. In this trial, researchers assessed the effect of DAPT on the incidence of stent thrombosis at 3 years in patients randomized to receive the Endeavor zotarolimus-eluting stent or the Cypher sirolimus-eluting stent.
After stent placement, patients were assigned to receive aspirin indefinitely and clopidogrel/ticlopidine for at least 3 months and up to 12 months.
Results in DAPT cohort
In the DAPT cohort, ischemia occurred in 348 patients (3.0%), and bleeding occurred in 215 (1.8%).
The researchers said the derivation cohort models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.70 and 0.68, respectively. After bootstrap internal validation, optimism-corrected c statistics were 0.68 and 0.66, respectively.
The researchers also compared patients with high DAPT scores (≥2 points) to those with lower scores (<2). As expected, continued DAPT was associated with larger reductions in ischemia and smaller increases in bleeding in the high-score group (n=5917) than in the low-score group (n=5731).
In the high-score group, the incidence of ischemia was 2.7% for continued DAPT and 5.7% for placebo plus aspirin (P<0.001). In the low-score group, the incidence was 1.7% for continued DAPT and 2.3% for placebo plus aspirin (P=0.07; interaction P<0.001).
In the high-score group, the incidence of bleeding was 1.8% for continued DAPT and 1.4% for placebo plus aspirin (P=0.26). In the low-score group, the incidence was 3.0% for continued DAPT and 1.4% for placebo plus aspirin (P<0.001; interaction P=0.02).
Results in PROTECT cohort
In the PROTECT cohort, ischemia occurred in 79 patients (1.0%) and bleeding in 37 patients (0.5%). Again, the models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.64 for both outcomes.
The rate of ischemia from 12 through 30 months after PCI was greater among the high-score patients (n=2848) than the low-score patients (n=5288). The rates were 1.5% and 0.7%, respectively. The hazard ratio was 2.01 (P=0.002).
Rates of moderate or severe bleeding were not significantly different by DAPT Score. The rates were 0.4% in the high-score patients and 0.5% in the low-score patients. The hazard ratio was 0.69 (P=0.31).
The researchers said that, based on these results, use of the DAPT Score should be cautious pending further validation.
“We haven’t prospectively validated the use of the score, and it’s only applicable to patients similar to those who were randomized in the DAPT study, so we still need to be cautious,” Dr Yeh said. “Nevertheless, we think it represents a significant step forward in understanding benefits and risks of treatment.” ![]()
Researchers believe a new tool could help physicians predict the risks and benefits of extended dual antiplatelet therapy (DAPT) in patients who have undergone percutaneous coronary intervention (PCI).
The team said the tool, known as the DAPT Score, exhibited “modest accuracy” for determining which patients were at high risk for late ischemic events and would therefore benefit most from longer-term DAPT therapy.
The DAPT Score also proved somewhat accurate for identifying patients who were at high risk of late bleeding events and might be harmed by continuing DAPT for more than a year after PCI.
Still, the researchers said the scoring system requires further validation and prospective evaluation to assess its potential effects on patient care.
Robert W. Yeh, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts, and his colleagues reported these results in JAMA.
“Dual antiplatelet therapy is standard for patients following coronary stent procedures, but we haven’t had good tools to help us determine how long we should be treating individual patients,” Dr Yeh said.
So he and his colleagues set out to identify factors that would predict whether the expected benefit of reduced ischemia would outweigh the expected increase in bleeding associated with continuing DAPT for more than a year after PCI.
The team used 11,648 patients treated on the DAPT study to create the DAPT Score. Patients in this trial had a drug-eluting stent placed, then received 12 months of open-label thienopyridine plus aspirin. After that, they were randomized to 18 months of continued thienopyridine plus aspirin or placebo plus aspirin.
The DAPT Score was designed to distinguish ischemic and bleeding risk 12 to 30 months after PCI. Patients are given a numerical score (-2 to 10) based on certain risk factors. They receive:
- 1 point each for myocardial infarction at presentation, prior myocardial infarction or PCI, diabetes, stent diameter less than 3 mm, smoking, and paclitaxel-eluting stent
- 2 points each for history of congestive heart failure/low ejection fraction and vein graft intervention
- −1 point for age 65 to younger than 75
- −2 points for age 75 or older.
The researchers validated the DAPT Score in 8136 patients from the PROTECT trial. In this trial, researchers assessed the effect of DAPT on the incidence of stent thrombosis at 3 years in patients randomized to receive the Endeavor zotarolimus-eluting stent or the Cypher sirolimus-eluting stent.
After stent placement, patients were assigned to receive aspirin indefinitely and clopidogrel/ticlopidine for at least 3 months and up to 12 months.
Results in DAPT cohort
In the DAPT cohort, ischemia occurred in 348 patients (3.0%), and bleeding occurred in 215 (1.8%).
The researchers said the derivation cohort models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.70 and 0.68, respectively. After bootstrap internal validation, optimism-corrected c statistics were 0.68 and 0.66, respectively.
The researchers also compared patients with high DAPT scores (≥2 points) to those with lower scores (<2). As expected, continued DAPT was associated with larger reductions in ischemia and smaller increases in bleeding in the high-score group (n=5917) than in the low-score group (n=5731).
In the high-score group, the incidence of ischemia was 2.7% for continued DAPT and 5.7% for placebo plus aspirin (P<0.001). In the low-score group, the incidence was 1.7% for continued DAPT and 2.3% for placebo plus aspirin (P=0.07; interaction P<0.001).
In the high-score group, the incidence of bleeding was 1.8% for continued DAPT and 1.4% for placebo plus aspirin (P=0.26). In the low-score group, the incidence was 3.0% for continued DAPT and 1.4% for placebo plus aspirin (P<0.001; interaction P=0.02).
Results in PROTECT cohort
In the PROTECT cohort, ischemia occurred in 79 patients (1.0%) and bleeding in 37 patients (0.5%). Again, the models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.64 for both outcomes.
The rate of ischemia from 12 through 30 months after PCI was greater among the high-score patients (n=2848) than the low-score patients (n=5288). The rates were 1.5% and 0.7%, respectively. The hazard ratio was 2.01 (P=0.002).
Rates of moderate or severe bleeding were not significantly different by DAPT Score. The rates were 0.4% in the high-score patients and 0.5% in the low-score patients. The hazard ratio was 0.69 (P=0.31).
The researchers said that, based on these results, use of the DAPT Score should be cautious pending further validation.
“We haven’t prospectively validated the use of the score, and it’s only applicable to patients similar to those who were randomized in the DAPT study, so we still need to be cautious,” Dr Yeh said. “Nevertheless, we think it represents a significant step forward in understanding benefits and risks of treatment.” ![]()
Researchers believe a new tool could help physicians predict the risks and benefits of extended dual antiplatelet therapy (DAPT) in patients who have undergone percutaneous coronary intervention (PCI).
The team said the tool, known as the DAPT Score, exhibited “modest accuracy” for determining which patients were at high risk for late ischemic events and would therefore benefit most from longer-term DAPT therapy.
The DAPT Score also proved somewhat accurate for identifying patients who were at high risk of late bleeding events and might be harmed by continuing DAPT for more than a year after PCI.
Still, the researchers said the scoring system requires further validation and prospective evaluation to assess its potential effects on patient care.
Robert W. Yeh, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts, and his colleagues reported these results in JAMA.
“Dual antiplatelet therapy is standard for patients following coronary stent procedures, but we haven’t had good tools to help us determine how long we should be treating individual patients,” Dr Yeh said.
So he and his colleagues set out to identify factors that would predict whether the expected benefit of reduced ischemia would outweigh the expected increase in bleeding associated with continuing DAPT for more than a year after PCI.
The team used 11,648 patients treated on the DAPT study to create the DAPT Score. Patients in this trial had a drug-eluting stent placed, then received 12 months of open-label thienopyridine plus aspirin. After that, they were randomized to 18 months of continued thienopyridine plus aspirin or placebo plus aspirin.
The DAPT Score was designed to distinguish ischemic and bleeding risk 12 to 30 months after PCI. Patients are given a numerical score (-2 to 10) based on certain risk factors. They receive:
- 1 point each for myocardial infarction at presentation, prior myocardial infarction or PCI, diabetes, stent diameter less than 3 mm, smoking, and paclitaxel-eluting stent
- 2 points each for history of congestive heart failure/low ejection fraction and vein graft intervention
- −1 point for age 65 to younger than 75
- −2 points for age 75 or older.
The researchers validated the DAPT Score in 8136 patients from the PROTECT trial. In this trial, researchers assessed the effect of DAPT on the incidence of stent thrombosis at 3 years in patients randomized to receive the Endeavor zotarolimus-eluting stent or the Cypher sirolimus-eluting stent.
After stent placement, patients were assigned to receive aspirin indefinitely and clopidogrel/ticlopidine for at least 3 months and up to 12 months.
Results in DAPT cohort
In the DAPT cohort, ischemia occurred in 348 patients (3.0%), and bleeding occurred in 215 (1.8%).
The researchers said the derivation cohort models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.70 and 0.68, respectively. After bootstrap internal validation, optimism-corrected c statistics were 0.68 and 0.66, respectively.
The researchers also compared patients with high DAPT scores (≥2 points) to those with lower scores (<2). As expected, continued DAPT was associated with larger reductions in ischemia and smaller increases in bleeding in the high-score group (n=5917) than in the low-score group (n=5731).
In the high-score group, the incidence of ischemia was 2.7% for continued DAPT and 5.7% for placebo plus aspirin (P<0.001). In the low-score group, the incidence was 1.7% for continued DAPT and 2.3% for placebo plus aspirin (P=0.07; interaction P<0.001).
In the high-score group, the incidence of bleeding was 1.8% for continued DAPT and 1.4% for placebo plus aspirin (P=0.26). In the low-score group, the incidence was 3.0% for continued DAPT and 1.4% for placebo plus aspirin (P<0.001; interaction P=0.02).
Results in PROTECT cohort
In the PROTECT cohort, ischemia occurred in 79 patients (1.0%) and bleeding in 37 patients (0.5%). Again, the models predicting ischemia and bleeding had moderate discrimination, with c statistics of 0.64 for both outcomes.
The rate of ischemia from 12 through 30 months after PCI was greater among the high-score patients (n=2848) than the low-score patients (n=5288). The rates were 1.5% and 0.7%, respectively. The hazard ratio was 2.01 (P=0.002).
Rates of moderate or severe bleeding were not significantly different by DAPT Score. The rates were 0.4% in the high-score patients and 0.5% in the low-score patients. The hazard ratio was 0.69 (P=0.31).
The researchers said that, based on these results, use of the DAPT Score should be cautious pending further validation.
“We haven’t prospectively validated the use of the score, and it’s only applicable to patients similar to those who were randomized in the DAPT study, so we still need to be cautious,” Dr Yeh said. “Nevertheless, we think it represents a significant step forward in understanding benefits and risks of treatment.” ![]()
PET probe could aid treatment for leukemia

Image by Jens Langner
A PET probe known as [18F]CFA could be used to aid the treatment of leukemias and other cancers, according to research published in PNAS.
Investigators say [18F]CFA can detect the activity of deoxycytidine kinase (dCK) in humans more effectively than existing probes.
dCK is a rate-limiting enzyme in the cytosolic deoxyribonucleoside salvage pathway and is considered an important therapeutic and PET-imaging target in certain cancers.
Research has shown that dCK is highly expressed in acute leukemia cells and activated lymphocytes. And the enzyme plays an integral role in allowing drugs such as clofarabine, cytarabine, and fludarabine to treat certain leukemias.
“This enzyme is essential for the therapeutic activity of an entire class of anticancer drugs and even for some antiviral drugs,” said study author Caius Radu, MD, of the University of California, Los Angeles.
“It can take an inactive drug and activate it. If you trick a cancer cell or virus to activate the drug, it would be toxic for the cancer cell or viral genome.”
Until recently, PET technology was only able to clearly detect dCK in mice due to the metabolic instability of the available probes and cross-reactivity with a dCK-related enzyme in humans.
However, Dr Radu and his colleagues showed that [18F]CFA can clearly detect dCK in humans.
The team found that [18F]CFA accumulation in leukemia cells correlated with dCK expression, and they were able to inhibit [18F]CFA accumulation with a dCK inhibitor.
Experiments with [18F]CFA PET/CT in humans showed probe accumulation in tissues with high dCK expression, such as hematopoietic bone marrow and secondary lymphoid organs.
“We are able to clearly see tissues, including tumor tissues, with high dCK activity that we haven’t seen before in humans using any of the other probes previously developed for this enzyme,” Dr Radu said.
He added that, since activated immune cells increase their expression of dCK, [18F]CFA could also be used to monitor the effectiveness of immunotherapeutic interventions.
The investigators hope to begin clinical trials with [18F]CFA in the near future.
Dr Radu and his team invented [18F]CFA and its analogs, which were patented by the University of California and have been licensed to Sofie Biosciences, a company founded by Dr Radu and his team. The University of California also patented additional intellectual property for small-molecule dCK inhibitors. ![]()
Image by Jens Langner
A PET probe known as [18F]CFA could be used to aid the treatment of leukemias and other cancers, according to research published in PNAS.
Investigators say [18F]CFA can detect the activity of deoxycytidine kinase (dCK) in humans more effectively than existing probes.
dCK is a rate-limiting enzyme in the cytosolic deoxyribonucleoside salvage pathway and is considered an important therapeutic and PET-imaging target in certain cancers.
Research has shown that dCK is highly expressed in acute leukemia cells and activated lymphocytes. And the enzyme plays an integral role in allowing drugs such as clofarabine, cytarabine, and fludarabine to treat certain leukemias.
“This enzyme is essential for the therapeutic activity of an entire class of anticancer drugs and even for some antiviral drugs,” said study author Caius Radu, MD, of the University of California, Los Angeles.
“It can take an inactive drug and activate it. If you trick a cancer cell or virus to activate the drug, it would be toxic for the cancer cell or viral genome.”
Until recently, PET technology was only able to clearly detect dCK in mice due to the metabolic instability of the available probes and cross-reactivity with a dCK-related enzyme in humans.
However, Dr Radu and his colleagues showed that [18F]CFA can clearly detect dCK in humans.
The team found that [18F]CFA accumulation in leukemia cells correlated with dCK expression, and they were able to inhibit [18F]CFA accumulation with a dCK inhibitor.
Experiments with [18F]CFA PET/CT in humans showed probe accumulation in tissues with high dCK expression, such as hematopoietic bone marrow and secondary lymphoid organs.
“We are able to clearly see tissues, including tumor tissues, with high dCK activity that we haven’t seen before in humans using any of the other probes previously developed for this enzyme,” Dr Radu said.
He added that, since activated immune cells increase their expression of dCK, [18F]CFA could also be used to monitor the effectiveness of immunotherapeutic interventions.
The investigators hope to begin clinical trials with [18F]CFA in the near future.
Dr Radu and his team invented [18F]CFA and its analogs, which were patented by the University of California and have been licensed to Sofie Biosciences, a company founded by Dr Radu and his team. The University of California also patented additional intellectual property for small-molecule dCK inhibitors. ![]()
Image by Jens Langner
A PET probe known as [18F]CFA could be used to aid the treatment of leukemias and other cancers, according to research published in PNAS.
Investigators say [18F]CFA can detect the activity of deoxycytidine kinase (dCK) in humans more effectively than existing probes.
dCK is a rate-limiting enzyme in the cytosolic deoxyribonucleoside salvage pathway and is considered an important therapeutic and PET-imaging target in certain cancers.
Research has shown that dCK is highly expressed in acute leukemia cells and activated lymphocytes. And the enzyme plays an integral role in allowing drugs such as clofarabine, cytarabine, and fludarabine to treat certain leukemias.
“This enzyme is essential for the therapeutic activity of an entire class of anticancer drugs and even for some antiviral drugs,” said study author Caius Radu, MD, of the University of California, Los Angeles.
“It can take an inactive drug and activate it. If you trick a cancer cell or virus to activate the drug, it would be toxic for the cancer cell or viral genome.”
Until recently, PET technology was only able to clearly detect dCK in mice due to the metabolic instability of the available probes and cross-reactivity with a dCK-related enzyme in humans.
However, Dr Radu and his colleagues showed that [18F]CFA can clearly detect dCK in humans.
The team found that [18F]CFA accumulation in leukemia cells correlated with dCK expression, and they were able to inhibit [18F]CFA accumulation with a dCK inhibitor.
Experiments with [18F]CFA PET/CT in humans showed probe accumulation in tissues with high dCK expression, such as hematopoietic bone marrow and secondary lymphoid organs.
“We are able to clearly see tissues, including tumor tissues, with high dCK activity that we haven’t seen before in humans using any of the other probes previously developed for this enzyme,” Dr Radu said.
He added that, since activated immune cells increase their expression of dCK, [18F]CFA could also be used to monitor the effectiveness of immunotherapeutic interventions.
The investigators hope to begin clinical trials with [18F]CFA in the near future.
Dr Radu and his team invented [18F]CFA and its analogs, which were patented by the University of California and have been licensed to Sofie Biosciences, a company founded by Dr Radu and his team. The University of California also patented additional intellectual property for small-molecule dCK inhibitors. ![]()
Blood culture panel cleared by FDA

Staphylococcus infection
Photo by Bill Branson
The US Food and Drug Administration (FDA) has granted 510(k) clearance for a blood culture panel that detects sepsis caused by methicillin-resistant Staphylococcus aureus (MRSA) and other Staphylococcus species.
The Staph ID/R Blood Culture Panel is a product of Great Basin Scientific, Inc.
It is an automated, DNA multiplex assay used to identify Staphylococcus species directly from positive blood cultures in about 2 hours.
The panel also detects the mecA gene, a drug-resistance marker that confers resistance to methicillin and other beta-lactams and creates MRSA.
In addition, the Staph ID/R Blood Culture Panel identifies coagulase-negative staphylococci.
According to the US Centers for Disease Control and Prevention, 20% to 50% of all positive blood cultures are likely false positives due to contamination caused by coagulase-negative staphylococci, many of which are part of the normal flora of human skin and are not dangerous.
The Staph ID/R Blood Culture Panel is run on the Great Basin Analyzer. The company says the assay requires less than a minute of hands-on time and no results interpretation due to electronic results reporting. ![]()
Staphylococcus infection
Photo by Bill Branson
The US Food and Drug Administration (FDA) has granted 510(k) clearance for a blood culture panel that detects sepsis caused by methicillin-resistant Staphylococcus aureus (MRSA) and other Staphylococcus species.
The Staph ID/R Blood Culture Panel is a product of Great Basin Scientific, Inc.
It is an automated, DNA multiplex assay used to identify Staphylococcus species directly from positive blood cultures in about 2 hours.
The panel also detects the mecA gene, a drug-resistance marker that confers resistance to methicillin and other beta-lactams and creates MRSA.
In addition, the Staph ID/R Blood Culture Panel identifies coagulase-negative staphylococci.
According to the US Centers for Disease Control and Prevention, 20% to 50% of all positive blood cultures are likely false positives due to contamination caused by coagulase-negative staphylococci, many of which are part of the normal flora of human skin and are not dangerous.
The Staph ID/R Blood Culture Panel is run on the Great Basin Analyzer. The company says the assay requires less than a minute of hands-on time and no results interpretation due to electronic results reporting. ![]()
Staphylococcus infection
Photo by Bill Branson
The US Food and Drug Administration (FDA) has granted 510(k) clearance for a blood culture panel that detects sepsis caused by methicillin-resistant Staphylococcus aureus (MRSA) and other Staphylococcus species.
The Staph ID/R Blood Culture Panel is a product of Great Basin Scientific, Inc.
It is an automated, DNA multiplex assay used to identify Staphylococcus species directly from positive blood cultures in about 2 hours.
The panel also detects the mecA gene, a drug-resistance marker that confers resistance to methicillin and other beta-lactams and creates MRSA.
In addition, the Staph ID/R Blood Culture Panel identifies coagulase-negative staphylococci.
According to the US Centers for Disease Control and Prevention, 20% to 50% of all positive blood cultures are likely false positives due to contamination caused by coagulase-negative staphylococci, many of which are part of the normal flora of human skin and are not dangerous.
The Staph ID/R Blood Culture Panel is run on the Great Basin Analyzer. The company says the assay requires less than a minute of hands-on time and no results interpretation due to electronic results reporting. ![]()
Accuracy of blood test results varies

Photo by Graham Colm
A comparison of commercially available blood tests has revealed more variability than expected, according to researchers.
The group compared basic blood tests run by commercial laboratories and found the testing service, type of test, and time of collection all influenced the accuracy of results.
Given that these tests can be used for disease diagnosis or to determine whether a patient’s medication is working, the researchers said this study highlights the importance of knowing the accuracy and variability of blood test results.
“While most of the variability we found was within clinically accepted ranges, there were several cases where inaccurate results would have led to incorrect medical decisions,” said Joel Dudley, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“We hope this study will inspire the biomedical community to take a critical look at all testing variables to ensure that lab results are as robust and reproducible as possible.”
Dr Dudley and his colleagues described this study in the Journal of Clinical Investigation.
The researchers collected peripheral blood samples from 60 healthy adults at 4 separate time points within a 6.5-hour window. The samples were collected in Phoenix, Arizona, at an ambulatory clinic and at retail outlets with point-of-care services.
The team collected 14 samples per subject and used those samples to compare 22 common clinical lab tests conducted at 3 commercial labs. One lab, Theranos, offered blood tests obtained from a finger prick, and the other 2, Quest and LabCorp, required standard venipuncture draws.
More than half of the test results showed significant differences between test providers. Of the 22 tests, 15 (68%) showed significant variability between labs (P<0.002).
Triglyceride levels and red blood cell counts were among the most consistent results, while white blood cell counts and overall cholesterol levels were among the most variable.
Test results from Theranos were flagged by Theranos as abnormal 1.6 times more often than tests from LabCorp or Quest (P<0.0001). The percentages for measurements outside their normal range were 8.3% for LabCorp, 7.5% for Quest, and 12.2% for Theranos.
In addition, the researchers noted that, although they controlled subjects’ eating and physical activity, data from blood samples collected earlier in the day were sometimes significantly different from samples taken from the same subjects later in the day.
There were significant difference between measurements collected at time points 1 and 2 vs time points 3 and 4 for 13 of the 22 tests (P<0.002).
“These testing disparities occurred despite rigorous laboratory certification and proficiency standards designed to ensure consistency,” said study author Eric Schadt, PhD, of Mount Sinai.
“Our results suggest the need for greater transparency in lab technologies and procedures, as well as a much more thorough investigation of biological mechanisms that may contribute to more dynamic levels than we currently understand.” ![]()
Photo by Graham Colm
A comparison of commercially available blood tests has revealed more variability than expected, according to researchers.
The group compared basic blood tests run by commercial laboratories and found the testing service, type of test, and time of collection all influenced the accuracy of results.
Given that these tests can be used for disease diagnosis or to determine whether a patient’s medication is working, the researchers said this study highlights the importance of knowing the accuracy and variability of blood test results.
“While most of the variability we found was within clinically accepted ranges, there were several cases where inaccurate results would have led to incorrect medical decisions,” said Joel Dudley, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“We hope this study will inspire the biomedical community to take a critical look at all testing variables to ensure that lab results are as robust and reproducible as possible.”
Dr Dudley and his colleagues described this study in the Journal of Clinical Investigation.
The researchers collected peripheral blood samples from 60 healthy adults at 4 separate time points within a 6.5-hour window. The samples were collected in Phoenix, Arizona, at an ambulatory clinic and at retail outlets with point-of-care services.
The team collected 14 samples per subject and used those samples to compare 22 common clinical lab tests conducted at 3 commercial labs. One lab, Theranos, offered blood tests obtained from a finger prick, and the other 2, Quest and LabCorp, required standard venipuncture draws.
More than half of the test results showed significant differences between test providers. Of the 22 tests, 15 (68%) showed significant variability between labs (P<0.002).
Triglyceride levels and red blood cell counts were among the most consistent results, while white blood cell counts and overall cholesterol levels were among the most variable.
Test results from Theranos were flagged by Theranos as abnormal 1.6 times more often than tests from LabCorp or Quest (P<0.0001). The percentages for measurements outside their normal range were 8.3% for LabCorp, 7.5% for Quest, and 12.2% for Theranos.
In addition, the researchers noted that, although they controlled subjects’ eating and physical activity, data from blood samples collected earlier in the day were sometimes significantly different from samples taken from the same subjects later in the day.
There were significant difference between measurements collected at time points 1 and 2 vs time points 3 and 4 for 13 of the 22 tests (P<0.002).
“These testing disparities occurred despite rigorous laboratory certification and proficiency standards designed to ensure consistency,” said study author Eric Schadt, PhD, of Mount Sinai.
“Our results suggest the need for greater transparency in lab technologies and procedures, as well as a much more thorough investigation of biological mechanisms that may contribute to more dynamic levels than we currently understand.” ![]()
Photo by Graham Colm
A comparison of commercially available blood tests has revealed more variability than expected, according to researchers.
The group compared basic blood tests run by commercial laboratories and found the testing service, type of test, and time of collection all influenced the accuracy of results.
Given that these tests can be used for disease diagnosis or to determine whether a patient’s medication is working, the researchers said this study highlights the importance of knowing the accuracy and variability of blood test results.
“While most of the variability we found was within clinically accepted ranges, there were several cases where inaccurate results would have led to incorrect medical decisions,” said Joel Dudley, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“We hope this study will inspire the biomedical community to take a critical look at all testing variables to ensure that lab results are as robust and reproducible as possible.”
Dr Dudley and his colleagues described this study in the Journal of Clinical Investigation.
The researchers collected peripheral blood samples from 60 healthy adults at 4 separate time points within a 6.5-hour window. The samples were collected in Phoenix, Arizona, at an ambulatory clinic and at retail outlets with point-of-care services.
The team collected 14 samples per subject and used those samples to compare 22 common clinical lab tests conducted at 3 commercial labs. One lab, Theranos, offered blood tests obtained from a finger prick, and the other 2, Quest and LabCorp, required standard venipuncture draws.
More than half of the test results showed significant differences between test providers. Of the 22 tests, 15 (68%) showed significant variability between labs (P<0.002).
Triglyceride levels and red blood cell counts were among the most consistent results, while white blood cell counts and overall cholesterol levels were among the most variable.
Test results from Theranos were flagged by Theranos as abnormal 1.6 times more often than tests from LabCorp or Quest (P<0.0001). The percentages for measurements outside their normal range were 8.3% for LabCorp, 7.5% for Quest, and 12.2% for Theranos.
In addition, the researchers noted that, although they controlled subjects’ eating and physical activity, data from blood samples collected earlier in the day were sometimes significantly different from samples taken from the same subjects later in the day.
There were significant difference between measurements collected at time points 1 and 2 vs time points 3 and 4 for 13 of the 22 tests (P<0.002).
“These testing disparities occurred despite rigorous laboratory certification and proficiency standards designed to ensure consistency,” said study author Eric Schadt, PhD, of Mount Sinai.
“Our results suggest the need for greater transparency in lab technologies and procedures, as well as a much more thorough investigation of biological mechanisms that may contribute to more dynamic levels than we currently understand.” ![]()
An unconventional approach to chest wall pain
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
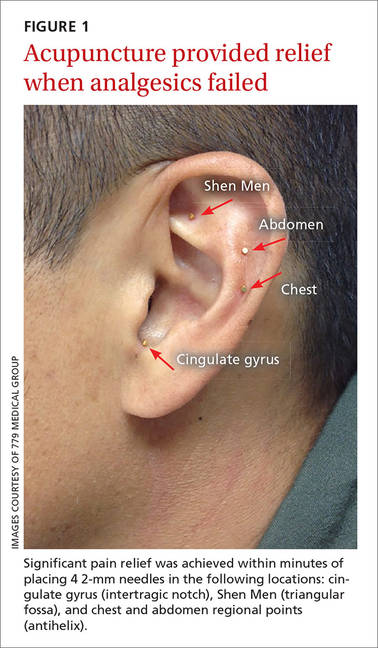
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
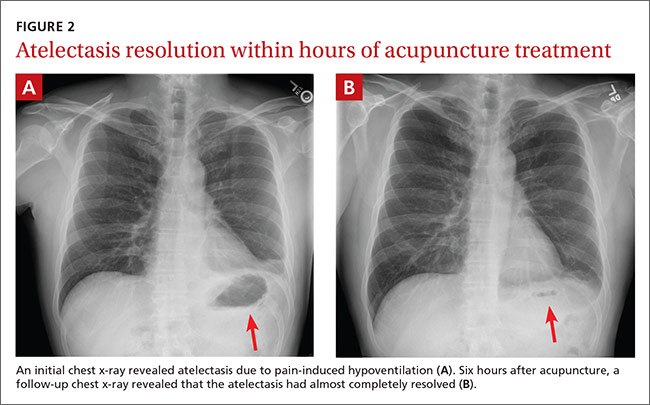
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.
Uninjured athlete with edematous arm • Dx?
THE CASE
A 16-year-old boy presented to the emergency room (ER) with pain, redness, and swelling of his right upper arm that had been bothering him for 2 days. He was the quarterback of his high school football team, a sport that he’d been playing since he was 8 years old. He indicated that his football training—which involved repetitive throwing with his right arm—had intensified over the previous 2 months.
Prior to the ER visit, the patient was healthy and active with no significant medical history. He’d had no shoulder trauma and there was no family history of any coagulopathies, venous thrombosis, or pulmonary embolism. He denied chest pain, shortness of breath, palpitations, and fever, and said that he did not smoke cigarettes or drink alcohol.
On physical examination, his blood pressure was 118/70 mm Hg and his heart rate was 74 beats per minute. He had nonpitting edema and erythema of his right upper arm. His radial and brachial pulses were strong and equal in both arms. Assessment of neurologic and vascular integrity produced positive Wright’s and Adson’s tests, but a negative Halstead’s test. (For more on these tests, see: Wright’s test, Adson’s test, and Halstead’s test.) The circumference of the patient’s right upper arm was 2.5 cm greater than the left upper arm. The remainder of the physical exam was normal.
THE DIAGNOSIS
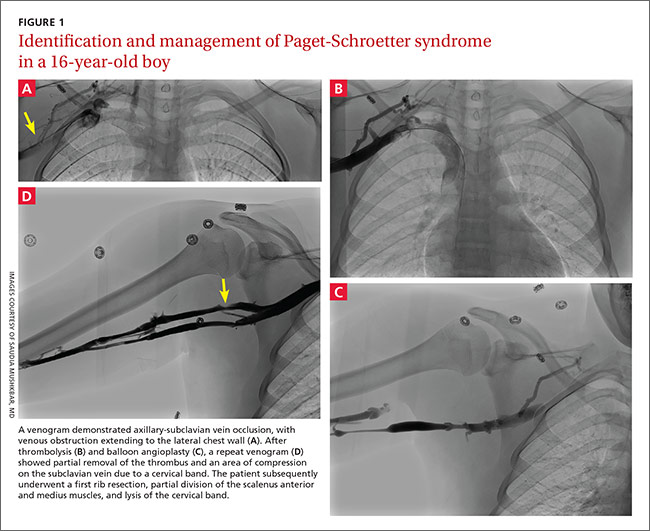
A duplex ultrasound of the right upper arm revealed an acute occlusive thrombus in the axillary vein. We started the patient on intravenous heparin. A venogram confirmed thrombosis of the axillary-subclavian vein (FIGURE 1A). Based on the patient’s clinical presentation and the results of the venogram, we diagnosed Paget-Schroetter syndrome. The venogram was followed by thrombolysis with alteplase (FIGURE 1B) and a balloon angioplasty (FIGURE 1C). One week later, a repeat venogram demonstrated partial removal of the thrombus and an area of compression on the inferior aspect of the subclavian vein due to a cervical band (FIGURE 1D).
DISCUSSION
Paget-Schroetter syndrome (PSS), or effort thrombosis of the upper extremities, is defined as spontaneous thrombus in the axillary and subclavian veins that occurs as a consequence of strenuous upper-extremity activity. It is a rare condition with an incidence of one to 2 cases per 100,000 people per year, and represents 1% to 4% of all cases of deep vein thrombosis (DVT).1
Spontaneous thrombosis of the upper extremities typically presents in young, otherwise healthy individuals. It has been described in athletes who are involved in ball games, games with rackets or clubs, aquatic sports, combatant sports, and in violin players.2 The repetitive movements used in these activities can lead to compression of the axillary and subclavian veins by hypertrophied muscles. Repetitive trauma causes intimal damage and thrombogenesis.3
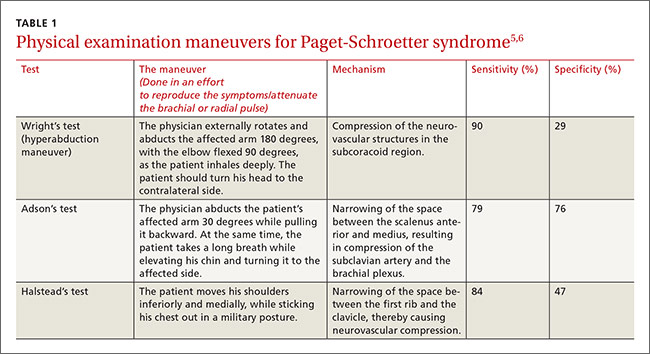
PSS is characterized by the abrupt, spontaneous swelling of the entire arm, cyanosis, and pain that occurs with use or overhead positioning. Enlarged subcutaneous veins are present in the upper arm, around the shoulder, or in the upper anterior chest wall (Urschel’s sign). The classic presentation is acute onset of upper extremity pain and swelling in the dominant arm following a particularly strenuous activity.4 A low-grade fever, superficial thrombophlebitis, or neurologic symptoms may coexist. Certain provocative maneuvers can help reproduce the symptoms (TABLE 15,6). Complications of PSS include pulmonary embolism, postthrombotic syndrome (pain, heaviness, and swelling), and recurrent thrombosis.7
Contrast venography best shows the extent of thrombosis
Duplex ultrasound, with its high sensitivity and specificity, is the initial, noninvasive test of choice (TABLE 24,8-11). However, duplex ultrasound has a false-negative rate of 30% because it is highly technician-dependent and can be complicated by acoustic shadows from the clavicle or sternum.8
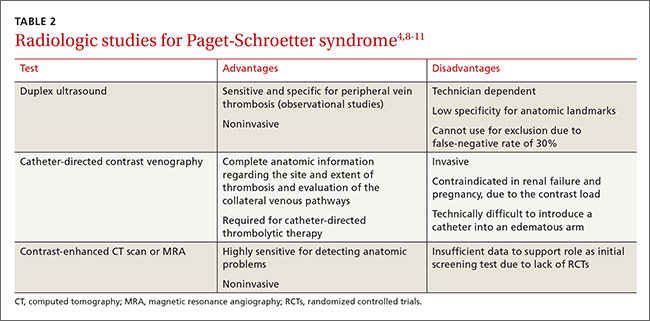
The most direct and definitive means to confirm the diagnosis of PSS is catheter-directed contrast venography.9 This method provides complete anatomic information regarding the site and extent of thrombosis, allows definitive evaluation of the collateral venous pathways, and is a necessary step toward the use of thrombolytic therapy. Contrast load, however, contraindicates the procedure in patients with renal failure and in those who are pregnant.
Contrast-enhanced computed tomography (CT) and magnetic resonance angiography (MRA) are also highly sensitive for detecting focal stenosis at the level of the first rib, the presence or absence of enlarged collateral veins, and the chronicity of any thrombus present. However, the usefulness of CT and magnetic resonance venography in initial screening is unclear, due to a lack of randomized controlled trials.
Treatment involves anticoagulants, thrombolytics, and possibly surgery
Prompt use of anticoagulation is indicated in PSS. Initial anticoagulation with low molecular weight unfractionated heparin or a direct thrombin inhibitor followed by warfarin for a minimum of 3 to 6 months is recommended.12
Patients treated with anticoagulation alone have a higher incidence of long-term residual symptoms, disability, and recurrent thrombosis.7 As a result, a more aggressive approach with the use of thrombolytic therapy is indicated, especially in young, active patients, to minimize long-term consequences. Alteplase or reteplase are used for this purpose. Thrombolysis is less likely to be beneficial if the thrombus is more than 2 weeks old or if there are inflammatory changes in the vein. The use of catheter-directed thrombolysis minimizes the risk of systemic adverse effects and achieves higher clot resolution rates.13
Because PSS is caused by compression of the vein, rather than a disorder of blood clotting, there is still a 50% to 70% risk of recurrent thrombosis despite thrombolysis and anticoagulation.14 Therefore, the most definitive management approach remains surgical treatment. Patients with recent thrombosis who are within the first several weeks of undergoing successful thrombolytic therapy are excellent candidates for surgery. Operative treatment for PSS includes first rib resection, scalene muscle removal, or subclavius muscle removal, along with removal of constricting scar tissue from around the vein.7
THE TAKEAWAY
PSS is characterized by upper-extremity DVT resulting from repetitive trauma to the subclavian-axillary vein. Early diagnosis of PSS with contrast venography and prompt use of anticoagulation can effectively restore venous patency, reduce the risk of rethrombosis, and return the patient to normal function. Primary care physicians should be aware of this condition, because delayed recognition in a high-functioning person can be potentially disabling.
Our patient had a first rib resection, partial division of the scalenus anterior and medius muscles, and lysis of the cervical band. Follow-up venography confirmed resolution of thrombosis without any complications. The patient was continued on anticoagulation with warfarin for 3 months.
1. Isma N, Svensson PJ, Gottsäter A, et al. Upper extremity deep venous thrombosis in the population-based Malmö thrombophilia study (MATS). Epidemiology, risk factors, recurrence risk, and mortality. Thromb Res. 2010;125:e335-e338.
2. DiFelice GS, Paletta GA Jr, Phillips BB, et al. Effort thrombosis in the elite throwing athlete. Am J Sports Med. 2002;30:708-712.
3. Thompson JF, Winterborn RJ, Bays S, et al. Venous thoracic outlet compression and the Paget-Schroetter syndrome: a review and recommendations for management. Cardiovasc Intervent Radiol. 2011;34:903-910.
4. Joffe HV, Kucher N, Tapson VF, et al; Deep vein thrombosis (DVT) FREE steering committee. Upper-extremity deep vein thrombosis: a prospective registry of 592 patients. Circulation. 2004;110:1605-1611.
5. Osterman AL, Lincoski C. Thoracic outlet syndrome. In: Skirven TM, Osterman AL, Fedorczyk JM, et al, eds. Rehabilitation of the Hand and Upper Extremity. 6th ed. Philadelphia, Pa: Mosby, Inc; 2011:723-732.
6. Laker S, Sullivan WJ, Whitehill TA. Thoracic outlet syndrome. In: Akuthota V, Herring SA, eds. Nerve and vascular injuries in sports medicine. New York, NY: Springer; 2009:117.
7. Urschel HC Jr, Patel AN. Surgery remains the most effective treatment for Paget-Schroetter syndrome: 50 years’ experience. Ann Thorac Surg. 2008;86:254-260; discussion 260.
8. Melby SJ, Vedantham S, Narra VR, et al. Comprehensive surgical management of the competitive athlete with effort thrombosis of the subclavian vein (Paget-Schroetter syndrome). J Vasc Surg. 2008;47:809-820; discussion 821.
9. Di Nisio M, Van Sluis GL, Bossuyt PM, et al. Accuracy of diagnostic tests for clinically suspected upper extremity deep vein thrombosis: a systematic review. J Thromb Haemost. 2010;8:684-692.
10. Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol. 2012;29:44-51.
11. Desjardins B, Rybicki FJ, Kim HS, et al. ACR Appropriateness Criteria® Suspected upper extremity deep vein thrombosis. J Am Coll Radiol. 2012;9:613-619.
12. Savage KJ, Wells PS, Schulz V, et al. Outpatient use of low molecular weight heparin (Dalteparin) for the treatment of deep vein thrombosis of the upper extremity. Thromb Haemost. 1999;82:1008-1010.
13. Machleder HI. Evaluation of a new treatment strategy for Paget-Schroetter syndrome: spontaneous thrombosis of the axillary-subclavian vein. J Vasc Surg. 1993;17:305-315; discussion 316-317.
14. Thomas IH, Zierler BK. An integrative review of outcomes in patients with acute primary upper extremity deep venous thrombosis following no treatment or treatment with anticoagulation, thrombolysis, or surgical algorithms. Vasc Endovascular Surg. 2005;39:163-174.
THE CASE
A 16-year-old boy presented to the emergency room (ER) with pain, redness, and swelling of his right upper arm that had been bothering him for 2 days. He was the quarterback of his high school football team, a sport that he’d been playing since he was 8 years old. He indicated that his football training—which involved repetitive throwing with his right arm—had intensified over the previous 2 months.
Prior to the ER visit, the patient was healthy and active with no significant medical history. He’d had no shoulder trauma and there was no family history of any coagulopathies, venous thrombosis, or pulmonary embolism. He denied chest pain, shortness of breath, palpitations, and fever, and said that he did not smoke cigarettes or drink alcohol.
On physical examination, his blood pressure was 118/70 mm Hg and his heart rate was 74 beats per minute. He had nonpitting edema and erythema of his right upper arm. His radial and brachial pulses were strong and equal in both arms. Assessment of neurologic and vascular integrity produced positive Wright’s and Adson’s tests, but a negative Halstead’s test. (For more on these tests, see: Wright’s test, Adson’s test, and Halstead’s test.) The circumference of the patient’s right upper arm was 2.5 cm greater than the left upper arm. The remainder of the physical exam was normal.
THE DIAGNOSIS
A duplex ultrasound of the right upper arm revealed an acute occlusive thrombus in the axillary vein. We started the patient on intravenous heparin. A venogram confirmed thrombosis of the axillary-subclavian vein (FIGURE 1A). Based on the patient’s clinical presentation and the results of the venogram, we diagnosed Paget-Schroetter syndrome. The venogram was followed by thrombolysis with alteplase (FIGURE 1B) and a balloon angioplasty (FIGURE 1C). One week later, a repeat venogram demonstrated partial removal of the thrombus and an area of compression on the inferior aspect of the subclavian vein due to a cervical band (FIGURE 1D).
DISCUSSION
Paget-Schroetter syndrome (PSS), or effort thrombosis of the upper extremities, is defined as spontaneous thrombus in the axillary and subclavian veins that occurs as a consequence of strenuous upper-extremity activity. It is a rare condition with an incidence of one to 2 cases per 100,000 people per year, and represents 1% to 4% of all cases of deep vein thrombosis (DVT).1
Spontaneous thrombosis of the upper extremities typically presents in young, otherwise healthy individuals. It has been described in athletes who are involved in ball games, games with rackets or clubs, aquatic sports, combatant sports, and in violin players.2 The repetitive movements used in these activities can lead to compression of the axillary and subclavian veins by hypertrophied muscles. Repetitive trauma causes intimal damage and thrombogenesis.3
PSS is characterized by the abrupt, spontaneous swelling of the entire arm, cyanosis, and pain that occurs with use or overhead positioning. Enlarged subcutaneous veins are present in the upper arm, around the shoulder, or in the upper anterior chest wall (Urschel’s sign). The classic presentation is acute onset of upper extremity pain and swelling in the dominant arm following a particularly strenuous activity.4 A low-grade fever, superficial thrombophlebitis, or neurologic symptoms may coexist. Certain provocative maneuvers can help reproduce the symptoms (TABLE 15,6). Complications of PSS include pulmonary embolism, postthrombotic syndrome (pain, heaviness, and swelling), and recurrent thrombosis.7
Contrast venography best shows the extent of thrombosis
Duplex ultrasound, with its high sensitivity and specificity, is the initial, noninvasive test of choice (TABLE 24,8-11). However, duplex ultrasound has a false-negative rate of 30% because it is highly technician-dependent and can be complicated by acoustic shadows from the clavicle or sternum.8
The most direct and definitive means to confirm the diagnosis of PSS is catheter-directed contrast venography.9 This method provides complete anatomic information regarding the site and extent of thrombosis, allows definitive evaluation of the collateral venous pathways, and is a necessary step toward the use of thrombolytic therapy. Contrast load, however, contraindicates the procedure in patients with renal failure and in those who are pregnant.
Contrast-enhanced computed tomography (CT) and magnetic resonance angiography (MRA) are also highly sensitive for detecting focal stenosis at the level of the first rib, the presence or absence of enlarged collateral veins, and the chronicity of any thrombus present. However, the usefulness of CT and magnetic resonance venography in initial screening is unclear, due to a lack of randomized controlled trials.
Treatment involves anticoagulants, thrombolytics, and possibly surgery
Prompt use of anticoagulation is indicated in PSS. Initial anticoagulation with low molecular weight unfractionated heparin or a direct thrombin inhibitor followed by warfarin for a minimum of 3 to 6 months is recommended.12
Patients treated with anticoagulation alone have a higher incidence of long-term residual symptoms, disability, and recurrent thrombosis.7 As a result, a more aggressive approach with the use of thrombolytic therapy is indicated, especially in young, active patients, to minimize long-term consequences. Alteplase or reteplase are used for this purpose. Thrombolysis is less likely to be beneficial if the thrombus is more than 2 weeks old or if there are inflammatory changes in the vein. The use of catheter-directed thrombolysis minimizes the risk of systemic adverse effects and achieves higher clot resolution rates.13
Because PSS is caused by compression of the vein, rather than a disorder of blood clotting, there is still a 50% to 70% risk of recurrent thrombosis despite thrombolysis and anticoagulation.14 Therefore, the most definitive management approach remains surgical treatment. Patients with recent thrombosis who are within the first several weeks of undergoing successful thrombolytic therapy are excellent candidates for surgery. Operative treatment for PSS includes first rib resection, scalene muscle removal, or subclavius muscle removal, along with removal of constricting scar tissue from around the vein.7
THE TAKEAWAY
PSS is characterized by upper-extremity DVT resulting from repetitive trauma to the subclavian-axillary vein. Early diagnosis of PSS with contrast venography and prompt use of anticoagulation can effectively restore venous patency, reduce the risk of rethrombosis, and return the patient to normal function. Primary care physicians should be aware of this condition, because delayed recognition in a high-functioning person can be potentially disabling.
Our patient had a first rib resection, partial division of the scalenus anterior and medius muscles, and lysis of the cervical band. Follow-up venography confirmed resolution of thrombosis without any complications. The patient was continued on anticoagulation with warfarin for 3 months.
THE CASE
A 16-year-old boy presented to the emergency room (ER) with pain, redness, and swelling of his right upper arm that had been bothering him for 2 days. He was the quarterback of his high school football team, a sport that he’d been playing since he was 8 years old. He indicated that his football training—which involved repetitive throwing with his right arm—had intensified over the previous 2 months.
Prior to the ER visit, the patient was healthy and active with no significant medical history. He’d had no shoulder trauma and there was no family history of any coagulopathies, venous thrombosis, or pulmonary embolism. He denied chest pain, shortness of breath, palpitations, and fever, and said that he did not smoke cigarettes or drink alcohol.
On physical examination, his blood pressure was 118/70 mm Hg and his heart rate was 74 beats per minute. He had nonpitting edema and erythema of his right upper arm. His radial and brachial pulses were strong and equal in both arms. Assessment of neurologic and vascular integrity produced positive Wright’s and Adson’s tests, but a negative Halstead’s test. (For more on these tests, see: Wright’s test, Adson’s test, and Halstead’s test.) The circumference of the patient’s right upper arm was 2.5 cm greater than the left upper arm. The remainder of the physical exam was normal.
THE DIAGNOSIS
A duplex ultrasound of the right upper arm revealed an acute occlusive thrombus in the axillary vein. We started the patient on intravenous heparin. A venogram confirmed thrombosis of the axillary-subclavian vein (FIGURE 1A). Based on the patient’s clinical presentation and the results of the venogram, we diagnosed Paget-Schroetter syndrome. The venogram was followed by thrombolysis with alteplase (FIGURE 1B) and a balloon angioplasty (FIGURE 1C). One week later, a repeat venogram demonstrated partial removal of the thrombus and an area of compression on the inferior aspect of the subclavian vein due to a cervical band (FIGURE 1D).
DISCUSSION
Paget-Schroetter syndrome (PSS), or effort thrombosis of the upper extremities, is defined as spontaneous thrombus in the axillary and subclavian veins that occurs as a consequence of strenuous upper-extremity activity. It is a rare condition with an incidence of one to 2 cases per 100,000 people per year, and represents 1% to 4% of all cases of deep vein thrombosis (DVT).1
Spontaneous thrombosis of the upper extremities typically presents in young, otherwise healthy individuals. It has been described in athletes who are involved in ball games, games with rackets or clubs, aquatic sports, combatant sports, and in violin players.2 The repetitive movements used in these activities can lead to compression of the axillary and subclavian veins by hypertrophied muscles. Repetitive trauma causes intimal damage and thrombogenesis.3
PSS is characterized by the abrupt, spontaneous swelling of the entire arm, cyanosis, and pain that occurs with use or overhead positioning. Enlarged subcutaneous veins are present in the upper arm, around the shoulder, or in the upper anterior chest wall (Urschel’s sign). The classic presentation is acute onset of upper extremity pain and swelling in the dominant arm following a particularly strenuous activity.4 A low-grade fever, superficial thrombophlebitis, or neurologic symptoms may coexist. Certain provocative maneuvers can help reproduce the symptoms (TABLE 15,6). Complications of PSS include pulmonary embolism, postthrombotic syndrome (pain, heaviness, and swelling), and recurrent thrombosis.7
Contrast venography best shows the extent of thrombosis
Duplex ultrasound, with its high sensitivity and specificity, is the initial, noninvasive test of choice (TABLE 24,8-11). However, duplex ultrasound has a false-negative rate of 30% because it is highly technician-dependent and can be complicated by acoustic shadows from the clavicle or sternum.8
The most direct and definitive means to confirm the diagnosis of PSS is catheter-directed contrast venography.9 This method provides complete anatomic information regarding the site and extent of thrombosis, allows definitive evaluation of the collateral venous pathways, and is a necessary step toward the use of thrombolytic therapy. Contrast load, however, contraindicates the procedure in patients with renal failure and in those who are pregnant.
Contrast-enhanced computed tomography (CT) and magnetic resonance angiography (MRA) are also highly sensitive for detecting focal stenosis at the level of the first rib, the presence or absence of enlarged collateral veins, and the chronicity of any thrombus present. However, the usefulness of CT and magnetic resonance venography in initial screening is unclear, due to a lack of randomized controlled trials.
Treatment involves anticoagulants, thrombolytics, and possibly surgery
Prompt use of anticoagulation is indicated in PSS. Initial anticoagulation with low molecular weight unfractionated heparin or a direct thrombin inhibitor followed by warfarin for a minimum of 3 to 6 months is recommended.12
Patients treated with anticoagulation alone have a higher incidence of long-term residual symptoms, disability, and recurrent thrombosis.7 As a result, a more aggressive approach with the use of thrombolytic therapy is indicated, especially in young, active patients, to minimize long-term consequences. Alteplase or reteplase are used for this purpose. Thrombolysis is less likely to be beneficial if the thrombus is more than 2 weeks old or if there are inflammatory changes in the vein. The use of catheter-directed thrombolysis minimizes the risk of systemic adverse effects and achieves higher clot resolution rates.13
Because PSS is caused by compression of the vein, rather than a disorder of blood clotting, there is still a 50% to 70% risk of recurrent thrombosis despite thrombolysis and anticoagulation.14 Therefore, the most definitive management approach remains surgical treatment. Patients with recent thrombosis who are within the first several weeks of undergoing successful thrombolytic therapy are excellent candidates for surgery. Operative treatment for PSS includes first rib resection, scalene muscle removal, or subclavius muscle removal, along with removal of constricting scar tissue from around the vein.7
THE TAKEAWAY
PSS is characterized by upper-extremity DVT resulting from repetitive trauma to the subclavian-axillary vein. Early diagnosis of PSS with contrast venography and prompt use of anticoagulation can effectively restore venous patency, reduce the risk of rethrombosis, and return the patient to normal function. Primary care physicians should be aware of this condition, because delayed recognition in a high-functioning person can be potentially disabling.
Our patient had a first rib resection, partial division of the scalenus anterior and medius muscles, and lysis of the cervical band. Follow-up venography confirmed resolution of thrombosis without any complications. The patient was continued on anticoagulation with warfarin for 3 months.
1. Isma N, Svensson PJ, Gottsäter A, et al. Upper extremity deep venous thrombosis in the population-based Malmö thrombophilia study (MATS). Epidemiology, risk factors, recurrence risk, and mortality. Thromb Res. 2010;125:e335-e338.
2. DiFelice GS, Paletta GA Jr, Phillips BB, et al. Effort thrombosis in the elite throwing athlete. Am J Sports Med. 2002;30:708-712.
3. Thompson JF, Winterborn RJ, Bays S, et al. Venous thoracic outlet compression and the Paget-Schroetter syndrome: a review and recommendations for management. Cardiovasc Intervent Radiol. 2011;34:903-910.
4. Joffe HV, Kucher N, Tapson VF, et al; Deep vein thrombosis (DVT) FREE steering committee. Upper-extremity deep vein thrombosis: a prospective registry of 592 patients. Circulation. 2004;110:1605-1611.
5. Osterman AL, Lincoski C. Thoracic outlet syndrome. In: Skirven TM, Osterman AL, Fedorczyk JM, et al, eds. Rehabilitation of the Hand and Upper Extremity. 6th ed. Philadelphia, Pa: Mosby, Inc; 2011:723-732.
6. Laker S, Sullivan WJ, Whitehill TA. Thoracic outlet syndrome. In: Akuthota V, Herring SA, eds. Nerve and vascular injuries in sports medicine. New York, NY: Springer; 2009:117.
7. Urschel HC Jr, Patel AN. Surgery remains the most effective treatment for Paget-Schroetter syndrome: 50 years’ experience. Ann Thorac Surg. 2008;86:254-260; discussion 260.
8. Melby SJ, Vedantham S, Narra VR, et al. Comprehensive surgical management of the competitive athlete with effort thrombosis of the subclavian vein (Paget-Schroetter syndrome). J Vasc Surg. 2008;47:809-820; discussion 821.
9. Di Nisio M, Van Sluis GL, Bossuyt PM, et al. Accuracy of diagnostic tests for clinically suspected upper extremity deep vein thrombosis: a systematic review. J Thromb Haemost. 2010;8:684-692.
10. Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol. 2012;29:44-51.
11. Desjardins B, Rybicki FJ, Kim HS, et al. ACR Appropriateness Criteria® Suspected upper extremity deep vein thrombosis. J Am Coll Radiol. 2012;9:613-619.
12. Savage KJ, Wells PS, Schulz V, et al. Outpatient use of low molecular weight heparin (Dalteparin) for the treatment of deep vein thrombosis of the upper extremity. Thromb Haemost. 1999;82:1008-1010.
13. Machleder HI. Evaluation of a new treatment strategy for Paget-Schroetter syndrome: spontaneous thrombosis of the axillary-subclavian vein. J Vasc Surg. 1993;17:305-315; discussion 316-317.
14. Thomas IH, Zierler BK. An integrative review of outcomes in patients with acute primary upper extremity deep venous thrombosis following no treatment or treatment with anticoagulation, thrombolysis, or surgical algorithms. Vasc Endovascular Surg. 2005;39:163-174.
1. Isma N, Svensson PJ, Gottsäter A, et al. Upper extremity deep venous thrombosis in the population-based Malmö thrombophilia study (MATS). Epidemiology, risk factors, recurrence risk, and mortality. Thromb Res. 2010;125:e335-e338.
2. DiFelice GS, Paletta GA Jr, Phillips BB, et al. Effort thrombosis in the elite throwing athlete. Am J Sports Med. 2002;30:708-712.
3. Thompson JF, Winterborn RJ, Bays S, et al. Venous thoracic outlet compression and the Paget-Schroetter syndrome: a review and recommendations for management. Cardiovasc Intervent Radiol. 2011;34:903-910.
4. Joffe HV, Kucher N, Tapson VF, et al; Deep vein thrombosis (DVT) FREE steering committee. Upper-extremity deep vein thrombosis: a prospective registry of 592 patients. Circulation. 2004;110:1605-1611.
5. Osterman AL, Lincoski C. Thoracic outlet syndrome. In: Skirven TM, Osterman AL, Fedorczyk JM, et al, eds. Rehabilitation of the Hand and Upper Extremity. 6th ed. Philadelphia, Pa: Mosby, Inc; 2011:723-732.
6. Laker S, Sullivan WJ, Whitehill TA. Thoracic outlet syndrome. In: Akuthota V, Herring SA, eds. Nerve and vascular injuries in sports medicine. New York, NY: Springer; 2009:117.
7. Urschel HC Jr, Patel AN. Surgery remains the most effective treatment for Paget-Schroetter syndrome: 50 years’ experience. Ann Thorac Surg. 2008;86:254-260; discussion 260.
8. Melby SJ, Vedantham S, Narra VR, et al. Comprehensive surgical management of the competitive athlete with effort thrombosis of the subclavian vein (Paget-Schroetter syndrome). J Vasc Surg. 2008;47:809-820; discussion 821.
9. Di Nisio M, Van Sluis GL, Bossuyt PM, et al. Accuracy of diagnostic tests for clinically suspected upper extremity deep vein thrombosis: a systematic review. J Thromb Haemost. 2010;8:684-692.
10. Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol. 2012;29:44-51.
11. Desjardins B, Rybicki FJ, Kim HS, et al. ACR Appropriateness Criteria® Suspected upper extremity deep vein thrombosis. J Am Coll Radiol. 2012;9:613-619.
12. Savage KJ, Wells PS, Schulz V, et al. Outpatient use of low molecular weight heparin (Dalteparin) for the treatment of deep vein thrombosis of the upper extremity. Thromb Haemost. 1999;82:1008-1010.
13. Machleder HI. Evaluation of a new treatment strategy for Paget-Schroetter syndrome: spontaneous thrombosis of the axillary-subclavian vein. J Vasc Surg. 1993;17:305-315; discussion 316-317.
14. Thomas IH, Zierler BK. An integrative review of outcomes in patients with acute primary upper extremity deep venous thrombosis following no treatment or treatment with anticoagulation, thrombolysis, or surgical algorithms. Vasc Endovascular Surg. 2005;39:163-174.

Are IV fluids better than oral rehydration for children with acute diarrhea and vomiting?
Intravenous fluid therapy (IVF) has a slightly lower failure rate than oral replacement therapy (ORT) in children with acute gastroenteritis, but the clinical significance is questionable. IVF takes longer to initiate than ORT and lengthens the hospital stay (strength of recommendation: B, meta-analysis of poor-to-moderate-quality trials).
Shorter hospital stay with oral replacement therapy
A 2006 systematic review compared ORT and IVF in 1811 children 0 to 18 years of age with viral gastroenteritis who were treated for failure to rehydrate in both outpatient and inpatient settings (18 randomized controlled trials [RCTs] of poor to moderate quality).1 The primary outcome was “continued failure to rehydrate,” which varied by study and included persistent vomiting, persistent dehydration, shock, or seizures.
Overall, the risk of failure to rehydrate was 4.9% for ORT and 1.3% for IVF (risk difference [RD]=4%; 95% confidence interval [CI], 1%-7%; number needed to treat [NNT]=25). The length of stay (24-hour observation unit or inpatient hospitalization) was shorter for ORT than IVF (6 studies, 526 patients; weighted mean difference (WMD)= −1.2 days; 95% CI, −2.38 to −0.02). Investigators found no difference in weight gain, hyponatremia, hypernatremia, duration of diarrhea, or total fluid intake at 24 hours.
ORT can be started more quickly than IVF
An RCT conducted in an urban emergency department evaluated ORT and IVF for 4 hours in 72 children ages 8 weeks to 3 years with moderate dehydration from viral gastroenteritis.2 This trial was included in the previously described review but evaluated additional outcomes: time required to initiate either ORT or IVF, improvement in symptoms at 2 hours, hospitalization rate, and preference for ORT in the future.
The authors also used a 10-point dehydration scoring system that included: decreased skin elasticity, capillary refill >2 seconds, general appearance, absence of tears, abnormal respirations, dry mucous membranes, sunken eyes, abnormal radial pulse, tachycardia >150 beats per minute, and decreased urine output. Details on the type of ORT or IVF were not reported.
ORT was initiated faster than IVF (mean difference [MD]=21 minutes; 95% CI, 10-32 minutes). No difference in improvement in dehydration scores was observed at 2 hours (ORT 78% vs IVF 80%; MD=1.2%; 95% CI, −20.5% to 18%). Nor was the hospitalization rate significantly different (IVF 48.7% and ORT 30.6%; MD=−18.1%; 95% CI, −40.1% to 4.1%). Most patients preferred to have the same therapy, whether ORT or IVF, with the next episode of gastroenteritis (61.3% vs 51.4%; MD=9.9%; 95% CI, −14 to 34).
1. Hartling L, Bellmare S, Wiebe N, et al. Oral versus intravenous rehydration for treating dehydration due to gastroenteritis in children. Cochrane Database Syst Rev. 2006;(3):CD004390.
2. Spandorfer PR, Alessandrini EA, Joffe MD, et al. Oral versus intravenous rehydration of moderately dehydrated children: a randomized, controlled trial. Pediatrics. 2005;115:295-301.
Intravenous fluid therapy (IVF) has a slightly lower failure rate than oral replacement therapy (ORT) in children with acute gastroenteritis, but the clinical significance is questionable. IVF takes longer to initiate than ORT and lengthens the hospital stay (strength of recommendation: B, meta-analysis of poor-to-moderate-quality trials).
Shorter hospital stay with oral replacement therapy
A 2006 systematic review compared ORT and IVF in 1811 children 0 to 18 years of age with viral gastroenteritis who were treated for failure to rehydrate in both outpatient and inpatient settings (18 randomized controlled trials [RCTs] of poor to moderate quality).1 The primary outcome was “continued failure to rehydrate,” which varied by study and included persistent vomiting, persistent dehydration, shock, or seizures.
Overall, the risk of failure to rehydrate was 4.9% for ORT and 1.3% for IVF (risk difference [RD]=4%; 95% confidence interval [CI], 1%-7%; number needed to treat [NNT]=25). The length of stay (24-hour observation unit or inpatient hospitalization) was shorter for ORT than IVF (6 studies, 526 patients; weighted mean difference (WMD)= −1.2 days; 95% CI, −2.38 to −0.02). Investigators found no difference in weight gain, hyponatremia, hypernatremia, duration of diarrhea, or total fluid intake at 24 hours.
ORT can be started more quickly than IVF
An RCT conducted in an urban emergency department evaluated ORT and IVF for 4 hours in 72 children ages 8 weeks to 3 years with moderate dehydration from viral gastroenteritis.2 This trial was included in the previously described review but evaluated additional outcomes: time required to initiate either ORT or IVF, improvement in symptoms at 2 hours, hospitalization rate, and preference for ORT in the future.
The authors also used a 10-point dehydration scoring system that included: decreased skin elasticity, capillary refill >2 seconds, general appearance, absence of tears, abnormal respirations, dry mucous membranes, sunken eyes, abnormal radial pulse, tachycardia >150 beats per minute, and decreased urine output. Details on the type of ORT or IVF were not reported.
ORT was initiated faster than IVF (mean difference [MD]=21 minutes; 95% CI, 10-32 minutes). No difference in improvement in dehydration scores was observed at 2 hours (ORT 78% vs IVF 80%; MD=1.2%; 95% CI, −20.5% to 18%). Nor was the hospitalization rate significantly different (IVF 48.7% and ORT 30.6%; MD=−18.1%; 95% CI, −40.1% to 4.1%). Most patients preferred to have the same therapy, whether ORT or IVF, with the next episode of gastroenteritis (61.3% vs 51.4%; MD=9.9%; 95% CI, −14 to 34).
Intravenous fluid therapy (IVF) has a slightly lower failure rate than oral replacement therapy (ORT) in children with acute gastroenteritis, but the clinical significance is questionable. IVF takes longer to initiate than ORT and lengthens the hospital stay (strength of recommendation: B, meta-analysis of poor-to-moderate-quality trials).
Shorter hospital stay with oral replacement therapy
A 2006 systematic review compared ORT and IVF in 1811 children 0 to 18 years of age with viral gastroenteritis who were treated for failure to rehydrate in both outpatient and inpatient settings (18 randomized controlled trials [RCTs] of poor to moderate quality).1 The primary outcome was “continued failure to rehydrate,” which varied by study and included persistent vomiting, persistent dehydration, shock, or seizures.
Overall, the risk of failure to rehydrate was 4.9% for ORT and 1.3% for IVF (risk difference [RD]=4%; 95% confidence interval [CI], 1%-7%; number needed to treat [NNT]=25). The length of stay (24-hour observation unit or inpatient hospitalization) was shorter for ORT than IVF (6 studies, 526 patients; weighted mean difference (WMD)= −1.2 days; 95% CI, −2.38 to −0.02). Investigators found no difference in weight gain, hyponatremia, hypernatremia, duration of diarrhea, or total fluid intake at 24 hours.
ORT can be started more quickly than IVF
An RCT conducted in an urban emergency department evaluated ORT and IVF for 4 hours in 72 children ages 8 weeks to 3 years with moderate dehydration from viral gastroenteritis.2 This trial was included in the previously described review but evaluated additional outcomes: time required to initiate either ORT or IVF, improvement in symptoms at 2 hours, hospitalization rate, and preference for ORT in the future.
The authors also used a 10-point dehydration scoring system that included: decreased skin elasticity, capillary refill >2 seconds, general appearance, absence of tears, abnormal respirations, dry mucous membranes, sunken eyes, abnormal radial pulse, tachycardia >150 beats per minute, and decreased urine output. Details on the type of ORT or IVF were not reported.
ORT was initiated faster than IVF (mean difference [MD]=21 minutes; 95% CI, 10-32 minutes). No difference in improvement in dehydration scores was observed at 2 hours (ORT 78% vs IVF 80%; MD=1.2%; 95% CI, −20.5% to 18%). Nor was the hospitalization rate significantly different (IVF 48.7% and ORT 30.6%; MD=−18.1%; 95% CI, −40.1% to 4.1%). Most patients preferred to have the same therapy, whether ORT or IVF, with the next episode of gastroenteritis (61.3% vs 51.4%; MD=9.9%; 95% CI, −14 to 34).
1. Hartling L, Bellmare S, Wiebe N, et al. Oral versus intravenous rehydration for treating dehydration due to gastroenteritis in children. Cochrane Database Syst Rev. 2006;(3):CD004390.
2. Spandorfer PR, Alessandrini EA, Joffe MD, et al. Oral versus intravenous rehydration of moderately dehydrated children: a randomized, controlled trial. Pediatrics. 2005;115:295-301.
1. Hartling L, Bellmare S, Wiebe N, et al. Oral versus intravenous rehydration for treating dehydration due to gastroenteritis in children. Cochrane Database Syst Rev. 2006;(3):CD004390.
2. Spandorfer PR, Alessandrini EA, Joffe MD, et al. Oral versus intravenous rehydration of moderately dehydrated children: a randomized, controlled trial. Pediatrics. 2005;115:295-301.
Evidence-based answers from the Family Physicians Inquiries Network

Parkinson’s disease psychosis drug gets favorable review from FDA advisory panel
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.
Parkinson’s disease psychosis drug gets favorable review from FDA advisory panel
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
![]()
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
![]()
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.
The lack of available treatments that adequately treat Parkinson’s disease psychosis proved to be a big motivating factor for a majority of members of the Food and Drug Administration’s Psychopharmacologic Drugs Advisory Committee, who voted at a meeting March 29 that the benefits of the novel drug pimavanserin outweigh its risks.
The panel voted 12-2 in support of the benefit-to-risk ratio for pimavanserin, a selective 5-hydroxytryptamine2A (5-HT2A) inverse agonist that does not affect the dopaminergic, histaminergic, adrenergic, or muscarinic systems, according to its developer, Acadia Pharmaceuticals.
![]()
Although Acadia submitted just one positive phase III trial out of a total of four 6-week, randomized, placebo-controlled trials of pimavanserin, committee members voted 12-2 that the company “provided substantial evidence of the effectiveness” of the drug for the treatment of psychosis associated with Parkinsons’s disease (PDP). Another 11-3 vote supported the question of whether pimavanersin’s safety profile was “adequately characterized.”
Results from the single phase III trial conducted in 199 patients with Parkinsons’s disease psychosis (PDP) unequivocally showed that 34 mg/day pimavanserin improved scores on an abbreviated, 9-item version of the 20-item Scale for the Assessment of Positive Symptoms–Hallucinations and Delusions score, called the SAPS-PD. After 6 weeks, SAPS-PD scores declined by a statistically significant 3.1 points or 23.1% on active treatment versus placebo, which was an absolute decrease of about 6 points from baseline. One of the questions brought up by FDA reviewers and panelists was whether the 3.1-point difference (on the SAPS-PD’s 45-point scale) seen between active treatment and placebo was of great enough clinical benefit to outweigh the higher rate of serious adverse events observed with pimavanserin versus placebo across all of the 6-week trials.
Across all four 6-week studies, serious adverse events occurred in 16 (7.9%) of 202 patients who took 34 mg pimavanserin and in 8 (3.5%) of 231 placebo-treated patients. Three deaths occurred in the patients who received pimavanserin, and one in the placebo arms. However, none of the deaths were considered to be a drug-related event, and the deaths were not pathologically unique relative to what is expected in the disease course of patients with PDP. The death of another patient who had received 10 mg pimavanserin in an earlier uncontrolled trial also was reported.
Meanwhile, the drug did not worsen motor symptoms of Parkinson’s disease.
FDA analyses showed that 11 patients would need to be treated in order for 1 patient to have a 50% reduction in the SAPS-PD, which corresponds to “much improvement,” whereas 22 patients would need to be treated for 1 to be harmed with a serious adverse event (SAE). This means that for every two patients who have a 50% reduction in the SAPS-PD, one will have a serious adverse event attributable to pimavanserin. Overall, 37.2% of patients in the pimavanserin arm of the phase III trial had a 50% decline in the SAPS-PD after 6 weeks, compared with 27.8% in the placebo arm.
However, the number needed to harm/number needed to treat ratio for SAEs had wide confidence intervals, and there was a high degree of uncertainty about its magnitude such that the inclusion of just one or two more SAEs would substantially change the ratio, many panelists agreed.
Some panelists voiced concern about pimavanserin being called an antipsychotic, even though it has demonstrated no proof of efficacy in conditions with classical symptoms of psychosis, such as schizophrenia, and worried about its off-label use in patients with other conditions who have psychotic symptoms. They also called for a postmarketing observational study to track the safety of the drug if it is approved.
Pimavanserin’s application received breakthrough drug status from the FDA and was fast tracked, and a decision is expected from the agency by May 1. If approved, pimavanserin would be marketed under the trade name Nuplazid.