User login
High-dose vitamin D improves heart structure, function in chronic heart failure
High-dose oral vitamin D supplements taken for one year significantly improved cardiac structure and function in patients with chronic heart failure (CHF) secondary to left ventricular systolic dysfunction, according to results from a new study published online in the Journal of the American College of Cardiology. However, the study, led by Dr. Klaus Witte of the University of Leeds (England), found that 6-minute walk-distance—the study’s primary outcome measure—was not improved after a year’s supplementation with vitamin D. For more on the study, go to Cardiology News: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/high-dose-vitamin-d-improves-heart-structure-function-in-chronic-heart-failure/ddee3f3aef17d20293b99a606045ef98.html.
High-dose oral vitamin D supplements taken for one year significantly improved cardiac structure and function in patients with chronic heart failure (CHF) secondary to left ventricular systolic dysfunction, according to results from a new study published online in the Journal of the American College of Cardiology. However, the study, led by Dr. Klaus Witte of the University of Leeds (England), found that 6-minute walk-distance—the study’s primary outcome measure—was not improved after a year’s supplementation with vitamin D. For more on the study, go to Cardiology News: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/high-dose-vitamin-d-improves-heart-structure-function-in-chronic-heart-failure/ddee3f3aef17d20293b99a606045ef98.html.
High-dose oral vitamin D supplements taken for one year significantly improved cardiac structure and function in patients with chronic heart failure (CHF) secondary to left ventricular systolic dysfunction, according to results from a new study published online in the Journal of the American College of Cardiology. However, the study, led by Dr. Klaus Witte of the University of Leeds (England), found that 6-minute walk-distance—the study’s primary outcome measure—was not improved after a year’s supplementation with vitamin D. For more on the study, go to Cardiology News: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/high-dose-vitamin-d-improves-heart-structure-function-in-chronic-heart-failure/ddee3f3aef17d20293b99a606045ef98.html.
Diabetes drug appears to reduce recurrent vascular events
Pioglitazone, which is used to treat type 2 diabetes, may reduce the risk of recurrent stroke and heart attacks by 24% in people who are insulin resistant but do not have diabetes, according to findings from the Insulin Resistance Intervention after Stroke (IRIS) trial. The study, supported by the National Institute of Neurological Disorders and Stroke, is the first to provide evidence that suggests a drug that targets cell metabolism may be protective against recurrent vascular events even before diabetes develops. More information on the study is available at Federal Practitioner: http://www.fedprac.com/the-publication/issue-single-view/diabetes-drug-reduces-recurrent-vascular-events/bd40f959f882ada3b88cfaa670c4fa44/ocregister.html.
Pioglitazone, which is used to treat type 2 diabetes, may reduce the risk of recurrent stroke and heart attacks by 24% in people who are insulin resistant but do not have diabetes, according to findings from the Insulin Resistance Intervention after Stroke (IRIS) trial. The study, supported by the National Institute of Neurological Disorders and Stroke, is the first to provide evidence that suggests a drug that targets cell metabolism may be protective against recurrent vascular events even before diabetes develops. More information on the study is available at Federal Practitioner: http://www.fedprac.com/the-publication/issue-single-view/diabetes-drug-reduces-recurrent-vascular-events/bd40f959f882ada3b88cfaa670c4fa44/ocregister.html.
Pioglitazone, which is used to treat type 2 diabetes, may reduce the risk of recurrent stroke and heart attacks by 24% in people who are insulin resistant but do not have diabetes, according to findings from the Insulin Resistance Intervention after Stroke (IRIS) trial. The study, supported by the National Institute of Neurological Disorders and Stroke, is the first to provide evidence that suggests a drug that targets cell metabolism may be protective against recurrent vascular events even before diabetes develops. More information on the study is available at Federal Practitioner: http://www.fedprac.com/the-publication/issue-single-view/diabetes-drug-reduces-recurrent-vascular-events/bd40f959f882ada3b88cfaa670c4fa44/ocregister.html.
Laser Best Practices for Darker Skin Types

What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.
What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.
What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.

Cardiovascular consequences of extreme prematurity persist into late adolescence
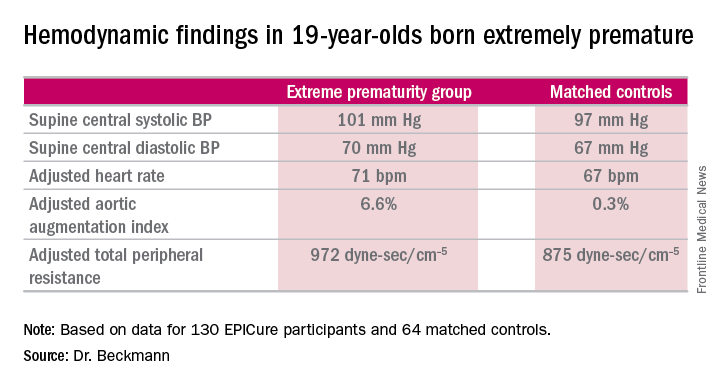
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
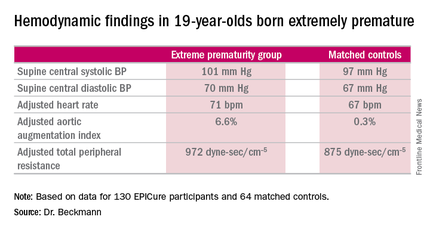
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
AT ACC 16
Key clinical point: At age 19 years, persons born extremely premature still show significant abnormalities in arterial hemodynamics and peripheral resistance.
Major finding: The adjusted aortic augmentation index was 6.6% in 19-year-olds born at 22-25 weeks gestation compared with 0.3% in matched controls.
Data source: EPICure, a longitudinal study of health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks gestation in the United Kingdom during 1995-1996.
Disclosures: EPICure is funded by the Medical Research Council. The presenter reported having no financial conflicts of interest.
Physicians, Residents, Students Can Learn High-Value, Cost-Conscious Care
Clinical question: What are the factors that promote education in delivering high-value, cost-conscious care?

Background: Healthcare costs are increasing, with most recent numbers showing U.S. expenditures on healthcare of more than $3 trillion, almost 18% of the gross domestic product. High-value care focuses on understanding the benefits, risks, and costs of care and promoting interventions that add value.
Study design: Systematic review.
Setting: Physicians, resident physicians, and medical students in North America, Asia, and Oceania.
Synopsis: Seventy-nine articles were included in the analysis, with 14 being RCTs. Most of the studies were conducted in North America (78.5%) and used a pre-post interventional design (58.2%). Practicing physicians (36.7%) made up the majority of participants in the study, with residents (15.2%) and medical students (6.3%) in smaller numbers. Analysis of the studies identified three factors for successful learning:
- effective transmission of knowledge about prices of services and general health economics, scientific evidence, and patient preferences;
- facilitation of reflective practice through feedback and/or stimulating reflection; and
- creation of a supportive environment.
Bottom line: The most-effective interventions in educating physicians, resident physicians, and medical students on high-value, cost-conscious care are effective transmission of knowledge, reflective practice, and supportive environment.
Citation: Stammen LA, Stalmeijer RE, Paternotte E, et al. Training physicians to provide high-value, cost-conscious care: a systematic review. JAMA. 2015;314(22):2384-2400.
Clinical question: What are the factors that promote education in delivering high-value, cost-conscious care?
Background: Healthcare costs are increasing, with most recent numbers showing U.S. expenditures on healthcare of more than $3 trillion, almost 18% of the gross domestic product. High-value care focuses on understanding the benefits, risks, and costs of care and promoting interventions that add value.
Study design: Systematic review.
Setting: Physicians, resident physicians, and medical students in North America, Asia, and Oceania.
Synopsis: Seventy-nine articles were included in the analysis, with 14 being RCTs. Most of the studies were conducted in North America (78.5%) and used a pre-post interventional design (58.2%). Practicing physicians (36.7%) made up the majority of participants in the study, with residents (15.2%) and medical students (6.3%) in smaller numbers. Analysis of the studies identified three factors for successful learning:
- effective transmission of knowledge about prices of services and general health economics, scientific evidence, and patient preferences;
- facilitation of reflective practice through feedback and/or stimulating reflection; and
- creation of a supportive environment.
Bottom line: The most-effective interventions in educating physicians, resident physicians, and medical students on high-value, cost-conscious care are effective transmission of knowledge, reflective practice, and supportive environment.
Citation: Stammen LA, Stalmeijer RE, Paternotte E, et al. Training physicians to provide high-value, cost-conscious care: a systematic review. JAMA. 2015;314(22):2384-2400.
Clinical question: What are the factors that promote education in delivering high-value, cost-conscious care?
Background: Healthcare costs are increasing, with most recent numbers showing U.S. expenditures on healthcare of more than $3 trillion, almost 18% of the gross domestic product. High-value care focuses on understanding the benefits, risks, and costs of care and promoting interventions that add value.
Study design: Systematic review.
Setting: Physicians, resident physicians, and medical students in North America, Asia, and Oceania.
Synopsis: Seventy-nine articles were included in the analysis, with 14 being RCTs. Most of the studies were conducted in North America (78.5%) and used a pre-post interventional design (58.2%). Practicing physicians (36.7%) made up the majority of participants in the study, with residents (15.2%) and medical students (6.3%) in smaller numbers. Analysis of the studies identified three factors for successful learning:
- effective transmission of knowledge about prices of services and general health economics, scientific evidence, and patient preferences;
- facilitation of reflective practice through feedback and/or stimulating reflection; and
- creation of a supportive environment.
Bottom line: The most-effective interventions in educating physicians, resident physicians, and medical students on high-value, cost-conscious care are effective transmission of knowledge, reflective practice, and supportive environment.
Citation: Stammen LA, Stalmeijer RE, Paternotte E, et al. Training physicians to provide high-value, cost-conscious care: a systematic review. JAMA. 2015;314(22):2384-2400.

Data Show Patients Are More Likely to Die at Night, on Weekends
Clinical question: Is there a clinical difference in rates of return of spontaneous circulation (ROSC) and survival to discharge in patients with in-hospital cardiac arrest (IHCA) depending on time of day and day of the week?
Background: Current U.S. data from the American Hospital Association’s “Get with the Guidelines-Resuscitation” (AHA GWTG-R) show hospital survival is lower at night and on the weekends. However, little data exist in the U.K. describing patients already hospitalized and the outcomes of in-hospital cardiac arrest with respect to time of day and day of the week.
Study design: Observational cohort study.
Setting: One hundred forty-six hospitals in the United Kingdom.
Synopsis: Study investigators included 27,700 patients ≥16 years of age receiving chest compressions and/or defibrillation from the U.K. National Cardiac Arrest Audit (NCAA) from April 2011 to September 2013. When compared to weekday daytime, the risk-adjusted rates of ROSC were worse for weekend daytime (odds ratio [OR] ROSC >20 min. 0.88; 95% CI, 0.81–0.95) and nighttime (OR ROSC >20 min. 0.72; 95% CI, 0.68–0.76). Hospital survival had similar trends, with OR for the weekend daytime of 0.72 (95% CI, 0.64–0.80) and OR for nighttime 0.58 (95% CI, 0.54–0.63; P value for all was <0.001).
IHCAs were equally likely to occur during the day and night, and the patients were broadly similar, thus suggesting differences in outcomes were secondary to care differences. However, unmeasured patient characteristics may have affected the outcomes. Given that the study was observational, it is difficult to attribute causality, but results are similar to the large, multicenter study published by the AHA GWTG-R registry.
Bottom line: IHCAs that occur during the night or on weekends have increased odds of worse outcomes.
Citation: Robinson EJ, Smith GB, Power GS, et al. Risk-adjusted survival for adults following in-hospital cardiac arrest by day of week and time of day: observational cohort study [published online ahead of print December 11, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-004223.
Short Take
USPSTF Recommends Statins for More Americans
The U.S. Preventive Services Task Force recommends a low- to moderate-dose statin for adults ages 40–75 with no history of cardiovascular disease and a calculated 10-year cardiovascular disease event risk of ≥10%.
Citation: U.S. Preventive Services Task Force. Draft recommendation statement: statin use for the primary prevention of cardiovascular disease in adults: preventive medication. Available at:
Clinical question: Is there a clinical difference in rates of return of spontaneous circulation (ROSC) and survival to discharge in patients with in-hospital cardiac arrest (IHCA) depending on time of day and day of the week?
Background: Current U.S. data from the American Hospital Association’s “Get with the Guidelines-Resuscitation” (AHA GWTG-R) show hospital survival is lower at night and on the weekends. However, little data exist in the U.K. describing patients already hospitalized and the outcomes of in-hospital cardiac arrest with respect to time of day and day of the week.
Study design: Observational cohort study.
Setting: One hundred forty-six hospitals in the United Kingdom.
Synopsis: Study investigators included 27,700 patients ≥16 years of age receiving chest compressions and/or defibrillation from the U.K. National Cardiac Arrest Audit (NCAA) from April 2011 to September 2013. When compared to weekday daytime, the risk-adjusted rates of ROSC were worse for weekend daytime (odds ratio [OR] ROSC >20 min. 0.88; 95% CI, 0.81–0.95) and nighttime (OR ROSC >20 min. 0.72; 95% CI, 0.68–0.76). Hospital survival had similar trends, with OR for the weekend daytime of 0.72 (95% CI, 0.64–0.80) and OR for nighttime 0.58 (95% CI, 0.54–0.63; P value for all was <0.001).
IHCAs were equally likely to occur during the day and night, and the patients were broadly similar, thus suggesting differences in outcomes were secondary to care differences. However, unmeasured patient characteristics may have affected the outcomes. Given that the study was observational, it is difficult to attribute causality, but results are similar to the large, multicenter study published by the AHA GWTG-R registry.
Bottom line: IHCAs that occur during the night or on weekends have increased odds of worse outcomes.
Citation: Robinson EJ, Smith GB, Power GS, et al. Risk-adjusted survival for adults following in-hospital cardiac arrest by day of week and time of day: observational cohort study [published online ahead of print December 11, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-004223.
Short Take
USPSTF Recommends Statins for More Americans
The U.S. Preventive Services Task Force recommends a low- to moderate-dose statin for adults ages 40–75 with no history of cardiovascular disease and a calculated 10-year cardiovascular disease event risk of ≥10%.
Citation: U.S. Preventive Services Task Force. Draft recommendation statement: statin use for the primary prevention of cardiovascular disease in adults: preventive medication. Available at:
Clinical question: Is there a clinical difference in rates of return of spontaneous circulation (ROSC) and survival to discharge in patients with in-hospital cardiac arrest (IHCA) depending on time of day and day of the week?
Background: Current U.S. data from the American Hospital Association’s “Get with the Guidelines-Resuscitation” (AHA GWTG-R) show hospital survival is lower at night and on the weekends. However, little data exist in the U.K. describing patients already hospitalized and the outcomes of in-hospital cardiac arrest with respect to time of day and day of the week.
Study design: Observational cohort study.
Setting: One hundred forty-six hospitals in the United Kingdom.
Synopsis: Study investigators included 27,700 patients ≥16 years of age receiving chest compressions and/or defibrillation from the U.K. National Cardiac Arrest Audit (NCAA) from April 2011 to September 2013. When compared to weekday daytime, the risk-adjusted rates of ROSC were worse for weekend daytime (odds ratio [OR] ROSC >20 min. 0.88; 95% CI, 0.81–0.95) and nighttime (OR ROSC >20 min. 0.72; 95% CI, 0.68–0.76). Hospital survival had similar trends, with OR for the weekend daytime of 0.72 (95% CI, 0.64–0.80) and OR for nighttime 0.58 (95% CI, 0.54–0.63; P value for all was <0.001).
IHCAs were equally likely to occur during the day and night, and the patients were broadly similar, thus suggesting differences in outcomes were secondary to care differences. However, unmeasured patient characteristics may have affected the outcomes. Given that the study was observational, it is difficult to attribute causality, but results are similar to the large, multicenter study published by the AHA GWTG-R registry.
Bottom line: IHCAs that occur during the night or on weekends have increased odds of worse outcomes.
Citation: Robinson EJ, Smith GB, Power GS, et al. Risk-adjusted survival for adults following in-hospital cardiac arrest by day of week and time of day: observational cohort study [published online ahead of print December 11, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-004223.
Short Take
USPSTF Recommends Statins for More Americans
The U.S. Preventive Services Task Force recommends a low- to moderate-dose statin for adults ages 40–75 with no history of cardiovascular disease and a calculated 10-year cardiovascular disease event risk of ≥10%.
Citation: U.S. Preventive Services Task Force. Draft recommendation statement: statin use for the primary prevention of cardiovascular disease in adults: preventive medication. Available at:
Medicare 'Hospital Star Rating' May Correspond to Patient Outcomes
The Centers for Medicare and Medicaid Services has been letting patients grade their hospital experiences, and those "patient experience scores" may give some insight into a hospital's health outcomes, a new study suggests.
Some people have been concerned that patient experience isn't the most important factor to measure, said coauthor Dr. Ashish K. Jha, of the Harvard T. H. Chan School of Public Health in Boston.
"Medicare has been putting a lot of data out for a long time, but the broad consensus has been it's very hard for consumers to use this info," Jha told Reuters Health by phone. "CMS responded by giving out star ratings that consumers can understand easily."
The five-star rating system is based on patients' answers to 27 questions about a recent hospital stay. Questions cover communication with nurses and doctors, the responsiveness of hospital staff, the hospital's cleanliness and quietness, pain management, communication about medicines, discharge
information, and would they recommend the hospital.
The survey is administered to a random sample of adult patients between 48 hours and six weeks after hospital discharge. Consumers can compare their local hospitals online.
For the new study, the researchers compared the CMS patient-experience ratings at more than 3,000 hospitals in October 2015 to data from those hospitals on death or readmission within 30 days of discharge.
Patients in the study had been hospitalized for myocardial infarction, pneumonia or heart failure.
Of the 3,000 hospitals, 125 had five stars, more than 2,000 had three or four stars, 623 had two stars, and 76 had only one star.
Four and five-star hospitals tended to be small rural nonteaching hospitals in the Midwest.
Five-star hospitals had the lowest average patient death rate, 9.8 percent over the 30 days following discharge, while four three and two-star hospitals all had just over 10 percent mortality rates and one-star hospitals had an average 11.2 percent mortality rate, as reported in a research letter online April 10 in JAMA Internal Medicine.
Five-star hospitals also readmitted less than 20 percent of patients over the next month, while other hospitals all readmitted at least that many.
The data only included Medicare patients, who are older andmay not have the same results as younger patients, and there was not much difference between two, three and four-star hospitals, the authors note.
"If you use the star rating you're more likely to end up at a high quality hospital," Jha said. "But I wouldn't use only the star rating to choose a hospital."
"I don't think these data are enough to by themselves to suggest that (patients) should use the star rating as a single guide to choose an institution," agreed Dr. Joshua J. Fenton of the University of California, Davis, who was not part of the new study.
No large hospitals had five stars, and more than half of the five-star facilities didn't have an intensive care unit, Fenton told Reuters Health by phone.
"I can say from practicing in a rural hospital for a few years and we did not have an ICU, when we hospitalized someone with pneumonia or congestive heart failure, we would certainly not have kept them there if we thought it was likely there would be a complication," he said.
Smaller rural hospitals "select" less acute patients, he said. The authors of the new study tried to account for that, but it may still have affected the results.
The Centers for Medicare and Medicaid Services has been letting patients grade their hospital experiences, and those "patient experience scores" may give some insight into a hospital's health outcomes, a new study suggests.
Some people have been concerned that patient experience isn't the most important factor to measure, said coauthor Dr. Ashish K. Jha, of the Harvard T. H. Chan School of Public Health in Boston.
"Medicare has been putting a lot of data out for a long time, but the broad consensus has been it's very hard for consumers to use this info," Jha told Reuters Health by phone. "CMS responded by giving out star ratings that consumers can understand easily."
The five-star rating system is based on patients' answers to 27 questions about a recent hospital stay. Questions cover communication with nurses and doctors, the responsiveness of hospital staff, the hospital's cleanliness and quietness, pain management, communication about medicines, discharge
information, and would they recommend the hospital.
The survey is administered to a random sample of adult patients between 48 hours and six weeks after hospital discharge. Consumers can compare their local hospitals online.
For the new study, the researchers compared the CMS patient-experience ratings at more than 3,000 hospitals in October 2015 to data from those hospitals on death or readmission within 30 days of discharge.
Patients in the study had been hospitalized for myocardial infarction, pneumonia or heart failure.
Of the 3,000 hospitals, 125 had five stars, more than 2,000 had three or four stars, 623 had two stars, and 76 had only one star.
Four and five-star hospitals tended to be small rural nonteaching hospitals in the Midwest.
Five-star hospitals had the lowest average patient death rate, 9.8 percent over the 30 days following discharge, while four three and two-star hospitals all had just over 10 percent mortality rates and one-star hospitals had an average 11.2 percent mortality rate, as reported in a research letter online April 10 in JAMA Internal Medicine.
Five-star hospitals also readmitted less than 20 percent of patients over the next month, while other hospitals all readmitted at least that many.
The data only included Medicare patients, who are older andmay not have the same results as younger patients, and there was not much difference between two, three and four-star hospitals, the authors note.
"If you use the star rating you're more likely to end up at a high quality hospital," Jha said. "But I wouldn't use only the star rating to choose a hospital."
"I don't think these data are enough to by themselves to suggest that (patients) should use the star rating as a single guide to choose an institution," agreed Dr. Joshua J. Fenton of the University of California, Davis, who was not part of the new study.
No large hospitals had five stars, and more than half of the five-star facilities didn't have an intensive care unit, Fenton told Reuters Health by phone.
"I can say from practicing in a rural hospital for a few years and we did not have an ICU, when we hospitalized someone with pneumonia or congestive heart failure, we would certainly not have kept them there if we thought it was likely there would be a complication," he said.
Smaller rural hospitals "select" less acute patients, he said. The authors of the new study tried to account for that, but it may still have affected the results.
The Centers for Medicare and Medicaid Services has been letting patients grade their hospital experiences, and those "patient experience scores" may give some insight into a hospital's health outcomes, a new study suggests.
Some people have been concerned that patient experience isn't the most important factor to measure, said coauthor Dr. Ashish K. Jha, of the Harvard T. H. Chan School of Public Health in Boston.
"Medicare has been putting a lot of data out for a long time, but the broad consensus has been it's very hard for consumers to use this info," Jha told Reuters Health by phone. "CMS responded by giving out star ratings that consumers can understand easily."
The five-star rating system is based on patients' answers to 27 questions about a recent hospital stay. Questions cover communication with nurses and doctors, the responsiveness of hospital staff, the hospital's cleanliness and quietness, pain management, communication about medicines, discharge
information, and would they recommend the hospital.
The survey is administered to a random sample of adult patients between 48 hours and six weeks after hospital discharge. Consumers can compare their local hospitals online.
For the new study, the researchers compared the CMS patient-experience ratings at more than 3,000 hospitals in October 2015 to data from those hospitals on death or readmission within 30 days of discharge.
Patients in the study had been hospitalized for myocardial infarction, pneumonia or heart failure.
Of the 3,000 hospitals, 125 had five stars, more than 2,000 had three or four stars, 623 had two stars, and 76 had only one star.
Four and five-star hospitals tended to be small rural nonteaching hospitals in the Midwest.
Five-star hospitals had the lowest average patient death rate, 9.8 percent over the 30 days following discharge, while four three and two-star hospitals all had just over 10 percent mortality rates and one-star hospitals had an average 11.2 percent mortality rate, as reported in a research letter online April 10 in JAMA Internal Medicine.
Five-star hospitals also readmitted less than 20 percent of patients over the next month, while other hospitals all readmitted at least that many.
The data only included Medicare patients, who are older andmay not have the same results as younger patients, and there was not much difference between two, three and four-star hospitals, the authors note.
"If you use the star rating you're more likely to end up at a high quality hospital," Jha said. "But I wouldn't use only the star rating to choose a hospital."
"I don't think these data are enough to by themselves to suggest that (patients) should use the star rating as a single guide to choose an institution," agreed Dr. Joshua J. Fenton of the University of California, Davis, who was not part of the new study.
No large hospitals had five stars, and more than half of the five-star facilities didn't have an intensive care unit, Fenton told Reuters Health by phone.
"I can say from practicing in a rural hospital for a few years and we did not have an ICU, when we hospitalized someone with pneumonia or congestive heart failure, we would certainly not have kept them there if we thought it was likely there would be a complication," he said.
Smaller rural hospitals "select" less acute patients, he said. The authors of the new study tried to account for that, but it may still have affected the results.
All-oral combo extends PFS in rel/ref MM

Photo courtesy of ASH
In the phase 3 TOURMALINE-MM1 trial, adding the oral proteasome inhibitor ixazomib to treatment with lenalidomide and dexamethasone significantly extended progression-free survival (PFS), with limited additional toxicity, in patients with relapsed/refractory multiple myeloma (MM).
The median PFS was about 21 months for patients who received ixazomib, lenalidomide, and dexamethasone (IRd) and about 15 months for those who received placebo, lenalidomide, and dexamethasone (Rd).
Gastrointestinal adverse events (AEs), rash, and grade 3/4 thrombocytopenia were more common in the IRd arm than the Rd arm.
These results were published in NEJM. The study was sponsored by Millennium Pharmaceuticals, Inc. Results from this trial were previously presented at ASH 2015, but the data in NEJM differ slightly from that presentation.
“NEJM has published the results of the first phase 3 study supporting an all-oral triplet regimen containing a proteasome inhibitor in multiple myeloma,” said study author Philippe Moreau, MD, of University of Nantes in France.
“The TOURMALINE-MM1 results demonstrated that ixazomib in combination with lenalidomide and dexamethasone is an effective and tolerable oral regimen with a manageable safety profile for patients with relapsed and/or refractory multiple myeloma.”
TOURMALINE-MM1 enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive IRd (n=360) or Rd (n=362). Baseline patient characteristics were similar between the treatment arms. The median age was 66 in both arms (overall range, 30-91), and nearly 60% of patients were male.
About 60% of patients in both arms had received 1 prior therapy, roughly 30% had received 2, and about 10% had received 3. Seventy percent of patients in both arms had received prior treatment with a proteasome inhibitor, and about 55% had received an immunomodulatory drug.
Efficacy
The study’s primary endpoint was PFS. And the researchers saw a significant improvement in PFS for the IRd arm compared to the Rd arm. The median PFS was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
There was a benefit in PFS in the IRd arm across pre-specified patient subgroups, including patients with poor prognosis, such as elderly patients, those who had received 2 or 3 prior therapies, those with advanced stage disease, and those with high-risk cytogenetic abnormalities.
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
The overall response rates were 78% in the IRd arm and 72% in the Rd arm. The complete response rates were 12% and 7%, respectively, and the stringent complete response rates were 2% and <1%, respectively.
The median time to response was 1.1 months in the IRd arm and 1.9 months in the Rd arm. The median duration of response was 20.5 months and 15.0 months, respectively.
Safety
AEs occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively, serious AEs occurred in 47% and 49%, respectively, and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia was more frequent in the IRd arm (12% and 7%, respectively) than in the Rd arm (5% and 4%, respectively). Rash also occurred more frequently in the IRd arm than in the Rd arm (36% and 23%, respectively).
Gastrointestinal AEs were more frequent in the IRd arm than the Rd arm, including diarrhea (45% vs 39%), constipation (35% vs 26%), nausea (29% vs 22%), and vomiting (23% vs 12%).
The incidence of peripheral neuropathy was 27% in the IRd arm and 22% in the Rd arm. Grade 3 events occurred in 2% of patients in each arm, and no grade 4 events were reported.
Roughly the same percentage of patients developed new primary malignant tumors—5% in the IRd arm and 4% in the Rd arm. ![]()
Photo courtesy of ASH
In the phase 3 TOURMALINE-MM1 trial, adding the oral proteasome inhibitor ixazomib to treatment with lenalidomide and dexamethasone significantly extended progression-free survival (PFS), with limited additional toxicity, in patients with relapsed/refractory multiple myeloma (MM).
The median PFS was about 21 months for patients who received ixazomib, lenalidomide, and dexamethasone (IRd) and about 15 months for those who received placebo, lenalidomide, and dexamethasone (Rd).
Gastrointestinal adverse events (AEs), rash, and grade 3/4 thrombocytopenia were more common in the IRd arm than the Rd arm.
These results were published in NEJM. The study was sponsored by Millennium Pharmaceuticals, Inc. Results from this trial were previously presented at ASH 2015, but the data in NEJM differ slightly from that presentation.
“NEJM has published the results of the first phase 3 study supporting an all-oral triplet regimen containing a proteasome inhibitor in multiple myeloma,” said study author Philippe Moreau, MD, of University of Nantes in France.
“The TOURMALINE-MM1 results demonstrated that ixazomib in combination with lenalidomide and dexamethasone is an effective and tolerable oral regimen with a manageable safety profile for patients with relapsed and/or refractory multiple myeloma.”
TOURMALINE-MM1 enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive IRd (n=360) or Rd (n=362). Baseline patient characteristics were similar between the treatment arms. The median age was 66 in both arms (overall range, 30-91), and nearly 60% of patients were male.
About 60% of patients in both arms had received 1 prior therapy, roughly 30% had received 2, and about 10% had received 3. Seventy percent of patients in both arms had received prior treatment with a proteasome inhibitor, and about 55% had received an immunomodulatory drug.
Efficacy
The study’s primary endpoint was PFS. And the researchers saw a significant improvement in PFS for the IRd arm compared to the Rd arm. The median PFS was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
There was a benefit in PFS in the IRd arm across pre-specified patient subgroups, including patients with poor prognosis, such as elderly patients, those who had received 2 or 3 prior therapies, those with advanced stage disease, and those with high-risk cytogenetic abnormalities.
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
The overall response rates were 78% in the IRd arm and 72% in the Rd arm. The complete response rates were 12% and 7%, respectively, and the stringent complete response rates were 2% and <1%, respectively.
The median time to response was 1.1 months in the IRd arm and 1.9 months in the Rd arm. The median duration of response was 20.5 months and 15.0 months, respectively.
Safety
AEs occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively, serious AEs occurred in 47% and 49%, respectively, and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia was more frequent in the IRd arm (12% and 7%, respectively) than in the Rd arm (5% and 4%, respectively). Rash also occurred more frequently in the IRd arm than in the Rd arm (36% and 23%, respectively).
Gastrointestinal AEs were more frequent in the IRd arm than the Rd arm, including diarrhea (45% vs 39%), constipation (35% vs 26%), nausea (29% vs 22%), and vomiting (23% vs 12%).
The incidence of peripheral neuropathy was 27% in the IRd arm and 22% in the Rd arm. Grade 3 events occurred in 2% of patients in each arm, and no grade 4 events were reported.
Roughly the same percentage of patients developed new primary malignant tumors—5% in the IRd arm and 4% in the Rd arm. ![]()
Photo courtesy of ASH
In the phase 3 TOURMALINE-MM1 trial, adding the oral proteasome inhibitor ixazomib to treatment with lenalidomide and dexamethasone significantly extended progression-free survival (PFS), with limited additional toxicity, in patients with relapsed/refractory multiple myeloma (MM).
The median PFS was about 21 months for patients who received ixazomib, lenalidomide, and dexamethasone (IRd) and about 15 months for those who received placebo, lenalidomide, and dexamethasone (Rd).
Gastrointestinal adverse events (AEs), rash, and grade 3/4 thrombocytopenia were more common in the IRd arm than the Rd arm.
These results were published in NEJM. The study was sponsored by Millennium Pharmaceuticals, Inc. Results from this trial were previously presented at ASH 2015, but the data in NEJM differ slightly from that presentation.
“NEJM has published the results of the first phase 3 study supporting an all-oral triplet regimen containing a proteasome inhibitor in multiple myeloma,” said study author Philippe Moreau, MD, of University of Nantes in France.
“The TOURMALINE-MM1 results demonstrated that ixazomib in combination with lenalidomide and dexamethasone is an effective and tolerable oral regimen with a manageable safety profile for patients with relapsed and/or refractory multiple myeloma.”
TOURMALINE-MM1 enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive IRd (n=360) or Rd (n=362). Baseline patient characteristics were similar between the treatment arms. The median age was 66 in both arms (overall range, 30-91), and nearly 60% of patients were male.
About 60% of patients in both arms had received 1 prior therapy, roughly 30% had received 2, and about 10% had received 3. Seventy percent of patients in both arms had received prior treatment with a proteasome inhibitor, and about 55% had received an immunomodulatory drug.
Efficacy
The study’s primary endpoint was PFS. And the researchers saw a significant improvement in PFS for the IRd arm compared to the Rd arm. The median PFS was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
There was a benefit in PFS in the IRd arm across pre-specified patient subgroups, including patients with poor prognosis, such as elderly patients, those who had received 2 or 3 prior therapies, those with advanced stage disease, and those with high-risk cytogenetic abnormalities.
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
The overall response rates were 78% in the IRd arm and 72% in the Rd arm. The complete response rates were 12% and 7%, respectively, and the stringent complete response rates were 2% and <1%, respectively.
The median time to response was 1.1 months in the IRd arm and 1.9 months in the Rd arm. The median duration of response was 20.5 months and 15.0 months, respectively.
Safety
AEs occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively, serious AEs occurred in 47% and 49%, respectively, and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia was more frequent in the IRd arm (12% and 7%, respectively) than in the Rd arm (5% and 4%, respectively). Rash also occurred more frequently in the IRd arm than in the Rd arm (36% and 23%, respectively).
Gastrointestinal AEs were more frequent in the IRd arm than the Rd arm, including diarrhea (45% vs 39%), constipation (35% vs 26%), nausea (29% vs 22%), and vomiting (23% vs 12%).
The incidence of peripheral neuropathy was 27% in the IRd arm and 22% in the Rd arm. Grade 3 events occurred in 2% of patients in each arm, and no grade 4 events were reported.
Roughly the same percentage of patients developed new primary malignant tumors—5% in the IRd arm and 4% in the Rd arm. ![]()
Biomarker may predict sensitivity to PIs in MM

in a thermal cycler
Photo by Karl Mumm
Measuring expression of the gene TJP1 could help determine which multiple myeloma (MM) patients are most likely to benefit from treatment with proteasome inhibitors (PIs), according to a study published in Cancer Cell.
Investigators found that TJP1 enhanced PI sensitivity in vitro and in vivo.
When they analyzed patient data, the team found that high TJP1 expression in patients’ MM cells was associated with a significantly higher likelihood of responding to bortezomib and a longer response duration.
“Proteasome inhibitors form the cornerstone of our standard therapy for multiple myeloma,” said study author Robert Orlowski, MD, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“However, no biomarkers have been clinically validated that can identify patients most likely to respond to this treatment. Our findings provide a rationale for use of TJP1 as the first biomarker to select patients who are most and least likely to benefit from proteasome inhibitors.”
At the start of this study, Dr Orlowski and his colleagues examined gene-expression profiles of ANBL-6 and KAS-6/1 wild-type and bortezomib-resistant MM cells and found that TJP1 was downregulated in the resistant cells.
To further study the role of TJP1 in PI resistance, the investigators conducted experiments with RPMI 8226 and U266 MM cell lines (models that expressed high TJP1 levels) and MOLP-8 (a model that expressed low levels).
They found that knocking down TJP1 in RPMI 8226 and U266 cells with short hairpin RNA (shRNA) preserved the cells’ viability after exposure to bortezomib or carfilzomib. On the other hand, TJP1 overexpression sensitized MOLP-8 cells to the PIs.
In mice, RPMI 8226/TJP1 shRNA tumors were less sensitive to bortezomib than RPMI 8226/control tumors. And mice with MOLP-8/TJP1 shRNA tumors had a greater reduction in tumor growth after bortezomib treatment than MOLP-8/control mice.
Further investigation revealed that TJP1 modulates signaling through a pathway involving EGFR, JAK1, and STAT3. This finding supports the hypothesis that plasma cells expressing low TJP1 levels have both high EGFR/JAK1/STAT3 activity and high proteasome content.
“Therefore, these plasma cells were resistant to proteasome inhibitors,” Dr Orlowski explained. “Moreover, they demonstrated a previously unknown role for EGFR signaling in myeloma and for STAT3 in controlling the level of proteasomes in cells and, therefore, the cell’s ability to break down proteins.”
“This study allows us to identify promising future directions to overcome proteasome inhibitor resistance in patients with high signaling through the EGFR/JAK1/STAT3 pathway by offering combination therapies such as bortezomib with either the EGFR inhibitor erlotinib or a JAK1 inhibitor such as ruxolitinib.”
Finally, Dr Orlowski and his colleagues found that patients whose MM cells expressed low TJP1 levels were significantly less likely to achieve a response or benefit from bortezomib.
Patients who achieved a response after bortezomib across multiple studies had significantly higher TJP1 expression than nonresponders. And patients with the highest TJP1 expression levels had the longest time to progression. ![]()
in a thermal cycler
Photo by Karl Mumm
Measuring expression of the gene TJP1 could help determine which multiple myeloma (MM) patients are most likely to benefit from treatment with proteasome inhibitors (PIs), according to a study published in Cancer Cell.
Investigators found that TJP1 enhanced PI sensitivity in vitro and in vivo.
When they analyzed patient data, the team found that high TJP1 expression in patients’ MM cells was associated with a significantly higher likelihood of responding to bortezomib and a longer response duration.
“Proteasome inhibitors form the cornerstone of our standard therapy for multiple myeloma,” said study author Robert Orlowski, MD, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“However, no biomarkers have been clinically validated that can identify patients most likely to respond to this treatment. Our findings provide a rationale for use of TJP1 as the first biomarker to select patients who are most and least likely to benefit from proteasome inhibitors.”
At the start of this study, Dr Orlowski and his colleagues examined gene-expression profiles of ANBL-6 and KAS-6/1 wild-type and bortezomib-resistant MM cells and found that TJP1 was downregulated in the resistant cells.
To further study the role of TJP1 in PI resistance, the investigators conducted experiments with RPMI 8226 and U266 MM cell lines (models that expressed high TJP1 levels) and MOLP-8 (a model that expressed low levels).
They found that knocking down TJP1 in RPMI 8226 and U266 cells with short hairpin RNA (shRNA) preserved the cells’ viability after exposure to bortezomib or carfilzomib. On the other hand, TJP1 overexpression sensitized MOLP-8 cells to the PIs.
In mice, RPMI 8226/TJP1 shRNA tumors were less sensitive to bortezomib than RPMI 8226/control tumors. And mice with MOLP-8/TJP1 shRNA tumors had a greater reduction in tumor growth after bortezomib treatment than MOLP-8/control mice.
Further investigation revealed that TJP1 modulates signaling through a pathway involving EGFR, JAK1, and STAT3. This finding supports the hypothesis that plasma cells expressing low TJP1 levels have both high EGFR/JAK1/STAT3 activity and high proteasome content.
“Therefore, these plasma cells were resistant to proteasome inhibitors,” Dr Orlowski explained. “Moreover, they demonstrated a previously unknown role for EGFR signaling in myeloma and for STAT3 in controlling the level of proteasomes in cells and, therefore, the cell’s ability to break down proteins.”
“This study allows us to identify promising future directions to overcome proteasome inhibitor resistance in patients with high signaling through the EGFR/JAK1/STAT3 pathway by offering combination therapies such as bortezomib with either the EGFR inhibitor erlotinib or a JAK1 inhibitor such as ruxolitinib.”
Finally, Dr Orlowski and his colleagues found that patients whose MM cells expressed low TJP1 levels were significantly less likely to achieve a response or benefit from bortezomib.
Patients who achieved a response after bortezomib across multiple studies had significantly higher TJP1 expression than nonresponders. And patients with the highest TJP1 expression levels had the longest time to progression. ![]()
in a thermal cycler
Photo by Karl Mumm
Measuring expression of the gene TJP1 could help determine which multiple myeloma (MM) patients are most likely to benefit from treatment with proteasome inhibitors (PIs), according to a study published in Cancer Cell.
Investigators found that TJP1 enhanced PI sensitivity in vitro and in vivo.
When they analyzed patient data, the team found that high TJP1 expression in patients’ MM cells was associated with a significantly higher likelihood of responding to bortezomib and a longer response duration.
“Proteasome inhibitors form the cornerstone of our standard therapy for multiple myeloma,” said study author Robert Orlowski, MD, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“However, no biomarkers have been clinically validated that can identify patients most likely to respond to this treatment. Our findings provide a rationale for use of TJP1 as the first biomarker to select patients who are most and least likely to benefit from proteasome inhibitors.”
At the start of this study, Dr Orlowski and his colleagues examined gene-expression profiles of ANBL-6 and KAS-6/1 wild-type and bortezomib-resistant MM cells and found that TJP1 was downregulated in the resistant cells.
To further study the role of TJP1 in PI resistance, the investigators conducted experiments with RPMI 8226 and U266 MM cell lines (models that expressed high TJP1 levels) and MOLP-8 (a model that expressed low levels).
They found that knocking down TJP1 in RPMI 8226 and U266 cells with short hairpin RNA (shRNA) preserved the cells’ viability after exposure to bortezomib or carfilzomib. On the other hand, TJP1 overexpression sensitized MOLP-8 cells to the PIs.
In mice, RPMI 8226/TJP1 shRNA tumors were less sensitive to bortezomib than RPMI 8226/control tumors. And mice with MOLP-8/TJP1 shRNA tumors had a greater reduction in tumor growth after bortezomib treatment than MOLP-8/control mice.
Further investigation revealed that TJP1 modulates signaling through a pathway involving EGFR, JAK1, and STAT3. This finding supports the hypothesis that plasma cells expressing low TJP1 levels have both high EGFR/JAK1/STAT3 activity and high proteasome content.
“Therefore, these plasma cells were resistant to proteasome inhibitors,” Dr Orlowski explained. “Moreover, they demonstrated a previously unknown role for EGFR signaling in myeloma and for STAT3 in controlling the level of proteasomes in cells and, therefore, the cell’s ability to break down proteins.”
“This study allows us to identify promising future directions to overcome proteasome inhibitor resistance in patients with high signaling through the EGFR/JAK1/STAT3 pathway by offering combination therapies such as bortezomib with either the EGFR inhibitor erlotinib or a JAK1 inhibitor such as ruxolitinib.”
Finally, Dr Orlowski and his colleagues found that patients whose MM cells expressed low TJP1 levels were significantly less likely to achieve a response or benefit from bortezomib.
Patients who achieved a response after bortezomib across multiple studies had significantly higher TJP1 expression than nonresponders. And patients with the highest TJP1 expression levels had the longest time to progression. ![]()
Cancer diagnosis linked to mental health disorders

A recent cancer diagnosis is associated with an increased risk for mental health disorders and increased use of psychiatric medications, according to a large, nationwide study conducted in Sweden.
Overall, there was an increased risk of mental health disorders from 10 months before a cancer diagnosis that peaked during the first week after diagnosis and decreased after that, although the risk remained elevated at 10 years after diagnosis.
In addition, there was an increased use of psychiatric medications from 1 month before cancer diagnosis that peaked at about 3 months after diagnosis and remained elevated 2 years after diagnosis.
Donghao Lu, MD, of the Karolinska Institutet in Stockholm, Sweden and colleagues conducted this study and reported the results in JAMA Oncology.
The study included 304,118 patients with cancer and 3,041,174 cancer-free individuals randomly selected from the Swedish population for comparison.
The researchers investigated changes in risk for several common and potentially stress-related mental disorders—including depression, anxiety, substance abuse, somatoform/conversion disorder, and stress reaction/adjustment disorder—from the cancer diagnostic workup through to post-diagnosis.
They found the relative rate for all of the mental disorders studied started to increase from 10 months before cancer diagnosis, with a hazard ratio [HR] of 1.1 (95%CI, 1.1-1.2).
The rate peaked during the first week after diagnosis, with an HR of 6.7 (95%CI, 6.1-7.4). It decreased rapidly thereafter but was still elevated 10 years after diagnosis, with an HR of 1.1 (95%CI, 1.1-1.2).
The rate elevation was clear for all of the main cancers, including hematologic malignancies, except for nonmelanoma skin cancer.
Among the cancer patients, the mental disorder with the highest cumulative incidence was depression. This was followed by anxiety and stress reaction/adjustment disorder.
When compared to controls, the cancer patients had a higher cumulative incidence of most of the mental disorders. The exception was somatoform/conversion disorder.
The researchers also examined the use of psychiatric medications for patients with cancer to assess milder mental health conditions and symptoms.
The team found an increased use of psychiatric medications in cancer patients compared to controls, from 1 month before diagnosis—12.2% vs 11.7% (P=0.04)—that peaked at about 3 months after diagnosis—18.1% vs 11.9% (P<0.001)—and was still elevated 2 years after diagnosis—15.4% vs 12.7% (P<0.001).
The researchers said the results of this study support the existing guidelines of integrating psychological management into cancer care and call for extended vigilance for multiple mental disorders starting from the time of the cancer diagnostic workup. ![]()
A recent cancer diagnosis is associated with an increased risk for mental health disorders and increased use of psychiatric medications, according to a large, nationwide study conducted in Sweden.
Overall, there was an increased risk of mental health disorders from 10 months before a cancer diagnosis that peaked during the first week after diagnosis and decreased after that, although the risk remained elevated at 10 years after diagnosis.
In addition, there was an increased use of psychiatric medications from 1 month before cancer diagnosis that peaked at about 3 months after diagnosis and remained elevated 2 years after diagnosis.
Donghao Lu, MD, of the Karolinska Institutet in Stockholm, Sweden and colleagues conducted this study and reported the results in JAMA Oncology.
The study included 304,118 patients with cancer and 3,041,174 cancer-free individuals randomly selected from the Swedish population for comparison.
The researchers investigated changes in risk for several common and potentially stress-related mental disorders—including depression, anxiety, substance abuse, somatoform/conversion disorder, and stress reaction/adjustment disorder—from the cancer diagnostic workup through to post-diagnosis.
They found the relative rate for all of the mental disorders studied started to increase from 10 months before cancer diagnosis, with a hazard ratio [HR] of 1.1 (95%CI, 1.1-1.2).
The rate peaked during the first week after diagnosis, with an HR of 6.7 (95%CI, 6.1-7.4). It decreased rapidly thereafter but was still elevated 10 years after diagnosis, with an HR of 1.1 (95%CI, 1.1-1.2).
The rate elevation was clear for all of the main cancers, including hematologic malignancies, except for nonmelanoma skin cancer.
Among the cancer patients, the mental disorder with the highest cumulative incidence was depression. This was followed by anxiety and stress reaction/adjustment disorder.
When compared to controls, the cancer patients had a higher cumulative incidence of most of the mental disorders. The exception was somatoform/conversion disorder.
The researchers also examined the use of psychiatric medications for patients with cancer to assess milder mental health conditions and symptoms.
The team found an increased use of psychiatric medications in cancer patients compared to controls, from 1 month before diagnosis—12.2% vs 11.7% (P=0.04)—that peaked at about 3 months after diagnosis—18.1% vs 11.9% (P<0.001)—and was still elevated 2 years after diagnosis—15.4% vs 12.7% (P<0.001).
The researchers said the results of this study support the existing guidelines of integrating psychological management into cancer care and call for extended vigilance for multiple mental disorders starting from the time of the cancer diagnostic workup. ![]()
A recent cancer diagnosis is associated with an increased risk for mental health disorders and increased use of psychiatric medications, according to a large, nationwide study conducted in Sweden.
Overall, there was an increased risk of mental health disorders from 10 months before a cancer diagnosis that peaked during the first week after diagnosis and decreased after that, although the risk remained elevated at 10 years after diagnosis.
In addition, there was an increased use of psychiatric medications from 1 month before cancer diagnosis that peaked at about 3 months after diagnosis and remained elevated 2 years after diagnosis.
Donghao Lu, MD, of the Karolinska Institutet in Stockholm, Sweden and colleagues conducted this study and reported the results in JAMA Oncology.
The study included 304,118 patients with cancer and 3,041,174 cancer-free individuals randomly selected from the Swedish population for comparison.
The researchers investigated changes in risk for several common and potentially stress-related mental disorders—including depression, anxiety, substance abuse, somatoform/conversion disorder, and stress reaction/adjustment disorder—from the cancer diagnostic workup through to post-diagnosis.
They found the relative rate for all of the mental disorders studied started to increase from 10 months before cancer diagnosis, with a hazard ratio [HR] of 1.1 (95%CI, 1.1-1.2).
The rate peaked during the first week after diagnosis, with an HR of 6.7 (95%CI, 6.1-7.4). It decreased rapidly thereafter but was still elevated 10 years after diagnosis, with an HR of 1.1 (95%CI, 1.1-1.2).
The rate elevation was clear for all of the main cancers, including hematologic malignancies, except for nonmelanoma skin cancer.
Among the cancer patients, the mental disorder with the highest cumulative incidence was depression. This was followed by anxiety and stress reaction/adjustment disorder.
When compared to controls, the cancer patients had a higher cumulative incidence of most of the mental disorders. The exception was somatoform/conversion disorder.
The researchers also examined the use of psychiatric medications for patients with cancer to assess milder mental health conditions and symptoms.
The team found an increased use of psychiatric medications in cancer patients compared to controls, from 1 month before diagnosis—12.2% vs 11.7% (P=0.04)—that peaked at about 3 months after diagnosis—18.1% vs 11.9% (P<0.001)—and was still elevated 2 years after diagnosis—15.4% vs 12.7% (P<0.001).
The researchers said the results of this study support the existing guidelines of integrating psychological management into cancer care and call for extended vigilance for multiple mental disorders starting from the time of the cancer diagnostic workup. ![]()