User login
Ectopic pregnancy misdiagnosed

Ectopic pregnancy misdiagnosed
When a patient called her ObGyn (Dr. A) to report that she was 6 weeks' pregnant and had lower abdominal pain, she was seen by his partner (Dr. B). Dr. B could not identify an intrauterine pregnancy using ultrasonography (US), but the patient's hCG level was highly suggestive of an ectopic pregnancy. The next day, Dr. B performed exploratory laparoscopy, found no evidence of an ectopic pregnancy, and removed the patient's appendix. He continued to be concerned about the possibility of an ectopic pregnancy and suggested that the patient terminate the pregnancy. The next day he prescribed methotrexate. A week later, US revealed a fetus in utero with a beating heart. Because of the likelihood of birth defects after methotrexate use, Dr. B recommended terminating the pregnancy; an abortion was performed a month later.
PATIENT’S CLAIM:
Dr. B should have waited for the pathology report on the appendix and repeated the US before rushing into advising termination of pregnancy.
PHYSICIAN’S CLAIM :
Dr. B acted reasonably based on the patient's symptoms.
VERDICT:
A Kentucky defense verdict was returned.
Related article:
Stop using the hCG discriminatory zone of 1,500 to 2,000 mIU/mL to guide intervention during early pregnancy
Hemorrhage after trocar insertion
A gynecologist performed laparoscopic hysterectomy on his 46-year-old patient. During trocar insertion, the patient's iliac artery, iliac vein, and small bowel were injured. The patient hemorrhaged and went into cardiac arrest. The patient was given several transfusions and the injuries were repaired.
One day after discharge, she returned to the hospital with symptoms of an embolism; she was treated with anticoagulants for 1 year. A year after surgery, she was informed that she was transfused during surgery with HIV-positive blood. Her initial HIV test came back negative.
PATIENT’S CLAIM:
The gynecologist deviated from the standard of care by performing a "blind" trocar insertion, which caused the major vessels to be more susceptible to injury.
PHYSICIAN’S DEFENSE:
There was no deviation from the standard of care. Blind insertion of a trocar is an acceptable procedure.
VERDICT:
A $383,000 Illinois verdict was returned.
Related article:
How to avoid major vessel injury during gynecologic laparoscopy
Delay in ovarian cancer diagnosis: $1.9M settlement
A 64-year-old woman reported worsening abdominal pain, fatigue, and unexplained weight loss to her primary care physician. The physician did not order tests to assess the patient's status; he diagnosed gastritis. Several months later the patient saw another physician, who ordered imaging and identified stage IV ovarian clear cell carcinoma.
PATIENT’S CLAIM:
Timely imaging would have diagnosed ovarian cancer at stage I or II and given her a 90% survival rate at 10 years. Due to the diagnostic delay, her survival rate was less than 10% at 10 years.
PHYSICIAN’S DEFENSE:
The case settled before trial.
VERDICT:
A $1.9 million Illinois settlement was reached.
Late breast cancer diagnosis: $1.7M settlement
When a 25-year-old woman found a lump in her left breast she saw her gynecologist, who recommended US and fine-needle aspiration biopsy. US results indicated possible cancer; biopsy results were reported as negative for cancer. No further action was taken.
Eight months later, a second physician diagnosed stage IV breast cancer requiring chemotherapy, radiation therapy, and multiple surgeries.
PATIENT’S CLAIM:
The radiologist misread the fine-needle aspiration biopsy results. The gynecologist should have ordered a core needle biopsy because it is more reliable.
PHYSICIAN’S DEFENSE:
The case was settled during the trial.
VERDICT:
A $3.5 million Illinois settlement was reached.
Perforated colon after oophorectomy
A 55-year-old woman underwent laparoscopic oophorectomy to address pelvic pain and a right ovarian mass. Following surgery she developed peritonitis and sepsis. She underwent a colon resection with colostomy and had severe keloid scarring.
PATIENT’S CLAIM:
The surgeon was well aware of her history of extensive pelvic adhesions. Given her medical history, he should have performed an open laparotomy.
PHYSICIAN’S DEFENSE:
The case settled during trial.
VERDICT:
A $700,000 Illinois settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Ectopic pregnancy misdiagnosed
When a patient called her ObGyn (Dr. A) to report that she was 6 weeks' pregnant and had lower abdominal pain, she was seen by his partner (Dr. B). Dr. B could not identify an intrauterine pregnancy using ultrasonography (US), but the patient's hCG level was highly suggestive of an ectopic pregnancy. The next day, Dr. B performed exploratory laparoscopy, found no evidence of an ectopic pregnancy, and removed the patient's appendix. He continued to be concerned about the possibility of an ectopic pregnancy and suggested that the patient terminate the pregnancy. The next day he prescribed methotrexate. A week later, US revealed a fetus in utero with a beating heart. Because of the likelihood of birth defects after methotrexate use, Dr. B recommended terminating the pregnancy; an abortion was performed a month later.
PATIENT’S CLAIM:
Dr. B should have waited for the pathology report on the appendix and repeated the US before rushing into advising termination of pregnancy.
PHYSICIAN’S CLAIM :
Dr. B acted reasonably based on the patient's symptoms.
VERDICT:
A Kentucky defense verdict was returned.
Related article:
Stop using the hCG discriminatory zone of 1,500 to 2,000 mIU/mL to guide intervention during early pregnancy
Hemorrhage after trocar insertion
A gynecologist performed laparoscopic hysterectomy on his 46-year-old patient. During trocar insertion, the patient's iliac artery, iliac vein, and small bowel were injured. The patient hemorrhaged and went into cardiac arrest. The patient was given several transfusions and the injuries were repaired.
One day after discharge, she returned to the hospital with symptoms of an embolism; she was treated with anticoagulants for 1 year. A year after surgery, she was informed that she was transfused during surgery with HIV-positive blood. Her initial HIV test came back negative.
PATIENT’S CLAIM:
The gynecologist deviated from the standard of care by performing a "blind" trocar insertion, which caused the major vessels to be more susceptible to injury.
PHYSICIAN’S DEFENSE:
There was no deviation from the standard of care. Blind insertion of a trocar is an acceptable procedure.
VERDICT:
A $383,000 Illinois verdict was returned.
Related article:
How to avoid major vessel injury during gynecologic laparoscopy
Delay in ovarian cancer diagnosis: $1.9M settlement
A 64-year-old woman reported worsening abdominal pain, fatigue, and unexplained weight loss to her primary care physician. The physician did not order tests to assess the patient's status; he diagnosed gastritis. Several months later the patient saw another physician, who ordered imaging and identified stage IV ovarian clear cell carcinoma.
PATIENT’S CLAIM:
Timely imaging would have diagnosed ovarian cancer at stage I or II and given her a 90% survival rate at 10 years. Due to the diagnostic delay, her survival rate was less than 10% at 10 years.
PHYSICIAN’S DEFENSE:
The case settled before trial.
VERDICT:
A $1.9 million Illinois settlement was reached.
Late breast cancer diagnosis: $1.7M settlement
When a 25-year-old woman found a lump in her left breast she saw her gynecologist, who recommended US and fine-needle aspiration biopsy. US results indicated possible cancer; biopsy results were reported as negative for cancer. No further action was taken.
Eight months later, a second physician diagnosed stage IV breast cancer requiring chemotherapy, radiation therapy, and multiple surgeries.
PATIENT’S CLAIM:
The radiologist misread the fine-needle aspiration biopsy results. The gynecologist should have ordered a core needle biopsy because it is more reliable.
PHYSICIAN’S DEFENSE:
The case was settled during the trial.
VERDICT:
A $3.5 million Illinois settlement was reached.
Perforated colon after oophorectomy
A 55-year-old woman underwent laparoscopic oophorectomy to address pelvic pain and a right ovarian mass. Following surgery she developed peritonitis and sepsis. She underwent a colon resection with colostomy and had severe keloid scarring.
PATIENT’S CLAIM:
The surgeon was well aware of her history of extensive pelvic adhesions. Given her medical history, he should have performed an open laparotomy.
PHYSICIAN’S DEFENSE:
The case settled during trial.
VERDICT:
A $700,000 Illinois settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Ectopic pregnancy misdiagnosed
When a patient called her ObGyn (Dr. A) to report that she was 6 weeks' pregnant and had lower abdominal pain, she was seen by his partner (Dr. B). Dr. B could not identify an intrauterine pregnancy using ultrasonography (US), but the patient's hCG level was highly suggestive of an ectopic pregnancy. The next day, Dr. B performed exploratory laparoscopy, found no evidence of an ectopic pregnancy, and removed the patient's appendix. He continued to be concerned about the possibility of an ectopic pregnancy and suggested that the patient terminate the pregnancy. The next day he prescribed methotrexate. A week later, US revealed a fetus in utero with a beating heart. Because of the likelihood of birth defects after methotrexate use, Dr. B recommended terminating the pregnancy; an abortion was performed a month later.
PATIENT’S CLAIM:
Dr. B should have waited for the pathology report on the appendix and repeated the US before rushing into advising termination of pregnancy.
PHYSICIAN’S CLAIM :
Dr. B acted reasonably based on the patient's symptoms.
VERDICT:
A Kentucky defense verdict was returned.
Related article:
Stop using the hCG discriminatory zone of 1,500 to 2,000 mIU/mL to guide intervention during early pregnancy
Hemorrhage after trocar insertion
A gynecologist performed laparoscopic hysterectomy on his 46-year-old patient. During trocar insertion, the patient's iliac artery, iliac vein, and small bowel were injured. The patient hemorrhaged and went into cardiac arrest. The patient was given several transfusions and the injuries were repaired.
One day after discharge, she returned to the hospital with symptoms of an embolism; she was treated with anticoagulants for 1 year. A year after surgery, she was informed that she was transfused during surgery with HIV-positive blood. Her initial HIV test came back negative.
PATIENT’S CLAIM:
The gynecologist deviated from the standard of care by performing a "blind" trocar insertion, which caused the major vessels to be more susceptible to injury.
PHYSICIAN’S DEFENSE:
There was no deviation from the standard of care. Blind insertion of a trocar is an acceptable procedure.
VERDICT:
A $383,000 Illinois verdict was returned.
Related article:
How to avoid major vessel injury during gynecologic laparoscopy
Delay in ovarian cancer diagnosis: $1.9M settlement
A 64-year-old woman reported worsening abdominal pain, fatigue, and unexplained weight loss to her primary care physician. The physician did not order tests to assess the patient's status; he diagnosed gastritis. Several months later the patient saw another physician, who ordered imaging and identified stage IV ovarian clear cell carcinoma.
PATIENT’S CLAIM:
Timely imaging would have diagnosed ovarian cancer at stage I or II and given her a 90% survival rate at 10 years. Due to the diagnostic delay, her survival rate was less than 10% at 10 years.
PHYSICIAN’S DEFENSE:
The case settled before trial.
VERDICT:
A $1.9 million Illinois settlement was reached.
Late breast cancer diagnosis: $1.7M settlement
When a 25-year-old woman found a lump in her left breast she saw her gynecologist, who recommended US and fine-needle aspiration biopsy. US results indicated possible cancer; biopsy results were reported as negative for cancer. No further action was taken.
Eight months later, a second physician diagnosed stage IV breast cancer requiring chemotherapy, radiation therapy, and multiple surgeries.
PATIENT’S CLAIM:
The radiologist misread the fine-needle aspiration biopsy results. The gynecologist should have ordered a core needle biopsy because it is more reliable.
PHYSICIAN’S DEFENSE:
The case was settled during the trial.
VERDICT:
A $3.5 million Illinois settlement was reached.
Perforated colon after oophorectomy
A 55-year-old woman underwent laparoscopic oophorectomy to address pelvic pain and a right ovarian mass. Following surgery she developed peritonitis and sepsis. She underwent a colon resection with colostomy and had severe keloid scarring.
PATIENT’S CLAIM:
The surgeon was well aware of her history of extensive pelvic adhesions. Given her medical history, he should have performed an open laparotomy.
PHYSICIAN’S DEFENSE:
The case settled during trial.
VERDICT:
A $700,000 Illinois settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The New Face of Personalized Medicine in Headache Therapy
RIVIERA BEACH, FL—“How do we take care of patients in 2016?” asked Robert Cowan, MD, at the 43rd Annual Meeting of the Southern Clinical Neurological Society. “We’re using the same model for healthcare delivery we have been using since 2500 BC,” he said. In headache medicine, a patient starts out with a headache and goes to see a primary care doctor. Based on the fund of knowledge that the doctor has in headache, he or she will come up with what hopefully is a reasonable differential diagnosis, work-up, and treatment plan. This approach may be successful or it may not. If it isn’t successful, more time will elapse before the patient is referred to a neurologist or headache specialist.

Robert Cowan, MD
At Stanford University, where Dr. Cowan is a Professor of Neurology, they looked at the patients coming in for headache care. “On average, it took 18 months from the time they went to their primary care doctor with a complaint of headache to the time they were seen at Stanford,” Dr. Cowan said. Eighteen months and a cost of around $12,000, he added.
There are just over 500 board-certified headache specialists in the United States. There are about 60 million people with headache, about 37 million people with migraine, and about 4% of those patients have chronic migraine. “Right now there are not enough specialists,” Dr. Cowan said. “The challenges are economic, geographical, and institutional.” And in some areas of the world, the situation is far worse.
Beyond the problem of scale—the patient population versus the health care providers available to diagnose and treat them—there is, according to Dr. Cowan, a triage problem. Which patients with headache are easily managed and which ones require specialist care? “To be seen at Stanford, there is about a three-month wait right now, despite the fact that we have six board-certified headache specialists in our division,” Dr. Cowan said. “We don’t have effective ways of triaging from primary care through subspecialists.” The solution has been to try to turn primary care doctors into specialists. “It doesn’t make sense to keep turning to the primary care doctor as a gatekeeper for every patient.”
From a time-management and economic perspective, headache care can be viewed as neurology’s loss leader. “On average, a physician spends seven to 20 minutes with a patient,” Dr. Cowan said. “With a complex patient, I can’t get a decent history in an hour. I don’t know how I can get a decent history in seven minutes. If I’m practicing in India or China, I have 2.5 minutes to get a decent history and formulate a treatment plan. There is a disincentive to provide good care. If you are a fee-for-service physician, spending more time costs you money. If you are a salary-based physician, why would you want to see more patients per day? We don’t have great incentives for physicians to fix this.”
Online Patient Prescreening
Technology can help address some of these problems. One solution is prescreening, Dr. Cowan said. “We can collect data before the patient gets the appointment.” Dr. Cowan, Alan Rapoport, MD, and Jim Blythe, PhD, have created a detailed online questionnaire that is very detailed. It takes, in general, about an hour to complete. It generates a narrative report that is tied to a rule engine. The elements in the patient history are compared with International Classification of Headache Disorders (ICHD) diagnostic criteria, and a clinical impression similar to a differential diagnosis is generated. It documents diagnostic red flags, medication history, and other elements. For example, “There are elements in your history that suggest you may have a secondary headache. Here they are. You might want to discuss these with your physician.” The patient can either send that report electronically to his or her primary care physician or print it out as a PDF and carry it. The questionnaire can also be done with voice activation over the phone and faxed to the clinic—a benefit in countries without access to computers or smartphones. One benefit of this online tool is that it saves the physician the time of having to ask basic questions that are already covered in the narrative report.
The online questionnaire Dr. Cowan referred to is part of BonTriage, a start-up he and Drs. Rapoport and Blythe created. It is designed to help triage and monitor patients with headache and bring specialized care to underserved patient populations. At present, the service is free to patients.
“This is not intended as a replacement for an in-person history,” Dr. Cowan said. “But it does save a lot of time. The other advantage of it is that you have expert opinion in advance of the visit. You’ve got a differential that you know is tied to hard data.”
Automated Patient Monitoring
Technology can also facilitate patient monitoring between office visits. There are apps in development that give patients a push notification on their phone—a text message—that asks, “Did you have a headache today?” A yes or no response is recorded and, as appropriate, additional questions are asked. For example, “Did you have trigger exposures?” Some patients say, “My headaches are tied to the weather. I have no control over them.” The same app includes technology to monitor barometric pressure changes, so correlations can be drawn between headaches and weather changes. Another example is sleep. “Every smartphone can monitor your sleep. If you have an iPhone, it has that technology in it. If you put the phone under your pillow it can tell you, using movement as a correlation, how well you slept,” Dr. Cowan said. “It is not as good as a sleep study, but it will, at least, in general terms, tell you if you had good quality sleep.” That data can then be correlated with headache days.
Predictive Modeling
Predictive modeling is also currently available. An iPhone can provide a push notification that says, “You didn’t sleep well last night, there’s a storm front coming in, you might want to skip red wine with dinner because all of these are risk factors for you.” Wearable technology such as Fitbit or Up can monitor heart rate variability and other autonomic changes and suggest that there is an imminent migraine ahead. “By imminent, I mean within the next hour,” Dr. Cowan said. If patients were wearing something similar to the Zecuity patch, they could actually have their phone say, “You’ve got a headache coming, do you want medication?” If the patient responds yes, the patch could be activated and medication delivered. “This is off-the-shelf technology that is available now that we don’t take advantage of,” Dr. Cowan said.
“The app that I was just describing can send information to the cloud that can then be accessed by the physician at any point. For example, the physician could receive an email saying, ‘Patient X had 13 headache days this month, and it is only the 13th day of the month. Last month, she had 13 headache days in the whole month. She had five triptan days last month, already nine triptan days this month. Things are not going well.’” Alerts can be generated. “It is possible to monitor patients in real time without having to bring them into the office,” Dr. Cowan said.
Also in development is a calendar app that can correlate data at the end of each month and generate a printout that can, for example, observe, “More headaches this month. Not responding to acute care medication.” The treating physician can then say, “More headaches? Preventive medicine. Not responding? Change the acute care.” And those clinical decisions can be based on the patient’s own personal data.
Patient Compliance
Technology can also help increase compliance. A company called Proteus has an ingestible sensor that can be put on any pill. When the pill reaches the stomach, the sensor sends a message to a smartphone and the cloud. “So, compliance is no longer subjective. You can actually see when patients are taking their medications and tie that information to data from a wearable device and information entered by the patient,” Dr. Cowan said. This technology is also capable of sending messages to patients saying, when appropriate, “Missed your pill. You might want to take that pill.”
In summary, Dr. Cowan said, “That’s a glimpse as to where we are and what is just around the corner. Everything I described could be happening for every patient today. It is not, but this is what we can do technologically.”
—Glenn S. Williams
RIVIERA BEACH, FL—“How do we take care of patients in 2016?” asked Robert Cowan, MD, at the 43rd Annual Meeting of the Southern Clinical Neurological Society. “We’re using the same model for healthcare delivery we have been using since 2500 BC,” he said. In headache medicine, a patient starts out with a headache and goes to see a primary care doctor. Based on the fund of knowledge that the doctor has in headache, he or she will come up with what hopefully is a reasonable differential diagnosis, work-up, and treatment plan. This approach may be successful or it may not. If it isn’t successful, more time will elapse before the patient is referred to a neurologist or headache specialist.
Robert Cowan, MD
At Stanford University, where Dr. Cowan is a Professor of Neurology, they looked at the patients coming in for headache care. “On average, it took 18 months from the time they went to their primary care doctor with a complaint of headache to the time they were seen at Stanford,” Dr. Cowan said. Eighteen months and a cost of around $12,000, he added.
There are just over 500 board-certified headache specialists in the United States. There are about 60 million people with headache, about 37 million people with migraine, and about 4% of those patients have chronic migraine. “Right now there are not enough specialists,” Dr. Cowan said. “The challenges are economic, geographical, and institutional.” And in some areas of the world, the situation is far worse.
Beyond the problem of scale—the patient population versus the health care providers available to diagnose and treat them—there is, according to Dr. Cowan, a triage problem. Which patients with headache are easily managed and which ones require specialist care? “To be seen at Stanford, there is about a three-month wait right now, despite the fact that we have six board-certified headache specialists in our division,” Dr. Cowan said. “We don’t have effective ways of triaging from primary care through subspecialists.” The solution has been to try to turn primary care doctors into specialists. “It doesn’t make sense to keep turning to the primary care doctor as a gatekeeper for every patient.”
From a time-management and economic perspective, headache care can be viewed as neurology’s loss leader. “On average, a physician spends seven to 20 minutes with a patient,” Dr. Cowan said. “With a complex patient, I can’t get a decent history in an hour. I don’t know how I can get a decent history in seven minutes. If I’m practicing in India or China, I have 2.5 minutes to get a decent history and formulate a treatment plan. There is a disincentive to provide good care. If you are a fee-for-service physician, spending more time costs you money. If you are a salary-based physician, why would you want to see more patients per day? We don’t have great incentives for physicians to fix this.”
Online Patient Prescreening
Technology can help address some of these problems. One solution is prescreening, Dr. Cowan said. “We can collect data before the patient gets the appointment.” Dr. Cowan, Alan Rapoport, MD, and Jim Blythe, PhD, have created a detailed online questionnaire that is very detailed. It takes, in general, about an hour to complete. It generates a narrative report that is tied to a rule engine. The elements in the patient history are compared with International Classification of Headache Disorders (ICHD) diagnostic criteria, and a clinical impression similar to a differential diagnosis is generated. It documents diagnostic red flags, medication history, and other elements. For example, “There are elements in your history that suggest you may have a secondary headache. Here they are. You might want to discuss these with your physician.” The patient can either send that report electronically to his or her primary care physician or print it out as a PDF and carry it. The questionnaire can also be done with voice activation over the phone and faxed to the clinic—a benefit in countries without access to computers or smartphones. One benefit of this online tool is that it saves the physician the time of having to ask basic questions that are already covered in the narrative report.
The online questionnaire Dr. Cowan referred to is part of BonTriage, a start-up he and Drs. Rapoport and Blythe created. It is designed to help triage and monitor patients with headache and bring specialized care to underserved patient populations. At present, the service is free to patients.
“This is not intended as a replacement for an in-person history,” Dr. Cowan said. “But it does save a lot of time. The other advantage of it is that you have expert opinion in advance of the visit. You’ve got a differential that you know is tied to hard data.”
Automated Patient Monitoring
Technology can also facilitate patient monitoring between office visits. There are apps in development that give patients a push notification on their phone—a text message—that asks, “Did you have a headache today?” A yes or no response is recorded and, as appropriate, additional questions are asked. For example, “Did you have trigger exposures?” Some patients say, “My headaches are tied to the weather. I have no control over them.” The same app includes technology to monitor barometric pressure changes, so correlations can be drawn between headaches and weather changes. Another example is sleep. “Every smartphone can monitor your sleep. If you have an iPhone, it has that technology in it. If you put the phone under your pillow it can tell you, using movement as a correlation, how well you slept,” Dr. Cowan said. “It is not as good as a sleep study, but it will, at least, in general terms, tell you if you had good quality sleep.” That data can then be correlated with headache days.
Predictive Modeling
Predictive modeling is also currently available. An iPhone can provide a push notification that says, “You didn’t sleep well last night, there’s a storm front coming in, you might want to skip red wine with dinner because all of these are risk factors for you.” Wearable technology such as Fitbit or Up can monitor heart rate variability and other autonomic changes and suggest that there is an imminent migraine ahead. “By imminent, I mean within the next hour,” Dr. Cowan said. If patients were wearing something similar to the Zecuity patch, they could actually have their phone say, “You’ve got a headache coming, do you want medication?” If the patient responds yes, the patch could be activated and medication delivered. “This is off-the-shelf technology that is available now that we don’t take advantage of,” Dr. Cowan said.
“The app that I was just describing can send information to the cloud that can then be accessed by the physician at any point. For example, the physician could receive an email saying, ‘Patient X had 13 headache days this month, and it is only the 13th day of the month. Last month, she had 13 headache days in the whole month. She had five triptan days last month, already nine triptan days this month. Things are not going well.’” Alerts can be generated. “It is possible to monitor patients in real time without having to bring them into the office,” Dr. Cowan said.
Also in development is a calendar app that can correlate data at the end of each month and generate a printout that can, for example, observe, “More headaches this month. Not responding to acute care medication.” The treating physician can then say, “More headaches? Preventive medicine. Not responding? Change the acute care.” And those clinical decisions can be based on the patient’s own personal data.
Patient Compliance
Technology can also help increase compliance. A company called Proteus has an ingestible sensor that can be put on any pill. When the pill reaches the stomach, the sensor sends a message to a smartphone and the cloud. “So, compliance is no longer subjective. You can actually see when patients are taking their medications and tie that information to data from a wearable device and information entered by the patient,” Dr. Cowan said. This technology is also capable of sending messages to patients saying, when appropriate, “Missed your pill. You might want to take that pill.”
In summary, Dr. Cowan said, “That’s a glimpse as to where we are and what is just around the corner. Everything I described could be happening for every patient today. It is not, but this is what we can do technologically.”
—Glenn S. Williams
RIVIERA BEACH, FL—“How do we take care of patients in 2016?” asked Robert Cowan, MD, at the 43rd Annual Meeting of the Southern Clinical Neurological Society. “We’re using the same model for healthcare delivery we have been using since 2500 BC,” he said. In headache medicine, a patient starts out with a headache and goes to see a primary care doctor. Based on the fund of knowledge that the doctor has in headache, he or she will come up with what hopefully is a reasonable differential diagnosis, work-up, and treatment plan. This approach may be successful or it may not. If it isn’t successful, more time will elapse before the patient is referred to a neurologist or headache specialist.
Robert Cowan, MD
At Stanford University, where Dr. Cowan is a Professor of Neurology, they looked at the patients coming in for headache care. “On average, it took 18 months from the time they went to their primary care doctor with a complaint of headache to the time they were seen at Stanford,” Dr. Cowan said. Eighteen months and a cost of around $12,000, he added.
There are just over 500 board-certified headache specialists in the United States. There are about 60 million people with headache, about 37 million people with migraine, and about 4% of those patients have chronic migraine. “Right now there are not enough specialists,” Dr. Cowan said. “The challenges are economic, geographical, and institutional.” And in some areas of the world, the situation is far worse.
Beyond the problem of scale—the patient population versus the health care providers available to diagnose and treat them—there is, according to Dr. Cowan, a triage problem. Which patients with headache are easily managed and which ones require specialist care? “To be seen at Stanford, there is about a three-month wait right now, despite the fact that we have six board-certified headache specialists in our division,” Dr. Cowan said. “We don’t have effective ways of triaging from primary care through subspecialists.” The solution has been to try to turn primary care doctors into specialists. “It doesn’t make sense to keep turning to the primary care doctor as a gatekeeper for every patient.”
From a time-management and economic perspective, headache care can be viewed as neurology’s loss leader. “On average, a physician spends seven to 20 minutes with a patient,” Dr. Cowan said. “With a complex patient, I can’t get a decent history in an hour. I don’t know how I can get a decent history in seven minutes. If I’m practicing in India or China, I have 2.5 minutes to get a decent history and formulate a treatment plan. There is a disincentive to provide good care. If you are a fee-for-service physician, spending more time costs you money. If you are a salary-based physician, why would you want to see more patients per day? We don’t have great incentives for physicians to fix this.”
Online Patient Prescreening
Technology can help address some of these problems. One solution is prescreening, Dr. Cowan said. “We can collect data before the patient gets the appointment.” Dr. Cowan, Alan Rapoport, MD, and Jim Blythe, PhD, have created a detailed online questionnaire that is very detailed. It takes, in general, about an hour to complete. It generates a narrative report that is tied to a rule engine. The elements in the patient history are compared with International Classification of Headache Disorders (ICHD) diagnostic criteria, and a clinical impression similar to a differential diagnosis is generated. It documents diagnostic red flags, medication history, and other elements. For example, “There are elements in your history that suggest you may have a secondary headache. Here they are. You might want to discuss these with your physician.” The patient can either send that report electronically to his or her primary care physician or print it out as a PDF and carry it. The questionnaire can also be done with voice activation over the phone and faxed to the clinic—a benefit in countries without access to computers or smartphones. One benefit of this online tool is that it saves the physician the time of having to ask basic questions that are already covered in the narrative report.
The online questionnaire Dr. Cowan referred to is part of BonTriage, a start-up he and Drs. Rapoport and Blythe created. It is designed to help triage and monitor patients with headache and bring specialized care to underserved patient populations. At present, the service is free to patients.
“This is not intended as a replacement for an in-person history,” Dr. Cowan said. “But it does save a lot of time. The other advantage of it is that you have expert opinion in advance of the visit. You’ve got a differential that you know is tied to hard data.”
Automated Patient Monitoring
Technology can also facilitate patient monitoring between office visits. There are apps in development that give patients a push notification on their phone—a text message—that asks, “Did you have a headache today?” A yes or no response is recorded and, as appropriate, additional questions are asked. For example, “Did you have trigger exposures?” Some patients say, “My headaches are tied to the weather. I have no control over them.” The same app includes technology to monitor barometric pressure changes, so correlations can be drawn between headaches and weather changes. Another example is sleep. “Every smartphone can monitor your sleep. If you have an iPhone, it has that technology in it. If you put the phone under your pillow it can tell you, using movement as a correlation, how well you slept,” Dr. Cowan said. “It is not as good as a sleep study, but it will, at least, in general terms, tell you if you had good quality sleep.” That data can then be correlated with headache days.
Predictive Modeling
Predictive modeling is also currently available. An iPhone can provide a push notification that says, “You didn’t sleep well last night, there’s a storm front coming in, you might want to skip red wine with dinner because all of these are risk factors for you.” Wearable technology such as Fitbit or Up can monitor heart rate variability and other autonomic changes and suggest that there is an imminent migraine ahead. “By imminent, I mean within the next hour,” Dr. Cowan said. If patients were wearing something similar to the Zecuity patch, they could actually have their phone say, “You’ve got a headache coming, do you want medication?” If the patient responds yes, the patch could be activated and medication delivered. “This is off-the-shelf technology that is available now that we don’t take advantage of,” Dr. Cowan said.
“The app that I was just describing can send information to the cloud that can then be accessed by the physician at any point. For example, the physician could receive an email saying, ‘Patient X had 13 headache days this month, and it is only the 13th day of the month. Last month, she had 13 headache days in the whole month. She had five triptan days last month, already nine triptan days this month. Things are not going well.’” Alerts can be generated. “It is possible to monitor patients in real time without having to bring them into the office,” Dr. Cowan said.
Also in development is a calendar app that can correlate data at the end of each month and generate a printout that can, for example, observe, “More headaches this month. Not responding to acute care medication.” The treating physician can then say, “More headaches? Preventive medicine. Not responding? Change the acute care.” And those clinical decisions can be based on the patient’s own personal data.
Patient Compliance
Technology can also help increase compliance. A company called Proteus has an ingestible sensor that can be put on any pill. When the pill reaches the stomach, the sensor sends a message to a smartphone and the cloud. “So, compliance is no longer subjective. You can actually see when patients are taking their medications and tie that information to data from a wearable device and information entered by the patient,” Dr. Cowan said. This technology is also capable of sending messages to patients saying, when appropriate, “Missed your pill. You might want to take that pill.”
In summary, Dr. Cowan said, “That’s a glimpse as to where we are and what is just around the corner. Everything I described could be happening for every patient today. It is not, but this is what we can do technologically.”
—Glenn S. Williams

FDA approves changing brand name of Brintellix to Trintellix
To avoid confusion with another drug, the Food and Drug Administration has approved a name change request for the antidepressant Brintellix (vortioxetine), according to a press release.
In a Medwatch alert in July 2015, the FDA noted that prescribing and dispensing errors had occurred because of the similarity in names of Brintellix and the blood thinner Brilinta (ticagrelor). Because of the large difference in purpose between the two drugs, Brintellix manufacturer Takeda Pharmaceuticals has renamed the drug to Trintellix, expected to become available in June 2016.
No additional changes will be made to the label or packaging of Trintellix, and the medicine will not change. Drug information content publishers and medication-related electronic system administrators should note that Trintellix will receive a new National Drug Code number.
“Health care professionals should check carefully to make sure they have prescribed or dispensed the correct medicine. During the transition to the new name change from Brintellix to Trintellix, prescribers can reduce the risk of name confusion by including the generic name of the medication they are ordering, in addition to the brand name and indication for use,” the FDA said in its press release.
To avoid confusion with another drug, the Food and Drug Administration has approved a name change request for the antidepressant Brintellix (vortioxetine), according to a press release.
In a Medwatch alert in July 2015, the FDA noted that prescribing and dispensing errors had occurred because of the similarity in names of Brintellix and the blood thinner Brilinta (ticagrelor). Because of the large difference in purpose between the two drugs, Brintellix manufacturer Takeda Pharmaceuticals has renamed the drug to Trintellix, expected to become available in June 2016.
No additional changes will be made to the label or packaging of Trintellix, and the medicine will not change. Drug information content publishers and medication-related electronic system administrators should note that Trintellix will receive a new National Drug Code number.
“Health care professionals should check carefully to make sure they have prescribed or dispensed the correct medicine. During the transition to the new name change from Brintellix to Trintellix, prescribers can reduce the risk of name confusion by including the generic name of the medication they are ordering, in addition to the brand name and indication for use,” the FDA said in its press release.
To avoid confusion with another drug, the Food and Drug Administration has approved a name change request for the antidepressant Brintellix (vortioxetine), according to a press release.
In a Medwatch alert in July 2015, the FDA noted that prescribing and dispensing errors had occurred because of the similarity in names of Brintellix and the blood thinner Brilinta (ticagrelor). Because of the large difference in purpose between the two drugs, Brintellix manufacturer Takeda Pharmaceuticals has renamed the drug to Trintellix, expected to become available in June 2016.
No additional changes will be made to the label or packaging of Trintellix, and the medicine will not change. Drug information content publishers and medication-related electronic system administrators should note that Trintellix will receive a new National Drug Code number.
“Health care professionals should check carefully to make sure they have prescribed or dispensed the correct medicine. During the transition to the new name change from Brintellix to Trintellix, prescribers can reduce the risk of name confusion by including the generic name of the medication they are ordering, in addition to the brand name and indication for use,” the FDA said in its press release.
Webcast: Providing LARC methods of contraception to adolescents
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Emergency contraception: How to choose the right one for your patient
- Contraceptive considerations for women with headache and migraine
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Emergency contraception: How to choose the right one for your patient
- Contraceptive considerations for women with headache and migraine
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Emergency contraception: How to choose the right one for your patient
- Contraceptive considerations for women with headache and migraine
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
Study eyes mortality among octogenarians after emergency Hartmann’s procedure
LOS ANGELES – Patients over the age of 80 who present with diverticulitis requiring an emergent Hartmann’s procedure have a 30-day mortality rate of 20%, results from a study of national data demonstrated.
“Given the high morbidity and mortality described in this study, further work to elucidate whether an elective surgical therapy should be pursued in the octogenarian population is warranted,” lead study author Dr. Ian C. Bostock said in an interview in advance of the annual meeting of the American Society of Colon and Rectal Surgeons.

In an effort to investigate the 30-day outcomes for patients undergoing emergent Hartmann’s procedures for diverticular disease, Dr. Bostock of the department of general surgery at Dartmouth Hitchcock Medical Center, Lebanon, N.H., and his associates queried the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2013 to identify all patients aged 80 years or older who underwent an open and laparoscopic Hartmann’s procedure in an emergency setting for diverticular disease. They divided patients into two groups: those with 30-day postoperative mortality (expired) and those alive after 30 days (alive), and used univariate analysis to assess the risk of mortality and to identify associated risk factors.
Of the 464 patients who met inclusion criteria, 91 expired within 30 days postoperatively, for a mortality rate of 20%. No statistically significant differences were observed between the expired and alive groups in terms of age, gender distribution, body mass index, smoking status, alcohol use, prior chemotherapy/radiotherapy, comorbid conditions such as diabetes, hypertension, current hemodialysis use, and operative time. Factors identified to be associated with a higher risk for death were congestive heart failure (odds ratio, 3.0), steroid use (OR, 3.0), chronic obstructive pulmonary disease (OR, 2.1), and ASA classification of greater than 3 (OR, 2.9). Additionally, the development of postoperative cardiac arrest (OR, 22.9), MI (OR, 8.7), renal failure (OR, 6.3), respiratory failure (OR, 4.7), and septic shock (OR, 5.6) were associated with death. A laparoscopic procedure was shown to have a protective effect (0.169).
“Interestingly, the most common complication in both groups was respiratory failure,” Dr. Bostock said. “These results suggest that the elderly are more prone to respiratory complications as a whole. These results have been corroborated in prior studies in patients exposed to major abdominal operations.”
Dr. Bostock acknowledged certain limitations of the study, including the fact that ACS-NSQIP is unable to track procedure-specific complications that might occur after surgery. “It mainly helps us to determine the morbidity rate after specific types of procedures,” he said. “Additionally, the exact indication for emergent operation in the patients included in our analysis is unknown since we don’t have any access to specific patient data and/or chart review.”
The researchers reported having no financial disclosures.
LOS ANGELES – Patients over the age of 80 who present with diverticulitis requiring an emergent Hartmann’s procedure have a 30-day mortality rate of 20%, results from a study of national data demonstrated.
“Given the high morbidity and mortality described in this study, further work to elucidate whether an elective surgical therapy should be pursued in the octogenarian population is warranted,” lead study author Dr. Ian C. Bostock said in an interview in advance of the annual meeting of the American Society of Colon and Rectal Surgeons.
In an effort to investigate the 30-day outcomes for patients undergoing emergent Hartmann’s procedures for diverticular disease, Dr. Bostock of the department of general surgery at Dartmouth Hitchcock Medical Center, Lebanon, N.H., and his associates queried the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2013 to identify all patients aged 80 years or older who underwent an open and laparoscopic Hartmann’s procedure in an emergency setting for diverticular disease. They divided patients into two groups: those with 30-day postoperative mortality (expired) and those alive after 30 days (alive), and used univariate analysis to assess the risk of mortality and to identify associated risk factors.
Of the 464 patients who met inclusion criteria, 91 expired within 30 days postoperatively, for a mortality rate of 20%. No statistically significant differences were observed between the expired and alive groups in terms of age, gender distribution, body mass index, smoking status, alcohol use, prior chemotherapy/radiotherapy, comorbid conditions such as diabetes, hypertension, current hemodialysis use, and operative time. Factors identified to be associated with a higher risk for death were congestive heart failure (odds ratio, 3.0), steroid use (OR, 3.0), chronic obstructive pulmonary disease (OR, 2.1), and ASA classification of greater than 3 (OR, 2.9). Additionally, the development of postoperative cardiac arrest (OR, 22.9), MI (OR, 8.7), renal failure (OR, 6.3), respiratory failure (OR, 4.7), and septic shock (OR, 5.6) were associated with death. A laparoscopic procedure was shown to have a protective effect (0.169).
“Interestingly, the most common complication in both groups was respiratory failure,” Dr. Bostock said. “These results suggest that the elderly are more prone to respiratory complications as a whole. These results have been corroborated in prior studies in patients exposed to major abdominal operations.”
Dr. Bostock acknowledged certain limitations of the study, including the fact that ACS-NSQIP is unable to track procedure-specific complications that might occur after surgery. “It mainly helps us to determine the morbidity rate after specific types of procedures,” he said. “Additionally, the exact indication for emergent operation in the patients included in our analysis is unknown since we don’t have any access to specific patient data and/or chart review.”
The researchers reported having no financial disclosures.
LOS ANGELES – Patients over the age of 80 who present with diverticulitis requiring an emergent Hartmann’s procedure have a 30-day mortality rate of 20%, results from a study of national data demonstrated.
“Given the high morbidity and mortality described in this study, further work to elucidate whether an elective surgical therapy should be pursued in the octogenarian population is warranted,” lead study author Dr. Ian C. Bostock said in an interview in advance of the annual meeting of the American Society of Colon and Rectal Surgeons.
In an effort to investigate the 30-day outcomes for patients undergoing emergent Hartmann’s procedures for diverticular disease, Dr. Bostock of the department of general surgery at Dartmouth Hitchcock Medical Center, Lebanon, N.H., and his associates queried the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2013 to identify all patients aged 80 years or older who underwent an open and laparoscopic Hartmann’s procedure in an emergency setting for diverticular disease. They divided patients into two groups: those with 30-day postoperative mortality (expired) and those alive after 30 days (alive), and used univariate analysis to assess the risk of mortality and to identify associated risk factors.
Of the 464 patients who met inclusion criteria, 91 expired within 30 days postoperatively, for a mortality rate of 20%. No statistically significant differences were observed between the expired and alive groups in terms of age, gender distribution, body mass index, smoking status, alcohol use, prior chemotherapy/radiotherapy, comorbid conditions such as diabetes, hypertension, current hemodialysis use, and operative time. Factors identified to be associated with a higher risk for death were congestive heart failure (odds ratio, 3.0), steroid use (OR, 3.0), chronic obstructive pulmonary disease (OR, 2.1), and ASA classification of greater than 3 (OR, 2.9). Additionally, the development of postoperative cardiac arrest (OR, 22.9), MI (OR, 8.7), renal failure (OR, 6.3), respiratory failure (OR, 4.7), and septic shock (OR, 5.6) were associated with death. A laparoscopic procedure was shown to have a protective effect (0.169).
“Interestingly, the most common complication in both groups was respiratory failure,” Dr. Bostock said. “These results suggest that the elderly are more prone to respiratory complications as a whole. These results have been corroborated in prior studies in patients exposed to major abdominal operations.”
Dr. Bostock acknowledged certain limitations of the study, including the fact that ACS-NSQIP is unable to track procedure-specific complications that might occur after surgery. “It mainly helps us to determine the morbidity rate after specific types of procedures,” he said. “Additionally, the exact indication for emergent operation in the patients included in our analysis is unknown since we don’t have any access to specific patient data and/or chart review.”
The researchers reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: One in five octogenarians with diverticulitis who undergo an emergency Hartmann’s procedure die within 30 days postoperatively.
Major finding: The 30-day postoperative mortality rate for octogenarians who underwent an emergency Hartmann’s procedure for diverticular disease was 20%.
Data source: An analysis of American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) data from 464 patients aged 80 and older who underwent an open and laparoscopic Hartmann’s procedure in an emergency setting for diverticular disease.
Disclosures: Dr. Bostock reported having no financial disclosures.

Aspirin lowers bile duct cancer risk
Regular aspirin use is associated with an approximately threefold reduction in risk for the three major subtypes of cholangiocarcinoma, results of a case-control study indicate.
In a study comparing patients with bile duct cancers with matched controls, aspirin use was associated with a 65% reduction in risk for intrahepatic cholangiocarcinoma (CCA), 66% reduction in risk for perihilar CCA, and 71% reduction in risk for distal CCA, reported Dr. Jonggi Choi and colleagues from the Mayo Medical School in Rochester, Minn.
“This is one of the largest hospital-based case-control studies evaluating risk factors for CCA in Western populations. We found that aspirin use had a significant inverse association with CCA development,” they wrote in Hepatology (2016. doi: 10.1002/hep.28529).
They also found that other disorders, including primary sclerosing cholangitis (PSC), non–PSC related cirrhosis, biliary tract diseases, hepatitis B infections, and diabetes, as well as smoking, were associated with varying magnitudes of risk for different CCA subtypes.
“This supports the hypothesis that the three CCA subtypes are distinct diseases and that each subtype thus has its own susceptibility to risk factors,” they wrote.
The investigators conducted a case-control study to look at various risk factors for CCA using data on all patients seen for CCA at the Mayo Clinic in Rochester from 2000 through 2014. Each case was matched by age, race, sex, and residence to two controls, chosen from among patients enrolled in the Mayo Clinic Biobank.

There were a total of 2,395 cases (1,169 with intrahepatic CCA, 995 with perihilar CCA, and 231 with distal CCA) and 4,769 controls. In all, 24.7% of cases and 44.6% of controls had used aspirin.
In multivariate logistic regression analysis controlling for demographic factors, obesity, hypertension, diabetes, stroke, coronary artery disease, peripheral vascular disease, atrial fibrillation, nonalcoholic fatty liver disease/nonalcoholic steatohepatitis, PSC, cirrhosis, irritable bowel disease, and smoking status, aspirin was significantly associated with a reduction in risk for all CCA subtypes with adjusted odds ratios (AOR) of 0.35 for intrahepatic CCA, 0.34 for perihilar cancer, and 0.29 for distal CCA (P for all less than .001).
In addition, they found that PSC was strongly associated with risk for perihilar CCA (AOR 453; P less than .001), intrahepatic CCA (AOR 93.4, P less than .001), and distal CCA (AOR 34.0, P = .002).
Cirrhosis not related to PSC was also associated with intrahepatic and perihilar CCA (AOR 13.8 and 14.1, respectively, P less than .001 for each), but not with distal CCA. Isolated inflammatory bowel disease without PSC was not associated with elevated risk of any CCA subtype.
Regular aspirin use is associated with an approximately threefold reduction in risk for the three major subtypes of cholangiocarcinoma, results of a case-control study indicate.
In a study comparing patients with bile duct cancers with matched controls, aspirin use was associated with a 65% reduction in risk for intrahepatic cholangiocarcinoma (CCA), 66% reduction in risk for perihilar CCA, and 71% reduction in risk for distal CCA, reported Dr. Jonggi Choi and colleagues from the Mayo Medical School in Rochester, Minn.
“This is one of the largest hospital-based case-control studies evaluating risk factors for CCA in Western populations. We found that aspirin use had a significant inverse association with CCA development,” they wrote in Hepatology (2016. doi: 10.1002/hep.28529).
They also found that other disorders, including primary sclerosing cholangitis (PSC), non–PSC related cirrhosis, biliary tract diseases, hepatitis B infections, and diabetes, as well as smoking, were associated with varying magnitudes of risk for different CCA subtypes.
“This supports the hypothesis that the three CCA subtypes are distinct diseases and that each subtype thus has its own susceptibility to risk factors,” they wrote.
The investigators conducted a case-control study to look at various risk factors for CCA using data on all patients seen for CCA at the Mayo Clinic in Rochester from 2000 through 2014. Each case was matched by age, race, sex, and residence to two controls, chosen from among patients enrolled in the Mayo Clinic Biobank.
There were a total of 2,395 cases (1,169 with intrahepatic CCA, 995 with perihilar CCA, and 231 with distal CCA) and 4,769 controls. In all, 24.7% of cases and 44.6% of controls had used aspirin.
In multivariate logistic regression analysis controlling for demographic factors, obesity, hypertension, diabetes, stroke, coronary artery disease, peripheral vascular disease, atrial fibrillation, nonalcoholic fatty liver disease/nonalcoholic steatohepatitis, PSC, cirrhosis, irritable bowel disease, and smoking status, aspirin was significantly associated with a reduction in risk for all CCA subtypes with adjusted odds ratios (AOR) of 0.35 for intrahepatic CCA, 0.34 for perihilar cancer, and 0.29 for distal CCA (P for all less than .001).
In addition, they found that PSC was strongly associated with risk for perihilar CCA (AOR 453; P less than .001), intrahepatic CCA (AOR 93.4, P less than .001), and distal CCA (AOR 34.0, P = .002).
Cirrhosis not related to PSC was also associated with intrahepatic and perihilar CCA (AOR 13.8 and 14.1, respectively, P less than .001 for each), but not with distal CCA. Isolated inflammatory bowel disease without PSC was not associated with elevated risk of any CCA subtype.
Regular aspirin use is associated with an approximately threefold reduction in risk for the three major subtypes of cholangiocarcinoma, results of a case-control study indicate.
In a study comparing patients with bile duct cancers with matched controls, aspirin use was associated with a 65% reduction in risk for intrahepatic cholangiocarcinoma (CCA), 66% reduction in risk for perihilar CCA, and 71% reduction in risk for distal CCA, reported Dr. Jonggi Choi and colleagues from the Mayo Medical School in Rochester, Minn.
“This is one of the largest hospital-based case-control studies evaluating risk factors for CCA in Western populations. We found that aspirin use had a significant inverse association with CCA development,” they wrote in Hepatology (2016. doi: 10.1002/hep.28529).
They also found that other disorders, including primary sclerosing cholangitis (PSC), non–PSC related cirrhosis, biliary tract diseases, hepatitis B infections, and diabetes, as well as smoking, were associated with varying magnitudes of risk for different CCA subtypes.
“This supports the hypothesis that the three CCA subtypes are distinct diseases and that each subtype thus has its own susceptibility to risk factors,” they wrote.
The investigators conducted a case-control study to look at various risk factors for CCA using data on all patients seen for CCA at the Mayo Clinic in Rochester from 2000 through 2014. Each case was matched by age, race, sex, and residence to two controls, chosen from among patients enrolled in the Mayo Clinic Biobank.
There were a total of 2,395 cases (1,169 with intrahepatic CCA, 995 with perihilar CCA, and 231 with distal CCA) and 4,769 controls. In all, 24.7% of cases and 44.6% of controls had used aspirin.
In multivariate logistic regression analysis controlling for demographic factors, obesity, hypertension, diabetes, stroke, coronary artery disease, peripheral vascular disease, atrial fibrillation, nonalcoholic fatty liver disease/nonalcoholic steatohepatitis, PSC, cirrhosis, irritable bowel disease, and smoking status, aspirin was significantly associated with a reduction in risk for all CCA subtypes with adjusted odds ratios (AOR) of 0.35 for intrahepatic CCA, 0.34 for perihilar cancer, and 0.29 for distal CCA (P for all less than .001).
In addition, they found that PSC was strongly associated with risk for perihilar CCA (AOR 453; P less than .001), intrahepatic CCA (AOR 93.4, P less than .001), and distal CCA (AOR 34.0, P = .002).
Cirrhosis not related to PSC was also associated with intrahepatic and perihilar CCA (AOR 13.8 and 14.1, respectively, P less than .001 for each), but not with distal CCA. Isolated inflammatory bowel disease without PSC was not associated with elevated risk of any CCA subtype.
FROM HEPATOLOGY
Key clinical point: Aspirin use is associated with an approximately threefold reduction in risk for the three cholangiocarcinoma (CCA) subtypes.
Major finding: Respective adjusted odds ratios for aspirin and intrahepatic, perihilar, and distal CCA were 0.35, 0.34, and 0.29.
Data source: Case-control study including 2,395 patients with CCA and 4,769 controls.
Disclosures: The study was supported by the National Institutes of Health, Mayo Clinic, Mayo Foundation, and the Cholangiocarcinoma Foundation. The authors reported no conflicts of interest.

How Genetic Epilepsy Testing Can Impact Clinical Care and Practice
PHILADELPHIA—Genetic epilepsy testing can impact clinical care and practice by providing diagnostic certainty and suggesting an approach to medical management, said Annapurna Poduri, MD, MPH, in a lecture at the 69th Annual Meeting of the American Epilepsy Society.

Annapurna Poduri, MD, MPH
With a precise genetic diagnosis, neurologists might be able to give more information about a patient’s prognosis. In addition, a genetic diagnosis can end a patient’s “diagnostic odyssey,” which can entail the burden of blood tests, lumbar punctures, and repeated imaging, said Dr. Poduri, Associate Professor of Neurology at Harvard Medical School in Boston.
“There are a small but growing number of genes associated with specific treatment recommendations,” she said. “We might be able to move toward precision medicine in epilepsy.”
New Evidence
Epilepsy genetics is “not a new topic, but it’s one where we have a lot of new evidence.” Twin studies and family studies helped establish the role of genetics in epilepsy, and in the 1990s, researchers identified several genes associated with epilepsy, including SCN1A, SCN1B, CHRNA4, and GABRB2.
When the human genome was sequenced, large association studies were not initially revealing about new causes of epilepsy. New sequencing technologies and the ability to assess copy number variation, however, have led to further advances. “In 2010, there were three papers showing us the role of copy number variation in epilepsy that had previously not had an identified etiology,” Dr. Poduri said.
Researchers found that as many as 3% of cases of genetic generalized epilepsy, formerly called idiopathic generalized epilepsy, might have deletions in the regions 15q11.2, 15q13.3, or 16p13.11. “You might say … that’s not a lot of our cases in epilepsy. But in fact, there hadn’t been this sort of robust evidence for the role of copy number variation in genetic generalized epilepsy and some of the focal epilepsies until this point,” said Dr. Poduri. “These were seminal discoveries that paved the way for further testing.”
The Epi4K Consortium and Epilepsy Phenome/Genome Project, which involved 26 institutions, undertook one effort that identified additional epilepsy-related mutations and genes. The project initially looked at individuals with infantile spasms and Lennox-Gastaut syndrome. Sequencing the exomes of 264 patients and their parents “allowed us to enlist the power of having a relatively large group of these otherwise rare disorders,” said Dr. Poduri. Among the known epilepsy genes identified by the study was SCN1A. “If we hadn’t already known … that SCN1A is an important gene for epilepsy, this is the sort of study that could tell us.” The study broadened the phenotype associated with mutations in STXBP1, which previously had been associated with Ohtahara syndrome. The investigators also identified a new epilepsy gene: DNM1. This gene did not achieve genome-wide significance in the initial study, but when researchers added about a hundred trios from a European cohort, EuroEPINOMICS, DNM1 rose to significance, said Dr. Poduri. “There were a total of five cases across these 356 trios, and a robust analysis of all of these data together through the Epi4K and EuroEPINOMICS Consortia was able to put this gene robustly on the map.”
The Effect on Practice
Such discoveries can affect clinical practice and patient management. “When you have enough data pointing to a new gene like [DNM1]—this is a synaptic gene, it makes sense, but previously was not on our radar—it means that gene testing panels are going to incorporate genes like this and be able to find more mutations like this,” said Dr. Poduri.
Certain genes are associated with specific phenotypes. The patients with de novo mutations in DNM1 had infantile spasms, and four of the five patients developed Lennox-Gastaut syndrome. “All of them had severe to profound intellectual disability and hypotonia,” said Dr. Poduri. “It gives you some sense of [the] prognosis.” Likewise, if a patient had a mutation that “uniformly was associated with a benign course, that might give us some reassurance that it’s not a progressive disorder,” she said. Findings like this might help to give physicians and patients’ families some diagnostic certainty.
Some genes suggest specific treatments to pursue or avoid. For example, in treating patients with Dravet syndrome and mutations in SCN1A, “we tend to avoid lamotrigine and phenytoin,” Dr. Poduri said. In general, neurologists avoid these sodium channel agents because they have seen patient worsening, although these recommendations are not universal, she said.
According to recent case reports, patients with SCN2A- and SCN8A- associated encephalopathies have responded to high-dose phenytoin. Mutations in SLC2A1 are associated with glucose transporter type 1 deficiency, which can be treated with the ketogenic diet. Mutations in ALDH7A1 are associated with pyridoxine deficiency, and mutations in PNPO are associated with a pyridoxal-5-phosphate deficiency. Rectifying the deficiencies may affect seizures in some cases, Dr. Poduri said.
Pierson et al reported in 2014 the case of a child with a GRIN2A mutation that changed leucine to methionine at amino acid position 812. This change increased the potency of the NMDA agonists glutamate and glycine. Investigators found that, with this mutation, memantine can block the excessive gain of function response. With adjunctive memantine therapy, the child had a dramatic reduction in seizures, although not a dramatic improvement in development, Dr. Poduri said. The child had been receiving treatment with lacosamide, rufinamide, and valproic acid. After starting memantine, lacosamide and rufinamide were tapered off.
A precise genetic diagnosis also might influence the decision between epilepsy surgery and medical treatment. For example, if a patient with infantile spasms and a mutation in SCN1A has a focal lesion, a neurologist may consider surgery, but some studies suggest that outcomes are not always favorable for these patients, Dr. Poduri said.
Need for Awareness
Neurologists should pursue updated genetic testing for their patients to take advantage of the latest genetic discoveries, Dr. Poduri said. They should learn which genes are associated with epilepsy syndromes, and bear in mind that the list of identified genes is growing.
Dr. Poduri hopes clinical practices will engage with clinical researchers and gene discovery efforts, which can lead to clinically relevant models, preclinical trials, and eventually precision medicine. “This may seem like a bit of a dream, but I think it’s really where we’re moving, and we actually have traction now in all of these areas,” she said.
—Jake Remaly
PHILADELPHIA—Genetic epilepsy testing can impact clinical care and practice by providing diagnostic certainty and suggesting an approach to medical management, said Annapurna Poduri, MD, MPH, in a lecture at the 69th Annual Meeting of the American Epilepsy Society.
Annapurna Poduri, MD, MPH
With a precise genetic diagnosis, neurologists might be able to give more information about a patient’s prognosis. In addition, a genetic diagnosis can end a patient’s “diagnostic odyssey,” which can entail the burden of blood tests, lumbar punctures, and repeated imaging, said Dr. Poduri, Associate Professor of Neurology at Harvard Medical School in Boston.
“There are a small but growing number of genes associated with specific treatment recommendations,” she said. “We might be able to move toward precision medicine in epilepsy.”
New Evidence
Epilepsy genetics is “not a new topic, but it’s one where we have a lot of new evidence.” Twin studies and family studies helped establish the role of genetics in epilepsy, and in the 1990s, researchers identified several genes associated with epilepsy, including SCN1A, SCN1B, CHRNA4, and GABRB2.
When the human genome was sequenced, large association studies were not initially revealing about new causes of epilepsy. New sequencing technologies and the ability to assess copy number variation, however, have led to further advances. “In 2010, there were three papers showing us the role of copy number variation in epilepsy that had previously not had an identified etiology,” Dr. Poduri said.
Researchers found that as many as 3% of cases of genetic generalized epilepsy, formerly called idiopathic generalized epilepsy, might have deletions in the regions 15q11.2, 15q13.3, or 16p13.11. “You might say … that’s not a lot of our cases in epilepsy. But in fact, there hadn’t been this sort of robust evidence for the role of copy number variation in genetic generalized epilepsy and some of the focal epilepsies until this point,” said Dr. Poduri. “These were seminal discoveries that paved the way for further testing.”
The Epi4K Consortium and Epilepsy Phenome/Genome Project, which involved 26 institutions, undertook one effort that identified additional epilepsy-related mutations and genes. The project initially looked at individuals with infantile spasms and Lennox-Gastaut syndrome. Sequencing the exomes of 264 patients and their parents “allowed us to enlist the power of having a relatively large group of these otherwise rare disorders,” said Dr. Poduri. Among the known epilepsy genes identified by the study was SCN1A. “If we hadn’t already known … that SCN1A is an important gene for epilepsy, this is the sort of study that could tell us.” The study broadened the phenotype associated with mutations in STXBP1, which previously had been associated with Ohtahara syndrome. The investigators also identified a new epilepsy gene: DNM1. This gene did not achieve genome-wide significance in the initial study, but when researchers added about a hundred trios from a European cohort, EuroEPINOMICS, DNM1 rose to significance, said Dr. Poduri. “There were a total of five cases across these 356 trios, and a robust analysis of all of these data together through the Epi4K and EuroEPINOMICS Consortia was able to put this gene robustly on the map.”
The Effect on Practice
Such discoveries can affect clinical practice and patient management. “When you have enough data pointing to a new gene like [DNM1]—this is a synaptic gene, it makes sense, but previously was not on our radar—it means that gene testing panels are going to incorporate genes like this and be able to find more mutations like this,” said Dr. Poduri.
Certain genes are associated with specific phenotypes. The patients with de novo mutations in DNM1 had infantile spasms, and four of the five patients developed Lennox-Gastaut syndrome. “All of them had severe to profound intellectual disability and hypotonia,” said Dr. Poduri. “It gives you some sense of [the] prognosis.” Likewise, if a patient had a mutation that “uniformly was associated with a benign course, that might give us some reassurance that it’s not a progressive disorder,” she said. Findings like this might help to give physicians and patients’ families some diagnostic certainty.
Some genes suggest specific treatments to pursue or avoid. For example, in treating patients with Dravet syndrome and mutations in SCN1A, “we tend to avoid lamotrigine and phenytoin,” Dr. Poduri said. In general, neurologists avoid these sodium channel agents because they have seen patient worsening, although these recommendations are not universal, she said.
According to recent case reports, patients with SCN2A- and SCN8A- associated encephalopathies have responded to high-dose phenytoin. Mutations in SLC2A1 are associated with glucose transporter type 1 deficiency, which can be treated with the ketogenic diet. Mutations in ALDH7A1 are associated with pyridoxine deficiency, and mutations in PNPO are associated with a pyridoxal-5-phosphate deficiency. Rectifying the deficiencies may affect seizures in some cases, Dr. Poduri said.
Pierson et al reported in 2014 the case of a child with a GRIN2A mutation that changed leucine to methionine at amino acid position 812. This change increased the potency of the NMDA agonists glutamate and glycine. Investigators found that, with this mutation, memantine can block the excessive gain of function response. With adjunctive memantine therapy, the child had a dramatic reduction in seizures, although not a dramatic improvement in development, Dr. Poduri said. The child had been receiving treatment with lacosamide, rufinamide, and valproic acid. After starting memantine, lacosamide and rufinamide were tapered off.
A precise genetic diagnosis also might influence the decision between epilepsy surgery and medical treatment. For example, if a patient with infantile spasms and a mutation in SCN1A has a focal lesion, a neurologist may consider surgery, but some studies suggest that outcomes are not always favorable for these patients, Dr. Poduri said.
Need for Awareness
Neurologists should pursue updated genetic testing for their patients to take advantage of the latest genetic discoveries, Dr. Poduri said. They should learn which genes are associated with epilepsy syndromes, and bear in mind that the list of identified genes is growing.
Dr. Poduri hopes clinical practices will engage with clinical researchers and gene discovery efforts, which can lead to clinically relevant models, preclinical trials, and eventually precision medicine. “This may seem like a bit of a dream, but I think it’s really where we’re moving, and we actually have traction now in all of these areas,” she said.
—Jake Remaly
PHILADELPHIA—Genetic epilepsy testing can impact clinical care and practice by providing diagnostic certainty and suggesting an approach to medical management, said Annapurna Poduri, MD, MPH, in a lecture at the 69th Annual Meeting of the American Epilepsy Society.
Annapurna Poduri, MD, MPH
With a precise genetic diagnosis, neurologists might be able to give more information about a patient’s prognosis. In addition, a genetic diagnosis can end a patient’s “diagnostic odyssey,” which can entail the burden of blood tests, lumbar punctures, and repeated imaging, said Dr. Poduri, Associate Professor of Neurology at Harvard Medical School in Boston.
“There are a small but growing number of genes associated with specific treatment recommendations,” she said. “We might be able to move toward precision medicine in epilepsy.”
New Evidence
Epilepsy genetics is “not a new topic, but it’s one where we have a lot of new evidence.” Twin studies and family studies helped establish the role of genetics in epilepsy, and in the 1990s, researchers identified several genes associated with epilepsy, including SCN1A, SCN1B, CHRNA4, and GABRB2.
When the human genome was sequenced, large association studies were not initially revealing about new causes of epilepsy. New sequencing technologies and the ability to assess copy number variation, however, have led to further advances. “In 2010, there were three papers showing us the role of copy number variation in epilepsy that had previously not had an identified etiology,” Dr. Poduri said.
Researchers found that as many as 3% of cases of genetic generalized epilepsy, formerly called idiopathic generalized epilepsy, might have deletions in the regions 15q11.2, 15q13.3, or 16p13.11. “You might say … that’s not a lot of our cases in epilepsy. But in fact, there hadn’t been this sort of robust evidence for the role of copy number variation in genetic generalized epilepsy and some of the focal epilepsies until this point,” said Dr. Poduri. “These were seminal discoveries that paved the way for further testing.”
The Epi4K Consortium and Epilepsy Phenome/Genome Project, which involved 26 institutions, undertook one effort that identified additional epilepsy-related mutations and genes. The project initially looked at individuals with infantile spasms and Lennox-Gastaut syndrome. Sequencing the exomes of 264 patients and their parents “allowed us to enlist the power of having a relatively large group of these otherwise rare disorders,” said Dr. Poduri. Among the known epilepsy genes identified by the study was SCN1A. “If we hadn’t already known … that SCN1A is an important gene for epilepsy, this is the sort of study that could tell us.” The study broadened the phenotype associated with mutations in STXBP1, which previously had been associated with Ohtahara syndrome. The investigators also identified a new epilepsy gene: DNM1. This gene did not achieve genome-wide significance in the initial study, but when researchers added about a hundred trios from a European cohort, EuroEPINOMICS, DNM1 rose to significance, said Dr. Poduri. “There were a total of five cases across these 356 trios, and a robust analysis of all of these data together through the Epi4K and EuroEPINOMICS Consortia was able to put this gene robustly on the map.”
The Effect on Practice
Such discoveries can affect clinical practice and patient management. “When you have enough data pointing to a new gene like [DNM1]—this is a synaptic gene, it makes sense, but previously was not on our radar—it means that gene testing panels are going to incorporate genes like this and be able to find more mutations like this,” said Dr. Poduri.
Certain genes are associated with specific phenotypes. The patients with de novo mutations in DNM1 had infantile spasms, and four of the five patients developed Lennox-Gastaut syndrome. “All of them had severe to profound intellectual disability and hypotonia,” said Dr. Poduri. “It gives you some sense of [the] prognosis.” Likewise, if a patient had a mutation that “uniformly was associated with a benign course, that might give us some reassurance that it’s not a progressive disorder,” she said. Findings like this might help to give physicians and patients’ families some diagnostic certainty.
Some genes suggest specific treatments to pursue or avoid. For example, in treating patients with Dravet syndrome and mutations in SCN1A, “we tend to avoid lamotrigine and phenytoin,” Dr. Poduri said. In general, neurologists avoid these sodium channel agents because they have seen patient worsening, although these recommendations are not universal, she said.
According to recent case reports, patients with SCN2A- and SCN8A- associated encephalopathies have responded to high-dose phenytoin. Mutations in SLC2A1 are associated with glucose transporter type 1 deficiency, which can be treated with the ketogenic diet. Mutations in ALDH7A1 are associated with pyridoxine deficiency, and mutations in PNPO are associated with a pyridoxal-5-phosphate deficiency. Rectifying the deficiencies may affect seizures in some cases, Dr. Poduri said.
Pierson et al reported in 2014 the case of a child with a GRIN2A mutation that changed leucine to methionine at amino acid position 812. This change increased the potency of the NMDA agonists glutamate and glycine. Investigators found that, with this mutation, memantine can block the excessive gain of function response. With adjunctive memantine therapy, the child had a dramatic reduction in seizures, although not a dramatic improvement in development, Dr. Poduri said. The child had been receiving treatment with lacosamide, rufinamide, and valproic acid. After starting memantine, lacosamide and rufinamide were tapered off.
A precise genetic diagnosis also might influence the decision between epilepsy surgery and medical treatment. For example, if a patient with infantile spasms and a mutation in SCN1A has a focal lesion, a neurologist may consider surgery, but some studies suggest that outcomes are not always favorable for these patients, Dr. Poduri said.
Need for Awareness
Neurologists should pursue updated genetic testing for their patients to take advantage of the latest genetic discoveries, Dr. Poduri said. They should learn which genes are associated with epilepsy syndromes, and bear in mind that the list of identified genes is growing.
Dr. Poduri hopes clinical practices will engage with clinical researchers and gene discovery efforts, which can lead to clinically relevant models, preclinical trials, and eventually precision medicine. “This may seem like a bit of a dream, but I think it’s really where we’re moving, and we actually have traction now in all of these areas,” she said.
—Jake Remaly

Acute heart failure mortality climbs with severity of peripheral edema
CHICAGO – Breathlessness typically results in hospital admission for patients with heart failure, but peripheral edema is what prolongs their stay, according to Dr. John G.F. Cleland.
Moreover, it’s not only hospital length of stay that climbs with increasing severity of peripheral edema on admission. So does mortality, both during the index admission and long term, Dr. Cleland reported at the annual meeting of the American College of Cardiology.
He presented a retrospective analysis of 121,229 patients admitted with a primary diagnosis of heart failure to more than 90% of the hospitals in England and Wales during 2007-2013.
“It turns out that the majority of patients we’re seeing admitted with heart failure at U.K. hospitals are not admitted because of severe breathlessness at rest; they’re admitted for increasing fluid retention. They have lots of peripheral edema, which is actually associated with bad outcome. The patients who are very breathless tend to have the better outcome because they have left heart failure. The ones who are full of peripheral edema have more renal dysfunction and anemia, and they’re more likely to have right heart failure,” said Dr. Cleland, professor of cardiology at Imperial College London.
“I’m not saying the breathless group isn’t a target, but this group with peripheral edema is a bigger target – and we’re not designing trials to address their problems,” he added.
Compared with patients with no peripheral edema on hospital admission, the risk of mortality during that hospitalization and up to 3 years of subsequent follow-up was increased 1.2-fold in those with mild peripheral edema, 1.48-fold with moderate peripheral edema, and 1.89-fold in those with severe peripheral edema.
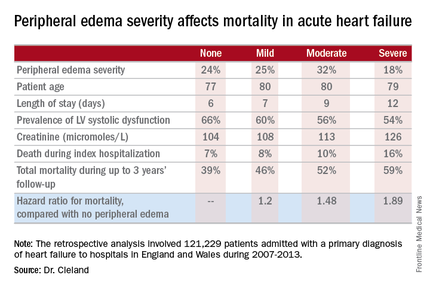
“We’re designing all the big clinical trials in acute heart failure to capture what I regard as neither fish nor fowl. They’re recruiting patients 6-12 hours after admission for acute heart failure. But by that point they’ve pretty well responded to their intravenous diuretics, and we’re just catching the tail end of their breathlessness. They’re not an emergency. The problem is really their peripheral edema, and that’s a day 2/day 3 problem. The first 6 hours of care really isn’t relevant to this group,” according to the internationally renowned heart failure researcher.
Indeed, he said he’d like to see the term “acute heart failure” laid to rest.
“If you think of acute decompensated heart failure, you think of patients wearing an oxygen mask coming in by an ambulance with blue lights flashing, and it’s an emergency. We need to move the mind-set. We shouldn’t call it acute heart failure at all, we should start talking about hospitalized heart failure, of which some is acute but much of it is subacute in people who have been deteriorating over several weeks and have just gotten to the point where they’re not coping at home anymore. They call a taxi or a friend who takes them to the hospital. Then they take a wheelchair from the taxi to the ER, but they don’t really need an ER at all,” Dr. Cleland said.
Many of these patients could be redirected to a different sort of facility at great cost savings, he added.
“In the United Kingdom and I think in the States, we’re now talking about furosemide lounges where, rather than admit the patient, you can bring them up as a day case, give them intravenous therapy, then [have them] go home at night, perhaps coming back for 3 or 4 days if needed. People are also now looking at home infusion services, and there’s a nice device for giving subcutaneous doses of furosemide as well,” the cardiologist said.
Apart from diuretics, there really aren’t any effective medications at present for peripheral edema in heart failure. But there are novel investigational agents worthy of evaluation, according to Dr. Cleland, including drugs aimed at improving mitochondrial function, agents that inhibit channels that allow edema to gather, and iron therapy.
The study was supported by the British Society for Heart Failure and the National Institute for Cardiovascular Outcomes Research. Dr. Cleland reported having no relevant financial conflicts.
CHICAGO – Breathlessness typically results in hospital admission for patients with heart failure, but peripheral edema is what prolongs their stay, according to Dr. John G.F. Cleland.
Moreover, it’s not only hospital length of stay that climbs with increasing severity of peripheral edema on admission. So does mortality, both during the index admission and long term, Dr. Cleland reported at the annual meeting of the American College of Cardiology.
He presented a retrospective analysis of 121,229 patients admitted with a primary diagnosis of heart failure to more than 90% of the hospitals in England and Wales during 2007-2013.
“It turns out that the majority of patients we’re seeing admitted with heart failure at U.K. hospitals are not admitted because of severe breathlessness at rest; they’re admitted for increasing fluid retention. They have lots of peripheral edema, which is actually associated with bad outcome. The patients who are very breathless tend to have the better outcome because they have left heart failure. The ones who are full of peripheral edema have more renal dysfunction and anemia, and they’re more likely to have right heart failure,” said Dr. Cleland, professor of cardiology at Imperial College London.
“I’m not saying the breathless group isn’t a target, but this group with peripheral edema is a bigger target – and we’re not designing trials to address their problems,” he added.
Compared with patients with no peripheral edema on hospital admission, the risk of mortality during that hospitalization and up to 3 years of subsequent follow-up was increased 1.2-fold in those with mild peripheral edema, 1.48-fold with moderate peripheral edema, and 1.89-fold in those with severe peripheral edema.
“We’re designing all the big clinical trials in acute heart failure to capture what I regard as neither fish nor fowl. They’re recruiting patients 6-12 hours after admission for acute heart failure. But by that point they’ve pretty well responded to their intravenous diuretics, and we’re just catching the tail end of their breathlessness. They’re not an emergency. The problem is really their peripheral edema, and that’s a day 2/day 3 problem. The first 6 hours of care really isn’t relevant to this group,” according to the internationally renowned heart failure researcher.
Indeed, he said he’d like to see the term “acute heart failure” laid to rest.
“If you think of acute decompensated heart failure, you think of patients wearing an oxygen mask coming in by an ambulance with blue lights flashing, and it’s an emergency. We need to move the mind-set. We shouldn’t call it acute heart failure at all, we should start talking about hospitalized heart failure, of which some is acute but much of it is subacute in people who have been deteriorating over several weeks and have just gotten to the point where they’re not coping at home anymore. They call a taxi or a friend who takes them to the hospital. Then they take a wheelchair from the taxi to the ER, but they don’t really need an ER at all,” Dr. Cleland said.
Many of these patients could be redirected to a different sort of facility at great cost savings, he added.
“In the United Kingdom and I think in the States, we’re now talking about furosemide lounges where, rather than admit the patient, you can bring them up as a day case, give them intravenous therapy, then [have them] go home at night, perhaps coming back for 3 or 4 days if needed. People are also now looking at home infusion services, and there’s a nice device for giving subcutaneous doses of furosemide as well,” the cardiologist said.
Apart from diuretics, there really aren’t any effective medications at present for peripheral edema in heart failure. But there are novel investigational agents worthy of evaluation, according to Dr. Cleland, including drugs aimed at improving mitochondrial function, agents that inhibit channels that allow edema to gather, and iron therapy.
The study was supported by the British Society for Heart Failure and the National Institute for Cardiovascular Outcomes Research. Dr. Cleland reported having no relevant financial conflicts.
CHICAGO – Breathlessness typically results in hospital admission for patients with heart failure, but peripheral edema is what prolongs their stay, according to Dr. John G.F. Cleland.
Moreover, it’s not only hospital length of stay that climbs with increasing severity of peripheral edema on admission. So does mortality, both during the index admission and long term, Dr. Cleland reported at the annual meeting of the American College of Cardiology.
He presented a retrospective analysis of 121,229 patients admitted with a primary diagnosis of heart failure to more than 90% of the hospitals in England and Wales during 2007-2013.
“It turns out that the majority of patients we’re seeing admitted with heart failure at U.K. hospitals are not admitted because of severe breathlessness at rest; they’re admitted for increasing fluid retention. They have lots of peripheral edema, which is actually associated with bad outcome. The patients who are very breathless tend to have the better outcome because they have left heart failure. The ones who are full of peripheral edema have more renal dysfunction and anemia, and they’re more likely to have right heart failure,” said Dr. Cleland, professor of cardiology at Imperial College London.
“I’m not saying the breathless group isn’t a target, but this group with peripheral edema is a bigger target – and we’re not designing trials to address their problems,” he added.
Compared with patients with no peripheral edema on hospital admission, the risk of mortality during that hospitalization and up to 3 years of subsequent follow-up was increased 1.2-fold in those with mild peripheral edema, 1.48-fold with moderate peripheral edema, and 1.89-fold in those with severe peripheral edema.
“We’re designing all the big clinical trials in acute heart failure to capture what I regard as neither fish nor fowl. They’re recruiting patients 6-12 hours after admission for acute heart failure. But by that point they’ve pretty well responded to their intravenous diuretics, and we’re just catching the tail end of their breathlessness. They’re not an emergency. The problem is really their peripheral edema, and that’s a day 2/day 3 problem. The first 6 hours of care really isn’t relevant to this group,” according to the internationally renowned heart failure researcher.
Indeed, he said he’d like to see the term “acute heart failure” laid to rest.
“If you think of acute decompensated heart failure, you think of patients wearing an oxygen mask coming in by an ambulance with blue lights flashing, and it’s an emergency. We need to move the mind-set. We shouldn’t call it acute heart failure at all, we should start talking about hospitalized heart failure, of which some is acute but much of it is subacute in people who have been deteriorating over several weeks and have just gotten to the point where they’re not coping at home anymore. They call a taxi or a friend who takes them to the hospital. Then they take a wheelchair from the taxi to the ER, but they don’t really need an ER at all,” Dr. Cleland said.
Many of these patients could be redirected to a different sort of facility at great cost savings, he added.
“In the United Kingdom and I think in the States, we’re now talking about furosemide lounges where, rather than admit the patient, you can bring them up as a day case, give them intravenous therapy, then [have them] go home at night, perhaps coming back for 3 or 4 days if needed. People are also now looking at home infusion services, and there’s a nice device for giving subcutaneous doses of furosemide as well,” the cardiologist said.
Apart from diuretics, there really aren’t any effective medications at present for peripheral edema in heart failure. But there are novel investigational agents worthy of evaluation, according to Dr. Cleland, including drugs aimed at improving mitochondrial function, agents that inhibit channels that allow edema to gather, and iron therapy.
The study was supported by the British Society for Heart Failure and the National Institute for Cardiovascular Outcomes Research. Dr. Cleland reported having no relevant financial conflicts.
AT ACC 16
Key clinical point: Leg swelling warrants greater attention in patients hospitalized for acute heart failure.
Major finding: In-hospital mortality was more than twice as great in patients admitted for acute heart failure with severe peripheral edema, compared with no leg swelling.
Data source: A retrospective study of more than 121,000 patients hospitalized for acute heart failure in England and Wales.
Disclosures: The study was supported by the British Society for Heart Failure and the National Institute for Cardiovascular Outcomes Research. The presenter reported having no relevant financial conflicts.
Cosmetic Corner: Dermatologists Weigh in on Tinted Moisturizers
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Evidence Builds for Mesenchymal Stem Cell Therapy in Multiple Sclerosis
NEW ORLEANS—In an uncontrolled, prospective study, repeated intrathecal administration of autologous mesenchymal bone marrow–derived stromal stem cells to treat multiple sclerosis was safe and induced accelerated beneficial effects in some patients.
Of 28 patients with either secondary progressive or relapsing-progressive multiple sclerosis who were experiencing severe clinical deterioration and failure to respond to first- and second-line immunomodulatory treatments, 25 experienced either stable or improved Expanded Disability Status Scale (EDSS) scores following autologous mesenchymal stem cell (MSC) injections. The mean score decreased from 6.76 at study entry to 6.57 at a mean follow-up of 3.6 years, Panayiota Petrou, MD, of Hadassah University Hospital in Jerusalem, and her colleagues reported at the ACTRIMS 2016 Forum.
In addition, 17 patients experienced improvements in at least one functional system of the EDSS, including 14 who experienced improved motor function, five who experienced improved speech or bulbar functions, four who experienced improved urinary function, and six who experienced improved cerebellar function. Eight patients remained stable during the entire follow-up period.
In a prior pilot trial, intrathecal administration of MSCs was shown to be safe and provided “some indications of potentially clinically meaningful beneficial effects on the progression of the disease,” said the investigators.
The current study provides further support for those findings. It included patients who experienced severe clinical deterioration of at least 0.5 points on the EDSS during the year prior to study enrollment, or who had at least one major relapse without sufficient recovery following steroid treatment. Study subjects had a mean age of 56 and mean disease duration of 15.4 years. They received at least two courses and up to 10 injections with 1 million cells/kg; most patients received two injections (eight patients) or three injections (nine patients), and the participants were followed for up to six years. No serious side effects were observed during long-term follow-up. Eight patients experienced headaches or fever in the hours and days after injection; two patients experienced symptoms of encephalopathy that resolved within a few hours. One patient experienced back pain, and one patient had neck rigidity. No long-term side effects were reported.
Immunologic follow-up showed a transient up-regulation of regulatory T cells and down-regulation of the proliferative ability of lymphocytes and of several immune activation surface markers for up to three months.
—Sharon Worcester
NEW ORLEANS—In an uncontrolled, prospective study, repeated intrathecal administration of autologous mesenchymal bone marrow–derived stromal stem cells to treat multiple sclerosis was safe and induced accelerated beneficial effects in some patients.
Of 28 patients with either secondary progressive or relapsing-progressive multiple sclerosis who were experiencing severe clinical deterioration and failure to respond to first- and second-line immunomodulatory treatments, 25 experienced either stable or improved Expanded Disability Status Scale (EDSS) scores following autologous mesenchymal stem cell (MSC) injections. The mean score decreased from 6.76 at study entry to 6.57 at a mean follow-up of 3.6 years, Panayiota Petrou, MD, of Hadassah University Hospital in Jerusalem, and her colleagues reported at the ACTRIMS 2016 Forum.
In addition, 17 patients experienced improvements in at least one functional system of the EDSS, including 14 who experienced improved motor function, five who experienced improved speech or bulbar functions, four who experienced improved urinary function, and six who experienced improved cerebellar function. Eight patients remained stable during the entire follow-up period.
In a prior pilot trial, intrathecal administration of MSCs was shown to be safe and provided “some indications of potentially clinically meaningful beneficial effects on the progression of the disease,” said the investigators.
The current study provides further support for those findings. It included patients who experienced severe clinical deterioration of at least 0.5 points on the EDSS during the year prior to study enrollment, or who had at least one major relapse without sufficient recovery following steroid treatment. Study subjects had a mean age of 56 and mean disease duration of 15.4 years. They received at least two courses and up to 10 injections with 1 million cells/kg; most patients received two injections (eight patients) or three injections (nine patients), and the participants were followed for up to six years. No serious side effects were observed during long-term follow-up. Eight patients experienced headaches or fever in the hours and days after injection; two patients experienced symptoms of encephalopathy that resolved within a few hours. One patient experienced back pain, and one patient had neck rigidity. No long-term side effects were reported.
Immunologic follow-up showed a transient up-regulation of regulatory T cells and down-regulation of the proliferative ability of lymphocytes and of several immune activation surface markers for up to three months.
—Sharon Worcester
NEW ORLEANS—In an uncontrolled, prospective study, repeated intrathecal administration of autologous mesenchymal bone marrow–derived stromal stem cells to treat multiple sclerosis was safe and induced accelerated beneficial effects in some patients.
Of 28 patients with either secondary progressive or relapsing-progressive multiple sclerosis who were experiencing severe clinical deterioration and failure to respond to first- and second-line immunomodulatory treatments, 25 experienced either stable or improved Expanded Disability Status Scale (EDSS) scores following autologous mesenchymal stem cell (MSC) injections. The mean score decreased from 6.76 at study entry to 6.57 at a mean follow-up of 3.6 years, Panayiota Petrou, MD, of Hadassah University Hospital in Jerusalem, and her colleagues reported at the ACTRIMS 2016 Forum.
In addition, 17 patients experienced improvements in at least one functional system of the EDSS, including 14 who experienced improved motor function, five who experienced improved speech or bulbar functions, four who experienced improved urinary function, and six who experienced improved cerebellar function. Eight patients remained stable during the entire follow-up period.
In a prior pilot trial, intrathecal administration of MSCs was shown to be safe and provided “some indications of potentially clinically meaningful beneficial effects on the progression of the disease,” said the investigators.
The current study provides further support for those findings. It included patients who experienced severe clinical deterioration of at least 0.5 points on the EDSS during the year prior to study enrollment, or who had at least one major relapse without sufficient recovery following steroid treatment. Study subjects had a mean age of 56 and mean disease duration of 15.4 years. They received at least two courses and up to 10 injections with 1 million cells/kg; most patients received two injections (eight patients) or three injections (nine patients), and the participants were followed for up to six years. No serious side effects were observed during long-term follow-up. Eight patients experienced headaches or fever in the hours and days after injection; two patients experienced symptoms of encephalopathy that resolved within a few hours. One patient experienced back pain, and one patient had neck rigidity. No long-term side effects were reported.
Immunologic follow-up showed a transient up-regulation of regulatory T cells and down-regulation of the proliferative ability of lymphocytes and of several immune activation surface markers for up to three months.
—Sharon Worcester