User login
FDA is investigating Zecuity sumatriptan patch for reports of serious burns
The Food and Drug Administration is evaluating patient reports of serious burns and potential permanent scarring that have occurred with the use of the Zecuity patch (sumatriptan iontophoretic transdermal system) to relieve migraine headaches.
Since September 2015, a large number of patients using the Zecuity patch have reported that they have experienced burns or scars on the skin where the patch was worn. Severe redness, pain, skin discoloration, blistering, and cracked skin were reported, according to the agency’s June 2 drug safety announcement.
The Zecuity patch contains sumatriptan which is a prescription medicine used to treat acute migraine headaches in adults. It is designed to give a dose of medicine by way of a single-use, battery-powered patch that is wrapped around the upper arm or thigh.
“Health care professionals should advise patients who complain of moderate to severe pain at the application site to remove the Zecuity patch immediately,” the safety report states. “Consider a different formulation of sumatriptan or switch these patients to an alternative migraine medicine.”
It is advised that patients should not bathe, shower, or swim while wearing the patch. Patients and health care professionals should report possible side effects involving the Zecuity patch to the FDA MedWatch program.
The Food and Drug Administration is evaluating patient reports of serious burns and potential permanent scarring that have occurred with the use of the Zecuity patch (sumatriptan iontophoretic transdermal system) to relieve migraine headaches.
Since September 2015, a large number of patients using the Zecuity patch have reported that they have experienced burns or scars on the skin where the patch was worn. Severe redness, pain, skin discoloration, blistering, and cracked skin were reported, according to the agency’s June 2 drug safety announcement.
The Zecuity patch contains sumatriptan which is a prescription medicine used to treat acute migraine headaches in adults. It is designed to give a dose of medicine by way of a single-use, battery-powered patch that is wrapped around the upper arm or thigh.
“Health care professionals should advise patients who complain of moderate to severe pain at the application site to remove the Zecuity patch immediately,” the safety report states. “Consider a different formulation of sumatriptan or switch these patients to an alternative migraine medicine.”
It is advised that patients should not bathe, shower, or swim while wearing the patch. Patients and health care professionals should report possible side effects involving the Zecuity patch to the FDA MedWatch program.
The Food and Drug Administration is evaluating patient reports of serious burns and potential permanent scarring that have occurred with the use of the Zecuity patch (sumatriptan iontophoretic transdermal system) to relieve migraine headaches.
Since September 2015, a large number of patients using the Zecuity patch have reported that they have experienced burns or scars on the skin where the patch was worn. Severe redness, pain, skin discoloration, blistering, and cracked skin were reported, according to the agency’s June 2 drug safety announcement.
The Zecuity patch contains sumatriptan which is a prescription medicine used to treat acute migraine headaches in adults. It is designed to give a dose of medicine by way of a single-use, battery-powered patch that is wrapped around the upper arm or thigh.
“Health care professionals should advise patients who complain of moderate to severe pain at the application site to remove the Zecuity patch immediately,” the safety report states. “Consider a different formulation of sumatriptan or switch these patients to an alternative migraine medicine.”
It is advised that patients should not bathe, shower, or swim while wearing the patch. Patients and health care professionals should report possible side effects involving the Zecuity patch to the FDA MedWatch program.
Starting with combination diabetes therapy beats initial monotherapy
ORLANDO – Whether to start a patient with newly diagnosed type 2 diabetes mellitus on combination therapy or monotherapy should be based on experimentation and observation rather than expert opinion, according to Dr. Alan Garber, president of the American College of Endocrinology and professor of medicine, biochemistry, and molecular and cellular biology at Baylor College of Medicine in Houston.
Monotherapy for type 2 diabetes with stepwise addition of other antihyperglycemic agents has long been the accepted way to initiate therapy in this population. Beginning in the 1990s, investigators began to compare the efficacy of monotherapy with combination therapy, first with metformin and glyburide alone or together, and then testing metformin in combination with glipizide, rosiglitazone, and sitagliptin, he said.
For metformin and glyburide, each agent alone lowered glycated hemoglobin (HbA1c), compared with placebo, but adding one to the other enhanced lowering. Combining the two drugs had the greatest benefit for higher HbA1c entry levels (e.g., HbA1c strata of 9%-9.9% or 10% or greater vs. less than 8%). At the highest-entry HbA1c levels, half doses of each of metformin and glyburide (250 mg/1.25 mg, respectively) were more efficacious than full doses of each (500 mg/2.5 mg). “This is called drug sparing,” he said.
In a trial of metformin and rosiglitazone, the combination was superior to either alone, producing significantly greater mean reductions in HbA1c and in fasting plasma glucose (FPG) at 32 weeks from their respective baselines, again, with greater reductions for higher-entry HbA1c levels. The combination was also better than either drug alone in the speed of reducing HbA1c or FPG, and in the final attained levels.
The combination of metformin and a sulfonylurea presents a risk of hypoglycemia, but Dr. Garber said the results are “much cleaner” using combinations of metformin with agents such as a thiazolidinedione, a dipeptidyl peptidase-4 inhibitor, or a sodium/glucose cotransporter-2 inhibitor.
Also noteworthy are findings from the EDICT (Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes) trial using insulin-sensitizing and insulin-secreting agents metformin/pioglitazone/exenatide in combination vs. escalating doses of metformin with sequential addition of a sulfonylurea and glargine insulin to treat patients with newly diagnosed type 2 diabetes. Over 2 years, the subjects receiving combination therapy had lower HbA1c, a mean weight loss, compared with weight gain, in the sequential therapy group, and a 7.5-fold lower rate of hypoglycemia, compared with the sequential treatment group (Diabetes Obes Metab. 2015;17:268-75).
Although the agents used in the two treatment strategies were not strictly equivalent, “it’s clear that testing multiple therapeutic mechanisms tends to produce better outcomes than fewer therapeutic mechanisms,” Dr. Garber said. The conclusions are fairly straightforward. “Look for evidence to support what strategies you want to use for your patients’ care.”
Using the Kaiser Permanente database, investigators found that the mean time of having an HbA1c above 8% was 3 years before a second agent was added, and the mean HbA1c was 9%. Many people have ascribed this sort of delay to a problem with the physician. But Dr. Garber said it is more related to patients, who often resist prescriptions for more drugs. So starting with two drugs may produce better efficacy faster as well as overcome the psychological issues of trying to add another one later (Am J Manag Care. 2003;9:213-7).

Session moderator Dr. Daniel Einhorn, medical director of the Scripps Whittier Diabetes Institute in La Jolla, California, raised the possibility of “subtraction therapy, where you start with three agents no matter what, and then if things go well, you subtract. And so you reverse the situation that Alan discussed.” In the patient’s view, “you have a celebration that night instead of a wake,” he said.
Dr. Garber has received honoraria or consulting fees as a member of the advisory boards of Novo Nordisk, Janssen, and Merck. Dr. Einhorn is on the scientific advisory boards of Eli Lilly, Novo Nordisk, Janssen, Boehringer Ingelheim, Sanofi, and Adocia, is a consultant for Halozyme, Glysens, Freedom-Meditech, and Epitracker, and has research funding from Lilly, Novo, Janssen, AstraZeneca, Mannkind, Freedom-Meditech, Merck, Sanofi, and Boehringer Ingelheim.
ORLANDO – Whether to start a patient with newly diagnosed type 2 diabetes mellitus on combination therapy or monotherapy should be based on experimentation and observation rather than expert opinion, according to Dr. Alan Garber, president of the American College of Endocrinology and professor of medicine, biochemistry, and molecular and cellular biology at Baylor College of Medicine in Houston.
Monotherapy for type 2 diabetes with stepwise addition of other antihyperglycemic agents has long been the accepted way to initiate therapy in this population. Beginning in the 1990s, investigators began to compare the efficacy of monotherapy with combination therapy, first with metformin and glyburide alone or together, and then testing metformin in combination with glipizide, rosiglitazone, and sitagliptin, he said.
For metformin and glyburide, each agent alone lowered glycated hemoglobin (HbA1c), compared with placebo, but adding one to the other enhanced lowering. Combining the two drugs had the greatest benefit for higher HbA1c entry levels (e.g., HbA1c strata of 9%-9.9% or 10% or greater vs. less than 8%). At the highest-entry HbA1c levels, half doses of each of metformin and glyburide (250 mg/1.25 mg, respectively) were more efficacious than full doses of each (500 mg/2.5 mg). “This is called drug sparing,” he said.
In a trial of metformin and rosiglitazone, the combination was superior to either alone, producing significantly greater mean reductions in HbA1c and in fasting plasma glucose (FPG) at 32 weeks from their respective baselines, again, with greater reductions for higher-entry HbA1c levels. The combination was also better than either drug alone in the speed of reducing HbA1c or FPG, and in the final attained levels.
The combination of metformin and a sulfonylurea presents a risk of hypoglycemia, but Dr. Garber said the results are “much cleaner” using combinations of metformin with agents such as a thiazolidinedione, a dipeptidyl peptidase-4 inhibitor, or a sodium/glucose cotransporter-2 inhibitor.
Also noteworthy are findings from the EDICT (Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes) trial using insulin-sensitizing and insulin-secreting agents metformin/pioglitazone/exenatide in combination vs. escalating doses of metformin with sequential addition of a sulfonylurea and glargine insulin to treat patients with newly diagnosed type 2 diabetes. Over 2 years, the subjects receiving combination therapy had lower HbA1c, a mean weight loss, compared with weight gain, in the sequential therapy group, and a 7.5-fold lower rate of hypoglycemia, compared with the sequential treatment group (Diabetes Obes Metab. 2015;17:268-75).
Although the agents used in the two treatment strategies were not strictly equivalent, “it’s clear that testing multiple therapeutic mechanisms tends to produce better outcomes than fewer therapeutic mechanisms,” Dr. Garber said. The conclusions are fairly straightforward. “Look for evidence to support what strategies you want to use for your patients’ care.”
Using the Kaiser Permanente database, investigators found that the mean time of having an HbA1c above 8% was 3 years before a second agent was added, and the mean HbA1c was 9%. Many people have ascribed this sort of delay to a problem with the physician. But Dr. Garber said it is more related to patients, who often resist prescriptions for more drugs. So starting with two drugs may produce better efficacy faster as well as overcome the psychological issues of trying to add another one later (Am J Manag Care. 2003;9:213-7).
Session moderator Dr. Daniel Einhorn, medical director of the Scripps Whittier Diabetes Institute in La Jolla, California, raised the possibility of “subtraction therapy, where you start with three agents no matter what, and then if things go well, you subtract. And so you reverse the situation that Alan discussed.” In the patient’s view, “you have a celebration that night instead of a wake,” he said.
Dr. Garber has received honoraria or consulting fees as a member of the advisory boards of Novo Nordisk, Janssen, and Merck. Dr. Einhorn is on the scientific advisory boards of Eli Lilly, Novo Nordisk, Janssen, Boehringer Ingelheim, Sanofi, and Adocia, is a consultant for Halozyme, Glysens, Freedom-Meditech, and Epitracker, and has research funding from Lilly, Novo, Janssen, AstraZeneca, Mannkind, Freedom-Meditech, Merck, Sanofi, and Boehringer Ingelheim.
ORLANDO – Whether to start a patient with newly diagnosed type 2 diabetes mellitus on combination therapy or monotherapy should be based on experimentation and observation rather than expert opinion, according to Dr. Alan Garber, president of the American College of Endocrinology and professor of medicine, biochemistry, and molecular and cellular biology at Baylor College of Medicine in Houston.
Monotherapy for type 2 diabetes with stepwise addition of other antihyperglycemic agents has long been the accepted way to initiate therapy in this population. Beginning in the 1990s, investigators began to compare the efficacy of monotherapy with combination therapy, first with metformin and glyburide alone or together, and then testing metformin in combination with glipizide, rosiglitazone, and sitagliptin, he said.
For metformin and glyburide, each agent alone lowered glycated hemoglobin (HbA1c), compared with placebo, but adding one to the other enhanced lowering. Combining the two drugs had the greatest benefit for higher HbA1c entry levels (e.g., HbA1c strata of 9%-9.9% or 10% or greater vs. less than 8%). At the highest-entry HbA1c levels, half doses of each of metformin and glyburide (250 mg/1.25 mg, respectively) were more efficacious than full doses of each (500 mg/2.5 mg). “This is called drug sparing,” he said.
In a trial of metformin and rosiglitazone, the combination was superior to either alone, producing significantly greater mean reductions in HbA1c and in fasting plasma glucose (FPG) at 32 weeks from their respective baselines, again, with greater reductions for higher-entry HbA1c levels. The combination was also better than either drug alone in the speed of reducing HbA1c or FPG, and in the final attained levels.
The combination of metformin and a sulfonylurea presents a risk of hypoglycemia, but Dr. Garber said the results are “much cleaner” using combinations of metformin with agents such as a thiazolidinedione, a dipeptidyl peptidase-4 inhibitor, or a sodium/glucose cotransporter-2 inhibitor.
Also noteworthy are findings from the EDICT (Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes) trial using insulin-sensitizing and insulin-secreting agents metformin/pioglitazone/exenatide in combination vs. escalating doses of metformin with sequential addition of a sulfonylurea and glargine insulin to treat patients with newly diagnosed type 2 diabetes. Over 2 years, the subjects receiving combination therapy had lower HbA1c, a mean weight loss, compared with weight gain, in the sequential therapy group, and a 7.5-fold lower rate of hypoglycemia, compared with the sequential treatment group (Diabetes Obes Metab. 2015;17:268-75).
Although the agents used in the two treatment strategies were not strictly equivalent, “it’s clear that testing multiple therapeutic mechanisms tends to produce better outcomes than fewer therapeutic mechanisms,” Dr. Garber said. The conclusions are fairly straightforward. “Look for evidence to support what strategies you want to use for your patients’ care.”
Using the Kaiser Permanente database, investigators found that the mean time of having an HbA1c above 8% was 3 years before a second agent was added, and the mean HbA1c was 9%. Many people have ascribed this sort of delay to a problem with the physician. But Dr. Garber said it is more related to patients, who often resist prescriptions for more drugs. So starting with two drugs may produce better efficacy faster as well as overcome the psychological issues of trying to add another one later (Am J Manag Care. 2003;9:213-7).
Session moderator Dr. Daniel Einhorn, medical director of the Scripps Whittier Diabetes Institute in La Jolla, California, raised the possibility of “subtraction therapy, where you start with three agents no matter what, and then if things go well, you subtract. And so you reverse the situation that Alan discussed.” In the patient’s view, “you have a celebration that night instead of a wake,” he said.
Dr. Garber has received honoraria or consulting fees as a member of the advisory boards of Novo Nordisk, Janssen, and Merck. Dr. Einhorn is on the scientific advisory boards of Eli Lilly, Novo Nordisk, Janssen, Boehringer Ingelheim, Sanofi, and Adocia, is a consultant for Halozyme, Glysens, Freedom-Meditech, and Epitracker, and has research funding from Lilly, Novo, Janssen, AstraZeneca, Mannkind, Freedom-Meditech, Merck, Sanofi, and Boehringer Ingelheim.
EXPERT ANALYSIS AT AACE 2016
RF ablation successfully treats focal adrenal tumors
ORLANDO – Radiofrequency (RF) ablation is a safe and effective procedure for treating focal adrenal tumors in patients who are poor surgical candidates or who refuse adrenalectomy. With a short treatment time and minimal hospital stay, RF ablation can provide rapid clinical and biochemical improvement.
Dr. Lima Lawrence, an internal medicine resident at the University of Illinois at Chicago/Advocate Christ Medical Center in Oak Lawn, presented a case report and a review of the literature during an oral abstract session at the annual meeting of the American Association of Clinical Endocrinologists. The patient was a 65-year-old woman who presented with weight gain, decreased energy, and muscle weakness. On physical exam, she was hypertensive, anxious, obese, and had prominent supraclavicular fat pads. Salivary cortisol and overnight dexamethasone suppression tests were both elevated, and ACTH levels were depressed, confirming the diagnosis of a cortisol-secreting tumor causing adrenal Cushing’s syndrome. Computed tomography (CT) surveillance showed a progressively enlarging right-sided adrenal mass. A peritoneal biopsy revealed a low-grade serous neoplasm of peritoneal origin.
Her medical history included type 2 diabetes, uncontrolled hypertension, mixed connective tissue disease, depression, and total abdominal hysterectomy with bilateral salpingo-oophorectomy for ovarian cancer.
Dr. Lawrence said the patient had been scheduled for adrenalectomy, but it was not performed because of an intraoperative finding of peritoneal studding from what turned out to be metastatic ovarian cancer. Therefore, she underwent CT-guided RF ablation of the adrenal mass using a 14-gauge probe that heated a 3.5-cm ablation zone to 50-60 C for 8-10 minutes to achieve complete tumor necrosis.
The patient showed dramatic “clinical and biochemical improvement,” Dr. Lawrence said. The patient had no procedural complications and no blood loss and was observed for 23 hours before being discharged to home. A CT scan 8 weeks later showed a slightly decreased mass with marked decreased radiographic attenuation post-contrast from 30.2 Hounsfield Units (HU) preoperatively to 17 HU on follow-up.

Potential adverse outcomes using RF ablation include a risk of pneumothorax, hemothorax, and tumor seeding along the catheter track, but this last possibility can be mitigated by continuing to heat the RF probe as it is withdrawn.
Published evidence supports use of RF ablation. “To date there have been no randomized clinical trials comparing the safety, efficacy, and survival benefits of adrenalectomy vs. radio frequency ablation,” she said. It may not be feasible to do a randomized trial. But a review of the literature generally supports the efficacy of the technique although the publications each involved a small series of patients, Dr. Lawrence said in an interview.
A 2003 series (Cancer. 2003;97:554-60) of 15 primary or metastatic adrenal cell carcinomas that were unresectable or were in patients who were not surgical candidates showed nonenhancement and no growth in 8 (53%) at a mean follow-up of 10.3 months. Eight of the 12 tumors of 5 cm or smaller had complete loss of radiographic enhancement and a decrease in size.
From a retrospective series of 13 patients with functional adrenal neoplasms over 7 years, there was 100% resolution of biochemical abnormalities and clinical symptoms at a mean follow-up of 21.2 months. One small pneumothorax and one limited hemothorax occurred, neither of which required hospital admission. There were two instances of transient, self-remitting hypertension associated with the procedures (Radiology. 2011;258:308-16).
In 2015, one group of investigators followed 11 patients for 12 weeks postprocedure. Eight of nine patients with Conn’s syndrome attained normal serum aldosterone levels. One with a nodule close to the inferior vena cava had incomplete ablation. Two of two Cushing’s patients had normal cortisol levels after the procedure (J Vasc Interv Radiol. 2015;26:1459-64).
A retrospective analysis of 16 adrenal metastases showed that 13 (81%) had no local progression over 14 months after ablation. In two of three functional adrenal neoplasms, clinical and biochemical abnormalities resolved (Eur J Radiol. 2012.81:1717-23).
A retrospective series of 10 adrenal metastases showed that one recurred at 7 months after image-guided thermal ablation, with no recurrence of the rest at 26.6 months. There was no tumor recurrence for any of the cases of metastatic disease localized to the RF ablation site (J Vasc Interv Radiol. 2014;25:593-8).
Results were somewhat less good in a retrospective evaluation of 35 patients with unresectable adrenal masses over 9 years. Although 33 of 35 (94%) lost tumor enhancement after the initial adrenal RF ablation, there was local tumor progression in 8 of 35 (23%) patients at a mean follow-up of 30.1 months (Radiology. 2015;277:584-93).
Finally, Dr. Lawrence discussed a systematic literature review on adrenalectomy vs. stereotactic ablative body radiotherapy (SABR) and percutaneous catheter ablation (PCA) in the treatment of adrenal metastases: 30 papers on adrenalectomy on 818 patients; 9 papers on SABR on 178 patients; and 6 papers on PCA, including RF ablation, on 51 patients. The authors concluded that there was “insufficient evidence to determine the best local treatment modality for isolated or limited adrenal metastases.” Adrenalectomy appeared to be a reasonable treatment for suitable patients. SABR was a valid alternative for nonsurgical candidates, but they did not recommend PCA until more long-term outcomes were available (Cancer Treat Rev. 2014;40:838-46).
Dr. Lawrence concurred, based on her case study and literature review. She said RF ablation “offers patients a minimally invasive option for treating focal adrenal tumors” and is a “safe and effective procedure … in patients who are poor surgical candidates or refuse adrenalectomy.” More long-term follow-up studies are needed before RF ablation could replace adrenalectomy, she noted.
ORLANDO – Radiofrequency (RF) ablation is a safe and effective procedure for treating focal adrenal tumors in patients who are poor surgical candidates or who refuse adrenalectomy. With a short treatment time and minimal hospital stay, RF ablation can provide rapid clinical and biochemical improvement.
Dr. Lima Lawrence, an internal medicine resident at the University of Illinois at Chicago/Advocate Christ Medical Center in Oak Lawn, presented a case report and a review of the literature during an oral abstract session at the annual meeting of the American Association of Clinical Endocrinologists. The patient was a 65-year-old woman who presented with weight gain, decreased energy, and muscle weakness. On physical exam, she was hypertensive, anxious, obese, and had prominent supraclavicular fat pads. Salivary cortisol and overnight dexamethasone suppression tests were both elevated, and ACTH levels were depressed, confirming the diagnosis of a cortisol-secreting tumor causing adrenal Cushing’s syndrome. Computed tomography (CT) surveillance showed a progressively enlarging right-sided adrenal mass. A peritoneal biopsy revealed a low-grade serous neoplasm of peritoneal origin.
Her medical history included type 2 diabetes, uncontrolled hypertension, mixed connective tissue disease, depression, and total abdominal hysterectomy with bilateral salpingo-oophorectomy for ovarian cancer.
Dr. Lawrence said the patient had been scheduled for adrenalectomy, but it was not performed because of an intraoperative finding of peritoneal studding from what turned out to be metastatic ovarian cancer. Therefore, she underwent CT-guided RF ablation of the adrenal mass using a 14-gauge probe that heated a 3.5-cm ablation zone to 50-60 C for 8-10 minutes to achieve complete tumor necrosis.
The patient showed dramatic “clinical and biochemical improvement,” Dr. Lawrence said. The patient had no procedural complications and no blood loss and was observed for 23 hours before being discharged to home. A CT scan 8 weeks later showed a slightly decreased mass with marked decreased radiographic attenuation post-contrast from 30.2 Hounsfield Units (HU) preoperatively to 17 HU on follow-up.
Potential adverse outcomes using RF ablation include a risk of pneumothorax, hemothorax, and tumor seeding along the catheter track, but this last possibility can be mitigated by continuing to heat the RF probe as it is withdrawn.
Published evidence supports use of RF ablation. “To date there have been no randomized clinical trials comparing the safety, efficacy, and survival benefits of adrenalectomy vs. radio frequency ablation,” she said. It may not be feasible to do a randomized trial. But a review of the literature generally supports the efficacy of the technique although the publications each involved a small series of patients, Dr. Lawrence said in an interview.
A 2003 series (Cancer. 2003;97:554-60) of 15 primary or metastatic adrenal cell carcinomas that were unresectable or were in patients who were not surgical candidates showed nonenhancement and no growth in 8 (53%) at a mean follow-up of 10.3 months. Eight of the 12 tumors of 5 cm or smaller had complete loss of radiographic enhancement and a decrease in size.
From a retrospective series of 13 patients with functional adrenal neoplasms over 7 years, there was 100% resolution of biochemical abnormalities and clinical symptoms at a mean follow-up of 21.2 months. One small pneumothorax and one limited hemothorax occurred, neither of which required hospital admission. There were two instances of transient, self-remitting hypertension associated with the procedures (Radiology. 2011;258:308-16).
In 2015, one group of investigators followed 11 patients for 12 weeks postprocedure. Eight of nine patients with Conn’s syndrome attained normal serum aldosterone levels. One with a nodule close to the inferior vena cava had incomplete ablation. Two of two Cushing’s patients had normal cortisol levels after the procedure (J Vasc Interv Radiol. 2015;26:1459-64).
A retrospective analysis of 16 adrenal metastases showed that 13 (81%) had no local progression over 14 months after ablation. In two of three functional adrenal neoplasms, clinical and biochemical abnormalities resolved (Eur J Radiol. 2012.81:1717-23).
A retrospective series of 10 adrenal metastases showed that one recurred at 7 months after image-guided thermal ablation, with no recurrence of the rest at 26.6 months. There was no tumor recurrence for any of the cases of metastatic disease localized to the RF ablation site (J Vasc Interv Radiol. 2014;25:593-8).
Results were somewhat less good in a retrospective evaluation of 35 patients with unresectable adrenal masses over 9 years. Although 33 of 35 (94%) lost tumor enhancement after the initial adrenal RF ablation, there was local tumor progression in 8 of 35 (23%) patients at a mean follow-up of 30.1 months (Radiology. 2015;277:584-93).
Finally, Dr. Lawrence discussed a systematic literature review on adrenalectomy vs. stereotactic ablative body radiotherapy (SABR) and percutaneous catheter ablation (PCA) in the treatment of adrenal metastases: 30 papers on adrenalectomy on 818 patients; 9 papers on SABR on 178 patients; and 6 papers on PCA, including RF ablation, on 51 patients. The authors concluded that there was “insufficient evidence to determine the best local treatment modality for isolated or limited adrenal metastases.” Adrenalectomy appeared to be a reasonable treatment for suitable patients. SABR was a valid alternative for nonsurgical candidates, but they did not recommend PCA until more long-term outcomes were available (Cancer Treat Rev. 2014;40:838-46).
Dr. Lawrence concurred, based on her case study and literature review. She said RF ablation “offers patients a minimally invasive option for treating focal adrenal tumors” and is a “safe and effective procedure … in patients who are poor surgical candidates or refuse adrenalectomy.” More long-term follow-up studies are needed before RF ablation could replace adrenalectomy, she noted.
ORLANDO – Radiofrequency (RF) ablation is a safe and effective procedure for treating focal adrenal tumors in patients who are poor surgical candidates or who refuse adrenalectomy. With a short treatment time and minimal hospital stay, RF ablation can provide rapid clinical and biochemical improvement.
Dr. Lima Lawrence, an internal medicine resident at the University of Illinois at Chicago/Advocate Christ Medical Center in Oak Lawn, presented a case report and a review of the literature during an oral abstract session at the annual meeting of the American Association of Clinical Endocrinologists. The patient was a 65-year-old woman who presented with weight gain, decreased energy, and muscle weakness. On physical exam, she was hypertensive, anxious, obese, and had prominent supraclavicular fat pads. Salivary cortisol and overnight dexamethasone suppression tests were both elevated, and ACTH levels were depressed, confirming the diagnosis of a cortisol-secreting tumor causing adrenal Cushing’s syndrome. Computed tomography (CT) surveillance showed a progressively enlarging right-sided adrenal mass. A peritoneal biopsy revealed a low-grade serous neoplasm of peritoneal origin.
Her medical history included type 2 diabetes, uncontrolled hypertension, mixed connective tissue disease, depression, and total abdominal hysterectomy with bilateral salpingo-oophorectomy for ovarian cancer.
Dr. Lawrence said the patient had been scheduled for adrenalectomy, but it was not performed because of an intraoperative finding of peritoneal studding from what turned out to be metastatic ovarian cancer. Therefore, she underwent CT-guided RF ablation of the adrenal mass using a 14-gauge probe that heated a 3.5-cm ablation zone to 50-60 C for 8-10 minutes to achieve complete tumor necrosis.
The patient showed dramatic “clinical and biochemical improvement,” Dr. Lawrence said. The patient had no procedural complications and no blood loss and was observed for 23 hours before being discharged to home. A CT scan 8 weeks later showed a slightly decreased mass with marked decreased radiographic attenuation post-contrast from 30.2 Hounsfield Units (HU) preoperatively to 17 HU on follow-up.
Potential adverse outcomes using RF ablation include a risk of pneumothorax, hemothorax, and tumor seeding along the catheter track, but this last possibility can be mitigated by continuing to heat the RF probe as it is withdrawn.
Published evidence supports use of RF ablation. “To date there have been no randomized clinical trials comparing the safety, efficacy, and survival benefits of adrenalectomy vs. radio frequency ablation,” she said. It may not be feasible to do a randomized trial. But a review of the literature generally supports the efficacy of the technique although the publications each involved a small series of patients, Dr. Lawrence said in an interview.
A 2003 series (Cancer. 2003;97:554-60) of 15 primary or metastatic adrenal cell carcinomas that were unresectable or were in patients who were not surgical candidates showed nonenhancement and no growth in 8 (53%) at a mean follow-up of 10.3 months. Eight of the 12 tumors of 5 cm or smaller had complete loss of radiographic enhancement and a decrease in size.
From a retrospective series of 13 patients with functional adrenal neoplasms over 7 years, there was 100% resolution of biochemical abnormalities and clinical symptoms at a mean follow-up of 21.2 months. One small pneumothorax and one limited hemothorax occurred, neither of which required hospital admission. There were two instances of transient, self-remitting hypertension associated with the procedures (Radiology. 2011;258:308-16).
In 2015, one group of investigators followed 11 patients for 12 weeks postprocedure. Eight of nine patients with Conn’s syndrome attained normal serum aldosterone levels. One with a nodule close to the inferior vena cava had incomplete ablation. Two of two Cushing’s patients had normal cortisol levels after the procedure (J Vasc Interv Radiol. 2015;26:1459-64).
A retrospective analysis of 16 adrenal metastases showed that 13 (81%) had no local progression over 14 months after ablation. In two of three functional adrenal neoplasms, clinical and biochemical abnormalities resolved (Eur J Radiol. 2012.81:1717-23).
A retrospective series of 10 adrenal metastases showed that one recurred at 7 months after image-guided thermal ablation, with no recurrence of the rest at 26.6 months. There was no tumor recurrence for any of the cases of metastatic disease localized to the RF ablation site (J Vasc Interv Radiol. 2014;25:593-8).
Results were somewhat less good in a retrospective evaluation of 35 patients with unresectable adrenal masses over 9 years. Although 33 of 35 (94%) lost tumor enhancement after the initial adrenal RF ablation, there was local tumor progression in 8 of 35 (23%) patients at a mean follow-up of 30.1 months (Radiology. 2015;277:584-93).
Finally, Dr. Lawrence discussed a systematic literature review on adrenalectomy vs. stereotactic ablative body radiotherapy (SABR) and percutaneous catheter ablation (PCA) in the treatment of adrenal metastases: 30 papers on adrenalectomy on 818 patients; 9 papers on SABR on 178 patients; and 6 papers on PCA, including RF ablation, on 51 patients. The authors concluded that there was “insufficient evidence to determine the best local treatment modality for isolated or limited adrenal metastases.” Adrenalectomy appeared to be a reasonable treatment for suitable patients. SABR was a valid alternative for nonsurgical candidates, but they did not recommend PCA until more long-term outcomes were available (Cancer Treat Rev. 2014;40:838-46).
Dr. Lawrence concurred, based on her case study and literature review. She said RF ablation “offers patients a minimally invasive option for treating focal adrenal tumors” and is a “safe and effective procedure … in patients who are poor surgical candidates or refuse adrenalectomy.” More long-term follow-up studies are needed before RF ablation could replace adrenalectomy, she noted.
EXPERT ANALYSIS AT AACE 2016

Give serious thought before starting antipsychotics in elders
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
Low-FODMAP diet eased abdominal symptoms in IBS
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
AT DDW® 2016
Key clinical point: A diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols was associated with significant and clinically meaningful improvements in the abdominal symptoms of diarrhea-predominant irritable bowel syndrome.
Major finding: About half of patients on the low-FODMAP diet improved, compared with about a quarter of patients on a common-sense control diet.
Data source: A prospective, single-center, single-blind randomized controlled trial of 92 adults with IBS with diarrhea (Rome III).
Disclosures: Dr. Eswaren had no disclosures.
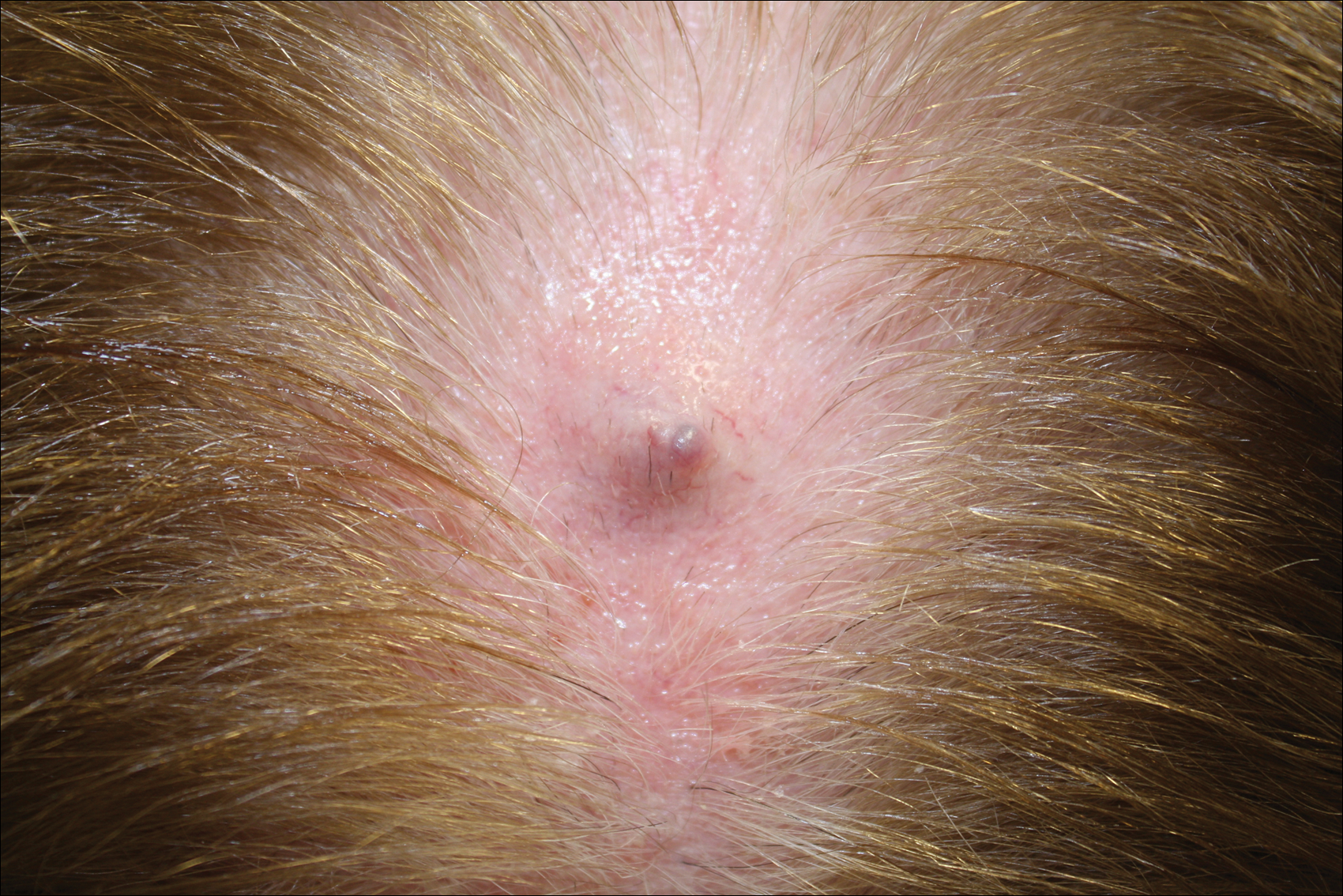
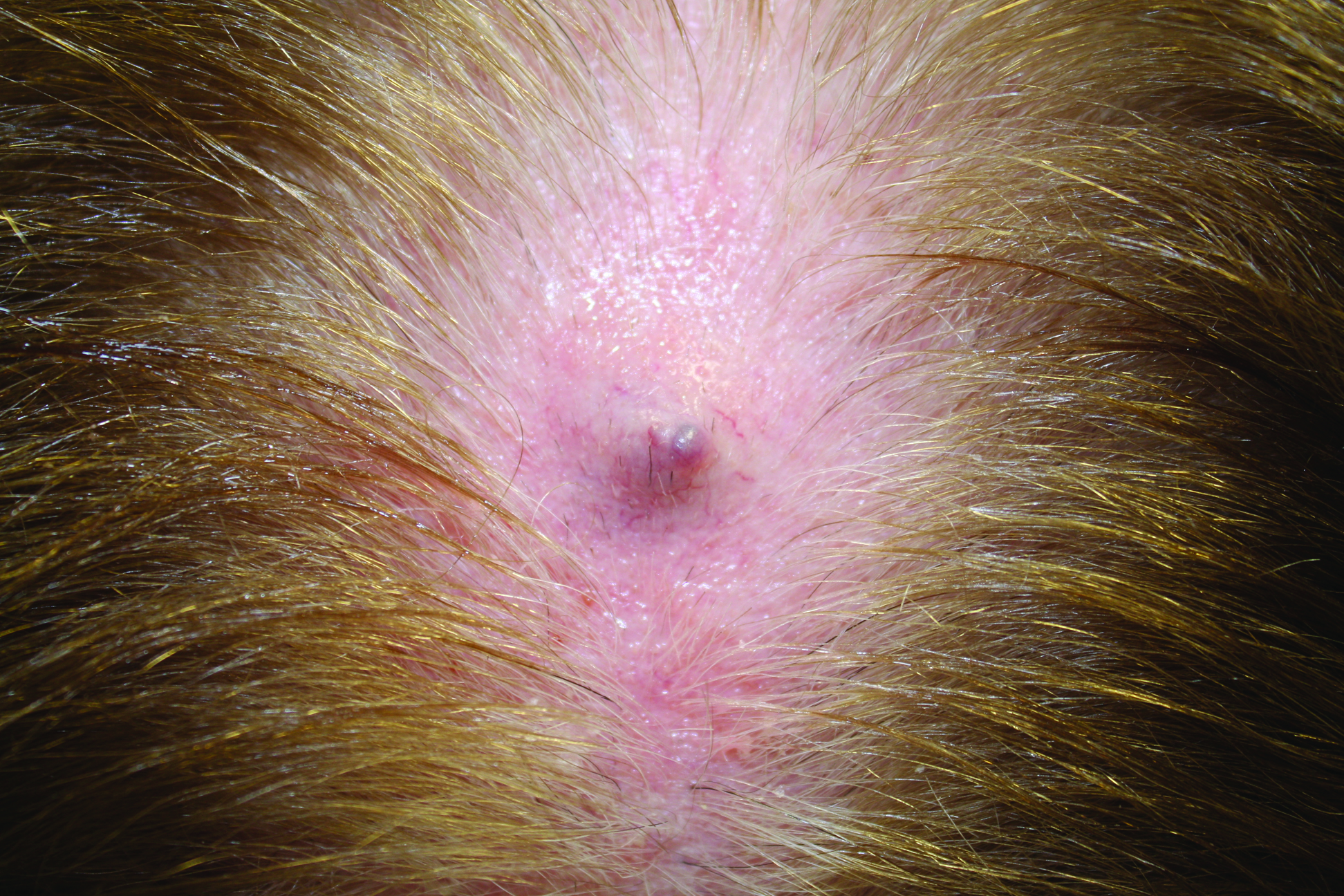
Firm Gray Nodule on the Scalp
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
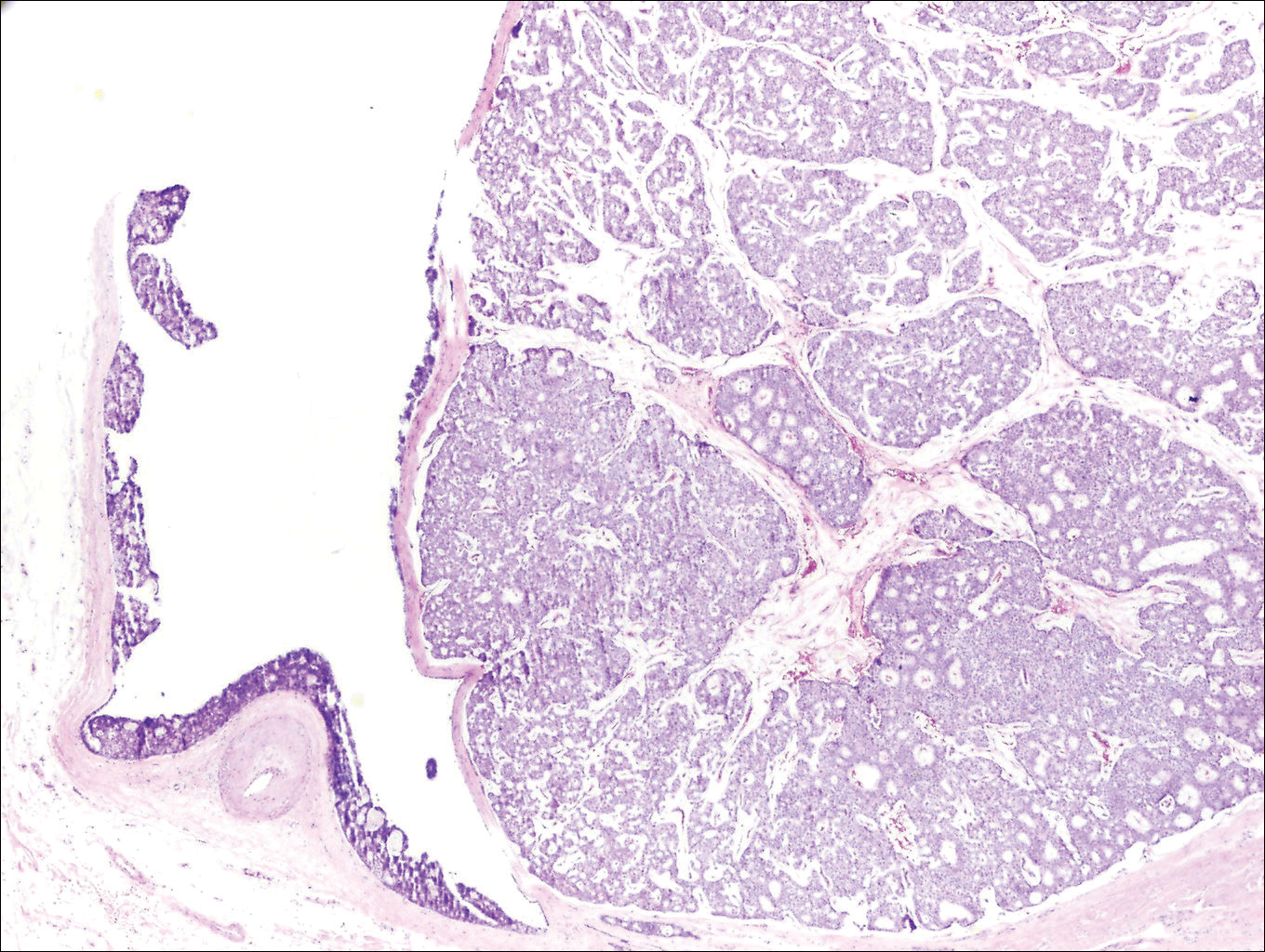
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
Dimethyl Fumarate and Fingolimod May Decrease Relapse Rate More Than Other DMTs
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.

Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.
Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.
Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson

Alemtuzumab-Associated Improvement Is Sustained for More Than Five Years
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.

Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.
Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.
Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson

BENEFIT 11: An 11-Year Follow-Up of Early Treatment With Interferon Beta-1b
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.

Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.
Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.
Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams

Primary Herpes Simplex Virus Infection of the Nipple in a Breastfeeding Woman
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.

The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
Practice Points
- Herpes mastitis should be included in the differential diagnosis for breast pain during lactation.
- Children of breastfeeding women diagnosed with herpes mastitis require immediate evaluation for a possible source of the infection, as complications of herpes viral infection in infants can be severe and life threatening.
