User login
Nurse-Managed Protocols Offer Benefits in the Outpatient Management of Adults with Chronic Illness
Study Overview
Objective. To determine whether nurse-managed protocols are effective for the outpatient management of adults with diabetes, hypertension, and hyperlipidemia.
Study design. Systematic review and meta-analysis.
Data sources. The authors searched MEDLINE, Cochrane Central Register of Controlled Trials, EMBASE, and CINAHL for English-language peer-reviewed studies published between January 1980 and January 2014 that evaluated interventions that compared nurse-managed protocols with usual care in investigations targeting adults with chronic conditions. Two reviewers used eligibility criteria to assess titles, abstracts, and full texts, and resolved their disagreements by discussion or by consulting a third reviewer. Eligibility criteria included the involvement of an RN or LPN functioning beyond the usual scope of practice, such as adjusting medications, and conducting interventions based on a written protocol.
Main outcome measures. The effects of nurse-managed protocols on biophysical markers, patient treatment adherence, nurse protocol adherence, adverse effects, and resource use. When quantitative synthesis was feasible, dichotomous outcomes were combined using odds ratios and continuous outcomes were combined using mean differences in random-effects models. When quantitative synthesis was not feasible, the authors annualized data qualitatively, giving more weight to evidence from higher-quality studies. They evaluated overall strength of evidence (SOE) by assessing risk of bias, consistency, directness, and precision, and assigned a rating of high, moderate, or low SOE, or insufficient evidence.
Main results. Of the 2954 studies in the search results, 18 were ultimately eligible and included in the review, 16 randomized controlled trials and 2 before and after diabetes studies. Eleven were done in Western Europe and 7 in the United States. An RN or non-US equivalent was the interventionist in all studies (none used an LPN). In only 11 of the 18 studies were nurses independently allowed to initiate new medications. The meta-analysis found that hemoglobin A1c (HbA1c) level decreased by 0.4% (moderate SOE) (95% confidence interval {CI}, 0.1% to 0.7%) (n = 8), systolic and diastolic blood pressure decreased by 3.68 mm Hg (CI, 1.05 to 6.31) and 1.56 mm Hg (CI, 0.36 to 2.76), respectively (moderate SOE) (n = 12); total cholesterol level decreased by 9.37 mg/dL (20.77-mg/dL decrease to 2.02-mg/dL increase) (n = 9); and low-density-lipoprotein cholesterol level decreased by 12.07 mg/dL (CI, 28.27-mg/dL decrease to 4.13-mg/dL increase) (low SOE) (n = 6). The SOE was insufficient to estimate a treatment effect for all other outcomes.
Conclusion. A team approach that uses nurse-managed protocols may have positive effects on the outpatient management of adults with chronic conditions such as diabetes, hypertension, and hyperlipidemia.
Commentary
Hypertension, diabetes, and hyperlipidemia are major causes of morbidity and mortality worldwide and are widely prevalent in the United States. These chronic illnesses require long-term medical management, often requiring management of multiple medications and patient lifestyle changes and self-monitoring [1]. The patient-centered medical home, which involves a team approach, is increasingly being recognized as a promising model for delivering effective chronic disease care. Likewise, expanding the role of nurses as part of team care is increasingly being explored to help achieve high quality patient outcomes. The use of nurse-managed protocols can be an appropriate strategy in this scenario.
In this study, the researchers aimed to determine whether nurse-managed protocols are effective for outpatient management of adults with diabetes, hypertension, and hyperlipidemia and performed a systematic review and meta-analysis. Researchers followed a standardized procedure to conduct their search and carefully reviewed the studies, including contacting authors for missing data or clarification. They followed the approach recommended by the Agency for Healthcare Research and Quality (AHRQ) to evaluate the overall strength of the body of evidence [2].
However, some limitations must be taken into account. They acknowledge that they may have missed studies in which nurses had autonomy to practice in capacities beyond their scope of practice. In addition, the literature lacked details about the interventions and protocols used. Also, the researchers searched for studies across a 34-year range (1980–2014). Changes occurring in the nursing profession over these years may have impacted the findings.
Applications for Clinical Practice
Team-based care that includes nurse-managed protocols for titrating medications can be beneficial in the management of chronic conditions in primary care patients. With physician shortages predicted, which will impact primary care more than other specialties, team approaches using nurse-managed protocols have the potential to help lighten physician workloads and ensure quality care.
—Paloma Cesar de Sales, BN, RN, MS
1. Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the Chronic Care Model in the new millennium. Health Aff (Millwood) 2009;28:75–85.
2. Agency for Healthcare Research and Quality. Methods guide for effectiveness and comparative effectiveness reviews. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
Study Overview
Objective. To determine whether nurse-managed protocols are effective for the outpatient management of adults with diabetes, hypertension, and hyperlipidemia.
Study design. Systematic review and meta-analysis.
Data sources. The authors searched MEDLINE, Cochrane Central Register of Controlled Trials, EMBASE, and CINAHL for English-language peer-reviewed studies published between January 1980 and January 2014 that evaluated interventions that compared nurse-managed protocols with usual care in investigations targeting adults with chronic conditions. Two reviewers used eligibility criteria to assess titles, abstracts, and full texts, and resolved their disagreements by discussion or by consulting a third reviewer. Eligibility criteria included the involvement of an RN or LPN functioning beyond the usual scope of practice, such as adjusting medications, and conducting interventions based on a written protocol.
Main outcome measures. The effects of nurse-managed protocols on biophysical markers, patient treatment adherence, nurse protocol adherence, adverse effects, and resource use. When quantitative synthesis was feasible, dichotomous outcomes were combined using odds ratios and continuous outcomes were combined using mean differences in random-effects models. When quantitative synthesis was not feasible, the authors annualized data qualitatively, giving more weight to evidence from higher-quality studies. They evaluated overall strength of evidence (SOE) by assessing risk of bias, consistency, directness, and precision, and assigned a rating of high, moderate, or low SOE, or insufficient evidence.
Main results. Of the 2954 studies in the search results, 18 were ultimately eligible and included in the review, 16 randomized controlled trials and 2 before and after diabetes studies. Eleven were done in Western Europe and 7 in the United States. An RN or non-US equivalent was the interventionist in all studies (none used an LPN). In only 11 of the 18 studies were nurses independently allowed to initiate new medications. The meta-analysis found that hemoglobin A1c (HbA1c) level decreased by 0.4% (moderate SOE) (95% confidence interval {CI}, 0.1% to 0.7%) (n = 8), systolic and diastolic blood pressure decreased by 3.68 mm Hg (CI, 1.05 to 6.31) and 1.56 mm Hg (CI, 0.36 to 2.76), respectively (moderate SOE) (n = 12); total cholesterol level decreased by 9.37 mg/dL (20.77-mg/dL decrease to 2.02-mg/dL increase) (n = 9); and low-density-lipoprotein cholesterol level decreased by 12.07 mg/dL (CI, 28.27-mg/dL decrease to 4.13-mg/dL increase) (low SOE) (n = 6). The SOE was insufficient to estimate a treatment effect for all other outcomes.
Conclusion. A team approach that uses nurse-managed protocols may have positive effects on the outpatient management of adults with chronic conditions such as diabetes, hypertension, and hyperlipidemia.
Commentary
Hypertension, diabetes, and hyperlipidemia are major causes of morbidity and mortality worldwide and are widely prevalent in the United States. These chronic illnesses require long-term medical management, often requiring management of multiple medications and patient lifestyle changes and self-monitoring [1]. The patient-centered medical home, which involves a team approach, is increasingly being recognized as a promising model for delivering effective chronic disease care. Likewise, expanding the role of nurses as part of team care is increasingly being explored to help achieve high quality patient outcomes. The use of nurse-managed protocols can be an appropriate strategy in this scenario.
In this study, the researchers aimed to determine whether nurse-managed protocols are effective for outpatient management of adults with diabetes, hypertension, and hyperlipidemia and performed a systematic review and meta-analysis. Researchers followed a standardized procedure to conduct their search and carefully reviewed the studies, including contacting authors for missing data or clarification. They followed the approach recommended by the Agency for Healthcare Research and Quality (AHRQ) to evaluate the overall strength of the body of evidence [2].
However, some limitations must be taken into account. They acknowledge that they may have missed studies in which nurses had autonomy to practice in capacities beyond their scope of practice. In addition, the literature lacked details about the interventions and protocols used. Also, the researchers searched for studies across a 34-year range (1980–2014). Changes occurring in the nursing profession over these years may have impacted the findings.
Applications for Clinical Practice
Team-based care that includes nurse-managed protocols for titrating medications can be beneficial in the management of chronic conditions in primary care patients. With physician shortages predicted, which will impact primary care more than other specialties, team approaches using nurse-managed protocols have the potential to help lighten physician workloads and ensure quality care.
—Paloma Cesar de Sales, BN, RN, MS
Study Overview
Objective. To determine whether nurse-managed protocols are effective for the outpatient management of adults with diabetes, hypertension, and hyperlipidemia.
Study design. Systematic review and meta-analysis.
Data sources. The authors searched MEDLINE, Cochrane Central Register of Controlled Trials, EMBASE, and CINAHL for English-language peer-reviewed studies published between January 1980 and January 2014 that evaluated interventions that compared nurse-managed protocols with usual care in investigations targeting adults with chronic conditions. Two reviewers used eligibility criteria to assess titles, abstracts, and full texts, and resolved their disagreements by discussion or by consulting a third reviewer. Eligibility criteria included the involvement of an RN or LPN functioning beyond the usual scope of practice, such as adjusting medications, and conducting interventions based on a written protocol.
Main outcome measures. The effects of nurse-managed protocols on biophysical markers, patient treatment adherence, nurse protocol adherence, adverse effects, and resource use. When quantitative synthesis was feasible, dichotomous outcomes were combined using odds ratios and continuous outcomes were combined using mean differences in random-effects models. When quantitative synthesis was not feasible, the authors annualized data qualitatively, giving more weight to evidence from higher-quality studies. They evaluated overall strength of evidence (SOE) by assessing risk of bias, consistency, directness, and precision, and assigned a rating of high, moderate, or low SOE, or insufficient evidence.
Main results. Of the 2954 studies in the search results, 18 were ultimately eligible and included in the review, 16 randomized controlled trials and 2 before and after diabetes studies. Eleven were done in Western Europe and 7 in the United States. An RN or non-US equivalent was the interventionist in all studies (none used an LPN). In only 11 of the 18 studies were nurses independently allowed to initiate new medications. The meta-analysis found that hemoglobin A1c (HbA1c) level decreased by 0.4% (moderate SOE) (95% confidence interval {CI}, 0.1% to 0.7%) (n = 8), systolic and diastolic blood pressure decreased by 3.68 mm Hg (CI, 1.05 to 6.31) and 1.56 mm Hg (CI, 0.36 to 2.76), respectively (moderate SOE) (n = 12); total cholesterol level decreased by 9.37 mg/dL (20.77-mg/dL decrease to 2.02-mg/dL increase) (n = 9); and low-density-lipoprotein cholesterol level decreased by 12.07 mg/dL (CI, 28.27-mg/dL decrease to 4.13-mg/dL increase) (low SOE) (n = 6). The SOE was insufficient to estimate a treatment effect for all other outcomes.
Conclusion. A team approach that uses nurse-managed protocols may have positive effects on the outpatient management of adults with chronic conditions such as diabetes, hypertension, and hyperlipidemia.
Commentary
Hypertension, diabetes, and hyperlipidemia are major causes of morbidity and mortality worldwide and are widely prevalent in the United States. These chronic illnesses require long-term medical management, often requiring management of multiple medications and patient lifestyle changes and self-monitoring [1]. The patient-centered medical home, which involves a team approach, is increasingly being recognized as a promising model for delivering effective chronic disease care. Likewise, expanding the role of nurses as part of team care is increasingly being explored to help achieve high quality patient outcomes. The use of nurse-managed protocols can be an appropriate strategy in this scenario.
In this study, the researchers aimed to determine whether nurse-managed protocols are effective for outpatient management of adults with diabetes, hypertension, and hyperlipidemia and performed a systematic review and meta-analysis. Researchers followed a standardized procedure to conduct their search and carefully reviewed the studies, including contacting authors for missing data or clarification. They followed the approach recommended by the Agency for Healthcare Research and Quality (AHRQ) to evaluate the overall strength of the body of evidence [2].
However, some limitations must be taken into account. They acknowledge that they may have missed studies in which nurses had autonomy to practice in capacities beyond their scope of practice. In addition, the literature lacked details about the interventions and protocols used. Also, the researchers searched for studies across a 34-year range (1980–2014). Changes occurring in the nursing profession over these years may have impacted the findings.
Applications for Clinical Practice
Team-based care that includes nurse-managed protocols for titrating medications can be beneficial in the management of chronic conditions in primary care patients. With physician shortages predicted, which will impact primary care more than other specialties, team approaches using nurse-managed protocols have the potential to help lighten physician workloads and ensure quality care.
—Paloma Cesar de Sales, BN, RN, MS
1. Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the Chronic Care Model in the new millennium. Health Aff (Millwood) 2009;28:75–85.
2. Agency for Healthcare Research and Quality. Methods guide for effectiveness and comparative effectiveness reviews. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
1. Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the Chronic Care Model in the new millennium. Health Aff (Millwood) 2009;28:75–85.
2. Agency for Healthcare Research and Quality. Methods guide for effectiveness and comparative effectiveness reviews. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
Increased Dementia Risk Among Men and Women With Posttraumatic Stress Disorder
TORONTO—Posttraumatic stress disorder (PTSD) is a risk factor for dementia in men and women. Among men, PTSD is associated with a 90% increased risk of incident dementia, according to research presented at the Alzheimer’s Association International Conference.
Women and PTSD
Previous studies indicate that women are at a higher risk of PTSD, but little research is available concerning the risk of dementia in women diagnosed with PTSD. “They are more likely to experience trauma, maybe from domestic abuse, violence, [and] rape … so I think this is a huge area that needs research,” said Jason Flatt, PhD, MPH, Assistant Professor of Health and Aging at the University of California, San Francisco. To analyze the link between PTSD and dementia in both genders, Dr. Flatt and colleagues examined data from a diverse population.
“The objectives of the study were to look at the effect of PTSD on the risk of dementia over 13 years among older men and women and see if the association is explained by medical comorbidities like depression and traumatic brain injury,” said Dr. Flatt.
Diverse Population Sample
Participants were selected from the Kaiser Permanente Northern California healthcare system and were age 60 or older in January 2002. Women made up 54.7% of the population, 68% of the population was white, 5.5% was black, 6.5% was Hispanic, and 9% was Asian. Mean age at baseline was 71. The dementia diagnoses were collected from medical records for January 1, 2002 through December 31, 2014. Mean follow-up was approximately eight years.
Investigators evaluated the association between PTSD and dementia using gender-modified models adjusted for age, race, diabetes, and stroke, with censoring for death and gaps in health coverage of greater than 90 days. In all, 1,147 patients were diagnosed with PTSD. In addition, researchers found that during the 13-year follow-up period, 11.8% of subjects received a diagnosis of dementia.
People with PTSD were more likely to experience traumatic brain injuries and depression. Patients with PTSD also had a 56% increased risk of developing dementia, compared with controls without PTSD. Men with PTSD had a 90% increase in dementia risk, and women with PTSD had a 41% increase in dementia risk, compared with controls.
“This is the first large study of PTSD and risk of dementia in women, and results suggest that PTSD is a risk factor in both genders,” said Dr. Flatt.
Strengths of this study include its longitudinal design, diverse sample, and 13-year follow-up period. Dementia was diagnosed by physicians, however, and as a result, researchers were unable to observe dementia subtypes.
“Future research should think about these mechanisms and how to link and better understand how PTSD may be involved in dementia risk,” said Dr. Flatt.
Suggested Reading
Wang TY, Wei HT, Liou YJ et al. Risk for developing dementia among patients with posttraumatic stress disorder: A nationwide longitudinal study. J Affect Disord. 2016 Aug 16 [Epub ahead of print].
McCartney JR, Severson K. Sexual violence, post-traumatic stress disorder and dementia. J Am Geriatr Soc. 1997; 45(1):76-78.
TORONTO—Posttraumatic stress disorder (PTSD) is a risk factor for dementia in men and women. Among men, PTSD is associated with a 90% increased risk of incident dementia, according to research presented at the Alzheimer’s Association International Conference.
Women and PTSD
Previous studies indicate that women are at a higher risk of PTSD, but little research is available concerning the risk of dementia in women diagnosed with PTSD. “They are more likely to experience trauma, maybe from domestic abuse, violence, [and] rape … so I think this is a huge area that needs research,” said Jason Flatt, PhD, MPH, Assistant Professor of Health and Aging at the University of California, San Francisco. To analyze the link between PTSD and dementia in both genders, Dr. Flatt and colleagues examined data from a diverse population.
“The objectives of the study were to look at the effect of PTSD on the risk of dementia over 13 years among older men and women and see if the association is explained by medical comorbidities like depression and traumatic brain injury,” said Dr. Flatt.
Diverse Population Sample
Participants were selected from the Kaiser Permanente Northern California healthcare system and were age 60 or older in January 2002. Women made up 54.7% of the population, 68% of the population was white, 5.5% was black, 6.5% was Hispanic, and 9% was Asian. Mean age at baseline was 71. The dementia diagnoses were collected from medical records for January 1, 2002 through December 31, 2014. Mean follow-up was approximately eight years.
Investigators evaluated the association between PTSD and dementia using gender-modified models adjusted for age, race, diabetes, and stroke, with censoring for death and gaps in health coverage of greater than 90 days. In all, 1,147 patients were diagnosed with PTSD. In addition, researchers found that during the 13-year follow-up period, 11.8% of subjects received a diagnosis of dementia.
People with PTSD were more likely to experience traumatic brain injuries and depression. Patients with PTSD also had a 56% increased risk of developing dementia, compared with controls without PTSD. Men with PTSD had a 90% increase in dementia risk, and women with PTSD had a 41% increase in dementia risk, compared with controls.
“This is the first large study of PTSD and risk of dementia in women, and results suggest that PTSD is a risk factor in both genders,” said Dr. Flatt.
Strengths of this study include its longitudinal design, diverse sample, and 13-year follow-up period. Dementia was diagnosed by physicians, however, and as a result, researchers were unable to observe dementia subtypes.
“Future research should think about these mechanisms and how to link and better understand how PTSD may be involved in dementia risk,” said Dr. Flatt.
Suggested Reading
Wang TY, Wei HT, Liou YJ et al. Risk for developing dementia among patients with posttraumatic stress disorder: A nationwide longitudinal study. J Affect Disord. 2016 Aug 16 [Epub ahead of print].
McCartney JR, Severson K. Sexual violence, post-traumatic stress disorder and dementia. J Am Geriatr Soc. 1997; 45(1):76-78.
TORONTO—Posttraumatic stress disorder (PTSD) is a risk factor for dementia in men and women. Among men, PTSD is associated with a 90% increased risk of incident dementia, according to research presented at the Alzheimer’s Association International Conference.
Women and PTSD
Previous studies indicate that women are at a higher risk of PTSD, but little research is available concerning the risk of dementia in women diagnosed with PTSD. “They are more likely to experience trauma, maybe from domestic abuse, violence, [and] rape … so I think this is a huge area that needs research,” said Jason Flatt, PhD, MPH, Assistant Professor of Health and Aging at the University of California, San Francisco. To analyze the link between PTSD and dementia in both genders, Dr. Flatt and colleagues examined data from a diverse population.
“The objectives of the study were to look at the effect of PTSD on the risk of dementia over 13 years among older men and women and see if the association is explained by medical comorbidities like depression and traumatic brain injury,” said Dr. Flatt.
Diverse Population Sample
Participants were selected from the Kaiser Permanente Northern California healthcare system and were age 60 or older in January 2002. Women made up 54.7% of the population, 68% of the population was white, 5.5% was black, 6.5% was Hispanic, and 9% was Asian. Mean age at baseline was 71. The dementia diagnoses were collected from medical records for January 1, 2002 through December 31, 2014. Mean follow-up was approximately eight years.
Investigators evaluated the association between PTSD and dementia using gender-modified models adjusted for age, race, diabetes, and stroke, with censoring for death and gaps in health coverage of greater than 90 days. In all, 1,147 patients were diagnosed with PTSD. In addition, researchers found that during the 13-year follow-up period, 11.8% of subjects received a diagnosis of dementia.
People with PTSD were more likely to experience traumatic brain injuries and depression. Patients with PTSD also had a 56% increased risk of developing dementia, compared with controls without PTSD. Men with PTSD had a 90% increase in dementia risk, and women with PTSD had a 41% increase in dementia risk, compared with controls.
“This is the first large study of PTSD and risk of dementia in women, and results suggest that PTSD is a risk factor in both genders,” said Dr. Flatt.
Strengths of this study include its longitudinal design, diverse sample, and 13-year follow-up period. Dementia was diagnosed by physicians, however, and as a result, researchers were unable to observe dementia subtypes.
“Future research should think about these mechanisms and how to link and better understand how PTSD may be involved in dementia risk,” said Dr. Flatt.
Suggested Reading
Wang TY, Wei HT, Liou YJ et al. Risk for developing dementia among patients with posttraumatic stress disorder: A nationwide longitudinal study. J Affect Disord. 2016 Aug 16 [Epub ahead of print].
McCartney JR, Severson K. Sexual violence, post-traumatic stress disorder and dementia. J Am Geriatr Soc. 1997; 45(1):76-78.
Glymphatic System May Play Key Role in Removing Brain Waste
SAN DIEGO—A recently discovered system known as the glymphatic system clears waste from the brain. It is most active during sleep and may have implications in headache and in neurodegenerative diseases associated with pathologic protein aggregation, including Parkinson’s disease and Alzheimer’s disease, said Helene Benveniste, MD, PhD, Professor of Anesthesiology and Vice Chair for Research at Stony Brook School of Medicine in New York. Data suggest that sleep, posture, and brain injury may affect this waste removal system.

“We look at the glymphatic pathway as a bit of an overlooked compartment of the vasculature or the perivascular space that is … facilitating solute and waste removal,” Dr. Benveniste said at the 58th Annual Scientific Meeting of the American Headache Society. Although most studies of the glymphatic system so far have been performed in rodents, “data are starting to come out showing that this system is also present in humans,” she said.
A Brainwide Pathway
The glymphatic system, which gets its name from the glial cells and lymphatic system that it mimics, may explain how the brain—one of the most metabolically active organs—clears excess fluids, solutes, and waste products without authentic lymph vessels, Dr. Benveniste said. The system consists of a brainwide pathway that facilitates the exchange of CSF with interstitial fluid to clear interstitial waste from the brain parenchyma. The waste is moved into perivenous pathways and ultimately cleared via cervical lymphatic vessels.
Researchers first described the concept of the glymphatic system in Science Translational Medicine in 2012. They injected fluorescent tracers into the cisterna magna and fluorescent-tagged amyloid beta into brain parenchyma of mice and observed distribution of the tracers along the glymphatic pathway using two-photon imaging. The paper’s senior author, Maiken Nedergaard, MD, DMSc, Professor of Neurosurgery and Translational Neuromedicine at the University of Rochester in New York, contacted Dr. Benveniste to develop a way to visualize the system using MRI, which they accomplished using a 9.4-T system and small molecular weight contrast dye injected via an intrathecal catheter inserted in the cisterna magna.
In 2015, researchers in Norway published a case report in Acta Radiologica Open supporting the existence of a glymphatic system in humans. They administered intrathecal gadobutrol to diagnose a CSF leak in a patient. The patient underwent 3D T1-weighted imaging at one hour and 4.5 hours. The distribution of gadobutrol into the brain was consistent with that observed in rodents and supports the concept of a glymphatic pathway in the human brain, the authors concluded.
Researchers still are evaluating the glymphatic system’s role in maintaining brain health and how it differs in humans and rodents. Aquaporin channels, which are crucial in facilitating CSF transport from the periarterial space and into the interstitial space to drive waste removal via the glymphatic pathway, may be positioned differently in rodents and humans, Dr. Benveniste said. In addition, waste clearance may be orders of magnitude slower in humans due to brain size and complexity, she said.
Factors Affecting Glymphatic Flow
In mice genetically modified to lack aquaporin channels, convective flow and waste removal via the glymphatic pathway are slowed down immensely.
After traumatic brain injury, glymphatic pathway function was reduced by approximately 60% in mice for at least one month, Iliff et al reported in the Journal of Neuroscience in 2014. In mice without aquaporin channels, however, glymphatic pathway dysfunction was further exacerbated, and those animals developed neurofibrillary pathology and neurodegeneration.
One of the most important factors affecting glymphatic flow is interstitial space volume, which increases by 40% to 60% during sleep, Dr. Benveniste said. Natural sleep and certain types of anesthetics dramatically increase interstitial space volume, Xie et al reported in Science in 2013. Likewise, awaking sleeping mice sharply reduces glymphatic flow. The authors concluded, “the restorative function of sleep may be a consequence of the enhanced removal of potentially neurotoxic waste products that accumulate in the awake CNS.”
Injecting a norepinephrine receptor antagonist intrathecally can stimulate intense glymphatic transport in animals in the awake state, indicating that noradrenergic tone may be responsible for the process, Dr. Benveniste said.
She and her colleagues studied glymphatic clearance in mice anesthetized with dexmedetomidine, which induces a state similar to stage 2 sleep, versus the inhalational anesthetic isoflurane. Glymphatic processing was much greater in rodents that received dexmedetomidine.
Sleep Position
Hedok Lee, PhD, Clinical Assistant Professor of Anesthesiology at Stony Brook School of Medicine, Dr. Benveniste, and colleagues studied the effect of body posture on brain glymphatic transport in rats. They found that glymphatic transport and amyloid beta clearance were most efficient in the lateral and supine positions, while the prone position (ie, most upright and mimicking awake posture) resulted in slower clearance.
“Right lateral seems to be the position where you have got the best efflux and influx,” Dr. Benveniste said. The findings suggest that sleep position’s effect on the glymphatic system may be relevant for imaging the system in humans, and ultimately for patient care.
—Jake Remaly
Suggested Reading
Eide PK, Ringstad G. MRI with intrathecal MRI gadolinium contrast medium administration: a possible method to assess glymphatic function in human brain. Acta Radiol Open. 2015;4(11):2058460115609635.
Iliff JJ, Chen MJ, Plog BA, et al. Impairment of glymphatic pathway function promotes tau pathology after traumatic brain injury. J Neurosci. 2014;34(49):16180-16193.
Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111.
Lee H, Xie L, Yu M, et al. The effect of body posture on brain glymphatic transport. J Neurosci. 2015;35(31):11034-11044.
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
SAN DIEGO—A recently discovered system known as the glymphatic system clears waste from the brain. It is most active during sleep and may have implications in headache and in neurodegenerative diseases associated with pathologic protein aggregation, including Parkinson’s disease and Alzheimer’s disease, said Helene Benveniste, MD, PhD, Professor of Anesthesiology and Vice Chair for Research at Stony Brook School of Medicine in New York. Data suggest that sleep, posture, and brain injury may affect this waste removal system.
“We look at the glymphatic pathway as a bit of an overlooked compartment of the vasculature or the perivascular space that is … facilitating solute and waste removal,” Dr. Benveniste said at the 58th Annual Scientific Meeting of the American Headache Society. Although most studies of the glymphatic system so far have been performed in rodents, “data are starting to come out showing that this system is also present in humans,” she said.
A Brainwide Pathway
The glymphatic system, which gets its name from the glial cells and lymphatic system that it mimics, may explain how the brain—one of the most metabolically active organs—clears excess fluids, solutes, and waste products without authentic lymph vessels, Dr. Benveniste said. The system consists of a brainwide pathway that facilitates the exchange of CSF with interstitial fluid to clear interstitial waste from the brain parenchyma. The waste is moved into perivenous pathways and ultimately cleared via cervical lymphatic vessels.
Researchers first described the concept of the glymphatic system in Science Translational Medicine in 2012. They injected fluorescent tracers into the cisterna magna and fluorescent-tagged amyloid beta into brain parenchyma of mice and observed distribution of the tracers along the glymphatic pathway using two-photon imaging. The paper’s senior author, Maiken Nedergaard, MD, DMSc, Professor of Neurosurgery and Translational Neuromedicine at the University of Rochester in New York, contacted Dr. Benveniste to develop a way to visualize the system using MRI, which they accomplished using a 9.4-T system and small molecular weight contrast dye injected via an intrathecal catheter inserted in the cisterna magna.
In 2015, researchers in Norway published a case report in Acta Radiologica Open supporting the existence of a glymphatic system in humans. They administered intrathecal gadobutrol to diagnose a CSF leak in a patient. The patient underwent 3D T1-weighted imaging at one hour and 4.5 hours. The distribution of gadobutrol into the brain was consistent with that observed in rodents and supports the concept of a glymphatic pathway in the human brain, the authors concluded.
Researchers still are evaluating the glymphatic system’s role in maintaining brain health and how it differs in humans and rodents. Aquaporin channels, which are crucial in facilitating CSF transport from the periarterial space and into the interstitial space to drive waste removal via the glymphatic pathway, may be positioned differently in rodents and humans, Dr. Benveniste said. In addition, waste clearance may be orders of magnitude slower in humans due to brain size and complexity, she said.
Factors Affecting Glymphatic Flow
In mice genetically modified to lack aquaporin channels, convective flow and waste removal via the glymphatic pathway are slowed down immensely.
After traumatic brain injury, glymphatic pathway function was reduced by approximately 60% in mice for at least one month, Iliff et al reported in the Journal of Neuroscience in 2014. In mice without aquaporin channels, however, glymphatic pathway dysfunction was further exacerbated, and those animals developed neurofibrillary pathology and neurodegeneration.
One of the most important factors affecting glymphatic flow is interstitial space volume, which increases by 40% to 60% during sleep, Dr. Benveniste said. Natural sleep and certain types of anesthetics dramatically increase interstitial space volume, Xie et al reported in Science in 2013. Likewise, awaking sleeping mice sharply reduces glymphatic flow. The authors concluded, “the restorative function of sleep may be a consequence of the enhanced removal of potentially neurotoxic waste products that accumulate in the awake CNS.”
Injecting a norepinephrine receptor antagonist intrathecally can stimulate intense glymphatic transport in animals in the awake state, indicating that noradrenergic tone may be responsible for the process, Dr. Benveniste said.
She and her colleagues studied glymphatic clearance in mice anesthetized with dexmedetomidine, which induces a state similar to stage 2 sleep, versus the inhalational anesthetic isoflurane. Glymphatic processing was much greater in rodents that received dexmedetomidine.
Sleep Position
Hedok Lee, PhD, Clinical Assistant Professor of Anesthesiology at Stony Brook School of Medicine, Dr. Benveniste, and colleagues studied the effect of body posture on brain glymphatic transport in rats. They found that glymphatic transport and amyloid beta clearance were most efficient in the lateral and supine positions, while the prone position (ie, most upright and mimicking awake posture) resulted in slower clearance.
“Right lateral seems to be the position where you have got the best efflux and influx,” Dr. Benveniste said. The findings suggest that sleep position’s effect on the glymphatic system may be relevant for imaging the system in humans, and ultimately for patient care.
—Jake Remaly
Suggested Reading
Eide PK, Ringstad G. MRI with intrathecal MRI gadolinium contrast medium administration: a possible method to assess glymphatic function in human brain. Acta Radiol Open. 2015;4(11):2058460115609635.
Iliff JJ, Chen MJ, Plog BA, et al. Impairment of glymphatic pathway function promotes tau pathology after traumatic brain injury. J Neurosci. 2014;34(49):16180-16193.
Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111.
Lee H, Xie L, Yu M, et al. The effect of body posture on brain glymphatic transport. J Neurosci. 2015;35(31):11034-11044.
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
SAN DIEGO—A recently discovered system known as the glymphatic system clears waste from the brain. It is most active during sleep and may have implications in headache and in neurodegenerative diseases associated with pathologic protein aggregation, including Parkinson’s disease and Alzheimer’s disease, said Helene Benveniste, MD, PhD, Professor of Anesthesiology and Vice Chair for Research at Stony Brook School of Medicine in New York. Data suggest that sleep, posture, and brain injury may affect this waste removal system.
“We look at the glymphatic pathway as a bit of an overlooked compartment of the vasculature or the perivascular space that is … facilitating solute and waste removal,” Dr. Benveniste said at the 58th Annual Scientific Meeting of the American Headache Society. Although most studies of the glymphatic system so far have been performed in rodents, “data are starting to come out showing that this system is also present in humans,” she said.
A Brainwide Pathway
The glymphatic system, which gets its name from the glial cells and lymphatic system that it mimics, may explain how the brain—one of the most metabolically active organs—clears excess fluids, solutes, and waste products without authentic lymph vessels, Dr. Benveniste said. The system consists of a brainwide pathway that facilitates the exchange of CSF with interstitial fluid to clear interstitial waste from the brain parenchyma. The waste is moved into perivenous pathways and ultimately cleared via cervical lymphatic vessels.
Researchers first described the concept of the glymphatic system in Science Translational Medicine in 2012. They injected fluorescent tracers into the cisterna magna and fluorescent-tagged amyloid beta into brain parenchyma of mice and observed distribution of the tracers along the glymphatic pathway using two-photon imaging. The paper’s senior author, Maiken Nedergaard, MD, DMSc, Professor of Neurosurgery and Translational Neuromedicine at the University of Rochester in New York, contacted Dr. Benveniste to develop a way to visualize the system using MRI, which they accomplished using a 9.4-T system and small molecular weight contrast dye injected via an intrathecal catheter inserted in the cisterna magna.
In 2015, researchers in Norway published a case report in Acta Radiologica Open supporting the existence of a glymphatic system in humans. They administered intrathecal gadobutrol to diagnose a CSF leak in a patient. The patient underwent 3D T1-weighted imaging at one hour and 4.5 hours. The distribution of gadobutrol into the brain was consistent with that observed in rodents and supports the concept of a glymphatic pathway in the human brain, the authors concluded.
Researchers still are evaluating the glymphatic system’s role in maintaining brain health and how it differs in humans and rodents. Aquaporin channels, which are crucial in facilitating CSF transport from the periarterial space and into the interstitial space to drive waste removal via the glymphatic pathway, may be positioned differently in rodents and humans, Dr. Benveniste said. In addition, waste clearance may be orders of magnitude slower in humans due to brain size and complexity, she said.
Factors Affecting Glymphatic Flow
In mice genetically modified to lack aquaporin channels, convective flow and waste removal via the glymphatic pathway are slowed down immensely.
After traumatic brain injury, glymphatic pathway function was reduced by approximately 60% in mice for at least one month, Iliff et al reported in the Journal of Neuroscience in 2014. In mice without aquaporin channels, however, glymphatic pathway dysfunction was further exacerbated, and those animals developed neurofibrillary pathology and neurodegeneration.
One of the most important factors affecting glymphatic flow is interstitial space volume, which increases by 40% to 60% during sleep, Dr. Benveniste said. Natural sleep and certain types of anesthetics dramatically increase interstitial space volume, Xie et al reported in Science in 2013. Likewise, awaking sleeping mice sharply reduces glymphatic flow. The authors concluded, “the restorative function of sleep may be a consequence of the enhanced removal of potentially neurotoxic waste products that accumulate in the awake CNS.”
Injecting a norepinephrine receptor antagonist intrathecally can stimulate intense glymphatic transport in animals in the awake state, indicating that noradrenergic tone may be responsible for the process, Dr. Benveniste said.
She and her colleagues studied glymphatic clearance in mice anesthetized with dexmedetomidine, which induces a state similar to stage 2 sleep, versus the inhalational anesthetic isoflurane. Glymphatic processing was much greater in rodents that received dexmedetomidine.
Sleep Position
Hedok Lee, PhD, Clinical Assistant Professor of Anesthesiology at Stony Brook School of Medicine, Dr. Benveniste, and colleagues studied the effect of body posture on brain glymphatic transport in rats. They found that glymphatic transport and amyloid beta clearance were most efficient in the lateral and supine positions, while the prone position (ie, most upright and mimicking awake posture) resulted in slower clearance.
“Right lateral seems to be the position where you have got the best efflux and influx,” Dr. Benveniste said. The findings suggest that sleep position’s effect on the glymphatic system may be relevant for imaging the system in humans, and ultimately for patient care.
—Jake Remaly
Suggested Reading
Eide PK, Ringstad G. MRI with intrathecal MRI gadolinium contrast medium administration: a possible method to assess glymphatic function in human brain. Acta Radiol Open. 2015;4(11):2058460115609635.
Iliff JJ, Chen MJ, Plog BA, et al. Impairment of glymphatic pathway function promotes tau pathology after traumatic brain injury. J Neurosci. 2014;34(49):16180-16193.
Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111.
Lee H, Xie L, Yu M, et al. The effect of body posture on brain glymphatic transport. J Neurosci. 2015;35(31):11034-11044.
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
Clinical Considerations of New and Pending MS Treatments
HILTON HEAD, SC—Managing patient expectations is important when discussing new and pending treatments for multiple sclerosis (MS), according to a lecture given at the 39th Annual Contemporary Clinical Neurology Symposium. The FDA’s recent approval of daclizumab and ongoing priority review of ocrelizumab mean that neurologists likely will be discussing these therapies with patients in their clinics. Conversations may revolve around efficacy, laboratory monitoring, and risk of adverse events.
In the case of daclizumab (Zinbryta), which was approved in May 2016, patient counseling may focus on monthly laboratory monitoring requirements that are part of the drug’s risk evaluation and mitigation strategy (REMS) program and the potential for adverse events at any time during treatment, said Harold Moses Jr, MD, Associate Professor of Neurology at Vanderbilt University in Nashville.

Ocrelizumab (Ocrevus) could be the first drug approved for primary progressive MS and a new treatment option for patients with relapsing MS. Neurologists may need to temper patients’ expectations regarding the drug’s efficacy in patients with more advanced progressive disease.
“If this drug gets approved for progressive MS, you are going to have a number of patients coming to your clinics to ask for this drug,” he said. It is unclear, however, how beneficial the treatment might be for patients with advanced disease, based on the clinical trial conducted in primary progressive MS. “In my opinion, if someone is 65 to 70 years old and has had primary progressive MS for 15 to 20 years and has been wheelchair-confined for five or more years, it is unlikely that this drug is going to be very meaningful for them. Although, I do not know that for a fact. Therefore, my plan is to offer this [treatment], probably for approximately a year, and see what happens. We will continue to follow them and make a decision together about continuing therapy or stopping.”
“Remember, half the people in the world who have MS have progressive disease,” Dr. Moses said. “They have seen more than 20 years of therapies [approved] for relapsing MS, so they have a lot of pent-up expectations about a treatment option, and rightfully so. I just think this potential treatment has to be discussed in a broader context of how the study was done.”
Daclizumab
Daclizumab is an interleukin-2 receptor blocking humanized monoclonal antibody approved for use in relapsing forms of MS. It is self-administered as a subcutaneous injection once per month at a dose of 150 mg/mL. The drug’s label notes, “Because of its safety profile, the use of Zinbryta should generally be reserved for patients who have had an inadequate response to two or more drugs indicated for the treatment of MS.” This FDA guidance is similar to that for alemtuzumab. “With more than a dozen drugs for MS, it is not too surprising we are seeing this,” Dr. Moses said.
The efficacy of the drug was demonstrated in two randomized, double-blind studies. One study compared daclizumab with interferon beta-1a. The other study compared daclizumab and placebo.
In the active comparator study, 919 patients received daclizumab and 922 received interferon beta-1a. Compared with interferon beta-1a, daclizumab had a statistically significant effect on annualized relapse rate (0.393 vs 0.216; relative reduction, 45%) and on the number of new or newly enlarging T2 hyperintense lesions. Treatment did not significantly affect 12-week confirmed disability progression.
In some patients, daclizumab has a significant impact on the liver. As a result, physicians are asked to assess transaminase levels and total bilirubin monthly during treatment and for six months after stopping therapy, Dr. Moses said.
Autoimmune hepatitis and other immune-mediated disorders, including lymphadenopathy, noninfectious colitis, and cutaneous adverse events, were seen with daclizumab treatment.
Dermatologic reactions to daclizumab can range from mild rashes to serious reactions, and can include psoriasiform nail changes, erythematous changes and swelling, and desquamation and erythema of the palms. Neurologists should advise patients that these reactions “could happen at any point while they are taking this medication,” Dr. Moses said. Some patients experienced reactions after receiving the therapy for nearly three years.Patients also experienced adverse events related to infection, including nasopharyngitis, bronchitis, and tonsillitis. “Daclizumab is the newest approved drug for relapsing MS,” Dr. Moses said. “It has a unique mechanism of action and a favorable dosing schedule. Challenges exist with monitoring requirements and potential serious adverse events.”
Ocrelizumab
Ocrelizumab is a humanized monoclonal antibody that depletes CD20+ B cells.
Two identical studies, OPERA I and II, evaluated ocrelizumab in patients with relapsing MS. Another trial, ORATORIO, assessed ocrelizumab in patients with primary progressive MS. In the trials, patients received 600 mg of ocrelizumab by IV infusion every 24 weeks.
In OPERA I and II, treatment with ocrelizumab resulted in a 46% and 47% reduction in annualized relapse rate, respectively, compared with interferon beta-1a. In addition, ocrelizumab reduced the risk of confirmed disability progression for 12 weeks by 43% and 37%, respectively. Ocrelizumab also dramatically reduced the number of T1 gadolinium-enhancing lesions and the number of new or enlarging T2 hyperintense lesions, compared with interferon beta-1a.
The ORATORIO study included 732 patients with primary progressive MS who received ocrelizumab or placebo. Patients were ages 18 to 55, had an Expanded Disability Status Scale score of 3.0 to 6.5, and had abnormal CSF. Patients were treated for at least 120 weeks. Investigators measured slowing of disability progression as the primary outcome. There was a 24% reduction in clinical disability sustained for at least 12 weeks, compared with placebo.
Ocrelizumab generally was well tolerated. In the clinical trials, a similar proportion of patients treated with ocrelizumab and controls experienced adverse events. In OPERA I and II, the most common adverse event associated with ocrelizumab was infusion-related reactions, which occurred in 34.3% of patients in the ocrelizumab arm, compared with 9.7% of patients in the interferon beta-1a arm.
In ORATORIO, more malignancies were reported in patients treated with ocrelizumab, compared with patients who received placebo (11 vs 2). The implications of that finding are unclear. “We will see how that plays out in terms of what the FDA thinks about that,” Dr. Moses said.
The FDA has granted a priority review designation to ocrelizumab, with a targeted action date of December 28, 2016. “Ocrelizumab remains on the horizon with a potential role in both relapsing and progressive MS,” Dr. Moses said.
—Jake Remaly
HILTON HEAD, SC—Managing patient expectations is important when discussing new and pending treatments for multiple sclerosis (MS), according to a lecture given at the 39th Annual Contemporary Clinical Neurology Symposium. The FDA’s recent approval of daclizumab and ongoing priority review of ocrelizumab mean that neurologists likely will be discussing these therapies with patients in their clinics. Conversations may revolve around efficacy, laboratory monitoring, and risk of adverse events.
In the case of daclizumab (Zinbryta), which was approved in May 2016, patient counseling may focus on monthly laboratory monitoring requirements that are part of the drug’s risk evaluation and mitigation strategy (REMS) program and the potential for adverse events at any time during treatment, said Harold Moses Jr, MD, Associate Professor of Neurology at Vanderbilt University in Nashville.
Ocrelizumab (Ocrevus) could be the first drug approved for primary progressive MS and a new treatment option for patients with relapsing MS. Neurologists may need to temper patients’ expectations regarding the drug’s efficacy in patients with more advanced progressive disease.
“If this drug gets approved for progressive MS, you are going to have a number of patients coming to your clinics to ask for this drug,” he said. It is unclear, however, how beneficial the treatment might be for patients with advanced disease, based on the clinical trial conducted in primary progressive MS. “In my opinion, if someone is 65 to 70 years old and has had primary progressive MS for 15 to 20 years and has been wheelchair-confined for five or more years, it is unlikely that this drug is going to be very meaningful for them. Although, I do not know that for a fact. Therefore, my plan is to offer this [treatment], probably for approximately a year, and see what happens. We will continue to follow them and make a decision together about continuing therapy or stopping.”
“Remember, half the people in the world who have MS have progressive disease,” Dr. Moses said. “They have seen more than 20 years of therapies [approved] for relapsing MS, so they have a lot of pent-up expectations about a treatment option, and rightfully so. I just think this potential treatment has to be discussed in a broader context of how the study was done.”
Daclizumab
Daclizumab is an interleukin-2 receptor blocking humanized monoclonal antibody approved for use in relapsing forms of MS. It is self-administered as a subcutaneous injection once per month at a dose of 150 mg/mL. The drug’s label notes, “Because of its safety profile, the use of Zinbryta should generally be reserved for patients who have had an inadequate response to two or more drugs indicated for the treatment of MS.” This FDA guidance is similar to that for alemtuzumab. “With more than a dozen drugs for MS, it is not too surprising we are seeing this,” Dr. Moses said.
The efficacy of the drug was demonstrated in two randomized, double-blind studies. One study compared daclizumab with interferon beta-1a. The other study compared daclizumab and placebo.
In the active comparator study, 919 patients received daclizumab and 922 received interferon beta-1a. Compared with interferon beta-1a, daclizumab had a statistically significant effect on annualized relapse rate (0.393 vs 0.216; relative reduction, 45%) and on the number of new or newly enlarging T2 hyperintense lesions. Treatment did not significantly affect 12-week confirmed disability progression.
In some patients, daclizumab has a significant impact on the liver. As a result, physicians are asked to assess transaminase levels and total bilirubin monthly during treatment and for six months after stopping therapy, Dr. Moses said.
Autoimmune hepatitis and other immune-mediated disorders, including lymphadenopathy, noninfectious colitis, and cutaneous adverse events, were seen with daclizumab treatment.
Dermatologic reactions to daclizumab can range from mild rashes to serious reactions, and can include psoriasiform nail changes, erythematous changes and swelling, and desquamation and erythema of the palms. Neurologists should advise patients that these reactions “could happen at any point while they are taking this medication,” Dr. Moses said. Some patients experienced reactions after receiving the therapy for nearly three years.Patients also experienced adverse events related to infection, including nasopharyngitis, bronchitis, and tonsillitis. “Daclizumab is the newest approved drug for relapsing MS,” Dr. Moses said. “It has a unique mechanism of action and a favorable dosing schedule. Challenges exist with monitoring requirements and potential serious adverse events.”
Ocrelizumab
Ocrelizumab is a humanized monoclonal antibody that depletes CD20+ B cells.
Two identical studies, OPERA I and II, evaluated ocrelizumab in patients with relapsing MS. Another trial, ORATORIO, assessed ocrelizumab in patients with primary progressive MS. In the trials, patients received 600 mg of ocrelizumab by IV infusion every 24 weeks.
In OPERA I and II, treatment with ocrelizumab resulted in a 46% and 47% reduction in annualized relapse rate, respectively, compared with interferon beta-1a. In addition, ocrelizumab reduced the risk of confirmed disability progression for 12 weeks by 43% and 37%, respectively. Ocrelizumab also dramatically reduced the number of T1 gadolinium-enhancing lesions and the number of new or enlarging T2 hyperintense lesions, compared with interferon beta-1a.
The ORATORIO study included 732 patients with primary progressive MS who received ocrelizumab or placebo. Patients were ages 18 to 55, had an Expanded Disability Status Scale score of 3.0 to 6.5, and had abnormal CSF. Patients were treated for at least 120 weeks. Investigators measured slowing of disability progression as the primary outcome. There was a 24% reduction in clinical disability sustained for at least 12 weeks, compared with placebo.
Ocrelizumab generally was well tolerated. In the clinical trials, a similar proportion of patients treated with ocrelizumab and controls experienced adverse events. In OPERA I and II, the most common adverse event associated with ocrelizumab was infusion-related reactions, which occurred in 34.3% of patients in the ocrelizumab arm, compared with 9.7% of patients in the interferon beta-1a arm.
In ORATORIO, more malignancies were reported in patients treated with ocrelizumab, compared with patients who received placebo (11 vs 2). The implications of that finding are unclear. “We will see how that plays out in terms of what the FDA thinks about that,” Dr. Moses said.
The FDA has granted a priority review designation to ocrelizumab, with a targeted action date of December 28, 2016. “Ocrelizumab remains on the horizon with a potential role in both relapsing and progressive MS,” Dr. Moses said.
—Jake Remaly
HILTON HEAD, SC—Managing patient expectations is important when discussing new and pending treatments for multiple sclerosis (MS), according to a lecture given at the 39th Annual Contemporary Clinical Neurology Symposium. The FDA’s recent approval of daclizumab and ongoing priority review of ocrelizumab mean that neurologists likely will be discussing these therapies with patients in their clinics. Conversations may revolve around efficacy, laboratory monitoring, and risk of adverse events.
In the case of daclizumab (Zinbryta), which was approved in May 2016, patient counseling may focus on monthly laboratory monitoring requirements that are part of the drug’s risk evaluation and mitigation strategy (REMS) program and the potential for adverse events at any time during treatment, said Harold Moses Jr, MD, Associate Professor of Neurology at Vanderbilt University in Nashville.
Ocrelizumab (Ocrevus) could be the first drug approved for primary progressive MS and a new treatment option for patients with relapsing MS. Neurologists may need to temper patients’ expectations regarding the drug’s efficacy in patients with more advanced progressive disease.
“If this drug gets approved for progressive MS, you are going to have a number of patients coming to your clinics to ask for this drug,” he said. It is unclear, however, how beneficial the treatment might be for patients with advanced disease, based on the clinical trial conducted in primary progressive MS. “In my opinion, if someone is 65 to 70 years old and has had primary progressive MS for 15 to 20 years and has been wheelchair-confined for five or more years, it is unlikely that this drug is going to be very meaningful for them. Although, I do not know that for a fact. Therefore, my plan is to offer this [treatment], probably for approximately a year, and see what happens. We will continue to follow them and make a decision together about continuing therapy or stopping.”
“Remember, half the people in the world who have MS have progressive disease,” Dr. Moses said. “They have seen more than 20 years of therapies [approved] for relapsing MS, so they have a lot of pent-up expectations about a treatment option, and rightfully so. I just think this potential treatment has to be discussed in a broader context of how the study was done.”
Daclizumab
Daclizumab is an interleukin-2 receptor blocking humanized monoclonal antibody approved for use in relapsing forms of MS. It is self-administered as a subcutaneous injection once per month at a dose of 150 mg/mL. The drug’s label notes, “Because of its safety profile, the use of Zinbryta should generally be reserved for patients who have had an inadequate response to two or more drugs indicated for the treatment of MS.” This FDA guidance is similar to that for alemtuzumab. “With more than a dozen drugs for MS, it is not too surprising we are seeing this,” Dr. Moses said.
The efficacy of the drug was demonstrated in two randomized, double-blind studies. One study compared daclizumab with interferon beta-1a. The other study compared daclizumab and placebo.
In the active comparator study, 919 patients received daclizumab and 922 received interferon beta-1a. Compared with interferon beta-1a, daclizumab had a statistically significant effect on annualized relapse rate (0.393 vs 0.216; relative reduction, 45%) and on the number of new or newly enlarging T2 hyperintense lesions. Treatment did not significantly affect 12-week confirmed disability progression.
In some patients, daclizumab has a significant impact on the liver. As a result, physicians are asked to assess transaminase levels and total bilirubin monthly during treatment and for six months after stopping therapy, Dr. Moses said.
Autoimmune hepatitis and other immune-mediated disorders, including lymphadenopathy, noninfectious colitis, and cutaneous adverse events, were seen with daclizumab treatment.
Dermatologic reactions to daclizumab can range from mild rashes to serious reactions, and can include psoriasiform nail changes, erythematous changes and swelling, and desquamation and erythema of the palms. Neurologists should advise patients that these reactions “could happen at any point while they are taking this medication,” Dr. Moses said. Some patients experienced reactions after receiving the therapy for nearly three years.Patients also experienced adverse events related to infection, including nasopharyngitis, bronchitis, and tonsillitis. “Daclizumab is the newest approved drug for relapsing MS,” Dr. Moses said. “It has a unique mechanism of action and a favorable dosing schedule. Challenges exist with monitoring requirements and potential serious adverse events.”
Ocrelizumab
Ocrelizumab is a humanized monoclonal antibody that depletes CD20+ B cells.
Two identical studies, OPERA I and II, evaluated ocrelizumab in patients with relapsing MS. Another trial, ORATORIO, assessed ocrelizumab in patients with primary progressive MS. In the trials, patients received 600 mg of ocrelizumab by IV infusion every 24 weeks.
In OPERA I and II, treatment with ocrelizumab resulted in a 46% and 47% reduction in annualized relapse rate, respectively, compared with interferon beta-1a. In addition, ocrelizumab reduced the risk of confirmed disability progression for 12 weeks by 43% and 37%, respectively. Ocrelizumab also dramatically reduced the number of T1 gadolinium-enhancing lesions and the number of new or enlarging T2 hyperintense lesions, compared with interferon beta-1a.
The ORATORIO study included 732 patients with primary progressive MS who received ocrelizumab or placebo. Patients were ages 18 to 55, had an Expanded Disability Status Scale score of 3.0 to 6.5, and had abnormal CSF. Patients were treated for at least 120 weeks. Investigators measured slowing of disability progression as the primary outcome. There was a 24% reduction in clinical disability sustained for at least 12 weeks, compared with placebo.
Ocrelizumab generally was well tolerated. In the clinical trials, a similar proportion of patients treated with ocrelizumab and controls experienced adverse events. In OPERA I and II, the most common adverse event associated with ocrelizumab was infusion-related reactions, which occurred in 34.3% of patients in the ocrelizumab arm, compared with 9.7% of patients in the interferon beta-1a arm.
In ORATORIO, more malignancies were reported in patients treated with ocrelizumab, compared with patients who received placebo (11 vs 2). The implications of that finding are unclear. “We will see how that plays out in terms of what the FDA thinks about that,” Dr. Moses said.
The FDA has granted a priority review designation to ocrelizumab, with a targeted action date of December 28, 2016. “Ocrelizumab remains on the horizon with a potential role in both relapsing and progressive MS,” Dr. Moses said.
—Jake Remaly

Take steps to relieve ataxia in patients with alcohol use disorder
Ataxia is a well-known complication of chronic alcohol abuse, which is attributed to degeneration of the cerebellar vermis. However, effective treatment approaches, as well as the timing and level of recovery, remain unclear. One cross-sectional study found that long-term abstainers from alcohol had less severe ataxia than short-term abstainers,1 suggesting that improvement is possible with continued sobriety. However, a recent longitudinal study contradicts this finding, reporting no improvement in ataxia in patients abstinent for 10 weeks to 1 year.2
CASE REPORT
Unable to walk, heavy alcohol use
Mr. G, a 59-year-old white male with a history of daily, heavy alcohol use, presents to the emergency room reporting that he has “not been able to walk right” for 3 weeks. He is in a wheelchair because of ataxia and difficulty balancing. He denies headaches, visual changes, weakness, numbness, and difficulty speaking or swallowing.
Mr. G reports drinking one 40-oz bottle of malt liquor and 2 pints of vodka per day for more than 40 years. His alcohol abuse led to homelessness, unemployment, and divorce. Despite heavy drinking, he denies signs of withdrawal, including shaking, sweating, seizures, and delirium.
Mr. G has no other medical conditions. He denies a family history of neurologic disorders or substance abuse.
His pulse is 100 beats per minute, respirations of 16 breaths per minute, temperature of 37°C, and blood pressure of 143/89 mm Hg. Physical examination reveals a wide-based gait.
Mr. G is admitted to the inpatient psychiatric unit to monitor and treat his alcohol withdrawal and to undergo further workup of the gait disturbance.
A head CT scan shows non-specific changes; an EEG also is within normal limits. Complete blood count, basic metabolic panel, liver function test, HIV test, acute hepatitis panel, thyroid function test, erythrocyte sedimentation rate, and vitamin B12 tests are within normal ranges.
A full neurologic exam reveals a wide-based gait, impaired heel-shin test, and dysmetria on finger-nose-finger test. Mr. G is given a diagnosis of ataxia due to alcoholic cerebellar degeneration. Thiamine repletion is suggested.
Treatment and outcome
Mr. G continues on thiamine, 100 mg, twice daily, and oxazepam, 15 mg, as needed, to manage withdrawal symptoms. He receives gait training 3 times per week.
Approximately 10 days after admission, Mr. G is able to ambulate with a walker. Three weeks after admission, his gait has improved and he walks with a cane. (See the video at CurrentPsychiatry.com for an illustration of this progressive recovery.)
After discharge, Mr. G is referred to an addiction psychiatrist and addiction psychotherapist for ongoing treatment of alcohol use disorder.
Making the diagnosis
In a patient complaining of balance difficulties, consider ataxia secondary to cerebellar degeneration.
- Take a complete history. Ask about the onset and progression of ataxia.
- Obtain a family history. Some types of ataxia are genetic.
- Perform a neurologic examination, which may reveal signs of cerebellar deficits, particularly characteristic wide-based gait. These patients will have difficulty when walking in tandem. Other impairments on the neurologic exam that may raise suspicion for a cerebellar disorder include: impaired heel-shin test, impaired finger-nose-finger test (dysmetria), impaired rapid alternating movements (dysdiadochokinesia), nystagmus, impaired smooth pursuits, intention tremor, or speech abnormalities.
- Perform head imaging, such as a CT scan or MRI. In patients with ataxia secondary to alcohol abuse, imaging might reveal degeneration of the cerebellar vermis.
- Perform laboratory tests, such as inflammatory markers, vitamin levels, and thyroid function testing to detect possible toxic-metabolic or inflammatory causes.
Alcohol-induced ataxia can be diagnosed in patients with a history of heavy drinking if the workup does not reveal another possible cause for the gait disturbance. Other less common deficits associated with alcohol-induced cerebellar injury include:
- dysarthria
- abnormal rate and force of movement
- limb ataxia.3
Recommendations
- Be able to recognize the characteristic gait of patients with alcohol-induced ataxia.
- Provide thiamine supplementation.
- Refer patients to physical therapy.
- Educate your patients that their gait will not improve and may worsen if they continue to drink.
- Refer patients for ongoing treatment for alcohol use disorder, including medication management and psychotherapy.
Our experience suggests that patients with alcohol use disorder with cerebellar ataxia could have a good prognosis for ambulation. Improvement could occur over several weeks; it is unclear whether further gains can be expected with months or years of abstinence.
1. Smith S, Fein G. Persistent but less severe ataxia in long-term versus short-term abstinent alcoholic men and women: a cross-sectional analysis. Alcohol Clin Exp Res. 2011;35(12):2184-2192.
2. Fein G, Greenstein D. Gait and balance deficits in chronic alcoholics: no improvement from 10 weeks through 1 year abstinence. Alcohol Clin Exp Res. 2013;37(1):86-95.
3. Fitzpatrick LE, Jackson M, Crowe SF. Characterization of cerebellar ataxia in chronic alcoholics using the International Cooperative Ataxia Rating Scale (ICARS). Alcohol Clin Exp Res. 2012;36(11):1942-1951.
Ataxia is a well-known complication of chronic alcohol abuse, which is attributed to degeneration of the cerebellar vermis. However, effective treatment approaches, as well as the timing and level of recovery, remain unclear. One cross-sectional study found that long-term abstainers from alcohol had less severe ataxia than short-term abstainers,1 suggesting that improvement is possible with continued sobriety. However, a recent longitudinal study contradicts this finding, reporting no improvement in ataxia in patients abstinent for 10 weeks to 1 year.2
CASE REPORT
Unable to walk, heavy alcohol use
Mr. G, a 59-year-old white male with a history of daily, heavy alcohol use, presents to the emergency room reporting that he has “not been able to walk right” for 3 weeks. He is in a wheelchair because of ataxia and difficulty balancing. He denies headaches, visual changes, weakness, numbness, and difficulty speaking or swallowing.
Mr. G reports drinking one 40-oz bottle of malt liquor and 2 pints of vodka per day for more than 40 years. His alcohol abuse led to homelessness, unemployment, and divorce. Despite heavy drinking, he denies signs of withdrawal, including shaking, sweating, seizures, and delirium.
Mr. G has no other medical conditions. He denies a family history of neurologic disorders or substance abuse.
His pulse is 100 beats per minute, respirations of 16 breaths per minute, temperature of 37°C, and blood pressure of 143/89 mm Hg. Physical examination reveals a wide-based gait.
Mr. G is admitted to the inpatient psychiatric unit to monitor and treat his alcohol withdrawal and to undergo further workup of the gait disturbance.
A head CT scan shows non-specific changes; an EEG also is within normal limits. Complete blood count, basic metabolic panel, liver function test, HIV test, acute hepatitis panel, thyroid function test, erythrocyte sedimentation rate, and vitamin B12 tests are within normal ranges.
A full neurologic exam reveals a wide-based gait, impaired heel-shin test, and dysmetria on finger-nose-finger test. Mr. G is given a diagnosis of ataxia due to alcoholic cerebellar degeneration. Thiamine repletion is suggested.
Treatment and outcome
Mr. G continues on thiamine, 100 mg, twice daily, and oxazepam, 15 mg, as needed, to manage withdrawal symptoms. He receives gait training 3 times per week.
Approximately 10 days after admission, Mr. G is able to ambulate with a walker. Three weeks after admission, his gait has improved and he walks with a cane. (See the video at CurrentPsychiatry.com for an illustration of this progressive recovery.)
After discharge, Mr. G is referred to an addiction psychiatrist and addiction psychotherapist for ongoing treatment of alcohol use disorder.
Making the diagnosis
In a patient complaining of balance difficulties, consider ataxia secondary to cerebellar degeneration.
- Take a complete history. Ask about the onset and progression of ataxia.
- Obtain a family history. Some types of ataxia are genetic.
- Perform a neurologic examination, which may reveal signs of cerebellar deficits, particularly characteristic wide-based gait. These patients will have difficulty when walking in tandem. Other impairments on the neurologic exam that may raise suspicion for a cerebellar disorder include: impaired heel-shin test, impaired finger-nose-finger test (dysmetria), impaired rapid alternating movements (dysdiadochokinesia), nystagmus, impaired smooth pursuits, intention tremor, or speech abnormalities.
- Perform head imaging, such as a CT scan or MRI. In patients with ataxia secondary to alcohol abuse, imaging might reveal degeneration of the cerebellar vermis.
- Perform laboratory tests, such as inflammatory markers, vitamin levels, and thyroid function testing to detect possible toxic-metabolic or inflammatory causes.
Alcohol-induced ataxia can be diagnosed in patients with a history of heavy drinking if the workup does not reveal another possible cause for the gait disturbance. Other less common deficits associated with alcohol-induced cerebellar injury include:
- dysarthria
- abnormal rate and force of movement
- limb ataxia.3
Recommendations
- Be able to recognize the characteristic gait of patients with alcohol-induced ataxia.
- Provide thiamine supplementation.
- Refer patients to physical therapy.
- Educate your patients that their gait will not improve and may worsen if they continue to drink.
- Refer patients for ongoing treatment for alcohol use disorder, including medication management and psychotherapy.
Our experience suggests that patients with alcohol use disorder with cerebellar ataxia could have a good prognosis for ambulation. Improvement could occur over several weeks; it is unclear whether further gains can be expected with months or years of abstinence.
Ataxia is a well-known complication of chronic alcohol abuse, which is attributed to degeneration of the cerebellar vermis. However, effective treatment approaches, as well as the timing and level of recovery, remain unclear. One cross-sectional study found that long-term abstainers from alcohol had less severe ataxia than short-term abstainers,1 suggesting that improvement is possible with continued sobriety. However, a recent longitudinal study contradicts this finding, reporting no improvement in ataxia in patients abstinent for 10 weeks to 1 year.2
CASE REPORT
Unable to walk, heavy alcohol use
Mr. G, a 59-year-old white male with a history of daily, heavy alcohol use, presents to the emergency room reporting that he has “not been able to walk right” for 3 weeks. He is in a wheelchair because of ataxia and difficulty balancing. He denies headaches, visual changes, weakness, numbness, and difficulty speaking or swallowing.
Mr. G reports drinking one 40-oz bottle of malt liquor and 2 pints of vodka per day for more than 40 years. His alcohol abuse led to homelessness, unemployment, and divorce. Despite heavy drinking, he denies signs of withdrawal, including shaking, sweating, seizures, and delirium.
Mr. G has no other medical conditions. He denies a family history of neurologic disorders or substance abuse.
His pulse is 100 beats per minute, respirations of 16 breaths per minute, temperature of 37°C, and blood pressure of 143/89 mm Hg. Physical examination reveals a wide-based gait.
Mr. G is admitted to the inpatient psychiatric unit to monitor and treat his alcohol withdrawal and to undergo further workup of the gait disturbance.
A head CT scan shows non-specific changes; an EEG also is within normal limits. Complete blood count, basic metabolic panel, liver function test, HIV test, acute hepatitis panel, thyroid function test, erythrocyte sedimentation rate, and vitamin B12 tests are within normal ranges.
A full neurologic exam reveals a wide-based gait, impaired heel-shin test, and dysmetria on finger-nose-finger test. Mr. G is given a diagnosis of ataxia due to alcoholic cerebellar degeneration. Thiamine repletion is suggested.
Treatment and outcome
Mr. G continues on thiamine, 100 mg, twice daily, and oxazepam, 15 mg, as needed, to manage withdrawal symptoms. He receives gait training 3 times per week.
Approximately 10 days after admission, Mr. G is able to ambulate with a walker. Three weeks after admission, his gait has improved and he walks with a cane. (See the video at CurrentPsychiatry.com for an illustration of this progressive recovery.)
After discharge, Mr. G is referred to an addiction psychiatrist and addiction psychotherapist for ongoing treatment of alcohol use disorder.
Making the diagnosis
In a patient complaining of balance difficulties, consider ataxia secondary to cerebellar degeneration.
- Take a complete history. Ask about the onset and progression of ataxia.
- Obtain a family history. Some types of ataxia are genetic.
- Perform a neurologic examination, which may reveal signs of cerebellar deficits, particularly characteristic wide-based gait. These patients will have difficulty when walking in tandem. Other impairments on the neurologic exam that may raise suspicion for a cerebellar disorder include: impaired heel-shin test, impaired finger-nose-finger test (dysmetria), impaired rapid alternating movements (dysdiadochokinesia), nystagmus, impaired smooth pursuits, intention tremor, or speech abnormalities.
- Perform head imaging, such as a CT scan or MRI. In patients with ataxia secondary to alcohol abuse, imaging might reveal degeneration of the cerebellar vermis.
- Perform laboratory tests, such as inflammatory markers, vitamin levels, and thyroid function testing to detect possible toxic-metabolic or inflammatory causes.
Alcohol-induced ataxia can be diagnosed in patients with a history of heavy drinking if the workup does not reveal another possible cause for the gait disturbance. Other less common deficits associated with alcohol-induced cerebellar injury include:
- dysarthria
- abnormal rate and force of movement
- limb ataxia.3
Recommendations
- Be able to recognize the characteristic gait of patients with alcohol-induced ataxia.
- Provide thiamine supplementation.
- Refer patients to physical therapy.
- Educate your patients that their gait will not improve and may worsen if they continue to drink.
- Refer patients for ongoing treatment for alcohol use disorder, including medication management and psychotherapy.
Our experience suggests that patients with alcohol use disorder with cerebellar ataxia could have a good prognosis for ambulation. Improvement could occur over several weeks; it is unclear whether further gains can be expected with months or years of abstinence.
1. Smith S, Fein G. Persistent but less severe ataxia in long-term versus short-term abstinent alcoholic men and women: a cross-sectional analysis. Alcohol Clin Exp Res. 2011;35(12):2184-2192.
2. Fein G, Greenstein D. Gait and balance deficits in chronic alcoholics: no improvement from 10 weeks through 1 year abstinence. Alcohol Clin Exp Res. 2013;37(1):86-95.
3. Fitzpatrick LE, Jackson M, Crowe SF. Characterization of cerebellar ataxia in chronic alcoholics using the International Cooperative Ataxia Rating Scale (ICARS). Alcohol Clin Exp Res. 2012;36(11):1942-1951.
1. Smith S, Fein G. Persistent but less severe ataxia in long-term versus short-term abstinent alcoholic men and women: a cross-sectional analysis. Alcohol Clin Exp Res. 2011;35(12):2184-2192.
2. Fein G, Greenstein D. Gait and balance deficits in chronic alcoholics: no improvement from 10 weeks through 1 year abstinence. Alcohol Clin Exp Res. 2013;37(1):86-95.
3. Fitzpatrick LE, Jackson M, Crowe SF. Characterization of cerebellar ataxia in chronic alcoholics using the International Cooperative Ataxia Rating Scale (ICARS). Alcohol Clin Exp Res. 2012;36(11):1942-1951.
No more 'stickies'!: Help your patients bring their ‘to-do’ list into the 21st century
Difficulty with time management and organization is one of the most common complaints of patients with attention-deficit/hyperactivity disorder (ADHD). Being unproductive and inefficient also is anxiety-producing and depressing, leaving patients with additional comorbidity.
Although medication can help improve a person’s focus, if the patient is focusing on a set of poorly designed systems, he (she) will see little improvement. A comprehensive approach to improving day-to-day task management, similar to the one I describe here and use with my patients, is therefore as important as medication.
Needed: An ‘organizing principle’
Imagine that supermarkets displayed food in the order it arrives from the food distributors and producers. You’d walk in to the store and see a display of food that lacks hierarchy—1 random item placed next to another. The experience would be jarring, and shopping would be a much slower chore. Furthermore, what if you had to go to 5 stores to cover all your needs?
Yet, that is how most “to-do” lists are executed: A thought comes in, a thought goes down on paper. Or on a sticky note. Or in an app. Or in a calendar. Or all of the above! Often, there is neither an organizing principle (other than perhaps chronological order) or a central repository. No wonder it’s hard to feel present and clear-minded. Add to this disorganization the volume of information coming in from the environment—e-mails, voice mails, texts, notifications, dings, beeps, buzzes, and maybe even snail mail—and the feeling of being overwhelmed grows.
Unconscious motives for maintaining poor systems also might play a role. People with a “need to please” personality type or who are more passive-aggressive in their communication are more likely to overcommit, and then forget or be late completing their tasks, rather than saying “No” from the outset or delegating the work.
Survival basics for time management
Assuming there is simply a skills deficit, you can teach basic time and project management skills to patients with ADHD (and to any patient with suboptimal executive functioning). Here are basic principles to adopt:
- If you can forget it, you will, so all tasks should go onto the to-do list.
- You should keep only 1 list. Adding on “stickies” is not allowed.
- Your list is like an extra lobe of your brain: It should be present at all times, whether you keep it in “the Cloud,” on your desktop, or on paper.
- Review your list and clean it up at least daily. This takes time, but it also saves time—in spades—when you can call upon the right task, at the right time, with energy and drive.
- The first action you should take in the daily review is to weed out or delegate tasks.
- Next, categorize remaining tasks. (Note: The free smartphone app Evernote allows you to do this with “tags.”) Categorizing allows you to process sets of tasks in buckets that can be tackled as a bundle and, therefore, more efficiently. For example, having all of your errands, items to research, and telephone calls that need to be returned in separate buckets allows for speedier processing—as opposed to veering back and forth between line items.
- Then, move remaining high-priority items to the top of the list. However, remember that, if everything is urgent, nothing is. Items that are low-hanging fruit that you can cross off the list in a matter of minutes can be prioritized even if they are not as urgent. By doing that, your list becomes more manageable and your brain can dive deeper into more complex tasks.
- Block out calendar time for each of your buckets with this formula: (1) Estimate how much time you’ll need to complete the tasks in each bucket, then add 50% for each bucket. (2) Add in commuting, set-up, or wind-down time, if you need it, to the grand total for all buckets, and then add 50% more than you’ve estimated
Set the brain free!
This process will seem like a burden at the beginning, when the synapses underneath it still need to get stronger (much like how the body responds to exercise). However, as long as these principles are put into action daily, they will become a trusted, second-nature system that frees the brain from distraction and anxiety—and, ultimately,
Difficulty with time management and organization is one of the most common complaints of patients with attention-deficit/hyperactivity disorder (ADHD). Being unproductive and inefficient also is anxiety-producing and depressing, leaving patients with additional comorbidity.
Although medication can help improve a person’s focus, if the patient is focusing on a set of poorly designed systems, he (she) will see little improvement. A comprehensive approach to improving day-to-day task management, similar to the one I describe here and use with my patients, is therefore as important as medication.
Needed: An ‘organizing principle’
Imagine that supermarkets displayed food in the order it arrives from the food distributors and producers. You’d walk in to the store and see a display of food that lacks hierarchy—1 random item placed next to another. The experience would be jarring, and shopping would be a much slower chore. Furthermore, what if you had to go to 5 stores to cover all your needs?
Yet, that is how most “to-do” lists are executed: A thought comes in, a thought goes down on paper. Or on a sticky note. Or in an app. Or in a calendar. Or all of the above! Often, there is neither an organizing principle (other than perhaps chronological order) or a central repository. No wonder it’s hard to feel present and clear-minded. Add to this disorganization the volume of information coming in from the environment—e-mails, voice mails, texts, notifications, dings, beeps, buzzes, and maybe even snail mail—and the feeling of being overwhelmed grows.
Unconscious motives for maintaining poor systems also might play a role. People with a “need to please” personality type or who are more passive-aggressive in their communication are more likely to overcommit, and then forget or be late completing their tasks, rather than saying “No” from the outset or delegating the work.
Survival basics for time management
Assuming there is simply a skills deficit, you can teach basic time and project management skills to patients with ADHD (and to any patient with suboptimal executive functioning). Here are basic principles to adopt:
- If you can forget it, you will, so all tasks should go onto the to-do list.
- You should keep only 1 list. Adding on “stickies” is not allowed.
- Your list is like an extra lobe of your brain: It should be present at all times, whether you keep it in “the Cloud,” on your desktop, or on paper.
- Review your list and clean it up at least daily. This takes time, but it also saves time—in spades—when you can call upon the right task, at the right time, with energy and drive.
- The first action you should take in the daily review is to weed out or delegate tasks.
- Next, categorize remaining tasks. (Note: The free smartphone app Evernote allows you to do this with “tags.”) Categorizing allows you to process sets of tasks in buckets that can be tackled as a bundle and, therefore, more efficiently. For example, having all of your errands, items to research, and telephone calls that need to be returned in separate buckets allows for speedier processing—as opposed to veering back and forth between line items.
- Then, move remaining high-priority items to the top of the list. However, remember that, if everything is urgent, nothing is. Items that are low-hanging fruit that you can cross off the list in a matter of minutes can be prioritized even if they are not as urgent. By doing that, your list becomes more manageable and your brain can dive deeper into more complex tasks.
- Block out calendar time for each of your buckets with this formula: (1) Estimate how much time you’ll need to complete the tasks in each bucket, then add 50% for each bucket. (2) Add in commuting, set-up, or wind-down time, if you need it, to the grand total for all buckets, and then add 50% more than you’ve estimated
Set the brain free!
This process will seem like a burden at the beginning, when the synapses underneath it still need to get stronger (much like how the body responds to exercise). However, as long as these principles are put into action daily, they will become a trusted, second-nature system that frees the brain from distraction and anxiety—and, ultimately,
Difficulty with time management and organization is one of the most common complaints of patients with attention-deficit/hyperactivity disorder (ADHD). Being unproductive and inefficient also is anxiety-producing and depressing, leaving patients with additional comorbidity.
Although medication can help improve a person’s focus, if the patient is focusing on a set of poorly designed systems, he (she) will see little improvement. A comprehensive approach to improving day-to-day task management, similar to the one I describe here and use with my patients, is therefore as important as medication.
Needed: An ‘organizing principle’
Imagine that supermarkets displayed food in the order it arrives from the food distributors and producers. You’d walk in to the store and see a display of food that lacks hierarchy—1 random item placed next to another. The experience would be jarring, and shopping would be a much slower chore. Furthermore, what if you had to go to 5 stores to cover all your needs?
Yet, that is how most “to-do” lists are executed: A thought comes in, a thought goes down on paper. Or on a sticky note. Or in an app. Or in a calendar. Or all of the above! Often, there is neither an organizing principle (other than perhaps chronological order) or a central repository. No wonder it’s hard to feel present and clear-minded. Add to this disorganization the volume of information coming in from the environment—e-mails, voice mails, texts, notifications, dings, beeps, buzzes, and maybe even snail mail—and the feeling of being overwhelmed grows.
Unconscious motives for maintaining poor systems also might play a role. People with a “need to please” personality type or who are more passive-aggressive in their communication are more likely to overcommit, and then forget or be late completing their tasks, rather than saying “No” from the outset or delegating the work.
Survival basics for time management
Assuming there is simply a skills deficit, you can teach basic time and project management skills to patients with ADHD (and to any patient with suboptimal executive functioning). Here are basic principles to adopt:
- If you can forget it, you will, so all tasks should go onto the to-do list.
- You should keep only 1 list. Adding on “stickies” is not allowed.
- Your list is like an extra lobe of your brain: It should be present at all times, whether you keep it in “the Cloud,” on your desktop, or on paper.
- Review your list and clean it up at least daily. This takes time, but it also saves time—in spades—when you can call upon the right task, at the right time, with energy and drive.
- The first action you should take in the daily review is to weed out or delegate tasks.
- Next, categorize remaining tasks. (Note: The free smartphone app Evernote allows you to do this with “tags.”) Categorizing allows you to process sets of tasks in buckets that can be tackled as a bundle and, therefore, more efficiently. For example, having all of your errands, items to research, and telephone calls that need to be returned in separate buckets allows for speedier processing—as opposed to veering back and forth between line items.
- Then, move remaining high-priority items to the top of the list. However, remember that, if everything is urgent, nothing is. Items that are low-hanging fruit that you can cross off the list in a matter of minutes can be prioritized even if they are not as urgent. By doing that, your list becomes more manageable and your brain can dive deeper into more complex tasks.
- Block out calendar time for each of your buckets with this formula: (1) Estimate how much time you’ll need to complete the tasks in each bucket, then add 50% for each bucket. (2) Add in commuting, set-up, or wind-down time, if you need it, to the grand total for all buckets, and then add 50% more than you’ve estimated
Set the brain free!
This process will seem like a burden at the beginning, when the synapses underneath it still need to get stronger (much like how the body responds to exercise). However, as long as these principles are put into action daily, they will become a trusted, second-nature system that frees the brain from distraction and anxiety—and, ultimately,
Ataxia due to alcohol abuse
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Sanofi Gets $43 M U.S. Funding to Spur Zika Vaccine Development
(Reuters) - Sanofi SA said on Monday the U.S. Department of Health and Human Services (HHS) approved $43.18 million in funding to accelerate the development of a Zika vaccine, as efforts to prevent the infection gather momentum.
The funding from the HHS' Biomedical Advanced Research and Development Authority (BARDA) will be used for mid-stage trials, expected to begin in the first half of 2018, and for manufacturing, the French drugmaker said.
The contract runs through June 2022, but if the data is positive, the contract includes an option for up to additional $130.45 million for late-stage trials necessary for eventual approval.
Work on the vaccine began in March as a collaborative effort between the U.S. Department Of Defense's Walter Reed Army Institute of Research (WRAIR), BARDA and the National Institutes of Health. Sanofi in July teamed up with WRAIR to co-develop the vaccine.
Earlier this month, BARDA gave Japanese drugmaker Takeda Pharmaceutical Co nearly $20 million in initial funding to develop a Zika vaccine.
Sanofi is one of the many companies around the world looking to develop a vaccine against the virus that has spread rapidly since the current outbreak was first detected last year in Brazil.
Hundreds of thousands of people are estimated to have been infected with Zika in the Americas and parts of Asia. Most have no symptoms or experience only a mild illness.
The virus can penetrate the womb in pregnant women, causing a rare but crippling birth defect known as microcephaly. In adults, it has been linked to Guillain-Barre syndrome, a form of temporary paralysis.
Zika, a member of the flavivirus species that includes dengue, yellow fever and West Nile virus, is typically spread by the bite of the Aedes aegypti mosquito.
It can be also passed on through sex, a unique characteristic among mosquito-borne viruses.
Sanofi Pasteur, the vaccine unit of Sanofi, already has several vaccines approved for others flaviviruses, such as yellow fever, dengue and Japanese encephalitis.
As of September, the HHS has awarded at least $433 million in repurposed funds to support Zika response and preparedness activities.
(Reuters) - Sanofi SA said on Monday the U.S. Department of Health and Human Services (HHS) approved $43.18 million in funding to accelerate the development of a Zika vaccine, as efforts to prevent the infection gather momentum.
The funding from the HHS' Biomedical Advanced Research and Development Authority (BARDA) will be used for mid-stage trials, expected to begin in the first half of 2018, and for manufacturing, the French drugmaker said.
The contract runs through June 2022, but if the data is positive, the contract includes an option for up to additional $130.45 million for late-stage trials necessary for eventual approval.
Work on the vaccine began in March as a collaborative effort between the U.S. Department Of Defense's Walter Reed Army Institute of Research (WRAIR), BARDA and the National Institutes of Health. Sanofi in July teamed up with WRAIR to co-develop the vaccine.
Earlier this month, BARDA gave Japanese drugmaker Takeda Pharmaceutical Co nearly $20 million in initial funding to develop a Zika vaccine.
Sanofi is one of the many companies around the world looking to develop a vaccine against the virus that has spread rapidly since the current outbreak was first detected last year in Brazil.
Hundreds of thousands of people are estimated to have been infected with Zika in the Americas and parts of Asia. Most have no symptoms or experience only a mild illness.
The virus can penetrate the womb in pregnant women, causing a rare but crippling birth defect known as microcephaly. In adults, it has been linked to Guillain-Barre syndrome, a form of temporary paralysis.
Zika, a member of the flavivirus species that includes dengue, yellow fever and West Nile virus, is typically spread by the bite of the Aedes aegypti mosquito.
It can be also passed on through sex, a unique characteristic among mosquito-borne viruses.
Sanofi Pasteur, the vaccine unit of Sanofi, already has several vaccines approved for others flaviviruses, such as yellow fever, dengue and Japanese encephalitis.
As of September, the HHS has awarded at least $433 million in repurposed funds to support Zika response and preparedness activities.
(Reuters) - Sanofi SA said on Monday the U.S. Department of Health and Human Services (HHS) approved $43.18 million in funding to accelerate the development of a Zika vaccine, as efforts to prevent the infection gather momentum.
The funding from the HHS' Biomedical Advanced Research and Development Authority (BARDA) will be used for mid-stage trials, expected to begin in the first half of 2018, and for manufacturing, the French drugmaker said.
The contract runs through June 2022, but if the data is positive, the contract includes an option for up to additional $130.45 million for late-stage trials necessary for eventual approval.
Work on the vaccine began in March as a collaborative effort between the U.S. Department Of Defense's Walter Reed Army Institute of Research (WRAIR), BARDA and the National Institutes of Health. Sanofi in July teamed up with WRAIR to co-develop the vaccine.
Earlier this month, BARDA gave Japanese drugmaker Takeda Pharmaceutical Co nearly $20 million in initial funding to develop a Zika vaccine.
Sanofi is one of the many companies around the world looking to develop a vaccine against the virus that has spread rapidly since the current outbreak was first detected last year in Brazil.
Hundreds of thousands of people are estimated to have been infected with Zika in the Americas and parts of Asia. Most have no symptoms or experience only a mild illness.
The virus can penetrate the womb in pregnant women, causing a rare but crippling birth defect known as microcephaly. In adults, it has been linked to Guillain-Barre syndrome, a form of temporary paralysis.
Zika, a member of the flavivirus species that includes dengue, yellow fever and West Nile virus, is typically spread by the bite of the Aedes aegypti mosquito.
It can be also passed on through sex, a unique characteristic among mosquito-borne viruses.
Sanofi Pasteur, the vaccine unit of Sanofi, already has several vaccines approved for others flaviviruses, such as yellow fever, dengue and Japanese encephalitis.
As of September, the HHS has awarded at least $433 million in repurposed funds to support Zika response and preparedness activities.
Coordinating Better Care for Opioid-Addicted Women and Their Children
Caring for a woman who is addicted to opioids—and who is a mother or about to be—can be challenging. But child welfare systems are reporting heavier caseloads, primarily among infants and young children. Moreover, hospitals are reporting increasing numbers of infants born with neonatal abstinence syndrome.
As part of HHS’s overall initiative to address the many public health problems posed by the opioid disorder crisis, SAMHSA, with the Administration on Children, Youth, and Families, is releasing A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders.
The guide is aimed at promoting a coordinated multisystemic approach among agencies and providers, including child welfare, medical, and substance abuse treatment, grounded in early identification and interventions to support families.
The publication covers the extent of opioid use by pregnant women and its effects on their fetus. It offers evidence-based recommendations for treatment approaches, along with recommendations for collaborative planning and tools to conduct a needs-and-gap analysis to develop a collaborative action plan.
SAMHSA also publishes Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance. This report summarizes the evidence review and rating processes SAMHSA used to establish appropriate interventions.
Caring for a woman who is addicted to opioids—and who is a mother or about to be—can be challenging. But child welfare systems are reporting heavier caseloads, primarily among infants and young children. Moreover, hospitals are reporting increasing numbers of infants born with neonatal abstinence syndrome.
As part of HHS’s overall initiative to address the many public health problems posed by the opioid disorder crisis, SAMHSA, with the Administration on Children, Youth, and Families, is releasing A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders.
The guide is aimed at promoting a coordinated multisystemic approach among agencies and providers, including child welfare, medical, and substance abuse treatment, grounded in early identification and interventions to support families.
The publication covers the extent of opioid use by pregnant women and its effects on their fetus. It offers evidence-based recommendations for treatment approaches, along with recommendations for collaborative planning and tools to conduct a needs-and-gap analysis to develop a collaborative action plan.
SAMHSA also publishes Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance. This report summarizes the evidence review and rating processes SAMHSA used to establish appropriate interventions.
Caring for a woman who is addicted to opioids—and who is a mother or about to be—can be challenging. But child welfare systems are reporting heavier caseloads, primarily among infants and young children. Moreover, hospitals are reporting increasing numbers of infants born with neonatal abstinence syndrome.
As part of HHS’s overall initiative to address the many public health problems posed by the opioid disorder crisis, SAMHSA, with the Administration on Children, Youth, and Families, is releasing A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders.
The guide is aimed at promoting a coordinated multisystemic approach among agencies and providers, including child welfare, medical, and substance abuse treatment, grounded in early identification and interventions to support families.
The publication covers the extent of opioid use by pregnant women and its effects on their fetus. It offers evidence-based recommendations for treatment approaches, along with recommendations for collaborative planning and tools to conduct a needs-and-gap analysis to develop a collaborative action plan.
SAMHSA also publishes Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance. This report summarizes the evidence review and rating processes SAMHSA used to establish appropriate interventions.
An Atypical Angiomyomatous Hamartoma With Unexplained Hepatosplenomegaly
Angiomyomatous hamartoma (AMH) of the lymph node is an extremely uncommon vascular disorder of unknown etiology, first described by Chan and colleagues in 1992.1-3 Angiomyomatous hamartoma particularly involves inguinal and femoral lymph nodes, with few cases reported in the cervical, popliteal, and submandibular lymph nodes.1 Angiomyomatous hamartoma can occasionally be associated with edema of the ipsilateral limb. To the authors’ knowledge, to date only 18 cases of AMH have been reported.4
Case Presentation
A 40-year-old white man started to have a left inguinal and scrotal pain along with left thigh swelling at age 22 while serving in the U.S. Army.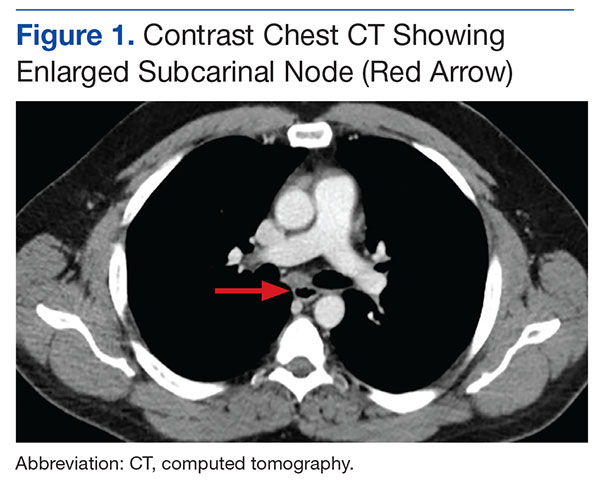

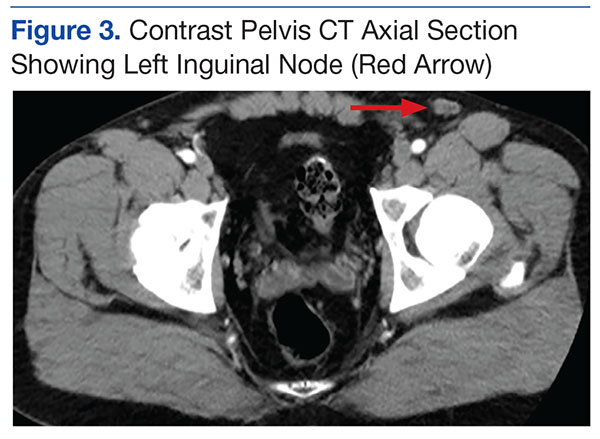
An abdominal Doppler ultrasound did not show any evidence of portal hypertension. A thoraco-abdomino-pelvic computed tomography (CT) scan showed bilateral axillary, subcarinal (Figure 1), mesenteric and retroperitoneal (Figure 2), and left inguinal (Figure 3) lymphadenopathy. Excisional biopsy of a 3.5 x 2.5 x 1.5 cm left inguinal lymph node was performed, and histopathology showed extensive smooth muscle and vascular proliferation replacing most of the lymph node (Figure 4), a finding consistent with AMH. A trichrome staining (Figure 5) and immunohistochemical study for smooth muscle actin (Figure 6) were performed and supported the diagnosis. Due to persistent pain in the scrotal area, the patient underwent a left spermatic cord denervation. Currently, the patient has persistent left thigh swelling. His condition remains stable with a regular follow-up CT scan showing unchanged lymphadenopathy.
Discussion
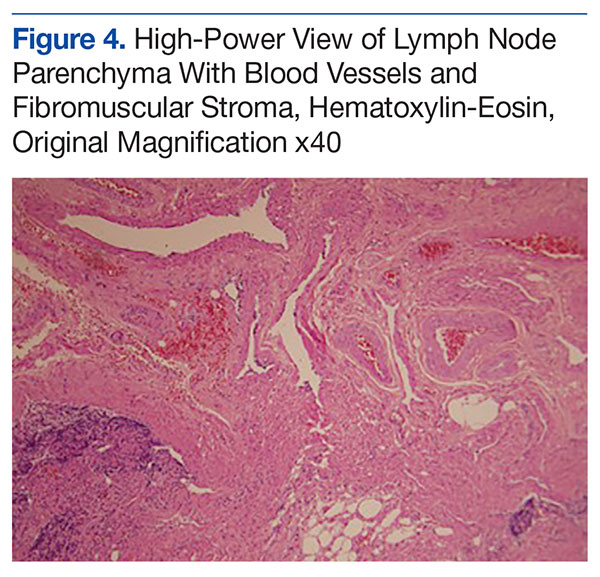
Angiomyomatous hamartoma is a rare, primary vascular tumor of the lymph nodes occurring almost exclusively in the inguinal and femoral lymph nodes and occasionally associated with edema of the ipsilateral limb.1 A few cases with popliteal and cervical lymph node involvement have been reported.1 There are no prior reports of cases with either generalized adenopathy or hepatosplenomegaly.
The histopathogenesis of AMH remains unclear. Chan and colleagues first reported this distinct clinicopathologic entity in 1992 as a primary vascular tumor of the lymph node.1-3 The hamartomatous nature of the disease was postulated by the authors on the basis of a disorganized growth pattern of smooth muscle cells and blood vessels noted on pathology.2,3 The AMH could represent a localized malformation in a congenitally damaged lymphatic vessel system.5 Other hypothesis suggests lymphedema as a possible etiology of AMH through continuous stimulation of lymphatic vessels, which triggers vasoproliferation and eventually the vascular transformation of the lymph nodes.5
Differential diagnoses of AMH include nodal lymphangiomyomatosis, which is most prevalent in women, particularly presenting with thoracic and intra-abdominal lymph nodes and plumper HMB45 (human melanoma black 45) -positive tumor cells6; leiomyomato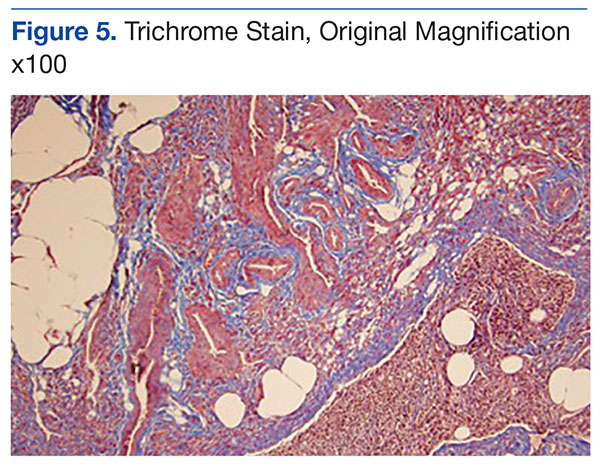
Treatment is either conservative or surgical, depending on clinical judgment. This is only the 19th case of AMH reported so far in the literature and the fifth reported case in which the patient presented with ipsilateral lymphedema of the limb. Importantly, it is the first reported case with generalized (axillary, subcarinal, mesenteric, inguinal and retroperitoneal) lymphadenopathy and unexplained hepatosplenomegaly.
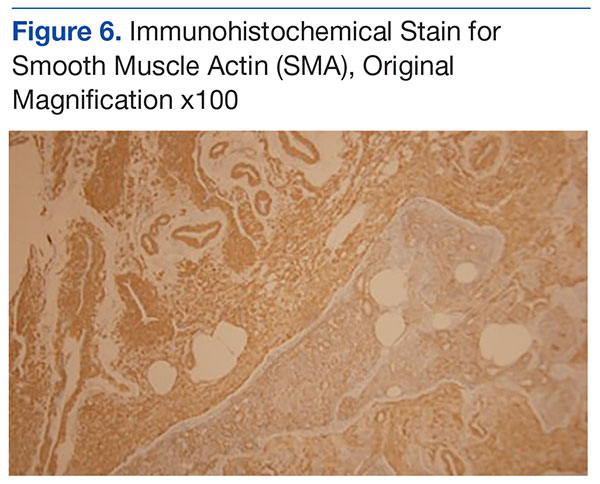
Conclusion
Angiomyomatous hamartoma of the lymph nodes is an exceedingly rare diagnosis but should be considered when evaluating patients with lymphatic tumors. This patient remains relatively asymptomatic and on observation at this time and seems to have more extensive disease than prior reports in the literature.
1. Mridha AR, Ranjan R, Kinra P, Ray R, Khan SA, Shivanand G. Angiomyomatous hamartoma of popliteal lymph node: an unusual entity. J Pathol Transl Med. 2015;49(2):156-158.
2. Dargent JL, Lespagnard L, Verdebout JM, Bourgeois P, Munck D. Glomeruloid microvascular proliferation in angiomyomatous hamartoma of the lymph node. Virchows Arch. 2004;445(3):320-322.
3. Chan JK, Frizzera G, Fletcher CD, Rosai J. Primary vascular tumors of lymph nodes other than Kaposi’s sarcoma. Analysis of 39 cases and delineation of two new entities. Am J Surg Pathol. 1992;16(4):335-350.
4. Ram M, Alsanjari N, Ansari N. Angiomyomatous hamartoma: a rare case report with review of the literature. Rare Tumors. 2009;1(2):e25.
5. Piedimonte A, De Nictolis M, Lorenzini P, Sperti V, Bertani A. Angiomyomatous hamartoma of inguinal lymph nodes. Plast Reconstr Surg. 2006;117(2):714-716.
6. Lee CH, Chang TC, Ku JW. Angiomyomatous hamartoma in an inguinal lymph node with proliferating pericytes/smooth muscle cells, plexiform vessel tangles, and ectopic calcification. Indian J Pathol Microbiol. 2015;58(2):226-228.
Angiomyomatous hamartoma (AMH) of the lymph node is an extremely uncommon vascular disorder of unknown etiology, first described by Chan and colleagues in 1992.1-3 Angiomyomatous hamartoma particularly involves inguinal and femoral lymph nodes, with few cases reported in the cervical, popliteal, and submandibular lymph nodes.1 Angiomyomatous hamartoma can occasionally be associated with edema of the ipsilateral limb. To the authors’ knowledge, to date only 18 cases of AMH have been reported.4
Case Presentation
A 40-year-old white man started to have a left inguinal and scrotal pain along with left thigh swelling at age 22 while serving in the U.S. Army.
An abdominal Doppler ultrasound did not show any evidence of portal hypertension. A thoraco-abdomino-pelvic computed tomography (CT) scan showed bilateral axillary, subcarinal (Figure 1), mesenteric and retroperitoneal (Figure 2), and left inguinal (Figure 3) lymphadenopathy. Excisional biopsy of a 3.5 x 2.5 x 1.5 cm left inguinal lymph node was performed, and histopathology showed extensive smooth muscle and vascular proliferation replacing most of the lymph node (Figure 4), a finding consistent with AMH. A trichrome staining (Figure 5) and immunohistochemical study for smooth muscle actin (Figure 6) were performed and supported the diagnosis. Due to persistent pain in the scrotal area, the patient underwent a left spermatic cord denervation. Currently, the patient has persistent left thigh swelling. His condition remains stable with a regular follow-up CT scan showing unchanged lymphadenopathy.
Discussion
Angiomyomatous hamartoma is a rare, primary vascular tumor of the lymph nodes occurring almost exclusively in the inguinal and femoral lymph nodes and occasionally associated with edema of the ipsilateral limb.1 A few cases with popliteal and cervical lymph node involvement have been reported.1 There are no prior reports of cases with either generalized adenopathy or hepatosplenomegaly.
The histopathogenesis of AMH remains unclear. Chan and colleagues first reported this distinct clinicopathologic entity in 1992 as a primary vascular tumor of the lymph node.1-3 The hamartomatous nature of the disease was postulated by the authors on the basis of a disorganized growth pattern of smooth muscle cells and blood vessels noted on pathology.2,3 The AMH could represent a localized malformation in a congenitally damaged lymphatic vessel system.5 Other hypothesis suggests lymphedema as a possible etiology of AMH through continuous stimulation of lymphatic vessels, which triggers vasoproliferation and eventually the vascular transformation of the lymph nodes.5
Differential diagnoses of AMH include nodal lymphangiomyomatosis, which is most prevalent in women, particularly presenting with thoracic and intra-abdominal lymph nodes and plumper HMB45 (human melanoma black 45) -positive tumor cells6; leiomyomato
Treatment is either conservative or surgical, depending on clinical judgment. This is only the 19th case of AMH reported so far in the literature and the fifth reported case in which the patient presented with ipsilateral lymphedema of the limb. Importantly, it is the first reported case with generalized (axillary, subcarinal, mesenteric, inguinal and retroperitoneal) lymphadenopathy and unexplained hepatosplenomegaly.
Conclusion
Angiomyomatous hamartoma of the lymph nodes is an exceedingly rare diagnosis but should be considered when evaluating patients with lymphatic tumors. This patient remains relatively asymptomatic and on observation at this time and seems to have more extensive disease than prior reports in the literature.
Angiomyomatous hamartoma (AMH) of the lymph node is an extremely uncommon vascular disorder of unknown etiology, first described by Chan and colleagues in 1992.1-3 Angiomyomatous hamartoma particularly involves inguinal and femoral lymph nodes, with few cases reported in the cervical, popliteal, and submandibular lymph nodes.1 Angiomyomatous hamartoma can occasionally be associated with edema of the ipsilateral limb. To the authors’ knowledge, to date only 18 cases of AMH have been reported.4
Case Presentation
A 40-year-old white man started to have a left inguinal and scrotal pain along with left thigh swelling at age 22 while serving in the U.S. Army.
An abdominal Doppler ultrasound did not show any evidence of portal hypertension. A thoraco-abdomino-pelvic computed tomography (CT) scan showed bilateral axillary, subcarinal (Figure 1), mesenteric and retroperitoneal (Figure 2), and left inguinal (Figure 3) lymphadenopathy. Excisional biopsy of a 3.5 x 2.5 x 1.5 cm left inguinal lymph node was performed, and histopathology showed extensive smooth muscle and vascular proliferation replacing most of the lymph node (Figure 4), a finding consistent with AMH. A trichrome staining (Figure 5) and immunohistochemical study for smooth muscle actin (Figure 6) were performed and supported the diagnosis. Due to persistent pain in the scrotal area, the patient underwent a left spermatic cord denervation. Currently, the patient has persistent left thigh swelling. His condition remains stable with a regular follow-up CT scan showing unchanged lymphadenopathy.
Discussion
Angiomyomatous hamartoma is a rare, primary vascular tumor of the lymph nodes occurring almost exclusively in the inguinal and femoral lymph nodes and occasionally associated with edema of the ipsilateral limb.1 A few cases with popliteal and cervical lymph node involvement have been reported.1 There are no prior reports of cases with either generalized adenopathy or hepatosplenomegaly.
The histopathogenesis of AMH remains unclear. Chan and colleagues first reported this distinct clinicopathologic entity in 1992 as a primary vascular tumor of the lymph node.1-3 The hamartomatous nature of the disease was postulated by the authors on the basis of a disorganized growth pattern of smooth muscle cells and blood vessels noted on pathology.2,3 The AMH could represent a localized malformation in a congenitally damaged lymphatic vessel system.5 Other hypothesis suggests lymphedema as a possible etiology of AMH through continuous stimulation of lymphatic vessels, which triggers vasoproliferation and eventually the vascular transformation of the lymph nodes.5
Differential diagnoses of AMH include nodal lymphangiomyomatosis, which is most prevalent in women, particularly presenting with thoracic and intra-abdominal lymph nodes and plumper HMB45 (human melanoma black 45) -positive tumor cells6; leiomyomato
Treatment is either conservative or surgical, depending on clinical judgment. This is only the 19th case of AMH reported so far in the literature and the fifth reported case in which the patient presented with ipsilateral lymphedema of the limb. Importantly, it is the first reported case with generalized (axillary, subcarinal, mesenteric, inguinal and retroperitoneal) lymphadenopathy and unexplained hepatosplenomegaly.
Conclusion
Angiomyomatous hamartoma of the lymph nodes is an exceedingly rare diagnosis but should be considered when evaluating patients with lymphatic tumors. This patient remains relatively asymptomatic and on observation at this time and seems to have more extensive disease than prior reports in the literature.
1. Mridha AR, Ranjan R, Kinra P, Ray R, Khan SA, Shivanand G. Angiomyomatous hamartoma of popliteal lymph node: an unusual entity. J Pathol Transl Med. 2015;49(2):156-158.
2. Dargent JL, Lespagnard L, Verdebout JM, Bourgeois P, Munck D. Glomeruloid microvascular proliferation in angiomyomatous hamartoma of the lymph node. Virchows Arch. 2004;445(3):320-322.
3. Chan JK, Frizzera G, Fletcher CD, Rosai J. Primary vascular tumors of lymph nodes other than Kaposi’s sarcoma. Analysis of 39 cases and delineation of two new entities. Am J Surg Pathol. 1992;16(4):335-350.
4. Ram M, Alsanjari N, Ansari N. Angiomyomatous hamartoma: a rare case report with review of the literature. Rare Tumors. 2009;1(2):e25.
5. Piedimonte A, De Nictolis M, Lorenzini P, Sperti V, Bertani A. Angiomyomatous hamartoma of inguinal lymph nodes. Plast Reconstr Surg. 2006;117(2):714-716.
6. Lee CH, Chang TC, Ku JW. Angiomyomatous hamartoma in an inguinal lymph node with proliferating pericytes/smooth muscle cells, plexiform vessel tangles, and ectopic calcification. Indian J Pathol Microbiol. 2015;58(2):226-228.
1. Mridha AR, Ranjan R, Kinra P, Ray R, Khan SA, Shivanand G. Angiomyomatous hamartoma of popliteal lymph node: an unusual entity. J Pathol Transl Med. 2015;49(2):156-158.
2. Dargent JL, Lespagnard L, Verdebout JM, Bourgeois P, Munck D. Glomeruloid microvascular proliferation in angiomyomatous hamartoma of the lymph node. Virchows Arch. 2004;445(3):320-322.
3. Chan JK, Frizzera G, Fletcher CD, Rosai J. Primary vascular tumors of lymph nodes other than Kaposi’s sarcoma. Analysis of 39 cases and delineation of two new entities. Am J Surg Pathol. 1992;16(4):335-350.
4. Ram M, Alsanjari N, Ansari N. Angiomyomatous hamartoma: a rare case report with review of the literature. Rare Tumors. 2009;1(2):e25.
5. Piedimonte A, De Nictolis M, Lorenzini P, Sperti V, Bertani A. Angiomyomatous hamartoma of inguinal lymph nodes. Plast Reconstr Surg. 2006;117(2):714-716.
6. Lee CH, Chang TC, Ku JW. Angiomyomatous hamartoma in an inguinal lymph node with proliferating pericytes/smooth muscle cells, plexiform vessel tangles, and ectopic calcification. Indian J Pathol Microbiol. 2015;58(2):226-228.