User login
Mental Health: A Forgotten Facet of Primary Care
One of the biggest disparities in health care today is the separate treatment of mind and body, despite their known integration.1 While mental and behavioral health conditions are frequently diagnosed and treated within primary care settings, fragmentation persists between the mental and physical health care systems—creating barriers in the quality, outcome, and efficiency of care.2 Since half of Americans with mental health conditions go without essential care, reform of our nation’s mental health system is a priority issue for NPs and PAs and the patients we serve.
Some progress has been made to implement change—the Now Is the Time initiative, launched in 2013, increased federal funding for behavioral health care workforce training in an effort to support more providers in mental and substance use disorder treatment. The Affordable Care Act (ACA) has worked to improve behavioral health coverage for Americans in three ways: ending insurance company discrimination based on pre-existing conditions, requiring health insurance coverage for mental and substance use disorder services, and expanding mental health parity. This has improved coverage and access to mental and substance abuse services for more than 60 million Americans.3 In January 2016, President Obama proposed a $500 million investment to increase access to mental health care.4 The most recent presidential election creates an uncertain future for
Regardless, more work has to be done to guarantee that Americans have the access they need. Sadly, even with these advancements in behavioral health coverage, only about half of children and less than half of adults with diagnosable mental health disorders get the treatment they need.4 A 2016 report from the Rural Health Research Center revealed that more than 15 million Americans face behavioral health issues without access to the necessary care.5
Psychiatric providers (like most other specialists) tend to be located in urban areas, limiting access in rural areas and even some underserved urban communities. Only 43% of family physicians in this country provide mental health care.6 The team-based care that NPs and PAs provide has great potential for bridging this gap in mental health coverage.
NPs and PAs are an important but underutilized resource for improving mental health care access—but how can primary care NPs and PAs work to enhance the delivery of mental health care in our country? In the preprofessional area, it would be prudent to entice qualified individuals in the mental health field—particularly those who are licensed clinical social workers, licensed professional counselors, or marriage and family therapists—into NP and PA programs with preference.
Clinical rotations in behavioral health (BH)/psychiatry should be encouraged—even mandated—in professional education. We should ensure this content is taught in the didactic portion of NP/PA professional education, as well as bolstering psychiatric pharmacology in coursework.
Postprofessional education should encourage primary care NPs and PAs to gain additional self-directed education in BH/psychiatry. This can be achieved via a focused psychiatry “boot camp” (for PAs following the CAQ blueprint, found at www.nccpa.net/psychiatry) or a competency-based online postprofessional certificate in BH/psychiatry (such as—shameless plug—the one offered at my institution; www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online).7,8
This psychiatric background is fundamental throughout primary care but is crucial in community health centers, correctional health care centers, and Veterans Administration hospitals. Of course, in order to make a difference, we must remove the barriers that prevent psychiatric NPs and PAs from being considered mental health providers and adjust reimbursement accordingly.
Do you have ideas on how to increase the knowledge base of primary care NPs and PAs and enhance the provision of mental health services in this country? Will the political change in leadership in January 2017 increase opportunities to make a difference in mental health care? Please share your thoughts by contacting me at PAEditor@frontlinemedcom.com.
1. deGruy F. Mental health care in the primary care setting. In: Donaldson MS, Yordy KD, Lohr KN, Vanselow NA, eds. Primary Care: America’s Health in a New Era. Washington, DC: Institute of Medicine; 1996.
2. Simon GE, Katon WJ, VonKorff M, et al. Cost-effectiveness of a collaborative care program for primary care patients with persistent depression. Am J Psychiatry. 2001;158(10): 1638-1644.
3. Enomoto K. Improving access to mental health services - President’s FY 2017 Budget proposes new investments to increase access. http://abilitychicagoinfo.blogspot.com/2016/02/improving-access-to-mental-health.html. Accessed November 3, 2016.
4. Enomoto K. Improving access to mental health services. www.hhs.gov/blog/2016/02/09/improving-access-mental-health-services.html. Accessed November 3, 2016.
5. Rural Health Research Center. Supply and distribution of the behavioral health workforce in rural America. http://depts.washington.edu/fammed/rhrc/wp-content/uploads/sites/4/2016/09/RHRC_DB160_Larson.pdf. Accessed November 3, 2016.
6. Miller BF, Druss B. The role of family physicians in mental health care delivery in the United States: implications for health reform. J Am Board Fam Med. 2013;26(2): 111-113.
7. National Commission on Certification of Physician Assistants. Psychiatry CAQ. www.nccpa.net/psychiatry. Accessed November 3, 2016.
8. A.T. Still University. Postgraduate certificate in psychiatry and behavioral health online. www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online. Accessed November 3, 2016.

One of the biggest disparities in health care today is the separate treatment of mind and body, despite their known integration.1 While mental and behavioral health conditions are frequently diagnosed and treated within primary care settings, fragmentation persists between the mental and physical health care systems—creating barriers in the quality, outcome, and efficiency of care.2 Since half of Americans with mental health conditions go without essential care, reform of our nation’s mental health system is a priority issue for NPs and PAs and the patients we serve.
Some progress has been made to implement change—the Now Is the Time initiative, launched in 2013, increased federal funding for behavioral health care workforce training in an effort to support more providers in mental and substance use disorder treatment. The Affordable Care Act (ACA) has worked to improve behavioral health coverage for Americans in three ways: ending insurance company discrimination based on pre-existing conditions, requiring health insurance coverage for mental and substance use disorder services, and expanding mental health parity. This has improved coverage and access to mental and substance abuse services for more than 60 million Americans.3 In January 2016, President Obama proposed a $500 million investment to increase access to mental health care.4 The most recent presidential election creates an uncertain future for
Regardless, more work has to be done to guarantee that Americans have the access they need. Sadly, even with these advancements in behavioral health coverage, only about half of children and less than half of adults with diagnosable mental health disorders get the treatment they need.4 A 2016 report from the Rural Health Research Center revealed that more than 15 million Americans face behavioral health issues without access to the necessary care.5
Psychiatric providers (like most other specialists) tend to be located in urban areas, limiting access in rural areas and even some underserved urban communities. Only 43% of family physicians in this country provide mental health care.6 The team-based care that NPs and PAs provide has great potential for bridging this gap in mental health coverage.
NPs and PAs are an important but underutilized resource for improving mental health care access—but how can primary care NPs and PAs work to enhance the delivery of mental health care in our country? In the preprofessional area, it would be prudent to entice qualified individuals in the mental health field—particularly those who are licensed clinical social workers, licensed professional counselors, or marriage and family therapists—into NP and PA programs with preference.
Clinical rotations in behavioral health (BH)/psychiatry should be encouraged—even mandated—in professional education. We should ensure this content is taught in the didactic portion of NP/PA professional education, as well as bolstering psychiatric pharmacology in coursework.
Postprofessional education should encourage primary care NPs and PAs to gain additional self-directed education in BH/psychiatry. This can be achieved via a focused psychiatry “boot camp” (for PAs following the CAQ blueprint, found at www.nccpa.net/psychiatry) or a competency-based online postprofessional certificate in BH/psychiatry (such as—shameless plug—the one offered at my institution; www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online).7,8
This psychiatric background is fundamental throughout primary care but is crucial in community health centers, correctional health care centers, and Veterans Administration hospitals. Of course, in order to make a difference, we must remove the barriers that prevent psychiatric NPs and PAs from being considered mental health providers and adjust reimbursement accordingly.
Do you have ideas on how to increase the knowledge base of primary care NPs and PAs and enhance the provision of mental health services in this country? Will the political change in leadership in January 2017 increase opportunities to make a difference in mental health care? Please share your thoughts by contacting me at PAEditor@frontlinemedcom.com.
One of the biggest disparities in health care today is the separate treatment of mind and body, despite their known integration.1 While mental and behavioral health conditions are frequently diagnosed and treated within primary care settings, fragmentation persists between the mental and physical health care systems—creating barriers in the quality, outcome, and efficiency of care.2 Since half of Americans with mental health conditions go without essential care, reform of our nation’s mental health system is a priority issue for NPs and PAs and the patients we serve.
Some progress has been made to implement change—the Now Is the Time initiative, launched in 2013, increased federal funding for behavioral health care workforce training in an effort to support more providers in mental and substance use disorder treatment. The Affordable Care Act (ACA) has worked to improve behavioral health coverage for Americans in three ways: ending insurance company discrimination based on pre-existing conditions, requiring health insurance coverage for mental and substance use disorder services, and expanding mental health parity. This has improved coverage and access to mental and substance abuse services for more than 60 million Americans.3 In January 2016, President Obama proposed a $500 million investment to increase access to mental health care.4 The most recent presidential election creates an uncertain future for
Regardless, more work has to be done to guarantee that Americans have the access they need. Sadly, even with these advancements in behavioral health coverage, only about half of children and less than half of adults with diagnosable mental health disorders get the treatment they need.4 A 2016 report from the Rural Health Research Center revealed that more than 15 million Americans face behavioral health issues without access to the necessary care.5
Psychiatric providers (like most other specialists) tend to be located in urban areas, limiting access in rural areas and even some underserved urban communities. Only 43% of family physicians in this country provide mental health care.6 The team-based care that NPs and PAs provide has great potential for bridging this gap in mental health coverage.
NPs and PAs are an important but underutilized resource for improving mental health care access—but how can primary care NPs and PAs work to enhance the delivery of mental health care in our country? In the preprofessional area, it would be prudent to entice qualified individuals in the mental health field—particularly those who are licensed clinical social workers, licensed professional counselors, or marriage and family therapists—into NP and PA programs with preference.
Clinical rotations in behavioral health (BH)/psychiatry should be encouraged—even mandated—in professional education. We should ensure this content is taught in the didactic portion of NP/PA professional education, as well as bolstering psychiatric pharmacology in coursework.
Postprofessional education should encourage primary care NPs and PAs to gain additional self-directed education in BH/psychiatry. This can be achieved via a focused psychiatry “boot camp” (for PAs following the CAQ blueprint, found at www.nccpa.net/psychiatry) or a competency-based online postprofessional certificate in BH/psychiatry (such as—shameless plug—the one offered at my institution; www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online).7,8
This psychiatric background is fundamental throughout primary care but is crucial in community health centers, correctional health care centers, and Veterans Administration hospitals. Of course, in order to make a difference, we must remove the barriers that prevent psychiatric NPs and PAs from being considered mental health providers and adjust reimbursement accordingly.
Do you have ideas on how to increase the knowledge base of primary care NPs and PAs and enhance the provision of mental health services in this country? Will the political change in leadership in January 2017 increase opportunities to make a difference in mental health care? Please share your thoughts by contacting me at PAEditor@frontlinemedcom.com.
1. deGruy F. Mental health care in the primary care setting. In: Donaldson MS, Yordy KD, Lohr KN, Vanselow NA, eds. Primary Care: America’s Health in a New Era. Washington, DC: Institute of Medicine; 1996.
2. Simon GE, Katon WJ, VonKorff M, et al. Cost-effectiveness of a collaborative care program for primary care patients with persistent depression. Am J Psychiatry. 2001;158(10): 1638-1644.
3. Enomoto K. Improving access to mental health services - President’s FY 2017 Budget proposes new investments to increase access. http://abilitychicagoinfo.blogspot.com/2016/02/improving-access-to-mental-health.html. Accessed November 3, 2016.
4. Enomoto K. Improving access to mental health services. www.hhs.gov/blog/2016/02/09/improving-access-mental-health-services.html. Accessed November 3, 2016.
5. Rural Health Research Center. Supply and distribution of the behavioral health workforce in rural America. http://depts.washington.edu/fammed/rhrc/wp-content/uploads/sites/4/2016/09/RHRC_DB160_Larson.pdf. Accessed November 3, 2016.
6. Miller BF, Druss B. The role of family physicians in mental health care delivery in the United States: implications for health reform. J Am Board Fam Med. 2013;26(2): 111-113.
7. National Commission on Certification of Physician Assistants. Psychiatry CAQ. www.nccpa.net/psychiatry. Accessed November 3, 2016.
8. A.T. Still University. Postgraduate certificate in psychiatry and behavioral health online. www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online. Accessed November 3, 2016.
1. deGruy F. Mental health care in the primary care setting. In: Donaldson MS, Yordy KD, Lohr KN, Vanselow NA, eds. Primary Care: America’s Health in a New Era. Washington, DC: Institute of Medicine; 1996.
2. Simon GE, Katon WJ, VonKorff M, et al. Cost-effectiveness of a collaborative care program for primary care patients with persistent depression. Am J Psychiatry. 2001;158(10): 1638-1644.
3. Enomoto K. Improving access to mental health services - President’s FY 2017 Budget proposes new investments to increase access. http://abilitychicagoinfo.blogspot.com/2016/02/improving-access-to-mental-health.html. Accessed November 3, 2016.
4. Enomoto K. Improving access to mental health services. www.hhs.gov/blog/2016/02/09/improving-access-mental-health-services.html. Accessed November 3, 2016.
5. Rural Health Research Center. Supply and distribution of the behavioral health workforce in rural America. http://depts.washington.edu/fammed/rhrc/wp-content/uploads/sites/4/2016/09/RHRC_DB160_Larson.pdf. Accessed November 3, 2016.
6. Miller BF, Druss B. The role of family physicians in mental health care delivery in the United States: implications for health reform. J Am Board Fam Med. 2013;26(2): 111-113.
7. National Commission on Certification of Physician Assistants. Psychiatry CAQ. www.nccpa.net/psychiatry. Accessed November 3, 2016.
8. A.T. Still University. Postgraduate certificate in psychiatry and behavioral health online. www.atsu.edu/postgraduate-certificate-in-psychiatry-and-behavioral-health-online. Accessed November 3, 2016.
Diagnosis & assessment of pain: Refining your approach
![]()
Louis Kuritzky, MD
Clinical Assistant Professor Emeritus
Department of Community Health & Family Medicine
University of Florida, Gainesville
![]()
Louis Kuritzky, MD
Clinical Assistant Professor Emeritus
Department of Community Health & Family Medicine
University of Florida, Gainesville
![]()
Louis Kuritzky, MD
Clinical Assistant Professor Emeritus
Department of Community Health & Family Medicine
University of Florida, Gainesville
Pediatric update: 2 vaccine changes and the latest word on media time

VIDEO: No difference between PPI and H2RA for low-dose aspirin gastroprotection
Among patients on low-dose aspirin at risk for recurrent GI bleeding, there were slightly fewer GI bleeds or ulcers when patients were on the proton pump inhibitor rabeprazole (Aciphex) instead of the histamine2-receptor antagonist famotidine (Pepcid), but the difference was not statistically significant according to a study reported in the January issue of Gastroenterology.
SOURCE: American Gastroenterological Association
In a 270-subject, double-blind, randomized trial in Hong Kong and Japan led by Francis Chan, MD, of the Chinese University of Hong Kong, investigators found, “Among high-risk aspirin users, the incidence of recurrent bleeding is comparable with either use of PPI [proton pump inhibitor] or H2RA [H2-receptor antagonist].” However, “since a small difference in efficacy cannot be excluded, PPI probably remains the preferred treatment for long-term protection against upper GI bleeding in high-risk aspirin users” (Gastroenterology. 2016 Sep 15. doi: 10.1053/j.gastro.2016.09.006).
Even so, “our findings suggest that famotidine may be a reasonable alternative option for aspirin users who disfavor long-term PPI therapy,” they said.
Because of concerns about the long-term safety of PPIs, including the association between PPIs and increased risk of serious cardiovascular events in patients on clopidogrel (Plavix), clinicians have been looking for alternatives. The findings reassure that H2RAs are a reasonable choice; many clinicians have already turned to them.
All 270 subjects had previously had endoscopically confirmed ulcer bleeding while on low-dose aspirin (325 mg or less per day). “Considering clinicians will be most concerned with the adequacy of gastroprotective treatment effect in aspirin users with the highest risk, we exclusively enrolled patients with endoscopy-proven upper GI bleeding,” Dr. Chan and his colleagues said.
After the ulcers healed, the subjects resumed aspirin (80 mg) daily and were randomized to either famotidine 40 mg once daily (n = 132) or rabeprazole 20 mg daily (n = 138) for up to 12 months. Helicobacter pylori was eradicated prior to randomization in patients who tested positive. Subjects were evaluated every 2 months, with repeat endoscopy for symptoms of upper GI bleeding or significant drops in hemoglobin, as well as at the end of the study.
During the 12-month study period, upper GI bleeding recurred in one patient receiving rabeprazole (0.7%) and four receiving famotidine (3.1%; P = .16). The composite endpoint of recurrent bleeding or endoscopic ulcers at month 12 was reached by nine patients in the rabeprazole group (7.9%) and 13 receiving famotidine (12.4%; P = .26).
“Our findings indicate that both treatments are comparable in preventing recurrent upper GI bleeding in high-risk aspirin users, although a small difference in efficacy cannot be excluded,” the investigators said.
Over two-thirds of the subjects were men, and the mean age was 73 years. About a quarter in the PPI group and almost 40% in the H2RA group had H. pylori cleared before randomization.
The Research Grant Council of Hong Kong funded the work. Dr. Chan has served as a consultant to Pfizer, Eisai, Takeda, and Otsuka, and has received research grants from Pfizer and lecture fees from Pfizer, AstraZeneca, and Takeda. Several other authors reported similar industry disclosures.
Aspirin is widely used for primary and secondary prophylaxis of cardiovascular disease. Dr. Chan and colleagues present a randomized, controlled trial comparing rabeprazole 20 mg once a day to famotidine 40 mg once a day in preventing recurrent GI hemorrhage and endoscopic ulcers in low-dose (less than 325 mg) aspirin users. The authors conclude that no statistical difference was found between the two agents. The study contrasts with another study from Hong Kong, which found that proton pump inhibitors were more effective.
The authors are to be complimented on this important addition to the literature but the reader should not conclude that H2-receptor antagonists and proton pump inhibitors are equivalent in preventing recurrent bleeding from aspirin-induced ulcers.
Nimish Vakil, MD, AGAF, is clinical professor of medicine at the University of Wisconsin–Madison. He has consulted for Ironwood and AstraZeneca.
Aspirin is widely used for primary and secondary prophylaxis of cardiovascular disease. Dr. Chan and colleagues present a randomized, controlled trial comparing rabeprazole 20 mg once a day to famotidine 40 mg once a day in preventing recurrent GI hemorrhage and endoscopic ulcers in low-dose (less than 325 mg) aspirin users. The authors conclude that no statistical difference was found between the two agents. The study contrasts with another study from Hong Kong, which found that proton pump inhibitors were more effective.
The authors are to be complimented on this important addition to the literature but the reader should not conclude that H2-receptor antagonists and proton pump inhibitors are equivalent in preventing recurrent bleeding from aspirin-induced ulcers.
Nimish Vakil, MD, AGAF, is clinical professor of medicine at the University of Wisconsin–Madison. He has consulted for Ironwood and AstraZeneca.
Aspirin is widely used for primary and secondary prophylaxis of cardiovascular disease. Dr. Chan and colleagues present a randomized, controlled trial comparing rabeprazole 20 mg once a day to famotidine 40 mg once a day in preventing recurrent GI hemorrhage and endoscopic ulcers in low-dose (less than 325 mg) aspirin users. The authors conclude that no statistical difference was found between the two agents. The study contrasts with another study from Hong Kong, which found that proton pump inhibitors were more effective.
The authors are to be complimented on this important addition to the literature but the reader should not conclude that H2-receptor antagonists and proton pump inhibitors are equivalent in preventing recurrent bleeding from aspirin-induced ulcers.
Nimish Vakil, MD, AGAF, is clinical professor of medicine at the University of Wisconsin–Madison. He has consulted for Ironwood and AstraZeneca.
Among patients on low-dose aspirin at risk for recurrent GI bleeding, there were slightly fewer GI bleeds or ulcers when patients were on the proton pump inhibitor rabeprazole (Aciphex) instead of the histamine2-receptor antagonist famotidine (Pepcid), but the difference was not statistically significant according to a study reported in the January issue of Gastroenterology.
SOURCE: American Gastroenterological Association
In a 270-subject, double-blind, randomized trial in Hong Kong and Japan led by Francis Chan, MD, of the Chinese University of Hong Kong, investigators found, “Among high-risk aspirin users, the incidence of recurrent bleeding is comparable with either use of PPI [proton pump inhibitor] or H2RA [H2-receptor antagonist].” However, “since a small difference in efficacy cannot be excluded, PPI probably remains the preferred treatment for long-term protection against upper GI bleeding in high-risk aspirin users” (Gastroenterology. 2016 Sep 15. doi: 10.1053/j.gastro.2016.09.006).
Even so, “our findings suggest that famotidine may be a reasonable alternative option for aspirin users who disfavor long-term PPI therapy,” they said.
Because of concerns about the long-term safety of PPIs, including the association between PPIs and increased risk of serious cardiovascular events in patients on clopidogrel (Plavix), clinicians have been looking for alternatives. The findings reassure that H2RAs are a reasonable choice; many clinicians have already turned to them.
All 270 subjects had previously had endoscopically confirmed ulcer bleeding while on low-dose aspirin (325 mg or less per day). “Considering clinicians will be most concerned with the adequacy of gastroprotective treatment effect in aspirin users with the highest risk, we exclusively enrolled patients with endoscopy-proven upper GI bleeding,” Dr. Chan and his colleagues said.
After the ulcers healed, the subjects resumed aspirin (80 mg) daily and were randomized to either famotidine 40 mg once daily (n = 132) or rabeprazole 20 mg daily (n = 138) for up to 12 months. Helicobacter pylori was eradicated prior to randomization in patients who tested positive. Subjects were evaluated every 2 months, with repeat endoscopy for symptoms of upper GI bleeding or significant drops in hemoglobin, as well as at the end of the study.
During the 12-month study period, upper GI bleeding recurred in one patient receiving rabeprazole (0.7%) and four receiving famotidine (3.1%; P = .16). The composite endpoint of recurrent bleeding or endoscopic ulcers at month 12 was reached by nine patients in the rabeprazole group (7.9%) and 13 receiving famotidine (12.4%; P = .26).
“Our findings indicate that both treatments are comparable in preventing recurrent upper GI bleeding in high-risk aspirin users, although a small difference in efficacy cannot be excluded,” the investigators said.
Over two-thirds of the subjects were men, and the mean age was 73 years. About a quarter in the PPI group and almost 40% in the H2RA group had H. pylori cleared before randomization.
The Research Grant Council of Hong Kong funded the work. Dr. Chan has served as a consultant to Pfizer, Eisai, Takeda, and Otsuka, and has received research grants from Pfizer and lecture fees from Pfizer, AstraZeneca, and Takeda. Several other authors reported similar industry disclosures.
Among patients on low-dose aspirin at risk for recurrent GI bleeding, there were slightly fewer GI bleeds or ulcers when patients were on the proton pump inhibitor rabeprazole (Aciphex) instead of the histamine2-receptor antagonist famotidine (Pepcid), but the difference was not statistically significant according to a study reported in the January issue of Gastroenterology.
SOURCE: American Gastroenterological Association
In a 270-subject, double-blind, randomized trial in Hong Kong and Japan led by Francis Chan, MD, of the Chinese University of Hong Kong, investigators found, “Among high-risk aspirin users, the incidence of recurrent bleeding is comparable with either use of PPI [proton pump inhibitor] or H2RA [H2-receptor antagonist].” However, “since a small difference in efficacy cannot be excluded, PPI probably remains the preferred treatment for long-term protection against upper GI bleeding in high-risk aspirin users” (Gastroenterology. 2016 Sep 15. doi: 10.1053/j.gastro.2016.09.006).
Even so, “our findings suggest that famotidine may be a reasonable alternative option for aspirin users who disfavor long-term PPI therapy,” they said.
Because of concerns about the long-term safety of PPIs, including the association between PPIs and increased risk of serious cardiovascular events in patients on clopidogrel (Plavix), clinicians have been looking for alternatives. The findings reassure that H2RAs are a reasonable choice; many clinicians have already turned to them.
All 270 subjects had previously had endoscopically confirmed ulcer bleeding while on low-dose aspirin (325 mg or less per day). “Considering clinicians will be most concerned with the adequacy of gastroprotective treatment effect in aspirin users with the highest risk, we exclusively enrolled patients with endoscopy-proven upper GI bleeding,” Dr. Chan and his colleagues said.
After the ulcers healed, the subjects resumed aspirin (80 mg) daily and were randomized to either famotidine 40 mg once daily (n = 132) or rabeprazole 20 mg daily (n = 138) for up to 12 months. Helicobacter pylori was eradicated prior to randomization in patients who tested positive. Subjects were evaluated every 2 months, with repeat endoscopy for symptoms of upper GI bleeding or significant drops in hemoglobin, as well as at the end of the study.
During the 12-month study period, upper GI bleeding recurred in one patient receiving rabeprazole (0.7%) and four receiving famotidine (3.1%; P = .16). The composite endpoint of recurrent bleeding or endoscopic ulcers at month 12 was reached by nine patients in the rabeprazole group (7.9%) and 13 receiving famotidine (12.4%; P = .26).
“Our findings indicate that both treatments are comparable in preventing recurrent upper GI bleeding in high-risk aspirin users, although a small difference in efficacy cannot be excluded,” the investigators said.
Over two-thirds of the subjects were men, and the mean age was 73 years. About a quarter in the PPI group and almost 40% in the H2RA group had H. pylori cleared before randomization.
The Research Grant Council of Hong Kong funded the work. Dr. Chan has served as a consultant to Pfizer, Eisai, Takeda, and Otsuka, and has received research grants from Pfizer and lecture fees from Pfizer, AstraZeneca, and Takeda. Several other authors reported similar industry disclosures.
FROM GASTROENTEROLOGY
Key clinical point:
Major finding: During the 12-month study period, upper GI bleeding recurred in one patient receiving rabeprazole (0.7%) and four receiving famotidine (3.1%; P = .16). The composite endpoint of recurrent bleeding or endoscopic ulcers at month 12 was reached by nine patients in the rabeprazole group (7.9%) and 13 receiving famotidine (12.4%; P = .26).
Data source: A 270-subject, double-blind, randomized trial in Hong Kong and Japan.
Disclosures: The Research Grant Council of Hong Kong funded the work. The lead investigator has served as a consultant to Pfizer, Eisai, Takeda, and Otsuka, and has received research grants from Pfizer and lecture fees from Pfizer, AstraZeneca, and Takeda. Several other authors reported similar industry disclosures.

In lung cancer screening, patient education works
A counseling and shared decision-making visit improved patient knowledge of the eligibility criteria, benefits, and potential risks of lung cancer screening via a low-radiation chest CT scan.
The Center for Medicare & Medicaid Services has added the type of visit addressed in this study to Medicare’s preventive services benefits for individuals meeting certain criteria, but no previous study had looked at how the implementation of such a visit impacted a patient’s knowledge and understanding.
The researchers noted significant improvement in all questions before and after a counseling session (P = .03 to P less than .0001). Those improvements lessened at 1 month, but were still higher than precounseling scores.
The percentages of participants who knew the age criteria for lung cancer screening before counseling, immediately after counseling, and 1 month after counseling, for example, were 8.8% (11 patients), 59.2% (74 patients), and 21.4% (24 patients), respectively. The percentage of participants able to identify at least one of the potential hazards of screening increased by a similar amount immediately after receiving counseling, as did the percentage of participants able to identify the age criteria for lung cancer screening immediately after receiving counseling. The percentages of patients able to identify at least one of the potential hazards of screening were 38.4% before counseling and 90.4% immediately after receiving counseling. One month following counseling, the percentage of patients with such knowledge remained fairly high, dropping to 78.6%.
“Showing the value of these visits is very important to encourage policymakers and payers to continue to support the counseling and shared decision-making visit,” Peter J. Mazzone, MD, MPH, who led the study, said in an interview.
These types of conversations are important because of the uncertainties surrounding lung cancer screening, which leads to about a 20% reduction in mortality risk. That translates to the need to screen about 250 people to save 1 life. “I think the public sometimes doesn’t realize that the effectiveness of some of these preventive screenings may not be as large as they think they are,” said David Grossman, vice chair of the US Preventive Services Task Force and a senior investigator at the Group Health Research Institute, Seattle, who was not involved in the study.
The researchers developed a centralized counseling and shared decision-making visit that included a narrated slide show and individualized risk assessment. They approached 423 consecutive patients who had been identified by their primary care provider or a specialist as potential candidates for screening. Of those 423 patients, 125 agreed to participate in the study (Chest. 2016 Nov 1. doi: 10.1016/j.chest.2016.10.027).
The session delivered expected improvements in patient knowledge, but there were some surprises. “The starting point of knowledge was perhaps less than we would have anticipated, and the gains, though very substantial, weren’t perfect,” said Dr. Mazzone, who is also director of the lung cancer screening program at the Cleveland Clinic.
The drop in knowledge at 1 month suggests that the information needs to be reinforced, possibly each time patients come in for an annual screening visit, Dr. Mazzone added.
Counseling sessions can also help convince patients to quit smoking, if tobacco use is a concern. “It’s not appropriate to screen for lung cancer without making a commitment to try to quit,” said Dr. Grossman.
No funding source was disclosed. Dr. Mazzone and Dr. Grossman reported having no financial disclosures.
A counseling and shared decision-making visit improved patient knowledge of the eligibility criteria, benefits, and potential risks of lung cancer screening via a low-radiation chest CT scan.
The Center for Medicare & Medicaid Services has added the type of visit addressed in this study to Medicare’s preventive services benefits for individuals meeting certain criteria, but no previous study had looked at how the implementation of such a visit impacted a patient’s knowledge and understanding.
The researchers noted significant improvement in all questions before and after a counseling session (P = .03 to P less than .0001). Those improvements lessened at 1 month, but were still higher than precounseling scores.
The percentages of participants who knew the age criteria for lung cancer screening before counseling, immediately after counseling, and 1 month after counseling, for example, were 8.8% (11 patients), 59.2% (74 patients), and 21.4% (24 patients), respectively. The percentage of participants able to identify at least one of the potential hazards of screening increased by a similar amount immediately after receiving counseling, as did the percentage of participants able to identify the age criteria for lung cancer screening immediately after receiving counseling. The percentages of patients able to identify at least one of the potential hazards of screening were 38.4% before counseling and 90.4% immediately after receiving counseling. One month following counseling, the percentage of patients with such knowledge remained fairly high, dropping to 78.6%.
“Showing the value of these visits is very important to encourage policymakers and payers to continue to support the counseling and shared decision-making visit,” Peter J. Mazzone, MD, MPH, who led the study, said in an interview.
These types of conversations are important because of the uncertainties surrounding lung cancer screening, which leads to about a 20% reduction in mortality risk. That translates to the need to screen about 250 people to save 1 life. “I think the public sometimes doesn’t realize that the effectiveness of some of these preventive screenings may not be as large as they think they are,” said David Grossman, vice chair of the US Preventive Services Task Force and a senior investigator at the Group Health Research Institute, Seattle, who was not involved in the study.
The researchers developed a centralized counseling and shared decision-making visit that included a narrated slide show and individualized risk assessment. They approached 423 consecutive patients who had been identified by their primary care provider or a specialist as potential candidates for screening. Of those 423 patients, 125 agreed to participate in the study (Chest. 2016 Nov 1. doi: 10.1016/j.chest.2016.10.027).
The session delivered expected improvements in patient knowledge, but there were some surprises. “The starting point of knowledge was perhaps less than we would have anticipated, and the gains, though very substantial, weren’t perfect,” said Dr. Mazzone, who is also director of the lung cancer screening program at the Cleveland Clinic.
The drop in knowledge at 1 month suggests that the information needs to be reinforced, possibly each time patients come in for an annual screening visit, Dr. Mazzone added.
Counseling sessions can also help convince patients to quit smoking, if tobacco use is a concern. “It’s not appropriate to screen for lung cancer without making a commitment to try to quit,” said Dr. Grossman.
No funding source was disclosed. Dr. Mazzone and Dr. Grossman reported having no financial disclosures.
A counseling and shared decision-making visit improved patient knowledge of the eligibility criteria, benefits, and potential risks of lung cancer screening via a low-radiation chest CT scan.
The Center for Medicare & Medicaid Services has added the type of visit addressed in this study to Medicare’s preventive services benefits for individuals meeting certain criteria, but no previous study had looked at how the implementation of such a visit impacted a patient’s knowledge and understanding.
The researchers noted significant improvement in all questions before and after a counseling session (P = .03 to P less than .0001). Those improvements lessened at 1 month, but were still higher than precounseling scores.
The percentages of participants who knew the age criteria for lung cancer screening before counseling, immediately after counseling, and 1 month after counseling, for example, were 8.8% (11 patients), 59.2% (74 patients), and 21.4% (24 patients), respectively. The percentage of participants able to identify at least one of the potential hazards of screening increased by a similar amount immediately after receiving counseling, as did the percentage of participants able to identify the age criteria for lung cancer screening immediately after receiving counseling. The percentages of patients able to identify at least one of the potential hazards of screening were 38.4% before counseling and 90.4% immediately after receiving counseling. One month following counseling, the percentage of patients with such knowledge remained fairly high, dropping to 78.6%.
“Showing the value of these visits is very important to encourage policymakers and payers to continue to support the counseling and shared decision-making visit,” Peter J. Mazzone, MD, MPH, who led the study, said in an interview.
These types of conversations are important because of the uncertainties surrounding lung cancer screening, which leads to about a 20% reduction in mortality risk. That translates to the need to screen about 250 people to save 1 life. “I think the public sometimes doesn’t realize that the effectiveness of some of these preventive screenings may not be as large as they think they are,” said David Grossman, vice chair of the US Preventive Services Task Force and a senior investigator at the Group Health Research Institute, Seattle, who was not involved in the study.
The researchers developed a centralized counseling and shared decision-making visit that included a narrated slide show and individualized risk assessment. They approached 423 consecutive patients who had been identified by their primary care provider or a specialist as potential candidates for screening. Of those 423 patients, 125 agreed to participate in the study (Chest. 2016 Nov 1. doi: 10.1016/j.chest.2016.10.027).
The session delivered expected improvements in patient knowledge, but there were some surprises. “The starting point of knowledge was perhaps less than we would have anticipated, and the gains, though very substantial, weren’t perfect,” said Dr. Mazzone, who is also director of the lung cancer screening program at the Cleveland Clinic.
The drop in knowledge at 1 month suggests that the information needs to be reinforced, possibly each time patients come in for an annual screening visit, Dr. Mazzone added.
Counseling sessions can also help convince patients to quit smoking, if tobacco use is a concern. “It’s not appropriate to screen for lung cancer without making a commitment to try to quit,” said Dr. Grossman.
No funding source was disclosed. Dr. Mazzone and Dr. Grossman reported having no financial disclosures.
FROM CHEST
Key clinical point:
Major finding: Failure to identify potential harm dropped from 61.6% to 21.4%.
Data source: Prospective study of 125 patients.
Disclosures: No funding source was disclosed. Dr. Mazzone and Dr. Grossman reported having no financial disclosures.
Ultrasound effective in diagnosing occult hernia in women
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Key clinical point:
Major finding: About 53% of women with chronic pelvic pain were diagnosed with an occult hernia following physical exam and ultrasound. Surgeons confirmed the hernia diagnosis in 34 out of 35 patients who consented to surgery.
Data source: A retrospective cohort study of 96 women with chronic pelvic pain and focal inguinal tenderness.
Disclosures: Dr. Aoun reported having no relevant financial disclosures.
Dapivirine vaginal ring cuts new HIV-1 infections
The dapivirine vaginal ring reduced the rate of new HIV-1 infection by 31% in a phase III clinical trial involving 1,959 high-risk women in sub-Saharan Africa, according to a report published in the New England Journal of Medicine.
The dapivirine-containing ring is replaced every month and was used in this study for up to 2 years. It was not associated with any safety concerns, said Annalene Nel, MD, PhD, of the International Partnership for Microbicides, Silver Spring, Md., and her associates.
The International Partnership for Microbicides is a nonprofit group that developed the ring, which can be self-inserted and removed and which provides a sustained release of the antiretroviral drug for at least 4 weeks. QPharma of Malmö, Sweden, manufactures the rings and donated the ones used in this study, but was not otherwise involved in the trial.
The study participants were sexually active women aged 18-45 years (mean age, 26) treated at seven research centers in South Africa and Uganda. Almost all of them (98%) had only one male sexual partner. For the purposes of this trial, the women were asked to attend the participating clinics every 4 weeks to have the rings replaced and to provide a plasma sample. This allowed the researchers to measure the residual amount of dapivirine in the used rings and to measure plasma levels of the drug, both of which were indicators of compliance.
A total of 1,307 women were randomly assigned to receive dapivirine rings and 652 to receive placebo rings. At the data cutoff point, 615 women (31.4%) were still in the trial and 761 (38.8%) had completed it; 583 women (29.8%) had discontinued early. All the participants at one medical center were withdrawn by the sponsor because of high rates of protocol violation at that facility and corresponding high rates of patient nonadherence with the device.
The primary efficacy endpoint – the rate of HIV-1 seroconversion during follow-up – was 4.1 per 100 person-years with the dapivirine ring, compared with 6.1 per 100 person-years with the placebo ring. This represents a 31% lower infection rate with the active treatment (hazard ratio, 0.69). A subgroup analysis that excluded participants at the protocol-violating facility showed a seroconversion rate of 3.6 per 100 person-years with the active treatment vs. 5.4 per 100 person-years with the placebo, a 30% reduction in the infection rate, the investigators said (N Engl J Med. 2016 Dec 1. doi: 10.1056/NEJMoa1602046).
The findings were consistent across other subgroup analyses, including those that categorized the participants according to their adherence levels, as measured by plasma levels and residual ring levels of dapivirine.
The cumulative incidence of adverse events was similar between the two study groups (87.4% and 85.7%, respectively), as was the incidence of grade 3 or 4 adverse events. None of the more serious adverse events were judged to be related to the devices. Mild product-related adverse events occurred in 5 women (0.4%) in the dapivirine group and 3 (0.5%) in the placebo group. There also were no significant differences between the two study groups in the incidence of laboratory abnormalities, rates of sexually transmitted and other genital infections, or pregnancy rates.
The study was funded by the International Partnership for Microbicides, which is supported by the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the U.K. Department for International Development, the U.S. Agency for International Development, and the President’s Emergency Plan for AIDS Relief.
Dr. Nel reported having no relevant financial disclosures; one of her associates reported ties to Janssen and Johnson & Johnson.
The dapivirine vaginal ring reduced the rate of new HIV-1 infection by 31% in a phase III clinical trial involving 1,959 high-risk women in sub-Saharan Africa, according to a report published in the New England Journal of Medicine.
The dapivirine-containing ring is replaced every month and was used in this study for up to 2 years. It was not associated with any safety concerns, said Annalene Nel, MD, PhD, of the International Partnership for Microbicides, Silver Spring, Md., and her associates.
The International Partnership for Microbicides is a nonprofit group that developed the ring, which can be self-inserted and removed and which provides a sustained release of the antiretroviral drug for at least 4 weeks. QPharma of Malmö, Sweden, manufactures the rings and donated the ones used in this study, but was not otherwise involved in the trial.
The study participants were sexually active women aged 18-45 years (mean age, 26) treated at seven research centers in South Africa and Uganda. Almost all of them (98%) had only one male sexual partner. For the purposes of this trial, the women were asked to attend the participating clinics every 4 weeks to have the rings replaced and to provide a plasma sample. This allowed the researchers to measure the residual amount of dapivirine in the used rings and to measure plasma levels of the drug, both of which were indicators of compliance.
A total of 1,307 women were randomly assigned to receive dapivirine rings and 652 to receive placebo rings. At the data cutoff point, 615 women (31.4%) were still in the trial and 761 (38.8%) had completed it; 583 women (29.8%) had discontinued early. All the participants at one medical center were withdrawn by the sponsor because of high rates of protocol violation at that facility and corresponding high rates of patient nonadherence with the device.
The primary efficacy endpoint – the rate of HIV-1 seroconversion during follow-up – was 4.1 per 100 person-years with the dapivirine ring, compared with 6.1 per 100 person-years with the placebo ring. This represents a 31% lower infection rate with the active treatment (hazard ratio, 0.69). A subgroup analysis that excluded participants at the protocol-violating facility showed a seroconversion rate of 3.6 per 100 person-years with the active treatment vs. 5.4 per 100 person-years with the placebo, a 30% reduction in the infection rate, the investigators said (N Engl J Med. 2016 Dec 1. doi: 10.1056/NEJMoa1602046).
The findings were consistent across other subgroup analyses, including those that categorized the participants according to their adherence levels, as measured by plasma levels and residual ring levels of dapivirine.
The cumulative incidence of adverse events was similar between the two study groups (87.4% and 85.7%, respectively), as was the incidence of grade 3 or 4 adverse events. None of the more serious adverse events were judged to be related to the devices. Mild product-related adverse events occurred in 5 women (0.4%) in the dapivirine group and 3 (0.5%) in the placebo group. There also were no significant differences between the two study groups in the incidence of laboratory abnormalities, rates of sexually transmitted and other genital infections, or pregnancy rates.
The study was funded by the International Partnership for Microbicides, which is supported by the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the U.K. Department for International Development, the U.S. Agency for International Development, and the President’s Emergency Plan for AIDS Relief.
Dr. Nel reported having no relevant financial disclosures; one of her associates reported ties to Janssen and Johnson & Johnson.
The dapivirine vaginal ring reduced the rate of new HIV-1 infection by 31% in a phase III clinical trial involving 1,959 high-risk women in sub-Saharan Africa, according to a report published in the New England Journal of Medicine.
The dapivirine-containing ring is replaced every month and was used in this study for up to 2 years. It was not associated with any safety concerns, said Annalene Nel, MD, PhD, of the International Partnership for Microbicides, Silver Spring, Md., and her associates.
The International Partnership for Microbicides is a nonprofit group that developed the ring, which can be self-inserted and removed and which provides a sustained release of the antiretroviral drug for at least 4 weeks. QPharma of Malmö, Sweden, manufactures the rings and donated the ones used in this study, but was not otherwise involved in the trial.
The study participants were sexually active women aged 18-45 years (mean age, 26) treated at seven research centers in South Africa and Uganda. Almost all of them (98%) had only one male sexual partner. For the purposes of this trial, the women were asked to attend the participating clinics every 4 weeks to have the rings replaced and to provide a plasma sample. This allowed the researchers to measure the residual amount of dapivirine in the used rings and to measure plasma levels of the drug, both of which were indicators of compliance.
A total of 1,307 women were randomly assigned to receive dapivirine rings and 652 to receive placebo rings. At the data cutoff point, 615 women (31.4%) were still in the trial and 761 (38.8%) had completed it; 583 women (29.8%) had discontinued early. All the participants at one medical center were withdrawn by the sponsor because of high rates of protocol violation at that facility and corresponding high rates of patient nonadherence with the device.
The primary efficacy endpoint – the rate of HIV-1 seroconversion during follow-up – was 4.1 per 100 person-years with the dapivirine ring, compared with 6.1 per 100 person-years with the placebo ring. This represents a 31% lower infection rate with the active treatment (hazard ratio, 0.69). A subgroup analysis that excluded participants at the protocol-violating facility showed a seroconversion rate of 3.6 per 100 person-years with the active treatment vs. 5.4 per 100 person-years with the placebo, a 30% reduction in the infection rate, the investigators said (N Engl J Med. 2016 Dec 1. doi: 10.1056/NEJMoa1602046).
The findings were consistent across other subgroup analyses, including those that categorized the participants according to their adherence levels, as measured by plasma levels and residual ring levels of dapivirine.
The cumulative incidence of adverse events was similar between the two study groups (87.4% and 85.7%, respectively), as was the incidence of grade 3 or 4 adverse events. None of the more serious adverse events were judged to be related to the devices. Mild product-related adverse events occurred in 5 women (0.4%) in the dapivirine group and 3 (0.5%) in the placebo group. There also were no significant differences between the two study groups in the incidence of laboratory abnormalities, rates of sexually transmitted and other genital infections, or pregnancy rates.
The study was funded by the International Partnership for Microbicides, which is supported by the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the U.K. Department for International Development, the U.S. Agency for International Development, and the President’s Emergency Plan for AIDS Relief.
Dr. Nel reported having no relevant financial disclosures; one of her associates reported ties to Janssen and Johnson & Johnson.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: The dapivirine vaginal ring reduced the rate of new HIV-1 infection by 31% in a phase III trial involving 1,959 high-risk women in sub-Saharan Africa.
Major finding: The primary efficacy endpoint – the rate of HIV-1 seroconversion during follow-up – was 4.1 per 100 person-years with the dapivirine ring, compared with 6.1 per 100 person-years with the placebo ring.
Data source: A multicenter randomized double-blind placebo-controlled phase III trial involving 1,959 high-risk women in South Africa and Uganda.
Disclosures: This study was supported by the International Partnership for Microbicides, a nonprofit group that developed the dapivirine vaginal ring and is supported by the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the U.K. Department for International Development, the U.S. Agency for International Development, and the President’s Emergency Plan for AIDS Relief. Dr. Nel reported having no relevant financial disclosures; one of her associates reported ties to Janssen and Johnson & Johnson.
Can bioprosthetics work for large airway defects?
Large and complex airway defects that primary repair cannot fully close require alternative surgical approaches and techniques that are far more difficult to perform, but bioprosthetic materials may be an option to repair large tracheal and bronchial defects that has achieved good results, without postoperative death or defect recurrence, in a small cohort of patients at Massachusetts General Hospital, in Boston.
Brooks Udelsman, MD, and his coauthors reported their results of bioprosthetic repair of central airway defects in eight patients in the Journal of Thoracic and Cardiovascular Surgery (2016 Nov;152:1388-97). “Although our results are derived from a limited number of heterogeneous patients, they suggest that closure of noncircumferential large airway defects with bioprosthetic materials is feasible, safe and reliable,” Dr. Udelsman said. He previously reported the results at the annual meeting of the American Association for Thoracic Surgery, May 14-18, 2016, in Baltimore.
These complex defects typically exceed 5 cm and can involve communication with the esophagus. For repair of smaller defects, surgeons can use a more conventional approach that involves neck flexion, laryngeal release, airway mobilization, and hilar release, but in larger defects, these techniques increase the risk of too much tension on the anastomosis and dehiscence along with airway failure. Large and complex defects occur in patients who have had a previous airway operation or radiation exposure, requiring alternative strategies, the researchers wrote. “Patients in this rare category should be referred to a high-volume center for careful evaluation by a surgeon experienced in complex airway reconstruction before the decision to abandon primary repair is made,” he said. Among the advantages that bioprosthetic materials have over synthetic materials for airway defect repair are easier handling, minimal immunogenic response, and potential for tissue ingrowth, Dr. Udelsman and his coauthors said.
All eight patients in this study, who underwent repair from 2008 to 2015, had significant comorbidities, including previous surgery of the trachea, esophagus, or thyroid. The etiology of the airway defect included HIV-AIDS–associated esophagitis, malignancy, mesh erosion, and complications from extended intubation. Three patients had previous radiation therapy to the neck or chest. Five patients had defects localized to the membranous tracheal wall, two had defects of the mainstem bronchus or bronchus intermedius, and one patient had a defect of the anterior wall of the trachea.
Dr. Udelsman and his coauthors used both aortic homograft and acellular dermal matrix to repair large defects. Their experience confirmed previous reports of the formation of granulation tissue with aortic autografts, underscoring the importance of frequent bronchoscopy and debridement when necessary. And while previous reports have claimed human acellular dermis resists granulation formation, that wasn’t the case in this study. “The exact histologic basis of bioprosthetic incorporation and reepithelialization in these patients is still elusive and will require further study,” the researchers said.
This study also employed the controversial muscle buttress repair in six patients, which helped, at least theoretically, to secure the repairs when leaks occur, to separate suture lines when both the airway and esophagus were repaired and to support the bioprosthetic material to prevent tissue softening, Dr. Udelsman and his coauthors said.
Postoperative examinations confirmed that the operations successfully closed the airway defects in all eight patients. Long term, most resumed oral intake, but three did not for various reasons: one had a pharyngostomy; another had neurocognitive issues preoperatively; and a third with a tracheoesophageal fistula repair and cervical esophagostomy could resume oral intake but depended on tube feeds to meet caloric needs.
All patients developed granulation at the repair site, two of whom required further debridement and one who underwent balloon dilation. Pneumonia was the most common complication within 30 days of surgery, occurring in two patients. Three patients died within 120 days from metastatic disease, and a fourth patient progressed to end-stage AIDS 6 years after the operation and eventually died.
Dr. Udelsman and his coauthors reported having no financial disclosures.
In his invited commentary, Raja Flores, MD, of Mount Sinai Health System in New York said this study demonstrated “modest success” with bioprosthetic materials for repair of large airway deficits – the same level of success he ascribes to human studies of other surgical approaches to large airway deficits (J Thorac Cardiovasc Surg. 2016 Nov;152:1233-4).
But progress has been slow and animal studies of large airway deficit repair have been “wastefully repetitive” without any advances. “We must build on what these human studies have taught us and not continue unsuccessfully to reinvent the same malfunctioning [airways],” Dr. Flores said.

When surgeons encounter such patients, surgery isn’t necessary for their survival, Dr. Flores said. “T-tubes work just fine.” The goal is to improve their quality of life. “Unless we can provide a reliable, long-lasting solution, an unpredictable life-threatening experimental surgical intervention is not justified to treat a stable, functional patient,” he said.
And while Dr. Udelsman and his colleagues have shown “some progress” in their study, he cautioned surgeons to heed the words of a tracheal surgery pioneer Hermes Grillo, MD, at Boston’s Massachusetts General Hospital and Harvard Medical School: “Success has been announced episodically over the decades in each of these categories, but thus far no one replacement method has held for the long term in any safe and practicable manner.” Dr. Flores added: “This still holds true today.”
Dr. Flores reported having no financial disclosures.
In his invited commentary, Raja Flores, MD, of Mount Sinai Health System in New York said this study demonstrated “modest success” with bioprosthetic materials for repair of large airway deficits – the same level of success he ascribes to human studies of other surgical approaches to large airway deficits (J Thorac Cardiovasc Surg. 2016 Nov;152:1233-4).
But progress has been slow and animal studies of large airway deficit repair have been “wastefully repetitive” without any advances. “We must build on what these human studies have taught us and not continue unsuccessfully to reinvent the same malfunctioning [airways],” Dr. Flores said.
When surgeons encounter such patients, surgery isn’t necessary for their survival, Dr. Flores said. “T-tubes work just fine.” The goal is to improve their quality of life. “Unless we can provide a reliable, long-lasting solution, an unpredictable life-threatening experimental surgical intervention is not justified to treat a stable, functional patient,” he said.
And while Dr. Udelsman and his colleagues have shown “some progress” in their study, he cautioned surgeons to heed the words of a tracheal surgery pioneer Hermes Grillo, MD, at Boston’s Massachusetts General Hospital and Harvard Medical School: “Success has been announced episodically over the decades in each of these categories, but thus far no one replacement method has held for the long term in any safe and practicable manner.” Dr. Flores added: “This still holds true today.”
Dr. Flores reported having no financial disclosures.
In his invited commentary, Raja Flores, MD, of Mount Sinai Health System in New York said this study demonstrated “modest success” with bioprosthetic materials for repair of large airway deficits – the same level of success he ascribes to human studies of other surgical approaches to large airway deficits (J Thorac Cardiovasc Surg. 2016 Nov;152:1233-4).
But progress has been slow and animal studies of large airway deficit repair have been “wastefully repetitive” without any advances. “We must build on what these human studies have taught us and not continue unsuccessfully to reinvent the same malfunctioning [airways],” Dr. Flores said.
When surgeons encounter such patients, surgery isn’t necessary for their survival, Dr. Flores said. “T-tubes work just fine.” The goal is to improve their quality of life. “Unless we can provide a reliable, long-lasting solution, an unpredictable life-threatening experimental surgical intervention is not justified to treat a stable, functional patient,” he said.
And while Dr. Udelsman and his colleagues have shown “some progress” in their study, he cautioned surgeons to heed the words of a tracheal surgery pioneer Hermes Grillo, MD, at Boston’s Massachusetts General Hospital and Harvard Medical School: “Success has been announced episodically over the decades in each of these categories, but thus far no one replacement method has held for the long term in any safe and practicable manner.” Dr. Flores added: “This still holds true today.”
Dr. Flores reported having no financial disclosures.
Large and complex airway defects that primary repair cannot fully close require alternative surgical approaches and techniques that are far more difficult to perform, but bioprosthetic materials may be an option to repair large tracheal and bronchial defects that has achieved good results, without postoperative death or defect recurrence, in a small cohort of patients at Massachusetts General Hospital, in Boston.
Brooks Udelsman, MD, and his coauthors reported their results of bioprosthetic repair of central airway defects in eight patients in the Journal of Thoracic and Cardiovascular Surgery (2016 Nov;152:1388-97). “Although our results are derived from a limited number of heterogeneous patients, they suggest that closure of noncircumferential large airway defects with bioprosthetic materials is feasible, safe and reliable,” Dr. Udelsman said. He previously reported the results at the annual meeting of the American Association for Thoracic Surgery, May 14-18, 2016, in Baltimore.
These complex defects typically exceed 5 cm and can involve communication with the esophagus. For repair of smaller defects, surgeons can use a more conventional approach that involves neck flexion, laryngeal release, airway mobilization, and hilar release, but in larger defects, these techniques increase the risk of too much tension on the anastomosis and dehiscence along with airway failure. Large and complex defects occur in patients who have had a previous airway operation or radiation exposure, requiring alternative strategies, the researchers wrote. “Patients in this rare category should be referred to a high-volume center for careful evaluation by a surgeon experienced in complex airway reconstruction before the decision to abandon primary repair is made,” he said. Among the advantages that bioprosthetic materials have over synthetic materials for airway defect repair are easier handling, minimal immunogenic response, and potential for tissue ingrowth, Dr. Udelsman and his coauthors said.
All eight patients in this study, who underwent repair from 2008 to 2015, had significant comorbidities, including previous surgery of the trachea, esophagus, or thyroid. The etiology of the airway defect included HIV-AIDS–associated esophagitis, malignancy, mesh erosion, and complications from extended intubation. Three patients had previous radiation therapy to the neck or chest. Five patients had defects localized to the membranous tracheal wall, two had defects of the mainstem bronchus or bronchus intermedius, and one patient had a defect of the anterior wall of the trachea.
Dr. Udelsman and his coauthors used both aortic homograft and acellular dermal matrix to repair large defects. Their experience confirmed previous reports of the formation of granulation tissue with aortic autografts, underscoring the importance of frequent bronchoscopy and debridement when necessary. And while previous reports have claimed human acellular dermis resists granulation formation, that wasn’t the case in this study. “The exact histologic basis of bioprosthetic incorporation and reepithelialization in these patients is still elusive and will require further study,” the researchers said.
This study also employed the controversial muscle buttress repair in six patients, which helped, at least theoretically, to secure the repairs when leaks occur, to separate suture lines when both the airway and esophagus were repaired and to support the bioprosthetic material to prevent tissue softening, Dr. Udelsman and his coauthors said.
Postoperative examinations confirmed that the operations successfully closed the airway defects in all eight patients. Long term, most resumed oral intake, but three did not for various reasons: one had a pharyngostomy; another had neurocognitive issues preoperatively; and a third with a tracheoesophageal fistula repair and cervical esophagostomy could resume oral intake but depended on tube feeds to meet caloric needs.
All patients developed granulation at the repair site, two of whom required further debridement and one who underwent balloon dilation. Pneumonia was the most common complication within 30 days of surgery, occurring in two patients. Three patients died within 120 days from metastatic disease, and a fourth patient progressed to end-stage AIDS 6 years after the operation and eventually died.
Dr. Udelsman and his coauthors reported having no financial disclosures.
Large and complex airway defects that primary repair cannot fully close require alternative surgical approaches and techniques that are far more difficult to perform, but bioprosthetic materials may be an option to repair large tracheal and bronchial defects that has achieved good results, without postoperative death or defect recurrence, in a small cohort of patients at Massachusetts General Hospital, in Boston.
Brooks Udelsman, MD, and his coauthors reported their results of bioprosthetic repair of central airway defects in eight patients in the Journal of Thoracic and Cardiovascular Surgery (2016 Nov;152:1388-97). “Although our results are derived from a limited number of heterogeneous patients, they suggest that closure of noncircumferential large airway defects with bioprosthetic materials is feasible, safe and reliable,” Dr. Udelsman said. He previously reported the results at the annual meeting of the American Association for Thoracic Surgery, May 14-18, 2016, in Baltimore.
These complex defects typically exceed 5 cm and can involve communication with the esophagus. For repair of smaller defects, surgeons can use a more conventional approach that involves neck flexion, laryngeal release, airway mobilization, and hilar release, but in larger defects, these techniques increase the risk of too much tension on the anastomosis and dehiscence along with airway failure. Large and complex defects occur in patients who have had a previous airway operation or radiation exposure, requiring alternative strategies, the researchers wrote. “Patients in this rare category should be referred to a high-volume center for careful evaluation by a surgeon experienced in complex airway reconstruction before the decision to abandon primary repair is made,” he said. Among the advantages that bioprosthetic materials have over synthetic materials for airway defect repair are easier handling, minimal immunogenic response, and potential for tissue ingrowth, Dr. Udelsman and his coauthors said.
All eight patients in this study, who underwent repair from 2008 to 2015, had significant comorbidities, including previous surgery of the trachea, esophagus, or thyroid. The etiology of the airway defect included HIV-AIDS–associated esophagitis, malignancy, mesh erosion, and complications from extended intubation. Three patients had previous radiation therapy to the neck or chest. Five patients had defects localized to the membranous tracheal wall, two had defects of the mainstem bronchus or bronchus intermedius, and one patient had a defect of the anterior wall of the trachea.
Dr. Udelsman and his coauthors used both aortic homograft and acellular dermal matrix to repair large defects. Their experience confirmed previous reports of the formation of granulation tissue with aortic autografts, underscoring the importance of frequent bronchoscopy and debridement when necessary. And while previous reports have claimed human acellular dermis resists granulation formation, that wasn’t the case in this study. “The exact histologic basis of bioprosthetic incorporation and reepithelialization in these patients is still elusive and will require further study,” the researchers said.
This study also employed the controversial muscle buttress repair in six patients, which helped, at least theoretically, to secure the repairs when leaks occur, to separate suture lines when both the airway and esophagus were repaired and to support the bioprosthetic material to prevent tissue softening, Dr. Udelsman and his coauthors said.
Postoperative examinations confirmed that the operations successfully closed the airway defects in all eight patients. Long term, most resumed oral intake, but three did not for various reasons: one had a pharyngostomy; another had neurocognitive issues preoperatively; and a third with a tracheoesophageal fistula repair and cervical esophagostomy could resume oral intake but depended on tube feeds to meet caloric needs.
All patients developed granulation at the repair site, two of whom required further debridement and one who underwent balloon dilation. Pneumonia was the most common complication within 30 days of surgery, occurring in two patients. Three patients died within 120 days from metastatic disease, and a fourth patient progressed to end-stage AIDS 6 years after the operation and eventually died.
Dr. Udelsman and his coauthors reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Bioprosthetic materials show progress for reconstruction of large airway defects.
Major finding: Airway defects were successfully closed in all patients, with no postoperative deaths or recurrence of airway defect.
Data source: Eight patients who underwent closure of complex central airway defects with bioprosthetic materials between 2008 and 2015.
Disclosures: Dr. Udelsman and coauthors reported having no relevant financial disclosures.
Oral Fixed Drug Eruption Due to Tinidazole
To the Editor:
A 50-year-old man presented with a painful ulcer and a burning sensation on the tongue of 2 days’ duration (Figure, A). The ulcer had a yellowish white appearance with erythematous borders. The patient started taking tinidazole 500 mg twice daily 2 days prior, which was prescribed by his primary care physician for an episode of gastroenteritis. He was not taking any other medications and did not smoke or drink. Routine laboratory test results did not reveal any abnormalities. Based on the physical examination as well as the patient’s medical and medication history, a provisional diagnosis of fixed drug eruption (FDE) due to tinidazole was made. Tinidazole was immediately withdrawn and the patient was prescribed beclomethasone dipropionate ointment twice daily to relieve the burning sensation. A punch biopsy of the lesion was recommended; however, the patient opted to wait a week after discontinuing the drug. At follow-up 1 week later, complete healing of the ulcer was observed with no scarring and the burning sensation had resolved (Figure, B). After obtaining informed consent from the patient, an oral challenge test was conducted in the office with 50 mg of tinidazole. Four hours after taking the drug orally, the patient felt a burning sensation and a small ulcerative lesion was observed on the tongue at the same site the next day. The patient was informed of the fixed drug reaction to tinidazole, a drug belonging to the nitroimidazole group, and this information also was conveyed to the patient’s primary care physician.
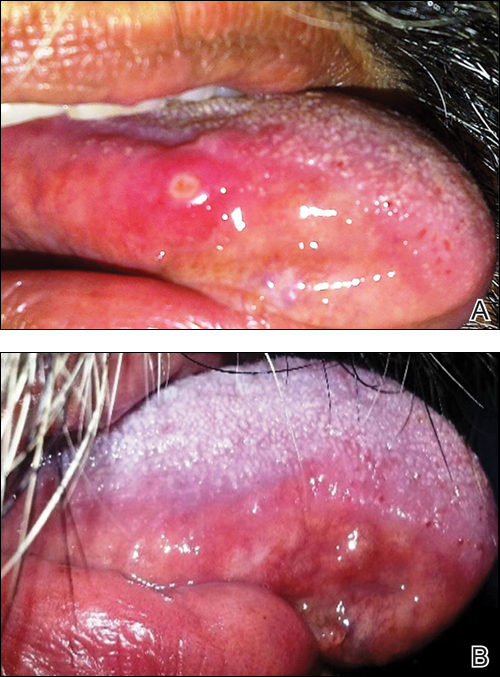
Tinidazole is a synthetic antiprotozoal and antibacterial agent used primarily in infections such as amebiasis, giardiasis, and trichomoniasis.1 Tinidazole may be a therapeutic alternative to metronidazole. Fixed drug eruption is a distinctive variant of drug eruption with characteristic recurrence at the same site of skin or mucous membranes. It is characterized by onset of round/oval, erythematous, well-defined macules on the skin and/or mucosa associated with itching and burning.1 Fixed drug eruption generally is restricted to the mucous membrane and skin, with the lips, palms, soles, glans penis, and groin area being the most common sites. Intraoral involvement, excluding the lips, of FDE is rare. The tongue is a rare site of an FDE.2 Fixed drug eruption on the tongue has been reported with clarithromycin.3 Dental clinicians have to be aware of the possibility of FDE due to commonly used drugs such tinidazole, which would help in prompt diagnosis of these lesions.
- Prieto A, De Barrio M, Infante S, et al. Recurrent fixed drug eruption due to metronidazole elicited by patch test with tinidazole. Contact Dermatitis. 2005;53:169-170.
- Dhar S, Kanwar AJ. Fixed drug eruption on the tongue of a 4-year-old boy. Pediatr Dermatol. 1995;12:51-52.
- Alonso JC, Melgosa AC, Gonzalo MJ, et al. Fixed drug eruption on the tongue due to clarithromycin. Contact Dermatitis. 2005;53:121-122.
To the Editor:
A 50-year-old man presented with a painful ulcer and a burning sensation on the tongue of 2 days’ duration (Figure, A). The ulcer had a yellowish white appearance with erythematous borders. The patient started taking tinidazole 500 mg twice daily 2 days prior, which was prescribed by his primary care physician for an episode of gastroenteritis. He was not taking any other medications and did not smoke or drink. Routine laboratory test results did not reveal any abnormalities. Based on the physical examination as well as the patient’s medical and medication history, a provisional diagnosis of fixed drug eruption (FDE) due to tinidazole was made. Tinidazole was immediately withdrawn and the patient was prescribed beclomethasone dipropionate ointment twice daily to relieve the burning sensation. A punch biopsy of the lesion was recommended; however, the patient opted to wait a week after discontinuing the drug. At follow-up 1 week later, complete healing of the ulcer was observed with no scarring and the burning sensation had resolved (Figure, B). After obtaining informed consent from the patient, an oral challenge test was conducted in the office with 50 mg of tinidazole. Four hours after taking the drug orally, the patient felt a burning sensation and a small ulcerative lesion was observed on the tongue at the same site the next day. The patient was informed of the fixed drug reaction to tinidazole, a drug belonging to the nitroimidazole group, and this information also was conveyed to the patient’s primary care physician.
Tinidazole is a synthetic antiprotozoal and antibacterial agent used primarily in infections such as amebiasis, giardiasis, and trichomoniasis.1 Tinidazole may be a therapeutic alternative to metronidazole. Fixed drug eruption is a distinctive variant of drug eruption with characteristic recurrence at the same site of skin or mucous membranes. It is characterized by onset of round/oval, erythematous, well-defined macules on the skin and/or mucosa associated with itching and burning.1 Fixed drug eruption generally is restricted to the mucous membrane and skin, with the lips, palms, soles, glans penis, and groin area being the most common sites. Intraoral involvement, excluding the lips, of FDE is rare. The tongue is a rare site of an FDE.2 Fixed drug eruption on the tongue has been reported with clarithromycin.3 Dental clinicians have to be aware of the possibility of FDE due to commonly used drugs such tinidazole, which would help in prompt diagnosis of these lesions.
To the Editor:
A 50-year-old man presented with a painful ulcer and a burning sensation on the tongue of 2 days’ duration (Figure, A). The ulcer had a yellowish white appearance with erythematous borders. The patient started taking tinidazole 500 mg twice daily 2 days prior, which was prescribed by his primary care physician for an episode of gastroenteritis. He was not taking any other medications and did not smoke or drink. Routine laboratory test results did not reveal any abnormalities. Based on the physical examination as well as the patient’s medical and medication history, a provisional diagnosis of fixed drug eruption (FDE) due to tinidazole was made. Tinidazole was immediately withdrawn and the patient was prescribed beclomethasone dipropionate ointment twice daily to relieve the burning sensation. A punch biopsy of the lesion was recommended; however, the patient opted to wait a week after discontinuing the drug. At follow-up 1 week later, complete healing of the ulcer was observed with no scarring and the burning sensation had resolved (Figure, B). After obtaining informed consent from the patient, an oral challenge test was conducted in the office with 50 mg of tinidazole. Four hours after taking the drug orally, the patient felt a burning sensation and a small ulcerative lesion was observed on the tongue at the same site the next day. The patient was informed of the fixed drug reaction to tinidazole, a drug belonging to the nitroimidazole group, and this information also was conveyed to the patient’s primary care physician.
Tinidazole is a synthetic antiprotozoal and antibacterial agent used primarily in infections such as amebiasis, giardiasis, and trichomoniasis.1 Tinidazole may be a therapeutic alternative to metronidazole. Fixed drug eruption is a distinctive variant of drug eruption with characteristic recurrence at the same site of skin or mucous membranes. It is characterized by onset of round/oval, erythematous, well-defined macules on the skin and/or mucosa associated with itching and burning.1 Fixed drug eruption generally is restricted to the mucous membrane and skin, with the lips, palms, soles, glans penis, and groin area being the most common sites. Intraoral involvement, excluding the lips, of FDE is rare. The tongue is a rare site of an FDE.2 Fixed drug eruption on the tongue has been reported with clarithromycin.3 Dental clinicians have to be aware of the possibility of FDE due to commonly used drugs such tinidazole, which would help in prompt diagnosis of these lesions.
- Prieto A, De Barrio M, Infante S, et al. Recurrent fixed drug eruption due to metronidazole elicited by patch test with tinidazole. Contact Dermatitis. 2005;53:169-170.
- Dhar S, Kanwar AJ. Fixed drug eruption on the tongue of a 4-year-old boy. Pediatr Dermatol. 1995;12:51-52.
- Alonso JC, Melgosa AC, Gonzalo MJ, et al. Fixed drug eruption on the tongue due to clarithromycin. Contact Dermatitis. 2005;53:121-122.
- Prieto A, De Barrio M, Infante S, et al. Recurrent fixed drug eruption due to metronidazole elicited by patch test with tinidazole. Contact Dermatitis. 2005;53:169-170.
- Dhar S, Kanwar AJ. Fixed drug eruption on the tongue of a 4-year-old boy. Pediatr Dermatol. 1995;12:51-52.
- Alonso JC, Melgosa AC, Gonzalo MJ, et al. Fixed drug eruption on the tongue due to clarithromycin. Contact Dermatitis. 2005;53:121-122.
Practice Points
- Fixed drug eruption (FDE) is characterized by onset of round/oval, erythematous, well-defined macules on the skin and/or mucosa associated with itching and burning.
- Intraoral involvement of FDE is rare.
- Tinidazole may cause FDE and should be suspected in patients with a spontaneous eruption of macules on mucous membranes.
Sore throat and ear pain
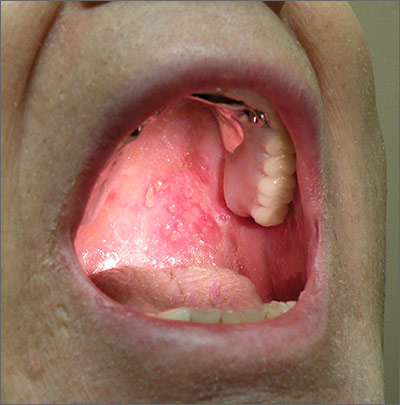
Based on the patient’s clinical presentation, he was given a diagnosis of herpes zoster oticus—also known as Ramsay Hunt syndrome. Patients with Ramsay Hunt syndrome typically develop unilateral facial paralysis and erythematous vesicles that appear ipsilaterally on the ear and/or in the mouth. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.
An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected. Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.
Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus. Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1, Epstein-Barr virus, group A Streptococcus, and measles.
A diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis, polymerase chain reaction (PCR) testing, or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity. PCR has a higher sensitivity (92%), is widely available, and is the diagnostic test of choice, according to the Centers for Disease Control and Prevention.
Treatment with an oral steroid, such as prednisone, in addition to an antiviral such as acyclovir or valacyclovir, may reduce the likelihood of postherpetic neuralgia and improve facial motor function. However, these benefits have not been demonstrated in randomized controlled trials.
In this case, the FP prescribed oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days for the patient. After one week of treatment, the patient’s symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
Adapted from: Moss DA, Crawford P. Sore throat and left ear pain. J Fam Pract. 2015;64:117-119.
Based on the patient’s clinical presentation, he was given a diagnosis of herpes zoster oticus—also known as Ramsay Hunt syndrome. Patients with Ramsay Hunt syndrome typically develop unilateral facial paralysis and erythematous vesicles that appear ipsilaterally on the ear and/or in the mouth. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.
An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected. Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.
Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus. Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1, Epstein-Barr virus, group A Streptococcus, and measles.
A diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis, polymerase chain reaction (PCR) testing, or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity. PCR has a higher sensitivity (92%), is widely available, and is the diagnostic test of choice, according to the Centers for Disease Control and Prevention.
Treatment with an oral steroid, such as prednisone, in addition to an antiviral such as acyclovir or valacyclovir, may reduce the likelihood of postherpetic neuralgia and improve facial motor function. However, these benefits have not been demonstrated in randomized controlled trials.
In this case, the FP prescribed oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days for the patient. After one week of treatment, the patient’s symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
Adapted from: Moss DA, Crawford P. Sore throat and left ear pain. J Fam Pract. 2015;64:117-119.
Based on the patient’s clinical presentation, he was given a diagnosis of herpes zoster oticus—also known as Ramsay Hunt syndrome. Patients with Ramsay Hunt syndrome typically develop unilateral facial paralysis and erythematous vesicles that appear ipsilaterally on the ear and/or in the mouth. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.
An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected. Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.
Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus. Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1, Epstein-Barr virus, group A Streptococcus, and measles.
A diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis, polymerase chain reaction (PCR) testing, or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity. PCR has a higher sensitivity (92%), is widely available, and is the diagnostic test of choice, according to the Centers for Disease Control and Prevention.
Treatment with an oral steroid, such as prednisone, in addition to an antiviral such as acyclovir or valacyclovir, may reduce the likelihood of postherpetic neuralgia and improve facial motor function. However, these benefits have not been demonstrated in randomized controlled trials.
In this case, the FP prescribed oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days for the patient. After one week of treatment, the patient’s symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
Adapted from: Moss DA, Crawford P. Sore throat and left ear pain. J Fam Pract. 2015;64:117-119.
