User login
It isn’t over until it’s over
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.

On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”

I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.
On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”
I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.
On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”
I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Intermittent breaks from sunitinib feasible in metastatic RCC
Intermittent breaks from sunitinib therapy are feasible and don’t appear to compromise the agent’s clinical efficacy against metastatic renal cell carcinoma, according to investigators.
One of the greatest challenges in treating this cancer is balancing treatment-related toxicity against efficacy “in a setting ... in which patients are largely incurable and thus subjected to chronic therapy,” said Moshe C. Ornstein, MD, and his associates at the Cleveland Clinic Taussig Cancer Institute.
They performed a single-center phase II study that they described as the first prospective trial to assess treatment interruptions whenever tumor burden was reduced by 10% or more, followed by resumption of treatment if tumors then progressed 10% or more. This approach “may result in reduced toxicities, improved quality of life, cost savings, and potentially improved clinical outcomes.”
The study involved 37 adults (median age, 63 years) who were given 50 mg sunitinib once daily for the first 28 days of a 42-day cycle, with dose adjustments allowed to minimize toxicities. Twenty patients (54%) who showed a 10% or greater reduction in tumor burden after four cycles suspended treatment until scans showed a 10% or greater progression, at which point treatment was resumed. These 20 patients were able to take up to 11 treatment breaks (median, 3 breaks per patient), with each break having a median duration of more than 8 weeks (range, 4.7-192.1 weeks).
Seven patients were able to have extended drug holidays lasting 3-43 months, and three have never had to resume sunitinib therapy after their first break. “The overall sum of all the breaks was 1,296.6 weeks, which corresponds to 216 6-week cycles with a median of 9 saved cycles per patient,” Dr. Ornstein and his associates said (J Clin Oncol. 2017 Jan 23. doi: 10.1200/JCO.2016.71.1184).
Given that the average wholesale price of sunitinib is $17,811.83 per 28-day cycle, “the 9 cycles saved per patient translates into a median cost saving of $160,302 per patient and $3.85 million overall, not including the cost of toxicity management that may have been incurred without breaks,” they noted.
The median progression-free survival was 22.4 months for the entire study cohort and 37.6 months for the 20 patients who had intermittent therapy.
Patients who showed tumor progression during a treatment break were transitioned back to standard dosing without showing any adverse clinical effects. This suggests that “with close clinical and radiographic monitoring, patients can safely take a therapy break for extended periods of time,” the investigators said.
Intermittent breaks from sunitinib therapy are feasible and don’t appear to compromise the agent’s clinical efficacy against metastatic renal cell carcinoma, according to investigators.
One of the greatest challenges in treating this cancer is balancing treatment-related toxicity against efficacy “in a setting ... in which patients are largely incurable and thus subjected to chronic therapy,” said Moshe C. Ornstein, MD, and his associates at the Cleveland Clinic Taussig Cancer Institute.
They performed a single-center phase II study that they described as the first prospective trial to assess treatment interruptions whenever tumor burden was reduced by 10% or more, followed by resumption of treatment if tumors then progressed 10% or more. This approach “may result in reduced toxicities, improved quality of life, cost savings, and potentially improved clinical outcomes.”
The study involved 37 adults (median age, 63 years) who were given 50 mg sunitinib once daily for the first 28 days of a 42-day cycle, with dose adjustments allowed to minimize toxicities. Twenty patients (54%) who showed a 10% or greater reduction in tumor burden after four cycles suspended treatment until scans showed a 10% or greater progression, at which point treatment was resumed. These 20 patients were able to take up to 11 treatment breaks (median, 3 breaks per patient), with each break having a median duration of more than 8 weeks (range, 4.7-192.1 weeks).
Seven patients were able to have extended drug holidays lasting 3-43 months, and three have never had to resume sunitinib therapy after their first break. “The overall sum of all the breaks was 1,296.6 weeks, which corresponds to 216 6-week cycles with a median of 9 saved cycles per patient,” Dr. Ornstein and his associates said (J Clin Oncol. 2017 Jan 23. doi: 10.1200/JCO.2016.71.1184).
Given that the average wholesale price of sunitinib is $17,811.83 per 28-day cycle, “the 9 cycles saved per patient translates into a median cost saving of $160,302 per patient and $3.85 million overall, not including the cost of toxicity management that may have been incurred without breaks,” they noted.
The median progression-free survival was 22.4 months for the entire study cohort and 37.6 months for the 20 patients who had intermittent therapy.
Patients who showed tumor progression during a treatment break were transitioned back to standard dosing without showing any adverse clinical effects. This suggests that “with close clinical and radiographic monitoring, patients can safely take a therapy break for extended periods of time,” the investigators said.
Intermittent breaks from sunitinib therapy are feasible and don’t appear to compromise the agent’s clinical efficacy against metastatic renal cell carcinoma, according to investigators.
One of the greatest challenges in treating this cancer is balancing treatment-related toxicity against efficacy “in a setting ... in which patients are largely incurable and thus subjected to chronic therapy,” said Moshe C. Ornstein, MD, and his associates at the Cleveland Clinic Taussig Cancer Institute.
They performed a single-center phase II study that they described as the first prospective trial to assess treatment interruptions whenever tumor burden was reduced by 10% or more, followed by resumption of treatment if tumors then progressed 10% or more. This approach “may result in reduced toxicities, improved quality of life, cost savings, and potentially improved clinical outcomes.”
The study involved 37 adults (median age, 63 years) who were given 50 mg sunitinib once daily for the first 28 days of a 42-day cycle, with dose adjustments allowed to minimize toxicities. Twenty patients (54%) who showed a 10% or greater reduction in tumor burden after four cycles suspended treatment until scans showed a 10% or greater progression, at which point treatment was resumed. These 20 patients were able to take up to 11 treatment breaks (median, 3 breaks per patient), with each break having a median duration of more than 8 weeks (range, 4.7-192.1 weeks).
Seven patients were able to have extended drug holidays lasting 3-43 months, and three have never had to resume sunitinib therapy after their first break. “The overall sum of all the breaks was 1,296.6 weeks, which corresponds to 216 6-week cycles with a median of 9 saved cycles per patient,” Dr. Ornstein and his associates said (J Clin Oncol. 2017 Jan 23. doi: 10.1200/JCO.2016.71.1184).
Given that the average wholesale price of sunitinib is $17,811.83 per 28-day cycle, “the 9 cycles saved per patient translates into a median cost saving of $160,302 per patient and $3.85 million overall, not including the cost of toxicity management that may have been incurred without breaks,” they noted.
The median progression-free survival was 22.4 months for the entire study cohort and 37.6 months for the 20 patients who had intermittent therapy.
Patients who showed tumor progression during a treatment break were transitioned back to standard dosing without showing any adverse clinical effects. This suggests that “with close clinical and radiographic monitoring, patients can safely take a therapy break for extended periods of time,” the investigators said.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Intermittent breaks from sunitinib therapy are feasible and don’t appear to compromise the agent’s clinical efficacy against metastatic renal cell carcinoma.
Major finding: Twenty patients were able to take up to 11 treatment breaks (median, 3 drug holidays per patient), with each break having a median duration of more than 8 weeks (range, 5-192 weeks).
Data source: A 2-year single-center prospective phase II trial involving 37 adults with metastatic renal cell carcinoma.
Disclosures: The Cleveland Clinic Taussig Cancer Institute supported the trial. Dr. Ornstein reported having no relevant financial disclosures; some of his associates reported ties to numerous industry sources.
What Are the Key Elements of an Initial Pediatric Concussion Evaluation?
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.

Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.
Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.
Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.

Charging for medical records: For whom and at what cost?
Do you charge for medical records?
You probably do, and so do I, at times.
Generally, I’m willing to give a patient one copy of their records or transfer them to another doctor for continuation of care, at no charge. People move away. They change insurance or doctors. They have urgent hospital admissions. To me, charging to forward records in these cases is like withholding care.
That’s not to say I don’t lose money on them. It takes a few minutes (or more) of staff time to print them up and fax them. If they need to be mailed, postage costs money. And then there’s paper, printer ink, and so on. I’m sure it adds up to something over the course of the year, although I have no idea how much.

How much you can charge is a more complex issue, with each state setting its own rules. A recent article published in JAMA Internal Medicine noted that a patient in Georgia could pay up to $111.68 for a 100-page record. Hitting someone up for that amount, who’s already having health problems and may be relocating or trying to find a new doctor, seems like making an already difficult situation worse.
But we’re in the digital age now. So how much does it cost to send records? Most files (.doc, .pdf, .jpg, and so on) are interchangeable between Mac and Windows.
Things get iffy here. I mean, it’s easy to send a .pdf file by email, but that’s not particularly secure. And I hate having to sign up and create passwords for the many allegedly safer file-sharing services out there.
Burning records on a CD or DVD certainly saves postage, though takes about the same amount of computer time as printing them up. Not only that, but this seems to be a format that’s on its way out. The last three computers I’ve bought didn’t even have optical drives. CD/DVD’s are starting to resemble VHS tapes in the late 1990s.
Flash drives are the present and immediate future of transferred records. Small, lightweight, and capable of holding a lot. But they still need to be mailed, and are more expensive than paper. They also have security risks that concern me. When a patient hands me one and asks me to plug it in, I never do. There could be a virus or spyware that can compromise the security and privacy of my office, and cost a fortune to reverse the damage.
And so, at the end of that chain of thought, paper still appears to be king. It’s not going to carry ransomware into my office. It can be mailed or faxed, and is easily adaptable to any system (like mine) with a scanner. The paper world may hypothetically no longer exist, but for many things in medicine it still does, and is critical.
Some ultimate solutions, such as a universal database of health care data on all patients or a complete interchangeability between systems, sound great. No one would need to transfer records between doctors and all would have access to their own charts. But at this point in time, while technologically achievable, the privacy concerns and high-stakes security risks make such a thing impossible.
It’s easy to hope that the age of electronic medical records will lead to, as the article states, “easy, inexpensive” reproduction of medical records. But things never seem to be that simple, for some of the reasons I’ve mentioned above.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Do you charge for medical records?
You probably do, and so do I, at times.
Generally, I’m willing to give a patient one copy of their records or transfer them to another doctor for continuation of care, at no charge. People move away. They change insurance or doctors. They have urgent hospital admissions. To me, charging to forward records in these cases is like withholding care.
That’s not to say I don’t lose money on them. It takes a few minutes (or more) of staff time to print them up and fax them. If they need to be mailed, postage costs money. And then there’s paper, printer ink, and so on. I’m sure it adds up to something over the course of the year, although I have no idea how much.
How much you can charge is a more complex issue, with each state setting its own rules. A recent article published in JAMA Internal Medicine noted that a patient in Georgia could pay up to $111.68 for a 100-page record. Hitting someone up for that amount, who’s already having health problems and may be relocating or trying to find a new doctor, seems like making an already difficult situation worse.
But we’re in the digital age now. So how much does it cost to send records? Most files (.doc, .pdf, .jpg, and so on) are interchangeable between Mac and Windows.
Things get iffy here. I mean, it’s easy to send a .pdf file by email, but that’s not particularly secure. And I hate having to sign up and create passwords for the many allegedly safer file-sharing services out there.
Burning records on a CD or DVD certainly saves postage, though takes about the same amount of computer time as printing them up. Not only that, but this seems to be a format that’s on its way out. The last three computers I’ve bought didn’t even have optical drives. CD/DVD’s are starting to resemble VHS tapes in the late 1990s.
Flash drives are the present and immediate future of transferred records. Small, lightweight, and capable of holding a lot. But they still need to be mailed, and are more expensive than paper. They also have security risks that concern me. When a patient hands me one and asks me to plug it in, I never do. There could be a virus or spyware that can compromise the security and privacy of my office, and cost a fortune to reverse the damage.
And so, at the end of that chain of thought, paper still appears to be king. It’s not going to carry ransomware into my office. It can be mailed or faxed, and is easily adaptable to any system (like mine) with a scanner. The paper world may hypothetically no longer exist, but for many things in medicine it still does, and is critical.
Some ultimate solutions, such as a universal database of health care data on all patients or a complete interchangeability between systems, sound great. No one would need to transfer records between doctors and all would have access to their own charts. But at this point in time, while technologically achievable, the privacy concerns and high-stakes security risks make such a thing impossible.
It’s easy to hope that the age of electronic medical records will lead to, as the article states, “easy, inexpensive” reproduction of medical records. But things never seem to be that simple, for some of the reasons I’ve mentioned above.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Do you charge for medical records?
You probably do, and so do I, at times.
Generally, I’m willing to give a patient one copy of their records or transfer them to another doctor for continuation of care, at no charge. People move away. They change insurance or doctors. They have urgent hospital admissions. To me, charging to forward records in these cases is like withholding care.
That’s not to say I don’t lose money on them. It takes a few minutes (or more) of staff time to print them up and fax them. If they need to be mailed, postage costs money. And then there’s paper, printer ink, and so on. I’m sure it adds up to something over the course of the year, although I have no idea how much.
How much you can charge is a more complex issue, with each state setting its own rules. A recent article published in JAMA Internal Medicine noted that a patient in Georgia could pay up to $111.68 for a 100-page record. Hitting someone up for that amount, who’s already having health problems and may be relocating or trying to find a new doctor, seems like making an already difficult situation worse.
But we’re in the digital age now. So how much does it cost to send records? Most files (.doc, .pdf, .jpg, and so on) are interchangeable between Mac and Windows.
Things get iffy here. I mean, it’s easy to send a .pdf file by email, but that’s not particularly secure. And I hate having to sign up and create passwords for the many allegedly safer file-sharing services out there.
Burning records on a CD or DVD certainly saves postage, though takes about the same amount of computer time as printing them up. Not only that, but this seems to be a format that’s on its way out. The last three computers I’ve bought didn’t even have optical drives. CD/DVD’s are starting to resemble VHS tapes in the late 1990s.
Flash drives are the present and immediate future of transferred records. Small, lightweight, and capable of holding a lot. But they still need to be mailed, and are more expensive than paper. They also have security risks that concern me. When a patient hands me one and asks me to plug it in, I never do. There could be a virus or spyware that can compromise the security and privacy of my office, and cost a fortune to reverse the damage.
And so, at the end of that chain of thought, paper still appears to be king. It’s not going to carry ransomware into my office. It can be mailed or faxed, and is easily adaptable to any system (like mine) with a scanner. The paper world may hypothetically no longer exist, but for many things in medicine it still does, and is critical.
Some ultimate solutions, such as a universal database of health care data on all patients or a complete interchangeability between systems, sound great. No one would need to transfer records between doctors and all would have access to their own charts. But at this point in time, while technologically achievable, the privacy concerns and high-stakes security risks make such a thing impossible.
It’s easy to hope that the age of electronic medical records will lead to, as the article states, “easy, inexpensive” reproduction of medical records. But things never seem to be that simple, for some of the reasons I’ve mentioned above.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Substantial long-term increase seen in multiple myeloma survival
The 5-year survival rate for multiple myeloma increased eightfold over an approximately 60-year span starting in the early 1950s, said Ali H. Mokdad, PhD, and his associates.
Patients with multiple myeloma had a 5-year relative survival rate of 6% in 1950-1954, compared with 49.8% in 2008-2013, according to data from the Surveillance, Epidemiology, and End Results Program (JAMA 2017;317[4]:388-406).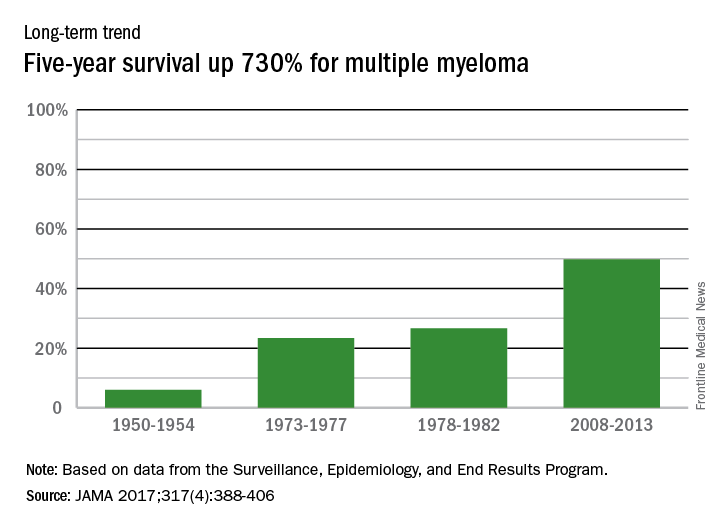
In 2014, there were about 13,000 deaths resulting from multiple myeloma, with 219,000 years of life lost, which ranked 17th among the 29 selected cancers, noted Dr. Mokdad and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
The 5-year survival rate for multiple myeloma increased eightfold over an approximately 60-year span starting in the early 1950s, said Ali H. Mokdad, PhD, and his associates.
Patients with multiple myeloma had a 5-year relative survival rate of 6% in 1950-1954, compared with 49.8% in 2008-2013, according to data from the Surveillance, Epidemiology, and End Results Program (JAMA 2017;317[4]:388-406).
In 2014, there were about 13,000 deaths resulting from multiple myeloma, with 219,000 years of life lost, which ranked 17th among the 29 selected cancers, noted Dr. Mokdad and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
The 5-year survival rate for multiple myeloma increased eightfold over an approximately 60-year span starting in the early 1950s, said Ali H. Mokdad, PhD, and his associates.
Patients with multiple myeloma had a 5-year relative survival rate of 6% in 1950-1954, compared with 49.8% in 2008-2013, according to data from the Surveillance, Epidemiology, and End Results Program (JAMA 2017;317[4]:388-406).
In 2014, there were about 13,000 deaths resulting from multiple myeloma, with 219,000 years of life lost, which ranked 17th among the 29 selected cancers, noted Dr. Mokdad and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
FROM JAMA
AML leads percent gains in 5-year survival among leukemias
Over the 60-year span from the early 1950s to 2013, the 5-year survival rate for all leukemias increased by 500%, according to data from the Surveillance, Epidemiology, and End Results Program.
For 2008-2013, the 5-year relative survival rate for all leukemias was 60.1%, compared with 10% during 1950-1954, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle (JAMA 2017;317[4]:388-406).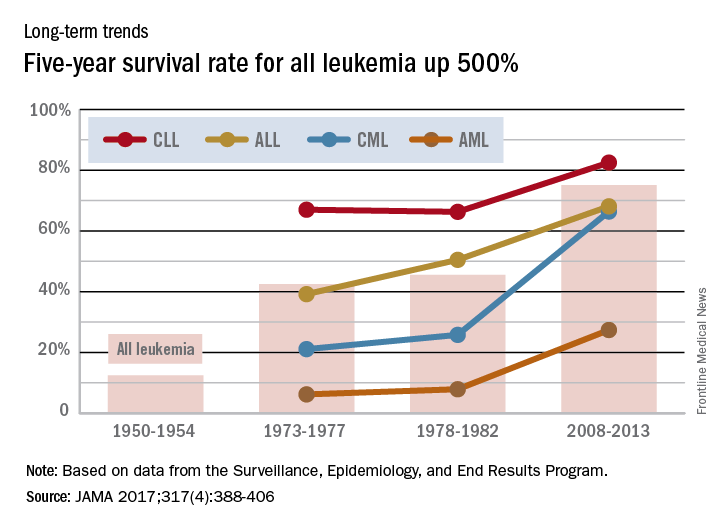
Over the 60-year span from the early 1950s to 2013, the 5-year survival rate for all leukemias increased by 500%, according to data from the Surveillance, Epidemiology, and End Results Program.
For 2008-2013, the 5-year relative survival rate for all leukemias was 60.1%, compared with 10% during 1950-1954, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle (JAMA 2017;317[4]:388-406).
Over the 60-year span from the early 1950s to 2013, the 5-year survival rate for all leukemias increased by 500%, according to data from the Surveillance, Epidemiology, and End Results Program.
For 2008-2013, the 5-year relative survival rate for all leukemias was 60.1%, compared with 10% during 1950-1954, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle (JAMA 2017;317[4]:388-406).
Long view shows doubling of survival in non-Hodgkin lymphoma
Five-year survival for patients with non-Hodgkin lymphoma has more than doubled since the early 1950s, according to Ali H. Mokdad, PhD, and his associates.
Data from the Surveillance, Epidemiology, and End Results Program show that the 5-year relative survival rate for non-Hodgkin lymphoma in the United States went from 33% in 1950-1954 to 71.2% in 2008-2013, an increase of 116%, Dr. Mokdad and his associates reported (JAMA 2017;317[4]:388-406).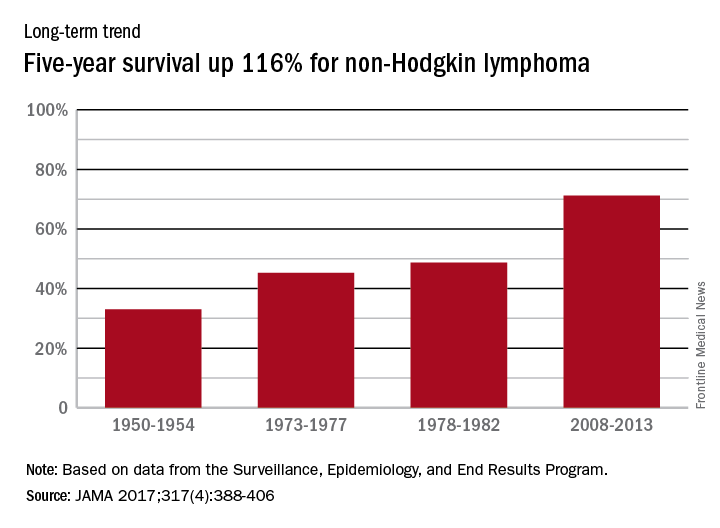
In 2014, mortality for non-Hodgkin lymphoma was the 7th highest among the 29 cancers included in the study, and more than 487,000 years of life were lost, which put it 6th among the 29 cancers, said Dr. Mokdad and his associates from the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
Five-year survival for patients with non-Hodgkin lymphoma has more than doubled since the early 1950s, according to Ali H. Mokdad, PhD, and his associates.
Data from the Surveillance, Epidemiology, and End Results Program show that the 5-year relative survival rate for non-Hodgkin lymphoma in the United States went from 33% in 1950-1954 to 71.2% in 2008-2013, an increase of 116%, Dr. Mokdad and his associates reported (JAMA 2017;317[4]:388-406).
In 2014, mortality for non-Hodgkin lymphoma was the 7th highest among the 29 cancers included in the study, and more than 487,000 years of life were lost, which put it 6th among the 29 cancers, said Dr. Mokdad and his associates from the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
Five-year survival for patients with non-Hodgkin lymphoma has more than doubled since the early 1950s, according to Ali H. Mokdad, PhD, and his associates.
Data from the Surveillance, Epidemiology, and End Results Program show that the 5-year relative survival rate for non-Hodgkin lymphoma in the United States went from 33% in 1950-1954 to 71.2% in 2008-2013, an increase of 116%, Dr. Mokdad and his associates reported (JAMA 2017;317[4]:388-406).
In 2014, mortality for non-Hodgkin lymphoma was the 7th highest among the 29 cancers included in the study, and more than 487,000 years of life were lost, which put it 6th among the 29 cancers, said Dr. Mokdad and his associates from the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
FROM JAMA
How Do Patients With Epilepsy Use Herbal and Botanical Therapies?
HOUSTON—Many people with epilepsy use herbal and botanical therapies. Some patients use them to help control their seizures, while others use them to treat medication side effects or co-occurring symptoms, such as depression, anxiety, and memory problems.
“Ask your patients about the use of botanicals because they are probably using them,” said Dana Ekstein, MD, PhD, a senior neurologist at Hadassah Medical Center in Jerusalem, in an overview provided at the 70th Annual Meeting of the American Epilepsy Society. “Be ready to advise on the safety of their use.”

Efficacy and safety data for many of the treatments are limited, but educational resources are available to keep neurologists up to date. In addition, neurologists should ensure that botanicals do not interfere with conventional medication.
Widely Used
According to the 2012 American National Health Interview Survey, about a third of the population uses complementary medicine. Herbal and botanical medicines (ie, nonvitamin, nonmineral natural products) are the most commonly used complementary medicines and are used by about 18% of the population. Among people with epilepsy, studies have found that about half of adults and a third of children use complementary therapies. Patients often do not report the use of complementary medicine to their physicians, Dr. Ekstein said.
Massot-Tarrús and McLachlan examined the use of cannabis by people with epilepsy who were admitted to an epilepsy monitoring unit in Canada. More than half of them had tried marijuana. Many of them—59% of patients with epilepsy and 33% of patients with psychogenic nonepileptic seizures—used cannabis daily.Although botanicals were the mainstay of epilepsy treatment for centuries, modern data on botanicals in epilepsy are limited, Dr. Ekstein said. A 2009 Cochrane review of traditional Chinese medicine for epilepsy included only five unblinded single-center controlled studies. Although the studies reported some benefit, the probability of selection, detection, and performance bias meant that the treatment’s effect could not reliably be evaluated.
Cannabis
A 2014 Cochrane review of cannabinoids for epilepsy considered four randomized controlled trials with a total of 48 patients. Each trial included between nine and 15 patients, and investigators followed patients for between one and 12 months. The studies failed to provide efficacy evidence. In another review that considered all published studies with more than one patient, researchers analyzed eight studies with a total of 105 children and adults. Patients received placebo or cannabis compounds. Of the patients who received cannabis, 61% experienced improvement.
A retrospective trial of medical cannabis oil in Israel published in 2016 included 74 pediatric patients. Fifty-two percent of the patients had a 50% or greater reduction in seizure frequency, and one patient became seizure-free. Sixty percent of patients reported other benefits, such as improved behavior, alertness, language, communication, motor skills, and sleep.
A prospective open-label study by Devinsky et al enrolled 214 patients from 11 centers in the United States. The study included patients with drug-resistant epilepsy with onset in childhood who had at least four seizures per month. Patients received cannabidiol and were followed for three months. Of 137 patients included in the efficacy analysis, 39% had a 50% or greater reduction in seizure frequency.
Mushroom May Treat Depression
A Chinese mushroom called Xylaria nigripes has been studied for the treatment of depression in patients with epilepsy, Dr. Ekstein said. Peng et al conducted a randomized double-blind placebo-controlled trial that included 104 patients with epilepsy and depression. The mushroom significantly improved Hamilton Depression Rating Scale and quality of life scores, compared with placebo.
Although not studied in patients with epilepsy, research has shown that St. John’s wort effectively treats mild to moderate depression; kava treats generalized anxiety; and rosenroot improves attention, fatigue, mild depression, and mental performance, she said.
Safety
Many patients assume that natural products are safe, but there are important safety considerations, Dr. Ekstein said. Some botanicals have been associated with seizures, including ephedra, St. John’s wort, and ginkgo biloba. Cannabinoids, especially tetrahydrocannabinol (THC), may induce memory and executive function impairment and psychiatric symptoms. Cannabinoids also may impair plasticity in the developing brain.
Side effects in cannabis trials have been relatively common. In the retrospective Israeli trial, 46% of patients experienced adverse events (eg, seizure aggravation, somnolence, fatigue, and gastrointestinal disturbances). In the trial by Devinsky et al, 79% of patients experienced adverse events. Although most of the adverse events were mild to moderate and transient, 30% were serious adverse events (eg, status epilepticus, diarrhea, pneumonia, and weight loss).
Interactions between botanicals and antiepileptic drugs also should be taken into account, she said. Some botanicals may decrease or increase bioavailability of antiepileptic drugs. For example, cannabidiol increases concentrations of clobazam.
More clinical trials are needed to establish the efficacy and safety of botanical therapies. Cannabinoids are “on the right path” in terms of receiving further study. “There are almost no planned trials” of other botanicals, however, Dr. Ekstein said. The medical community should prioritize botanicals for further study, and neurologists should offer patients participation in clinical studies when they are available, she said.
Neurologists generally should be better educated regarding the use of botanical therapies. Online resources, such as those provided by the National Center for Complementary and Integrative Health, provide information about botanical therapies. The International League Against Epilepsy recently created the Web-based Epilepsy Naturapedia to provide information about the use of natural products in the treatment of epilepsy, Dr. Ekstein said.
—Jake Remaly
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Ekstein D, Schachter SC. Natural products in epilepsy-the present situation and perspectives for the future. Pharmaceuticals (Basel). 2010;3(5):1426-1445.
Gloss D, Vickrey B. Cannabinoids for epilepsy. Cochrane Database Syst Rev. 2014;(3):CD009270.
Li Q, Chen X, He L, Zhou D. Traditional Chinese medicine for epilepsy. Cochrane Database Syst Rev. 2009;(3):CD006454.
Massot-Tarrús A, McLachlan RS. Marijuana use in adults admitted to a Canadian epilepsy monitoring unit. Epilepsy Behav. 2016;63:73-78.
Peng WF, Wang X, Hong Z, et al. The anti-depression effect of Xylaria nigripes in patients with epilepsy: A multicenter randomized double-blind study. Seizure. 2015;29:26-33.
Szaflarski JP, Bebin EM. Cannabis, cannabidiol, and epilepsy--from receptors to clinical response. Epilepsy Behav. 2014;41:277-282.
Tzadok M, Uliel-Siboni S, Linder I, et al. CBD-enriched medical cannabis for intractable pediatric epilepsy: the current Israeli experience. Seizure. 2016;35:41-44.
HOUSTON—Many people with epilepsy use herbal and botanical therapies. Some patients use them to help control their seizures, while others use them to treat medication side effects or co-occurring symptoms, such as depression, anxiety, and memory problems.
“Ask your patients about the use of botanicals because they are probably using them,” said Dana Ekstein, MD, PhD, a senior neurologist at Hadassah Medical Center in Jerusalem, in an overview provided at the 70th Annual Meeting of the American Epilepsy Society. “Be ready to advise on the safety of their use.”
Efficacy and safety data for many of the treatments are limited, but educational resources are available to keep neurologists up to date. In addition, neurologists should ensure that botanicals do not interfere with conventional medication.
Widely Used
According to the 2012 American National Health Interview Survey, about a third of the population uses complementary medicine. Herbal and botanical medicines (ie, nonvitamin, nonmineral natural products) are the most commonly used complementary medicines and are used by about 18% of the population. Among people with epilepsy, studies have found that about half of adults and a third of children use complementary therapies. Patients often do not report the use of complementary medicine to their physicians, Dr. Ekstein said.
Massot-Tarrús and McLachlan examined the use of cannabis by people with epilepsy who were admitted to an epilepsy monitoring unit in Canada. More than half of them had tried marijuana. Many of them—59% of patients with epilepsy and 33% of patients with psychogenic nonepileptic seizures—used cannabis daily.Although botanicals were the mainstay of epilepsy treatment for centuries, modern data on botanicals in epilepsy are limited, Dr. Ekstein said. A 2009 Cochrane review of traditional Chinese medicine for epilepsy included only five unblinded single-center controlled studies. Although the studies reported some benefit, the probability of selection, detection, and performance bias meant that the treatment’s effect could not reliably be evaluated.
Cannabis
A 2014 Cochrane review of cannabinoids for epilepsy considered four randomized controlled trials with a total of 48 patients. Each trial included between nine and 15 patients, and investigators followed patients for between one and 12 months. The studies failed to provide efficacy evidence. In another review that considered all published studies with more than one patient, researchers analyzed eight studies with a total of 105 children and adults. Patients received placebo or cannabis compounds. Of the patients who received cannabis, 61% experienced improvement.
A retrospective trial of medical cannabis oil in Israel published in 2016 included 74 pediatric patients. Fifty-two percent of the patients had a 50% or greater reduction in seizure frequency, and one patient became seizure-free. Sixty percent of patients reported other benefits, such as improved behavior, alertness, language, communication, motor skills, and sleep.
A prospective open-label study by Devinsky et al enrolled 214 patients from 11 centers in the United States. The study included patients with drug-resistant epilepsy with onset in childhood who had at least four seizures per month. Patients received cannabidiol and were followed for three months. Of 137 patients included in the efficacy analysis, 39% had a 50% or greater reduction in seizure frequency.
Mushroom May Treat Depression
A Chinese mushroom called Xylaria nigripes has been studied for the treatment of depression in patients with epilepsy, Dr. Ekstein said. Peng et al conducted a randomized double-blind placebo-controlled trial that included 104 patients with epilepsy and depression. The mushroom significantly improved Hamilton Depression Rating Scale and quality of life scores, compared with placebo.
Although not studied in patients with epilepsy, research has shown that St. John’s wort effectively treats mild to moderate depression; kava treats generalized anxiety; and rosenroot improves attention, fatigue, mild depression, and mental performance, she said.
Safety
Many patients assume that natural products are safe, but there are important safety considerations, Dr. Ekstein said. Some botanicals have been associated with seizures, including ephedra, St. John’s wort, and ginkgo biloba. Cannabinoids, especially tetrahydrocannabinol (THC), may induce memory and executive function impairment and psychiatric symptoms. Cannabinoids also may impair plasticity in the developing brain.
Side effects in cannabis trials have been relatively common. In the retrospective Israeli trial, 46% of patients experienced adverse events (eg, seizure aggravation, somnolence, fatigue, and gastrointestinal disturbances). In the trial by Devinsky et al, 79% of patients experienced adverse events. Although most of the adverse events were mild to moderate and transient, 30% were serious adverse events (eg, status epilepticus, diarrhea, pneumonia, and weight loss).
Interactions between botanicals and antiepileptic drugs also should be taken into account, she said. Some botanicals may decrease or increase bioavailability of antiepileptic drugs. For example, cannabidiol increases concentrations of clobazam.
More clinical trials are needed to establish the efficacy and safety of botanical therapies. Cannabinoids are “on the right path” in terms of receiving further study. “There are almost no planned trials” of other botanicals, however, Dr. Ekstein said. The medical community should prioritize botanicals for further study, and neurologists should offer patients participation in clinical studies when they are available, she said.
Neurologists generally should be better educated regarding the use of botanical therapies. Online resources, such as those provided by the National Center for Complementary and Integrative Health, provide information about botanical therapies. The International League Against Epilepsy recently created the Web-based Epilepsy Naturapedia to provide information about the use of natural products in the treatment of epilepsy, Dr. Ekstein said.
—Jake Remaly
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Ekstein D, Schachter SC. Natural products in epilepsy-the present situation and perspectives for the future. Pharmaceuticals (Basel). 2010;3(5):1426-1445.
Gloss D, Vickrey B. Cannabinoids for epilepsy. Cochrane Database Syst Rev. 2014;(3):CD009270.
Li Q, Chen X, He L, Zhou D. Traditional Chinese medicine for epilepsy. Cochrane Database Syst Rev. 2009;(3):CD006454.
Massot-Tarrús A, McLachlan RS. Marijuana use in adults admitted to a Canadian epilepsy monitoring unit. Epilepsy Behav. 2016;63:73-78.
Peng WF, Wang X, Hong Z, et al. The anti-depression effect of Xylaria nigripes in patients with epilepsy: A multicenter randomized double-blind study. Seizure. 2015;29:26-33.
Szaflarski JP, Bebin EM. Cannabis, cannabidiol, and epilepsy--from receptors to clinical response. Epilepsy Behav. 2014;41:277-282.
Tzadok M, Uliel-Siboni S, Linder I, et al. CBD-enriched medical cannabis for intractable pediatric epilepsy: the current Israeli experience. Seizure. 2016;35:41-44.
HOUSTON—Many people with epilepsy use herbal and botanical therapies. Some patients use them to help control their seizures, while others use them to treat medication side effects or co-occurring symptoms, such as depression, anxiety, and memory problems.
“Ask your patients about the use of botanicals because they are probably using them,” said Dana Ekstein, MD, PhD, a senior neurologist at Hadassah Medical Center in Jerusalem, in an overview provided at the 70th Annual Meeting of the American Epilepsy Society. “Be ready to advise on the safety of their use.”
Efficacy and safety data for many of the treatments are limited, but educational resources are available to keep neurologists up to date. In addition, neurologists should ensure that botanicals do not interfere with conventional medication.
Widely Used
According to the 2012 American National Health Interview Survey, about a third of the population uses complementary medicine. Herbal and botanical medicines (ie, nonvitamin, nonmineral natural products) are the most commonly used complementary medicines and are used by about 18% of the population. Among people with epilepsy, studies have found that about half of adults and a third of children use complementary therapies. Patients often do not report the use of complementary medicine to their physicians, Dr. Ekstein said.
Massot-Tarrús and McLachlan examined the use of cannabis by people with epilepsy who were admitted to an epilepsy monitoring unit in Canada. More than half of them had tried marijuana. Many of them—59% of patients with epilepsy and 33% of patients with psychogenic nonepileptic seizures—used cannabis daily.Although botanicals were the mainstay of epilepsy treatment for centuries, modern data on botanicals in epilepsy are limited, Dr. Ekstein said. A 2009 Cochrane review of traditional Chinese medicine for epilepsy included only five unblinded single-center controlled studies. Although the studies reported some benefit, the probability of selection, detection, and performance bias meant that the treatment’s effect could not reliably be evaluated.
Cannabis
A 2014 Cochrane review of cannabinoids for epilepsy considered four randomized controlled trials with a total of 48 patients. Each trial included between nine and 15 patients, and investigators followed patients for between one and 12 months. The studies failed to provide efficacy evidence. In another review that considered all published studies with more than one patient, researchers analyzed eight studies with a total of 105 children and adults. Patients received placebo or cannabis compounds. Of the patients who received cannabis, 61% experienced improvement.
A retrospective trial of medical cannabis oil in Israel published in 2016 included 74 pediatric patients. Fifty-two percent of the patients had a 50% or greater reduction in seizure frequency, and one patient became seizure-free. Sixty percent of patients reported other benefits, such as improved behavior, alertness, language, communication, motor skills, and sleep.
A prospective open-label study by Devinsky et al enrolled 214 patients from 11 centers in the United States. The study included patients with drug-resistant epilepsy with onset in childhood who had at least four seizures per month. Patients received cannabidiol and were followed for three months. Of 137 patients included in the efficacy analysis, 39% had a 50% or greater reduction in seizure frequency.
Mushroom May Treat Depression
A Chinese mushroom called Xylaria nigripes has been studied for the treatment of depression in patients with epilepsy, Dr. Ekstein said. Peng et al conducted a randomized double-blind placebo-controlled trial that included 104 patients with epilepsy and depression. The mushroom significantly improved Hamilton Depression Rating Scale and quality of life scores, compared with placebo.
Although not studied in patients with epilepsy, research has shown that St. John’s wort effectively treats mild to moderate depression; kava treats generalized anxiety; and rosenroot improves attention, fatigue, mild depression, and mental performance, she said.
Safety
Many patients assume that natural products are safe, but there are important safety considerations, Dr. Ekstein said. Some botanicals have been associated with seizures, including ephedra, St. John’s wort, and ginkgo biloba. Cannabinoids, especially tetrahydrocannabinol (THC), may induce memory and executive function impairment and psychiatric symptoms. Cannabinoids also may impair plasticity in the developing brain.
Side effects in cannabis trials have been relatively common. In the retrospective Israeli trial, 46% of patients experienced adverse events (eg, seizure aggravation, somnolence, fatigue, and gastrointestinal disturbances). In the trial by Devinsky et al, 79% of patients experienced adverse events. Although most of the adverse events were mild to moderate and transient, 30% were serious adverse events (eg, status epilepticus, diarrhea, pneumonia, and weight loss).
Interactions between botanicals and antiepileptic drugs also should be taken into account, she said. Some botanicals may decrease or increase bioavailability of antiepileptic drugs. For example, cannabidiol increases concentrations of clobazam.
More clinical trials are needed to establish the efficacy and safety of botanical therapies. Cannabinoids are “on the right path” in terms of receiving further study. “There are almost no planned trials” of other botanicals, however, Dr. Ekstein said. The medical community should prioritize botanicals for further study, and neurologists should offer patients participation in clinical studies when they are available, she said.
Neurologists generally should be better educated regarding the use of botanical therapies. Online resources, such as those provided by the National Center for Complementary and Integrative Health, provide information about botanical therapies. The International League Against Epilepsy recently created the Web-based Epilepsy Naturapedia to provide information about the use of natural products in the treatment of epilepsy, Dr. Ekstein said.
—Jake Remaly
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Ekstein D, Schachter SC. Natural products in epilepsy-the present situation and perspectives for the future. Pharmaceuticals (Basel). 2010;3(5):1426-1445.
Gloss D, Vickrey B. Cannabinoids for epilepsy. Cochrane Database Syst Rev. 2014;(3):CD009270.
Li Q, Chen X, He L, Zhou D. Traditional Chinese medicine for epilepsy. Cochrane Database Syst Rev. 2009;(3):CD006454.
Massot-Tarrús A, McLachlan RS. Marijuana use in adults admitted to a Canadian epilepsy monitoring unit. Epilepsy Behav. 2016;63:73-78.
Peng WF, Wang X, Hong Z, et al. The anti-depression effect of Xylaria nigripes in patients with epilepsy: A multicenter randomized double-blind study. Seizure. 2015;29:26-33.
Szaflarski JP, Bebin EM. Cannabis, cannabidiol, and epilepsy--from receptors to clinical response. Epilepsy Behav. 2014;41:277-282.
Tzadok M, Uliel-Siboni S, Linder I, et al. CBD-enriched medical cannabis for intractable pediatric epilepsy: the current Israeli experience. Seizure. 2016;35:41-44.

Hodgkin lymphoma survival has nearly tripled since the 1950s
Five-year relative survival for Hodgkin lymphoma increased 189% over the approximately 60 years from the early 1950s to 2013, according to investigators looking at data from the Surveillance, Epidemiology, and End Results Program.
During 1950-1954, the 5-year relative survival rate for Hodgkin lymphoma was 30%, compared with 86.6% in 2008-2013, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.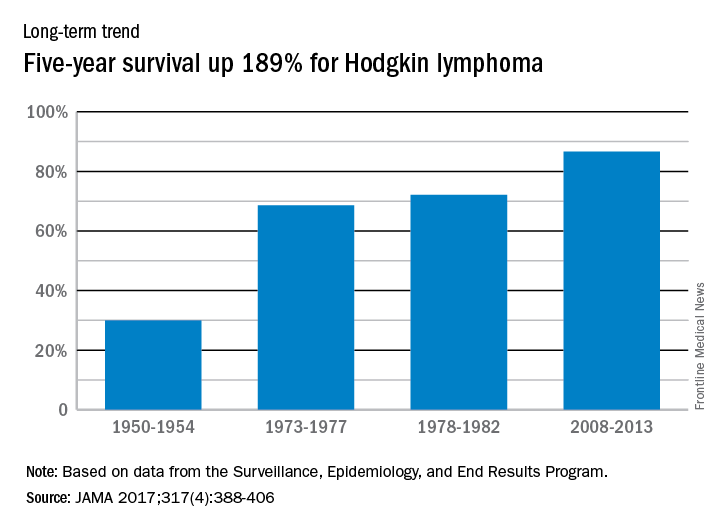
In 2014, mortality for Hodgkin lymphoma was 0.4 per 100,000 population, which put it 27th among the 29 included cancers, with about 36,000 years of life lost, which was 26th of the 29 cancers, Dr. Mokdad and his associates said. This part of their study used deidentified death records from the National Center for Health Statistics and population counts from the Census Bureau, the NCHS, and the Human Mortality Database.
Five-year relative survival for Hodgkin lymphoma increased 189% over the approximately 60 years from the early 1950s to 2013, according to investigators looking at data from the Surveillance, Epidemiology, and End Results Program.
During 1950-1954, the 5-year relative survival rate for Hodgkin lymphoma was 30%, compared with 86.6% in 2008-2013, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
In 2014, mortality for Hodgkin lymphoma was 0.4 per 100,000 population, which put it 27th among the 29 included cancers, with about 36,000 years of life lost, which was 26th of the 29 cancers, Dr. Mokdad and his associates said. This part of their study used deidentified death records from the National Center for Health Statistics and population counts from the Census Bureau, the NCHS, and the Human Mortality Database.
Five-year relative survival for Hodgkin lymphoma increased 189% over the approximately 60 years from the early 1950s to 2013, according to investigators looking at data from the Surveillance, Epidemiology, and End Results Program.
During 1950-1954, the 5-year relative survival rate for Hodgkin lymphoma was 30%, compared with 86.6% in 2008-2013, said Ali H. Mokdad, PhD, and his associates at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle.
In 2014, mortality for Hodgkin lymphoma was 0.4 per 100,000 population, which put it 27th among the 29 included cancers, with about 36,000 years of life lost, which was 26th of the 29 cancers, Dr. Mokdad and his associates said. This part of their study used deidentified death records from the National Center for Health Statistics and population counts from the Census Bureau, the NCHS, and the Human Mortality Database.
FROM JAMA
Sterile fecal filtrate effectively treated recurrent CDI
Sterile fecal filtrate transplantation (FFT) effectively treated five cases of symptomatic chronic-relapsing Clostridium difficile infection, investigators reported.
The procedure restored normal bowel habits and eliminated symptoms through the end of the study – that is, for at least 6 months – in all patients, Stephan J. Ott, MD, and his associates wrote (Gastroenterology. 2019. doi: 10.1053/j.gastro.2016.11.010).
Proteome analyses did not identify proteins likely to explain this efficacy, but 16S rRNA gene sequencing did demonstrate diverse bacterial DNA signatures in the filtrates, and tests of virus-like particles yielded “a complex signature of macrophages,” Dr. Ott and his associates reported. Additional tests suggested that recipients’ microbiomes continued to change weeks after FFT. “This open-label series strongly suggests that FFT should be evaluated in a controlled setting in comparison with standard fecal microbiota transplantation,” the researchers concluded.
Fecal microbiota transplantation (FMT) effectively treats recurrent Clostridium difficile infection (CDI), but even “the most rigorous and costly donor screening procedures, or defined panels of bacteria, cannot exclude the risk of transferring unknown pathogens or undetectable functional characteristics within the living microorganisms to the recipient, including bacterial or viral risk factors for metabolic diseases, cancer, atopy, or autoimmunity,” the investigators wrote.
Therefore, they performed sterile FFT in five patients who were positive on at least two of three tests: enzyme-linked immunosorbent assay for C. difficile–specific glutamate dehydrogenase; C. difficile toxin enzyme-linked immunosorbent assay; and culture of toxin-producing C. difficile. Patients chose their own stool donors, who were then screened based on published guidelines (Clin Gastroenterol Hepatol. 2011;9[12]:1044-49). Next, “slurries” were prepared from donor stool and filtered with a custom-built air pressure filtration system, yielding a “light brown, clear liquid with a subjectively less unpleasant and intensive odor” than conventional FMT stool preparations. Bacterial cultures of these filtrates yielded no growth, whereas donor stool cultures showed profuse growth of aerobic and anaerobic bacterial colonies, Dr. Ott and his associates said.
Patients became symptom-free 2-4 days after undergoing FFT. Notably, one patient had previously undergone FMT, which led to acute fever and diarrhea and recurrence of baseline symptoms after 3 months. This patient did not develop fever or diarrhea after FFT, was symptom-free after 3 days, and remained symptom-free until the study ended 2 years later, the researchers said. All other patients also remained symptom-free through the end of the study, that is, for 6 months to more than 2 years.
Analyses of 16S rRNA revealed substantial longitudinal shifts after FFT that often were present by week 1 and remained stable until week 6, the investigators said. Further tests confirmed marked shifts in bacterial phylotypes and in their relative abundance over time. Repeated virus analyses of one patient also showed that the phageome shifted over time to resemble that of the donor.
Patients were between 49 and 75 years old, three were female and two were male, and all had received more than one antibiotic before their first episode of CDI. Antibiotics for CDI had included metronidazole, vancomycin, and rifaximin. Comorbidities included pseudomembranous colitis, renal failure, HIV infection, epilepsy, and chronic heart failure, and medical histories included recurrent diverticulitis with sigmoid resection, gastric carcinoma, and colon cancer.
“It is important to keep in mind that, in contrast to conventional FMT, transferring sterile FFT filtrates cannot be expected to establish a microbiota similar to that of the donor in the receiving patient,” Dr. Ott and his associates noted. Instead, bacterial DNA in the filtrate might trigger the re-establishment of the recipient microbiome, they said. Bacterial cell wall fragments or bacteriophages also might play a role, they added.
The German Excellence Cluster and CONARIS Research Institute AG supported the work. Dr. Ott reported having lectured for Allergosan. Two coinvestigators reported employment with CONARIS. A third coinvestigator reported shareholder relationships with CONARIS, Allergosan, Danone, and Nestle and lectureship compensation from Allergosan. The other eight coinvestigators had no relevant conflicts of interest.
The remarkable efficacy of fecal microbial transplant in recurrent C. difficile infection provides a compelling example of ecologic microbiome-based therapy. Its mechanism is widely considered to be the restoration of select microbial species that suppress C. difficile colonization and virulence in healthy individuals. Identification of such suppressive microbiota is still at an early stage, with empirical studies revealing effective synthetic microbial consortia, and evidence of some modes of action, such as bile salt metabolism (Nature 2015;517:205-8; PLoS Pathog. 2012;8:e1002995).
Clouding this elegant concept is the provocative new study of Dr. Ott and his colleagues. Prompted by long-term safety concerns, they evaluated the efficacy of a donor fecal microfiltrate lacking viable intact organisms. Indeed, in five patients, long-term eradication of C. difficile was achieved with a single dose. This observation indicates that the initial action of fecal transplant may not require restoration of viable organisms into the antibiotic-damaged ecosystem.
What mechanisms might account for the therapeutic action of organism-free fecal microfiltrate? First, this material is laden with a complex, potentially distinct mix of microbial products and particulates (Cell. 2016;165[5]:1106-19) from donor origin or ex vivo processing. These biologicals may induce immune processes to promote control of C. difficile directly or via changes in other commensals of the patient's microbiome. Second, the microfiltrate retains abundant and diverse bacteria-targeting viruses of the fecal stream. Perhaps certain viruses, deficient in patients, target C. difficile and/or beneficially reshape microbial composition (Cell Mol Gastroenterol Hepatol. 2015;1[1]:28-40). So, C. difficile challenges us once more into the breach with new insights ahead for the principles and practice of ecologic microbiome therapy.
Jonathan Braun, MD, PhD, is professor and chair of pathology and laboratory medicine at the University of California, Los Angeles. He has no conflicts of interest.
The remarkable efficacy of fecal microbial transplant in recurrent C. difficile infection provides a compelling example of ecologic microbiome-based therapy. Its mechanism is widely considered to be the restoration of select microbial species that suppress C. difficile colonization and virulence in healthy individuals. Identification of such suppressive microbiota is still at an early stage, with empirical studies revealing effective synthetic microbial consortia, and evidence of some modes of action, such as bile salt metabolism (Nature 2015;517:205-8; PLoS Pathog. 2012;8:e1002995).
Clouding this elegant concept is the provocative new study of Dr. Ott and his colleagues. Prompted by long-term safety concerns, they evaluated the efficacy of a donor fecal microfiltrate lacking viable intact organisms. Indeed, in five patients, long-term eradication of C. difficile was achieved with a single dose. This observation indicates that the initial action of fecal transplant may not require restoration of viable organisms into the antibiotic-damaged ecosystem.
What mechanisms might account for the therapeutic action of organism-free fecal microfiltrate? First, this material is laden with a complex, potentially distinct mix of microbial products and particulates (Cell. 2016;165[5]:1106-19) from donor origin or ex vivo processing. These biologicals may induce immune processes to promote control of C. difficile directly or via changes in other commensals of the patient's microbiome. Second, the microfiltrate retains abundant and diverse bacteria-targeting viruses of the fecal stream. Perhaps certain viruses, deficient in patients, target C. difficile and/or beneficially reshape microbial composition (Cell Mol Gastroenterol Hepatol. 2015;1[1]:28-40). So, C. difficile challenges us once more into the breach with new insights ahead for the principles and practice of ecologic microbiome therapy.
Jonathan Braun, MD, PhD, is professor and chair of pathology and laboratory medicine at the University of California, Los Angeles. He has no conflicts of interest.
The remarkable efficacy of fecal microbial transplant in recurrent C. difficile infection provides a compelling example of ecologic microbiome-based therapy. Its mechanism is widely considered to be the restoration of select microbial species that suppress C. difficile colonization and virulence in healthy individuals. Identification of such suppressive microbiota is still at an early stage, with empirical studies revealing effective synthetic microbial consortia, and evidence of some modes of action, such as bile salt metabolism (Nature 2015;517:205-8; PLoS Pathog. 2012;8:e1002995).
Clouding this elegant concept is the provocative new study of Dr. Ott and his colleagues. Prompted by long-term safety concerns, they evaluated the efficacy of a donor fecal microfiltrate lacking viable intact organisms. Indeed, in five patients, long-term eradication of C. difficile was achieved with a single dose. This observation indicates that the initial action of fecal transplant may not require restoration of viable organisms into the antibiotic-damaged ecosystem.
What mechanisms might account for the therapeutic action of organism-free fecal microfiltrate? First, this material is laden with a complex, potentially distinct mix of microbial products and particulates (Cell. 2016;165[5]:1106-19) from donor origin or ex vivo processing. These biologicals may induce immune processes to promote control of C. difficile directly or via changes in other commensals of the patient's microbiome. Second, the microfiltrate retains abundant and diverse bacteria-targeting viruses of the fecal stream. Perhaps certain viruses, deficient in patients, target C. difficile and/or beneficially reshape microbial composition (Cell Mol Gastroenterol Hepatol. 2015;1[1]:28-40). So, C. difficile challenges us once more into the breach with new insights ahead for the principles and practice of ecologic microbiome therapy.
Jonathan Braun, MD, PhD, is professor and chair of pathology and laboratory medicine at the University of California, Los Angeles. He has no conflicts of interest.
Sterile fecal filtrate transplantation (FFT) effectively treated five cases of symptomatic chronic-relapsing Clostridium difficile infection, investigators reported.
The procedure restored normal bowel habits and eliminated symptoms through the end of the study – that is, for at least 6 months – in all patients, Stephan J. Ott, MD, and his associates wrote (Gastroenterology. 2019. doi: 10.1053/j.gastro.2016.11.010).
Proteome analyses did not identify proteins likely to explain this efficacy, but 16S rRNA gene sequencing did demonstrate diverse bacterial DNA signatures in the filtrates, and tests of virus-like particles yielded “a complex signature of macrophages,” Dr. Ott and his associates reported. Additional tests suggested that recipients’ microbiomes continued to change weeks after FFT. “This open-label series strongly suggests that FFT should be evaluated in a controlled setting in comparison with standard fecal microbiota transplantation,” the researchers concluded.
Fecal microbiota transplantation (FMT) effectively treats recurrent Clostridium difficile infection (CDI), but even “the most rigorous and costly donor screening procedures, or defined panels of bacteria, cannot exclude the risk of transferring unknown pathogens or undetectable functional characteristics within the living microorganisms to the recipient, including bacterial or viral risk factors for metabolic diseases, cancer, atopy, or autoimmunity,” the investigators wrote.
Therefore, they performed sterile FFT in five patients who were positive on at least two of three tests: enzyme-linked immunosorbent assay for C. difficile–specific glutamate dehydrogenase; C. difficile toxin enzyme-linked immunosorbent assay; and culture of toxin-producing C. difficile. Patients chose their own stool donors, who were then screened based on published guidelines (Clin Gastroenterol Hepatol. 2011;9[12]:1044-49). Next, “slurries” were prepared from donor stool and filtered with a custom-built air pressure filtration system, yielding a “light brown, clear liquid with a subjectively less unpleasant and intensive odor” than conventional FMT stool preparations. Bacterial cultures of these filtrates yielded no growth, whereas donor stool cultures showed profuse growth of aerobic and anaerobic bacterial colonies, Dr. Ott and his associates said.
Patients became symptom-free 2-4 days after undergoing FFT. Notably, one patient had previously undergone FMT, which led to acute fever and diarrhea and recurrence of baseline symptoms after 3 months. This patient did not develop fever or diarrhea after FFT, was symptom-free after 3 days, and remained symptom-free until the study ended 2 years later, the researchers said. All other patients also remained symptom-free through the end of the study, that is, for 6 months to more than 2 years.
Analyses of 16S rRNA revealed substantial longitudinal shifts after FFT that often were present by week 1 and remained stable until week 6, the investigators said. Further tests confirmed marked shifts in bacterial phylotypes and in their relative abundance over time. Repeated virus analyses of one patient also showed that the phageome shifted over time to resemble that of the donor.
Patients were between 49 and 75 years old, three were female and two were male, and all had received more than one antibiotic before their first episode of CDI. Antibiotics for CDI had included metronidazole, vancomycin, and rifaximin. Comorbidities included pseudomembranous colitis, renal failure, HIV infection, epilepsy, and chronic heart failure, and medical histories included recurrent diverticulitis with sigmoid resection, gastric carcinoma, and colon cancer.
“It is important to keep in mind that, in contrast to conventional FMT, transferring sterile FFT filtrates cannot be expected to establish a microbiota similar to that of the donor in the receiving patient,” Dr. Ott and his associates noted. Instead, bacterial DNA in the filtrate might trigger the re-establishment of the recipient microbiome, they said. Bacterial cell wall fragments or bacteriophages also might play a role, they added.
The German Excellence Cluster and CONARIS Research Institute AG supported the work. Dr. Ott reported having lectured for Allergosan. Two coinvestigators reported employment with CONARIS. A third coinvestigator reported shareholder relationships with CONARIS, Allergosan, Danone, and Nestle and lectureship compensation from Allergosan. The other eight coinvestigators had no relevant conflicts of interest.
Sterile fecal filtrate transplantation (FFT) effectively treated five cases of symptomatic chronic-relapsing Clostridium difficile infection, investigators reported.
The procedure restored normal bowel habits and eliminated symptoms through the end of the study – that is, for at least 6 months – in all patients, Stephan J. Ott, MD, and his associates wrote (Gastroenterology. 2019. doi: 10.1053/j.gastro.2016.11.010).
Proteome analyses did not identify proteins likely to explain this efficacy, but 16S rRNA gene sequencing did demonstrate diverse bacterial DNA signatures in the filtrates, and tests of virus-like particles yielded “a complex signature of macrophages,” Dr. Ott and his associates reported. Additional tests suggested that recipients’ microbiomes continued to change weeks after FFT. “This open-label series strongly suggests that FFT should be evaluated in a controlled setting in comparison with standard fecal microbiota transplantation,” the researchers concluded.
Fecal microbiota transplantation (FMT) effectively treats recurrent Clostridium difficile infection (CDI), but even “the most rigorous and costly donor screening procedures, or defined panels of bacteria, cannot exclude the risk of transferring unknown pathogens or undetectable functional characteristics within the living microorganisms to the recipient, including bacterial or viral risk factors for metabolic diseases, cancer, atopy, or autoimmunity,” the investigators wrote.
Therefore, they performed sterile FFT in five patients who were positive on at least two of three tests: enzyme-linked immunosorbent assay for C. difficile–specific glutamate dehydrogenase; C. difficile toxin enzyme-linked immunosorbent assay; and culture of toxin-producing C. difficile. Patients chose their own stool donors, who were then screened based on published guidelines (Clin Gastroenterol Hepatol. 2011;9[12]:1044-49). Next, “slurries” were prepared from donor stool and filtered with a custom-built air pressure filtration system, yielding a “light brown, clear liquid with a subjectively less unpleasant and intensive odor” than conventional FMT stool preparations. Bacterial cultures of these filtrates yielded no growth, whereas donor stool cultures showed profuse growth of aerobic and anaerobic bacterial colonies, Dr. Ott and his associates said.
Patients became symptom-free 2-4 days after undergoing FFT. Notably, one patient had previously undergone FMT, which led to acute fever and diarrhea and recurrence of baseline symptoms after 3 months. This patient did not develop fever or diarrhea after FFT, was symptom-free after 3 days, and remained symptom-free until the study ended 2 years later, the researchers said. All other patients also remained symptom-free through the end of the study, that is, for 6 months to more than 2 years.
Analyses of 16S rRNA revealed substantial longitudinal shifts after FFT that often were present by week 1 and remained stable until week 6, the investigators said. Further tests confirmed marked shifts in bacterial phylotypes and in their relative abundance over time. Repeated virus analyses of one patient also showed that the phageome shifted over time to resemble that of the donor.
Patients were between 49 and 75 years old, three were female and two were male, and all had received more than one antibiotic before their first episode of CDI. Antibiotics for CDI had included metronidazole, vancomycin, and rifaximin. Comorbidities included pseudomembranous colitis, renal failure, HIV infection, epilepsy, and chronic heart failure, and medical histories included recurrent diverticulitis with sigmoid resection, gastric carcinoma, and colon cancer.
“It is important to keep in mind that, in contrast to conventional FMT, transferring sterile FFT filtrates cannot be expected to establish a microbiota similar to that of the donor in the receiving patient,” Dr. Ott and his associates noted. Instead, bacterial DNA in the filtrate might trigger the re-establishment of the recipient microbiome, they said. Bacterial cell wall fragments or bacteriophages also might play a role, they added.
The German Excellence Cluster and CONARIS Research Institute AG supported the work. Dr. Ott reported having lectured for Allergosan. Two coinvestigators reported employment with CONARIS. A third coinvestigator reported shareholder relationships with CONARIS, Allergosan, Danone, and Nestle and lectureship compensation from Allergosan. The other eight coinvestigators had no relevant conflicts of interest.
FROM GASTROENTEROLOGY
Key clinical point: Sterile fecal filtrate transplantation effectively treated symptomatic chronic-relapsing Clostridium difficile infection.
Major finding: For all patients, transplantation restored normal bowel habits within 2-4 days and eliminated symptoms for at least 6 months.
Data source: A single-center cases series of five patients with recurrent symptomatic CDI.
Disclosures: The German Excellence Cluster and CONARIS Research Institute AG supported the work. Dr. Ott reported having lectured for Allergosan. Two coinvestigators reported employment with CONARIS. A third coinvestigator reported shareholder relationships with CONARIS, Allergosan, Danone, and Nestle and lectureship compensation from Allergosan. The other eight coinvestigators had no relevant conflicts of interest.