User login
VIDEO: Nonsteroidal topical expands options for pediatric AD
WAILEA, HAWAII – In an interview, pediatric dermatologist Lawrence F. Eichenfield, MD, discusses a recently approved topical therapy for atopic dermatitis, which provides a nonsteroidal option for treating the disease in young patients.
“We’re really excited to have a new topical agent” for AD, Dr. Eichenfield said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The product, crisaborole (Eucrisa), is a phosphodiesterase 4 (PDE-4) inhibitor, a new type of chemical entity “based on a different pathway of decreasing inflammation,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego. Crisaborole, the first new chemical entity to become available for treating AD since 2001, blocks PDE-4 and decreases cytokines, thereby reducing the inflammation in AD, he explained.
In the United States, the product is approved for the topical treatment of mild to moderate AD for patients aged 2 years and older. No serious adverse events attributed to crisaborole have been reported so far, in phase II and III studies and in a 1-year study, he said.
Dr. Eichenfield disclosed relationships with companies including Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka. Crisaborole is manufactured by Anacor. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In an interview, pediatric dermatologist Lawrence F. Eichenfield, MD, discusses a recently approved topical therapy for atopic dermatitis, which provides a nonsteroidal option for treating the disease in young patients.
“We’re really excited to have a new topical agent” for AD, Dr. Eichenfield said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The product, crisaborole (Eucrisa), is a phosphodiesterase 4 (PDE-4) inhibitor, a new type of chemical entity “based on a different pathway of decreasing inflammation,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego. Crisaborole, the first new chemical entity to become available for treating AD since 2001, blocks PDE-4 and decreases cytokines, thereby reducing the inflammation in AD, he explained.
In the United States, the product is approved for the topical treatment of mild to moderate AD for patients aged 2 years and older. No serious adverse events attributed to crisaborole have been reported so far, in phase II and III studies and in a 1-year study, he said.
Dr. Eichenfield disclosed relationships with companies including Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka. Crisaborole is manufactured by Anacor. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In an interview, pediatric dermatologist Lawrence F. Eichenfield, MD, discusses a recently approved topical therapy for atopic dermatitis, which provides a nonsteroidal option for treating the disease in young patients.
“We’re really excited to have a new topical agent” for AD, Dr. Eichenfield said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The product, crisaborole (Eucrisa), is a phosphodiesterase 4 (PDE-4) inhibitor, a new type of chemical entity “based on a different pathway of decreasing inflammation,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego. Crisaborole, the first new chemical entity to become available for treating AD since 2001, blocks PDE-4 and decreases cytokines, thereby reducing the inflammation in AD, he explained.
In the United States, the product is approved for the topical treatment of mild to moderate AD for patients aged 2 years and older. No serious adverse events attributed to crisaborole have been reported so far, in phase II and III studies and in a 1-year study, he said.
Dr. Eichenfield disclosed relationships with companies including Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka. Crisaborole is manufactured by Anacor. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

AGA, other medical organizations respond to Trump’s immigration order
Organizations representing physicians and medical students have expressed their concern regarding President Trump’s executive order of Jan. 27 that curtails entry into the United States by travelers from seven Muslim-majority countries. The order also suspends for 120 days entry into the United States for all persons seeking refugee status, and it bars refugees from Syria indefinitely.
Following are direct excerpts from statements issued by medical organizations.
American Gastroenterological Association
Science and illness ignore borders and political divides. That is why AGA is concerned that the recent U.S. executive order on immigration could limit scientific exchange, delay patient care, and impair medical training.
AGA is committed to diversity, which we define as inclusive of race, ethnicity, and national origin. Diversity within training programs and laboratories in the United States built today’s practice of gastroenterology. Scientists from around the world publish in our journals, work in our laboratories, train in our programs, and present data at Digestive Disease Week.® This exchange leads to better patient care, and very sick patients travel to the U.S. from around the world for the best digestive health care.
In light of these concerns, AGA adds our support to a growing number of medical institutions urging the administration to consider the devastating impact of the executive order on the health of the nation that will result from turning away patients, health professionals, and researchers. The recent immigration policy is clearly detrimental to America’s leadership role in advancing health care, and to the standing of the United States within the international community.
American Academy of Family Physicians
“We are deeply concerned that steps your Administration has taken will have a chilling effect on our nation’s physician workforce, biomedical research, and global health. It is often America’s physicians who answer the call to assist people around the world when a public health crisis occurs. Imagine a world where physicians fail to answer the call of the needy because they fear they may not be able to return to their home and families in the United States.
Many family physicians are international medical graduates (IMG), who have completed all or part of their education and training in the United States. They are professionals who dedicate their careers to the service of their patients in communities large and small, urban and rural. In fact, 20% of our membership and over 25% of family medicine residents [comprise] IMGs. The AAFP applauds and supports wholly the contributions of these individual family physicians to their patients and communities and we celebrate their diversity.
We recognize that one of your primary responsibilities as President is to ensure the safety and security of the country and its citizens. This is, without question, a daunting responsibility. But we strongly urge that the methods of doing so be examined carefully, so that the many people who can add so much to our country through immigration have the opportunity to do so, and those who are doing so already are treated with the respect and dignity they deserve.”
American Academy of Pediatrics
“The executive orders signed today are harmful to immigrant children and families throughout our country. Many of the children who will be most affected are the victims of unspeakable violence and have been exposed to trauma. Children do not immigrate, they flee. They are coming to the United States seeking safe haven in our country and they need our compassion and assistance. Broad scale expansion of family detention only exacerbates their suffering ... The AAP is non-partisan and pro-children. We urge President Trump and his administration to ensure that children and families who are fleeing violence and adversity can continue to seek refuge in our country. Immigrant children and families are an integral part of our communities and our nation, and they deserve to be cared for, treated with compassion, and celebrated. Most of all, they deserve to be healthy and safe. Pediatricians stand with the immigrant families we care for and will continue to advocate that their needs are met and prioritized.”
American Association of Medical Colleges
“The United States is facing a serious shortage of physicians. IMGs play an important role in U.S. health care, representing roughly 25% of the workforce. Current immigration pathways – including student, exchange-visitor, and employment visas – provide a balanced solution that improves health care access across the country through programs like the National Interest Waiver and the Conrad 30 J-1 Visa Waiver. In the last decade, Conrad 30 alone has directed nearly 10,000 physicians into rural and urban underserved communities. Impeding these U.S. immigration pathways jeopardizes critical access to high-quality physician care for our nation’s most vulnerable populations.
Our ability to attract top talent from around the world also enriches the research laboratories at medical schools and teaching hospitals that are working toward cures and has helped position the United States as a global leader in medical research, strengthening our economy and bolstering the public’s health. Because disease knows no geographic boundaries, it is essential to ensure that we continue to foster, rather than impede, scientific cooperation with physicians and researchers of all nationalities, as we strive to keep our country healthy.”
American College of Cardiology
“The ability to share ideas and knowledge necessary to address [the global epidemic of cardiovascular disease] is imperative. Policies that impede this free-flow of ideas will have a detrimental impact on scientific discovery, as well as the lives of patients around the world. If we are to realize a future where cardiovascular disease is no longer the number one killer of men and women worldwide we must ensure that our system of scientific exchange allows for health care professionals to learn from each other regardless of their nationality.
Additionally, IMGs, naturalized citizens, and legal residents make up a significant portion of the health care workforce in hospitals and practices across the country. More than 25% of current practicing physicians are IMGs, with cardiology ranking among the top when broken down by medical specialty. Policies that bring the immigration status of those already here into question, while also limiting the ability of others to legally train in the United States going forward, will only serve to exacerbate the already existing cardiovascular workforce shortage, especially in rural America. Such policies also threaten the care continuum of patients who rely on these providers for their medical care.”
American College of Physicians
“The executive order could deny entry or reentry to tens of thousands more persons, including medical students and physicians who are being trained in the United States and/or are delivering direct patient care. ... It also creates a precedent for barring entry of IMGs based on their religion and country of origin. ... Approximately 30% of ACP members are IMGs.”
American Society of Clinical Oncology
ASCO is deeply concerned about the potential impact of the recent executive order on cancer research, patient care, and international scientific collaboration.
Our more than 40,000 members in 148 countries lead the charge to conquer cancer in all its forms and in every nation. Tens of thousands of people from more than 100 countries participate in our scientific meetings to exchange advances and ideas to improve patient care. Millions of cancer survivors are alive today because of the progress made possible by scientific collaboration. Progress against this disease will falter if the close-knit global community of cancer care providers is divided by policies that bar members of certain nationalities from entering the United States to conduct research, care for people with cancer, or participate in scientific and medical conferences.
American Society of Hematology
We express our deep concern about the Administration’s executive order that has denied U.S. entry to people who bring unique expertise to the practice of medicine and the conduct of cancer and biomedical research. Our nation depends on the contributions of the greatest minds from around the world to maintain the high quality of our biomedical research enterprise and health care services.
The benefits of scientific collaborations are amplified by our diversity. Limiting the exchange of ideas, practices, and data across cultures has the potential to significantly retard scientific progress and adversely affect public health. Any loss of researchers and physicians will render the United States less competitive over time, and our traditionally strong research institutions and the patients they serve will be negatively affected.
We remain deeply concerned that restricting travel will prohibit participation in scientific meetings, where cutting-edge science and treatment methods are often first introduced. These in-person meetings and other global exchanges are vitally important because they provide unparalleled opportunities for collaborations and information-sharing. Such scientific and medical meetings are absolutely essential to the conquest of cancer and blood diseases.
(Statement issued on behalf of ASH, American Association for Cancer Research, Association of American Cancer Institutes, American Society for Radiation Oncology, The American Society for Pediatric Hematology/Oncology, and LUNGevity Foundation.)
The text of the executive order can be found on the White House website.
dfulton@frontlinemedcom.com
On Twitter @denisefulton
Organizations representing physicians and medical students have expressed their concern regarding President Trump’s executive order of Jan. 27 that curtails entry into the United States by travelers from seven Muslim-majority countries. The order also suspends for 120 days entry into the United States for all persons seeking refugee status, and it bars refugees from Syria indefinitely.
Following are direct excerpts from statements issued by medical organizations.
American Gastroenterological Association
Science and illness ignore borders and political divides. That is why AGA is concerned that the recent U.S. executive order on immigration could limit scientific exchange, delay patient care, and impair medical training.
AGA is committed to diversity, which we define as inclusive of race, ethnicity, and national origin. Diversity within training programs and laboratories in the United States built today’s practice of gastroenterology. Scientists from around the world publish in our journals, work in our laboratories, train in our programs, and present data at Digestive Disease Week.® This exchange leads to better patient care, and very sick patients travel to the U.S. from around the world for the best digestive health care.
In light of these concerns, AGA adds our support to a growing number of medical institutions urging the administration to consider the devastating impact of the executive order on the health of the nation that will result from turning away patients, health professionals, and researchers. The recent immigration policy is clearly detrimental to America’s leadership role in advancing health care, and to the standing of the United States within the international community.
American Academy of Family Physicians
“We are deeply concerned that steps your Administration has taken will have a chilling effect on our nation’s physician workforce, biomedical research, and global health. It is often America’s physicians who answer the call to assist people around the world when a public health crisis occurs. Imagine a world where physicians fail to answer the call of the needy because they fear they may not be able to return to their home and families in the United States.
Many family physicians are international medical graduates (IMG), who have completed all or part of their education and training in the United States. They are professionals who dedicate their careers to the service of their patients in communities large and small, urban and rural. In fact, 20% of our membership and over 25% of family medicine residents [comprise] IMGs. The AAFP applauds and supports wholly the contributions of these individual family physicians to their patients and communities and we celebrate their diversity.
We recognize that one of your primary responsibilities as President is to ensure the safety and security of the country and its citizens. This is, without question, a daunting responsibility. But we strongly urge that the methods of doing so be examined carefully, so that the many people who can add so much to our country through immigration have the opportunity to do so, and those who are doing so already are treated with the respect and dignity they deserve.”
American Academy of Pediatrics
“The executive orders signed today are harmful to immigrant children and families throughout our country. Many of the children who will be most affected are the victims of unspeakable violence and have been exposed to trauma. Children do not immigrate, they flee. They are coming to the United States seeking safe haven in our country and they need our compassion and assistance. Broad scale expansion of family detention only exacerbates their suffering ... The AAP is non-partisan and pro-children. We urge President Trump and his administration to ensure that children and families who are fleeing violence and adversity can continue to seek refuge in our country. Immigrant children and families are an integral part of our communities and our nation, and they deserve to be cared for, treated with compassion, and celebrated. Most of all, they deserve to be healthy and safe. Pediatricians stand with the immigrant families we care for and will continue to advocate that their needs are met and prioritized.”
American Association of Medical Colleges
“The United States is facing a serious shortage of physicians. IMGs play an important role in U.S. health care, representing roughly 25% of the workforce. Current immigration pathways – including student, exchange-visitor, and employment visas – provide a balanced solution that improves health care access across the country through programs like the National Interest Waiver and the Conrad 30 J-1 Visa Waiver. In the last decade, Conrad 30 alone has directed nearly 10,000 physicians into rural and urban underserved communities. Impeding these U.S. immigration pathways jeopardizes critical access to high-quality physician care for our nation’s most vulnerable populations.
Our ability to attract top talent from around the world also enriches the research laboratories at medical schools and teaching hospitals that are working toward cures and has helped position the United States as a global leader in medical research, strengthening our economy and bolstering the public’s health. Because disease knows no geographic boundaries, it is essential to ensure that we continue to foster, rather than impede, scientific cooperation with physicians and researchers of all nationalities, as we strive to keep our country healthy.”
American College of Cardiology
“The ability to share ideas and knowledge necessary to address [the global epidemic of cardiovascular disease] is imperative. Policies that impede this free-flow of ideas will have a detrimental impact on scientific discovery, as well as the lives of patients around the world. If we are to realize a future where cardiovascular disease is no longer the number one killer of men and women worldwide we must ensure that our system of scientific exchange allows for health care professionals to learn from each other regardless of their nationality.
Additionally, IMGs, naturalized citizens, and legal residents make up a significant portion of the health care workforce in hospitals and practices across the country. More than 25% of current practicing physicians are IMGs, with cardiology ranking among the top when broken down by medical specialty. Policies that bring the immigration status of those already here into question, while also limiting the ability of others to legally train in the United States going forward, will only serve to exacerbate the already existing cardiovascular workforce shortage, especially in rural America. Such policies also threaten the care continuum of patients who rely on these providers for their medical care.”
American College of Physicians
“The executive order could deny entry or reentry to tens of thousands more persons, including medical students and physicians who are being trained in the United States and/or are delivering direct patient care. ... It also creates a precedent for barring entry of IMGs based on their religion and country of origin. ... Approximately 30% of ACP members are IMGs.”
American Society of Clinical Oncology
ASCO is deeply concerned about the potential impact of the recent executive order on cancer research, patient care, and international scientific collaboration.
Our more than 40,000 members in 148 countries lead the charge to conquer cancer in all its forms and in every nation. Tens of thousands of people from more than 100 countries participate in our scientific meetings to exchange advances and ideas to improve patient care. Millions of cancer survivors are alive today because of the progress made possible by scientific collaboration. Progress against this disease will falter if the close-knit global community of cancer care providers is divided by policies that bar members of certain nationalities from entering the United States to conduct research, care for people with cancer, or participate in scientific and medical conferences.
American Society of Hematology
We express our deep concern about the Administration’s executive order that has denied U.S. entry to people who bring unique expertise to the practice of medicine and the conduct of cancer and biomedical research. Our nation depends on the contributions of the greatest minds from around the world to maintain the high quality of our biomedical research enterprise and health care services.
The benefits of scientific collaborations are amplified by our diversity. Limiting the exchange of ideas, practices, and data across cultures has the potential to significantly retard scientific progress and adversely affect public health. Any loss of researchers and physicians will render the United States less competitive over time, and our traditionally strong research institutions and the patients they serve will be negatively affected.
We remain deeply concerned that restricting travel will prohibit participation in scientific meetings, where cutting-edge science and treatment methods are often first introduced. These in-person meetings and other global exchanges are vitally important because they provide unparalleled opportunities for collaborations and information-sharing. Such scientific and medical meetings are absolutely essential to the conquest of cancer and blood diseases.
(Statement issued on behalf of ASH, American Association for Cancer Research, Association of American Cancer Institutes, American Society for Radiation Oncology, The American Society for Pediatric Hematology/Oncology, and LUNGevity Foundation.)
The text of the executive order can be found on the White House website.
dfulton@frontlinemedcom.com
On Twitter @denisefulton
Organizations representing physicians and medical students have expressed their concern regarding President Trump’s executive order of Jan. 27 that curtails entry into the United States by travelers from seven Muslim-majority countries. The order also suspends for 120 days entry into the United States for all persons seeking refugee status, and it bars refugees from Syria indefinitely.
Following are direct excerpts from statements issued by medical organizations.
American Gastroenterological Association
Science and illness ignore borders and political divides. That is why AGA is concerned that the recent U.S. executive order on immigration could limit scientific exchange, delay patient care, and impair medical training.
AGA is committed to diversity, which we define as inclusive of race, ethnicity, and national origin. Diversity within training programs and laboratories in the United States built today’s practice of gastroenterology. Scientists from around the world publish in our journals, work in our laboratories, train in our programs, and present data at Digestive Disease Week.® This exchange leads to better patient care, and very sick patients travel to the U.S. from around the world for the best digestive health care.
In light of these concerns, AGA adds our support to a growing number of medical institutions urging the administration to consider the devastating impact of the executive order on the health of the nation that will result from turning away patients, health professionals, and researchers. The recent immigration policy is clearly detrimental to America’s leadership role in advancing health care, and to the standing of the United States within the international community.
American Academy of Family Physicians
“We are deeply concerned that steps your Administration has taken will have a chilling effect on our nation’s physician workforce, biomedical research, and global health. It is often America’s physicians who answer the call to assist people around the world when a public health crisis occurs. Imagine a world where physicians fail to answer the call of the needy because they fear they may not be able to return to their home and families in the United States.
Many family physicians are international medical graduates (IMG), who have completed all or part of their education and training in the United States. They are professionals who dedicate their careers to the service of their patients in communities large and small, urban and rural. In fact, 20% of our membership and over 25% of family medicine residents [comprise] IMGs. The AAFP applauds and supports wholly the contributions of these individual family physicians to their patients and communities and we celebrate their diversity.
We recognize that one of your primary responsibilities as President is to ensure the safety and security of the country and its citizens. This is, without question, a daunting responsibility. But we strongly urge that the methods of doing so be examined carefully, so that the many people who can add so much to our country through immigration have the opportunity to do so, and those who are doing so already are treated with the respect and dignity they deserve.”
American Academy of Pediatrics
“The executive orders signed today are harmful to immigrant children and families throughout our country. Many of the children who will be most affected are the victims of unspeakable violence and have been exposed to trauma. Children do not immigrate, they flee. They are coming to the United States seeking safe haven in our country and they need our compassion and assistance. Broad scale expansion of family detention only exacerbates their suffering ... The AAP is non-partisan and pro-children. We urge President Trump and his administration to ensure that children and families who are fleeing violence and adversity can continue to seek refuge in our country. Immigrant children and families are an integral part of our communities and our nation, and they deserve to be cared for, treated with compassion, and celebrated. Most of all, they deserve to be healthy and safe. Pediatricians stand with the immigrant families we care for and will continue to advocate that their needs are met and prioritized.”
American Association of Medical Colleges
“The United States is facing a serious shortage of physicians. IMGs play an important role in U.S. health care, representing roughly 25% of the workforce. Current immigration pathways – including student, exchange-visitor, and employment visas – provide a balanced solution that improves health care access across the country through programs like the National Interest Waiver and the Conrad 30 J-1 Visa Waiver. In the last decade, Conrad 30 alone has directed nearly 10,000 physicians into rural and urban underserved communities. Impeding these U.S. immigration pathways jeopardizes critical access to high-quality physician care for our nation’s most vulnerable populations.
Our ability to attract top talent from around the world also enriches the research laboratories at medical schools and teaching hospitals that are working toward cures and has helped position the United States as a global leader in medical research, strengthening our economy and bolstering the public’s health. Because disease knows no geographic boundaries, it is essential to ensure that we continue to foster, rather than impede, scientific cooperation with physicians and researchers of all nationalities, as we strive to keep our country healthy.”
American College of Cardiology
“The ability to share ideas and knowledge necessary to address [the global epidemic of cardiovascular disease] is imperative. Policies that impede this free-flow of ideas will have a detrimental impact on scientific discovery, as well as the lives of patients around the world. If we are to realize a future where cardiovascular disease is no longer the number one killer of men and women worldwide we must ensure that our system of scientific exchange allows for health care professionals to learn from each other regardless of their nationality.
Additionally, IMGs, naturalized citizens, and legal residents make up a significant portion of the health care workforce in hospitals and practices across the country. More than 25% of current practicing physicians are IMGs, with cardiology ranking among the top when broken down by medical specialty. Policies that bring the immigration status of those already here into question, while also limiting the ability of others to legally train in the United States going forward, will only serve to exacerbate the already existing cardiovascular workforce shortage, especially in rural America. Such policies also threaten the care continuum of patients who rely on these providers for their medical care.”
American College of Physicians
“The executive order could deny entry or reentry to tens of thousands more persons, including medical students and physicians who are being trained in the United States and/or are delivering direct patient care. ... It also creates a precedent for barring entry of IMGs based on their religion and country of origin. ... Approximately 30% of ACP members are IMGs.”
American Society of Clinical Oncology
ASCO is deeply concerned about the potential impact of the recent executive order on cancer research, patient care, and international scientific collaboration.
Our more than 40,000 members in 148 countries lead the charge to conquer cancer in all its forms and in every nation. Tens of thousands of people from more than 100 countries participate in our scientific meetings to exchange advances and ideas to improve patient care. Millions of cancer survivors are alive today because of the progress made possible by scientific collaboration. Progress against this disease will falter if the close-knit global community of cancer care providers is divided by policies that bar members of certain nationalities from entering the United States to conduct research, care for people with cancer, or participate in scientific and medical conferences.
American Society of Hematology
We express our deep concern about the Administration’s executive order that has denied U.S. entry to people who bring unique expertise to the practice of medicine and the conduct of cancer and biomedical research. Our nation depends on the contributions of the greatest minds from around the world to maintain the high quality of our biomedical research enterprise and health care services.
The benefits of scientific collaborations are amplified by our diversity. Limiting the exchange of ideas, practices, and data across cultures has the potential to significantly retard scientific progress and adversely affect public health. Any loss of researchers and physicians will render the United States less competitive over time, and our traditionally strong research institutions and the patients they serve will be negatively affected.
We remain deeply concerned that restricting travel will prohibit participation in scientific meetings, where cutting-edge science and treatment methods are often first introduced. These in-person meetings and other global exchanges are vitally important because they provide unparalleled opportunities for collaborations and information-sharing. Such scientific and medical meetings are absolutely essential to the conquest of cancer and blood diseases.
(Statement issued on behalf of ASH, American Association for Cancer Research, Association of American Cancer Institutes, American Society for Radiation Oncology, The American Society for Pediatric Hematology/Oncology, and LUNGevity Foundation.)
The text of the executive order can be found on the White House website.
dfulton@frontlinemedcom.com
On Twitter @denisefulton
Congenital Hemangioma
Hemangiomas are the most common benign tumors of childhood. In recent years, subsets of hemangiomas that are fully formed at birth have been recognized as clinically and biologically distinct from the classic infantile hemangioma (IH). Congenital hemangiomas (CHs) are classified based on clinical course as rapidly involuting CHs (RICHs) or noninvoluting CHs (NICHs). The aim of this retrospective study was to describe the epidemiology, clinical aspects, and clinical outcome of CH over a 5-year period.
Methods
Using electronic medical records from the department of dermatology (Hedi Chaker Hospital, Sfax, Tunisia) for a 5-year period (2008-2012), we searched for hemangioma. After collecting those records, we identified patients with CHs. We studied the epidemiologic (eg, sex, age), clinical course (eg, location, size, number, color, surrounding skin), and evolutionary aspects in these patients.
Results
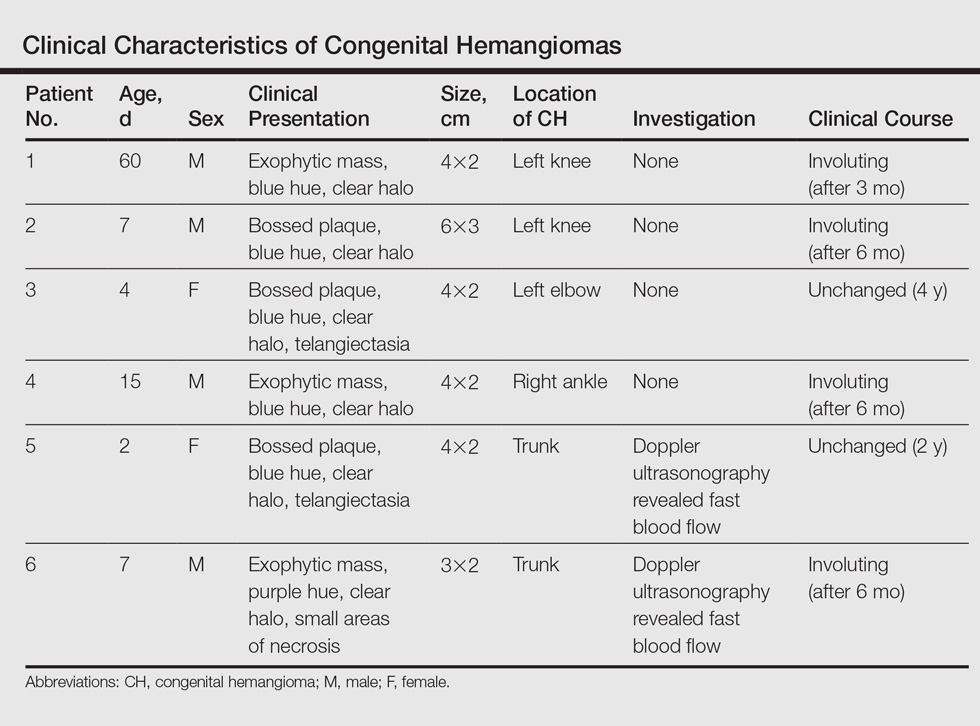
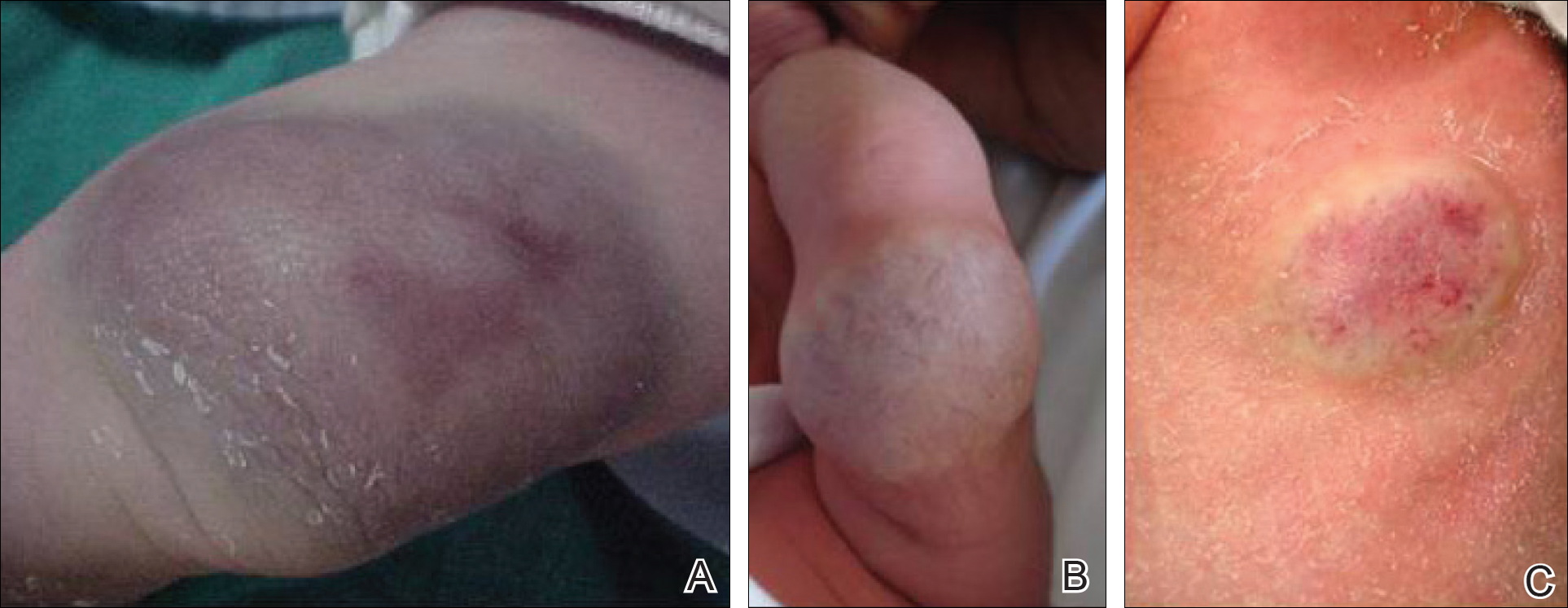
Twenty IHs were identified, 6 (30%) of which were considered CHs. The clinical characteristics of the 6 patients are summarized in the Table. We identified 2 females and 4 males aged 2 to 60 days (mean age, 16 days). Four patients had CHs involving the limbs (knee [n=2]; ankle [n=1]; elbow [n=1]) and 2 patients had CHs involving the trunk. Congenital hemangiomas were singular, oval shaped, and surrounded by a clear halo in all 6 patients. They presented as exophytic masses (n=3) or bossed plaques (n=3). A blue hue was noted in 5 patients and a purple hue in 1 patient. In some cases, telangiectasia (n=2) or small areas of necrosis (n=1) were noted at the center of the CHs. The CHs ranged in size from 3 to 6 cm (mean, 4 cm). Doppler ultrasonography was performed in 2 patients and showed fast blood flow. It is well known that manipulating a CH when it is ulcerative may cause a fatal hemorrhage. Thus, parents/guardians should be cautious when cleaning and dressing the lesions. Regular follow-up was recommended to all patients as noted in the medical records. The lesion involuted in4 patients after a mean period of 6 months, which allowed us to classify the lesions as RICHs (Figure, A). Two CHs were persistent after 2-year (Figure, B) and 4-year (Figure, C) follow-up, which was consistent with NICH classification.
Comment
Since 1996, vascular anomalies have been classified either as tumors or malformations.1 Infantile hemangioma is the most common vascular tumor and presents as an endothelial cellular proliferation that develops within days after birth. Congenital hemangiomas are fully developed at birth2,3 and are classified as RICHs and NICHs according to their clinical outcome.
As expected, our analysis revealed that CH usually is solitary and may present as a small lesion (eg, a few millimeters) but also may be large in size.4 Congenital hemangioma has an equal sex distribution and a predilection for the head and limbs near a joint. In contrast, IH exhibits female predilection and can occur anywhere on the body.4-6 In our study, CHs were more common in males and had a predilection for the limbs. Three patients presented with exophytic masses with a clear halo and overlying telangiectasia, which are commonly described features in CH.4,6
In the classification of vascular anomalies, RICHs and NICHs are fast-flow lesions that are indistinguishable at birth.7,8 Untreated, RICHs usually resolve in the first 14 months of life, often resulting in an area of atrophic or excess skin.8,9 Noninvoluting CHs persist and grow in proportion with the patient.10-12
When Doppler ultrasonography findings are inconsistent with a CH, an early biopsy from the periphery of the lesion may be performed to exclude an uncommon soft-tissue tumor such as infantile myofibromatosis or sarcoma.8,9,12 Because of the presence of a clear halo in all cases and mainly rapid involution of CHs, these differential diagnoses were dismissed. The histologic appearance of RICH differed from NICH and common IH, but some overlap was noted among the 3 lesions. Rapidly involuting CH was composed of small to large lobules of capillaries with moderately plump endothelial cells and pericytes; the lobules were surrounded by abundant fibrous tissue.9
Despite the notable differences in natural history between RICHs and NICHs, as RICHs regress within months while NICHs do not, both classes of CH share an important immunohistochemical phenotype; they do not express glucose transporter 1, the marker of IH.13 Tests for this marker were not performed in our study. The prognosis of CH generally is good, and special management is not required.
Conclusion
Rapidly involuting CHs and NICHs have many similarities, such as appearance, location, and sex distribution. The obvious differences in behavior serve to differentiate RICHs, NICHs, and common IHs. Infantile hemangiomas are not fully developed at birth and need many years to regress.
- Boon LM, Enjolras O, Mulliken JB. Congenital hemangioma: evidence of accelerated involution. J Pediatr. 1996;128:329-335.
- Neri I, Balestri R, Patrizi A. Hemangiomas: new insight and medical treatment. Dermatol Ther. 2012;25:322-334.
- Enjolras O, Mulliken JB. Vascular tumors and vascular malformations (new issues). Adv Dermatol. 1997;13:375-423.
- Mulliken JB, Enjolras O. Congenital hemangiomas and infantile hemangioma: missing links. J Am Acad Dermatol. 2004:50:875-882.
- Frieden IJ, Haggstrom AN, Drolet BA, et al. Infantile hemangiomas: current knowledge, future directions. proceedings of a research workshop on infantile hemangiomas, April 7-9, 2005, Bethesda, Maryland, USA. Pediatr Dermatol. 2005;22:383-406.
- Enjolras O, Picard A, Soupre V. Congenital haemangiomas and other rare infantile vascular tumours [in French]. Ann Chir Plast Esthet. 2006;51:339-346.
- Gorincour G, Kokta V, Rypens F, et al. Imaging characteristics of two subtypes of congenital hemangiomas: rapidly involuting congenital hemangiomas and non-involuting congenital hemangiomas. Pediatr Radiol. 2005;35:1178-1185.
- Rogers M, Lam A, Fischer G. Sonographic findings in a series of rapidly involuting congenital hemangiomas (RICH). Pediatr Dermatol. 2002;19:5-11.
- Berenguer B, Mulliken JB, Enjolras O, et al. Rapidly involuting congenital hemangioma: clinical and histopathologic features. Pediatr Dev Pathol. 2003;6:495-510.
- North PE, Waner M, James CA, et al. Congenital nonprogressive hemangioma: a distinct clinicopathologic entity unlike infantile hemangioma. Arch Dermatol. 2001;137:1607-1620.
- Chiavérini C, Kurzenne JY, Rogopoulos A, et al. Noninvoluting congenital hemangioma: 2 cases [in French]. Ann Dermatol Venerol. 2002;129:735-737.
- Enjolras O, Mulliken JB, Boon LM, et al. Noninvoluting congenital hemangioma: a rare cutaneous vascular anomaly. Plast Reconstr Surg. 2001;107:1647-1654.
- North PE, Waner M, Mizeracki A, et al. GLUT1: a newly discovered immunohistochemical marker for juvenile hemangiomas. Hum Pathol. 2000;31:11-22.
Hemangiomas are the most common benign tumors of childhood. In recent years, subsets of hemangiomas that are fully formed at birth have been recognized as clinically and biologically distinct from the classic infantile hemangioma (IH). Congenital hemangiomas (CHs) are classified based on clinical course as rapidly involuting CHs (RICHs) or noninvoluting CHs (NICHs). The aim of this retrospective study was to describe the epidemiology, clinical aspects, and clinical outcome of CH over a 5-year period.
Methods
Using electronic medical records from the department of dermatology (Hedi Chaker Hospital, Sfax, Tunisia) for a 5-year period (2008-2012), we searched for hemangioma. After collecting those records, we identified patients with CHs. We studied the epidemiologic (eg, sex, age), clinical course (eg, location, size, number, color, surrounding skin), and evolutionary aspects in these patients.
Results
Twenty IHs were identified, 6 (30%) of which were considered CHs. The clinical characteristics of the 6 patients are summarized in the Table. We identified 2 females and 4 males aged 2 to 60 days (mean age, 16 days). Four patients had CHs involving the limbs (knee [n=2]; ankle [n=1]; elbow [n=1]) and 2 patients had CHs involving the trunk. Congenital hemangiomas were singular, oval shaped, and surrounded by a clear halo in all 6 patients. They presented as exophytic masses (n=3) or bossed plaques (n=3). A blue hue was noted in 5 patients and a purple hue in 1 patient. In some cases, telangiectasia (n=2) or small areas of necrosis (n=1) were noted at the center of the CHs. The CHs ranged in size from 3 to 6 cm (mean, 4 cm). Doppler ultrasonography was performed in 2 patients and showed fast blood flow. It is well known that manipulating a CH when it is ulcerative may cause a fatal hemorrhage. Thus, parents/guardians should be cautious when cleaning and dressing the lesions. Regular follow-up was recommended to all patients as noted in the medical records. The lesion involuted in4 patients after a mean period of 6 months, which allowed us to classify the lesions as RICHs (Figure, A). Two CHs were persistent after 2-year (Figure, B) and 4-year (Figure, C) follow-up, which was consistent with NICH classification.
Comment
Since 1996, vascular anomalies have been classified either as tumors or malformations.1 Infantile hemangioma is the most common vascular tumor and presents as an endothelial cellular proliferation that develops within days after birth. Congenital hemangiomas are fully developed at birth2,3 and are classified as RICHs and NICHs according to their clinical outcome.
As expected, our analysis revealed that CH usually is solitary and may present as a small lesion (eg, a few millimeters) but also may be large in size.4 Congenital hemangioma has an equal sex distribution and a predilection for the head and limbs near a joint. In contrast, IH exhibits female predilection and can occur anywhere on the body.4-6 In our study, CHs were more common in males and had a predilection for the limbs. Three patients presented with exophytic masses with a clear halo and overlying telangiectasia, which are commonly described features in CH.4,6
In the classification of vascular anomalies, RICHs and NICHs are fast-flow lesions that are indistinguishable at birth.7,8 Untreated, RICHs usually resolve in the first 14 months of life, often resulting in an area of atrophic or excess skin.8,9 Noninvoluting CHs persist and grow in proportion with the patient.10-12
When Doppler ultrasonography findings are inconsistent with a CH, an early biopsy from the periphery of the lesion may be performed to exclude an uncommon soft-tissue tumor such as infantile myofibromatosis or sarcoma.8,9,12 Because of the presence of a clear halo in all cases and mainly rapid involution of CHs, these differential diagnoses were dismissed. The histologic appearance of RICH differed from NICH and common IH, but some overlap was noted among the 3 lesions. Rapidly involuting CH was composed of small to large lobules of capillaries with moderately plump endothelial cells and pericytes; the lobules were surrounded by abundant fibrous tissue.9
Despite the notable differences in natural history between RICHs and NICHs, as RICHs regress within months while NICHs do not, both classes of CH share an important immunohistochemical phenotype; they do not express glucose transporter 1, the marker of IH.13 Tests for this marker were not performed in our study. The prognosis of CH generally is good, and special management is not required.
Conclusion
Rapidly involuting CHs and NICHs have many similarities, such as appearance, location, and sex distribution. The obvious differences in behavior serve to differentiate RICHs, NICHs, and common IHs. Infantile hemangiomas are not fully developed at birth and need many years to regress.
Hemangiomas are the most common benign tumors of childhood. In recent years, subsets of hemangiomas that are fully formed at birth have been recognized as clinically and biologically distinct from the classic infantile hemangioma (IH). Congenital hemangiomas (CHs) are classified based on clinical course as rapidly involuting CHs (RICHs) or noninvoluting CHs (NICHs). The aim of this retrospective study was to describe the epidemiology, clinical aspects, and clinical outcome of CH over a 5-year period.
Methods
Using electronic medical records from the department of dermatology (Hedi Chaker Hospital, Sfax, Tunisia) for a 5-year period (2008-2012), we searched for hemangioma. After collecting those records, we identified patients with CHs. We studied the epidemiologic (eg, sex, age), clinical course (eg, location, size, number, color, surrounding skin), and evolutionary aspects in these patients.
Results
Twenty IHs were identified, 6 (30%) of which were considered CHs. The clinical characteristics of the 6 patients are summarized in the Table. We identified 2 females and 4 males aged 2 to 60 days (mean age, 16 days). Four patients had CHs involving the limbs (knee [n=2]; ankle [n=1]; elbow [n=1]) and 2 patients had CHs involving the trunk. Congenital hemangiomas were singular, oval shaped, and surrounded by a clear halo in all 6 patients. They presented as exophytic masses (n=3) or bossed plaques (n=3). A blue hue was noted in 5 patients and a purple hue in 1 patient. In some cases, telangiectasia (n=2) or small areas of necrosis (n=1) were noted at the center of the CHs. The CHs ranged in size from 3 to 6 cm (mean, 4 cm). Doppler ultrasonography was performed in 2 patients and showed fast blood flow. It is well known that manipulating a CH when it is ulcerative may cause a fatal hemorrhage. Thus, parents/guardians should be cautious when cleaning and dressing the lesions. Regular follow-up was recommended to all patients as noted in the medical records. The lesion involuted in4 patients after a mean period of 6 months, which allowed us to classify the lesions as RICHs (Figure, A). Two CHs were persistent after 2-year (Figure, B) and 4-year (Figure, C) follow-up, which was consistent with NICH classification.
Comment
Since 1996, vascular anomalies have been classified either as tumors or malformations.1 Infantile hemangioma is the most common vascular tumor and presents as an endothelial cellular proliferation that develops within days after birth. Congenital hemangiomas are fully developed at birth2,3 and are classified as RICHs and NICHs according to their clinical outcome.
As expected, our analysis revealed that CH usually is solitary and may present as a small lesion (eg, a few millimeters) but also may be large in size.4 Congenital hemangioma has an equal sex distribution and a predilection for the head and limbs near a joint. In contrast, IH exhibits female predilection and can occur anywhere on the body.4-6 In our study, CHs were more common in males and had a predilection for the limbs. Three patients presented with exophytic masses with a clear halo and overlying telangiectasia, which are commonly described features in CH.4,6
In the classification of vascular anomalies, RICHs and NICHs are fast-flow lesions that are indistinguishable at birth.7,8 Untreated, RICHs usually resolve in the first 14 months of life, often resulting in an area of atrophic or excess skin.8,9 Noninvoluting CHs persist and grow in proportion with the patient.10-12
When Doppler ultrasonography findings are inconsistent with a CH, an early biopsy from the periphery of the lesion may be performed to exclude an uncommon soft-tissue tumor such as infantile myofibromatosis or sarcoma.8,9,12 Because of the presence of a clear halo in all cases and mainly rapid involution of CHs, these differential diagnoses were dismissed. The histologic appearance of RICH differed from NICH and common IH, but some overlap was noted among the 3 lesions. Rapidly involuting CH was composed of small to large lobules of capillaries with moderately plump endothelial cells and pericytes; the lobules were surrounded by abundant fibrous tissue.9
Despite the notable differences in natural history between RICHs and NICHs, as RICHs regress within months while NICHs do not, both classes of CH share an important immunohistochemical phenotype; they do not express glucose transporter 1, the marker of IH.13 Tests for this marker were not performed in our study. The prognosis of CH generally is good, and special management is not required.
Conclusion
Rapidly involuting CHs and NICHs have many similarities, such as appearance, location, and sex distribution. The obvious differences in behavior serve to differentiate RICHs, NICHs, and common IHs. Infantile hemangiomas are not fully developed at birth and need many years to regress.
- Boon LM, Enjolras O, Mulliken JB. Congenital hemangioma: evidence of accelerated involution. J Pediatr. 1996;128:329-335.
- Neri I, Balestri R, Patrizi A. Hemangiomas: new insight and medical treatment. Dermatol Ther. 2012;25:322-334.
- Enjolras O, Mulliken JB. Vascular tumors and vascular malformations (new issues). Adv Dermatol. 1997;13:375-423.
- Mulliken JB, Enjolras O. Congenital hemangiomas and infantile hemangioma: missing links. J Am Acad Dermatol. 2004:50:875-882.
- Frieden IJ, Haggstrom AN, Drolet BA, et al. Infantile hemangiomas: current knowledge, future directions. proceedings of a research workshop on infantile hemangiomas, April 7-9, 2005, Bethesda, Maryland, USA. Pediatr Dermatol. 2005;22:383-406.
- Enjolras O, Picard A, Soupre V. Congenital haemangiomas and other rare infantile vascular tumours [in French]. Ann Chir Plast Esthet. 2006;51:339-346.
- Gorincour G, Kokta V, Rypens F, et al. Imaging characteristics of two subtypes of congenital hemangiomas: rapidly involuting congenital hemangiomas and non-involuting congenital hemangiomas. Pediatr Radiol. 2005;35:1178-1185.
- Rogers M, Lam A, Fischer G. Sonographic findings in a series of rapidly involuting congenital hemangiomas (RICH). Pediatr Dermatol. 2002;19:5-11.
- Berenguer B, Mulliken JB, Enjolras O, et al. Rapidly involuting congenital hemangioma: clinical and histopathologic features. Pediatr Dev Pathol. 2003;6:495-510.
- North PE, Waner M, James CA, et al. Congenital nonprogressive hemangioma: a distinct clinicopathologic entity unlike infantile hemangioma. Arch Dermatol. 2001;137:1607-1620.
- Chiavérini C, Kurzenne JY, Rogopoulos A, et al. Noninvoluting congenital hemangioma: 2 cases [in French]. Ann Dermatol Venerol. 2002;129:735-737.
- Enjolras O, Mulliken JB, Boon LM, et al. Noninvoluting congenital hemangioma: a rare cutaneous vascular anomaly. Plast Reconstr Surg. 2001;107:1647-1654.
- North PE, Waner M, Mizeracki A, et al. GLUT1: a newly discovered immunohistochemical marker for juvenile hemangiomas. Hum Pathol. 2000;31:11-22.
- Boon LM, Enjolras O, Mulliken JB. Congenital hemangioma: evidence of accelerated involution. J Pediatr. 1996;128:329-335.
- Neri I, Balestri R, Patrizi A. Hemangiomas: new insight and medical treatment. Dermatol Ther. 2012;25:322-334.
- Enjolras O, Mulliken JB. Vascular tumors and vascular malformations (new issues). Adv Dermatol. 1997;13:375-423.
- Mulliken JB, Enjolras O. Congenital hemangiomas and infantile hemangioma: missing links. J Am Acad Dermatol. 2004:50:875-882.
- Frieden IJ, Haggstrom AN, Drolet BA, et al. Infantile hemangiomas: current knowledge, future directions. proceedings of a research workshop on infantile hemangiomas, April 7-9, 2005, Bethesda, Maryland, USA. Pediatr Dermatol. 2005;22:383-406.
- Enjolras O, Picard A, Soupre V. Congenital haemangiomas and other rare infantile vascular tumours [in French]. Ann Chir Plast Esthet. 2006;51:339-346.
- Gorincour G, Kokta V, Rypens F, et al. Imaging characteristics of two subtypes of congenital hemangiomas: rapidly involuting congenital hemangiomas and non-involuting congenital hemangiomas. Pediatr Radiol. 2005;35:1178-1185.
- Rogers M, Lam A, Fischer G. Sonographic findings in a series of rapidly involuting congenital hemangiomas (RICH). Pediatr Dermatol. 2002;19:5-11.
- Berenguer B, Mulliken JB, Enjolras O, et al. Rapidly involuting congenital hemangioma: clinical and histopathologic features. Pediatr Dev Pathol. 2003;6:495-510.
- North PE, Waner M, James CA, et al. Congenital nonprogressive hemangioma: a distinct clinicopathologic entity unlike infantile hemangioma. Arch Dermatol. 2001;137:1607-1620.
- Chiavérini C, Kurzenne JY, Rogopoulos A, et al. Noninvoluting congenital hemangioma: 2 cases [in French]. Ann Dermatol Venerol. 2002;129:735-737.
- Enjolras O, Mulliken JB, Boon LM, et al. Noninvoluting congenital hemangioma: a rare cutaneous vascular anomaly. Plast Reconstr Surg. 2001;107:1647-1654.
- North PE, Waner M, Mizeracki A, et al. GLUT1: a newly discovered immunohistochemical marker for juvenile hemangiomas. Hum Pathol. 2000;31:11-22.
Practice Points
- Congenital hemangiomas (CHs) are fully developed hemangiomas that are present at birth.
- In our study, CHs were more common in males, with a predilection for the limbs.
- Infantile hemangiomas are not fully developed at birth and need many years to regress.

Burnout: No laughing matter
Much has been written about burnout in U.S. physicians over the course of many years. Burnout is a syndrome that is exemplified by emotional exhaustion, depersonalization, and a low sense of personal accomplishment. It appears that hospitalists are particularly prone to burnout, being at the very front line of patient care. In addition, the prevalence of burnout appears to be getting worse. According to a survey from the American Medical Association, the prevalence of burnout in 2011 was 45%. Three years later in 2014 the prevalence was up to 55%.1,2
Although triggers for the onset and intensity of burnout likely vary by specialty, a recent Medscape Lifestyle Report found the most common causes of burnout among physicians included (see graphic):3
• Bureaucratic tasks.
• Work hours.
• Computerization.
• Compensation.

• Lower work satisfaction.
• Disrupted personal relationships.
• Substance misuse.
• Depression.
• Suicide.
Burnout also leads to lower productivity, higher job turnover, and early retirement. In addition, from a systems perspective, burnout is associated with higher medical errors, reduced quality of patient care, and lower patient satisfaction. And, at its most extreme, burnout is deadly: Sadly, every year, 300-400 physicians in the United States commit suicide. Female physicians are 2.3 times more likely to commit suicide than are female nonphysicians; for males, the risk is 1.4 times higher among physicians compared to the general population.1
Proactive approaches
Despite all these sobering statistics on the prevalence and outcomes of burnout among physicians, the ongoing question is, what can we do about it? Although awareness and recognition of burnout has grown substantially over time, successful interventions to prevent or mitigate burnout have not. Many potential interventions and ideas have surfaced and have been published, but none have had impressive impacts or have been adopted widely within or across institutions. According to a Modern Healthcare survey of approximately 100 health care CEOs, only about one-third reported that their organization had programs to address physician burnout, although about another one-third reported attempts to develop such programs.1
The good news is that at least there is a lot of activity around trying new interventions to reduce burnout, including in medical schools and graduate training programs. The thought is that if you can employ healthy resilience tactics during training, these can be carried throughout a career to diminish the risk and/or severity of burnout, despite any challenges that arise along the way.
Some of these interventions are aimed at individuals (to enhance personal resilience and coping skills) while others are aimed at the level of organizations (to reduce organizational stress and/or workload). A recent Modern Healthcare article found several good examples:1
• New York’s Albert Einstein College of Medicine’s WellMed program has been designed to help students develop healthy and balanced habits and attitudes, and to enhance their personal resilience, for the short and the long term.
• Baystate Health in Massachusetts hosts a physician leadership academy that offers training in communication, unconscious bias, strategy, and other management skills, to enhance individual resilience and organizational engagement.
• HealthPartners, a not-for-profit, Minnesota-based health care organization, has specific programs to engage physicians and allow them to have organizational impact, as well as programs to simplify technology use.
Organization efforts are key to prevent, treat
The key to reducing burnout does seem to be employing a combination of self-directed and organization-directed interventions, each of which enhances resilience and reduces workplace stressors (i.e., administrative tasks and workload). Specific to hospitalists, Leslie Flores, MBA, recently wrote about burnout at The Hospital Leader blog. Her list included several specific examples to reduce the top causes of burnout among busy hospitalists:4
• Modifying the skill mix in hospital medicine groups so that less costly support staff are doing much of the work not requiring a physician’s expertise, freeing up hospitalists to provide better care to more patients.
• Reducing unnecessary interruptions and the stress they cause, via both technology and process improvement.
• Paying deliberate attention to hospitalist personal and professional well-being.
• Adjusting hospitalist schedules and work flow so that hospitalists can be more efficient (that is, do less low-value work and re-work) and have better work-life balance.
• Ensuring that hospitalists have the training, clinical competencies, and support to comfortably perform in expanded clinical roles.
Many of these systemic solutions were recently validated as likely able to have an impact on burnout (and seem to be more effective than interventions focused on individual resilience).5 A recent meta-analysis found that physician-directed interventions were associated with small but significant reductions in burnout; these were primarily mindfulness-based stress reduction techniques, educational interventions targeting physicians self-confidence and communication skills, exercise, or a combination of these features. More impactful were organization-directed interventions, which were associated with more significant reductions in burnout; these were primarily aimed at reducing workload and enhancing teamwork and leadership.
In sum
It is important for all of us hospitalists to understand and try to mitigate burnout within our teams. Although individual-focused interventions can have some effect, most efforts should primarily be focused on system-based interventions, to reduce administrative burdens and workload. Through such system design and redesign, we can likely reduce burnout amongst our teams, and therefore improve the sustainability of our specialty.
References
1.http://www.modernhealthcare.com/article/20161029/MAGAZINE/310299983
2. http://www.mayoclinicproceedings.org/article/S0025-6196(15)00716-8/abstract
3.http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview#page=5
4. http://blogs.hospitalmedicine.org/Blog/making-hospital-medicine-a-sustainable-specialty/
5.http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2588814
Much has been written about burnout in U.S. physicians over the course of many years. Burnout is a syndrome that is exemplified by emotional exhaustion, depersonalization, and a low sense of personal accomplishment. It appears that hospitalists are particularly prone to burnout, being at the very front line of patient care. In addition, the prevalence of burnout appears to be getting worse. According to a survey from the American Medical Association, the prevalence of burnout in 2011 was 45%. Three years later in 2014 the prevalence was up to 55%.1,2
Although triggers for the onset and intensity of burnout likely vary by specialty, a recent Medscape Lifestyle Report found the most common causes of burnout among physicians included (see graphic):3
• Bureaucratic tasks.
• Work hours.
• Computerization.
• Compensation.
• Lower work satisfaction.
• Disrupted personal relationships.
• Substance misuse.
• Depression.
• Suicide.
Burnout also leads to lower productivity, higher job turnover, and early retirement. In addition, from a systems perspective, burnout is associated with higher medical errors, reduced quality of patient care, and lower patient satisfaction. And, at its most extreme, burnout is deadly: Sadly, every year, 300-400 physicians in the United States commit suicide. Female physicians are 2.3 times more likely to commit suicide than are female nonphysicians; for males, the risk is 1.4 times higher among physicians compared to the general population.1
Proactive approaches
Despite all these sobering statistics on the prevalence and outcomes of burnout among physicians, the ongoing question is, what can we do about it? Although awareness and recognition of burnout has grown substantially over time, successful interventions to prevent or mitigate burnout have not. Many potential interventions and ideas have surfaced and have been published, but none have had impressive impacts or have been adopted widely within or across institutions. According to a Modern Healthcare survey of approximately 100 health care CEOs, only about one-third reported that their organization had programs to address physician burnout, although about another one-third reported attempts to develop such programs.1
The good news is that at least there is a lot of activity around trying new interventions to reduce burnout, including in medical schools and graduate training programs. The thought is that if you can employ healthy resilience tactics during training, these can be carried throughout a career to diminish the risk and/or severity of burnout, despite any challenges that arise along the way.
Some of these interventions are aimed at individuals (to enhance personal resilience and coping skills) while others are aimed at the level of organizations (to reduce organizational stress and/or workload). A recent Modern Healthcare article found several good examples:1
• New York’s Albert Einstein College of Medicine’s WellMed program has been designed to help students develop healthy and balanced habits and attitudes, and to enhance their personal resilience, for the short and the long term.
• Baystate Health in Massachusetts hosts a physician leadership academy that offers training in communication, unconscious bias, strategy, and other management skills, to enhance individual resilience and organizational engagement.
• HealthPartners, a not-for-profit, Minnesota-based health care organization, has specific programs to engage physicians and allow them to have organizational impact, as well as programs to simplify technology use.
Organization efforts are key to prevent, treat
The key to reducing burnout does seem to be employing a combination of self-directed and organization-directed interventions, each of which enhances resilience and reduces workplace stressors (i.e., administrative tasks and workload). Specific to hospitalists, Leslie Flores, MBA, recently wrote about burnout at The Hospital Leader blog. Her list included several specific examples to reduce the top causes of burnout among busy hospitalists:4
• Modifying the skill mix in hospital medicine groups so that less costly support staff are doing much of the work not requiring a physician’s expertise, freeing up hospitalists to provide better care to more patients.
• Reducing unnecessary interruptions and the stress they cause, via both technology and process improvement.
• Paying deliberate attention to hospitalist personal and professional well-being.
• Adjusting hospitalist schedules and work flow so that hospitalists can be more efficient (that is, do less low-value work and re-work) and have better work-life balance.
• Ensuring that hospitalists have the training, clinical competencies, and support to comfortably perform in expanded clinical roles.
Many of these systemic solutions were recently validated as likely able to have an impact on burnout (and seem to be more effective than interventions focused on individual resilience).5 A recent meta-analysis found that physician-directed interventions were associated with small but significant reductions in burnout; these were primarily mindfulness-based stress reduction techniques, educational interventions targeting physicians self-confidence and communication skills, exercise, or a combination of these features. More impactful were organization-directed interventions, which were associated with more significant reductions in burnout; these were primarily aimed at reducing workload and enhancing teamwork and leadership.
In sum
It is important for all of us hospitalists to understand and try to mitigate burnout within our teams. Although individual-focused interventions can have some effect, most efforts should primarily be focused on system-based interventions, to reduce administrative burdens and workload. Through such system design and redesign, we can likely reduce burnout amongst our teams, and therefore improve the sustainability of our specialty.
References
1.http://www.modernhealthcare.com/article/20161029/MAGAZINE/310299983
2. http://www.mayoclinicproceedings.org/article/S0025-6196(15)00716-8/abstract
3.http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview#page=5
4. http://blogs.hospitalmedicine.org/Blog/making-hospital-medicine-a-sustainable-specialty/
5.http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2588814
Much has been written about burnout in U.S. physicians over the course of many years. Burnout is a syndrome that is exemplified by emotional exhaustion, depersonalization, and a low sense of personal accomplishment. It appears that hospitalists are particularly prone to burnout, being at the very front line of patient care. In addition, the prevalence of burnout appears to be getting worse. According to a survey from the American Medical Association, the prevalence of burnout in 2011 was 45%. Three years later in 2014 the prevalence was up to 55%.1,2
Although triggers for the onset and intensity of burnout likely vary by specialty, a recent Medscape Lifestyle Report found the most common causes of burnout among physicians included (see graphic):3
• Bureaucratic tasks.
• Work hours.
• Computerization.
• Compensation.
• Lower work satisfaction.
• Disrupted personal relationships.
• Substance misuse.
• Depression.
• Suicide.
Burnout also leads to lower productivity, higher job turnover, and early retirement. In addition, from a systems perspective, burnout is associated with higher medical errors, reduced quality of patient care, and lower patient satisfaction. And, at its most extreme, burnout is deadly: Sadly, every year, 300-400 physicians in the United States commit suicide. Female physicians are 2.3 times more likely to commit suicide than are female nonphysicians; for males, the risk is 1.4 times higher among physicians compared to the general population.1
Proactive approaches
Despite all these sobering statistics on the prevalence and outcomes of burnout among physicians, the ongoing question is, what can we do about it? Although awareness and recognition of burnout has grown substantially over time, successful interventions to prevent or mitigate burnout have not. Many potential interventions and ideas have surfaced and have been published, but none have had impressive impacts or have been adopted widely within or across institutions. According to a Modern Healthcare survey of approximately 100 health care CEOs, only about one-third reported that their organization had programs to address physician burnout, although about another one-third reported attempts to develop such programs.1
The good news is that at least there is a lot of activity around trying new interventions to reduce burnout, including in medical schools and graduate training programs. The thought is that if you can employ healthy resilience tactics during training, these can be carried throughout a career to diminish the risk and/or severity of burnout, despite any challenges that arise along the way.
Some of these interventions are aimed at individuals (to enhance personal resilience and coping skills) while others are aimed at the level of organizations (to reduce organizational stress and/or workload). A recent Modern Healthcare article found several good examples:1
• New York’s Albert Einstein College of Medicine’s WellMed program has been designed to help students develop healthy and balanced habits and attitudes, and to enhance their personal resilience, for the short and the long term.
• Baystate Health in Massachusetts hosts a physician leadership academy that offers training in communication, unconscious bias, strategy, and other management skills, to enhance individual resilience and organizational engagement.
• HealthPartners, a not-for-profit, Minnesota-based health care organization, has specific programs to engage physicians and allow them to have organizational impact, as well as programs to simplify technology use.
Organization efforts are key to prevent, treat
The key to reducing burnout does seem to be employing a combination of self-directed and organization-directed interventions, each of which enhances resilience and reduces workplace stressors (i.e., administrative tasks and workload). Specific to hospitalists, Leslie Flores, MBA, recently wrote about burnout at The Hospital Leader blog. Her list included several specific examples to reduce the top causes of burnout among busy hospitalists:4
• Modifying the skill mix in hospital medicine groups so that less costly support staff are doing much of the work not requiring a physician’s expertise, freeing up hospitalists to provide better care to more patients.
• Reducing unnecessary interruptions and the stress they cause, via both technology and process improvement.
• Paying deliberate attention to hospitalist personal and professional well-being.
• Adjusting hospitalist schedules and work flow so that hospitalists can be more efficient (that is, do less low-value work and re-work) and have better work-life balance.
• Ensuring that hospitalists have the training, clinical competencies, and support to comfortably perform in expanded clinical roles.
Many of these systemic solutions were recently validated as likely able to have an impact on burnout (and seem to be more effective than interventions focused on individual resilience).5 A recent meta-analysis found that physician-directed interventions were associated with small but significant reductions in burnout; these were primarily mindfulness-based stress reduction techniques, educational interventions targeting physicians self-confidence and communication skills, exercise, or a combination of these features. More impactful were organization-directed interventions, which were associated with more significant reductions in burnout; these were primarily aimed at reducing workload and enhancing teamwork and leadership.
In sum
It is important for all of us hospitalists to understand and try to mitigate burnout within our teams. Although individual-focused interventions can have some effect, most efforts should primarily be focused on system-based interventions, to reduce administrative burdens and workload. Through such system design and redesign, we can likely reduce burnout amongst our teams, and therefore improve the sustainability of our specialty.
References
1.http://www.modernhealthcare.com/article/20161029/MAGAZINE/310299983
2. http://www.mayoclinicproceedings.org/article/S0025-6196(15)00716-8/abstract
3.http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview#page=5
4. http://blogs.hospitalmedicine.org/Blog/making-hospital-medicine-a-sustainable-specialty/
5.http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2588814
AATS Week 2017 Registration Now Open
AATS Week 2017 will bring together the world’s foremost CT surgery scientists and medical professionals for seven days at three important events:
Mitral Conclave
April 27 – 28, 2017
New York, NY
AATS Innovation Summit
April 29, 2017
Boston, MA
The AATS Centennial
April 29 – May 3
Boston, MA
Registration is now open.
Choose from one of several registration packages:
AATS Week 2017 Package
Register and receive a $100 discount*
*Discount does not apply to Residents/Fellows or Medical Students. The discount is applied to the AATS Mitral Conclave registration fee.
Genius Pass
The Genius Pass provides access to almost every offering at the AATS Centennial. The package includes:
** Access to Saturday Skills Courses and Sunday Symposia
** Access to all simulation sessions (Monday – Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday & Tuesday)
** Welcome Reception
Innovation Pass
Ignite your spirit for innovation with Course Director W. Randolph Chitwood Jr. at this one-day program assisting cardiothoracic surgeons to develop new clinically applicable technology by obtaining the cross-specialty knowledge needed for novel idea generation, protecting intellectual property, developmental funding, clinical trials, regulatory pathways and industry relations.
Innovation Pass Registration includes:
** Registration for the Saturday AATS Innovation Summit
** Access to all Sunday Symposia
** Access to all simulations sessions (Monday- Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday and Tuesday)
** Welcome Reception
Note: You can only attend the AATS Innovation Summit or the Saturday Skills Courses. You cannot choose to attend both events on Saturday.
Resident/Fellows and Medical Students: Can only attend the AATS Centennial by choosing the AATS Genius or Innovation Pass.
Separate registration is required for: Saturday hands-on sessions, Member for a Day session, Survival Guide for the Cardiothoracic Surgical Team, MOC Breakfast, Cardiothoracic Residents & Ethics Forum Luncheons, and all social events and tours.
Conference Flex Pass
This pass is best suited for those who want to attend some, but not all, offerings.
Customize your AATS Centennial participation by adding individual educational events to your cart — any combination of the Saturday Courses, Sunday Symposia, and Monday-Wednesday simultaneous sessions.
Saturday Courses and Sunday Symposium Registration
Register for a Saturday course and/or a Sunday symposium and receive access to all other courses/symposia taking place that day.
Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting registration rate.
Registration & Housing information
AATS Week 2017 will bring together the world’s foremost CT surgery scientists and medical professionals for seven days at three important events:
Mitral Conclave
April 27 – 28, 2017
New York, NY
AATS Innovation Summit
April 29, 2017
Boston, MA
The AATS Centennial
April 29 – May 3
Boston, MA
Registration is now open.
Choose from one of several registration packages:
AATS Week 2017 Package
Register and receive a $100 discount*
*Discount does not apply to Residents/Fellows or Medical Students. The discount is applied to the AATS Mitral Conclave registration fee.
Genius Pass
The Genius Pass provides access to almost every offering at the AATS Centennial. The package includes:
** Access to Saturday Skills Courses and Sunday Symposia
** Access to all simulation sessions (Monday – Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday & Tuesday)
** Welcome Reception
Innovation Pass
Ignite your spirit for innovation with Course Director W. Randolph Chitwood Jr. at this one-day program assisting cardiothoracic surgeons to develop new clinically applicable technology by obtaining the cross-specialty knowledge needed for novel idea generation, protecting intellectual property, developmental funding, clinical trials, regulatory pathways and industry relations.
Innovation Pass Registration includes:
** Registration for the Saturday AATS Innovation Summit
** Access to all Sunday Symposia
** Access to all simulations sessions (Monday- Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday and Tuesday)
** Welcome Reception
Note: You can only attend the AATS Innovation Summit or the Saturday Skills Courses. You cannot choose to attend both events on Saturday.
Resident/Fellows and Medical Students: Can only attend the AATS Centennial by choosing the AATS Genius or Innovation Pass.
Separate registration is required for: Saturday hands-on sessions, Member for a Day session, Survival Guide for the Cardiothoracic Surgical Team, MOC Breakfast, Cardiothoracic Residents & Ethics Forum Luncheons, and all social events and tours.
Conference Flex Pass
This pass is best suited for those who want to attend some, but not all, offerings.
Customize your AATS Centennial participation by adding individual educational events to your cart — any combination of the Saturday Courses, Sunday Symposia, and Monday-Wednesday simultaneous sessions.
Saturday Courses and Sunday Symposium Registration
Register for a Saturday course and/or a Sunday symposium and receive access to all other courses/symposia taking place that day.
Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting registration rate.
Registration & Housing information
AATS Week 2017 will bring together the world’s foremost CT surgery scientists and medical professionals for seven days at three important events:
Mitral Conclave
April 27 – 28, 2017
New York, NY
AATS Innovation Summit
April 29, 2017
Boston, MA
The AATS Centennial
April 29 – May 3
Boston, MA
Registration is now open.
Choose from one of several registration packages:
AATS Week 2017 Package
Register and receive a $100 discount*
*Discount does not apply to Residents/Fellows or Medical Students. The discount is applied to the AATS Mitral Conclave registration fee.
Genius Pass
The Genius Pass provides access to almost every offering at the AATS Centennial. The package includes:
** Access to Saturday Skills Courses and Sunday Symposia
** Access to all simulation sessions (Monday – Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday & Tuesday)
** Welcome Reception
Innovation Pass
Ignite your spirit for innovation with Course Director W. Randolph Chitwood Jr. at this one-day program assisting cardiothoracic surgeons to develop new clinically applicable technology by obtaining the cross-specialty knowledge needed for novel idea generation, protecting intellectual property, developmental funding, clinical trials, regulatory pathways and industry relations.
Innovation Pass Registration includes:
** Registration for the Saturday AATS Innovation Summit
** Access to all Sunday Symposia
** Access to all simulations sessions (Monday- Wednesday)
** Exhibit Hall admission
** Lunch in the Exhibit Hall (Monday and Tuesday)
** Welcome Reception
Note: You can only attend the AATS Innovation Summit or the Saturday Skills Courses. You cannot choose to attend both events on Saturday.
Resident/Fellows and Medical Students: Can only attend the AATS Centennial by choosing the AATS Genius or Innovation Pass.
Separate registration is required for: Saturday hands-on sessions, Member for a Day session, Survival Guide for the Cardiothoracic Surgical Team, MOC Breakfast, Cardiothoracic Residents & Ethics Forum Luncheons, and all social events and tours.
Conference Flex Pass
This pass is best suited for those who want to attend some, but not all, offerings.
Customize your AATS Centennial participation by adding individual educational events to your cart — any combination of the Saturday Courses, Sunday Symposia, and Monday-Wednesday simultaneous sessions.
Saturday Courses and Sunday Symposium Registration
Register for a Saturday course and/or a Sunday symposium and receive access to all other courses/symposia taking place that day.
Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting registration rate.
Registration & Housing information
Don’t Miss the Celebration: AATS Centennial
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Hydroxychloroquine dosing guidelines have little impact in clinical practice
A substantial number of rheumatology patients are receiving excess starting and maintenance doses of hydroxychloroquine despite the existence of dosing guidelines, a group of ophthalmologists has reported.
The report raises some concerns because hydroxychloroquine has well-established ocular side effects and toxicities that makes screening by a ophthalmologist necessary for all patients on long-term therapy.
Rebekah A. Braslow, MD, and her colleagues in the division of ophthalmology at NorthShore University HealthSystem in Illinois conducted a retrospective review of the records of 554 rheumatology patients who were prescribed hydroxychloroquine during 2009-2016 and seen by a NorthShore ophthalmologist. They found that about half of the patients were on excess initial doses of the disease-modifying antirheumatic drug, according to retinal toxicity guidelines published by the American Academy of Ophthalmology (AAO) in 2011. There was no difference in the percentage of patients on an excess starting dose before the 2011 guidelines were published (54% of 92 patients) or after (49% of 462). The maintenance dose 1 year after beginning treatment was the same as the starting dose in 84% of patients, with reductions in 7% and increases in 9% (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
The AAO revised the guidelines in 2016 to define excess doses of hydroxychloroquine as greater than 5.0 mg/kg of actual body weight (Ophthalmology. 2016;123:1386-94). Based on these new guidelines, the investigators found that 56% of 527 patients who were currently receiving hydroxychloroquine were taking excess doses, and 43% of the 527 patients were still receiving doses that are more than 50 mg in excess of the calculated target dose that is recommended by the guidelines.
“The published ophthalmology screening guidelines have had no appreciable impact on clinical practice, highlighting a persistent deficiency in patient care and a significant medico-legal risk,” they concluded.
“Our findings are particularly concerning given that choosing a proper starting dose is the single safest, simplest, and most cost-effective measure available,” they wrote.
According to the authors, there were several reasons for the widespread inaccurate dosing. Firstly, the guidelines were published in ophthalmology literature and were therefore unlikely to be seen by rheumatologists. Secondly, the formulation of the drug, currently available only in 200-mg tablet form, made it difficult to adjust doses according to a patient’s weight.
This particular issue could be addressed if the drug manufacturers expanded formulation options, or by alternating daily dosing regimens or involving compound pharmacies, they suggested.
System-wide education and prompts via electronic medical records would also go some way toward ensuring that patients are prescribed the correct dose, they added.
The study was supported by intramural research funds within the division of ophthalmology in NorthShore University Health System.
A substantial number of rheumatology patients are receiving excess starting and maintenance doses of hydroxychloroquine despite the existence of dosing guidelines, a group of ophthalmologists has reported.
The report raises some concerns because hydroxychloroquine has well-established ocular side effects and toxicities that makes screening by a ophthalmologist necessary for all patients on long-term therapy.
Rebekah A. Braslow, MD, and her colleagues in the division of ophthalmology at NorthShore University HealthSystem in Illinois conducted a retrospective review of the records of 554 rheumatology patients who were prescribed hydroxychloroquine during 2009-2016 and seen by a NorthShore ophthalmologist. They found that about half of the patients were on excess initial doses of the disease-modifying antirheumatic drug, according to retinal toxicity guidelines published by the American Academy of Ophthalmology (AAO) in 2011. There was no difference in the percentage of patients on an excess starting dose before the 2011 guidelines were published (54% of 92 patients) or after (49% of 462). The maintenance dose 1 year after beginning treatment was the same as the starting dose in 84% of patients, with reductions in 7% and increases in 9% (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
The AAO revised the guidelines in 2016 to define excess doses of hydroxychloroquine as greater than 5.0 mg/kg of actual body weight (Ophthalmology. 2016;123:1386-94). Based on these new guidelines, the investigators found that 56% of 527 patients who were currently receiving hydroxychloroquine were taking excess doses, and 43% of the 527 patients were still receiving doses that are more than 50 mg in excess of the calculated target dose that is recommended by the guidelines.
“The published ophthalmology screening guidelines have had no appreciable impact on clinical practice, highlighting a persistent deficiency in patient care and a significant medico-legal risk,” they concluded.
“Our findings are particularly concerning given that choosing a proper starting dose is the single safest, simplest, and most cost-effective measure available,” they wrote.
According to the authors, there were several reasons for the widespread inaccurate dosing. Firstly, the guidelines were published in ophthalmology literature and were therefore unlikely to be seen by rheumatologists. Secondly, the formulation of the drug, currently available only in 200-mg tablet form, made it difficult to adjust doses according to a patient’s weight.
This particular issue could be addressed if the drug manufacturers expanded formulation options, or by alternating daily dosing regimens or involving compound pharmacies, they suggested.
System-wide education and prompts via electronic medical records would also go some way toward ensuring that patients are prescribed the correct dose, they added.
The study was supported by intramural research funds within the division of ophthalmology in NorthShore University Health System.
A substantial number of rheumatology patients are receiving excess starting and maintenance doses of hydroxychloroquine despite the existence of dosing guidelines, a group of ophthalmologists has reported.
The report raises some concerns because hydroxychloroquine has well-established ocular side effects and toxicities that makes screening by a ophthalmologist necessary for all patients on long-term therapy.
Rebekah A. Braslow, MD, and her colleagues in the division of ophthalmology at NorthShore University HealthSystem in Illinois conducted a retrospective review of the records of 554 rheumatology patients who were prescribed hydroxychloroquine during 2009-2016 and seen by a NorthShore ophthalmologist. They found that about half of the patients were on excess initial doses of the disease-modifying antirheumatic drug, according to retinal toxicity guidelines published by the American Academy of Ophthalmology (AAO) in 2011. There was no difference in the percentage of patients on an excess starting dose before the 2011 guidelines were published (54% of 92 patients) or after (49% of 462). The maintenance dose 1 year after beginning treatment was the same as the starting dose in 84% of patients, with reductions in 7% and increases in 9% (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
The AAO revised the guidelines in 2016 to define excess doses of hydroxychloroquine as greater than 5.0 mg/kg of actual body weight (Ophthalmology. 2016;123:1386-94). Based on these new guidelines, the investigators found that 56% of 527 patients who were currently receiving hydroxychloroquine were taking excess doses, and 43% of the 527 patients were still receiving doses that are more than 50 mg in excess of the calculated target dose that is recommended by the guidelines.
“The published ophthalmology screening guidelines have had no appreciable impact on clinical practice, highlighting a persistent deficiency in patient care and a significant medico-legal risk,” they concluded.
“Our findings are particularly concerning given that choosing a proper starting dose is the single safest, simplest, and most cost-effective measure available,” they wrote.
According to the authors, there were several reasons for the widespread inaccurate dosing. Firstly, the guidelines were published in ophthalmology literature and were therefore unlikely to be seen by rheumatologists. Secondly, the formulation of the drug, currently available only in 200-mg tablet form, made it difficult to adjust doses according to a patient’s weight.
This particular issue could be addressed if the drug manufacturers expanded formulation options, or by alternating daily dosing regimens or involving compound pharmacies, they suggested.
System-wide education and prompts via electronic medical records would also go some way toward ensuring that patients are prescribed the correct dose, they added.
The study was supported by intramural research funds within the division of ophthalmology in NorthShore University Health System.
FROM OPHTHALMOLOGY
Key clinical point:
Major finding: Nearly half of the patients seen by rheumatologist in a health system were prescribed excess initial doses of hydroxychloroquine and just over half of the patients (56%) were taking excess maintenance doses, according to 2016 dosing guidelines.
Data source: A retrospective review of the electronic medical records of 554 rheumatology patients.
Disclosures: The study was supported by intramural research funds within the division of ophthalmology in NorthShore University HealthSystem.
Intermediate nature of ‘incomplete’ lupus shown in large study
People with incomplete lupus erythematosus exhibit nearly as many disease-related symptoms as do those with systemic lupus erythematosus and often receive many of the same treatments, according to findings reported from a cohort study of 3,837 patients registered with the Lupus Family Registry and Repository.
The study found that while individuals with incomplete lupus erythematosus (ILE) generally have fewer biomarkers of lupus, a subset are at risk of permanent organ damage and may transition to systemic lupus erythematosus (SLE).
“No risk stratification protocols or treatment recommendations for ILE currently exist, and clinical care is largely derived from SLE experience, in part due to the lack of consensus on what constitutes ILE,” wrote Teresa Aberle of the Oklahoma Medical Research Foundation, Oklahoma City, and her coauthors.
The treatments that ILE patients received also ran the gamut from hydroxychloroquine and steroids to immunosuppressants of varying potency.
The investigators classified participants as having ILE if they met three of the 1997 American College of Rheumatology SLE classification criteria, and were classified as having SLE if they met four or more of those criteria. Overall, 440 individuals had ILE and 3,397 had SLE, with ILE patients on average older than SLE patients and less likely to be African American (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23201).
Among those with ILE, 97.3% were ANA positive, compared with 99.3% of patients with SLE, but fewer ILE patients had ANA titers of 1:1,080 or higher (10.5% vs. 19.5%; odds ratio, 2.03; P less than .0001). ILE patients were also more than three times less likely to show anti-dsDNA antibodies than were SLE patients, but a similar percentage – approximately 42% – of both groups had anti-cardiolipin antibodies.
The researchers also examined plasma levels of B-lymphocyte stimulator, hypothesizing that lower antibody levels and fewer autoantibody specificities in ILE patients might connect with autoantibody production. In a subset of 72 ILE patients, 100 SLE patients, and 172 healthy controls, they observed that median B-lymphocyte stimulator levels were significantly lower in ILE patients, compared with SLE patients, although they were still higher than those in healthy controls. Around one-third of ILE patients had B-lymphocyte stimulator levels that exceeded the positive cutoff value, compared with 54% of SLE patients and 9% of healthy controls.
When it came to symptoms, the researchers found that each lupus classification criterion was seen in at least some ILE patients, although SLE patients were significantly more likely to have protein in urine (65.1% vs. 50%; OR, 1.9; P less than .0001), low blood counts (76.6% vs. 66%; OR, 1.7; P less than .0001), and experience seizures (19.4% vs. 14.4%; OR, 1.4; P = .012). Patients with SLE were also more likely to have pleurisy (58.2% vs. 51.9%; P = .012) and exhibit rapid hair loss (52.2% vs. 47.2%; P = .049) than were those with ILE.
Nearly one in five patients with ILE were affected by at least one clinical criterion of the disease linked to multiple indicators of disease severity, which included criteria such as serositis, renal symptoms, neurologic symptoms, hemolytic anemia, and thrombocytopenia. The investigators also noted that African Americans with ILE showed a higher rate of major clinical manifestations than did European Americans with ILE (25.7% vs. 14.9%).
“Given the association between renal disease and future transition to classified SLE, these observations suggest that patients of non-European American ancestry would likely benefit from careful monitoring and inclusion in future longitudinal studies of early or incomplete lupus,” they wrote.
While ILE patients used fewer medication types and were less likely to have used each type of medication, 65.2% of them had been treated with hydroxychloroquine and 70.7% had been treated with steroids. More than a quarter of ILE patients had used immunosuppressants and 14.8% had used major immunosuppressants, such as mycophenolate mofetil and cyclophosphamide.
“These results show that in clinical practice, ILE is often treated with hydroxychloroquine and/or steroids and occasionally may warrant treatment with potent immunosuppressants,” the authors wrote.
The authors also noted that while some patients with ILE have more severe clinical presentations and require more aggressive treatments, others with less severe disease who are at low risk of transitioning to SLE may be at risk of overtreatment.
“These results reinforce the need for new strategies to personalize disease management in ILE based on individual presentation and risk factors.”
The National Institutes of Health and the U.S. Department of Veterans Affairs supported the study. One author reported grants from pharmaceutical companies outside of the submitted work, and there were no other conflicts of interest declared.

Where the study from Ms. Aberle and her colleagues most advances knowledge of these intermediate phenotype ILE patients is in the more sophisticated interrogation of the immunologic features of ILE vs. SLE patients than has been performed in past studies. These findings are consistent with the conception of ILE as an intermediate state between health and “complete lupus” with similar, but less immune dysregulation than patients classified with SLE.

Karen H. Costenbader, MD, is with the division of rheumatology, immunology and allergy at Brigham and Women’s Hospital, Boston, and David I. Daikh, MD, is with the division of rheumatology at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23196). No conflicts of interest were declared.
Where the study from Ms. Aberle and her colleagues most advances knowledge of these intermediate phenotype ILE patients is in the more sophisticated interrogation of the immunologic features of ILE vs. SLE patients than has been performed in past studies. These findings are consistent with the conception of ILE as an intermediate state between health and “complete lupus” with similar, but less immune dysregulation than patients classified with SLE.
Karen H. Costenbader, MD, is with the division of rheumatology, immunology and allergy at Brigham and Women’s Hospital, Boston, and David I. Daikh, MD, is with the division of rheumatology at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23196). No conflicts of interest were declared.
Where the study from Ms. Aberle and her colleagues most advances knowledge of these intermediate phenotype ILE patients is in the more sophisticated interrogation of the immunologic features of ILE vs. SLE patients than has been performed in past studies. These findings are consistent with the conception of ILE as an intermediate state between health and “complete lupus” with similar, but less immune dysregulation than patients classified with SLE.
Karen H. Costenbader, MD, is with the division of rheumatology, immunology and allergy at Brigham and Women’s Hospital, Boston, and David I. Daikh, MD, is with the division of rheumatology at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23196). No conflicts of interest were declared.
People with incomplete lupus erythematosus exhibit nearly as many disease-related symptoms as do those with systemic lupus erythematosus and often receive many of the same treatments, according to findings reported from a cohort study of 3,837 patients registered with the Lupus Family Registry and Repository.
The study found that while individuals with incomplete lupus erythematosus (ILE) generally have fewer biomarkers of lupus, a subset are at risk of permanent organ damage and may transition to systemic lupus erythematosus (SLE).
“No risk stratification protocols or treatment recommendations for ILE currently exist, and clinical care is largely derived from SLE experience, in part due to the lack of consensus on what constitutes ILE,” wrote Teresa Aberle of the Oklahoma Medical Research Foundation, Oklahoma City, and her coauthors.
The treatments that ILE patients received also ran the gamut from hydroxychloroquine and steroids to immunosuppressants of varying potency.
The investigators classified participants as having ILE if they met three of the 1997 American College of Rheumatology SLE classification criteria, and were classified as having SLE if they met four or more of those criteria. Overall, 440 individuals had ILE and 3,397 had SLE, with ILE patients on average older than SLE patients and less likely to be African American (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23201).
Among those with ILE, 97.3% were ANA positive, compared with 99.3% of patients with SLE, but fewer ILE patients had ANA titers of 1:1,080 or higher (10.5% vs. 19.5%; odds ratio, 2.03; P less than .0001). ILE patients were also more than three times less likely to show anti-dsDNA antibodies than were SLE patients, but a similar percentage – approximately 42% – of both groups had anti-cardiolipin antibodies.
The researchers also examined plasma levels of B-lymphocyte stimulator, hypothesizing that lower antibody levels and fewer autoantibody specificities in ILE patients might connect with autoantibody production. In a subset of 72 ILE patients, 100 SLE patients, and 172 healthy controls, they observed that median B-lymphocyte stimulator levels were significantly lower in ILE patients, compared with SLE patients, although they were still higher than those in healthy controls. Around one-third of ILE patients had B-lymphocyte stimulator levels that exceeded the positive cutoff value, compared with 54% of SLE patients and 9% of healthy controls.
When it came to symptoms, the researchers found that each lupus classification criterion was seen in at least some ILE patients, although SLE patients were significantly more likely to have protein in urine (65.1% vs. 50%; OR, 1.9; P less than .0001), low blood counts (76.6% vs. 66%; OR, 1.7; P less than .0001), and experience seizures (19.4% vs. 14.4%; OR, 1.4; P = .012). Patients with SLE were also more likely to have pleurisy (58.2% vs. 51.9%; P = .012) and exhibit rapid hair loss (52.2% vs. 47.2%; P = .049) than were those with ILE.
Nearly one in five patients with ILE were affected by at least one clinical criterion of the disease linked to multiple indicators of disease severity, which included criteria such as serositis, renal symptoms, neurologic symptoms, hemolytic anemia, and thrombocytopenia. The investigators also noted that African Americans with ILE showed a higher rate of major clinical manifestations than did European Americans with ILE (25.7% vs. 14.9%).
“Given the association between renal disease and future transition to classified SLE, these observations suggest that patients of non-European American ancestry would likely benefit from careful monitoring and inclusion in future longitudinal studies of early or incomplete lupus,” they wrote.
While ILE patients used fewer medication types and were less likely to have used each type of medication, 65.2% of them had been treated with hydroxychloroquine and 70.7% had been treated with steroids. More than a quarter of ILE patients had used immunosuppressants and 14.8% had used major immunosuppressants, such as mycophenolate mofetil and cyclophosphamide.
“These results show that in clinical practice, ILE is often treated with hydroxychloroquine and/or steroids and occasionally may warrant treatment with potent immunosuppressants,” the authors wrote.
The authors also noted that while some patients with ILE have more severe clinical presentations and require more aggressive treatments, others with less severe disease who are at low risk of transitioning to SLE may be at risk of overtreatment.
“These results reinforce the need for new strategies to personalize disease management in ILE based on individual presentation and risk factors.”
The National Institutes of Health and the U.S. Department of Veterans Affairs supported the study. One author reported grants from pharmaceutical companies outside of the submitted work, and there were no other conflicts of interest declared.
People with incomplete lupus erythematosus exhibit nearly as many disease-related symptoms as do those with systemic lupus erythematosus and often receive many of the same treatments, according to findings reported from a cohort study of 3,837 patients registered with the Lupus Family Registry and Repository.
The study found that while individuals with incomplete lupus erythematosus (ILE) generally have fewer biomarkers of lupus, a subset are at risk of permanent organ damage and may transition to systemic lupus erythematosus (SLE).
“No risk stratification protocols or treatment recommendations for ILE currently exist, and clinical care is largely derived from SLE experience, in part due to the lack of consensus on what constitutes ILE,” wrote Teresa Aberle of the Oklahoma Medical Research Foundation, Oklahoma City, and her coauthors.
The treatments that ILE patients received also ran the gamut from hydroxychloroquine and steroids to immunosuppressants of varying potency.
The investigators classified participants as having ILE if they met three of the 1997 American College of Rheumatology SLE classification criteria, and were classified as having SLE if they met four or more of those criteria. Overall, 440 individuals had ILE and 3,397 had SLE, with ILE patients on average older than SLE patients and less likely to be African American (Arthritis Care Res. 2017 Jan 24. doi: 10.1002/acr.23201).
Among those with ILE, 97.3% were ANA positive, compared with 99.3% of patients with SLE, but fewer ILE patients had ANA titers of 1:1,080 or higher (10.5% vs. 19.5%; odds ratio, 2.03; P less than .0001). ILE patients were also more than three times less likely to show anti-dsDNA antibodies than were SLE patients, but a similar percentage – approximately 42% – of both groups had anti-cardiolipin antibodies.
The researchers also examined plasma levels of B-lymphocyte stimulator, hypothesizing that lower antibody levels and fewer autoantibody specificities in ILE patients might connect with autoantibody production. In a subset of 72 ILE patients, 100 SLE patients, and 172 healthy controls, they observed that median B-lymphocyte stimulator levels were significantly lower in ILE patients, compared with SLE patients, although they were still higher than those in healthy controls. Around one-third of ILE patients had B-lymphocyte stimulator levels that exceeded the positive cutoff value, compared with 54% of SLE patients and 9% of healthy controls.
When it came to symptoms, the researchers found that each lupus classification criterion was seen in at least some ILE patients, although SLE patients were significantly more likely to have protein in urine (65.1% vs. 50%; OR, 1.9; P less than .0001), low blood counts (76.6% vs. 66%; OR, 1.7; P less than .0001), and experience seizures (19.4% vs. 14.4%; OR, 1.4; P = .012). Patients with SLE were also more likely to have pleurisy (58.2% vs. 51.9%; P = .012) and exhibit rapid hair loss (52.2% vs. 47.2%; P = .049) than were those with ILE.
Nearly one in five patients with ILE were affected by at least one clinical criterion of the disease linked to multiple indicators of disease severity, which included criteria such as serositis, renal symptoms, neurologic symptoms, hemolytic anemia, and thrombocytopenia. The investigators also noted that African Americans with ILE showed a higher rate of major clinical manifestations than did European Americans with ILE (25.7% vs. 14.9%).
“Given the association between renal disease and future transition to classified SLE, these observations suggest that patients of non-European American ancestry would likely benefit from careful monitoring and inclusion in future longitudinal studies of early or incomplete lupus,” they wrote.
While ILE patients used fewer medication types and were less likely to have used each type of medication, 65.2% of them had been treated with hydroxychloroquine and 70.7% had been treated with steroids. More than a quarter of ILE patients had used immunosuppressants and 14.8% had used major immunosuppressants, such as mycophenolate mofetil and cyclophosphamide.
“These results show that in clinical practice, ILE is often treated with hydroxychloroquine and/or steroids and occasionally may warrant treatment with potent immunosuppressants,” the authors wrote.
The authors also noted that while some patients with ILE have more severe clinical presentations and require more aggressive treatments, others with less severe disease who are at low risk of transitioning to SLE may be at risk of overtreatment.
“These results reinforce the need for new strategies to personalize disease management in ILE based on individual presentation and risk factors.”
The National Institutes of Health and the U.S. Department of Veterans Affairs supported the study. One author reported grants from pharmaceutical companies outside of the submitted work, and there were no other conflicts of interest declared.
Key clinical point:
Major finding: Each lupus classification criterion was seen in at least some incomplete lupus erythematosus patients, although systemic lupus erythematosus patients were significantly more likely to have protein in urine, low blood counts, and experience seizures.
Data source: A cohort study of 3,837 patients registered with the Lupus Family Registry and Repository.
Disclosures: The National Institutes of Health and the U.S. Department of Veterans Affairs supported the study. One author reported grants from pharmaceutical companies outside of the submitted work, and there were no other conflicts of interest declared.
VIDEO: Dosing an important consideration when using neuromodulators in men
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR

VIDEO: Patient survey data yield useful information on acne and different contraceptives
WAILEA, HAWAII – A study that used patient-reported outcomes to assess the impact of different contraceptive methods on acne provided “fascinating results,” Lawrence F. Eichenfield, MD, said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“Progestins are present in birth control for the birth control, but they’re not usually good for the acne,” Dr. Eichenfield said in a video interview at the meeting.
Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and his colleagues reviewed patient reports from an Internet-based survey of more than 2,000 adolescent and young adult acne patients asking whether they were on any contraceptive, and if so, how they thought the contraceptive method affected their acne.
Overall, hormonal progestin-only IUDs and some progestin-only implants correlated with worse acne. Of the combined oral contraceptives, those on the OCs containing drospirenone performed best, he said. Also of interest, the triphasic OCs, with the progestin in three phases, had a better impact on the acne than did the dual ones, he added.
The review of patient-reported outcomes can not only inform clinicians on how they should prescribe hormonal therapy, but also raises awareness of the impact of contraceptives on acne in general, Dr. Eichenfield said.
The results were published last year (J Drugs Dermatol. 2016 Jun 1;15[6]:670-4).
Dr. Eichenfield disclosed relationships with Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – A study that used patient-reported outcomes to assess the impact of different contraceptive methods on acne provided “fascinating results,” Lawrence F. Eichenfield, MD, said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“Progestins are present in birth control for the birth control, but they’re not usually good for the acne,” Dr. Eichenfield said in a video interview at the meeting.
Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and his colleagues reviewed patient reports from an Internet-based survey of more than 2,000 adolescent and young adult acne patients asking whether they were on any contraceptive, and if so, how they thought the contraceptive method affected their acne.
Overall, hormonal progestin-only IUDs and some progestin-only implants correlated with worse acne. Of the combined oral contraceptives, those on the OCs containing drospirenone performed best, he said. Also of interest, the triphasic OCs, with the progestin in three phases, had a better impact on the acne than did the dual ones, he added.
The review of patient-reported outcomes can not only inform clinicians on how they should prescribe hormonal therapy, but also raises awareness of the impact of contraceptives on acne in general, Dr. Eichenfield said.
The results were published last year (J Drugs Dermatol. 2016 Jun 1;15[6]:670-4).
Dr. Eichenfield disclosed relationships with Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – A study that used patient-reported outcomes to assess the impact of different contraceptive methods on acne provided “fascinating results,” Lawrence F. Eichenfield, MD, said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“Progestins are present in birth control for the birth control, but they’re not usually good for the acne,” Dr. Eichenfield said in a video interview at the meeting.
Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and his colleagues reviewed patient reports from an Internet-based survey of more than 2,000 adolescent and young adult acne patients asking whether they were on any contraceptive, and if so, how they thought the contraceptive method affected their acne.
Overall, hormonal progestin-only IUDs and some progestin-only implants correlated with worse acne. Of the combined oral contraceptives, those on the OCs containing drospirenone performed best, he said. Also of interest, the triphasic OCs, with the progestin in three phases, had a better impact on the acne than did the dual ones, he added.
The review of patient-reported outcomes can not only inform clinicians on how they should prescribe hormonal therapy, but also raises awareness of the impact of contraceptives on acne in general, Dr. Eichenfield said.
The results were published last year (J Drugs Dermatol. 2016 Jun 1;15[6]:670-4).
Dr. Eichenfield disclosed relationships with Anacor/Pfizer, Genentech, Lilly, Regeneron/Sanofi, Medimetriks, and Otsuka.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
