User login
Simple blood test plus AI may flag early-stage Alzheimer’s disease
, raising the prospect of early intervention when effective treatments become available.
In a study, investigators used six AI methodologies, including Deep Learning, to assess blood leukocyte epigenomic biomarkers. They found more than 150 genetic differences among study participants with Alzheimer’s disease in comparison with participants who did not have Alzheimer’s disease.
All of the AI platforms were effective in predicting Alzheimer’s disease. Deep Learning’s assessment of intragenic cytosine-phosphate-guanines (CpGs) had sensitivity and specificity rates of 97%.
“It’s almost as if the leukocytes have become a newspaper to tell us, ‘This is what is going on in the brain,’ “ lead author Ray Bahado-Singh, MD, chair of the department of obstetrics and gynecology, Oakland University, Auburn Hills, Mich., said in a news release.
The researchers noted that the findings, if replicated in future studies, may help in providing Alzheimer’s disease diagnoses “much earlier” in the disease process. “The holy grail is to identify patients in the preclinical stage so effective early interventions, including new medications, can be studied and ultimately used,” Dr. Bahado-Singh said.
“This certainly isn’t the final step in Alzheimer’s research, but I think this represents a significant change in direction,” he told attendees at a press briefing.
The findings were published online March 31 in PLOS ONE.
Silver tsunami
The investigators noted that Alzheimer’s disease is often diagnosed when the disease is in its later stages, after irreversible brain damage has occurred. “There is currently no cure for the disease, and the treatment is limited to drugs that attempt to treat symptoms and have little effect on the disease’s progression,” they noted.
Coinvestigator Khaled Imam, MD, director of geriatric medicine for Beaumont Health in Michigan, pointed out that although MRI and lumbar puncture can identify Alzheimer’s disease early on, the processes are expensive and/or invasive.
“Having biomarkers in the blood ... and being able to identify [Alzheimer’s disease] years before symptoms start, hopefully we’d be able to intervene early on in the process of the disease,” Dr. Imam said.
It is estimated that the number of Americans aged 85 and older will triple by 2050. This impending “silver tsunami,” which will come with a commensurate increase in Alzheimer’s disease cases, makes it even more important to be able to diagnose the disease early on, he noted.
The study included 24 individuals with late-onset Alzheimer’s disease (70.8% women; mean age, 83 years); 24 were deemed to be “cognitively healthy” (66.7% women; mean age, 80 years). About 500 ng of genomic DNA was extracted from whole-blood samples from each participant.
The researchers used the Infinium MethylationEPIC BeadChip array, and the samples were then examined for markers of methylation that would “indicate the disease process has started,” they noted.
In addition to Deep Learning, the five other AI platforms were the Support Vector Machine, Generalized Linear Model, Prediction Analysis for Microarrays, Random Forest, and Linear Discriminant Analysis.
These platforms were used to assess leukocyte genome changes. To predict Alzheimer’s disease, the researchers also used Ingenuity Pathway Analysis.
Significant “chemical changes”
Results showed that the Alzheimer’s disease group had 152 significantly differentially methylated CpGs in 171 genes in comparison with the non-Alzheimer’s disease group (false discovery rate P value < .05).
As a whole, using intragenic and intergenic/extragenic CpGs, the AI platforms were effective in predicting who had Alzheimer’s disease (area under the curve [AUC], ≥ 0.93). Using intragenic markers, the AUC for Deep Learning was 0.99.
“We looked at close to a million different sites, and we saw some chemical changes that we know are associated with alteration or change in gene function,” Dr. Bahado-Singh said.
Altered genes that were found in the Alzheimer’s disease group included CR1L, CTSV, S1PR1, and LTB4R – all of which “have been previously linked with Alzheimer’s disease and dementia,” the researchers noted. They also found the methylated genes CTSV and PRMT5, both of which have been previously associated with cardiovascular disease.
“A significant strength of our study is the novelty, i.e. the use of blood leukocytes to accurately detect Alzheimer’s disease and also for interrogating the pathogenesis of Alzheimer’s disease,” the investigators wrote.
Dr. Bahado-Singh said that the test let them identify changes in cells in the blood, “giving us a comprehensive account not only of the fact that the brain is being affected by Alzheimer’s disease but it’s telling us what kinds of processes are going on in the brain.
“Normally you don’t have access to the brain. This gives us a simple blood test to get an ongoing reading of the course of events in the brain – and potentially tell us very early on before the onset of symptoms,” he added.
Cautiously optimistic
During the question-and-answer session following his presentation at the briefing, Dr. Bahado-Singh reiterated that they are at a very early stage in the research and were not able to make clinical recommendations at this point. However, he added, “There was evidence that DNA methylation change could likely precede the onset of abnormalities in the cells that give rise to the disease.”
Coinvestigator Stewart Graham, PhD, director of Alzheimer’s research at Beaumont Health, added that although the initial study findings led to some excitement for the team, “we have to be very conservative with what we say.”
He noted that the findings need to be replicated in a more diverse population. Still, “we’re excited at the moment and looking forward to seeing what the future results hold,” Dr. Graham said.
Dr. Bahado-Singh said that if larger studies confirm the findings and the test is viable, it would make sense to use it as a screen for individuals older than 65. He noted that because of the aging of the population, “this subset of individuals will constitute a larger and larger fraction of the population globally.”
Still early days
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that the investigators used an “interesting” diagnostic process.
“It was a unique approach to looking at and trying to understand what might be some of the biological underpinnings and using these tools and technologies to determine if they’re able to differentiate individuals with Alzheimer’s disease” from those without Alzheimer’s disease, said Dr. Snyder, who was not involved with the research.
“Ultimately, we want to know who is at greater risk, who may have some of the changing biology at the earliest time point so that we can intervene to stop the progression of the disease,” she said.
She pointed out that a number of types of biomarker tests are currently under investigation, many of which are measuring different outcomes. “And that’s what we want to see going forward. We want to have as many tools in our toolbox that allow us to accurately diagnose at that earliest time point,” Dr. Snyder said.
“At this point, [the current study] is still pretty early, so it needs to be replicated and then expanded to larger groups to really understand what they may be seeing,” she added.
Dr. Bahado-Singh, Dr. Imam, Dr. Graham, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, raising the prospect of early intervention when effective treatments become available.
In a study, investigators used six AI methodologies, including Deep Learning, to assess blood leukocyte epigenomic biomarkers. They found more than 150 genetic differences among study participants with Alzheimer’s disease in comparison with participants who did not have Alzheimer’s disease.
All of the AI platforms were effective in predicting Alzheimer’s disease. Deep Learning’s assessment of intragenic cytosine-phosphate-guanines (CpGs) had sensitivity and specificity rates of 97%.
“It’s almost as if the leukocytes have become a newspaper to tell us, ‘This is what is going on in the brain,’ “ lead author Ray Bahado-Singh, MD, chair of the department of obstetrics and gynecology, Oakland University, Auburn Hills, Mich., said in a news release.
The researchers noted that the findings, if replicated in future studies, may help in providing Alzheimer’s disease diagnoses “much earlier” in the disease process. “The holy grail is to identify patients in the preclinical stage so effective early interventions, including new medications, can be studied and ultimately used,” Dr. Bahado-Singh said.
“This certainly isn’t the final step in Alzheimer’s research, but I think this represents a significant change in direction,” he told attendees at a press briefing.
The findings were published online March 31 in PLOS ONE.
Silver tsunami
The investigators noted that Alzheimer’s disease is often diagnosed when the disease is in its later stages, after irreversible brain damage has occurred. “There is currently no cure for the disease, and the treatment is limited to drugs that attempt to treat symptoms and have little effect on the disease’s progression,” they noted.
Coinvestigator Khaled Imam, MD, director of geriatric medicine for Beaumont Health in Michigan, pointed out that although MRI and lumbar puncture can identify Alzheimer’s disease early on, the processes are expensive and/or invasive.
“Having biomarkers in the blood ... and being able to identify [Alzheimer’s disease] years before symptoms start, hopefully we’d be able to intervene early on in the process of the disease,” Dr. Imam said.
It is estimated that the number of Americans aged 85 and older will triple by 2050. This impending “silver tsunami,” which will come with a commensurate increase in Alzheimer’s disease cases, makes it even more important to be able to diagnose the disease early on, he noted.
The study included 24 individuals with late-onset Alzheimer’s disease (70.8% women; mean age, 83 years); 24 were deemed to be “cognitively healthy” (66.7% women; mean age, 80 years). About 500 ng of genomic DNA was extracted from whole-blood samples from each participant.
The researchers used the Infinium MethylationEPIC BeadChip array, and the samples were then examined for markers of methylation that would “indicate the disease process has started,” they noted.
In addition to Deep Learning, the five other AI platforms were the Support Vector Machine, Generalized Linear Model, Prediction Analysis for Microarrays, Random Forest, and Linear Discriminant Analysis.
These platforms were used to assess leukocyte genome changes. To predict Alzheimer’s disease, the researchers also used Ingenuity Pathway Analysis.
Significant “chemical changes”
Results showed that the Alzheimer’s disease group had 152 significantly differentially methylated CpGs in 171 genes in comparison with the non-Alzheimer’s disease group (false discovery rate P value < .05).
As a whole, using intragenic and intergenic/extragenic CpGs, the AI platforms were effective in predicting who had Alzheimer’s disease (area under the curve [AUC], ≥ 0.93). Using intragenic markers, the AUC for Deep Learning was 0.99.
“We looked at close to a million different sites, and we saw some chemical changes that we know are associated with alteration or change in gene function,” Dr. Bahado-Singh said.
Altered genes that were found in the Alzheimer’s disease group included CR1L, CTSV, S1PR1, and LTB4R – all of which “have been previously linked with Alzheimer’s disease and dementia,” the researchers noted. They also found the methylated genes CTSV and PRMT5, both of which have been previously associated with cardiovascular disease.
“A significant strength of our study is the novelty, i.e. the use of blood leukocytes to accurately detect Alzheimer’s disease and also for interrogating the pathogenesis of Alzheimer’s disease,” the investigators wrote.
Dr. Bahado-Singh said that the test let them identify changes in cells in the blood, “giving us a comprehensive account not only of the fact that the brain is being affected by Alzheimer’s disease but it’s telling us what kinds of processes are going on in the brain.
“Normally you don’t have access to the brain. This gives us a simple blood test to get an ongoing reading of the course of events in the brain – and potentially tell us very early on before the onset of symptoms,” he added.
Cautiously optimistic
During the question-and-answer session following his presentation at the briefing, Dr. Bahado-Singh reiterated that they are at a very early stage in the research and were not able to make clinical recommendations at this point. However, he added, “There was evidence that DNA methylation change could likely precede the onset of abnormalities in the cells that give rise to the disease.”
Coinvestigator Stewart Graham, PhD, director of Alzheimer’s research at Beaumont Health, added that although the initial study findings led to some excitement for the team, “we have to be very conservative with what we say.”
He noted that the findings need to be replicated in a more diverse population. Still, “we’re excited at the moment and looking forward to seeing what the future results hold,” Dr. Graham said.
Dr. Bahado-Singh said that if larger studies confirm the findings and the test is viable, it would make sense to use it as a screen for individuals older than 65. He noted that because of the aging of the population, “this subset of individuals will constitute a larger and larger fraction of the population globally.”
Still early days
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that the investigators used an “interesting” diagnostic process.
“It was a unique approach to looking at and trying to understand what might be some of the biological underpinnings and using these tools and technologies to determine if they’re able to differentiate individuals with Alzheimer’s disease” from those without Alzheimer’s disease, said Dr. Snyder, who was not involved with the research.
“Ultimately, we want to know who is at greater risk, who may have some of the changing biology at the earliest time point so that we can intervene to stop the progression of the disease,” she said.
She pointed out that a number of types of biomarker tests are currently under investigation, many of which are measuring different outcomes. “And that’s what we want to see going forward. We want to have as many tools in our toolbox that allow us to accurately diagnose at that earliest time point,” Dr. Snyder said.
“At this point, [the current study] is still pretty early, so it needs to be replicated and then expanded to larger groups to really understand what they may be seeing,” she added.
Dr. Bahado-Singh, Dr. Imam, Dr. Graham, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, raising the prospect of early intervention when effective treatments become available.
In a study, investigators used six AI methodologies, including Deep Learning, to assess blood leukocyte epigenomic biomarkers. They found more than 150 genetic differences among study participants with Alzheimer’s disease in comparison with participants who did not have Alzheimer’s disease.
All of the AI platforms were effective in predicting Alzheimer’s disease. Deep Learning’s assessment of intragenic cytosine-phosphate-guanines (CpGs) had sensitivity and specificity rates of 97%.
“It’s almost as if the leukocytes have become a newspaper to tell us, ‘This is what is going on in the brain,’ “ lead author Ray Bahado-Singh, MD, chair of the department of obstetrics and gynecology, Oakland University, Auburn Hills, Mich., said in a news release.
The researchers noted that the findings, if replicated in future studies, may help in providing Alzheimer’s disease diagnoses “much earlier” in the disease process. “The holy grail is to identify patients in the preclinical stage so effective early interventions, including new medications, can be studied and ultimately used,” Dr. Bahado-Singh said.
“This certainly isn’t the final step in Alzheimer’s research, but I think this represents a significant change in direction,” he told attendees at a press briefing.
The findings were published online March 31 in PLOS ONE.
Silver tsunami
The investigators noted that Alzheimer’s disease is often diagnosed when the disease is in its later stages, after irreversible brain damage has occurred. “There is currently no cure for the disease, and the treatment is limited to drugs that attempt to treat symptoms and have little effect on the disease’s progression,” they noted.
Coinvestigator Khaled Imam, MD, director of geriatric medicine for Beaumont Health in Michigan, pointed out that although MRI and lumbar puncture can identify Alzheimer’s disease early on, the processes are expensive and/or invasive.
“Having biomarkers in the blood ... and being able to identify [Alzheimer’s disease] years before symptoms start, hopefully we’d be able to intervene early on in the process of the disease,” Dr. Imam said.
It is estimated that the number of Americans aged 85 and older will triple by 2050. This impending “silver tsunami,” which will come with a commensurate increase in Alzheimer’s disease cases, makes it even more important to be able to diagnose the disease early on, he noted.
The study included 24 individuals with late-onset Alzheimer’s disease (70.8% women; mean age, 83 years); 24 were deemed to be “cognitively healthy” (66.7% women; mean age, 80 years). About 500 ng of genomic DNA was extracted from whole-blood samples from each participant.
The researchers used the Infinium MethylationEPIC BeadChip array, and the samples were then examined for markers of methylation that would “indicate the disease process has started,” they noted.
In addition to Deep Learning, the five other AI platforms were the Support Vector Machine, Generalized Linear Model, Prediction Analysis for Microarrays, Random Forest, and Linear Discriminant Analysis.
These platforms were used to assess leukocyte genome changes. To predict Alzheimer’s disease, the researchers also used Ingenuity Pathway Analysis.
Significant “chemical changes”
Results showed that the Alzheimer’s disease group had 152 significantly differentially methylated CpGs in 171 genes in comparison with the non-Alzheimer’s disease group (false discovery rate P value < .05).
As a whole, using intragenic and intergenic/extragenic CpGs, the AI platforms were effective in predicting who had Alzheimer’s disease (area under the curve [AUC], ≥ 0.93). Using intragenic markers, the AUC for Deep Learning was 0.99.
“We looked at close to a million different sites, and we saw some chemical changes that we know are associated with alteration or change in gene function,” Dr. Bahado-Singh said.
Altered genes that were found in the Alzheimer’s disease group included CR1L, CTSV, S1PR1, and LTB4R – all of which “have been previously linked with Alzheimer’s disease and dementia,” the researchers noted. They also found the methylated genes CTSV and PRMT5, both of which have been previously associated with cardiovascular disease.
“A significant strength of our study is the novelty, i.e. the use of blood leukocytes to accurately detect Alzheimer’s disease and also for interrogating the pathogenesis of Alzheimer’s disease,” the investigators wrote.
Dr. Bahado-Singh said that the test let them identify changes in cells in the blood, “giving us a comprehensive account not only of the fact that the brain is being affected by Alzheimer’s disease but it’s telling us what kinds of processes are going on in the brain.
“Normally you don’t have access to the brain. This gives us a simple blood test to get an ongoing reading of the course of events in the brain – and potentially tell us very early on before the onset of symptoms,” he added.
Cautiously optimistic
During the question-and-answer session following his presentation at the briefing, Dr. Bahado-Singh reiterated that they are at a very early stage in the research and were not able to make clinical recommendations at this point. However, he added, “There was evidence that DNA methylation change could likely precede the onset of abnormalities in the cells that give rise to the disease.”
Coinvestigator Stewart Graham, PhD, director of Alzheimer’s research at Beaumont Health, added that although the initial study findings led to some excitement for the team, “we have to be very conservative with what we say.”
He noted that the findings need to be replicated in a more diverse population. Still, “we’re excited at the moment and looking forward to seeing what the future results hold,” Dr. Graham said.
Dr. Bahado-Singh said that if larger studies confirm the findings and the test is viable, it would make sense to use it as a screen for individuals older than 65. He noted that because of the aging of the population, “this subset of individuals will constitute a larger and larger fraction of the population globally.”
Still early days
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that the investigators used an “interesting” diagnostic process.
“It was a unique approach to looking at and trying to understand what might be some of the biological underpinnings and using these tools and technologies to determine if they’re able to differentiate individuals with Alzheimer’s disease” from those without Alzheimer’s disease, said Dr. Snyder, who was not involved with the research.
“Ultimately, we want to know who is at greater risk, who may have some of the changing biology at the earliest time point so that we can intervene to stop the progression of the disease,” she said.
She pointed out that a number of types of biomarker tests are currently under investigation, many of which are measuring different outcomes. “And that’s what we want to see going forward. We want to have as many tools in our toolbox that allow us to accurately diagnose at that earliest time point,” Dr. Snyder said.
“At this point, [the current study] is still pretty early, so it needs to be replicated and then expanded to larger groups to really understand what they may be seeing,” she added.
Dr. Bahado-Singh, Dr. Imam, Dr. Graham, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PLOS ONE
Habitual fish intake may prevent frailty in RA patients
Key clinical point: Frailty is positively associated with disease activity in rheumatoid arthritis (RA), and habitual fish intake may help prevent progression of frailty and RA.
Major finding: The presence of frailty was significantly associated with the disease activity score (Disease Activity Score 28-erythrocyte sedimentation rate; odds ratio [OR], 1.70; P less than .0001). Patients who consumed fish more than twice per week had a lower prevalence of frailty than those who consumed fish twice per week or lesser (OR, 0.35; P = .00060).
Study details: The data come from a cross-sectional study of 306 female outpatients with RA from the KURAMA cohort database.
Disclosures: KURAMA cohort study was supported by AMED and a grant from the Daiichi Sankyo Co. Ltd. M. Hashimoto, R Watanabe, K Nishitani, H Ito, K Ohmura, and S Matsuda reported to receive grants and/or speaker fees from various pharmaceutical companies including Bristol-Meyers, Mitsubishi Tanabe Pharma, Asahi-Kasei Pharma, Daiichi-Sankyo, etc. Some of the authors declared no conflicts of interest.
Source: Minamino H et al. Sci Rep. 2021 Mar 3. doi: 10.1038/s41598-021-84479-0.
Key clinical point: Frailty is positively associated with disease activity in rheumatoid arthritis (RA), and habitual fish intake may help prevent progression of frailty and RA.
Major finding: The presence of frailty was significantly associated with the disease activity score (Disease Activity Score 28-erythrocyte sedimentation rate; odds ratio [OR], 1.70; P less than .0001). Patients who consumed fish more than twice per week had a lower prevalence of frailty than those who consumed fish twice per week or lesser (OR, 0.35; P = .00060).
Study details: The data come from a cross-sectional study of 306 female outpatients with RA from the KURAMA cohort database.
Disclosures: KURAMA cohort study was supported by AMED and a grant from the Daiichi Sankyo Co. Ltd. M. Hashimoto, R Watanabe, K Nishitani, H Ito, K Ohmura, and S Matsuda reported to receive grants and/or speaker fees from various pharmaceutical companies including Bristol-Meyers, Mitsubishi Tanabe Pharma, Asahi-Kasei Pharma, Daiichi-Sankyo, etc. Some of the authors declared no conflicts of interest.
Source: Minamino H et al. Sci Rep. 2021 Mar 3. doi: 10.1038/s41598-021-84479-0.
Key clinical point: Frailty is positively associated with disease activity in rheumatoid arthritis (RA), and habitual fish intake may help prevent progression of frailty and RA.
Major finding: The presence of frailty was significantly associated with the disease activity score (Disease Activity Score 28-erythrocyte sedimentation rate; odds ratio [OR], 1.70; P less than .0001). Patients who consumed fish more than twice per week had a lower prevalence of frailty than those who consumed fish twice per week or lesser (OR, 0.35; P = .00060).
Study details: The data come from a cross-sectional study of 306 female outpatients with RA from the KURAMA cohort database.
Disclosures: KURAMA cohort study was supported by AMED and a grant from the Daiichi Sankyo Co. Ltd. M. Hashimoto, R Watanabe, K Nishitani, H Ito, K Ohmura, and S Matsuda reported to receive grants and/or speaker fees from various pharmaceutical companies including Bristol-Meyers, Mitsubishi Tanabe Pharma, Asahi-Kasei Pharma, Daiichi-Sankyo, etc. Some of the authors declared no conflicts of interest.
Source: Minamino H et al. Sci Rep. 2021 Mar 3. doi: 10.1038/s41598-021-84479-0.
RA tied to worse long-term outcomes after myocardial infarction
Key clinical point: Rheumatoid arthritis (RA) is associated with poor long-term prognosis after myocardial infarction (MI).
Major finding: At 14-year follow-up after MI, the cumulative all-cause mortality risk was significantly higher among patients with vs. without RA (80.4% vs. 72.3%; hazard ratio [HR], 1.25; P less than .0001). Patients with RA had a higher risk for new MI (HR, 1.22; P = .0001) and revascularization (HR, 1.27; P = .002) after discharge from index MI.
Study details: This was a nationwide, multicenter, cohort register study of real-life MI patients with RA (n=1,614) retrospectively compared with propensity score-matched MI patients without RA (n=8,070).
Disclosures: This study was supported by grant funding from the Finnish Cultural Foundation, the Paulo Foundation, and the Finnish Governmental VTR-funding. A Palomäki, AM Kerola, M Malmberg, and V Kytö reported relevant relationships with various pharmaceutical companies and/or research organizations. The other author declared no conflicts of interest.
Source: Palomäki A et al. Rheumatology (Oxford). 2021 Mar 1. doi: 10.1093/rheumatology/keab204.
Key clinical point: Rheumatoid arthritis (RA) is associated with poor long-term prognosis after myocardial infarction (MI).
Major finding: At 14-year follow-up after MI, the cumulative all-cause mortality risk was significantly higher among patients with vs. without RA (80.4% vs. 72.3%; hazard ratio [HR], 1.25; P less than .0001). Patients with RA had a higher risk for new MI (HR, 1.22; P = .0001) and revascularization (HR, 1.27; P = .002) after discharge from index MI.
Study details: This was a nationwide, multicenter, cohort register study of real-life MI patients with RA (n=1,614) retrospectively compared with propensity score-matched MI patients without RA (n=8,070).
Disclosures: This study was supported by grant funding from the Finnish Cultural Foundation, the Paulo Foundation, and the Finnish Governmental VTR-funding. A Palomäki, AM Kerola, M Malmberg, and V Kytö reported relevant relationships with various pharmaceutical companies and/or research organizations. The other author declared no conflicts of interest.
Source: Palomäki A et al. Rheumatology (Oxford). 2021 Mar 1. doi: 10.1093/rheumatology/keab204.
Key clinical point: Rheumatoid arthritis (RA) is associated with poor long-term prognosis after myocardial infarction (MI).
Major finding: At 14-year follow-up after MI, the cumulative all-cause mortality risk was significantly higher among patients with vs. without RA (80.4% vs. 72.3%; hazard ratio [HR], 1.25; P less than .0001). Patients with RA had a higher risk for new MI (HR, 1.22; P = .0001) and revascularization (HR, 1.27; P = .002) after discharge from index MI.
Study details: This was a nationwide, multicenter, cohort register study of real-life MI patients with RA (n=1,614) retrospectively compared with propensity score-matched MI patients without RA (n=8,070).
Disclosures: This study was supported by grant funding from the Finnish Cultural Foundation, the Paulo Foundation, and the Finnish Governmental VTR-funding. A Palomäki, AM Kerola, M Malmberg, and V Kytö reported relevant relationships with various pharmaceutical companies and/or research organizations. The other author declared no conflicts of interest.
Source: Palomäki A et al. Rheumatology (Oxford). 2021 Mar 1. doi: 10.1093/rheumatology/keab204.
MBDA score not sufficiently responsive to assess RA disease activity
Key clinical point: Multi-Biomarker Disease Activity (MBDA) should not be preferred to assess clinically meaningful improvements in disease activity after repository corticotropin injection (RCI) therapy in patients with active rheumatoid arthritis (RA).
Major finding: RCI-mediated improvements in Disease Activity Score 28-erythrocyte sedimentation rate and Clinical Disease Activity Index scores suggested clinically meaningful improvement with more than 84% of patients meeting the minimal clinically important difference/minimally important difference criteria, which ranged from 26.3% to 34.7% for MBDA.
Study details: The data come from a multicenter, randomized, placebo-controlled study of 259 patients with active RA despite treatment with stable glucocorticoid dose and 1 or 2 disease-modifying anti-rheumatic drugs. Patients achieving low disease activity during open-label period were randomly assigned to either 80 U of RCI (n=77) or placebo (n=76) during the 12-week double-blind period.
Disclosures: This study was funded by Mallinckrodt Pharmaceuticals. R Fleischmann, DE Furst, and OG Segurado reported receiving clinical trial grants and consulting fees from various pharmaceutical companies including Mallinckrodt Pharmaceuticals. J Liu and J Zhu declared being employees of Mallinckrodt Pharmaceuticals.
Source: Fleischmann R et al. Arthritis Care Res (Hoboken). 2021 Feb 28. doi: 10.1002/acr.24583.
Key clinical point: Multi-Biomarker Disease Activity (MBDA) should not be preferred to assess clinically meaningful improvements in disease activity after repository corticotropin injection (RCI) therapy in patients with active rheumatoid arthritis (RA).
Major finding: RCI-mediated improvements in Disease Activity Score 28-erythrocyte sedimentation rate and Clinical Disease Activity Index scores suggested clinically meaningful improvement with more than 84% of patients meeting the minimal clinically important difference/minimally important difference criteria, which ranged from 26.3% to 34.7% for MBDA.
Study details: The data come from a multicenter, randomized, placebo-controlled study of 259 patients with active RA despite treatment with stable glucocorticoid dose and 1 or 2 disease-modifying anti-rheumatic drugs. Patients achieving low disease activity during open-label period were randomly assigned to either 80 U of RCI (n=77) or placebo (n=76) during the 12-week double-blind period.
Disclosures: This study was funded by Mallinckrodt Pharmaceuticals. R Fleischmann, DE Furst, and OG Segurado reported receiving clinical trial grants and consulting fees from various pharmaceutical companies including Mallinckrodt Pharmaceuticals. J Liu and J Zhu declared being employees of Mallinckrodt Pharmaceuticals.
Source: Fleischmann R et al. Arthritis Care Res (Hoboken). 2021 Feb 28. doi: 10.1002/acr.24583.
Key clinical point: Multi-Biomarker Disease Activity (MBDA) should not be preferred to assess clinically meaningful improvements in disease activity after repository corticotropin injection (RCI) therapy in patients with active rheumatoid arthritis (RA).
Major finding: RCI-mediated improvements in Disease Activity Score 28-erythrocyte sedimentation rate and Clinical Disease Activity Index scores suggested clinically meaningful improvement with more than 84% of patients meeting the minimal clinically important difference/minimally important difference criteria, which ranged from 26.3% to 34.7% for MBDA.
Study details: The data come from a multicenter, randomized, placebo-controlled study of 259 patients with active RA despite treatment with stable glucocorticoid dose and 1 or 2 disease-modifying anti-rheumatic drugs. Patients achieving low disease activity during open-label period were randomly assigned to either 80 U of RCI (n=77) or placebo (n=76) during the 12-week double-blind period.
Disclosures: This study was funded by Mallinckrodt Pharmaceuticals. R Fleischmann, DE Furst, and OG Segurado reported receiving clinical trial grants and consulting fees from various pharmaceutical companies including Mallinckrodt Pharmaceuticals. J Liu and J Zhu declared being employees of Mallinckrodt Pharmaceuticals.
Source: Fleischmann R et al. Arthritis Care Res (Hoboken). 2021 Feb 28. doi: 10.1002/acr.24583.
Durability of tocilizumab response in patients with RA
Key clinical point: Median durability of tocilizumab (TCZ) response was more than 3 years when measured as maintenance of minimum clinically important difference (MCID) in Clinical Disease Activity Index (CDAI) score in patients with RA initiating TCZ.
Major finding: Overall, durability of response among patients who initiated TCZ and achieved MCID in CDAI remained more than 50% after 3 years of follow-up. The proportion of patients maintaining MCID durability at 1, 2, and 3 years was 64.4% (95% CI, 59.2%-69.6%), 56.0% (95% CI, 50.0%-62.0%), and 51.8% (95% CI, 44.7%-58.9%), respectively.
Study details: The findings are from an observational study of 1,789 patients with RA who initiated TCZ and were enrolled in the US-based Corrona RA Registry.
Disclosures: This study was sponsored by Corrona LLC, and the analysis was funded by Genentech, Inc. DA Pappas, T Blachley, and K Emeanuru declared being employees and/or shareholders of Corrona, LLC. JH Best, WG Reiss, and S Zlotnick declared being current/former employees and/or shareholders of Genentech, Inc.
Source: Pappas DA et al. Rheumatol Ther. 2021 Feb 25. doi: 10.1007/s40744-021-00285-0.
Key clinical point: Median durability of tocilizumab (TCZ) response was more than 3 years when measured as maintenance of minimum clinically important difference (MCID) in Clinical Disease Activity Index (CDAI) score in patients with RA initiating TCZ.
Major finding: Overall, durability of response among patients who initiated TCZ and achieved MCID in CDAI remained more than 50% after 3 years of follow-up. The proportion of patients maintaining MCID durability at 1, 2, and 3 years was 64.4% (95% CI, 59.2%-69.6%), 56.0% (95% CI, 50.0%-62.0%), and 51.8% (95% CI, 44.7%-58.9%), respectively.
Study details: The findings are from an observational study of 1,789 patients with RA who initiated TCZ and were enrolled in the US-based Corrona RA Registry.
Disclosures: This study was sponsored by Corrona LLC, and the analysis was funded by Genentech, Inc. DA Pappas, T Blachley, and K Emeanuru declared being employees and/or shareholders of Corrona, LLC. JH Best, WG Reiss, and S Zlotnick declared being current/former employees and/or shareholders of Genentech, Inc.
Source: Pappas DA et al. Rheumatol Ther. 2021 Feb 25. doi: 10.1007/s40744-021-00285-0.
Key clinical point: Median durability of tocilizumab (TCZ) response was more than 3 years when measured as maintenance of minimum clinically important difference (MCID) in Clinical Disease Activity Index (CDAI) score in patients with RA initiating TCZ.
Major finding: Overall, durability of response among patients who initiated TCZ and achieved MCID in CDAI remained more than 50% after 3 years of follow-up. The proportion of patients maintaining MCID durability at 1, 2, and 3 years was 64.4% (95% CI, 59.2%-69.6%), 56.0% (95% CI, 50.0%-62.0%), and 51.8% (95% CI, 44.7%-58.9%), respectively.
Study details: The findings are from an observational study of 1,789 patients with RA who initiated TCZ and were enrolled in the US-based Corrona RA Registry.
Disclosures: This study was sponsored by Corrona LLC, and the analysis was funded by Genentech, Inc. DA Pappas, T Blachley, and K Emeanuru declared being employees and/or shareholders of Corrona, LLC. JH Best, WG Reiss, and S Zlotnick declared being current/former employees and/or shareholders of Genentech, Inc.
Source: Pappas DA et al. Rheumatol Ther. 2021 Feb 25. doi: 10.1007/s40744-021-00285-0.
Additional iguratimod may allow tapering MTX dose in RA with remission
Key clinical point: The addition of iguratimod (IGU) can effectively reduce methotrexate (MTX) dose required by rheumatoid arthritis (RA) patients with long-term clinical remission.
Major finding: MTX dose could be reduced from 8.6±2.4 mg/week to 4.7±2.2 mg/week at 36 weeks. Despite MTX dose reduction, disease activity score 28-erythrocyte sedimentation rate was maintained at 1.48 at baseline and 1.69 at 36 weeks (P = .911). Other than drug discontinuation by 2 patients in the IGU addition group, no other adverse events were observed.
Study details: Findings are from a prospective analysis of 47 patients with RA who had sustained clinical remission with MTX for more than 24 weeks. Patients either continued constant MTX dose (n=25) or were treated with additional IGU and tapered MTX dose (n=22).
Disclosures: No source of funding was declared. The authors declared no conflicts of interest.
Source: Yoshikawa A et al. Mod Rheumatol. 2021 Mar 16. doi: 10.1080/14397595.2021.1892945.
Key clinical point: The addition of iguratimod (IGU) can effectively reduce methotrexate (MTX) dose required by rheumatoid arthritis (RA) patients with long-term clinical remission.
Major finding: MTX dose could be reduced from 8.6±2.4 mg/week to 4.7±2.2 mg/week at 36 weeks. Despite MTX dose reduction, disease activity score 28-erythrocyte sedimentation rate was maintained at 1.48 at baseline and 1.69 at 36 weeks (P = .911). Other than drug discontinuation by 2 patients in the IGU addition group, no other adverse events were observed.
Study details: Findings are from a prospective analysis of 47 patients with RA who had sustained clinical remission with MTX for more than 24 weeks. Patients either continued constant MTX dose (n=25) or were treated with additional IGU and tapered MTX dose (n=22).
Disclosures: No source of funding was declared. The authors declared no conflicts of interest.
Source: Yoshikawa A et al. Mod Rheumatol. 2021 Mar 16. doi: 10.1080/14397595.2021.1892945.
Key clinical point: The addition of iguratimod (IGU) can effectively reduce methotrexate (MTX) dose required by rheumatoid arthritis (RA) patients with long-term clinical remission.
Major finding: MTX dose could be reduced from 8.6±2.4 mg/week to 4.7±2.2 mg/week at 36 weeks. Despite MTX dose reduction, disease activity score 28-erythrocyte sedimentation rate was maintained at 1.48 at baseline and 1.69 at 36 weeks (P = .911). Other than drug discontinuation by 2 patients in the IGU addition group, no other adverse events were observed.
Study details: Findings are from a prospective analysis of 47 patients with RA who had sustained clinical remission with MTX for more than 24 weeks. Patients either continued constant MTX dose (n=25) or were treated with additional IGU and tapered MTX dose (n=22).
Disclosures: No source of funding was declared. The authors declared no conflicts of interest.
Source: Yoshikawa A et al. Mod Rheumatol. 2021 Mar 16. doi: 10.1080/14397595.2021.1892945.
JAK inhibitors vs. rituximab in patients with RA and pulmonary disease
Key clinical point: Janus kinase inhibitors (JAKis: baricitinib or tofacitinib) vs. rituximab for the treatment of rheumatoid arthritis (RA) in patients with concurrent interstitial lung disease (ILD) or bronchiectasis did not increase the rate of hospitalization or mortality because of a respiratory cause.
Major finding: Respiratory events were reported in 5 patients treated with JAKi (18%; 7 hospitalizations, 2 of whom died) and 4 patients treated with rituximab (21%; 4 hospitalizations, 1 of whom died). Respiratory event survival (hazard ratio [HR], 1.38; P = .64) and the rate of drug discontinuation HR, 1.9; P = .251) did not differ significantly between groups.
Study details: A retrospective analysis of patients with RA and concurrent ILD or bronchiectasis who received JAKis (n=28: baricitinib, n=26; tofacitinib, n=2) or rituximab (n=19) for a mean of 1.1 and 2.14 years, respectively.
Disclosures: The study did not receive any funding. The lead author received sponsorship from Lilly and Pfizer to attend educational conferences. The other authors declared no conflicts of interest.
Citation: Cronin O et al. Rheumatol Int. 2021 Mar 15. doi: 10.1007/s00296-021-04835-1.
Key clinical point: Janus kinase inhibitors (JAKis: baricitinib or tofacitinib) vs. rituximab for the treatment of rheumatoid arthritis (RA) in patients with concurrent interstitial lung disease (ILD) or bronchiectasis did not increase the rate of hospitalization or mortality because of a respiratory cause.
Major finding: Respiratory events were reported in 5 patients treated with JAKi (18%; 7 hospitalizations, 2 of whom died) and 4 patients treated with rituximab (21%; 4 hospitalizations, 1 of whom died). Respiratory event survival (hazard ratio [HR], 1.38; P = .64) and the rate of drug discontinuation HR, 1.9; P = .251) did not differ significantly between groups.
Study details: A retrospective analysis of patients with RA and concurrent ILD or bronchiectasis who received JAKis (n=28: baricitinib, n=26; tofacitinib, n=2) or rituximab (n=19) for a mean of 1.1 and 2.14 years, respectively.
Disclosures: The study did not receive any funding. The lead author received sponsorship from Lilly and Pfizer to attend educational conferences. The other authors declared no conflicts of interest.
Citation: Cronin O et al. Rheumatol Int. 2021 Mar 15. doi: 10.1007/s00296-021-04835-1.
Key clinical point: Janus kinase inhibitors (JAKis: baricitinib or tofacitinib) vs. rituximab for the treatment of rheumatoid arthritis (RA) in patients with concurrent interstitial lung disease (ILD) or bronchiectasis did not increase the rate of hospitalization or mortality because of a respiratory cause.
Major finding: Respiratory events were reported in 5 patients treated with JAKi (18%; 7 hospitalizations, 2 of whom died) and 4 patients treated with rituximab (21%; 4 hospitalizations, 1 of whom died). Respiratory event survival (hazard ratio [HR], 1.38; P = .64) and the rate of drug discontinuation HR, 1.9; P = .251) did not differ significantly between groups.
Study details: A retrospective analysis of patients with RA and concurrent ILD or bronchiectasis who received JAKis (n=28: baricitinib, n=26; tofacitinib, n=2) or rituximab (n=19) for a mean of 1.1 and 2.14 years, respectively.
Disclosures: The study did not receive any funding. The lead author received sponsorship from Lilly and Pfizer to attend educational conferences. The other authors declared no conflicts of interest.
Citation: Cronin O et al. Rheumatol Int. 2021 Mar 15. doi: 10.1007/s00296-021-04835-1.
Peficitinib safe and effective for long-term management of RA
Key clinical point: Peficitinib (ASP015K) showed improvement in clinical outcomes, which was maintained throughout the treatment duration of 32 months along with a generally tolerable safety profile in patients with rheumatoid arthritis (RA).
Major finding: The American College of Rheumatology (ACR)20, ACR50, and ACR70 response rates were maintained throughout from baseline (71.6%, 52.1%, and 34.7%, respectively) to the end of treatment (78.7%, 63.3%, and 44.1%, respectively). Treatment-emergent adverse events, mostly grade 1 or 2 in severity, were experienced by 94.4% of patients, leading to drug discontinuation in 16.6% of patients.
Study details: Findings are from the final analysis of an open-label long-term extension study involving 843 Asian patients with RA who previously completed phase 2b and phase 3 studies of peficitinib.
Disclosures: This work was funded by the Astellas Pharma, Inc. The authors including the lead author reported receiving grants, speaker’s fees, consultancy fees, personal fees, and/or honoraria from various sources including Astellas Pharma, Inc. Four of the authors reported being employees of Astellas Pharma, Inc.
Source: Takeuchi T et al. Rheumatol Ther. 2021 Mar 3. doi: 10.1007/s40744-021-00280-5.
Key clinical point: Peficitinib (ASP015K) showed improvement in clinical outcomes, which was maintained throughout the treatment duration of 32 months along with a generally tolerable safety profile in patients with rheumatoid arthritis (RA).
Major finding: The American College of Rheumatology (ACR)20, ACR50, and ACR70 response rates were maintained throughout from baseline (71.6%, 52.1%, and 34.7%, respectively) to the end of treatment (78.7%, 63.3%, and 44.1%, respectively). Treatment-emergent adverse events, mostly grade 1 or 2 in severity, were experienced by 94.4% of patients, leading to drug discontinuation in 16.6% of patients.
Study details: Findings are from the final analysis of an open-label long-term extension study involving 843 Asian patients with RA who previously completed phase 2b and phase 3 studies of peficitinib.
Disclosures: This work was funded by the Astellas Pharma, Inc. The authors including the lead author reported receiving grants, speaker’s fees, consultancy fees, personal fees, and/or honoraria from various sources including Astellas Pharma, Inc. Four of the authors reported being employees of Astellas Pharma, Inc.
Source: Takeuchi T et al. Rheumatol Ther. 2021 Mar 3. doi: 10.1007/s40744-021-00280-5.
Key clinical point: Peficitinib (ASP015K) showed improvement in clinical outcomes, which was maintained throughout the treatment duration of 32 months along with a generally tolerable safety profile in patients with rheumatoid arthritis (RA).
Major finding: The American College of Rheumatology (ACR)20, ACR50, and ACR70 response rates were maintained throughout from baseline (71.6%, 52.1%, and 34.7%, respectively) to the end of treatment (78.7%, 63.3%, and 44.1%, respectively). Treatment-emergent adverse events, mostly grade 1 or 2 in severity, were experienced by 94.4% of patients, leading to drug discontinuation in 16.6% of patients.
Study details: Findings are from the final analysis of an open-label long-term extension study involving 843 Asian patients with RA who previously completed phase 2b and phase 3 studies of peficitinib.
Disclosures: This work was funded by the Astellas Pharma, Inc. The authors including the lead author reported receiving grants, speaker’s fees, consultancy fees, personal fees, and/or honoraria from various sources including Astellas Pharma, Inc. Four of the authors reported being employees of Astellas Pharma, Inc.
Source: Takeuchi T et al. Rheumatol Ther. 2021 Mar 3. doi: 10.1007/s40744-021-00280-5.
Sustained remission more likely with biological vs. triple therapy after inadequate response to MTX
Key clinical point: Patients with early rheumatoid arthritis (RA) who initiated biological vs. triple therapy after inadequate response to methotrexate (MTX) were more likely to achieve sustained remission (SR).
Major finding: Patients initiating biological vs. triple therapy were more likely to achieve short-term and long-term SR at 1 year (adjusted odds ratio [aOR], 1.79; 95% confidence interval [CI], 1.18-2.71 and aOR, 1.86; 95% CI, 1.00-3.48, respectively) and 2 years (aOR, 1.92; 95% CI, 1.21-3.06 and aOR, 1.62; 95% CI, 0.94-2.79, respectively) from treatment initiation.
Study details: Findings are from an analysis of 1,502 patients with relatively early RA who initiated biological (biological disease-modifying antirheumatic drugs+MTX; n=1,155) or triple (MTX+sulfasalazine+hydroxychloroquine/chloroquine; n=347) therapy as the first treatment strategy after inadequate response to MTX monotherapy.
Disclosures: This work funded by the Swedish Rheumatism Association, the Medical Faculty of Lund University, Alfred Österlund ́s Foundation, Greta and Johan Kock ́s foundation, the King Gustaf V Foundation, Lund University Hospital, Professor Nanna Svartz Foundation, and Anna-Greta Crafoord Foundation. The authors declared no conflicts of interest.
Source: Källmark H et al. Arthritis Rheumatol. 2021 Mar 7. doi: 10.1002/art.41720.
Key clinical point: Patients with early rheumatoid arthritis (RA) who initiated biological vs. triple therapy after inadequate response to methotrexate (MTX) were more likely to achieve sustained remission (SR).
Major finding: Patients initiating biological vs. triple therapy were more likely to achieve short-term and long-term SR at 1 year (adjusted odds ratio [aOR], 1.79; 95% confidence interval [CI], 1.18-2.71 and aOR, 1.86; 95% CI, 1.00-3.48, respectively) and 2 years (aOR, 1.92; 95% CI, 1.21-3.06 and aOR, 1.62; 95% CI, 0.94-2.79, respectively) from treatment initiation.
Study details: Findings are from an analysis of 1,502 patients with relatively early RA who initiated biological (biological disease-modifying antirheumatic drugs+MTX; n=1,155) or triple (MTX+sulfasalazine+hydroxychloroquine/chloroquine; n=347) therapy as the first treatment strategy after inadequate response to MTX monotherapy.
Disclosures: This work funded by the Swedish Rheumatism Association, the Medical Faculty of Lund University, Alfred Österlund ́s Foundation, Greta and Johan Kock ́s foundation, the King Gustaf V Foundation, Lund University Hospital, Professor Nanna Svartz Foundation, and Anna-Greta Crafoord Foundation. The authors declared no conflicts of interest.
Source: Källmark H et al. Arthritis Rheumatol. 2021 Mar 7. doi: 10.1002/art.41720.
Key clinical point: Patients with early rheumatoid arthritis (RA) who initiated biological vs. triple therapy after inadequate response to methotrexate (MTX) were more likely to achieve sustained remission (SR).
Major finding: Patients initiating biological vs. triple therapy were more likely to achieve short-term and long-term SR at 1 year (adjusted odds ratio [aOR], 1.79; 95% confidence interval [CI], 1.18-2.71 and aOR, 1.86; 95% CI, 1.00-3.48, respectively) and 2 years (aOR, 1.92; 95% CI, 1.21-3.06 and aOR, 1.62; 95% CI, 0.94-2.79, respectively) from treatment initiation.
Study details: Findings are from an analysis of 1,502 patients with relatively early RA who initiated biological (biological disease-modifying antirheumatic drugs+MTX; n=1,155) or triple (MTX+sulfasalazine+hydroxychloroquine/chloroquine; n=347) therapy as the first treatment strategy after inadequate response to MTX monotherapy.
Disclosures: This work funded by the Swedish Rheumatism Association, the Medical Faculty of Lund University, Alfred Österlund ́s Foundation, Greta and Johan Kock ́s foundation, the King Gustaf V Foundation, Lund University Hospital, Professor Nanna Svartz Foundation, and Anna-Greta Crafoord Foundation. The authors declared no conflicts of interest.
Source: Källmark H et al. Arthritis Rheumatol. 2021 Mar 7. doi: 10.1002/art.41720.
Vesicles and Bullae on the Leg
The Diagnosis: Cutaneous B-cell Lymphoma
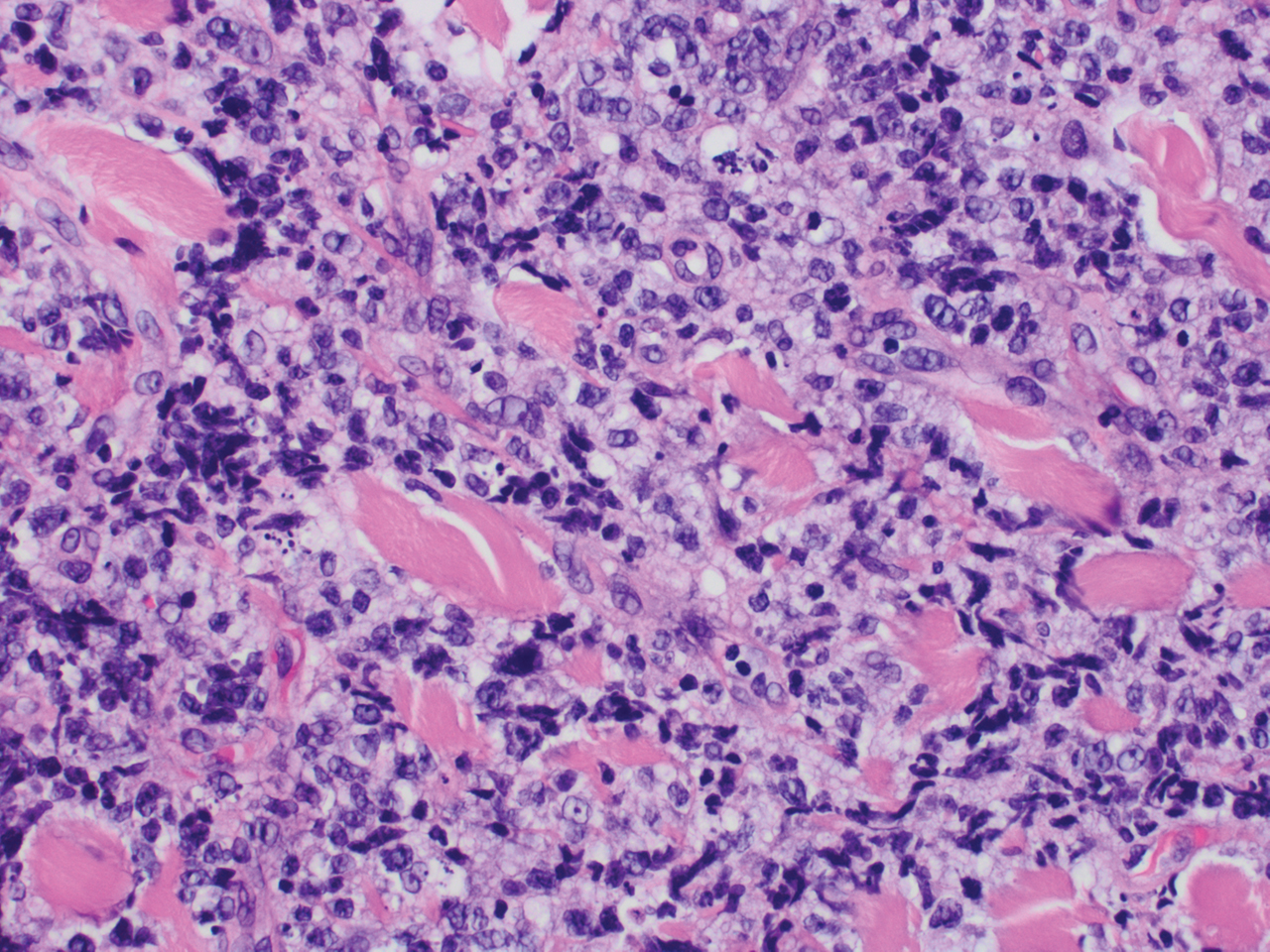
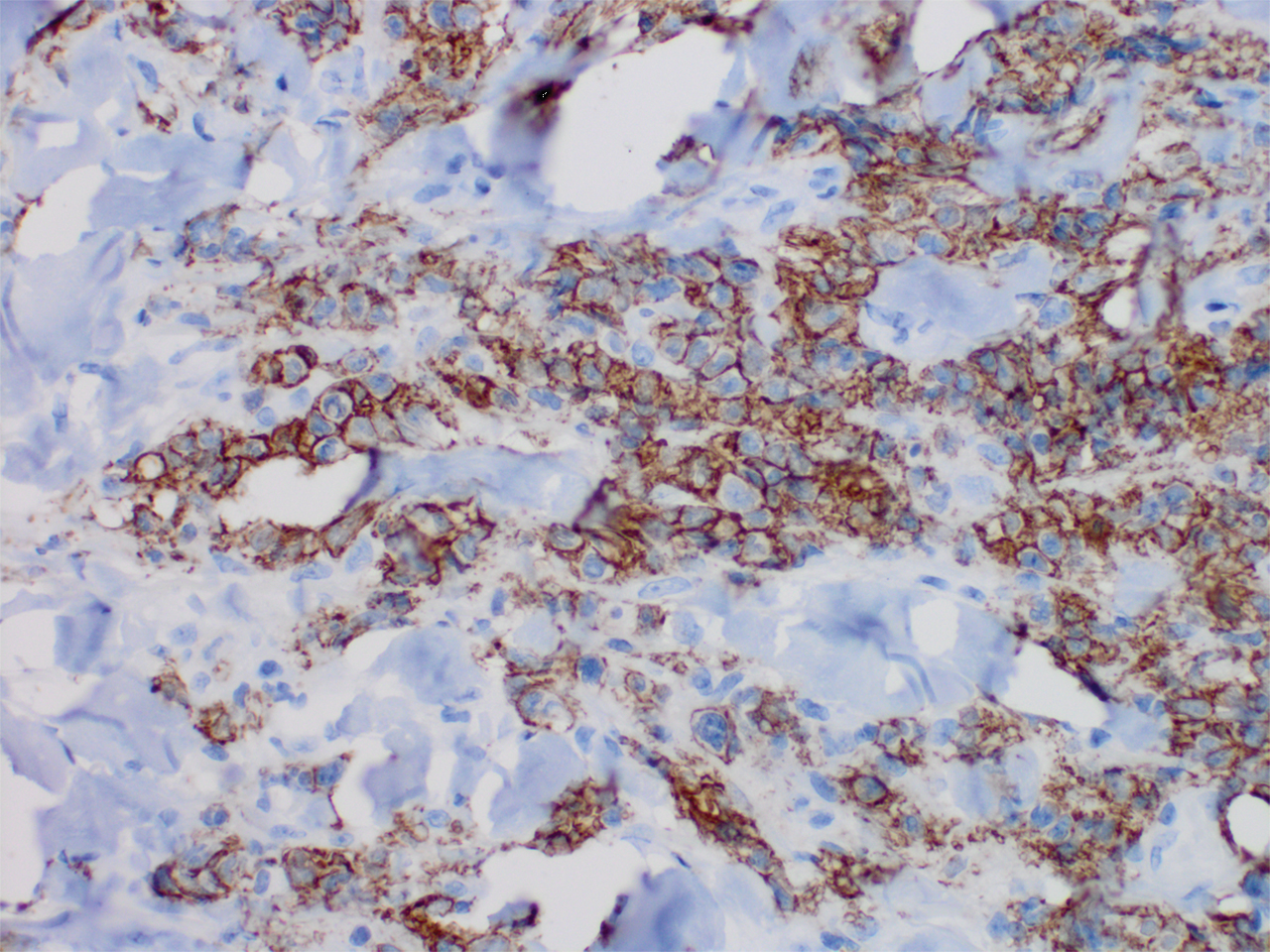
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.
The Diagnosis: Cutaneous B-cell Lymphoma
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
The Diagnosis: Cutaneous B-cell Lymphoma
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.

A 60-year-old man presented to the emergency department with slowly progressing edema of the lower legs of 3 months’ duration. In the week prior to presentation to the emergency department, he noticed a sudden eruption of vesicles and bullae on the right leg that drained clear fluid and healed with brown crust. The lesions were associated with mild burning, pruritus, and pain. He denied fever, chills, recent travel, or injury. His medical history was notable for poorly controlled diabetes mellitus, congestive heart failure, hypertension, chronic kidney disease, hyperlipidemia, and chronic anemia. Physical examination revealed multiple scattered erythematous vesicles and bullae on the right leg on a background of hyperpigmentation. Bilateral 2+ pitting edema of the legs also was present. A punch biopsy of a lesion was performed.
