User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Rare Neurological Disease Special Report

Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
COVID-19 update: Transmission 5% or less among close contacts
The transmission rate of coronavirus disease 2019 (COVID-19) was 1%-5% among 38,000 Chinese people in close contact with infected patients, according to the chief epidemiologist of the Chinese Centers for Disease Control and Prevention, Beijing, Zunyou Wu, MD, PhD, who gave an update on the epidemic at the Conference on Retroviruses & Opportunistic Infections.
The rate of spread to family members – the driver of the infection in China – was 10% early in the outbreak, but fell to 3% with quicker recognition and isolation. The overall numbers are lower than might have been expected, and an important insight for clinicians trying to contain the outbreak in the United States.
, but their ability to spread the infection dropped after that, Dr. Wu and others said at a special COVID-19 session at the meeting, which was scheduled to be in Boston, but was held online instead because of concerns about spreading the virus. The session has been posted.
Transmission from presymptomatic people is rare. Shedding persists to some degree for 7-12 days in mild/moderate cases, but 2 weeks or more in severe cases.
Dr. Wu said the numbers in China are moving in the right direction, which means that containment efforts there have worked.
The virus emerged in Wuhan, the capital of Hubei province in central China, in connection with a wildlife food market in December 2019. Bats are thought to be the reservoir, with perhaps an intermediate step between civet cats and raccoon dogs. Officials shut down the market.
Essentially, the entire population of China, more than a billion people, was told to stay home for 10 days to interrupt the transmission cycle after the virus spread throughout the country in a few weeks, and almost 60 million people in Hubei were put behind a cordon sanitaire, where they have been for 50 days and will remain “for a while,” Dr. Wu said.
It’s led to a steep drop in new cases and deaths in China since mid-February; both are now more common outside China than inside, and international numbers are lower than they were at the peak in China.
Meanwhile, there’s been no evidence of perinatal transmission; the virus has not been detected in amniotic fluid, cord blood, neonatal throat swabs, or breast milk. Maternal morbidity appears to be similar to uninfected women. “The data around pregnancy are reassuring,” said John Brooks, MD, chief medical officers for HIV/AIDS prevention at the Centers for Disease Control and Prevention, Atlanta, who has been involved with CDC’s containment efforts.
There’s no data yet for immunocompromised people, but for people with HIV, he said, “we think the risk of severe illness would be greater” with lower CD4 counts and unsuppressed viral loads. “People living with HIV should take precautions against this new virus,” including having at least a 30-day supply of HIV medications; keeping up flu and pneumonia vaccinations; and having a care plan if quarantined. Setting up telemedicine might be a good idea.
The usual incubation period for COVID-19 is 4-6 days but can be longer. Recovery time is about 2 weeks in mild cases and 3-6 weeks in more severe cases. People who die do so within 2 months of symptom onset.
The most common symptoms among hospitalized patients in China are fever, dry cough, fatigue, and headache. Truly asymptomatic cases are not common; most go on to develop symptoms. There have been reports of diarrhea before other symptoms by a day or two, but it’s probably a red herring. The virus has been isolated from stool, but there is no evidence of fecal-oral transmission, Dr. Wu said.
Eighty percent of COVID-19 cases are mild or moderate and most patients recover spontaneously, especially middle aged and younger people. There is no meaningful difference in distribution between the sexes.
There are limited pediatric data perhaps due to underreporting, “but we know [children] experience milder illness than adults,” the CDC’s Dr. Brooks said.
He pegged the latest case fatality estimate at 0.5% to 3.5%, which is considerably higher than seasonal flu, but might well drop as more mild cases are detected and added to the denominator, he said.
For now, death rates top 5% in adults over 60 years old and climb further with increasing age, approaching 16% in people 80 years or older. Patients with hypertension, diabetes, cardiovascular disease, and chronic respiratory illness are at increased risk. The ultimate cause of death is acute respiratory distress syndrome, said Ralph Baric, PhD, a coronavirus expert and epidemiology professor at the University of North Carolina, Chapel Hill, who also presented at the meeting.
Several drug and vaccine candidates are under study for the infection. An intriguing possibility is that angiotensin converting enzyme (ACE) inhibitors might help. Hypertension is a known risk factor for severe infection; the virus makes use of ACE receptor pathways to infect airway epithelial cells; and there have been reports of ACE inhibitors having effect against the virus that caused severe acute respiratory syndrome (SARS), another coronavirus outbreak in 2003.
“I think it’s a very good idea to go back and re-explore use of these drugs,” Dr. Baric said.
The presenters didn’t have any relevant disclosures.
The transmission rate of coronavirus disease 2019 (COVID-19) was 1%-5% among 38,000 Chinese people in close contact with infected patients, according to the chief epidemiologist of the Chinese Centers for Disease Control and Prevention, Beijing, Zunyou Wu, MD, PhD, who gave an update on the epidemic at the Conference on Retroviruses & Opportunistic Infections.
The rate of spread to family members – the driver of the infection in China – was 10% early in the outbreak, but fell to 3% with quicker recognition and isolation. The overall numbers are lower than might have been expected, and an important insight for clinicians trying to contain the outbreak in the United States.
, but their ability to spread the infection dropped after that, Dr. Wu and others said at a special COVID-19 session at the meeting, which was scheduled to be in Boston, but was held online instead because of concerns about spreading the virus. The session has been posted.
Transmission from presymptomatic people is rare. Shedding persists to some degree for 7-12 days in mild/moderate cases, but 2 weeks or more in severe cases.
Dr. Wu said the numbers in China are moving in the right direction, which means that containment efforts there have worked.
The virus emerged in Wuhan, the capital of Hubei province in central China, in connection with a wildlife food market in December 2019. Bats are thought to be the reservoir, with perhaps an intermediate step between civet cats and raccoon dogs. Officials shut down the market.
Essentially, the entire population of China, more than a billion people, was told to stay home for 10 days to interrupt the transmission cycle after the virus spread throughout the country in a few weeks, and almost 60 million people in Hubei were put behind a cordon sanitaire, where they have been for 50 days and will remain “for a while,” Dr. Wu said.
It’s led to a steep drop in new cases and deaths in China since mid-February; both are now more common outside China than inside, and international numbers are lower than they were at the peak in China.
Meanwhile, there’s been no evidence of perinatal transmission; the virus has not been detected in amniotic fluid, cord blood, neonatal throat swabs, or breast milk. Maternal morbidity appears to be similar to uninfected women. “The data around pregnancy are reassuring,” said John Brooks, MD, chief medical officers for HIV/AIDS prevention at the Centers for Disease Control and Prevention, Atlanta, who has been involved with CDC’s containment efforts.
There’s no data yet for immunocompromised people, but for people with HIV, he said, “we think the risk of severe illness would be greater” with lower CD4 counts and unsuppressed viral loads. “People living with HIV should take precautions against this new virus,” including having at least a 30-day supply of HIV medications; keeping up flu and pneumonia vaccinations; and having a care plan if quarantined. Setting up telemedicine might be a good idea.
The usual incubation period for COVID-19 is 4-6 days but can be longer. Recovery time is about 2 weeks in mild cases and 3-6 weeks in more severe cases. People who die do so within 2 months of symptom onset.
The most common symptoms among hospitalized patients in China are fever, dry cough, fatigue, and headache. Truly asymptomatic cases are not common; most go on to develop symptoms. There have been reports of diarrhea before other symptoms by a day or two, but it’s probably a red herring. The virus has been isolated from stool, but there is no evidence of fecal-oral transmission, Dr. Wu said.
Eighty percent of COVID-19 cases are mild or moderate and most patients recover spontaneously, especially middle aged and younger people. There is no meaningful difference in distribution between the sexes.
There are limited pediatric data perhaps due to underreporting, “but we know [children] experience milder illness than adults,” the CDC’s Dr. Brooks said.
He pegged the latest case fatality estimate at 0.5% to 3.5%, which is considerably higher than seasonal flu, but might well drop as more mild cases are detected and added to the denominator, he said.
For now, death rates top 5% in adults over 60 years old and climb further with increasing age, approaching 16% in people 80 years or older. Patients with hypertension, diabetes, cardiovascular disease, and chronic respiratory illness are at increased risk. The ultimate cause of death is acute respiratory distress syndrome, said Ralph Baric, PhD, a coronavirus expert and epidemiology professor at the University of North Carolina, Chapel Hill, who also presented at the meeting.
Several drug and vaccine candidates are under study for the infection. An intriguing possibility is that angiotensin converting enzyme (ACE) inhibitors might help. Hypertension is a known risk factor for severe infection; the virus makes use of ACE receptor pathways to infect airway epithelial cells; and there have been reports of ACE inhibitors having effect against the virus that caused severe acute respiratory syndrome (SARS), another coronavirus outbreak in 2003.
“I think it’s a very good idea to go back and re-explore use of these drugs,” Dr. Baric said.
The presenters didn’t have any relevant disclosures.
The transmission rate of coronavirus disease 2019 (COVID-19) was 1%-5% among 38,000 Chinese people in close contact with infected patients, according to the chief epidemiologist of the Chinese Centers for Disease Control and Prevention, Beijing, Zunyou Wu, MD, PhD, who gave an update on the epidemic at the Conference on Retroviruses & Opportunistic Infections.
The rate of spread to family members – the driver of the infection in China – was 10% early in the outbreak, but fell to 3% with quicker recognition and isolation. The overall numbers are lower than might have been expected, and an important insight for clinicians trying to contain the outbreak in the United States.
, but their ability to spread the infection dropped after that, Dr. Wu and others said at a special COVID-19 session at the meeting, which was scheduled to be in Boston, but was held online instead because of concerns about spreading the virus. The session has been posted.
Transmission from presymptomatic people is rare. Shedding persists to some degree for 7-12 days in mild/moderate cases, but 2 weeks or more in severe cases.
Dr. Wu said the numbers in China are moving in the right direction, which means that containment efforts there have worked.
The virus emerged in Wuhan, the capital of Hubei province in central China, in connection with a wildlife food market in December 2019. Bats are thought to be the reservoir, with perhaps an intermediate step between civet cats and raccoon dogs. Officials shut down the market.
Essentially, the entire population of China, more than a billion people, was told to stay home for 10 days to interrupt the transmission cycle after the virus spread throughout the country in a few weeks, and almost 60 million people in Hubei were put behind a cordon sanitaire, where they have been for 50 days and will remain “for a while,” Dr. Wu said.
It’s led to a steep drop in new cases and deaths in China since mid-February; both are now more common outside China than inside, and international numbers are lower than they were at the peak in China.
Meanwhile, there’s been no evidence of perinatal transmission; the virus has not been detected in amniotic fluid, cord blood, neonatal throat swabs, or breast milk. Maternal morbidity appears to be similar to uninfected women. “The data around pregnancy are reassuring,” said John Brooks, MD, chief medical officers for HIV/AIDS prevention at the Centers for Disease Control and Prevention, Atlanta, who has been involved with CDC’s containment efforts.
There’s no data yet for immunocompromised people, but for people with HIV, he said, “we think the risk of severe illness would be greater” with lower CD4 counts and unsuppressed viral loads. “People living with HIV should take precautions against this new virus,” including having at least a 30-day supply of HIV medications; keeping up flu and pneumonia vaccinations; and having a care plan if quarantined. Setting up telemedicine might be a good idea.
The usual incubation period for COVID-19 is 4-6 days but can be longer. Recovery time is about 2 weeks in mild cases and 3-6 weeks in more severe cases. People who die do so within 2 months of symptom onset.
The most common symptoms among hospitalized patients in China are fever, dry cough, fatigue, and headache. Truly asymptomatic cases are not common; most go on to develop symptoms. There have been reports of diarrhea before other symptoms by a day or two, but it’s probably a red herring. The virus has been isolated from stool, but there is no evidence of fecal-oral transmission, Dr. Wu said.
Eighty percent of COVID-19 cases are mild or moderate and most patients recover spontaneously, especially middle aged and younger people. There is no meaningful difference in distribution between the sexes.
There are limited pediatric data perhaps due to underreporting, “but we know [children] experience milder illness than adults,” the CDC’s Dr. Brooks said.
He pegged the latest case fatality estimate at 0.5% to 3.5%, which is considerably higher than seasonal flu, but might well drop as more mild cases are detected and added to the denominator, he said.
For now, death rates top 5% in adults over 60 years old and climb further with increasing age, approaching 16% in people 80 years or older. Patients with hypertension, diabetes, cardiovascular disease, and chronic respiratory illness are at increased risk. The ultimate cause of death is acute respiratory distress syndrome, said Ralph Baric, PhD, a coronavirus expert and epidemiology professor at the University of North Carolina, Chapel Hill, who also presented at the meeting.
Several drug and vaccine candidates are under study for the infection. An intriguing possibility is that angiotensin converting enzyme (ACE) inhibitors might help. Hypertension is a known risk factor for severe infection; the virus makes use of ACE receptor pathways to infect airway epithelial cells; and there have been reports of ACE inhibitors having effect against the virus that caused severe acute respiratory syndrome (SARS), another coronavirus outbreak in 2003.
“I think it’s a very good idea to go back and re-explore use of these drugs,” Dr. Baric said.
The presenters didn’t have any relevant disclosures.
FROM CROI 2020
Serum GFAP may indicate disease severity in NMOSD
WEST PALM BEACH, FLA. – (NMOSD), according to research presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Treatment with inebilizumab decreases serum GFAP concentrations and reduces the risk of an NMOSD attack, the investigators said.
In NMOSD, autoantibodies often target aquaporin-4, a protein expressed on astrocytes. This immune response destroys astrocytes and increases levels of GFAP in cerebrospinal fluid and serum. In the N-MOmentum trial, inebilizumab reduced the risk of attacks by 73%, compared with placebo, in patients with NMOSD. Bruce Cree, MD, PhD, professor of neurology at the University of California, San Francisco, Weill Institute for Neurosciences and colleagues analyzed the data from this trial to examine the relationship between serum GFAP concentrations and disease activity.
In the study, the investigators prospectively collected 1,260 serum samples from 215 participants, 25 healthy donors, and 23 patients with relapsing-remitting multiple sclerosis (MS). Serum GFAP concentration was measured using a single-molecule array assay. The researchers and an independent adjudication committee evaluated attacks during the 28-week randomized controlled study period using predefined criteria.
The median serum GFAP concentration was higher in patients with NMOSD (128.3 pg/mL) than in patients with relapsing-remitting MS (97.5 pg/mL) and healthy controls (73.3 pg/mL). At baseline, 29% of patients with NMOSD and 9% of patients with MS had a serum GFAP concentration that was three or more standard deviations above the mean level in healthy donors.
During the study, patients with a high baseline concentration of serum GFAP were three times more likely to have an adjudicated NMOSD attack than patients with lower serum GFAP concentrations. Concentrations of serum GFAP increased within 1 week of an adjudicated attack during the randomized controlled period. Furthermore, serum GFAP concentration was significantly higher in patients with major adjudicated attacks, compared with those who had minor adjudicated attacks. This finding was true for all organ domains, including for attacks that affected only the optic nerve.
Compared with placebo, inebilizumab reduced the risk of an adjudicated attack by 79% in patients with a normal baseline serum GFAP concentration and by 61% in patients with an elevated baseline serum GFAP concentration. The increase in serum GFAP concentration following an adjudicated attack was significant in patients receiving placebo, but not in patients receiving inebilizumab. Seven samples taken during an adjudicated attack from patients receiving inebilizumab had serum GFAP concentrations within the normal range. One sample taken during an attack from a patient receiving placebo had a serum GFAP concentration within the normal range. In addition, serum GFAP concentrations decreased from baseline among patients receiving inebilizumab who did not have an adjudicated attack.
“These observations suggest that serum GFAP could be a clinically useful biomarker of disease activity and increased attack risk in NMOSD,” said Dr. Cree and colleagues.
Viela Bio, which is developing inebilizumab, and MedImmune sponsored the study. Dr. Cree has received compensation for consulting services that he provided to Alexion, Atara, Biogen, EMD Serono, Novartis, and TG Therapeutics.
SOURCE: Hartung H et al. ACTRIMS 2020, Abstract P205.
WEST PALM BEACH, FLA. – (NMOSD), according to research presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Treatment with inebilizumab decreases serum GFAP concentrations and reduces the risk of an NMOSD attack, the investigators said.
In NMOSD, autoantibodies often target aquaporin-4, a protein expressed on astrocytes. This immune response destroys astrocytes and increases levels of GFAP in cerebrospinal fluid and serum. In the N-MOmentum trial, inebilizumab reduced the risk of attacks by 73%, compared with placebo, in patients with NMOSD. Bruce Cree, MD, PhD, professor of neurology at the University of California, San Francisco, Weill Institute for Neurosciences and colleagues analyzed the data from this trial to examine the relationship between serum GFAP concentrations and disease activity.
In the study, the investigators prospectively collected 1,260 serum samples from 215 participants, 25 healthy donors, and 23 patients with relapsing-remitting multiple sclerosis (MS). Serum GFAP concentration was measured using a single-molecule array assay. The researchers and an independent adjudication committee evaluated attacks during the 28-week randomized controlled study period using predefined criteria.
The median serum GFAP concentration was higher in patients with NMOSD (128.3 pg/mL) than in patients with relapsing-remitting MS (97.5 pg/mL) and healthy controls (73.3 pg/mL). At baseline, 29% of patients with NMOSD and 9% of patients with MS had a serum GFAP concentration that was three or more standard deviations above the mean level in healthy donors.
During the study, patients with a high baseline concentration of serum GFAP were three times more likely to have an adjudicated NMOSD attack than patients with lower serum GFAP concentrations. Concentrations of serum GFAP increased within 1 week of an adjudicated attack during the randomized controlled period. Furthermore, serum GFAP concentration was significantly higher in patients with major adjudicated attacks, compared with those who had minor adjudicated attacks. This finding was true for all organ domains, including for attacks that affected only the optic nerve.
Compared with placebo, inebilizumab reduced the risk of an adjudicated attack by 79% in patients with a normal baseline serum GFAP concentration and by 61% in patients with an elevated baseline serum GFAP concentration. The increase in serum GFAP concentration following an adjudicated attack was significant in patients receiving placebo, but not in patients receiving inebilizumab. Seven samples taken during an adjudicated attack from patients receiving inebilizumab had serum GFAP concentrations within the normal range. One sample taken during an attack from a patient receiving placebo had a serum GFAP concentration within the normal range. In addition, serum GFAP concentrations decreased from baseline among patients receiving inebilizumab who did not have an adjudicated attack.
“These observations suggest that serum GFAP could be a clinically useful biomarker of disease activity and increased attack risk in NMOSD,” said Dr. Cree and colleagues.
Viela Bio, which is developing inebilizumab, and MedImmune sponsored the study. Dr. Cree has received compensation for consulting services that he provided to Alexion, Atara, Biogen, EMD Serono, Novartis, and TG Therapeutics.
SOURCE: Hartung H et al. ACTRIMS 2020, Abstract P205.
WEST PALM BEACH, FLA. – (NMOSD), according to research presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Treatment with inebilizumab decreases serum GFAP concentrations and reduces the risk of an NMOSD attack, the investigators said.
In NMOSD, autoantibodies often target aquaporin-4, a protein expressed on astrocytes. This immune response destroys astrocytes and increases levels of GFAP in cerebrospinal fluid and serum. In the N-MOmentum trial, inebilizumab reduced the risk of attacks by 73%, compared with placebo, in patients with NMOSD. Bruce Cree, MD, PhD, professor of neurology at the University of California, San Francisco, Weill Institute for Neurosciences and colleagues analyzed the data from this trial to examine the relationship between serum GFAP concentrations and disease activity.
In the study, the investigators prospectively collected 1,260 serum samples from 215 participants, 25 healthy donors, and 23 patients with relapsing-remitting multiple sclerosis (MS). Serum GFAP concentration was measured using a single-molecule array assay. The researchers and an independent adjudication committee evaluated attacks during the 28-week randomized controlled study period using predefined criteria.
The median serum GFAP concentration was higher in patients with NMOSD (128.3 pg/mL) than in patients with relapsing-remitting MS (97.5 pg/mL) and healthy controls (73.3 pg/mL). At baseline, 29% of patients with NMOSD and 9% of patients with MS had a serum GFAP concentration that was three or more standard deviations above the mean level in healthy donors.
During the study, patients with a high baseline concentration of serum GFAP were three times more likely to have an adjudicated NMOSD attack than patients with lower serum GFAP concentrations. Concentrations of serum GFAP increased within 1 week of an adjudicated attack during the randomized controlled period. Furthermore, serum GFAP concentration was significantly higher in patients with major adjudicated attacks, compared with those who had minor adjudicated attacks. This finding was true for all organ domains, including for attacks that affected only the optic nerve.
Compared with placebo, inebilizumab reduced the risk of an adjudicated attack by 79% in patients with a normal baseline serum GFAP concentration and by 61% in patients with an elevated baseline serum GFAP concentration. The increase in serum GFAP concentration following an adjudicated attack was significant in patients receiving placebo, but not in patients receiving inebilizumab. Seven samples taken during an adjudicated attack from patients receiving inebilizumab had serum GFAP concentrations within the normal range. One sample taken during an attack from a patient receiving placebo had a serum GFAP concentration within the normal range. In addition, serum GFAP concentrations decreased from baseline among patients receiving inebilizumab who did not have an adjudicated attack.
“These observations suggest that serum GFAP could be a clinically useful biomarker of disease activity and increased attack risk in NMOSD,” said Dr. Cree and colleagues.
Viela Bio, which is developing inebilizumab, and MedImmune sponsored the study. Dr. Cree has received compensation for consulting services that he provided to Alexion, Atara, Biogen, EMD Serono, Novartis, and TG Therapeutics.
SOURCE: Hartung H et al. ACTRIMS 2020, Abstract P205.
REPORTING FROM ACTRIMS FORUM 2020
FDA cancels or postpones meetings amid COVID-19 concerns
Officials at the Food and Drug Administration’s Center for Drug Evaluation and Research are taking the precautionary step of canceling or postponing advisory committee meetings and limiting staff travel in an effort to help curb the spread of the COVID-19.

“The outbreak of respiratory illness caused by a novel coronavirus, COVID-19, that started in China is spreading to other countries, including the United States,” CDER Director Janet Woodcock, MD, said in a memo to CDER staff. “As a precaution, FDA is canceling foreign official agency travel and limiting domestic travel to mission critical only, effective immediately and through April.”
Additionally, the memo notes that “CDER-organized external meetings, conferences, and workshops will be postponed or canceled from March 10 through April.”
“To mitigate the impact on our work, I encourage you to hold meetings with external stakeholders through teleconference, when possible,” she wrote.
Thus far, only a few CDER events on the FDA’s meeting webpage are listed as being canceled or postponed. Some of the affected meetings include a March 10 public meeting on patient-focused drug development for stimulant-use disorder, a March 11 meeting of the Nonprescription Drug Advisory Committee, and a March 30 public meeting on patient-focused drug development for vitiligo, all of which are postponed until further notice. The Center for Biologics Evaluation and Research also has postponed until further notice its U.S.–Japan Cellular and Gene Therapy Conference, originally scheduled for March 12.
Dr. Woodcock also noted in the memo that in relation to inspections, “we plan to use technology and established agreements with our foreign counterparts to minimize disruptions to the drug supply chain and to applications under review, so that Americans can continue to get their medications.”
Officials at the Food and Drug Administration’s Center for Drug Evaluation and Research are taking the precautionary step of canceling or postponing advisory committee meetings and limiting staff travel in an effort to help curb the spread of the COVID-19.
“The outbreak of respiratory illness caused by a novel coronavirus, COVID-19, that started in China is spreading to other countries, including the United States,” CDER Director Janet Woodcock, MD, said in a memo to CDER staff. “As a precaution, FDA is canceling foreign official agency travel and limiting domestic travel to mission critical only, effective immediately and through April.”
Additionally, the memo notes that “CDER-organized external meetings, conferences, and workshops will be postponed or canceled from March 10 through April.”
“To mitigate the impact on our work, I encourage you to hold meetings with external stakeholders through teleconference, when possible,” she wrote.
Thus far, only a few CDER events on the FDA’s meeting webpage are listed as being canceled or postponed. Some of the affected meetings include a March 10 public meeting on patient-focused drug development for stimulant-use disorder, a March 11 meeting of the Nonprescription Drug Advisory Committee, and a March 30 public meeting on patient-focused drug development for vitiligo, all of which are postponed until further notice. The Center for Biologics Evaluation and Research also has postponed until further notice its U.S.–Japan Cellular and Gene Therapy Conference, originally scheduled for March 12.
Dr. Woodcock also noted in the memo that in relation to inspections, “we plan to use technology and established agreements with our foreign counterparts to minimize disruptions to the drug supply chain and to applications under review, so that Americans can continue to get their medications.”
Officials at the Food and Drug Administration’s Center for Drug Evaluation and Research are taking the precautionary step of canceling or postponing advisory committee meetings and limiting staff travel in an effort to help curb the spread of the COVID-19.
“The outbreak of respiratory illness caused by a novel coronavirus, COVID-19, that started in China is spreading to other countries, including the United States,” CDER Director Janet Woodcock, MD, said in a memo to CDER staff. “As a precaution, FDA is canceling foreign official agency travel and limiting domestic travel to mission critical only, effective immediately and through April.”
Additionally, the memo notes that “CDER-organized external meetings, conferences, and workshops will be postponed or canceled from March 10 through April.”
“To mitigate the impact on our work, I encourage you to hold meetings with external stakeholders through teleconference, when possible,” she wrote.
Thus far, only a few CDER events on the FDA’s meeting webpage are listed as being canceled or postponed. Some of the affected meetings include a March 10 public meeting on patient-focused drug development for stimulant-use disorder, a March 11 meeting of the Nonprescription Drug Advisory Committee, and a March 30 public meeting on patient-focused drug development for vitiligo, all of which are postponed until further notice. The Center for Biologics Evaluation and Research also has postponed until further notice its U.S.–Japan Cellular and Gene Therapy Conference, originally scheduled for March 12.
Dr. Woodcock also noted in the memo that in relation to inspections, “we plan to use technology and established agreements with our foreign counterparts to minimize disruptions to the drug supply chain and to applications under review, so that Americans can continue to get their medications.”
Age does not appear to affect efficacy of siponimod in secondary progressive MS
WEST PALM BEACH, FLA. – (MS), according to data presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Siponimod’s tolerability also does not vary with age, the researchers said.

Although many effective treatments for relapsing-remitting MS are available, patients still have a high risk of developing secondary progressive MS. Increasing age is associated with disability accumulation, regardless of disease duration. This accumulation of disability could affect treatment outcomes.
Siponimod is an approved treatment for adults with relapsing forms of MS, including clinically isolated syndrome and active secondary progressive MS. Compared with placebo, siponimod significantly reduced the risk of confirmed disability progression in the phase 3 EXPAND trial.
Efficacy was similar between age groups
Le Hua, MD, a neurologist at the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, and colleagues sought to evaluate the safety and efficacy of siponimod by age in patients with active secondary progressive MS who participated in the EXPAND study. The investigators defined active disease as a relapse in the 2 years before screening or one or more T1 gadolinium–enhancing lesions at baseline. Time to 3- and 6-month confirmed disability progression, defined using Expanded Disability Status Scale (EDSS) scores, were the efficacy endpoints of this analysis. Dr. Hua and colleagues also examined adverse events, serious adverse events, and adverse events leading to treatment discontinuation.
Of the 1,651 patients included in EXPAND, 779 had active secondary progressive MS. Dr. Hua and colleagues categorized this group as younger than 45 years (306 patients) or 45 years or older (473 patients). In the overall EXPAND population, siponimod reduced the risk of 3-month confirmed disability progression by 21% and the risk of 6-month confirmed disability progression by 26%, compared with placebo. Among patients younger than 45 years, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 32% and 40%, respectively. Among patients aged 45 years or older, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 31% and 33%, respectively.
Siponimod’s safety profile was similar between age groups. Among participants younger than 45 years, the rate of any adverse event was 82.6% for siponimod and 82.8% for placebo. In patients age 45 years or older, the rate of any adverse event was 89.8% for siponimod and 75.9% for placebo. The rate of serious adverse events was lower for siponimod than for placebo in both age groups. Among patients younger than 45 years, the rate was 12.7% for siponimod and 15.1% for placebo. Among patients age 45 years or older, the rate was 18.2% for siponimod and 19.4% for placebo. The rate of adverse events leading to discontinuation, however, was slightly higher among older patients. For younger patients, the rate was 3.3% for siponimod and 4.3% for placebo. For older patients, the rate was 7.6% for siponimod and 7.1% for placebo.
Real-world data will provide clearer answers
Rates of adverse events, serious adverse events, and adverse events leading to discontinuation were all higher in patients aged 45 or older. “This was not a surprising finding,” said Dr. Hua. “The differences appeared small, and the study was not powered to detect if these differences were significant. ... In general, older patients are more likely to have more cardiac events and infections than younger patients.”
Few studies have analyzed the efficacy and safety of MS therapy by age, said Dr. Hua. In 2015, Matell et al. evaluated the effectiveness of natalizumab in patients over age 50 years. In that study, a greater number of older patients, compared with younger patients, stopped treatment because of lack of effectiveness. Studies of other disease-modifying therapies (DMTs) have included subgroup analyses based on age, “but subgroup analyses are limited in the ability to make any strong conclusions regarding significant differences in safety,” said Dr. Hua. “A recent meta-analysis of published clinical trials of all DMTs performed by Weideman et al. indicated that the efficacy of DMTs appears to wane after age 53 years. However, there are limitations in interpreting this data, as they weren’t able to evaluate the raw data. And in most clinical trials, the age cutoff is usually 55 years, which limits generalizations. Real-world data analyses are needed to truly understand efficacy and safety of DMT in older patients.”
Novartis funded the study. Dr. Hua received fees from Novartis, Biogen, Celgene, EMD Serono, Genentech, and Genzyme.
SOURCE: Hua L et al. ACTRIMS FORUM 2020, Abstract P029.
WEST PALM BEACH, FLA. – (MS), according to data presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Siponimod’s tolerability also does not vary with age, the researchers said.
Although many effective treatments for relapsing-remitting MS are available, patients still have a high risk of developing secondary progressive MS. Increasing age is associated with disability accumulation, regardless of disease duration. This accumulation of disability could affect treatment outcomes.
Siponimod is an approved treatment for adults with relapsing forms of MS, including clinically isolated syndrome and active secondary progressive MS. Compared with placebo, siponimod significantly reduced the risk of confirmed disability progression in the phase 3 EXPAND trial.
Efficacy was similar between age groups
Le Hua, MD, a neurologist at the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, and colleagues sought to evaluate the safety and efficacy of siponimod by age in patients with active secondary progressive MS who participated in the EXPAND study. The investigators defined active disease as a relapse in the 2 years before screening or one or more T1 gadolinium–enhancing lesions at baseline. Time to 3- and 6-month confirmed disability progression, defined using Expanded Disability Status Scale (EDSS) scores, were the efficacy endpoints of this analysis. Dr. Hua and colleagues also examined adverse events, serious adverse events, and adverse events leading to treatment discontinuation.
Of the 1,651 patients included in EXPAND, 779 had active secondary progressive MS. Dr. Hua and colleagues categorized this group as younger than 45 years (306 patients) or 45 years or older (473 patients). In the overall EXPAND population, siponimod reduced the risk of 3-month confirmed disability progression by 21% and the risk of 6-month confirmed disability progression by 26%, compared with placebo. Among patients younger than 45 years, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 32% and 40%, respectively. Among patients aged 45 years or older, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 31% and 33%, respectively.
Siponimod’s safety profile was similar between age groups. Among participants younger than 45 years, the rate of any adverse event was 82.6% for siponimod and 82.8% for placebo. In patients age 45 years or older, the rate of any adverse event was 89.8% for siponimod and 75.9% for placebo. The rate of serious adverse events was lower for siponimod than for placebo in both age groups. Among patients younger than 45 years, the rate was 12.7% for siponimod and 15.1% for placebo. Among patients age 45 years or older, the rate was 18.2% for siponimod and 19.4% for placebo. The rate of adverse events leading to discontinuation, however, was slightly higher among older patients. For younger patients, the rate was 3.3% for siponimod and 4.3% for placebo. For older patients, the rate was 7.6% for siponimod and 7.1% for placebo.
Real-world data will provide clearer answers
Rates of adverse events, serious adverse events, and adverse events leading to discontinuation were all higher in patients aged 45 or older. “This was not a surprising finding,” said Dr. Hua. “The differences appeared small, and the study was not powered to detect if these differences were significant. ... In general, older patients are more likely to have more cardiac events and infections than younger patients.”
Few studies have analyzed the efficacy and safety of MS therapy by age, said Dr. Hua. In 2015, Matell et al. evaluated the effectiveness of natalizumab in patients over age 50 years. In that study, a greater number of older patients, compared with younger patients, stopped treatment because of lack of effectiveness. Studies of other disease-modifying therapies (DMTs) have included subgroup analyses based on age, “but subgroup analyses are limited in the ability to make any strong conclusions regarding significant differences in safety,” said Dr. Hua. “A recent meta-analysis of published clinical trials of all DMTs performed by Weideman et al. indicated that the efficacy of DMTs appears to wane after age 53 years. However, there are limitations in interpreting this data, as they weren’t able to evaluate the raw data. And in most clinical trials, the age cutoff is usually 55 years, which limits generalizations. Real-world data analyses are needed to truly understand efficacy and safety of DMT in older patients.”
Novartis funded the study. Dr. Hua received fees from Novartis, Biogen, Celgene, EMD Serono, Genentech, and Genzyme.
SOURCE: Hua L et al. ACTRIMS FORUM 2020, Abstract P029.
WEST PALM BEACH, FLA. – (MS), according to data presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis. Siponimod’s tolerability also does not vary with age, the researchers said.
Although many effective treatments for relapsing-remitting MS are available, patients still have a high risk of developing secondary progressive MS. Increasing age is associated with disability accumulation, regardless of disease duration. This accumulation of disability could affect treatment outcomes.
Siponimod is an approved treatment for adults with relapsing forms of MS, including clinically isolated syndrome and active secondary progressive MS. Compared with placebo, siponimod significantly reduced the risk of confirmed disability progression in the phase 3 EXPAND trial.
Efficacy was similar between age groups
Le Hua, MD, a neurologist at the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, and colleagues sought to evaluate the safety and efficacy of siponimod by age in patients with active secondary progressive MS who participated in the EXPAND study. The investigators defined active disease as a relapse in the 2 years before screening or one or more T1 gadolinium–enhancing lesions at baseline. Time to 3- and 6-month confirmed disability progression, defined using Expanded Disability Status Scale (EDSS) scores, were the efficacy endpoints of this analysis. Dr. Hua and colleagues also examined adverse events, serious adverse events, and adverse events leading to treatment discontinuation.
Of the 1,651 patients included in EXPAND, 779 had active secondary progressive MS. Dr. Hua and colleagues categorized this group as younger than 45 years (306 patients) or 45 years or older (473 patients). In the overall EXPAND population, siponimod reduced the risk of 3-month confirmed disability progression by 21% and the risk of 6-month confirmed disability progression by 26%, compared with placebo. Among patients younger than 45 years, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 32% and 40%, respectively. Among patients aged 45 years or older, siponimod reduced the risks of 3- and 6-month confirmed disability progression by 31% and 33%, respectively.
Siponimod’s safety profile was similar between age groups. Among participants younger than 45 years, the rate of any adverse event was 82.6% for siponimod and 82.8% for placebo. In patients age 45 years or older, the rate of any adverse event was 89.8% for siponimod and 75.9% for placebo. The rate of serious adverse events was lower for siponimod than for placebo in both age groups. Among patients younger than 45 years, the rate was 12.7% for siponimod and 15.1% for placebo. Among patients age 45 years or older, the rate was 18.2% for siponimod and 19.4% for placebo. The rate of adverse events leading to discontinuation, however, was slightly higher among older patients. For younger patients, the rate was 3.3% for siponimod and 4.3% for placebo. For older patients, the rate was 7.6% for siponimod and 7.1% for placebo.
Real-world data will provide clearer answers
Rates of adverse events, serious adverse events, and adverse events leading to discontinuation were all higher in patients aged 45 or older. “This was not a surprising finding,” said Dr. Hua. “The differences appeared small, and the study was not powered to detect if these differences were significant. ... In general, older patients are more likely to have more cardiac events and infections than younger patients.”
Few studies have analyzed the efficacy and safety of MS therapy by age, said Dr. Hua. In 2015, Matell et al. evaluated the effectiveness of natalizumab in patients over age 50 years. In that study, a greater number of older patients, compared with younger patients, stopped treatment because of lack of effectiveness. Studies of other disease-modifying therapies (DMTs) have included subgroup analyses based on age, “but subgroup analyses are limited in the ability to make any strong conclusions regarding significant differences in safety,” said Dr. Hua. “A recent meta-analysis of published clinical trials of all DMTs performed by Weideman et al. indicated that the efficacy of DMTs appears to wane after age 53 years. However, there are limitations in interpreting this data, as they weren’t able to evaluate the raw data. And in most clinical trials, the age cutoff is usually 55 years, which limits generalizations. Real-world data analyses are needed to truly understand efficacy and safety of DMT in older patients.”
Novartis funded the study. Dr. Hua received fees from Novartis, Biogen, Celgene, EMD Serono, Genentech, and Genzyme.
SOURCE: Hua L et al. ACTRIMS FORUM 2020, Abstract P029.
REPORTING FROM ACTRIMS FORUM 2020

American Headache Society updates guideline on neuroimaging for migraine
Migraine with atypical features may require neuroimaging, according to the guideline. These include an unusual aura; change in clinical features; a first or worst migraine; a migraine that presents with brainstem aura, confusion, or motor manifestation; migraine accompaniments in later life; headaches that are side-locked or posttraumatic; and aura that presents without headache.
Assessing the evidence
The recommendation to avoid MRI or CT in otherwise neurologically normal patients with migraine carried a grade A recommendation from the American Headache Society, while the specific considerations for neuroimaging was based on consensus and carried a grade C recommendation, according to lead author Randolph W. Evans, MD, of the department of neurology at Baylor College of Medicine in Houston, and colleagues.
The recommendations, published in the journal Headache (2020 Feb;60(2):318-36), came from a systematic review of 23 studies of adults at least 18 years old who underwent MRI or CT during outpatient treatment for migraine between 1973 and 2018. Ten studies looked at CT neuroimaging in patients with migraine, nine studies examined MRI neuroimaging alone in patients with migraine, and four studies contained adults with headache or migraine who underwent either MRI or CT. The majority of studies analyzed were retrospective or cross-sectional in nature, while four studies were prospective observational studies.
Dr. Evans and colleagues noted that neuroimaging for patients with suspected migraine is ordered for a variety of reasons, such as excluding conditions that aren’t migraine, diagnostic certainty, cognitive bias, practice workflow, medicolegal concerns, addressing patient and family anxiety, and addressing clinician anxiety. Neuroimaging also can be costly, they said, adding up to an estimated $1 billion annually according to one study, and can lead to additional testing from findings that may not be clinically significant.
Good advice, with caveats
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, said that while he generally does not like broad guideline recommendations, the recommendation made by the American Headache Society to avoid neuroimaging in patients with a normal neurological examination without any atypical features and red flags “takes most of the important factors into consideration and will work almost all the time.” The recommendation made by consensus for specific considerations of neuroimaging was issued by top headache specialists in the United States who reviewed the data, and it is unlikely a patient with a migraine as diagnosed by the International Classification of Headache Disorders with a normal neurological examination would have a significant abnormality that would appear with imaging, Dr. Rapoport said.
“If everyone caring for migraine patients knew these recommendations, and used them unless the patients fit the exclusions mentioned, we would have more efficient clinical practice and save lots of money on unnecessary scanning,” he said.
However, Dr. Rapoport, clinical professor of neurology at the University of California, Los Angeles, founder of the New England Center for Headache, and past president of The International Headache Society, said that not all clinicians will be convinced by the American Headache Society’s recommendations.
“Various third parties often jump on society recommendations or guidelines and prevent smart clinicians from doing what they need to do when they want to disregard the recommendation or guideline,” he explained. “More importantly, if a physician feels the need to think out of the box and image a patient without a clear reason, and the patient cannot pay for the scan when a medical insurance company refuses to authorize it, there can be a bad result if the patient does not get the study.”
Dr. Rapoport noted that the guideline does not address situations where neuroimaging may not pick up conditions that lead to migraine, such as a subarachnoid or subdural hemorrhage, reversible cerebral vasoconstriction syndrome, or early aspects of low cerebrospinal fluid pressure syndrome. Anxiety on the part of the patient or the clinician is another area that can be addressed by future research, he said.
“If the clinician does a good job of explaining the odds of anything significant being found with a typical migraine history and normal examination, and the patient says [they] need an MRI with contrast to be sure, it will be difficult to dissuade them,” said Dr. Rapoport. “If you don’t order one, they will find a way to get one. If it is abnormal, you could be in trouble. Also, if the clinician has no good reason to do a scan but has anxiety about what is being missed, it will probably get done.”
There was no funding source for the guidelines. The authors reported personal and institutional relationships in the form of advisory board memberships, investigator appointments, speakers bureau positions, research support, and consultancies for a variety of pharmaceutical companies, agencies, institutions, publishers, and other organizations.
Migraine with atypical features may require neuroimaging, according to the guideline. These include an unusual aura; change in clinical features; a first or worst migraine; a migraine that presents with brainstem aura, confusion, or motor manifestation; migraine accompaniments in later life; headaches that are side-locked or posttraumatic; and aura that presents without headache.
Assessing the evidence
The recommendation to avoid MRI or CT in otherwise neurologically normal patients with migraine carried a grade A recommendation from the American Headache Society, while the specific considerations for neuroimaging was based on consensus and carried a grade C recommendation, according to lead author Randolph W. Evans, MD, of the department of neurology at Baylor College of Medicine in Houston, and colleagues.
The recommendations, published in the journal Headache (2020 Feb;60(2):318-36), came from a systematic review of 23 studies of adults at least 18 years old who underwent MRI or CT during outpatient treatment for migraine between 1973 and 2018. Ten studies looked at CT neuroimaging in patients with migraine, nine studies examined MRI neuroimaging alone in patients with migraine, and four studies contained adults with headache or migraine who underwent either MRI or CT. The majority of studies analyzed were retrospective or cross-sectional in nature, while four studies were prospective observational studies.
Dr. Evans and colleagues noted that neuroimaging for patients with suspected migraine is ordered for a variety of reasons, such as excluding conditions that aren’t migraine, diagnostic certainty, cognitive bias, practice workflow, medicolegal concerns, addressing patient and family anxiety, and addressing clinician anxiety. Neuroimaging also can be costly, they said, adding up to an estimated $1 billion annually according to one study, and can lead to additional testing from findings that may not be clinically significant.
Good advice, with caveats
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, said that while he generally does not like broad guideline recommendations, the recommendation made by the American Headache Society to avoid neuroimaging in patients with a normal neurological examination without any atypical features and red flags “takes most of the important factors into consideration and will work almost all the time.” The recommendation made by consensus for specific considerations of neuroimaging was issued by top headache specialists in the United States who reviewed the data, and it is unlikely a patient with a migraine as diagnosed by the International Classification of Headache Disorders with a normal neurological examination would have a significant abnormality that would appear with imaging, Dr. Rapoport said.
“If everyone caring for migraine patients knew these recommendations, and used them unless the patients fit the exclusions mentioned, we would have more efficient clinical practice and save lots of money on unnecessary scanning,” he said.
However, Dr. Rapoport, clinical professor of neurology at the University of California, Los Angeles, founder of the New England Center for Headache, and past president of The International Headache Society, said that not all clinicians will be convinced by the American Headache Society’s recommendations.
“Various third parties often jump on society recommendations or guidelines and prevent smart clinicians from doing what they need to do when they want to disregard the recommendation or guideline,” he explained. “More importantly, if a physician feels the need to think out of the box and image a patient without a clear reason, and the patient cannot pay for the scan when a medical insurance company refuses to authorize it, there can be a bad result if the patient does not get the study.”
Dr. Rapoport noted that the guideline does not address situations where neuroimaging may not pick up conditions that lead to migraine, such as a subarachnoid or subdural hemorrhage, reversible cerebral vasoconstriction syndrome, or early aspects of low cerebrospinal fluid pressure syndrome. Anxiety on the part of the patient or the clinician is another area that can be addressed by future research, he said.
“If the clinician does a good job of explaining the odds of anything significant being found with a typical migraine history and normal examination, and the patient says [they] need an MRI with contrast to be sure, it will be difficult to dissuade them,” said Dr. Rapoport. “If you don’t order one, they will find a way to get one. If it is abnormal, you could be in trouble. Also, if the clinician has no good reason to do a scan but has anxiety about what is being missed, it will probably get done.”
There was no funding source for the guidelines. The authors reported personal and institutional relationships in the form of advisory board memberships, investigator appointments, speakers bureau positions, research support, and consultancies for a variety of pharmaceutical companies, agencies, institutions, publishers, and other organizations.
Migraine with atypical features may require neuroimaging, according to the guideline. These include an unusual aura; change in clinical features; a first or worst migraine; a migraine that presents with brainstem aura, confusion, or motor manifestation; migraine accompaniments in later life; headaches that are side-locked or posttraumatic; and aura that presents without headache.
Assessing the evidence
The recommendation to avoid MRI or CT in otherwise neurologically normal patients with migraine carried a grade A recommendation from the American Headache Society, while the specific considerations for neuroimaging was based on consensus and carried a grade C recommendation, according to lead author Randolph W. Evans, MD, of the department of neurology at Baylor College of Medicine in Houston, and colleagues.
The recommendations, published in the journal Headache (2020 Feb;60(2):318-36), came from a systematic review of 23 studies of adults at least 18 years old who underwent MRI or CT during outpatient treatment for migraine between 1973 and 2018. Ten studies looked at CT neuroimaging in patients with migraine, nine studies examined MRI neuroimaging alone in patients with migraine, and four studies contained adults with headache or migraine who underwent either MRI or CT. The majority of studies analyzed were retrospective or cross-sectional in nature, while four studies were prospective observational studies.
Dr. Evans and colleagues noted that neuroimaging for patients with suspected migraine is ordered for a variety of reasons, such as excluding conditions that aren’t migraine, diagnostic certainty, cognitive bias, practice workflow, medicolegal concerns, addressing patient and family anxiety, and addressing clinician anxiety. Neuroimaging also can be costly, they said, adding up to an estimated $1 billion annually according to one study, and can lead to additional testing from findings that may not be clinically significant.
Good advice, with caveats
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, said that while he generally does not like broad guideline recommendations, the recommendation made by the American Headache Society to avoid neuroimaging in patients with a normal neurological examination without any atypical features and red flags “takes most of the important factors into consideration and will work almost all the time.” The recommendation made by consensus for specific considerations of neuroimaging was issued by top headache specialists in the United States who reviewed the data, and it is unlikely a patient with a migraine as diagnosed by the International Classification of Headache Disorders with a normal neurological examination would have a significant abnormality that would appear with imaging, Dr. Rapoport said.
“If everyone caring for migraine patients knew these recommendations, and used them unless the patients fit the exclusions mentioned, we would have more efficient clinical practice and save lots of money on unnecessary scanning,” he said.
However, Dr. Rapoport, clinical professor of neurology at the University of California, Los Angeles, founder of the New England Center for Headache, and past president of The International Headache Society, said that not all clinicians will be convinced by the American Headache Society’s recommendations.
“Various third parties often jump on society recommendations or guidelines and prevent smart clinicians from doing what they need to do when they want to disregard the recommendation or guideline,” he explained. “More importantly, if a physician feels the need to think out of the box and image a patient without a clear reason, and the patient cannot pay for the scan when a medical insurance company refuses to authorize it, there can be a bad result if the patient does not get the study.”
Dr. Rapoport noted that the guideline does not address situations where neuroimaging may not pick up conditions that lead to migraine, such as a subarachnoid or subdural hemorrhage, reversible cerebral vasoconstriction syndrome, or early aspects of low cerebrospinal fluid pressure syndrome. Anxiety on the part of the patient or the clinician is another area that can be addressed by future research, he said.
“If the clinician does a good job of explaining the odds of anything significant being found with a typical migraine history and normal examination, and the patient says [they] need an MRI with contrast to be sure, it will be difficult to dissuade them,” said Dr. Rapoport. “If you don’t order one, they will find a way to get one. If it is abnormal, you could be in trouble. Also, if the clinician has no good reason to do a scan but has anxiety about what is being missed, it will probably get done.”
There was no funding source for the guidelines. The authors reported personal and institutional relationships in the form of advisory board memberships, investigator appointments, speakers bureau positions, research support, and consultancies for a variety of pharmaceutical companies, agencies, institutions, publishers, and other organizations.
FROM HEADACHE
Hyperlipidemia occurs earlier in patients with MS
WEST PALM BEACH, FLA. – Onset of hyperlipidemia tends to occur earlier in patients with multiple sclerosis (MS), compared with matched controls, according to new research. Among females and African Americans, the effect of MS on age of hyperlipidemia onset may be especially pronounced, said Diane Krill, PhD, professor of biological sciences at Point Park University, Pittsburgh, and colleagues.
Many patients with MS have hyperlipidemia, and adverse lipid profiles correlate with physical and cognitive impairment in this population. “There is evidence of endothelial dysfunction and inflammation in both MS and hyperlipidemia, but the timing of onset of hyperlipidemia is not known,” the researchers said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To assess whether patients with MS have hyperlipidemia diagnosed at an earlier age, relative to matched controls, Dr. Krill and colleagues analyzed data from the Cleveland Clinic health system. They included in their analyses patients with at least two hyperlipidemia diagnoses and at least five encounters with a primary care physician. They matched each patient with MS to four patients without MS using variables such as birth year, sex, race, and year of first encounter. In all, the study included 669 patients with MS and 2,676 controls. The investigators examined age of hyperlipidemia onset using multivariable Cox proportional hazard models that adjusted for sex, race, smoking, and body mass index.
Patients with MS had a 20% increased risk for earlier onset of hyperlipidemia, relative to matched controls. The effect was greater among females (hazard ratio, 1.22) and African Americans (HR, 1.42). Patients with MS have earlier onset of hyperlipidemia “irrespective of the relationship with age of MS onset,” Dr. Krill and colleagues noted. “Additional research is warranted to further characterize the temporal relationships between MS and hyperlipidemia, as well as considerations for timing of disease-modifying therapies.”
The researchers had no relevant disclosures.
SOURCE: Krill D et al. ACTRIMS Forum 2020, Abstract P085.
WEST PALM BEACH, FLA. – Onset of hyperlipidemia tends to occur earlier in patients with multiple sclerosis (MS), compared with matched controls, according to new research. Among females and African Americans, the effect of MS on age of hyperlipidemia onset may be especially pronounced, said Diane Krill, PhD, professor of biological sciences at Point Park University, Pittsburgh, and colleagues.
Many patients with MS have hyperlipidemia, and adverse lipid profiles correlate with physical and cognitive impairment in this population. “There is evidence of endothelial dysfunction and inflammation in both MS and hyperlipidemia, but the timing of onset of hyperlipidemia is not known,” the researchers said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To assess whether patients with MS have hyperlipidemia diagnosed at an earlier age, relative to matched controls, Dr. Krill and colleagues analyzed data from the Cleveland Clinic health system. They included in their analyses patients with at least two hyperlipidemia diagnoses and at least five encounters with a primary care physician. They matched each patient with MS to four patients without MS using variables such as birth year, sex, race, and year of first encounter. In all, the study included 669 patients with MS and 2,676 controls. The investigators examined age of hyperlipidemia onset using multivariable Cox proportional hazard models that adjusted for sex, race, smoking, and body mass index.
Patients with MS had a 20% increased risk for earlier onset of hyperlipidemia, relative to matched controls. The effect was greater among females (hazard ratio, 1.22) and African Americans (HR, 1.42). Patients with MS have earlier onset of hyperlipidemia “irrespective of the relationship with age of MS onset,” Dr. Krill and colleagues noted. “Additional research is warranted to further characterize the temporal relationships between MS and hyperlipidemia, as well as considerations for timing of disease-modifying therapies.”
The researchers had no relevant disclosures.
SOURCE: Krill D et al. ACTRIMS Forum 2020, Abstract P085.
WEST PALM BEACH, FLA. – Onset of hyperlipidemia tends to occur earlier in patients with multiple sclerosis (MS), compared with matched controls, according to new research. Among females and African Americans, the effect of MS on age of hyperlipidemia onset may be especially pronounced, said Diane Krill, PhD, professor of biological sciences at Point Park University, Pittsburgh, and colleagues.
Many patients with MS have hyperlipidemia, and adverse lipid profiles correlate with physical and cognitive impairment in this population. “There is evidence of endothelial dysfunction and inflammation in both MS and hyperlipidemia, but the timing of onset of hyperlipidemia is not known,” the researchers said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To assess whether patients with MS have hyperlipidemia diagnosed at an earlier age, relative to matched controls, Dr. Krill and colleagues analyzed data from the Cleveland Clinic health system. They included in their analyses patients with at least two hyperlipidemia diagnoses and at least five encounters with a primary care physician. They matched each patient with MS to four patients without MS using variables such as birth year, sex, race, and year of first encounter. In all, the study included 669 patients with MS and 2,676 controls. The investigators examined age of hyperlipidemia onset using multivariable Cox proportional hazard models that adjusted for sex, race, smoking, and body mass index.
Patients with MS had a 20% increased risk for earlier onset of hyperlipidemia, relative to matched controls. The effect was greater among females (hazard ratio, 1.22) and African Americans (HR, 1.42). Patients with MS have earlier onset of hyperlipidemia “irrespective of the relationship with age of MS onset,” Dr. Krill and colleagues noted. “Additional research is warranted to further characterize the temporal relationships between MS and hyperlipidemia, as well as considerations for timing of disease-modifying therapies.”
The researchers had no relevant disclosures.
SOURCE: Krill D et al. ACTRIMS Forum 2020, Abstract P085.
REPORTING FROM ACTRIMS FORUM 2020
Some infected patients could show COVID-19 symptoms after quarantine
Although a 14-day quarantine after exposure to novel coronavirus is “well supported” by evidence, some infected individuals will not become symptomatic until after that period, according to authors of a recent analysis published in Annals of Internal Medicine.
Most individuals infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will develop symptoms by day 12 of the infection, which is within the 14-day period of active monitoring currently recommended by the Centers for Disease Control and Prevention, the authors wrote.
However, an estimated 101 out of 10,000 cases could become symptomatic after the end of that 14-day monitoring period, they cautioned.
“Our analyses do not preclude that estimate from being higher,” said the investigators, led by Stephen A. Lauer, PhD, MD, of Johns Hopkins Bloomberg School of Public Health, Baltimore.
The analysis, based on 181 confirmed cases of coronavirus disease 2019 (COVID-19) that were documented outside of the outbreak epicenter, Wuhan, China, makes “more conservative assumptions” about the window of symptom onset and potential for continued exposure, compared with analyses in previous studies, the researchers wrote.
The estimated incubation period for SARS-CoV-2 in the 181-patient study was a median of 5.1 days, which is comparable with previous estimates based on COVID-19 cases outside of Wuhan and consistent with other known human coronavirus diseases, such as SARS, which had a reported mean incubation period of 5 days, Dr. Lauer and colleagues noted.
Symptoms developed within 11.5 days for 97.5% of patients in the study.
Whether it’s acceptable to have 101 out of 10,000 cases becoming symptomatic beyond the recommended quarantine window depends on two factors, according to the authors. The first is the expected infection risk in the population that is being monitored, and the second is “judgment about the cost of missing cases,” wrote the authors.
In an interview, Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau, Oceanside, N.Y., said that in practical terms, the results suggest that the majority of patients with COVID-19 will be identified within 14 days, with an “outside chance” of an infected individual leaving quarantine and transmitting virus for a short period of time before becoming symptomatic.
“I think the proper message to give those patients [who are asymptomatic upon leaving quarantine] is, ‘after 14 days, we’re pretty sure you’re out of the woods, but should you get any symptoms, immediately requarantine yourself and seek medical care,” he said.
Study coauthor Kyra H. Grantz, a doctoral graduate student at the Johns Hopkins Bloomberg School of Public Health, said that extending a quarantine beyond 14 days might be considered in the highest-risk scenarios, though the benefits of doing so would have to be weighed against the costs to public health and to the individuals under quarantine.
“Our estimate of the incubation period definitely supports the 14-day recommendation that the CDC has been using,” she said in an interview.
Dr. Grantz emphasized that the estimate of 101 out of 10,000 cases developing symptoms after day 14 of active monitoring – representing the 99th percentile of cases – assumes the “most conservative, worst-case scenario” in a population that is fully infected.
“If you’re looking at a following a cohort of 1,000 people whom you think may have been exposed, only a certain percentage will be infected, and only a certain percentage of those will even develop symptoms – before we get to this idea of how many people would we miss,” she said.
The study was supported by the Centers for Disease Control and Prevention, the National Institute of Allergy and Infectious Diseases, the National Institute of General Medical Sciences, and the Alexander von Humboldt Foundation. Four authors reported disclosures related to those entities, and the remaining five reported no conflicts of interest.
SOURCE: Lauer SA et al. Ann Intern Med. 2020 Mar 9. doi:10.1101/2020.02.02.20020016.
Although a 14-day quarantine after exposure to novel coronavirus is “well supported” by evidence, some infected individuals will not become symptomatic until after that period, according to authors of a recent analysis published in Annals of Internal Medicine.
Most individuals infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will develop symptoms by day 12 of the infection, which is within the 14-day period of active monitoring currently recommended by the Centers for Disease Control and Prevention, the authors wrote.
However, an estimated 101 out of 10,000 cases could become symptomatic after the end of that 14-day monitoring period, they cautioned.
“Our analyses do not preclude that estimate from being higher,” said the investigators, led by Stephen A. Lauer, PhD, MD, of Johns Hopkins Bloomberg School of Public Health, Baltimore.
The analysis, based on 181 confirmed cases of coronavirus disease 2019 (COVID-19) that were documented outside of the outbreak epicenter, Wuhan, China, makes “more conservative assumptions” about the window of symptom onset and potential for continued exposure, compared with analyses in previous studies, the researchers wrote.
The estimated incubation period for SARS-CoV-2 in the 181-patient study was a median of 5.1 days, which is comparable with previous estimates based on COVID-19 cases outside of Wuhan and consistent with other known human coronavirus diseases, such as SARS, which had a reported mean incubation period of 5 days, Dr. Lauer and colleagues noted.
Symptoms developed within 11.5 days for 97.5% of patients in the study.
Whether it’s acceptable to have 101 out of 10,000 cases becoming symptomatic beyond the recommended quarantine window depends on two factors, according to the authors. The first is the expected infection risk in the population that is being monitored, and the second is “judgment about the cost of missing cases,” wrote the authors.
In an interview, Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau, Oceanside, N.Y., said that in practical terms, the results suggest that the majority of patients with COVID-19 will be identified within 14 days, with an “outside chance” of an infected individual leaving quarantine and transmitting virus for a short period of time before becoming symptomatic.
“I think the proper message to give those patients [who are asymptomatic upon leaving quarantine] is, ‘after 14 days, we’re pretty sure you’re out of the woods, but should you get any symptoms, immediately requarantine yourself and seek medical care,” he said.
Study coauthor Kyra H. Grantz, a doctoral graduate student at the Johns Hopkins Bloomberg School of Public Health, said that extending a quarantine beyond 14 days might be considered in the highest-risk scenarios, though the benefits of doing so would have to be weighed against the costs to public health and to the individuals under quarantine.
“Our estimate of the incubation period definitely supports the 14-day recommendation that the CDC has been using,” she said in an interview.
Dr. Grantz emphasized that the estimate of 101 out of 10,000 cases developing symptoms after day 14 of active monitoring – representing the 99th percentile of cases – assumes the “most conservative, worst-case scenario” in a population that is fully infected.
“If you’re looking at a following a cohort of 1,000 people whom you think may have been exposed, only a certain percentage will be infected, and only a certain percentage of those will even develop symptoms – before we get to this idea of how many people would we miss,” she said.
The study was supported by the Centers for Disease Control and Prevention, the National Institute of Allergy and Infectious Diseases, the National Institute of General Medical Sciences, and the Alexander von Humboldt Foundation. Four authors reported disclosures related to those entities, and the remaining five reported no conflicts of interest.
SOURCE: Lauer SA et al. Ann Intern Med. 2020 Mar 9. doi:10.1101/2020.02.02.20020016.
Although a 14-day quarantine after exposure to novel coronavirus is “well supported” by evidence, some infected individuals will not become symptomatic until after that period, according to authors of a recent analysis published in Annals of Internal Medicine.
Most individuals infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will develop symptoms by day 12 of the infection, which is within the 14-day period of active monitoring currently recommended by the Centers for Disease Control and Prevention, the authors wrote.
However, an estimated 101 out of 10,000 cases could become symptomatic after the end of that 14-day monitoring period, they cautioned.
“Our analyses do not preclude that estimate from being higher,” said the investigators, led by Stephen A. Lauer, PhD, MD, of Johns Hopkins Bloomberg School of Public Health, Baltimore.
The analysis, based on 181 confirmed cases of coronavirus disease 2019 (COVID-19) that were documented outside of the outbreak epicenter, Wuhan, China, makes “more conservative assumptions” about the window of symptom onset and potential for continued exposure, compared with analyses in previous studies, the researchers wrote.
The estimated incubation period for SARS-CoV-2 in the 181-patient study was a median of 5.1 days, which is comparable with previous estimates based on COVID-19 cases outside of Wuhan and consistent with other known human coronavirus diseases, such as SARS, which had a reported mean incubation period of 5 days, Dr. Lauer and colleagues noted.
Symptoms developed within 11.5 days for 97.5% of patients in the study.
Whether it’s acceptable to have 101 out of 10,000 cases becoming symptomatic beyond the recommended quarantine window depends on two factors, according to the authors. The first is the expected infection risk in the population that is being monitored, and the second is “judgment about the cost of missing cases,” wrote the authors.
In an interview, Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau, Oceanside, N.Y., said that in practical terms, the results suggest that the majority of patients with COVID-19 will be identified within 14 days, with an “outside chance” of an infected individual leaving quarantine and transmitting virus for a short period of time before becoming symptomatic.
“I think the proper message to give those patients [who are asymptomatic upon leaving quarantine] is, ‘after 14 days, we’re pretty sure you’re out of the woods, but should you get any symptoms, immediately requarantine yourself and seek medical care,” he said.
Study coauthor Kyra H. Grantz, a doctoral graduate student at the Johns Hopkins Bloomberg School of Public Health, said that extending a quarantine beyond 14 days might be considered in the highest-risk scenarios, though the benefits of doing so would have to be weighed against the costs to public health and to the individuals under quarantine.
“Our estimate of the incubation period definitely supports the 14-day recommendation that the CDC has been using,” she said in an interview.
Dr. Grantz emphasized that the estimate of 101 out of 10,000 cases developing symptoms after day 14 of active monitoring – representing the 99th percentile of cases – assumes the “most conservative, worst-case scenario” in a population that is fully infected.
“If you’re looking at a following a cohort of 1,000 people whom you think may have been exposed, only a certain percentage will be infected, and only a certain percentage of those will even develop symptoms – before we get to this idea of how many people would we miss,” she said.
The study was supported by the Centers for Disease Control and Prevention, the National Institute of Allergy and Infectious Diseases, the National Institute of General Medical Sciences, and the Alexander von Humboldt Foundation. Four authors reported disclosures related to those entities, and the remaining five reported no conflicts of interest.
SOURCE: Lauer SA et al. Ann Intern Med. 2020 Mar 9. doi:10.1101/2020.02.02.20020016.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Some individuals who are infected with the novel coronavirus could become symptomatic after the active 14-day quarantine period.
Major finding: The median incubation period was 5.1 days, with 97.5% of patients developing symptoms within 11.5 days, implying that 101 of every 10,000 cases (99th percentile) would develop symptoms beyond the quarantine period.
Study details: Analysis of 181 confirmed COVID-19 cases identified outside of the outbreak epicenter, Wuhan, China.
Disclosures: The study was supported by the U.S. Centers for Disease Control and Prevention, the National Institute of Allergy and Infectious Diseases, the National Institute of General Medical Sciences, and the Alexander von Humboldt Foundation. Four authors reported disclosures related to those entities, and the remaining five reported no conflicts of interest.
Source: Lauer SA et al. Ann Intern Med. 2020 Mar 9. doi: 10.1101/2020.02.02.20020016.
Is there empathy erosion?
You learned a lot of things in medical school. But there must have been some things that you unlearned on the way to your degree. For instance, you unlearned that you could catch a cold by playing outside on a cold damp day without your jacket. You unlearned that handling a toad would give you warts.

The authors of a recent study suggest that over your 4 years in medical school you also unlearned how to be empathetic (“Does Empathy Decline in the Clinical Phase of Medical Education? A Nationwide, Multi-institutional, Cross-Sectional Study of Students at DO-Granting Medical Schools,” Acad Med. 2020 Jan 21. doi: 10.1097/ACM.0000000000003175). The researchers surveyed more than 10,000 medical students at nearly 50 DO-granting medical schools using standardized questionnaire called the Jefferson Scale of Empathy. They discovered that the students in the clinical phase (years 3 and 4) had lower “empathy scores” than the students in the preclinical phase of their education (years 1 and 2). This decline was statistically significant but “negligible” in magnitude. One wonders why they even chose to publish their results, particularly when the number of respondents to the web-based survey declined with each successive year in medical school. Having looked at the a sample of some of the questions being asked, I can understand why third- and fourth-year students couldn’t be bothered to respond. They were too busy to answer a few dozen “lame” questions.
There may be a decline in empathy over the course our medical training, but I’m not sure that this study can speak to it. An older study found that although medical students scores on a self-administered scale declined between the second and third year, the observed empathetic behavior actually increased. If I had to choose, I would lean more heavily on the results of the behavioral observations.
Certainly, we all changed over the course of our medical education. Including postgraduate training, it may have lasted a decade or more. We saw hundreds of patients, observed life and death on a scale and with an intensity that most of us previously had never experienced. Our perspective changed from being a naive observer to playing the role of an active participant. Did that change include a decline in our capacity for empathy?
Something had to change. We found quickly that we didn’t have the time or emotional energy to learn as much about the person hiding behind every complaint as we once thought we should. We had to cut corners. Sometimes we cut too many. On the other hand, as we saw more patients we may have learned more efficient ways of discovering what we needed to know about them to become an effective and caring physician. If we found ourselves in a specialty in which patients have a high mortality, we were forced to learn ways of protecting ourselves from the emotional damage.
What would you call this process? Was it empathy erosion? Was it a hardening or toughening? Or was it simply maturation? Whatever term you use, it was an obligatory process if we hoped to survive. However, not all of us have done it well. Some of us have narrowed our focus to see only the complaint and the diagnosis, and we too often fail to see the human hiding in plain sight.

For those of us who completed our training with our empathy intact, was this the result of a genetic gift or the atmosphere our parents had created at home? I suspect that in most cases our capacity for empathy as physicians was nurtured and enhanced by the role models we encountered during our training. The mentors we most revered were those who had already been through the annealing process of medical school and specialty training and become even more skilled at caring than when they left college. It is an intangible that can’t be taught. Sadly, there is no way of guaranteeing that everyone who enters medical school will be exposed to or benefit from even one of these master physicians.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
You learned a lot of things in medical school. But there must have been some things that you unlearned on the way to your degree. For instance, you unlearned that you could catch a cold by playing outside on a cold damp day without your jacket. You unlearned that handling a toad would give you warts.
The authors of a recent study suggest that over your 4 years in medical school you also unlearned how to be empathetic (“Does Empathy Decline in the Clinical Phase of Medical Education? A Nationwide, Multi-institutional, Cross-Sectional Study of Students at DO-Granting Medical Schools,” Acad Med. 2020 Jan 21. doi: 10.1097/ACM.0000000000003175). The researchers surveyed more than 10,000 medical students at nearly 50 DO-granting medical schools using standardized questionnaire called the Jefferson Scale of Empathy. They discovered that the students in the clinical phase (years 3 and 4) had lower “empathy scores” than the students in the preclinical phase of their education (years 1 and 2). This decline was statistically significant but “negligible” in magnitude. One wonders why they even chose to publish their results, particularly when the number of respondents to the web-based survey declined with each successive year in medical school. Having looked at the a sample of some of the questions being asked, I can understand why third- and fourth-year students couldn’t be bothered to respond. They were too busy to answer a few dozen “lame” questions.
There may be a decline in empathy over the course our medical training, but I’m not sure that this study can speak to it. An older study found that although medical students scores on a self-administered scale declined between the second and third year, the observed empathetic behavior actually increased. If I had to choose, I would lean more heavily on the results of the behavioral observations.
Certainly, we all changed over the course of our medical education. Including postgraduate training, it may have lasted a decade or more. We saw hundreds of patients, observed life and death on a scale and with an intensity that most of us previously had never experienced. Our perspective changed from being a naive observer to playing the role of an active participant. Did that change include a decline in our capacity for empathy?
Something had to change. We found quickly that we didn’t have the time or emotional energy to learn as much about the person hiding behind every complaint as we once thought we should. We had to cut corners. Sometimes we cut too many. On the other hand, as we saw more patients we may have learned more efficient ways of discovering what we needed to know about them to become an effective and caring physician. If we found ourselves in a specialty in which patients have a high mortality, we were forced to learn ways of protecting ourselves from the emotional damage.
What would you call this process? Was it empathy erosion? Was it a hardening or toughening? Or was it simply maturation? Whatever term you use, it was an obligatory process if we hoped to survive. However, not all of us have done it well. Some of us have narrowed our focus to see only the complaint and the diagnosis, and we too often fail to see the human hiding in plain sight.
For those of us who completed our training with our empathy intact, was this the result of a genetic gift or the atmosphere our parents had created at home? I suspect that in most cases our capacity for empathy as physicians was nurtured and enhanced by the role models we encountered during our training. The mentors we most revered were those who had already been through the annealing process of medical school and specialty training and become even more skilled at caring than when they left college. It is an intangible that can’t be taught. Sadly, there is no way of guaranteeing that everyone who enters medical school will be exposed to or benefit from even one of these master physicians.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
You learned a lot of things in medical school. But there must have been some things that you unlearned on the way to your degree. For instance, you unlearned that you could catch a cold by playing outside on a cold damp day without your jacket. You unlearned that handling a toad would give you warts.
The authors of a recent study suggest that over your 4 years in medical school you also unlearned how to be empathetic (“Does Empathy Decline in the Clinical Phase of Medical Education? A Nationwide, Multi-institutional, Cross-Sectional Study of Students at DO-Granting Medical Schools,” Acad Med. 2020 Jan 21. doi: 10.1097/ACM.0000000000003175). The researchers surveyed more than 10,000 medical students at nearly 50 DO-granting medical schools using standardized questionnaire called the Jefferson Scale of Empathy. They discovered that the students in the clinical phase (years 3 and 4) had lower “empathy scores” than the students in the preclinical phase of their education (years 1 and 2). This decline was statistically significant but “negligible” in magnitude. One wonders why they even chose to publish their results, particularly when the number of respondents to the web-based survey declined with each successive year in medical school. Having looked at the a sample of some of the questions being asked, I can understand why third- and fourth-year students couldn’t be bothered to respond. They were too busy to answer a few dozen “lame” questions.
There may be a decline in empathy over the course our medical training, but I’m not sure that this study can speak to it. An older study found that although medical students scores on a self-administered scale declined between the second and third year, the observed empathetic behavior actually increased. If I had to choose, I would lean more heavily on the results of the behavioral observations.
Certainly, we all changed over the course of our medical education. Including postgraduate training, it may have lasted a decade or more. We saw hundreds of patients, observed life and death on a scale and with an intensity that most of us previously had never experienced. Our perspective changed from being a naive observer to playing the role of an active participant. Did that change include a decline in our capacity for empathy?
Something had to change. We found quickly that we didn’t have the time or emotional energy to learn as much about the person hiding behind every complaint as we once thought we should. We had to cut corners. Sometimes we cut too many. On the other hand, as we saw more patients we may have learned more efficient ways of discovering what we needed to know about them to become an effective and caring physician. If we found ourselves in a specialty in which patients have a high mortality, we were forced to learn ways of protecting ourselves from the emotional damage.
What would you call this process? Was it empathy erosion? Was it a hardening or toughening? Or was it simply maturation? Whatever term you use, it was an obligatory process if we hoped to survive. However, not all of us have done it well. Some of us have narrowed our focus to see only the complaint and the diagnosis, and we too often fail to see the human hiding in plain sight.
For those of us who completed our training with our empathy intact, was this the result of a genetic gift or the atmosphere our parents had created at home? I suspect that in most cases our capacity for empathy as physicians was nurtured and enhanced by the role models we encountered during our training. The mentors we most revered were those who had already been through the annealing process of medical school and specialty training and become even more skilled at caring than when they left college. It is an intangible that can’t be taught. Sadly, there is no way of guaranteeing that everyone who enters medical school will be exposed to or benefit from even one of these master physicians.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
TBI deaths from falls on the rise
A 17% surge in mortality from fall-related traumatic brain injuries from 2008 to 2017 was driven largely by increases among those aged 75 years and older, according to investigators from the Centers for Disease Control and Prevention.
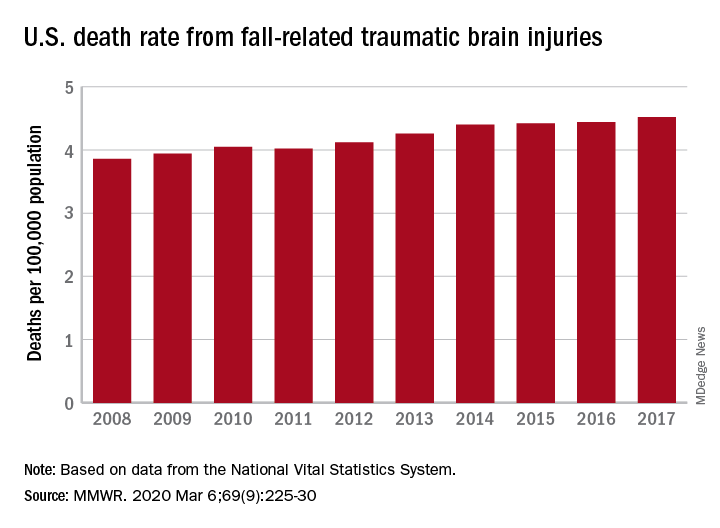
Nationally, the rate of deaths from traumatic brain injuries (TBIs) caused by unintentional falls rose from 3.86 per 100,000 population in 2008 to 4.52 per 100,000 in 2017, as the number of deaths went from 12,311 to 17,408, said Alexis B. Peterson, PhD, and Scott R. Kegler, PhD, of the CDC’s National Center for Injury Prevention and Control in Atlanta.
“This increase might be explained by longer survival following the onset of common diseases such as stroke, cancer, and heart disease or be attributable to the increasing population of older adults in the United States,” they suggested in the Mortality and Morbidity Weekly Report.
The rate of fall-related TBI among Americans aged 75 years and older increased by an average of 2.6% per year from 2008 to 2017, compared with 1.8% in those aged 55-74. Over that same time, death rates dropped for those aged 35-44 (–0.3%), 18-34 (–1.1%), and 0-17 (–4.3%), they said, based on data from the National Vital Statistics System’s multiple cause-of-death database.
The death rate increased fastest in residents of rural areas (2.9% per year), but deaths from fall-related TBI were up at all levels of urbanization. The largest central cities and fringe metro areas were up by 1.4% a year, with larger annual increases seen in medium-size cities (2.1%), small cities (2.2%), and small towns (2.1%), Dr. Peterson and Dr. Kegler said.
Rates of TBI-related mortality in general are higher in rural areas, they noted, and “heterogeneity in the availability and accessibility of resources (e.g., access to high-level trauma centers and rehabilitative services) can result in disparities in postinjury outcomes.”
State-specific rates increased in 45 states, although Alaska was excluded from the analysis because of its small number of cases (less than 20). Increases were significant in 29 states, but none of the changes were significant in the 4 states with lower rates at the end of the study period, the investigators reported.
“In older adults, evidence-based fall prevention strategies can prevent falls and avert costly medical expenditures,” Dr. Peterson and Dr. Kegler said, suggesting that health care providers “consider prescribing exercises that incorporate balance, strength and gait activities, such as tai chi, and reviewing and managing medications linked to falls.”
SOURCE: Peterson AB, Kegler SR. MMWR. 2019 Mar 6;69(9):225-30.
A 17% surge in mortality from fall-related traumatic brain injuries from 2008 to 2017 was driven largely by increases among those aged 75 years and older, according to investigators from the Centers for Disease Control and Prevention.
Nationally, the rate of deaths from traumatic brain injuries (TBIs) caused by unintentional falls rose from 3.86 per 100,000 population in 2008 to 4.52 per 100,000 in 2017, as the number of deaths went from 12,311 to 17,408, said Alexis B. Peterson, PhD, and Scott R. Kegler, PhD, of the CDC’s National Center for Injury Prevention and Control in Atlanta.
“This increase might be explained by longer survival following the onset of common diseases such as stroke, cancer, and heart disease or be attributable to the increasing population of older adults in the United States,” they suggested in the Mortality and Morbidity Weekly Report.
The rate of fall-related TBI among Americans aged 75 years and older increased by an average of 2.6% per year from 2008 to 2017, compared with 1.8% in those aged 55-74. Over that same time, death rates dropped for those aged 35-44 (–0.3%), 18-34 (–1.1%), and 0-17 (–4.3%), they said, based on data from the National Vital Statistics System’s multiple cause-of-death database.
The death rate increased fastest in residents of rural areas (2.9% per year), but deaths from fall-related TBI were up at all levels of urbanization. The largest central cities and fringe metro areas were up by 1.4% a year, with larger annual increases seen in medium-size cities (2.1%), small cities (2.2%), and small towns (2.1%), Dr. Peterson and Dr. Kegler said.
Rates of TBI-related mortality in general are higher in rural areas, they noted, and “heterogeneity in the availability and accessibility of resources (e.g., access to high-level trauma centers and rehabilitative services) can result in disparities in postinjury outcomes.”
State-specific rates increased in 45 states, although Alaska was excluded from the analysis because of its small number of cases (less than 20). Increases were significant in 29 states, but none of the changes were significant in the 4 states with lower rates at the end of the study period, the investigators reported.
“In older adults, evidence-based fall prevention strategies can prevent falls and avert costly medical expenditures,” Dr. Peterson and Dr. Kegler said, suggesting that health care providers “consider prescribing exercises that incorporate balance, strength and gait activities, such as tai chi, and reviewing and managing medications linked to falls.”
SOURCE: Peterson AB, Kegler SR. MMWR. 2019 Mar 6;69(9):225-30.
A 17% surge in mortality from fall-related traumatic brain injuries from 2008 to 2017 was driven largely by increases among those aged 75 years and older, according to investigators from the Centers for Disease Control and Prevention.
Nationally, the rate of deaths from traumatic brain injuries (TBIs) caused by unintentional falls rose from 3.86 per 100,000 population in 2008 to 4.52 per 100,000 in 2017, as the number of deaths went from 12,311 to 17,408, said Alexis B. Peterson, PhD, and Scott R. Kegler, PhD, of the CDC’s National Center for Injury Prevention and Control in Atlanta.
“This increase might be explained by longer survival following the onset of common diseases such as stroke, cancer, and heart disease or be attributable to the increasing population of older adults in the United States,” they suggested in the Mortality and Morbidity Weekly Report.
The rate of fall-related TBI among Americans aged 75 years and older increased by an average of 2.6% per year from 2008 to 2017, compared with 1.8% in those aged 55-74. Over that same time, death rates dropped for those aged 35-44 (–0.3%), 18-34 (–1.1%), and 0-17 (–4.3%), they said, based on data from the National Vital Statistics System’s multiple cause-of-death database.
The death rate increased fastest in residents of rural areas (2.9% per year), but deaths from fall-related TBI were up at all levels of urbanization. The largest central cities and fringe metro areas were up by 1.4% a year, with larger annual increases seen in medium-size cities (2.1%), small cities (2.2%), and small towns (2.1%), Dr. Peterson and Dr. Kegler said.
Rates of TBI-related mortality in general are higher in rural areas, they noted, and “heterogeneity in the availability and accessibility of resources (e.g., access to high-level trauma centers and rehabilitative services) can result in disparities in postinjury outcomes.”
State-specific rates increased in 45 states, although Alaska was excluded from the analysis because of its small number of cases (less than 20). Increases were significant in 29 states, but none of the changes were significant in the 4 states with lower rates at the end of the study period, the investigators reported.
“In older adults, evidence-based fall prevention strategies can prevent falls and avert costly medical expenditures,” Dr. Peterson and Dr. Kegler said, suggesting that health care providers “consider prescribing exercises that incorporate balance, strength and gait activities, such as tai chi, and reviewing and managing medications linked to falls.”
SOURCE: Peterson AB, Kegler SR. MMWR. 2019 Mar 6;69(9):225-30.
FROM MMWR