User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Medical identity theft
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.

– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.

Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.
– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.
Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.
– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.
Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Scientific community ‘shocked’ by loss of MIND diet pioneer
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
Early GI symptoms in COVID-19 may indicate fecal transmission
Fecal-oral transmission may be part of the COVID-19 clinical picture, according to two reports published in Gastroenterology. The researchers find that RNA and proteins from SARS-CoV-2, the viral cause of COVID-19, are shed in feces early in infection and persist after respiratory symptoms abate.
But the discovery is preliminary. “There is evidence of the virus in stool, but not evidence of infectious virus,” David A. Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine in Norfolk, told Medscape Medical News.
The findings are not entirely unexpected. Both of the coronaviruses behind SARS and MERS are shed in stool, Jinyang Gu, MD, from Shanghai Jiao Tong University School of Medicine in Shanghai, China, and colleagues, note in one of the newly published articles.
In addition, as COVID-19 spread beyond China, clinicians began noticing initial mild gastrointestinal (GI) symptoms in some patients, including diarrhea, nausea, vomiting, and abdominal pain, preceding the hallmark fever, dry cough, and dyspnea. The first patient diagnosed in the United States with COVID-19 reported having 2 days of nausea and vomiting, with viral RNA detected in fecal and respiratory specimens, according to an earlier report.
Gu and colleagues warn that initial investigations would likely have not considered cases that manifested initially only as mild gastrointestinal symptoms.
Although early reports indicated that only about 10% of people with COVID-19 have GI symptoms, it isn’t known whether some infected individuals have only GI symptoms, Johnson said.
The GI manifestations are consistent with the distribution of ACE2 receptors, which serve as entry points for SARS-CoV-2, as well as SARS-CoV-1, which causes SARS. The receptors are most abundant in the cell membranes of lung AT2 cells, as well as in enterocytes in the ileum and colon.
“Altogether, many efforts should be made to be alert on the initial digestive symptoms of COVID-19 for early detection, early diagnosis, early isolation and early intervention,” Gu and colleagues conclude.
But Johnson cautions, “gastroenterologists are not the ones managing diagnosis of COVID-19. It is diagnosed as a respiratory illness, but we are seeing concomitant gastrointestinal shedding in stool and saliva, and GI symptoms.”
Samples From 73 Patients Studied
In the second article published, Fei Xiao, MD, of Sun Yat-sen University in Guangdong Province, China, and colleagues report detecting viral RNA in samples from the mouths, noses, throats, urine, and feces of 73 patients hospitalized during the first 2 weeks of February.
Of the 73 hospitalized patients, 39 (53.24%; 25 males and 14 females) had viral RNA in their feces, present from 1 to 12 days. Seventeen (23.29%) of the patients continued to have viral RNA in their stool after respiratory symptoms had improved.
One patient underwent endoscopy. There was no evidence of damage to the GI epithelium, but the clinicians detected slightly elevated levels of lymphocytes and plasma cells.
The researcher used laser scanning confocal microscopy to analyze samples taken during the endoscopy. They found evidence of both ACE2 receptors and viral nucleocapsid proteins in the gastric, duodenal, and rectal glandular epithelial cells.
Finding evidence of SARS-CoV-2 throughout the GI system, if not direct infectivity, suggests a fecal-oral route of transmission, the researchers conclude. “Our immunofluorescent data showed that ACE2 protein, a cell receptor for SARS-CoV-2, is abundantly expressed in the glandular cells of gastric, duodenal and rectal epithelia, supporting the entry of SARS-CoV-2 into the host cells.”
Detection of viral RNA at different time points in infection, they write, suggests that the virions are continually secreted and therefore likely infectious, which is under investigation. “Prevention of fecal-oral transmission should be taken into consideration to control the spread of the virus,” they write.
Current recommendations do not require that patients’ fecal samples be tested before being considered noninfectious. However, given their findings and evidence from other studies, Xiao and colleagues recommend that real-time reverse transcriptase-polymerase chain reaction (rRT-PCR) testing of fecal samples be added to current protocols.
Johnson offers practical suggestions based on the “potty hygiene” suggestions he gives to patients dealing with fecal shedding in Clostridioides difficile infection.
“To combat the microaerosolization of C. diff spores, I have patients do a complete bacteriocidal washing out of the toilet bowl, as well as clean surface areas and especially toothbrushes.” Keeping the bowl closed when not in use is important too in preventing “fecal-oral transmission of remnants” of toilet contents, he adds.
The new papers add to other reports suggesting that virus-bearing droplets may reach people in various ways, Johnson said. “Maybe the virus isn’t only spread by a cough or a sneeze.”
The researchers and commentator have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fecal-oral transmission may be part of the COVID-19 clinical picture, according to two reports published in Gastroenterology. The researchers find that RNA and proteins from SARS-CoV-2, the viral cause of COVID-19, are shed in feces early in infection and persist after respiratory symptoms abate.
But the discovery is preliminary. “There is evidence of the virus in stool, but not evidence of infectious virus,” David A. Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine in Norfolk, told Medscape Medical News.
The findings are not entirely unexpected. Both of the coronaviruses behind SARS and MERS are shed in stool, Jinyang Gu, MD, from Shanghai Jiao Tong University School of Medicine in Shanghai, China, and colleagues, note in one of the newly published articles.
In addition, as COVID-19 spread beyond China, clinicians began noticing initial mild gastrointestinal (GI) symptoms in some patients, including diarrhea, nausea, vomiting, and abdominal pain, preceding the hallmark fever, dry cough, and dyspnea. The first patient diagnosed in the United States with COVID-19 reported having 2 days of nausea and vomiting, with viral RNA detected in fecal and respiratory specimens, according to an earlier report.
Gu and colleagues warn that initial investigations would likely have not considered cases that manifested initially only as mild gastrointestinal symptoms.
Although early reports indicated that only about 10% of people with COVID-19 have GI symptoms, it isn’t known whether some infected individuals have only GI symptoms, Johnson said.
The GI manifestations are consistent with the distribution of ACE2 receptors, which serve as entry points for SARS-CoV-2, as well as SARS-CoV-1, which causes SARS. The receptors are most abundant in the cell membranes of lung AT2 cells, as well as in enterocytes in the ileum and colon.
“Altogether, many efforts should be made to be alert on the initial digestive symptoms of COVID-19 for early detection, early diagnosis, early isolation and early intervention,” Gu and colleagues conclude.
But Johnson cautions, “gastroenterologists are not the ones managing diagnosis of COVID-19. It is diagnosed as a respiratory illness, but we are seeing concomitant gastrointestinal shedding in stool and saliva, and GI symptoms.”
Samples From 73 Patients Studied
In the second article published, Fei Xiao, MD, of Sun Yat-sen University in Guangdong Province, China, and colleagues report detecting viral RNA in samples from the mouths, noses, throats, urine, and feces of 73 patients hospitalized during the first 2 weeks of February.
Of the 73 hospitalized patients, 39 (53.24%; 25 males and 14 females) had viral RNA in their feces, present from 1 to 12 days. Seventeen (23.29%) of the patients continued to have viral RNA in their stool after respiratory symptoms had improved.
One patient underwent endoscopy. There was no evidence of damage to the GI epithelium, but the clinicians detected slightly elevated levels of lymphocytes and plasma cells.
The researcher used laser scanning confocal microscopy to analyze samples taken during the endoscopy. They found evidence of both ACE2 receptors and viral nucleocapsid proteins in the gastric, duodenal, and rectal glandular epithelial cells.
Finding evidence of SARS-CoV-2 throughout the GI system, if not direct infectivity, suggests a fecal-oral route of transmission, the researchers conclude. “Our immunofluorescent data showed that ACE2 protein, a cell receptor for SARS-CoV-2, is abundantly expressed in the glandular cells of gastric, duodenal and rectal epithelia, supporting the entry of SARS-CoV-2 into the host cells.”
Detection of viral RNA at different time points in infection, they write, suggests that the virions are continually secreted and therefore likely infectious, which is under investigation. “Prevention of fecal-oral transmission should be taken into consideration to control the spread of the virus,” they write.
Current recommendations do not require that patients’ fecal samples be tested before being considered noninfectious. However, given their findings and evidence from other studies, Xiao and colleagues recommend that real-time reverse transcriptase-polymerase chain reaction (rRT-PCR) testing of fecal samples be added to current protocols.
Johnson offers practical suggestions based on the “potty hygiene” suggestions he gives to patients dealing with fecal shedding in Clostridioides difficile infection.
“To combat the microaerosolization of C. diff spores, I have patients do a complete bacteriocidal washing out of the toilet bowl, as well as clean surface areas and especially toothbrushes.” Keeping the bowl closed when not in use is important too in preventing “fecal-oral transmission of remnants” of toilet contents, he adds.
The new papers add to other reports suggesting that virus-bearing droplets may reach people in various ways, Johnson said. “Maybe the virus isn’t only spread by a cough or a sneeze.”
The researchers and commentator have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fecal-oral transmission may be part of the COVID-19 clinical picture, according to two reports published in Gastroenterology. The researchers find that RNA and proteins from SARS-CoV-2, the viral cause of COVID-19, are shed in feces early in infection and persist after respiratory symptoms abate.
But the discovery is preliminary. “There is evidence of the virus in stool, but not evidence of infectious virus,” David A. Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine in Norfolk, told Medscape Medical News.
The findings are not entirely unexpected. Both of the coronaviruses behind SARS and MERS are shed in stool, Jinyang Gu, MD, from Shanghai Jiao Tong University School of Medicine in Shanghai, China, and colleagues, note in one of the newly published articles.
In addition, as COVID-19 spread beyond China, clinicians began noticing initial mild gastrointestinal (GI) symptoms in some patients, including diarrhea, nausea, vomiting, and abdominal pain, preceding the hallmark fever, dry cough, and dyspnea. The first patient diagnosed in the United States with COVID-19 reported having 2 days of nausea and vomiting, with viral RNA detected in fecal and respiratory specimens, according to an earlier report.
Gu and colleagues warn that initial investigations would likely have not considered cases that manifested initially only as mild gastrointestinal symptoms.
Although early reports indicated that only about 10% of people with COVID-19 have GI symptoms, it isn’t known whether some infected individuals have only GI symptoms, Johnson said.
The GI manifestations are consistent with the distribution of ACE2 receptors, which serve as entry points for SARS-CoV-2, as well as SARS-CoV-1, which causes SARS. The receptors are most abundant in the cell membranes of lung AT2 cells, as well as in enterocytes in the ileum and colon.
“Altogether, many efforts should be made to be alert on the initial digestive symptoms of COVID-19 for early detection, early diagnosis, early isolation and early intervention,” Gu and colleagues conclude.
But Johnson cautions, “gastroenterologists are not the ones managing diagnosis of COVID-19. It is diagnosed as a respiratory illness, but we are seeing concomitant gastrointestinal shedding in stool and saliva, and GI symptoms.”
Samples From 73 Patients Studied
In the second article published, Fei Xiao, MD, of Sun Yat-sen University in Guangdong Province, China, and colleagues report detecting viral RNA in samples from the mouths, noses, throats, urine, and feces of 73 patients hospitalized during the first 2 weeks of February.
Of the 73 hospitalized patients, 39 (53.24%; 25 males and 14 females) had viral RNA in their feces, present from 1 to 12 days. Seventeen (23.29%) of the patients continued to have viral RNA in their stool after respiratory symptoms had improved.
One patient underwent endoscopy. There was no evidence of damage to the GI epithelium, but the clinicians detected slightly elevated levels of lymphocytes and plasma cells.
The researcher used laser scanning confocal microscopy to analyze samples taken during the endoscopy. They found evidence of both ACE2 receptors and viral nucleocapsid proteins in the gastric, duodenal, and rectal glandular epithelial cells.
Finding evidence of SARS-CoV-2 throughout the GI system, if not direct infectivity, suggests a fecal-oral route of transmission, the researchers conclude. “Our immunofluorescent data showed that ACE2 protein, a cell receptor for SARS-CoV-2, is abundantly expressed in the glandular cells of gastric, duodenal and rectal epithelia, supporting the entry of SARS-CoV-2 into the host cells.”
Detection of viral RNA at different time points in infection, they write, suggests that the virions are continually secreted and therefore likely infectious, which is under investigation. “Prevention of fecal-oral transmission should be taken into consideration to control the spread of the virus,” they write.
Current recommendations do not require that patients’ fecal samples be tested before being considered noninfectious. However, given their findings and evidence from other studies, Xiao and colleagues recommend that real-time reverse transcriptase-polymerase chain reaction (rRT-PCR) testing of fecal samples be added to current protocols.
Johnson offers practical suggestions based on the “potty hygiene” suggestions he gives to patients dealing with fecal shedding in Clostridioides difficile infection.
“To combat the microaerosolization of C. diff spores, I have patients do a complete bacteriocidal washing out of the toilet bowl, as well as clean surface areas and especially toothbrushes.” Keeping the bowl closed when not in use is important too in preventing “fecal-oral transmission of remnants” of toilet contents, he adds.
The new papers add to other reports suggesting that virus-bearing droplets may reach people in various ways, Johnson said. “Maybe the virus isn’t only spread by a cough or a sneeze.”
The researchers and commentator have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Risk factors for death from COVID-19 identified in Wuhan patients
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
Does misplaced faith in modern medicine run at odds against healthier lifestyles?
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.

This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.

Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.
This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.
Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.
This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.
Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
WHO declares COVID-19 outbreak a pandemic
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
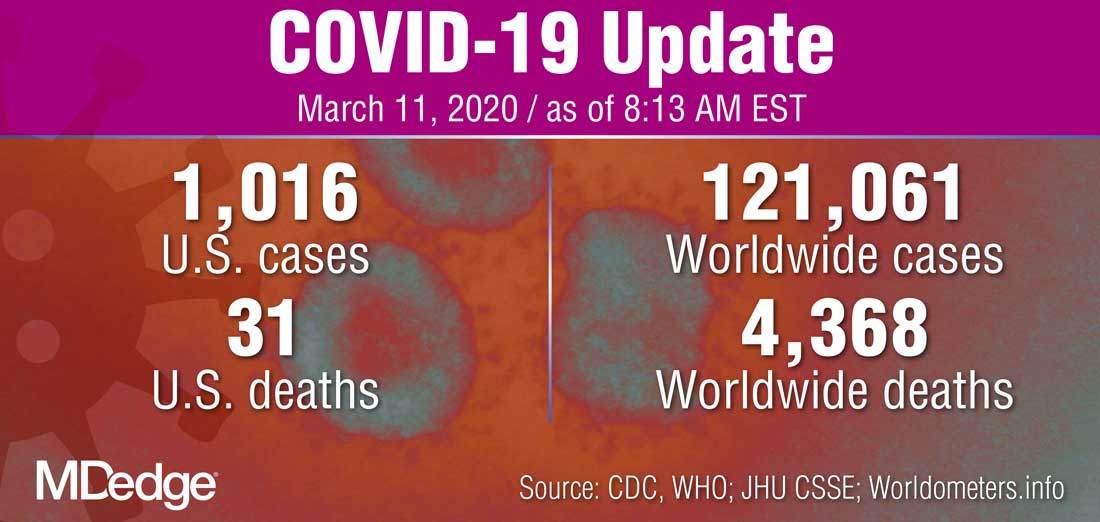
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.
Young women with insomnia at higher risk for car accidents
and reported daytime sleepiness represent a subpopulation at specific risk, according to an analysis of a 5-year population sample. The new research was published online in Sleep and led by Charles Morin, PhD, of Laval University, Quebec City.

The risks of daytime sleepiness and MVA are generally thought of in the context of obstructive sleep apnea (OSA) or men, but the results of the new work suggest that insomnia should not be overlooked, according to Krishna Sundar, MD, clinical professor of pulmonary, critical care, and sleep medicine, and medical director of the Sleep-Wake Center, at the University of Utah, Salt Lake City.
“The notion has been that it may keep them more hypervigilant and less prone to motor vehicle accidents because they are less able to fall asleep even if they want to during the daytime, as compared to other conditions like sleep apnea where there is a higher tendency to doze off,” Dr. Sundar said in an interview.
It should also be remembered that patients aren’t always completely reliable when it comes to self-assessment, according to Brandon M. Seay, MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. “Most people with insomnia won’t say they are sleepy in the daytime, but when you objectively look, you do see an element of daytime sleepiness even if it’s not perceived that well by insomnia patients,” said Dr. Seay.

The heightened risks in young women with insomnia is notable, according to Dr. Sundar. Insomnia is more common in women, and they may also be more susceptible to unintended consequences of sleep medications because they metabolize them more slowly. “Especially for younger women, if they are insomniac and on prescription medicines, and if they have excess daytime sleepiness, this [risk of MVA] needs to be factored in,” said Dr. Sundar.
Insomnia is a condition that waxes and wanes over time, and can vary in its presentation across age groups, which is why the authors chose to conduct a prospective longitudinal study in a Canadian sample. They recruited 3,413 adults with insomnia (median age, 49.0 years; range, 18-96; 61.5% female). After 5 years, the retention rate was 68.7%.
After filling out baseline information, participants were asked every 6 months about MVAs and what role they believed daytime consequences of insomnia played if an accident occurred. Prescription and over-the-counter medication use were also self-reported.
In the first 2 years of the study, 8.2% of women aged 18-29 reported MVAs, which was the highest of any demographic (range, 2.3%-4.3%). By the third year, the frequency in this group overlapped that of men in the same age group, and both remained higher than older age groups.
Participants judged that insomnia consequences played a role in 39.4% of reported MVA. In 17.2% of accidents, participants said insomnia consequences contributed at least 50% of the cause.
MVA risk was associated individually with presence of insomnia symptoms (hazard ratio [HR], 1.20; 95% confidence interval, 1.00-1.45) and daytime fatigue (HR, 1.21; 95% CI, 1.01-1.47), but there were only trends toward associations with sleeping fewer than 6 hours (P = .16) and excessive daytime sleepiness (P = .06). MVAs were associated with reported past-year use of prescribed sleep medications (HR, 1.50; 95% CI, 1.17-1.91) and reported use of OTC medications (HR, 1.42; 95% CI, 1.02-1.98).
In women aged 18-29, MVAs were associated with insomnia symptoms (HR, 1.83; 95% CI, 1.13-2.98) and excessive daytime sleepiness (HR, 2.42; 95% CI, 1.11-5.24).
The study was limited by its reliance on self-reporting and lack of data on specific medications used.
The study was funded by the Canadian Institutes of Health.
SOURCE: Morin C et al. Sleep. 2020 Feb 29. DOI: 10.1093/sleep/zsaa032.
and reported daytime sleepiness represent a subpopulation at specific risk, according to an analysis of a 5-year population sample. The new research was published online in Sleep and led by Charles Morin, PhD, of Laval University, Quebec City.
The risks of daytime sleepiness and MVA are generally thought of in the context of obstructive sleep apnea (OSA) or men, but the results of the new work suggest that insomnia should not be overlooked, according to Krishna Sundar, MD, clinical professor of pulmonary, critical care, and sleep medicine, and medical director of the Sleep-Wake Center, at the University of Utah, Salt Lake City.
“The notion has been that it may keep them more hypervigilant and less prone to motor vehicle accidents because they are less able to fall asleep even if they want to during the daytime, as compared to other conditions like sleep apnea where there is a higher tendency to doze off,” Dr. Sundar said in an interview.
It should also be remembered that patients aren’t always completely reliable when it comes to self-assessment, according to Brandon M. Seay, MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. “Most people with insomnia won’t say they are sleepy in the daytime, but when you objectively look, you do see an element of daytime sleepiness even if it’s not perceived that well by insomnia patients,” said Dr. Seay.
The heightened risks in young women with insomnia is notable, according to Dr. Sundar. Insomnia is more common in women, and they may also be more susceptible to unintended consequences of sleep medications because they metabolize them more slowly. “Especially for younger women, if they are insomniac and on prescription medicines, and if they have excess daytime sleepiness, this [risk of MVA] needs to be factored in,” said Dr. Sundar.
Insomnia is a condition that waxes and wanes over time, and can vary in its presentation across age groups, which is why the authors chose to conduct a prospective longitudinal study in a Canadian sample. They recruited 3,413 adults with insomnia (median age, 49.0 years; range, 18-96; 61.5% female). After 5 years, the retention rate was 68.7%.
After filling out baseline information, participants were asked every 6 months about MVAs and what role they believed daytime consequences of insomnia played if an accident occurred. Prescription and over-the-counter medication use were also self-reported.
In the first 2 years of the study, 8.2% of women aged 18-29 reported MVAs, which was the highest of any demographic (range, 2.3%-4.3%). By the third year, the frequency in this group overlapped that of men in the same age group, and both remained higher than older age groups.
Participants judged that insomnia consequences played a role in 39.4% of reported MVA. In 17.2% of accidents, participants said insomnia consequences contributed at least 50% of the cause.
MVA risk was associated individually with presence of insomnia symptoms (hazard ratio [HR], 1.20; 95% confidence interval, 1.00-1.45) and daytime fatigue (HR, 1.21; 95% CI, 1.01-1.47), but there were only trends toward associations with sleeping fewer than 6 hours (P = .16) and excessive daytime sleepiness (P = .06). MVAs were associated with reported past-year use of prescribed sleep medications (HR, 1.50; 95% CI, 1.17-1.91) and reported use of OTC medications (HR, 1.42; 95% CI, 1.02-1.98).
In women aged 18-29, MVAs were associated with insomnia symptoms (HR, 1.83; 95% CI, 1.13-2.98) and excessive daytime sleepiness (HR, 2.42; 95% CI, 1.11-5.24).
The study was limited by its reliance on self-reporting and lack of data on specific medications used.
The study was funded by the Canadian Institutes of Health.
SOURCE: Morin C et al. Sleep. 2020 Feb 29. DOI: 10.1093/sleep/zsaa032.
and reported daytime sleepiness represent a subpopulation at specific risk, according to an analysis of a 5-year population sample. The new research was published online in Sleep and led by Charles Morin, PhD, of Laval University, Quebec City.
The risks of daytime sleepiness and MVA are generally thought of in the context of obstructive sleep apnea (OSA) or men, but the results of the new work suggest that insomnia should not be overlooked, according to Krishna Sundar, MD, clinical professor of pulmonary, critical care, and sleep medicine, and medical director of the Sleep-Wake Center, at the University of Utah, Salt Lake City.
“The notion has been that it may keep them more hypervigilant and less prone to motor vehicle accidents because they are less able to fall asleep even if they want to during the daytime, as compared to other conditions like sleep apnea where there is a higher tendency to doze off,” Dr. Sundar said in an interview.
It should also be remembered that patients aren’t always completely reliable when it comes to self-assessment, according to Brandon M. Seay, MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. “Most people with insomnia won’t say they are sleepy in the daytime, but when you objectively look, you do see an element of daytime sleepiness even if it’s not perceived that well by insomnia patients,” said Dr. Seay.
The heightened risks in young women with insomnia is notable, according to Dr. Sundar. Insomnia is more common in women, and they may also be more susceptible to unintended consequences of sleep medications because they metabolize them more slowly. “Especially for younger women, if they are insomniac and on prescription medicines, and if they have excess daytime sleepiness, this [risk of MVA] needs to be factored in,” said Dr. Sundar.
Insomnia is a condition that waxes and wanes over time, and can vary in its presentation across age groups, which is why the authors chose to conduct a prospective longitudinal study in a Canadian sample. They recruited 3,413 adults with insomnia (median age, 49.0 years; range, 18-96; 61.5% female). After 5 years, the retention rate was 68.7%.
After filling out baseline information, participants were asked every 6 months about MVAs and what role they believed daytime consequences of insomnia played if an accident occurred. Prescription and over-the-counter medication use were also self-reported.
In the first 2 years of the study, 8.2% of women aged 18-29 reported MVAs, which was the highest of any demographic (range, 2.3%-4.3%). By the third year, the frequency in this group overlapped that of men in the same age group, and both remained higher than older age groups.
Participants judged that insomnia consequences played a role in 39.4% of reported MVA. In 17.2% of accidents, participants said insomnia consequences contributed at least 50% of the cause.
MVA risk was associated individually with presence of insomnia symptoms (hazard ratio [HR], 1.20; 95% confidence interval, 1.00-1.45) and daytime fatigue (HR, 1.21; 95% CI, 1.01-1.47), but there were only trends toward associations with sleeping fewer than 6 hours (P = .16) and excessive daytime sleepiness (P = .06). MVAs were associated with reported past-year use of prescribed sleep medications (HR, 1.50; 95% CI, 1.17-1.91) and reported use of OTC medications (HR, 1.42; 95% CI, 1.02-1.98).
In women aged 18-29, MVAs were associated with insomnia symptoms (HR, 1.83; 95% CI, 1.13-2.98) and excessive daytime sleepiness (HR, 2.42; 95% CI, 1.11-5.24).
The study was limited by its reliance on self-reporting and lack of data on specific medications used.
The study was funded by the Canadian Institutes of Health.
SOURCE: Morin C et al. Sleep. 2020 Feb 29. DOI: 10.1093/sleep/zsaa032.
FROM SLEEP
Manual dexterity may decline more rapidly in pediatric-onset MS
WEST PALM BEACH, FLA. – (AOMS), according to an analysis presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.

When MS onset occurs before the patient is age 18 years, the patient is considered to have POMS. Compared with AOMS, POMS is less prevalent and has distinct features. To determine whether changes in physical performance differ between POMS and AOMS, Sarah M. Planchon, PhD, a project scientist at the Mellen Center for MS at the Cleveland Clinic, and colleagues analyzed data cut 9 from the MS PATHS (MS Partners Advancing Technology and Health Solutions) initiative. As part of this initiative, which is sponsored by Biogen, investigators collect MS performance measures longitudinally at each patient visit. Among these measures are the manual dexterity test (MDT), an iPad version of the Nine-Hole Peg Test, and the walking speed test (WST), which is the iPad version of the Timed 25-Foot Walk.
Dr. Planchon and colleagues matched each patient with POMS to five patients with AOMS according to disease duration. They calculated descriptive statistics for the sample and performed Tukey’s honestly significant difference test to compare patient groups on several categorical variables.
Overall, function was better in POMS than in AOMS
The investigators included 3 years’ worth of data from 6,457 patients in their analysis. The average age was approximately 50 years for patients with AOMS and 31 years for patients with POMS. The time elapsed since diagnosis was approximately 14 years in the AOMS group and 17 years in the POMS group. The proportion of female patients was about 74% in the AOMS group and 73% in the POMS group. Compared with the AOMS group, the POMS group had higher proportions of patients who were Asian (0.5% vs 2.6%), black (9.3% vs 11.5%), and other race (2.8% vs 9.3%).
Overall, patients with POMS performed better than patients with AOMS by 1.39 seconds on the MDT and by 0.79 seconds on the WST. Regression analyses indicated that with increasing age, patients with AOMS declined more quickly on the MDT and the WST than patients with POMS did. When the investigators stratified the results by disease duration, however, patients with POMS declined more rapidly on the MDT than did patients with AOMS. There was no significant difference between groups in WST in this analysis. When Dr. Planchon and colleagues performed linear regression and adjusted for variables such as age, sex, race, education, insurance, employment, MS phenotype, disease duration, number of relapses, and Patient-Determined Disease Steps (PDDS), the MS onset type did not significantly affect outcomes. Age, sex, PDDS, and MS type were significant covariates for both tests.
The role of occupational and physical therapy
“POMS patients tend to have a greater dysfunction of the cerebellar and brainstem regions of the brain, both of which may impact motor skills to a greater degree than other regions of the brain,” said Dr. Planchon. The increased rate of manual impairment in POMS, compared with AOMS, does not necessarily indicate more severe disease, she added. Getting a true picture of disease severity would require consideration of factors such as ambulation, cognitive functioning, vision, fatigue, and depression.
“We would recommend introducing POMS patients to occupational and physical therapy early in their disease course, before significant deficits accrue,” said Dr. Planchon. “Early familiarity with rehabilitation services should help the patient and family optimize what exercises are being done to improve and maintain function.”
The optimal pharmacologic treatment for POMS is unknown. One therapy (i.e., fingolimod) has Food and Drug Administration approval, and clinical trials of other treatments are ongoing. Some MS treatments not indicated for a pediatric population are used off label in children.
“We plan to delve deeper into the data set, including using regression modeling to try to better define differences between individuals with POMS and AOMS that may lead to the functional outcome changes we have already observed,” said Dr. Planchon. “We also plan to investigate further the impact of POMS on cognition and quality of life measures and to better understand disease-modifying therapy prescribing patterns and benefits in individuals with POMS. We will look for associations in the MRI imaging findings and various biomarkers to help us understand the disease process in this special population of MS.”
Dr. Planchon has received research support from the Guthy-Jackson Charitable Foundation. Her coinvestigators received funding from Biogen, Genentech, Genzyme, MedImmune, Novartis, Serono, and Teva.
SOURCE: Planchon SM et al. ACTRIMS 2020. Abstract P043.
WEST PALM BEACH, FLA. – (AOMS), according to an analysis presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
When MS onset occurs before the patient is age 18 years, the patient is considered to have POMS. Compared with AOMS, POMS is less prevalent and has distinct features. To determine whether changes in physical performance differ between POMS and AOMS, Sarah M. Planchon, PhD, a project scientist at the Mellen Center for MS at the Cleveland Clinic, and colleagues analyzed data cut 9 from the MS PATHS (MS Partners Advancing Technology and Health Solutions) initiative. As part of this initiative, which is sponsored by Biogen, investigators collect MS performance measures longitudinally at each patient visit. Among these measures are the manual dexterity test (MDT), an iPad version of the Nine-Hole Peg Test, and the walking speed test (WST), which is the iPad version of the Timed 25-Foot Walk.
Dr. Planchon and colleagues matched each patient with POMS to five patients with AOMS according to disease duration. They calculated descriptive statistics for the sample and performed Tukey’s honestly significant difference test to compare patient groups on several categorical variables.
Overall, function was better in POMS than in AOMS
The investigators included 3 years’ worth of data from 6,457 patients in their analysis. The average age was approximately 50 years for patients with AOMS and 31 years for patients with POMS. The time elapsed since diagnosis was approximately 14 years in the AOMS group and 17 years in the POMS group. The proportion of female patients was about 74% in the AOMS group and 73% in the POMS group. Compared with the AOMS group, the POMS group had higher proportions of patients who were Asian (0.5% vs 2.6%), black (9.3% vs 11.5%), and other race (2.8% vs 9.3%).
Overall, patients with POMS performed better than patients with AOMS by 1.39 seconds on the MDT and by 0.79 seconds on the WST. Regression analyses indicated that with increasing age, patients with AOMS declined more quickly on the MDT and the WST than patients with POMS did. When the investigators stratified the results by disease duration, however, patients with POMS declined more rapidly on the MDT than did patients with AOMS. There was no significant difference between groups in WST in this analysis. When Dr. Planchon and colleagues performed linear regression and adjusted for variables such as age, sex, race, education, insurance, employment, MS phenotype, disease duration, number of relapses, and Patient-Determined Disease Steps (PDDS), the MS onset type did not significantly affect outcomes. Age, sex, PDDS, and MS type were significant covariates for both tests.
The role of occupational and physical therapy
“POMS patients tend to have a greater dysfunction of the cerebellar and brainstem regions of the brain, both of which may impact motor skills to a greater degree than other regions of the brain,” said Dr. Planchon. The increased rate of manual impairment in POMS, compared with AOMS, does not necessarily indicate more severe disease, she added. Getting a true picture of disease severity would require consideration of factors such as ambulation, cognitive functioning, vision, fatigue, and depression.
“We would recommend introducing POMS patients to occupational and physical therapy early in their disease course, before significant deficits accrue,” said Dr. Planchon. “Early familiarity with rehabilitation services should help the patient and family optimize what exercises are being done to improve and maintain function.”
The optimal pharmacologic treatment for POMS is unknown. One therapy (i.e., fingolimod) has Food and Drug Administration approval, and clinical trials of other treatments are ongoing. Some MS treatments not indicated for a pediatric population are used off label in children.
“We plan to delve deeper into the data set, including using regression modeling to try to better define differences between individuals with POMS and AOMS that may lead to the functional outcome changes we have already observed,” said Dr. Planchon. “We also plan to investigate further the impact of POMS on cognition and quality of life measures and to better understand disease-modifying therapy prescribing patterns and benefits in individuals with POMS. We will look for associations in the MRI imaging findings and various biomarkers to help us understand the disease process in this special population of MS.”
Dr. Planchon has received research support from the Guthy-Jackson Charitable Foundation. Her coinvestigators received funding from Biogen, Genentech, Genzyme, MedImmune, Novartis, Serono, and Teva.
SOURCE: Planchon SM et al. ACTRIMS 2020. Abstract P043.
WEST PALM BEACH, FLA. – (AOMS), according to an analysis presented at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
When MS onset occurs before the patient is age 18 years, the patient is considered to have POMS. Compared with AOMS, POMS is less prevalent and has distinct features. To determine whether changes in physical performance differ between POMS and AOMS, Sarah M. Planchon, PhD, a project scientist at the Mellen Center for MS at the Cleveland Clinic, and colleagues analyzed data cut 9 from the MS PATHS (MS Partners Advancing Technology and Health Solutions) initiative. As part of this initiative, which is sponsored by Biogen, investigators collect MS performance measures longitudinally at each patient visit. Among these measures are the manual dexterity test (MDT), an iPad version of the Nine-Hole Peg Test, and the walking speed test (WST), which is the iPad version of the Timed 25-Foot Walk.
Dr. Planchon and colleagues matched each patient with POMS to five patients with AOMS according to disease duration. They calculated descriptive statistics for the sample and performed Tukey’s honestly significant difference test to compare patient groups on several categorical variables.
Overall, function was better in POMS than in AOMS
The investigators included 3 years’ worth of data from 6,457 patients in their analysis. The average age was approximately 50 years for patients with AOMS and 31 years for patients with POMS. The time elapsed since diagnosis was approximately 14 years in the AOMS group and 17 years in the POMS group. The proportion of female patients was about 74% in the AOMS group and 73% in the POMS group. Compared with the AOMS group, the POMS group had higher proportions of patients who were Asian (0.5% vs 2.6%), black (9.3% vs 11.5%), and other race (2.8% vs 9.3%).
Overall, patients with POMS performed better than patients with AOMS by 1.39 seconds on the MDT and by 0.79 seconds on the WST. Regression analyses indicated that with increasing age, patients with AOMS declined more quickly on the MDT and the WST than patients with POMS did. When the investigators stratified the results by disease duration, however, patients with POMS declined more rapidly on the MDT than did patients with AOMS. There was no significant difference between groups in WST in this analysis. When Dr. Planchon and colleagues performed linear regression and adjusted for variables such as age, sex, race, education, insurance, employment, MS phenotype, disease duration, number of relapses, and Patient-Determined Disease Steps (PDDS), the MS onset type did not significantly affect outcomes. Age, sex, PDDS, and MS type were significant covariates for both tests.
The role of occupational and physical therapy
“POMS patients tend to have a greater dysfunction of the cerebellar and brainstem regions of the brain, both of which may impact motor skills to a greater degree than other regions of the brain,” said Dr. Planchon. The increased rate of manual impairment in POMS, compared with AOMS, does not necessarily indicate more severe disease, she added. Getting a true picture of disease severity would require consideration of factors such as ambulation, cognitive functioning, vision, fatigue, and depression.
“We would recommend introducing POMS patients to occupational and physical therapy early in their disease course, before significant deficits accrue,” said Dr. Planchon. “Early familiarity with rehabilitation services should help the patient and family optimize what exercises are being done to improve and maintain function.”
The optimal pharmacologic treatment for POMS is unknown. One therapy (i.e., fingolimod) has Food and Drug Administration approval, and clinical trials of other treatments are ongoing. Some MS treatments not indicated for a pediatric population are used off label in children.
“We plan to delve deeper into the data set, including using regression modeling to try to better define differences between individuals with POMS and AOMS that may lead to the functional outcome changes we have already observed,” said Dr. Planchon. “We also plan to investigate further the impact of POMS on cognition and quality of life measures and to better understand disease-modifying therapy prescribing patterns and benefits in individuals with POMS. We will look for associations in the MRI imaging findings and various biomarkers to help us understand the disease process in this special population of MS.”
Dr. Planchon has received research support from the Guthy-Jackson Charitable Foundation. Her coinvestigators received funding from Biogen, Genentech, Genzyme, MedImmune, Novartis, Serono, and Teva.
SOURCE: Planchon SM et al. ACTRIMS 2020. Abstract P043.
REPORTING FROM ACTRIMS FORUM 2020
Managing children’s fear, anxiety in the age of COVID-19
With coronavirus disease (COVID-19) reaching epidemic proportions, many US children are growing increasingly anxious about what this means for their own health and safety and that of their friends and family.
The constantly changing numbers of people affected by the virus and the evolving situation mean daily life for many children is affected in some way, with school trips, sports tournaments, and family vacations being postponed or canceled.
All children may have a heightened level of worry, and some who are normally anxious might be obsessing more about handwashing or getting sick.
Experts say there are ways to manage this fear to help children feel safe and appropriately informed.
Clinicians and other adults should provide children with honest and accurate information geared to their age and developmental level, said David Fassler, MD, clinical professor of psychiatry, University of Vermont Larner College of Medicine, Burlington, and member of the Consumer Issues Committee of the American Academy of Child and Adolescent Psychiatry.
That said, it’s also acceptable to let children know that some questions can’t be answered, said Fassler.
Be truthful, calm
“This is partly because the information keeps changing as we learn more about how the virus spreads, how to best protect communities, and how to treat people who get sick,” he added.
Clinicians and parents should remind children “that there are a lot of adults who are working very hard to keep them safe,” said Eli R. Lebowitz, PhD, associate professor in the Child Study Center, Yale School of Medicine, New Haven, Connecticut, who directs a program for anxiety.
It’s important for adults to pay attention not only to what they say to children but also how they say it, said Lebowitz. He highlighted the importance of talking about the virus “in a calm and matter-of-fact way” rather than in an anxious way.
“If you look scared or tense or your voice is conveying that you’re really scared, the child is going to absorb that and feel anxious as well,” he noted.
This advice also applies when adults are discussing the issue among themselves. They should be aware that “children are listening” and are picking up any anxiety or panic adults are expressing.
Children are soaking up information about this virus from the Internet, the media, friends, teachers, and elsewhere. Lebowitz suggests asking children what they have already heard, which provides an opportunity to correct rumors and inaccurate information.
“A child might have a very inflated sense of what the actual risk is. For example, they may think that anyone who gets the virus dies,” he said.
Myth busting
Adults should let children know that not everything they hear from friends or on the Internet “is necessarily correct,” he added.
Some children who have experienced serious illness or losses may be particularly vulnerable to experiencing intense reactions to graphic news reports or images of illness or death and may need extra support, said Fassler.
Adults could use the “framework of knowledge” that children already have, said Lebowitz. He noted that all children are aware of sickness.
“They know people get sick, and they themselves have probably been sick, so you can tell them that this is a sickness like a bad flu,” he said.
Children should be encouraged to approach adults they trust, such as their pediatrician, a parent, or a teacher, with their questions, said Lebowitz. “Those are the people who are able to give them the most accurate information.”
Fassler noted that accurate, up-to-date information is available via fact sheets developed by the Centers for Disease Control and Prevention and the World Health Organization.
Although it’s helpful and appropriate to be reassuring, Fassler advises not to make unrealistic promises.
“It’s fine to tell kids that you’ll deal with whatever happens, even if it means altering travel plans or work schedules, but you can’t promise that no one in your state or community will get sick,” he said.
Maintain healthy habits
Physicians and other adults can tell children “in an age-appropriate way” how the virus is transmitted and what the symptoms are, but it’s important to emphasize that most people who are sick don’t have COVID-19, said Lebowitz.
“I would emphasize that the people who are the sickest are the elderly who are already sick, rather than healthy younger people,” he said.
Lebowitz recommends continuing to follow guidelines on staying healthy, including coughing into a sleeve instead of your hand and regular handwashing.
It’s also important at this time for children to maintain healthy habits – getting enough physical activity and sleep, eating well, and being outside – because this regime will go a long way toward reducing anxiety, said Lebowitz. Deep breathing and muscle-relaxing exercises can also help, he said.
Lebowitz also suggests maintaining a supportive attitude and showing “some acceptance and validation of what children are feeling, as well as some confidence that they can cope and tolerate feeling uncomfortable sometimes, that they can handle some anxiety.”
While accepting that the child could be anxious, it’s important not to encourage excessive avoidance or unhealthy coping strategies. Fassler and Lebowitz agree that children who are overly anxious or preoccupied with concerns about the coronavirus should be evaluated by a trained, qualified mental health professional.
Signs that a child may need additional help include ongoing sleep difficulties, intrusive thoughts or worries, obsessive-compulsive behaviors, or reluctance or refusal to go to school, said Fassler.
The good news is that most children are resilient, said Fassler. “They’ll adjust, adapt, and go on with their lives.”
This article first appeared on Medscape.com.
With coronavirus disease (COVID-19) reaching epidemic proportions, many US children are growing increasingly anxious about what this means for their own health and safety and that of their friends and family.
The constantly changing numbers of people affected by the virus and the evolving situation mean daily life for many children is affected in some way, with school trips, sports tournaments, and family vacations being postponed or canceled.
All children may have a heightened level of worry, and some who are normally anxious might be obsessing more about handwashing or getting sick.
Experts say there are ways to manage this fear to help children feel safe and appropriately informed.
Clinicians and other adults should provide children with honest and accurate information geared to their age and developmental level, said David Fassler, MD, clinical professor of psychiatry, University of Vermont Larner College of Medicine, Burlington, and member of the Consumer Issues Committee of the American Academy of Child and Adolescent Psychiatry.
That said, it’s also acceptable to let children know that some questions can’t be answered, said Fassler.
Be truthful, calm
“This is partly because the information keeps changing as we learn more about how the virus spreads, how to best protect communities, and how to treat people who get sick,” he added.
Clinicians and parents should remind children “that there are a lot of adults who are working very hard to keep them safe,” said Eli R. Lebowitz, PhD, associate professor in the Child Study Center, Yale School of Medicine, New Haven, Connecticut, who directs a program for anxiety.
It’s important for adults to pay attention not only to what they say to children but also how they say it, said Lebowitz. He highlighted the importance of talking about the virus “in a calm and matter-of-fact way” rather than in an anxious way.
“If you look scared or tense or your voice is conveying that you’re really scared, the child is going to absorb that and feel anxious as well,” he noted.
This advice also applies when adults are discussing the issue among themselves. They should be aware that “children are listening” and are picking up any anxiety or panic adults are expressing.
Children are soaking up information about this virus from the Internet, the media, friends, teachers, and elsewhere. Lebowitz suggests asking children what they have already heard, which provides an opportunity to correct rumors and inaccurate information.
“A child might have a very inflated sense of what the actual risk is. For example, they may think that anyone who gets the virus dies,” he said.
Myth busting
Adults should let children know that not everything they hear from friends or on the Internet “is necessarily correct,” he added.
Some children who have experienced serious illness or losses may be particularly vulnerable to experiencing intense reactions to graphic news reports or images of illness or death and may need extra support, said Fassler.
Adults could use the “framework of knowledge” that children already have, said Lebowitz. He noted that all children are aware of sickness.
“They know people get sick, and they themselves have probably been sick, so you can tell them that this is a sickness like a bad flu,” he said.
Children should be encouraged to approach adults they trust, such as their pediatrician, a parent, or a teacher, with their questions, said Lebowitz. “Those are the people who are able to give them the most accurate information.”
Fassler noted that accurate, up-to-date information is available via fact sheets developed by the Centers for Disease Control and Prevention and the World Health Organization.
Although it’s helpful and appropriate to be reassuring, Fassler advises not to make unrealistic promises.
“It’s fine to tell kids that you’ll deal with whatever happens, even if it means altering travel plans or work schedules, but you can’t promise that no one in your state or community will get sick,” he said.
Maintain healthy habits
Physicians and other adults can tell children “in an age-appropriate way” how the virus is transmitted and what the symptoms are, but it’s important to emphasize that most people who are sick don’t have COVID-19, said Lebowitz.
“I would emphasize that the people who are the sickest are the elderly who are already sick, rather than healthy younger people,” he said.
Lebowitz recommends continuing to follow guidelines on staying healthy, including coughing into a sleeve instead of your hand and regular handwashing.
It’s also important at this time for children to maintain healthy habits – getting enough physical activity and sleep, eating well, and being outside – because this regime will go a long way toward reducing anxiety, said Lebowitz. Deep breathing and muscle-relaxing exercises can also help, he said.
Lebowitz also suggests maintaining a supportive attitude and showing “some acceptance and validation of what children are feeling, as well as some confidence that they can cope and tolerate feeling uncomfortable sometimes, that they can handle some anxiety.”
While accepting that the child could be anxious, it’s important not to encourage excessive avoidance or unhealthy coping strategies. Fassler and Lebowitz agree that children who are overly anxious or preoccupied with concerns about the coronavirus should be evaluated by a trained, qualified mental health professional.
Signs that a child may need additional help include ongoing sleep difficulties, intrusive thoughts or worries, obsessive-compulsive behaviors, or reluctance or refusal to go to school, said Fassler.
The good news is that most children are resilient, said Fassler. “They’ll adjust, adapt, and go on with their lives.”
This article first appeared on Medscape.com.
With coronavirus disease (COVID-19) reaching epidemic proportions, many US children are growing increasingly anxious about what this means for their own health and safety and that of their friends and family.
The constantly changing numbers of people affected by the virus and the evolving situation mean daily life for many children is affected in some way, with school trips, sports tournaments, and family vacations being postponed or canceled.
All children may have a heightened level of worry, and some who are normally anxious might be obsessing more about handwashing or getting sick.
Experts say there are ways to manage this fear to help children feel safe and appropriately informed.
Clinicians and other adults should provide children with honest and accurate information geared to their age and developmental level, said David Fassler, MD, clinical professor of psychiatry, University of Vermont Larner College of Medicine, Burlington, and member of the Consumer Issues Committee of the American Academy of Child and Adolescent Psychiatry.
That said, it’s also acceptable to let children know that some questions can’t be answered, said Fassler.
Be truthful, calm
“This is partly because the information keeps changing as we learn more about how the virus spreads, how to best protect communities, and how to treat people who get sick,” he added.
Clinicians and parents should remind children “that there are a lot of adults who are working very hard to keep them safe,” said Eli R. Lebowitz, PhD, associate professor in the Child Study Center, Yale School of Medicine, New Haven, Connecticut, who directs a program for anxiety.
It’s important for adults to pay attention not only to what they say to children but also how they say it, said Lebowitz. He highlighted the importance of talking about the virus “in a calm and matter-of-fact way” rather than in an anxious way.
“If you look scared or tense or your voice is conveying that you’re really scared, the child is going to absorb that and feel anxious as well,” he noted.
This advice also applies when adults are discussing the issue among themselves. They should be aware that “children are listening” and are picking up any anxiety or panic adults are expressing.
Children are soaking up information about this virus from the Internet, the media, friends, teachers, and elsewhere. Lebowitz suggests asking children what they have already heard, which provides an opportunity to correct rumors and inaccurate information.
“A child might have a very inflated sense of what the actual risk is. For example, they may think that anyone who gets the virus dies,” he said.
Myth busting
Adults should let children know that not everything they hear from friends or on the Internet “is necessarily correct,” he added.
Some children who have experienced serious illness or losses may be particularly vulnerable to experiencing intense reactions to graphic news reports or images of illness or death and may need extra support, said Fassler.
Adults could use the “framework of knowledge” that children already have, said Lebowitz. He noted that all children are aware of sickness.
“They know people get sick, and they themselves have probably been sick, so you can tell them that this is a sickness like a bad flu,” he said.
Children should be encouraged to approach adults they trust, such as their pediatrician, a parent, or a teacher, with their questions, said Lebowitz. “Those are the people who are able to give them the most accurate information.”
Fassler noted that accurate, up-to-date information is available via fact sheets developed by the Centers for Disease Control and Prevention and the World Health Organization.
Although it’s helpful and appropriate to be reassuring, Fassler advises not to make unrealistic promises.
“It’s fine to tell kids that you’ll deal with whatever happens, even if it means altering travel plans or work schedules, but you can’t promise that no one in your state or community will get sick,” he said.
Maintain healthy habits
Physicians and other adults can tell children “in an age-appropriate way” how the virus is transmitted and what the symptoms are, but it’s important to emphasize that most people who are sick don’t have COVID-19, said Lebowitz.
“I would emphasize that the people who are the sickest are the elderly who are already sick, rather than healthy younger people,” he said.
Lebowitz recommends continuing to follow guidelines on staying healthy, including coughing into a sleeve instead of your hand and regular handwashing.
It’s also important at this time for children to maintain healthy habits – getting enough physical activity and sleep, eating well, and being outside – because this regime will go a long way toward reducing anxiety, said Lebowitz. Deep breathing and muscle-relaxing exercises can also help, he said.
Lebowitz also suggests maintaining a supportive attitude and showing “some acceptance and validation of what children are feeling, as well as some confidence that they can cope and tolerate feeling uncomfortable sometimes, that they can handle some anxiety.”
While accepting that the child could be anxious, it’s important not to encourage excessive avoidance or unhealthy coping strategies. Fassler and Lebowitz agree that children who are overly anxious or preoccupied with concerns about the coronavirus should be evaluated by a trained, qualified mental health professional.
Signs that a child may need additional help include ongoing sleep difficulties, intrusive thoughts or worries, obsessive-compulsive behaviors, or reluctance or refusal to go to school, said Fassler.
The good news is that most children are resilient, said Fassler. “They’ll adjust, adapt, and go on with their lives.”
This article first appeared on Medscape.com.
DMT use is common in older patients with MS
WEST PALM BEACH, FLA. –
MS disease activity typically declines with age. At the same time, evidence to support the efficacy of MS drugs in older patients is limited, said Yinan Zhang, MD, a researcher at Icahn School of Medicine at Mount Sinai, New York. Clinical trials have tended to enroll younger patients and to include only patients with active disease, which is not representative of most older patients in the real world, Dr. Zhang said.
“DMTs for MS may be less efficacious in the elderly, especially in the absence of active disease, yet real-world prescribing patterns still show widespread use of DMTs in older patients,” Dr. Zhang and colleagues said. Physicians may be able to use the presence of disease activity to identify older patients who should receive therapy. “Continuing DMTs in elderly patients who have no evidence of disease activity should be questioned rather than accepted,” they said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To investigate whether age affects the efficacy of DMTs in patients with relapsing-remitting MS and how often DMTs are used in different age groups, Dr. Zhang and coinvestigators conducted a meta-analysis of group-level data from clinical trial, analyzed individual-level data from one of the trials, and reviewed survey data from two registries.
The meta-analysis included 26 clinical trials of 13 DMTs with more than 12,400 patients. Participants had an average age of about 37 years. “An age-dependent relationship of DMTs on relapse rate in RRMS [relapsing-remitting MS] cannot be established with currently published aggregate summary data,” the researchers said. “The meta-analysis was limited by the use of group-level data resulting in a narrow range of mean age.”
In an effort to overcome the limitations of group-level data, they analyzed individual-level data from approximately 1,000 patients in the CombiRx trial, which compared interferon beta-1a plus glatiramer acetate versus the agents alone. Thirty-seven of the patients were aged 55 years or older. The results suggest that each “1-year increase in baseline age was associated with a 3.2% reduction in the odds of having a relapse” during the trial, the investigators said. Change in annualized relapse rate was not significantly associated with age group, which may have resulted from “enrollment criteria selecting for patients with active disease, where DMTs are expected to show the greatest efficacy,” the researchers said.
Finally, Dr. Zhang and colleagues reviewed data on DMT use by age group from the North American Research Committee on Multiple Sclerosis (NARCOMS) and the Multiple Sclerosis Surveillance Registry (MSSR) from Veterans Affairs. In a 2018 survey of nearly 7,000 patients in the NARCOMS registry, 39.2% of patients older than 60 years were taking a DMT, including 44.5% of patients aged 61-70, 28.6% of patients aged 71-80, and 11% of patients aged 81 years and older. In comparison, about 62% of patients aged 41-50 years were taking DMT.
A 2019 survey of about 1,700 veterans in the MSSR found that 36.3% of patients older than 60 years were taking a DMT, including 41.1% of patients aged 61-70, 27.2% of patients aged 71-80, and 7.1% of patients aged 81 years and older. Among patients aged 41-50 years, more than 72% were taking a DMT. “The continued use of DMTs in the elderly may be the result of the perceived notion that disease inactivity is due to the effect of DMTs rather than the natural disease course with aging,” they said.
Dr. Zhang had no relevant disclosures. Coauthors disclosed consulting for and grant support from various pharmaceutical companies.
SOURCE: Zhang Y et al. ACTRIMS Forum 2020. Abstract P263.
WEST PALM BEACH, FLA. –
MS disease activity typically declines with age. At the same time, evidence to support the efficacy of MS drugs in older patients is limited, said Yinan Zhang, MD, a researcher at Icahn School of Medicine at Mount Sinai, New York. Clinical trials have tended to enroll younger patients and to include only patients with active disease, which is not representative of most older patients in the real world, Dr. Zhang said.
“DMTs for MS may be less efficacious in the elderly, especially in the absence of active disease, yet real-world prescribing patterns still show widespread use of DMTs in older patients,” Dr. Zhang and colleagues said. Physicians may be able to use the presence of disease activity to identify older patients who should receive therapy. “Continuing DMTs in elderly patients who have no evidence of disease activity should be questioned rather than accepted,” they said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To investigate whether age affects the efficacy of DMTs in patients with relapsing-remitting MS and how often DMTs are used in different age groups, Dr. Zhang and coinvestigators conducted a meta-analysis of group-level data from clinical trial, analyzed individual-level data from one of the trials, and reviewed survey data from two registries.
The meta-analysis included 26 clinical trials of 13 DMTs with more than 12,400 patients. Participants had an average age of about 37 years. “An age-dependent relationship of DMTs on relapse rate in RRMS [relapsing-remitting MS] cannot be established with currently published aggregate summary data,” the researchers said. “The meta-analysis was limited by the use of group-level data resulting in a narrow range of mean age.”
In an effort to overcome the limitations of group-level data, they analyzed individual-level data from approximately 1,000 patients in the CombiRx trial, which compared interferon beta-1a plus glatiramer acetate versus the agents alone. Thirty-seven of the patients were aged 55 years or older. The results suggest that each “1-year increase in baseline age was associated with a 3.2% reduction in the odds of having a relapse” during the trial, the investigators said. Change in annualized relapse rate was not significantly associated with age group, which may have resulted from “enrollment criteria selecting for patients with active disease, where DMTs are expected to show the greatest efficacy,” the researchers said.
Finally, Dr. Zhang and colleagues reviewed data on DMT use by age group from the North American Research Committee on Multiple Sclerosis (NARCOMS) and the Multiple Sclerosis Surveillance Registry (MSSR) from Veterans Affairs. In a 2018 survey of nearly 7,000 patients in the NARCOMS registry, 39.2% of patients older than 60 years were taking a DMT, including 44.5% of patients aged 61-70, 28.6% of patients aged 71-80, and 11% of patients aged 81 years and older. In comparison, about 62% of patients aged 41-50 years were taking DMT.
A 2019 survey of about 1,700 veterans in the MSSR found that 36.3% of patients older than 60 years were taking a DMT, including 41.1% of patients aged 61-70, 27.2% of patients aged 71-80, and 7.1% of patients aged 81 years and older. Among patients aged 41-50 years, more than 72% were taking a DMT. “The continued use of DMTs in the elderly may be the result of the perceived notion that disease inactivity is due to the effect of DMTs rather than the natural disease course with aging,” they said.
Dr. Zhang had no relevant disclosures. Coauthors disclosed consulting for and grant support from various pharmaceutical companies.
SOURCE: Zhang Y et al. ACTRIMS Forum 2020. Abstract P263.
WEST PALM BEACH, FLA. –
MS disease activity typically declines with age. At the same time, evidence to support the efficacy of MS drugs in older patients is limited, said Yinan Zhang, MD, a researcher at Icahn School of Medicine at Mount Sinai, New York. Clinical trials have tended to enroll younger patients and to include only patients with active disease, which is not representative of most older patients in the real world, Dr. Zhang said.
“DMTs for MS may be less efficacious in the elderly, especially in the absence of active disease, yet real-world prescribing patterns still show widespread use of DMTs in older patients,” Dr. Zhang and colleagues said. Physicians may be able to use the presence of disease activity to identify older patients who should receive therapy. “Continuing DMTs in elderly patients who have no evidence of disease activity should be questioned rather than accepted,” they said at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
To investigate whether age affects the efficacy of DMTs in patients with relapsing-remitting MS and how often DMTs are used in different age groups, Dr. Zhang and coinvestigators conducted a meta-analysis of group-level data from clinical trial, analyzed individual-level data from one of the trials, and reviewed survey data from two registries.
The meta-analysis included 26 clinical trials of 13 DMTs with more than 12,400 patients. Participants had an average age of about 37 years. “An age-dependent relationship of DMTs on relapse rate in RRMS [relapsing-remitting MS] cannot be established with currently published aggregate summary data,” the researchers said. “The meta-analysis was limited by the use of group-level data resulting in a narrow range of mean age.”
In an effort to overcome the limitations of group-level data, they analyzed individual-level data from approximately 1,000 patients in the CombiRx trial, which compared interferon beta-1a plus glatiramer acetate versus the agents alone. Thirty-seven of the patients were aged 55 years or older. The results suggest that each “1-year increase in baseline age was associated with a 3.2% reduction in the odds of having a relapse” during the trial, the investigators said. Change in annualized relapse rate was not significantly associated with age group, which may have resulted from “enrollment criteria selecting for patients with active disease, where DMTs are expected to show the greatest efficacy,” the researchers said.
Finally, Dr. Zhang and colleagues reviewed data on DMT use by age group from the North American Research Committee on Multiple Sclerosis (NARCOMS) and the Multiple Sclerosis Surveillance Registry (MSSR) from Veterans Affairs. In a 2018 survey of nearly 7,000 patients in the NARCOMS registry, 39.2% of patients older than 60 years were taking a DMT, including 44.5% of patients aged 61-70, 28.6% of patients aged 71-80, and 11% of patients aged 81 years and older. In comparison, about 62% of patients aged 41-50 years were taking DMT.
A 2019 survey of about 1,700 veterans in the MSSR found that 36.3% of patients older than 60 years were taking a DMT, including 41.1% of patients aged 61-70, 27.2% of patients aged 71-80, and 7.1% of patients aged 81 years and older. Among patients aged 41-50 years, more than 72% were taking a DMT. “The continued use of DMTs in the elderly may be the result of the perceived notion that disease inactivity is due to the effect of DMTs rather than the natural disease course with aging,” they said.
Dr. Zhang had no relevant disclosures. Coauthors disclosed consulting for and grant support from various pharmaceutical companies.
SOURCE: Zhang Y et al. ACTRIMS Forum 2020. Abstract P263.
REPORTING FROM ACTRIMS FORUM 2020