User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Preserving civility in trying times
Recently I was in a minor car accident. No injuries, just some bent metal and scratched paint from a low-speed parking lot mishap.

The other driver and I got out of our cars, made sure we were both okay, and then I said “Let’s exchange insurance information.” We got our insurance cards out; I took a picture of her card, and she wrote down my info. Then we drove off and went on with our days. The whole thing took a few minutes.
Why am I writing about this?
Because it was all handled very politely. There were no angry words, name calling, or heated exchanges. We checked the damage, made sure the other was okay, and exchanged insurance cards ... without a single impolite phrase or gesture.
To me this is a good thing. In a world in which people yell (and sometimes brandish weapons) over imagined and minor offenses, in which political candidates exchange crude insults rather then debate policy, and in which an opposing viewpoint is treated as blasphemy rather than an honest difference of opinion, it was nice to have a polite, adult, exchange under unpleasant circumstances.
Perhaps it’s sad to find relief in such a minor event, but it’s also reassuring. In medicine (especially hospital work) we often see people at their very worst, and dealing with them can be a challenge. We live in a world of at-times seemingly endless rudeness, one-upping, and “problem-solving” with yelling, threats, and intimidation.
So I was glad the minor incident resulted in nothing more serious at the time than a brief, polite, conversation.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has nothing to disclose.
Recently I was in a minor car accident. No injuries, just some bent metal and scratched paint from a low-speed parking lot mishap.
The other driver and I got out of our cars, made sure we were both okay, and then I said “Let’s exchange insurance information.” We got our insurance cards out; I took a picture of her card, and she wrote down my info. Then we drove off and went on with our days. The whole thing took a few minutes.
Why am I writing about this?
Because it was all handled very politely. There were no angry words, name calling, or heated exchanges. We checked the damage, made sure the other was okay, and exchanged insurance cards ... without a single impolite phrase or gesture.
To me this is a good thing. In a world in which people yell (and sometimes brandish weapons) over imagined and minor offenses, in which political candidates exchange crude insults rather then debate policy, and in which an opposing viewpoint is treated as blasphemy rather than an honest difference of opinion, it was nice to have a polite, adult, exchange under unpleasant circumstances.
Perhaps it’s sad to find relief in such a minor event, but it’s also reassuring. In medicine (especially hospital work) we often see people at their very worst, and dealing with them can be a challenge. We live in a world of at-times seemingly endless rudeness, one-upping, and “problem-solving” with yelling, threats, and intimidation.
So I was glad the minor incident resulted in nothing more serious at the time than a brief, polite, conversation.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has nothing to disclose.
Recently I was in a minor car accident. No injuries, just some bent metal and scratched paint from a low-speed parking lot mishap.
The other driver and I got out of our cars, made sure we were both okay, and then I said “Let’s exchange insurance information.” We got our insurance cards out; I took a picture of her card, and she wrote down my info. Then we drove off and went on with our days. The whole thing took a few minutes.
Why am I writing about this?
Because it was all handled very politely. There were no angry words, name calling, or heated exchanges. We checked the damage, made sure the other was okay, and exchanged insurance cards ... without a single impolite phrase or gesture.
To me this is a good thing. In a world in which people yell (and sometimes brandish weapons) over imagined and minor offenses, in which political candidates exchange crude insults rather then debate policy, and in which an opposing viewpoint is treated as blasphemy rather than an honest difference of opinion, it was nice to have a polite, adult, exchange under unpleasant circumstances.
Perhaps it’s sad to find relief in such a minor event, but it’s also reassuring. In medicine (especially hospital work) we often see people at their very worst, and dealing with them can be a challenge. We live in a world of at-times seemingly endless rudeness, one-upping, and “problem-solving” with yelling, threats, and intimidation.
So I was glad the minor incident resulted in nothing more serious at the time than a brief, polite, conversation.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has nothing to disclose.
Children’s share of new COVID-19 cases is on the rise
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
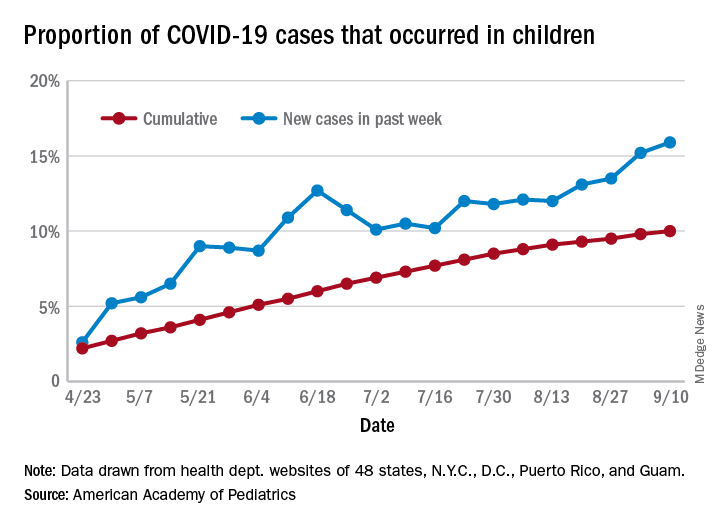
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
FROM PEDIATRICS
MS Highlights from AAN & CMSC

- Initial high-efficacy MS therapy is associated with less disability later
- Serum NfL in early MS can help predict clinical course
- No benefit of three commonly used medications for MS fatigue
- Telerehabilitation may be effective in MS
- CMSC MRI guidelines evolve into international consensus protocol
- Newest oral DMTs haven’t yet made a big impact in the MS world
Read the supplement.
- Initial high-efficacy MS therapy is associated with less disability later
- Serum NfL in early MS can help predict clinical course
- No benefit of three commonly used medications for MS fatigue
- Telerehabilitation may be effective in MS
- CMSC MRI guidelines evolve into international consensus protocol
- Newest oral DMTs haven’t yet made a big impact in the MS world
Read the supplement.
- Initial high-efficacy MS therapy is associated with less disability later
- Serum NfL in early MS can help predict clinical course
- No benefit of three commonly used medications for MS fatigue
- Telerehabilitation may be effective in MS
- CMSC MRI guidelines evolve into international consensus protocol
- Newest oral DMTs haven’t yet made a big impact in the MS world
Read the supplement.
Pandemic poses new challenges for rural doctors
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.

Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.

In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.

Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.

He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.
Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.
In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.
Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.
He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.
Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.
In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.
Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.
He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
Lower rituximab doses may be as effective, safer in MS
Further data suggesting that (MS), according to a new observational study. “We showed similar numbers of relapses, MRI new/active lesions, and effects on disability with a higher and lower dose of rituximab over a median follow of 16 months,” said lead author, Luciana Midaglia, MD, Multiple Sclerosis Centre of Catalonia (Cemcat) at Vall d’Hebron University Hospital, Barcelona. “But adverse effects – particularly frequency of infection – were increased in the high-dose group.”
Dr. Midaglia presented the findings at the recent Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“There haven’t been large studies of rituximab in MS as the company [Genentech/Roche] prioritized development of ocrelizumab over rituximab,” she explained. Rituximab has, therefore, never been approved for this indication. But it is available for several other conditions, and it is often used off label for MS.
“Although we now have a lot of experience with rituximab in MS, a dosage regimen has not been standardized,” Dr. Midaglia noted.
The current study was conducted to compare the efficacy and safety of two different dosage regimens of rituximab used at two different Catalan MS centers.
In the Barcelona center, 249 patients received a regimen of 2 g IV for the first three 6-month cycles followed by 1 g every 6 months thereafter (higher-dose group). In the Girona center, 54 patients received just one loading dose of 2 g followed by 500 mg every 6 months thereafter (lower-dose group).
Patients were followed up clinically every 6 months, and MRI brain scans were performed at baseline and yearly thereafter. Blood samples for safety and B cell/immunoglobulin monitoring were drawn at 3 months after rituximab infusions.
Results showed that the annualized relapse rate reduced by 87% (from 0.4 to 0.05; P < .001) in the higher-dose cohort, and by 90% (from 0.31 to 0.03; P = .018) in the lower-dose cohort.
The Expanded Disability Status Scale score remained stable or improved in 83% of the higher-dose group versus 72% of the lower-dose group (P = .09).
Contrast-enhancing lesions were reduced by 92% by 12 months and by 100% by 36 months in the higher-dose group and by 81% and 100%, respectively, in the lower-dose group.
New T2 lesions were present in 19% of patients at 12 months and in 12% at 36 months in the higher-dose group and in 16% and 0%, respectively, in the lower-dose group.
Reductions in B cell levels were similar with both doses. However, a reduced rate of adverse effects, mainly infections, was seen in the lower-dose group.
Infections were reported in 7.2% of the higher-dose group and 3.7% of the lower-dose group at 1 year, in 9.7% versus 0% in the second year, and in 9.7% versus 0% in the third year. Urinary tract infections, followed by respiratory infections, were the most prevalent.
A randomized phase 3 study is now underway testing an even lower dose of rituximab. The trial, known as RIDOSE-MS, is comparing maintenance doses of 500 mg every 6 months and 500 mg every 12 months.
Dr. Midaglia said that most centers are using higher doses of rituximab – similar to the Barcelona cohort in this study.
“After this study, we will we now start a new protocol and use the lower dose for all MS patients,” she said.
She reported that her hospital has been using rituximab extensively in MS.
“There were delays to ocrelizumab being introduced in Spain, and while we were waiting, we started using rituximab,” she said. “We believe it is similarly effective to ocrelizumab. It has exactly the same mechanism of action. The only difference is that rituximab is a chimeric antibody while ocrelizumab is fully humanized.”
While rituximab has not had the validation of a full phase 3 trial, she added, “there are data available from several smaller studies and we feel we have learned how to use it in the real world, but we don’t have an approved dosage schedule. We started off using the dose approved for use in rheumatological and hematological conditions.”
Now that ocrelizumab is approved, Dr. Midaglia said they are using that drug for the patients who meet the approved criteria, but there are many patients who don’t qualify.
“For example, in progressive MS, ocrelizumab has quite a narrow indication – it is not reimbursed for patients without any inflammatory activity. So for these patients, we tend to use rituximab,” she noted.
“While there is no good data on its efficacy in these patients, we believe it has some effect and there is no other option at present. Rituximab is an inexpensive drug and has a long safety record in other conditions, so we feel it’s worth a try,” Dr. Midaglia concluded. “And now we have better data on the optimal dosage.”
Commenting on the study, Daniel Ontaneda, MD, comoderator of the session at which the study was presented, said: “Rituximab is not an [Food and Drug Administration]–approved medication for MS, but it has been used in clinical practice quite extensively in the U.S. and also in Europe. The study is of interest as it showed that the lower dose of rituximab achieved good control of disease activity.”
Dr. Ontaneda, a neurologist at the Mellen Center for MS at the Cleveland Clinic, Ohio, added: “Many centers have been using lower doses or less frequent infusions and this study supports this practice. Some degree of residual confounding in the study in the differences in side effects may be related to the two different sites, but overall I think these results add to the real-world observational data now available for anti-CD20 therapies.”
Dr. Midaglia reported receiving travel funding from Genzyme, Roche, Biogen Idec, and Novartis, and personal fees for lectures from Roche.
A version of this article originally appeared on Medscape.com.
Further data suggesting that (MS), according to a new observational study. “We showed similar numbers of relapses, MRI new/active lesions, and effects on disability with a higher and lower dose of rituximab over a median follow of 16 months,” said lead author, Luciana Midaglia, MD, Multiple Sclerosis Centre of Catalonia (Cemcat) at Vall d’Hebron University Hospital, Barcelona. “But adverse effects – particularly frequency of infection – were increased in the high-dose group.”
Dr. Midaglia presented the findings at the recent Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“There haven’t been large studies of rituximab in MS as the company [Genentech/Roche] prioritized development of ocrelizumab over rituximab,” she explained. Rituximab has, therefore, never been approved for this indication. But it is available for several other conditions, and it is often used off label for MS.
“Although we now have a lot of experience with rituximab in MS, a dosage regimen has not been standardized,” Dr. Midaglia noted.
The current study was conducted to compare the efficacy and safety of two different dosage regimens of rituximab used at two different Catalan MS centers.
In the Barcelona center, 249 patients received a regimen of 2 g IV for the first three 6-month cycles followed by 1 g every 6 months thereafter (higher-dose group). In the Girona center, 54 patients received just one loading dose of 2 g followed by 500 mg every 6 months thereafter (lower-dose group).
Patients were followed up clinically every 6 months, and MRI brain scans were performed at baseline and yearly thereafter. Blood samples for safety and B cell/immunoglobulin monitoring were drawn at 3 months after rituximab infusions.
Results showed that the annualized relapse rate reduced by 87% (from 0.4 to 0.05; P < .001) in the higher-dose cohort, and by 90% (from 0.31 to 0.03; P = .018) in the lower-dose cohort.
The Expanded Disability Status Scale score remained stable or improved in 83% of the higher-dose group versus 72% of the lower-dose group (P = .09).
Contrast-enhancing lesions were reduced by 92% by 12 months and by 100% by 36 months in the higher-dose group and by 81% and 100%, respectively, in the lower-dose group.
New T2 lesions were present in 19% of patients at 12 months and in 12% at 36 months in the higher-dose group and in 16% and 0%, respectively, in the lower-dose group.
Reductions in B cell levels were similar with both doses. However, a reduced rate of adverse effects, mainly infections, was seen in the lower-dose group.
Infections were reported in 7.2% of the higher-dose group and 3.7% of the lower-dose group at 1 year, in 9.7% versus 0% in the second year, and in 9.7% versus 0% in the third year. Urinary tract infections, followed by respiratory infections, were the most prevalent.
A randomized phase 3 study is now underway testing an even lower dose of rituximab. The trial, known as RIDOSE-MS, is comparing maintenance doses of 500 mg every 6 months and 500 mg every 12 months.
Dr. Midaglia said that most centers are using higher doses of rituximab – similar to the Barcelona cohort in this study.
“After this study, we will we now start a new protocol and use the lower dose for all MS patients,” she said.
She reported that her hospital has been using rituximab extensively in MS.
“There were delays to ocrelizumab being introduced in Spain, and while we were waiting, we started using rituximab,” she said. “We believe it is similarly effective to ocrelizumab. It has exactly the same mechanism of action. The only difference is that rituximab is a chimeric antibody while ocrelizumab is fully humanized.”
While rituximab has not had the validation of a full phase 3 trial, she added, “there are data available from several smaller studies and we feel we have learned how to use it in the real world, but we don’t have an approved dosage schedule. We started off using the dose approved for use in rheumatological and hematological conditions.”
Now that ocrelizumab is approved, Dr. Midaglia said they are using that drug for the patients who meet the approved criteria, but there are many patients who don’t qualify.
“For example, in progressive MS, ocrelizumab has quite a narrow indication – it is not reimbursed for patients without any inflammatory activity. So for these patients, we tend to use rituximab,” she noted.
“While there is no good data on its efficacy in these patients, we believe it has some effect and there is no other option at present. Rituximab is an inexpensive drug and has a long safety record in other conditions, so we feel it’s worth a try,” Dr. Midaglia concluded. “And now we have better data on the optimal dosage.”
Commenting on the study, Daniel Ontaneda, MD, comoderator of the session at which the study was presented, said: “Rituximab is not an [Food and Drug Administration]–approved medication for MS, but it has been used in clinical practice quite extensively in the U.S. and also in Europe. The study is of interest as it showed that the lower dose of rituximab achieved good control of disease activity.”
Dr. Ontaneda, a neurologist at the Mellen Center for MS at the Cleveland Clinic, Ohio, added: “Many centers have been using lower doses or less frequent infusions and this study supports this practice. Some degree of residual confounding in the study in the differences in side effects may be related to the two different sites, but overall I think these results add to the real-world observational data now available for anti-CD20 therapies.”
Dr. Midaglia reported receiving travel funding from Genzyme, Roche, Biogen Idec, and Novartis, and personal fees for lectures from Roche.
A version of this article originally appeared on Medscape.com.
Further data suggesting that (MS), according to a new observational study. “We showed similar numbers of relapses, MRI new/active lesions, and effects on disability with a higher and lower dose of rituximab over a median follow of 16 months,” said lead author, Luciana Midaglia, MD, Multiple Sclerosis Centre of Catalonia (Cemcat) at Vall d’Hebron University Hospital, Barcelona. “But adverse effects – particularly frequency of infection – were increased in the high-dose group.”
Dr. Midaglia presented the findings at the recent Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“There haven’t been large studies of rituximab in MS as the company [Genentech/Roche] prioritized development of ocrelizumab over rituximab,” she explained. Rituximab has, therefore, never been approved for this indication. But it is available for several other conditions, and it is often used off label for MS.
“Although we now have a lot of experience with rituximab in MS, a dosage regimen has not been standardized,” Dr. Midaglia noted.
The current study was conducted to compare the efficacy and safety of two different dosage regimens of rituximab used at two different Catalan MS centers.
In the Barcelona center, 249 patients received a regimen of 2 g IV for the first three 6-month cycles followed by 1 g every 6 months thereafter (higher-dose group). In the Girona center, 54 patients received just one loading dose of 2 g followed by 500 mg every 6 months thereafter (lower-dose group).
Patients were followed up clinically every 6 months, and MRI brain scans were performed at baseline and yearly thereafter. Blood samples for safety and B cell/immunoglobulin monitoring were drawn at 3 months after rituximab infusions.
Results showed that the annualized relapse rate reduced by 87% (from 0.4 to 0.05; P < .001) in the higher-dose cohort, and by 90% (from 0.31 to 0.03; P = .018) in the lower-dose cohort.
The Expanded Disability Status Scale score remained stable or improved in 83% of the higher-dose group versus 72% of the lower-dose group (P = .09).
Contrast-enhancing lesions were reduced by 92% by 12 months and by 100% by 36 months in the higher-dose group and by 81% and 100%, respectively, in the lower-dose group.
New T2 lesions were present in 19% of patients at 12 months and in 12% at 36 months in the higher-dose group and in 16% and 0%, respectively, in the lower-dose group.
Reductions in B cell levels were similar with both doses. However, a reduced rate of adverse effects, mainly infections, was seen in the lower-dose group.
Infections were reported in 7.2% of the higher-dose group and 3.7% of the lower-dose group at 1 year, in 9.7% versus 0% in the second year, and in 9.7% versus 0% in the third year. Urinary tract infections, followed by respiratory infections, were the most prevalent.
A randomized phase 3 study is now underway testing an even lower dose of rituximab. The trial, known as RIDOSE-MS, is comparing maintenance doses of 500 mg every 6 months and 500 mg every 12 months.
Dr. Midaglia said that most centers are using higher doses of rituximab – similar to the Barcelona cohort in this study.
“After this study, we will we now start a new protocol and use the lower dose for all MS patients,” she said.
She reported that her hospital has been using rituximab extensively in MS.
“There were delays to ocrelizumab being introduced in Spain, and while we were waiting, we started using rituximab,” she said. “We believe it is similarly effective to ocrelizumab. It has exactly the same mechanism of action. The only difference is that rituximab is a chimeric antibody while ocrelizumab is fully humanized.”
While rituximab has not had the validation of a full phase 3 trial, she added, “there are data available from several smaller studies and we feel we have learned how to use it in the real world, but we don’t have an approved dosage schedule. We started off using the dose approved for use in rheumatological and hematological conditions.”
Now that ocrelizumab is approved, Dr. Midaglia said they are using that drug for the patients who meet the approved criteria, but there are many patients who don’t qualify.
“For example, in progressive MS, ocrelizumab has quite a narrow indication – it is not reimbursed for patients without any inflammatory activity. So for these patients, we tend to use rituximab,” she noted.
“While there is no good data on its efficacy in these patients, we believe it has some effect and there is no other option at present. Rituximab is an inexpensive drug and has a long safety record in other conditions, so we feel it’s worth a try,” Dr. Midaglia concluded. “And now we have better data on the optimal dosage.”
Commenting on the study, Daniel Ontaneda, MD, comoderator of the session at which the study was presented, said: “Rituximab is not an [Food and Drug Administration]–approved medication for MS, but it has been used in clinical practice quite extensively in the U.S. and also in Europe. The study is of interest as it showed that the lower dose of rituximab achieved good control of disease activity.”
Dr. Ontaneda, a neurologist at the Mellen Center for MS at the Cleveland Clinic, Ohio, added: “Many centers have been using lower doses or less frequent infusions and this study supports this practice. Some degree of residual confounding in the study in the differences in side effects may be related to the two different sites, but overall I think these results add to the real-world observational data now available for anti-CD20 therapies.”
Dr. Midaglia reported receiving travel funding from Genzyme, Roche, Biogen Idec, and Novartis, and personal fees for lectures from Roche.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020
Prior autoimmunity does not predict adverse events of alemtuzumab
a new study has shown.
These latest data were reported by Alasdair J. Coles, MD, University of Cambridge (England), at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Dr. Coles, who led the initial research to develop alemtuzumab in partnership with Genzyme, explained that autoimmune disease is a well-described and common adverse event with the drug, manifesting mainly as autoimmune thyroid events that can occur in up to 40% of patients.
But as postmarketing experience has grown, it has become clear that there is a low frequency of more serious autoimmune disease, he noted. In an effort to understand this better, regulators have suggested that the presence of non–multiple sclerosis (MS) autoimmune disease before alemtuzumab treatment and the emergence of autoimmune disease after alemtuzumab treatment may define a group that is at higher risk of one of the rare but serious autoimmune events for those on the drug.
To investigate if this was the case, Dr. Coles and colleagues analyzed data on 1,216 patients who received alemtuzumab in the clinical development program. Of these, 96 had preexisting non-MS autoimmunity.
Results showed that up to 9 years after alemtuzumab initiation, the percentage of patients with new autoimmune disease was similar in those with (35.4%) versus without (35.3%) preexisting autoimmunity.
Similar percentages of patients with versus without preexisting autoimmunity had two or more new autoimmune events (5.2% vs. 8.2%, respectively). And most patients with thyroid disorders at baseline did not experience new autoimmunity after alemtuzumab.
In addition, treatment-emergent thyroid autoimmunity after the first alemtuzumab course was not associated with subsequent nonthyroid autoimmunity after the second course. Similarly, thyroid autoimmunity after the second course did not predict non-thyroid autoimmunity after the third course.
In another analysis of the incidence of serious autoimmune events from postmarketing data on 25,292 patients treated with alemtuzumab, immune thrombocytopenic purpura was reported in 43 patients, newly identified autoimmune hepatitis in 11 patients, and hemophagocytic lymphohistiocytosis in 9 patients.
There was “no hint at all” that baseline thyroid disorders or postalemtuzumab thyroid disorders are associated with increased risk of these serious autoimmune adverse events, Dr. Coles said.
He calculated that the incidence of serious autoimmune diseases that could be life-threatening after alemtuzumab treatment was 10.7 per 10,000 patients treated for autoimmune hepatitis and 2.7 per 10,000 patients treated for hemophagocytic lymphohistiocytosis.
“From two separate data sources – phase 2/3 trials populations combined and postmarketing data – there is no evidence to support the hypothesis that preexisting non-MS autoimmunity predisposes to the serious but rare autoimmune events that have newly been described, nor does thyroid autoimmunity following the use of alemtuzumab,” Dr. Coles stated.
“In my opinion it is not appropriate to preclude the use of alemtuzumab to patients who have had previous autoimmune disease before treatment or who develop thyroid autoimmunity after alemtuzumab,” he said.
“It remains in my view a reasonable treatment option for patients with active MS to receive this highly effective therapy in the face of well-managed, well-understood thyroid autoimmunity and the very unlikely, rare, but serious autoimmune disease,” he concluded.
Risk stratification
Commenting on the presentation, Robert J. Fox, MD, a neurologist at the Mellen Center for Multiple Sclerosis, Cleveland Clinic, Ohio, explained that, whenever there is a serious risk of a complication, clinicians like to try to stratify that risk.
“We like to identify those at higher risk [and perhaps not use the therapy] and those at lower risk [and perhaps consider more likely the use of that therapy],” he said.
With regard to alemtuzumab, Dr. Fox noted: “We’d like to stratify the risk of autoimmune complications, which could help guide us regarding the patients in whom therapy may be safer. Unfortunately, these findings did not point to a risk stratification to help guide its use towards lower-risk patients.
“I view this as an unfortunate result, because it leaves me without a way to stratify the risks of alemtuzumab, which are quite significant and currently limit my use of that MS therapy only to those with no other treatment options,” he added.
On Dr. Coles’ view of alemtuzumab as a “reasonable” treatment option, Dr. Fox commented: “I guess it depends upon how that’s interpreted. Given the risks of serious, life-threatening immune and infectious complications, I only consider alemtuzumab when all other immune-modulating therapies have been tried or are not a reasonable treatment option. So, yes, I see it as ‘reasonable,’ but only when there are no other available treatment options.”
The current work was supported by Sanofi and Bayer HealthCare. Dr. Coles reported sitting on advisory boards for Genzyme (Sanofi). He is credited as an inventor on several patents related to the technology on which alemtuzumab is based. Dr. Fox has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new study has shown.
These latest data were reported by Alasdair J. Coles, MD, University of Cambridge (England), at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Dr. Coles, who led the initial research to develop alemtuzumab in partnership with Genzyme, explained that autoimmune disease is a well-described and common adverse event with the drug, manifesting mainly as autoimmune thyroid events that can occur in up to 40% of patients.
But as postmarketing experience has grown, it has become clear that there is a low frequency of more serious autoimmune disease, he noted. In an effort to understand this better, regulators have suggested that the presence of non–multiple sclerosis (MS) autoimmune disease before alemtuzumab treatment and the emergence of autoimmune disease after alemtuzumab treatment may define a group that is at higher risk of one of the rare but serious autoimmune events for those on the drug.
To investigate if this was the case, Dr. Coles and colleagues analyzed data on 1,216 patients who received alemtuzumab in the clinical development program. Of these, 96 had preexisting non-MS autoimmunity.
Results showed that up to 9 years after alemtuzumab initiation, the percentage of patients with new autoimmune disease was similar in those with (35.4%) versus without (35.3%) preexisting autoimmunity.
Similar percentages of patients with versus without preexisting autoimmunity had two or more new autoimmune events (5.2% vs. 8.2%, respectively). And most patients with thyroid disorders at baseline did not experience new autoimmunity after alemtuzumab.
In addition, treatment-emergent thyroid autoimmunity after the first alemtuzumab course was not associated with subsequent nonthyroid autoimmunity after the second course. Similarly, thyroid autoimmunity after the second course did not predict non-thyroid autoimmunity after the third course.
In another analysis of the incidence of serious autoimmune events from postmarketing data on 25,292 patients treated with alemtuzumab, immune thrombocytopenic purpura was reported in 43 patients, newly identified autoimmune hepatitis in 11 patients, and hemophagocytic lymphohistiocytosis in 9 patients.
There was “no hint at all” that baseline thyroid disorders or postalemtuzumab thyroid disorders are associated with increased risk of these serious autoimmune adverse events, Dr. Coles said.
He calculated that the incidence of serious autoimmune diseases that could be life-threatening after alemtuzumab treatment was 10.7 per 10,000 patients treated for autoimmune hepatitis and 2.7 per 10,000 patients treated for hemophagocytic lymphohistiocytosis.
“From two separate data sources – phase 2/3 trials populations combined and postmarketing data – there is no evidence to support the hypothesis that preexisting non-MS autoimmunity predisposes to the serious but rare autoimmune events that have newly been described, nor does thyroid autoimmunity following the use of alemtuzumab,” Dr. Coles stated.
“In my opinion it is not appropriate to preclude the use of alemtuzumab to patients who have had previous autoimmune disease before treatment or who develop thyroid autoimmunity after alemtuzumab,” he said.
“It remains in my view a reasonable treatment option for patients with active MS to receive this highly effective therapy in the face of well-managed, well-understood thyroid autoimmunity and the very unlikely, rare, but serious autoimmune disease,” he concluded.
Risk stratification
Commenting on the presentation, Robert J. Fox, MD, a neurologist at the Mellen Center for Multiple Sclerosis, Cleveland Clinic, Ohio, explained that, whenever there is a serious risk of a complication, clinicians like to try to stratify that risk.
“We like to identify those at higher risk [and perhaps not use the therapy] and those at lower risk [and perhaps consider more likely the use of that therapy],” he said.
With regard to alemtuzumab, Dr. Fox noted: “We’d like to stratify the risk of autoimmune complications, which could help guide us regarding the patients in whom therapy may be safer. Unfortunately, these findings did not point to a risk stratification to help guide its use towards lower-risk patients.
“I view this as an unfortunate result, because it leaves me without a way to stratify the risks of alemtuzumab, which are quite significant and currently limit my use of that MS therapy only to those with no other treatment options,” he added.
On Dr. Coles’ view of alemtuzumab as a “reasonable” treatment option, Dr. Fox commented: “I guess it depends upon how that’s interpreted. Given the risks of serious, life-threatening immune and infectious complications, I only consider alemtuzumab when all other immune-modulating therapies have been tried or are not a reasonable treatment option. So, yes, I see it as ‘reasonable,’ but only when there are no other available treatment options.”
The current work was supported by Sanofi and Bayer HealthCare. Dr. Coles reported sitting on advisory boards for Genzyme (Sanofi). He is credited as an inventor on several patents related to the technology on which alemtuzumab is based. Dr. Fox has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new study has shown.
These latest data were reported by Alasdair J. Coles, MD, University of Cambridge (England), at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Dr. Coles, who led the initial research to develop alemtuzumab in partnership with Genzyme, explained that autoimmune disease is a well-described and common adverse event with the drug, manifesting mainly as autoimmune thyroid events that can occur in up to 40% of patients.
But as postmarketing experience has grown, it has become clear that there is a low frequency of more serious autoimmune disease, he noted. In an effort to understand this better, regulators have suggested that the presence of non–multiple sclerosis (MS) autoimmune disease before alemtuzumab treatment and the emergence of autoimmune disease after alemtuzumab treatment may define a group that is at higher risk of one of the rare but serious autoimmune events for those on the drug.
To investigate if this was the case, Dr. Coles and colleagues analyzed data on 1,216 patients who received alemtuzumab in the clinical development program. Of these, 96 had preexisting non-MS autoimmunity.
Results showed that up to 9 years after alemtuzumab initiation, the percentage of patients with new autoimmune disease was similar in those with (35.4%) versus without (35.3%) preexisting autoimmunity.
Similar percentages of patients with versus without preexisting autoimmunity had two or more new autoimmune events (5.2% vs. 8.2%, respectively). And most patients with thyroid disorders at baseline did not experience new autoimmunity after alemtuzumab.
In addition, treatment-emergent thyroid autoimmunity after the first alemtuzumab course was not associated with subsequent nonthyroid autoimmunity after the second course. Similarly, thyroid autoimmunity after the second course did not predict non-thyroid autoimmunity after the third course.
In another analysis of the incidence of serious autoimmune events from postmarketing data on 25,292 patients treated with alemtuzumab, immune thrombocytopenic purpura was reported in 43 patients, newly identified autoimmune hepatitis in 11 patients, and hemophagocytic lymphohistiocytosis in 9 patients.
There was “no hint at all” that baseline thyroid disorders or postalemtuzumab thyroid disorders are associated with increased risk of these serious autoimmune adverse events, Dr. Coles said.
He calculated that the incidence of serious autoimmune diseases that could be life-threatening after alemtuzumab treatment was 10.7 per 10,000 patients treated for autoimmune hepatitis and 2.7 per 10,000 patients treated for hemophagocytic lymphohistiocytosis.
“From two separate data sources – phase 2/3 trials populations combined and postmarketing data – there is no evidence to support the hypothesis that preexisting non-MS autoimmunity predisposes to the serious but rare autoimmune events that have newly been described, nor does thyroid autoimmunity following the use of alemtuzumab,” Dr. Coles stated.
“In my opinion it is not appropriate to preclude the use of alemtuzumab to patients who have had previous autoimmune disease before treatment or who develop thyroid autoimmunity after alemtuzumab,” he said.
“It remains in my view a reasonable treatment option for patients with active MS to receive this highly effective therapy in the face of well-managed, well-understood thyroid autoimmunity and the very unlikely, rare, but serious autoimmune disease,” he concluded.
Risk stratification
Commenting on the presentation, Robert J. Fox, MD, a neurologist at the Mellen Center for Multiple Sclerosis, Cleveland Clinic, Ohio, explained that, whenever there is a serious risk of a complication, clinicians like to try to stratify that risk.
“We like to identify those at higher risk [and perhaps not use the therapy] and those at lower risk [and perhaps consider more likely the use of that therapy],” he said.
With regard to alemtuzumab, Dr. Fox noted: “We’d like to stratify the risk of autoimmune complications, which could help guide us regarding the patients in whom therapy may be safer. Unfortunately, these findings did not point to a risk stratification to help guide its use towards lower-risk patients.
“I view this as an unfortunate result, because it leaves me without a way to stratify the risks of alemtuzumab, which are quite significant and currently limit my use of that MS therapy only to those with no other treatment options,” he added.
On Dr. Coles’ view of alemtuzumab as a “reasonable” treatment option, Dr. Fox commented: “I guess it depends upon how that’s interpreted. Given the risks of serious, life-threatening immune and infectious complications, I only consider alemtuzumab when all other immune-modulating therapies have been tried or are not a reasonable treatment option. So, yes, I see it as ‘reasonable,’ but only when there are no other available treatment options.”
The current work was supported by Sanofi and Bayer HealthCare. Dr. Coles reported sitting on advisory boards for Genzyme (Sanofi). He is credited as an inventor on several patents related to the technology on which alemtuzumab is based. Dr. Fox has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020
B-cell test predicts alemtuzumab autoimmunity in MS
a new study suggests.
“Alemtuzumab has proven to be an effective treatment for patients with highly active remitting relapsing MS, but adverse events may limit the use of this drug, particularly autoimmune adverse events, which are the most prevalent, occurring in about 30% of patients. Reliable biomarkers to assess patient risk for developing this complication would be of great importance,” said lead author Paulette Walo, MD.
“Our results suggest that a higher percentage of total B cells, and in particular plasmablasts, could be a very predictive biomarker for autoimmunity after alemtuzumab treatment. This could help us in choosing the patients for this drug,” said Dr. Walo, an immunologist at Ramon y Cajal University Hospital, Madrid. She presented the findings at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The objective of this study was to explore if patient blood lymphocyte profile before alemtuzumab treatment initiation can identify patients with an increased risk of developing later autoimmunity, Dr. Walo explained.
The study included 54 patients from five hospitals throughout Spain who had received treatment with alemtuzumab. Of these, the vast majority had received the normal two-dose cycle and two patients had received a third dose because of worsening MS activity.
Blood samples were collected before initiating treatment with alemtuzumab. Peripheral blood mononuclear cells were obtained and cryopreserved. Leukocyte populations were assessed by flow cytometry.
Autoimmune adverse events were defined as the development, at any point within 2 years of follow-up, of any autoimmune thyroid-associated event, immune thrombocytopenia, and/or autoimmune nephropathy.
Over the 2 years of follow-up, 14 patients (25.9%) experienced autoimmune adverse events, all of which were dysthyroidism. No immune thrombocytopenia or nephropathies were observed.
No statistical differences were found in clinical and demographic characteristics between patients who developed autoimmune adverse events and those who did not. Previous treatments did not influence B-cell percentages.
Analysis of blood lymphocyte profiles showed no difference in T-cell subsets between those who had an autoimmune event and those who did not.
Still, there were important differences in the B-cell profile, Dr. Walo said. “Total B cells were higher in patients who had an autoimmune event mainly due to naive B cells and plasmablasts.”
Patients who experienced autoimmune adverse events before treatment onset had a higher percentage of blood CD19+ B cells (P = .001), with a higher relative percentage of naive B cells and plasmablasts.
When individual types of cell numbers were explored, only plasmablast levels remained significant (P = .02).
The researchers calculated a CD19+ B-cell predictive value for autoimmunity of 7.6%. If patients had more than 7.6% B cells, they were at higher risk of an autoimmune adverse event after alemtuzumab treatment versus those with lower levels (odds ratio, 14.67; P ≤ .0001).
Similarly, the predictive value for plasmablasts was 0.13%. If patients had levels higher than 0.13% they had a higher risk of an autoimmune event after alemtuzumab treatment (P = .002). Plasmablasts are a category of B cells which are very differentiated and have the capacity to produce antibodies; they are a very active and aggressive subtype of B cells, Dr. Walo noted.
She explained that, as was the case in this study, autoimmune events after alemtuzumab treatment normally manifests as the development of antibodies against the thyroid gland, with the development of either hyperthyroidism or hypothyroidism, necessitating long-term treatment to manage these conditions.
“Autoimmunity develops at variable timescales. It can appear in the first year after alemtuzumab treatment but it can also appear later on,” she said.
Dr. Walo’s group is hoping to validate their results in a larger study. “This is only a small study so we need to replicate these findings in a larger cohort. We are in the process of doing this, collaborating with other hospitals,” she commented.
She said that, if the results are validated, then patients could undergo blood tests before alemtuzumab treatment to analyze their B-cell counts.
“For those with high levels of B cells – and particularly plasmablasts – alemtuzumab may not be the best treatment to choose,” Dr. Walo said.
Personalized strategy
During the postpresentation discussion, the suggestion was raised of giving an anti–B-cell drug before alemtuzumab to try and prevent autoimmunity. Dr. Walo responded that this is a possibility. “This is something that we are going to look into. If our larger study validates our initial results, then we would plan a study to give an anti–B-cell treatment such as rituximab before alemtuzumab and see whether this reduces the risk of autoimmunity.”
Commenting on the study, session comoderator Darin Okuda, MD, professor in the department of neurology and neurotherapeutics at the University of Texas Southwestern Medical Center, Dallas, said: “This is an intriguing approach and suggests a more personalized strategy for sure if we can identify patients who are at higher risk of developing autoimmunity.”
Also commenting, ACTRIMS president Jeffrey Cohen, MD, said: “One of the main drawbacks of alemtuzumab is the risk of antibody-mediated autoimmune conditions, so the ability to predict who is at risk for autoimmune adverse events prior to initiating alemtuzumab would be useful. Not surprisingly, factors related to B-cell number and profile were predictive.”
Dr. Cohen, who is a director of experimental neurotherapeutics at the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, added however that the suggestion of pretreating patients with an anti-CD20 monoclonal antibody “does not seem tenable to me,” because of the potential cost of such a strategy, and “no efficacy advantage for most patients over an anti-CD20 antibody alone.”
Commenting on this presentation, Alasdair J. Coles, MD, University of Cambridge (England), who was one of the co-inventors of alemtuzumab, said observations of an increased B-cell count before treatment as a risk predictor of thyroid autoimmunity after alemtuzumab had not been replicated in the clinical trial datasets of the drug. “So I fear we still do not have a reliable biomarker,” he added.
The study had no specific funding listed. Dr. Walo has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new study suggests.
“Alemtuzumab has proven to be an effective treatment for patients with highly active remitting relapsing MS, but adverse events may limit the use of this drug, particularly autoimmune adverse events, which are the most prevalent, occurring in about 30% of patients. Reliable biomarkers to assess patient risk for developing this complication would be of great importance,” said lead author Paulette Walo, MD.
“Our results suggest that a higher percentage of total B cells, and in particular plasmablasts, could be a very predictive biomarker for autoimmunity after alemtuzumab treatment. This could help us in choosing the patients for this drug,” said Dr. Walo, an immunologist at Ramon y Cajal University Hospital, Madrid. She presented the findings at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The objective of this study was to explore if patient blood lymphocyte profile before alemtuzumab treatment initiation can identify patients with an increased risk of developing later autoimmunity, Dr. Walo explained.
The study included 54 patients from five hospitals throughout Spain who had received treatment with alemtuzumab. Of these, the vast majority had received the normal two-dose cycle and two patients had received a third dose because of worsening MS activity.
Blood samples were collected before initiating treatment with alemtuzumab. Peripheral blood mononuclear cells were obtained and cryopreserved. Leukocyte populations were assessed by flow cytometry.
Autoimmune adverse events were defined as the development, at any point within 2 years of follow-up, of any autoimmune thyroid-associated event, immune thrombocytopenia, and/or autoimmune nephropathy.
Over the 2 years of follow-up, 14 patients (25.9%) experienced autoimmune adverse events, all of which were dysthyroidism. No immune thrombocytopenia or nephropathies were observed.
No statistical differences were found in clinical and demographic characteristics between patients who developed autoimmune adverse events and those who did not. Previous treatments did not influence B-cell percentages.
Analysis of blood lymphocyte profiles showed no difference in T-cell subsets between those who had an autoimmune event and those who did not.
Still, there were important differences in the B-cell profile, Dr. Walo said. “Total B cells were higher in patients who had an autoimmune event mainly due to naive B cells and plasmablasts.”
Patients who experienced autoimmune adverse events before treatment onset had a higher percentage of blood CD19+ B cells (P = .001), with a higher relative percentage of naive B cells and plasmablasts.
When individual types of cell numbers were explored, only plasmablast levels remained significant (P = .02).
The researchers calculated a CD19+ B-cell predictive value for autoimmunity of 7.6%. If patients had more than 7.6% B cells, they were at higher risk of an autoimmune adverse event after alemtuzumab treatment versus those with lower levels (odds ratio, 14.67; P ≤ .0001).
Similarly, the predictive value for plasmablasts was 0.13%. If patients had levels higher than 0.13% they had a higher risk of an autoimmune event after alemtuzumab treatment (P = .002). Plasmablasts are a category of B cells which are very differentiated and have the capacity to produce antibodies; they are a very active and aggressive subtype of B cells, Dr. Walo noted.
She explained that, as was the case in this study, autoimmune events after alemtuzumab treatment normally manifests as the development of antibodies against the thyroid gland, with the development of either hyperthyroidism or hypothyroidism, necessitating long-term treatment to manage these conditions.
“Autoimmunity develops at variable timescales. It can appear in the first year after alemtuzumab treatment but it can also appear later on,” she said.
Dr. Walo’s group is hoping to validate their results in a larger study. “This is only a small study so we need to replicate these findings in a larger cohort. We are in the process of doing this, collaborating with other hospitals,” she commented.
She said that, if the results are validated, then patients could undergo blood tests before alemtuzumab treatment to analyze their B-cell counts.
“For those with high levels of B cells – and particularly plasmablasts – alemtuzumab may not be the best treatment to choose,” Dr. Walo said.
Personalized strategy
During the postpresentation discussion, the suggestion was raised of giving an anti–B-cell drug before alemtuzumab to try and prevent autoimmunity. Dr. Walo responded that this is a possibility. “This is something that we are going to look into. If our larger study validates our initial results, then we would plan a study to give an anti–B-cell treatment such as rituximab before alemtuzumab and see whether this reduces the risk of autoimmunity.”
Commenting on the study, session comoderator Darin Okuda, MD, professor in the department of neurology and neurotherapeutics at the University of Texas Southwestern Medical Center, Dallas, said: “This is an intriguing approach and suggests a more personalized strategy for sure if we can identify patients who are at higher risk of developing autoimmunity.”
Also commenting, ACTRIMS president Jeffrey Cohen, MD, said: “One of the main drawbacks of alemtuzumab is the risk of antibody-mediated autoimmune conditions, so the ability to predict who is at risk for autoimmune adverse events prior to initiating alemtuzumab would be useful. Not surprisingly, factors related to B-cell number and profile were predictive.”
Dr. Cohen, who is a director of experimental neurotherapeutics at the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, added however that the suggestion of pretreating patients with an anti-CD20 monoclonal antibody “does not seem tenable to me,” because of the potential cost of such a strategy, and “no efficacy advantage for most patients over an anti-CD20 antibody alone.”
Commenting on this presentation, Alasdair J. Coles, MD, University of Cambridge (England), who was one of the co-inventors of alemtuzumab, said observations of an increased B-cell count before treatment as a risk predictor of thyroid autoimmunity after alemtuzumab had not been replicated in the clinical trial datasets of the drug. “So I fear we still do not have a reliable biomarker,” he added.
The study had no specific funding listed. Dr. Walo has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new study suggests.
“Alemtuzumab has proven to be an effective treatment for patients with highly active remitting relapsing MS, but adverse events may limit the use of this drug, particularly autoimmune adverse events, which are the most prevalent, occurring in about 30% of patients. Reliable biomarkers to assess patient risk for developing this complication would be of great importance,” said lead author Paulette Walo, MD.
“Our results suggest that a higher percentage of total B cells, and in particular plasmablasts, could be a very predictive biomarker for autoimmunity after alemtuzumab treatment. This could help us in choosing the patients for this drug,” said Dr. Walo, an immunologist at Ramon y Cajal University Hospital, Madrid. She presented the findings at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The objective of this study was to explore if patient blood lymphocyte profile before alemtuzumab treatment initiation can identify patients with an increased risk of developing later autoimmunity, Dr. Walo explained.
The study included 54 patients from five hospitals throughout Spain who had received treatment with alemtuzumab. Of these, the vast majority had received the normal two-dose cycle and two patients had received a third dose because of worsening MS activity.
Blood samples were collected before initiating treatment with alemtuzumab. Peripheral blood mononuclear cells were obtained and cryopreserved. Leukocyte populations were assessed by flow cytometry.
Autoimmune adverse events were defined as the development, at any point within 2 years of follow-up, of any autoimmune thyroid-associated event, immune thrombocytopenia, and/or autoimmune nephropathy.
Over the 2 years of follow-up, 14 patients (25.9%) experienced autoimmune adverse events, all of which were dysthyroidism. No immune thrombocytopenia or nephropathies were observed.
No statistical differences were found in clinical and demographic characteristics between patients who developed autoimmune adverse events and those who did not. Previous treatments did not influence B-cell percentages.
Analysis of blood lymphocyte profiles showed no difference in T-cell subsets between those who had an autoimmune event and those who did not.
Still, there were important differences in the B-cell profile, Dr. Walo said. “Total B cells were higher in patients who had an autoimmune event mainly due to naive B cells and plasmablasts.”
Patients who experienced autoimmune adverse events before treatment onset had a higher percentage of blood CD19+ B cells (P = .001), with a higher relative percentage of naive B cells and plasmablasts.
When individual types of cell numbers were explored, only plasmablast levels remained significant (P = .02).
The researchers calculated a CD19+ B-cell predictive value for autoimmunity of 7.6%. If patients had more than 7.6% B cells, they were at higher risk of an autoimmune adverse event after alemtuzumab treatment versus those with lower levels (odds ratio, 14.67; P ≤ .0001).
Similarly, the predictive value for plasmablasts was 0.13%. If patients had levels higher than 0.13% they had a higher risk of an autoimmune event after alemtuzumab treatment (P = .002). Plasmablasts are a category of B cells which are very differentiated and have the capacity to produce antibodies; they are a very active and aggressive subtype of B cells, Dr. Walo noted.
She explained that, as was the case in this study, autoimmune events after alemtuzumab treatment normally manifests as the development of antibodies against the thyroid gland, with the development of either hyperthyroidism or hypothyroidism, necessitating long-term treatment to manage these conditions.
“Autoimmunity develops at variable timescales. It can appear in the first year after alemtuzumab treatment but it can also appear later on,” she said.
Dr. Walo’s group is hoping to validate their results in a larger study. “This is only a small study so we need to replicate these findings in a larger cohort. We are in the process of doing this, collaborating with other hospitals,” she commented.
She said that, if the results are validated, then patients could undergo blood tests before alemtuzumab treatment to analyze their B-cell counts.
“For those with high levels of B cells – and particularly plasmablasts – alemtuzumab may not be the best treatment to choose,” Dr. Walo said.
Personalized strategy
During the postpresentation discussion, the suggestion was raised of giving an anti–B-cell drug before alemtuzumab to try and prevent autoimmunity. Dr. Walo responded that this is a possibility. “This is something that we are going to look into. If our larger study validates our initial results, then we would plan a study to give an anti–B-cell treatment such as rituximab before alemtuzumab and see whether this reduces the risk of autoimmunity.”
Commenting on the study, session comoderator Darin Okuda, MD, professor in the department of neurology and neurotherapeutics at the University of Texas Southwestern Medical Center, Dallas, said: “This is an intriguing approach and suggests a more personalized strategy for sure if we can identify patients who are at higher risk of developing autoimmunity.”
Also commenting, ACTRIMS president Jeffrey Cohen, MD, said: “One of the main drawbacks of alemtuzumab is the risk of antibody-mediated autoimmune conditions, so the ability to predict who is at risk for autoimmune adverse events prior to initiating alemtuzumab would be useful. Not surprisingly, factors related to B-cell number and profile were predictive.”
Dr. Cohen, who is a director of experimental neurotherapeutics at the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, added however that the suggestion of pretreating patients with an anti-CD20 monoclonal antibody “does not seem tenable to me,” because of the potential cost of such a strategy, and “no efficacy advantage for most patients over an anti-CD20 antibody alone.”
Commenting on this presentation, Alasdair J. Coles, MD, University of Cambridge (England), who was one of the co-inventors of alemtuzumab, said observations of an increased B-cell count before treatment as a risk predictor of thyroid autoimmunity after alemtuzumab had not been replicated in the clinical trial datasets of the drug. “So I fear we still do not have a reliable biomarker,” he added.
The study had no specific funding listed. Dr. Walo has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020
J&J’s one-shot COVID-19 vaccine advances to phase 3 testing
The National Institute of Allergy and Infectious Diseases, which is aiding Johnson & Johnson with development, described this in a news release as the fourth phase 3 clinical trial of evaluating an investigational vaccine for coronavirus disease.
This NIAID tally tracks products likely to be presented soon for Food and Drug Administration approval. (The World Health Organization’s COVID vaccine tracker lists nine candidates as having reached this stage, including products developed in Russia and China.)
As many as 60,000 volunteers will be enrolled in the trial, with about 215 clinical research sites expected to participate, NIAID said. The vaccine will be tested in the United States and abroad.
The start of this test, known as the ENSEMBLE trial, follows positive results from a Phase 1/2a clinical study, which involved a single vaccination. The results of this study have been submitted to medRxiv and are set to be published online imminently.
New Brunswick, N.J–based J&J said it intends to offer the vaccine on “a not-for-profit basis for emergency pandemic use.” If testing proceeds well, J&J might seek an emergency use clearance for the vaccine, which could possibly allow the first batches to be made available in early 2021.
J&J’s vaccine is unusual in that it will be tested based on a single dose, while other advanced candidates have been tested in two-dose regimens.
J&J on Wednesday also released the study protocol for its phase 3 test. The developers of the other late-stage COVID vaccine candidates also have done this, as reported by Medscape Medical News. Because of the great interest in the COVID vaccine, the American Medical Association had last month asked the FDA to keep physicians informed of their COVID-19 vaccine review process.
Trials and tribulations
One of these experimental COVID vaccines already has had a setback in phase 3 testing, which is a fairly routine occurrence in drug development. But with a pandemic still causing deaths and disrupting lives around the world, there has been intense interest in each step of the effort to develop a COVID vaccine.
AstraZeneca PLC earlier this month announced a temporary cessation of all their coronavirus vaccine trials to investigate an “unexplained illness” that arose in a participant, as reported by Medscape Medical News.
On September 12, AstraZeneca announced that clinical trials for the AZD1222, which it developed with Oxford University, had resumed in the United Kingdom. On Wednesday, CNBC said Health and Human Services Secretary Alex Azar told the news station that AstraZeneca’s late-stage coronavirus vaccine trial in the United States remains on hold until safety concerns are resolved, a critical issue with all the fast-track COVID vaccines now being tested.
“Look at the AstraZeneca program, phase 3 clinical trial, a lot of hope. [A] single serious adverse event report in the United Kingdom, global shutdown, and [a] hold of the clinical trials,” Mr. Azar told CNBC.
The New York Times has reported on concerns stemming from serious neurologic illnesses in two participants, both women, who received AstraZeneca’s experimental vaccine in Britain.
The Senate Health, Education, Labor and Pensions Committee on Wednesday separately held a hearing with the leaders of the FDA and the Centers of Disease Control and Prevention, allowing an airing of lawmakers’ concerns about a potential rush to approve a COVID vaccine.
Details of J&J trial
The J&J trial is designed primarily to determine if the investigational vaccine can prevent moderate to severe COVID-19 after a single dose. It also is designed to examine whether the vaccine can prevent COVID-19 requiring medical intervention and if the vaccine can prevent milder cases of COVID-19 and asymptomatic SARS-CoV-2 infection, NIAID said.
Principal investigators for the phase 3 trial of the J & J vaccine are Paul A. Goepfert, MD, director of the Alabama Vaccine Research Clinic at the University of Alabama in Birmingham; Beatriz Grinsztejn, MD, PhD, director of the Laboratory of Clinical Research on HIV/AIDS at the Evandro Chagas National Institute of Infectious Diseases-Oswaldo Cruz Foundation in Rio de Janeiro, Brazil; and Glenda E. Gray, MBBCh, president and chief executive officer of the South African Medical Research Council and coprincipal investigator of the HIV Vaccine Trials Network.
This article first appeared on Medscape.com.
The National Institute of Allergy and Infectious Diseases, which is aiding Johnson & Johnson with development, described this in a news release as the fourth phase 3 clinical trial of evaluating an investigational vaccine for coronavirus disease.
This NIAID tally tracks products likely to be presented soon for Food and Drug Administration approval. (The World Health Organization’s COVID vaccine tracker lists nine candidates as having reached this stage, including products developed in Russia and China.)
As many as 60,000 volunteers will be enrolled in the trial, with about 215 clinical research sites expected to participate, NIAID said. The vaccine will be tested in the United States and abroad.
The start of this test, known as the ENSEMBLE trial, follows positive results from a Phase 1/2a clinical study, which involved a single vaccination. The results of this study have been submitted to medRxiv and are set to be published online imminently.
New Brunswick, N.J–based J&J said it intends to offer the vaccine on “a not-for-profit basis for emergency pandemic use.” If testing proceeds well, J&J might seek an emergency use clearance for the vaccine, which could possibly allow the first batches to be made available in early 2021.
J&J’s vaccine is unusual in that it will be tested based on a single dose, while other advanced candidates have been tested in two-dose regimens.
J&J on Wednesday also released the study protocol for its phase 3 test. The developers of the other late-stage COVID vaccine candidates also have done this, as reported by Medscape Medical News. Because of the great interest in the COVID vaccine, the American Medical Association had last month asked the FDA to keep physicians informed of their COVID-19 vaccine review process.
Trials and tribulations
One of these experimental COVID vaccines already has had a setback in phase 3 testing, which is a fairly routine occurrence in drug development. But with a pandemic still causing deaths and disrupting lives around the world, there has been intense interest in each step of the effort to develop a COVID vaccine.
AstraZeneca PLC earlier this month announced a temporary cessation of all their coronavirus vaccine trials to investigate an “unexplained illness” that arose in a participant, as reported by Medscape Medical News.
On September 12, AstraZeneca announced that clinical trials for the AZD1222, which it developed with Oxford University, had resumed in the United Kingdom. On Wednesday, CNBC said Health and Human Services Secretary Alex Azar told the news station that AstraZeneca’s late-stage coronavirus vaccine trial in the United States remains on hold until safety concerns are resolved, a critical issue with all the fast-track COVID vaccines now being tested.
“Look at the AstraZeneca program, phase 3 clinical trial, a lot of hope. [A] single serious adverse event report in the United Kingdom, global shutdown, and [a] hold of the clinical trials,” Mr. Azar told CNBC.
The New York Times has reported on concerns stemming from serious neurologic illnesses in two participants, both women, who received AstraZeneca’s experimental vaccine in Britain.
The Senate Health, Education, Labor and Pensions Committee on Wednesday separately held a hearing with the leaders of the FDA and the Centers of Disease Control and Prevention, allowing an airing of lawmakers’ concerns about a potential rush to approve a COVID vaccine.
Details of J&J trial
The J&J trial is designed primarily to determine if the investigational vaccine can prevent moderate to severe COVID-19 after a single dose. It also is designed to examine whether the vaccine can prevent COVID-19 requiring medical intervention and if the vaccine can prevent milder cases of COVID-19 and asymptomatic SARS-CoV-2 infection, NIAID said.
Principal investigators for the phase 3 trial of the J & J vaccine are Paul A. Goepfert, MD, director of the Alabama Vaccine Research Clinic at the University of Alabama in Birmingham; Beatriz Grinsztejn, MD, PhD, director of the Laboratory of Clinical Research on HIV/AIDS at the Evandro Chagas National Institute of Infectious Diseases-Oswaldo Cruz Foundation in Rio de Janeiro, Brazil; and Glenda E. Gray, MBBCh, president and chief executive officer of the South African Medical Research Council and coprincipal investigator of the HIV Vaccine Trials Network.
This article first appeared on Medscape.com.
The National Institute of Allergy and Infectious Diseases, which is aiding Johnson & Johnson with development, described this in a news release as the fourth phase 3 clinical trial of evaluating an investigational vaccine for coronavirus disease.
This NIAID tally tracks products likely to be presented soon for Food and Drug Administration approval. (The World Health Organization’s COVID vaccine tracker lists nine candidates as having reached this stage, including products developed in Russia and China.)
As many as 60,000 volunteers will be enrolled in the trial, with about 215 clinical research sites expected to participate, NIAID said. The vaccine will be tested in the United States and abroad.
The start of this test, known as the ENSEMBLE trial, follows positive results from a Phase 1/2a clinical study, which involved a single vaccination. The results of this study have been submitted to medRxiv and are set to be published online imminently.
New Brunswick, N.J–based J&J said it intends to offer the vaccine on “a not-for-profit basis for emergency pandemic use.” If testing proceeds well, J&J might seek an emergency use clearance for the vaccine, which could possibly allow the first batches to be made available in early 2021.
J&J’s vaccine is unusual in that it will be tested based on a single dose, while other advanced candidates have been tested in two-dose regimens.
J&J on Wednesday also released the study protocol for its phase 3 test. The developers of the other late-stage COVID vaccine candidates also have done this, as reported by Medscape Medical News. Because of the great interest in the COVID vaccine, the American Medical Association had last month asked the FDA to keep physicians informed of their COVID-19 vaccine review process.
Trials and tribulations
One of these experimental COVID vaccines already has had a setback in phase 3 testing, which is a fairly routine occurrence in drug development. But with a pandemic still causing deaths and disrupting lives around the world, there has been intense interest in each step of the effort to develop a COVID vaccine.
AstraZeneca PLC earlier this month announced a temporary cessation of all their coronavirus vaccine trials to investigate an “unexplained illness” that arose in a participant, as reported by Medscape Medical News.
On September 12, AstraZeneca announced that clinical trials for the AZD1222, which it developed with Oxford University, had resumed in the United Kingdom. On Wednesday, CNBC said Health and Human Services Secretary Alex Azar told the news station that AstraZeneca’s late-stage coronavirus vaccine trial in the United States remains on hold until safety concerns are resolved, a critical issue with all the fast-track COVID vaccines now being tested.
“Look at the AstraZeneca program, phase 3 clinical trial, a lot of hope. [A] single serious adverse event report in the United Kingdom, global shutdown, and [a] hold of the clinical trials,” Mr. Azar told CNBC.
The New York Times has reported on concerns stemming from serious neurologic illnesses in two participants, both women, who received AstraZeneca’s experimental vaccine in Britain.
The Senate Health, Education, Labor and Pensions Committee on Wednesday separately held a hearing with the leaders of the FDA and the Centers of Disease Control and Prevention, allowing an airing of lawmakers’ concerns about a potential rush to approve a COVID vaccine.
Details of J&J trial
The J&J trial is designed primarily to determine if the investigational vaccine can prevent moderate to severe COVID-19 after a single dose. It also is designed to examine whether the vaccine can prevent COVID-19 requiring medical intervention and if the vaccine can prevent milder cases of COVID-19 and asymptomatic SARS-CoV-2 infection, NIAID said.
Principal investigators for the phase 3 trial of the J & J vaccine are Paul A. Goepfert, MD, director of the Alabama Vaccine Research Clinic at the University of Alabama in Birmingham; Beatriz Grinsztejn, MD, PhD, director of the Laboratory of Clinical Research on HIV/AIDS at the Evandro Chagas National Institute of Infectious Diseases-Oswaldo Cruz Foundation in Rio de Janeiro, Brazil; and Glenda E. Gray, MBBCh, president and chief executive officer of the South African Medical Research Council and coprincipal investigator of the HIV Vaccine Trials Network.
This article first appeared on Medscape.com.
CDC playbook prepares states for rollout of COVID-19 vaccine if one is approved
States have begun preparing to distribute a COVID-19 vaccine if one is approved, a CDC official said today.
The CDC released guidance for states on Sept. 16 titled COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. The document discusses vaccine ordering, storage, and handling and says that states should submit their plans for vaccine distribution to the agency by Oct. 16.
“Every jurisdiction is heavily involved right now in their plan development,” CDC official Janell Routh, MD, told the Advisory Committee on Immunization Practices during its Sept. 22 meeting. “It was really impressive to me that, even though the playbook only went out last week, states and jurisdictions have been thinking about this for quite some time.”
However, one committee member suggested that setting a deadline before more safety, efficacy, and storage information is known may be premature.
“I cannot imagine that we will actually know the final storage requirements for this vaccine by Oct. 16, which makes me a little concerned about finalizing state plans,” said Helen “Keipp” Talbot, MD, MPH, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. “We also don’t know the best populations yet when it comes to efficacy and safety.”
Dr. Routh said the CDC is asking states to plan on the basis of assumptions. “We know those plans will constantly be improving, changing, as we learn more information,” Dr. Routh said. States agreed to return a plan 30 days after the playbook was released, which is how the Oct. 16 deadline was established, she said.
States are encouraged to think broadly. Plans may include contingencies for a product that requires ultracold storage or for distributing more than one vaccine product, Dr. Routh said.
“One goal is to be ready on the first day that we can actually distribute vaccine,” Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during the meeting. “Our colleagues in Operation Warp Speed say that they expect there will be vaccine as early as November, and therefore we need to be ready so there is no delay in distributing that vaccine. And that phase, that early phase, is really close upon us.”
Many states have already developed plans, and the CDC is providing technical assistance as needed to monitor the plans regularly, Dr. Routh said.
Key issues identified
From holding pilot meetings with five jurisdictions, officials learned that public confidence in the vaccine is among states’ greatest concerns, Dr. Routh said. In addition, distribution is resource intensive, and social distancing adds logistical complexity.
Specific guidance on whom to vaccinate in the early stages will smooth the process, officials suggested during the pilot meetings. For the first several weeks, vaccine doses may be limited to priority populations, such as health care workers.
“This interim playbook is a living document,” Dr. Routh emphasized. “We definitely plan to update the content regularly as we learn more information about what vaccines and when they will be released.”
During the early stages of COVID-19 vaccination, officials plan to implement an enhanced monitoring program in which vaccine recipients would complete surveys about adverse events, in addition to the traditional vaccine safety monitoring programs that already exist, officials said.
A version of this article originally appeared on Medscape.com.
States have begun preparing to distribute a COVID-19 vaccine if one is approved, a CDC official said today.
The CDC released guidance for states on Sept. 16 titled COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. The document discusses vaccine ordering, storage, and handling and says that states should submit their plans for vaccine distribution to the agency by Oct. 16.
“Every jurisdiction is heavily involved right now in their plan development,” CDC official Janell Routh, MD, told the Advisory Committee on Immunization Practices during its Sept. 22 meeting. “It was really impressive to me that, even though the playbook only went out last week, states and jurisdictions have been thinking about this for quite some time.”
However, one committee member suggested that setting a deadline before more safety, efficacy, and storage information is known may be premature.
“I cannot imagine that we will actually know the final storage requirements for this vaccine by Oct. 16, which makes me a little concerned about finalizing state plans,” said Helen “Keipp” Talbot, MD, MPH, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. “We also don’t know the best populations yet when it comes to efficacy and safety.”
Dr. Routh said the CDC is asking states to plan on the basis of assumptions. “We know those plans will constantly be improving, changing, as we learn more information,” Dr. Routh said. States agreed to return a plan 30 days after the playbook was released, which is how the Oct. 16 deadline was established, she said.
States are encouraged to think broadly. Plans may include contingencies for a product that requires ultracold storage or for distributing more than one vaccine product, Dr. Routh said.
“One goal is to be ready on the first day that we can actually distribute vaccine,” Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during the meeting. “Our colleagues in Operation Warp Speed say that they expect there will be vaccine as early as November, and therefore we need to be ready so there is no delay in distributing that vaccine. And that phase, that early phase, is really close upon us.”
Many states have already developed plans, and the CDC is providing technical assistance as needed to monitor the plans regularly, Dr. Routh said.
Key issues identified
From holding pilot meetings with five jurisdictions, officials learned that public confidence in the vaccine is among states’ greatest concerns, Dr. Routh said. In addition, distribution is resource intensive, and social distancing adds logistical complexity.
Specific guidance on whom to vaccinate in the early stages will smooth the process, officials suggested during the pilot meetings. For the first several weeks, vaccine doses may be limited to priority populations, such as health care workers.
“This interim playbook is a living document,” Dr. Routh emphasized. “We definitely plan to update the content regularly as we learn more information about what vaccines and when they will be released.”
During the early stages of COVID-19 vaccination, officials plan to implement an enhanced monitoring program in which vaccine recipients would complete surveys about adverse events, in addition to the traditional vaccine safety monitoring programs that already exist, officials said.
A version of this article originally appeared on Medscape.com.
States have begun preparing to distribute a COVID-19 vaccine if one is approved, a CDC official said today.
The CDC released guidance for states on Sept. 16 titled COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. The document discusses vaccine ordering, storage, and handling and says that states should submit their plans for vaccine distribution to the agency by Oct. 16.
“Every jurisdiction is heavily involved right now in their plan development,” CDC official Janell Routh, MD, told the Advisory Committee on Immunization Practices during its Sept. 22 meeting. “It was really impressive to me that, even though the playbook only went out last week, states and jurisdictions have been thinking about this for quite some time.”
However, one committee member suggested that setting a deadline before more safety, efficacy, and storage information is known may be premature.
“I cannot imagine that we will actually know the final storage requirements for this vaccine by Oct. 16, which makes me a little concerned about finalizing state plans,” said Helen “Keipp” Talbot, MD, MPH, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. “We also don’t know the best populations yet when it comes to efficacy and safety.”
Dr. Routh said the CDC is asking states to plan on the basis of assumptions. “We know those plans will constantly be improving, changing, as we learn more information,” Dr. Routh said. States agreed to return a plan 30 days after the playbook was released, which is how the Oct. 16 deadline was established, she said.
States are encouraged to think broadly. Plans may include contingencies for a product that requires ultracold storage or for distributing more than one vaccine product, Dr. Routh said.
“One goal is to be ready on the first day that we can actually distribute vaccine,” Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during the meeting. “Our colleagues in Operation Warp Speed say that they expect there will be vaccine as early as November, and therefore we need to be ready so there is no delay in distributing that vaccine. And that phase, that early phase, is really close upon us.”
Many states have already developed plans, and the CDC is providing technical assistance as needed to monitor the plans regularly, Dr. Routh said.
Key issues identified
From holding pilot meetings with five jurisdictions, officials learned that public confidence in the vaccine is among states’ greatest concerns, Dr. Routh said. In addition, distribution is resource intensive, and social distancing adds logistical complexity.
Specific guidance on whom to vaccinate in the early stages will smooth the process, officials suggested during the pilot meetings. For the first several weeks, vaccine doses may be limited to priority populations, such as health care workers.
“This interim playbook is a living document,” Dr. Routh emphasized. “We definitely plan to update the content regularly as we learn more information about what vaccines and when they will be released.”
During the early stages of COVID-19 vaccination, officials plan to implement an enhanced monitoring program in which vaccine recipients would complete surveys about adverse events, in addition to the traditional vaccine safety monitoring programs that already exist, officials said.
A version of this article originally appeared on Medscape.com.
Three major COVID vaccine developers release detailed trial protocols
Typically, manufacturers guard the specifics of preclinical vaccine trials. This rare move follows calls for greater transparency. For example, the American Medical Association wrote a letter in late August asking the Food and Drug Administration to keep physicians informed of their COVID-19 vaccine review process.
On September 17, ModernaTx released the phase 3 trial protocol for its mRNA-1273 SARS-CoV-2 vaccine. In short order, on September 19, Pfizer/BioNTech shared their phase 1/2/3 trial vaccine protocol. AstraZeneca, which is developing a vaccine along with Oxford University, also released its protocol.
The AstraZeneca vaccine trial made headlines recently for having to be temporarily halted because of unexpected illnesses that arose in two participants, according to the New York Times and other sources.
“I applaud the release of the clinical trial protocols by the companies. The public trust in any COVID-19 vaccine is paramount, especially given the fast timeline and perceived political pressures of these candidates,” Robert Kruse, MD, PhD, told Medscape Medical News when asked to comment.
AstraZeneca takes a shot at transparency
The three primary objectives of the AstraZeneca AZD1222 trial outlined in the 110-page protocol include estimating the efficacy, safety, tolerability, and reactogenicity associated with two intramuscular doses of the vaccine in comparison with placebo in adults.
The projected enrollment is 30,000 participants, and the estimated primary completion date is Dec. 2, 2020, according to information on clinicaltrials.gov.
“Given the unprecedented global impact of the coronavirus pandemic and the need for public information, AstraZeneca has published the detailed protocol and design of our AZD1222 clinical trial,” the company said in a statement. “As with most clinical development, protocols are not typically shared publicly due to the importance of maintaining confidentiality and integrity of trials.
“AstraZeneca continues to work with industry peers to ensure a consistent approach to sharing timely clinical trial information,” the company added.
Moderna methodology
The ModernaTX 135-page protocol outlines the primary trial objectives of evaluating efficacy, safety, and reactogenicity of two injections of the vaccine administered 28 days apart. Researchers also plan to randomly assign 30,000 adults to receive either vaccine or placebo. The estimated primary completion date is Oct. 27, 2022.
A statement that was requested from ModernaTX was not received by press time.
Pfizer protocol
In the Pfizer/BioNTech vaccine trial, researchers plan to evaluate different doses in different age groups in a multistep protocol. The trial features 20 primary safety objectives, which include reporting adverse events and serious adverse events, including any local or systemic events.
Efficacy endpoints are secondary objectives. The estimated enrollment is 29,481 adults; the estimated primary completion date is April 19, 2021.
“Pfizer and BioNTech recognize that the COVID-19 pandemic is a unique circumstance, and the need for transparency is clear,” Pfizer spokesperson Sharon Castillo told Medscape Medical News. By making the full protocol available, “we believe this will reinforce our long-standing commitment to scientific and regulatory rigor that benefits patients,” she said.
“Based on current infection rates, Pfizer and BioNTech continue to expect that a conclusive read-out on efficacy is likely by the end of October. Neither Pfizer nor the FDA can move faster than the data we are generating through our clinical trial,” Castillo said.
If clinical work and regulatory approval or authorization proceed as planned, Pfizer and BioNTech expect to supply up to 100 million doses worldwide by the end of 2020 and approximately 1.3 billion doses worldwide by the end of 2021.
Pfizer is not willing to sacrifice safety and efficacy in the name of expediency, Castillo said. “We will not cut corners in this pursuit. Patient safety is our highest priority, and Pfizer will not bring a vaccine to market without adequate evidence of safety and efficacy.”
A positive move
“COVID-19 vaccines will only be useful if many people are willing to receive them,” said Kruse, a postgraduate year 3 resident in the Department of Pathology at Johns Hopkins Medicine in Baltimore, Maryland.
“By giving the general public along with other scientists and physicians the opportunity to critique the protocols, everyone can understand what the metrics would be for an early look at efficacy,” Kruse said. He noted that information could help inform a potential FDA emergency use authorization.
Kruse has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Typically, manufacturers guard the specifics of preclinical vaccine trials. This rare move follows calls for greater transparency. For example, the American Medical Association wrote a letter in late August asking the Food and Drug Administration to keep physicians informed of their COVID-19 vaccine review process.
On September 17, ModernaTx released the phase 3 trial protocol for its mRNA-1273 SARS-CoV-2 vaccine. In short order, on September 19, Pfizer/BioNTech shared their phase 1/2/3 trial vaccine protocol. AstraZeneca, which is developing a vaccine along with Oxford University, also released its protocol.
The AstraZeneca vaccine trial made headlines recently for having to be temporarily halted because of unexpected illnesses that arose in two participants, according to the New York Times and other sources.
“I applaud the release of the clinical trial protocols by the companies. The public trust in any COVID-19 vaccine is paramount, especially given the fast timeline and perceived political pressures of these candidates,” Robert Kruse, MD, PhD, told Medscape Medical News when asked to comment.
AstraZeneca takes a shot at transparency
The three primary objectives of the AstraZeneca AZD1222 trial outlined in the 110-page protocol include estimating the efficacy, safety, tolerability, and reactogenicity associated with two intramuscular doses of the vaccine in comparison with placebo in adults.
The projected enrollment is 30,000 participants, and the estimated primary completion date is Dec. 2, 2020, according to information on clinicaltrials.gov.
“Given the unprecedented global impact of the coronavirus pandemic and the need for public information, AstraZeneca has published the detailed protocol and design of our AZD1222 clinical trial,” the company said in a statement. “As with most clinical development, protocols are not typically shared publicly due to the importance of maintaining confidentiality and integrity of trials.
“AstraZeneca continues to work with industry peers to ensure a consistent approach to sharing timely clinical trial information,” the company added.
Moderna methodology
The ModernaTX 135-page protocol outlines the primary trial objectives of evaluating efficacy, safety, and reactogenicity of two injections of the vaccine administered 28 days apart. Researchers also plan to randomly assign 30,000 adults to receive either vaccine or placebo. The estimated primary completion date is Oct. 27, 2022.
A statement that was requested from ModernaTX was not received by press time.
Pfizer protocol
In the Pfizer/BioNTech vaccine trial, researchers plan to evaluate different doses in different age groups in a multistep protocol. The trial features 20 primary safety objectives, which include reporting adverse events and serious adverse events, including any local or systemic events.
Efficacy endpoints are secondary objectives. The estimated enrollment is 29,481 adults; the estimated primary completion date is April 19, 2021.
“Pfizer and BioNTech recognize that the COVID-19 pandemic is a unique circumstance, and the need for transparency is clear,” Pfizer spokesperson Sharon Castillo told Medscape Medical News. By making the full protocol available, “we believe this will reinforce our long-standing commitment to scientific and regulatory rigor that benefits patients,” she said.
“Based on current infection rates, Pfizer and BioNTech continue to expect that a conclusive read-out on efficacy is likely by the end of October. Neither Pfizer nor the FDA can move faster than the data we are generating through our clinical trial,” Castillo said.
If clinical work and regulatory approval or authorization proceed as planned, Pfizer and BioNTech expect to supply up to 100 million doses worldwide by the end of 2020 and approximately 1.3 billion doses worldwide by the end of 2021.
Pfizer is not willing to sacrifice safety and efficacy in the name of expediency, Castillo said. “We will not cut corners in this pursuit. Patient safety is our highest priority, and Pfizer will not bring a vaccine to market without adequate evidence of safety and efficacy.”
A positive move
“COVID-19 vaccines will only be useful if many people are willing to receive them,” said Kruse, a postgraduate year 3 resident in the Department of Pathology at Johns Hopkins Medicine in Baltimore, Maryland.
“By giving the general public along with other scientists and physicians the opportunity to critique the protocols, everyone can understand what the metrics would be for an early look at efficacy,” Kruse said. He noted that information could help inform a potential FDA emergency use authorization.
Kruse has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Typically, manufacturers guard the specifics of preclinical vaccine trials. This rare move follows calls for greater transparency. For example, the American Medical Association wrote a letter in late August asking the Food and Drug Administration to keep physicians informed of their COVID-19 vaccine review process.
On September 17, ModernaTx released the phase 3 trial protocol for its mRNA-1273 SARS-CoV-2 vaccine. In short order, on September 19, Pfizer/BioNTech shared their phase 1/2/3 trial vaccine protocol. AstraZeneca, which is developing a vaccine along with Oxford University, also released its protocol.
The AstraZeneca vaccine trial made headlines recently for having to be temporarily halted because of unexpected illnesses that arose in two participants, according to the New York Times and other sources.
“I applaud the release of the clinical trial protocols by the companies. The public trust in any COVID-19 vaccine is paramount, especially given the fast timeline and perceived political pressures of these candidates,” Robert Kruse, MD, PhD, told Medscape Medical News when asked to comment.
AstraZeneca takes a shot at transparency
The three primary objectives of the AstraZeneca AZD1222 trial outlined in the 110-page protocol include estimating the efficacy, safety, tolerability, and reactogenicity associated with two intramuscular doses of the vaccine in comparison with placebo in adults.
The projected enrollment is 30,000 participants, and the estimated primary completion date is Dec. 2, 2020, according to information on clinicaltrials.gov.
“Given the unprecedented global impact of the coronavirus pandemic and the need for public information, AstraZeneca has published the detailed protocol and design of our AZD1222 clinical trial,” the company said in a statement. “As with most clinical development, protocols are not typically shared publicly due to the importance of maintaining confidentiality and integrity of trials.
“AstraZeneca continues to work with industry peers to ensure a consistent approach to sharing timely clinical trial information,” the company added.
Moderna methodology
The ModernaTX 135-page protocol outlines the primary trial objectives of evaluating efficacy, safety, and reactogenicity of two injections of the vaccine administered 28 days apart. Researchers also plan to randomly assign 30,000 adults to receive either vaccine or placebo. The estimated primary completion date is Oct. 27, 2022.
A statement that was requested from ModernaTX was not received by press time.
Pfizer protocol
In the Pfizer/BioNTech vaccine trial, researchers plan to evaluate different doses in different age groups in a multistep protocol. The trial features 20 primary safety objectives, which include reporting adverse events and serious adverse events, including any local or systemic events.
Efficacy endpoints are secondary objectives. The estimated enrollment is 29,481 adults; the estimated primary completion date is April 19, 2021.
“Pfizer and BioNTech recognize that the COVID-19 pandemic is a unique circumstance, and the need for transparency is clear,” Pfizer spokesperson Sharon Castillo told Medscape Medical News. By making the full protocol available, “we believe this will reinforce our long-standing commitment to scientific and regulatory rigor that benefits patients,” she said.
“Based on current infection rates, Pfizer and BioNTech continue to expect that a conclusive read-out on efficacy is likely by the end of October. Neither Pfizer nor the FDA can move faster than the data we are generating through our clinical trial,” Castillo said.
If clinical work and regulatory approval or authorization proceed as planned, Pfizer and BioNTech expect to supply up to 100 million doses worldwide by the end of 2020 and approximately 1.3 billion doses worldwide by the end of 2021.
Pfizer is not willing to sacrifice safety and efficacy in the name of expediency, Castillo said. “We will not cut corners in this pursuit. Patient safety is our highest priority, and Pfizer will not bring a vaccine to market without adequate evidence of safety and efficacy.”
A positive move
“COVID-19 vaccines will only be useful if many people are willing to receive them,” said Kruse, a postgraduate year 3 resident in the Department of Pathology at Johns Hopkins Medicine in Baltimore, Maryland.
“By giving the general public along with other scientists and physicians the opportunity to critique the protocols, everyone can understand what the metrics would be for an early look at efficacy,” Kruse said. He noted that information could help inform a potential FDA emergency use authorization.
Kruse has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.