User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Exercise later in the day for better blood glucose control?
The data come from 775 participants with a mean body mass index (BMI) of 26.2 kg/m2 in the observational Netherlands Epidemiology of Obesity (NEO) study. Use of activity monitors for four consecutive days showed that performance of MVPA (defined as activity with intensity of > 3 metabolic equivalents of task) in the afternoon or evening was associated with up to 25% reduced insulin resistance compared with an even distribution of activity during the day.
“This is one of the first studies where in humans the relation between timing of physical activity and insulin resistance was examined,” lead author Jeroen van der Velde of the department of clinical epidemiology, Leiden (the Netherlands) University Medical Center, said in an interview.
Moreover, he noted that, while previous intervention studies have shown greater blood glucose reduction with high-intensity exercise performed in the afternoon, compared with the morning, in people with impaired glucose metabolism or type 2 diabetes, “as far as I am aware, we were the first to use a population-based study in a general population to study this.”
Katarina Kos, MD, PhD, senior lecturer in diabetes and obesity, University of Exeter (England), said: “This study is novel in that it relates the timing of physical activity if performed in the morning, afternoon, or evening to insulin resistance and fat content. This is from a cohort of middle-aged Dutch people between ages 45-65 studied 10 years ago and based on self-reports of weight and eating behavior and who were found to be generally overweight.”
Is it down to circadian rhythm?
“The results are of interest in that if the chosen timing was in the afternoon [63% of studied population] or evening (8% of the studied population), it seemed to relate with improved metabolism when compared to the morning exercising [16% of population]. ... Whether this was due to the (timing) of activity is yet to be shown,” Dr. Kos told the UK Science Media Centre.
Mr. van der Velde agrees that the effect may be explained at least in part by the circadian rhythm of the body. “Physical activity may act as ... a cue for the activation of clock genes. Previous research has suggested that our body’s muscular system and oxidative system are also affected by our circadian rhythm and their peak activity seems to be in the late afternoon. So, being mostly active in this time period ... may elicit greater metabolic responses compared to being active in the morning.”
But, he cautioned, “I think it is important to realize that we are just beginning to understand the potential impact of physical activity timing. At this stage, I believe it is most important to be physically active in general. So ... if the morning is the only time of the day to go for a walk or a run, certainly do this.”
Dr. Kos concurred: “As this is not an intervention study, further research is needed to explain the cause of the observed association.”
Mr. van der Velde also added that it’s not yet clear which individuals or subgroups might experience additional benefits from timed activities. That’s the current research focus of a large consortium of several research institutes in the Netherlands and Canada.
Timed exercise reduces insulin resistance but not liver fat
The findings were published online in Diabetologia.
The study population included men and women living in the greater Leiden area in the western Netherlands who were aged 45-65 years and self-reported a BMI of 27 or higher. A second cohort included inhabitants of one municipality who were invited to participate regardless of their BMI. All wore the activity monitors for 4 consecutive days and nights during their usual activities.
Neither sedentary time nor breaks in sedentary time (defined as a period of activity with an acceleration greater than 0.75 m/s2 following a sedentary period) were associated with lower insulin resistance, as calculated by blood sampling.
However, the number of breaks in sedentary time was associated with a significant 22% higher liver fat content, assessed with proton magnetic resonance spectroscopy.
One reason for the lack of effect of breaks on insulin resistance, the authors theorized, is that this was a real-world observational study where regular breaks aren’t common. Alternatively, people might not have been intensively active enough during breaks to make a difference.
After adjustment for total body fat, an additional hour of MVPA was associated with a 5% drop in insulin resistance. An additional hour of MVPA in 5-minute bouts was associated with 9% lower insulin resistance.
Also after adjustments, insulin resistance was reduced significantly in participants who were most active in the afternoon, by 18%, or evening, by 25%, whereas insulin resistance was not affected among those who were most active in the morning (–3%), all compared with people who distributed their MVPA throughout the day.
Timing of MVPA was not associated with liver fat content, and there were no significant differences in liver fat content and insulin resistance between groups based on timing of light physical activity.
“This is just speculation, but perhaps for fat accumulation in the liver the circadian system is less involved. Or perhaps timing of other lifestyle variables are more important here, such as dietary intake,” Mr. van der Velde said.
Finally, he observed, “timing of physical activity is most likely just a piece of the puzzle. Timing of other lifestyle behavior, such as sleep, and food intake are important cues for our circadian system as well, and it is likely that all these behaviors interact with each other.”
The NEO study is supported by Leiden University Medical Center, the Netherlands Cardiovascular Research Initiative, an initiative supported by the Dutch Heart Foundation, and the Netherlands Organisation for Health Research and Development/Partnership Diabetes/Dutch Diabetes foundation Breakthrough. Mr. van der Velde has reported no further disclosures.
A version of this article first appeared on Medscape.com.
The data come from 775 participants with a mean body mass index (BMI) of 26.2 kg/m2 in the observational Netherlands Epidemiology of Obesity (NEO) study. Use of activity monitors for four consecutive days showed that performance of MVPA (defined as activity with intensity of > 3 metabolic equivalents of task) in the afternoon or evening was associated with up to 25% reduced insulin resistance compared with an even distribution of activity during the day.
“This is one of the first studies where in humans the relation between timing of physical activity and insulin resistance was examined,” lead author Jeroen van der Velde of the department of clinical epidemiology, Leiden (the Netherlands) University Medical Center, said in an interview.
Moreover, he noted that, while previous intervention studies have shown greater blood glucose reduction with high-intensity exercise performed in the afternoon, compared with the morning, in people with impaired glucose metabolism or type 2 diabetes, “as far as I am aware, we were the first to use a population-based study in a general population to study this.”
Katarina Kos, MD, PhD, senior lecturer in diabetes and obesity, University of Exeter (England), said: “This study is novel in that it relates the timing of physical activity if performed in the morning, afternoon, or evening to insulin resistance and fat content. This is from a cohort of middle-aged Dutch people between ages 45-65 studied 10 years ago and based on self-reports of weight and eating behavior and who were found to be generally overweight.”
Is it down to circadian rhythm?
“The results are of interest in that if the chosen timing was in the afternoon [63% of studied population] or evening (8% of the studied population), it seemed to relate with improved metabolism when compared to the morning exercising [16% of population]. ... Whether this was due to the (timing) of activity is yet to be shown,” Dr. Kos told the UK Science Media Centre.
Mr. van der Velde agrees that the effect may be explained at least in part by the circadian rhythm of the body. “Physical activity may act as ... a cue for the activation of clock genes. Previous research has suggested that our body’s muscular system and oxidative system are also affected by our circadian rhythm and their peak activity seems to be in the late afternoon. So, being mostly active in this time period ... may elicit greater metabolic responses compared to being active in the morning.”
But, he cautioned, “I think it is important to realize that we are just beginning to understand the potential impact of physical activity timing. At this stage, I believe it is most important to be physically active in general. So ... if the morning is the only time of the day to go for a walk or a run, certainly do this.”
Dr. Kos concurred: “As this is not an intervention study, further research is needed to explain the cause of the observed association.”
Mr. van der Velde also added that it’s not yet clear which individuals or subgroups might experience additional benefits from timed activities. That’s the current research focus of a large consortium of several research institutes in the Netherlands and Canada.
Timed exercise reduces insulin resistance but not liver fat
The findings were published online in Diabetologia.
The study population included men and women living in the greater Leiden area in the western Netherlands who were aged 45-65 years and self-reported a BMI of 27 or higher. A second cohort included inhabitants of one municipality who were invited to participate regardless of their BMI. All wore the activity monitors for 4 consecutive days and nights during their usual activities.
Neither sedentary time nor breaks in sedentary time (defined as a period of activity with an acceleration greater than 0.75 m/s2 following a sedentary period) were associated with lower insulin resistance, as calculated by blood sampling.
However, the number of breaks in sedentary time was associated with a significant 22% higher liver fat content, assessed with proton magnetic resonance spectroscopy.
One reason for the lack of effect of breaks on insulin resistance, the authors theorized, is that this was a real-world observational study where regular breaks aren’t common. Alternatively, people might not have been intensively active enough during breaks to make a difference.
After adjustment for total body fat, an additional hour of MVPA was associated with a 5% drop in insulin resistance. An additional hour of MVPA in 5-minute bouts was associated with 9% lower insulin resistance.
Also after adjustments, insulin resistance was reduced significantly in participants who were most active in the afternoon, by 18%, or evening, by 25%, whereas insulin resistance was not affected among those who were most active in the morning (–3%), all compared with people who distributed their MVPA throughout the day.
Timing of MVPA was not associated with liver fat content, and there were no significant differences in liver fat content and insulin resistance between groups based on timing of light physical activity.
“This is just speculation, but perhaps for fat accumulation in the liver the circadian system is less involved. Or perhaps timing of other lifestyle variables are more important here, such as dietary intake,” Mr. van der Velde said.
Finally, he observed, “timing of physical activity is most likely just a piece of the puzzle. Timing of other lifestyle behavior, such as sleep, and food intake are important cues for our circadian system as well, and it is likely that all these behaviors interact with each other.”
The NEO study is supported by Leiden University Medical Center, the Netherlands Cardiovascular Research Initiative, an initiative supported by the Dutch Heart Foundation, and the Netherlands Organisation for Health Research and Development/Partnership Diabetes/Dutch Diabetes foundation Breakthrough. Mr. van der Velde has reported no further disclosures.
A version of this article first appeared on Medscape.com.
The data come from 775 participants with a mean body mass index (BMI) of 26.2 kg/m2 in the observational Netherlands Epidemiology of Obesity (NEO) study. Use of activity monitors for four consecutive days showed that performance of MVPA (defined as activity with intensity of > 3 metabolic equivalents of task) in the afternoon or evening was associated with up to 25% reduced insulin resistance compared with an even distribution of activity during the day.
“This is one of the first studies where in humans the relation between timing of physical activity and insulin resistance was examined,” lead author Jeroen van der Velde of the department of clinical epidemiology, Leiden (the Netherlands) University Medical Center, said in an interview.
Moreover, he noted that, while previous intervention studies have shown greater blood glucose reduction with high-intensity exercise performed in the afternoon, compared with the morning, in people with impaired glucose metabolism or type 2 diabetes, “as far as I am aware, we were the first to use a population-based study in a general population to study this.”
Katarina Kos, MD, PhD, senior lecturer in diabetes and obesity, University of Exeter (England), said: “This study is novel in that it relates the timing of physical activity if performed in the morning, afternoon, or evening to insulin resistance and fat content. This is from a cohort of middle-aged Dutch people between ages 45-65 studied 10 years ago and based on self-reports of weight and eating behavior and who were found to be generally overweight.”
Is it down to circadian rhythm?
“The results are of interest in that if the chosen timing was in the afternoon [63% of studied population] or evening (8% of the studied population), it seemed to relate with improved metabolism when compared to the morning exercising [16% of population]. ... Whether this was due to the (timing) of activity is yet to be shown,” Dr. Kos told the UK Science Media Centre.
Mr. van der Velde agrees that the effect may be explained at least in part by the circadian rhythm of the body. “Physical activity may act as ... a cue for the activation of clock genes. Previous research has suggested that our body’s muscular system and oxidative system are also affected by our circadian rhythm and their peak activity seems to be in the late afternoon. So, being mostly active in this time period ... may elicit greater metabolic responses compared to being active in the morning.”
But, he cautioned, “I think it is important to realize that we are just beginning to understand the potential impact of physical activity timing. At this stage, I believe it is most important to be physically active in general. So ... if the morning is the only time of the day to go for a walk or a run, certainly do this.”
Dr. Kos concurred: “As this is not an intervention study, further research is needed to explain the cause of the observed association.”
Mr. van der Velde also added that it’s not yet clear which individuals or subgroups might experience additional benefits from timed activities. That’s the current research focus of a large consortium of several research institutes in the Netherlands and Canada.
Timed exercise reduces insulin resistance but not liver fat
The findings were published online in Diabetologia.
The study population included men and women living in the greater Leiden area in the western Netherlands who were aged 45-65 years and self-reported a BMI of 27 or higher. A second cohort included inhabitants of one municipality who were invited to participate regardless of their BMI. All wore the activity monitors for 4 consecutive days and nights during their usual activities.
Neither sedentary time nor breaks in sedentary time (defined as a period of activity with an acceleration greater than 0.75 m/s2 following a sedentary period) were associated with lower insulin resistance, as calculated by blood sampling.
However, the number of breaks in sedentary time was associated with a significant 22% higher liver fat content, assessed with proton magnetic resonance spectroscopy.
One reason for the lack of effect of breaks on insulin resistance, the authors theorized, is that this was a real-world observational study where regular breaks aren’t common. Alternatively, people might not have been intensively active enough during breaks to make a difference.
After adjustment for total body fat, an additional hour of MVPA was associated with a 5% drop in insulin resistance. An additional hour of MVPA in 5-minute bouts was associated with 9% lower insulin resistance.
Also after adjustments, insulin resistance was reduced significantly in participants who were most active in the afternoon, by 18%, or evening, by 25%, whereas insulin resistance was not affected among those who were most active in the morning (–3%), all compared with people who distributed their MVPA throughout the day.
Timing of MVPA was not associated with liver fat content, and there were no significant differences in liver fat content and insulin resistance between groups based on timing of light physical activity.
“This is just speculation, but perhaps for fat accumulation in the liver the circadian system is less involved. Or perhaps timing of other lifestyle variables are more important here, such as dietary intake,” Mr. van der Velde said.
Finally, he observed, “timing of physical activity is most likely just a piece of the puzzle. Timing of other lifestyle behavior, such as sleep, and food intake are important cues for our circadian system as well, and it is likely that all these behaviors interact with each other.”
The NEO study is supported by Leiden University Medical Center, the Netherlands Cardiovascular Research Initiative, an initiative supported by the Dutch Heart Foundation, and the Netherlands Organisation for Health Research and Development/Partnership Diabetes/Dutch Diabetes foundation Breakthrough. Mr. van der Velde has reported no further disclosures.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
‘Unappreciated’ ties between COVID and gut dysbiosis
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
FROM NATURE COMMUNICATIONS
Access to abortion clinics declines sharply
Estimated travel time to abortion facilities in the United States has increased significantly since the Supreme Court overturned Roe v. Wade, according to results from an original investigation published online in JAMA.
In the wake of the ruling, many clinics have closed and now 33.3% of females of reproductive age live more than an hour from an abortion facility, more than double the 14.6% who lived that far before the Dobbs v. Jackson Women’s Health Organization court ruling, the paper states.
A 2022 study found that when people live 50 miles or more from an abortion facility they “were more likely to still be seeking an abortion on a 4-week follow-up than those who lived closer to an abortion facility,” wrote the authors, led by Benjamin Rader, MPH, from the Computational Epidemiology Lab at Boston Children’s Hospital.
Of 1,134 abortion facilities in the United States, 749 were considered active before the ruling and 671 were considered active in a simulated post-Dobbs period.
More than 15 states have total or partial bans
The researchers accounted for the closure of abortion facilities in states with total bans or 6-week abortion bans, compared with the period before the ruling, “during which all facilities providing abortions in 2021 were considered active.” The authors noted that more than 15 states have such bans.
Researchers found median and mean travel times to abortion facilities were estimated to be 10.9 minutes (interquartile ratio, 4.3-32.4) and 27.8 (standard deviation, 42.0) minutes before the ruling and used a paired sample t test (P < .001) to estimate the increase to a median of 17.0 (IQR, 4.9-124.5) minutes and a mean 100.4 (SD, 161.5) minutes after the ruling.
The numbers “highlight the catastrophe in terms of where we are,” Catherine Cansino, MD, MPH, professor, obstetrics and gynecology at the University of California, Davis, said in an interview.
Behind those numbers, she said, are brick walls for people who can’t take off work to drive that far or can’t leave their responsibilities of care for dependents or don’t have a car or even a driver’s license. It also calculates only land travel (car or public transportation) and doesn’t capture the financial and logistical burdens for some to fly to other states.
Dr. Cansino serves on the board of the Society of Family Planning, which publishes #WeCount, a national reporting effort that attempts to capture the effect of the Dobbs decision on abortion access. In a report published Oct. 28, #WeCount stated the numbers show that since the decision, there were 5,270 fewer abortions in July and 5,400 fewer in August, for a total of 10,670 fewer people in the United States who had abortions in the 2 months.
For Dr. Cansino, the numbers are only one measure of the wider problem.
“If it affects one person, it’s really the spirit of the consequence,” she said. “It’s difficult to wrap your mind around these numbers but the bottom line is that someone other than the person experiencing this health issue is making a decision for them.
“You will see physicians leaving states,” she said, “because their hands are tied in giving care.”
Glimpse of future from Texas example
The experience of abortion restrictions in Texas, described in another original investigation published in JAMA, provides a window into what could happen as access to abortions continues to decrease.
Texas has banned abortions after detectable embryonic cardiac activity since Sept. 1, 2021. Researchers obtained data on 80,107 abortions performed between September 2020 and February 2022.
In the first month following implementation of the Texas law, SB-8, the number of abortions in Texas dropped by 50%, compared with September 2020, and many pregnant Texas residents traveled out of state for abortion care.
But out-of-state abortions didn’t fully offset the overall drop in facility-based abortions.
“This decrease in facility-based abortion care suggests that many Texas residents continued their pregnancies, traveled beyond a neighboring state, or self-managed their abortion,” the authors wrote.
Increased time comes with costs
Sarah W. Prager, MD, professor in obstetrics and gynecology at University of Washington, Seattle, and director of the family planning division, explained that the travel time has to be seen in addition to the time it takes to complete the procedure.
Depending on state law, an abortion may take more than one visit to a clinic, which may mean adding lodging costs and overnight hours, or taking time off work, or finding childcare.
“A typical time to be at a clinic is upwards of 6 hours,” Dr. Prager explained, including paperwork, counseling, consent, the procedure, and recovery. That time is growing as active clinics overbook with others closing, she noted.
“We already know that 75% of people getting abortions are economically burdened at baseline. Gas is super expensive so the farther they have to drive – if they have their own car – that’s going to be expensive,” she noted.
In Washington, she said, abortion access is centralized in the western part of the state and located primarily between Seattle and Olympia. Though Oregon to the south has some of the nation’s most supportive laws for abortion, the other surrounding states have restrictive laws.
People in Alaska, Wyoming, Idaho, and Montana all have restrictive access, she noted, so people seeking abortions from those states have long distances to drive to western Washington and Oregon.
“Even for people living in eastern Washington, they are sometimes driving hours to get abortion care,” she said. “We’re really looking at health care that is dictated by geography, not by evidence, medicine, or science.”
The study by Dr. White and colleagues was supported by grants from the Susan Thompson Buffett Foundation and Collaborative for Gender + Reproductive Equity, as well as a center grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development awarded to the Population Research Center at the University of Texas at Austin. One coauthor reported receiving compensation from the University of Texas at Austin for providing data during the conduct of the study, as well as grants from Merck and Gynuity Health Projects and personal fees from Merck and Organon outside the submitted work; another reported being named plaintiff in the case Planned Parenthood of Montana v State of Montana, a lawsuit challenging abortion restrictions in that state. No other disclosures were reported. Dr. Cansino and Dr. Prager reported no relevant financial relationships.
Estimated travel time to abortion facilities in the United States has increased significantly since the Supreme Court overturned Roe v. Wade, according to results from an original investigation published online in JAMA.
In the wake of the ruling, many clinics have closed and now 33.3% of females of reproductive age live more than an hour from an abortion facility, more than double the 14.6% who lived that far before the Dobbs v. Jackson Women’s Health Organization court ruling, the paper states.
A 2022 study found that when people live 50 miles or more from an abortion facility they “were more likely to still be seeking an abortion on a 4-week follow-up than those who lived closer to an abortion facility,” wrote the authors, led by Benjamin Rader, MPH, from the Computational Epidemiology Lab at Boston Children’s Hospital.
Of 1,134 abortion facilities in the United States, 749 were considered active before the ruling and 671 were considered active in a simulated post-Dobbs period.
More than 15 states have total or partial bans
The researchers accounted for the closure of abortion facilities in states with total bans or 6-week abortion bans, compared with the period before the ruling, “during which all facilities providing abortions in 2021 were considered active.” The authors noted that more than 15 states have such bans.
Researchers found median and mean travel times to abortion facilities were estimated to be 10.9 minutes (interquartile ratio, 4.3-32.4) and 27.8 (standard deviation, 42.0) minutes before the ruling and used a paired sample t test (P < .001) to estimate the increase to a median of 17.0 (IQR, 4.9-124.5) minutes and a mean 100.4 (SD, 161.5) minutes after the ruling.
The numbers “highlight the catastrophe in terms of where we are,” Catherine Cansino, MD, MPH, professor, obstetrics and gynecology at the University of California, Davis, said in an interview.
Behind those numbers, she said, are brick walls for people who can’t take off work to drive that far or can’t leave their responsibilities of care for dependents or don’t have a car or even a driver’s license. It also calculates only land travel (car or public transportation) and doesn’t capture the financial and logistical burdens for some to fly to other states.
Dr. Cansino serves on the board of the Society of Family Planning, which publishes #WeCount, a national reporting effort that attempts to capture the effect of the Dobbs decision on abortion access. In a report published Oct. 28, #WeCount stated the numbers show that since the decision, there were 5,270 fewer abortions in July and 5,400 fewer in August, for a total of 10,670 fewer people in the United States who had abortions in the 2 months.
For Dr. Cansino, the numbers are only one measure of the wider problem.
“If it affects one person, it’s really the spirit of the consequence,” she said. “It’s difficult to wrap your mind around these numbers but the bottom line is that someone other than the person experiencing this health issue is making a decision for them.
“You will see physicians leaving states,” she said, “because their hands are tied in giving care.”
Glimpse of future from Texas example
The experience of abortion restrictions in Texas, described in another original investigation published in JAMA, provides a window into what could happen as access to abortions continues to decrease.
Texas has banned abortions after detectable embryonic cardiac activity since Sept. 1, 2021. Researchers obtained data on 80,107 abortions performed between September 2020 and February 2022.
In the first month following implementation of the Texas law, SB-8, the number of abortions in Texas dropped by 50%, compared with September 2020, and many pregnant Texas residents traveled out of state for abortion care.
But out-of-state abortions didn’t fully offset the overall drop in facility-based abortions.
“This decrease in facility-based abortion care suggests that many Texas residents continued their pregnancies, traveled beyond a neighboring state, or self-managed their abortion,” the authors wrote.
Increased time comes with costs
Sarah W. Prager, MD, professor in obstetrics and gynecology at University of Washington, Seattle, and director of the family planning division, explained that the travel time has to be seen in addition to the time it takes to complete the procedure.
Depending on state law, an abortion may take more than one visit to a clinic, which may mean adding lodging costs and overnight hours, or taking time off work, or finding childcare.
“A typical time to be at a clinic is upwards of 6 hours,” Dr. Prager explained, including paperwork, counseling, consent, the procedure, and recovery. That time is growing as active clinics overbook with others closing, she noted.
“We already know that 75% of people getting abortions are economically burdened at baseline. Gas is super expensive so the farther they have to drive – if they have their own car – that’s going to be expensive,” she noted.
In Washington, she said, abortion access is centralized in the western part of the state and located primarily between Seattle and Olympia. Though Oregon to the south has some of the nation’s most supportive laws for abortion, the other surrounding states have restrictive laws.
People in Alaska, Wyoming, Idaho, and Montana all have restrictive access, she noted, so people seeking abortions from those states have long distances to drive to western Washington and Oregon.
“Even for people living in eastern Washington, they are sometimes driving hours to get abortion care,” she said. “We’re really looking at health care that is dictated by geography, not by evidence, medicine, or science.”
The study by Dr. White and colleagues was supported by grants from the Susan Thompson Buffett Foundation and Collaborative for Gender + Reproductive Equity, as well as a center grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development awarded to the Population Research Center at the University of Texas at Austin. One coauthor reported receiving compensation from the University of Texas at Austin for providing data during the conduct of the study, as well as grants from Merck and Gynuity Health Projects and personal fees from Merck and Organon outside the submitted work; another reported being named plaintiff in the case Planned Parenthood of Montana v State of Montana, a lawsuit challenging abortion restrictions in that state. No other disclosures were reported. Dr. Cansino and Dr. Prager reported no relevant financial relationships.
Estimated travel time to abortion facilities in the United States has increased significantly since the Supreme Court overturned Roe v. Wade, according to results from an original investigation published online in JAMA.
In the wake of the ruling, many clinics have closed and now 33.3% of females of reproductive age live more than an hour from an abortion facility, more than double the 14.6% who lived that far before the Dobbs v. Jackson Women’s Health Organization court ruling, the paper states.
A 2022 study found that when people live 50 miles or more from an abortion facility they “were more likely to still be seeking an abortion on a 4-week follow-up than those who lived closer to an abortion facility,” wrote the authors, led by Benjamin Rader, MPH, from the Computational Epidemiology Lab at Boston Children’s Hospital.
Of 1,134 abortion facilities in the United States, 749 were considered active before the ruling and 671 were considered active in a simulated post-Dobbs period.
More than 15 states have total or partial bans
The researchers accounted for the closure of abortion facilities in states with total bans or 6-week abortion bans, compared with the period before the ruling, “during which all facilities providing abortions in 2021 were considered active.” The authors noted that more than 15 states have such bans.
Researchers found median and mean travel times to abortion facilities were estimated to be 10.9 minutes (interquartile ratio, 4.3-32.4) and 27.8 (standard deviation, 42.0) minutes before the ruling and used a paired sample t test (P < .001) to estimate the increase to a median of 17.0 (IQR, 4.9-124.5) minutes and a mean 100.4 (SD, 161.5) minutes after the ruling.
The numbers “highlight the catastrophe in terms of where we are,” Catherine Cansino, MD, MPH, professor, obstetrics and gynecology at the University of California, Davis, said in an interview.
Behind those numbers, she said, are brick walls for people who can’t take off work to drive that far or can’t leave their responsibilities of care for dependents or don’t have a car or even a driver’s license. It also calculates only land travel (car or public transportation) and doesn’t capture the financial and logistical burdens for some to fly to other states.
Dr. Cansino serves on the board of the Society of Family Planning, which publishes #WeCount, a national reporting effort that attempts to capture the effect of the Dobbs decision on abortion access. In a report published Oct. 28, #WeCount stated the numbers show that since the decision, there were 5,270 fewer abortions in July and 5,400 fewer in August, for a total of 10,670 fewer people in the United States who had abortions in the 2 months.
For Dr. Cansino, the numbers are only one measure of the wider problem.
“If it affects one person, it’s really the spirit of the consequence,” she said. “It’s difficult to wrap your mind around these numbers but the bottom line is that someone other than the person experiencing this health issue is making a decision for them.
“You will see physicians leaving states,” she said, “because their hands are tied in giving care.”
Glimpse of future from Texas example
The experience of abortion restrictions in Texas, described in another original investigation published in JAMA, provides a window into what could happen as access to abortions continues to decrease.
Texas has banned abortions after detectable embryonic cardiac activity since Sept. 1, 2021. Researchers obtained data on 80,107 abortions performed between September 2020 and February 2022.
In the first month following implementation of the Texas law, SB-8, the number of abortions in Texas dropped by 50%, compared with September 2020, and many pregnant Texas residents traveled out of state for abortion care.
But out-of-state abortions didn’t fully offset the overall drop in facility-based abortions.
“This decrease in facility-based abortion care suggests that many Texas residents continued their pregnancies, traveled beyond a neighboring state, or self-managed their abortion,” the authors wrote.
Increased time comes with costs
Sarah W. Prager, MD, professor in obstetrics and gynecology at University of Washington, Seattle, and director of the family planning division, explained that the travel time has to be seen in addition to the time it takes to complete the procedure.
Depending on state law, an abortion may take more than one visit to a clinic, which may mean adding lodging costs and overnight hours, or taking time off work, or finding childcare.
“A typical time to be at a clinic is upwards of 6 hours,” Dr. Prager explained, including paperwork, counseling, consent, the procedure, and recovery. That time is growing as active clinics overbook with others closing, she noted.
“We already know that 75% of people getting abortions are economically burdened at baseline. Gas is super expensive so the farther they have to drive – if they have their own car – that’s going to be expensive,” she noted.
In Washington, she said, abortion access is centralized in the western part of the state and located primarily between Seattle and Olympia. Though Oregon to the south has some of the nation’s most supportive laws for abortion, the other surrounding states have restrictive laws.
People in Alaska, Wyoming, Idaho, and Montana all have restrictive access, she noted, so people seeking abortions from those states have long distances to drive to western Washington and Oregon.
“Even for people living in eastern Washington, they are sometimes driving hours to get abortion care,” she said. “We’re really looking at health care that is dictated by geography, not by evidence, medicine, or science.”
The study by Dr. White and colleagues was supported by grants from the Susan Thompson Buffett Foundation and Collaborative for Gender + Reproductive Equity, as well as a center grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development awarded to the Population Research Center at the University of Texas at Austin. One coauthor reported receiving compensation from the University of Texas at Austin for providing data during the conduct of the study, as well as grants from Merck and Gynuity Health Projects and personal fees from Merck and Organon outside the submitted work; another reported being named plaintiff in the case Planned Parenthood of Montana v State of Montana, a lawsuit challenging abortion restrictions in that state. No other disclosures were reported. Dr. Cansino and Dr. Prager reported no relevant financial relationships.
FROM JAMA
Children and COVID: Weekly cases can’t sustain downward trend
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.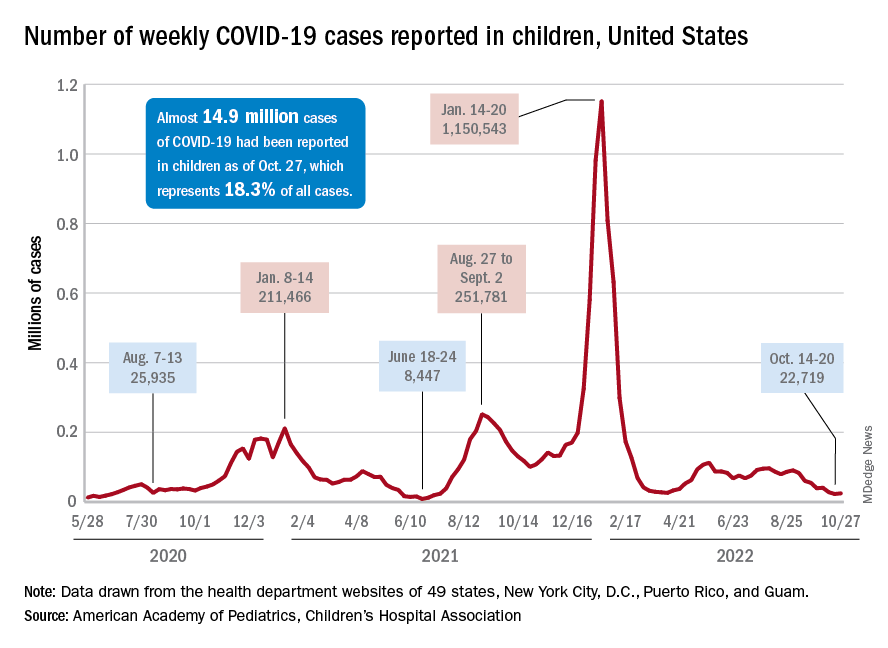
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
Best anticoagulant for minimizing bleeding risk identified
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
FROM ANNALS OF INTERNAL MEDICINE
Recurrent urinary tract infections: What’s good prophylaxis?
For those affected, recurrent urinary tract infections (UTIs) are sometimes stressful. However, even an informative discussion about risk factors and the imparting of behavioral recommendations can be very helpful for many women. Antibiotic prophylaxis should only be considered once all nonantibiotic therapy options have been exhausted.
One in seven women suffers at least once a year from cystitis. Around a third of those women develop a further urinary tract infection 6-12 months after the first infection. A urinary tract infection is classified as recurrent if two symptomatic episodes have occurred within the last 6 months or if three episodes have occurred within the last 12 months.
There are many different approaches to reducing the recurrence rate of urinary tract infections, Daniel Klussmann and Florian Wagenlehner, MD, of the department and outpatient clinic for urology at the University of Giessen (Germany) wrote in DMW Klinischer Fortschritt. Aside from general information and advice,
Fluids and D-mannose
An individual consultation discussion is the most important nonantibiotic strategy. Studies have shown that this strategy alone can lower the frequency of recurrent UTIs. According to the authors, special education programs on the causes and behavioral measures are especially helpful. Included in these programs is the recommendation to drink a sufficient, but not excessive, amount of fluids: approximately 1.5 liters per day. In one randomized study, this level of consumption halved UTI frequency. However, drinking an excessive amount of fluids should also be avoided, otherwise the antimicrobial peptides present in the urine become overly diluted.
The regular consumption of fruit juice, especially of that from berries, is also beneficial, according to the authors. However, study results on long-term prevention using cranberry products are inconsistent, and they are not recommended in the updated guideline. Like cranberries, D-mannose also inhibits the fimbriae of the Escherichia coli bacteria and therefore the bacteria’s ability to bind to the bladder epithelium. The authors cite a study in which, following the intake of 2 g of D-mannose dissolved in a glass of water every day, the rate of urinary tract infections dropped significantly, compared with consumption of placebo.
Additional recommendations in the S3 guideline include various phytotherapeutic products such as bearberry leaves, nasturtium herb, or horseradish root, although studies on the comparability of phytotherapeutic agents are very difficult to execute, the authors conceded.
It is already known that there is a positive correlation (by a factor of 60) between the recurrence rate of UTIs and the frequency of sexual intercourse. Even with contraceptive methods (such as vaginal suppositories, diaphragms or condoms coated with spermicide, and intrauterine devices), the risk of urinary tract infections increases by a factor of 2-14. Sexual abstinence, even if temporary, can be a remedy. Evidence for the recommendation to urinate immediately after coitus is contradictory in the literature, however. Excessive intimate hygiene clearly damages the local protective environment.
Estrogen substitution beneficial
For postmenopausal women, there is also the option of local estriol substitution (0.5 mg/day) as another nonantibiotic method of prophylaxis. This treatment serves as therapy for vaginal atrophy and reduces both vaginal colonization with uropathogens and the vaginal pH level. The authors cite Scandinavian studies that detected no increase in the risk of breast cancer from the local application of estriol.
Furthermore, the current guidelines recommend oral immunostimulation with bacterial cell wall components from uropathogenic strains of E. coli (OM-89, Uro-Vaxom). The authors reported on two meta-studies in which the average recurrence rate was reduced by 39%, compared with placebo. In addition, the treatment time for breakthrough infections decreased significantly, and prevention with OM-89 could even be started during acute therapy. Also recommended is parenteral immunostimulation with inactivated pathogens (StroVac). Acupuncture as cutaneous immunostimulation has also displayed a positive protective effect.
Only when nonantibiotic therapy fails and the patient is under a high amount of psychological strain should antibiotic prophylaxis be initiated, according to the authors. A period of 3-6 months should be the target here. When choosing an antibiotic and before starting therapy, the corresponding pathogen should be confirmed through a urine culture, and resistance testing should be performed. On the other hand, single-use, postcoital antibiotic prevention could be an alternative, particularly for women in whom a correlation between recurrent UTIs and sexual intercourse has been suspected, the authors wrote.
This article was translated from Univadis Germany. A version appeared on Medscape.com.
For those affected, recurrent urinary tract infections (UTIs) are sometimes stressful. However, even an informative discussion about risk factors and the imparting of behavioral recommendations can be very helpful for many women. Antibiotic prophylaxis should only be considered once all nonantibiotic therapy options have been exhausted.
One in seven women suffers at least once a year from cystitis. Around a third of those women develop a further urinary tract infection 6-12 months after the first infection. A urinary tract infection is classified as recurrent if two symptomatic episodes have occurred within the last 6 months or if three episodes have occurred within the last 12 months.
There are many different approaches to reducing the recurrence rate of urinary tract infections, Daniel Klussmann and Florian Wagenlehner, MD, of the department and outpatient clinic for urology at the University of Giessen (Germany) wrote in DMW Klinischer Fortschritt. Aside from general information and advice,
Fluids and D-mannose
An individual consultation discussion is the most important nonantibiotic strategy. Studies have shown that this strategy alone can lower the frequency of recurrent UTIs. According to the authors, special education programs on the causes and behavioral measures are especially helpful. Included in these programs is the recommendation to drink a sufficient, but not excessive, amount of fluids: approximately 1.5 liters per day. In one randomized study, this level of consumption halved UTI frequency. However, drinking an excessive amount of fluids should also be avoided, otherwise the antimicrobial peptides present in the urine become overly diluted.
The regular consumption of fruit juice, especially of that from berries, is also beneficial, according to the authors. However, study results on long-term prevention using cranberry products are inconsistent, and they are not recommended in the updated guideline. Like cranberries, D-mannose also inhibits the fimbriae of the Escherichia coli bacteria and therefore the bacteria’s ability to bind to the bladder epithelium. The authors cite a study in which, following the intake of 2 g of D-mannose dissolved in a glass of water every day, the rate of urinary tract infections dropped significantly, compared with consumption of placebo.
Additional recommendations in the S3 guideline include various phytotherapeutic products such as bearberry leaves, nasturtium herb, or horseradish root, although studies on the comparability of phytotherapeutic agents are very difficult to execute, the authors conceded.
It is already known that there is a positive correlation (by a factor of 60) between the recurrence rate of UTIs and the frequency of sexual intercourse. Even with contraceptive methods (such as vaginal suppositories, diaphragms or condoms coated with spermicide, and intrauterine devices), the risk of urinary tract infections increases by a factor of 2-14. Sexual abstinence, even if temporary, can be a remedy. Evidence for the recommendation to urinate immediately after coitus is contradictory in the literature, however. Excessive intimate hygiene clearly damages the local protective environment.
Estrogen substitution beneficial
For postmenopausal women, there is also the option of local estriol substitution (0.5 mg/day) as another nonantibiotic method of prophylaxis. This treatment serves as therapy for vaginal atrophy and reduces both vaginal colonization with uropathogens and the vaginal pH level. The authors cite Scandinavian studies that detected no increase in the risk of breast cancer from the local application of estriol.
Furthermore, the current guidelines recommend oral immunostimulation with bacterial cell wall components from uropathogenic strains of E. coli (OM-89, Uro-Vaxom). The authors reported on two meta-studies in which the average recurrence rate was reduced by 39%, compared with placebo. In addition, the treatment time for breakthrough infections decreased significantly, and prevention with OM-89 could even be started during acute therapy. Also recommended is parenteral immunostimulation with inactivated pathogens (StroVac). Acupuncture as cutaneous immunostimulation has also displayed a positive protective effect.
Only when nonantibiotic therapy fails and the patient is under a high amount of psychological strain should antibiotic prophylaxis be initiated, according to the authors. A period of 3-6 months should be the target here. When choosing an antibiotic and before starting therapy, the corresponding pathogen should be confirmed through a urine culture, and resistance testing should be performed. On the other hand, single-use, postcoital antibiotic prevention could be an alternative, particularly for women in whom a correlation between recurrent UTIs and sexual intercourse has been suspected, the authors wrote.
This article was translated from Univadis Germany. A version appeared on Medscape.com.
For those affected, recurrent urinary tract infections (UTIs) are sometimes stressful. However, even an informative discussion about risk factors and the imparting of behavioral recommendations can be very helpful for many women. Antibiotic prophylaxis should only be considered once all nonantibiotic therapy options have been exhausted.
One in seven women suffers at least once a year from cystitis. Around a third of those women develop a further urinary tract infection 6-12 months after the first infection. A urinary tract infection is classified as recurrent if two symptomatic episodes have occurred within the last 6 months or if three episodes have occurred within the last 12 months.
There are many different approaches to reducing the recurrence rate of urinary tract infections, Daniel Klussmann and Florian Wagenlehner, MD, of the department and outpatient clinic for urology at the University of Giessen (Germany) wrote in DMW Klinischer Fortschritt. Aside from general information and advice,
Fluids and D-mannose
An individual consultation discussion is the most important nonantibiotic strategy. Studies have shown that this strategy alone can lower the frequency of recurrent UTIs. According to the authors, special education programs on the causes and behavioral measures are especially helpful. Included in these programs is the recommendation to drink a sufficient, but not excessive, amount of fluids: approximately 1.5 liters per day. In one randomized study, this level of consumption halved UTI frequency. However, drinking an excessive amount of fluids should also be avoided, otherwise the antimicrobial peptides present in the urine become overly diluted.
The regular consumption of fruit juice, especially of that from berries, is also beneficial, according to the authors. However, study results on long-term prevention using cranberry products are inconsistent, and they are not recommended in the updated guideline. Like cranberries, D-mannose also inhibits the fimbriae of the Escherichia coli bacteria and therefore the bacteria’s ability to bind to the bladder epithelium. The authors cite a study in which, following the intake of 2 g of D-mannose dissolved in a glass of water every day, the rate of urinary tract infections dropped significantly, compared with consumption of placebo.
Additional recommendations in the S3 guideline include various phytotherapeutic products such as bearberry leaves, nasturtium herb, or horseradish root, although studies on the comparability of phytotherapeutic agents are very difficult to execute, the authors conceded.
It is already known that there is a positive correlation (by a factor of 60) between the recurrence rate of UTIs and the frequency of sexual intercourse. Even with contraceptive methods (such as vaginal suppositories, diaphragms or condoms coated with spermicide, and intrauterine devices), the risk of urinary tract infections increases by a factor of 2-14. Sexual abstinence, even if temporary, can be a remedy. Evidence for the recommendation to urinate immediately after coitus is contradictory in the literature, however. Excessive intimate hygiene clearly damages the local protective environment.
Estrogen substitution beneficial
For postmenopausal women, there is also the option of local estriol substitution (0.5 mg/day) as another nonantibiotic method of prophylaxis. This treatment serves as therapy for vaginal atrophy and reduces both vaginal colonization with uropathogens and the vaginal pH level. The authors cite Scandinavian studies that detected no increase in the risk of breast cancer from the local application of estriol.
Furthermore, the current guidelines recommend oral immunostimulation with bacterial cell wall components from uropathogenic strains of E. coli (OM-89, Uro-Vaxom). The authors reported on two meta-studies in which the average recurrence rate was reduced by 39%, compared with placebo. In addition, the treatment time for breakthrough infections decreased significantly, and prevention with OM-89 could even be started during acute therapy. Also recommended is parenteral immunostimulation with inactivated pathogens (StroVac). Acupuncture as cutaneous immunostimulation has also displayed a positive protective effect.
Only when nonantibiotic therapy fails and the patient is under a high amount of psychological strain should antibiotic prophylaxis be initiated, according to the authors. A period of 3-6 months should be the target here. When choosing an antibiotic and before starting therapy, the corresponding pathogen should be confirmed through a urine culture, and resistance testing should be performed. On the other hand, single-use, postcoital antibiotic prevention could be an alternative, particularly for women in whom a correlation between recurrent UTIs and sexual intercourse has been suspected, the authors wrote.
This article was translated from Univadis Germany. A version appeared on Medscape.com.
FROM DMW KLINISCHER FORTSCHRITT
Kidney function may help docs pick antiplatelet mix after stroke
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
FROM ANNALS OF INTERNAL MEDICINE
Original COVID-19 vaccines fall short against Omicron subvariants for the immunocompromised
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
FROM MMWR
Intensive BP lowering harmful in acute ischemic stroke: ENCHANTED2/MT
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
FROM THE WORLD STROKE CONGRESS
Thyroid dysfunction may linger a year after severe COVID-19
MONTREAL – Patients hospitalized with severe COVID-19 and no prior history of thyroid dysfunction show signs of thyroiditis that, although asymptomatic, continue to persist for up to a year after infection, according to research that adds to evidence on the complex involvement of the thyroid in COVID-19.
“To our knowledge these findings are novel,” first author Ilaria Muller, MD, PhD, an assistant professor in endocrinology in the department of clinical sciences and community health, University of Milan, told this news organization.
“Little has been written about the long-term follow-up of thyroid function after severe COVID-19 disease, and we have followed patients up to 1 year after infection.”
The effects are seen in about 10%-15% of patients, and “[while] the thyroid dysfunction is transient, ultrasound areas of thyroiditis may persist after 1 year, even if they progressively shrink,” said Dr. Muller, who presented the findings at the American Thyroid Association annual meeting.
Immunological scars? Clinical implications unclear
The nature and implications of the persistent thyroiditis areas are uncertain, Dr. Muller noted. “These areas of thyroiditis are likely a sort of ‘immunologic scar’ of the previous SARS-CoV-2 infection,” she explained. “We still don’t know if there are clinical implications, even if they seem unlikely.”
Of note, increases in autoimmune processes or a higher incidence of thyroid dysfunction after COVID-19 have not been observed, and the shrinkage of the areas of thyroiditis over time is encouraging, she said.
The reasons why some patients develop atypical thyroiditis and others don’t are also unclear, with Dr. Muller’s team investigating further. Importantly, similar effects have been associated with other severe infections, not just COVID-19. “It is well known that in classic subacute thyroiditis due to other viral infections, the areas of thyroiditis persist for months, so this phenomenon might not be unique to COVID-19,” she explained.
Commenting on the story, Jeffrey R. Garber, MD, also noted that such thyroiditis areas stemming from other types of infection may persist – but go unnoticed.
“Resolution is the clinical rule, [and] we generally do not restudy in detail those who clinically recover,” he said in an interview. “However, there is evidence of impaired thyroid reserve in those who recover from viral thyroiditis due to other sources.”
“Thyroid symptoms are often not specific, so ‘atypical’ [cases] are common, [and] resolution with restoring thyroid status to normal is mixed,” noted Dr. Garber, an associate professor of medicine at Harvard Medical School and chief of the division of endocrinology at Atrius Health, Boston.
In terms of clinical practice, while such issues should be kept in mind when evaluating abnormal thyroid tests during severe COVID-19, “it is not a call for routinely checking it in the absence of clinical suspicion,” he observed.
Study details
Dr. Muller and her team previously observed that patients hospitalized in intensive care with COVID-19 often had low or suppressed serum thyroid-stimulating hormone (TSH) levels, with and without elevated free thyroxine (FT4) concentrations, suggestive of thyrotoxicosis.
Upon investigating those cases, they found, as in their previous study reported by this news organization, that a painless, atypical thyroiditis occurs with nonthyroidal illness syndrome among patients hospitalized with severe COVID-19. The atypical thyroiditis was slightly more common in men and was associated with lymphopenia.
To further investigate those cases and follow patients up to 1 year, the team conducted a longitudinal study of 183 patients hospitalized with severe COVID-19 in Italy. The patients, who had no known prior history of thyroid dysfunction, were assessed for serum thyroid function, autoantibodies, and inflammatory markers.
At baseline, 10% of the patients were found to have thyrotoxicosis, and ultrasound performed within 2-3 months postinfection on 65 patients showed that 18 (28%) had areas of thyroiditis.
Importantly, 60% of those patients with the areas of thyroiditis had low TSH levels, while 25% had normal TSH levels (P = .034).
In addition, those showing the presence of thyroiditis on ultrasound at 23 months were more likely to have elevated serum concentrations of FT4 (P = .018) and higher levels of interleukin-26 (P = .016), compared with those with normal ultrasound readings.
In a longitudinal analysis further following patients post infection, among 15 patients who were evaluated at 6 months, most, 13 (87%), still had areas of thyroiditis, and 6 of 12 (50%) had thyroiditis areas that, though reduced in size, still persisted even at 12 months.
In terms of thyroid uptake, at 3 months, 14 of 17 patients (82%) had diffused or focal areas of a reduction of uptake. After 6 months, there was a recovery, with a median of 28% of thyroid uptake recovered, however, 67% of patients still had some focal or diffused reduction in thyroid uptake.
Of note, the indications of thyroiditis on imaging persisted even though patients’ TSH levels had quickly normalized at the end of infection and remained normal up to 1 year of follow-up.
The patients showed no apparent development of thyroglobulin antibody, thyroid peroxidase antibodies, or TSH receptor antibodies.
A further fine needle aspiration analysis of eight patients with atypical thyroiditis at 3 months after infection showed that those patients had tissue resident memory T cells (CD4+/CD8+/CD103+/CD69+) within the thyroid, but not in the blood as expected.
Additional assessments at 8 months after infection showed those tissue resident memory T cells continued to be present on imaging.
The results showed “SARS-CoV-2–specific T cells were enriched within the thyroid compared with the blood, many with a tissue resident phenotype,” Dr. Muller explained.
The findings are notable in that “such an in-depth characterization of areas of thyroiditis triggered by SARS-CoV-2 infection combining ultrasound, scintigraphy, and immunological phenotyping has not been performed so far,” she said.
“In particular, SARS-CoV-2–specific tissue-resident memory T lymphocytes have not been described before in the thyroid gland.”
Dr. Muller and Dr. Garber have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – Patients hospitalized with severe COVID-19 and no prior history of thyroid dysfunction show signs of thyroiditis that, although asymptomatic, continue to persist for up to a year after infection, according to research that adds to evidence on the complex involvement of the thyroid in COVID-19.
“To our knowledge these findings are novel,” first author Ilaria Muller, MD, PhD, an assistant professor in endocrinology in the department of clinical sciences and community health, University of Milan, told this news organization.
“Little has been written about the long-term follow-up of thyroid function after severe COVID-19 disease, and we have followed patients up to 1 year after infection.”
The effects are seen in about 10%-15% of patients, and “[while] the thyroid dysfunction is transient, ultrasound areas of thyroiditis may persist after 1 year, even if they progressively shrink,” said Dr. Muller, who presented the findings at the American Thyroid Association annual meeting.
Immunological scars? Clinical implications unclear
The nature and implications of the persistent thyroiditis areas are uncertain, Dr. Muller noted. “These areas of thyroiditis are likely a sort of ‘immunologic scar’ of the previous SARS-CoV-2 infection,” she explained. “We still don’t know if there are clinical implications, even if they seem unlikely.”
Of note, increases in autoimmune processes or a higher incidence of thyroid dysfunction after COVID-19 have not been observed, and the shrinkage of the areas of thyroiditis over time is encouraging, she said.
The reasons why some patients develop atypical thyroiditis and others don’t are also unclear, with Dr. Muller’s team investigating further. Importantly, similar effects have been associated with other severe infections, not just COVID-19. “It is well known that in classic subacute thyroiditis due to other viral infections, the areas of thyroiditis persist for months, so this phenomenon might not be unique to COVID-19,” she explained.
Commenting on the story, Jeffrey R. Garber, MD, also noted that such thyroiditis areas stemming from other types of infection may persist – but go unnoticed.
“Resolution is the clinical rule, [and] we generally do not restudy in detail those who clinically recover,” he said in an interview. “However, there is evidence of impaired thyroid reserve in those who recover from viral thyroiditis due to other sources.”
“Thyroid symptoms are often not specific, so ‘atypical’ [cases] are common, [and] resolution with restoring thyroid status to normal is mixed,” noted Dr. Garber, an associate professor of medicine at Harvard Medical School and chief of the division of endocrinology at Atrius Health, Boston.
In terms of clinical practice, while such issues should be kept in mind when evaluating abnormal thyroid tests during severe COVID-19, “it is not a call for routinely checking it in the absence of clinical suspicion,” he observed.
Study details
Dr. Muller and her team previously observed that patients hospitalized in intensive care with COVID-19 often had low or suppressed serum thyroid-stimulating hormone (TSH) levels, with and without elevated free thyroxine (FT4) concentrations, suggestive of thyrotoxicosis.
Upon investigating those cases, they found, as in their previous study reported by this news organization, that a painless, atypical thyroiditis occurs with nonthyroidal illness syndrome among patients hospitalized with severe COVID-19. The atypical thyroiditis was slightly more common in men and was associated with lymphopenia.
To further investigate those cases and follow patients up to 1 year, the team conducted a longitudinal study of 183 patients hospitalized with severe COVID-19 in Italy. The patients, who had no known prior history of thyroid dysfunction, were assessed for serum thyroid function, autoantibodies, and inflammatory markers.
At baseline, 10% of the patients were found to have thyrotoxicosis, and ultrasound performed within 2-3 months postinfection on 65 patients showed that 18 (28%) had areas of thyroiditis.
Importantly, 60% of those patients with the areas of thyroiditis had low TSH levels, while 25% had normal TSH levels (P = .034).
In addition, those showing the presence of thyroiditis on ultrasound at 23 months were more likely to have elevated serum concentrations of FT4 (P = .018) and higher levels of interleukin-26 (P = .016), compared with those with normal ultrasound readings.
In a longitudinal analysis further following patients post infection, among 15 patients who were evaluated at 6 months, most, 13 (87%), still had areas of thyroiditis, and 6 of 12 (50%) had thyroiditis areas that, though reduced in size, still persisted even at 12 months.
In terms of thyroid uptake, at 3 months, 14 of 17 patients (82%) had diffused or focal areas of a reduction of uptake. After 6 months, there was a recovery, with a median of 28% of thyroid uptake recovered, however, 67% of patients still had some focal or diffused reduction in thyroid uptake.
Of note, the indications of thyroiditis on imaging persisted even though patients’ TSH levels had quickly normalized at the end of infection and remained normal up to 1 year of follow-up.
The patients showed no apparent development of thyroglobulin antibody, thyroid peroxidase antibodies, or TSH receptor antibodies.
A further fine needle aspiration analysis of eight patients with atypical thyroiditis at 3 months after infection showed that those patients had tissue resident memory T cells (CD4+/CD8+/CD103+/CD69+) within the thyroid, but not in the blood as expected.
Additional assessments at 8 months after infection showed those tissue resident memory T cells continued to be present on imaging.
The results showed “SARS-CoV-2–specific T cells were enriched within the thyroid compared with the blood, many with a tissue resident phenotype,” Dr. Muller explained.
The findings are notable in that “such an in-depth characterization of areas of thyroiditis triggered by SARS-CoV-2 infection combining ultrasound, scintigraphy, and immunological phenotyping has not been performed so far,” she said.
“In particular, SARS-CoV-2–specific tissue-resident memory T lymphocytes have not been described before in the thyroid gland.”
Dr. Muller and Dr. Garber have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – Patients hospitalized with severe COVID-19 and no prior history of thyroid dysfunction show signs of thyroiditis that, although asymptomatic, continue to persist for up to a year after infection, according to research that adds to evidence on the complex involvement of the thyroid in COVID-19.
“To our knowledge these findings are novel,” first author Ilaria Muller, MD, PhD, an assistant professor in endocrinology in the department of clinical sciences and community health, University of Milan, told this news organization.
“Little has been written about the long-term follow-up of thyroid function after severe COVID-19 disease, and we have followed patients up to 1 year after infection.”
The effects are seen in about 10%-15% of patients, and “[while] the thyroid dysfunction is transient, ultrasound areas of thyroiditis may persist after 1 year, even if they progressively shrink,” said Dr. Muller, who presented the findings at the American Thyroid Association annual meeting.
Immunological scars? Clinical implications unclear
The nature and implications of the persistent thyroiditis areas are uncertain, Dr. Muller noted. “These areas of thyroiditis are likely a sort of ‘immunologic scar’ of the previous SARS-CoV-2 infection,” she explained. “We still don’t know if there are clinical implications, even if they seem unlikely.”
Of note, increases in autoimmune processes or a higher incidence of thyroid dysfunction after COVID-19 have not been observed, and the shrinkage of the areas of thyroiditis over time is encouraging, she said.
The reasons why some patients develop atypical thyroiditis and others don’t are also unclear, with Dr. Muller’s team investigating further. Importantly, similar effects have been associated with other severe infections, not just COVID-19. “It is well known that in classic subacute thyroiditis due to other viral infections, the areas of thyroiditis persist for months, so this phenomenon might not be unique to COVID-19,” she explained.
Commenting on the story, Jeffrey R. Garber, MD, also noted that such thyroiditis areas stemming from other types of infection may persist – but go unnoticed.
“Resolution is the clinical rule, [and] we generally do not restudy in detail those who clinically recover,” he said in an interview. “However, there is evidence of impaired thyroid reserve in those who recover from viral thyroiditis due to other sources.”
“Thyroid symptoms are often not specific, so ‘atypical’ [cases] are common, [and] resolution with restoring thyroid status to normal is mixed,” noted Dr. Garber, an associate professor of medicine at Harvard Medical School and chief of the division of endocrinology at Atrius Health, Boston.
In terms of clinical practice, while such issues should be kept in mind when evaluating abnormal thyroid tests during severe COVID-19, “it is not a call for routinely checking it in the absence of clinical suspicion,” he observed.
Study details
Dr. Muller and her team previously observed that patients hospitalized in intensive care with COVID-19 often had low or suppressed serum thyroid-stimulating hormone (TSH) levels, with and without elevated free thyroxine (FT4) concentrations, suggestive of thyrotoxicosis.
Upon investigating those cases, they found, as in their previous study reported by this news organization, that a painless, atypical thyroiditis occurs with nonthyroidal illness syndrome among patients hospitalized with severe COVID-19. The atypical thyroiditis was slightly more common in men and was associated with lymphopenia.
To further investigate those cases and follow patients up to 1 year, the team conducted a longitudinal study of 183 patients hospitalized with severe COVID-19 in Italy. The patients, who had no known prior history of thyroid dysfunction, were assessed for serum thyroid function, autoantibodies, and inflammatory markers.
At baseline, 10% of the patients were found to have thyrotoxicosis, and ultrasound performed within 2-3 months postinfection on 65 patients showed that 18 (28%) had areas of thyroiditis.
Importantly, 60% of those patients with the areas of thyroiditis had low TSH levels, while 25% had normal TSH levels (P = .034).
In addition, those showing the presence of thyroiditis on ultrasound at 23 months were more likely to have elevated serum concentrations of FT4 (P = .018) and higher levels of interleukin-26 (P = .016), compared with those with normal ultrasound readings.
In a longitudinal analysis further following patients post infection, among 15 patients who were evaluated at 6 months, most, 13 (87%), still had areas of thyroiditis, and 6 of 12 (50%) had thyroiditis areas that, though reduced in size, still persisted even at 12 months.
In terms of thyroid uptake, at 3 months, 14 of 17 patients (82%) had diffused or focal areas of a reduction of uptake. After 6 months, there was a recovery, with a median of 28% of thyroid uptake recovered, however, 67% of patients still had some focal or diffused reduction in thyroid uptake.
Of note, the indications of thyroiditis on imaging persisted even though patients’ TSH levels had quickly normalized at the end of infection and remained normal up to 1 year of follow-up.
The patients showed no apparent development of thyroglobulin antibody, thyroid peroxidase antibodies, or TSH receptor antibodies.
A further fine needle aspiration analysis of eight patients with atypical thyroiditis at 3 months after infection showed that those patients had tissue resident memory T cells (CD4+/CD8+/CD103+/CD69+) within the thyroid, but not in the blood as expected.
Additional assessments at 8 months after infection showed those tissue resident memory T cells continued to be present on imaging.
The results showed “SARS-CoV-2–specific T cells were enriched within the thyroid compared with the blood, many with a tissue resident phenotype,” Dr. Muller explained.
The findings are notable in that “such an in-depth characterization of areas of thyroiditis triggered by SARS-CoV-2 infection combining ultrasound, scintigraphy, and immunological phenotyping has not been performed so far,” she said.
“In particular, SARS-CoV-2–specific tissue-resident memory T lymphocytes have not been described before in the thyroid gland.”
Dr. Muller and Dr. Garber have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ATA 2022