User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Sexual activities in seniors: Experts advise on what to ask
Sexual activity in older adults is something of a taboo, rarely discussed and largely ignored by researchers.
But failing to address human sexuality in old age can lead doctors to ask seniors the wrong questions about sex – if they ask at all.
When researchers do look at the issue, they find surprises, as Janie Steckenrider, PhD, has learned. In a new study presented at the annual scientific meeting of the Gerontological Society of America, Dr. Steckenrider, a professor of political science at Loyola Marymount University, Los Angeles, found that previous attempts to qualify the sexual activities of seniors appear to be limited largely to partnered sex – despite the fact that many older people tend to practice “solo sex,” another term for masturbation.
“Maybe they don’t have a partner, or their partner has sexual dysfunction, or has died. There could be pain involved,” Dr. Steckenrider said. “In the hierarchy of sexual activity, penetrative sex is the cultural norm. As people get older, penetrative sex becomes less important. The hierarchy shifts to include more emotional intimacy like touching and fondling.”
Of the 17 survey questionnaires Dr. Steckenrider analyzed, 11 had questions that focused exclusively on sex with a partner. Nine defined sexual activity and just five included questions about masturbation.
Take, for example, a 2018 poll by researchers at the University of Michigan, Ann Arbor, who found that 40% of people ages 65-80 said they were sexually active. Meanwhile, nearly two thirds of older adults said they were interested in sex, and more than half said sex was important to their quality of life.
But Dr. Steckenrider said this poll, like others, left the term “sexually active” undefined – raising questions about the meaning of the findings.
Sheryl A. Kingsberg, PhD, chief of behavioral medicine in the department of obstetrics and gynecology at University Hospitals Cleveland Medical Center, said she was surprised so few of the studies analyzed by Dr. Steckenrider included masturbation in their definition of sex.
“Clinical trials of potential treatments for female sexual problems, like hypoactive sexual desire disorder or painful sex, include both definitions of sexual activity and questions about masturbation, she said. “Definitions also should not assume partnered sex is male or female,” she added.
Dr. Steckenrider and Dr. Kingsberg encouraged healthcare providers to address the sexual health of their patients by asking questions about their sexual health and concerns.
“Health care professionals cannot address sexual concerns if they don’t acknowledge their patients as sexual beings and inquire about sexual problems,” Dr. Kingsberg said.
The key, according to Dr. Steckenrider, is for clinicians to ask the right questions. But which ones?
Detail is crucial.
“I think that’s far better than asking whether they are sexually active, yes or no,” she said. “Ask: ‘How often have you engaged in these types of sexual activities?’ If you are looking for frequency, and be specific about the types of sex: kissing, fondling, or masturbation.”
A version of this article first appeared on Medscape.com.
Sexual activity in older adults is something of a taboo, rarely discussed and largely ignored by researchers.
But failing to address human sexuality in old age can lead doctors to ask seniors the wrong questions about sex – if they ask at all.
When researchers do look at the issue, they find surprises, as Janie Steckenrider, PhD, has learned. In a new study presented at the annual scientific meeting of the Gerontological Society of America, Dr. Steckenrider, a professor of political science at Loyola Marymount University, Los Angeles, found that previous attempts to qualify the sexual activities of seniors appear to be limited largely to partnered sex – despite the fact that many older people tend to practice “solo sex,” another term for masturbation.
“Maybe they don’t have a partner, or their partner has sexual dysfunction, or has died. There could be pain involved,” Dr. Steckenrider said. “In the hierarchy of sexual activity, penetrative sex is the cultural norm. As people get older, penetrative sex becomes less important. The hierarchy shifts to include more emotional intimacy like touching and fondling.”
Of the 17 survey questionnaires Dr. Steckenrider analyzed, 11 had questions that focused exclusively on sex with a partner. Nine defined sexual activity and just five included questions about masturbation.
Take, for example, a 2018 poll by researchers at the University of Michigan, Ann Arbor, who found that 40% of people ages 65-80 said they were sexually active. Meanwhile, nearly two thirds of older adults said they were interested in sex, and more than half said sex was important to their quality of life.
But Dr. Steckenrider said this poll, like others, left the term “sexually active” undefined – raising questions about the meaning of the findings.
Sheryl A. Kingsberg, PhD, chief of behavioral medicine in the department of obstetrics and gynecology at University Hospitals Cleveland Medical Center, said she was surprised so few of the studies analyzed by Dr. Steckenrider included masturbation in their definition of sex.
“Clinical trials of potential treatments for female sexual problems, like hypoactive sexual desire disorder or painful sex, include both definitions of sexual activity and questions about masturbation, she said. “Definitions also should not assume partnered sex is male or female,” she added.
Dr. Steckenrider and Dr. Kingsberg encouraged healthcare providers to address the sexual health of their patients by asking questions about their sexual health and concerns.
“Health care professionals cannot address sexual concerns if they don’t acknowledge their patients as sexual beings and inquire about sexual problems,” Dr. Kingsberg said.
The key, according to Dr. Steckenrider, is for clinicians to ask the right questions. But which ones?
Detail is crucial.
“I think that’s far better than asking whether they are sexually active, yes or no,” she said. “Ask: ‘How often have you engaged in these types of sexual activities?’ If you are looking for frequency, and be specific about the types of sex: kissing, fondling, or masturbation.”
A version of this article first appeared on Medscape.com.
Sexual activity in older adults is something of a taboo, rarely discussed and largely ignored by researchers.
But failing to address human sexuality in old age can lead doctors to ask seniors the wrong questions about sex – if they ask at all.
When researchers do look at the issue, they find surprises, as Janie Steckenrider, PhD, has learned. In a new study presented at the annual scientific meeting of the Gerontological Society of America, Dr. Steckenrider, a professor of political science at Loyola Marymount University, Los Angeles, found that previous attempts to qualify the sexual activities of seniors appear to be limited largely to partnered sex – despite the fact that many older people tend to practice “solo sex,” another term for masturbation.
“Maybe they don’t have a partner, or their partner has sexual dysfunction, or has died. There could be pain involved,” Dr. Steckenrider said. “In the hierarchy of sexual activity, penetrative sex is the cultural norm. As people get older, penetrative sex becomes less important. The hierarchy shifts to include more emotional intimacy like touching and fondling.”
Of the 17 survey questionnaires Dr. Steckenrider analyzed, 11 had questions that focused exclusively on sex with a partner. Nine defined sexual activity and just five included questions about masturbation.
Take, for example, a 2018 poll by researchers at the University of Michigan, Ann Arbor, who found that 40% of people ages 65-80 said they were sexually active. Meanwhile, nearly two thirds of older adults said they were interested in sex, and more than half said sex was important to their quality of life.
But Dr. Steckenrider said this poll, like others, left the term “sexually active” undefined – raising questions about the meaning of the findings.
Sheryl A. Kingsberg, PhD, chief of behavioral medicine in the department of obstetrics and gynecology at University Hospitals Cleveland Medical Center, said she was surprised so few of the studies analyzed by Dr. Steckenrider included masturbation in their definition of sex.
“Clinical trials of potential treatments for female sexual problems, like hypoactive sexual desire disorder or painful sex, include both definitions of sexual activity and questions about masturbation, she said. “Definitions also should not assume partnered sex is male or female,” she added.
Dr. Steckenrider and Dr. Kingsberg encouraged healthcare providers to address the sexual health of their patients by asking questions about their sexual health and concerns.
“Health care professionals cannot address sexual concerns if they don’t acknowledge their patients as sexual beings and inquire about sexual problems,” Dr. Kingsberg said.
The key, according to Dr. Steckenrider, is for clinicians to ask the right questions. But which ones?
Detail is crucial.
“I think that’s far better than asking whether they are sexually active, yes or no,” she said. “Ask: ‘How often have you engaged in these types of sexual activities?’ If you are looking for frequency, and be specific about the types of sex: kissing, fondling, or masturbation.”
A version of this article first appeared on Medscape.com.
New research confirms recommendations on COVID-19 boosters in MS
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From ECTRIMS 2022
Single dose of psilocybin for major depression tied to short-term remission
, new research shows.
In the largest study of psilocybin for TRD to date, results of the phase 2b randomized, double-blind trial show participants in the 25-mg dose group experienced a significant reduction in depressive symptoms for at least 3 weeks vs. patients in the 10-mg or 1-mg group, which served as the control group.
Investigators found that 29% of participants who received the 25-mg dose were in remission 3 weeks after the treatment and 37% had at least a 50% drop in depression scores. However, at the 3-month mark, only 20% of those on the 25-mg dose experienced significant improvement.
The change from baseline to week 3 in the Montgomery–Åsberg Depression Rating Scale (MADRS) total score was significantly better with a 25-mg dose than with a 1-mg dose; there was no significant difference between the 10-mg dose and the 1-mg dose, the investigators reported.
The response rate was high for those receiving the 25-mg dose, lead investigator Guy Goodwin, MD, DPhil, told reporters attending a press briefing.
“It’s important to understand that response rates in these patients are usually somewhere between 10% and 20%, and we are seeing remission rates at three weeks of 30%,” he said.
Dr. Goodwin is chief medical officer of COMPASS Pathways, the company that funded the trial and created COMP360, the synthetic formulation of psilocybin used in the trial, and professor emeritus of psychiatry at the University of Oxford, England.
Based on the results of the trial it was announced that a phase 3 trial will launch in December.
The study was published online in the New England Journal of Medicine.
Further research planned
Psilocybin has been under investigation for TRD for some time, including one study that compared it with the antidepressant escitalopram (Lexapro) with promising results.
In the current study the researchers sought to find an acceptable, efficacious dose and the safety of a synthetic formulation of the drug administered in combination with psychological support.
The multicenter study was conducted at 22 sites in 10 countries and included 233 participants with TRD and evaluated the safety and efficacy of one of three doses. The study’s primary endpoint was change from baseline to 3 weeks in MADRS scores in patients with TRD. The scale runs from 0 to 60 with higher scores indicating more severe depression.
Participants were randomly assigned to receive 25 mg of psilocybin (n = 79), 10 mg (n = 75) or 1 mg (n = 79). Those taking medications discontinued them at least 2 weeks before the baseline visit. The mean MADRS score was 32 or 33 in each study group.
There was a 3- to 6-week run-up period to the study in which each participant met with a study therapist about three times to build trust and prepare for the psychedelic experience.
On the day of psilocybin administration, each participant listened to a tailored music playlist and wore eye shades while reclining in a comfortable chair to direct attention inwardly.
The psychotherapy sessions lasted 6-8 hours, and two therapists were always present. The following day, participants returned for an “integration” session with the therapists that was designed to help the participants explore insights from their session.
MADRS scores were measured at baseline, the day following psilocybin administration, and at weeks 1, 3, 6, 9, and 12.
Participants were asked to stay off standard antidepressant treatment during the first 3 weeks of the trial but could be restarted at any time if deemed necessary by a trial investigator.
Mean changes from baseline to week 3 in MADRS scores were −12.0 for 25-mg, −7.9 for 10-mg, and −5.4 for 1-mg groups. The difference between the 25-mg group and 1-mg group was −6.6 (95% confidence interval [CI], −10.2 to −2.9; P < .001 and between the 10-mg group and 1-mg group was −2.5 (95% CI, −6.2 to 1.2; P = .18).
The investigators reported that in the 25-mg group, the incidences of response and remission at 3 weeks, but not sustained response at 12 weeks, were generally supportive of the primary results.
Up to 84% of those who received the 25-mg dosage reported adverse events, with the occurrence dropping slightly with each dosage group. The most frequent adverse events included headache, nausea, dizziness, and fatigue, and occurred only on administration day.
Among those who received the 25-mg dose of psilocybin, two participants reported suicidal thoughts during the 3 weeks following treatment, and 3 months post treatment, three patients exhibited suicidal behavior.
Dr. Goodwin noted that these participants had a prior history of suicidal behavior. Two participants in the 10-mg group also had suicidal thoughts. However, the investigators also noted that suicidal ideation, behavior, or self-injury occurred in all dose groups.
The researchers noted that longer and larger trials, including comparisons with existing depression treatments, are needed to determine the safety and efficacy of psilocybin for TRD.
Intriguing, sobering
In an accompanying editorial, Bertha Madras, PhD, McLean Hospital, Belmont, Mass., and Harvard Medical School, Boston, noted “the findings are both intriguing and sobering. The highest dose (25 mg), but not the intermediate dose (10 mg), resulted in significantly lower levels of depressive symptoms after 3 weeks than the lowest dose (1 mg, which served as a control), but the 37% incidence of response with the 25-mg dose was numerically lower than that in large trials of conventional antidepressants and less robust than in a trial showing similar efficacies of psilocybin and a selective serotonin reuptake inhibitor.”
Also sobering, she noted, were the high percentages of adverse events in the 25-mg group and suicidal ideation and behavior. Dr. Madras also wondered if “legalization and commercialization [of psychedelics] are allied with the medical movement, psychedelic shops and ‘clinics’ could proliferate even for vulnerable populations, and rigorously designed medical protocols will be compromised.
“Nevertheless,” she concluded, “it is provocative that these agents show some short-term benefit for depression in selected populations.”
Dr. Goodwin is CMO of Compass Pathways, which funded the study. He and several coauthors disclosed relationships with industry. Dr. Madras reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
In the largest study of psilocybin for TRD to date, results of the phase 2b randomized, double-blind trial show participants in the 25-mg dose group experienced a significant reduction in depressive symptoms for at least 3 weeks vs. patients in the 10-mg or 1-mg group, which served as the control group.
Investigators found that 29% of participants who received the 25-mg dose were in remission 3 weeks after the treatment and 37% had at least a 50% drop in depression scores. However, at the 3-month mark, only 20% of those on the 25-mg dose experienced significant improvement.
The change from baseline to week 3 in the Montgomery–Åsberg Depression Rating Scale (MADRS) total score was significantly better with a 25-mg dose than with a 1-mg dose; there was no significant difference between the 10-mg dose and the 1-mg dose, the investigators reported.
The response rate was high for those receiving the 25-mg dose, lead investigator Guy Goodwin, MD, DPhil, told reporters attending a press briefing.
“It’s important to understand that response rates in these patients are usually somewhere between 10% and 20%, and we are seeing remission rates at three weeks of 30%,” he said.
Dr. Goodwin is chief medical officer of COMPASS Pathways, the company that funded the trial and created COMP360, the synthetic formulation of psilocybin used in the trial, and professor emeritus of psychiatry at the University of Oxford, England.
Based on the results of the trial it was announced that a phase 3 trial will launch in December.
The study was published online in the New England Journal of Medicine.
Further research planned
Psilocybin has been under investigation for TRD for some time, including one study that compared it with the antidepressant escitalopram (Lexapro) with promising results.
In the current study the researchers sought to find an acceptable, efficacious dose and the safety of a synthetic formulation of the drug administered in combination with psychological support.
The multicenter study was conducted at 22 sites in 10 countries and included 233 participants with TRD and evaluated the safety and efficacy of one of three doses. The study’s primary endpoint was change from baseline to 3 weeks in MADRS scores in patients with TRD. The scale runs from 0 to 60 with higher scores indicating more severe depression.
Participants were randomly assigned to receive 25 mg of psilocybin (n = 79), 10 mg (n = 75) or 1 mg (n = 79). Those taking medications discontinued them at least 2 weeks before the baseline visit. The mean MADRS score was 32 or 33 in each study group.
There was a 3- to 6-week run-up period to the study in which each participant met with a study therapist about three times to build trust and prepare for the psychedelic experience.
On the day of psilocybin administration, each participant listened to a tailored music playlist and wore eye shades while reclining in a comfortable chair to direct attention inwardly.
The psychotherapy sessions lasted 6-8 hours, and two therapists were always present. The following day, participants returned for an “integration” session with the therapists that was designed to help the participants explore insights from their session.
MADRS scores were measured at baseline, the day following psilocybin administration, and at weeks 1, 3, 6, 9, and 12.
Participants were asked to stay off standard antidepressant treatment during the first 3 weeks of the trial but could be restarted at any time if deemed necessary by a trial investigator.
Mean changes from baseline to week 3 in MADRS scores were −12.0 for 25-mg, −7.9 for 10-mg, and −5.4 for 1-mg groups. The difference between the 25-mg group and 1-mg group was −6.6 (95% confidence interval [CI], −10.2 to −2.9; P < .001 and between the 10-mg group and 1-mg group was −2.5 (95% CI, −6.2 to 1.2; P = .18).
The investigators reported that in the 25-mg group, the incidences of response and remission at 3 weeks, but not sustained response at 12 weeks, were generally supportive of the primary results.
Up to 84% of those who received the 25-mg dosage reported adverse events, with the occurrence dropping slightly with each dosage group. The most frequent adverse events included headache, nausea, dizziness, and fatigue, and occurred only on administration day.
Among those who received the 25-mg dose of psilocybin, two participants reported suicidal thoughts during the 3 weeks following treatment, and 3 months post treatment, three patients exhibited suicidal behavior.
Dr. Goodwin noted that these participants had a prior history of suicidal behavior. Two participants in the 10-mg group also had suicidal thoughts. However, the investigators also noted that suicidal ideation, behavior, or self-injury occurred in all dose groups.
The researchers noted that longer and larger trials, including comparisons with existing depression treatments, are needed to determine the safety and efficacy of psilocybin for TRD.
Intriguing, sobering
In an accompanying editorial, Bertha Madras, PhD, McLean Hospital, Belmont, Mass., and Harvard Medical School, Boston, noted “the findings are both intriguing and sobering. The highest dose (25 mg), but not the intermediate dose (10 mg), resulted in significantly lower levels of depressive symptoms after 3 weeks than the lowest dose (1 mg, which served as a control), but the 37% incidence of response with the 25-mg dose was numerically lower than that in large trials of conventional antidepressants and less robust than in a trial showing similar efficacies of psilocybin and a selective serotonin reuptake inhibitor.”
Also sobering, she noted, were the high percentages of adverse events in the 25-mg group and suicidal ideation and behavior. Dr. Madras also wondered if “legalization and commercialization [of psychedelics] are allied with the medical movement, psychedelic shops and ‘clinics’ could proliferate even for vulnerable populations, and rigorously designed medical protocols will be compromised.
“Nevertheless,” she concluded, “it is provocative that these agents show some short-term benefit for depression in selected populations.”
Dr. Goodwin is CMO of Compass Pathways, which funded the study. He and several coauthors disclosed relationships with industry. Dr. Madras reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
In the largest study of psilocybin for TRD to date, results of the phase 2b randomized, double-blind trial show participants in the 25-mg dose group experienced a significant reduction in depressive symptoms for at least 3 weeks vs. patients in the 10-mg or 1-mg group, which served as the control group.
Investigators found that 29% of participants who received the 25-mg dose were in remission 3 weeks after the treatment and 37% had at least a 50% drop in depression scores. However, at the 3-month mark, only 20% of those on the 25-mg dose experienced significant improvement.
The change from baseline to week 3 in the Montgomery–Åsberg Depression Rating Scale (MADRS) total score was significantly better with a 25-mg dose than with a 1-mg dose; there was no significant difference between the 10-mg dose and the 1-mg dose, the investigators reported.
The response rate was high for those receiving the 25-mg dose, lead investigator Guy Goodwin, MD, DPhil, told reporters attending a press briefing.
“It’s important to understand that response rates in these patients are usually somewhere between 10% and 20%, and we are seeing remission rates at three weeks of 30%,” he said.
Dr. Goodwin is chief medical officer of COMPASS Pathways, the company that funded the trial and created COMP360, the synthetic formulation of psilocybin used in the trial, and professor emeritus of psychiatry at the University of Oxford, England.
Based on the results of the trial it was announced that a phase 3 trial will launch in December.
The study was published online in the New England Journal of Medicine.
Further research planned
Psilocybin has been under investigation for TRD for some time, including one study that compared it with the antidepressant escitalopram (Lexapro) with promising results.
In the current study the researchers sought to find an acceptable, efficacious dose and the safety of a synthetic formulation of the drug administered in combination with psychological support.
The multicenter study was conducted at 22 sites in 10 countries and included 233 participants with TRD and evaluated the safety and efficacy of one of three doses. The study’s primary endpoint was change from baseline to 3 weeks in MADRS scores in patients with TRD. The scale runs from 0 to 60 with higher scores indicating more severe depression.
Participants were randomly assigned to receive 25 mg of psilocybin (n = 79), 10 mg (n = 75) or 1 mg (n = 79). Those taking medications discontinued them at least 2 weeks before the baseline visit. The mean MADRS score was 32 or 33 in each study group.
There was a 3- to 6-week run-up period to the study in which each participant met with a study therapist about three times to build trust and prepare for the psychedelic experience.
On the day of psilocybin administration, each participant listened to a tailored music playlist and wore eye shades while reclining in a comfortable chair to direct attention inwardly.
The psychotherapy sessions lasted 6-8 hours, and two therapists were always present. The following day, participants returned for an “integration” session with the therapists that was designed to help the participants explore insights from their session.
MADRS scores were measured at baseline, the day following psilocybin administration, and at weeks 1, 3, 6, 9, and 12.
Participants were asked to stay off standard antidepressant treatment during the first 3 weeks of the trial but could be restarted at any time if deemed necessary by a trial investigator.
Mean changes from baseline to week 3 in MADRS scores were −12.0 for 25-mg, −7.9 for 10-mg, and −5.4 for 1-mg groups. The difference between the 25-mg group and 1-mg group was −6.6 (95% confidence interval [CI], −10.2 to −2.9; P < .001 and between the 10-mg group and 1-mg group was −2.5 (95% CI, −6.2 to 1.2; P = .18).
The investigators reported that in the 25-mg group, the incidences of response and remission at 3 weeks, but not sustained response at 12 weeks, were generally supportive of the primary results.
Up to 84% of those who received the 25-mg dosage reported adverse events, with the occurrence dropping slightly with each dosage group. The most frequent adverse events included headache, nausea, dizziness, and fatigue, and occurred only on administration day.
Among those who received the 25-mg dose of psilocybin, two participants reported suicidal thoughts during the 3 weeks following treatment, and 3 months post treatment, three patients exhibited suicidal behavior.
Dr. Goodwin noted that these participants had a prior history of suicidal behavior. Two participants in the 10-mg group also had suicidal thoughts. However, the investigators also noted that suicidal ideation, behavior, or self-injury occurred in all dose groups.
The researchers noted that longer and larger trials, including comparisons with existing depression treatments, are needed to determine the safety and efficacy of psilocybin for TRD.
Intriguing, sobering
In an accompanying editorial, Bertha Madras, PhD, McLean Hospital, Belmont, Mass., and Harvard Medical School, Boston, noted “the findings are both intriguing and sobering. The highest dose (25 mg), but not the intermediate dose (10 mg), resulted in significantly lower levels of depressive symptoms after 3 weeks than the lowest dose (1 mg, which served as a control), but the 37% incidence of response with the 25-mg dose was numerically lower than that in large trials of conventional antidepressants and less robust than in a trial showing similar efficacies of psilocybin and a selective serotonin reuptake inhibitor.”
Also sobering, she noted, were the high percentages of adverse events in the 25-mg group and suicidal ideation and behavior. Dr. Madras also wondered if “legalization and commercialization [of psychedelics] are allied with the medical movement, psychedelic shops and ‘clinics’ could proliferate even for vulnerable populations, and rigorously designed medical protocols will be compromised.
“Nevertheless,” she concluded, “it is provocative that these agents show some short-term benefit for depression in selected populations.”
Dr. Goodwin is CMO of Compass Pathways, which funded the study. He and several coauthors disclosed relationships with industry. Dr. Madras reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE

STEP TEENS: Semaglutide ‘gives hope’ to adolescents with obesity
Attendees at ObesityWeek® 2022 listened with much excitement to the results of the STEP TEENS phase 3 trial of once-weekly subcutaneous semaglutide 2.4 mg (Wegovy) in adolescents aged 12 up to 18 years old with obesity.
When a session panel member said that clinical trials of weight-loss medications for adolescents with obesity should henceforth stop using placebo controls – implying that comparison with the once-weekly injection semaglutide would be more informative – the audience applauded.
The results were also simultaneously published in the New England Journal of Medicine to coincide with the presentation.
The research “gives hope” to adolescents with obesity, their parents, and their doctors, the trial’s principal investigator, Daniel Weghuber, MD, said in an interview.
“Many of them have been struggling for such a long time – both the parents and the kids themselves,” said Dr. Weghuber, from the department of pediatrics, Paracelsus Medical University, Salzburg, Austria.
“It’s not an issue of lack of willpower,” he stressed. “That’s a major misunderstanding.”
“This drug [semaglutide] seems to enable people who are living with obesity to adhere to the recommendations that they may have been following for years and years but were [still] not able to achieve their goal,” he said. It “enables people to achieve their goals.”
Asked about any potential negative impact on normal growth, Dr. Weghuber pointed out that the average weight of study participants was 107 kg (236 lb). “I’m really not afraid of a 15-year-old with 107 kg losing 10%, 15%, 20%” of their weight, he said. There was no indication of a problem regarding normal growth or development in the study.
, he summarized.
Senior study author, Silva Arslanian, MD, who holds the Richard L. Day Endowed Chair in Pediatrics at the University of Pittsburgh, agreed. “The results are amazing,” said Dr. Arslanian in a press release issued by the University of Pittsburgh. “For a person who is 5 foot, 5 inches tall and weighs 240 pounds, the average reduction in BMI equates to shedding about 40 pounds.”
‘Mind-blowing, awesome’ results
The session at ObesityWeek® 2022, the annual meeting of the Obesity Society, was chaired by Aaron S. Kelly, PhD, professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota, Minneapolis.
Dr. Kelly led the SCALE TEENS clinical trial of liraglutide (Saxenda), also a glucagon-like peptide (GLP-1) agonist like semaglutide, for adolescents aged 12 up to 18 years with obesity, which assigned 125 participants to the daily injectable liraglutide group and 126 to the placebo group. SCALE TEENS was presented and published in May 2020, leading to the approval of liraglutide for obesity in this age group, in December 2020.
Dr. Kelly called on two experts who were not involved in the research to offer their comments, starting with Claudia K. Fox, MD, MPH.
“These results are mind-blowing,” said Dr. Fox, who is associate professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota.
“We are getting close to bariatric surgery results” in these adolescent patients with obesity, added Dr. Fox, who is an American Board of Obesity Medicine diplomate. To have 40% of patients attain normal weight, “that’s massive” and “life-changing,” she said. And improvement in quality of life is what families care most about. “I am super excited,” she commented.
Next, Dr. Kelly called on Sarah C. Armstrong, MD, director of the Duke Children’s Healthy Lifestyles Program, Duke University, Durham, N.C.
Dr. Armstrong is a member of the executive committee for the American Academy of Pediatrics Section on Obesity and a coauthor of the upcoming clinical practice guidelines that are being published.
Looking at more than 16,000 abstracts at the meeting shows that “watchful waiting is not effective,” Dr. Armstrong said.
200 teens with obesity, only 1 with overweight
Obesity affects almost one in five children and adolescents worldwide. The chronic disease is linked with decreased life expectancy and higher risk of developing serious health problems such as type 2 diabetes, heart disease, nonalcoholic fatty liver disease, sleep apnea, and certain cancers. Teenagers with obesity are also more likely to have depression, anxiety, poor self-esteem, and other psychological issues.
STEP TEENS enrolled 201 adolescents aged 12 up to 18 years with obesity (body mass index [BMI] ≥ 95th percentile) or overweight (BMI ≥ 85th percentile) plus at least one weight-related comorbidity.
Only one recruited patient fit the latter category; the rest had obesity.
Most patients (62%) were female. They had a mean age of 15.4 years, a mean BMI of 37 kg/m2, and a mean waist circumference of 110 cm (43 inches).
Patients were randomized 2:1 to receive a once-weekly 2.4-mg subcutaneous injection of semaglutide or placebo for 68 weeks, plus lifestyle intervention.
Dr. Weghuber noted that 89.6% of patients in the semaglutide group completed treatment.
The primary endpoint, mean change in BMI from baseline to week 68, was −16.1% with semaglutide and +0.6% with placebo (estimated difference, −16.7 percentage points; P < .001).
A second confirmatory endpoint, at least 5% weight loss at week 68, was met by 73% of patients in the semaglutide group versus 18% of patients in the placebo group (P < .001).
Reductions in body weight and improvements in waist circumference, A1c, lipids (except HDL cholesterol), and the liver enzyme alanine aminotransferase were greater with semaglutide than placebo.
The Impact of Weight on Quality of Life – Kids (IWQOL-Kids) questionnaire total score as well as scores for body esteem, family relation, physical comfort, and social life were better in the semaglutide group.
However, the incidence of gastrointestinal adverse events was greater with semaglutide than placebo (62% versus 42%).
Five participants (4%) in the semaglutide group and none in the placebo group developed gallstones (cholelithiasis).
Serious adverse events were reported in 11% of patients in the semaglutide group and 9% of patients in the placebo group.
‘Big change’ coming in guidelines for obesity in teens
Commenting on the upcoming new recommendations for adolescents, Dr. Armstrong noted “there’s going to be a strong recommendation” for therapy in the new guidelines for pediatric obesity. “That’s a big change,” she said.
In the lively question-and-answer session that followed, a clinician wanted to know what explained the very high rate of study completion during the COVID-19 pandemic (when STEP TEENS was conducted). “What can we learn?” he asked.
“The bottom line is the relationship” and “close communication” between study investigators and patients, Dr. Weghuber replied.
“The fast track is likely to lead to approval in adolescents,” another member of the audience noted. He wanted to know if the company is planning a trial of semaglutide in younger children.
They are, Dr. Weghuber replied, and one with liraglutide is already underway.
The SCALE KIDS clinical trial of liraglutide is randomizing 78 participants aged 6 up to 12 years for 56 weeks of treatment and 26 weeks of follow-up, with an estimated primary completion date of July 7, 2023.
The last words went to Dr. Fox. The current results “are indeed very awesome,” she said, yet “thousands of providers are hesitant” to prescribe medications for adolescents with obesity.
The trial was funded by Novo Nordisk. Dr. Weghuber has reported being a consultant for Novo Nordisk and member of the Global Pediatric Obesity Expert Panel for the company. Disclosures for the other authors are listed with the article. Dr. Kelly has reported receiving donated drugs from AstraZeneca and travel support from Novo Nordisk and serving as an unpaid consultant for Novo Nordisk, Orexigen Therapeutics, VIVUS, and WW (formerly Weight Watchers).
A version of this article first appeared on Medscape.com.
Attendees at ObesityWeek® 2022 listened with much excitement to the results of the STEP TEENS phase 3 trial of once-weekly subcutaneous semaglutide 2.4 mg (Wegovy) in adolescents aged 12 up to 18 years old with obesity.
When a session panel member said that clinical trials of weight-loss medications for adolescents with obesity should henceforth stop using placebo controls – implying that comparison with the once-weekly injection semaglutide would be more informative – the audience applauded.
The results were also simultaneously published in the New England Journal of Medicine to coincide with the presentation.
The research “gives hope” to adolescents with obesity, their parents, and their doctors, the trial’s principal investigator, Daniel Weghuber, MD, said in an interview.
“Many of them have been struggling for such a long time – both the parents and the kids themselves,” said Dr. Weghuber, from the department of pediatrics, Paracelsus Medical University, Salzburg, Austria.
“It’s not an issue of lack of willpower,” he stressed. “That’s a major misunderstanding.”
“This drug [semaglutide] seems to enable people who are living with obesity to adhere to the recommendations that they may have been following for years and years but were [still] not able to achieve their goal,” he said. It “enables people to achieve their goals.”
Asked about any potential negative impact on normal growth, Dr. Weghuber pointed out that the average weight of study participants was 107 kg (236 lb). “I’m really not afraid of a 15-year-old with 107 kg losing 10%, 15%, 20%” of their weight, he said. There was no indication of a problem regarding normal growth or development in the study.
, he summarized.
Senior study author, Silva Arslanian, MD, who holds the Richard L. Day Endowed Chair in Pediatrics at the University of Pittsburgh, agreed. “The results are amazing,” said Dr. Arslanian in a press release issued by the University of Pittsburgh. “For a person who is 5 foot, 5 inches tall and weighs 240 pounds, the average reduction in BMI equates to shedding about 40 pounds.”
‘Mind-blowing, awesome’ results
The session at ObesityWeek® 2022, the annual meeting of the Obesity Society, was chaired by Aaron S. Kelly, PhD, professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota, Minneapolis.
Dr. Kelly led the SCALE TEENS clinical trial of liraglutide (Saxenda), also a glucagon-like peptide (GLP-1) agonist like semaglutide, for adolescents aged 12 up to 18 years with obesity, which assigned 125 participants to the daily injectable liraglutide group and 126 to the placebo group. SCALE TEENS was presented and published in May 2020, leading to the approval of liraglutide for obesity in this age group, in December 2020.
Dr. Kelly called on two experts who were not involved in the research to offer their comments, starting with Claudia K. Fox, MD, MPH.
“These results are mind-blowing,” said Dr. Fox, who is associate professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota.
“We are getting close to bariatric surgery results” in these adolescent patients with obesity, added Dr. Fox, who is an American Board of Obesity Medicine diplomate. To have 40% of patients attain normal weight, “that’s massive” and “life-changing,” she said. And improvement in quality of life is what families care most about. “I am super excited,” she commented.
Next, Dr. Kelly called on Sarah C. Armstrong, MD, director of the Duke Children’s Healthy Lifestyles Program, Duke University, Durham, N.C.
Dr. Armstrong is a member of the executive committee for the American Academy of Pediatrics Section on Obesity and a coauthor of the upcoming clinical practice guidelines that are being published.
Looking at more than 16,000 abstracts at the meeting shows that “watchful waiting is not effective,” Dr. Armstrong said.
200 teens with obesity, only 1 with overweight
Obesity affects almost one in five children and adolescents worldwide. The chronic disease is linked with decreased life expectancy and higher risk of developing serious health problems such as type 2 diabetes, heart disease, nonalcoholic fatty liver disease, sleep apnea, and certain cancers. Teenagers with obesity are also more likely to have depression, anxiety, poor self-esteem, and other psychological issues.
STEP TEENS enrolled 201 adolescents aged 12 up to 18 years with obesity (body mass index [BMI] ≥ 95th percentile) or overweight (BMI ≥ 85th percentile) plus at least one weight-related comorbidity.
Only one recruited patient fit the latter category; the rest had obesity.
Most patients (62%) were female. They had a mean age of 15.4 years, a mean BMI of 37 kg/m2, and a mean waist circumference of 110 cm (43 inches).
Patients were randomized 2:1 to receive a once-weekly 2.4-mg subcutaneous injection of semaglutide or placebo for 68 weeks, plus lifestyle intervention.
Dr. Weghuber noted that 89.6% of patients in the semaglutide group completed treatment.
The primary endpoint, mean change in BMI from baseline to week 68, was −16.1% with semaglutide and +0.6% with placebo (estimated difference, −16.7 percentage points; P < .001).
A second confirmatory endpoint, at least 5% weight loss at week 68, was met by 73% of patients in the semaglutide group versus 18% of patients in the placebo group (P < .001).
Reductions in body weight and improvements in waist circumference, A1c, lipids (except HDL cholesterol), and the liver enzyme alanine aminotransferase were greater with semaglutide than placebo.
The Impact of Weight on Quality of Life – Kids (IWQOL-Kids) questionnaire total score as well as scores for body esteem, family relation, physical comfort, and social life were better in the semaglutide group.
However, the incidence of gastrointestinal adverse events was greater with semaglutide than placebo (62% versus 42%).
Five participants (4%) in the semaglutide group and none in the placebo group developed gallstones (cholelithiasis).
Serious adverse events were reported in 11% of patients in the semaglutide group and 9% of patients in the placebo group.
‘Big change’ coming in guidelines for obesity in teens
Commenting on the upcoming new recommendations for adolescents, Dr. Armstrong noted “there’s going to be a strong recommendation” for therapy in the new guidelines for pediatric obesity. “That’s a big change,” she said.
In the lively question-and-answer session that followed, a clinician wanted to know what explained the very high rate of study completion during the COVID-19 pandemic (when STEP TEENS was conducted). “What can we learn?” he asked.
“The bottom line is the relationship” and “close communication” between study investigators and patients, Dr. Weghuber replied.
“The fast track is likely to lead to approval in adolescents,” another member of the audience noted. He wanted to know if the company is planning a trial of semaglutide in younger children.
They are, Dr. Weghuber replied, and one with liraglutide is already underway.
The SCALE KIDS clinical trial of liraglutide is randomizing 78 participants aged 6 up to 12 years for 56 weeks of treatment and 26 weeks of follow-up, with an estimated primary completion date of July 7, 2023.
The last words went to Dr. Fox. The current results “are indeed very awesome,” she said, yet “thousands of providers are hesitant” to prescribe medications for adolescents with obesity.
The trial was funded by Novo Nordisk. Dr. Weghuber has reported being a consultant for Novo Nordisk and member of the Global Pediatric Obesity Expert Panel for the company. Disclosures for the other authors are listed with the article. Dr. Kelly has reported receiving donated drugs from AstraZeneca and travel support from Novo Nordisk and serving as an unpaid consultant for Novo Nordisk, Orexigen Therapeutics, VIVUS, and WW (formerly Weight Watchers).
A version of this article first appeared on Medscape.com.
Attendees at ObesityWeek® 2022 listened with much excitement to the results of the STEP TEENS phase 3 trial of once-weekly subcutaneous semaglutide 2.4 mg (Wegovy) in adolescents aged 12 up to 18 years old with obesity.
When a session panel member said that clinical trials of weight-loss medications for adolescents with obesity should henceforth stop using placebo controls – implying that comparison with the once-weekly injection semaglutide would be more informative – the audience applauded.
The results were also simultaneously published in the New England Journal of Medicine to coincide with the presentation.
The research “gives hope” to adolescents with obesity, their parents, and their doctors, the trial’s principal investigator, Daniel Weghuber, MD, said in an interview.
“Many of them have been struggling for such a long time – both the parents and the kids themselves,” said Dr. Weghuber, from the department of pediatrics, Paracelsus Medical University, Salzburg, Austria.
“It’s not an issue of lack of willpower,” he stressed. “That’s a major misunderstanding.”
“This drug [semaglutide] seems to enable people who are living with obesity to adhere to the recommendations that they may have been following for years and years but were [still] not able to achieve their goal,” he said. It “enables people to achieve their goals.”
Asked about any potential negative impact on normal growth, Dr. Weghuber pointed out that the average weight of study participants was 107 kg (236 lb). “I’m really not afraid of a 15-year-old with 107 kg losing 10%, 15%, 20%” of their weight, he said. There was no indication of a problem regarding normal growth or development in the study.
, he summarized.
Senior study author, Silva Arslanian, MD, who holds the Richard L. Day Endowed Chair in Pediatrics at the University of Pittsburgh, agreed. “The results are amazing,” said Dr. Arslanian in a press release issued by the University of Pittsburgh. “For a person who is 5 foot, 5 inches tall and weighs 240 pounds, the average reduction in BMI equates to shedding about 40 pounds.”
‘Mind-blowing, awesome’ results
The session at ObesityWeek® 2022, the annual meeting of the Obesity Society, was chaired by Aaron S. Kelly, PhD, professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota, Minneapolis.
Dr. Kelly led the SCALE TEENS clinical trial of liraglutide (Saxenda), also a glucagon-like peptide (GLP-1) agonist like semaglutide, for adolescents aged 12 up to 18 years with obesity, which assigned 125 participants to the daily injectable liraglutide group and 126 to the placebo group. SCALE TEENS was presented and published in May 2020, leading to the approval of liraglutide for obesity in this age group, in December 2020.
Dr. Kelly called on two experts who were not involved in the research to offer their comments, starting with Claudia K. Fox, MD, MPH.
“These results are mind-blowing,” said Dr. Fox, who is associate professor of pediatrics and codirector of the center for pediatric obesity medicine at the University of Minnesota.
“We are getting close to bariatric surgery results” in these adolescent patients with obesity, added Dr. Fox, who is an American Board of Obesity Medicine diplomate. To have 40% of patients attain normal weight, “that’s massive” and “life-changing,” she said. And improvement in quality of life is what families care most about. “I am super excited,” she commented.
Next, Dr. Kelly called on Sarah C. Armstrong, MD, director of the Duke Children’s Healthy Lifestyles Program, Duke University, Durham, N.C.
Dr. Armstrong is a member of the executive committee for the American Academy of Pediatrics Section on Obesity and a coauthor of the upcoming clinical practice guidelines that are being published.
Looking at more than 16,000 abstracts at the meeting shows that “watchful waiting is not effective,” Dr. Armstrong said.
200 teens with obesity, only 1 with overweight
Obesity affects almost one in five children and adolescents worldwide. The chronic disease is linked with decreased life expectancy and higher risk of developing serious health problems such as type 2 diabetes, heart disease, nonalcoholic fatty liver disease, sleep apnea, and certain cancers. Teenagers with obesity are also more likely to have depression, anxiety, poor self-esteem, and other psychological issues.
STEP TEENS enrolled 201 adolescents aged 12 up to 18 years with obesity (body mass index [BMI] ≥ 95th percentile) or overweight (BMI ≥ 85th percentile) plus at least one weight-related comorbidity.
Only one recruited patient fit the latter category; the rest had obesity.
Most patients (62%) were female. They had a mean age of 15.4 years, a mean BMI of 37 kg/m2, and a mean waist circumference of 110 cm (43 inches).
Patients were randomized 2:1 to receive a once-weekly 2.4-mg subcutaneous injection of semaglutide or placebo for 68 weeks, plus lifestyle intervention.
Dr. Weghuber noted that 89.6% of patients in the semaglutide group completed treatment.
The primary endpoint, mean change in BMI from baseline to week 68, was −16.1% with semaglutide and +0.6% with placebo (estimated difference, −16.7 percentage points; P < .001).
A second confirmatory endpoint, at least 5% weight loss at week 68, was met by 73% of patients in the semaglutide group versus 18% of patients in the placebo group (P < .001).
Reductions in body weight and improvements in waist circumference, A1c, lipids (except HDL cholesterol), and the liver enzyme alanine aminotransferase were greater with semaglutide than placebo.
The Impact of Weight on Quality of Life – Kids (IWQOL-Kids) questionnaire total score as well as scores for body esteem, family relation, physical comfort, and social life were better in the semaglutide group.
However, the incidence of gastrointestinal adverse events was greater with semaglutide than placebo (62% versus 42%).
Five participants (4%) in the semaglutide group and none in the placebo group developed gallstones (cholelithiasis).
Serious adverse events were reported in 11% of patients in the semaglutide group and 9% of patients in the placebo group.
‘Big change’ coming in guidelines for obesity in teens
Commenting on the upcoming new recommendations for adolescents, Dr. Armstrong noted “there’s going to be a strong recommendation” for therapy in the new guidelines for pediatric obesity. “That’s a big change,” she said.
In the lively question-and-answer session that followed, a clinician wanted to know what explained the very high rate of study completion during the COVID-19 pandemic (when STEP TEENS was conducted). “What can we learn?” he asked.
“The bottom line is the relationship” and “close communication” between study investigators and patients, Dr. Weghuber replied.
“The fast track is likely to lead to approval in adolescents,” another member of the audience noted. He wanted to know if the company is planning a trial of semaglutide in younger children.
They are, Dr. Weghuber replied, and one with liraglutide is already underway.
The SCALE KIDS clinical trial of liraglutide is randomizing 78 participants aged 6 up to 12 years for 56 weeks of treatment and 26 weeks of follow-up, with an estimated primary completion date of July 7, 2023.
The last words went to Dr. Fox. The current results “are indeed very awesome,” she said, yet “thousands of providers are hesitant” to prescribe medications for adolescents with obesity.
The trial was funded by Novo Nordisk. Dr. Weghuber has reported being a consultant for Novo Nordisk and member of the Global Pediatric Obesity Expert Panel for the company. Disclosures for the other authors are listed with the article. Dr. Kelly has reported receiving donated drugs from AstraZeneca and travel support from Novo Nordisk and serving as an unpaid consultant for Novo Nordisk, Orexigen Therapeutics, VIVUS, and WW (formerly Weight Watchers).
A version of this article first appeared on Medscape.com.
FROM OBESITYWEEK® 2022
Microplastics and health risks: What do we really know?
You eat a credit card’s worth of plastic in a week. That may bother you. But does it harm you?
The answer depends on who you ask. Awareness of microplastics in general is certainly increasing; the most recent news is the detection of microplastics in human breast milk. Other research has suggested that we may be consuming up to 5 grams of plastic each week from our food, water, and certain consumer products.
The World Health Organization has been releasing reports on microplastics and human health since 2019. Their most recent report was released in late August 2022.
“Although the limited data provide little evidence that nano- and microplastic particles have adverse effects in humans, there is increasing public awareness and an overwhelming consensus among all stakeholders that plastics do not belong in the environment, and measures should be taken to mitigate exposure,” the WHO said at the time.
The WHO can’t go beyond what the data shows, of course. If microplastics are wreaking long-term havoc in our bodies as we speak, science hasn’t connected the dots enough to definitively say “this is the problem.”
But some researchers are willing to speculate – and, at the very least, the risks are becoming impossible to ignore. Dick Vethaak, PhD, a microplastics researcher and emeritus professor of ecotoxicology at Vrije Universiteit, Amsterdam, is blunt, calling them “a plastic time bomb.”
The plastic problem
Every piece of plastic that has ever been created is still on our planet today, apart from what has been burned. Past estimates show we only recycle about 9% of all plastic, leaving 9 billion tons in our landfills, oceans, and ecosystems. For context, that amount is 1,500 times heavier than the Great Pyramid of Khufu.
New data is even more dire. A 2022 report from Greenpeace showed a 5% U.S. recycling rate in 2021, with a large portion of what consumers think of as “recycled” still winding up in garbage piles or bodies of water.
And this plastic doesn’t disappear. Instead, it breaks down into smaller and smaller pieces known as microplastics and nanoplastics.
Microplastics have been confirmed in human blood, lung tissue, colons, placentas, stool, and breast milk. But how they impact our health is still unknown.
To assess risk, we must ask: “How hazardous is the material?” said Flemming Cassee, PhD, professor of inhalation toxicology at Utrecht (the Netherlands) University and coauthor of the WHO’s recent microplastics report.
There are three potential hazards of microplastics: their physical presence in our bodies, what they’re made of, and what they carry. To determine the extent of these risks, we need to know how much we’re exposed to, said Dr. Cassee.
The first initiative to research the impact of microplastics on human health came from the European Union in 2018. Although microplastics were around before then, we were unable to detect them, said Dr. Cassee.
That’s the real problem: warned Dr. Vethaak.
What, exactly, are microplastics?
Microplastics are plastic particles between 5 mm and 100 nm in diameter, or the width of a pencil eraser and something 10 times thinner than a human hair. Anything smaller than that is known as a nanoplastic.
“Microplastics include a wide range of different materials, different sizes, different shapes, different densities, and different colors,” said Evangelos Danopoulos, PhD, a microplastics researcher at Hull York (England) Medical School.
“Primary” microplastics are manufactured to be small and used in things like cosmetics and paints. “Secondary” microplastics result from the breaking down of larger plastic materials, like water bottles and plastic bags.
Secondary microplastics are more diverse than primary microplastics and can take forms ranging from fibers shed from synthetic clothing (like polyester) to pieces of a plastic spoon left in our rivers, lakes, and oceans. Any plastic in the environment will eventually become a secondary microplastic as natural forces such as wind, water currents, and UV radiation break it down into smaller and smaller pieces.
Plastic is a diverse material. Heather Leslie, PhD, senior researcher in Vrije Universiteit’s department of environment and health, likens it to spaghetti with sauce. The noodles are the long polymer backbone that all plastic shares. The sauces are “the pigments, the antioxidants, the flame retardants, etc., that make it functional,” she said.
What makes microplastics dangerous?
There are more than 10,000 different chemicals, or “sauces,” used to alter a plastic’s physical characteristics – making it softer, more rigid, or more flexible, said Hanna Dusza, PhD, of the Institute for Risk Assessment Sciences at Utrecht University.
As plastics degrade and become microplastics, these chemicals likely remain. Recent research has shown that microplastics leach these chemicals locally in human tissues, or other areas of accumulation, said Dr. Dusza. Some 2,400 of the 10,000 chemical additives were classified as substances of potential concern, meeting the European Union’s criteria for persistence, bioaccumulation, or toxicity.
Many of these chemicals also act as endocrine-disrupting compounds, or toxicants that imitate hormones when they enter the body. Hormones are active at very low concentrations in your bloodstream, explained Dr. Leslie. To your body, some chemical additives in plastic resemble hormones, so the body responds.
“Sometimes even a low dose of some of these additives can cause unwanted effects,” said Dr. Leslie.
Bisphenol A (BPA), for example, is one of the more infamous endocrine disruptors. It is used as an additive to make plastics more rigid and can be found in any number of plastic products, though areas of concern have been plastic water bottles, baby bottles, and the protective coatings in canned foods.
BPA may mimic estrogen, the female sex hormone essential for reproduction, neurodevelopment, and bone density. In men, estrogen regulates sperm count, sex drive, and erectile function. BPA exposure has been linked with – but not proven to cause – multiple cancer types, ADHD, obesity, and low sperm count. Most everyone has some amount of BPA circulating within their blood, but microplastics may retain BPA as they degrade, potentially increasing our exposure, leading to its unwanted consequences, said Dr. Dusza.
And BPA is just one of those 2,400 substances of “potential concern.”
The inflammation problem
A potentially larger health issue emerges from our bodies yet again doing what they are supposed to do when encountering microplastics. Particles can trigger an immune response when they enter your bloodstream, explains Nienke Vrisekoop, PhD, assistant professor at UMC Utrecht.
White blood cells have no issue breaking down things like bacteria, but microplastics cannot be degraded. When a white blood cell engulfs a certain mass of microplastics – either many small particles or a singular large one – it dies, releasing its enzymes and causing local inflammation.
Meanwhile, the plastic particle remains. So more white blood cells attack.
“This triggers continual activation that can result in various adverse effects, including oxidative stress and the release of cytokines that trigger inflammatory reactions, said Dr. Vethaak.
And “chronic inflammation is the prelude to chronic diseases,” said Dr. Leslie. “Every chronic disease, like cancer, heart disease, and even neuropsychiatric diseases like Parkinson’s or major depression, begins with inflammation.”
Meanwhile, inhaling microplastic particles can lead to respiratory diseases and cancer.
“The smallest particles – less than one-tenth of a micrometer – penetrate deep into the lungs and even into the bloodstream, causing damage to the heart, blood vessels and brain,” said Dr. Vetaak. “The only direct evidence comes from workers in the textile and plastic industries that had been exposed to very high amounts of plastic fibrous dust.”
Microplastics as carriers
Microplastics can also pick up harmful substances and deliver them into your body.
“When they’re in an environment, they basically can suck up [chemicals] like a sponge,” said Dr. Dusza. “These chemicals are known environmental pollutants, like pesticides, fluorinated compounds, flame retardants, and so on.”
Once in the body, these chemicals can be released, potentially leading to cancer, chronic inflammation, or other unknown effects.
Particles can also act as a vector for microbes, bacteria, and viruses. A September 2022 study found that infectious viruses can survive for 3 days in fresh water by “hitchhiking” on microplastics. Their porous nature provides microbes with a perfect environment in which to live and reproduce, said Dr. Dusza. If you ingest the plastics, you ingest the microbes.
How to minimize exposure
There is no way to avoid microplastics. They’re in the air we breathe, the products we use, the water we drink, and the food we eat.
Dr. Danopoulos reviewed 72 studies to quantify our consumption of microplastics in drinking water, salt, and seafood.
“We are exposed to millions of microplastics every year, and I was only looking at three food sources, so there are really a lot more,” he said. “Once plastic waste is mismanaged and it enters the environment, there is very little we can do to extract it.”
That said, we can take steps to lower our exposure and keep the problem from getting worse.
Water filtration is one option, though it is not perfect. Research has shown that municipal water treatment can be effective. An October 2021 study found that two methods – electrocoagulation-electroflotation and membrane filtration – can be 100% effective in removing microplastics from treated water. The problem? Not all municipal water treatment uses these methods – and you would have to investigate to find out if your locality does.
As for at-home filtration methods, they can be effective but can also be dicey. Some consumer brands claim they remove microplastics, but how well depends on not just the type of filter but the size of the particles in the water. Meanwhile, how do you know if a filter is working on your water without testing it, something few people will do? Best not to take a brand’s claims on face-value, but look for independent testing on at-home brands.
A longer-term project: Reduce our risk by reusing and recycling plastic waste. Limiting our consumption of plastic, especially single use plastic, decreases the amount available to become micro- and nanoplastics.
We must all learn to not treat plastic as waste, but rather as a renewable material, said Dr. Cassee. But if that seems like a tall order, it’s because it is.
“You’re a human being and you have a voice and there are a lot of other humans out there with voices,” said Dr. Leslie.
“You sign a petition in your community. You talk about it with your friends at the pub. If you’re a teacher, you discuss it in your class. You call your elected representatives and tell them what you think and how you want them to vote on bills.”
When people start working together, you can really amplify that voice, said Dr. Leslie.
What’s the bottom line right now, today?
Numerous sources have declared microplastics do not impact human health. But that’s largely because no direct evidence of this exists yet.
Even the WHO in its report suggests that progress must happen if we’re to fully understand the scope of the problem.
“Strengthening of the evidence necessary for reliable characterization and quantification of the risks to human health posed by [nano- and microplastics] will require active participation by all stakeholders,” it said.
All researchers interviewed for this article agree we don’t have enough evidence to draw any definite conclusions. But “if you look at the wrong endpoints, things will look safe, until you look at the endpoint where it’s really causing the problem,” said Dr. Leslie.
We must research our blind spots and continually ask: Where could we be wrong?
“It is a problem; it’s not going to go away,” said Dr. Danopoulos. “It’s going to get worse, and will continue to get worse, not by something that we are doing now but by something we did 5 years ago.”
Perhaps the question to be asked, then, is the hardest to answer: Are we willing to wait for the science?
A version of this article first appeared on WebMD.com.
You eat a credit card’s worth of plastic in a week. That may bother you. But does it harm you?
The answer depends on who you ask. Awareness of microplastics in general is certainly increasing; the most recent news is the detection of microplastics in human breast milk. Other research has suggested that we may be consuming up to 5 grams of plastic each week from our food, water, and certain consumer products.
The World Health Organization has been releasing reports on microplastics and human health since 2019. Their most recent report was released in late August 2022.
“Although the limited data provide little evidence that nano- and microplastic particles have adverse effects in humans, there is increasing public awareness and an overwhelming consensus among all stakeholders that plastics do not belong in the environment, and measures should be taken to mitigate exposure,” the WHO said at the time.
The WHO can’t go beyond what the data shows, of course. If microplastics are wreaking long-term havoc in our bodies as we speak, science hasn’t connected the dots enough to definitively say “this is the problem.”
But some researchers are willing to speculate – and, at the very least, the risks are becoming impossible to ignore. Dick Vethaak, PhD, a microplastics researcher and emeritus professor of ecotoxicology at Vrije Universiteit, Amsterdam, is blunt, calling them “a plastic time bomb.”
The plastic problem
Every piece of plastic that has ever been created is still on our planet today, apart from what has been burned. Past estimates show we only recycle about 9% of all plastic, leaving 9 billion tons in our landfills, oceans, and ecosystems. For context, that amount is 1,500 times heavier than the Great Pyramid of Khufu.
New data is even more dire. A 2022 report from Greenpeace showed a 5% U.S. recycling rate in 2021, with a large portion of what consumers think of as “recycled” still winding up in garbage piles or bodies of water.
And this plastic doesn’t disappear. Instead, it breaks down into smaller and smaller pieces known as microplastics and nanoplastics.
Microplastics have been confirmed in human blood, lung tissue, colons, placentas, stool, and breast milk. But how they impact our health is still unknown.
To assess risk, we must ask: “How hazardous is the material?” said Flemming Cassee, PhD, professor of inhalation toxicology at Utrecht (the Netherlands) University and coauthor of the WHO’s recent microplastics report.
There are three potential hazards of microplastics: their physical presence in our bodies, what they’re made of, and what they carry. To determine the extent of these risks, we need to know how much we’re exposed to, said Dr. Cassee.
The first initiative to research the impact of microplastics on human health came from the European Union in 2018. Although microplastics were around before then, we were unable to detect them, said Dr. Cassee.
That’s the real problem: warned Dr. Vethaak.
What, exactly, are microplastics?
Microplastics are plastic particles between 5 mm and 100 nm in diameter, or the width of a pencil eraser and something 10 times thinner than a human hair. Anything smaller than that is known as a nanoplastic.
“Microplastics include a wide range of different materials, different sizes, different shapes, different densities, and different colors,” said Evangelos Danopoulos, PhD, a microplastics researcher at Hull York (England) Medical School.
“Primary” microplastics are manufactured to be small and used in things like cosmetics and paints. “Secondary” microplastics result from the breaking down of larger plastic materials, like water bottles and plastic bags.
Secondary microplastics are more diverse than primary microplastics and can take forms ranging from fibers shed from synthetic clothing (like polyester) to pieces of a plastic spoon left in our rivers, lakes, and oceans. Any plastic in the environment will eventually become a secondary microplastic as natural forces such as wind, water currents, and UV radiation break it down into smaller and smaller pieces.
Plastic is a diverse material. Heather Leslie, PhD, senior researcher in Vrije Universiteit’s department of environment and health, likens it to spaghetti with sauce. The noodles are the long polymer backbone that all plastic shares. The sauces are “the pigments, the antioxidants, the flame retardants, etc., that make it functional,” she said.
What makes microplastics dangerous?
There are more than 10,000 different chemicals, or “sauces,” used to alter a plastic’s physical characteristics – making it softer, more rigid, or more flexible, said Hanna Dusza, PhD, of the Institute for Risk Assessment Sciences at Utrecht University.
As plastics degrade and become microplastics, these chemicals likely remain. Recent research has shown that microplastics leach these chemicals locally in human tissues, or other areas of accumulation, said Dr. Dusza. Some 2,400 of the 10,000 chemical additives were classified as substances of potential concern, meeting the European Union’s criteria for persistence, bioaccumulation, or toxicity.
Many of these chemicals also act as endocrine-disrupting compounds, or toxicants that imitate hormones when they enter the body. Hormones are active at very low concentrations in your bloodstream, explained Dr. Leslie. To your body, some chemical additives in plastic resemble hormones, so the body responds.
“Sometimes even a low dose of some of these additives can cause unwanted effects,” said Dr. Leslie.
Bisphenol A (BPA), for example, is one of the more infamous endocrine disruptors. It is used as an additive to make plastics more rigid and can be found in any number of plastic products, though areas of concern have been plastic water bottles, baby bottles, and the protective coatings in canned foods.
BPA may mimic estrogen, the female sex hormone essential for reproduction, neurodevelopment, and bone density. In men, estrogen regulates sperm count, sex drive, and erectile function. BPA exposure has been linked with – but not proven to cause – multiple cancer types, ADHD, obesity, and low sperm count. Most everyone has some amount of BPA circulating within their blood, but microplastics may retain BPA as they degrade, potentially increasing our exposure, leading to its unwanted consequences, said Dr. Dusza.
And BPA is just one of those 2,400 substances of “potential concern.”
The inflammation problem
A potentially larger health issue emerges from our bodies yet again doing what they are supposed to do when encountering microplastics. Particles can trigger an immune response when they enter your bloodstream, explains Nienke Vrisekoop, PhD, assistant professor at UMC Utrecht.
White blood cells have no issue breaking down things like bacteria, but microplastics cannot be degraded. When a white blood cell engulfs a certain mass of microplastics – either many small particles or a singular large one – it dies, releasing its enzymes and causing local inflammation.
Meanwhile, the plastic particle remains. So more white blood cells attack.
“This triggers continual activation that can result in various adverse effects, including oxidative stress and the release of cytokines that trigger inflammatory reactions, said Dr. Vethaak.
And “chronic inflammation is the prelude to chronic diseases,” said Dr. Leslie. “Every chronic disease, like cancer, heart disease, and even neuropsychiatric diseases like Parkinson’s or major depression, begins with inflammation.”
Meanwhile, inhaling microplastic particles can lead to respiratory diseases and cancer.
“The smallest particles – less than one-tenth of a micrometer – penetrate deep into the lungs and even into the bloodstream, causing damage to the heart, blood vessels and brain,” said Dr. Vetaak. “The only direct evidence comes from workers in the textile and plastic industries that had been exposed to very high amounts of plastic fibrous dust.”
Microplastics as carriers
Microplastics can also pick up harmful substances and deliver them into your body.
“When they’re in an environment, they basically can suck up [chemicals] like a sponge,” said Dr. Dusza. “These chemicals are known environmental pollutants, like pesticides, fluorinated compounds, flame retardants, and so on.”
Once in the body, these chemicals can be released, potentially leading to cancer, chronic inflammation, or other unknown effects.
Particles can also act as a vector for microbes, bacteria, and viruses. A September 2022 study found that infectious viruses can survive for 3 days in fresh water by “hitchhiking” on microplastics. Their porous nature provides microbes with a perfect environment in which to live and reproduce, said Dr. Dusza. If you ingest the plastics, you ingest the microbes.
How to minimize exposure
There is no way to avoid microplastics. They’re in the air we breathe, the products we use, the water we drink, and the food we eat.
Dr. Danopoulos reviewed 72 studies to quantify our consumption of microplastics in drinking water, salt, and seafood.
“We are exposed to millions of microplastics every year, and I was only looking at three food sources, so there are really a lot more,” he said. “Once plastic waste is mismanaged and it enters the environment, there is very little we can do to extract it.”
That said, we can take steps to lower our exposure and keep the problem from getting worse.
Water filtration is one option, though it is not perfect. Research has shown that municipal water treatment can be effective. An October 2021 study found that two methods – electrocoagulation-electroflotation and membrane filtration – can be 100% effective in removing microplastics from treated water. The problem? Not all municipal water treatment uses these methods – and you would have to investigate to find out if your locality does.
As for at-home filtration methods, they can be effective but can also be dicey. Some consumer brands claim they remove microplastics, but how well depends on not just the type of filter but the size of the particles in the water. Meanwhile, how do you know if a filter is working on your water without testing it, something few people will do? Best not to take a brand’s claims on face-value, but look for independent testing on at-home brands.
A longer-term project: Reduce our risk by reusing and recycling plastic waste. Limiting our consumption of plastic, especially single use plastic, decreases the amount available to become micro- and nanoplastics.
We must all learn to not treat plastic as waste, but rather as a renewable material, said Dr. Cassee. But if that seems like a tall order, it’s because it is.
“You’re a human being and you have a voice and there are a lot of other humans out there with voices,” said Dr. Leslie.
“You sign a petition in your community. You talk about it with your friends at the pub. If you’re a teacher, you discuss it in your class. You call your elected representatives and tell them what you think and how you want them to vote on bills.”
When people start working together, you can really amplify that voice, said Dr. Leslie.
What’s the bottom line right now, today?
Numerous sources have declared microplastics do not impact human health. But that’s largely because no direct evidence of this exists yet.
Even the WHO in its report suggests that progress must happen if we’re to fully understand the scope of the problem.
“Strengthening of the evidence necessary for reliable characterization and quantification of the risks to human health posed by [nano- and microplastics] will require active participation by all stakeholders,” it said.
All researchers interviewed for this article agree we don’t have enough evidence to draw any definite conclusions. But “if you look at the wrong endpoints, things will look safe, until you look at the endpoint where it’s really causing the problem,” said Dr. Leslie.
We must research our blind spots and continually ask: Where could we be wrong?
“It is a problem; it’s not going to go away,” said Dr. Danopoulos. “It’s going to get worse, and will continue to get worse, not by something that we are doing now but by something we did 5 years ago.”
Perhaps the question to be asked, then, is the hardest to answer: Are we willing to wait for the science?
A version of this article first appeared on WebMD.com.
You eat a credit card’s worth of plastic in a week. That may bother you. But does it harm you?
The answer depends on who you ask. Awareness of microplastics in general is certainly increasing; the most recent news is the detection of microplastics in human breast milk. Other research has suggested that we may be consuming up to 5 grams of plastic each week from our food, water, and certain consumer products.
The World Health Organization has been releasing reports on microplastics and human health since 2019. Their most recent report was released in late August 2022.
“Although the limited data provide little evidence that nano- and microplastic particles have adverse effects in humans, there is increasing public awareness and an overwhelming consensus among all stakeholders that plastics do not belong in the environment, and measures should be taken to mitigate exposure,” the WHO said at the time.
The WHO can’t go beyond what the data shows, of course. If microplastics are wreaking long-term havoc in our bodies as we speak, science hasn’t connected the dots enough to definitively say “this is the problem.”
But some researchers are willing to speculate – and, at the very least, the risks are becoming impossible to ignore. Dick Vethaak, PhD, a microplastics researcher and emeritus professor of ecotoxicology at Vrije Universiteit, Amsterdam, is blunt, calling them “a plastic time bomb.”
The plastic problem
Every piece of plastic that has ever been created is still on our planet today, apart from what has been burned. Past estimates show we only recycle about 9% of all plastic, leaving 9 billion tons in our landfills, oceans, and ecosystems. For context, that amount is 1,500 times heavier than the Great Pyramid of Khufu.
New data is even more dire. A 2022 report from Greenpeace showed a 5% U.S. recycling rate in 2021, with a large portion of what consumers think of as “recycled” still winding up in garbage piles or bodies of water.
And this plastic doesn’t disappear. Instead, it breaks down into smaller and smaller pieces known as microplastics and nanoplastics.
Microplastics have been confirmed in human blood, lung tissue, colons, placentas, stool, and breast milk. But how they impact our health is still unknown.
To assess risk, we must ask: “How hazardous is the material?” said Flemming Cassee, PhD, professor of inhalation toxicology at Utrecht (the Netherlands) University and coauthor of the WHO’s recent microplastics report.
There are three potential hazards of microplastics: their physical presence in our bodies, what they’re made of, and what they carry. To determine the extent of these risks, we need to know how much we’re exposed to, said Dr. Cassee.
The first initiative to research the impact of microplastics on human health came from the European Union in 2018. Although microplastics were around before then, we were unable to detect them, said Dr. Cassee.
That’s the real problem: warned Dr. Vethaak.
What, exactly, are microplastics?
Microplastics are plastic particles between 5 mm and 100 nm in diameter, or the width of a pencil eraser and something 10 times thinner than a human hair. Anything smaller than that is known as a nanoplastic.
“Microplastics include a wide range of different materials, different sizes, different shapes, different densities, and different colors,” said Evangelos Danopoulos, PhD, a microplastics researcher at Hull York (England) Medical School.
“Primary” microplastics are manufactured to be small and used in things like cosmetics and paints. “Secondary” microplastics result from the breaking down of larger plastic materials, like water bottles and plastic bags.
Secondary microplastics are more diverse than primary microplastics and can take forms ranging from fibers shed from synthetic clothing (like polyester) to pieces of a plastic spoon left in our rivers, lakes, and oceans. Any plastic in the environment will eventually become a secondary microplastic as natural forces such as wind, water currents, and UV radiation break it down into smaller and smaller pieces.
Plastic is a diverse material. Heather Leslie, PhD, senior researcher in Vrije Universiteit’s department of environment and health, likens it to spaghetti with sauce. The noodles are the long polymer backbone that all plastic shares. The sauces are “the pigments, the antioxidants, the flame retardants, etc., that make it functional,” she said.
What makes microplastics dangerous?
There are more than 10,000 different chemicals, or “sauces,” used to alter a plastic’s physical characteristics – making it softer, more rigid, or more flexible, said Hanna Dusza, PhD, of the Institute for Risk Assessment Sciences at Utrecht University.
As plastics degrade and become microplastics, these chemicals likely remain. Recent research has shown that microplastics leach these chemicals locally in human tissues, or other areas of accumulation, said Dr. Dusza. Some 2,400 of the 10,000 chemical additives were classified as substances of potential concern, meeting the European Union’s criteria for persistence, bioaccumulation, or toxicity.
Many of these chemicals also act as endocrine-disrupting compounds, or toxicants that imitate hormones when they enter the body. Hormones are active at very low concentrations in your bloodstream, explained Dr. Leslie. To your body, some chemical additives in plastic resemble hormones, so the body responds.
“Sometimes even a low dose of some of these additives can cause unwanted effects,” said Dr. Leslie.
Bisphenol A (BPA), for example, is one of the more infamous endocrine disruptors. It is used as an additive to make plastics more rigid and can be found in any number of plastic products, though areas of concern have been plastic water bottles, baby bottles, and the protective coatings in canned foods.
BPA may mimic estrogen, the female sex hormone essential for reproduction, neurodevelopment, and bone density. In men, estrogen regulates sperm count, sex drive, and erectile function. BPA exposure has been linked with – but not proven to cause – multiple cancer types, ADHD, obesity, and low sperm count. Most everyone has some amount of BPA circulating within their blood, but microplastics may retain BPA as they degrade, potentially increasing our exposure, leading to its unwanted consequences, said Dr. Dusza.
And BPA is just one of those 2,400 substances of “potential concern.”
The inflammation problem
A potentially larger health issue emerges from our bodies yet again doing what they are supposed to do when encountering microplastics. Particles can trigger an immune response when they enter your bloodstream, explains Nienke Vrisekoop, PhD, assistant professor at UMC Utrecht.
White blood cells have no issue breaking down things like bacteria, but microplastics cannot be degraded. When a white blood cell engulfs a certain mass of microplastics – either many small particles or a singular large one – it dies, releasing its enzymes and causing local inflammation.
Meanwhile, the plastic particle remains. So more white blood cells attack.
“This triggers continual activation that can result in various adverse effects, including oxidative stress and the release of cytokines that trigger inflammatory reactions, said Dr. Vethaak.
And “chronic inflammation is the prelude to chronic diseases,” said Dr. Leslie. “Every chronic disease, like cancer, heart disease, and even neuropsychiatric diseases like Parkinson’s or major depression, begins with inflammation.”
Meanwhile, inhaling microplastic particles can lead to respiratory diseases and cancer.
“The smallest particles – less than one-tenth of a micrometer – penetrate deep into the lungs and even into the bloodstream, causing damage to the heart, blood vessels and brain,” said Dr. Vetaak. “The only direct evidence comes from workers in the textile and plastic industries that had been exposed to very high amounts of plastic fibrous dust.”
Microplastics as carriers
Microplastics can also pick up harmful substances and deliver them into your body.
“When they’re in an environment, they basically can suck up [chemicals] like a sponge,” said Dr. Dusza. “These chemicals are known environmental pollutants, like pesticides, fluorinated compounds, flame retardants, and so on.”
Once in the body, these chemicals can be released, potentially leading to cancer, chronic inflammation, or other unknown effects.
Particles can also act as a vector for microbes, bacteria, and viruses. A September 2022 study found that infectious viruses can survive for 3 days in fresh water by “hitchhiking” on microplastics. Their porous nature provides microbes with a perfect environment in which to live and reproduce, said Dr. Dusza. If you ingest the plastics, you ingest the microbes.
How to minimize exposure
There is no way to avoid microplastics. They’re in the air we breathe, the products we use, the water we drink, and the food we eat.
Dr. Danopoulos reviewed 72 studies to quantify our consumption of microplastics in drinking water, salt, and seafood.
“We are exposed to millions of microplastics every year, and I was only looking at three food sources, so there are really a lot more,” he said. “Once plastic waste is mismanaged and it enters the environment, there is very little we can do to extract it.”
That said, we can take steps to lower our exposure and keep the problem from getting worse.
Water filtration is one option, though it is not perfect. Research has shown that municipal water treatment can be effective. An October 2021 study found that two methods – electrocoagulation-electroflotation and membrane filtration – can be 100% effective in removing microplastics from treated water. The problem? Not all municipal water treatment uses these methods – and you would have to investigate to find out if your locality does.
As for at-home filtration methods, they can be effective but can also be dicey. Some consumer brands claim they remove microplastics, but how well depends on not just the type of filter but the size of the particles in the water. Meanwhile, how do you know if a filter is working on your water without testing it, something few people will do? Best not to take a brand’s claims on face-value, but look for independent testing on at-home brands.
A longer-term project: Reduce our risk by reusing and recycling plastic waste. Limiting our consumption of plastic, especially single use plastic, decreases the amount available to become micro- and nanoplastics.
We must all learn to not treat plastic as waste, but rather as a renewable material, said Dr. Cassee. But if that seems like a tall order, it’s because it is.
“You’re a human being and you have a voice and there are a lot of other humans out there with voices,” said Dr. Leslie.
“You sign a petition in your community. You talk about it with your friends at the pub. If you’re a teacher, you discuss it in your class. You call your elected representatives and tell them what you think and how you want them to vote on bills.”
When people start working together, you can really amplify that voice, said Dr. Leslie.
What’s the bottom line right now, today?
Numerous sources have declared microplastics do not impact human health. But that’s largely because no direct evidence of this exists yet.
Even the WHO in its report suggests that progress must happen if we’re to fully understand the scope of the problem.
“Strengthening of the evidence necessary for reliable characterization and quantification of the risks to human health posed by [nano- and microplastics] will require active participation by all stakeholders,” it said.
All researchers interviewed for this article agree we don’t have enough evidence to draw any definite conclusions. But “if you look at the wrong endpoints, things will look safe, until you look at the endpoint where it’s really causing the problem,” said Dr. Leslie.
We must research our blind spots and continually ask: Where could we be wrong?
“It is a problem; it’s not going to go away,” said Dr. Danopoulos. “It’s going to get worse, and will continue to get worse, not by something that we are doing now but by something we did 5 years ago.”
Perhaps the question to be asked, then, is the hardest to answer: Are we willing to wait for the science?
A version of this article first appeared on WebMD.com.
Uptake of high-sensitivity troponin assays lags in U.S. hospitals
Most hospitals in the United States have yet to transition from conventional to high-sensitivity cardiac troponin (hs-cTn) assays, despite their greater sensitivity for myocardial injury, a new National Cardiovascular Data Registry (NCDR) registry study indicates.
hs-cTn assays have been used in routine clinical practice in Europe, Canada, and Australia since 2010, but the first such assay did not gain approval in the United States until 2017. Although single-center studies have examined their efficacy and potential downstream consequences, few data exist on hs-cTn implementation nationally, explained study author Cian McCarthy, MB, BCh, BAO, Massachusetts General Hospital, Boston.
The results were published online in the Journal of the American College of Cardiology and will be presented Nov. 5 at the American Heart Association scientific sessions.
For the study, Dr. McCarthy and colleagues examined 550 hospitals participating in the NCDR Chest Pain-MI registry from January 2019 through September 2021.
Of the 251,000 patients included in the analysis (mean age, 64 years; 41.5% female), 155,049 had a non–ST-segment myocardial infarction (NSTEMI), 15,989 had unstable angina, and 79,962 had low-risk chest pain.
The hs-cTn assays included Roche Diagnostic’s Elecsys Gen5 STAT troponin T assay (23%); Abbott’s ARCHITECT STAT (17%); Beckman Coulter’s ACCESS (21%); and Siemens’ Atellica IM (18%), Dimension VISTA (14%), Dimension EXL (4%), and ADVIA Centaur (2%) troponin I assays.
During the study period, 11.5% of patients were evaluated with hs-cTn assays and the remainder were evaluated with conventional troponin assays. These patients were slightly older (65.0 vs. 64.0 years), more commonly White (83.1% vs. 79.9%), less likely to be of Hispanic or Latino ethnicity (8.9% vs. 10.0%), and less likely to be uninsured (6.8% vs. 8.3%; P for all < .001).
A slightly higher proportion of patients evaluated with hs-cTn assays were diagnosed with unstable angina (7.1% vs. 6.3%), a lower proportion with NSTEMI (61.1% vs. 61.9%), and a similar proportion with low-risk chest pain (31.8% vs. 31.9%) compared with those evaluated by conventional troponin assays.
Implementation, defined as at least 25% of patients evaluated by hs-cTn in each quarter, increased from 3.3% in the first quarter of 2019 to 32.6% in the third quarter of 2021 (P trend < .001).
Using higher implementation thresholds of at least 50% and 75% of patients evaluated by hs-cTn, the prevalence in 2021 was 28.9% and 24.7%, respectively.
“So still, the majority of the hospitals by the end of the third quarter 2021 were not using these assays,” Dr. McCarthy said.
Potential explanations for the slow uptake are that prospective comparative effectiveness trials of These assays have predominantly been in international populations and real-world data on U.S. implementation have been limited to integrated health networks at academic institutions.
Approval of several assays was also delayed and the study data cut off just before the October publication of the 2021 AHA/ACC Chest Pain guideline. “So, whether the chest pain guideline with the new class 1 recommendation for hs-cTn will lead to further uptake is something that will need to be looked at in the future,” he said.
Downstream testing
In adjusted analyses, hs-cTn use was associated with more echocardiography among patients with non-ST elevation–acute coronary syndrome (NSTE-ACS) (82.4% vs. 75.0%; odds ratio [OR], 1.43; 95% confidence interval [CI], 1.19-1.73), but not among those with low-risk chest pain (19.7% vs. 19.4%; OR, 0.93; 95% CI, 0.71-1.22) compared with conventional cTn assays.
Importantly, hs-cTn was not associated with a difference in stress testing or CT coronary angiography utilization.
Use of hs-cTn was associated with lower use of invasive coronary angiography among patients with low-risk chest pain (3.7% vs. 4.5%; OR, 0.73, 95% CI, 0.58-0.92) but similar use for NSTE-ACS (96.3% vs. 95.8%; OR, 0.99, 95% CI, 0.82-1.19).
Among patients with NSTE-ACS, there also was no difference in revascularization with percutaneous coronary intervention (PCI) (52.7% vs. 52.3%; OR, 0.99; 95% CI, 0.94-1.04) or coronary bypass graft surgery (9.4% vs. 9.1%; OR, 1.06; 95% CI, 0.94-1.18).
PCI (0.1% vs. 0.2%; P = .05) and bypass graft surgery (both 0.1%) were uncommon among patients with low-risk chest pain.
In-hospital mortality was similar among patients with low-risk chest pain evaluated using hs-cTn assays vs. conventional troponin assays (0% vs. 0.02%; P = .16) and among patients with NSTE-ACS (2.8% vs. 3.2%; OR, 0.98, 95% CI, 0.87-1.11).
Length of stay was slightly shorter with hs-cTn use for patients with low-risk chest pain (median, 5.8 vs. 6.2 hours; P < .001) and patients with NSTE-ACS (66.9 vs. 67.8 hours; P = .01).
“There was always a concern that maybe high-sensitivity cardiac troponin would dramatically increase testing and could even increase length of stay, but I think these data are reassuring, in that this study suggests high-sensitivity cardiac troponin is associated with a small reduction in length of stay and possibly more appropriate use of testing with echocardiography in STEMI and a reduction in invasive angiography in low-risk patients,” Dr. McCarthy said. “But the majority of hospitals haven’t implemented the assay.”
The authors pointed out that because registry entry of patients with low-risk chest pain and unstable angina is optional for participating sites, the percentage of patients with NSTEMI is higher than in typical chest pain analyses. This higher pretest probability for MI may thus affect post-test accuracy for a true positive result. “That stated, this is the exact scenario where higher sensitivity might be associated with favorable impact on utilization.”
Among other limitations: There was the potential for unmeasured confounders, the accuracy of diagnoses could not be confirmed, patients with type 2 MI were excluded from the registry, and post-discharge safety was not assessed.
“These data indicate further opportunities to more widely and effectively implement hs-cTn in the U.S. hospitals persist that could optimize care for patients with possible or definitive ACS,” Dr. McCarthy and colleagues concluded.
The study was funded by the American College of Cardiology’s National Cardiovascular Data Registry. Dr. McCarthy is supported by the National Heart, Lung, and Blood Institute and has received consulting income from Abbott Laboratories.
A version of this article first appeared on Medscape.com.
Most hospitals in the United States have yet to transition from conventional to high-sensitivity cardiac troponin (hs-cTn) assays, despite their greater sensitivity for myocardial injury, a new National Cardiovascular Data Registry (NCDR) registry study indicates.
hs-cTn assays have been used in routine clinical practice in Europe, Canada, and Australia since 2010, but the first such assay did not gain approval in the United States until 2017. Although single-center studies have examined their efficacy and potential downstream consequences, few data exist on hs-cTn implementation nationally, explained study author Cian McCarthy, MB, BCh, BAO, Massachusetts General Hospital, Boston.
The results were published online in the Journal of the American College of Cardiology and will be presented Nov. 5 at the American Heart Association scientific sessions.
For the study, Dr. McCarthy and colleagues examined 550 hospitals participating in the NCDR Chest Pain-MI registry from January 2019 through September 2021.
Of the 251,000 patients included in the analysis (mean age, 64 years; 41.5% female), 155,049 had a non–ST-segment myocardial infarction (NSTEMI), 15,989 had unstable angina, and 79,962 had low-risk chest pain.
The hs-cTn assays included Roche Diagnostic’s Elecsys Gen5 STAT troponin T assay (23%); Abbott’s ARCHITECT STAT (17%); Beckman Coulter’s ACCESS (21%); and Siemens’ Atellica IM (18%), Dimension VISTA (14%), Dimension EXL (4%), and ADVIA Centaur (2%) troponin I assays.
During the study period, 11.5% of patients were evaluated with hs-cTn assays and the remainder were evaluated with conventional troponin assays. These patients were slightly older (65.0 vs. 64.0 years), more commonly White (83.1% vs. 79.9%), less likely to be of Hispanic or Latino ethnicity (8.9% vs. 10.0%), and less likely to be uninsured (6.8% vs. 8.3%; P for all < .001).
A slightly higher proportion of patients evaluated with hs-cTn assays were diagnosed with unstable angina (7.1% vs. 6.3%), a lower proportion with NSTEMI (61.1% vs. 61.9%), and a similar proportion with low-risk chest pain (31.8% vs. 31.9%) compared with those evaluated by conventional troponin assays.
Implementation, defined as at least 25% of patients evaluated by hs-cTn in each quarter, increased from 3.3% in the first quarter of 2019 to 32.6% in the third quarter of 2021 (P trend < .001).
Using higher implementation thresholds of at least 50% and 75% of patients evaluated by hs-cTn, the prevalence in 2021 was 28.9% and 24.7%, respectively.
“So still, the majority of the hospitals by the end of the third quarter 2021 were not using these assays,” Dr. McCarthy said.
Potential explanations for the slow uptake are that prospective comparative effectiveness trials of These assays have predominantly been in international populations and real-world data on U.S. implementation have been limited to integrated health networks at academic institutions.
Approval of several assays was also delayed and the study data cut off just before the October publication of the 2021 AHA/ACC Chest Pain guideline. “So, whether the chest pain guideline with the new class 1 recommendation for hs-cTn will lead to further uptake is something that will need to be looked at in the future,” he said.
Downstream testing
In adjusted analyses, hs-cTn use was associated with more echocardiography among patients with non-ST elevation–acute coronary syndrome (NSTE-ACS) (82.4% vs. 75.0%; odds ratio [OR], 1.43; 95% confidence interval [CI], 1.19-1.73), but not among those with low-risk chest pain (19.7% vs. 19.4%; OR, 0.93; 95% CI, 0.71-1.22) compared with conventional cTn assays.
Importantly, hs-cTn was not associated with a difference in stress testing or CT coronary angiography utilization.
Use of hs-cTn was associated with lower use of invasive coronary angiography among patients with low-risk chest pain (3.7% vs. 4.5%; OR, 0.73, 95% CI, 0.58-0.92) but similar use for NSTE-ACS (96.3% vs. 95.8%; OR, 0.99, 95% CI, 0.82-1.19).
Among patients with NSTE-ACS, there also was no difference in revascularization with percutaneous coronary intervention (PCI) (52.7% vs. 52.3%; OR, 0.99; 95% CI, 0.94-1.04) or coronary bypass graft surgery (9.4% vs. 9.1%; OR, 1.06; 95% CI, 0.94-1.18).
PCI (0.1% vs. 0.2%; P = .05) and bypass graft surgery (both 0.1%) were uncommon among patients with low-risk chest pain.
In-hospital mortality was similar among patients with low-risk chest pain evaluated using hs-cTn assays vs. conventional troponin assays (0% vs. 0.02%; P = .16) and among patients with NSTE-ACS (2.8% vs. 3.2%; OR, 0.98, 95% CI, 0.87-1.11).
Length of stay was slightly shorter with hs-cTn use for patients with low-risk chest pain (median, 5.8 vs. 6.2 hours; P < .001) and patients with NSTE-ACS (66.9 vs. 67.8 hours; P = .01).
“There was always a concern that maybe high-sensitivity cardiac troponin would dramatically increase testing and could even increase length of stay, but I think these data are reassuring, in that this study suggests high-sensitivity cardiac troponin is associated with a small reduction in length of stay and possibly more appropriate use of testing with echocardiography in STEMI and a reduction in invasive angiography in low-risk patients,” Dr. McCarthy said. “But the majority of hospitals haven’t implemented the assay.”
The authors pointed out that because registry entry of patients with low-risk chest pain and unstable angina is optional for participating sites, the percentage of patients with NSTEMI is higher than in typical chest pain analyses. This higher pretest probability for MI may thus affect post-test accuracy for a true positive result. “That stated, this is the exact scenario where higher sensitivity might be associated with favorable impact on utilization.”
Among other limitations: There was the potential for unmeasured confounders, the accuracy of diagnoses could not be confirmed, patients with type 2 MI were excluded from the registry, and post-discharge safety was not assessed.
“These data indicate further opportunities to more widely and effectively implement hs-cTn in the U.S. hospitals persist that could optimize care for patients with possible or definitive ACS,” Dr. McCarthy and colleagues concluded.
The study was funded by the American College of Cardiology’s National Cardiovascular Data Registry. Dr. McCarthy is supported by the National Heart, Lung, and Blood Institute and has received consulting income from Abbott Laboratories.
A version of this article first appeared on Medscape.com.
Most hospitals in the United States have yet to transition from conventional to high-sensitivity cardiac troponin (hs-cTn) assays, despite their greater sensitivity for myocardial injury, a new National Cardiovascular Data Registry (NCDR) registry study indicates.
hs-cTn assays have been used in routine clinical practice in Europe, Canada, and Australia since 2010, but the first such assay did not gain approval in the United States until 2017. Although single-center studies have examined their efficacy and potential downstream consequences, few data exist on hs-cTn implementation nationally, explained study author Cian McCarthy, MB, BCh, BAO, Massachusetts General Hospital, Boston.
The results were published online in the Journal of the American College of Cardiology and will be presented Nov. 5 at the American Heart Association scientific sessions.
For the study, Dr. McCarthy and colleagues examined 550 hospitals participating in the NCDR Chest Pain-MI registry from January 2019 through September 2021.
Of the 251,000 patients included in the analysis (mean age, 64 years; 41.5% female), 155,049 had a non–ST-segment myocardial infarction (NSTEMI), 15,989 had unstable angina, and 79,962 had low-risk chest pain.
The hs-cTn assays included Roche Diagnostic’s Elecsys Gen5 STAT troponin T assay (23%); Abbott’s ARCHITECT STAT (17%); Beckman Coulter’s ACCESS (21%); and Siemens’ Atellica IM (18%), Dimension VISTA (14%), Dimension EXL (4%), and ADVIA Centaur (2%) troponin I assays.
During the study period, 11.5% of patients were evaluated with hs-cTn assays and the remainder were evaluated with conventional troponin assays. These patients were slightly older (65.0 vs. 64.0 years), more commonly White (83.1% vs. 79.9%), less likely to be of Hispanic or Latino ethnicity (8.9% vs. 10.0%), and less likely to be uninsured (6.8% vs. 8.3%; P for all < .001).
A slightly higher proportion of patients evaluated with hs-cTn assays were diagnosed with unstable angina (7.1% vs. 6.3%), a lower proportion with NSTEMI (61.1% vs. 61.9%), and a similar proportion with low-risk chest pain (31.8% vs. 31.9%) compared with those evaluated by conventional troponin assays.
Implementation, defined as at least 25% of patients evaluated by hs-cTn in each quarter, increased from 3.3% in the first quarter of 2019 to 32.6% in the third quarter of 2021 (P trend < .001).
Using higher implementation thresholds of at least 50% and 75% of patients evaluated by hs-cTn, the prevalence in 2021 was 28.9% and 24.7%, respectively.
“So still, the majority of the hospitals by the end of the third quarter 2021 were not using these assays,” Dr. McCarthy said.
Potential explanations for the slow uptake are that prospective comparative effectiveness trials of These assays have predominantly been in international populations and real-world data on U.S. implementation have been limited to integrated health networks at academic institutions.
Approval of several assays was also delayed and the study data cut off just before the October publication of the 2021 AHA/ACC Chest Pain guideline. “So, whether the chest pain guideline with the new class 1 recommendation for hs-cTn will lead to further uptake is something that will need to be looked at in the future,” he said.
Downstream testing
In adjusted analyses, hs-cTn use was associated with more echocardiography among patients with non-ST elevation–acute coronary syndrome (NSTE-ACS) (82.4% vs. 75.0%; odds ratio [OR], 1.43; 95% confidence interval [CI], 1.19-1.73), but not among those with low-risk chest pain (19.7% vs. 19.4%; OR, 0.93; 95% CI, 0.71-1.22) compared with conventional cTn assays.
Importantly, hs-cTn was not associated with a difference in stress testing or CT coronary angiography utilization.
Use of hs-cTn was associated with lower use of invasive coronary angiography among patients with low-risk chest pain (3.7% vs. 4.5%; OR, 0.73, 95% CI, 0.58-0.92) but similar use for NSTE-ACS (96.3% vs. 95.8%; OR, 0.99, 95% CI, 0.82-1.19).
Among patients with NSTE-ACS, there also was no difference in revascularization with percutaneous coronary intervention (PCI) (52.7% vs. 52.3%; OR, 0.99; 95% CI, 0.94-1.04) or coronary bypass graft surgery (9.4% vs. 9.1%; OR, 1.06; 95% CI, 0.94-1.18).
PCI (0.1% vs. 0.2%; P = .05) and bypass graft surgery (both 0.1%) were uncommon among patients with low-risk chest pain.
In-hospital mortality was similar among patients with low-risk chest pain evaluated using hs-cTn assays vs. conventional troponin assays (0% vs. 0.02%; P = .16) and among patients with NSTE-ACS (2.8% vs. 3.2%; OR, 0.98, 95% CI, 0.87-1.11).
Length of stay was slightly shorter with hs-cTn use for patients with low-risk chest pain (median, 5.8 vs. 6.2 hours; P < .001) and patients with NSTE-ACS (66.9 vs. 67.8 hours; P = .01).
“There was always a concern that maybe high-sensitivity cardiac troponin would dramatically increase testing and could even increase length of stay, but I think these data are reassuring, in that this study suggests high-sensitivity cardiac troponin is associated with a small reduction in length of stay and possibly more appropriate use of testing with echocardiography in STEMI and a reduction in invasive angiography in low-risk patients,” Dr. McCarthy said. “But the majority of hospitals haven’t implemented the assay.”
The authors pointed out that because registry entry of patients with low-risk chest pain and unstable angina is optional for participating sites, the percentage of patients with NSTEMI is higher than in typical chest pain analyses. This higher pretest probability for MI may thus affect post-test accuracy for a true positive result. “That stated, this is the exact scenario where higher sensitivity might be associated with favorable impact on utilization.”
Among other limitations: There was the potential for unmeasured confounders, the accuracy of diagnoses could not be confirmed, patients with type 2 MI were excluded from the registry, and post-discharge safety was not assessed.
“These data indicate further opportunities to more widely and effectively implement hs-cTn in the U.S. hospitals persist that could optimize care for patients with possible or definitive ACS,” Dr. McCarthy and colleagues concluded.
The study was funded by the American College of Cardiology’s National Cardiovascular Data Registry. Dr. McCarthy is supported by the National Heart, Lung, and Blood Institute and has received consulting income from Abbott Laboratories.
A version of this article first appeared on Medscape.com.
FROM AHA 2022
Race and gender: Tailoring treatment for sleep disorders is preferred and better
While trials of various interventions for obstructive sleep apnea and insomnia were effective, there was a strong suggestion that tailoring them according to the race/gender of the target populations strengthens engagement and improvements, according to a presentation by Dayna A. Johnson, PhD, MPH, at the annual meeting of the American College of Chest Physicians (CHEST).
Dr. Johnson, assistant professor at Emory University in Atlanta, stated that determinants of sleep disparities are multifactorial across the lifespan, from in utero to aging, but it was also important to focus on social determinants of poor sleep.
The complexity of factors, she said, calls for multilevel interventions beyond screening and treatment. In addition, neighborhood factors including safety, noise and light pollution, ventilation, and thermal comfort come into play.
Dr. Johnson cited the example of parents who work multiple jobs to provide for their families: “Minimum wage is not a livable wage, and parents may not be available to ensure that children have consistent bedtimes.” Interventions, she added, may have to be at the neighborhood level, including placing sleep specialists in the local neighborhood “where the need is.” Cleaning up a neighborhood reduces crime and overall health, while light shielding in public housing can lower light pollution.
Observing that African Americans have higher rates of obstructive sleep apnea, Dr. Johnson and colleagues designed a screening tool specifically for African Americans with five prediction models with increasing levels of factor measurements (from 4 to 10). The prediction accuracy across the models ascended in lockstep with the number of measures from 74.0% to 76.1%, with the simplest model including only age, body mass index, male sex, and snoring. The latter model added witnessed apneas, high depressive symptoms, two measures of waist and neck size, and sleepiness. Dr. Johnson pointed out that accuracy for well-established predictive models is notably lower: STOP-Bang score ranges from 56% to 66%; NoSAS ranges from 58% to 66% and the HCHS prediction model accuracy is 70%. Dr. Johnson said that a Latino model they developed was more accurate than the traditional models, but not as accurate as their model for African Americans.
Turning to specific interventions, and underscoring higher levels of stress and anxiety among African American and Hispanic populations, Dr. Johnson cited MINDS (Mindfulness Intervention to Improve Sleep and Reduce Diabetes Risk Among a Diverse Sample in Atlanta), her study at Emory University of mindfulness meditation. Although prior studies have confirmed sleep benefits of mindfulness meditation, studies tailored for African American or Hispanic populations have been lacking.
The MINDS pilot study investigators enrolled 17 individuals (mostly women, with a mixture of racial and ethnic groups comprising Black, White, Asian and Hispanic patients) with poor sleep quality as measured by the Pittsburgh Sleep Quality Index (PSQI). Most patients, Dr. Johnson said, were overweight. Because of COVID restrictions on clinic visits, the diabetes portion of the study was dropped. All participants received at least 3 days of instruction on mindfulness meditation, on dealing with stress and anxiety, and on optimum sleep health practices. While PSQI scores higher than 5 are considered to indicate poor sleep quality, the mean PSQI score at study outset in MINDS was 9.2, she stated.
After 30 days of the intervention, stress (on a perceived stress scale) was improved, as were PSQI scores and actigraphy measures of sleep duration, efficiency and wakefulness after sleep onset, Dr. Johnson reported. “Participants found the mindfulness app to be acceptable and appropriate, and to reduce time to falling asleep,” Dr. Johnson said.
Qualitative data gathered post intervention from four focus groups (two to six participants in each; 1-1.5 hours in length), revealed general acceptability of the MINDS app. It showed also that among those with 50% or more adherence to the intervention, time to falling asleep was reduced, as were sleep awakenings at night. The most striking finding, Dr. Johnson said, was that individuals from among racial/ethnic minorities expressed appreciation of the diversity of the meditation instructors, and said that they preferred instruction from a person of their own race and sex. Findings would be even more striking with a larger sample size, Dr. Johnson speculated.
Citing TASHE (Tailored Approach to Sleep Health Education), a further observational study on obstructive sleep apnea knowledge conducted at New York University, Dr. Johnson addressed the fact that current messages are not tailored to race/ethnic minorities with low-to-moderate symptom knowledge. Also, a 3-arm randomized clinical trial of Internet-delivered treatment (Sleep Healthy or SHUTI) with a version revised for Black women (SHUTI-BWHS) showed findings similar to those of other studies cited and suggested: “Tailoring may be necessary to increase uptake and sustainability and to improve sleep among racial/ethnic minorities.”
Dr. Johnson noted, in closing, that Black/African American individuals have higher risk for obstructive sleep apnea than that of their White counterparts and lower rates of screening for treatment.
Dr. Johnson’s research was funded by the National Institutes of Health; National Heart, Lung, and Blood Institute; Woodruff Health Sciences Center; Synergy Award; Rollins School of Public Health Dean’s Pilot and Innovation Award; and Georgia Center for Diabetes Translation Research Pilot and Feasibility award program. She reported no relevant conflicts.
While trials of various interventions for obstructive sleep apnea and insomnia were effective, there was a strong suggestion that tailoring them according to the race/gender of the target populations strengthens engagement and improvements, according to a presentation by Dayna A. Johnson, PhD, MPH, at the annual meeting of the American College of Chest Physicians (CHEST).
Dr. Johnson, assistant professor at Emory University in Atlanta, stated that determinants of sleep disparities are multifactorial across the lifespan, from in utero to aging, but it was also important to focus on social determinants of poor sleep.
The complexity of factors, she said, calls for multilevel interventions beyond screening and treatment. In addition, neighborhood factors including safety, noise and light pollution, ventilation, and thermal comfort come into play.
Dr. Johnson cited the example of parents who work multiple jobs to provide for their families: “Minimum wage is not a livable wage, and parents may not be available to ensure that children have consistent bedtimes.” Interventions, she added, may have to be at the neighborhood level, including placing sleep specialists in the local neighborhood “where the need is.” Cleaning up a neighborhood reduces crime and overall health, while light shielding in public housing can lower light pollution.
Observing that African Americans have higher rates of obstructive sleep apnea, Dr. Johnson and colleagues designed a screening tool specifically for African Americans with five prediction models with increasing levels of factor measurements (from 4 to 10). The prediction accuracy across the models ascended in lockstep with the number of measures from 74.0% to 76.1%, with the simplest model including only age, body mass index, male sex, and snoring. The latter model added witnessed apneas, high depressive symptoms, two measures of waist and neck size, and sleepiness. Dr. Johnson pointed out that accuracy for well-established predictive models is notably lower: STOP-Bang score ranges from 56% to 66%; NoSAS ranges from 58% to 66% and the HCHS prediction model accuracy is 70%. Dr. Johnson said that a Latino model they developed was more accurate than the traditional models, but not as accurate as their model for African Americans.
Turning to specific interventions, and underscoring higher levels of stress and anxiety among African American and Hispanic populations, Dr. Johnson cited MINDS (Mindfulness Intervention to Improve Sleep and Reduce Diabetes Risk Among a Diverse Sample in Atlanta), her study at Emory University of mindfulness meditation. Although prior studies have confirmed sleep benefits of mindfulness meditation, studies tailored for African American or Hispanic populations have been lacking.
The MINDS pilot study investigators enrolled 17 individuals (mostly women, with a mixture of racial and ethnic groups comprising Black, White, Asian and Hispanic patients) with poor sleep quality as measured by the Pittsburgh Sleep Quality Index (PSQI). Most patients, Dr. Johnson said, were overweight. Because of COVID restrictions on clinic visits, the diabetes portion of the study was dropped. All participants received at least 3 days of instruction on mindfulness meditation, on dealing with stress and anxiety, and on optimum sleep health practices. While PSQI scores higher than 5 are considered to indicate poor sleep quality, the mean PSQI score at study outset in MINDS was 9.2, she stated.
After 30 days of the intervention, stress (on a perceived stress scale) was improved, as were PSQI scores and actigraphy measures of sleep duration, efficiency and wakefulness after sleep onset, Dr. Johnson reported. “Participants found the mindfulness app to be acceptable and appropriate, and to reduce time to falling asleep,” Dr. Johnson said.
Qualitative data gathered post intervention from four focus groups (two to six participants in each; 1-1.5 hours in length), revealed general acceptability of the MINDS app. It showed also that among those with 50% or more adherence to the intervention, time to falling asleep was reduced, as were sleep awakenings at night. The most striking finding, Dr. Johnson said, was that individuals from among racial/ethnic minorities expressed appreciation of the diversity of the meditation instructors, and said that they preferred instruction from a person of their own race and sex. Findings would be even more striking with a larger sample size, Dr. Johnson speculated.
Citing TASHE (Tailored Approach to Sleep Health Education), a further observational study on obstructive sleep apnea knowledge conducted at New York University, Dr. Johnson addressed the fact that current messages are not tailored to race/ethnic minorities with low-to-moderate symptom knowledge. Also, a 3-arm randomized clinical trial of Internet-delivered treatment (Sleep Healthy or SHUTI) with a version revised for Black women (SHUTI-BWHS) showed findings similar to those of other studies cited and suggested: “Tailoring may be necessary to increase uptake and sustainability and to improve sleep among racial/ethnic minorities.”
Dr. Johnson noted, in closing, that Black/African American individuals have higher risk for obstructive sleep apnea than that of their White counterparts and lower rates of screening for treatment.
Dr. Johnson’s research was funded by the National Institutes of Health; National Heart, Lung, and Blood Institute; Woodruff Health Sciences Center; Synergy Award; Rollins School of Public Health Dean’s Pilot and Innovation Award; and Georgia Center for Diabetes Translation Research Pilot and Feasibility award program. She reported no relevant conflicts.
While trials of various interventions for obstructive sleep apnea and insomnia were effective, there was a strong suggestion that tailoring them according to the race/gender of the target populations strengthens engagement and improvements, according to a presentation by Dayna A. Johnson, PhD, MPH, at the annual meeting of the American College of Chest Physicians (CHEST).
Dr. Johnson, assistant professor at Emory University in Atlanta, stated that determinants of sleep disparities are multifactorial across the lifespan, from in utero to aging, but it was also important to focus on social determinants of poor sleep.
The complexity of factors, she said, calls for multilevel interventions beyond screening and treatment. In addition, neighborhood factors including safety, noise and light pollution, ventilation, and thermal comfort come into play.
Dr. Johnson cited the example of parents who work multiple jobs to provide for their families: “Minimum wage is not a livable wage, and parents may not be available to ensure that children have consistent bedtimes.” Interventions, she added, may have to be at the neighborhood level, including placing sleep specialists in the local neighborhood “where the need is.” Cleaning up a neighborhood reduces crime and overall health, while light shielding in public housing can lower light pollution.
Observing that African Americans have higher rates of obstructive sleep apnea, Dr. Johnson and colleagues designed a screening tool specifically for African Americans with five prediction models with increasing levels of factor measurements (from 4 to 10). The prediction accuracy across the models ascended in lockstep with the number of measures from 74.0% to 76.1%, with the simplest model including only age, body mass index, male sex, and snoring. The latter model added witnessed apneas, high depressive symptoms, two measures of waist and neck size, and sleepiness. Dr. Johnson pointed out that accuracy for well-established predictive models is notably lower: STOP-Bang score ranges from 56% to 66%; NoSAS ranges from 58% to 66% and the HCHS prediction model accuracy is 70%. Dr. Johnson said that a Latino model they developed was more accurate than the traditional models, but not as accurate as their model for African Americans.
Turning to specific interventions, and underscoring higher levels of stress and anxiety among African American and Hispanic populations, Dr. Johnson cited MINDS (Mindfulness Intervention to Improve Sleep and Reduce Diabetes Risk Among a Diverse Sample in Atlanta), her study at Emory University of mindfulness meditation. Although prior studies have confirmed sleep benefits of mindfulness meditation, studies tailored for African American or Hispanic populations have been lacking.
The MINDS pilot study investigators enrolled 17 individuals (mostly women, with a mixture of racial and ethnic groups comprising Black, White, Asian and Hispanic patients) with poor sleep quality as measured by the Pittsburgh Sleep Quality Index (PSQI). Most patients, Dr. Johnson said, were overweight. Because of COVID restrictions on clinic visits, the diabetes portion of the study was dropped. All participants received at least 3 days of instruction on mindfulness meditation, on dealing with stress and anxiety, and on optimum sleep health practices. While PSQI scores higher than 5 are considered to indicate poor sleep quality, the mean PSQI score at study outset in MINDS was 9.2, she stated.
After 30 days of the intervention, stress (on a perceived stress scale) was improved, as were PSQI scores and actigraphy measures of sleep duration, efficiency and wakefulness after sleep onset, Dr. Johnson reported. “Participants found the mindfulness app to be acceptable and appropriate, and to reduce time to falling asleep,” Dr. Johnson said.
Qualitative data gathered post intervention from four focus groups (two to six participants in each; 1-1.5 hours in length), revealed general acceptability of the MINDS app. It showed also that among those with 50% or more adherence to the intervention, time to falling asleep was reduced, as were sleep awakenings at night. The most striking finding, Dr. Johnson said, was that individuals from among racial/ethnic minorities expressed appreciation of the diversity of the meditation instructors, and said that they preferred instruction from a person of their own race and sex. Findings would be even more striking with a larger sample size, Dr. Johnson speculated.
Citing TASHE (Tailored Approach to Sleep Health Education), a further observational study on obstructive sleep apnea knowledge conducted at New York University, Dr. Johnson addressed the fact that current messages are not tailored to race/ethnic minorities with low-to-moderate symptom knowledge. Also, a 3-arm randomized clinical trial of Internet-delivered treatment (Sleep Healthy or SHUTI) with a version revised for Black women (SHUTI-BWHS) showed findings similar to those of other studies cited and suggested: “Tailoring may be necessary to increase uptake and sustainability and to improve sleep among racial/ethnic minorities.”
Dr. Johnson noted, in closing, that Black/African American individuals have higher risk for obstructive sleep apnea than that of their White counterparts and lower rates of screening for treatment.
Dr. Johnson’s research was funded by the National Institutes of Health; National Heart, Lung, and Blood Institute; Woodruff Health Sciences Center; Synergy Award; Rollins School of Public Health Dean’s Pilot and Innovation Award; and Georgia Center for Diabetes Translation Research Pilot and Feasibility award program. She reported no relevant conflicts.
FROM CHEST 2022
Mid-October flulike illness cases higher than past 5 years
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”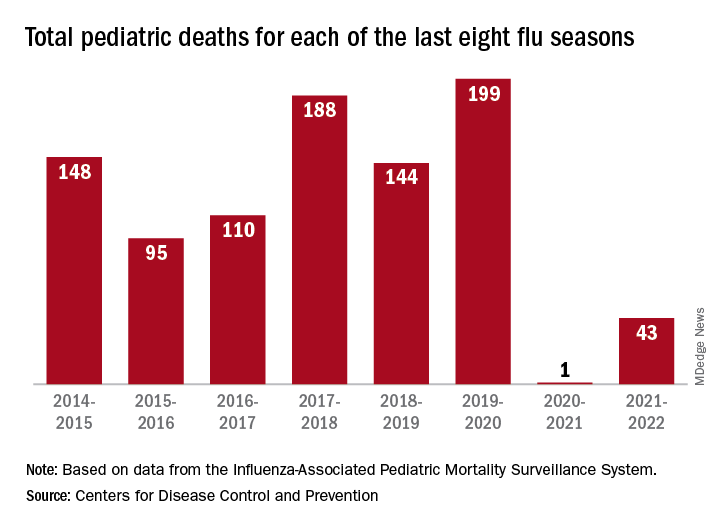
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Major depression treatments boost brain connectivity
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ECNP 2022
Medicare fines for high hospital readmissions drop, but nearly 2,300 facilities are still penalized
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.