User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Without guidelines, docs make their own long-COVID protocols
Treating the condition requires equal combinations of skill, experience, and intuition, and doctors waiting for guidelines have started cobbling together treatment plans designed to ease the worst symptoms.
Their work is urgent. In the United States alone, as many as 29 million people have long COVID, according to estimates from the American Academy of Physical Medicine and Rehabilitation.
“Patients with long COVID have on average at least 14 different symptoms involving nine or more different organ systems, so a holistic approach to treatment is essential,” said Janna Friedly, MD, executive director of the Post-COVID Rehabilitation and Recovery Clinic at the University of Washington in Seattle.
For acute COVID cases, the National Institutes of Health has treatment guidelines that are taking a lot of the guesswork out of managing patients’ complex mix of symptoms. This has made it easier for primary care providers to manage people with milder cases and for specialists to come up with effective treatment plans for those with severe illness. But no such guidelines exist for long COVID, and this is making it harder for many doctors – particularly in primary care – to determine the best treatment.
While there isn’t a single treatment that is effective for all long-COVID symptoms – and nothing is approved by the Food and Drug Administration specifically for this syndrome – doctors do have tools, Dr. Friedly said.
“We always start with the basics – making sure we help patients get enough restorative sleep, optimizing their nutrition, ensuring proper hydration, reducing stress, breathing exercises, and restorative exercise – because all of these are critically important to helping people’s immune system stay as healthy as possible,” she said. “In addition, we help people manage the anxiety and depression that may be exacerbating their symptoms.”
Fatigue is an obvious target. Widely available screening tools, including assessments that have been used in cancer patients and people with chronic fatigue syndrome, can pinpoint how bad symptoms are in long-COVID patients.
“Fatigue is generally the No. 1 symptom,” said Monica Verduzco-Gutierrez, MD, chair of rehabilitation medicine and director of the COVID-19 Recovery Clinic at the University of Texas Health Science Center in San Antonio. “If a patient has this, then their therapy program has to look very different, because they actually do better with pacing themselves.”
This was the first symptom tackled in a series of long-COVID treatment guidelines issued by the medical society representing many of the providers on the front lines with these patients every day – the American Academy of Physical Medicine and Rehabilitation. These fatigue guidelines stress the importance of rest, energy conservation, and proper hydration.
For patients with only mild fatigue who can still keep up with essential activities like work and school, activity programs may begin with a gradual return to daily routines such as housework or going out with friends. As long as they have no setbacks, patients can also start with light aerobic exercise and make it more intense and frequent over time. As long as they have no setbacks in symptoms, they can ramp up exercise by about 10% every 10 days.
But with severe fatigue, this is too much, too soon. Activity plans are more apt to start with only light stretching and progress to light muscle strengthening before any aerobic exercise enters the picture.
“Traditional exercise programs may be harmful to some patients with long COVID,” said Dr. Verduzco-Gutierrez. “Many cannot tolerate graded exercise [where exertion slowly ramps up], and it actually can make them worse.”
There’s less consensus on other options for treating fatigue, like prescription medications, dietary supplements, and acupuncture. Some doctors have tried prescription drugs like the antiviral and movement disorder medication amantadine, the narcolepsy drug modafinil, and the stimulant methylphenidate, which have been studied for managing fatigue in patients with other conditions like cancer, multiple sclerosis, traumatic brain injuries, and Parkinson’s disease. But there isn’t yet clear evidence from clinical trials about how well these options work for long COVID.
Similarly, interventions to tackle neurological symptoms and cognitive problems borrow a page from treatments used for other conditions like stroke and dementia – but require changes to meet the needs of those with long COVID. Four in five long-COVID patients with neurological and cognitive issues have brain fog, while more than two-thirds have headaches, and more than half have numbness and tingling in their extremities, loss of taste, loss of smell, and muscle pain, one study suggests.
Patients with deficits in areas like memory, attention, executive function, and visual and spatial planning may get speech therapy or occupational therapy, for example – both approaches that are common in people with cognitive decline caused by other medical conditions.
Doctors also promote good sleep practices and treating any mood disorders – both of which can contribute to cognitive problems. But they often have to skip one of the best interventions for improving brain function – exercise – because so many long-COVID patients struggle with fatigue and exertion or have cardiovascular issues that limit their exercise.
The lack of formal guidelines is especially a problem because there aren’t nearly enough specialists to manage the surge of patients who need treatment for issues like fatigue and brain fog. And without guidelines, primary care providers lack a reliable road map to guide referrals that many patients may need.
“Given the complexity of long COVID and the wide range of symptoms and medical issues associated with long COVID, most physicians, regardless of specialty, will need to evaluate and treat long-COVID symptoms,” said Dr. Friedly. “And yet, most do not have the knowledge or experience to effectively manage long-COVID symptoms, so having guidelines that can be updated as more research is conducted is critical.”
One barrier to developing guidelines for long COVID is the lack of research into the biological causes of fatigue and autonomic dysfunction – nervous system damage that can impact critical things like blood pressure, digestion, and body temperature – that affect so many long-COVID patients, said Alba Miranda Azola, MD, codirector of the Post-Acute COVID-19 Team at Johns Hopkins University in Baltimore.
Research is also progressing much more slowly for long COVID than it did for those hospitalized with severe acute infections. The logistics of running rigorous studies to prove which treatments work best for specific symptoms – information needed to create definitive treatment guidelines – are much more complicated for people with long COVID who live at home and may be too exhausted or too preoccupied with their daily lives to take part in research.
The vast number of symptoms, surfacing in different ways for each patient, also make it hard to isolate specific ways to manage specific long-COVID symptoms. Even when two patients have fatigue and brain fog, they may still need different treatments based on the complex mix of other symptoms they have.
“All long-COVID patients are not equal, and it is critical that research focuses on establishing specific descriptions of the disease,” Dr. Azola said.
The National Institutes of Health is working on this through its long-COVID Recover Initiative. It’s unclear how long it will take for this research to yield enough definitive information to inform long-COVID treatment guidelines similar to what the agency produced for acute coronavirus infections, and it didn’t respond to questions about the timeline.
But over the next few months, the National Institutes of Health expects to begin several clinical trials focused on some of the symptoms that doctors are seeing most often in their clinics, like fatigue, brain fog, exercise intolerance, sleep disturbances, and changes in the nervous system’s ability to regulate key functions like heart rate and body temperature.
One trial starting in January will examine whether the COVID-19 drug Paxlovid can help. A recent preprint Department of Veterans Affairs study showed patients treated with Paxlovid were less likely to get long COVID in the first place.
Some professionals aren’t waiting for the agency. The LongCovid Research Consortium links researchers from Harvard and Stanford universities; the University of California, San Francisco; the J. Craig Venter Institute; Johns Hopkins University; the University of Pennsylvania; Mount Sinai; Cardiff; and Yale who are studying, for instance, whether tiny blood clots contribute to long COVID and whether drugs can reduce or eliminate them.
“Given the widespread and diverse impact the virus has on the human body, it is unlikely that there will be one cure, one treatment,” said Gary H. Gibbons, MD, director of the National Heart, Lung, and Blood Institute at the National Institutes of Health. “This is why there will be multiple clinical trials over the coming months that study a range of symptoms, underlying causes, risk factors, outcomes, and potential strategies for treatment and prevention, in people of all races, ethnicities, genders, and ages.”
A version of this article first appeared on WebMD.com.
Treating the condition requires equal combinations of skill, experience, and intuition, and doctors waiting for guidelines have started cobbling together treatment plans designed to ease the worst symptoms.
Their work is urgent. In the United States alone, as many as 29 million people have long COVID, according to estimates from the American Academy of Physical Medicine and Rehabilitation.
“Patients with long COVID have on average at least 14 different symptoms involving nine or more different organ systems, so a holistic approach to treatment is essential,” said Janna Friedly, MD, executive director of the Post-COVID Rehabilitation and Recovery Clinic at the University of Washington in Seattle.
For acute COVID cases, the National Institutes of Health has treatment guidelines that are taking a lot of the guesswork out of managing patients’ complex mix of symptoms. This has made it easier for primary care providers to manage people with milder cases and for specialists to come up with effective treatment plans for those with severe illness. But no such guidelines exist for long COVID, and this is making it harder for many doctors – particularly in primary care – to determine the best treatment.
While there isn’t a single treatment that is effective for all long-COVID symptoms – and nothing is approved by the Food and Drug Administration specifically for this syndrome – doctors do have tools, Dr. Friedly said.
“We always start with the basics – making sure we help patients get enough restorative sleep, optimizing their nutrition, ensuring proper hydration, reducing stress, breathing exercises, and restorative exercise – because all of these are critically important to helping people’s immune system stay as healthy as possible,” she said. “In addition, we help people manage the anxiety and depression that may be exacerbating their symptoms.”
Fatigue is an obvious target. Widely available screening tools, including assessments that have been used in cancer patients and people with chronic fatigue syndrome, can pinpoint how bad symptoms are in long-COVID patients.
“Fatigue is generally the No. 1 symptom,” said Monica Verduzco-Gutierrez, MD, chair of rehabilitation medicine and director of the COVID-19 Recovery Clinic at the University of Texas Health Science Center in San Antonio. “If a patient has this, then their therapy program has to look very different, because they actually do better with pacing themselves.”
This was the first symptom tackled in a series of long-COVID treatment guidelines issued by the medical society representing many of the providers on the front lines with these patients every day – the American Academy of Physical Medicine and Rehabilitation. These fatigue guidelines stress the importance of rest, energy conservation, and proper hydration.
For patients with only mild fatigue who can still keep up with essential activities like work and school, activity programs may begin with a gradual return to daily routines such as housework or going out with friends. As long as they have no setbacks, patients can also start with light aerobic exercise and make it more intense and frequent over time. As long as they have no setbacks in symptoms, they can ramp up exercise by about 10% every 10 days.
But with severe fatigue, this is too much, too soon. Activity plans are more apt to start with only light stretching and progress to light muscle strengthening before any aerobic exercise enters the picture.
“Traditional exercise programs may be harmful to some patients with long COVID,” said Dr. Verduzco-Gutierrez. “Many cannot tolerate graded exercise [where exertion slowly ramps up], and it actually can make them worse.”
There’s less consensus on other options for treating fatigue, like prescription medications, dietary supplements, and acupuncture. Some doctors have tried prescription drugs like the antiviral and movement disorder medication amantadine, the narcolepsy drug modafinil, and the stimulant methylphenidate, which have been studied for managing fatigue in patients with other conditions like cancer, multiple sclerosis, traumatic brain injuries, and Parkinson’s disease. But there isn’t yet clear evidence from clinical trials about how well these options work for long COVID.
Similarly, interventions to tackle neurological symptoms and cognitive problems borrow a page from treatments used for other conditions like stroke and dementia – but require changes to meet the needs of those with long COVID. Four in five long-COVID patients with neurological and cognitive issues have brain fog, while more than two-thirds have headaches, and more than half have numbness and tingling in their extremities, loss of taste, loss of smell, and muscle pain, one study suggests.
Patients with deficits in areas like memory, attention, executive function, and visual and spatial planning may get speech therapy or occupational therapy, for example – both approaches that are common in people with cognitive decline caused by other medical conditions.
Doctors also promote good sleep practices and treating any mood disorders – both of which can contribute to cognitive problems. But they often have to skip one of the best interventions for improving brain function – exercise – because so many long-COVID patients struggle with fatigue and exertion or have cardiovascular issues that limit their exercise.
The lack of formal guidelines is especially a problem because there aren’t nearly enough specialists to manage the surge of patients who need treatment for issues like fatigue and brain fog. And without guidelines, primary care providers lack a reliable road map to guide referrals that many patients may need.
“Given the complexity of long COVID and the wide range of symptoms and medical issues associated with long COVID, most physicians, regardless of specialty, will need to evaluate and treat long-COVID symptoms,” said Dr. Friedly. “And yet, most do not have the knowledge or experience to effectively manage long-COVID symptoms, so having guidelines that can be updated as more research is conducted is critical.”
One barrier to developing guidelines for long COVID is the lack of research into the biological causes of fatigue and autonomic dysfunction – nervous system damage that can impact critical things like blood pressure, digestion, and body temperature – that affect so many long-COVID patients, said Alba Miranda Azola, MD, codirector of the Post-Acute COVID-19 Team at Johns Hopkins University in Baltimore.
Research is also progressing much more slowly for long COVID than it did for those hospitalized with severe acute infections. The logistics of running rigorous studies to prove which treatments work best for specific symptoms – information needed to create definitive treatment guidelines – are much more complicated for people with long COVID who live at home and may be too exhausted or too preoccupied with their daily lives to take part in research.
The vast number of symptoms, surfacing in different ways for each patient, also make it hard to isolate specific ways to manage specific long-COVID symptoms. Even when two patients have fatigue and brain fog, they may still need different treatments based on the complex mix of other symptoms they have.
“All long-COVID patients are not equal, and it is critical that research focuses on establishing specific descriptions of the disease,” Dr. Azola said.
The National Institutes of Health is working on this through its long-COVID Recover Initiative. It’s unclear how long it will take for this research to yield enough definitive information to inform long-COVID treatment guidelines similar to what the agency produced for acute coronavirus infections, and it didn’t respond to questions about the timeline.
But over the next few months, the National Institutes of Health expects to begin several clinical trials focused on some of the symptoms that doctors are seeing most often in their clinics, like fatigue, brain fog, exercise intolerance, sleep disturbances, and changes in the nervous system’s ability to regulate key functions like heart rate and body temperature.
One trial starting in January will examine whether the COVID-19 drug Paxlovid can help. A recent preprint Department of Veterans Affairs study showed patients treated with Paxlovid were less likely to get long COVID in the first place.
Some professionals aren’t waiting for the agency. The LongCovid Research Consortium links researchers from Harvard and Stanford universities; the University of California, San Francisco; the J. Craig Venter Institute; Johns Hopkins University; the University of Pennsylvania; Mount Sinai; Cardiff; and Yale who are studying, for instance, whether tiny blood clots contribute to long COVID and whether drugs can reduce or eliminate them.
“Given the widespread and diverse impact the virus has on the human body, it is unlikely that there will be one cure, one treatment,” said Gary H. Gibbons, MD, director of the National Heart, Lung, and Blood Institute at the National Institutes of Health. “This is why there will be multiple clinical trials over the coming months that study a range of symptoms, underlying causes, risk factors, outcomes, and potential strategies for treatment and prevention, in people of all races, ethnicities, genders, and ages.”
A version of this article first appeared on WebMD.com.
Treating the condition requires equal combinations of skill, experience, and intuition, and doctors waiting for guidelines have started cobbling together treatment plans designed to ease the worst symptoms.
Their work is urgent. In the United States alone, as many as 29 million people have long COVID, according to estimates from the American Academy of Physical Medicine and Rehabilitation.
“Patients with long COVID have on average at least 14 different symptoms involving nine or more different organ systems, so a holistic approach to treatment is essential,” said Janna Friedly, MD, executive director of the Post-COVID Rehabilitation and Recovery Clinic at the University of Washington in Seattle.
For acute COVID cases, the National Institutes of Health has treatment guidelines that are taking a lot of the guesswork out of managing patients’ complex mix of symptoms. This has made it easier for primary care providers to manage people with milder cases and for specialists to come up with effective treatment plans for those with severe illness. But no such guidelines exist for long COVID, and this is making it harder for many doctors – particularly in primary care – to determine the best treatment.
While there isn’t a single treatment that is effective for all long-COVID symptoms – and nothing is approved by the Food and Drug Administration specifically for this syndrome – doctors do have tools, Dr. Friedly said.
“We always start with the basics – making sure we help patients get enough restorative sleep, optimizing their nutrition, ensuring proper hydration, reducing stress, breathing exercises, and restorative exercise – because all of these are critically important to helping people’s immune system stay as healthy as possible,” she said. “In addition, we help people manage the anxiety and depression that may be exacerbating their symptoms.”
Fatigue is an obvious target. Widely available screening tools, including assessments that have been used in cancer patients and people with chronic fatigue syndrome, can pinpoint how bad symptoms are in long-COVID patients.
“Fatigue is generally the No. 1 symptom,” said Monica Verduzco-Gutierrez, MD, chair of rehabilitation medicine and director of the COVID-19 Recovery Clinic at the University of Texas Health Science Center in San Antonio. “If a patient has this, then their therapy program has to look very different, because they actually do better with pacing themselves.”
This was the first symptom tackled in a series of long-COVID treatment guidelines issued by the medical society representing many of the providers on the front lines with these patients every day – the American Academy of Physical Medicine and Rehabilitation. These fatigue guidelines stress the importance of rest, energy conservation, and proper hydration.
For patients with only mild fatigue who can still keep up with essential activities like work and school, activity programs may begin with a gradual return to daily routines such as housework or going out with friends. As long as they have no setbacks, patients can also start with light aerobic exercise and make it more intense and frequent over time. As long as they have no setbacks in symptoms, they can ramp up exercise by about 10% every 10 days.
But with severe fatigue, this is too much, too soon. Activity plans are more apt to start with only light stretching and progress to light muscle strengthening before any aerobic exercise enters the picture.
“Traditional exercise programs may be harmful to some patients with long COVID,” said Dr. Verduzco-Gutierrez. “Many cannot tolerate graded exercise [where exertion slowly ramps up], and it actually can make them worse.”
There’s less consensus on other options for treating fatigue, like prescription medications, dietary supplements, and acupuncture. Some doctors have tried prescription drugs like the antiviral and movement disorder medication amantadine, the narcolepsy drug modafinil, and the stimulant methylphenidate, which have been studied for managing fatigue in patients with other conditions like cancer, multiple sclerosis, traumatic brain injuries, and Parkinson’s disease. But there isn’t yet clear evidence from clinical trials about how well these options work for long COVID.
Similarly, interventions to tackle neurological symptoms and cognitive problems borrow a page from treatments used for other conditions like stroke and dementia – but require changes to meet the needs of those with long COVID. Four in five long-COVID patients with neurological and cognitive issues have brain fog, while more than two-thirds have headaches, and more than half have numbness and tingling in their extremities, loss of taste, loss of smell, and muscle pain, one study suggests.
Patients with deficits in areas like memory, attention, executive function, and visual and spatial planning may get speech therapy or occupational therapy, for example – both approaches that are common in people with cognitive decline caused by other medical conditions.
Doctors also promote good sleep practices and treating any mood disorders – both of which can contribute to cognitive problems. But they often have to skip one of the best interventions for improving brain function – exercise – because so many long-COVID patients struggle with fatigue and exertion or have cardiovascular issues that limit their exercise.
The lack of formal guidelines is especially a problem because there aren’t nearly enough specialists to manage the surge of patients who need treatment for issues like fatigue and brain fog. And without guidelines, primary care providers lack a reliable road map to guide referrals that many patients may need.
“Given the complexity of long COVID and the wide range of symptoms and medical issues associated with long COVID, most physicians, regardless of specialty, will need to evaluate and treat long-COVID symptoms,” said Dr. Friedly. “And yet, most do not have the knowledge or experience to effectively manage long-COVID symptoms, so having guidelines that can be updated as more research is conducted is critical.”
One barrier to developing guidelines for long COVID is the lack of research into the biological causes of fatigue and autonomic dysfunction – nervous system damage that can impact critical things like blood pressure, digestion, and body temperature – that affect so many long-COVID patients, said Alba Miranda Azola, MD, codirector of the Post-Acute COVID-19 Team at Johns Hopkins University in Baltimore.
Research is also progressing much more slowly for long COVID than it did for those hospitalized with severe acute infections. The logistics of running rigorous studies to prove which treatments work best for specific symptoms – information needed to create definitive treatment guidelines – are much more complicated for people with long COVID who live at home and may be too exhausted or too preoccupied with their daily lives to take part in research.
The vast number of symptoms, surfacing in different ways for each patient, also make it hard to isolate specific ways to manage specific long-COVID symptoms. Even when two patients have fatigue and brain fog, they may still need different treatments based on the complex mix of other symptoms they have.
“All long-COVID patients are not equal, and it is critical that research focuses on establishing specific descriptions of the disease,” Dr. Azola said.
The National Institutes of Health is working on this through its long-COVID Recover Initiative. It’s unclear how long it will take for this research to yield enough definitive information to inform long-COVID treatment guidelines similar to what the agency produced for acute coronavirus infections, and it didn’t respond to questions about the timeline.
But over the next few months, the National Institutes of Health expects to begin several clinical trials focused on some of the symptoms that doctors are seeing most often in their clinics, like fatigue, brain fog, exercise intolerance, sleep disturbances, and changes in the nervous system’s ability to regulate key functions like heart rate and body temperature.
One trial starting in January will examine whether the COVID-19 drug Paxlovid can help. A recent preprint Department of Veterans Affairs study showed patients treated with Paxlovid were less likely to get long COVID in the first place.
Some professionals aren’t waiting for the agency. The LongCovid Research Consortium links researchers from Harvard and Stanford universities; the University of California, San Francisco; the J. Craig Venter Institute; Johns Hopkins University; the University of Pennsylvania; Mount Sinai; Cardiff; and Yale who are studying, for instance, whether tiny blood clots contribute to long COVID and whether drugs can reduce or eliminate them.
“Given the widespread and diverse impact the virus has on the human body, it is unlikely that there will be one cure, one treatment,” said Gary H. Gibbons, MD, director of the National Heart, Lung, and Blood Institute at the National Institutes of Health. “This is why there will be multiple clinical trials over the coming months that study a range of symptoms, underlying causes, risk factors, outcomes, and potential strategies for treatment and prevention, in people of all races, ethnicities, genders, and ages.”
A version of this article first appeared on WebMD.com.
Opt-out HIV testing in EDs can help identify undiagnosed cases
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
COPD care bundle curbs all-cause readmissions
at 30, 60, and 90 days, based on data from approximately 300 patients.
COPD remains a leading cause of mortality and a leading contributor to health care costs, but data suggest that adoption of an interdisciplinary care bundle could reduce hospital readmission for COPD patients, Sibyl Cherian, PharmD, BCPS, of Overlook Medical Center, Summit, N.J., and colleagues wrote. The Centers for Medicare & Medicaid Services has introduced both penalties and bundled payments for hospitals with excess all-cause readmission rates after hospitalizations, but more data are needed on the ability of a COPD care bundle to reduce readmission for COPD.
In a study published in the Journal of the American Pharmacists Association, the researchers assigned 127 individuals with COPD to a COPD care bundle arm and 189 to a control arm for treatment at a single center. The standard of care group was admitted between Jan. 1 and Dec. 31, 2017; the COPD care bundle group was admitted between Jan. 1 and Dec. 31, 2018. The mean age of the participants across both groups was 72 years, and more than 70% of patients in each group were White. The COPD care bundle was managed by a team including pulmonologists, hospitalists, care managers, advanced practice nurses, pharmacists, respiratory care practitioners, physical therapists, documentation specialists, quality improvement experts, social workers, and dietitians.
The primary outcome was 30-day all-cause readmission among adults with acute exacerbation of COPD.
Overall, the rate of 30-day all-cause readmissions was significantly lower in the COPD care bundle arm versus the control arm (11.8% vs. 21.7%; P = .017). Similar differences appeared between the care bundle group and control group for all-cause readmissions at 60 days (8.7% vs. 18%; P = .013) and 90 days (4.7% vs. 19.6%; P < .001).
Reasons for reduced readmissions after implementation of the COPD care bundle included pulmonary follow-up appointments of 7 days or less, significantly increased physical therapy consults, and significant escalation of COPD maintenance therapy, the researchers wrote.
Notably, pharmacists consulted with 68.5% of patients overall and assisted with access to outpatient medications for 45.7% of those in the care bundle arm, the researchers wrote. Patients in the COPD care bundle group were significantly more likely to have an escalation in maintenance therapy versus the control patients (44.9% vs. 22.2%; P < .001), which illustrates the importance of interventions by pharmacists in escalating therapy to reduce readmissions.
The study findings were limited by several factors including the retrospective design and use of data from a single center, the researchers noted. Other limitations included the lack of data on the need for therapy escalation in the control group and by the lack of controlling for socioeconomic status, which is a known risk factor for hospital readmission.
However, the results support the value of a COPD care bundle for reducing readmissions, and that such a bundle can be replicated at other hospitals, although more research is needed to evaluate the impact of other COPD care strategies, they emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose.
at 30, 60, and 90 days, based on data from approximately 300 patients.
COPD remains a leading cause of mortality and a leading contributor to health care costs, but data suggest that adoption of an interdisciplinary care bundle could reduce hospital readmission for COPD patients, Sibyl Cherian, PharmD, BCPS, of Overlook Medical Center, Summit, N.J., and colleagues wrote. The Centers for Medicare & Medicaid Services has introduced both penalties and bundled payments for hospitals with excess all-cause readmission rates after hospitalizations, but more data are needed on the ability of a COPD care bundle to reduce readmission for COPD.
In a study published in the Journal of the American Pharmacists Association, the researchers assigned 127 individuals with COPD to a COPD care bundle arm and 189 to a control arm for treatment at a single center. The standard of care group was admitted between Jan. 1 and Dec. 31, 2017; the COPD care bundle group was admitted between Jan. 1 and Dec. 31, 2018. The mean age of the participants across both groups was 72 years, and more than 70% of patients in each group were White. The COPD care bundle was managed by a team including pulmonologists, hospitalists, care managers, advanced practice nurses, pharmacists, respiratory care practitioners, physical therapists, documentation specialists, quality improvement experts, social workers, and dietitians.
The primary outcome was 30-day all-cause readmission among adults with acute exacerbation of COPD.
Overall, the rate of 30-day all-cause readmissions was significantly lower in the COPD care bundle arm versus the control arm (11.8% vs. 21.7%; P = .017). Similar differences appeared between the care bundle group and control group for all-cause readmissions at 60 days (8.7% vs. 18%; P = .013) and 90 days (4.7% vs. 19.6%; P < .001).
Reasons for reduced readmissions after implementation of the COPD care bundle included pulmonary follow-up appointments of 7 days or less, significantly increased physical therapy consults, and significant escalation of COPD maintenance therapy, the researchers wrote.
Notably, pharmacists consulted with 68.5% of patients overall and assisted with access to outpatient medications for 45.7% of those in the care bundle arm, the researchers wrote. Patients in the COPD care bundle group were significantly more likely to have an escalation in maintenance therapy versus the control patients (44.9% vs. 22.2%; P < .001), which illustrates the importance of interventions by pharmacists in escalating therapy to reduce readmissions.
The study findings were limited by several factors including the retrospective design and use of data from a single center, the researchers noted. Other limitations included the lack of data on the need for therapy escalation in the control group and by the lack of controlling for socioeconomic status, which is a known risk factor for hospital readmission.
However, the results support the value of a COPD care bundle for reducing readmissions, and that such a bundle can be replicated at other hospitals, although more research is needed to evaluate the impact of other COPD care strategies, they emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose.
at 30, 60, and 90 days, based on data from approximately 300 patients.
COPD remains a leading cause of mortality and a leading contributor to health care costs, but data suggest that adoption of an interdisciplinary care bundle could reduce hospital readmission for COPD patients, Sibyl Cherian, PharmD, BCPS, of Overlook Medical Center, Summit, N.J., and colleagues wrote. The Centers for Medicare & Medicaid Services has introduced both penalties and bundled payments for hospitals with excess all-cause readmission rates after hospitalizations, but more data are needed on the ability of a COPD care bundle to reduce readmission for COPD.
In a study published in the Journal of the American Pharmacists Association, the researchers assigned 127 individuals with COPD to a COPD care bundle arm and 189 to a control arm for treatment at a single center. The standard of care group was admitted between Jan. 1 and Dec. 31, 2017; the COPD care bundle group was admitted between Jan. 1 and Dec. 31, 2018. The mean age of the participants across both groups was 72 years, and more than 70% of patients in each group were White. The COPD care bundle was managed by a team including pulmonologists, hospitalists, care managers, advanced practice nurses, pharmacists, respiratory care practitioners, physical therapists, documentation specialists, quality improvement experts, social workers, and dietitians.
The primary outcome was 30-day all-cause readmission among adults with acute exacerbation of COPD.
Overall, the rate of 30-day all-cause readmissions was significantly lower in the COPD care bundle arm versus the control arm (11.8% vs. 21.7%; P = .017). Similar differences appeared between the care bundle group and control group for all-cause readmissions at 60 days (8.7% vs. 18%; P = .013) and 90 days (4.7% vs. 19.6%; P < .001).
Reasons for reduced readmissions after implementation of the COPD care bundle included pulmonary follow-up appointments of 7 days or less, significantly increased physical therapy consults, and significant escalation of COPD maintenance therapy, the researchers wrote.
Notably, pharmacists consulted with 68.5% of patients overall and assisted with access to outpatient medications for 45.7% of those in the care bundle arm, the researchers wrote. Patients in the COPD care bundle group were significantly more likely to have an escalation in maintenance therapy versus the control patients (44.9% vs. 22.2%; P < .001), which illustrates the importance of interventions by pharmacists in escalating therapy to reduce readmissions.
The study findings were limited by several factors including the retrospective design and use of data from a single center, the researchers noted. Other limitations included the lack of data on the need for therapy escalation in the control group and by the lack of controlling for socioeconomic status, which is a known risk factor for hospital readmission.
However, the results support the value of a COPD care bundle for reducing readmissions, and that such a bundle can be replicated at other hospitals, although more research is needed to evaluate the impact of other COPD care strategies, they emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN PHARMACISTS ASSOCIATION
The right indoor relative humidity could ward off COVID
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF THE ROYAL SOCIETY INTERFACE
Patient safety in hospitals improved in past decade: Report
, according to the 10th annual report from nonprofit the Leapfrog Group, a national nonprofit organization focused on health care safety and quality.
For five outcome measures, the safety improvements saved an estimated 16,000 lives during the 10-year period, the report said. These included two “never” events that both declined by approximately 25%: incidents of falls and trauma and incidents of objects unintentionally left in a body after surgery.
There were also decreases in three health care–associated infections, including methicillin-resistant Staphylococcus aureus (MRSA), which decreased by 22%; central line–associated bloodstream infection (CLABSI), which fell by 43%; and Clostridioides difficile infection (C. Diff), which declined by 8%.
The patient safety record of U.S. hospitals improved over the past decade, according to the report.
“Never in history have we seen across-the-board improvement in patient safety until this last decade, coinciding with the history of the [Leapfrog] Hospital Safety Grade,” said Leah Binder, president and CEO of the Leapfrog Group, in a news release. “We salute hospitals for this milestone and encourage them to accelerate their hard work saving patient lives.”
During the past decade, the report noted, hospitals have widely adopted technology and staffing strategies that can protect patients from preventable harm and death. Leapfrog cited a nearly sevenfold increase in the adoption of computerized provider order entry, which can reduce medication errors by more than 40%.
However, federal health officials separately have reported that the pandemic may have eroded some of those gains.
The Leapfrog report also cited a recent study, published in JAMA, that found that the rates of preventable adverse events in hospitalized patients – including adverse drug events, hospital-acquired infections, postprocedure events, and hospital-acquired pressure ulcers and falls – significantly declined between 2010 and 2019.
That study pointed to specific decreases in the rates of adverse events for patients admitted for myocardial infarction, heart failure, pneumonia, and major surgical procedures. There were also significant drops in adverse events for all other conditions, the study found.
Quality improvement efforts targeting those four conditions might have partly accounted for the lower rates of adverse events in patients with the conditions, the study observed. But “similar interventions did not occur for most of the conditions represented in the ‘all other conditions’ group,” it said.
In a 2019 report by the U.S. Agency for Healthcare Research and Quality (AHRQ), the agency noted that from 2000 to 2017, there had been gains in nearly two-thirds of patient-safety measures in acute, post-acute, and ambulatory care. Hospital safety improved on nine metrics and was unchanged on three. For example, from 2014 to 2017, the number of some hospital-acquired conditions, including adverse drug events and C. Diff infections, dropped about 20%.
However, in an article this past February, officials of the Centers for Medicare & Medicaid Services (CMS) said they had observed deterioration on multiple patient-safety metrics since the start of the pandemic. For example, central line infections, which had dropped by 31% in the five years before the COVID-19 outbreak, jumped 28% in the second quarter of 2020, compared with the prior-year period.
Commenting on these developments, the CMS authors said “the fact that the pandemic degraded patient safety so quickly and severely suggests that our health care system lacks a sufficiently resilient safety culture and infrastructure.”
A version of this article first appeared on Medscape.com.
, according to the 10th annual report from nonprofit the Leapfrog Group, a national nonprofit organization focused on health care safety and quality.
For five outcome measures, the safety improvements saved an estimated 16,000 lives during the 10-year period, the report said. These included two “never” events that both declined by approximately 25%: incidents of falls and trauma and incidents of objects unintentionally left in a body after surgery.
There were also decreases in three health care–associated infections, including methicillin-resistant Staphylococcus aureus (MRSA), which decreased by 22%; central line–associated bloodstream infection (CLABSI), which fell by 43%; and Clostridioides difficile infection (C. Diff), which declined by 8%.
The patient safety record of U.S. hospitals improved over the past decade, according to the report.
“Never in history have we seen across-the-board improvement in patient safety until this last decade, coinciding with the history of the [Leapfrog] Hospital Safety Grade,” said Leah Binder, president and CEO of the Leapfrog Group, in a news release. “We salute hospitals for this milestone and encourage them to accelerate their hard work saving patient lives.”
During the past decade, the report noted, hospitals have widely adopted technology and staffing strategies that can protect patients from preventable harm and death. Leapfrog cited a nearly sevenfold increase in the adoption of computerized provider order entry, which can reduce medication errors by more than 40%.
However, federal health officials separately have reported that the pandemic may have eroded some of those gains.
The Leapfrog report also cited a recent study, published in JAMA, that found that the rates of preventable adverse events in hospitalized patients – including adverse drug events, hospital-acquired infections, postprocedure events, and hospital-acquired pressure ulcers and falls – significantly declined between 2010 and 2019.
That study pointed to specific decreases in the rates of adverse events for patients admitted for myocardial infarction, heart failure, pneumonia, and major surgical procedures. There were also significant drops in adverse events for all other conditions, the study found.
Quality improvement efforts targeting those four conditions might have partly accounted for the lower rates of adverse events in patients with the conditions, the study observed. But “similar interventions did not occur for most of the conditions represented in the ‘all other conditions’ group,” it said.
In a 2019 report by the U.S. Agency for Healthcare Research and Quality (AHRQ), the agency noted that from 2000 to 2017, there had been gains in nearly two-thirds of patient-safety measures in acute, post-acute, and ambulatory care. Hospital safety improved on nine metrics and was unchanged on three. For example, from 2014 to 2017, the number of some hospital-acquired conditions, including adverse drug events and C. Diff infections, dropped about 20%.
However, in an article this past February, officials of the Centers for Medicare & Medicaid Services (CMS) said they had observed deterioration on multiple patient-safety metrics since the start of the pandemic. For example, central line infections, which had dropped by 31% in the five years before the COVID-19 outbreak, jumped 28% in the second quarter of 2020, compared with the prior-year period.
Commenting on these developments, the CMS authors said “the fact that the pandemic degraded patient safety so quickly and severely suggests that our health care system lacks a sufficiently resilient safety culture and infrastructure.”
A version of this article first appeared on Medscape.com.
, according to the 10th annual report from nonprofit the Leapfrog Group, a national nonprofit organization focused on health care safety and quality.
For five outcome measures, the safety improvements saved an estimated 16,000 lives during the 10-year period, the report said. These included two “never” events that both declined by approximately 25%: incidents of falls and trauma and incidents of objects unintentionally left in a body after surgery.
There were also decreases in three health care–associated infections, including methicillin-resistant Staphylococcus aureus (MRSA), which decreased by 22%; central line–associated bloodstream infection (CLABSI), which fell by 43%; and Clostridioides difficile infection (C. Diff), which declined by 8%.
The patient safety record of U.S. hospitals improved over the past decade, according to the report.
“Never in history have we seen across-the-board improvement in patient safety until this last decade, coinciding with the history of the [Leapfrog] Hospital Safety Grade,” said Leah Binder, president and CEO of the Leapfrog Group, in a news release. “We salute hospitals for this milestone and encourage them to accelerate their hard work saving patient lives.”
During the past decade, the report noted, hospitals have widely adopted technology and staffing strategies that can protect patients from preventable harm and death. Leapfrog cited a nearly sevenfold increase in the adoption of computerized provider order entry, which can reduce medication errors by more than 40%.
However, federal health officials separately have reported that the pandemic may have eroded some of those gains.
The Leapfrog report also cited a recent study, published in JAMA, that found that the rates of preventable adverse events in hospitalized patients – including adverse drug events, hospital-acquired infections, postprocedure events, and hospital-acquired pressure ulcers and falls – significantly declined between 2010 and 2019.
That study pointed to specific decreases in the rates of adverse events for patients admitted for myocardial infarction, heart failure, pneumonia, and major surgical procedures. There were also significant drops in adverse events for all other conditions, the study found.
Quality improvement efforts targeting those four conditions might have partly accounted for the lower rates of adverse events in patients with the conditions, the study observed. But “similar interventions did not occur for most of the conditions represented in the ‘all other conditions’ group,” it said.
In a 2019 report by the U.S. Agency for Healthcare Research and Quality (AHRQ), the agency noted that from 2000 to 2017, there had been gains in nearly two-thirds of patient-safety measures in acute, post-acute, and ambulatory care. Hospital safety improved on nine metrics and was unchanged on three. For example, from 2014 to 2017, the number of some hospital-acquired conditions, including adverse drug events and C. Diff infections, dropped about 20%.
However, in an article this past February, officials of the Centers for Medicare & Medicaid Services (CMS) said they had observed deterioration on multiple patient-safety metrics since the start of the pandemic. For example, central line infections, which had dropped by 31% in the five years before the COVID-19 outbreak, jumped 28% in the second quarter of 2020, compared with the prior-year period.
Commenting on these developments, the CMS authors said “the fact that the pandemic degraded patient safety so quickly and severely suggests that our health care system lacks a sufficiently resilient safety culture and infrastructure.”
A version of this article first appeared on Medscape.com.
Meet the JCOM Author with Dr. Barkoudah: Neurosurgery Operating Room Efficiency During the COVID-19 Era
Meet the JCOM Author with Dr. Barkoudah: Quality of Life and Population Health in Behavioral Health Care

HDL cholesterol not linked to CHD risk in Blacks: REGARDS
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”

Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”
Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”
Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Children and COVID: Weekly cases maintain a low-level plateau
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.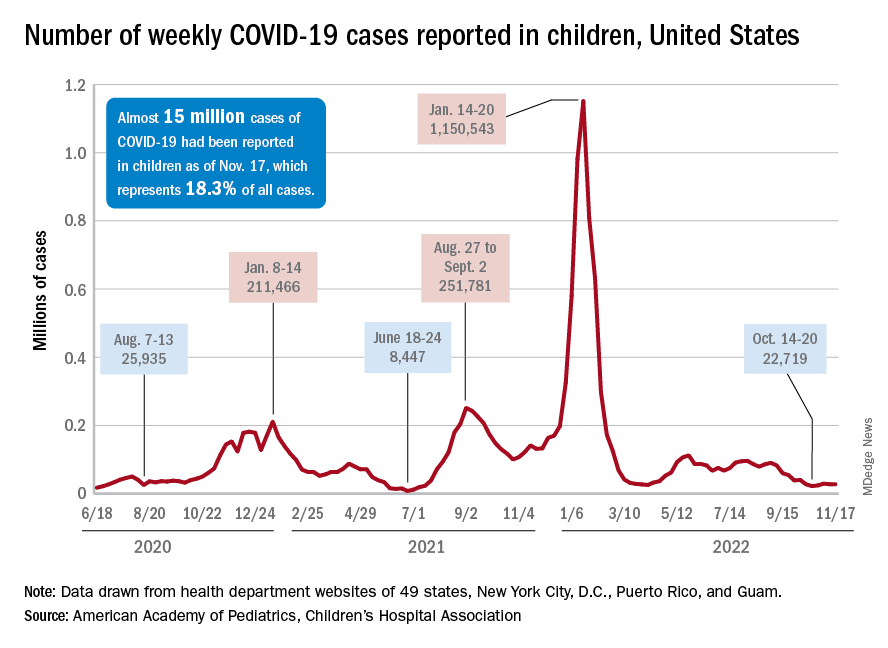
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
Will ICER review aid bid for Medicare to pay for obesity drugs?
A report from a well-respected nonprofit group may bolster efforts to have Medicare, the largest U.S. purchaser of prescription drugs, cover obesity medicines, for which there has been accumulating evidence of significant benefit.
The Institute for Clinical and Economic Review (ICER) released a report last month on obesity medicines, based on extensive review of research done to date and input from clinicians, drug-makers, and members of the public.
Of the treatments reviewed, the ICER report gave the best ratings to two Novo Nordisk products, a B+ for semaglutide (Wegovy) and a B for liraglutide (Saxenda), while also making the case for price cuts. At an annual U.S. net price estimated at $13,618, semaglutide exceeds what ICER considers typical cost-effectiveness thresholds. ICER suggested a benchmark annual price range for semaglutide of between $7,500 and $9,800.
The ICER report also directs insurers in general to provide more generous coverage of obesity medicines, with a specific recommendation for the U.S. Congress to pass a pending bill known as the Treat and Reduce Obesity Act of 2021. The bill would undo a restriction on weight-loss drugs in the Medicare Part D plans, which covered about 49 million people last year. Sen. Tom Carper (D-Del.) and Sen. Bill Cassidy, MD, (R-La.) have repeatedly introduced versions of the bill since 2013.
“In both chambers of Congress and with bipartisan support, we’ve pushed to expand Medicare coverage of additional therapies and medications to treat obesity,” Sen. Cassidy said in an email. “This report confirms what we’ve worked on for nearly a decade – our legislation will help improve lives.”
The current House version of the bill has the backing of more than a third of the members of that chamber, with 113 Democratic and 40 Republican cosponsors. The Senate version has 22 sponsors.
Changing views
The ICER report comes amid a broader change in how clinicians view obesity.
The American Academy of Pediatrics is readying a new Clinical Practice Guideline for the Evaluation and Treatment of Pediatric Obesity that will mark a major shift in approach. Aaron S. Kelly, PhD, a professor of pediatrics at the University of Minnesota, Minneapolis, described it as a “sea change,” with obesity now seen as “a chronic, refractory, relapsing disease,” for which watchful waiting is no longer appropriate.
But the field of obesity treatment looked quite different in the early 2000s when Congress worked on a plan to add a pharmacy benefit to Medicare.
The deliberate omission of obesity medicine in the Medicare Part D benefit reflected both the state of science at the time and U.S. experience with a dangerous weight-loss drug combo in the late 1990s.
Initial expectations for weight-loss pills were high after the Food and Drug Administration cleared dexfenfluramine HCl (Redux) in 1996, which was part of the popular fen-phen combination. “Newly Approved Diet Drug Promises to Help Millions of Obese Americans – But Is No Magic Bullet,” read a headline about the Redux approval in The Washington Post
When work began in the 2000s to create a Medicare pharmacy benefit, lawmakers and congressional staff had a pool of about $400 billion available to establish what became the Part D program, Joel White, a former House staffer who helped draft the law, told this news organization in an email exchange.
Given the state of obesity research at the time, it seemed to make sense to exclude weight-loss medications, wrote Mr. White. Mr. White is now chief executive of the consulting firm Horizon, which has clients in the drug industry including the Pharmaceutical Research and Manufacturers of America.
“Now we know that obesity is a chronic disease of epidemic proportions. Decades of research have produced a series of advances in the way we understand and treat obesity. While scientists and many who work directly with those impacted by this epidemic understand how treatments have advanced, the law lags behind,” Mr. White said.
XXXCurrent payment policies for obesity treatments are based on “outdated information and ongoing misperception,” he noted. “While Part D has been a resounding success, our Medicare approach to obesity is not.”
“In addition, it makes no sense that Medicare covers the most drastic procedure (bariatric surgery) but not less-invasive, effective treatments,” he added. “We should have long ago lifted restrictions based on advances in science and medicine.”
Overcoming the stigma
Scott Kahan, MD, MPH, agreed and hopes that the new ICER report will help more patients secure needed medications, raising a “call to arms” about the need for better coverage of obesity drugs.
Dr. Kahan is director of the National Center for Weight and Wellness, a private clinic in Washington, and chair of the clinical committee for The Obesity Society. He also served as a member of a policy roundtable that ICER convened as part of research on the report on obesity drugs. Dr. Kahan, who also serves on the faculty at the Johns Hopkins Bloomberg School of Public Health, Baltimore, has received fees from drug makers such as Eli Lilly.
The ICER report may help what Dr. Kahan described as well-founded caution about obesity treatments in general.
“When it comes to weight loss, there are all of these magical treatments that are sold on social media and traditional media. There are a lot of bad actors in terms of people calling themselves experts and gurus and promising all kinds of crazy stuff,” said Dr. Kahan.
And there are long-standing stigmas about obesity, he stressed.
“That underlies a lot of the backward policies, including poor coverage for medications and the noncoverage by Medicare,” Dr. Kahan said. “There’s a societal ingrained set of beliefs and misperceptions and biases. That takes time to unwind, and I think we’re on the way, but we’re not quite there yet.”
Lifestyle changes not enough to tackle obesity
AHIP (formerly America’s Health Insurance Plans) told this news organization its members consider ICER reports when making decisions about which products to cover. “And health plans already cover obesity treatments that they consider medically necessary,” said David Allen, an AHIP spokesperson.
“It is important to note that every treatment does not work for every patient, and many patients experience adverse events and may discontinue treatment,” he added in an email. “Health insurance providers play an important role in helping [health care] providers and patients identify the treatment options that are most likely to be effective as well as affordable.”
Separately, the nonprofit watchdog group Public Citizen cautioned against liraglutide on its Worst Pills, Best Pills website. In its view, the drug is minimally effective and has many dangerous adverse effects, which are even more frequent with the higher-dose weight-loss version (a lower-dose version is approved for type 2 diabetes).
“There is currently no medication that can be used safely to achieve weight loss effortlessly and without dangerous adverse effects,” the group said. “Rather than focus on losing weight by turning to risky drugs, overweight and obese adults seeking to achieve better health should make reasonable and sustainable changes to their lifestyle, such as eating a healthy diet and getting regular exercise.”
Yet, many people find there is little help available for making lifestyle changes, and some patients and physicians say these modifications by themselves are not enough.
“The vast majority of people with obesity cannot achieve sustained weight loss through diet and exercise alone,” said David Rind, MD, chief medical officer of ICER, in an Oct. 20 statement. “As such, obesity, and its resulting physical health, mental health, and social burdens, is not a choice or failing, but a medical condition.”
The focus should now be on assuring that effective medications “are priced in alignment with their benefits so that they are accessible and affordable across U.S. society,” Dr. Rind urges.
‘My own demise with a fork and knife’
ICER sought public feedback on a draft version of the report before finalizing it.
In their comments on ICER’s work, several pharmaceutical researchers and Novo Nordisk questioned the calculations used in making judgments about the value of obesity drugs. In a statement, Novo Nordisk told this news organization that the company’s view is that ICER’s modeling “does not adequately address the real-world complexities of obesity, and consequently underestimates the health and societal impact medical treatments can have.”
Commenters also dug into aspects of ICER’s calculations, including ones that consider quality-adjusted life-years (QALYs). ICER describes QALY as an academic standard for measuring how well all different types of medical treatments can extend or improve patients’ lives. In an explainer on its website, ICER says this metric has served as a fundamental component of cost-effectiveness analyses in the United States and around the world for more than 30 years.
ICER and drug makers have been at odds for some time, with PhRMA having criticized the nonprofit group. A 2020 Reuters article detailed public relations strategies used by firms paid by drug makers to raise questions about ICER’s work. Critics accuse it of allying with insurers.
ICER’s list of its recent financial supporters includes Blue Cross Blue Shield of Massachusetts and the Kaiser Foundation Health Plan, but also many other groups, such as the U.S. Department of Veterans Affairs, the American Academy of Neurology, and the American College of Rheumatology.
The public comments on the ICER report also include one from an unidentified woman who wrote of her past struggles to lose weight.
She said her health plan wouldn’t cover behavioral programs or semaglutide as a weight-loss drug but did cover it eventually because of signs that she had developed insulin resistance. The patient said the drug worked for her, whereas other approaches to control weight had failed.
“To put it simply, I now experience hunger and satiety in a way that I can only assume people with normal metabolism do. I am 49 years old and approaching the age where serious comorbidities associated with obesity begin to manifest,” the patient wrote.
“I no longer worry about bringing about my own demise with a fork and knife because of misfiring hunger cues.”
A version of this article first appeared on Medscape.com.
A report from a well-respected nonprofit group may bolster efforts to have Medicare, the largest U.S. purchaser of prescription drugs, cover obesity medicines, for which there has been accumulating evidence of significant benefit.
The Institute for Clinical and Economic Review (ICER) released a report last month on obesity medicines, based on extensive review of research done to date and input from clinicians, drug-makers, and members of the public.
Of the treatments reviewed, the ICER report gave the best ratings to two Novo Nordisk products, a B+ for semaglutide (Wegovy) and a B for liraglutide (Saxenda), while also making the case for price cuts. At an annual U.S. net price estimated at $13,618, semaglutide exceeds what ICER considers typical cost-effectiveness thresholds. ICER suggested a benchmark annual price range for semaglutide of between $7,500 and $9,800.
The ICER report also directs insurers in general to provide more generous coverage of obesity medicines, with a specific recommendation for the U.S. Congress to pass a pending bill known as the Treat and Reduce Obesity Act of 2021. The bill would undo a restriction on weight-loss drugs in the Medicare Part D plans, which covered about 49 million people last year. Sen. Tom Carper (D-Del.) and Sen. Bill Cassidy, MD, (R-La.) have repeatedly introduced versions of the bill since 2013.
“In both chambers of Congress and with bipartisan support, we’ve pushed to expand Medicare coverage of additional therapies and medications to treat obesity,” Sen. Cassidy said in an email. “This report confirms what we’ve worked on for nearly a decade – our legislation will help improve lives.”
The current House version of the bill has the backing of more than a third of the members of that chamber, with 113 Democratic and 40 Republican cosponsors. The Senate version has 22 sponsors.
Changing views
The ICER report comes amid a broader change in how clinicians view obesity.
The American Academy of Pediatrics is readying a new Clinical Practice Guideline for the Evaluation and Treatment of Pediatric Obesity that will mark a major shift in approach. Aaron S. Kelly, PhD, a professor of pediatrics at the University of Minnesota, Minneapolis, described it as a “sea change,” with obesity now seen as “a chronic, refractory, relapsing disease,” for which watchful waiting is no longer appropriate.
But the field of obesity treatment looked quite different in the early 2000s when Congress worked on a plan to add a pharmacy benefit to Medicare.
The deliberate omission of obesity medicine in the Medicare Part D benefit reflected both the state of science at the time and U.S. experience with a dangerous weight-loss drug combo in the late 1990s.
Initial expectations for weight-loss pills were high after the Food and Drug Administration cleared dexfenfluramine HCl (Redux) in 1996, which was part of the popular fen-phen combination. “Newly Approved Diet Drug Promises to Help Millions of Obese Americans – But Is No Magic Bullet,” read a headline about the Redux approval in The Washington Post
When work began in the 2000s to create a Medicare pharmacy benefit, lawmakers and congressional staff had a pool of about $400 billion available to establish what became the Part D program, Joel White, a former House staffer who helped draft the law, told this news organization in an email exchange.
Given the state of obesity research at the time, it seemed to make sense to exclude weight-loss medications, wrote Mr. White. Mr. White is now chief executive of the consulting firm Horizon, which has clients in the drug industry including the Pharmaceutical Research and Manufacturers of America.
“Now we know that obesity is a chronic disease of epidemic proportions. Decades of research have produced a series of advances in the way we understand and treat obesity. While scientists and many who work directly with those impacted by this epidemic understand how treatments have advanced, the law lags behind,” Mr. White said.
XXXCurrent payment policies for obesity treatments are based on “outdated information and ongoing misperception,” he noted. “While Part D has been a resounding success, our Medicare approach to obesity is not.”
“In addition, it makes no sense that Medicare covers the most drastic procedure (bariatric surgery) but not less-invasive, effective treatments,” he added. “We should have long ago lifted restrictions based on advances in science and medicine.”
Overcoming the stigma
Scott Kahan, MD, MPH, agreed and hopes that the new ICER report will help more patients secure needed medications, raising a “call to arms” about the need for better coverage of obesity drugs.
Dr. Kahan is director of the National Center for Weight and Wellness, a private clinic in Washington, and chair of the clinical committee for The Obesity Society. He also served as a member of a policy roundtable that ICER convened as part of research on the report on obesity drugs. Dr. Kahan, who also serves on the faculty at the Johns Hopkins Bloomberg School of Public Health, Baltimore, has received fees from drug makers such as Eli Lilly.
The ICER report may help what Dr. Kahan described as well-founded caution about obesity treatments in general.
“When it comes to weight loss, there are all of these magical treatments that are sold on social media and traditional media. There are a lot of bad actors in terms of people calling themselves experts and gurus and promising all kinds of crazy stuff,” said Dr. Kahan.
And there are long-standing stigmas about obesity, he stressed.
“That underlies a lot of the backward policies, including poor coverage for medications and the noncoverage by Medicare,” Dr. Kahan said. “There’s a societal ingrained set of beliefs and misperceptions and biases. That takes time to unwind, and I think we’re on the way, but we’re not quite there yet.”
Lifestyle changes not enough to tackle obesity
AHIP (formerly America’s Health Insurance Plans) told this news organization its members consider ICER reports when making decisions about which products to cover. “And health plans already cover obesity treatments that they consider medically necessary,” said David Allen, an AHIP spokesperson.
“It is important to note that every treatment does not work for every patient, and many patients experience adverse events and may discontinue treatment,” he added in an email. “Health insurance providers play an important role in helping [health care] providers and patients identify the treatment options that are most likely to be effective as well as affordable.”
Separately, the nonprofit watchdog group Public Citizen cautioned against liraglutide on its Worst Pills, Best Pills website. In its view, the drug is minimally effective and has many dangerous adverse effects, which are even more frequent with the higher-dose weight-loss version (a lower-dose version is approved for type 2 diabetes).
“There is currently no medication that can be used safely to achieve weight loss effortlessly and without dangerous adverse effects,” the group said. “Rather than focus on losing weight by turning to risky drugs, overweight and obese adults seeking to achieve better health should make reasonable and sustainable changes to their lifestyle, such as eating a healthy diet and getting regular exercise.”
Yet, many people find there is little help available for making lifestyle changes, and some patients and physicians say these modifications by themselves are not enough.
“The vast majority of people with obesity cannot achieve sustained weight loss through diet and exercise alone,” said David Rind, MD, chief medical officer of ICER, in an Oct. 20 statement. “As such, obesity, and its resulting physical health, mental health, and social burdens, is not a choice or failing, but a medical condition.”
The focus should now be on assuring that effective medications “are priced in alignment with their benefits so that they are accessible and affordable across U.S. society,” Dr. Rind urges.
‘My own demise with a fork and knife’
ICER sought public feedback on a draft version of the report before finalizing it.
In their comments on ICER’s work, several pharmaceutical researchers and Novo Nordisk questioned the calculations used in making judgments about the value of obesity drugs. In a statement, Novo Nordisk told this news organization that the company’s view is that ICER’s modeling “does not adequately address the real-world complexities of obesity, and consequently underestimates the health and societal impact medical treatments can have.”
Commenters also dug into aspects of ICER’s calculations, including ones that consider quality-adjusted life-years (QALYs). ICER describes QALY as an academic standard for measuring how well all different types of medical treatments can extend or improve patients’ lives. In an explainer on its website, ICER says this metric has served as a fundamental component of cost-effectiveness analyses in the United States and around the world for more than 30 years.
ICER and drug makers have been at odds for some time, with PhRMA having criticized the nonprofit group. A 2020 Reuters article detailed public relations strategies used by firms paid by drug makers to raise questions about ICER’s work. Critics accuse it of allying with insurers.
ICER’s list of its recent financial supporters includes Blue Cross Blue Shield of Massachusetts and the Kaiser Foundation Health Plan, but also many other groups, such as the U.S. Department of Veterans Affairs, the American Academy of Neurology, and the American College of Rheumatology.
The public comments on the ICER report also include one from an unidentified woman who wrote of her past struggles to lose weight.
She said her health plan wouldn’t cover behavioral programs or semaglutide as a weight-loss drug but did cover it eventually because of signs that she had developed insulin resistance. The patient said the drug worked for her, whereas other approaches to control weight had failed.
“To put it simply, I now experience hunger and satiety in a way that I can only assume people with normal metabolism do. I am 49 years old and approaching the age where serious comorbidities associated with obesity begin to manifest,” the patient wrote.
“I no longer worry about bringing about my own demise with a fork and knife because of misfiring hunger cues.”
A version of this article first appeared on Medscape.com.
A report from a well-respected nonprofit group may bolster efforts to have Medicare, the largest U.S. purchaser of prescription drugs, cover obesity medicines, for which there has been accumulating evidence of significant benefit.
The Institute for Clinical and Economic Review (ICER) released a report last month on obesity medicines, based on extensive review of research done to date and input from clinicians, drug-makers, and members of the public.
Of the treatments reviewed, the ICER report gave the best ratings to two Novo Nordisk products, a B+ for semaglutide (Wegovy) and a B for liraglutide (Saxenda), while also making the case for price cuts. At an annual U.S. net price estimated at $13,618, semaglutide exceeds what ICER considers typical cost-effectiveness thresholds. ICER suggested a benchmark annual price range for semaglutide of between $7,500 and $9,800.
The ICER report also directs insurers in general to provide more generous coverage of obesity medicines, with a specific recommendation for the U.S. Congress to pass a pending bill known as the Treat and Reduce Obesity Act of 2021. The bill would undo a restriction on weight-loss drugs in the Medicare Part D plans, which covered about 49 million people last year. Sen. Tom Carper (D-Del.) and Sen. Bill Cassidy, MD, (R-La.) have repeatedly introduced versions of the bill since 2013.
“In both chambers of Congress and with bipartisan support, we’ve pushed to expand Medicare coverage of additional therapies and medications to treat obesity,” Sen. Cassidy said in an email. “This report confirms what we’ve worked on for nearly a decade – our legislation will help improve lives.”
The current House version of the bill has the backing of more than a third of the members of that chamber, with 113 Democratic and 40 Republican cosponsors. The Senate version has 22 sponsors.
Changing views
The ICER report comes amid a broader change in how clinicians view obesity.
The American Academy of Pediatrics is readying a new Clinical Practice Guideline for the Evaluation and Treatment of Pediatric Obesity that will mark a major shift in approach. Aaron S. Kelly, PhD, a professor of pediatrics at the University of Minnesota, Minneapolis, described it as a “sea change,” with obesity now seen as “a chronic, refractory, relapsing disease,” for which watchful waiting is no longer appropriate.
But the field of obesity treatment looked quite different in the early 2000s when Congress worked on a plan to add a pharmacy benefit to Medicare.
The deliberate omission of obesity medicine in the Medicare Part D benefit reflected both the state of science at the time and U.S. experience with a dangerous weight-loss drug combo in the late 1990s.
Initial expectations for weight-loss pills were high after the Food and Drug Administration cleared dexfenfluramine HCl (Redux) in 1996, which was part of the popular fen-phen combination. “Newly Approved Diet Drug Promises to Help Millions of Obese Americans – But Is No Magic Bullet,” read a headline about the Redux approval in The Washington Post
When work began in the 2000s to create a Medicare pharmacy benefit, lawmakers and congressional staff had a pool of about $400 billion available to establish what became the Part D program, Joel White, a former House staffer who helped draft the law, told this news organization in an email exchange.
Given the state of obesity research at the time, it seemed to make sense to exclude weight-loss medications, wrote Mr. White. Mr. White is now chief executive of the consulting firm Horizon, which has clients in the drug industry including the Pharmaceutical Research and Manufacturers of America.
“Now we know that obesity is a chronic disease of epidemic proportions. Decades of research have produced a series of advances in the way we understand and treat obesity. While scientists and many who work directly with those impacted by this epidemic understand how treatments have advanced, the law lags behind,” Mr. White said.
XXXCurrent payment policies for obesity treatments are based on “outdated information and ongoing misperception,” he noted. “While Part D has been a resounding success, our Medicare approach to obesity is not.”
“In addition, it makes no sense that Medicare covers the most drastic procedure (bariatric surgery) but not less-invasive, effective treatments,” he added. “We should have long ago lifted restrictions based on advances in science and medicine.”
Overcoming the stigma
Scott Kahan, MD, MPH, agreed and hopes that the new ICER report will help more patients secure needed medications, raising a “call to arms” about the need for better coverage of obesity drugs.
Dr. Kahan is director of the National Center for Weight and Wellness, a private clinic in Washington, and chair of the clinical committee for The Obesity Society. He also served as a member of a policy roundtable that ICER convened as part of research on the report on obesity drugs. Dr. Kahan, who also serves on the faculty at the Johns Hopkins Bloomberg School of Public Health, Baltimore, has received fees from drug makers such as Eli Lilly.
The ICER report may help what Dr. Kahan described as well-founded caution about obesity treatments in general.
“When it comes to weight loss, there are all of these magical treatments that are sold on social media and traditional media. There are a lot of bad actors in terms of people calling themselves experts and gurus and promising all kinds of crazy stuff,” said Dr. Kahan.
And there are long-standing stigmas about obesity, he stressed.
“That underlies a lot of the backward policies, including poor coverage for medications and the noncoverage by Medicare,” Dr. Kahan said. “There’s a societal ingrained set of beliefs and misperceptions and biases. That takes time to unwind, and I think we’re on the way, but we’re not quite there yet.”
Lifestyle changes not enough to tackle obesity
AHIP (formerly America’s Health Insurance Plans) told this news organization its members consider ICER reports when making decisions about which products to cover. “And health plans already cover obesity treatments that they consider medically necessary,” said David Allen, an AHIP spokesperson.
“It is important to note that every treatment does not work for every patient, and many patients experience adverse events and may discontinue treatment,” he added in an email. “Health insurance providers play an important role in helping [health care] providers and patients identify the treatment options that are most likely to be effective as well as affordable.”
Separately, the nonprofit watchdog group Public Citizen cautioned against liraglutide on its Worst Pills, Best Pills website. In its view, the drug is minimally effective and has many dangerous adverse effects, which are even more frequent with the higher-dose weight-loss version (a lower-dose version is approved for type 2 diabetes).
“There is currently no medication that can be used safely to achieve weight loss effortlessly and without dangerous adverse effects,” the group said. “Rather than focus on losing weight by turning to risky drugs, overweight and obese adults seeking to achieve better health should make reasonable and sustainable changes to their lifestyle, such as eating a healthy diet and getting regular exercise.”
Yet, many people find there is little help available for making lifestyle changes, and some patients and physicians say these modifications by themselves are not enough.
“The vast majority of people with obesity cannot achieve sustained weight loss through diet and exercise alone,” said David Rind, MD, chief medical officer of ICER, in an Oct. 20 statement. “As such, obesity, and its resulting physical health, mental health, and social burdens, is not a choice or failing, but a medical condition.”
The focus should now be on assuring that effective medications “are priced in alignment with their benefits so that they are accessible and affordable across U.S. society,” Dr. Rind urges.
‘My own demise with a fork and knife’
ICER sought public feedback on a draft version of the report before finalizing it.
In their comments on ICER’s work, several pharmaceutical researchers and Novo Nordisk questioned the calculations used in making judgments about the value of obesity drugs. In a statement, Novo Nordisk told this news organization that the company’s view is that ICER’s modeling “does not adequately address the real-world complexities of obesity, and consequently underestimates the health and societal impact medical treatments can have.”
Commenters also dug into aspects of ICER’s calculations, including ones that consider quality-adjusted life-years (QALYs). ICER describes QALY as an academic standard for measuring how well all different types of medical treatments can extend or improve patients’ lives. In an explainer on its website, ICER says this metric has served as a fundamental component of cost-effectiveness analyses in the United States and around the world for more than 30 years.
ICER and drug makers have been at odds for some time, with PhRMA having criticized the nonprofit group. A 2020 Reuters article detailed public relations strategies used by firms paid by drug makers to raise questions about ICER’s work. Critics accuse it of allying with insurers.
ICER’s list of its recent financial supporters includes Blue Cross Blue Shield of Massachusetts and the Kaiser Foundation Health Plan, but also many other groups, such as the U.S. Department of Veterans Affairs, the American Academy of Neurology, and the American College of Rheumatology.
The public comments on the ICER report also include one from an unidentified woman who wrote of her past struggles to lose weight.
She said her health plan wouldn’t cover behavioral programs or semaglutide as a weight-loss drug but did cover it eventually because of signs that she had developed insulin resistance. The patient said the drug worked for her, whereas other approaches to control weight had failed.
“To put it simply, I now experience hunger and satiety in a way that I can only assume people with normal metabolism do. I am 49 years old and approaching the age where serious comorbidities associated with obesity begin to manifest,” the patient wrote.
“I no longer worry about bringing about my own demise with a fork and knife because of misfiring hunger cues.”
A version of this article first appeared on Medscape.com.