User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Tips for connecting with your patients
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.

Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.
Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.
Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
Children and COVID: Weekly cases down by more than half
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.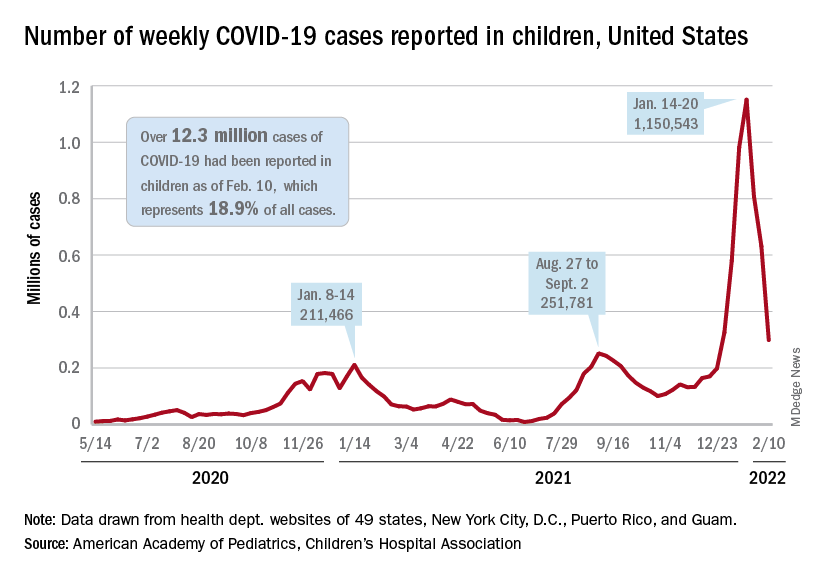
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
Long COVID symptoms linked to effects on vagus nerve
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Can periodontal treatment reduce cardiovascular events in stroke patients?
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
FROM ISC 2022
Tenecteplase for stroke linked to reduced ICH risk
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
FROM ISC 2022
‘Remarkable’ benefit with intra-arterial tPA after stroke thrombectomy: CHOICE
in a new study.
The phase 2b CHOICE study was presented at the International Stroke Conference by Ángel Chamorro, MD, University of Barcelona, who received a round of applause as the results were revealed.
The study was also published online in JAMA to coincide with the presentation at the ISC.
The main results showed a remarkable and significant 18.4% absolute increase in the number of patients achieving an excellent neurologic outcome, defined as modified Rankin Scale (mRS) score of 0-1, after treatment with intra-arterial alteplase immediately following thrombectomy. This was despite the fact that the study was stopped early because of difficulty obtaining placebo supplies during the pandemic, having only enrolled 121 of the planned 200 patients.
This benefit was achieved without any increase in intracranial hemorrhage, which Dr. Chamorro described as “reassuring.”
He explained that although mechanical thrombectomy gives a high rate of successful reperfusion, only about 27% of patients achieve complete freedom of disability (mRS 0-1) at 3 months. He suggested that this may be the result of impaired reperfusion of the microcirculation despite complete recanalization of the occluded vessel.
The researchers postulated that thrombi could persist within the microcirculation in patients with normal or nearly normal cerebral angiograms at the end of thrombectomy and that these smaller thrombi may be dissolved by a dose of intra-arterial thrombolysis.
‘Dramatic and exciting results’
The CHOICE study was greeted with enthusiasm from commentators at the ISC meeting, which was presented by the American Stroke Association, a division of the American Heart Association. Louise McCullough, MD, chair of the late-breaking science session at which the study was presented and ISC program chair, described the results as “very dramatic and very exciting.”
“The CHOICE trial is going to be a highlight of the meeting because it could change care now,” Dr. McCullough said. “By just giving a little adjunctive tPA after the main clot is out, everybody seems to benefit, and there was no increased risk in bleeding. I think that’s the one that people are going to take back to their practice. But it was a very small trial, so you have to be cautious.”
And Peter Panagos, MD, professor of emergency medicine and neurology at Washington University School of Medicine, St. Louis, said: “It’s great to see this study. The 18% treatment effect is very impressive.”
Dr. Panagos added: “This study addresses a well-described finding from many of the interventional trials, that despite excellent outcomes in recanalization, patients don’t do as well as predicted. The thought is that either re-stenosis or propagation of smaller clots downstream from the original clot in small-caliber vessels [is what] causes additional, unintended damage. The use of intra-arterial thrombolysis after recanalization may assist in dissolving those smaller, downstream clots and debris and improve outcomes.”
But he pointed out that enthusiasm over these results must be matched with some concerns, including the small study size and wide confidence intervals – so larger, randomized studies will be required to confirm and change current clinical practice.
An abbreviated phase 2b trial
The CHOICE trial was conducted in seven centers in Catalonia, Spain.
For the study, patients with large vessel occlusion acute ischemic stroke treated with thrombectomy within 24 hours after stroke onset and who had achieved successful reperfusion (an expanded TICI angiographic score of 2b50 to 3) were randomly assigned to receive intra-arterial alteplase (0.225 mg/kg; maximum dose, 22.5 mg) infused over 15 to 30 minutes or placebo.
Because of the lack of continued availability of placebo supplies, the study had to be stopped early after 121 patients were enrolled (65 alteplase; 56 placebo), and after a few dropouts who did not receive treatment, the analysis was performed on 61 patients who received alteplase and 52 given placebo.
Results showed that the proportion of patients with an mRS score of 0 or 1 at 90 days was 59% (36/61) with alteplase and 40.4% (21/52) with placebo (adjusted risk difference, 18.4%; 95% confidence interval, 0.3%-36.4%; P = .047).
The proportion of patients with symptomatic intracranial hemorrhage within 24 hours was 0% with alteplase and 3.8% with placebo (risk difference, −3.8%; 95% CI, −13.2% to 2.5%).
Mortality at 90 days was 8% with alteplase and 15% with placebo (risk difference, −7.2%; 95% CI, −19.2% to 4.8%).
The improved clinical outcomes in the alteplase group were seen despite only minor differences between the treatment groups in angiographic scores or in other surrogate imaging, Dr. Chamorro pointed out, suggesting that the improved functional outcome may be explained by an amelioration in the microcirculatory reperfusion.
He said the study also supported the safety of intra-arterial alteplase infusion for 15-30 minutes at the dose used. Of note, 60% of the study population had also received IV alteplase before thrombectomy.
In the JAMA study, the authors report that current guidelines recommend that all eligible patients receive intravenous alteplase before thrombectomy, and the results of this trial do not contradict this recommendation.
“The study results support the safety of adjunct intra-arterial alteplase in patients with successful reperfusion at the end of thrombectomy, including in patients treated previously with intravenous alteplase, although the findings on effectiveness should be interpreted as preliminary, requiring replication before any recommendations for practice change,” they concluded.
Dr. Chamorro said that his group was now planning a second larger trial, CHOICE-2.
In an accompanying editorial in JAMA, Pooja Khatri, MD, MSc, University of Cincinnati, said “the 18% treatment effect observed in this 113-patient trial is remarkable.”
However, she cautions that consideration of its clinical implications must be tempered because of the lack of precision of the effect estimate, given wide 95% confidence intervals, the small sample size, and the observation that trials with early termination are well known to overestimate treatment effect.
But she acknowledges that the results suggest “that additional reperfusion therapy may be warranted after relatively successful mechanical thrombectomy of large vessel occlusions, whether to treat the residual primary thrombus, more distal arterial occlusions, or perhaps even microthromboses.”
Dr. Khatri noted that this approach runs counter to the recent movement to consider bypass of intravenous alteplase altogether in thrombectomy-eligible patients and suggests that additional or perhaps more targeted thrombolysis will be the most beneficial approach.
Further studies testing current thrombolytic agents, novel clot-dissolving agents, and other adjunctive antithrombotic and anti-inflammatory agents are needed, she concluded.
A version of this article first appeared on Medscape.com.
in a new study.
The phase 2b CHOICE study was presented at the International Stroke Conference by Ángel Chamorro, MD, University of Barcelona, who received a round of applause as the results were revealed.
The study was also published online in JAMA to coincide with the presentation at the ISC.
The main results showed a remarkable and significant 18.4% absolute increase in the number of patients achieving an excellent neurologic outcome, defined as modified Rankin Scale (mRS) score of 0-1, after treatment with intra-arterial alteplase immediately following thrombectomy. This was despite the fact that the study was stopped early because of difficulty obtaining placebo supplies during the pandemic, having only enrolled 121 of the planned 200 patients.
This benefit was achieved without any increase in intracranial hemorrhage, which Dr. Chamorro described as “reassuring.”
He explained that although mechanical thrombectomy gives a high rate of successful reperfusion, only about 27% of patients achieve complete freedom of disability (mRS 0-1) at 3 months. He suggested that this may be the result of impaired reperfusion of the microcirculation despite complete recanalization of the occluded vessel.
The researchers postulated that thrombi could persist within the microcirculation in patients with normal or nearly normal cerebral angiograms at the end of thrombectomy and that these smaller thrombi may be dissolved by a dose of intra-arterial thrombolysis.
‘Dramatic and exciting results’
The CHOICE study was greeted with enthusiasm from commentators at the ISC meeting, which was presented by the American Stroke Association, a division of the American Heart Association. Louise McCullough, MD, chair of the late-breaking science session at which the study was presented and ISC program chair, described the results as “very dramatic and very exciting.”
“The CHOICE trial is going to be a highlight of the meeting because it could change care now,” Dr. McCullough said. “By just giving a little adjunctive tPA after the main clot is out, everybody seems to benefit, and there was no increased risk in bleeding. I think that’s the one that people are going to take back to their practice. But it was a very small trial, so you have to be cautious.”
And Peter Panagos, MD, professor of emergency medicine and neurology at Washington University School of Medicine, St. Louis, said: “It’s great to see this study. The 18% treatment effect is very impressive.”
Dr. Panagos added: “This study addresses a well-described finding from many of the interventional trials, that despite excellent outcomes in recanalization, patients don’t do as well as predicted. The thought is that either re-stenosis or propagation of smaller clots downstream from the original clot in small-caliber vessels [is what] causes additional, unintended damage. The use of intra-arterial thrombolysis after recanalization may assist in dissolving those smaller, downstream clots and debris and improve outcomes.”
But he pointed out that enthusiasm over these results must be matched with some concerns, including the small study size and wide confidence intervals – so larger, randomized studies will be required to confirm and change current clinical practice.
An abbreviated phase 2b trial
The CHOICE trial was conducted in seven centers in Catalonia, Spain.
For the study, patients with large vessel occlusion acute ischemic stroke treated with thrombectomy within 24 hours after stroke onset and who had achieved successful reperfusion (an expanded TICI angiographic score of 2b50 to 3) were randomly assigned to receive intra-arterial alteplase (0.225 mg/kg; maximum dose, 22.5 mg) infused over 15 to 30 minutes or placebo.
Because of the lack of continued availability of placebo supplies, the study had to be stopped early after 121 patients were enrolled (65 alteplase; 56 placebo), and after a few dropouts who did not receive treatment, the analysis was performed on 61 patients who received alteplase and 52 given placebo.
Results showed that the proportion of patients with an mRS score of 0 or 1 at 90 days was 59% (36/61) with alteplase and 40.4% (21/52) with placebo (adjusted risk difference, 18.4%; 95% confidence interval, 0.3%-36.4%; P = .047).
The proportion of patients with symptomatic intracranial hemorrhage within 24 hours was 0% with alteplase and 3.8% with placebo (risk difference, −3.8%; 95% CI, −13.2% to 2.5%).
Mortality at 90 days was 8% with alteplase and 15% with placebo (risk difference, −7.2%; 95% CI, −19.2% to 4.8%).
The improved clinical outcomes in the alteplase group were seen despite only minor differences between the treatment groups in angiographic scores or in other surrogate imaging, Dr. Chamorro pointed out, suggesting that the improved functional outcome may be explained by an amelioration in the microcirculatory reperfusion.
He said the study also supported the safety of intra-arterial alteplase infusion for 15-30 minutes at the dose used. Of note, 60% of the study population had also received IV alteplase before thrombectomy.
In the JAMA study, the authors report that current guidelines recommend that all eligible patients receive intravenous alteplase before thrombectomy, and the results of this trial do not contradict this recommendation.
“The study results support the safety of adjunct intra-arterial alteplase in patients with successful reperfusion at the end of thrombectomy, including in patients treated previously with intravenous alteplase, although the findings on effectiveness should be interpreted as preliminary, requiring replication before any recommendations for practice change,” they concluded.
Dr. Chamorro said that his group was now planning a second larger trial, CHOICE-2.
In an accompanying editorial in JAMA, Pooja Khatri, MD, MSc, University of Cincinnati, said “the 18% treatment effect observed in this 113-patient trial is remarkable.”
However, she cautions that consideration of its clinical implications must be tempered because of the lack of precision of the effect estimate, given wide 95% confidence intervals, the small sample size, and the observation that trials with early termination are well known to overestimate treatment effect.
But she acknowledges that the results suggest “that additional reperfusion therapy may be warranted after relatively successful mechanical thrombectomy of large vessel occlusions, whether to treat the residual primary thrombus, more distal arterial occlusions, or perhaps even microthromboses.”
Dr. Khatri noted that this approach runs counter to the recent movement to consider bypass of intravenous alteplase altogether in thrombectomy-eligible patients and suggests that additional or perhaps more targeted thrombolysis will be the most beneficial approach.
Further studies testing current thrombolytic agents, novel clot-dissolving agents, and other adjunctive antithrombotic and anti-inflammatory agents are needed, she concluded.
A version of this article first appeared on Medscape.com.
in a new study.
The phase 2b CHOICE study was presented at the International Stroke Conference by Ángel Chamorro, MD, University of Barcelona, who received a round of applause as the results were revealed.
The study was also published online in JAMA to coincide with the presentation at the ISC.
The main results showed a remarkable and significant 18.4% absolute increase in the number of patients achieving an excellent neurologic outcome, defined as modified Rankin Scale (mRS) score of 0-1, after treatment with intra-arterial alteplase immediately following thrombectomy. This was despite the fact that the study was stopped early because of difficulty obtaining placebo supplies during the pandemic, having only enrolled 121 of the planned 200 patients.
This benefit was achieved without any increase in intracranial hemorrhage, which Dr. Chamorro described as “reassuring.”
He explained that although mechanical thrombectomy gives a high rate of successful reperfusion, only about 27% of patients achieve complete freedom of disability (mRS 0-1) at 3 months. He suggested that this may be the result of impaired reperfusion of the microcirculation despite complete recanalization of the occluded vessel.
The researchers postulated that thrombi could persist within the microcirculation in patients with normal or nearly normal cerebral angiograms at the end of thrombectomy and that these smaller thrombi may be dissolved by a dose of intra-arterial thrombolysis.
‘Dramatic and exciting results’
The CHOICE study was greeted with enthusiasm from commentators at the ISC meeting, which was presented by the American Stroke Association, a division of the American Heart Association. Louise McCullough, MD, chair of the late-breaking science session at which the study was presented and ISC program chair, described the results as “very dramatic and very exciting.”
“The CHOICE trial is going to be a highlight of the meeting because it could change care now,” Dr. McCullough said. “By just giving a little adjunctive tPA after the main clot is out, everybody seems to benefit, and there was no increased risk in bleeding. I think that’s the one that people are going to take back to their practice. But it was a very small trial, so you have to be cautious.”
And Peter Panagos, MD, professor of emergency medicine and neurology at Washington University School of Medicine, St. Louis, said: “It’s great to see this study. The 18% treatment effect is very impressive.”
Dr. Panagos added: “This study addresses a well-described finding from many of the interventional trials, that despite excellent outcomes in recanalization, patients don’t do as well as predicted. The thought is that either re-stenosis or propagation of smaller clots downstream from the original clot in small-caliber vessels [is what] causes additional, unintended damage. The use of intra-arterial thrombolysis after recanalization may assist in dissolving those smaller, downstream clots and debris and improve outcomes.”
But he pointed out that enthusiasm over these results must be matched with some concerns, including the small study size and wide confidence intervals – so larger, randomized studies will be required to confirm and change current clinical practice.
An abbreviated phase 2b trial
The CHOICE trial was conducted in seven centers in Catalonia, Spain.
For the study, patients with large vessel occlusion acute ischemic stroke treated with thrombectomy within 24 hours after stroke onset and who had achieved successful reperfusion (an expanded TICI angiographic score of 2b50 to 3) were randomly assigned to receive intra-arterial alteplase (0.225 mg/kg; maximum dose, 22.5 mg) infused over 15 to 30 minutes or placebo.
Because of the lack of continued availability of placebo supplies, the study had to be stopped early after 121 patients were enrolled (65 alteplase; 56 placebo), and after a few dropouts who did not receive treatment, the analysis was performed on 61 patients who received alteplase and 52 given placebo.
Results showed that the proportion of patients with an mRS score of 0 or 1 at 90 days was 59% (36/61) with alteplase and 40.4% (21/52) with placebo (adjusted risk difference, 18.4%; 95% confidence interval, 0.3%-36.4%; P = .047).
The proportion of patients with symptomatic intracranial hemorrhage within 24 hours was 0% with alteplase and 3.8% with placebo (risk difference, −3.8%; 95% CI, −13.2% to 2.5%).
Mortality at 90 days was 8% with alteplase and 15% with placebo (risk difference, −7.2%; 95% CI, −19.2% to 4.8%).
The improved clinical outcomes in the alteplase group were seen despite only minor differences between the treatment groups in angiographic scores or in other surrogate imaging, Dr. Chamorro pointed out, suggesting that the improved functional outcome may be explained by an amelioration in the microcirculatory reperfusion.
He said the study also supported the safety of intra-arterial alteplase infusion for 15-30 minutes at the dose used. Of note, 60% of the study population had also received IV alteplase before thrombectomy.
In the JAMA study, the authors report that current guidelines recommend that all eligible patients receive intravenous alteplase before thrombectomy, and the results of this trial do not contradict this recommendation.
“The study results support the safety of adjunct intra-arterial alteplase in patients with successful reperfusion at the end of thrombectomy, including in patients treated previously with intravenous alteplase, although the findings on effectiveness should be interpreted as preliminary, requiring replication before any recommendations for practice change,” they concluded.
Dr. Chamorro said that his group was now planning a second larger trial, CHOICE-2.
In an accompanying editorial in JAMA, Pooja Khatri, MD, MSc, University of Cincinnati, said “the 18% treatment effect observed in this 113-patient trial is remarkable.”
However, she cautions that consideration of its clinical implications must be tempered because of the lack of precision of the effect estimate, given wide 95% confidence intervals, the small sample size, and the observation that trials with early termination are well known to overestimate treatment effect.
But she acknowledges that the results suggest “that additional reperfusion therapy may be warranted after relatively successful mechanical thrombectomy of large vessel occlusions, whether to treat the residual primary thrombus, more distal arterial occlusions, or perhaps even microthromboses.”
Dr. Khatri noted that this approach runs counter to the recent movement to consider bypass of intravenous alteplase altogether in thrombectomy-eligible patients and suggests that additional or perhaps more targeted thrombolysis will be the most beneficial approach.
Further studies testing current thrombolytic agents, novel clot-dissolving agents, and other adjunctive antithrombotic and anti-inflammatory agents are needed, she concluded.
A version of this article first appeared on Medscape.com.
FROM ISC 2022
Is mild cognitive impairment reversible?
new research shows.
The investigators found individuals with these factors, which are all markers of cognitive reserve, had a significantly greater chance of reversion from MCI to normal cognition (NC) than progression from MCI to dementia.
In a cohort study of more than 600 women aged 75 years or older, about a third of those with MCI reverted to NC at some point during follow-up, which sends “an encouraging message,” study author Suzanne Tyas, PhD, associate professor, University of Waterloo (Ont.), said in an interview.
“That’s a positive thing for people to keep in mind when they’re thinking about prognosis. Some of these novel characteristics we’ve identified might be useful in thinking about how likely a particular patient might be to improve versus decline cognitively,” Dr. Tyas added.
The findings were published online Feb. 4, 2022, in the journal Neurology.
Highly educated cohort
As the population ages, the number of individuals experiencing age-related conditions, including dementia, increases. There is no cure for most dementia types so prevention is key – and preventing dementia requires understanding its risk factors, Dr. Tyas noted.
The analysis included participants from the Nun Study, a longitudinal study of aging and cognition among members of the School Sisters of Notre Dame in the United States. All were 75 and older at baseline, which was from 1991 to 1993; about 14.5% were older than 90 years.
Participants were generally highly educated, with 84.5% attaining an undergraduate or graduate degree. They also had a similar socioeconomic status, level of social supports, marital and reproductive history, and alcohol and tobacco use.
Researchers examined cognitive function at baseline and then about annually until death or end of the 12th round of assessments. They used five measures from the Consortium to Establish a Registry for Alzheimer’s Disease neuropsychological battery to categorize subjects into NC, MCI, or dementia: Delayed Word Recall, Verbal Fluency, Boston Naming, Constructional Praxis, and the Mini-Mental State Exam.
The current analysis focused on the 619 participants with data on apolipoprotein E (apo E) epsilon-4 genotyping and education. From convent archives, investigators also had access to the nuns’ early high school academic performance in English, Latin, algebra, and geometry.
“Typically we only have data for [overall] education. But I know from teaching that there’s a difference between people who just pass my courses and graduate with a university degree versus those who really excel,” Dr. Tyas said.
The researchers also assessed handwriting samples from before the participants entered the religious order. From these, they scored “idea density,” which is the number of ideas contained in the writing and “grammatical complexity,” which includes structure, use of clauses, subclauses, and so on.
Dementia not inevitable
Results showed 472 of the 619 participants had MCI during the study period. About 30.3% of these showed at least one reverse transition from MCI to NC during a mean follow-up of 8.6 years; 83.9% went on to develop dementia.
This shows converting from MCI to NC occurs relatively frequently, Dr. Tyas noted.
“This is encouraging because some people think that if they have a diagnosis of MCI they are inevitably going to decline to dementia,” she added.
The researchers also used complicated modeling of transition rates over time between NC, MCI, and dementia and adjusted for participants who died. They estimated relative risk of reversion versus progression for age, apo E, and potential cognitive reserve indicators.
Not surprisingly, younger age (90 years or less) and absence of apo E epsilon-4 allele contributed to a significantly higher rate for reversion from MCI to NC versus progression from MCI to dementia.
However, although age and apo E are known risk factors for dementia, these have not been examined in the context of whether individuals with MCI are more likely to improve or decline, said Dr. Tyas.
Higher educational attainment, the traditional indicator of cognitive reserve, was associated with a significantly higher relative risk for reversion from MCI to NC versus progression from MCI to dementia (RR, 2.6) for a bachelor’s degree versus less education.
There was a greater RR for even higher education after adjusting for age and apo E epsilon-4 status.
Language skills key
Interestingly, the investigators also found a significant association with good grades in high school English but not other subjects (RR for higher vs. lower English grades, 1.83; 95% confidence interval, 1.07-3.14).
In addition, they found both characteristics of written language skills (idea density and grammatical complexity) were significant predictors of conversion to NC.
“Those with high levels of idea density were four times more likely to improve to normal cognition than progress to dementia, and the effect was even stronger for grammatical structure. Those individuals with higher levels were almost six times more likely to improve than decline,” Dr. Tyas reported.
The RR for higher versus lower idea density was 3.93 (95% CI, 1.3-11.9) and the RR for higher versus lower grammatical complexity was 5.78 (95% CI, 1.56-21.42).
These new results could be useful when planning future clinical trials, Dr. Tyas noted. “MCI in some people is going to improve even without any treatment, and this should be taken into consideration when recruiting participants to a study and when interpreting the results.
“You don’t want something to look like it’s a benefit of the treatment when in fact these individuals would have just reverted on their own,” she added.
Research implications
Commenting on the findings, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, noted that, in “this study of highly educated, older women,” transitions from MCI to NC “were about equally common” as transitions from MCI to dementia.
“As advances are made in early detection of dementia, and treatments are developed and marketed for people living with MCI, this article’s findings are important to inform discussions of prognosis with patients and [to the] design of clinical trials,” Dr. Sexton said.
The study was funded by the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada. Funding for the Nun Study at the University of Kentucky was provided by the U.S. National Institute of Aging and the Kleberg Foundation. Dr. Tyas has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research shows.
The investigators found individuals with these factors, which are all markers of cognitive reserve, had a significantly greater chance of reversion from MCI to normal cognition (NC) than progression from MCI to dementia.
In a cohort study of more than 600 women aged 75 years or older, about a third of those with MCI reverted to NC at some point during follow-up, which sends “an encouraging message,” study author Suzanne Tyas, PhD, associate professor, University of Waterloo (Ont.), said in an interview.
“That’s a positive thing for people to keep in mind when they’re thinking about prognosis. Some of these novel characteristics we’ve identified might be useful in thinking about how likely a particular patient might be to improve versus decline cognitively,” Dr. Tyas added.
The findings were published online Feb. 4, 2022, in the journal Neurology.
Highly educated cohort
As the population ages, the number of individuals experiencing age-related conditions, including dementia, increases. There is no cure for most dementia types so prevention is key – and preventing dementia requires understanding its risk factors, Dr. Tyas noted.
The analysis included participants from the Nun Study, a longitudinal study of aging and cognition among members of the School Sisters of Notre Dame in the United States. All were 75 and older at baseline, which was from 1991 to 1993; about 14.5% were older than 90 years.
Participants were generally highly educated, with 84.5% attaining an undergraduate or graduate degree. They also had a similar socioeconomic status, level of social supports, marital and reproductive history, and alcohol and tobacco use.
Researchers examined cognitive function at baseline and then about annually until death or end of the 12th round of assessments. They used five measures from the Consortium to Establish a Registry for Alzheimer’s Disease neuropsychological battery to categorize subjects into NC, MCI, or dementia: Delayed Word Recall, Verbal Fluency, Boston Naming, Constructional Praxis, and the Mini-Mental State Exam.
The current analysis focused on the 619 participants with data on apolipoprotein E (apo E) epsilon-4 genotyping and education. From convent archives, investigators also had access to the nuns’ early high school academic performance in English, Latin, algebra, and geometry.
“Typically we only have data for [overall] education. But I know from teaching that there’s a difference between people who just pass my courses and graduate with a university degree versus those who really excel,” Dr. Tyas said.
The researchers also assessed handwriting samples from before the participants entered the religious order. From these, they scored “idea density,” which is the number of ideas contained in the writing and “grammatical complexity,” which includes structure, use of clauses, subclauses, and so on.
Dementia not inevitable
Results showed 472 of the 619 participants had MCI during the study period. About 30.3% of these showed at least one reverse transition from MCI to NC during a mean follow-up of 8.6 years; 83.9% went on to develop dementia.
This shows converting from MCI to NC occurs relatively frequently, Dr. Tyas noted.
“This is encouraging because some people think that if they have a diagnosis of MCI they are inevitably going to decline to dementia,” she added.
The researchers also used complicated modeling of transition rates over time between NC, MCI, and dementia and adjusted for participants who died. They estimated relative risk of reversion versus progression for age, apo E, and potential cognitive reserve indicators.
Not surprisingly, younger age (90 years or less) and absence of apo E epsilon-4 allele contributed to a significantly higher rate for reversion from MCI to NC versus progression from MCI to dementia.
However, although age and apo E are known risk factors for dementia, these have not been examined in the context of whether individuals with MCI are more likely to improve or decline, said Dr. Tyas.
Higher educational attainment, the traditional indicator of cognitive reserve, was associated with a significantly higher relative risk for reversion from MCI to NC versus progression from MCI to dementia (RR, 2.6) for a bachelor’s degree versus less education.
There was a greater RR for even higher education after adjusting for age and apo E epsilon-4 status.
Language skills key
Interestingly, the investigators also found a significant association with good grades in high school English but not other subjects (RR for higher vs. lower English grades, 1.83; 95% confidence interval, 1.07-3.14).
In addition, they found both characteristics of written language skills (idea density and grammatical complexity) were significant predictors of conversion to NC.
“Those with high levels of idea density were four times more likely to improve to normal cognition than progress to dementia, and the effect was even stronger for grammatical structure. Those individuals with higher levels were almost six times more likely to improve than decline,” Dr. Tyas reported.
The RR for higher versus lower idea density was 3.93 (95% CI, 1.3-11.9) and the RR for higher versus lower grammatical complexity was 5.78 (95% CI, 1.56-21.42).
These new results could be useful when planning future clinical trials, Dr. Tyas noted. “MCI in some people is going to improve even without any treatment, and this should be taken into consideration when recruiting participants to a study and when interpreting the results.
“You don’t want something to look like it’s a benefit of the treatment when in fact these individuals would have just reverted on their own,” she added.
Research implications
Commenting on the findings, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, noted that, in “this study of highly educated, older women,” transitions from MCI to NC “were about equally common” as transitions from MCI to dementia.
“As advances are made in early detection of dementia, and treatments are developed and marketed for people living with MCI, this article’s findings are important to inform discussions of prognosis with patients and [to the] design of clinical trials,” Dr. Sexton said.
The study was funded by the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada. Funding for the Nun Study at the University of Kentucky was provided by the U.S. National Institute of Aging and the Kleberg Foundation. Dr. Tyas has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research shows.
The investigators found individuals with these factors, which are all markers of cognitive reserve, had a significantly greater chance of reversion from MCI to normal cognition (NC) than progression from MCI to dementia.
In a cohort study of more than 600 women aged 75 years or older, about a third of those with MCI reverted to NC at some point during follow-up, which sends “an encouraging message,” study author Suzanne Tyas, PhD, associate professor, University of Waterloo (Ont.), said in an interview.
“That’s a positive thing for people to keep in mind when they’re thinking about prognosis. Some of these novel characteristics we’ve identified might be useful in thinking about how likely a particular patient might be to improve versus decline cognitively,” Dr. Tyas added.
The findings were published online Feb. 4, 2022, in the journal Neurology.
Highly educated cohort
As the population ages, the number of individuals experiencing age-related conditions, including dementia, increases. There is no cure for most dementia types so prevention is key – and preventing dementia requires understanding its risk factors, Dr. Tyas noted.
The analysis included participants from the Nun Study, a longitudinal study of aging and cognition among members of the School Sisters of Notre Dame in the United States. All were 75 and older at baseline, which was from 1991 to 1993; about 14.5% were older than 90 years.
Participants were generally highly educated, with 84.5% attaining an undergraduate or graduate degree. They also had a similar socioeconomic status, level of social supports, marital and reproductive history, and alcohol and tobacco use.
Researchers examined cognitive function at baseline and then about annually until death or end of the 12th round of assessments. They used five measures from the Consortium to Establish a Registry for Alzheimer’s Disease neuropsychological battery to categorize subjects into NC, MCI, or dementia: Delayed Word Recall, Verbal Fluency, Boston Naming, Constructional Praxis, and the Mini-Mental State Exam.
The current analysis focused on the 619 participants with data on apolipoprotein E (apo E) epsilon-4 genotyping and education. From convent archives, investigators also had access to the nuns’ early high school academic performance in English, Latin, algebra, and geometry.
“Typically we only have data for [overall] education. But I know from teaching that there’s a difference between people who just pass my courses and graduate with a university degree versus those who really excel,” Dr. Tyas said.
The researchers also assessed handwriting samples from before the participants entered the religious order. From these, they scored “idea density,” which is the number of ideas contained in the writing and “grammatical complexity,” which includes structure, use of clauses, subclauses, and so on.
Dementia not inevitable
Results showed 472 of the 619 participants had MCI during the study period. About 30.3% of these showed at least one reverse transition from MCI to NC during a mean follow-up of 8.6 years; 83.9% went on to develop dementia.
This shows converting from MCI to NC occurs relatively frequently, Dr. Tyas noted.
“This is encouraging because some people think that if they have a diagnosis of MCI they are inevitably going to decline to dementia,” she added.
The researchers also used complicated modeling of transition rates over time between NC, MCI, and dementia and adjusted for participants who died. They estimated relative risk of reversion versus progression for age, apo E, and potential cognitive reserve indicators.
Not surprisingly, younger age (90 years or less) and absence of apo E epsilon-4 allele contributed to a significantly higher rate for reversion from MCI to NC versus progression from MCI to dementia.
However, although age and apo E are known risk factors for dementia, these have not been examined in the context of whether individuals with MCI are more likely to improve or decline, said Dr. Tyas.
Higher educational attainment, the traditional indicator of cognitive reserve, was associated with a significantly higher relative risk for reversion from MCI to NC versus progression from MCI to dementia (RR, 2.6) for a bachelor’s degree versus less education.
There was a greater RR for even higher education after adjusting for age and apo E epsilon-4 status.
Language skills key
Interestingly, the investigators also found a significant association with good grades in high school English but not other subjects (RR for higher vs. lower English grades, 1.83; 95% confidence interval, 1.07-3.14).
In addition, they found both characteristics of written language skills (idea density and grammatical complexity) were significant predictors of conversion to NC.
“Those with high levels of idea density were four times more likely to improve to normal cognition than progress to dementia, and the effect was even stronger for grammatical structure. Those individuals with higher levels were almost six times more likely to improve than decline,” Dr. Tyas reported.
The RR for higher versus lower idea density was 3.93 (95% CI, 1.3-11.9) and the RR for higher versus lower grammatical complexity was 5.78 (95% CI, 1.56-21.42).
These new results could be useful when planning future clinical trials, Dr. Tyas noted. “MCI in some people is going to improve even without any treatment, and this should be taken into consideration when recruiting participants to a study and when interpreting the results.
“You don’t want something to look like it’s a benefit of the treatment when in fact these individuals would have just reverted on their own,” she added.
Research implications
Commenting on the findings, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, noted that, in “this study of highly educated, older women,” transitions from MCI to NC “were about equally common” as transitions from MCI to dementia.
“As advances are made in early detection of dementia, and treatments are developed and marketed for people living with MCI, this article’s findings are important to inform discussions of prognosis with patients and [to the] design of clinical trials,” Dr. Sexton said.
The study was funded by the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada. Funding for the Nun Study at the University of Kentucky was provided by the U.S. National Institute of Aging and the Kleberg Foundation. Dr. Tyas has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Can cancer patients get approved COVID therapies?
In mid-November, Kevin Billingsley, MD, MBA, chief medical officer at Yale Cancer Center, New Haven, Conn., was keeping a close eye on the new COVID variant sweeping across South Africa. Six weeks later, the Omicron variant had become the dominant strain in the U.S. – and the Yale health system was no exception.
“As we entered January, we had a breathtaking rate of infection in our hospital,” said Dr. Billingsley, who also leads clinical care at the Smilow Cancer Hospital. “Some of the newly authorized COVID agents were available but not widely enough to make a clinically meaningful impact to protect all high-risk individuals during this surge.”
That left the team at Yale with difficult decisions about who would receive these treatments and who wouldn’t.
The health system convened a COVID-19 immunocompromised working group to identify which patients should get priority access to one of the promising drugs authorized to treat the infection – the monoclonal antibody sotrovimab and antiviral pills Paxlovid and molnupiravir – or the sole available option to prevent it, Evusheld.
“Although clinically sound, none of these decisions have been easy,” Dr. Billingsley told this news organization. “We have done a lot of case-by-case reviewing and a lot of handwringing. Omicron has been a wild ride for us all, and we have been doing the best we can with limited resources.”
‘We’re seeing incredible variability’
The team at Yale is not alone. The restricted supply of COVID-19 treatments has led many oncologists and other experts across the U.S. to create carefully curated lists of their most vulnerable patients.
In late December, the National Institutes of Health published broad criteria to help clinicians prioritize patients most likely to benefit from these therapies. A handful of state health departments, including those in Michigan and Minnesota, established their own standards. Patients with cancer – specifically those with hematologic malignancies and receiving oncology therapies that compromise the immune system – appeared at the top of everyone’s list.
But ultimately individual decisions about who receives these drugs and how they’re allocated fell to institutions.
“Overall, what we’re seeing is incredible variability across the country, because there’s no uniform agreement on what comprises best practices on allocating scarce resources,” said Matthew Wynia, MD, MPH, professor of medicine and director of the Center for Bioethics and Humanities at the University of Colorado, Aurora. “There are so many people at the top of most lists, and the drugs are in such short supply, that there’s no guarantee even those in the top tier will get it.”
This news organization spoke to experts across the country about their experiences accessing these treatments during the Omicron surge and their strategies prioritizing patients with cancer.
Dealing with limited supply
Overall, the limited supply of COVID-19 drugs means not every patient who’s eligible to receive a treatment will get one.
A snapshot of the past 2 weeks, for instance, shows that the count of new infections hit almost 4.3 million, while distribution of the two antiviral pills Paxlovid and molnupiravir and the monoclonal antibody sotrovimab reached just over 600,000 courses.
Since receiving emergency use authorization in early December, almost 500,000 courses of the pre-exposure prophylactic agent Evusheld – which offers about 6 months of protection for immunocompromised individuals – have been distributed; however, about 7 million adults in the U.S. could potentially benefit from it.
In addition, the distribution of drugs is uneven. The federal government manages the overall distribution to states, but states then decide how to divvy up these allocations to hospitals, pharmacies, and medical centers. In Ohio, for instance, the antivirals go to providers who already receive monoclonal antibodies, while in Tennessee, the supply of antiviral agents only goes to Walmart pharmacies.
This strategy, Dr. Wynia explained, can leave clinicians at the mercy of where and how much states decide to allocate to each location. “I’ve heard of some hospitals and health systems in Colorado that aren’t using all they’ve got, but most don’t have nearly enough,” Dr. Wynia said. However, he noted, “some of that is inevitable. We will never get a perfect distribution of these drugs when there is such variable need and demand.”
And, according to Nicolette Louissaint, PhD, MBA, senior vice president of policy and strategic planning at the Healthcare Distribution Alliance in Arlington, Virginia, “we can take some comfort that the federal government is actively looking at cases from week to week and working with state and local health departments to see who needs these products, which means the process is constantly being reviewed and adjusted.”
Plus, not every positive COVID-19 case, even among immunocompromised individuals, necessarily warrants treatment. “If, for instance, an individual with cancer has a mild case of COVID-19, their provider may not deem it necessary for them to receive treatment,” Dr. Louissaint noted.
Still, given the limited and unpredictable supply, “we have had to be thoughtful about who gets these drugs,” said Derek Raghavan, MD, PhD, president of the Levine Cancer Institute, part of the 40-hospital Atrium Health system in Charlotte, North Carolina.
Dr. Raghavan said the highest priority goes to patients with hematologic malignancies, those receiving or coming off chemotherapy or experiencing myelosuppression and immune paresis, as well as those who have undergone organ transplants. Age and other comorbidities, such as diabetes or obesity, play into the lineup as well.
To further hone their priority list, the Levine Cancer Institute has implemented a cancer-centered Hospital at Home initiative. The program includes 40 oncology nurse navigators who routinely screen and score all cancer patients who test positive for COVID-19 by their symptoms and risk factors. For a time-sensitive treatment like Paxlovid, this close monitoring allows patients with COVID to access the pills within 5 days of symptom onset.
Ultimately, “the decision regarding who gets these drugs is [made] by a team to overcome any risk of personal bias, and some of it just comes down to the interface between clinical judgment and available data,” Dr. Raghavan told this news organization. “Although we’d like to have more COVID drugs available and fewer patients with COVID, we have been able to get adequate supplies for our most at-risk patients.”
Like Dr. Raghavan, Karen Bloch, MD, MPH, the medical director for the COVID Infusion Clinic at Vanderbilt University Medical Center (VUMC), said the clinic has had to be highly selective about which patients would benefit most from the COVID monoclonal antibodies. For patients with cancer, her team prioritizes individuals who would be least able to develop antibodies through vaccination or natural infection – which includes patients with B cell malignancies, acute myeloid leukemia, or multiple myeloma receiving active treatment, as well as those who recently received an allogeneic or autologous stem cell transplant.
“Since our criteria for treatment with therapies such as sotrovimab and Evusheld are pretty stringent, we have had sufficient supply to treat those who meet our internal ‘category 1’ predetermined criteria,” said Dr. Bloch, professor of medicine and associate division director for clinical affairs at VUMC, Nashville. “More recently, as the supply chain has begun to open up, we’ve been able to loosen our criteria for sotrovimab, though not for Evusheld yet.”
The Yale team described a similar evolution. “Initially, only a small subset of oncology patients could get these drugs,” said Osama (Sam) Abdelghany, PharmD, MHA, associate director of Oncology Pharmacy Services at Smilow Cancer Hospital. But as the caseload has diminished, Dr. Abdelghany noted, “we have been able to reach many more patients with COVID-19.”
An equitable system?
Dr. Wynia, who has written many reports on crisis standards of care, has spent thousands of hours delving into the ethics of allocating scarce resources during a disaster.
A core problem arises when there are too many people who need a scarce resource and no way of differentiating among them.
In response to the limited supply of COVID-19 treatments, some institutions, such as the University of Pittsburgh Medical Center and Massachusetts General Hospital, have created a lottery system. Others, such as Johns Hopkins Medicine, have opted for first come, first served. Each strategy comes with caveats.
“First come, first served prioritization may be quicker, but it gives more well-resourced people an advantage and lends itself to people abusing the system or exacerbating existing disparities,” Dr. Wynia said.
While a lottery system may be more equitable, this strategy often comes at the price of efficiency. “The practicality of doing a lottery when you have to make a decision about whether or not to treat the patient sitting in front of you comes with its own challenges,” Dr. Wynia said.
At the University of Colorado, he explained, the health center constantly scans medical records for patients who have been diagnosed with COVID and fall into a high-risk group. That way clinicians can call or email those most likely to benefit from these drugs.
“It ends up being a bit of a first come, first served strategy,” Dr. Wynia said. “But we also do not have a huge supply coming in each week, so reaching out to the most eligible people when we have the drugs in hand means more privileged patients are less likely to game the system.”
To manage the supply of Evusheld, Timothy Kubal, MD, MBA, and colleagues also reach out to patients most likely to benefit – specifically, those who can’t mount an adequate antibody response after vaccination.
“We screen all of our patients who have been receiving anti-CD20 agents and other chemotherapy agents known to suppress antibody response,” Dr. Kubal, a medical oncologist/hematologist at the Moffitt Institute in Tampa, Florida, said in an interview. “We then test those patients for antibodies and deliver Evusheld if they have no evidence of antibodies.”
Fortunately, in the coming months, distribution of these drugs should improve significantly. Pfizer says it expects to deliver 10 million courses of Paxlovid by the end of June, and another 10 million by the end of September. More than 1 million courses of sotrovimab should be distributed by GlaxoSmithKline through the end of March. And, recently, the Biden administration announced it purchased 1.2 million courses of Evusheld from AstraZeneca.
“Every few weeks, because the COVID picture changes, the demand changes,” said Dr. Louissaint. “With vaccination rates going up and cases going down, fewer patients will need these products.”
Still, the constant barrage of supply shortages over the past 2 years – from COVID tests, ventilators, and personal protective equipment early on to COVID vaccines a year later and more recently health care staff and COVID tests once again – has taken its toll.
“We have faced supply challenge after challenge and have had to be creative in each situation,” said Lisa Barbarotta, MSN, APRN, program director of Oncology Education and Clinical Practice at Smilow Cancer Hospital. “Nothing has been easy about this.”
And, Dr. Bloch cautioned, even with broader access to COVID-19 drugs on the horizon, there is still no substitute for vaccination. “Getting vaccinated is the best and first line of defense for most people,” she said.
A version of this article first appeared on Medscape.com.
In mid-November, Kevin Billingsley, MD, MBA, chief medical officer at Yale Cancer Center, New Haven, Conn., was keeping a close eye on the new COVID variant sweeping across South Africa. Six weeks later, the Omicron variant had become the dominant strain in the U.S. – and the Yale health system was no exception.
“As we entered January, we had a breathtaking rate of infection in our hospital,” said Dr. Billingsley, who also leads clinical care at the Smilow Cancer Hospital. “Some of the newly authorized COVID agents were available but not widely enough to make a clinically meaningful impact to protect all high-risk individuals during this surge.”
That left the team at Yale with difficult decisions about who would receive these treatments and who wouldn’t.
The health system convened a COVID-19 immunocompromised working group to identify which patients should get priority access to one of the promising drugs authorized to treat the infection – the monoclonal antibody sotrovimab and antiviral pills Paxlovid and molnupiravir – or the sole available option to prevent it, Evusheld.
“Although clinically sound, none of these decisions have been easy,” Dr. Billingsley told this news organization. “We have done a lot of case-by-case reviewing and a lot of handwringing. Omicron has been a wild ride for us all, and we have been doing the best we can with limited resources.”
‘We’re seeing incredible variability’
The team at Yale is not alone. The restricted supply of COVID-19 treatments has led many oncologists and other experts across the U.S. to create carefully curated lists of their most vulnerable patients.
In late December, the National Institutes of Health published broad criteria to help clinicians prioritize patients most likely to benefit from these therapies. A handful of state health departments, including those in Michigan and Minnesota, established their own standards. Patients with cancer – specifically those with hematologic malignancies and receiving oncology therapies that compromise the immune system – appeared at the top of everyone’s list.
But ultimately individual decisions about who receives these drugs and how they’re allocated fell to institutions.
“Overall, what we’re seeing is incredible variability across the country, because there’s no uniform agreement on what comprises best practices on allocating scarce resources,” said Matthew Wynia, MD, MPH, professor of medicine and director of the Center for Bioethics and Humanities at the University of Colorado, Aurora. “There are so many people at the top of most lists, and the drugs are in such short supply, that there’s no guarantee even those in the top tier will get it.”
This news organization spoke to experts across the country about their experiences accessing these treatments during the Omicron surge and their strategies prioritizing patients with cancer.
Dealing with limited supply
Overall, the limited supply of COVID-19 drugs means not every patient who’s eligible to receive a treatment will get one.
A snapshot of the past 2 weeks, for instance, shows that the count of new infections hit almost 4.3 million, while distribution of the two antiviral pills Paxlovid and molnupiravir and the monoclonal antibody sotrovimab reached just over 600,000 courses.
Since receiving emergency use authorization in early December, almost 500,000 courses of the pre-exposure prophylactic agent Evusheld – which offers about 6 months of protection for immunocompromised individuals – have been distributed; however, about 7 million adults in the U.S. could potentially benefit from it.
In addition, the distribution of drugs is uneven. The federal government manages the overall distribution to states, but states then decide how to divvy up these allocations to hospitals, pharmacies, and medical centers. In Ohio, for instance, the antivirals go to providers who already receive monoclonal antibodies, while in Tennessee, the supply of antiviral agents only goes to Walmart pharmacies.
This strategy, Dr. Wynia explained, can leave clinicians at the mercy of where and how much states decide to allocate to each location. “I’ve heard of some hospitals and health systems in Colorado that aren’t using all they’ve got, but most don’t have nearly enough,” Dr. Wynia said. However, he noted, “some of that is inevitable. We will never get a perfect distribution of these drugs when there is such variable need and demand.”
And, according to Nicolette Louissaint, PhD, MBA, senior vice president of policy and strategic planning at the Healthcare Distribution Alliance in Arlington, Virginia, “we can take some comfort that the federal government is actively looking at cases from week to week and working with state and local health departments to see who needs these products, which means the process is constantly being reviewed and adjusted.”
Plus, not every positive COVID-19 case, even among immunocompromised individuals, necessarily warrants treatment. “If, for instance, an individual with cancer has a mild case of COVID-19, their provider may not deem it necessary for them to receive treatment,” Dr. Louissaint noted.
Still, given the limited and unpredictable supply, “we have had to be thoughtful about who gets these drugs,” said Derek Raghavan, MD, PhD, president of the Levine Cancer Institute, part of the 40-hospital Atrium Health system in Charlotte, North Carolina.
Dr. Raghavan said the highest priority goes to patients with hematologic malignancies, those receiving or coming off chemotherapy or experiencing myelosuppression and immune paresis, as well as those who have undergone organ transplants. Age and other comorbidities, such as diabetes or obesity, play into the lineup as well.
To further hone their priority list, the Levine Cancer Institute has implemented a cancer-centered Hospital at Home initiative. The program includes 40 oncology nurse navigators who routinely screen and score all cancer patients who test positive for COVID-19 by their symptoms and risk factors. For a time-sensitive treatment like Paxlovid, this close monitoring allows patients with COVID to access the pills within 5 days of symptom onset.
Ultimately, “the decision regarding who gets these drugs is [made] by a team to overcome any risk of personal bias, and some of it just comes down to the interface between clinical judgment and available data,” Dr. Raghavan told this news organization. “Although we’d like to have more COVID drugs available and fewer patients with COVID, we have been able to get adequate supplies for our most at-risk patients.”
Like Dr. Raghavan, Karen Bloch, MD, MPH, the medical director for the COVID Infusion Clinic at Vanderbilt University Medical Center (VUMC), said the clinic has had to be highly selective about which patients would benefit most from the COVID monoclonal antibodies. For patients with cancer, her team prioritizes individuals who would be least able to develop antibodies through vaccination or natural infection – which includes patients with B cell malignancies, acute myeloid leukemia, or multiple myeloma receiving active treatment, as well as those who recently received an allogeneic or autologous stem cell transplant.
“Since our criteria for treatment with therapies such as sotrovimab and Evusheld are pretty stringent, we have had sufficient supply to treat those who meet our internal ‘category 1’ predetermined criteria,” said Dr. Bloch, professor of medicine and associate division director for clinical affairs at VUMC, Nashville. “More recently, as the supply chain has begun to open up, we’ve been able to loosen our criteria for sotrovimab, though not for Evusheld yet.”
The Yale team described a similar evolution. “Initially, only a small subset of oncology patients could get these drugs,” said Osama (Sam) Abdelghany, PharmD, MHA, associate director of Oncology Pharmacy Services at Smilow Cancer Hospital. But as the caseload has diminished, Dr. Abdelghany noted, “we have been able to reach many more patients with COVID-19.”
An equitable system?
Dr. Wynia, who has written many reports on crisis standards of care, has spent thousands of hours delving into the ethics of allocating scarce resources during a disaster.
A core problem arises when there are too many people who need a scarce resource and no way of differentiating among them.
In response to the limited supply of COVID-19 treatments, some institutions, such as the University of Pittsburgh Medical Center and Massachusetts General Hospital, have created a lottery system. Others, such as Johns Hopkins Medicine, have opted for first come, first served. Each strategy comes with caveats.
“First come, first served prioritization may be quicker, but it gives more well-resourced people an advantage and lends itself to people abusing the system or exacerbating existing disparities,” Dr. Wynia said.
While a lottery system may be more equitable, this strategy often comes at the price of efficiency. “The practicality of doing a lottery when you have to make a decision about whether or not to treat the patient sitting in front of you comes with its own challenges,” Dr. Wynia said.
At the University of Colorado, he explained, the health center constantly scans medical records for patients who have been diagnosed with COVID and fall into a high-risk group. That way clinicians can call or email those most likely to benefit from these drugs.
“It ends up being a bit of a first come, first served strategy,” Dr. Wynia said. “But we also do not have a huge supply coming in each week, so reaching out to the most eligible people when we have the drugs in hand means more privileged patients are less likely to game the system.”
To manage the supply of Evusheld, Timothy Kubal, MD, MBA, and colleagues also reach out to patients most likely to benefit – specifically, those who can’t mount an adequate antibody response after vaccination.
“We screen all of our patients who have been receiving anti-CD20 agents and other chemotherapy agents known to suppress antibody response,” Dr. Kubal, a medical oncologist/hematologist at the Moffitt Institute in Tampa, Florida, said in an interview. “We then test those patients for antibodies and deliver Evusheld if they have no evidence of antibodies.”
Fortunately, in the coming months, distribution of these drugs should improve significantly. Pfizer says it expects to deliver 10 million courses of Paxlovid by the end of June, and another 10 million by the end of September. More than 1 million courses of sotrovimab should be distributed by GlaxoSmithKline through the end of March. And, recently, the Biden administration announced it purchased 1.2 million courses of Evusheld from AstraZeneca.
“Every few weeks, because the COVID picture changes, the demand changes,” said Dr. Louissaint. “With vaccination rates going up and cases going down, fewer patients will need these products.”
Still, the constant barrage of supply shortages over the past 2 years – from COVID tests, ventilators, and personal protective equipment early on to COVID vaccines a year later and more recently health care staff and COVID tests once again – has taken its toll.
“We have faced supply challenge after challenge and have had to be creative in each situation,” said Lisa Barbarotta, MSN, APRN, program director of Oncology Education and Clinical Practice at Smilow Cancer Hospital. “Nothing has been easy about this.”
And, Dr. Bloch cautioned, even with broader access to COVID-19 drugs on the horizon, there is still no substitute for vaccination. “Getting vaccinated is the best and first line of defense for most people,” she said.
A version of this article first appeared on Medscape.com.
In mid-November, Kevin Billingsley, MD, MBA, chief medical officer at Yale Cancer Center, New Haven, Conn., was keeping a close eye on the new COVID variant sweeping across South Africa. Six weeks later, the Omicron variant had become the dominant strain in the U.S. – and the Yale health system was no exception.
“As we entered January, we had a breathtaking rate of infection in our hospital,” said Dr. Billingsley, who also leads clinical care at the Smilow Cancer Hospital. “Some of the newly authorized COVID agents were available but not widely enough to make a clinically meaningful impact to protect all high-risk individuals during this surge.”
That left the team at Yale with difficult decisions about who would receive these treatments and who wouldn’t.
The health system convened a COVID-19 immunocompromised working group to identify which patients should get priority access to one of the promising drugs authorized to treat the infection – the monoclonal antibody sotrovimab and antiviral pills Paxlovid and molnupiravir – or the sole available option to prevent it, Evusheld.
“Although clinically sound, none of these decisions have been easy,” Dr. Billingsley told this news organization. “We have done a lot of case-by-case reviewing and a lot of handwringing. Omicron has been a wild ride for us all, and we have been doing the best we can with limited resources.”
‘We’re seeing incredible variability’
The team at Yale is not alone. The restricted supply of COVID-19 treatments has led many oncologists and other experts across the U.S. to create carefully curated lists of their most vulnerable patients.
In late December, the National Institutes of Health published broad criteria to help clinicians prioritize patients most likely to benefit from these therapies. A handful of state health departments, including those in Michigan and Minnesota, established their own standards. Patients with cancer – specifically those with hematologic malignancies and receiving oncology therapies that compromise the immune system – appeared at the top of everyone’s list.
But ultimately individual decisions about who receives these drugs and how they’re allocated fell to institutions.
“Overall, what we’re seeing is incredible variability across the country, because there’s no uniform agreement on what comprises best practices on allocating scarce resources,” said Matthew Wynia, MD, MPH, professor of medicine and director of the Center for Bioethics and Humanities at the University of Colorado, Aurora. “There are so many people at the top of most lists, and the drugs are in such short supply, that there’s no guarantee even those in the top tier will get it.”
This news organization spoke to experts across the country about their experiences accessing these treatments during the Omicron surge and their strategies prioritizing patients with cancer.
Dealing with limited supply
Overall, the limited supply of COVID-19 drugs means not every patient who’s eligible to receive a treatment will get one.
A snapshot of the past 2 weeks, for instance, shows that the count of new infections hit almost 4.3 million, while distribution of the two antiviral pills Paxlovid and molnupiravir and the monoclonal antibody sotrovimab reached just over 600,000 courses.
Since receiving emergency use authorization in early December, almost 500,000 courses of the pre-exposure prophylactic agent Evusheld – which offers about 6 months of protection for immunocompromised individuals – have been distributed; however, about 7 million adults in the U.S. could potentially benefit from it.
In addition, the distribution of drugs is uneven. The federal government manages the overall distribution to states, but states then decide how to divvy up these allocations to hospitals, pharmacies, and medical centers. In Ohio, for instance, the antivirals go to providers who already receive monoclonal antibodies, while in Tennessee, the supply of antiviral agents only goes to Walmart pharmacies.
This strategy, Dr. Wynia explained, can leave clinicians at the mercy of where and how much states decide to allocate to each location. “I’ve heard of some hospitals and health systems in Colorado that aren’t using all they’ve got, but most don’t have nearly enough,” Dr. Wynia said. However, he noted, “some of that is inevitable. We will never get a perfect distribution of these drugs when there is such variable need and demand.”
And, according to Nicolette Louissaint, PhD, MBA, senior vice president of policy and strategic planning at the Healthcare Distribution Alliance in Arlington, Virginia, “we can take some comfort that the federal government is actively looking at cases from week to week and working with state and local health departments to see who needs these products, which means the process is constantly being reviewed and adjusted.”
Plus, not every positive COVID-19 case, even among immunocompromised individuals, necessarily warrants treatment. “If, for instance, an individual with cancer has a mild case of COVID-19, their provider may not deem it necessary for them to receive treatment,” Dr. Louissaint noted.
Still, given the limited and unpredictable supply, “we have had to be thoughtful about who gets these drugs,” said Derek Raghavan, MD, PhD, president of the Levine Cancer Institute, part of the 40-hospital Atrium Health system in Charlotte, North Carolina.
Dr. Raghavan said the highest priority goes to patients with hematologic malignancies, those receiving or coming off chemotherapy or experiencing myelosuppression and immune paresis, as well as those who have undergone organ transplants. Age and other comorbidities, such as diabetes or obesity, play into the lineup as well.
To further hone their priority list, the Levine Cancer Institute has implemented a cancer-centered Hospital at Home initiative. The program includes 40 oncology nurse navigators who routinely screen and score all cancer patients who test positive for COVID-19 by their symptoms and risk factors. For a time-sensitive treatment like Paxlovid, this close monitoring allows patients with COVID to access the pills within 5 days of symptom onset.
Ultimately, “the decision regarding who gets these drugs is [made] by a team to overcome any risk of personal bias, and some of it just comes down to the interface between clinical judgment and available data,” Dr. Raghavan told this news organization. “Although we’d like to have more COVID drugs available and fewer patients with COVID, we have been able to get adequate supplies for our most at-risk patients.”
Like Dr. Raghavan, Karen Bloch, MD, MPH, the medical director for the COVID Infusion Clinic at Vanderbilt University Medical Center (VUMC), said the clinic has had to be highly selective about which patients would benefit most from the COVID monoclonal antibodies. For patients with cancer, her team prioritizes individuals who would be least able to develop antibodies through vaccination or natural infection – which includes patients with B cell malignancies, acute myeloid leukemia, or multiple myeloma receiving active treatment, as well as those who recently received an allogeneic or autologous stem cell transplant.
“Since our criteria for treatment with therapies such as sotrovimab and Evusheld are pretty stringent, we have had sufficient supply to treat those who meet our internal ‘category 1’ predetermined criteria,” said Dr. Bloch, professor of medicine and associate division director for clinical affairs at VUMC, Nashville. “More recently, as the supply chain has begun to open up, we’ve been able to loosen our criteria for sotrovimab, though not for Evusheld yet.”
The Yale team described a similar evolution. “Initially, only a small subset of oncology patients could get these drugs,” said Osama (Sam) Abdelghany, PharmD, MHA, associate director of Oncology Pharmacy Services at Smilow Cancer Hospital. But as the caseload has diminished, Dr. Abdelghany noted, “we have been able to reach many more patients with COVID-19.”
An equitable system?
Dr. Wynia, who has written many reports on crisis standards of care, has spent thousands of hours delving into the ethics of allocating scarce resources during a disaster.
A core problem arises when there are too many people who need a scarce resource and no way of differentiating among them.
In response to the limited supply of COVID-19 treatments, some institutions, such as the University of Pittsburgh Medical Center and Massachusetts General Hospital, have created a lottery system. Others, such as Johns Hopkins Medicine, have opted for first come, first served. Each strategy comes with caveats.
“First come, first served prioritization may be quicker, but it gives more well-resourced people an advantage and lends itself to people abusing the system or exacerbating existing disparities,” Dr. Wynia said.
While a lottery system may be more equitable, this strategy often comes at the price of efficiency. “The practicality of doing a lottery when you have to make a decision about whether or not to treat the patient sitting in front of you comes with its own challenges,” Dr. Wynia said.
At the University of Colorado, he explained, the health center constantly scans medical records for patients who have been diagnosed with COVID and fall into a high-risk group. That way clinicians can call or email those most likely to benefit from these drugs.
“It ends up being a bit of a first come, first served strategy,” Dr. Wynia said. “But we also do not have a huge supply coming in each week, so reaching out to the most eligible people when we have the drugs in hand means more privileged patients are less likely to game the system.”
To manage the supply of Evusheld, Timothy Kubal, MD, MBA, and colleagues also reach out to patients most likely to benefit – specifically, those who can’t mount an adequate antibody response after vaccination.
“We screen all of our patients who have been receiving anti-CD20 agents and other chemotherapy agents known to suppress antibody response,” Dr. Kubal, a medical oncologist/hematologist at the Moffitt Institute in Tampa, Florida, said in an interview. “We then test those patients for antibodies and deliver Evusheld if they have no evidence of antibodies.”
Fortunately, in the coming months, distribution of these drugs should improve significantly. Pfizer says it expects to deliver 10 million courses of Paxlovid by the end of June, and another 10 million by the end of September. More than 1 million courses of sotrovimab should be distributed by GlaxoSmithKline through the end of March. And, recently, the Biden administration announced it purchased 1.2 million courses of Evusheld from AstraZeneca.
“Every few weeks, because the COVID picture changes, the demand changes,” said Dr. Louissaint. “With vaccination rates going up and cases going down, fewer patients will need these products.”
Still, the constant barrage of supply shortages over the past 2 years – from COVID tests, ventilators, and personal protective equipment early on to COVID vaccines a year later and more recently health care staff and COVID tests once again – has taken its toll.
“We have faced supply challenge after challenge and have had to be creative in each situation,” said Lisa Barbarotta, MSN, APRN, program director of Oncology Education and Clinical Practice at Smilow Cancer Hospital. “Nothing has been easy about this.”
And, Dr. Bloch cautioned, even with broader access to COVID-19 drugs on the horizon, there is still no substitute for vaccination. “Getting vaccinated is the best and first line of defense for most people,” she said.
A version of this article first appeared on Medscape.com.
Fewer diabetes complications with NOACs in patients with AFib
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
FROM ANNALS OF INTERNAL MEDICINE
Early-onset severe COPD: Similar physical symptoms, but higher depression rates
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
FROM CLINICAL NUTRITION