User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Exploring the relationship of COVID-19 vaccines and fertility
Introduction
Amidst an aggressive vaccination campaign for COVID-19, misinformation has spread over the Internet, affecting public perception and making some people hesitant to participate in ongoing immunization campaigns. Of chief concern are issues pertaining to fertility or viability of sperm – information circulating on social networks posits that the coronavirus vaccine may influence infertility in men, which, according to physicians, is not grounded in reality. From the perspective of evidence-based medicine, there is a dearth of information suggesting an untoward effect of the vaccine on male fertility. The risk of adverse reactions arising from approved vaccines is negligible, with mild, albeit controllable, side effects demonstrated by patients in clinical trials. Therefore, there is no plausible reason for the general public to avoid vaccinations.1
Infertility following vaccination
The source of confusion can be traced back to a study conducted by researchers at the University of Miami Miller School of Medicine; the general public has conflated a side effect of the virus, namely, infertility and erectile dysfunction, with that of the vaccine.2 According to Ranjith Ramasamy, MD, director of the urology program at Miller, “We were the first to demonstrate that the COVID virus, itself, can affect male fertility and be a potential cause for erectile dysfunction. We are now the first to examine if there is any impact of the COVID vaccine on male fertility potential, which we did not find.”3
Coronavirus can indeed cause significant damage to the testicular tissue of infected men by means of mediating ACE2 expression on Leydig and Sertoli cells of the testis. It should be noted that COVID-19 may potentially attack any type of cell in the body that expresses the enzyme ACE2. However, it is particularly harmful to cells with high levels of expression of this enzyme, such as testicular cells. The spermatogenesis process can be affected, thereby posing a risk to male fertility.4
Expanding on the theme of fertility during the pandemic, a number of false claims5-7 about the vaccine and its overall effect on the placenta and fertility have also emerged as a contentious topic for debate on social media; doctors continue to explain why the theories are not reasonable or a cause for concern. The World Health Organization (WHO) provides recommendations on COVID-19 vaccinations for pregnant and/or lactating women and encourages a shared decision process involving risk/benefit assessment with the prescribing physician.5 Pregnant women, especially those with underlying comorbid conditions, are susceptible to developing severe symptom manifestations of COVID-19 with the disease also being associated with an increased likelihood of premature birth. As far as lactating women are concerned, the evidence thus far has indicated that the risk of side effects of the vaccine is very low, suggesting that these women could be vaccinated.5
The vaccine is the best option
While more studies are needed to ascertain the relationship between COVID-19 and male infertility, the vaccine is currently the best option for those who are concerned about their fertility from exposure to the coronavirus. Because of delayed wholesale acceptance of vaccines by the general population, clinicians should continue to emphasize the importance of preventive care with respect to disease exposure.6
In addition, those who are concerned with fertility can opt for ways to preserve their reproductive capacity, such as the removal of semen for freezing sperm, albeit with adherence to sperm-washing procedures to preclude cross-contamination from viruses.8,9 For the preservation of sperm, the noninvasive method is often performed, preferably collected in several samples. Then, the semen is cryopreserved.8 In some instances, the sperm can also be removed directly from the testicles with a simple needle or by means of a minor surgical procedure.
A wait and try approach is advocated by clinicians for individuals who have already experienced COVID-19 symptoms and are therefore concerned about the prospect of childbearing.10 If the couple is unable to conceive after a year of trying, it is recommended that they consult a reproductive specialist; the clinician can carry out a comprehensive evaluation and order a series of tests to identify the source of the problem, indicating whether there are alternative methods for helping the couple to start a family (addressing the underlying factors involved in infertility, or treating via assisted reproduction procedures, such as in vitro fertilization).11
Dr. Aman is faculty member at the biology department of City Colleges of Chicago, and a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF). She disclosed no relevant financial relationships. Dr. Islam is a medical writer for the IMCHF, Montreal, is based in New York, and disclosed no relevant financial relationships. Mr. Choudhry is a research assistant at the IMCHF and he has no disclosures. Dr. Zia Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. Berry SD et al. J Am Geriatr Soc. 2021 May;69(5):1140-6.
2. Achua JK et al. World J Men’s Health. 2021 Jan;39(1):65-74.
3. Broderick JM. Urology Times. 2021 June.
4. Huang C et al. Andrology. 2021 Jan;9(1):80-7.
5. Sajjadi NB et al. J Osteopath Med. 2021 Apr 12;121(6):583-7.
6. Sallam M et al. Vaccines. 2021 Jan;9(1):42.
7. Islam MS et al. PloS One. 2021 May 12;16(5):e0251605.
8. Tesarik J. J Fertil Preserv. 2021;2:art246111.
9. Adiga SK et al. Reprod BioMed Online. 2020 Dec;41(6):991-7.
10. FAQs related to COVID-19. Q: If I get sick or test positive for COVID-19, when is it safe to become pregnant? American Society for Reproductive Medicine.
11. Cross C. Wellness and Prevention: Why can’t I get pregnant? John Hopkins Medicine.
Introduction
Amidst an aggressive vaccination campaign for COVID-19, misinformation has spread over the Internet, affecting public perception and making some people hesitant to participate in ongoing immunization campaigns. Of chief concern are issues pertaining to fertility or viability of sperm – information circulating on social networks posits that the coronavirus vaccine may influence infertility in men, which, according to physicians, is not grounded in reality. From the perspective of evidence-based medicine, there is a dearth of information suggesting an untoward effect of the vaccine on male fertility. The risk of adverse reactions arising from approved vaccines is negligible, with mild, albeit controllable, side effects demonstrated by patients in clinical trials. Therefore, there is no plausible reason for the general public to avoid vaccinations.1
Infertility following vaccination
The source of confusion can be traced back to a study conducted by researchers at the University of Miami Miller School of Medicine; the general public has conflated a side effect of the virus, namely, infertility and erectile dysfunction, with that of the vaccine.2 According to Ranjith Ramasamy, MD, director of the urology program at Miller, “We were the first to demonstrate that the COVID virus, itself, can affect male fertility and be a potential cause for erectile dysfunction. We are now the first to examine if there is any impact of the COVID vaccine on male fertility potential, which we did not find.”3
Coronavirus can indeed cause significant damage to the testicular tissue of infected men by means of mediating ACE2 expression on Leydig and Sertoli cells of the testis. It should be noted that COVID-19 may potentially attack any type of cell in the body that expresses the enzyme ACE2. However, it is particularly harmful to cells with high levels of expression of this enzyme, such as testicular cells. The spermatogenesis process can be affected, thereby posing a risk to male fertility.4
Expanding on the theme of fertility during the pandemic, a number of false claims5-7 about the vaccine and its overall effect on the placenta and fertility have also emerged as a contentious topic for debate on social media; doctors continue to explain why the theories are not reasonable or a cause for concern. The World Health Organization (WHO) provides recommendations on COVID-19 vaccinations for pregnant and/or lactating women and encourages a shared decision process involving risk/benefit assessment with the prescribing physician.5 Pregnant women, especially those with underlying comorbid conditions, are susceptible to developing severe symptom manifestations of COVID-19 with the disease also being associated with an increased likelihood of premature birth. As far as lactating women are concerned, the evidence thus far has indicated that the risk of side effects of the vaccine is very low, suggesting that these women could be vaccinated.5
The vaccine is the best option
While more studies are needed to ascertain the relationship between COVID-19 and male infertility, the vaccine is currently the best option for those who are concerned about their fertility from exposure to the coronavirus. Because of delayed wholesale acceptance of vaccines by the general population, clinicians should continue to emphasize the importance of preventive care with respect to disease exposure.6
In addition, those who are concerned with fertility can opt for ways to preserve their reproductive capacity, such as the removal of semen for freezing sperm, albeit with adherence to sperm-washing procedures to preclude cross-contamination from viruses.8,9 For the preservation of sperm, the noninvasive method is often performed, preferably collected in several samples. Then, the semen is cryopreserved.8 In some instances, the sperm can also be removed directly from the testicles with a simple needle or by means of a minor surgical procedure.
A wait and try approach is advocated by clinicians for individuals who have already experienced COVID-19 symptoms and are therefore concerned about the prospect of childbearing.10 If the couple is unable to conceive after a year of trying, it is recommended that they consult a reproductive specialist; the clinician can carry out a comprehensive evaluation and order a series of tests to identify the source of the problem, indicating whether there are alternative methods for helping the couple to start a family (addressing the underlying factors involved in infertility, or treating via assisted reproduction procedures, such as in vitro fertilization).11
Dr. Aman is faculty member at the biology department of City Colleges of Chicago, and a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF). She disclosed no relevant financial relationships. Dr. Islam is a medical writer for the IMCHF, Montreal, is based in New York, and disclosed no relevant financial relationships. Mr. Choudhry is a research assistant at the IMCHF and he has no disclosures. Dr. Zia Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. Berry SD et al. J Am Geriatr Soc. 2021 May;69(5):1140-6.
2. Achua JK et al. World J Men’s Health. 2021 Jan;39(1):65-74.
3. Broderick JM. Urology Times. 2021 June.
4. Huang C et al. Andrology. 2021 Jan;9(1):80-7.
5. Sajjadi NB et al. J Osteopath Med. 2021 Apr 12;121(6):583-7.
6. Sallam M et al. Vaccines. 2021 Jan;9(1):42.
7. Islam MS et al. PloS One. 2021 May 12;16(5):e0251605.
8. Tesarik J. J Fertil Preserv. 2021;2:art246111.
9. Adiga SK et al. Reprod BioMed Online. 2020 Dec;41(6):991-7.
10. FAQs related to COVID-19. Q: If I get sick or test positive for COVID-19, when is it safe to become pregnant? American Society for Reproductive Medicine.
11. Cross C. Wellness and Prevention: Why can’t I get pregnant? John Hopkins Medicine.
Introduction
Amidst an aggressive vaccination campaign for COVID-19, misinformation has spread over the Internet, affecting public perception and making some people hesitant to participate in ongoing immunization campaigns. Of chief concern are issues pertaining to fertility or viability of sperm – information circulating on social networks posits that the coronavirus vaccine may influence infertility in men, which, according to physicians, is not grounded in reality. From the perspective of evidence-based medicine, there is a dearth of information suggesting an untoward effect of the vaccine on male fertility. The risk of adverse reactions arising from approved vaccines is negligible, with mild, albeit controllable, side effects demonstrated by patients in clinical trials. Therefore, there is no plausible reason for the general public to avoid vaccinations.1
Infertility following vaccination
The source of confusion can be traced back to a study conducted by researchers at the University of Miami Miller School of Medicine; the general public has conflated a side effect of the virus, namely, infertility and erectile dysfunction, with that of the vaccine.2 According to Ranjith Ramasamy, MD, director of the urology program at Miller, “We were the first to demonstrate that the COVID virus, itself, can affect male fertility and be a potential cause for erectile dysfunction. We are now the first to examine if there is any impact of the COVID vaccine on male fertility potential, which we did not find.”3
Coronavirus can indeed cause significant damage to the testicular tissue of infected men by means of mediating ACE2 expression on Leydig and Sertoli cells of the testis. It should be noted that COVID-19 may potentially attack any type of cell in the body that expresses the enzyme ACE2. However, it is particularly harmful to cells with high levels of expression of this enzyme, such as testicular cells. The spermatogenesis process can be affected, thereby posing a risk to male fertility.4
Expanding on the theme of fertility during the pandemic, a number of false claims5-7 about the vaccine and its overall effect on the placenta and fertility have also emerged as a contentious topic for debate on social media; doctors continue to explain why the theories are not reasonable or a cause for concern. The World Health Organization (WHO) provides recommendations on COVID-19 vaccinations for pregnant and/or lactating women and encourages a shared decision process involving risk/benefit assessment with the prescribing physician.5 Pregnant women, especially those with underlying comorbid conditions, are susceptible to developing severe symptom manifestations of COVID-19 with the disease also being associated with an increased likelihood of premature birth. As far as lactating women are concerned, the evidence thus far has indicated that the risk of side effects of the vaccine is very low, suggesting that these women could be vaccinated.5
The vaccine is the best option
While more studies are needed to ascertain the relationship between COVID-19 and male infertility, the vaccine is currently the best option for those who are concerned about their fertility from exposure to the coronavirus. Because of delayed wholesale acceptance of vaccines by the general population, clinicians should continue to emphasize the importance of preventive care with respect to disease exposure.6
In addition, those who are concerned with fertility can opt for ways to preserve their reproductive capacity, such as the removal of semen for freezing sperm, albeit with adherence to sperm-washing procedures to preclude cross-contamination from viruses.8,9 For the preservation of sperm, the noninvasive method is often performed, preferably collected in several samples. Then, the semen is cryopreserved.8 In some instances, the sperm can also be removed directly from the testicles with a simple needle or by means of a minor surgical procedure.
A wait and try approach is advocated by clinicians for individuals who have already experienced COVID-19 symptoms and are therefore concerned about the prospect of childbearing.10 If the couple is unable to conceive after a year of trying, it is recommended that they consult a reproductive specialist; the clinician can carry out a comprehensive evaluation and order a series of tests to identify the source of the problem, indicating whether there are alternative methods for helping the couple to start a family (addressing the underlying factors involved in infertility, or treating via assisted reproduction procedures, such as in vitro fertilization).11
Dr. Aman is faculty member at the biology department of City Colleges of Chicago, and a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF). She disclosed no relevant financial relationships. Dr. Islam is a medical writer for the IMCHF, Montreal, is based in New York, and disclosed no relevant financial relationships. Mr. Choudhry is a research assistant at the IMCHF and he has no disclosures. Dr. Zia Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. Berry SD et al. J Am Geriatr Soc. 2021 May;69(5):1140-6.
2. Achua JK et al. World J Men’s Health. 2021 Jan;39(1):65-74.
3. Broderick JM. Urology Times. 2021 June.
4. Huang C et al. Andrology. 2021 Jan;9(1):80-7.
5. Sajjadi NB et al. J Osteopath Med. 2021 Apr 12;121(6):583-7.
6. Sallam M et al. Vaccines. 2021 Jan;9(1):42.
7. Islam MS et al. PloS One. 2021 May 12;16(5):e0251605.
8. Tesarik J. J Fertil Preserv. 2021;2:art246111.
9. Adiga SK et al. Reprod BioMed Online. 2020 Dec;41(6):991-7.
10. FAQs related to COVID-19. Q: If I get sick or test positive for COVID-19, when is it safe to become pregnant? American Society for Reproductive Medicine.
11. Cross C. Wellness and Prevention: Why can’t I get pregnant? John Hopkins Medicine.
USPSTF tweaks primary prevention statin recommendations in new draft guidance
Given the expansive contemporary role of statins for primary cardiovascular disease (CVD) prevention, the language in the new U.S. Preventive Services Task Force draft guidance on their use in that setting may seem conservative. Even so, the proposed recommendations, open to public comment until March 21, take more recent data into account but don’t substantially vary from the 2016 USPSTF document they are intended to replace.
The task force concluded “with moderate certainty” that a statin prescription will clinically benefit adults aged 40-75 years without CVD but with at least one of several risk factors, such as dyslipidemia or diabetes, who have a 10-year CVD risk of at least 7.5%.
the new report states. That, says an accompanying USPSTF press release, means such people “may benefit from statin use and should decide with their clinician if taking a statin is right for them.”
Also, notes the report, the net benefit of statin therapy is “at least moderate” for individuals with a 10% or greater CVD risk over the next decade who, the press release states, “should take a statin to prevent a first heart attack or stroke.”
The evidence review on which the task force based the guidance, the report says, lacked sufficient basis for determining statin benefit versus risk in adults older than 75 years without a history of CVD. “In the absence of this evidence, clinicians should use their judgment as to whether to offer a statin to a patient in this age group,” according to the press release.
The review focused on 22 clinical trials for data on the statin benefits and saw significantly decreased associated risks for death from any cause, fatal or nonfatal stroke, and fatal or nonfatal myocardial infarction with treatment. The combined trial populations exceeded 85,000 for assessing all-cause mortality and 76,000 for each of the other two endpoints.
To assess any potential statin therapy harms, the evidence review covered 19 clinical trials with a combined enrollment of about 75,000 – two more trials than considered in the 2016 document – plus three observational studies with more than 400,000 participants. Statins were found not to be associated with an increased risk for study withdrawal because of adverse events, nor were there signs of greater risk for myalgia or new-onset diabetes, compared with placebo.
“A majority of the trials reviewed by the USPSTF used moderate-intensity statin therapy,” the report states. “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CVD in most persons.”
A version of this article first appeared on Medscape.com.
Given the expansive contemporary role of statins for primary cardiovascular disease (CVD) prevention, the language in the new U.S. Preventive Services Task Force draft guidance on their use in that setting may seem conservative. Even so, the proposed recommendations, open to public comment until March 21, take more recent data into account but don’t substantially vary from the 2016 USPSTF document they are intended to replace.
The task force concluded “with moderate certainty” that a statin prescription will clinically benefit adults aged 40-75 years without CVD but with at least one of several risk factors, such as dyslipidemia or diabetes, who have a 10-year CVD risk of at least 7.5%.
the new report states. That, says an accompanying USPSTF press release, means such people “may benefit from statin use and should decide with their clinician if taking a statin is right for them.”
Also, notes the report, the net benefit of statin therapy is “at least moderate” for individuals with a 10% or greater CVD risk over the next decade who, the press release states, “should take a statin to prevent a first heart attack or stroke.”
The evidence review on which the task force based the guidance, the report says, lacked sufficient basis for determining statin benefit versus risk in adults older than 75 years without a history of CVD. “In the absence of this evidence, clinicians should use their judgment as to whether to offer a statin to a patient in this age group,” according to the press release.
The review focused on 22 clinical trials for data on the statin benefits and saw significantly decreased associated risks for death from any cause, fatal or nonfatal stroke, and fatal or nonfatal myocardial infarction with treatment. The combined trial populations exceeded 85,000 for assessing all-cause mortality and 76,000 for each of the other two endpoints.
To assess any potential statin therapy harms, the evidence review covered 19 clinical trials with a combined enrollment of about 75,000 – two more trials than considered in the 2016 document – plus three observational studies with more than 400,000 participants. Statins were found not to be associated with an increased risk for study withdrawal because of adverse events, nor were there signs of greater risk for myalgia or new-onset diabetes, compared with placebo.
“A majority of the trials reviewed by the USPSTF used moderate-intensity statin therapy,” the report states. “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CVD in most persons.”
A version of this article first appeared on Medscape.com.
Given the expansive contemporary role of statins for primary cardiovascular disease (CVD) prevention, the language in the new U.S. Preventive Services Task Force draft guidance on their use in that setting may seem conservative. Even so, the proposed recommendations, open to public comment until March 21, take more recent data into account but don’t substantially vary from the 2016 USPSTF document they are intended to replace.
The task force concluded “with moderate certainty” that a statin prescription will clinically benefit adults aged 40-75 years without CVD but with at least one of several risk factors, such as dyslipidemia or diabetes, who have a 10-year CVD risk of at least 7.5%.
the new report states. That, says an accompanying USPSTF press release, means such people “may benefit from statin use and should decide with their clinician if taking a statin is right for them.”
Also, notes the report, the net benefit of statin therapy is “at least moderate” for individuals with a 10% or greater CVD risk over the next decade who, the press release states, “should take a statin to prevent a first heart attack or stroke.”
The evidence review on which the task force based the guidance, the report says, lacked sufficient basis for determining statin benefit versus risk in adults older than 75 years without a history of CVD. “In the absence of this evidence, clinicians should use their judgment as to whether to offer a statin to a patient in this age group,” according to the press release.
The review focused on 22 clinical trials for data on the statin benefits and saw significantly decreased associated risks for death from any cause, fatal or nonfatal stroke, and fatal or nonfatal myocardial infarction with treatment. The combined trial populations exceeded 85,000 for assessing all-cause mortality and 76,000 for each of the other two endpoints.
To assess any potential statin therapy harms, the evidence review covered 19 clinical trials with a combined enrollment of about 75,000 – two more trials than considered in the 2016 document – plus three observational studies with more than 400,000 participants. Statins were found not to be associated with an increased risk for study withdrawal because of adverse events, nor were there signs of greater risk for myalgia or new-onset diabetes, compared with placebo.
“A majority of the trials reviewed by the USPSTF used moderate-intensity statin therapy,” the report states. “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CVD in most persons.”
A version of this article first appeared on Medscape.com.
‘In the presence of kindness’: humanitarian Paul Farmer dies
Renowned infectious disease specialist, humanitarian, and healthcare champion for many of the world’s most vulnerable patient populations, Paul Edward Farmer, MD, died suddenly in his sleep from an acute cardiac event on Feb. 21 in Rwanda, where he had been teaching. He was 62.
Dr. Farmer cofounded the Boston-based global nonprofit Partners In Health and spent decades providing healthcare to impoverished communities worldwide, fighting on the frontline to protect underserved communities against deadly pandemics.
Dr. Farmer was the Kolokotrones University Professor and chair of the department of global health and social medicine in the Blavatnik Institute at Harvard Medical School, Boston. He served as chief of the division of global health equity at Brigham and Women’s Hospital, also in Boston.
“Paul dedicated his life to improving human health and advocating for health equity and social justice on a global scale,” said HMS dean George Q. Daley in a letter to the HMS community. “I am particularly shaken by his passing because he was not only a consummate colleague and a beloved mentor, but a close friend. To me, Paul represented the heart and soul of Harvard Medical School.”
He was also chancellor and cofounder of the University of Global Health Equity in Kigali, Rwanda. Before his death, he spent several weeks teaching at the university.
“Paul Farmer’s loss is devastating, but his vision for the world will live on through Partners In Health,” said Partners In Health CEO Sheila Davis in a statement. “Paul taught all those around him the power of accompaniment, love for one another, and solidarity. Our deepest sympathies are with his family.”
Dr. Farmer was born in North Adams, Mass., and grew up in Florida with his parents and five siblings. He attended Duke University on a Benjamin N. Duke Scholarship and received his medical degree in 1988, followed by his PhD in 1990 from Harvard University.
His humanitarian work began when he was a college student volunteering in Haiti in 1983 working with dispossessed farmers. In 1987, he cofounded Partners In Health with the goal of helping patients in poverty-stricken corners of the world.
Under Dr. Farmer’s leadership, the nonprofit tackled major public health crises: Haiti’s devastating 2010 earthquake, drug-resistant tuberculosis in Peru and other countries, and an Ebola outbreak that tore through West Africa.
Dr. Farmer documented his 2014-2015 experience treating Africa’s Ebola patients in a book called “Fevers, Feuds, and Diamonds: Ebola and the Ravages of History.”
He wrote that by the time he arrived, “western Sierra Leone was ground zero of the epidemic, and Upper West Africa was just about the worst place in the world to be critically ill or injured.”
One of his greatest qualities was his ability to connect with patients – to treat them “not like ones who suffered, but like a pal you’d joke with,” said Pardis Sabeti, MD, PhD, a Harvard University geneticist who also spent time in Africa and famously sequenced samples of the Ebola virus’ genome.
Dr. Sabeti and Dr. Farmer bonded over their love for Sierra Leone, and their grief over losing a close colleague to Ebola, Sheik Humarr Khan, who was one of the area’s leading infectious disease experts.
Dr. Sabeti first met Dr. Farmer years earlier as a first-year Harvard medical student when she enrolled in one of his courses. She said students introduced themselves, one by one, each veering into heartfelt testimonies about what Dr. Farmer’s work had meant to them.
Dr. Farmer and Dr. Sabeti were just texting on Feb. 19, and the two were “goofing around in our usual way, and scheming about how to make the world better, as we always did.”
Dr. Farmer was funny, mischievous, and above all, exactly what you would expect upon meeting him, Dr. Sabeti said.
“It’s cliché, but the energetic kick you get from just being in his presence, it’s almost otherworldly,” she said. “It’s not even otherworldly in the sense of: ‘I just came across – greatness.’ It’s more: ‘I just came across kindness.’ ”
Dr. Farmer’s work has been widely distributed in publications including Bulletin of the World Health Organization, The Lancet, the New England Journal of Medicine, Clinical Infectious Diseases, and Social Science & Medicine.
He was awarded the 2020 Berggruen Prize for Philosophy & Culture, the Margaret Mead Award from the American Anthropological Association, the American Medical Association’s Outstanding International Physician (Nathan Davis) Award, and, with his Partners In Health colleagues, the Hilton Humanitarian Prize.
He is survived by his wife, Didi Bertrand Farmer, and their three children.
A verison of this article first appeared on Medscape.com.
Renowned infectious disease specialist, humanitarian, and healthcare champion for many of the world’s most vulnerable patient populations, Paul Edward Farmer, MD, died suddenly in his sleep from an acute cardiac event on Feb. 21 in Rwanda, where he had been teaching. He was 62.
Dr. Farmer cofounded the Boston-based global nonprofit Partners In Health and spent decades providing healthcare to impoverished communities worldwide, fighting on the frontline to protect underserved communities against deadly pandemics.
Dr. Farmer was the Kolokotrones University Professor and chair of the department of global health and social medicine in the Blavatnik Institute at Harvard Medical School, Boston. He served as chief of the division of global health equity at Brigham and Women’s Hospital, also in Boston.
“Paul dedicated his life to improving human health and advocating for health equity and social justice on a global scale,” said HMS dean George Q. Daley in a letter to the HMS community. “I am particularly shaken by his passing because he was not only a consummate colleague and a beloved mentor, but a close friend. To me, Paul represented the heart and soul of Harvard Medical School.”
He was also chancellor and cofounder of the University of Global Health Equity in Kigali, Rwanda. Before his death, he spent several weeks teaching at the university.
“Paul Farmer’s loss is devastating, but his vision for the world will live on through Partners In Health,” said Partners In Health CEO Sheila Davis in a statement. “Paul taught all those around him the power of accompaniment, love for one another, and solidarity. Our deepest sympathies are with his family.”
Dr. Farmer was born in North Adams, Mass., and grew up in Florida with his parents and five siblings. He attended Duke University on a Benjamin N. Duke Scholarship and received his medical degree in 1988, followed by his PhD in 1990 from Harvard University.
His humanitarian work began when he was a college student volunteering in Haiti in 1983 working with dispossessed farmers. In 1987, he cofounded Partners In Health with the goal of helping patients in poverty-stricken corners of the world.
Under Dr. Farmer’s leadership, the nonprofit tackled major public health crises: Haiti’s devastating 2010 earthquake, drug-resistant tuberculosis in Peru and other countries, and an Ebola outbreak that tore through West Africa.
Dr. Farmer documented his 2014-2015 experience treating Africa’s Ebola patients in a book called “Fevers, Feuds, and Diamonds: Ebola and the Ravages of History.”
He wrote that by the time he arrived, “western Sierra Leone was ground zero of the epidemic, and Upper West Africa was just about the worst place in the world to be critically ill or injured.”
One of his greatest qualities was his ability to connect with patients – to treat them “not like ones who suffered, but like a pal you’d joke with,” said Pardis Sabeti, MD, PhD, a Harvard University geneticist who also spent time in Africa and famously sequenced samples of the Ebola virus’ genome.
Dr. Sabeti and Dr. Farmer bonded over their love for Sierra Leone, and their grief over losing a close colleague to Ebola, Sheik Humarr Khan, who was one of the area’s leading infectious disease experts.
Dr. Sabeti first met Dr. Farmer years earlier as a first-year Harvard medical student when she enrolled in one of his courses. She said students introduced themselves, one by one, each veering into heartfelt testimonies about what Dr. Farmer’s work had meant to them.
Dr. Farmer and Dr. Sabeti were just texting on Feb. 19, and the two were “goofing around in our usual way, and scheming about how to make the world better, as we always did.”
Dr. Farmer was funny, mischievous, and above all, exactly what you would expect upon meeting him, Dr. Sabeti said.
“It’s cliché, but the energetic kick you get from just being in his presence, it’s almost otherworldly,” she said. “It’s not even otherworldly in the sense of: ‘I just came across – greatness.’ It’s more: ‘I just came across kindness.’ ”
Dr. Farmer’s work has been widely distributed in publications including Bulletin of the World Health Organization, The Lancet, the New England Journal of Medicine, Clinical Infectious Diseases, and Social Science & Medicine.
He was awarded the 2020 Berggruen Prize for Philosophy & Culture, the Margaret Mead Award from the American Anthropological Association, the American Medical Association’s Outstanding International Physician (Nathan Davis) Award, and, with his Partners In Health colleagues, the Hilton Humanitarian Prize.
He is survived by his wife, Didi Bertrand Farmer, and their three children.
A verison of this article first appeared on Medscape.com.
Renowned infectious disease specialist, humanitarian, and healthcare champion for many of the world’s most vulnerable patient populations, Paul Edward Farmer, MD, died suddenly in his sleep from an acute cardiac event on Feb. 21 in Rwanda, where he had been teaching. He was 62.
Dr. Farmer cofounded the Boston-based global nonprofit Partners In Health and spent decades providing healthcare to impoverished communities worldwide, fighting on the frontline to protect underserved communities against deadly pandemics.
Dr. Farmer was the Kolokotrones University Professor and chair of the department of global health and social medicine in the Blavatnik Institute at Harvard Medical School, Boston. He served as chief of the division of global health equity at Brigham and Women’s Hospital, also in Boston.
“Paul dedicated his life to improving human health and advocating for health equity and social justice on a global scale,” said HMS dean George Q. Daley in a letter to the HMS community. “I am particularly shaken by his passing because he was not only a consummate colleague and a beloved mentor, but a close friend. To me, Paul represented the heart and soul of Harvard Medical School.”
He was also chancellor and cofounder of the University of Global Health Equity in Kigali, Rwanda. Before his death, he spent several weeks teaching at the university.
“Paul Farmer’s loss is devastating, but his vision for the world will live on through Partners In Health,” said Partners In Health CEO Sheila Davis in a statement. “Paul taught all those around him the power of accompaniment, love for one another, and solidarity. Our deepest sympathies are with his family.”
Dr. Farmer was born in North Adams, Mass., and grew up in Florida with his parents and five siblings. He attended Duke University on a Benjamin N. Duke Scholarship and received his medical degree in 1988, followed by his PhD in 1990 from Harvard University.
His humanitarian work began when he was a college student volunteering in Haiti in 1983 working with dispossessed farmers. In 1987, he cofounded Partners In Health with the goal of helping patients in poverty-stricken corners of the world.
Under Dr. Farmer’s leadership, the nonprofit tackled major public health crises: Haiti’s devastating 2010 earthquake, drug-resistant tuberculosis in Peru and other countries, and an Ebola outbreak that tore through West Africa.
Dr. Farmer documented his 2014-2015 experience treating Africa’s Ebola patients in a book called “Fevers, Feuds, and Diamonds: Ebola and the Ravages of History.”
He wrote that by the time he arrived, “western Sierra Leone was ground zero of the epidemic, and Upper West Africa was just about the worst place in the world to be critically ill or injured.”
One of his greatest qualities was his ability to connect with patients – to treat them “not like ones who suffered, but like a pal you’d joke with,” said Pardis Sabeti, MD, PhD, a Harvard University geneticist who also spent time in Africa and famously sequenced samples of the Ebola virus’ genome.
Dr. Sabeti and Dr. Farmer bonded over their love for Sierra Leone, and their grief over losing a close colleague to Ebola, Sheik Humarr Khan, who was one of the area’s leading infectious disease experts.
Dr. Sabeti first met Dr. Farmer years earlier as a first-year Harvard medical student when she enrolled in one of his courses. She said students introduced themselves, one by one, each veering into heartfelt testimonies about what Dr. Farmer’s work had meant to them.
Dr. Farmer and Dr. Sabeti were just texting on Feb. 19, and the two were “goofing around in our usual way, and scheming about how to make the world better, as we always did.”
Dr. Farmer was funny, mischievous, and above all, exactly what you would expect upon meeting him, Dr. Sabeti said.
“It’s cliché, but the energetic kick you get from just being in his presence, it’s almost otherworldly,” she said. “It’s not even otherworldly in the sense of: ‘I just came across – greatness.’ It’s more: ‘I just came across kindness.’ ”
Dr. Farmer’s work has been widely distributed in publications including Bulletin of the World Health Organization, The Lancet, the New England Journal of Medicine, Clinical Infectious Diseases, and Social Science & Medicine.
He was awarded the 2020 Berggruen Prize for Philosophy & Culture, the Margaret Mead Award from the American Anthropological Association, the American Medical Association’s Outstanding International Physician (Nathan Davis) Award, and, with his Partners In Health colleagues, the Hilton Humanitarian Prize.
He is survived by his wife, Didi Bertrand Farmer, and their three children.
A verison of this article first appeared on Medscape.com.
Children and COVID: The Omicron surge has become a retreat
The Omicron decline continued for a fourth consecutive week as new cases of COVID-19 in children fell by 42% from the week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That 42% represents a drop from the 299,000 new cases reported for Feb. 4-10 down to 174,000 for the most recent week, Feb. 11-17. 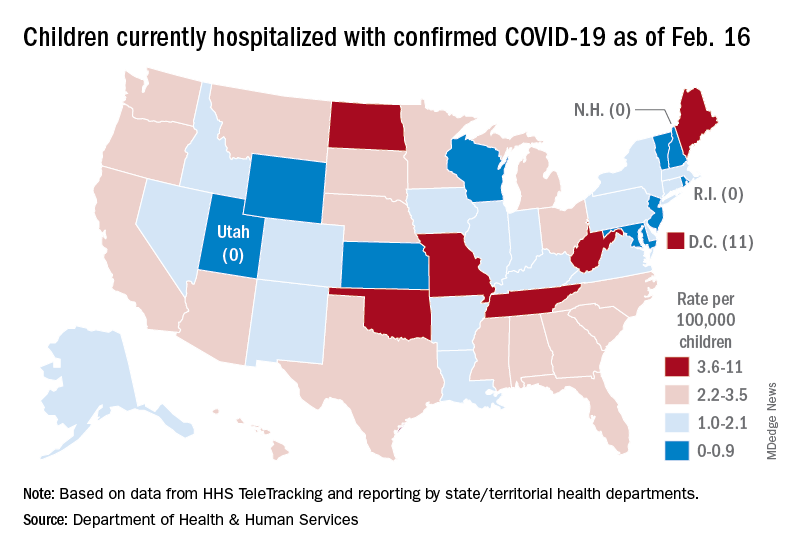
The overall count of COVID-19 cases in children is 12.5 million over the course of the pandemic, and that represents 19% of cases reported among all ages, the AAP and CHA said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Hospital admissions also continued to fall, with the rate for children aged 0-17 at 0.43 per 100,000 population as of Feb. 20, down by almost 66% from the peak of 1.25 per 100,000 reached on Jan. 16, the Centers for Disease Control and Prevention reported.
A snapshot of the hospitalization situation shows that 1,687 children were occupying inpatient beds on Feb. 16, compared with 4,070 on Jan. 19, which appears to be the peak of the Omicron surge, according to data from the Department of Health & Human Services.
The state with the highest rate – 5.6 per 100,000 children – on Feb. 16 was North Dakota, although the District of Columbia came in at 11.0 per 100,000. They were followed by Oklahoma (5.3), Missouri (5.2), and West Virginia (4.1). There were three states – New Hampshire, Rhode Island, and Utah – with no children in the hospital on that date, the HHS said.
New vaccinations in children aged 5-11 years, which declined in mid- and late January, even as Omicron surged, continued to decline, as did vaccine completions. Vaccinations also fell among children aged 12-17 for the latest reporting week, Feb. 10-16, the AAP said in a separate report.
As more states and school districts drop mask mandates, data from the CDC indicate that 32.5% of 5- to 11-year olds and 67.4% of 12- to 17-year-olds have gotten at least one dose of the COVID-19 vaccine and that 25.1% and 57.3%, respectively, are fully vaccinated. Meanwhile, 20.5% of those fully vaccinated 12- to 17-year-olds have gotten a booster dose, the CDC said.
The Omicron decline continued for a fourth consecutive week as new cases of COVID-19 in children fell by 42% from the week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That 42% represents a drop from the 299,000 new cases reported for Feb. 4-10 down to 174,000 for the most recent week, Feb. 11-17.
The overall count of COVID-19 cases in children is 12.5 million over the course of the pandemic, and that represents 19% of cases reported among all ages, the AAP and CHA said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Hospital admissions also continued to fall, with the rate for children aged 0-17 at 0.43 per 100,000 population as of Feb. 20, down by almost 66% from the peak of 1.25 per 100,000 reached on Jan. 16, the Centers for Disease Control and Prevention reported.
A snapshot of the hospitalization situation shows that 1,687 children were occupying inpatient beds on Feb. 16, compared with 4,070 on Jan. 19, which appears to be the peak of the Omicron surge, according to data from the Department of Health & Human Services.
The state with the highest rate – 5.6 per 100,000 children – on Feb. 16 was North Dakota, although the District of Columbia came in at 11.0 per 100,000. They were followed by Oklahoma (5.3), Missouri (5.2), and West Virginia (4.1). There were three states – New Hampshire, Rhode Island, and Utah – with no children in the hospital on that date, the HHS said.
New vaccinations in children aged 5-11 years, which declined in mid- and late January, even as Omicron surged, continued to decline, as did vaccine completions. Vaccinations also fell among children aged 12-17 for the latest reporting week, Feb. 10-16, the AAP said in a separate report.
As more states and school districts drop mask mandates, data from the CDC indicate that 32.5% of 5- to 11-year olds and 67.4% of 12- to 17-year-olds have gotten at least one dose of the COVID-19 vaccine and that 25.1% and 57.3%, respectively, are fully vaccinated. Meanwhile, 20.5% of those fully vaccinated 12- to 17-year-olds have gotten a booster dose, the CDC said.
The Omicron decline continued for a fourth consecutive week as new cases of COVID-19 in children fell by 42% from the week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That 42% represents a drop from the 299,000 new cases reported for Feb. 4-10 down to 174,000 for the most recent week, Feb. 11-17.
The overall count of COVID-19 cases in children is 12.5 million over the course of the pandemic, and that represents 19% of cases reported among all ages, the AAP and CHA said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Hospital admissions also continued to fall, with the rate for children aged 0-17 at 0.43 per 100,000 population as of Feb. 20, down by almost 66% from the peak of 1.25 per 100,000 reached on Jan. 16, the Centers for Disease Control and Prevention reported.
A snapshot of the hospitalization situation shows that 1,687 children were occupying inpatient beds on Feb. 16, compared with 4,070 on Jan. 19, which appears to be the peak of the Omicron surge, according to data from the Department of Health & Human Services.
The state with the highest rate – 5.6 per 100,000 children – on Feb. 16 was North Dakota, although the District of Columbia came in at 11.0 per 100,000. They were followed by Oklahoma (5.3), Missouri (5.2), and West Virginia (4.1). There were three states – New Hampshire, Rhode Island, and Utah – with no children in the hospital on that date, the HHS said.
New vaccinations in children aged 5-11 years, which declined in mid- and late January, even as Omicron surged, continued to decline, as did vaccine completions. Vaccinations also fell among children aged 12-17 for the latest reporting week, Feb. 10-16, the AAP said in a separate report.
As more states and school districts drop mask mandates, data from the CDC indicate that 32.5% of 5- to 11-year olds and 67.4% of 12- to 17-year-olds have gotten at least one dose of the COVID-19 vaccine and that 25.1% and 57.3%, respectively, are fully vaccinated. Meanwhile, 20.5% of those fully vaccinated 12- to 17-year-olds have gotten a booster dose, the CDC said.
Burnout rates rising among psychiatrists
The lingering effects of the COVID-19 pandemic continue to take a toll on the happiness, well-being, and lifestyles of many segments of the population, especially those in the health care field, including psychiatrists.
The newly released Medscape Psychiatrist Lifestyle, Happiness & Burnout Report 2022 explores psychiatrists’ happiness in their personal and professional lives and how they are maintaining mental and physical health.
Prior to the global pandemic, 79% of psychiatrists said they were “very” or “somewhat” happy outside of work, like physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Higher in women
In last year’s report, overall 42% of psychiatrists reported burnout; that’s risen to 47% this year.
When it comes to burnout, psychiatrists are in the lower range of burned-out physicians. Perhaps not surprising, given the challenges of the COVID-19 pandemic, burnout rates are highest in emergency medicine and critical care specialists.
About half of psychiatrists (52%) reported that they were more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About one-third said their burnout was the same.
Female psychiatrists reported being burned out at a greater rate than their male colleagues (46% vs. 30%).
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.

“Often women assumed more of the childcare and home schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main contributor to psychiatrist burnout (69%), even more so than for physicians overall (60%).
Too many work hours, lack of respect from colleagues, lack of control or autonomy, and increasing use of electronic health records (EHRs) and other technology are also major drivers of burnout in this year’s report.
To quell burnout, psychiatrists reduce their hours on the job and participate in meditation or other stress-reduction techniques.
Thirty-eight percent of psychiatrists feel that their personality type contributes to their burnout. Nearly seven in 10 psychiatrists say burnout affects their relationships, about the same proportion as for physicians overall (68%).
Work-life balance
More than half of psychiatrists (53%) report they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time. This is similar among physicians overall (55%).
More than one-third (39%) of psychiatrists reported clinical depression (severe depression lasting some time and not caused by grief), while 44% reported colloquial depression (feeling down, blue, sad).
About half of depressed psychiatrists said their depression does not have an impact on relationships with patients. Of those who saw an impact, the major behaviors they reported were being easily exasperated with patients and feeling less motivated to take patient notes carefully.
To maintain happiness and mental health, psychiatrists choose to spend time with loved ones, do the things they enjoy, exercise, and get plenty of sleep.
Perhaps not surprisingly, more psychiatrists were happy with their work-life balance before the pandemic (68% vs. 54%). The same holds for physicians overall.
Before the pandemic, 17% of psychiatrists reported being unhappy with their work-life balance. That has risen to 29% this year.
The vast majority of psychiatrists are currently in a committed relationship, with 76% either married or living with a partner. A somewhat higher percentage (83%) of physicians overall report being in a committed relationship.
About eight in 10 psychiatrists (81%) describe their marriage as good or very good – the same as last year.
A little more than half of psychiatrists have life partners who do not work in medicine. This is similar to the proportion among all physicians (56%).
Among psychiatrists balancing parenthood and a medical career, female psychiatrists noted feeling conflicted more often than their male counterparts (36% vs. 22% were “very conflicted” or “conflicted”).
This general attitude is reflected in almost all occupations, according to a Pew Research survey, which found that larger shares of mothers than fathers struggled with childcare responsibilities during the pandemic.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29 and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
The lingering effects of the COVID-19 pandemic continue to take a toll on the happiness, well-being, and lifestyles of many segments of the population, especially those in the health care field, including psychiatrists.
The newly released Medscape Psychiatrist Lifestyle, Happiness & Burnout Report 2022 explores psychiatrists’ happiness in their personal and professional lives and how they are maintaining mental and physical health.
Prior to the global pandemic, 79% of psychiatrists said they were “very” or “somewhat” happy outside of work, like physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Higher in women
In last year’s report, overall 42% of psychiatrists reported burnout; that’s risen to 47% this year.
When it comes to burnout, psychiatrists are in the lower range of burned-out physicians. Perhaps not surprising, given the challenges of the COVID-19 pandemic, burnout rates are highest in emergency medicine and critical care specialists.
About half of psychiatrists (52%) reported that they were more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About one-third said their burnout was the same.
Female psychiatrists reported being burned out at a greater rate than their male colleagues (46% vs. 30%).
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.
“Often women assumed more of the childcare and home schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main contributor to psychiatrist burnout (69%), even more so than for physicians overall (60%).
Too many work hours, lack of respect from colleagues, lack of control or autonomy, and increasing use of electronic health records (EHRs) and other technology are also major drivers of burnout in this year’s report.
To quell burnout, psychiatrists reduce their hours on the job and participate in meditation or other stress-reduction techniques.
Thirty-eight percent of psychiatrists feel that their personality type contributes to their burnout. Nearly seven in 10 psychiatrists say burnout affects their relationships, about the same proportion as for physicians overall (68%).
Work-life balance
More than half of psychiatrists (53%) report they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time. This is similar among physicians overall (55%).
More than one-third (39%) of psychiatrists reported clinical depression (severe depression lasting some time and not caused by grief), while 44% reported colloquial depression (feeling down, blue, sad).
About half of depressed psychiatrists said their depression does not have an impact on relationships with patients. Of those who saw an impact, the major behaviors they reported were being easily exasperated with patients and feeling less motivated to take patient notes carefully.
To maintain happiness and mental health, psychiatrists choose to spend time with loved ones, do the things they enjoy, exercise, and get plenty of sleep.
Perhaps not surprisingly, more psychiatrists were happy with their work-life balance before the pandemic (68% vs. 54%). The same holds for physicians overall.
Before the pandemic, 17% of psychiatrists reported being unhappy with their work-life balance. That has risen to 29% this year.
The vast majority of psychiatrists are currently in a committed relationship, with 76% either married or living with a partner. A somewhat higher percentage (83%) of physicians overall report being in a committed relationship.
About eight in 10 psychiatrists (81%) describe their marriage as good or very good – the same as last year.
A little more than half of psychiatrists have life partners who do not work in medicine. This is similar to the proportion among all physicians (56%).
Among psychiatrists balancing parenthood and a medical career, female psychiatrists noted feeling conflicted more often than their male counterparts (36% vs. 22% were “very conflicted” or “conflicted”).
This general attitude is reflected in almost all occupations, according to a Pew Research survey, which found that larger shares of mothers than fathers struggled with childcare responsibilities during the pandemic.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29 and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
The lingering effects of the COVID-19 pandemic continue to take a toll on the happiness, well-being, and lifestyles of many segments of the population, especially those in the health care field, including psychiatrists.
The newly released Medscape Psychiatrist Lifestyle, Happiness & Burnout Report 2022 explores psychiatrists’ happiness in their personal and professional lives and how they are maintaining mental and physical health.
Prior to the global pandemic, 79% of psychiatrists said they were “very” or “somewhat” happy outside of work, like physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Higher in women
In last year’s report, overall 42% of psychiatrists reported burnout; that’s risen to 47% this year.
When it comes to burnout, psychiatrists are in the lower range of burned-out physicians. Perhaps not surprising, given the challenges of the COVID-19 pandemic, burnout rates are highest in emergency medicine and critical care specialists.
About half of psychiatrists (52%) reported that they were more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About one-third said their burnout was the same.
Female psychiatrists reported being burned out at a greater rate than their male colleagues (46% vs. 30%).
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.
“Often women assumed more of the childcare and home schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main contributor to psychiatrist burnout (69%), even more so than for physicians overall (60%).
Too many work hours, lack of respect from colleagues, lack of control or autonomy, and increasing use of electronic health records (EHRs) and other technology are also major drivers of burnout in this year’s report.
To quell burnout, psychiatrists reduce their hours on the job and participate in meditation or other stress-reduction techniques.
Thirty-eight percent of psychiatrists feel that their personality type contributes to their burnout. Nearly seven in 10 psychiatrists say burnout affects their relationships, about the same proportion as for physicians overall (68%).
Work-life balance
More than half of psychiatrists (53%) report they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time. This is similar among physicians overall (55%).
More than one-third (39%) of psychiatrists reported clinical depression (severe depression lasting some time and not caused by grief), while 44% reported colloquial depression (feeling down, blue, sad).
About half of depressed psychiatrists said their depression does not have an impact on relationships with patients. Of those who saw an impact, the major behaviors they reported were being easily exasperated with patients and feeling less motivated to take patient notes carefully.
To maintain happiness and mental health, psychiatrists choose to spend time with loved ones, do the things they enjoy, exercise, and get plenty of sleep.
Perhaps not surprisingly, more psychiatrists were happy with their work-life balance before the pandemic (68% vs. 54%). The same holds for physicians overall.
Before the pandemic, 17% of psychiatrists reported being unhappy with their work-life balance. That has risen to 29% this year.
The vast majority of psychiatrists are currently in a committed relationship, with 76% either married or living with a partner. A somewhat higher percentage (83%) of physicians overall report being in a committed relationship.
About eight in 10 psychiatrists (81%) describe their marriage as good or very good – the same as last year.
A little more than half of psychiatrists have life partners who do not work in medicine. This is similar to the proportion among all physicians (56%).
Among psychiatrists balancing parenthood and a medical career, female psychiatrists noted feeling conflicted more often than their male counterparts (36% vs. 22% were “very conflicted” or “conflicted”).
This general attitude is reflected in almost all occupations, according to a Pew Research survey, which found that larger shares of mothers than fathers struggled with childcare responsibilities during the pandemic.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29 and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
Healthy gut tied to better cognition
Investigators conducted cognitive testing and analyzed stool samples in close to 600 adults and found that beta-diversity, which is a between-person measure of gut microbial community composition, was significantly associated with cognitive scores.
Three specific bacterial genera showed a positive association with performance on at least one cognitive test, while one showed a negative association.
“Data from our study support an association between the gut microbial community and measure of cognitive function – results that are consistent with findings from other human and animal research,” study investigator Katie Meyer, ScD, assistant professor, department of nutrition, UNC Gillings School of Public Health, Chapel Hill, N.C., told this news organization.
“However, it is also important to recognize that we are still learning about how to characterize the role of this dynamic ecological community and delineate mechanistic pathways,” she said.
The study was published online Feb 8 in JAMA Network Open.
‘Novel’ research
“Communication pathways between gut bacteria and neurologic function (referred to as the ‘gut-brain axis’) have emerged as a novel area of research into potential mechanisms regulating brain health through immunologic, metabolic, and endocrine pathways,” the authors wrote.
A number of studies have “shown associations between gut microbial measures and neurological outcomes, including cognitive function and dementia,” but mechanisms underlying these associations “have not been fully established.”
Animal and small-scale human studies have suggested that reduced microbial diversity is associated with poorer cognition, but studies have not been conducted in community-based large and diverse populations.
The researchers therefore examined cross-sectional associations of gut microbial diversity and taxonomic composition with cognitive status in a large group of community-dwelling, sociodemographically diverse Black and White adults living in four metropolitan areas who were participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
They hypothesized that microbial diversity would be positively associated with global as well as domain-specific cognitive status and that higher cognitive status would be associated with specific taxonomic groups involved in short-chain fatty acid production.
The CARDIA’s year 30 follow-up examination took place during 2015-2016, when the original participants ranged in age from 48 to 60 years. During that examination, participants took a battery of cognitive assessments, and 615 also provided a stool sample for a microbiome substudy; of these, 597 (mean [SD] age, 55.2 [3.5] years, 44.7% Black, 45.2% White) had both stool DNA available for sequencing and a complete complement of cognitive tests and were included in the current study.
The cognitive tests included the Digit Symbol Substitution Test (DSST); Rey-Auditory Verbal Learning Test (RAVLT); the timed Stroop test; letter fluency and category fluency; and the Montreal Cognitive Assessment (MoCA).
Covariates that might confound associations between microbial and cognitive measures, including body mass index, diabetes, age, sex, race, field center, education, physical activity, current smoking, diet quality, number of medications, and hypertension, were included in the analyses.
The investigators conducted three standard microbial analyses: within-person alpha-diversity; between-person beta-diversity; and individual taxa.
Potential pathways
The strongest associations in the variance tests for beta-diversity, which were significant for all cognition measures in multivariable-adjusted principal coordinates analysis (all Ps = .001 except for the Stroop, which was .007). However, the association with letter fluency was not deemed significant (P = .07).
After fully adjusting for sociodemographic variables, health behaviors, and clinical covariates, the researchers found that three genera were positively associated, while one was negatively associated with cognitive measures.
“The strongest results from our study were from a multivariate analysis that can be considered a test of the overall community,” said Dr. Meyer.
She pointed to several pathways through which gut microbiota can contribute to brain health.
“We know from mechanistic studies in animal models that the gut microbiota is involved in systemic inflammation, which is a risk factor for brain pathology,” she said.
Moreover, “the gut microbiota is involved in the production of metabolites that may impact the brain, including tryptophan metabolites and short-chain fatty acids, many of which derive from dietary components, which may help explain associations between diet and cognition (e.g., the Mediterranean-style diet can be protective),” she added.
Starting point
Commenting for this news organization, Timothy Dinan, MD, PhD, professor of psychiatry and an investigator, APC Microbiome Institute, University College Cork, Ireland, said, “This is an important study, adding to the growing body of evidence that gut microbes influence brain function.”
Dr. Dinan, who was not involved with the study, continued: “In an impressively large sample, an association between cognition and gut microbiota architecture was demonstrated.”
He cautioned that the study “is limited by the fact that it is cross-sectional, and the relationships are correlational.” Nevertheless, “despite these obvious caveats, the paper undoubtedly advances the field.”
Dr. Meyer agreed, noting that there is “a paucity of biomarkers that can be used to predict cognitive decline and dementia,” but because their study was cross-sectional, “we cannot assess temporality (i.e., whether gut microbiota predicts cognitive decline); but, as a start, we can assess associations.”
She added that “at this point, we know far more about modifiable risk factors that have been shown to be positively associated with cognitive function,” including eating a Mediterranean diet and engaging in physical activity.
“It is possible that protective effects of diet and activity may, in part, operate thorough the gut microbiota,” Dr. Meyer suggested.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute, the Intramural Research Program of the National Institute on Aging, and the University of North Carolina Nutrition Research Institute. Dr. Meyer and coauthors and Dr. Dinan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators conducted cognitive testing and analyzed stool samples in close to 600 adults and found that beta-diversity, which is a between-person measure of gut microbial community composition, was significantly associated with cognitive scores.
Three specific bacterial genera showed a positive association with performance on at least one cognitive test, while one showed a negative association.
“Data from our study support an association between the gut microbial community and measure of cognitive function – results that are consistent with findings from other human and animal research,” study investigator Katie Meyer, ScD, assistant professor, department of nutrition, UNC Gillings School of Public Health, Chapel Hill, N.C., told this news organization.
“However, it is also important to recognize that we are still learning about how to characterize the role of this dynamic ecological community and delineate mechanistic pathways,” she said.
The study was published online Feb 8 in JAMA Network Open.
‘Novel’ research
“Communication pathways between gut bacteria and neurologic function (referred to as the ‘gut-brain axis’) have emerged as a novel area of research into potential mechanisms regulating brain health through immunologic, metabolic, and endocrine pathways,” the authors wrote.
A number of studies have “shown associations between gut microbial measures and neurological outcomes, including cognitive function and dementia,” but mechanisms underlying these associations “have not been fully established.”
Animal and small-scale human studies have suggested that reduced microbial diversity is associated with poorer cognition, but studies have not been conducted in community-based large and diverse populations.
The researchers therefore examined cross-sectional associations of gut microbial diversity and taxonomic composition with cognitive status in a large group of community-dwelling, sociodemographically diverse Black and White adults living in four metropolitan areas who were participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
They hypothesized that microbial diversity would be positively associated with global as well as domain-specific cognitive status and that higher cognitive status would be associated with specific taxonomic groups involved in short-chain fatty acid production.
The CARDIA’s year 30 follow-up examination took place during 2015-2016, when the original participants ranged in age from 48 to 60 years. During that examination, participants took a battery of cognitive assessments, and 615 also provided a stool sample for a microbiome substudy; of these, 597 (mean [SD] age, 55.2 [3.5] years, 44.7% Black, 45.2% White) had both stool DNA available for sequencing and a complete complement of cognitive tests and were included in the current study.
The cognitive tests included the Digit Symbol Substitution Test (DSST); Rey-Auditory Verbal Learning Test (RAVLT); the timed Stroop test; letter fluency and category fluency; and the Montreal Cognitive Assessment (MoCA).
Covariates that might confound associations between microbial and cognitive measures, including body mass index, diabetes, age, sex, race, field center, education, physical activity, current smoking, diet quality, number of medications, and hypertension, were included in the analyses.
The investigators conducted three standard microbial analyses: within-person alpha-diversity; between-person beta-diversity; and individual taxa.
Potential pathways
The strongest associations in the variance tests for beta-diversity, which were significant for all cognition measures in multivariable-adjusted principal coordinates analysis (all Ps = .001 except for the Stroop, which was .007). However, the association with letter fluency was not deemed significant (P = .07).
After fully adjusting for sociodemographic variables, health behaviors, and clinical covariates, the researchers found that three genera were positively associated, while one was negatively associated with cognitive measures.
“The strongest results from our study were from a multivariate analysis that can be considered a test of the overall community,” said Dr. Meyer.
She pointed to several pathways through which gut microbiota can contribute to brain health.
“We know from mechanistic studies in animal models that the gut microbiota is involved in systemic inflammation, which is a risk factor for brain pathology,” she said.
Moreover, “the gut microbiota is involved in the production of metabolites that may impact the brain, including tryptophan metabolites and short-chain fatty acids, many of which derive from dietary components, which may help explain associations between diet and cognition (e.g., the Mediterranean-style diet can be protective),” she added.
Starting point
Commenting for this news organization, Timothy Dinan, MD, PhD, professor of psychiatry and an investigator, APC Microbiome Institute, University College Cork, Ireland, said, “This is an important study, adding to the growing body of evidence that gut microbes influence brain function.”
Dr. Dinan, who was not involved with the study, continued: “In an impressively large sample, an association between cognition and gut microbiota architecture was demonstrated.”
He cautioned that the study “is limited by the fact that it is cross-sectional, and the relationships are correlational.” Nevertheless, “despite these obvious caveats, the paper undoubtedly advances the field.”
Dr. Meyer agreed, noting that there is “a paucity of biomarkers that can be used to predict cognitive decline and dementia,” but because their study was cross-sectional, “we cannot assess temporality (i.e., whether gut microbiota predicts cognitive decline); but, as a start, we can assess associations.”
She added that “at this point, we know far more about modifiable risk factors that have been shown to be positively associated with cognitive function,” including eating a Mediterranean diet and engaging in physical activity.
“It is possible that protective effects of diet and activity may, in part, operate thorough the gut microbiota,” Dr. Meyer suggested.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute, the Intramural Research Program of the National Institute on Aging, and the University of North Carolina Nutrition Research Institute. Dr. Meyer and coauthors and Dr. Dinan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators conducted cognitive testing and analyzed stool samples in close to 600 adults and found that beta-diversity, which is a between-person measure of gut microbial community composition, was significantly associated with cognitive scores.
Three specific bacterial genera showed a positive association with performance on at least one cognitive test, while one showed a negative association.
“Data from our study support an association between the gut microbial community and measure of cognitive function – results that are consistent with findings from other human and animal research,” study investigator Katie Meyer, ScD, assistant professor, department of nutrition, UNC Gillings School of Public Health, Chapel Hill, N.C., told this news organization.
“However, it is also important to recognize that we are still learning about how to characterize the role of this dynamic ecological community and delineate mechanistic pathways,” she said.
The study was published online Feb 8 in JAMA Network Open.
‘Novel’ research
“Communication pathways between gut bacteria and neurologic function (referred to as the ‘gut-brain axis’) have emerged as a novel area of research into potential mechanisms regulating brain health through immunologic, metabolic, and endocrine pathways,” the authors wrote.
A number of studies have “shown associations between gut microbial measures and neurological outcomes, including cognitive function and dementia,” but mechanisms underlying these associations “have not been fully established.”
Animal and small-scale human studies have suggested that reduced microbial diversity is associated with poorer cognition, but studies have not been conducted in community-based large and diverse populations.
The researchers therefore examined cross-sectional associations of gut microbial diversity and taxonomic composition with cognitive status in a large group of community-dwelling, sociodemographically diverse Black and White adults living in four metropolitan areas who were participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
They hypothesized that microbial diversity would be positively associated with global as well as domain-specific cognitive status and that higher cognitive status would be associated with specific taxonomic groups involved in short-chain fatty acid production.
The CARDIA’s year 30 follow-up examination took place during 2015-2016, when the original participants ranged in age from 48 to 60 years. During that examination, participants took a battery of cognitive assessments, and 615 also provided a stool sample for a microbiome substudy; of these, 597 (mean [SD] age, 55.2 [3.5] years, 44.7% Black, 45.2% White) had both stool DNA available for sequencing and a complete complement of cognitive tests and were included in the current study.
The cognitive tests included the Digit Symbol Substitution Test (DSST); Rey-Auditory Verbal Learning Test (RAVLT); the timed Stroop test; letter fluency and category fluency; and the Montreal Cognitive Assessment (MoCA).
Covariates that might confound associations between microbial and cognitive measures, including body mass index, diabetes, age, sex, race, field center, education, physical activity, current smoking, diet quality, number of medications, and hypertension, were included in the analyses.
The investigators conducted three standard microbial analyses: within-person alpha-diversity; between-person beta-diversity; and individual taxa.
Potential pathways
The strongest associations in the variance tests for beta-diversity, which were significant for all cognition measures in multivariable-adjusted principal coordinates analysis (all Ps = .001 except for the Stroop, which was .007). However, the association with letter fluency was not deemed significant (P = .07).
After fully adjusting for sociodemographic variables, health behaviors, and clinical covariates, the researchers found that three genera were positively associated, while one was negatively associated with cognitive measures.
“The strongest results from our study were from a multivariate analysis that can be considered a test of the overall community,” said Dr. Meyer.
She pointed to several pathways through which gut microbiota can contribute to brain health.
“We know from mechanistic studies in animal models that the gut microbiota is involved in systemic inflammation, which is a risk factor for brain pathology,” she said.
Moreover, “the gut microbiota is involved in the production of metabolites that may impact the brain, including tryptophan metabolites and short-chain fatty acids, many of which derive from dietary components, which may help explain associations between diet and cognition (e.g., the Mediterranean-style diet can be protective),” she added.
Starting point
Commenting for this news organization, Timothy Dinan, MD, PhD, professor of psychiatry and an investigator, APC Microbiome Institute, University College Cork, Ireland, said, “This is an important study, adding to the growing body of evidence that gut microbes influence brain function.”
Dr. Dinan, who was not involved with the study, continued: “In an impressively large sample, an association between cognition and gut microbiota architecture was demonstrated.”
He cautioned that the study “is limited by the fact that it is cross-sectional, and the relationships are correlational.” Nevertheless, “despite these obvious caveats, the paper undoubtedly advances the field.”
Dr. Meyer agreed, noting that there is “a paucity of biomarkers that can be used to predict cognitive decline and dementia,” but because their study was cross-sectional, “we cannot assess temporality (i.e., whether gut microbiota predicts cognitive decline); but, as a start, we can assess associations.”
She added that “at this point, we know far more about modifiable risk factors that have been shown to be positively associated with cognitive function,” including eating a Mediterranean diet and engaging in physical activity.
“It is possible that protective effects of diet and activity may, in part, operate thorough the gut microbiota,” Dr. Meyer suggested.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute, the Intramural Research Program of the National Institute on Aging, and the University of North Carolina Nutrition Research Institute. Dr. Meyer and coauthors and Dr. Dinan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Twitter storm over ‘reprehensible behavior’ at conference podium
, held in San Francisco and also online. One of the panelists was accused of being less than professional in handling questions from the floor.
It began with a tweet from Sumanta Pal, MD, of the City of Hope, when he called out the behavior, although he did not identify the perpetrator.
“Yesterday we saw some reprehensible behavior emanating from the @ASCO #GU22 podium, with a well known investigator insulting (in a manner deeply imbued w microaggressions) an esteemed colleague at the mic. It’s a teachable moment & the lesson is simple: be kind to ur colleagues.”
It was not immediately clear what had occurred, and several people asked him to identify the people involved. One physician responded, “If it was bad enough to infer and share on Twitter, name the name.”
But even without details, the post provoked a reaction.
Erika Hamilton, MD, wrote, “I am not aware of this incident, but I always wonder ... if someone would do that from the podium, what would they/have they done and said when they didn’t think everyone was watching?”
Another tweet questioned why there were no codes of conduct in place, so that situations like this one wouldn’t happen.
“[It is] about time professional societies had codes of conduct in place for invited speakers, moderators of sessions etc,” wrote Deborah Verran, MD. “Then if it is breached the individual concerned is not invited back. This kind of incident also needs to be mentioned as part of the conference feedback process.”
As the number of clinicians chiming in increased, it soon became apparent that others were aware of the incident, and one posted a video clip, putting the mystery to rest.
Moderator quips, ‘Behave ... children’
The exchange occurred immediately following the oral abstract presentations on prostate cancer on Feb. 17. Two of these abstracts featured new data from large clinical trials investigating the use of PARP inhibitors in metastatic prostate cancer, which had slightly different results, leading to some debate. The PROpel trial with olaparib showed a benefit in all patients, irrespective of gene mutation status, but the MAGNITUDE trial with niraparib showed a benefit only in patients with gene alterations, and especially in those with BRCA1/2 mutations.
The invited discussant, Celestia Higano, MD, from the University of British Columbia, Vancouver, compared and contrasted the two trials and the differing results.
During the question-and-answer session that followed, Neeraj Agarwal, MD, from the Huntsman Cancer Institute, University of Utah, directed a question to Fred Saad, MD, who had presented the results of the PROpel trial.*
“As a practicing oncologist, I am very intrigued by the different results of the MAGNITUDE and PROpel trials. I am trying to figure out what do I do in my practice,” Dr. Agarwal began.
He continued on, explaining that he didn’t think that olaparib and niraparib were that different from one another for the two studies to have such differing results, when both of the drugs were given in combination with abiraterone.
The inclusion criteria for PROpel stipulated that patients undergo testing by ctDNA to determine if they were biomarker positive or not, but he pointed out that it is possible for testing to miss patients who might otherwise be positive for homologous recombination repair (HRR) gene alterations. He posed the question, could some of the patients deemed biomarker negative in fact have been positive but whose status was not detected by ctDNA testing?
At that point, Dr. Higano interrupted him before he had completed his question and asked, “Can I make a comment? Were you listening to my discussion?”
She then continued, pointing out that “you can’t talk about comparing olaparib and niraparib – these two trials had two very different populations.”
She emphasized that this was about the combinations in the populations being studied and not about olaparib and niraparib. “I clearly wasn’t very clear,” she said.
Dr. Agarwal then repeated that he wanted to know what to do with his patients and asked again about the accuracy of ctDNA testing.
“That’s a good question,” Dr. Higano said, “But the other comments you made weren’t.”
At that point, the moderator chimed in. “Let’s all calm down ... children.”
After a brief applause following the moderator’s comment, Dr. Saad then addressed the question.
When the video clip of this exchange was posted, a flood of tweets poured in, supporting Dr. Pal’s initial summation of the situation.
Alison Birtle, MD, tweeted, “I’m even more appalled having seen this exchange. Unacceptable. You don’t humiliate either the speaker or the delegate and the questions were entirely valid in my opinion. Basically what do I do tomorrow with these data so why ask were you listening. That’s just rude.”
Jason Kovac, MD, tweeted: “It’s absolutely not a proper way to behave. Whether it’s behind the scenes or to your face. You can hear the arrogance from everyone including the moderator with his children comment. This is the true face of medicine.”
Jarey Wang, MD, PhD, however, liked the moderator’s input. “Love it. ‘Let’s all calm down children.’ Good for the moderator.”
Several of the physicians who commented thought that the issue should have been addressed at the time it happened. Don S. Dizon, MD, wrote, “Calling out microagressions as they occur is so important. And very difficult. Agree, the teachable moment must be met with bravery. But it should happen in real time too.”
After 2 days of bantering on Twitter, with the thread growing increasingly longer and with the vast majority of posts supporting Dr. Pal’s initial assessment, Dr. Higano finally entered the discussion and defended her comments: “What you do not know is that the questioner and I are good colleagues,” she tweeted. “I have been involved in two of his academic promotions. My main concern was his comment re: how the two trials could have ‘so different results with the same combination.’ I sought to rectify wrong message.”
There were no direct replies to Dr. Higano’s tweet.
Perhaps the line to draw under this affair is the tweet from Simon Kim, MD, MPH, who wrote: “We can do better!”
A version of this article first appeared on Medscape.com.
Correction, 2/24/22: Dr. Fred Saad's name was misstated in an earlier version of this article.
, held in San Francisco and also online. One of the panelists was accused of being less than professional in handling questions from the floor.
It began with a tweet from Sumanta Pal, MD, of the City of Hope, when he called out the behavior, although he did not identify the perpetrator.
“Yesterday we saw some reprehensible behavior emanating from the @ASCO #GU22 podium, with a well known investigator insulting (in a manner deeply imbued w microaggressions) an esteemed colleague at the mic. It’s a teachable moment & the lesson is simple: be kind to ur colleagues.”
It was not immediately clear what had occurred, and several people asked him to identify the people involved. One physician responded, “If it was bad enough to infer and share on Twitter, name the name.”
But even without details, the post provoked a reaction.
Erika Hamilton, MD, wrote, “I am not aware of this incident, but I always wonder ... if someone would do that from the podium, what would they/have they done and said when they didn’t think everyone was watching?”
Another tweet questioned why there were no codes of conduct in place, so that situations like this one wouldn’t happen.
“[It is] about time professional societies had codes of conduct in place for invited speakers, moderators of sessions etc,” wrote Deborah Verran, MD. “Then if it is breached the individual concerned is not invited back. This kind of incident also needs to be mentioned as part of the conference feedback process.”
As the number of clinicians chiming in increased, it soon became apparent that others were aware of the incident, and one posted a video clip, putting the mystery to rest.
Moderator quips, ‘Behave ... children’
The exchange occurred immediately following the oral abstract presentations on prostate cancer on Feb. 17. Two of these abstracts featured new data from large clinical trials investigating the use of PARP inhibitors in metastatic prostate cancer, which had slightly different results, leading to some debate. The PROpel trial with olaparib showed a benefit in all patients, irrespective of gene mutation status, but the MAGNITUDE trial with niraparib showed a benefit only in patients with gene alterations, and especially in those with BRCA1/2 mutations.
The invited discussant, Celestia Higano, MD, from the University of British Columbia, Vancouver, compared and contrasted the two trials and the differing results.
During the question-and-answer session that followed, Neeraj Agarwal, MD, from the Huntsman Cancer Institute, University of Utah, directed a question to Fred Saad, MD, who had presented the results of the PROpel trial.*
“As a practicing oncologist, I am very intrigued by the different results of the MAGNITUDE and PROpel trials. I am trying to figure out what do I do in my practice,” Dr. Agarwal began.
He continued on, explaining that he didn’t think that olaparib and niraparib were that different from one another for the two studies to have such differing results, when both of the drugs were given in combination with abiraterone.
The inclusion criteria for PROpel stipulated that patients undergo testing by ctDNA to determine if they were biomarker positive or not, but he pointed out that it is possible for testing to miss patients who might otherwise be positive for homologous recombination repair (HRR) gene alterations. He posed the question, could some of the patients deemed biomarker negative in fact have been positive but whose status was not detected by ctDNA testing?
At that point, Dr. Higano interrupted him before he had completed his question and asked, “Can I make a comment? Were you listening to my discussion?”
She then continued, pointing out that “you can’t talk about comparing olaparib and niraparib – these two trials had two very different populations.”
She emphasized that this was about the combinations in the populations being studied and not about olaparib and niraparib. “I clearly wasn’t very clear,” she said.
Dr. Agarwal then repeated that he wanted to know what to do with his patients and asked again about the accuracy of ctDNA testing.
“That’s a good question,” Dr. Higano said, “But the other comments you made weren’t.”
At that point, the moderator chimed in. “Let’s all calm down ... children.”
After a brief applause following the moderator’s comment, Dr. Saad then addressed the question.
When the video clip of this exchange was posted, a flood of tweets poured in, supporting Dr. Pal’s initial summation of the situation.
Alison Birtle, MD, tweeted, “I’m even more appalled having seen this exchange. Unacceptable. You don’t humiliate either the speaker or the delegate and the questions were entirely valid in my opinion. Basically what do I do tomorrow with these data so why ask were you listening. That’s just rude.”
Jason Kovac, MD, tweeted: “It’s absolutely not a proper way to behave. Whether it’s behind the scenes or to your face. You can hear the arrogance from everyone including the moderator with his children comment. This is the true face of medicine.”
Jarey Wang, MD, PhD, however, liked the moderator’s input. “Love it. ‘Let’s all calm down children.’ Good for the moderator.”
Several of the physicians who commented thought that the issue should have been addressed at the time it happened. Don S. Dizon, MD, wrote, “Calling out microagressions as they occur is so important. And very difficult. Agree, the teachable moment must be met with bravery. But it should happen in real time too.”
After 2 days of bantering on Twitter, with the thread growing increasingly longer and with the vast majority of posts supporting Dr. Pal’s initial assessment, Dr. Higano finally entered the discussion and defended her comments: “What you do not know is that the questioner and I are good colleagues,” she tweeted. “I have been involved in two of his academic promotions. My main concern was his comment re: how the two trials could have ‘so different results with the same combination.’ I sought to rectify wrong message.”
There were no direct replies to Dr. Higano’s tweet.
Perhaps the line to draw under this affair is the tweet from Simon Kim, MD, MPH, who wrote: “We can do better!”
A version of this article first appeared on Medscape.com.
Correction, 2/24/22: Dr. Fred Saad's name was misstated in an earlier version of this article.
, held in San Francisco and also online. One of the panelists was accused of being less than professional in handling questions from the floor.
It began with a tweet from Sumanta Pal, MD, of the City of Hope, when he called out the behavior, although he did not identify the perpetrator.
“Yesterday we saw some reprehensible behavior emanating from the @ASCO #GU22 podium, with a well known investigator insulting (in a manner deeply imbued w microaggressions) an esteemed colleague at the mic. It’s a teachable moment & the lesson is simple: be kind to ur colleagues.”
It was not immediately clear what had occurred, and several people asked him to identify the people involved. One physician responded, “If it was bad enough to infer and share on Twitter, name the name.”
But even without details, the post provoked a reaction.
Erika Hamilton, MD, wrote, “I am not aware of this incident, but I always wonder ... if someone would do that from the podium, what would they/have they done and said when they didn’t think everyone was watching?”
Another tweet questioned why there were no codes of conduct in place, so that situations like this one wouldn’t happen.
“[It is] about time professional societies had codes of conduct in place for invited speakers, moderators of sessions etc,” wrote Deborah Verran, MD. “Then if it is breached the individual concerned is not invited back. This kind of incident also needs to be mentioned as part of the conference feedback process.”
As the number of clinicians chiming in increased, it soon became apparent that others were aware of the incident, and one posted a video clip, putting the mystery to rest.
Moderator quips, ‘Behave ... children’
The exchange occurred immediately following the oral abstract presentations on prostate cancer on Feb. 17. Two of these abstracts featured new data from large clinical trials investigating the use of PARP inhibitors in metastatic prostate cancer, which had slightly different results, leading to some debate. The PROpel trial with olaparib showed a benefit in all patients, irrespective of gene mutation status, but the MAGNITUDE trial with niraparib showed a benefit only in patients with gene alterations, and especially in those with BRCA1/2 mutations.
The invited discussant, Celestia Higano, MD, from the University of British Columbia, Vancouver, compared and contrasted the two trials and the differing results.
During the question-and-answer session that followed, Neeraj Agarwal, MD, from the Huntsman Cancer Institute, University of Utah, directed a question to Fred Saad, MD, who had presented the results of the PROpel trial.*
“As a practicing oncologist, I am very intrigued by the different results of the MAGNITUDE and PROpel trials. I am trying to figure out what do I do in my practice,” Dr. Agarwal began.
He continued on, explaining that he didn’t think that olaparib and niraparib were that different from one another for the two studies to have such differing results, when both of the drugs were given in combination with abiraterone.
The inclusion criteria for PROpel stipulated that patients undergo testing by ctDNA to determine if they were biomarker positive or not, but he pointed out that it is possible for testing to miss patients who might otherwise be positive for homologous recombination repair (HRR) gene alterations. He posed the question, could some of the patients deemed biomarker negative in fact have been positive but whose status was not detected by ctDNA testing?
At that point, Dr. Higano interrupted him before he had completed his question and asked, “Can I make a comment? Were you listening to my discussion?”
She then continued, pointing out that “you can’t talk about comparing olaparib and niraparib – these two trials had two very different populations.”
She emphasized that this was about the combinations in the populations being studied and not about olaparib and niraparib. “I clearly wasn’t very clear,” she said.
Dr. Agarwal then repeated that he wanted to know what to do with his patients and asked again about the accuracy of ctDNA testing.
“That’s a good question,” Dr. Higano said, “But the other comments you made weren’t.”
At that point, the moderator chimed in. “Let’s all calm down ... children.”
After a brief applause following the moderator’s comment, Dr. Saad then addressed the question.
When the video clip of this exchange was posted, a flood of tweets poured in, supporting Dr. Pal’s initial summation of the situation.
Alison Birtle, MD, tweeted, “I’m even more appalled having seen this exchange. Unacceptable. You don’t humiliate either the speaker or the delegate and the questions were entirely valid in my opinion. Basically what do I do tomorrow with these data so why ask were you listening. That’s just rude.”
Jason Kovac, MD, tweeted: “It’s absolutely not a proper way to behave. Whether it’s behind the scenes or to your face. You can hear the arrogance from everyone including the moderator with his children comment. This is the true face of medicine.”
Jarey Wang, MD, PhD, however, liked the moderator’s input. “Love it. ‘Let’s all calm down children.’ Good for the moderator.”
Several of the physicians who commented thought that the issue should have been addressed at the time it happened. Don S. Dizon, MD, wrote, “Calling out microagressions as they occur is so important. And very difficult. Agree, the teachable moment must be met with bravery. But it should happen in real time too.”
After 2 days of bantering on Twitter, with the thread growing increasingly longer and with the vast majority of posts supporting Dr. Pal’s initial assessment, Dr. Higano finally entered the discussion and defended her comments: “What you do not know is that the questioner and I are good colleagues,” she tweeted. “I have been involved in two of his academic promotions. My main concern was his comment re: how the two trials could have ‘so different results with the same combination.’ I sought to rectify wrong message.”
There were no direct replies to Dr. Higano’s tweet.
Perhaps the line to draw under this affair is the tweet from Simon Kim, MD, MPH, who wrote: “We can do better!”
A version of this article first appeared on Medscape.com.
Correction, 2/24/22: Dr. Fred Saad's name was misstated in an earlier version of this article.
FROM ASCO GU 2022
Alarming rates of self-harm in adults with autism expose a broken system
When a recent study from Columbia University reported that suicide and self-harm were nearly four times more likely in adults with autism spectrum disorder (ASD) than in the general population, the findings were sobering. But to many in the field, they were not surprising.
Previous analyses showed individuals with ASD were up to six times more likely to attempt suicide and nearly eight times as likely to succeed. However, the recent study published in JAMA Network Open is one of only a few on self-harm and suicide in autism spectrum disorder (ASD) to include a focus on adults.
“Previously there was relatively little information about adults with autism in general and on injury risk among adults with autism specifically,” study investigator Guohua Li, DrPH, MD, professor of epidemiology at Columbia University Mailman School of Public Health, New York, told this news organization.
“How to continue to provide social support and health care services to adults with autism presents a real challenge to society and is a public health issue,” Dr. Li said.
Falling off a ‘services cliff’
The ASD rate among children is at a record-high in the United States, which means the number of adults on the spectrum will also continue to climb. The incidence of adults with newly diagnosed ASD, who are sometimes described as the “lost generation,” is also increasing. Despite these realities, adults with ASD remain largely underserved and understudied.
The data that are available paint a concerning picture. Adolescents with ASD face a “services cliff” as they transition to adulthood and fall into a landscape with a serious lack of services, support, and clinicians trained to treat adults with ASD.
Compared with young adults without ASD, those on the spectrum have significantly lower college graduation rates, have a harder time finding and keeping a job, are more likely to have a co-occurring mental illness, and are far less likely to live independently.
Before 2020, there were no national data on the number of U.S. adults with autism. That year, the Centers for Disease Control and Prevention released its first-ever report on adult autism prevalence, estimated to be 5.4 million.
That figure is almost definitely low, Matthew Maenner, PhD, autism surveillance team lead with the CDC’s National Center on Birth Defects and Developmental Disabilities, told this news organization.
Researchers use school and medical records to calculate child ASD rates, but counting adults with the disorder is far more difficult.
The CDC’s estimate was based on modeling reports from 2017 state-based population and mortality records and parent-reported survey data of U.S. children diagnosed with ASD. It was inexact, said Dr. Maenner, but it was a start.
“There are no good data on the prevalence of autism in adults. Anywhere,” he added.
Masking and camouflaging
Only about 3.5% of published studies on autism focus on adults, one review showed. In the recently published “The Lancet Commission on the future of care and clinical research in autism,” the section on research on adolescents and adults was a mere 189 words long.
“The brevity of this paragraph reflects the little data available in this area, not its importance” the authors write.
The recent report of higher self-harm risk in adults on the spectrum offers further evidence that “there just aren’t enough services and research on adults on [the] autism spectrum,” Edward S. Brodkin, MD, associate professor of psychiatry and director of the Adult Autism Spectrum Program at the University of Pennsylvania Perelman School of Medicine in Philadelphia, told this news organization.
Founded by Dr. Brodkin in 2013, the program provides ASD diagnostic and support services for adults with ASD. Like others in the field, Dr. Brodkin has noted a sharp increase in the number of previously undiagnosed adults seeking evaluation for possible ASD.
Many of his patients have recently diagnosed children and realized they share some of the same ASD symptoms. Others have long recognized traits common in autism but have engaged in what clinicians call “masking” or “camouflaging.” This is particularly true in women, who are diagnosed with autism at far lower rates than men.
The “lost generation” of adults who receive an ASD diagnosis later in life have a lower quality of life, studies suggest, and have the highest risk for suicide among all individuals with autism.
The recent study from Dr. Li and colleagues offers new evidence in both children and adults. But although the systematic review and meta-analysis of 31 studies showed high rates of self-injurious behavior and suicidality in both groups, Dr. Li said it’s the data on adults that was most alarming.
The OR of suicidality in children was 2.53, but the risk in adults was significantly higher, with an odds ratio (OR) of 3.84.
Adults were at greater risk for self-harm than children (OR, 1.45; 95% confidence interval, 1.04-2.03), with higher odds of self-injurious behavior (OR, 3.38; 95% CI, 2.54-4.50) and suicidality (OR, 3.84; 95% CI, 2.78-5.30), compared with children (OR, 2.99; 95% CI, 1.93-4.64 for self-injurious behavior, and OR, 2.53; 95% CI, 1.70-3.76 for suicidality).
Lightbulb moment?
Commenting for this news organization, Brenna Maddox, PhD, assistant professor of psychiatry at UNC Chapel Hill and co-chair of the American Association of Suicidology’s Autism and Suicide Committee, said “the sad reality” is that these findings won’t be surprising to many who work in the field.

“But for some clinicians and the public, this will be a lightbulb kind of moment, increasing awareness about a problem many of us have been talking about for a while,” said Dr. Maddox, who was not involved with the current research.
In January, she launched a 5-year, $9 million study to compare the efficacy of two suicide intervention programs in adolescents and young adults with autism.
The interventions use a well-known suicide prevention tool that has been newly modified for use in people with autism. One program would rely on the intervention alone, and the other would add a structured clinical follow-up.
“There has to be much more than awareness. We need more training for clinicians, we need more tools, we need to know which tools are going to work,” Dr. Maddox said.
Her new project could address all of those needs. Funded by the nonprofit Patient-Centered Outcomes Research Institute (PCORI), it will train 150 clinicians at centers in four states to identify suicidal risk among young adults with autism, utilize the prevention tool, and collect data on its efficacy alone or with follow-up.
Clinician training will begin this spring, and researchers hope to have the first patient data in the fall.
Scaling the ‘services cliff’
While Dr. Maddox’s study could yield a potential suicide prevention tool, she is quick to point out that the ultimate goal would be to have fewer people reach the point where such a tool is needed. However, that will take a multidisciplinary approach that begins with access to clinical care, including mental health care, she noted.
“Our mental health care system in general is not great for people on the spectrum, but it’s even worse for adults,” Dr. Maddox said.
Compared with neurotypical adults, adults with autism use more mental health services, have higher hospitalization rates, and are more likely to use primary care services, one recent study showed. The problem, Dr. Maddox notes, is that there are too few clinicians in those areas who are trained in autism care.
One way to address that issue is to mandate autism instruction in the medical curriculum, Catherine Lord, PhD, told this news organization when asked for comment. Dr. Lord is cochair of The Lancet commission on the future of care and clinical research in autism and professor of psychiatry at the Semel Institute for Neuroscience and Human Behavior at UCLA.
“Medical schools offer very little training on ASD, even in standard psychiatry training. For people who don’t specialize in child or adolescence psychiatry, there’s almost none,” Dr. Lord said.
Dr. Maddox agrees. One goal of the PCORI study is to turn their findings into a transportable training program, perhaps available via a webinar for clinicians, crisis center staff, and others who may encounter an adult with autism who is contemplating suicide.
“This is a life and death situation,” Dr. Maddox said. “We have to marshal every resource we have, and we have to do it now. We can’t waste time.”
Dr. Li’s study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health. Study authors and other sources reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When a recent study from Columbia University reported that suicide and self-harm were nearly four times more likely in adults with autism spectrum disorder (ASD) than in the general population, the findings were sobering. But to many in the field, they were not surprising.
Previous analyses showed individuals with ASD were up to six times more likely to attempt suicide and nearly eight times as likely to succeed. However, the recent study published in JAMA Network Open is one of only a few on self-harm and suicide in autism spectrum disorder (ASD) to include a focus on adults.
“Previously there was relatively little information about adults with autism in general and on injury risk among adults with autism specifically,” study investigator Guohua Li, DrPH, MD, professor of epidemiology at Columbia University Mailman School of Public Health, New York, told this news organization.
“How to continue to provide social support and health care services to adults with autism presents a real challenge to society and is a public health issue,” Dr. Li said.
Falling off a ‘services cliff’
The ASD rate among children is at a record-high in the United States, which means the number of adults on the spectrum will also continue to climb. The incidence of adults with newly diagnosed ASD, who are sometimes described as the “lost generation,” is also increasing. Despite these realities, adults with ASD remain largely underserved and understudied.
The data that are available paint a concerning picture. Adolescents with ASD face a “services cliff” as they transition to adulthood and fall into a landscape with a serious lack of services, support, and clinicians trained to treat adults with ASD.
Compared with young adults without ASD, those on the spectrum have significantly lower college graduation rates, have a harder time finding and keeping a job, are more likely to have a co-occurring mental illness, and are far less likely to live independently.
Before 2020, there were no national data on the number of U.S. adults with autism. That year, the Centers for Disease Control and Prevention released its first-ever report on adult autism prevalence, estimated to be 5.4 million.
That figure is almost definitely low, Matthew Maenner, PhD, autism surveillance team lead with the CDC’s National Center on Birth Defects and Developmental Disabilities, told this news organization.
Researchers use school and medical records to calculate child ASD rates, but counting adults with the disorder is far more difficult.
The CDC’s estimate was based on modeling reports from 2017 state-based population and mortality records and parent-reported survey data of U.S. children diagnosed with ASD. It was inexact, said Dr. Maenner, but it was a start.
“There are no good data on the prevalence of autism in adults. Anywhere,” he added.
Masking and camouflaging
Only about 3.5% of published studies on autism focus on adults, one review showed. In the recently published “The Lancet Commission on the future of care and clinical research in autism,” the section on research on adolescents and adults was a mere 189 words long.
“The brevity of this paragraph reflects the little data available in this area, not its importance” the authors write.
The recent report of higher self-harm risk in adults on the spectrum offers further evidence that “there just aren’t enough services and research on adults on [the] autism spectrum,” Edward S. Brodkin, MD, associate professor of psychiatry and director of the Adult Autism Spectrum Program at the University of Pennsylvania Perelman School of Medicine in Philadelphia, told this news organization.
Founded by Dr. Brodkin in 2013, the program provides ASD diagnostic and support services for adults with ASD. Like others in the field, Dr. Brodkin has noted a sharp increase in the number of previously undiagnosed adults seeking evaluation for possible ASD.
Many of his patients have recently diagnosed children and realized they share some of the same ASD symptoms. Others have long recognized traits common in autism but have engaged in what clinicians call “masking” or “camouflaging.” This is particularly true in women, who are diagnosed with autism at far lower rates than men.
The “lost generation” of adults who receive an ASD diagnosis later in life have a lower quality of life, studies suggest, and have the highest risk for suicide among all individuals with autism.
The recent study from Dr. Li and colleagues offers new evidence in both children and adults. But although the systematic review and meta-analysis of 31 studies showed high rates of self-injurious behavior and suicidality in both groups, Dr. Li said it’s the data on adults that was most alarming.
The OR of suicidality in children was 2.53, but the risk in adults was significantly higher, with an odds ratio (OR) of 3.84.
Adults were at greater risk for self-harm than children (OR, 1.45; 95% confidence interval, 1.04-2.03), with higher odds of self-injurious behavior (OR, 3.38; 95% CI, 2.54-4.50) and suicidality (OR, 3.84; 95% CI, 2.78-5.30), compared with children (OR, 2.99; 95% CI, 1.93-4.64 for self-injurious behavior, and OR, 2.53; 95% CI, 1.70-3.76 for suicidality).
Lightbulb moment?
Commenting for this news organization, Brenna Maddox, PhD, assistant professor of psychiatry at UNC Chapel Hill and co-chair of the American Association of Suicidology’s Autism and Suicide Committee, said “the sad reality” is that these findings won’t be surprising to many who work in the field.
“But for some clinicians and the public, this will be a lightbulb kind of moment, increasing awareness about a problem many of us have been talking about for a while,” said Dr. Maddox, who was not involved with the current research.
In January, she launched a 5-year, $9 million study to compare the efficacy of two suicide intervention programs in adolescents and young adults with autism.
The interventions use a well-known suicide prevention tool that has been newly modified for use in people with autism. One program would rely on the intervention alone, and the other would add a structured clinical follow-up.
“There has to be much more than awareness. We need more training for clinicians, we need more tools, we need to know which tools are going to work,” Dr. Maddox said.
Her new project could address all of those needs. Funded by the nonprofit Patient-Centered Outcomes Research Institute (PCORI), it will train 150 clinicians at centers in four states to identify suicidal risk among young adults with autism, utilize the prevention tool, and collect data on its efficacy alone or with follow-up.
Clinician training will begin this spring, and researchers hope to have the first patient data in the fall.
Scaling the ‘services cliff’
While Dr. Maddox’s study could yield a potential suicide prevention tool, she is quick to point out that the ultimate goal would be to have fewer people reach the point where such a tool is needed. However, that will take a multidisciplinary approach that begins with access to clinical care, including mental health care, she noted.
“Our mental health care system in general is not great for people on the spectrum, but it’s even worse for adults,” Dr. Maddox said.
Compared with neurotypical adults, adults with autism use more mental health services, have higher hospitalization rates, and are more likely to use primary care services, one recent study showed. The problem, Dr. Maddox notes, is that there are too few clinicians in those areas who are trained in autism care.
One way to address that issue is to mandate autism instruction in the medical curriculum, Catherine Lord, PhD, told this news organization when asked for comment. Dr. Lord is cochair of The Lancet commission on the future of care and clinical research in autism and professor of psychiatry at the Semel Institute for Neuroscience and Human Behavior at UCLA.
“Medical schools offer very little training on ASD, even in standard psychiatry training. For people who don’t specialize in child or adolescence psychiatry, there’s almost none,” Dr. Lord said.
Dr. Maddox agrees. One goal of the PCORI study is to turn their findings into a transportable training program, perhaps available via a webinar for clinicians, crisis center staff, and others who may encounter an adult with autism who is contemplating suicide.
“This is a life and death situation,” Dr. Maddox said. “We have to marshal every resource we have, and we have to do it now. We can’t waste time.”
Dr. Li’s study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health. Study authors and other sources reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When a recent study from Columbia University reported that suicide and self-harm were nearly four times more likely in adults with autism spectrum disorder (ASD) than in the general population, the findings were sobering. But to many in the field, they were not surprising.
Previous analyses showed individuals with ASD were up to six times more likely to attempt suicide and nearly eight times as likely to succeed. However, the recent study published in JAMA Network Open is one of only a few on self-harm and suicide in autism spectrum disorder (ASD) to include a focus on adults.
“Previously there was relatively little information about adults with autism in general and on injury risk among adults with autism specifically,” study investigator Guohua Li, DrPH, MD, professor of epidemiology at Columbia University Mailman School of Public Health, New York, told this news organization.
“How to continue to provide social support and health care services to adults with autism presents a real challenge to society and is a public health issue,” Dr. Li said.
Falling off a ‘services cliff’
The ASD rate among children is at a record-high in the United States, which means the number of adults on the spectrum will also continue to climb. The incidence of adults with newly diagnosed ASD, who are sometimes described as the “lost generation,” is also increasing. Despite these realities, adults with ASD remain largely underserved and understudied.
The data that are available paint a concerning picture. Adolescents with ASD face a “services cliff” as they transition to adulthood and fall into a landscape with a serious lack of services, support, and clinicians trained to treat adults with ASD.
Compared with young adults without ASD, those on the spectrum have significantly lower college graduation rates, have a harder time finding and keeping a job, are more likely to have a co-occurring mental illness, and are far less likely to live independently.
Before 2020, there were no national data on the number of U.S. adults with autism. That year, the Centers for Disease Control and Prevention released its first-ever report on adult autism prevalence, estimated to be 5.4 million.
That figure is almost definitely low, Matthew Maenner, PhD, autism surveillance team lead with the CDC’s National Center on Birth Defects and Developmental Disabilities, told this news organization.
Researchers use school and medical records to calculate child ASD rates, but counting adults with the disorder is far more difficult.
The CDC’s estimate was based on modeling reports from 2017 state-based population and mortality records and parent-reported survey data of U.S. children diagnosed with ASD. It was inexact, said Dr. Maenner, but it was a start.
“There are no good data on the prevalence of autism in adults. Anywhere,” he added.
Masking and camouflaging
Only about 3.5% of published studies on autism focus on adults, one review showed. In the recently published “The Lancet Commission on the future of care and clinical research in autism,” the section on research on adolescents and adults was a mere 189 words long.
“The brevity of this paragraph reflects the little data available in this area, not its importance” the authors write.
The recent report of higher self-harm risk in adults on the spectrum offers further evidence that “there just aren’t enough services and research on adults on [the] autism spectrum,” Edward S. Brodkin, MD, associate professor of psychiatry and director of the Adult Autism Spectrum Program at the University of Pennsylvania Perelman School of Medicine in Philadelphia, told this news organization.
Founded by Dr. Brodkin in 2013, the program provides ASD diagnostic and support services for adults with ASD. Like others in the field, Dr. Brodkin has noted a sharp increase in the number of previously undiagnosed adults seeking evaluation for possible ASD.
Many of his patients have recently diagnosed children and realized they share some of the same ASD symptoms. Others have long recognized traits common in autism but have engaged in what clinicians call “masking” or “camouflaging.” This is particularly true in women, who are diagnosed with autism at far lower rates than men.
The “lost generation” of adults who receive an ASD diagnosis later in life have a lower quality of life, studies suggest, and have the highest risk for suicide among all individuals with autism.
The recent study from Dr. Li and colleagues offers new evidence in both children and adults. But although the systematic review and meta-analysis of 31 studies showed high rates of self-injurious behavior and suicidality in both groups, Dr. Li said it’s the data on adults that was most alarming.
The OR of suicidality in children was 2.53, but the risk in adults was significantly higher, with an odds ratio (OR) of 3.84.
Adults were at greater risk for self-harm than children (OR, 1.45; 95% confidence interval, 1.04-2.03), with higher odds of self-injurious behavior (OR, 3.38; 95% CI, 2.54-4.50) and suicidality (OR, 3.84; 95% CI, 2.78-5.30), compared with children (OR, 2.99; 95% CI, 1.93-4.64 for self-injurious behavior, and OR, 2.53; 95% CI, 1.70-3.76 for suicidality).
Lightbulb moment?
Commenting for this news organization, Brenna Maddox, PhD, assistant professor of psychiatry at UNC Chapel Hill and co-chair of the American Association of Suicidology’s Autism and Suicide Committee, said “the sad reality” is that these findings won’t be surprising to many who work in the field.
“But for some clinicians and the public, this will be a lightbulb kind of moment, increasing awareness about a problem many of us have been talking about for a while,” said Dr. Maddox, who was not involved with the current research.
In January, she launched a 5-year, $9 million study to compare the efficacy of two suicide intervention programs in adolescents and young adults with autism.
The interventions use a well-known suicide prevention tool that has been newly modified for use in people with autism. One program would rely on the intervention alone, and the other would add a structured clinical follow-up.
“There has to be much more than awareness. We need more training for clinicians, we need more tools, we need to know which tools are going to work,” Dr. Maddox said.
Her new project could address all of those needs. Funded by the nonprofit Patient-Centered Outcomes Research Institute (PCORI), it will train 150 clinicians at centers in four states to identify suicidal risk among young adults with autism, utilize the prevention tool, and collect data on its efficacy alone or with follow-up.
Clinician training will begin this spring, and researchers hope to have the first patient data in the fall.
Scaling the ‘services cliff’
While Dr. Maddox’s study could yield a potential suicide prevention tool, she is quick to point out that the ultimate goal would be to have fewer people reach the point where such a tool is needed. However, that will take a multidisciplinary approach that begins with access to clinical care, including mental health care, she noted.
“Our mental health care system in general is not great for people on the spectrum, but it’s even worse for adults,” Dr. Maddox said.
Compared with neurotypical adults, adults with autism use more mental health services, have higher hospitalization rates, and are more likely to use primary care services, one recent study showed. The problem, Dr. Maddox notes, is that there are too few clinicians in those areas who are trained in autism care.
One way to address that issue is to mandate autism instruction in the medical curriculum, Catherine Lord, PhD, told this news organization when asked for comment. Dr. Lord is cochair of The Lancet commission on the future of care and clinical research in autism and professor of psychiatry at the Semel Institute for Neuroscience and Human Behavior at UCLA.
“Medical schools offer very little training on ASD, even in standard psychiatry training. For people who don’t specialize in child or adolescence psychiatry, there’s almost none,” Dr. Lord said.
Dr. Maddox agrees. One goal of the PCORI study is to turn their findings into a transportable training program, perhaps available via a webinar for clinicians, crisis center staff, and others who may encounter an adult with autism who is contemplating suicide.
“This is a life and death situation,” Dr. Maddox said. “We have to marshal every resource we have, and we have to do it now. We can’t waste time.”
Dr. Li’s study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health. Study authors and other sources reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New MIS-C guidance addresses diagnostic challenges, cardiac care
Updated guidance for health care providers on multisystem inflammatory syndrome in children (MIS-C) recognizes the evolving nature of the disease and offers strategies for pediatric rheumatologists, who also may be asked to recommend treatment for hyperinflammation in children with acute COVID-19.
Guidance is needed for many reasons, including the variable case definitions for MIS-C, the presence of MIS-C features in other infections and childhood rheumatic diseases, the extrapolation of treatment strategies from other conditions with similar presentations, and the issue of myocardial dysfunction, wrote Lauren A. Henderson, MD, MMSC, of Boston Children’s Hospital, and members of the American College of Rheumatology MIS-C and COVID-19–Related Hyperinflammation Task Force.

However, “modifications to treatment plans, particularly in patients with complex conditions, are highly disease, patient, geography, and time specific, and therefore must be individualized as part of a shared decision-making process,” the authors said. The updated guidance was published in Arthritis & Rheumatology.
Update needed in wake of Omicron
“We continue to see cases of MIS-C across the United States due to the spike in SARS-CoV-2 infections from the Omicron variant,” and therefore updated guidance is important at this time, Dr. Henderson told this news organization.
“MIS-C remains a serious complication of COVID-19 in children and the ACR wanted to continue to provide pediatricians with up-to-date recommendations for the management of MIS-C,” she said.
“Children began to present with MIS-C in April 2020. At that time, little was known about this entity. Most of the recommendations in the first version of the MIS-C guidance were based on expert opinion,” she explained. However, “over the last 2 years, pediatricians have worked very hard to conduct high-quality research studies to better understand MIS-C, so we now have more scientific evidence to guide our recommendations.
“In version three of the MIS-C guidance, there are new recommendations on treatment. Previously, it was unclear what medications should be used for first-line treatment in patients with MIS-C. Some children were given intravenous immunoglobulin while others were given IVIg and steroids together. Several new studies show that children with MIS-C who are treated with a combination of IVIg and steroids have better outcomes. Accordingly, the MIS-C guidance now recommends dual therapy with IVIg and steroids in children with MIS-C.”
Diagnostic evaluation
The guidance calls for maintaining a broad differential diagnosis of MIS-C, given that the condition remains rare, and that most children with COVID-19 present with mild symptoms and have excellent outcomes, the authors noted. The range of clinical features associated with MIS-C include fever, mucocutaneous findings, myocardial dysfunction, cardiac conduction abnormalities, shock, gastrointestinal symptoms, and lymphadenopathy.
Some patients also experience neurologic involvement in the form of severe headache, altered mental status, seizures, cranial nerve palsies, meningismus, cerebral edema, and ischemic or hemorrhagic stroke. Given the nonspecific nature of these symptoms, “it is imperative that a diagnostic evaluation for MIS-C include investigation for other possible causes, as deemed appropriate by the treating provider,” the authors emphasized. Other diagnostic considerations include the prevalence and chronology of COVID-19 in the community, which may change over time.
MIS-C and Kawasaki disease phenotypes
Earlier in the pandemic, when MIS-C first emerged, it was compared with Kawasaki disease (KD). “However, a closer examination of the literature shows that only about one-quarter to half of patients with a reported diagnosis of MIS-C meet the full diagnostic criteria for KD,” the authors wrote. Key features that separate MIS-C from KD include the greater incidence of KD among children in Japan and East Asia versus the higher incidence of MIS-C among non-Hispanic Black children. In addition, children with MIS-C have shown a wider age range, more prominent gastrointestinal and neurologic symptoms, and more frequent cardiac dysfunction, compared with those with KD.
Cardiac management
Close follow-up with cardiology is essential for children with MIS-C, according to the authors. The recommendations call for repeat echocardiograms for all children with MIS-C at a minimum of 7-14 days, then again at 4-6 weeks after the initial presentation. The authors also recommended additional echocardiograms for children with left ventricular dysfunction and cardiac aortic aneurysms.
MIS-C treatment
Current treatment recommendations emphasize that patients under investigation for MIS-C with life-threatening manifestations may need immunomodulatory therapy before a full diagnostic evaluation is complete, the authors said. However, patients without life-threatening manifestations should be evaluated before starting immunomodulatory treatment to avoid potentially harmful therapies for pediatric patients who don’t need them.
When MIS-C is refractory to initial immunomodulatory treatment, a second dose of IVIg is not recommended, but intensification therapy is advised with either high-dose (10-30 mg/kg per day) glucocorticoids, anakinra, or infliximab. However, there is little evidence available for selecting a specific agent for intensification therapy.
The task force also advises giving low-dose aspirin (3-5 mg/kg per day, up to 81 mg once daily) to all MIS-C patients without active bleeding or significant bleeding risk until normalization of the platelet count and confirmed normal coronary arteries at least 4 weeks after diagnosis.
COVID-19 and hyperinflammation
The task force also noted a distinction between MIS-C and severe COVID-19 in children. Although many children with MIS-C are previously healthy, most children who develop severe COVID-19 during an initial infection have complex conditions or comorbidities such as developmental delay or genetic anomaly, or chronic conditions such as congenital heart disease, type 1 diabetes, or asthma, the authors said. They recommend that “hospitalized children with COVID-19 requiring supplemental oxygen or respiratory support should be considered for immunomodulatory therapy in addition to supportive care and antiviral medications.”
The authors acknowledged the limitations and evolving nature of the recommendations, which will continue to change and do not replace clinical judgment for the management of individual patients. In the meantime, the ACR will support the task force in reviewing new evidence and providing revised versions of the current document.
Many questions about MIS-C remain, Dr. Henderson said in an interview. “It can be very hard to diagnose children with MIS-C because many of the symptoms are similar to those seen in other febrile illness of childhood. We need to identify better biomarkers to help us make the diagnosis of MIS-C. In addition, we need studies to provide information about what treatments should be used if children fail to respond to IVIg and steroids. Finally, it appears that vaccination [against SARS-CoV-2] protects against severe forms of MIS-C, and studies are needed to see how vaccination protects children from MIS-C.”
The development of the guidance was supported by the American College of Rheumatology. Dr. Henderson disclosed relationships with companies including Sobi, Pfizer, and Adaptive Biotechnologies (less than $10,000) and research support from the Childhood Arthritis and Rheumatology Research Alliance and research grant support from Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
Updated guidance for health care providers on multisystem inflammatory syndrome in children (MIS-C) recognizes the evolving nature of the disease and offers strategies for pediatric rheumatologists, who also may be asked to recommend treatment for hyperinflammation in children with acute COVID-19.
Guidance is needed for many reasons, including the variable case definitions for MIS-C, the presence of MIS-C features in other infections and childhood rheumatic diseases, the extrapolation of treatment strategies from other conditions with similar presentations, and the issue of myocardial dysfunction, wrote Lauren A. Henderson, MD, MMSC, of Boston Children’s Hospital, and members of the American College of Rheumatology MIS-C and COVID-19–Related Hyperinflammation Task Force.
However, “modifications to treatment plans, particularly in patients with complex conditions, are highly disease, patient, geography, and time specific, and therefore must be individualized as part of a shared decision-making process,” the authors said. The updated guidance was published in Arthritis & Rheumatology.
Update needed in wake of Omicron
“We continue to see cases of MIS-C across the United States due to the spike in SARS-CoV-2 infections from the Omicron variant,” and therefore updated guidance is important at this time, Dr. Henderson told this news organization.
“MIS-C remains a serious complication of COVID-19 in children and the ACR wanted to continue to provide pediatricians with up-to-date recommendations for the management of MIS-C,” she said.
“Children began to present with MIS-C in April 2020. At that time, little was known about this entity. Most of the recommendations in the first version of the MIS-C guidance were based on expert opinion,” she explained. However, “over the last 2 years, pediatricians have worked very hard to conduct high-quality research studies to better understand MIS-C, so we now have more scientific evidence to guide our recommendations.
“In version three of the MIS-C guidance, there are new recommendations on treatment. Previously, it was unclear what medications should be used for first-line treatment in patients with MIS-C. Some children were given intravenous immunoglobulin while others were given IVIg and steroids together. Several new studies show that children with MIS-C who are treated with a combination of IVIg and steroids have better outcomes. Accordingly, the MIS-C guidance now recommends dual therapy with IVIg and steroids in children with MIS-C.”
Diagnostic evaluation
The guidance calls for maintaining a broad differential diagnosis of MIS-C, given that the condition remains rare, and that most children with COVID-19 present with mild symptoms and have excellent outcomes, the authors noted. The range of clinical features associated with MIS-C include fever, mucocutaneous findings, myocardial dysfunction, cardiac conduction abnormalities, shock, gastrointestinal symptoms, and lymphadenopathy.
Some patients also experience neurologic involvement in the form of severe headache, altered mental status, seizures, cranial nerve palsies, meningismus, cerebral edema, and ischemic or hemorrhagic stroke. Given the nonspecific nature of these symptoms, “it is imperative that a diagnostic evaluation for MIS-C include investigation for other possible causes, as deemed appropriate by the treating provider,” the authors emphasized. Other diagnostic considerations include the prevalence and chronology of COVID-19 in the community, which may change over time.
MIS-C and Kawasaki disease phenotypes
Earlier in the pandemic, when MIS-C first emerged, it was compared with Kawasaki disease (KD). “However, a closer examination of the literature shows that only about one-quarter to half of patients with a reported diagnosis of MIS-C meet the full diagnostic criteria for KD,” the authors wrote. Key features that separate MIS-C from KD include the greater incidence of KD among children in Japan and East Asia versus the higher incidence of MIS-C among non-Hispanic Black children. In addition, children with MIS-C have shown a wider age range, more prominent gastrointestinal and neurologic symptoms, and more frequent cardiac dysfunction, compared with those with KD.
Cardiac management
Close follow-up with cardiology is essential for children with MIS-C, according to the authors. The recommendations call for repeat echocardiograms for all children with MIS-C at a minimum of 7-14 days, then again at 4-6 weeks after the initial presentation. The authors also recommended additional echocardiograms for children with left ventricular dysfunction and cardiac aortic aneurysms.
MIS-C treatment
Current treatment recommendations emphasize that patients under investigation for MIS-C with life-threatening manifestations may need immunomodulatory therapy before a full diagnostic evaluation is complete, the authors said. However, patients without life-threatening manifestations should be evaluated before starting immunomodulatory treatment to avoid potentially harmful therapies for pediatric patients who don’t need them.
When MIS-C is refractory to initial immunomodulatory treatment, a second dose of IVIg is not recommended, but intensification therapy is advised with either high-dose (10-30 mg/kg per day) glucocorticoids, anakinra, or infliximab. However, there is little evidence available for selecting a specific agent for intensification therapy.
The task force also advises giving low-dose aspirin (3-5 mg/kg per day, up to 81 mg once daily) to all MIS-C patients without active bleeding or significant bleeding risk until normalization of the platelet count and confirmed normal coronary arteries at least 4 weeks after diagnosis.
COVID-19 and hyperinflammation
The task force also noted a distinction between MIS-C and severe COVID-19 in children. Although many children with MIS-C are previously healthy, most children who develop severe COVID-19 during an initial infection have complex conditions or comorbidities such as developmental delay or genetic anomaly, or chronic conditions such as congenital heart disease, type 1 diabetes, or asthma, the authors said. They recommend that “hospitalized children with COVID-19 requiring supplemental oxygen or respiratory support should be considered for immunomodulatory therapy in addition to supportive care and antiviral medications.”
The authors acknowledged the limitations and evolving nature of the recommendations, which will continue to change and do not replace clinical judgment for the management of individual patients. In the meantime, the ACR will support the task force in reviewing new evidence and providing revised versions of the current document.
Many questions about MIS-C remain, Dr. Henderson said in an interview. “It can be very hard to diagnose children with MIS-C because many of the symptoms are similar to those seen in other febrile illness of childhood. We need to identify better biomarkers to help us make the diagnosis of MIS-C. In addition, we need studies to provide information about what treatments should be used if children fail to respond to IVIg and steroids. Finally, it appears that vaccination [against SARS-CoV-2] protects against severe forms of MIS-C, and studies are needed to see how vaccination protects children from MIS-C.”
The development of the guidance was supported by the American College of Rheumatology. Dr. Henderson disclosed relationships with companies including Sobi, Pfizer, and Adaptive Biotechnologies (less than $10,000) and research support from the Childhood Arthritis and Rheumatology Research Alliance and research grant support from Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
Updated guidance for health care providers on multisystem inflammatory syndrome in children (MIS-C) recognizes the evolving nature of the disease and offers strategies for pediatric rheumatologists, who also may be asked to recommend treatment for hyperinflammation in children with acute COVID-19.
Guidance is needed for many reasons, including the variable case definitions for MIS-C, the presence of MIS-C features in other infections and childhood rheumatic diseases, the extrapolation of treatment strategies from other conditions with similar presentations, and the issue of myocardial dysfunction, wrote Lauren A. Henderson, MD, MMSC, of Boston Children’s Hospital, and members of the American College of Rheumatology MIS-C and COVID-19–Related Hyperinflammation Task Force.
However, “modifications to treatment plans, particularly in patients with complex conditions, are highly disease, patient, geography, and time specific, and therefore must be individualized as part of a shared decision-making process,” the authors said. The updated guidance was published in Arthritis & Rheumatology.
Update needed in wake of Omicron
“We continue to see cases of MIS-C across the United States due to the spike in SARS-CoV-2 infections from the Omicron variant,” and therefore updated guidance is important at this time, Dr. Henderson told this news organization.
“MIS-C remains a serious complication of COVID-19 in children and the ACR wanted to continue to provide pediatricians with up-to-date recommendations for the management of MIS-C,” she said.
“Children began to present with MIS-C in April 2020. At that time, little was known about this entity. Most of the recommendations in the first version of the MIS-C guidance were based on expert opinion,” she explained. However, “over the last 2 years, pediatricians have worked very hard to conduct high-quality research studies to better understand MIS-C, so we now have more scientific evidence to guide our recommendations.
“In version three of the MIS-C guidance, there are new recommendations on treatment. Previously, it was unclear what medications should be used for first-line treatment in patients with MIS-C. Some children were given intravenous immunoglobulin while others were given IVIg and steroids together. Several new studies show that children with MIS-C who are treated with a combination of IVIg and steroids have better outcomes. Accordingly, the MIS-C guidance now recommends dual therapy with IVIg and steroids in children with MIS-C.”
Diagnostic evaluation
The guidance calls for maintaining a broad differential diagnosis of MIS-C, given that the condition remains rare, and that most children with COVID-19 present with mild symptoms and have excellent outcomes, the authors noted. The range of clinical features associated with MIS-C include fever, mucocutaneous findings, myocardial dysfunction, cardiac conduction abnormalities, shock, gastrointestinal symptoms, and lymphadenopathy.
Some patients also experience neurologic involvement in the form of severe headache, altered mental status, seizures, cranial nerve palsies, meningismus, cerebral edema, and ischemic or hemorrhagic stroke. Given the nonspecific nature of these symptoms, “it is imperative that a diagnostic evaluation for MIS-C include investigation for other possible causes, as deemed appropriate by the treating provider,” the authors emphasized. Other diagnostic considerations include the prevalence and chronology of COVID-19 in the community, which may change over time.
MIS-C and Kawasaki disease phenotypes
Earlier in the pandemic, when MIS-C first emerged, it was compared with Kawasaki disease (KD). “However, a closer examination of the literature shows that only about one-quarter to half of patients with a reported diagnosis of MIS-C meet the full diagnostic criteria for KD,” the authors wrote. Key features that separate MIS-C from KD include the greater incidence of KD among children in Japan and East Asia versus the higher incidence of MIS-C among non-Hispanic Black children. In addition, children with MIS-C have shown a wider age range, more prominent gastrointestinal and neurologic symptoms, and more frequent cardiac dysfunction, compared with those with KD.
Cardiac management
Close follow-up with cardiology is essential for children with MIS-C, according to the authors. The recommendations call for repeat echocardiograms for all children with MIS-C at a minimum of 7-14 days, then again at 4-6 weeks after the initial presentation. The authors also recommended additional echocardiograms for children with left ventricular dysfunction and cardiac aortic aneurysms.
MIS-C treatment
Current treatment recommendations emphasize that patients under investigation for MIS-C with life-threatening manifestations may need immunomodulatory therapy before a full diagnostic evaluation is complete, the authors said. However, patients without life-threatening manifestations should be evaluated before starting immunomodulatory treatment to avoid potentially harmful therapies for pediatric patients who don’t need them.
When MIS-C is refractory to initial immunomodulatory treatment, a second dose of IVIg is not recommended, but intensification therapy is advised with either high-dose (10-30 mg/kg per day) glucocorticoids, anakinra, or infliximab. However, there is little evidence available for selecting a specific agent for intensification therapy.
The task force also advises giving low-dose aspirin (3-5 mg/kg per day, up to 81 mg once daily) to all MIS-C patients without active bleeding or significant bleeding risk until normalization of the platelet count and confirmed normal coronary arteries at least 4 weeks after diagnosis.
COVID-19 and hyperinflammation
The task force also noted a distinction between MIS-C and severe COVID-19 in children. Although many children with MIS-C are previously healthy, most children who develop severe COVID-19 during an initial infection have complex conditions or comorbidities such as developmental delay or genetic anomaly, or chronic conditions such as congenital heart disease, type 1 diabetes, or asthma, the authors said. They recommend that “hospitalized children with COVID-19 requiring supplemental oxygen or respiratory support should be considered for immunomodulatory therapy in addition to supportive care and antiviral medications.”
The authors acknowledged the limitations and evolving nature of the recommendations, which will continue to change and do not replace clinical judgment for the management of individual patients. In the meantime, the ACR will support the task force in reviewing new evidence and providing revised versions of the current document.
Many questions about MIS-C remain, Dr. Henderson said in an interview. “It can be very hard to diagnose children with MIS-C because many of the symptoms are similar to those seen in other febrile illness of childhood. We need to identify better biomarkers to help us make the diagnosis of MIS-C. In addition, we need studies to provide information about what treatments should be used if children fail to respond to IVIg and steroids. Finally, it appears that vaccination [against SARS-CoV-2] protects against severe forms of MIS-C, and studies are needed to see how vaccination protects children from MIS-C.”
The development of the guidance was supported by the American College of Rheumatology. Dr. Henderson disclosed relationships with companies including Sobi, Pfizer, and Adaptive Biotechnologies (less than $10,000) and research support from the Childhood Arthritis and Rheumatology Research Alliance and research grant support from Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS AND RHEUMATOLOGY
Subvariant may be more dangerous than original Omicron strain
, a lab study from Japan says.
“Our multiscale investigations suggest that the risk of BA.2 for global health is potentially higher than that of BA.1,” the researchers said in the study published on the preprint server bioRxiv. The study has not been peer-reviewed.
The researchers infected hamsters with BA.1 and BA.2. The hamsters infected with BA.2 got sicker, with more lung damage and loss of body weight. Results were similar when mice were infected with BA.1 and BA.2.
“Infection experiments using hamsters show that BA.2 is more pathogenic than BA.1,” the study said.
BA.1 and BA.2 both appear to evade immunity created by COVID-19 vaccines, the study said. But a booster shot makes illness after infection 74% less likely, CNN said.
What’s more, therapeutic monoclonal antibodies used to treat people infected with COVID didn’t have much effect on BA.2.
BA.2 was “almost completely resistant” to casirivimab and imdevimab and was 35 times more resistant to sotrovimab, compared to the original B.1.1 virus, the researchers wrote.
“In summary, our data suggest the possibility that BA.2 would be the most concerned variant to global health,” the researchers wrote. “Currently, both BA.2 and BA.1 are recognised together as Omicron and these are almost undistinguishable. Based on our findings, we propose that BA.2 should be recognised as a unique variant of concern, and this SARS-CoV-2 variant should be monitored in depth.”
If the World Health Organization recognized BA.2 as a “unique variant of concern,” it would be given its own Greek letter.
But some scientists noted that findings in the lab don’t always reflect what’s happening in the real world of people.
“I think it’s always hard to translate differences in animal and cell culture models to what’s going on with regards to human disease,” Jeremy Kamil, PhD, an associate professor of microbiology and immunology at Louisiana State University Health Shreveport, told Newsweek. “That said, the differences do look real.”
“It might be, from a human’s perspective, a worse virus than BA.1 and might be able to transmit better and cause worse disease,” Daniel Rhoads, MD, section head of microbiology at the Cleveland Clinic in Ohio, told CNN. He reviewed the Japanese study but was not involved in it.
Another scientist who reviewed the study but was not involved in the research noted that human immune systems are evolving along with the COVID variants.
“One of the caveats that we have to think about, as we get new variants that might seem more dangerous, is the fact that there’s two sides to the story,” Deborah Fuller, PhD, a virologist at the University of Washington School of Medicine, told CNN. “Our immune system is evolving as well. And so that’s pushing back on things.”
Scientists have already established that BA.2 is more transmissible than BA.1. The Omicron subvariant has been detected in 74 countries and 47 U.S. states, according to CNN. About 4% of Americans with COVID were infected with BA.2, the outlet reported, citing the CDC, but it’s now the dominant strain in other nations.
It’s not clear yet if BA.2 causes more severe illness in people. While BA.2 spreads faster than BA.1, there’s no evidence the subvariant makes people any sicker, an official with the World Health Organization said, according to CNBC.
A version of this article first appeared on WebMD.com.
, a lab study from Japan says.
“Our multiscale investigations suggest that the risk of BA.2 for global health is potentially higher than that of BA.1,” the researchers said in the study published on the preprint server bioRxiv. The study has not been peer-reviewed.
The researchers infected hamsters with BA.1 and BA.2. The hamsters infected with BA.2 got sicker, with more lung damage and loss of body weight. Results were similar when mice were infected with BA.1 and BA.2.
“Infection experiments using hamsters show that BA.2 is more pathogenic than BA.1,” the study said.
BA.1 and BA.2 both appear to evade immunity created by COVID-19 vaccines, the study said. But a booster shot makes illness after infection 74% less likely, CNN said.
What’s more, therapeutic monoclonal antibodies used to treat people infected with COVID didn’t have much effect on BA.2.
BA.2 was “almost completely resistant” to casirivimab and imdevimab and was 35 times more resistant to sotrovimab, compared to the original B.1.1 virus, the researchers wrote.
“In summary, our data suggest the possibility that BA.2 would be the most concerned variant to global health,” the researchers wrote. “Currently, both BA.2 and BA.1 are recognised together as Omicron and these are almost undistinguishable. Based on our findings, we propose that BA.2 should be recognised as a unique variant of concern, and this SARS-CoV-2 variant should be monitored in depth.”
If the World Health Organization recognized BA.2 as a “unique variant of concern,” it would be given its own Greek letter.
But some scientists noted that findings in the lab don’t always reflect what’s happening in the real world of people.
“I think it’s always hard to translate differences in animal and cell culture models to what’s going on with regards to human disease,” Jeremy Kamil, PhD, an associate professor of microbiology and immunology at Louisiana State University Health Shreveport, told Newsweek. “That said, the differences do look real.”
“It might be, from a human’s perspective, a worse virus than BA.1 and might be able to transmit better and cause worse disease,” Daniel Rhoads, MD, section head of microbiology at the Cleveland Clinic in Ohio, told CNN. He reviewed the Japanese study but was not involved in it.
Another scientist who reviewed the study but was not involved in the research noted that human immune systems are evolving along with the COVID variants.
“One of the caveats that we have to think about, as we get new variants that might seem more dangerous, is the fact that there’s two sides to the story,” Deborah Fuller, PhD, a virologist at the University of Washington School of Medicine, told CNN. “Our immune system is evolving as well. And so that’s pushing back on things.”
Scientists have already established that BA.2 is more transmissible than BA.1. The Omicron subvariant has been detected in 74 countries and 47 U.S. states, according to CNN. About 4% of Americans with COVID were infected with BA.2, the outlet reported, citing the CDC, but it’s now the dominant strain in other nations.
It’s not clear yet if BA.2 causes more severe illness in people. While BA.2 spreads faster than BA.1, there’s no evidence the subvariant makes people any sicker, an official with the World Health Organization said, according to CNBC.
A version of this article first appeared on WebMD.com.
, a lab study from Japan says.
“Our multiscale investigations suggest that the risk of BA.2 for global health is potentially higher than that of BA.1,” the researchers said in the study published on the preprint server bioRxiv. The study has not been peer-reviewed.
The researchers infected hamsters with BA.1 and BA.2. The hamsters infected with BA.2 got sicker, with more lung damage and loss of body weight. Results were similar when mice were infected with BA.1 and BA.2.
“Infection experiments using hamsters show that BA.2 is more pathogenic than BA.1,” the study said.
BA.1 and BA.2 both appear to evade immunity created by COVID-19 vaccines, the study said. But a booster shot makes illness after infection 74% less likely, CNN said.
What’s more, therapeutic monoclonal antibodies used to treat people infected with COVID didn’t have much effect on BA.2.
BA.2 was “almost completely resistant” to casirivimab and imdevimab and was 35 times more resistant to sotrovimab, compared to the original B.1.1 virus, the researchers wrote.
“In summary, our data suggest the possibility that BA.2 would be the most concerned variant to global health,” the researchers wrote. “Currently, both BA.2 and BA.1 are recognised together as Omicron and these are almost undistinguishable. Based on our findings, we propose that BA.2 should be recognised as a unique variant of concern, and this SARS-CoV-2 variant should be monitored in depth.”
If the World Health Organization recognized BA.2 as a “unique variant of concern,” it would be given its own Greek letter.
But some scientists noted that findings in the lab don’t always reflect what’s happening in the real world of people.
“I think it’s always hard to translate differences in animal and cell culture models to what’s going on with regards to human disease,” Jeremy Kamil, PhD, an associate professor of microbiology and immunology at Louisiana State University Health Shreveport, told Newsweek. “That said, the differences do look real.”
“It might be, from a human’s perspective, a worse virus than BA.1 and might be able to transmit better and cause worse disease,” Daniel Rhoads, MD, section head of microbiology at the Cleveland Clinic in Ohio, told CNN. He reviewed the Japanese study but was not involved in it.
Another scientist who reviewed the study but was not involved in the research noted that human immune systems are evolving along with the COVID variants.
“One of the caveats that we have to think about, as we get new variants that might seem more dangerous, is the fact that there’s two sides to the story,” Deborah Fuller, PhD, a virologist at the University of Washington School of Medicine, told CNN. “Our immune system is evolving as well. And so that’s pushing back on things.”
Scientists have already established that BA.2 is more transmissible than BA.1. The Omicron subvariant has been detected in 74 countries and 47 U.S. states, according to CNN. About 4% of Americans with COVID were infected with BA.2, the outlet reported, citing the CDC, but it’s now the dominant strain in other nations.
It’s not clear yet if BA.2 causes more severe illness in people. While BA.2 spreads faster than BA.1, there’s no evidence the subvariant makes people any sicker, an official with the World Health Organization said, according to CNBC.
A version of this article first appeared on WebMD.com.