User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Stroke is ‘not a common complication’ in COVID-19
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
From AAN 2021
Ten reasons airborne transmission of SARS-CoV-2 appears airtight
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
Children’s share of COVID-19 burden has never been higher
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
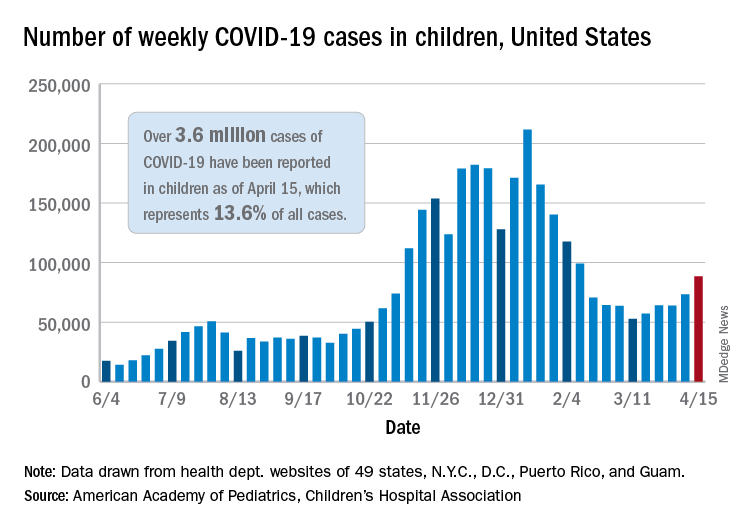
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
What COVID did to MD income in 2020
, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Almost 18,000 physicians in more than 29 specialties told Medscape about their income, hours worked, greatest challenges, and the unexpected impact of COVID-19 on their compensation.
How many physicians avoided massive losses
When the pandemic started around March 2020, “a great many physicians saw reductions in volume at first,” says Robert Pearl, MD, former CEO of the Permanente Medical Group and a professor at Stanford (Calif.) University.
Medscape’s survey report shows that a staggering 44% saw a 1%-25% reduction in patient volume, and 9% saw a 26%-50% decline. “That is indeed breathtaking,” Dr. Pearl says.
Several key factors saved many practices from hemorrhaging money, says Michael Belkin, JD, divisional vice president at Merritt Hawkins and Associates in Dallas. “Many physicians used the federal Paycheck Protection Program [PPP] to help keep themselves afloat,” he says. “A large percentage reduced their staff, which reduced their expenses, and many got some of their volume back by transitioning to telemedicine.”
In a 2020 survey for the Physicians Foundation, conducted by Merritt Hawkins, 48% of physicians said their practice had received PPP support, and most of those said the support was enough to allow them to stay open without reducing staff. Only 6% of practices that received PPP support did not stay open.
Telemedicine helped many practices
Early in the pandemic, Medicare reimbursements for telemedicine were equal with those for face-to-face visits. “Since telemedicine takes a third less time than an inpatient visit, doctors could see more patients,” Dr. Pearl says.
The switch was almost instantaneous in some practices. Within 3 days, a 200-provider multispecialty practice in Wilmington, N.C., went from not using telehealth to its being used by all physicians, the Medical Group Management Association reported. By late April, the practice was already back up to about 70% of normal overall production.
However, telemedicine could not help every specialty equally. “Generally, allergists can’t do their allergy testing virtually, and patients with mild problems probably put off visits,” Dr. Pearl says. Allergists experienced a large percentage decline in compensation, according to Medscape’s survey. For some, income fell from $301,000 the prior year to $274,000 this year.
Primary care struggled
Primary care physicians posted lower compensation than they did the prior year, but most rebounded to some degree. A study released in June 2020 projected that, even with telemedicine, primary care physicians would lose an average of $67,774 for the year.
However, Medscape’s survey found that internists’ average compensation declined from $251,000 in the prior year to $248,000, and average family physicians’ compensation actually rose from $234,000.
Pediatricians had a harder slog. Their average compensation sank from $232,000 to $221,000, according to the report. Even with telemedicine, parents of young children were not contacting the doctor. In May 2020, visits by children aged 3-5 years were down by 56%.
Many proceduralists recovered
Procedure-oriented specialties were particularly hard-hit at first, because many hospitals and some states banned all elective surgeries at the beginning of the pandemic.
“In March and April, ophthalmology practices were virtually at a standstill,” says John B. Pinto, an ophthalmology practice management consultant in San Diego. “But by the fourth quarter, operations were back to normal. Practices were fully open, and patients were coming back in.”
Medscape’s survey shows that, by year’s end, compensation was about the same as the year before for orthopedic surgeons ($511,000 in both the 2020 and 2021 reports); cardiologists actually did better ($438,000 in our 2020 report and $459,000 in 2021); and ophthalmologists’ compensation was about the same ($378,000 in our prior report and $379,000 in 2021).
Some other proceduralists, however, did not do as well. Otolaryngologists’ compensation fell to $417,000, the second-biggest percentage drop. “This may be because otolaryngologists’ chief procedures are tonsillectomies, sinus surgery, and nasal surgery, which can be put off,” Dr. Pearl says.
Anesthesiologists, who depend on surgical volume, also did not earn as much in 2020. Their compensation declined from $398,000 in our 2020 report to $378,000 in Medscape’s 2021 report.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day,” an independent anesthesiology practice in Alabama told the MGMA early in the pandemic.
Plastic surgeons now the top earners
The biggest increase in compensation by far was made by plastic surgeons, whose income rose 9.8% over the year before, to $526,000. This put them at the top of the list
Dr. Pearl adds that plastic surgeons can perform their procedures in their offices, rather than in a hospital, where elective surgeries were often canceled.
Mr. Belkin says specialties other than plastic surgery had been offering more boutique cosmetic care even before the pandemic. In 2020, nonsurgical cosmetic procedures such as neurotoxin therapy, dermal filler procedures, chemical peels, and hair removal earned $3.1 billion in revenue, according to a survey by the Aesthetic Society.
Other specialties that earned more even during COVID
In Medscape’s survey, several specialties actually earned more during the pandemic than in 2019. Some specialties, such as critical care and public health, were integral in managing COVID patients and the pandemic.
However, some specialties involved in COVID care did not see an increase. Compensation for infectious disease specialists (at $245,000) and emergency medicine specialists (at $354,000) remained basically unchanged from the prior year, and for pulmonologists, it was slightly down.
Emergency departments reported decreases in volume of 40% or more early in the pandemic, according to the American College of Emergency Physicians. It was reported that patients were avoiding EDs for fear of contracting COVID, and car accidents were down because people ventured out less.
In this year’s report, psychiatrists saw a modest rise in compensation, to $275,000. “There has been an increase in mental health visits in the pandemic,” Dr. Pearl says. In 2020, about 4 in 10 adults in the United States reported symptoms of anxiety or depressive disorder, up from 1 in 10 adults the prior year. In addition, psychiatrists were third on the list of Merritt Hawkins’ most requested recruiting engagements.
Oncologists saw a rise in compensation, from $377,000 to $403,000. “Volume likely did not fall because cancer patients would go through with their chemotherapy in spite of the pandemic,” Dr. Pearl says. “The increase in income might have to do with the usual inflation in the cost of chemotherapy drugs.” Dr. Pinto saw the same trend for retinal surgeons, whose care also cannot be delayed.
Medscape’s survey also reports increases in compensation for rheumatologists, endocrinologists, and neurologists, but it reports small declines among dermatologists, radiologists, and gastroenterologists.
Gender-based pay gap remains in place
The gender-based pay gap in this year’s report is similar to that seen in Medscape’s report for the prior year. Men earned 27% more than women in 2021, compared with 25% more the year before. Some physicians commented that more women physicians maintained flexible or shorter work schedules to help with children who could not go into school.
“Having to be a full-time physician, full-time mom, and full-time teacher during our surge was unbelievable,” a primary care pediatrician in group practice and mother of two reported in November. “I felt pulled in all directions and didn’t do anything well.”
In addition, “men dominate some specialties that seem to have seen a smaller drop in volume in the pandemic, such as emergency medicine, infectious disease, pulmonology, and oncology,” says Halee Fischer-Wright, MD, CEO of MGMA.
Employed physicians shared their employers’ pain
Employed physicians, who typically work at hospitals, shared the financial pains of their institutions, particularly in the early stages of the pandemic. In April, hospital admissions were 34.1% below prepandemic levels, according to a study published in Health Affairs. That figure had risen by June, but it was still 8.3% below prepandemic volume.
By the end of the year, many hospitals and hospital systems were in the black, thanks in large part to generous federal subsidies, but actual operations still lost money for the year. Altogether, 42% of them posted an operational loss in 2020, up from the 23% in 2019, according to a survey by Moody’s Investors Service.
Medscape’s report shows that many employed physicians lost pay in 2020, and for many, pay had not returned to pre-COVID levels. Only 28% of primary care physicians and 32% of specialists who lost pay have seen it restored, according to the report. In addition, 15% of surveyed physicians did not receive an annual raise.
Many employed doctors are paid on the basis of relative value units (RVUs), which is a measure of the value of their work. In many cases, there was not enough work to reach RVU thresholds. Would hospitals and other employers lower RVU targets to meet the problem? “I haven’t seen our clients make concessions to providers along those lines,” Mr. Belkin says.
Physicians had to work longer hours
The Medscape report also found that in 2020, physicians saw fewer patients because each visit took longer.
“With the threat of COVID, in-person visits take more time than before,” Mr. Belkin says. “Physicians and staff have to prepare the exam room after each visit, and doctors must spend more time answering patients’ questions about COVID.”
“The new protocols to keep everyone safe add time between patients, and physicians have to answer patients’ questions about the pandemic and vaccines,” Dr. Fischer-Wright says. “You might see a 20% increase in time spent just on these non–revenue-generating COVID activities.”
Physicians still like their specialty
Although 2020 was a challenging year for physicians, the percentage of those who were satisfied with their specialty choice generally did not slip from the year before. It actually rose for several specialties – most notably, rheumatology, pulmonology, physical medicine and rehabilitation, and nephrology.
One specialty saw a decline in satisfaction with their specialty choice, and that was public health and preventive medicine, which plummeted 16 percentage points to 67% – putting it at the bottom of the list.
Even before the pandemic, many public health departments were chronically underfunded. This problem was possibly exacerbated by the pressures to keep up with COVID reporting and testing responsibilities.
Conclusion
Although 2020 was a wild ride for many physicians, many came out of it with only minor reductions in overall compensation, and some saw increases. Still, some specialties and many individuals experienced terrible financial stress and had to make changes in their lives and their spending in order to stay afloat.
“The biggest inhibitor to getting back to normal had to do with doctors who did not want to return because they did not want to risk getting COVID,” Dr. Pinto reports. But he notes that by February 2021 most doctors were completely vaccinated and could feel safe again.
A version of this article first appeared on Medscape.com.
, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Almost 18,000 physicians in more than 29 specialties told Medscape about their income, hours worked, greatest challenges, and the unexpected impact of COVID-19 on their compensation.
How many physicians avoided massive losses
When the pandemic started around March 2020, “a great many physicians saw reductions in volume at first,” says Robert Pearl, MD, former CEO of the Permanente Medical Group and a professor at Stanford (Calif.) University.
Medscape’s survey report shows that a staggering 44% saw a 1%-25% reduction in patient volume, and 9% saw a 26%-50% decline. “That is indeed breathtaking,” Dr. Pearl says.
Several key factors saved many practices from hemorrhaging money, says Michael Belkin, JD, divisional vice president at Merritt Hawkins and Associates in Dallas. “Many physicians used the federal Paycheck Protection Program [PPP] to help keep themselves afloat,” he says. “A large percentage reduced their staff, which reduced their expenses, and many got some of their volume back by transitioning to telemedicine.”
In a 2020 survey for the Physicians Foundation, conducted by Merritt Hawkins, 48% of physicians said their practice had received PPP support, and most of those said the support was enough to allow them to stay open without reducing staff. Only 6% of practices that received PPP support did not stay open.
Telemedicine helped many practices
Early in the pandemic, Medicare reimbursements for telemedicine were equal with those for face-to-face visits. “Since telemedicine takes a third less time than an inpatient visit, doctors could see more patients,” Dr. Pearl says.
The switch was almost instantaneous in some practices. Within 3 days, a 200-provider multispecialty practice in Wilmington, N.C., went from not using telehealth to its being used by all physicians, the Medical Group Management Association reported. By late April, the practice was already back up to about 70% of normal overall production.
However, telemedicine could not help every specialty equally. “Generally, allergists can’t do their allergy testing virtually, and patients with mild problems probably put off visits,” Dr. Pearl says. Allergists experienced a large percentage decline in compensation, according to Medscape’s survey. For some, income fell from $301,000 the prior year to $274,000 this year.
Primary care struggled
Primary care physicians posted lower compensation than they did the prior year, but most rebounded to some degree. A study released in June 2020 projected that, even with telemedicine, primary care physicians would lose an average of $67,774 for the year.
However, Medscape’s survey found that internists’ average compensation declined from $251,000 in the prior year to $248,000, and average family physicians’ compensation actually rose from $234,000.
Pediatricians had a harder slog. Their average compensation sank from $232,000 to $221,000, according to the report. Even with telemedicine, parents of young children were not contacting the doctor. In May 2020, visits by children aged 3-5 years were down by 56%.
Many proceduralists recovered
Procedure-oriented specialties were particularly hard-hit at first, because many hospitals and some states banned all elective surgeries at the beginning of the pandemic.
“In March and April, ophthalmology practices were virtually at a standstill,” says John B. Pinto, an ophthalmology practice management consultant in San Diego. “But by the fourth quarter, operations were back to normal. Practices were fully open, and patients were coming back in.”
Medscape’s survey shows that, by year’s end, compensation was about the same as the year before for orthopedic surgeons ($511,000 in both the 2020 and 2021 reports); cardiologists actually did better ($438,000 in our 2020 report and $459,000 in 2021); and ophthalmologists’ compensation was about the same ($378,000 in our prior report and $379,000 in 2021).
Some other proceduralists, however, did not do as well. Otolaryngologists’ compensation fell to $417,000, the second-biggest percentage drop. “This may be because otolaryngologists’ chief procedures are tonsillectomies, sinus surgery, and nasal surgery, which can be put off,” Dr. Pearl says.
Anesthesiologists, who depend on surgical volume, also did not earn as much in 2020. Their compensation declined from $398,000 in our 2020 report to $378,000 in Medscape’s 2021 report.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day,” an independent anesthesiology practice in Alabama told the MGMA early in the pandemic.
Plastic surgeons now the top earners
The biggest increase in compensation by far was made by plastic surgeons, whose income rose 9.8% over the year before, to $526,000. This put them at the top of the list
Dr. Pearl adds that plastic surgeons can perform their procedures in their offices, rather than in a hospital, where elective surgeries were often canceled.
Mr. Belkin says specialties other than plastic surgery had been offering more boutique cosmetic care even before the pandemic. In 2020, nonsurgical cosmetic procedures such as neurotoxin therapy, dermal filler procedures, chemical peels, and hair removal earned $3.1 billion in revenue, according to a survey by the Aesthetic Society.
Other specialties that earned more even during COVID
In Medscape’s survey, several specialties actually earned more during the pandemic than in 2019. Some specialties, such as critical care and public health, were integral in managing COVID patients and the pandemic.
However, some specialties involved in COVID care did not see an increase. Compensation for infectious disease specialists (at $245,000) and emergency medicine specialists (at $354,000) remained basically unchanged from the prior year, and for pulmonologists, it was slightly down.
Emergency departments reported decreases in volume of 40% or more early in the pandemic, according to the American College of Emergency Physicians. It was reported that patients were avoiding EDs for fear of contracting COVID, and car accidents were down because people ventured out less.
In this year’s report, psychiatrists saw a modest rise in compensation, to $275,000. “There has been an increase in mental health visits in the pandemic,” Dr. Pearl says. In 2020, about 4 in 10 adults in the United States reported symptoms of anxiety or depressive disorder, up from 1 in 10 adults the prior year. In addition, psychiatrists were third on the list of Merritt Hawkins’ most requested recruiting engagements.
Oncologists saw a rise in compensation, from $377,000 to $403,000. “Volume likely did not fall because cancer patients would go through with their chemotherapy in spite of the pandemic,” Dr. Pearl says. “The increase in income might have to do with the usual inflation in the cost of chemotherapy drugs.” Dr. Pinto saw the same trend for retinal surgeons, whose care also cannot be delayed.
Medscape’s survey also reports increases in compensation for rheumatologists, endocrinologists, and neurologists, but it reports small declines among dermatologists, radiologists, and gastroenterologists.
Gender-based pay gap remains in place
The gender-based pay gap in this year’s report is similar to that seen in Medscape’s report for the prior year. Men earned 27% more than women in 2021, compared with 25% more the year before. Some physicians commented that more women physicians maintained flexible or shorter work schedules to help with children who could not go into school.
“Having to be a full-time physician, full-time mom, and full-time teacher during our surge was unbelievable,” a primary care pediatrician in group practice and mother of two reported in November. “I felt pulled in all directions and didn’t do anything well.”
In addition, “men dominate some specialties that seem to have seen a smaller drop in volume in the pandemic, such as emergency medicine, infectious disease, pulmonology, and oncology,” says Halee Fischer-Wright, MD, CEO of MGMA.
Employed physicians shared their employers’ pain
Employed physicians, who typically work at hospitals, shared the financial pains of their institutions, particularly in the early stages of the pandemic. In April, hospital admissions were 34.1% below prepandemic levels, according to a study published in Health Affairs. That figure had risen by June, but it was still 8.3% below prepandemic volume.
By the end of the year, many hospitals and hospital systems were in the black, thanks in large part to generous federal subsidies, but actual operations still lost money for the year. Altogether, 42% of them posted an operational loss in 2020, up from the 23% in 2019, according to a survey by Moody’s Investors Service.
Medscape’s report shows that many employed physicians lost pay in 2020, and for many, pay had not returned to pre-COVID levels. Only 28% of primary care physicians and 32% of specialists who lost pay have seen it restored, according to the report. In addition, 15% of surveyed physicians did not receive an annual raise.
Many employed doctors are paid on the basis of relative value units (RVUs), which is a measure of the value of their work. In many cases, there was not enough work to reach RVU thresholds. Would hospitals and other employers lower RVU targets to meet the problem? “I haven’t seen our clients make concessions to providers along those lines,” Mr. Belkin says.
Physicians had to work longer hours
The Medscape report also found that in 2020, physicians saw fewer patients because each visit took longer.
“With the threat of COVID, in-person visits take more time than before,” Mr. Belkin says. “Physicians and staff have to prepare the exam room after each visit, and doctors must spend more time answering patients’ questions about COVID.”
“The new protocols to keep everyone safe add time between patients, and physicians have to answer patients’ questions about the pandemic and vaccines,” Dr. Fischer-Wright says. “You might see a 20% increase in time spent just on these non–revenue-generating COVID activities.”
Physicians still like their specialty
Although 2020 was a challenging year for physicians, the percentage of those who were satisfied with their specialty choice generally did not slip from the year before. It actually rose for several specialties – most notably, rheumatology, pulmonology, physical medicine and rehabilitation, and nephrology.
One specialty saw a decline in satisfaction with their specialty choice, and that was public health and preventive medicine, which plummeted 16 percentage points to 67% – putting it at the bottom of the list.
Even before the pandemic, many public health departments were chronically underfunded. This problem was possibly exacerbated by the pressures to keep up with COVID reporting and testing responsibilities.
Conclusion
Although 2020 was a wild ride for many physicians, many came out of it with only minor reductions in overall compensation, and some saw increases. Still, some specialties and many individuals experienced terrible financial stress and had to make changes in their lives and their spending in order to stay afloat.
“The biggest inhibitor to getting back to normal had to do with doctors who did not want to return because they did not want to risk getting COVID,” Dr. Pinto reports. But he notes that by February 2021 most doctors were completely vaccinated and could feel safe again.
A version of this article first appeared on Medscape.com.
, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Almost 18,000 physicians in more than 29 specialties told Medscape about their income, hours worked, greatest challenges, and the unexpected impact of COVID-19 on their compensation.
How many physicians avoided massive losses
When the pandemic started around March 2020, “a great many physicians saw reductions in volume at first,” says Robert Pearl, MD, former CEO of the Permanente Medical Group and a professor at Stanford (Calif.) University.
Medscape’s survey report shows that a staggering 44% saw a 1%-25% reduction in patient volume, and 9% saw a 26%-50% decline. “That is indeed breathtaking,” Dr. Pearl says.
Several key factors saved many practices from hemorrhaging money, says Michael Belkin, JD, divisional vice president at Merritt Hawkins and Associates in Dallas. “Many physicians used the federal Paycheck Protection Program [PPP] to help keep themselves afloat,” he says. “A large percentage reduced their staff, which reduced their expenses, and many got some of their volume back by transitioning to telemedicine.”
In a 2020 survey for the Physicians Foundation, conducted by Merritt Hawkins, 48% of physicians said their practice had received PPP support, and most of those said the support was enough to allow them to stay open without reducing staff. Only 6% of practices that received PPP support did not stay open.
Telemedicine helped many practices
Early in the pandemic, Medicare reimbursements for telemedicine were equal with those for face-to-face visits. “Since telemedicine takes a third less time than an inpatient visit, doctors could see more patients,” Dr. Pearl says.
The switch was almost instantaneous in some practices. Within 3 days, a 200-provider multispecialty practice in Wilmington, N.C., went from not using telehealth to its being used by all physicians, the Medical Group Management Association reported. By late April, the practice was already back up to about 70% of normal overall production.
However, telemedicine could not help every specialty equally. “Generally, allergists can’t do their allergy testing virtually, and patients with mild problems probably put off visits,” Dr. Pearl says. Allergists experienced a large percentage decline in compensation, according to Medscape’s survey. For some, income fell from $301,000 the prior year to $274,000 this year.
Primary care struggled
Primary care physicians posted lower compensation than they did the prior year, but most rebounded to some degree. A study released in June 2020 projected that, even with telemedicine, primary care physicians would lose an average of $67,774 for the year.
However, Medscape’s survey found that internists’ average compensation declined from $251,000 in the prior year to $248,000, and average family physicians’ compensation actually rose from $234,000.
Pediatricians had a harder slog. Their average compensation sank from $232,000 to $221,000, according to the report. Even with telemedicine, parents of young children were not contacting the doctor. In May 2020, visits by children aged 3-5 years were down by 56%.
Many proceduralists recovered
Procedure-oriented specialties were particularly hard-hit at first, because many hospitals and some states banned all elective surgeries at the beginning of the pandemic.
“In March and April, ophthalmology practices were virtually at a standstill,” says John B. Pinto, an ophthalmology practice management consultant in San Diego. “But by the fourth quarter, operations were back to normal. Practices were fully open, and patients were coming back in.”
Medscape’s survey shows that, by year’s end, compensation was about the same as the year before for orthopedic surgeons ($511,000 in both the 2020 and 2021 reports); cardiologists actually did better ($438,000 in our 2020 report and $459,000 in 2021); and ophthalmologists’ compensation was about the same ($378,000 in our prior report and $379,000 in 2021).
Some other proceduralists, however, did not do as well. Otolaryngologists’ compensation fell to $417,000, the second-biggest percentage drop. “This may be because otolaryngologists’ chief procedures are tonsillectomies, sinus surgery, and nasal surgery, which can be put off,” Dr. Pearl says.
Anesthesiologists, who depend on surgical volume, also did not earn as much in 2020. Their compensation declined from $398,000 in our 2020 report to $378,000 in Medscape’s 2021 report.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day,” an independent anesthesiology practice in Alabama told the MGMA early in the pandemic.
Plastic surgeons now the top earners
The biggest increase in compensation by far was made by plastic surgeons, whose income rose 9.8% over the year before, to $526,000. This put them at the top of the list
Dr. Pearl adds that plastic surgeons can perform their procedures in their offices, rather than in a hospital, where elective surgeries were often canceled.
Mr. Belkin says specialties other than plastic surgery had been offering more boutique cosmetic care even before the pandemic. In 2020, nonsurgical cosmetic procedures such as neurotoxin therapy, dermal filler procedures, chemical peels, and hair removal earned $3.1 billion in revenue, according to a survey by the Aesthetic Society.
Other specialties that earned more even during COVID
In Medscape’s survey, several specialties actually earned more during the pandemic than in 2019. Some specialties, such as critical care and public health, were integral in managing COVID patients and the pandemic.
However, some specialties involved in COVID care did not see an increase. Compensation for infectious disease specialists (at $245,000) and emergency medicine specialists (at $354,000) remained basically unchanged from the prior year, and for pulmonologists, it was slightly down.
Emergency departments reported decreases in volume of 40% or more early in the pandemic, according to the American College of Emergency Physicians. It was reported that patients were avoiding EDs for fear of contracting COVID, and car accidents were down because people ventured out less.
In this year’s report, psychiatrists saw a modest rise in compensation, to $275,000. “There has been an increase in mental health visits in the pandemic,” Dr. Pearl says. In 2020, about 4 in 10 adults in the United States reported symptoms of anxiety or depressive disorder, up from 1 in 10 adults the prior year. In addition, psychiatrists were third on the list of Merritt Hawkins’ most requested recruiting engagements.
Oncologists saw a rise in compensation, from $377,000 to $403,000. “Volume likely did not fall because cancer patients would go through with their chemotherapy in spite of the pandemic,” Dr. Pearl says. “The increase in income might have to do with the usual inflation in the cost of chemotherapy drugs.” Dr. Pinto saw the same trend for retinal surgeons, whose care also cannot be delayed.
Medscape’s survey also reports increases in compensation for rheumatologists, endocrinologists, and neurologists, but it reports small declines among dermatologists, radiologists, and gastroenterologists.
Gender-based pay gap remains in place
The gender-based pay gap in this year’s report is similar to that seen in Medscape’s report for the prior year. Men earned 27% more than women in 2021, compared with 25% more the year before. Some physicians commented that more women physicians maintained flexible or shorter work schedules to help with children who could not go into school.
“Having to be a full-time physician, full-time mom, and full-time teacher during our surge was unbelievable,” a primary care pediatrician in group practice and mother of two reported in November. “I felt pulled in all directions and didn’t do anything well.”
In addition, “men dominate some specialties that seem to have seen a smaller drop in volume in the pandemic, such as emergency medicine, infectious disease, pulmonology, and oncology,” says Halee Fischer-Wright, MD, CEO of MGMA.
Employed physicians shared their employers’ pain
Employed physicians, who typically work at hospitals, shared the financial pains of their institutions, particularly in the early stages of the pandemic. In April, hospital admissions were 34.1% below prepandemic levels, according to a study published in Health Affairs. That figure had risen by June, but it was still 8.3% below prepandemic volume.
By the end of the year, many hospitals and hospital systems were in the black, thanks in large part to generous federal subsidies, but actual operations still lost money for the year. Altogether, 42% of them posted an operational loss in 2020, up from the 23% in 2019, according to a survey by Moody’s Investors Service.
Medscape’s report shows that many employed physicians lost pay in 2020, and for many, pay had not returned to pre-COVID levels. Only 28% of primary care physicians and 32% of specialists who lost pay have seen it restored, according to the report. In addition, 15% of surveyed physicians did not receive an annual raise.
Many employed doctors are paid on the basis of relative value units (RVUs), which is a measure of the value of their work. In many cases, there was not enough work to reach RVU thresholds. Would hospitals and other employers lower RVU targets to meet the problem? “I haven’t seen our clients make concessions to providers along those lines,” Mr. Belkin says.
Physicians had to work longer hours
The Medscape report also found that in 2020, physicians saw fewer patients because each visit took longer.
“With the threat of COVID, in-person visits take more time than before,” Mr. Belkin says. “Physicians and staff have to prepare the exam room after each visit, and doctors must spend more time answering patients’ questions about COVID.”
“The new protocols to keep everyone safe add time between patients, and physicians have to answer patients’ questions about the pandemic and vaccines,” Dr. Fischer-Wright says. “You might see a 20% increase in time spent just on these non–revenue-generating COVID activities.”
Physicians still like their specialty
Although 2020 was a challenging year for physicians, the percentage of those who were satisfied with their specialty choice generally did not slip from the year before. It actually rose for several specialties – most notably, rheumatology, pulmonology, physical medicine and rehabilitation, and nephrology.
One specialty saw a decline in satisfaction with their specialty choice, and that was public health and preventive medicine, which plummeted 16 percentage points to 67% – putting it at the bottom of the list.
Even before the pandemic, many public health departments were chronically underfunded. This problem was possibly exacerbated by the pressures to keep up with COVID reporting and testing responsibilities.
Conclusion
Although 2020 was a wild ride for many physicians, many came out of it with only minor reductions in overall compensation, and some saw increases. Still, some specialties and many individuals experienced terrible financial stress and had to make changes in their lives and their spending in order to stay afloat.
“The biggest inhibitor to getting back to normal had to do with doctors who did not want to return because they did not want to risk getting COVID,” Dr. Pinto reports. But he notes that by February 2021 most doctors were completely vaccinated and could feel safe again.
A version of this article first appeared on Medscape.com.
Twenty percent of dialysis patients are hesitant about COVID-19 vaccine
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
CLL patients: Diagnostic difficulties, treatment confusion with COVID-19
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
FROM LEUKEMIA RESEARCH REPORTS
CDC: STI rates rise for sixth year in a row
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
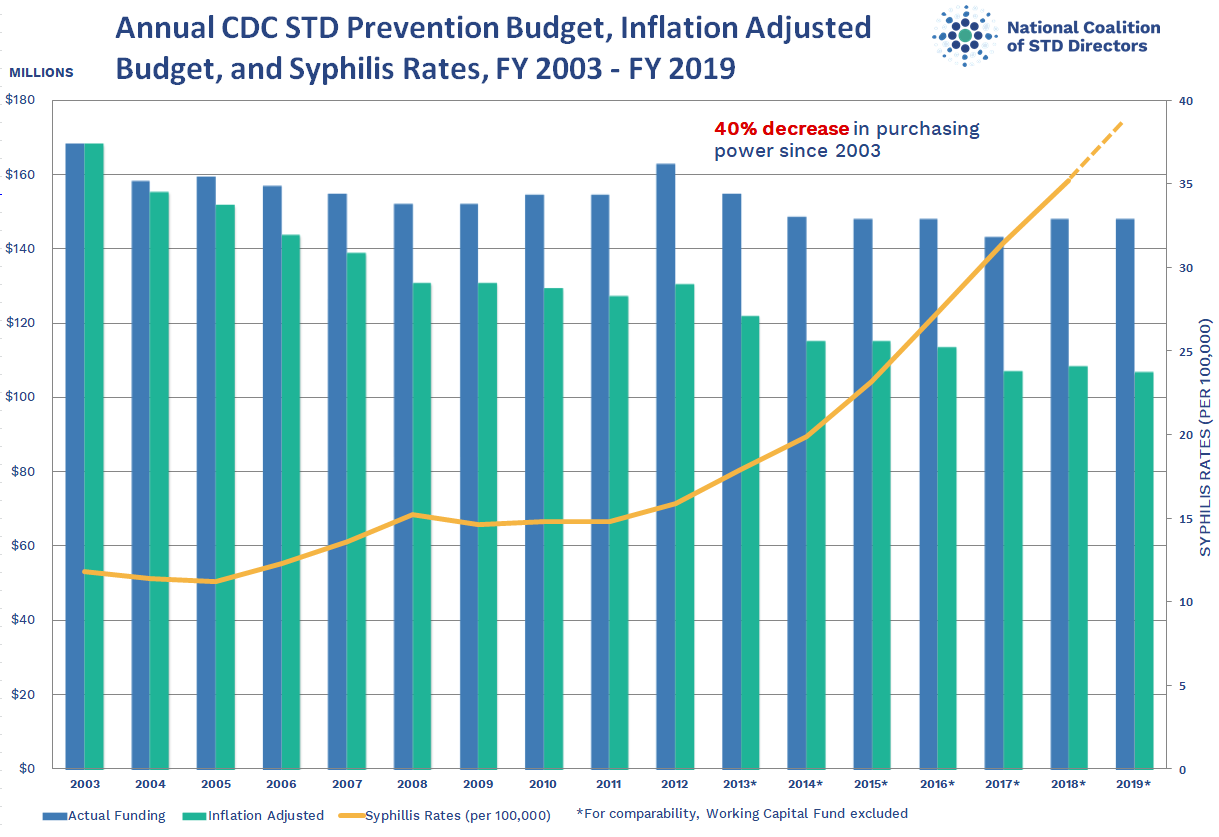{kind=link}
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
COVID-19–related inflammatory syndrome tied to neurologic symptoms in children
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Phage-targeting PCR test picks up early Lyme disease
An investigational polymerase chain reaction (PCR) test that detects the presence of a viral gene in Lyme disease–causing bacteria can distinguish between early and late infection, according to the results of a study that the authors described as “systematic and comprehensive.”

“The current way of diagnosing Lyme disease is struggling to reflect the ‘true’ incidence of Lyme disease,” study investigator Jinyu Shan, PhD, said in an interview. Although there are tests for Lyme disease approved by the Food and Drug Administration, they are based on the development of antibodies in the blood, and the problem is that antibodies might not develop until several weeks after an infection.
Diagnosis therefore still relies heavily on the clinician’s experience. There are often telltale signs – such as a “bullseye” skin rash or having been to an area known to be infested with ticks that carry Lyme disease – but this might not always be the case.
For the new test, “we’re not targeting bacteria. We’re targeting bacteriophages,” said Dr. Shan, a research fellow in the department of genetics and genome biology at the University of Leicester (England).
Fortunately, there’s high correlation between the presence of the terL gene and the presence of Borrelia burgdorferi, the spirochete that causes Lyme disease. “If you find the bacteriophages, the bacteria are there,” said Dr. Shan.
“Importantly, there are 10 times more bacteriophages, compared with the bacteria, so you have a lot more targets,” he added.
In an evaluation of a total of 312 samples (156 whole blood and 156 serum samples), significantly fewer copies of the terL gene were found in samples from people with early Lyme disease than in those with late Lyme disease, whereas the fewest copies of terL were seen in healthy volunteers.
Most pathogenic bacteria carry viral DNA either as multiple complete or partial prophages, Dr. Shan explained. Knowing the prophage sequences means that quantitative PCR primers and probes can be designed and used to detect the presence of the associated bacteria.
Although the novel test still needs evaluation in a clinical trial, it could represent a “step-change” in the detection of Lyme disease, Dr. Shan and associates suggested in their report published in Frontiers in Microbiology.
Early treatment is key to the prevention of longer-term consequences of Lyme disease. Clinicians familiar with the treatment of Lyme disease might choose to initiate antibiotic treatment without a positive lab test. However, the lack of a test that can pick out people with Lyme disease in the first few weeks of infection means that many people are not diagnosed or treated early enough.
The new phage-based PCR test Dr. Shan and associates have developed could change all that. With only 0.3 mL of blood being needed, it can potentially be developed as a simple point-of-care test, but that’s a long way off.
At this stage, the research is very much a “proof of concept,” Dr. Shan said. One of the things he plans to try to work out next is whether the test can distinguish between active and dormant disease, which is a “big question” in the diagnosis of Lyme disease.
“Bacteriophages can only be sustained by actively growing bacteria,” explained Dr. Shan, so there is a chance that if they are present in a substantive amount the disease is active, and if they are not – or are in very low numbers – then the disease is dormant. The cutoff value, however, “is not trivial to establish, but we are working toward it,” added Dr. Shan.
Over the past 2 years, Dr. Shan and associates have been working with the Belgian-based diagnostics company, R.E.D Laboratories, to see how the test will fare in a real-world environment. This relationship is providing useful information to add to their bid to perform a clinical trial for which they are now seeking additional sponsorship.
“The lack of an early and effective diagnosis of Lyme disease remains a major cause of misdiagnosis and long-term patient suffering,” commented Rosie Milsom, charity manager for Caudwell LymeCo Charity in the United Kingdom.
It could be a game changer if the test passes the necessary clinical trial testing and validation stages, noted Ms. Milsom, who was not involved in the research.
“Not only would the test help to establish the level or length of infection,” she said, “but it could also act as a way to test after treatment to see if the infection levels are decreasing.” If levels are still high, “you would know more treatment is needed.
The research is being funded by the charity Phelix Research and Development with support from the University of Leicester and the Dutch-based Lyme Fund, Lymefonds. Dr. Shan is named as coinventor of the phage-targeting PCR test, alongside Martha R.J. Clokie, professor of microbiology at the University of Leicester and the senior author of the study. Dr. Shan is chief scientific officer for Phelix Research and Development. Ms. Clokie and other coauthors hold key positions within the medical research charity.
A version of this article first appeared on Medscape.com.
An investigational polymerase chain reaction (PCR) test that detects the presence of a viral gene in Lyme disease–causing bacteria can distinguish between early and late infection, according to the results of a study that the authors described as “systematic and comprehensive.”
“The current way of diagnosing Lyme disease is struggling to reflect the ‘true’ incidence of Lyme disease,” study investigator Jinyu Shan, PhD, said in an interview. Although there are tests for Lyme disease approved by the Food and Drug Administration, they are based on the development of antibodies in the blood, and the problem is that antibodies might not develop until several weeks after an infection.
Diagnosis therefore still relies heavily on the clinician’s experience. There are often telltale signs – such as a “bullseye” skin rash or having been to an area known to be infested with ticks that carry Lyme disease – but this might not always be the case.
For the new test, “we’re not targeting bacteria. We’re targeting bacteriophages,” said Dr. Shan, a research fellow in the department of genetics and genome biology at the University of Leicester (England).
Fortunately, there’s high correlation between the presence of the terL gene and the presence of Borrelia burgdorferi, the spirochete that causes Lyme disease. “If you find the bacteriophages, the bacteria are there,” said Dr. Shan.
“Importantly, there are 10 times more bacteriophages, compared with the bacteria, so you have a lot more targets,” he added.
In an evaluation of a total of 312 samples (156 whole blood and 156 serum samples), significantly fewer copies of the terL gene were found in samples from people with early Lyme disease than in those with late Lyme disease, whereas the fewest copies of terL were seen in healthy volunteers.
Most pathogenic bacteria carry viral DNA either as multiple complete or partial prophages, Dr. Shan explained. Knowing the prophage sequences means that quantitative PCR primers and probes can be designed and used to detect the presence of the associated bacteria.
Although the novel test still needs evaluation in a clinical trial, it could represent a “step-change” in the detection of Lyme disease, Dr. Shan and associates suggested in their report published in Frontiers in Microbiology.
Early treatment is key to the prevention of longer-term consequences of Lyme disease. Clinicians familiar with the treatment of Lyme disease might choose to initiate antibiotic treatment without a positive lab test. However, the lack of a test that can pick out people with Lyme disease in the first few weeks of infection means that many people are not diagnosed or treated early enough.
The new phage-based PCR test Dr. Shan and associates have developed could change all that. With only 0.3 mL of blood being needed, it can potentially be developed as a simple point-of-care test, but that’s a long way off.
At this stage, the research is very much a “proof of concept,” Dr. Shan said. One of the things he plans to try to work out next is whether the test can distinguish between active and dormant disease, which is a “big question” in the diagnosis of Lyme disease.
“Bacteriophages can only be sustained by actively growing bacteria,” explained Dr. Shan, so there is a chance that if they are present in a substantive amount the disease is active, and if they are not – or are in very low numbers – then the disease is dormant. The cutoff value, however, “is not trivial to establish, but we are working toward it,” added Dr. Shan.
Over the past 2 years, Dr. Shan and associates have been working with the Belgian-based diagnostics company, R.E.D Laboratories, to see how the test will fare in a real-world environment. This relationship is providing useful information to add to their bid to perform a clinical trial for which they are now seeking additional sponsorship.
“The lack of an early and effective diagnosis of Lyme disease remains a major cause of misdiagnosis and long-term patient suffering,” commented Rosie Milsom, charity manager for Caudwell LymeCo Charity in the United Kingdom.
It could be a game changer if the test passes the necessary clinical trial testing and validation stages, noted Ms. Milsom, who was not involved in the research.
“Not only would the test help to establish the level or length of infection,” she said, “but it could also act as a way to test after treatment to see if the infection levels are decreasing.” If levels are still high, “you would know more treatment is needed.
The research is being funded by the charity Phelix Research and Development with support from the University of Leicester and the Dutch-based Lyme Fund, Lymefonds. Dr. Shan is named as coinventor of the phage-targeting PCR test, alongside Martha R.J. Clokie, professor of microbiology at the University of Leicester and the senior author of the study. Dr. Shan is chief scientific officer for Phelix Research and Development. Ms. Clokie and other coauthors hold key positions within the medical research charity.
A version of this article first appeared on Medscape.com.
An investigational polymerase chain reaction (PCR) test that detects the presence of a viral gene in Lyme disease–causing bacteria can distinguish between early and late infection, according to the results of a study that the authors described as “systematic and comprehensive.”
“The current way of diagnosing Lyme disease is struggling to reflect the ‘true’ incidence of Lyme disease,” study investigator Jinyu Shan, PhD, said in an interview. Although there are tests for Lyme disease approved by the Food and Drug Administration, they are based on the development of antibodies in the blood, and the problem is that antibodies might not develop until several weeks after an infection.
Diagnosis therefore still relies heavily on the clinician’s experience. There are often telltale signs – such as a “bullseye” skin rash or having been to an area known to be infested with ticks that carry Lyme disease – but this might not always be the case.
For the new test, “we’re not targeting bacteria. We’re targeting bacteriophages,” said Dr. Shan, a research fellow in the department of genetics and genome biology at the University of Leicester (England).
Fortunately, there’s high correlation between the presence of the terL gene and the presence of Borrelia burgdorferi, the spirochete that causes Lyme disease. “If you find the bacteriophages, the bacteria are there,” said Dr. Shan.
“Importantly, there are 10 times more bacteriophages, compared with the bacteria, so you have a lot more targets,” he added.
In an evaluation of a total of 312 samples (156 whole blood and 156 serum samples), significantly fewer copies of the terL gene were found in samples from people with early Lyme disease than in those with late Lyme disease, whereas the fewest copies of terL were seen in healthy volunteers.
Most pathogenic bacteria carry viral DNA either as multiple complete or partial prophages, Dr. Shan explained. Knowing the prophage sequences means that quantitative PCR primers and probes can be designed and used to detect the presence of the associated bacteria.
Although the novel test still needs evaluation in a clinical trial, it could represent a “step-change” in the detection of Lyme disease, Dr. Shan and associates suggested in their report published in Frontiers in Microbiology.
Early treatment is key to the prevention of longer-term consequences of Lyme disease. Clinicians familiar with the treatment of Lyme disease might choose to initiate antibiotic treatment without a positive lab test. However, the lack of a test that can pick out people with Lyme disease in the first few weeks of infection means that many people are not diagnosed or treated early enough.
The new phage-based PCR test Dr. Shan and associates have developed could change all that. With only 0.3 mL of blood being needed, it can potentially be developed as a simple point-of-care test, but that’s a long way off.
At this stage, the research is very much a “proof of concept,” Dr. Shan said. One of the things he plans to try to work out next is whether the test can distinguish between active and dormant disease, which is a “big question” in the diagnosis of Lyme disease.
“Bacteriophages can only be sustained by actively growing bacteria,” explained Dr. Shan, so there is a chance that if they are present in a substantive amount the disease is active, and if they are not – or are in very low numbers – then the disease is dormant. The cutoff value, however, “is not trivial to establish, but we are working toward it,” added Dr. Shan.
Over the past 2 years, Dr. Shan and associates have been working with the Belgian-based diagnostics company, R.E.D Laboratories, to see how the test will fare in a real-world environment. This relationship is providing useful information to add to their bid to perform a clinical trial for which they are now seeking additional sponsorship.
“The lack of an early and effective diagnosis of Lyme disease remains a major cause of misdiagnosis and long-term patient suffering,” commented Rosie Milsom, charity manager for Caudwell LymeCo Charity in the United Kingdom.
It could be a game changer if the test passes the necessary clinical trial testing and validation stages, noted Ms. Milsom, who was not involved in the research.
“Not only would the test help to establish the level or length of infection,” she said, “but it could also act as a way to test after treatment to see if the infection levels are decreasing.” If levels are still high, “you would know more treatment is needed.
The research is being funded by the charity Phelix Research and Development with support from the University of Leicester and the Dutch-based Lyme Fund, Lymefonds. Dr. Shan is named as coinventor of the phage-targeting PCR test, alongside Martha R.J. Clokie, professor of microbiology at the University of Leicester and the senior author of the study. Dr. Shan is chief scientific officer for Phelix Research and Development. Ms. Clokie and other coauthors hold key positions within the medical research charity.
A version of this article first appeared on Medscape.com.
Let me tell you about my vaccine
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.

For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.

And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.
For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.
And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.
For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.
And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.