User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Study Highlights Melanoma Survival Disparities in Rural vs Urban Settings
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SID 2024
Chemo May Benefit Some Older Patients With Metastatic Pancreatic Cancer
TOPLINE:
METHODOLOGY:
Pancreatic cancer is most often diagnosed in adults aged 65 years or older. Providing cancer treatment for this older, often vulnerable, population comes with significant challenges and can lead to worse survival.
To examine real-world outcomes of older adults with untreated metastatic pancreatic cancer, researchers recruited patients aged 70 years or older and performed a geriatric assessment to identify comorbidities, cognitive issues, and other geriatric abnormalities.
Those who were deemed “fit” (ie, with no geriatric abnormalities) were assigned to receive off-study standard-of-care treatment, whereas those classified as “frail” (ie, with severe abnormalities) received off-study supportive care.
The remaining 176 “vulnerable” patients with mild to moderate geriatric abnormalities completed a geriatric and quality-of-life assessment and were then randomly assigned to receive either dose-reduced 5-fluorouracil (5-FU), leucovorin plus liposomal irinotecan (n = 88) or modified gemcitabine plus nab-paclitaxel (n = 88) every 2 weeks. Ultimately, 79 patients started the 5-FU combination and 75 received gemcitabine plus nab-paclitaxel. Patients were assessed every 8 weeks until disease progression or intolerance.
Overall, patients had a median age of 77 years; 61.9% were aged 75 years or older. About half were female, and 81.5% were White. The majority (87.5%) had a performance status of 0 or 1.
TAKEAWAY:
- Median overall survival was 4.7 months in the gemcitabine plus nab-paclitaxel arm and 4.4 months in the 5-FU combination group, with no significant survival difference observed between the two arms (P = .72).
- When the overall survival analysis was restricted to patients who received at least 4 weeks, or two cycles, of treatment (about 62% of patients), the median overall survival across the two treatment arms reached 8.0 months, in line with expectations for these regimens.
- Patient stratification revealed that those with a performance status of 2 had significantly worse overall survival than those with a status of 0: 1.4 months vs 6.9 months, respectively (hazard ratio [HR], 2.77; P < .001). A similar divide was seen when patients were stratified by physical/functional status and well-being. Age, however, did not significantly influence the results.
- Overall, more than half of patients experienced grade 3 or higher adverse events. Just over 38% of patients received only one to three cycles of therapy, whereas 26% remained on treatment for 12 or more cycles. The adverse event rates were similar between the two regimens, but the toxicity profile was slightly different — the researchers, for instance, observed more peripheral neuropathy with gemcitabine plus nab-paclitaxel and more diarrhea in the 5-FU combination arm.
IN PRACTICE:
- Overall, the “survival outcomes among vulnerable older patients were lower than expected, with high percentage of patients not able to start treatment, or complete one month of therapy due to clinical deterioration,” said study presenter Efrat Dotan, MD, chief, Division of Gastrointestinal Medical Oncology, Fox Chase Cancer Center, Philadelphia.
- “For vulnerable older adults who can tolerate treatment, these two regimens provide clinicians with options for tailoring therapy based on toxicity profile,” Dr. Dotan added. But “tools are needed to better identify patients who can benefit from treatment.”
- The results underline the need to perform geriatric assessments, as opposed to merely looking at performance status, commented David F. Chang, PhD, MS, MBBS, professor of Surgical Oncology, University of Glasgow, Scotland, who was not involved in the study.
SOURCE:
The research, presented at the 2024 annual meeting of the American Society of Clinical Oncology, was funded by the National Cancer Institute and the Eastern Cooperative Oncology Group.
LIMITATIONS:
Dr. Chang noted that the study did not reveal which treatment regimen was more effective.
DISCLOSURES:
Dr. Dotan declared relationships with Agenus, Amgen, G1 Therapeutics, Incyte, Olympus, and Taiho Pharmaceutical and institutional relationships with Dragonfly Therapeutics, Gilead Sciences, Ipsen, Kinnate Biopharma, Leap Therapeutics, Lilly, Lutris, NGM Biopharmaceuticals, Relay Therapeutics, and Zymeworks. Dr. Chang declared relationships with Immodulon Therapeutics and Mylan and institutional relationships with AstraZeneca, BMS GmbH & Co. KG, Immodulon Therapeutics, and Merck.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
Pancreatic cancer is most often diagnosed in adults aged 65 years or older. Providing cancer treatment for this older, often vulnerable, population comes with significant challenges and can lead to worse survival.
To examine real-world outcomes of older adults with untreated metastatic pancreatic cancer, researchers recruited patients aged 70 years or older and performed a geriatric assessment to identify comorbidities, cognitive issues, and other geriatric abnormalities.
Those who were deemed “fit” (ie, with no geriatric abnormalities) were assigned to receive off-study standard-of-care treatment, whereas those classified as “frail” (ie, with severe abnormalities) received off-study supportive care.
The remaining 176 “vulnerable” patients with mild to moderate geriatric abnormalities completed a geriatric and quality-of-life assessment and were then randomly assigned to receive either dose-reduced 5-fluorouracil (5-FU), leucovorin plus liposomal irinotecan (n = 88) or modified gemcitabine plus nab-paclitaxel (n = 88) every 2 weeks. Ultimately, 79 patients started the 5-FU combination and 75 received gemcitabine plus nab-paclitaxel. Patients were assessed every 8 weeks until disease progression or intolerance.
Overall, patients had a median age of 77 years; 61.9% were aged 75 years or older. About half were female, and 81.5% were White. The majority (87.5%) had a performance status of 0 or 1.
TAKEAWAY:
- Median overall survival was 4.7 months in the gemcitabine plus nab-paclitaxel arm and 4.4 months in the 5-FU combination group, with no significant survival difference observed between the two arms (P = .72).
- When the overall survival analysis was restricted to patients who received at least 4 weeks, or two cycles, of treatment (about 62% of patients), the median overall survival across the two treatment arms reached 8.0 months, in line with expectations for these regimens.
- Patient stratification revealed that those with a performance status of 2 had significantly worse overall survival than those with a status of 0: 1.4 months vs 6.9 months, respectively (hazard ratio [HR], 2.77; P < .001). A similar divide was seen when patients were stratified by physical/functional status and well-being. Age, however, did not significantly influence the results.
- Overall, more than half of patients experienced grade 3 or higher adverse events. Just over 38% of patients received only one to three cycles of therapy, whereas 26% remained on treatment for 12 or more cycles. The adverse event rates were similar between the two regimens, but the toxicity profile was slightly different — the researchers, for instance, observed more peripheral neuropathy with gemcitabine plus nab-paclitaxel and more diarrhea in the 5-FU combination arm.
IN PRACTICE:
- Overall, the “survival outcomes among vulnerable older patients were lower than expected, with high percentage of patients not able to start treatment, or complete one month of therapy due to clinical deterioration,” said study presenter Efrat Dotan, MD, chief, Division of Gastrointestinal Medical Oncology, Fox Chase Cancer Center, Philadelphia.
- “For vulnerable older adults who can tolerate treatment, these two regimens provide clinicians with options for tailoring therapy based on toxicity profile,” Dr. Dotan added. But “tools are needed to better identify patients who can benefit from treatment.”
- The results underline the need to perform geriatric assessments, as opposed to merely looking at performance status, commented David F. Chang, PhD, MS, MBBS, professor of Surgical Oncology, University of Glasgow, Scotland, who was not involved in the study.
SOURCE:
The research, presented at the 2024 annual meeting of the American Society of Clinical Oncology, was funded by the National Cancer Institute and the Eastern Cooperative Oncology Group.
LIMITATIONS:
Dr. Chang noted that the study did not reveal which treatment regimen was more effective.
DISCLOSURES:
Dr. Dotan declared relationships with Agenus, Amgen, G1 Therapeutics, Incyte, Olympus, and Taiho Pharmaceutical and institutional relationships with Dragonfly Therapeutics, Gilead Sciences, Ipsen, Kinnate Biopharma, Leap Therapeutics, Lilly, Lutris, NGM Biopharmaceuticals, Relay Therapeutics, and Zymeworks. Dr. Chang declared relationships with Immodulon Therapeutics and Mylan and institutional relationships with AstraZeneca, BMS GmbH & Co. KG, Immodulon Therapeutics, and Merck.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
Pancreatic cancer is most often diagnosed in adults aged 65 years or older. Providing cancer treatment for this older, often vulnerable, population comes with significant challenges and can lead to worse survival.
To examine real-world outcomes of older adults with untreated metastatic pancreatic cancer, researchers recruited patients aged 70 years or older and performed a geriatric assessment to identify comorbidities, cognitive issues, and other geriatric abnormalities.
Those who were deemed “fit” (ie, with no geriatric abnormalities) were assigned to receive off-study standard-of-care treatment, whereas those classified as “frail” (ie, with severe abnormalities) received off-study supportive care.
The remaining 176 “vulnerable” patients with mild to moderate geriatric abnormalities completed a geriatric and quality-of-life assessment and were then randomly assigned to receive either dose-reduced 5-fluorouracil (5-FU), leucovorin plus liposomal irinotecan (n = 88) or modified gemcitabine plus nab-paclitaxel (n = 88) every 2 weeks. Ultimately, 79 patients started the 5-FU combination and 75 received gemcitabine plus nab-paclitaxel. Patients were assessed every 8 weeks until disease progression or intolerance.
Overall, patients had a median age of 77 years; 61.9% were aged 75 years or older. About half were female, and 81.5% were White. The majority (87.5%) had a performance status of 0 or 1.
TAKEAWAY:
- Median overall survival was 4.7 months in the gemcitabine plus nab-paclitaxel arm and 4.4 months in the 5-FU combination group, with no significant survival difference observed between the two arms (P = .72).
- When the overall survival analysis was restricted to patients who received at least 4 weeks, or two cycles, of treatment (about 62% of patients), the median overall survival across the two treatment arms reached 8.0 months, in line with expectations for these regimens.
- Patient stratification revealed that those with a performance status of 2 had significantly worse overall survival than those with a status of 0: 1.4 months vs 6.9 months, respectively (hazard ratio [HR], 2.77; P < .001). A similar divide was seen when patients were stratified by physical/functional status and well-being. Age, however, did not significantly influence the results.
- Overall, more than half of patients experienced grade 3 or higher adverse events. Just over 38% of patients received only one to three cycles of therapy, whereas 26% remained on treatment for 12 or more cycles. The adverse event rates were similar between the two regimens, but the toxicity profile was slightly different — the researchers, for instance, observed more peripheral neuropathy with gemcitabine plus nab-paclitaxel and more diarrhea in the 5-FU combination arm.
IN PRACTICE:
- Overall, the “survival outcomes among vulnerable older patients were lower than expected, with high percentage of patients not able to start treatment, or complete one month of therapy due to clinical deterioration,” said study presenter Efrat Dotan, MD, chief, Division of Gastrointestinal Medical Oncology, Fox Chase Cancer Center, Philadelphia.
- “For vulnerable older adults who can tolerate treatment, these two regimens provide clinicians with options for tailoring therapy based on toxicity profile,” Dr. Dotan added. But “tools are needed to better identify patients who can benefit from treatment.”
- The results underline the need to perform geriatric assessments, as opposed to merely looking at performance status, commented David F. Chang, PhD, MS, MBBS, professor of Surgical Oncology, University of Glasgow, Scotland, who was not involved in the study.
SOURCE:
The research, presented at the 2024 annual meeting of the American Society of Clinical Oncology, was funded by the National Cancer Institute and the Eastern Cooperative Oncology Group.
LIMITATIONS:
Dr. Chang noted that the study did not reveal which treatment regimen was more effective.
DISCLOSURES:
Dr. Dotan declared relationships with Agenus, Amgen, G1 Therapeutics, Incyte, Olympus, and Taiho Pharmaceutical and institutional relationships with Dragonfly Therapeutics, Gilead Sciences, Ipsen, Kinnate Biopharma, Leap Therapeutics, Lilly, Lutris, NGM Biopharmaceuticals, Relay Therapeutics, and Zymeworks. Dr. Chang declared relationships with Immodulon Therapeutics and Mylan and institutional relationships with AstraZeneca, BMS GmbH & Co. KG, Immodulon Therapeutics, and Merck.
A version of this article appeared on Medscape.com.
Overuse of Hematocrit Testing After Elective General Surgery at a Veterans Affairs Medical Center
It is common practice to routinely measure postoperative hematocrit levels at US Department of Veterans Affairs (VA) hospitals for a wide range of elective general surgeries. While hematocrit measurement is a low-cost test, the high frequency with which these tests are performed may drastically increase overall costs.
Numerous studies have suggested that physicians overuse laboratory testing.1-10 Kohli and colleagues recommended that the routine practice of obtaining postoperative hematocrit tests following elective gynecologic surgery be abandoned.1 A similar recommendation was made by Olus and colleagues after studying uneventful, unplanned cesarean sections and by Wu and colleagues after investigating routine laboratory tests post total hip arthroplasty.2,3
To our knowledge, a study assessing routine postoperative hematocrit testing in elective general surgery has not yet been conducted. Many laboratory tests ordered in the perioperative period are not indicated, including complete blood count (CBC), electrolytes, and coagulation studies.4 Based on the results of these studies, we expected that the routine measurement of postoperative hematocrit levels after elective general surgeries at VA medical centers would not be cost effective. A PubMed search for articles published from 1990 to 2023 using the search terms “hematocrit,” “hemoglobin,” “general,” “surgery,” “routine,” and “cost” or “cost-effectiveness,” suggests that the clinical usefulness of postoperative hematocrit testing has not been well studied in the general surgery setting. The purpose of this study was to determine the clinical utility and associated cost of measuring routine postoperative hematocrit levels in order to generate a guide as to when the practice is warranted following common elective general surgery.
Although gynecologic textbooks may describe recommendations of routine hematocrit checking after elective gynecologic operations, one has difficulty finding the same recommendations in general surgery textbooks.1 However, it is common practice for surgical residents and attending surgeons to routinely order hematocrit on postoperative day-1 to ensure that the operation did not result in unsuspected anemia that then would need treatment (either with fluids or a blood transfusion). Many other surgeons rely on clinical factors such as tachycardia, oliguria, or hypotension to trigger a hematocrit (and other laboratory) tests. Our hypothesis is that the latter group has chosen the most cost-effective and prudent practice. One problem with checking the hematocrit routinely, as with any other screening test, is what to do with an abnormal result, assuming an asymptomatic patient? If the postoperative hematocrit is lower than expected given the estimated blood loss (EBL), what is one to do?
Methods
This retrospective case-control study conducted at the New Mexico VA Health Care System (NMVAHCS) in Albuquerque compared data for patients who received transfusion within 72 hours of elective surgeries vs patients who did not. Patients who underwent elective general surgery from January 2011 through December 2014 were included. An elective general surgery was defined as surgery performed following an outpatient preoperative anesthesia evaluation ≥ 30 days prior to operation. Patients who underwent emergency operations, and those with baseline anemia (preoperative hematocrit < 30%), and those transfused > 72 hours after their operation were excluded. The NMVAHCSInstitutional Review Board approved this study (No. 15-H184).
A detailed record review was conducted to collect data on demographics and other preoperative risk factors, including age, sex, body mass index (BMI), race and ethnicity, cardiac and pulmonary comorbidities, tobacco use, alcohol intake, diabetes, American Society of Anesthesiologists Physical Status Classification, metabolic equivalent of task, hematologic conditions, and renal disease.
For each procedure, we recorded the type of elective general surgery performed, the diagnosis/indication, pre- and postoperative hemoglobin/hematocrit, intraoperative EBL, length of operation, surgical wound class, length of hospital stay (LOS), intensive care unit (ICU) status, number of hematocrit tests, cardiovascular risk of operation (defined by anesthesia assessment), presence or absence of malignancy, preoperative platelet count, albumin level, preoperative prothrombin time/activated partial thromboplastin time (aPTT), international normalized ratio (INR), hemoglobin A1c, and incidence of transfusion. Signs and symptoms of anemia were recorded as present if the postoperative vital signs suggested low intravascular volume (pulse > 120 beats/minute, systolic blood pressure < 90 mm Hg, or vasoactive medication requirement [per anesthesia postoperative note]) or if the patient reported or exhibited symptoms of dizziness or fatigue or evidence of clinically apparent bleeding (ie, hematoma formation). Laboratory charges for hematocrit tests and CBC at the NMAVAHCS were used to assess cost.11
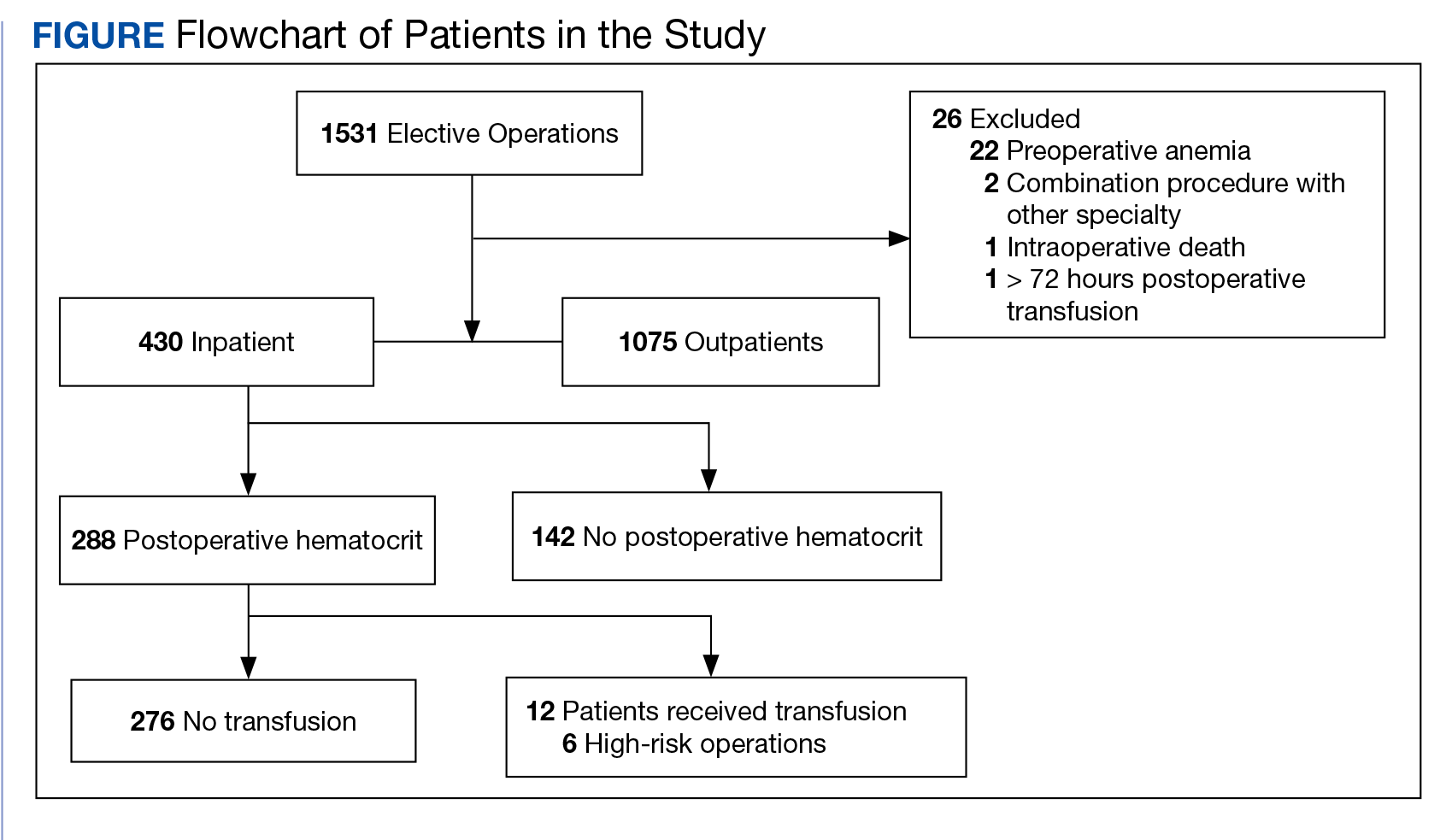
To stratify the transfusion risk, patients were distributed among 3 groups based on the following criteria: discharged home the same day as surgery; admitted but did not have postoperative hematocrit testing; and admitted and had postoperative hematocrit testing. We also stratified operations into low or high risk based on the risk for postoperative transfusion (Figure). Recognizing that the American College of Chest Physicians guidelines for perioperative management of antithrombotic therapy places bowel resection in a high-risk category, we designated a surgery as high risk when ≥ 2 patients in the transfusion group had that type of surgery over the 4 years of the study.12 Otherwise, the operations were deemed low risk.
Statistical Analysis
Numeric analysis used t tests and Binary and categorical variables used Fisher exact tests. P value ≤ .05 was considered statistically significant. SAS software was used for all statistical analyses.
Results
From 2011 through 2014, 1531 patients had elective general surgery at NMVAHCS. Twenty-two patients with preoperative anemia (hematocrit < 30%) and 1 patient who received a transfusion > 72 hours after the operation were excluded. Most elective operations (70%, n = 1075) were performed on an outpatient basis; none involved transfusion. Inguinal hernia repair was most common with 479 operations; 17 patients were treated inpatient of which 2 patients had routine postoperative hematocrit checks; (neither received transfusion). One patient with inguinal hernia surgery received transfusion without routine postoperative hematocrit monitoring.
Of 112 partial colon resections, 1 patient had a postoperative transfusion; and all but 3 received postoperative hematocrit monitoring. Nineteen patients undergoing partial colon resection had a clinical indication for postoperative hematocrit monitoring. None of the 5 patients with partial gastrectomy received a postoperative transfusion. Of 121 elective cholecystectomies, no patients had postoperative transfusion, whereas 34 had postoperative hematocrit monitoring; only 2 patients had a clinical reason for the hematocrit monitoring.
Of 430 elective inpatient operations, 12 received transfusions and 288 patients had ≥ 1 postoperative hematocrit test (67%). All hematocrit tests were requested by the attending surgeon, resident surgeon, or the surgical ICU team. Of the group that had postoperative hematocrit monitoring, there was an average of 4.4 postoperative hematocrit tests per patient (range, 1-44).
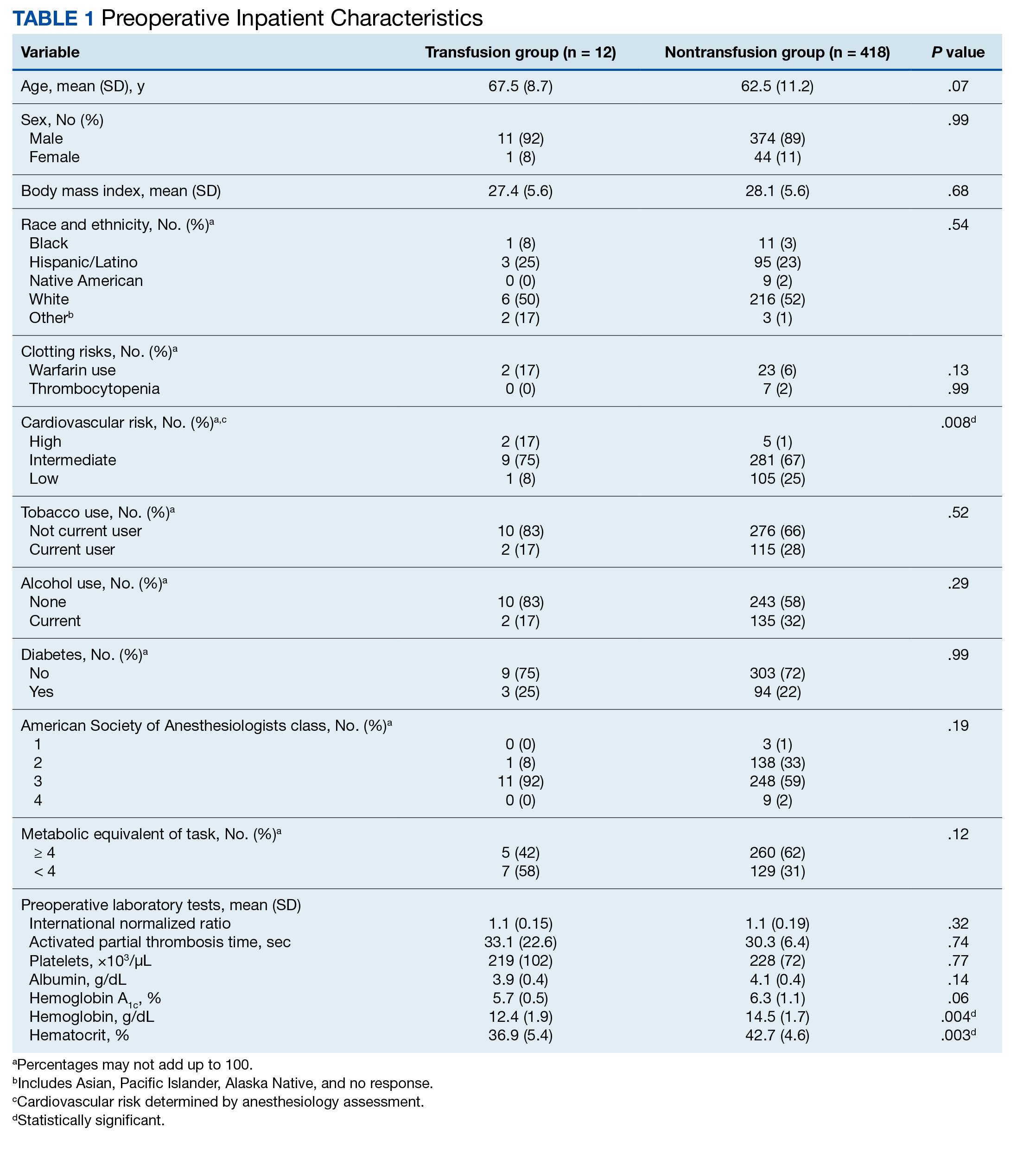
There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 Five of the 12 patients received intraoperative transfusions while 7 were transfused within 72 hours postoperation. All but 1 patient receiving transfusion had EBL > 199 mL (range, 5-3000; mean, 950 mL; median, 500 mL) and/or signs or symptoms of anemia or other indications for measurement of the postoperative hematocrit. There were no statistically significant differences in patients’ age, sex, BMI, or race and ethnicity between groups receiving and not receiving transfusion (Table 1).
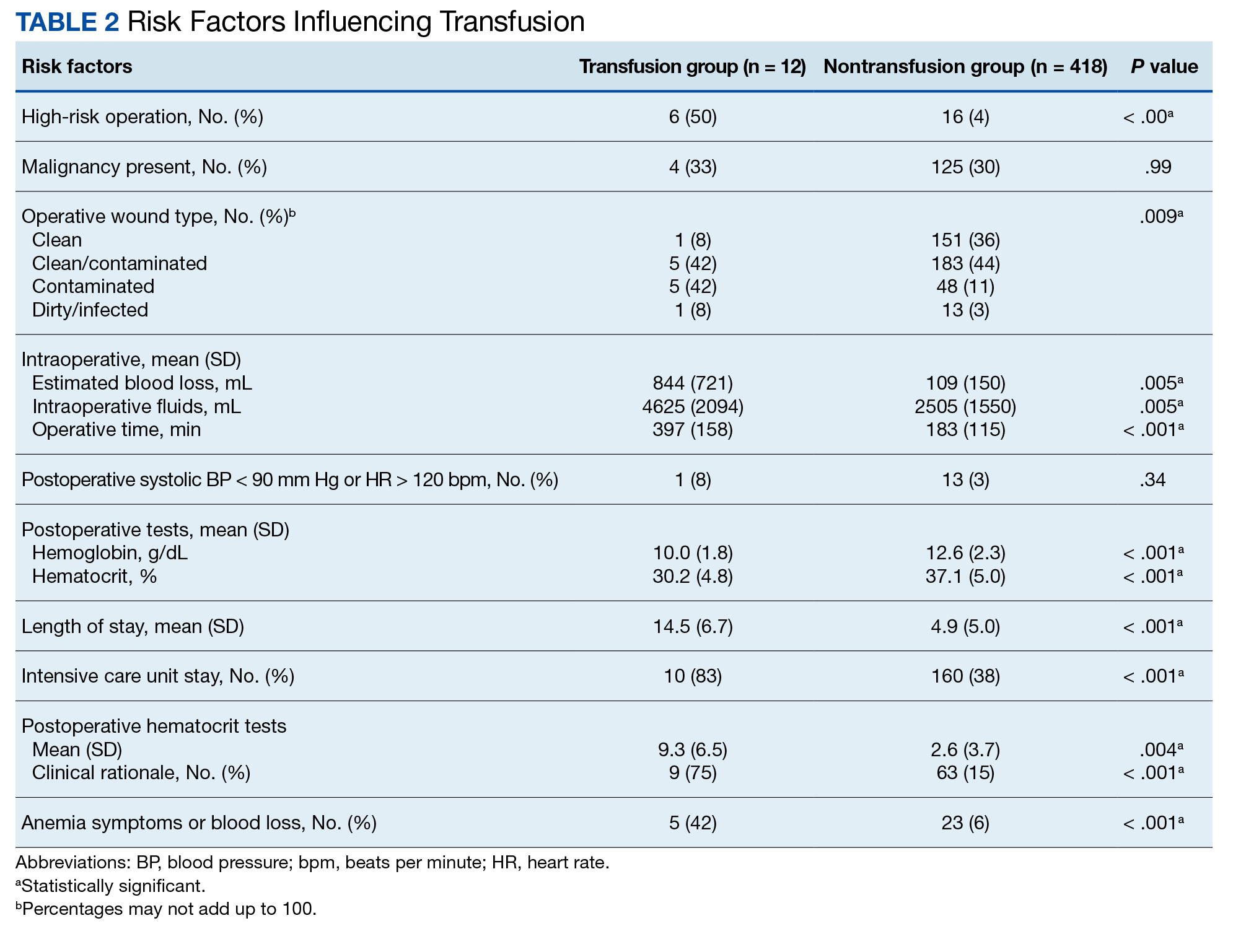
When comparing the transfusion vs the nontransfusion groups (after excluding those with clinical preoperative anemia) the risk factors for transfusion included: relatively low mean preoperative hematocrit (mean, 36.9% vs 42.7%, respectively; P = .003), low postoperative hematocrit (mean, 30.2% vs 37.1%, respectively; P < .001), high EBL (mean, 844 mL vs 109 mL, respectively; P = .005), large infusion of intraoperative fluids (mean, 4625 mL vs 2505 mL, respectively; P = .005), longer duration of operation (mean, 397 min vs 183 min, respectively; P < .001), and longer LOS (mean, 14.5 d vs 4.9 d, respectively; P < .001) (Table 2). Similarly, we found an increased risk for transfusion with high/intermediate cardiovascular risk (vs low), any wound not classified as clean, ICU stay, and postoperative symptoms of anemia.
We found no increased risk for transfusion with ethanol, tobacco, warfarin, or clopidogrel use; polycythemia; thrombocytopenia; preoperative INR; preoperative aPTT; preoperative albumin; Hemoglobin A1c; or diabetes mellitus; or for operations performed for malignancy. Ten patients in the ICU received transfusion (5.8%) compared with 2 patients (0.8%) not admitted to the ICU.
Operations were deemed high risk when ≥ 2 of patients having that operation received transfusions within 72 hours of their operation. There were 15 abdominoperineal resections; 3 of these received transfusions (20%). There were 7 total abdominal colectomies; 3 of these received transfusions (43%). We therefore had 22 high-risk operations, 6 of which were transfused (27%).
Discussion
Routine measurement of postoperative hematocrit levels after elective general surgery at NMVAHCS was not necessary. There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 We found that routine postoperative hematocrit measurements to assess anemia had little or no effect on clinical decision-making or clinical outcomes.
According to our results, 88% of initial hematocrit tests after elective partial colectomies could have been eliminated; only 32 of 146 patients demonstrated a clinical reason for postoperative hematocrit testing. Similarly, 36 of 40 postcholecystectomy hematocrit tests (90%) could have been eliminated had the surgeons relied on clinical signs indicating possible postoperative anemia (none were transfused). Excluding patients with major intraoperative blood loss (> 300 mL), only 29 of 288 (10%) patients who had postoperative hematocrit tests had a clinical indication for a postoperative hematocrit test (ie, symptoms of anemia and/or active bleeding). One patient with inguinal hernia surgery who received transfusion was taking an anticoagulant and had a clinically indicated hematocrit test for a large hematoma that eventually required reoperation.
Our study found that routine hematocrit checks may actually increase the risk that a patient would receive an unnecessary transfusion. For instance, one elderly patient, after a right colectomy, had 6 hematocrit levels while on a heparin drip and received transfusion despite being asymptomatic. His lowest hematocrit level prior to transfusion was 23.7%. This patient had a total of 18 hematocrit tests. His EBL was 350 mL and his first postoperative HCT level was 33.1%. In another instance, a patient undergoing abdominoperineal resection had a transfusion on postoperative day 1, despite being hypertensive, with a hematocrit that ranged from 26% before transfusion to 31% after the transfusion. These 2 cases illustrate what has been shown in a recent study: A substantial number of patients with colorectal cancer receive unnecessary transfusions.14 On the other hand, one ileostomy closure patient had 33 hematocrit tests, yet his initial postoperative hematocrit was 37%, and he never received a transfusion. With low-risk surgeries, clinical judgment should dictate when a postoperative hematocrit level is needed. This strategy would have eliminated 206 unnecessary initial postoperative hematocrit tests (72%), could have decreased the number of unnecessary transfusions, and would have saved NMVAHCS about $1600 annually.
Abdominoperineal resections and total abdominal colectomies accounted for a high proportion of transfusions in our study. Inpatient elective operations can be risk stratified and have routine hematocrit tests ordered for patients at high risk. The probability of transfusion was greater in high-risk vs low-risk surgeries; 27% (6 of 22 patients) vs 2% (6 of 408 patients), respectively (P < .001). Since 14 of the 22 patients undergoing high-risk operation already had clinical reasons for a postoperative hematocrit test, we only need to add the remaining 8 patients with high-risk operations to the 74 who had a clinical reason for a hematocrit test and conclude that 82 of 430 patients (19%) had a clinical reason for a hematocrit test, either from signs or symptoms of blood loss or because they were in a high-risk group.
While our elective general surgery cases may not represent many general surgery programs in the US and VA health care systems, we can extrapolate cost savings using the same cost analyses outlined by Kohli and colleagues.1 Assuming 1.9 million elective inpatient general surgeries per year in the United States with an average cost of $21 per CBC, the annual cost of universal postoperative hematocrit testing would be $40 million.11,15 If postoperative hematocrit testing were 70% consistent with our findings, the annual cost for hematocrit tests on 51% of the inpatient general surgeries would be approximately $20.4 million. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our finding that 19% were deemed necessary) results in an annual savings of $30 million. This conservative estimate could be even higher since there were 4.4 hematocrit tests per patient; therefore, we have about $132 million in savings.
Assuming 181,384 elective VA inpatient general surgeries each year, costing $7.14 per CBC (the NMVAHCS cost), the VA could save $1.3 million annually. If postoperative HCT testing were 70% consistent with our findings, the annual cost for hematocrit tests on 50.4% of inpatient general surgery operations would be about $653,000. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our 19%) results in annual VA savings of $330,000. This conservative estimate could be even higher since there were on average 4.4 hematocrit levels per patient; therefore, we estimate that annual savings for the VA of about $1.45 million.
Limitations
The retrospective chart review nature of this study may have led to selection bias. Only a small number of patients received a transfusion, which may have skewed the data. This study population comes from a single VA medical center; this patient population may not be reflective of other VA medical centers or the US population as a whole. Given that NMVAHCS does not perform hepatic, esophageal, pancreas, or transplant operations, the potential savings to both the US and the VA may be overestimated, but this could be studied in the future by VA medical centers that perform more complex operations.
Conclusions
This study found that over a 4-year period routine postoperative hematocrit tests for patients undergoing elective general surgery at a VA medical center were not necessary. General surgeons routinely order various pre- and postoperative laboratory tests despite their limited utility. Reduction in unneeded routine tests could result in notable savings to the VA without compromising quality of care.
Only general surgery patients undergoing operations that carry a high risk for needing a blood transfusion should have a routine postoperative hematocrit testing. In our study population, the chance of an elective colectomy, cholecystectomy, or hernia patient needing a transfusion was rare. This strategy could eliminate a considerable number of unnecessary blood tests and would potentially yield significant savings.
1. Kohli N, Mallipeddi PK, Neff JM, Sze EH, Roat TW. Routine hematocrit after elective gynecologic surgery. Obstet Gynecol. 2000;95(6 Pt 1):847-850. doi:10.1016/s0029-7844(00)00796-1
2. Olus A, Orhan, U, Murat A, et al. Do asymptomatic patients require routine hemoglobin testing following uneventful, unplanned cesarean sections? Arch Gynecol Obstet. 2010;281(2):195-199. doi:10.1007/s00404-009-1093-1
3. Wu XD, Zhu ZL, Xiao P, Liu JC, Wang JW, Huang W. Are routine postoperative laboratory tests necessary after primary total hip arthroplasty? J Arthroplasty. 2020;35(10):2892-2898. doi:10.1016/j.arth.2020.04.097
4. Kumar A, Srivastava U. Role of routine laboratory investigations in preoperative evaluation. J Anesthesiol Clin Pharmacol. 2011;27(2):174-179. doi:10.4103/0970-9185.81824
5. Aghajanian A, Grimes DA. Routine prothrombin time determination before elective gynecologic operations. Obstet Gynecol. 1991;78(5 Pt 1):837-839.
6. Ransom SB, McNeeley SG, Malone JM Jr. A cost-effectiveness evaluation of preoperative type-and-screen testing for vaginal hysterectomy. Am J Obstet Gynecol. 1996;175(5):1201-1203. doi:10.1016/s0002-9378(96)70028-5
7. Ransom SB, McNeeley SG, Hosseini RB. Cost-effectiveness of routine blood type and screen testing before elective laparoscopy. Obstet Gynecol. 1995;86(3):346-348. doi:10.1016/0029-7844(95)00187-V
8. Committee on Standards and Practice Parameters, Apfelbaum JL, Connis RT, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116(3):522-538. doi:10.1097/ALN.0b013e31823c1067
9. Weil IA, Seicean S, Neuhauser D, Schiltz NK, Seicean A. Use and utility of hemostatic screening in adults undergoing elective, non-cardiac surgery. PLoS One. 2015;10(12):e0139139. doi:10.1371/journal.pone.0139139
10. Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing non-cardiac surgery. JAMA. 2007;297(22):2481-2488. doi:10.1001/jama.297.22.2481
11. Healthcare Bluebook. Complete blood count (CBC) with differential. Accessed March 28, 2024. https://www.healthcarebluebook.com/page_ProcedureDetails.aspx?id=214&dataset=lab
12. Douketis JD, Spyropoulos AC, Murad MH, et al. Perioperative management of antithrombotic therapy: an American College of Chest Physicians Clinical Practice Guideline. Chest. 2022;162(5):e207-e243. doi:10.1016/j.chest.2022.07.025
13. Randall JA, Wagner KT, Brody F. Perioperative transfusions in veterans following noncardiac procedures. J Laparoendosc Adv Surg Tech A. 2023;33(10):923-931. doi:10.1089/lap. 2023.0307
14. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115. doi:10.1046/j.1537-2995.1985.25285169199.x
15. Steiner CA, Karaca Z, Moore BJ, Imshaug MC, Pickens G. Surgeries in hospital-based ambulatory surgery and hospital inpatient settings, 2014. Healthcare Cost and Utilization Project statistical brief #223. May 2017. Revised July 2020. Agency for Healthcare Research and Quality. Accessed February 26, 2024. https://hcup-us.ahrq.gov/reports/statbriefs/sb223-Ambulatory-Inpatient-Surgeries-2014.pdf
16. US Department of Veterans Affairs, National Surgery Office. Quarterly report: Q3 of fiscal year 2017. VISN operative complexity summary [Source not verified].
It is common practice to routinely measure postoperative hematocrit levels at US Department of Veterans Affairs (VA) hospitals for a wide range of elective general surgeries. While hematocrit measurement is a low-cost test, the high frequency with which these tests are performed may drastically increase overall costs.
Numerous studies have suggested that physicians overuse laboratory testing.1-10 Kohli and colleagues recommended that the routine practice of obtaining postoperative hematocrit tests following elective gynecologic surgery be abandoned.1 A similar recommendation was made by Olus and colleagues after studying uneventful, unplanned cesarean sections and by Wu and colleagues after investigating routine laboratory tests post total hip arthroplasty.2,3
To our knowledge, a study assessing routine postoperative hematocrit testing in elective general surgery has not yet been conducted. Many laboratory tests ordered in the perioperative period are not indicated, including complete blood count (CBC), electrolytes, and coagulation studies.4 Based on the results of these studies, we expected that the routine measurement of postoperative hematocrit levels after elective general surgeries at VA medical centers would not be cost effective. A PubMed search for articles published from 1990 to 2023 using the search terms “hematocrit,” “hemoglobin,” “general,” “surgery,” “routine,” and “cost” or “cost-effectiveness,” suggests that the clinical usefulness of postoperative hematocrit testing has not been well studied in the general surgery setting. The purpose of this study was to determine the clinical utility and associated cost of measuring routine postoperative hematocrit levels in order to generate a guide as to when the practice is warranted following common elective general surgery.
Although gynecologic textbooks may describe recommendations of routine hematocrit checking after elective gynecologic operations, one has difficulty finding the same recommendations in general surgery textbooks.1 However, it is common practice for surgical residents and attending surgeons to routinely order hematocrit on postoperative day-1 to ensure that the operation did not result in unsuspected anemia that then would need treatment (either with fluids or a blood transfusion). Many other surgeons rely on clinical factors such as tachycardia, oliguria, or hypotension to trigger a hematocrit (and other laboratory) tests. Our hypothesis is that the latter group has chosen the most cost-effective and prudent practice. One problem with checking the hematocrit routinely, as with any other screening test, is what to do with an abnormal result, assuming an asymptomatic patient? If the postoperative hematocrit is lower than expected given the estimated blood loss (EBL), what is one to do?
Methods
This retrospective case-control study conducted at the New Mexico VA Health Care System (NMVAHCS) in Albuquerque compared data for patients who received transfusion within 72 hours of elective surgeries vs patients who did not. Patients who underwent elective general surgery from January 2011 through December 2014 were included. An elective general surgery was defined as surgery performed following an outpatient preoperative anesthesia evaluation ≥ 30 days prior to operation. Patients who underwent emergency operations, and those with baseline anemia (preoperative hematocrit < 30%), and those transfused > 72 hours after their operation were excluded. The NMVAHCSInstitutional Review Board approved this study (No. 15-H184).
A detailed record review was conducted to collect data on demographics and other preoperative risk factors, including age, sex, body mass index (BMI), race and ethnicity, cardiac and pulmonary comorbidities, tobacco use, alcohol intake, diabetes, American Society of Anesthesiologists Physical Status Classification, metabolic equivalent of task, hematologic conditions, and renal disease.
For each procedure, we recorded the type of elective general surgery performed, the diagnosis/indication, pre- and postoperative hemoglobin/hematocrit, intraoperative EBL, length of operation, surgical wound class, length of hospital stay (LOS), intensive care unit (ICU) status, number of hematocrit tests, cardiovascular risk of operation (defined by anesthesia assessment), presence or absence of malignancy, preoperative platelet count, albumin level, preoperative prothrombin time/activated partial thromboplastin time (aPTT), international normalized ratio (INR), hemoglobin A1c, and incidence of transfusion. Signs and symptoms of anemia were recorded as present if the postoperative vital signs suggested low intravascular volume (pulse > 120 beats/minute, systolic blood pressure < 90 mm Hg, or vasoactive medication requirement [per anesthesia postoperative note]) or if the patient reported or exhibited symptoms of dizziness or fatigue or evidence of clinically apparent bleeding (ie, hematoma formation). Laboratory charges for hematocrit tests and CBC at the NMAVAHCS were used to assess cost.11
To stratify the transfusion risk, patients were distributed among 3 groups based on the following criteria: discharged home the same day as surgery; admitted but did not have postoperative hematocrit testing; and admitted and had postoperative hematocrit testing. We also stratified operations into low or high risk based on the risk for postoperative transfusion (Figure). Recognizing that the American College of Chest Physicians guidelines for perioperative management of antithrombotic therapy places bowel resection in a high-risk category, we designated a surgery as high risk when ≥ 2 patients in the transfusion group had that type of surgery over the 4 years of the study.12 Otherwise, the operations were deemed low risk.
Statistical Analysis
Numeric analysis used t tests and Binary and categorical variables used Fisher exact tests. P value ≤ .05 was considered statistically significant. SAS software was used for all statistical analyses.
Results
From 2011 through 2014, 1531 patients had elective general surgery at NMVAHCS. Twenty-two patients with preoperative anemia (hematocrit < 30%) and 1 patient who received a transfusion > 72 hours after the operation were excluded. Most elective operations (70%, n = 1075) were performed on an outpatient basis; none involved transfusion. Inguinal hernia repair was most common with 479 operations; 17 patients were treated inpatient of which 2 patients had routine postoperative hematocrit checks; (neither received transfusion). One patient with inguinal hernia surgery received transfusion without routine postoperative hematocrit monitoring.
Of 112 partial colon resections, 1 patient had a postoperative transfusion; and all but 3 received postoperative hematocrit monitoring. Nineteen patients undergoing partial colon resection had a clinical indication for postoperative hematocrit monitoring. None of the 5 patients with partial gastrectomy received a postoperative transfusion. Of 121 elective cholecystectomies, no patients had postoperative transfusion, whereas 34 had postoperative hematocrit monitoring; only 2 patients had a clinical reason for the hematocrit monitoring.
Of 430 elective inpatient operations, 12 received transfusions and 288 patients had ≥ 1 postoperative hematocrit test (67%). All hematocrit tests were requested by the attending surgeon, resident surgeon, or the surgical ICU team. Of the group that had postoperative hematocrit monitoring, there was an average of 4.4 postoperative hematocrit tests per patient (range, 1-44).
There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 Five of the 12 patients received intraoperative transfusions while 7 were transfused within 72 hours postoperation. All but 1 patient receiving transfusion had EBL > 199 mL (range, 5-3000; mean, 950 mL; median, 500 mL) and/or signs or symptoms of anemia or other indications for measurement of the postoperative hematocrit. There were no statistically significant differences in patients’ age, sex, BMI, or race and ethnicity between groups receiving and not receiving transfusion (Table 1).
When comparing the transfusion vs the nontransfusion groups (after excluding those with clinical preoperative anemia) the risk factors for transfusion included: relatively low mean preoperative hematocrit (mean, 36.9% vs 42.7%, respectively; P = .003), low postoperative hematocrit (mean, 30.2% vs 37.1%, respectively; P < .001), high EBL (mean, 844 mL vs 109 mL, respectively; P = .005), large infusion of intraoperative fluids (mean, 4625 mL vs 2505 mL, respectively; P = .005), longer duration of operation (mean, 397 min vs 183 min, respectively; P < .001), and longer LOS (mean, 14.5 d vs 4.9 d, respectively; P < .001) (Table 2). Similarly, we found an increased risk for transfusion with high/intermediate cardiovascular risk (vs low), any wound not classified as clean, ICU stay, and postoperative symptoms of anemia.
We found no increased risk for transfusion with ethanol, tobacco, warfarin, or clopidogrel use; polycythemia; thrombocytopenia; preoperative INR; preoperative aPTT; preoperative albumin; Hemoglobin A1c; or diabetes mellitus; or for operations performed for malignancy. Ten patients in the ICU received transfusion (5.8%) compared with 2 patients (0.8%) not admitted to the ICU.
Operations were deemed high risk when ≥ 2 of patients having that operation received transfusions within 72 hours of their operation. There were 15 abdominoperineal resections; 3 of these received transfusions (20%). There were 7 total abdominal colectomies; 3 of these received transfusions (43%). We therefore had 22 high-risk operations, 6 of which were transfused (27%).
Discussion
Routine measurement of postoperative hematocrit levels after elective general surgery at NMVAHCS was not necessary. There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 We found that routine postoperative hematocrit measurements to assess anemia had little or no effect on clinical decision-making or clinical outcomes.
According to our results, 88% of initial hematocrit tests after elective partial colectomies could have been eliminated; only 32 of 146 patients demonstrated a clinical reason for postoperative hematocrit testing. Similarly, 36 of 40 postcholecystectomy hematocrit tests (90%) could have been eliminated had the surgeons relied on clinical signs indicating possible postoperative anemia (none were transfused). Excluding patients with major intraoperative blood loss (> 300 mL), only 29 of 288 (10%) patients who had postoperative hematocrit tests had a clinical indication for a postoperative hematocrit test (ie, symptoms of anemia and/or active bleeding). One patient with inguinal hernia surgery who received transfusion was taking an anticoagulant and had a clinically indicated hematocrit test for a large hematoma that eventually required reoperation.
Our study found that routine hematocrit checks may actually increase the risk that a patient would receive an unnecessary transfusion. For instance, one elderly patient, after a right colectomy, had 6 hematocrit levels while on a heparin drip and received transfusion despite being asymptomatic. His lowest hematocrit level prior to transfusion was 23.7%. This patient had a total of 18 hematocrit tests. His EBL was 350 mL and his first postoperative HCT level was 33.1%. In another instance, a patient undergoing abdominoperineal resection had a transfusion on postoperative day 1, despite being hypertensive, with a hematocrit that ranged from 26% before transfusion to 31% after the transfusion. These 2 cases illustrate what has been shown in a recent study: A substantial number of patients with colorectal cancer receive unnecessary transfusions.14 On the other hand, one ileostomy closure patient had 33 hematocrit tests, yet his initial postoperative hematocrit was 37%, and he never received a transfusion. With low-risk surgeries, clinical judgment should dictate when a postoperative hematocrit level is needed. This strategy would have eliminated 206 unnecessary initial postoperative hematocrit tests (72%), could have decreased the number of unnecessary transfusions, and would have saved NMVAHCS about $1600 annually.
Abdominoperineal resections and total abdominal colectomies accounted for a high proportion of transfusions in our study. Inpatient elective operations can be risk stratified and have routine hematocrit tests ordered for patients at high risk. The probability of transfusion was greater in high-risk vs low-risk surgeries; 27% (6 of 22 patients) vs 2% (6 of 408 patients), respectively (P < .001). Since 14 of the 22 patients undergoing high-risk operation already had clinical reasons for a postoperative hematocrit test, we only need to add the remaining 8 patients with high-risk operations to the 74 who had a clinical reason for a hematocrit test and conclude that 82 of 430 patients (19%) had a clinical reason for a hematocrit test, either from signs or symptoms of blood loss or because they were in a high-risk group.
While our elective general surgery cases may not represent many general surgery programs in the US and VA health care systems, we can extrapolate cost savings using the same cost analyses outlined by Kohli and colleagues.1 Assuming 1.9 million elective inpatient general surgeries per year in the United States with an average cost of $21 per CBC, the annual cost of universal postoperative hematocrit testing would be $40 million.11,15 If postoperative hematocrit testing were 70% consistent with our findings, the annual cost for hematocrit tests on 51% of the inpatient general surgeries would be approximately $20.4 million. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our finding that 19% were deemed necessary) results in an annual savings of $30 million. This conservative estimate could be even higher since there were 4.4 hematocrit tests per patient; therefore, we have about $132 million in savings.
Assuming 181,384 elective VA inpatient general surgeries each year, costing $7.14 per CBC (the NMVAHCS cost), the VA could save $1.3 million annually. If postoperative HCT testing were 70% consistent with our findings, the annual cost for hematocrit tests on 50.4% of inpatient general surgery operations would be about $653,000. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our 19%) results in annual VA savings of $330,000. This conservative estimate could be even higher since there were on average 4.4 hematocrit levels per patient; therefore, we estimate that annual savings for the VA of about $1.45 million.
Limitations
The retrospective chart review nature of this study may have led to selection bias. Only a small number of patients received a transfusion, which may have skewed the data. This study population comes from a single VA medical center; this patient population may not be reflective of other VA medical centers or the US population as a whole. Given that NMVAHCS does not perform hepatic, esophageal, pancreas, or transplant operations, the potential savings to both the US and the VA may be overestimated, but this could be studied in the future by VA medical centers that perform more complex operations.
Conclusions
This study found that over a 4-year period routine postoperative hematocrit tests for patients undergoing elective general surgery at a VA medical center were not necessary. General surgeons routinely order various pre- and postoperative laboratory tests despite their limited utility. Reduction in unneeded routine tests could result in notable savings to the VA without compromising quality of care.
Only general surgery patients undergoing operations that carry a high risk for needing a blood transfusion should have a routine postoperative hematocrit testing. In our study population, the chance of an elective colectomy, cholecystectomy, or hernia patient needing a transfusion was rare. This strategy could eliminate a considerable number of unnecessary blood tests and would potentially yield significant savings.
It is common practice to routinely measure postoperative hematocrit levels at US Department of Veterans Affairs (VA) hospitals for a wide range of elective general surgeries. While hematocrit measurement is a low-cost test, the high frequency with which these tests are performed may drastically increase overall costs.
Numerous studies have suggested that physicians overuse laboratory testing.1-10 Kohli and colleagues recommended that the routine practice of obtaining postoperative hematocrit tests following elective gynecologic surgery be abandoned.1 A similar recommendation was made by Olus and colleagues after studying uneventful, unplanned cesarean sections and by Wu and colleagues after investigating routine laboratory tests post total hip arthroplasty.2,3
To our knowledge, a study assessing routine postoperative hematocrit testing in elective general surgery has not yet been conducted. Many laboratory tests ordered in the perioperative period are not indicated, including complete blood count (CBC), electrolytes, and coagulation studies.4 Based on the results of these studies, we expected that the routine measurement of postoperative hematocrit levels after elective general surgeries at VA medical centers would not be cost effective. A PubMed search for articles published from 1990 to 2023 using the search terms “hematocrit,” “hemoglobin,” “general,” “surgery,” “routine,” and “cost” or “cost-effectiveness,” suggests that the clinical usefulness of postoperative hematocrit testing has not been well studied in the general surgery setting. The purpose of this study was to determine the clinical utility and associated cost of measuring routine postoperative hematocrit levels in order to generate a guide as to when the practice is warranted following common elective general surgery.
Although gynecologic textbooks may describe recommendations of routine hematocrit checking after elective gynecologic operations, one has difficulty finding the same recommendations in general surgery textbooks.1 However, it is common practice for surgical residents and attending surgeons to routinely order hematocrit on postoperative day-1 to ensure that the operation did not result in unsuspected anemia that then would need treatment (either with fluids or a blood transfusion). Many other surgeons rely on clinical factors such as tachycardia, oliguria, or hypotension to trigger a hematocrit (and other laboratory) tests. Our hypothesis is that the latter group has chosen the most cost-effective and prudent practice. One problem with checking the hematocrit routinely, as with any other screening test, is what to do with an abnormal result, assuming an asymptomatic patient? If the postoperative hematocrit is lower than expected given the estimated blood loss (EBL), what is one to do?
Methods
This retrospective case-control study conducted at the New Mexico VA Health Care System (NMVAHCS) in Albuquerque compared data for patients who received transfusion within 72 hours of elective surgeries vs patients who did not. Patients who underwent elective general surgery from January 2011 through December 2014 were included. An elective general surgery was defined as surgery performed following an outpatient preoperative anesthesia evaluation ≥ 30 days prior to operation. Patients who underwent emergency operations, and those with baseline anemia (preoperative hematocrit < 30%), and those transfused > 72 hours after their operation were excluded. The NMVAHCSInstitutional Review Board approved this study (No. 15-H184).
A detailed record review was conducted to collect data on demographics and other preoperative risk factors, including age, sex, body mass index (BMI), race and ethnicity, cardiac and pulmonary comorbidities, tobacco use, alcohol intake, diabetes, American Society of Anesthesiologists Physical Status Classification, metabolic equivalent of task, hematologic conditions, and renal disease.
For each procedure, we recorded the type of elective general surgery performed, the diagnosis/indication, pre- and postoperative hemoglobin/hematocrit, intraoperative EBL, length of operation, surgical wound class, length of hospital stay (LOS), intensive care unit (ICU) status, number of hematocrit tests, cardiovascular risk of operation (defined by anesthesia assessment), presence or absence of malignancy, preoperative platelet count, albumin level, preoperative prothrombin time/activated partial thromboplastin time (aPTT), international normalized ratio (INR), hemoglobin A1c, and incidence of transfusion. Signs and symptoms of anemia were recorded as present if the postoperative vital signs suggested low intravascular volume (pulse > 120 beats/minute, systolic blood pressure < 90 mm Hg, or vasoactive medication requirement [per anesthesia postoperative note]) or if the patient reported or exhibited symptoms of dizziness or fatigue or evidence of clinically apparent bleeding (ie, hematoma formation). Laboratory charges for hematocrit tests and CBC at the NMAVAHCS were used to assess cost.11
To stratify the transfusion risk, patients were distributed among 3 groups based on the following criteria: discharged home the same day as surgery; admitted but did not have postoperative hematocrit testing; and admitted and had postoperative hematocrit testing. We also stratified operations into low or high risk based on the risk for postoperative transfusion (Figure). Recognizing that the American College of Chest Physicians guidelines for perioperative management of antithrombotic therapy places bowel resection in a high-risk category, we designated a surgery as high risk when ≥ 2 patients in the transfusion group had that type of surgery over the 4 years of the study.12 Otherwise, the operations were deemed low risk.
Statistical Analysis
Numeric analysis used t tests and Binary and categorical variables used Fisher exact tests. P value ≤ .05 was considered statistically significant. SAS software was used for all statistical analyses.
Results
From 2011 through 2014, 1531 patients had elective general surgery at NMVAHCS. Twenty-two patients with preoperative anemia (hematocrit < 30%) and 1 patient who received a transfusion > 72 hours after the operation were excluded. Most elective operations (70%, n = 1075) were performed on an outpatient basis; none involved transfusion. Inguinal hernia repair was most common with 479 operations; 17 patients were treated inpatient of which 2 patients had routine postoperative hematocrit checks; (neither received transfusion). One patient with inguinal hernia surgery received transfusion without routine postoperative hematocrit monitoring.
Of 112 partial colon resections, 1 patient had a postoperative transfusion; and all but 3 received postoperative hematocrit monitoring. Nineteen patients undergoing partial colon resection had a clinical indication for postoperative hematocrit monitoring. None of the 5 patients with partial gastrectomy received a postoperative transfusion. Of 121 elective cholecystectomies, no patients had postoperative transfusion, whereas 34 had postoperative hematocrit monitoring; only 2 patients had a clinical reason for the hematocrit monitoring.
Of 430 elective inpatient operations, 12 received transfusions and 288 patients had ≥ 1 postoperative hematocrit test (67%). All hematocrit tests were requested by the attending surgeon, resident surgeon, or the surgical ICU team. Of the group that had postoperative hematocrit monitoring, there was an average of 4.4 postoperative hematocrit tests per patient (range, 1-44).
There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 Five of the 12 patients received intraoperative transfusions while 7 were transfused within 72 hours postoperation. All but 1 patient receiving transfusion had EBL > 199 mL (range, 5-3000; mean, 950 mL; median, 500 mL) and/or signs or symptoms of anemia or other indications for measurement of the postoperative hematocrit. There were no statistically significant differences in patients’ age, sex, BMI, or race and ethnicity between groups receiving and not receiving transfusion (Table 1).
When comparing the transfusion vs the nontransfusion groups (after excluding those with clinical preoperative anemia) the risk factors for transfusion included: relatively low mean preoperative hematocrit (mean, 36.9% vs 42.7%, respectively; P = .003), low postoperative hematocrit (mean, 30.2% vs 37.1%, respectively; P < .001), high EBL (mean, 844 mL vs 109 mL, respectively; P = .005), large infusion of intraoperative fluids (mean, 4625 mL vs 2505 mL, respectively; P = .005), longer duration of operation (mean, 397 min vs 183 min, respectively; P < .001), and longer LOS (mean, 14.5 d vs 4.9 d, respectively; P < .001) (Table 2). Similarly, we found an increased risk for transfusion with high/intermediate cardiovascular risk (vs low), any wound not classified as clean, ICU stay, and postoperative symptoms of anemia.
We found no increased risk for transfusion with ethanol, tobacco, warfarin, or clopidogrel use; polycythemia; thrombocytopenia; preoperative INR; preoperative aPTT; preoperative albumin; Hemoglobin A1c; or diabetes mellitus; or for operations performed for malignancy. Ten patients in the ICU received transfusion (5.8%) compared with 2 patients (0.8%) not admitted to the ICU.
Operations were deemed high risk when ≥ 2 of patients having that operation received transfusions within 72 hours of their operation. There were 15 abdominoperineal resections; 3 of these received transfusions (20%). There were 7 total abdominal colectomies; 3 of these received transfusions (43%). We therefore had 22 high-risk operations, 6 of which were transfused (27%).
Discussion
Routine measurement of postoperative hematocrit levels after elective general surgery at NMVAHCS was not necessary. There were 12 transfusions for inpatients (2.8%), which is similar to the findings of a recent study of VA general surgery (2.3%).13 We found that routine postoperative hematocrit measurements to assess anemia had little or no effect on clinical decision-making or clinical outcomes.
According to our results, 88% of initial hematocrit tests after elective partial colectomies could have been eliminated; only 32 of 146 patients demonstrated a clinical reason for postoperative hematocrit testing. Similarly, 36 of 40 postcholecystectomy hematocrit tests (90%) could have been eliminated had the surgeons relied on clinical signs indicating possible postoperative anemia (none were transfused). Excluding patients with major intraoperative blood loss (> 300 mL), only 29 of 288 (10%) patients who had postoperative hematocrit tests had a clinical indication for a postoperative hematocrit test (ie, symptoms of anemia and/or active bleeding). One patient with inguinal hernia surgery who received transfusion was taking an anticoagulant and had a clinically indicated hematocrit test for a large hematoma that eventually required reoperation.
Our study found that routine hematocrit checks may actually increase the risk that a patient would receive an unnecessary transfusion. For instance, one elderly patient, after a right colectomy, had 6 hematocrit levels while on a heparin drip and received transfusion despite being asymptomatic. His lowest hematocrit level prior to transfusion was 23.7%. This patient had a total of 18 hematocrit tests. His EBL was 350 mL and his first postoperative HCT level was 33.1%. In another instance, a patient undergoing abdominoperineal resection had a transfusion on postoperative day 1, despite being hypertensive, with a hematocrit that ranged from 26% before transfusion to 31% after the transfusion. These 2 cases illustrate what has been shown in a recent study: A substantial number of patients with colorectal cancer receive unnecessary transfusions.14 On the other hand, one ileostomy closure patient had 33 hematocrit tests, yet his initial postoperative hematocrit was 37%, and he never received a transfusion. With low-risk surgeries, clinical judgment should dictate when a postoperative hematocrit level is needed. This strategy would have eliminated 206 unnecessary initial postoperative hematocrit tests (72%), could have decreased the number of unnecessary transfusions, and would have saved NMVAHCS about $1600 annually.
Abdominoperineal resections and total abdominal colectomies accounted for a high proportion of transfusions in our study. Inpatient elective operations can be risk stratified and have routine hematocrit tests ordered for patients at high risk. The probability of transfusion was greater in high-risk vs low-risk surgeries; 27% (6 of 22 patients) vs 2% (6 of 408 patients), respectively (P < .001). Since 14 of the 22 patients undergoing high-risk operation already had clinical reasons for a postoperative hematocrit test, we only need to add the remaining 8 patients with high-risk operations to the 74 who had a clinical reason for a hematocrit test and conclude that 82 of 430 patients (19%) had a clinical reason for a hematocrit test, either from signs or symptoms of blood loss or because they were in a high-risk group.
While our elective general surgery cases may not represent many general surgery programs in the US and VA health care systems, we can extrapolate cost savings using the same cost analyses outlined by Kohli and colleagues.1 Assuming 1.9 million elective inpatient general surgeries per year in the United States with an average cost of $21 per CBC, the annual cost of universal postoperative hematocrit testing would be $40 million.11,15 If postoperative hematocrit testing were 70% consistent with our findings, the annual cost for hematocrit tests on 51% of the inpatient general surgeries would be approximately $20.4 million. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our finding that 19% were deemed necessary) results in an annual savings of $30 million. This conservative estimate could be even higher since there were 4.4 hematocrit tests per patient; therefore, we have about $132 million in savings.
Assuming 181,384 elective VA inpatient general surgeries each year, costing $7.14 per CBC (the NMVAHCS cost), the VA could save $1.3 million annually. If postoperative HCT testing were 70% consistent with our findings, the annual cost for hematocrit tests on 50.4% of inpatient general surgery operations would be about $653,000. A reduction in routine hematocrit testing to 25% of all inpatient general surgeries (vs our 19%) results in annual VA savings of $330,000. This conservative estimate could be even higher since there were on average 4.4 hematocrit levels per patient; therefore, we estimate that annual savings for the VA of about $1.45 million.
Limitations
The retrospective chart review nature of this study may have led to selection bias. Only a small number of patients received a transfusion, which may have skewed the data. This study population comes from a single VA medical center; this patient population may not be reflective of other VA medical centers or the US population as a whole. Given that NMVAHCS does not perform hepatic, esophageal, pancreas, or transplant operations, the potential savings to both the US and the VA may be overestimated, but this could be studied in the future by VA medical centers that perform more complex operations.
Conclusions
This study found that over a 4-year period routine postoperative hematocrit tests for patients undergoing elective general surgery at a VA medical center were not necessary. General surgeons routinely order various pre- and postoperative laboratory tests despite their limited utility. Reduction in unneeded routine tests could result in notable savings to the VA without compromising quality of care.
Only general surgery patients undergoing operations that carry a high risk for needing a blood transfusion should have a routine postoperative hematocrit testing. In our study population, the chance of an elective colectomy, cholecystectomy, or hernia patient needing a transfusion was rare. This strategy could eliminate a considerable number of unnecessary blood tests and would potentially yield significant savings.
1. Kohli N, Mallipeddi PK, Neff JM, Sze EH, Roat TW. Routine hematocrit after elective gynecologic surgery. Obstet Gynecol. 2000;95(6 Pt 1):847-850. doi:10.1016/s0029-7844(00)00796-1
2. Olus A, Orhan, U, Murat A, et al. Do asymptomatic patients require routine hemoglobin testing following uneventful, unplanned cesarean sections? Arch Gynecol Obstet. 2010;281(2):195-199. doi:10.1007/s00404-009-1093-1
3. Wu XD, Zhu ZL, Xiao P, Liu JC, Wang JW, Huang W. Are routine postoperative laboratory tests necessary after primary total hip arthroplasty? J Arthroplasty. 2020;35(10):2892-2898. doi:10.1016/j.arth.2020.04.097
4. Kumar A, Srivastava U. Role of routine laboratory investigations in preoperative evaluation. J Anesthesiol Clin Pharmacol. 2011;27(2):174-179. doi:10.4103/0970-9185.81824
5. Aghajanian A, Grimes DA. Routine prothrombin time determination before elective gynecologic operations. Obstet Gynecol. 1991;78(5 Pt 1):837-839.
6. Ransom SB, McNeeley SG, Malone JM Jr. A cost-effectiveness evaluation of preoperative type-and-screen testing for vaginal hysterectomy. Am J Obstet Gynecol. 1996;175(5):1201-1203. doi:10.1016/s0002-9378(96)70028-5
7. Ransom SB, McNeeley SG, Hosseini RB. Cost-effectiveness of routine blood type and screen testing before elective laparoscopy. Obstet Gynecol. 1995;86(3):346-348. doi:10.1016/0029-7844(95)00187-V
8. Committee on Standards and Practice Parameters, Apfelbaum JL, Connis RT, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116(3):522-538. doi:10.1097/ALN.0b013e31823c1067
9. Weil IA, Seicean S, Neuhauser D, Schiltz NK, Seicean A. Use and utility of hemostatic screening in adults undergoing elective, non-cardiac surgery. PLoS One. 2015;10(12):e0139139. doi:10.1371/journal.pone.0139139
10. Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing non-cardiac surgery. JAMA. 2007;297(22):2481-2488. doi:10.1001/jama.297.22.2481
11. Healthcare Bluebook. Complete blood count (CBC) with differential. Accessed March 28, 2024. https://www.healthcarebluebook.com/page_ProcedureDetails.aspx?id=214&dataset=lab
12. Douketis JD, Spyropoulos AC, Murad MH, et al. Perioperative management of antithrombotic therapy: an American College of Chest Physicians Clinical Practice Guideline. Chest. 2022;162(5):e207-e243. doi:10.1016/j.chest.2022.07.025
13. Randall JA, Wagner KT, Brody F. Perioperative transfusions in veterans following noncardiac procedures. J Laparoendosc Adv Surg Tech A. 2023;33(10):923-931. doi:10.1089/lap. 2023.0307
14. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115. doi:10.1046/j.1537-2995.1985.25285169199.x
15. Steiner CA, Karaca Z, Moore BJ, Imshaug MC, Pickens G. Surgeries in hospital-based ambulatory surgery and hospital inpatient settings, 2014. Healthcare Cost and Utilization Project statistical brief #223. May 2017. Revised July 2020. Agency for Healthcare Research and Quality. Accessed February 26, 2024. https://hcup-us.ahrq.gov/reports/statbriefs/sb223-Ambulatory-Inpatient-Surgeries-2014.pdf
16. US Department of Veterans Affairs, National Surgery Office. Quarterly report: Q3 of fiscal year 2017. VISN operative complexity summary [Source not verified].
1. Kohli N, Mallipeddi PK, Neff JM, Sze EH, Roat TW. Routine hematocrit after elective gynecologic surgery. Obstet Gynecol. 2000;95(6 Pt 1):847-850. doi:10.1016/s0029-7844(00)00796-1
2. Olus A, Orhan, U, Murat A, et al. Do asymptomatic patients require routine hemoglobin testing following uneventful, unplanned cesarean sections? Arch Gynecol Obstet. 2010;281(2):195-199. doi:10.1007/s00404-009-1093-1
3. Wu XD, Zhu ZL, Xiao P, Liu JC, Wang JW, Huang W. Are routine postoperative laboratory tests necessary after primary total hip arthroplasty? J Arthroplasty. 2020;35(10):2892-2898. doi:10.1016/j.arth.2020.04.097
4. Kumar A, Srivastava U. Role of routine laboratory investigations in preoperative evaluation. J Anesthesiol Clin Pharmacol. 2011;27(2):174-179. doi:10.4103/0970-9185.81824
5. Aghajanian A, Grimes DA. Routine prothrombin time determination before elective gynecologic operations. Obstet Gynecol. 1991;78(5 Pt 1):837-839.
6. Ransom SB, McNeeley SG, Malone JM Jr. A cost-effectiveness evaluation of preoperative type-and-screen testing for vaginal hysterectomy. Am J Obstet Gynecol. 1996;175(5):1201-1203. doi:10.1016/s0002-9378(96)70028-5
7. Ransom SB, McNeeley SG, Hosseini RB. Cost-effectiveness of routine blood type and screen testing before elective laparoscopy. Obstet Gynecol. 1995;86(3):346-348. doi:10.1016/0029-7844(95)00187-V
8. Committee on Standards and Practice Parameters, Apfelbaum JL, Connis RT, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116(3):522-538. doi:10.1097/ALN.0b013e31823c1067
9. Weil IA, Seicean S, Neuhauser D, Schiltz NK, Seicean A. Use and utility of hemostatic screening in adults undergoing elective, non-cardiac surgery. PLoS One. 2015;10(12):e0139139. doi:10.1371/journal.pone.0139139
10. Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing non-cardiac surgery. JAMA. 2007;297(22):2481-2488. doi:10.1001/jama.297.22.2481
11. Healthcare Bluebook. Complete blood count (CBC) with differential. Accessed March 28, 2024. https://www.healthcarebluebook.com/page_ProcedureDetails.aspx?id=214&dataset=lab
12. Douketis JD, Spyropoulos AC, Murad MH, et al. Perioperative management of antithrombotic therapy: an American College of Chest Physicians Clinical Practice Guideline. Chest. 2022;162(5):e207-e243. doi:10.1016/j.chest.2022.07.025
13. Randall JA, Wagner KT, Brody F. Perioperative transfusions in veterans following noncardiac procedures. J Laparoendosc Adv Surg Tech A. 2023;33(10):923-931. doi:10.1089/lap. 2023.0307
14. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115. doi:10.1046/j.1537-2995.1985.25285169199.x
15. Steiner CA, Karaca Z, Moore BJ, Imshaug MC, Pickens G. Surgeries in hospital-based ambulatory surgery and hospital inpatient settings, 2014. Healthcare Cost and Utilization Project statistical brief #223. May 2017. Revised July 2020. Agency for Healthcare Research and Quality. Accessed February 26, 2024. https://hcup-us.ahrq.gov/reports/statbriefs/sb223-Ambulatory-Inpatient-Surgeries-2014.pdf
16. US Department of Veterans Affairs, National Surgery Office. Quarterly report: Q3 of fiscal year 2017. VISN operative complexity summary [Source not verified].
T-DXd Moves Toward First Line for HER2-Low Metastatic BC
HER2-low cancers express levels of human epidermal growth factor receptor 2 that are below standard thresholds for HER2-positive immunohistochemistry. In 2022, results from the DESTINY-Breast04 trial showed T-DXd (Enhertu, AstraZeneca) to be an effective second-line chemotherapy in patients with HER2-low metastatic breast cancer.
The highly awaited new findings, from the manufacturer-sponsored, open-label Phase 3 DESTINY-Breast06 trial, were presented at the annual meeting of the American Society of Clinical Oncology (ASCO) in Chicago, Illinois.
The findings not only definitively establish a role for T-DXd earlier in the treatment sequence for HER2-low cancers, they also suggest benefit in a group of patients designated for the purposes of this trial to be HER2-ultralow. These patients have cancers with only faintly detectable HER2 expression on currently used assays (J Clin Oncol 42, 2024 [suppl 17; abstr LBA 1000]).
In a separate set of findings also presented at ASCO, from the randomized phase 1B open-label study, DESTINY-Breast07, T-Dxd showed efficacy in previously untreated HER2-positive metastatic breast cancer patients both alone and in combination with the monoclonal antibody pertuzumab (Perjeta, Genentech).
DESTINY-Breast06 Methods and Results
The DESTINY-Breast06 findings were presented by lead investigator Guiseppe Curigliano, MD, PhD, of the University of Milan and European Institute of Oncology. Dr. Curigliano and his colleagues randomized 866 patients with metastatic breast cancer: 436 to intravenous T-Dxd and 430 to the investigator’s choice of capecitabine, nab-paclitaxel, or paclitaxel chemotherapy. The investigators chose capecitabine 60% of the time.
Most patients had cancers classed as HER2 low (immunohistochemistry 1+ or 2+), while 153 had cancers classed by investigators as HER2-ultralow (IHC 0 with membrane staining or IHC under 1+). Patients enrolled in the study were those whose disease had progressed after endocrine therapy with or without targeted therapy. Patients’ median age was between 57 and 58, and all were chemotherapy-naive in the metastatic breast cancer setting.
The main outcome of the study was median progression-free survival in the HER2-low group. T-Dxd was seen improving progression-free survival, with median 13.2 months vs. 8.1 months (hazard ratio, 0.62; 95% confidence interval, 0.51-0.74; P < .0001). In the intention-to-treat population, which included the HER2 ultralow patients, the benefit was the same (HR, 0.63; 95% CI, 0.53-0.75; P < .0001). This suggested that T-DXd is also effective in these patients, and it will be extremely important going forward to identify the lowest level of HER2 expression in metastatic breast cancers that can still benefit from therapy with T-DxD, Dr. Curigliano said.
Overall survival could not be assessed in the study cohort because complete data were not yet available, Dr. Curigliano said. However, trends pointed to an advantage for T-DXd, and tumor response rates were markedly higher with T-DXd: 57% compared with 31% for standard chemotherapy in the full cohort.
Serious treatment-emergent adverse events were more common in the T-Dxd–treated patients, with 11% of that arm developing drug-related interstitial lung disease, and three patients dying of it. Five patients in the T-DXd arm died of adverse events deemed treatment-related, and none died from treatment-related adverse events in the standard chemotherapy arm. Altogether 11 patients died in the T-DXd arm and 6 in the chemotherapy arm.
Clinical Implications of DESTINY-Breast06
The DESTINY-Breast06 data show that “we have to again change how we think about HER2 expression. Even very low levels of HER2 expression matter, and they can be leveraged to improve the treatment for our patients,” said Ian Krop, MD, PhD, of the Yale Cancer Center in New Haven, Connecticut, during the session where the results were presented.
But T-DXd may not be an appropriate first choice for all patients, especially given the safety concerns associated with T-DXd, he continued. With overall survival and quality-of-life data still lacking, clinicians will have to determine on a case-by-case basis who should get T-DXd in the first line.
“For patients who have symptomatic metastatic disease, who need a response to address those symptoms, those in whom you think chemotherapy may not work as well because they had, for example, a short recurrence interval after their adjuvant chemotherapy — using T-DXd in that first-line setting makes perfect sense to take advantage of the substantially higher response rate compared to chemo,” Dr. Krop said. “But for patients who have asymptomatic low burdens of disease, it seems very reasonable to consider using a well-tolerated chemotherapy like capecitabine in the first line, and then using T-DXd in the second line.”
In an interview, Erica Mayer, MD, of the Dana Farber Cancer Institute in Boston, Massachusetts, said patient choice will also matter in determining whether T-DXd is a first-line option. The known toxicity of T-DXd was underscored by the latest findings, she noted, while capecitabine, one of the chemotherapy choices in the control arm of the study, “really reflects what the majority of breast cancer doctors tend to offer, both because of the efficacy of the drug, but also because it’s oral, it’s well tolerated, and you don’t lose your hair.”
DESTINY-Breast07 Results
The DESTINY-Breast07 findings, from a Phase 1B open-label trial measuring safety and tolerability, were presented by Fabrice Andre, MD, PhD, of Université Paris Saclay in Paris, France. Dr. Andre and his colleagues presented the first data comparing T-DXd monotherapy and T-DXd with pertuzumab — a monoclonal antibody targeting HER2 — as a first-line treatment in patients with HER2-overexpressing (immunohistochemistry 3 and above) metastatic breast cancer. (J Clin Oncol 42, 2024 [suppl 16; abstr 1009]).
Current first-line standard of care for these patients is pertuzumab, trastuzumab, and docetaxel, based on results from the 2015 CLEOPATRA trial. T-DXd is currently approved as a second-line treatment.
Dr. Andre and his colleagues randomized 75 patients to monotherapy with T-DXd and 50 to combined therapy, with a median follow-up of 2 years.
After 1 year of treatment, combination of T-DXd and pertuzumab was seen to be associated with a progression-free survival of 89% at 1 year (80% CI, 81.9-93.9), compared with 80% in patients treated with T-DXd alone (80% CI, 73.7-86.1). Objective tumor response rate was 84% for the combined therapy at 12 weeks, with 20% of patients seeing a complete response, compared with 76% and 8%, respectively, for monotherapy.
As in the DESTINY-Breast06 trial, adverse events were high, with interstitial lung disease seen in 9% of patients in the monotherapy group and in 14% of the combined-therapy patients, although no treatment-related deaths occurred.
A randomized phase 3 trial, DESTINY Breast09, will now compare the monotherapy and the combined therapy with standard care.
T-DXd has seen a rapidly expanding role in treating breast and other solid tumors. The DESTINY Breast06 findings will move up its place in the treatment algorithm for metastatic breast cancer, “allowing us to now offer T-DXd as the first chemotherapy choice for patients who are making that transition to chemotherapy over many of the traditional provider choices that we previously have offered,” Dr. Mayer said.
The results “support the use of not only this specific agent, but also the concept of antibody drug conjugates as a very effective way to treat malignancy,” she added.
Dr. Curigliano reported receiving speaker’s fees, research funding, and other support from AstraZeneca and Daiichi Sankyo, among other companies, as did most of his co-authors, of whom three were AstraZeneca employees. Dr. Fabrice disclosed receiving research funding, travel compensation, and/or advisory fees from AstraZeneca and other entities, as did several of his co-authors. Two of his co-authors were employed by AstraZeneca and Roche, manufacturers of the study drugs. Dr. Krop and Dr. Mayer disclosed relationships with AstraZeneca and others.
HER2-low cancers express levels of human epidermal growth factor receptor 2 that are below standard thresholds for HER2-positive immunohistochemistry. In 2022, results from the DESTINY-Breast04 trial showed T-DXd (Enhertu, AstraZeneca) to be an effective second-line chemotherapy in patients with HER2-low metastatic breast cancer.
The highly awaited new findings, from the manufacturer-sponsored, open-label Phase 3 DESTINY-Breast06 trial, were presented at the annual meeting of the American Society of Clinical Oncology (ASCO) in Chicago, Illinois.
The findings not only definitively establish a role for T-DXd earlier in the treatment sequence for HER2-low cancers, they also suggest benefit in a group of patients designated for the purposes of this trial to be HER2-ultralow. These patients have cancers with only faintly detectable HER2 expression on currently used assays (J Clin Oncol 42, 2024 [suppl 17; abstr LBA 1000]).
In a separate set of findings also presented at ASCO, from the randomized phase 1B open-label study, DESTINY-Breast07, T-Dxd showed efficacy in previously untreated HER2-positive metastatic breast cancer patients both alone and in combination with the monoclonal antibody pertuzumab (Perjeta, Genentech).
DESTINY-Breast06 Methods and Results
The DESTINY-Breast06 findings were presented by lead investigator Guiseppe Curigliano, MD, PhD, of the University of Milan and European Institute of Oncology. Dr. Curigliano and his colleagues randomized 866 patients with metastatic breast cancer: 436 to intravenous T-Dxd and 430 to the investigator’s choice of capecitabine, nab-paclitaxel, or paclitaxel chemotherapy. The investigators chose capecitabine 60% of the time.
Most patients had cancers classed as HER2 low (immunohistochemistry 1+ or 2+), while 153 had cancers classed by investigators as HER2-ultralow (IHC 0 with membrane staining or IHC under 1+). Patients enrolled in the study were those whose disease had progressed after endocrine therapy with or without targeted therapy. Patients’ median age was between 57 and 58, and all were chemotherapy-naive in the metastatic breast cancer setting.
The main outcome of the study was median progression-free survival in the HER2-low group. T-Dxd was seen improving progression-free survival, with median 13.2 months vs. 8.1 months (hazard ratio, 0.62; 95% confidence interval, 0.51-0.74; P < .0001). In the intention-to-treat population, which included the HER2 ultralow patients, the benefit was the same (HR, 0.63; 95% CI, 0.53-0.75; P < .0001). This suggested that T-DXd is also effective in these patients, and it will be extremely important going forward to identify the lowest level of HER2 expression in metastatic breast cancers that can still benefit from therapy with T-DxD, Dr. Curigliano said.
Overall survival could not be assessed in the study cohort because complete data were not yet available, Dr. Curigliano said. However, trends pointed to an advantage for T-DXd, and tumor response rates were markedly higher with T-DXd: 57% compared with 31% for standard chemotherapy in the full cohort.
Serious treatment-emergent adverse events were more common in the T-Dxd–treated patients, with 11% of that arm developing drug-related interstitial lung disease, and three patients dying of it. Five patients in the T-DXd arm died of adverse events deemed treatment-related, and none died from treatment-related adverse events in the standard chemotherapy arm. Altogether 11 patients died in the T-DXd arm and 6 in the chemotherapy arm.
Clinical Implications of DESTINY-Breast06
The DESTINY-Breast06 data show that “we have to again change how we think about HER2 expression. Even very low levels of HER2 expression matter, and they can be leveraged to improve the treatment for our patients,” said Ian Krop, MD, PhD, of the Yale Cancer Center in New Haven, Connecticut, during the session where the results were presented.
But T-DXd may not be an appropriate first choice for all patients, especially given the safety concerns associated with T-DXd, he continued. With overall survival and quality-of-life data still lacking, clinicians will have to determine on a case-by-case basis who should get T-DXd in the first line.
“For patients who have symptomatic metastatic disease, who need a response to address those symptoms, those in whom you think chemotherapy may not work as well because they had, for example, a short recurrence interval after their adjuvant chemotherapy — using T-DXd in that first-line setting makes perfect sense to take advantage of the substantially higher response rate compared to chemo,” Dr. Krop said. “But for patients who have asymptomatic low burdens of disease, it seems very reasonable to consider using a well-tolerated chemotherapy like capecitabine in the first line, and then using T-DXd in the second line.”
In an interview, Erica Mayer, MD, of the Dana Farber Cancer Institute in Boston, Massachusetts, said patient choice will also matter in determining whether T-DXd is a first-line option. The known toxicity of T-DXd was underscored by the latest findings, she noted, while capecitabine, one of the chemotherapy choices in the control arm of the study, “really reflects what the majority of breast cancer doctors tend to offer, both because of the efficacy of the drug, but also because it’s oral, it’s well tolerated, and you don’t lose your hair.”
DESTINY-Breast07 Results
The DESTINY-Breast07 findings, from a Phase 1B open-label trial measuring safety and tolerability, were presented by Fabrice Andre, MD, PhD, of Université Paris Saclay in Paris, France. Dr. Andre and his colleagues presented the first data comparing T-DXd monotherapy and T-DXd with pertuzumab — a monoclonal antibody targeting HER2 — as a first-line treatment in patients with HER2-overexpressing (immunohistochemistry 3 and above) metastatic breast cancer. (J Clin Oncol 42, 2024 [suppl 16; abstr 1009]).
Current first-line standard of care for these patients is pertuzumab, trastuzumab, and docetaxel, based on results from the 2015 CLEOPATRA trial. T-DXd is currently approved as a second-line treatment.
Dr. Andre and his colleagues randomized 75 patients to monotherapy with T-DXd and 50 to combined therapy, with a median follow-up of 2 years.
After 1 year of treatment, combination of T-DXd and pertuzumab was seen to be associated with a progression-free survival of 89% at 1 year (80% CI, 81.9-93.9), compared with 80% in patients treated with T-DXd alone (80% CI, 73.7-86.1). Objective tumor response rate was 84% for the combined therapy at 12 weeks, with 20% of patients seeing a complete response, compared with 76% and 8%, respectively, for monotherapy.
As in the DESTINY-Breast06 trial, adverse events were high, with interstitial lung disease seen in 9% of patients in the monotherapy group and in 14% of the combined-therapy patients, although no treatment-related deaths occurred.
A randomized phase 3 trial, DESTINY Breast09, will now compare the monotherapy and the combined therapy with standard care.
T-DXd has seen a rapidly expanding role in treating breast and other solid tumors. The DESTINY Breast06 findings will move up its place in the treatment algorithm for metastatic breast cancer, “allowing us to now offer T-DXd as the first chemotherapy choice for patients who are making that transition to chemotherapy over many of the traditional provider choices that we previously have offered,” Dr. Mayer said.
The results “support the use of not only this specific agent, but also the concept of antibody drug conjugates as a very effective way to treat malignancy,” she added.
Dr. Curigliano reported receiving speaker’s fees, research funding, and other support from AstraZeneca and Daiichi Sankyo, among other companies, as did most of his co-authors, of whom three were AstraZeneca employees. Dr. Fabrice disclosed receiving research funding, travel compensation, and/or advisory fees from AstraZeneca and other entities, as did several of his co-authors. Two of his co-authors were employed by AstraZeneca and Roche, manufacturers of the study drugs. Dr. Krop and Dr. Mayer disclosed relationships with AstraZeneca and others.
HER2-low cancers express levels of human epidermal growth factor receptor 2 that are below standard thresholds for HER2-positive immunohistochemistry. In 2022, results from the DESTINY-Breast04 trial showed T-DXd (Enhertu, AstraZeneca) to be an effective second-line chemotherapy in patients with HER2-low metastatic breast cancer.
The highly awaited new findings, from the manufacturer-sponsored, open-label Phase 3 DESTINY-Breast06 trial, were presented at the annual meeting of the American Society of Clinical Oncology (ASCO) in Chicago, Illinois.
The findings not only definitively establish a role for T-DXd earlier in the treatment sequence for HER2-low cancers, they also suggest benefit in a group of patients designated for the purposes of this trial to be HER2-ultralow. These patients have cancers with only faintly detectable HER2 expression on currently used assays (J Clin Oncol 42, 2024 [suppl 17; abstr LBA 1000]).
In a separate set of findings also presented at ASCO, from the randomized phase 1B open-label study, DESTINY-Breast07, T-Dxd showed efficacy in previously untreated HER2-positive metastatic breast cancer patients both alone and in combination with the monoclonal antibody pertuzumab (Perjeta, Genentech).
DESTINY-Breast06 Methods and Results
The DESTINY-Breast06 findings were presented by lead investigator Guiseppe Curigliano, MD, PhD, of the University of Milan and European Institute of Oncology. Dr. Curigliano and his colleagues randomized 866 patients with metastatic breast cancer: 436 to intravenous T-Dxd and 430 to the investigator’s choice of capecitabine, nab-paclitaxel, or paclitaxel chemotherapy. The investigators chose capecitabine 60% of the time.
Most patients had cancers classed as HER2 low (immunohistochemistry 1+ or 2+), while 153 had cancers classed by investigators as HER2-ultralow (IHC 0 with membrane staining or IHC under 1+). Patients enrolled in the study were those whose disease had progressed after endocrine therapy with or without targeted therapy. Patients’ median age was between 57 and 58, and all were chemotherapy-naive in the metastatic breast cancer setting.
The main outcome of the study was median progression-free survival in the HER2-low group. T-Dxd was seen improving progression-free survival, with median 13.2 months vs. 8.1 months (hazard ratio, 0.62; 95% confidence interval, 0.51-0.74; P < .0001). In the intention-to-treat population, which included the HER2 ultralow patients, the benefit was the same (HR, 0.63; 95% CI, 0.53-0.75; P < .0001). This suggested that T-DXd is also effective in these patients, and it will be extremely important going forward to identify the lowest level of HER2 expression in metastatic breast cancers that can still benefit from therapy with T-DxD, Dr. Curigliano said.
Overall survival could not be assessed in the study cohort because complete data were not yet available, Dr. Curigliano said. However, trends pointed to an advantage for T-DXd, and tumor response rates were markedly higher with T-DXd: 57% compared with 31% for standard chemotherapy in the full cohort.
Serious treatment-emergent adverse events were more common in the T-Dxd–treated patients, with 11% of that arm developing drug-related interstitial lung disease, and three patients dying of it. Five patients in the T-DXd arm died of adverse events deemed treatment-related, and none died from treatment-related adverse events in the standard chemotherapy arm. Altogether 11 patients died in the T-DXd arm and 6 in the chemotherapy arm.
Clinical Implications of DESTINY-Breast06
The DESTINY-Breast06 data show that “we have to again change how we think about HER2 expression. Even very low levels of HER2 expression matter, and they can be leveraged to improve the treatment for our patients,” said Ian Krop, MD, PhD, of the Yale Cancer Center in New Haven, Connecticut, during the session where the results were presented.
But T-DXd may not be an appropriate first choice for all patients, especially given the safety concerns associated with T-DXd, he continued. With overall survival and quality-of-life data still lacking, clinicians will have to determine on a case-by-case basis who should get T-DXd in the first line.
“For patients who have symptomatic metastatic disease, who need a response to address those symptoms, those in whom you think chemotherapy may not work as well because they had, for example, a short recurrence interval after their adjuvant chemotherapy — using T-DXd in that first-line setting makes perfect sense to take advantage of the substantially higher response rate compared to chemo,” Dr. Krop said. “But for patients who have asymptomatic low burdens of disease, it seems very reasonable to consider using a well-tolerated chemotherapy like capecitabine in the first line, and then using T-DXd in the second line.”
In an interview, Erica Mayer, MD, of the Dana Farber Cancer Institute in Boston, Massachusetts, said patient choice will also matter in determining whether T-DXd is a first-line option. The known toxicity of T-DXd was underscored by the latest findings, she noted, while capecitabine, one of the chemotherapy choices in the control arm of the study, “really reflects what the majority of breast cancer doctors tend to offer, both because of the efficacy of the drug, but also because it’s oral, it’s well tolerated, and you don’t lose your hair.”
DESTINY-Breast07 Results
The DESTINY-Breast07 findings, from a Phase 1B open-label trial measuring safety and tolerability, were presented by Fabrice Andre, MD, PhD, of Université Paris Saclay in Paris, France. Dr. Andre and his colleagues presented the first data comparing T-DXd monotherapy and T-DXd with pertuzumab — a monoclonal antibody targeting HER2 — as a first-line treatment in patients with HER2-overexpressing (immunohistochemistry 3 and above) metastatic breast cancer. (J Clin Oncol 42, 2024 [suppl 16; abstr 1009]).
Current first-line standard of care for these patients is pertuzumab, trastuzumab, and docetaxel, based on results from the 2015 CLEOPATRA trial. T-DXd is currently approved as a second-line treatment.
Dr. Andre and his colleagues randomized 75 patients to monotherapy with T-DXd and 50 to combined therapy, with a median follow-up of 2 years.
After 1 year of treatment, combination of T-DXd and pertuzumab was seen to be associated with a progression-free survival of 89% at 1 year (80% CI, 81.9-93.9), compared with 80% in patients treated with T-DXd alone (80% CI, 73.7-86.1). Objective tumor response rate was 84% for the combined therapy at 12 weeks, with 20% of patients seeing a complete response, compared with 76% and 8%, respectively, for monotherapy.
As in the DESTINY-Breast06 trial, adverse events were high, with interstitial lung disease seen in 9% of patients in the monotherapy group and in 14% of the combined-therapy patients, although no treatment-related deaths occurred.
A randomized phase 3 trial, DESTINY Breast09, will now compare the monotherapy and the combined therapy with standard care.
T-DXd has seen a rapidly expanding role in treating breast and other solid tumors. The DESTINY Breast06 findings will move up its place in the treatment algorithm for metastatic breast cancer, “allowing us to now offer T-DXd as the first chemotherapy choice for patients who are making that transition to chemotherapy over many of the traditional provider choices that we previously have offered,” Dr. Mayer said.
The results “support the use of not only this specific agent, but also the concept of antibody drug conjugates as a very effective way to treat malignancy,” she added.
Dr. Curigliano reported receiving speaker’s fees, research funding, and other support from AstraZeneca and Daiichi Sankyo, among other companies, as did most of his co-authors, of whom three were AstraZeneca employees. Dr. Fabrice disclosed receiving research funding, travel compensation, and/or advisory fees from AstraZeneca and other entities, as did several of his co-authors. Two of his co-authors were employed by AstraZeneca and Roche, manufacturers of the study drugs. Dr. Krop and Dr. Mayer disclosed relationships with AstraZeneca and others.
FROM ASCO
Young People’s Gut Bacteria May Drive Colorectal Cancer Risk
CHICAGO — Genetics and diet have been among the top theories for what may be fueling the troubling rise of colorectal cancer in young adults. Now,
The findings were presented at the annual meeting of the American Society for Clinical Oncology (ASCO) by researchers from Ohio State University. For the analysis, they analyzed genetic data on tumors.
The researchers found signs that a high-fat, low-fiber diet may increase inflammation in the gut that prevents it from naturally suppressing tumors. The cells of young people with colorectal cancer also appeared to have aged more quickly — by 15 years on average — than a person’s actual age. That’s unusual, because older people with colorectal cancer don’t have the same boost in cellular aging.
The rate of colorectal cancer among young people has been rising at an alarming rate, according to a 2023 report from the American Cancer Society. In 2019, one in five colorectal cancer cases were among people younger than 55. That’s up from 1 in 10 in 1995, which means the rate has doubled in less than 30 years.
Need Colon Cancer Screening?
Who needs a colorectal cancer screening? Ask colorectal cancer specialist Nancy Kemeny, MD.
A 2017 analysis estimated that a person’s risk of colorectal cancer increased 12% by eating 3.5 ounces of red or processed meat daily, which is the equivalent of the size of a deck of playing cards. The same study also linked colorectal cancer risk to alcohol intake, citing its ethanol content. Eating a diet high in fiber can reduce a person’s risk.
This latest study aligned with previous findings that link bacteria called Fusobacterium to colorectal cancer. It’s not unusual for Fusobacterium to be present in a person’s mouth, but it is more likely to be found in the intestines of colorectal cancer patients, compared with those of healthy people. One study even found that people with colorectal cancer were five times more likely to have Fusobacterium in their stool, compared with healthy people.
Colorectal cancer is more common among men than women, “likely reflecting differences in risk factor prevalence, such as excess body weight and processed meat consumption,” the authors of the 2023 American Cancer Society report explained.
People younger than 45 should alert their medical provider if they have constipation, rectal bleeding, or sudden changes in bowel movements, which can be symptoms of colorectal cancer. Screening for colorectal cancer should begin for most people at age 45.
A version of this article appeared on WebMD.com.
CHICAGO — Genetics and diet have been among the top theories for what may be fueling the troubling rise of colorectal cancer in young adults. Now,
The findings were presented at the annual meeting of the American Society for Clinical Oncology (ASCO) by researchers from Ohio State University. For the analysis, they analyzed genetic data on tumors.
The researchers found signs that a high-fat, low-fiber diet may increase inflammation in the gut that prevents it from naturally suppressing tumors. The cells of young people with colorectal cancer also appeared to have aged more quickly — by 15 years on average — than a person’s actual age. That’s unusual, because older people with colorectal cancer don’t have the same boost in cellular aging.
The rate of colorectal cancer among young people has been rising at an alarming rate, according to a 2023 report from the American Cancer Society. In 2019, one in five colorectal cancer cases were among people younger than 55. That’s up from 1 in 10 in 1995, which means the rate has doubled in less than 30 years.
Need Colon Cancer Screening?
Who needs a colorectal cancer screening? Ask colorectal cancer specialist Nancy Kemeny, MD.
A 2017 analysis estimated that a person’s risk of colorectal cancer increased 12% by eating 3.5 ounces of red or processed meat daily, which is the equivalent of the size of a deck of playing cards. The same study also linked colorectal cancer risk to alcohol intake, citing its ethanol content. Eating a diet high in fiber can reduce a person’s risk.
This latest study aligned with previous findings that link bacteria called Fusobacterium to colorectal cancer. It’s not unusual for Fusobacterium to be present in a person’s mouth, but it is more likely to be found in the intestines of colorectal cancer patients, compared with those of healthy people. One study even found that people with colorectal cancer were five times more likely to have Fusobacterium in their stool, compared with healthy people.
Colorectal cancer is more common among men than women, “likely reflecting differences in risk factor prevalence, such as excess body weight and processed meat consumption,” the authors of the 2023 American Cancer Society report explained.
People younger than 45 should alert their medical provider if they have constipation, rectal bleeding, or sudden changes in bowel movements, which can be symptoms of colorectal cancer. Screening for colorectal cancer should begin for most people at age 45.
A version of this article appeared on WebMD.com.
CHICAGO — Genetics and diet have been among the top theories for what may be fueling the troubling rise of colorectal cancer in young adults. Now,
The findings were presented at the annual meeting of the American Society for Clinical Oncology (ASCO) by researchers from Ohio State University. For the analysis, they analyzed genetic data on tumors.
The researchers found signs that a high-fat, low-fiber diet may increase inflammation in the gut that prevents it from naturally suppressing tumors. The cells of young people with colorectal cancer also appeared to have aged more quickly — by 15 years on average — than a person’s actual age. That’s unusual, because older people with colorectal cancer don’t have the same boost in cellular aging.
The rate of colorectal cancer among young people has been rising at an alarming rate, according to a 2023 report from the American Cancer Society. In 2019, one in five colorectal cancer cases were among people younger than 55. That’s up from 1 in 10 in 1995, which means the rate has doubled in less than 30 years.
Need Colon Cancer Screening?
Who needs a colorectal cancer screening? Ask colorectal cancer specialist Nancy Kemeny, MD.
A 2017 analysis estimated that a person’s risk of colorectal cancer increased 12% by eating 3.5 ounces of red or processed meat daily, which is the equivalent of the size of a deck of playing cards. The same study also linked colorectal cancer risk to alcohol intake, citing its ethanol content. Eating a diet high in fiber can reduce a person’s risk.
This latest study aligned with previous findings that link bacteria called Fusobacterium to colorectal cancer. It’s not unusual for Fusobacterium to be present in a person’s mouth, but it is more likely to be found in the intestines of colorectal cancer patients, compared with those of healthy people. One study even found that people with colorectal cancer were five times more likely to have Fusobacterium in their stool, compared with healthy people.
Colorectal cancer is more common among men than women, “likely reflecting differences in risk factor prevalence, such as excess body weight and processed meat consumption,” the authors of the 2023 American Cancer Society report explained.
People younger than 45 should alert their medical provider if they have constipation, rectal bleeding, or sudden changes in bowel movements, which can be symptoms of colorectal cancer. Screening for colorectal cancer should begin for most people at age 45.
A version of this article appeared on WebMD.com.
FROM ASCO 2024
Red Flags for Early-Onset Colorectal Cancer Identified
TOPLINE:
Patients with early-onset colorectal cancer (EOCRC) often present with hematochezia or abdominal pain, symptoms frequently overlooked in younger populations, leading to delays in diagnosis of 4-6 months, a new analysis showed.
METHODOLOGY:
- As the number of cases of EOCRC, defined as colorectal cancer (CRC) diagnosed before age 50, continues to rise, early detection has become increasingly important. Improved recognition of presenting signs and symptoms associated with EOCRC could lead to a more timely diagnosis and better clinical outcomes.
- In a systematic review and meta-analysis of 81 studies with 24.9 million EOCRC cases, researchers sought to determine the most common presenting signs and symptoms, their association with EOCRC risk, and the time from presentation to diagnosis.
- Data extraction and quality assessment were performed independently in duplicate using PRISMA guidelines, and Joanna Briggs Institute critical appraisal tools were used to measure the risk of bias.
TAKEAWAY:
- Hematochezia was the most common presenting sign/symptom, with a pooled prevalence of 45%, followed by abdominal pain, with a pooled prevalence of 40%.
- Altered bowel habits, which included constipation, diarrhea, and alternating bowel habits, were the third most common presenting sign/symptom (pooled prevalence of 27%), followed by unexplained weight loss (pooled prevalence of 17%).
- The likelihood of EOCRC was estimated to be fivefold to 54-fold higher with hematochezia and 1.3-fold to sixfold higher with abdominal pain.
- The mean time from sign or symptom onset to EOCRC diagnosis was 6.4 months (range, 1.8-13.7 months).
IN PRACTICE:
“These findings and the increasing risk of CRC in individuals younger than 50 years highlight the urgent need to educate clinicians and patients about these signs and symptoms to ensure that diagnostic workup and resolution are not delayed. Adapting current clinical practice to identify and address these signs and symptoms through careful clinical triage and follow-up could help limit morbidity and mortality associated with EOCRC,” the authors wrote.
SOURCE:
The study, with Joshua Demb, PhD, MPH, division of gastroenterology, department of medicine, University of California, San Diego, was published online May 24 in JAMA Network Open.
LIMITATIONS:
Significant heterogeneity across studies affected the ability to meta-analyze some results. The cross-sectional data limited the ability to stratify by age, sex, race and ethnicity, or genetic ancestry. It was not possible to evaluate the impact of time to diagnosis on CRC outcomes due to a limited number of studies answering this question. Researchers were unable to examine the constellation of signs and symptoms because they lacked individual-level data from each study.
DISCLOSURES:
The authors disclosed no relevant conflicts of interest. No specific funding was disclosed.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with early-onset colorectal cancer (EOCRC) often present with hematochezia or abdominal pain, symptoms frequently overlooked in younger populations, leading to delays in diagnosis of 4-6 months, a new analysis showed.
METHODOLOGY:
- As the number of cases of EOCRC, defined as colorectal cancer (CRC) diagnosed before age 50, continues to rise, early detection has become increasingly important. Improved recognition of presenting signs and symptoms associated with EOCRC could lead to a more timely diagnosis and better clinical outcomes.
- In a systematic review and meta-analysis of 81 studies with 24.9 million EOCRC cases, researchers sought to determine the most common presenting signs and symptoms, their association with EOCRC risk, and the time from presentation to diagnosis.
- Data extraction and quality assessment were performed independently in duplicate using PRISMA guidelines, and Joanna Briggs Institute critical appraisal tools were used to measure the risk of bias.
TAKEAWAY:
- Hematochezia was the most common presenting sign/symptom, with a pooled prevalence of 45%, followed by abdominal pain, with a pooled prevalence of 40%.
- Altered bowel habits, which included constipation, diarrhea, and alternating bowel habits, were the third most common presenting sign/symptom (pooled prevalence of 27%), followed by unexplained weight loss (pooled prevalence of 17%).
- The likelihood of EOCRC was estimated to be fivefold to 54-fold higher with hematochezia and 1.3-fold to sixfold higher with abdominal pain.
- The mean time from sign or symptom onset to EOCRC diagnosis was 6.4 months (range, 1.8-13.7 months).
IN PRACTICE:
“These findings and the increasing risk of CRC in individuals younger than 50 years highlight the urgent need to educate clinicians and patients about these signs and symptoms to ensure that diagnostic workup and resolution are not delayed. Adapting current clinical practice to identify and address these signs and symptoms through careful clinical triage and follow-up could help limit morbidity and mortality associated with EOCRC,” the authors wrote.
SOURCE:
The study, with Joshua Demb, PhD, MPH, division of gastroenterology, department of medicine, University of California, San Diego, was published online May 24 in JAMA Network Open.
LIMITATIONS:
Significant heterogeneity across studies affected the ability to meta-analyze some results. The cross-sectional data limited the ability to stratify by age, sex, race and ethnicity, or genetic ancestry. It was not possible to evaluate the impact of time to diagnosis on CRC outcomes due to a limited number of studies answering this question. Researchers were unable to examine the constellation of signs and symptoms because they lacked individual-level data from each study.
DISCLOSURES:
The authors disclosed no relevant conflicts of interest. No specific funding was disclosed.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with early-onset colorectal cancer (EOCRC) often present with hematochezia or abdominal pain, symptoms frequently overlooked in younger populations, leading to delays in diagnosis of 4-6 months, a new analysis showed.
METHODOLOGY:
- As the number of cases of EOCRC, defined as colorectal cancer (CRC) diagnosed before age 50, continues to rise, early detection has become increasingly important. Improved recognition of presenting signs and symptoms associated with EOCRC could lead to a more timely diagnosis and better clinical outcomes.
- In a systematic review and meta-analysis of 81 studies with 24.9 million EOCRC cases, researchers sought to determine the most common presenting signs and symptoms, their association with EOCRC risk, and the time from presentation to diagnosis.
- Data extraction and quality assessment were performed independently in duplicate using PRISMA guidelines, and Joanna Briggs Institute critical appraisal tools were used to measure the risk of bias.
TAKEAWAY:
- Hematochezia was the most common presenting sign/symptom, with a pooled prevalence of 45%, followed by abdominal pain, with a pooled prevalence of 40%.
- Altered bowel habits, which included constipation, diarrhea, and alternating bowel habits, were the third most common presenting sign/symptom (pooled prevalence of 27%), followed by unexplained weight loss (pooled prevalence of 17%).
- The likelihood of EOCRC was estimated to be fivefold to 54-fold higher with hematochezia and 1.3-fold to sixfold higher with abdominal pain.
- The mean time from sign or symptom onset to EOCRC diagnosis was 6.4 months (range, 1.8-13.7 months).
IN PRACTICE:
“These findings and the increasing risk of CRC in individuals younger than 50 years highlight the urgent need to educate clinicians and patients about these signs and symptoms to ensure that diagnostic workup and resolution are not delayed. Adapting current clinical practice to identify and address these signs and symptoms through careful clinical triage and follow-up could help limit morbidity and mortality associated with EOCRC,” the authors wrote.
SOURCE:
The study, with Joshua Demb, PhD, MPH, division of gastroenterology, department of medicine, University of California, San Diego, was published online May 24 in JAMA Network Open.
LIMITATIONS:
Significant heterogeneity across studies affected the ability to meta-analyze some results. The cross-sectional data limited the ability to stratify by age, sex, race and ethnicity, or genetic ancestry. It was not possible to evaluate the impact of time to diagnosis on CRC outcomes due to a limited number of studies answering this question. Researchers were unable to examine the constellation of signs and symptoms because they lacked individual-level data from each study.
DISCLOSURES:
The authors disclosed no relevant conflicts of interest. No specific funding was disclosed.
A version of this article appeared on Medscape.com.
‘Groundbreaking’ Trial Shows Survival Benefits in Lung Cancer
These are results of the ADRIATIC trial, the first planned interim analysis of the randomized, phase 3, double-blind, placebo-controlled multicenter study comparing the PD-L 1 antibody durvalumab vs placebo in patients with stage I-III limited stage disease and prior concurrent chemoradiotherapy.
Lead author David R. Spigel, MD, drew several rounds of applause from an enthusiastic audience when he presented this data, at the plenary session of the annual meeting of the American Society for Clinical Oncology (ASCO) in Chicago.
“ADRIATIC is the first positive, global phase 3 trial of immunotherapy in limited stage SCLC,” said Lauren Byers, MD, the discussant in the session.
“This groundbreaking trial sets a new standard of care with consolidative durvalumab following concurrent chemoradiation,” continued Dr. Byers, who is professor and thoracic section chief in the Department of Thoracic/Head and Neck Medical Oncology at the University of Texas MD Andersen Cancer Center in Houston, Texas.
ADRIATIC Methods and Results
The new study enrolled 730 patients and randomized them between 1 and 42 days after concurrent chemoradiation to one of three treatments: durvalumab 1500 mg; durvalumab plus tremelimumab 75 mg; or placebo. Treatment was continued for a maximum of 24 months, or until progression or intolerable toxicity.
The study had dual primary endpoints of overall survival (OS) and progression-free survival (PFS) for durvalumab vs placebo. The researchers have not yet looked at the results for the secondary endpoints of OS and PFS for patients treated with durvalumab plus tremelimumab vs placebo.
After a median follow-up of 3 years, there was a median OS of 55.9 months in the durvalumab-treated patients, compared with 33.4 months in the placebo arm (hazard ratio [HR], 0.73), and, at a median follow-up of 2 years, there was median PFS of 16.6 months vs 9.2 months respectively (HR, 0.76).
New Standard of Care for Patients with LS-SCLC
“This study had a very good safety profile,” said Dr. Spigel, who is also a medical oncologist and the chief scientific officer at Sarah Cannon Research Institute in Nashville, Tennessee, during his presentation.
“Looking at severe grade 3 or 4 events, these were nearly identical in either arm at 24%. Looking at any-grade immune-mediated AEs, these were 31.2% and 10.2% respectively, and then looking at radiation pneumonitis or pneumonitis, the rates were 38.2% in the durvalumab arm, compared with 30.2% in the placebo arm,” Dr. Spigel said.
Noting that there have been no major advances in the treatment of LS-SCLC for several decades, with most patients experiencing recurrences within 2 years of the cCRT standard of care, Dr. Spigel said “consolidation durvalumab will become the new standard of care for patients with LS-SCLC who have not progressed after cCRT.”
Toby Campbell, MD, a thoracic oncologist, who is professor and chief of Palliative Care at the University of Wisconsin, in Madison, Wisconsin, agrees.
“I take care of patients with small cell lung cancer, an aggressive cancer with high symptom burden that devastates patients and families in its wake,” said Dr. Campbell, during an interview. “About 15% of patients luckily present when the cancer is still contained in the chest and is potentially curable. However, with current treatments we give, which include chemotherapy together with radiation, we are ‘successful’ at curing one in four people.
“This study presents a new treatment option which makes a big difference to patients like mine,” Dr. Campbell continued. “For example, at the 2-year time point, nearly half of patients are still cancer-free. These folks have the opportunity to live their lives more fully, unburdened by the symptoms and dread this disease brings. If approved, I think this treatment would immediately be appropriate to use in clinic.
“Further, oncologists are comfortable using this medication as it is already FDA-approved and used similarly in non–small cell lung cancer.”
The study was funded by AstraZeneca. Dr. Spigel discloses consulting or advisory roles with Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, GlaxoSmithKline, Ipsen, Jazz Pharmaceuticals, Lyell Immunopharma, MedImmune, Monte Rosa Therapeutics, Novartis, Novocure, and Sanofi/Aventis. He has also received research funding from many companies, and travel, accommodations, and other expense reimbursements from AstraZeneca, Genentech, and Novartis.
Dr. Byers discloses honoraria from and consulting or advisory roles with Abbvie, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Beigene, Boehringer Ingelheim, Chugai Pharma, Daiichi Sankyo, Genentech, Jazz Pharmaceuticals, Merck, Dohme, Novartis, and Puma Biotechnology. He also has received research funding from Amgen, AstraZeneca, and Jazz Pharmaceuticals.
Dr. Campbell has served as an advisor for Novocure and Genentech.
These are results of the ADRIATIC trial, the first planned interim analysis of the randomized, phase 3, double-blind, placebo-controlled multicenter study comparing the PD-L 1 antibody durvalumab vs placebo in patients with stage I-III limited stage disease and prior concurrent chemoradiotherapy.
Lead author David R. Spigel, MD, drew several rounds of applause from an enthusiastic audience when he presented this data, at the plenary session of the annual meeting of the American Society for Clinical Oncology (ASCO) in Chicago.
“ADRIATIC is the first positive, global phase 3 trial of immunotherapy in limited stage SCLC,” said Lauren Byers, MD, the discussant in the session.
“This groundbreaking trial sets a new standard of care with consolidative durvalumab following concurrent chemoradiation,” continued Dr. Byers, who is professor and thoracic section chief in the Department of Thoracic/Head and Neck Medical Oncology at the University of Texas MD Andersen Cancer Center in Houston, Texas.
ADRIATIC Methods and Results
The new study enrolled 730 patients and randomized them between 1 and 42 days after concurrent chemoradiation to one of three treatments: durvalumab 1500 mg; durvalumab plus tremelimumab 75 mg; or placebo. Treatment was continued for a maximum of 24 months, or until progression or intolerable toxicity.
The study had dual primary endpoints of overall survival (OS) and progression-free survival (PFS) for durvalumab vs placebo. The researchers have not yet looked at the results for the secondary endpoints of OS and PFS for patients treated with durvalumab plus tremelimumab vs placebo.
After a median follow-up of 3 years, there was a median OS of 55.9 months in the durvalumab-treated patients, compared with 33.4 months in the placebo arm (hazard ratio [HR], 0.73), and, at a median follow-up of 2 years, there was median PFS of 16.6 months vs 9.2 months respectively (HR, 0.76).
New Standard of Care for Patients with LS-SCLC
“This study had a very good safety profile,” said Dr. Spigel, who is also a medical oncologist and the chief scientific officer at Sarah Cannon Research Institute in Nashville, Tennessee, during his presentation.
“Looking at severe grade 3 or 4 events, these were nearly identical in either arm at 24%. Looking at any-grade immune-mediated AEs, these were 31.2% and 10.2% respectively, and then looking at radiation pneumonitis or pneumonitis, the rates were 38.2% in the durvalumab arm, compared with 30.2% in the placebo arm,” Dr. Spigel said.
Noting that there have been no major advances in the treatment of LS-SCLC for several decades, with most patients experiencing recurrences within 2 years of the cCRT standard of care, Dr. Spigel said “consolidation durvalumab will become the new standard of care for patients with LS-SCLC who have not progressed after cCRT.”
Toby Campbell, MD, a thoracic oncologist, who is professor and chief of Palliative Care at the University of Wisconsin, in Madison, Wisconsin, agrees.
“I take care of patients with small cell lung cancer, an aggressive cancer with high symptom burden that devastates patients and families in its wake,” said Dr. Campbell, during an interview. “About 15% of patients luckily present when the cancer is still contained in the chest and is potentially curable. However, with current treatments we give, which include chemotherapy together with radiation, we are ‘successful’ at curing one in four people.
“This study presents a new treatment option which makes a big difference to patients like mine,” Dr. Campbell continued. “For example, at the 2-year time point, nearly half of patients are still cancer-free. These folks have the opportunity to live their lives more fully, unburdened by the symptoms and dread this disease brings. If approved, I think this treatment would immediately be appropriate to use in clinic.
“Further, oncologists are comfortable using this medication as it is already FDA-approved and used similarly in non–small cell lung cancer.”
The study was funded by AstraZeneca. Dr. Spigel discloses consulting or advisory roles with Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, GlaxoSmithKline, Ipsen, Jazz Pharmaceuticals, Lyell Immunopharma, MedImmune, Monte Rosa Therapeutics, Novartis, Novocure, and Sanofi/Aventis. He has also received research funding from many companies, and travel, accommodations, and other expense reimbursements from AstraZeneca, Genentech, and Novartis.
Dr. Byers discloses honoraria from and consulting or advisory roles with Abbvie, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Beigene, Boehringer Ingelheim, Chugai Pharma, Daiichi Sankyo, Genentech, Jazz Pharmaceuticals, Merck, Dohme, Novartis, and Puma Biotechnology. He also has received research funding from Amgen, AstraZeneca, and Jazz Pharmaceuticals.
Dr. Campbell has served as an advisor for Novocure and Genentech.
These are results of the ADRIATIC trial, the first planned interim analysis of the randomized, phase 3, double-blind, placebo-controlled multicenter study comparing the PD-L 1 antibody durvalumab vs placebo in patients with stage I-III limited stage disease and prior concurrent chemoradiotherapy.
Lead author David R. Spigel, MD, drew several rounds of applause from an enthusiastic audience when he presented this data, at the plenary session of the annual meeting of the American Society for Clinical Oncology (ASCO) in Chicago.
“ADRIATIC is the first positive, global phase 3 trial of immunotherapy in limited stage SCLC,” said Lauren Byers, MD, the discussant in the session.
“This groundbreaking trial sets a new standard of care with consolidative durvalumab following concurrent chemoradiation,” continued Dr. Byers, who is professor and thoracic section chief in the Department of Thoracic/Head and Neck Medical Oncology at the University of Texas MD Andersen Cancer Center in Houston, Texas.
ADRIATIC Methods and Results
The new study enrolled 730 patients and randomized them between 1 and 42 days after concurrent chemoradiation to one of three treatments: durvalumab 1500 mg; durvalumab plus tremelimumab 75 mg; or placebo. Treatment was continued for a maximum of 24 months, or until progression or intolerable toxicity.
The study had dual primary endpoints of overall survival (OS) and progression-free survival (PFS) for durvalumab vs placebo. The researchers have not yet looked at the results for the secondary endpoints of OS and PFS for patients treated with durvalumab plus tremelimumab vs placebo.
After a median follow-up of 3 years, there was a median OS of 55.9 months in the durvalumab-treated patients, compared with 33.4 months in the placebo arm (hazard ratio [HR], 0.73), and, at a median follow-up of 2 years, there was median PFS of 16.6 months vs 9.2 months respectively (HR, 0.76).
New Standard of Care for Patients with LS-SCLC
“This study had a very good safety profile,” said Dr. Spigel, who is also a medical oncologist and the chief scientific officer at Sarah Cannon Research Institute in Nashville, Tennessee, during his presentation.
“Looking at severe grade 3 or 4 events, these were nearly identical in either arm at 24%. Looking at any-grade immune-mediated AEs, these were 31.2% and 10.2% respectively, and then looking at radiation pneumonitis or pneumonitis, the rates were 38.2% in the durvalumab arm, compared with 30.2% in the placebo arm,” Dr. Spigel said.
Noting that there have been no major advances in the treatment of LS-SCLC for several decades, with most patients experiencing recurrences within 2 years of the cCRT standard of care, Dr. Spigel said “consolidation durvalumab will become the new standard of care for patients with LS-SCLC who have not progressed after cCRT.”
Toby Campbell, MD, a thoracic oncologist, who is professor and chief of Palliative Care at the University of Wisconsin, in Madison, Wisconsin, agrees.
“I take care of patients with small cell lung cancer, an aggressive cancer with high symptom burden that devastates patients and families in its wake,” said Dr. Campbell, during an interview. “About 15% of patients luckily present when the cancer is still contained in the chest and is potentially curable. However, with current treatments we give, which include chemotherapy together with radiation, we are ‘successful’ at curing one in four people.
“This study presents a new treatment option which makes a big difference to patients like mine,” Dr. Campbell continued. “For example, at the 2-year time point, nearly half of patients are still cancer-free. These folks have the opportunity to live their lives more fully, unburdened by the symptoms and dread this disease brings. If approved, I think this treatment would immediately be appropriate to use in clinic.
“Further, oncologists are comfortable using this medication as it is already FDA-approved and used similarly in non–small cell lung cancer.”
The study was funded by AstraZeneca. Dr. Spigel discloses consulting or advisory roles with Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, GlaxoSmithKline, Ipsen, Jazz Pharmaceuticals, Lyell Immunopharma, MedImmune, Monte Rosa Therapeutics, Novartis, Novocure, and Sanofi/Aventis. He has also received research funding from many companies, and travel, accommodations, and other expense reimbursements from AstraZeneca, Genentech, and Novartis.
Dr. Byers discloses honoraria from and consulting or advisory roles with Abbvie, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Beigene, Boehringer Ingelheim, Chugai Pharma, Daiichi Sankyo, Genentech, Jazz Pharmaceuticals, Merck, Dohme, Novartis, and Puma Biotechnology. He also has received research funding from Amgen, AstraZeneca, and Jazz Pharmaceuticals.
Dr. Campbell has served as an advisor for Novocure and Genentech.
FROM ASCO 2024
Neoadjuvant Checkpoint Inhibition Study Sets New Standard of Care in Melanoma
These results set a new standard of care in this patient population, the study’s lead author, Christian U. Blank, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology in Chicago.
Dr. Blank, a hematologist/oncologist from the Netherlands Cancer Institute in Amsterdam, called the result “very special,” noting that the trial included an active comparator, rather than a placebo control.
“When we treat these patients with surgery only, the outcome … is very bad: The 5-year relapse-free survival is only 30% and the overall survival is only 50%. Adjuvant therapy improves relapse-free survival but not overall survival ...Thus, there is an urgent need for these patients for novel therapy approaches,” he said during a press conference at the meeting.
Study Methods and Results
The study included 423 patients with stage III de novo or recurrent pathologically proven resectable melanoma with at least 1 lymph node metastasis. Patients were randomized to either the experimental neoadjuvant arm (n = 212), or the standard treatment control arm (n = 211), which consisted of therapeutic lymph node dissection (TLND) followed by 12 cycles of adjuvant nivolumab (NIVO 480 mg every 4 weeks).
Patients in the experimental arm received two cycles of neoadjuvant ipilimumab (IPI 80 mg every 3 weeks) plus NIVO 240 mg for 3 weeks followed by TLND. Those with a major pathologic response (MPR), defined as less than 10% vital tumor cells in the post-neoadjuvant resection specimen, went straight to follow-up.
Those without an MPR received adjuvant therapy. For patients with BRAF wild-type, this involved 11 cycles of adjuvant NIVO (480 mg every 4 weeks), while BRAF-mutated patients received dabrafenib plus trametinib (150 mg b.i.d./2 mg once a day; 46 weeks).
The study met its primary endpoint — event-free survival (EFS) — at the first interim analysis. After a median follow-up of 9.9 months, the estimated EFS was 83.7% for neoadjuvant immunotherapy versus 57.2% for standard of care, (P less than .0001, hazard ratio [HR] = 0.32).
“When we look into the subgroups, for example BRAF-mutated status or BRAF-wild-type status ... you see for both groups also a highly statistically significant outcome favoring the neoadjuvant therapy with hazard ratios of 0.29 and 0.35,” said Dr. Blank.
In total, 59% of patients in the experimental arm had an MPR needing no further treatment. “This is important, because the patients that achieve a major pathologic response have excellent outcomes, with an EFS of 95%,” said Dr. Blank.
He added that those with a partial response had an EFS of 76%, and among those who had “nonresponse,” the EFS was 57% — the same as that of patients in the control arm.
Toxicities were considered transient and acceptable, with systemic treatment-related grade 3 or 4 events in 29.7% of the neoadjuvant arm and 14.7% of the adjuvant arm.
NADINA is the first neoadjuvant checkpoint inhibitor phase 3 study in melanoma and the first phase 3 trial in oncology testing a checkpoint inhibitor without chemotherapy, noted Dr. Blank.
“At the moment we see only additions of immunotherapy to the chemotherapy neoadjuvant arms, but here you see that we can also treat patients with pure immunotherapy.”
Neoadjuvant Therapy Defined as Standard of Care
When considered along with evidence from the phase 2 SWOG 1801 study (N Engl J Med. 2023;388:813-8), “NADINA defines neoadjuvant therapy as the new standard of care for macroscopic stage III melanoma “which means that all trials currently ongoing need to be amended from adjuvant comparators to neoadjuvant comparators,” he said.
Dr. Blank called the trial a “new template for other malignancies implementing a neoadjuvant immunotherapy regimen followed by a response-driven adjuvant therapy.
“I think we see at the moment only sandwich designs, and this is more sales driven than patient driven, because what we have seen is that if a patient achieves a really deep response, the patient doesn’t need an adjuvant part,” he said.
Commenting during the press conference, Michael Lowe, MD, said the result “confirms and shows for the first time in a phase 3 study that giving immunotherapy before surgery results in superior outcomes to giving immunotherapy only after surgery.”
Dr. Lowe, associate professor in the Division of Surgical Oncology, at Emory University School of Medicine, Atlanta, added that the study “also confirms that giving two immunotherapy drugs before surgery results in excellent responses.”
However, he cautioned that “we cannot make comparisons to trials in which patients only got one immunotherapy. But this study confirms that consistency that patients who receive ipilimumab and nivolumab have superior responses compared to single-agent immunotherapy.”
He noted that all of the patients in the new study had all of their lymph nodes removed and called for doing that to remain the standard of care in terms of surgical approach.
“With short follow-up, it is too early to tell if some patients may have benefited from that adjuvant therapy. However, NADINA confirms that immunotherapy should be given to all patients with advanced melanoma before surgery, when possible, and establishes dual therapy with nivolumab and ipilimumab, as the standard of care in the appropriate patient,” Dr. Lowe said.
EFS Improvement Exceeds Expectations
In an interview, Rodabe N. Amaria, MD, a medical oncologist and professor at The University of Texas MD Anderson Cancer Center in Houston, agreed with Dr. Lowe’s assessment of the findings.
“For years we have been doing neoadjuvant immunotherapy trials, all with favorable results, but all relatively small, with data that was intriguing, but not necessarily definitive,” she said. “I see the data from the NADINA trial as being definitive and true evidence of the many advantages of neoadjuvant immunotherapy for clinical stage 3 melanoma ... This work builds on the data from the SWOG 1801 trial but also exceeds expectations with the 68% improvement in EFS appreciated with the dual combination immunotherapy regimen compared to adjuvant nivolumab.”
Additionally, the approximately 30% grade 3 or higher immune-mediated toxicity is reasonable and in keeping with known data, and this trial demonstrates clearly that neoadjuvant immunotherapy does not increase the rate of surgical complications, she said.
Dr. Amaria also considered that 59% of patients who achieved a major pathologic response were observed in the neoadjuvant setting to be a key finding.
This indicates thats “over half the patients could be spared additional immunotherapy and risk of further immune-mediated toxicities by having only two doses of neoadjuvant immunotherapy, she said.
The results “demonstrate the superiority of a neoadjuvant combination immunotherapy approach for patients with clinical stage III melanoma,” she added.
The study was funded by Bristol Myers-Squibb and the Australian government.
Dr. Blank disclosed ties with Immagene, Signature Oncology, AstraZeneca, Bristol-Myers Squibb, GenMab, GlaxoSmithKline, Lilly, MSD Oncology, Novartis, Pfizer, Pierre Fabre, Roche/Genentech, Third Rock Ventures, 4SC, NanoString Technologies, WO 2021/177822 A1, and Freshfields Bruckhaus Deringer. No other experts reported any relevant disclosures.
These results set a new standard of care in this patient population, the study’s lead author, Christian U. Blank, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology in Chicago.
Dr. Blank, a hematologist/oncologist from the Netherlands Cancer Institute in Amsterdam, called the result “very special,” noting that the trial included an active comparator, rather than a placebo control.
“When we treat these patients with surgery only, the outcome … is very bad: The 5-year relapse-free survival is only 30% and the overall survival is only 50%. Adjuvant therapy improves relapse-free survival but not overall survival ...Thus, there is an urgent need for these patients for novel therapy approaches,” he said during a press conference at the meeting.
Study Methods and Results
The study included 423 patients with stage III de novo or recurrent pathologically proven resectable melanoma with at least 1 lymph node metastasis. Patients were randomized to either the experimental neoadjuvant arm (n = 212), or the standard treatment control arm (n = 211), which consisted of therapeutic lymph node dissection (TLND) followed by 12 cycles of adjuvant nivolumab (NIVO 480 mg every 4 weeks).
Patients in the experimental arm received two cycles of neoadjuvant ipilimumab (IPI 80 mg every 3 weeks) plus NIVO 240 mg for 3 weeks followed by TLND. Those with a major pathologic response (MPR), defined as less than 10% vital tumor cells in the post-neoadjuvant resection specimen, went straight to follow-up.
Those without an MPR received adjuvant therapy. For patients with BRAF wild-type, this involved 11 cycles of adjuvant NIVO (480 mg every 4 weeks), while BRAF-mutated patients received dabrafenib plus trametinib (150 mg b.i.d./2 mg once a day; 46 weeks).
The study met its primary endpoint — event-free survival (EFS) — at the first interim analysis. After a median follow-up of 9.9 months, the estimated EFS was 83.7% for neoadjuvant immunotherapy versus 57.2% for standard of care, (P less than .0001, hazard ratio [HR] = 0.32).
“When we look into the subgroups, for example BRAF-mutated status or BRAF-wild-type status ... you see for both groups also a highly statistically significant outcome favoring the neoadjuvant therapy with hazard ratios of 0.29 and 0.35,” said Dr. Blank.
In total, 59% of patients in the experimental arm had an MPR needing no further treatment. “This is important, because the patients that achieve a major pathologic response have excellent outcomes, with an EFS of 95%,” said Dr. Blank.
He added that those with a partial response had an EFS of 76%, and among those who had “nonresponse,” the EFS was 57% — the same as that of patients in the control arm.
Toxicities were considered transient and acceptable, with systemic treatment-related grade 3 or 4 events in 29.7% of the neoadjuvant arm and 14.7% of the adjuvant arm.
NADINA is the first neoadjuvant checkpoint inhibitor phase 3 study in melanoma and the first phase 3 trial in oncology testing a checkpoint inhibitor without chemotherapy, noted Dr. Blank.
“At the moment we see only additions of immunotherapy to the chemotherapy neoadjuvant arms, but here you see that we can also treat patients with pure immunotherapy.”
Neoadjuvant Therapy Defined as Standard of Care
When considered along with evidence from the phase 2 SWOG 1801 study (N Engl J Med. 2023;388:813-8), “NADINA defines neoadjuvant therapy as the new standard of care for macroscopic stage III melanoma “which means that all trials currently ongoing need to be amended from adjuvant comparators to neoadjuvant comparators,” he said.
Dr. Blank called the trial a “new template for other malignancies implementing a neoadjuvant immunotherapy regimen followed by a response-driven adjuvant therapy.
“I think we see at the moment only sandwich designs, and this is more sales driven than patient driven, because what we have seen is that if a patient achieves a really deep response, the patient doesn’t need an adjuvant part,” he said.
Commenting during the press conference, Michael Lowe, MD, said the result “confirms and shows for the first time in a phase 3 study that giving immunotherapy before surgery results in superior outcomes to giving immunotherapy only after surgery.”
Dr. Lowe, associate professor in the Division of Surgical Oncology, at Emory University School of Medicine, Atlanta, added that the study “also confirms that giving two immunotherapy drugs before surgery results in excellent responses.”
However, he cautioned that “we cannot make comparisons to trials in which patients only got one immunotherapy. But this study confirms that consistency that patients who receive ipilimumab and nivolumab have superior responses compared to single-agent immunotherapy.”
He noted that all of the patients in the new study had all of their lymph nodes removed and called for doing that to remain the standard of care in terms of surgical approach.
“With short follow-up, it is too early to tell if some patients may have benefited from that adjuvant therapy. However, NADINA confirms that immunotherapy should be given to all patients with advanced melanoma before surgery, when possible, and establishes dual therapy with nivolumab and ipilimumab, as the standard of care in the appropriate patient,” Dr. Lowe said.
EFS Improvement Exceeds Expectations
In an interview, Rodabe N. Amaria, MD, a medical oncologist and professor at The University of Texas MD Anderson Cancer Center in Houston, agreed with Dr. Lowe’s assessment of the findings.
“For years we have been doing neoadjuvant immunotherapy trials, all with favorable results, but all relatively small, with data that was intriguing, but not necessarily definitive,” she said. “I see the data from the NADINA trial as being definitive and true evidence of the many advantages of neoadjuvant immunotherapy for clinical stage 3 melanoma ... This work builds on the data from the SWOG 1801 trial but also exceeds expectations with the 68% improvement in EFS appreciated with the dual combination immunotherapy regimen compared to adjuvant nivolumab.”
Additionally, the approximately 30% grade 3 or higher immune-mediated toxicity is reasonable and in keeping with known data, and this trial demonstrates clearly that neoadjuvant immunotherapy does not increase the rate of surgical complications, she said.
Dr. Amaria also considered that 59% of patients who achieved a major pathologic response were observed in the neoadjuvant setting to be a key finding.
This indicates thats “over half the patients could be spared additional immunotherapy and risk of further immune-mediated toxicities by having only two doses of neoadjuvant immunotherapy, she said.
The results “demonstrate the superiority of a neoadjuvant combination immunotherapy approach for patients with clinical stage III melanoma,” she added.
The study was funded by Bristol Myers-Squibb and the Australian government.
Dr. Blank disclosed ties with Immagene, Signature Oncology, AstraZeneca, Bristol-Myers Squibb, GenMab, GlaxoSmithKline, Lilly, MSD Oncology, Novartis, Pfizer, Pierre Fabre, Roche/Genentech, Third Rock Ventures, 4SC, NanoString Technologies, WO 2021/177822 A1, and Freshfields Bruckhaus Deringer. No other experts reported any relevant disclosures.
These results set a new standard of care in this patient population, the study’s lead author, Christian U. Blank, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology in Chicago.
Dr. Blank, a hematologist/oncologist from the Netherlands Cancer Institute in Amsterdam, called the result “very special,” noting that the trial included an active comparator, rather than a placebo control.
“When we treat these patients with surgery only, the outcome … is very bad: The 5-year relapse-free survival is only 30% and the overall survival is only 50%. Adjuvant therapy improves relapse-free survival but not overall survival ...Thus, there is an urgent need for these patients for novel therapy approaches,” he said during a press conference at the meeting.
Study Methods and Results
The study included 423 patients with stage III de novo or recurrent pathologically proven resectable melanoma with at least 1 lymph node metastasis. Patients were randomized to either the experimental neoadjuvant arm (n = 212), or the standard treatment control arm (n = 211), which consisted of therapeutic lymph node dissection (TLND) followed by 12 cycles of adjuvant nivolumab (NIVO 480 mg every 4 weeks).
Patients in the experimental arm received two cycles of neoadjuvant ipilimumab (IPI 80 mg every 3 weeks) plus NIVO 240 mg for 3 weeks followed by TLND. Those with a major pathologic response (MPR), defined as less than 10% vital tumor cells in the post-neoadjuvant resection specimen, went straight to follow-up.
Those without an MPR received adjuvant therapy. For patients with BRAF wild-type, this involved 11 cycles of adjuvant NIVO (480 mg every 4 weeks), while BRAF-mutated patients received dabrafenib plus trametinib (150 mg b.i.d./2 mg once a day; 46 weeks).
The study met its primary endpoint — event-free survival (EFS) — at the first interim analysis. After a median follow-up of 9.9 months, the estimated EFS was 83.7% for neoadjuvant immunotherapy versus 57.2% for standard of care, (P less than .0001, hazard ratio [HR] = 0.32).
“When we look into the subgroups, for example BRAF-mutated status or BRAF-wild-type status ... you see for both groups also a highly statistically significant outcome favoring the neoadjuvant therapy with hazard ratios of 0.29 and 0.35,” said Dr. Blank.
In total, 59% of patients in the experimental arm had an MPR needing no further treatment. “This is important, because the patients that achieve a major pathologic response have excellent outcomes, with an EFS of 95%,” said Dr. Blank.
He added that those with a partial response had an EFS of 76%, and among those who had “nonresponse,” the EFS was 57% — the same as that of patients in the control arm.
Toxicities were considered transient and acceptable, with systemic treatment-related grade 3 or 4 events in 29.7% of the neoadjuvant arm and 14.7% of the adjuvant arm.
NADINA is the first neoadjuvant checkpoint inhibitor phase 3 study in melanoma and the first phase 3 trial in oncology testing a checkpoint inhibitor without chemotherapy, noted Dr. Blank.
“At the moment we see only additions of immunotherapy to the chemotherapy neoadjuvant arms, but here you see that we can also treat patients with pure immunotherapy.”
Neoadjuvant Therapy Defined as Standard of Care
When considered along with evidence from the phase 2 SWOG 1801 study (N Engl J Med. 2023;388:813-8), “NADINA defines neoadjuvant therapy as the new standard of care for macroscopic stage III melanoma “which means that all trials currently ongoing need to be amended from adjuvant comparators to neoadjuvant comparators,” he said.
Dr. Blank called the trial a “new template for other malignancies implementing a neoadjuvant immunotherapy regimen followed by a response-driven adjuvant therapy.
“I think we see at the moment only sandwich designs, and this is more sales driven than patient driven, because what we have seen is that if a patient achieves a really deep response, the patient doesn’t need an adjuvant part,” he said.
Commenting during the press conference, Michael Lowe, MD, said the result “confirms and shows for the first time in a phase 3 study that giving immunotherapy before surgery results in superior outcomes to giving immunotherapy only after surgery.”
Dr. Lowe, associate professor in the Division of Surgical Oncology, at Emory University School of Medicine, Atlanta, added that the study “also confirms that giving two immunotherapy drugs before surgery results in excellent responses.”
However, he cautioned that “we cannot make comparisons to trials in which patients only got one immunotherapy. But this study confirms that consistency that patients who receive ipilimumab and nivolumab have superior responses compared to single-agent immunotherapy.”
He noted that all of the patients in the new study had all of their lymph nodes removed and called for doing that to remain the standard of care in terms of surgical approach.
“With short follow-up, it is too early to tell if some patients may have benefited from that adjuvant therapy. However, NADINA confirms that immunotherapy should be given to all patients with advanced melanoma before surgery, when possible, and establishes dual therapy with nivolumab and ipilimumab, as the standard of care in the appropriate patient,” Dr. Lowe said.
EFS Improvement Exceeds Expectations
In an interview, Rodabe N. Amaria, MD, a medical oncologist and professor at The University of Texas MD Anderson Cancer Center in Houston, agreed with Dr. Lowe’s assessment of the findings.
“For years we have been doing neoadjuvant immunotherapy trials, all with favorable results, but all relatively small, with data that was intriguing, but not necessarily definitive,” she said. “I see the data from the NADINA trial as being definitive and true evidence of the many advantages of neoadjuvant immunotherapy for clinical stage 3 melanoma ... This work builds on the data from the SWOG 1801 trial but also exceeds expectations with the 68% improvement in EFS appreciated with the dual combination immunotherapy regimen compared to adjuvant nivolumab.”
Additionally, the approximately 30% grade 3 or higher immune-mediated toxicity is reasonable and in keeping with known data, and this trial demonstrates clearly that neoadjuvant immunotherapy does not increase the rate of surgical complications, she said.
Dr. Amaria also considered that 59% of patients who achieved a major pathologic response were observed in the neoadjuvant setting to be a key finding.
This indicates thats “over half the patients could be spared additional immunotherapy and risk of further immune-mediated toxicities by having only two doses of neoadjuvant immunotherapy, she said.
The results “demonstrate the superiority of a neoadjuvant combination immunotherapy approach for patients with clinical stage III melanoma,” she added.
The study was funded by Bristol Myers-Squibb and the Australian government.
Dr. Blank disclosed ties with Immagene, Signature Oncology, AstraZeneca, Bristol-Myers Squibb, GenMab, GlaxoSmithKline, Lilly, MSD Oncology, Novartis, Pfizer, Pierre Fabre, Roche/Genentech, Third Rock Ventures, 4SC, NanoString Technologies, WO 2021/177822 A1, and Freshfields Bruckhaus Deringer. No other experts reported any relevant disclosures.
FROM ASCO 2024
New Drug Combo Boosts PFS
At a median follow-up of 4 years, progression-free survival for the new treatment, known as BrECADD, was 94.3% vs. 90.9% for BEACOPP (hazard ratio, 0.66, 95% CI, P = .035), researchers led by Peter Borchmann, MD, assistant medical director of hematology and oncology at the University Hospital of Cologne, Germany, reported at the annual meeting of the American Society of Clinical Oncology (ASCO).
“These results are really striking,” said hematologist-oncologist Oreofe O. Odejide, MD, MPH, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, who was not involved in the study and commented on it during an ASCO news briefing. “This is really poised to impact the standard-of-care treatment for patients with advanced-stage classical Hodgkin lymphoma.”
As Dr. Borchmann explained at the briefing, Hodgkin lymphoma is the most common cancer among young adults. “The median age at onset is around 30 years, and it can be primarily cured with chemotherapy. Intensified chemotherapy probably is better primary lymphoma control than less intensive treatment, but this comes at the cost of treatment-related adverse events.”
Dr. Borchmann and colleagues developed the existing treatment known as BEACOPP, a combination of bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone. “It’s our standard of care due to its high primary cure rate, which is reflected by compelling progression-free survival,” he said.
However, he said, “it’s a high burden of treatment.” The investigational treatment, BrECADD, includes six drugs instead of seven: brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone. Two of the additions — brentuximab vedotin and dacarbazine — are cancer drugs, and dexamethasone is a steroid. There is one fewer cancer drug in the new formulation.
In the international HD21 trial (9 countries, 233 sites), researchers recruited patients aged 18-60 who received four or six cycles of either BEACOPP or BrECADD. The doses were guided by PET2 findings.
In the intention-to-treat cohort of 1,482 subjects (median age 31.1, 44% female), 742 were assigned to BrECADD and 740 to BEACOPP.
There were few early treatment failures in the BrECADD group vs. BEACOPP. The numbers who had primary progression within the first 3 months were 5 vs. 15, respectively, and the numbers reaching early relapse between months 3 and 12 were 11 vs. 23, respectively.
Four-year overall survival rates in the groups were nearly identical at 98.5% for BrECADD and 98.2% for BEACOPP. In regard to fertility, follicle-stimulating hormone recovery rates after 1 year were higher in the BrECADD group in both men (67% vs. 24%, respectively) and women (89% vs. 68%, respectively). Birth rates were also higher in the BrECADD group (n = 60 vs. n = 43 in the BEACOPP group).
Nearly two-thirds of those in BrECADD group (64%) required 12 weeks of therapy — four cycles. As for treatment-related morbidity toxicities, they were less common in the BrECADD group vs. the BEACOPP group (42% vs. 59%, respectively, P < .0001), and 1% of BrECADD-treated had them at 1 year.
Oncologist Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, welcomed the findings at the ACO news briefing. “By replacing some pretty toxic chemo with an antibody-drug conjugate [brentuximab vedotin], and changing the regimen a bit, and using PET scan to determine the number of cycles received, the long-term outcomes were maintained, if not even improved upon,” said Dr. Dr. Gralow, who was not involved in the study.
In addition, she said, the findings about fertility are good news because “these are young people who probably haven’t started a family yet, and we’re increasing the odds that they will be able to do so after survival.”
Moving forward, she said, “we will need to have some discussion on how this relates to ABVD, which is a more commonly used regimen in the United States right now.” ABVD refers to a combination of doxorubicin hydrochloride, bleomycin sulfate, vinblastine sulfate, and dacarbazine.
Takeda funded the study. Dr. Borchmann reported ties with BMS, GmbH & Co, Incyte, MSD/Merck, Roche, Takeda/Millennium, Miltenyi, Amgen, and Novartis. Some of the other study authors reported various disclosures. Dr. Odejide and Dr. Gralow have no disclosures.
At a median follow-up of 4 years, progression-free survival for the new treatment, known as BrECADD, was 94.3% vs. 90.9% for BEACOPP (hazard ratio, 0.66, 95% CI, P = .035), researchers led by Peter Borchmann, MD, assistant medical director of hematology and oncology at the University Hospital of Cologne, Germany, reported at the annual meeting of the American Society of Clinical Oncology (ASCO).
“These results are really striking,” said hematologist-oncologist Oreofe O. Odejide, MD, MPH, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, who was not involved in the study and commented on it during an ASCO news briefing. “This is really poised to impact the standard-of-care treatment for patients with advanced-stage classical Hodgkin lymphoma.”
As Dr. Borchmann explained at the briefing, Hodgkin lymphoma is the most common cancer among young adults. “The median age at onset is around 30 years, and it can be primarily cured with chemotherapy. Intensified chemotherapy probably is better primary lymphoma control than less intensive treatment, but this comes at the cost of treatment-related adverse events.”
Dr. Borchmann and colleagues developed the existing treatment known as BEACOPP, a combination of bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone. “It’s our standard of care due to its high primary cure rate, which is reflected by compelling progression-free survival,” he said.
However, he said, “it’s a high burden of treatment.” The investigational treatment, BrECADD, includes six drugs instead of seven: brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone. Two of the additions — brentuximab vedotin and dacarbazine — are cancer drugs, and dexamethasone is a steroid. There is one fewer cancer drug in the new formulation.
In the international HD21 trial (9 countries, 233 sites), researchers recruited patients aged 18-60 who received four or six cycles of either BEACOPP or BrECADD. The doses were guided by PET2 findings.
In the intention-to-treat cohort of 1,482 subjects (median age 31.1, 44% female), 742 were assigned to BrECADD and 740 to BEACOPP.
There were few early treatment failures in the BrECADD group vs. BEACOPP. The numbers who had primary progression within the first 3 months were 5 vs. 15, respectively, and the numbers reaching early relapse between months 3 and 12 were 11 vs. 23, respectively.
Four-year overall survival rates in the groups were nearly identical at 98.5% for BrECADD and 98.2% for BEACOPP. In regard to fertility, follicle-stimulating hormone recovery rates after 1 year were higher in the BrECADD group in both men (67% vs. 24%, respectively) and women (89% vs. 68%, respectively). Birth rates were also higher in the BrECADD group (n = 60 vs. n = 43 in the BEACOPP group).
Nearly two-thirds of those in BrECADD group (64%) required 12 weeks of therapy — four cycles. As for treatment-related morbidity toxicities, they were less common in the BrECADD group vs. the BEACOPP group (42% vs. 59%, respectively, P < .0001), and 1% of BrECADD-treated had them at 1 year.
Oncologist Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, welcomed the findings at the ACO news briefing. “By replacing some pretty toxic chemo with an antibody-drug conjugate [brentuximab vedotin], and changing the regimen a bit, and using PET scan to determine the number of cycles received, the long-term outcomes were maintained, if not even improved upon,” said Dr. Dr. Gralow, who was not involved in the study.
In addition, she said, the findings about fertility are good news because “these are young people who probably haven’t started a family yet, and we’re increasing the odds that they will be able to do so after survival.”
Moving forward, she said, “we will need to have some discussion on how this relates to ABVD, which is a more commonly used regimen in the United States right now.” ABVD refers to a combination of doxorubicin hydrochloride, bleomycin sulfate, vinblastine sulfate, and dacarbazine.
Takeda funded the study. Dr. Borchmann reported ties with BMS, GmbH & Co, Incyte, MSD/Merck, Roche, Takeda/Millennium, Miltenyi, Amgen, and Novartis. Some of the other study authors reported various disclosures. Dr. Odejide and Dr. Gralow have no disclosures.
At a median follow-up of 4 years, progression-free survival for the new treatment, known as BrECADD, was 94.3% vs. 90.9% for BEACOPP (hazard ratio, 0.66, 95% CI, P = .035), researchers led by Peter Borchmann, MD, assistant medical director of hematology and oncology at the University Hospital of Cologne, Germany, reported at the annual meeting of the American Society of Clinical Oncology (ASCO).
“These results are really striking,” said hematologist-oncologist Oreofe O. Odejide, MD, MPH, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, who was not involved in the study and commented on it during an ASCO news briefing. “This is really poised to impact the standard-of-care treatment for patients with advanced-stage classical Hodgkin lymphoma.”
As Dr. Borchmann explained at the briefing, Hodgkin lymphoma is the most common cancer among young adults. “The median age at onset is around 30 years, and it can be primarily cured with chemotherapy. Intensified chemotherapy probably is better primary lymphoma control than less intensive treatment, but this comes at the cost of treatment-related adverse events.”
Dr. Borchmann and colleagues developed the existing treatment known as BEACOPP, a combination of bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone. “It’s our standard of care due to its high primary cure rate, which is reflected by compelling progression-free survival,” he said.
However, he said, “it’s a high burden of treatment.” The investigational treatment, BrECADD, includes six drugs instead of seven: brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone. Two of the additions — brentuximab vedotin and dacarbazine — are cancer drugs, and dexamethasone is a steroid. There is one fewer cancer drug in the new formulation.
In the international HD21 trial (9 countries, 233 sites), researchers recruited patients aged 18-60 who received four or six cycles of either BEACOPP or BrECADD. The doses were guided by PET2 findings.
In the intention-to-treat cohort of 1,482 subjects (median age 31.1, 44% female), 742 were assigned to BrECADD and 740 to BEACOPP.
There were few early treatment failures in the BrECADD group vs. BEACOPP. The numbers who had primary progression within the first 3 months were 5 vs. 15, respectively, and the numbers reaching early relapse between months 3 and 12 were 11 vs. 23, respectively.
Four-year overall survival rates in the groups were nearly identical at 98.5% for BrECADD and 98.2% for BEACOPP. In regard to fertility, follicle-stimulating hormone recovery rates after 1 year were higher in the BrECADD group in both men (67% vs. 24%, respectively) and women (89% vs. 68%, respectively). Birth rates were also higher in the BrECADD group (n = 60 vs. n = 43 in the BEACOPP group).
Nearly two-thirds of those in BrECADD group (64%) required 12 weeks of therapy — four cycles. As for treatment-related morbidity toxicities, they were less common in the BrECADD group vs. the BEACOPP group (42% vs. 59%, respectively, P < .0001), and 1% of BrECADD-treated had them at 1 year.
Oncologist Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, welcomed the findings at the ACO news briefing. “By replacing some pretty toxic chemo with an antibody-drug conjugate [brentuximab vedotin], and changing the regimen a bit, and using PET scan to determine the number of cycles received, the long-term outcomes were maintained, if not even improved upon,” said Dr. Dr. Gralow, who was not involved in the study.
In addition, she said, the findings about fertility are good news because “these are young people who probably haven’t started a family yet, and we’re increasing the odds that they will be able to do so after survival.”
Moving forward, she said, “we will need to have some discussion on how this relates to ABVD, which is a more commonly used regimen in the United States right now.” ABVD refers to a combination of doxorubicin hydrochloride, bleomycin sulfate, vinblastine sulfate, and dacarbazine.
Takeda funded the study. Dr. Borchmann reported ties with BMS, GmbH & Co, Incyte, MSD/Merck, Roche, Takeda/Millennium, Miltenyi, Amgen, and Novartis. Some of the other study authors reported various disclosures. Dr. Odejide and Dr. Gralow have no disclosures.
FROM ASCO 2024
Role of JAK2 in Polycythemia Vera

How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.
How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.
How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.