User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Five things most physicians don’t know about radiation oncology
As a field, radiation oncology is perhaps one of medicine’s best kept secrets. Sometimes, even our own colleagues don’t know where our department exists in the hospital or exactly what we do.
As two radiation oncologists who are, in fact, the children of radiation oncologists, we will admit that it’s possible we are a tiny bit biased. We cannot lie, though: Our field is a hidden gem.
What is well known is that radiation oncologists have a symbiotic relationship with our treatment technology. The evolution of treatment machines and radiation precision allows us to deliver patient-tailored treatment down to the millimeter. What may get lost in the discussions of isodose lines and penumbra, however, is that we’ve also got cutting-edge research and personalized patient care within a specialized team in the depths of the hospital.
Because the inner workings of what happens to patients as they come in and out of our office remains a mystery,
1. Nobody knows what goes on in the basement.
Misconceptions about our subspecialty are common, even among other oncologists. A frequent misconception is that a radiation oncologist’s involvement in patient care is limited, and radiation is delivered in a standardized manner. This essentially renders radiation oncologists technicians of expensive machines.
In reality however, radiation oncologists touch every aspect of a patient’s care, and customized radiation therapy may be indicated for virtually every cancer site in both curative and palliative settings. We strive to deliver precision medicine and practice truly patient-centered care.
To cure cancer, radiation may be used in the neoadjuvant (prior to local surgical resection), definitive (as the primary local therapy), and adjuvant (postsurgical) setting. In palliative cases, radiation can be used to treat areas of metastatic spread as well as primary unresectable tumors to alleviate obstruction and/or bleeding symptoms. Referral to radiation oncology, therefore, can be appropriate at many different points of time on the continuum of cancer care.
For many treating radiation oncologists, the close personal connections that we form with our patients is one of the primary reasons we went into this field. Not only are we making patient-centered clinical decisions during every step of the treatment plan evaluation and optimization but we also see our patients weekly for clinical visits and then ongoing in visits that may span many years of survivorship.
Our deep commitment to addressing patient needs as they are receiving treatment and responsibility for late radiation effects is absolutely an integral part of our training and lifelong practice.
2. We get down in the details.
The workflow from consultation to radiation delivery can be confusing for anyone outside our specialized field.
Once seen in consult and considered a good candidate for radiation, patients will enter the essential next step: the treatment planning imaging – or “simulation.”
The simulation scan – mostly CT, although occasionally fused MRI or PET – involves a separate appointment and another hour or so of arranging and scanning patients in the exact position that they will be treated. Given the precision of modern radiation, the simulation often includes making a customized mold so patients have minimal movement during treatment. These simulation images allow the radiation oncology team to create a treatment plan that is customized to each patient and precisely reproducible during their course of radiation treatments – what’s known as fractions.
Creating a treatment plan involves a radiation oncologist literally drawing – or contouring – on pictures of the patient’s internal anatomy in three dimensions. Radiation oncologists contour exactly where the cancer is – or where it was if the treatment is given postoperatively – and identify the surrounding organs so that the doses can be preferentially directed to the cancer target and minimize risk to nearby organs. This precision is within millimeters and accounts for microscopic disease, organ motion, and patient setup. Ultimately, we create colorful heat gradient volumes of the anticipated radiation dose delivery and optimize these to reflect our planning priorities.
We use advanced technologies to shape the beams of radiation to treat the tumor and avoid delivering high doses to the neighboring tissues with techniques such as intensity modulated radiation therapy (IMRT), stereotactic ablative radiation therapy (SABR or SBRT), and stereotactic radiosurgery. We can also take advantage of the unique properties of different modalities, such as proton therapy and electron therapy, to achieve these same goals if indicated. Radiation oncologists live for precision medicine in every aspect of their workflow.
3. We roll deep.
Radiation oncology is exemplary of “the art of medicine.” We fuse anatomy-based treatment design with advanced technology and orchestrate the daily functions of a large medical team.
But, the treatment plan and delivery would not be possible without the input and care given within a large multi- and intradisciplinary team of oncologists, medical physicists, dosimetrists, radiation therapists, nurses, social workers, and other support staff. Radiation oncologists participate in regular tumor boards with surgeons, medical oncologists, pathologists, and radiologists to optimize interdisciplinary management of complex patients, providing a thoughtful tumor localization and treatment plan, as well as to better understand an individual’s ongoing symptoms and well-being as a whole. Considering all aspects of what a patient may need involves communication with fellow physicians, nurse navigators, and social workers.
Within our own department, treatment plan creation and quality checking or verification can sometimes take over 2 weeks, with detailed input from dosimetrists and medical physicists. The actual treatment delivery involves daily communication with the radiation therapists who are dedicated to each treatment machine – like the linear accelerator – and symptom management with clinic nurses and supportive staff, such as physical therapists and registered dietitians.
This massive team effort is required to get each patient through daily radiation treatments that can last 7 weeks and may require rapid replanning if the tumor shrinks or the patient loses weight.
As part of this team, radiation oncologists are uniquely positioned to quarterback each play and guide the entire game strategy.
4. Radiation therapy takes a lot of heat.
Radiation therapy is often blamed for issues unrelated to the treatment. Irradiating the pelvis for prostate cancer, for instance, does not cause a headache or heartburn during or after treatment.
Other than fatigue, associated side effects are localized and related to the total radiation dose and fraction size – how much and how fast – that reaches the surrounding tissues.
Our colleagues often swap stories of the bizarre things radiation therapy has been blamed for, including dental problems in someone receiving vaginal cylinder treatment, heart dysfunction in someone treated for rectal cancer, and hip fracture in someone treated for breast cancer because the radiation “destroyed” their bones. At best, these are humorous stories, but at worst, they can delay diagnosis and treatment of what is truly causing someone’s symptoms.
5. We truly believe that less is more.
One of the most fundamental aspects of radiation oncology is our drive to optimize treatment delivery and continually improve patient care – sometimes at our own field’s economic detriment. We’re dedicated to showing that patients may get the same benefit from less and less radiation.
In the past 2 decades, the evolution and adoption of photon IMRT and proton therapy has allowed radiation plans to successfully spare surrounding tissue while improving our targeting. This evolution is coupled with technological and imaging advances that allow us to delivery of doses to certain tumors via SABR/SBRT in one to five total fractions.
A prime example: Treatment to eradicate lung or gastrointestinal tumors, which used to span up to 6 weeks, can now potentially be delivered in as little as 1 week.
For other common cancers, hypofractionation – slightly higher radiation doses per fraction at fewer total fractions overall – has revolutionized patient care, providing less radiation without impacting survival or increasing treatment toxicity.
Take breast cancer care: 50 years ago, virtually all patients with breast cancer received a mastectomy and lymph node dissections. Today, surgical techniques for lumpectomy paired with radiation therapy to the whole breast now allows us to preserve disease-free survival for those who elected to keep their breasts.
Over the past 20 years, the standards of care have shifted from 6-7 weeks of treatment to 3-4 weeks using a hypofractionated model that involves daily whole-breast radiation. The most recent clinical trials have shown that whole-breast radiation can be delivered safely and effectively for select women in as few as five fractions with either whole or partial breast targeting. Additional research driven by the idea of “right sizing” radiation treatment has even shown that certain women may not need radiation at all.
This evolution in radiation therapy illustrates how our subspecialty is constantly working to improve survival and patient well-being, form deep connections with our patients, and push the boundaries of medical innovations.
We are proud to be radiation oncologists and happy to share more. Want to know more about what goes on in the basement? Come on down, we’re happy to show you around.
Dr. Giap is a resident in the department of radiation oncology at the University of Florida, Gainesville. Dr. Chino is an assistant attending in the department of radiation oncology at Memorial Sloan Kettering Cancer Center, New York. Neither reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
As a field, radiation oncology is perhaps one of medicine’s best kept secrets. Sometimes, even our own colleagues don’t know where our department exists in the hospital or exactly what we do.
As two radiation oncologists who are, in fact, the children of radiation oncologists, we will admit that it’s possible we are a tiny bit biased. We cannot lie, though: Our field is a hidden gem.
What is well known is that radiation oncologists have a symbiotic relationship with our treatment technology. The evolution of treatment machines and radiation precision allows us to deliver patient-tailored treatment down to the millimeter. What may get lost in the discussions of isodose lines and penumbra, however, is that we’ve also got cutting-edge research and personalized patient care within a specialized team in the depths of the hospital.
Because the inner workings of what happens to patients as they come in and out of our office remains a mystery,
1. Nobody knows what goes on in the basement.
Misconceptions about our subspecialty are common, even among other oncologists. A frequent misconception is that a radiation oncologist’s involvement in patient care is limited, and radiation is delivered in a standardized manner. This essentially renders radiation oncologists technicians of expensive machines.
In reality however, radiation oncologists touch every aspect of a patient’s care, and customized radiation therapy may be indicated for virtually every cancer site in both curative and palliative settings. We strive to deliver precision medicine and practice truly patient-centered care.
To cure cancer, radiation may be used in the neoadjuvant (prior to local surgical resection), definitive (as the primary local therapy), and adjuvant (postsurgical) setting. In palliative cases, radiation can be used to treat areas of metastatic spread as well as primary unresectable tumors to alleviate obstruction and/or bleeding symptoms. Referral to radiation oncology, therefore, can be appropriate at many different points of time on the continuum of cancer care.
For many treating radiation oncologists, the close personal connections that we form with our patients is one of the primary reasons we went into this field. Not only are we making patient-centered clinical decisions during every step of the treatment plan evaluation and optimization but we also see our patients weekly for clinical visits and then ongoing in visits that may span many years of survivorship.
Our deep commitment to addressing patient needs as they are receiving treatment and responsibility for late radiation effects is absolutely an integral part of our training and lifelong practice.
2. We get down in the details.
The workflow from consultation to radiation delivery can be confusing for anyone outside our specialized field.
Once seen in consult and considered a good candidate for radiation, patients will enter the essential next step: the treatment planning imaging – or “simulation.”
The simulation scan – mostly CT, although occasionally fused MRI or PET – involves a separate appointment and another hour or so of arranging and scanning patients in the exact position that they will be treated. Given the precision of modern radiation, the simulation often includes making a customized mold so patients have minimal movement during treatment. These simulation images allow the radiation oncology team to create a treatment plan that is customized to each patient and precisely reproducible during their course of radiation treatments – what’s known as fractions.
Creating a treatment plan involves a radiation oncologist literally drawing – or contouring – on pictures of the patient’s internal anatomy in three dimensions. Radiation oncologists contour exactly where the cancer is – or where it was if the treatment is given postoperatively – and identify the surrounding organs so that the doses can be preferentially directed to the cancer target and minimize risk to nearby organs. This precision is within millimeters and accounts for microscopic disease, organ motion, and patient setup. Ultimately, we create colorful heat gradient volumes of the anticipated radiation dose delivery and optimize these to reflect our planning priorities.
We use advanced technologies to shape the beams of radiation to treat the tumor and avoid delivering high doses to the neighboring tissues with techniques such as intensity modulated radiation therapy (IMRT), stereotactic ablative radiation therapy (SABR or SBRT), and stereotactic radiosurgery. We can also take advantage of the unique properties of different modalities, such as proton therapy and electron therapy, to achieve these same goals if indicated. Radiation oncologists live for precision medicine in every aspect of their workflow.
3. We roll deep.
Radiation oncology is exemplary of “the art of medicine.” We fuse anatomy-based treatment design with advanced technology and orchestrate the daily functions of a large medical team.
But, the treatment plan and delivery would not be possible without the input and care given within a large multi- and intradisciplinary team of oncologists, medical physicists, dosimetrists, radiation therapists, nurses, social workers, and other support staff. Radiation oncologists participate in regular tumor boards with surgeons, medical oncologists, pathologists, and radiologists to optimize interdisciplinary management of complex patients, providing a thoughtful tumor localization and treatment plan, as well as to better understand an individual’s ongoing symptoms and well-being as a whole. Considering all aspects of what a patient may need involves communication with fellow physicians, nurse navigators, and social workers.
Within our own department, treatment plan creation and quality checking or verification can sometimes take over 2 weeks, with detailed input from dosimetrists and medical physicists. The actual treatment delivery involves daily communication with the radiation therapists who are dedicated to each treatment machine – like the linear accelerator – and symptom management with clinic nurses and supportive staff, such as physical therapists and registered dietitians.
This massive team effort is required to get each patient through daily radiation treatments that can last 7 weeks and may require rapid replanning if the tumor shrinks or the patient loses weight.
As part of this team, radiation oncologists are uniquely positioned to quarterback each play and guide the entire game strategy.
4. Radiation therapy takes a lot of heat.
Radiation therapy is often blamed for issues unrelated to the treatment. Irradiating the pelvis for prostate cancer, for instance, does not cause a headache or heartburn during or after treatment.
Other than fatigue, associated side effects are localized and related to the total radiation dose and fraction size – how much and how fast – that reaches the surrounding tissues.
Our colleagues often swap stories of the bizarre things radiation therapy has been blamed for, including dental problems in someone receiving vaginal cylinder treatment, heart dysfunction in someone treated for rectal cancer, and hip fracture in someone treated for breast cancer because the radiation “destroyed” their bones. At best, these are humorous stories, but at worst, they can delay diagnosis and treatment of what is truly causing someone’s symptoms.
5. We truly believe that less is more.
One of the most fundamental aspects of radiation oncology is our drive to optimize treatment delivery and continually improve patient care – sometimes at our own field’s economic detriment. We’re dedicated to showing that patients may get the same benefit from less and less radiation.
In the past 2 decades, the evolution and adoption of photon IMRT and proton therapy has allowed radiation plans to successfully spare surrounding tissue while improving our targeting. This evolution is coupled with technological and imaging advances that allow us to delivery of doses to certain tumors via SABR/SBRT in one to five total fractions.
A prime example: Treatment to eradicate lung or gastrointestinal tumors, which used to span up to 6 weeks, can now potentially be delivered in as little as 1 week.
For other common cancers, hypofractionation – slightly higher radiation doses per fraction at fewer total fractions overall – has revolutionized patient care, providing less radiation without impacting survival or increasing treatment toxicity.
Take breast cancer care: 50 years ago, virtually all patients with breast cancer received a mastectomy and lymph node dissections. Today, surgical techniques for lumpectomy paired with radiation therapy to the whole breast now allows us to preserve disease-free survival for those who elected to keep their breasts.
Over the past 20 years, the standards of care have shifted from 6-7 weeks of treatment to 3-4 weeks using a hypofractionated model that involves daily whole-breast radiation. The most recent clinical trials have shown that whole-breast radiation can be delivered safely and effectively for select women in as few as five fractions with either whole or partial breast targeting. Additional research driven by the idea of “right sizing” radiation treatment has even shown that certain women may not need radiation at all.
This evolution in radiation therapy illustrates how our subspecialty is constantly working to improve survival and patient well-being, form deep connections with our patients, and push the boundaries of medical innovations.
We are proud to be radiation oncologists and happy to share more. Want to know more about what goes on in the basement? Come on down, we’re happy to show you around.
Dr. Giap is a resident in the department of radiation oncology at the University of Florida, Gainesville. Dr. Chino is an assistant attending in the department of radiation oncology at Memorial Sloan Kettering Cancer Center, New York. Neither reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
As a field, radiation oncology is perhaps one of medicine’s best kept secrets. Sometimes, even our own colleagues don’t know where our department exists in the hospital or exactly what we do.
As two radiation oncologists who are, in fact, the children of radiation oncologists, we will admit that it’s possible we are a tiny bit biased. We cannot lie, though: Our field is a hidden gem.
What is well known is that radiation oncologists have a symbiotic relationship with our treatment technology. The evolution of treatment machines and radiation precision allows us to deliver patient-tailored treatment down to the millimeter. What may get lost in the discussions of isodose lines and penumbra, however, is that we’ve also got cutting-edge research and personalized patient care within a specialized team in the depths of the hospital.
Because the inner workings of what happens to patients as they come in and out of our office remains a mystery,
1. Nobody knows what goes on in the basement.
Misconceptions about our subspecialty are common, even among other oncologists. A frequent misconception is that a radiation oncologist’s involvement in patient care is limited, and radiation is delivered in a standardized manner. This essentially renders radiation oncologists technicians of expensive machines.
In reality however, radiation oncologists touch every aspect of a patient’s care, and customized radiation therapy may be indicated for virtually every cancer site in both curative and palliative settings. We strive to deliver precision medicine and practice truly patient-centered care.
To cure cancer, radiation may be used in the neoadjuvant (prior to local surgical resection), definitive (as the primary local therapy), and adjuvant (postsurgical) setting. In palliative cases, radiation can be used to treat areas of metastatic spread as well as primary unresectable tumors to alleviate obstruction and/or bleeding symptoms. Referral to radiation oncology, therefore, can be appropriate at many different points of time on the continuum of cancer care.
For many treating radiation oncologists, the close personal connections that we form with our patients is one of the primary reasons we went into this field. Not only are we making patient-centered clinical decisions during every step of the treatment plan evaluation and optimization but we also see our patients weekly for clinical visits and then ongoing in visits that may span many years of survivorship.
Our deep commitment to addressing patient needs as they are receiving treatment and responsibility for late radiation effects is absolutely an integral part of our training and lifelong practice.
2. We get down in the details.
The workflow from consultation to radiation delivery can be confusing for anyone outside our specialized field.
Once seen in consult and considered a good candidate for radiation, patients will enter the essential next step: the treatment planning imaging – or “simulation.”
The simulation scan – mostly CT, although occasionally fused MRI or PET – involves a separate appointment and another hour or so of arranging and scanning patients in the exact position that they will be treated. Given the precision of modern radiation, the simulation often includes making a customized mold so patients have minimal movement during treatment. These simulation images allow the radiation oncology team to create a treatment plan that is customized to each patient and precisely reproducible during their course of radiation treatments – what’s known as fractions.
Creating a treatment plan involves a radiation oncologist literally drawing – or contouring – on pictures of the patient’s internal anatomy in three dimensions. Radiation oncologists contour exactly where the cancer is – or where it was if the treatment is given postoperatively – and identify the surrounding organs so that the doses can be preferentially directed to the cancer target and minimize risk to nearby organs. This precision is within millimeters and accounts for microscopic disease, organ motion, and patient setup. Ultimately, we create colorful heat gradient volumes of the anticipated radiation dose delivery and optimize these to reflect our planning priorities.
We use advanced technologies to shape the beams of radiation to treat the tumor and avoid delivering high doses to the neighboring tissues with techniques such as intensity modulated radiation therapy (IMRT), stereotactic ablative radiation therapy (SABR or SBRT), and stereotactic radiosurgery. We can also take advantage of the unique properties of different modalities, such as proton therapy and electron therapy, to achieve these same goals if indicated. Radiation oncologists live for precision medicine in every aspect of their workflow.
3. We roll deep.
Radiation oncology is exemplary of “the art of medicine.” We fuse anatomy-based treatment design with advanced technology and orchestrate the daily functions of a large medical team.
But, the treatment plan and delivery would not be possible without the input and care given within a large multi- and intradisciplinary team of oncologists, medical physicists, dosimetrists, radiation therapists, nurses, social workers, and other support staff. Radiation oncologists participate in regular tumor boards with surgeons, medical oncologists, pathologists, and radiologists to optimize interdisciplinary management of complex patients, providing a thoughtful tumor localization and treatment plan, as well as to better understand an individual’s ongoing symptoms and well-being as a whole. Considering all aspects of what a patient may need involves communication with fellow physicians, nurse navigators, and social workers.
Within our own department, treatment plan creation and quality checking or verification can sometimes take over 2 weeks, with detailed input from dosimetrists and medical physicists. The actual treatment delivery involves daily communication with the radiation therapists who are dedicated to each treatment machine – like the linear accelerator – and symptom management with clinic nurses and supportive staff, such as physical therapists and registered dietitians.
This massive team effort is required to get each patient through daily radiation treatments that can last 7 weeks and may require rapid replanning if the tumor shrinks or the patient loses weight.
As part of this team, radiation oncologists are uniquely positioned to quarterback each play and guide the entire game strategy.
4. Radiation therapy takes a lot of heat.
Radiation therapy is often blamed for issues unrelated to the treatment. Irradiating the pelvis for prostate cancer, for instance, does not cause a headache or heartburn during or after treatment.
Other than fatigue, associated side effects are localized and related to the total radiation dose and fraction size – how much and how fast – that reaches the surrounding tissues.
Our colleagues often swap stories of the bizarre things radiation therapy has been blamed for, including dental problems in someone receiving vaginal cylinder treatment, heart dysfunction in someone treated for rectal cancer, and hip fracture in someone treated for breast cancer because the radiation “destroyed” their bones. At best, these are humorous stories, but at worst, they can delay diagnosis and treatment of what is truly causing someone’s symptoms.
5. We truly believe that less is more.
One of the most fundamental aspects of radiation oncology is our drive to optimize treatment delivery and continually improve patient care – sometimes at our own field’s economic detriment. We’re dedicated to showing that patients may get the same benefit from less and less radiation.
In the past 2 decades, the evolution and adoption of photon IMRT and proton therapy has allowed radiation plans to successfully spare surrounding tissue while improving our targeting. This evolution is coupled with technological and imaging advances that allow us to delivery of doses to certain tumors via SABR/SBRT in one to five total fractions.
A prime example: Treatment to eradicate lung or gastrointestinal tumors, which used to span up to 6 weeks, can now potentially be delivered in as little as 1 week.
For other common cancers, hypofractionation – slightly higher radiation doses per fraction at fewer total fractions overall – has revolutionized patient care, providing less radiation without impacting survival or increasing treatment toxicity.
Take breast cancer care: 50 years ago, virtually all patients with breast cancer received a mastectomy and lymph node dissections. Today, surgical techniques for lumpectomy paired with radiation therapy to the whole breast now allows us to preserve disease-free survival for those who elected to keep their breasts.
Over the past 20 years, the standards of care have shifted from 6-7 weeks of treatment to 3-4 weeks using a hypofractionated model that involves daily whole-breast radiation. The most recent clinical trials have shown that whole-breast radiation can be delivered safely and effectively for select women in as few as five fractions with either whole or partial breast targeting. Additional research driven by the idea of “right sizing” radiation treatment has even shown that certain women may not need radiation at all.
This evolution in radiation therapy illustrates how our subspecialty is constantly working to improve survival and patient well-being, form deep connections with our patients, and push the boundaries of medical innovations.
We are proud to be radiation oncologists and happy to share more. Want to know more about what goes on in the basement? Come on down, we’re happy to show you around.
Dr. Giap is a resident in the department of radiation oncology at the University of Florida, Gainesville. Dr. Chino is an assistant attending in the department of radiation oncology at Memorial Sloan Kettering Cancer Center, New York. Neither reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Marital status plays modest role in gastric cancer overall survival
, according to research published in the Journal of Investigative Medicine.
Tumor size remained the largest contributor to overall survival, but marital status was among several other significant factors, such as age, race, gender, treatment style, and pathologic stage, that can provide insight into a patient’s likelihood of overall survival, as it does with several other cancers.
“Married patients had the best prognosis, followed by single patients, and the prognosis of separated patients was the worst,” write Lixiang Zhang and colleagues at the First Affiliated Hospital of Anhui Medical University, Hefei, China. “We speculate that this might be due to the fact that married patients had better financial conditions and emotional encouragement, while separated patients might be more likely to experience financial difficulties [and] emotional loss.”
The results were not necessarily surprising to Richard M. Peek, Jr., MD, director of the division of gastroenterology and a professor of medicine at Vanderbilt University Medical Center, who was not involved in the research.
“Marital status is a reflection of support systems, and a strong support system is a prognosticator for increased compliance with medical appointments and medical therapies,” Dr. Peek told this news organization. “It is something to consider when somebody is being treated for gastric cancer, because if they don’t have a strong support system – and marital status can be a proxy for that – then they may need more intensive follow-up and surveillance, for example, than somebody who does not have that support system.”
Exploring the marital status–cancer survival connection
Gastric cancer is the third leading cause of cancer deaths across the world, causing 780,000 deaths in 2018, the authors note. Yet it’s difficult to accurately predict the prognosis in patients who undergo treatment for early stage gastric cancer. Previous research has found marital status to be associated with survival in prostate, cervical, and rectal cancers.
Mark A. Lewis, MD, director of gastrointestinal oncology at Intermountain Healthcare Cancer Center, Utah, told this news organization that the connection between marital status and cancer outcomes has been described previously, including in an even larger analysis using the U.S. Surveillance, Epidemiology, and End Results (SEER) database from 2013. That study found that “unmarried patients are at significantly higher risk of presentation with metastatic cancer, undertreatment, and death resulting from their cancer.”
In this study, the researchers compared marital status and survival rates among 3,647 patients with early-stage gastric cancer, using data from the SEER database. The study only included patients with tumors in the lamina propria, mucosa, and submucosa and excluded those with distant metastasis or distant lymph node metastases, a second cancer, no data on chemotherapy received, or unknown survival time.
Because they were using a nomogram and building a new predictive nomogram that would include marital status, the researchers divided the patient population into a training set of 2,719 patients and a testing set of 928 patients. Using overall survival as the primary endpoint, the analysis included the variables of “age at diagnosis, race, gender, tumor location, histology, grade, stage_T and stage_N, surgery in the primary site, lymph node dissection, chemotherapy, radiation, tumor size, insurance, and marital status,” the authors report.
Among the study population, 53.7% were married, 17.3% were widowed, 14% were single and never married, 7.5% were divorced, 1.1% were separated, and the status of 6.4% was unknown. Age at diagnosis, race, gender, histology, tumor grade, stage T, stage N, surgery type, tumor size, and insurance status were all significantly different between the marital status subgroups.
Married patients had the best prognosis, with an average overall survival of 72 months, compared with an average 60 months in widowed persons, the group with the poorest overall survival. Overall survival was higher in married women (76 months) than in married men (69 months). The same pattern held for women (62 months) and men (52 months) who had been widowed.
“It is worthy to note that survival was significantly better in divorced female patients than in divorced male patients,” the authors report. “Survival was better in female patients than in male patients” across all marital groups.
What long-term relationships reveal
These findings do not mean that simply getting married changes one’s likelihood of survival, however. Rather, a long-term relationship is revealing about other aspects in a person’s life.
“I think it represents more stability in the supportive relationship that you need to really deal with a serious disease like cancer,” Dr. Peek said.
If a patient does not have a long-term partner, their care team can ask other questions to get a sense of what their support network is like, Dr. Peek added. “We want to know, does anybody else live in the house with them? Do they have adequate transportation? Can they make medical appointments? Do they have somebody who can help with the medical issues that are going to come up? Do they have family in the area?”
Cancer treatment requires a multidisciplinary approach, and having someone other than just the patient around to help bring together the different aspects of care from different care teams can make a difference in how the patient fares, Dr. Peek explained. Patients without a strong support system may need closer follow-up and other accommodations, he said.
Providers “may schedule their clinical appointments closer together if they don’t have a support system, or they may be able to reach out and offer transportation assistance and those kinds of things that somebody living alone may need,” Dr. Peek said. Outside resources may be a higher priority for those who lack a support system at home, he added.
Dr. Peek also noted other factors that may play a role in a patient’s survival that these researchers did not have the data to address, such as socioeconomic status, employment, alcohol use, smoking, and infection with Helicobacter pylori, the strongest known risk factor for gastric cancer.
A potentially relevant limitation of the study is that it probably has some selection bias, because the patients who were included probably had the means to have received an earlier diagnosis, said Dr. Lewis, who was not involved in the research.
“Furthermore, just in terms of the group sizes, the baseline characteristics section makes it clear that the preponderance of patients were married, lending that group more statistical weight,” Dr. Lewis said.
“Of the seven attributes in the nomogram, the impact of the marital status seems comparatively meager relative to conventional clinicopathology risk factors like T stage,” he added.
“All in all, I think this study reinforces our awareness that socioeconomic status and social determinants of health play a huge role in cancer outcomes, but it’s not entirely clear that’s modifiable just by getting married,” Dr. Lewis said. “There is a saying in oncology that ‘expensive liquor causes less cancer than cheap liquor,’ which is not negating the carcinogenicity of alcohol but rather identifying different outcomes by socioeconomic status.”
The research was funded by the Natural Science Foundation of Anhui Province. The authors report no relevant financial relationships. Dr. Peek reports no relevant financial relationships. Dr. Lewis reports receiving speaking fees for AstraZeneca/Daiichi Sankyo and having done educational videos for Astellas.
A version of this article first appeared on Medscape.com.
, according to research published in the Journal of Investigative Medicine.
Tumor size remained the largest contributor to overall survival, but marital status was among several other significant factors, such as age, race, gender, treatment style, and pathologic stage, that can provide insight into a patient’s likelihood of overall survival, as it does with several other cancers.
“Married patients had the best prognosis, followed by single patients, and the prognosis of separated patients was the worst,” write Lixiang Zhang and colleagues at the First Affiliated Hospital of Anhui Medical University, Hefei, China. “We speculate that this might be due to the fact that married patients had better financial conditions and emotional encouragement, while separated patients might be more likely to experience financial difficulties [and] emotional loss.”
The results were not necessarily surprising to Richard M. Peek, Jr., MD, director of the division of gastroenterology and a professor of medicine at Vanderbilt University Medical Center, who was not involved in the research.
“Marital status is a reflection of support systems, and a strong support system is a prognosticator for increased compliance with medical appointments and medical therapies,” Dr. Peek told this news organization. “It is something to consider when somebody is being treated for gastric cancer, because if they don’t have a strong support system – and marital status can be a proxy for that – then they may need more intensive follow-up and surveillance, for example, than somebody who does not have that support system.”
Exploring the marital status–cancer survival connection
Gastric cancer is the third leading cause of cancer deaths across the world, causing 780,000 deaths in 2018, the authors note. Yet it’s difficult to accurately predict the prognosis in patients who undergo treatment for early stage gastric cancer. Previous research has found marital status to be associated with survival in prostate, cervical, and rectal cancers.
Mark A. Lewis, MD, director of gastrointestinal oncology at Intermountain Healthcare Cancer Center, Utah, told this news organization that the connection between marital status and cancer outcomes has been described previously, including in an even larger analysis using the U.S. Surveillance, Epidemiology, and End Results (SEER) database from 2013. That study found that “unmarried patients are at significantly higher risk of presentation with metastatic cancer, undertreatment, and death resulting from their cancer.”
In this study, the researchers compared marital status and survival rates among 3,647 patients with early-stage gastric cancer, using data from the SEER database. The study only included patients with tumors in the lamina propria, mucosa, and submucosa and excluded those with distant metastasis or distant lymph node metastases, a second cancer, no data on chemotherapy received, or unknown survival time.
Because they were using a nomogram and building a new predictive nomogram that would include marital status, the researchers divided the patient population into a training set of 2,719 patients and a testing set of 928 patients. Using overall survival as the primary endpoint, the analysis included the variables of “age at diagnosis, race, gender, tumor location, histology, grade, stage_T and stage_N, surgery in the primary site, lymph node dissection, chemotherapy, radiation, tumor size, insurance, and marital status,” the authors report.
Among the study population, 53.7% were married, 17.3% were widowed, 14% were single and never married, 7.5% were divorced, 1.1% were separated, and the status of 6.4% was unknown. Age at diagnosis, race, gender, histology, tumor grade, stage T, stage N, surgery type, tumor size, and insurance status were all significantly different between the marital status subgroups.
Married patients had the best prognosis, with an average overall survival of 72 months, compared with an average 60 months in widowed persons, the group with the poorest overall survival. Overall survival was higher in married women (76 months) than in married men (69 months). The same pattern held for women (62 months) and men (52 months) who had been widowed.
“It is worthy to note that survival was significantly better in divorced female patients than in divorced male patients,” the authors report. “Survival was better in female patients than in male patients” across all marital groups.
What long-term relationships reveal
These findings do not mean that simply getting married changes one’s likelihood of survival, however. Rather, a long-term relationship is revealing about other aspects in a person’s life.
“I think it represents more stability in the supportive relationship that you need to really deal with a serious disease like cancer,” Dr. Peek said.
If a patient does not have a long-term partner, their care team can ask other questions to get a sense of what their support network is like, Dr. Peek added. “We want to know, does anybody else live in the house with them? Do they have adequate transportation? Can they make medical appointments? Do they have somebody who can help with the medical issues that are going to come up? Do they have family in the area?”
Cancer treatment requires a multidisciplinary approach, and having someone other than just the patient around to help bring together the different aspects of care from different care teams can make a difference in how the patient fares, Dr. Peek explained. Patients without a strong support system may need closer follow-up and other accommodations, he said.
Providers “may schedule their clinical appointments closer together if they don’t have a support system, or they may be able to reach out and offer transportation assistance and those kinds of things that somebody living alone may need,” Dr. Peek said. Outside resources may be a higher priority for those who lack a support system at home, he added.
Dr. Peek also noted other factors that may play a role in a patient’s survival that these researchers did not have the data to address, such as socioeconomic status, employment, alcohol use, smoking, and infection with Helicobacter pylori, the strongest known risk factor for gastric cancer.
A potentially relevant limitation of the study is that it probably has some selection bias, because the patients who were included probably had the means to have received an earlier diagnosis, said Dr. Lewis, who was not involved in the research.
“Furthermore, just in terms of the group sizes, the baseline characteristics section makes it clear that the preponderance of patients were married, lending that group more statistical weight,” Dr. Lewis said.
“Of the seven attributes in the nomogram, the impact of the marital status seems comparatively meager relative to conventional clinicopathology risk factors like T stage,” he added.
“All in all, I think this study reinforces our awareness that socioeconomic status and social determinants of health play a huge role in cancer outcomes, but it’s not entirely clear that’s modifiable just by getting married,” Dr. Lewis said. “There is a saying in oncology that ‘expensive liquor causes less cancer than cheap liquor,’ which is not negating the carcinogenicity of alcohol but rather identifying different outcomes by socioeconomic status.”
The research was funded by the Natural Science Foundation of Anhui Province. The authors report no relevant financial relationships. Dr. Peek reports no relevant financial relationships. Dr. Lewis reports receiving speaking fees for AstraZeneca/Daiichi Sankyo and having done educational videos for Astellas.
A version of this article first appeared on Medscape.com.
, according to research published in the Journal of Investigative Medicine.
Tumor size remained the largest contributor to overall survival, but marital status was among several other significant factors, such as age, race, gender, treatment style, and pathologic stage, that can provide insight into a patient’s likelihood of overall survival, as it does with several other cancers.
“Married patients had the best prognosis, followed by single patients, and the prognosis of separated patients was the worst,” write Lixiang Zhang and colleagues at the First Affiliated Hospital of Anhui Medical University, Hefei, China. “We speculate that this might be due to the fact that married patients had better financial conditions and emotional encouragement, while separated patients might be more likely to experience financial difficulties [and] emotional loss.”
The results were not necessarily surprising to Richard M. Peek, Jr., MD, director of the division of gastroenterology and a professor of medicine at Vanderbilt University Medical Center, who was not involved in the research.
“Marital status is a reflection of support systems, and a strong support system is a prognosticator for increased compliance with medical appointments and medical therapies,” Dr. Peek told this news organization. “It is something to consider when somebody is being treated for gastric cancer, because if they don’t have a strong support system – and marital status can be a proxy for that – then they may need more intensive follow-up and surveillance, for example, than somebody who does not have that support system.”
Exploring the marital status–cancer survival connection
Gastric cancer is the third leading cause of cancer deaths across the world, causing 780,000 deaths in 2018, the authors note. Yet it’s difficult to accurately predict the prognosis in patients who undergo treatment for early stage gastric cancer. Previous research has found marital status to be associated with survival in prostate, cervical, and rectal cancers.
Mark A. Lewis, MD, director of gastrointestinal oncology at Intermountain Healthcare Cancer Center, Utah, told this news organization that the connection between marital status and cancer outcomes has been described previously, including in an even larger analysis using the U.S. Surveillance, Epidemiology, and End Results (SEER) database from 2013. That study found that “unmarried patients are at significantly higher risk of presentation with metastatic cancer, undertreatment, and death resulting from their cancer.”
In this study, the researchers compared marital status and survival rates among 3,647 patients with early-stage gastric cancer, using data from the SEER database. The study only included patients with tumors in the lamina propria, mucosa, and submucosa and excluded those with distant metastasis or distant lymph node metastases, a second cancer, no data on chemotherapy received, or unknown survival time.
Because they were using a nomogram and building a new predictive nomogram that would include marital status, the researchers divided the patient population into a training set of 2,719 patients and a testing set of 928 patients. Using overall survival as the primary endpoint, the analysis included the variables of “age at diagnosis, race, gender, tumor location, histology, grade, stage_T and stage_N, surgery in the primary site, lymph node dissection, chemotherapy, radiation, tumor size, insurance, and marital status,” the authors report.
Among the study population, 53.7% were married, 17.3% were widowed, 14% were single and never married, 7.5% were divorced, 1.1% were separated, and the status of 6.4% was unknown. Age at diagnosis, race, gender, histology, tumor grade, stage T, stage N, surgery type, tumor size, and insurance status were all significantly different between the marital status subgroups.
Married patients had the best prognosis, with an average overall survival of 72 months, compared with an average 60 months in widowed persons, the group with the poorest overall survival. Overall survival was higher in married women (76 months) than in married men (69 months). The same pattern held for women (62 months) and men (52 months) who had been widowed.
“It is worthy to note that survival was significantly better in divorced female patients than in divorced male patients,” the authors report. “Survival was better in female patients than in male patients” across all marital groups.
What long-term relationships reveal
These findings do not mean that simply getting married changes one’s likelihood of survival, however. Rather, a long-term relationship is revealing about other aspects in a person’s life.
“I think it represents more stability in the supportive relationship that you need to really deal with a serious disease like cancer,” Dr. Peek said.
If a patient does not have a long-term partner, their care team can ask other questions to get a sense of what their support network is like, Dr. Peek added. “We want to know, does anybody else live in the house with them? Do they have adequate transportation? Can they make medical appointments? Do they have somebody who can help with the medical issues that are going to come up? Do they have family in the area?”
Cancer treatment requires a multidisciplinary approach, and having someone other than just the patient around to help bring together the different aspects of care from different care teams can make a difference in how the patient fares, Dr. Peek explained. Patients without a strong support system may need closer follow-up and other accommodations, he said.
Providers “may schedule their clinical appointments closer together if they don’t have a support system, or they may be able to reach out and offer transportation assistance and those kinds of things that somebody living alone may need,” Dr. Peek said. Outside resources may be a higher priority for those who lack a support system at home, he added.
Dr. Peek also noted other factors that may play a role in a patient’s survival that these researchers did not have the data to address, such as socioeconomic status, employment, alcohol use, smoking, and infection with Helicobacter pylori, the strongest known risk factor for gastric cancer.
A potentially relevant limitation of the study is that it probably has some selection bias, because the patients who were included probably had the means to have received an earlier diagnosis, said Dr. Lewis, who was not involved in the research.
“Furthermore, just in terms of the group sizes, the baseline characteristics section makes it clear that the preponderance of patients were married, lending that group more statistical weight,” Dr. Lewis said.
“Of the seven attributes in the nomogram, the impact of the marital status seems comparatively meager relative to conventional clinicopathology risk factors like T stage,” he added.
“All in all, I think this study reinforces our awareness that socioeconomic status and social determinants of health play a huge role in cancer outcomes, but it’s not entirely clear that’s modifiable just by getting married,” Dr. Lewis said. “There is a saying in oncology that ‘expensive liquor causes less cancer than cheap liquor,’ which is not negating the carcinogenicity of alcohol but rather identifying different outcomes by socioeconomic status.”
The research was funded by the Natural Science Foundation of Anhui Province. The authors report no relevant financial relationships. Dr. Peek reports no relevant financial relationships. Dr. Lewis reports receiving speaking fees for AstraZeneca/Daiichi Sankyo and having done educational videos for Astellas.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF INVESTIGATIVE MEDICINE
Drug shortages plague hematology, but preparedness helps
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.
The shifting sands of lung cancer screening
An analysis of trends in lung cancer screening since March 2021 when the U.S. Preventive Services Task Force (USPSTF) expanded the eligibility criteria for lung cancer screening, shows that significantly more Black men have been screened for lung cancer, but not women or undereducated people.
The eligibility for lung cancer screening was expanded in 2021 to include men and women under 50 years old and people who smoke at least one pack of cigarettes a day for the last 20 years. “
“Expansion of screening criteria is a critical first step to achieving equity in lung cancer screening for all high-risk populations, but myriad challenges remain before individuals enter the door for screening,” wrote the authors, led by Julie A. Barta, MD, Thomas Jefferson University, Philadelphia. “Health policy changes must occur simultaneously with efforts to expand community outreach, overcome logistical barriers, and facilitate screening adherence. Only after comprehensive strategies to dismantle screening barriers are identified, validated, and implemented can there be a truly equitable landscape for lung cancer screening.”
For the study, published in JAMA Open Network, researchers examined rates of centralized lung cancer screening in the Baltimore area. In addition to expanding lung cancer screening generally, there was hope that the expanded criteria might increase uptake of screening in populations that are traditionally underserved, such as African American, Hispanic, and female patients. Of 815 people screened during the study period (March-December 2021), 161 were newly eligible for screening under the 2021 criteria.
“There’s been quite a bit of work in the field demonstrating that Black men and women develop lung cancer at more advanced stages of disease, and they often are diagnosed at younger ages and have fewer pack-years of smoking. So the hypothesis was that this would reduce some of the disparities seen in lung cancer screening by making more people eligible,” Dr. Barta said in an interview.
The researchers categorized participants as those who would have been eligible for screening under the USPSTF 2013 guideline (age 55 or older, 30 or more pack-years, quit within the past 15 years), and those who would be eligible under the 2021 guideline (age 50 or older, 20 or more pack-years, quit within the past 15 years). Of the 2021 cohort, 54.5% were African American, versus 39.5% of the 2013 cohort (P = .002). There were no differences between the cohorts with respect to education level or gender.
“Although we’ve seen some encouraging improvement in terms of getting more eligible patients into our screening program, there’s still a lot of work to be done in the field,” Dr. Barta said. “Diagnosing lung cancer at earlier stages of disease is more cost effective in general for the health care system than fighting lung cancer at advanced stages, which requires more complex and multimodal and prolonged therapies.”
New evidence: Chest CTs for lung cancer screening reduces incidence of advanced lung cancer
In an analysis of the SEER database presented in June at the annual meeting of the American Society of Clinical Oncology, the adoption of low-dose chest computed tomography (LDCT) led to fewer diagnoses of advanced lung cancer, although these declines varied significantly by race and ethnicity. Non-Hispanic Blacks seemed to benefit the most with a 55% decline (P < .01), while Hispanics had the lowest rate of decline at 41% (P < .01). The change was recommended by USPSTF in 2013 after the National Lung Screening Trial revealed a 20% relative reduction in mortality when CT scans were used instead of chest radiography. The Centers for Medicare and Medicaid Services approved coverage of the screen in 2015.
The SEER study looked at data from 400,343 individuals from 2004-2014 (preintervention) and 2015-2018 (postintervention). The age-adjusted incidence of advanced lung cancer declined during both periods, but the decline was sharper between 2015 and 2018, with three fewer cases per 100,000 people than 2004-2014 (P < .01). Similar patterns were seen in subanalyses of males and females, non-Hispanic Whites, non-Hispanic Blacks, and Hispanics. The relative declines were largest in women, non-Hispanic Blacks, and people who lived outside of Metropolitan areas.
During a Q&A session that followed the presentation, Robert Smith, PhD, pointed out that the bar for eligibility of lung cancer risk has been set quite high, following the eligibility criteria for clinical trials. He noted that . “We are missing opportunities to prevent avertable lung cancer deaths,” said Dr. Smith, senior vice president of cancer screening at the American Cancer Society.
On the other hand, screening-prompted biopsies have the potential to cause harm, particularly in patients who already have lung disease, said Douglas Allen Arenberg, MD, professor at the University of Michigan, Ann Arbor. “I think that’s what scares most people is the potential downside, which is very hard to measure outside of a clinical trial,” said Dr. Arenberg, who served as a discussant for the presentation.
One way to reduce that risk is to identify biomarkers, either for screens or for incidentally-detected nodules, that have good negative predictive value. “If I had a blood test that is as good as a negative PET scan, I’m going to be much more likely to say, ‘Yeah, you’re 40 and your grandfather had lung cancer. Maybe you should get a CT. If we had that, we could screen a lot more people. Right now, I would discourage anybody who is at low risk from getting screened because when they come to me, the biggest opportunity I have to do harm is when I do a biopsy, and you always remember the ones that go wrong,” he said.
Dr. Arenberg also called for improvements in electronic medical records to better flag at-risk patients. “I think we as physicians have to demand more of the software developers that create these EMRs for us,” he said.
Another study in the same session used data from 1,391,088 patients drawn from the National Cancer Database between 2010 and 2017 to examine trends in diagnosis of stage I cancer. In 2010, 23.5% of patients were diagnosed as stage I, versus 29.1% in 2017. Stage I incidence increased from 25.8% to 31.7% in non–small cell lung cancer, but there was no statistically significant change in small cell lung cancer. As with the SEER database study, the researchers noted that the shift toward stage I diagnoses predated the recommendation of LDCT.
Dr. Arenberg suggested that the trend may come down to increased frequency of CT scans, which often collect incidental images of the lungs. He added that better access to care may also be helping to drive the change. “How much of that might have had something to do with the introduction 5 or 10 years earlier of the Affordable Care Act and people just simply having access to care and taking advantage of that?” Dr. Arenberg said.
But Dr. Arenberg said that not even screening can explain all the data. He referenced a stage shift in patients of all age groups in the National Cancer Database study, even those too young to be eligible for screening. “There’s something else going on here. It would be nice for us to understand what caused these trends, so perhaps we could accentuate that trend even more, but stage shifts are clearly occurring in lung cancer,” Dr. Arenberg said.
Dr. Barta has received grants from Genentech Health Equity Innovations Fund. Dr. Arenberg has no relevant financial disclosures. Dr. Smith’s potential disclosures could not be ascertained.
An analysis of trends in lung cancer screening since March 2021 when the U.S. Preventive Services Task Force (USPSTF) expanded the eligibility criteria for lung cancer screening, shows that significantly more Black men have been screened for lung cancer, but not women or undereducated people.
The eligibility for lung cancer screening was expanded in 2021 to include men and women under 50 years old and people who smoke at least one pack of cigarettes a day for the last 20 years. “
“Expansion of screening criteria is a critical first step to achieving equity in lung cancer screening for all high-risk populations, but myriad challenges remain before individuals enter the door for screening,” wrote the authors, led by Julie A. Barta, MD, Thomas Jefferson University, Philadelphia. “Health policy changes must occur simultaneously with efforts to expand community outreach, overcome logistical barriers, and facilitate screening adherence. Only after comprehensive strategies to dismantle screening barriers are identified, validated, and implemented can there be a truly equitable landscape for lung cancer screening.”
For the study, published in JAMA Open Network, researchers examined rates of centralized lung cancer screening in the Baltimore area. In addition to expanding lung cancer screening generally, there was hope that the expanded criteria might increase uptake of screening in populations that are traditionally underserved, such as African American, Hispanic, and female patients. Of 815 people screened during the study period (March-December 2021), 161 were newly eligible for screening under the 2021 criteria.
“There’s been quite a bit of work in the field demonstrating that Black men and women develop lung cancer at more advanced stages of disease, and they often are diagnosed at younger ages and have fewer pack-years of smoking. So the hypothesis was that this would reduce some of the disparities seen in lung cancer screening by making more people eligible,” Dr. Barta said in an interview.
The researchers categorized participants as those who would have been eligible for screening under the USPSTF 2013 guideline (age 55 or older, 30 or more pack-years, quit within the past 15 years), and those who would be eligible under the 2021 guideline (age 50 or older, 20 or more pack-years, quit within the past 15 years). Of the 2021 cohort, 54.5% were African American, versus 39.5% of the 2013 cohort (P = .002). There were no differences between the cohorts with respect to education level or gender.
“Although we’ve seen some encouraging improvement in terms of getting more eligible patients into our screening program, there’s still a lot of work to be done in the field,” Dr. Barta said. “Diagnosing lung cancer at earlier stages of disease is more cost effective in general for the health care system than fighting lung cancer at advanced stages, which requires more complex and multimodal and prolonged therapies.”
New evidence: Chest CTs for lung cancer screening reduces incidence of advanced lung cancer
In an analysis of the SEER database presented in June at the annual meeting of the American Society of Clinical Oncology, the adoption of low-dose chest computed tomography (LDCT) led to fewer diagnoses of advanced lung cancer, although these declines varied significantly by race and ethnicity. Non-Hispanic Blacks seemed to benefit the most with a 55% decline (P < .01), while Hispanics had the lowest rate of decline at 41% (P < .01). The change was recommended by USPSTF in 2013 after the National Lung Screening Trial revealed a 20% relative reduction in mortality when CT scans were used instead of chest radiography. The Centers for Medicare and Medicaid Services approved coverage of the screen in 2015.
The SEER study looked at data from 400,343 individuals from 2004-2014 (preintervention) and 2015-2018 (postintervention). The age-adjusted incidence of advanced lung cancer declined during both periods, but the decline was sharper between 2015 and 2018, with three fewer cases per 100,000 people than 2004-2014 (P < .01). Similar patterns were seen in subanalyses of males and females, non-Hispanic Whites, non-Hispanic Blacks, and Hispanics. The relative declines were largest in women, non-Hispanic Blacks, and people who lived outside of Metropolitan areas.
During a Q&A session that followed the presentation, Robert Smith, PhD, pointed out that the bar for eligibility of lung cancer risk has been set quite high, following the eligibility criteria for clinical trials. He noted that . “We are missing opportunities to prevent avertable lung cancer deaths,” said Dr. Smith, senior vice president of cancer screening at the American Cancer Society.
On the other hand, screening-prompted biopsies have the potential to cause harm, particularly in patients who already have lung disease, said Douglas Allen Arenberg, MD, professor at the University of Michigan, Ann Arbor. “I think that’s what scares most people is the potential downside, which is very hard to measure outside of a clinical trial,” said Dr. Arenberg, who served as a discussant for the presentation.
One way to reduce that risk is to identify biomarkers, either for screens or for incidentally-detected nodules, that have good negative predictive value. “If I had a blood test that is as good as a negative PET scan, I’m going to be much more likely to say, ‘Yeah, you’re 40 and your grandfather had lung cancer. Maybe you should get a CT. If we had that, we could screen a lot more people. Right now, I would discourage anybody who is at low risk from getting screened because when they come to me, the biggest opportunity I have to do harm is when I do a biopsy, and you always remember the ones that go wrong,” he said.
Dr. Arenberg also called for improvements in electronic medical records to better flag at-risk patients. “I think we as physicians have to demand more of the software developers that create these EMRs for us,” he said.
Another study in the same session used data from 1,391,088 patients drawn from the National Cancer Database between 2010 and 2017 to examine trends in diagnosis of stage I cancer. In 2010, 23.5% of patients were diagnosed as stage I, versus 29.1% in 2017. Stage I incidence increased from 25.8% to 31.7% in non–small cell lung cancer, but there was no statistically significant change in small cell lung cancer. As with the SEER database study, the researchers noted that the shift toward stage I diagnoses predated the recommendation of LDCT.
Dr. Arenberg suggested that the trend may come down to increased frequency of CT scans, which often collect incidental images of the lungs. He added that better access to care may also be helping to drive the change. “How much of that might have had something to do with the introduction 5 or 10 years earlier of the Affordable Care Act and people just simply having access to care and taking advantage of that?” Dr. Arenberg said.
But Dr. Arenberg said that not even screening can explain all the data. He referenced a stage shift in patients of all age groups in the National Cancer Database study, even those too young to be eligible for screening. “There’s something else going on here. It would be nice for us to understand what caused these trends, so perhaps we could accentuate that trend even more, but stage shifts are clearly occurring in lung cancer,” Dr. Arenberg said.
Dr. Barta has received grants from Genentech Health Equity Innovations Fund. Dr. Arenberg has no relevant financial disclosures. Dr. Smith’s potential disclosures could not be ascertained.
An analysis of trends in lung cancer screening since March 2021 when the U.S. Preventive Services Task Force (USPSTF) expanded the eligibility criteria for lung cancer screening, shows that significantly more Black men have been screened for lung cancer, but not women or undereducated people.
The eligibility for lung cancer screening was expanded in 2021 to include men and women under 50 years old and people who smoke at least one pack of cigarettes a day for the last 20 years. “
“Expansion of screening criteria is a critical first step to achieving equity in lung cancer screening for all high-risk populations, but myriad challenges remain before individuals enter the door for screening,” wrote the authors, led by Julie A. Barta, MD, Thomas Jefferson University, Philadelphia. “Health policy changes must occur simultaneously with efforts to expand community outreach, overcome logistical barriers, and facilitate screening adherence. Only after comprehensive strategies to dismantle screening barriers are identified, validated, and implemented can there be a truly equitable landscape for lung cancer screening.”
For the study, published in JAMA Open Network, researchers examined rates of centralized lung cancer screening in the Baltimore area. In addition to expanding lung cancer screening generally, there was hope that the expanded criteria might increase uptake of screening in populations that are traditionally underserved, such as African American, Hispanic, and female patients. Of 815 people screened during the study period (March-December 2021), 161 were newly eligible for screening under the 2021 criteria.
“There’s been quite a bit of work in the field demonstrating that Black men and women develop lung cancer at more advanced stages of disease, and they often are diagnosed at younger ages and have fewer pack-years of smoking. So the hypothesis was that this would reduce some of the disparities seen in lung cancer screening by making more people eligible,” Dr. Barta said in an interview.
The researchers categorized participants as those who would have been eligible for screening under the USPSTF 2013 guideline (age 55 or older, 30 or more pack-years, quit within the past 15 years), and those who would be eligible under the 2021 guideline (age 50 or older, 20 or more pack-years, quit within the past 15 years). Of the 2021 cohort, 54.5% were African American, versus 39.5% of the 2013 cohort (P = .002). There were no differences between the cohorts with respect to education level or gender.
“Although we’ve seen some encouraging improvement in terms of getting more eligible patients into our screening program, there’s still a lot of work to be done in the field,” Dr. Barta said. “Diagnosing lung cancer at earlier stages of disease is more cost effective in general for the health care system than fighting lung cancer at advanced stages, which requires more complex and multimodal and prolonged therapies.”
New evidence: Chest CTs for lung cancer screening reduces incidence of advanced lung cancer
In an analysis of the SEER database presented in June at the annual meeting of the American Society of Clinical Oncology, the adoption of low-dose chest computed tomography (LDCT) led to fewer diagnoses of advanced lung cancer, although these declines varied significantly by race and ethnicity. Non-Hispanic Blacks seemed to benefit the most with a 55% decline (P < .01), while Hispanics had the lowest rate of decline at 41% (P < .01). The change was recommended by USPSTF in 2013 after the National Lung Screening Trial revealed a 20% relative reduction in mortality when CT scans were used instead of chest radiography. The Centers for Medicare and Medicaid Services approved coverage of the screen in 2015.
The SEER study looked at data from 400,343 individuals from 2004-2014 (preintervention) and 2015-2018 (postintervention). The age-adjusted incidence of advanced lung cancer declined during both periods, but the decline was sharper between 2015 and 2018, with three fewer cases per 100,000 people than 2004-2014 (P < .01). Similar patterns were seen in subanalyses of males and females, non-Hispanic Whites, non-Hispanic Blacks, and Hispanics. The relative declines were largest in women, non-Hispanic Blacks, and people who lived outside of Metropolitan areas.
During a Q&A session that followed the presentation, Robert Smith, PhD, pointed out that the bar for eligibility of lung cancer risk has been set quite high, following the eligibility criteria for clinical trials. He noted that . “We are missing opportunities to prevent avertable lung cancer deaths,” said Dr. Smith, senior vice president of cancer screening at the American Cancer Society.
On the other hand, screening-prompted biopsies have the potential to cause harm, particularly in patients who already have lung disease, said Douglas Allen Arenberg, MD, professor at the University of Michigan, Ann Arbor. “I think that’s what scares most people is the potential downside, which is very hard to measure outside of a clinical trial,” said Dr. Arenberg, who served as a discussant for the presentation.
One way to reduce that risk is to identify biomarkers, either for screens or for incidentally-detected nodules, that have good negative predictive value. “If I had a blood test that is as good as a negative PET scan, I’m going to be much more likely to say, ‘Yeah, you’re 40 and your grandfather had lung cancer. Maybe you should get a CT. If we had that, we could screen a lot more people. Right now, I would discourage anybody who is at low risk from getting screened because when they come to me, the biggest opportunity I have to do harm is when I do a biopsy, and you always remember the ones that go wrong,” he said.
Dr. Arenberg also called for improvements in electronic medical records to better flag at-risk patients. “I think we as physicians have to demand more of the software developers that create these EMRs for us,” he said.
Another study in the same session used data from 1,391,088 patients drawn from the National Cancer Database between 2010 and 2017 to examine trends in diagnosis of stage I cancer. In 2010, 23.5% of patients were diagnosed as stage I, versus 29.1% in 2017. Stage I incidence increased from 25.8% to 31.7% in non–small cell lung cancer, but there was no statistically significant change in small cell lung cancer. As with the SEER database study, the researchers noted that the shift toward stage I diagnoses predated the recommendation of LDCT.
Dr. Arenberg suggested that the trend may come down to increased frequency of CT scans, which often collect incidental images of the lungs. He added that better access to care may also be helping to drive the change. “How much of that might have had something to do with the introduction 5 or 10 years earlier of the Affordable Care Act and people just simply having access to care and taking advantage of that?” Dr. Arenberg said.
But Dr. Arenberg said that not even screening can explain all the data. He referenced a stage shift in patients of all age groups in the National Cancer Database study, even those too young to be eligible for screening. “There’s something else going on here. It would be nice for us to understand what caused these trends, so perhaps we could accentuate that trend even more, but stage shifts are clearly occurring in lung cancer,” Dr. Arenberg said.
Dr. Barta has received grants from Genentech Health Equity Innovations Fund. Dr. Arenberg has no relevant financial disclosures. Dr. Smith’s potential disclosures could not be ascertained.
FROM JAMA NETWORK OPEN
Moderate drinking shows more benefit for older vs. younger adults
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.

“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.
“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.
“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
FROM THE LANCET
Risky business: Most cancer drugs don’t reach the market
, a new analysis suggests.
The researchers also found that about 8% of approved agents were subsequently taken off the market.
“The 6% is not a big surprise to us, since a few other studies using different methodologies and foci have estimated similar percentages,” Alyson Haslam, PhD, University of California, San Francisco, told this news organization. “When you look at drug development, it makes sense that you have to test a lot of drugs to get one that works, but sometimes it is nice to quantify the actual percentage in order to fully appreciate the process.”
The fact that 8% were withdrawn, however, “elicits the question of how the approval process can be improved to avoid ineffective or harmful drugs from coming onto the market,” Dr. Haslam added.
The study was published online in the International Journal of Cancer.
More desirable features?
Monitoring trends over time helps oncologists assess whether more drugs are making it to market and if certain factors make some drugs more likely to get approved.
Prior published estimates put the likelihood of approval between 6.7% and 13.4%, but these estimates were for drugs tested more than a decade ago.
To provide updated estimates, the researchers searched the literature for all oncology drugs tested in phase 1 studies during 2015 and evaluated their fate in subsequent phase 2/3 studies through FDA clearance.
Overall, the team found 803 phase 1 studies that met initial inclusion criteria; 48 trials that included only Japanese participants were excluded because these studies often evaluated drugs already approved in the United States, leaving 755 studies for the analysis.
The most common tumor types were solid/multiple tumors (24.2%), leukemias (12.8%), and lung cancer (8.5%). Just under half (47%) of the trials tested a drug as monotherapy; 43% were combination trials with one dose-escalated drug; and about 10% were combination trials with both drugs dose-escalated.
The FDA approved 51 drugs during the study period. Four (7.8%) were subsequently withdrawn: nivolumab (Opdivo) and pembrolizumab (Keytruda) for small cell lung cancer, olaratumab (Lartruvo) for soft tissue sarcoma, and melflufen (Pepaxto) for multiple myeloma. These four were not counted in the overall number of approvals.
“We really wanted to look at the end fate of drugs (within a reasonable time frame), which is why we did not include the four drugs that were initially approved but later withdrawn, although this had little impact on the main finding,” Dr. Haslam explained.
The estimated probability of any drug or drug combination tested in a phase 1 trial published in 2015 and approved that year was 1.7% and reached 6.2% by the end of 2021, the researchers found.
Monoclonal antibodies had a higher probability of being approved (15.3%), compared with inhibitors (5.1%) and chemotherapy drugs (4.2%).
The FDA was also more apt to green-light drugs tested as monotherapy, compared with drug combinations (odds ratio, 0.22). Drugs tested in monotherapy had a 9.4% probability of approval versus those tested in combination, which had a 5.6% probability of being approved when pairing a novel drug with one or more established agents, as well as when combining two novel drugs. The probability of approval was less than 1% for trials testing two established drug combinations.
Other factors that boosted the odds of FDA approval include having a response rate over 40% in phase 1 testing, demonstrating an overall survival benefit in phase 3 testing, and having the trial sponsored by a top-20 drug company, compared with a non–top-20 drug company.
Dr. Haslam found the last finding rather surprising, given the recent trend for bigger companies to invest in smaller companies who are developing promising drugs, rather than doing all of the development themselves. “In fact, a recent analysis found that only 25% of new drugs are sponsored by larger companies,” she noted.
Reached for comment, Jeff Allen, PhD, who wasn’t involved in the study, noted that “these types of landscape analyses are quite helpful in understanding the current state of oncology science and drug development.”
When looking at a 6.2% success rate for phase 1–tested oncology drugs, “it can be difficult holistically to determine all factors for which development didn’t continue,” said Dr. Allen, president and CEO of the nonprofit Friends of Cancer Research.
For instance, lack of approval may not signal the drug was a failure “but rather an artifact of circumstances such as resource limitations or reprioritization,” Dr. Allen said.
Plus, he commented, “I don’t think that we should expect all these early studies to lead to eventual approvals, but it’s clear from the authors’ findings that continued efforts to improve the overall success rate in developing new cancer medicines are greatly needed.”
The study was funded by Arnold Ventures. Dr. Haslam and Dr. Allen have no relevant disclosures. Study author Vinay Prasad, MD, MPH, receives royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The researchers also found that about 8% of approved agents were subsequently taken off the market.
“The 6% is not a big surprise to us, since a few other studies using different methodologies and foci have estimated similar percentages,” Alyson Haslam, PhD, University of California, San Francisco, told this news organization. “When you look at drug development, it makes sense that you have to test a lot of drugs to get one that works, but sometimes it is nice to quantify the actual percentage in order to fully appreciate the process.”
The fact that 8% were withdrawn, however, “elicits the question of how the approval process can be improved to avoid ineffective or harmful drugs from coming onto the market,” Dr. Haslam added.
The study was published online in the International Journal of Cancer.
More desirable features?
Monitoring trends over time helps oncologists assess whether more drugs are making it to market and if certain factors make some drugs more likely to get approved.
Prior published estimates put the likelihood of approval between 6.7% and 13.4%, but these estimates were for drugs tested more than a decade ago.
To provide updated estimates, the researchers searched the literature for all oncology drugs tested in phase 1 studies during 2015 and evaluated their fate in subsequent phase 2/3 studies through FDA clearance.
Overall, the team found 803 phase 1 studies that met initial inclusion criteria; 48 trials that included only Japanese participants were excluded because these studies often evaluated drugs already approved in the United States, leaving 755 studies for the analysis.
The most common tumor types were solid/multiple tumors (24.2%), leukemias (12.8%), and lung cancer (8.5%). Just under half (47%) of the trials tested a drug as monotherapy; 43% were combination trials with one dose-escalated drug; and about 10% were combination trials with both drugs dose-escalated.
The FDA approved 51 drugs during the study period. Four (7.8%) were subsequently withdrawn: nivolumab (Opdivo) and pembrolizumab (Keytruda) for small cell lung cancer, olaratumab (Lartruvo) for soft tissue sarcoma, and melflufen (Pepaxto) for multiple myeloma. These four were not counted in the overall number of approvals.
“We really wanted to look at the end fate of drugs (within a reasonable time frame), which is why we did not include the four drugs that were initially approved but later withdrawn, although this had little impact on the main finding,” Dr. Haslam explained.
The estimated probability of any drug or drug combination tested in a phase 1 trial published in 2015 and approved that year was 1.7% and reached 6.2% by the end of 2021, the researchers found.
Monoclonal antibodies had a higher probability of being approved (15.3%), compared with inhibitors (5.1%) and chemotherapy drugs (4.2%).
The FDA was also more apt to green-light drugs tested as monotherapy, compared with drug combinations (odds ratio, 0.22). Drugs tested in monotherapy had a 9.4% probability of approval versus those tested in combination, which had a 5.6% probability of being approved when pairing a novel drug with one or more established agents, as well as when combining two novel drugs. The probability of approval was less than 1% for trials testing two established drug combinations.
Other factors that boosted the odds of FDA approval include having a response rate over 40% in phase 1 testing, demonstrating an overall survival benefit in phase 3 testing, and having the trial sponsored by a top-20 drug company, compared with a non–top-20 drug company.
Dr. Haslam found the last finding rather surprising, given the recent trend for bigger companies to invest in smaller companies who are developing promising drugs, rather than doing all of the development themselves. “In fact, a recent analysis found that only 25% of new drugs are sponsored by larger companies,” she noted.
Reached for comment, Jeff Allen, PhD, who wasn’t involved in the study, noted that “these types of landscape analyses are quite helpful in understanding the current state of oncology science and drug development.”
When looking at a 6.2% success rate for phase 1–tested oncology drugs, “it can be difficult holistically to determine all factors for which development didn’t continue,” said Dr. Allen, president and CEO of the nonprofit Friends of Cancer Research.
For instance, lack of approval may not signal the drug was a failure “but rather an artifact of circumstances such as resource limitations or reprioritization,” Dr. Allen said.
Plus, he commented, “I don’t think that we should expect all these early studies to lead to eventual approvals, but it’s clear from the authors’ findings that continued efforts to improve the overall success rate in developing new cancer medicines are greatly needed.”
The study was funded by Arnold Ventures. Dr. Haslam and Dr. Allen have no relevant disclosures. Study author Vinay Prasad, MD, MPH, receives royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The researchers also found that about 8% of approved agents were subsequently taken off the market.
“The 6% is not a big surprise to us, since a few other studies using different methodologies and foci have estimated similar percentages,” Alyson Haslam, PhD, University of California, San Francisco, told this news organization. “When you look at drug development, it makes sense that you have to test a lot of drugs to get one that works, but sometimes it is nice to quantify the actual percentage in order to fully appreciate the process.”
The fact that 8% were withdrawn, however, “elicits the question of how the approval process can be improved to avoid ineffective or harmful drugs from coming onto the market,” Dr. Haslam added.
The study was published online in the International Journal of Cancer.
More desirable features?
Monitoring trends over time helps oncologists assess whether more drugs are making it to market and if certain factors make some drugs more likely to get approved.
Prior published estimates put the likelihood of approval between 6.7% and 13.4%, but these estimates were for drugs tested more than a decade ago.
To provide updated estimates, the researchers searched the literature for all oncology drugs tested in phase 1 studies during 2015 and evaluated their fate in subsequent phase 2/3 studies through FDA clearance.
Overall, the team found 803 phase 1 studies that met initial inclusion criteria; 48 trials that included only Japanese participants were excluded because these studies often evaluated drugs already approved in the United States, leaving 755 studies for the analysis.
The most common tumor types were solid/multiple tumors (24.2%), leukemias (12.8%), and lung cancer (8.5%). Just under half (47%) of the trials tested a drug as monotherapy; 43% were combination trials with one dose-escalated drug; and about 10% were combination trials with both drugs dose-escalated.
The FDA approved 51 drugs during the study period. Four (7.8%) were subsequently withdrawn: nivolumab (Opdivo) and pembrolizumab (Keytruda) for small cell lung cancer, olaratumab (Lartruvo) for soft tissue sarcoma, and melflufen (Pepaxto) for multiple myeloma. These four were not counted in the overall number of approvals.
“We really wanted to look at the end fate of drugs (within a reasonable time frame), which is why we did not include the four drugs that were initially approved but later withdrawn, although this had little impact on the main finding,” Dr. Haslam explained.
The estimated probability of any drug or drug combination tested in a phase 1 trial published in 2015 and approved that year was 1.7% and reached 6.2% by the end of 2021, the researchers found.
Monoclonal antibodies had a higher probability of being approved (15.3%), compared with inhibitors (5.1%) and chemotherapy drugs (4.2%).
The FDA was also more apt to green-light drugs tested as monotherapy, compared with drug combinations (odds ratio, 0.22). Drugs tested in monotherapy had a 9.4% probability of approval versus those tested in combination, which had a 5.6% probability of being approved when pairing a novel drug with one or more established agents, as well as when combining two novel drugs. The probability of approval was less than 1% for trials testing two established drug combinations.
Other factors that boosted the odds of FDA approval include having a response rate over 40% in phase 1 testing, demonstrating an overall survival benefit in phase 3 testing, and having the trial sponsored by a top-20 drug company, compared with a non–top-20 drug company.
Dr. Haslam found the last finding rather surprising, given the recent trend for bigger companies to invest in smaller companies who are developing promising drugs, rather than doing all of the development themselves. “In fact, a recent analysis found that only 25% of new drugs are sponsored by larger companies,” she noted.
Reached for comment, Jeff Allen, PhD, who wasn’t involved in the study, noted that “these types of landscape analyses are quite helpful in understanding the current state of oncology science and drug development.”
When looking at a 6.2% success rate for phase 1–tested oncology drugs, “it can be difficult holistically to determine all factors for which development didn’t continue,” said Dr. Allen, president and CEO of the nonprofit Friends of Cancer Research.
For instance, lack of approval may not signal the drug was a failure “but rather an artifact of circumstances such as resource limitations or reprioritization,” Dr. Allen said.
Plus, he commented, “I don’t think that we should expect all these early studies to lead to eventual approvals, but it’s clear from the authors’ findings that continued efforts to improve the overall success rate in developing new cancer medicines are greatly needed.”
The study was funded by Arnold Ventures. Dr. Haslam and Dr. Allen have no relevant disclosures. Study author Vinay Prasad, MD, MPH, receives royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
FROM INTERNATIONAL JOURNAL OF CANCER
U.S. hot, cold spots of young-onset CRC may help target interventions
The so-called hot and cold spots of mortality from young-onset CRC differed slightly for people younger than 50 and those younger than 35, report the researchers, who say such studies may lead to better understanding of the underlying factors as well as to targeted interventions.
The authors suggest that deaths in the youngest young-onset CRC individuals “may be driven by a distinct set of factors, compared with deaths among older young-onset CRC and average-onset CRC patients.”
They add that “unmeasured factors ... may drive anomalous young-onset CRC mortality rates, either independently or in conjunction with demographic [and] modifiable variables accounted for here.”
The research was published online in Gastroenterology.
Incidence, mortality rates on the rise
The incidence and mortality rates of young-onset CRC have been increasing for decades, the authors write, but it has only recently begun to attract public health attention.
Risk factors and prognostic indicators, such as smoking, obesity, alcohol consumption, diabetes, sex, race, and socioeconomic factors, have been implicated in the development of the condition.
Geospatial distribution of young-onset CRC adds an “important [layer] for understanding the underlying drivers of mortality and allocating public health resources,” the authors write.
It is “too soon” to draw conclusions about the cause of the hot and cold spots, cautioned senior author Stephanie L. Schmit, PhD, vice chair of the Genomic Medicine Institute at the Lerner Research Institute, Cleveland Clinic.
Speaking to this news organization, she said, “Additional factors like proximity to primary care, gastroenterology, and cancer care facilities or novel environmental exposures may contribute to hot spots.”
On the other hand, “lifestyle factors like diet and exercise might contribute to some extent to cold spots,” she added.
While Dr. Schmit said it would be “challenging” to replicate the findings nationally, “further analyses at more granular geographic levels would be incredibly helpful.”
Exploring the geographical distribution
To explore the geographical distribution of young-onset CRC mortality, the researchers gathered 20 years of data on more than 1 million CRC deaths from 3,036 U.S. counties. With aggregated county-level information from 1999 to 2019, they derived mortality rates from CDC WONDER underlying cause of death data.
Over the study period, there were 69,976 deaths from CRC among individuals diagnosed before age 50, including 7,325 persons diagnosed younger than 35. Most CRC deaths (1,033,541) occurred in people diagnosed at age 50 and older.
The researchers calculated an average county-level young-onset CRC mortality rate of 1.78 deaths per 100,000 population, compared with a CRC mortality rate of 56.82 per 100,000 population among individuals 50 and older.
Overall, for individuals younger than 50 at diagnosis, the researchers found two hot spots – in the Southeast (relative risk, 1.24) and in the Great Lakes region (RR, 1.10). They identified cold spots in lower Wisconsin (RR, 0.87), the Northeast (RR, 0.92), southwest Texas (RR, 0.90), and Western counties more broadly, including Alaska (RR, 0.82).
Further analysis of those diagnosed when younger than 35 revealed two significant young-onset CRC mortality hot spots – in the Northeast (RR, 1.25) and the upper Midwest (RR, 1.11). In this youngest group, the team also found three significant cold spots – in the Southwest (RR, 0.74), in California (RR, 0.78), and in the Mountain West (RR, 0.82).
Among those aged 35-49 years at diagnosis, researchers found three hot spots – two in the Southeast (RR,1.20 and 1.16) and in the Great Lakes region (RR, 1.12). Several cold spots emerged from the mortality data on young-onset CRC in this age group – in the Pacific/Mountain West (RR, 0.90), in California (RR, 0.82), southern Texas (RR, 0.89), and the Southwest more broadly (RR, 0.86).
“Though cold spots were similar across strata, young-onset CRC hot spots shifted southward in the 35-49 age stratum in comparison to the less than 35 group,” the team notes.
They acknowledge several limitations to the study, including its “ecological nature” and the lack of adjustment for stage at diagnosis.
In comments to this news organization, Andrew T. Chan, MD, MPH, of Massachusetts General Hospital and Harvard Medical School, Boston, said the approach used by the researchers was “very interesting.”
Dr. Chan said that this is “one of the first studies that has given us insight into whether there is potential geographic variation in the incidence of young-onset colorectal cancer.”
This, he continued, is “very helpful in terms of thinking about potential risk factors for early-onset cancer and giving us more information about where we might want to focus our efforts in terms of prevention.”
Dr. Chan added that another interesting aspect of the study was that “the patterns might be different, depending on how you define early-onset cancer,” whether as “very-early onset,” defined as onset in those younger than 35, or the “less stringent definition” of 35-49 years.
He said that, “within the group that we’re calling very-early onset, there may be enriched factors,” compared with people who are “a little bit older.”
The research was supported by a National Cancer Institute of the National Institutes of Health grant to Case Comprehensive Cancer Center. Dr. Schmit reports no relevant financial relationships. Other authors have relationships with Exelixis, Tempus, Olympus, Anthos, Bayer, BMS, Janssen, Nektar Therapeutics, Pfizer, Sanofi, and WebMD/Medscape. Dr. Chan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The so-called hot and cold spots of mortality from young-onset CRC differed slightly for people younger than 50 and those younger than 35, report the researchers, who say such studies may lead to better understanding of the underlying factors as well as to targeted interventions.
The authors suggest that deaths in the youngest young-onset CRC individuals “may be driven by a distinct set of factors, compared with deaths among older young-onset CRC and average-onset CRC patients.”
They add that “unmeasured factors ... may drive anomalous young-onset CRC mortality rates, either independently or in conjunction with demographic [and] modifiable variables accounted for here.”
The research was published online in Gastroenterology.
Incidence, mortality rates on the rise
The incidence and mortality rates of young-onset CRC have been increasing for decades, the authors write, but it has only recently begun to attract public health attention.
Risk factors and prognostic indicators, such as smoking, obesity, alcohol consumption, diabetes, sex, race, and socioeconomic factors, have been implicated in the development of the condition.
Geospatial distribution of young-onset CRC adds an “important [layer] for understanding the underlying drivers of mortality and allocating public health resources,” the authors write.
It is “too soon” to draw conclusions about the cause of the hot and cold spots, cautioned senior author Stephanie L. Schmit, PhD, vice chair of the Genomic Medicine Institute at the Lerner Research Institute, Cleveland Clinic.
Speaking to this news organization, she said, “Additional factors like proximity to primary care, gastroenterology, and cancer care facilities or novel environmental exposures may contribute to hot spots.”
On the other hand, “lifestyle factors like diet and exercise might contribute to some extent to cold spots,” she added.
While Dr. Schmit said it would be “challenging” to replicate the findings nationally, “further analyses at more granular geographic levels would be incredibly helpful.”
Exploring the geographical distribution
To explore the geographical distribution of young-onset CRC mortality, the researchers gathered 20 years of data on more than 1 million CRC deaths from 3,036 U.S. counties. With aggregated county-level information from 1999 to 2019, they derived mortality rates from CDC WONDER underlying cause of death data.
Over the study period, there were 69,976 deaths from CRC among individuals diagnosed before age 50, including 7,325 persons diagnosed younger than 35. Most CRC deaths (1,033,541) occurred in people diagnosed at age 50 and older.
The researchers calculated an average county-level young-onset CRC mortality rate of 1.78 deaths per 100,000 population, compared with a CRC mortality rate of 56.82 per 100,000 population among individuals 50 and older.
Overall, for individuals younger than 50 at diagnosis, the researchers found two hot spots – in the Southeast (relative risk, 1.24) and in the Great Lakes region (RR, 1.10). They identified cold spots in lower Wisconsin (RR, 0.87), the Northeast (RR, 0.92), southwest Texas (RR, 0.90), and Western counties more broadly, including Alaska (RR, 0.82).
Further analysis of those diagnosed when younger than 35 revealed two significant young-onset CRC mortality hot spots – in the Northeast (RR, 1.25) and the upper Midwest (RR, 1.11). In this youngest group, the team also found three significant cold spots – in the Southwest (RR, 0.74), in California (RR, 0.78), and in the Mountain West (RR, 0.82).
Among those aged 35-49 years at diagnosis, researchers found three hot spots – two in the Southeast (RR,1.20 and 1.16) and in the Great Lakes region (RR, 1.12). Several cold spots emerged from the mortality data on young-onset CRC in this age group – in the Pacific/Mountain West (RR, 0.90), in California (RR, 0.82), southern Texas (RR, 0.89), and the Southwest more broadly (RR, 0.86).
“Though cold spots were similar across strata, young-onset CRC hot spots shifted southward in the 35-49 age stratum in comparison to the less than 35 group,” the team notes.
They acknowledge several limitations to the study, including its “ecological nature” and the lack of adjustment for stage at diagnosis.
In comments to this news organization, Andrew T. Chan, MD, MPH, of Massachusetts General Hospital and Harvard Medical School, Boston, said the approach used by the researchers was “very interesting.”
Dr. Chan said that this is “one of the first studies that has given us insight into whether there is potential geographic variation in the incidence of young-onset colorectal cancer.”
This, he continued, is “very helpful in terms of thinking about potential risk factors for early-onset cancer and giving us more information about where we might want to focus our efforts in terms of prevention.”
Dr. Chan added that another interesting aspect of the study was that “the patterns might be different, depending on how you define early-onset cancer,” whether as “very-early onset,” defined as onset in those younger than 35, or the “less stringent definition” of 35-49 years.
He said that, “within the group that we’re calling very-early onset, there may be enriched factors,” compared with people who are “a little bit older.”
The research was supported by a National Cancer Institute of the National Institutes of Health grant to Case Comprehensive Cancer Center. Dr. Schmit reports no relevant financial relationships. Other authors have relationships with Exelixis, Tempus, Olympus, Anthos, Bayer, BMS, Janssen, Nektar Therapeutics, Pfizer, Sanofi, and WebMD/Medscape. Dr. Chan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The so-called hot and cold spots of mortality from young-onset CRC differed slightly for people younger than 50 and those younger than 35, report the researchers, who say such studies may lead to better understanding of the underlying factors as well as to targeted interventions.
The authors suggest that deaths in the youngest young-onset CRC individuals “may be driven by a distinct set of factors, compared with deaths among older young-onset CRC and average-onset CRC patients.”
They add that “unmeasured factors ... may drive anomalous young-onset CRC mortality rates, either independently or in conjunction with demographic [and] modifiable variables accounted for here.”
The research was published online in Gastroenterology.
Incidence, mortality rates on the rise
The incidence and mortality rates of young-onset CRC have been increasing for decades, the authors write, but it has only recently begun to attract public health attention.
Risk factors and prognostic indicators, such as smoking, obesity, alcohol consumption, diabetes, sex, race, and socioeconomic factors, have been implicated in the development of the condition.
Geospatial distribution of young-onset CRC adds an “important [layer] for understanding the underlying drivers of mortality and allocating public health resources,” the authors write.
It is “too soon” to draw conclusions about the cause of the hot and cold spots, cautioned senior author Stephanie L. Schmit, PhD, vice chair of the Genomic Medicine Institute at the Lerner Research Institute, Cleveland Clinic.
Speaking to this news organization, she said, “Additional factors like proximity to primary care, gastroenterology, and cancer care facilities or novel environmental exposures may contribute to hot spots.”
On the other hand, “lifestyle factors like diet and exercise might contribute to some extent to cold spots,” she added.
While Dr. Schmit said it would be “challenging” to replicate the findings nationally, “further analyses at more granular geographic levels would be incredibly helpful.”
Exploring the geographical distribution
To explore the geographical distribution of young-onset CRC mortality, the researchers gathered 20 years of data on more than 1 million CRC deaths from 3,036 U.S. counties. With aggregated county-level information from 1999 to 2019, they derived mortality rates from CDC WONDER underlying cause of death data.
Over the study period, there were 69,976 deaths from CRC among individuals diagnosed before age 50, including 7,325 persons diagnosed younger than 35. Most CRC deaths (1,033,541) occurred in people diagnosed at age 50 and older.
The researchers calculated an average county-level young-onset CRC mortality rate of 1.78 deaths per 100,000 population, compared with a CRC mortality rate of 56.82 per 100,000 population among individuals 50 and older.
Overall, for individuals younger than 50 at diagnosis, the researchers found two hot spots – in the Southeast (relative risk, 1.24) and in the Great Lakes region (RR, 1.10). They identified cold spots in lower Wisconsin (RR, 0.87), the Northeast (RR, 0.92), southwest Texas (RR, 0.90), and Western counties more broadly, including Alaska (RR, 0.82).
Further analysis of those diagnosed when younger than 35 revealed two significant young-onset CRC mortality hot spots – in the Northeast (RR, 1.25) and the upper Midwest (RR, 1.11). In this youngest group, the team also found three significant cold spots – in the Southwest (RR, 0.74), in California (RR, 0.78), and in the Mountain West (RR, 0.82).
Among those aged 35-49 years at diagnosis, researchers found three hot spots – two in the Southeast (RR,1.20 and 1.16) and in the Great Lakes region (RR, 1.12). Several cold spots emerged from the mortality data on young-onset CRC in this age group – in the Pacific/Mountain West (RR, 0.90), in California (RR, 0.82), southern Texas (RR, 0.89), and the Southwest more broadly (RR, 0.86).
“Though cold spots were similar across strata, young-onset CRC hot spots shifted southward in the 35-49 age stratum in comparison to the less than 35 group,” the team notes.
They acknowledge several limitations to the study, including its “ecological nature” and the lack of adjustment for stage at diagnosis.
In comments to this news organization, Andrew T. Chan, MD, MPH, of Massachusetts General Hospital and Harvard Medical School, Boston, said the approach used by the researchers was “very interesting.”
Dr. Chan said that this is “one of the first studies that has given us insight into whether there is potential geographic variation in the incidence of young-onset colorectal cancer.”
This, he continued, is “very helpful in terms of thinking about potential risk factors for early-onset cancer and giving us more information about where we might want to focus our efforts in terms of prevention.”
Dr. Chan added that another interesting aspect of the study was that “the patterns might be different, depending on how you define early-onset cancer,” whether as “very-early onset,” defined as onset in those younger than 35, or the “less stringent definition” of 35-49 years.
He said that, “within the group that we’re calling very-early onset, there may be enriched factors,” compared with people who are “a little bit older.”
The research was supported by a National Cancer Institute of the National Institutes of Health grant to Case Comprehensive Cancer Center. Dr. Schmit reports no relevant financial relationships. Other authors have relationships with Exelixis, Tempus, Olympus, Anthos, Bayer, BMS, Janssen, Nektar Therapeutics, Pfizer, Sanofi, and WebMD/Medscape. Dr. Chan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM GASTROENTEROLOGY
Amazon involved with new cancer vaccine clinical trial
The trial is aimed at finding “personalized vaccines” to treat breast cancer and melanoma. The phase 1 trial is recruiting 20 people over the age of 18 to study the safety of the vaccines, according to CNBC.
The Fred Hutchinson Cancer Research Center and University of Washington Cancer Consortium are listed as the researchers of the clinical trial, and Amazon is listed as a collaborator, according to a filing on the ClinicalTrials.gov database.
“Amazon is contributing scientific and machine learning expertise to a partnership with Fred Hutch to explore the development of a personalized treatment for certain forms of cancer,” an Amazon spokesperson told CNBC.
“It’s very early, but Fred Hutch recently received permission from the U.S. Food and Drug Administration to proceed with a phase 1 clinical trial, and it’s unclear whether it will be successful,” the spokesperson said. “This will be a long, multiyear process – should it progress, we would be open to working with other organizations in health care and life sciences that might also be interested in similar efforts.”
In recent years, Amazon has grown its presence in the health care industry, CNBC reported. The company launched an online pharmacy in 2020, developed a telehealth service called Amazon Care, and released its own COVID-19 test during the pandemic.
A research and development group inside Amazon, known as Grand Challenge, oversaw the company’s early cancer vaccine effort, according to Business Insider. It’s now under the purview of a cancer research team that reports to Robert Williams, the company’s vice president of devices.
The study was first posted on ClinicalTrials.gov in October 2021 and began recruiting patients on June 9, according to the filing. The phase 1 trial is expected to run through November 2023.
The phase 1 trial will study the safety of personalized vaccines to treat patients with late-stage melanoma or hormone receptor-positive HER2-negative breast cancer which has either spread to other parts of the body or doesn’t respond to treatment.
More information about the study can be found on ClinicalTrials.gov under the identifier NCT05098210.
A version of this article first appeared on WebMD.com.
The trial is aimed at finding “personalized vaccines” to treat breast cancer and melanoma. The phase 1 trial is recruiting 20 people over the age of 18 to study the safety of the vaccines, according to CNBC.
The Fred Hutchinson Cancer Research Center and University of Washington Cancer Consortium are listed as the researchers of the clinical trial, and Amazon is listed as a collaborator, according to a filing on the ClinicalTrials.gov database.
“Amazon is contributing scientific and machine learning expertise to a partnership with Fred Hutch to explore the development of a personalized treatment for certain forms of cancer,” an Amazon spokesperson told CNBC.
“It’s very early, but Fred Hutch recently received permission from the U.S. Food and Drug Administration to proceed with a phase 1 clinical trial, and it’s unclear whether it will be successful,” the spokesperson said. “This will be a long, multiyear process – should it progress, we would be open to working with other organizations in health care and life sciences that might also be interested in similar efforts.”
In recent years, Amazon has grown its presence in the health care industry, CNBC reported. The company launched an online pharmacy in 2020, developed a telehealth service called Amazon Care, and released its own COVID-19 test during the pandemic.
A research and development group inside Amazon, known as Grand Challenge, oversaw the company’s early cancer vaccine effort, according to Business Insider. It’s now under the purview of a cancer research team that reports to Robert Williams, the company’s vice president of devices.
The study was first posted on ClinicalTrials.gov in October 2021 and began recruiting patients on June 9, according to the filing. The phase 1 trial is expected to run through November 2023.
The phase 1 trial will study the safety of personalized vaccines to treat patients with late-stage melanoma or hormone receptor-positive HER2-negative breast cancer which has either spread to other parts of the body or doesn’t respond to treatment.
More information about the study can be found on ClinicalTrials.gov under the identifier NCT05098210.
A version of this article first appeared on WebMD.com.
The trial is aimed at finding “personalized vaccines” to treat breast cancer and melanoma. The phase 1 trial is recruiting 20 people over the age of 18 to study the safety of the vaccines, according to CNBC.
The Fred Hutchinson Cancer Research Center and University of Washington Cancer Consortium are listed as the researchers of the clinical trial, and Amazon is listed as a collaborator, according to a filing on the ClinicalTrials.gov database.
“Amazon is contributing scientific and machine learning expertise to a partnership with Fred Hutch to explore the development of a personalized treatment for certain forms of cancer,” an Amazon spokesperson told CNBC.
“It’s very early, but Fred Hutch recently received permission from the U.S. Food and Drug Administration to proceed with a phase 1 clinical trial, and it’s unclear whether it will be successful,” the spokesperson said. “This will be a long, multiyear process – should it progress, we would be open to working with other organizations in health care and life sciences that might also be interested in similar efforts.”
In recent years, Amazon has grown its presence in the health care industry, CNBC reported. The company launched an online pharmacy in 2020, developed a telehealth service called Amazon Care, and released its own COVID-19 test during the pandemic.
A research and development group inside Amazon, known as Grand Challenge, oversaw the company’s early cancer vaccine effort, according to Business Insider. It’s now under the purview of a cancer research team that reports to Robert Williams, the company’s vice president of devices.
The study was first posted on ClinicalTrials.gov in October 2021 and began recruiting patients on June 9, according to the filing. The phase 1 trial is expected to run through November 2023.
The phase 1 trial will study the safety of personalized vaccines to treat patients with late-stage melanoma or hormone receptor-positive HER2-negative breast cancer which has either spread to other parts of the body or doesn’t respond to treatment.
More information about the study can be found on ClinicalTrials.gov under the identifier NCT05098210.
A version of this article first appeared on WebMD.com.
Surgical Treatment of Nonmelanoma Skin Cancer in Older Adult Veterans
Skin cancer is the most diagnosed cancer in the United States. Nonmelanoma skin cancers (NMSC), which include basal cell carcinoma and squamous cell carcinoma, are usually cured with removal.1 The incidence of NMSC increases with age and is commonly found in nursing homes and geriatric units. These cancers are not usually metastatic or fatal but can cause local destruction and disfigurement if neglected.2 The current standard of care is to treat diagnosed NMSC; however, the dermatology and geriatric care literature have questioned the logic of treating asymptomatic skin cancers that will not affect a patient’s life expectancy.2-4
Forty-seven percent of the current living veteran population is aged ≥ 65 years.5 Older adult patients are frequently referred to the US Department of Veterans Affairs (VA) surgical service for the treatment of NMSC. The veteran population includes a higher percentage of individuals at an elevated risk of skin cancers (older, White, and male) compared with the general population.6 World War II veterans deployed in regions closer to the equator have been found to have an elevated risk of melanoma and nonmelanoma skin carcinomas.7 A retrospective study of Vietnam veterans exposed to Agent Orange (2,3,7,8-tetrachlorodibenzodioxin) found a significantly higher risk of invasive NMSC in Fitzpatrick skin types I-IV compared with an age-matched subset of the general population.8 Younger veterans who were deployed in Afghanistan and Iraq for Operation Enduring Freedom/Operation Iraqi Freedom worked at more equatorial latitudes than the rest of the US population and may be at increased risk of NMSC. Inadequate sunscreen access, immediate safety concerns, outdoor recreational activities, harsh weather, and insufficient emphasis on sun protection have created a multifactorial challenge for the military population. Riemenschneider and colleagues recommended targeted screening for at-risk veteran patients and prioritizing annual skin cancer screenings during medical mission physical examinations for active military.7
The plastic surgery service regularly receives consults from dermatology, general surgery, and primary care to remove skin cancers on the face, scalp, hands, and forearms. Skin cancer treatment can create serious hardships for older adult patients and their families with multiple appointments for the consult, procedure, and follow-up. Patients are often told to hold their anticoagulant medications when the surgery will be performed on a highly vascular region, such as the scalp or face. This can create wide swings in their laboratory test values and result in life-threatening complications from either bleeding or clotting. The appropriateness of offering surgery to patients with serious comorbidities and a limited life expectancy has been questioned.2-4 The purpose of this study was to measure the morbidity and unrelated 5-year mortality for patients with skin cancer referred to the plastic surgery service to help patients and families make a more informed treatment decision, particularly when the patients are aged > 80 years and have significant life-threatening comorbidities.
Methods
The University of Florida and Malcom Randall VA Medical Center Institutional review board in Gainesville, approved a retrospective review of all consults completed by the plastic surgery service for the treatment of NMSC performed from July 1, 2011 to June 30, 2015. Data collected included age and common life-limiting comorbidities at the time of referral. Morbidities were found on the electronic health record, including coronary artery disease (CAD), congestive heart failure (CHF), cerebral vascular disease (CVD), peripheral vascular disease, dementia, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), tobacco use, diabetes mellitus (DM), liver disease, alcohol use, and obstructive sleep apnea.
Treatment, complications, and 5-year mortality were recorded. A χ2 analysis with P value < .05 was used to determine statistical significance between individual risk factors and 5-year mortality. The relative risk of 5-year mortality was calculated by combining advanced age (aged > 80 years) with the individual comorbidities.
Results
Over 4 years, 800 consults for NMSC were completed by the plastic surgery service. Treatment decisions included 210 excisions (with or without reconstruction) in the operating room, 402 excisions (with or without reconstruction) under local anesthesia in clinic, 55 Mohs surgical dermatology referrals, 21 other service or hospital referrals, and 112 patient who were observed, declined intervention, or died prior to intervention. Five-year mortality was 28.6%. No patients died of NMSC. The median age at consult submission for patients deceased 5 years later was 78 years. Complication rate was 5% and included wound infection, dehiscence, bleeding, or graft loss. Two patients, both deceased within 5 years, had unplanned admissions due to bleeding from either a skin graft donor site or recipient bleeding. Aged ≥ 80 years, CAD, CHF, CVD, peripheral vascular disease, dementia, CKD, COPD, and DM were all found individually to be statistically significant predictors of 5-year mortality (Table 1). Combining aged ≥ 80 years plus CAD, CHF, or dementia all increased the 5-year mortality by a relative risk of > 3 (Table 2).
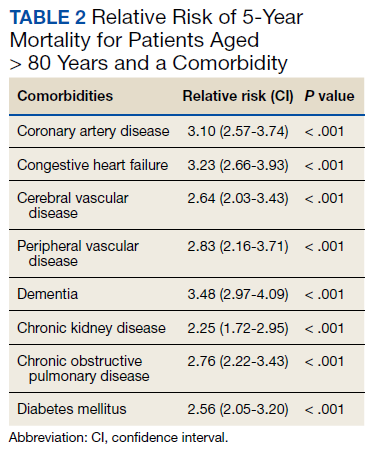
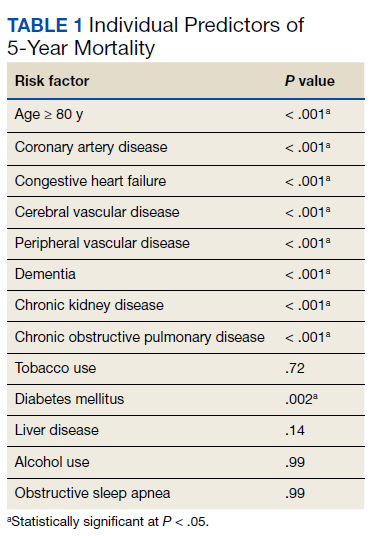
Discussion
The standard of care is to treat NMSC. Most NMSCs are treated surgically without consideration of patient age or life expectancy.2,4,9,10 A prospective cohort study involving a university-based private practice and a VA medical center in San Francisco found a 22.6% overall 5-year mortality and a 43.3% mortality in the group defined as limited life expectancy (LLE) based on age (≥ 85 years) and medical comorbidities. None died due to the NMSC. Leading cause of death was cardiac, cerebrovascular, and respiratory disease, lung and prostate cancer, and Alzheimer disease. The authors suggested the LLE group may be exposed to wound complications without benefiting from the treatment.4
Another study of 440 patients receiving excision for biopsy-proven facial NMSC at the Roudebush VA Medical Center in Indianapolis, Indiana, found no residual carcinoma in 35.3% of excisions, and in patients aged > 90 years, more than half of the excisions had no residual carcinoma. More than half of the patients aged > 90 years died within 1 year, not as a result of the NMSC. The authors argued for watchful waiting in select patients to maximize comfort and outcomes.10
NMSCs are often asymptomatic and not immediately life threatening. Although NMSCs tend to have a favorable prognosis, studies have found that NMSC may be a marker for other poor health outcomes. A significant increased risk for all-cause mortality was found for patients with a history of SCC, which may be attributed to immune status.11 The aging veteran population has more complex health care needs to be considered when developing surgical treatment plans. These medical problems may limit their life expectancy much sooner than the skin cancer will become symptomatic. We found that individuals aged ≥ 80 years who had CAD, CHF, or dementia had a relative risk of 3 or higher for 5-year mortality. The leading cause of death in the United States in years 2011 to 2015 was heart disease. Alzheimer disease was the sixth leading cause of death in those same years.12-14
Skin cancer excisions do not typically require general anesthesia, deep sedation, or large fluid shifts; however, studies have found that when frail patients undergo low-risk procedures, they tend to have a higher mortality rate than their healthier counterparts.15 Frailty is a concept that identifies patients who are at increased risk of dying in 6 to 60 months due to a decline in their physical reserve. Frail patients have increased rates of perioperative mortality and complications. Various tools have been used to assess the components of physical performance, speed, mobility, nutrition status, mental health, and cognition.16 Frailty screening has been initiated in several VA hospitals, including our own in Gainesville, Florida, with the goal of decreasing postoperative morbidity and mortality in older adult patients.17 The patients are given a 1-page screening assessment that asks about their living situation, medical conditions, nutrition status, cognition, and activities of daily living. The results can trigger the clinician to rethink the surgical plan and mobilize more resources to optimize the patient’s health. This study period precedes the initiative at our institution.
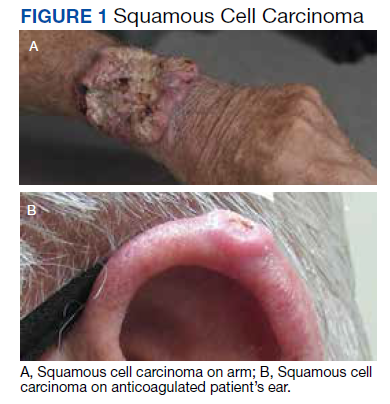
The plastic surgery service’s routine practice is to excise skin cancers in the operating room if sedation or general anesthesia will be needed (Figure 1A), for optimal control of bleeding (Figure 1B) in a patient who cannot safely stop blood thinners, or for excision of a highly vascularized area such as the scalp. Surgery is offered in an office-based setting if the area can be closed primarily, left open to close secondarily, or closed with a small skin graft under local anesthesia only (Figure 2). We prefer treating frail patients in the minor procedure clinic, when possible, to avoid the risks of sedation and the additional preoperative visits and transportation requirements. NMSC with unclear margins (Figure 3A) or in cosmetically sensitive areas where tissue needs to be preserved (Figure 3B) are referred to the Mohs dermatologist. The skin cancers in this study were most frequently found on the face, scalp, hands, and forearms based on referral patterns.
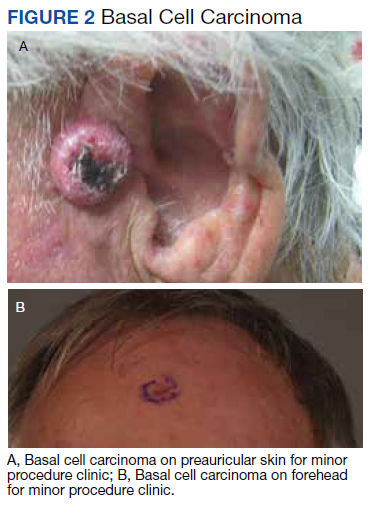
Other treatment options for NMSC include curettage and electrodessication, cryotherapy, and radiation; however, ours is a surgical service and patients are typically referred to us by primary care or dermatology when those are not reasonable or desirable options.18 Published complication rates of patients having skin cancer surgery without age restriction have a rate of 3% to 6%, which is consistent with our study of 5%.19-21 Two bleeding complications that needed to be admitted did not require more than a bedside procedure and neither required transfusions. One patient had been instructed to continue taking coumadin during the perioperative office-based procedure due to a recent carotid stent placement in the setting of a rapidly growing basal cell on an easily accessible location.
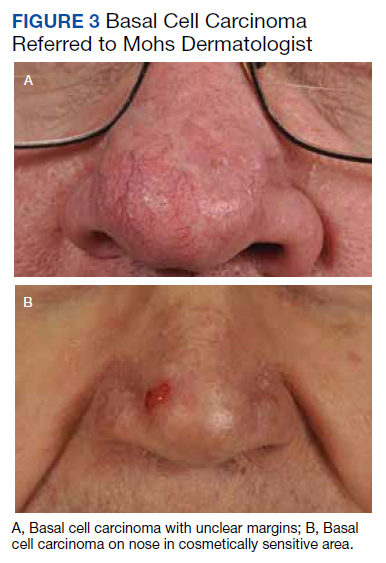
The most noted comorbidity in patients with wound complications was found to be DM; however, this was not found to be a statistically significant risk factor for wound complications (P = .10). We do not have a set rule for advising for or against NMSC surgery. We do counsel frail patients and their families that not all cancer is immediately life threatening and will work with them to do whatever makes the most sense to achieve their goals, occasionally accepting positive margins in order to debulk a symptomatic growth. The objective of this paper is to contribute to the discussion of performing invasive procedures on older adult veterans with life-limiting comorbidities. Patients and their families will have different thresholds for what they feel needs intervention, especially if other medical problems are consuming much of their time. We also have the community care referral option for patients whose treatment decisions are being dictated by travel hardships.
Strengths and Limitations
A strength of this study is that the data were obtained from a closed system. Patients tend to stay long-term within the VA and their health record is accessible throughout the country as long as they are seen at a VA facility. Complications, therefore, return to the treating service or primary care, who would route the patient back to the surgeon.
One limitation of the study is that this is a retrospective review from 2011. The authors are limited to data that are recorded in the patient record. Multiple health care professionals saw the patients and notes lack consistency in detail. Size of the lesions were not consistently recorded and did not get logged into our database for that reason.
Conclusions
Treatment of NMSC in older adult patients has a low morbidity but needs to be balanced against a patient and family’s goals when the patient presents with life-limiting comorbidities. An elevated 5-year mortality in patients aged > 80 years with serious unrelated medical conditions is intuitive, but this study may help put treatment plans into perspective for families and health care professionals who want to provide an indicated service while maximizing patient quality of life.
Acknowledgments
This manuscript is the result of work supported with resources and the use of facilities at the North Florida/South Georgia Veterans Health System, Gainesville, Florida.
1. American Cancer Society. Cancer Facts & Figures 2021. Accessed May 26, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf
2. Albert A, Knoll MA, Conti JA, Zbar RIS. Non-melanoma skin cancers in the older patient. Curr Oncol Rep. 2019;21(9):79. Published 2019 Jul 29. doi:10.1007/s11912-019-0828-9
3. Linos E, Chren MM, Stijacic Cenzer I, Covinsky KE. Skin cancer in U.S. elderly adults: does life expectancy play a role in treatment decisions? J Am Geriatr Soc. 2016;64(8):1610-1615. doi:10.1111/jgs.14202
4. Linos E, Parvataneni R, Stuart SE, Boscardin WJ, Landefeld CS, Chren MM. Treatment of nonfatal conditions at the end of life: nonmelanoma skin cancer. JAMA Intern Med. 2013;173(11):1006-1012. doi:10.1001/jamainternmed.2013.639
5. O’Malley KA, Vinson L, Kaiser AP, Sager Z, Hinrichs K. Mental health and aging veterans: how the Veterans Health Administration meets the needs of aging veterans. Public Policy Aging Rep. 2020;30(1):19-23. doi:10.1093/ppar/prz027
6. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Profile of veterans: 2017. Accessed May 26, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf 7. Riemenschneider K, Liu J, Powers JG. Skin cancer in the military: a systematic review of melanoma and nonmelanoma skin cancer incidence, prevention, and screening among active duty and veteran personnel. J Am Acad Dermatol. 2018;78(6):1185-1192. doi:10.1016/j.jaad.2017.11.062
8. Clemens MW, Kochuba AL, Carter ME, Han K, Liu J, Evans K. Association between Agent Orange exposure and nonmelanotic invasive skin cancer: a pilot study. Plast Reconstr Surg. 2014;133(2):432-437. doi:10.1097/01.prs.0000436859.40151.cf
9. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-317. doi:10.1016/j.jaad.2018.03.060
10. Chauhan R, Munger BN, Chu MW, et al. Age at diagnosis as a relative contraindication for intervention in facial nonmelanoma skin cancer. JAMA Surg. 2018;153(4):390-392. doi:10.1001/jamasurg.2017.5073
11. Barton V, Armeson K, Hampras S, et al. Nonmelanoma skin cancer and risk of all-cause and cancer-related mortality: a systematic review. Arch Dermatol Res. 2017;309(4):243-251. doi:10.1007/s00403-017-1724-5
12. Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2013. NCHS Data Brief 178. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db178.htm
13. Xu JQ, Kochanek KD, Murphy SL, Arias E. Mortality in the United States, 2012. NCHS Data Brief 168. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db168.htm
14. Xu JQ, Murphy SL, Kochanek KD, Arias E. Mortality in the United States, 2015. NCHS Data Brief 267. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db267.htm
15. Varley PR , Borrebach JD, Arya S, et al. Clinical utility of the risk analysis index as a prospective frailty screening tool within a multi-practice, multi-hospital integrated healthcare system. Ann Surg. 2021;274(6):e1230-e1237. doi:10.1097/SLA.0000000000003808
16. Hall DE, Arya S , Schmid KK, et al. Development and initial validation of the risk analysis index for measuring frailty in surgical populations. JAMA Surg. 2017;152(2):175-182. doi:10.1001/jamasurg.2016.4202
17. US Department of Veterans Affairs, Health Services Research & Development. Improving healthcare for aging veterans. Updated August 30, 2017. Accessed May 26, 2022. https://www.hsrd.research.va.gov/news/feature/aging0917.cfm
18. Leus AJG, Frie M, Haisma MS, et al. Treatment of keratinocyte carcinoma in elderly patients – a review of the current literature. J Eur Acad Dermatol Venereol. 2020;34(9):1932-1943. doi:10.1111/jdv.16268
19. Amici JM, Rogues AM, Lasheras A, et al. A prospective study of the incidence of complications associated with dermatological surgery. Br J Dermatol. 2005;153(5):967-971. doi:10.1111/j.1365-2133.2005.06861.x
20. Arguello-Guerra L, Vargas-Chandomid E, Díaz-González JM, Méndez-Flores S, Ruelas-Villavicencio A, Domínguez-Cherit J. Incidence of complications in dermatological surgery of melanoma and non-melanoma skin cancer in patients with multiple comorbidity and/or antiplatelet-anticoagulants. Five-year experience in our hospital. Cir Cir. 2019;86(1):15-23. doi:10.24875/CIRUE.M18000003
21. Keith DJ, de Berker DA, Bray AP, Cheung ST, Brain A, Mohd Mustapa MF. British Association of Dermatologists’ national audit on nonmelanoma skin cancer excision, 2014. Clin Exp Dermatol. 2017;42(1):46-53. doi:10.1111/ced.12990
Skin cancer is the most diagnosed cancer in the United States. Nonmelanoma skin cancers (NMSC), which include basal cell carcinoma and squamous cell carcinoma, are usually cured with removal.1 The incidence of NMSC increases with age and is commonly found in nursing homes and geriatric units. These cancers are not usually metastatic or fatal but can cause local destruction and disfigurement if neglected.2 The current standard of care is to treat diagnosed NMSC; however, the dermatology and geriatric care literature have questioned the logic of treating asymptomatic skin cancers that will not affect a patient’s life expectancy.2-4
Forty-seven percent of the current living veteran population is aged ≥ 65 years.5 Older adult patients are frequently referred to the US Department of Veterans Affairs (VA) surgical service for the treatment of NMSC. The veteran population includes a higher percentage of individuals at an elevated risk of skin cancers (older, White, and male) compared with the general population.6 World War II veterans deployed in regions closer to the equator have been found to have an elevated risk of melanoma and nonmelanoma skin carcinomas.7 A retrospective study of Vietnam veterans exposed to Agent Orange (2,3,7,8-tetrachlorodibenzodioxin) found a significantly higher risk of invasive NMSC in Fitzpatrick skin types I-IV compared with an age-matched subset of the general population.8 Younger veterans who were deployed in Afghanistan and Iraq for Operation Enduring Freedom/Operation Iraqi Freedom worked at more equatorial latitudes than the rest of the US population and may be at increased risk of NMSC. Inadequate sunscreen access, immediate safety concerns, outdoor recreational activities, harsh weather, and insufficient emphasis on sun protection have created a multifactorial challenge for the military population. Riemenschneider and colleagues recommended targeted screening for at-risk veteran patients and prioritizing annual skin cancer screenings during medical mission physical examinations for active military.7
The plastic surgery service regularly receives consults from dermatology, general surgery, and primary care to remove skin cancers on the face, scalp, hands, and forearms. Skin cancer treatment can create serious hardships for older adult patients and their families with multiple appointments for the consult, procedure, and follow-up. Patients are often told to hold their anticoagulant medications when the surgery will be performed on a highly vascular region, such as the scalp or face. This can create wide swings in their laboratory test values and result in life-threatening complications from either bleeding or clotting. The appropriateness of offering surgery to patients with serious comorbidities and a limited life expectancy has been questioned.2-4 The purpose of this study was to measure the morbidity and unrelated 5-year mortality for patients with skin cancer referred to the plastic surgery service to help patients and families make a more informed treatment decision, particularly when the patients are aged > 80 years and have significant life-threatening comorbidities.
Methods
The University of Florida and Malcom Randall VA Medical Center Institutional review board in Gainesville, approved a retrospective review of all consults completed by the plastic surgery service for the treatment of NMSC performed from July 1, 2011 to June 30, 2015. Data collected included age and common life-limiting comorbidities at the time of referral. Morbidities were found on the electronic health record, including coronary artery disease (CAD), congestive heart failure (CHF), cerebral vascular disease (CVD), peripheral vascular disease, dementia, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), tobacco use, diabetes mellitus (DM), liver disease, alcohol use, and obstructive sleep apnea.
Treatment, complications, and 5-year mortality were recorded. A χ2 analysis with P value < .05 was used to determine statistical significance between individual risk factors and 5-year mortality. The relative risk of 5-year mortality was calculated by combining advanced age (aged > 80 years) with the individual comorbidities.
Results
Over 4 years, 800 consults for NMSC were completed by the plastic surgery service. Treatment decisions included 210 excisions (with or without reconstruction) in the operating room, 402 excisions (with or without reconstruction) under local anesthesia in clinic, 55 Mohs surgical dermatology referrals, 21 other service or hospital referrals, and 112 patient who were observed, declined intervention, or died prior to intervention. Five-year mortality was 28.6%. No patients died of NMSC. The median age at consult submission for patients deceased 5 years later was 78 years. Complication rate was 5% and included wound infection, dehiscence, bleeding, or graft loss. Two patients, both deceased within 5 years, had unplanned admissions due to bleeding from either a skin graft donor site or recipient bleeding. Aged ≥ 80 years, CAD, CHF, CVD, peripheral vascular disease, dementia, CKD, COPD, and DM were all found individually to be statistically significant predictors of 5-year mortality (Table 1). Combining aged ≥ 80 years plus CAD, CHF, or dementia all increased the 5-year mortality by a relative risk of > 3 (Table 2).
Discussion
The standard of care is to treat NMSC. Most NMSCs are treated surgically without consideration of patient age or life expectancy.2,4,9,10 A prospective cohort study involving a university-based private practice and a VA medical center in San Francisco found a 22.6% overall 5-year mortality and a 43.3% mortality in the group defined as limited life expectancy (LLE) based on age (≥ 85 years) and medical comorbidities. None died due to the NMSC. Leading cause of death was cardiac, cerebrovascular, and respiratory disease, lung and prostate cancer, and Alzheimer disease. The authors suggested the LLE group may be exposed to wound complications without benefiting from the treatment.4
Another study of 440 patients receiving excision for biopsy-proven facial NMSC at the Roudebush VA Medical Center in Indianapolis, Indiana, found no residual carcinoma in 35.3% of excisions, and in patients aged > 90 years, more than half of the excisions had no residual carcinoma. More than half of the patients aged > 90 years died within 1 year, not as a result of the NMSC. The authors argued for watchful waiting in select patients to maximize comfort and outcomes.10
NMSCs are often asymptomatic and not immediately life threatening. Although NMSCs tend to have a favorable prognosis, studies have found that NMSC may be a marker for other poor health outcomes. A significant increased risk for all-cause mortality was found for patients with a history of SCC, which may be attributed to immune status.11 The aging veteran population has more complex health care needs to be considered when developing surgical treatment plans. These medical problems may limit their life expectancy much sooner than the skin cancer will become symptomatic. We found that individuals aged ≥ 80 years who had CAD, CHF, or dementia had a relative risk of 3 or higher for 5-year mortality. The leading cause of death in the United States in years 2011 to 2015 was heart disease. Alzheimer disease was the sixth leading cause of death in those same years.12-14
Skin cancer excisions do not typically require general anesthesia, deep sedation, or large fluid shifts; however, studies have found that when frail patients undergo low-risk procedures, they tend to have a higher mortality rate than their healthier counterparts.15 Frailty is a concept that identifies patients who are at increased risk of dying in 6 to 60 months due to a decline in their physical reserve. Frail patients have increased rates of perioperative mortality and complications. Various tools have been used to assess the components of physical performance, speed, mobility, nutrition status, mental health, and cognition.16 Frailty screening has been initiated in several VA hospitals, including our own in Gainesville, Florida, with the goal of decreasing postoperative morbidity and mortality in older adult patients.17 The patients are given a 1-page screening assessment that asks about their living situation, medical conditions, nutrition status, cognition, and activities of daily living. The results can trigger the clinician to rethink the surgical plan and mobilize more resources to optimize the patient’s health. This study period precedes the initiative at our institution.
The plastic surgery service’s routine practice is to excise skin cancers in the operating room if sedation or general anesthesia will be needed (Figure 1A), for optimal control of bleeding (Figure 1B) in a patient who cannot safely stop blood thinners, or for excision of a highly vascularized area such as the scalp. Surgery is offered in an office-based setting if the area can be closed primarily, left open to close secondarily, or closed with a small skin graft under local anesthesia only (Figure 2). We prefer treating frail patients in the minor procedure clinic, when possible, to avoid the risks of sedation and the additional preoperative visits and transportation requirements. NMSC with unclear margins (Figure 3A) or in cosmetically sensitive areas where tissue needs to be preserved (Figure 3B) are referred to the Mohs dermatologist. The skin cancers in this study were most frequently found on the face, scalp, hands, and forearms based on referral patterns.
Other treatment options for NMSC include curettage and electrodessication, cryotherapy, and radiation; however, ours is a surgical service and patients are typically referred to us by primary care or dermatology when those are not reasonable or desirable options.18 Published complication rates of patients having skin cancer surgery without age restriction have a rate of 3% to 6%, which is consistent with our study of 5%.19-21 Two bleeding complications that needed to be admitted did not require more than a bedside procedure and neither required transfusions. One patient had been instructed to continue taking coumadin during the perioperative office-based procedure due to a recent carotid stent placement in the setting of a rapidly growing basal cell on an easily accessible location.
The most noted comorbidity in patients with wound complications was found to be DM; however, this was not found to be a statistically significant risk factor for wound complications (P = .10). We do not have a set rule for advising for or against NMSC surgery. We do counsel frail patients and their families that not all cancer is immediately life threatening and will work with them to do whatever makes the most sense to achieve their goals, occasionally accepting positive margins in order to debulk a symptomatic growth. The objective of this paper is to contribute to the discussion of performing invasive procedures on older adult veterans with life-limiting comorbidities. Patients and their families will have different thresholds for what they feel needs intervention, especially if other medical problems are consuming much of their time. We also have the community care referral option for patients whose treatment decisions are being dictated by travel hardships.
Strengths and Limitations
A strength of this study is that the data were obtained from a closed system. Patients tend to stay long-term within the VA and their health record is accessible throughout the country as long as they are seen at a VA facility. Complications, therefore, return to the treating service or primary care, who would route the patient back to the surgeon.
One limitation of the study is that this is a retrospective review from 2011. The authors are limited to data that are recorded in the patient record. Multiple health care professionals saw the patients and notes lack consistency in detail. Size of the lesions were not consistently recorded and did not get logged into our database for that reason.
Conclusions
Treatment of NMSC in older adult patients has a low morbidity but needs to be balanced against a patient and family’s goals when the patient presents with life-limiting comorbidities. An elevated 5-year mortality in patients aged > 80 years with serious unrelated medical conditions is intuitive, but this study may help put treatment plans into perspective for families and health care professionals who want to provide an indicated service while maximizing patient quality of life.
Acknowledgments
This manuscript is the result of work supported with resources and the use of facilities at the North Florida/South Georgia Veterans Health System, Gainesville, Florida.
Skin cancer is the most diagnosed cancer in the United States. Nonmelanoma skin cancers (NMSC), which include basal cell carcinoma and squamous cell carcinoma, are usually cured with removal.1 The incidence of NMSC increases with age and is commonly found in nursing homes and geriatric units. These cancers are not usually metastatic or fatal but can cause local destruction and disfigurement if neglected.2 The current standard of care is to treat diagnosed NMSC; however, the dermatology and geriatric care literature have questioned the logic of treating asymptomatic skin cancers that will not affect a patient’s life expectancy.2-4
Forty-seven percent of the current living veteran population is aged ≥ 65 years.5 Older adult patients are frequently referred to the US Department of Veterans Affairs (VA) surgical service for the treatment of NMSC. The veteran population includes a higher percentage of individuals at an elevated risk of skin cancers (older, White, and male) compared with the general population.6 World War II veterans deployed in regions closer to the equator have been found to have an elevated risk of melanoma and nonmelanoma skin carcinomas.7 A retrospective study of Vietnam veterans exposed to Agent Orange (2,3,7,8-tetrachlorodibenzodioxin) found a significantly higher risk of invasive NMSC in Fitzpatrick skin types I-IV compared with an age-matched subset of the general population.8 Younger veterans who were deployed in Afghanistan and Iraq for Operation Enduring Freedom/Operation Iraqi Freedom worked at more equatorial latitudes than the rest of the US population and may be at increased risk of NMSC. Inadequate sunscreen access, immediate safety concerns, outdoor recreational activities, harsh weather, and insufficient emphasis on sun protection have created a multifactorial challenge for the military population. Riemenschneider and colleagues recommended targeted screening for at-risk veteran patients and prioritizing annual skin cancer screenings during medical mission physical examinations for active military.7
The plastic surgery service regularly receives consults from dermatology, general surgery, and primary care to remove skin cancers on the face, scalp, hands, and forearms. Skin cancer treatment can create serious hardships for older adult patients and their families with multiple appointments for the consult, procedure, and follow-up. Patients are often told to hold their anticoagulant medications when the surgery will be performed on a highly vascular region, such as the scalp or face. This can create wide swings in their laboratory test values and result in life-threatening complications from either bleeding or clotting. The appropriateness of offering surgery to patients with serious comorbidities and a limited life expectancy has been questioned.2-4 The purpose of this study was to measure the morbidity and unrelated 5-year mortality for patients with skin cancer referred to the plastic surgery service to help patients and families make a more informed treatment decision, particularly when the patients are aged > 80 years and have significant life-threatening comorbidities.
Methods
The University of Florida and Malcom Randall VA Medical Center Institutional review board in Gainesville, approved a retrospective review of all consults completed by the plastic surgery service for the treatment of NMSC performed from July 1, 2011 to June 30, 2015. Data collected included age and common life-limiting comorbidities at the time of referral. Morbidities were found on the electronic health record, including coronary artery disease (CAD), congestive heart failure (CHF), cerebral vascular disease (CVD), peripheral vascular disease, dementia, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), tobacco use, diabetes mellitus (DM), liver disease, alcohol use, and obstructive sleep apnea.
Treatment, complications, and 5-year mortality were recorded. A χ2 analysis with P value < .05 was used to determine statistical significance between individual risk factors and 5-year mortality. The relative risk of 5-year mortality was calculated by combining advanced age (aged > 80 years) with the individual comorbidities.
Results
Over 4 years, 800 consults for NMSC were completed by the plastic surgery service. Treatment decisions included 210 excisions (with or without reconstruction) in the operating room, 402 excisions (with or without reconstruction) under local anesthesia in clinic, 55 Mohs surgical dermatology referrals, 21 other service or hospital referrals, and 112 patient who were observed, declined intervention, or died prior to intervention. Five-year mortality was 28.6%. No patients died of NMSC. The median age at consult submission for patients deceased 5 years later was 78 years. Complication rate was 5% and included wound infection, dehiscence, bleeding, or graft loss. Two patients, both deceased within 5 years, had unplanned admissions due to bleeding from either a skin graft donor site or recipient bleeding. Aged ≥ 80 years, CAD, CHF, CVD, peripheral vascular disease, dementia, CKD, COPD, and DM were all found individually to be statistically significant predictors of 5-year mortality (Table 1). Combining aged ≥ 80 years plus CAD, CHF, or dementia all increased the 5-year mortality by a relative risk of > 3 (Table 2).
Discussion
The standard of care is to treat NMSC. Most NMSCs are treated surgically without consideration of patient age or life expectancy.2,4,9,10 A prospective cohort study involving a university-based private practice and a VA medical center in San Francisco found a 22.6% overall 5-year mortality and a 43.3% mortality in the group defined as limited life expectancy (LLE) based on age (≥ 85 years) and medical comorbidities. None died due to the NMSC. Leading cause of death was cardiac, cerebrovascular, and respiratory disease, lung and prostate cancer, and Alzheimer disease. The authors suggested the LLE group may be exposed to wound complications without benefiting from the treatment.4
Another study of 440 patients receiving excision for biopsy-proven facial NMSC at the Roudebush VA Medical Center in Indianapolis, Indiana, found no residual carcinoma in 35.3% of excisions, and in patients aged > 90 years, more than half of the excisions had no residual carcinoma. More than half of the patients aged > 90 years died within 1 year, not as a result of the NMSC. The authors argued for watchful waiting in select patients to maximize comfort and outcomes.10
NMSCs are often asymptomatic and not immediately life threatening. Although NMSCs tend to have a favorable prognosis, studies have found that NMSC may be a marker for other poor health outcomes. A significant increased risk for all-cause mortality was found for patients with a history of SCC, which may be attributed to immune status.11 The aging veteran population has more complex health care needs to be considered when developing surgical treatment plans. These medical problems may limit their life expectancy much sooner than the skin cancer will become symptomatic. We found that individuals aged ≥ 80 years who had CAD, CHF, or dementia had a relative risk of 3 or higher for 5-year mortality. The leading cause of death in the United States in years 2011 to 2015 was heart disease. Alzheimer disease was the sixth leading cause of death in those same years.12-14
Skin cancer excisions do not typically require general anesthesia, deep sedation, or large fluid shifts; however, studies have found that when frail patients undergo low-risk procedures, they tend to have a higher mortality rate than their healthier counterparts.15 Frailty is a concept that identifies patients who are at increased risk of dying in 6 to 60 months due to a decline in their physical reserve. Frail patients have increased rates of perioperative mortality and complications. Various tools have been used to assess the components of physical performance, speed, mobility, nutrition status, mental health, and cognition.16 Frailty screening has been initiated in several VA hospitals, including our own in Gainesville, Florida, with the goal of decreasing postoperative morbidity and mortality in older adult patients.17 The patients are given a 1-page screening assessment that asks about their living situation, medical conditions, nutrition status, cognition, and activities of daily living. The results can trigger the clinician to rethink the surgical plan and mobilize more resources to optimize the patient’s health. This study period precedes the initiative at our institution.
The plastic surgery service’s routine practice is to excise skin cancers in the operating room if sedation or general anesthesia will be needed (Figure 1A), for optimal control of bleeding (Figure 1B) in a patient who cannot safely stop blood thinners, or for excision of a highly vascularized area such as the scalp. Surgery is offered in an office-based setting if the area can be closed primarily, left open to close secondarily, or closed with a small skin graft under local anesthesia only (Figure 2). We prefer treating frail patients in the minor procedure clinic, when possible, to avoid the risks of sedation and the additional preoperative visits and transportation requirements. NMSC with unclear margins (Figure 3A) or in cosmetically sensitive areas where tissue needs to be preserved (Figure 3B) are referred to the Mohs dermatologist. The skin cancers in this study were most frequently found on the face, scalp, hands, and forearms based on referral patterns.
Other treatment options for NMSC include curettage and electrodessication, cryotherapy, and radiation; however, ours is a surgical service and patients are typically referred to us by primary care or dermatology when those are not reasonable or desirable options.18 Published complication rates of patients having skin cancer surgery without age restriction have a rate of 3% to 6%, which is consistent with our study of 5%.19-21 Two bleeding complications that needed to be admitted did not require more than a bedside procedure and neither required transfusions. One patient had been instructed to continue taking coumadin during the perioperative office-based procedure due to a recent carotid stent placement in the setting of a rapidly growing basal cell on an easily accessible location.
The most noted comorbidity in patients with wound complications was found to be DM; however, this was not found to be a statistically significant risk factor for wound complications (P = .10). We do not have a set rule for advising for or against NMSC surgery. We do counsel frail patients and their families that not all cancer is immediately life threatening and will work with them to do whatever makes the most sense to achieve their goals, occasionally accepting positive margins in order to debulk a symptomatic growth. The objective of this paper is to contribute to the discussion of performing invasive procedures on older adult veterans with life-limiting comorbidities. Patients and their families will have different thresholds for what they feel needs intervention, especially if other medical problems are consuming much of their time. We also have the community care referral option for patients whose treatment decisions are being dictated by travel hardships.
Strengths and Limitations
A strength of this study is that the data were obtained from a closed system. Patients tend to stay long-term within the VA and their health record is accessible throughout the country as long as they are seen at a VA facility. Complications, therefore, return to the treating service or primary care, who would route the patient back to the surgeon.
One limitation of the study is that this is a retrospective review from 2011. The authors are limited to data that are recorded in the patient record. Multiple health care professionals saw the patients and notes lack consistency in detail. Size of the lesions were not consistently recorded and did not get logged into our database for that reason.
Conclusions
Treatment of NMSC in older adult patients has a low morbidity but needs to be balanced against a patient and family’s goals when the patient presents with life-limiting comorbidities. An elevated 5-year mortality in patients aged > 80 years with serious unrelated medical conditions is intuitive, but this study may help put treatment plans into perspective for families and health care professionals who want to provide an indicated service while maximizing patient quality of life.
Acknowledgments
This manuscript is the result of work supported with resources and the use of facilities at the North Florida/South Georgia Veterans Health System, Gainesville, Florida.
1. American Cancer Society. Cancer Facts & Figures 2021. Accessed May 26, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf
2. Albert A, Knoll MA, Conti JA, Zbar RIS. Non-melanoma skin cancers in the older patient. Curr Oncol Rep. 2019;21(9):79. Published 2019 Jul 29. doi:10.1007/s11912-019-0828-9
3. Linos E, Chren MM, Stijacic Cenzer I, Covinsky KE. Skin cancer in U.S. elderly adults: does life expectancy play a role in treatment decisions? J Am Geriatr Soc. 2016;64(8):1610-1615. doi:10.1111/jgs.14202
4. Linos E, Parvataneni R, Stuart SE, Boscardin WJ, Landefeld CS, Chren MM. Treatment of nonfatal conditions at the end of life: nonmelanoma skin cancer. JAMA Intern Med. 2013;173(11):1006-1012. doi:10.1001/jamainternmed.2013.639
5. O’Malley KA, Vinson L, Kaiser AP, Sager Z, Hinrichs K. Mental health and aging veterans: how the Veterans Health Administration meets the needs of aging veterans. Public Policy Aging Rep. 2020;30(1):19-23. doi:10.1093/ppar/prz027
6. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Profile of veterans: 2017. Accessed May 26, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf 7. Riemenschneider K, Liu J, Powers JG. Skin cancer in the military: a systematic review of melanoma and nonmelanoma skin cancer incidence, prevention, and screening among active duty and veteran personnel. J Am Acad Dermatol. 2018;78(6):1185-1192. doi:10.1016/j.jaad.2017.11.062
8. Clemens MW, Kochuba AL, Carter ME, Han K, Liu J, Evans K. Association between Agent Orange exposure and nonmelanotic invasive skin cancer: a pilot study. Plast Reconstr Surg. 2014;133(2):432-437. doi:10.1097/01.prs.0000436859.40151.cf
9. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-317. doi:10.1016/j.jaad.2018.03.060
10. Chauhan R, Munger BN, Chu MW, et al. Age at diagnosis as a relative contraindication for intervention in facial nonmelanoma skin cancer. JAMA Surg. 2018;153(4):390-392. doi:10.1001/jamasurg.2017.5073
11. Barton V, Armeson K, Hampras S, et al. Nonmelanoma skin cancer and risk of all-cause and cancer-related mortality: a systematic review. Arch Dermatol Res. 2017;309(4):243-251. doi:10.1007/s00403-017-1724-5
12. Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2013. NCHS Data Brief 178. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db178.htm
13. Xu JQ, Kochanek KD, Murphy SL, Arias E. Mortality in the United States, 2012. NCHS Data Brief 168. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db168.htm
14. Xu JQ, Murphy SL, Kochanek KD, Arias E. Mortality in the United States, 2015. NCHS Data Brief 267. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db267.htm
15. Varley PR , Borrebach JD, Arya S, et al. Clinical utility of the risk analysis index as a prospective frailty screening tool within a multi-practice, multi-hospital integrated healthcare system. Ann Surg. 2021;274(6):e1230-e1237. doi:10.1097/SLA.0000000000003808
16. Hall DE, Arya S , Schmid KK, et al. Development and initial validation of the risk analysis index for measuring frailty in surgical populations. JAMA Surg. 2017;152(2):175-182. doi:10.1001/jamasurg.2016.4202
17. US Department of Veterans Affairs, Health Services Research & Development. Improving healthcare for aging veterans. Updated August 30, 2017. Accessed May 26, 2022. https://www.hsrd.research.va.gov/news/feature/aging0917.cfm
18. Leus AJG, Frie M, Haisma MS, et al. Treatment of keratinocyte carcinoma in elderly patients – a review of the current literature. J Eur Acad Dermatol Venereol. 2020;34(9):1932-1943. doi:10.1111/jdv.16268
19. Amici JM, Rogues AM, Lasheras A, et al. A prospective study of the incidence of complications associated with dermatological surgery. Br J Dermatol. 2005;153(5):967-971. doi:10.1111/j.1365-2133.2005.06861.x
20. Arguello-Guerra L, Vargas-Chandomid E, Díaz-González JM, Méndez-Flores S, Ruelas-Villavicencio A, Domínguez-Cherit J. Incidence of complications in dermatological surgery of melanoma and non-melanoma skin cancer in patients with multiple comorbidity and/or antiplatelet-anticoagulants. Five-year experience in our hospital. Cir Cir. 2019;86(1):15-23. doi:10.24875/CIRUE.M18000003
21. Keith DJ, de Berker DA, Bray AP, Cheung ST, Brain A, Mohd Mustapa MF. British Association of Dermatologists’ national audit on nonmelanoma skin cancer excision, 2014. Clin Exp Dermatol. 2017;42(1):46-53. doi:10.1111/ced.12990
1. American Cancer Society. Cancer Facts & Figures 2021. Accessed May 26, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf
2. Albert A, Knoll MA, Conti JA, Zbar RIS. Non-melanoma skin cancers in the older patient. Curr Oncol Rep. 2019;21(9):79. Published 2019 Jul 29. doi:10.1007/s11912-019-0828-9
3. Linos E, Chren MM, Stijacic Cenzer I, Covinsky KE. Skin cancer in U.S. elderly adults: does life expectancy play a role in treatment decisions? J Am Geriatr Soc. 2016;64(8):1610-1615. doi:10.1111/jgs.14202
4. Linos E, Parvataneni R, Stuart SE, Boscardin WJ, Landefeld CS, Chren MM. Treatment of nonfatal conditions at the end of life: nonmelanoma skin cancer. JAMA Intern Med. 2013;173(11):1006-1012. doi:10.1001/jamainternmed.2013.639
5. O’Malley KA, Vinson L, Kaiser AP, Sager Z, Hinrichs K. Mental health and aging veterans: how the Veterans Health Administration meets the needs of aging veterans. Public Policy Aging Rep. 2020;30(1):19-23. doi:10.1093/ppar/prz027
6. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Profile of veterans: 2017. Accessed May 26, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf 7. Riemenschneider K, Liu J, Powers JG. Skin cancer in the military: a systematic review of melanoma and nonmelanoma skin cancer incidence, prevention, and screening among active duty and veteran personnel. J Am Acad Dermatol. 2018;78(6):1185-1192. doi:10.1016/j.jaad.2017.11.062
8. Clemens MW, Kochuba AL, Carter ME, Han K, Liu J, Evans K. Association between Agent Orange exposure and nonmelanotic invasive skin cancer: a pilot study. Plast Reconstr Surg. 2014;133(2):432-437. doi:10.1097/01.prs.0000436859.40151.cf
9. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-317. doi:10.1016/j.jaad.2018.03.060
10. Chauhan R, Munger BN, Chu MW, et al. Age at diagnosis as a relative contraindication for intervention in facial nonmelanoma skin cancer. JAMA Surg. 2018;153(4):390-392. doi:10.1001/jamasurg.2017.5073
11. Barton V, Armeson K, Hampras S, et al. Nonmelanoma skin cancer and risk of all-cause and cancer-related mortality: a systematic review. Arch Dermatol Res. 2017;309(4):243-251. doi:10.1007/s00403-017-1724-5
12. Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2013. NCHS Data Brief 178. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db178.htm
13. Xu JQ, Kochanek KD, Murphy SL, Arias E. Mortality in the United States, 2012. NCHS Data Brief 168. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db168.htm
14. Xu JQ, Murphy SL, Kochanek KD, Arias E. Mortality in the United States, 2015. NCHS Data Brief 267. Accessed May 26, 2022. https://www.cdc.gov/nchs/products/databriefs/db267.htm
15. Varley PR , Borrebach JD, Arya S, et al. Clinical utility of the risk analysis index as a prospective frailty screening tool within a multi-practice, multi-hospital integrated healthcare system. Ann Surg. 2021;274(6):e1230-e1237. doi:10.1097/SLA.0000000000003808
16. Hall DE, Arya S , Schmid KK, et al. Development and initial validation of the risk analysis index for measuring frailty in surgical populations. JAMA Surg. 2017;152(2):175-182. doi:10.1001/jamasurg.2016.4202
17. US Department of Veterans Affairs, Health Services Research & Development. Improving healthcare for aging veterans. Updated August 30, 2017. Accessed May 26, 2022. https://www.hsrd.research.va.gov/news/feature/aging0917.cfm
18. Leus AJG, Frie M, Haisma MS, et al. Treatment of keratinocyte carcinoma in elderly patients – a review of the current literature. J Eur Acad Dermatol Venereol. 2020;34(9):1932-1943. doi:10.1111/jdv.16268
19. Amici JM, Rogues AM, Lasheras A, et al. A prospective study of the incidence of complications associated with dermatological surgery. Br J Dermatol. 2005;153(5):967-971. doi:10.1111/j.1365-2133.2005.06861.x
20. Arguello-Guerra L, Vargas-Chandomid E, Díaz-González JM, Méndez-Flores S, Ruelas-Villavicencio A, Domínguez-Cherit J. Incidence of complications in dermatological surgery of melanoma and non-melanoma skin cancer in patients with multiple comorbidity and/or antiplatelet-anticoagulants. Five-year experience in our hospital. Cir Cir. 2019;86(1):15-23. doi:10.24875/CIRUE.M18000003
21. Keith DJ, de Berker DA, Bray AP, Cheung ST, Brain A, Mohd Mustapa MF. British Association of Dermatologists’ national audit on nonmelanoma skin cancer excision, 2014. Clin Exp Dermatol. 2017;42(1):46-53. doi:10.1111/ced.12990
Nodular Sclerosing Hodgkin Lymphoma With Paraneoplastic Cerebellar Degeneration
Paraneoplastic syndrome is a rare disorder involving manifestations of immune dysregulation triggered by malignancy. The immune system develops antibodies to the malignancy, which can cause cross reactivation with various tissues in the body, resulting in an autoimmune response. Paraneoplastic cerebellar degeneration (PCD) is a rare condition caused by immune-mediated damage to the Purkinje cells of the cerebellar tract. Symptoms may include gait instability, double vision, decreased fine motor skills, and ataxia, with progression to brainstem-associated symptoms, such as nystagmus, dysarthria, and dysphagia. Early detection and treatment of the underlying malignancy is critical to halt the progression of autoimmune-mediated destruction. We present a case of a young adult female patient with PCD caused by Purkinje cell cytoplasmic–Tr (PCA-Tr) antibody with Hodgkin lymphoma.
Case Presentation
A 20-year-old previously healthy active-duty female patient presented to the emergency department with acute worsening of chronic intermittent, recurrent episodes of lightheadedness and vertigo. Symptoms persisted for 9 months until acutely worsening over the 2 weeks prior to presentation. She reported left eye double vision but did not report seeing spots, photophobia, tinnitus, or headache. She felt off-balance, leaning on nearby objects to remain standing. Symptoms primarily occurred during ambulation; however, occasionally they happened at rest. Episodes lasted up to several minutes and occurred up to 15 times a day. The patient reported no fever, night sweats, unexplained weight loss, muscle aches, weakness, numbness or tingling, loss of bowel or bladder function, or rash. She had no recent illnesses, changes to medications, or recent travel. Oral intake to include food and water was adequate and unchanged. The patient had a remote history of mild concussions without loss of consciousness while playing sports 4 years previously. She reported no recent trauma. Nine months before, she received treatment for benign paroxysmal positional vertigo (BPPV) with the Epley maneuver with full resolution of symptoms lasting several days. She reported no prescription or over-the-counter medications, herbal remedies, or supplements. She reported no other medical or surgical history and no pertinent social or family history.
Physical examination revealed a nontoxic-appearing female patient with intermittent conversational dysarthria, saccadic pursuits, horizontal nystagmus with lateral gaze, and vertical nystagmus with vertical gaze. The patient exhibited dysdiadochokinesia, or impaired ability to perform rapid alternating hand movements with repetition. Finger-to-nose testing was impaired and heel-to-shin motion remained intact. A Romberg test was positive, and the patient had tandem gait instability. Strength testing, sensation, reflexes, and cranial nerves were otherwise intact. Initial laboratory testing was unremarkable except for mild normocytic anemia. Her infectious workup, including testing for venereal disease, HIV, COVID-19, and Coccidioidies was negative. Heavy metals analysis and urine drug screen were negative. Ophthalmology was consulted and workup revealed small amplitude downbeat nystagmus in primary gaze, sustained gaze evoked lateral beating jerk nystagmus with rebound nystagmus R>L gaze, but there was no evidence of afferent package defect and optic nerve function remained intact. Magnetic resonance imaging of the brain demonstrated cerebellar vermis hypoplasia with prominence of the superior cerebellar folia. Due to concerns for autoimmune encephalitis, a lumbar puncture was performed. Antibody testing revealed PCA-Tr antibodies, which is commonly associated with Hodgkin lymphoma, prompting further evaluation for malignancy.
Computed tomography (CT) of the chest with contrast demonstrated multiple mediastinal masses with a conglomeration of lymph nodes along the right paratracheal region. Further evaluation was performed with a positron emission tomography (PET)–CT, revealing a large conglomeration of hypermetabolic pretracheal, mediastinal, and right supraclavicular lymph that were suggestive of lymphoma. Mediastinoscopy with excisional lymph node biopsy was performed with immunohistochemical staining confirming diagnosis of a nodular sclerosing variant of Hodgkin lymphoma. The patient was treated with IV immunoglobulin at 0.4g/kg daily for 5 days. A central venous catheter was placed into the patient’s right internal jugular vein and a chemotherapy regimen of doxorubicin 46 mg, vinblastine 11 mg, bleomycin 19 units, and dacarbazine 700 mg was initiated. The patient’s symptoms improved with resolution of dysarthria; however, her visual impairment and gait instability persisted. Repeat PET-CT imaging 2 months later revealed interval improvement with decreased intensity and extent of the hypermetabolic lymph nodes and no new hypermetabolic foci.
Discussion
PCA-Tr antibodies affect the delta/notchlike epidermal growth factor–related receptor, expressed on the dendrites of cerebellar Purkinje cells.1 These fibers are the only output neurons of the cerebellar cortex and are critical to the coordination of motor movements, accounting for the ataxia experienced by patients with this subtype of PCD.2 The link between Hodgkin lymphoma and PCA-Tr antibodies has been established; however, most reports involve men with a median age of 61 years with lymphoma-associated symptoms (such as lymphadenopathy) or systemic symptoms (fever, night sweats, or weight loss) preceding neurologic manifestations in 80% of cases.3
Our patient was a young, previously healthy adult female who initially presented with vertigo, a common concern with frequently benign origins. Although there was temporary resolution of symptoms after Epley maneuvers, symptoms recurred and progressed over several months to include brainstem manifestations of nystagmus, diplopia, and dysarthria. Previous reports indicate that after remission of the Hodgkin lymphoma, PCA-Tr antibodies disappear and symptoms can improve or resolve.4,5 Treatment has just begun for our patient and although there has been initial clinical improvement, given the chronicity of symptoms, it is unclear if complete resolution will be achieved.
Conclusions
PCD can result in debilitating neurologic dysfunction and may be associated with malignancy such as Hodgkin lymphoma. This case offers unique insight due to the patient’s demographics and presentation, which involved brainstem pathology typically associated with late-onset disease and preceded by constitutional symptoms. Clinical suspicion of this rare disorder should be considered in all ages, especially if symptoms are progressive or neurologic manifestations arise, as early detection and treatment of the underlying malignancy are paramount to the prevention of significant disability.
1. de Graaff E, Maat P, Hulsenboom E, et al. Identification of delta/notch-like epidermal growth factor-related receptor as the Tr antigen in paraneoplastic cerebellar degeneration. Ann Neurol. 2012;71(6):815-824. doi:10.1002/ana.23550
2. MacKenzie-Graham A, Tiwari-Woodruff SK, Sharma G, et al. Purkinje cell loss in experimental autoimmune encephalomyelitis. Neuroimage. 2009;48(4):637-651. doi:10.1016/j.neuroimage.2009.06.073
3. Bernal F, Shams’ili S, Rojas I, et al. Anti-Tr antibodies as markers of paraneoplastic cerebellar degeneration and Hodgkin’s disease. Neurology. 2003;60(2):230-234. doi:10.1212/01.wnl.0000041495.87539.98
4. Graus F, Ariño H, Dalmau J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood. 2014;123(21):3230-3238. doi:10.1182/blood-2014-03-537506
5. Aly R, Emmady PD. Paraneoplastic cerebellar degeneration. Updated May 8, 2022. Accessed March 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK560638
Paraneoplastic syndrome is a rare disorder involving manifestations of immune dysregulation triggered by malignancy. The immune system develops antibodies to the malignancy, which can cause cross reactivation with various tissues in the body, resulting in an autoimmune response. Paraneoplastic cerebellar degeneration (PCD) is a rare condition caused by immune-mediated damage to the Purkinje cells of the cerebellar tract. Symptoms may include gait instability, double vision, decreased fine motor skills, and ataxia, with progression to brainstem-associated symptoms, such as nystagmus, dysarthria, and dysphagia. Early detection and treatment of the underlying malignancy is critical to halt the progression of autoimmune-mediated destruction. We present a case of a young adult female patient with PCD caused by Purkinje cell cytoplasmic–Tr (PCA-Tr) antibody with Hodgkin lymphoma.
Case Presentation
A 20-year-old previously healthy active-duty female patient presented to the emergency department with acute worsening of chronic intermittent, recurrent episodes of lightheadedness and vertigo. Symptoms persisted for 9 months until acutely worsening over the 2 weeks prior to presentation. She reported left eye double vision but did not report seeing spots, photophobia, tinnitus, or headache. She felt off-balance, leaning on nearby objects to remain standing. Symptoms primarily occurred during ambulation; however, occasionally they happened at rest. Episodes lasted up to several minutes and occurred up to 15 times a day. The patient reported no fever, night sweats, unexplained weight loss, muscle aches, weakness, numbness or tingling, loss of bowel or bladder function, or rash. She had no recent illnesses, changes to medications, or recent travel. Oral intake to include food and water was adequate and unchanged. The patient had a remote history of mild concussions without loss of consciousness while playing sports 4 years previously. She reported no recent trauma. Nine months before, she received treatment for benign paroxysmal positional vertigo (BPPV) with the Epley maneuver with full resolution of symptoms lasting several days. She reported no prescription or over-the-counter medications, herbal remedies, or supplements. She reported no other medical or surgical history and no pertinent social or family history.
Physical examination revealed a nontoxic-appearing female patient with intermittent conversational dysarthria, saccadic pursuits, horizontal nystagmus with lateral gaze, and vertical nystagmus with vertical gaze. The patient exhibited dysdiadochokinesia, or impaired ability to perform rapid alternating hand movements with repetition. Finger-to-nose testing was impaired and heel-to-shin motion remained intact. A Romberg test was positive, and the patient had tandem gait instability. Strength testing, sensation, reflexes, and cranial nerves were otherwise intact. Initial laboratory testing was unremarkable except for mild normocytic anemia. Her infectious workup, including testing for venereal disease, HIV, COVID-19, and Coccidioidies was negative. Heavy metals analysis and urine drug screen were negative. Ophthalmology was consulted and workup revealed small amplitude downbeat nystagmus in primary gaze, sustained gaze evoked lateral beating jerk nystagmus with rebound nystagmus R>L gaze, but there was no evidence of afferent package defect and optic nerve function remained intact. Magnetic resonance imaging of the brain demonstrated cerebellar vermis hypoplasia with prominence of the superior cerebellar folia. Due to concerns for autoimmune encephalitis, a lumbar puncture was performed. Antibody testing revealed PCA-Tr antibodies, which is commonly associated with Hodgkin lymphoma, prompting further evaluation for malignancy.
Computed tomography (CT) of the chest with contrast demonstrated multiple mediastinal masses with a conglomeration of lymph nodes along the right paratracheal region. Further evaluation was performed with a positron emission tomography (PET)–CT, revealing a large conglomeration of hypermetabolic pretracheal, mediastinal, and right supraclavicular lymph that were suggestive of lymphoma. Mediastinoscopy with excisional lymph node biopsy was performed with immunohistochemical staining confirming diagnosis of a nodular sclerosing variant of Hodgkin lymphoma. The patient was treated with IV immunoglobulin at 0.4g/kg daily for 5 days. A central venous catheter was placed into the patient’s right internal jugular vein and a chemotherapy regimen of doxorubicin 46 mg, vinblastine 11 mg, bleomycin 19 units, and dacarbazine 700 mg was initiated. The patient’s symptoms improved with resolution of dysarthria; however, her visual impairment and gait instability persisted. Repeat PET-CT imaging 2 months later revealed interval improvement with decreased intensity and extent of the hypermetabolic lymph nodes and no new hypermetabolic foci.
Discussion
PCA-Tr antibodies affect the delta/notchlike epidermal growth factor–related receptor, expressed on the dendrites of cerebellar Purkinje cells.1 These fibers are the only output neurons of the cerebellar cortex and are critical to the coordination of motor movements, accounting for the ataxia experienced by patients with this subtype of PCD.2 The link between Hodgkin lymphoma and PCA-Tr antibodies has been established; however, most reports involve men with a median age of 61 years with lymphoma-associated symptoms (such as lymphadenopathy) or systemic symptoms (fever, night sweats, or weight loss) preceding neurologic manifestations in 80% of cases.3
Our patient was a young, previously healthy adult female who initially presented with vertigo, a common concern with frequently benign origins. Although there was temporary resolution of symptoms after Epley maneuvers, symptoms recurred and progressed over several months to include brainstem manifestations of nystagmus, diplopia, and dysarthria. Previous reports indicate that after remission of the Hodgkin lymphoma, PCA-Tr antibodies disappear and symptoms can improve or resolve.4,5 Treatment has just begun for our patient and although there has been initial clinical improvement, given the chronicity of symptoms, it is unclear if complete resolution will be achieved.
Conclusions
PCD can result in debilitating neurologic dysfunction and may be associated with malignancy such as Hodgkin lymphoma. This case offers unique insight due to the patient’s demographics and presentation, which involved brainstem pathology typically associated with late-onset disease and preceded by constitutional symptoms. Clinical suspicion of this rare disorder should be considered in all ages, especially if symptoms are progressive or neurologic manifestations arise, as early detection and treatment of the underlying malignancy are paramount to the prevention of significant disability.
Paraneoplastic syndrome is a rare disorder involving manifestations of immune dysregulation triggered by malignancy. The immune system develops antibodies to the malignancy, which can cause cross reactivation with various tissues in the body, resulting in an autoimmune response. Paraneoplastic cerebellar degeneration (PCD) is a rare condition caused by immune-mediated damage to the Purkinje cells of the cerebellar tract. Symptoms may include gait instability, double vision, decreased fine motor skills, and ataxia, with progression to brainstem-associated symptoms, such as nystagmus, dysarthria, and dysphagia. Early detection and treatment of the underlying malignancy is critical to halt the progression of autoimmune-mediated destruction. We present a case of a young adult female patient with PCD caused by Purkinje cell cytoplasmic–Tr (PCA-Tr) antibody with Hodgkin lymphoma.
Case Presentation
A 20-year-old previously healthy active-duty female patient presented to the emergency department with acute worsening of chronic intermittent, recurrent episodes of lightheadedness and vertigo. Symptoms persisted for 9 months until acutely worsening over the 2 weeks prior to presentation. She reported left eye double vision but did not report seeing spots, photophobia, tinnitus, or headache. She felt off-balance, leaning on nearby objects to remain standing. Symptoms primarily occurred during ambulation; however, occasionally they happened at rest. Episodes lasted up to several minutes and occurred up to 15 times a day. The patient reported no fever, night sweats, unexplained weight loss, muscle aches, weakness, numbness or tingling, loss of bowel or bladder function, or rash. She had no recent illnesses, changes to medications, or recent travel. Oral intake to include food and water was adequate and unchanged. The patient had a remote history of mild concussions without loss of consciousness while playing sports 4 years previously. She reported no recent trauma. Nine months before, she received treatment for benign paroxysmal positional vertigo (BPPV) with the Epley maneuver with full resolution of symptoms lasting several days. She reported no prescription or over-the-counter medications, herbal remedies, or supplements. She reported no other medical or surgical history and no pertinent social or family history.
Physical examination revealed a nontoxic-appearing female patient with intermittent conversational dysarthria, saccadic pursuits, horizontal nystagmus with lateral gaze, and vertical nystagmus with vertical gaze. The patient exhibited dysdiadochokinesia, or impaired ability to perform rapid alternating hand movements with repetition. Finger-to-nose testing was impaired and heel-to-shin motion remained intact. A Romberg test was positive, and the patient had tandem gait instability. Strength testing, sensation, reflexes, and cranial nerves were otherwise intact. Initial laboratory testing was unremarkable except for mild normocytic anemia. Her infectious workup, including testing for venereal disease, HIV, COVID-19, and Coccidioidies was negative. Heavy metals analysis and urine drug screen were negative. Ophthalmology was consulted and workup revealed small amplitude downbeat nystagmus in primary gaze, sustained gaze evoked lateral beating jerk nystagmus with rebound nystagmus R>L gaze, but there was no evidence of afferent package defect and optic nerve function remained intact. Magnetic resonance imaging of the brain demonstrated cerebellar vermis hypoplasia with prominence of the superior cerebellar folia. Due to concerns for autoimmune encephalitis, a lumbar puncture was performed. Antibody testing revealed PCA-Tr antibodies, which is commonly associated with Hodgkin lymphoma, prompting further evaluation for malignancy.
Computed tomography (CT) of the chest with contrast demonstrated multiple mediastinal masses with a conglomeration of lymph nodes along the right paratracheal region. Further evaluation was performed with a positron emission tomography (PET)–CT, revealing a large conglomeration of hypermetabolic pretracheal, mediastinal, and right supraclavicular lymph that were suggestive of lymphoma. Mediastinoscopy with excisional lymph node biopsy was performed with immunohistochemical staining confirming diagnosis of a nodular sclerosing variant of Hodgkin lymphoma. The patient was treated with IV immunoglobulin at 0.4g/kg daily for 5 days. A central venous catheter was placed into the patient’s right internal jugular vein and a chemotherapy regimen of doxorubicin 46 mg, vinblastine 11 mg, bleomycin 19 units, and dacarbazine 700 mg was initiated. The patient’s symptoms improved with resolution of dysarthria; however, her visual impairment and gait instability persisted. Repeat PET-CT imaging 2 months later revealed interval improvement with decreased intensity and extent of the hypermetabolic lymph nodes and no new hypermetabolic foci.
Discussion
PCA-Tr antibodies affect the delta/notchlike epidermal growth factor–related receptor, expressed on the dendrites of cerebellar Purkinje cells.1 These fibers are the only output neurons of the cerebellar cortex and are critical to the coordination of motor movements, accounting for the ataxia experienced by patients with this subtype of PCD.2 The link between Hodgkin lymphoma and PCA-Tr antibodies has been established; however, most reports involve men with a median age of 61 years with lymphoma-associated symptoms (such as lymphadenopathy) or systemic symptoms (fever, night sweats, or weight loss) preceding neurologic manifestations in 80% of cases.3
Our patient was a young, previously healthy adult female who initially presented with vertigo, a common concern with frequently benign origins. Although there was temporary resolution of symptoms after Epley maneuvers, symptoms recurred and progressed over several months to include brainstem manifestations of nystagmus, diplopia, and dysarthria. Previous reports indicate that after remission of the Hodgkin lymphoma, PCA-Tr antibodies disappear and symptoms can improve or resolve.4,5 Treatment has just begun for our patient and although there has been initial clinical improvement, given the chronicity of symptoms, it is unclear if complete resolution will be achieved.
Conclusions
PCD can result in debilitating neurologic dysfunction and may be associated with malignancy such as Hodgkin lymphoma. This case offers unique insight due to the patient’s demographics and presentation, which involved brainstem pathology typically associated with late-onset disease and preceded by constitutional symptoms. Clinical suspicion of this rare disorder should be considered in all ages, especially if symptoms are progressive or neurologic manifestations arise, as early detection and treatment of the underlying malignancy are paramount to the prevention of significant disability.
1. de Graaff E, Maat P, Hulsenboom E, et al. Identification of delta/notch-like epidermal growth factor-related receptor as the Tr antigen in paraneoplastic cerebellar degeneration. Ann Neurol. 2012;71(6):815-824. doi:10.1002/ana.23550
2. MacKenzie-Graham A, Tiwari-Woodruff SK, Sharma G, et al. Purkinje cell loss in experimental autoimmune encephalomyelitis. Neuroimage. 2009;48(4):637-651. doi:10.1016/j.neuroimage.2009.06.073
3. Bernal F, Shams’ili S, Rojas I, et al. Anti-Tr antibodies as markers of paraneoplastic cerebellar degeneration and Hodgkin’s disease. Neurology. 2003;60(2):230-234. doi:10.1212/01.wnl.0000041495.87539.98
4. Graus F, Ariño H, Dalmau J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood. 2014;123(21):3230-3238. doi:10.1182/blood-2014-03-537506
5. Aly R, Emmady PD. Paraneoplastic cerebellar degeneration. Updated May 8, 2022. Accessed March 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK560638
1. de Graaff E, Maat P, Hulsenboom E, et al. Identification of delta/notch-like epidermal growth factor-related receptor as the Tr antigen in paraneoplastic cerebellar degeneration. Ann Neurol. 2012;71(6):815-824. doi:10.1002/ana.23550
2. MacKenzie-Graham A, Tiwari-Woodruff SK, Sharma G, et al. Purkinje cell loss in experimental autoimmune encephalomyelitis. Neuroimage. 2009;48(4):637-651. doi:10.1016/j.neuroimage.2009.06.073
3. Bernal F, Shams’ili S, Rojas I, et al. Anti-Tr antibodies as markers of paraneoplastic cerebellar degeneration and Hodgkin’s disease. Neurology. 2003;60(2):230-234. doi:10.1212/01.wnl.0000041495.87539.98
4. Graus F, Ariño H, Dalmau J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood. 2014;123(21):3230-3238. doi:10.1182/blood-2014-03-537506
5. Aly R, Emmady PD. Paraneoplastic cerebellar degeneration. Updated May 8, 2022. Accessed March 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK560638