User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
COVID-19 and risk of clotting: ‘Be proactive about prevention’
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.

The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.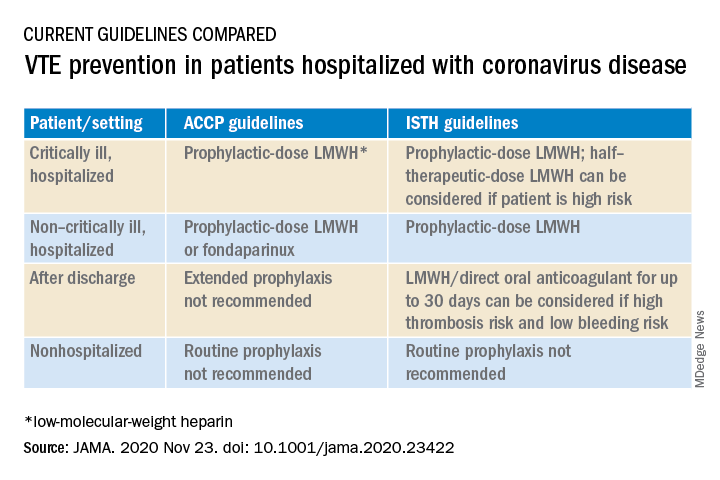
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
New residency matching sets record, says NRMP
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
Biden chooses California Attorney General Xavier Becerra to head HHS

If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
If confirmed by the US Senate, Becerra will face the challenge of overseeing the federal agency charged with protecting the health of all Americans in the midst of the COVID-19 pandemic. At the time of the announcement, nearly 15 million Americans had tested positive for COVID-19 and more than 280,000 had died.
Becerra served 12 terms in Congress, representing the Los Angeles area. Although his public health experience is limited, he served on the Congressional Ways and Means Committee overseeing health-related issues. Becerra is known as an advocate for the health and well-being of women in particular.
The American College of Physicians, American Academy of Pediatrics, American College of Obstetricians & Gynecologists, American Academy of Family Physicians, and the American Psychiatric Association wrote a letter to Biden on December 3 urging him to select leaders with medical and healthcare expertise, in particular physicians.
“We believe that your administration and the country would be well-served by the appointment of qualified physicians to serve in key positions critical to advancing the health of our nation,” they wrote. “Therefore, our organizations, which represent more than 400,000 front-line physicians practicing in the United States, write to request that you identify and appoint physicians to healthcare leadership positions within your administration.”
Recent advocacy
Becerra has worked with Republican attorneys general to lobby HHS to increase access to remdesivir to treat people with COVID-19.
As attorney general, Becerra filed more than 100 lawsuits against the Trump administration. In November, he also represented more than 20 states in arguments supporting the Affordable Care Act before the Supreme Court.
On December 4, Becerra joined with attorneys general from 23 states and the District of Columbia opposing a proposed rule from the outgoing Trump administration. The rule would deregulate HHS and “sunset”many agency provisions before Trump leaves office next month.
Becerra will be the first Latino appointed as HHS secretary, which furthers Biden’s goal to create a diverse cabinet. Becerra has been attorney general of California since 2017, replacing Vice President-elect Kamala Harris when she became senator.
Biden’s choice of Becerra was unexpected, according to The New York Times, and he was not the only candidate. Speculation was that Biden initially considered Vivek Murthy, MD, later chosen as the next US surgeon general, as well New Mexico Gov. Michelle Lujan Grisham and Rhode Island Gov. Gina Raimondo.
A huge undertaking
As HHS secretary, Becerra would oversee a wide range of federal agencies, including the US Food and Drug Administration, the Centers for Disease Control and Prevention, the National Institutes of Health, and the Centers for Medicare & Medicaid Services.
The fiscal year 2021 budget proposed for HHS includes $94.5 billion in discretionary budget authority and $1.3 trillion in mandatory funding. Overall, HHS controls nearly one quarter of all federal expenditures and provides more grant money than all other federal agencies combined.
Becerra, 62, grew up in Sacramento, California. He was the first in his family to graduate from college. He received his undergraduate and law degrees from Stanford University.
This article first appeared on Medscape.com.
PPE shortage crisis continues at most hospitals, survey shows
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
Infant’s COVID-19–related myocardial injury reversed
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.

and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
FROM JACC CASE REPORTS
Key clinical point: Children presenting with COVID-19 should be tested for heart failure.
Major finding: A 2-month-old infant with COVID-19 had acute but reversible myocardial injury.
Study details: Single case report.
Disclosures: Dr. Sharma, MD, has no relevant financial relationships to disclose.
Source: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
FDA clears first drug for rare genetic causes of severe obesity
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has approved setmelanotide (Imcivree, Rhythm Pharmaceuticals) for weight management in adults and children as young as 6 years with obesity because of proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing.
Individuals with these rare genetic causes of severe obesity have a normal weight at birth but develop persistent severe obesity within months because of insatiable hunger (hyperphagia).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for these disorders.
“Many patients and families who live with these diseases face an often-burdensome stigma associated with severe obesity. To manage this obesity and control disruptive food-seeking behavior, caregivers often lock cabinets and refrigerators and significantly limit social activities,” said Jennifer Miller, MD, a pediatric endocrinologist at University of Florida Health, Gainesville, in a press release issued by the company.
“This FDA approval marks an important turning point, providing a much needed therapy and supporting the use of genetic testing to identify and properly diagnose patients with these rare genetic diseases of obesity,” she noted.
David Meeker, MD, chair, president, and CEO of Rhythm Pharmaceuticals, added: “We are advancing a first-in-class, precision medicine that is designed to directly address the underlying cause of obesities driven by genetic deficits in the MC4R pathway.”
Setmelanotide was evaluated in two phase 3 clinical trials. In one trial, 80% of patients with obesity caused by POMC or PCSK1 deficiency achieved greater than 10% weight loss after 1 year of treatment.
In the other trial, 45.5% of patients with obesity caused by LEPR deficiency achieved greater than 10% weight loss with 1 year of treatment.
Results for the two trials were recently published in The Lancet Diabetes & Endocrinology and discussed at the ObesityWeek Interactive 2020 meeting.
Setmelanotide was generally well tolerated in both trials. The most common adverse events were injection-site reactions, skin hyperpigmentation, and nausea.
The drug label notes that disturbances in sexual arousal, depression, and suicidal ideation; skin pigmentation; and darkening of preexisting nevi may occur with setmelanotide treatment.
The drug label also notes a risk for serious adverse reactions because of benzyl alcohol preservative in neonates and low-birth-weight infants. Setmelanotide is not approved for use in neonates or infants.
The company expects the drug to be commercially available in the United States in the first quarter of 2021.
Setmelanotide for the treatment of obesity associated with rare genetic defects had FDA breakthrough therapy designation as well as orphan drug designation.
The company is also evaluating setmelanotide for reduction in hunger and body weight in a pivotal phase 3 trial in people living with Bardet-Biedl or Alström syndrome, and top-line data are due soon.
A version of this article originally appeared on Medscape.com.
Understanding and addressing suicide risk in LGBTQ+ youth
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
Even as dozens of state legislature bills attempt to limit the rights of sexual-diverse and gender-diverse youth, researchers are learning more and more that can help pediatricians better support this population in their practices, according to David Inwards-Breland, MD, MPH, a professor of clinical pediatrics at the University of California, San Diego.
Dr. Inwards-Breland highlighted two key studies in recent years during the LGBTQ+ section at the annual meeting of the American Academy of Pediatrics, held virtually in 2020.
High suicide rates among sexual minority youth
Past research has found that adolescents who identify as sexual minorities have nearly five times the rate of suicide attempts, compared with their heterosexual peers, Dr. Inwards-Breland said as he introduced a recent study on disparities in adolescent suicide.
“This may be from a disproportionate burden of poor mental health that has been linked to stigma,” he said, adding that an estimated 125 state bills have been introduced in the United States that would restrict the rights of sexual minorities.
The study, published in Pediatrics in March 2020, compiled data from 110,243 adolescents in six states on sexual orientation identity; 25,994 adolescents in four states on same-sex sexual contact and sexual assault; and 20,655 adolescents in three states on sexual orientation identity, the sex of sexual contacts, and sexual assault.
The authors found that heterosexual identity dropped from 93% to 86% between 2009 and 2017, but sexual minority youth accounted for an increasing share of suicide attempts over the same period. A quarter of adolescents who attempted suicide in 2009 were sexual minorities, which increased to 36% in 2017. Similarly, among sexually active teens who attempted suicide, the proportion of those who had same-sex contact nearly doubled, from 16% to 30%.
The good news, Dr. Inwards-Breland said, was that overall suicide attempts declined among sexual minorities, but they remain three times as likely to attempt suicide, compared with their heterosexual counterparts.
“As the number of adolescents increase in our country, there will be increasing numbers of adolescents identifying as sexual minorities or who have had same-sex sexual contact,” Dr. Inwards-Breland said. “Therefore, providing confidential services is even more important to allow youth to feel comfortable with their health care provider.” He also emphasized the importance of consistent universal depression screening and advocacy to eliminate and prevent policies that harm these youth.
Using youths’ chosen names
Transgender and nonbinary youth – those who do not identify as male or female – have a higher risk of poor mental health and higher levels of suicidal ideation and behaviors, compared with their “cis” peers, those who identify with the gender they were assigned at birth, Dr. Inwards-Breland said. However, using the chosen, or assertive, name of transgender and nonbinary youth predicted fewer depressive symptoms and less suicidal ideation and behavior in a study published in the Journal of Adolescent Health in October 2018.
“Choosing a name is an important part of social transition of transgender individuals, yet they’re unable to use their name because of interpersonal or institutional barriers,” he said. In addition, using a name other than their legally given name can subject them to discrimination and victimization.
The study, drawing from a larger cohort of LGBTQ youth, involved 129 transgender and nonbinary adolescents, aged 15-21, of whom 74 had a chosen name. No other differences in personal characteristics were associated with depressive symptoms or suicidal ideation besides increased use of their assertive name in different life contexts.
An increase in one context where chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior, the study found. All three outcomes were at their lowest levels when chosen names were used in all four contexts explored in the study.
“The chosen name affirms their gender identity,” Dr. Inwards-Breland said, but “the legal name change process is very onerous.” He highlighted the need for institutions to adjust regulations and information systems, for policies that promote the transition process, and for youths’ names to be affirmed in multiple contexts.
“We as pediatricians, specialists, and primary care doctors can support families as they adjust the transition process by helping them with assertive names and pronouns and giving them resources,” Dr. Inwards-Breland said. He also called for school policies and teacher/staff training that promote the use of assertive names and pronouns, and ensuring that the assertive name and pronouns are in the medical record and used by office staff and other medical professionals.
‘A light in the dark’ for LGBTQ+ youth
Clair Kronk of the University of Cincinnati and Cincinnati Children’s Hospital and Medical Center attended the LGBTQ+ section at the AAP meeting because of concerns about she and her transgender siblings have been treated by the medical community.
“It has always been important to be ‘on the pulse’ of what is happening in the medical community, especially with new, more discriminatory policies being passed seemingly willy-nilly these days, both in the medical realm and outside of it,” Ms. Kronk said in an interview. “I was overjoyed to see how many people seemed to care so much about the transgender community and LGBTQIA+ people generally.”
As an ontologist and bioinformatician, she did not recall many big clinical takeaways for her particular work, but she appreciated how many areas the session covered, especially given the dearth of instruction about LGBTQ+ care in medical training.
“This session was a bit of a light in the dark given the state of LGBTQIA+ health care rights,” she said. “There is a lot at stake in the next year or so, and providers’ and LGBTQIA+ persons’ voices need to be heard right now more than ever.”
Sonia Khan, MD, a pediatrician and the medical director of the substance use disorder counseling program in the department of health and human services in Fremont, Calif., also attended the session and came away feeling invigorated.
“These data make me feel more optimistic than I have been in ages in terms of increasing the safety of young people being able to come out,” Dr. Khan said in the comments during the session. “These last 4 years felt so regressive. [It’s] good to get the big picture.”
The presenters and commentators had no disclosures.
FROM AAP 2020
Obesity, hypoxia predict severity in children with COVID-19
based on data from 281 patients at 8 locations.
Manifestations of COVID-19 in children include respiratory disease similar to that seen in adults, but the full spectrum of disease in children has been studied mainly in single settings or with a focus on one clinical manifestation, wrote Danielle M. Fernandes, MD, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in the Journal of Pediatrics, the researchers identified 281 children hospitalized with COVID-19 and/or multisystem inflammatory syndrome in children (MIS-C) at 8 sites in Connecticut, New Jersey, and New York. A total of 143 (51%) had respiratory disease, 69 (25%) had MIS-C, and 69 (25%) had other manifestations of illness including 32 patients with gastrointestinal problems, 21 infants with fever, 6 cases of neurologic disease, 6 cases of diabetic ketoacidosis, and 4 patients with other indications. The median age of the patients was 10 years, 60% were male, 51% were Hispanic, and 23% were non-Hispanic Black. The most common comorbidities were obesity (34%) and asthma (14%).
Independent predictors of disease severity in children found
After controlling for multiple variables, obesity and hypoxia at hospital admission were significant independent predictors of severe respiratory disease, with odds ratios of 3.39 and 4.01, respectively. In addition, lower absolute lymphocyte count (OR, 8.33 per unit decrease in 109 cells/L) and higher C-reactive protein (OR, 1.06 per unit increase in mg/dL) were significantly predictive of severe MIS-C (P = .001 and P = .017, respectively).
“The association between weight and severe respiratory COVID-19 is consistent with the adult literature; however, the mechanisms of this association require further study,” Dr. Fernandes and associates noted.
Overall, children with MIS-C were significantly more likely to be non-Hispanic Black, compared with children with respiratory disease, an 18% difference. However, neither race/ethnicity nor socioeconomic status were significant predictors of disease severity, the researchers wrote.
During the study period, 7 patients (2%) died and 114 (41%) were admitted to the ICU.
“We found a wide array of clinical manifestations in children and youth hospitalized with SARS-CoV-2,” Dr. Fernandes and associates wrote. Notably, gastrointestinal symptoms, ocular symptoms, and dermatologic symptoms have rarely been noted in adults with COVID-19, but occurred in more than 30% of the pediatric patients.
“We also found that SARS-CoV-2 can be an incidental finding in a substantial number of hospitalized pediatric patients,” the researchers said.
The findings were limited by several factors including a population of patients only from Connecticut, New Jersey, and New York, and the possibility that decisions on hospital and ICU admission may have varied by location, the researchers said. In addition, approaches may have varied in the absence of data on the optimal treatment of MIS-C.
“This study builds on the growing body of evidence showing that mortality in hospitalized pediatric patients is low, compared with adults,” Dr. Fernandes and associates said. “However, it highlights that the young population is not universally spared from morbidity, and that even previously healthy children and youth can develop severe disease requiring supportive therapy.”
Findings confirm other clinical experience
The study was important to show that, “although most children are spared severe illness from COVID-19, some children are hospitalized both with acute COVID-19 respiratory disease, with MIS-C and with a range of other complications,” Adrienne Randolph, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, said in an interview.
Dr. Randolph said she was not surprised by the study findings, “as we are also seeing these types of complications at Boston Children’s Hospital where I work.”
Additional research is needed on the outcomes of these patients, “especially the longer-term sequelae of having COVID-19 or MIS-C early in life,” she emphasized.
The take-home message to clinicians from the findings at this time is to be aware that children and adolescents can become severely ill from COVID-19–related complications, said Dr. Randolph. “Some of the laboratory values on presentation appear to be associated with disease severity.”
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Randolph disclosed funding from the Centers for Disease Control and Prevention to lead the Overcoming COVID-19 Study in U.S. Children and Adults.
SOURCE: Fernandes DM et al. J Pediatr. 2020 Nov 13. doi: 10.1016/j.jpeds.2020.11.016.
based on data from 281 patients at 8 locations.
Manifestations of COVID-19 in children include respiratory disease similar to that seen in adults, but the full spectrum of disease in children has been studied mainly in single settings or with a focus on one clinical manifestation, wrote Danielle M. Fernandes, MD, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in the Journal of Pediatrics, the researchers identified 281 children hospitalized with COVID-19 and/or multisystem inflammatory syndrome in children (MIS-C) at 8 sites in Connecticut, New Jersey, and New York. A total of 143 (51%) had respiratory disease, 69 (25%) had MIS-C, and 69 (25%) had other manifestations of illness including 32 patients with gastrointestinal problems, 21 infants with fever, 6 cases of neurologic disease, 6 cases of diabetic ketoacidosis, and 4 patients with other indications. The median age of the patients was 10 years, 60% were male, 51% were Hispanic, and 23% were non-Hispanic Black. The most common comorbidities were obesity (34%) and asthma (14%).
Independent predictors of disease severity in children found
After controlling for multiple variables, obesity and hypoxia at hospital admission were significant independent predictors of severe respiratory disease, with odds ratios of 3.39 and 4.01, respectively. In addition, lower absolute lymphocyte count (OR, 8.33 per unit decrease in 109 cells/L) and higher C-reactive protein (OR, 1.06 per unit increase in mg/dL) were significantly predictive of severe MIS-C (P = .001 and P = .017, respectively).
“The association between weight and severe respiratory COVID-19 is consistent with the adult literature; however, the mechanisms of this association require further study,” Dr. Fernandes and associates noted.
Overall, children with MIS-C were significantly more likely to be non-Hispanic Black, compared with children with respiratory disease, an 18% difference. However, neither race/ethnicity nor socioeconomic status were significant predictors of disease severity, the researchers wrote.
During the study period, 7 patients (2%) died and 114 (41%) were admitted to the ICU.
“We found a wide array of clinical manifestations in children and youth hospitalized with SARS-CoV-2,” Dr. Fernandes and associates wrote. Notably, gastrointestinal symptoms, ocular symptoms, and dermatologic symptoms have rarely been noted in adults with COVID-19, but occurred in more than 30% of the pediatric patients.
“We also found that SARS-CoV-2 can be an incidental finding in a substantial number of hospitalized pediatric patients,” the researchers said.
The findings were limited by several factors including a population of patients only from Connecticut, New Jersey, and New York, and the possibility that decisions on hospital and ICU admission may have varied by location, the researchers said. In addition, approaches may have varied in the absence of data on the optimal treatment of MIS-C.
“This study builds on the growing body of evidence showing that mortality in hospitalized pediatric patients is low, compared with adults,” Dr. Fernandes and associates said. “However, it highlights that the young population is not universally spared from morbidity, and that even previously healthy children and youth can develop severe disease requiring supportive therapy.”
Findings confirm other clinical experience
The study was important to show that, “although most children are spared severe illness from COVID-19, some children are hospitalized both with acute COVID-19 respiratory disease, with MIS-C and with a range of other complications,” Adrienne Randolph, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, said in an interview.
Dr. Randolph said she was not surprised by the study findings, “as we are also seeing these types of complications at Boston Children’s Hospital where I work.”
Additional research is needed on the outcomes of these patients, “especially the longer-term sequelae of having COVID-19 or MIS-C early in life,” she emphasized.
The take-home message to clinicians from the findings at this time is to be aware that children and adolescents can become severely ill from COVID-19–related complications, said Dr. Randolph. “Some of the laboratory values on presentation appear to be associated with disease severity.”
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Randolph disclosed funding from the Centers for Disease Control and Prevention to lead the Overcoming COVID-19 Study in U.S. Children and Adults.
SOURCE: Fernandes DM et al. J Pediatr. 2020 Nov 13. doi: 10.1016/j.jpeds.2020.11.016.
based on data from 281 patients at 8 locations.
Manifestations of COVID-19 in children include respiratory disease similar to that seen in adults, but the full spectrum of disease in children has been studied mainly in single settings or with a focus on one clinical manifestation, wrote Danielle M. Fernandes, MD, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in the Journal of Pediatrics, the researchers identified 281 children hospitalized with COVID-19 and/or multisystem inflammatory syndrome in children (MIS-C) at 8 sites in Connecticut, New Jersey, and New York. A total of 143 (51%) had respiratory disease, 69 (25%) had MIS-C, and 69 (25%) had other manifestations of illness including 32 patients with gastrointestinal problems, 21 infants with fever, 6 cases of neurologic disease, 6 cases of diabetic ketoacidosis, and 4 patients with other indications. The median age of the patients was 10 years, 60% were male, 51% were Hispanic, and 23% were non-Hispanic Black. The most common comorbidities were obesity (34%) and asthma (14%).
Independent predictors of disease severity in children found
After controlling for multiple variables, obesity and hypoxia at hospital admission were significant independent predictors of severe respiratory disease, with odds ratios of 3.39 and 4.01, respectively. In addition, lower absolute lymphocyte count (OR, 8.33 per unit decrease in 109 cells/L) and higher C-reactive protein (OR, 1.06 per unit increase in mg/dL) were significantly predictive of severe MIS-C (P = .001 and P = .017, respectively).
“The association between weight and severe respiratory COVID-19 is consistent with the adult literature; however, the mechanisms of this association require further study,” Dr. Fernandes and associates noted.
Overall, children with MIS-C were significantly more likely to be non-Hispanic Black, compared with children with respiratory disease, an 18% difference. However, neither race/ethnicity nor socioeconomic status were significant predictors of disease severity, the researchers wrote.
During the study period, 7 patients (2%) died and 114 (41%) were admitted to the ICU.
“We found a wide array of clinical manifestations in children and youth hospitalized with SARS-CoV-2,” Dr. Fernandes and associates wrote. Notably, gastrointestinal symptoms, ocular symptoms, and dermatologic symptoms have rarely been noted in adults with COVID-19, but occurred in more than 30% of the pediatric patients.
“We also found that SARS-CoV-2 can be an incidental finding in a substantial number of hospitalized pediatric patients,” the researchers said.
The findings were limited by several factors including a population of patients only from Connecticut, New Jersey, and New York, and the possibility that decisions on hospital and ICU admission may have varied by location, the researchers said. In addition, approaches may have varied in the absence of data on the optimal treatment of MIS-C.
“This study builds on the growing body of evidence showing that mortality in hospitalized pediatric patients is low, compared with adults,” Dr. Fernandes and associates said. “However, it highlights that the young population is not universally spared from morbidity, and that even previously healthy children and youth can develop severe disease requiring supportive therapy.”
Findings confirm other clinical experience
The study was important to show that, “although most children are spared severe illness from COVID-19, some children are hospitalized both with acute COVID-19 respiratory disease, with MIS-C and with a range of other complications,” Adrienne Randolph, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, said in an interview.
Dr. Randolph said she was not surprised by the study findings, “as we are also seeing these types of complications at Boston Children’s Hospital where I work.”
Additional research is needed on the outcomes of these patients, “especially the longer-term sequelae of having COVID-19 or MIS-C early in life,” she emphasized.
The take-home message to clinicians from the findings at this time is to be aware that children and adolescents can become severely ill from COVID-19–related complications, said Dr. Randolph. “Some of the laboratory values on presentation appear to be associated with disease severity.”
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Randolph disclosed funding from the Centers for Disease Control and Prevention to lead the Overcoming COVID-19 Study in U.S. Children and Adults.
SOURCE: Fernandes DM et al. J Pediatr. 2020 Nov 13. doi: 10.1016/j.jpeds.2020.11.016.
FROM THE JOURNAL OF PEDIATRICS
Age no barrier to weight loss in those with morbid obesity
Older adults should be recommended for hospital-based lifestyle interventions to reduce weight, say U.K. investigators after finding there was no difference in weight loss between older and younger individuals in their program for those with morbid obesity.
Thomas M. Barber, PhD, and colleagues looked back at nearly 250 randomly selected adults who attended their obesity service over an 11-year period.
Older individuals, defined as aged 60 years and over, had higher rates of type 2 diabetes but experienced a similar percentage weight loss and reduction in body mass index (BMI) as younger patients over the course of around 40 months.
“Age should be no barrier to lifestyle management of obesity,” said Dr. Barber, of University Hospitals Coventry (England) and Warwickshire, in a news release from his institution. “Rather than putting up barriers to older people accessing weight-loss programs, we should be proactively facilitating that process. To do otherwise would risk further and unnecessary neglect of older people through societal ageist misconceptions.”
He urged service providers and policy makers to “appreciate the importance of weight loss in older people with obesity for the maintenance of health and well-being and the facilitation of healthy aging. Furthermore, age per se should not contribute toward clinical decisions regarding the implementation of lifestyle management of older people.”
The research was published online Nov. 22 in Clinical Endocrinology.
Real-world data will inform clinical practice
Jason Halford, PhD, a professor of biological psychology and health behavior, said in an interview: “The fear is that older patients are perceived not to respond” to lifestyle interventions to control obesity, “and that’s clearly a fallacy, according to this study.”
The findings are strengthened by the fact that these are real-world data, “and so it will inform clinical practice,” he added.
And one of the “more interesting” findings was that [type 2] diabetes was “more prevalent” in the older group “but they’re still losing weight,” he noted.
“Traditionally it’s been thought that people with type 2 diabetes find it more difficult to lose weight because you’re trying to manage two conditions,” said Dr. Halford, of the University of Leeds (England), who is also president-elect of the European Association for the Study of Obesity.
Don’t discount older patients
The researchers note that many of the comorbidities associated with obesity “develop over time” and that “no one is immune to obesity,” regardless of their age, sex, ethnicity, and socioeconomic status.
Barber said there are “a number of reasons” why health care professionals “may discount weight loss in older people,” including “an ‘ageist’ perspective that weight-loss is not relevant to older people and misconceptions of reduced ability of older people to lose weight through dietary modification and increased exercise.”
And “older people may feel that hospital-based obesity services are not for them,” he noted.
To determine the effect of age on the ability to lose weight through lifestyle interventions, Dr. Barber and colleagues randomly selected 242 patients with morbid obesity who attended their hospital-based service between 2005 and 2016.
Of these, 167 were aged 18-60 years and 75 were aged 60 years and older. Most participants were women (75.4% of the younger patients and 60.0% of the older patients).
The proportion of patients with confirmed diabetes was markedly higher in the older group, compared with the younger group, at 62.7% versus 35.3%, although older patients had a significantly lower baseline BMI, at 46.9 versus 49.7 kg/m2 (P < .05).
The average duration of the lifestyle intervention was over 3 years (41.5 months) in the younger patients and 33.6 months in the older patients.
There was no significant difference in percentage weight loss between younger and older patients, at 6.9% and 7.3%, respectively, and no difference in percentage reduction in BMI, at 8.1% versus 7.8%.
Further analysis demonstrated that there was no significant correlation between age at referral to the hospital-based service and percentage weight loss (correlation coefficient, –0.13).
Dr. Halford said it would have been “useful” to know the proportion of patients achieving 5% and 10% weight loss because, if a third of patients lost more than 10% of their weight, “even in an elderly population, that would suggest there’d be real benefits in terms of things like type 2 diabetes,” he noted.
And he would like to have seen more data around how long participants had been struggling with obesity, as it’s “just an assumption that the second group is further down the path because they’re older, but we can’t be 100% sure.”
The team noted the study is limited by being retrospective and including a random selection of patients attending the service rather than the entire cohort.
Dr. Halford agreed but said the analysis is a “starting point” and could be used as a platform to conduct “much more systematic research on this area.”
No funding or relevant financial relationships were declared.
A version of this article originally appeared on Medscape.com.
Older adults should be recommended for hospital-based lifestyle interventions to reduce weight, say U.K. investigators after finding there was no difference in weight loss between older and younger individuals in their program for those with morbid obesity.
Thomas M. Barber, PhD, and colleagues looked back at nearly 250 randomly selected adults who attended their obesity service over an 11-year period.
Older individuals, defined as aged 60 years and over, had higher rates of type 2 diabetes but experienced a similar percentage weight loss and reduction in body mass index (BMI) as younger patients over the course of around 40 months.
“Age should be no barrier to lifestyle management of obesity,” said Dr. Barber, of University Hospitals Coventry (England) and Warwickshire, in a news release from his institution. “Rather than putting up barriers to older people accessing weight-loss programs, we should be proactively facilitating that process. To do otherwise would risk further and unnecessary neglect of older people through societal ageist misconceptions.”
He urged service providers and policy makers to “appreciate the importance of weight loss in older people with obesity for the maintenance of health and well-being and the facilitation of healthy aging. Furthermore, age per se should not contribute toward clinical decisions regarding the implementation of lifestyle management of older people.”
The research was published online Nov. 22 in Clinical Endocrinology.
Real-world data will inform clinical practice
Jason Halford, PhD, a professor of biological psychology and health behavior, said in an interview: “The fear is that older patients are perceived not to respond” to lifestyle interventions to control obesity, “and that’s clearly a fallacy, according to this study.”
The findings are strengthened by the fact that these are real-world data, “and so it will inform clinical practice,” he added.
And one of the “more interesting” findings was that [type 2] diabetes was “more prevalent” in the older group “but they’re still losing weight,” he noted.
“Traditionally it’s been thought that people with type 2 diabetes find it more difficult to lose weight because you’re trying to manage two conditions,” said Dr. Halford, of the University of Leeds (England), who is also president-elect of the European Association for the Study of Obesity.
Don’t discount older patients
The researchers note that many of the comorbidities associated with obesity “develop over time” and that “no one is immune to obesity,” regardless of their age, sex, ethnicity, and socioeconomic status.
Barber said there are “a number of reasons” why health care professionals “may discount weight loss in older people,” including “an ‘ageist’ perspective that weight-loss is not relevant to older people and misconceptions of reduced ability of older people to lose weight through dietary modification and increased exercise.”
And “older people may feel that hospital-based obesity services are not for them,” he noted.
To determine the effect of age on the ability to lose weight through lifestyle interventions, Dr. Barber and colleagues randomly selected 242 patients with morbid obesity who attended their hospital-based service between 2005 and 2016.
Of these, 167 were aged 18-60 years and 75 were aged 60 years and older. Most participants were women (75.4% of the younger patients and 60.0% of the older patients).
The proportion of patients with confirmed diabetes was markedly higher in the older group, compared with the younger group, at 62.7% versus 35.3%, although older patients had a significantly lower baseline BMI, at 46.9 versus 49.7 kg/m2 (P < .05).
The average duration of the lifestyle intervention was over 3 years (41.5 months) in the younger patients and 33.6 months in the older patients.
There was no significant difference in percentage weight loss between younger and older patients, at 6.9% and 7.3%, respectively, and no difference in percentage reduction in BMI, at 8.1% versus 7.8%.
Further analysis demonstrated that there was no significant correlation between age at referral to the hospital-based service and percentage weight loss (correlation coefficient, –0.13).
Dr. Halford said it would have been “useful” to know the proportion of patients achieving 5% and 10% weight loss because, if a third of patients lost more than 10% of their weight, “even in an elderly population, that would suggest there’d be real benefits in terms of things like type 2 diabetes,” he noted.
And he would like to have seen more data around how long participants had been struggling with obesity, as it’s “just an assumption that the second group is further down the path because they’re older, but we can’t be 100% sure.”
The team noted the study is limited by being retrospective and including a random selection of patients attending the service rather than the entire cohort.
Dr. Halford agreed but said the analysis is a “starting point” and could be used as a platform to conduct “much more systematic research on this area.”
No funding or relevant financial relationships were declared.
A version of this article originally appeared on Medscape.com.
Older adults should be recommended for hospital-based lifestyle interventions to reduce weight, say U.K. investigators after finding there was no difference in weight loss between older and younger individuals in their program for those with morbid obesity.
Thomas M. Barber, PhD, and colleagues looked back at nearly 250 randomly selected adults who attended their obesity service over an 11-year period.
Older individuals, defined as aged 60 years and over, had higher rates of type 2 diabetes but experienced a similar percentage weight loss and reduction in body mass index (BMI) as younger patients over the course of around 40 months.
“Age should be no barrier to lifestyle management of obesity,” said Dr. Barber, of University Hospitals Coventry (England) and Warwickshire, in a news release from his institution. “Rather than putting up barriers to older people accessing weight-loss programs, we should be proactively facilitating that process. To do otherwise would risk further and unnecessary neglect of older people through societal ageist misconceptions.”
He urged service providers and policy makers to “appreciate the importance of weight loss in older people with obesity for the maintenance of health and well-being and the facilitation of healthy aging. Furthermore, age per se should not contribute toward clinical decisions regarding the implementation of lifestyle management of older people.”
The research was published online Nov. 22 in Clinical Endocrinology.
Real-world data will inform clinical practice
Jason Halford, PhD, a professor of biological psychology and health behavior, said in an interview: “The fear is that older patients are perceived not to respond” to lifestyle interventions to control obesity, “and that’s clearly a fallacy, according to this study.”
The findings are strengthened by the fact that these are real-world data, “and so it will inform clinical practice,” he added.
And one of the “more interesting” findings was that [type 2] diabetes was “more prevalent” in the older group “but they’re still losing weight,” he noted.
“Traditionally it’s been thought that people with type 2 diabetes find it more difficult to lose weight because you’re trying to manage two conditions,” said Dr. Halford, of the University of Leeds (England), who is also president-elect of the European Association for the Study of Obesity.
Don’t discount older patients
The researchers note that many of the comorbidities associated with obesity “develop over time” and that “no one is immune to obesity,” regardless of their age, sex, ethnicity, and socioeconomic status.
Barber said there are “a number of reasons” why health care professionals “may discount weight loss in older people,” including “an ‘ageist’ perspective that weight-loss is not relevant to older people and misconceptions of reduced ability of older people to lose weight through dietary modification and increased exercise.”
And “older people may feel that hospital-based obesity services are not for them,” he noted.
To determine the effect of age on the ability to lose weight through lifestyle interventions, Dr. Barber and colleagues randomly selected 242 patients with morbid obesity who attended their hospital-based service between 2005 and 2016.
Of these, 167 were aged 18-60 years and 75 were aged 60 years and older. Most participants were women (75.4% of the younger patients and 60.0% of the older patients).
The proportion of patients with confirmed diabetes was markedly higher in the older group, compared with the younger group, at 62.7% versus 35.3%, although older patients had a significantly lower baseline BMI, at 46.9 versus 49.7 kg/m2 (P < .05).
The average duration of the lifestyle intervention was over 3 years (41.5 months) in the younger patients and 33.6 months in the older patients.
There was no significant difference in percentage weight loss between younger and older patients, at 6.9% and 7.3%, respectively, and no difference in percentage reduction in BMI, at 8.1% versus 7.8%.
Further analysis demonstrated that there was no significant correlation between age at referral to the hospital-based service and percentage weight loss (correlation coefficient, –0.13).
Dr. Halford said it would have been “useful” to know the proportion of patients achieving 5% and 10% weight loss because, if a third of patients lost more than 10% of their weight, “even in an elderly population, that would suggest there’d be real benefits in terms of things like type 2 diabetes,” he noted.
And he would like to have seen more data around how long participants had been struggling with obesity, as it’s “just an assumption that the second group is further down the path because they’re older, but we can’t be 100% sure.”
The team noted the study is limited by being retrospective and including a random selection of patients attending the service rather than the entire cohort.
Dr. Halford agreed but said the analysis is a “starting point” and could be used as a platform to conduct “much more systematic research on this area.”
No funding or relevant financial relationships were declared.
A version of this article originally appeared on Medscape.com.
Obesity phenotyping matches patients with more effective interventions
A phenotype-guided strategy for systematically matching weight-loss patients to their potentially ideal weight-loss drug roughly doubled treatment efficacy, compared with usual practice, in a single-center, randomized study with 268 patients.

In contrast, in 200 patients who received weight loss–drug therapy selected by routine means, 35% achieved greater than 10% loss compared with their starting weight, Andres J. Acosta, MD, said at the virtual ObesityWeek® Interactive 2020 meeting.
The phenotype-guided strategy also led to an average 16% weight loss from baseline after 12 months, compared with a 9% average loss among the usual-care controls, reported Dr. Acosta, a gastroenterologist at the Mayo Clinic in Rochester, Minn.
A “one-size-fits-all approach to weight loss treatment is not working,” he declared. “Our long-term goal is to develop a personalized approach to obesity management.”
Personalized weight loss treatment isn’t new
“The better we can match treatment to a patient’s needs, the more likely it will succeed. That’s not a brand new idea. They are trying to standardize the way that we classify the disorders that play a role in why a person gains weight or has trouble losing weight,” commented John D. Clark III, MD, an internal medicine physician and weight-management specialist at UT Southwestern Medical Center in Dallas.
The increased weight loss levels that Dr. Acosta reported in patients who underwent the study’s phenotyping protocol and received tailored treatment “are similar to the numbers we see when a patient’s treatment is the right fit for them. You see weight loss in these ranges,” Dr. Clark said in an interview.
The study run by Dr. Acosta and his associates consisted of two phases. First, they established normal and abnormal ranges for four different obesity phenotypes by studying 100 patients with obesity. The patients underwent an extensive and uniform workup designed to classify their obesity phenotype.
Four obesity phenotypes
The researchers categorized patients into one of four types:
- Disordered initial eating satiation, called ‘hungry brain,” and assessed by measuring food intake at a buffet, ad libidum meal.
- Disordered maintenance of satiety, called “hungry gut,” assessed by both a gastric-emptying study as well as patient self-assessment for postprandial fullness.
- “Emotional hunger,” assessed with two questionnaires.
- Disordered energy expenditure, called “slow burn,” assessed by measuring basal metabolic rate, and self-reports of both exercise and nonexercise activity.
Dr. Acosta estimated that the complete workup to assess all four potential phenotypes costs about $1,200.
The researchers then applied the 75th percentile value from each of these assessments to 450 patients with obesity in their clinic to see the prevalence of the four phenotypes. They identified a single phenotype in 58% of these patients, including 18% with hungry gut, 16% with hungry brain, 12% with emotional hunger, and 12% with slow burn. An additional 27% of the patients were positive for two or more phenotypes (including 9% who were positive for all four phenotypes), and 15% did not test positive for any of the four phenotypes.
Phenotype-guided treatments
They then applied their findings in a prospective randomized study that matched a drug intervention to each of the four phenotypes during a year-long, comprehensive weight-loss program at the Mayo Clinic’s Weight Management Clinic. The study randomized 100 patients to the phenotype-driven arm, with 68 of these patients receiving their assigned drug, and 200 patients served as controls. Patients averaged about 47 years old, and their average body mass index was about 41 kg/m2.
The investigational arm included 30 patients classified as having a hungry brain, with 20 of these patients treated with phentermine plus topiramate and 10 treated with lorcaserin (before it was withdrawn by the Food and Drug Administration); 12 with hungry gut and treated with liraglutide (Saxenda); 19 with emotional hunger who received naltrexone SR/bupropion SR (Contrave); and seven with slow burn who received phentermine.
The control arm included 200 patients seeking weight loss treatment at Mayo who did not undergo phenotyping and received their drug treatment based on their personal preference in consultation with their Mayo physician. In this group, drug treatment broke down as 106 patients (53%) on phentermine plus topiramate, 41 (21%) on liraglutide, 34 (17%) on phentermine alone, 14 (7%) on naltrexone SR/bupropion SR, and 5 patients (3%) on locaserin (percentages total 101% because of rounding).
Overall, phenotyping led to more patients treated with naltrexone SR/buproprion SR and lorcaserin and fewer treated with phentermine or phentermine and topiramate ER. All patients were eligible to also receive behavioral interventions as needed.
“We do a lot of testing to identify the phenotype,” in addition to gathering additional clues from a detailed history, said Dr. Acosta. Patients identified with more than one phenotype in routine practice at Mayo are often begun on more than one drug. When phenotyping fails to classify a patient, Dr. Acosta puts the patient on a low-calorie diet and then does a follow-up assessment “to see if the phenotype pops up as a metabolic adaptation.”
“This is something we’re all working toward” in the obesity management field. “How can we better identify the underlying causes in a way that can fit into the work flow. How can we move from research to things we can use daily in the clinic,” observed Dr. Clark. “We need a lot more investigation to determine how well this works in the real world. Are there other tools we can use that are not as expensive” as what Dr. Acosta used for this study?
“For this proof of concept study, it made sense to be very rigorous, but that probably is not realistic for every patient. What are other ways to get this information, or perhaps only use an extensive workup when initial weight loss attempts are unsuccessful,” Dr. Clark suggested.
A phenotype-guided strategy for systematically matching weight-loss patients to their potentially ideal weight-loss drug roughly doubled treatment efficacy, compared with usual practice, in a single-center, randomized study with 268 patients.
In contrast, in 200 patients who received weight loss–drug therapy selected by routine means, 35% achieved greater than 10% loss compared with their starting weight, Andres J. Acosta, MD, said at the virtual ObesityWeek® Interactive 2020 meeting.
The phenotype-guided strategy also led to an average 16% weight loss from baseline after 12 months, compared with a 9% average loss among the usual-care controls, reported Dr. Acosta, a gastroenterologist at the Mayo Clinic in Rochester, Minn.
A “one-size-fits-all approach to weight loss treatment is not working,” he declared. “Our long-term goal is to develop a personalized approach to obesity management.”
Personalized weight loss treatment isn’t new
“The better we can match treatment to a patient’s needs, the more likely it will succeed. That’s not a brand new idea. They are trying to standardize the way that we classify the disorders that play a role in why a person gains weight or has trouble losing weight,” commented John D. Clark III, MD, an internal medicine physician and weight-management specialist at UT Southwestern Medical Center in Dallas.
The increased weight loss levels that Dr. Acosta reported in patients who underwent the study’s phenotyping protocol and received tailored treatment “are similar to the numbers we see when a patient’s treatment is the right fit for them. You see weight loss in these ranges,” Dr. Clark said in an interview.
The study run by Dr. Acosta and his associates consisted of two phases. First, they established normal and abnormal ranges for four different obesity phenotypes by studying 100 patients with obesity. The patients underwent an extensive and uniform workup designed to classify their obesity phenotype.
Four obesity phenotypes
The researchers categorized patients into one of four types:
- Disordered initial eating satiation, called ‘hungry brain,” and assessed by measuring food intake at a buffet, ad libidum meal.
- Disordered maintenance of satiety, called “hungry gut,” assessed by both a gastric-emptying study as well as patient self-assessment for postprandial fullness.
- “Emotional hunger,” assessed with two questionnaires.
- Disordered energy expenditure, called “slow burn,” assessed by measuring basal metabolic rate, and self-reports of both exercise and nonexercise activity.
Dr. Acosta estimated that the complete workup to assess all four potential phenotypes costs about $1,200.
The researchers then applied the 75th percentile value from each of these assessments to 450 patients with obesity in their clinic to see the prevalence of the four phenotypes. They identified a single phenotype in 58% of these patients, including 18% with hungry gut, 16% with hungry brain, 12% with emotional hunger, and 12% with slow burn. An additional 27% of the patients were positive for two or more phenotypes (including 9% who were positive for all four phenotypes), and 15% did not test positive for any of the four phenotypes.
Phenotype-guided treatments
They then applied their findings in a prospective randomized study that matched a drug intervention to each of the four phenotypes during a year-long, comprehensive weight-loss program at the Mayo Clinic’s Weight Management Clinic. The study randomized 100 patients to the phenotype-driven arm, with 68 of these patients receiving their assigned drug, and 200 patients served as controls. Patients averaged about 47 years old, and their average body mass index was about 41 kg/m2.
The investigational arm included 30 patients classified as having a hungry brain, with 20 of these patients treated with phentermine plus topiramate and 10 treated with lorcaserin (before it was withdrawn by the Food and Drug Administration); 12 with hungry gut and treated with liraglutide (Saxenda); 19 with emotional hunger who received naltrexone SR/bupropion SR (Contrave); and seven with slow burn who received phentermine.
The control arm included 200 patients seeking weight loss treatment at Mayo who did not undergo phenotyping and received their drug treatment based on their personal preference in consultation with their Mayo physician. In this group, drug treatment broke down as 106 patients (53%) on phentermine plus topiramate, 41 (21%) on liraglutide, 34 (17%) on phentermine alone, 14 (7%) on naltrexone SR/bupropion SR, and 5 patients (3%) on locaserin (percentages total 101% because of rounding).
Overall, phenotyping led to more patients treated with naltrexone SR/buproprion SR and lorcaserin and fewer treated with phentermine or phentermine and topiramate ER. All patients were eligible to also receive behavioral interventions as needed.
“We do a lot of testing to identify the phenotype,” in addition to gathering additional clues from a detailed history, said Dr. Acosta. Patients identified with more than one phenotype in routine practice at Mayo are often begun on more than one drug. When phenotyping fails to classify a patient, Dr. Acosta puts the patient on a low-calorie diet and then does a follow-up assessment “to see if the phenotype pops up as a metabolic adaptation.”
“This is something we’re all working toward” in the obesity management field. “How can we better identify the underlying causes in a way that can fit into the work flow. How can we move from research to things we can use daily in the clinic,” observed Dr. Clark. “We need a lot more investigation to determine how well this works in the real world. Are there other tools we can use that are not as expensive” as what Dr. Acosta used for this study?
“For this proof of concept study, it made sense to be very rigorous, but that probably is not realistic for every patient. What are other ways to get this information, or perhaps only use an extensive workup when initial weight loss attempts are unsuccessful,” Dr. Clark suggested.
A phenotype-guided strategy for systematically matching weight-loss patients to their potentially ideal weight-loss drug roughly doubled treatment efficacy, compared with usual practice, in a single-center, randomized study with 268 patients.
In contrast, in 200 patients who received weight loss–drug therapy selected by routine means, 35% achieved greater than 10% loss compared with their starting weight, Andres J. Acosta, MD, said at the virtual ObesityWeek® Interactive 2020 meeting.
The phenotype-guided strategy also led to an average 16% weight loss from baseline after 12 months, compared with a 9% average loss among the usual-care controls, reported Dr. Acosta, a gastroenterologist at the Mayo Clinic in Rochester, Minn.
A “one-size-fits-all approach to weight loss treatment is not working,” he declared. “Our long-term goal is to develop a personalized approach to obesity management.”
Personalized weight loss treatment isn’t new
“The better we can match treatment to a patient’s needs, the more likely it will succeed. That’s not a brand new idea. They are trying to standardize the way that we classify the disorders that play a role in why a person gains weight or has trouble losing weight,” commented John D. Clark III, MD, an internal medicine physician and weight-management specialist at UT Southwestern Medical Center in Dallas.
The increased weight loss levels that Dr. Acosta reported in patients who underwent the study’s phenotyping protocol and received tailored treatment “are similar to the numbers we see when a patient’s treatment is the right fit for them. You see weight loss in these ranges,” Dr. Clark said in an interview.
The study run by Dr. Acosta and his associates consisted of two phases. First, they established normal and abnormal ranges for four different obesity phenotypes by studying 100 patients with obesity. The patients underwent an extensive and uniform workup designed to classify their obesity phenotype.
Four obesity phenotypes
The researchers categorized patients into one of four types:
- Disordered initial eating satiation, called ‘hungry brain,” and assessed by measuring food intake at a buffet, ad libidum meal.
- Disordered maintenance of satiety, called “hungry gut,” assessed by both a gastric-emptying study as well as patient self-assessment for postprandial fullness.
- “Emotional hunger,” assessed with two questionnaires.
- Disordered energy expenditure, called “slow burn,” assessed by measuring basal metabolic rate, and self-reports of both exercise and nonexercise activity.
Dr. Acosta estimated that the complete workup to assess all four potential phenotypes costs about $1,200.
The researchers then applied the 75th percentile value from each of these assessments to 450 patients with obesity in their clinic to see the prevalence of the four phenotypes. They identified a single phenotype in 58% of these patients, including 18% with hungry gut, 16% with hungry brain, 12% with emotional hunger, and 12% with slow burn. An additional 27% of the patients were positive for two or more phenotypes (including 9% who were positive for all four phenotypes), and 15% did not test positive for any of the four phenotypes.
Phenotype-guided treatments
They then applied their findings in a prospective randomized study that matched a drug intervention to each of the four phenotypes during a year-long, comprehensive weight-loss program at the Mayo Clinic’s Weight Management Clinic. The study randomized 100 patients to the phenotype-driven arm, with 68 of these patients receiving their assigned drug, and 200 patients served as controls. Patients averaged about 47 years old, and their average body mass index was about 41 kg/m2.
The investigational arm included 30 patients classified as having a hungry brain, with 20 of these patients treated with phentermine plus topiramate and 10 treated with lorcaserin (before it was withdrawn by the Food and Drug Administration); 12 with hungry gut and treated with liraglutide (Saxenda); 19 with emotional hunger who received naltrexone SR/bupropion SR (Contrave); and seven with slow burn who received phentermine.
The control arm included 200 patients seeking weight loss treatment at Mayo who did not undergo phenotyping and received their drug treatment based on their personal preference in consultation with their Mayo physician. In this group, drug treatment broke down as 106 patients (53%) on phentermine plus topiramate, 41 (21%) on liraglutide, 34 (17%) on phentermine alone, 14 (7%) on naltrexone SR/bupropion SR, and 5 patients (3%) on locaserin (percentages total 101% because of rounding).
Overall, phenotyping led to more patients treated with naltrexone SR/buproprion SR and lorcaserin and fewer treated with phentermine or phentermine and topiramate ER. All patients were eligible to also receive behavioral interventions as needed.
“We do a lot of testing to identify the phenotype,” in addition to gathering additional clues from a detailed history, said Dr. Acosta. Patients identified with more than one phenotype in routine practice at Mayo are often begun on more than one drug. When phenotyping fails to classify a patient, Dr. Acosta puts the patient on a low-calorie diet and then does a follow-up assessment “to see if the phenotype pops up as a metabolic adaptation.”
“This is something we’re all working toward” in the obesity management field. “How can we better identify the underlying causes in a way that can fit into the work flow. How can we move from research to things we can use daily in the clinic,” observed Dr. Clark. “We need a lot more investigation to determine how well this works in the real world. Are there other tools we can use that are not as expensive” as what Dr. Acosta used for this study?
“For this proof of concept study, it made sense to be very rigorous, but that probably is not realistic for every patient. What are other ways to get this information, or perhaps only use an extensive workup when initial weight loss attempts are unsuccessful,” Dr. Clark suggested.
FROM OBESITY WEEK 2020