User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
A call to revamp revascularization trial endpoints
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.

In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”

MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.
In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”
MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.
In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”
MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Why the approval of MiniMed 780G is a ‘quantum leap’ forward
This transcript has been edited for clarity.
There is wonderful news in the field of hybrid closed-loop pump technology because the Medtronic 780G system was just approved. I can’t tell you how happy this makes me because we’ve all been waiting for this seemingly forever and ever. This isn’t just a small upgrade from the 770G. It’s a quantum leap from the 770G to the 780G. The 780G has newer algorithms, a new sensor, and a longer-lasting infusion set.

It’s been used since 2020 in Europe, so we have good data on how well it works. Frankly, I think it works really well. We’ve seen nice improvements in [hemoglobin] A1c, time in range, other glycemic metrics, and patient satisfaction in studies done in Europe.
Now, I’ve never had the system to use in one of my patients. I always say I never know a system until I see it in use in my own patients, but let me tell you what I’ve read.
First, it has something called meal-detection technology with autocorrection boluses every 5 minutes. If this works, it can be a huge win for our patients because the problem my patients have is with mealtime dosing. They often dose late, or they may not dose enough insulin for the carbohydrates. That’s where the issues are.
All these hybrid closed-loop systems, this one included, show that the best improvements in glycemia are overnight. I’m hoping that this one shows some nice improvements in daytime glycemia as well. Stay tuned and I’ll let you know once I’ve been using it.
Next, it has adjustable targets down to 100. This is the lowest target for any hybrid closed-loop system. It has an extended-wear infusion set that lasts for 7 days. This infusion set is already available but works with this new system.
Finally, it has a new sensor. It looks like the old sensors, but it’s the Guardian 4, which requires much fewer finger sticks. Now, I’m not entirely sure about how often one has to do a finger stick. I know one has to do with finger sticking to initiate auto mode, or what they call SmartGuard, but I don’t know whether you ever have to do it again. I know for sure that you have to do it again if you fall out of the automated mode into manual mode. Once you’re in SmartGuard, I believe there are no further finger-stick calibrations required.
If people are already on the 770G system, this is just a software update that is presumably easy to upgrade to the 780G. Now, the physical pieces ... If someone doesn’t already have the Guardian 4 sensor or the extended-wear infusion set, they’ll have to get those. The software update to make the 770G increase to the 780G should just come through the cloud. I don’t know when that’s going to happen.
I do know that preorders for this system, if you want to buy the new physical system, start on May 15. The shipping of the new 780G system should occur in the United States toward the end of this summer.
I’m so excited. I think this is really going to benefit my patients. I can’t wait to start using it and letting patients see how these algorithms work and how they really help patients improve their glucose control.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with Abbott Diabetes Care, Becton Dickinson, Boehringer Ingelheim, Eli Lilly, Lexicon Pharmaceuticals, Livongo, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, Zafgen, Dexcom, MannKind, and AstraZeneca.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There is wonderful news in the field of hybrid closed-loop pump technology because the Medtronic 780G system was just approved. I can’t tell you how happy this makes me because we’ve all been waiting for this seemingly forever and ever. This isn’t just a small upgrade from the 770G. It’s a quantum leap from the 770G to the 780G. The 780G has newer algorithms, a new sensor, and a longer-lasting infusion set.
It’s been used since 2020 in Europe, so we have good data on how well it works. Frankly, I think it works really well. We’ve seen nice improvements in [hemoglobin] A1c, time in range, other glycemic metrics, and patient satisfaction in studies done in Europe.
Now, I’ve never had the system to use in one of my patients. I always say I never know a system until I see it in use in my own patients, but let me tell you what I’ve read.
First, it has something called meal-detection technology with autocorrection boluses every 5 minutes. If this works, it can be a huge win for our patients because the problem my patients have is with mealtime dosing. They often dose late, or they may not dose enough insulin for the carbohydrates. That’s where the issues are.
All these hybrid closed-loop systems, this one included, show that the best improvements in glycemia are overnight. I’m hoping that this one shows some nice improvements in daytime glycemia as well. Stay tuned and I’ll let you know once I’ve been using it.
Next, it has adjustable targets down to 100. This is the lowest target for any hybrid closed-loop system. It has an extended-wear infusion set that lasts for 7 days. This infusion set is already available but works with this new system.
Finally, it has a new sensor. It looks like the old sensors, but it’s the Guardian 4, which requires much fewer finger sticks. Now, I’m not entirely sure about how often one has to do a finger stick. I know one has to do with finger sticking to initiate auto mode, or what they call SmartGuard, but I don’t know whether you ever have to do it again. I know for sure that you have to do it again if you fall out of the automated mode into manual mode. Once you’re in SmartGuard, I believe there are no further finger-stick calibrations required.
If people are already on the 770G system, this is just a software update that is presumably easy to upgrade to the 780G. Now, the physical pieces ... If someone doesn’t already have the Guardian 4 sensor or the extended-wear infusion set, they’ll have to get those. The software update to make the 770G increase to the 780G should just come through the cloud. I don’t know when that’s going to happen.
I do know that preorders for this system, if you want to buy the new physical system, start on May 15. The shipping of the new 780G system should occur in the United States toward the end of this summer.
I’m so excited. I think this is really going to benefit my patients. I can’t wait to start using it and letting patients see how these algorithms work and how they really help patients improve their glucose control.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with Abbott Diabetes Care, Becton Dickinson, Boehringer Ingelheim, Eli Lilly, Lexicon Pharmaceuticals, Livongo, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, Zafgen, Dexcom, MannKind, and AstraZeneca.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There is wonderful news in the field of hybrid closed-loop pump technology because the Medtronic 780G system was just approved. I can’t tell you how happy this makes me because we’ve all been waiting for this seemingly forever and ever. This isn’t just a small upgrade from the 770G. It’s a quantum leap from the 770G to the 780G. The 780G has newer algorithms, a new sensor, and a longer-lasting infusion set.
It’s been used since 2020 in Europe, so we have good data on how well it works. Frankly, I think it works really well. We’ve seen nice improvements in [hemoglobin] A1c, time in range, other glycemic metrics, and patient satisfaction in studies done in Europe.
Now, I’ve never had the system to use in one of my patients. I always say I never know a system until I see it in use in my own patients, but let me tell you what I’ve read.
First, it has something called meal-detection technology with autocorrection boluses every 5 minutes. If this works, it can be a huge win for our patients because the problem my patients have is with mealtime dosing. They often dose late, or they may not dose enough insulin for the carbohydrates. That’s where the issues are.
All these hybrid closed-loop systems, this one included, show that the best improvements in glycemia are overnight. I’m hoping that this one shows some nice improvements in daytime glycemia as well. Stay tuned and I’ll let you know once I’ve been using it.
Next, it has adjustable targets down to 100. This is the lowest target for any hybrid closed-loop system. It has an extended-wear infusion set that lasts for 7 days. This infusion set is already available but works with this new system.
Finally, it has a new sensor. It looks like the old sensors, but it’s the Guardian 4, which requires much fewer finger sticks. Now, I’m not entirely sure about how often one has to do a finger stick. I know one has to do with finger sticking to initiate auto mode, or what they call SmartGuard, but I don’t know whether you ever have to do it again. I know for sure that you have to do it again if you fall out of the automated mode into manual mode. Once you’re in SmartGuard, I believe there are no further finger-stick calibrations required.
If people are already on the 770G system, this is just a software update that is presumably easy to upgrade to the 780G. Now, the physical pieces ... If someone doesn’t already have the Guardian 4 sensor or the extended-wear infusion set, they’ll have to get those. The software update to make the 770G increase to the 780G should just come through the cloud. I don’t know when that’s going to happen.
I do know that preorders for this system, if you want to buy the new physical system, start on May 15. The shipping of the new 780G system should occur in the United States toward the end of this summer.
I’m so excited. I think this is really going to benefit my patients. I can’t wait to start using it and letting patients see how these algorithms work and how they really help patients improve their glucose control.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with Abbott Diabetes Care, Becton Dickinson, Boehringer Ingelheim, Eli Lilly, Lexicon Pharmaceuticals, Livongo, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, Zafgen, Dexcom, MannKind, and AstraZeneca.
A version of this article first appeared on Medscape.com.
Statin misinformation on social media flagged by AI
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Stroke scale cutoff might not be ideal guide for ordering CTA and detecting large vessel occlusions
BOSTON – (LVO), according to large body of data presented at the 2023 annual meeting of the American Academy of Neurology.
If the goal is not to miss any LVOs, there is no NIHSS score below which these do not occur, according to Theresa Sevilis, DO, regional medical director, TeleSpecialists, Fort Myers, Fla.
For example, her evaluation of a large and nationally representative dataset shows that more than 10% of the LVOs eventually identified and accepted for intervention would be missed with a cutoff of NIHSS score of 6 or higher. Moving the cutoff NIHSS score to 4 or greater, 6% of LVOs among the 23,166 strokes evaluated would have gone undetected.
“The current guidelines do not address low NIHSS score largely due to a paucity of data,” according to Dr. Sevilis, who showed data indicating that there is great variation among institutions in regard to ordering computed tomography angiography (CTA). She indicated that CTA is the current imaging standard for detecting LVO.
Large prospective dataset
The data for this study were derived from the TeleCare database, which captures acute stroke consultations in the emergency departments in 227 facilities in 27 states. Stroke consultations over a 6-month period from July through December 2021 were evaluated. The prospectively collected data were subjected to a multivariate analysis to determine the odds ratio for a CTA performed and LVO found at each NIHSS score of 0 to 5. Scores 6 or above served as the reference.
“Only consults performed within 24 hours [of presentation] were included,” Dr. Sevilis said.
After excluding cases in which no NIHSS score was captured, which represented less than 1% of cases, more than 10,500 cases underwent CTA, providing a rate of 45.5%. The rate of CTA for the whole dataset was 45.5%. Of the study population, 24.6% had a NIHSS score of 6 or above.
“When you are discussing when to perform CTA in patients with a low NIHSS score, you are discussing the majority of patients,” Dr. Sevilis said.
Of those with a NIHSS stroke of 6 or below, 28.2% had a score of 0. Not surprisingly, these were the least likely to have a CTA performed on the basis of an odds ratio of 0.14 and the least likely to have a LVO detected (OR, 0.1). With the exception of a NIHSS stroke score of 1, the likelihood of CTA and LVO climbed incrementally with higher stroke scores. These odds ratios were, respectively, 0.16 and 0.09 for a score of 1; 0.27 and 0.16 for a score of 2; 0.33 and 0.14 for a score of 3; 0.49 and 0.24 for a score of 4; and 0.71 and 0.27 for a score of 5.
In the group with NIHSS score of 6 or above, 24.1% were found to have an LVO. Of these, the proportion accepted for a mechanical thrombectomy was less than half. The intervention acceptance rate for mechanical intervention among LVOs in patients with lower NIHSS scores again fell incrementally by score. The acceptance rate was about 35% among LVO patients with a NIHSS score of 3 or 4 and 25% for those with a score of 0-2.
The interpretation of these data “depends on goals,” Dr. Sevilis said. “If the goal is to not miss a single LVO, then it is important to consider the balance between benefits and risks.”
No consistent cutoff
In participating facilities, the protocol for considering CTA to detect and treat LVOs ranges from neurologist choice to cutoffs of NIHSS scores of 2, 4, and 6, according to Dr. Sevilis. Where the data suggest that a cutoff of 4 or above might be reasonable, she said that NIHSS scoring is not a useful tool for those “who do not want to miss any LVOs.”
These data are based on emergency room stroke consultations and not on confirmed strokes,” Dr. Sevilis emphasized. Indeed, she noted that the final discharge diagnosis was not available. Recognizing that the analysis was not performed on a population with confirmed strokes is particularly important for understanding the limited rate of CTAs performed even in those with relatively high NIHSS scores. She noted this could be explained by many different reasons, including suspicion of hemorrhage or clinical features that took the workup in a different direction.
Reconsidering protocols
Based on the large sample size, Dr. Sevilis contended that it is likely that these data are representative, but she considers this study a first step toward considering protocols and developing guidelines for addressing stroke alerts in the emergency department.
A more important step will be ongoing trials designed specifically to generate data to answer this question. Pascal Jabbour, MD, chief of the division of neurovascular and endovascular neurosurgery, Thomas Jefferson University Hospitals, Philadelphia, is participating in one of these trials. He agreed with the premise that better evidence-based criteria are needed when evaluating acute stroke patients with a potential LVO.
The trial in which he is a coinvestigator, called ENDOLOW, is testing the hypothesis that outcomes will be better if acute stroke patients with a LVO and a low baseline NIHSS score (< 5) are treated with immediate thrombectomy rather than medical management. If this hypothesis is confirmed in the randomized ENDOLOW, it will provide an evidence basis for an approach already being practiced at some centers.
“There should be a very low threshold for CTA,” said Dr. Jabbour in an interview. This imaging “takes less than 2 minutes and it can provide the basis for a life-saving endovascular thrombectomy if a LVO is found.”
It is already well known that LVO is not restricted only to patients with an elevated NIHSS score, he said.
For determining whether to order a CTA, “I do not agree with NIHSS score of 6 or above. There is no absolute number below which risk of missing a LVO is eliminated,” Dr. Jabbour said. He also argued against relying on NIHSS score without considering other clinical features, particularly cortical signs, which should raise suspicion of a LVO regardless of NIHSS score.
One problem is that NIHSS scores are not static. Decompensation can be rapid with the NIHSS score quickly climbing. When this happens, the delay in treatment might lead to a preventable adverse outcome.
“There is a change in the paradigm now that we have more evidence of a benefit from aggressive treatment in the right candidates,” according to Dr. Jabbour, referring to the recently published SELECT2 trial. In that trial, on which Dr. Jabbour served as a coauthor, patients with LVO and large territory infarct were randomized to thrombectomy or medical care within 24 hours of a stroke. It was stopped early for efficacy because of the increased functional independence (20% vs. 7%) in the surgical intervention group.
If the ongoing trials establish better criteria for ruling in or out the presence of LVO in patients with acute stroke, Dr. Jabbour predicted that guidelines will be written to standardize practice.
Dr. Sevilis reports no potential conflicts of interest. Dr. Jabbour has financial relationships with Cerenovus, Medtronic, and Microvention.
BOSTON – (LVO), according to large body of data presented at the 2023 annual meeting of the American Academy of Neurology.
If the goal is not to miss any LVOs, there is no NIHSS score below which these do not occur, according to Theresa Sevilis, DO, regional medical director, TeleSpecialists, Fort Myers, Fla.
For example, her evaluation of a large and nationally representative dataset shows that more than 10% of the LVOs eventually identified and accepted for intervention would be missed with a cutoff of NIHSS score of 6 or higher. Moving the cutoff NIHSS score to 4 or greater, 6% of LVOs among the 23,166 strokes evaluated would have gone undetected.
“The current guidelines do not address low NIHSS score largely due to a paucity of data,” according to Dr. Sevilis, who showed data indicating that there is great variation among institutions in regard to ordering computed tomography angiography (CTA). She indicated that CTA is the current imaging standard for detecting LVO.
Large prospective dataset
The data for this study were derived from the TeleCare database, which captures acute stroke consultations in the emergency departments in 227 facilities in 27 states. Stroke consultations over a 6-month period from July through December 2021 were evaluated. The prospectively collected data were subjected to a multivariate analysis to determine the odds ratio for a CTA performed and LVO found at each NIHSS score of 0 to 5. Scores 6 or above served as the reference.
“Only consults performed within 24 hours [of presentation] were included,” Dr. Sevilis said.
After excluding cases in which no NIHSS score was captured, which represented less than 1% of cases, more than 10,500 cases underwent CTA, providing a rate of 45.5%. The rate of CTA for the whole dataset was 45.5%. Of the study population, 24.6% had a NIHSS score of 6 or above.
“When you are discussing when to perform CTA in patients with a low NIHSS score, you are discussing the majority of patients,” Dr. Sevilis said.
Of those with a NIHSS stroke of 6 or below, 28.2% had a score of 0. Not surprisingly, these were the least likely to have a CTA performed on the basis of an odds ratio of 0.14 and the least likely to have a LVO detected (OR, 0.1). With the exception of a NIHSS stroke score of 1, the likelihood of CTA and LVO climbed incrementally with higher stroke scores. These odds ratios were, respectively, 0.16 and 0.09 for a score of 1; 0.27 and 0.16 for a score of 2; 0.33 and 0.14 for a score of 3; 0.49 and 0.24 for a score of 4; and 0.71 and 0.27 for a score of 5.
In the group with NIHSS score of 6 or above, 24.1% were found to have an LVO. Of these, the proportion accepted for a mechanical thrombectomy was less than half. The intervention acceptance rate for mechanical intervention among LVOs in patients with lower NIHSS scores again fell incrementally by score. The acceptance rate was about 35% among LVO patients with a NIHSS score of 3 or 4 and 25% for those with a score of 0-2.
The interpretation of these data “depends on goals,” Dr. Sevilis said. “If the goal is to not miss a single LVO, then it is important to consider the balance between benefits and risks.”
No consistent cutoff
In participating facilities, the protocol for considering CTA to detect and treat LVOs ranges from neurologist choice to cutoffs of NIHSS scores of 2, 4, and 6, according to Dr. Sevilis. Where the data suggest that a cutoff of 4 or above might be reasonable, she said that NIHSS scoring is not a useful tool for those “who do not want to miss any LVOs.”
These data are based on emergency room stroke consultations and not on confirmed strokes,” Dr. Sevilis emphasized. Indeed, she noted that the final discharge diagnosis was not available. Recognizing that the analysis was not performed on a population with confirmed strokes is particularly important for understanding the limited rate of CTAs performed even in those with relatively high NIHSS scores. She noted this could be explained by many different reasons, including suspicion of hemorrhage or clinical features that took the workup in a different direction.
Reconsidering protocols
Based on the large sample size, Dr. Sevilis contended that it is likely that these data are representative, but she considers this study a first step toward considering protocols and developing guidelines for addressing stroke alerts in the emergency department.
A more important step will be ongoing trials designed specifically to generate data to answer this question. Pascal Jabbour, MD, chief of the division of neurovascular and endovascular neurosurgery, Thomas Jefferson University Hospitals, Philadelphia, is participating in one of these trials. He agreed with the premise that better evidence-based criteria are needed when evaluating acute stroke patients with a potential LVO.
The trial in which he is a coinvestigator, called ENDOLOW, is testing the hypothesis that outcomes will be better if acute stroke patients with a LVO and a low baseline NIHSS score (< 5) are treated with immediate thrombectomy rather than medical management. If this hypothesis is confirmed in the randomized ENDOLOW, it will provide an evidence basis for an approach already being practiced at some centers.
“There should be a very low threshold for CTA,” said Dr. Jabbour in an interview. This imaging “takes less than 2 minutes and it can provide the basis for a life-saving endovascular thrombectomy if a LVO is found.”
It is already well known that LVO is not restricted only to patients with an elevated NIHSS score, he said.
For determining whether to order a CTA, “I do not agree with NIHSS score of 6 or above. There is no absolute number below which risk of missing a LVO is eliminated,” Dr. Jabbour said. He also argued against relying on NIHSS score without considering other clinical features, particularly cortical signs, which should raise suspicion of a LVO regardless of NIHSS score.
One problem is that NIHSS scores are not static. Decompensation can be rapid with the NIHSS score quickly climbing. When this happens, the delay in treatment might lead to a preventable adverse outcome.
“There is a change in the paradigm now that we have more evidence of a benefit from aggressive treatment in the right candidates,” according to Dr. Jabbour, referring to the recently published SELECT2 trial. In that trial, on which Dr. Jabbour served as a coauthor, patients with LVO and large territory infarct were randomized to thrombectomy or medical care within 24 hours of a stroke. It was stopped early for efficacy because of the increased functional independence (20% vs. 7%) in the surgical intervention group.
If the ongoing trials establish better criteria for ruling in or out the presence of LVO in patients with acute stroke, Dr. Jabbour predicted that guidelines will be written to standardize practice.
Dr. Sevilis reports no potential conflicts of interest. Dr. Jabbour has financial relationships with Cerenovus, Medtronic, and Microvention.
BOSTON – (LVO), according to large body of data presented at the 2023 annual meeting of the American Academy of Neurology.
If the goal is not to miss any LVOs, there is no NIHSS score below which these do not occur, according to Theresa Sevilis, DO, regional medical director, TeleSpecialists, Fort Myers, Fla.
For example, her evaluation of a large and nationally representative dataset shows that more than 10% of the LVOs eventually identified and accepted for intervention would be missed with a cutoff of NIHSS score of 6 or higher. Moving the cutoff NIHSS score to 4 or greater, 6% of LVOs among the 23,166 strokes evaluated would have gone undetected.
“The current guidelines do not address low NIHSS score largely due to a paucity of data,” according to Dr. Sevilis, who showed data indicating that there is great variation among institutions in regard to ordering computed tomography angiography (CTA). She indicated that CTA is the current imaging standard for detecting LVO.
Large prospective dataset
The data for this study were derived from the TeleCare database, which captures acute stroke consultations in the emergency departments in 227 facilities in 27 states. Stroke consultations over a 6-month period from July through December 2021 were evaluated. The prospectively collected data were subjected to a multivariate analysis to determine the odds ratio for a CTA performed and LVO found at each NIHSS score of 0 to 5. Scores 6 or above served as the reference.
“Only consults performed within 24 hours [of presentation] were included,” Dr. Sevilis said.
After excluding cases in which no NIHSS score was captured, which represented less than 1% of cases, more than 10,500 cases underwent CTA, providing a rate of 45.5%. The rate of CTA for the whole dataset was 45.5%. Of the study population, 24.6% had a NIHSS score of 6 or above.
“When you are discussing when to perform CTA in patients with a low NIHSS score, you are discussing the majority of patients,” Dr. Sevilis said.
Of those with a NIHSS stroke of 6 or below, 28.2% had a score of 0. Not surprisingly, these were the least likely to have a CTA performed on the basis of an odds ratio of 0.14 and the least likely to have a LVO detected (OR, 0.1). With the exception of a NIHSS stroke score of 1, the likelihood of CTA and LVO climbed incrementally with higher stroke scores. These odds ratios were, respectively, 0.16 and 0.09 for a score of 1; 0.27 and 0.16 for a score of 2; 0.33 and 0.14 for a score of 3; 0.49 and 0.24 for a score of 4; and 0.71 and 0.27 for a score of 5.
In the group with NIHSS score of 6 or above, 24.1% were found to have an LVO. Of these, the proportion accepted for a mechanical thrombectomy was less than half. The intervention acceptance rate for mechanical intervention among LVOs in patients with lower NIHSS scores again fell incrementally by score. The acceptance rate was about 35% among LVO patients with a NIHSS score of 3 or 4 and 25% for those with a score of 0-2.
The interpretation of these data “depends on goals,” Dr. Sevilis said. “If the goal is to not miss a single LVO, then it is important to consider the balance between benefits and risks.”
No consistent cutoff
In participating facilities, the protocol for considering CTA to detect and treat LVOs ranges from neurologist choice to cutoffs of NIHSS scores of 2, 4, and 6, according to Dr. Sevilis. Where the data suggest that a cutoff of 4 or above might be reasonable, she said that NIHSS scoring is not a useful tool for those “who do not want to miss any LVOs.”
These data are based on emergency room stroke consultations and not on confirmed strokes,” Dr. Sevilis emphasized. Indeed, she noted that the final discharge diagnosis was not available. Recognizing that the analysis was not performed on a population with confirmed strokes is particularly important for understanding the limited rate of CTAs performed even in those with relatively high NIHSS scores. She noted this could be explained by many different reasons, including suspicion of hemorrhage or clinical features that took the workup in a different direction.
Reconsidering protocols
Based on the large sample size, Dr. Sevilis contended that it is likely that these data are representative, but she considers this study a first step toward considering protocols and developing guidelines for addressing stroke alerts in the emergency department.
A more important step will be ongoing trials designed specifically to generate data to answer this question. Pascal Jabbour, MD, chief of the division of neurovascular and endovascular neurosurgery, Thomas Jefferson University Hospitals, Philadelphia, is participating in one of these trials. He agreed with the premise that better evidence-based criteria are needed when evaluating acute stroke patients with a potential LVO.
The trial in which he is a coinvestigator, called ENDOLOW, is testing the hypothesis that outcomes will be better if acute stroke patients with a LVO and a low baseline NIHSS score (< 5) are treated with immediate thrombectomy rather than medical management. If this hypothesis is confirmed in the randomized ENDOLOW, it will provide an evidence basis for an approach already being practiced at some centers.
“There should be a very low threshold for CTA,” said Dr. Jabbour in an interview. This imaging “takes less than 2 minutes and it can provide the basis for a life-saving endovascular thrombectomy if a LVO is found.”
It is already well known that LVO is not restricted only to patients with an elevated NIHSS score, he said.
For determining whether to order a CTA, “I do not agree with NIHSS score of 6 or above. There is no absolute number below which risk of missing a LVO is eliminated,” Dr. Jabbour said. He also argued against relying on NIHSS score without considering other clinical features, particularly cortical signs, which should raise suspicion of a LVO regardless of NIHSS score.
One problem is that NIHSS scores are not static. Decompensation can be rapid with the NIHSS score quickly climbing. When this happens, the delay in treatment might lead to a preventable adverse outcome.
“There is a change in the paradigm now that we have more evidence of a benefit from aggressive treatment in the right candidates,” according to Dr. Jabbour, referring to the recently published SELECT2 trial. In that trial, on which Dr. Jabbour served as a coauthor, patients with LVO and large territory infarct were randomized to thrombectomy or medical care within 24 hours of a stroke. It was stopped early for efficacy because of the increased functional independence (20% vs. 7%) in the surgical intervention group.
If the ongoing trials establish better criteria for ruling in or out the presence of LVO in patients with acute stroke, Dr. Jabbour predicted that guidelines will be written to standardize practice.
Dr. Sevilis reports no potential conflicts of interest. Dr. Jabbour has financial relationships with Cerenovus, Medtronic, and Microvention.
FROM AAN 2023
Expert discusses which diets are best, based on the evidence
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
AT INTERNAL MEDICINE 2023
LAA closure outcomes improve with CCTA: Swiss-Apero subanalysis
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
Statins tied to lower stroke risk in atrial fibrillation
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM EHRA 2023
Lifestyle med experts tell how to deprescribe diabetes meds
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM CLINICAL DIABETES
Active older women show heightened AFib risk
Older women with high levels of physical activity showed twice the risk of atrial fibrillation (AFib) over 10 years as they did for cardiac disease or stroke, based on data from 46 cross-country skiers.
Although previous research suggests that women derive greater health benefits from endurance sports, compared with men, women are generally underrepresented in sports cardiology research, and most previous studies have focused on younger women, Marius Myrstad, MD, of Baerum Hospital, Gjettum, Norway, said in a presentation at the annual congress of the European Association of Preventive Cardiology.
Previous research also has shown an increased risk of AFib in male endurance athletes, but similar data on women are lacking, Dr. Myrstad said.
The researchers reviewed data from the Birkebeiner Ageing Study, a study of Norwegian cross-country skiers aged 65 years and older who were followed for 10 years. The participants were competitors in the 2009/2010 Birkebeiner race, a 54-km cross country ski race in Norway.
Participants responded to a questionnaire addressing cardiovascular disease risk factors, exercise habits, and other health issues. The mean age at baseline was 67.5 year. A total of 34 participants (76%) were available for follow-up visits in 2014, and 36 attended a follow-up visit in 2020. Cumulative exposure to exercise was 26 years.
A total of 86% of the women reported moderate to vigorous exercise in the past year at baseline; 61% did so at the 2020 follow-up visit. One of the participants died during the study period.
“The baseline prevalence of cardiovascular conditions was very low,” Dr. Myrstad noted.
However, despite a low prevalence of cardiovascular risk factors, the risk of AFib in the study population was twice as high as for other cardiac diseases and stroke (15.6%, 7.1%, and 7.1%, respectively).
The mechanism of action for the increased AFib remains unclear, but the current study highlights the need for large, prospective studies of female athletes to address not only AFib, but also exercise-induced cardiac remodeling and cardiovascular health in general, said Dr. Myrstad.
The findings were limited by the small sample size and use of self-reports, Dr. Myrstad said, and more research is needed to clarify the association between increased AFib and high-level athletic activity in women.
“We should strive to close the gap between female and male athletes in sports cardiology research,” he added.
Consider the big picture of AFib risk
This study is important because of the growing recognition that atrial fibrillation may be a preventable disease, said Gregory Marcus, MD, a cardiologist at the University of California, San Francisco, said in an interview.

“Various behaviors or exposures that are under the control of the individual patient may reveal especially powerful means to help reduce risk,” he added.
Dr. Marcus said he was not surprised by the current study findings, as they reflect those of other studies suggesting a heightened risk for atrial fibrillation associated with very excessive exercise. However, the study was limited by the relatively small size and lack of a comparison group, he said. In addition, “The study was observational, and therefore the possibility that factors other than the predictor of interest, in this case intensive endurance exercise, were truly causal of atrial fibrillation could not be excluded,” he noted.
“It is very important to place this specialized analysis in the greater context of the full weight of evidence related to physical activity and atrial fibrillation,” said Dr. Marcus. “Specifically, when it comes to the general public and the great majority of patients we see in clinical practice, encouraging more physical activity is generally the best approach to reduce risks of atrial fibrillation,” he said. “It appears to be only in extraordinarily rigorous and prolonged endurance exercise that higher risks of atrial fibrillation may result,” he noted.
However, “Exercise also has many other benefits, related to overall cardiovascular health, brain health, bone health, and even cancer risk reduction, such that, even among the highly trained endurance athletes, the net benefit versus risk remains unknown,” he said.
“While the risk of atrial fibrillation in these highly trained endurance athletes was higher than expected, it still occurred in the minority,” Dr. Marcus said. “Therefore, there are certainly other factors yet to be identified that influence this heightened atrial fibrillation risk, and future research aimed at elucidating these other factors may help identify individuals more or less prone to atrial fibrillation or other behaviors that can help mitigate that risk.”
Dr. Myrstad disclosed lecture fees from Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, MSD, and Pfizer unrelated to the current study. Dr. Marcus disclosed serving as a consultant for Johnson and Johnson and InCarda, and holding equity as a cofounder of InCarda.
Older women with high levels of physical activity showed twice the risk of atrial fibrillation (AFib) over 10 years as they did for cardiac disease or stroke, based on data from 46 cross-country skiers.
Although previous research suggests that women derive greater health benefits from endurance sports, compared with men, women are generally underrepresented in sports cardiology research, and most previous studies have focused on younger women, Marius Myrstad, MD, of Baerum Hospital, Gjettum, Norway, said in a presentation at the annual congress of the European Association of Preventive Cardiology.
Previous research also has shown an increased risk of AFib in male endurance athletes, but similar data on women are lacking, Dr. Myrstad said.
The researchers reviewed data from the Birkebeiner Ageing Study, a study of Norwegian cross-country skiers aged 65 years and older who were followed for 10 years. The participants were competitors in the 2009/2010 Birkebeiner race, a 54-km cross country ski race in Norway.
Participants responded to a questionnaire addressing cardiovascular disease risk factors, exercise habits, and other health issues. The mean age at baseline was 67.5 year. A total of 34 participants (76%) were available for follow-up visits in 2014, and 36 attended a follow-up visit in 2020. Cumulative exposure to exercise was 26 years.
A total of 86% of the women reported moderate to vigorous exercise in the past year at baseline; 61% did so at the 2020 follow-up visit. One of the participants died during the study period.
“The baseline prevalence of cardiovascular conditions was very low,” Dr. Myrstad noted.
However, despite a low prevalence of cardiovascular risk factors, the risk of AFib in the study population was twice as high as for other cardiac diseases and stroke (15.6%, 7.1%, and 7.1%, respectively).
The mechanism of action for the increased AFib remains unclear, but the current study highlights the need for large, prospective studies of female athletes to address not only AFib, but also exercise-induced cardiac remodeling and cardiovascular health in general, said Dr. Myrstad.
The findings were limited by the small sample size and use of self-reports, Dr. Myrstad said, and more research is needed to clarify the association between increased AFib and high-level athletic activity in women.
“We should strive to close the gap between female and male athletes in sports cardiology research,” he added.
Consider the big picture of AFib risk
This study is important because of the growing recognition that atrial fibrillation may be a preventable disease, said Gregory Marcus, MD, a cardiologist at the University of California, San Francisco, said in an interview.
“Various behaviors or exposures that are under the control of the individual patient may reveal especially powerful means to help reduce risk,” he added.
Dr. Marcus said he was not surprised by the current study findings, as they reflect those of other studies suggesting a heightened risk for atrial fibrillation associated with very excessive exercise. However, the study was limited by the relatively small size and lack of a comparison group, he said. In addition, “The study was observational, and therefore the possibility that factors other than the predictor of interest, in this case intensive endurance exercise, were truly causal of atrial fibrillation could not be excluded,” he noted.
“It is very important to place this specialized analysis in the greater context of the full weight of evidence related to physical activity and atrial fibrillation,” said Dr. Marcus. “Specifically, when it comes to the general public and the great majority of patients we see in clinical practice, encouraging more physical activity is generally the best approach to reduce risks of atrial fibrillation,” he said. “It appears to be only in extraordinarily rigorous and prolonged endurance exercise that higher risks of atrial fibrillation may result,” he noted.
However, “Exercise also has many other benefits, related to overall cardiovascular health, brain health, bone health, and even cancer risk reduction, such that, even among the highly trained endurance athletes, the net benefit versus risk remains unknown,” he said.
“While the risk of atrial fibrillation in these highly trained endurance athletes was higher than expected, it still occurred in the minority,” Dr. Marcus said. “Therefore, there are certainly other factors yet to be identified that influence this heightened atrial fibrillation risk, and future research aimed at elucidating these other factors may help identify individuals more or less prone to atrial fibrillation or other behaviors that can help mitigate that risk.”
Dr. Myrstad disclosed lecture fees from Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, MSD, and Pfizer unrelated to the current study. Dr. Marcus disclosed serving as a consultant for Johnson and Johnson and InCarda, and holding equity as a cofounder of InCarda.
Older women with high levels of physical activity showed twice the risk of atrial fibrillation (AFib) over 10 years as they did for cardiac disease or stroke, based on data from 46 cross-country skiers.
Although previous research suggests that women derive greater health benefits from endurance sports, compared with men, women are generally underrepresented in sports cardiology research, and most previous studies have focused on younger women, Marius Myrstad, MD, of Baerum Hospital, Gjettum, Norway, said in a presentation at the annual congress of the European Association of Preventive Cardiology.
Previous research also has shown an increased risk of AFib in male endurance athletes, but similar data on women are lacking, Dr. Myrstad said.
The researchers reviewed data from the Birkebeiner Ageing Study, a study of Norwegian cross-country skiers aged 65 years and older who were followed for 10 years. The participants were competitors in the 2009/2010 Birkebeiner race, a 54-km cross country ski race in Norway.
Participants responded to a questionnaire addressing cardiovascular disease risk factors, exercise habits, and other health issues. The mean age at baseline was 67.5 year. A total of 34 participants (76%) were available for follow-up visits in 2014, and 36 attended a follow-up visit in 2020. Cumulative exposure to exercise was 26 years.
A total of 86% of the women reported moderate to vigorous exercise in the past year at baseline; 61% did so at the 2020 follow-up visit. One of the participants died during the study period.
“The baseline prevalence of cardiovascular conditions was very low,” Dr. Myrstad noted.
However, despite a low prevalence of cardiovascular risk factors, the risk of AFib in the study population was twice as high as for other cardiac diseases and stroke (15.6%, 7.1%, and 7.1%, respectively).
The mechanism of action for the increased AFib remains unclear, but the current study highlights the need for large, prospective studies of female athletes to address not only AFib, but also exercise-induced cardiac remodeling and cardiovascular health in general, said Dr. Myrstad.
The findings were limited by the small sample size and use of self-reports, Dr. Myrstad said, and more research is needed to clarify the association between increased AFib and high-level athletic activity in women.
“We should strive to close the gap between female and male athletes in sports cardiology research,” he added.
Consider the big picture of AFib risk
This study is important because of the growing recognition that atrial fibrillation may be a preventable disease, said Gregory Marcus, MD, a cardiologist at the University of California, San Francisco, said in an interview.
“Various behaviors or exposures that are under the control of the individual patient may reveal especially powerful means to help reduce risk,” he added.
Dr. Marcus said he was not surprised by the current study findings, as they reflect those of other studies suggesting a heightened risk for atrial fibrillation associated with very excessive exercise. However, the study was limited by the relatively small size and lack of a comparison group, he said. In addition, “The study was observational, and therefore the possibility that factors other than the predictor of interest, in this case intensive endurance exercise, were truly causal of atrial fibrillation could not be excluded,” he noted.
“It is very important to place this specialized analysis in the greater context of the full weight of evidence related to physical activity and atrial fibrillation,” said Dr. Marcus. “Specifically, when it comes to the general public and the great majority of patients we see in clinical practice, encouraging more physical activity is generally the best approach to reduce risks of atrial fibrillation,” he said. “It appears to be only in extraordinarily rigorous and prolonged endurance exercise that higher risks of atrial fibrillation may result,” he noted.
However, “Exercise also has many other benefits, related to overall cardiovascular health, brain health, bone health, and even cancer risk reduction, such that, even among the highly trained endurance athletes, the net benefit versus risk remains unknown,” he said.
“While the risk of atrial fibrillation in these highly trained endurance athletes was higher than expected, it still occurred in the minority,” Dr. Marcus said. “Therefore, there are certainly other factors yet to be identified that influence this heightened atrial fibrillation risk, and future research aimed at elucidating these other factors may help identify individuals more or less prone to atrial fibrillation or other behaviors that can help mitigate that risk.”
Dr. Myrstad disclosed lecture fees from Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, MSD, and Pfizer unrelated to the current study. Dr. Marcus disclosed serving as a consultant for Johnson and Johnson and InCarda, and holding equity as a cofounder of InCarda.
FROM ESC PREVENTIVE CARDIOLOGY 2023
Medical-level empathy? Yup, ChatGPT can fake that
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?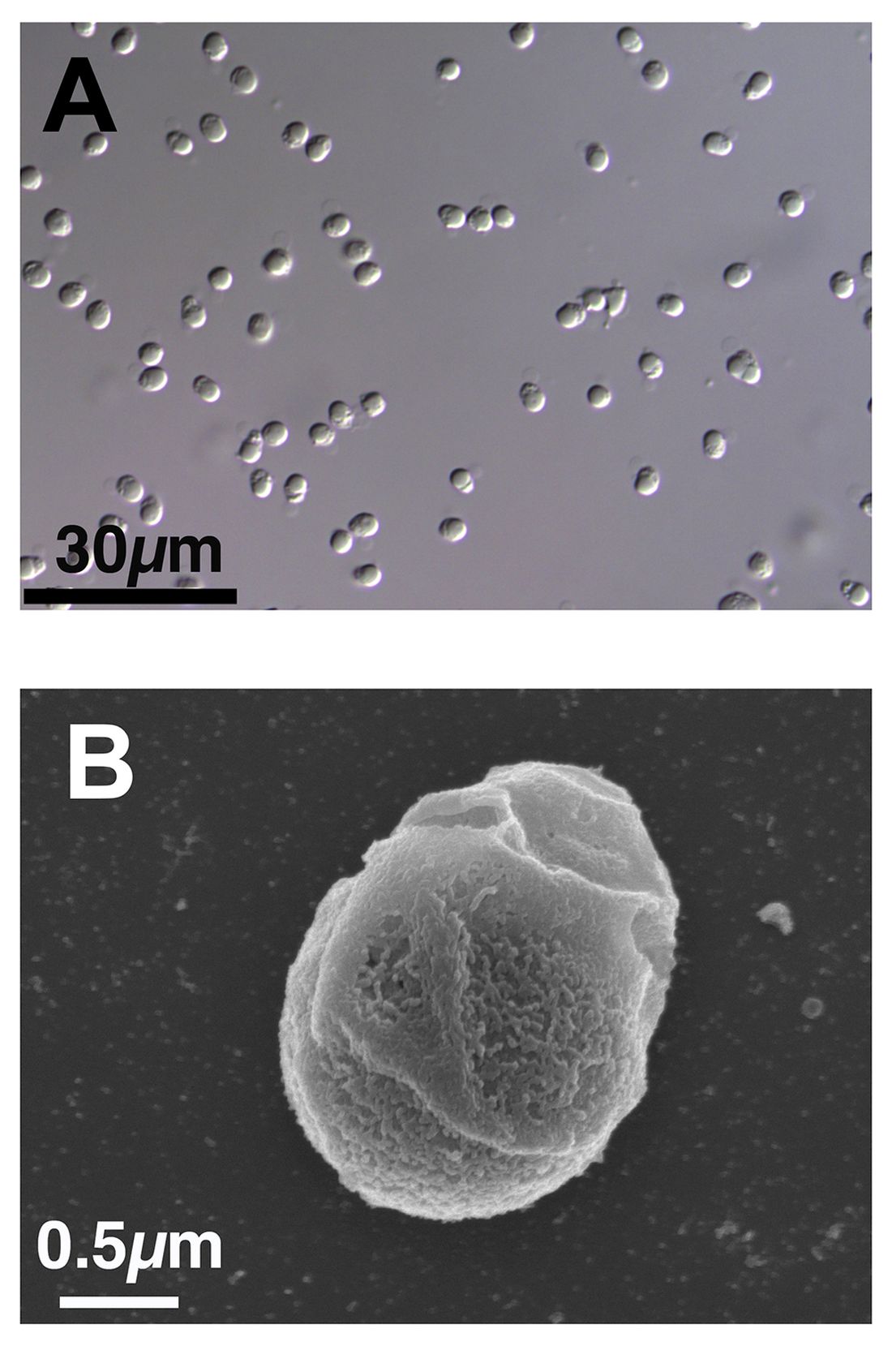
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.