User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
AI at the office: Are clinicians prepared?
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AT SGIM 2023
Pop this question to improve medication adherence
AURORA, COLO. – How often do you talk with patients about how to lower their out-of-pocket costs for medical care?
For most clinicians, the answer is: not often enough. But having those conversations can improve medication adherence and strengthen the patient-clinician relationship, according to panelists at the annual meeting of the Society of General Internal Medicine.
The inverse association between out-of-pocket expenditures and fidelity to prescriptions is clear. A 2020 study by the IQVIA Institute for Human Data Science, for example, found that rates of prescription abandonment are less than 5% when a given medication carries no out-of-pocket cost for patients. That figure rises to 45% when the cost is more than $125, and to 60% when it exceeds $500. One in five Americans said cost prevented them from adhering to medication regimens, according to a new study in JAMA Network Open.
The researchers surveyed more than 2,000 men and women, 40.4% of whom were aged 75 or older. They found that nearly 90% of respondents said they would not be uncomfortable being asked about drug costs before a visit with a physician. A similar share (89.5%) said they would welcome the use by their physician of a real-time tool to determine the cost of their medication.
But the survey results contained a note of warning for clinicians: A significant number of respondents said they would be “extremely” upset if the cost of their medication exceeded the estimate from the pricing tool. And many also said they would be “moderately” or “extremely” angry if their physician used a pricing tool but failed to share the results with them.
“Real-time benefit tools may support medication cost conversations and cost-conscious prescribing, and patients are enthusiastic about their use,” the authors write. “However, if disclosed prices are inaccurate, there is potential for harm through loss of confidence in the physician and nonadherence to prescribed medications.”
While having conversations about cost can be difficult for both clinicians and patients, studies have shown that patients who discuss cost concerns with their doctors feel as if they have stronger relationships as a result.
Clinicians often avoid conversations about out-of-pocket expenses because they don’t know specific price information, they lack solutions to address cost, or they are uncomfortable bringing up the issue.
One member of the audience at the SGIM meeting recalled a patient who worked in a warehouse for a large company. The man, who had type 2 diabetes, had medical insurance, but even with insurance, insulin was going to cost him $150 per month. He struggled to afford the necessary treatment.
“He looked at me and said, ‘What do they want me to do? Do they want me to actually not be able to work for them and not manage my diabetes?’ ”
The clinician said he offered empathy in the moment but felt he could do little else.
Panelists acknowledged that clinicians are crunched on time when seeing patients, but being willing to initiate conversations about cost with patients and to offer resources can help patients get necessary treatment.
Start the conversation
Panel member Caroline Sloan, MD, an assistant professor of medicine at Duke University, Durham, N.C., said making patients aware that you know cost can make a big difference.
The American College of Physicians advises clinicians to ask patients whether they are worried about the cost of care and to not assume which patients may have concerns.
The conversation could be started like this: “I’d like to discuss any concerns you might have about the cost of your health care.”
Normalize the concern by making it more general, and reassure your patient that your goal is to get them the best care. Say something like, “I’ve heard from many patients the cost of medications or tests is becoming hard to manage.”
Once a patient’s concerns are clear, you can direct them to resources for assistance in reducing their costs, Dr. Sloan said, such as ClearHealthCosts, FAIR Health, Healthcare Bluebook, New Choice Health, GoodRx, PharmacyChecker, HealthWell Foundation, Patient Advocate Foundation, Good Days, Good Health Will, Mercy Medical Angels, and the American Association of Family Physicians Neighborhood Navigator.
Dr. Sloan said she knows clinicians don’t have time to understand every insurance plan and other issues related to cost. “But at least know to ask about costs,” she said. “Practice, practice, practice. It feels awkward at first, but it gets easier every time.”
A version of this article first appeared on Medscape.com.
AURORA, COLO. – How often do you talk with patients about how to lower their out-of-pocket costs for medical care?
For most clinicians, the answer is: not often enough. But having those conversations can improve medication adherence and strengthen the patient-clinician relationship, according to panelists at the annual meeting of the Society of General Internal Medicine.
The inverse association between out-of-pocket expenditures and fidelity to prescriptions is clear. A 2020 study by the IQVIA Institute for Human Data Science, for example, found that rates of prescription abandonment are less than 5% when a given medication carries no out-of-pocket cost for patients. That figure rises to 45% when the cost is more than $125, and to 60% when it exceeds $500. One in five Americans said cost prevented them from adhering to medication regimens, according to a new study in JAMA Network Open.
The researchers surveyed more than 2,000 men and women, 40.4% of whom were aged 75 or older. They found that nearly 90% of respondents said they would not be uncomfortable being asked about drug costs before a visit with a physician. A similar share (89.5%) said they would welcome the use by their physician of a real-time tool to determine the cost of their medication.
But the survey results contained a note of warning for clinicians: A significant number of respondents said they would be “extremely” upset if the cost of their medication exceeded the estimate from the pricing tool. And many also said they would be “moderately” or “extremely” angry if their physician used a pricing tool but failed to share the results with them.
“Real-time benefit tools may support medication cost conversations and cost-conscious prescribing, and patients are enthusiastic about their use,” the authors write. “However, if disclosed prices are inaccurate, there is potential for harm through loss of confidence in the physician and nonadherence to prescribed medications.”
While having conversations about cost can be difficult for both clinicians and patients, studies have shown that patients who discuss cost concerns with their doctors feel as if they have stronger relationships as a result.
Clinicians often avoid conversations about out-of-pocket expenses because they don’t know specific price information, they lack solutions to address cost, or they are uncomfortable bringing up the issue.
One member of the audience at the SGIM meeting recalled a patient who worked in a warehouse for a large company. The man, who had type 2 diabetes, had medical insurance, but even with insurance, insulin was going to cost him $150 per month. He struggled to afford the necessary treatment.
“He looked at me and said, ‘What do they want me to do? Do they want me to actually not be able to work for them and not manage my diabetes?’ ”
The clinician said he offered empathy in the moment but felt he could do little else.
Panelists acknowledged that clinicians are crunched on time when seeing patients, but being willing to initiate conversations about cost with patients and to offer resources can help patients get necessary treatment.
Start the conversation
Panel member Caroline Sloan, MD, an assistant professor of medicine at Duke University, Durham, N.C., said making patients aware that you know cost can make a big difference.
The American College of Physicians advises clinicians to ask patients whether they are worried about the cost of care and to not assume which patients may have concerns.
The conversation could be started like this: “I’d like to discuss any concerns you might have about the cost of your health care.”
Normalize the concern by making it more general, and reassure your patient that your goal is to get them the best care. Say something like, “I’ve heard from many patients the cost of medications or tests is becoming hard to manage.”
Once a patient’s concerns are clear, you can direct them to resources for assistance in reducing their costs, Dr. Sloan said, such as ClearHealthCosts, FAIR Health, Healthcare Bluebook, New Choice Health, GoodRx, PharmacyChecker, HealthWell Foundation, Patient Advocate Foundation, Good Days, Good Health Will, Mercy Medical Angels, and the American Association of Family Physicians Neighborhood Navigator.
Dr. Sloan said she knows clinicians don’t have time to understand every insurance plan and other issues related to cost. “But at least know to ask about costs,” she said. “Practice, practice, practice. It feels awkward at first, but it gets easier every time.”
A version of this article first appeared on Medscape.com.
AURORA, COLO. – How often do you talk with patients about how to lower their out-of-pocket costs for medical care?
For most clinicians, the answer is: not often enough. But having those conversations can improve medication adherence and strengthen the patient-clinician relationship, according to panelists at the annual meeting of the Society of General Internal Medicine.
The inverse association between out-of-pocket expenditures and fidelity to prescriptions is clear. A 2020 study by the IQVIA Institute for Human Data Science, for example, found that rates of prescription abandonment are less than 5% when a given medication carries no out-of-pocket cost for patients. That figure rises to 45% when the cost is more than $125, and to 60% when it exceeds $500. One in five Americans said cost prevented them from adhering to medication regimens, according to a new study in JAMA Network Open.
The researchers surveyed more than 2,000 men and women, 40.4% of whom were aged 75 or older. They found that nearly 90% of respondents said they would not be uncomfortable being asked about drug costs before a visit with a physician. A similar share (89.5%) said they would welcome the use by their physician of a real-time tool to determine the cost of their medication.
But the survey results contained a note of warning for clinicians: A significant number of respondents said they would be “extremely” upset if the cost of their medication exceeded the estimate from the pricing tool. And many also said they would be “moderately” or “extremely” angry if their physician used a pricing tool but failed to share the results with them.
“Real-time benefit tools may support medication cost conversations and cost-conscious prescribing, and patients are enthusiastic about their use,” the authors write. “However, if disclosed prices are inaccurate, there is potential for harm through loss of confidence in the physician and nonadherence to prescribed medications.”
While having conversations about cost can be difficult for both clinicians and patients, studies have shown that patients who discuss cost concerns with their doctors feel as if they have stronger relationships as a result.
Clinicians often avoid conversations about out-of-pocket expenses because they don’t know specific price information, they lack solutions to address cost, or they are uncomfortable bringing up the issue.
One member of the audience at the SGIM meeting recalled a patient who worked in a warehouse for a large company. The man, who had type 2 diabetes, had medical insurance, but even with insurance, insulin was going to cost him $150 per month. He struggled to afford the necessary treatment.
“He looked at me and said, ‘What do they want me to do? Do they want me to actually not be able to work for them and not manage my diabetes?’ ”
The clinician said he offered empathy in the moment but felt he could do little else.
Panelists acknowledged that clinicians are crunched on time when seeing patients, but being willing to initiate conversations about cost with patients and to offer resources can help patients get necessary treatment.
Start the conversation
Panel member Caroline Sloan, MD, an assistant professor of medicine at Duke University, Durham, N.C., said making patients aware that you know cost can make a big difference.
The American College of Physicians advises clinicians to ask patients whether they are worried about the cost of care and to not assume which patients may have concerns.
The conversation could be started like this: “I’d like to discuss any concerns you might have about the cost of your health care.”
Normalize the concern by making it more general, and reassure your patient that your goal is to get them the best care. Say something like, “I’ve heard from many patients the cost of medications or tests is becoming hard to manage.”
Once a patient’s concerns are clear, you can direct them to resources for assistance in reducing their costs, Dr. Sloan said, such as ClearHealthCosts, FAIR Health, Healthcare Bluebook, New Choice Health, GoodRx, PharmacyChecker, HealthWell Foundation, Patient Advocate Foundation, Good Days, Good Health Will, Mercy Medical Angels, and the American Association of Family Physicians Neighborhood Navigator.
Dr. Sloan said she knows clinicians don’t have time to understand every insurance plan and other issues related to cost. “But at least know to ask about costs,” she said. “Practice, practice, practice. It feels awkward at first, but it gets easier every time.”
A version of this article first appeared on Medscape.com.
AT SGIM 2023
Age-specific cut-offs needed for cardiac troponin tests?
The study shows that the 99th percentile for the upper reference limit (used to define myocardial injury) for high-sensitivity (hs)–troponin T in the new analysis matched those reported by manufacturers. However, the same threshold for hs–troponin I was lower than was manufacturer-reported levels when considering the whole population.
And for both hs–troponin T and hs–troponin I, there were significant differences in 99th percentile levels by age.
“Our data suggest that some cases of myocardial injury may be missed in the whole population by using current non–age specific thresholds of troponin I,” lead author, John McEvoy, MB, University of Galway (Ireland), said in an interview. “If the non–age specific threshold was lowered to that in our cohort, then we would pick up more people with myocardial injury.”
“However,” Dr. McEvoy added, “if age-specific thresholds were deployed, then our data suggest that thresholds used to diagnose myocardial injury would need to be higher in older adults, somewhat lower in middle-aged individuals and much lower in younger people.”
The study was published online in the Journal of the American College of Cardiology.
The authors explain that the 99th percentile upper–reference limit threshold is the common benchmark of abnormality for all troponin assays. Five high-sensitivity cardiac troponin assays have been cleared by the Food and Drug Administration for clinical use and allow for earlier diagnosis of MI.
However, there has been variability in the approach used to define the 99th percentile upper reference limits for these assays, with definitions of healthy reference populations differing and the various assays available are not standardized or harmonized. So troponin concentrations at 99th percentiles do not align across assays, and the generalizability of manufacturer-reported reference upper reference limits for hs-troponin assays to the U.S. adult population is unknown.
They note that though sex-specific 99th percentile upper reference limits for hs-troponin have been recommended since 2018, age-specific thresholds are not yet endorsed, and whether thresholds differ by race or ethnicity is also controversial.
They aimed to investigate these issues using stored serum samples from adults aged 18 or older who participated in the 1999-2004 National Health and Nutrition Examination Survey (NHANES).
Dr. McEvoy described the NHANES database as “the gold standard cohort for representation of the U.S. adult population,” noting that other studies conducted by the manufacturers of the troponin tests have often used convenience samples from patients attending hospital clinics and blood donors, which he said were not representative of the whole population.
For the study, the researchers estimated that the 99th percentile upper reference limit for four hs-troponin assays (one troponin T and three troponin I) in a strictly defined healthy reference subgroup of 2,746 individuals from the NHANES cohort.
Results showed that the NHANES 99th percentile upper reference limit for hs–troponin T (19 ng/L) matched the manufacturer-reported level (19 ng/L). But, the NHANES upper reference levels for three troponin I assays were lower than were levels stated by the manufacturers.
The NHANES levels were 13 ng/L for the Abbott hs–troponin I assay (manufacturer: 28 ng/L); 5 ng/L for the Ortho hs–troponin I assay (manufacturer: 11 ng/L); and 37 ng/L for the Siemens hs–troponin I assay (manufacturer: 46.5 ng/L).
Furthermore, the 99th percentile upper reference limits for all four hs-troponin assays were statistically significantly lower in healthy adults younger than 40 years, compared with healthy adults older than 60 years.
There were also significant differences in upper reference limits by sex, but none by race/ethnicity.
Dr. McEvoy explained that NHANES is a very well phenotyped database with information on individuals’ health, body mass index, and other biomarkers. “This allows us to define a completely healthy subgroup of people, which could explain why the 99th percentile threshold for hs–troponin I was lower than previously reported from other cohorts,” he added.
Though there may be concern that such a healthy subgroup would mean the sample is enriched with younger people, whereas the typical person having their troponin measured would be older, Dr. McEvoy pointed out that there were more than 400 people older than 60 years in the healthy group. “This is probably the biggest cohort of super healthy older U.S. adults ever sampled in this regard,” he commented.
Dr. McEvoy said that the overall results from the study suggested that different thresholds might need to be considered for troponin I. “This could lead to threshold levels used to diagnose myocardial injury being cut in the population as a whole.”
But, he said a more important message was the need for age-specific thresholds.
“We found that troponin levels track with age. Even in individuals who age in a very healthy way, their troponin levels are greater than in younger people. This is the first time this has been shown with such clear statistical significance,” Dr. McEvoy said. “We think this data provides a compelling case for the use of age-specific cut-offs.”
He explained that, if age-specific thresholds were used to diagnose myocardial injury, the cut point from the current data would be higher than it would be from current manufacturers’ recommendations in those older than 60 years, so fewer people in this age group would be labeled as having myocardial injury.
“Our results suggest that, at present, we are seeing more false positives in older people leading to more unnecessary tests.” Using age-specific cut off points will reduce the number of false positives in older people. Dr. McEvoy noted a similar change in the way D-Dimer blood tests have been used to diagnose pulmonary embolism in recent years.
Using age-specific cut-offs for hs-troponin would also reduce the number of false negatives in younger people, Dr. McEvoy added.
Further studies needed?
In an accompanying editorial, Cian McCarthy, MB, Austin Vyas, and James Januzzi, MD, of Massachusetts General Hospital, Boston, note that though there are substantial shortcomings to using the 99th percentile upper reference limit of troponins for the diagnosis of cardiac injury, they believe this measurement should persist as a central component of the MI diagnostic criteria, with the caveat that this is only one component of the definition of MI and does not alone define it.
“Cardiac troponin measurement is one of the most commonly utilized blood tests in hospital-based settings, and yet important questions remain about what exactly is a normal value for this test,” the editorialists comment.
They say this new study emphasizes the importance of age and sex in interpretation of troponin levels.
“Although the use of such cut-offs may further complicate MI diagnostic criteria, this is superseded by the benefits of improved diagnostic accuracy in younger and female patients (a critical health equity step) while reducing MI overdiagnosis in the elderly, with the resultant harms that might follow, adverse psychosocial patient impact, and unnecessary health care expenditure from cascade testing,” they write.
They conclude that further large studies derived from healthy cohorts should be conducted to answer this question in a definitive fashion.
A version of this article first appeared on Medscape.com.
The study shows that the 99th percentile for the upper reference limit (used to define myocardial injury) for high-sensitivity (hs)–troponin T in the new analysis matched those reported by manufacturers. However, the same threshold for hs–troponin I was lower than was manufacturer-reported levels when considering the whole population.
And for both hs–troponin T and hs–troponin I, there were significant differences in 99th percentile levels by age.
“Our data suggest that some cases of myocardial injury may be missed in the whole population by using current non–age specific thresholds of troponin I,” lead author, John McEvoy, MB, University of Galway (Ireland), said in an interview. “If the non–age specific threshold was lowered to that in our cohort, then we would pick up more people with myocardial injury.”
“However,” Dr. McEvoy added, “if age-specific thresholds were deployed, then our data suggest that thresholds used to diagnose myocardial injury would need to be higher in older adults, somewhat lower in middle-aged individuals and much lower in younger people.”
The study was published online in the Journal of the American College of Cardiology.
The authors explain that the 99th percentile upper–reference limit threshold is the common benchmark of abnormality for all troponin assays. Five high-sensitivity cardiac troponin assays have been cleared by the Food and Drug Administration for clinical use and allow for earlier diagnosis of MI.
However, there has been variability in the approach used to define the 99th percentile upper reference limits for these assays, with definitions of healthy reference populations differing and the various assays available are not standardized or harmonized. So troponin concentrations at 99th percentiles do not align across assays, and the generalizability of manufacturer-reported reference upper reference limits for hs-troponin assays to the U.S. adult population is unknown.
They note that though sex-specific 99th percentile upper reference limits for hs-troponin have been recommended since 2018, age-specific thresholds are not yet endorsed, and whether thresholds differ by race or ethnicity is also controversial.
They aimed to investigate these issues using stored serum samples from adults aged 18 or older who participated in the 1999-2004 National Health and Nutrition Examination Survey (NHANES).
Dr. McEvoy described the NHANES database as “the gold standard cohort for representation of the U.S. adult population,” noting that other studies conducted by the manufacturers of the troponin tests have often used convenience samples from patients attending hospital clinics and blood donors, which he said were not representative of the whole population.
For the study, the researchers estimated that the 99th percentile upper reference limit for four hs-troponin assays (one troponin T and three troponin I) in a strictly defined healthy reference subgroup of 2,746 individuals from the NHANES cohort.
Results showed that the NHANES 99th percentile upper reference limit for hs–troponin T (19 ng/L) matched the manufacturer-reported level (19 ng/L). But, the NHANES upper reference levels for three troponin I assays were lower than were levels stated by the manufacturers.
The NHANES levels were 13 ng/L for the Abbott hs–troponin I assay (manufacturer: 28 ng/L); 5 ng/L for the Ortho hs–troponin I assay (manufacturer: 11 ng/L); and 37 ng/L for the Siemens hs–troponin I assay (manufacturer: 46.5 ng/L).
Furthermore, the 99th percentile upper reference limits for all four hs-troponin assays were statistically significantly lower in healthy adults younger than 40 years, compared with healthy adults older than 60 years.
There were also significant differences in upper reference limits by sex, but none by race/ethnicity.
Dr. McEvoy explained that NHANES is a very well phenotyped database with information on individuals’ health, body mass index, and other biomarkers. “This allows us to define a completely healthy subgroup of people, which could explain why the 99th percentile threshold for hs–troponin I was lower than previously reported from other cohorts,” he added.
Though there may be concern that such a healthy subgroup would mean the sample is enriched with younger people, whereas the typical person having their troponin measured would be older, Dr. McEvoy pointed out that there were more than 400 people older than 60 years in the healthy group. “This is probably the biggest cohort of super healthy older U.S. adults ever sampled in this regard,” he commented.
Dr. McEvoy said that the overall results from the study suggested that different thresholds might need to be considered for troponin I. “This could lead to threshold levels used to diagnose myocardial injury being cut in the population as a whole.”
But, he said a more important message was the need for age-specific thresholds.
“We found that troponin levels track with age. Even in individuals who age in a very healthy way, their troponin levels are greater than in younger people. This is the first time this has been shown with such clear statistical significance,” Dr. McEvoy said. “We think this data provides a compelling case for the use of age-specific cut-offs.”
He explained that, if age-specific thresholds were used to diagnose myocardial injury, the cut point from the current data would be higher than it would be from current manufacturers’ recommendations in those older than 60 years, so fewer people in this age group would be labeled as having myocardial injury.
“Our results suggest that, at present, we are seeing more false positives in older people leading to more unnecessary tests.” Using age-specific cut off points will reduce the number of false positives in older people. Dr. McEvoy noted a similar change in the way D-Dimer blood tests have been used to diagnose pulmonary embolism in recent years.
Using age-specific cut-offs for hs-troponin would also reduce the number of false negatives in younger people, Dr. McEvoy added.
Further studies needed?
In an accompanying editorial, Cian McCarthy, MB, Austin Vyas, and James Januzzi, MD, of Massachusetts General Hospital, Boston, note that though there are substantial shortcomings to using the 99th percentile upper reference limit of troponins for the diagnosis of cardiac injury, they believe this measurement should persist as a central component of the MI diagnostic criteria, with the caveat that this is only one component of the definition of MI and does not alone define it.
“Cardiac troponin measurement is one of the most commonly utilized blood tests in hospital-based settings, and yet important questions remain about what exactly is a normal value for this test,” the editorialists comment.
They say this new study emphasizes the importance of age and sex in interpretation of troponin levels.
“Although the use of such cut-offs may further complicate MI diagnostic criteria, this is superseded by the benefits of improved diagnostic accuracy in younger and female patients (a critical health equity step) while reducing MI overdiagnosis in the elderly, with the resultant harms that might follow, adverse psychosocial patient impact, and unnecessary health care expenditure from cascade testing,” they write.
They conclude that further large studies derived from healthy cohorts should be conducted to answer this question in a definitive fashion.
A version of this article first appeared on Medscape.com.
The study shows that the 99th percentile for the upper reference limit (used to define myocardial injury) for high-sensitivity (hs)–troponin T in the new analysis matched those reported by manufacturers. However, the same threshold for hs–troponin I was lower than was manufacturer-reported levels when considering the whole population.
And for both hs–troponin T and hs–troponin I, there were significant differences in 99th percentile levels by age.
“Our data suggest that some cases of myocardial injury may be missed in the whole population by using current non–age specific thresholds of troponin I,” lead author, John McEvoy, MB, University of Galway (Ireland), said in an interview. “If the non–age specific threshold was lowered to that in our cohort, then we would pick up more people with myocardial injury.”
“However,” Dr. McEvoy added, “if age-specific thresholds were deployed, then our data suggest that thresholds used to diagnose myocardial injury would need to be higher in older adults, somewhat lower in middle-aged individuals and much lower in younger people.”
The study was published online in the Journal of the American College of Cardiology.
The authors explain that the 99th percentile upper–reference limit threshold is the common benchmark of abnormality for all troponin assays. Five high-sensitivity cardiac troponin assays have been cleared by the Food and Drug Administration for clinical use and allow for earlier diagnosis of MI.
However, there has been variability in the approach used to define the 99th percentile upper reference limits for these assays, with definitions of healthy reference populations differing and the various assays available are not standardized or harmonized. So troponin concentrations at 99th percentiles do not align across assays, and the generalizability of manufacturer-reported reference upper reference limits for hs-troponin assays to the U.S. adult population is unknown.
They note that though sex-specific 99th percentile upper reference limits for hs-troponin have been recommended since 2018, age-specific thresholds are not yet endorsed, and whether thresholds differ by race or ethnicity is also controversial.
They aimed to investigate these issues using stored serum samples from adults aged 18 or older who participated in the 1999-2004 National Health and Nutrition Examination Survey (NHANES).
Dr. McEvoy described the NHANES database as “the gold standard cohort for representation of the U.S. adult population,” noting that other studies conducted by the manufacturers of the troponin tests have often used convenience samples from patients attending hospital clinics and blood donors, which he said were not representative of the whole population.
For the study, the researchers estimated that the 99th percentile upper reference limit for four hs-troponin assays (one troponin T and three troponin I) in a strictly defined healthy reference subgroup of 2,746 individuals from the NHANES cohort.
Results showed that the NHANES 99th percentile upper reference limit for hs–troponin T (19 ng/L) matched the manufacturer-reported level (19 ng/L). But, the NHANES upper reference levels for three troponin I assays were lower than were levels stated by the manufacturers.
The NHANES levels were 13 ng/L for the Abbott hs–troponin I assay (manufacturer: 28 ng/L); 5 ng/L for the Ortho hs–troponin I assay (manufacturer: 11 ng/L); and 37 ng/L for the Siemens hs–troponin I assay (manufacturer: 46.5 ng/L).
Furthermore, the 99th percentile upper reference limits for all four hs-troponin assays were statistically significantly lower in healthy adults younger than 40 years, compared with healthy adults older than 60 years.
There were also significant differences in upper reference limits by sex, but none by race/ethnicity.
Dr. McEvoy explained that NHANES is a very well phenotyped database with information on individuals’ health, body mass index, and other biomarkers. “This allows us to define a completely healthy subgroup of people, which could explain why the 99th percentile threshold for hs–troponin I was lower than previously reported from other cohorts,” he added.
Though there may be concern that such a healthy subgroup would mean the sample is enriched with younger people, whereas the typical person having their troponin measured would be older, Dr. McEvoy pointed out that there were more than 400 people older than 60 years in the healthy group. “This is probably the biggest cohort of super healthy older U.S. adults ever sampled in this regard,” he commented.
Dr. McEvoy said that the overall results from the study suggested that different thresholds might need to be considered for troponin I. “This could lead to threshold levels used to diagnose myocardial injury being cut in the population as a whole.”
But, he said a more important message was the need for age-specific thresholds.
“We found that troponin levels track with age. Even in individuals who age in a very healthy way, their troponin levels are greater than in younger people. This is the first time this has been shown with such clear statistical significance,” Dr. McEvoy said. “We think this data provides a compelling case for the use of age-specific cut-offs.”
He explained that, if age-specific thresholds were used to diagnose myocardial injury, the cut point from the current data would be higher than it would be from current manufacturers’ recommendations in those older than 60 years, so fewer people in this age group would be labeled as having myocardial injury.
“Our results suggest that, at present, we are seeing more false positives in older people leading to more unnecessary tests.” Using age-specific cut off points will reduce the number of false positives in older people. Dr. McEvoy noted a similar change in the way D-Dimer blood tests have been used to diagnose pulmonary embolism in recent years.
Using age-specific cut-offs for hs-troponin would also reduce the number of false negatives in younger people, Dr. McEvoy added.
Further studies needed?
In an accompanying editorial, Cian McCarthy, MB, Austin Vyas, and James Januzzi, MD, of Massachusetts General Hospital, Boston, note that though there are substantial shortcomings to using the 99th percentile upper reference limit of troponins for the diagnosis of cardiac injury, they believe this measurement should persist as a central component of the MI diagnostic criteria, with the caveat that this is only one component of the definition of MI and does not alone define it.
“Cardiac troponin measurement is one of the most commonly utilized blood tests in hospital-based settings, and yet important questions remain about what exactly is a normal value for this test,” the editorialists comment.
They say this new study emphasizes the importance of age and sex in interpretation of troponin levels.
“Although the use of such cut-offs may further complicate MI diagnostic criteria, this is superseded by the benefits of improved diagnostic accuracy in younger and female patients (a critical health equity step) while reducing MI overdiagnosis in the elderly, with the resultant harms that might follow, adverse psychosocial patient impact, and unnecessary health care expenditure from cascade testing,” they write.
They conclude that further large studies derived from healthy cohorts should be conducted to answer this question in a definitive fashion.
A version of this article first appeared on Medscape.com.
FROM JACC
Half of teens drop below obesity cutoff with semaglutide
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.

“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.
“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.
“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
FROM ECO 2023
Morning PT
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.

Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.
Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.
Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Review supports continued mask-wearing in health care visits
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
FROM ANNALS OF INTERNAL MEDICINE
Evidence of TAVR benefit extends to cardiogenic shock
Early risks outweighed at 1 year
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
Early risks outweighed at 1 year
Early risks outweighed at 1 year
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
FROM EUROPCR 2023
The antimicrobial peptide that even Pharma can love
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.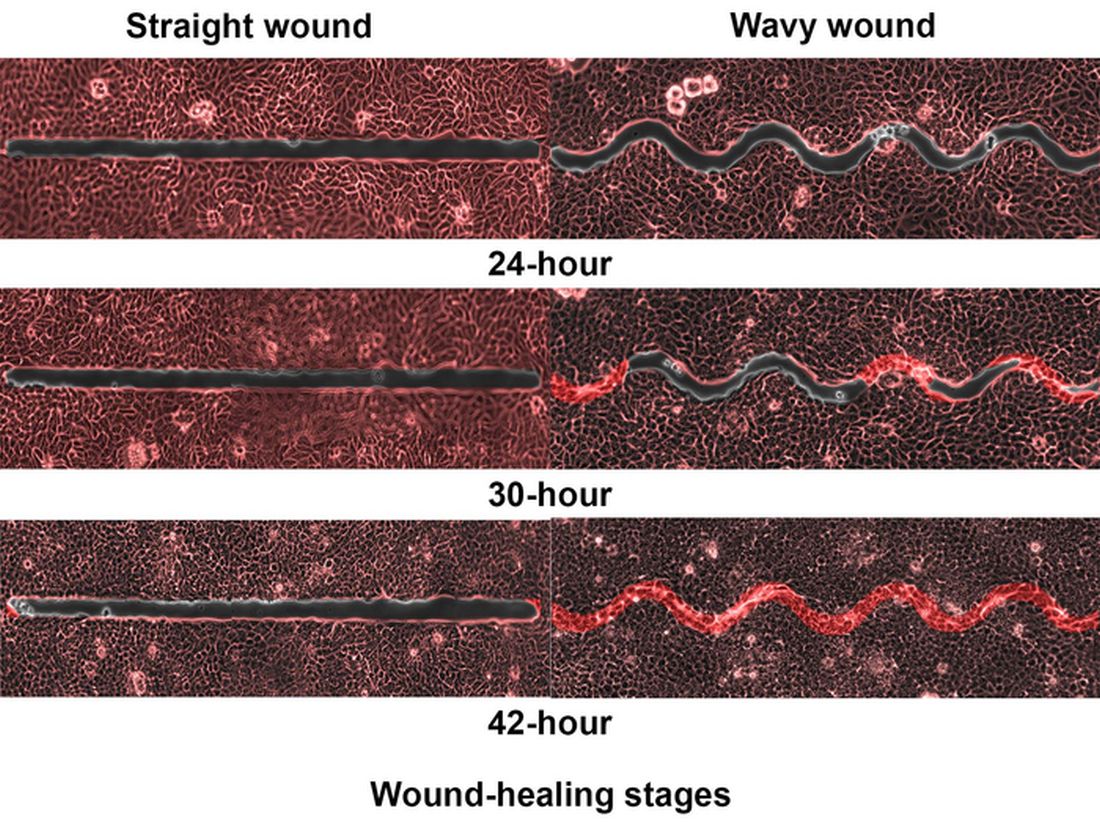
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Redo-TAVR in U.S. database yields good news: Outcomes rival first intervention
Data support redo if needed.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
Data support redo if needed.
Data support redo if needed.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
FROM EUROPCR 2023
Docs fervently hope federal ban on noncompete clauses goes through
The Federal Trade Commission’s proposed regulation that would ban noncompete agreements across the country seems like potential good news for doctors. Of course, many hospitals and employers are against it. As a result, the FTC’s sweeping proposal has tongues wagging on both sides of the issue.
Many physicians are thrilled that they may soon have more control over their career and not be stuck in jobs where they feel frustrated, underpaid, or blocked in their progress.
As of 2018, as many as 45% of primary care physicians had inked such agreements with their employers.
Typically, the agreements prevent physicians from practicing medicine with a new employer for a defined period within a specific geographic area. No matter how attractive an alternate offer of employment might be, doctors are bound by the agreements to say no if the offer exists in that defined area and time period.
The period for public comment on the proposed regulation ended on April 19, and there is currently no set date for a decision.
In a Medscape poll of 558 physicians, more than 9 out of 10 respondents said that they were either currently bound by a noncompete clause or that they had been bound by one in the past that had forced them to temporarily stop working, commute long distances, move to a different area, or switch fields.
The new proposal would make it illegal for an employer, such as a hospital or large group, to enter a noncompete with a worker; maintain a noncompete with a worker; or represent to a worker, under certain circumstances, that the worker is subject to a noncompete.
It also would not only ban future noncompete agreements but also retroactively invalidate existing ones. The FTC reasons that noncompete clauses could potentially increase worker earnings as well as lower health care costs by billions of dollars. If the ruling were to move forward, it would represent part of President Biden’s “worker-forward” priorities, focusing on how competition can be a good thing for employees. The President billed the FTC’s announcement as a “huge win for workers.”
In its statements on the proposed ban, the FTC claimed that it could lower consumer prices across the board by as much as $150 billion per year and return nearly $300 million to workers each year.
However, even if passed, the draft rule would keep in place nonsolicitation rules that many health care organizations have put into place. That means that, if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to switch to him or her in the new job.
Within that clause, however, the FTC has specified that if such nonsolicitation agreement has the “equivalent effect” of a noncompete, the agency would deem it such. That means, even if that rule stays, it could be contested and may be interpreted as violating the noncompete law. So there’s value in reading all the fine print should the ban move forward.
Could the ban bring potential downsides?
Most physicians view the potential to break free of a noncompete agreement as a victory. Peter Glennon, an employment litigation attorney with The Glennon Law Firm in Rochester, N.Y., says not so fast. “If you ask anyone if they’d prefer a noncompete agreement, of course they’re going to say no,” he said in an interview. “It sounds like a restriction, one that can hold you back.”
Mr. Glennon believes that there are actually upsides to physician noncompetes. For instance, many noncompetes come with sign-on bonuses that could potentially disappear without the agreements. There’s also the fact that when some physicians sign a noncompete agreement, they then receive pro bono training and continuing education along with marketing and promotion of their skills. Without signing a noncompete, employers may be less incentivized to provide all those benefits to their physician employers.
Those benefits – and the noncompetes – also vary by specialty, Mr. Glennon said. “In 2021, Washington, DC, banned noncompetes for doctors making less than $250,000. So, most generalists there can walk across the street and get a new job. For specialists like cardiologists or neurosurgeons, however, advanced training and marketing benefits matter, so many of them don’t want to lose noncompetes.”
Still, most physicians hope that the FTC’s ban takes hold. Manan Shah, MD, founder, and chief medical officer at Wyndly, an allergy relief startup practice, is one of them.
“Initially, it might disincentivize hospital systems from helping new physicians build up their name and practice because they might be concerned about a physician leaving and starting anew,” he said. “But in the long term, hospitals require physicians to bring their patients to them for care, so the best hospitals will always compete for the best physicians and support them as they build up their practice.”
Dr. Shah views noncompetes as overly prohibitive to physicians. “Right now, if a physician starts a job at a large hospital system and realizes they want to switch jobs, the noncompete distances are so wide they often have to move cities to continue practicing,” he said. “Picking up and starting over in a new city isn’t an option for everyone and can be especially difficult for someone with a family.”
Where Mr. Glennon argued that a physician leaving a team-based practice might harm patients, Shah takes a different perspective. “Imagine you have a doctor whom you trust and have been working with,” he said. “If something changes at their hospital and they decide to move, you literally have to find a new doctor instead of just being able to see them at another location down the street.”
Another potential burden of the noncompete agreements is that they could possibly squelch doctor’s desires to hang up their own shingle. According to Dr. Shah, the agreements make it so that if a physician wants to work independently, it’s nearly impossible to fly solo. “This is frustrating because independent practices have been shown to be more cost effective and allow patients to build better relationships with their doctors,” he claimed.
A 2016 study from Annals of Family Medicine supports that claim, at least for small general practices. Another study appearing in JAMA concurred. It does point out, however, that the cost equation is nuanced and that benefits of larger systems include more resilience to economic downturns and can provide more specialized care.
Will nonprofit hospitals be subject to this noncompete ban?
Further complicating the noncompete ban issue is how it might impact nonprofit institutions versus their for-profit peers. Most hospitals structured as nonprofits would be exempt from the rule because the FTC Act provides that it can enforce against “persons, partnerships, or corporations,” which are further defined as entities “organized to carry on business for their own profit or that of their members.”
The fallout from this, said Dr. Shah, is that it “would disproportionately affect health care providers, since many hospital systems are nonprofits. This is disconcerting because we know that many nonprofit systems make large profits anyway and can offer executive teams’ lucrative packages, while the nurses, assistants, and physicians providing the care are generally not well compensated.”
So far, about nine states plus Washington, D.C., have already put noncompete bans in place, and they may serve as a harbinger of things to come should the federal ban go into effect. Each varies in its specifics. Some, like Indiana, outright ban them, whereas others limit them based on variables like income and industry. “We’re seeing these states responding to local market conditions,” said Darryl Drevna, senior director of regulatory affairs at the American Medical Group Association. “Health care is a hyperlocal market. Depending on the situation, the bans adapt and respond specific to those states.”
Should the federal ban take hold, however, it will supersede whatever rules the individual states have in place.
Some opponents of the federal ban proposal question its authority to begin with, however, Mr. Glennon included. “Many people believe the FTC is overstepping,” he said. “Some people believe that Section 5 of the FTC Act does not give it the authority to police labor markets.”
Mr. Drevna noted that the FTC has taken an aggressive stance, one that will ultimately wind up in the courts. “How it works out is anyone’s guess,” he said. “Ideally, the FTC will consider the comments and concerns of groups like AMGA and realize that states are best suited to regulate in this area.”
In general, the ban’s supporters are employees/physicians; those who oppose it are their employers. Joining the AMGA in speaking out against the noncompete ban is the American Hospital Association, whereas the American College of Emergency Physicians has come out largely in support of the ban.
Still, doctors like Dr. Shah remain hopeful. “I am optimistic that perhaps my colleagues will not continue to be stuck in overrestrictive noncompetes, but I am also realistic,” he said. “Hospital systems are already coming out strongly against this and they have deep pockets, so I won’t be surprised if it does not come to pass.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s proposed regulation that would ban noncompete agreements across the country seems like potential good news for doctors. Of course, many hospitals and employers are against it. As a result, the FTC’s sweeping proposal has tongues wagging on both sides of the issue.
Many physicians are thrilled that they may soon have more control over their career and not be stuck in jobs where they feel frustrated, underpaid, or blocked in their progress.
As of 2018, as many as 45% of primary care physicians had inked such agreements with their employers.
Typically, the agreements prevent physicians from practicing medicine with a new employer for a defined period within a specific geographic area. No matter how attractive an alternate offer of employment might be, doctors are bound by the agreements to say no if the offer exists in that defined area and time period.
The period for public comment on the proposed regulation ended on April 19, and there is currently no set date for a decision.
In a Medscape poll of 558 physicians, more than 9 out of 10 respondents said that they were either currently bound by a noncompete clause or that they had been bound by one in the past that had forced them to temporarily stop working, commute long distances, move to a different area, or switch fields.
The new proposal would make it illegal for an employer, such as a hospital or large group, to enter a noncompete with a worker; maintain a noncompete with a worker; or represent to a worker, under certain circumstances, that the worker is subject to a noncompete.
It also would not only ban future noncompete agreements but also retroactively invalidate existing ones. The FTC reasons that noncompete clauses could potentially increase worker earnings as well as lower health care costs by billions of dollars. If the ruling were to move forward, it would represent part of President Biden’s “worker-forward” priorities, focusing on how competition can be a good thing for employees. The President billed the FTC’s announcement as a “huge win for workers.”
In its statements on the proposed ban, the FTC claimed that it could lower consumer prices across the board by as much as $150 billion per year and return nearly $300 million to workers each year.
However, even if passed, the draft rule would keep in place nonsolicitation rules that many health care organizations have put into place. That means that, if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to switch to him or her in the new job.
Within that clause, however, the FTC has specified that if such nonsolicitation agreement has the “equivalent effect” of a noncompete, the agency would deem it such. That means, even if that rule stays, it could be contested and may be interpreted as violating the noncompete law. So there’s value in reading all the fine print should the ban move forward.
Could the ban bring potential downsides?
Most physicians view the potential to break free of a noncompete agreement as a victory. Peter Glennon, an employment litigation attorney with The Glennon Law Firm in Rochester, N.Y., says not so fast. “If you ask anyone if they’d prefer a noncompete agreement, of course they’re going to say no,” he said in an interview. “It sounds like a restriction, one that can hold you back.”
Mr. Glennon believes that there are actually upsides to physician noncompetes. For instance, many noncompetes come with sign-on bonuses that could potentially disappear without the agreements. There’s also the fact that when some physicians sign a noncompete agreement, they then receive pro bono training and continuing education along with marketing and promotion of their skills. Without signing a noncompete, employers may be less incentivized to provide all those benefits to their physician employers.
Those benefits – and the noncompetes – also vary by specialty, Mr. Glennon said. “In 2021, Washington, DC, banned noncompetes for doctors making less than $250,000. So, most generalists there can walk across the street and get a new job. For specialists like cardiologists or neurosurgeons, however, advanced training and marketing benefits matter, so many of them don’t want to lose noncompetes.”
Still, most physicians hope that the FTC’s ban takes hold. Manan Shah, MD, founder, and chief medical officer at Wyndly, an allergy relief startup practice, is one of them.
“Initially, it might disincentivize hospital systems from helping new physicians build up their name and practice because they might be concerned about a physician leaving and starting anew,” he said. “But in the long term, hospitals require physicians to bring their patients to them for care, so the best hospitals will always compete for the best physicians and support them as they build up their practice.”
Dr. Shah views noncompetes as overly prohibitive to physicians. “Right now, if a physician starts a job at a large hospital system and realizes they want to switch jobs, the noncompete distances are so wide they often have to move cities to continue practicing,” he said. “Picking up and starting over in a new city isn’t an option for everyone and can be especially difficult for someone with a family.”
Where Mr. Glennon argued that a physician leaving a team-based practice might harm patients, Shah takes a different perspective. “Imagine you have a doctor whom you trust and have been working with,” he said. “If something changes at their hospital and they decide to move, you literally have to find a new doctor instead of just being able to see them at another location down the street.”
Another potential burden of the noncompete agreements is that they could possibly squelch doctor’s desires to hang up their own shingle. According to Dr. Shah, the agreements make it so that if a physician wants to work independently, it’s nearly impossible to fly solo. “This is frustrating because independent practices have been shown to be more cost effective and allow patients to build better relationships with their doctors,” he claimed.
A 2016 study from Annals of Family Medicine supports that claim, at least for small general practices. Another study appearing in JAMA concurred. It does point out, however, that the cost equation is nuanced and that benefits of larger systems include more resilience to economic downturns and can provide more specialized care.
Will nonprofit hospitals be subject to this noncompete ban?
Further complicating the noncompete ban issue is how it might impact nonprofit institutions versus their for-profit peers. Most hospitals structured as nonprofits would be exempt from the rule because the FTC Act provides that it can enforce against “persons, partnerships, or corporations,” which are further defined as entities “organized to carry on business for their own profit or that of their members.”
The fallout from this, said Dr. Shah, is that it “would disproportionately affect health care providers, since many hospital systems are nonprofits. This is disconcerting because we know that many nonprofit systems make large profits anyway and can offer executive teams’ lucrative packages, while the nurses, assistants, and physicians providing the care are generally not well compensated.”
So far, about nine states plus Washington, D.C., have already put noncompete bans in place, and they may serve as a harbinger of things to come should the federal ban go into effect. Each varies in its specifics. Some, like Indiana, outright ban them, whereas others limit them based on variables like income and industry. “We’re seeing these states responding to local market conditions,” said Darryl Drevna, senior director of regulatory affairs at the American Medical Group Association. “Health care is a hyperlocal market. Depending on the situation, the bans adapt and respond specific to those states.”
Should the federal ban take hold, however, it will supersede whatever rules the individual states have in place.
Some opponents of the federal ban proposal question its authority to begin with, however, Mr. Glennon included. “Many people believe the FTC is overstepping,” he said. “Some people believe that Section 5 of the FTC Act does not give it the authority to police labor markets.”
Mr. Drevna noted that the FTC has taken an aggressive stance, one that will ultimately wind up in the courts. “How it works out is anyone’s guess,” he said. “Ideally, the FTC will consider the comments and concerns of groups like AMGA and realize that states are best suited to regulate in this area.”
In general, the ban’s supporters are employees/physicians; those who oppose it are their employers. Joining the AMGA in speaking out against the noncompete ban is the American Hospital Association, whereas the American College of Emergency Physicians has come out largely in support of the ban.
Still, doctors like Dr. Shah remain hopeful. “I am optimistic that perhaps my colleagues will not continue to be stuck in overrestrictive noncompetes, but I am also realistic,” he said. “Hospital systems are already coming out strongly against this and they have deep pockets, so I won’t be surprised if it does not come to pass.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s proposed regulation that would ban noncompete agreements across the country seems like potential good news for doctors. Of course, many hospitals and employers are against it. As a result, the FTC’s sweeping proposal has tongues wagging on both sides of the issue.
Many physicians are thrilled that they may soon have more control over their career and not be stuck in jobs where they feel frustrated, underpaid, or blocked in their progress.
As of 2018, as many as 45% of primary care physicians had inked such agreements with their employers.
Typically, the agreements prevent physicians from practicing medicine with a new employer for a defined period within a specific geographic area. No matter how attractive an alternate offer of employment might be, doctors are bound by the agreements to say no if the offer exists in that defined area and time period.
The period for public comment on the proposed regulation ended on April 19, and there is currently no set date for a decision.
In a Medscape poll of 558 physicians, more than 9 out of 10 respondents said that they were either currently bound by a noncompete clause or that they had been bound by one in the past that had forced them to temporarily stop working, commute long distances, move to a different area, or switch fields.
The new proposal would make it illegal for an employer, such as a hospital or large group, to enter a noncompete with a worker; maintain a noncompete with a worker; or represent to a worker, under certain circumstances, that the worker is subject to a noncompete.
It also would not only ban future noncompete agreements but also retroactively invalidate existing ones. The FTC reasons that noncompete clauses could potentially increase worker earnings as well as lower health care costs by billions of dollars. If the ruling were to move forward, it would represent part of President Biden’s “worker-forward” priorities, focusing on how competition can be a good thing for employees. The President billed the FTC’s announcement as a “huge win for workers.”
In its statements on the proposed ban, the FTC claimed that it could lower consumer prices across the board by as much as $150 billion per year and return nearly $300 million to workers each year.
However, even if passed, the draft rule would keep in place nonsolicitation rules that many health care organizations have put into place. That means that, if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to switch to him or her in the new job.
Within that clause, however, the FTC has specified that if such nonsolicitation agreement has the “equivalent effect” of a noncompete, the agency would deem it such. That means, even if that rule stays, it could be contested and may be interpreted as violating the noncompete law. So there’s value in reading all the fine print should the ban move forward.
Could the ban bring potential downsides?
Most physicians view the potential to break free of a noncompete agreement as a victory. Peter Glennon, an employment litigation attorney with The Glennon Law Firm in Rochester, N.Y., says not so fast. “If you ask anyone if they’d prefer a noncompete agreement, of course they’re going to say no,” he said in an interview. “It sounds like a restriction, one that can hold you back.”
Mr. Glennon believes that there are actually upsides to physician noncompetes. For instance, many noncompetes come with sign-on bonuses that could potentially disappear without the agreements. There’s also the fact that when some physicians sign a noncompete agreement, they then receive pro bono training and continuing education along with marketing and promotion of their skills. Without signing a noncompete, employers may be less incentivized to provide all those benefits to their physician employers.
Those benefits – and the noncompetes – also vary by specialty, Mr. Glennon said. “In 2021, Washington, DC, banned noncompetes for doctors making less than $250,000. So, most generalists there can walk across the street and get a new job. For specialists like cardiologists or neurosurgeons, however, advanced training and marketing benefits matter, so many of them don’t want to lose noncompetes.”
Still, most physicians hope that the FTC’s ban takes hold. Manan Shah, MD, founder, and chief medical officer at Wyndly, an allergy relief startup practice, is one of them.
“Initially, it might disincentivize hospital systems from helping new physicians build up their name and practice because they might be concerned about a physician leaving and starting anew,” he said. “But in the long term, hospitals require physicians to bring their patients to them for care, so the best hospitals will always compete for the best physicians and support them as they build up their practice.”
Dr. Shah views noncompetes as overly prohibitive to physicians. “Right now, if a physician starts a job at a large hospital system and realizes they want to switch jobs, the noncompete distances are so wide they often have to move cities to continue practicing,” he said. “Picking up and starting over in a new city isn’t an option for everyone and can be especially difficult for someone with a family.”
Where Mr. Glennon argued that a physician leaving a team-based practice might harm patients, Shah takes a different perspective. “Imagine you have a doctor whom you trust and have been working with,” he said. “If something changes at their hospital and they decide to move, you literally have to find a new doctor instead of just being able to see them at another location down the street.”
Another potential burden of the noncompete agreements is that they could possibly squelch doctor’s desires to hang up their own shingle. According to Dr. Shah, the agreements make it so that if a physician wants to work independently, it’s nearly impossible to fly solo. “This is frustrating because independent practices have been shown to be more cost effective and allow patients to build better relationships with their doctors,” he claimed.
A 2016 study from Annals of Family Medicine supports that claim, at least for small general practices. Another study appearing in JAMA concurred. It does point out, however, that the cost equation is nuanced and that benefits of larger systems include more resilience to economic downturns and can provide more specialized care.
Will nonprofit hospitals be subject to this noncompete ban?
Further complicating the noncompete ban issue is how it might impact nonprofit institutions versus their for-profit peers. Most hospitals structured as nonprofits would be exempt from the rule because the FTC Act provides that it can enforce against “persons, partnerships, or corporations,” which are further defined as entities “organized to carry on business for their own profit or that of their members.”
The fallout from this, said Dr. Shah, is that it “would disproportionately affect health care providers, since many hospital systems are nonprofits. This is disconcerting because we know that many nonprofit systems make large profits anyway and can offer executive teams’ lucrative packages, while the nurses, assistants, and physicians providing the care are generally not well compensated.”
So far, about nine states plus Washington, D.C., have already put noncompete bans in place, and they may serve as a harbinger of things to come should the federal ban go into effect. Each varies in its specifics. Some, like Indiana, outright ban them, whereas others limit them based on variables like income and industry. “We’re seeing these states responding to local market conditions,” said Darryl Drevna, senior director of regulatory affairs at the American Medical Group Association. “Health care is a hyperlocal market. Depending on the situation, the bans adapt and respond specific to those states.”
Should the federal ban take hold, however, it will supersede whatever rules the individual states have in place.
Some opponents of the federal ban proposal question its authority to begin with, however, Mr. Glennon included. “Many people believe the FTC is overstepping,” he said. “Some people believe that Section 5 of the FTC Act does not give it the authority to police labor markets.”
Mr. Drevna noted that the FTC has taken an aggressive stance, one that will ultimately wind up in the courts. “How it works out is anyone’s guess,” he said. “Ideally, the FTC will consider the comments and concerns of groups like AMGA and realize that states are best suited to regulate in this area.”
In general, the ban’s supporters are employees/physicians; those who oppose it are their employers. Joining the AMGA in speaking out against the noncompete ban is the American Hospital Association, whereas the American College of Emergency Physicians has come out largely in support of the ban.
Still, doctors like Dr. Shah remain hopeful. “I am optimistic that perhaps my colleagues will not continue to be stuck in overrestrictive noncompetes, but I am also realistic,” he said. “Hospital systems are already coming out strongly against this and they have deep pockets, so I won’t be surprised if it does not come to pass.”
A version of this article first appeared on Medscape.com.