User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Losing weight may bolster AFib ablation’s chances for success: LEAF interim results
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.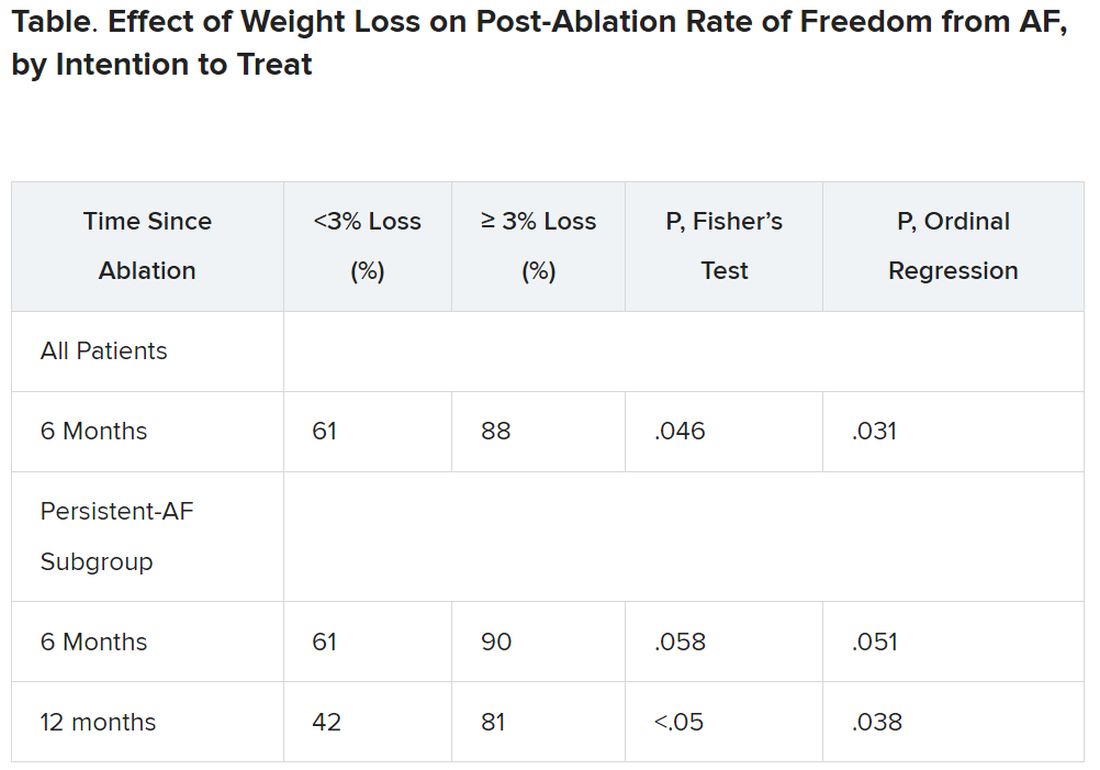
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HEART RHYTHM 2023
Novel antibody safe, promising for ATTR in phase 1 trial
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
FROM ESC HEART FAILURE 2023
Coronary artery calcium score bests polygenic risk score in CHD prediction
As a predictor of coronary heart disease (CHD) events, the coronary artery calcium (CAC) score on computed tomography had better risk discrimination than the polygenic risk score, a binational study found. And when added to classic cardiovascular risk factors, the CAC score significantly improved risk classification while the polygenic risk factor score did not.

These findings emerged from two large cohorts of middle-aged and older White adults from the United States and the Netherlands in the first head-to-head comparison of these two approaches. Led by Sadiya S. Kahn, MD, MSc, an assistant professor of medicine (cardiology) and preventive medicine (epidemiology) at Northwestern University, Chicago, the study was published online in JAMA.
There has been much interest in using both genetic factors and CT imaging to better identify individuals at risk for heart disease. “Each approach has advantages and disadvantages, and we wanted to better understand the comparative predictive utility to provide support for what the preferred approach should be,” Dr. Kahn said in an interview. “We focused on middle-aged to older adults for whom current risk prediction equations are relevant in estimating risk with the Pooled Cohort Equation, or PCE.”
The superiority of the CT-imaged coronary artery risk score may be because of its direct visualization of calcification in the arteries and the subclinical disease burden rather than a focus on common genetic variants, Dr. Kahn explained. “In addition, prior studies have demonstrated that genetics, or inherited risk, is not destiny, so this score may not perform as well for risk discrimination as the traditional risk factors themselves along with CT.”
The study
Study participants came from the U.S. Multi-Ethnic Study of Atherosclerosis (MESA, n = 1,991) and the Dutch Rotterdam Study (RS, n = 1,217). Ages ranged from 45 to 79, with the medians in the two cohorts 61 and 68 years, respectively. Slightly more than half of participants in both groups were female.
Traditional risk factors were used to calculate CHD risk with pooled cohort equations, while computed tomography was used to determine the CAC score and genotyped samples for a validated polygenic risk score.
Both scores were significantly associated with 10-year risk of incident CHD.
The median predicted atherosclerotic disease risk based on traditional risk factors was 6.99% in MESA and 5.93% in RS. During the total available follow-up in MESA (median, 16.0 years) and RS (median, 14.2 years), incident CHD occurred in 187 participants (9.4%) and 98 participants (8.1%), respectively.
C (concordance) statistics for the two scores showed the superiority of the CAC. This statistic measures a model’s ability to rank patients from high to low risk, with a value of 1 being perfect risk fit or concordance and 0.70 or more indicating good concordance and risk discrimination. The CAC score had a C statistic of 0.76 (95% confidence interval, 0.71-0.79) vs. 0.69 for the polygenic risk score (95% CI, 0.63-0.71).
When each score was added to PCEs, the C statistics changed as follows: CAC score, 0.09 (95% CI, 0.06-0.13); polygenic risk score, 0.02 (95% CI, 0.00-0.04); and 0.10 (95% CI, 0.07-0.14) for both.
Net reclassification significantly improved with the CAC plus PCEs by the following values: 0.19 (95% CI, 0.06-0.28). The change was not significant, however, with the polygenic risk score plus PCEs: 0.04 (95% CI, –0.05-0.10).
In the clinical setting, Dr. Kahn said, “The use of CT in patients who are at intermediate risk for heart disease can be helpful in refining risk estimation and guiding recommendations for lipid-lowering therapy. Polygenic risk scores are not helpful in middle-aged to older adults above and beyond traditional risk factors for predicting risk of heart disease.”
This study was supported by the National Heart, Lung, and Blood Institute. MESA is supported by the NHLBI. The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University Rotterdam; the Netherlands Organization for Scientific Research; the Netherlands Organization for Health Research and Development; the Research Institute for Diseases in the Elderly; the Netherlands Genomics Initiative; the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. Dr. Khan reported grants from the NHLBI and the NIH during the study and outside of the submitted work. Several coauthors reported grant support from, variously, the NIH, the NHLBI, and the American Heart Association.
As a predictor of coronary heart disease (CHD) events, the coronary artery calcium (CAC) score on computed tomography had better risk discrimination than the polygenic risk score, a binational study found. And when added to classic cardiovascular risk factors, the CAC score significantly improved risk classification while the polygenic risk factor score did not.
These findings emerged from two large cohorts of middle-aged and older White adults from the United States and the Netherlands in the first head-to-head comparison of these two approaches. Led by Sadiya S. Kahn, MD, MSc, an assistant professor of medicine (cardiology) and preventive medicine (epidemiology) at Northwestern University, Chicago, the study was published online in JAMA.
There has been much interest in using both genetic factors and CT imaging to better identify individuals at risk for heart disease. “Each approach has advantages and disadvantages, and we wanted to better understand the comparative predictive utility to provide support for what the preferred approach should be,” Dr. Kahn said in an interview. “We focused on middle-aged to older adults for whom current risk prediction equations are relevant in estimating risk with the Pooled Cohort Equation, or PCE.”
The superiority of the CT-imaged coronary artery risk score may be because of its direct visualization of calcification in the arteries and the subclinical disease burden rather than a focus on common genetic variants, Dr. Kahn explained. “In addition, prior studies have demonstrated that genetics, or inherited risk, is not destiny, so this score may not perform as well for risk discrimination as the traditional risk factors themselves along with CT.”
The study
Study participants came from the U.S. Multi-Ethnic Study of Atherosclerosis (MESA, n = 1,991) and the Dutch Rotterdam Study (RS, n = 1,217). Ages ranged from 45 to 79, with the medians in the two cohorts 61 and 68 years, respectively. Slightly more than half of participants in both groups were female.
Traditional risk factors were used to calculate CHD risk with pooled cohort equations, while computed tomography was used to determine the CAC score and genotyped samples for a validated polygenic risk score.
Both scores were significantly associated with 10-year risk of incident CHD.
The median predicted atherosclerotic disease risk based on traditional risk factors was 6.99% in MESA and 5.93% in RS. During the total available follow-up in MESA (median, 16.0 years) and RS (median, 14.2 years), incident CHD occurred in 187 participants (9.4%) and 98 participants (8.1%), respectively.
C (concordance) statistics for the two scores showed the superiority of the CAC. This statistic measures a model’s ability to rank patients from high to low risk, with a value of 1 being perfect risk fit or concordance and 0.70 or more indicating good concordance and risk discrimination. The CAC score had a C statistic of 0.76 (95% confidence interval, 0.71-0.79) vs. 0.69 for the polygenic risk score (95% CI, 0.63-0.71).
When each score was added to PCEs, the C statistics changed as follows: CAC score, 0.09 (95% CI, 0.06-0.13); polygenic risk score, 0.02 (95% CI, 0.00-0.04); and 0.10 (95% CI, 0.07-0.14) for both.
Net reclassification significantly improved with the CAC plus PCEs by the following values: 0.19 (95% CI, 0.06-0.28). The change was not significant, however, with the polygenic risk score plus PCEs: 0.04 (95% CI, –0.05-0.10).
In the clinical setting, Dr. Kahn said, “The use of CT in patients who are at intermediate risk for heart disease can be helpful in refining risk estimation and guiding recommendations for lipid-lowering therapy. Polygenic risk scores are not helpful in middle-aged to older adults above and beyond traditional risk factors for predicting risk of heart disease.”
This study was supported by the National Heart, Lung, and Blood Institute. MESA is supported by the NHLBI. The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University Rotterdam; the Netherlands Organization for Scientific Research; the Netherlands Organization for Health Research and Development; the Research Institute for Diseases in the Elderly; the Netherlands Genomics Initiative; the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. Dr. Khan reported grants from the NHLBI and the NIH during the study and outside of the submitted work. Several coauthors reported grant support from, variously, the NIH, the NHLBI, and the American Heart Association.
As a predictor of coronary heart disease (CHD) events, the coronary artery calcium (CAC) score on computed tomography had better risk discrimination than the polygenic risk score, a binational study found. And when added to classic cardiovascular risk factors, the CAC score significantly improved risk classification while the polygenic risk factor score did not.
These findings emerged from two large cohorts of middle-aged and older White adults from the United States and the Netherlands in the first head-to-head comparison of these two approaches. Led by Sadiya S. Kahn, MD, MSc, an assistant professor of medicine (cardiology) and preventive medicine (epidemiology) at Northwestern University, Chicago, the study was published online in JAMA.
There has been much interest in using both genetic factors and CT imaging to better identify individuals at risk for heart disease. “Each approach has advantages and disadvantages, and we wanted to better understand the comparative predictive utility to provide support for what the preferred approach should be,” Dr. Kahn said in an interview. “We focused on middle-aged to older adults for whom current risk prediction equations are relevant in estimating risk with the Pooled Cohort Equation, or PCE.”
The superiority of the CT-imaged coronary artery risk score may be because of its direct visualization of calcification in the arteries and the subclinical disease burden rather than a focus on common genetic variants, Dr. Kahn explained. “In addition, prior studies have demonstrated that genetics, or inherited risk, is not destiny, so this score may not perform as well for risk discrimination as the traditional risk factors themselves along with CT.”
The study
Study participants came from the U.S. Multi-Ethnic Study of Atherosclerosis (MESA, n = 1,991) and the Dutch Rotterdam Study (RS, n = 1,217). Ages ranged from 45 to 79, with the medians in the two cohorts 61 and 68 years, respectively. Slightly more than half of participants in both groups were female.
Traditional risk factors were used to calculate CHD risk with pooled cohort equations, while computed tomography was used to determine the CAC score and genotyped samples for a validated polygenic risk score.
Both scores were significantly associated with 10-year risk of incident CHD.
The median predicted atherosclerotic disease risk based on traditional risk factors was 6.99% in MESA and 5.93% in RS. During the total available follow-up in MESA (median, 16.0 years) and RS (median, 14.2 years), incident CHD occurred in 187 participants (9.4%) and 98 participants (8.1%), respectively.
C (concordance) statistics for the two scores showed the superiority of the CAC. This statistic measures a model’s ability to rank patients from high to low risk, with a value of 1 being perfect risk fit or concordance and 0.70 or more indicating good concordance and risk discrimination. The CAC score had a C statistic of 0.76 (95% confidence interval, 0.71-0.79) vs. 0.69 for the polygenic risk score (95% CI, 0.63-0.71).
When each score was added to PCEs, the C statistics changed as follows: CAC score, 0.09 (95% CI, 0.06-0.13); polygenic risk score, 0.02 (95% CI, 0.00-0.04); and 0.10 (95% CI, 0.07-0.14) for both.
Net reclassification significantly improved with the CAC plus PCEs by the following values: 0.19 (95% CI, 0.06-0.28). The change was not significant, however, with the polygenic risk score plus PCEs: 0.04 (95% CI, –0.05-0.10).
In the clinical setting, Dr. Kahn said, “The use of CT in patients who are at intermediate risk for heart disease can be helpful in refining risk estimation and guiding recommendations for lipid-lowering therapy. Polygenic risk scores are not helpful in middle-aged to older adults above and beyond traditional risk factors for predicting risk of heart disease.”
This study was supported by the National Heart, Lung, and Blood Institute. MESA is supported by the NHLBI. The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University Rotterdam; the Netherlands Organization for Scientific Research; the Netherlands Organization for Health Research and Development; the Research Institute for Diseases in the Elderly; the Netherlands Genomics Initiative; the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. Dr. Khan reported grants from the NHLBI and the NIH during the study and outside of the submitted work. Several coauthors reported grant support from, variously, the NIH, the NHLBI, and the American Heart Association.
FROM JAMA
Noninferior to DES, novel bioadaptable stent may improve target vessel physiology
Stent is not a “me-too” device
Moving in a very different direction from past coronary stent designs, at 12 months in a randomized controlled trial.
“The device restored vessel motion, which we think is the reason that we saw plaque stabilization and regression,” reported Shigero Saito, MD, director of the catheterization laboratory at Shonan Kamakura (Japan) General Hospital.
The principal features of the bioadaptable design are cobalt-chromium metal helical strands to provide indefinite scaffolding support coupled with a biodegradable sirolimus-containing poly(D,L-lacti-co-glycolic acid) (PLGA) topcoat and a biodegradable poly-L-lactic acid (PLLA) bottom coat to “uncage” the vessel once these materials are resorbed, said Dr. Saito.
Twelve-month data from the randomized BIOADAPTOR trial, presented as a late breaker at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, provide the first evidence that this uncaging of the vessel is an advantage.
Compared head-to-head in a contemporary drug-eluting stent (DES) in a randomized trial, the bioadaptable stent, as predicted in prior studies, “improved hemodynamics and supported plaque stabilization and positive remodeling,” said Dr. Saito.
In BIOADAPTOR, 445 patients in Japan, Germany, Belgium, and New Zealand were randomized to the novel stent, called DynamX, or to the Resolute Onyx. The trial has a planned follow-up of 5 years.
While the primary endpoint at 12 months was noninferiority for target lesion failure (TLF), it was a series of secondary imaging endpoints that suggest an important impact of uncaging the vessel. This includes better vessel function potentially relevant to resistance to restenosis.
As a result of numerically lower TLF in the DynamX group (1.8% vs. 2.8%), the new device easily demonstrated noninferiority at a high level of significance (P < .001). A numerical advantage for most events, including cardiovascular death (0% vs. 0.9%) and target-vessel myocardial infarction (1.4% vs. 1.9%), favored the novel device, but event rates were low in both arms and none of these differences were statistically significant.
However, the secondary imaging analyses at 12 months suggested major differences between the two devices from “uncaging” the vessel.
These differences included a highly significant improvement at 12 months in vessel pulsatility (P < .001) within the DynamX stent relative to the Onyx stent in all measured segments (proximal, mid, and distal).
In addition, compliance remained suppressed relative to both the proximal (P < .001) and distal (P < .001) vessels of patients fitted with Onyx device. Conversely, there was no significant relative difference in this measure among those fitted with the DynamX device.
At 12 months, the plaque volume change behind the stent of noncalcified lesions increased 9% in the Onyx group but was reduced 4% in the DynamX group (P = .028).
While there was a 13% gain overall in percent diameter stenosis within the stent of patients receiving the DynamX device, it was consistently lower than that observed in the Onyx group. This difference was only a trend overall (12.7% vs. 17.3%; P = .051), but the advantage reached significance, favoring DynamX, for the left anterior descending (LAD) artery (12.1% vs. 19.0%; P = .006), small vessels (13.0% vs. 18.3%; P = .045), and long lesions (13.0% vs. 22.9%; P = .008).
The same relative advantage for DynamX was seen on late lumen loss at 6 months. In this case, the overall advantage of DynamX (0.09 vs. 0.25; P = .038) did reach significance, and there was an advantage for the LAD (–0.02 vs. 0.24; P = .007) and long lesions (–0.06 vs. 0.38; P = .016). The difference did not reach significance for small vessels (0.08 vs. 0.26; P = .121).
All of these advantages on the secondary endpoints can be directly attributed to the effect of uncaging the vessel, according to Dr. Saito, who said this new design “addresses the shortcomings” of both previous drug-eluting and biodegradable stents.
Pointing out that the nonplateauing of late events has persisted regardless of stent design after “more than 20 years of innovation in design and materials,” Dr. Saito said all current stents have weaknesses. While biodegradable stents have not improved long-term outcomes relative to DES “as a result of loss of long-term vessel dynamic support,” DES are flawed due to “permanent caging of the vessel and loss of vessel motion and function.”
This novel hybrid design, employing both metal and biodegradable components, “is a completely different concept,” said Ron Waksman, MD, associate director, division of cardiology, Medstar Hospital Center, Washington. He was particularly impressed by the improvements in pulsatility and compliance in target vessels along with the favorable effects on plaque volume.
“The reduction in plaque volume is something we have not seen before. Usually we see the opposite,” Dr. Waksman said.

“Clearly, the Bioadaptor device is not a me-too stent,” he said. He was not surprised that there was no difference in hard outcomes given both the small sample size and the fact that the advantages of uncaging the vessel are likely to accrue over time.
“We need to look at what happens after 1 year. We still have not seen the potential of this device,” he said, adding he was “impressed” by the features of this novel concept. However, he suggested the advantages remain theoretical from the clinical standpoint, advising Dr. Saito that “you still need to demonstrate the clinical benefits.”
Dr. Saito reports a financial relationship with Elixir Medical, which funded the BIOADAPTOR trial. Dr. Waksman reports financial relationships with 19 pharmaceutical companies including those that manufacture cardiovascular stents.
Stent is not a “me-too” device
Stent is not a “me-too” device
Moving in a very different direction from past coronary stent designs, at 12 months in a randomized controlled trial.
“The device restored vessel motion, which we think is the reason that we saw plaque stabilization and regression,” reported Shigero Saito, MD, director of the catheterization laboratory at Shonan Kamakura (Japan) General Hospital.
The principal features of the bioadaptable design are cobalt-chromium metal helical strands to provide indefinite scaffolding support coupled with a biodegradable sirolimus-containing poly(D,L-lacti-co-glycolic acid) (PLGA) topcoat and a biodegradable poly-L-lactic acid (PLLA) bottom coat to “uncage” the vessel once these materials are resorbed, said Dr. Saito.
Twelve-month data from the randomized BIOADAPTOR trial, presented as a late breaker at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, provide the first evidence that this uncaging of the vessel is an advantage.
Compared head-to-head in a contemporary drug-eluting stent (DES) in a randomized trial, the bioadaptable stent, as predicted in prior studies, “improved hemodynamics and supported plaque stabilization and positive remodeling,” said Dr. Saito.
In BIOADAPTOR, 445 patients in Japan, Germany, Belgium, and New Zealand were randomized to the novel stent, called DynamX, or to the Resolute Onyx. The trial has a planned follow-up of 5 years.
While the primary endpoint at 12 months was noninferiority for target lesion failure (TLF), it was a series of secondary imaging endpoints that suggest an important impact of uncaging the vessel. This includes better vessel function potentially relevant to resistance to restenosis.
As a result of numerically lower TLF in the DynamX group (1.8% vs. 2.8%), the new device easily demonstrated noninferiority at a high level of significance (P < .001). A numerical advantage for most events, including cardiovascular death (0% vs. 0.9%) and target-vessel myocardial infarction (1.4% vs. 1.9%), favored the novel device, but event rates were low in both arms and none of these differences were statistically significant.
However, the secondary imaging analyses at 12 months suggested major differences between the two devices from “uncaging” the vessel.
These differences included a highly significant improvement at 12 months in vessel pulsatility (P < .001) within the DynamX stent relative to the Onyx stent in all measured segments (proximal, mid, and distal).
In addition, compliance remained suppressed relative to both the proximal (P < .001) and distal (P < .001) vessels of patients fitted with Onyx device. Conversely, there was no significant relative difference in this measure among those fitted with the DynamX device.
At 12 months, the plaque volume change behind the stent of noncalcified lesions increased 9% in the Onyx group but was reduced 4% in the DynamX group (P = .028).
While there was a 13% gain overall in percent diameter stenosis within the stent of patients receiving the DynamX device, it was consistently lower than that observed in the Onyx group. This difference was only a trend overall (12.7% vs. 17.3%; P = .051), but the advantage reached significance, favoring DynamX, for the left anterior descending (LAD) artery (12.1% vs. 19.0%; P = .006), small vessels (13.0% vs. 18.3%; P = .045), and long lesions (13.0% vs. 22.9%; P = .008).
The same relative advantage for DynamX was seen on late lumen loss at 6 months. In this case, the overall advantage of DynamX (0.09 vs. 0.25; P = .038) did reach significance, and there was an advantage for the LAD (–0.02 vs. 0.24; P = .007) and long lesions (–0.06 vs. 0.38; P = .016). The difference did not reach significance for small vessels (0.08 vs. 0.26; P = .121).
All of these advantages on the secondary endpoints can be directly attributed to the effect of uncaging the vessel, according to Dr. Saito, who said this new design “addresses the shortcomings” of both previous drug-eluting and biodegradable stents.
Pointing out that the nonplateauing of late events has persisted regardless of stent design after “more than 20 years of innovation in design and materials,” Dr. Saito said all current stents have weaknesses. While biodegradable stents have not improved long-term outcomes relative to DES “as a result of loss of long-term vessel dynamic support,” DES are flawed due to “permanent caging of the vessel and loss of vessel motion and function.”
This novel hybrid design, employing both metal and biodegradable components, “is a completely different concept,” said Ron Waksman, MD, associate director, division of cardiology, Medstar Hospital Center, Washington. He was particularly impressed by the improvements in pulsatility and compliance in target vessels along with the favorable effects on plaque volume.
“The reduction in plaque volume is something we have not seen before. Usually we see the opposite,” Dr. Waksman said.
“Clearly, the Bioadaptor device is not a me-too stent,” he said. He was not surprised that there was no difference in hard outcomes given both the small sample size and the fact that the advantages of uncaging the vessel are likely to accrue over time.
“We need to look at what happens after 1 year. We still have not seen the potential of this device,” he said, adding he was “impressed” by the features of this novel concept. However, he suggested the advantages remain theoretical from the clinical standpoint, advising Dr. Saito that “you still need to demonstrate the clinical benefits.”
Dr. Saito reports a financial relationship with Elixir Medical, which funded the BIOADAPTOR trial. Dr. Waksman reports financial relationships with 19 pharmaceutical companies including those that manufacture cardiovascular stents.
Moving in a very different direction from past coronary stent designs, at 12 months in a randomized controlled trial.
“The device restored vessel motion, which we think is the reason that we saw plaque stabilization and regression,” reported Shigero Saito, MD, director of the catheterization laboratory at Shonan Kamakura (Japan) General Hospital.
The principal features of the bioadaptable design are cobalt-chromium metal helical strands to provide indefinite scaffolding support coupled with a biodegradable sirolimus-containing poly(D,L-lacti-co-glycolic acid) (PLGA) topcoat and a biodegradable poly-L-lactic acid (PLLA) bottom coat to “uncage” the vessel once these materials are resorbed, said Dr. Saito.
Twelve-month data from the randomized BIOADAPTOR trial, presented as a late breaker at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, provide the first evidence that this uncaging of the vessel is an advantage.
Compared head-to-head in a contemporary drug-eluting stent (DES) in a randomized trial, the bioadaptable stent, as predicted in prior studies, “improved hemodynamics and supported plaque stabilization and positive remodeling,” said Dr. Saito.
In BIOADAPTOR, 445 patients in Japan, Germany, Belgium, and New Zealand were randomized to the novel stent, called DynamX, or to the Resolute Onyx. The trial has a planned follow-up of 5 years.
While the primary endpoint at 12 months was noninferiority for target lesion failure (TLF), it was a series of secondary imaging endpoints that suggest an important impact of uncaging the vessel. This includes better vessel function potentially relevant to resistance to restenosis.
As a result of numerically lower TLF in the DynamX group (1.8% vs. 2.8%), the new device easily demonstrated noninferiority at a high level of significance (P < .001). A numerical advantage for most events, including cardiovascular death (0% vs. 0.9%) and target-vessel myocardial infarction (1.4% vs. 1.9%), favored the novel device, but event rates were low in both arms and none of these differences were statistically significant.
However, the secondary imaging analyses at 12 months suggested major differences between the two devices from “uncaging” the vessel.
These differences included a highly significant improvement at 12 months in vessel pulsatility (P < .001) within the DynamX stent relative to the Onyx stent in all measured segments (proximal, mid, and distal).
In addition, compliance remained suppressed relative to both the proximal (P < .001) and distal (P < .001) vessels of patients fitted with Onyx device. Conversely, there was no significant relative difference in this measure among those fitted with the DynamX device.
At 12 months, the plaque volume change behind the stent of noncalcified lesions increased 9% in the Onyx group but was reduced 4% in the DynamX group (P = .028).
While there was a 13% gain overall in percent diameter stenosis within the stent of patients receiving the DynamX device, it was consistently lower than that observed in the Onyx group. This difference was only a trend overall (12.7% vs. 17.3%; P = .051), but the advantage reached significance, favoring DynamX, for the left anterior descending (LAD) artery (12.1% vs. 19.0%; P = .006), small vessels (13.0% vs. 18.3%; P = .045), and long lesions (13.0% vs. 22.9%; P = .008).
The same relative advantage for DynamX was seen on late lumen loss at 6 months. In this case, the overall advantage of DynamX (0.09 vs. 0.25; P = .038) did reach significance, and there was an advantage for the LAD (–0.02 vs. 0.24; P = .007) and long lesions (–0.06 vs. 0.38; P = .016). The difference did not reach significance for small vessels (0.08 vs. 0.26; P = .121).
All of these advantages on the secondary endpoints can be directly attributed to the effect of uncaging the vessel, according to Dr. Saito, who said this new design “addresses the shortcomings” of both previous drug-eluting and biodegradable stents.
Pointing out that the nonplateauing of late events has persisted regardless of stent design after “more than 20 years of innovation in design and materials,” Dr. Saito said all current stents have weaknesses. While biodegradable stents have not improved long-term outcomes relative to DES “as a result of loss of long-term vessel dynamic support,” DES are flawed due to “permanent caging of the vessel and loss of vessel motion and function.”
This novel hybrid design, employing both metal and biodegradable components, “is a completely different concept,” said Ron Waksman, MD, associate director, division of cardiology, Medstar Hospital Center, Washington. He was particularly impressed by the improvements in pulsatility and compliance in target vessels along with the favorable effects on plaque volume.
“The reduction in plaque volume is something we have not seen before. Usually we see the opposite,” Dr. Waksman said.
“Clearly, the Bioadaptor device is not a me-too stent,” he said. He was not surprised that there was no difference in hard outcomes given both the small sample size and the fact that the advantages of uncaging the vessel are likely to accrue over time.
“We need to look at what happens after 1 year. We still have not seen the potential of this device,” he said, adding he was “impressed” by the features of this novel concept. However, he suggested the advantages remain theoretical from the clinical standpoint, advising Dr. Saito that “you still need to demonstrate the clinical benefits.”
Dr. Saito reports a financial relationship with Elixir Medical, which funded the BIOADAPTOR trial. Dr. Waksman reports financial relationships with 19 pharmaceutical companies including those that manufacture cardiovascular stents.
FROM EUROPCR 2023
Distal radial access doesn’t harm hand function at 1 year
Outcomes equal to proximal approach
In what may be the first randomized trial to compare coronary intervention access using the distal or proximal radial arteries, researchers have found no significant differences between the two in hand function a year after the procedure.
The distal radial artery (DRA) access point is just below the thumb on the inside of the wrist. The proximal radial artery (PRA) entry is in the inside lower forearm above the wrist.
“There has been growing interest in the use of distal radial access given its ease of hemostasis, lower incidence of radial artery occlusions, as well as the more ergonomic favorable setup for a left radial access, which is typically utilized in patients with prior CABG who undergo a cardiac catheterization when used as alternative to femoral artery access,” Karim Al-Azizi, MD, of Texas A&M University, an interventional cardiologist and associate program director of the cardiology fellowship at Baylor Scott & White Health, in Plano, Tex., said in an interview.

Dr Al-Azizi presented the late-breaking 1-year results of the DIPRA–for Distal vs. Proximal Radial Artery–study at the Society for Cardiovascular Angiography & Interventions annual scientific sessions. The 30-day results of the DIPRA trial were presented in 2022 at this meeting.
Dr. Al-Azizi said DIPRA is the first randomized, controlled trial comparing hand function outcomes with the two approaches. “I think the biggest question for most investigators and most practitioners is that, is this safe on the hand? Are we doing the right thing by going into the radial artery in the anatomical snuff box in proximity to the radial nerve and would that affect motor function?” he said. “And it does not seem like it from a head-to-head comparison of proximal versus distal access.”
The DIPRA study randomized 300 patients 1:1 to cardiac catheterization through either the distal or proximal access. Of those, 216 completed 1-year follow-up, 112 randomized to DRA and 104 to PRA.
The study used three metrics to evaluate hand function: hand-grip strength; pinch test, which measured the strength of a pinch between the thumb and index finger; and QuickDASH, an abbreviated version of the Disabilities of the Arm, Shoulder, and Hand questionnaire, in which participants self-evaluate their hand function. Study protocol mandated that operators use ultrasound guidance for DRA access.
The 1-year results of all three measures showed no significant difference in change of hand function from baseline between the two groups. The composite average score change was –0.07 (–0.41, 0.44) for the DRA patients and –0.03. (–0.36, 0.44) for the PRA group (P = .59).
One-year change for the specific hand function measures for DRA and PRA, respectively, were: hand grip, 0.7 (–3, 4.5) vs. 1.3 (–2, 4.3) kg (P = .57); pinch grip, –0.1 (–1.1, 1) vs. –0.3 (–1, 0.7) kg (P = .66); and none for change in the QuickDASH score (–6.6, 2.3 vs. –4.6, 2.9) points (P = .58).
Outcomes at intervention were also similar. Bleeding incidence was 0% and 1.4% (P = .25) in the respective groups. Successful RA access was achieved in 96.7% and 98% (P = .72).
Baseline characteristics were balanced between the two groups: 75% were male; mean age was 66.6 ± 9.6 years; 32% had diabetes; 77% had hypertension; and 19% had a previous percutaneous coronary intervention.
One key strength of the DIPRA study Dr. Al-Azizi noted is that it included some investigators who were at the early stage of the learning curve with the procedure. A limitation is that it didn’t evaluate hand numbness or tingling, but hand sensory testing is “very subjective,” he said. “To avoid confusion, we decided to go with the more repeatable questionnaire rather than a sensation or sensory test,” he added.
The next step for his research team is to conduct a meta-analysis of studies that have evaluated DRA and PRA, Dr. Al-Azizi said.
‘Slow to the party’
U.S. interventional cardiologists have been “slow to the party” in adopting radial artery access for PCI, said David A. Cox, MD, of Sanger Heart and Vascular Institute in Charlotte, N.C., and SCAI communications committee chair. Even now uptake is low, compared with the rest of the world, he said.
“I can tell you what patients care about: Did you have to stick my groin?” he said at a SCAI press conference. “What they just want to know is that there are no issues with hand function.”
Some patients who need fine motor hand function would still opt for femoral access, he said.
“Are we looking at the right metric?” he asked Dr. Al-Azizi. “It took a long time to get American doctors to stick the radial, so why would I want to learn distal radial artery if I’m really pretty good at proximal and if it’s not inferior?”
Dr. Al-Azizi noted that previous studies showed a trend toward a lower incidence of radial artery occlusion (RAO) with DRA access. It also better preserves the renal arteries for dialysis and CABG, he said.
“The metric that would move the needle,” Dr. Cox noted, “is if you had radial artery occlusion rates vs. snuff box occlusion rates, and we don’t have that rate.”
Dr. Al-Azizi has no relevant financial disclosures. Dr. Cox disclosed financial relationships with Medtronic.
Outcomes equal to proximal approach
Outcomes equal to proximal approach
In what may be the first randomized trial to compare coronary intervention access using the distal or proximal radial arteries, researchers have found no significant differences between the two in hand function a year after the procedure.
The distal radial artery (DRA) access point is just below the thumb on the inside of the wrist. The proximal radial artery (PRA) entry is in the inside lower forearm above the wrist.
“There has been growing interest in the use of distal radial access given its ease of hemostasis, lower incidence of radial artery occlusions, as well as the more ergonomic favorable setup for a left radial access, which is typically utilized in patients with prior CABG who undergo a cardiac catheterization when used as alternative to femoral artery access,” Karim Al-Azizi, MD, of Texas A&M University, an interventional cardiologist and associate program director of the cardiology fellowship at Baylor Scott & White Health, in Plano, Tex., said in an interview.
Dr Al-Azizi presented the late-breaking 1-year results of the DIPRA–for Distal vs. Proximal Radial Artery–study at the Society for Cardiovascular Angiography & Interventions annual scientific sessions. The 30-day results of the DIPRA trial were presented in 2022 at this meeting.
Dr. Al-Azizi said DIPRA is the first randomized, controlled trial comparing hand function outcomes with the two approaches. “I think the biggest question for most investigators and most practitioners is that, is this safe on the hand? Are we doing the right thing by going into the radial artery in the anatomical snuff box in proximity to the radial nerve and would that affect motor function?” he said. “And it does not seem like it from a head-to-head comparison of proximal versus distal access.”
The DIPRA study randomized 300 patients 1:1 to cardiac catheterization through either the distal or proximal access. Of those, 216 completed 1-year follow-up, 112 randomized to DRA and 104 to PRA.
The study used three metrics to evaluate hand function: hand-grip strength; pinch test, which measured the strength of a pinch between the thumb and index finger; and QuickDASH, an abbreviated version of the Disabilities of the Arm, Shoulder, and Hand questionnaire, in which participants self-evaluate their hand function. Study protocol mandated that operators use ultrasound guidance for DRA access.
The 1-year results of all three measures showed no significant difference in change of hand function from baseline between the two groups. The composite average score change was –0.07 (–0.41, 0.44) for the DRA patients and –0.03. (–0.36, 0.44) for the PRA group (P = .59).
One-year change for the specific hand function measures for DRA and PRA, respectively, were: hand grip, 0.7 (–3, 4.5) vs. 1.3 (–2, 4.3) kg (P = .57); pinch grip, –0.1 (–1.1, 1) vs. –0.3 (–1, 0.7) kg (P = .66); and none for change in the QuickDASH score (–6.6, 2.3 vs. –4.6, 2.9) points (P = .58).
Outcomes at intervention were also similar. Bleeding incidence was 0% and 1.4% (P = .25) in the respective groups. Successful RA access was achieved in 96.7% and 98% (P = .72).
Baseline characteristics were balanced between the two groups: 75% were male; mean age was 66.6 ± 9.6 years; 32% had diabetes; 77% had hypertension; and 19% had a previous percutaneous coronary intervention.
One key strength of the DIPRA study Dr. Al-Azizi noted is that it included some investigators who were at the early stage of the learning curve with the procedure. A limitation is that it didn’t evaluate hand numbness or tingling, but hand sensory testing is “very subjective,” he said. “To avoid confusion, we decided to go with the more repeatable questionnaire rather than a sensation or sensory test,” he added.
The next step for his research team is to conduct a meta-analysis of studies that have evaluated DRA and PRA, Dr. Al-Azizi said.
‘Slow to the party’
U.S. interventional cardiologists have been “slow to the party” in adopting radial artery access for PCI, said David A. Cox, MD, of Sanger Heart and Vascular Institute in Charlotte, N.C., and SCAI communications committee chair. Even now uptake is low, compared with the rest of the world, he said.
“I can tell you what patients care about: Did you have to stick my groin?” he said at a SCAI press conference. “What they just want to know is that there are no issues with hand function.”
Some patients who need fine motor hand function would still opt for femoral access, he said.
“Are we looking at the right metric?” he asked Dr. Al-Azizi. “It took a long time to get American doctors to stick the radial, so why would I want to learn distal radial artery if I’m really pretty good at proximal and if it’s not inferior?”
Dr. Al-Azizi noted that previous studies showed a trend toward a lower incidence of radial artery occlusion (RAO) with DRA access. It also better preserves the renal arteries for dialysis and CABG, he said.
“The metric that would move the needle,” Dr. Cox noted, “is if you had radial artery occlusion rates vs. snuff box occlusion rates, and we don’t have that rate.”
Dr. Al-Azizi has no relevant financial disclosures. Dr. Cox disclosed financial relationships with Medtronic.
In what may be the first randomized trial to compare coronary intervention access using the distal or proximal radial arteries, researchers have found no significant differences between the two in hand function a year after the procedure.
The distal radial artery (DRA) access point is just below the thumb on the inside of the wrist. The proximal radial artery (PRA) entry is in the inside lower forearm above the wrist.
“There has been growing interest in the use of distal radial access given its ease of hemostasis, lower incidence of radial artery occlusions, as well as the more ergonomic favorable setup for a left radial access, which is typically utilized in patients with prior CABG who undergo a cardiac catheterization when used as alternative to femoral artery access,” Karim Al-Azizi, MD, of Texas A&M University, an interventional cardiologist and associate program director of the cardiology fellowship at Baylor Scott & White Health, in Plano, Tex., said in an interview.
Dr Al-Azizi presented the late-breaking 1-year results of the DIPRA–for Distal vs. Proximal Radial Artery–study at the Society for Cardiovascular Angiography & Interventions annual scientific sessions. The 30-day results of the DIPRA trial were presented in 2022 at this meeting.
Dr. Al-Azizi said DIPRA is the first randomized, controlled trial comparing hand function outcomes with the two approaches. “I think the biggest question for most investigators and most practitioners is that, is this safe on the hand? Are we doing the right thing by going into the radial artery in the anatomical snuff box in proximity to the radial nerve and would that affect motor function?” he said. “And it does not seem like it from a head-to-head comparison of proximal versus distal access.”
The DIPRA study randomized 300 patients 1:1 to cardiac catheterization through either the distal or proximal access. Of those, 216 completed 1-year follow-up, 112 randomized to DRA and 104 to PRA.
The study used three metrics to evaluate hand function: hand-grip strength; pinch test, which measured the strength of a pinch between the thumb and index finger; and QuickDASH, an abbreviated version of the Disabilities of the Arm, Shoulder, and Hand questionnaire, in which participants self-evaluate their hand function. Study protocol mandated that operators use ultrasound guidance for DRA access.
The 1-year results of all three measures showed no significant difference in change of hand function from baseline between the two groups. The composite average score change was –0.07 (–0.41, 0.44) for the DRA patients and –0.03. (–0.36, 0.44) for the PRA group (P = .59).
One-year change for the specific hand function measures for DRA and PRA, respectively, were: hand grip, 0.7 (–3, 4.5) vs. 1.3 (–2, 4.3) kg (P = .57); pinch grip, –0.1 (–1.1, 1) vs. –0.3 (–1, 0.7) kg (P = .66); and none for change in the QuickDASH score (–6.6, 2.3 vs. –4.6, 2.9) points (P = .58).
Outcomes at intervention were also similar. Bleeding incidence was 0% and 1.4% (P = .25) in the respective groups. Successful RA access was achieved in 96.7% and 98% (P = .72).
Baseline characteristics were balanced between the two groups: 75% were male; mean age was 66.6 ± 9.6 years; 32% had diabetes; 77% had hypertension; and 19% had a previous percutaneous coronary intervention.
One key strength of the DIPRA study Dr. Al-Azizi noted is that it included some investigators who were at the early stage of the learning curve with the procedure. A limitation is that it didn’t evaluate hand numbness or tingling, but hand sensory testing is “very subjective,” he said. “To avoid confusion, we decided to go with the more repeatable questionnaire rather than a sensation or sensory test,” he added.
The next step for his research team is to conduct a meta-analysis of studies that have evaluated DRA and PRA, Dr. Al-Azizi said.
‘Slow to the party’
U.S. interventional cardiologists have been “slow to the party” in adopting radial artery access for PCI, said David A. Cox, MD, of Sanger Heart and Vascular Institute in Charlotte, N.C., and SCAI communications committee chair. Even now uptake is low, compared with the rest of the world, he said.
“I can tell you what patients care about: Did you have to stick my groin?” he said at a SCAI press conference. “What they just want to know is that there are no issues with hand function.”
Some patients who need fine motor hand function would still opt for femoral access, he said.
“Are we looking at the right metric?” he asked Dr. Al-Azizi. “It took a long time to get American doctors to stick the radial, so why would I want to learn distal radial artery if I’m really pretty good at proximal and if it’s not inferior?”
Dr. Al-Azizi noted that previous studies showed a trend toward a lower incidence of radial artery occlusion (RAO) with DRA access. It also better preserves the renal arteries for dialysis and CABG, he said.
“The metric that would move the needle,” Dr. Cox noted, “is if you had radial artery occlusion rates vs. snuff box occlusion rates, and we don’t have that rate.”
Dr. Al-Azizi has no relevant financial disclosures. Dr. Cox disclosed financial relationships with Medtronic.
FROM SCAI 2023
Machine-learning model improves MI diagnosis
Use of a machine-learning model that incorporates information from a single troponin test as well as other clinical data was superior to current practice as an aid to the diagnosis of myocardial infarction in the emergency department in a new study.
“Our results suggest that and free up space in the emergency department,” senior author Nicholas L. Mills, MD, University of Edinburgh, Scotland, said in an interview.

“And, perhaps even more importantly, use of this model could also increase the proportion of patients who are correctly identified as at a high probability of having an MI,” he added.
The study was published online in Nature Medicine.
The authors explained that at present, the likelihood of an MI diagnosis for patients presenting to the emergency department with chest pain is based on a fixed troponin threshold in serial tests at specific time points, but there are several problems with this approach.
First, a fixed troponin threshold is generally used for all patients, which does not account for age, sex, or comorbidities that are known to influence cardiac troponin concentrations. Second, the need to perform tests at specific time points for serial testing can be challenging in busy emergency departments.
And third, patients are categorized as being at low, intermediate, or high risk of MI on the basis of troponin thresholds alone, and the test does not take into account other important factors, such as the time of symptom onset or findings on the electrocardiogram.
“Our current practice of using the same threshold to rule in and rule out an MI for everyone, regardless of whether they are an 18-year-old female without a history of heart disease or an 85-year-old male with known heart failure, doesn’t perform well, and there’s a significant risk of misdiagnosis. There is also a high likelihood for inequalities in care, particularly between men and women,” Dr. Mills said.
The current study evaluated whether use of a machine learning model known as CoDE-ACS to guide decision-making could overcome some of these challenges.
The machine learning model assesses the whole spectrum of troponin levels as a continuous variable (rather than use of a single threshold) and turns this measurement into a probability that an individual patient is having an MI after accounting for other factors, including age, sex, comorbidities, and time from symptom onset.
For the current study, the CoDE-ACS model was trained in 10,000 patients with suspected acute coronary syndrome (ACS) who presented to 10 hospitals in Scotland as part of the High-STEACS trial evaluating the implementation of a high-sensitivity cardiac troponin I assay. The results were then validated in another 10,000 patients from six countries around the world.
“Using this model, the patient can have a troponin test on arrival at the emergency department. The other information on age, sex, clinical history, and time since symptom onset is keyed in, and it gives a probability on a scale of 0–100 as to whether the patient is having an MI,” Dr. Mills noted.
“It also has the capacity to incorporate more information over time. So, if there is a second troponin measurement made, then the model automatically refines the probability score,” he added.
The current study showed that use of the CoDE-ACS model identified more patients at presentation as having a low probability of having an MI than fixed cardiac troponin thresholds (61% vs. 27%) with a similar negative predictive value.
It also identified fewer patients as having a high probability of having an MI (10% vs. 16%) with a greater positive predictive value.
Among patients who were identified as having a low probability of MI, the rate of cardiac death was lower than the rate among those with intermediate or high probability at 30 days (0.1% vs. 0.5% and 1.8%) and 1 year (0.3% vs. 2.8% and 4.2%).
“The results show that the machine learning model doubles the proportion of patients who can be discharged with a single test compared to the current practice of using the threshold approach. It really is a game changer in terms of its potential to improve health efficiency,” Dr. Mills said.
In terms of ruling patients in as possibly having an MI, he pointed out that troponin levels are increased in patients with a wide range of other conditions, including heart failure, kidney failure, and atrial fibrillation.
“When using the threshold approach, only one in four patients with an elevated troponin level will actually be having an MI, and that leads to confusion,” he said. “This model takes into consideration these other conditions and so it can correctly identify three out of four patients with a high probability of having an MI. We can therefore be more confident that it is appropriate to refer those patients to cardiology and save a lot of potentially unnecessary investigations and treatments in the others.”
Dr. Mills said the model also seems to work when assessing patients early on.
“Around one-third of patients present within 3 hours of symptom onset, and actually these are a high-risk group because people who have genuine cardiac pain are normally extremely uncomfortable and tend to present quickly. Current guidelines require that we do two tests in all these individuals, but this new model incorporates the time of symptom onset into its estimates of probability and therefore allows us to rule out patients even when they present very early.”
He reported that a second test is required in only one in five patients – those whose first test indicated intermediate probability.
“The second test allows us to refine the probability further, allowing us to rule another half of those patients out. We are then left with a small proportion of patients – about 1 in 10 – who remain of intermediate probability and will require additional clinical judgment.”
Should improve inequities in MI diagnosis
Dr. Mills said the CoDE-ACS model will improve current inequities in MI diagnosis, because of which MI is underrecognized in women and younger people.
“Women have troponin concentrations that are half those of men, and although sex-specific troponin thresholds are recommended in the guidelines, they are not widely used. This automatically leads to underrecognition of heart disease in women. But this new machine learning model performs identically in men and women because it has been trained to recognize the different normal levels in men and women,” he explained.
“It will also help us not to underdiagnose MI in younger people who often have a less classical presentation of MI, and they also generally have very low concentrations of troponin, so any increase in troponin way below the current diagnostic threshold may be very relevant to their risk,” he added.
The researchers are planning a randomized trial of the new model to demonstrate the impact it could have on equality of care and overcrowding in the emergency department. In the trial, patients will be randomly assigned to undergo decision-making on the basis of troponin thresholds (current practice) or to undergo decision-making through the CoDE-ACS model.
“The hope is that this trial will show reductions in unnecessary hospital admissions and length of stay in the emergency department,” Dr. Mills said. Results are expected sometime next year.
“This algorithm is very well trained. It has learned on 20,000 patients, so it has a lot more experience than I have, and I have been a professor of cardiology for 20 years,” Dr. Mills said.
He said he believes these models will get even smarter in the future as more data are added.
“I think the future for good decision-making in emergency care will be informed by clinical decision support from well-trained machine learning algorithms and they will help us guide not just the diagnosis of MI but also heart failure and other important cardiac conditions,” he said.
‘Elegant and exciting’ data
Commenting on the study, John W. McEvoy, MB, University of Galway, Ireland, said: “These are elegant and exciting data; however, the inputs into the machine learning algorithm include all the necessary information to actually diagnose MI. So why predict MI, when a human diagnosis can just be made directly? The answer to this question may depend on whether we trust machines more than humans.”
Dr. Mills noted that clinical judgment will always be an important part of MI diagnosis.
“Currently, using the troponin threshold approach, experienced clinicians will be able to nuance the results, but invariably, there is disagreement on this, and this can be a major source of tension within clinical care. By providing more individualized information, this will help enormously in the decision-making process,” he said.
“This model is not about replacing clinical decision-making. It’s more about augmenting decision-making and giving clinicians guidance to be able to improve efficiency and reduce inequality,” he added.
The study was funded with support from the National Institute for Health Research and NHSX, the British Heart Foundation, and Wellcome Leap. Dr. Mills has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. He is employed by the University of Edinburgh, which has filed a patent on the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome score.
A version of this article first appeared on Medscape.com.
Use of a machine-learning model that incorporates information from a single troponin test as well as other clinical data was superior to current practice as an aid to the diagnosis of myocardial infarction in the emergency department in a new study.
“Our results suggest that and free up space in the emergency department,” senior author Nicholas L. Mills, MD, University of Edinburgh, Scotland, said in an interview.
“And, perhaps even more importantly, use of this model could also increase the proportion of patients who are correctly identified as at a high probability of having an MI,” he added.
The study was published online in Nature Medicine.
The authors explained that at present, the likelihood of an MI diagnosis for patients presenting to the emergency department with chest pain is based on a fixed troponin threshold in serial tests at specific time points, but there are several problems with this approach.
First, a fixed troponin threshold is generally used for all patients, which does not account for age, sex, or comorbidities that are known to influence cardiac troponin concentrations. Second, the need to perform tests at specific time points for serial testing can be challenging in busy emergency departments.
And third, patients are categorized as being at low, intermediate, or high risk of MI on the basis of troponin thresholds alone, and the test does not take into account other important factors, such as the time of symptom onset or findings on the electrocardiogram.
“Our current practice of using the same threshold to rule in and rule out an MI for everyone, regardless of whether they are an 18-year-old female without a history of heart disease or an 85-year-old male with known heart failure, doesn’t perform well, and there’s a significant risk of misdiagnosis. There is also a high likelihood for inequalities in care, particularly between men and women,” Dr. Mills said.
The current study evaluated whether use of a machine learning model known as CoDE-ACS to guide decision-making could overcome some of these challenges.
The machine learning model assesses the whole spectrum of troponin levels as a continuous variable (rather than use of a single threshold) and turns this measurement into a probability that an individual patient is having an MI after accounting for other factors, including age, sex, comorbidities, and time from symptom onset.
For the current study, the CoDE-ACS model was trained in 10,000 patients with suspected acute coronary syndrome (ACS) who presented to 10 hospitals in Scotland as part of the High-STEACS trial evaluating the implementation of a high-sensitivity cardiac troponin I assay. The results were then validated in another 10,000 patients from six countries around the world.
“Using this model, the patient can have a troponin test on arrival at the emergency department. The other information on age, sex, clinical history, and time since symptom onset is keyed in, and it gives a probability on a scale of 0–100 as to whether the patient is having an MI,” Dr. Mills noted.
“It also has the capacity to incorporate more information over time. So, if there is a second troponin measurement made, then the model automatically refines the probability score,” he added.
The current study showed that use of the CoDE-ACS model identified more patients at presentation as having a low probability of having an MI than fixed cardiac troponin thresholds (61% vs. 27%) with a similar negative predictive value.
It also identified fewer patients as having a high probability of having an MI (10% vs. 16%) with a greater positive predictive value.
Among patients who were identified as having a low probability of MI, the rate of cardiac death was lower than the rate among those with intermediate or high probability at 30 days (0.1% vs. 0.5% and 1.8%) and 1 year (0.3% vs. 2.8% and 4.2%).
“The results show that the machine learning model doubles the proportion of patients who can be discharged with a single test compared to the current practice of using the threshold approach. It really is a game changer in terms of its potential to improve health efficiency,” Dr. Mills said.
In terms of ruling patients in as possibly having an MI, he pointed out that troponin levels are increased in patients with a wide range of other conditions, including heart failure, kidney failure, and atrial fibrillation.
“When using the threshold approach, only one in four patients with an elevated troponin level will actually be having an MI, and that leads to confusion,” he said. “This model takes into consideration these other conditions and so it can correctly identify three out of four patients with a high probability of having an MI. We can therefore be more confident that it is appropriate to refer those patients to cardiology and save a lot of potentially unnecessary investigations and treatments in the others.”
Dr. Mills said the model also seems to work when assessing patients early on.
“Around one-third of patients present within 3 hours of symptom onset, and actually these are a high-risk group because people who have genuine cardiac pain are normally extremely uncomfortable and tend to present quickly. Current guidelines require that we do two tests in all these individuals, but this new model incorporates the time of symptom onset into its estimates of probability and therefore allows us to rule out patients even when they present very early.”
He reported that a second test is required in only one in five patients – those whose first test indicated intermediate probability.
“The second test allows us to refine the probability further, allowing us to rule another half of those patients out. We are then left with a small proportion of patients – about 1 in 10 – who remain of intermediate probability and will require additional clinical judgment.”
Should improve inequities in MI diagnosis
Dr. Mills said the CoDE-ACS model will improve current inequities in MI diagnosis, because of which MI is underrecognized in women and younger people.
“Women have troponin concentrations that are half those of men, and although sex-specific troponin thresholds are recommended in the guidelines, they are not widely used. This automatically leads to underrecognition of heart disease in women. But this new machine learning model performs identically in men and women because it has been trained to recognize the different normal levels in men and women,” he explained.
“It will also help us not to underdiagnose MI in younger people who often have a less classical presentation of MI, and they also generally have very low concentrations of troponin, so any increase in troponin way below the current diagnostic threshold may be very relevant to their risk,” he added.
The researchers are planning a randomized trial of the new model to demonstrate the impact it could have on equality of care and overcrowding in the emergency department. In the trial, patients will be randomly assigned to undergo decision-making on the basis of troponin thresholds (current practice) or to undergo decision-making through the CoDE-ACS model.
“The hope is that this trial will show reductions in unnecessary hospital admissions and length of stay in the emergency department,” Dr. Mills said. Results are expected sometime next year.
“This algorithm is very well trained. It has learned on 20,000 patients, so it has a lot more experience than I have, and I have been a professor of cardiology for 20 years,” Dr. Mills said.
He said he believes these models will get even smarter in the future as more data are added.
“I think the future for good decision-making in emergency care will be informed by clinical decision support from well-trained machine learning algorithms and they will help us guide not just the diagnosis of MI but also heart failure and other important cardiac conditions,” he said.
‘Elegant and exciting’ data
Commenting on the study, John W. McEvoy, MB, University of Galway, Ireland, said: “These are elegant and exciting data; however, the inputs into the machine learning algorithm include all the necessary information to actually diagnose MI. So why predict MI, when a human diagnosis can just be made directly? The answer to this question may depend on whether we trust machines more than humans.”
Dr. Mills noted that clinical judgment will always be an important part of MI diagnosis.
“Currently, using the troponin threshold approach, experienced clinicians will be able to nuance the results, but invariably, there is disagreement on this, and this can be a major source of tension within clinical care. By providing more individualized information, this will help enormously in the decision-making process,” he said.
“This model is not about replacing clinical decision-making. It’s more about augmenting decision-making and giving clinicians guidance to be able to improve efficiency and reduce inequality,” he added.
The study was funded with support from the National Institute for Health Research and NHSX, the British Heart Foundation, and Wellcome Leap. Dr. Mills has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. He is employed by the University of Edinburgh, which has filed a patent on the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome score.
A version of this article first appeared on Medscape.com.
Use of a machine-learning model that incorporates information from a single troponin test as well as other clinical data was superior to current practice as an aid to the diagnosis of myocardial infarction in the emergency department in a new study.
“Our results suggest that and free up space in the emergency department,” senior author Nicholas L. Mills, MD, University of Edinburgh, Scotland, said in an interview.
“And, perhaps even more importantly, use of this model could also increase the proportion of patients who are correctly identified as at a high probability of having an MI,” he added.
The study was published online in Nature Medicine.
The authors explained that at present, the likelihood of an MI diagnosis for patients presenting to the emergency department with chest pain is based on a fixed troponin threshold in serial tests at specific time points, but there are several problems with this approach.
First, a fixed troponin threshold is generally used for all patients, which does not account for age, sex, or comorbidities that are known to influence cardiac troponin concentrations. Second, the need to perform tests at specific time points for serial testing can be challenging in busy emergency departments.
And third, patients are categorized as being at low, intermediate, or high risk of MI on the basis of troponin thresholds alone, and the test does not take into account other important factors, such as the time of symptom onset or findings on the electrocardiogram.
“Our current practice of using the same threshold to rule in and rule out an MI for everyone, regardless of whether they are an 18-year-old female without a history of heart disease or an 85-year-old male with known heart failure, doesn’t perform well, and there’s a significant risk of misdiagnosis. There is also a high likelihood for inequalities in care, particularly between men and women,” Dr. Mills said.
The current study evaluated whether use of a machine learning model known as CoDE-ACS to guide decision-making could overcome some of these challenges.
The machine learning model assesses the whole spectrum of troponin levels as a continuous variable (rather than use of a single threshold) and turns this measurement into a probability that an individual patient is having an MI after accounting for other factors, including age, sex, comorbidities, and time from symptom onset.
For the current study, the CoDE-ACS model was trained in 10,000 patients with suspected acute coronary syndrome (ACS) who presented to 10 hospitals in Scotland as part of the High-STEACS trial evaluating the implementation of a high-sensitivity cardiac troponin I assay. The results were then validated in another 10,000 patients from six countries around the world.
“Using this model, the patient can have a troponin test on arrival at the emergency department. The other information on age, sex, clinical history, and time since symptom onset is keyed in, and it gives a probability on a scale of 0–100 as to whether the patient is having an MI,” Dr. Mills noted.
“It also has the capacity to incorporate more information over time. So, if there is a second troponin measurement made, then the model automatically refines the probability score,” he added.
The current study showed that use of the CoDE-ACS model identified more patients at presentation as having a low probability of having an MI than fixed cardiac troponin thresholds (61% vs. 27%) with a similar negative predictive value.
It also identified fewer patients as having a high probability of having an MI (10% vs. 16%) with a greater positive predictive value.
Among patients who were identified as having a low probability of MI, the rate of cardiac death was lower than the rate among those with intermediate or high probability at 30 days (0.1% vs. 0.5% and 1.8%) and 1 year (0.3% vs. 2.8% and 4.2%).
“The results show that the machine learning model doubles the proportion of patients who can be discharged with a single test compared to the current practice of using the threshold approach. It really is a game changer in terms of its potential to improve health efficiency,” Dr. Mills said.
In terms of ruling patients in as possibly having an MI, he pointed out that troponin levels are increased in patients with a wide range of other conditions, including heart failure, kidney failure, and atrial fibrillation.
“When using the threshold approach, only one in four patients with an elevated troponin level will actually be having an MI, and that leads to confusion,” he said. “This model takes into consideration these other conditions and so it can correctly identify three out of four patients with a high probability of having an MI. We can therefore be more confident that it is appropriate to refer those patients to cardiology and save a lot of potentially unnecessary investigations and treatments in the others.”
Dr. Mills said the model also seems to work when assessing patients early on.
“Around one-third of patients present within 3 hours of symptom onset, and actually these are a high-risk group because people who have genuine cardiac pain are normally extremely uncomfortable and tend to present quickly. Current guidelines require that we do two tests in all these individuals, but this new model incorporates the time of symptom onset into its estimates of probability and therefore allows us to rule out patients even when they present very early.”
He reported that a second test is required in only one in five patients – those whose first test indicated intermediate probability.
“The second test allows us to refine the probability further, allowing us to rule another half of those patients out. We are then left with a small proportion of patients – about 1 in 10 – who remain of intermediate probability and will require additional clinical judgment.”
Should improve inequities in MI diagnosis
Dr. Mills said the CoDE-ACS model will improve current inequities in MI diagnosis, because of which MI is underrecognized in women and younger people.
“Women have troponin concentrations that are half those of men, and although sex-specific troponin thresholds are recommended in the guidelines, they are not widely used. This automatically leads to underrecognition of heart disease in women. But this new machine learning model performs identically in men and women because it has been trained to recognize the different normal levels in men and women,” he explained.
“It will also help us not to underdiagnose MI in younger people who often have a less classical presentation of MI, and they also generally have very low concentrations of troponin, so any increase in troponin way below the current diagnostic threshold may be very relevant to their risk,” he added.
The researchers are planning a randomized trial of the new model to demonstrate the impact it could have on equality of care and overcrowding in the emergency department. In the trial, patients will be randomly assigned to undergo decision-making on the basis of troponin thresholds (current practice) or to undergo decision-making through the CoDE-ACS model.
“The hope is that this trial will show reductions in unnecessary hospital admissions and length of stay in the emergency department,” Dr. Mills said. Results are expected sometime next year.
“This algorithm is very well trained. It has learned on 20,000 patients, so it has a lot more experience than I have, and I have been a professor of cardiology for 20 years,” Dr. Mills said.
He said he believes these models will get even smarter in the future as more data are added.
“I think the future for good decision-making in emergency care will be informed by clinical decision support from well-trained machine learning algorithms and they will help us guide not just the diagnosis of MI but also heart failure and other important cardiac conditions,” he said.
‘Elegant and exciting’ data
Commenting on the study, John W. McEvoy, MB, University of Galway, Ireland, said: “These are elegant and exciting data; however, the inputs into the machine learning algorithm include all the necessary information to actually diagnose MI. So why predict MI, when a human diagnosis can just be made directly? The answer to this question may depend on whether we trust machines more than humans.”
Dr. Mills noted that clinical judgment will always be an important part of MI diagnosis.
“Currently, using the troponin threshold approach, experienced clinicians will be able to nuance the results, but invariably, there is disagreement on this, and this can be a major source of tension within clinical care. By providing more individualized information, this will help enormously in the decision-making process,” he said.
“This model is not about replacing clinical decision-making. It’s more about augmenting decision-making and giving clinicians guidance to be able to improve efficiency and reduce inequality,” he added.
The study was funded with support from the National Institute for Health Research and NHSX, the British Heart Foundation, and Wellcome Leap. Dr. Mills has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. He is employed by the University of Edinburgh, which has filed a patent on the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome score.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
Anticipating FDA action, SCAI drafts guidance for adoption of renal denervation
Anticipating Food and Drug Administration approval of at least one investigational device for renal denervation (RDN) as a treatment for hypertension (HTN) refractory to medical therapies, the Society for Cardiovascular Angiography and Interventions is asking its members and the public to provide input on a draft position statement to guide use of the procedure.
SCAI is requesting feedback by June 14.
“With the anticipated FDA approval of renal denervation, there will be a need for SCAI to formulate an official position around clinical competence and training standards, best practices, and institutional and operator requirements for RDN,” Herbert D. Aronow, MD, MPH, chair of the statement writing committee, said in an interview.
RDN is an endoscopic procedure that disrupts the sympathetic nerves near the renal arteries. A number of studies, including sham-controlled, randomized trials, have shown that RDN can achieve short-term reductions in blood pressure for patients for whom HTN medications don’t work. Two devices are awaiting FDA premarket approval: the Paradise uRDN system, by ReCor Medical; and the Symplicity Spyral device, by Medtronic.
However, the trajectory of RDN has been uneven, said Dr. Aronow, president of the Society for Vascular Medicine and medical director for heart and vascular services and Benson Ford Chair in cardiology at Henry Ford Health, Detroit.
“Despite supportive early animal and human data, the first sham-controlled randomized trial of RDN was negative on its primary endpoint,” he said. “Modifications to patient inclusion/exclusion criteria, refinements in denervation technology and protocols, and selection of more appropriate study endpoints resulted in a series of positive randomized, sham-controlled trials. These second-generation trials found that RDN, when compared with sham therapy, substantially reduced ambulatory and office blood pressures.”
The draft is available for review at the SCAI website. Comments may be submitted via a link to a questionnaire.
“Through the open comment process, we are hoping to gain broad perspective from stakeholders, including clinicians, hospitals, payers, professional societies, industry and patients,” Dr. Aronow said. “By incorporating this feedback, we hope to enhance the quality of the document before we submit it for publication.”
The bulk of the SCAI draft position statement is devoted to patient selection and procedural and technical considerations. “We believe it will serve as a road map for the successful launch of RDN programs around the United States,” Dr. Aronow said.
Patient selection considerations
The draft statement notes that RDN for all patients with uncontrolled HTN “would not currently be practical.” The average age of patients for whom RDN showed effectiveness in the cited clinical trials was less than 60 years. The effectiveness of RDN for patients in whom arterial stiffness is a primary driver of HTN “is less certain.”
Patients who may benefit most from RDN are those with limited medical treatment options. Initially, RDN was tried on patients who had continued to experience resistant HTN despite taking three or more medications, including a diuretic, the statement noted. But even nonadherent patients may derive some potential benefit from RDN.
The statement also added that RDN isn’t a panacea; about one-third of trial patients didn’t respond to the procedure. The most reliable predictor of response may be higher levels of baseline systolic blood pressure, otherwise known as Wilder’s principle. The statement listed other potential markers of success, including higher nocturnal blood pressure and wider swings in nocturnal blood pressure.
Procedural and technical considerations
The statement also provided direction on a protocol for RDN procedures. The preprocedure evaluation should include noninvasive imaging to rule out disqualifying secondary causes of HTN, such as renal artery stenosis or fibromuscular dysplasia.
Patient characteristics should drive the selection of imaging modality, and availability as well as local expertise should be taken into account. The statement gave CT angiography or magnetic resonance angiography the edge over duplex ultrasound.
The statement also noted a number of anatomic considerations, citing preclinical analyses that “consistently reinforce” circumferential, perivascular RDN to ablate the renal nerves. In planning the procedure, consideration should be given to accessory renal arteries.
Additionally, operators should have training in obtaining access, and they should be familiar with different catheters and console devices as well as troubleshooting.
Training, competency, and institutional requirements
Interventional cardiologists who want to perform RDN should demonstrate proficiency in a number of specific skill sets germane to the procedure, from arterial vascular access and hemostasis to recognizing and treating potential renovascular complications.
For institutions that want to offer RDN, the statement offered a number of requirements. One is to designate a primary physician stakeholder who’s well versed in HTN management to oversee the long-term management of RDN patients.
The institution must have a dedicated HTN program and a multidisciplinary team to manage treated patients. Requirements for RDN referral centers range from operators experienced with FDA-approved RDN devices to an infrastructure that includes CT or MR angiography to identify appropriate candidates.
“Renal denervation has been a long time coming, and it’s a great example of how academicians, clinicians and industry leaders can partner to move the cardiovascular field forward, addressing a major public health issue for which alternative solutions are greatly needed,” Dr. Aronow said.
Dr. Aronow has served as an unpaid council member for Medtronic and as a paid moderator for ReCor.
A version of this article first appeared on Medscape.com.
Anticipating Food and Drug Administration approval of at least one investigational device for renal denervation (RDN) as a treatment for hypertension (HTN) refractory to medical therapies, the Society for Cardiovascular Angiography and Interventions is asking its members and the public to provide input on a draft position statement to guide use of the procedure.
SCAI is requesting feedback by June 14.
“With the anticipated FDA approval of renal denervation, there will be a need for SCAI to formulate an official position around clinical competence and training standards, best practices, and institutional and operator requirements for RDN,” Herbert D. Aronow, MD, MPH, chair of the statement writing committee, said in an interview.
RDN is an endoscopic procedure that disrupts the sympathetic nerves near the renal arteries. A number of studies, including sham-controlled, randomized trials, have shown that RDN can achieve short-term reductions in blood pressure for patients for whom HTN medications don’t work. Two devices are awaiting FDA premarket approval: the Paradise uRDN system, by ReCor Medical; and the Symplicity Spyral device, by Medtronic.
However, the trajectory of RDN has been uneven, said Dr. Aronow, president of the Society for Vascular Medicine and medical director for heart and vascular services and Benson Ford Chair in cardiology at Henry Ford Health, Detroit.
“Despite supportive early animal and human data, the first sham-controlled randomized trial of RDN was negative on its primary endpoint,” he said. “Modifications to patient inclusion/exclusion criteria, refinements in denervation technology and protocols, and selection of more appropriate study endpoints resulted in a series of positive randomized, sham-controlled trials. These second-generation trials found that RDN, when compared with sham therapy, substantially reduced ambulatory and office blood pressures.”
The draft is available for review at the SCAI website. Comments may be submitted via a link to a questionnaire.
“Through the open comment process, we are hoping to gain broad perspective from stakeholders, including clinicians, hospitals, payers, professional societies, industry and patients,” Dr. Aronow said. “By incorporating this feedback, we hope to enhance the quality of the document before we submit it for publication.”
The bulk of the SCAI draft position statement is devoted to patient selection and procedural and technical considerations. “We believe it will serve as a road map for the successful launch of RDN programs around the United States,” Dr. Aronow said.
Patient selection considerations
The draft statement notes that RDN for all patients with uncontrolled HTN “would not currently be practical.” The average age of patients for whom RDN showed effectiveness in the cited clinical trials was less than 60 years. The effectiveness of RDN for patients in whom arterial stiffness is a primary driver of HTN “is less certain.”
Patients who may benefit most from RDN are those with limited medical treatment options. Initially, RDN was tried on patients who had continued to experience resistant HTN despite taking three or more medications, including a diuretic, the statement noted. But even nonadherent patients may derive some potential benefit from RDN.
The statement also added that RDN isn’t a panacea; about one-third of trial patients didn’t respond to the procedure. The most reliable predictor of response may be higher levels of baseline systolic blood pressure, otherwise known as Wilder’s principle. The statement listed other potential markers of success, including higher nocturnal blood pressure and wider swings in nocturnal blood pressure.
Procedural and technical considerations
The statement also provided direction on a protocol for RDN procedures. The preprocedure evaluation should include noninvasive imaging to rule out disqualifying secondary causes of HTN, such as renal artery stenosis or fibromuscular dysplasia.
Patient characteristics should drive the selection of imaging modality, and availability as well as local expertise should be taken into account. The statement gave CT angiography or magnetic resonance angiography the edge over duplex ultrasound.
The statement also noted a number of anatomic considerations, citing preclinical analyses that “consistently reinforce” circumferential, perivascular RDN to ablate the renal nerves. In planning the procedure, consideration should be given to accessory renal arteries.
Additionally, operators should have training in obtaining access, and they should be familiar with different catheters and console devices as well as troubleshooting.
Training, competency, and institutional requirements
Interventional cardiologists who want to perform RDN should demonstrate proficiency in a number of specific skill sets germane to the procedure, from arterial vascular access and hemostasis to recognizing and treating potential renovascular complications.
For institutions that want to offer RDN, the statement offered a number of requirements. One is to designate a primary physician stakeholder who’s well versed in HTN management to oversee the long-term management of RDN patients.
The institution must have a dedicated HTN program and a multidisciplinary team to manage treated patients. Requirements for RDN referral centers range from operators experienced with FDA-approved RDN devices to an infrastructure that includes CT or MR angiography to identify appropriate candidates.
“Renal denervation has been a long time coming, and it’s a great example of how academicians, clinicians and industry leaders can partner to move the cardiovascular field forward, addressing a major public health issue for which alternative solutions are greatly needed,” Dr. Aronow said.
Dr. Aronow has served as an unpaid council member for Medtronic and as a paid moderator for ReCor.
A version of this article first appeared on Medscape.com.
Anticipating Food and Drug Administration approval of at least one investigational device for renal denervation (RDN) as a treatment for hypertension (HTN) refractory to medical therapies, the Society for Cardiovascular Angiography and Interventions is asking its members and the public to provide input on a draft position statement to guide use of the procedure.
SCAI is requesting feedback by June 14.
“With the anticipated FDA approval of renal denervation, there will be a need for SCAI to formulate an official position around clinical competence and training standards, best practices, and institutional and operator requirements for RDN,” Herbert D. Aronow, MD, MPH, chair of the statement writing committee, said in an interview.
RDN is an endoscopic procedure that disrupts the sympathetic nerves near the renal arteries. A number of studies, including sham-controlled, randomized trials, have shown that RDN can achieve short-term reductions in blood pressure for patients for whom HTN medications don’t work. Two devices are awaiting FDA premarket approval: the Paradise uRDN system, by ReCor Medical; and the Symplicity Spyral device, by Medtronic.
However, the trajectory of RDN has been uneven, said Dr. Aronow, president of the Society for Vascular Medicine and medical director for heart and vascular services and Benson Ford Chair in cardiology at Henry Ford Health, Detroit.
“Despite supportive early animal and human data, the first sham-controlled randomized trial of RDN was negative on its primary endpoint,” he said. “Modifications to patient inclusion/exclusion criteria, refinements in denervation technology and protocols, and selection of more appropriate study endpoints resulted in a series of positive randomized, sham-controlled trials. These second-generation trials found that RDN, when compared with sham therapy, substantially reduced ambulatory and office blood pressures.”
The draft is available for review at the SCAI website. Comments may be submitted via a link to a questionnaire.
“Through the open comment process, we are hoping to gain broad perspective from stakeholders, including clinicians, hospitals, payers, professional societies, industry and patients,” Dr. Aronow said. “By incorporating this feedback, we hope to enhance the quality of the document before we submit it for publication.”
The bulk of the SCAI draft position statement is devoted to patient selection and procedural and technical considerations. “We believe it will serve as a road map for the successful launch of RDN programs around the United States,” Dr. Aronow said.
Patient selection considerations
The draft statement notes that RDN for all patients with uncontrolled HTN “would not currently be practical.” The average age of patients for whom RDN showed effectiveness in the cited clinical trials was less than 60 years. The effectiveness of RDN for patients in whom arterial stiffness is a primary driver of HTN “is less certain.”
Patients who may benefit most from RDN are those with limited medical treatment options. Initially, RDN was tried on patients who had continued to experience resistant HTN despite taking three or more medications, including a diuretic, the statement noted. But even nonadherent patients may derive some potential benefit from RDN.
The statement also added that RDN isn’t a panacea; about one-third of trial patients didn’t respond to the procedure. The most reliable predictor of response may be higher levels of baseline systolic blood pressure, otherwise known as Wilder’s principle. The statement listed other potential markers of success, including higher nocturnal blood pressure and wider swings in nocturnal blood pressure.
Procedural and technical considerations
The statement also provided direction on a protocol for RDN procedures. The preprocedure evaluation should include noninvasive imaging to rule out disqualifying secondary causes of HTN, such as renal artery stenosis or fibromuscular dysplasia.
Patient characteristics should drive the selection of imaging modality, and availability as well as local expertise should be taken into account. The statement gave CT angiography or magnetic resonance angiography the edge over duplex ultrasound.
The statement also noted a number of anatomic considerations, citing preclinical analyses that “consistently reinforce” circumferential, perivascular RDN to ablate the renal nerves. In planning the procedure, consideration should be given to accessory renal arteries.
Additionally, operators should have training in obtaining access, and they should be familiar with different catheters and console devices as well as troubleshooting.
Training, competency, and institutional requirements
Interventional cardiologists who want to perform RDN should demonstrate proficiency in a number of specific skill sets germane to the procedure, from arterial vascular access and hemostasis to recognizing and treating potential renovascular complications.
For institutions that want to offer RDN, the statement offered a number of requirements. One is to designate a primary physician stakeholder who’s well versed in HTN management to oversee the long-term management of RDN patients.
The institution must have a dedicated HTN program and a multidisciplinary team to manage treated patients. Requirements for RDN referral centers range from operators experienced with FDA-approved RDN devices to an infrastructure that includes CT or MR angiography to identify appropriate candidates.
“Renal denervation has been a long time coming, and it’s a great example of how academicians, clinicians and industry leaders can partner to move the cardiovascular field forward, addressing a major public health issue for which alternative solutions are greatly needed,” Dr. Aronow said.
Dr. Aronow has served as an unpaid council member for Medtronic and as a paid moderator for ReCor.
A version of this article first appeared on Medscape.com.
Marijuana linked to higher PAD risk
But death, intervention rates same
PHOENIX – although there was no greater risk of death from myocardial infarction or other cardiac causes or need for revascularization.

The researchers noted, however, that the study population was young, with an average age of 37.4 years, and that the study period, from 2016 to 2019, predates the legalization of recreational marijuana in a number of states.
Nonetheless, even in this young study population, marijuana users’ risk of developing peripheral artery disease (PAD) was 3.68 times greater (P < .001) than that of nonusers. PAD at a young age could precede worse outcomes later in life, the study authors said.
“Basically, marijuana users were at increased risk of being diagnosed with peripheral artery disease, but there was no increased risk for them requiring any intervention, such as a peripheral vascular intervention, nor were they at increased risk of death from what we found,” said Hirva Vyas, DO, an internal medicine resident at Hackensack University Medical Center in New Jersey, who presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
The study used data on 623,768 marijuana users from the National Inpatient Sample, a nationwide database of inpatient visits covered by all public and commercial payers, then extracted a diagnosis for PAD from all 30 million–plus patient encounters to compare PAD rates between marijuana users and nonusers. Marijuana users were more likely to be White and to have elective rather than emergency admissions (P < .001). The researchers used diagnostic codes to identify marijuana users and PAD patients.
Recreational marijuana is legal in 22 states and the District of Columbia, according to ProCon.org. Since 2019, the last year of the study, 11 states have legalized marijuana for recreational use. “It’s a data point that we studied at one point in time, only from 2016 to 2019,” Dr. Vyas said in an interview.
“As we’ve seen over the past 4-5 years, legalization has skyrocketed and recreational use has become more and more favorable not only among younger folks but older folks,” study coauthor Harsh Jain, MD, a second-year internal medicine resident at Montefiore Medical Center in New York, said in the interview. “It would be really refreshing to see how these data change as we look at endpoints from 2019 to 2023.”
Because of the young age of the study population, Dr. Jain said, these findings may not accurately represent the true cardiovascular risks of marijuana use, especially later in life.
“One of the biggest secondary endpoints that we wanted to study was the development of chronic conditions that lead to multiple rehospitalizations, the most significant one of which would be the development of heart failure,” Dr. Jain said. “However, it was difficult to stratify because, again, many of these patients were very young and so they did not carry the diagnosis for heart failure, so we couldn’t complete that subset analysis.”
The goal is to extend the study period out to 2023, Dr. Jain said. “We know that these are very crude and rudimentary data findings that we presented so far, but we’re hoping that the final paper gives us a chance to flesh out all the details of our study and also gives us a chance to expand going forward,” he said.
The findings are in line with other research into the effects of marijuana and cardiovascular disease, said Carl “Chip” Lavie, MD, medical director for cardiac rehabilitation and prevention at the John Ochsner Heart and Vascular Institute in New Orleans who’s published a number of studies on PAD and substance use, including marijuana.
“It is known that cannabis is associated with more vasoconstriction, has sympathomimetic effects, causes endothelial dysfunction and increased platelet aggregation, and is known to increase the risk of acute myocardial infarction, especially in the hour or so after use,” he said in written comments sent to this news organization.
“It is also well known to be a cause of thromboangiitis obliterans, which is in the PAD family,” he added. “Based on these mechanisms, one would expect an increased PAD and, especially, PAD events. The 3.7-fold increased risk is supportive of this increased PAD.”
One study strength, Dr. Lavie pointed out, is that it’s one of the few studies that found an association between marijuana and PAD, which hasn’t been studied as well as other cardiovascular endpoints. “However,” he said, “the limitation is this is just an inpatient sample, and it is all based on coding – e.g., a patient could have PAD and it may not have been coded.”
But death, intervention rates same
But death, intervention rates same
PHOENIX – although there was no greater risk of death from myocardial infarction or other cardiac causes or need for revascularization.
The researchers noted, however, that the study population was young, with an average age of 37.4 years, and that the study period, from 2016 to 2019, predates the legalization of recreational marijuana in a number of states.
Nonetheless, even in this young study population, marijuana users’ risk of developing peripheral artery disease (PAD) was 3.68 times greater (P < .001) than that of nonusers. PAD at a young age could precede worse outcomes later in life, the study authors said.
“Basically, marijuana users were at increased risk of being diagnosed with peripheral artery disease, but there was no increased risk for them requiring any intervention, such as a peripheral vascular intervention, nor were they at increased risk of death from what we found,” said Hirva Vyas, DO, an internal medicine resident at Hackensack University Medical Center in New Jersey, who presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
The study used data on 623,768 marijuana users from the National Inpatient Sample, a nationwide database of inpatient visits covered by all public and commercial payers, then extracted a diagnosis for PAD from all 30 million–plus patient encounters to compare PAD rates between marijuana users and nonusers. Marijuana users were more likely to be White and to have elective rather than emergency admissions (P < .001). The researchers used diagnostic codes to identify marijuana users and PAD patients.
Recreational marijuana is legal in 22 states and the District of Columbia, according to ProCon.org. Since 2019, the last year of the study, 11 states have legalized marijuana for recreational use. “It’s a data point that we studied at one point in time, only from 2016 to 2019,” Dr. Vyas said in an interview.
“As we’ve seen over the past 4-5 years, legalization has skyrocketed and recreational use has become more and more favorable not only among younger folks but older folks,” study coauthor Harsh Jain, MD, a second-year internal medicine resident at Montefiore Medical Center in New York, said in the interview. “It would be really refreshing to see how these data change as we look at endpoints from 2019 to 2023.”
Because of the young age of the study population, Dr. Jain said, these findings may not accurately represent the true cardiovascular risks of marijuana use, especially later in life.
“One of the biggest secondary endpoints that we wanted to study was the development of chronic conditions that lead to multiple rehospitalizations, the most significant one of which would be the development of heart failure,” Dr. Jain said. “However, it was difficult to stratify because, again, many of these patients were very young and so they did not carry the diagnosis for heart failure, so we couldn’t complete that subset analysis.”
The goal is to extend the study period out to 2023, Dr. Jain said. “We know that these are very crude and rudimentary data findings that we presented so far, but we’re hoping that the final paper gives us a chance to flesh out all the details of our study and also gives us a chance to expand going forward,” he said.
The findings are in line with other research into the effects of marijuana and cardiovascular disease, said Carl “Chip” Lavie, MD, medical director for cardiac rehabilitation and prevention at the John Ochsner Heart and Vascular Institute in New Orleans who’s published a number of studies on PAD and substance use, including marijuana.
“It is known that cannabis is associated with more vasoconstriction, has sympathomimetic effects, causes endothelial dysfunction and increased platelet aggregation, and is known to increase the risk of acute myocardial infarction, especially in the hour or so after use,” he said in written comments sent to this news organization.
“It is also well known to be a cause of thromboangiitis obliterans, which is in the PAD family,” he added. “Based on these mechanisms, one would expect an increased PAD and, especially, PAD events. The 3.7-fold increased risk is supportive of this increased PAD.”
One study strength, Dr. Lavie pointed out, is that it’s one of the few studies that found an association between marijuana and PAD, which hasn’t been studied as well as other cardiovascular endpoints. “However,” he said, “the limitation is this is just an inpatient sample, and it is all based on coding – e.g., a patient could have PAD and it may not have been coded.”
PHOENIX – although there was no greater risk of death from myocardial infarction or other cardiac causes or need for revascularization.
The researchers noted, however, that the study population was young, with an average age of 37.4 years, and that the study period, from 2016 to 2019, predates the legalization of recreational marijuana in a number of states.
Nonetheless, even in this young study population, marijuana users’ risk of developing peripheral artery disease (PAD) was 3.68 times greater (P < .001) than that of nonusers. PAD at a young age could precede worse outcomes later in life, the study authors said.
“Basically, marijuana users were at increased risk of being diagnosed with peripheral artery disease, but there was no increased risk for them requiring any intervention, such as a peripheral vascular intervention, nor were they at increased risk of death from what we found,” said Hirva Vyas, DO, an internal medicine resident at Hackensack University Medical Center in New Jersey, who presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
The study used data on 623,768 marijuana users from the National Inpatient Sample, a nationwide database of inpatient visits covered by all public and commercial payers, then extracted a diagnosis for PAD from all 30 million–plus patient encounters to compare PAD rates between marijuana users and nonusers. Marijuana users were more likely to be White and to have elective rather than emergency admissions (P < .001). The researchers used diagnostic codes to identify marijuana users and PAD patients.
Recreational marijuana is legal in 22 states and the District of Columbia, according to ProCon.org. Since 2019, the last year of the study, 11 states have legalized marijuana for recreational use. “It’s a data point that we studied at one point in time, only from 2016 to 2019,” Dr. Vyas said in an interview.
“As we’ve seen over the past 4-5 years, legalization has skyrocketed and recreational use has become more and more favorable not only among younger folks but older folks,” study coauthor Harsh Jain, MD, a second-year internal medicine resident at Montefiore Medical Center in New York, said in the interview. “It would be really refreshing to see how these data change as we look at endpoints from 2019 to 2023.”
Because of the young age of the study population, Dr. Jain said, these findings may not accurately represent the true cardiovascular risks of marijuana use, especially later in life.
“One of the biggest secondary endpoints that we wanted to study was the development of chronic conditions that lead to multiple rehospitalizations, the most significant one of which would be the development of heart failure,” Dr. Jain said. “However, it was difficult to stratify because, again, many of these patients were very young and so they did not carry the diagnosis for heart failure, so we couldn’t complete that subset analysis.”
The goal is to extend the study period out to 2023, Dr. Jain said. “We know that these are very crude and rudimentary data findings that we presented so far, but we’re hoping that the final paper gives us a chance to flesh out all the details of our study and also gives us a chance to expand going forward,” he said.
The findings are in line with other research into the effects of marijuana and cardiovascular disease, said Carl “Chip” Lavie, MD, medical director for cardiac rehabilitation and prevention at the John Ochsner Heart and Vascular Institute in New Orleans who’s published a number of studies on PAD and substance use, including marijuana.
“It is known that cannabis is associated with more vasoconstriction, has sympathomimetic effects, causes endothelial dysfunction and increased platelet aggregation, and is known to increase the risk of acute myocardial infarction, especially in the hour or so after use,” he said in written comments sent to this news organization.
“It is also well known to be a cause of thromboangiitis obliterans, which is in the PAD family,” he added. “Based on these mechanisms, one would expect an increased PAD and, especially, PAD events. The 3.7-fold increased risk is supportive of this increased PAD.”
One study strength, Dr. Lavie pointed out, is that it’s one of the few studies that found an association between marijuana and PAD, which hasn’t been studied as well as other cardiovascular endpoints. “However,” he said, “the limitation is this is just an inpatient sample, and it is all based on coding – e.g., a patient could have PAD and it may not have been coded.”
AT SCAI 2023
Transcatheter tricuspid valve repair in real-world setting replicates trials
Data support benefit and safety
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
Data support benefit and safety
Data support benefit and safety
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
FROM EUROPCR 2023
MACE, VTE rates compared between TNF and JAK inhibitors for AxSpA and PsA
CLEVELAND – Patients with axial spondyloarthritis or psoriatic arthritis who used Janus kinase (JAK) inhibitors did not have higher risk of myocardial infarction, stroke, or venous thromboembolism (VTE), compared with those who used tumor necrosis factor inhibitors (TNFi), according to new research.
The information was presented in a poster at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
Patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) have increased cardiovascular risk compared with the general population. Emerging evidence has suggested that TNFi may protect the cardiovascular system and that there are cardiovascular and thrombotic concerns with JAK inhibitors.
Sali Merjanah, MD, a rheumatology fellow at Boston University, and colleagues, compared how drugs in the two treatment classes affected the likelihood of major adverse cardiovascular events (MACE) or VTE. MACE in this study were myocardial infarction and stroke.
In a search of the Marketscan Database during 2006-2021, the researchers identified 1,621 TNFi and 47 JAK inhibitor users with 273 and 8 cases of MACE, respectively. They identified 2,507 TNFi and 96 JAK users with 452 and 26 cases of VTE, respectively. Patients were aged 18-65 years and had at least one inpatient or two outpatient axSpA or PsA ICD-9 or ICD-10 diagnosis codes separated by at least 7 days.
The likelihood of MACE was 14% lower among JAK inhibitor users than TNFi users (the reference group), whereas the likelihood of VTE was 39% higher for JAK inhibitor users, but neither comparison was statistically significant. JAK/TNFi nonusers had a statistically significant 27% greater likelihood of MACE than did TNFi users. The likelihood for VTE was 12% higher for JAK/TNFi nonusers, compared with TNFi users, but this finding was not statistically significant. The researchers adjusted comparisons for age, medications, and comorbidities.
Small numbers complicate the research
Lianne Gensler, MD, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco, who was not part of the study, said the limitations the authors list are important to note. The researchers said that the study’s small number of JAK inhibitor users, short duration of exposure, and low event rate limit its precision, and there is potential misclassification of TNF/JAK inhibitor exposure, as well as confounding by indication.

Dr. Gensler noted that these same limitations apply to studies of patients with RA as well that try to answer the question of risk for MACE and malignancy when using these drugs,
“MACE is a rare event, malignancy is a rare event. So it’s like finding a needle in a haystack, and the haystack is really big. You either have to enrich the haystack with more needles or you have to make a smaller haystack,” Dr. Gensler said.
Nevertheless, she said, she credits the researchers for bringing the available information to light.
“I think we have to do this many different ways to try to get at the answer in a partial way,” she said.
The data were drawn from 2006 to 2021, but JAK inhibitors have only been approved for axSpA in the last one and a half years and for PsA at the end of 2017.
Additionally, the people taking JAK inhibitors would have likely already failed TNFis, she said, adding that this can make it hard to tell whether an event was linked with the JAK or the TNFi.
Nonusers may have other risk factors
She pointed out that in this study patients who were not using TNF or JAK inhibitors had slightly higher risk numerically for both MACE and VTE than did those using TNFis.
“There, the assumption is always that this is confounding by indication, meaning it is likely that the people who are nonusers have other risk factors for MACE, which is why we’re not giving them these drugs.”
Having heart failure, for instance, is a contraindication for using a TNF inhibitor, she noted. “So it’s not that these are protective compared to nonusers. It’s probably that the nonuser has higher risk and is not getting treated with these drugs to begin with.”
The authors properly concluded from the data that patients using JAK inhibitors did not have higher risk of MACE or VTE, compared with those who used TNFis, she said, but larger studies with more follow-up are needed.
“No evidence doesn’t mean no effect,” she said. “Part of it depends on the [statistical] power and the population you’re studying.”
Dr. Gensler is a consultant for AbbVie, Acceleron, Eli Lilly, Janssen, Novartis, Pfizer, and UCB; and has received grant support from Novartis and UCB. The authors’ financial relationships were not available.
CLEVELAND – Patients with axial spondyloarthritis or psoriatic arthritis who used Janus kinase (JAK) inhibitors did not have higher risk of myocardial infarction, stroke, or venous thromboembolism (VTE), compared with those who used tumor necrosis factor inhibitors (TNFi), according to new research.
The information was presented in a poster at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
Patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) have increased cardiovascular risk compared with the general population. Emerging evidence has suggested that TNFi may protect the cardiovascular system and that there are cardiovascular and thrombotic concerns with JAK inhibitors.
Sali Merjanah, MD, a rheumatology fellow at Boston University, and colleagues, compared how drugs in the two treatment classes affected the likelihood of major adverse cardiovascular events (MACE) or VTE. MACE in this study were myocardial infarction and stroke.
In a search of the Marketscan Database during 2006-2021, the researchers identified 1,621 TNFi and 47 JAK inhibitor users with 273 and 8 cases of MACE, respectively. They identified 2,507 TNFi and 96 JAK users with 452 and 26 cases of VTE, respectively. Patients were aged 18-65 years and had at least one inpatient or two outpatient axSpA or PsA ICD-9 or ICD-10 diagnosis codes separated by at least 7 days.
The likelihood of MACE was 14% lower among JAK inhibitor users than TNFi users (the reference group), whereas the likelihood of VTE was 39% higher for JAK inhibitor users, but neither comparison was statistically significant. JAK/TNFi nonusers had a statistically significant 27% greater likelihood of MACE than did TNFi users. The likelihood for VTE was 12% higher for JAK/TNFi nonusers, compared with TNFi users, but this finding was not statistically significant. The researchers adjusted comparisons for age, medications, and comorbidities.
Small numbers complicate the research
Lianne Gensler, MD, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco, who was not part of the study, said the limitations the authors list are important to note. The researchers said that the study’s small number of JAK inhibitor users, short duration of exposure, and low event rate limit its precision, and there is potential misclassification of TNF/JAK inhibitor exposure, as well as confounding by indication.
Dr. Gensler noted that these same limitations apply to studies of patients with RA as well that try to answer the question of risk for MACE and malignancy when using these drugs,
“MACE is a rare event, malignancy is a rare event. So it’s like finding a needle in a haystack, and the haystack is really big. You either have to enrich the haystack with more needles or you have to make a smaller haystack,” Dr. Gensler said.
Nevertheless, she said, she credits the researchers for bringing the available information to light.
“I think we have to do this many different ways to try to get at the answer in a partial way,” she said.
The data were drawn from 2006 to 2021, but JAK inhibitors have only been approved for axSpA in the last one and a half years and for PsA at the end of 2017.
Additionally, the people taking JAK inhibitors would have likely already failed TNFis, she said, adding that this can make it hard to tell whether an event was linked with the JAK or the TNFi.
Nonusers may have other risk factors
She pointed out that in this study patients who were not using TNF or JAK inhibitors had slightly higher risk numerically for both MACE and VTE than did those using TNFis.
“There, the assumption is always that this is confounding by indication, meaning it is likely that the people who are nonusers have other risk factors for MACE, which is why we’re not giving them these drugs.”
Having heart failure, for instance, is a contraindication for using a TNF inhibitor, she noted. “So it’s not that these are protective compared to nonusers. It’s probably that the nonuser has higher risk and is not getting treated with these drugs to begin with.”
The authors properly concluded from the data that patients using JAK inhibitors did not have higher risk of MACE or VTE, compared with those who used TNFis, she said, but larger studies with more follow-up are needed.
“No evidence doesn’t mean no effect,” she said. “Part of it depends on the [statistical] power and the population you’re studying.”
Dr. Gensler is a consultant for AbbVie, Acceleron, Eli Lilly, Janssen, Novartis, Pfizer, and UCB; and has received grant support from Novartis and UCB. The authors’ financial relationships were not available.
CLEVELAND – Patients with axial spondyloarthritis or psoriatic arthritis who used Janus kinase (JAK) inhibitors did not have higher risk of myocardial infarction, stroke, or venous thromboembolism (VTE), compared with those who used tumor necrosis factor inhibitors (TNFi), according to new research.
The information was presented in a poster at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
Patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) have increased cardiovascular risk compared with the general population. Emerging evidence has suggested that TNFi may protect the cardiovascular system and that there are cardiovascular and thrombotic concerns with JAK inhibitors.
Sali Merjanah, MD, a rheumatology fellow at Boston University, and colleagues, compared how drugs in the two treatment classes affected the likelihood of major adverse cardiovascular events (MACE) or VTE. MACE in this study were myocardial infarction and stroke.
In a search of the Marketscan Database during 2006-2021, the researchers identified 1,621 TNFi and 47 JAK inhibitor users with 273 and 8 cases of MACE, respectively. They identified 2,507 TNFi and 96 JAK users with 452 and 26 cases of VTE, respectively. Patients were aged 18-65 years and had at least one inpatient or two outpatient axSpA or PsA ICD-9 or ICD-10 diagnosis codes separated by at least 7 days.
The likelihood of MACE was 14% lower among JAK inhibitor users than TNFi users (the reference group), whereas the likelihood of VTE was 39% higher for JAK inhibitor users, but neither comparison was statistically significant. JAK/TNFi nonusers had a statistically significant 27% greater likelihood of MACE than did TNFi users. The likelihood for VTE was 12% higher for JAK/TNFi nonusers, compared with TNFi users, but this finding was not statistically significant. The researchers adjusted comparisons for age, medications, and comorbidities.
Small numbers complicate the research
Lianne Gensler, MD, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco, who was not part of the study, said the limitations the authors list are important to note. The researchers said that the study’s small number of JAK inhibitor users, short duration of exposure, and low event rate limit its precision, and there is potential misclassification of TNF/JAK inhibitor exposure, as well as confounding by indication.
Dr. Gensler noted that these same limitations apply to studies of patients with RA as well that try to answer the question of risk for MACE and malignancy when using these drugs,
“MACE is a rare event, malignancy is a rare event. So it’s like finding a needle in a haystack, and the haystack is really big. You either have to enrich the haystack with more needles or you have to make a smaller haystack,” Dr. Gensler said.
Nevertheless, she said, she credits the researchers for bringing the available information to light.
“I think we have to do this many different ways to try to get at the answer in a partial way,” she said.
The data were drawn from 2006 to 2021, but JAK inhibitors have only been approved for axSpA in the last one and a half years and for PsA at the end of 2017.
Additionally, the people taking JAK inhibitors would have likely already failed TNFis, she said, adding that this can make it hard to tell whether an event was linked with the JAK or the TNFi.
Nonusers may have other risk factors
She pointed out that in this study patients who were not using TNF or JAK inhibitors had slightly higher risk numerically for both MACE and VTE than did those using TNFis.
“There, the assumption is always that this is confounding by indication, meaning it is likely that the people who are nonusers have other risk factors for MACE, which is why we’re not giving them these drugs.”
Having heart failure, for instance, is a contraindication for using a TNF inhibitor, she noted. “So it’s not that these are protective compared to nonusers. It’s probably that the nonuser has higher risk and is not getting treated with these drugs to begin with.”
The authors properly concluded from the data that patients using JAK inhibitors did not have higher risk of MACE or VTE, compared with those who used TNFis, she said, but larger studies with more follow-up are needed.
“No evidence doesn’t mean no effect,” she said. “Part of it depends on the [statistical] power and the population you’re studying.”
Dr. Gensler is a consultant for AbbVie, Acceleron, Eli Lilly, Janssen, Novartis, Pfizer, and UCB; and has received grant support from Novartis and UCB. The authors’ financial relationships were not available.
AT SPARTAN 2023