User login
Buprenorphine Care Uncovers New Illnesses
Major Finding: Treating opioid dependence in primary care offices identified new chronic medical problems in 36 (27%) of 135 patients and led to initiation of treatment in 70% of 172 previously known chronic medical problems that were not being treated.
Data Source: Retrospective review of patients presenting to a primary care clinic for treatment of opioid dependence who received a prescription for sublingual buprenorphine.
Disclosures: Dr. Rowe said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO – Treating patients for opioid dependence with sublingual buprenorphine in a primary care clinic helped providers identify chronic medical conditions that were not being treated.
Among 135 new patients who presented to a primary care office for help with opioid dependence and who received a prescription for sublingual buprenorphine within a month of their visit, 69% had no primary care provider until that visit. Newly diagnosed chronic medical conditions were identified in 36 (27%) of patients, Dr. Theresa Rowe reported in a poster presentation at the annual meeting of the American Society of Addiction Medicine.
Patients started treatment for 41 (95%) of 43 newly diagnosed chronic medical conditions within a year, said Dr. Rowe of Johns Hopkins University, and her study associate, Dr. Darius Rastegar, of the Johns Hopkins Bayview Medical Center, both in Baltimore.
The most common new diagnoses were hepatitis C in 11 patients, hypertension in 10, psychiatric disorders in 8, hyperlipidemia in 6, and diabetes in 3 patients. All of these conditions, except the hepatitis C infections, were treated within the year.
In addition, 74% of patients had previously diagnosed chronic medical conditions, but 70% of the 172 previously identified diagnoses were not being treated at the time they sought help for opioid dependence.
Major Finding: Treating opioid dependence in primary care offices identified new chronic medical problems in 36 (27%) of 135 patients and led to initiation of treatment in 70% of 172 previously known chronic medical problems that were not being treated.
Data Source: Retrospective review of patients presenting to a primary care clinic for treatment of opioid dependence who received a prescription for sublingual buprenorphine.
Disclosures: Dr. Rowe said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO – Treating patients for opioid dependence with sublingual buprenorphine in a primary care clinic helped providers identify chronic medical conditions that were not being treated.
Among 135 new patients who presented to a primary care office for help with opioid dependence and who received a prescription for sublingual buprenorphine within a month of their visit, 69% had no primary care provider until that visit. Newly diagnosed chronic medical conditions were identified in 36 (27%) of patients, Dr. Theresa Rowe reported in a poster presentation at the annual meeting of the American Society of Addiction Medicine.
Patients started treatment for 41 (95%) of 43 newly diagnosed chronic medical conditions within a year, said Dr. Rowe of Johns Hopkins University, and her study associate, Dr. Darius Rastegar, of the Johns Hopkins Bayview Medical Center, both in Baltimore.
The most common new diagnoses were hepatitis C in 11 patients, hypertension in 10, psychiatric disorders in 8, hyperlipidemia in 6, and diabetes in 3 patients. All of these conditions, except the hepatitis C infections, were treated within the year.
In addition, 74% of patients had previously diagnosed chronic medical conditions, but 70% of the 172 previously identified diagnoses were not being treated at the time they sought help for opioid dependence.
Major Finding: Treating opioid dependence in primary care offices identified new chronic medical problems in 36 (27%) of 135 patients and led to initiation of treatment in 70% of 172 previously known chronic medical problems that were not being treated.
Data Source: Retrospective review of patients presenting to a primary care clinic for treatment of opioid dependence who received a prescription for sublingual buprenorphine.
Disclosures: Dr. Rowe said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO – Treating patients for opioid dependence with sublingual buprenorphine in a primary care clinic helped providers identify chronic medical conditions that were not being treated.
Among 135 new patients who presented to a primary care office for help with opioid dependence and who received a prescription for sublingual buprenorphine within a month of their visit, 69% had no primary care provider until that visit. Newly diagnosed chronic medical conditions were identified in 36 (27%) of patients, Dr. Theresa Rowe reported in a poster presentation at the annual meeting of the American Society of Addiction Medicine.
Patients started treatment for 41 (95%) of 43 newly diagnosed chronic medical conditions within a year, said Dr. Rowe of Johns Hopkins University, and her study associate, Dr. Darius Rastegar, of the Johns Hopkins Bayview Medical Center, both in Baltimore.
The most common new diagnoses were hepatitis C in 11 patients, hypertension in 10, psychiatric disorders in 8, hyperlipidemia in 6, and diabetes in 3 patients. All of these conditions, except the hepatitis C infections, were treated within the year.
In addition, 74% of patients had previously diagnosed chronic medical conditions, but 70% of the 172 previously identified diagnoses were not being treated at the time they sought help for opioid dependence.
Compliance Is Spoiler in Cocaine Dependence Drug Trial
SAN FRANCISCO – A trial of the anticonvulsant vigabatrin to treat cocaine dependence may have failed because the patients weren't taking it, not because the drug didn't work, the study results have shown.
The National Institute on Drug Abuse will repeat the trial, but this time the investigators will try to enroll people who appear motivated to stop cocaine use so that adherence to treatment can be better measured, Dr. Eugene C. Somoza said at the meeting.
“The trial failed, but we don't think that the drug failed,” said Dr. Somoza of the University of Cincinnati. Vigabatrin is currently indicated for adjunctive treatment of complex partial seizures and infantile spasms. The original double-blind, placebo-controlled trial randomized 186 adults with cocaine dependence to 12 weeks of treatment with placebo or 3 g daily of vigabatrin in two divided doses. The investigators assessed cocaine use during the study through patient self-report and measurements of benzoylecgonine, a long-acting metabolite of cocaine in the urine. Cocaine use did not differ significantly between the groups, suggesting that vigabatrin failed to decrease use of the drug.
Dr. Somoza said he was “very surprised that it didn't work,” because vigabatrin had decreased cocaine use in a similar study of 103 patients in Mexico. In that study, however, investigators observed patients ingesting the drug on 29% of the treatment days. The American study relied on pill counts and patient self-reports to measure treatment adherence, which was rated as 85%.
A subsequent analysis of urine samples retained from the study showed that fewer than 40% of 53 patients in the vigabatrin arm who completed the 12-week study had urine drug levels that would indicate adherence to the medication regimen. The subsequent urinalyses suggested that at 5 of the 11 study sites, fewer than half of the patients had taken the medication as prescribed.
After lack of adherence to the treatment regimen was controlled for, the findings indicated that patients who took vigabatrin used less cocaine than did those who were on placebo, Dr. Somoza said.
The Mexican study enrolled participants who were seeking treatment for their cocaine dependence and who may have been more motivated to adhere to treatment than were participants in the American study, he added.
The study was funded by Catalyst Pharmaceutical Partners, which makes the vigabatrin formulation used in the study. Two of Dr. Somoza's research associates in the study work for the company.
SAN FRANCISCO – A trial of the anticonvulsant vigabatrin to treat cocaine dependence may have failed because the patients weren't taking it, not because the drug didn't work, the study results have shown.
The National Institute on Drug Abuse will repeat the trial, but this time the investigators will try to enroll people who appear motivated to stop cocaine use so that adherence to treatment can be better measured, Dr. Eugene C. Somoza said at the meeting.
“The trial failed, but we don't think that the drug failed,” said Dr. Somoza of the University of Cincinnati. Vigabatrin is currently indicated for adjunctive treatment of complex partial seizures and infantile spasms. The original double-blind, placebo-controlled trial randomized 186 adults with cocaine dependence to 12 weeks of treatment with placebo or 3 g daily of vigabatrin in two divided doses. The investigators assessed cocaine use during the study through patient self-report and measurements of benzoylecgonine, a long-acting metabolite of cocaine in the urine. Cocaine use did not differ significantly between the groups, suggesting that vigabatrin failed to decrease use of the drug.
Dr. Somoza said he was “very surprised that it didn't work,” because vigabatrin had decreased cocaine use in a similar study of 103 patients in Mexico. In that study, however, investigators observed patients ingesting the drug on 29% of the treatment days. The American study relied on pill counts and patient self-reports to measure treatment adherence, which was rated as 85%.
A subsequent analysis of urine samples retained from the study showed that fewer than 40% of 53 patients in the vigabatrin arm who completed the 12-week study had urine drug levels that would indicate adherence to the medication regimen. The subsequent urinalyses suggested that at 5 of the 11 study sites, fewer than half of the patients had taken the medication as prescribed.
After lack of adherence to the treatment regimen was controlled for, the findings indicated that patients who took vigabatrin used less cocaine than did those who were on placebo, Dr. Somoza said.
The Mexican study enrolled participants who were seeking treatment for their cocaine dependence and who may have been more motivated to adhere to treatment than were participants in the American study, he added.
The study was funded by Catalyst Pharmaceutical Partners, which makes the vigabatrin formulation used in the study. Two of Dr. Somoza's research associates in the study work for the company.
SAN FRANCISCO – A trial of the anticonvulsant vigabatrin to treat cocaine dependence may have failed because the patients weren't taking it, not because the drug didn't work, the study results have shown.
The National Institute on Drug Abuse will repeat the trial, but this time the investigators will try to enroll people who appear motivated to stop cocaine use so that adherence to treatment can be better measured, Dr. Eugene C. Somoza said at the meeting.
“The trial failed, but we don't think that the drug failed,” said Dr. Somoza of the University of Cincinnati. Vigabatrin is currently indicated for adjunctive treatment of complex partial seizures and infantile spasms. The original double-blind, placebo-controlled trial randomized 186 adults with cocaine dependence to 12 weeks of treatment with placebo or 3 g daily of vigabatrin in two divided doses. The investigators assessed cocaine use during the study through patient self-report and measurements of benzoylecgonine, a long-acting metabolite of cocaine in the urine. Cocaine use did not differ significantly between the groups, suggesting that vigabatrin failed to decrease use of the drug.
Dr. Somoza said he was “very surprised that it didn't work,” because vigabatrin had decreased cocaine use in a similar study of 103 patients in Mexico. In that study, however, investigators observed patients ingesting the drug on 29% of the treatment days. The American study relied on pill counts and patient self-reports to measure treatment adherence, which was rated as 85%.
A subsequent analysis of urine samples retained from the study showed that fewer than 40% of 53 patients in the vigabatrin arm who completed the 12-week study had urine drug levels that would indicate adherence to the medication regimen. The subsequent urinalyses suggested that at 5 of the 11 study sites, fewer than half of the patients had taken the medication as prescribed.
After lack of adherence to the treatment regimen was controlled for, the findings indicated that patients who took vigabatrin used less cocaine than did those who were on placebo, Dr. Somoza said.
The Mexican study enrolled participants who were seeking treatment for their cocaine dependence and who may have been more motivated to adhere to treatment than were participants in the American study, he added.
The study was funded by Catalyst Pharmaceutical Partners, which makes the vigabatrin formulation used in the study. Two of Dr. Somoza's research associates in the study work for the company.
HPV Vaccine Reduced Abnormal Pap Results
SAN FRANCISCO - A vaccine for human papillomavirus decreased the risk for cytologic abnormalities over a 3-year period by 56%-68%, compared with placebo vaccine, a secondary analysis of data on 17,347 women in a phase III clinical trial found.
The analysis looked at vaccination with all three doses of Cervarix, the atropine sulfate–adjuvanted vaccine for human papillomavirus types 16 and 18 (HPV-16/18), in 8,665 young, predominantly sexually active women compared with a control group of 8,682 women who got hepatitis A vaccine.
The primary results of the Papilloma Trial Against Cancer in Young Adults (PATRICIA), reported last year, showed that the vaccine was highly prophylactic against grade II cervical intraepithelial neoplasia (CIN2) associated with HPV-16/18 and against several oncogenic non-vaccine types of HPV (Lancet 2009;374:301-14).
Dr. Mark G. Martens reported at the meeting on a secondary end point built into the PATRICIA trial to assess vaccine efficacy in preventing abnormal Pap smear results and subsequent reduction in colposcopy referrals and cervical excision procedures.
Cervical samples were collected every 6 months for HPV DNA genotyping, and the women underwent yearly gynecology and cytologic examinations. The rate of atypical squamous cells of undetermined significance (ASCUS) with HPV-16/18 was 57% lower in the vaccine group compared with the control group during 3 years of follow-up, said Dr. Martens, who conducted the analysis while at Oklahoma State University, Tulsa, and now practices at Jersey Shore University Medical Center, Neptune, N.J.
The rate of low-grade squamous intraepithelial lesions (LSILs) with HPV-16/18 was 68% lower than in the control group, and the rate of high-grade squamous intraepithelial lesions (HSILs) with HPV-16/18 was 56% lower than in the control group, he said.
Absolute rates of ASCUS with HPV-16/18 were 2% in the vaccine group and 4% in the control group (percentages are rounded). LSILs with HPV-16/18 were detected in 2% of the vaccine group and 6% of the control group. HSILs with HPV-16/18 were present in 0.2% of the vaccine group and 0.5% of the control group.
There was a statistically significant difference between groups for HSILs with HPV-16 (0.1% in the vaccine group vs. 0.4% in the control group) but not for HSILs with HPV-18 (0.05% and 0.1%).
Irrespective of HPV type, the vaccine reduced the risk for ASCUS by 8%, the risk for LSILs by 14%, and the risk for HSILs by 41%, he added.
The risk for CIN2 and CIN3 was 30% and 33% lower than in the control group. “That means the lesions we’re going to act upon”— HSILs, CIN2 and CIN3—“were 30%-40% lower with the vaccine,” Dr. Martens said.
HSILs were found in 0.5% of the vaccine group, irrespective of HPV type, and 0.9% of the control group. CIN2 was detected in 2.5% of the vaccine group and 3.7% of the control group. The rate of CIN3 was 0.8% in the vaccine group and 1.3% in the control group.
Compared with the control group, colposcopy referrals were reduced by 10% and cervical excision procedures were reduced by 25% in the vaccine group, he reported.
Dr. Martens said he did an extra calculation for one state—Ohio—and estimated that each physician performing Pap smears in the state would see 20 fewer cases of CIN2/3 per year if patients were vaccinated. Nationally, the vaccine could result in 5 million fewer Pap smears per year because there would be less abnormal cytology, he added.
Women were included in the analysis regardless of their HPV DNA status, HPV serostatus, or cytology at baseline. Evidence of past or current infection with HPV-16/18 was present at baseline in 26% of women, but only 98 participants (less than 1%) were DNA positive for both HPV-16 and HPV-18.
SAN FRANCISCO - A vaccine for human papillomavirus decreased the risk for cytologic abnormalities over a 3-year period by 56%-68%, compared with placebo vaccine, a secondary analysis of data on 17,347 women in a phase III clinical trial found.
The analysis looked at vaccination with all three doses of Cervarix, the atropine sulfate–adjuvanted vaccine for human papillomavirus types 16 and 18 (HPV-16/18), in 8,665 young, predominantly sexually active women compared with a control group of 8,682 women who got hepatitis A vaccine.
The primary results of the Papilloma Trial Against Cancer in Young Adults (PATRICIA), reported last year, showed that the vaccine was highly prophylactic against grade II cervical intraepithelial neoplasia (CIN2) associated with HPV-16/18 and against several oncogenic non-vaccine types of HPV (Lancet 2009;374:301-14).
Dr. Mark G. Martens reported at the meeting on a secondary end point built into the PATRICIA trial to assess vaccine efficacy in preventing abnormal Pap smear results and subsequent reduction in colposcopy referrals and cervical excision procedures.
Cervical samples were collected every 6 months for HPV DNA genotyping, and the women underwent yearly gynecology and cytologic examinations. The rate of atypical squamous cells of undetermined significance (ASCUS) with HPV-16/18 was 57% lower in the vaccine group compared with the control group during 3 years of follow-up, said Dr. Martens, who conducted the analysis while at Oklahoma State University, Tulsa, and now practices at Jersey Shore University Medical Center, Neptune, N.J.
The rate of low-grade squamous intraepithelial lesions (LSILs) with HPV-16/18 was 68% lower than in the control group, and the rate of high-grade squamous intraepithelial lesions (HSILs) with HPV-16/18 was 56% lower than in the control group, he said.
Absolute rates of ASCUS with HPV-16/18 were 2% in the vaccine group and 4% in the control group (percentages are rounded). LSILs with HPV-16/18 were detected in 2% of the vaccine group and 6% of the control group. HSILs with HPV-16/18 were present in 0.2% of the vaccine group and 0.5% of the control group.
There was a statistically significant difference between groups for HSILs with HPV-16 (0.1% in the vaccine group vs. 0.4% in the control group) but not for HSILs with HPV-18 (0.05% and 0.1%).
Irrespective of HPV type, the vaccine reduced the risk for ASCUS by 8%, the risk for LSILs by 14%, and the risk for HSILs by 41%, he added.
The risk for CIN2 and CIN3 was 30% and 33% lower than in the control group. “That means the lesions we’re going to act upon”— HSILs, CIN2 and CIN3—“were 30%-40% lower with the vaccine,” Dr. Martens said.
HSILs were found in 0.5% of the vaccine group, irrespective of HPV type, and 0.9% of the control group. CIN2 was detected in 2.5% of the vaccine group and 3.7% of the control group. The rate of CIN3 was 0.8% in the vaccine group and 1.3% in the control group.
Compared with the control group, colposcopy referrals were reduced by 10% and cervical excision procedures were reduced by 25% in the vaccine group, he reported.
Dr. Martens said he did an extra calculation for one state—Ohio—and estimated that each physician performing Pap smears in the state would see 20 fewer cases of CIN2/3 per year if patients were vaccinated. Nationally, the vaccine could result in 5 million fewer Pap smears per year because there would be less abnormal cytology, he added.
Women were included in the analysis regardless of their HPV DNA status, HPV serostatus, or cytology at baseline. Evidence of past or current infection with HPV-16/18 was present at baseline in 26% of women, but only 98 participants (less than 1%) were DNA positive for both HPV-16 and HPV-18.
SAN FRANCISCO - A vaccine for human papillomavirus decreased the risk for cytologic abnormalities over a 3-year period by 56%-68%, compared with placebo vaccine, a secondary analysis of data on 17,347 women in a phase III clinical trial found.
The analysis looked at vaccination with all three doses of Cervarix, the atropine sulfate–adjuvanted vaccine for human papillomavirus types 16 and 18 (HPV-16/18), in 8,665 young, predominantly sexually active women compared with a control group of 8,682 women who got hepatitis A vaccine.
The primary results of the Papilloma Trial Against Cancer in Young Adults (PATRICIA), reported last year, showed that the vaccine was highly prophylactic against grade II cervical intraepithelial neoplasia (CIN2) associated with HPV-16/18 and against several oncogenic non-vaccine types of HPV (Lancet 2009;374:301-14).
Dr. Mark G. Martens reported at the meeting on a secondary end point built into the PATRICIA trial to assess vaccine efficacy in preventing abnormal Pap smear results and subsequent reduction in colposcopy referrals and cervical excision procedures.
Cervical samples were collected every 6 months for HPV DNA genotyping, and the women underwent yearly gynecology and cytologic examinations. The rate of atypical squamous cells of undetermined significance (ASCUS) with HPV-16/18 was 57% lower in the vaccine group compared with the control group during 3 years of follow-up, said Dr. Martens, who conducted the analysis while at Oklahoma State University, Tulsa, and now practices at Jersey Shore University Medical Center, Neptune, N.J.
The rate of low-grade squamous intraepithelial lesions (LSILs) with HPV-16/18 was 68% lower than in the control group, and the rate of high-grade squamous intraepithelial lesions (HSILs) with HPV-16/18 was 56% lower than in the control group, he said.
Absolute rates of ASCUS with HPV-16/18 were 2% in the vaccine group and 4% in the control group (percentages are rounded). LSILs with HPV-16/18 were detected in 2% of the vaccine group and 6% of the control group. HSILs with HPV-16/18 were present in 0.2% of the vaccine group and 0.5% of the control group.
There was a statistically significant difference between groups for HSILs with HPV-16 (0.1% in the vaccine group vs. 0.4% in the control group) but not for HSILs with HPV-18 (0.05% and 0.1%).
Irrespective of HPV type, the vaccine reduced the risk for ASCUS by 8%, the risk for LSILs by 14%, and the risk for HSILs by 41%, he added.
The risk for CIN2 and CIN3 was 30% and 33% lower than in the control group. “That means the lesions we’re going to act upon”— HSILs, CIN2 and CIN3—“were 30%-40% lower with the vaccine,” Dr. Martens said.
HSILs were found in 0.5% of the vaccine group, irrespective of HPV type, and 0.9% of the control group. CIN2 was detected in 2.5% of the vaccine group and 3.7% of the control group. The rate of CIN3 was 0.8% in the vaccine group and 1.3% in the control group.
Compared with the control group, colposcopy referrals were reduced by 10% and cervical excision procedures were reduced by 25% in the vaccine group, he reported.
Dr. Martens said he did an extra calculation for one state—Ohio—and estimated that each physician performing Pap smears in the state would see 20 fewer cases of CIN2/3 per year if patients were vaccinated. Nationally, the vaccine could result in 5 million fewer Pap smears per year because there would be less abnormal cytology, he added.
Women were included in the analysis regardless of their HPV DNA status, HPV serostatus, or cytology at baseline. Evidence of past or current infection with HPV-16/18 was present at baseline in 26% of women, but only 98 participants (less than 1%) were DNA positive for both HPV-16 and HPV-18.
From the annual meeting of the American College of Obstetricians and Gynecologists.
Major Finding: The atropine sulfate–adjuvanted vaccine for human papillomavirus types 16 and 18 (Cervarix) significantly reduced the risk of abnormal Pap test results over a 3-year period by 56%-68% depending on the type of abnormality.
Data Source: Secondary analysis of data on 17,347 women from a phase III efficacy trial in 14 countries.
Disclosures: Dr. Martens has been a consultant for and received research funds, honoraria, and conference sponsorship from Merck & Co. and from GlaxoSmithKline Biologicals, which makes the vaccine and funded the study.
Saucerization Advocated for Atypical Pigmented Lesion
Monterey, Calif. — When Dr. Kenneth G. Gross wants to biopsy an atypical pigmented lesion, he reaches for an old-fashioned razor blade.
Not for a shave biopsy, mind you. He prefers a saucerization biopsy to a shave, punch, or blunt excisional biopsy for these lesions.
“The reason I prefer saucerization for atypical pigmented lesions—and even more for lentigo maligna—is that it takes the least amount of normal tissue. It allows the smallest wide re-excision. It’s fast. It’s easy—there’s no undermining—and it gives adequate histostaging,” he said at the annual meeting of the American Society for Mohs Surgery
He also likes that it requires the biopsy-taker to “engage your brain before you engage your blade,” said Dr. Gross, a dermatologic surgeon practicing in San Diego. “You’ve got to ask yourself, what information do I need to histostage this lesion?” to decide how you’ll bend the razor blade to get the depth and shape of biopsy required to provide the needed information.
A saucerization biopsy leaves a round defect that heals by secondary intention, and the lack of undermining makes wide re-excision relatively simple. A blunt excisional biopsy, on the other hand, takes longer, may violate the deep tissue plane that’s optimal for wide re-excision, and magnifies the size of the eventual wide re-excision.
“Are you really doing your patient a favor to take an excisional biopsy down to the base of the fat? Do you really need to go that far? To me, the answer is, ‘No,’ ” he said.
For his saucerization biopsies, Dr. Gross uses Personna stainless steel, double-edge prep blades designed for old-fashioned razors. Fold the two-blade package in half before opening, and the blades snap in half, providing one blunt edge to hold and a sharp edge for cutting.
“The nice thing about these little blades is that they’re sterile when they come out of the factory, and I have yet to see an infection in a biopsy site using these,” he said.
Fold the blade to any degree desired to do a very small, deep biopsy—“almost like a punch” biopsy—or a wider or more shallow biopsy, he explained. “For a lesion like lentigo maligna, you want a larger but more superficial biopsy.”
To avoid “flipping” a biopsy specimen, unbend the blade and lay it flat immediately after taking the specimen. “I’ve never flipped one yet,” he said.
On one patient with what looked on dermoscopy like a superficial spreading malignant melanoma, Dr. Gross took a saucerization biopsy with a 1- to 2-mm margin down to the middermis. Under the microscope, it looked to be a 0.7-mm superficial melanoma, so he did a wide re-excision. There was no residual tumor on the pathology report, “nor would I expect there to be any residual melanoma in most of these, because this is a saucerization-type excisional biopsy, if you will. It’s not a shave biopsy,” Dr. Gross said.
Razors are not only sharper than scalpel blades, they’re easier to use and can be curved either up or down for convex or concave surfaces, he added. The blades can be used virtually anywhere on the skin, on any type of tissue, to get specimens that are adequate for both diagnosis and histostaging.
Another patient had a lesion in the nail bed. “The patient has had this dystrophic nail for a while, notes some changes in the base, and I want to do a matrix biopsy. I want to see if there is any squamous cell carcinoma going on here,” Dr. Gross explains. “This is really simple task with this blade. I can fold it to any depth I want, any width. It is a simple, quick procedure.”
A small, not-so-deep saucerization biopsy was adequate for another patient with an atypical nevus that was growing and changing rapidly but looked like a benign lesion, and proved to be so. With the saucerization, though, “we’ve got enough depth here to make the diagnosis, and if it were melanoma, to do histostaging,” he noted.
Disclosures: Dr. Gross said he has no pertinent conflicts of interest.
Monterey, Calif. — When Dr. Kenneth G. Gross wants to biopsy an atypical pigmented lesion, he reaches for an old-fashioned razor blade.
Not for a shave biopsy, mind you. He prefers a saucerization biopsy to a shave, punch, or blunt excisional biopsy for these lesions.
“The reason I prefer saucerization for atypical pigmented lesions—and even more for lentigo maligna—is that it takes the least amount of normal tissue. It allows the smallest wide re-excision. It’s fast. It’s easy—there’s no undermining—and it gives adequate histostaging,” he said at the annual meeting of the American Society for Mohs Surgery
He also likes that it requires the biopsy-taker to “engage your brain before you engage your blade,” said Dr. Gross, a dermatologic surgeon practicing in San Diego. “You’ve got to ask yourself, what information do I need to histostage this lesion?” to decide how you’ll bend the razor blade to get the depth and shape of biopsy required to provide the needed information.
A saucerization biopsy leaves a round defect that heals by secondary intention, and the lack of undermining makes wide re-excision relatively simple. A blunt excisional biopsy, on the other hand, takes longer, may violate the deep tissue plane that’s optimal for wide re-excision, and magnifies the size of the eventual wide re-excision.
“Are you really doing your patient a favor to take an excisional biopsy down to the base of the fat? Do you really need to go that far? To me, the answer is, ‘No,’ ” he said.
For his saucerization biopsies, Dr. Gross uses Personna stainless steel, double-edge prep blades designed for old-fashioned razors. Fold the two-blade package in half before opening, and the blades snap in half, providing one blunt edge to hold and a sharp edge for cutting.
“The nice thing about these little blades is that they’re sterile when they come out of the factory, and I have yet to see an infection in a biopsy site using these,” he said.
Fold the blade to any degree desired to do a very small, deep biopsy—“almost like a punch” biopsy—or a wider or more shallow biopsy, he explained. “For a lesion like lentigo maligna, you want a larger but more superficial biopsy.”
To avoid “flipping” a biopsy specimen, unbend the blade and lay it flat immediately after taking the specimen. “I’ve never flipped one yet,” he said.
On one patient with what looked on dermoscopy like a superficial spreading malignant melanoma, Dr. Gross took a saucerization biopsy with a 1- to 2-mm margin down to the middermis. Under the microscope, it looked to be a 0.7-mm superficial melanoma, so he did a wide re-excision. There was no residual tumor on the pathology report, “nor would I expect there to be any residual melanoma in most of these, because this is a saucerization-type excisional biopsy, if you will. It’s not a shave biopsy,” Dr. Gross said.
Razors are not only sharper than scalpel blades, they’re easier to use and can be curved either up or down for convex or concave surfaces, he added. The blades can be used virtually anywhere on the skin, on any type of tissue, to get specimens that are adequate for both diagnosis and histostaging.
Another patient had a lesion in the nail bed. “The patient has had this dystrophic nail for a while, notes some changes in the base, and I want to do a matrix biopsy. I want to see if there is any squamous cell carcinoma going on here,” Dr. Gross explains. “This is really simple task with this blade. I can fold it to any depth I want, any width. It is a simple, quick procedure.”
A small, not-so-deep saucerization biopsy was adequate for another patient with an atypical nevus that was growing and changing rapidly but looked like a benign lesion, and proved to be so. With the saucerization, though, “we’ve got enough depth here to make the diagnosis, and if it were melanoma, to do histostaging,” he noted.
Disclosures: Dr. Gross said he has no pertinent conflicts of interest.
Monterey, Calif. — When Dr. Kenneth G. Gross wants to biopsy an atypical pigmented lesion, he reaches for an old-fashioned razor blade.
Not for a shave biopsy, mind you. He prefers a saucerization biopsy to a shave, punch, or blunt excisional biopsy for these lesions.
“The reason I prefer saucerization for atypical pigmented lesions—and even more for lentigo maligna—is that it takes the least amount of normal tissue. It allows the smallest wide re-excision. It’s fast. It’s easy—there’s no undermining—and it gives adequate histostaging,” he said at the annual meeting of the American Society for Mohs Surgery
He also likes that it requires the biopsy-taker to “engage your brain before you engage your blade,” said Dr. Gross, a dermatologic surgeon practicing in San Diego. “You’ve got to ask yourself, what information do I need to histostage this lesion?” to decide how you’ll bend the razor blade to get the depth and shape of biopsy required to provide the needed information.
A saucerization biopsy leaves a round defect that heals by secondary intention, and the lack of undermining makes wide re-excision relatively simple. A blunt excisional biopsy, on the other hand, takes longer, may violate the deep tissue plane that’s optimal for wide re-excision, and magnifies the size of the eventual wide re-excision.
“Are you really doing your patient a favor to take an excisional biopsy down to the base of the fat? Do you really need to go that far? To me, the answer is, ‘No,’ ” he said.
For his saucerization biopsies, Dr. Gross uses Personna stainless steel, double-edge prep blades designed for old-fashioned razors. Fold the two-blade package in half before opening, and the blades snap in half, providing one blunt edge to hold and a sharp edge for cutting.
“The nice thing about these little blades is that they’re sterile when they come out of the factory, and I have yet to see an infection in a biopsy site using these,” he said.
Fold the blade to any degree desired to do a very small, deep biopsy—“almost like a punch” biopsy—or a wider or more shallow biopsy, he explained. “For a lesion like lentigo maligna, you want a larger but more superficial biopsy.”
To avoid “flipping” a biopsy specimen, unbend the blade and lay it flat immediately after taking the specimen. “I’ve never flipped one yet,” he said.
On one patient with what looked on dermoscopy like a superficial spreading malignant melanoma, Dr. Gross took a saucerization biopsy with a 1- to 2-mm margin down to the middermis. Under the microscope, it looked to be a 0.7-mm superficial melanoma, so he did a wide re-excision. There was no residual tumor on the pathology report, “nor would I expect there to be any residual melanoma in most of these, because this is a saucerization-type excisional biopsy, if you will. It’s not a shave biopsy,” Dr. Gross said.
Razors are not only sharper than scalpel blades, they’re easier to use and can be curved either up or down for convex or concave surfaces, he added. The blades can be used virtually anywhere on the skin, on any type of tissue, to get specimens that are adequate for both diagnosis and histostaging.
Another patient had a lesion in the nail bed. “The patient has had this dystrophic nail for a while, notes some changes in the base, and I want to do a matrix biopsy. I want to see if there is any squamous cell carcinoma going on here,” Dr. Gross explains. “This is really simple task with this blade. I can fold it to any depth I want, any width. It is a simple, quick procedure.”
A small, not-so-deep saucerization biopsy was adequate for another patient with an atypical nevus that was growing and changing rapidly but looked like a benign lesion, and proved to be so. With the saucerization, though, “we’ve got enough depth here to make the diagnosis, and if it were melanoma, to do histostaging,” he noted.
Disclosures: Dr. Gross said he has no pertinent conflicts of interest.
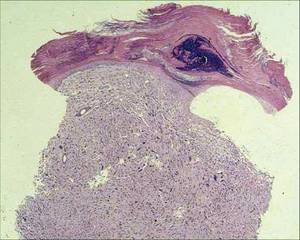
Deadly Doppelganger for Atypical Fibroxanthoma
Monterey, Calif. - If there is a doppelganger in dermatology, malignant fibrous histiocytoma is it, according to Dr. Henry W. Randle at a meeting of the American Society for Mohs Surgery.
By immunohistochemistry, MFH is a dead ringer for atypical fibroxanthoma (AFX). Compared with rare mortality from AFX, however, approximately 38% of patients with MFH die within 3.5 years, said Dr. Randle.

Histologically, we can’t tell them apart. They look the same, but they behave very differently,” and require different treatment approaches, said Dr. Randle of the Mayo Clinic, Jacksonville, Fla.
The two main treatments for AFX are excision with a 1- to 2-cm margin that includes subcutaneous tissue or Mohs surgery.
For MFH, treatment involves tumor staging and wide excision to several centimeters, with consideration of node dissection, radiation, and chemotherapy. Mohs surgery is not the best option. “You’re brave if you do that” for MFH, he said. “This is a different animal.”
The problem lies in telling the two apart. Even the histologic diagnosis of AFX can be challenging, because no specific marker or test exists to identify AFX. Diagnosis requires excluding spindle cell squamous cell carcinomas, melanomas of the spindle cells, and other spindle cell malignancies.

The only identifiable characteristics that separate the relatively innocuous AFX from the more lethal MFH are the more superficial location of AFX and the fact that AFX typically appears on the head and neck, whereas MFH more typically occurs on the extremities and trunk, but not on the face.
A recent retrospective series of 89 patients with a histologic diagnosis of AFX claimed that no patients developed metastases, but that was because the authors decided not to include three cases with metastases because they acted differently from the other 86, Dr. Randle noted (Derm. Surg. 2009;35:765-772). Had the authors included those three cases, the metastases rate would be 3%.
“It is this small subset that is the problem,” he said.
Dr. Randle reserves the term AFX for small tumors that are less than 1.5 cm in diameter, that are based in the dermis and do not extend into the fat, and that occur in sun-damaged skin with no more than minimal involvement of the subcutis. Any diagnosis of AFX that did not analyze subcutaneous tissue with some fat has the potential for regional or distant spread, and may not be AFX, he said.
Consider the tumor to be MFH or another spindle cell tumor if it extends into the subcutis, shows vascular invasion, or has tumor necrosis, which does not occur with AFX. “I do not do Mohs if it has these features,” Dr. Randle said.
Visually, AFX usually looks like a rapidly growing red nodule, often ulcerated, on the sun-damaged head or neck skin of an elderly patient. It is twice as common in men as in women. Histologically, it’s a nonencapsulated cellular tumor, contiguous with the epidermis, with pleomorphic and atypical cells. It often has spindle-shaped cells with prominent, vesicular nuclei.
Reported recurrence rates range from 7% to 12% depending on the type of surgical treatment. Rare metastases in the regional node typically come from large, deep, recurrent tumors that are inadequately excised. In Dr. Randle’s personal experience with 56 AFX tumors in the past 20 years, 4 recurred (7%), one with metastasis. For MFH, the reported recurrence rate is 43%, he added.
Patients who have undergone organ transplants have higher prevalences of both AFX and MFH.
Disclosures: Dr. Randle reported having no relevant conflicts of interest.
Monterey, Calif. - If there is a doppelganger in dermatology, malignant fibrous histiocytoma is it, according to Dr. Henry W. Randle at a meeting of the American Society for Mohs Surgery.
By immunohistochemistry, MFH is a dead ringer for atypical fibroxanthoma (AFX). Compared with rare mortality from AFX, however, approximately 38% of patients with MFH die within 3.5 years, said Dr. Randle.
Histologically, we can’t tell them apart. They look the same, but they behave very differently,” and require different treatment approaches, said Dr. Randle of the Mayo Clinic, Jacksonville, Fla.
The two main treatments for AFX are excision with a 1- to 2-cm margin that includes subcutaneous tissue or Mohs surgery.
For MFH, treatment involves tumor staging and wide excision to several centimeters, with consideration of node dissection, radiation, and chemotherapy. Mohs surgery is not the best option. “You’re brave if you do that” for MFH, he said. “This is a different animal.”
The problem lies in telling the two apart. Even the histologic diagnosis of AFX can be challenging, because no specific marker or test exists to identify AFX. Diagnosis requires excluding spindle cell squamous cell carcinomas, melanomas of the spindle cells, and other spindle cell malignancies.
The only identifiable characteristics that separate the relatively innocuous AFX from the more lethal MFH are the more superficial location of AFX and the fact that AFX typically appears on the head and neck, whereas MFH more typically occurs on the extremities and trunk, but not on the face.
A recent retrospective series of 89 patients with a histologic diagnosis of AFX claimed that no patients developed metastases, but that was because the authors decided not to include three cases with metastases because they acted differently from the other 86, Dr. Randle noted (Derm. Surg. 2009;35:765-772). Had the authors included those three cases, the metastases rate would be 3%.
“It is this small subset that is the problem,” he said.
Dr. Randle reserves the term AFX for small tumors that are less than 1.5 cm in diameter, that are based in the dermis and do not extend into the fat, and that occur in sun-damaged skin with no more than minimal involvement of the subcutis. Any diagnosis of AFX that did not analyze subcutaneous tissue with some fat has the potential for regional or distant spread, and may not be AFX, he said.
Consider the tumor to be MFH or another spindle cell tumor if it extends into the subcutis, shows vascular invasion, or has tumor necrosis, which does not occur with AFX. “I do not do Mohs if it has these features,” Dr. Randle said.
Visually, AFX usually looks like a rapidly growing red nodule, often ulcerated, on the sun-damaged head or neck skin of an elderly patient. It is twice as common in men as in women. Histologically, it’s a nonencapsulated cellular tumor, contiguous with the epidermis, with pleomorphic and atypical cells. It often has spindle-shaped cells with prominent, vesicular nuclei.
Reported recurrence rates range from 7% to 12% depending on the type of surgical treatment. Rare metastases in the regional node typically come from large, deep, recurrent tumors that are inadequately excised. In Dr. Randle’s personal experience with 56 AFX tumors in the past 20 years, 4 recurred (7%), one with metastasis. For MFH, the reported recurrence rate is 43%, he added.
Patients who have undergone organ transplants have higher prevalences of both AFX and MFH.
Disclosures: Dr. Randle reported having no relevant conflicts of interest.
Monterey, Calif. - If there is a doppelganger in dermatology, malignant fibrous histiocytoma is it, according to Dr. Henry W. Randle at a meeting of the American Society for Mohs Surgery.
By immunohistochemistry, MFH is a dead ringer for atypical fibroxanthoma (AFX). Compared with rare mortality from AFX, however, approximately 38% of patients with MFH die within 3.5 years, said Dr. Randle.
Histologically, we can’t tell them apart. They look the same, but they behave very differently,” and require different treatment approaches, said Dr. Randle of the Mayo Clinic, Jacksonville, Fla.
The two main treatments for AFX are excision with a 1- to 2-cm margin that includes subcutaneous tissue or Mohs surgery.
For MFH, treatment involves tumor staging and wide excision to several centimeters, with consideration of node dissection, radiation, and chemotherapy. Mohs surgery is not the best option. “You’re brave if you do that” for MFH, he said. “This is a different animal.”
The problem lies in telling the two apart. Even the histologic diagnosis of AFX can be challenging, because no specific marker or test exists to identify AFX. Diagnosis requires excluding spindle cell squamous cell carcinomas, melanomas of the spindle cells, and other spindle cell malignancies.
The only identifiable characteristics that separate the relatively innocuous AFX from the more lethal MFH are the more superficial location of AFX and the fact that AFX typically appears on the head and neck, whereas MFH more typically occurs on the extremities and trunk, but not on the face.
A recent retrospective series of 89 patients with a histologic diagnosis of AFX claimed that no patients developed metastases, but that was because the authors decided not to include three cases with metastases because they acted differently from the other 86, Dr. Randle noted (Derm. Surg. 2009;35:765-772). Had the authors included those three cases, the metastases rate would be 3%.
“It is this small subset that is the problem,” he said.
Dr. Randle reserves the term AFX for small tumors that are less than 1.5 cm in diameter, that are based in the dermis and do not extend into the fat, and that occur in sun-damaged skin with no more than minimal involvement of the subcutis. Any diagnosis of AFX that did not analyze subcutaneous tissue with some fat has the potential for regional or distant spread, and may not be AFX, he said.
Consider the tumor to be MFH or another spindle cell tumor if it extends into the subcutis, shows vascular invasion, or has tumor necrosis, which does not occur with AFX. “I do not do Mohs if it has these features,” Dr. Randle said.
Visually, AFX usually looks like a rapidly growing red nodule, often ulcerated, on the sun-damaged head or neck skin of an elderly patient. It is twice as common in men as in women. Histologically, it’s a nonencapsulated cellular tumor, contiguous with the epidermis, with pleomorphic and atypical cells. It often has spindle-shaped cells with prominent, vesicular nuclei.
Reported recurrence rates range from 7% to 12% depending on the type of surgical treatment. Rare metastases in the regional node typically come from large, deep, recurrent tumors that are inadequately excised. In Dr. Randle’s personal experience with 56 AFX tumors in the past 20 years, 4 recurred (7%), one with metastasis. For MFH, the reported recurrence rate is 43%, he added.
Patients who have undergone organ transplants have higher prevalences of both AFX and MFH.
Disclosures: Dr. Randle reported having no relevant conflicts of interest.
Efficacy of Midurethral Slings Similar After 1 Year
Major Finding: One year after surgery for urinary incontinence with retropubic or transobturator midurethral slings, results were similar in objective cure rates (81% vs. 78%) and subjective cure rates (62% vs. 56%), but various adverse events differed significantly between groups.
Data Source: Randomized, multicenter trial in 597 women.
Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and by the National Institute of Child Health and Human Development. Dr. Richter said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO — One year after surgery for stress urinary incontinence with retropubic or transobturator midurethral slings, objective and subjective cure rates were equivalent for the two approaches but rates of various adverse events differed significantly in a randomized, multicenter trial in 597 women.
“This trial gives us more information regarding equivalency in certain outcomes and gives us much more information regarding how to counsel our patients with respect to choosing treatment” by considering their risks for various adverse events, Dr. Holly E. Richter said at the meeting.
Unadjusted rates for objective cure were 81% for the retropubic group and 78% for the transobturator group. Objective cure rates after the site of surgery was controlled for were 82% for the retropubic group and 80% for the transobturator group, reported Dr. Richter of the University of Alabama at Birmingham. Objective cure was defined as a negative stress test result, a negative 24-hour pad test result, and no retreatment.
Subjective cure rates were 62% in the retropubic group and 56% in the transobturator group, both for the unadjusted rate and after the surgery site was controlled for. Subjective cure was defined as no patient reports of stress urinary incontinence symptoms, no leakage episodes in a 3-day voiding diary, and no retreatment.
Patient satisfaction was similar between groups—86% with retropubic midurethral sling and 90% with transobturator midurethral sling, Dr. Richter and her associates in the Urinary Incontinence Treatment Network found.
Adverse events that occurred significantly more often in the retropubic group compared with the transobturator group included voiding dysfunction requiring surgical intervention (9 events vs. none), and postoperative urinary tract infection (46 events vs. 27). Only patients in the retropubic group had bladder perforations—15 events vs. none in the transobturator group, Dr. Richter reported.
Adverse events that occurred significantly more often in the transobturator group than in the retropubic group included neurologic symptoms (31 events vs. 15), with the majority in the upper leg (20 and 4 events, respectively). Vaginal perforations were more likely in the transobturator group—13 events vs. 6—with in-to-out perforations more common (10 and 3 events) than out-to-in perforations.
“What this trial gives us is more information with which to counsel our patients and individualize treatment. There may be some patients, for example, that have some baseline neurologic symptoms, and you want to stay away from a transobturator approach. And there may be some women, for example, that are Valsalva voiders. They have a problem with voiding after a sling procedure, and you may want to stay away from a retropubic approach,” Dr. Richter said.
Women could enroll in the trial if they had predominant stress urinary incontinence symptoms, demonstrated leakage on cough stress tests, and were clinically eligible for both procedures. The only significant difference at baseline between groups was in the mean Valsalva leak point pressure—114 cm of water in the retropubic group vs. 124 cm of water in the transobturator group.
Major Finding: One year after surgery for urinary incontinence with retropubic or transobturator midurethral slings, results were similar in objective cure rates (81% vs. 78%) and subjective cure rates (62% vs. 56%), but various adverse events differed significantly between groups.
Data Source: Randomized, multicenter trial in 597 women.
Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and by the National Institute of Child Health and Human Development. Dr. Richter said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO — One year after surgery for stress urinary incontinence with retropubic or transobturator midurethral slings, objective and subjective cure rates were equivalent for the two approaches but rates of various adverse events differed significantly in a randomized, multicenter trial in 597 women.
“This trial gives us more information regarding equivalency in certain outcomes and gives us much more information regarding how to counsel our patients with respect to choosing treatment” by considering their risks for various adverse events, Dr. Holly E. Richter said at the meeting.
Unadjusted rates for objective cure were 81% for the retropubic group and 78% for the transobturator group. Objective cure rates after the site of surgery was controlled for were 82% for the retropubic group and 80% for the transobturator group, reported Dr. Richter of the University of Alabama at Birmingham. Objective cure was defined as a negative stress test result, a negative 24-hour pad test result, and no retreatment.
Subjective cure rates were 62% in the retropubic group and 56% in the transobturator group, both for the unadjusted rate and after the surgery site was controlled for. Subjective cure was defined as no patient reports of stress urinary incontinence symptoms, no leakage episodes in a 3-day voiding diary, and no retreatment.
Patient satisfaction was similar between groups—86% with retropubic midurethral sling and 90% with transobturator midurethral sling, Dr. Richter and her associates in the Urinary Incontinence Treatment Network found.
Adverse events that occurred significantly more often in the retropubic group compared with the transobturator group included voiding dysfunction requiring surgical intervention (9 events vs. none), and postoperative urinary tract infection (46 events vs. 27). Only patients in the retropubic group had bladder perforations—15 events vs. none in the transobturator group, Dr. Richter reported.
Adverse events that occurred significantly more often in the transobturator group than in the retropubic group included neurologic symptoms (31 events vs. 15), with the majority in the upper leg (20 and 4 events, respectively). Vaginal perforations were more likely in the transobturator group—13 events vs. 6—with in-to-out perforations more common (10 and 3 events) than out-to-in perforations.
“What this trial gives us is more information with which to counsel our patients and individualize treatment. There may be some patients, for example, that have some baseline neurologic symptoms, and you want to stay away from a transobturator approach. And there may be some women, for example, that are Valsalva voiders. They have a problem with voiding after a sling procedure, and you may want to stay away from a retropubic approach,” Dr. Richter said.
Women could enroll in the trial if they had predominant stress urinary incontinence symptoms, demonstrated leakage on cough stress tests, and were clinically eligible for both procedures. The only significant difference at baseline between groups was in the mean Valsalva leak point pressure—114 cm of water in the retropubic group vs. 124 cm of water in the transobturator group.
Major Finding: One year after surgery for urinary incontinence with retropubic or transobturator midurethral slings, results were similar in objective cure rates (81% vs. 78%) and subjective cure rates (62% vs. 56%), but various adverse events differed significantly between groups.
Data Source: Randomized, multicenter trial in 597 women.
Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and by the National Institute of Child Health and Human Development. Dr. Richter said the investigators have no pertinent conflicts of interest.
SAN FRANCISCO — One year after surgery for stress urinary incontinence with retropubic or transobturator midurethral slings, objective and subjective cure rates were equivalent for the two approaches but rates of various adverse events differed significantly in a randomized, multicenter trial in 597 women.
“This trial gives us more information regarding equivalency in certain outcomes and gives us much more information regarding how to counsel our patients with respect to choosing treatment” by considering their risks for various adverse events, Dr. Holly E. Richter said at the meeting.
Unadjusted rates for objective cure were 81% for the retropubic group and 78% for the transobturator group. Objective cure rates after the site of surgery was controlled for were 82% for the retropubic group and 80% for the transobturator group, reported Dr. Richter of the University of Alabama at Birmingham. Objective cure was defined as a negative stress test result, a negative 24-hour pad test result, and no retreatment.
Subjective cure rates were 62% in the retropubic group and 56% in the transobturator group, both for the unadjusted rate and after the surgery site was controlled for. Subjective cure was defined as no patient reports of stress urinary incontinence symptoms, no leakage episodes in a 3-day voiding diary, and no retreatment.
Patient satisfaction was similar between groups—86% with retropubic midurethral sling and 90% with transobturator midurethral sling, Dr. Richter and her associates in the Urinary Incontinence Treatment Network found.
Adverse events that occurred significantly more often in the retropubic group compared with the transobturator group included voiding dysfunction requiring surgical intervention (9 events vs. none), and postoperative urinary tract infection (46 events vs. 27). Only patients in the retropubic group had bladder perforations—15 events vs. none in the transobturator group, Dr. Richter reported.
Adverse events that occurred significantly more often in the transobturator group than in the retropubic group included neurologic symptoms (31 events vs. 15), with the majority in the upper leg (20 and 4 events, respectively). Vaginal perforations were more likely in the transobturator group—13 events vs. 6—with in-to-out perforations more common (10 and 3 events) than out-to-in perforations.
“What this trial gives us is more information with which to counsel our patients and individualize treatment. There may be some patients, for example, that have some baseline neurologic symptoms, and you want to stay away from a transobturator approach. And there may be some women, for example, that are Valsalva voiders. They have a problem with voiding after a sling procedure, and you may want to stay away from a retropubic approach,” Dr. Richter said.
Women could enroll in the trial if they had predominant stress urinary incontinence symptoms, demonstrated leakage on cough stress tests, and were clinically eligible for both procedures. The only significant difference at baseline between groups was in the mean Valsalva leak point pressure—114 cm of water in the retropubic group vs. 124 cm of water in the transobturator group.
From the Annual Meeting of the American College of Obstetricians and Gynecologists
Fortified OC Raised Blood Folate Levels
SAN FRANCISCO — A folate-fortified oral contraceptive significantly improved folate levels in red blood cells and plasma compared with a conventional oral contraceptive after 24 weeks, in a preliminary randomized, double-blind trial of 379 healthy U.S. women seeking contraception.
The study randomized 94 women to take the oral contraceptive Yaz (ethinyl estradiol 0.02 mg plus 3 mg drospirenone) and 285 women to take an experimental version of Yaz that also contained 0.451 mg levomefolate calcium, the calcium salt of L-5-methyltetrahydrofolate, the most prevalent form of dietary folate. During each of six treatment cycles, they got fortified Yaz or conventional Yaz for 24 days, followed by 4 days of levomefolate calcium alone in the fortified group or placebo in the control group.
Seventy women in the control group and 203 in the fortified group completed the 24 weeks of treatment, at which time average red blood cell folate levels were 1,406 nmol/L in the fortified group and 1,024 nmol/L in the control group. Plasma folate levels averaged 61 nmol/L in the fortified group and 41 nmol/L in the control group, Dr. Stephan Bart reported at the meeting.
The differences between groups were statistically significant, said Dr. Bart, a contract researcher at SNBL Clinical Pharmacology Center, Baltimore. Overall rates of adverse events were similar between groups.
The study did not restrict the use of additional folate-containing supplements, and U.S. women generally consume folate-fortified foods, emphasizing that a folate-fortified contraceptive could increase folate levels even in populations already exposed to sources of folate, he noted.
“These results support the concept that folate-fortified oral contraceptives would improve the folate status of all women of childbearing potential,” Dr. Bart said.
Among the women, aged 18-40 years, one or more adverse events were reported in 56% of the fortified group and 57% of the control group. Most adverse events were mild or moderate in intensity and consisted mainly of upper respiratory tract infections (10% of each group) or increases in low-density lipoprotein cholesterol (6% of the fortified group and 9% of the control group), Dr. Bart said.
Disclosures: Bayer Healthcare Pharmaceuticals, which markets Yaz and is developing the folate-fortified version, funded the trial and Dr. Bart's travel to the meeting. His associates in the study all were employees of divisions of Bayer.
SAN FRANCISCO — A folate-fortified oral contraceptive significantly improved folate levels in red blood cells and plasma compared with a conventional oral contraceptive after 24 weeks, in a preliminary randomized, double-blind trial of 379 healthy U.S. women seeking contraception.
The study randomized 94 women to take the oral contraceptive Yaz (ethinyl estradiol 0.02 mg plus 3 mg drospirenone) and 285 women to take an experimental version of Yaz that also contained 0.451 mg levomefolate calcium, the calcium salt of L-5-methyltetrahydrofolate, the most prevalent form of dietary folate. During each of six treatment cycles, they got fortified Yaz or conventional Yaz for 24 days, followed by 4 days of levomefolate calcium alone in the fortified group or placebo in the control group.
Seventy women in the control group and 203 in the fortified group completed the 24 weeks of treatment, at which time average red blood cell folate levels were 1,406 nmol/L in the fortified group and 1,024 nmol/L in the control group. Plasma folate levels averaged 61 nmol/L in the fortified group and 41 nmol/L in the control group, Dr. Stephan Bart reported at the meeting.
The differences between groups were statistically significant, said Dr. Bart, a contract researcher at SNBL Clinical Pharmacology Center, Baltimore. Overall rates of adverse events were similar between groups.
The study did not restrict the use of additional folate-containing supplements, and U.S. women generally consume folate-fortified foods, emphasizing that a folate-fortified contraceptive could increase folate levels even in populations already exposed to sources of folate, he noted.
“These results support the concept that folate-fortified oral contraceptives would improve the folate status of all women of childbearing potential,” Dr. Bart said.
Among the women, aged 18-40 years, one or more adverse events were reported in 56% of the fortified group and 57% of the control group. Most adverse events were mild or moderate in intensity and consisted mainly of upper respiratory tract infections (10% of each group) or increases in low-density lipoprotein cholesterol (6% of the fortified group and 9% of the control group), Dr. Bart said.
Disclosures: Bayer Healthcare Pharmaceuticals, which markets Yaz and is developing the folate-fortified version, funded the trial and Dr. Bart's travel to the meeting. His associates in the study all were employees of divisions of Bayer.
SAN FRANCISCO — A folate-fortified oral contraceptive significantly improved folate levels in red blood cells and plasma compared with a conventional oral contraceptive after 24 weeks, in a preliminary randomized, double-blind trial of 379 healthy U.S. women seeking contraception.
The study randomized 94 women to take the oral contraceptive Yaz (ethinyl estradiol 0.02 mg plus 3 mg drospirenone) and 285 women to take an experimental version of Yaz that also contained 0.451 mg levomefolate calcium, the calcium salt of L-5-methyltetrahydrofolate, the most prevalent form of dietary folate. During each of six treatment cycles, they got fortified Yaz or conventional Yaz for 24 days, followed by 4 days of levomefolate calcium alone in the fortified group or placebo in the control group.
Seventy women in the control group and 203 in the fortified group completed the 24 weeks of treatment, at which time average red blood cell folate levels were 1,406 nmol/L in the fortified group and 1,024 nmol/L in the control group. Plasma folate levels averaged 61 nmol/L in the fortified group and 41 nmol/L in the control group, Dr. Stephan Bart reported at the meeting.
The differences between groups were statistically significant, said Dr. Bart, a contract researcher at SNBL Clinical Pharmacology Center, Baltimore. Overall rates of adverse events were similar between groups.
The study did not restrict the use of additional folate-containing supplements, and U.S. women generally consume folate-fortified foods, emphasizing that a folate-fortified contraceptive could increase folate levels even in populations already exposed to sources of folate, he noted.
“These results support the concept that folate-fortified oral contraceptives would improve the folate status of all women of childbearing potential,” Dr. Bart said.
Among the women, aged 18-40 years, one or more adverse events were reported in 56% of the fortified group and 57% of the control group. Most adverse events were mild or moderate in intensity and consisted mainly of upper respiratory tract infections (10% of each group) or increases in low-density lipoprotein cholesterol (6% of the fortified group and 9% of the control group), Dr. Bart said.
Disclosures: Bayer Healthcare Pharmaceuticals, which markets Yaz and is developing the folate-fortified version, funded the trial and Dr. Bart's travel to the meeting. His associates in the study all were employees of divisions of Bayer.
From The Annual Meeting of the American College of Obstetricians and Gynecologists
Same-Day Discharge Safe in Lap. Hysterectomy
Major Finding: Among 287 patients who underwent supracervical laparoscopic hysterectomy, only 0.7% were readmitted within 48 hours, and 3.4% within 3 months. Among 241 patients who underwent total laparoscopic hysterectomy, only 0.4% were readmitted within 48 hours, and 4.1% within 3 months.
Data Source: Retrospective case series of all women undergoing a laparoscopic hysterectomy for benign indications, performed by ob.gyn. generalists.
Disclosures: None was reported.
SAN FRANCISCO — Only 0.6% of 528 women who were discharged from the hospital the same day that they underwent a laparoscopic hysterectomy were readmitted within 48 hours, and 3.8% were readmitted within 3 months, results of a retrospective study found.
Using previous large studies on hysterectomies as a reference, any readmission rate less than 6% could be considered acceptable, and readmission rates in the current study were significantly lower than that, Dr. Miya Yamamoto reported in a prize-winning poster. Same-day discharge after laparoscopic hysterectomy appears to be safe, and could significantly decrease costs and health care use by eliminating postprocedure hospital stays, she and her colleagues said.
Hysterectomy is the most common gynecologic surgery in the United States, and an increasing number are being performed laparoscopically. No previous large studies have evaluated the safety of same-day discharge after laparoscopic hysterectomy. Many patients are admitted for an overnight hospital stay after the procedure, but a growing number are discharged on the same day, they said.
Dr. Yamamoto of Oakland, Calif., and her associates at Kaiser Permanente Northern California studied records on women at their institutions who underwent a laparoscopic hysterectomy for benign indications in 2007-2009 and were discharged the same day. The surgeries were performed by generalists in ob.gyn. and included 287 supracervical laparoscopic hysterectomies and 241 total laparoscopic hysterectomies. Overall, 1.5% had urgent clinic visits after their hysterectomy and discharge. Four percent visited the emergency department within 48 hours of the procedure, mainly for nausea or vomiting, urinary retention, or pain.
Of patients who underwent supracervical laparoscopic hysterectomy, 0.7% were readmitted within 48 hours, and 3.4% within 3 months. In those who underwent total laparoscopic hysterectomy, 0.4% were readmitted within 48 hours, and 4.1% within 3 months. The two subgroups did not differ significantly in any outcomes.
Records from the hysterectomies showed a mean operating time of 157 minutes, a median estimated blood loss of 50 mL, and a mean uterine weight of 222 g. Hysterectomies were performed because of fibroids in 46% of patients, for menorrhagia in 27%, for pain in 15%, and for other reasons in 12%.
Patients in the current study had a median age of 45 years and a median body mass index of 28 kg/m
Major Finding: Among 287 patients who underwent supracervical laparoscopic hysterectomy, only 0.7% were readmitted within 48 hours, and 3.4% within 3 months. Among 241 patients who underwent total laparoscopic hysterectomy, only 0.4% were readmitted within 48 hours, and 4.1% within 3 months.
Data Source: Retrospective case series of all women undergoing a laparoscopic hysterectomy for benign indications, performed by ob.gyn. generalists.
Disclosures: None was reported.
SAN FRANCISCO — Only 0.6% of 528 women who were discharged from the hospital the same day that they underwent a laparoscopic hysterectomy were readmitted within 48 hours, and 3.8% were readmitted within 3 months, results of a retrospective study found.
Using previous large studies on hysterectomies as a reference, any readmission rate less than 6% could be considered acceptable, and readmission rates in the current study were significantly lower than that, Dr. Miya Yamamoto reported in a prize-winning poster. Same-day discharge after laparoscopic hysterectomy appears to be safe, and could significantly decrease costs and health care use by eliminating postprocedure hospital stays, she and her colleagues said.
Hysterectomy is the most common gynecologic surgery in the United States, and an increasing number are being performed laparoscopically. No previous large studies have evaluated the safety of same-day discharge after laparoscopic hysterectomy. Many patients are admitted for an overnight hospital stay after the procedure, but a growing number are discharged on the same day, they said.
Dr. Yamamoto of Oakland, Calif., and her associates at Kaiser Permanente Northern California studied records on women at their institutions who underwent a laparoscopic hysterectomy for benign indications in 2007-2009 and were discharged the same day. The surgeries were performed by generalists in ob.gyn. and included 287 supracervical laparoscopic hysterectomies and 241 total laparoscopic hysterectomies. Overall, 1.5% had urgent clinic visits after their hysterectomy and discharge. Four percent visited the emergency department within 48 hours of the procedure, mainly for nausea or vomiting, urinary retention, or pain.
Of patients who underwent supracervical laparoscopic hysterectomy, 0.7% were readmitted within 48 hours, and 3.4% within 3 months. In those who underwent total laparoscopic hysterectomy, 0.4% were readmitted within 48 hours, and 4.1% within 3 months. The two subgroups did not differ significantly in any outcomes.
Records from the hysterectomies showed a mean operating time of 157 minutes, a median estimated blood loss of 50 mL, and a mean uterine weight of 222 g. Hysterectomies were performed because of fibroids in 46% of patients, for menorrhagia in 27%, for pain in 15%, and for other reasons in 12%.
Patients in the current study had a median age of 45 years and a median body mass index of 28 kg/m
Major Finding: Among 287 patients who underwent supracervical laparoscopic hysterectomy, only 0.7% were readmitted within 48 hours, and 3.4% within 3 months. Among 241 patients who underwent total laparoscopic hysterectomy, only 0.4% were readmitted within 48 hours, and 4.1% within 3 months.
Data Source: Retrospective case series of all women undergoing a laparoscopic hysterectomy for benign indications, performed by ob.gyn. generalists.
Disclosures: None was reported.
SAN FRANCISCO — Only 0.6% of 528 women who were discharged from the hospital the same day that they underwent a laparoscopic hysterectomy were readmitted within 48 hours, and 3.8% were readmitted within 3 months, results of a retrospective study found.
Using previous large studies on hysterectomies as a reference, any readmission rate less than 6% could be considered acceptable, and readmission rates in the current study were significantly lower than that, Dr. Miya Yamamoto reported in a prize-winning poster. Same-day discharge after laparoscopic hysterectomy appears to be safe, and could significantly decrease costs and health care use by eliminating postprocedure hospital stays, she and her colleagues said.
Hysterectomy is the most common gynecologic surgery in the United States, and an increasing number are being performed laparoscopically. No previous large studies have evaluated the safety of same-day discharge after laparoscopic hysterectomy. Many patients are admitted for an overnight hospital stay after the procedure, but a growing number are discharged on the same day, they said.
Dr. Yamamoto of Oakland, Calif., and her associates at Kaiser Permanente Northern California studied records on women at their institutions who underwent a laparoscopic hysterectomy for benign indications in 2007-2009 and were discharged the same day. The surgeries were performed by generalists in ob.gyn. and included 287 supracervical laparoscopic hysterectomies and 241 total laparoscopic hysterectomies. Overall, 1.5% had urgent clinic visits after their hysterectomy and discharge. Four percent visited the emergency department within 48 hours of the procedure, mainly for nausea or vomiting, urinary retention, or pain.
Of patients who underwent supracervical laparoscopic hysterectomy, 0.7% were readmitted within 48 hours, and 3.4% within 3 months. In those who underwent total laparoscopic hysterectomy, 0.4% were readmitted within 48 hours, and 4.1% within 3 months. The two subgroups did not differ significantly in any outcomes.
Records from the hysterectomies showed a mean operating time of 157 minutes, a median estimated blood loss of 50 mL, and a mean uterine weight of 222 g. Hysterectomies were performed because of fibroids in 46% of patients, for menorrhagia in 27%, for pain in 15%, and for other reasons in 12%.
Patients in the current study had a median age of 45 years and a median body mass index of 28 kg/m
From the Annual Meeting of the American College of Obstetricians and Gynecologists
Cervical Length Measurement Predicts Preterm Delivery
Major Finding: Measurements of vaginal cervical length using a disposable probe were similar to fetal fibronectin tests in predicting the likelihood of preterm delivery in women with threatened preterm labor.
Data Source: Study of 52 women with threatened preterm labor.
Disclosures: One of Dr. Burwick's associates in the study, Dr. Michael Ross, is medical director of CerviLenz Inc., the company that makes the device, and provided it free to the study. The investigators reported having no other conflicts of interest.
SAN FRANCISCO — A disposable probe that measures vaginal cervical length during speculum examination appeared to be similar in efficacy to fetal fibronectin testing for predicting the likelihood of preterm delivery, in a study of 52 at-risk women.
A cervical length less than 30 mm as measured by the CerviLenz probe correlated with fetal fibronectin positivity and with preterm birth within 7 days, Dr. Richard M. Burwick reported at the meeting.
The sensitivity for preterm delivery within 7 days was 67% with either a CerviLenz measurement of less than 30 mm or fetal fibronectin positivity. The specificity was 83% with the CerviLenz probe and 78% with fetal fibronectin, reported Dr. Burwick, who led the study at Harbor-UCLA Medical Center before moving to Brigham and Women's Hospital, Boston.
The positive predictive value for preterm delivery within 7 days was 22% with a CerviLenz measurement of less than 30 mm and 17% with fetal fibronectin positivity, and the negative predictive value was 97% in each group.
Both measures were less accurate in predicting delivery prior to 37 weeks' gestation. Sensitivity was 29% with a CerviLenz measurement of vaginal cervical length less than 30 mm and 40% with fetal fibronectin positivity. Specificity was 81% and 80%, respectively. The positive predictive value for delivery before 37 weeks was 22% with the CerviLenz measure and 33% with fetal fibronectin results, and the negative predictive value was 85% and 84%, respectively.
“Symptomatic women with a CerviLenz cervical length of less than 30 mm should undergo further observation and consideration of tocolytic and maternal glucocorticoid therapy,” Dr. Burwick said.
Immediate and quantifiable measures of cervical length using the CerviLenz probe may be less variable than the most common way of measuring—by digital exam—and speedier than waiting for fetal fibronectin results, he suggested. The CerviLenz probe also can be used after intercourse or bleeding, he added.
In a previous study by some of the same investigators in the current study, the CerviLenz probe had good predictive value compared with transvaginal ultrasound in identifying women with a cervix shorter than 30 mm (J. Reprod. Med. 2007;52:385-9).
The study enrolled women with singletons at 24-34 weeks' gestational age who were at risk for preterm delivery, with uterine contractions, less than 3 cm cervical dilation, intact membranes, and no vaginal bleeding or recent intercourse. During a speculum examination, fetal fibronectin was collected, cervical length was measured by the CerviLenz probe, and cervical cultures were taken in most patients.
Fetal fibronectin tests in 49 patients were positive in 12 (24%), and CerviLenz measurements were less than 30 mm in 9 of 43 patients (21%). The mean cervical length measurement was 34 mm. The cohort was predominantly Hispanic (38 patients), and 15 patients had a prior preterm birth.
Previous data have shown that only 21%-27% of women with symptoms of preterm labor will have preterm births. Cervical length and cervical effacement help assess preterm birth risk in symptomatic women.
In asymptomatic women, cervical length shorter than 25 mm has been linked to a sixfold increase in risk for preterm birth.
{kind=link}
Sensitivity for preterm delivery within 7 days was 67% with either the CerviLenz probe or fetal fibronectin.
Source DR. BURWICK
Major Finding: Measurements of vaginal cervical length using a disposable probe were similar to fetal fibronectin tests in predicting the likelihood of preterm delivery in women with threatened preterm labor.
Data Source: Study of 52 women with threatened preterm labor.
Disclosures: One of Dr. Burwick's associates in the study, Dr. Michael Ross, is medical director of CerviLenz Inc., the company that makes the device, and provided it free to the study. The investigators reported having no other conflicts of interest.
SAN FRANCISCO — A disposable probe that measures vaginal cervical length during speculum examination appeared to be similar in efficacy to fetal fibronectin testing for predicting the likelihood of preterm delivery, in a study of 52 at-risk women.
A cervical length less than 30 mm as measured by the CerviLenz probe correlated with fetal fibronectin positivity and with preterm birth within 7 days, Dr. Richard M. Burwick reported at the meeting.
The sensitivity for preterm delivery within 7 days was 67% with either a CerviLenz measurement of less than 30 mm or fetal fibronectin positivity. The specificity was 83% with the CerviLenz probe and 78% with fetal fibronectin, reported Dr. Burwick, who led the study at Harbor-UCLA Medical Center before moving to Brigham and Women's Hospital, Boston.
The positive predictive value for preterm delivery within 7 days was 22% with a CerviLenz measurement of less than 30 mm and 17% with fetal fibronectin positivity, and the negative predictive value was 97% in each group.
Both measures were less accurate in predicting delivery prior to 37 weeks' gestation. Sensitivity was 29% with a CerviLenz measurement of vaginal cervical length less than 30 mm and 40% with fetal fibronectin positivity. Specificity was 81% and 80%, respectively. The positive predictive value for delivery before 37 weeks was 22% with the CerviLenz measure and 33% with fetal fibronectin results, and the negative predictive value was 85% and 84%, respectively.
“Symptomatic women with a CerviLenz cervical length of less than 30 mm should undergo further observation and consideration of tocolytic and maternal glucocorticoid therapy,” Dr. Burwick said.
Immediate and quantifiable measures of cervical length using the CerviLenz probe may be less variable than the most common way of measuring—by digital exam—and speedier than waiting for fetal fibronectin results, he suggested. The CerviLenz probe also can be used after intercourse or bleeding, he added.
In a previous study by some of the same investigators in the current study, the CerviLenz probe had good predictive value compared with transvaginal ultrasound in identifying women with a cervix shorter than 30 mm (J. Reprod. Med. 2007;52:385-9).
The study enrolled women with singletons at 24-34 weeks' gestational age who were at risk for preterm delivery, with uterine contractions, less than 3 cm cervical dilation, intact membranes, and no vaginal bleeding or recent intercourse. During a speculum examination, fetal fibronectin was collected, cervical length was measured by the CerviLenz probe, and cervical cultures were taken in most patients.
Fetal fibronectin tests in 49 patients were positive in 12 (24%), and CerviLenz measurements were less than 30 mm in 9 of 43 patients (21%). The mean cervical length measurement was 34 mm. The cohort was predominantly Hispanic (38 patients), and 15 patients had a prior preterm birth.
Previous data have shown that only 21%-27% of women with symptoms of preterm labor will have preterm births. Cervical length and cervical effacement help assess preterm birth risk in symptomatic women.
In asymptomatic women, cervical length shorter than 25 mm has been linked to a sixfold increase in risk for preterm birth.
Sensitivity for preterm delivery within 7 days was 67% with either the CerviLenz probe or fetal fibronectin.
Source DR. BURWICK
Major Finding: Measurements of vaginal cervical length using a disposable probe were similar to fetal fibronectin tests in predicting the likelihood of preterm delivery in women with threatened preterm labor.
Data Source: Study of 52 women with threatened preterm labor.
Disclosures: One of Dr. Burwick's associates in the study, Dr. Michael Ross, is medical director of CerviLenz Inc., the company that makes the device, and provided it free to the study. The investigators reported having no other conflicts of interest.
SAN FRANCISCO — A disposable probe that measures vaginal cervical length during speculum examination appeared to be similar in efficacy to fetal fibronectin testing for predicting the likelihood of preterm delivery, in a study of 52 at-risk women.
A cervical length less than 30 mm as measured by the CerviLenz probe correlated with fetal fibronectin positivity and with preterm birth within 7 days, Dr. Richard M. Burwick reported at the meeting.
The sensitivity for preterm delivery within 7 days was 67% with either a CerviLenz measurement of less than 30 mm or fetal fibronectin positivity. The specificity was 83% with the CerviLenz probe and 78% with fetal fibronectin, reported Dr. Burwick, who led the study at Harbor-UCLA Medical Center before moving to Brigham and Women's Hospital, Boston.
The positive predictive value for preterm delivery within 7 days was 22% with a CerviLenz measurement of less than 30 mm and 17% with fetal fibronectin positivity, and the negative predictive value was 97% in each group.
Both measures were less accurate in predicting delivery prior to 37 weeks' gestation. Sensitivity was 29% with a CerviLenz measurement of vaginal cervical length less than 30 mm and 40% with fetal fibronectin positivity. Specificity was 81% and 80%, respectively. The positive predictive value for delivery before 37 weeks was 22% with the CerviLenz measure and 33% with fetal fibronectin results, and the negative predictive value was 85% and 84%, respectively.
“Symptomatic women with a CerviLenz cervical length of less than 30 mm should undergo further observation and consideration of tocolytic and maternal glucocorticoid therapy,” Dr. Burwick said.
Immediate and quantifiable measures of cervical length using the CerviLenz probe may be less variable than the most common way of measuring—by digital exam—and speedier than waiting for fetal fibronectin results, he suggested. The CerviLenz probe also can be used after intercourse or bleeding, he added.
In a previous study by some of the same investigators in the current study, the CerviLenz probe had good predictive value compared with transvaginal ultrasound in identifying women with a cervix shorter than 30 mm (J. Reprod. Med. 2007;52:385-9).
The study enrolled women with singletons at 24-34 weeks' gestational age who were at risk for preterm delivery, with uterine contractions, less than 3 cm cervical dilation, intact membranes, and no vaginal bleeding or recent intercourse. During a speculum examination, fetal fibronectin was collected, cervical length was measured by the CerviLenz probe, and cervical cultures were taken in most patients.
Fetal fibronectin tests in 49 patients were positive in 12 (24%), and CerviLenz measurements were less than 30 mm in 9 of 43 patients (21%). The mean cervical length measurement was 34 mm. The cohort was predominantly Hispanic (38 patients), and 15 patients had a prior preterm birth.
Previous data have shown that only 21%-27% of women with symptoms of preterm labor will have preterm births. Cervical length and cervical effacement help assess preterm birth risk in symptomatic women.
In asymptomatic women, cervical length shorter than 25 mm has been linked to a sixfold increase in risk for preterm birth.
Sensitivity for preterm delivery within 7 days was 67% with either the CerviLenz probe or fetal fibronectin.
Source DR. BURWICK
From the Annual Meeting of the American College of Obstetricians and Gynecologists
Use of Form Improves Dystocia Documentation
Major Finding: Before use of the form, 39% of physicians documented estimated fetal weight, compared with 84% after adoption. The rate of documenting the head-to-shoulder delivery interval increased from 15% in the earlier time period to 77% after adoption of the form.
Data Source: Comparison of records for 100 deliveries with shoulder dystocia before use of the standardized form and 80 deliveries with shoulder dystocia afterward at one institution.
Disclosures: None was reported.
SAN FRANCISCO — Adoption of a standardized form for use during deliveries involving shoulder dystocia significantly improved documentation of some information at one institution, according to Dr. Vasiliki A. Moragianni.
A comparison of charts for 100 patients with deliveries involving shoulder dystocia before implementation of the standardized form in August 2003 and charts for 80 patients after adoption of the form found significant increases in the proportion of charts documenting the head-to-shoulder delivery interval and the estimated fetal weight.
Better documentation of shoulder dystocia cases could reduce legal risk, said Dr. Moragianni, whose presentation earned a second-place prize for clinical investigation at the meeting.
Before use of the form, 39 of 100 physicians (39%) documented estimated fetal weight, compared with 67 of 80 physicians (84%) after adoption of the form. The rate of documenting the head-to-shoulder delivery interval increased from 15 physicians (15%) in the earlier time period to 62 of 80 (77%) after adoption of the form.
The results show that adding a standardized form for shoulder dystocia cases improves documentation beyond what's recorded in standardized delivery forms already in use, she said. The standardized form for shoulder dystocia improved documentation of an item already included in the delivery form (estimated fetal weight) and an item not previously included (head-to-shoulder delivery interval), reported Dr. Moragianni of Beth Israel Deaconess Medical Center, Boston.
The investigators selected charts from the 2% of deliveries that involve shoulder dystocia at Abington (Pa.) Memorial Hospital, where Dr. Moragianni completed her residency training. The new form included documentation of estimated fetal weight, umbilical cord pH, the maneuvers used in managing shoulder dystocia, the head-to-shoulder delivery interval, the duration of the second stage of labor, and estimated blood loss.
Except for the head-to-shoulder delivery interval and estimated fetal weight, documentation did not change significantly between the two time periods.
Documentation of maneuvers used for shoulder dystocia included the type and the order of maneuvers tried, and adjuncts to maneuvers, but not the exact timing of maneuvers. The form did include records of delivery times for the head and shoulders.
The study's findings may be limited by the small number of cases, the retrospective design, and the concurrent “drills” for managing shoulder dystocia that were held at the hospital, she said.
The form might be improved by adding documentation of the team members involved in managing the case of shoulder dystocia and their training levels, the fetal head position (whether the presenting shoulder was anterior or posterior), and the condition of the infant's arms immediately following surgery, Dr. Moragianni added.
“Every obstetrician in the hospital is completing the form,” she noted.
Shoulder dystocia was the third-leading cause of obstetric litigation in one analysis, accounting for 14% of obstetric lawsuits. Poor documentation drove 54% of these cases, which resulted in an average payout of $429,000 (Obstet. Gynecol. 2008;112:1279-83), she noted.
{kind=link}
Shoulder dystocia was the third-leading causeof obstetric litigation in one analysis.
Source DR. MORAGIANNI
Major Finding: Before use of the form, 39% of physicians documented estimated fetal weight, compared with 84% after adoption. The rate of documenting the head-to-shoulder delivery interval increased from 15% in the earlier time period to 77% after adoption of the form.
Data Source: Comparison of records for 100 deliveries with shoulder dystocia before use of the standardized form and 80 deliveries with shoulder dystocia afterward at one institution.
Disclosures: None was reported.
SAN FRANCISCO — Adoption of a standardized form for use during deliveries involving shoulder dystocia significantly improved documentation of some information at one institution, according to Dr. Vasiliki A. Moragianni.
A comparison of charts for 100 patients with deliveries involving shoulder dystocia before implementation of the standardized form in August 2003 and charts for 80 patients after adoption of the form found significant increases in the proportion of charts documenting the head-to-shoulder delivery interval and the estimated fetal weight.
Better documentation of shoulder dystocia cases could reduce legal risk, said Dr. Moragianni, whose presentation earned a second-place prize for clinical investigation at the meeting.
Before use of the form, 39 of 100 physicians (39%) documented estimated fetal weight, compared with 67 of 80 physicians (84%) after adoption of the form. The rate of documenting the head-to-shoulder delivery interval increased from 15 physicians (15%) in the earlier time period to 62 of 80 (77%) after adoption of the form.
The results show that adding a standardized form for shoulder dystocia cases improves documentation beyond what's recorded in standardized delivery forms already in use, she said. The standardized form for shoulder dystocia improved documentation of an item already included in the delivery form (estimated fetal weight) and an item not previously included (head-to-shoulder delivery interval), reported Dr. Moragianni of Beth Israel Deaconess Medical Center, Boston.
The investigators selected charts from the 2% of deliveries that involve shoulder dystocia at Abington (Pa.) Memorial Hospital, where Dr. Moragianni completed her residency training. The new form included documentation of estimated fetal weight, umbilical cord pH, the maneuvers used in managing shoulder dystocia, the head-to-shoulder delivery interval, the duration of the second stage of labor, and estimated blood loss.
Except for the head-to-shoulder delivery interval and estimated fetal weight, documentation did not change significantly between the two time periods.
Documentation of maneuvers used for shoulder dystocia included the type and the order of maneuvers tried, and adjuncts to maneuvers, but not the exact timing of maneuvers. The form did include records of delivery times for the head and shoulders.
The study's findings may be limited by the small number of cases, the retrospective design, and the concurrent “drills” for managing shoulder dystocia that were held at the hospital, she said.
The form might be improved by adding documentation of the team members involved in managing the case of shoulder dystocia and their training levels, the fetal head position (whether the presenting shoulder was anterior or posterior), and the condition of the infant's arms immediately following surgery, Dr. Moragianni added.
“Every obstetrician in the hospital is completing the form,” she noted.
Shoulder dystocia was the third-leading cause of obstetric litigation in one analysis, accounting for 14% of obstetric lawsuits. Poor documentation drove 54% of these cases, which resulted in an average payout of $429,000 (Obstet. Gynecol. 2008;112:1279-83), she noted.
Shoulder dystocia was the third-leading causeof obstetric litigation in one analysis.
Source DR. MORAGIANNI
Major Finding: Before use of the form, 39% of physicians documented estimated fetal weight, compared with 84% after adoption. The rate of documenting the head-to-shoulder delivery interval increased from 15% in the earlier time period to 77% after adoption of the form.
Data Source: Comparison of records for 100 deliveries with shoulder dystocia before use of the standardized form and 80 deliveries with shoulder dystocia afterward at one institution.
Disclosures: None was reported.
SAN FRANCISCO — Adoption of a standardized form for use during deliveries involving shoulder dystocia significantly improved documentation of some information at one institution, according to Dr. Vasiliki A. Moragianni.
A comparison of charts for 100 patients with deliveries involving shoulder dystocia before implementation of the standardized form in August 2003 and charts for 80 patients after adoption of the form found significant increases in the proportion of charts documenting the head-to-shoulder delivery interval and the estimated fetal weight.
Better documentation of shoulder dystocia cases could reduce legal risk, said Dr. Moragianni, whose presentation earned a second-place prize for clinical investigation at the meeting.
Before use of the form, 39 of 100 physicians (39%) documented estimated fetal weight, compared with 67 of 80 physicians (84%) after adoption of the form. The rate of documenting the head-to-shoulder delivery interval increased from 15 physicians (15%) in the earlier time period to 62 of 80 (77%) after adoption of the form.
The results show that adding a standardized form for shoulder dystocia cases improves documentation beyond what's recorded in standardized delivery forms already in use, she said. The standardized form for shoulder dystocia improved documentation of an item already included in the delivery form (estimated fetal weight) and an item not previously included (head-to-shoulder delivery interval), reported Dr. Moragianni of Beth Israel Deaconess Medical Center, Boston.
The investigators selected charts from the 2% of deliveries that involve shoulder dystocia at Abington (Pa.) Memorial Hospital, where Dr. Moragianni completed her residency training. The new form included documentation of estimated fetal weight, umbilical cord pH, the maneuvers used in managing shoulder dystocia, the head-to-shoulder delivery interval, the duration of the second stage of labor, and estimated blood loss.
Except for the head-to-shoulder delivery interval and estimated fetal weight, documentation did not change significantly between the two time periods.
Documentation of maneuvers used for shoulder dystocia included the type and the order of maneuvers tried, and adjuncts to maneuvers, but not the exact timing of maneuvers. The form did include records of delivery times for the head and shoulders.
The study's findings may be limited by the small number of cases, the retrospective design, and the concurrent “drills” for managing shoulder dystocia that were held at the hospital, she said.
The form might be improved by adding documentation of the team members involved in managing the case of shoulder dystocia and their training levels, the fetal head position (whether the presenting shoulder was anterior or posterior), and the condition of the infant's arms immediately following surgery, Dr. Moragianni added.
“Every obstetrician in the hospital is completing the form,” she noted.
Shoulder dystocia was the third-leading cause of obstetric litigation in one analysis, accounting for 14% of obstetric lawsuits. Poor documentation drove 54% of these cases, which resulted in an average payout of $429,000 (Obstet. Gynecol. 2008;112:1279-83), she noted.
Shoulder dystocia was the third-leading causeof obstetric litigation in one analysis.
Source DR. MORAGIANNI
From the Annual Meeting of the American College of Obstetricians and Gynecologists