User login
Toxic Erythema of Chemotherapy Called By Many Names
PASADENA, Calif. - Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum - toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
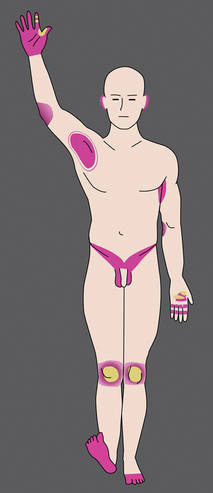
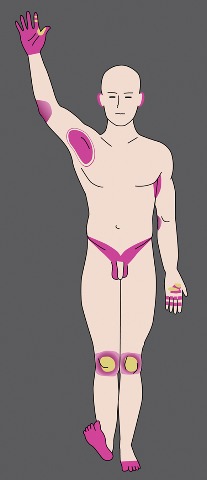
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.

“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
PASADENA, Calif. - Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum - toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
PASADENA, Calif. - Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum - toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
Toxic Erythema of Chemotherapy By Any Other Name
PASADENA, Calif. – Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum—toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC (see list below) include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.

Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
TEC a Better Term than Many
These diagnoses all fall under the umbrella of (TEC), and all should be called TEC, Dr. Bolognia said:
Erythrodysesthesia
Acral erythrodysesthesia
Palmar-plantar (palmoplantar) erythrodysesthesia
Acral erythema
Chemotherapy-induced acral erythema
Hand-food syndrome
AraC (cytarabine) ears
Chemotherapy-induced eccrine squamous syringometaplasia
Epidermal dysmaturation
Intertriginous eruption associated with chemotherapy
Chemotherapy-associated neutrophilic eccrine hidradenitis
Drug-induced eccrine hidradenitis
Chemotherapy-induced hidradenitis
Pseudocellulitis (erysipeloid reaction to chemotherapy)
PASADENA, Calif. – Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum—toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC (see list below) include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
TEC a Better Term than Many
These diagnoses all fall under the umbrella of (TEC), and all should be called TEC, Dr. Bolognia said:
Erythrodysesthesia
Acral erythrodysesthesia
Palmar-plantar (palmoplantar) erythrodysesthesia
Acral erythema
Chemotherapy-induced acral erythema
Hand-food syndrome
AraC (cytarabine) ears
Chemotherapy-induced eccrine squamous syringometaplasia
Epidermal dysmaturation
Intertriginous eruption associated with chemotherapy
Chemotherapy-associated neutrophilic eccrine hidradenitis
Drug-induced eccrine hidradenitis
Chemotherapy-induced hidradenitis
Pseudocellulitis (erysipeloid reaction to chemotherapy)
PASADENA, Calif. – Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum—toxic erythema of chemotherapy.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC (see list below) include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.
Pseudocellulitis (or erysipeloid reaction) also falls within the spectrum of TEC. Large patches or plaques of burning erythema appear and tense bullae may develop. The bullae do not spontaneously slough, and there is no Nikolsky’s sign. Pseudocellulitis is seen primarily following exposure to gemcitabine, but also to clofarabine, a newer drug being used as a second- or third-line agent for leukemia.
Lastly, chemotherapy-induced eccrine hidradenitis clearly falls within the histologic spectrum of TEC, she said, but clinically there are some patients who have a Sweet’s syndrome–like presentation, and these could be categorized separately.
TEC can be misdiagnosed as several other entities including cellulitis, herpetic viral infections, vasculitis, graft-versus-host disease (especially when the patient also has diarrhea), or a hypersensitivity drug reaction. It is important to note that TEC can be a skin sign of systemic disease in that severe cutaneous disease can be associated with severe cytotoxicity of the bowel, leading to sepsis caused by GI flora, she said. The team caring for the patient should be made aware of this possibility.
Disclosures: Dr. Bolognia said she has no pertinent conflicts of interest.
TEC a Better Term than Many
These diagnoses all fall under the umbrella of (TEC), and all should be called TEC, Dr. Bolognia said:
Erythrodysesthesia
Acral erythrodysesthesia
Palmar-plantar (palmoplantar) erythrodysesthesia
Acral erythema
Chemotherapy-induced acral erythema
Hand-food syndrome
AraC (cytarabine) ears
Chemotherapy-induced eccrine squamous syringometaplasia
Epidermal dysmaturation
Intertriginous eruption associated with chemotherapy
Chemotherapy-associated neutrophilic eccrine hidradenitis
Drug-induced eccrine hidradenitis
Chemotherapy-induced hidradenitis
Pseudocellulitis (erysipeloid reaction to chemotherapy)
Listen First, Don’t Rush in Lip Augmentation
Pasadena, Calif. - No one lip architecture is inherently more beautiful than another, and there are many aesthetically pleasing shapes for lips.
With that said, bigger is not necessarily better. Really listen to what patients are asking for—even watch body language to understand expectations. Don’t rush. Don’t do anything out of your comfort level. And make it painless, said Dr. Roberta D. Sengelmann. It’s not so much what you do. but how you do it that counts.

Ask patients to bring in photos or fashion magazines with images of lips that they like, and address their expectations, she suggested.
Fillers for lip augmentation are used off-label, so explaining the risks and getting informed consent from patients are essential. A dozen or more potential adverse outcomes can range from a shorter-than-expected duration of the bulking effect to infection, necrosis, or scaring.
To meet a patient’s desire for more pleasing lips, keep in mind widely accepted characteristics of a “beautiful” face and mouth, she advised.
Lips are symmetrical. The width of the lips is 30%-50% of facial width, and the width between the oral commissures equals the distance between the medial limbi. The upper lip is slightly thinner than the lower one—making the upper lip too big looks unnatural. The commissures should angle up slightly.
With age, the mouth starts to angle down and to look smaller (the lips “cave in”), radial lip lines develop, 3-D volume decreases, and there’s inversion of the lip’s white roll, said Dr. Sengelmann, a dermatologic surgeon in private practice in Santa Barbara, Calif.
Pay attention to anatomy to plan your approach to lip augmentation. The first step is to elevate the oral commissures. If you run out of product or need to stop, the patient still will look better, said Dr. Sengelmann.
If you can do more, define the vermilion border or white roll. Then add volume to the pink part of the lip. If needed, redefine the philtral columns. And, if you have some product left, ablate vertical lip lines. One main caveat applies: The patient’s desires take precedence in deciding which of those steps to address, she said.
Consider antiviral prophylaxis before lip injections, and definitely use it treat anyone who’s had more than six annual outbreaks of herpes simplex virus, she advised. If the patient is on blood-thinning medication, discontinue it a week before lip augmentation. “I don’t treat people on Coumadin, ever,” she said.
Before you start injecting, remove any makeup, and evaluate the patient at rest and in motion. Take photos before and after the first treatment. Mark the philtral columns with an eyeliner pencil, because they can be difficult to see once filled. Review your plans and the patient’s expectations before you begin.
“You can’t rush this technique,” Dr. Sengelmann said. Make it as painless as possible by applying ice, topical anesthesia, or nerve blocks. Consider local anesthesia at the commissures. Vibration seems to work, too, but “I’m not comfortable” using it, she added.
Use only the finest fillers when injecting into dermis, and more viscous fillers for potential space under the skin. Dr. Sengelmann avoids Radiesse for lips because nodules can be a problem, she cautioned. Again, use a slow hand. “Hasty injectors have a much higher complication rate,” Dr. Sengelmann said.
For augmenting the angle of the mouth, she uses Radiesse, Juvéderm Ultra Plus, Perlane, or Restylane. For the vermilion border and philtral columns or to augment the pink lip, she prefers Juvéderm Ultra, Restylane, Juvéderm Ultra Plus, or Perlane. For radial lines, she injects Prevelle Silk, Restylane, or Juvéderm Ultra using a 32-gauge needle.
After treatment, assess lip symmetry before the product is gone—consider saving a little as leftover in case it is needed. Massaging and molding the injected area may help distribution, “but remember, you can’t correct for poor technique,” she said. Apply ice packs after the procedure and have the patient rest for about 6 hours, with no exercise of vigorous activity for the rest of the day.
For a patient whose only complaint is dynamic lip lines (with no vertical lines at rest), botulinum toxin alone may soften those lines, provide some lip eversion, and give the perception of fullness to lips, Dr. Sengelmann suggested.
She advised using caution when considering lip augmentation for a patient with a long upper lip, inverted white roll, coarse radial lip lines, or deep Marionette lines. Other features that should inspire caution include very thin lips, lip incompetence, recessed bone or dentition, lip asymmetry, and unrealistic expectations.
Disclosures: Dr. Sengelmann has been an advisor to Allergan (Juvéderm), BioForm Medical (maker of Radiesse), and MicroAire (formally Coapt Systems), and has received research support from MicroAire.
Pasadena, Calif. - No one lip architecture is inherently more beautiful than another, and there are many aesthetically pleasing shapes for lips.
With that said, bigger is not necessarily better. Really listen to what patients are asking for—even watch body language to understand expectations. Don’t rush. Don’t do anything out of your comfort level. And make it painless, said Dr. Roberta D. Sengelmann. It’s not so much what you do. but how you do it that counts.
Ask patients to bring in photos or fashion magazines with images of lips that they like, and address their expectations, she suggested.
Fillers for lip augmentation are used off-label, so explaining the risks and getting informed consent from patients are essential. A dozen or more potential adverse outcomes can range from a shorter-than-expected duration of the bulking effect to infection, necrosis, or scaring.
To meet a patient’s desire for more pleasing lips, keep in mind widely accepted characteristics of a “beautiful” face and mouth, she advised.
Lips are symmetrical. The width of the lips is 30%-50% of facial width, and the width between the oral commissures equals the distance between the medial limbi. The upper lip is slightly thinner than the lower one—making the upper lip too big looks unnatural. The commissures should angle up slightly.
With age, the mouth starts to angle down and to look smaller (the lips “cave in”), radial lip lines develop, 3-D volume decreases, and there’s inversion of the lip’s white roll, said Dr. Sengelmann, a dermatologic surgeon in private practice in Santa Barbara, Calif.
Pay attention to anatomy to plan your approach to lip augmentation. The first step is to elevate the oral commissures. If you run out of product or need to stop, the patient still will look better, said Dr. Sengelmann.
If you can do more, define the vermilion border or white roll. Then add volume to the pink part of the lip. If needed, redefine the philtral columns. And, if you have some product left, ablate vertical lip lines. One main caveat applies: The patient’s desires take precedence in deciding which of those steps to address, she said.
Consider antiviral prophylaxis before lip injections, and definitely use it treat anyone who’s had more than six annual outbreaks of herpes simplex virus, she advised. If the patient is on blood-thinning medication, discontinue it a week before lip augmentation. “I don’t treat people on Coumadin, ever,” she said.
Before you start injecting, remove any makeup, and evaluate the patient at rest and in motion. Take photos before and after the first treatment. Mark the philtral columns with an eyeliner pencil, because they can be difficult to see once filled. Review your plans and the patient’s expectations before you begin.
“You can’t rush this technique,” Dr. Sengelmann said. Make it as painless as possible by applying ice, topical anesthesia, or nerve blocks. Consider local anesthesia at the commissures. Vibration seems to work, too, but “I’m not comfortable” using it, she added.
Use only the finest fillers when injecting into dermis, and more viscous fillers for potential space under the skin. Dr. Sengelmann avoids Radiesse for lips because nodules can be a problem, she cautioned. Again, use a slow hand. “Hasty injectors have a much higher complication rate,” Dr. Sengelmann said.
For augmenting the angle of the mouth, she uses Radiesse, Juvéderm Ultra Plus, Perlane, or Restylane. For the vermilion border and philtral columns or to augment the pink lip, she prefers Juvéderm Ultra, Restylane, Juvéderm Ultra Plus, or Perlane. For radial lines, she injects Prevelle Silk, Restylane, or Juvéderm Ultra using a 32-gauge needle.
After treatment, assess lip symmetry before the product is gone—consider saving a little as leftover in case it is needed. Massaging and molding the injected area may help distribution, “but remember, you can’t correct for poor technique,” she said. Apply ice packs after the procedure and have the patient rest for about 6 hours, with no exercise of vigorous activity for the rest of the day.
For a patient whose only complaint is dynamic lip lines (with no vertical lines at rest), botulinum toxin alone may soften those lines, provide some lip eversion, and give the perception of fullness to lips, Dr. Sengelmann suggested.
She advised using caution when considering lip augmentation for a patient with a long upper lip, inverted white roll, coarse radial lip lines, or deep Marionette lines. Other features that should inspire caution include very thin lips, lip incompetence, recessed bone or dentition, lip asymmetry, and unrealistic expectations.
Disclosures: Dr. Sengelmann has been an advisor to Allergan (Juvéderm), BioForm Medical (maker of Radiesse), and MicroAire (formally Coapt Systems), and has received research support from MicroAire.
Pasadena, Calif. - No one lip architecture is inherently more beautiful than another, and there are many aesthetically pleasing shapes for lips.
With that said, bigger is not necessarily better. Really listen to what patients are asking for—even watch body language to understand expectations. Don’t rush. Don’t do anything out of your comfort level. And make it painless, said Dr. Roberta D. Sengelmann. It’s not so much what you do. but how you do it that counts.
Ask patients to bring in photos or fashion magazines with images of lips that they like, and address their expectations, she suggested.
Fillers for lip augmentation are used off-label, so explaining the risks and getting informed consent from patients are essential. A dozen or more potential adverse outcomes can range from a shorter-than-expected duration of the bulking effect to infection, necrosis, or scaring.
To meet a patient’s desire for more pleasing lips, keep in mind widely accepted characteristics of a “beautiful” face and mouth, she advised.
Lips are symmetrical. The width of the lips is 30%-50% of facial width, and the width between the oral commissures equals the distance between the medial limbi. The upper lip is slightly thinner than the lower one—making the upper lip too big looks unnatural. The commissures should angle up slightly.
With age, the mouth starts to angle down and to look smaller (the lips “cave in”), radial lip lines develop, 3-D volume decreases, and there’s inversion of the lip’s white roll, said Dr. Sengelmann, a dermatologic surgeon in private practice in Santa Barbara, Calif.
Pay attention to anatomy to plan your approach to lip augmentation. The first step is to elevate the oral commissures. If you run out of product or need to stop, the patient still will look better, said Dr. Sengelmann.
If you can do more, define the vermilion border or white roll. Then add volume to the pink part of the lip. If needed, redefine the philtral columns. And, if you have some product left, ablate vertical lip lines. One main caveat applies: The patient’s desires take precedence in deciding which of those steps to address, she said.
Consider antiviral prophylaxis before lip injections, and definitely use it treat anyone who’s had more than six annual outbreaks of herpes simplex virus, she advised. If the patient is on blood-thinning medication, discontinue it a week before lip augmentation. “I don’t treat people on Coumadin, ever,” she said.
Before you start injecting, remove any makeup, and evaluate the patient at rest and in motion. Take photos before and after the first treatment. Mark the philtral columns with an eyeliner pencil, because they can be difficult to see once filled. Review your plans and the patient’s expectations before you begin.
“You can’t rush this technique,” Dr. Sengelmann said. Make it as painless as possible by applying ice, topical anesthesia, or nerve blocks. Consider local anesthesia at the commissures. Vibration seems to work, too, but “I’m not comfortable” using it, she added.
Use only the finest fillers when injecting into dermis, and more viscous fillers for potential space under the skin. Dr. Sengelmann avoids Radiesse for lips because nodules can be a problem, she cautioned. Again, use a slow hand. “Hasty injectors have a much higher complication rate,” Dr. Sengelmann said.
For augmenting the angle of the mouth, she uses Radiesse, Juvéderm Ultra Plus, Perlane, or Restylane. For the vermilion border and philtral columns or to augment the pink lip, she prefers Juvéderm Ultra, Restylane, Juvéderm Ultra Plus, or Perlane. For radial lines, she injects Prevelle Silk, Restylane, or Juvéderm Ultra using a 32-gauge needle.
After treatment, assess lip symmetry before the product is gone—consider saving a little as leftover in case it is needed. Massaging and molding the injected area may help distribution, “but remember, you can’t correct for poor technique,” she said. Apply ice packs after the procedure and have the patient rest for about 6 hours, with no exercise of vigorous activity for the rest of the day.
For a patient whose only complaint is dynamic lip lines (with no vertical lines at rest), botulinum toxin alone may soften those lines, provide some lip eversion, and give the perception of fullness to lips, Dr. Sengelmann suggested.
She advised using caution when considering lip augmentation for a patient with a long upper lip, inverted white roll, coarse radial lip lines, or deep Marionette lines. Other features that should inspire caution include very thin lips, lip incompetence, recessed bone or dentition, lip asymmetry, and unrealistic expectations.
Disclosures: Dr. Sengelmann has been an advisor to Allergan (Juvéderm), BioForm Medical (maker of Radiesse), and MicroAire (formally Coapt Systems), and has received research support from MicroAire.
Stem Cells a Growth Area in Cosmetic Dermatology
PASADENA, Calif. - Stem cell therapies, molecular medicine, less-invasive procedures and robotic surgery might play prominent roles in the future of cosmetic dermatology.
That's what Dr. Ronald Moy sees when he looks into his figurative crystal ball. And it means many, many cosmetic procedures, he said at the annual meeting of the Pacific Dermatologic Association.

"Stem cell research is most exciting," said Dr. Moy, who practices in Beverly Hills, Calif. and is president-elect of the American Academy of Dermatology. As many as an eighth to a quarter of presentations at cosmetic surgery meetings these days mention stem cells, he estimated. Cosmetic procedures in general have increased by 228% since 1997 in the United States, he said.
Dermatologists in his area who do a lot of marketing are advertising "stem cell facelifts," he added. In his own office, he or his partner may extract fat from a patient and then centrifuge or decant it to get fat for reinjecting, and that fat contains some stem cells. Fat injections can improve skin quality over the injection area and may add volume; however, volume results are not as predictable, compared with injections of other fillers.
Once researchers find a way to extract stem cells reliably, they might replace use of these fillers in many cases, he suggested. Stem cells also might be used in the future to grow skin, fat, and hair. "Fillers that we are using might be considered archaic; it will be people’s own skin" used in procedures and, hair cloning and gene therapy will replace hair transplants, he predicted.
A forerunner of this scenario that is widely used today is the biostimulator Sculptra, an injectable poly-l-lactic acid, he said. Sculptra can help thicken the skin and stimulate collagen production.
Molecular tools also will be part of cosmetic dermatologists' armamentarium, switching genes on and off via synthetic medicines individualized to patients. These "are in the near future," Dr. Moy predicted.
Cocktails of immunostimulants that cure skin cancer are close at hand and probably will replace surgical treatments, he added: "Many of our Mohs surgeons and probably many of our skin cancer surgeons will probably be dinosaurs in the near future."
As baby boomers age, they’ll want less-invasive procedures, so radiofrequency devices that tighten the skin and fractional laser resurfacing to remove some wrinkles and sun-damaged skin will be used more and more, he believes. The results aren't as dramatic as with phenol peels or conventional carbon dioxide laser resurfacing, but those techniques require longer recovery times and carry a higher risk for complications. When surgery is used for brow lifts, facelifts, or fat removal, the trend will be toward smaller incisions.
Lasers will evolve like other mobile devices to become hand-held and used by patients to remove hair, fat, wrinkles, lentigos, and more, Dr. Moy said.
More muscle-relaxing products will come on the market to compete with Botox or Dysport, including a topical version that’s now being tested and seems to work well for superficial areas, he said.
He also foresees new concoctions of creams that will go beyond sunscreens to prevent skin cancers, adding that prevention already is a booming trend, with some emphasis shifting toward greater attention to the molecular benefits of nutrition in preventing skin problems, he said. "Nutrition is important, and we haven't thought about that much in dermatology," he remarked.
Still, much of cosmetic dermatology will continue to involve new and expensive technology, which will affect not just how patients are treated, but how dermatologists practice, he said. Machines that cost $100,000 will be hard for solo practitioners to afford. "Unless you're practicing as a group, it's going to be very difficult" to offer the most modern services."
Dr. Moy made no disclosures.
PASADENA, Calif. - Stem cell therapies, molecular medicine, less-invasive procedures and robotic surgery might play prominent roles in the future of cosmetic dermatology.
That's what Dr. Ronald Moy sees when he looks into his figurative crystal ball. And it means many, many cosmetic procedures, he said at the annual meeting of the Pacific Dermatologic Association.
"Stem cell research is most exciting," said Dr. Moy, who practices in Beverly Hills, Calif. and is president-elect of the American Academy of Dermatology. As many as an eighth to a quarter of presentations at cosmetic surgery meetings these days mention stem cells, he estimated. Cosmetic procedures in general have increased by 228% since 1997 in the United States, he said.
Dermatologists in his area who do a lot of marketing are advertising "stem cell facelifts," he added. In his own office, he or his partner may extract fat from a patient and then centrifuge or decant it to get fat for reinjecting, and that fat contains some stem cells. Fat injections can improve skin quality over the injection area and may add volume; however, volume results are not as predictable, compared with injections of other fillers.
Once researchers find a way to extract stem cells reliably, they might replace use of these fillers in many cases, he suggested. Stem cells also might be used in the future to grow skin, fat, and hair. "Fillers that we are using might be considered archaic; it will be people’s own skin" used in procedures and, hair cloning and gene therapy will replace hair transplants, he predicted.
A forerunner of this scenario that is widely used today is the biostimulator Sculptra, an injectable poly-l-lactic acid, he said. Sculptra can help thicken the skin and stimulate collagen production.
Molecular tools also will be part of cosmetic dermatologists' armamentarium, switching genes on and off via synthetic medicines individualized to patients. These "are in the near future," Dr. Moy predicted.
Cocktails of immunostimulants that cure skin cancer are close at hand and probably will replace surgical treatments, he added: "Many of our Mohs surgeons and probably many of our skin cancer surgeons will probably be dinosaurs in the near future."
As baby boomers age, they’ll want less-invasive procedures, so radiofrequency devices that tighten the skin and fractional laser resurfacing to remove some wrinkles and sun-damaged skin will be used more and more, he believes. The results aren't as dramatic as with phenol peels or conventional carbon dioxide laser resurfacing, but those techniques require longer recovery times and carry a higher risk for complications. When surgery is used for brow lifts, facelifts, or fat removal, the trend will be toward smaller incisions.
Lasers will evolve like other mobile devices to become hand-held and used by patients to remove hair, fat, wrinkles, lentigos, and more, Dr. Moy said.
More muscle-relaxing products will come on the market to compete with Botox or Dysport, including a topical version that’s now being tested and seems to work well for superficial areas, he said.
He also foresees new concoctions of creams that will go beyond sunscreens to prevent skin cancers, adding that prevention already is a booming trend, with some emphasis shifting toward greater attention to the molecular benefits of nutrition in preventing skin problems, he said. "Nutrition is important, and we haven't thought about that much in dermatology," he remarked.
Still, much of cosmetic dermatology will continue to involve new and expensive technology, which will affect not just how patients are treated, but how dermatologists practice, he said. Machines that cost $100,000 will be hard for solo practitioners to afford. "Unless you're practicing as a group, it's going to be very difficult" to offer the most modern services."
Dr. Moy made no disclosures.
PASADENA, Calif. - Stem cell therapies, molecular medicine, less-invasive procedures and robotic surgery might play prominent roles in the future of cosmetic dermatology.
That's what Dr. Ronald Moy sees when he looks into his figurative crystal ball. And it means many, many cosmetic procedures, he said at the annual meeting of the Pacific Dermatologic Association.
"Stem cell research is most exciting," said Dr. Moy, who practices in Beverly Hills, Calif. and is president-elect of the American Academy of Dermatology. As many as an eighth to a quarter of presentations at cosmetic surgery meetings these days mention stem cells, he estimated. Cosmetic procedures in general have increased by 228% since 1997 in the United States, he said.
Dermatologists in his area who do a lot of marketing are advertising "stem cell facelifts," he added. In his own office, he or his partner may extract fat from a patient and then centrifuge or decant it to get fat for reinjecting, and that fat contains some stem cells. Fat injections can improve skin quality over the injection area and may add volume; however, volume results are not as predictable, compared with injections of other fillers.
Once researchers find a way to extract stem cells reliably, they might replace use of these fillers in many cases, he suggested. Stem cells also might be used in the future to grow skin, fat, and hair. "Fillers that we are using might be considered archaic; it will be people’s own skin" used in procedures and, hair cloning and gene therapy will replace hair transplants, he predicted.
A forerunner of this scenario that is widely used today is the biostimulator Sculptra, an injectable poly-l-lactic acid, he said. Sculptra can help thicken the skin and stimulate collagen production.
Molecular tools also will be part of cosmetic dermatologists' armamentarium, switching genes on and off via synthetic medicines individualized to patients. These "are in the near future," Dr. Moy predicted.
Cocktails of immunostimulants that cure skin cancer are close at hand and probably will replace surgical treatments, he added: "Many of our Mohs surgeons and probably many of our skin cancer surgeons will probably be dinosaurs in the near future."
As baby boomers age, they’ll want less-invasive procedures, so radiofrequency devices that tighten the skin and fractional laser resurfacing to remove some wrinkles and sun-damaged skin will be used more and more, he believes. The results aren't as dramatic as with phenol peels or conventional carbon dioxide laser resurfacing, but those techniques require longer recovery times and carry a higher risk for complications. When surgery is used for brow lifts, facelifts, or fat removal, the trend will be toward smaller incisions.
Lasers will evolve like other mobile devices to become hand-held and used by patients to remove hair, fat, wrinkles, lentigos, and more, Dr. Moy said.
More muscle-relaxing products will come on the market to compete with Botox or Dysport, including a topical version that’s now being tested and seems to work well for superficial areas, he said.
He also foresees new concoctions of creams that will go beyond sunscreens to prevent skin cancers, adding that prevention already is a booming trend, with some emphasis shifting toward greater attention to the molecular benefits of nutrition in preventing skin problems, he said. "Nutrition is important, and we haven't thought about that much in dermatology," he remarked.
Still, much of cosmetic dermatology will continue to involve new and expensive technology, which will affect not just how patients are treated, but how dermatologists practice, he said. Machines that cost $100,000 will be hard for solo practitioners to afford. "Unless you're practicing as a group, it's going to be very difficult" to offer the most modern services."
Dr. Moy made no disclosures.
GDC-0449 and Itraconazole Look Promising for Basal Cell Carcinomas
PASADENA, Calif. - Two drugs - one old, one new - are showing promise in early clinical trials for the treatment of basal cell carcinomas.
If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.

“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial - and randomized to 18 months of treatment with GDC-0449 or placebo - 23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
PASADENA, Calif. - Two drugs - one old, one new - are showing promise in early clinical trials for the treatment of basal cell carcinomas.
If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.
“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial - and randomized to 18 months of treatment with GDC-0449 or placebo - 23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
PASADENA, Calif. - Two drugs - one old, one new - are showing promise in early clinical trials for the treatment of basal cell carcinomas.
If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.
“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial - and randomized to 18 months of treatment with GDC-0449 or placebo - 23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
Major Finding: Group A patients started with a median of 252 BCCs and had 127 at the most recent follow-up.
Data Source: Phase II trial of 41 patients recruited thus far with basal cell nevus syndrome.
Disclosures: Genentech is sponsoring the GDC-0449 trial and provided free medication and travel funds for patients. The investigators have no other conflicts of interest, Dr. Tang said.
Two Promising Drugs Identified for Basal Cell Carcinomas
PASADENA, Calif. - Two drugs—one old, one new—are showing promise in early clinical trials for the treatment of basal cell carcinomas.

If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.
“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial—and randomized to 18 months of treatment with GDC-0449 or placebo—23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
PASADENA, Calif. - Two drugs—one old, one new—are showing promise in early clinical trials for the treatment of basal cell carcinomas.
If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.
“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial—and randomized to 18 months of treatment with GDC-0449 or placebo—23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
PASADENA, Calif. - Two drugs—one old, one new—are showing promise in early clinical trials for the treatment of basal cell carcinomas.
If they prove to be useful, clinicians can thank scientists whose years of research successfully identified abnormalities in the hedgehog signaling pathway as the mechanism of disease for basal cell carcinoma (BCC), Dr. Jean Tang said at the annual meeting of the Pacific Dermatologic Association.
“Every major pharmaceutical company is now interested in the hedgehog pathway, so we may see a lot of treatments in the near future” for BCC and other cancers that have aberrations in this pathway, said Dr. Tang of Stanford (Calif.) University.
She and her associates are conducting a phase II trial of the experimental Genentech drug GDC-0449 in patients with many BCCs from basal cell nevus syndrome (Gorlin’s syndrome), and a separate proof-of-concept study of the antifungal drug itraconazole in patients with small numbers of BCCs who do not have basal cell nevus syndrome. Dr. Tang said she is pleased by the early results with both drugs so far.
For GDC-0449, a previous phase I study in 33 patients with locally advanced or metastatic BCC who took the drug for a median of 10 months found that 50%-60% had partial or complete responses and the drug was generally well tolerated (N. Engl. J. Med. 2009;361:1,164-72).
Of the 41 patients with basal cell nevus syndrome recruited thus far for the phase II trial—and randomized to 18 months of treatment with GDC-0449 or placebo—23 patients (with 953 BCC tumors) have more than 1 month of data.
Although the study is still blinded, 15 patients in group A have developed a median of one new BCC during that month, compared with a median of 10 new BCCs in each of the 8 patients in group B, a significant difference that suggests group A may have received the drug and it may be working, Dr. Tang suggested.
In group A, patients started with a median of 252 BCCs and had 127 at the most recent follow-up, a 50% decline. In group B, patients started with 217 BCCs and had 267 at follow-up, a 23% increase in BCCs.
The difference between groups is significant, she said. The existing BCCs in group A also seem to have decreased in size.
“In the patients who have responded, it has changed their lives,” Dr. Tang said. “We are really excited about it.”
Patients in group A, however, were significantly more likely to develop dysgeusia (decreased taste sensation). The condition was seen in 14 of 15 patients, compared with none in group B. Seven patients in group A and none in group B reported some hair loss, though this difference was not statistically significant. Two patients in group A stopped treatment due to dysgeusia and hair loss, compared with no patient cessation in group A. Myalgia was also reported in group A but not group B.
These side effects may be acceptable to patients with basal cell nevus syndrome but probably not to patients with only one or two BCCs, Dr. Tang noted.
For the latter group, a proof-of-concept trial has randomized eight patients thus far to 1 month of treatment with 400 mg/day of oral itraconazole, a drug that has been on the market for approximately 2 decades and is considered relatively safe, she said. Patients are followed clinically for changes in their BCCs, and they undergo tumor biopsies before and after the 1-month therapy to measure the treatment’s effects on the hedgehog signaling pathway.
Preliminary data are “somewhat promising” in reducing BCC size, Dr. Tang said. The effect has not been as dramatic as with the GDC-0449 study, but neither have the side effects.
“This is very preliminary data but I wanted to share it with the other dermatologists in case some of them would like to put some patients on itraconazole, and, collectively, we can figure out whether or not it has a true effect” on BCC, she said.
In addition to the studies on itraconazole and GDC-0449, studies are underway by other investigators on experimental oral or topical agents by Novartis, Exelixis, and Infinity Pharmaceuticals that address aberrations in the hedgehog signaling pathway for the treatment of BCC.
Major Finding: Group A patients started with a median of 252 BCCs and had 127 at the most recent follow-up.
Data Source: Phase II trial of 41 patients recruited thus far with basal cell nevus syndrome.
Disclosures: Genentech is sponsoring the GDC-0449 trial and provided free medication and travel funds for patients. The investigators have no other conflicts of interest, Dr. Tang said.
Open Mesenteric Approach Still Useful
SCOTTSDALE, ARIZ. -- Despite the fact that open surgery for patients with chronic mesenteric ischemia tends to be reserved for sicker, more complicated patients who aren't good candidates for endovascular revascularization, outcomes have not declined over time.
A single-center review of 116 patients with 203 obstructed mesenteric arteries who underwent open repairs since 1998 found no significant differences in outcomes in 58 patients treated before endovascular treatment became the norm and 58 treated with open surgery during the endovascular era. "We believe that open revascularization still plays an important role in the treatment of this disease," Dr. Evan Ryer and his associates reported at the annual meeting of the Society for Clinical Vascular Surgery.
All patients were symptomatic and had open surgery at the Mayo Clinic, Rochester, Minn., which adopted endovascular treatment in 2002 for most cases of chronic mesenteric ischemia. Starting in that year, approximately 70% of patients with the disease were treated using endovascular revascularization.
"Since 2002, open mesenteric revascularization has been used in only 58 of 176 patients (33%) treated for chronic mesenteric ischemia at the Mayo Clinic," Dr. Ryer said in an interview. "Endovascular revascularization, which is our primary modality of treatment in most patients with suitable lesions, was not performed in these cases because it had failed previously or the anatomy was considered unfavorable because of chronic occlusion, severe calcification, or long-segment stenosis," he explained.
Patients in the pre-endovascular era (1998-2001) and post-endovascular era (2002-2009) who underwent open surgery reported similar durations of symptoms and degrees of weight loss. Compared with the pre-endovascular era patients, however, the post-endovascular era group had significantly higher rates of hypertension (86% vs. 66%), hyperlipidemia (76% vs. 36%), coronary artery disease requiring intervention (29% vs. 14%), cardiac dysrhythmias (28% vs. 7%), postprandial pain (88% vs. 72%), food fear (71% vs. 45%), and need for total parenteral nutrition (10% vs. 2%), as well as higher Society for Vascular Surgery comorbidity severity scores (7 vs. 5).
The extent of disease was greater in post-endovascular era patients, who were more likely to have three-vessel disease (79% vs. 59%) and occluded superior mesenteric arteries (67% vs. 45%) compared with pre-endovascular era patients, Dr. Ryer said. Two-vessel disease accounted for 81% of cases in the pre-endovascular era and 69% of cases in the post-endovascular era. Only 1% of patients in the post-endovascular era and none in the earlier time period had single-vessel disease. The differences between eras in two- and single-vessel disease rates were not significant.
The two time periods did not differ significantly in the technical details of the open procedures or in any outcomes, he added.
In the pre- and post-endovascular eras, patients averaged 4 and 5 days in the intensive care unit, respectively, and 13 and 12 days in the hospital. Among short-term outcomes, symptoms improved in 56% and 54% of patients treated in the pre- and post-endovascular eras, respectively. Two patients in the earlier era and three patients in the more recent era died, and major complications developed in 17 and 21 patients, respectively. These differences between groups were not significant.
After 5 years of follow-up, survival rates were 84% for pre-endovascular era patients and 78% for those in the post-endovascular era. Recurrence-free survival rates were 84% and 76%, respectively, primary patency rates were 82% and 81%, and secondary patency rates were 86% and 82%. None of the differences in outcomes were significant between groups.
The investigators declared they had no conflicts.
SCOTTSDALE, ARIZ. -- Despite the fact that open surgery for patients with chronic mesenteric ischemia tends to be reserved for sicker, more complicated patients who aren't good candidates for endovascular revascularization, outcomes have not declined over time.
A single-center review of 116 patients with 203 obstructed mesenteric arteries who underwent open repairs since 1998 found no significant differences in outcomes in 58 patients treated before endovascular treatment became the norm and 58 treated with open surgery during the endovascular era. "We believe that open revascularization still plays an important role in the treatment of this disease," Dr. Evan Ryer and his associates reported at the annual meeting of the Society for Clinical Vascular Surgery.
All patients were symptomatic and had open surgery at the Mayo Clinic, Rochester, Minn., which adopted endovascular treatment in 2002 for most cases of chronic mesenteric ischemia. Starting in that year, approximately 70% of patients with the disease were treated using endovascular revascularization.
"Since 2002, open mesenteric revascularization has been used in only 58 of 176 patients (33%) treated for chronic mesenteric ischemia at the Mayo Clinic," Dr. Ryer said in an interview. "Endovascular revascularization, which is our primary modality of treatment in most patients with suitable lesions, was not performed in these cases because it had failed previously or the anatomy was considered unfavorable because of chronic occlusion, severe calcification, or long-segment stenosis," he explained.
Patients in the pre-endovascular era (1998-2001) and post-endovascular era (2002-2009) who underwent open surgery reported similar durations of symptoms and degrees of weight loss. Compared with the pre-endovascular era patients, however, the post-endovascular era group had significantly higher rates of hypertension (86% vs. 66%), hyperlipidemia (76% vs. 36%), coronary artery disease requiring intervention (29% vs. 14%), cardiac dysrhythmias (28% vs. 7%), postprandial pain (88% vs. 72%), food fear (71% vs. 45%), and need for total parenteral nutrition (10% vs. 2%), as well as higher Society for Vascular Surgery comorbidity severity scores (7 vs. 5).
The extent of disease was greater in post-endovascular era patients, who were more likely to have three-vessel disease (79% vs. 59%) and occluded superior mesenteric arteries (67% vs. 45%) compared with pre-endovascular era patients, Dr. Ryer said. Two-vessel disease accounted for 81% of cases in the pre-endovascular era and 69% of cases in the post-endovascular era. Only 1% of patients in the post-endovascular era and none in the earlier time period had single-vessel disease. The differences between eras in two- and single-vessel disease rates were not significant.
The two time periods did not differ significantly in the technical details of the open procedures or in any outcomes, he added.
In the pre- and post-endovascular eras, patients averaged 4 and 5 days in the intensive care unit, respectively, and 13 and 12 days in the hospital. Among short-term outcomes, symptoms improved in 56% and 54% of patients treated in the pre- and post-endovascular eras, respectively. Two patients in the earlier era and three patients in the more recent era died, and major complications developed in 17 and 21 patients, respectively. These differences between groups were not significant.
After 5 years of follow-up, survival rates were 84% for pre-endovascular era patients and 78% for those in the post-endovascular era. Recurrence-free survival rates were 84% and 76%, respectively, primary patency rates were 82% and 81%, and secondary patency rates were 86% and 82%. None of the differences in outcomes were significant between groups.
The investigators declared they had no conflicts.
SCOTTSDALE, ARIZ. -- Despite the fact that open surgery for patients with chronic mesenteric ischemia tends to be reserved for sicker, more complicated patients who aren't good candidates for endovascular revascularization, outcomes have not declined over time.
A single-center review of 116 patients with 203 obstructed mesenteric arteries who underwent open repairs since 1998 found no significant differences in outcomes in 58 patients treated before endovascular treatment became the norm and 58 treated with open surgery during the endovascular era. "We believe that open revascularization still plays an important role in the treatment of this disease," Dr. Evan Ryer and his associates reported at the annual meeting of the Society for Clinical Vascular Surgery.
All patients were symptomatic and had open surgery at the Mayo Clinic, Rochester, Minn., which adopted endovascular treatment in 2002 for most cases of chronic mesenteric ischemia. Starting in that year, approximately 70% of patients with the disease were treated using endovascular revascularization.
"Since 2002, open mesenteric revascularization has been used in only 58 of 176 patients (33%) treated for chronic mesenteric ischemia at the Mayo Clinic," Dr. Ryer said in an interview. "Endovascular revascularization, which is our primary modality of treatment in most patients with suitable lesions, was not performed in these cases because it had failed previously or the anatomy was considered unfavorable because of chronic occlusion, severe calcification, or long-segment stenosis," he explained.
Patients in the pre-endovascular era (1998-2001) and post-endovascular era (2002-2009) who underwent open surgery reported similar durations of symptoms and degrees of weight loss. Compared with the pre-endovascular era patients, however, the post-endovascular era group had significantly higher rates of hypertension (86% vs. 66%), hyperlipidemia (76% vs. 36%), coronary artery disease requiring intervention (29% vs. 14%), cardiac dysrhythmias (28% vs. 7%), postprandial pain (88% vs. 72%), food fear (71% vs. 45%), and need for total parenteral nutrition (10% vs. 2%), as well as higher Society for Vascular Surgery comorbidity severity scores (7 vs. 5).
The extent of disease was greater in post-endovascular era patients, who were more likely to have three-vessel disease (79% vs. 59%) and occluded superior mesenteric arteries (67% vs. 45%) compared with pre-endovascular era patients, Dr. Ryer said. Two-vessel disease accounted for 81% of cases in the pre-endovascular era and 69% of cases in the post-endovascular era. Only 1% of patients in the post-endovascular era and none in the earlier time period had single-vessel disease. The differences between eras in two- and single-vessel disease rates were not significant.
The two time periods did not differ significantly in the technical details of the open procedures or in any outcomes, he added.
In the pre- and post-endovascular eras, patients averaged 4 and 5 days in the intensive care unit, respectively, and 13 and 12 days in the hospital. Among short-term outcomes, symptoms improved in 56% and 54% of patients treated in the pre- and post-endovascular eras, respectively. Two patients in the earlier era and three patients in the more recent era died, and major complications developed in 17 and 21 patients, respectively. These differences between groups were not significant.
After 5 years of follow-up, survival rates were 84% for pre-endovascular era patients and 78% for those in the post-endovascular era. Recurrence-free survival rates were 84% and 76%, respectively, primary patency rates were 82% and 81%, and secondary patency rates were 86% and 82%. None of the differences in outcomes were significant between groups.
The investigators declared they had no conflicts.
Massive Transfusion Protocol Ups RBCs, Plasma
SAN FRANCISCO — From the front lines of war comes a new protocol for preserving life during massive blood transfusion to treat maternal hemorrhage.
Physicians providing trauma care during the Iraq war noticed that giving fresh frozen plasma earlier to patients requiring massive transfusion and making a few other changes in conventional transfusion protocols decreased coagulopathy and improved the well-being of patients, Dr. Mark D. Rollins said at the meeting sponsored by the University of California, San Francisco.
Subsequent retrospective studies in civilians and a prospective study that was completed this year supported the military's suggestion that increasing ratios of plasma and platelets to red blood cells (RBCs) would improve survival in massive transfusions.
Responding to these new ideas, the California Maternal Quality Care Collaborative convened an Obstetric Hemorrhage Expert Task Force, which incorporated these cutting-edge recommendations into a free Obstetric Hemorrhage Toolkit (available at www.cmqcc.org/ob_hemorrhage
“I'm not saying we have a ton of evidence,” but the limited evidence available was sufficient to justify modifying protocols for managing maternal hemorrhage, said Dr. Rollins, an obstetric anesthesiologist at the university and a member of the California Maternal Hemorrhage Collaborative.
The military observations, published in 2007 (J. Trauma 2007;62:112-9), were followed by a retrospective study of 466 civilians who underwent massive transfusions at 16 U.S. trauma centers (Ann. Surg. 2008;248:447-59). That study found better survival using increased ratios of plasma and platelets to RBCs in massive transfusions.
Conventional guidelines called for a 1:3 ratio of plasma to RBCs, and the military called for a 1:1 ratio, with no recommendation for the ratio of platelets to RBCs. The civilian study found 30-day survival was 60% in patients who received more than 1 U of plasma or platelets with every 2 U of RBCs, compared with 40% survival with lower ratios of plasma or platelets to RBCs, so the investigators recommended a 1:1:1 ratio of plasma, platelets, and RBCs in massive transfusions.
A randomized, controlled trial of 214 civilian trauma patients, completed this year by Dr. Rollins and his associates, found significantly increased 30-day survival rates with higher ratios of plasma, platelets, or cryoprecipitate to RBCs in massive transfusions, defined as more than 10 RBC products transfused within 24 hours (Transfusion 2010;50:493-500).
Survival was 59% after transfusions with at least 1 U of plasma per 2 of RBCs, compared with 44% with ratios of 1:3 or more. For platelets, survival rates were 63% with at least 1:1 ratios, compared with 33% with ratios of 1:2 or more. Higher ratios of cryoprecipitate to RBCs improved survival, compared with lower ratios: 66% vs. 41%, respectively.
In developed countries, hemorrhage causes 13% of maternal deaths and is the third-leading cause of maternal death, with higher rates in other countries, according to a World Health Organization report (Lancet 2006;367:1066-74).
Death rates from postpartum hemorrhage have increased from approximately 2% in 1994 to 3% in 2006 in the United States, and from 4% to 5% in Canada during that time period.
“In the past couple of years, we've had two or three deaths right here in the San Francisco Bay Area in our hospitals from maternal hemorrhage,” he said.
Disclosures: He reported having no conflicts of interest related to these topics.
Managing Massive Transfusions
For best management of massive obstetric transfusions, consider these steps, Dr. Rollins said:
▸ Get into good communication with your blood bank, and ask for supplies for massive transfusions in packs of multiple units of RBCs and fresh frozen plasma—potentially even platelets—that arrive together. “This just helps remind everyone as those packs arrive that they should be giving the fresh frozen plasma with the red cells,” he said. Make sure the blood bank knows exactly which room you're in.
▸ Have a team ready to mobilize, including a second anesthesiologist, a second surgeon, additional nurses, and runners for laboratory tests and blood products.
▸ Move expeditiously to an operating room if you're not already in one.
▸ If you're considering options such as interventional radiology, call those teams early to give them time to set up.
▸ Place large-bore IVs (16-14 gauge). “I like to think that goes without saying, but plenty of times I've had people come in with just 20-gauge IVs put in, and you can't transfuse enough through them to make a difference,” Dr. Rollins said.
▸ Place invasive monitoring equipment.
▸ Repeat laboratory tests frequently, but don't wait for results to proceed with transfusion. Results will be useful later to assess how the case developed. Use point-of-care testing if it's available for faster results.
▸ Consider using fluid warmers and forced-air warmers to keep patients from becoming hypothermic and more coagulopathic.
▸ Have rapid infusion pumps or pressure bags available to speed the transfusion.
▸ Prepare for general anesthesia.
▸ Have vasopressors and uterotonics immediately available.
▸ Have a supply of calcium chloride on hand to prevent the low levels of ionized calcium that can occur after rapid transfusion. Citrates in blood products bind with calcium, increasing the risk of extreme hypotension and depressed heart function.
▸ Have a Foley catheter (for measuring urine output) and compression stockings available.
▸ Reserve an ICU bed.
▸ Ask for additional packs of blood products if needed.
▸ Consider giving cryoprecipitate (fibrinogen less than 100 mg/dL).
▸ Consider off-label treatment with recombinant factor VIIa only after the patient has received approximately 10 U of packed RBCs and full factor replacement. “It's not a first-line drug. There's plenty of morbidity and mortality that can occur” with factor VIIa, he noted. “Having said that, I do believe that it is very effective in certain situations.”
▸ Designate someone to tally and record the use of blood products and estimated blood loss.
▸ Bring the “code cart” into the OR early.
▸ Afterward, meet for 3-5 minutes with everyone who worked on the case to review what went well, what didn't, and ideas for improvement.
SAN FRANCISCO — From the front lines of war comes a new protocol for preserving life during massive blood transfusion to treat maternal hemorrhage.
Physicians providing trauma care during the Iraq war noticed that giving fresh frozen plasma earlier to patients requiring massive transfusion and making a few other changes in conventional transfusion protocols decreased coagulopathy and improved the well-being of patients, Dr. Mark D. Rollins said at the meeting sponsored by the University of California, San Francisco.
Subsequent retrospective studies in civilians and a prospective study that was completed this year supported the military's suggestion that increasing ratios of plasma and platelets to red blood cells (RBCs) would improve survival in massive transfusions.
Responding to these new ideas, the California Maternal Quality Care Collaborative convened an Obstetric Hemorrhage Expert Task Force, which incorporated these cutting-edge recommendations into a free Obstetric Hemorrhage Toolkit (available at www.cmqcc.org/ob_hemorrhage
“I'm not saying we have a ton of evidence,” but the limited evidence available was sufficient to justify modifying protocols for managing maternal hemorrhage, said Dr. Rollins, an obstetric anesthesiologist at the university and a member of the California Maternal Hemorrhage Collaborative.
The military observations, published in 2007 (J. Trauma 2007;62:112-9), were followed by a retrospective study of 466 civilians who underwent massive transfusions at 16 U.S. trauma centers (Ann. Surg. 2008;248:447-59). That study found better survival using increased ratios of plasma and platelets to RBCs in massive transfusions.
Conventional guidelines called for a 1:3 ratio of plasma to RBCs, and the military called for a 1:1 ratio, with no recommendation for the ratio of platelets to RBCs. The civilian study found 30-day survival was 60% in patients who received more than 1 U of plasma or platelets with every 2 U of RBCs, compared with 40% survival with lower ratios of plasma or platelets to RBCs, so the investigators recommended a 1:1:1 ratio of plasma, platelets, and RBCs in massive transfusions.
A randomized, controlled trial of 214 civilian trauma patients, completed this year by Dr. Rollins and his associates, found significantly increased 30-day survival rates with higher ratios of plasma, platelets, or cryoprecipitate to RBCs in massive transfusions, defined as more than 10 RBC products transfused within 24 hours (Transfusion 2010;50:493-500).
Survival was 59% after transfusions with at least 1 U of plasma per 2 of RBCs, compared with 44% with ratios of 1:3 or more. For platelets, survival rates were 63% with at least 1:1 ratios, compared with 33% with ratios of 1:2 or more. Higher ratios of cryoprecipitate to RBCs improved survival, compared with lower ratios: 66% vs. 41%, respectively.
In developed countries, hemorrhage causes 13% of maternal deaths and is the third-leading cause of maternal death, with higher rates in other countries, according to a World Health Organization report (Lancet 2006;367:1066-74).
Death rates from postpartum hemorrhage have increased from approximately 2% in 1994 to 3% in 2006 in the United States, and from 4% to 5% in Canada during that time period.
“In the past couple of years, we've had two or three deaths right here in the San Francisco Bay Area in our hospitals from maternal hemorrhage,” he said.
Disclosures: He reported having no conflicts of interest related to these topics.
Managing Massive Transfusions
For best management of massive obstetric transfusions, consider these steps, Dr. Rollins said:
▸ Get into good communication with your blood bank, and ask for supplies for massive transfusions in packs of multiple units of RBCs and fresh frozen plasma—potentially even platelets—that arrive together. “This just helps remind everyone as those packs arrive that they should be giving the fresh frozen plasma with the red cells,” he said. Make sure the blood bank knows exactly which room you're in.
▸ Have a team ready to mobilize, including a second anesthesiologist, a second surgeon, additional nurses, and runners for laboratory tests and blood products.
▸ Move expeditiously to an operating room if you're not already in one.
▸ If you're considering options such as interventional radiology, call those teams early to give them time to set up.
▸ Place large-bore IVs (16-14 gauge). “I like to think that goes without saying, but plenty of times I've had people come in with just 20-gauge IVs put in, and you can't transfuse enough through them to make a difference,” Dr. Rollins said.
▸ Place invasive monitoring equipment.
▸ Repeat laboratory tests frequently, but don't wait for results to proceed with transfusion. Results will be useful later to assess how the case developed. Use point-of-care testing if it's available for faster results.
▸ Consider using fluid warmers and forced-air warmers to keep patients from becoming hypothermic and more coagulopathic.
▸ Have rapid infusion pumps or pressure bags available to speed the transfusion.
▸ Prepare for general anesthesia.
▸ Have vasopressors and uterotonics immediately available.
▸ Have a supply of calcium chloride on hand to prevent the low levels of ionized calcium that can occur after rapid transfusion. Citrates in blood products bind with calcium, increasing the risk of extreme hypotension and depressed heart function.
▸ Have a Foley catheter (for measuring urine output) and compression stockings available.
▸ Reserve an ICU bed.
▸ Ask for additional packs of blood products if needed.
▸ Consider giving cryoprecipitate (fibrinogen less than 100 mg/dL).
▸ Consider off-label treatment with recombinant factor VIIa only after the patient has received approximately 10 U of packed RBCs and full factor replacement. “It's not a first-line drug. There's plenty of morbidity and mortality that can occur” with factor VIIa, he noted. “Having said that, I do believe that it is very effective in certain situations.”
▸ Designate someone to tally and record the use of blood products and estimated blood loss.
▸ Bring the “code cart” into the OR early.
▸ Afterward, meet for 3-5 minutes with everyone who worked on the case to review what went well, what didn't, and ideas for improvement.
SAN FRANCISCO — From the front lines of war comes a new protocol for preserving life during massive blood transfusion to treat maternal hemorrhage.
Physicians providing trauma care during the Iraq war noticed that giving fresh frozen plasma earlier to patients requiring massive transfusion and making a few other changes in conventional transfusion protocols decreased coagulopathy and improved the well-being of patients, Dr. Mark D. Rollins said at the meeting sponsored by the University of California, San Francisco.
Subsequent retrospective studies in civilians and a prospective study that was completed this year supported the military's suggestion that increasing ratios of plasma and platelets to red blood cells (RBCs) would improve survival in massive transfusions.
Responding to these new ideas, the California Maternal Quality Care Collaborative convened an Obstetric Hemorrhage Expert Task Force, which incorporated these cutting-edge recommendations into a free Obstetric Hemorrhage Toolkit (available at www.cmqcc.org/ob_hemorrhage
“I'm not saying we have a ton of evidence,” but the limited evidence available was sufficient to justify modifying protocols for managing maternal hemorrhage, said Dr. Rollins, an obstetric anesthesiologist at the university and a member of the California Maternal Hemorrhage Collaborative.
The military observations, published in 2007 (J. Trauma 2007;62:112-9), were followed by a retrospective study of 466 civilians who underwent massive transfusions at 16 U.S. trauma centers (Ann. Surg. 2008;248:447-59). That study found better survival using increased ratios of plasma and platelets to RBCs in massive transfusions.
Conventional guidelines called for a 1:3 ratio of plasma to RBCs, and the military called for a 1:1 ratio, with no recommendation for the ratio of platelets to RBCs. The civilian study found 30-day survival was 60% in patients who received more than 1 U of plasma or platelets with every 2 U of RBCs, compared with 40% survival with lower ratios of plasma or platelets to RBCs, so the investigators recommended a 1:1:1 ratio of plasma, platelets, and RBCs in massive transfusions.
A randomized, controlled trial of 214 civilian trauma patients, completed this year by Dr. Rollins and his associates, found significantly increased 30-day survival rates with higher ratios of plasma, platelets, or cryoprecipitate to RBCs in massive transfusions, defined as more than 10 RBC products transfused within 24 hours (Transfusion 2010;50:493-500).
Survival was 59% after transfusions with at least 1 U of plasma per 2 of RBCs, compared with 44% with ratios of 1:3 or more. For platelets, survival rates were 63% with at least 1:1 ratios, compared with 33% with ratios of 1:2 or more. Higher ratios of cryoprecipitate to RBCs improved survival, compared with lower ratios: 66% vs. 41%, respectively.
In developed countries, hemorrhage causes 13% of maternal deaths and is the third-leading cause of maternal death, with higher rates in other countries, according to a World Health Organization report (Lancet 2006;367:1066-74).
Death rates from postpartum hemorrhage have increased from approximately 2% in 1994 to 3% in 2006 in the United States, and from 4% to 5% in Canada during that time period.
“In the past couple of years, we've had two or three deaths right here in the San Francisco Bay Area in our hospitals from maternal hemorrhage,” he said.
Disclosures: He reported having no conflicts of interest related to these topics.
Managing Massive Transfusions
For best management of massive obstetric transfusions, consider these steps, Dr. Rollins said:
▸ Get into good communication with your blood bank, and ask for supplies for massive transfusions in packs of multiple units of RBCs and fresh frozen plasma—potentially even platelets—that arrive together. “This just helps remind everyone as those packs arrive that they should be giving the fresh frozen plasma with the red cells,” he said. Make sure the blood bank knows exactly which room you're in.
▸ Have a team ready to mobilize, including a second anesthesiologist, a second surgeon, additional nurses, and runners for laboratory tests and blood products.
▸ Move expeditiously to an operating room if you're not already in one.
▸ If you're considering options such as interventional radiology, call those teams early to give them time to set up.
▸ Place large-bore IVs (16-14 gauge). “I like to think that goes without saying, but plenty of times I've had people come in with just 20-gauge IVs put in, and you can't transfuse enough through them to make a difference,” Dr. Rollins said.
▸ Place invasive monitoring equipment.
▸ Repeat laboratory tests frequently, but don't wait for results to proceed with transfusion. Results will be useful later to assess how the case developed. Use point-of-care testing if it's available for faster results.
▸ Consider using fluid warmers and forced-air warmers to keep patients from becoming hypothermic and more coagulopathic.
▸ Have rapid infusion pumps or pressure bags available to speed the transfusion.
▸ Prepare for general anesthesia.
▸ Have vasopressors and uterotonics immediately available.
▸ Have a supply of calcium chloride on hand to prevent the low levels of ionized calcium that can occur after rapid transfusion. Citrates in blood products bind with calcium, increasing the risk of extreme hypotension and depressed heart function.
▸ Have a Foley catheter (for measuring urine output) and compression stockings available.
▸ Reserve an ICU bed.
▸ Ask for additional packs of blood products if needed.
▸ Consider giving cryoprecipitate (fibrinogen less than 100 mg/dL).
▸ Consider off-label treatment with recombinant factor VIIa only after the patient has received approximately 10 U of packed RBCs and full factor replacement. “It's not a first-line drug. There's plenty of morbidity and mortality that can occur” with factor VIIa, he noted. “Having said that, I do believe that it is very effective in certain situations.”
▸ Designate someone to tally and record the use of blood products and estimated blood loss.
▸ Bring the “code cart” into the OR early.
▸ Afterward, meet for 3-5 minutes with everyone who worked on the case to review what went well, what didn't, and ideas for improvement.
From a meeting on Antepartum and Intrapartum Management
Injury History Associated With Comorbidities in Migraineurs
Major Finding: Adults with migraines and a history of head or neck injury had more frequent headaches than did migraineurs without injuries (16 vs. 13 days/month, respectively) as well as disabling headaches (mean score on the Headache Impact Test-6, 60 vs. 54, respectively) and higher rates of various comorbidities.
Data Source: Self-administered electronic questionnaires completed by 1,348 clinic patients.
Disclosures: Dr. Tietjen has received research grants from GlaxoSmithKline and consulting fees and honoraria from MAP Pharmaceuticals. A grant from the American Headache Society's Women's Issues Section funded the study.
LOS ANGELES — Migraine patients with a history of head or neck injury reported more frequent and disabling headaches and higher rates of a variety of comorbidities than did migraineurs without head or neck injuries in a survey of 1,348 adult patients.
Some migraine features differed significantly between patients with or without a history of head or neck injury, according to responses to electronic questionnaires that were completed by patients seen in clinics for their migraine headaches, Dr. Gretchen E. Tietjen reported.
In the survey, Dr. Tietjen and her associates gathered information from 373 patients with a history of head or neck injury. They averaged 16 days with headaches per month, compared with 13 days per month in 975 noninjured patients. Chronic headaches (defined as headaches occurring more than 15 days/month) were a problem for 42% of patients with a history of injury and 31% of those who had not been injured. Scores on the Headache Impact Test–6 averaged 60 in the injured group and 54 in the noninjured group, suggesting a greater impact of headaches on daily life in the injured group.
Comparing the injured group with the noninjured group, prevalence rates were 52% vs. 35% for depression, 40% vs. 27% for anxiety, 37% vs. 21% for arthritis, and 30% vs. 21% for irritable bowel syndrome. Other differences in prevalence rates were 16% vs. 7% for fibromyalgia, 11% vs. 6% for sleep apnea, 9% vs. 5% for interstitial cystitis, and 17% vs. 10% for uterine fibroids, respectively. Each of these differences between groups was statistically significant.
Patients developed symptoms of these comorbidities and were diagnosed at an earlier age if they had a history of injury than if they had not been injured. The onset of depression, anxiety, sleep apnea, and fibromyalgia occurred at a significantly earlier age in those who had been injured than in those who had not, said Dr. Tietjen, professor and chair of neurology at the University of Toledo (Ohio).
Patients with a history of injury were significantly more likely to have a history of substance abuse (24%), compared with noninjured patients (16%), and to have an education level no higher than high school (32% vs. 25%, respectively).
Among patients with a history of head or neck injury in whom the timing of the injury was known, the 45 patients whose migraines started concurrently with the injury were less likely to have migraine with aura, compared with the 170 patients whose migraines started prior to the injury or the 109 patients whose migraines began after the injury. The migraines came with aura in 22% of the subgroup with concurrent-onset migraine, 45% of the subgroup with migraine before their injury, and 47% of those with migraine after their injury.
Patients in the concurrent-onset group also were significantly younger (average age, 40 years), compared with the patients whose migraines started before the injury (42 years) or patients whose migraines started after injury (44 years).
The questionnaire did not ask about the nature or causes of the head and neck injuries. Patients were asked about the number of head and neck injuries, their age at the first one, their age at the worst injury, whether or not there was a loss of consciousness associated with the injury, and when they were diagnosed with migraine headache.
A physician in the audience asked whether the head injuries might have contributed to the development of psychosomatic syndromes that increased the prevalence of comorbidities. Dr. Tietjen doubted that this was the case, given the wide nature of the comorbidities that included conditions such as uterine fibroids.
{kind=link}
The prevalence of depression was 52% in the injured group vs. 35% in the noninjured group.
Source DR. TIETJEN
Major Finding: Adults with migraines and a history of head or neck injury had more frequent headaches than did migraineurs without injuries (16 vs. 13 days/month, respectively) as well as disabling headaches (mean score on the Headache Impact Test-6, 60 vs. 54, respectively) and higher rates of various comorbidities.
Data Source: Self-administered electronic questionnaires completed by 1,348 clinic patients.
Disclosures: Dr. Tietjen has received research grants from GlaxoSmithKline and consulting fees and honoraria from MAP Pharmaceuticals. A grant from the American Headache Society's Women's Issues Section funded the study.
LOS ANGELES — Migraine patients with a history of head or neck injury reported more frequent and disabling headaches and higher rates of a variety of comorbidities than did migraineurs without head or neck injuries in a survey of 1,348 adult patients.
Some migraine features differed significantly between patients with or without a history of head or neck injury, according to responses to electronic questionnaires that were completed by patients seen in clinics for their migraine headaches, Dr. Gretchen E. Tietjen reported.
In the survey, Dr. Tietjen and her associates gathered information from 373 patients with a history of head or neck injury. They averaged 16 days with headaches per month, compared with 13 days per month in 975 noninjured patients. Chronic headaches (defined as headaches occurring more than 15 days/month) were a problem for 42% of patients with a history of injury and 31% of those who had not been injured. Scores on the Headache Impact Test–6 averaged 60 in the injured group and 54 in the noninjured group, suggesting a greater impact of headaches on daily life in the injured group.
Comparing the injured group with the noninjured group, prevalence rates were 52% vs. 35% for depression, 40% vs. 27% for anxiety, 37% vs. 21% for arthritis, and 30% vs. 21% for irritable bowel syndrome. Other differences in prevalence rates were 16% vs. 7% for fibromyalgia, 11% vs. 6% for sleep apnea, 9% vs. 5% for interstitial cystitis, and 17% vs. 10% for uterine fibroids, respectively. Each of these differences between groups was statistically significant.
Patients developed symptoms of these comorbidities and were diagnosed at an earlier age if they had a history of injury than if they had not been injured. The onset of depression, anxiety, sleep apnea, and fibromyalgia occurred at a significantly earlier age in those who had been injured than in those who had not, said Dr. Tietjen, professor and chair of neurology at the University of Toledo (Ohio).
Patients with a history of injury were significantly more likely to have a history of substance abuse (24%), compared with noninjured patients (16%), and to have an education level no higher than high school (32% vs. 25%, respectively).
Among patients with a history of head or neck injury in whom the timing of the injury was known, the 45 patients whose migraines started concurrently with the injury were less likely to have migraine with aura, compared with the 170 patients whose migraines started prior to the injury or the 109 patients whose migraines began after the injury. The migraines came with aura in 22% of the subgroup with concurrent-onset migraine, 45% of the subgroup with migraine before their injury, and 47% of those with migraine after their injury.
Patients in the concurrent-onset group also were significantly younger (average age, 40 years), compared with the patients whose migraines started before the injury (42 years) or patients whose migraines started after injury (44 years).
The questionnaire did not ask about the nature or causes of the head and neck injuries. Patients were asked about the number of head and neck injuries, their age at the first one, their age at the worst injury, whether or not there was a loss of consciousness associated with the injury, and when they were diagnosed with migraine headache.
A physician in the audience asked whether the head injuries might have contributed to the development of psychosomatic syndromes that increased the prevalence of comorbidities. Dr. Tietjen doubted that this was the case, given the wide nature of the comorbidities that included conditions such as uterine fibroids.
The prevalence of depression was 52% in the injured group vs. 35% in the noninjured group.
Source DR. TIETJEN
Major Finding: Adults with migraines and a history of head or neck injury had more frequent headaches than did migraineurs without injuries (16 vs. 13 days/month, respectively) as well as disabling headaches (mean score on the Headache Impact Test-6, 60 vs. 54, respectively) and higher rates of various comorbidities.
Data Source: Self-administered electronic questionnaires completed by 1,348 clinic patients.
Disclosures: Dr. Tietjen has received research grants from GlaxoSmithKline and consulting fees and honoraria from MAP Pharmaceuticals. A grant from the American Headache Society's Women's Issues Section funded the study.
LOS ANGELES — Migraine patients with a history of head or neck injury reported more frequent and disabling headaches and higher rates of a variety of comorbidities than did migraineurs without head or neck injuries in a survey of 1,348 adult patients.
Some migraine features differed significantly between patients with or without a history of head or neck injury, according to responses to electronic questionnaires that were completed by patients seen in clinics for their migraine headaches, Dr. Gretchen E. Tietjen reported.
In the survey, Dr. Tietjen and her associates gathered information from 373 patients with a history of head or neck injury. They averaged 16 days with headaches per month, compared with 13 days per month in 975 noninjured patients. Chronic headaches (defined as headaches occurring more than 15 days/month) were a problem for 42% of patients with a history of injury and 31% of those who had not been injured. Scores on the Headache Impact Test–6 averaged 60 in the injured group and 54 in the noninjured group, suggesting a greater impact of headaches on daily life in the injured group.
Comparing the injured group with the noninjured group, prevalence rates were 52% vs. 35% for depression, 40% vs. 27% for anxiety, 37% vs. 21% for arthritis, and 30% vs. 21% for irritable bowel syndrome. Other differences in prevalence rates were 16% vs. 7% for fibromyalgia, 11% vs. 6% for sleep apnea, 9% vs. 5% for interstitial cystitis, and 17% vs. 10% for uterine fibroids, respectively. Each of these differences between groups was statistically significant.
Patients developed symptoms of these comorbidities and were diagnosed at an earlier age if they had a history of injury than if they had not been injured. The onset of depression, anxiety, sleep apnea, and fibromyalgia occurred at a significantly earlier age in those who had been injured than in those who had not, said Dr. Tietjen, professor and chair of neurology at the University of Toledo (Ohio).
Patients with a history of injury were significantly more likely to have a history of substance abuse (24%), compared with noninjured patients (16%), and to have an education level no higher than high school (32% vs. 25%, respectively).
Among patients with a history of head or neck injury in whom the timing of the injury was known, the 45 patients whose migraines started concurrently with the injury were less likely to have migraine with aura, compared with the 170 patients whose migraines started prior to the injury or the 109 patients whose migraines began after the injury. The migraines came with aura in 22% of the subgroup with concurrent-onset migraine, 45% of the subgroup with migraine before their injury, and 47% of those with migraine after their injury.
Patients in the concurrent-onset group also were significantly younger (average age, 40 years), compared with the patients whose migraines started before the injury (42 years) or patients whose migraines started after injury (44 years).
The questionnaire did not ask about the nature or causes of the head and neck injuries. Patients were asked about the number of head and neck injuries, their age at the first one, their age at the worst injury, whether or not there was a loss of consciousness associated with the injury, and when they were diagnosed with migraine headache.
A physician in the audience asked whether the head injuries might have contributed to the development of psychosomatic syndromes that increased the prevalence of comorbidities. Dr. Tietjen doubted that this was the case, given the wide nature of the comorbidities that included conditions such as uterine fibroids.
The prevalence of depression was 52% in the injured group vs. 35% in the noninjured group.
Source DR. TIETJEN
Headaches Persist Long Term in TBI Patients
Major Finding: Headaches, initially reported by 46% of patients soon after injury, still occurred in 48% at 3 months, 44% at 6 months, and 46% at 12 months.
Data Source: Prospective study of 377 consecutive admissions to acute rehabilitation facilities for traumatic brain injury.
Disclosures: Dr. Lucas said she has no relevant conflicts of interest. The National Institute on Disability and Rehabilitation Research funded the study.
LOS ANGELES — Nearly half of 377 patients with traumatic brain injury reported postinjury headaches that persisted during a year of follow-up in a prospective study.
The prevalence of headaches in the cohort increased from 18% before the injury to 46% soon after injury, according to patient reports during rehabilitation hospitalization for TBI. In phone interviews after discharge at 3, 6, and 12 months post injury, headaches were reported by 48%, 44%, and 46%, respectively.
The persistence of the headaches took senior investigator Dr. Sylvia Lucas and her colleagues by surprise, because previous data have suggested that 18%-22% of posttraumatic headaches are chronic problems.
Dr. Lucas said that she and her associates also were surprised that most of the headaches in the current study were classified as migraine or tension-type headache, that the presence of preinjury headache seemed to be a risk factor for postinjury headache, and that women were at higher risk for postinjury headache.
The findings on types of headache and their persistence could have “important implications for treatment” of posttraumatic headache, said Dr. Lucas, founder and director of the headache center at the University of Washington, Seattle.
Posttraumatic headache is one of the most common persisting symptoms after TBI, occurring in 30%-90% of patients, previous studies suggest. Although most familiar as a salient symptom in soldiers who were exposed to explosive blasts, “it's becoming of great interest in adolescent children who've been in sports concussion injuries,” she said at the meeting.
The study included consecutive admissions of patients older than 16 years at seven acute rehabilitation facilities for TBI, excluding 79 patients who could not provide consent or answer questions themselves without their families' acting as proxy.
The cause of injury was vehicular trauma in approximately 56%, falls or impacts with flying objects in 28%, violence in 9%, and sports or pedestrian accidents in 4% each. (Percentages were rounded.)
Based on descriptions of symptoms by patients who reported headache, 60% of preinjury headaches were classified as migraine or probable migraine, compared with 48% soon after injury and 54% a year later. Although 25% of preinjury headaches and 37% of headaches soon after injury were deemed “unclassifiable” by investigators using patients' descriptions, over time they gained features that allowed them to be classified in one of the primary headache classifications, so that the proportion of “unclassified” headaches fell to 19% by 12 months post injury.
“Mostly, patients were classified as migraine with or without aura, or as tension-type headache, which is also surprising given the fact that most of these were vehicular injuries,” Dr. Lucas said. Headaches were classified as tension-type in 12% before injury, in 7% soon after injury, and in 19% at 12 months. Headaches were classified as cervicogenic in 4% before injury, in 8% soon after injury, and in 5% at 12 months.
Among patients who said they suffered headaches before the injury, 48% reported postinjury headache, compared with 23% of patients who said they did not have headaches before the injury. “Preinjury headache may be a risk factor for posttraumatic headache. This may argue for a common underlying mechanism,” Dr. Lucas said.
The cohort was 71% male and 75% white. Patients had an average age of 43 years, and 84% were able to be discharged to home. The injury caused posttraumatic amnesia for less than a day in 7% (indicative of a milder head injury), for 1-7 days in 21%, for 8-28 days in 42%, and for 29 or more days in 30%.
“This was primarily a male group; however, along all the time points studied—at baseline, 3 months, 6 months, and 12 months—there was a significant difference in women having more posttraumatic headache than men,” as well as a higher incidence of preinjury headache, she said. About 40% of men had headache at all follow-up times after injury, vs. 60% of women.
A physician in the audience asked if there was any relationship between insurance claims and reports that the headaches were persisting. “At the time of our study, that information was not available,” she responded.
{kind=link}
More attention is being directed to adolescent children who've been in sports concussion injuries.
Source DR. LUCAS
Major Finding: Headaches, initially reported by 46% of patients soon after injury, still occurred in 48% at 3 months, 44% at 6 months, and 46% at 12 months.
Data Source: Prospective study of 377 consecutive admissions to acute rehabilitation facilities for traumatic brain injury.
Disclosures: Dr. Lucas said she has no relevant conflicts of interest. The National Institute on Disability and Rehabilitation Research funded the study.
LOS ANGELES — Nearly half of 377 patients with traumatic brain injury reported postinjury headaches that persisted during a year of follow-up in a prospective study.
The prevalence of headaches in the cohort increased from 18% before the injury to 46% soon after injury, according to patient reports during rehabilitation hospitalization for TBI. In phone interviews after discharge at 3, 6, and 12 months post injury, headaches were reported by 48%, 44%, and 46%, respectively.
The persistence of the headaches took senior investigator Dr. Sylvia Lucas and her colleagues by surprise, because previous data have suggested that 18%-22% of posttraumatic headaches are chronic problems.
Dr. Lucas said that she and her associates also were surprised that most of the headaches in the current study were classified as migraine or tension-type headache, that the presence of preinjury headache seemed to be a risk factor for postinjury headache, and that women were at higher risk for postinjury headache.
The findings on types of headache and their persistence could have “important implications for treatment” of posttraumatic headache, said Dr. Lucas, founder and director of the headache center at the University of Washington, Seattle.
Posttraumatic headache is one of the most common persisting symptoms after TBI, occurring in 30%-90% of patients, previous studies suggest. Although most familiar as a salient symptom in soldiers who were exposed to explosive blasts, “it's becoming of great interest in adolescent children who've been in sports concussion injuries,” she said at the meeting.
The study included consecutive admissions of patients older than 16 years at seven acute rehabilitation facilities for TBI, excluding 79 patients who could not provide consent or answer questions themselves without their families' acting as proxy.
The cause of injury was vehicular trauma in approximately 56%, falls or impacts with flying objects in 28%, violence in 9%, and sports or pedestrian accidents in 4% each. (Percentages were rounded.)
Based on descriptions of symptoms by patients who reported headache, 60% of preinjury headaches were classified as migraine or probable migraine, compared with 48% soon after injury and 54% a year later. Although 25% of preinjury headaches and 37% of headaches soon after injury were deemed “unclassifiable” by investigators using patients' descriptions, over time they gained features that allowed them to be classified in one of the primary headache classifications, so that the proportion of “unclassified” headaches fell to 19% by 12 months post injury.
“Mostly, patients were classified as migraine with or without aura, or as tension-type headache, which is also surprising given the fact that most of these were vehicular injuries,” Dr. Lucas said. Headaches were classified as tension-type in 12% before injury, in 7% soon after injury, and in 19% at 12 months. Headaches were classified as cervicogenic in 4% before injury, in 8% soon after injury, and in 5% at 12 months.
Among patients who said they suffered headaches before the injury, 48% reported postinjury headache, compared with 23% of patients who said they did not have headaches before the injury. “Preinjury headache may be a risk factor for posttraumatic headache. This may argue for a common underlying mechanism,” Dr. Lucas said.
The cohort was 71% male and 75% white. Patients had an average age of 43 years, and 84% were able to be discharged to home. The injury caused posttraumatic amnesia for less than a day in 7% (indicative of a milder head injury), for 1-7 days in 21%, for 8-28 days in 42%, and for 29 or more days in 30%.
“This was primarily a male group; however, along all the time points studied—at baseline, 3 months, 6 months, and 12 months—there was a significant difference in women having more posttraumatic headache than men,” as well as a higher incidence of preinjury headache, she said. About 40% of men had headache at all follow-up times after injury, vs. 60% of women.
A physician in the audience asked if there was any relationship between insurance claims and reports that the headaches were persisting. “At the time of our study, that information was not available,” she responded.
More attention is being directed to adolescent children who've been in sports concussion injuries.
Source DR. LUCAS
Major Finding: Headaches, initially reported by 46% of patients soon after injury, still occurred in 48% at 3 months, 44% at 6 months, and 46% at 12 months.
Data Source: Prospective study of 377 consecutive admissions to acute rehabilitation facilities for traumatic brain injury.
Disclosures: Dr. Lucas said she has no relevant conflicts of interest. The National Institute on Disability and Rehabilitation Research funded the study.
LOS ANGELES — Nearly half of 377 patients with traumatic brain injury reported postinjury headaches that persisted during a year of follow-up in a prospective study.
The prevalence of headaches in the cohort increased from 18% before the injury to 46% soon after injury, according to patient reports during rehabilitation hospitalization for TBI. In phone interviews after discharge at 3, 6, and 12 months post injury, headaches were reported by 48%, 44%, and 46%, respectively.
The persistence of the headaches took senior investigator Dr. Sylvia Lucas and her colleagues by surprise, because previous data have suggested that 18%-22% of posttraumatic headaches are chronic problems.
Dr. Lucas said that she and her associates also were surprised that most of the headaches in the current study were classified as migraine or tension-type headache, that the presence of preinjury headache seemed to be a risk factor for postinjury headache, and that women were at higher risk for postinjury headache.
The findings on types of headache and their persistence could have “important implications for treatment” of posttraumatic headache, said Dr. Lucas, founder and director of the headache center at the University of Washington, Seattle.
Posttraumatic headache is one of the most common persisting symptoms after TBI, occurring in 30%-90% of patients, previous studies suggest. Although most familiar as a salient symptom in soldiers who were exposed to explosive blasts, “it's becoming of great interest in adolescent children who've been in sports concussion injuries,” she said at the meeting.
The study included consecutive admissions of patients older than 16 years at seven acute rehabilitation facilities for TBI, excluding 79 patients who could not provide consent or answer questions themselves without their families' acting as proxy.
The cause of injury was vehicular trauma in approximately 56%, falls or impacts with flying objects in 28%, violence in 9%, and sports or pedestrian accidents in 4% each. (Percentages were rounded.)
Based on descriptions of symptoms by patients who reported headache, 60% of preinjury headaches were classified as migraine or probable migraine, compared with 48% soon after injury and 54% a year later. Although 25% of preinjury headaches and 37% of headaches soon after injury were deemed “unclassifiable” by investigators using patients' descriptions, over time they gained features that allowed them to be classified in one of the primary headache classifications, so that the proportion of “unclassified” headaches fell to 19% by 12 months post injury.
“Mostly, patients were classified as migraine with or without aura, or as tension-type headache, which is also surprising given the fact that most of these were vehicular injuries,” Dr. Lucas said. Headaches were classified as tension-type in 12% before injury, in 7% soon after injury, and in 19% at 12 months. Headaches were classified as cervicogenic in 4% before injury, in 8% soon after injury, and in 5% at 12 months.
Among patients who said they suffered headaches before the injury, 48% reported postinjury headache, compared with 23% of patients who said they did not have headaches before the injury. “Preinjury headache may be a risk factor for posttraumatic headache. This may argue for a common underlying mechanism,” Dr. Lucas said.
The cohort was 71% male and 75% white. Patients had an average age of 43 years, and 84% were able to be discharged to home. The injury caused posttraumatic amnesia for less than a day in 7% (indicative of a milder head injury), for 1-7 days in 21%, for 8-28 days in 42%, and for 29 or more days in 30%.
“This was primarily a male group; however, along all the time points studied—at baseline, 3 months, 6 months, and 12 months—there was a significant difference in women having more posttraumatic headache than men,” as well as a higher incidence of preinjury headache, she said. About 40% of men had headache at all follow-up times after injury, vs. 60% of women.
A physician in the audience asked if there was any relationship between insurance claims and reports that the headaches were persisting. “At the time of our study, that information was not available,” she responded.
More attention is being directed to adolescent children who've been in sports concussion injuries.
Source DR. LUCAS