User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Under Pressure
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
New Medicare Rule Reduces Retroactive Billing Period
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
More Money, More Problems
Hospitalists should be mindful that President Obama's half-billion-dollar commitment to new funding for community health centers (CHCs) could translate into unexpected compensation and burnout issues in the coming years, according to an SHM Public Policy Committee member.
Felix Aguirre, MD, FHM, vice president of medical affairs for IPC: The Hospitalist Company, says that until long-term healthcare reform is implemented, Obama’s $493 million in CHC grants "should be a wash."
Dr. Aguirre cautions that American Recovery and Reinvestment Act funding could have unintended consequences. For example, some clinics might raise compensation standards to retain or recruit hospitalists in order to deal with increased patient census. That increase could force local bidding wars for hospitalists at a time when supply is short.
“They will have a bit more money to attract those hospitalists,” Dr. Aguirre says.
In San Antonio, where Dr. Aguirre works, the effect could be even more pronounced, as one in four Texans are uninsured and more likely to take advantage of federally qualified health centers. In fact, 2007 federal data show roughly 40% of CHC patients were uninsured.
U.S. Health and Human Services officials say the stimulus money will provide care to nearly 3 million additional patients in the next two years, including roughly 1 million people without insurance. The added workload could cause burnout in hospitalists serving those institutions but who specialize in HM in part for the quality of life and scheduling perks that it affords.
"The ones that work with the CHCs would have more volume, but less chance of collecting on it, unless they have some arrangement to collect on that," Dr. Aguirre says. "There will be stress with increased volume."
Hospitalists should be mindful that President Obama's half-billion-dollar commitment to new funding for community health centers (CHCs) could translate into unexpected compensation and burnout issues in the coming years, according to an SHM Public Policy Committee member.
Felix Aguirre, MD, FHM, vice president of medical affairs for IPC: The Hospitalist Company, says that until long-term healthcare reform is implemented, Obama’s $493 million in CHC grants "should be a wash."
Dr. Aguirre cautions that American Recovery and Reinvestment Act funding could have unintended consequences. For example, some clinics might raise compensation standards to retain or recruit hospitalists in order to deal with increased patient census. That increase could force local bidding wars for hospitalists at a time when supply is short.
“They will have a bit more money to attract those hospitalists,” Dr. Aguirre says.
In San Antonio, where Dr. Aguirre works, the effect could be even more pronounced, as one in four Texans are uninsured and more likely to take advantage of federally qualified health centers. In fact, 2007 federal data show roughly 40% of CHC patients were uninsured.
U.S. Health and Human Services officials say the stimulus money will provide care to nearly 3 million additional patients in the next two years, including roughly 1 million people without insurance. The added workload could cause burnout in hospitalists serving those institutions but who specialize in HM in part for the quality of life and scheduling perks that it affords.
"The ones that work with the CHCs would have more volume, but less chance of collecting on it, unless they have some arrangement to collect on that," Dr. Aguirre says. "There will be stress with increased volume."
Hospitalists should be mindful that President Obama's half-billion-dollar commitment to new funding for community health centers (CHCs) could translate into unexpected compensation and burnout issues in the coming years, according to an SHM Public Policy Committee member.
Felix Aguirre, MD, FHM, vice president of medical affairs for IPC: The Hospitalist Company, says that until long-term healthcare reform is implemented, Obama’s $493 million in CHC grants "should be a wash."
Dr. Aguirre cautions that American Recovery and Reinvestment Act funding could have unintended consequences. For example, some clinics might raise compensation standards to retain or recruit hospitalists in order to deal with increased patient census. That increase could force local bidding wars for hospitalists at a time when supply is short.
“They will have a bit more money to attract those hospitalists,” Dr. Aguirre says.
In San Antonio, where Dr. Aguirre works, the effect could be even more pronounced, as one in four Texans are uninsured and more likely to take advantage of federally qualified health centers. In fact, 2007 federal data show roughly 40% of CHC patients were uninsured.
U.S. Health and Human Services officials say the stimulus money will provide care to nearly 3 million additional patients in the next two years, including roughly 1 million people without insurance. The added workload could cause burnout in hospitalists serving those institutions but who specialize in HM in part for the quality of life and scheduling perks that it affords.
"The ones that work with the CHCs would have more volume, but less chance of collecting on it, unless they have some arrangement to collect on that," Dr. Aguirre says. "There will be stress with increased volume."
Advertise at Your Own Risk

“The issue for hospitalists really isn’t different from anybody else,” says Erin A. Egan, MD, JD, a hospitalist at the University of Colorado at Denver and chair of SHM’s Ethics Committee. “If you can claim something quantifiable, you better be able to back it up. If you claim something qualitative, essentially you’re offering an opinion, and opinions don’t have to be based in fact.”
Virtua Health in Voorhees, N.J., and Cooper Health System, based in Camden, N.J., have been engaged in a legal battle since February. Virtua’s advertising claims the hospital has the most “Top Docs” in the region. After Cooper launched a legal challenge to the validity of the claim, a state judge ruled that Virtua could continue to say it had the most “Top Docs,” a claim based on a compilation of rankings from four regional magazines. The judge did, however, rule that Virtua had to withdraw wording from advertising that claimed the findings were made by an "independent" source, as Virtua had hired a group to compile the rankings. The judge also told Virtua to remove Web links to sites that explained how the figures were tallied. A federal case is pending.
Dr. Egan notes that few HM advertising tiffs result in similar legal claims unless they involve fraud. She adds that such battles often are costly and fruitless. For this reason, she urges advertisers to ensure their promotions are legally defensible. She offers these tips for any HM group when creating a marketing campaign:
- Use subjective language for subjective claims;
- Make sure you can back up all factual claims; and
- Think about the response you will give if you are challenged.
“The issue for hospitalists really isn’t different from anybody else,” says Erin A. Egan, MD, JD, a hospitalist at the University of Colorado at Denver and chair of SHM’s Ethics Committee. “If you can claim something quantifiable, you better be able to back it up. If you claim something qualitative, essentially you’re offering an opinion, and opinions don’t have to be based in fact.”
Virtua Health in Voorhees, N.J., and Cooper Health System, based in Camden, N.J., have been engaged in a legal battle since February. Virtua’s advertising claims the hospital has the most “Top Docs” in the region. After Cooper launched a legal challenge to the validity of the claim, a state judge ruled that Virtua could continue to say it had the most “Top Docs,” a claim based on a compilation of rankings from four regional magazines. The judge did, however, rule that Virtua had to withdraw wording from advertising that claimed the findings were made by an "independent" source, as Virtua had hired a group to compile the rankings. The judge also told Virtua to remove Web links to sites that explained how the figures were tallied. A federal case is pending.
Dr. Egan notes that few HM advertising tiffs result in similar legal claims unless they involve fraud. She adds that such battles often are costly and fruitless. For this reason, she urges advertisers to ensure their promotions are legally defensible. She offers these tips for any HM group when creating a marketing campaign:
- Use subjective language for subjective claims;
- Make sure you can back up all factual claims; and
- Think about the response you will give if you are challenged.
“The issue for hospitalists really isn’t different from anybody else,” says Erin A. Egan, MD, JD, a hospitalist at the University of Colorado at Denver and chair of SHM’s Ethics Committee. “If you can claim something quantifiable, you better be able to back it up. If you claim something qualitative, essentially you’re offering an opinion, and opinions don’t have to be based in fact.”
Virtua Health in Voorhees, N.J., and Cooper Health System, based in Camden, N.J., have been engaged in a legal battle since February. Virtua’s advertising claims the hospital has the most “Top Docs” in the region. After Cooper launched a legal challenge to the validity of the claim, a state judge ruled that Virtua could continue to say it had the most “Top Docs,” a claim based on a compilation of rankings from four regional magazines. The judge did, however, rule that Virtua had to withdraw wording from advertising that claimed the findings were made by an "independent" source, as Virtua had hired a group to compile the rankings. The judge also told Virtua to remove Web links to sites that explained how the figures were tallied. A federal case is pending.
Dr. Egan notes that few HM advertising tiffs result in similar legal claims unless they involve fraud. She adds that such battles often are costly and fruitless. For this reason, she urges advertisers to ensure their promotions are legally defensible. She offers these tips for any HM group when creating a marketing campaign:
- Use subjective language for subjective claims;
- Make sure you can back up all factual claims; and
- Think about the response you will give if you are challenged.
EMR System Shortage Means HM Opportunity
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
There Until the End
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
Eliminate Inconsistency
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
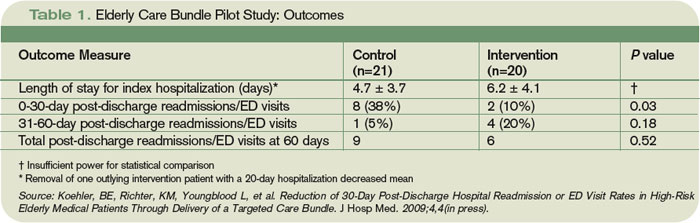
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.

—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.
—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.
—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
Fine-Tuning the Discharge Process
The first metrics from SHM's Project BOOST mentorship program won't be ready until later this year, but the recent addition of more intervention sites comes as pilot institutions are reporting success in changing the discharge culture.
SHM recently announced 24 new sites for Project BOOST (Better Outcomes for Older Adults through Safe Transitions), bringing the number of participating institutions to 30. Each site features SHM mentors working with hospitalists to improve transitional care via a discharge planning toolkit.
Emmanuel King, MD, director of the Nurse Practitioner Hospitalist Service at the Hospital of the University of Pennsylvania in Philadelphia, says a major shift is implementing the "7P Risk Scale," a transitional-care checklist. Dr. King says some of his staff initially balked at depression screening and questions about health literacy, but when the tools were introduced and the checklist items were embraced, hospitalists felt "included in and comfortable with the process."
"Tweaking it to meet the needs of the team was a great idea," says Dr. King, assistant professor of clinical at UPenn's School of Medicine. "We've been able to get the team to buy in."
Tina Budnitz, MPH, SHM senior advisor for quality initiatives, says some early responses to Project BOOST have been better than expected, especially in the area of follow-up tasks.
"I was expecting people to say they were incredibly time-intensive," Budnitz says. "Some of the hospitalists got back to us and said, 'We think it's a good idea to call every patient, regardless of their risk status.' "
The first metrics from SHM's Project BOOST mentorship program won't be ready until later this year, but the recent addition of more intervention sites comes as pilot institutions are reporting success in changing the discharge culture.
SHM recently announced 24 new sites for Project BOOST (Better Outcomes for Older Adults through Safe Transitions), bringing the number of participating institutions to 30. Each site features SHM mentors working with hospitalists to improve transitional care via a discharge planning toolkit.
Emmanuel King, MD, director of the Nurse Practitioner Hospitalist Service at the Hospital of the University of Pennsylvania in Philadelphia, says a major shift is implementing the "7P Risk Scale," a transitional-care checklist. Dr. King says some of his staff initially balked at depression screening and questions about health literacy, but when the tools were introduced and the checklist items were embraced, hospitalists felt "included in and comfortable with the process."
"Tweaking it to meet the needs of the team was a great idea," says Dr. King, assistant professor of clinical at UPenn's School of Medicine. "We've been able to get the team to buy in."
Tina Budnitz, MPH, SHM senior advisor for quality initiatives, says some early responses to Project BOOST have been better than expected, especially in the area of follow-up tasks.
"I was expecting people to say they were incredibly time-intensive," Budnitz says. "Some of the hospitalists got back to us and said, 'We think it's a good idea to call every patient, regardless of their risk status.' "
The first metrics from SHM's Project BOOST mentorship program won't be ready until later this year, but the recent addition of more intervention sites comes as pilot institutions are reporting success in changing the discharge culture.
SHM recently announced 24 new sites for Project BOOST (Better Outcomes for Older Adults through Safe Transitions), bringing the number of participating institutions to 30. Each site features SHM mentors working with hospitalists to improve transitional care via a discharge planning toolkit.
Emmanuel King, MD, director of the Nurse Practitioner Hospitalist Service at the Hospital of the University of Pennsylvania in Philadelphia, says a major shift is implementing the "7P Risk Scale," a transitional-care checklist. Dr. King says some of his staff initially balked at depression screening and questions about health literacy, but when the tools were introduced and the checklist items were embraced, hospitalists felt "included in and comfortable with the process."
"Tweaking it to meet the needs of the team was a great idea," says Dr. King, assistant professor of clinical at UPenn's School of Medicine. "We've been able to get the team to buy in."
Tina Budnitz, MPH, SHM senior advisor for quality initiatives, says some early responses to Project BOOST have been better than expected, especially in the area of follow-up tasks.
"I was expecting people to say they were incredibly time-intensive," Budnitz says. "Some of the hospitalists got back to us and said, 'We think it's a good idea to call every patient, regardless of their risk status.' "
HM Spreads Its Wings
Hospitalists are not just general internists anymore, having successfully branched out into such subspecialties as cardiology, pulmonology, and gastroenterology, according to a March 12 study in the New England Journal of Medicine (2009;360:1102-12).
In the first quantitative national review to study hospitalists based on Medicare payment data, a team of researchers at the University of Texas Medical Branch at Galveston calculated that the percentage of internal medicine physicians practicing as hospitalists jumped to 19% in 2006 from 5.9% in 1995.
Perhaps more interesting is the number of cardiologists, pulmonologists, gastroenterologists, family physicians, and general practitioners who work as hospitalists totaled roughly 20% in 2006. The study defined hospitalists as those who generated more than 90% of their E/M claims from hospitalized patients.
HM appears to have even more room to grow, as more physicians move toward the HM model and away from primary care, according to an editorial accompanying the NEJM study. The editorial debated the value-adds and the complications caused by the presence of hospitalists in all phases of the care continuum. The authors also acknowledged the model is widely accepted as beneficial.
"The economic and practical forces that promoted the growth in the care of patients by hospitalists are intensifying, not lessening, and hospitalists are here to stay," according to the editorial, written by a trio of NEJM editors, including editor-in-chief Jeffrey M. Drazen, MD. "It is time to focus on how to enhance the value."
Hospitalists are not just general internists anymore, having successfully branched out into such subspecialties as cardiology, pulmonology, and gastroenterology, according to a March 12 study in the New England Journal of Medicine (2009;360:1102-12).
In the first quantitative national review to study hospitalists based on Medicare payment data, a team of researchers at the University of Texas Medical Branch at Galveston calculated that the percentage of internal medicine physicians practicing as hospitalists jumped to 19% in 2006 from 5.9% in 1995.
Perhaps more interesting is the number of cardiologists, pulmonologists, gastroenterologists, family physicians, and general practitioners who work as hospitalists totaled roughly 20% in 2006. The study defined hospitalists as those who generated more than 90% of their E/M claims from hospitalized patients.
HM appears to have even more room to grow, as more physicians move toward the HM model and away from primary care, according to an editorial accompanying the NEJM study. The editorial debated the value-adds and the complications caused by the presence of hospitalists in all phases of the care continuum. The authors also acknowledged the model is widely accepted as beneficial.
"The economic and practical forces that promoted the growth in the care of patients by hospitalists are intensifying, not lessening, and hospitalists are here to stay," according to the editorial, written by a trio of NEJM editors, including editor-in-chief Jeffrey M. Drazen, MD. "It is time to focus on how to enhance the value."
Hospitalists are not just general internists anymore, having successfully branched out into such subspecialties as cardiology, pulmonology, and gastroenterology, according to a March 12 study in the New England Journal of Medicine (2009;360:1102-12).
In the first quantitative national review to study hospitalists based on Medicare payment data, a team of researchers at the University of Texas Medical Branch at Galveston calculated that the percentage of internal medicine physicians practicing as hospitalists jumped to 19% in 2006 from 5.9% in 1995.
Perhaps more interesting is the number of cardiologists, pulmonologists, gastroenterologists, family physicians, and general practitioners who work as hospitalists totaled roughly 20% in 2006. The study defined hospitalists as those who generated more than 90% of their E/M claims from hospitalized patients.
HM appears to have even more room to grow, as more physicians move toward the HM model and away from primary care, according to an editorial accompanying the NEJM study. The editorial debated the value-adds and the complications caused by the presence of hospitalists in all phases of the care continuum. The authors also acknowledged the model is widely accepted as beneficial.
"The economic and practical forces that promoted the growth in the care of patients by hospitalists are intensifying, not lessening, and hospitalists are here to stay," according to the editorial, written by a trio of NEJM editors, including editor-in-chief Jeffrey M. Drazen, MD. "It is time to focus on how to enhance the value."
Head of the Class
Brian Tyson, MD, was named medical director of the hospitalist program at St. Bernardine Medical Center in San Bernardino, Calif., about a year ago, but he still can't learn enough about business drivers, communication, and leadership skills. That's why he attended SHM's Leadership Academy last week in Honolulu.
"I needed some things to work on. ...I think we all need to," says Dr. Tyson, whose HM program is operated by Cogent Healthcare. "This is that opportunity. When people have done things and run things, you don't need to reinvent the wheel. It's easier sometimes to get the keys to success from someone who’s been there."
More than a hundred hospitalists apparently agreed, joining Dr. Tyson at the four-day session. Dr. Tyson found the insights into business particularly helpful, especially because fiscal matters are not a major focus of medical school. Analyzing his managerial personality and identifying his program's strengths and weaknesses were "eye opening," as was the chance to discuss staffing and budget issues with HM directors from different parts of the country.
The leadership program offers two tracks, and the first course must be completed before taking the advanced level. A first-time attendee, Dr. Tyson says he is looking forward to completing the second part of the academy.
"Medicine is changing so much, this helps us manage our programs," he says. "Having the tools to be able to do that is absolutely necessary."
Brian Tyson, MD, was named medical director of the hospitalist program at St. Bernardine Medical Center in San Bernardino, Calif., about a year ago, but he still can't learn enough about business drivers, communication, and leadership skills. That's why he attended SHM's Leadership Academy last week in Honolulu.
"I needed some things to work on. ...I think we all need to," says Dr. Tyson, whose HM program is operated by Cogent Healthcare. "This is that opportunity. When people have done things and run things, you don't need to reinvent the wheel. It's easier sometimes to get the keys to success from someone who’s been there."
More than a hundred hospitalists apparently agreed, joining Dr. Tyson at the four-day session. Dr. Tyson found the insights into business particularly helpful, especially because fiscal matters are not a major focus of medical school. Analyzing his managerial personality and identifying his program's strengths and weaknesses were "eye opening," as was the chance to discuss staffing and budget issues with HM directors from different parts of the country.
The leadership program offers two tracks, and the first course must be completed before taking the advanced level. A first-time attendee, Dr. Tyson says he is looking forward to completing the second part of the academy.
"Medicine is changing so much, this helps us manage our programs," he says. "Having the tools to be able to do that is absolutely necessary."
Brian Tyson, MD, was named medical director of the hospitalist program at St. Bernardine Medical Center in San Bernardino, Calif., about a year ago, but he still can't learn enough about business drivers, communication, and leadership skills. That's why he attended SHM's Leadership Academy last week in Honolulu.
"I needed some things to work on. ...I think we all need to," says Dr. Tyson, whose HM program is operated by Cogent Healthcare. "This is that opportunity. When people have done things and run things, you don't need to reinvent the wheel. It's easier sometimes to get the keys to success from someone who’s been there."
More than a hundred hospitalists apparently agreed, joining Dr. Tyson at the four-day session. Dr. Tyson found the insights into business particularly helpful, especially because fiscal matters are not a major focus of medical school. Analyzing his managerial personality and identifying his program's strengths and weaknesses were "eye opening," as was the chance to discuss staffing and budget issues with HM directors from different parts of the country.
The leadership program offers two tracks, and the first course must be completed before taking the advanced level. A first-time attendee, Dr. Tyson says he is looking forward to completing the second part of the academy.
"Medicine is changing so much, this helps us manage our programs," he says. "Having the tools to be able to do that is absolutely necessary."