User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Team Effort to Combat Fractures
A joint venture between a hospitalist and an orthopedist in rural Minnesota is targeting geriatric fracture patients, and aims to reduce lengths of stay and morbidity.
The program, created by Northern Orthopedics and St. Joseph's Medical Center in Brainerd, Minn., has developed a toolkit for elderly fracture patients. The kit includes a pictorial guidebook, postoperative instructions and rehabilitation information, and early discharge planning. Only a half-dozen or so patients have used the service since its January launch, but developers say the purpose is to pair a surgeon with a hospitalist soon after a patient's admission to ensure that other medical problems are treated alongside any fractures.
"The fracture is not really the biggest problem," says Ben Robertson, MD, a surgeon with Northern Orthopedics. "The surgeon can deal with that. These patients, after we fix their hip fracture ... there's a whole host of medical problems that can happen."
That's where St. Joseph's hospitalist Jim Baumgartner, MD, steps in. The early introduction of a hospitalist allows Dr. Baumgartner to know a patient's treatment history, keep an eye out for medical-related complications, and set up corresponding treatment programs. Dr. Baumgartner says the Minnesota program—modeled after one at the University of Rochester—could be replicated at other hospitals to produce better functional outcomes.
"Everybody works together from the beginning," Dr. Baumgartner says. "The results are patients getting better faster, shorter lengths of stay, and much more efficient resource utilization. This is what hospitalists are geared for."
A joint venture between a hospitalist and an orthopedist in rural Minnesota is targeting geriatric fracture patients, and aims to reduce lengths of stay and morbidity.
The program, created by Northern Orthopedics and St. Joseph's Medical Center in Brainerd, Minn., has developed a toolkit for elderly fracture patients. The kit includes a pictorial guidebook, postoperative instructions and rehabilitation information, and early discharge planning. Only a half-dozen or so patients have used the service since its January launch, but developers say the purpose is to pair a surgeon with a hospitalist soon after a patient's admission to ensure that other medical problems are treated alongside any fractures.
"The fracture is not really the biggest problem," says Ben Robertson, MD, a surgeon with Northern Orthopedics. "The surgeon can deal with that. These patients, after we fix their hip fracture ... there's a whole host of medical problems that can happen."
That's where St. Joseph's hospitalist Jim Baumgartner, MD, steps in. The early introduction of a hospitalist allows Dr. Baumgartner to know a patient's treatment history, keep an eye out for medical-related complications, and set up corresponding treatment programs. Dr. Baumgartner says the Minnesota program—modeled after one at the University of Rochester—could be replicated at other hospitals to produce better functional outcomes.
"Everybody works together from the beginning," Dr. Baumgartner says. "The results are patients getting better faster, shorter lengths of stay, and much more efficient resource utilization. This is what hospitalists are geared for."
A joint venture between a hospitalist and an orthopedist in rural Minnesota is targeting geriatric fracture patients, and aims to reduce lengths of stay and morbidity.
The program, created by Northern Orthopedics and St. Joseph's Medical Center in Brainerd, Minn., has developed a toolkit for elderly fracture patients. The kit includes a pictorial guidebook, postoperative instructions and rehabilitation information, and early discharge planning. Only a half-dozen or so patients have used the service since its January launch, but developers say the purpose is to pair a surgeon with a hospitalist soon after a patient's admission to ensure that other medical problems are treated alongside any fractures.
"The fracture is not really the biggest problem," says Ben Robertson, MD, a surgeon with Northern Orthopedics. "The surgeon can deal with that. These patients, after we fix their hip fracture ... there's a whole host of medical problems that can happen."
That's where St. Joseph's hospitalist Jim Baumgartner, MD, steps in. The early introduction of a hospitalist allows Dr. Baumgartner to know a patient's treatment history, keep an eye out for medical-related complications, and set up corresponding treatment programs. Dr. Baumgartner says the Minnesota program—modeled after one at the University of Rochester—could be replicated at other hospitals to produce better functional outcomes.
"Everybody works together from the beginning," Dr. Baumgartner says. "The results are patients getting better faster, shorter lengths of stay, and much more efficient resource utilization. This is what hospitalists are geared for."
HHS Nominee: Take Two
The so-far fitful process of choosing a U.S. Department of Health and Human Services (HHS) secretary may not delay meaningful healthcare reform—if President Obama remains committed to making the overhaul a top priority, says one of SHM's co-founders.
"On the one hand, he hasn't been able to get anything done in the first 100 days," says Hospitalist Win Whitcomb, MD, vice president of quality improvement at Mercy Medical Center in Springfield, Mass. "That's not as concerning as if he did not prioritize the first year of his presidency. If he doesn't lay the groundwork for meaningful reform in healthcare, that's concerning."
Dr. Whitcomb's comments came as Obama picked Kansas Gov. Kathleen Sebelius as his new HHS secretary nominee. Obama's original choice, former Sen. Tom Daschle, withdrew from consideration amid questions about his taxes. Sebelius, a Democratic governor in a conservative state, could face a contentious Senate confirmation because of her anti-abortion critics. Obama, however, already has filled the other job Daschle was to hold with Nancy-Ann DeParle, a former health policy official during the Clinton administration. She will lead the White House Office on Health Reform; the appointment does not require Senate approval.
What this means for hospitalists is that Obama's goals to expand health insurance coverage, help install electronic record systems, and establish pay for performance in care delivery are receiving significant Oval Office attention. All were discussion topics last week as SHM officials met with congressional leaders on Capitol Hill.
"Any sort of reform that's going to be affecting hospitals, we'll be the key role players in making those changes," Dr. Whitcomb says. "We're in the hospital all the time and [among] the most invested."
For more on Obama's healthcare agenda visit http://www.whitehouse.gov/agenda/health_care.
The so-far fitful process of choosing a U.S. Department of Health and Human Services (HHS) secretary may not delay meaningful healthcare reform—if President Obama remains committed to making the overhaul a top priority, says one of SHM's co-founders.
"On the one hand, he hasn't been able to get anything done in the first 100 days," says Hospitalist Win Whitcomb, MD, vice president of quality improvement at Mercy Medical Center in Springfield, Mass. "That's not as concerning as if he did not prioritize the first year of his presidency. If he doesn't lay the groundwork for meaningful reform in healthcare, that's concerning."
Dr. Whitcomb's comments came as Obama picked Kansas Gov. Kathleen Sebelius as his new HHS secretary nominee. Obama's original choice, former Sen. Tom Daschle, withdrew from consideration amid questions about his taxes. Sebelius, a Democratic governor in a conservative state, could face a contentious Senate confirmation because of her anti-abortion critics. Obama, however, already has filled the other job Daschle was to hold with Nancy-Ann DeParle, a former health policy official during the Clinton administration. She will lead the White House Office on Health Reform; the appointment does not require Senate approval.
What this means for hospitalists is that Obama's goals to expand health insurance coverage, help install electronic record systems, and establish pay for performance in care delivery are receiving significant Oval Office attention. All were discussion topics last week as SHM officials met with congressional leaders on Capitol Hill.
"Any sort of reform that's going to be affecting hospitals, we'll be the key role players in making those changes," Dr. Whitcomb says. "We're in the hospital all the time and [among] the most invested."
For more on Obama's healthcare agenda visit http://www.whitehouse.gov/agenda/health_care.
The so-far fitful process of choosing a U.S. Department of Health and Human Services (HHS) secretary may not delay meaningful healthcare reform—if President Obama remains committed to making the overhaul a top priority, says one of SHM's co-founders.
"On the one hand, he hasn't been able to get anything done in the first 100 days," says Hospitalist Win Whitcomb, MD, vice president of quality improvement at Mercy Medical Center in Springfield, Mass. "That's not as concerning as if he did not prioritize the first year of his presidency. If he doesn't lay the groundwork for meaningful reform in healthcare, that's concerning."
Dr. Whitcomb's comments came as Obama picked Kansas Gov. Kathleen Sebelius as his new HHS secretary nominee. Obama's original choice, former Sen. Tom Daschle, withdrew from consideration amid questions about his taxes. Sebelius, a Democratic governor in a conservative state, could face a contentious Senate confirmation because of her anti-abortion critics. Obama, however, already has filled the other job Daschle was to hold with Nancy-Ann DeParle, a former health policy official during the Clinton administration. She will lead the White House Office on Health Reform; the appointment does not require Senate approval.
What this means for hospitalists is that Obama's goals to expand health insurance coverage, help install electronic record systems, and establish pay for performance in care delivery are receiving significant Oval Office attention. All were discussion topics last week as SHM officials met with congressional leaders on Capitol Hill.
"Any sort of reform that's going to be affecting hospitals, we'll be the key role players in making those changes," Dr. Whitcomb says. "We're in the hospital all the time and [among] the most invested."
For more on Obama's healthcare agenda visit http://www.whitehouse.gov/agenda/health_care.
Model's Death Sheds Spotlight on Sepsis Treatment
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
Discharge Development
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
Back to School
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Transparent Hospitalists
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Crunch Time
Before his recent promotion, hospitalist Garth King, MD, medical director of the Schumacher Group at Southwest Medical Center in Lafayette, La., had hoped to add a fourth full-time doctor to his roster. The hiring made sense at the time. As recently as last summer, the group’s three full-time doctors were averaging 35 to 40 patient encounters a day, enough to warrant the additional hospitalist position. But the group’s census dropped 25% in the fourth quarter of 2008, and these days, Dr. King simply can’t justify the math to bring on another six-figure salary.
“Over the past two, three months, patient slowdown has pushed off the ability” to add staff, Dr. King explains. “We’ll wait until things ramp up again, once we get the numbers to where they were before.”
Dr. King could be in for a long wait. The fiscal meltdown that began in 2007 and last year mushroomed into a full-blown recession has taken hold in the world of hospital medicine. More and more, hospitals are reporting decreased revenues and increased levels of charity care. The result: Planned group expansions have been put on hold, open positions are going unfilled, and some hospitalists have been laid off.
Constituencies from health-system executives to rank-and-file hospitalists to economists remain cautious of acting too boldly before President Obama and the new Congress unveil much-anticipated changes to Medicare billing and reimbursement schedules. Aggressive reforms, such as extending health coverage to more than 45 million uninsured Americans, could swamp hospitals with new patients and lead to cuts in reimbursement rates. A more temperate approach by the new administration could leave a relative status quo.
Either way, hospital medicine has never endured a recession so deep that some healthcare economists liken it to the Great Depression, so the practical effect on the industry is difficult to forecast with accuracy. Hospitalists and their observers agree on one thing, though: This is the year hospital medicine will have to prove its worth more empirically than ever. Positive public relations and studies proclaiming reduced lengths of stay and sped-up emergency department throughput have given the industry a “rarified position as a specialty,” one researcher says. But in constrictive economic times, those figures likely will be revisited, says Mark Pauly, professor of healthcare management at The Wharton School at the University of Pennsylvania. “When revenues are falling, you go back and look at that evidence again,” Pauly says. “Is it really bulletproof?”
Still, the prognosis for economic health is not all bad. Many hospital medicine leaders think the concerns over whether chief financial officers will look to hospital contracts as places to cut spending might spawn improved coding and billing, create new partnerships between hospital medicine groups, and push new revenue streams, such as preoperative clinics or inpatient palliative-care initiatives. This also is a time for hospital groups to reaffirm to their respective C-suites—through a deft combination of data and intangible relationships—that they are an indispensable staffing measure that their respective institutions cannot do without.
“This is an opportunity for hospitalists,” says Joe Miller, SHM’s executive advisor to the CEO. “The problem is we’ve got young, inexperienced leaders. Can they see this? Can they recognize this and not see this as a challenge?”
Problem Identification
Hospitalist Marc Westle, DO, FACP, president and managing partner of Asheville Hospital Group in North Carolina, thinks tracking, collating, and reporting quantifiable metrics is the fastest way to convince hospital executives that hospitalists are not the place to cut spending. And when those same executives are looking at staff reductions—53% of hospitals already are cutting or considering cuts, according to the most recent American Hospital Association data—hospital medicine leaders need to be able to point to specific numbers to prove their worth. Detailed information on coding, cost of capture, revenue production, and patient referrals generated are data points that can strengthen a presentation, especially if an argument shows that revenue production and collection is maximized.
“Don’t leave money on the table,” Dr. Westle says. “Your billing department is only going to bill what your physicians tell them to bill. For hospital groups that have not mentioned both the upfront E&M coding by their doctors and the back-end billing efficiency, those are definite things they need to do, today or yesterday. That efficiency may not have hurt them before, but it could hurt them in the next 12 to 18 months.”
Dr. Westle and others also note that hospitalists have to see the economic downturn through the eyes of hospital executives—and the hospital’s bottom line. Recent AHA data show 29% of hospitals are reporting moderate decreases in admissions, and another 9% of hospitals categorize those drops as significant. More than 3 in 10 hospitals have reported a noticeable reduction in elective procedures.
Pauly, the Wharton professor, also cautions that a tightened economy might force primary-care physicians (PCPs) back into hospitals, taking away patients now in the hospitalists’ purview. Hospital medicine’s beginnings trace to those PCPs acquiescing hospital rounds to a new intermediary—hospitalists—in return for the ability to focus more on their daily practices, Pauly says. Ancillary benefits included not being on call 24 hours a day, seven days a week.
“A lower income may change that willingness,” Pauly notes. “Leisure is a luxury good, and if your revenue is falling, you may want to get that business back.”
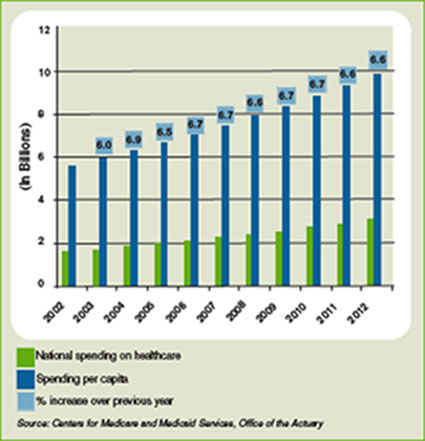
Another part of the equation is the rising tide of the uninsured, currently estimated at 47 million. It remains to be seen what effect the uninsured have on overall healthcare spending in the U.S., which is projected to rise 6.6% in 2009 to $2.6 trillion, according to the most recent data available from the Centers for Medicare and Medicaid Services (see Figure 1, below). Those projections, however, were released nearly a year ago, long before the severity of the current financial crisis became clear. Pauly says adjusted numbers released this winter, which assumedly will reflect the nation’s ever-deepening financial hole, should be a better gauge on whether healthcare remains as recession-proof as some think it is.
Hoangmai Pham, a senior health researcher at the Center for Studying Health System Change and lead author of a study on how the hospitalist model has focused attention on patient-care coordination, says changes at the federal level will be a driving factor in the strength of healthcare. Roughly 50% to 80% of a hospitalist’s annual salary comes from clinical billings, according to SHM data. The balance comes from hospital subsidies, in the form of annual contracts, monthly stipends, or pay-for-performance bonuses. Drastic changes in payment policy could have drastic implications on those subsidies.
“The ground is very fluid right now, in terms of where payment policy is going,” Pham says. “If I were hospitalists, part of the nervousness would be I’m not sure what direction things are heading in.”
Potential Solutions
Many hospitalists, however, see positives in the economic morass. Hospitalist Troy Ahlstrom, MD, is financial director of Hospitalists of Northwest Michigan in Traverse City, which serves roughly 400 beds at Munson Medical Center. He says groups can prove their worth by showing how they make it easier for other specialists—cardiologists, orthopedists, etc.—to perform the more lucrative procedures on which hospitals rely for higher reimbursements. Then, the group can negotiate for a piece of the savings under a pay-for-performance contracting model.
“What can we do to help make you more efficient, so you can do two extra surgical cases a week?” Dr. Ahlstrom says. “What if the hospital itself realizes a 15% increase in efficiency? Work out a deal that if we save you 15% … you give us a cut.”
Dr. Westle suggests analyzing cost accounting as another way to offer evidence of productivity. Paying overtime for back-office staff is ineffective if your salary overhead is greater than your billing collection. He also recommends a virtual office to employ billing specialists who work from home and doctors without off-site offices, eliminating real estate, utility, and infectious-waste-disposal costs that can cost private practices 55% to 60% in overhead costs.
Partnerships and reinvention are other avenues for cost-effectiveness. Some smaller, single-hospitalist groups might merge to cut costs through economies of scale, but SHM’s Miller thinks there is an opportunity to create a cooperative structure in which hospital medicine groups maintain individual identifies yet share certain functions, such as a common billing service.
Dr. King, the medical director who was promoted in November, is running a long-term acute-care center (LTAC) to help generate a parallel revenue stream. The center opened in May; during periods of decreased patient traffic at Southwest Medical Center, it affords his hospitalists another place to work, encountering patients and billing services. It also creates a referral stream for his hospital. He also has engaged in preliminary discussions for opening and staffing a pre-operative clinic or a wound-care clinic, but those discussions are in the early stages. King is sitting down with PCPs his group has little history with to increase referrals, and he is meeting with the hospital’s specialists to inform them that earlier consults with hospitalists could allow for streamlined service, shorter stays, and greater revenue.
“If you stop your research and development (R&D) during the hard times, 18 months from now, everyone else has stopped their R&D,” Dr. Westle says. “But if you continued your R&D, you’re 18 months ahead of everyone else.”
Dr. Westle refers to his method as “weaving yourself into the fabric of the health system.” Caring for the unassigned adult population and handling internal medicine assignments is low-hanging fruit for hospital medicine groups. He suggests creating programs to teach residents who are participating in hospital quality committees or other panels to deal with coding and billing, staffing LTACs, and improving the referral process for smaller, outlying hospitals to send patients to larger hospitals.
And, of course, there is relationship-building. Although tight economic times will require hospitalists to provide more quantitative data to prove their worth, the hospitalist model thrives on doctor-to-doctor interactions. Connections built with proceduralists and nurses, who can vouch for the value of a hospital medicine group, can mean a lot when hospital boards are searching for areas to trim costs.
“If you talk to seasoned directors of hospitalist programs, you win over hearts and minds one at a time,” Pham says. Most hospital executives “know there is value beyond that which can be proven on the balance sheet. It’s difficult to price things like convenience, satisfaction.”
What’s Next
Doug Cutler, MD, a hospitalist at Banner Sun City Hospitalists in Arizona, which serves 800-plus beds in two hospitals in Sun City and Sun City West, has watched economics change his situation. His old employer, Banner Health, recently merged its two hospitals with Sun Health. The new owners are learning how Cutler’s group works, talking to both hospitalists and other hospital staff. They have the group’s documentation to review, but individual doctors now have the opportunity to prove themselves as standouts.
“Find out the needs and service them the best you can,” Dr. Cutler says. “If it’s a throughput issue, work with them on that. Are you on committees? Are you on the quality committee? Pharmacy and therapeutics? Find what they need and fill a niche. Talk to medical directors, work with case managers. Don’t be the one that they hate to page; be the one they’re not worried about stopping in the hallways because you’re the go-to physician.”
SHM’s Miller agrees that individual hospitalists should take every opportunity to stand out. Whether it’s making sure hospital executives know your name, earning as many certifications as applicable, or applying for the society’s new Fellow in Hospital Medicine program, each doctor has to look at the economic crisis from a professional and personal viewpoint.
And while some could reason that Dr. Cutler’s situation—working for a hospital-owned group as opposed to a large multistate group or multispecialty practice—gives him more job security, he could argue the lack of negotiating leverage might give him less. But as he often tells his patients when they ask for a diagnosis: It’s hard to see 10 seconds into the future.
“I don’t want to think I’m sitting here fat, dumb, and happy and they won’t let me go,” Cutler says, knocking on wood. “I just don’t know. Every company … realistically needs to look at everything if they want to survive. We’re potentially on the chopping block, but do you lop off something that costs a million dollars when it saves you five? Are you willing to go back to a time before that?” TH
Richard Quinn is a freelance writer based in New Jersey.
Before his recent promotion, hospitalist Garth King, MD, medical director of the Schumacher Group at Southwest Medical Center in Lafayette, La., had hoped to add a fourth full-time doctor to his roster. The hiring made sense at the time. As recently as last summer, the group’s three full-time doctors were averaging 35 to 40 patient encounters a day, enough to warrant the additional hospitalist position. But the group’s census dropped 25% in the fourth quarter of 2008, and these days, Dr. King simply can’t justify the math to bring on another six-figure salary.
“Over the past two, three months, patient slowdown has pushed off the ability” to add staff, Dr. King explains. “We’ll wait until things ramp up again, once we get the numbers to where they were before.”
Dr. King could be in for a long wait. The fiscal meltdown that began in 2007 and last year mushroomed into a full-blown recession has taken hold in the world of hospital medicine. More and more, hospitals are reporting decreased revenues and increased levels of charity care. The result: Planned group expansions have been put on hold, open positions are going unfilled, and some hospitalists have been laid off.
Constituencies from health-system executives to rank-and-file hospitalists to economists remain cautious of acting too boldly before President Obama and the new Congress unveil much-anticipated changes to Medicare billing and reimbursement schedules. Aggressive reforms, such as extending health coverage to more than 45 million uninsured Americans, could swamp hospitals with new patients and lead to cuts in reimbursement rates. A more temperate approach by the new administration could leave a relative status quo.
Either way, hospital medicine has never endured a recession so deep that some healthcare economists liken it to the Great Depression, so the practical effect on the industry is difficult to forecast with accuracy. Hospitalists and their observers agree on one thing, though: This is the year hospital medicine will have to prove its worth more empirically than ever. Positive public relations and studies proclaiming reduced lengths of stay and sped-up emergency department throughput have given the industry a “rarified position as a specialty,” one researcher says. But in constrictive economic times, those figures likely will be revisited, says Mark Pauly, professor of healthcare management at The Wharton School at the University of Pennsylvania. “When revenues are falling, you go back and look at that evidence again,” Pauly says. “Is it really bulletproof?”
Still, the prognosis for economic health is not all bad. Many hospital medicine leaders think the concerns over whether chief financial officers will look to hospital contracts as places to cut spending might spawn improved coding and billing, create new partnerships between hospital medicine groups, and push new revenue streams, such as preoperative clinics or inpatient palliative-care initiatives. This also is a time for hospital groups to reaffirm to their respective C-suites—through a deft combination of data and intangible relationships—that they are an indispensable staffing measure that their respective institutions cannot do without.
“This is an opportunity for hospitalists,” says Joe Miller, SHM’s executive advisor to the CEO. “The problem is we’ve got young, inexperienced leaders. Can they see this? Can they recognize this and not see this as a challenge?”
Problem Identification
Hospitalist Marc Westle, DO, FACP, president and managing partner of Asheville Hospital Group in North Carolina, thinks tracking, collating, and reporting quantifiable metrics is the fastest way to convince hospital executives that hospitalists are not the place to cut spending. And when those same executives are looking at staff reductions—53% of hospitals already are cutting or considering cuts, according to the most recent American Hospital Association data—hospital medicine leaders need to be able to point to specific numbers to prove their worth. Detailed information on coding, cost of capture, revenue production, and patient referrals generated are data points that can strengthen a presentation, especially if an argument shows that revenue production and collection is maximized.
“Don’t leave money on the table,” Dr. Westle says. “Your billing department is only going to bill what your physicians tell them to bill. For hospital groups that have not mentioned both the upfront E&M coding by their doctors and the back-end billing efficiency, those are definite things they need to do, today or yesterday. That efficiency may not have hurt them before, but it could hurt them in the next 12 to 18 months.”
Dr. Westle and others also note that hospitalists have to see the economic downturn through the eyes of hospital executives—and the hospital’s bottom line. Recent AHA data show 29% of hospitals are reporting moderate decreases in admissions, and another 9% of hospitals categorize those drops as significant. More than 3 in 10 hospitals have reported a noticeable reduction in elective procedures.
Pauly, the Wharton professor, also cautions that a tightened economy might force primary-care physicians (PCPs) back into hospitals, taking away patients now in the hospitalists’ purview. Hospital medicine’s beginnings trace to those PCPs acquiescing hospital rounds to a new intermediary—hospitalists—in return for the ability to focus more on their daily practices, Pauly says. Ancillary benefits included not being on call 24 hours a day, seven days a week.
“A lower income may change that willingness,” Pauly notes. “Leisure is a luxury good, and if your revenue is falling, you may want to get that business back.”
Another part of the equation is the rising tide of the uninsured, currently estimated at 47 million. It remains to be seen what effect the uninsured have on overall healthcare spending in the U.S., which is projected to rise 6.6% in 2009 to $2.6 trillion, according to the most recent data available from the Centers for Medicare and Medicaid Services (see Figure 1, below). Those projections, however, were released nearly a year ago, long before the severity of the current financial crisis became clear. Pauly says adjusted numbers released this winter, which assumedly will reflect the nation’s ever-deepening financial hole, should be a better gauge on whether healthcare remains as recession-proof as some think it is.
Hoangmai Pham, a senior health researcher at the Center for Studying Health System Change and lead author of a study on how the hospitalist model has focused attention on patient-care coordination, says changes at the federal level will be a driving factor in the strength of healthcare. Roughly 50% to 80% of a hospitalist’s annual salary comes from clinical billings, according to SHM data. The balance comes from hospital subsidies, in the form of annual contracts, monthly stipends, or pay-for-performance bonuses. Drastic changes in payment policy could have drastic implications on those subsidies.
“The ground is very fluid right now, in terms of where payment policy is going,” Pham says. “If I were hospitalists, part of the nervousness would be I’m not sure what direction things are heading in.”
Potential Solutions
Many hospitalists, however, see positives in the economic morass. Hospitalist Troy Ahlstrom, MD, is financial director of Hospitalists of Northwest Michigan in Traverse City, which serves roughly 400 beds at Munson Medical Center. He says groups can prove their worth by showing how they make it easier for other specialists—cardiologists, orthopedists, etc.—to perform the more lucrative procedures on which hospitals rely for higher reimbursements. Then, the group can negotiate for a piece of the savings under a pay-for-performance contracting model.
“What can we do to help make you more efficient, so you can do two extra surgical cases a week?” Dr. Ahlstrom says. “What if the hospital itself realizes a 15% increase in efficiency? Work out a deal that if we save you 15% … you give us a cut.”
Dr. Westle suggests analyzing cost accounting as another way to offer evidence of productivity. Paying overtime for back-office staff is ineffective if your salary overhead is greater than your billing collection. He also recommends a virtual office to employ billing specialists who work from home and doctors without off-site offices, eliminating real estate, utility, and infectious-waste-disposal costs that can cost private practices 55% to 60% in overhead costs.
Partnerships and reinvention are other avenues for cost-effectiveness. Some smaller, single-hospitalist groups might merge to cut costs through economies of scale, but SHM’s Miller thinks there is an opportunity to create a cooperative structure in which hospital medicine groups maintain individual identifies yet share certain functions, such as a common billing service.
Dr. King, the medical director who was promoted in November, is running a long-term acute-care center (LTAC) to help generate a parallel revenue stream. The center opened in May; during periods of decreased patient traffic at Southwest Medical Center, it affords his hospitalists another place to work, encountering patients and billing services. It also creates a referral stream for his hospital. He also has engaged in preliminary discussions for opening and staffing a pre-operative clinic or a wound-care clinic, but those discussions are in the early stages. King is sitting down with PCPs his group has little history with to increase referrals, and he is meeting with the hospital’s specialists to inform them that earlier consults with hospitalists could allow for streamlined service, shorter stays, and greater revenue.
“If you stop your research and development (R&D) during the hard times, 18 months from now, everyone else has stopped their R&D,” Dr. Westle says. “But if you continued your R&D, you’re 18 months ahead of everyone else.”
Dr. Westle refers to his method as “weaving yourself into the fabric of the health system.” Caring for the unassigned adult population and handling internal medicine assignments is low-hanging fruit for hospital medicine groups. He suggests creating programs to teach residents who are participating in hospital quality committees or other panels to deal with coding and billing, staffing LTACs, and improving the referral process for smaller, outlying hospitals to send patients to larger hospitals.
And, of course, there is relationship-building. Although tight economic times will require hospitalists to provide more quantitative data to prove their worth, the hospitalist model thrives on doctor-to-doctor interactions. Connections built with proceduralists and nurses, who can vouch for the value of a hospital medicine group, can mean a lot when hospital boards are searching for areas to trim costs.
“If you talk to seasoned directors of hospitalist programs, you win over hearts and minds one at a time,” Pham says. Most hospital executives “know there is value beyond that which can be proven on the balance sheet. It’s difficult to price things like convenience, satisfaction.”
What’s Next
Doug Cutler, MD, a hospitalist at Banner Sun City Hospitalists in Arizona, which serves 800-plus beds in two hospitals in Sun City and Sun City West, has watched economics change his situation. His old employer, Banner Health, recently merged its two hospitals with Sun Health. The new owners are learning how Cutler’s group works, talking to both hospitalists and other hospital staff. They have the group’s documentation to review, but individual doctors now have the opportunity to prove themselves as standouts.
“Find out the needs and service them the best you can,” Dr. Cutler says. “If it’s a throughput issue, work with them on that. Are you on committees? Are you on the quality committee? Pharmacy and therapeutics? Find what they need and fill a niche. Talk to medical directors, work with case managers. Don’t be the one that they hate to page; be the one they’re not worried about stopping in the hallways because you’re the go-to physician.”
SHM’s Miller agrees that individual hospitalists should take every opportunity to stand out. Whether it’s making sure hospital executives know your name, earning as many certifications as applicable, or applying for the society’s new Fellow in Hospital Medicine program, each doctor has to look at the economic crisis from a professional and personal viewpoint.
And while some could reason that Dr. Cutler’s situation—working for a hospital-owned group as opposed to a large multistate group or multispecialty practice—gives him more job security, he could argue the lack of negotiating leverage might give him less. But as he often tells his patients when they ask for a diagnosis: It’s hard to see 10 seconds into the future.
“I don’t want to think I’m sitting here fat, dumb, and happy and they won’t let me go,” Cutler says, knocking on wood. “I just don’t know. Every company … realistically needs to look at everything if they want to survive. We’re potentially on the chopping block, but do you lop off something that costs a million dollars when it saves you five? Are you willing to go back to a time before that?” TH
Richard Quinn is a freelance writer based in New Jersey.
Before his recent promotion, hospitalist Garth King, MD, medical director of the Schumacher Group at Southwest Medical Center in Lafayette, La., had hoped to add a fourth full-time doctor to his roster. The hiring made sense at the time. As recently as last summer, the group’s three full-time doctors were averaging 35 to 40 patient encounters a day, enough to warrant the additional hospitalist position. But the group’s census dropped 25% in the fourth quarter of 2008, and these days, Dr. King simply can’t justify the math to bring on another six-figure salary.
“Over the past two, three months, patient slowdown has pushed off the ability” to add staff, Dr. King explains. “We’ll wait until things ramp up again, once we get the numbers to where they were before.”
Dr. King could be in for a long wait. The fiscal meltdown that began in 2007 and last year mushroomed into a full-blown recession has taken hold in the world of hospital medicine. More and more, hospitals are reporting decreased revenues and increased levels of charity care. The result: Planned group expansions have been put on hold, open positions are going unfilled, and some hospitalists have been laid off.
Constituencies from health-system executives to rank-and-file hospitalists to economists remain cautious of acting too boldly before President Obama and the new Congress unveil much-anticipated changes to Medicare billing and reimbursement schedules. Aggressive reforms, such as extending health coverage to more than 45 million uninsured Americans, could swamp hospitals with new patients and lead to cuts in reimbursement rates. A more temperate approach by the new administration could leave a relative status quo.
Either way, hospital medicine has never endured a recession so deep that some healthcare economists liken it to the Great Depression, so the practical effect on the industry is difficult to forecast with accuracy. Hospitalists and their observers agree on one thing, though: This is the year hospital medicine will have to prove its worth more empirically than ever. Positive public relations and studies proclaiming reduced lengths of stay and sped-up emergency department throughput have given the industry a “rarified position as a specialty,” one researcher says. But in constrictive economic times, those figures likely will be revisited, says Mark Pauly, professor of healthcare management at The Wharton School at the University of Pennsylvania. “When revenues are falling, you go back and look at that evidence again,” Pauly says. “Is it really bulletproof?”
Still, the prognosis for economic health is not all bad. Many hospital medicine leaders think the concerns over whether chief financial officers will look to hospital contracts as places to cut spending might spawn improved coding and billing, create new partnerships between hospital medicine groups, and push new revenue streams, such as preoperative clinics or inpatient palliative-care initiatives. This also is a time for hospital groups to reaffirm to their respective C-suites—through a deft combination of data and intangible relationships—that they are an indispensable staffing measure that their respective institutions cannot do without.
“This is an opportunity for hospitalists,” says Joe Miller, SHM’s executive advisor to the CEO. “The problem is we’ve got young, inexperienced leaders. Can they see this? Can they recognize this and not see this as a challenge?”
Problem Identification
Hospitalist Marc Westle, DO, FACP, president and managing partner of Asheville Hospital Group in North Carolina, thinks tracking, collating, and reporting quantifiable metrics is the fastest way to convince hospital executives that hospitalists are not the place to cut spending. And when those same executives are looking at staff reductions—53% of hospitals already are cutting or considering cuts, according to the most recent American Hospital Association data—hospital medicine leaders need to be able to point to specific numbers to prove their worth. Detailed information on coding, cost of capture, revenue production, and patient referrals generated are data points that can strengthen a presentation, especially if an argument shows that revenue production and collection is maximized.
“Don’t leave money on the table,” Dr. Westle says. “Your billing department is only going to bill what your physicians tell them to bill. For hospital groups that have not mentioned both the upfront E&M coding by their doctors and the back-end billing efficiency, those are definite things they need to do, today or yesterday. That efficiency may not have hurt them before, but it could hurt them in the next 12 to 18 months.”
Dr. Westle and others also note that hospitalists have to see the economic downturn through the eyes of hospital executives—and the hospital’s bottom line. Recent AHA data show 29% of hospitals are reporting moderate decreases in admissions, and another 9% of hospitals categorize those drops as significant. More than 3 in 10 hospitals have reported a noticeable reduction in elective procedures.
Pauly, the Wharton professor, also cautions that a tightened economy might force primary-care physicians (PCPs) back into hospitals, taking away patients now in the hospitalists’ purview. Hospital medicine’s beginnings trace to those PCPs acquiescing hospital rounds to a new intermediary—hospitalists—in return for the ability to focus more on their daily practices, Pauly says. Ancillary benefits included not being on call 24 hours a day, seven days a week.
“A lower income may change that willingness,” Pauly notes. “Leisure is a luxury good, and if your revenue is falling, you may want to get that business back.”
Another part of the equation is the rising tide of the uninsured, currently estimated at 47 million. It remains to be seen what effect the uninsured have on overall healthcare spending in the U.S., which is projected to rise 6.6% in 2009 to $2.6 trillion, according to the most recent data available from the Centers for Medicare and Medicaid Services (see Figure 1, below). Those projections, however, were released nearly a year ago, long before the severity of the current financial crisis became clear. Pauly says adjusted numbers released this winter, which assumedly will reflect the nation’s ever-deepening financial hole, should be a better gauge on whether healthcare remains as recession-proof as some think it is.
Hoangmai Pham, a senior health researcher at the Center for Studying Health System Change and lead author of a study on how the hospitalist model has focused attention on patient-care coordination, says changes at the federal level will be a driving factor in the strength of healthcare. Roughly 50% to 80% of a hospitalist’s annual salary comes from clinical billings, according to SHM data. The balance comes from hospital subsidies, in the form of annual contracts, monthly stipends, or pay-for-performance bonuses. Drastic changes in payment policy could have drastic implications on those subsidies.
“The ground is very fluid right now, in terms of where payment policy is going,” Pham says. “If I were hospitalists, part of the nervousness would be I’m not sure what direction things are heading in.”
Potential Solutions
Many hospitalists, however, see positives in the economic morass. Hospitalist Troy Ahlstrom, MD, is financial director of Hospitalists of Northwest Michigan in Traverse City, which serves roughly 400 beds at Munson Medical Center. He says groups can prove their worth by showing how they make it easier for other specialists—cardiologists, orthopedists, etc.—to perform the more lucrative procedures on which hospitals rely for higher reimbursements. Then, the group can negotiate for a piece of the savings under a pay-for-performance contracting model.
“What can we do to help make you more efficient, so you can do two extra surgical cases a week?” Dr. Ahlstrom says. “What if the hospital itself realizes a 15% increase in efficiency? Work out a deal that if we save you 15% … you give us a cut.”
Dr. Westle suggests analyzing cost accounting as another way to offer evidence of productivity. Paying overtime for back-office staff is ineffective if your salary overhead is greater than your billing collection. He also recommends a virtual office to employ billing specialists who work from home and doctors without off-site offices, eliminating real estate, utility, and infectious-waste-disposal costs that can cost private practices 55% to 60% in overhead costs.
Partnerships and reinvention are other avenues for cost-effectiveness. Some smaller, single-hospitalist groups might merge to cut costs through economies of scale, but SHM’s Miller thinks there is an opportunity to create a cooperative structure in which hospital medicine groups maintain individual identifies yet share certain functions, such as a common billing service.
Dr. King, the medical director who was promoted in November, is running a long-term acute-care center (LTAC) to help generate a parallel revenue stream. The center opened in May; during periods of decreased patient traffic at Southwest Medical Center, it affords his hospitalists another place to work, encountering patients and billing services. It also creates a referral stream for his hospital. He also has engaged in preliminary discussions for opening and staffing a pre-operative clinic or a wound-care clinic, but those discussions are in the early stages. King is sitting down with PCPs his group has little history with to increase referrals, and he is meeting with the hospital’s specialists to inform them that earlier consults with hospitalists could allow for streamlined service, shorter stays, and greater revenue.
“If you stop your research and development (R&D) during the hard times, 18 months from now, everyone else has stopped their R&D,” Dr. Westle says. “But if you continued your R&D, you’re 18 months ahead of everyone else.”
Dr. Westle refers to his method as “weaving yourself into the fabric of the health system.” Caring for the unassigned adult population and handling internal medicine assignments is low-hanging fruit for hospital medicine groups. He suggests creating programs to teach residents who are participating in hospital quality committees or other panels to deal with coding and billing, staffing LTACs, and improving the referral process for smaller, outlying hospitals to send patients to larger hospitals.
And, of course, there is relationship-building. Although tight economic times will require hospitalists to provide more quantitative data to prove their worth, the hospitalist model thrives on doctor-to-doctor interactions. Connections built with proceduralists and nurses, who can vouch for the value of a hospital medicine group, can mean a lot when hospital boards are searching for areas to trim costs.
“If you talk to seasoned directors of hospitalist programs, you win over hearts and minds one at a time,” Pham says. Most hospital executives “know there is value beyond that which can be proven on the balance sheet. It’s difficult to price things like convenience, satisfaction.”
What’s Next
Doug Cutler, MD, a hospitalist at Banner Sun City Hospitalists in Arizona, which serves 800-plus beds in two hospitals in Sun City and Sun City West, has watched economics change his situation. His old employer, Banner Health, recently merged its two hospitals with Sun Health. The new owners are learning how Cutler’s group works, talking to both hospitalists and other hospital staff. They have the group’s documentation to review, but individual doctors now have the opportunity to prove themselves as standouts.
“Find out the needs and service them the best you can,” Dr. Cutler says. “If it’s a throughput issue, work with them on that. Are you on committees? Are you on the quality committee? Pharmacy and therapeutics? Find what they need and fill a niche. Talk to medical directors, work with case managers. Don’t be the one that they hate to page; be the one they’re not worried about stopping in the hallways because you’re the go-to physician.”
SHM’s Miller agrees that individual hospitalists should take every opportunity to stand out. Whether it’s making sure hospital executives know your name, earning as many certifications as applicable, or applying for the society’s new Fellow in Hospital Medicine program, each doctor has to look at the economic crisis from a professional and personal viewpoint.
And while some could reason that Dr. Cutler’s situation—working for a hospital-owned group as opposed to a large multistate group or multispecialty practice—gives him more job security, he could argue the lack of negotiating leverage might give him less. But as he often tells his patients when they ask for a diagnosis: It’s hard to see 10 seconds into the future.
“I don’t want to think I’m sitting here fat, dumb, and happy and they won’t let me go,” Cutler says, knocking on wood. “I just don’t know. Every company … realistically needs to look at everything if they want to survive. We’re potentially on the chopping block, but do you lop off something that costs a million dollars when it saves you five? Are you willing to go back to a time before that?” TH
Richard Quinn is a freelance writer based in New Jersey.
Plane Crash Highlights Hospitalists' Role in MCIs
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
Onward and Upward
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
A New Revenue Source?
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."