User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Regulated Relationship?
As the American Medical Association (AMA) develops a toolkit to help physicians implement contracts that govern the professional relationship between physicians and non-physician providers (NPPs), one SHM committee member says the trade group should keep an open mind on the pros and cons of such agreements.
The AMA House of Delegates last month tasked its staff to develop the toolkit after several delegates expressed concerns that without the so-called “practice agreements,” NPPs and physicians do not have clear boundaries on the scope of practice responsibilities, according to American Medical News, the society’s newspaper.
Lorraine Britting, MS, NP-C, a member of SHM’s Non-Physician Provider Committee, says the agreements can be a framework for certain practices but might be seen as burdensome to HM groups that have worked for years without the contracts in place.
“In the states that already have practice agreements mandated, you put these regulations in place and they work well. That being said, if new requirements are too restrictive, there is certainly potential for there to be some conflict between the physicians and the nurse practitioners,” says Britting, lead nurse practitioner in the department of cardiology medicine at the Cardiovascular Institute at Beth Israel Deaconess Medical Center in Boston.
Britting notes that many HM groups already have practice agreements in place and that she has never worked without one because Massachusetts requires them. She says professional relationships between doctors and NPPs could be helped by rules on who is responsible for what—but only if those agreements are developed with input from all stakeholders.
“It’s hard to make a blanket statement. Someone who has 10 years’ experience working in hospital medicine versus somebody who just graduated ... their needs are going to be very different,” Britting says. “It has to be individually tailored.”
As the American Medical Association (AMA) develops a toolkit to help physicians implement contracts that govern the professional relationship between physicians and non-physician providers (NPPs), one SHM committee member says the trade group should keep an open mind on the pros and cons of such agreements.
The AMA House of Delegates last month tasked its staff to develop the toolkit after several delegates expressed concerns that without the so-called “practice agreements,” NPPs and physicians do not have clear boundaries on the scope of practice responsibilities, according to American Medical News, the society’s newspaper.
Lorraine Britting, MS, NP-C, a member of SHM’s Non-Physician Provider Committee, says the agreements can be a framework for certain practices but might be seen as burdensome to HM groups that have worked for years without the contracts in place.
“In the states that already have practice agreements mandated, you put these regulations in place and they work well. That being said, if new requirements are too restrictive, there is certainly potential for there to be some conflict between the physicians and the nurse practitioners,” says Britting, lead nurse practitioner in the department of cardiology medicine at the Cardiovascular Institute at Beth Israel Deaconess Medical Center in Boston.
Britting notes that many HM groups already have practice agreements in place and that she has never worked without one because Massachusetts requires them. She says professional relationships between doctors and NPPs could be helped by rules on who is responsible for what—but only if those agreements are developed with input from all stakeholders.
“It’s hard to make a blanket statement. Someone who has 10 years’ experience working in hospital medicine versus somebody who just graduated ... their needs are going to be very different,” Britting says. “It has to be individually tailored.”
As the American Medical Association (AMA) develops a toolkit to help physicians implement contracts that govern the professional relationship between physicians and non-physician providers (NPPs), one SHM committee member says the trade group should keep an open mind on the pros and cons of such agreements.
The AMA House of Delegates last month tasked its staff to develop the toolkit after several delegates expressed concerns that without the so-called “practice agreements,” NPPs and physicians do not have clear boundaries on the scope of practice responsibilities, according to American Medical News, the society’s newspaper.
Lorraine Britting, MS, NP-C, a member of SHM’s Non-Physician Provider Committee, says the agreements can be a framework for certain practices but might be seen as burdensome to HM groups that have worked for years without the contracts in place.
“In the states that already have practice agreements mandated, you put these regulations in place and they work well. That being said, if new requirements are too restrictive, there is certainly potential for there to be some conflict between the physicians and the nurse practitioners,” says Britting, lead nurse practitioner in the department of cardiology medicine at the Cardiovascular Institute at Beth Israel Deaconess Medical Center in Boston.
Britting notes that many HM groups already have practice agreements in place and that she has never worked without one because Massachusetts requires them. She says professional relationships between doctors and NPPs could be helped by rules on who is responsible for what—but only if those agreements are developed with input from all stakeholders.
“It’s hard to make a blanket statement. Someone who has 10 years’ experience working in hospital medicine versus somebody who just graduated ... their needs are going to be very different,” Britting says. “It has to be individually tailored.”
Caution Urged in Interpreting Glargine Cancer Risk
A series of studies reported last month by a European health organization has questioned whether the use of insulin glargine, known commercially as Lantus, inflates a patient’s risk of cancer. But according to one source, hospitalists with a large census of diabetic or hypoglycemic patients shouldn’t pull their patients off the treatment just yet.
Four different population-based studies were reported on the Web site for Diabetologia, the journal of the European Association of the Study of Diabetes. A German study of 127,000 patients in an insurance database found that for every 100 patients taking Lantus, there was one more person diagnosed with cancer when compared with 100 patients taking similar doses of human insulin. The risk increased with the dosage, the study reported.
But the American Diabetes Association quickly released a statement calling the studies “conflicting and confusing.”
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, who estimates one-third of his patients are either diabetic or hypoglycemic, agrees, saying that observational studies make it hard to draw any conclusions.
“I tell patients we don’t know enough,” says Dr. Schnipper, director of clinical research and associate physician in the Division of General Medicine at Brigham and Women’s Hospital Hospitalist Service in Boston. “Right now, there’s no good strong evidence that Lantus is worse than any other alternative.”
Dr. Schnipper cautioned fellow hospitalists to not overreact to the reports, noting that without a randomized trial to follow through on the hypotheses raised, there is no resolution to the confounding-by-indication bias that can plague observational studies.
“There’s an adage in medicine that you never want to be the first person or the last person to use a drug,” Dr. Schnipper says. “I would say you should never be the first person or the last person to stop using a drug.”
A series of studies reported last month by a European health organization has questioned whether the use of insulin glargine, known commercially as Lantus, inflates a patient’s risk of cancer. But according to one source, hospitalists with a large census of diabetic or hypoglycemic patients shouldn’t pull their patients off the treatment just yet.
Four different population-based studies were reported on the Web site for Diabetologia, the journal of the European Association of the Study of Diabetes. A German study of 127,000 patients in an insurance database found that for every 100 patients taking Lantus, there was one more person diagnosed with cancer when compared with 100 patients taking similar doses of human insulin. The risk increased with the dosage, the study reported.
But the American Diabetes Association quickly released a statement calling the studies “conflicting and confusing.”
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, who estimates one-third of his patients are either diabetic or hypoglycemic, agrees, saying that observational studies make it hard to draw any conclusions.
“I tell patients we don’t know enough,” says Dr. Schnipper, director of clinical research and associate physician in the Division of General Medicine at Brigham and Women’s Hospital Hospitalist Service in Boston. “Right now, there’s no good strong evidence that Lantus is worse than any other alternative.”
Dr. Schnipper cautioned fellow hospitalists to not overreact to the reports, noting that without a randomized trial to follow through on the hypotheses raised, there is no resolution to the confounding-by-indication bias that can plague observational studies.
“There’s an adage in medicine that you never want to be the first person or the last person to use a drug,” Dr. Schnipper says. “I would say you should never be the first person or the last person to stop using a drug.”
A series of studies reported last month by a European health organization has questioned whether the use of insulin glargine, known commercially as Lantus, inflates a patient’s risk of cancer. But according to one source, hospitalists with a large census of diabetic or hypoglycemic patients shouldn’t pull their patients off the treatment just yet.
Four different population-based studies were reported on the Web site for Diabetologia, the journal of the European Association of the Study of Diabetes. A German study of 127,000 patients in an insurance database found that for every 100 patients taking Lantus, there was one more person diagnosed with cancer when compared with 100 patients taking similar doses of human insulin. The risk increased with the dosage, the study reported.
But the American Diabetes Association quickly released a statement calling the studies “conflicting and confusing.”
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, who estimates one-third of his patients are either diabetic or hypoglycemic, agrees, saying that observational studies make it hard to draw any conclusions.
“I tell patients we don’t know enough,” says Dr. Schnipper, director of clinical research and associate physician in the Division of General Medicine at Brigham and Women’s Hospital Hospitalist Service in Boston. “Right now, there’s no good strong evidence that Lantus is worse than any other alternative.”
Dr. Schnipper cautioned fellow hospitalists to not overreact to the reports, noting that without a randomized trial to follow through on the hypotheses raised, there is no resolution to the confounding-by-indication bias that can plague observational studies.
“There’s an adage in medicine that you never want to be the first person or the last person to use a drug,” Dr. Schnipper says. “I would say you should never be the first person or the last person to stop using a drug.”
A Sickle Cell Primer
Sickle cell anemia is a prototypical single gene deletion disorder familiar to medical students everywhere. Most physicians recall that it is a devastating disorder that starts with a single substitution of valine for glutamic acid in the beta-globin gene of the hemoglobin molecule, rendering the hemoglobin molecule unstable in its de-oxygenated state. This leads to polymerization of hemoglobin molecules within the red cell, deformation of the cell membrane, and sickling. Sickling, in turn, causes blood vessel damage, vaso-occlusion, and various other physiologic effects, which lead to both micro- and macro-vascular protean complications.1
Despite extensive basic research in sickle cell disease (SCD), clinical research into the optimal management of this complex disease has lagged behind. Many adult hospitalists may be unfamiliar with the care of adult SCD patients because most of these patients are cared for in academic centers by hematologists.
In this article we review the common complications of sickle cell anemia in adult patients, the management of associated conditions, and the evidence base for treatment guidelines.
Overview
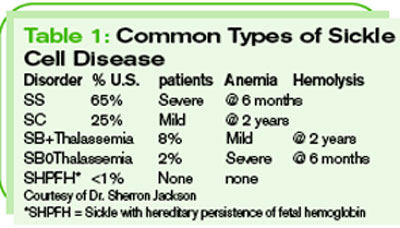
Sickle cell anemia is not just one disorder, but is, rather, a collection of related disorders involving mutations of the hemoglobin molecule. (These disorders are categorized in Table 1, p. 40) In the United States, SCD primarily affects black Americans, with about 9% of this population having sickle trait.2 One in 600 black Americans has sickle cell anemia, also known as hemoglobin SS disease, and there are an estimated 72,000 patients with SCD in the United States.2
In the early 1970s, the average life expectancy for patients with SCD was estimated to be 14.3 years.3 At that time, more than half of SCD patients died before age five, primarily from infectious complications such as pneumococcal sepsis. Twenty years later, the Cooperative Study of SCD documented a much better life expectancy: an average of 42 for males and 48 for females with homozygous S disease (the set of patients with two copies of the defective hemoglobin S mutation).
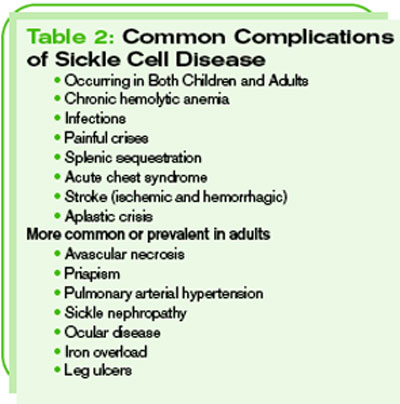
On average, patients with hemoglobin SCD routinely survive into their 60s. Many factors, including earlier diagnosis of SCD through universal screening programs, better vaccines and vaccination rates, prophylactic antibiotics in infancy and young childhood, and aggressive treatment of fever in infants, as well as other advances in care, have contributed to this progress. A longer life expectancy in this population has heralded the extension of common complications into adulthood, however, along with the emergence of other adult-specific complications of SCD. (See Table 2, p. 40.) In order to best treat adults with SCD, hospitalists should be aware of these complications, as well as of the advances that have been achieved.
Extension of Pediatric Complications
Perhaps the most common manifestation of SCD in children and adults is the painful crisis. This manifests in infants as a painful swelling in the digits of the hands and feet known as dactylitis. In older children and adults, pain occurs more often in the long bones of the arms and legs and in the sternum, vertebrae, and pelvic bones. Risk factors for painful crises include higher hematocrit values and higher sickle fractions, typically greater than 30%.4 Frequent painful crises are a marker of disease severity and an independent risk factor for death in SCD.
Hospitalists who regularly admit SCD patients are familiar with a subset of “frequent flyers” who experience recurrent painful crises. Remember that this is a small fraction of the total SCD population. In fact, 40% of SCD patients don’t suffer any painful crises requiring medical attention in a given year, and only 1% face more than six such events.5 Pain management in SCD is perhaps beyond the scope of this article, and there are no widely accepted guidelines. A few expert reviews are available for guidance, however.6,7
Treatment Options for Painful Crises
The most beneficial new treatment for painful crisis in the past two decades has been the use of hydroxyurea. After early studies showed promise, a phase III clinical trial in adults with SCD who suffered frequent painful crises (i.e., more than four per year) and who were given doses of up to 35 mg/kg/day of hydroxyurea showed a dramatic decrease in painful episodes. These patients also endured fewer episodes of acute chest syndrome, with a relative risk of 0.44, and experienced a reduced need for transfusions, with a relative risk of 0.64. This trial was stopped early (at 21 months average follow-up) due to the striking findings.8 Subsequent longer-term trials have not shown any of the feared theoretical complications of hydroxyurea, including cytopenias (when the production of one or more blood cell types ceases or is greatly reduced) or secondary malignancies.9 (See Table 3, p. 40.)

Childhood Complications
Some SCD complications are more prominent or more severe in early childhood than in adulthood. Two examples of this phenomenon are infectious complications and splenic sequestration. Pediatricians and parents of children with SCD live in fear of febrile illness because overwhelming infections such as pneumococcal sepsis remain the primary reason for death in children with SCD. This was especially true before Hemophilus influenza type b (Hib) and pneumococcal conjugate vaccines were introduced and before penicillin prophylaxis from birth through age five became universal.
Though functionally asplenic, adult patients are at a relatively low risk for overwhelming infections because their immune systems have matured enough to allow type-specific antibody production to polysaccharide antigens.7 Still, adults with SCD should be aggressively evaluated for infectious etiology of any febrile illness and routinely administered empiric antibiotics to cover strep species.
Splenic sequestration occurs when sickled cells are caught up in the spleen; this causes massive hemolysis, splenic enlargement, and cardiovascular compromise, and it is most common in SCD patients younger than five. Thankfully, this is rare in adults with SS and SB0Thal; however, the notable exception to this rule is in patients with hemoglobin SC disease or SB+Thal, where complete splenic infarction does not routinely occur.
Acute chest syndrome (ACS) is perhaps the most feared complication in both children and adults with SCD—and with good reason. It is the second most common cause for hospital admission in SCD patients, and it is an independent risk factor for death in SCD.7,10 Occurring more often in children, ACS is typically more severe in adults, in whom ACS can progress rapidly to an acute respiratory distress syndrome (ARDS)-like picture, with mortality reaching 5%-9%.11
ACS involves a classic triad of fever, chest pain, and new pulmonary infiltrates on chest X-ray, but patients are invariably hypoxic and dyspneic as well. The etiology of ACS varies. In one series, 54% of patients had an identified infectious pathogen, most commonly chlamydia or mycoplasma. Bronchoalveolar lavage (BAL) showed lipid-laden macrophages in about 16%, suggesting fat embolism after bony infarcts. The remainder of patients were presumed to have primary pulmonary infarctions.11 The treatment of ACS involves broad-spectrum antibiotics, especially atypical coverage, along with transfusion (simple versus exchange), supplemental oxygen, pain control, and judicious use of IV fluids.
The second most feared complication in SCD is stroke, which can be devastating in both children and young adults. Eleven percent of patients younger than 20 have ischemic strokes, with a risk of stroke that is 200 times higher than that of age-matched peers.9,12 The peak incidence of ischemic stroke occurs before 10 and after 30. These patients are also susceptible to hemorrhagic strokes, the incidence of which peaks in the third decade, for reasons that are unclear.13
Management of acute ischemic stroke in patients with SCD is similar to that used with general patients: antiplatelet therapy, careful attention to normo-glycemia and normovolemia, and maintenance of cerebral perfusion pressure. In addition, SCD patients should receive emergent transfusion to reduce the sickle fraction to less than 30%. Patients with prior transient ischemic attack (TIA) or stroke should be on a chronic monthly transfusion regimen. Also, based on the results of the 1997 STOP I trial (Stroke Prevention Trial in Sickle Cell Anemia), children with SCD should be screened with transcranial Doppler for high velocity flow (>200 cm/second) in the internal jugular and vertebral arteries.14 Children with high velocity flow who were treated with preventative transfusion regimens had a 90% absolute risk reduction in the incidence of first stroke.
In 2001-2006, a follow-up trial (STOP 2) revealed that among patients receiving at least 30 months of chronic transfusion to prevent a first stroke 39% of those randomized to discontinue transfusion had a reversion to high risk Doppler or suffered a stroke within an average of 4.5 months. This has led many to believe that prophylactic transfusion should be a lifelong treatment.15
Complications Seen Primarily in Adults
As the SCD population in this country has grown older, some previously uncommon complications have become more prominent. One predominantly adult complication of SCD is avascular necrosis of the femoral and humeral heads. Though clearly recognized in younger children in whom the incidence is estimated at about 3%, the major burden of femoral osteonecrosis is seen in adults older than 35, in whom prevalence reaches 50%.16 Necrosis of the humeral head can affect nearly 20% of SCD adults as well.17
It is important to recognize this complication as a new or different type of pain, separate from the vaso-occlusive pain usually experienced by SCD patients because it benefits from different therapies. Diagnosis by plain radiography is possible in the late stages, when evidence of remodeling, cystic changes, and sclerosis can be seen, but MRI has become the gold standard, with an estimated diagnostic accuracy of 90%.16 Conservative treatments include NSAIDs and steroid joint injections, but many afflicted patients may need orthopedic referral for joint replacement.
While acute chest syndrome remains a primary cause of mortality in SCD, adults with SCD are also at high risk for the chronic effects of pulmonary arterial hypertension (PAH). Thought to be uncommon in children, PAH affects up to one-third of adult SCD patients.18 Suspicion of this condition can be based on worsened fatigue, new resting hypoxemia, or increased painful crises, but experts advocate universal screening using transthoracic echocardiography. Patients with a tricuspid regurgitant jet velocity of 2.5 m/sec meet diagnostic criteria, and it is notable that the relative risk of death is 7.4 compared with SCD patients without PAH. This correlates with only moderate elevation of pulmonary pressures, suggesting that SCD patients tolerate PAH less well than other populations. Treatment options advocated include hydroxyurea, chronic transfusions, oxygen, pulmonary vasodilators such as prostacyclin and bosentan, and phosphodiesterase inhibitors such as sildenafil.
As SCD patients age, kidney disease is seen with increasing frequency, and three primary mechanisms are recognized. First, ischemic damage in the tubules causes tubular necrosis, which leads to hematuria.19 This condition can range from microscopic to severe gross hematuria, threatening urinary obstruction. Second, damage in the collecting duct impairs the body’s ability to concentrate urine, a condition that is called hyposthenuria. This condition makes SCD patients susceptible to dehydration, especially during physical exertion or in hot weather.
Interestingly, these first two mechanisms of kidney damage are also seen in patients with sickle cell trait. Finally, and most importantly, medullary interstitial fibrosis damages the glomerulus. Clinically, this is the most important mechanism because it leads to nephritic syndrome and chronic kidney disease as well as end-stage renal disease (ESRD).19
Priapism is the persistent, painful erection of the penis in post-pubertal SCD males not associated with sexual desire or relieved by orgasm; this condition is typically defined as lasting more than four to six hours.20 It is particularly common in younger males, with a yearly incidence of 6%-27%; the incidence of priapism in adults approaches 42%. In addition to being extremely painful, prolonged or repeated episodes can lead to impotence. Unfortunately, there are few well-studied treatment options; expert opinion suggests supportive care, including IV fluids, oxygen, ice, elevation, narcotic pain control, and even red cell transfusion in selected cases. Medications used include oral terbutaline, pseudoephedrine, and even stilboestrol, as well as injected phenylephrine, epinephrine, methylene blue, and tenecteplase (TNK-tPA). Surgical procedures attempted have included dorsal penile nerve block, cavernous aspiration, and the Winter procedure, which involves creating a vascular shunt from the corpora cavernosa to the glans penis. Urology consultation is often required for severe cases.
Several forms of eye disease occur in SCD patients. They can be broadly grouped into non-proliferative and proliferative diseases. In the former group, ocular trauma should be recognized as a visual emergency because patients are at risk for developing hyphema, occlusion of the trabeculae in the anterior chamber, and acute glaucoma. SCD patients of all ages are also at risk for acute retinal artery occlusion. Older SCD patients are at greatest risk, however, for a proliferative retinopathy similar to that seen in diabetes.21
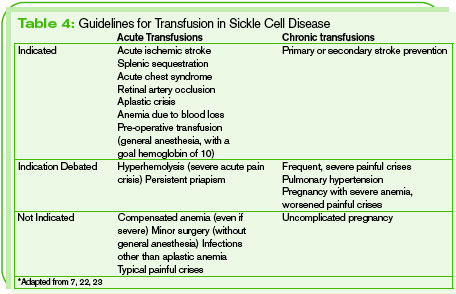
Though red blood cell transfusions are helpful in many SCD patients, repeated transfusions can result in infections, immunologic consequences, and iron overload. (See Table 4, p. 41.) Infections that may result include parvovirus B19, HIV, human T-lymphotropic viruses (HTLV) I and II, and viral hepatitides. Immunologic consequences include alloimmunization, which occurs in up to 50% of SCD patients, and potentially fatal acute hemolytic reactions.22 Finally, patients who require frequent transfusions develop iron overload, which in turn causes fatigue, cardiomyopathy, diabetes mellitus, and cirrhosis. This necessitates iron chelators such as deferoxamine, which are disappointingly difficult to administer, requiring either IV or subcutaneous infusion over 12-24 hours daily. One bright note is the recent approval of deferasirox, an iron chelator that is taken orally once daily.
Conclusion
SCD is a complex genetic disease that affects multiple organs. Advances in medical care have increased longevity for SCD patients, and there are currently more adults living with the disease than ever before. Though patients often receive their care in academic centers, hospitalists may encounter them in routine practice. It is useful to have an understanding of the complications of SCD commonly seen in adults and to review the evidence base for care. TH
References
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Quinn CT, Rogers ZR, Buchanan GR. Survival of children with sickle cell disease. Blood. 2004 Jun 1;103(11):4023-4027.
- Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease. Life expectancy and risk factors for early death. [See comment.] N Engl J Med. 1994 Oct 13;331(15):1022-1023.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease: rates and risk factors. N Engl J Med. 1991 Jul 4;325(1):11-16.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease. rates and risk factors. [See comment.] N Engl J Med. 1991;325(24):1747-1748.
- Ballas SK. Pain management of sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):785-802.
- National Institutes of Health. The Management of Sickle Cell Disease. 4th ed. Washington, DC: National Heart, Lung, and Blood Institute; 2002. NIH publication No. 02-2117.
- Charache S, Terrin ML, Moore RD, et al. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. [See comment.] N Engl J Med. 1995 May 18;332(20):1317-1322.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987, ix. Review.
- Johnson CS. The acute chest syndrome. Hematol Oncol Clin North Am. 2005;19(5):857-879, vi-vii.
- Vichinsky EP, Neumayr LD, Earles AN, et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N Engl J Med. 2000 Sep 14;342(25):1855-65.
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998 Jan;91(1):288-294.
- Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. [See comment.] N Engl J Med. 1998 Jul;339(20):1477-1478.
- Adams RJ, Brambilla D. Optimizing Primary Stroke Prevention in Sickle Cell Anemia (STOP 2) Trial Investigators. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. [See comment.] N Engl J Med. 2005;353(26):2743-2745.
- Aguilar C, Vichinsky E, Neumayr L. Bone and joint disease in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):929-941, viii. Review.
- Milner PF, Kraus AP, Sebes JI, et al. Osteonecrosis of the humeral head in sickle cell disease. Clin Orthop Relat Res. 1993;289:136-143.
- Castro O, Gladwin MT. Pulmonary hypertension in sickle cell disease: mechanisms, diagnosis, and management. Hematol Oncol Clin North Am. 2005;19(5):881-896, vii.
- Saborio P, Scheinman JI. Sickle cell nephropathy. J Am Soc Nephrol. 1999 Jan;10(1):187-192. Review.
- Vilke GM, Harrigan RA, Ufberg JW, et al. Emergency evaluation and treatment of priapism. J Emerg Med. 2004 Apr;26(3):325-329. Review.
- Charache S. Eye disease in sickling disorders. Hematol Oncol Clin North Am. 1996;10(6): 1357-1362.
- Wanko SO, Telen MJ. Transfusion management in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):803-826, v-vi.
- Ohene-Frempong K. Indications for red cell transfusion in sickle cell disease. Semin Hematol. 2001 Jan;38(1 Suppl 1):5-13.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. [See comment.] N Engl J Med. 1995 Jul 27;333(4):206-213.
- Piga A, Galanello R, Cappellini, MD, et al. Phase II study of oral chelator ICL670 in thalassaemia patients with transfusional iron overload: efficacy, safety, pharmacokinetics (PK) and pharmacodynamics (PD) after 6 months of therapy. Blood. 2002;100:5a (abstract).
Sickle cell anemia is a prototypical single gene deletion disorder familiar to medical students everywhere. Most physicians recall that it is a devastating disorder that starts with a single substitution of valine for glutamic acid in the beta-globin gene of the hemoglobin molecule, rendering the hemoglobin molecule unstable in its de-oxygenated state. This leads to polymerization of hemoglobin molecules within the red cell, deformation of the cell membrane, and sickling. Sickling, in turn, causes blood vessel damage, vaso-occlusion, and various other physiologic effects, which lead to both micro- and macro-vascular protean complications.1
Despite extensive basic research in sickle cell disease (SCD), clinical research into the optimal management of this complex disease has lagged behind. Many adult hospitalists may be unfamiliar with the care of adult SCD patients because most of these patients are cared for in academic centers by hematologists.
In this article we review the common complications of sickle cell anemia in adult patients, the management of associated conditions, and the evidence base for treatment guidelines.
Overview
Sickle cell anemia is not just one disorder, but is, rather, a collection of related disorders involving mutations of the hemoglobin molecule. (These disorders are categorized in Table 1, p. 40) In the United States, SCD primarily affects black Americans, with about 9% of this population having sickle trait.2 One in 600 black Americans has sickle cell anemia, also known as hemoglobin SS disease, and there are an estimated 72,000 patients with SCD in the United States.2
In the early 1970s, the average life expectancy for patients with SCD was estimated to be 14.3 years.3 At that time, more than half of SCD patients died before age five, primarily from infectious complications such as pneumococcal sepsis. Twenty years later, the Cooperative Study of SCD documented a much better life expectancy: an average of 42 for males and 48 for females with homozygous S disease (the set of patients with two copies of the defective hemoglobin S mutation).
On average, patients with hemoglobin SCD routinely survive into their 60s. Many factors, including earlier diagnosis of SCD through universal screening programs, better vaccines and vaccination rates, prophylactic antibiotics in infancy and young childhood, and aggressive treatment of fever in infants, as well as other advances in care, have contributed to this progress. A longer life expectancy in this population has heralded the extension of common complications into adulthood, however, along with the emergence of other adult-specific complications of SCD. (See Table 2, p. 40.) In order to best treat adults with SCD, hospitalists should be aware of these complications, as well as of the advances that have been achieved.
Extension of Pediatric Complications
Perhaps the most common manifestation of SCD in children and adults is the painful crisis. This manifests in infants as a painful swelling in the digits of the hands and feet known as dactylitis. In older children and adults, pain occurs more often in the long bones of the arms and legs and in the sternum, vertebrae, and pelvic bones. Risk factors for painful crises include higher hematocrit values and higher sickle fractions, typically greater than 30%.4 Frequent painful crises are a marker of disease severity and an independent risk factor for death in SCD.
Hospitalists who regularly admit SCD patients are familiar with a subset of “frequent flyers” who experience recurrent painful crises. Remember that this is a small fraction of the total SCD population. In fact, 40% of SCD patients don’t suffer any painful crises requiring medical attention in a given year, and only 1% face more than six such events.5 Pain management in SCD is perhaps beyond the scope of this article, and there are no widely accepted guidelines. A few expert reviews are available for guidance, however.6,7
Treatment Options for Painful Crises
The most beneficial new treatment for painful crisis in the past two decades has been the use of hydroxyurea. After early studies showed promise, a phase III clinical trial in adults with SCD who suffered frequent painful crises (i.e., more than four per year) and who were given doses of up to 35 mg/kg/day of hydroxyurea showed a dramatic decrease in painful episodes. These patients also endured fewer episodes of acute chest syndrome, with a relative risk of 0.44, and experienced a reduced need for transfusions, with a relative risk of 0.64. This trial was stopped early (at 21 months average follow-up) due to the striking findings.8 Subsequent longer-term trials have not shown any of the feared theoretical complications of hydroxyurea, including cytopenias (when the production of one or more blood cell types ceases or is greatly reduced) or secondary malignancies.9 (See Table 3, p. 40.)
Childhood Complications
Some SCD complications are more prominent or more severe in early childhood than in adulthood. Two examples of this phenomenon are infectious complications and splenic sequestration. Pediatricians and parents of children with SCD live in fear of febrile illness because overwhelming infections such as pneumococcal sepsis remain the primary reason for death in children with SCD. This was especially true before Hemophilus influenza type b (Hib) and pneumococcal conjugate vaccines were introduced and before penicillin prophylaxis from birth through age five became universal.
Though functionally asplenic, adult patients are at a relatively low risk for overwhelming infections because their immune systems have matured enough to allow type-specific antibody production to polysaccharide antigens.7 Still, adults with SCD should be aggressively evaluated for infectious etiology of any febrile illness and routinely administered empiric antibiotics to cover strep species.
Splenic sequestration occurs when sickled cells are caught up in the spleen; this causes massive hemolysis, splenic enlargement, and cardiovascular compromise, and it is most common in SCD patients younger than five. Thankfully, this is rare in adults with SS and SB0Thal; however, the notable exception to this rule is in patients with hemoglobin SC disease or SB+Thal, where complete splenic infarction does not routinely occur.
Acute chest syndrome (ACS) is perhaps the most feared complication in both children and adults with SCD—and with good reason. It is the second most common cause for hospital admission in SCD patients, and it is an independent risk factor for death in SCD.7,10 Occurring more often in children, ACS is typically more severe in adults, in whom ACS can progress rapidly to an acute respiratory distress syndrome (ARDS)-like picture, with mortality reaching 5%-9%.11
ACS involves a classic triad of fever, chest pain, and new pulmonary infiltrates on chest X-ray, but patients are invariably hypoxic and dyspneic as well. The etiology of ACS varies. In one series, 54% of patients had an identified infectious pathogen, most commonly chlamydia or mycoplasma. Bronchoalveolar lavage (BAL) showed lipid-laden macrophages in about 16%, suggesting fat embolism after bony infarcts. The remainder of patients were presumed to have primary pulmonary infarctions.11 The treatment of ACS involves broad-spectrum antibiotics, especially atypical coverage, along with transfusion (simple versus exchange), supplemental oxygen, pain control, and judicious use of IV fluids.
The second most feared complication in SCD is stroke, which can be devastating in both children and young adults. Eleven percent of patients younger than 20 have ischemic strokes, with a risk of stroke that is 200 times higher than that of age-matched peers.9,12 The peak incidence of ischemic stroke occurs before 10 and after 30. These patients are also susceptible to hemorrhagic strokes, the incidence of which peaks in the third decade, for reasons that are unclear.13
Management of acute ischemic stroke in patients with SCD is similar to that used with general patients: antiplatelet therapy, careful attention to normo-glycemia and normovolemia, and maintenance of cerebral perfusion pressure. In addition, SCD patients should receive emergent transfusion to reduce the sickle fraction to less than 30%. Patients with prior transient ischemic attack (TIA) or stroke should be on a chronic monthly transfusion regimen. Also, based on the results of the 1997 STOP I trial (Stroke Prevention Trial in Sickle Cell Anemia), children with SCD should be screened with transcranial Doppler for high velocity flow (>200 cm/second) in the internal jugular and vertebral arteries.14 Children with high velocity flow who were treated with preventative transfusion regimens had a 90% absolute risk reduction in the incidence of first stroke.
In 2001-2006, a follow-up trial (STOP 2) revealed that among patients receiving at least 30 months of chronic transfusion to prevent a first stroke 39% of those randomized to discontinue transfusion had a reversion to high risk Doppler or suffered a stroke within an average of 4.5 months. This has led many to believe that prophylactic transfusion should be a lifelong treatment.15
Complications Seen Primarily in Adults
As the SCD population in this country has grown older, some previously uncommon complications have become more prominent. One predominantly adult complication of SCD is avascular necrosis of the femoral and humeral heads. Though clearly recognized in younger children in whom the incidence is estimated at about 3%, the major burden of femoral osteonecrosis is seen in adults older than 35, in whom prevalence reaches 50%.16 Necrosis of the humeral head can affect nearly 20% of SCD adults as well.17
It is important to recognize this complication as a new or different type of pain, separate from the vaso-occlusive pain usually experienced by SCD patients because it benefits from different therapies. Diagnosis by plain radiography is possible in the late stages, when evidence of remodeling, cystic changes, and sclerosis can be seen, but MRI has become the gold standard, with an estimated diagnostic accuracy of 90%.16 Conservative treatments include NSAIDs and steroid joint injections, but many afflicted patients may need orthopedic referral for joint replacement.
While acute chest syndrome remains a primary cause of mortality in SCD, adults with SCD are also at high risk for the chronic effects of pulmonary arterial hypertension (PAH). Thought to be uncommon in children, PAH affects up to one-third of adult SCD patients.18 Suspicion of this condition can be based on worsened fatigue, new resting hypoxemia, or increased painful crises, but experts advocate universal screening using transthoracic echocardiography. Patients with a tricuspid regurgitant jet velocity of 2.5 m/sec meet diagnostic criteria, and it is notable that the relative risk of death is 7.4 compared with SCD patients without PAH. This correlates with only moderate elevation of pulmonary pressures, suggesting that SCD patients tolerate PAH less well than other populations. Treatment options advocated include hydroxyurea, chronic transfusions, oxygen, pulmonary vasodilators such as prostacyclin and bosentan, and phosphodiesterase inhibitors such as sildenafil.
As SCD patients age, kidney disease is seen with increasing frequency, and three primary mechanisms are recognized. First, ischemic damage in the tubules causes tubular necrosis, which leads to hematuria.19 This condition can range from microscopic to severe gross hematuria, threatening urinary obstruction. Second, damage in the collecting duct impairs the body’s ability to concentrate urine, a condition that is called hyposthenuria. This condition makes SCD patients susceptible to dehydration, especially during physical exertion or in hot weather.
Interestingly, these first two mechanisms of kidney damage are also seen in patients with sickle cell trait. Finally, and most importantly, medullary interstitial fibrosis damages the glomerulus. Clinically, this is the most important mechanism because it leads to nephritic syndrome and chronic kidney disease as well as end-stage renal disease (ESRD).19
Priapism is the persistent, painful erection of the penis in post-pubertal SCD males not associated with sexual desire or relieved by orgasm; this condition is typically defined as lasting more than four to six hours.20 It is particularly common in younger males, with a yearly incidence of 6%-27%; the incidence of priapism in adults approaches 42%. In addition to being extremely painful, prolonged or repeated episodes can lead to impotence. Unfortunately, there are few well-studied treatment options; expert opinion suggests supportive care, including IV fluids, oxygen, ice, elevation, narcotic pain control, and even red cell transfusion in selected cases. Medications used include oral terbutaline, pseudoephedrine, and even stilboestrol, as well as injected phenylephrine, epinephrine, methylene blue, and tenecteplase (TNK-tPA). Surgical procedures attempted have included dorsal penile nerve block, cavernous aspiration, and the Winter procedure, which involves creating a vascular shunt from the corpora cavernosa to the glans penis. Urology consultation is often required for severe cases.
Several forms of eye disease occur in SCD patients. They can be broadly grouped into non-proliferative and proliferative diseases. In the former group, ocular trauma should be recognized as a visual emergency because patients are at risk for developing hyphema, occlusion of the trabeculae in the anterior chamber, and acute glaucoma. SCD patients of all ages are also at risk for acute retinal artery occlusion. Older SCD patients are at greatest risk, however, for a proliferative retinopathy similar to that seen in diabetes.21
Though red blood cell transfusions are helpful in many SCD patients, repeated transfusions can result in infections, immunologic consequences, and iron overload. (See Table 4, p. 41.) Infections that may result include parvovirus B19, HIV, human T-lymphotropic viruses (HTLV) I and II, and viral hepatitides. Immunologic consequences include alloimmunization, which occurs in up to 50% of SCD patients, and potentially fatal acute hemolytic reactions.22 Finally, patients who require frequent transfusions develop iron overload, which in turn causes fatigue, cardiomyopathy, diabetes mellitus, and cirrhosis. This necessitates iron chelators such as deferoxamine, which are disappointingly difficult to administer, requiring either IV or subcutaneous infusion over 12-24 hours daily. One bright note is the recent approval of deferasirox, an iron chelator that is taken orally once daily.
Conclusion
SCD is a complex genetic disease that affects multiple organs. Advances in medical care have increased longevity for SCD patients, and there are currently more adults living with the disease than ever before. Though patients often receive their care in academic centers, hospitalists may encounter them in routine practice. It is useful to have an understanding of the complications of SCD commonly seen in adults and to review the evidence base for care. TH
References
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Quinn CT, Rogers ZR, Buchanan GR. Survival of children with sickle cell disease. Blood. 2004 Jun 1;103(11):4023-4027.
- Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease. Life expectancy and risk factors for early death. [See comment.] N Engl J Med. 1994 Oct 13;331(15):1022-1023.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease: rates and risk factors. N Engl J Med. 1991 Jul 4;325(1):11-16.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease. rates and risk factors. [See comment.] N Engl J Med. 1991;325(24):1747-1748.
- Ballas SK. Pain management of sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):785-802.
- National Institutes of Health. The Management of Sickle Cell Disease. 4th ed. Washington, DC: National Heart, Lung, and Blood Institute; 2002. NIH publication No. 02-2117.
- Charache S, Terrin ML, Moore RD, et al. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. [See comment.] N Engl J Med. 1995 May 18;332(20):1317-1322.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987, ix. Review.
- Johnson CS. The acute chest syndrome. Hematol Oncol Clin North Am. 2005;19(5):857-879, vi-vii.
- Vichinsky EP, Neumayr LD, Earles AN, et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N Engl J Med. 2000 Sep 14;342(25):1855-65.
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998 Jan;91(1):288-294.
- Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. [See comment.] N Engl J Med. 1998 Jul;339(20):1477-1478.
- Adams RJ, Brambilla D. Optimizing Primary Stroke Prevention in Sickle Cell Anemia (STOP 2) Trial Investigators. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. [See comment.] N Engl J Med. 2005;353(26):2743-2745.
- Aguilar C, Vichinsky E, Neumayr L. Bone and joint disease in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):929-941, viii. Review.
- Milner PF, Kraus AP, Sebes JI, et al. Osteonecrosis of the humeral head in sickle cell disease. Clin Orthop Relat Res. 1993;289:136-143.
- Castro O, Gladwin MT. Pulmonary hypertension in sickle cell disease: mechanisms, diagnosis, and management. Hematol Oncol Clin North Am. 2005;19(5):881-896, vii.
- Saborio P, Scheinman JI. Sickle cell nephropathy. J Am Soc Nephrol. 1999 Jan;10(1):187-192. Review.
- Vilke GM, Harrigan RA, Ufberg JW, et al. Emergency evaluation and treatment of priapism. J Emerg Med. 2004 Apr;26(3):325-329. Review.
- Charache S. Eye disease in sickling disorders. Hematol Oncol Clin North Am. 1996;10(6): 1357-1362.
- Wanko SO, Telen MJ. Transfusion management in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):803-826, v-vi.
- Ohene-Frempong K. Indications for red cell transfusion in sickle cell disease. Semin Hematol. 2001 Jan;38(1 Suppl 1):5-13.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. [See comment.] N Engl J Med. 1995 Jul 27;333(4):206-213.
- Piga A, Galanello R, Cappellini, MD, et al. Phase II study of oral chelator ICL670 in thalassaemia patients with transfusional iron overload: efficacy, safety, pharmacokinetics (PK) and pharmacodynamics (PD) after 6 months of therapy. Blood. 2002;100:5a (abstract).
Sickle cell anemia is a prototypical single gene deletion disorder familiar to medical students everywhere. Most physicians recall that it is a devastating disorder that starts with a single substitution of valine for glutamic acid in the beta-globin gene of the hemoglobin molecule, rendering the hemoglobin molecule unstable in its de-oxygenated state. This leads to polymerization of hemoglobin molecules within the red cell, deformation of the cell membrane, and sickling. Sickling, in turn, causes blood vessel damage, vaso-occlusion, and various other physiologic effects, which lead to both micro- and macro-vascular protean complications.1
Despite extensive basic research in sickle cell disease (SCD), clinical research into the optimal management of this complex disease has lagged behind. Many adult hospitalists may be unfamiliar with the care of adult SCD patients because most of these patients are cared for in academic centers by hematologists.
In this article we review the common complications of sickle cell anemia in adult patients, the management of associated conditions, and the evidence base for treatment guidelines.
Overview
Sickle cell anemia is not just one disorder, but is, rather, a collection of related disorders involving mutations of the hemoglobin molecule. (These disorders are categorized in Table 1, p. 40) In the United States, SCD primarily affects black Americans, with about 9% of this population having sickle trait.2 One in 600 black Americans has sickle cell anemia, also known as hemoglobin SS disease, and there are an estimated 72,000 patients with SCD in the United States.2
In the early 1970s, the average life expectancy for patients with SCD was estimated to be 14.3 years.3 At that time, more than half of SCD patients died before age five, primarily from infectious complications such as pneumococcal sepsis. Twenty years later, the Cooperative Study of SCD documented a much better life expectancy: an average of 42 for males and 48 for females with homozygous S disease (the set of patients with two copies of the defective hemoglobin S mutation).
On average, patients with hemoglobin SCD routinely survive into their 60s. Many factors, including earlier diagnosis of SCD through universal screening programs, better vaccines and vaccination rates, prophylactic antibiotics in infancy and young childhood, and aggressive treatment of fever in infants, as well as other advances in care, have contributed to this progress. A longer life expectancy in this population has heralded the extension of common complications into adulthood, however, along with the emergence of other adult-specific complications of SCD. (See Table 2, p. 40.) In order to best treat adults with SCD, hospitalists should be aware of these complications, as well as of the advances that have been achieved.
Extension of Pediatric Complications
Perhaps the most common manifestation of SCD in children and adults is the painful crisis. This manifests in infants as a painful swelling in the digits of the hands and feet known as dactylitis. In older children and adults, pain occurs more often in the long bones of the arms and legs and in the sternum, vertebrae, and pelvic bones. Risk factors for painful crises include higher hematocrit values and higher sickle fractions, typically greater than 30%.4 Frequent painful crises are a marker of disease severity and an independent risk factor for death in SCD.
Hospitalists who regularly admit SCD patients are familiar with a subset of “frequent flyers” who experience recurrent painful crises. Remember that this is a small fraction of the total SCD population. In fact, 40% of SCD patients don’t suffer any painful crises requiring medical attention in a given year, and only 1% face more than six such events.5 Pain management in SCD is perhaps beyond the scope of this article, and there are no widely accepted guidelines. A few expert reviews are available for guidance, however.6,7
Treatment Options for Painful Crises
The most beneficial new treatment for painful crisis in the past two decades has been the use of hydroxyurea. After early studies showed promise, a phase III clinical trial in adults with SCD who suffered frequent painful crises (i.e., more than four per year) and who were given doses of up to 35 mg/kg/day of hydroxyurea showed a dramatic decrease in painful episodes. These patients also endured fewer episodes of acute chest syndrome, with a relative risk of 0.44, and experienced a reduced need for transfusions, with a relative risk of 0.64. This trial was stopped early (at 21 months average follow-up) due to the striking findings.8 Subsequent longer-term trials have not shown any of the feared theoretical complications of hydroxyurea, including cytopenias (when the production of one or more blood cell types ceases or is greatly reduced) or secondary malignancies.9 (See Table 3, p. 40.)
Childhood Complications
Some SCD complications are more prominent or more severe in early childhood than in adulthood. Two examples of this phenomenon are infectious complications and splenic sequestration. Pediatricians and parents of children with SCD live in fear of febrile illness because overwhelming infections such as pneumococcal sepsis remain the primary reason for death in children with SCD. This was especially true before Hemophilus influenza type b (Hib) and pneumococcal conjugate vaccines were introduced and before penicillin prophylaxis from birth through age five became universal.
Though functionally asplenic, adult patients are at a relatively low risk for overwhelming infections because their immune systems have matured enough to allow type-specific antibody production to polysaccharide antigens.7 Still, adults with SCD should be aggressively evaluated for infectious etiology of any febrile illness and routinely administered empiric antibiotics to cover strep species.
Splenic sequestration occurs when sickled cells are caught up in the spleen; this causes massive hemolysis, splenic enlargement, and cardiovascular compromise, and it is most common in SCD patients younger than five. Thankfully, this is rare in adults with SS and SB0Thal; however, the notable exception to this rule is in patients with hemoglobin SC disease or SB+Thal, where complete splenic infarction does not routinely occur.
Acute chest syndrome (ACS) is perhaps the most feared complication in both children and adults with SCD—and with good reason. It is the second most common cause for hospital admission in SCD patients, and it is an independent risk factor for death in SCD.7,10 Occurring more often in children, ACS is typically more severe in adults, in whom ACS can progress rapidly to an acute respiratory distress syndrome (ARDS)-like picture, with mortality reaching 5%-9%.11
ACS involves a classic triad of fever, chest pain, and new pulmonary infiltrates on chest X-ray, but patients are invariably hypoxic and dyspneic as well. The etiology of ACS varies. In one series, 54% of patients had an identified infectious pathogen, most commonly chlamydia or mycoplasma. Bronchoalveolar lavage (BAL) showed lipid-laden macrophages in about 16%, suggesting fat embolism after bony infarcts. The remainder of patients were presumed to have primary pulmonary infarctions.11 The treatment of ACS involves broad-spectrum antibiotics, especially atypical coverage, along with transfusion (simple versus exchange), supplemental oxygen, pain control, and judicious use of IV fluids.
The second most feared complication in SCD is stroke, which can be devastating in both children and young adults. Eleven percent of patients younger than 20 have ischemic strokes, with a risk of stroke that is 200 times higher than that of age-matched peers.9,12 The peak incidence of ischemic stroke occurs before 10 and after 30. These patients are also susceptible to hemorrhagic strokes, the incidence of which peaks in the third decade, for reasons that are unclear.13
Management of acute ischemic stroke in patients with SCD is similar to that used with general patients: antiplatelet therapy, careful attention to normo-glycemia and normovolemia, and maintenance of cerebral perfusion pressure. In addition, SCD patients should receive emergent transfusion to reduce the sickle fraction to less than 30%. Patients with prior transient ischemic attack (TIA) or stroke should be on a chronic monthly transfusion regimen. Also, based on the results of the 1997 STOP I trial (Stroke Prevention Trial in Sickle Cell Anemia), children with SCD should be screened with transcranial Doppler for high velocity flow (>200 cm/second) in the internal jugular and vertebral arteries.14 Children with high velocity flow who were treated with preventative transfusion regimens had a 90% absolute risk reduction in the incidence of first stroke.
In 2001-2006, a follow-up trial (STOP 2) revealed that among patients receiving at least 30 months of chronic transfusion to prevent a first stroke 39% of those randomized to discontinue transfusion had a reversion to high risk Doppler or suffered a stroke within an average of 4.5 months. This has led many to believe that prophylactic transfusion should be a lifelong treatment.15
Complications Seen Primarily in Adults
As the SCD population in this country has grown older, some previously uncommon complications have become more prominent. One predominantly adult complication of SCD is avascular necrosis of the femoral and humeral heads. Though clearly recognized in younger children in whom the incidence is estimated at about 3%, the major burden of femoral osteonecrosis is seen in adults older than 35, in whom prevalence reaches 50%.16 Necrosis of the humeral head can affect nearly 20% of SCD adults as well.17
It is important to recognize this complication as a new or different type of pain, separate from the vaso-occlusive pain usually experienced by SCD patients because it benefits from different therapies. Diagnosis by plain radiography is possible in the late stages, when evidence of remodeling, cystic changes, and sclerosis can be seen, but MRI has become the gold standard, with an estimated diagnostic accuracy of 90%.16 Conservative treatments include NSAIDs and steroid joint injections, but many afflicted patients may need orthopedic referral for joint replacement.
While acute chest syndrome remains a primary cause of mortality in SCD, adults with SCD are also at high risk for the chronic effects of pulmonary arterial hypertension (PAH). Thought to be uncommon in children, PAH affects up to one-third of adult SCD patients.18 Suspicion of this condition can be based on worsened fatigue, new resting hypoxemia, or increased painful crises, but experts advocate universal screening using transthoracic echocardiography. Patients with a tricuspid regurgitant jet velocity of 2.5 m/sec meet diagnostic criteria, and it is notable that the relative risk of death is 7.4 compared with SCD patients without PAH. This correlates with only moderate elevation of pulmonary pressures, suggesting that SCD patients tolerate PAH less well than other populations. Treatment options advocated include hydroxyurea, chronic transfusions, oxygen, pulmonary vasodilators such as prostacyclin and bosentan, and phosphodiesterase inhibitors such as sildenafil.
As SCD patients age, kidney disease is seen with increasing frequency, and three primary mechanisms are recognized. First, ischemic damage in the tubules causes tubular necrosis, which leads to hematuria.19 This condition can range from microscopic to severe gross hematuria, threatening urinary obstruction. Second, damage in the collecting duct impairs the body’s ability to concentrate urine, a condition that is called hyposthenuria. This condition makes SCD patients susceptible to dehydration, especially during physical exertion or in hot weather.
Interestingly, these first two mechanisms of kidney damage are also seen in patients with sickle cell trait. Finally, and most importantly, medullary interstitial fibrosis damages the glomerulus. Clinically, this is the most important mechanism because it leads to nephritic syndrome and chronic kidney disease as well as end-stage renal disease (ESRD).19
Priapism is the persistent, painful erection of the penis in post-pubertal SCD males not associated with sexual desire or relieved by orgasm; this condition is typically defined as lasting more than four to six hours.20 It is particularly common in younger males, with a yearly incidence of 6%-27%; the incidence of priapism in adults approaches 42%. In addition to being extremely painful, prolonged or repeated episodes can lead to impotence. Unfortunately, there are few well-studied treatment options; expert opinion suggests supportive care, including IV fluids, oxygen, ice, elevation, narcotic pain control, and even red cell transfusion in selected cases. Medications used include oral terbutaline, pseudoephedrine, and even stilboestrol, as well as injected phenylephrine, epinephrine, methylene blue, and tenecteplase (TNK-tPA). Surgical procedures attempted have included dorsal penile nerve block, cavernous aspiration, and the Winter procedure, which involves creating a vascular shunt from the corpora cavernosa to the glans penis. Urology consultation is often required for severe cases.
Several forms of eye disease occur in SCD patients. They can be broadly grouped into non-proliferative and proliferative diseases. In the former group, ocular trauma should be recognized as a visual emergency because patients are at risk for developing hyphema, occlusion of the trabeculae in the anterior chamber, and acute glaucoma. SCD patients of all ages are also at risk for acute retinal artery occlusion. Older SCD patients are at greatest risk, however, for a proliferative retinopathy similar to that seen in diabetes.21
Though red blood cell transfusions are helpful in many SCD patients, repeated transfusions can result in infections, immunologic consequences, and iron overload. (See Table 4, p. 41.) Infections that may result include parvovirus B19, HIV, human T-lymphotropic viruses (HTLV) I and II, and viral hepatitides. Immunologic consequences include alloimmunization, which occurs in up to 50% of SCD patients, and potentially fatal acute hemolytic reactions.22 Finally, patients who require frequent transfusions develop iron overload, which in turn causes fatigue, cardiomyopathy, diabetes mellitus, and cirrhosis. This necessitates iron chelators such as deferoxamine, which are disappointingly difficult to administer, requiring either IV or subcutaneous infusion over 12-24 hours daily. One bright note is the recent approval of deferasirox, an iron chelator that is taken orally once daily.
Conclusion
SCD is a complex genetic disease that affects multiple organs. Advances in medical care have increased longevity for SCD patients, and there are currently more adults living with the disease than ever before. Though patients often receive their care in academic centers, hospitalists may encounter them in routine practice. It is useful to have an understanding of the complications of SCD commonly seen in adults and to review the evidence base for care. TH
References
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Quinn CT, Rogers ZR, Buchanan GR. Survival of children with sickle cell disease. Blood. 2004 Jun 1;103(11):4023-4027.
- Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease. Life expectancy and risk factors for early death. [See comment.] N Engl J Med. 1994 Oct 13;331(15):1022-1023.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease: rates and risk factors. N Engl J Med. 1991 Jul 4;325(1):11-16.
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease. rates and risk factors. [See comment.] N Engl J Med. 1991;325(24):1747-1748.
- Ballas SK. Pain management of sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):785-802.
- National Institutes of Health. The Management of Sickle Cell Disease. 4th ed. Washington, DC: National Heart, Lung, and Blood Institute; 2002. NIH publication No. 02-2117.
- Charache S, Terrin ML, Moore RD, et al. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. [See comment.] N Engl J Med. 1995 May 18;332(20):1317-1322.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987, ix. Review.
- Johnson CS. The acute chest syndrome. Hematol Oncol Clin North Am. 2005;19(5):857-879, vi-vii.
- Vichinsky EP, Neumayr LD, Earles AN, et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N Engl J Med. 2000 Sep 14;342(25):1855-65.
- Platt OS. Preventing stroke in sickle cell anemia. N Engl J Med. 2005 Dec 29;353(26): 2743-2745.
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998 Jan;91(1):288-294.
- Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. [See comment.] N Engl J Med. 1998 Jul;339(20):1477-1478.
- Adams RJ, Brambilla D. Optimizing Primary Stroke Prevention in Sickle Cell Anemia (STOP 2) Trial Investigators. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. [See comment.] N Engl J Med. 2005;353(26):2743-2745.
- Aguilar C, Vichinsky E, Neumayr L. Bone and joint disease in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):929-941, viii. Review.
- Milner PF, Kraus AP, Sebes JI, et al. Osteonecrosis of the humeral head in sickle cell disease. Clin Orthop Relat Res. 1993;289:136-143.
- Castro O, Gladwin MT. Pulmonary hypertension in sickle cell disease: mechanisms, diagnosis, and management. Hematol Oncol Clin North Am. 2005;19(5):881-896, vii.
- Saborio P, Scheinman JI. Sickle cell nephropathy. J Am Soc Nephrol. 1999 Jan;10(1):187-192. Review.
- Vilke GM, Harrigan RA, Ufberg JW, et al. Emergency evaluation and treatment of priapism. J Emerg Med. 2004 Apr;26(3):325-329. Review.
- Charache S. Eye disease in sickling disorders. Hematol Oncol Clin North Am. 1996;10(6): 1357-1362.
- Wanko SO, Telen MJ. Transfusion management in sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):803-826, v-vi.
- Ohene-Frempong K. Indications for red cell transfusion in sickle cell disease. Semin Hematol. 2001 Jan;38(1 Suppl 1):5-13.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. [See comment.] N Engl J Med. 1995 Jul 27;333(4):206-213.
- Piga A, Galanello R, Cappellini, MD, et al. Phase II study of oral chelator ICL670 in thalassaemia patients with transfusional iron overload: efficacy, safety, pharmacokinetics (PK) and pharmacodynamics (PD) after 6 months of therapy. Blood. 2002;100:5a (abstract).
Initial Impact
The Journal of Hospital Medicine’s debut impact factor (IF) ranks it in the top 20% of its cohort—no small achievement for a peer-reviewed medical journal in its fourth year of publication.
JHM’s 2008 IF is 3.163, a stronger-than-expected showing that Editor-in-Chief Mark V. Williams, MD, FACP, FHM, hopes will translate into increased submissions.
JHM ranks No. 21 out of 107 journals in the Medicine, General, and Internal subject category. Impact factors are an industry metric used as a rough average of citations received by peer-reviewed journals. For comparison's sake, the IF for the Journal of General Internal Medicine is 2.72; the IF for the Annals of Internal Medicine is 17.457; and the IF for the New England Journal of Medicine is 50.017.
“In context of other journals of similar editorial scope … an [IF score] does indicate something about its influence,” says James Testa, senior director of editorial development and publisher relations for Thomson Reuters, which calculates the score.
Dr. Williams is a little more effusive. The IF, he says, “tells us we need to keep doing what we’re doing. ... There are journals that are 20 years old that don’t have impact factors as high as we do.” Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM's top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development, a supplement published with Volume 1, Issue 1. The supplement's clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development and methodologies.
"SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM.
The Journal of Hospital Medicine’s debut impact factor (IF) ranks it in the top 20% of its cohort—no small achievement for a peer-reviewed medical journal in its fourth year of publication.
JHM’s 2008 IF is 3.163, a stronger-than-expected showing that Editor-in-Chief Mark V. Williams, MD, FACP, FHM, hopes will translate into increased submissions.
JHM ranks No. 21 out of 107 journals in the Medicine, General, and Internal subject category. Impact factors are an industry metric used as a rough average of citations received by peer-reviewed journals. For comparison's sake, the IF for the Journal of General Internal Medicine is 2.72; the IF for the Annals of Internal Medicine is 17.457; and the IF for the New England Journal of Medicine is 50.017.
“In context of other journals of similar editorial scope … an [IF score] does indicate something about its influence,” says James Testa, senior director of editorial development and publisher relations for Thomson Reuters, which calculates the score.
Dr. Williams is a little more effusive. The IF, he says, “tells us we need to keep doing what we’re doing. ... There are journals that are 20 years old that don’t have impact factors as high as we do.” Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM's top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development, a supplement published with Volume 1, Issue 1. The supplement's clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development and methodologies.
"SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM.
The Journal of Hospital Medicine’s debut impact factor (IF) ranks it in the top 20% of its cohort—no small achievement for a peer-reviewed medical journal in its fourth year of publication.
JHM’s 2008 IF is 3.163, a stronger-than-expected showing that Editor-in-Chief Mark V. Williams, MD, FACP, FHM, hopes will translate into increased submissions.
JHM ranks No. 21 out of 107 journals in the Medicine, General, and Internal subject category. Impact factors are an industry metric used as a rough average of citations received by peer-reviewed journals. For comparison's sake, the IF for the Journal of General Internal Medicine is 2.72; the IF for the Annals of Internal Medicine is 17.457; and the IF for the New England Journal of Medicine is 50.017.
“In context of other journals of similar editorial scope … an [IF score] does indicate something about its influence,” says James Testa, senior director of editorial development and publisher relations for Thomson Reuters, which calculates the score.
Dr. Williams is a little more effusive. The IF, he says, “tells us we need to keep doing what we’re doing. ... There are journals that are 20 years old that don’t have impact factors as high as we do.” Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM's top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development, a supplement published with Volume 1, Issue 1. The supplement's clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development and methodologies.
"SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM.
Relational Growth
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
Detail-Oriented
While President Obama made a splash last week with his first stump speeches for healthcare reform, SHM policy leaders want to hear more—a lot more. Those hospitalists say HM advocates need to stay on top of the details that will emerge in coming months about “accountable healthcare,” the bundling of Medicare reimbursement payments, and other sensitive issues.
"Reform is going to happen," says Eric Siegal, MD, FHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison and the chair of SHM’s Public Policy Committee. “The scope of what it is remains to be seen. ... The devil is absolutely in the details."
Dr. Siegal resisted focusing on Obama's opposition to cap malpractice awards. "While tort reform is important and should be addressed, medical malpractice is not the root cause of our dysfunctional healthcare system." Dr. Siegal agrees "conceptually" with the administration’s plans to bundle payments, encourage more medical students to enter primary care, and hold healthcare organizations accountable. But he and other SHM leaders want pilot programs to test the efficacy of such initiatives before any broad changes are implemented.
Some policy wonks wonder how fast HM leaders might see the impact of Obama’s proposal to cut $600 billion from Medicare and Medicaid by 2019. SHM policy committee member Bradley Flansbaum, DO, MPH, said if cuts are implemented quickly, then hospitalists could see hospital subsidies to their programs reduced, or could simply be competing with other specialists for a shrinking fiscal pie.
“Short-term, I would be concerned,” says Dr. Flansbaum, chief of hospitalist services at Lenox Hill Hospital in New York City. “What he’s proposing is more or less ... a haircut. Depending on how quickly the system is worked out, there could be a lot of pain on the hospital medicine side.”
For more public policy information, visit SHM’s Advocacy Website.
While President Obama made a splash last week with his first stump speeches for healthcare reform, SHM policy leaders want to hear more—a lot more. Those hospitalists say HM advocates need to stay on top of the details that will emerge in coming months about “accountable healthcare,” the bundling of Medicare reimbursement payments, and other sensitive issues.
"Reform is going to happen," says Eric Siegal, MD, FHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison and the chair of SHM’s Public Policy Committee. “The scope of what it is remains to be seen. ... The devil is absolutely in the details."
Dr. Siegal resisted focusing on Obama's opposition to cap malpractice awards. "While tort reform is important and should be addressed, medical malpractice is not the root cause of our dysfunctional healthcare system." Dr. Siegal agrees "conceptually" with the administration’s plans to bundle payments, encourage more medical students to enter primary care, and hold healthcare organizations accountable. But he and other SHM leaders want pilot programs to test the efficacy of such initiatives before any broad changes are implemented.
Some policy wonks wonder how fast HM leaders might see the impact of Obama’s proposal to cut $600 billion from Medicare and Medicaid by 2019. SHM policy committee member Bradley Flansbaum, DO, MPH, said if cuts are implemented quickly, then hospitalists could see hospital subsidies to their programs reduced, or could simply be competing with other specialists for a shrinking fiscal pie.
“Short-term, I would be concerned,” says Dr. Flansbaum, chief of hospitalist services at Lenox Hill Hospital in New York City. “What he’s proposing is more or less ... a haircut. Depending on how quickly the system is worked out, there could be a lot of pain on the hospital medicine side.”
For more public policy information, visit SHM’s Advocacy Website.
While President Obama made a splash last week with his first stump speeches for healthcare reform, SHM policy leaders want to hear more—a lot more. Those hospitalists say HM advocates need to stay on top of the details that will emerge in coming months about “accountable healthcare,” the bundling of Medicare reimbursement payments, and other sensitive issues.
"Reform is going to happen," says Eric Siegal, MD, FHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison and the chair of SHM’s Public Policy Committee. “The scope of what it is remains to be seen. ... The devil is absolutely in the details."
Dr. Siegal resisted focusing on Obama's opposition to cap malpractice awards. "While tort reform is important and should be addressed, medical malpractice is not the root cause of our dysfunctional healthcare system." Dr. Siegal agrees "conceptually" with the administration’s plans to bundle payments, encourage more medical students to enter primary care, and hold healthcare organizations accountable. But he and other SHM leaders want pilot programs to test the efficacy of such initiatives before any broad changes are implemented.
Some policy wonks wonder how fast HM leaders might see the impact of Obama’s proposal to cut $600 billion from Medicare and Medicaid by 2019. SHM policy committee member Bradley Flansbaum, DO, MPH, said if cuts are implemented quickly, then hospitalists could see hospital subsidies to their programs reduced, or could simply be competing with other specialists for a shrinking fiscal pie.
“Short-term, I would be concerned,” says Dr. Flansbaum, chief of hospitalist services at Lenox Hill Hospital in New York City. “What he’s proposing is more or less ... a haircut. Depending on how quickly the system is worked out, there could be a lot of pain on the hospital medicine side.”
For more public policy information, visit SHM’s Advocacy Website.
A Hospitalist Is Born
The hospitalist business model has been adopted nationwide to help stem the tide of obstetrician/gynecologists who forgo delivering babies at hospitals—or providing emergency obstetric care—because of skyrocketing malpractice costs and a frustration with on-call schedules. Like the familiar HM model, a new class of OB-GYN has cropped up to work in medical centers.
Called laborists or OB hospitalists, this breed resembles hospital-based physicians: They work out of their respective institutions but don’t have private-practice patients. Hospitals like the arrangement because they have trained delivery staff in-house, and private-practice physicians don't mind giving up hospital calls because they can earn more cycling patients through their office.
The OB Hospitalist Group of Greenville, S.C., already has placed 60 OB hospitalists in six states, including Texas, California, and Florida. Group president Chris Swain, MD, hopes to place 100 by year's end, but only if he can find enough qualified candidates to manage both deliveries and OB emergencies.
"If you're going to be in a hospital 24 hours a day, you want to be able to handle all the emergencies that come in," Dr. Swain says. “You can't take time to look it up. You need to know it."
Dr. Swain's group pays for that knowledge. The average OB-GYN makes about $280,000 per year; Dr. Swain's OB hospitalists earn roughly $300,000 a year. In exchange for the higher salaries and defined work schedules, OB Hospitalist Group requires board certification, monitoring courses, and continued training. "We want our doctors to be the experts in emergency obstetrics care," Dr. Swain says. "We pay our doctors more; we expect more out of them."
The hospitalist business model has been adopted nationwide to help stem the tide of obstetrician/gynecologists who forgo delivering babies at hospitals—or providing emergency obstetric care—because of skyrocketing malpractice costs and a frustration with on-call schedules. Like the familiar HM model, a new class of OB-GYN has cropped up to work in medical centers.
Called laborists or OB hospitalists, this breed resembles hospital-based physicians: They work out of their respective institutions but don’t have private-practice patients. Hospitals like the arrangement because they have trained delivery staff in-house, and private-practice physicians don't mind giving up hospital calls because they can earn more cycling patients through their office.
The OB Hospitalist Group of Greenville, S.C., already has placed 60 OB hospitalists in six states, including Texas, California, and Florida. Group president Chris Swain, MD, hopes to place 100 by year's end, but only if he can find enough qualified candidates to manage both deliveries and OB emergencies.
"If you're going to be in a hospital 24 hours a day, you want to be able to handle all the emergencies that come in," Dr. Swain says. “You can't take time to look it up. You need to know it."
Dr. Swain's group pays for that knowledge. The average OB-GYN makes about $280,000 per year; Dr. Swain's OB hospitalists earn roughly $300,000 a year. In exchange for the higher salaries and defined work schedules, OB Hospitalist Group requires board certification, monitoring courses, and continued training. "We want our doctors to be the experts in emergency obstetrics care," Dr. Swain says. "We pay our doctors more; we expect more out of them."
The hospitalist business model has been adopted nationwide to help stem the tide of obstetrician/gynecologists who forgo delivering babies at hospitals—or providing emergency obstetric care—because of skyrocketing malpractice costs and a frustration with on-call schedules. Like the familiar HM model, a new class of OB-GYN has cropped up to work in medical centers.
Called laborists or OB hospitalists, this breed resembles hospital-based physicians: They work out of their respective institutions but don’t have private-practice patients. Hospitals like the arrangement because they have trained delivery staff in-house, and private-practice physicians don't mind giving up hospital calls because they can earn more cycling patients through their office.
The OB Hospitalist Group of Greenville, S.C., already has placed 60 OB hospitalists in six states, including Texas, California, and Florida. Group president Chris Swain, MD, hopes to place 100 by year's end, but only if he can find enough qualified candidates to manage both deliveries and OB emergencies.
"If you're going to be in a hospital 24 hours a day, you want to be able to handle all the emergencies that come in," Dr. Swain says. “You can't take time to look it up. You need to know it."
Dr. Swain's group pays for that knowledge. The average OB-GYN makes about $280,000 per year; Dr. Swain's OB hospitalists earn roughly $300,000 a year. In exchange for the higher salaries and defined work schedules, OB Hospitalist Group requires board certification, monitoring courses, and continued training. "We want our doctors to be the experts in emergency obstetrics care," Dr. Swain says. "We pay our doctors more; we expect more out of them."
Team Approach to Patient Care
Hospitalists find themselves working with nonphysician providers (NPP) more and more as institutions spread workloads and cut costs. The work arrangement can be panaceas when they work well, barely palatable when they don’t.
Several sessions at HM09 in Chicago explored the best practices of HM groups that use nurse practitioners (NPs) and physician assistants (PAs). A particularly popular session examined case studies that showed two main trends: NPP programs run into trouble when the people involved view their positions as competition; programs succeed when there is buy-in from all stakeholders.
“There are things DOs and MDs do better than NPs and PAs, and there are things NPs and PAs do better than DOs and MDs,” says Mitch Wilson, MD, FHM, corporate medical director for Eagle Hospital Physicians in Atlanta. "It’s all about understanding the cumulative skill set.”
Dr. Wilson and Tracy Cardin, ACNP, at the University of Chicago Medical Center, used care stories as teaching tools for hospitals looking to implement new programs. The first cautionary tale failed because an “old school” culture left a new NPP so isolated from physicians and nursing staff that she quit. Two other cases showed NPPs integrate more easily because of mutual respect, defined responsibilities, and an alignment of expectations between both hospitalists and NPPs.
Mac McCormick, MD, vice president of clinical services at Eagle Hospital Physicians in Atlanta, offers the following suggestions to best utilize NPPs:
•Conduct an analysis of your practice environment, bylaws, staff experience, and pre-existing attitudes to identify potential barriers and optimal opportunities in hiring NPPs;
•Avoid pigeonholing NPPs into such narrow roles as completing discharge summaries or collecting data. Tasks that tend not to utilize their skills set might lead to professional dissatisfaction and likely aren't the most cost-efficient use of resources; and
•Approach things in a team model. Shared visits are one way to accomplish this. Keep communication lines open to make sure accurate and timely information is available to all.
Hospitalists find themselves working with nonphysician providers (NPP) more and more as institutions spread workloads and cut costs. The work arrangement can be panaceas when they work well, barely palatable when they don’t.
Several sessions at HM09 in Chicago explored the best practices of HM groups that use nurse practitioners (NPs) and physician assistants (PAs). A particularly popular session examined case studies that showed two main trends: NPP programs run into trouble when the people involved view their positions as competition; programs succeed when there is buy-in from all stakeholders.
“There are things DOs and MDs do better than NPs and PAs, and there are things NPs and PAs do better than DOs and MDs,” says Mitch Wilson, MD, FHM, corporate medical director for Eagle Hospital Physicians in Atlanta. "It’s all about understanding the cumulative skill set.”
Dr. Wilson and Tracy Cardin, ACNP, at the University of Chicago Medical Center, used care stories as teaching tools for hospitals looking to implement new programs. The first cautionary tale failed because an “old school” culture left a new NPP so isolated from physicians and nursing staff that she quit. Two other cases showed NPPs integrate more easily because of mutual respect, defined responsibilities, and an alignment of expectations between both hospitalists and NPPs.
Mac McCormick, MD, vice president of clinical services at Eagle Hospital Physicians in Atlanta, offers the following suggestions to best utilize NPPs:
•Conduct an analysis of your practice environment, bylaws, staff experience, and pre-existing attitudes to identify potential barriers and optimal opportunities in hiring NPPs;
•Avoid pigeonholing NPPs into such narrow roles as completing discharge summaries or collecting data. Tasks that tend not to utilize their skills set might lead to professional dissatisfaction and likely aren't the most cost-efficient use of resources; and
•Approach things in a team model. Shared visits are one way to accomplish this. Keep communication lines open to make sure accurate and timely information is available to all.
Hospitalists find themselves working with nonphysician providers (NPP) more and more as institutions spread workloads and cut costs. The work arrangement can be panaceas when they work well, barely palatable when they don’t.
Several sessions at HM09 in Chicago explored the best practices of HM groups that use nurse practitioners (NPs) and physician assistants (PAs). A particularly popular session examined case studies that showed two main trends: NPP programs run into trouble when the people involved view their positions as competition; programs succeed when there is buy-in from all stakeholders.
“There are things DOs and MDs do better than NPs and PAs, and there are things NPs and PAs do better than DOs and MDs,” says Mitch Wilson, MD, FHM, corporate medical director for Eagle Hospital Physicians in Atlanta. "It’s all about understanding the cumulative skill set.”
Dr. Wilson and Tracy Cardin, ACNP, at the University of Chicago Medical Center, used care stories as teaching tools for hospitals looking to implement new programs. The first cautionary tale failed because an “old school” culture left a new NPP so isolated from physicians and nursing staff that she quit. Two other cases showed NPPs integrate more easily because of mutual respect, defined responsibilities, and an alignment of expectations between both hospitalists and NPPs.
Mac McCormick, MD, vice president of clinical services at Eagle Hospital Physicians in Atlanta, offers the following suggestions to best utilize NPPs:
•Conduct an analysis of your practice environment, bylaws, staff experience, and pre-existing attitudes to identify potential barriers and optimal opportunities in hiring NPPs;
•Avoid pigeonholing NPPs into such narrow roles as completing discharge summaries or collecting data. Tasks that tend not to utilize their skills set might lead to professional dissatisfaction and likely aren't the most cost-efficient use of resources; and
•Approach things in a team model. Shared visits are one way to accomplish this. Keep communication lines open to make sure accurate and timely information is available to all.
New Tools of the Trade
Andrew Fishmann, MD, FCCP, FACP, listened for more than an hour as an award-winning hospitalist talked about strategies to improve communication between physicians and administrators. Brian Bossard, MD, FACP, FHM, gleaned lessons from case studies of how two HM groups (HMGs) navigated the adolescent years. And dozens more hospitalists sat still for the bulk of an hour as they were given a nuts-and-bolts tutorial of HM finances.
Welcome to SHM’s new practice management track, a three-day series of training sessions that debuted at HM09 and focuses on the inner workings of HMGs—from startup to coding and billing to expansion. “There’s always a quality track, there’s always a clinical track, and there’s always a leadership track,” says Kimberly Dickinson, vice president of operations for Cogent Healthcare in Brentwood, Tenn., and an SHM Career Satisfaction Task Force member. “This was trying to bring together some of the nonclinical aspects.”
The experiment drew positive reviews, if rooms crowded with physicians—some lined up along the walls—are any indication. Dr. Fishmann, a Cogent co-founder who is practicing as a hospitalist with California Lung Associates in Los Angeles, says the courses give younger hospitalists different perspectives. “It’s taking doctors a little out of the hospital and putting them in the boardroom,” he says. “You don’t have a choice. … You need to be involved and have more input.”
The practice management courses are structured to give a broad overview of nearly every facet of opening and operating an HMG. One popular course, which ran nearly 15 minutes long because of participant questions, focused on managing HMG growth. Another session spent more than an hour taking physicians through comanagement issues that arise during collaborations with surgeons.
Real-Life Experiences
Most of the courses were led by familiar SHM leaders. But several attendees said they enjoyed sessions that were led by rank-and-file hospitalists and administrators who live the front-line struggles every day.
The “Case Studies in Managing Program Growth” course featured detailed explanations of the growing pains of HM programs in Michigan and Massachusetts. In the former case, Carole Montgomery, MD, talked about how the Michigan Medical PC group she helped start in western Michigan struggled to formalize certain procedures when it signed its first contract with a hospital in 2002. The group doubled its hospitalist roster and instantly went from an informal HM practice in which everyone knew each other and had relatively similar opinions to a business in which it was unclear who would make major decisions.
In response, Dr. Montgomery’s group crafted a mission statement, created a hospitalist executive committee to make routine operational decisions, and changed how it negotiated contracts with hospitals. Soon after, the group fired its first physician. Last year, the group instituted “internal governance guidelines” to make management decisions clearer. Dr. Montgomery says each of the developments taught her that solving major issues takes patience and a willingness to continually adapt. “I thought I was done each time,” she says. “Now I realize it’s an interactive process.”

Results-Oriented
Peter Short, MD, FAAP, CPE, medical director of Northeast Hospital Corp., shared his recent struggles to hire one hospitalist and expand night coverage. Hospitalists in Dr. Short’s service, who practice at Beverly Hospital in Beverly, Mass., resisted the change at first, not wanting to add additional night-shift responsibility. Dr. Short also spoke about financial concerns to the group and the hospital. After explaining the pros and cons of hiring a sixth rounder, the hospitalists embraced the idea. So far, hospital administrators have had zero complaints, as the first three months of data show a reduction in length of stay by 0.3 days and an average cost decrease of roughly $500 per case.
Dr. Short also explained an unexpected byproduct of the hiring: Night work proved so popular that the hospitalists have demanded that they receive a specified number of overnight shifts a year. “They went from not wanting it to fighting for it,” Dr. Short says proudly. “There is no one-size-fits-all for hospital programs.”
Dr. Bossard, who founded Inpatient Physician Associates in Lincoln, Neb., says the types of detail-oriented presentations made by Drs. Montgomery and Short are useful if physicians learn lessons they can take home and adapt to their practice. “If it’s a lot of smoke without an action item or a bullet point we can latch on to,” he says, “it’s not as helpful.”
Richard Quinn is a freelance writer based in New Jersey.
Andrew Fishmann, MD, FCCP, FACP, listened for more than an hour as an award-winning hospitalist talked about strategies to improve communication between physicians and administrators. Brian Bossard, MD, FACP, FHM, gleaned lessons from case studies of how two HM groups (HMGs) navigated the adolescent years. And dozens more hospitalists sat still for the bulk of an hour as they were given a nuts-and-bolts tutorial of HM finances.
Welcome to SHM’s new practice management track, a three-day series of training sessions that debuted at HM09 and focuses on the inner workings of HMGs—from startup to coding and billing to expansion. “There’s always a quality track, there’s always a clinical track, and there’s always a leadership track,” says Kimberly Dickinson, vice president of operations for Cogent Healthcare in Brentwood, Tenn., and an SHM Career Satisfaction Task Force member. “This was trying to bring together some of the nonclinical aspects.”
The experiment drew positive reviews, if rooms crowded with physicians—some lined up along the walls—are any indication. Dr. Fishmann, a Cogent co-founder who is practicing as a hospitalist with California Lung Associates in Los Angeles, says the courses give younger hospitalists different perspectives. “It’s taking doctors a little out of the hospital and putting them in the boardroom,” he says. “You don’t have a choice. … You need to be involved and have more input.”
The practice management courses are structured to give a broad overview of nearly every facet of opening and operating an HMG. One popular course, which ran nearly 15 minutes long because of participant questions, focused on managing HMG growth. Another session spent more than an hour taking physicians through comanagement issues that arise during collaborations with surgeons.
Real-Life Experiences
Most of the courses were led by familiar SHM leaders. But several attendees said they enjoyed sessions that were led by rank-and-file hospitalists and administrators who live the front-line struggles every day.
The “Case Studies in Managing Program Growth” course featured detailed explanations of the growing pains of HM programs in Michigan and Massachusetts. In the former case, Carole Montgomery, MD, talked about how the Michigan Medical PC group she helped start in western Michigan struggled to formalize certain procedures when it signed its first contract with a hospital in 2002. The group doubled its hospitalist roster and instantly went from an informal HM practice in which everyone knew each other and had relatively similar opinions to a business in which it was unclear who would make major decisions.
In response, Dr. Montgomery’s group crafted a mission statement, created a hospitalist executive committee to make routine operational decisions, and changed how it negotiated contracts with hospitals. Soon after, the group fired its first physician. Last year, the group instituted “internal governance guidelines” to make management decisions clearer. Dr. Montgomery says each of the developments taught her that solving major issues takes patience and a willingness to continually adapt. “I thought I was done each time,” she says. “Now I realize it’s an interactive process.”
Results-Oriented
Peter Short, MD, FAAP, CPE, medical director of Northeast Hospital Corp., shared his recent struggles to hire one hospitalist and expand night coverage. Hospitalists in Dr. Short’s service, who practice at Beverly Hospital in Beverly, Mass., resisted the change at first, not wanting to add additional night-shift responsibility. Dr. Short also spoke about financial concerns to the group and the hospital. After explaining the pros and cons of hiring a sixth rounder, the hospitalists embraced the idea. So far, hospital administrators have had zero complaints, as the first three months of data show a reduction in length of stay by 0.3 days and an average cost decrease of roughly $500 per case.
Dr. Short also explained an unexpected byproduct of the hiring: Night work proved so popular that the hospitalists have demanded that they receive a specified number of overnight shifts a year. “They went from not wanting it to fighting for it,” Dr. Short says proudly. “There is no one-size-fits-all for hospital programs.”
Dr. Bossard, who founded Inpatient Physician Associates in Lincoln, Neb., says the types of detail-oriented presentations made by Drs. Montgomery and Short are useful if physicians learn lessons they can take home and adapt to their practice. “If it’s a lot of smoke without an action item or a bullet point we can latch on to,” he says, “it’s not as helpful.”
Richard Quinn is a freelance writer based in New Jersey.
Andrew Fishmann, MD, FCCP, FACP, listened for more than an hour as an award-winning hospitalist talked about strategies to improve communication between physicians and administrators. Brian Bossard, MD, FACP, FHM, gleaned lessons from case studies of how two HM groups (HMGs) navigated the adolescent years. And dozens more hospitalists sat still for the bulk of an hour as they were given a nuts-and-bolts tutorial of HM finances.
Welcome to SHM’s new practice management track, a three-day series of training sessions that debuted at HM09 and focuses on the inner workings of HMGs—from startup to coding and billing to expansion. “There’s always a quality track, there’s always a clinical track, and there’s always a leadership track,” says Kimberly Dickinson, vice president of operations for Cogent Healthcare in Brentwood, Tenn., and an SHM Career Satisfaction Task Force member. “This was trying to bring together some of the nonclinical aspects.”
The experiment drew positive reviews, if rooms crowded with physicians—some lined up along the walls—are any indication. Dr. Fishmann, a Cogent co-founder who is practicing as a hospitalist with California Lung Associates in Los Angeles, says the courses give younger hospitalists different perspectives. “It’s taking doctors a little out of the hospital and putting them in the boardroom,” he says. “You don’t have a choice. … You need to be involved and have more input.”
The practice management courses are structured to give a broad overview of nearly every facet of opening and operating an HMG. One popular course, which ran nearly 15 minutes long because of participant questions, focused on managing HMG growth. Another session spent more than an hour taking physicians through comanagement issues that arise during collaborations with surgeons.
Real-Life Experiences
Most of the courses were led by familiar SHM leaders. But several attendees said they enjoyed sessions that were led by rank-and-file hospitalists and administrators who live the front-line struggles every day.
The “Case Studies in Managing Program Growth” course featured detailed explanations of the growing pains of HM programs in Michigan and Massachusetts. In the former case, Carole Montgomery, MD, talked about how the Michigan Medical PC group she helped start in western Michigan struggled to formalize certain procedures when it signed its first contract with a hospital in 2002. The group doubled its hospitalist roster and instantly went from an informal HM practice in which everyone knew each other and had relatively similar opinions to a business in which it was unclear who would make major decisions.
In response, Dr. Montgomery’s group crafted a mission statement, created a hospitalist executive committee to make routine operational decisions, and changed how it negotiated contracts with hospitals. Soon after, the group fired its first physician. Last year, the group instituted “internal governance guidelines” to make management decisions clearer. Dr. Montgomery says each of the developments taught her that solving major issues takes patience and a willingness to continually adapt. “I thought I was done each time,” she says. “Now I realize it’s an interactive process.”
Results-Oriented
Peter Short, MD, FAAP, CPE, medical director of Northeast Hospital Corp., shared his recent struggles to hire one hospitalist and expand night coverage. Hospitalists in Dr. Short’s service, who practice at Beverly Hospital in Beverly, Mass., resisted the change at first, not wanting to add additional night-shift responsibility. Dr. Short also spoke about financial concerns to the group and the hospital. After explaining the pros and cons of hiring a sixth rounder, the hospitalists embraced the idea. So far, hospital administrators have had zero complaints, as the first three months of data show a reduction in length of stay by 0.3 days and an average cost decrease of roughly $500 per case.
Dr. Short also explained an unexpected byproduct of the hiring: Night work proved so popular that the hospitalists have demanded that they receive a specified number of overnight shifts a year. “They went from not wanting it to fighting for it,” Dr. Short says proudly. “There is no one-size-fits-all for hospital programs.”
Dr. Bossard, who founded Inpatient Physician Associates in Lincoln, Neb., says the types of detail-oriented presentations made by Drs. Montgomery and Short are useful if physicians learn lessons they can take home and adapt to their practice. “If it’s a lot of smoke without an action item or a bullet point we can latch on to,” he says, “it’s not as helpful.”
Richard Quinn is a freelance writer based in New Jersey.
New Path to Primary Care?
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."