User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Physician Engagement
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.

—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.
—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.
—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
New Jersey Cracks Down on Never Events
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”
Hospitals Look to Future with White House Deal
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
Digital Dilemma
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.

The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.
The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.
The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
Hospitalized Patients Take MRSA Home
A new report on how hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) spreads after patients are discharged has at least one hospitalist wondering whether HM could, or should, take a leading role in reducing MRSA transfers.
The study, "Carriage of Methicillin-Resistant Staphylococcus aureus in Home Care Settings," identified MRSA in 191 of the 1,501 patients (12.7%) who were screened before discharge from French hospitals in 2003 and 2004. Researchers reported that 19% of relatives and caretakers who came into contact with the patients identified with MRSA also acquired the bacteria (Arch Intern Med. 2009;169(15)1372-1378).
Hospitalist and infectious-disease specialist James Pile, MD, FACP, FHM, interim director of the Division of Hospital Medicine at CWRU/MetroHealth Medical Center in Cleveland, says the study might be most important for the questions it raises regarding the degree to which community-acquired MRSA (CA-MRSA) is colonizing household contacts of discharged patients, as the burden of clinical disease in those individuals is likely to be greater than in those colonized with traditional, healthcare-associated MRSA (HA-MRSA). CA-MRSA appears to be supplanting HA-MRSA in many hospitals, Dr. Pile says, and the simple intervention of more rigorous hand washing by caregivers and other household contacts of patients discharged with MRSA infections could help limit the associated fallout.
“This is a chance for healthcare professionals, and hospitalists specifically, to recognize that and to counsel that as patients leave the hospital,” Dr. Pile says.
The authors note that “because none of the household contacts who acquired MRSA developed an infection, it is unclear whether this transmission represents a serious health problem.”
To that end, Dr. Pile says HM should wait for more definitive studies before committing to potentially time-consuming QI projects focused on MRSA transmissions to the home. “Before hospitalists galvanize their resources to try to tackle this problem,” Dr. Pile says, “we want to make sure there is enough bang for the buck.”
A new report on how hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) spreads after patients are discharged has at least one hospitalist wondering whether HM could, or should, take a leading role in reducing MRSA transfers.
The study, "Carriage of Methicillin-Resistant Staphylococcus aureus in Home Care Settings," identified MRSA in 191 of the 1,501 patients (12.7%) who were screened before discharge from French hospitals in 2003 and 2004. Researchers reported that 19% of relatives and caretakers who came into contact with the patients identified with MRSA also acquired the bacteria (Arch Intern Med. 2009;169(15)1372-1378).
Hospitalist and infectious-disease specialist James Pile, MD, FACP, FHM, interim director of the Division of Hospital Medicine at CWRU/MetroHealth Medical Center in Cleveland, says the study might be most important for the questions it raises regarding the degree to which community-acquired MRSA (CA-MRSA) is colonizing household contacts of discharged patients, as the burden of clinical disease in those individuals is likely to be greater than in those colonized with traditional, healthcare-associated MRSA (HA-MRSA). CA-MRSA appears to be supplanting HA-MRSA in many hospitals, Dr. Pile says, and the simple intervention of more rigorous hand washing by caregivers and other household contacts of patients discharged with MRSA infections could help limit the associated fallout.
“This is a chance for healthcare professionals, and hospitalists specifically, to recognize that and to counsel that as patients leave the hospital,” Dr. Pile says.
The authors note that “because none of the household contacts who acquired MRSA developed an infection, it is unclear whether this transmission represents a serious health problem.”
To that end, Dr. Pile says HM should wait for more definitive studies before committing to potentially time-consuming QI projects focused on MRSA transmissions to the home. “Before hospitalists galvanize their resources to try to tackle this problem,” Dr. Pile says, “we want to make sure there is enough bang for the buck.”
A new report on how hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) spreads after patients are discharged has at least one hospitalist wondering whether HM could, or should, take a leading role in reducing MRSA transfers.
The study, "Carriage of Methicillin-Resistant Staphylococcus aureus in Home Care Settings," identified MRSA in 191 of the 1,501 patients (12.7%) who were screened before discharge from French hospitals in 2003 and 2004. Researchers reported that 19% of relatives and caretakers who came into contact with the patients identified with MRSA also acquired the bacteria (Arch Intern Med. 2009;169(15)1372-1378).
Hospitalist and infectious-disease specialist James Pile, MD, FACP, FHM, interim director of the Division of Hospital Medicine at CWRU/MetroHealth Medical Center in Cleveland, says the study might be most important for the questions it raises regarding the degree to which community-acquired MRSA (CA-MRSA) is colonizing household contacts of discharged patients, as the burden of clinical disease in those individuals is likely to be greater than in those colonized with traditional, healthcare-associated MRSA (HA-MRSA). CA-MRSA appears to be supplanting HA-MRSA in many hospitals, Dr. Pile says, and the simple intervention of more rigorous hand washing by caregivers and other household contacts of patients discharged with MRSA infections could help limit the associated fallout.
“This is a chance for healthcare professionals, and hospitalists specifically, to recognize that and to counsel that as patients leave the hospital,” Dr. Pile says.
The authors note that “because none of the household contacts who acquired MRSA developed an infection, it is unclear whether this transmission represents a serious health problem.”
To that end, Dr. Pile says HM should wait for more definitive studies before committing to potentially time-consuming QI projects focused on MRSA transmissions to the home. “Before hospitalists galvanize their resources to try to tackle this problem,” Dr. Pile says, “we want to make sure there is enough bang for the buck.”
A Shorter, Sweeter Stay
A hospitalist-orthopedic comanagement model at Loyola University Medical Center in Maywood, Ill., improves both patient care and satisfaction, according to a study published in the July issue of Orthopedics (2009;32:495).
The approach, which dedicates two hospitalists to work with the orthopedists, was the culmination of a joint effort that began in 2005 to address communication issues between the hospitalist consultation service and the orthopedic surgery team, says Edward Gurza, MD, associate professor of medicine and director of the Division of General Internal Medicine at Loyola's Stritch School of Medicine in Chicago. “The idea was to have the same group of people to take care of patients pre-operatively, peri-operatively, and post-operatively,” Dr. Gurza says. “That’s absolutely critical. With orthopedics, one of the big issues is lack of continuity in the coordination of care.”
The study reports that the length of hospital stays was 0.693 days for 86 high-risk, comanaged patients with multiple comorbidities compared with 0.862 days for 54 patients in the control group. The severity of illness and risk of mortality scores were higher in the study group. The analysis found little effect on costs of care, but patient satisfaction scores for the test groups rose by 5% and 14%, respectively, in the categories of “communication with doctors” and “doctors treated you with respect.”
Dr. Gurza says the program needed no new funding, just a commitment from HM group leaders to dedicate staff to the concept. Hospitalists breed familiarity that cements a bond between physician and patient. “It flows naturally,” he says. “You’re not going out to specifically charm a patient. Hopefully, if you’re doing your job as an internist delivering proper care, patients understand that.”
A hospitalist-orthopedic comanagement model at Loyola University Medical Center in Maywood, Ill., improves both patient care and satisfaction, according to a study published in the July issue of Orthopedics (2009;32:495).
The approach, which dedicates two hospitalists to work with the orthopedists, was the culmination of a joint effort that began in 2005 to address communication issues between the hospitalist consultation service and the orthopedic surgery team, says Edward Gurza, MD, associate professor of medicine and director of the Division of General Internal Medicine at Loyola's Stritch School of Medicine in Chicago. “The idea was to have the same group of people to take care of patients pre-operatively, peri-operatively, and post-operatively,” Dr. Gurza says. “That’s absolutely critical. With orthopedics, one of the big issues is lack of continuity in the coordination of care.”
The study reports that the length of hospital stays was 0.693 days for 86 high-risk, comanaged patients with multiple comorbidities compared with 0.862 days for 54 patients in the control group. The severity of illness and risk of mortality scores were higher in the study group. The analysis found little effect on costs of care, but patient satisfaction scores for the test groups rose by 5% and 14%, respectively, in the categories of “communication with doctors” and “doctors treated you with respect.”
Dr. Gurza says the program needed no new funding, just a commitment from HM group leaders to dedicate staff to the concept. Hospitalists breed familiarity that cements a bond between physician and patient. “It flows naturally,” he says. “You’re not going out to specifically charm a patient. Hopefully, if you’re doing your job as an internist delivering proper care, patients understand that.”
A hospitalist-orthopedic comanagement model at Loyola University Medical Center in Maywood, Ill., improves both patient care and satisfaction, according to a study published in the July issue of Orthopedics (2009;32:495).
The approach, which dedicates two hospitalists to work with the orthopedists, was the culmination of a joint effort that began in 2005 to address communication issues between the hospitalist consultation service and the orthopedic surgery team, says Edward Gurza, MD, associate professor of medicine and director of the Division of General Internal Medicine at Loyola's Stritch School of Medicine in Chicago. “The idea was to have the same group of people to take care of patients pre-operatively, peri-operatively, and post-operatively,” Dr. Gurza says. “That’s absolutely critical. With orthopedics, one of the big issues is lack of continuity in the coordination of care.”
The study reports that the length of hospital stays was 0.693 days for 86 high-risk, comanaged patients with multiple comorbidities compared with 0.862 days for 54 patients in the control group. The severity of illness and risk of mortality scores were higher in the study group. The analysis found little effect on costs of care, but patient satisfaction scores for the test groups rose by 5% and 14%, respectively, in the categories of “communication with doctors” and “doctors treated you with respect.”
Dr. Gurza says the program needed no new funding, just a commitment from HM group leaders to dedicate staff to the concept. Hospitalists breed familiarity that cements a bond between physician and patient. “It flows naturally,” he says. “You’re not going out to specifically charm a patient. Hopefully, if you’re doing your job as an internist delivering proper care, patients understand that.”
The Happiness Factor
HM groups are built—in part—on the theory of work-life balance. But what about work-work balance?
A study published this spring found that faculty physicians at academic medical centers might be more satisfied if they spend at least one day per week on the part of their job that is most meaningful to them (Arch Intern Med, 2009;169(10):990-995).
“The notion of ‘job fit’ is clearly important,” says Noah Harris, MD, FHM, a hospitalist at Presbyterian Hospital in Albuquerque, N.M., and a member of SHM’s Career Satisfaction Task Force. “Since most physicians are drawn to medicine for the notion of patient care, the other activities may be troublesome for many of us.”
To improve employees’ job satisfaction, Dr. Harris and Chad Whelan, MD, FHM, chair of SHM’s career task force, suggest HM leaders do the following:
- Understand what your group has to offer. Let physicians explore parts of the practice unfamiliar to them—and if they find something they have a passion for, encourage it.
- Identify hospitalists who are at risk for burnout and guide them to potential opportunities. Be proactive before dissatisfaction sets in.
- Don’t push people into leadership roles they don’t want. Some people want clinical posts, while others want to be medical directors who meet with administration daily.
- Recognize the importance of flexibility. As HM groups evolve, there are chances to offer new schedules or build in new clinical and nonclinical initiatives.
- Support staff members via mentoring and professional development to make them feel as if they’re doing work they want to do.
“A common mistake, though, is to simply pay people a stipend for doing more,” says Dr. Whelan, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine. “If their professional time is already fully taken with other activities, a stipend will not provide time to appropriately pursue those meaningful activities.”
HM groups are built—in part—on the theory of work-life balance. But what about work-work balance?
A study published this spring found that faculty physicians at academic medical centers might be more satisfied if they spend at least one day per week on the part of their job that is most meaningful to them (Arch Intern Med, 2009;169(10):990-995).
“The notion of ‘job fit’ is clearly important,” says Noah Harris, MD, FHM, a hospitalist at Presbyterian Hospital in Albuquerque, N.M., and a member of SHM’s Career Satisfaction Task Force. “Since most physicians are drawn to medicine for the notion of patient care, the other activities may be troublesome for many of us.”
To improve employees’ job satisfaction, Dr. Harris and Chad Whelan, MD, FHM, chair of SHM’s career task force, suggest HM leaders do the following:
- Understand what your group has to offer. Let physicians explore parts of the practice unfamiliar to them—and if they find something they have a passion for, encourage it.
- Identify hospitalists who are at risk for burnout and guide them to potential opportunities. Be proactive before dissatisfaction sets in.
- Don’t push people into leadership roles they don’t want. Some people want clinical posts, while others want to be medical directors who meet with administration daily.
- Recognize the importance of flexibility. As HM groups evolve, there are chances to offer new schedules or build in new clinical and nonclinical initiatives.
- Support staff members via mentoring and professional development to make them feel as if they’re doing work they want to do.
“A common mistake, though, is to simply pay people a stipend for doing more,” says Dr. Whelan, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine. “If their professional time is already fully taken with other activities, a stipend will not provide time to appropriately pursue those meaningful activities.”
HM groups are built—in part—on the theory of work-life balance. But what about work-work balance?
A study published this spring found that faculty physicians at academic medical centers might be more satisfied if they spend at least one day per week on the part of their job that is most meaningful to them (Arch Intern Med, 2009;169(10):990-995).
“The notion of ‘job fit’ is clearly important,” says Noah Harris, MD, FHM, a hospitalist at Presbyterian Hospital in Albuquerque, N.M., and a member of SHM’s Career Satisfaction Task Force. “Since most physicians are drawn to medicine for the notion of patient care, the other activities may be troublesome for many of us.”
To improve employees’ job satisfaction, Dr. Harris and Chad Whelan, MD, FHM, chair of SHM’s career task force, suggest HM leaders do the following:
- Understand what your group has to offer. Let physicians explore parts of the practice unfamiliar to them—and if they find something they have a passion for, encourage it.
- Identify hospitalists who are at risk for burnout and guide them to potential opportunities. Be proactive before dissatisfaction sets in.
- Don’t push people into leadership roles they don’t want. Some people want clinical posts, while others want to be medical directors who meet with administration daily.
- Recognize the importance of flexibility. As HM groups evolve, there are chances to offer new schedules or build in new clinical and nonclinical initiatives.
- Support staff members via mentoring and professional development to make them feel as if they’re doing work they want to do.
“A common mistake, though, is to simply pay people a stipend for doing more,” says Dr. Whelan, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine. “If their professional time is already fully taken with other activities, a stipend will not provide time to appropriately pursue those meaningful activities.”
New Initiative: Defibrillator Delays
A new report that hints stress factors like case volume and academic status of a hospital do not explain the wide disparities in defibrillation response times in hospitals has at least one hospitalist convinced HM leaders can help solve the problem.
Traditional hospital pressures do not predict whether patients with cardiac arrest are likely to experience delays in receiving defibrillation, according to a July 27 report in the Archives of Internal Medicine (2009;169(14):1260-1261). Such factors as the number of beds and where the cardiac unit was located were found to have more impact, the study found.
“This is a very simple thing,” says hospitalist Jason Persoff, MD, FHM, assistant professor of medicine at the Mayo Clinic in Jacksonville, Fla. "What are the barriers to shocking the patient? This doesn’t require huge committees. The question is, 'Why isn’t this happening?' … This paper is a call to arms."
According to the study, rates of delayed defibrillation, which were defined as longer than the two-minute standard, ranged from 2.4% to 50.9%. The authors state that standardizing defibrillation times to meet the two-minute standard set by the American Hospital Association could be a quality initiative focus for HM groups.
“Now that we’ve identified the problem, that helps us identify how to move forward,” Dr. Persoff says. “We are in dire need of improving our system when it comes to cardiac care. The hospitalists are in the best position to do that because we are able to work closest with the nurses.”
Jane Kelly-Cummings, RN, CPHQ, SHM's senior director of quality initiatives, agrees there is room for improvement in the survival rate of in-hospital cardiac patients. "In order to make those improvements, hospitals will need to make changes to their cardiac resuscitation processes and procedures," she says. "Hospitalists are integral and central players on cardiac resuscitation teams at a great majority of hospitals with hospital medicine programs. They act as change agents at these and many other facilities."
For more information on HM's role in cardiac resuscitation of hospitalized patients, visit the Emergency Procedures section of the "Core Competencies in Hospital Medicine."a
A new report that hints stress factors like case volume and academic status of a hospital do not explain the wide disparities in defibrillation response times in hospitals has at least one hospitalist convinced HM leaders can help solve the problem.
Traditional hospital pressures do not predict whether patients with cardiac arrest are likely to experience delays in receiving defibrillation, according to a July 27 report in the Archives of Internal Medicine (2009;169(14):1260-1261). Such factors as the number of beds and where the cardiac unit was located were found to have more impact, the study found.
“This is a very simple thing,” says hospitalist Jason Persoff, MD, FHM, assistant professor of medicine at the Mayo Clinic in Jacksonville, Fla. "What are the barriers to shocking the patient? This doesn’t require huge committees. The question is, 'Why isn’t this happening?' … This paper is a call to arms."
According to the study, rates of delayed defibrillation, which were defined as longer than the two-minute standard, ranged from 2.4% to 50.9%. The authors state that standardizing defibrillation times to meet the two-minute standard set by the American Hospital Association could be a quality initiative focus for HM groups.
“Now that we’ve identified the problem, that helps us identify how to move forward,” Dr. Persoff says. “We are in dire need of improving our system when it comes to cardiac care. The hospitalists are in the best position to do that because we are able to work closest with the nurses.”
Jane Kelly-Cummings, RN, CPHQ, SHM's senior director of quality initiatives, agrees there is room for improvement in the survival rate of in-hospital cardiac patients. "In order to make those improvements, hospitals will need to make changes to their cardiac resuscitation processes and procedures," she says. "Hospitalists are integral and central players on cardiac resuscitation teams at a great majority of hospitals with hospital medicine programs. They act as change agents at these and many other facilities."
For more information on HM's role in cardiac resuscitation of hospitalized patients, visit the Emergency Procedures section of the "Core Competencies in Hospital Medicine."a
A new report that hints stress factors like case volume and academic status of a hospital do not explain the wide disparities in defibrillation response times in hospitals has at least one hospitalist convinced HM leaders can help solve the problem.
Traditional hospital pressures do not predict whether patients with cardiac arrest are likely to experience delays in receiving defibrillation, according to a July 27 report in the Archives of Internal Medicine (2009;169(14):1260-1261). Such factors as the number of beds and where the cardiac unit was located were found to have more impact, the study found.
“This is a very simple thing,” says hospitalist Jason Persoff, MD, FHM, assistant professor of medicine at the Mayo Clinic in Jacksonville, Fla. "What are the barriers to shocking the patient? This doesn’t require huge committees. The question is, 'Why isn’t this happening?' … This paper is a call to arms."
According to the study, rates of delayed defibrillation, which were defined as longer than the two-minute standard, ranged from 2.4% to 50.9%. The authors state that standardizing defibrillation times to meet the two-minute standard set by the American Hospital Association could be a quality initiative focus for HM groups.
“Now that we’ve identified the problem, that helps us identify how to move forward,” Dr. Persoff says. “We are in dire need of improving our system when it comes to cardiac care. The hospitalists are in the best position to do that because we are able to work closest with the nurses.”
Jane Kelly-Cummings, RN, CPHQ, SHM's senior director of quality initiatives, agrees there is room for improvement in the survival rate of in-hospital cardiac patients. "In order to make those improvements, hospitals will need to make changes to their cardiac resuscitation processes and procedures," she says. "Hospitalists are integral and central players on cardiac resuscitation teams at a great majority of hospitals with hospital medicine programs. They act as change agents at these and many other facilities."
For more information on HM's role in cardiac resuscitation of hospitalized patients, visit the Emergency Procedures section of the "Core Competencies in Hospital Medicine."a
JHM Makes Immediate Industry Impact

On June 19, the Journal of Hospital Medicine (JHM) received a higher-than-expected first Impact Factor score, the measure of citations received in 2008 to articles published in 2006 and 2007. The 3.613 initial score ranks JHM No. 21 out of 107 journals in the Internal and General Medicine subject category.
Impact Factor scores are used as a proxy for the importance of a journal to its field. Academic researchers are evaluated on the “impact” of their publications based on this score.
“There are journals that are 20 years old that don’t have impact factors as high as we do,” says Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago and editor of JHM. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM’s top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development (www.hospitalmedicine.org/ResourceRoomRedesign/RR_Main/html/Core_Competencies.cfm). The clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development, and methodology.
“SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM. TH
Freelance Writer Richard Quinn contributed to this report.
Letters
SHM Should Support Reform Measures to Medicare System
As part of healthcare reform, I believe SHM should support the following ideas for Medicare reform:
- Primary-care physician (PCP) reimbursement should increase by 25%;
- Surgical reimbursement should decrease by 10%;
- Medical subspecialist reimbursement should decrease by 10%;
- All HIV/AIDS patients should be covered under Medicaid;
- All end-stage renal disease (ESRD) should be covered under Medicaid;
- Community health center funding should be covered under Medicaid;
- Children’s Health Insurance Plan (CHIP) funding should not come out of the Medicare fund;
- National Institutes of Health (NIH) funding should not come out of the Medicare fund;
- The Medicare tax on income before deductions should have no income ceiling; and
- The Social Security tax should be higher for those earning more than $250,000 per year before any deductions.
These changes would strengthen the Medicare fund to provide for our senior citizens’ healthcare and retirement. The above will be better than budget-neutral. Those to be covered (above) under Medicaid (HIV, ESRD, CHC, etc.) will actually have to pay less out of pocket for medications, services, procedures, and hospitalization.
The disproportionately low reimbursement to PCPs would be partially corrected in line with the medical home program concept. Partial financial correction of the overcompensated specialists and procedurists who dominate the rate commission would be accomplished with only a small amount of financial distress, which PCPs have been suffering for more than a decade.
Robert Beshany, MD,
SHM charter member,
Colorado Springs, Colo.
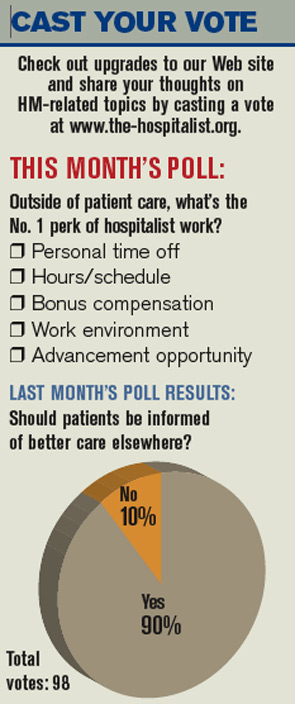
SHM responds:
SHM advocates for reforms that increase access to affordable healthcare and deliver safer, higher-quality, and more cost-effective healthcare to all Americans. Over the past five years, SHM has become widely respected for our progressive and collaborative approach to healthcare payment reform.
We advocate for:
- Improved care coordination, particularly during transitions of care. We have met with MedPAC, key Congressional leaders, and CMS to advocate for reimbursement that supports better care transitions and reduces unnecessary rehospitalizations.
- Incentive alignment. Providers, hospitals, and payors must have aligned incentives that consistently reward quality as well as evidence-based, cost-effective care. To that end, we have strongly supported such pay-for-performance initiatives as the Physician Quality Reporting Initiative and Hospital Value Based Purchasing. We also support exploration of new payment methodologies, such as bundled payments to accountable-care organizations, which is still at the demonstration project stage. Properly structured, these new reimbursement models could spur innovation, reduce compartmentalization of care, and decrease costs.
- Expanded federal support for the Agency for Healthcare Research and Quality, as well as robust funding for comparative effectiveness research.
- Incentives supporting the adoption of e-prescribing and health information technology.
- Replacement of the flawed Sustainable Growth Rate with a stable, predictable payment methodology.
- Support for initiatives that encourage physicians to choose generalist tracks.
We encourage our members to visit our Legislative Advocacy Web site (www.hospitalmedicine.org/advocacy) to see where we stand on healthcare reform.
Eric M. Siegal, MD, FHM,
chairman, SHM Public
Policy Committee
On June 19, the Journal of Hospital Medicine (JHM) received a higher-than-expected first Impact Factor score, the measure of citations received in 2008 to articles published in 2006 and 2007. The 3.613 initial score ranks JHM No. 21 out of 107 journals in the Internal and General Medicine subject category.
Impact Factor scores are used as a proxy for the importance of a journal to its field. Academic researchers are evaluated on the “impact” of their publications based on this score.
“There are journals that are 20 years old that don’t have impact factors as high as we do,” says Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago and editor of JHM. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM’s top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development (www.hospitalmedicine.org/ResourceRoomRedesign/RR_Main/html/Core_Competencies.cfm). The clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development, and methodology.
“SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM. TH
Freelance Writer Richard Quinn contributed to this report.
Letters
SHM Should Support Reform Measures to Medicare System
As part of healthcare reform, I believe SHM should support the following ideas for Medicare reform:
- Primary-care physician (PCP) reimbursement should increase by 25%;
- Surgical reimbursement should decrease by 10%;
- Medical subspecialist reimbursement should decrease by 10%;
- All HIV/AIDS patients should be covered under Medicaid;
- All end-stage renal disease (ESRD) should be covered under Medicaid;
- Community health center funding should be covered under Medicaid;
- Children’s Health Insurance Plan (CHIP) funding should not come out of the Medicare fund;
- National Institutes of Health (NIH) funding should not come out of the Medicare fund;
- The Medicare tax on income before deductions should have no income ceiling; and
- The Social Security tax should be higher for those earning more than $250,000 per year before any deductions.
These changes would strengthen the Medicare fund to provide for our senior citizens’ healthcare and retirement. The above will be better than budget-neutral. Those to be covered (above) under Medicaid (HIV, ESRD, CHC, etc.) will actually have to pay less out of pocket for medications, services, procedures, and hospitalization.
The disproportionately low reimbursement to PCPs would be partially corrected in line with the medical home program concept. Partial financial correction of the overcompensated specialists and procedurists who dominate the rate commission would be accomplished with only a small amount of financial distress, which PCPs have been suffering for more than a decade.
Robert Beshany, MD,
SHM charter member,
Colorado Springs, Colo.
SHM responds:
SHM advocates for reforms that increase access to affordable healthcare and deliver safer, higher-quality, and more cost-effective healthcare to all Americans. Over the past five years, SHM has become widely respected for our progressive and collaborative approach to healthcare payment reform.
We advocate for:
- Improved care coordination, particularly during transitions of care. We have met with MedPAC, key Congressional leaders, and CMS to advocate for reimbursement that supports better care transitions and reduces unnecessary rehospitalizations.
- Incentive alignment. Providers, hospitals, and payors must have aligned incentives that consistently reward quality as well as evidence-based, cost-effective care. To that end, we have strongly supported such pay-for-performance initiatives as the Physician Quality Reporting Initiative and Hospital Value Based Purchasing. We also support exploration of new payment methodologies, such as bundled payments to accountable-care organizations, which is still at the demonstration project stage. Properly structured, these new reimbursement models could spur innovation, reduce compartmentalization of care, and decrease costs.
- Expanded federal support for the Agency for Healthcare Research and Quality, as well as robust funding for comparative effectiveness research.
- Incentives supporting the adoption of e-prescribing and health information technology.
- Replacement of the flawed Sustainable Growth Rate with a stable, predictable payment methodology.
- Support for initiatives that encourage physicians to choose generalist tracks.
We encourage our members to visit our Legislative Advocacy Web site (www.hospitalmedicine.org/advocacy) to see where we stand on healthcare reform.
Eric M. Siegal, MD, FHM,
chairman, SHM Public
Policy Committee
On June 19, the Journal of Hospital Medicine (JHM) received a higher-than-expected first Impact Factor score, the measure of citations received in 2008 to articles published in 2006 and 2007. The 3.613 initial score ranks JHM No. 21 out of 107 journals in the Internal and General Medicine subject category.
Impact Factor scores are used as a proxy for the importance of a journal to its field. Academic researchers are evaluated on the “impact” of their publications based on this score.
“There are journals that are 20 years old that don’t have impact factors as high as we do,” says Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago and editor of JHM. “Hopefully, this will lead to academicians across the world being interested in submitting their scholarly work.”
JHM’s top-cited source is Core Competencies in Hospital Medicine: A Framework for Curriculum Development (www.hospitalmedicine.org/ResourceRoomRedesign/RR_Main/html/Core_Competencies.cfm). The clinical content is an essential tool for practicing hospitalists, providing guidance in the areas of clinical conditions, procedures, healthcare systems, development, and methodology.
“SHM is very proud of our journal, JHM, and getting such a sterling impact factor is a further acknowledgement of JHM’s credibility, reach, and world-class content,” says Larry Wellikson, MD, FHM, CEO of SHM. TH
Freelance Writer Richard Quinn contributed to this report.
Letters
SHM Should Support Reform Measures to Medicare System
As part of healthcare reform, I believe SHM should support the following ideas for Medicare reform:
- Primary-care physician (PCP) reimbursement should increase by 25%;
- Surgical reimbursement should decrease by 10%;
- Medical subspecialist reimbursement should decrease by 10%;
- All HIV/AIDS patients should be covered under Medicaid;
- All end-stage renal disease (ESRD) should be covered under Medicaid;
- Community health center funding should be covered under Medicaid;
- Children’s Health Insurance Plan (CHIP) funding should not come out of the Medicare fund;
- National Institutes of Health (NIH) funding should not come out of the Medicare fund;
- The Medicare tax on income before deductions should have no income ceiling; and
- The Social Security tax should be higher for those earning more than $250,000 per year before any deductions.
These changes would strengthen the Medicare fund to provide for our senior citizens’ healthcare and retirement. The above will be better than budget-neutral. Those to be covered (above) under Medicaid (HIV, ESRD, CHC, etc.) will actually have to pay less out of pocket for medications, services, procedures, and hospitalization.
The disproportionately low reimbursement to PCPs would be partially corrected in line with the medical home program concept. Partial financial correction of the overcompensated specialists and procedurists who dominate the rate commission would be accomplished with only a small amount of financial distress, which PCPs have been suffering for more than a decade.
Robert Beshany, MD,
SHM charter member,
Colorado Springs, Colo.
SHM responds:
SHM advocates for reforms that increase access to affordable healthcare and deliver safer, higher-quality, and more cost-effective healthcare to all Americans. Over the past five years, SHM has become widely respected for our progressive and collaborative approach to healthcare payment reform.
We advocate for:
- Improved care coordination, particularly during transitions of care. We have met with MedPAC, key Congressional leaders, and CMS to advocate for reimbursement that supports better care transitions and reduces unnecessary rehospitalizations.
- Incentive alignment. Providers, hospitals, and payors must have aligned incentives that consistently reward quality as well as evidence-based, cost-effective care. To that end, we have strongly supported such pay-for-performance initiatives as the Physician Quality Reporting Initiative and Hospital Value Based Purchasing. We also support exploration of new payment methodologies, such as bundled payments to accountable-care organizations, which is still at the demonstration project stage. Properly structured, these new reimbursement models could spur innovation, reduce compartmentalization of care, and decrease costs.
- Expanded federal support for the Agency for Healthcare Research and Quality, as well as robust funding for comparative effectiveness research.
- Incentives supporting the adoption of e-prescribing and health information technology.
- Replacement of the flawed Sustainable Growth Rate with a stable, predictable payment methodology.
- Support for initiatives that encourage physicians to choose generalist tracks.
We encourage our members to visit our Legislative Advocacy Web site (www.hospitalmedicine.org/advocacy) to see where we stand on healthcare reform.
Eric M. Siegal, MD, FHM,
chairman, SHM Public
Policy Committee
Lack of Evidence
In the late 1940s, Patricia Sanchez remembers sleeping on a cot in her oldest son’s bedroom most winter nights, listening for the vaporizer to run out of water so she could quickly refill it. The flu or even a bad cold invariably exacerbated his asthma, often causing him to wheeze and gasp for breath.
“We didn’t have any good medicines. It was a scary time,” she says. “I think we had to take him to the emergency department almost every winter.”
Today, with such medical advances as inhaled corticosteroids, many hospitalizations for asthma-related conditions can be avoided. Similarly, the use of ondansetron (Zofran) in children with gastroenteritis has decreased hospitalization rates. Many such medications originally developed for adults are helping to advance the treatment of childhood diseases, especially in oncology. But has the attraction of newer, stronger medications contributed to overuse for certain pediatric diseases?
A number of pediatric hospitalists think it has. Medication use in children has—for the most part—not received enough study. Therefore, hospitalists don’t always have enough evidence to guide their treatment decisions for young patients. Until the research catches up with the medications, hospitalists should be cautious.
HM physicians must stay abreast of the latest drug information and treatment guidelines. More importantly, they need to maintain clear lines of communication and outline reasonable expectations with their patients and their patients’ families.
Too Much, Too Soon?
Overuse of antibiotics and the growing threat of methicillin-resistant Staphylococcus aureus (MRSA) and other resistant strains frequently affect hospitalists in their practices, says Jack Percelay, MD, MPH, FAAP, FHM, a pediatric hospitalist with E.L.M.O. Pediatrics in New York City and a member of SHM’s board of directors. So does pressure from worried parents who want to employ whatever it takes to make their child better. “We want to be really careful about giving kids antibiotics,” he says, “and not use the biggest, newest guns in the hospital when they are not necessary.”

—Brian Alverson, MD, pediatric hospitalist, Hasbro Children’s Hospital, Providence, R.I.
Knowing how young and how much is safe and effective isn’t easy. Samir S. Shah, MD, MSCE, assistant professor of pediatrics and epidemiology at the University of Pennsylvania School of Medicine and attending physician in the divisions of infectious diseases and general pediatrics at The Children’s Hospital of Philadelphia, and his colleagues examined the use of adjuvant corticosteroids in children with bacterial meningitis. What they found was a worrisome upward trend of increased steroid administration, even though current evidence does not warrant the approach.1 When bacterial meningitis is caused by Haemophilus influenzae type B, adjuvant corticosteroids show a reduction in hearing loss in children, but studies conducted in the current era (when Streptococcus pneumoniae and Neisseria meningitidies are common causes of bacterial meningitis) do not show similar benefit.
In childhood cancer, oncology physicians and researchers have done an excellent job of refining treatment protocols, says Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, and pediatric editor of The Hospitalist. Nearly 70% of all children with cancer in the U.S. are enrolled in clinical trials, which allows for expanded evidence on treatments and outcomes.
In other settings, it might be too early to tell whether children are being overmedicated, undermedicated, or appropriately medicated. The real question: What will the consequences of long-term medication be?
Direct-to-consumer advertising; expansion of the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder; and the acceptance of “biological psychiatry” as the theoretical basis for the etiology of behavioral and emotional disorders all contribute to the increased use of psychotropics, says Julie M. Zito, PhD, professor of pharmacy and psychiatry in the Pharmaceutical Health Services Research Department at the University of Maryland at Baltimore. Using Medicaid administrative claims data for Texas youth in foster care in 2004, Dr. Zito and colleagues found that more than a third of these children (37.9%) had been prescribed a psychotropic medication.2 Of those receiving medications, 41.3% were receiving at least three different classes of drugs, most frequently antidepressants, ADHD drugs, and anti-psychotic agents.
Although the foster child population is relatively small (513,000 children in the U.S. were in foster care in 2005, according to the Department of Health and Human Services), the trend seen in this population is concerning. Medco Health Solutions’ 2007 survey of drug trends predicts that prescriptions for medications to treat ADHD will continue to increase at a rate of about 3% per year.3
Another concern is that the use of atypical antipsychotic medications to treat behavioral or bipolar disorders in children could result in weight gain (as it does in adults), which can trigger metabolic syndrome and increased risk of diabetes.
A Florida study that Dr. Zito co-authored demonstrated increased cardiovascular visits to the ED in Medicaid-insured children who had received stimulants.4 “It’s clear that we need to know more about safety and efficacy [of these medications in children],” Dr. Zito says.
The Parent Trap
Daniel Coghlin, MD, a general pediatrician for eight years and now a pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., believes parents’ expectations of their physicians—and medications—often are too high. Many think the doctor should provide a solution to all of their children’s illnesses, and the expected solution often entails a prescription.
Does parental pressure influence prescribing patterns? One study showed that pediatricians would prescribe antimicrobials 62% of the time if they thought the parents wanted them—even for a presumed viral illness.5
Dr. Shah points out that physicians might misunderstand the parents’ expectations; he suggests having a frank discussion about efficacy of antibiotics. “Studies have also shown that if the physician explains that antibiotics won’t work against viruses, that there is no benefit but there is potential harm, [then] that’s an answer that’s acceptable to most parents,” he says.
To be fair, says Brian Alverson, MD, also a pediatric hospitalist at Hasbro Children’s Hospital, physicians also contribute to overuse of antibiotics by ordering tests that drive up their inappropriate use. An X-ray might show small areas of lung atelectasis, which could be interpreted as pneumonia. A CBC test with an elevated white count could trigger an antimicrobial order. For the record, Dr. Alverson says neither test is indicated on a routine basis in the setting of bronchiolitis.
Over-the-Counter Risk
American consumers purchase 95 million packages of over-the-counter (OTC) cough and cold preparations for their sick children each year, according to the Consumer Healthcare Products Association. Many in the scientific community, including the American Academy of Pediatrics (AAP) and Wayne Snodgrass, MD, of the University of Texas Medical Branch’s department of pharmacology in Galveston, have pressed for more regulatory action, pointing to published evidence that ingredients such as brompheniramine are no more effective than a placebo in stopping a cough.6,7 Prompted by reports of two deaths in children, the FDA last October recommended that OTC cough-and-cold products not be given to infants or children under age 2. The FDA also is reviewing its recommendations for children ages 2 to 11.
Since initiation of the Pediatric Exclusivity Provision, which extends six months of patent exclusivity for products undergoing testing in children, and passage of the Best Pharmaceuticals for Children Act (BPCA) in 2002, more than 133 labeling changes have resulted from 300 pediatric-specific studies. (For a comprehensive list of the labeling changes, visit www.fda.gov/oc/opt/pediatriclabeling.html.)
In addition, National Institutes of Health prioritization of medications for future research studies in youth now consider frequency-of-use data from insured populations, Dr. Zito says. These changes have led to some improvements—for example, “black box” warnings against stimulants given for ADHD and selective serotonin reuptake inhibitors (SSRIs) prescribed for depression. The moves also underline the need for more research.
Key safety questions remain in the pediatric community. For example, is it acceptable to calculate smaller doses by weight of drugs approved safe for adults? On this subject, pediatric hospitalists “are woefully, inadequately armed with evidence,” Dr. Alverson says. “We routinely use medications in children where the dosing is arbitrarily guessed at.”
A 2007 study conducted by Dr. Shah and colleagues validates this point. The study found that most of the children hospitalized at 31 tertiary-care pediatric hospitals received at least one medication outside the FDA product license indication.8 Although the finding does not necessarily mean the medications were inappropriate, it highlights the dearth of studies establishing the proper dosages and uses of medications in children, and the long-term outcomes of their usage.
One way in which hospitalists can help is educating parents about the perils of OTC medicines, Dr. Shen says. An example of a safety concern is parents giving their children acetaminophen (Tylenol) and ibuprofen (Motrin) together; evidence shows that this kind of dosing error by parents is relatively common.
Fill the Knowledge Gap
When it comes to choosing medications and dosages for children, pediatric hospitalists often make treatment decisions based on their clinical experience, observational studies, or by extrapolating data from adult studies.
“There are countless examples of places where evidence-based physicians must still make educated guesses,” Dr. Alverson says.
However, experts point out that children are not “little adults.” Extrapolating from adult data can lead to unpredictable clinical responses and the possibility of overmedication. Going forward, the trick will be to tease out, with rigorous research, which medications—and at which dosages—are best for which kids.
Dr. Alverson suggests hospitalists stay on top of the literature, take advantage of all available CME, and plug into a listserv, such as the American Academy of Pediatrics’ HM listserv (download instructions and an enrollment form at www.aap.org/sections/hospcare/listservSOHM.pdf).
Above all, the key to dealing with families, he says, is to give them an open assessment of risks, benefits, and gaps in the scientific knowledge. TH
Gretchen Henkel is a freelance writer based in California.
References
- Mongelluzzo J, Mohamad Z, Ten Have TR, Shah SS. Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048-2055.
- Zito JM, Safer DJ, Sai D, et al. Psychotropic medication patterns among youth in foster care. Pediatrics. 2008;121(1):e157-163.
- Drug Trend Report 2008. Medco Corporate Web site. Available at: www.medcohealth.com/medco/corporate/home.jsp?ltSess=y&articleID=DT_2008_Report_Pdf<Sess=y. Accessed April 1, 2009.
- Winterstein AG, Gerhard T, Shuster J, et al. Cardiac safety of central nervous system stimulants in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics. 2007;120(6):e1494-1501.
- Mangione-Smith R, McGlynn EA, Elliott MN, Krogstad P, Brook RH. The relationship between perceived parental expectations and physician antimicrobial prescribing behavior. Pediatrics. 1999;103(4 Pt 1):711-718.
- Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar—pediatric cough and cold medications. N Engl J Med. 2007;357(23): 2321-2324.
- Clemens CJ, Taylor JA, Almquist JR, Quinn HC, Mehta A, Naylor GS. Is an antihistamine-decongestant combination effective in temporarily relieving symptoms of the common cold in preschool children? J Pediatr. 1997;130(3):463-466.
- Shah SS, Hall M, Goodman DM, et al. Off-label drug use in hospitalized children. Arch Pediatr Adolesc Med. 2007;161(3):282-290.
In the late 1940s, Patricia Sanchez remembers sleeping on a cot in her oldest son’s bedroom most winter nights, listening for the vaporizer to run out of water so she could quickly refill it. The flu or even a bad cold invariably exacerbated his asthma, often causing him to wheeze and gasp for breath.
“We didn’t have any good medicines. It was a scary time,” she says. “I think we had to take him to the emergency department almost every winter.”
Today, with such medical advances as inhaled corticosteroids, many hospitalizations for asthma-related conditions can be avoided. Similarly, the use of ondansetron (Zofran) in children with gastroenteritis has decreased hospitalization rates. Many such medications originally developed for adults are helping to advance the treatment of childhood diseases, especially in oncology. But has the attraction of newer, stronger medications contributed to overuse for certain pediatric diseases?
A number of pediatric hospitalists think it has. Medication use in children has—for the most part—not received enough study. Therefore, hospitalists don’t always have enough evidence to guide their treatment decisions for young patients. Until the research catches up with the medications, hospitalists should be cautious.
HM physicians must stay abreast of the latest drug information and treatment guidelines. More importantly, they need to maintain clear lines of communication and outline reasonable expectations with their patients and their patients’ families.
Too Much, Too Soon?
Overuse of antibiotics and the growing threat of methicillin-resistant Staphylococcus aureus (MRSA) and other resistant strains frequently affect hospitalists in their practices, says Jack Percelay, MD, MPH, FAAP, FHM, a pediatric hospitalist with E.L.M.O. Pediatrics in New York City and a member of SHM’s board of directors. So does pressure from worried parents who want to employ whatever it takes to make their child better. “We want to be really careful about giving kids antibiotics,” he says, “and not use the biggest, newest guns in the hospital when they are not necessary.”
—Brian Alverson, MD, pediatric hospitalist, Hasbro Children’s Hospital, Providence, R.I.
Knowing how young and how much is safe and effective isn’t easy. Samir S. Shah, MD, MSCE, assistant professor of pediatrics and epidemiology at the University of Pennsylvania School of Medicine and attending physician in the divisions of infectious diseases and general pediatrics at The Children’s Hospital of Philadelphia, and his colleagues examined the use of adjuvant corticosteroids in children with bacterial meningitis. What they found was a worrisome upward trend of increased steroid administration, even though current evidence does not warrant the approach.1 When bacterial meningitis is caused by Haemophilus influenzae type B, adjuvant corticosteroids show a reduction in hearing loss in children, but studies conducted in the current era (when Streptococcus pneumoniae and Neisseria meningitidies are common causes of bacterial meningitis) do not show similar benefit.
In childhood cancer, oncology physicians and researchers have done an excellent job of refining treatment protocols, says Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, and pediatric editor of The Hospitalist. Nearly 70% of all children with cancer in the U.S. are enrolled in clinical trials, which allows for expanded evidence on treatments and outcomes.
In other settings, it might be too early to tell whether children are being overmedicated, undermedicated, or appropriately medicated. The real question: What will the consequences of long-term medication be?
Direct-to-consumer advertising; expansion of the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder; and the acceptance of “biological psychiatry” as the theoretical basis for the etiology of behavioral and emotional disorders all contribute to the increased use of psychotropics, says Julie M. Zito, PhD, professor of pharmacy and psychiatry in the Pharmaceutical Health Services Research Department at the University of Maryland at Baltimore. Using Medicaid administrative claims data for Texas youth in foster care in 2004, Dr. Zito and colleagues found that more than a third of these children (37.9%) had been prescribed a psychotropic medication.2 Of those receiving medications, 41.3% were receiving at least three different classes of drugs, most frequently antidepressants, ADHD drugs, and anti-psychotic agents.
Although the foster child population is relatively small (513,000 children in the U.S. were in foster care in 2005, according to the Department of Health and Human Services), the trend seen in this population is concerning. Medco Health Solutions’ 2007 survey of drug trends predicts that prescriptions for medications to treat ADHD will continue to increase at a rate of about 3% per year.3
Another concern is that the use of atypical antipsychotic medications to treat behavioral or bipolar disorders in children could result in weight gain (as it does in adults), which can trigger metabolic syndrome and increased risk of diabetes.
A Florida study that Dr. Zito co-authored demonstrated increased cardiovascular visits to the ED in Medicaid-insured children who had received stimulants.4 “It’s clear that we need to know more about safety and efficacy [of these medications in children],” Dr. Zito says.
The Parent Trap
Daniel Coghlin, MD, a general pediatrician for eight years and now a pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., believes parents’ expectations of their physicians—and medications—often are too high. Many think the doctor should provide a solution to all of their children’s illnesses, and the expected solution often entails a prescription.
Does parental pressure influence prescribing patterns? One study showed that pediatricians would prescribe antimicrobials 62% of the time if they thought the parents wanted them—even for a presumed viral illness.5
Dr. Shah points out that physicians might misunderstand the parents’ expectations; he suggests having a frank discussion about efficacy of antibiotics. “Studies have also shown that if the physician explains that antibiotics won’t work against viruses, that there is no benefit but there is potential harm, [then] that’s an answer that’s acceptable to most parents,” he says.
To be fair, says Brian Alverson, MD, also a pediatric hospitalist at Hasbro Children’s Hospital, physicians also contribute to overuse of antibiotics by ordering tests that drive up their inappropriate use. An X-ray might show small areas of lung atelectasis, which could be interpreted as pneumonia. A CBC test with an elevated white count could trigger an antimicrobial order. For the record, Dr. Alverson says neither test is indicated on a routine basis in the setting of bronchiolitis.
Over-the-Counter Risk
American consumers purchase 95 million packages of over-the-counter (OTC) cough and cold preparations for their sick children each year, according to the Consumer Healthcare Products Association. Many in the scientific community, including the American Academy of Pediatrics (AAP) and Wayne Snodgrass, MD, of the University of Texas Medical Branch’s department of pharmacology in Galveston, have pressed for more regulatory action, pointing to published evidence that ingredients such as brompheniramine are no more effective than a placebo in stopping a cough.6,7 Prompted by reports of two deaths in children, the FDA last October recommended that OTC cough-and-cold products not be given to infants or children under age 2. The FDA also is reviewing its recommendations for children ages 2 to 11.
Since initiation of the Pediatric Exclusivity Provision, which extends six months of patent exclusivity for products undergoing testing in children, and passage of the Best Pharmaceuticals for Children Act (BPCA) in 2002, more than 133 labeling changes have resulted from 300 pediatric-specific studies. (For a comprehensive list of the labeling changes, visit www.fda.gov/oc/opt/pediatriclabeling.html.)
In addition, National Institutes of Health prioritization of medications for future research studies in youth now consider frequency-of-use data from insured populations, Dr. Zito says. These changes have led to some improvements—for example, “black box” warnings against stimulants given for ADHD and selective serotonin reuptake inhibitors (SSRIs) prescribed for depression. The moves also underline the need for more research.
Key safety questions remain in the pediatric community. For example, is it acceptable to calculate smaller doses by weight of drugs approved safe for adults? On this subject, pediatric hospitalists “are woefully, inadequately armed with evidence,” Dr. Alverson says. “We routinely use medications in children where the dosing is arbitrarily guessed at.”
A 2007 study conducted by Dr. Shah and colleagues validates this point. The study found that most of the children hospitalized at 31 tertiary-care pediatric hospitals received at least one medication outside the FDA product license indication.8 Although the finding does not necessarily mean the medications were inappropriate, it highlights the dearth of studies establishing the proper dosages and uses of medications in children, and the long-term outcomes of their usage.
One way in which hospitalists can help is educating parents about the perils of OTC medicines, Dr. Shen says. An example of a safety concern is parents giving their children acetaminophen (Tylenol) and ibuprofen (Motrin) together; evidence shows that this kind of dosing error by parents is relatively common.
Fill the Knowledge Gap
When it comes to choosing medications and dosages for children, pediatric hospitalists often make treatment decisions based on their clinical experience, observational studies, or by extrapolating data from adult studies.
“There are countless examples of places where evidence-based physicians must still make educated guesses,” Dr. Alverson says.
However, experts point out that children are not “little adults.” Extrapolating from adult data can lead to unpredictable clinical responses and the possibility of overmedication. Going forward, the trick will be to tease out, with rigorous research, which medications—and at which dosages—are best for which kids.
Dr. Alverson suggests hospitalists stay on top of the literature, take advantage of all available CME, and plug into a listserv, such as the American Academy of Pediatrics’ HM listserv (download instructions and an enrollment form at www.aap.org/sections/hospcare/listservSOHM.pdf).
Above all, the key to dealing with families, he says, is to give them an open assessment of risks, benefits, and gaps in the scientific knowledge. TH
Gretchen Henkel is a freelance writer based in California.
References
- Mongelluzzo J, Mohamad Z, Ten Have TR, Shah SS. Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048-2055.
- Zito JM, Safer DJ, Sai D, et al. Psychotropic medication patterns among youth in foster care. Pediatrics. 2008;121(1):e157-163.
- Drug Trend Report 2008. Medco Corporate Web site. Available at: www.medcohealth.com/medco/corporate/home.jsp?ltSess=y&articleID=DT_2008_Report_Pdf<Sess=y. Accessed April 1, 2009.
- Winterstein AG, Gerhard T, Shuster J, et al. Cardiac safety of central nervous system stimulants in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics. 2007;120(6):e1494-1501.
- Mangione-Smith R, McGlynn EA, Elliott MN, Krogstad P, Brook RH. The relationship between perceived parental expectations and physician antimicrobial prescribing behavior. Pediatrics. 1999;103(4 Pt 1):711-718.
- Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar—pediatric cough and cold medications. N Engl J Med. 2007;357(23): 2321-2324.
- Clemens CJ, Taylor JA, Almquist JR, Quinn HC, Mehta A, Naylor GS. Is an antihistamine-decongestant combination effective in temporarily relieving symptoms of the common cold in preschool children? J Pediatr. 1997;130(3):463-466.
- Shah SS, Hall M, Goodman DM, et al. Off-label drug use in hospitalized children. Arch Pediatr Adolesc Med. 2007;161(3):282-290.
In the late 1940s, Patricia Sanchez remembers sleeping on a cot in her oldest son’s bedroom most winter nights, listening for the vaporizer to run out of water so she could quickly refill it. The flu or even a bad cold invariably exacerbated his asthma, often causing him to wheeze and gasp for breath.
“We didn’t have any good medicines. It was a scary time,” she says. “I think we had to take him to the emergency department almost every winter.”
Today, with such medical advances as inhaled corticosteroids, many hospitalizations for asthma-related conditions can be avoided. Similarly, the use of ondansetron (Zofran) in children with gastroenteritis has decreased hospitalization rates. Many such medications originally developed for adults are helping to advance the treatment of childhood diseases, especially in oncology. But has the attraction of newer, stronger medications contributed to overuse for certain pediatric diseases?
A number of pediatric hospitalists think it has. Medication use in children has—for the most part—not received enough study. Therefore, hospitalists don’t always have enough evidence to guide their treatment decisions for young patients. Until the research catches up with the medications, hospitalists should be cautious.
HM physicians must stay abreast of the latest drug information and treatment guidelines. More importantly, they need to maintain clear lines of communication and outline reasonable expectations with their patients and their patients’ families.
Too Much, Too Soon?
Overuse of antibiotics and the growing threat of methicillin-resistant Staphylococcus aureus (MRSA) and other resistant strains frequently affect hospitalists in their practices, says Jack Percelay, MD, MPH, FAAP, FHM, a pediatric hospitalist with E.L.M.O. Pediatrics in New York City and a member of SHM’s board of directors. So does pressure from worried parents who want to employ whatever it takes to make their child better. “We want to be really careful about giving kids antibiotics,” he says, “and not use the biggest, newest guns in the hospital when they are not necessary.”
—Brian Alverson, MD, pediatric hospitalist, Hasbro Children’s Hospital, Providence, R.I.
Knowing how young and how much is safe and effective isn’t easy. Samir S. Shah, MD, MSCE, assistant professor of pediatrics and epidemiology at the University of Pennsylvania School of Medicine and attending physician in the divisions of infectious diseases and general pediatrics at The Children’s Hospital of Philadelphia, and his colleagues examined the use of adjuvant corticosteroids in children with bacterial meningitis. What they found was a worrisome upward trend of increased steroid administration, even though current evidence does not warrant the approach.1 When bacterial meningitis is caused by Haemophilus influenzae type B, adjuvant corticosteroids show a reduction in hearing loss in children, but studies conducted in the current era (when Streptococcus pneumoniae and Neisseria meningitidies are common causes of bacterial meningitis) do not show similar benefit.
In childhood cancer, oncology physicians and researchers have done an excellent job of refining treatment protocols, says Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, and pediatric editor of The Hospitalist. Nearly 70% of all children with cancer in the U.S. are enrolled in clinical trials, which allows for expanded evidence on treatments and outcomes.
In other settings, it might be too early to tell whether children are being overmedicated, undermedicated, or appropriately medicated. The real question: What will the consequences of long-term medication be?
Direct-to-consumer advertising; expansion of the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder; and the acceptance of “biological psychiatry” as the theoretical basis for the etiology of behavioral and emotional disorders all contribute to the increased use of psychotropics, says Julie M. Zito, PhD, professor of pharmacy and psychiatry in the Pharmaceutical Health Services Research Department at the University of Maryland at Baltimore. Using Medicaid administrative claims data for Texas youth in foster care in 2004, Dr. Zito and colleagues found that more than a third of these children (37.9%) had been prescribed a psychotropic medication.2 Of those receiving medications, 41.3% were receiving at least three different classes of drugs, most frequently antidepressants, ADHD drugs, and anti-psychotic agents.
Although the foster child population is relatively small (513,000 children in the U.S. were in foster care in 2005, according to the Department of Health and Human Services), the trend seen in this population is concerning. Medco Health Solutions’ 2007 survey of drug trends predicts that prescriptions for medications to treat ADHD will continue to increase at a rate of about 3% per year.3
Another concern is that the use of atypical antipsychotic medications to treat behavioral or bipolar disorders in children could result in weight gain (as it does in adults), which can trigger metabolic syndrome and increased risk of diabetes.
A Florida study that Dr. Zito co-authored demonstrated increased cardiovascular visits to the ED in Medicaid-insured children who had received stimulants.4 “It’s clear that we need to know more about safety and efficacy [of these medications in children],” Dr. Zito says.
The Parent Trap
Daniel Coghlin, MD, a general pediatrician for eight years and now a pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., believes parents’ expectations of their physicians—and medications—often are too high. Many think the doctor should provide a solution to all of their children’s illnesses, and the expected solution often entails a prescription.
Does parental pressure influence prescribing patterns? One study showed that pediatricians would prescribe antimicrobials 62% of the time if they thought the parents wanted them—even for a presumed viral illness.5
Dr. Shah points out that physicians might misunderstand the parents’ expectations; he suggests having a frank discussion about efficacy of antibiotics. “Studies have also shown that if the physician explains that antibiotics won’t work against viruses, that there is no benefit but there is potential harm, [then] that’s an answer that’s acceptable to most parents,” he says.
To be fair, says Brian Alverson, MD, also a pediatric hospitalist at Hasbro Children’s Hospital, physicians also contribute to overuse of antibiotics by ordering tests that drive up their inappropriate use. An X-ray might show small areas of lung atelectasis, which could be interpreted as pneumonia. A CBC test with an elevated white count could trigger an antimicrobial order. For the record, Dr. Alverson says neither test is indicated on a routine basis in the setting of bronchiolitis.
Over-the-Counter Risk
American consumers purchase 95 million packages of over-the-counter (OTC) cough and cold preparations for their sick children each year, according to the Consumer Healthcare Products Association. Many in the scientific community, including the American Academy of Pediatrics (AAP) and Wayne Snodgrass, MD, of the University of Texas Medical Branch’s department of pharmacology in Galveston, have pressed for more regulatory action, pointing to published evidence that ingredients such as brompheniramine are no more effective than a placebo in stopping a cough.6,7 Prompted by reports of two deaths in children, the FDA last October recommended that OTC cough-and-cold products not be given to infants or children under age 2. The FDA also is reviewing its recommendations for children ages 2 to 11.
Since initiation of the Pediatric Exclusivity Provision, which extends six months of patent exclusivity for products undergoing testing in children, and passage of the Best Pharmaceuticals for Children Act (BPCA) in 2002, more than 133 labeling changes have resulted from 300 pediatric-specific studies. (For a comprehensive list of the labeling changes, visit www.fda.gov/oc/opt/pediatriclabeling.html.)
In addition, National Institutes of Health prioritization of medications for future research studies in youth now consider frequency-of-use data from insured populations, Dr. Zito says. These changes have led to some improvements—for example, “black box” warnings against stimulants given for ADHD and selective serotonin reuptake inhibitors (SSRIs) prescribed for depression. The moves also underline the need for more research.
Key safety questions remain in the pediatric community. For example, is it acceptable to calculate smaller doses by weight of drugs approved safe for adults? On this subject, pediatric hospitalists “are woefully, inadequately armed with evidence,” Dr. Alverson says. “We routinely use medications in children where the dosing is arbitrarily guessed at.”
A 2007 study conducted by Dr. Shah and colleagues validates this point. The study found that most of the children hospitalized at 31 tertiary-care pediatric hospitals received at least one medication outside the FDA product license indication.8 Although the finding does not necessarily mean the medications were inappropriate, it highlights the dearth of studies establishing the proper dosages and uses of medications in children, and the long-term outcomes of their usage.
One way in which hospitalists can help is educating parents about the perils of OTC medicines, Dr. Shen says. An example of a safety concern is parents giving their children acetaminophen (Tylenol) and ibuprofen (Motrin) together; evidence shows that this kind of dosing error by parents is relatively common.
Fill the Knowledge Gap
When it comes to choosing medications and dosages for children, pediatric hospitalists often make treatment decisions based on their clinical experience, observational studies, or by extrapolating data from adult studies.
“There are countless examples of places where evidence-based physicians must still make educated guesses,” Dr. Alverson says.
However, experts point out that children are not “little adults.” Extrapolating from adult data can lead to unpredictable clinical responses and the possibility of overmedication. Going forward, the trick will be to tease out, with rigorous research, which medications—and at which dosages—are best for which kids.
Dr. Alverson suggests hospitalists stay on top of the literature, take advantage of all available CME, and plug into a listserv, such as the American Academy of Pediatrics’ HM listserv (download instructions and an enrollment form at www.aap.org/sections/hospcare/listservSOHM.pdf).
Above all, the key to dealing with families, he says, is to give them an open assessment of risks, benefits, and gaps in the scientific knowledge. TH
Gretchen Henkel is a freelance writer based in California.
References
- Mongelluzzo J, Mohamad Z, Ten Have TR, Shah SS. Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048-2055.
- Zito JM, Safer DJ, Sai D, et al. Psychotropic medication patterns among youth in foster care. Pediatrics. 2008;121(1):e157-163.
- Drug Trend Report 2008. Medco Corporate Web site. Available at: www.medcohealth.com/medco/corporate/home.jsp?ltSess=y&articleID=DT_2008_Report_Pdf<Sess=y. Accessed April 1, 2009.
- Winterstein AG, Gerhard T, Shuster J, et al. Cardiac safety of central nervous system stimulants in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics. 2007;120(6):e1494-1501.
- Mangione-Smith R, McGlynn EA, Elliott MN, Krogstad P, Brook RH. The relationship between perceived parental expectations and physician antimicrobial prescribing behavior. Pediatrics. 1999;103(4 Pt 1):711-718.
- Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar—pediatric cough and cold medications. N Engl J Med. 2007;357(23): 2321-2324.
- Clemens CJ, Taylor JA, Almquist JR, Quinn HC, Mehta A, Naylor GS. Is an antihistamine-decongestant combination effective in temporarily relieving symptoms of the common cold in preschool children? J Pediatr. 1997;130(3):463-466.
- Shah SS, Hall M, Goodman DM, et al. Off-label drug use in hospitalized children. Arch Pediatr Adolesc Med. 2007;161(3):282-290.