User login
TOPPS: Limit prophylactic platelets to select groups
ATLANTA – The broad use of prophylactic platelet transfusions in adults with hematologic malignancies and severe thrombocytopenia will likely be narrowed in the wake of the randomized, international TOPPS trial.
The primary endpoint of grade 2 or higher bleeding, by World Health Organization criteria, was seen in 50% with no prophylaxis (151 of 300) and 43% receiving a prophylactic platelet transfusion (128 of 298). The adjusted difference in proportions was 8.4%, which fell below the 15.2% upper limit for confidence interval set for TOPPS (Trial of Prophylactic Platelet Transfusions).

"This multicenter trial has not shown that a no-prophylaxis platelet transfusion policy is noninferior to prophylaxis," lead author Dr. Simon Stanworth said at the annual meeting of the American Society of Hematology.
A predefined subgroup analysis, however, found a significant difference in the primary endpoint between patients undergoing autologous stem cell transplantation (ASCT), who comprised 70% of the study population, and those receiving other treatments such as induction chemotherapy for acute myeloid leukemia (AML) or allogeneic bone marrow transplantation (P value = .04).
The rate of grade 2 or higher bleeding was very similar among patients undergoing autologous transplantation with or without prophylaxis (45% vs. 47%), while a clear benefit signal was seen in the subgroup of AML and allograft patients receiving treatment plus prophylaxis, compared with no prophylaxis (38% vs. 58%).
"Based on the results, the role of prophylactic platelet transfusions in different patient groups is varied and needs to be considered further," said Dr. Stanworth, a consultant hematologist with National Health Service Blood and Transplant, Oxford (England) University Hospital.
The finding that prophylactic platelets confer no advantage among those getting autologous transplants, however, could open up the opportunity to save millions of dollars in health care costs by skipping this unbeneficial treatment. An estimated 2 million platelets were transfused in the United States in 2008, a significant 16.7% increase from 2006, according to the latest National Blood Collection and Utilization Survey Report.
The results of TOPPS will likely change practice, but it will take time, Dr. Walter Dzik, codirector of the blood transfusion service at Massachusetts General Hospital, Boston, said in an interview.
"It takes quite some time, months to years, for knowledge transfer to occur and for well-established practices to change, but the end result will be to decrease the use of prophylactic platelets in autologous stem cell transplant patients," he said.
Prophylactic platelet transfusions are overused in the United States, in part because many clinicians transfuse their oncologic patients before they reach the recommended platelet prophylaxis threshold of 10 x 109 platelets per liter (Transfusion 2007;47:201-5). Thousands of doses of platelets are also used each year outside of the context of hematology/oncology, in patients undergoing surgery or cardiac procedures, without evidenced-based indications.
During his formal introduction of the plenary abstract, Dr. Dzik said a study published 2 years ago begs the question of whether prophylactic platelets are needed at all, reporting that the number of platelets in a prophylactic transfusion had no effect on the incidence of hemorrhage in patients with hypoproliferative thrombocytopenia (N. Engl. J. Med. 2010;362:600-13).
He pointed out that a recent open-label German trial, however, agrees with the TOPPS data, also finding no advantage from prophylactic platelets in autologous transplants, and all of the advantage resting in allogeneic transplants and AML patients. There was an "unmistakable" reduction in WHO grade 2 bleeding overall, but there was no advantage with the prophylaxis in the amount of red blood cells used per patient, number of days in the hospital, or overall survival (Lancet 2012;380:1309-16). It is against this background that clinicians looked to the TOPPS trial for additional insights, Dr. Dzik observed.
TOPPS enrolled 600 patients with a hematologic malignancy who were receiving or expected to receive chemotherapy or stem cell transplant, and expected to be thrombocytopenic for at least 5 days. Patients were randomly assigned to receive prophylactic platelet transfusion if their platelet count fell below 10x109/L, or no prophylaxis. Therapeutic platelets were given only after documented signs or symptoms of bleeding, prior to invasive procedures or at physician discretion.
Patients in the no-prophylaxis group were significantly less likely to receive a transfusion (59% vs. 89%), received fewer transfusions per patient (mean 1.7 vs. 3.0), and had more days with platelets less than 10,000/microL (mean 3.6 days vs. 1.8 days; all P less than .001, Dr. Stanworth reported.
Patients in the no-prophylaxis group averaged 1.7 days with a grade 2-4 bleed during follow-up vs. 1.2 days in the prophylaxis group (P value = .004), and developed an initial grade 2-4 bleed 2 days earlier than those receiving prophylaxis (hazard ratio 1.30; P = .02).
Still, there was no significant difference between the two groups in time to recovery from thrombocytopenia or a range of other outcomes including number of days in hospital or adverse events, Dr. Stanworth said.
Serious grade 3 or 4 bleeds occurred in one patient in the prophylaxis group (0.3%) and six in the no-prophylaxis group (2%). The difference did not reach statistical significance, but represents a sixfold increase in these sometimes life-threatening events (odds ratio 6.05; P = .13).
One intracranial bleed occurred in the no-prophylaxis group. Only two of the seven patients had a platelet count below 10x109/L at the onset of grade 3-4 bleeding, and both were receiving induction chemotherapy for AML, he said.
During a discussion of the results, an audience member described the difference in bleeding between subgroups as remarkable, and suggested that AML patients should be taken far more seriously with regard to platelet prophylaxis because they may be especially predisposed to serious bleeding events because of endothelial damage during therapy. Dr. Stanworth concurred.
In his conclusion, Dr. Stanworth said there is clearly a need for new strategies to minimize the high burden of bleeding, and suggested that antifibrinolytics and the role of tranexamic acid should be explored.
For his part, Dr. Dzik said, "We need to stop approaching all patients as if they were the same and develop a risk score to identify those patients at higher risk of bleeding. The first question on the score will be ‘Are you an autologous stem cell case?’ and then tailor the degree of hemostatic support to match the risk of the patient."
TOPPS was funded by the National Health Service Blood and Transplant. Dr. Stanworth and Dr. Dzik reported no disclosures.
ATLANTA – The broad use of prophylactic platelet transfusions in adults with hematologic malignancies and severe thrombocytopenia will likely be narrowed in the wake of the randomized, international TOPPS trial.
The primary endpoint of grade 2 or higher bleeding, by World Health Organization criteria, was seen in 50% with no prophylaxis (151 of 300) and 43% receiving a prophylactic platelet transfusion (128 of 298). The adjusted difference in proportions was 8.4%, which fell below the 15.2% upper limit for confidence interval set for TOPPS (Trial of Prophylactic Platelet Transfusions).
"This multicenter trial has not shown that a no-prophylaxis platelet transfusion policy is noninferior to prophylaxis," lead author Dr. Simon Stanworth said at the annual meeting of the American Society of Hematology.
A predefined subgroup analysis, however, found a significant difference in the primary endpoint between patients undergoing autologous stem cell transplantation (ASCT), who comprised 70% of the study population, and those receiving other treatments such as induction chemotherapy for acute myeloid leukemia (AML) or allogeneic bone marrow transplantation (P value = .04).
The rate of grade 2 or higher bleeding was very similar among patients undergoing autologous transplantation with or without prophylaxis (45% vs. 47%), while a clear benefit signal was seen in the subgroup of AML and allograft patients receiving treatment plus prophylaxis, compared with no prophylaxis (38% vs. 58%).
"Based on the results, the role of prophylactic platelet transfusions in different patient groups is varied and needs to be considered further," said Dr. Stanworth, a consultant hematologist with National Health Service Blood and Transplant, Oxford (England) University Hospital.
The finding that prophylactic platelets confer no advantage among those getting autologous transplants, however, could open up the opportunity to save millions of dollars in health care costs by skipping this unbeneficial treatment. An estimated 2 million platelets were transfused in the United States in 2008, a significant 16.7% increase from 2006, according to the latest National Blood Collection and Utilization Survey Report.
The results of TOPPS will likely change practice, but it will take time, Dr. Walter Dzik, codirector of the blood transfusion service at Massachusetts General Hospital, Boston, said in an interview.
"It takes quite some time, months to years, for knowledge transfer to occur and for well-established practices to change, but the end result will be to decrease the use of prophylactic platelets in autologous stem cell transplant patients," he said.
Prophylactic platelet transfusions are overused in the United States, in part because many clinicians transfuse their oncologic patients before they reach the recommended platelet prophylaxis threshold of 10 x 109 platelets per liter (Transfusion 2007;47:201-5). Thousands of doses of platelets are also used each year outside of the context of hematology/oncology, in patients undergoing surgery or cardiac procedures, without evidenced-based indications.
During his formal introduction of the plenary abstract, Dr. Dzik said a study published 2 years ago begs the question of whether prophylactic platelets are needed at all, reporting that the number of platelets in a prophylactic transfusion had no effect on the incidence of hemorrhage in patients with hypoproliferative thrombocytopenia (N. Engl. J. Med. 2010;362:600-13).
He pointed out that a recent open-label German trial, however, agrees with the TOPPS data, also finding no advantage from prophylactic platelets in autologous transplants, and all of the advantage resting in allogeneic transplants and AML patients. There was an "unmistakable" reduction in WHO grade 2 bleeding overall, but there was no advantage with the prophylaxis in the amount of red blood cells used per patient, number of days in the hospital, or overall survival (Lancet 2012;380:1309-16). It is against this background that clinicians looked to the TOPPS trial for additional insights, Dr. Dzik observed.
TOPPS enrolled 600 patients with a hematologic malignancy who were receiving or expected to receive chemotherapy or stem cell transplant, and expected to be thrombocytopenic for at least 5 days. Patients were randomly assigned to receive prophylactic platelet transfusion if their platelet count fell below 10x109/L, or no prophylaxis. Therapeutic platelets were given only after documented signs or symptoms of bleeding, prior to invasive procedures or at physician discretion.
Patients in the no-prophylaxis group were significantly less likely to receive a transfusion (59% vs. 89%), received fewer transfusions per patient (mean 1.7 vs. 3.0), and had more days with platelets less than 10,000/microL (mean 3.6 days vs. 1.8 days; all P less than .001, Dr. Stanworth reported.
Patients in the no-prophylaxis group averaged 1.7 days with a grade 2-4 bleed during follow-up vs. 1.2 days in the prophylaxis group (P value = .004), and developed an initial grade 2-4 bleed 2 days earlier than those receiving prophylaxis (hazard ratio 1.30; P = .02).
Still, there was no significant difference between the two groups in time to recovery from thrombocytopenia or a range of other outcomes including number of days in hospital or adverse events, Dr. Stanworth said.
Serious grade 3 or 4 bleeds occurred in one patient in the prophylaxis group (0.3%) and six in the no-prophylaxis group (2%). The difference did not reach statistical significance, but represents a sixfold increase in these sometimes life-threatening events (odds ratio 6.05; P = .13).
One intracranial bleed occurred in the no-prophylaxis group. Only two of the seven patients had a platelet count below 10x109/L at the onset of grade 3-4 bleeding, and both were receiving induction chemotherapy for AML, he said.
During a discussion of the results, an audience member described the difference in bleeding between subgroups as remarkable, and suggested that AML patients should be taken far more seriously with regard to platelet prophylaxis because they may be especially predisposed to serious bleeding events because of endothelial damage during therapy. Dr. Stanworth concurred.
In his conclusion, Dr. Stanworth said there is clearly a need for new strategies to minimize the high burden of bleeding, and suggested that antifibrinolytics and the role of tranexamic acid should be explored.
For his part, Dr. Dzik said, "We need to stop approaching all patients as if they were the same and develop a risk score to identify those patients at higher risk of bleeding. The first question on the score will be ‘Are you an autologous stem cell case?’ and then tailor the degree of hemostatic support to match the risk of the patient."
TOPPS was funded by the National Health Service Blood and Transplant. Dr. Stanworth and Dr. Dzik reported no disclosures.
ATLANTA – The broad use of prophylactic platelet transfusions in adults with hematologic malignancies and severe thrombocytopenia will likely be narrowed in the wake of the randomized, international TOPPS trial.
The primary endpoint of grade 2 or higher bleeding, by World Health Organization criteria, was seen in 50% with no prophylaxis (151 of 300) and 43% receiving a prophylactic platelet transfusion (128 of 298). The adjusted difference in proportions was 8.4%, which fell below the 15.2% upper limit for confidence interval set for TOPPS (Trial of Prophylactic Platelet Transfusions).
"This multicenter trial has not shown that a no-prophylaxis platelet transfusion policy is noninferior to prophylaxis," lead author Dr. Simon Stanworth said at the annual meeting of the American Society of Hematology.
A predefined subgroup analysis, however, found a significant difference in the primary endpoint between patients undergoing autologous stem cell transplantation (ASCT), who comprised 70% of the study population, and those receiving other treatments such as induction chemotherapy for acute myeloid leukemia (AML) or allogeneic bone marrow transplantation (P value = .04).
The rate of grade 2 or higher bleeding was very similar among patients undergoing autologous transplantation with or without prophylaxis (45% vs. 47%), while a clear benefit signal was seen in the subgroup of AML and allograft patients receiving treatment plus prophylaxis, compared with no prophylaxis (38% vs. 58%).
"Based on the results, the role of prophylactic platelet transfusions in different patient groups is varied and needs to be considered further," said Dr. Stanworth, a consultant hematologist with National Health Service Blood and Transplant, Oxford (England) University Hospital.
The finding that prophylactic platelets confer no advantage among those getting autologous transplants, however, could open up the opportunity to save millions of dollars in health care costs by skipping this unbeneficial treatment. An estimated 2 million platelets were transfused in the United States in 2008, a significant 16.7% increase from 2006, according to the latest National Blood Collection and Utilization Survey Report.
The results of TOPPS will likely change practice, but it will take time, Dr. Walter Dzik, codirector of the blood transfusion service at Massachusetts General Hospital, Boston, said in an interview.
"It takes quite some time, months to years, for knowledge transfer to occur and for well-established practices to change, but the end result will be to decrease the use of prophylactic platelets in autologous stem cell transplant patients," he said.
Prophylactic platelet transfusions are overused in the United States, in part because many clinicians transfuse their oncologic patients before they reach the recommended platelet prophylaxis threshold of 10 x 109 platelets per liter (Transfusion 2007;47:201-5). Thousands of doses of platelets are also used each year outside of the context of hematology/oncology, in patients undergoing surgery or cardiac procedures, without evidenced-based indications.
During his formal introduction of the plenary abstract, Dr. Dzik said a study published 2 years ago begs the question of whether prophylactic platelets are needed at all, reporting that the number of platelets in a prophylactic transfusion had no effect on the incidence of hemorrhage in patients with hypoproliferative thrombocytopenia (N. Engl. J. Med. 2010;362:600-13).
He pointed out that a recent open-label German trial, however, agrees with the TOPPS data, also finding no advantage from prophylactic platelets in autologous transplants, and all of the advantage resting in allogeneic transplants and AML patients. There was an "unmistakable" reduction in WHO grade 2 bleeding overall, but there was no advantage with the prophylaxis in the amount of red blood cells used per patient, number of days in the hospital, or overall survival (Lancet 2012;380:1309-16). It is against this background that clinicians looked to the TOPPS trial for additional insights, Dr. Dzik observed.
TOPPS enrolled 600 patients with a hematologic malignancy who were receiving or expected to receive chemotherapy or stem cell transplant, and expected to be thrombocytopenic for at least 5 days. Patients were randomly assigned to receive prophylactic platelet transfusion if their platelet count fell below 10x109/L, or no prophylaxis. Therapeutic platelets were given only after documented signs or symptoms of bleeding, prior to invasive procedures or at physician discretion.
Patients in the no-prophylaxis group were significantly less likely to receive a transfusion (59% vs. 89%), received fewer transfusions per patient (mean 1.7 vs. 3.0), and had more days with platelets less than 10,000/microL (mean 3.6 days vs. 1.8 days; all P less than .001, Dr. Stanworth reported.
Patients in the no-prophylaxis group averaged 1.7 days with a grade 2-4 bleed during follow-up vs. 1.2 days in the prophylaxis group (P value = .004), and developed an initial grade 2-4 bleed 2 days earlier than those receiving prophylaxis (hazard ratio 1.30; P = .02).
Still, there was no significant difference between the two groups in time to recovery from thrombocytopenia or a range of other outcomes including number of days in hospital or adverse events, Dr. Stanworth said.
Serious grade 3 or 4 bleeds occurred in one patient in the prophylaxis group (0.3%) and six in the no-prophylaxis group (2%). The difference did not reach statistical significance, but represents a sixfold increase in these sometimes life-threatening events (odds ratio 6.05; P = .13).
One intracranial bleed occurred in the no-prophylaxis group. Only two of the seven patients had a platelet count below 10x109/L at the onset of grade 3-4 bleeding, and both were receiving induction chemotherapy for AML, he said.
During a discussion of the results, an audience member described the difference in bleeding between subgroups as remarkable, and suggested that AML patients should be taken far more seriously with regard to platelet prophylaxis because they may be especially predisposed to serious bleeding events because of endothelial damage during therapy. Dr. Stanworth concurred.
In his conclusion, Dr. Stanworth said there is clearly a need for new strategies to minimize the high burden of bleeding, and suggested that antifibrinolytics and the role of tranexamic acid should be explored.
For his part, Dr. Dzik said, "We need to stop approaching all patients as if they were the same and develop a risk score to identify those patients at higher risk of bleeding. The first question on the score will be ‘Are you an autologous stem cell case?’ and then tailor the degree of hemostatic support to match the risk of the patient."
TOPPS was funded by the National Health Service Blood and Transplant. Dr. Stanworth and Dr. Dzik reported no disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: The primary endpoint of WHO grade 2 or higher bleeding was seen in 50% with no prophylaxis (151 of 300) and 43% receiving prophylactic platelet transfusion (128 of 298).
Data Source: Randomized controlled trial of prophylactic vs. nonprophylactic platelet transfusions in patients with hematologic malignancies.
Disclosures: TOPPS was funded by the National Health Service Blood and Transplant. Dr. Stanworth and Dr. Dzik reported no disclosures.

Pomalidomide: A new option for relapsed myeloma
ATLANTA – Patients with refractory multiple myeloma, including those with heavily pretreated disease, lived significantly longer with the immunomodulatory drug pomalidomide plus low-dose dexamethasone than with high-dose dexamethasone alone in a phase III, head-to-head study.
Patients given pomalidomide (Pomalyst) and low-dose dexamethasone (Decadron) lived a median of 3.2 months without progression, compared with 1.7 months for patients on high-dose dexamethasone (hazard ratio, 0.45; P less than .001).
Moreover, the combination was equally beneficial in patients refractory to both lenalidomide (Revlimid) and bortezomib (Velcade) (3.2 vs. 1.7 months; HR, 0.48; P less than .001), who comprised three-fourths of the study cohort. Such patients are currently without standard treatment options and frequently receive only palliative care, Dr. Meletios Dimopoulos reported in a late-breaking abstract session at the annual meeting of the American Society of Hematology.
An interim survival analysis also showed a statistically significant improvement in overall survival with the combination compared with high-dose dexamethasone (median not reached vs. 7.8 months; HR, 0.53; P less than .001), prompting the data-monitoring committee to recommend that patients in the control arm be allowed to cross over to pomalidomide plus low-dose dexamethasone.
"We believe that pomalidomide and low-dose dexamethasone should be considered as a new treatment option for these patients," said Dr. Dimopoulos of Alexandra Hospital, Athens.
Dr. Martin Tallman, chief of the leukemia service at Memorial Sloan-Kettering Cancer Center in New York and comoderator of the session, described the MM-003 trial as a large, well-done "definitive" study.
"It’s a very active new agent, pomalidomide, a new IMiD, and I think it will emerge as a new standard of care for relapsed and refractory patients – a population for whom, as Dr. Dimopoulous indicated, we don’t have very good therapies" he said in an interview.
Pomalidomide, a derivative of thalidomide that acts as an immunomodulator, is expected to be approved in early 2013 in the United States, with a decision by European regulatory authorities in the second half of 2013, according to Celgene.
Dr. Dimopoulos said MM-003 did not address whether pomalidomide is more potent as a rescue therapy than carfilzomib (Kyprolis), a second-generation proteasome inhibitor granted accelerated approval in July 2012, for patients with multiple myeloma progressing after at least 2 prior therapies, including bortezomib and an IMiD. The approval was based on response rate only, with clinical benefit such as improved survival not yet verified.
"It is not possible to compare two different drugs from two different trials; however, as the myeloma community, we are encouraged that we now have carfilzomib and pomalidomide with low-dose dexamethasone that could be used to salvage, to rescue and help some patients with an unmet need in multiple myeloma," he said in an interview.
The MM-003 trial randomly assigned 455 patients with relapsed or refractory multiple myeloma to 4 mg oral pomalidomide on days 1-21 of a 28-day cycle plus oral dexamethasone 40 mg weekly, or to 40 mg high-dose dexamethasone on days 1-4, 9-12, and 17-20 of a 28-day cycle until disease progression. Patients older than 75 years in each arm received 20 mg dexamethasone on the same schedules.
All 302 patients in the experimental arm and 153 patients in the control arm had received prior lenalidomide and bortezomib, with 75% refractory to both. The median number of prior therapies was five in each arm, including dexamethasone, thalidomide, and stem cell transplant. One-third of all patients had renal impairment, defined by a creatinine clearance of less than 60 mL/min. The median age of patients in each arm was 64 and 65, respectively.
The overall response rate, defined as at least a partial response, was significantly higher in the experimental arm than the control arm at 21% vs. 3%, reaching 24% vs. 3% among patients randomized for at least 6 months (P less than .001), Dr. Dimopoulos reported.
Progression-free survival, the study’s primary endpoint, was significantly longer in patients on pomalidomide plus low-dose dexamethasone regardless of whether patients’ last prior treatment was bortezomib (median 3.6 vs. 1.8 months; HR, 0.47) or lenalidomide (median 3.7 vs. 1.8 months; HR, 0.38), or whether they had renal impairment (median 3.2 vs. 1.6 months; HR, 0.44; P less than .001 for all comparisons).
The combination therapy was generally well tolerated, although roughly one-third of patients experienced grade 3/4 neutropenia, an expected complication of pomalidomide (42% vs. 15% of controls), Dr. Dimopoulos observed.
Rates of any grade venous thromboembolism were low at 3% vs. 2% in controls, as were exacerbations of peripheral neuropathy at 12% vs. 11%. In all, 7% of patients discontinued pomalidomide plus low-dose dexamethasone, compared with 6% on high-dose dexamethasone, he said.
Session comoderator Dr. Agnes Lee of the University of British Columbia and Vancouver Coastal Health said her colleagues who enrolled patients in the trial are thrilled with having a possible new option for relapsed/refractory myeloma and very surprised with the minimal amount of toxicity they’ve seen. "Right now we’re just waiting for the next step – will this drug be available, especially here in Canada ... and whether it will now be investigated in earlier disease, especially when it’s so well tolerated."
Dr. Dimopoulos reported honoraria from the study sponsor, Celgene. Several of his coauthors reported commercial relationships with Celgene including employment and equity ownership. Dr. Tallman and Dr. Lee reported no relevant financial conflicts.
Dimopoulos, M.A. et al. Pomalidomide in combination with low-dose dexamethasone: Demonstrates a significant progression-free survival and overall survival advantage in relapsed/refractory MM: A phase 3, multicenter, randomized, open-label study. LBA-6.
ATLANTA – Patients with refractory multiple myeloma, including those with heavily pretreated disease, lived significantly longer with the immunomodulatory drug pomalidomide plus low-dose dexamethasone than with high-dose dexamethasone alone in a phase III, head-to-head study.
Patients given pomalidomide (Pomalyst) and low-dose dexamethasone (Decadron) lived a median of 3.2 months without progression, compared with 1.7 months for patients on high-dose dexamethasone (hazard ratio, 0.45; P less than .001).
Moreover, the combination was equally beneficial in patients refractory to both lenalidomide (Revlimid) and bortezomib (Velcade) (3.2 vs. 1.7 months; HR, 0.48; P less than .001), who comprised three-fourths of the study cohort. Such patients are currently without standard treatment options and frequently receive only palliative care, Dr. Meletios Dimopoulos reported in a late-breaking abstract session at the annual meeting of the American Society of Hematology.
An interim survival analysis also showed a statistically significant improvement in overall survival with the combination compared with high-dose dexamethasone (median not reached vs. 7.8 months; HR, 0.53; P less than .001), prompting the data-monitoring committee to recommend that patients in the control arm be allowed to cross over to pomalidomide plus low-dose dexamethasone.
"We believe that pomalidomide and low-dose dexamethasone should be considered as a new treatment option for these patients," said Dr. Dimopoulos of Alexandra Hospital, Athens.
Dr. Martin Tallman, chief of the leukemia service at Memorial Sloan-Kettering Cancer Center in New York and comoderator of the session, described the MM-003 trial as a large, well-done "definitive" study.
"It’s a very active new agent, pomalidomide, a new IMiD, and I think it will emerge as a new standard of care for relapsed and refractory patients – a population for whom, as Dr. Dimopoulous indicated, we don’t have very good therapies" he said in an interview.
Pomalidomide, a derivative of thalidomide that acts as an immunomodulator, is expected to be approved in early 2013 in the United States, with a decision by European regulatory authorities in the second half of 2013, according to Celgene.
Dr. Dimopoulos said MM-003 did not address whether pomalidomide is more potent as a rescue therapy than carfilzomib (Kyprolis), a second-generation proteasome inhibitor granted accelerated approval in July 2012, for patients with multiple myeloma progressing after at least 2 prior therapies, including bortezomib and an IMiD. The approval was based on response rate only, with clinical benefit such as improved survival not yet verified.
"It is not possible to compare two different drugs from two different trials; however, as the myeloma community, we are encouraged that we now have carfilzomib and pomalidomide with low-dose dexamethasone that could be used to salvage, to rescue and help some patients with an unmet need in multiple myeloma," he said in an interview.
The MM-003 trial randomly assigned 455 patients with relapsed or refractory multiple myeloma to 4 mg oral pomalidomide on days 1-21 of a 28-day cycle plus oral dexamethasone 40 mg weekly, or to 40 mg high-dose dexamethasone on days 1-4, 9-12, and 17-20 of a 28-day cycle until disease progression. Patients older than 75 years in each arm received 20 mg dexamethasone on the same schedules.
All 302 patients in the experimental arm and 153 patients in the control arm had received prior lenalidomide and bortezomib, with 75% refractory to both. The median number of prior therapies was five in each arm, including dexamethasone, thalidomide, and stem cell transplant. One-third of all patients had renal impairment, defined by a creatinine clearance of less than 60 mL/min. The median age of patients in each arm was 64 and 65, respectively.
The overall response rate, defined as at least a partial response, was significantly higher in the experimental arm than the control arm at 21% vs. 3%, reaching 24% vs. 3% among patients randomized for at least 6 months (P less than .001), Dr. Dimopoulos reported.
Progression-free survival, the study’s primary endpoint, was significantly longer in patients on pomalidomide plus low-dose dexamethasone regardless of whether patients’ last prior treatment was bortezomib (median 3.6 vs. 1.8 months; HR, 0.47) or lenalidomide (median 3.7 vs. 1.8 months; HR, 0.38), or whether they had renal impairment (median 3.2 vs. 1.6 months; HR, 0.44; P less than .001 for all comparisons).
The combination therapy was generally well tolerated, although roughly one-third of patients experienced grade 3/4 neutropenia, an expected complication of pomalidomide (42% vs. 15% of controls), Dr. Dimopoulos observed.
Rates of any grade venous thromboembolism were low at 3% vs. 2% in controls, as were exacerbations of peripheral neuropathy at 12% vs. 11%. In all, 7% of patients discontinued pomalidomide plus low-dose dexamethasone, compared with 6% on high-dose dexamethasone, he said.
Session comoderator Dr. Agnes Lee of the University of British Columbia and Vancouver Coastal Health said her colleagues who enrolled patients in the trial are thrilled with having a possible new option for relapsed/refractory myeloma and very surprised with the minimal amount of toxicity they’ve seen. "Right now we’re just waiting for the next step – will this drug be available, especially here in Canada ... and whether it will now be investigated in earlier disease, especially when it’s so well tolerated."
Dr. Dimopoulos reported honoraria from the study sponsor, Celgene. Several of his coauthors reported commercial relationships with Celgene including employment and equity ownership. Dr. Tallman and Dr. Lee reported no relevant financial conflicts.
Dimopoulos, M.A. et al. Pomalidomide in combination with low-dose dexamethasone: Demonstrates a significant progression-free survival and overall survival advantage in relapsed/refractory MM: A phase 3, multicenter, randomized, open-label study. LBA-6.
ATLANTA – Patients with refractory multiple myeloma, including those with heavily pretreated disease, lived significantly longer with the immunomodulatory drug pomalidomide plus low-dose dexamethasone than with high-dose dexamethasone alone in a phase III, head-to-head study.
Patients given pomalidomide (Pomalyst) and low-dose dexamethasone (Decadron) lived a median of 3.2 months without progression, compared with 1.7 months for patients on high-dose dexamethasone (hazard ratio, 0.45; P less than .001).
Moreover, the combination was equally beneficial in patients refractory to both lenalidomide (Revlimid) and bortezomib (Velcade) (3.2 vs. 1.7 months; HR, 0.48; P less than .001), who comprised three-fourths of the study cohort. Such patients are currently without standard treatment options and frequently receive only palliative care, Dr. Meletios Dimopoulos reported in a late-breaking abstract session at the annual meeting of the American Society of Hematology.
An interim survival analysis also showed a statistically significant improvement in overall survival with the combination compared with high-dose dexamethasone (median not reached vs. 7.8 months; HR, 0.53; P less than .001), prompting the data-monitoring committee to recommend that patients in the control arm be allowed to cross over to pomalidomide plus low-dose dexamethasone.
"We believe that pomalidomide and low-dose dexamethasone should be considered as a new treatment option for these patients," said Dr. Dimopoulos of Alexandra Hospital, Athens.
Dr. Martin Tallman, chief of the leukemia service at Memorial Sloan-Kettering Cancer Center in New York and comoderator of the session, described the MM-003 trial as a large, well-done "definitive" study.
"It’s a very active new agent, pomalidomide, a new IMiD, and I think it will emerge as a new standard of care for relapsed and refractory patients – a population for whom, as Dr. Dimopoulous indicated, we don’t have very good therapies" he said in an interview.
Pomalidomide, a derivative of thalidomide that acts as an immunomodulator, is expected to be approved in early 2013 in the United States, with a decision by European regulatory authorities in the second half of 2013, according to Celgene.
Dr. Dimopoulos said MM-003 did not address whether pomalidomide is more potent as a rescue therapy than carfilzomib (Kyprolis), a second-generation proteasome inhibitor granted accelerated approval in July 2012, for patients with multiple myeloma progressing after at least 2 prior therapies, including bortezomib and an IMiD. The approval was based on response rate only, with clinical benefit such as improved survival not yet verified.
"It is not possible to compare two different drugs from two different trials; however, as the myeloma community, we are encouraged that we now have carfilzomib and pomalidomide with low-dose dexamethasone that could be used to salvage, to rescue and help some patients with an unmet need in multiple myeloma," he said in an interview.
The MM-003 trial randomly assigned 455 patients with relapsed or refractory multiple myeloma to 4 mg oral pomalidomide on days 1-21 of a 28-day cycle plus oral dexamethasone 40 mg weekly, or to 40 mg high-dose dexamethasone on days 1-4, 9-12, and 17-20 of a 28-day cycle until disease progression. Patients older than 75 years in each arm received 20 mg dexamethasone on the same schedules.
All 302 patients in the experimental arm and 153 patients in the control arm had received prior lenalidomide and bortezomib, with 75% refractory to both. The median number of prior therapies was five in each arm, including dexamethasone, thalidomide, and stem cell transplant. One-third of all patients had renal impairment, defined by a creatinine clearance of less than 60 mL/min. The median age of patients in each arm was 64 and 65, respectively.
The overall response rate, defined as at least a partial response, was significantly higher in the experimental arm than the control arm at 21% vs. 3%, reaching 24% vs. 3% among patients randomized for at least 6 months (P less than .001), Dr. Dimopoulos reported.
Progression-free survival, the study’s primary endpoint, was significantly longer in patients on pomalidomide plus low-dose dexamethasone regardless of whether patients’ last prior treatment was bortezomib (median 3.6 vs. 1.8 months; HR, 0.47) or lenalidomide (median 3.7 vs. 1.8 months; HR, 0.38), or whether they had renal impairment (median 3.2 vs. 1.6 months; HR, 0.44; P less than .001 for all comparisons).
The combination therapy was generally well tolerated, although roughly one-third of patients experienced grade 3/4 neutropenia, an expected complication of pomalidomide (42% vs. 15% of controls), Dr. Dimopoulos observed.
Rates of any grade venous thromboembolism were low at 3% vs. 2% in controls, as were exacerbations of peripheral neuropathy at 12% vs. 11%. In all, 7% of patients discontinued pomalidomide plus low-dose dexamethasone, compared with 6% on high-dose dexamethasone, he said.
Session comoderator Dr. Agnes Lee of the University of British Columbia and Vancouver Coastal Health said her colleagues who enrolled patients in the trial are thrilled with having a possible new option for relapsed/refractory myeloma and very surprised with the minimal amount of toxicity they’ve seen. "Right now we’re just waiting for the next step – will this drug be available, especially here in Canada ... and whether it will now be investigated in earlier disease, especially when it’s so well tolerated."
Dr. Dimopoulos reported honoraria from the study sponsor, Celgene. Several of his coauthors reported commercial relationships with Celgene including employment and equity ownership. Dr. Tallman and Dr. Lee reported no relevant financial conflicts.
Dimopoulos, M.A. et al. Pomalidomide in combination with low-dose dexamethasone: Demonstrates a significant progression-free survival and overall survival advantage in relapsed/refractory MM: A phase 3, multicenter, randomized, open-label study. LBA-6.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Progression-free survival was nearly doubled from 1.7 months with high-dose dexamethasone to 3.2 months with pomalidomide plus low-dose dexamethasone (HR, 0.45; P less than .001).
Data Source: Phase III, open-label study in 455 patients with relapsed or refractory multiple myeloma.
Disclosures: Dr. Dimopoulos reported honoraria from the study sponsor, Celgene. Several of his coauthors reported commercial relationships with Celgene including employment and equity ownership. Dr. Tallman and Dr. Lee reported no relevant financial conflicts.

Chemo-free combo tames 'worst of the worst' acute leukemia
ATLANTA – Cytotoxic chemotherapy is not needed to achieve excellent results in the first-line treatment of acute promyelocytic leukemia, a most aggressive form of acute leukemia.
A phase III trial achieved a 2-year event-free survival rate of 86.7% with all-trans retinoic acid (ATRA) and chemotherapy, the current standard, and 97% with ATRA plus arsenic trioxide (ATO), a small-molecule arsenic compound (P = .03).

The new chemotherapy-free regimen represents "the demolition of a dogma" by showing that cancer is not an irreversible condition and that malignant cells can be transformed rather than killed with chemotherapy, Dr. Francesco Lo-Coco said at a press briefing during the annual meeting of the American Society of Hematology.
ASH president Armand Keating said that the groundbreaking study highlights novel approaches – in this case a targeted combination with roots in ancient Chinese medicine – that can produce comparable efficacy with far less toxicity than chemotherapy.
"This, I think, is an exciting development because it is a shift in the way we think of treating potentially fatal diseases, quite remarkable," Dr. Keating said during a teleconference with reporters.
He pointed out that, 30-40 years ago, before ATRA and chemotherapy transformed the treatment of acute promyelocytic leukemia (APL), mortality was 100%, with most patients dying within a week.
ATRA and cytotoxic chemotherapy, typically containing anthracyclines, produce remission rates of 85%-90% in APL, but early death and relapse among high-risk groups such as the elderly remain problematic in the management of APL.
"I found this study amazing, frankly. ... This [disease] used to be the worst of the worst," ASH Secretary Charles Abrahms said during the teleconference.
Both men remarked that the results will spur further research to elucidate how ATO works, not just in APL but in other diseases.
The current trial is the first randomized, prospective phase III trial to compare ATRA plus ATO against the standard of care, although earlier phase II trials have reported encouraging responses to ATO in combination with other drugs.
As for how the combination works, the altered protein present in APL has specific binding sites for ATO and ATRA, explained Dr. Lo-Coco of the University of Tor Vergata, Rome. ATRA, a derivative developed from Chinese herbal medicine, is thought to induce leukemia cell differentiation, whereas ATO, well known for its activity in treating relapsed APL, produces remissions at least in part by inducing apoptosis.
Dr. Lo-Coco and his coinvestigators in Italy and Germany enrolled 162 patients with newly diagnosed, non–high-risk APL; the median age was 45 years (range 18-70) and the median white blood cell count was 1.50 × 109/L.
Patients in the experimental arm received arsenic trioxide 0.15/kg plus oral ATRA 45 mg/m2 daily until complete remission, then ATO given 5 days per week, 4 weeks on and 4 weeks off, for a total of four courses and ATRA given 2 weeks on and 2 weeks off for a total of seven courses. Patients in the control arm received standard ATRA plus 12 mg/m2 idarubicin as induction, followed by three cycles of anthracycline-based chemotherapy plus ATRA consolidation and maintenance with low-dose chemotherapy and ATRA.
Of the 154 patients evaluable for response to induction, all 75 patients in the experimental arm and 75 of 79 in the control arm achieved complete remission, Dr. Lo-Coco reported in the plenary session.
Molecular complete remission per central review was seen in 141 of 142 evaluable patients after completing the third round of consolidation therapy.
After a median follow-up of 31 months, overall survival was 98.7% with ATRA plus ATO and 91.1% with ATRA plus chemotherapy (P = .02), he said.
Patients receiving ATRA and chemotherapy had significantly more episodes of fever lasting more than 15 days and grade 3 or higher neutropenia and thrombocytopenia than those receiving ATRA and ATO (P less than .001 for all differences).
The ATRA/ATO combination, however, induced QTc prolongation in two patients, requiring ATO discontinuation and study withdrawal for one of them, Dr. Lo-Coco reported.
Rates of APL differentiation syndrome and increased liver enzymes were similar in both groups. There was one death and two relapses in the experimental arm vs. seven deaths and four relapses in the control arm.
The success achieved with ATRA and ATO therapy is likely to raise new questions regarding use of ATO monotherapy in the first-line treatment of APL. The first study to take this approach reported a complete remission rate of 86% in treatment-naive patients (J. Clin. Oncol. 2011;29:2753-7), but the phase II study conducted in Iran prompted a backlash of criticism that it violated medical ethics by failing to provide standard treatment. An accompanying editorial, however, pointed out that treatment with ATRA, anthracyclines, and cytarabine is often "prohibitively expensive in the developing world" (J. Clin. Oncol. 2011;29:2743-6)
A more recent Chinese study pointed to benefits with single-agent ATO in the hard-to-treat elderly, with 88% of patients, aged 60 years or older, achieving a complete remission. The 10-year cumulative incidence of relapse was 10.3% after a median follow-up of 99 months, during which time no patient died of ATO-related toxicities (Cancer 2013;119:115-25).
Dr. Lo-Coco reported serving on the board of directors or advisory committees for Boehringer Ingelheim and as a speaker for Cephalon, the maker of Trisenox (arsenic trioxide). His coauthors reported relationships with several pharmaceutical firms.
ATLANTA – Cytotoxic chemotherapy is not needed to achieve excellent results in the first-line treatment of acute promyelocytic leukemia, a most aggressive form of acute leukemia.
A phase III trial achieved a 2-year event-free survival rate of 86.7% with all-trans retinoic acid (ATRA) and chemotherapy, the current standard, and 97% with ATRA plus arsenic trioxide (ATO), a small-molecule arsenic compound (P = .03).
The new chemotherapy-free regimen represents "the demolition of a dogma" by showing that cancer is not an irreversible condition and that malignant cells can be transformed rather than killed with chemotherapy, Dr. Francesco Lo-Coco said at a press briefing during the annual meeting of the American Society of Hematology.
ASH president Armand Keating said that the groundbreaking study highlights novel approaches – in this case a targeted combination with roots in ancient Chinese medicine – that can produce comparable efficacy with far less toxicity than chemotherapy.
"This, I think, is an exciting development because it is a shift in the way we think of treating potentially fatal diseases, quite remarkable," Dr. Keating said during a teleconference with reporters.
He pointed out that, 30-40 years ago, before ATRA and chemotherapy transformed the treatment of acute promyelocytic leukemia (APL), mortality was 100%, with most patients dying within a week.
ATRA and cytotoxic chemotherapy, typically containing anthracyclines, produce remission rates of 85%-90% in APL, but early death and relapse among high-risk groups such as the elderly remain problematic in the management of APL.
"I found this study amazing, frankly. ... This [disease] used to be the worst of the worst," ASH Secretary Charles Abrahms said during the teleconference.
Both men remarked that the results will spur further research to elucidate how ATO works, not just in APL but in other diseases.
The current trial is the first randomized, prospective phase III trial to compare ATRA plus ATO against the standard of care, although earlier phase II trials have reported encouraging responses to ATO in combination with other drugs.
As for how the combination works, the altered protein present in APL has specific binding sites for ATO and ATRA, explained Dr. Lo-Coco of the University of Tor Vergata, Rome. ATRA, a derivative developed from Chinese herbal medicine, is thought to induce leukemia cell differentiation, whereas ATO, well known for its activity in treating relapsed APL, produces remissions at least in part by inducing apoptosis.
Dr. Lo-Coco and his coinvestigators in Italy and Germany enrolled 162 patients with newly diagnosed, non–high-risk APL; the median age was 45 years (range 18-70) and the median white blood cell count was 1.50 × 109/L.
Patients in the experimental arm received arsenic trioxide 0.15/kg plus oral ATRA 45 mg/m2 daily until complete remission, then ATO given 5 days per week, 4 weeks on and 4 weeks off, for a total of four courses and ATRA given 2 weeks on and 2 weeks off for a total of seven courses. Patients in the control arm received standard ATRA plus 12 mg/m2 idarubicin as induction, followed by three cycles of anthracycline-based chemotherapy plus ATRA consolidation and maintenance with low-dose chemotherapy and ATRA.
Of the 154 patients evaluable for response to induction, all 75 patients in the experimental arm and 75 of 79 in the control arm achieved complete remission, Dr. Lo-Coco reported in the plenary session.
Molecular complete remission per central review was seen in 141 of 142 evaluable patients after completing the third round of consolidation therapy.
After a median follow-up of 31 months, overall survival was 98.7% with ATRA plus ATO and 91.1% with ATRA plus chemotherapy (P = .02), he said.
Patients receiving ATRA and chemotherapy had significantly more episodes of fever lasting more than 15 days and grade 3 or higher neutropenia and thrombocytopenia than those receiving ATRA and ATO (P less than .001 for all differences).
The ATRA/ATO combination, however, induced QTc prolongation in two patients, requiring ATO discontinuation and study withdrawal for one of them, Dr. Lo-Coco reported.
Rates of APL differentiation syndrome and increased liver enzymes were similar in both groups. There was one death and two relapses in the experimental arm vs. seven deaths and four relapses in the control arm.
The success achieved with ATRA and ATO therapy is likely to raise new questions regarding use of ATO monotherapy in the first-line treatment of APL. The first study to take this approach reported a complete remission rate of 86% in treatment-naive patients (J. Clin. Oncol. 2011;29:2753-7), but the phase II study conducted in Iran prompted a backlash of criticism that it violated medical ethics by failing to provide standard treatment. An accompanying editorial, however, pointed out that treatment with ATRA, anthracyclines, and cytarabine is often "prohibitively expensive in the developing world" (J. Clin. Oncol. 2011;29:2743-6)
A more recent Chinese study pointed to benefits with single-agent ATO in the hard-to-treat elderly, with 88% of patients, aged 60 years or older, achieving a complete remission. The 10-year cumulative incidence of relapse was 10.3% after a median follow-up of 99 months, during which time no patient died of ATO-related toxicities (Cancer 2013;119:115-25).
Dr. Lo-Coco reported serving on the board of directors or advisory committees for Boehringer Ingelheim and as a speaker for Cephalon, the maker of Trisenox (arsenic trioxide). His coauthors reported relationships with several pharmaceutical firms.
ATLANTA – Cytotoxic chemotherapy is not needed to achieve excellent results in the first-line treatment of acute promyelocytic leukemia, a most aggressive form of acute leukemia.
A phase III trial achieved a 2-year event-free survival rate of 86.7% with all-trans retinoic acid (ATRA) and chemotherapy, the current standard, and 97% with ATRA plus arsenic trioxide (ATO), a small-molecule arsenic compound (P = .03).
The new chemotherapy-free regimen represents "the demolition of a dogma" by showing that cancer is not an irreversible condition and that malignant cells can be transformed rather than killed with chemotherapy, Dr. Francesco Lo-Coco said at a press briefing during the annual meeting of the American Society of Hematology.
ASH president Armand Keating said that the groundbreaking study highlights novel approaches – in this case a targeted combination with roots in ancient Chinese medicine – that can produce comparable efficacy with far less toxicity than chemotherapy.
"This, I think, is an exciting development because it is a shift in the way we think of treating potentially fatal diseases, quite remarkable," Dr. Keating said during a teleconference with reporters.
He pointed out that, 30-40 years ago, before ATRA and chemotherapy transformed the treatment of acute promyelocytic leukemia (APL), mortality was 100%, with most patients dying within a week.
ATRA and cytotoxic chemotherapy, typically containing anthracyclines, produce remission rates of 85%-90% in APL, but early death and relapse among high-risk groups such as the elderly remain problematic in the management of APL.
"I found this study amazing, frankly. ... This [disease] used to be the worst of the worst," ASH Secretary Charles Abrahms said during the teleconference.
Both men remarked that the results will spur further research to elucidate how ATO works, not just in APL but in other diseases.
The current trial is the first randomized, prospective phase III trial to compare ATRA plus ATO against the standard of care, although earlier phase II trials have reported encouraging responses to ATO in combination with other drugs.
As for how the combination works, the altered protein present in APL has specific binding sites for ATO and ATRA, explained Dr. Lo-Coco of the University of Tor Vergata, Rome. ATRA, a derivative developed from Chinese herbal medicine, is thought to induce leukemia cell differentiation, whereas ATO, well known for its activity in treating relapsed APL, produces remissions at least in part by inducing apoptosis.
Dr. Lo-Coco and his coinvestigators in Italy and Germany enrolled 162 patients with newly diagnosed, non–high-risk APL; the median age was 45 years (range 18-70) and the median white blood cell count was 1.50 × 109/L.
Patients in the experimental arm received arsenic trioxide 0.15/kg plus oral ATRA 45 mg/m2 daily until complete remission, then ATO given 5 days per week, 4 weeks on and 4 weeks off, for a total of four courses and ATRA given 2 weeks on and 2 weeks off for a total of seven courses. Patients in the control arm received standard ATRA plus 12 mg/m2 idarubicin as induction, followed by three cycles of anthracycline-based chemotherapy plus ATRA consolidation and maintenance with low-dose chemotherapy and ATRA.
Of the 154 patients evaluable for response to induction, all 75 patients in the experimental arm and 75 of 79 in the control arm achieved complete remission, Dr. Lo-Coco reported in the plenary session.
Molecular complete remission per central review was seen in 141 of 142 evaluable patients after completing the third round of consolidation therapy.
After a median follow-up of 31 months, overall survival was 98.7% with ATRA plus ATO and 91.1% with ATRA plus chemotherapy (P = .02), he said.
Patients receiving ATRA and chemotherapy had significantly more episodes of fever lasting more than 15 days and grade 3 or higher neutropenia and thrombocytopenia than those receiving ATRA and ATO (P less than .001 for all differences).
The ATRA/ATO combination, however, induced QTc prolongation in two patients, requiring ATO discontinuation and study withdrawal for one of them, Dr. Lo-Coco reported.
Rates of APL differentiation syndrome and increased liver enzymes were similar in both groups. There was one death and two relapses in the experimental arm vs. seven deaths and four relapses in the control arm.
The success achieved with ATRA and ATO therapy is likely to raise new questions regarding use of ATO monotherapy in the first-line treatment of APL. The first study to take this approach reported a complete remission rate of 86% in treatment-naive patients (J. Clin. Oncol. 2011;29:2753-7), but the phase II study conducted in Iran prompted a backlash of criticism that it violated medical ethics by failing to provide standard treatment. An accompanying editorial, however, pointed out that treatment with ATRA, anthracyclines, and cytarabine is often "prohibitively expensive in the developing world" (J. Clin. Oncol. 2011;29:2743-6)
A more recent Chinese study pointed to benefits with single-agent ATO in the hard-to-treat elderly, with 88% of patients, aged 60 years or older, achieving a complete remission. The 10-year cumulative incidence of relapse was 10.3% after a median follow-up of 99 months, during which time no patient died of ATO-related toxicities (Cancer 2013;119:115-25).
Dr. Lo-Coco reported serving on the board of directors or advisory committees for Boehringer Ingelheim and as a speaker for Cephalon, the maker of Trisenox (arsenic trioxide). His coauthors reported relationships with several pharmaceutical firms.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Two-year event-free survival was 86.7% with all-trans retinoic acid (ATRA) and chemotherapy and 97% with ATRA plus arsenic trioxide (P = .03).
Data Source: Prospective, randomized, phase III trial in acute promyelocytic leukemia.
Disclosures: Dr. Lo-Coco reported serving on the board of directors or advisory committees for Boehringer Ingelheim and as a speaker for Cephalon, the maker of Trisenox (arsenic trioxide). His coauthors reported relationships with several pharmaceutical firms.

ADVANCE: TAVI survival remains high with CoreValve
At 1 year, overall survival after implantation with the transcatheter aortic CoreValve in the postmarket ADVANCE study was 82.1% and cardiovascular survival 88.2%. This compares with survival rates of 87.4% and 91.7% at 6 months and 95.5% and 96.6% at 30 days, principal investigator Dr. Axel Linke said at Transcatheter Cardiovascular Therapeutics 2012.
"If you put it into the perspective of the PARTNER A and B cohorts [in the pivotal trial in the Sapien transcatheter valve system], our mortality rate is, in absolute values, 8% to 13% lower," he said in an interview.
One explanation is that the 1,015-patient, postmarket ADVANCE study sought out centers experienced with transcatheter aortic valve implantation (TAVI). The 44 centers in Western Europe, Asia, and South America had to have performed at least 40 TAVI procedures, with some German centers having done as many as 500, to be certified by a TAVI proctor and to have a heart team in place. In comparison, some centers in the PARTNER trial of the Edwards Lifesciences Sapien valve contributed just six or seven patients and were selected based on their experience with general cardiologic intervention, he observed.
The 1-year survival rates in ADVANCE also surpass those from early registries, notably the French Aortic National CoreValve and Edwards Registry, where the initial experience with TAVI was associated with interventional mistakes, which were linked to early mortality, Dr. Linke said. The CoreValve System has been implanted in more than 30,000 patients since approval in the European Union in 2007, but is limited to investigational use in the United States.
No details were presented regarding mortality in various subgroups or complications such as stroke, paravalvular leaks or left bundle branch block (LBBB). A recent analysis raised concerns about LBBB, showing that one-third of 202 consecutive patients with no prior conduction disturbances developed new-onset LBBB after TAVI with a balloon-expandable valve (Sapien or Sapien XT). Although it resolved in 37.7% by hospital discharge and 57.3% at 6- to 12-month follow-up, patients with persistent LBBB had a significantly higher incidence of syncope and complete atrioventricular block requiring a permanent pacemaker (J. Am. Coll. Cardiol. 2012;60:1743-52 [doi:10.1016/j.jacc.2012.035].
The researchers will look at LBBB in detailed analyses expected from ADVANCE, but there’s been no evidence of a problem with LBBB in earlier follow-up in ADVANCE or from other CoreValve users.
Quality of life data from ADVANCE, reported in a separate poster session at the meeting, showed significant benefits with CoreValve, even in higher-risk patients. The access route used during TAVI had no impact on quality of life improvement at 6 months.
Dr. Linke has served as a consultant for Medtronic, the study sponsor.
At 1 year, overall survival after implantation with the transcatheter aortic CoreValve in the postmarket ADVANCE study was 82.1% and cardiovascular survival 88.2%. This compares with survival rates of 87.4% and 91.7% at 6 months and 95.5% and 96.6% at 30 days, principal investigator Dr. Axel Linke said at Transcatheter Cardiovascular Therapeutics 2012.
"If you put it into the perspective of the PARTNER A and B cohorts [in the pivotal trial in the Sapien transcatheter valve system], our mortality rate is, in absolute values, 8% to 13% lower," he said in an interview.
One explanation is that the 1,015-patient, postmarket ADVANCE study sought out centers experienced with transcatheter aortic valve implantation (TAVI). The 44 centers in Western Europe, Asia, and South America had to have performed at least 40 TAVI procedures, with some German centers having done as many as 500, to be certified by a TAVI proctor and to have a heart team in place. In comparison, some centers in the PARTNER trial of the Edwards Lifesciences Sapien valve contributed just six or seven patients and were selected based on their experience with general cardiologic intervention, he observed.
The 1-year survival rates in ADVANCE also surpass those from early registries, notably the French Aortic National CoreValve and Edwards Registry, where the initial experience with TAVI was associated with interventional mistakes, which were linked to early mortality, Dr. Linke said. The CoreValve System has been implanted in more than 30,000 patients since approval in the European Union in 2007, but is limited to investigational use in the United States.
No details were presented regarding mortality in various subgroups or complications such as stroke, paravalvular leaks or left bundle branch block (LBBB). A recent analysis raised concerns about LBBB, showing that one-third of 202 consecutive patients with no prior conduction disturbances developed new-onset LBBB after TAVI with a balloon-expandable valve (Sapien or Sapien XT). Although it resolved in 37.7% by hospital discharge and 57.3% at 6- to 12-month follow-up, patients with persistent LBBB had a significantly higher incidence of syncope and complete atrioventricular block requiring a permanent pacemaker (J. Am. Coll. Cardiol. 2012;60:1743-52 [doi:10.1016/j.jacc.2012.035].
The researchers will look at LBBB in detailed analyses expected from ADVANCE, but there’s been no evidence of a problem with LBBB in earlier follow-up in ADVANCE or from other CoreValve users.
Quality of life data from ADVANCE, reported in a separate poster session at the meeting, showed significant benefits with CoreValve, even in higher-risk patients. The access route used during TAVI had no impact on quality of life improvement at 6 months.
Dr. Linke has served as a consultant for Medtronic, the study sponsor.
At 1 year, overall survival after implantation with the transcatheter aortic CoreValve in the postmarket ADVANCE study was 82.1% and cardiovascular survival 88.2%. This compares with survival rates of 87.4% and 91.7% at 6 months and 95.5% and 96.6% at 30 days, principal investigator Dr. Axel Linke said at Transcatheter Cardiovascular Therapeutics 2012.
"If you put it into the perspective of the PARTNER A and B cohorts [in the pivotal trial in the Sapien transcatheter valve system], our mortality rate is, in absolute values, 8% to 13% lower," he said in an interview.
One explanation is that the 1,015-patient, postmarket ADVANCE study sought out centers experienced with transcatheter aortic valve implantation (TAVI). The 44 centers in Western Europe, Asia, and South America had to have performed at least 40 TAVI procedures, with some German centers having done as many as 500, to be certified by a TAVI proctor and to have a heart team in place. In comparison, some centers in the PARTNER trial of the Edwards Lifesciences Sapien valve contributed just six or seven patients and were selected based on their experience with general cardiologic intervention, he observed.
The 1-year survival rates in ADVANCE also surpass those from early registries, notably the French Aortic National CoreValve and Edwards Registry, where the initial experience with TAVI was associated with interventional mistakes, which were linked to early mortality, Dr. Linke said. The CoreValve System has been implanted in more than 30,000 patients since approval in the European Union in 2007, but is limited to investigational use in the United States.
No details were presented regarding mortality in various subgroups or complications such as stroke, paravalvular leaks or left bundle branch block (LBBB). A recent analysis raised concerns about LBBB, showing that one-third of 202 consecutive patients with no prior conduction disturbances developed new-onset LBBB after TAVI with a balloon-expandable valve (Sapien or Sapien XT). Although it resolved in 37.7% by hospital discharge and 57.3% at 6- to 12-month follow-up, patients with persistent LBBB had a significantly higher incidence of syncope and complete atrioventricular block requiring a permanent pacemaker (J. Am. Coll. Cardiol. 2012;60:1743-52 [doi:10.1016/j.jacc.2012.035].
The researchers will look at LBBB in detailed analyses expected from ADVANCE, but there’s been no evidence of a problem with LBBB in earlier follow-up in ADVANCE or from other CoreValve users.
Quality of life data from ADVANCE, reported in a separate poster session at the meeting, showed significant benefits with CoreValve, even in higher-risk patients. The access route used during TAVI had no impact on quality of life improvement at 6 months.
Dr. Linke has served as a consultant for Medtronic, the study sponsor.
Major Finding: At 1 year, overall survival was 82.1% and cardiovascular survival 88.2%.
Data Source: International, postmarket phase IV study of 1,015 patients with severe aortic stenosis implanted with the transcatheter CoreValve.
Disclosures: Dr. Linke reported serving as an advisor or consultant for Medtronic, which sponsored the study.
Bullets no match for dual-energy CT scrutiny
CHICAGO – Dual-energy computed tomography may have a role in clearing patients with embedded bullets and other metallic objects for magnetic resonance imaging who would otherwise be excluded because of safety concerns.
A Swiss analysis of bullets and shotgun pellets found that dual-energy CT had a high discriminatory power to distinguish between projectiles with and without ferromagnetic properties. MR safety depends on whether a metallic object has ferromagnetic properties – something that most patients don’t know or may be unable to communicate during an emergency evaluation, study author Dr. Sebastian Winklhofer said at the annual meeting of the Radiological Society of North America.

"Dual-energy measurements may contribute to MR safety and allow for MR imaging of patients with retained projectiles," he said.
Retained metallic objects such as bullets, shrapnel, and medical devices are frequently contraindicated for MRI, because they might move, dislodge, or accelerate at dangerously high velocities toward the scanner’s magnet. This has led to patient injury, and in some cases death, if the object is located near or in a critical anatomic structure.
Session comoderator Dr. Seppo Koskinen of Helsinki University Central Hospital, Finland, said he recently had to forgo MR imaging in a patient with a bullet lodged in the spinal canal because the patient didn’t know if it was lead or steel.
"We didn’t do an MR, but maybe with this system we could have," he said in an interview. "So it has a real clinical impact."
Unsafe exams and misinformed refusals to refer or scan a patient are also occurring as a result of confusion over the ever increasing number of metallic orthopedic and cardiovascular implants. For example, a device that is known to be safe on a 1.5 tesla scanner may be contraindicated on a more powerful 3T scanner or on other scanners using different settings.
When the American College of Radiology penned its Safe MR Practices guidelines in 2007, no cardiac pacemakers or implantable defibrillators were labeled as safe or conditionally safe for MR imaging, prompting the college to recommend that routine MRI is inadvisable in patients with these devices.
In its scientific statement on the controversial topic, the American Heart Association says data are available to support MR imaging in patients with cardiovascular devices, but recommends a series of precautions, including careful patient screening and an accurate determination of the device and its properties (Circulation 2007:116:2878-91).
Dual-energy CT has been used in research and clinical settings to assess the composition of various objects, said Dr. Winklhofer of University Hospital Zurich, Switzerland. He highlighted one study showing that dual-energy CT had a 98% specificity in differentiating between urinary stones that did or did not contain uric acid (Invest. Radiology 2010;45:1-6).
In the current study, nine bullets and two shotgun pellets were scanned in an ex vivo chest phantom using second-generation dual-source CT (SOMATOM Definition Flash, Siemens Healthcare), with tube voltages set at 80, 100, 120, and 140 kVp. Two readers, blinded to the ferromagnetic properties of the projectiles, independently assessed CT numbers on 44 images reconstructed using the extended CT scale technique, which helps overcome artifacts arising from metallic objects. A CT number is the density assigned to a voxel in a CT scan.
Dual-energy indices (DEI) were calculated from 80/140 kVP and 100/140 kVP pairs, and receiver operating characteristics analyses were fitted to predict ferromagnetic properties by means of DEI and CT numbers.
The bullets/pellets ranged in diameter from 2 mm to 14 mm; five were ferromagnetic and six nonferromagnetic.

Intrareader agreement was significantly correlated with mean CT number measurements (P less than .001), with excellent intraclass correlation coefficient agreement (Reader 1: ICC = 0.998; Reader 2: ICC = 0.963), Dr. Winklhofer said.
Interreader agreement was also significantly correlated (P less than .001), and again, there was excellent ICC agreement (both readers ICC = 0.988).
In contrast, when the same projectiles were scanned with single-energy CT, no significant differences in CT numbers for ferromagnetic vs. nonferromagnetic projectiles were observed, said Dr. Winklhofer, who received the RSNA Trainee Research prize for his work.
"Single-energy does not allow for differentiation between those types of projectiles, whereas the dual-energy results show it is possible to differentiate between ferromagnetic and nonferromagnetic projectiles," he said.
Finally, the dual-energy indices of ferromagnetic projectiles were significantly higher than were those of nonferromagnetic projectiles for both the 80/140 kVP and 100/140 kVP energy pairs (at a P value less than .10).
Before dual-energy CT is ready for prime time, however, additional studies are needed to prove that the technique is valid in phantoms of other body regions and in humans, Dr. Winklhofer said in an interview. The prospective study is currently underway.
Dr. Winklhofer and Dr. Koskinen reported no conflicts of interest.
CHICAGO – Dual-energy computed tomography may have a role in clearing patients with embedded bullets and other metallic objects for magnetic resonance imaging who would otherwise be excluded because of safety concerns.
A Swiss analysis of bullets and shotgun pellets found that dual-energy CT had a high discriminatory power to distinguish between projectiles with and without ferromagnetic properties. MR safety depends on whether a metallic object has ferromagnetic properties – something that most patients don’t know or may be unable to communicate during an emergency evaluation, study author Dr. Sebastian Winklhofer said at the annual meeting of the Radiological Society of North America.
"Dual-energy measurements may contribute to MR safety and allow for MR imaging of patients with retained projectiles," he said.
Retained metallic objects such as bullets, shrapnel, and medical devices are frequently contraindicated for MRI, because they might move, dislodge, or accelerate at dangerously high velocities toward the scanner’s magnet. This has led to patient injury, and in some cases death, if the object is located near or in a critical anatomic structure.
Session comoderator Dr. Seppo Koskinen of Helsinki University Central Hospital, Finland, said he recently had to forgo MR imaging in a patient with a bullet lodged in the spinal canal because the patient didn’t know if it was lead or steel.
"We didn’t do an MR, but maybe with this system we could have," he said in an interview. "So it has a real clinical impact."
Unsafe exams and misinformed refusals to refer or scan a patient are also occurring as a result of confusion over the ever increasing number of metallic orthopedic and cardiovascular implants. For example, a device that is known to be safe on a 1.5 tesla scanner may be contraindicated on a more powerful 3T scanner or on other scanners using different settings.
When the American College of Radiology penned its Safe MR Practices guidelines in 2007, no cardiac pacemakers or implantable defibrillators were labeled as safe or conditionally safe for MR imaging, prompting the college to recommend that routine MRI is inadvisable in patients with these devices.
In its scientific statement on the controversial topic, the American Heart Association says data are available to support MR imaging in patients with cardiovascular devices, but recommends a series of precautions, including careful patient screening and an accurate determination of the device and its properties (Circulation 2007:116:2878-91).
Dual-energy CT has been used in research and clinical settings to assess the composition of various objects, said Dr. Winklhofer of University Hospital Zurich, Switzerland. He highlighted one study showing that dual-energy CT had a 98% specificity in differentiating between urinary stones that did or did not contain uric acid (Invest. Radiology 2010;45:1-6).
In the current study, nine bullets and two shotgun pellets were scanned in an ex vivo chest phantom using second-generation dual-source CT (SOMATOM Definition Flash, Siemens Healthcare), with tube voltages set at 80, 100, 120, and 140 kVp. Two readers, blinded to the ferromagnetic properties of the projectiles, independently assessed CT numbers on 44 images reconstructed using the extended CT scale technique, which helps overcome artifacts arising from metallic objects. A CT number is the density assigned to a voxel in a CT scan.
Dual-energy indices (DEI) were calculated from 80/140 kVP and 100/140 kVP pairs, and receiver operating characteristics analyses were fitted to predict ferromagnetic properties by means of DEI and CT numbers.
The bullets/pellets ranged in diameter from 2 mm to 14 mm; five were ferromagnetic and six nonferromagnetic.
Intrareader agreement was significantly correlated with mean CT number measurements (P less than .001), with excellent intraclass correlation coefficient agreement (Reader 1: ICC = 0.998; Reader 2: ICC = 0.963), Dr. Winklhofer said.
Interreader agreement was also significantly correlated (P less than .001), and again, there was excellent ICC agreement (both readers ICC = 0.988).
In contrast, when the same projectiles were scanned with single-energy CT, no significant differences in CT numbers for ferromagnetic vs. nonferromagnetic projectiles were observed, said Dr. Winklhofer, who received the RSNA Trainee Research prize for his work.
"Single-energy does not allow for differentiation between those types of projectiles, whereas the dual-energy results show it is possible to differentiate between ferromagnetic and nonferromagnetic projectiles," he said.
Finally, the dual-energy indices of ferromagnetic projectiles were significantly higher than were those of nonferromagnetic projectiles for both the 80/140 kVP and 100/140 kVP energy pairs (at a P value less than .10).
Before dual-energy CT is ready for prime time, however, additional studies are needed to prove that the technique is valid in phantoms of other body regions and in humans, Dr. Winklhofer said in an interview. The prospective study is currently underway.
Dr. Winklhofer and Dr. Koskinen reported no conflicts of interest.
CHICAGO – Dual-energy computed tomography may have a role in clearing patients with embedded bullets and other metallic objects for magnetic resonance imaging who would otherwise be excluded because of safety concerns.
A Swiss analysis of bullets and shotgun pellets found that dual-energy CT had a high discriminatory power to distinguish between projectiles with and without ferromagnetic properties. MR safety depends on whether a metallic object has ferromagnetic properties – something that most patients don’t know or may be unable to communicate during an emergency evaluation, study author Dr. Sebastian Winklhofer said at the annual meeting of the Radiological Society of North America.
"Dual-energy measurements may contribute to MR safety and allow for MR imaging of patients with retained projectiles," he said.
Retained metallic objects such as bullets, shrapnel, and medical devices are frequently contraindicated for MRI, because they might move, dislodge, or accelerate at dangerously high velocities toward the scanner’s magnet. This has led to patient injury, and in some cases death, if the object is located near or in a critical anatomic structure.
Session comoderator Dr. Seppo Koskinen of Helsinki University Central Hospital, Finland, said he recently had to forgo MR imaging in a patient with a bullet lodged in the spinal canal because the patient didn’t know if it was lead or steel.
"We didn’t do an MR, but maybe with this system we could have," he said in an interview. "So it has a real clinical impact."
Unsafe exams and misinformed refusals to refer or scan a patient are also occurring as a result of confusion over the ever increasing number of metallic orthopedic and cardiovascular implants. For example, a device that is known to be safe on a 1.5 tesla scanner may be contraindicated on a more powerful 3T scanner or on other scanners using different settings.
When the American College of Radiology penned its Safe MR Practices guidelines in 2007, no cardiac pacemakers or implantable defibrillators were labeled as safe or conditionally safe for MR imaging, prompting the college to recommend that routine MRI is inadvisable in patients with these devices.
In its scientific statement on the controversial topic, the American Heart Association says data are available to support MR imaging in patients with cardiovascular devices, but recommends a series of precautions, including careful patient screening and an accurate determination of the device and its properties (Circulation 2007:116:2878-91).
Dual-energy CT has been used in research and clinical settings to assess the composition of various objects, said Dr. Winklhofer of University Hospital Zurich, Switzerland. He highlighted one study showing that dual-energy CT had a 98% specificity in differentiating between urinary stones that did or did not contain uric acid (Invest. Radiology 2010;45:1-6).
In the current study, nine bullets and two shotgun pellets were scanned in an ex vivo chest phantom using second-generation dual-source CT (SOMATOM Definition Flash, Siemens Healthcare), with tube voltages set at 80, 100, 120, and 140 kVp. Two readers, blinded to the ferromagnetic properties of the projectiles, independently assessed CT numbers on 44 images reconstructed using the extended CT scale technique, which helps overcome artifacts arising from metallic objects. A CT number is the density assigned to a voxel in a CT scan.
Dual-energy indices (DEI) were calculated from 80/140 kVP and 100/140 kVP pairs, and receiver operating characteristics analyses were fitted to predict ferromagnetic properties by means of DEI and CT numbers.
The bullets/pellets ranged in diameter from 2 mm to 14 mm; five were ferromagnetic and six nonferromagnetic.
Intrareader agreement was significantly correlated with mean CT number measurements (P less than .001), with excellent intraclass correlation coefficient agreement (Reader 1: ICC = 0.998; Reader 2: ICC = 0.963), Dr. Winklhofer said.
Interreader agreement was also significantly correlated (P less than .001), and again, there was excellent ICC agreement (both readers ICC = 0.988).
In contrast, when the same projectiles were scanned with single-energy CT, no significant differences in CT numbers for ferromagnetic vs. nonferromagnetic projectiles were observed, said Dr. Winklhofer, who received the RSNA Trainee Research prize for his work.
"Single-energy does not allow for differentiation between those types of projectiles, whereas the dual-energy results show it is possible to differentiate between ferromagnetic and nonferromagnetic projectiles," he said.
Finally, the dual-energy indices of ferromagnetic projectiles were significantly higher than were those of nonferromagnetic projectiles for both the 80/140 kVP and 100/140 kVP energy pairs (at a P value less than .10).
Before dual-energy CT is ready for prime time, however, additional studies are needed to prove that the technique is valid in phantoms of other body regions and in humans, Dr. Winklhofer said in an interview. The prospective study is currently underway.
Dr. Winklhofer and Dr. Koskinen reported no conflicts of interest.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Intrareader agreement was significantly correlated with mean CT number measurements (P less than .001), with excellent intraclass correlation coefficient agreement.
Data Source: Prospective analysis of ballistic projectiles.
Disclosures: Dr. Winklhofer and Dr. Koskinen reported no conflicts of interest.

Marshall score better predictor of early TBI death
CHICAGO – The Marshall CT classification system is a better predictor of early death in patients with traumatic brain injury than is the Rotterdam score, an award-winning study found.
As observed in previous reports, higher scores on both computed tomography–based scoring systems were significantly associated with early death among patients with mild to severe traumatic brain injury, or TBI (both P values less than .0001).
In a logistic regression analysis, however, only the Marshall scoring system was significantly associated with early death, defined as death at hospital discharge (P less than .002), Dr. Daddy Mata Mbemba reported at the annual meeting of the Radiological Society of North America.
This is likely because the two strongest independent predictors of early death – the absence of basal cistern and positive midline shift – are included in both CT scoring systems, while the next strongest predictor, hemorrhagic mass, is included in the Marshall score only, he explained.
Marshall and Rotterdam are the two most commonly used radiologic scoring systems, according to Dr. Mbemba, but they group CT findings differently. The Marshall score includes the status of basal cisterns, midline shift greater than 5 mm, and hemorrhagic mass, whereas the Rotterdam score includes basal cisterns, midline shift greater than 5 mm, subarachnoid hemorrhage and/or intraventricular hemorrhage, and epidural hemorrhage, but not hemorrhagic mass, explained Dr. Mbemba, a radiologist at Tohoku University, Sendai City, Japan.
He noted that several studies have suggested that increased intracranial pressure may lead to early death, while vasospasm associated with subarachnoid hemorrhage and/or intraventricular hemorrhage that decrease intracerebral circulation is associated with a worsening clinical outcome.
To assess whether the Marshall or Rotterdam scores are related to death at hospital discharge, investigators in the current study reviewed the initial CT scans and status at hospital discharge of 245 consecutive patients with mild to severe TBI. Mild cases, defined by a Glasgow Coma Scale score of 13-15, were included if a CT examination was recommended according to New Orleans Criteria and/or the Canadian CT Head Rule. Patients’ mean age was 49 years (range, 15-93 years), and 67% were men.
At hospital discharge, 25 patients had died and 220 were alive. The median time to death was 3 days (range, 1-83 days), said Dr. Mbemba, who earned a trainee research award from RSNA for his study.
In a logistic regression analysis, CT findings independently related to early death were basal cistern status (odds ratio, 771.5; P less than .001), positive midline shift (OR, 56.2; P = .0011), hemorrhagic mass (OR, 12.9; P = .0065), and subarachnoid hemorrhage and/or intraventricular hemorrhage (OR 3.8; P = .0394), Dr. Mbemba said. The presence or absence of an epidural hemorrhage was not a significant predictor.
In a recently published study, initial Marshall and Rotterdam scores were significantly associated with mortality after severe TBI, while Glasgow Coma Scale scores on admission were not (Neurosurgery 2012;70:1095-105). No relationship was observed, however, between any of the three scoring systems and ICU intracranial pressure or brain tissue oxygen tension, suggesting that factors associated with outcome, may not always predict a patient’s ICU course, especially intracranial physiology.
Dr. Mbemba and his coauthors reported no relevant financial disclosures.
computed tomography–based scoring systems, TBI, Dr. Daddy Mata Mbemba, Radiological Society of North America, vasospasm, associated with subarachnoid hemorrhage, intraventricular hemorrhage, intracerebral circulation,
CHICAGO – The Marshall CT classification system is a better predictor of early death in patients with traumatic brain injury than is the Rotterdam score, an award-winning study found.
As observed in previous reports, higher scores on both computed tomography–based scoring systems were significantly associated with early death among patients with mild to severe traumatic brain injury, or TBI (both P values less than .0001).
In a logistic regression analysis, however, only the Marshall scoring system was significantly associated with early death, defined as death at hospital discharge (P less than .002), Dr. Daddy Mata Mbemba reported at the annual meeting of the Radiological Society of North America.
This is likely because the two strongest independent predictors of early death – the absence of basal cistern and positive midline shift – are included in both CT scoring systems, while the next strongest predictor, hemorrhagic mass, is included in the Marshall score only, he explained.
Marshall and Rotterdam are the two most commonly used radiologic scoring systems, according to Dr. Mbemba, but they group CT findings differently. The Marshall score includes the status of basal cisterns, midline shift greater than 5 mm, and hemorrhagic mass, whereas the Rotterdam score includes basal cisterns, midline shift greater than 5 mm, subarachnoid hemorrhage and/or intraventricular hemorrhage, and epidural hemorrhage, but not hemorrhagic mass, explained Dr. Mbemba, a radiologist at Tohoku University, Sendai City, Japan.
He noted that several studies have suggested that increased intracranial pressure may lead to early death, while vasospasm associated with subarachnoid hemorrhage and/or intraventricular hemorrhage that decrease intracerebral circulation is associated with a worsening clinical outcome.
To assess whether the Marshall or Rotterdam scores are related to death at hospital discharge, investigators in the current study reviewed the initial CT scans and status at hospital discharge of 245 consecutive patients with mild to severe TBI. Mild cases, defined by a Glasgow Coma Scale score of 13-15, were included if a CT examination was recommended according to New Orleans Criteria and/or the Canadian CT Head Rule. Patients’ mean age was 49 years (range, 15-93 years), and 67% were men.
At hospital discharge, 25 patients had died and 220 were alive. The median time to death was 3 days (range, 1-83 days), said Dr. Mbemba, who earned a trainee research award from RSNA for his study.
In a logistic regression analysis, CT findings independently related to early death were basal cistern status (odds ratio, 771.5; P less than .001), positive midline shift (OR, 56.2; P = .0011), hemorrhagic mass (OR, 12.9; P = .0065), and subarachnoid hemorrhage and/or intraventricular hemorrhage (OR 3.8; P = .0394), Dr. Mbemba said. The presence or absence of an epidural hemorrhage was not a significant predictor.
In a recently published study, initial Marshall and Rotterdam scores were significantly associated with mortality after severe TBI, while Glasgow Coma Scale scores on admission were not (Neurosurgery 2012;70:1095-105). No relationship was observed, however, between any of the three scoring systems and ICU intracranial pressure or brain tissue oxygen tension, suggesting that factors associated with outcome, may not always predict a patient’s ICU course, especially intracranial physiology.
Dr. Mbemba and his coauthors reported no relevant financial disclosures.
CHICAGO – The Marshall CT classification system is a better predictor of early death in patients with traumatic brain injury than is the Rotterdam score, an award-winning study found.
As observed in previous reports, higher scores on both computed tomography–based scoring systems were significantly associated with early death among patients with mild to severe traumatic brain injury, or TBI (both P values less than .0001).
In a logistic regression analysis, however, only the Marshall scoring system was significantly associated with early death, defined as death at hospital discharge (P less than .002), Dr. Daddy Mata Mbemba reported at the annual meeting of the Radiological Society of North America.
This is likely because the two strongest independent predictors of early death – the absence of basal cistern and positive midline shift – are included in both CT scoring systems, while the next strongest predictor, hemorrhagic mass, is included in the Marshall score only, he explained.
Marshall and Rotterdam are the two most commonly used radiologic scoring systems, according to Dr. Mbemba, but they group CT findings differently. The Marshall score includes the status of basal cisterns, midline shift greater than 5 mm, and hemorrhagic mass, whereas the Rotterdam score includes basal cisterns, midline shift greater than 5 mm, subarachnoid hemorrhage and/or intraventricular hemorrhage, and epidural hemorrhage, but not hemorrhagic mass, explained Dr. Mbemba, a radiologist at Tohoku University, Sendai City, Japan.
He noted that several studies have suggested that increased intracranial pressure may lead to early death, while vasospasm associated with subarachnoid hemorrhage and/or intraventricular hemorrhage that decrease intracerebral circulation is associated with a worsening clinical outcome.
To assess whether the Marshall or Rotterdam scores are related to death at hospital discharge, investigators in the current study reviewed the initial CT scans and status at hospital discharge of 245 consecutive patients with mild to severe TBI. Mild cases, defined by a Glasgow Coma Scale score of 13-15, were included if a CT examination was recommended according to New Orleans Criteria and/or the Canadian CT Head Rule. Patients’ mean age was 49 years (range, 15-93 years), and 67% were men.
At hospital discharge, 25 patients had died and 220 were alive. The median time to death was 3 days (range, 1-83 days), said Dr. Mbemba, who earned a trainee research award from RSNA for his study.
In a logistic regression analysis, CT findings independently related to early death were basal cistern status (odds ratio, 771.5; P less than .001), positive midline shift (OR, 56.2; P = .0011), hemorrhagic mass (OR, 12.9; P = .0065), and subarachnoid hemorrhage and/or intraventricular hemorrhage (OR 3.8; P = .0394), Dr. Mbemba said. The presence or absence of an epidural hemorrhage was not a significant predictor.
In a recently published study, initial Marshall and Rotterdam scores were significantly associated with mortality after severe TBI, while Glasgow Coma Scale scores on admission were not (Neurosurgery 2012;70:1095-105). No relationship was observed, however, between any of the three scoring systems and ICU intracranial pressure or brain tissue oxygen tension, suggesting that factors associated with outcome, may not always predict a patient’s ICU course, especially intracranial physiology.
Dr. Mbemba and his coauthors reported no relevant financial disclosures.
computed tomography–based scoring systems, TBI, Dr. Daddy Mata Mbemba, Radiological Society of North America, vasospasm, associated with subarachnoid hemorrhage, intraventricular hemorrhage, intracerebral circulation,
computed tomography–based scoring systems, TBI, Dr. Daddy Mata Mbemba, Radiological Society of North America, vasospasm, associated with subarachnoid hemorrhage, intraventricular hemorrhage, intracerebral circulation,
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: In a logistic regression analysis, only the Marshall score was significantly associated with early death, defined as death at hospital discharge (P less than .002).
Data Source: Retrospective analysis involving 245 patients with traumatic brain injury.
Disclosures: Dr. Mbemba and his coauthors reported no relevant financial disclosures.
Two-Step Rule Sizes Up CT Pleural Effusions
CHICAGO – Researchers have developed and validated a simple two-step rule to quantify pleural effusion size on computed tomography – something currently not standardized.
Use of the rule significantly improved interobserver agreement, from a kappa coefficient of 0.56 to 0.79 (P less than .0001), among nine physicians ranging in skill from cardiothoracic radiologists and pulmonologists to radiology residents.
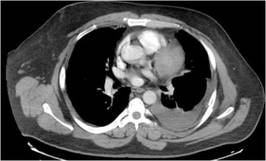
"It’s practical for any physician with access to the images and the referent tool, and conveys relevant information in terms of comparing effusion size and possibly guiding therapy," Dr. Matthew Moy said at the annual meeting of the Radiological Society of North America.
Computed tomography (CT) is highly sensitive for detecting small effusions, and differentiating pleural and parenchymal disease. The problem lies in the subjective grading of pleural effusion size and the wide variation in terminology between radiologists. These issues lead to confusion among physicians when reading CT reports or comparing effusions based on different reports, he said.
To illustrate his point, Dr. Moy showed three CT images of pleural effusions reported as being "small-moderate" to "moderate" to "large," although all three were similar in size.

In an effort to improve this communication, investigators at the Albert Einstein College of Medicine, New York, selected 34 adult CT scans, representing a wide range of pleural effusion sizes, and measured the volume of each effusion and ipsilateral hemithorax using a morphometric segmentation tool. The effusion and ipsilateral hemithorax were then manually traced on each axial slice, and the effusion volume calculated as a percent of the volume of the hemithorax to account for differences in body habitus, explained Dr. Moy.
The mean effusion volume was 37.42% of the hemithorax (range, 5.59%-89.05%). The patients’ mean age was 64 years, and 74% had undergone noncontrast CT.
Two cardiothoracic fellowship–trained radiologists then reviewed the CTs to identify qualitative and quantitative features that correlated with effusion volume. Several features emerged, but only anteroposterior (AP) quartile, maximum AP depth, and degree of atelectasis remained significant in multivariate analysis. The last was dropped, however, because it was not found to be useful for differentiating large effusions, said Dr. Moy, now with Massachusetts General Hospital in Boston.

AP quartile is calculated using the axial image where the effusion appears largest cephalad to the dome of the hemidiaphragm. The hemithorax is divided into four quartiles, and the AP quartile is then measured as the anterior-most quartile in which the effusion is seen, he explained. Maximum AP depth is measured in centimeters at the midclavicular line.
A classification rule was then developed in which first AP quartile (0%-25%) effusions are small, second quartile (25%-50%) effusions are moderate, and third or fourth AP quartile (50%-75% or 75%-100%) effusions are large. In borderline cases where it’s not easy to assess the quartile, AP depth can be measured using cutoffs of less than 3 cm (small), 3-10 cm (moderate), and more than 10 cm (large), Dr. Moy suggested.
To validate the rule, the 34 CT scans were then assessed by the nine physicians, who were not involved in the initial CT analysis. Interobserver agreement improved from a kappa of 0.59 to a kappa of 0.73 for radiology residents, 0.54 to 0.76 for pulmonologists, and 0.74 to 0.85 for cardiothoracic radiologists.

"This rule can elevate the level of agreement and consistency of both the novice radiologist and clinician to the level of cardiothoracic radiologists," Dr. Moy observed.
Session comoderator Dr. Reginald Munden, a professor of diagnostic radiology at the University of Texas M.D. Anderson Cancer Center in Houston, said in an interview, "I like anything we can do to standardize our reports, because we’re all over the place. This is particularly important, because a lot of smalls are insignificant and we don’t need to do anything with them.
"In our setting, with patients on chemotherapy, we see pleural effusions all the time," he added. "So it’s important when an effusion becomes large enough that it needs to be drained or it might be symptomatic for some other issue."
Dr. Munden went on to say that the grading scale needs to be validated in a larger population and should include a fourth subcategory, "present, but normal," to distinguish small effusions from those that are normal, but may be only 15 cc.
All effusions characterized as small in the analysis were less than 328 mL in absolute volume, Dr. Moy said in an interview. This is significant because malignant pleural effusions less than 1 cm in thickness on a lateral decubitus radiograph are a relative contraindication to thoracentesis, per American Thoracic Society guidelines (Am. J. Respir. Crit. Care Med. 2000;162:1987-2001). Pleural effusions greater than 1 cm on a lateral decubitus view have been shown to measure more than 300 mL in volume (Radiology 1994;191:681-4), he noted.
The new two-step rule is currently in use at Albert Einstein, and has been published online (Chest 2012 Nov. 8 [doi: 10.1378/chest.12-1292]).
Dr. Moy reported no conflicts of interest. A coauthor reported investments in Ortho Space and Kryon Systems.
CHICAGO – Researchers have developed and validated a simple two-step rule to quantify pleural effusion size on computed tomography – something currently not standardized.
Use of the rule significantly improved interobserver agreement, from a kappa coefficient of 0.56 to 0.79 (P less than .0001), among nine physicians ranging in skill from cardiothoracic radiologists and pulmonologists to radiology residents.
"It’s practical for any physician with access to the images and the referent tool, and conveys relevant information in terms of comparing effusion size and possibly guiding therapy," Dr. Matthew Moy said at the annual meeting of the Radiological Society of North America.
Computed tomography (CT) is highly sensitive for detecting small effusions, and differentiating pleural and parenchymal disease. The problem lies in the subjective grading of pleural effusion size and the wide variation in terminology between radiologists. These issues lead to confusion among physicians when reading CT reports or comparing effusions based on different reports, he said.
To illustrate his point, Dr. Moy showed three CT images of pleural effusions reported as being "small-moderate" to "moderate" to "large," although all three were similar in size.
In an effort to improve this communication, investigators at the Albert Einstein College of Medicine, New York, selected 34 adult CT scans, representing a wide range of pleural effusion sizes, and measured the volume of each effusion and ipsilateral hemithorax using a morphometric segmentation tool. The effusion and ipsilateral hemithorax were then manually traced on each axial slice, and the effusion volume calculated as a percent of the volume of the hemithorax to account for differences in body habitus, explained Dr. Moy.
The mean effusion volume was 37.42% of the hemithorax (range, 5.59%-89.05%). The patients’ mean age was 64 years, and 74% had undergone noncontrast CT.
Two cardiothoracic fellowship–trained radiologists then reviewed the CTs to identify qualitative and quantitative features that correlated with effusion volume. Several features emerged, but only anteroposterior (AP) quartile, maximum AP depth, and degree of atelectasis remained significant in multivariate analysis. The last was dropped, however, because it was not found to be useful for differentiating large effusions, said Dr. Moy, now with Massachusetts General Hospital in Boston.
AP quartile is calculated using the axial image where the effusion appears largest cephalad to the dome of the hemidiaphragm. The hemithorax is divided into four quartiles, and the AP quartile is then measured as the anterior-most quartile in which the effusion is seen, he explained. Maximum AP depth is measured in centimeters at the midclavicular line.
A classification rule was then developed in which first AP quartile (0%-25%) effusions are small, second quartile (25%-50%) effusions are moderate, and third or fourth AP quartile (50%-75% or 75%-100%) effusions are large. In borderline cases where it’s not easy to assess the quartile, AP depth can be measured using cutoffs of less than 3 cm (small), 3-10 cm (moderate), and more than 10 cm (large), Dr. Moy suggested.
To validate the rule, the 34 CT scans were then assessed by the nine physicians, who were not involved in the initial CT analysis. Interobserver agreement improved from a kappa of 0.59 to a kappa of 0.73 for radiology residents, 0.54 to 0.76 for pulmonologists, and 0.74 to 0.85 for cardiothoracic radiologists.
"This rule can elevate the level of agreement and consistency of both the novice radiologist and clinician to the level of cardiothoracic radiologists," Dr. Moy observed.
Session comoderator Dr. Reginald Munden, a professor of diagnostic radiology at the University of Texas M.D. Anderson Cancer Center in Houston, said in an interview, "I like anything we can do to standardize our reports, because we’re all over the place. This is particularly important, because a lot of smalls are insignificant and we don’t need to do anything with them.
"In our setting, with patients on chemotherapy, we see pleural effusions all the time," he added. "So it’s important when an effusion becomes large enough that it needs to be drained or it might be symptomatic for some other issue."
Dr. Munden went on to say that the grading scale needs to be validated in a larger population and should include a fourth subcategory, "present, but normal," to distinguish small effusions from those that are normal, but may be only 15 cc.
All effusions characterized as small in the analysis were less than 328 mL in absolute volume, Dr. Moy said in an interview. This is significant because malignant pleural effusions less than 1 cm in thickness on a lateral decubitus radiograph are a relative contraindication to thoracentesis, per American Thoracic Society guidelines (Am. J. Respir. Crit. Care Med. 2000;162:1987-2001). Pleural effusions greater than 1 cm on a lateral decubitus view have been shown to measure more than 300 mL in volume (Radiology 1994;191:681-4), he noted.
The new two-step rule is currently in use at Albert Einstein, and has been published online (Chest 2012 Nov. 8 [doi: 10.1378/chest.12-1292]).
Dr. Moy reported no conflicts of interest. A coauthor reported investments in Ortho Space and Kryon Systems.
CHICAGO – Researchers have developed and validated a simple two-step rule to quantify pleural effusion size on computed tomography – something currently not standardized.
Use of the rule significantly improved interobserver agreement, from a kappa coefficient of 0.56 to 0.79 (P less than .0001), among nine physicians ranging in skill from cardiothoracic radiologists and pulmonologists to radiology residents.
"It’s practical for any physician with access to the images and the referent tool, and conveys relevant information in terms of comparing effusion size and possibly guiding therapy," Dr. Matthew Moy said at the annual meeting of the Radiological Society of North America.
Computed tomography (CT) is highly sensitive for detecting small effusions, and differentiating pleural and parenchymal disease. The problem lies in the subjective grading of pleural effusion size and the wide variation in terminology between radiologists. These issues lead to confusion among physicians when reading CT reports or comparing effusions based on different reports, he said.
To illustrate his point, Dr. Moy showed three CT images of pleural effusions reported as being "small-moderate" to "moderate" to "large," although all three were similar in size.
In an effort to improve this communication, investigators at the Albert Einstein College of Medicine, New York, selected 34 adult CT scans, representing a wide range of pleural effusion sizes, and measured the volume of each effusion and ipsilateral hemithorax using a morphometric segmentation tool. The effusion and ipsilateral hemithorax were then manually traced on each axial slice, and the effusion volume calculated as a percent of the volume of the hemithorax to account for differences in body habitus, explained Dr. Moy.
The mean effusion volume was 37.42% of the hemithorax (range, 5.59%-89.05%). The patients’ mean age was 64 years, and 74% had undergone noncontrast CT.
Two cardiothoracic fellowship–trained radiologists then reviewed the CTs to identify qualitative and quantitative features that correlated with effusion volume. Several features emerged, but only anteroposterior (AP) quartile, maximum AP depth, and degree of atelectasis remained significant in multivariate analysis. The last was dropped, however, because it was not found to be useful for differentiating large effusions, said Dr. Moy, now with Massachusetts General Hospital in Boston.
AP quartile is calculated using the axial image where the effusion appears largest cephalad to the dome of the hemidiaphragm. The hemithorax is divided into four quartiles, and the AP quartile is then measured as the anterior-most quartile in which the effusion is seen, he explained. Maximum AP depth is measured in centimeters at the midclavicular line.
A classification rule was then developed in which first AP quartile (0%-25%) effusions are small, second quartile (25%-50%) effusions are moderate, and third or fourth AP quartile (50%-75% or 75%-100%) effusions are large. In borderline cases where it’s not easy to assess the quartile, AP depth can be measured using cutoffs of less than 3 cm (small), 3-10 cm (moderate), and more than 10 cm (large), Dr. Moy suggested.
To validate the rule, the 34 CT scans were then assessed by the nine physicians, who were not involved in the initial CT analysis. Interobserver agreement improved from a kappa of 0.59 to a kappa of 0.73 for radiology residents, 0.54 to 0.76 for pulmonologists, and 0.74 to 0.85 for cardiothoracic radiologists.
"This rule can elevate the level of agreement and consistency of both the novice radiologist and clinician to the level of cardiothoracic radiologists," Dr. Moy observed.
Session comoderator Dr. Reginald Munden, a professor of diagnostic radiology at the University of Texas M.D. Anderson Cancer Center in Houston, said in an interview, "I like anything we can do to standardize our reports, because we’re all over the place. This is particularly important, because a lot of smalls are insignificant and we don’t need to do anything with them.
"In our setting, with patients on chemotherapy, we see pleural effusions all the time," he added. "So it’s important when an effusion becomes large enough that it needs to be drained or it might be symptomatic for some other issue."
Dr. Munden went on to say that the grading scale needs to be validated in a larger population and should include a fourth subcategory, "present, but normal," to distinguish small effusions from those that are normal, but may be only 15 cc.
All effusions characterized as small in the analysis were less than 328 mL in absolute volume, Dr. Moy said in an interview. This is significant because malignant pleural effusions less than 1 cm in thickness on a lateral decubitus radiograph are a relative contraindication to thoracentesis, per American Thoracic Society guidelines (Am. J. Respir. Crit. Care Med. 2000;162:1987-2001). Pleural effusions greater than 1 cm on a lateral decubitus view have been shown to measure more than 300 mL in volume (Radiology 1994;191:681-4), he noted.
The new two-step rule is currently in use at Albert Einstein, and has been published online (Chest 2012 Nov. 8 [doi: 10.1378/chest.12-1292]).
Dr. Moy reported no conflicts of interest. A coauthor reported investments in Ortho Space and Kryon Systems.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Use of the rule significantly improved interobserver agreement from a kappa coefficient of 0.56 to 0.79 among nine cardiothoracic radiologists, pulmonologists, and radiology residents (P less than .0001).
Data Source: Analysis of 34 adult chest CT scans.
Disclosures: Dr. Moy reported no conflicts of interest. A coauthor reported investments in Ortho Space and Kryon Systems.
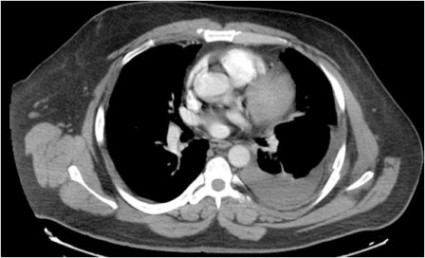
Targeted CT follow-up proposed for incidental lung nodules
CHICAGO – Limiting CT follow-up of incidental pulmonary nodules to a small area around the suspicious nodule may help resolve a common clinical dilemma and an Achilles heel of lung cancer screening, researchers suggest.
It could also reduce the radiation dose by more than 80%.
"Why should we radiate the entire thorax on follow-up?" Dr. Gregory D. Pearson asked rhetorically at the annual meeting of the Radiological Society of North America.
In the pivotal National Lung Cancer Screening Trial, annual low-dose CT reduced lung cancer deaths by 20% and all-cause mortality by 6.7% among heavy smokers, compared with traditional X-rays. Approximately 40% of the CT group, however, had findings of small, indeterminate pulmonary nodules considered suspicious for lung cancer on at least one scan, with 1.4% experiencing a complication as a result of additional testing (N. Engl. J. Med. 2011;365:395-409).

Several societies are working to devise the best protocol for further workup of detected nodules, but none have come up with the solution. The Fleischner Society, an international society for thoracic radiology, previously proposed serial follow-up imaging at intervals of less than 1 year for solid nodules smaller than 8 mm detected incidentally at nonscreening CT (Radiology 2005;237:395-400). For all semisolid nodules and ground-glass nodules at least 5 mm in size, researchers recommended a 3-month follow-up (Radiology 2005;237:395-400).
Follow-up CT scans, however, add costs and contribute to a patient’s cumulative radiation burden, said Dr. Pearson, a thoracic radiologist at New York-Presbyterian Hospital/Columbia University in New York City.
In an effort to develop a more practical solution, Dr. Pearson and his colleagues analyzed the variability in nodule location among 50 patients with subcentimeter nodules identified on CT screening for lung cancer and emphysema, and then devised a protocol for targeted CT follow-up that was validated in 50 additional patients.
Two experts and one novice reader, a medical student, independently measured the distances of the nodules from two anatomical landmarks, the lung apex and carina, on baseline and follow-up scans by cross-referencing the axial images with the CT scanogram on a PACS (picture archiving and communication system) workstation.
The interobserver variability was quite low, with mean differences of just 2-3 mm when the two experts were paired together or individually paired with the novice reader, Dr. Pearson said. Results were significantly better measuring from the apex than from the carina for two of the three reader pairings (P = .005 and .03), although the absolute difference was just 1 mm.
Interscan variability between the baseline and follow-up scans was slightly larger, averaging 5.3 mm from the apex and 6.2 mm from the carina. The maximal difference in nodule location between the two scans was 24 mm from the apex and 29 mm from the carina. Both outcomes significantly favored the measurement from the apex (P = .01).
"The measurements were highly reproducible, [there was] no benefit in measuring from the carina, and we figured that if the nodules were normally distributed throughout the lungs, that 99% of nodules should range between the mean plus 3 standard deviations, which would be about a 38-mm range," Dr. Pearson said.
To allow for a greater margin of error, measurements in the validation phase of the study were only from the ipsilateral lung apex and covered a 60-mm range. At baseline, the expert identified the nodule and placed a cut line on the scan to measure the distance from the apex. Medical students then measured the distance of the nodule from the apex on the follow-up scan, and reviewed a region of about 6 cm to determine whether the nodule would have been included in its entirety if the range of the CT scan had been narrowed to just 60 mm.
"The results here are pretty simple; 100% of the nodules in follow-up were scanned in their entirety," Dr. Pearson said.
The average craniocaudal coverage on follow-up CT was 363 mm.
By using a targeted 60-mm range, the average craniocaudal coverage and radiation dose would be reduced by 83%, although the actual dose reduction will depend on the location of the nodules, he added.
In addition, use of targeted CTs would cut interpretation and report times due to the decreased anatomical coverage, would not disrupt work flow, and would require minimal technologist training.
Still, the technique needs to be validated prospectively in larger groups, and would require buy-in from radiologists, medical societies, and Medicare and private insurers, Dr. Pearson said.

Session comoderator Dr. H. Page McAdams, division chief of cardiac and thoracic imaging at Duke University in Durham, N.C., said in an interview that the concept is intriguing, but raises a number of potential societal, reimbursement, and medical-legal issues. For example, what happens if a physician does a limited follow-up CT and misses a new nodule? The other question is, how many patients in these screening populations really have a simple nodule? If most of them have multiple nodules, it would obviate the benefits of targeted CT.
"I think it’s a great idea, but there’s a lot of work that still needs to be done in terms of answering those particular questions," Dr. McAdams said.
Roughly 75% of the 100 consecutive patients in the study had a single nodule, Dr. Pearson told this publication.
Dr. McAdams reported a research grant from General Electric, serving as a consultant for American College of Radiology Image Metrix, and working as an author for Reed Elsevier and UpToDate Inc.
CHICAGO – Limiting CT follow-up of incidental pulmonary nodules to a small area around the suspicious nodule may help resolve a common clinical dilemma and an Achilles heel of lung cancer screening, researchers suggest.
It could also reduce the radiation dose by more than 80%.
"Why should we radiate the entire thorax on follow-up?" Dr. Gregory D. Pearson asked rhetorically at the annual meeting of the Radiological Society of North America.
In the pivotal National Lung Cancer Screening Trial, annual low-dose CT reduced lung cancer deaths by 20% and all-cause mortality by 6.7% among heavy smokers, compared with traditional X-rays. Approximately 40% of the CT group, however, had findings of small, indeterminate pulmonary nodules considered suspicious for lung cancer on at least one scan, with 1.4% experiencing a complication as a result of additional testing (N. Engl. J. Med. 2011;365:395-409).
Several societies are working to devise the best protocol for further workup of detected nodules, but none have come up with the solution. The Fleischner Society, an international society for thoracic radiology, previously proposed serial follow-up imaging at intervals of less than 1 year for solid nodules smaller than 8 mm detected incidentally at nonscreening CT (Radiology 2005;237:395-400). For all semisolid nodules and ground-glass nodules at least 5 mm in size, researchers recommended a 3-month follow-up (Radiology 2005;237:395-400).
Follow-up CT scans, however, add costs and contribute to a patient’s cumulative radiation burden, said Dr. Pearson, a thoracic radiologist at New York-Presbyterian Hospital/Columbia University in New York City.
In an effort to develop a more practical solution, Dr. Pearson and his colleagues analyzed the variability in nodule location among 50 patients with subcentimeter nodules identified on CT screening for lung cancer and emphysema, and then devised a protocol for targeted CT follow-up that was validated in 50 additional patients.
Two experts and one novice reader, a medical student, independently measured the distances of the nodules from two anatomical landmarks, the lung apex and carina, on baseline and follow-up scans by cross-referencing the axial images with the CT scanogram on a PACS (picture archiving and communication system) workstation.
The interobserver variability was quite low, with mean differences of just 2-3 mm when the two experts were paired together or individually paired with the novice reader, Dr. Pearson said. Results were significantly better measuring from the apex than from the carina for two of the three reader pairings (P = .005 and .03), although the absolute difference was just 1 mm.
Interscan variability between the baseline and follow-up scans was slightly larger, averaging 5.3 mm from the apex and 6.2 mm from the carina. The maximal difference in nodule location between the two scans was 24 mm from the apex and 29 mm from the carina. Both outcomes significantly favored the measurement from the apex (P = .01).
"The measurements were highly reproducible, [there was] no benefit in measuring from the carina, and we figured that if the nodules were normally distributed throughout the lungs, that 99% of nodules should range between the mean plus 3 standard deviations, which would be about a 38-mm range," Dr. Pearson said.
To allow for a greater margin of error, measurements in the validation phase of the study were only from the ipsilateral lung apex and covered a 60-mm range. At baseline, the expert identified the nodule and placed a cut line on the scan to measure the distance from the apex. Medical students then measured the distance of the nodule from the apex on the follow-up scan, and reviewed a region of about 6 cm to determine whether the nodule would have been included in its entirety if the range of the CT scan had been narrowed to just 60 mm.
"The results here are pretty simple; 100% of the nodules in follow-up were scanned in their entirety," Dr. Pearson said.
The average craniocaudal coverage on follow-up CT was 363 mm.
By using a targeted 60-mm range, the average craniocaudal coverage and radiation dose would be reduced by 83%, although the actual dose reduction will depend on the location of the nodules, he added.
In addition, use of targeted CTs would cut interpretation and report times due to the decreased anatomical coverage, would not disrupt work flow, and would require minimal technologist training.
Still, the technique needs to be validated prospectively in larger groups, and would require buy-in from radiologists, medical societies, and Medicare and private insurers, Dr. Pearson said.
Session comoderator Dr. H. Page McAdams, division chief of cardiac and thoracic imaging at Duke University in Durham, N.C., said in an interview that the concept is intriguing, but raises a number of potential societal, reimbursement, and medical-legal issues. For example, what happens if a physician does a limited follow-up CT and misses a new nodule? The other question is, how many patients in these screening populations really have a simple nodule? If most of them have multiple nodules, it would obviate the benefits of targeted CT.
"I think it’s a great idea, but there’s a lot of work that still needs to be done in terms of answering those particular questions," Dr. McAdams said.
Roughly 75% of the 100 consecutive patients in the study had a single nodule, Dr. Pearson told this publication.
Dr. McAdams reported a research grant from General Electric, serving as a consultant for American College of Radiology Image Metrix, and working as an author for Reed Elsevier and UpToDate Inc.
CHICAGO – Limiting CT follow-up of incidental pulmonary nodules to a small area around the suspicious nodule may help resolve a common clinical dilemma and an Achilles heel of lung cancer screening, researchers suggest.
It could also reduce the radiation dose by more than 80%.
"Why should we radiate the entire thorax on follow-up?" Dr. Gregory D. Pearson asked rhetorically at the annual meeting of the Radiological Society of North America.
In the pivotal National Lung Cancer Screening Trial, annual low-dose CT reduced lung cancer deaths by 20% and all-cause mortality by 6.7% among heavy smokers, compared with traditional X-rays. Approximately 40% of the CT group, however, had findings of small, indeterminate pulmonary nodules considered suspicious for lung cancer on at least one scan, with 1.4% experiencing a complication as a result of additional testing (N. Engl. J. Med. 2011;365:395-409).
Several societies are working to devise the best protocol for further workup of detected nodules, but none have come up with the solution. The Fleischner Society, an international society for thoracic radiology, previously proposed serial follow-up imaging at intervals of less than 1 year for solid nodules smaller than 8 mm detected incidentally at nonscreening CT (Radiology 2005;237:395-400). For all semisolid nodules and ground-glass nodules at least 5 mm in size, researchers recommended a 3-month follow-up (Radiology 2005;237:395-400).
Follow-up CT scans, however, add costs and contribute to a patient’s cumulative radiation burden, said Dr. Pearson, a thoracic radiologist at New York-Presbyterian Hospital/Columbia University in New York City.
In an effort to develop a more practical solution, Dr. Pearson and his colleagues analyzed the variability in nodule location among 50 patients with subcentimeter nodules identified on CT screening for lung cancer and emphysema, and then devised a protocol for targeted CT follow-up that was validated in 50 additional patients.
Two experts and one novice reader, a medical student, independently measured the distances of the nodules from two anatomical landmarks, the lung apex and carina, on baseline and follow-up scans by cross-referencing the axial images with the CT scanogram on a PACS (picture archiving and communication system) workstation.
The interobserver variability was quite low, with mean differences of just 2-3 mm when the two experts were paired together or individually paired with the novice reader, Dr. Pearson said. Results were significantly better measuring from the apex than from the carina for two of the three reader pairings (P = .005 and .03), although the absolute difference was just 1 mm.
Interscan variability between the baseline and follow-up scans was slightly larger, averaging 5.3 mm from the apex and 6.2 mm from the carina. The maximal difference in nodule location between the two scans was 24 mm from the apex and 29 mm from the carina. Both outcomes significantly favored the measurement from the apex (P = .01).
"The measurements were highly reproducible, [there was] no benefit in measuring from the carina, and we figured that if the nodules were normally distributed throughout the lungs, that 99% of nodules should range between the mean plus 3 standard deviations, which would be about a 38-mm range," Dr. Pearson said.
To allow for a greater margin of error, measurements in the validation phase of the study were only from the ipsilateral lung apex and covered a 60-mm range. At baseline, the expert identified the nodule and placed a cut line on the scan to measure the distance from the apex. Medical students then measured the distance of the nodule from the apex on the follow-up scan, and reviewed a region of about 6 cm to determine whether the nodule would have been included in its entirety if the range of the CT scan had been narrowed to just 60 mm.
"The results here are pretty simple; 100% of the nodules in follow-up were scanned in their entirety," Dr. Pearson said.
The average craniocaudal coverage on follow-up CT was 363 mm.
By using a targeted 60-mm range, the average craniocaudal coverage and radiation dose would be reduced by 83%, although the actual dose reduction will depend on the location of the nodules, he added.
In addition, use of targeted CTs would cut interpretation and report times due to the decreased anatomical coverage, would not disrupt work flow, and would require minimal technologist training.
Still, the technique needs to be validated prospectively in larger groups, and would require buy-in from radiologists, medical societies, and Medicare and private insurers, Dr. Pearson said.
Session comoderator Dr. H. Page McAdams, division chief of cardiac and thoracic imaging at Duke University in Durham, N.C., said in an interview that the concept is intriguing, but raises a number of potential societal, reimbursement, and medical-legal issues. For example, what happens if a physician does a limited follow-up CT and misses a new nodule? The other question is, how many patients in these screening populations really have a simple nodule? If most of them have multiple nodules, it would obviate the benefits of targeted CT.
"I think it’s a great idea, but there’s a lot of work that still needs to be done in terms of answering those particular questions," Dr. McAdams said.
Roughly 75% of the 100 consecutive patients in the study had a single nodule, Dr. Pearson told this publication.
Dr. McAdams reported a research grant from General Electric, serving as a consultant for American College of Radiology Image Metrix, and working as an author for Reed Elsevier and UpToDate Inc.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: By using a targeted 60-mm range during CT follow-up of suspicious nodules, the average craniocaudal coverage and radiation dose would be reduced by 83%.
Data Source: Two-phase validation study in 100 consecutive patients with incidental subcentimeter lung nodules.
Disclosures: Dr. McAdams reported a research grant from General Electric, serving as a consultant for American College of Radiology Image Metrix, and working as an author for Reed Elsevier and UpToDate Inc.

Medicare Imaging Payments Fell 21% Since 2006
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."

Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."
Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."
Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Medicare Part B payments for noninvasive diagnostic imaging rose 101% from $5.9 million in 2000 to $11.9 billion in 2006, before falling 21% to $9.45 billion in 2010.
Data Source: Analysis of the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010.
Disclosures: Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
Targeting new myeloma pathway pays off with ARRY-520
ATLANTA – The experimental drug ARRY-520, the first kinesin spindle protein inhibitor in multiple myeloma, prompted responses in nearly one-fourth of heavily pretreated and triple-refractory patients in a phase II study.
The overall response rate to single-agent ARRY-520 was 16% in patients with a median of six prior regimens. It reached 22% when combined with dexamethasone in patients with a median of 10 prior regimens – all but one of whom was refractory to lenalidomide (Revlimid), bortezomib (Velcade), and dexamethasone (Decadron), Dr. Jatin Shah reported at the annual meeting of the American Society of Hematology.
Kinesin spindle protein (KSP) is a microtubule motor protein required for mitosis and separation of the mitotic spindle pole into a bipolar spindle pole. Inhibition of KSP prevents formation of the bipolar spindle, leading to cell death. Preclinical work shows that ARRY-520 also down-regulates myeloid cell leukemia-1 levels, a mechanism for dexamethasone resistance.

The investigators also identified a potential biomarker called alpha 1-acid glycoprotein (AAG) that may predict how well patients respond to ARRY-520.
Selecting patients by AAG serum results increased the response rate to 33% in the combination group, a population with an unmet clinical need, said Dr. Shah of the University of Texas M.D. Anderson Cancer Center in Houston.
"The assay isn’t a fancy test; it can be done actually at any commercial lab," he said in an interview. "The key is to validate that the labs are doing the assay in the same way."
Duration of response noted
Dr. Antonio Palumbo, chief of the myeloma unit at the University Hospital of Torino, Italy, who comoderated the session, said in an interview that ARRY-520 is "certainly an exciting new agent" in multiple myeloma, given its novel therapeutic target, partial responses of 20%-30% in such advanced disease and a potential biomarker.
"I think the biomarker was important and probably also the durability because this type of drug may have a major role in durability, more than on response," he said.
Median duration of response was 8.6 months with ARRY-520 monotherapy (range 1.4-20 months) and 5.4 months with combination therapy (2.5-9 months).
Dr. Angela Dispenzieri, hematologist and professor of medicine at Mayo Clinic, Rochester, Minn., and a member of the meeting’s scientific committee, was more effusive in her assessment of the results.
"Actually, I think it’s the best thing so far at ASH," she said after the session on the penultimate day of the meeting. "It’s novel.
"This is a new class and it actually has single-agent activity. That’s the beginning and that is very important. I was really impressed, and I’m really cynical."
Both Dr. Dispenzieri and Dr. Palumbo said results should be better if ARRY-520 is combined with other agents such as bortezomib, proteasome inhibitors or immunomodulatory drugs (IMiDs).
Preliminary results reported in a poster at the meeting show that one of six evaluable patients achieved a near complete response and four had stable disease after completing at least one cycle of ARRY-520 plus the proteasome inhibitor carfilzomib (Kyprolis), Dr. Shah reported.

"We’re already starting to see a signal there, and we’re going to go with IMiDs next," he said.
A phase Ib combination trial with bortezomib is also underway.
Fifty patients in two cohorts
The current phase II study included 32 patients who received single-agent ARRY-520 at 1.5 mg/m2 on days 1 and 2 every 2 weeks and 18 patients who also received low-dose dexamethasone 40 mg once weekly. Both groups received granulocyte–colony stimulating factor support.
The first cohort had relapsed and/or refractory multiple myeloma after receiving at least two prior rounds of therapy (range 2-19) that included bortezomib and an IMiD. Roughly half were bortezomib refractory (53%) and 41% were triple refractory.
Cohort two had also received at least two prior regimens (range 5-13), but progressed during or within 60 days of their last regimen, was refractory to lenalidomide, bortezomib, and dexamethasone (except one dexamethasone-refractory patient) and had received adequate prior alkylator therapy. High-risk cytogenetics were present in 17% vs. 9% of cohort one.

In cohort one, there were 5 partial responses, 6 minor plus partial responses, and 14 cases of stable disease, Dr. Shah said. The median time to response was 4.4 months and median progression-free survival was 3.7 months. The cohort had very durable responses at a median of 8.6 months (range 1.4-20 months), and an overall survival of 19 months, he said.
In cohort two, there were 4 partial responses, 6 minimal plus partial responses and 5 patients with stable disease. The median time on treatment about doubled from 2.1 in cohort one to 3.9 months, with a shorter time to response of 3.4 months. The median duration of response was shorter at 5.4 months, "but again this was a very different patient population," Dr. Shah said.
An analysis of baseline AAG levels in 45 patients revealed that patients with low AAG remained on study longer than did those with high AAG in both cohort one (3.4 months vs. 1.7 months) and cohort two (6.2 months vs. 1.6 months). Moreover, 24% of low-AAG patients on monotherapy and 22% on combination therapy achieved at least a partial response, whereas no patient with high AAG levels did so.
In vitro work has shown that increasing levels of AAG result in increased half maximal inhibitory concentration (IC50) of ARRY-520, suggesting that patients with elevated AAG may have subtherapeutic exposure to the drug, Dr. Shah explained. AAG does not bind to other standard multiple myeloma agents on the market, and is not correlated with prognostic markers in myeloma.
Nonhematologic adverse events were very low, including one case each of grade 4 fatigue and hypokalemia, and two cases of grade 4 pneumonia.
As expected from the biology of the drug, grade 3/4 hematologic events were more common, but generally reversible and not observed to be cumulative out to 3 years of therapy, Dr. Shah said. Grade 4 neutropenia, thrombocytopenia, and anemia were present in 28%, 25%, and 6% of patients in cohort one and in 38%, 19% and 5% of cohort two, respectively. Febrile neutropenia was grade 3 only, and reported in just one patient in each group, he noted.
Dr. Shah and coauthors reported relationships with study sponsor Array BioPharma, which is developing ARRY-520. Dr. Palumbo disclosed relationships with other companies.
Dr. Antonio Palumbo,
ATLANTA – The experimental drug ARRY-520, the first kinesin spindle protein inhibitor in multiple myeloma, prompted responses in nearly one-fourth of heavily pretreated and triple-refractory patients in a phase II study.
The overall response rate to single-agent ARRY-520 was 16% in patients with a median of six prior regimens. It reached 22% when combined with dexamethasone in patients with a median of 10 prior regimens – all but one of whom was refractory to lenalidomide (Revlimid), bortezomib (Velcade), and dexamethasone (Decadron), Dr. Jatin Shah reported at the annual meeting of the American Society of Hematology.
Kinesin spindle protein (KSP) is a microtubule motor protein required for mitosis and separation of the mitotic spindle pole into a bipolar spindle pole. Inhibition of KSP prevents formation of the bipolar spindle, leading to cell death. Preclinical work shows that ARRY-520 also down-regulates myeloid cell leukemia-1 levels, a mechanism for dexamethasone resistance.
The investigators also identified a potential biomarker called alpha 1-acid glycoprotein (AAG) that may predict how well patients respond to ARRY-520.
Selecting patients by AAG serum results increased the response rate to 33% in the combination group, a population with an unmet clinical need, said Dr. Shah of the University of Texas M.D. Anderson Cancer Center in Houston.
"The assay isn’t a fancy test; it can be done actually at any commercial lab," he said in an interview. "The key is to validate that the labs are doing the assay in the same way."
Duration of response noted
Dr. Antonio Palumbo, chief of the myeloma unit at the University Hospital of Torino, Italy, who comoderated the session, said in an interview that ARRY-520 is "certainly an exciting new agent" in multiple myeloma, given its novel therapeutic target, partial responses of 20%-30% in such advanced disease and a potential biomarker.
"I think the biomarker was important and probably also the durability because this type of drug may have a major role in durability, more than on response," he said.
Median duration of response was 8.6 months with ARRY-520 monotherapy (range 1.4-20 months) and 5.4 months with combination therapy (2.5-9 months).
Dr. Angela Dispenzieri, hematologist and professor of medicine at Mayo Clinic, Rochester, Minn., and a member of the meeting’s scientific committee, was more effusive in her assessment of the results.
"Actually, I think it’s the best thing so far at ASH," she said after the session on the penultimate day of the meeting. "It’s novel.
"This is a new class and it actually has single-agent activity. That’s the beginning and that is very important. I was really impressed, and I’m really cynical."
Both Dr. Dispenzieri and Dr. Palumbo said results should be better if ARRY-520 is combined with other agents such as bortezomib, proteasome inhibitors or immunomodulatory drugs (IMiDs).
Preliminary results reported in a poster at the meeting show that one of six evaluable patients achieved a near complete response and four had stable disease after completing at least one cycle of ARRY-520 plus the proteasome inhibitor carfilzomib (Kyprolis), Dr. Shah reported.
"We’re already starting to see a signal there, and we’re going to go with IMiDs next," he said.
A phase Ib combination trial with bortezomib is also underway.
Fifty patients in two cohorts
The current phase II study included 32 patients who received single-agent ARRY-520 at 1.5 mg/m2 on days 1 and 2 every 2 weeks and 18 patients who also received low-dose dexamethasone 40 mg once weekly. Both groups received granulocyte–colony stimulating factor support.
The first cohort had relapsed and/or refractory multiple myeloma after receiving at least two prior rounds of therapy (range 2-19) that included bortezomib and an IMiD. Roughly half were bortezomib refractory (53%) and 41% were triple refractory.
Cohort two had also received at least two prior regimens (range 5-13), but progressed during or within 60 days of their last regimen, was refractory to lenalidomide, bortezomib, and dexamethasone (except one dexamethasone-refractory patient) and had received adequate prior alkylator therapy. High-risk cytogenetics were present in 17% vs. 9% of cohort one.
In cohort one, there were 5 partial responses, 6 minor plus partial responses, and 14 cases of stable disease, Dr. Shah said. The median time to response was 4.4 months and median progression-free survival was 3.7 months. The cohort had very durable responses at a median of 8.6 months (range 1.4-20 months), and an overall survival of 19 months, he said.
In cohort two, there were 4 partial responses, 6 minimal plus partial responses and 5 patients with stable disease. The median time on treatment about doubled from 2.1 in cohort one to 3.9 months, with a shorter time to response of 3.4 months. The median duration of response was shorter at 5.4 months, "but again this was a very different patient population," Dr. Shah said.
An analysis of baseline AAG levels in 45 patients revealed that patients with low AAG remained on study longer than did those with high AAG in both cohort one (3.4 months vs. 1.7 months) and cohort two (6.2 months vs. 1.6 months). Moreover, 24% of low-AAG patients on monotherapy and 22% on combination therapy achieved at least a partial response, whereas no patient with high AAG levels did so.
In vitro work has shown that increasing levels of AAG result in increased half maximal inhibitory concentration (IC50) of ARRY-520, suggesting that patients with elevated AAG may have subtherapeutic exposure to the drug, Dr. Shah explained. AAG does not bind to other standard multiple myeloma agents on the market, and is not correlated with prognostic markers in myeloma.
Nonhematologic adverse events were very low, including one case each of grade 4 fatigue and hypokalemia, and two cases of grade 4 pneumonia.
As expected from the biology of the drug, grade 3/4 hematologic events were more common, but generally reversible and not observed to be cumulative out to 3 years of therapy, Dr. Shah said. Grade 4 neutropenia, thrombocytopenia, and anemia were present in 28%, 25%, and 6% of patients in cohort one and in 38%, 19% and 5% of cohort two, respectively. Febrile neutropenia was grade 3 only, and reported in just one patient in each group, he noted.
Dr. Shah and coauthors reported relationships with study sponsor Array BioPharma, which is developing ARRY-520. Dr. Palumbo disclosed relationships with other companies.
ATLANTA – The experimental drug ARRY-520, the first kinesin spindle protein inhibitor in multiple myeloma, prompted responses in nearly one-fourth of heavily pretreated and triple-refractory patients in a phase II study.
The overall response rate to single-agent ARRY-520 was 16% in patients with a median of six prior regimens. It reached 22% when combined with dexamethasone in patients with a median of 10 prior regimens – all but one of whom was refractory to lenalidomide (Revlimid), bortezomib (Velcade), and dexamethasone (Decadron), Dr. Jatin Shah reported at the annual meeting of the American Society of Hematology.
Kinesin spindle protein (KSP) is a microtubule motor protein required for mitosis and separation of the mitotic spindle pole into a bipolar spindle pole. Inhibition of KSP prevents formation of the bipolar spindle, leading to cell death. Preclinical work shows that ARRY-520 also down-regulates myeloid cell leukemia-1 levels, a mechanism for dexamethasone resistance.
The investigators also identified a potential biomarker called alpha 1-acid glycoprotein (AAG) that may predict how well patients respond to ARRY-520.
Selecting patients by AAG serum results increased the response rate to 33% in the combination group, a population with an unmet clinical need, said Dr. Shah of the University of Texas M.D. Anderson Cancer Center in Houston.
"The assay isn’t a fancy test; it can be done actually at any commercial lab," he said in an interview. "The key is to validate that the labs are doing the assay in the same way."
Duration of response noted
Dr. Antonio Palumbo, chief of the myeloma unit at the University Hospital of Torino, Italy, who comoderated the session, said in an interview that ARRY-520 is "certainly an exciting new agent" in multiple myeloma, given its novel therapeutic target, partial responses of 20%-30% in such advanced disease and a potential biomarker.
"I think the biomarker was important and probably also the durability because this type of drug may have a major role in durability, more than on response," he said.
Median duration of response was 8.6 months with ARRY-520 monotherapy (range 1.4-20 months) and 5.4 months with combination therapy (2.5-9 months).
Dr. Angela Dispenzieri, hematologist and professor of medicine at Mayo Clinic, Rochester, Minn., and a member of the meeting’s scientific committee, was more effusive in her assessment of the results.
"Actually, I think it’s the best thing so far at ASH," she said after the session on the penultimate day of the meeting. "It’s novel.
"This is a new class and it actually has single-agent activity. That’s the beginning and that is very important. I was really impressed, and I’m really cynical."
Both Dr. Dispenzieri and Dr. Palumbo said results should be better if ARRY-520 is combined with other agents such as bortezomib, proteasome inhibitors or immunomodulatory drugs (IMiDs).
Preliminary results reported in a poster at the meeting show that one of six evaluable patients achieved a near complete response and four had stable disease after completing at least one cycle of ARRY-520 plus the proteasome inhibitor carfilzomib (Kyprolis), Dr. Shah reported.
"We’re already starting to see a signal there, and we’re going to go with IMiDs next," he said.
A phase Ib combination trial with bortezomib is also underway.
Fifty patients in two cohorts
The current phase II study included 32 patients who received single-agent ARRY-520 at 1.5 mg/m2 on days 1 and 2 every 2 weeks and 18 patients who also received low-dose dexamethasone 40 mg once weekly. Both groups received granulocyte–colony stimulating factor support.
The first cohort had relapsed and/or refractory multiple myeloma after receiving at least two prior rounds of therapy (range 2-19) that included bortezomib and an IMiD. Roughly half were bortezomib refractory (53%) and 41% were triple refractory.
Cohort two had also received at least two prior regimens (range 5-13), but progressed during or within 60 days of their last regimen, was refractory to lenalidomide, bortezomib, and dexamethasone (except one dexamethasone-refractory patient) and had received adequate prior alkylator therapy. High-risk cytogenetics were present in 17% vs. 9% of cohort one.
In cohort one, there were 5 partial responses, 6 minor plus partial responses, and 14 cases of stable disease, Dr. Shah said. The median time to response was 4.4 months and median progression-free survival was 3.7 months. The cohort had very durable responses at a median of 8.6 months (range 1.4-20 months), and an overall survival of 19 months, he said.
In cohort two, there were 4 partial responses, 6 minimal plus partial responses and 5 patients with stable disease. The median time on treatment about doubled from 2.1 in cohort one to 3.9 months, with a shorter time to response of 3.4 months. The median duration of response was shorter at 5.4 months, "but again this was a very different patient population," Dr. Shah said.
An analysis of baseline AAG levels in 45 patients revealed that patients with low AAG remained on study longer than did those with high AAG in both cohort one (3.4 months vs. 1.7 months) and cohort two (6.2 months vs. 1.6 months). Moreover, 24% of low-AAG patients on monotherapy and 22% on combination therapy achieved at least a partial response, whereas no patient with high AAG levels did so.
In vitro work has shown that increasing levels of AAG result in increased half maximal inhibitory concentration (IC50) of ARRY-520, suggesting that patients with elevated AAG may have subtherapeutic exposure to the drug, Dr. Shah explained. AAG does not bind to other standard multiple myeloma agents on the market, and is not correlated with prognostic markers in myeloma.
Nonhematologic adverse events were very low, including one case each of grade 4 fatigue and hypokalemia, and two cases of grade 4 pneumonia.
As expected from the biology of the drug, grade 3/4 hematologic events were more common, but generally reversible and not observed to be cumulative out to 3 years of therapy, Dr. Shah said. Grade 4 neutropenia, thrombocytopenia, and anemia were present in 28%, 25%, and 6% of patients in cohort one and in 38%, 19% and 5% of cohort two, respectively. Febrile neutropenia was grade 3 only, and reported in just one patient in each group, he noted.
Dr. Shah and coauthors reported relationships with study sponsor Array BioPharma, which is developing ARRY-520. Dr. Palumbo disclosed relationships with other companies.
Dr. Antonio Palumbo,
Dr. Antonio Palumbo,
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: The overall response rate to single-agent ARRY-520 was 16% in patients with a median of 6 prior regimens and 22% when combined with dexamethasone in patients with a median of 10 prior regimens.
Data Source: Phase II study of ARRY-520 mono and combination therapy.
Disclosures: Dr. Shah and coauthors reported relationships with study sponsor Array BioPharma, which is developing ARRY-520. Dr. Palumbo disclosed relationships with other companies.
