User login
Hysterectomy Trendelenburg position: Less may be more
LAS VEGAS – Significantly reducing the degree of Trendelenburg position during robotic-assisted hysterectomy did not increase operative time and cut blood loss in half in a small retrospective analysis.
Surgeons spent an average of 66.5 minutes (range, 38-110 minutes) at the console when patients were placed in a minimum Trendelenburg position, compared with 79 minutes (range, 30-180 minutes) with a steep Trendelenburg position.
The difference in this primary outcome failed to achieve statistical significance (P = .105); however, the use of a minimum Trendelenburg position significantly reduced the average estimated blood loss from 101.3 mL to 50 mL (P = .007), Dr. Kelli Sasada reported at the 41st AAGL Global Congress.
A minimum degree of Trendelenburg position can be as effective as a steep Trendelenburg position in achieving adequate surgical exposure, thereby allowing safe completion of hysterectomy without increasing operative time, she said.
A steep Trendelenburg position, defined as at least 20 degrees in the anesthesia literature, improves the view of the surgical area during pelvic surgery by taking advantage of gravity to retract the bowels. It is common practice to use this approach during robotic-assisted hysterectomy because the patient’s position cannot conveniently be adjusted once the robot is docked, Dr. Sasada explained.
A steep Trendelenburg position, however, is often fraught with complications that can be severe and permanent, such as neural and retinal injuries, the patient moving or sliding off the table, ventilation concerns including airway access for the anesthesia provider, poor cardiopulmonary status, and alopecia, she added.
To explore the minimum degree of Trendelenburg necessary to complete the surgery safely, Dr. Sasada and her associate, Dr. Linda Mihalov, at Virginia Mason Medical Center in Seattle, took advantage of a new iPad app called clinometer HD (by plaincode) among 50 women undergoing da Vinci robotic-assisted benign total laparoscopic hysterectomy with or without bilateral salpingo-oophorectomy. Patients were secured in the dorsal lithotomy position, the abdomen was entered laparoscopically, and a brief survey was conducted to assess the size, position, and accessibility of the pelvic organs. The degree of Trendelenburg was determined by the surgeon and the iPad clinometer HD placed on the bed rail to measure the table tilt. The robot was then docked parallel to the patient’s side, and the surgery completed.
A steep Trendelenburg, defined as 30 degrees, was used in 38 women, and a minimum degree of Trendelenburg averaging 16.6 degrees (range, 13.8-19 degrees) used in 12 women, said Dr. Sasada, now with United Hospital System, St. Catherine’s Medical Center in Pleasant Prairie, Wis.
The average uterine weight was not significantly different between the steep and minimum Trendelenburg groups (215.4 g vs. 173.6 g; P = .21).
Body mass index also was similar at 28.5 kg/m2 vs. 25 kg/m2 (P = .071), with a wide range in both groups, she said.
There was one case of intraoperative bleeding (500 cc) and no postoperative complications in the steep Trendelenburg group, and one case of postoperative urinary retention and no intraoperative complications in the minimum Trendelenburg group.
During a discussion of the study, Dr. Sasada said it’s possible that the lower blood loss with the minimum Trendelenburg position could be due to chance, but that both surgeries were completed with the same four incisions and without bowel prep.
Dr. Sasada currently uses a minimum Trendelenburg position and an iPad when performing robotic-assisted hysterectomy and other pelvic surgeries, but not in all cases, as some OR beds have built-in clinometers. The advantage of the iPad technology is that it offers "ease of use in the OR by anesthesia or nursing staff, and reproducibility between OR beds," she said in an interview.
Dr. Sasada and Dr. Mihalov reported no relevant financial disclosures.
LAS VEGAS – Significantly reducing the degree of Trendelenburg position during robotic-assisted hysterectomy did not increase operative time and cut blood loss in half in a small retrospective analysis.
Surgeons spent an average of 66.5 minutes (range, 38-110 minutes) at the console when patients were placed in a minimum Trendelenburg position, compared with 79 minutes (range, 30-180 minutes) with a steep Trendelenburg position.
The difference in this primary outcome failed to achieve statistical significance (P = .105); however, the use of a minimum Trendelenburg position significantly reduced the average estimated blood loss from 101.3 mL to 50 mL (P = .007), Dr. Kelli Sasada reported at the 41st AAGL Global Congress.
A minimum degree of Trendelenburg position can be as effective as a steep Trendelenburg position in achieving adequate surgical exposure, thereby allowing safe completion of hysterectomy without increasing operative time, she said.
A steep Trendelenburg position, defined as at least 20 degrees in the anesthesia literature, improves the view of the surgical area during pelvic surgery by taking advantage of gravity to retract the bowels. It is common practice to use this approach during robotic-assisted hysterectomy because the patient’s position cannot conveniently be adjusted once the robot is docked, Dr. Sasada explained.
A steep Trendelenburg position, however, is often fraught with complications that can be severe and permanent, such as neural and retinal injuries, the patient moving or sliding off the table, ventilation concerns including airway access for the anesthesia provider, poor cardiopulmonary status, and alopecia, she added.
To explore the minimum degree of Trendelenburg necessary to complete the surgery safely, Dr. Sasada and her associate, Dr. Linda Mihalov, at Virginia Mason Medical Center in Seattle, took advantage of a new iPad app called clinometer HD (by plaincode) among 50 women undergoing da Vinci robotic-assisted benign total laparoscopic hysterectomy with or without bilateral salpingo-oophorectomy. Patients were secured in the dorsal lithotomy position, the abdomen was entered laparoscopically, and a brief survey was conducted to assess the size, position, and accessibility of the pelvic organs. The degree of Trendelenburg was determined by the surgeon and the iPad clinometer HD placed on the bed rail to measure the table tilt. The robot was then docked parallel to the patient’s side, and the surgery completed.
A steep Trendelenburg, defined as 30 degrees, was used in 38 women, and a minimum degree of Trendelenburg averaging 16.6 degrees (range, 13.8-19 degrees) used in 12 women, said Dr. Sasada, now with United Hospital System, St. Catherine’s Medical Center in Pleasant Prairie, Wis.
The average uterine weight was not significantly different between the steep and minimum Trendelenburg groups (215.4 g vs. 173.6 g; P = .21).
Body mass index also was similar at 28.5 kg/m2 vs. 25 kg/m2 (P = .071), with a wide range in both groups, she said.
There was one case of intraoperative bleeding (500 cc) and no postoperative complications in the steep Trendelenburg group, and one case of postoperative urinary retention and no intraoperative complications in the minimum Trendelenburg group.
During a discussion of the study, Dr. Sasada said it’s possible that the lower blood loss with the minimum Trendelenburg position could be due to chance, but that both surgeries were completed with the same four incisions and without bowel prep.
Dr. Sasada currently uses a minimum Trendelenburg position and an iPad when performing robotic-assisted hysterectomy and other pelvic surgeries, but not in all cases, as some OR beds have built-in clinometers. The advantage of the iPad technology is that it offers "ease of use in the OR by anesthesia or nursing staff, and reproducibility between OR beds," she said in an interview.
Dr. Sasada and Dr. Mihalov reported no relevant financial disclosures.
LAS VEGAS – Significantly reducing the degree of Trendelenburg position during robotic-assisted hysterectomy did not increase operative time and cut blood loss in half in a small retrospective analysis.
Surgeons spent an average of 66.5 minutes (range, 38-110 minutes) at the console when patients were placed in a minimum Trendelenburg position, compared with 79 minutes (range, 30-180 minutes) with a steep Trendelenburg position.
The difference in this primary outcome failed to achieve statistical significance (P = .105); however, the use of a minimum Trendelenburg position significantly reduced the average estimated blood loss from 101.3 mL to 50 mL (P = .007), Dr. Kelli Sasada reported at the 41st AAGL Global Congress.
A minimum degree of Trendelenburg position can be as effective as a steep Trendelenburg position in achieving adequate surgical exposure, thereby allowing safe completion of hysterectomy without increasing operative time, she said.
A steep Trendelenburg position, defined as at least 20 degrees in the anesthesia literature, improves the view of the surgical area during pelvic surgery by taking advantage of gravity to retract the bowels. It is common practice to use this approach during robotic-assisted hysterectomy because the patient’s position cannot conveniently be adjusted once the robot is docked, Dr. Sasada explained.
A steep Trendelenburg position, however, is often fraught with complications that can be severe and permanent, such as neural and retinal injuries, the patient moving or sliding off the table, ventilation concerns including airway access for the anesthesia provider, poor cardiopulmonary status, and alopecia, she added.
To explore the minimum degree of Trendelenburg necessary to complete the surgery safely, Dr. Sasada and her associate, Dr. Linda Mihalov, at Virginia Mason Medical Center in Seattle, took advantage of a new iPad app called clinometer HD (by plaincode) among 50 women undergoing da Vinci robotic-assisted benign total laparoscopic hysterectomy with or without bilateral salpingo-oophorectomy. Patients were secured in the dorsal lithotomy position, the abdomen was entered laparoscopically, and a brief survey was conducted to assess the size, position, and accessibility of the pelvic organs. The degree of Trendelenburg was determined by the surgeon and the iPad clinometer HD placed on the bed rail to measure the table tilt. The robot was then docked parallel to the patient’s side, and the surgery completed.
A steep Trendelenburg, defined as 30 degrees, was used in 38 women, and a minimum degree of Trendelenburg averaging 16.6 degrees (range, 13.8-19 degrees) used in 12 women, said Dr. Sasada, now with United Hospital System, St. Catherine’s Medical Center in Pleasant Prairie, Wis.
The average uterine weight was not significantly different between the steep and minimum Trendelenburg groups (215.4 g vs. 173.6 g; P = .21).
Body mass index also was similar at 28.5 kg/m2 vs. 25 kg/m2 (P = .071), with a wide range in both groups, she said.
There was one case of intraoperative bleeding (500 cc) and no postoperative complications in the steep Trendelenburg group, and one case of postoperative urinary retention and no intraoperative complications in the minimum Trendelenburg group.
During a discussion of the study, Dr. Sasada said it’s possible that the lower blood loss with the minimum Trendelenburg position could be due to chance, but that both surgeries were completed with the same four incisions and without bowel prep.
Dr. Sasada currently uses a minimum Trendelenburg position and an iPad when performing robotic-assisted hysterectomy and other pelvic surgeries, but not in all cases, as some OR beds have built-in clinometers. The advantage of the iPad technology is that it offers "ease of use in the OR by anesthesia or nursing staff, and reproducibility between OR beds," she said in an interview.
Dr. Sasada and Dr. Mihalov reported no relevant financial disclosures.
AT THE 41ST AAGL GLOBAL CONGRESS
Major Finding: Average estimated blood loss was 101.3 mL with the steep Trendelenburg position vs. 50 mL with the minimum Trendelenburg (P = .007).
Data Source: Retrospective chart study of 50 women undergoing robotic-assisted hysterectomy.
Disclosures: Dr. Sasada and Dr. Mihalov reported no relevant financial disclosures.
Good news for apixaban in recurrent VTE prevention
ATLANTA – An extra year of apixaban reduced the risk of recurrent events in patients with venous thromboembolism by 80%, while keeping major bleeding rates in line with placebo in the randomized AMPLIFY-EXT trial.
The number needed to treat with apixaban (Eliquis) to prevent one fatal or nonfatal recurrent VTE was only 14, while the number needed to treat to cause one episode of major or clinically relevant nonmajor bleeding was 200, Dr. Giancarlo Agnelli reported in a late-breaking abstract at the annual meeting of the American Society of Hematology.

"We really believe this study, for its design and results, is a remarkable achievement, and [may lead to a] change in clinical practice," he said during a press briefing at the meeting.
Apixaban was approved by the Food and Drug Administration in late December for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, based largely on data demonstrating superiority to warfarin in patients with AF in the ARISTOTLE trial.*
In the meantime, the results of AMPLIFY-EXT (Apixaban After the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy–Extended Treatment) provide some guidance for physicians uncertain about whether to extend or stop standard anticoagulation therapy in patients with VTE in the absence of recurrent events. Stopping warfarin therapy increases the risk of recurrent VTE by up to 10% in patients without reversible risk factors, but also requires frequent laboratory monitoring and increases the risk of bleeding.
Apixaban, an oral factor Xa inhibitor, is given in fixed doses without the need for laboratory monitoring, said Dr. Agnelli, director of the internal and cardiovascular medicine/stroke unit at the University of Perugia, Italy.
Given the efficacy demonstrated in AMPLIFY-EXT, apixaban may also be an attractive option for those VTE patients with renal impairment, because it is the least dependent on renal clearance compared with two other fixed-dose anticoagulants, rivaroxaban (Xarelto) and dabigatran (Pradaxa), said press briefing moderator Dr. Agnes Lee, medical director of the thrombosis program and associate professor of medicine at the University of British Columbia, Vancouver, and Vancouver Coastal Health.
Notably, a recent prespecified substudy of ARISTOLE demonstrated that apixaban produced 35%-52% fewer major bleeding events in patients with renal dysfunction and atrial fibrillation.
The double-blind AMPLIFY-EXT trial randomized 842 patients to apixaban 2.5 mg, 815 to apixaban 5 mg, and 829 to placebo, all twice daily for 12 months. Three-fourths had an initial diagnosis of deep vein thrombosis and one-fourth pulmonary embolism. All had received 6-12 months of anticoagulation therapy and reached clinical equipoise about the continuation or cessation of anticoagulation therapy.
VTE was associated with a transient or reversible risk factor in less than 10% of patients. Two patients from each apixaban group were excluded from the intention-to-treat efficacy analysis. Their average age was roughly 56.
The composite primary efficacy endpoint of symptomatic VTE recurrence or all-cause death occurred in 3.8% of patients on apixaban 2.5 mg and in 4.2% of patients on apixaban 5 mg, compared with 11.6% of patients given placebo, Dr. Agnelli said.
Symptomatic recurrent VTE or death from VTE occurred in 1.7% of patients in both apixaban groups vs. 8.8% of placebo-treated patients.
Major bleeding was reported in 0.2% of the 2.5-mg apixaban group, 0.1% of the 5-mg group, and 0.5% of the placebo group. Clinically relevant nonmajor bleeding rates were slightly higher at 3.0% and 4.2% in the apixaban groups vs. 2.3% in the placebo group, he said.
Further study will be needed to determine if the results can be directly applied to cancer patients who face an increased risk of VTE because of the disease, as only about 2% of the study population had active cancer, Dr. Agnelli said in an interview.
The study was simultaneously published in the New England Journal of Medicine (2012 Dec. 8 [doi: 10.1056/NEJMoa1207541]).
AMPLIFY-EXT was funded by Bristol-Myers Squibb and Pfizer. Dr. Agnelli reported commercial relationships with Bristol-Myers Squibb, Daiichi Sankyo, and other companies. His coauthors reported relationships with the study sponsors. Dr. Lee disclosed consulting for Bristol-Myers Squibb.
*This article was updated January 2, 2013.
ATLANTA – An extra year of apixaban reduced the risk of recurrent events in patients with venous thromboembolism by 80%, while keeping major bleeding rates in line with placebo in the randomized AMPLIFY-EXT trial.
The number needed to treat with apixaban (Eliquis) to prevent one fatal or nonfatal recurrent VTE was only 14, while the number needed to treat to cause one episode of major or clinically relevant nonmajor bleeding was 200, Dr. Giancarlo Agnelli reported in a late-breaking abstract at the annual meeting of the American Society of Hematology.
"We really believe this study, for its design and results, is a remarkable achievement, and [may lead to a] change in clinical practice," he said during a press briefing at the meeting.
Apixaban was approved by the Food and Drug Administration in late December for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, based largely on data demonstrating superiority to warfarin in patients with AF in the ARISTOTLE trial.*
In the meantime, the results of AMPLIFY-EXT (Apixaban After the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy–Extended Treatment) provide some guidance for physicians uncertain about whether to extend or stop standard anticoagulation therapy in patients with VTE in the absence of recurrent events. Stopping warfarin therapy increases the risk of recurrent VTE by up to 10% in patients without reversible risk factors, but also requires frequent laboratory monitoring and increases the risk of bleeding.
Apixaban, an oral factor Xa inhibitor, is given in fixed doses without the need for laboratory monitoring, said Dr. Agnelli, director of the internal and cardiovascular medicine/stroke unit at the University of Perugia, Italy.
Given the efficacy demonstrated in AMPLIFY-EXT, apixaban may also be an attractive option for those VTE patients with renal impairment, because it is the least dependent on renal clearance compared with two other fixed-dose anticoagulants, rivaroxaban (Xarelto) and dabigatran (Pradaxa), said press briefing moderator Dr. Agnes Lee, medical director of the thrombosis program and associate professor of medicine at the University of British Columbia, Vancouver, and Vancouver Coastal Health.
Notably, a recent prespecified substudy of ARISTOLE demonstrated that apixaban produced 35%-52% fewer major bleeding events in patients with renal dysfunction and atrial fibrillation.
The double-blind AMPLIFY-EXT trial randomized 842 patients to apixaban 2.5 mg, 815 to apixaban 5 mg, and 829 to placebo, all twice daily for 12 months. Three-fourths had an initial diagnosis of deep vein thrombosis and one-fourth pulmonary embolism. All had received 6-12 months of anticoagulation therapy and reached clinical equipoise about the continuation or cessation of anticoagulation therapy.
VTE was associated with a transient or reversible risk factor in less than 10% of patients. Two patients from each apixaban group were excluded from the intention-to-treat efficacy analysis. Their average age was roughly 56.
The composite primary efficacy endpoint of symptomatic VTE recurrence or all-cause death occurred in 3.8% of patients on apixaban 2.5 mg and in 4.2% of patients on apixaban 5 mg, compared with 11.6% of patients given placebo, Dr. Agnelli said.
Symptomatic recurrent VTE or death from VTE occurred in 1.7% of patients in both apixaban groups vs. 8.8% of placebo-treated patients.
Major bleeding was reported in 0.2% of the 2.5-mg apixaban group, 0.1% of the 5-mg group, and 0.5% of the placebo group. Clinically relevant nonmajor bleeding rates were slightly higher at 3.0% and 4.2% in the apixaban groups vs. 2.3% in the placebo group, he said.
Further study will be needed to determine if the results can be directly applied to cancer patients who face an increased risk of VTE because of the disease, as only about 2% of the study population had active cancer, Dr. Agnelli said in an interview.
The study was simultaneously published in the New England Journal of Medicine (2012 Dec. 8 [doi: 10.1056/NEJMoa1207541]).
AMPLIFY-EXT was funded by Bristol-Myers Squibb and Pfizer. Dr. Agnelli reported commercial relationships with Bristol-Myers Squibb, Daiichi Sankyo, and other companies. His coauthors reported relationships with the study sponsors. Dr. Lee disclosed consulting for Bristol-Myers Squibb.
*This article was updated January 2, 2013.
ATLANTA – An extra year of apixaban reduced the risk of recurrent events in patients with venous thromboembolism by 80%, while keeping major bleeding rates in line with placebo in the randomized AMPLIFY-EXT trial.
The number needed to treat with apixaban (Eliquis) to prevent one fatal or nonfatal recurrent VTE was only 14, while the number needed to treat to cause one episode of major or clinically relevant nonmajor bleeding was 200, Dr. Giancarlo Agnelli reported in a late-breaking abstract at the annual meeting of the American Society of Hematology.
"We really believe this study, for its design and results, is a remarkable achievement, and [may lead to a] change in clinical practice," he said during a press briefing at the meeting.
Apixaban was approved by the Food and Drug Administration in late December for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, based largely on data demonstrating superiority to warfarin in patients with AF in the ARISTOTLE trial.*
In the meantime, the results of AMPLIFY-EXT (Apixaban After the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy–Extended Treatment) provide some guidance for physicians uncertain about whether to extend or stop standard anticoagulation therapy in patients with VTE in the absence of recurrent events. Stopping warfarin therapy increases the risk of recurrent VTE by up to 10% in patients without reversible risk factors, but also requires frequent laboratory monitoring and increases the risk of bleeding.
Apixaban, an oral factor Xa inhibitor, is given in fixed doses without the need for laboratory monitoring, said Dr. Agnelli, director of the internal and cardiovascular medicine/stroke unit at the University of Perugia, Italy.
Given the efficacy demonstrated in AMPLIFY-EXT, apixaban may also be an attractive option for those VTE patients with renal impairment, because it is the least dependent on renal clearance compared with two other fixed-dose anticoagulants, rivaroxaban (Xarelto) and dabigatran (Pradaxa), said press briefing moderator Dr. Agnes Lee, medical director of the thrombosis program and associate professor of medicine at the University of British Columbia, Vancouver, and Vancouver Coastal Health.
Notably, a recent prespecified substudy of ARISTOLE demonstrated that apixaban produced 35%-52% fewer major bleeding events in patients with renal dysfunction and atrial fibrillation.
The double-blind AMPLIFY-EXT trial randomized 842 patients to apixaban 2.5 mg, 815 to apixaban 5 mg, and 829 to placebo, all twice daily for 12 months. Three-fourths had an initial diagnosis of deep vein thrombosis and one-fourth pulmonary embolism. All had received 6-12 months of anticoagulation therapy and reached clinical equipoise about the continuation or cessation of anticoagulation therapy.
VTE was associated with a transient or reversible risk factor in less than 10% of patients. Two patients from each apixaban group were excluded from the intention-to-treat efficacy analysis. Their average age was roughly 56.
The composite primary efficacy endpoint of symptomatic VTE recurrence or all-cause death occurred in 3.8% of patients on apixaban 2.5 mg and in 4.2% of patients on apixaban 5 mg, compared with 11.6% of patients given placebo, Dr. Agnelli said.
Symptomatic recurrent VTE or death from VTE occurred in 1.7% of patients in both apixaban groups vs. 8.8% of placebo-treated patients.
Major bleeding was reported in 0.2% of the 2.5-mg apixaban group, 0.1% of the 5-mg group, and 0.5% of the placebo group. Clinically relevant nonmajor bleeding rates were slightly higher at 3.0% and 4.2% in the apixaban groups vs. 2.3% in the placebo group, he said.
Further study will be needed to determine if the results can be directly applied to cancer patients who face an increased risk of VTE because of the disease, as only about 2% of the study population had active cancer, Dr. Agnelli said in an interview.
The study was simultaneously published in the New England Journal of Medicine (2012 Dec. 8 [doi: 10.1056/NEJMoa1207541]).
AMPLIFY-EXT was funded by Bristol-Myers Squibb and Pfizer. Dr. Agnelli reported commercial relationships with Bristol-Myers Squibb, Daiichi Sankyo, and other companies. His coauthors reported relationships with the study sponsors. Dr. Lee disclosed consulting for Bristol-Myers Squibb.
*This article was updated January 2, 2013.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: The composite primary efficacy endpoint of symptomatic VTE recurrence or all-cause death occurred in 3.8% of patients on apixaban 2.5 mg and 4.2% of patients on apixaban 5 mg, compared with 11.6% of patients given placebo.
Data Source: Double-blind, randomized trial in 2,486 patients with VTE.
Disclosures: AMPLIFY-EXT was funded by Bristol-Myers Squibb and Pfizer. Dr. Agnelli reported commercial relationships with Bristol-Myers Squibb, Daiichi Sankyo, and other companies. His coauthors reported relationships with the study sponsors. Dr. Lee disclosed consulting for Bristol-Myers Squibb.
Simple technique facilitates laparoscopic port closure
LAS VEGAS – Surgeons have developed a simple new suture technique using two S-retractors to close laparoscopic and robotic surgery ports without sacrificing visualization.
"This method involves minimal training and surgical skill, is quick to perform, and requires no additional instrumentation and no additional cost to the institution, surgeon, or patient," Dr. Homayara Aziz said at the 41st AAGL Global Congress.
No fewer than 29 original methods have been described in the literature for fascial closure, but many use assistance from inside the abdomen or extracorporeal assistance, and require additional ports. Others can be performed without an additional port, but may or may not provide direct visualization when securing the abdominal wall fascia and peritoneum.
With the new technique, devised at the State University of New York at Buffalo, the needle does not enter the peritoneal cavity blindly, where the bowel or other visceral organs may be present, Dr. Aziz said. Instead, the S-retractor functions as a barrier to protect the contents of the abdominal cavity, reducing the risk of visceral injuries.
The S-retractor also provides direct visualization of the different abdominal layers, exposing the needle tip during its course through the fascia. Because there is no needle tip in the intraperitoneal cavity, the procedure is safer, she said.
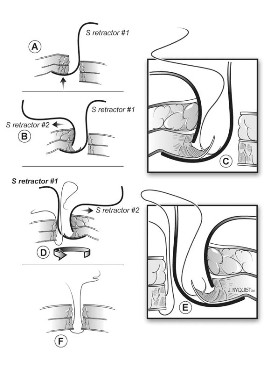
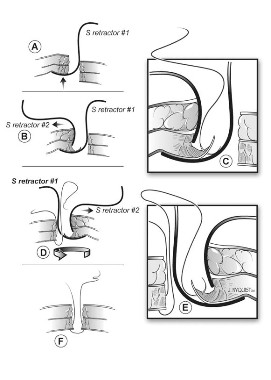
The two-step process starts with the surgeon inserting an S-retractor through the incision into the peritoneal cavity and then lifting the abdominal layers with the bottom of the retractor, creating a barrier between the fascia and the visceral contents. The assistant uses a second S-retractor to retract the skin, fat, and muscle in the opposite direction to expose the fascia. The surgeon then uses a needle suture to grasp the fascia, Dr. Aziz explained.
The first retractor is then rotated 180 degrees in the peritoneum by the surgeon to allow for work on the opposite side of the fascia. The second retractor, used by the assistant, is also moved to the opposite side of the abdominal wall layers to expose the fascia.
The surgeon again continues to grasp the opposite side of the fascia with the suture. The two ends are tied and the fascia is closed. If the fascial defect is greater than 10 mm, the surgeon may continue the same technique for another interrupted suture, figure of 8, or running closure, said Dr. Aziz, now a clinical instructor of obstetrics, gynecology, and reproductive science at the University of Maryland, Baltimore.
She reported on a prospective, consecutive case series involving 100 private and clinic patients in which this method was used over a 3-year period for fascial closure of total laparoscopic hysterectomies; bilateral or unilateral salpingo-oophorectomy where the port site was more than 12 mm to remove the specimen using an endocatch bag; and any robotic surgery where the ports are generally more than 8 mm.
There were no intraoperative incidents, nor was there added operative time or need to access costly instruments, she said.
No bowel injuries or port-site hernias were reported during a mean follow-up of 6 weeks post surgery and at 12-month annual follow-up.
"Closure of the fascia should remain simple, easy, cost-effective, and quick to apply," Dr. Aziz said. "It should also be safe and without any complications, and this technique described here fulfills all of these criteria."
The technique takes 5 minutes or less to learn, and has been used on at least 200 additional patients at both institutions since the current analysis was performed, Dr. Aziz said in an interview. "Many of my attendings at SUNY Buffalo call it ‘the Aziz technique’ and [it] has gained much popularity."
Dr. Aziz reported no relevant conflicts of interest.
LAS VEGAS – Surgeons have developed a simple new suture technique using two S-retractors to close laparoscopic and robotic surgery ports without sacrificing visualization.
"This method involves minimal training and surgical skill, is quick to perform, and requires no additional instrumentation and no additional cost to the institution, surgeon, or patient," Dr. Homayara Aziz said at the 41st AAGL Global Congress.
No fewer than 29 original methods have been described in the literature for fascial closure, but many use assistance from inside the abdomen or extracorporeal assistance, and require additional ports. Others can be performed without an additional port, but may or may not provide direct visualization when securing the abdominal wall fascia and peritoneum.
With the new technique, devised at the State University of New York at Buffalo, the needle does not enter the peritoneal cavity blindly, where the bowel or other visceral organs may be present, Dr. Aziz said. Instead, the S-retractor functions as a barrier to protect the contents of the abdominal cavity, reducing the risk of visceral injuries.
The S-retractor also provides direct visualization of the different abdominal layers, exposing the needle tip during its course through the fascia. Because there is no needle tip in the intraperitoneal cavity, the procedure is safer, she said.
The two-step process starts with the surgeon inserting an S-retractor through the incision into the peritoneal cavity and then lifting the abdominal layers with the bottom of the retractor, creating a barrier between the fascia and the visceral contents. The assistant uses a second S-retractor to retract the skin, fat, and muscle in the opposite direction to expose the fascia. The surgeon then uses a needle suture to grasp the fascia, Dr. Aziz explained.
The first retractor is then rotated 180 degrees in the peritoneum by the surgeon to allow for work on the opposite side of the fascia. The second retractor, used by the assistant, is also moved to the opposite side of the abdominal wall layers to expose the fascia.
The surgeon again continues to grasp the opposite side of the fascia with the suture. The two ends are tied and the fascia is closed. If the fascial defect is greater than 10 mm, the surgeon may continue the same technique for another interrupted suture, figure of 8, or running closure, said Dr. Aziz, now a clinical instructor of obstetrics, gynecology, and reproductive science at the University of Maryland, Baltimore.
She reported on a prospective, consecutive case series involving 100 private and clinic patients in which this method was used over a 3-year period for fascial closure of total laparoscopic hysterectomies; bilateral or unilateral salpingo-oophorectomy where the port site was more than 12 mm to remove the specimen using an endocatch bag; and any robotic surgery where the ports are generally more than 8 mm.
There were no intraoperative incidents, nor was there added operative time or need to access costly instruments, she said.
No bowel injuries or port-site hernias were reported during a mean follow-up of 6 weeks post surgery and at 12-month annual follow-up.
"Closure of the fascia should remain simple, easy, cost-effective, and quick to apply," Dr. Aziz said. "It should also be safe and without any complications, and this technique described here fulfills all of these criteria."
The technique takes 5 minutes or less to learn, and has been used on at least 200 additional patients at both institutions since the current analysis was performed, Dr. Aziz said in an interview. "Many of my attendings at SUNY Buffalo call it ‘the Aziz technique’ and [it] has gained much popularity."
Dr. Aziz reported no relevant conflicts of interest.
LAS VEGAS – Surgeons have developed a simple new suture technique using two S-retractors to close laparoscopic and robotic surgery ports without sacrificing visualization.
"This method involves minimal training and surgical skill, is quick to perform, and requires no additional instrumentation and no additional cost to the institution, surgeon, or patient," Dr. Homayara Aziz said at the 41st AAGL Global Congress.
No fewer than 29 original methods have been described in the literature for fascial closure, but many use assistance from inside the abdomen or extracorporeal assistance, and require additional ports. Others can be performed without an additional port, but may or may not provide direct visualization when securing the abdominal wall fascia and peritoneum.
With the new technique, devised at the State University of New York at Buffalo, the needle does not enter the peritoneal cavity blindly, where the bowel or other visceral organs may be present, Dr. Aziz said. Instead, the S-retractor functions as a barrier to protect the contents of the abdominal cavity, reducing the risk of visceral injuries.
The S-retractor also provides direct visualization of the different abdominal layers, exposing the needle tip during its course through the fascia. Because there is no needle tip in the intraperitoneal cavity, the procedure is safer, she said.
The two-step process starts with the surgeon inserting an S-retractor through the incision into the peritoneal cavity and then lifting the abdominal layers with the bottom of the retractor, creating a barrier between the fascia and the visceral contents. The assistant uses a second S-retractor to retract the skin, fat, and muscle in the opposite direction to expose the fascia. The surgeon then uses a needle suture to grasp the fascia, Dr. Aziz explained.
The first retractor is then rotated 180 degrees in the peritoneum by the surgeon to allow for work on the opposite side of the fascia. The second retractor, used by the assistant, is also moved to the opposite side of the abdominal wall layers to expose the fascia.
The surgeon again continues to grasp the opposite side of the fascia with the suture. The two ends are tied and the fascia is closed. If the fascial defect is greater than 10 mm, the surgeon may continue the same technique for another interrupted suture, figure of 8, or running closure, said Dr. Aziz, now a clinical instructor of obstetrics, gynecology, and reproductive science at the University of Maryland, Baltimore.
She reported on a prospective, consecutive case series involving 100 private and clinic patients in which this method was used over a 3-year period for fascial closure of total laparoscopic hysterectomies; bilateral or unilateral salpingo-oophorectomy where the port site was more than 12 mm to remove the specimen using an endocatch bag; and any robotic surgery where the ports are generally more than 8 mm.
There were no intraoperative incidents, nor was there added operative time or need to access costly instruments, she said.
No bowel injuries or port-site hernias were reported during a mean follow-up of 6 weeks post surgery and at 12-month annual follow-up.
"Closure of the fascia should remain simple, easy, cost-effective, and quick to apply," Dr. Aziz said. "It should also be safe and without any complications, and this technique described here fulfills all of these criteria."
The technique takes 5 minutes or less to learn, and has been used on at least 200 additional patients at both institutions since the current analysis was performed, Dr. Aziz said in an interview. "Many of my attendings at SUNY Buffalo call it ‘the Aziz technique’ and [it] has gained much popularity."
Dr. Aziz reported no relevant conflicts of interest.
AT THE 41ST AAGL GLOBAL CONGRESS
Major Finding: There were no intraoperative incidents, and no bowel injuries or port site hernias, during a mean follow-up of 6 weeks post surgery and at 12 months follow-up.
Data Source: Prospective, consecutive case series of 100 patients.
Disclosures: Dr. Aziz reported no relevant conflicts of interest.
Experimental Ibrutinib Could Change Treatment of CLL
ATLANTA – The experimental oral therapy ibrutinib produces dramatic responses but dodges the significant toxicity seen in conventional treatments for chronic lymphocytic leukemia and small lymphocytic lymphoma.
In one of two phase II trials, the overall response rate was 68% in previously untreated patients and 71% in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL).
The outcome was similar in patients with high-risk relapsed or refractory disease, with the possible exception of those with chromosome 17p deletion. However, with more than half responding, these patients still do better with ibrutinib than with any other therapy explored to date, said Dr. John C. Byrd, director of hematology at Ohio State Comprehensive Cancer Center in Columbus.
"Ibrutinib offers great potential to significantly change the treatment landscape of CLL," he said at a press briefing at the annual meeting of the American Society of Hematology.
In the second trial, combining ibrutinib with the anti-CD20 antibody rituximab (Rituxan) pushed the overall response rate to 83% in high-risk CLL and SLL, said Dr. Jan A. Burger, of the University of Texas M.D. Anderson Cancer Center in Houston.
He noted that several ongoing phase III trials are underway that should accelerate the development of ibrutinib for high-risk patients, who have a high unmet need for alternative treatments.
Ibrutinib is currently not available, even under compassionate use. Despite this, the drug is generating much enthusiasm among clinicians and patients, with some traveling great distances to get into these ongoing trials despite only a 50-50 chance of receiving the drug, said press briefing moderator Dr. Claire Dearden, head of the CLL unit at the Royal Marsden NHS Foundation Trust in London.
"It’s orally active, it’s well tolerated, it’s not chemo, and it produces excellent responses, particularly in patients who are elderly and frail and not necessarily suitable for the more intensive chemotherapy regimens that have become the first-line treatment for the younger, fitter patients," she said.
Ibrutinib, formerly known as PCI-32765, is the first irreversible inhibitor of Bruton’s tyrosine kinase (BTK) to enter clinical development. BTK is essential for B-cell receptor signaling, chemokine-mediated migration and adhesion, and toll-like receptor signaling.
96% Survival Estimates at 22 Months
Dr. Byrd reported new and updated results from 31 patients with treatment naive CLL or SLL, 61 with relapsed or refractory disease, and 24 with high-risk relapsed or refractory disease (defined as progression within 24 months of starting a regimen containing at least a nucleoside analogue or bendamustine in combination with a monoclonal antibody or failure to respond to such a regimen).
Patients were given ibrutinib 420 mg or 840 mg daily 2 hours before food until disease progression or intolerable toxicity. Their median age was 72.
After follow-up ranging from 14.7 months to 22.1 months, complete responses occurred in 10% of treatment-naive patients and 2% of relapsed or refractory patients, Dr. Byrd said. Partial responses occurred in 58% and 68%.
At 22 months, progression-free and overall survival estimates were both 96% among previously untreated patients. To put these results in perspective, he said, that with standard cytotoxic chemotherapy, one would expect this number to be 70% or less if patients are young and 50% or less if elderly. "So these are really dramatic results," he added.
In the relapsed or refractory group, progression-free survival was 76% and overall survival 85%.
Longer follow-up is needed to determine whether the remissions are durable once ibrutinib is stopped – something currently being studied more than a decade after clinicians began using another kinase inhibitor, imatinib (Gleevec), to treat chronic myeloid leukemia, Dr. Byrd said.
He reported 3 grade 3 and no grade 4 infections in treatment-naive patients, and 26 grade 3 infections and 4 grade 4 events in relapsed/refractory patients.
Nearly All Still on Study in Combination Trial
In the second trial, 40 patients received continuous ibrutinib 420 mg daily plus weekly rituximab 365 mg/m2 for 4 weeks, followed by daily ibrutinib plus monthly rituximab until month 6, followed by single-agent ibrutinib. High-risk CLL/SLL was defined as deletion 17p, TP53 mutation, deletion 11q, or less than 3 years remission after first-line chemo-immunotherapy. More than half of patients (58%) had stage IV disease.
After 3-6 months’ follow-up, there were 1 complete response, 32 partial responses, and 3 partial responses with lymphocytosis, Dr. Burger said. In all, 84% of patients experienced more than a 50% reduction in lymph node size.
At the time of the analysis, 95% of all patients and 90% with del 17p continued on therapy without disease progression.
Two patients came off study; one with pneumonia and an intracranial abscess, who died, and another who discontinued due to mucositis/ulcers after four cycles.
Severe toxicities were uncommon in both studies, particularly the considerable immunosuppression and serious infections associated with standard chemo-immunotherapy, the investigators said. The most common event was diarrhea, which was experienced by 54% of patients receiving ibrutinib monotherapy and was largely grade 1 or 2 and resolved after the first couple of cycles, Dr. Byrd said.
Other events included fatigue (29%), upper respiratory infection (29%), rash (28%), nausea (26%) and bone pain (25%). Rates were similar in the combination therapy trial, with bruising also seen in both trials
One of the ongoing phase III trials is the 350-patient RESONATE study evaluating ibrutinib versus ofatumumab (Arzerra) in patients with relapsed or refractory CLL or SLL.
Dr. Byrd disclosed research funding from the study sponsor Pharmacyclics, which is developing ibrutinib. Dr. Burger reported consulting for and research funding from Pharmacyclics. Co-authors of both studies are Pharmacyclics employees. Dr. Dearden disclosed no conflicts of interest.
ATLANTA – The experimental oral therapy ibrutinib produces dramatic responses but dodges the significant toxicity seen in conventional treatments for chronic lymphocytic leukemia and small lymphocytic lymphoma.
In one of two phase II trials, the overall response rate was 68% in previously untreated patients and 71% in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL).
The outcome was similar in patients with high-risk relapsed or refractory disease, with the possible exception of those with chromosome 17p deletion. However, with more than half responding, these patients still do better with ibrutinib than with any other therapy explored to date, said Dr. John C. Byrd, director of hematology at Ohio State Comprehensive Cancer Center in Columbus.
"Ibrutinib offers great potential to significantly change the treatment landscape of CLL," he said at a press briefing at the annual meeting of the American Society of Hematology.
In the second trial, combining ibrutinib with the anti-CD20 antibody rituximab (Rituxan) pushed the overall response rate to 83% in high-risk CLL and SLL, said Dr. Jan A. Burger, of the University of Texas M.D. Anderson Cancer Center in Houston.
He noted that several ongoing phase III trials are underway that should accelerate the development of ibrutinib for high-risk patients, who have a high unmet need for alternative treatments.
Ibrutinib is currently not available, even under compassionate use. Despite this, the drug is generating much enthusiasm among clinicians and patients, with some traveling great distances to get into these ongoing trials despite only a 50-50 chance of receiving the drug, said press briefing moderator Dr. Claire Dearden, head of the CLL unit at the Royal Marsden NHS Foundation Trust in London.
"It’s orally active, it’s well tolerated, it’s not chemo, and it produces excellent responses, particularly in patients who are elderly and frail and not necessarily suitable for the more intensive chemotherapy regimens that have become the first-line treatment for the younger, fitter patients," she said.
Ibrutinib, formerly known as PCI-32765, is the first irreversible inhibitor of Bruton’s tyrosine kinase (BTK) to enter clinical development. BTK is essential for B-cell receptor signaling, chemokine-mediated migration and adhesion, and toll-like receptor signaling.
96% Survival Estimates at 22 Months
Dr. Byrd reported new and updated results from 31 patients with treatment naive CLL or SLL, 61 with relapsed or refractory disease, and 24 with high-risk relapsed or refractory disease (defined as progression within 24 months of starting a regimen containing at least a nucleoside analogue or bendamustine in combination with a monoclonal antibody or failure to respond to such a regimen).
Patients were given ibrutinib 420 mg or 840 mg daily 2 hours before food until disease progression or intolerable toxicity. Their median age was 72.
After follow-up ranging from 14.7 months to 22.1 months, complete responses occurred in 10% of treatment-naive patients and 2% of relapsed or refractory patients, Dr. Byrd said. Partial responses occurred in 58% and 68%.
At 22 months, progression-free and overall survival estimates were both 96% among previously untreated patients. To put these results in perspective, he said, that with standard cytotoxic chemotherapy, one would expect this number to be 70% or less if patients are young and 50% or less if elderly. "So these are really dramatic results," he added.
In the relapsed or refractory group, progression-free survival was 76% and overall survival 85%.
Longer follow-up is needed to determine whether the remissions are durable once ibrutinib is stopped – something currently being studied more than a decade after clinicians began using another kinase inhibitor, imatinib (Gleevec), to treat chronic myeloid leukemia, Dr. Byrd said.
He reported 3 grade 3 and no grade 4 infections in treatment-naive patients, and 26 grade 3 infections and 4 grade 4 events in relapsed/refractory patients.
Nearly All Still on Study in Combination Trial
In the second trial, 40 patients received continuous ibrutinib 420 mg daily plus weekly rituximab 365 mg/m2 for 4 weeks, followed by daily ibrutinib plus monthly rituximab until month 6, followed by single-agent ibrutinib. High-risk CLL/SLL was defined as deletion 17p, TP53 mutation, deletion 11q, or less than 3 years remission after first-line chemo-immunotherapy. More than half of patients (58%) had stage IV disease.
After 3-6 months’ follow-up, there were 1 complete response, 32 partial responses, and 3 partial responses with lymphocytosis, Dr. Burger said. In all, 84% of patients experienced more than a 50% reduction in lymph node size.
At the time of the analysis, 95% of all patients and 90% with del 17p continued on therapy without disease progression.
Two patients came off study; one with pneumonia and an intracranial abscess, who died, and another who discontinued due to mucositis/ulcers after four cycles.
Severe toxicities were uncommon in both studies, particularly the considerable immunosuppression and serious infections associated with standard chemo-immunotherapy, the investigators said. The most common event was diarrhea, which was experienced by 54% of patients receiving ibrutinib monotherapy and was largely grade 1 or 2 and resolved after the first couple of cycles, Dr. Byrd said.
Other events included fatigue (29%), upper respiratory infection (29%), rash (28%), nausea (26%) and bone pain (25%). Rates were similar in the combination therapy trial, with bruising also seen in both trials
One of the ongoing phase III trials is the 350-patient RESONATE study evaluating ibrutinib versus ofatumumab (Arzerra) in patients with relapsed or refractory CLL or SLL.
Dr. Byrd disclosed research funding from the study sponsor Pharmacyclics, which is developing ibrutinib. Dr. Burger reported consulting for and research funding from Pharmacyclics. Co-authors of both studies are Pharmacyclics employees. Dr. Dearden disclosed no conflicts of interest.
ATLANTA – The experimental oral therapy ibrutinib produces dramatic responses but dodges the significant toxicity seen in conventional treatments for chronic lymphocytic leukemia and small lymphocytic lymphoma.
In one of two phase II trials, the overall response rate was 68% in previously untreated patients and 71% in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL).
The outcome was similar in patients with high-risk relapsed or refractory disease, with the possible exception of those with chromosome 17p deletion. However, with more than half responding, these patients still do better with ibrutinib than with any other therapy explored to date, said Dr. John C. Byrd, director of hematology at Ohio State Comprehensive Cancer Center in Columbus.
"Ibrutinib offers great potential to significantly change the treatment landscape of CLL," he said at a press briefing at the annual meeting of the American Society of Hematology.
In the second trial, combining ibrutinib with the anti-CD20 antibody rituximab (Rituxan) pushed the overall response rate to 83% in high-risk CLL and SLL, said Dr. Jan A. Burger, of the University of Texas M.D. Anderson Cancer Center in Houston.
He noted that several ongoing phase III trials are underway that should accelerate the development of ibrutinib for high-risk patients, who have a high unmet need for alternative treatments.
Ibrutinib is currently not available, even under compassionate use. Despite this, the drug is generating much enthusiasm among clinicians and patients, with some traveling great distances to get into these ongoing trials despite only a 50-50 chance of receiving the drug, said press briefing moderator Dr. Claire Dearden, head of the CLL unit at the Royal Marsden NHS Foundation Trust in London.
"It’s orally active, it’s well tolerated, it’s not chemo, and it produces excellent responses, particularly in patients who are elderly and frail and not necessarily suitable for the more intensive chemotherapy regimens that have become the first-line treatment for the younger, fitter patients," she said.
Ibrutinib, formerly known as PCI-32765, is the first irreversible inhibitor of Bruton’s tyrosine kinase (BTK) to enter clinical development. BTK is essential for B-cell receptor signaling, chemokine-mediated migration and adhesion, and toll-like receptor signaling.
96% Survival Estimates at 22 Months
Dr. Byrd reported new and updated results from 31 patients with treatment naive CLL or SLL, 61 with relapsed or refractory disease, and 24 with high-risk relapsed or refractory disease (defined as progression within 24 months of starting a regimen containing at least a nucleoside analogue or bendamustine in combination with a monoclonal antibody or failure to respond to such a regimen).
Patients were given ibrutinib 420 mg or 840 mg daily 2 hours before food until disease progression or intolerable toxicity. Their median age was 72.
After follow-up ranging from 14.7 months to 22.1 months, complete responses occurred in 10% of treatment-naive patients and 2% of relapsed or refractory patients, Dr. Byrd said. Partial responses occurred in 58% and 68%.
At 22 months, progression-free and overall survival estimates were both 96% among previously untreated patients. To put these results in perspective, he said, that with standard cytotoxic chemotherapy, one would expect this number to be 70% or less if patients are young and 50% or less if elderly. "So these are really dramatic results," he added.
In the relapsed or refractory group, progression-free survival was 76% and overall survival 85%.
Longer follow-up is needed to determine whether the remissions are durable once ibrutinib is stopped – something currently being studied more than a decade after clinicians began using another kinase inhibitor, imatinib (Gleevec), to treat chronic myeloid leukemia, Dr. Byrd said.
He reported 3 grade 3 and no grade 4 infections in treatment-naive patients, and 26 grade 3 infections and 4 grade 4 events in relapsed/refractory patients.
Nearly All Still on Study in Combination Trial
In the second trial, 40 patients received continuous ibrutinib 420 mg daily plus weekly rituximab 365 mg/m2 for 4 weeks, followed by daily ibrutinib plus monthly rituximab until month 6, followed by single-agent ibrutinib. High-risk CLL/SLL was defined as deletion 17p, TP53 mutation, deletion 11q, or less than 3 years remission after first-line chemo-immunotherapy. More than half of patients (58%) had stage IV disease.
After 3-6 months’ follow-up, there were 1 complete response, 32 partial responses, and 3 partial responses with lymphocytosis, Dr. Burger said. In all, 84% of patients experienced more than a 50% reduction in lymph node size.
At the time of the analysis, 95% of all patients and 90% with del 17p continued on therapy without disease progression.
Two patients came off study; one with pneumonia and an intracranial abscess, who died, and another who discontinued due to mucositis/ulcers after four cycles.
Severe toxicities were uncommon in both studies, particularly the considerable immunosuppression and serious infections associated with standard chemo-immunotherapy, the investigators said. The most common event was diarrhea, which was experienced by 54% of patients receiving ibrutinib monotherapy and was largely grade 1 or 2 and resolved after the first couple of cycles, Dr. Byrd said.
Other events included fatigue (29%), upper respiratory infection (29%), rash (28%), nausea (26%) and bone pain (25%). Rates were similar in the combination therapy trial, with bruising also seen in both trials
One of the ongoing phase III trials is the 350-patient RESONATE study evaluating ibrutinib versus ofatumumab (Arzerra) in patients with relapsed or refractory CLL or SLL.
Dr. Byrd disclosed research funding from the study sponsor Pharmacyclics, which is developing ibrutinib. Dr. Burger reported consulting for and research funding from Pharmacyclics. Co-authors of both studies are Pharmacyclics employees. Dr. Dearden disclosed no conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Ibrutinib monotherapy produced an overall response rate of 68% in previously untreated patients and 71% in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL).
Data Source: Phase Ib/II trial of ibrutinib monotherapy and phase II trial of ibrutinib in combination with rituximab.
Disclosures: Dr. Byrd disclosed research funding from the study sponsor Pharmacyclics, which is developing ibrutinib. Dr. Burger reported consulting for and research funding from Pharmacyclics. Coauthors of both studies are Pharmacyclics employees. Dr. Dearden disclosed no conflicts of interest.

PET/CT Pinpoints Physiological Evidence of Chemo Brain
CHICAGO – PET/CT scans routinely used in the care of oncology patients may prove useful in pinpointing physiological changes associated with chemo brain.
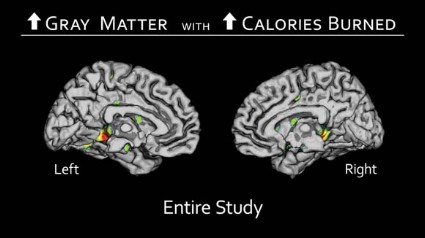
An analysis of 18F-fluorodeoxyglucose (18F-FDG) PET/CT images taken before and after chemotherapy in breast cancer patients revealed significant declines in glucose metabolism in two key regions of the brain. The affected areas were the superior medial frontal gyrus and temporal operculum, which are responsible for mental agility, problem solving, daily decision making, sequencing, and long-term memory, Dr. Rachel Lagos reported at the annual meeting of the Radiological Society of North America.

Interestingly, no changes in metabolism were observed in 61 other regions of the brain studied.
"If we can come up with an answer to explain why that is, or to reverse this, then we can solve the problem," Dr. Lagos said in an interview. "The good news is that we already know what these two areas do, so we know at a social level what to prepare women and their families for. We can give them some tools for coping, rather than just a pat on the hand."
Although many cancer patients complain of a mental fog or loss of coping skills, some clinicians remain skeptical without definitive scientific evidence. Previous studies have used magnetic resonance imaging, but this modality only allows clinicians to see anatomic details such as small losses in brain volume. With PET/CT, one can see the effects of chemotherapy on brain function over time, explained Dr. Lagos, a diagnostic radiology resident at West Virginia University in Morgantown.
The retrospective analysis involved PET/CT scans taken at the time of initial cancer staging and 12 months after chemotherapy from 116 women with advanced breast cancer, all of whom also received tamoxifen (Nolvadex, Soltamox). The investigators compared the scans to identify areas of reduced 18F-FDG uptake, representing lower glucose metabolism, and then plotted the changes as Z-score values. One patient with brain metastases was excluded from the analysis.
Statistically significant declines in glucose metabolism were observed post chemotherapy in the superior medial frontal gyrus as a whole (P = .025), when it was evaluated from left to right (P = .023), and in the temporal operculum (P = .036), Dr. Lagos said.
The investigators did not calculate an average value for the change in Z scores, but the decline in values ranged from 2.5 to 8.0 points, she said.
In 21 patients, the affected regions of the brain regained their metabolism, which corresponds to anecdotal information from patients that chemo brain lifts about 1-2 years after treatment.

"With the small data I’ve been able to accumulate so far, it’s hopeful that this kind of brain phenomenon is temporary," Dr. Lagos said.
The next step is to prospectively assess brain function starting at the time of cancer diagnosis and continuing throughout long-term follow-up, which potentially could lead to improved treatments or prevention, she said. In the meantime, the results provide physiologic evidence for chemo brain, and may prompt peers and counselors to use simple interventions such as creating lists for patients of their daily activities or meal plans to compensate for the mental fog.
Dr. Patrick J. Peller, a radiologist with the Mayo Clinic in Rochester, Minn., who hosted the poster session, said the study provides an understanding of the substrate for the often frustrating symptoms that patients experience, and could facilitate interventions to prevent chemo brain.
"Once you have a way to measure something, it sometimes drives your ability to treat it," he said in an interview. "We don’t have that treatment right now, just like we don’t have treatment for Alzheimer’s disease, but my sense is that it’s possible that our treatment for Alzheimer’s might work in some of these patients because it helps in compensation and not actually changing the underlying disease.
"If it improves the patient’s memory function, it might work in this situation, and you might be able to measure if it’s working with this technique."
Dr. Lagos and Dr. Peller reported no relevant financial disclosures.
CHICAGO – PET/CT scans routinely used in the care of oncology patients may prove useful in pinpointing physiological changes associated with chemo brain.
An analysis of 18F-fluorodeoxyglucose (18F-FDG) PET/CT images taken before and after chemotherapy in breast cancer patients revealed significant declines in glucose metabolism in two key regions of the brain. The affected areas were the superior medial frontal gyrus and temporal operculum, which are responsible for mental agility, problem solving, daily decision making, sequencing, and long-term memory, Dr. Rachel Lagos reported at the annual meeting of the Radiological Society of North America.
Interestingly, no changes in metabolism were observed in 61 other regions of the brain studied.
"If we can come up with an answer to explain why that is, or to reverse this, then we can solve the problem," Dr. Lagos said in an interview. "The good news is that we already know what these two areas do, so we know at a social level what to prepare women and their families for. We can give them some tools for coping, rather than just a pat on the hand."
Although many cancer patients complain of a mental fog or loss of coping skills, some clinicians remain skeptical without definitive scientific evidence. Previous studies have used magnetic resonance imaging, but this modality only allows clinicians to see anatomic details such as small losses in brain volume. With PET/CT, one can see the effects of chemotherapy on brain function over time, explained Dr. Lagos, a diagnostic radiology resident at West Virginia University in Morgantown.
The retrospective analysis involved PET/CT scans taken at the time of initial cancer staging and 12 months after chemotherapy from 116 women with advanced breast cancer, all of whom also received tamoxifen (Nolvadex, Soltamox). The investigators compared the scans to identify areas of reduced 18F-FDG uptake, representing lower glucose metabolism, and then plotted the changes as Z-score values. One patient with brain metastases was excluded from the analysis.
Statistically significant declines in glucose metabolism were observed post chemotherapy in the superior medial frontal gyrus as a whole (P = .025), when it was evaluated from left to right (P = .023), and in the temporal operculum (P = .036), Dr. Lagos said.
The investigators did not calculate an average value for the change in Z scores, but the decline in values ranged from 2.5 to 8.0 points, she said.
In 21 patients, the affected regions of the brain regained their metabolism, which corresponds to anecdotal information from patients that chemo brain lifts about 1-2 years after treatment.
"With the small data I’ve been able to accumulate so far, it’s hopeful that this kind of brain phenomenon is temporary," Dr. Lagos said.
The next step is to prospectively assess brain function starting at the time of cancer diagnosis and continuing throughout long-term follow-up, which potentially could lead to improved treatments or prevention, she said. In the meantime, the results provide physiologic evidence for chemo brain, and may prompt peers and counselors to use simple interventions such as creating lists for patients of their daily activities or meal plans to compensate for the mental fog.
Dr. Patrick J. Peller, a radiologist with the Mayo Clinic in Rochester, Minn., who hosted the poster session, said the study provides an understanding of the substrate for the often frustrating symptoms that patients experience, and could facilitate interventions to prevent chemo brain.
"Once you have a way to measure something, it sometimes drives your ability to treat it," he said in an interview. "We don’t have that treatment right now, just like we don’t have treatment for Alzheimer’s disease, but my sense is that it’s possible that our treatment for Alzheimer’s might work in some of these patients because it helps in compensation and not actually changing the underlying disease.
"If it improves the patient’s memory function, it might work in this situation, and you might be able to measure if it’s working with this technique."
Dr. Lagos and Dr. Peller reported no relevant financial disclosures.
CHICAGO – PET/CT scans routinely used in the care of oncology patients may prove useful in pinpointing physiological changes associated with chemo brain.
An analysis of 18F-fluorodeoxyglucose (18F-FDG) PET/CT images taken before and after chemotherapy in breast cancer patients revealed significant declines in glucose metabolism in two key regions of the brain. The affected areas were the superior medial frontal gyrus and temporal operculum, which are responsible for mental agility, problem solving, daily decision making, sequencing, and long-term memory, Dr. Rachel Lagos reported at the annual meeting of the Radiological Society of North America.
Interestingly, no changes in metabolism were observed in 61 other regions of the brain studied.
"If we can come up with an answer to explain why that is, or to reverse this, then we can solve the problem," Dr. Lagos said in an interview. "The good news is that we already know what these two areas do, so we know at a social level what to prepare women and their families for. We can give them some tools for coping, rather than just a pat on the hand."
Although many cancer patients complain of a mental fog or loss of coping skills, some clinicians remain skeptical without definitive scientific evidence. Previous studies have used magnetic resonance imaging, but this modality only allows clinicians to see anatomic details such as small losses in brain volume. With PET/CT, one can see the effects of chemotherapy on brain function over time, explained Dr. Lagos, a diagnostic radiology resident at West Virginia University in Morgantown.
The retrospective analysis involved PET/CT scans taken at the time of initial cancer staging and 12 months after chemotherapy from 116 women with advanced breast cancer, all of whom also received tamoxifen (Nolvadex, Soltamox). The investigators compared the scans to identify areas of reduced 18F-FDG uptake, representing lower glucose metabolism, and then plotted the changes as Z-score values. One patient with brain metastases was excluded from the analysis.
Statistically significant declines in glucose metabolism were observed post chemotherapy in the superior medial frontal gyrus as a whole (P = .025), when it was evaluated from left to right (P = .023), and in the temporal operculum (P = .036), Dr. Lagos said.
The investigators did not calculate an average value for the change in Z scores, but the decline in values ranged from 2.5 to 8.0 points, she said.
In 21 patients, the affected regions of the brain regained their metabolism, which corresponds to anecdotal information from patients that chemo brain lifts about 1-2 years after treatment.
"With the small data I’ve been able to accumulate so far, it’s hopeful that this kind of brain phenomenon is temporary," Dr. Lagos said.
The next step is to prospectively assess brain function starting at the time of cancer diagnosis and continuing throughout long-term follow-up, which potentially could lead to improved treatments or prevention, she said. In the meantime, the results provide physiologic evidence for chemo brain, and may prompt peers and counselors to use simple interventions such as creating lists for patients of their daily activities or meal plans to compensate for the mental fog.
Dr. Patrick J. Peller, a radiologist with the Mayo Clinic in Rochester, Minn., who hosted the poster session, said the study provides an understanding of the substrate for the often frustrating symptoms that patients experience, and could facilitate interventions to prevent chemo brain.
"Once you have a way to measure something, it sometimes drives your ability to treat it," he said in an interview. "We don’t have that treatment right now, just like we don’t have treatment for Alzheimer’s disease, but my sense is that it’s possible that our treatment for Alzheimer’s might work in some of these patients because it helps in compensation and not actually changing the underlying disease.
"If it improves the patient’s memory function, it might work in this situation, and you might be able to measure if it’s working with this technique."
Dr. Lagos and Dr. Peller reported no relevant financial disclosures.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Statistically significant declines in glucose metabolism were observed post chemotherapy in the superior medial frontal gyrus as a whole (P = .025), when it was evaluated from left to right (P = .023), and in the temporal operculum (P = .036).
Data Source: This was a retrospective analysis of PET/CT scans from 115 patients with advanced breast cancer.
Disclosures: Dr. Lagos and Dr. Peller reported no relevant financial disclosures.

Mammograms Dip in Wake of USPSTF Recommendations
CHICAGO – There has been a clear and abrupt decline in screening mammography in the wake of the controversial breast cancer screening recommendations by the U.S. Preventive Services Task Force.
After climbing steadily at a rate of about 1% per year since 2001, breast mammography among women on Medicare declined 4.3% in 2010, the first full year after the USPSTF recommendations came out.
The reasons for the decline aren’t entirely clear, but it may be that women over age 74 years began to follow the task force recommendations and no longer got screened, or that women aged 50-74 years extended their screening interval from 1 to 2 years, again according to task force recommendations, lead author Dr. David C. Levin said at the annual meeting of the Radiological Society of North America.

"What is clear is that the introduction of those recommendations in late 2009 had a chilling effect on the willingness of women to get screened," he said. "It remains to be seen whether this trend is going to continue and whether it will affect breast cancer mortality."
For the analysis, Dr. Levin reviewed film and digital screening mammography codes in the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2005 to 2010. The database provides volumes for each code each year.
From these data, he calculated that the screening mammography rate per 1,000 female Medicare beneficiaries had been growing in small increments each year from 311.6 in 2005 to 312.4 in 2006, 316.2 in 2007, 320.1 in 2008, and 322.9 in 2009. This represents a compound annual growth rate of 0.9%.
After the recommendations came out, the screening mammography rate fell to 309.1/1,000 women in 2010, representing a decline of 4.3% in a single year, said Dr. Levin, a radiologist and founder of the center for research on utilization of imaging services at Thomas Jefferson University Hospital in Philadelphia.
He pointed out that earlier this year, Mayo Clinic researchers reported a 5.7% decline in screening mammography in 2010 among women aged 40-64, based on data from almost 7.9 million women enrolled in nearly 100 health plans.
In a separate presentation at the meeting, investigators analyzed the outcomes of 43,351 screening mammograms performed between 2007 and 2010 to determine how the new USPSTF recommendations against screening in women 40-49 years could impact this age group.
The cross-sectional analysis included all patients presenting for a screening mammogram without clinical findings at New York Presbyterian Hospital–Weill Cornell Medical College (NYPH-WCMC) in New York City. Women aged 40-49 comprised 33.5% of the screening population.

During the 4 years, 205 breast cancers were detected (4.7/1,000). Women in their forties accounted for 19% of the cancers found, which would represent a substantial degree of underdiagnoses if they had been missed, reported Dr. Elizabeth Arleo, a radiologist at NYPH-WCMC.
Notably, only three of the women in their forties with screen-detected breast cancer had a first-degree relative with premenopausal breast cancer, thereby placing them at higher risk. More than half of the cancers in this subgroup, however, were invasive (21/39).
If the USPSTF recommendations had been enforced during the study years, these cancers may not have been detected until the patients’ baseline screening at age 50 or until the cancers had progressed to clinically evident, palpable disease, Dr. Arleo coauthors said.
Dr. Levin reported relationships with HealthHelp and Outpatient Imaging Affiliates. Dr. Arleo said she had no relevant financial disclosures.
CHICAGO – There has been a clear and abrupt decline in screening mammography in the wake of the controversial breast cancer screening recommendations by the U.S. Preventive Services Task Force.
After climbing steadily at a rate of about 1% per year since 2001, breast mammography among women on Medicare declined 4.3% in 2010, the first full year after the USPSTF recommendations came out.
The reasons for the decline aren’t entirely clear, but it may be that women over age 74 years began to follow the task force recommendations and no longer got screened, or that women aged 50-74 years extended their screening interval from 1 to 2 years, again according to task force recommendations, lead author Dr. David C. Levin said at the annual meeting of the Radiological Society of North America.
"What is clear is that the introduction of those recommendations in late 2009 had a chilling effect on the willingness of women to get screened," he said. "It remains to be seen whether this trend is going to continue and whether it will affect breast cancer mortality."
For the analysis, Dr. Levin reviewed film and digital screening mammography codes in the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2005 to 2010. The database provides volumes for each code each year.
From these data, he calculated that the screening mammography rate per 1,000 female Medicare beneficiaries had been growing in small increments each year from 311.6 in 2005 to 312.4 in 2006, 316.2 in 2007, 320.1 in 2008, and 322.9 in 2009. This represents a compound annual growth rate of 0.9%.
After the recommendations came out, the screening mammography rate fell to 309.1/1,000 women in 2010, representing a decline of 4.3% in a single year, said Dr. Levin, a radiologist and founder of the center for research on utilization of imaging services at Thomas Jefferson University Hospital in Philadelphia.
He pointed out that earlier this year, Mayo Clinic researchers reported a 5.7% decline in screening mammography in 2010 among women aged 40-64, based on data from almost 7.9 million women enrolled in nearly 100 health plans.
In a separate presentation at the meeting, investigators analyzed the outcomes of 43,351 screening mammograms performed between 2007 and 2010 to determine how the new USPSTF recommendations against screening in women 40-49 years could impact this age group.
The cross-sectional analysis included all patients presenting for a screening mammogram without clinical findings at New York Presbyterian Hospital–Weill Cornell Medical College (NYPH-WCMC) in New York City. Women aged 40-49 comprised 33.5% of the screening population.
During the 4 years, 205 breast cancers were detected (4.7/1,000). Women in their forties accounted for 19% of the cancers found, which would represent a substantial degree of underdiagnoses if they had been missed, reported Dr. Elizabeth Arleo, a radiologist at NYPH-WCMC.
Notably, only three of the women in their forties with screen-detected breast cancer had a first-degree relative with premenopausal breast cancer, thereby placing them at higher risk. More than half of the cancers in this subgroup, however, were invasive (21/39).
If the USPSTF recommendations had been enforced during the study years, these cancers may not have been detected until the patients’ baseline screening at age 50 or until the cancers had progressed to clinically evident, palpable disease, Dr. Arleo coauthors said.
Dr. Levin reported relationships with HealthHelp and Outpatient Imaging Affiliates. Dr. Arleo said she had no relevant financial disclosures.
CHICAGO – There has been a clear and abrupt decline in screening mammography in the wake of the controversial breast cancer screening recommendations by the U.S. Preventive Services Task Force.
After climbing steadily at a rate of about 1% per year since 2001, breast mammography among women on Medicare declined 4.3% in 2010, the first full year after the USPSTF recommendations came out.
The reasons for the decline aren’t entirely clear, but it may be that women over age 74 years began to follow the task force recommendations and no longer got screened, or that women aged 50-74 years extended their screening interval from 1 to 2 years, again according to task force recommendations, lead author Dr. David C. Levin said at the annual meeting of the Radiological Society of North America.
"What is clear is that the introduction of those recommendations in late 2009 had a chilling effect on the willingness of women to get screened," he said. "It remains to be seen whether this trend is going to continue and whether it will affect breast cancer mortality."
For the analysis, Dr. Levin reviewed film and digital screening mammography codes in the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2005 to 2010. The database provides volumes for each code each year.
From these data, he calculated that the screening mammography rate per 1,000 female Medicare beneficiaries had been growing in small increments each year from 311.6 in 2005 to 312.4 in 2006, 316.2 in 2007, 320.1 in 2008, and 322.9 in 2009. This represents a compound annual growth rate of 0.9%.
After the recommendations came out, the screening mammography rate fell to 309.1/1,000 women in 2010, representing a decline of 4.3% in a single year, said Dr. Levin, a radiologist and founder of the center for research on utilization of imaging services at Thomas Jefferson University Hospital in Philadelphia.
He pointed out that earlier this year, Mayo Clinic researchers reported a 5.7% decline in screening mammography in 2010 among women aged 40-64, based on data from almost 7.9 million women enrolled in nearly 100 health plans.
In a separate presentation at the meeting, investigators analyzed the outcomes of 43,351 screening mammograms performed between 2007 and 2010 to determine how the new USPSTF recommendations against screening in women 40-49 years could impact this age group.
The cross-sectional analysis included all patients presenting for a screening mammogram without clinical findings at New York Presbyterian Hospital–Weill Cornell Medical College (NYPH-WCMC) in New York City. Women aged 40-49 comprised 33.5% of the screening population.
During the 4 years, 205 breast cancers were detected (4.7/1,000). Women in their forties accounted for 19% of the cancers found, which would represent a substantial degree of underdiagnoses if they had been missed, reported Dr. Elizabeth Arleo, a radiologist at NYPH-WCMC.
Notably, only three of the women in their forties with screen-detected breast cancer had a first-degree relative with premenopausal breast cancer, thereby placing them at higher risk. More than half of the cancers in this subgroup, however, were invasive (21/39).
If the USPSTF recommendations had been enforced during the study years, these cancers may not have been detected until the patients’ baseline screening at age 50 or until the cancers had progressed to clinically evident, palpable disease, Dr. Arleo coauthors said.
Dr. Levin reported relationships with HealthHelp and Outpatient Imaging Affiliates. Dr. Arleo said she had no relevant financial disclosures.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Breast mammography among women on Medicare declined 4.3% in 2010, the first full year after the USPSTF recommendations came out.
Data Source: Findings are based on two retrospective analyses of women undergoing screening mammography.
Disclosures: Dr. Levin reported relationships with HealthHelp and Outpatient Imaging Affiliates. Dr. Arleo said she had no relevant financial disclosures.

Study: Uterus Preservation Feasible with Mesh POP Repair System
LAS VEGAS – The Elevate Anterior and Apical system – a transvaginal synthetic mesh repair system – was just as effective when pelvic organ prolapse repair was performed with or without uterine preservation in a prospective, multicenter trial.
Complication rates, including extrusion rates, were low, and there was long-term durability at 24 months, Dr. Edward J. Stanford said at the 41st AAGL Global Ccongress.

"In our opinion, the results support [the idea] that concomitant hysterectomy may not be, or is not, necessary in patients who, after informed consent, would like to preserve their uterus," he said.
The Elevate Anterior and Apical (EAA) transvaginal polypropylene mesh pelvic organ prolapse (POP) repair system is contraindicated in pregnant women and women planning future pregnancies, as the graft will not stretch significantly as the patient grows, according to the device manufacturer, American Medical Systems.
Concerns about the safety and efficacy of transvaginally placed synthetic mesh for POP prompted the American College of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) in late 2011 to recommend that such repairs be reserved for "high-risk patients in whom the benefit of mesh placement may justify the risk, such as those with recurrent prolapse" (Obstet. Gynecol. 2011;118:1459-64).
Dr. Stanford and his fellow investigators at 10 U.S. and 6 European sites sought to prospectively explore the efficacy of the EAA system when utilized with or without uterine preservation in 142 women with anterior vaginal prolapse and/or apical descent of at least stage II.
The primary outcome was treatment failure, defined as at least stage II of the Pelvic Organ Prolapse Quantification system (leading edge of prolapse within 1 cm of the hymenal ring) during follow-up, using the last observation carried forward method.
Three subgroups were analyzed: 61 women with a baseline, prior hysterectomy; 29 with a concomitant hysterectomy; and 51 with no hysterectomy. The groups were well balanced, although 10% of the concomitant group was current smokers, compared with roughly 2% in the other groups. Median gravity was 3 and median parity 2. Their average age was 64 years.
For the apical compartment, success at 24 months was reported in 29 patients with a prior hysterectomy (93.5%), 17 with a concomitant hysterectomy (94.4%), and 24 with no hysterectomy (100%), reported Dr. Stanford, a health care consultant in Las Vegas. Notably, data were missing for 30 of the 61 prior hysterectomy patients, 11 of the 29 concomitant patients, and 27 of the 51 uterine preservation patients.
For the anterior compartment, success was slightly lower at 79.6% with a prior hysterectomy (43 patients), 70.8% with a concomitant hysterectomy (17 patients), and 89% with uterine preservation (41 patients). Data were missing for 7, 5, and 5 patients, respectively.
There was no significant difference in success between the groups for the apical (P = .46) or anterior (P = .154) compartments, he said.
Dr. Stanford defended the use of the study’s methodology in an interview, and said that the last observation carried forward method was the best way to account for missing data.
"It penalized those groups with missing data, and our results were still good," he said.
Three patients in the prior and current hysterectomy groups experienced an intraoperative complication, as did seven patients with uterine preservation. Estimated blood loss was similar at a median of 50 mL in each group.
There was a nonsignificant trend toward higher mesh extrusion in women undergoing a concomitant hysterectomy (13.8%; 4 of 29), compared with those with a prior hysterectomy (5%; 3 of 61) or no hysterectomy (2%; 1 of 51), Dr. Stanford said.
"We are a little concerned that the higher extrusion rate with a concomitant hysterectomy, which has been seen in other studies, is coming true in this study as well," he added. "Perhaps, the higher number of smokers in that subgroup may be a factor."
Smoking and urogenital atrophy have been acknowledged as risk factors for mesh erosion. About 42% of patients were on vaginal or topical estrogen prior to surgery, and all received preoperative antibiotics, he said during a discussion of the study.
Almost all of the failures occurred early on, up to 3 months after surgery, with extrusion rates remaining stable from year 1 to year 2, Dr. Stanford said in an interview.
"A lot of experts are saying that late complications are happening on a regular basis, but we’re just not seeing it in our data or in other prolapse studies," he said.
Dr. Stanford contends that reported extrusion rates of 15% or more occurred primarily among surgeons still learning the technique. He credits the high success rate in the current study to the use of a standardized approach and the expertise of the surgeons, who were given specific training on the Elevate system and perform at least 100 vaginal mesh repairs annually.
"It’s a long learning curve, and you have to continue with an adequate volume and know how to do a proper dissection," he said. "You need about 25 to 50 cases to have a level of expertise, which is consistent with the surgical literature. We know that’s true of total laparoscopic hysterectomy as well."
In its joint communication, ACOG and AUGS recommended that surgeons placing vaginal mesh undergo training specific to each device, have experience with reconstructive surgical procedures, and have a thorough understanding of pelvic anatomy.
Based on the current limited data, the two groups said there is a "small, but significant group" of patients who experience permanent or life-altering sequelae as result of the transvaginal mesh placement.
In its updated July 2011 safety report, however, the Food and Drug Administration said that serious complications related to POP transvaginal mesh repair "are not rare," and that the procedure "may expose patients to greater risk" than traditional nonmesh repair.
The FDA’s Obstetrics and Gynecology Devices Panel subsequently called for postmarket studies to evaluate current products, and recommended that new vaginal mesh products for POP repair not be approved through the less rigorous Class II 501(k) process, but reclassified as Class III to ensure that premarket clinical studies are conducted.
Law firms are aggressively litigating cases against transvaginal mesh manufacturers, with commercials soliciting new clients airing on local television in Las Vegas throughout the AAGL meeting. American Medical Systems, which also manufactures the Apogee and Perigee mesh products, is one of several companies to be named in at least six ongoing multidistrict litigations.
Dr. Stanford said the current data are reassuring, and that there were no significant differences between women with or without uterine preservation in quality of life scores on the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12), Pelvic Floor Incontinence Questionnaire-7 (PFIQ-7), and Pelvic Floor Distress Inventory (PFDI).
Dr. Stanford disclosed a research grant from study sponsor American Medical Systems, maker of the Elevate system.
LAS VEGAS – The Elevate Anterior and Apical system – a transvaginal synthetic mesh repair system – was just as effective when pelvic organ prolapse repair was performed with or without uterine preservation in a prospective, multicenter trial.
Complication rates, including extrusion rates, were low, and there was long-term durability at 24 months, Dr. Edward J. Stanford said at the 41st AAGL Global Ccongress.
"In our opinion, the results support [the idea] that concomitant hysterectomy may not be, or is not, necessary in patients who, after informed consent, would like to preserve their uterus," he said.
The Elevate Anterior and Apical (EAA) transvaginal polypropylene mesh pelvic organ prolapse (POP) repair system is contraindicated in pregnant women and women planning future pregnancies, as the graft will not stretch significantly as the patient grows, according to the device manufacturer, American Medical Systems.
Concerns about the safety and efficacy of transvaginally placed synthetic mesh for POP prompted the American College of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) in late 2011 to recommend that such repairs be reserved for "high-risk patients in whom the benefit of mesh placement may justify the risk, such as those with recurrent prolapse" (Obstet. Gynecol. 2011;118:1459-64).
Dr. Stanford and his fellow investigators at 10 U.S. and 6 European sites sought to prospectively explore the efficacy of the EAA system when utilized with or without uterine preservation in 142 women with anterior vaginal prolapse and/or apical descent of at least stage II.
The primary outcome was treatment failure, defined as at least stage II of the Pelvic Organ Prolapse Quantification system (leading edge of prolapse within 1 cm of the hymenal ring) during follow-up, using the last observation carried forward method.
Three subgroups were analyzed: 61 women with a baseline, prior hysterectomy; 29 with a concomitant hysterectomy; and 51 with no hysterectomy. The groups were well balanced, although 10% of the concomitant group was current smokers, compared with roughly 2% in the other groups. Median gravity was 3 and median parity 2. Their average age was 64 years.
For the apical compartment, success at 24 months was reported in 29 patients with a prior hysterectomy (93.5%), 17 with a concomitant hysterectomy (94.4%), and 24 with no hysterectomy (100%), reported Dr. Stanford, a health care consultant in Las Vegas. Notably, data were missing for 30 of the 61 prior hysterectomy patients, 11 of the 29 concomitant patients, and 27 of the 51 uterine preservation patients.
For the anterior compartment, success was slightly lower at 79.6% with a prior hysterectomy (43 patients), 70.8% with a concomitant hysterectomy (17 patients), and 89% with uterine preservation (41 patients). Data were missing for 7, 5, and 5 patients, respectively.
There was no significant difference in success between the groups for the apical (P = .46) or anterior (P = .154) compartments, he said.
Dr. Stanford defended the use of the study’s methodology in an interview, and said that the last observation carried forward method was the best way to account for missing data.
"It penalized those groups with missing data, and our results were still good," he said.
Three patients in the prior and current hysterectomy groups experienced an intraoperative complication, as did seven patients with uterine preservation. Estimated blood loss was similar at a median of 50 mL in each group.
There was a nonsignificant trend toward higher mesh extrusion in women undergoing a concomitant hysterectomy (13.8%; 4 of 29), compared with those with a prior hysterectomy (5%; 3 of 61) or no hysterectomy (2%; 1 of 51), Dr. Stanford said.
"We are a little concerned that the higher extrusion rate with a concomitant hysterectomy, which has been seen in other studies, is coming true in this study as well," he added. "Perhaps, the higher number of smokers in that subgroup may be a factor."
Smoking and urogenital atrophy have been acknowledged as risk factors for mesh erosion. About 42% of patients were on vaginal or topical estrogen prior to surgery, and all received preoperative antibiotics, he said during a discussion of the study.
Almost all of the failures occurred early on, up to 3 months after surgery, with extrusion rates remaining stable from year 1 to year 2, Dr. Stanford said in an interview.
"A lot of experts are saying that late complications are happening on a regular basis, but we’re just not seeing it in our data or in other prolapse studies," he said.
Dr. Stanford contends that reported extrusion rates of 15% or more occurred primarily among surgeons still learning the technique. He credits the high success rate in the current study to the use of a standardized approach and the expertise of the surgeons, who were given specific training on the Elevate system and perform at least 100 vaginal mesh repairs annually.
"It’s a long learning curve, and you have to continue with an adequate volume and know how to do a proper dissection," he said. "You need about 25 to 50 cases to have a level of expertise, which is consistent with the surgical literature. We know that’s true of total laparoscopic hysterectomy as well."
In its joint communication, ACOG and AUGS recommended that surgeons placing vaginal mesh undergo training specific to each device, have experience with reconstructive surgical procedures, and have a thorough understanding of pelvic anatomy.
Based on the current limited data, the two groups said there is a "small, but significant group" of patients who experience permanent or life-altering sequelae as result of the transvaginal mesh placement.
In its updated July 2011 safety report, however, the Food and Drug Administration said that serious complications related to POP transvaginal mesh repair "are not rare," and that the procedure "may expose patients to greater risk" than traditional nonmesh repair.
The FDA’s Obstetrics and Gynecology Devices Panel subsequently called for postmarket studies to evaluate current products, and recommended that new vaginal mesh products for POP repair not be approved through the less rigorous Class II 501(k) process, but reclassified as Class III to ensure that premarket clinical studies are conducted.
Law firms are aggressively litigating cases against transvaginal mesh manufacturers, with commercials soliciting new clients airing on local television in Las Vegas throughout the AAGL meeting. American Medical Systems, which also manufactures the Apogee and Perigee mesh products, is one of several companies to be named in at least six ongoing multidistrict litigations.
Dr. Stanford said the current data are reassuring, and that there were no significant differences between women with or without uterine preservation in quality of life scores on the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12), Pelvic Floor Incontinence Questionnaire-7 (PFIQ-7), and Pelvic Floor Distress Inventory (PFDI).
Dr. Stanford disclosed a research grant from study sponsor American Medical Systems, maker of the Elevate system.
LAS VEGAS – The Elevate Anterior and Apical system – a transvaginal synthetic mesh repair system – was just as effective when pelvic organ prolapse repair was performed with or without uterine preservation in a prospective, multicenter trial.
Complication rates, including extrusion rates, were low, and there was long-term durability at 24 months, Dr. Edward J. Stanford said at the 41st AAGL Global Ccongress.
"In our opinion, the results support [the idea] that concomitant hysterectomy may not be, or is not, necessary in patients who, after informed consent, would like to preserve their uterus," he said.
The Elevate Anterior and Apical (EAA) transvaginal polypropylene mesh pelvic organ prolapse (POP) repair system is contraindicated in pregnant women and women planning future pregnancies, as the graft will not stretch significantly as the patient grows, according to the device manufacturer, American Medical Systems.
Concerns about the safety and efficacy of transvaginally placed synthetic mesh for POP prompted the American College of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) in late 2011 to recommend that such repairs be reserved for "high-risk patients in whom the benefit of mesh placement may justify the risk, such as those with recurrent prolapse" (Obstet. Gynecol. 2011;118:1459-64).
Dr. Stanford and his fellow investigators at 10 U.S. and 6 European sites sought to prospectively explore the efficacy of the EAA system when utilized with or without uterine preservation in 142 women with anterior vaginal prolapse and/or apical descent of at least stage II.
The primary outcome was treatment failure, defined as at least stage II of the Pelvic Organ Prolapse Quantification system (leading edge of prolapse within 1 cm of the hymenal ring) during follow-up, using the last observation carried forward method.
Three subgroups were analyzed: 61 women with a baseline, prior hysterectomy; 29 with a concomitant hysterectomy; and 51 with no hysterectomy. The groups were well balanced, although 10% of the concomitant group was current smokers, compared with roughly 2% in the other groups. Median gravity was 3 and median parity 2. Their average age was 64 years.
For the apical compartment, success at 24 months was reported in 29 patients with a prior hysterectomy (93.5%), 17 with a concomitant hysterectomy (94.4%), and 24 with no hysterectomy (100%), reported Dr. Stanford, a health care consultant in Las Vegas. Notably, data were missing for 30 of the 61 prior hysterectomy patients, 11 of the 29 concomitant patients, and 27 of the 51 uterine preservation patients.
For the anterior compartment, success was slightly lower at 79.6% with a prior hysterectomy (43 patients), 70.8% with a concomitant hysterectomy (17 patients), and 89% with uterine preservation (41 patients). Data were missing for 7, 5, and 5 patients, respectively.
There was no significant difference in success between the groups for the apical (P = .46) or anterior (P = .154) compartments, he said.
Dr. Stanford defended the use of the study’s methodology in an interview, and said that the last observation carried forward method was the best way to account for missing data.
"It penalized those groups with missing data, and our results were still good," he said.
Three patients in the prior and current hysterectomy groups experienced an intraoperative complication, as did seven patients with uterine preservation. Estimated blood loss was similar at a median of 50 mL in each group.
There was a nonsignificant trend toward higher mesh extrusion in women undergoing a concomitant hysterectomy (13.8%; 4 of 29), compared with those with a prior hysterectomy (5%; 3 of 61) or no hysterectomy (2%; 1 of 51), Dr. Stanford said.
"We are a little concerned that the higher extrusion rate with a concomitant hysterectomy, which has been seen in other studies, is coming true in this study as well," he added. "Perhaps, the higher number of smokers in that subgroup may be a factor."
Smoking and urogenital atrophy have been acknowledged as risk factors for mesh erosion. About 42% of patients were on vaginal or topical estrogen prior to surgery, and all received preoperative antibiotics, he said during a discussion of the study.
Almost all of the failures occurred early on, up to 3 months after surgery, with extrusion rates remaining stable from year 1 to year 2, Dr. Stanford said in an interview.
"A lot of experts are saying that late complications are happening on a regular basis, but we’re just not seeing it in our data or in other prolapse studies," he said.
Dr. Stanford contends that reported extrusion rates of 15% or more occurred primarily among surgeons still learning the technique. He credits the high success rate in the current study to the use of a standardized approach and the expertise of the surgeons, who were given specific training on the Elevate system and perform at least 100 vaginal mesh repairs annually.
"It’s a long learning curve, and you have to continue with an adequate volume and know how to do a proper dissection," he said. "You need about 25 to 50 cases to have a level of expertise, which is consistent with the surgical literature. We know that’s true of total laparoscopic hysterectomy as well."
In its joint communication, ACOG and AUGS recommended that surgeons placing vaginal mesh undergo training specific to each device, have experience with reconstructive surgical procedures, and have a thorough understanding of pelvic anatomy.
Based on the current limited data, the two groups said there is a "small, but significant group" of patients who experience permanent or life-altering sequelae as result of the transvaginal mesh placement.
In its updated July 2011 safety report, however, the Food and Drug Administration said that serious complications related to POP transvaginal mesh repair "are not rare," and that the procedure "may expose patients to greater risk" than traditional nonmesh repair.
The FDA’s Obstetrics and Gynecology Devices Panel subsequently called for postmarket studies to evaluate current products, and recommended that new vaginal mesh products for POP repair not be approved through the less rigorous Class II 501(k) process, but reclassified as Class III to ensure that premarket clinical studies are conducted.
Law firms are aggressively litigating cases against transvaginal mesh manufacturers, with commercials soliciting new clients airing on local television in Las Vegas throughout the AAGL meeting. American Medical Systems, which also manufactures the Apogee and Perigee mesh products, is one of several companies to be named in at least six ongoing multidistrict litigations.
Dr. Stanford said the current data are reassuring, and that there were no significant differences between women with or without uterine preservation in quality of life scores on the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12), Pelvic Floor Incontinence Questionnaire-7 (PFIQ-7), and Pelvic Floor Distress Inventory (PFDI).
Dr. Stanford disclosed a research grant from study sponsor American Medical Systems, maker of the Elevate system.
AT THE 41st AAGL GLOBAL CONGRESS
Major Finding: For the apical compartment, success at 24 months was reported in 93.5% of patients with a prior hysterectomy (29 patients), 94.4% of those with a concomitant hysterectomy (17), and 100% with no hysterectomy (24). For the anterior compartment, success was 79.6% with a prior hysterectomy (43 patients), 70.8% with a concomitant hysterectomy (17), and 89% with uterine preservation (41).
Data Source: This was a prospective, international study of 142 women treated with the Elevate Anterior and Apical Prolapse Repair System.
Disclosures: Dr. Stanford disclosed a research grant from study sponsor American Medical Systems, maker of the Elevate system.

Older Docs Still Balking at Minimally Invasive Hysterectomy
LAS VEGAS – Gynecologists who completed their residency more than 20 years ago are half as likely as more recent graduates to perform a laparoscopic hysterectomy, a survey has shown.
Total abdominal hysterectomy was the most commonly performed route for 35% of respondents, with 24% preferring a vaginal approach, and only 8% reporting total laparoscopic hysterectomy as their preferred method.

"Rates of laparoscopic hysterectomy are increasing, but as seen in other studies, the abdominal approach is still the preferred method," Dr. Terri Febbraro said at the 41st AAGL Global Congress.
Both a 2009 American College of Obstetricians and Gynecologists (ACOG) committee opinion and a 2010 AAGL position statement favor vaginal hysterectomy as the preferred route. Laparoscopic hysterectomy can be used as an alternative in the minority of cases when the vaginal approach is not feasible or indicated.
Still, the disconnect continues.
Total abdominal surgeries account for roughly two-thirds of hysterectomies in the United States (Obstet. Gynecol. 2007;110;1091-5), although that number may be declining. Only 8% of gynecologists, however, would choose an abdominal hysterectomy for themselves or their spouse (J. Minim. Invasive Gynecol. 2010;17:167-75), said Dr. February, a fourth-year resident at Brown University in Providence, R.I.
To explore the perceived barriers and contraindications among gynecologists to providing minimally invasive surgery (MIS), Dr. Febbraro and her associates sent a cross-sectional survey via the Web and mail to 802 ACOG fellows from October 2008 to May 2009. A total of 417 surveys (52%) were returned.
The majority of respondents practiced general ob.gyn. (94%) and were in private practice (82%). Almost half, or 42%, graduated residency more than 20 years ago and 31% graduated in the last 10 years. There was an equal gender split, and all geographic districts were represented.
Three-fourths of respondents (78%) reported performing an average of one to five hysterectomies per month, and 8% performed six or more, which was defined as high volume for the analysis.
In addition to the three approaches described above, 19% of respondents preferred laparoscopic-assisted vaginal, 11% supracervical laparoscopic, and 3% supracervical abdominal (3%) hysterectomy.
Physicians who reported performing laparoscopic hysterectomies most often were significantly more likely to have graduated from residency in the previous 10 years than were physicians who performed vaginal hysterectomies most often (52% vs. 26.2%; P = .03).
The odds of performing MIS, either vaginally or laparoscopically, increased with surgical volume (OR, 8.37) and specialized training (OR, 9.37). This was even more pronounced among physicians who reported performing laparoscopic hysterectomies most often (OR, 12.0, and OR, 16.4), Dr. Febbraro said.
Providers graduating from residency more than 20 years ago were half as likely to prefer a laparoscopic approach as were those graduating less than 10 years ago (OR, 0.44).
Providers who preferred an open abdominal approach were significantly more likely than those using MIS to cite minimal descent, narrow introitus, and a uterus more than 12 weeks in size as perceived contraindications to a vaginal hysterectomy, she said.
Prior exploratory laparotomy, endometriosis, and a uterus larger than 12 or 16 weeks were significantly more likely to be cited as contraindications to laparoscopic hysterectomy by providers preferring an open approach.
Those providers who preferred an abdominal approach also reported significantly more contraindications than did MIS providers to vaginal hysterectomy (mean 4.4 vs. 3.4; P = .0003) and laparoscopic hysterectomy (mean, 1.5 vs. 0.8; P less than .0001). The lower number of contraindications to laparoscopic hysterectomy is noteworthy, given that this approach was preferred by fewer respondents than either open or vaginal surgery, Dr. Febbraro noted.
"As surgical volume and specialized training increase, it is likely that perceived barriers and contraindications will decrease, prompting providers to offer minimally invasive surgeries more readily," she said. "Training programs addressing these factors could have an impact on providers’ choice of surgical approach."
During a discussion of the study, Dr. Febbraro said that she and her colleagues did not distinguish between rural and urban providers, but that no regional differences were observed.
Dr. Febbraro reported no relevant financial disclosures. One of her coauthors is an ACOG employee.
LAS VEGAS – Gynecologists who completed their residency more than 20 years ago are half as likely as more recent graduates to perform a laparoscopic hysterectomy, a survey has shown.
Total abdominal hysterectomy was the most commonly performed route for 35% of respondents, with 24% preferring a vaginal approach, and only 8% reporting total laparoscopic hysterectomy as their preferred method.
"Rates of laparoscopic hysterectomy are increasing, but as seen in other studies, the abdominal approach is still the preferred method," Dr. Terri Febbraro said at the 41st AAGL Global Congress.
Both a 2009 American College of Obstetricians and Gynecologists (ACOG) committee opinion and a 2010 AAGL position statement favor vaginal hysterectomy as the preferred route. Laparoscopic hysterectomy can be used as an alternative in the minority of cases when the vaginal approach is not feasible or indicated.
Still, the disconnect continues.
Total abdominal surgeries account for roughly two-thirds of hysterectomies in the United States (Obstet. Gynecol. 2007;110;1091-5), although that number may be declining. Only 8% of gynecologists, however, would choose an abdominal hysterectomy for themselves or their spouse (J. Minim. Invasive Gynecol. 2010;17:167-75), said Dr. February, a fourth-year resident at Brown University in Providence, R.I.
To explore the perceived barriers and contraindications among gynecologists to providing minimally invasive surgery (MIS), Dr. Febbraro and her associates sent a cross-sectional survey via the Web and mail to 802 ACOG fellows from October 2008 to May 2009. A total of 417 surveys (52%) were returned.
The majority of respondents practiced general ob.gyn. (94%) and were in private practice (82%). Almost half, or 42%, graduated residency more than 20 years ago and 31% graduated in the last 10 years. There was an equal gender split, and all geographic districts were represented.
Three-fourths of respondents (78%) reported performing an average of one to five hysterectomies per month, and 8% performed six or more, which was defined as high volume for the analysis.
In addition to the three approaches described above, 19% of respondents preferred laparoscopic-assisted vaginal, 11% supracervical laparoscopic, and 3% supracervical abdominal (3%) hysterectomy.
Physicians who reported performing laparoscopic hysterectomies most often were significantly more likely to have graduated from residency in the previous 10 years than were physicians who performed vaginal hysterectomies most often (52% vs. 26.2%; P = .03).
The odds of performing MIS, either vaginally or laparoscopically, increased with surgical volume (OR, 8.37) and specialized training (OR, 9.37). This was even more pronounced among physicians who reported performing laparoscopic hysterectomies most often (OR, 12.0, and OR, 16.4), Dr. Febbraro said.
Providers graduating from residency more than 20 years ago were half as likely to prefer a laparoscopic approach as were those graduating less than 10 years ago (OR, 0.44).
Providers who preferred an open abdominal approach were significantly more likely than those using MIS to cite minimal descent, narrow introitus, and a uterus more than 12 weeks in size as perceived contraindications to a vaginal hysterectomy, she said.
Prior exploratory laparotomy, endometriosis, and a uterus larger than 12 or 16 weeks were significantly more likely to be cited as contraindications to laparoscopic hysterectomy by providers preferring an open approach.
Those providers who preferred an abdominal approach also reported significantly more contraindications than did MIS providers to vaginal hysterectomy (mean 4.4 vs. 3.4; P = .0003) and laparoscopic hysterectomy (mean, 1.5 vs. 0.8; P less than .0001). The lower number of contraindications to laparoscopic hysterectomy is noteworthy, given that this approach was preferred by fewer respondents than either open or vaginal surgery, Dr. Febbraro noted.
"As surgical volume and specialized training increase, it is likely that perceived barriers and contraindications will decrease, prompting providers to offer minimally invasive surgeries more readily," she said. "Training programs addressing these factors could have an impact on providers’ choice of surgical approach."
During a discussion of the study, Dr. Febbraro said that she and her colleagues did not distinguish between rural and urban providers, but that no regional differences were observed.
Dr. Febbraro reported no relevant financial disclosures. One of her coauthors is an ACOG employee.
LAS VEGAS – Gynecologists who completed their residency more than 20 years ago are half as likely as more recent graduates to perform a laparoscopic hysterectomy, a survey has shown.
Total abdominal hysterectomy was the most commonly performed route for 35% of respondents, with 24% preferring a vaginal approach, and only 8% reporting total laparoscopic hysterectomy as their preferred method.
"Rates of laparoscopic hysterectomy are increasing, but as seen in other studies, the abdominal approach is still the preferred method," Dr. Terri Febbraro said at the 41st AAGL Global Congress.
Both a 2009 American College of Obstetricians and Gynecologists (ACOG) committee opinion and a 2010 AAGL position statement favor vaginal hysterectomy as the preferred route. Laparoscopic hysterectomy can be used as an alternative in the minority of cases when the vaginal approach is not feasible or indicated.
Still, the disconnect continues.
Total abdominal surgeries account for roughly two-thirds of hysterectomies in the United States (Obstet. Gynecol. 2007;110;1091-5), although that number may be declining. Only 8% of gynecologists, however, would choose an abdominal hysterectomy for themselves or their spouse (J. Minim. Invasive Gynecol. 2010;17:167-75), said Dr. February, a fourth-year resident at Brown University in Providence, R.I.
To explore the perceived barriers and contraindications among gynecologists to providing minimally invasive surgery (MIS), Dr. Febbraro and her associates sent a cross-sectional survey via the Web and mail to 802 ACOG fellows from October 2008 to May 2009. A total of 417 surveys (52%) were returned.
The majority of respondents practiced general ob.gyn. (94%) and were in private practice (82%). Almost half, or 42%, graduated residency more than 20 years ago and 31% graduated in the last 10 years. There was an equal gender split, and all geographic districts were represented.
Three-fourths of respondents (78%) reported performing an average of one to five hysterectomies per month, and 8% performed six or more, which was defined as high volume for the analysis.
In addition to the three approaches described above, 19% of respondents preferred laparoscopic-assisted vaginal, 11% supracervical laparoscopic, and 3% supracervical abdominal (3%) hysterectomy.
Physicians who reported performing laparoscopic hysterectomies most often were significantly more likely to have graduated from residency in the previous 10 years than were physicians who performed vaginal hysterectomies most often (52% vs. 26.2%; P = .03).
The odds of performing MIS, either vaginally or laparoscopically, increased with surgical volume (OR, 8.37) and specialized training (OR, 9.37). This was even more pronounced among physicians who reported performing laparoscopic hysterectomies most often (OR, 12.0, and OR, 16.4), Dr. Febbraro said.
Providers graduating from residency more than 20 years ago were half as likely to prefer a laparoscopic approach as were those graduating less than 10 years ago (OR, 0.44).
Providers who preferred an open abdominal approach were significantly more likely than those using MIS to cite minimal descent, narrow introitus, and a uterus more than 12 weeks in size as perceived contraindications to a vaginal hysterectomy, she said.
Prior exploratory laparotomy, endometriosis, and a uterus larger than 12 or 16 weeks were significantly more likely to be cited as contraindications to laparoscopic hysterectomy by providers preferring an open approach.
Those providers who preferred an abdominal approach also reported significantly more contraindications than did MIS providers to vaginal hysterectomy (mean 4.4 vs. 3.4; P = .0003) and laparoscopic hysterectomy (mean, 1.5 vs. 0.8; P less than .0001). The lower number of contraindications to laparoscopic hysterectomy is noteworthy, given that this approach was preferred by fewer respondents than either open or vaginal surgery, Dr. Febbraro noted.
"As surgical volume and specialized training increase, it is likely that perceived barriers and contraindications will decrease, prompting providers to offer minimally invasive surgeries more readily," she said. "Training programs addressing these factors could have an impact on providers’ choice of surgical approach."
During a discussion of the study, Dr. Febbraro said that she and her colleagues did not distinguish between rural and urban providers, but that no regional differences were observed.
Dr. Febbraro reported no relevant financial disclosures. One of her coauthors is an ACOG employee.
AT THE 41ST AAGL GLOBAL CONGRESS
Major Finding: Physicians who reported performing laparoscopic hysterectomies most often were significantly more likely to have graduated from residency in the previous 10 years than were physicians who performed vaginal hysterectomies most often (52% vs. 26.2%; P value = .03).
Data Source: Data are from a mixed-mode, cross-sectional survey sent to 802 ACOG fellows; 52% responded.
Disclosures: Dr. Febbraro reported no relevant financial disclosures. One of her coauthors is an ACOG employee.

Suture Method Linked to Vaginal Cuff Complications
LAS VEGAS – The risk of vaginal cuff complications was not influenced by the type of hysterectomy performed, although suture technique was a factor, in a retrospective analysis of 604 patients.
"In our study, the intracorporeal cuff suture was superior to the vaginal suture to prevent the vaginal cuff complications of evisceration and dehiscence in total laparoscopic hysterectomy," Dr. Yoon Byoung Kim said at the 41st AAGL Global Congress.
Although vaginal cuff dehiscence is a rare complication of hysterectomy, concerns have been raised that total laparoscopic hysterectomies may be associated with an increased risk of this potentially morbid complication.
Researchers at Beth Israel Deaconess Medical Center recently reported an updated incidence of vaginal cuff dehiscence of 1.35% after total laparoscopic hysterectomy, the highest rate among all hysterectomy modes evaluated (Obstet. Gynecol. 2011;118:794-801). This was dramatically lower, however, than the 4.93% incidence the group reported in a previous study (J. Minim. Invasive Gynecol. 2007;14:311-7).
Dr. Kim and her associates looked at the risk factors for vaginal cuff complications for six types of hysterectomies performed in 604 women between June 2007 and June 2011 at Korea University Anam Hospital, Seoul, Korea. The approach was robotic hysterectomy in 7, robotic radical hysterectomy and node dissection (RRHND) in 9, total laparoscopic hysterectomy (TLH) in 276, laparoscopically assisted vaginal hysterectomy (LAVH) in 238, laparoscopic radical hysterectomy and node dissection (LRHND) in 11, and abdominal radical hysterectomy in 63.
The suture technique was intracorporeal continuous for robotic hysterectomy, RRHND, and LRHND; intracorporeal or vaginal continuous locking for total laparoscopic hysterectomy; vaginal continuous locking for LAVH; and a 5-point suture with figure-8 vaginal suture for abdominal radical hysterectomy. Two TLH patients closed with a 3-point intracorporeal suture and figure-8 vaginal suture were excluded from the TLH analysis.
Among the remaining 274 TLH women, there were 1 case of evisceration and 4 cases of dehiscence with the intracorporeal continuous suture, compared with 0 cases of evisceration and 11 cases of dehiscence with the vaginal continuous locking suture (2.63% vs. 10.47%; P = .02).
In addition, the duration between surgery and the vaginal cuff complication was significantly longer with the intracorporeal suture than the vaginal suture (72.8 days vs. 23.6 days; P = .01), Dr. Kim said.
"The possible reasons for this result can be infection or delicate layering of the submucosal layer," she said.
Among all 604 women, there were 3 eviscerations (0.49%) and 21 cases of dehiscence (3.43%).
The incidence of evisceration was 0% for robotic hysterectomy, 11.1% for RRHND, 0.36% for total laparoscopic hysterectomy, 0% for LAVH, 0% for LRHND, and 1.5% for abdominal radical hysterectomy. The incidence of vaginal dehiscence was 0% for radical hysterectomy, 0% for RRHND, 5.43% for total laparoscopic hysterectomy, 1.68% for LAVH, 0% for LRHND, and 3.17% for abdominal radical hysterectomy.
Although total laparoscopic hysterectomy was associated with a higher incidence of cuff complications, the finding was not statistically significant, Dr. Kim said. Overall, there was no significant correlation between the incidence of cuff complications and the type of operation or suture technique.
The investigators then performed a subgroup analysis that included age, body mass index, operation time, estimated blood loss, postoperative fever, and antibiotic use. None of these risk factors correlated with dehiscence or evisceration (P = 0.99, 0.32, 0.46, 0.32, .06, and 0.42, respectively), Dr. Kim reported.
The limitations of the study were its small sample size, significant heterogeneity, and variation in sample size between groups, she said.
Dr. Kim reported no relevant financial disclosures.
LAS VEGAS – The risk of vaginal cuff complications was not influenced by the type of hysterectomy performed, although suture technique was a factor, in a retrospective analysis of 604 patients.
"In our study, the intracorporeal cuff suture was superior to the vaginal suture to prevent the vaginal cuff complications of evisceration and dehiscence in total laparoscopic hysterectomy," Dr. Yoon Byoung Kim said at the 41st AAGL Global Congress.
Although vaginal cuff dehiscence is a rare complication of hysterectomy, concerns have been raised that total laparoscopic hysterectomies may be associated with an increased risk of this potentially morbid complication.
Researchers at Beth Israel Deaconess Medical Center recently reported an updated incidence of vaginal cuff dehiscence of 1.35% after total laparoscopic hysterectomy, the highest rate among all hysterectomy modes evaluated (Obstet. Gynecol. 2011;118:794-801). This was dramatically lower, however, than the 4.93% incidence the group reported in a previous study (J. Minim. Invasive Gynecol. 2007;14:311-7).
Dr. Kim and her associates looked at the risk factors for vaginal cuff complications for six types of hysterectomies performed in 604 women between June 2007 and June 2011 at Korea University Anam Hospital, Seoul, Korea. The approach was robotic hysterectomy in 7, robotic radical hysterectomy and node dissection (RRHND) in 9, total laparoscopic hysterectomy (TLH) in 276, laparoscopically assisted vaginal hysterectomy (LAVH) in 238, laparoscopic radical hysterectomy and node dissection (LRHND) in 11, and abdominal radical hysterectomy in 63.
The suture technique was intracorporeal continuous for robotic hysterectomy, RRHND, and LRHND; intracorporeal or vaginal continuous locking for total laparoscopic hysterectomy; vaginal continuous locking for LAVH; and a 5-point suture with figure-8 vaginal suture for abdominal radical hysterectomy. Two TLH patients closed with a 3-point intracorporeal suture and figure-8 vaginal suture were excluded from the TLH analysis.
Among the remaining 274 TLH women, there were 1 case of evisceration and 4 cases of dehiscence with the intracorporeal continuous suture, compared with 0 cases of evisceration and 11 cases of dehiscence with the vaginal continuous locking suture (2.63% vs. 10.47%; P = .02).
In addition, the duration between surgery and the vaginal cuff complication was significantly longer with the intracorporeal suture than the vaginal suture (72.8 days vs. 23.6 days; P = .01), Dr. Kim said.
"The possible reasons for this result can be infection or delicate layering of the submucosal layer," she said.
Among all 604 women, there were 3 eviscerations (0.49%) and 21 cases of dehiscence (3.43%).
The incidence of evisceration was 0% for robotic hysterectomy, 11.1% for RRHND, 0.36% for total laparoscopic hysterectomy, 0% for LAVH, 0% for LRHND, and 1.5% for abdominal radical hysterectomy. The incidence of vaginal dehiscence was 0% for radical hysterectomy, 0% for RRHND, 5.43% for total laparoscopic hysterectomy, 1.68% for LAVH, 0% for LRHND, and 3.17% for abdominal radical hysterectomy.
Although total laparoscopic hysterectomy was associated with a higher incidence of cuff complications, the finding was not statistically significant, Dr. Kim said. Overall, there was no significant correlation between the incidence of cuff complications and the type of operation or suture technique.
The investigators then performed a subgroup analysis that included age, body mass index, operation time, estimated blood loss, postoperative fever, and antibiotic use. None of these risk factors correlated with dehiscence or evisceration (P = 0.99, 0.32, 0.46, 0.32, .06, and 0.42, respectively), Dr. Kim reported.
The limitations of the study were its small sample size, significant heterogeneity, and variation in sample size between groups, she said.
Dr. Kim reported no relevant financial disclosures.
LAS VEGAS – The risk of vaginal cuff complications was not influenced by the type of hysterectomy performed, although suture technique was a factor, in a retrospective analysis of 604 patients.
"In our study, the intracorporeal cuff suture was superior to the vaginal suture to prevent the vaginal cuff complications of evisceration and dehiscence in total laparoscopic hysterectomy," Dr. Yoon Byoung Kim said at the 41st AAGL Global Congress.
Although vaginal cuff dehiscence is a rare complication of hysterectomy, concerns have been raised that total laparoscopic hysterectomies may be associated with an increased risk of this potentially morbid complication.
Researchers at Beth Israel Deaconess Medical Center recently reported an updated incidence of vaginal cuff dehiscence of 1.35% after total laparoscopic hysterectomy, the highest rate among all hysterectomy modes evaluated (Obstet. Gynecol. 2011;118:794-801). This was dramatically lower, however, than the 4.93% incidence the group reported in a previous study (J. Minim. Invasive Gynecol. 2007;14:311-7).
Dr. Kim and her associates looked at the risk factors for vaginal cuff complications for six types of hysterectomies performed in 604 women between June 2007 and June 2011 at Korea University Anam Hospital, Seoul, Korea. The approach was robotic hysterectomy in 7, robotic radical hysterectomy and node dissection (RRHND) in 9, total laparoscopic hysterectomy (TLH) in 276, laparoscopically assisted vaginal hysterectomy (LAVH) in 238, laparoscopic radical hysterectomy and node dissection (LRHND) in 11, and abdominal radical hysterectomy in 63.
The suture technique was intracorporeal continuous for robotic hysterectomy, RRHND, and LRHND; intracorporeal or vaginal continuous locking for total laparoscopic hysterectomy; vaginal continuous locking for LAVH; and a 5-point suture with figure-8 vaginal suture for abdominal radical hysterectomy. Two TLH patients closed with a 3-point intracorporeal suture and figure-8 vaginal suture were excluded from the TLH analysis.
Among the remaining 274 TLH women, there were 1 case of evisceration and 4 cases of dehiscence with the intracorporeal continuous suture, compared with 0 cases of evisceration and 11 cases of dehiscence with the vaginal continuous locking suture (2.63% vs. 10.47%; P = .02).
In addition, the duration between surgery and the vaginal cuff complication was significantly longer with the intracorporeal suture than the vaginal suture (72.8 days vs. 23.6 days; P = .01), Dr. Kim said.
"The possible reasons for this result can be infection or delicate layering of the submucosal layer," she said.
Among all 604 women, there were 3 eviscerations (0.49%) and 21 cases of dehiscence (3.43%).
The incidence of evisceration was 0% for robotic hysterectomy, 11.1% for RRHND, 0.36% for total laparoscopic hysterectomy, 0% for LAVH, 0% for LRHND, and 1.5% for abdominal radical hysterectomy. The incidence of vaginal dehiscence was 0% for radical hysterectomy, 0% for RRHND, 5.43% for total laparoscopic hysterectomy, 1.68% for LAVH, 0% for LRHND, and 3.17% for abdominal radical hysterectomy.
Although total laparoscopic hysterectomy was associated with a higher incidence of cuff complications, the finding was not statistically significant, Dr. Kim said. Overall, there was no significant correlation between the incidence of cuff complications and the type of operation or suture technique.
The investigators then performed a subgroup analysis that included age, body mass index, operation time, estimated blood loss, postoperative fever, and antibiotic use. None of these risk factors correlated with dehiscence or evisceration (P = 0.99, 0.32, 0.46, 0.32, .06, and 0.42, respectively), Dr. Kim reported.
The limitations of the study were its small sample size, significant heterogeneity, and variation in sample size between groups, she said.
Dr. Kim reported no relevant financial disclosures.
AT THE 41ST AAGL GLOBAL CONGRESS
Major Finding: One case of evisceration and 4 cases of dehiscence occurred with the intracorporeal continuous suture vs. 11 cases of dehiscence with the vaginal continuous locking suture (2.63% vs. 10.47%; P value = .02)
Data Source: Data are from a retrospective, single-center analysis involving 604 women undergoing six types of hysterectomies.
Disclosures: Dr. Kim reported no relevant financial disclosures.
Active lifestyle boosts brain structure in older adults
CHICAGO – An active lifestyle positively influences brain volume in older adults with or without Alzheimer’s disease, a magnetic resonance imaging study revealed.
Among 876 individuals, the average gray matter volume was 663 mL in those with an active lifestyle, compared with 628 mL in those with an inactive lifestyle. That equates to a significant 5% difference (P value less than .05).
"That is a large number difference when you consider the tremendous biologic forces that have to be at work for gray matter volume to decrease," lead author Dr. Cyrus Raji said in a press briefing at the annual meeting of the Radiological Society of North America.
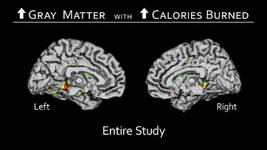
Prior research has looked at the influence of individual lifestyle factors such as obesity or walking on brain structure, but not a variety of activities, as was done in the current study. Improving lifestyle could reduce the risk for Alzheimer’s disease by 50%, resulting in 1.1 million fewer cases in the United States, said Dr. Raji, a radiology resident at the University of California, Los Angeles.
"In the United States, the lack of physical activity is the No. 1 most powerful lifestyle factor, contributing to 21% of cases of Alzheimer’s disease," he said. "Worldwide, it is the third most powerful risk factor after low educational attainment and smoking."
To determine how lifestyle influences brain structure, the investigators used MRI scans and clinical data collected over 20 years from 876 individuals enrolled at four sites in the Cardiovascular Health Study. The Minnesota Leisure Time Physical Activity Questionnaire was used to assess caloric expenditure during 15 different aerobic activities: swimming, hiking, aerobics, jogging, tennis, racquetball, walking, gardening, mowing, raking, golfing, bicycling, dancing, calisthenics, and riding an exercise bike. A technique called voxel-based morphology was used to quantify the amount of brain matter in the MRI scans.
The participants expended an average of 1,093 kcal/week. Overall, 42% were men, 88% were white, and about 25% had been diagnosed with Alzheimer’s disease or mild cognitive impairment (MCI). The cohort was largely overweight, with an average body mass index of 27 kg/m2. Their average age was 78 years.
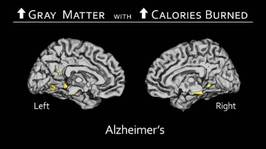
The analysis controlled for head size; age; gender; body mass index, which has been related to brain structure and atrophy; small vessel ischemic disease, which reflects processes like diabetes and hypertension that can affect the brain; Alzheimer’s or mild cognitive impairment (MCI) status; and study site.
The most active participants burned an average of 3,434 kcal/week, compared with 348 kcal/week in the least active participants.
There was larger bilateral gray matter volume in the cingulate gyrus, hippocampus, and temporal lobes – areas responsible for memory and learning – among individuals who burned the most calories per week, compared with those who burned the fewest, Dr. Raji said.
"That means the areas of the brain that are benefiting the most from this active lifestyle are also the areas affected in Alzheimer’s disease and are also responsible for cognition," he explained.

The same findings were observed in participants with Alzheimer’s disease or MCI. "People with Alzheimer’s who were more physically active in our study weren’t cured, but they had less deterioration in their brain matter volume, compared with the sedentary individuals," said Dr. Raji, who described the study as one of the largest voxel-based imaging studies of humans ever done.
Press briefing moderator Dr. Candice A. Johnstone of the Medical College of Wisconsin in Milwaukee said in an interview that what’s unique about the study is that it shows that physical activity actually changes brain volume and that this benefit can be obtained through a variety of activities. This is especially important when counseling patients who may have difficulty walking.
What the study fails to address, however, is whether an active lifestyle will have an impact on the symptoms of Alzheimer’s or MCI.
"Whether physical activity can significantly alter the course remains to be seen," she said. "It may be that people with changes in brain volume may be more likely to have [fewer] symptoms because their brain’s actively working to enhance those areas, but that’s the subject of future research. We do not know that."
Dr. Raji and Dr. Johnstone reported no conflicts of interest.
CHICAGO – An active lifestyle positively influences brain volume in older adults with or without Alzheimer’s disease, a magnetic resonance imaging study revealed.
Among 876 individuals, the average gray matter volume was 663 mL in those with an active lifestyle, compared with 628 mL in those with an inactive lifestyle. That equates to a significant 5% difference (P value less than .05).
"That is a large number difference when you consider the tremendous biologic forces that have to be at work for gray matter volume to decrease," lead author Dr. Cyrus Raji said in a press briefing at the annual meeting of the Radiological Society of North America.
Prior research has looked at the influence of individual lifestyle factors such as obesity or walking on brain structure, but not a variety of activities, as was done in the current study. Improving lifestyle could reduce the risk for Alzheimer’s disease by 50%, resulting in 1.1 million fewer cases in the United States, said Dr. Raji, a radiology resident at the University of California, Los Angeles.
"In the United States, the lack of physical activity is the No. 1 most powerful lifestyle factor, contributing to 21% of cases of Alzheimer’s disease," he said. "Worldwide, it is the third most powerful risk factor after low educational attainment and smoking."
To determine how lifestyle influences brain structure, the investigators used MRI scans and clinical data collected over 20 years from 876 individuals enrolled at four sites in the Cardiovascular Health Study. The Minnesota Leisure Time Physical Activity Questionnaire was used to assess caloric expenditure during 15 different aerobic activities: swimming, hiking, aerobics, jogging, tennis, racquetball, walking, gardening, mowing, raking, golfing, bicycling, dancing, calisthenics, and riding an exercise bike. A technique called voxel-based morphology was used to quantify the amount of brain matter in the MRI scans.
The participants expended an average of 1,093 kcal/week. Overall, 42% were men, 88% were white, and about 25% had been diagnosed with Alzheimer’s disease or mild cognitive impairment (MCI). The cohort was largely overweight, with an average body mass index of 27 kg/m2. Their average age was 78 years.
The analysis controlled for head size; age; gender; body mass index, which has been related to brain structure and atrophy; small vessel ischemic disease, which reflects processes like diabetes and hypertension that can affect the brain; Alzheimer’s or mild cognitive impairment (MCI) status; and study site.
The most active participants burned an average of 3,434 kcal/week, compared with 348 kcal/week in the least active participants.
There was larger bilateral gray matter volume in the cingulate gyrus, hippocampus, and temporal lobes – areas responsible for memory and learning – among individuals who burned the most calories per week, compared with those who burned the fewest, Dr. Raji said.
"That means the areas of the brain that are benefiting the most from this active lifestyle are also the areas affected in Alzheimer’s disease and are also responsible for cognition," he explained.
The same findings were observed in participants with Alzheimer’s disease or MCI. "People with Alzheimer’s who were more physically active in our study weren’t cured, but they had less deterioration in their brain matter volume, compared with the sedentary individuals," said Dr. Raji, who described the study as one of the largest voxel-based imaging studies of humans ever done.
Press briefing moderator Dr. Candice A. Johnstone of the Medical College of Wisconsin in Milwaukee said in an interview that what’s unique about the study is that it shows that physical activity actually changes brain volume and that this benefit can be obtained through a variety of activities. This is especially important when counseling patients who may have difficulty walking.
What the study fails to address, however, is whether an active lifestyle will have an impact on the symptoms of Alzheimer’s or MCI.
"Whether physical activity can significantly alter the course remains to be seen," she said. "It may be that people with changes in brain volume may be more likely to have [fewer] symptoms because their brain’s actively working to enhance those areas, but that’s the subject of future research. We do not know that."
Dr. Raji and Dr. Johnstone reported no conflicts of interest.
CHICAGO – An active lifestyle positively influences brain volume in older adults with or without Alzheimer’s disease, a magnetic resonance imaging study revealed.
Among 876 individuals, the average gray matter volume was 663 mL in those with an active lifestyle, compared with 628 mL in those with an inactive lifestyle. That equates to a significant 5% difference (P value less than .05).
"That is a large number difference when you consider the tremendous biologic forces that have to be at work for gray matter volume to decrease," lead author Dr. Cyrus Raji said in a press briefing at the annual meeting of the Radiological Society of North America.
Prior research has looked at the influence of individual lifestyle factors such as obesity or walking on brain structure, but not a variety of activities, as was done in the current study. Improving lifestyle could reduce the risk for Alzheimer’s disease by 50%, resulting in 1.1 million fewer cases in the United States, said Dr. Raji, a radiology resident at the University of California, Los Angeles.
"In the United States, the lack of physical activity is the No. 1 most powerful lifestyle factor, contributing to 21% of cases of Alzheimer’s disease," he said. "Worldwide, it is the third most powerful risk factor after low educational attainment and smoking."
To determine how lifestyle influences brain structure, the investigators used MRI scans and clinical data collected over 20 years from 876 individuals enrolled at four sites in the Cardiovascular Health Study. The Minnesota Leisure Time Physical Activity Questionnaire was used to assess caloric expenditure during 15 different aerobic activities: swimming, hiking, aerobics, jogging, tennis, racquetball, walking, gardening, mowing, raking, golfing, bicycling, dancing, calisthenics, and riding an exercise bike. A technique called voxel-based morphology was used to quantify the amount of brain matter in the MRI scans.
The participants expended an average of 1,093 kcal/week. Overall, 42% were men, 88% were white, and about 25% had been diagnosed with Alzheimer’s disease or mild cognitive impairment (MCI). The cohort was largely overweight, with an average body mass index of 27 kg/m2. Their average age was 78 years.
The analysis controlled for head size; age; gender; body mass index, which has been related to brain structure and atrophy; small vessel ischemic disease, which reflects processes like diabetes and hypertension that can affect the brain; Alzheimer’s or mild cognitive impairment (MCI) status; and study site.
The most active participants burned an average of 3,434 kcal/week, compared with 348 kcal/week in the least active participants.
There was larger bilateral gray matter volume in the cingulate gyrus, hippocampus, and temporal lobes – areas responsible for memory and learning – among individuals who burned the most calories per week, compared with those who burned the fewest, Dr. Raji said.
"That means the areas of the brain that are benefiting the most from this active lifestyle are also the areas affected in Alzheimer’s disease and are also responsible for cognition," he explained.
The same findings were observed in participants with Alzheimer’s disease or MCI. "People with Alzheimer’s who were more physically active in our study weren’t cured, but they had less deterioration in their brain matter volume, compared with the sedentary individuals," said Dr. Raji, who described the study as one of the largest voxel-based imaging studies of humans ever done.
Press briefing moderator Dr. Candice A. Johnstone of the Medical College of Wisconsin in Milwaukee said in an interview that what’s unique about the study is that it shows that physical activity actually changes brain volume and that this benefit can be obtained through a variety of activities. This is especially important when counseling patients who may have difficulty walking.
What the study fails to address, however, is whether an active lifestyle will have an impact on the symptoms of Alzheimer’s or MCI.
"Whether physical activity can significantly alter the course remains to be seen," she said. "It may be that people with changes in brain volume may be more likely to have [fewer] symptoms because their brain’s actively working to enhance those areas, but that’s the subject of future research. We do not know that."
Dr. Raji and Dr. Johnstone reported no conflicts of interest.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: There was larger bilateral gray matter volume in the cingulate gyrus, hippocampus, and temporal lobes – areas responsible for memory and learning – among individuals who burned the most calories per week (3,434 kcal), compared with those who burned the least (348 kcal).
Data Source: This study reviewed MRI scans and clinical data collected over 20 years from 876 individuals with normal cognition, Alzheimer’s disease, or mild cognitive impairment who were enrolled at four sites in the Cardiovascular Health Study.
Disclosures: Dr. Raji and Dr. Johnstone reported no conflicts of interest.