User login
VIDEO: Radioimmunotherapy eyed as possible HIV treatment
Radioimmunotherapy targeting the HIV gp41 glycoprotein destroyed residual reservoirs of HIV infected cells in the blood samples of patients treated with antiretrovirals. In an interview at the annual meeting of the Radiological Society of North America, Dr. Ekaterina Dadachova discusses the findings and the next steps for testing the approach in patients with HIV.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Radioimmunotherapy targeting the HIV gp41 glycoprotein destroyed residual reservoirs of HIV infected cells in the blood samples of patients treated with antiretrovirals. In an interview at the annual meeting of the Radiological Society of North America, Dr. Ekaterina Dadachova discusses the findings and the next steps for testing the approach in patients with HIV.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Radioimmunotherapy targeting the HIV gp41 glycoprotein destroyed residual reservoirs of HIV infected cells in the blood samples of patients treated with antiretrovirals. In an interview at the annual meeting of the Radiological Society of North America, Dr. Ekaterina Dadachova discusses the findings and the next steps for testing the approach in patients with HIV.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Breast tomosynthesis moving beyond clinical trials
CHICAGO – Screening all-comers with three-dimensional mammography increased breast cancer detection by 22.7% and reduced recall rates by 15.6% in a large observational study.
Although a 3D digital breast tomosynthesis (DBT) system was approved for breast cancer screening and diagnosis in the United States in 2011, DBT is typically a supplemental screening tool to standard 2D digital mammography.
In November 2011, however, the Hospital of the University of Pennsylvania, Philadelphia, took the plunge and began using DBT for every breast screening patient, regardless of age, cancer risk, breast density, or ability to pay.
Over a 17-month-period, DBT detected 82 cancers in 15,632 women, or 5.25 cancers per 1,000 cases, Dr. Emily F. Conant reported at the annual meeting of the Radiological Society of North America.

This compares with 46 cancers, or 4.28 cancers per 1,000 cases, detected with conventional mammography in 10,752 women in the 12 months prior to the switch.
The difference in cancer detection rates between 2D and 3D mammography did not reach statistical significance (P = .226), probably because of the small number of cases, Dr. Conant, a radiology professor at the hospital, said at a press briefing.
Compared with conventional mammography, however, DBT significantly improved the proportion of positive screening mammograms from which cancer was diagnosed by 45% (P = .036) and increased the detection of deadly invasive cancers by a nonsignificant 31%.
When asked whether the study showed that invasive lobular cancer can be better detected with DBT, Dr. Conant replied, "Yes. Those were the most remarkable cases, because those tumors tend to be large at presentation and notoriously difficult to detect because they don’t often form the mass that an invasive ductal carcinoma does."
Press briefing moderator Dr. Debra L. Somers Copit, chief of mammography and director of the Gershon-Cohen Breast Clinic at Einstein Medical Center, Philadelphia, described the improvements in cancer detection in the real-world cohort as "groundbreaking work for this modality that we hope will pan out across multiple institutions."

Reimbursement is problematic, however, as insurers will only pay for 2D mammography images taken as part of a tomosynthesis screening exam, she said in an interview.
Still, she personally believes tomosynthesis should now be the standard of care, adding, "I can’t imagine reading a mammogram without it."
Results from the current study are comparable with data reported recently from trials in the United States (Radiology 2013;269:694-700) and Norway (Eur. Radiol. 2013;23:2061-71) that paired 2D imaging with 3D tomosynthesis, Dr. Conant observed.
When the investigators looked at the independent risk factor of breast density, DBT also did a better job of detecting cancer than conventional mammography in fatty, scattered, heterogeneous, and extremely dense breasts, and it improved recall rates for all categories except extremely dense breasts, she said.
Overall, DBT significantly reduced the proportion of women recalled for additional imaging from 10.39% to 8.77% (P = .001).
DBT is an exciting improvement over 2D mammography and more economical than breast screening with magnetic resonance imaging, but it is "not the solution to everything," Dr. Conant said. The radiation dose for the average breast is within safety limits, but twice that of a regular mammogram.
"The cost to the patient is not monetary at our site; it may be at other sites," she said. "I think right now the dose is the biggest cost."
The May 2013 approval of Hologic’s C-View 2D imaging software, which eliminates the need for additional 2D exposures by generating 2D images from 3D tomosynthesis data, might address this, Dr. Conant added.
Dr. Conant reported consulting for Hologic. Her coauthors reported no financial disclosures. Dr. Copit is on Hologic’s scientific advisory board.
CHICAGO – Screening all-comers with three-dimensional mammography increased breast cancer detection by 22.7% and reduced recall rates by 15.6% in a large observational study.
Although a 3D digital breast tomosynthesis (DBT) system was approved for breast cancer screening and diagnosis in the United States in 2011, DBT is typically a supplemental screening tool to standard 2D digital mammography.
In November 2011, however, the Hospital of the University of Pennsylvania, Philadelphia, took the plunge and began using DBT for every breast screening patient, regardless of age, cancer risk, breast density, or ability to pay.
Over a 17-month-period, DBT detected 82 cancers in 15,632 women, or 5.25 cancers per 1,000 cases, Dr. Emily F. Conant reported at the annual meeting of the Radiological Society of North America.
This compares with 46 cancers, or 4.28 cancers per 1,000 cases, detected with conventional mammography in 10,752 women in the 12 months prior to the switch.
The difference in cancer detection rates between 2D and 3D mammography did not reach statistical significance (P = .226), probably because of the small number of cases, Dr. Conant, a radiology professor at the hospital, said at a press briefing.
Compared with conventional mammography, however, DBT significantly improved the proportion of positive screening mammograms from which cancer was diagnosed by 45% (P = .036) and increased the detection of deadly invasive cancers by a nonsignificant 31%.
When asked whether the study showed that invasive lobular cancer can be better detected with DBT, Dr. Conant replied, "Yes. Those were the most remarkable cases, because those tumors tend to be large at presentation and notoriously difficult to detect because they don’t often form the mass that an invasive ductal carcinoma does."
Press briefing moderator Dr. Debra L. Somers Copit, chief of mammography and director of the Gershon-Cohen Breast Clinic at Einstein Medical Center, Philadelphia, described the improvements in cancer detection in the real-world cohort as "groundbreaking work for this modality that we hope will pan out across multiple institutions."
Reimbursement is problematic, however, as insurers will only pay for 2D mammography images taken as part of a tomosynthesis screening exam, she said in an interview.
Still, she personally believes tomosynthesis should now be the standard of care, adding, "I can’t imagine reading a mammogram without it."
Results from the current study are comparable with data reported recently from trials in the United States (Radiology 2013;269:694-700) and Norway (Eur. Radiol. 2013;23:2061-71) that paired 2D imaging with 3D tomosynthesis, Dr. Conant observed.
When the investigators looked at the independent risk factor of breast density, DBT also did a better job of detecting cancer than conventional mammography in fatty, scattered, heterogeneous, and extremely dense breasts, and it improved recall rates for all categories except extremely dense breasts, she said.
Overall, DBT significantly reduced the proportion of women recalled for additional imaging from 10.39% to 8.77% (P = .001).
DBT is an exciting improvement over 2D mammography and more economical than breast screening with magnetic resonance imaging, but it is "not the solution to everything," Dr. Conant said. The radiation dose for the average breast is within safety limits, but twice that of a regular mammogram.
"The cost to the patient is not monetary at our site; it may be at other sites," she said. "I think right now the dose is the biggest cost."
The May 2013 approval of Hologic’s C-View 2D imaging software, which eliminates the need for additional 2D exposures by generating 2D images from 3D tomosynthesis data, might address this, Dr. Conant added.
Dr. Conant reported consulting for Hologic. Her coauthors reported no financial disclosures. Dr. Copit is on Hologic’s scientific advisory board.
CHICAGO – Screening all-comers with three-dimensional mammography increased breast cancer detection by 22.7% and reduced recall rates by 15.6% in a large observational study.
Although a 3D digital breast tomosynthesis (DBT) system was approved for breast cancer screening and diagnosis in the United States in 2011, DBT is typically a supplemental screening tool to standard 2D digital mammography.
In November 2011, however, the Hospital of the University of Pennsylvania, Philadelphia, took the plunge and began using DBT for every breast screening patient, regardless of age, cancer risk, breast density, or ability to pay.
Over a 17-month-period, DBT detected 82 cancers in 15,632 women, or 5.25 cancers per 1,000 cases, Dr. Emily F. Conant reported at the annual meeting of the Radiological Society of North America.
This compares with 46 cancers, or 4.28 cancers per 1,000 cases, detected with conventional mammography in 10,752 women in the 12 months prior to the switch.
The difference in cancer detection rates between 2D and 3D mammography did not reach statistical significance (P = .226), probably because of the small number of cases, Dr. Conant, a radiology professor at the hospital, said at a press briefing.
Compared with conventional mammography, however, DBT significantly improved the proportion of positive screening mammograms from which cancer was diagnosed by 45% (P = .036) and increased the detection of deadly invasive cancers by a nonsignificant 31%.
When asked whether the study showed that invasive lobular cancer can be better detected with DBT, Dr. Conant replied, "Yes. Those were the most remarkable cases, because those tumors tend to be large at presentation and notoriously difficult to detect because they don’t often form the mass that an invasive ductal carcinoma does."
Press briefing moderator Dr. Debra L. Somers Copit, chief of mammography and director of the Gershon-Cohen Breast Clinic at Einstein Medical Center, Philadelphia, described the improvements in cancer detection in the real-world cohort as "groundbreaking work for this modality that we hope will pan out across multiple institutions."
Reimbursement is problematic, however, as insurers will only pay for 2D mammography images taken as part of a tomosynthesis screening exam, she said in an interview.
Still, she personally believes tomosynthesis should now be the standard of care, adding, "I can’t imagine reading a mammogram without it."
Results from the current study are comparable with data reported recently from trials in the United States (Radiology 2013;269:694-700) and Norway (Eur. Radiol. 2013;23:2061-71) that paired 2D imaging with 3D tomosynthesis, Dr. Conant observed.
When the investigators looked at the independent risk factor of breast density, DBT also did a better job of detecting cancer than conventional mammography in fatty, scattered, heterogeneous, and extremely dense breasts, and it improved recall rates for all categories except extremely dense breasts, she said.
Overall, DBT significantly reduced the proportion of women recalled for additional imaging from 10.39% to 8.77% (P = .001).
DBT is an exciting improvement over 2D mammography and more economical than breast screening with magnetic resonance imaging, but it is "not the solution to everything," Dr. Conant said. The radiation dose for the average breast is within safety limits, but twice that of a regular mammogram.
"The cost to the patient is not monetary at our site; it may be at other sites," she said. "I think right now the dose is the biggest cost."
The May 2013 approval of Hologic’s C-View 2D imaging software, which eliminates the need for additional 2D exposures by generating 2D images from 3D tomosynthesis data, might address this, Dr. Conant added.
Dr. Conant reported consulting for Hologic. Her coauthors reported no financial disclosures. Dr. Copit is on Hologic’s scientific advisory board.
AT RSNA 2013
Major finding: Digital breast tomosynthesis detected 5.25 cancers per 1,000 cases over a 17-month period, compared with 4.28 cancers per 1,000 cases over 12 months with conventional mammography.
Data source: An observational study of 15,632 women screened using DBT and 10,752 women using 2-D digital mammography at the Hospital of the University of Pennsylvania.
Disclosures: Dr. Conant reported consulting for Hologic Inc. Her coauthors reported no financial disclosures. Dr. Copit is on Hologic’s scientific advisory board.

DTI detects long-term axonal injury in veterans with TBI
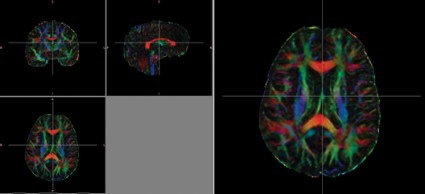
CHICAGO – Diffusion tensor imaging identified axonal damage in veterans more than 4 years after a blast-related traumatic brain injury in a phase I/II study.
None of the veterans had abnormalities on conventional CT or MRI, Thomas M. Malone reported at the annual meeting of the Radiological Society of North America.
Prior studies have shown that diffusion tensor imaging (DTI) identified white matter injuries in the middle cerebellar peduncles, cingulum bundles, and right orbitofrontal region of asymptomatic veterans with mild TBI less than 90 days post injury (N. Engl. J. Med. 2011;364:2091-100).

However, another study showed that the correlation between DTI findings and neuropsychological symptoms in the acute phase was inconsistent at 2.5 years (J. Neurotrauma 2010;27:683-94).
In the phase I portion of the current study, 10 veterans with blast-related mild TBI were evaluated at an average of 51.3 months after injury, along with 10 healthy controls.

Despite having normal findings on CT and MR imaging, veterans had significantly higher average DTI-derived fractional anisotropy (FA) values than did controls in the right posterior limb of the internal capsule (0.739 vs. 0.706; P less than .05) and left posterior limb of the internal capsule (0.777 vs. 0.716; P less than .05). FA values were similar between groups in the anterior limbs of the internal capsule and genu and splenium of the corpus callosum. These higher FA values differ from results found in DTI studies conducted during the acute phase of blast-related mild TBI, said Mr. Malone of St. Louis University.
Overall, veterans scored significantly lower than did controls on the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), immediate memory index (81.6 vs. 99.8; P less than .01), visual-constructional index (82.9 vs. 100.2; P less than .05), and delayed memory index (81.5 vs. 97.4; P less than .05).
Significant correlations were found between internal capsule FA values and neuropsychological tests measuring attention, memory, and motor functioning, including the RBANS and grooved pegboard test, Mr. Malone said.
For the phase II portion of the study, the investigators increased the cohort to 21 mild TBI and 8 moderate TBI veterans and 19 healthy controls, and removed outliers with FA values more than 2 standard deviations above or below the mean.

In this analysis, average FA values were significantly lower in the splenium of the corpus callosum among veterans than in controls (0.777 vs. 0.79; P less than .05).
"Decreased FA values among the TBI group are perhaps indicative of fiber damage and may explain the chronic deficits observed in mild blast injuries," Mr. Malone said.
Recovery from long-term axonal injury is possible, but the brain has somewhat limited capabilities in repairing itself, said senior author Dr. Richard Bucholz, professor and vice chair of neurosurgery at St. Louis University.
"My general feeling is if it doesn’t repair at 51 months, it probably never repairs," he said in an interview.
Although DTI findings of long-term axonal injury have important implications in terms of rehabilitation and continued problems associated with TBI injuries, both men urged caution in interpreting the results.
"I wouldn’t want to sell this as a diagnostic test," Mr. Malone said in a press briefing. "These were between-group differences."
Future studies will require larger numbers of veterans and the use of more robust preprocessing software such as Tortoise from the National Institutes of Health, automated segmentation, and voxel-based morphometry analysis.
Mr. Malone and his coauthors reported having no relevant financial disclosures.
CHICAGO – Diffusion tensor imaging identified axonal damage in veterans more than 4 years after a blast-related traumatic brain injury in a phase I/II study.
None of the veterans had abnormalities on conventional CT or MRI, Thomas M. Malone reported at the annual meeting of the Radiological Society of North America.
Prior studies have shown that diffusion tensor imaging (DTI) identified white matter injuries in the middle cerebellar peduncles, cingulum bundles, and right orbitofrontal region of asymptomatic veterans with mild TBI less than 90 days post injury (N. Engl. J. Med. 2011;364:2091-100).
However, another study showed that the correlation between DTI findings and neuropsychological symptoms in the acute phase was inconsistent at 2.5 years (J. Neurotrauma 2010;27:683-94).
In the phase I portion of the current study, 10 veterans with blast-related mild TBI were evaluated at an average of 51.3 months after injury, along with 10 healthy controls.
Despite having normal findings on CT and MR imaging, veterans had significantly higher average DTI-derived fractional anisotropy (FA) values than did controls in the right posterior limb of the internal capsule (0.739 vs. 0.706; P less than .05) and left posterior limb of the internal capsule (0.777 vs. 0.716; P less than .05). FA values were similar between groups in the anterior limbs of the internal capsule and genu and splenium of the corpus callosum. These higher FA values differ from results found in DTI studies conducted during the acute phase of blast-related mild TBI, said Mr. Malone of St. Louis University.
Overall, veterans scored significantly lower than did controls on the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), immediate memory index (81.6 vs. 99.8; P less than .01), visual-constructional index (82.9 vs. 100.2; P less than .05), and delayed memory index (81.5 vs. 97.4; P less than .05).
Significant correlations were found between internal capsule FA values and neuropsychological tests measuring attention, memory, and motor functioning, including the RBANS and grooved pegboard test, Mr. Malone said.
For the phase II portion of the study, the investigators increased the cohort to 21 mild TBI and 8 moderate TBI veterans and 19 healthy controls, and removed outliers with FA values more than 2 standard deviations above or below the mean.
In this analysis, average FA values were significantly lower in the splenium of the corpus callosum among veterans than in controls (0.777 vs. 0.79; P less than .05).
"Decreased FA values among the TBI group are perhaps indicative of fiber damage and may explain the chronic deficits observed in mild blast injuries," Mr. Malone said.
Recovery from long-term axonal injury is possible, but the brain has somewhat limited capabilities in repairing itself, said senior author Dr. Richard Bucholz, professor and vice chair of neurosurgery at St. Louis University.
"My general feeling is if it doesn’t repair at 51 months, it probably never repairs," he said in an interview.
Although DTI findings of long-term axonal injury have important implications in terms of rehabilitation and continued problems associated with TBI injuries, both men urged caution in interpreting the results.
"I wouldn’t want to sell this as a diagnostic test," Mr. Malone said in a press briefing. "These were between-group differences."
Future studies will require larger numbers of veterans and the use of more robust preprocessing software such as Tortoise from the National Institutes of Health, automated segmentation, and voxel-based morphometry analysis.
Mr. Malone and his coauthors reported having no relevant financial disclosures.
CHICAGO – Diffusion tensor imaging identified axonal damage in veterans more than 4 years after a blast-related traumatic brain injury in a phase I/II study.
None of the veterans had abnormalities on conventional CT or MRI, Thomas M. Malone reported at the annual meeting of the Radiological Society of North America.
Prior studies have shown that diffusion tensor imaging (DTI) identified white matter injuries in the middle cerebellar peduncles, cingulum bundles, and right orbitofrontal region of asymptomatic veterans with mild TBI less than 90 days post injury (N. Engl. J. Med. 2011;364:2091-100).
However, another study showed that the correlation between DTI findings and neuropsychological symptoms in the acute phase was inconsistent at 2.5 years (J. Neurotrauma 2010;27:683-94).
In the phase I portion of the current study, 10 veterans with blast-related mild TBI were evaluated at an average of 51.3 months after injury, along with 10 healthy controls.
Despite having normal findings on CT and MR imaging, veterans had significantly higher average DTI-derived fractional anisotropy (FA) values than did controls in the right posterior limb of the internal capsule (0.739 vs. 0.706; P less than .05) and left posterior limb of the internal capsule (0.777 vs. 0.716; P less than .05). FA values were similar between groups in the anterior limbs of the internal capsule and genu and splenium of the corpus callosum. These higher FA values differ from results found in DTI studies conducted during the acute phase of blast-related mild TBI, said Mr. Malone of St. Louis University.
Overall, veterans scored significantly lower than did controls on the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), immediate memory index (81.6 vs. 99.8; P less than .01), visual-constructional index (82.9 vs. 100.2; P less than .05), and delayed memory index (81.5 vs. 97.4; P less than .05).
Significant correlations were found between internal capsule FA values and neuropsychological tests measuring attention, memory, and motor functioning, including the RBANS and grooved pegboard test, Mr. Malone said.
For the phase II portion of the study, the investigators increased the cohort to 21 mild TBI and 8 moderate TBI veterans and 19 healthy controls, and removed outliers with FA values more than 2 standard deviations above or below the mean.
In this analysis, average FA values were significantly lower in the splenium of the corpus callosum among veterans than in controls (0.777 vs. 0.79; P less than .05).
"Decreased FA values among the TBI group are perhaps indicative of fiber damage and may explain the chronic deficits observed in mild blast injuries," Mr. Malone said.
Recovery from long-term axonal injury is possible, but the brain has somewhat limited capabilities in repairing itself, said senior author Dr. Richard Bucholz, professor and vice chair of neurosurgery at St. Louis University.
"My general feeling is if it doesn’t repair at 51 months, it probably never repairs," he said in an interview.
Although DTI findings of long-term axonal injury have important implications in terms of rehabilitation and continued problems associated with TBI injuries, both men urged caution in interpreting the results.
"I wouldn’t want to sell this as a diagnostic test," Mr. Malone said in a press briefing. "These were between-group differences."
Future studies will require larger numbers of veterans and the use of more robust preprocessing software such as Tortoise from the National Institutes of Health, automated segmentation, and voxel-based morphometry analysis.
Mr. Malone and his coauthors reported having no relevant financial disclosures.
AT RSNA 2013
Major finding: Veterans had significantly higher average diffusion tensor imaging–derived fractional anisotropy values than did healthy controls in the right posterior limb of the internal capsule (0.739 vs. 0.706; P less than .05) and left posterior limb of the internal capsule (0.777 vs. 0.716; P less than .05)
Data source: A retrospective phase I/II study in 39 veterans with traumatic brain injury and 29 healthy controls.
Disclosures: Mr. Malone and his coauthors reported having no relevant financial disclosures.
Energy drinks amp up heart contractility
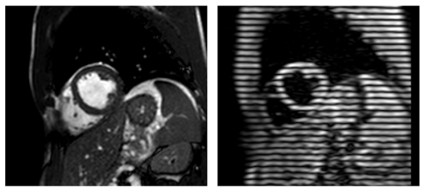
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.

Cardiac magnetic resonance imaging (MRI) was performed in 31 volunteers before and 1 hour after consuming an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time– increased by 6% (–1.19 to –1.26; P = .0032), said Dr. Dörner, with the University of Bonn, Germany.
No significant changes were found in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.

Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.
Cardiac magnetic resonance imaging (MRI) was performed in 31 volunteers before and 1 hour after consuming an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time– increased by 6% (–1.19 to –1.26; P = .0032), said Dr. Dörner, with the University of Bonn, Germany.
No significant changes were found in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.
Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.
Cardiac magnetic resonance imaging (MRI) was performed in 31 volunteers before and 1 hour after consuming an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time– increased by 6% (–1.19 to –1.26; P = .0032), said Dr. Dörner, with the University of Bonn, Germany.
No significant changes were found in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.
Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
AT RSNA 2013
Major finding: One hour after consumption of an energy drink containing caffeine and taurine, mean peak strain increased 7% from baseline and peak systolic strain rate increased 6%.
Data source: A prospective study of 31 healthy volunteers.
Disclosures: Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
Emerging imaging techniques target bronchial thermoplasty
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
AT CHEST 2013
Riociguat benefits persist in pulmonary hypertension
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
AT CHEST 2013
Major finding: Patients on continuous riociguat gained an average of 15 m on the 6-minute timed walk test after 1 year in CHEST-2 and 17 m in PATENT-2.
Data source: Prospective extension studies in 237 patients with chronic thromboembolic pulmonary hypertension and 434 patients with pulmonary arterial hypertension.
Disclosures: CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies, including Bayer.
LABA/LAMA combo beneficial in moderate, severe COPD
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.

Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.
Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.
Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
AT CHEST 2013
Major finding: Low- and high-dose formoterol combinations increased week-24 peak FEV1 by 87 mL and 108 mL, respectively, over aclidinium alone (P < .0001).
Data source: A prospective study of 1,692 patients with moderate to severe COPD.
Disclosures: Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.

IVC filter complications common, retrieval rare
CHICAGO – Penetration of the inferior vena cava and adjacent organs occurred with 46% of IVC filters placed among 262 patients, an award-winning analysis shows.
Grade 2 or 3 penetration was significantly associated with filter type (49% temporary vs. 5.3% permanent; P = .0001) and length of time in place (18.2% less than 30 days vs. 57.3% 30 days or more; P less than .0001).
"The majority of filters were placed for prophylaxis or relative indications and were temporary," Dr. Michael Go said at the annual meeting of the Midwestern Vascular Surgical Society.
The filter penetrated the aorta in 12 cases; duodenum in 26; and spine, colon, or kidney in 6; and simultaneously penetrated two organs in 7. Another 100 filters had struts immediately adjacent to the external aspect of the IVC, possibly indicating tenting of the cava.

Only 1.6% of temporary filters, however, were retrieved during the 3-year study period, he said.
A filter retrieval rate between 1.2% and 5.1% was cited in a recent Medicare data analysis, which reported an alarming 111% increase in the rate of IVC filter placement from 1999 through 2008 (J. Am. Coll. Radio. 2011;8:483-9).
"IVC filter placement is an epidemic because of the ever-increasing number of risk factors being identified for VTE [venous thromboembolism]," said Dr. Go, with the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
Other culprits behind the explosive growth of IVC filters are that angiography suites and catheter labs are now commonplace, the skill needed to insert a filter is easily disseminated, and temporary filters have decreased the threshold for placement.
A total of 591 patients had an IVC filter placed at Ohio State University between January 2006 and December 2009, with an adequate postfilter computed tomography (CT) scan available in 262. CT findings were graded, based on a modified, previously published scale (J. Vasc. Interv. Radiol. 2011;22:70-4), ranging from 0 (struts confined entirely within the IVC) to 3 (strut interacts with aorta, duodenum, or other organs).
Indications for filter placement were prophylaxis in 16.4% and VTE in 83.6%. Among the filters placed for VTE, 44.7% were for absolute indications (inability/failure of anticoagulation) and 55.3% for relative indications.
Grade 0 penetration occurred in 42 filters, grade 1 in 100, grade 2 in 83, and grade 3 in 37, Dr. Go said. Grade 2 or 3 penetration was present in 44.6% of Tulip filters, 74.4% of Celect, 5.3% of Greenfield, and 0% of Optease (P = .0000), according to the analysis, which won this year’s Pfeifer Venous Award from the society.
There was a trend toward increased grade 2 or 3 penetration with uniconical filters vs. biconical filters (46.7% vs. 0%; P = .0645).
In all, 32 patients sought clinical follow-up for abdominal or back pain, but none were conclusively tied to filter problems or penetration.
"It remains unclear if most penetrations caused clinically significant problems," he said.
Audience members asked whether efforts, such as percutaneous retrieval, were being undertaken.
"We have attempted to remove some of these filters, sometimes successfully, sometimes not," Dr. Go responded. "As far as our retrieval rate, I agree 1.6% is dismal. Vascular surgery put in 19% of the filters. We don’t have a specific protocol in place, other than hyperawareness amongst all of us partners about who has a filter in place and to bring them back when appropriate."
He also observed that even when retrieval is undertaken, technical failure rates are high at about 8.5% in the recent literature (Eur. J. Vasc. Endovasc. Surg. 2013;46:353-9).
Dr. Go and his coauthors reported no financial disclosures.
The results of this study speak for themselves – only a very small proportion of temporary filters are actually removed, and penetration of the inferior vena cava and adjacent structures by filter components is relatively common. It is particularly noteworthy that penetration was significantly more common with temporary filters vs. permanent filters, and the risk of penetration increased with time in place. These observations alone should inspire efforts to remove temporary filters as soon as clinically possible. The data presented also indicate that a large proportion of filters are being placed for prophylaxis or relative indications, suggesting that current evidence-based guidelines are not being followed.
However, in spite of the high observed penetration rate, this study does not provide much information on the clinical significance of this finding. In addition, this study represents a highly selected patient population, since a postfilter CT scan was available on less than half of all patients who received inferior vena cava filters during the study period. So while these results may not be completely generalizable, they certainly suggest that the majority of temporary filters become permanent filters, and a critical reappraisal of filter use is warranted.
Dr. R. Eugene Zierler is a professor of surgery at the University of Washington, Seattle, and an associate medical editor of Vascular Specialist.
The results of this study speak for themselves – only a very small proportion of temporary filters are actually removed, and penetration of the inferior vena cava and adjacent structures by filter components is relatively common. It is particularly noteworthy that penetration was significantly more common with temporary filters vs. permanent filters, and the risk of penetration increased with time in place. These observations alone should inspire efforts to remove temporary filters as soon as clinically possible. The data presented also indicate that a large proportion of filters are being placed for prophylaxis or relative indications, suggesting that current evidence-based guidelines are not being followed.
However, in spite of the high observed penetration rate, this study does not provide much information on the clinical significance of this finding. In addition, this study represents a highly selected patient population, since a postfilter CT scan was available on less than half of all patients who received inferior vena cava filters during the study period. So while these results may not be completely generalizable, they certainly suggest that the majority of temporary filters become permanent filters, and a critical reappraisal of filter use is warranted.
Dr. R. Eugene Zierler is a professor of surgery at the University of Washington, Seattle, and an associate medical editor of Vascular Specialist.
The results of this study speak for themselves – only a very small proportion of temporary filters are actually removed, and penetration of the inferior vena cava and adjacent structures by filter components is relatively common. It is particularly noteworthy that penetration was significantly more common with temporary filters vs. permanent filters, and the risk of penetration increased with time in place. These observations alone should inspire efforts to remove temporary filters as soon as clinically possible. The data presented also indicate that a large proportion of filters are being placed for prophylaxis or relative indications, suggesting that current evidence-based guidelines are not being followed.
However, in spite of the high observed penetration rate, this study does not provide much information on the clinical significance of this finding. In addition, this study represents a highly selected patient population, since a postfilter CT scan was available on less than half of all patients who received inferior vena cava filters during the study period. So while these results may not be completely generalizable, they certainly suggest that the majority of temporary filters become permanent filters, and a critical reappraisal of filter use is warranted.
Dr. R. Eugene Zierler is a professor of surgery at the University of Washington, Seattle, and an associate medical editor of Vascular Specialist.
CHICAGO – Penetration of the inferior vena cava and adjacent organs occurred with 46% of IVC filters placed among 262 patients, an award-winning analysis shows.
Grade 2 or 3 penetration was significantly associated with filter type (49% temporary vs. 5.3% permanent; P = .0001) and length of time in place (18.2% less than 30 days vs. 57.3% 30 days or more; P less than .0001).
"The majority of filters were placed for prophylaxis or relative indications and were temporary," Dr. Michael Go said at the annual meeting of the Midwestern Vascular Surgical Society.
The filter penetrated the aorta in 12 cases; duodenum in 26; and spine, colon, or kidney in 6; and simultaneously penetrated two organs in 7. Another 100 filters had struts immediately adjacent to the external aspect of the IVC, possibly indicating tenting of the cava.
Only 1.6% of temporary filters, however, were retrieved during the 3-year study period, he said.
A filter retrieval rate between 1.2% and 5.1% was cited in a recent Medicare data analysis, which reported an alarming 111% increase in the rate of IVC filter placement from 1999 through 2008 (J. Am. Coll. Radio. 2011;8:483-9).
"IVC filter placement is an epidemic because of the ever-increasing number of risk factors being identified for VTE [venous thromboembolism]," said Dr. Go, with the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
Other culprits behind the explosive growth of IVC filters are that angiography suites and catheter labs are now commonplace, the skill needed to insert a filter is easily disseminated, and temporary filters have decreased the threshold for placement.
A total of 591 patients had an IVC filter placed at Ohio State University between January 2006 and December 2009, with an adequate postfilter computed tomography (CT) scan available in 262. CT findings were graded, based on a modified, previously published scale (J. Vasc. Interv. Radiol. 2011;22:70-4), ranging from 0 (struts confined entirely within the IVC) to 3 (strut interacts with aorta, duodenum, or other organs).
Indications for filter placement were prophylaxis in 16.4% and VTE in 83.6%. Among the filters placed for VTE, 44.7% were for absolute indications (inability/failure of anticoagulation) and 55.3% for relative indications.
Grade 0 penetration occurred in 42 filters, grade 1 in 100, grade 2 in 83, and grade 3 in 37, Dr. Go said. Grade 2 or 3 penetration was present in 44.6% of Tulip filters, 74.4% of Celect, 5.3% of Greenfield, and 0% of Optease (P = .0000), according to the analysis, which won this year’s Pfeifer Venous Award from the society.
There was a trend toward increased grade 2 or 3 penetration with uniconical filters vs. biconical filters (46.7% vs. 0%; P = .0645).
In all, 32 patients sought clinical follow-up for abdominal or back pain, but none were conclusively tied to filter problems or penetration.
"It remains unclear if most penetrations caused clinically significant problems," he said.
Audience members asked whether efforts, such as percutaneous retrieval, were being undertaken.
"We have attempted to remove some of these filters, sometimes successfully, sometimes not," Dr. Go responded. "As far as our retrieval rate, I agree 1.6% is dismal. Vascular surgery put in 19% of the filters. We don’t have a specific protocol in place, other than hyperawareness amongst all of us partners about who has a filter in place and to bring them back when appropriate."
He also observed that even when retrieval is undertaken, technical failure rates are high at about 8.5% in the recent literature (Eur. J. Vasc. Endovasc. Surg. 2013;46:353-9).
Dr. Go and his coauthors reported no financial disclosures.
CHICAGO – Penetration of the inferior vena cava and adjacent organs occurred with 46% of IVC filters placed among 262 patients, an award-winning analysis shows.
Grade 2 or 3 penetration was significantly associated with filter type (49% temporary vs. 5.3% permanent; P = .0001) and length of time in place (18.2% less than 30 days vs. 57.3% 30 days or more; P less than .0001).
"The majority of filters were placed for prophylaxis or relative indications and were temporary," Dr. Michael Go said at the annual meeting of the Midwestern Vascular Surgical Society.
The filter penetrated the aorta in 12 cases; duodenum in 26; and spine, colon, or kidney in 6; and simultaneously penetrated two organs in 7. Another 100 filters had struts immediately adjacent to the external aspect of the IVC, possibly indicating tenting of the cava.
Only 1.6% of temporary filters, however, were retrieved during the 3-year study period, he said.
A filter retrieval rate between 1.2% and 5.1% was cited in a recent Medicare data analysis, which reported an alarming 111% increase in the rate of IVC filter placement from 1999 through 2008 (J. Am. Coll. Radio. 2011;8:483-9).
"IVC filter placement is an epidemic because of the ever-increasing number of risk factors being identified for VTE [venous thromboembolism]," said Dr. Go, with the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
Other culprits behind the explosive growth of IVC filters are that angiography suites and catheter labs are now commonplace, the skill needed to insert a filter is easily disseminated, and temporary filters have decreased the threshold for placement.
A total of 591 patients had an IVC filter placed at Ohio State University between January 2006 and December 2009, with an adequate postfilter computed tomography (CT) scan available in 262. CT findings were graded, based on a modified, previously published scale (J. Vasc. Interv. Radiol. 2011;22:70-4), ranging from 0 (struts confined entirely within the IVC) to 3 (strut interacts with aorta, duodenum, or other organs).
Indications for filter placement were prophylaxis in 16.4% and VTE in 83.6%. Among the filters placed for VTE, 44.7% were for absolute indications (inability/failure of anticoagulation) and 55.3% for relative indications.
Grade 0 penetration occurred in 42 filters, grade 1 in 100, grade 2 in 83, and grade 3 in 37, Dr. Go said. Grade 2 or 3 penetration was present in 44.6% of Tulip filters, 74.4% of Celect, 5.3% of Greenfield, and 0% of Optease (P = .0000), according to the analysis, which won this year’s Pfeifer Venous Award from the society.
There was a trend toward increased grade 2 or 3 penetration with uniconical filters vs. biconical filters (46.7% vs. 0%; P = .0645).
In all, 32 patients sought clinical follow-up for abdominal or back pain, but none were conclusively tied to filter problems or penetration.
"It remains unclear if most penetrations caused clinically significant problems," he said.
Audience members asked whether efforts, such as percutaneous retrieval, were being undertaken.
"We have attempted to remove some of these filters, sometimes successfully, sometimes not," Dr. Go responded. "As far as our retrieval rate, I agree 1.6% is dismal. Vascular surgery put in 19% of the filters. We don’t have a specific protocol in place, other than hyperawareness amongst all of us partners about who has a filter in place and to bring them back when appropriate."
He also observed that even when retrieval is undertaken, technical failure rates are high at about 8.5% in the recent literature (Eur. J. Vasc. Endovasc. Surg. 2013;46:353-9).
Dr. Go and his coauthors reported no financial disclosures.

A one-size-fits-all fenestrated graft for iliac aneurysms?
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.

"These people do well,extremely well," Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.
His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off-the-shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type 3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who co-moderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry.
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.
| |
Dr. John F. Eidt |
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of a "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather than discourage innovation in the develop- ment of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor of Vascular Specialist.
|
| |
Dr. John F. Eidt |
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of a "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather than discourage innovation in the develop- ment of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor of Vascular Specialist.
|
| |
Dr. John F. Eidt |
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of a "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather than discourage innovation in the develop- ment of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor of Vascular Specialist.
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
"These people do well,extremely well," Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.
His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off-the-shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type 3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who co-moderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry.
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
"These people do well,extremely well," Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.
His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off-the-shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type 3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who co-moderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry.
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.

Local anesthesia aids hemodynamic stability for CEA
CHICAGO – Patients undergoing carotid endarterectomy with cervical block anesthesia had fewer hemodynamic fluctuations and required less vasoactive medications than those under general anesthesia in a retrospective evaluation.
"Under cervical block anesthesia, carotid endarterectomy can be performed with a better hemodynamic profile," Dr. Marika Y. Gassner, a resident with Henry Ford Macomb Hospital, Clinton Township, Mich., said at the annual meeting of the Midwestern Vascular Surgical Society.
The practice switched in 2003 from using general anesthesia for the majority of carotid endarterectomy to performing more than 90% of cases under local cervical block anesthesia (CBA). Exceptions include patients who are extremely nervous, unable to communicate in English, or who have plaque extending above C2.

The investigators organized the retrospective cohort study after initial observations suggested patients under CBA had less intraoperative hypotension or fluctuations in mean arterial pressure below 65 mm Hg. Vasoactive therapy demands were also lower. For example, anesthesia records showed that several doses of beta-blockers and ephedrine were required for a patient under general anesthesia, while a patient under CBA had only a single dose of midazolam (Versed) early in the procedure, she said.
Other advantages of CBA include continuous feedback on neurologic status/cerebral perfusion, endotracheal intubation not required, shorter operative times, and reduced use of shunts, Dr. Gassner said.
The analysis included 651 patients who underwent carotid endarterectomy by a single surgeon at two suburban teaching hospitals, with 397 under general anesthesia (GA) and 254 under CBA.
The CBA and GA groups were similar in age (71.26 vs. 70.97 years) and incidence of coronary artery disease (57% vs. 56%), hypertension (77% vs. 75%), and renal failure (3.5% vs. 4.0%). The GA group, however, had significantly more females (39% vs. 46.6%), and a higher incidence of chronic obstructive pulmonary disease (16% vs. 23%), nicotine abuse, (50% vs. 63%), and symptomatic patients (41.3% vs. 54%).
The incidence of intraoperative hypotension (systolic BP less than 100 mm HG) was 0.52% with CBA and 17.84% with GA (P less than .001), Dr. Gassner said.
Mean arterial pressure changes of 20% or more per patient occurred in 20% and 41%, respectively (P less than .001).
Vasopressors were required during surgery in 51.13% of the GA group and 36.22% of the CBA group (P = .0002), and antihypertensive medications in 64% and 73.6% (P = .0085). Drugs from both categories were required by significantly fewer CBA patients (22.5% vs. 33.75%; P = .045), she said.
There were no deaths in either group. Postoperative complications were higher in the GA than the CBA group including myocardial infarction (4 vs. 0 events), stroke (6 vs. 0 events), hematoma (7 vs. 2 events), and return to the OR (7 vs. 0 events). The difference did not reach statistical significance because of the sample size, Dr. Gassner said.
Earlier in the presentation, she observed that there was no difference in the primary composite endpoint of stroke, myocardial infarction, or death at 30 days in the randomized GALA (general anaesthesia vs. local anaesthesia for carotid surgery) trial conducted at 95 centers in 24 countries (Lancet 2008;372:2132-42).
"If they couldn’t find it [a survival advantage] in GALA with 3,500 patients, we couldn’t find it here," Dr. Gassner said, adding that a randomized trial powered to look at late mortality is needed.
The group has no current plans to conduct such a study or a cost analysis, although a subsequent analysis of the GALA data revealed a cost savings of about $283 favoring carotid endarterectomy using local anesthesia (Br. J. Surg. 2010;97:1218-25).
Dr. Gassner and her coauthors reported having no financial disclosures.
CHICAGO – Patients undergoing carotid endarterectomy with cervical block anesthesia had fewer hemodynamic fluctuations and required less vasoactive medications than those under general anesthesia in a retrospective evaluation.
"Under cervical block anesthesia, carotid endarterectomy can be performed with a better hemodynamic profile," Dr. Marika Y. Gassner, a resident with Henry Ford Macomb Hospital, Clinton Township, Mich., said at the annual meeting of the Midwestern Vascular Surgical Society.
The practice switched in 2003 from using general anesthesia for the majority of carotid endarterectomy to performing more than 90% of cases under local cervical block anesthesia (CBA). Exceptions include patients who are extremely nervous, unable to communicate in English, or who have plaque extending above C2.
The investigators organized the retrospective cohort study after initial observations suggested patients under CBA had less intraoperative hypotension or fluctuations in mean arterial pressure below 65 mm Hg. Vasoactive therapy demands were also lower. For example, anesthesia records showed that several doses of beta-blockers and ephedrine were required for a patient under general anesthesia, while a patient under CBA had only a single dose of midazolam (Versed) early in the procedure, she said.
Other advantages of CBA include continuous feedback on neurologic status/cerebral perfusion, endotracheal intubation not required, shorter operative times, and reduced use of shunts, Dr. Gassner said.
The analysis included 651 patients who underwent carotid endarterectomy by a single surgeon at two suburban teaching hospitals, with 397 under general anesthesia (GA) and 254 under CBA.
The CBA and GA groups were similar in age (71.26 vs. 70.97 years) and incidence of coronary artery disease (57% vs. 56%), hypertension (77% vs. 75%), and renal failure (3.5% vs. 4.0%). The GA group, however, had significantly more females (39% vs. 46.6%), and a higher incidence of chronic obstructive pulmonary disease (16% vs. 23%), nicotine abuse, (50% vs. 63%), and symptomatic patients (41.3% vs. 54%).
The incidence of intraoperative hypotension (systolic BP less than 100 mm HG) was 0.52% with CBA and 17.84% with GA (P less than .001), Dr. Gassner said.
Mean arterial pressure changes of 20% or more per patient occurred in 20% and 41%, respectively (P less than .001).
Vasopressors were required during surgery in 51.13% of the GA group and 36.22% of the CBA group (P = .0002), and antihypertensive medications in 64% and 73.6% (P = .0085). Drugs from both categories were required by significantly fewer CBA patients (22.5% vs. 33.75%; P = .045), she said.
There were no deaths in either group. Postoperative complications were higher in the GA than the CBA group including myocardial infarction (4 vs. 0 events), stroke (6 vs. 0 events), hematoma (7 vs. 2 events), and return to the OR (7 vs. 0 events). The difference did not reach statistical significance because of the sample size, Dr. Gassner said.
Earlier in the presentation, she observed that there was no difference in the primary composite endpoint of stroke, myocardial infarction, or death at 30 days in the randomized GALA (general anaesthesia vs. local anaesthesia for carotid surgery) trial conducted at 95 centers in 24 countries (Lancet 2008;372:2132-42).
"If they couldn’t find it [a survival advantage] in GALA with 3,500 patients, we couldn’t find it here," Dr. Gassner said, adding that a randomized trial powered to look at late mortality is needed.
The group has no current plans to conduct such a study or a cost analysis, although a subsequent analysis of the GALA data revealed a cost savings of about $283 favoring carotid endarterectomy using local anesthesia (Br. J. Surg. 2010;97:1218-25).
Dr. Gassner and her coauthors reported having no financial disclosures.
CHICAGO – Patients undergoing carotid endarterectomy with cervical block anesthesia had fewer hemodynamic fluctuations and required less vasoactive medications than those under general anesthesia in a retrospective evaluation.
"Under cervical block anesthesia, carotid endarterectomy can be performed with a better hemodynamic profile," Dr. Marika Y. Gassner, a resident with Henry Ford Macomb Hospital, Clinton Township, Mich., said at the annual meeting of the Midwestern Vascular Surgical Society.
The practice switched in 2003 from using general anesthesia for the majority of carotid endarterectomy to performing more than 90% of cases under local cervical block anesthesia (CBA). Exceptions include patients who are extremely nervous, unable to communicate in English, or who have plaque extending above C2.
The investigators organized the retrospective cohort study after initial observations suggested patients under CBA had less intraoperative hypotension or fluctuations in mean arterial pressure below 65 mm Hg. Vasoactive therapy demands were also lower. For example, anesthesia records showed that several doses of beta-blockers and ephedrine were required for a patient under general anesthesia, while a patient under CBA had only a single dose of midazolam (Versed) early in the procedure, she said.
Other advantages of CBA include continuous feedback on neurologic status/cerebral perfusion, endotracheal intubation not required, shorter operative times, and reduced use of shunts, Dr. Gassner said.
The analysis included 651 patients who underwent carotid endarterectomy by a single surgeon at two suburban teaching hospitals, with 397 under general anesthesia (GA) and 254 under CBA.
The CBA and GA groups were similar in age (71.26 vs. 70.97 years) and incidence of coronary artery disease (57% vs. 56%), hypertension (77% vs. 75%), and renal failure (3.5% vs. 4.0%). The GA group, however, had significantly more females (39% vs. 46.6%), and a higher incidence of chronic obstructive pulmonary disease (16% vs. 23%), nicotine abuse, (50% vs. 63%), and symptomatic patients (41.3% vs. 54%).
The incidence of intraoperative hypotension (systolic BP less than 100 mm HG) was 0.52% with CBA and 17.84% with GA (P less than .001), Dr. Gassner said.
Mean arterial pressure changes of 20% or more per patient occurred in 20% and 41%, respectively (P less than .001).
Vasopressors were required during surgery in 51.13% of the GA group and 36.22% of the CBA group (P = .0002), and antihypertensive medications in 64% and 73.6% (P = .0085). Drugs from both categories were required by significantly fewer CBA patients (22.5% vs. 33.75%; P = .045), she said.
There were no deaths in either group. Postoperative complications were higher in the GA than the CBA group including myocardial infarction (4 vs. 0 events), stroke (6 vs. 0 events), hematoma (7 vs. 2 events), and return to the OR (7 vs. 0 events). The difference did not reach statistical significance because of the sample size, Dr. Gassner said.
Earlier in the presentation, she observed that there was no difference in the primary composite endpoint of stroke, myocardial infarction, or death at 30 days in the randomized GALA (general anaesthesia vs. local anaesthesia for carotid surgery) trial conducted at 95 centers in 24 countries (Lancet 2008;372:2132-42).
"If they couldn’t find it [a survival advantage] in GALA with 3,500 patients, we couldn’t find it here," Dr. Gassner said, adding that a randomized trial powered to look at late mortality is needed.
The group has no current plans to conduct such a study or a cost analysis, although a subsequent analysis of the GALA data revealed a cost savings of about $283 favoring carotid endarterectomy using local anesthesia (Br. J. Surg. 2010;97:1218-25).
Dr. Gassner and her coauthors reported having no financial disclosures.
