User login
Energy drinks amped up left ventricular contractility
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.
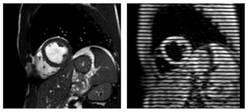
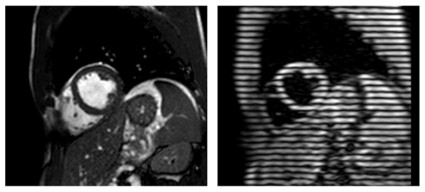
He and his colleagues performed cardiac magnetic resonance imaging (MRI) in 31 volunteers before and 1 hour after consumption of an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time – increased by 6% (–1.19 vs –1.26; P = .0032), reported Dr. Dörner, with the University of Bonn, Germany.
The investigators did not find any significant changes in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.

Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
Dr. Marcos I. Restrepo, FCCP, comments: This series of observations calls into attention the possible risks of the multiple energy drinks (and its contents) available in the market. The worry that high levels of caffeine and taurine found in energy drinks affect contractility in healthy volunteers should raise concerns in patients with comorbid conditions or unidentified heart problems. In addition, regular consumers of energy drinks may worry about potential heart problems, if the consumption occurs repetitively and for longer periods. There is hope that regulatory agencies consider these findings and promote more studies to address the possible risks related to ingestion of energy drinks.
Dr. Marcos I. Restrepo, FCCP, comments: This series of observations calls into attention the possible risks of the multiple energy drinks (and its contents) available in the market. The worry that high levels of caffeine and taurine found in energy drinks affect contractility in healthy volunteers should raise concerns in patients with comorbid conditions or unidentified heart problems. In addition, regular consumers of energy drinks may worry about potential heart problems, if the consumption occurs repetitively and for longer periods. There is hope that regulatory agencies consider these findings and promote more studies to address the possible risks related to ingestion of energy drinks.
Dr. Marcos I. Restrepo, FCCP, comments: This series of observations calls into attention the possible risks of the multiple energy drinks (and its contents) available in the market. The worry that high levels of caffeine and taurine found in energy drinks affect contractility in healthy volunteers should raise concerns in patients with comorbid conditions or unidentified heart problems. In addition, regular consumers of energy drinks may worry about potential heart problems, if the consumption occurs repetitively and for longer periods. There is hope that regulatory agencies consider these findings and promote more studies to address the possible risks related to ingestion of energy drinks.
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.
He and his colleagues performed cardiac magnetic resonance imaging (MRI) in 31 volunteers before and 1 hour after consumption of an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time – increased by 6% (–1.19 vs –1.26; P = .0032), reported Dr. Dörner, with the University of Bonn, Germany.
The investigators did not find any significant changes in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.
Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
CHICAGO – Consumption of an energy drink containing caffeine and taurine slightly, but significantly, altered left ventricular contractility in healthy volunteers, while consuming the same amount of caffeine alone did not lead to an alteration in contractility in a prospective study.
"A possible explanation for this finding could be the presence of taurine, which has been shown to increase the release of calcium in muscles," Dr. Jonas Dörner reported at the annual meeting of the Radiological Society of North America.
He and his colleagues performed cardiac magnetic resonance imaging (MRI) in 31 volunteers before and 1 hour after consumption of an energy drink containing caffeine (32 mg/100 mL) and taurine (400 mg/100 mL). The average patient age was 27.7 years.
Postconsumption images revealed that mean peak strain increased 7% from baseline (–22.84 vs. –24.35; P < .0001) and peak systolic strain rate – a measure of deformation with respect to time – increased by 6% (–1.19 vs –1.26; P = .0032), reported Dr. Dörner, with the University of Bonn, Germany.
The investigators did not find any significant changes in heart rate, systolic blood pressure, or left ventricular (LV) ejection fraction. LV end-diastolic volume and LV stroke volume increased significantly by 2% and 4%, respectively.
The same imaging protocol was repeated on a different day in 10 patients after consumption of caffeine only. No significant differences were seen in mean peak strain (–22.99 vs. –23.20) or mean peak systolic strain rate (–1.15 vs. –1.16) with caffeine alone, although diastolic blood pressure was significantly elevated and LV end-diastolic volume significantly decreased, Dr. Dörner said.
The current study took advantage of an MRI technique called complementary spatial modulation of magnetization (CSPAMM) for LV myocardial tagging. The technique is more exact than traditional ultrasound or speckle tracking and is able to measure very small differences in strain, he explained in an interview.
Although the differences in strain in the study were "subtle," the findings need to be taken into perspective because younger patients often consume higher doses of caffeine and taurine via energy drinks. According to the Food and Drug Administration, caffeinated sodas cannot contain more than 71 mg of caffeine per 12 fluid ounces (approximately 20 mg/100 mL), but energy drinks often contain three times that amount, he noted.
More than 500 brands of energy drinks are available worldwide, and 30%-50% are consumed by children, teenagers, and young adults. A report by the European Food Safety Authority found no adverse effects for up to 1 g of taurine per kilogram of body weight per day.
Further studies are needed to evaluate the effect of long-term energy drink consumption and the effect of these drinks on patients with heart disease and in combination with alcohol, Dr. Dörner said.
Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
Major finding: One hour after consumption of an energy drink containing caffeine and taurine, mean peak strain increased 7% from baseline and peak systolic strain rate increased 6%.
Data source: A prospective study of 31 healthy volunteers.
Disclosures: Dr. Dörner reported having no financial disclosures; a coauthor reported consulting for Medtronic.
Low event rates with real-world use of rivaroxaban in NOAC
NEW ORLEANS – Real-world use of rivaroxaban produced comparatively low rates of cardiovascular and major bleeding events when used for stroke prevention in unselected patients with atrial fibrillation.
The centrally adjudicated annual stroke rate was 1.4% among 1,194 patients given once-daily rivaroxaban (Xarelto) by 230 physicians from private practices and community hospitals across Saxony, Germany, in the prospective Dresden Novel Oral Anticoagulant (NOAC) registry.
This result falls within the annual stroke rate of 1.7% seen in the ROCKET-AF trial, which served as the basis for rivaroxaban’s November 2011 U.S. approval in this setting, Dr. Jan Beyer-Westendorf reported at the annual meeting of the American Society of Hematology.
Nonmajor, clinically relevant bleeding occurred in 21.6% of patients per year in the NOAC registry, while major bleeding was 3.4% per year.

Again, this is within the range of the phase III ROCKET-AF results (3.6% per year) and lower than the rate of up to 8% seen in the daily care of patients on vitamin K antagonists, he said. Gastrointestinal bleeding, a known side effect of rivaroxaban, was the most common major bleed. Intracranial bleeds were rare at three events.
Adherence to the oral direct factor Xa inhibitor was high at 12 months (13.7%), compared with up to 25% of patients who discontinue vitamin K antagonist therapy in the first year.
"In our population, the discontinuation rate was 14%, so basically we don’t have any concern that we put these patients at more risk in a daily care situation by treating them with rivaroxaban," said Dr. Beyer-Westendorf of the University Hospital Carl Gustav Carus, Dresden, Germany.
According to the analysis, 2,345 patients have been prospectively enrolled in the NOAC registry since October 2011; 1,194 with atrial fibrillation have been treated with anticoagulation to prevent venous thromboembolism (VTE) or stroke. No patients have been lost to follow-up, which now stands at 2,313 patient-years.
NOAC patients were slightly older at baseline than were those in ROCKET-AF (74.8 years vs. 73 years), less likely to have had prior vitamin K antagonists (37% vs. 62%), and had lower CHADS2 (Cardiac failure, Hypertension, Age, Diabetes Stroke system) scores (mean, 2.4 vs. 3.48). Higher CHADS2 scores are associated with worse outcomes, including higher rates of major bleeding.
During follow-up through October 2013, 53 NOAC patients (4.4%) experienced a major vascular event including 22 strokes, transient ischemic attacks (TIA), systemic emboli; 15 acute coronary syndromes; and four VTEs, he said. In all, 56 patients died (4.7%).
Patients on rivaroxaban 20 mg/day vs. 15 mg/day had a significantly lower annual stroke rate (0.9% vs. 2.3%; P = .052), defined as a new stroke, TIA, or systemic embolism.
Compared with those on rivaroxaban 20 mg, patients on the lower dose had higher baseline CHADS2 scores (mean, 2.8 vs. 2.2), were older (79 years vs. 73 years), more likely to have had a prior stroke (17% vs. 12.5%) or prior vitamin K antagonist therapy (40% vs. 36%), and took more concomitant drugs (mean, 6.4 vs. 5.4).
"It’s no surprise that these patients get a dose reduction because they have more comorbidities; they are at high risk of bleeding, and so it’s not a surprise that they have a slightly higher event rate," said Dr. Beyer-Westendorf, who noted that the lower dose did not reduce the risk of bleeding.
The NOAC registry is supported by scientific grants from Bayer Healthcare, Boehringer Ingelheim, and Pfizer. Dr. Beyer-Westendorf reported research funding from and serving as a speaker for these firms.
Bleeding complications detailed
In a separate presentation at ASH, Dr. Beyer-Westendorf detailed the pattern and management of bleeding complications in NOAC patients treated for stroke prevention in atrial fibrillation or VTE with rivaroxaban, dabigatran (Pradaxa), or apixaban (Eliquis).
These complications are a major concern for practitioners because there isn’t an emergency lab test available or rescue medications.
Of the 1,241 bleeding events that have occurred so far in 879 patients, 742 were minor (60%), 425 were nonmajor clinically relevant (34.2%), and 74 were major (6%).
Major bleeds per year of therapy were reported with rivaroxaban in 3.4% of patients with atrial fibrillation and in 4.4% with VTE. The major bleeding event rate with dabigatran in patients with atrial fibrillation was 2.6/100 patient-years at the 110-mg dose and 2.0/100 patient-years at the 150-mg dose. Short-term follow-up and low numbers of dabigatran and apixaban patients did not allow for sound event-rate calculations, according to Dr. Beyer-Westendorf, who stressed that no direct comparisons should be made between event rates for the different agents since the patients were in different cohorts and not in a randomized trial.
Most bleeds (93.3%) were managed conservatively with watchful waiting, compression, tamponade, or red blood cell transfusion. None of the minor bleeds and 16% (83/499) of the nonmajor clinically relevant and major bleeds required surgical or interventional treatment, he said.
Fresh frozen plasma and prothrombin complex concentrate were rarely used (seven patients each). No patient received recombinant activated factor VII.
Mortality was 0.4% for all patients with bleeding complications and 6.8% in those with major bleeds.
Death from any cause at 30 days and 90 days post bleeding occurred in 1 of 19 (5.3%) and 3 of 17 (17.6%) patients on dabigatran, respectively; in 5 of 99 (5%) and 6 of 88 (6.8%) on rivaroxaban; and in 1 of 2 (50%) at each time point for the few patients on apixaban.
With vitamin K antagonists, the case-fatality rates of major bleeding reach 14% at 90 days after bleeding leading to hospitalization and 18% within a week of discharge in atrial fibrillation patients, Dr. Beyer-Westendorf observed.
NEW ORLEANS – Real-world use of rivaroxaban produced comparatively low rates of cardiovascular and major bleeding events when used for stroke prevention in unselected patients with atrial fibrillation.
The centrally adjudicated annual stroke rate was 1.4% among 1,194 patients given once-daily rivaroxaban (Xarelto) by 230 physicians from private practices and community hospitals across Saxony, Germany, in the prospective Dresden Novel Oral Anticoagulant (NOAC) registry.
This result falls within the annual stroke rate of 1.7% seen in the ROCKET-AF trial, which served as the basis for rivaroxaban’s November 2011 U.S. approval in this setting, Dr. Jan Beyer-Westendorf reported at the annual meeting of the American Society of Hematology.
Nonmajor, clinically relevant bleeding occurred in 21.6% of patients per year in the NOAC registry, while major bleeding was 3.4% per year.
Again, this is within the range of the phase III ROCKET-AF results (3.6% per year) and lower than the rate of up to 8% seen in the daily care of patients on vitamin K antagonists, he said. Gastrointestinal bleeding, a known side effect of rivaroxaban, was the most common major bleed. Intracranial bleeds were rare at three events.
Adherence to the oral direct factor Xa inhibitor was high at 12 months (13.7%), compared with up to 25% of patients who discontinue vitamin K antagonist therapy in the first year.
"In our population, the discontinuation rate was 14%, so basically we don’t have any concern that we put these patients at more risk in a daily care situation by treating them with rivaroxaban," said Dr. Beyer-Westendorf of the University Hospital Carl Gustav Carus, Dresden, Germany.
According to the analysis, 2,345 patients have been prospectively enrolled in the NOAC registry since October 2011; 1,194 with atrial fibrillation have been treated with anticoagulation to prevent venous thromboembolism (VTE) or stroke. No patients have been lost to follow-up, which now stands at 2,313 patient-years.
NOAC patients were slightly older at baseline than were those in ROCKET-AF (74.8 years vs. 73 years), less likely to have had prior vitamin K antagonists (37% vs. 62%), and had lower CHADS2 (Cardiac failure, Hypertension, Age, Diabetes Stroke system) scores (mean, 2.4 vs. 3.48). Higher CHADS2 scores are associated with worse outcomes, including higher rates of major bleeding.
During follow-up through October 2013, 53 NOAC patients (4.4%) experienced a major vascular event including 22 strokes, transient ischemic attacks (TIA), systemic emboli; 15 acute coronary syndromes; and four VTEs, he said. In all, 56 patients died (4.7%).
Patients on rivaroxaban 20 mg/day vs. 15 mg/day had a significantly lower annual stroke rate (0.9% vs. 2.3%; P = .052), defined as a new stroke, TIA, or systemic embolism.
Compared with those on rivaroxaban 20 mg, patients on the lower dose had higher baseline CHADS2 scores (mean, 2.8 vs. 2.2), were older (79 years vs. 73 years), more likely to have had a prior stroke (17% vs. 12.5%) or prior vitamin K antagonist therapy (40% vs. 36%), and took more concomitant drugs (mean, 6.4 vs. 5.4).
"It’s no surprise that these patients get a dose reduction because they have more comorbidities; they are at high risk of bleeding, and so it’s not a surprise that they have a slightly higher event rate," said Dr. Beyer-Westendorf, who noted that the lower dose did not reduce the risk of bleeding.
The NOAC registry is supported by scientific grants from Bayer Healthcare, Boehringer Ingelheim, and Pfizer. Dr. Beyer-Westendorf reported research funding from and serving as a speaker for these firms.
Bleeding complications detailed
In a separate presentation at ASH, Dr. Beyer-Westendorf detailed the pattern and management of bleeding complications in NOAC patients treated for stroke prevention in atrial fibrillation or VTE with rivaroxaban, dabigatran (Pradaxa), or apixaban (Eliquis).
These complications are a major concern for practitioners because there isn’t an emergency lab test available or rescue medications.
Of the 1,241 bleeding events that have occurred so far in 879 patients, 742 were minor (60%), 425 were nonmajor clinically relevant (34.2%), and 74 were major (6%).
Major bleeds per year of therapy were reported with rivaroxaban in 3.4% of patients with atrial fibrillation and in 4.4% with VTE. The major bleeding event rate with dabigatran in patients with atrial fibrillation was 2.6/100 patient-years at the 110-mg dose and 2.0/100 patient-years at the 150-mg dose. Short-term follow-up and low numbers of dabigatran and apixaban patients did not allow for sound event-rate calculations, according to Dr. Beyer-Westendorf, who stressed that no direct comparisons should be made between event rates for the different agents since the patients were in different cohorts and not in a randomized trial.
Most bleeds (93.3%) were managed conservatively with watchful waiting, compression, tamponade, or red blood cell transfusion. None of the minor bleeds and 16% (83/499) of the nonmajor clinically relevant and major bleeds required surgical or interventional treatment, he said.
Fresh frozen plasma and prothrombin complex concentrate were rarely used (seven patients each). No patient received recombinant activated factor VII.
Mortality was 0.4% for all patients with bleeding complications and 6.8% in those with major bleeds.
Death from any cause at 30 days and 90 days post bleeding occurred in 1 of 19 (5.3%) and 3 of 17 (17.6%) patients on dabigatran, respectively; in 5 of 99 (5%) and 6 of 88 (6.8%) on rivaroxaban; and in 1 of 2 (50%) at each time point for the few patients on apixaban.
With vitamin K antagonists, the case-fatality rates of major bleeding reach 14% at 90 days after bleeding leading to hospitalization and 18% within a week of discharge in atrial fibrillation patients, Dr. Beyer-Westendorf observed.
NEW ORLEANS – Real-world use of rivaroxaban produced comparatively low rates of cardiovascular and major bleeding events when used for stroke prevention in unselected patients with atrial fibrillation.
The centrally adjudicated annual stroke rate was 1.4% among 1,194 patients given once-daily rivaroxaban (Xarelto) by 230 physicians from private practices and community hospitals across Saxony, Germany, in the prospective Dresden Novel Oral Anticoagulant (NOAC) registry.
This result falls within the annual stroke rate of 1.7% seen in the ROCKET-AF trial, which served as the basis for rivaroxaban’s November 2011 U.S. approval in this setting, Dr. Jan Beyer-Westendorf reported at the annual meeting of the American Society of Hematology.
Nonmajor, clinically relevant bleeding occurred in 21.6% of patients per year in the NOAC registry, while major bleeding was 3.4% per year.
Again, this is within the range of the phase III ROCKET-AF results (3.6% per year) and lower than the rate of up to 8% seen in the daily care of patients on vitamin K antagonists, he said. Gastrointestinal bleeding, a known side effect of rivaroxaban, was the most common major bleed. Intracranial bleeds were rare at three events.
Adherence to the oral direct factor Xa inhibitor was high at 12 months (13.7%), compared with up to 25% of patients who discontinue vitamin K antagonist therapy in the first year.
"In our population, the discontinuation rate was 14%, so basically we don’t have any concern that we put these patients at more risk in a daily care situation by treating them with rivaroxaban," said Dr. Beyer-Westendorf of the University Hospital Carl Gustav Carus, Dresden, Germany.
According to the analysis, 2,345 patients have been prospectively enrolled in the NOAC registry since October 2011; 1,194 with atrial fibrillation have been treated with anticoagulation to prevent venous thromboembolism (VTE) or stroke. No patients have been lost to follow-up, which now stands at 2,313 patient-years.
NOAC patients were slightly older at baseline than were those in ROCKET-AF (74.8 years vs. 73 years), less likely to have had prior vitamin K antagonists (37% vs. 62%), and had lower CHADS2 (Cardiac failure, Hypertension, Age, Diabetes Stroke system) scores (mean, 2.4 vs. 3.48). Higher CHADS2 scores are associated with worse outcomes, including higher rates of major bleeding.
During follow-up through October 2013, 53 NOAC patients (4.4%) experienced a major vascular event including 22 strokes, transient ischemic attacks (TIA), systemic emboli; 15 acute coronary syndromes; and four VTEs, he said. In all, 56 patients died (4.7%).
Patients on rivaroxaban 20 mg/day vs. 15 mg/day had a significantly lower annual stroke rate (0.9% vs. 2.3%; P = .052), defined as a new stroke, TIA, or systemic embolism.
Compared with those on rivaroxaban 20 mg, patients on the lower dose had higher baseline CHADS2 scores (mean, 2.8 vs. 2.2), were older (79 years vs. 73 years), more likely to have had a prior stroke (17% vs. 12.5%) or prior vitamin K antagonist therapy (40% vs. 36%), and took more concomitant drugs (mean, 6.4 vs. 5.4).
"It’s no surprise that these patients get a dose reduction because they have more comorbidities; they are at high risk of bleeding, and so it’s not a surprise that they have a slightly higher event rate," said Dr. Beyer-Westendorf, who noted that the lower dose did not reduce the risk of bleeding.
The NOAC registry is supported by scientific grants from Bayer Healthcare, Boehringer Ingelheim, and Pfizer. Dr. Beyer-Westendorf reported research funding from and serving as a speaker for these firms.
Bleeding complications detailed
In a separate presentation at ASH, Dr. Beyer-Westendorf detailed the pattern and management of bleeding complications in NOAC patients treated for stroke prevention in atrial fibrillation or VTE with rivaroxaban, dabigatran (Pradaxa), or apixaban (Eliquis).
These complications are a major concern for practitioners because there isn’t an emergency lab test available or rescue medications.
Of the 1,241 bleeding events that have occurred so far in 879 patients, 742 were minor (60%), 425 were nonmajor clinically relevant (34.2%), and 74 were major (6%).
Major bleeds per year of therapy were reported with rivaroxaban in 3.4% of patients with atrial fibrillation and in 4.4% with VTE. The major bleeding event rate with dabigatran in patients with atrial fibrillation was 2.6/100 patient-years at the 110-mg dose and 2.0/100 patient-years at the 150-mg dose. Short-term follow-up and low numbers of dabigatran and apixaban patients did not allow for sound event-rate calculations, according to Dr. Beyer-Westendorf, who stressed that no direct comparisons should be made between event rates for the different agents since the patients were in different cohorts and not in a randomized trial.
Most bleeds (93.3%) were managed conservatively with watchful waiting, compression, tamponade, or red blood cell transfusion. None of the minor bleeds and 16% (83/499) of the nonmajor clinically relevant and major bleeds required surgical or interventional treatment, he said.
Fresh frozen plasma and prothrombin complex concentrate were rarely used (seven patients each). No patient received recombinant activated factor VII.
Mortality was 0.4% for all patients with bleeding complications and 6.8% in those with major bleeds.
Death from any cause at 30 days and 90 days post bleeding occurred in 1 of 19 (5.3%) and 3 of 17 (17.6%) patients on dabigatran, respectively; in 5 of 99 (5%) and 6 of 88 (6.8%) on rivaroxaban; and in 1 of 2 (50%) at each time point for the few patients on apixaban.
With vitamin K antagonists, the case-fatality rates of major bleeding reach 14% at 90 days after bleeding leading to hospitalization and 18% within a week of discharge in atrial fibrillation patients, Dr. Beyer-Westendorf observed.
AT ASH 2013
Major finding: The annual stroke rate with once-daily rivaroxaban was 1.4% and the major bleeding rate was 3.4% among 1,194 patients with atrial fibrillation.
Data source: A prospective database of 2,345 patients treated with anticoagulation.
Disclosures: The NOAC registry is supported by scientific grants from Bayer Healthcare, Boehringer Ingelheim, and Pfizer. Dr. Beyer-Westendorf reported research funding from and serving as a speaker for these firms.

Cardiac CT angiography feasible at ultralow radiation doses
CHICAGO – Coronary computed tomography angiography with diagnostic image quality is feasible at an ultralow radiation dose of 0.2 millisievert using model-based iterative reconstruction.
This represents roughly an 80% reduction in radiation dose compared with standard coronary CT angiography, Dr. Julia Stehli said at the annual meeting of the Radiological Society of North America.
Increasing concerns about radiation exposure have prompted the use of prospective ECG triggering to reduce radiation doses from 20 mSv to 2 mSv or less. Several vendors also have developed new raw-data–based iterative reconstruction algorithms to further reduce radiation doses, but the trade-off can be increased image noise.
The model-based iterative reconstruction (MIBR) algorithm (GE Healthcare), however, has shown promising results for noise reduction, said Dr. Stehli of University Hospital Zurich. The technology, known as Veo, is already in use in the United States, Europe, and Asia for abdominal CT scans but is not yet commercially available for cardiac scans because of the added complexity of ECG triggering.

Dr. Stehli reported on the hospital’s first clinical experience with MIBR in 25 consecutive prospectively enrolled patients with suspected coronary artery disease who underwent standard low-dose coronary CT angiography (CCTA) and same-day ultralow-dose CCTA on a 64-slice CT scanner with prospective ECG triggering. Tube voltage and current were adapted to body mass index, which covered a wide range from 18.4 kg/m2 to 40.2 kg/m2. Contrast media volume and flow rate were adapted to body surface area. Intravenous beta-blockers were used prior to CCTA in 20 patients.
Standard CCTA was reconstructed using 30% of adaptive statistical iterative reconstruction (ASIR) according to usual hospital practice, while the ultralow-dose images were sent to the vendor for reconstruction with MIBR.
The effective radiation dose was 1.3 mSv with standard CCTA and 0.2 mSv in the ultralow-dose CCTA group (P less than .001), which is in the range reported for a postero-anterior and lateral chest X-ray, Dr. Stehli said.
A total of 100 vessels and 330 coronary artery segments were semiquantitatively assessed by two blinded, independent readers using a 4-point Likert scale, with 1 being nondiagnostic, 2 good, 3 adequate, and 4 excellent. The Kappa value for interobserver agreement of image quality was 0.8.
The average image quality score per segment was 3.3 with standard CCTA vs. 3.4 with ultralow-dose MBIR (P less than .05), she said.
Diagnostic image quality (score 2-4) was found in 319 segments (97%) and 317 segments (96%), respectively.
"These numbers are quite revolutionary," session comoderator Dr. Konstantin Nikolaou, professor of radiology at the University of Munich, said in an interview. "We’ve heard about 1.0 [mSv], so 0.2 [mSv] is great."
Still, more details are needed on exactly how the protocol works and the need to send images to the vendor for MBIR reconstruction, he said.
During a discussion of the results, Dr. Stehli said that reconstruction by the vendor typically took about 15 minutes, but Dr. Nikolau said that "it’s hard to say if that is feasible in routine clinical practice."
The ultimate test for the ultralow-dose protocol will be the clinical outcomes data, expected to be reported in 2014.
"If that proves to be robust and works in many patients and rates a good diagnostic accuracy, it would be great," Dr. Nikolau said.
The investigators would not release details on the clinical outcomes but said sensitivity and specificity for the new protocol are good.
"We believe this will have clinical applications in the near future," Dr. Stehli said in an interview.
Most patients in the study presented with chest pain (72%), and 56% were smokers, 44% had arterial hypertension, and 36% had a family history of cardiovascular disease. Their mean age was 58 years.
Dr. Stehli and her associates reported having no financial disclosures.
CHICAGO – Coronary computed tomography angiography with diagnostic image quality is feasible at an ultralow radiation dose of 0.2 millisievert using model-based iterative reconstruction.
This represents roughly an 80% reduction in radiation dose compared with standard coronary CT angiography, Dr. Julia Stehli said at the annual meeting of the Radiological Society of North America.
Increasing concerns about radiation exposure have prompted the use of prospective ECG triggering to reduce radiation doses from 20 mSv to 2 mSv or less. Several vendors also have developed new raw-data–based iterative reconstruction algorithms to further reduce radiation doses, but the trade-off can be increased image noise.
The model-based iterative reconstruction (MIBR) algorithm (GE Healthcare), however, has shown promising results for noise reduction, said Dr. Stehli of University Hospital Zurich. The technology, known as Veo, is already in use in the United States, Europe, and Asia for abdominal CT scans but is not yet commercially available for cardiac scans because of the added complexity of ECG triggering.
Dr. Stehli reported on the hospital’s first clinical experience with MIBR in 25 consecutive prospectively enrolled patients with suspected coronary artery disease who underwent standard low-dose coronary CT angiography (CCTA) and same-day ultralow-dose CCTA on a 64-slice CT scanner with prospective ECG triggering. Tube voltage and current were adapted to body mass index, which covered a wide range from 18.4 kg/m2 to 40.2 kg/m2. Contrast media volume and flow rate were adapted to body surface area. Intravenous beta-blockers were used prior to CCTA in 20 patients.
Standard CCTA was reconstructed using 30% of adaptive statistical iterative reconstruction (ASIR) according to usual hospital practice, while the ultralow-dose images were sent to the vendor for reconstruction with MIBR.
The effective radiation dose was 1.3 mSv with standard CCTA and 0.2 mSv in the ultralow-dose CCTA group (P less than .001), which is in the range reported for a postero-anterior and lateral chest X-ray, Dr. Stehli said.
A total of 100 vessels and 330 coronary artery segments were semiquantitatively assessed by two blinded, independent readers using a 4-point Likert scale, with 1 being nondiagnostic, 2 good, 3 adequate, and 4 excellent. The Kappa value for interobserver agreement of image quality was 0.8.
The average image quality score per segment was 3.3 with standard CCTA vs. 3.4 with ultralow-dose MBIR (P less than .05), she said.
Diagnostic image quality (score 2-4) was found in 319 segments (97%) and 317 segments (96%), respectively.
"These numbers are quite revolutionary," session comoderator Dr. Konstantin Nikolaou, professor of radiology at the University of Munich, said in an interview. "We’ve heard about 1.0 [mSv], so 0.2 [mSv] is great."
Still, more details are needed on exactly how the protocol works and the need to send images to the vendor for MBIR reconstruction, he said.
During a discussion of the results, Dr. Stehli said that reconstruction by the vendor typically took about 15 minutes, but Dr. Nikolau said that "it’s hard to say if that is feasible in routine clinical practice."
The ultimate test for the ultralow-dose protocol will be the clinical outcomes data, expected to be reported in 2014.
"If that proves to be robust and works in many patients and rates a good diagnostic accuracy, it would be great," Dr. Nikolau said.
The investigators would not release details on the clinical outcomes but said sensitivity and specificity for the new protocol are good.
"We believe this will have clinical applications in the near future," Dr. Stehli said in an interview.
Most patients in the study presented with chest pain (72%), and 56% were smokers, 44% had arterial hypertension, and 36% had a family history of cardiovascular disease. Their mean age was 58 years.
Dr. Stehli and her associates reported having no financial disclosures.
CHICAGO – Coronary computed tomography angiography with diagnostic image quality is feasible at an ultralow radiation dose of 0.2 millisievert using model-based iterative reconstruction.
This represents roughly an 80% reduction in radiation dose compared with standard coronary CT angiography, Dr. Julia Stehli said at the annual meeting of the Radiological Society of North America.
Increasing concerns about radiation exposure have prompted the use of prospective ECG triggering to reduce radiation doses from 20 mSv to 2 mSv or less. Several vendors also have developed new raw-data–based iterative reconstruction algorithms to further reduce radiation doses, but the trade-off can be increased image noise.
The model-based iterative reconstruction (MIBR) algorithm (GE Healthcare), however, has shown promising results for noise reduction, said Dr. Stehli of University Hospital Zurich. The technology, known as Veo, is already in use in the United States, Europe, and Asia for abdominal CT scans but is not yet commercially available for cardiac scans because of the added complexity of ECG triggering.
Dr. Stehli reported on the hospital’s first clinical experience with MIBR in 25 consecutive prospectively enrolled patients with suspected coronary artery disease who underwent standard low-dose coronary CT angiography (CCTA) and same-day ultralow-dose CCTA on a 64-slice CT scanner with prospective ECG triggering. Tube voltage and current were adapted to body mass index, which covered a wide range from 18.4 kg/m2 to 40.2 kg/m2. Contrast media volume and flow rate were adapted to body surface area. Intravenous beta-blockers were used prior to CCTA in 20 patients.
Standard CCTA was reconstructed using 30% of adaptive statistical iterative reconstruction (ASIR) according to usual hospital practice, while the ultralow-dose images were sent to the vendor for reconstruction with MIBR.
The effective radiation dose was 1.3 mSv with standard CCTA and 0.2 mSv in the ultralow-dose CCTA group (P less than .001), which is in the range reported for a postero-anterior and lateral chest X-ray, Dr. Stehli said.
A total of 100 vessels and 330 coronary artery segments were semiquantitatively assessed by two blinded, independent readers using a 4-point Likert scale, with 1 being nondiagnostic, 2 good, 3 adequate, and 4 excellent. The Kappa value for interobserver agreement of image quality was 0.8.
The average image quality score per segment was 3.3 with standard CCTA vs. 3.4 with ultralow-dose MBIR (P less than .05), she said.
Diagnostic image quality (score 2-4) was found in 319 segments (97%) and 317 segments (96%), respectively.
"These numbers are quite revolutionary," session comoderator Dr. Konstantin Nikolaou, professor of radiology at the University of Munich, said in an interview. "We’ve heard about 1.0 [mSv], so 0.2 [mSv] is great."
Still, more details are needed on exactly how the protocol works and the need to send images to the vendor for MBIR reconstruction, he said.
During a discussion of the results, Dr. Stehli said that reconstruction by the vendor typically took about 15 minutes, but Dr. Nikolau said that "it’s hard to say if that is feasible in routine clinical practice."
The ultimate test for the ultralow-dose protocol will be the clinical outcomes data, expected to be reported in 2014.
"If that proves to be robust and works in many patients and rates a good diagnostic accuracy, it would be great," Dr. Nikolau said.
The investigators would not release details on the clinical outcomes but said sensitivity and specificity for the new protocol are good.
"We believe this will have clinical applications in the near future," Dr. Stehli said in an interview.
Most patients in the study presented with chest pain (72%), and 56% were smokers, 44% had arterial hypertension, and 36% had a family history of cardiovascular disease. Their mean age was 58 years.
Dr. Stehli and her associates reported having no financial disclosures.
AT RSNA 2013
Major finding: The effective radiation dose was 1.3 mSv with standard CCTA and 0.2 mSv in the ultralow-dose CCTA group (P less than .001).
Data source: A prospective study of 25 patients with suspected coronary artery disease.
Disclosures: Dr. Stehli and her coauthors reported having no financial disclosures.

ONO-4059 makes waves in heavily pretreated CLL
NEW ORLEANS – Early data suggest that the second-generation oral BTK inhibitor ONO-4059 may give ibrutinib a run for its money in chronic lymphocytic leukemia.
The response rate to ONO-4059 monotherapy was 89% overall and 71% in those with the deleterious 17p deletion among 18 heavily pretreated patients with relapsed/refractory or high-risk CLL in a phase I, dose-escalation study.

Patients had already received a median of three prior therapies, including rituximab (84%) and fludarabine (95%), and had no higher priority therapy available to them, said Dr. Gilles Salles of Hospices Civils de Lyon (France), Universite Claude Bernard Lyon.
All patients had improved hemoglobin and platelet counts after 3 months on treatment and rapid reductions in lymph node size within the first 28-day cycle. Tumor burden was reduced by 50% for most patients, and all but one patient experienced a response that was detectable on a CT scan.
"This was true whatever their FISH status or 17p or 11q deletion status," Dr. Salles said at the annual meeting of the American Society of Hematology.
ONO-4059 is a highly selective Bruton’s tyrosine kinase (BTK) inhibitor with antitumor activity in several preclinical models.
No patients had received prior treatment with a P13 kinase or a BTK inhibitor, including ibrutinib (Imbruvica), which recently gained accelerated approval for previously treated mantle cell lymphoma.
ONO-4059 was given at daily doses ranging from 20 mg to 320 mg for up to 6 months, with the option of additional dosing up to 2 years. Sustained BTK inhibition was established at doses of 40 mg and higher.
Overall, the best response was a partial response in 14 patients, as well as two partial responses with lymphocytosis and one stable disease, he said. No complete responses occurred.
One patient progressed roughly 1 month after showing an initial response and complete disappearance of all palpable disease on physical exam. Richter’s syndrome was suspected.
"It’s very promising efficacy in this highly pretreated population," Dr. Salles said.
Patients with relapsed/refractory mantle cell lymphoma and diffuse large B-cell lymphoma, especially the ABC subtype, also appear sensitive to ONO-4059. Overall response rates were 43% and 75%, respectively, including three complete responses reported from the phase I study in a separate poster presentation at the meeting.
ONO-4059 had a favorable safety profile with a single dose-limiting toxicity observed in a patient who had Waldenstrom’s macroglobulinemia, was on the 320-mg dose, and was intolerant to all prior therapies. The maximum tolerated dose has not yet been reached.
The majority of adverse events in the CLL patients were grades 1 and 2. There were no clinically significant bleeding events or bruising, and there was a low incidence of diarrhea and rash, Dr. Salles said.
ONO-4059–related grade 3-4 events were independent of dose and included one grade 3 neutropenia at 20 mg and two grade 4 events at 20 mg and 320 mg. Four serious adverse events (febrile neutropenia, pyrexia, rash, and neutropenia) occurred in three patients, all of whom are still in the study and showing good clinical response, Dr. Salles said. Of the 30 patients dosed to date, 22 remain in the study.
No other trials are firmly planned, and pharmacokinetics/pharmacodynamics data continue to be explored in order to assess a phase II dosage, he said in an interview.
Dr. Salles reported consulting for and receiving honoraria from Roche. Several coauthors have financial ties, including employment with the study sponsor, Ono Pharmaceutical, which is developing ONO-4059.
NEW ORLEANS – Early data suggest that the second-generation oral BTK inhibitor ONO-4059 may give ibrutinib a run for its money in chronic lymphocytic leukemia.
The response rate to ONO-4059 monotherapy was 89% overall and 71% in those with the deleterious 17p deletion among 18 heavily pretreated patients with relapsed/refractory or high-risk CLL in a phase I, dose-escalation study.
Patients had already received a median of three prior therapies, including rituximab (84%) and fludarabine (95%), and had no higher priority therapy available to them, said Dr. Gilles Salles of Hospices Civils de Lyon (France), Universite Claude Bernard Lyon.
All patients had improved hemoglobin and platelet counts after 3 months on treatment and rapid reductions in lymph node size within the first 28-day cycle. Tumor burden was reduced by 50% for most patients, and all but one patient experienced a response that was detectable on a CT scan.
"This was true whatever their FISH status or 17p or 11q deletion status," Dr. Salles said at the annual meeting of the American Society of Hematology.
ONO-4059 is a highly selective Bruton’s tyrosine kinase (BTK) inhibitor with antitumor activity in several preclinical models.
No patients had received prior treatment with a P13 kinase or a BTK inhibitor, including ibrutinib (Imbruvica), which recently gained accelerated approval for previously treated mantle cell lymphoma.
ONO-4059 was given at daily doses ranging from 20 mg to 320 mg for up to 6 months, with the option of additional dosing up to 2 years. Sustained BTK inhibition was established at doses of 40 mg and higher.
Overall, the best response was a partial response in 14 patients, as well as two partial responses with lymphocytosis and one stable disease, he said. No complete responses occurred.
One patient progressed roughly 1 month after showing an initial response and complete disappearance of all palpable disease on physical exam. Richter’s syndrome was suspected.
"It’s very promising efficacy in this highly pretreated population," Dr. Salles said.
Patients with relapsed/refractory mantle cell lymphoma and diffuse large B-cell lymphoma, especially the ABC subtype, also appear sensitive to ONO-4059. Overall response rates were 43% and 75%, respectively, including three complete responses reported from the phase I study in a separate poster presentation at the meeting.
ONO-4059 had a favorable safety profile with a single dose-limiting toxicity observed in a patient who had Waldenstrom’s macroglobulinemia, was on the 320-mg dose, and was intolerant to all prior therapies. The maximum tolerated dose has not yet been reached.
The majority of adverse events in the CLL patients were grades 1 and 2. There were no clinically significant bleeding events or bruising, and there was a low incidence of diarrhea and rash, Dr. Salles said.
ONO-4059–related grade 3-4 events were independent of dose and included one grade 3 neutropenia at 20 mg and two grade 4 events at 20 mg and 320 mg. Four serious adverse events (febrile neutropenia, pyrexia, rash, and neutropenia) occurred in three patients, all of whom are still in the study and showing good clinical response, Dr. Salles said. Of the 30 patients dosed to date, 22 remain in the study.
No other trials are firmly planned, and pharmacokinetics/pharmacodynamics data continue to be explored in order to assess a phase II dosage, he said in an interview.
Dr. Salles reported consulting for and receiving honoraria from Roche. Several coauthors have financial ties, including employment with the study sponsor, Ono Pharmaceutical, which is developing ONO-4059.
NEW ORLEANS – Early data suggest that the second-generation oral BTK inhibitor ONO-4059 may give ibrutinib a run for its money in chronic lymphocytic leukemia.
The response rate to ONO-4059 monotherapy was 89% overall and 71% in those with the deleterious 17p deletion among 18 heavily pretreated patients with relapsed/refractory or high-risk CLL in a phase I, dose-escalation study.
Patients had already received a median of three prior therapies, including rituximab (84%) and fludarabine (95%), and had no higher priority therapy available to them, said Dr. Gilles Salles of Hospices Civils de Lyon (France), Universite Claude Bernard Lyon.
All patients had improved hemoglobin and platelet counts after 3 months on treatment and rapid reductions in lymph node size within the first 28-day cycle. Tumor burden was reduced by 50% for most patients, and all but one patient experienced a response that was detectable on a CT scan.
"This was true whatever their FISH status or 17p or 11q deletion status," Dr. Salles said at the annual meeting of the American Society of Hematology.
ONO-4059 is a highly selective Bruton’s tyrosine kinase (BTK) inhibitor with antitumor activity in several preclinical models.
No patients had received prior treatment with a P13 kinase or a BTK inhibitor, including ibrutinib (Imbruvica), which recently gained accelerated approval for previously treated mantle cell lymphoma.
ONO-4059 was given at daily doses ranging from 20 mg to 320 mg for up to 6 months, with the option of additional dosing up to 2 years. Sustained BTK inhibition was established at doses of 40 mg and higher.
Overall, the best response was a partial response in 14 patients, as well as two partial responses with lymphocytosis and one stable disease, he said. No complete responses occurred.
One patient progressed roughly 1 month after showing an initial response and complete disappearance of all palpable disease on physical exam. Richter’s syndrome was suspected.
"It’s very promising efficacy in this highly pretreated population," Dr. Salles said.
Patients with relapsed/refractory mantle cell lymphoma and diffuse large B-cell lymphoma, especially the ABC subtype, also appear sensitive to ONO-4059. Overall response rates were 43% and 75%, respectively, including three complete responses reported from the phase I study in a separate poster presentation at the meeting.
ONO-4059 had a favorable safety profile with a single dose-limiting toxicity observed in a patient who had Waldenstrom’s macroglobulinemia, was on the 320-mg dose, and was intolerant to all prior therapies. The maximum tolerated dose has not yet been reached.
The majority of adverse events in the CLL patients were grades 1 and 2. There were no clinically significant bleeding events or bruising, and there was a low incidence of diarrhea and rash, Dr. Salles said.
ONO-4059–related grade 3-4 events were independent of dose and included one grade 3 neutropenia at 20 mg and two grade 4 events at 20 mg and 320 mg. Four serious adverse events (febrile neutropenia, pyrexia, rash, and neutropenia) occurred in three patients, all of whom are still in the study and showing good clinical response, Dr. Salles said. Of the 30 patients dosed to date, 22 remain in the study.
No other trials are firmly planned, and pharmacokinetics/pharmacodynamics data continue to be explored in order to assess a phase II dosage, he said in an interview.
Dr. Salles reported consulting for and receiving honoraria from Roche. Several coauthors have financial ties, including employment with the study sponsor, Ono Pharmaceutical, which is developing ONO-4059.
AT ASH 2013
Major finding: The response rate was 89% overall and 71% for patients with 17p deletion.
Data source: A prospective, phase I dose-escalation study in 18 patients with relapsed/refractory or high-risk CLL.
Disclosures: Dr. Salles reported honoraria from Janssen, Gilead, and Celgene. Several coauthors have financial ties, including employment with the study sponsor, Ono Pharmaceutical, which is developing ONO-4059.

Anatomy’s role is elusive in carotid stenting risk
CHICAGO – Pinning down the anatomic characteristics that increase the risk of stroke with carotid artery stenting continues to be a challenge, as demonstrated by a database study and literature review presented at a symposium on vascular surgery sponsored by Northwestern University.
"I am absolutely convinced that certain anatomic and plaque characteristics increase the risk of a stroke for patients with carotid artery stenting," Dr. Melina R. Kibbe said in presenting her study. "The studies are not consistent in the literature, but there is a pattern."

She presented a prospective database review that evaluated no less than a dozen anatomic variables in 381 carotid arteries stented at the university from 2001 to 2010. The mostly male (75%), asymptomatic (70%), and moderate- to high-risk cohort had an average age of 70.5 years.
Within 30 days of carotid stenting, there were six strokes and eight transient ischemic attacks (TIAs), for an overall neurologic event rate of 3.7%, she said. Three patients had a heart attack, and two died.
The risk of perioperative stroke or TIA was significantly increased only in patients with a higher degree of internal carotid artery (ICA) stenosis (87% stenosis vs. 81% stenosis; P = .03).
It also trended higher, but fell short of significance, in those with greater arch calcification (P = .06).
Surprisingly, no statistical association was found between neurologic events and arch type (P = .16), despite the clinical belief that increasing arch type can be associated with more difficulty accessing the target lesion, said Dr. Kibbe, professor of vascular surgery and surgical research at Northwestern University, Chicago.
Other variables with trends that failed to reach statistical significance included internal to common carotid artery angulation, tortuous carotid artery, ipsilateral external carotid artery (ECA) stenosis, plaque calcification, and lesion length.
Turning to the literature for more answers, Dr. Kibbe and her colleagues performed a review of eight carotid stenting studies between 1993 and 2013. These studies included SAPPHIRE, which demonstrated an association between type II and III arches and increased stroke risk. Two other studies implicated type II, type III, and bovine arches, while three other studies, including a systematic review that incorporated the EVA-3S study (Stroke 2011;42:380-8), found no association between arch type and stroke.
Still, Dr. Kibbe said she’s convinced no two patients are alike when it comes to arterial anatomy and called for data from pivotal trials like CREST to be reanalyzed for stroke, based on arch type and plaque characteristics.
"Even better, I’d like to see a prospective, randomized study that excludes patients for carotid artery stenting based on their anatomy; for example, excluding all type III arches," she said. "My own personal bias is that patients with type III arches should not have carotid stenting. We don’t need to push the envelope."
Interestingly, no study in the review has shown ICA stenosis to be a risk factor for stroke or TIA, although lesions with a higher degree of stenosis would be expected to contribute to perioperative stroke risk.
Arch calcification, ECA stenosis, and plaque calcification also failed to register as risk factors, despite their potential to increase the risk of embolization with wire or catheter manipulation, Dr. Kibbe observed.
Two studies found that lesions longer than 1 cm or 1.5 cm were predictive of stroke, while one study (Catheter Cardiovasc. Interv. 2012;80:321-8) linked stroke with ICA tortuosity, defined as a distal ICA angle of more than 60 degrees.
Conventional thinking would suggest that right-sided carotid stenting would also confer a greater stroke risk because selecting the right ICA requires crossing the orifice of the left ICA, but only the SAPPHIRE trial reported more strokes with right-sided lesions, she said.
Finally, Dr. Kibbe highlighted an anatomic scoring system for carotid artery stenting developed by an international panel of seven vascular surgeons and five interventional radiologists (Stroke 2009;40:1698-703). Based on expert consensus, the greatest risk factor is type III arch, followed in descending order of risk by arch atheroma, diseased common carotid artery, ECA disease, angulated distal ICA, bovine arch, and pinhole stenosis. The resulting color-coded, traffic-light scoring system looks rather busy, but is relatively easy to use and provides guidance on carotid stenting suitability for the novice physician, she said.
Dr. Kibbe reported having no financial disclosures.
CHICAGO – Pinning down the anatomic characteristics that increase the risk of stroke with carotid artery stenting continues to be a challenge, as demonstrated by a database study and literature review presented at a symposium on vascular surgery sponsored by Northwestern University.
"I am absolutely convinced that certain anatomic and plaque characteristics increase the risk of a stroke for patients with carotid artery stenting," Dr. Melina R. Kibbe said in presenting her study. "The studies are not consistent in the literature, but there is a pattern."
She presented a prospective database review that evaluated no less than a dozen anatomic variables in 381 carotid arteries stented at the university from 2001 to 2010. The mostly male (75%), asymptomatic (70%), and moderate- to high-risk cohort had an average age of 70.5 years.
Within 30 days of carotid stenting, there were six strokes and eight transient ischemic attacks (TIAs), for an overall neurologic event rate of 3.7%, she said. Three patients had a heart attack, and two died.
The risk of perioperative stroke or TIA was significantly increased only in patients with a higher degree of internal carotid artery (ICA) stenosis (87% stenosis vs. 81% stenosis; P = .03).
It also trended higher, but fell short of significance, in those with greater arch calcification (P = .06).
Surprisingly, no statistical association was found between neurologic events and arch type (P = .16), despite the clinical belief that increasing arch type can be associated with more difficulty accessing the target lesion, said Dr. Kibbe, professor of vascular surgery and surgical research at Northwestern University, Chicago.
Other variables with trends that failed to reach statistical significance included internal to common carotid artery angulation, tortuous carotid artery, ipsilateral external carotid artery (ECA) stenosis, plaque calcification, and lesion length.
Turning to the literature for more answers, Dr. Kibbe and her colleagues performed a review of eight carotid stenting studies between 1993 and 2013. These studies included SAPPHIRE, which demonstrated an association between type II and III arches and increased stroke risk. Two other studies implicated type II, type III, and bovine arches, while three other studies, including a systematic review that incorporated the EVA-3S study (Stroke 2011;42:380-8), found no association between arch type and stroke.
Still, Dr. Kibbe said she’s convinced no two patients are alike when it comes to arterial anatomy and called for data from pivotal trials like CREST to be reanalyzed for stroke, based on arch type and plaque characteristics.
"Even better, I’d like to see a prospective, randomized study that excludes patients for carotid artery stenting based on their anatomy; for example, excluding all type III arches," she said. "My own personal bias is that patients with type III arches should not have carotid stenting. We don’t need to push the envelope."
Interestingly, no study in the review has shown ICA stenosis to be a risk factor for stroke or TIA, although lesions with a higher degree of stenosis would be expected to contribute to perioperative stroke risk.
Arch calcification, ECA stenosis, and plaque calcification also failed to register as risk factors, despite their potential to increase the risk of embolization with wire or catheter manipulation, Dr. Kibbe observed.
Two studies found that lesions longer than 1 cm or 1.5 cm were predictive of stroke, while one study (Catheter Cardiovasc. Interv. 2012;80:321-8) linked stroke with ICA tortuosity, defined as a distal ICA angle of more than 60 degrees.
Conventional thinking would suggest that right-sided carotid stenting would also confer a greater stroke risk because selecting the right ICA requires crossing the orifice of the left ICA, but only the SAPPHIRE trial reported more strokes with right-sided lesions, she said.
Finally, Dr. Kibbe highlighted an anatomic scoring system for carotid artery stenting developed by an international panel of seven vascular surgeons and five interventional radiologists (Stroke 2009;40:1698-703). Based on expert consensus, the greatest risk factor is type III arch, followed in descending order of risk by arch atheroma, diseased common carotid artery, ECA disease, angulated distal ICA, bovine arch, and pinhole stenosis. The resulting color-coded, traffic-light scoring system looks rather busy, but is relatively easy to use and provides guidance on carotid stenting suitability for the novice physician, she said.
Dr. Kibbe reported having no financial disclosures.
CHICAGO – Pinning down the anatomic characteristics that increase the risk of stroke with carotid artery stenting continues to be a challenge, as demonstrated by a database study and literature review presented at a symposium on vascular surgery sponsored by Northwestern University.
"I am absolutely convinced that certain anatomic and plaque characteristics increase the risk of a stroke for patients with carotid artery stenting," Dr. Melina R. Kibbe said in presenting her study. "The studies are not consistent in the literature, but there is a pattern."
She presented a prospective database review that evaluated no less than a dozen anatomic variables in 381 carotid arteries stented at the university from 2001 to 2010. The mostly male (75%), asymptomatic (70%), and moderate- to high-risk cohort had an average age of 70.5 years.
Within 30 days of carotid stenting, there were six strokes and eight transient ischemic attacks (TIAs), for an overall neurologic event rate of 3.7%, she said. Three patients had a heart attack, and two died.
The risk of perioperative stroke or TIA was significantly increased only in patients with a higher degree of internal carotid artery (ICA) stenosis (87% stenosis vs. 81% stenosis; P = .03).
It also trended higher, but fell short of significance, in those with greater arch calcification (P = .06).
Surprisingly, no statistical association was found between neurologic events and arch type (P = .16), despite the clinical belief that increasing arch type can be associated with more difficulty accessing the target lesion, said Dr. Kibbe, professor of vascular surgery and surgical research at Northwestern University, Chicago.
Other variables with trends that failed to reach statistical significance included internal to common carotid artery angulation, tortuous carotid artery, ipsilateral external carotid artery (ECA) stenosis, plaque calcification, and lesion length.
Turning to the literature for more answers, Dr. Kibbe and her colleagues performed a review of eight carotid stenting studies between 1993 and 2013. These studies included SAPPHIRE, which demonstrated an association between type II and III arches and increased stroke risk. Two other studies implicated type II, type III, and bovine arches, while three other studies, including a systematic review that incorporated the EVA-3S study (Stroke 2011;42:380-8), found no association between arch type and stroke.
Still, Dr. Kibbe said she’s convinced no two patients are alike when it comes to arterial anatomy and called for data from pivotal trials like CREST to be reanalyzed for stroke, based on arch type and plaque characteristics.
"Even better, I’d like to see a prospective, randomized study that excludes patients for carotid artery stenting based on their anatomy; for example, excluding all type III arches," she said. "My own personal bias is that patients with type III arches should not have carotid stenting. We don’t need to push the envelope."
Interestingly, no study in the review has shown ICA stenosis to be a risk factor for stroke or TIA, although lesions with a higher degree of stenosis would be expected to contribute to perioperative stroke risk.
Arch calcification, ECA stenosis, and plaque calcification also failed to register as risk factors, despite their potential to increase the risk of embolization with wire or catheter manipulation, Dr. Kibbe observed.
Two studies found that lesions longer than 1 cm or 1.5 cm were predictive of stroke, while one study (Catheter Cardiovasc. Interv. 2012;80:321-8) linked stroke with ICA tortuosity, defined as a distal ICA angle of more than 60 degrees.
Conventional thinking would suggest that right-sided carotid stenting would also confer a greater stroke risk because selecting the right ICA requires crossing the orifice of the left ICA, but only the SAPPHIRE trial reported more strokes with right-sided lesions, she said.
Finally, Dr. Kibbe highlighted an anatomic scoring system for carotid artery stenting developed by an international panel of seven vascular surgeons and five interventional radiologists (Stroke 2009;40:1698-703). Based on expert consensus, the greatest risk factor is type III arch, followed in descending order of risk by arch atheroma, diseased common carotid artery, ECA disease, angulated distal ICA, bovine arch, and pinhole stenosis. The resulting color-coded, traffic-light scoring system looks rather busy, but is relatively easy to use and provides guidance on carotid stenting suitability for the novice physician, she said.
Dr. Kibbe reported having no financial disclosures.
EXPERT ANALYSIS AT A NORTHWESTERN VASCULAR SYMPOSIUM
Major finding: The risk of perioperative stroke or TIA was significantly increased only in patients with a higher degree of internal carotid artery (ICA) stenosis (87% stenosis vs. 81% stenosis; P = .03).
Data source: A retrospective study of 381 carotid arteries and an analysis of eight published studies.
Disclosures: Dr. Kibbe reported having no financial disclosures.

Mild coronary artery disease is gender blind
CHICAGO – Men and women may not really be all that different when it comes to mild coronary artery disease.
A prospective, multinational registry analysis found that 1.2% of women and 1.1% of men with mild, nonobstructive coronary artery disease on coronary CT angiography experience a major adverse cardiovascular event, either heart attack or death, each year.

For those free of coronary artery disease (CAD), the event rate was 0.3% for both sexes, Dr. Jonathon A. Leipsic reported at the annual meeting of the Radiological Society of North America.
Women’s heart disease is typically viewed as different from men’s heart disease, in part because of women’s unique presenting symptomatology. Studies such as the Women’s Health Initiative have also reported that women with nonspecific or atypical chest pain have a twofold greater risk for nonfatal MI.
Importantly, all prior data has been reliant on invasive coronary angiography for anatomical coronary assessment, observed Dr. Leipsic, codirector of advanced cardiac imaging, Providence Health Care Heart Center at St. Paul’s Hospital, Vancouver, B.C.
The current analysis, however, used data from the prospective CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry, which tracks roughly 28,000 individuals in North America, Europe, and Asia who have undergone coronary CT angiography.
The results represent a major shift in thinking, Dr. Leipsic said in an interview.
"What we realize is that CT identifies mild disease in the wall in a way that the invasive angiogram does not," he said. "So suddenly, when you say you have a normal invasive angiogram, there may still be mild disease in the arteries, whereas when you have a normal CT in a woman, our data would suggest that those women do very well, even if they have symptoms."
Dr. Leipsic and his associates identified 18,158 patients in the CONFIRM registry with no disease or mild CAD with less than 50% stenosis. Propensity matching for risk factors, chest pain, and extent of disease left 11,462 patients.
Their average age was 55 years, 34% were asymptomatic, 45% had hypertension, 12% were diabetic, and 18% were current smokers.
Of these, 37 had an MI; 120 died; and 7 had an MI and died (1.4%).
The annual major adverse cardiovascular event (MACE) rate was 0.6% overall, and was significantly different between patients with a normal CT and those with nonobstructive disease (0.3% vs. 1.1%), Dr. Leipsic said.
"This mild disease we see on CT is not just incidental," he said during a press briefing at the meeting. "It actually identifies patients who are at increased risk of having a heart attack and dying, with an increased risk of 1.84 for the overall cohort (P = .001)."
Notably, 3-year MACE-free survival was similar among men and women without coronary plaque on CT as well as those with non-obstructive disease.
Dr. Leipsic commented that detractors of the data have argued that the analysis failed to focus on women at the greatest risk – those with atypical symptoms. A further sub-analysis, however, based on the presence or absence of symptoms and the type of symptoms (nonanginal chest pain, atypical angina, and typical angina), once again "found that men and women behave similarly," he said.
Event rates were lower in men and women with normal CT scans and elevated in both sexes in the setting of nonobstructive disease, "regardless of the nature of chest pain and even in the absence of chest pain," he noted.
Press briefing moderator Dr. Candice Johnstone of the Medical College of Wisconsin, Milwaukee, said in an interview, "Observational studies have limits, but at the same time, I think it may be a paradigm shift, in that it may be a new tool in our toolbox for people at lower risk of heart disease to avoid an invasive procedure."
Dr. Leipsic reported financial relationships with several entities including GE Healthcare, HeartFlow, Edwards LifeSciences, and TC3.
CHICAGO – Men and women may not really be all that different when it comes to mild coronary artery disease.
A prospective, multinational registry analysis found that 1.2% of women and 1.1% of men with mild, nonobstructive coronary artery disease on coronary CT angiography experience a major adverse cardiovascular event, either heart attack or death, each year.
For those free of coronary artery disease (CAD), the event rate was 0.3% for both sexes, Dr. Jonathon A. Leipsic reported at the annual meeting of the Radiological Society of North America.
Women’s heart disease is typically viewed as different from men’s heart disease, in part because of women’s unique presenting symptomatology. Studies such as the Women’s Health Initiative have also reported that women with nonspecific or atypical chest pain have a twofold greater risk for nonfatal MI.
Importantly, all prior data has been reliant on invasive coronary angiography for anatomical coronary assessment, observed Dr. Leipsic, codirector of advanced cardiac imaging, Providence Health Care Heart Center at St. Paul’s Hospital, Vancouver, B.C.
The current analysis, however, used data from the prospective CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry, which tracks roughly 28,000 individuals in North America, Europe, and Asia who have undergone coronary CT angiography.
The results represent a major shift in thinking, Dr. Leipsic said in an interview.
"What we realize is that CT identifies mild disease in the wall in a way that the invasive angiogram does not," he said. "So suddenly, when you say you have a normal invasive angiogram, there may still be mild disease in the arteries, whereas when you have a normal CT in a woman, our data would suggest that those women do very well, even if they have symptoms."
Dr. Leipsic and his associates identified 18,158 patients in the CONFIRM registry with no disease or mild CAD with less than 50% stenosis. Propensity matching for risk factors, chest pain, and extent of disease left 11,462 patients.
Their average age was 55 years, 34% were asymptomatic, 45% had hypertension, 12% were diabetic, and 18% were current smokers.
Of these, 37 had an MI; 120 died; and 7 had an MI and died (1.4%).
The annual major adverse cardiovascular event (MACE) rate was 0.6% overall, and was significantly different between patients with a normal CT and those with nonobstructive disease (0.3% vs. 1.1%), Dr. Leipsic said.
"This mild disease we see on CT is not just incidental," he said during a press briefing at the meeting. "It actually identifies patients who are at increased risk of having a heart attack and dying, with an increased risk of 1.84 for the overall cohort (P = .001)."
Notably, 3-year MACE-free survival was similar among men and women without coronary plaque on CT as well as those with non-obstructive disease.
Dr. Leipsic commented that detractors of the data have argued that the analysis failed to focus on women at the greatest risk – those with atypical symptoms. A further sub-analysis, however, based on the presence or absence of symptoms and the type of symptoms (nonanginal chest pain, atypical angina, and typical angina), once again "found that men and women behave similarly," he said.
Event rates were lower in men and women with normal CT scans and elevated in both sexes in the setting of nonobstructive disease, "regardless of the nature of chest pain and even in the absence of chest pain," he noted.
Press briefing moderator Dr. Candice Johnstone of the Medical College of Wisconsin, Milwaukee, said in an interview, "Observational studies have limits, but at the same time, I think it may be a paradigm shift, in that it may be a new tool in our toolbox for people at lower risk of heart disease to avoid an invasive procedure."
Dr. Leipsic reported financial relationships with several entities including GE Healthcare, HeartFlow, Edwards LifeSciences, and TC3.
CHICAGO – Men and women may not really be all that different when it comes to mild coronary artery disease.
A prospective, multinational registry analysis found that 1.2% of women and 1.1% of men with mild, nonobstructive coronary artery disease on coronary CT angiography experience a major adverse cardiovascular event, either heart attack or death, each year.
For those free of coronary artery disease (CAD), the event rate was 0.3% for both sexes, Dr. Jonathon A. Leipsic reported at the annual meeting of the Radiological Society of North America.
Women’s heart disease is typically viewed as different from men’s heart disease, in part because of women’s unique presenting symptomatology. Studies such as the Women’s Health Initiative have also reported that women with nonspecific or atypical chest pain have a twofold greater risk for nonfatal MI.
Importantly, all prior data has been reliant on invasive coronary angiography for anatomical coronary assessment, observed Dr. Leipsic, codirector of advanced cardiac imaging, Providence Health Care Heart Center at St. Paul’s Hospital, Vancouver, B.C.
The current analysis, however, used data from the prospective CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry, which tracks roughly 28,000 individuals in North America, Europe, and Asia who have undergone coronary CT angiography.
The results represent a major shift in thinking, Dr. Leipsic said in an interview.
"What we realize is that CT identifies mild disease in the wall in a way that the invasive angiogram does not," he said. "So suddenly, when you say you have a normal invasive angiogram, there may still be mild disease in the arteries, whereas when you have a normal CT in a woman, our data would suggest that those women do very well, even if they have symptoms."
Dr. Leipsic and his associates identified 18,158 patients in the CONFIRM registry with no disease or mild CAD with less than 50% stenosis. Propensity matching for risk factors, chest pain, and extent of disease left 11,462 patients.
Their average age was 55 years, 34% were asymptomatic, 45% had hypertension, 12% were diabetic, and 18% were current smokers.
Of these, 37 had an MI; 120 died; and 7 had an MI and died (1.4%).
The annual major adverse cardiovascular event (MACE) rate was 0.6% overall, and was significantly different between patients with a normal CT and those with nonobstructive disease (0.3% vs. 1.1%), Dr. Leipsic said.
"This mild disease we see on CT is not just incidental," he said during a press briefing at the meeting. "It actually identifies patients who are at increased risk of having a heart attack and dying, with an increased risk of 1.84 for the overall cohort (P = .001)."
Notably, 3-year MACE-free survival was similar among men and women without coronary plaque on CT as well as those with non-obstructive disease.
Dr. Leipsic commented that detractors of the data have argued that the analysis failed to focus on women at the greatest risk – those with atypical symptoms. A further sub-analysis, however, based on the presence or absence of symptoms and the type of symptoms (nonanginal chest pain, atypical angina, and typical angina), once again "found that men and women behave similarly," he said.
Event rates were lower in men and women with normal CT scans and elevated in both sexes in the setting of nonobstructive disease, "regardless of the nature of chest pain and even in the absence of chest pain," he noted.
Press briefing moderator Dr. Candice Johnstone of the Medical College of Wisconsin, Milwaukee, said in an interview, "Observational studies have limits, but at the same time, I think it may be a paradigm shift, in that it may be a new tool in our toolbox for people at lower risk of heart disease to avoid an invasive procedure."
Dr. Leipsic reported financial relationships with several entities including GE Healthcare, HeartFlow, Edwards LifeSciences, and TC3.
AT RSNA 2013
Major finding: In patients with mild, nonobstructive coronary disease, the annual MACE rate was 1.2% in women and 1.1% in men (P = .95).
Data source: An observational registry study in 11,462 patients with no disease or mild coronary disease with less than 50% stenosis.
Disclosures: Dr. Leipsic reported financial relationships with several entities including GE Healthcare, HeartFlow, Edwards LifeSciences, and TC3.

Zenith AAA fenestrated graft: 30-day outcomes match those seen in trial
CHICAGO – Real-world 30-day outcomes with the Zenith fenestrated endovascular graft compared well with those in the U.S. fenestrated trial for the treatment of juxtarenal aortic aneurysms, based on a multicenter, retrospective study of 57 patients.
The good results were seen despite higher rates of comorbidities and more challenging anatomy in the patients treated post approval. But "these are short-term outcomes and, ultimately, we’re going to need to know the long-term durability of this type of repair," Dr. Chandu Vemuri said at the annual meeting of the Midwestern Vascular Surgical Society.

The Zenith fenestrated AAA endovascular graft (zFEN) has been commercially available outside the United States since November 2002, and it gained federal approval in April 2012 based on the results of the pivotal U.S. fenestrated trial (USFT). The graft is indicated for the treatment of patients with abdominal aortic or aortoiliac aneurysms that have an infrarenal aortic neck at least 4 mm in length.
Notably, 47% of patients in the current analysis did not meet the USFT anatomic criteria of a 4- to 15-mm infrarenal neck. There were also significantly more mesenteric stents used in this group than in the USFT (13 vs. 0; P < .05), reflecting the higher anatomic complexity of these patients, said Dr. Vemuri, of Washington University, St. Louis.
Compared with the 42 USFT patients, study patients also had significantly higher rates of preoperative coronary artery disease (79% vs. 52%), myocardial infarction (60% vs. 24%), and renal insufficiency (26% vs. 9.5%); all P < .05).
Dr. Vemuri was quick to point out, however, that the results of the study may not broadly translate. The trial was conducted at institutions that had a high aortic volume, and involved highly experienced surgeons, many of whom took part in the USFT and were familiar with the zFEN device.
The technical success rate, with regard to aneurysm exclusion, was 100% in both the study and the USFT. In two study patients, the left renal artery (RA) fenestration was not able to be aligned. One patient had a kinked renal stent that was successfully restented, and one patient was converted to a unibody prosthesis with femoral-femoral bypass and an iliac plug, he said.
Other 30-day outcomes were similar between the study and USFT patients, including mortality (1 vs. 0), renal insufficiency (4 vs. 0), postoperative dialysis (1 vs. 0), and endoleak (10 vs. 9). Two of the 10 endoleaks were type III and 8 were type II.
The most common graft configuration was a scallop of the superior mesenteric artery (SMA) and bilateral RA fenestration in 40 patients, followed by bilateral RA fenestrations alone in 8, and a celiac scallop, SMA fenestration, and bilateral RA fenestration in 3, Dr. Vemuri observed.
One patient each had the following: right RA scallop plus left RA fenestration, right RA fenestration, right accessory RA fenestration, left RA fenestration, celiac scallop and SMA fenestration with a right RA fenestration, and an SMA scallop with left RA fenestration.
Total operative time averaged 250 minutes.
Audience members pressed Dr. Vemuri for details on the 47% of patients who did not meet the USFT anatomic criteria and whether the current cohort was really anatomically challenging or just consisted of on-label cases that were harder than usual.
Dr. Vemuri responded that the intervention was off-label in 27% of patients who did not have the minimum 4-mm infrarenal neck. One graft configuration was more complex than in the device’s instructions for use (IFU) document. All of the patients had a sufficient infrarenal neck for appropriate seal.
"I don’t think the purpose of this study is to endorse use outside the IFU of the device, but to report that when people do, this is what happens," he added.
Dr. Vemuri reported having no financial disclosures. His coauthors reported relationships including serving as consultants or researchers for Cook, which produces the Zenith graft.
CHICAGO – Real-world 30-day outcomes with the Zenith fenestrated endovascular graft compared well with those in the U.S. fenestrated trial for the treatment of juxtarenal aortic aneurysms, based on a multicenter, retrospective study of 57 patients.
The good results were seen despite higher rates of comorbidities and more challenging anatomy in the patients treated post approval. But "these are short-term outcomes and, ultimately, we’re going to need to know the long-term durability of this type of repair," Dr. Chandu Vemuri said at the annual meeting of the Midwestern Vascular Surgical Society.
The Zenith fenestrated AAA endovascular graft (zFEN) has been commercially available outside the United States since November 2002, and it gained federal approval in April 2012 based on the results of the pivotal U.S. fenestrated trial (USFT). The graft is indicated for the treatment of patients with abdominal aortic or aortoiliac aneurysms that have an infrarenal aortic neck at least 4 mm in length.
Notably, 47% of patients in the current analysis did not meet the USFT anatomic criteria of a 4- to 15-mm infrarenal neck. There were also significantly more mesenteric stents used in this group than in the USFT (13 vs. 0; P < .05), reflecting the higher anatomic complexity of these patients, said Dr. Vemuri, of Washington University, St. Louis.
Compared with the 42 USFT patients, study patients also had significantly higher rates of preoperative coronary artery disease (79% vs. 52%), myocardial infarction (60% vs. 24%), and renal insufficiency (26% vs. 9.5%); all P < .05).
Dr. Vemuri was quick to point out, however, that the results of the study may not broadly translate. The trial was conducted at institutions that had a high aortic volume, and involved highly experienced surgeons, many of whom took part in the USFT and were familiar with the zFEN device.
The technical success rate, with regard to aneurysm exclusion, was 100% in both the study and the USFT. In two study patients, the left renal artery (RA) fenestration was not able to be aligned. One patient had a kinked renal stent that was successfully restented, and one patient was converted to a unibody prosthesis with femoral-femoral bypass and an iliac plug, he said.
Other 30-day outcomes were similar between the study and USFT patients, including mortality (1 vs. 0), renal insufficiency (4 vs. 0), postoperative dialysis (1 vs. 0), and endoleak (10 vs. 9). Two of the 10 endoleaks were type III and 8 were type II.
The most common graft configuration was a scallop of the superior mesenteric artery (SMA) and bilateral RA fenestration in 40 patients, followed by bilateral RA fenestrations alone in 8, and a celiac scallop, SMA fenestration, and bilateral RA fenestration in 3, Dr. Vemuri observed.
One patient each had the following: right RA scallop plus left RA fenestration, right RA fenestration, right accessory RA fenestration, left RA fenestration, celiac scallop and SMA fenestration with a right RA fenestration, and an SMA scallop with left RA fenestration.
Total operative time averaged 250 minutes.
Audience members pressed Dr. Vemuri for details on the 47% of patients who did not meet the USFT anatomic criteria and whether the current cohort was really anatomically challenging or just consisted of on-label cases that were harder than usual.
Dr. Vemuri responded that the intervention was off-label in 27% of patients who did not have the minimum 4-mm infrarenal neck. One graft configuration was more complex than in the device’s instructions for use (IFU) document. All of the patients had a sufficient infrarenal neck for appropriate seal.
"I don’t think the purpose of this study is to endorse use outside the IFU of the device, but to report that when people do, this is what happens," he added.
Dr. Vemuri reported having no financial disclosures. His coauthors reported relationships including serving as consultants or researchers for Cook, which produces the Zenith graft.
CHICAGO – Real-world 30-day outcomes with the Zenith fenestrated endovascular graft compared well with those in the U.S. fenestrated trial for the treatment of juxtarenal aortic aneurysms, based on a multicenter, retrospective study of 57 patients.
The good results were seen despite higher rates of comorbidities and more challenging anatomy in the patients treated post approval. But "these are short-term outcomes and, ultimately, we’re going to need to know the long-term durability of this type of repair," Dr. Chandu Vemuri said at the annual meeting of the Midwestern Vascular Surgical Society.
The Zenith fenestrated AAA endovascular graft (zFEN) has been commercially available outside the United States since November 2002, and it gained federal approval in April 2012 based on the results of the pivotal U.S. fenestrated trial (USFT). The graft is indicated for the treatment of patients with abdominal aortic or aortoiliac aneurysms that have an infrarenal aortic neck at least 4 mm in length.
Notably, 47% of patients in the current analysis did not meet the USFT anatomic criteria of a 4- to 15-mm infrarenal neck. There were also significantly more mesenteric stents used in this group than in the USFT (13 vs. 0; P < .05), reflecting the higher anatomic complexity of these patients, said Dr. Vemuri, of Washington University, St. Louis.
Compared with the 42 USFT patients, study patients also had significantly higher rates of preoperative coronary artery disease (79% vs. 52%), myocardial infarction (60% vs. 24%), and renal insufficiency (26% vs. 9.5%); all P < .05).
Dr. Vemuri was quick to point out, however, that the results of the study may not broadly translate. The trial was conducted at institutions that had a high aortic volume, and involved highly experienced surgeons, many of whom took part in the USFT and were familiar with the zFEN device.
The technical success rate, with regard to aneurysm exclusion, was 100% in both the study and the USFT. In two study patients, the left renal artery (RA) fenestration was not able to be aligned. One patient had a kinked renal stent that was successfully restented, and one patient was converted to a unibody prosthesis with femoral-femoral bypass and an iliac plug, he said.
Other 30-day outcomes were similar between the study and USFT patients, including mortality (1 vs. 0), renal insufficiency (4 vs. 0), postoperative dialysis (1 vs. 0), and endoleak (10 vs. 9). Two of the 10 endoleaks were type III and 8 were type II.
The most common graft configuration was a scallop of the superior mesenteric artery (SMA) and bilateral RA fenestration in 40 patients, followed by bilateral RA fenestrations alone in 8, and a celiac scallop, SMA fenestration, and bilateral RA fenestration in 3, Dr. Vemuri observed.
One patient each had the following: right RA scallop plus left RA fenestration, right RA fenestration, right accessory RA fenestration, left RA fenestration, celiac scallop and SMA fenestration with a right RA fenestration, and an SMA scallop with left RA fenestration.
Total operative time averaged 250 minutes.
Audience members pressed Dr. Vemuri for details on the 47% of patients who did not meet the USFT anatomic criteria and whether the current cohort was really anatomically challenging or just consisted of on-label cases that were harder than usual.
Dr. Vemuri responded that the intervention was off-label in 27% of patients who did not have the minimum 4-mm infrarenal neck. One graft configuration was more complex than in the device’s instructions for use (IFU) document. All of the patients had a sufficient infrarenal neck for appropriate seal.
"I don’t think the purpose of this study is to endorse use outside the IFU of the device, but to report that when people do, this is what happens," he added.
Dr. Vemuri reported having no financial disclosures. His coauthors reported relationships including serving as consultants or researchers for Cook, which produces the Zenith graft.
AT MIDWESTERN VASCULAR 2013
Major finding: The technical success rate was 100%.
Data source: Retrospective study of 57 patients with juxtarenal aortic aneurysms treated post approval with the Zenith fenestrated endovascular graft.
Disclosures: Dr. Vemuri reported having no financial disclosures. His coauthors reported relationships including serving as consultants or researchers for Cook, which produces the Zenith graft.

Aortic arch repair outcomes held acceptable
CHICAGO – Repair of the isolated nontraumatic aortic arch aneurysm can be performed with acceptable early and late results, based on a 20-year review of 137 patients.
Early mortality was seen in nine patients (6.6%), and was similarly split between endovascular and open repair (7.3% vs. 6.5%, respectively).

Five-year survival did not differ between the endovascular- and open-repair groups (86% vs. 70%; P = .57), although the risk of reintervention was significantly higher with an endovascular strategy (94% vs. 77.5%; P = .02).
"These data support ongoing efforts to develop branched endografts specifically tailored for complex and difficult-to-treat pathology to potentially reduce the morbidity of therapy for this population," Dr. Himanshu J. Patel said at the annual meeting of the Midwestern Vascular Surgical Society.
Marginal landing zones and the need for complex arch debranching procedures to extend landing zones and facilitate repair can hinder endovascular repair, though open aortic repair is challenged by the frequent need for hypothermic circulatory arrest. Early and late results with either option are ill defined for this pathology, observed Dr. Patel, with the Cardiovascular Center, University of Michigan, Ann Arbor.
To investigate these outcomes, the authors evaluated data from 1993 to 2013 for 137 patients with nontraumatic aortic aneurysms located between the left and right pulmonary artery; 93 patients underwent open repair and 44 had an endovascular or hybrid repair.
The pathology was saccular in 39%, dissection in 11%, pseudoaneurysm in 18%, and anomalous arch in 11%. Rupture was identified in 14%. The average patient age was 59 years, and 46% were male.

In the open-repair group, 84 patients underwent a posterolateral thoracotomy and 9 had a median sternotomy. Extracorporeal perfusion was used in all, and 80 required deep hypothermic arrest.
In the endovascular group, the proximal extent of surgery was classified as Ishimaru zone 0 in 10 patients, zone 1 in 1, and zone 2 in 33. Treatment included full arch debranching and stent graft repair for zone 0 and zone 2 patients, respectively. A chimney stent of the carotid artery and left subclavian arterial bypass was used for the zone 1 patient.
Although the institutional preference is to utilize left subclavian artery (LSCA) revascularization for all, 76% of endovascular patients requiring LSCA coverage underwent preoperative bypass, Dr. Patel observed.
Significant differences existed at baseline between the two groups, with the endovascular group almost a full decade older than the open group (65 vs. 56 years). The endovascular group was also more likely to have saccular pathology (57% vs. 30%), and less likely to have a history of tobacco use (12% vs. 84%) or prior arch repair (16% vs. 36%).
Early morbidity included stroke in 6.6%, spinal cord ischemia in 0.7%, need for dialysis in 3.6%, and tracheostomy in 7.2%, Dr. Patel said.
The composite endpoint of stroke or early mortality was independently predicted by increasing age (odds ratio, 1.05; P = .055) and use of a hybrid procedure (OR, 6.4; P = .01).
Two-year freedom from aortic rupture or reintervention was 78% in the open group and 94% in the endovascular group (P = .02).
After a mean follow-up of 66 months, four patients had died of stroke, two from myocardial infarction, one from a proximal anastomosis disruption/rupture, and one from a type A dissection/rupture, Dr. Patel said.
The average survival was 145 months and 5-year survival rate was 59%.
Independent predictors of late mortality were increasing age (hazard ratio, 1.06; P = .001), peripheral vascular disease (HR, 2.4; P = .024), postoperative stroke (HR, 6.4; P less than .001), and postoperative dialysis (HR, 11.4; P less than .001). Notably, repair type was not predictive (P = .22), Dr. Patel said.
He cautioned the audience, however, that "cerebrovascular accidents remain an important cause of early and late mortality."
Dr. Patel reported consulting fees from W.L. Gore and Terumo.
CHICAGO – Repair of the isolated nontraumatic aortic arch aneurysm can be performed with acceptable early and late results, based on a 20-year review of 137 patients.
Early mortality was seen in nine patients (6.6%), and was similarly split between endovascular and open repair (7.3% vs. 6.5%, respectively).
Five-year survival did not differ between the endovascular- and open-repair groups (86% vs. 70%; P = .57), although the risk of reintervention was significantly higher with an endovascular strategy (94% vs. 77.5%; P = .02).
"These data support ongoing efforts to develop branched endografts specifically tailored for complex and difficult-to-treat pathology to potentially reduce the morbidity of therapy for this population," Dr. Himanshu J. Patel said at the annual meeting of the Midwestern Vascular Surgical Society.
Marginal landing zones and the need for complex arch debranching procedures to extend landing zones and facilitate repair can hinder endovascular repair, though open aortic repair is challenged by the frequent need for hypothermic circulatory arrest. Early and late results with either option are ill defined for this pathology, observed Dr. Patel, with the Cardiovascular Center, University of Michigan, Ann Arbor.
To investigate these outcomes, the authors evaluated data from 1993 to 2013 for 137 patients with nontraumatic aortic aneurysms located between the left and right pulmonary artery; 93 patients underwent open repair and 44 had an endovascular or hybrid repair.
The pathology was saccular in 39%, dissection in 11%, pseudoaneurysm in 18%, and anomalous arch in 11%. Rupture was identified in 14%. The average patient age was 59 years, and 46% were male.
In the open-repair group, 84 patients underwent a posterolateral thoracotomy and 9 had a median sternotomy. Extracorporeal perfusion was used in all, and 80 required deep hypothermic arrest.
In the endovascular group, the proximal extent of surgery was classified as Ishimaru zone 0 in 10 patients, zone 1 in 1, and zone 2 in 33. Treatment included full arch debranching and stent graft repair for zone 0 and zone 2 patients, respectively. A chimney stent of the carotid artery and left subclavian arterial bypass was used for the zone 1 patient.
Although the institutional preference is to utilize left subclavian artery (LSCA) revascularization for all, 76% of endovascular patients requiring LSCA coverage underwent preoperative bypass, Dr. Patel observed.
Significant differences existed at baseline between the two groups, with the endovascular group almost a full decade older than the open group (65 vs. 56 years). The endovascular group was also more likely to have saccular pathology (57% vs. 30%), and less likely to have a history of tobacco use (12% vs. 84%) or prior arch repair (16% vs. 36%).
Early morbidity included stroke in 6.6%, spinal cord ischemia in 0.7%, need for dialysis in 3.6%, and tracheostomy in 7.2%, Dr. Patel said.
The composite endpoint of stroke or early mortality was independently predicted by increasing age (odds ratio, 1.05; P = .055) and use of a hybrid procedure (OR, 6.4; P = .01).
Two-year freedom from aortic rupture or reintervention was 78% in the open group and 94% in the endovascular group (P = .02).
After a mean follow-up of 66 months, four patients had died of stroke, two from myocardial infarction, one from a proximal anastomosis disruption/rupture, and one from a type A dissection/rupture, Dr. Patel said.
The average survival was 145 months and 5-year survival rate was 59%.
Independent predictors of late mortality were increasing age (hazard ratio, 1.06; P = .001), peripheral vascular disease (HR, 2.4; P = .024), postoperative stroke (HR, 6.4; P less than .001), and postoperative dialysis (HR, 11.4; P less than .001). Notably, repair type was not predictive (P = .22), Dr. Patel said.
He cautioned the audience, however, that "cerebrovascular accidents remain an important cause of early and late mortality."
Dr. Patel reported consulting fees from W.L. Gore and Terumo.
CHICAGO – Repair of the isolated nontraumatic aortic arch aneurysm can be performed with acceptable early and late results, based on a 20-year review of 137 patients.
Early mortality was seen in nine patients (6.6%), and was similarly split between endovascular and open repair (7.3% vs. 6.5%, respectively).
Five-year survival did not differ between the endovascular- and open-repair groups (86% vs. 70%; P = .57), although the risk of reintervention was significantly higher with an endovascular strategy (94% vs. 77.5%; P = .02).
"These data support ongoing efforts to develop branched endografts specifically tailored for complex and difficult-to-treat pathology to potentially reduce the morbidity of therapy for this population," Dr. Himanshu J. Patel said at the annual meeting of the Midwestern Vascular Surgical Society.
Marginal landing zones and the need for complex arch debranching procedures to extend landing zones and facilitate repair can hinder endovascular repair, though open aortic repair is challenged by the frequent need for hypothermic circulatory arrest. Early and late results with either option are ill defined for this pathology, observed Dr. Patel, with the Cardiovascular Center, University of Michigan, Ann Arbor.
To investigate these outcomes, the authors evaluated data from 1993 to 2013 for 137 patients with nontraumatic aortic aneurysms located between the left and right pulmonary artery; 93 patients underwent open repair and 44 had an endovascular or hybrid repair.
The pathology was saccular in 39%, dissection in 11%, pseudoaneurysm in 18%, and anomalous arch in 11%. Rupture was identified in 14%. The average patient age was 59 years, and 46% were male.
In the open-repair group, 84 patients underwent a posterolateral thoracotomy and 9 had a median sternotomy. Extracorporeal perfusion was used in all, and 80 required deep hypothermic arrest.
In the endovascular group, the proximal extent of surgery was classified as Ishimaru zone 0 in 10 patients, zone 1 in 1, and zone 2 in 33. Treatment included full arch debranching and stent graft repair for zone 0 and zone 2 patients, respectively. A chimney stent of the carotid artery and left subclavian arterial bypass was used for the zone 1 patient.
Although the institutional preference is to utilize left subclavian artery (LSCA) revascularization for all, 76% of endovascular patients requiring LSCA coverage underwent preoperative bypass, Dr. Patel observed.
Significant differences existed at baseline between the two groups, with the endovascular group almost a full decade older than the open group (65 vs. 56 years). The endovascular group was also more likely to have saccular pathology (57% vs. 30%), and less likely to have a history of tobacco use (12% vs. 84%) or prior arch repair (16% vs. 36%).
Early morbidity included stroke in 6.6%, spinal cord ischemia in 0.7%, need for dialysis in 3.6%, and tracheostomy in 7.2%, Dr. Patel said.
The composite endpoint of stroke or early mortality was independently predicted by increasing age (odds ratio, 1.05; P = .055) and use of a hybrid procedure (OR, 6.4; P = .01).
Two-year freedom from aortic rupture or reintervention was 78% in the open group and 94% in the endovascular group (P = .02).
After a mean follow-up of 66 months, four patients had died of stroke, two from myocardial infarction, one from a proximal anastomosis disruption/rupture, and one from a type A dissection/rupture, Dr. Patel said.
The average survival was 145 months and 5-year survival rate was 59%.
Independent predictors of late mortality were increasing age (hazard ratio, 1.06; P = .001), peripheral vascular disease (HR, 2.4; P = .024), postoperative stroke (HR, 6.4; P less than .001), and postoperative dialysis (HR, 11.4; P less than .001). Notably, repair type was not predictive (P = .22), Dr. Patel said.
He cautioned the audience, however, that "cerebrovascular accidents remain an important cause of early and late mortality."
Dr. Patel reported consulting fees from W.L. Gore and Terumo.
AT MIDWESTERN VASCULAR 2013
Major finding: Five-year survival was 86% in the endovascular group and 70% in the open group (P = .57).
Data source: A retrospective study of 137 patients undergoing isolated aortic arch repair between 1993 and 2013.
Disclosures: Dr. Patel reported consulting fees from W.L. Gore and Terumo.

Renal injury taints proximal AAA repair
CHICAGO – Proximal abdominal aortic aneurysm repair can be achieved with a low perioperative mortality of about 3%, although renal dysfunction remains an Achilles’ heel, according to a 27-year review involving 245 patients.
In all, 60% of patients had postoperative acute kidney injury (AKI), 28% had persistent AKI at discharge, and 1.6% were discharged on hemodialysis. Persistent AKI at discharge was also associated with reduced long-term survival, Dr. Loay Kabbani said at the annual meeting of the Midwestern Vascular Surgical Society.

AKI stage was based on the Risk, Injury, Failure, Loss, and End-stage (RIFLE) kidney disease/Acute Kidney Injury Network (AKIN) classification system, with a change in serum creatinine of more than 0.3 mg/dL considered positive for injury. This is a much more sensitive criterion than what was used in previous studies, but is the new standard for reporting renal injury.
"This data should assist in establishing a benchmark for endovascular repair of these complex aneurysms," said Dr. Kabbani, a vascular surgeon at Henry Ford Hospital in Detroit.
The investigators identified 245 patients who underwent proximal AAA repair between 1986 and February 2013 at Henry Ford Hospital for juxtarenal (127), suprarenal (68), or type IV thoracoabdominal AAAs (50). The average aneurysm size was 6.4 cm (range, 3.1-14 cm), and mean preoperative estimated glomerular filtration rate was 62 mL/min per 1.73 m2 (range, 14-166 mL/min per 1.73 m2).
Most patients were male (69%), white (88.5%), and hypertensive (84%); 55% had chronic kidney disease based on a preoperative estimated glomerular filtration rate below 60 mL/min per 1.73 m2. Their average age was 71 years.
For most patients, the approach was retroperitoneal (48%) or thoracoabdominal (30%); the clamp was placed supraceliac (58%); and tube grafts were used (64%).
In-hospital mortality was 2.9% (7 patients) and 30-day mortality 3.3% (8 patients), Dr. Kabbani said.
Postoperative complications were AKI in 144 patients (60%), major pulmonary complications in 55 (22%), myocardial infarction in 9 (4%), return to the operating room for postoperative bleeding in 7 (3%), neurologic complications in 7 (3%), and bowel ischemia in 5 (2%).
Specifically, postoperative AKI was stage 1 (mild) in 35%, stage 2 (moderate) in 15%, and stage 3 (severe) in 10%, improving to 12%, 4%, and 3%, respectively, at discharge.
Though preoperative comorbidities were similar between patients with juxtarenal, suprarenal, and type IV aneurysms, postoperative complications increased significantly as the aneurysm extended more proximally (31% vs. 50% vs. 72%; P < .0001), Dr. Kabbani said.
Rates of AKI at discharge also followed the same pattern (18.2% vs. 35.4% vs. 43.8%; P less than .0012).
After a median follow-up of 54 months, the 5-year survival estimate was 70% and 10-year survival 43% based on a review of electronic medical records and the Social Security Death Index.
Cox regression analyses revealed no difference in long-term survival based on aneurysm type, but significantly worse survival based on increased aneurysm size (hazard ratio, 1.1; P = .01), preoperative chronic obstructive pulmonary disease (HR, 1.8; P = .002), congestive heart failure (HR, 3.5; P less than .001), history of stroke (HR, 1.9; P = .04), and persistent stage 2 (HR, 5.29; P = .001) and stage 3 AKI at discharge (HR, 2.71; P = .014), he said.
During a discussion of the results, Dr. Kabbani said the hospital usually uses mannitol (12.5-25 g) for renal protection and cold renal perfusion in select patients, although the latter did not jump out as a risk factor for CKI. The data were not broken down to see whether use of renal bypass during surgery affected outcomes for specific AAA types. Some attendees countered that renal protection should be used for all patients undergoing proximal AAA repair.
Dr. Kabbani reported having no financial disclosures.
CHICAGO – Proximal abdominal aortic aneurysm repair can be achieved with a low perioperative mortality of about 3%, although renal dysfunction remains an Achilles’ heel, according to a 27-year review involving 245 patients.
In all, 60% of patients had postoperative acute kidney injury (AKI), 28% had persistent AKI at discharge, and 1.6% were discharged on hemodialysis. Persistent AKI at discharge was also associated with reduced long-term survival, Dr. Loay Kabbani said at the annual meeting of the Midwestern Vascular Surgical Society.
AKI stage was based on the Risk, Injury, Failure, Loss, and End-stage (RIFLE) kidney disease/Acute Kidney Injury Network (AKIN) classification system, with a change in serum creatinine of more than 0.3 mg/dL considered positive for injury. This is a much more sensitive criterion than what was used in previous studies, but is the new standard for reporting renal injury.
"This data should assist in establishing a benchmark for endovascular repair of these complex aneurysms," said Dr. Kabbani, a vascular surgeon at Henry Ford Hospital in Detroit.
The investigators identified 245 patients who underwent proximal AAA repair between 1986 and February 2013 at Henry Ford Hospital for juxtarenal (127), suprarenal (68), or type IV thoracoabdominal AAAs (50). The average aneurysm size was 6.4 cm (range, 3.1-14 cm), and mean preoperative estimated glomerular filtration rate was 62 mL/min per 1.73 m2 (range, 14-166 mL/min per 1.73 m2).
Most patients were male (69%), white (88.5%), and hypertensive (84%); 55% had chronic kidney disease based on a preoperative estimated glomerular filtration rate below 60 mL/min per 1.73 m2. Their average age was 71 years.
For most patients, the approach was retroperitoneal (48%) or thoracoabdominal (30%); the clamp was placed supraceliac (58%); and tube grafts were used (64%).
In-hospital mortality was 2.9% (7 patients) and 30-day mortality 3.3% (8 patients), Dr. Kabbani said.
Postoperative complications were AKI in 144 patients (60%), major pulmonary complications in 55 (22%), myocardial infarction in 9 (4%), return to the operating room for postoperative bleeding in 7 (3%), neurologic complications in 7 (3%), and bowel ischemia in 5 (2%).
Specifically, postoperative AKI was stage 1 (mild) in 35%, stage 2 (moderate) in 15%, and stage 3 (severe) in 10%, improving to 12%, 4%, and 3%, respectively, at discharge.
Though preoperative comorbidities were similar between patients with juxtarenal, suprarenal, and type IV aneurysms, postoperative complications increased significantly as the aneurysm extended more proximally (31% vs. 50% vs. 72%; P < .0001), Dr. Kabbani said.
Rates of AKI at discharge also followed the same pattern (18.2% vs. 35.4% vs. 43.8%; P less than .0012).
After a median follow-up of 54 months, the 5-year survival estimate was 70% and 10-year survival 43% based on a review of electronic medical records and the Social Security Death Index.
Cox regression analyses revealed no difference in long-term survival based on aneurysm type, but significantly worse survival based on increased aneurysm size (hazard ratio, 1.1; P = .01), preoperative chronic obstructive pulmonary disease (HR, 1.8; P = .002), congestive heart failure (HR, 3.5; P less than .001), history of stroke (HR, 1.9; P = .04), and persistent stage 2 (HR, 5.29; P = .001) and stage 3 AKI at discharge (HR, 2.71; P = .014), he said.
During a discussion of the results, Dr. Kabbani said the hospital usually uses mannitol (12.5-25 g) for renal protection and cold renal perfusion in select patients, although the latter did not jump out as a risk factor for CKI. The data were not broken down to see whether use of renal bypass during surgery affected outcomes for specific AAA types. Some attendees countered that renal protection should be used for all patients undergoing proximal AAA repair.
Dr. Kabbani reported having no financial disclosures.
CHICAGO – Proximal abdominal aortic aneurysm repair can be achieved with a low perioperative mortality of about 3%, although renal dysfunction remains an Achilles’ heel, according to a 27-year review involving 245 patients.
In all, 60% of patients had postoperative acute kidney injury (AKI), 28% had persistent AKI at discharge, and 1.6% were discharged on hemodialysis. Persistent AKI at discharge was also associated with reduced long-term survival, Dr. Loay Kabbani said at the annual meeting of the Midwestern Vascular Surgical Society.
AKI stage was based on the Risk, Injury, Failure, Loss, and End-stage (RIFLE) kidney disease/Acute Kidney Injury Network (AKIN) classification system, with a change in serum creatinine of more than 0.3 mg/dL considered positive for injury. This is a much more sensitive criterion than what was used in previous studies, but is the new standard for reporting renal injury.
"This data should assist in establishing a benchmark for endovascular repair of these complex aneurysms," said Dr. Kabbani, a vascular surgeon at Henry Ford Hospital in Detroit.
The investigators identified 245 patients who underwent proximal AAA repair between 1986 and February 2013 at Henry Ford Hospital for juxtarenal (127), suprarenal (68), or type IV thoracoabdominal AAAs (50). The average aneurysm size was 6.4 cm (range, 3.1-14 cm), and mean preoperative estimated glomerular filtration rate was 62 mL/min per 1.73 m2 (range, 14-166 mL/min per 1.73 m2).
Most patients were male (69%), white (88.5%), and hypertensive (84%); 55% had chronic kidney disease based on a preoperative estimated glomerular filtration rate below 60 mL/min per 1.73 m2. Their average age was 71 years.
For most patients, the approach was retroperitoneal (48%) or thoracoabdominal (30%); the clamp was placed supraceliac (58%); and tube grafts were used (64%).
In-hospital mortality was 2.9% (7 patients) and 30-day mortality 3.3% (8 patients), Dr. Kabbani said.
Postoperative complications were AKI in 144 patients (60%), major pulmonary complications in 55 (22%), myocardial infarction in 9 (4%), return to the operating room for postoperative bleeding in 7 (3%), neurologic complications in 7 (3%), and bowel ischemia in 5 (2%).
Specifically, postoperative AKI was stage 1 (mild) in 35%, stage 2 (moderate) in 15%, and stage 3 (severe) in 10%, improving to 12%, 4%, and 3%, respectively, at discharge.
Though preoperative comorbidities were similar between patients with juxtarenal, suprarenal, and type IV aneurysms, postoperative complications increased significantly as the aneurysm extended more proximally (31% vs. 50% vs. 72%; P < .0001), Dr. Kabbani said.
Rates of AKI at discharge also followed the same pattern (18.2% vs. 35.4% vs. 43.8%; P less than .0012).
After a median follow-up of 54 months, the 5-year survival estimate was 70% and 10-year survival 43% based on a review of electronic medical records and the Social Security Death Index.
Cox regression analyses revealed no difference in long-term survival based on aneurysm type, but significantly worse survival based on increased aneurysm size (hazard ratio, 1.1; P = .01), preoperative chronic obstructive pulmonary disease (HR, 1.8; P = .002), congestive heart failure (HR, 3.5; P less than .001), history of stroke (HR, 1.9; P = .04), and persistent stage 2 (HR, 5.29; P = .001) and stage 3 AKI at discharge (HR, 2.71; P = .014), he said.
During a discussion of the results, Dr. Kabbani said the hospital usually uses mannitol (12.5-25 g) for renal protection and cold renal perfusion in select patients, although the latter did not jump out as a risk factor for CKI. The data were not broken down to see whether use of renal bypass during surgery affected outcomes for specific AAA types. Some attendees countered that renal protection should be used for all patients undergoing proximal AAA repair.
Dr. Kabbani reported having no financial disclosures.
AT MIDWESTERN VASCULAR 2013
Major finding: Perioperative mortality was 2.9%, but 60% of patients had postoperative acute kidney injury.
Data source: A retrospective analysis of 245 patients undergoing open proximal abdominal aortic aneurysm repair.
Disclosures: Dr. Kabbani reported having no financial disclosures.

Lower-dose quizartinib diminishes QT events
NEW ORLEANS – Lower doses of quizartinib reduced worrisome QT-interval prolongation events without a loss of efficacy in patients with FLT3-ITD–positive relapsed or refractory acute myeloid leukemia, a phase II study shows.
In a 76-patient study, grade 2 QT-interval prolongation (QTcF) of more than 480-500 msec occurred in two patients (5%) on oral quizartinib 30 mg/day and in five patients (14%) on 60 mg/day, with no differences between groups in QTcF events of more than 500 msec (5% vs. 3%).
In addition, an increase in QTcF from baseline of more than 60 msec was seen in 19% of patients on the 60-mg dose and in 3% of those on the 30-mg dose, Dr. Jorge Cortes reported at the annual meeting of the American Society of Hematology.
About a third of patients with acute myeloid leukemia (AML) will have FLT3 internal tandem duplications (FLT3-ITD), which are associated with early relapse and poor survival in AML. Quizartinib has shown the highest single-agent activity among FMS-like tyrosine kinase 3 (FLT3)-targeted agents in this population, according to Dr. Cortes.
At last year’s ASH meeting, investigators presented results from a phase II study in which the investigational agent elicited responses in both FLT3-positive and -negative relapsed/refractory AML. The unprecedented results at doses of 90, 135, and 200 mg were partially eclipsed, however, by respective 46%, 39%, and 92% increases in QTcF from baseline of more than 60 msec, noted Dr. Cortes, chair of the AML section, department of leukemia, University of Texas M.D. Anderson Cancer Center, Houston.
The current study randomized 76 patients to quizartinib 30 mg or 60 mg continuous daily dosing for primary AML or AML secondary to myelodysplastic syndrome that relapsed or was refractory to first-line salvage therapy or prior hematopoietic stem cell transplantation. The coprimary endpoints were rate of grade 2 QTc prolongation and the composite complete remission rate, which included complete remission (CR), CR with incomplete platelet recovery, and CR with incomplete hematologic recovery.
In all, 92% of patients had FLT3 internal tandem duplications, and 58 of 60 evaluable patients had intermediate or poor cytogenetic risk. Their mean age was 55 years. Two patients were randomized but not treated.
Treatment with the 30-mg and 60-mg doses resulted in a composite CR rate of 47%, Dr. Cortes said. The median duration of response was 4.1 weeks in the 30-mg group and 20 weeks in the 60-mg group.
Two patients (5%) on the 30-mg dose and 1 patient (3%) on the 60-mg dose achieved CR; 1 patient (3%) in the 60-mg group had a CR with incomplete platelet recovery; and 16 patients (42%) in each arm had a CR with incomplete hematologic recovery.
Partial responses were also seen in 5 patients (13%) in the 30-mg group and 9 (24%) in the 60-mg group.
These results compare favorably with composite CR rates of 47%, 45%, and 42% with the 90-, 135-, and 200-mg doses used in the earlier study, Dr. Cortes observed.
Median overall survival in the current study was 20.7 weeks in the lower-dose group and 25.4 weeks with the 60-mg dose.
Importantly, 34% of patients were successfully bridged to transplant, extending median survival to 31 weeks for those on 30 mg of quizartinib and to 28.1 weeks for those given 60 mg.
"This study demonstrates there is certainly sustained efficacy with these lower doses of quizartinib and a decreased QT signal at doses of 30 and 60 mg compared with the higher doses we’ve tested in the past," Dr. Cortes concluded.
Grade 3/4 adverse events were mainly anemia (39%) in the 30-mg group and febrile neutropenia (36%) in the 60-mg group. Three patients required dose reductions due to QTc prolongation.
A global phase III randomized study of quizartinib in FLT3-ITD–positive patients in first relapse is planned to start in early 2014, he said.
Development of quizartinib has been somewhat rocky, with Astellas Pharma announcing in March 2013 it was ending its collaboration with Ambit Biosciences to develop FLT3 inhibitors including quizartinib.
Dr. Cortes reported research funding from Astellas Pharma, Arog, Novartis, and Ambit Biosciences, which is developing quizartinib, and consulting for Astellas, Arog, and Ambit.
NEW ORLEANS – Lower doses of quizartinib reduced worrisome QT-interval prolongation events without a loss of efficacy in patients with FLT3-ITD–positive relapsed or refractory acute myeloid leukemia, a phase II study shows.
In a 76-patient study, grade 2 QT-interval prolongation (QTcF) of more than 480-500 msec occurred in two patients (5%) on oral quizartinib 30 mg/day and in five patients (14%) on 60 mg/day, with no differences between groups in QTcF events of more than 500 msec (5% vs. 3%).
In addition, an increase in QTcF from baseline of more than 60 msec was seen in 19% of patients on the 60-mg dose and in 3% of those on the 30-mg dose, Dr. Jorge Cortes reported at the annual meeting of the American Society of Hematology.
About a third of patients with acute myeloid leukemia (AML) will have FLT3 internal tandem duplications (FLT3-ITD), which are associated with early relapse and poor survival in AML. Quizartinib has shown the highest single-agent activity among FMS-like tyrosine kinase 3 (FLT3)-targeted agents in this population, according to Dr. Cortes.
At last year’s ASH meeting, investigators presented results from a phase II study in which the investigational agent elicited responses in both FLT3-positive and -negative relapsed/refractory AML. The unprecedented results at doses of 90, 135, and 200 mg were partially eclipsed, however, by respective 46%, 39%, and 92% increases in QTcF from baseline of more than 60 msec, noted Dr. Cortes, chair of the AML section, department of leukemia, University of Texas M.D. Anderson Cancer Center, Houston.
The current study randomized 76 patients to quizartinib 30 mg or 60 mg continuous daily dosing for primary AML or AML secondary to myelodysplastic syndrome that relapsed or was refractory to first-line salvage therapy or prior hematopoietic stem cell transplantation. The coprimary endpoints were rate of grade 2 QTc prolongation and the composite complete remission rate, which included complete remission (CR), CR with incomplete platelet recovery, and CR with incomplete hematologic recovery.
In all, 92% of patients had FLT3 internal tandem duplications, and 58 of 60 evaluable patients had intermediate or poor cytogenetic risk. Their mean age was 55 years. Two patients were randomized but not treated.
Treatment with the 30-mg and 60-mg doses resulted in a composite CR rate of 47%, Dr. Cortes said. The median duration of response was 4.1 weeks in the 30-mg group and 20 weeks in the 60-mg group.
Two patients (5%) on the 30-mg dose and 1 patient (3%) on the 60-mg dose achieved CR; 1 patient (3%) in the 60-mg group had a CR with incomplete platelet recovery; and 16 patients (42%) in each arm had a CR with incomplete hematologic recovery.
Partial responses were also seen in 5 patients (13%) in the 30-mg group and 9 (24%) in the 60-mg group.
These results compare favorably with composite CR rates of 47%, 45%, and 42% with the 90-, 135-, and 200-mg doses used in the earlier study, Dr. Cortes observed.
Median overall survival in the current study was 20.7 weeks in the lower-dose group and 25.4 weeks with the 60-mg dose.
Importantly, 34% of patients were successfully bridged to transplant, extending median survival to 31 weeks for those on 30 mg of quizartinib and to 28.1 weeks for those given 60 mg.
"This study demonstrates there is certainly sustained efficacy with these lower doses of quizartinib and a decreased QT signal at doses of 30 and 60 mg compared with the higher doses we’ve tested in the past," Dr. Cortes concluded.
Grade 3/4 adverse events were mainly anemia (39%) in the 30-mg group and febrile neutropenia (36%) in the 60-mg group. Three patients required dose reductions due to QTc prolongation.
A global phase III randomized study of quizartinib in FLT3-ITD–positive patients in first relapse is planned to start in early 2014, he said.
Development of quizartinib has been somewhat rocky, with Astellas Pharma announcing in March 2013 it was ending its collaboration with Ambit Biosciences to develop FLT3 inhibitors including quizartinib.
Dr. Cortes reported research funding from Astellas Pharma, Arog, Novartis, and Ambit Biosciences, which is developing quizartinib, and consulting for Astellas, Arog, and Ambit.
NEW ORLEANS – Lower doses of quizartinib reduced worrisome QT-interval prolongation events without a loss of efficacy in patients with FLT3-ITD–positive relapsed or refractory acute myeloid leukemia, a phase II study shows.
In a 76-patient study, grade 2 QT-interval prolongation (QTcF) of more than 480-500 msec occurred in two patients (5%) on oral quizartinib 30 mg/day and in five patients (14%) on 60 mg/day, with no differences between groups in QTcF events of more than 500 msec (5% vs. 3%).
In addition, an increase in QTcF from baseline of more than 60 msec was seen in 19% of patients on the 60-mg dose and in 3% of those on the 30-mg dose, Dr. Jorge Cortes reported at the annual meeting of the American Society of Hematology.
About a third of patients with acute myeloid leukemia (AML) will have FLT3 internal tandem duplications (FLT3-ITD), which are associated with early relapse and poor survival in AML. Quizartinib has shown the highest single-agent activity among FMS-like tyrosine kinase 3 (FLT3)-targeted agents in this population, according to Dr. Cortes.
At last year’s ASH meeting, investigators presented results from a phase II study in which the investigational agent elicited responses in both FLT3-positive and -negative relapsed/refractory AML. The unprecedented results at doses of 90, 135, and 200 mg were partially eclipsed, however, by respective 46%, 39%, and 92% increases in QTcF from baseline of more than 60 msec, noted Dr. Cortes, chair of the AML section, department of leukemia, University of Texas M.D. Anderson Cancer Center, Houston.
The current study randomized 76 patients to quizartinib 30 mg or 60 mg continuous daily dosing for primary AML or AML secondary to myelodysplastic syndrome that relapsed or was refractory to first-line salvage therapy or prior hematopoietic stem cell transplantation. The coprimary endpoints were rate of grade 2 QTc prolongation and the composite complete remission rate, which included complete remission (CR), CR with incomplete platelet recovery, and CR with incomplete hematologic recovery.
In all, 92% of patients had FLT3 internal tandem duplications, and 58 of 60 evaluable patients had intermediate or poor cytogenetic risk. Their mean age was 55 years. Two patients were randomized but not treated.
Treatment with the 30-mg and 60-mg doses resulted in a composite CR rate of 47%, Dr. Cortes said. The median duration of response was 4.1 weeks in the 30-mg group and 20 weeks in the 60-mg group.
Two patients (5%) on the 30-mg dose and 1 patient (3%) on the 60-mg dose achieved CR; 1 patient (3%) in the 60-mg group had a CR with incomplete platelet recovery; and 16 patients (42%) in each arm had a CR with incomplete hematologic recovery.
Partial responses were also seen in 5 patients (13%) in the 30-mg group and 9 (24%) in the 60-mg group.
These results compare favorably with composite CR rates of 47%, 45%, and 42% with the 90-, 135-, and 200-mg doses used in the earlier study, Dr. Cortes observed.
Median overall survival in the current study was 20.7 weeks in the lower-dose group and 25.4 weeks with the 60-mg dose.
Importantly, 34% of patients were successfully bridged to transplant, extending median survival to 31 weeks for those on 30 mg of quizartinib and to 28.1 weeks for those given 60 mg.
"This study demonstrates there is certainly sustained efficacy with these lower doses of quizartinib and a decreased QT signal at doses of 30 and 60 mg compared with the higher doses we’ve tested in the past," Dr. Cortes concluded.
Grade 3/4 adverse events were mainly anemia (39%) in the 30-mg group and febrile neutropenia (36%) in the 60-mg group. Three patients required dose reductions due to QTc prolongation.
A global phase III randomized study of quizartinib in FLT3-ITD–positive patients in first relapse is planned to start in early 2014, he said.
Development of quizartinib has been somewhat rocky, with Astellas Pharma announcing in March 2013 it was ending its collaboration with Ambit Biosciences to develop FLT3 inhibitors including quizartinib.
Dr. Cortes reported research funding from Astellas Pharma, Arog, Novartis, and Ambit Biosciences, which is developing quizartinib, and consulting for Astellas, Arog, and Ambit.
AT ASH 2013
Major finding: An increase in QTcF from baseline of more than 60 msec was seen in 19% of patients on quizartinib 60 mg and in 3% of those on 30 mg.
Data source: A prospective phase II study of 76 patients with relapsed/refractory AML.
Disclosures: Dr. Cortes reported research funding from Astellas Pharma, Arog, Novartis, and Ambit Biosciences, which is developing quizartinib, and consulting for Astellas, Arog, and Ambit.